Alzheimer disease pathology in cognitively healthy elderly: A genome-wide study
10
Neurobiology of Aging 32 (2011) 2113–2122 Alzheimer disease pathology in cognitively healthy elderly: A genome-wide study Patricia L. Kramer a,b,∗ , Haiyan Xu e , Randall L. Woltjer c , Shawn K. Westaway a,q , David Clark c , Deniz Erten-Lyons a , Jeffrey A. Kaye a,d , Kathleen A. Welsh-Bohmer f , Juan C. Troncoso g , William R. Markesbery h , Ronald C. Petersen i , R. Scott Turner j,k , Walter A. Kukull l , David A. Bennett m , Douglas Galasko n , John C. Morris o , Jurg Ott p a Department of Neurology, Oregon Health & Science University, Portland, OR 97239, USA b Department of Molecular and Medical Genetics, Oregon Health & Science University, Portland, OR 97239, USA c Department of Pathology, Oregon Health & Science University, Portland, OR 97239, USA d Department of Biomedical Engineering, Oregon Health & Science University, Portland, OR 97239, USA e Laboratory of Statistical Genetics, Rockefeller University, New York, NY 10065, USA f Department of Psychiatry and Medicine (Neurology), Duke University Medical Center, Durham, NC 27710, USA g Department of Pathology and Neurology, Johns Hopkins University, Baltimore, MD 21205, USA h Department of Pathology and Neurology, University of Kentucky, Lexington, KY 40536, USA i Department of Neurology, Mayo Clinic, Rochester, MN 55905, USA j Department of Neurology, University of Michigan, Ann Arbor, MI 48105, USA k Georgetown University Medical Center, Washington DC, 20057, USA l National Alzheimer Coordinating Center and Department of Epidemiology, Seattle, WA 98105, USA m Rush University Medical Center, Chicago, IL 60612, USA n Department of Neurosciences, University of California at San Diego, San Diego, CA 92037, USA o Department of Neurology, Washington University School of Medicine, St. Louis, MO 63108, USA p Beijing Institute of Genomics, Chinese Academy of Sciences, Beijing 100029, China q Department of Cardiology, Oregon Health & Science University, Portland, OR 97239, USA Received 23 November 2009; received in revised form 11 January 2010; accepted 14 January 2010 Available online 7 May 2010 Abstract Many elderly individuals remain dementia-free throughout their life. However, some of these individuals exhibit Alzheimer disease neu- ropathology on autopsy, evidenced by neurofibrillary tangles (NFTs) in AD-specific brain regions. We conducted a genome-wide association study to identify genetic mechanisms that distinguish non-demented elderly with a heavy NFT burden from those with a low NFT burden. The study included 299 non-demented subjects with autopsy (185 subjects with low and 114 with high NFT levels). Both a genotype test, using logistic regression, and an allele test provided consistent evidence that variants in the RELN gene are associated with neuropathology in the context of cognitive health. Immunohistochemical data for reelin expression in AD-related brain regions added support for these findings. Reelin signaling pathways modulate phosphorylation of tau, the major component of NFTs, either directly or through -amyloid pathways that influence tau phosphorylation. Our findings suggest that up-regulation of reelin may be a compensatory response to tau-related or beta-amyloid stress associated with AD even prior to the onset of dementia. © 2010 Elsevier Inc. All rights reserved. Keywords: Genome-wide association study; Alzheimer disease; Non-demented elderly with AD neuropathology; Non-demented elderly without AD neu- ropathology; Reelinneurofibrillary tangles ∗ Corresponding author at: Department of Neurology, CR131, Oregon Health & Science University, Portland, OR 97239, USA. Tel.: +1 503 494 7196; fax: +1 503 494 7499. E-mail address: [email protected] (P.L. Kramer). 0197-4580/$ – see front matter © 2010 Elsevier Inc. All rights reserved. doi:10.1016/j.neurobiolaging.2010.01.010
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Alzheimer disease pathology in cognitively healthy elderly: A genome-wide study

A
rsTutRis©
Kr
0d
Neurobiology of Aging 32 (2011) 2113–2122
Alzheimer disease pathology in cognitively healthy elderly:A genome-wide study
Patricia L. Kramer a,b,∗, Haiyan Xu e, Randall L. Woltjer c, Shawn K. Westaway a,q,David Clark c, Deniz Erten-Lyons a, Jeffrey A. Kaye a,d, Kathleen A. Welsh-Bohmer f,Juan C. Troncoso g, William R. Markesbery h, Ronald C. Petersen i, R. Scott Turner j,k,
Walter A. Kukull l, David A. Bennett m, Douglas Galasko n, John C. Morris o, Jurg Ott p
a Department of Neurology, Oregon Health & Science University, Portland, OR 97239, USAb Department of Molecular and Medical Genetics, Oregon Health & Science University, Portland, OR 97239, USA
c Department of Pathology, Oregon Health & Science University, Portland, OR 97239, USAd Department of Biomedical Engineering, Oregon Health & Science University, Portland, OR 97239, USA
e Laboratory of Statistical Genetics, Rockefeller University, New York, NY 10065, USAf Department of Psychiatry and Medicine (Neurology), Duke University Medical Center, Durham, NC 27710, USA
g Department of Pathology and Neurology, Johns Hopkins University, Baltimore, MD 21205, USAh Department of Pathology and Neurology, University of Kentucky, Lexington, KY 40536, USA
i Department of Neurology, Mayo Clinic, Rochester, MN 55905, USAj Department of Neurology, University of Michigan, Ann Arbor, MI 48105, USA
k Georgetown University Medical Center, Washington DC, 20057, USAl National Alzheimer Coordinating Center and Department of Epidemiology, Seattle, WA 98105, USA
m Rush University Medical Center, Chicago, IL 60612, USAn Department of Neurosciences, University of California at San Diego, San Diego, CA 92037, USAo Department of Neurology, Washington University School of Medicine, St. Louis, MO 63108, USA
p Beijing Institute of Genomics, Chinese Academy of Sciences, Beijing 100029, Chinaq Department of Cardiology, Oregon Health & Science University, Portland, OR 97239, USA
Received 23 November 2009; received in revised form 11 January 2010; accepted 14 January 2010Available online 7 May 2010
bstract
Many elderly individuals remain dementia-free throughout their life. However, some of these individuals exhibit Alzheimer disease neu-opathology on autopsy, evidenced by neurofibrillary tangles (NFTs) in AD-specific brain regions. We conducted a genome-wide associationtudy to identify genetic mechanisms that distinguish non-demented elderly with a heavy NFT burden from those with a low NFT burden.he study included 299 non-demented subjects with autopsy (185 subjects with low and 114 with high NFT levels). Both a genotype test,sing logistic regression, and an allele test provided consistent evidence that variants in the RELN gene are associated with neuropathology inhe context of cognitive health. Immunohistochemical data for reelin expression in AD-related brain regions added support for these findings.eelin signaling pathways modulate phosphorylation of tau, the major component of NFTs, either directly or through �-amyloid pathways that
nfluence tau phosphorylation. Our findings suggest that up-regulation of reelin may be a compensatory response to tau-related or beta-amyloidtress associated with AD even prior to the onset of dementia.
