
Alvimopan, a peripherally acting mu-opioid receptor (PAM-OR) antagonist for the treatment of...
13
Alvimopan, a peripherally acting mu-opioid receptor (PAM-OR) antagonist for the treatment of opioid-induced bowel dysfunction: Results from a randomized, double-blind, placebo-controlled, dose-finding study in subjects taking opioids for chronic non-cancer pain Lynn Webster a, * , Jan Peter Jansen b , John Peppin c , Ben Lasko d , Gordon Irving e , Bart Morlion f , Jerry Snidow g , Amy Pierce g , Eric Mortensen g , Christi Kleoudis g , Eric Carter g a Lifetree Clinical Research and Pain Clinic, 3838 South 700 East, Ste. 200, Salt Lake City, UT 84106, USA b Schwerpunktpraxis fu ¨ r Schmerztherapie und Ambulante Ana ¨ sthesie, Berlin, Germany c The Pain Treatment Center of the Bluegrass, Lexington, KY, USA d Manna Research, Toronto, Ont., Canada e Swedish Medical Center, Seattle, WA, USA f The Leuven Centre for Algology & Pain Management, University Hospital, Leuven, Belgium g GlaxoSmithKline, Research Triangle Park, NC, USA Received 2 February 2007; received in revised form 13 November 2007; accepted 14 November 2007 Abstract Our objective was to investigate the efficacy and safety of alvimopan, a peripherally acting mu-opioid receptor (PAM-OR) antagonist, in subjects with non-cancer pain and opioid-induced bowel dysfunction (OBD), and to identify at least one treatment regimen that improves OBD. Following a 2-week baseline period, 522 subjects reporting <3 spontaneous bowel movements (SBMs)/ week (with P25% accompanied by a sensation of incomplete evacuation, straining, or lumpy hard stools), requiring analgesia equiv- alent to P30 mg oral morphine/day were randomized to alvimopan 0.5 mg twice daily (BID), 1 mg once daily (QD), 1 mg BID, or placebo for 6 weeks. Compared with placebo, there was a statistically and clinically significant increase in mean weekly SBM frequency over the initial 3 weeks of treatment (primary endpoint) with alvimopan 0.5 mg BID (+1.71 mean SBMs/week), alvim- opan 1 mg QD (+1.64) and alvimopan 1 mg BID (+2.52); P < 0.001 for all comparisons. Increased SBM frequency and additional treatment effects, including improvements in symptoms such as straining, stool consistency, incomplete evacuation, abdominal bloating/discomfort, and decreased appetite, were sustained over 6 weeks. The most frequently reported adverse events were abdominal pain, nausea, and diarrhea, occurring more frequently in the higher dosage groups. The alvimopan 0.5 mg BID regimen demonstrated the best benefit-to-risk profile for managing OBD with alvimopan in this study population, with a side effect profile similar to that of placebo. There was no evidence of opioid analgesia antagonism. Competitive peripheral antagonism of opioids with alvimopan can restore GI function and relieve OBD without compromising analgesia. Ó 2007 International Association for the Study of Pain. Published by Elsevier B.V. All rights reserved. Keywords: Alvimopan; Antagonist; Opioid; Constipation; Gastrointestinal motility; Randomized controlled trial 0304-3959/$34.00 Ó 2007 International Association for the Study of Pain. Published by Elsevier B.V. All rights reserved. doi:10.1016/j.pain.2007.11.008 * Corresponding author. Tel.: +1 801 261 4988; fax: +1 801 269 9427. E-mail address: [email protected] (L. Webster). www.elsevier.com/locate/pain Pain 137 (2008) 428–440
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Alvimopan, a peripherally acting mu-opioid receptor (PAM-OR) antagonist for the treatment of...

www.elsevier.com/locate/pain
Pain 137 (2008) 428–440
Alvimopan, a peripherally acting mu-opioid receptor(PAM-OR) antagonist for the treatment of opioid-induced
bowel dysfunction: Results from a randomized,double-blind, placebo-controlled, dose-finding study
in subjects taking opioids for chronic non-cancer pain
Lynn Webster a,*, Jan Peter Jansen b, John Peppin c, Ben Lasko d,Gordon Irving e, Bart Morlion f, Jerry Snidow g, Amy Pierce g, Eric Mortensen g,
Christi Kleoudis g, Eric Carter g
a Lifetree Clinical Research and Pain Clinic, 3838 South 700 East, Ste. 200, Salt Lake City, UT 84106, USAb Schwerpunktpraxis fur Schmerztherapie und Ambulante Anasthesie, Berlin, Germany
c The Pain Treatment Center of the Bluegrass, Lexington, KY, USAd Manna Research, Toronto, Ont., Canada
e Swedish Medical Center, Seattle, WA, USAf The Leuven Centre for Algology & Pain Management, University Hospital, Leuven, Belgium
g GlaxoSmithKline, Research Triangle Park, NC, USA
Received 2 February 2007; received in revised form 13 November 2007; accepted 14 November 2007
Abstract
Our objective was to investigate the efficacy and safety of alvimopan, a peripherally acting mu-opioid receptor (PAM-OR)antagonist, in subjects with non-cancer pain and opioid-induced bowel dysfunction (OBD), and to identify at least one treatmentregimen that improves OBD. Following a 2-week baseline period, 522 subjects reporting <3 spontaneous bowel movements (SBMs)/week (with P25% accompanied by a sensation of incomplete evacuation, straining, or lumpy hard stools), requiring analgesia equiv-alent to P30 mg oral morphine/day were randomized to alvimopan 0.5 mg twice daily (BID), 1 mg once daily (QD), 1 mg BID, orplacebo for 6 weeks. Compared with placebo, there was a statistically and clinically significant increase in mean weekly SBMfrequency over the initial 3 weeks of treatment (primary endpoint) with alvimopan 0.5 mg BID (+1.71 mean SBMs/week), alvim-opan 1 mg QD (+1.64) and alvimopan 1 mg BID (+2.52); P < 0.001 for all comparisons. Increased SBM frequency and additionaltreatment effects, including improvements in symptoms such as straining, stool consistency, incomplete evacuation, abdominalbloating/discomfort, and decreased appetite, were sustained over 6 weeks. The most frequently reported adverse events wereabdominal pain, nausea, and diarrhea, occurring more frequently in the higher dosage groups. The alvimopan 0.5 mg BID regimendemonstrated the best benefit-to-risk profile for managing OBD with alvimopan in this study population, with a side effect profilesimilar to that of placebo. There was no evidence of opioid analgesia antagonism. Competitive peripheral antagonism of opioidswith alvimopan can restore GI function and relieve OBD without compromising analgesia.� 2007 International Association for the Study of Pain. Published by Elsevier B.V. All rights reserved.
Keywords: Alvimopan; Antagonist; Opioid; Constipation; Gastrointestinal motility; Randomized controlled trial
0304-3959/$34.00 � 2007 International Association for the Study of Pain. Published by Elsevier B.V. All rights reserved.
doi:10.1016/j.pain.2007.11.008
* Corresponding author. Tel.: +1 801 261 4988; fax: +1 801 269 9427.E-mail address: [email protected] (L. Webster).

L. Webster et al. / Pain 137 (2008) 428–440 429
1. Introduction
Opioids play a major role in the management ofchronic pain, acting via mu-opioid receptors in the cen-tral nervous system (CNS). However, activation of mu-opioid receptors in the enteric nervous system leads todecreased gastrointestinal (GI) propulsive activity[9,10,12,15,23]. This disruption of GI function manifestsas delayed gastric emptying; infrequent bowel move-ments and difficulty in rectal expulsion of stool; and var-ious associated symptoms such as gastric reflux,abdominal bloating, and abdominal pain [6,15,31]. Suchsymptoms are often persistent; tolerance rarely develops[19,27]. For many patients, such side effects can limitanalgesic dosing if left untreated [7,28]. Constipation isa common and bothersome side effect of opioid use[23,30]. Prospective, well-controlled studies or meta-analyses in non-cancer pain conditions suggest that20–60% of patients taking opioids report constipation[1,14,23]. This may be an underestimation, however,given that reported GI side effect rates are typicallybased upon spontaneously reported complaints ratherthan prospectively defined endpoints.
There is currently no approved therapy for the spe-cific management of opioid-induced bowel dysfunction.Treatment of constipation generally involves the use oflaxatives and stool softeners; however, efficacy can belimited and tolerability poor [23]. Laxative treatment isoften insufficient to manage all opioid-induced GI sideeffects or restore GI function [23], and can be compli-cated by side effects such as abdominal bloating/cramps[29]. Consequently, there is a need for a well-toleratedtherapy that helps patients taking opioids to maintainnormal bowel function.
