Altered T cell differentiation associated with loss of CD27 and CD28 in HIV infected Indian...
11
Cytometry Part B (Clinical Cytometry) 82B:43–53 (2012) Altered T Cell Differentiation Associated with Loss of CD27 and CD28 in HIV Infected Indian Individuals Kamalika Mojumdar, Madhu Vajpayee,* Neeraj Kumar Chauhan, Alpana Singh, Ravinder Singh, and Sravya Kurapati HIV & Immunology Laboratory, Department of Microbiology, All India Institute of Medical Sciences, New Delhi 110029, India Background: HIV-1 infection is associated with depletion of naı¨ve T cell subsets and skewed T cell differentiation and maturation, leading to accumulation of T cells at intermediate and end stages of dif- ferentiation. CD27 and CD28 expression have been utilized in assessing these population subsets. Methods: We characterized T cell subsets based on expression of CD45RA, CCR7, CD27, and CD28 and compared these subsets in HIV-1 infected Indian subjects and uninfected controls. Results: HIV-1 infection was associated with an increase in effector and memory T cell subsets and a concomitant decrease in naı¨ve T cells. HIV-1 infected subjects showed accumulation of intermediate CD8 T cell (CD271CD282) differentiation subsets, whereas CD4 T cells progressed to late stage differ- entiation (CD272CD282). These subsets were negatively associated with CD4 T cell counts and posi- tively associated with plasma viremia. CD57, an immunosenescence marker, was also increased on T cell subsets from HIV-1 infected individuals. Antiretroviral therapy resulted in partial restoration of dif- ferentiation status. Conclusion: Persistent HIV-1 replication and chronic immune activation, along with altered cytokine secretion profile, lead to impaired T cell differentiation and maturation. Detailed understanding of factors associated with differentiation defects in HIV-1 infected Indian individuals will strongly assist in Indian HIV-1 vaccine efforts and add to our knowledge of HIV-1 subtype C pathogenesis. V C 2011 International Clinical Cytometry Society Key terms: CD27; CD28; CD57; T cell differentiation; HIV-1 subtype C; India How to cite this article: Mojumdar K, Vajpayee M, Chauhan NK, Singh A, Singh R, Kurapati S. Altered T cell dif- ferentiation associated with loss of CD27 and CD28 in HIV infected Indian individuals. Cytometry Part B 2012; 82B: 43–53. HIV-1 infection is associated with destruction or impairment of factors associated with generation of opti- mal and effective immune response, CD4 T cell destruc- tion and impairment of antigen presenting cells (1,2), ultimately leading to failure of viral control and disease chronicity. Progressive HIV-1 infection is characterized by increased T cell turnover and decreased thymic out- put (3,4), an increase in the proportion of highly differ- entiated CD4 and CD8 T cells (5) with a corresponding decrease in naı ¨ve T cell numbers (6). T cell differentiation pathways have long been subject of intense research, with major emphasis on identifica- tion of molecular markers that help identify and isolate T cells sharing discrete stages of differentiation. Two markers CCR7 and CD45RA have long been used to classify four unique T cell populations: naı ¨ve (CD45RAþCCR7þ, N), central memory (CD45RAÀ CCR7þ, CM), effector memory (CD45RAÀCCR7À, EM), *Correspondence to: Associate Professor Dr. Madhu Vajpayee, Labo- ratory Head, HIV & Immunology Division, In charge, HIV National Ref- erence Laboratory & Integrated Counseling and Testing Center, Department of Microbiology, AIIMS, New Delhi 110029, India. E-mail: [email protected] Received 28 January 2011; Revision 23 May 2011; Accepted 1 June 2011 Published online 21 June 2011 in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/cyto.b.20610 Original Article V C 2011 International Clinical Cytometry Society
Transcript of Altered T cell differentiation associated with loss of CD27 and CD28 in HIV infected Indian...

Cytometry Part B (Clinical Cytometry) 82B:43–53 (2012)
Altered T Cell Differentiation Associated withLoss of CD27 and CD28 in HIV Infected
Indian Individuals
Kamalika Mojumdar, Madhu Vajpayee,* Neeraj Kumar Chauhan, Alpana Singh,Ravinder Singh, and Sravya Kurapati
HIV & Immunology Laboratory, Department of Microbiology, All India Institute of Medical Sciences,New Delhi 110029, India
Background: HIV-1 infection is associated with depletion of naı̈ve T cell subsets and skewed T celldifferentiation and maturation, leading to accumulation of T cells at intermediate and end stages of dif-ferentiation. CD27 and CD28 expression have been utilized in assessing these population subsets.
Methods: We characterized T cell subsets based on expression of CD45RA, CCR7, CD27, and CD28and compared these subsets in HIV-1 infected Indian subjects and uninfected controls.