2010 Elsevier Inc. All rights reserved.
ented e
eywords: Genome-wide association study; Alzheimer disease; Non-dem opathology; Reelinneurofibrillary tangles∗ Corresponding author at: Department of Neurology, CR131, Oregon Health & Sfax: +1 503 494 7499.
E-mail address: [email protected] (P.L. Kramer).
197-4580/$ – see front matter © 2010 Elsevier Inc. All rights reserved.oi:10.1016/j.neurobiolaging.2010.01.010
lderly with AD neuropathology; Non-demented elderly without AD neu-
cience University, Portland, OR 97239, USA. Tel.: +1 503 494 7196;

2 logy of
1
ststnrBicw
nvstvogin
(bnmfcmfielsesii
2
2
la((d(sgww
2
l(fd0nC
owiigL
(
(
(
(
1
2
ftwR
tj(su
114 P.L. Kramer et al. / Neurobio
. Introduction
Prevalence rates for Alzheimer disease (AD) climbteadily from ∼1% in 65-year-olds to as high as 40% byhe age of 85 (Hebert et al., 2003). Despite these dire figures,ome elderly individuals remain dementia-free throughoutheir life and, of these, a proportion exhibit substantial ADeuropathology, in the form of amyloid plaques and neurofib-illary tangles (NFTs), at autopsy (Erten-Lyons et al., 2009;ennett et al., 2005). Thus, individuals differ in their capac-
ty to maintain normative cognitive function even within theontext of neuropathological structural changes associatedith AD.There are a number of ways in which genetic mecha-
isms might promote cognitive health. On one hand, geneticariants may prevent development of the neuropathologicalubstrate that underlies susceptibility to cognitive dysfunc-ion. Alternatively, in the presence of neuropathology, geneticariants may mitigate the effects of AD-related lesions thattherwise result in cognitive decline. The first case providesreater guarantee of cognitive health. Thus, it is important todentify genetic variants associated with development of ADeuropathology within the context of cognitive resilience.
We conducted a genome-wide SNP association studyGWAS) to identify genetic mechanisms involved in healthyrain aging. This study was based on a sample ofon-demented, deceased subjects with autopsy who wereembers of longitudinal healthy aging cohorts at 10 NIA-
unded Alzheimer Disease Centers (ADC). These subjectsomprised one group with little or no evidence of NFT for-ation, and one with substantial or severe levels of NFT
ormation in critical brain regions. We report results thatmplicate variants in the glycoprotein reelin (RELN) as keylements in the molecular basis of AD-related neuropatho-ogical processes. We provide additional support for thesetatistical findings with immunohistochemical data for reelinxpression in AD-related brain regions in a subset of our studyubjects. To our knowledge, this is the first GWAS that specif-cally addresses genetic mechanisms of AD neuropathologyn non-demented elderly with post-mortem examinations.
. Methods
.1. Subjects
Subjects were recruited from aging research cohorts col-ected over the last two decades at 10 NIA-funded ADCscross the country. Eligibility criteria included the following:1) ≥65 years old at enrollment; (2) deceased, with autopsy;3) clinical diagnosis of “no dementia” at enrollment andeath; (4) ≥1 clinical evaluation within the year before death;5) DNA available; (6) Caucasian ancestry. A total of 412
ubjects met initial criteria. All subjects had been previouslyenotyped for apolipoproteinE (APOE) status and these dataere provided by the respective ADC Data Cores. The studyas approved by the IRB at OHSU.ssdd
Aging 32 (2011) 2113–2122
.2. Neuropathologic diagnosis
One of the hallmarks of AD is the occurrence of NFTs inimbic and neocortical regions of the brain. The Braak scoreBraak and Braak, 1991) is a measure of the location andrequency of NFTs and is a key to establishing the pathologiciagnosis of AD (NIA, 1997). Braak scores (BS) range from(no NFTs) to 6 (NFTs in primary motor and/or sensory
eocortex), and were obtained for all subjects from the ADClinical Data Cores.
We classified subjects on the basis of NFT burden tobtain subsets of individuals for analysis. Autopsy reportsere reviewed for consistency with the Braak score provided
n the data files from each ADC by a three-member teamncluding a neuropathologist (RW), a neurologist (JK) and aeneticist (PK). Subjects were classified into three groups:O Braak (≤2), MED Braak and HI Braak (≥4):
1) If the Braak score and information in the autopsy reportwere consistent with low NFT levels, the subject wasclassified as LO Braak (n = 182).
2) If the Braak score and information in the autopsy wereconsistent with high NFT levels, the subject was classi-fied as HI Braak (n = 105).
3) If the Braak score and autopsy information were at oddswith respect to classification of LO or HI NFT burden,preference was given to the autopsy (n = 12).
4) If the Braak score and autopsy information agreed witha Braak score of 3, the subjects was classified as MEDBraak (n = 73); furthermore, if the Braak score was 2,3 or 4, but the autopsy report lacked sufficient detail toconfirm these scores, the subject was also classified asMED Braak (n = 17). In order to maximize phenotypichomogeneity between groups, and thus increase power,we excluded this group from the initial analysis.
The final sample consisted of 299 subjects (185 LO Braak,14 HI Braak).
.3. Clinical diagnosis
All study subjects were deceased and had been evaluatedor cognitive decline and dementia within 12 months prioro death. Assessments for determining absence of dementiaere consistent with standardized protocols in the DSM-III-.