A substantial body of evidence now shows that mu-opioid receptor antagonists can accelerate bowel transitin patients with opioid-induced bowel dysfunction[3,15,17,24,32]. However, some agents have central
Fig. 1. Study design. Subjects who were randomized to the alvimopan 1 mg Btitrating to 1 mg BID on Day 4, and subjects who were randomized to the alvon Days 1–3, titrating to 1 mg QD on Day 4.
actions, and their practical use has been limited byantagonism of opioid analgesia and onset of withdrawalsymptoms [17,20]. Alvimopan is an orally administered,systemically available but peripherally acting mu-opioidreceptor (PAM-OR) antagonist, in development for thetreatment of opioid-induced bowel dysfunction[2,4]. Alvimopan does not cross the blood–brain barrierat clinically relevant dosages [26,33] and, unlike cen-trally acting opioid receptor antagonists, does notreverse analgesia or cause opioid withdrawal symptoms[16,25].
A 3-week study in subjects with opioid-induced boweldysfunction provided preliminary evidence that alvimo-pan restores bowel movements without compromisinganalgesia in patients with non-cancer pain [24]. Theobjective of the current study was to identify at leastone alvimopan treatment regimen that improved spon-taneous bowel movement frequency and relieved GIsymptoms over a 6-week treatment period comparedwith placebo, while maintaining an acceptable tolerabil-ity profile.
2. Methods
2.1. Subjects and study design
This phase IIb, randomized, double-blind, double-dummy,placebo-controlled, parallel-group study was conducted at 113centers in nine countries in 2003–4. It was carried out in accor-dance with the Declaration of Helsinki and guidelines onGood Clinical Practices. The study protocol and protocol-related documents were reviewed and approved by an Institu-tional Review Board or Independent Ethics Committee at eachcenter, and all subjects provided voluntary written informedconsent before a screening evaluation was performed. Thestudy included a 2-week baseline period (screening on Day-14 and randomization on Day 1), a 6-week treatment period(visits at Week 1, Week 3, and Week 6), and a 2-week fol-low-up period (final visit at Week 8) (Fig. 1).
ID group commenced dosing with alvimopan 0.5 mg BID on Days 1–3,imopan 1 mg QD group commenced dosing with alvimopan 0.5 mg QD

430 L. Webster et al. / Pain 137 (2008) 428–440
Male or female subjects aged P18 years at first screeningwere eligible for study participation if they had bowel dysfunc-tion resulting from chronic opioid treatment for the manage-ment of pain of a non-cancer origin. Opioid-induced boweldysfunction was defined as a history of decreased bowel move-ment frequency since initiating opioid therapy and P1 of the fol-lowing symptoms: incomplete evacuation, hard stools, orstraining, in P25% of bowel movements. Eligible subjects wererequired to be on a stable dose of a full opioid agonist (other thanmeperidine and propoxyphene) equivalent to a minimum of30 mg oral morphine, administered either orally, transdermally,intravenously, or subcutaneously, for P1 month prior to thefirst screening. All other routes of chronic administration wereexcluded, with the exception of intrathecal dosing. This was per-mitted only if the patient was also taking another chronicallydosed opioid that met all inclusion criteria, and the total dailydose of the intrathecally administered opioid was accuratelyrecorded.
Exclusion criteria included pregnancy or lactation inwomen; use of opioids for cancer-related pain or for manag-ing opioid addiction; use of mixed agonist/antagonist or par-tial agonist opioids; unwillingness to discontinue laxatives ormanual maneuvers to facilitate defecation at screening andthroughout the study; severe constipation that had not beenappropriately managed, leaving the patient at increasedimmediate risk of developing serious complications; GI orpelvic disorders that could affect bowel transit, produce GIobstruction, or contribute to bowel dysfunction; and boweldysfunction not considered to be caused by opioid use. Con-comitant medications known to cause constipation wereallowed at the discretion of the investigator only if opioidtherapy was considered to be the predominant cause ofconstipation.
Subjects were randomized to treatment if they experienceddecreased bowel movement frequency (<3 spontaneous bowelmovements and >0 total bowel movements per week; sponta-neous bowel movement defined as a bowel movement occur-ring in the absence of laxative use in the previous 24 h)during the 2-week baseline period, and at least one of the fol-lowing bowel symptoms for P25% of bowel movements: sen-sation of incomplete evacuation, straining, or lumpy hardstools or small pellets.
Eligible subjects were randomized in a 1:1:1:1 ratio to oralalvimopan 0.5 mg BID, 1 mg QD, 1 mg BID, or placebo cap-sules (Fig. 1). The rationale for dose selection was based lar-gely on findings of a previous phase II study [24] whichinvestigated the efficacy and safety of alvimopan at dosagesof 0.5 mg QD and 1 mg QD, and found that the lower dosehad limited efficacy compared with the higher dose. Therefore,in the current study, the lowest alvimopan dosage tested was atotal of 1 mg per day. In the study by Paulson et al., [24] alv-imopan 1 mg QD was associated with a higher rate of adverseevents than the lower dose. It was observed that, in the smallproportion of patients who discontinued alvimopan due toadverse events, these typically occurred within 3 h of dosingduring the first 2 days of drug administration, suggesting thatinfrequent transient intolerance on drug initiation might berelated to alvimopan peak concentrations. Therefore, the cur-rent trial explored different dosage regimes to optimize tolera-bility of alvimopan 1 mg per day, using either a single daily1 mg dose, or 0.5 mg BID. To attempt to avoid early discontin-
uations associated with higher dosages, subjects randomized toalvimopan 1 mg QD or BID received alvimopan 0.5 mg QD orBID, respectively, during the first 3 days of the treatment per-iod. On Day 4, subjects titrated up to the full dose regimen forthe remainder of the treatment period (Fig. 1). Compliancewith assigned therapy regimen was assessed by capsule countat each study visit.
To avoid the confounding influence that concomitant laxa-tives could have on interpreting the efficacy and safety data,subjects were instructed to discontinue all laxatives throughoutthe entire study period. Oral bisacodyl was provided as 5 mgtablets and permitted as rescue laxative medication, in a doserange of 10–30 mg, if the subject had no bowel movementfor 4 consecutive days and experienced unusual or significantdiscomfort. Consumption of whole foods or use of bulkingagents was permitted at a level consistent with, but not higherthan, pre-study dietary fiber levels. Subjects were encouragedto increase fluid intake, but were not required to record fiberor fluid intake.
2.2. Efficacy endpoints
The primary efficacy endpoint was a change in weekly spon-taneous bowel movement frequency during the first 3 weeks ofthe 6-week treatment period.
Secondary efficacy endpoints included: responders for Opi-oid-induced Bowel Dysfunction Global Improvement, definedas subjects describing their constipation as moderately or sub-stantially improved compared with baseline on a 7-point Lik-ert scale; weekly changes in subjective bowel movementsymptom rating scores (proportion of stools leaving subjectwith a sense of incomplete evacuation; stool consistency[loose/watery, semi-solid/soft, lumpy/hard, or small pellets];and straining [none, mild, moderate or severe]); changes inPatient Assessment of Constipation-Symptoms (PAC-SYM;[8]) questionnaire scores (total scores and scores on domainsof abdominal, rectal and stool symptoms); changes in weeklynumber of doses of rescue laxative used (including impact ofthe rescue laxative on bowel movement frequency, Opioid-induced Bowel Dysfunction Global Improvement, incompleteevacuation, stool consistency, and straining).
Exploratory efficacy analyses included: responders forspontaneous bowel movement frequency (defined as subjectswith P3 spontaneous bowel movements per week or subjectswith an increase from baseline of P1 spontaneous bowelmovement per week), and changes in severity of other opi-oid-induced bowel dysfunction-related symptoms (decreasedappetite, esophageal reflux, nausea, vomiting, headache,abdominal fullness, gas, and malaise; rated from absent to verysevere on a 5-point scale). Health outcomes endpoints includedresponders for overall satisfaction with treatment (defined assubjects giving a rating of satisfied or very satisfied with theirstudy treatment, on a 7-point Likert scale), or subjects report-ing ‘‘yes’’ that they would use their study treatment again,when asked at Week 6, and changes from baseline to Week 6in Patient Assessment of Constipation-Quality of Life (PAC-QOL) [18] total scores and domain scores.