Results: HIV-1 infection was associated with an increase in effector and memory T cell subsets and aconcomitant decrease in naı̈ve T cells. HIV-1 infected subjects showed accumulation of intermediateCD8 T cell (CD271CD282) differentiation subsets, whereas CD4 T cells progressed to late stage differ-entiation (CD272CD282). These subsets were negatively associated with CD4 T cell counts and posi-tively associated with plasma viremia. CD57, an immunosenescence marker, was also increased on Tcell subsets from HIV-1 infected individuals. Antiretroviral therapy resulted in partial restoration of dif-ferentiation status.
Conclusion: Persistent HIV-1 replication and chronic immune activation, along with altered cytokinesecretion profile, lead to impaired T cell differentiation and maturation. Detailed understanding of factorsassociated with differentiation defects in HIV-1 infected Indian individuals will strongly assist in IndianHIV-1 vaccine efforts and add to our knowledge of HIV-1 subtype C pathogenesis. VC 2011 International
Clinical Cytometry Society
Key terms: CD27; CD28; CD57; T cell differentiation; HIV-1 subtype C; India
How to cite this article: Mojumdar K, Vajpayee M, Chauhan NK, Singh A, Singh R, Kurapati S. Altered T cell dif-ferentiation associated with loss of CD27 and CD28 in HIV infected Indian individuals. Cytometry Part B 2012;82B: 43–53.
HIV-1 infection is associated with destruction orimpairment of factors associated with generation of opti-mal and effective immune response, CD4 T cell destruc-tion and impairment of antigen presenting cells (1,2),ultimately leading to failure of viral control and diseasechronicity. Progressive HIV-1 infection is characterizedby increased T cell turnover and decreased thymic out-put (3,4), an increase in the proportion of highly differ-entiated CD4 and CD8 T cells (5) with a correspondingdecrease in naı̈ve T cell numbers (6).
T cell differentiation pathways have long been subjectof intense research, with major emphasis on identifica-tion of molecular markers that help identify and isolateT cells sharing discrete stages of differentiation. Two
markers CCR7 and CD45RA have long been used toclassify four unique T cell populations: naı̈ve(CD45RAþCCR7þ, N), central memory (CD45RA�CCR7þ, CM), effector memory (CD45RA�CCR7�, EM),
*Correspondence to: Associate Professor Dr. Madhu Vajpayee, Labo-
ratory Head, HIV & Immunology Division, In charge, HIV National Ref-
erence Laboratory & Integrated Counseling and Testing Center,
Department of Microbiology, AIIMS, New Delhi 110029, India.
E-mail: [email protected]
Received 28 January 2011; Revision 23 May 2011; Accepted 1
June 2011
Published online 21 June 2011 in Wiley Online Library
(wileyonlinelibrary.com).
DOI: 10.1002/cyto.b.20610
Original Article
VC 2011 International Clinical Cytometry Society

and terminally differentiated effectors (CD45RAþ CCR7�,TEMRA). Naı̈ve T cells, on encountering antigen, divideand differentiate into effector T cell population, whichexert their immune function by direct cytolysis and alsothrough secretion of cytokines like IFN-c and TNF-a. Onantigen clearance, the effector population contracts, leavingbehind a small but effective population of memory T cellswhich form the basis of ‘‘immunological memory’’ (7).
However, an inclusion of major T cell co-stimulatorymolecules CD27 and CD28 in a five color analysis hasrevealed two additional pre-effector CD8 T cell subsets(8) and five major CD4 subsets (9). Romero et al. intheir study have further classified the EM subset intofour functionally distinct populations based on theirexpression of CD27 and CD28, leading to a total of 9unique T cell differentiation subsets (10). Based on thismodel, a study by Koch et al. has revealed skewed distri-bution of CD4 and CD8 T cells in various differentiationcompartments as a result of ageing (11).
Several studies have highlighted T cell maturation anddifferentiation defects (12,13) in HIV-1 infected subjects,with these defects found to be associated with HIV-1induced immune activation (14). Recent studies havecompared HIV-1 induced T cell differentiation defectswith patterns witnessed in ageing, a process called asimmunosenescence (15,16). According to these studies,chronic immune activation resulting from continuous vi-ral replication results in a scenario similar to ageing,causing accelerated T cell senescence (17). T cell immu-nosenescence has also been associated with increasedexpression of CD57 on T cells. These CD57þ cells arelate stage cells, and a study by Brenchley et al. hasshown them to have proliferative defects (18). CD57expression has been known to increase on CD8 T cellsin both ageing (19) and HIV-1 infection (20).
Though a number of studies have focused on dissectingT cell differentiation defects in HIV-1 infection, most ofthese studies have investigated either the CD4 or CD8 Tcell compartment. Further, there are no reports detailingthe effect of HIV-1 infection on T cell differentiation sub-sets in Indian HIV-1 infected subjects. With a diverse HLAbackground, different HIV-1 transmission route, and pre-existing background infections, the need for similar stud-ies in the Indian population still remains a necessity. Withthis background, we aimed at dissecting the HIV-1induced changes in these differentiation subsets in HIV-1infected Indian population. We also aimed at studying theexpression levels of CD57 on these subsets, and theirassociation, if any, with disease progression. Our resultsshow an increase in intermediate differentiation subsetsin CD8 T cells from HIV-1 infected subjects, and a partialrestoration to normal differentiation stage phenotypeswith successful antiretroviral therapy.