To minimize the extent of any cognitive impairment in thewo groups, we obtained longitudinal clinical data for all sub-ects, consisting of Clinical Dementia Rating (CDR) scoresMorris, 1993) and/or Mini-Mental State Exam (MMSE)cores (Folstein et al., 1975), from the time of enrollmentntil death. The CDR is a dementia staging-tool in which a
core of 0 represents no cognitive impairment, .5 may repre-ent some cognitive impairment, and a score ≥1 representsementia; MMSE scores ≥26 are generally indicative of noementia.
logy of
2(ABLsCsM
2
uDwGtd
jHfmc
2
2
rcref(ardta
2
batSaosgewc
vt
aiatrrbtpeBS
sta1
aaiscmgttpofoagwr2cpr
2
i(p
2For particular SNPs of interest, we conducted a post hoc
P.L. Kramer et al. / Neurobio
Longitudinal CDR scores were available for 134 of the99 subjects. Of these, 116 (87%) had no CDR scores >0; 1813%) had one CDR of .5 at some point during participation.mong these 18, 13 were in the LO Braak and 5 in the HIraak group. In the majority of these 18 subjects – 10 in theO and 2 in the HI Braak group – the CDR of .5 occurred atome point prior to the last evaluation and was followed byDRs of 0 in subsequent evaluations. Longitudinal MMSE
cores were available for the remaining 165 subjects. All hadMSE ≥26 at death (mean = 28.4; sd = 1.3).
.4. Genotyping
DNA was extracted from blood in 85 of the 299 subjects,sing standard procedures. For the remaining 214 subjects,NA was extracted from frozen brain tissue. Genomic DNAas extracted from 100 mg of brain tissue using the Wizardenomic DNA Purification Kit according to the manufac-
urer (Promega, Inc.). DNA quality and concentration wereetermined using a Biomate-3 spectrophotometer.
Genotyping was performed by deCODE Genetics (Reyk-avik, Iceland). Genotypes were obtained using the IlluminaumanCNV370v1 C array from 750 ng of genomic DNA
ollowing manufacturer’s protocols (Illumina, Inc.). Illu-ina’s BeadStudio3.1.14 genotyping module was used to
luster, call genotypes, and assign confidence scores.
.5. Analysis
.5.1. Quality controlWe included only individuals with a missing genotype
ate <2%. Since SNPs with low call rates may inflate asso-iation statistics (Plenge et al., 2007), only SNPs with callates ≥99% across the entire sample were used (19,310 SNPsxcluded due to low call rates). Only SNPs with a minor allelerequency (MAF) >0.05 in cases and controls were included18,882 SNPs excluded for low MAF). We also requiredbsence of strong deviation from Hardy-Weinberg equilib-ium (HWE) (p < .001) in controls; (728 SNPs excluded foreviation from HWE). As a result of these quality con-rol measures, a total of 307,992 SNPs were used in thisnalysis.
.5.2. Association analysisTwo different methods were used to test for the association
etween SNPs and the phenotype-association at the genotypend at the allele level. The former was carried out via logis-ic regression analysis with covariates and the latter with theet Association approach (Hoh et al., 2001) without covari-tes. We tested the effect of putative non-genetic risk factorsn the phenotype, and found that sex and age-at-death had aignificant impact. Thus in the logistic regression approach,
enotypes at a given SNP (a categorical variable), sex (a cat-gorical variable) and age of death (a continuous variable)ere included as independent variables, and the Braak scoreategory, HI (“case”) vs. LO (“control”), as the dependent
atov
Aging 32 (2011) 2113–2122 2115
ariable. The logistic regression analysis was carried out withhe PLINK program (Purcell et al., 2007).
We chose a genotypic model because it is a general model,nd is sensitive to different types of association. It is alsodeally suited for logistic regression analysis, in which wellow for the total effects of genotypes and non-genetic fac-ors, the latter of which act on individuals (i.e., genotypes)ather than alleles. Since the logistic regression result is mostobust when all three possible genotypes are represented inoth comparison groups, we only included SNPs in whichhis was the case; of the 299,081 autosomal SNPs whichassed quality control measures described above, 6906 werexcluded because there were <3 genotype classes in the HIraak and/or LO Braak groups. Thus, the total number ofNPs in the logistic regression analysis was 292,175.
To estimate the genomic control factor, lambda «use lc Gkymbol», we initially carried out 1 df chi-square tests in 2 × 2ables of alleles for each of the 292,175 SNPs and constructedQ–Q plot for the resulting chi-square values using the Systat2 statistics package (http://www.systat.com/).
In Set Association analysis (Hoh et al., 2001), we evalu-ted the combined effects of multiple SNPs. The combinedssociation of a given number of SNPs (wherever they aren the genome) was measured by the sum of their corre-ponding test statistics. As the SNP-specific test statistic, wehose the absolute difference between cases and controls ofean genotype codes, where codes of 0, 1, and 2 represented
enotypes AA, AB, and BB, respectively. Thus, the geno-ype code reflects the number of B alleles in the genotype sohat the mean absolute difference of genotype codes is thearametric equivalent of the Armitage trend test. We focusedn the most significant m SNPs, with m ranging successivelyrom 1 through 10. Significance levels for each such sumf test statistics were evaluated with permutation analysis,nd the smallest p-value for these sums was taken as theenome-wide overall test statistic, whose significance levelas again evaluated in randomization samples. This approach
epresents an approximation to multivariate analysis (Manly,007) and, thus, assesses the joint effects of the most signifi-ant SNPs on disease association. In this analysis, the sumstatrogram was used with 10,000 randomization samples perun (http://linkage.rockefeller.edu/ott/sumstat.html).
.5.3. Population stratificationWe used the agglomerative clustering method based on
dentity by state (IBS), as implemented in PLINK v1.05Purcell et al., 2007) (http://pngu.mgh.harvard.edu/∼purcell/link/) to test for population stratification in our data.
.5.4. Post hoc analysis
nalysis in which allelic association to the phenotype wasested with a likelihood ratio (LR), chi-square test, and thedds ratio (OR) were calculated with a 95% confidence inter-al (CI).