Data for evaluation of efficacy endpoints were collected pri-marily via an interactive voice response system (IVRS) using atouch-tone telephone data entry system. This was used on adaily basis to record number of bowel movements, associated

L. Webster et al. / Pain 137 (2008) 428–440 431
symptoms (incomplete evacuation, straining and stool consis-tency) and rescue laxative use. Subjects were instructed to callinto the system at the same time each day to ensure that thereporting period was consistent. In addition to these dailyassessments, the IVRS was used for weekly assessment of Opi-oid-induced Bowel Dysfunction Global Improvement. Ques-tionnaires were administered at clinic visits: PAC-SYM atbaseline, Weeks 1, 3, and 6, and at the end of follow-up (Week8, or on withdrawal from the study); PAC-QOL at baselineand Week 6 (or on withdrawal from the study); and treatmentsatisfaction and willingness to use again at Week 6 (or onwithdrawal).
2.3. Safety endpoints
Safety endpoints included: incidence of reported adverseevents, including serious adverse events; incidence of treat-ment-limiting toxicities, including both clinical and laboratoryadverse events; changes in weekly pain intensity score; changesin the morphine equivalents of opioids used; presence andseverity of withdrawal symptoms; and changes in laboratoryparameters.
Adverse events were coded using the International Confer-ence on Harmonization Medical Dictionary for RegulatoryActivities (ICH MedDRA�), and severity was graded by theinvestigator as mild (easily tolerated by the subject, causingminimal discomfort and not interfering with everydayactivities); moderate (sufficiently discomforting to interferewith normal everyday activities); or severe (prevents normaleveryday activities). Investigators also determined whethercausality of the adverse event was likely to be attributed tothe study treatment. Treatment-limiting adverse events weredefined as those that required withdrawal from drug treat-ment. Serious adverse events were defined as: any event thatresulted in death; was life-threatening; required hospitalizationor caused prolongation of existing hospitalization; resulted indisability/incapacity; was a congenital anomaly/birth defect;or which in the judgment of the investigator had potential tojeopardize the subject or require medical or surgical interven-tion to prevent one of the outcomes listed in the abovedefinition.
Pain intensity was scored each week on a 0–10 scale;patients reported their subjective ratings of average pain inten-sity and worst pain experienced through the week via theIVRS. Opioid consumption was also reported via the IVRS,on a daily basis. Systemic opioid withdrawal was assessed atclinic visits using a modified Himmelsbach scale to measureeach of the following signs: yawning, lacrimation, rhinorrhea,perspiration, tremor, mydriasis, piloerection, and restlessness,on a 4-point scale (none, mild, moderate, or severe) [5,11].At all visits, vital signs were measured and standard laboratorytests were performed.
2.4. Statistical analysis
Efficacy analyses were performed for the intent-to-treat(ITT) population, which included all randomized subjects.The safety population comprised of all subjects in the ITTpopulation who received at least one dose of study medication.Where data were missing, the last observation carried forward(LOCF) method was used to replace missing values with the
last previous non-missing value. Pairwise comparisons betweeneach alvimopan group and placebo for non-parametric contin-uous data were made using Wilcoxon rank sum tests withadjustment for multiple comparisons using Hommel’s generalmultiple Simes procedure [13]. The Fisher’s exact test was usedto compare alvimopan and placebo for categorical data.
Control of the type I error rate for statistical inferenceamong the secondary endpoints for a particular dose groupwas managed by assessing these endpoints over the first 3weeks of the treatment period in the following orderedsequence: (1) global improvement of opioid-induced boweldysfunction symptoms; (2) incomplete evacuation; (3) strain-ing; (4) stool consistency; and (5) PAC-SYM. These endpointswere assessed initially over the first 3 weeks during the treat-ment period, and if significance was demonstrated for thisinterval, weekly change from baseline and average change overthe entire 6-week treatment period were assessed for clinicalsignificance. Subsequently, if at least one of the secondary end-points was significant, interpretation of significance precededto the health outcomes endpoints in the following order: (1)overall satisfaction with treatment at Week 6; (2) willingnessto use treatment at Week 6; and (3) PAC-QOL at Week 6.No further multiple comparison adjustments were made forsupportive or explanatory efficacy endpoints nor to safetyendpoints.
Calculation of the required sample size was based on esti-mates of variability and treatment differences in the changefrom baseline in average weekly bowel movement frequencyfrom previous studies of alvimopan in opioid-induced boweldysfunction. Assuming a standard deviation of 3 spontaneousbowel movements per week, and aiming to detect an increaseof 1.25 spontaneous bowel movements per week in thealvimopan groups relative to placebo, it was calculatedthat a sample size of 125 patients per treatment group wasrequired to provide 90% power for a two-sided test at thea = 0.05 level.
3. Results
3.1. Subject characteristics
Of the 1108 subjects screened for study participation,522 were randomized to alvimopan 0.5 mg BID(n = 130), 1 mg QD (n = 133) or 1 mg BID (n = 130),or placebo (n = 129) (Fig. 2). The main reason fornon-randomization was ineligibility (n = 465; 79%),primarily from failure to report decreased bowelmovement frequency (average of <3 spontaneous bowelmovements but >0 total bowel movements per week) ornon-compliance with the IVRS system during the2-week baseline period.
Overall, 17% of randomized subjects did not com-plete the study; reasons for withdrawal are shown inFig. 2. There were no significant differences in reasonsfor withdrawal between groups.
No clinically relevant differences in demographiccharacteristics were observed between treatment groups(Table 1). The primary pain condition in each group wasback pain (55–62%). Subjects experienced pain for a

Fig. 2. Flowchart describing progress of participants through trial.
432 L. Webster et al. / Pain 137 (2008) 428–440
mean of 10.1–11.4 years, received chronic opioid treat-ment for a mean of 6.2–7.8 years, and had been takingtheir current opioid for a mean of 2.5–2.7 years. Thestudy population reported use of various opioids atbaseline, most commonly oxycodone and morphine,and a number of laxative preparations (discontinued atscreening) (Table 2).
Regarding compliance with study medication, P95%of subjects demonstrated P80% compliance withtreatment.
3.2. Efficacy parameters
3.2.1. Change in spontaneous bowel movement frequency
The change in spontaneous bowel movement fre-quency during the first 3 weeks of the treatment period(the primary efficacy endpoint) was significantly greaterin all alvimopan groups than the placebo group(P < 0.001 for all comparisons). The treatment differ-ence compared with placebo in mean weekly spontane-ous bowel movement frequency during this period was1.71 (95% CI 0.83–2.58) for alvimopan 0.5 mg BID,1.64 (0.88–2.40) for alvimopan 1 mg QD, and 2.52(1.40–3.64) for alvimopan 1 mg BID.
The average weekly frequency of spontaneous bowelmovements was significantly greater at all time pointsduring the treatment period for all alvimopan dosesthan for placebo (P 6 0.01 for all comparisons;Fig. 3). The overall mean change in spontaneousbowel movements during the 6-week treatment periodwas significantly greater in the alvimopan groups thanthe placebo group (P < 0.001 for all comparisons).Increases in spontaneous bowel movement frequencyin all alvimopan groups relative to placebo wereapparent within the first treatment week; indeed, onthe first day of treatment, 31% of patients in each alv-imopan group had at least one spontaneous bowelmovement, compared with 18% of patients in the pla-cebo group (P < 0.05). Increased spontaneous bowelmovement frequency was sustained throughout the 6-week treatment period, and the frequency decreasedtowards baseline in all treatment groups during the2-week follow-up period following treatment discontin-uation (Fig. 3).
On inspection of observed data and an analysis inwhich missing values were set to no change (M = NC),as opposed to LOCF, the change from baseline in spon-taneous bowel movement frequency was only greater

Table 1Subject demographics and pain history at baseline
Placebo (n = 129) Alvimopan
0.5 mg BID (n = 130) 1 mg QD (n = 133) 1 mg BID (n = 130)
GenderFemale 84 (65%) 77 (59%) 84 (63%) 88 (68%)Male 45 (35%) 53 (41%) 49 (37%) 42 (32%)
Mean age, years (SD) 51.3 (11.2) 49.7 (10.5) 51.5 (10.1) 48.6 (10.6)
RaceWhite 120 (93%) 125 (96%) 119 (89%) 116 (89%)
Primary pain conditionBack pain 60% 62% 55% 56%Neuralgia 7% 7% 8% 11%Fibromyalgia 8% 8% 8% 7%Arthritis 9% 5% 7% 8%Joint pain 3% 5% 6% 3%Headache 2% <1% 4% 6%CRPS 2% 3% 3% 3%Othera 10% 8% 10% 6%
Mean duration of pain condition, years (SD) 11.4 (10.5) 10.1 (8.0) 11.2 (9.9) 11.1 (7.9)
Mean lifetime chronic opioid use, years (SD) 7.4 (6.8) 6.2 (4.8) 6.4 (5.6) 7.8 (6.9)
Mean duration of current opioid for condition, years (SD) 2.7 (3.7) 2.5 (2.3) 2.5 (3.2) 2.6 (2.3)
Mean duration of stable use of current opioid (SD) 1.5 (2.1) 1.4 (1.6) 1.7 (3.1) 1.4 (1.7)
CRPS, complex regional pain syndrome.a Includes limb pain, myofascial pain, post-inflammatory pain, visceral pain, bone pain, multiple sclerosis, osteoporosis.
Table 2Opioid and laxative use at baseline
Placebo (n = 129) Alvimopan
0.5 mg BID (n = 130) 1 mg QD (n=133) 1 mg BID (n=130)
Opioid medication, % patientsOxycodone 43 42 35 40Morphine 33 37 32 41Fentanyl 16 22 23 14Methadone 18 12 21 19Hydrocodone 19 22 11 17Hydromorphone 7 8 6 5Codeine 6 4 8 5Tramadol <1 3 3 2Other <1 <1 <1 2
Mean oral morphine equivalent total daily dose, mg (SD)a,b 235.5 (381.3) 401.0 (909.4) 291.3 (315.1) 223.7 (245.2)
Laxative medication, % patientsc
Stimulant 50 42 50 48Stool softener 16 26 23 22Hyperosmotic 16 20 23 14Osmotic 16 10 11 15Bulk-forming agent 6 13 6 10Emollient 5 3 2 5Herbal 2 <1 2 0Miscellaneous 3 <1 <1 0
a Subjects may be taking more than one opioid.b Includes 6 subjects receiving intrathecal opioids (1, 4, and 1 in the placebo, alvimopan 0.5 mg BID and alvimopan 1 mg BID groups, respectively).
The elevated mean opioid consumption in the alvimopan 0.5 mg BID group is attributable to the contribution of the 4 intrathecally dosed subjects.c Subjects may be taking more than one laxative.
L. Webster et al. / Pain 137 (2008) 428–440 433
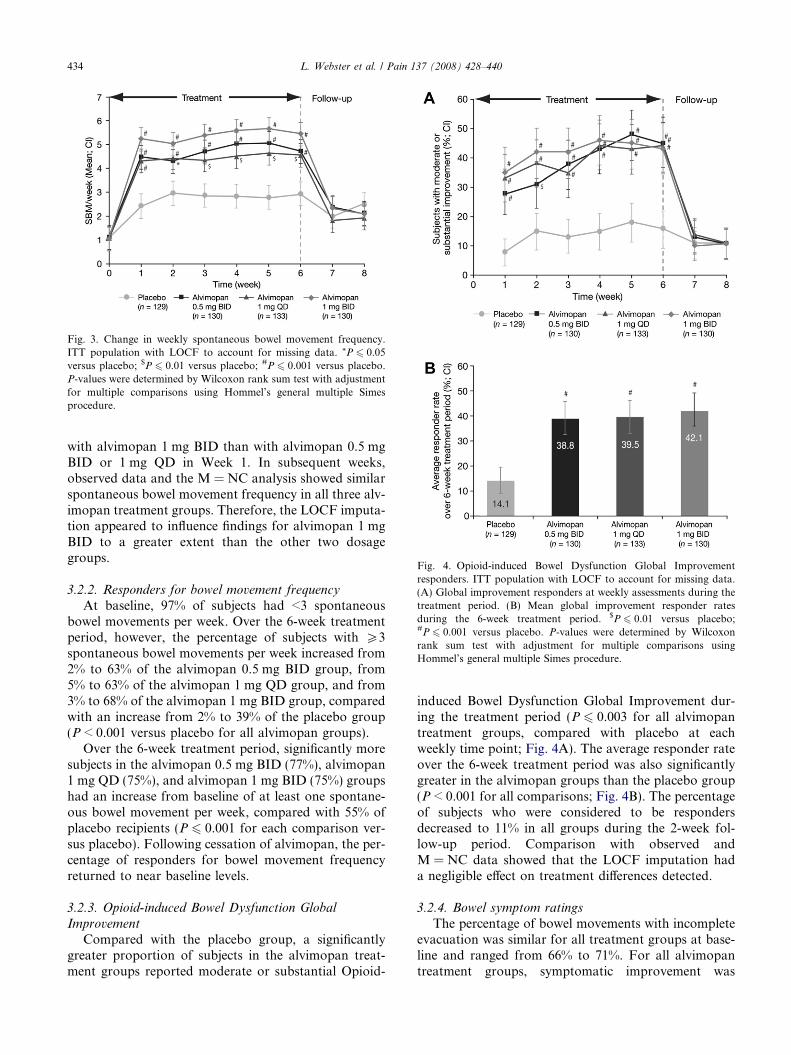
Fig. 3. Change in weekly spontaneous bowel movement frequency.ITT population with LOCF to account for missing data. *P 6 0.05versus placebo; $P 6 0.01 versus placebo; #P 6 0.001 versus placebo.P-values were determined by Wilcoxon rank sum test with adjustmentfor multiple comparisons using Hommel’s general multiple Simesprocedure.
Fig. 4. Opioid-induced Bowel Dysfunction Global Improvementresponders. ITT population with LOCF to account for missing data.(A) Global improvement responders at weekly assessments during thetreatment period. (B) Mean global improvement responder ratesduring the 6-week treatment period. $P 6 0.01 versus placebo;#P 6 0.001 versus placebo. P-values were determined by Wilcoxonrank sum test with adjustment for multiple comparisons usingHommel’s general multiple Simes procedure.
434 L. Webster et al. / Pain 137 (2008) 428–440
with alvimopan 1 mg BID than with alvimopan 0.5 mgBID or 1 mg QD in Week 1. In subsequent weeks,observed data and the M = NC analysis showed similarspontaneous bowel movement frequency in all three alv-imopan treatment groups. Therefore, the LOCF imputa-tion appeared to influence findings for alvimopan 1 mgBID to a greater extent than the other two dosagegroups.
3.2.2. Responders for bowel movement frequency
At baseline, 97% of subjects had <3 spontaneousbowel movements per week. Over the 6-week treatmentperiod, however, the percentage of subjects with P3spontaneous bowel movements per week increased from2% to 63% of the alvimopan 0.5 mg BID group, from5% to 63% of the alvimopan 1 mg QD group, and from3% to 68% of the alvimopan 1 mg BID group, comparedwith an increase from 2% to 39% of the placebo group(P < 0.001 versus placebo for all alvimopan groups).
Over the 6-week treatment period, significantly moresubjects in the alvimopan 0.5 mg BID (77%), alvimopan1 mg QD (75%), and alvimopan 1 mg BID (75%) groupshad an increase from baseline of at least one spontane-ous bowel movement per week, compared with 55% ofplacebo recipients (P 6 0.001 for each comparison ver-sus placebo). Following cessation of alvimopan, the per-centage of responders for bowel movement frequencyreturned to near baseline levels.
3.2.3. Opioid-induced Bowel Dysfunction Global
Improvement
Compared with the placebo group, a significantlygreater proportion of subjects in the alvimopan treat-ment groups reported moderate or substantial Opioid-
induced Bowel Dysfunction Global Improvement dur-ing the treatment period (P 6 0.003 for all alvimopantreatment groups, compared with placebo at eachweekly time point; Fig. 4A). The average responder rateover the 6-week treatment period was also significantlygreater in the alvimopan groups than the placebo group(P < 0.001 for all comparisons; Fig. 4B). The percentageof subjects who were considered to be respondersdecreased to 11% in all groups during the 2-week fol-low-up period. Comparison with observed andM = NC data showed that the LOCF imputation hada negligible effect on treatment differences detected.