2 logy of Aging 32 (2011) 2113–2122
2
fwfi2pap8wCwLnpbtpbc3mwh
3
3
it(i(apc(
bBpwlo
3
twtn
Fc
Sltaicusei
tSetrcc
arwnntrOag
116 P.L. Kramer et al. / Neurobio
.5.5. ImmunohistochemistryImmunohistochemistry for reelin expression was per-
ormed on cases with autopsy performed at OHSU and forhich the postmortem interval was less than 24 h. Brains werexed in neutral-buffered formaldehyde solution for at leastweeks and fixed hippocampal sections were processed in
araffin 7-�m sections, deparaffinized, subjected to standardntigen retrieval techniques (5 min treatment at room tem-erature with 95% formic acid, followed by incubation at5–90 ◦C in citrate buffer, pH 6.0 for 30 min) and stainedith antibody to reelin (Santa Cruz Biotechnology, Santaruz, CA, antibody H221 used at 1:200 dilution). Sectionsere developed using the Vectastain ABC technique (Vectoraboratories, Burlingame, CA). Reelin staining of pyramidaleurons was evaluated in CA1-4 regions of the hippocam-us and in subiculum by a neuropathologist (RLW) who waslinded to case status. A semiquantitative score was assignedo reelin positivity in pyramidal neurons in each hippocam-al sector (0 = no detectable reelin staining, 1 = cytoplasmiclush staining detectable at 40× magnification, 2 = clearytoplasmic staining identifiable at 10× magnification, and= pyramidal neurons identified as strong band of cytoplas-ic staining visible at 4× magnification. Total reelin stainingas calculated as the sum of the score in each region ofippocampus.
. Results
.1. Sample characteristics
Sample characteristics of the two groups are providedn Table 1. The proportion of females is increased inhe HI Braak group, and the difference is significantp = 0.031). Subjects in the HI Braak category were signif-cantly older at death than those in the LO Braak groupp < .0001); thus, we incorporated both gender and age-t-death as covariates. APOE allele frequencies (based onre-determined APOE genotypes) did not differ signifi-antly between groups (p = .756), nor did education levelp = .090).
The distribution of neuritic plaque density was differentetween groups (p < 0.031). Only 29% of subjects in the LOraak category had “frequent” or “moderate” plaques, com-ared to 68% in the HI category. Hence, although Braak scoreas used to stratify groups by AD-associated neuropatho-
ogical features, stratification by neuritic plaque burden alsoccurred.
.2. Analysis
Results of the test for population stratification indicated
hat all subjects were assigned to the same cluster, and thereas no significant difference between pair-wise IBS dis-ances in the LO and HI Braak groups. Thus, we detectedo evidence for population stratification.
hsg
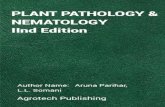
ig. 1. Q–Q plot based on nominal p-values resulting from the allelic asso-iation test.
Allelic association for one SNP at a time resulted in oneNP, rs4298437 on chromosome 7, showing a significance
evel of p = 0.0833 (corrected for multiple testing by permu-ation testing). Results for the ten SNPs with lowest p-valuesre shown in Table 2. The Q–Q plot for the chi-square testn Fig. 1 for all 292,175 SNPs demonstrates that most of thehi-square values perfectly follow theoretically expected val-es, thus confirming the conclusion of absence of populationtratification. The plot also shows that at least ten SNPs havelevated test statistics, although none of them is significantndividually.
In the Set Association analysis, the sum of test statis-ics (mean absolute differences of genotype codes) forNPs (Table 2; pSum) ranked 1–6 exhibited the small-st significance level, pmin = 0.0182. This analysis indicatedhat approximately six SNPs jointly contribute to AD neu-opathology. The significance level associated with pmin,orrected for testing 10 sums, was p = 0.0397). This resultonfirms an analogous conclusion based on the Q–Q plot.
For the logistic regression controlling for age of deathnd sex, the genome-wide distribution of all SNPs and theiregression p-values are presented in Fig. 2. The ten SNPsith the lowest p-values for an association with the ADeuropathology phenotype are listed in Table 3. Althougho SNPs reached significance with the overly conserva-ive Bonferroni correction, three of the four top SNPs,s4298437, rs6951875 and rs6943822, are in reelin (RELN).ne SNP, rs6951875, is in the promoter region of RELN,
nd the other two SNPs are located in the 5′ end of theene.
In the post hoc analysis all three reelin SNPs showed
ighly significant allelic association with the phenotype, ashown in Table 4. Alleles associated with the HI Braakroup are the A allele of rs4298437 (OR = 2.44), the G allele
P.L. Kramer et al. / Neurobiology of Aging 32 (2011) 2113–2122 2117
Table 1Sample characteristics.
LO Braak (n = 185) HI Braak (n = 114) p-value
Sex, n (%) Male 92 (50%) 42 (37%) .031Female 93 (50%) 72 (63%) Fisher’s exact, 2-tailed
Age at death: (years) Mean (sd) 83.96 (7.69) 87.96 (6.01) <.0001Range 65–104 72–106 t-test
Education: (years) Mean (sd) 16.26 (3.17) 16.96 (3.58) .09Range t-test
APOE allele 2 frequency, n (%) �2 37 (10%) 22 (10%) .756�3 287(80%) 174 (78%) χ2 = 0.562 df�4 38 (10%) 28 (2%)
Neuritic plaque density: Frequent 9 (5%) 28 (25%) <.0001Moderate 44 (24%) 49 (43%) χ2 = 51.1, 3dfSparse 37 (20%) 15 (13%)None 93 (51%) 21 (19%)
Table 2Results of the allele association tests, showing the ten best SNPs, listed in order of significance.
Rank SNP ch Position pRanda pSumb Genec Location
1 rs4298437 7 103413113 0.0833 0.0833 RELN Intron2 rs6951875 7 103419411 0.1222 0.0367 RELN Promotor3 rs894520 9 38179527 0.2754 0.0270 Unknown4 rs6943822 7 103385907 0.3644 0.0196 RELN Intron5 rs6734151 2 5387284 0.6341 0.0193 Unknown6 rs11782819 8 10372191 0.6955 0.0182 MSRA 45 kb downstream7 rs1278881 14 31458332 0.9751 0.0222 NUBPL 50 kb upstream8 rs9530579 13 76123603 0.9757 0.0247 Unknown9 rs9285657 5 143077331 0.9888 0.0279 HMHB1 90 kb upstream
10 rs1600790 8 26820864 0.9942 0.0317 ADRA1A 50 kb upstreama pRand = p-value computed in 10,000 randomization samples.b pSum = p-value associated with test statistic (mean absolute differences of genotype codes).c Data from NCBI MapViewer Build 36.3 (http://www.ncbi.nlm.nih.gov/mapview/).