3.2.4. Bowel symptom ratings
The percentage of bowel movements with incompleteevacuation was similar for all treatment groups at base-line and ranged from 66% to 71%. For all alvimopantreatment groups, symptomatic improvement was
L. Webster et al. / Pain 137 (2008) 428–440 435
apparent by Week 1, and was maintained throughoutthe 6-week treatment period (P 6 0.009). A post hocanalysis was performed to address the clinical relevanceof these findings by determining the response rate forimprovement in incomplete evacuation (<25% of bowelmovements with incomplete evacuation). Over the 6-week treatment period, significantly more alvimopan0.5 mg BID and 1 mg QD recipients were responders(<25% of bowel movements with incomplete evacua-
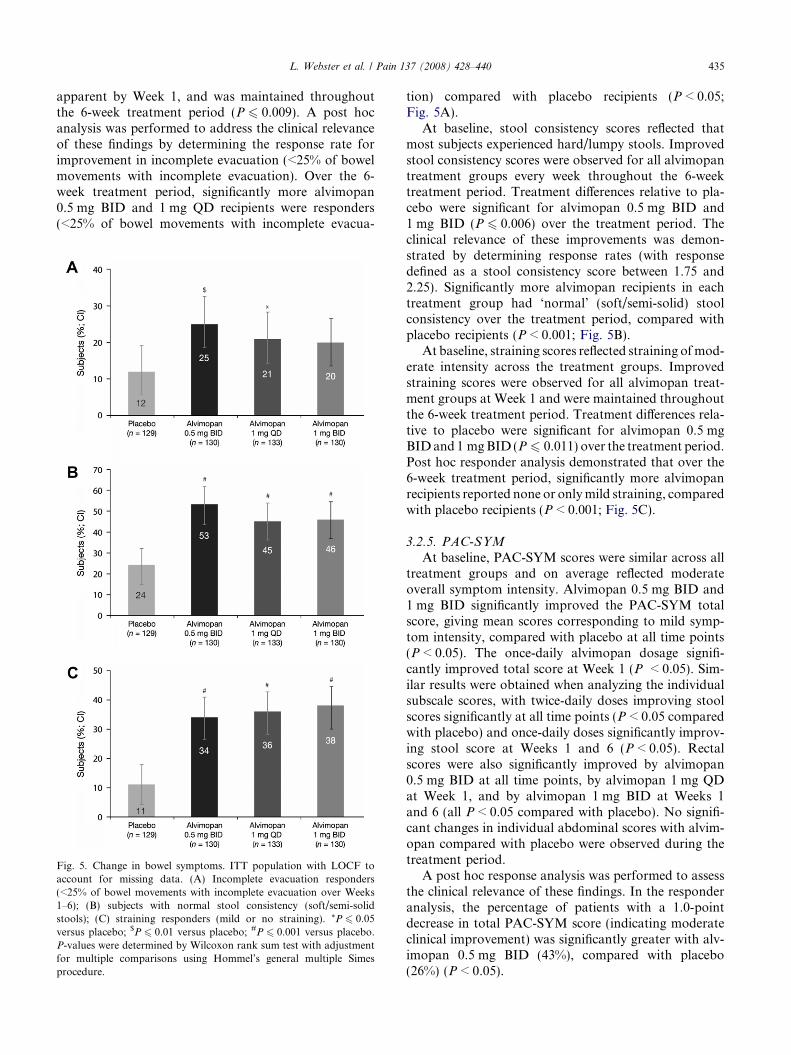
Fig. 5. Change in bowel symptoms. ITT population with LOCF toaccount for missing data. (A) Incomplete evacuation responders(<25% of bowel movements with incomplete evacuation over Weeks1–6); (B) subjects with normal stool consistency (soft/semi-solidstools); (C) straining responders (mild or no straining). *P 6 0.05versus placebo; $P 6 0.01 versus placebo; #P 6 0.001 versus placebo.P-values were determined by Wilcoxon rank sum test with adjustmentfor multiple comparisons using Hommel’s general multiple Simesprocedure.
tion) compared with placebo recipients (P < 0.05;Fig. 5A).
At baseline, stool consistency scores reflected thatmost subjects experienced hard/lumpy stools. Improvedstool consistency scores were observed for all alvimopantreatment groups every week throughout the 6-weektreatment period. Treatment differences relative to pla-cebo were significant for alvimopan 0.5 mg BID and1 mg BID (P 6 0.006) over the treatment period. Theclinical relevance of these improvements was demon-strated by determining response rates (with responsedefined as a stool consistency score between 1.75 and2.25). Significantly more alvimopan recipients in eachtreatment group had ‘normal’ (soft/semi-solid) stoolconsistency over the treatment period, compared withplacebo recipients (P < 0.001; Fig. 5B).
At baseline, straining scores reflected straining of mod-erate intensity across the treatment groups. Improvedstraining scores were observed for all alvimopan treat-ment groups at Week 1 and were maintained throughoutthe 6-week treatment period. Treatment differences rela-tive to placebo were significant for alvimopan 0.5 mgBID and 1 mg BID (P 6 0.011) over the treatment period.Post hoc responder analysis demonstrated that over the6-week treatment period, significantly more alvimopanrecipients reported none or only mild straining, comparedwith placebo recipients (P < 0.001; Fig. 5C).
3.2.5. PAC-SYM
At baseline, PAC-SYM scores were similar across alltreatment groups and on average reflected moderateoverall symptom intensity. Alvimopan 0.5 mg BID and1 mg BID significantly improved the PAC-SYM totalscore, giving mean scores corresponding to mild symp-tom intensity, compared with placebo at all time points(P < 0.05). The once-daily alvimopan dosage signifi-cantly improved total score at Week 1 (P < 0.05). Sim-ilar results were obtained when analyzing the individualsubscale scores, with twice-daily doses improving stoolscores significantly at all time points (P < 0.05 comparedwith placebo) and once-daily doses significantly improv-ing stool score at Weeks 1 and 6 (P < 0.05). Rectalscores were also significantly improved by alvimopan0.5 mg BID at all time points, by alvimopan 1 mg QDat Week 1, and by alvimopan 1 mg BID at Weeks 1and 6 (all P < 0.05 compared with placebo). No signifi-cant changes in individual abdominal scores with alvim-opan compared with placebo were observed during thetreatment period.
A post hoc response analysis was performed to assessthe clinical relevance of these findings. In the responderanalysis, the percentage of patients with a 1.0-pointdecrease in total PAC-SYM score (indicating moderateclinical improvement) was significantly greater with alv-imopan 0.5 mg BID (43%), compared with placebo(26%) (P < 0.05).

436 L. Webster et al. / Pain 137 (2008) 428–440
3.2.6. Rescue laxative use
Over the 6-week treatment period, alvimopan recipi-ents used significantly fewer rescue laxatives comparedwith placebo recipients (a treatment difference of�1.12, �1.28, and �0.78 tablets per week for alvimopan0.5 mg BID, 1 mg QD, and 1 mg BID, respectively, ver-sus a mean of approximately 2.9 tablets per week withplacebo; P = 0.01 for each comparison).
3.2.7. Opioid-induced bowel dysfunction-related
symptoms
Opioid-induced bowel dysfunction-related symptomsof decreased appetite, reflux, nausea, vomiting andheadache tended to be mild at baseline, whereas malaisewas of mild-to-moderate severity, and abdominal full-ness and gas were of moderate severity. Alvimopan pro-duced statistically significant improvements relative toplacebo for abdominal fullness (all dosage regimens)and decreased appetite (0.5 mg BID and 1 mg BID) atWeeks 1–6. Significant improvements with alvimopanin nausea (0.5 mg BID and 1 mg BID), gas (1 mgBID), and general malaise (1 mg BID) were alsoreported (Table 3).
3.2.8. Correlation analyses
Opioid-induced Bowel Dysfunction Global Improve-ment was significantly correlated with spontaneousbowel movement frequency at each week (P < 0.001for all comparisons), bowel movement symptoms (P< 0.001 for all comparisons), GI side effect-relatedsymptoms (P < 0.001 for all comparisons), constipationsymptoms (PAC-SYM) (P < 0.001 for all comparisons)and HRQoL (PAC-QOL) (P < 0.001 for all compari-sons). Bowel movement frequency was significantlyincreased in Opioid-induced Bowel Dysfunction GlobalImprovement responders versus non-responders, andsignificantly more responders than non-responders
Table 3Change in opioid-induced bowel dysfunction-related symptoms scoreat Week 6 from baseline
Placebo(n = 129)
Alvimopan
0.5 mgBID(n = 130)
1 mgQD(n = 133)
1 mgBID(n = 130)
Decreased appetite �0.18 �0.60*** �0.31 �0.45*
Reflux �0.10 �0.20 �0.29 �0.33Nausea �0.09 �0.40* �0.25 �0.38*
Vomiting �0.06 �0.04 �0.03 0.00Abdominal fullness �0.41 �0.86** �0.85** �0.88***
Gas �0.32 �0.34 �0.40 �0.67*
Headache �0.17 �0.18 �0.27 �0.16Malaise �0.21 �0.51 �0.45 �0.57*
* P < 0.05.** P < 0.01.