Table 3Results of the genotype association test using logistic regression analysis with covariates, showing the ten SNPs with the lowest p-values, in order of significance.
SNP Chr Position pNoma Geneb Location
rs4298437c 7 103413113 1.53E−06 RELN Intronrs11782819c 8 10372191 3.23E−06 MSRA 45 kb downstreamrs6951875c 7 103419411 5.15E−06 RELN Promoterrs6943822c 7 103385907 1.21E−05 RELN Intronrs7278439 21 41899403 1.33E−05 TMPRSS2 150 kb upstreamrs10956170 8 125381841 1.57E−05 TMEM65 10 kb downstreamrs877874 17 75450416 1.74E−05 C1QTNF1 20 kb upstreamrs11649538 16 24415618 2.00E−05 RBBP6 50 kb upstreamrs1481650 8 26829428 2.52E−05 ADRA1 50 kb upstreamrs9530579c 13 76123603 3.03E−05 Unknown
a pNom = nominal p-value.b Data from NCBI MapViewer Build 36.3 (http://www.ncbi.nlm.nih.gov/mapview/).c Gene (in which SNP is located) appears also in the list of significant genes obtained in the allele association analysis (Table 2).
Table 4Results of post hoc allelic association analysis of SNPs in RELN.
SNP Pearson’s χ2 p-value Freq allele 1 HI Freq allele 1 LO Freq allele 2 HI Freq allele 2 LO Odds ratio 95% CI
rs4298437 5.84e−07 G(0.54) G(0.74) A(0.46) A(0.26) 2.44 1.70–3.52rs6951875 2.95e−06 A(0.31) A(0.51) G(0.69) G(0.49) 2.30 1.61–3.31rs6943822 9.22e−06 G(0.32) G(0.51) A(0.68) A(0.49) 2.19 1.54–3.15

2118 P.L. Kramer et al. / Neurobiology of Aging 32 (2011) 2113–2122
Fig. 2. Manhattan plot showing the distribution of analyzed SNPs and their corresponding genotypic association p-values from logistic regression. The SNPsa (numb(
o(
apStaitwl
wpctfaTsHefd
s
rlnsyof studies that suggest that the positive association betweenAPOEε4 and AD declines after the age of 85 years (Juva et al.,2000). In order to further validate this finding, we examined
Table 5Frequencies of RELN SNP genotypes in Braak score categories (n, %).
Genotype rs4298437
LO Braak MED Braak HI Braak
AA 10 (.05) 9 (.10) 24 (.20)AG 78 (.41) 44 (.49) 62 (.52)GG 104 (.54) 37 (.41) 33 (.28)Total 192 90 119
rs6951875AA 46 (.24) 17 (.19) 10 (.08)AG 105 (.56) 45 (.50) 55 (.47)GG 38 (.20) 28 (.31) 53 (.45)Total 189 90 118
rs6943822AA 45 (.23) 28 (.31) 51 (.43)
re ordered by their positions on the chromosomes, and the chromosomesp-value).
f rs6951875 (OR = 2.30) and the A allele of rs6943822OR = 2.19).
There was modest overlap between the results of the allelicssociation test and the logistic regression analysis. Mostrominently, the three RELN SNPs were among the top fourNPs in both analyses. Only two other SNPs occur among
he ten most significant SNPs in both Tables 2 and 3. Wettribute two reasons to this apparent discrepancy. First, wencorporated age-at-death and sex as covariates in the logis-ic regression analysis, whereas the allele test was carried outithout inclusion of covariates. Also, the allele test may be
ess powerful than the genotype test.At the outset of this study, we excluded 90 subjects
ith mid-range (MED) Braak scores in order to maximizehenotypic differences between groups and avoid potentialonfounding effects of including subjects in this transi-ional category. Following the analysis, we examined therequency of the RELN genotypes in rs4298437, rs6951875nd rs6943822 in this group of subjects. As indicated inable 5, frequencies for all three SNPs in the MED Braakubjects were intermediate between those of the LO andI Braak subjects. This substantiates our approach of using
xtreme phenotypes rather than introducing the potential con-ounding effect of choosing an arbitrary mid-range value for
ichotomizing groups.Despite differences in AD neuropathology, there was noignificant difference between HI and LO Braak subjects with
AGT
ers 1–22 from left to right) are alternately colored. The y axis is −log10
espect to the frequency of the APOEε4 allele (Table 1). Thisack of association between the ε4 allele and high levels of ADeuropathology may be related to the advanced age of theseubjects (mean age at death in the HI Braak group = 87.96ears; Table 1). This would be consistent with a number
G 94 (.49) 42 (.47) 58 (.49)G 53 (.28) 20 (.22) 10 (.08)otal 192 90 119

logy of Aging 32 (2011) 2113–2122 2119
tnSeSo
3
pLrwsewwpRsncrstGevl
gpspprna
tse(gcSn
4
sht2
pbe
twee
nA
PO
E�
4fr
eque
ncy
and
RE
LN
geno
type
s.
437
#Su
bjec
tsw
/≥1
�4
alle
le#
Subj
ects
w/n
o�
4al
lele
SNP
rs69
5187
5ge
noty
peb
#Su
bjec
tsw
/≥1
�4
alle
le#
Subj
ects
w/n
o�
4al
lele
SNP
rs69
4382
2ge
noty
pec
#Su
bjec
tsw
/≥1
�4
alle
le#
Subj
ects
w/n
o�
4al
lele
22(.
35)
104
(.45
)G
G21
(.33
)69
(.30
)G
G9
(.14
)49
(.21
)30
(.48
)10
3(.
45)
AG
32(.
51)
119
(.52
)A
G32
(.51
)10
9(.
47)
11(.
17)
23(.
10)
AA
10(.
16)
41(.
18)
AA
22(.