*** P 6 0.001 versus placebo (Wilcoxon rank sum test).
reported improvements in bowel movement symptomsand GI side effect-related symptoms. Evaluation of Opi-oid-induced Bowel Dysfunction Global Improvementresponders versus non-responders also showed that Opi-oid-induced Bowel Dysfunction Global Improvementwas correlated with improved PAC-SYM and PAC-QOL total and subscale scores.
3.3. Health outcomes endpoints
3.3.1. Overall satisfaction with treatment
By Week 6, a higher percentage of patients reportedbeing satisfied or very satisfied with treatment in the alv-imopan groups versus placebo. The difference reachedstatistical significance for the twice-daily dosing regi-mens [placebo 34%; alvimopan 0.5 mg BID 56%(P = 0.001); 1 mg QD 46%; 1 mg BID 55%(P = 0.002)]. At Week 6, 69%, 66%, and 72% of alvimo-pan 0.5 mg BID, 1 mg QD, and 1 mg BID recipients,respectively, would be willing to continue treatment,compared with 55% of placebo recipients (P = 0.026for alvimopan 0.5 mg QD and P = 0.007 for alvimopan1 mg BID).
3.3.2. PAC-QOL
Baseline total PAC-QOL overall scores were similarin all groups, ranging from 1.87 to 2.1, indicating mod-erate impact of constipation on HRQoL. Comparedwith placebo, there were significant improvements inPAC-QOL overall scores with all three alvimopan doseregimens (�0.25 with 0.5 mg BID, �0.23 with 1 mg QD,and �0.39 with 1 mg BID; P 6 0.014). Furthermore,compared with placebo, there were significant improve-ments (P < 0.05) in all four subscale scores with alvimo-pan 0.5 mg BID and 1 mg BID. With alvimopan 1 mgQD, the improvements were significant for the worriesand concerns (P = 0.007) and the satisfaction(P = 0.031) subscale scores.
3.4. Safety
Overall, the incidence of treatment-emergent adverseevents in the alvimopan treatment groups was similar tothe placebo group (Table 4). The most frequentlyreported adverse events in this study were GI-related,consistent with the targeted action of alvimopan, andpredominantly included abdominal pain, nausea, anddiarrhea. A higher frequency of abdominal pain anddiarrhea occurred in the alvimopan 1 mg QD or BIDdosage groups, compared with alvimopan 0.5 mg BIDor placebo. When adverse events judged by investigatorsto be potentially related to treatment were considered, asimilar profile was observed.
No deaths were reported during the study. Seriousadverse events were experienced by 3% of the placebogroup and 5%, 8%, and 4% of the alvimopan 0.5 mg

Table 4Treatment-emergent adverse events occurring in P10% of subjects in any treatment group
Preferred term, n (%) Placebo (n = 129) Alvimopan 0.5 mgBID (n = 130)
Alvimopan 1 mgQD (n = 133)
Alvimopan 1 mgBID (n = 130)
Any adverse event 85 (66) 92 (71) 87 (65) 87 (67)Any GI-related adverse event 47 (36) 39 (30) 50 (38) 56 (43)Abdominal paina 19 (15) 22 (17) 29 (22) 36 (28)Diarrhea 7 (5) 9 (7) 14 (11) 18 (14)Nausea 12 (9) 9 (7) 12 (9) 13 (10)Flatulence 6 (5) 8 (6) 11 (8) 10 (8)Headache 8 (6) 15 (12) 8 (6) 9 (7)Hyperhidrosis 5 (4) 10 (8) 7 (5) 4 (3)Abdominal distension 8 (6) 4 (3) 5 (4) 8 (6)Back pain 4 (3) 8 (6) 7 (5) 5 (4)Vomiting 5 (4) 6 (5) 7 (5) 5 (4)Fatigue 6 (5) 8 (6) 3 (2) 2 (2)Weight increase 6 (5) 6 (5) 1 (<1) 5 (4)Rhinorrhea 3 (2) 6 (5) 1 (<1) 2 (2)Nasopharyngitis 0 3 (2) 6 (5) 1 (<1)
a Composite of abdominal pain, abdominal pain upper, and abdominal pain lower preferred terms.
L. Webster et al. / Pain 137 (2008) 428–440 437
BID, 1 mg QD, and 1 mg BID groups, respectively, withno statistically significant differences observed betweengroups. Of the 37 serious adverse events that occurredduring the trial, four were considered to be possiblyrelated to the investigational product: abdominal painresulting in hospitalization in two subjects in the alvim-opan 1 mg BID group (leading to study withdrawal);diarrhea in one subject in the alvimopan 1 mg QD group(which did not require study withdrawal) and hepatitisin one subject in the placebo group (who was withdrawnfollowing the subsequent development of urosepsis, notconsidered to be related to treatment). A total of threeserious cardiac adverse events occurred during the trial:one case of bradycardia in the alvimopan 0.5 mg BIDgroup, and one case of unstable angina and one caseof acute myocardial infarction in the alvimopan 1 mgQD group. None of these events were judged to havebeen related to study medication.
In the placebo group, 9% of subjects withdrew as aresult of adverse events, compared with 5%, 11%, and13% of the alvimopan 0.5 mg BID, 1 mg QD, and 1 mgBID groups, respectively (Fig. 2). The most commonevents leading to withdrawal were GI-related andincluded abdominal pain, diarrhea, and nausea. Themajority of adverse events that led to withdrawal fromthe study occurred within the first 2 weeks of treatment,with a higher rate in the alvimopan 1 mg QD and 1 mgBID groups within the first 3 days of therapy, despitethe fact that all subjects received alvimopan 0.5 mg QDor BID during this period in accordance with the step-up regimen.
There were no clinically relevant differences in routinelaboratory monitoring, vital signs and physical examin-ations between the four treatment groups.
Subjects in all randomized groups rated average painintensity as 5.8 at baseline, which did not change signif-icantly throughout the study period. The total daily dose
of opioid did not change significantly throughout thestudy period for any of the randomized groups. Meantotal Himmelsbach scores remained <1 (maximum pos-sible score 24) for all treatment arms from baseline tofollow-up, with no statistically significant differencesbetween any alvimopan dosage and placebo.
4. Discussion
This study demonstrates that specific, competitiveperipheral mu-opioid antagonism by alvimopan canrestore GI function and relieve opioid-induced boweldysfunction, without compromising analgesia, inpatients receiving chronic opioid therapy for non-malig-nant pain. The study findings also suggest that alvimo-pan 0.5 mg BID is the regimen that provides the mostfavorable benefit-to-risk profile for treatment of opi-oid-induced bowel dysfunction with alvimopan in thispatient population.
Alvimopan is a PAM-OR antagonist that specificallyblocks the actions of opioids on mu-opioid receptorslocated on the enteric neurons that innervate the smoothmuscle and submucosal layers of the GI tract [15]. In thepresent study, alvimopan was shown to improve GI func-tion in patients with non-cancer pain using opioids, with-out reversing analgesia or inducing opioid withdrawalsymptoms. All alvimopan dosage regimens were associ-ated with statistically significantly greater mean weeklyfrequency of spontaneous bowel movements within thefirst 3 weeks of treatment, compared with placebo(P < 0.001). This beneficial effect was sustained over the6-week treatment period, with spontaneous bowel move-ment frequency increasing by a mean of 3.4–4.3 per weekin the alvimopan treatment groups (P < 0.001), comparedwith a mean of 1.7 per week in the placebo group. The useof alvimopan resulted in a bowel movement on anaverage of 4–5 days per week without the use of laxatives.

438 L. Webster et al. / Pain 137 (2008) 428–440
Furthermore, once alvimopan therapy was stopped,bowel dysfunction returned to baseline levels.
The primary objective of this study was to determinethe most appropriate alvimopan regimen to provide thebest benefit-to-risk profile. For subjects who did nothave complete data sets available, the last recordedobservation for each endpoint was carried forward(LOCF) for statistical analysis. Using the LOCF impu-tation, higher alvimopan dosages produced numericallybetter improvements in spontaneous bowel movementfrequency, compared with the other dosing regimens.This would suggest that there was a dose-related benefitobserved with alvimopan. However, when missing datawere assigned a value of no change (M = NC imputa-tion) rather than LOCF, a dose-related benefit was nolonger observed. This suggested that treatment differ-ences in the higher alvimopan dosage groups may havebeen affected to a greater extent by the LOCF analysis,perhaps due to increased spontaneous bowel movementfrequency being carried forward for a larger proportionof subjects who withdrew early in these groups, com-pared with alvimopan 0.5 mg BID or placebo.