35)
72(.
31)
6323
0To
tal
6322
9To
tal
6323
0
P.L. Kramer et al. / Neurobio
he frequency of APOEε4 carriers (at least one ε4 allele) vs.on-carriers among the three genotypes for all three RELNNPs. As shown in Table 6, there were no significant differ-nces in the frequency of ε4 carriers and non-carriers acrossNP genotypes for rs4298437 (p = .16), rs6951875 (p = .86)r rs6943822 (p = .46).
.3. Reelin immunohistochemistry
Reelin immunohistochemistry was performed on hip-ocampal sections from 18 (9 from the HI and 9 from theO Braak group) subjects. Immunohistochemical staining for
eelin was also performed on hippocampi from four subjectsith clinical and neuropathological diagnoses of AD (Braak
tage VI with moderate to frequent neuritic plaques). In gen-ral, reelin expression was confined to pyramidal neuronshere it was present as variably intense cytoplasmic stainingith highest expression in the CA2/3 sector of the hippocam-us as previously described (Martinez-Cerdeno et al., 2002).eelin expression tended to be very pronounced in AD with
trong staining encountered especially in regions with manyeurons undergoing granulovacuolar degeneration (GVD), aytoplasmic feature associated with AD (Fig. 3, top). Neu-ons with mild to moderate GVD in particular tended to havetrong cytoplasmic reelin expression; granules and vacuoleshemselves did not contain reelin and neurons with markedVD tended to express less reelin due to extensive degen-
ration in general and to replacement of cytoplasmic withacuolar lesions in particular. Reelin staining of neurofibril-ary tangles and neuritic plaques was not conspicuous.
In contrast, cognitively intact subjects in the LO Braakroup tended to have lower reelin expression in the hippocam-us, whereas reelin expression in the HI Braak group wasimilar to that observed in AD hippocampi. Hippocampalyramidal neurons in both the LO and HI Braak groups dis-layed less GVD than in AD, but the tendency for increasedeelin expression in the HI Braak group was still notable ineurons in which GVD was not present or was present to onlyvery limited extent (Fig. 3, bottom).
Total reelin expression was quantified as described in Sec-ion 2. In both HI and LO Braak categories, subjects weretratified by rs4298437 genotype. Total hippocampal reelinxpression was significantly reduced in the LO Braak groupp = 0.031; Fig. 4). In addition, when the LO and HI Braakroups were combined, there was a suggestion of an asso-iation between GG homozygotes (for either or both reelinNPs) and reduced reelin expression, although this trend didot reach statistical significance (p = 0.090).
. Discussion
We identified three variants in the RELN gene that are con-
istently associated with AD neuropathology in cognitivelyealthy elderly individuals. Analysis of allelic association inhree SNPs in RELN generated significant ORs, ranging from.19 to 2.44, for the alleles associated with the HI Braak cat- Table
6R
elat
ions
hi
SNP
rs42
98ge
noty
pea
GG
AG
AA
Tota
la
p=
.16.
bp
=.8
6.c
p=
.46.

2120 P.L. Kramer et al. / Neurobiology of Aging 32 (2011) 2113–2122
Fig. 3. Reelin expression in hippocampal pyramidal neurons. Hippocampal immunohistochemistry was performed on paraffin sections of hippocampus andrepresentative pyramidal neurons from the CA2 region are depicted in AD (upper panel) and in non-demented subjects (lower panel). Strong cytoplasmicstaining was noted in pyramidal neurons in AD, especially in regions in which significant granulovacuolar degeneration (GVD) was noted. Neuritic plaquesand neurofibrillary tangles (NFTs) did not stain strongly for reelin. Cytoplasmic expression of reelin in pyramidal neurons was also present in non-dementeds imilar tc
ei2pbpe
b
F(wteirw
aDcump
ubjects with HI Braak stages as defined in the text (lower right panel), sonspicuous (lower left panel).
gory. A significant association with SNPs in RELN was alsodentified in a study of female AD patients (Seripa et al.,008). The region of RELN we found associated with NFTathology and the region found in Seripa et al. (2008) areoth near promoter elements, which have been postulated tolay a role in hypermethylation and therefore modification in
xpression of this gene (Chin et al., 2007; Dong et al., 2005).Reelin is an extracellular matrix glycoprotein, encodedy the RELN gene, which is secreted throughout the CNS
ig. 4. Analysis of reelin expression in hippocampus. ImmunohistochemicalIHC) expression of reelin was scored in the hippocampus of OHSU casesith postmortem interval less than 24 h. Scores are the sum of semiquanti-
ative assessments of cytoplasmic reelin positivity of pyramidal neurons inach sector as described in the text. Cases were stratified by Braak group-ng and by genotype. Two-way ANOVA showed a significant association ofeelin expression with HI vs. LO Braak stage (p = 0.031) but no associationith genotype.
seRpeiiroitoanhtsy
ATTtNr
o that observed in AD. Expression of reelin in LO Braak stages was less
nd is important in neuronal development (Bar et al., 2000;’Arcangelo, 2006). It is a ligand for at least three classes of
ell membrane receptors involved in actin cytoskeleton reg-lation/reorganization and in tau phosphorylation. Tau is aicrotubule-associated protein abundant in neurons and the
rimary component of NFTs. Normal reelin levels are neces-ary to prevent abnormal phosphorylation of tau (Hiesbergert al., 1999; Ohkubo et al., 2003; Trommsdorff et al., 1999).eelin is also associated with plaques in �-amyloid precursorrotein/presenilin-1 double-transgenic mouse brains (Wirthst al., 2001). A recent report (Durakoglugil et al., 2009)ndicates a role for reelin in protecting against beta-amyloid-nduced suppression of long-term potentiation and NMDAeceptors. Thus, reelin may play key roles in AD pathol-gy both extracellularly with its involvement in plaques andntracellularly via inhibition of tau phosphorylation. Sinceau phosphorylation is a key step in the formation of NFTs,ur finding of an association between RELN polymorphismsnd high levels of AD neuropathology is compelling. Weote that the three RELN SNPs found to be associated withigh levels of AD pathology in this study are probably nothe actual functional SNPs in this regard, but instead are introng linkage disequilibrium with other causative variantset to be identified.