The effects of alvimopan on other bowel-relatedsymptoms, including straining, incomplete evacuation,and abnormal stool consistency, were explored withsymptom-specific questions as well as the PAC-SYMquestionnaire. Alvimopan improved stool consistency,with almost half of alvimopan recipients characterizingtheir stool consistency as ‘normal’ at the end of treat-ment, compared with only one-quarter of placebo recip-ients. Straining scores were consistently lower withalvimopan, indicating less effort, and a sense of incom-plete evacuation occurred less frequently in the treat-ment groups. Consistent with these effects onsymptoms, scores on the PAC-SYM were consistentlyand significantly better with alvimopan versus placebofor each domain (abdominal, rectal, and stool symp-toms) and for the composite score.
Because opioid receptors are present throughout theGI tract [6], opioids may induce other GI side effects.Individuals treated with opioids may be prone to nau-sea, vomiting, reflux, or bloating [15,21,23]. Upperabdominal symptoms were evaluated with an opioid-induced bowel dysfunction-related symptoms question-naire. At baseline, these symptoms were generally mild(as would be expected, given that these symptoms tendto be most prominent at the start of opioid treatmentand subjects had received stable opioid therapy for atleast 1 month prior to entering the trial); therefore, themagnitude of difference following administration of alv-imopan and placebo is of uncertain clinical significance.However, notable improvements in abdominal fullness,nausea, appetite and gas were observed with alvimopanrelative to placebo; this exploratory analysis thereforeindicates that alvimopan may have a beneficial effecton other opioid-induced bowel dysfunction-related
symptoms affecting the upper GI tract. Further investi-gation is warranted to determine whether this benefitis independent of effects on constipation. In addition,since the incidence of opioid-induced constipation mayvary between different opioids, further studies on theeffect of alvimopan in homogenous patient groups tak-ing the same opioid, or in patients taking partial opioidagonists such as buprenorphine, may be of interest.
The effect of opioid-induced bowel dysfunction onsubjects’ quality of life has not been studied extensively.One survey demonstrated that non-cancer pain subjectsmay prefer to tolerate inadequate pain relief without GIside effects rather than achieve effective pain relief ifassociated with constipation [22]. In the current study,patients’ HRQoL was found to be moderately impairedat baseline, as assessed by the PAC-QOL instrument.Treatment with alvimopan significantly improved over-all PAC-QOL score, compared with placebo. Improve-ment in quality of life may encourage subjects tocontinue their opioid treatment.
Critical to the hypothesis that the mechanism ofaction of alvimopan centers on selective antagonism ofperipheral mu-opioid receptors is the demonstrationthat alvimopan did not reverse opioid analgesia orinduce opioid withdrawal phenomena. Pain scores weresimilar for all treatment arms and remained stablethroughout the baseline, treatment, and follow-up peri-ods. Changes from baseline in opioid consumption,expressed in oral morphine equivalents, were small anddid not differ significantly among the treatment arms. Inaddition, alvimopan did not induce an opioid abstinencesyndrome, as demonstrated by the low Himmelsbachscores in all treatment arms. This is in contrast to previ-ous studies with oral naloxone, an opioid receptorantagonist that crosses the blood–brain barrier, wherewithdrawal signs occurred quickly with initiation oftherapy or escalation of dosing, and commonly includedrestlessness, anxiety, perspiration, and pain [5]. Therewere no indications in this 6-week study of a waningof alvimopan effect. Efficacy was durable over timeand there was no evidence of the development of toler-ance; indeed, the drug’s mechanism of action as a recep-tor antagonist would suggest that this is unlikely tooccur. Long-term (12-week and 12-month) studies willfurther elucidate the apparent lack of development oftolerance to alvimopan.
Laxatives are often associated with GI side effectssuch as abdominal cramping [29]. In this study, as in aprevious study [24], alvimopan was not associated witha significant increase in GI side effects, compared withplacebo (30–43% versus 36%). A small numericalincrease in the incidence of some GI side effects wasobserved with alvimopan 1 mg QD and BID comparedwith placebo, despite the use of alvimopan 0.5 mg inthe 3-day step-up regimen at the start of the treatmentperiod; the frequency of abdominal pain and diarrhea

L. Webster et al. / Pain 137 (2008) 428–440 439
was higher in the alvimopan 1 mg QD and BID groups,compared with alvimopan 0.5 mg BID and placebogroups. Higher peak alvimopan concentrations follow-ing dosing with 1 mg than with 0.5 mg capsules mayresult in more opioid being displaced from the periphe-ral mu-opioid receptors, resulting in localized manifesta-tions of withdrawal in the opioid-adapted gut. Thisobservation of increased GI side effects with higher alv-imopan dose is consistent with an earlier study [24]. Inthis study, alvimopan was shown to be well tolerated,with a safety profile similar to placebo. Incidence ofall adverse events was similar in the alvimopan 0.5 mgBID group to the placebo group, and fewer subjects inthe alvimopan 0.5 mg BID group withdrew from thestudy because of adverse events. In conjunction withprevious data demonstrating limited efficacy of a0.5 mg QD regimen [24], the current study results indi-cate that the alvimopan 0.5 mg BID regimen providesthe most favorable benefit-to-risk profile in this studypopulation.
These results demonstrate that competitive peripheralantagonism of opioid analgesics with alvimopan canrestore GI function and relieve opioid-induced boweldysfunction without compromising analgesia in patientstreated with chronic opioids for non-cancer pain. Spe-cific peripheral mu-opioid receptor antagonism mayoffer improved prospects for the use of adequate opioiddosages to provide optimal pain relief and functionalimprovement in this population. These findings alsoestablish the alvimopan 0.5 mg BID regimen as the mostappropriate alvimopan dosing regimen for this studypopulation. A phase III program confirming the effectsof alvimopan in this population is currently underwayand should provide further insight into the role of alvim-opan in treating opioid-induced bowel dysfunction.
Acknowledgments
Study SB-767905/011 was initiated and sponsored byGlaxoSmithKline.
The authors were assisted in manuscript preparationand collation of author contributions by professionalmedical writers at Gardiner-Caldwell London. Financialassistance to support this service was provided byGlaxoSmithKline R&D.
The following investigators and institutions partici-pated in Study SB-767905/011: Australia: Milton Cohen,Michael Cousins, David Cherry, Lindy Roberts; Bel-gium: Bart Morlion, Leon Plaghki, Guy Hans; Canada:Naresh Aggarwal, Steve Blitzer, Guy Boudreau, JohnClark, Ian Cowan, Brently Dickson, Rafat Faraawi,Howard Intrater, Ben Lasko, Robert Welch, LindaWynne, Zlotnik Gregorio, Allan Gordon, RichardAudet, Brian Ramjattan, Line Routhier; Denmark:Michael Edward Crawford, Michael Kamp-Jensen,
Torsten Jonsson, Gitte Handberg; Germany: ThomasBlock, Thomas Floter, Hartmut Goebel, Jan-Peter Jansen,Gerhard Muller-Schwefe, Thomas Nolte, Christoph Rie-masch-Becker, Helmut Staudenmayer, Dago Mazur,Rainer Sabatowski, Achim Bechtold, Christoph Wach-ter, Hans-Detlev Stahl, Bastian Steinberg, Kai Her-manns, Jan Bek, Martin Ehmer, Hans-HermannNaegelein, Anette Herzner; Greece: Ioanna Siafaka,Eleni Plessia, Misel Ammari; Italy: Sergio Boncinelli,Laura Demartini, Paolo Marchettini, Vincenzo Mont-rone, Biagio Panascia, William Raffaeli, Gianluigi Zep-petella, Paulo Pinato; Portugal: Beatriz CraveiroLopes, Maria Georgina Coucelo, Rosario Alonso, Lau-rinda Lemos; United States: Omer Abdullah, James Be-retta, Daniel Brookoff, Steven Charapata, Diane Chau,Michael Drass, John Ervin, Jay Ferns, Theresa Ferrer-Brechner, Michael Gibson, Cynthia Guy, Joseph Holt-man, James Honet, Gordon Irving, Navnit Kaur, JakeLennard, Donald Lipkis, Mark Matsunaga, Paul Matz,Edward Michna, Thomas O’Barr, John Peppin, GeorgeRaad, Lowell Reynolds, Albert Razzetti, Dennis Riff,Mark Ringold, Jeffrey Rosen, Richard Smith, EgiliusLH Spierings, Rajbala Thakur, Charles Argoff, MiroslavBackonja, Richard Blonsky, Clifton Cage, Neal Slatkin,Marvin Tark, Zahid Bajwa, Michael Goldstein, SudhirDiwan, John Kelly, Joseph Bruzzese, Abraham Rivera,Lee Rocamora, Thalia Segal, Bhasker Venkateswaralu,Ronald Pucillo, Pamela Vick, Kevin Wingert, RonicaKluge, Michael Edwards, Robert Finnegan, StephenZellner, Stephen Elliot, Rajiv Parti, Michael Ellerbusch,Royal Anspach, Carlos Saad, Ronald Emkey, LynnWebster, Scott Segal, Martin Mollen, Donna DeSantis,Andrew Klymiuk, David McLain, Harold Minkowitz,Michael Gibson, Denise Lester, Michael Fairfax, Ber-nard Michlin, John Park, Rachakonda Prabhu, WilliamRenaudin, Craig Scoville, James Vogt, Arnold Weil, BretWittmer, Phyllis Troia, Karen Kolba, Howard Adel-glass, Mark Fisher, James Greenwald, John Huff, TudorJianu, Arifulla Khan, Greg Marc Silver, M Scott Touger,William Keeton, Parimal Parikh, Richard Rosenthal,Warren Rizzo, Gary Fink, Charles Bova.