Evidence for direct involvement in pathways related toD neuropathology is less apparent for other genes listed inables 2 and 3. Possible roles for the transmembrane protein,MEM65, methionine sulfoxide reductase A, MSRA, and
he Fe/S cluster-mitochondrial complex I assembler protein,UBPL, are conceivable. Variants in these genes, or others
epresented in the tables, may function in as yet unknown

logy of
wa
miu�tipt
thfbwnpttricSir
ddaioaitio
cesatcor
W
i
D
tCapocsfMAh
A
fodtCDCPaaPaAtaHHctPARAoS3
R
B
B
P.L. Kramer et al. / Neurobio
ays to either prevent or promote the formation of NFTsnd/or amyloid plaques.
Our discovery of increased expression of reelin in pyra-idal neurons of the hippocampus in AD and in cognitively
ntact controls with AD-associated pathology suggests thatp-regulation of reelin may be a compensatory response to-amyloid or tau-related stress associated with AD even prior
o the onset of dementia. If so, polymorphisms in RELN maynfluence the capacity for up-regulation in affected neuronalopulations and thereby exert effects on cognitive reserve inhe context of AD-associated stressors and pathologic lesions.
The purpose of this study was to identify genetic variantshat distinguish cognitively healthy, elderly individuals with aeavy NFT burden from those with minimal NFT burden. Theormer group also had a significantly greater amyloid plaqueurden than the latter. There are three broad mechanismshereby genetic variants could mediate NFT burden in cog-itively healthy individuals. They could act directly throughathways related to tau, indirectly through pathways relatedo �-amyloid pathology (which, in turn influences tau), orhrough other mechanisms that affect brain reserve (e.g., neu-onal or synaptic plasticity). One interpretation of this studys that genetic variants in RELN result in perturbations asso-iated with the development of NFTs (and amyloid plaques).ince these subjects were cognitively healthy, the implication
s that other genetic variants and/or environmental factors areequired for the development of cognitive dysfunction.
This is the first GWAS that specifically addresses geneticifferences related to AD neuropathology in clinically non-emented elderly. This is important because these individualsre traditionally used as control subjects in case-control stud-es of AD, under the assumption that, as a group, they are freef genetic factors related to AD pathophysiology. If, as thisnalysis suggests, a proportion of clinically non-dementedndividuals harbor genetic variants that predispose them tohe underlying neuropathology that characterizes AD, includ-ng them in a control group will likely confound the resultsf genetic case-control studies.
These findings require replication in larger datasets withomparable phenotypes. Well-characterized, non-dementedlderly with autopsy are difficult to obtain. The NIH isponsoring the AD Genetics Consortium to assemble andnalyze a comprehensive collection of AD cases and con-rols representing the collective resources of the AD researchommunity. This collection will provide an outstandingpportunity for confirmation and expansion of the resultseported here.
eb references
Plink, http://pngu.mgh.harvard.edu/∼purcell/plink/.
R, http://cran.cnr.berkeley.edu/web/packages/qvalue/ndex.html.Sumstat, http://www.big.ac.cn/genemapping/sumstat.html.Systat, http://www.systat.com/.
B
Aging 32 (2011) 2113–2122 2121
isclosure
Dr. Ronald Petersen serves as Chair of the Safety Moni-oring Committee and consultant for Elan Pharmaceuticals,hair of Safety Monitoring for Wyeth Pharmaceuticalsnd consultant for GE Healthcare.Dr. John Morris hasarticipated or is currently participating in clinical trialsf antidementia drugs sponsored by Elan Pharmaceuti-als, Eli Lilly and Wyeth Pharmaceuticals. Dr. Morris haserved as a consultant or has received speaking honorariarom AstraZeneca, Bristol-Myers Squibb, Genentech, Lilly,
erck, Novartis, Pfizer, Schering Plough, Wyeth, and Elan.ppropriate approval and procedures were used concerninguman subjects.
cknowledgements
The authors would like to thank the following individualsor their generous and varied contributions to the productionf this report, including clinical and neuropathologicalata verification, DNA and brain tissue procurement andransportation, and data organization and transmission:harles DeCarli MD, at the University of California atavis; Marilyn Albert MD, at Johns Hopkins University;hristine Hulette MD, James Burke MD, Jeffrey BrowndykehD, John Ervin, Michelle McCart and Mari Szmanski RNt Duke University Medical Center; Alison Goate PhD,t the Washington University School of Medicine; Josepharisi MD and Kris Johnson RN, at Mayo Clinic, Rochester,nd Dennis Dixon at Mayo Clinic, Jacksonville; Sonyanderson at the University of Kentucky; Mary Sundsmo at
he University of California at San Diego; Eszter Gombosit the University of Michigan; Jamie Laut at Oregonealth & Science University. We thank Dr. Chungshenge, Rockefeller University, for writing an R program to
reate the Manhattan plot. This work was supported byhe National Institute on Aging (grants R01-AG026916,30-AG028377, P50-AG005146, P30-AG028383, P50-G16574, U01-AG06786, P30-AG008017, P30-AG10161,01-AG17917, P30-AG10129, P50-AG05131, P50-G08671, P50-AG05681, P01-AG03991, U01-AG016976)f the National Institutes of Health, and by the Naturalcience Foundation of China NSFC, project number and0700442 (to JO).
eferences
ar, I., Lambert de Rouvroit, C., Goffinet, A.M., 2000. The evolution ofcortical development. An hypothesis based on the role of the Reelinsignaling pathway. Trends Neurosci. 23 (12), 633–638.
ennett, D.A., Schneider, J.A., Bienias, J.L., Evans, D.A., Wilson, R.S.,
2005. Mild cognitive impairment is related to Alzheimer disease pathol-ogy and cerebral infarctions. Neurology 64 (5), 834–841.raak, H., Braak, E., 1991. Neuropathological stageing of Alzheimer-relatedchanges. Acta Neuropathol. 82 (4), 239–259.

2 logy of
C
D
D
D
E
F
H
H
H
J
M
M
M
N
O
P
P
S
T
122 P.L. Kramer et al. / Neurobio
hin, J., Massaro, C.M., Palop, J.J., Thwin, M.T., Yu, G.Q., Bien-Ly, N.,Bender, A., Mucke, L., 2007. Reelin depletion in the entorhinal cortexof human amyloid precursor protein transgenic mice and humans withAlzheimer’s disease. J. Neurosci. 27 (11), 2727–2733.
’Arcangelo, G., 2006. Reelin mouse mutants as models of cortical devel-opment disorders. Epilepsy Behav. 8 (1), 81–90.
ong, E., Agis-Balboa, R.C., Simonini, M.V., Grayson, D.R., Costa, E.,Guidotti, A., 2005. Reelin and glutamic acid decarboxylase67 pro-moter remodeling in an epigenetic methionine-induced mouse modelof schizophrenia. Proc. Natl. Acad. Sci. U.S.A. 102 (35), 12578–12583.
urakoglugil, M.S., Chen, Y., White, C.L., Kavalali, E.T., Herz, J., 2009.Reelin signaling antagonizes beta-amyloid at the synapse. Proc. Natl.Acad. Sci. U.S.A. 106 (37), 15938–15943.
rten-Lyons, D., Woltjer, R.L., Dodge, H., Nixon, R., Vorobik, R., Calvert,J.F., Leahy, M., Montine, T., Kaye, J., 2009. Factors associated with resis-tance to dementia despite high Alzheimer disease pathology. Neurology72 (4), 354–360.
olstein, M.F., Folstein, S.E., McHugh, P.R., 1975. “Mini-mental state”.A practical method for grading the cognitive state of patients for theclinician. J. Psychiatry Res. 12 (3), 189–198.
ebert, L.E., Scherr, P.A., Bienias, J.L., Bennett, D.A., Evans, D.A., 2003.Alzheimer disease in the US population: prevalence estimates using the2000 census. Arch. Neurol. 60 (8), 1119–1122.
iesberger, T., Trommsdorff, M., Howell, B.W., Goffinet, A., Mumby, M.C.,Cooper, J.A., Herz, J., 1999. Direct binding of Reelin to VLDL receptorand ApoE receptor 2 induces tyrosine phosphorylation of disabled-1 andmodulates tau phosphorylation. Neuron 24 (2), 481–489.
oh, J., Wille, A., Ott, J., 2001. Trimming, weighting, and groupingSNPs in human case-control association studies. Genome Res. 11 (12),2115–2119.
uva, K., Verkkoniemi, A., Viramo, P., Polvikoski, T., Kainulainen, K.,Kontula, K., Sulkava, R., 2000. APOE epsilon4 does not predict mortal-ity, cognitive decline, or dementia in the oldest old. Neurology 54 (2),412–415.
anly, B.F.J., 2007. Randomization, Bootstrap, and Monte Carlo Methodsin Biology. Chapman & Hall/CRC, Boca Raton, FL.
artinez-Cerdeno, V., Galazo, M.J., Cavada, C., Clasca, F., 2002. Reelinimmunoreactivity in the adult primate brain: intracellular localization inprojecting and local circuit neurons of the cerebral cortex, hippocampusand subcortical regions. Cereb. Cortex 12 (12), 1298–1311.
W
Aging 32 (2011) 2113–2122
orris, J.C., 1993. The Clinical Dementia Rating (CDR): current versionand scoring rules. Neurology 43 (11), 2412–2414.
IA. The National Institute on Aging, and Reagan Institute WorkingGroup on Diagnostic Criteria for the Neuropathological Assessmentof Alzheimer’s Disease, 1997. Consensus recommendations for thepostmortem diagnosis of Alzheimer’s disease. Neurobiol. Aging 18 (4Suppl.), S1–S2.
hkubo, N., Lee, Y.D., Morishima, A., Terashima, T., Kikkawa, S.,Tohyama, M., Sakanaka, M., Tanaka, J., Maeda, N., Vitek, M.P.,Mitsuda, N., 2003. Apolipoprotein E and Reelin ligands modulatetau phosphorylation through an apolipoprotein E receptor/disabled-1/glycogen synthase kinase-3beta cascade. FASEB J. 17 (2),295–297.
lenge, R.M., Cotsapas, C., Davies, L., Price, A.L., de Bakker, P.I., Maller,J., Pe’er, I., Burtt, N.P., Blumenstiel, B., DeFelice, M., Parkin, M., Barry,R., Winslow, W., Healy, C., Graham, R.R., Neale, B.M., Izmailova, E.,Roubenoff, R., Parker, A.N., Glass, R., Karlson, E.W., Maher, N., Hafler,D.A., Lee, D.M., Seldin, M.F., Remmers, E.F., Lee, A.T., Padyukov, L.,Alfredsson, L., Coblyn, J., Weinblatt, M.E., Gabriel, S.B., Purcell, S.,Klareskog, L., Gregersen, P.K., Shadick, N.A., Daly, M.J., Altshuler, D.,2007. Two independent alleles at 6q23 associated with risk of rheumatoidarthritis. Nat. Genet. 39 (12), 1477–1482.
urcell, S., Neale, B., Todd-Brown, K., Thomas, L., Ferreira, M.A.,Bender, D., Maller, J., Sklar, P., de Bakker, P.I., Daly, M.J., Sham,P.C., 2007. PLINK: a tool set for whole-genome association andpopulation-based linkage analyses. Am. J. Hum. Genet. 81 (3),559–575.
eripa, D., Matera, M.G., Franceschi, M., Daniele, A., Bizzarro, A., Rinaldi,M., Panza, F., Fazio, V.M., Gravina, C., D’Onofrio, G., Solfrizzi, V.,Masullo, C., Pilotto, A., 2008. The RELN locus in Alzheimer’s disease.J. Alzheimer’s Dis. 14 (3), 335–344.
rommsdorff, M., Gotthardt, M., Hiesberger, T., Shelton, J., Stockinger,W., Nimpf, J., Hammer, R.E., Richardson, J.A., Herz, J., 1999.Reeler/Disabled-like disruption of neuronal migration in knockoutmice lacking the VLDL receptor and ApoE receptor 2. Cell 97 (6),689–701.
irths, O., Multhaup, G., Czech, C., Blanchard, V., Tremp, G., Pradier, L.,Beyreuther, K., Bayer, T.A., 2001. Reelin in plaques of beta-amyloidprecursor protein and presenilin-1 double-transgenic mice. Neurosci.Lett. 316 (3), 145–148.