Appendix A. Supplementary data
Supplementary data associated with this article canbe found, in the online version, at doi:10.1016/j.pain.2007.11.008.
References
[1] Allan L, Hays H, Jensen NH, Le Polain de Waroux B, Bolt M,Donald R, et al. Randomized crossover trial of transdermalfentanyl and sustained release oral morphine for treating chronicnon-cancer pain. BMJ 2001;322:1154–8.
[2] Azodo IA, Ehrenpreis ED. Alvimopan. Curr Opin Investig Drugs2002;3:1496–501.

440 L. Webster et al. / Pain 137 (2008) 428–440
[3] Bates JJ, Foss JF, Murphy DB. Are peripheral opioid antagoniststhe solution to opioid side effects? Anesth Analg 2004;98:116–22.
[4] Camilleri M. Alvimopan, a selective peripherally acting l-opioidantagonist. Neurogastroenterol Motil 2005;17:157–65.
[5] Culpepper-Morgan JA, Inturrisi CE, Portenoy RK, Foley K,Houde RW, Marsh F, et al. Treatment of opioid-inducedconstipation with oral naloxone: a pilot study. Clin PharmacolTher 1992;52:90–5.
[6] De Luca A, Coupar IM. Insights into opioid action in theintestinal tract. Pharmacol Ther 1996;69:103–15.
[7] Fallon MT. Constipation in cancer patients: prevalence, patho-genesis, and cost-related issues. Eur J Pain 1999;3:3–7.
[8] Frank L, Kleinman L, Farup C, Taylor L, Miner Jr P.Psychometric validation of a constipation symptom assessmentquestionnaire. Scand J Gastroenterol 1999;34:870–7.
[9] Friedman JD, Dello Buono FA. Opioid antagonists in thetreatment of opioid-induced constipation and pruritus. AnnPharmacother 2001;35:85–91.
[10] Gutstein HB, Akil H. Opioid analgesics. In: Hardman JG,Limbird LE, Gilman AG, editors. Goodman and Gilman’s Thepharmacological basis of therapeutics. New York, NY: Mc-Graw-Hill Medical Publishing Division; 2001. p. 569–619.
[11] Himmelsbach CK. The morphine abstinence syndrome, its natureand treatment. Ann Int Med 1941;15:829–39.
[12] Holzer P. Opioids and opioid receptors in the enteric nervoussystem: from a problem in opioid analgesia to a possible newprokinetic therapy in humans. Neurosci Lett 2004;361:192–5.
[13] Hommel G. A stagewise rejective multiple test procedure based ona modified Bonferroni test. Biometrika 1988;75:383–6.
[14] Kalso E, Edwards JE, Moore RA, McQuay HJ. Opioids inchronic non-cancer pain: systematic review of efficacy and safety.Pain 2004;112:372–80.
[15] Kurz A, Sessler DI. Opioid-induced bowel dysfunction: patho-physiology and potential new therapies. Drugs 2003;63:649–71.
[16] Liberto JG, Herschler JA, Jaffe JH, Norbeck JH, Carpenter RL.Effects of ADL 8-2698, a peripherally restricted mu opioidantagonist, on gut motility in methadone and LAAM-dependentpatients with opioid-induced constipation: a dose-ranging study.Drug Alcohol Depend 2001;63:S91.
[17] Liu M, Wittbrodt E. Low-dose oral naloxone reverses opioid-induced constipation and analgesia. J Pain Symptom Manage2002;23:48–53.
[18] Marquis P, De La Loge C, Dubois D, McDermott A, ChassanyO. Development and validation of the Patient Assessment ofConstipation Quality of Life questionnaire. Scand J Gastroenterol2005;40:540–51.
[19] McNicol E, Horowicz-Mehler N, Fisk RA, Bennett K, Gialeli-Goudas M, Chew PW, et al. Management of opioid side effects in
cancer-related and chronic noncancer pain: a systematic review. JPain 2003;4:231–56.
[20] Meissner W, Schmidt U, Hartmann M, Kath R, Reinhart K. Oralnaloxone reverses opioid-associated constipation. Pain2000;84:105–9.
[21] Moore RA, McQuay HJ. Prevalence of opioid adverse eventsin chronic non-malignant pain: systematic review of random-ised trials of oral opioids. Arthritis Res Ther 2005;7:R1046–51.
[22] Palmer CS, Ingham M, Schmier J, Flood E, Gourlay G, Dodd SL.Utility assessments of opioid treatment for patients with chronicnon-cancer pain. In: Presented at the 20th Annual Scientificmeeting of the American Pain Society, Phoenix, AZ, April 19–22;2001 [Abstract 790].
[23] Pappagallo M. Incidence, prevalence, and management of opioidbowel dysfunction. Am J Surg 2001;182:11S–8S.
[24] Paulson DM, Kennedy DT, Donovick RA, Carpenter RL,Cherubini M, Techner L, et al. Alvimopan: an oral, peripherallyacting, l-opioid receptor antagonist for the treatment of opioid-induced bowel dysfunction – a 21-day treatment-randomizedclinical trial. J Pain 2005;6:184–92.
[25] Rauck RL, Southern JP, Carpenter RL. Use of alvimopan, aperipherally restricted mu-opioid antagonist to speed gastrointes-tinal transit in patients with opioid induced bowel dysfunction. In:Presented at the 10th World Congress on Pain, San Diego, CA,August 17–22; 2002 [Abstract 1669].
[26] Schmidt WK. Alvimopan (ADL 8-2698) is a novel peripheralopioid antagonist. Am J Surg 2001;182:27S–38S.
[27] Schug SA, Zech D, Grond S. Adverse effects of systemic opioidanalgesics. Drug Safety 1992;7:200–13.
[28] Thorpe DM. Management of opioid-induced constipation. CurrPain Headache Rep 2001;5:237–40.
[29] Van Orden H. Constipation: an overview of treatment. J PediatrHealth Care 2004;18:320–2.
[30] Walsh TD. Prevention of opioid side effects. J Pain SymptomManage 1990;5:362–7.
[31] Wood JD, Galligan JJ. Function of opioids in the enteric nervoussystem. Neurogastroenterol Motil 2004;16:17–28.
[32] Yuan CS, Wei G, Foss JF, O’Connor M, Karrison T, OsinskiJ. Effects of subcutaneous methylnaltrexone on morphine-induced peripherally mediated side effects: a double-blindrandomized placebo-controlled trial. J Pharmacol Exp Ther2002;300:118–23.
[33] Zimmerman DM, Gidda JS, Cantrell BE, Schoepp DD, JohnsonBG, Leander JD. Discovery of a potent, peripherally selectivetrans-3,4-dimethyl-4-(3-hydroxyphenyl)piperidine opioid antago-nist for the treatment of gastrointestinal motility disorders. J MedChem 1994;37:2262–5.




