MATERIALS AND METHODS
Study Population
Thirty-nine consecutive HIV-1 infected individuals, 30untreated (18 males and 12 females) and nine treated
individuals (median duration of treatment, 13 months),at different stages of infection (21), were recruited fromthe AIDS Clinic of the Department of Microbiology atAll India Institute of Medical Sciences, New Delhi (fromMay 2010 to July 2010). The study was approved by theInstitute Ethics Committee and all patients gave writteninformed consent prior to inclusion in the study. Wealso included eight HIV-1-sero negative healthy individu-als (three females and five males) as study controls.
Immunophenotyping
T cell subset phenotyping was performed on freshblood samples, as described previously (22). The follow-ing monoclonal antibody panel was used for staining:allophycocynanin-H7 (APC-H7) labeled CD3, Pacific Bluelabeled CD45RA, allophycocyanin (APC) labeled CD28,AmCyan labeled CD8 or CD4, phycoerythrin (PE) la-beled CCR7, peridinin chlorophyll protein (PerCP)-Cy5.5labeled CD27, and fluorescein isothiocyanate (FITC)-la-beled CD57 or CD38, and APC labeled HLA-DR. (BectonDickinson, USA). The stained samples were furtherwashed, lysed, and resuspended in 250 ll of paraformal-dehyde before acquisition.
A total of 100,000–500,000 lymphocyte events wereacquired for each tube on a LSR II (Becton Dickinson,San Jose, USA) flow cytometer within 2 h of processingthe blood samples. Unstained cells or fluorescenceminus one (FMO) controls were used to set all gates.Gating scheme used for identification of T cell subsets isdepicted in Figure 1. The expression of CD27, CD28,and senescence marker (CD57) were then examined onthe CD4 and CD8 T cell subsets and correlated withexpression of activation markers (CD38, HLA-DR) onCD4 and CD8 T cells. FlowJo (TreeStar) software wasused for flow cytometric data analysis.
HIV-1 Viral RNA Quantification
HIV-1 viral RNA was extracted from plasma samplesof study subjects and quantified using COBAS TaqManHIV-1 Test version 2.0 (Roche Diagnostics, Meylan,France) with a lower limit of detection of 40 copies/ml.
Statistical Analysis
The Mann-Whitney U test was used for comparisonsbetween HIV-1-infected and uninfected control subjects.Kruskall-Wallis test was used for studying the differencein various T cell subsets between uninfected controls,HAART naı̈ve, and HAART treated subjects. Associationof CD4 T cell counts and HIV-1 viral load with T cellsubset proportions and expression of CD57 and withactivation marker expression on CD4 and CD8 T cellswas calculated using Spearman’s q. A p value of 0.05 orless was considered significant. All the statistical analy-ses were performed using SPSS software version 17(Chicago, IL).
RESULTS
The study population consisted of 30 treatment naı̈veHIV-1 seropositive patients (median age: 32; range, 22–
44 MOJUMDAR ET AL.
Cytometry Part B: Clinical Cytometry

55 years), and nine HAART-receiving patients (medianage: 36; range, 30–46 years). These were comparable tothe median age of HIV-1 uninfected control group (me-dian age: 30; range, 28–52 years; p ¼ 0.15). Studypatient characteristics are enumerated in Table 1.
CD27 and CD28 Expression on T Cells
In healthy subjects, 83.9% (range: 75.1%; 91.5%) CD4T cells and 58.4% (range: 42.7%; 95.4%) CD8 T cellsexpressed CD27, while 94.6% (range: 92%; 98%) CD4 Tcells and 58.8% (range: 43.6%; 94%) CD8 T cellsexpressed CD28. HIV-1 infection resulted in a significantdecrease in CD27 and CD28 expression on both CD4and CD8 T cells (CD27 expression on CD4 T cells,76.6%, p ¼ 0.018; CD27 expression on CD8 T cells,55.4%, p ¼ ns; CD28 expression on CD4 T cells, 86.3%,p ¼ 0.003; CD28 expression on CD8 T cells, 32.1%, p <0.001), with the decrease being more pronounced forCD28 expression. HAART treated subjects had higherCD27 and CD28 expression on CD4 and CD8 T cellscompared to HAART naı̈ve study subjects, although sta-tistical significance was observed for CD27 and CD28
MFI on CD4 and CD8 T cells, and not on percentage ofcells expressing these molecules (Fig. 2).
Association of CD27 and CD28 Expression with DiseaseMarkers
Percentage of CD27 and CD28 expressing CD4 cellsand various CD4 T cell subsets correlated positivelywith CD4 count and negatively with viral load. Of thesestatistically significant associations were observed forCD27 and CD28 expression on TEMRA and naı̈ve CD4 Tcell subsets. CD28 MFI on CD4 T cells correlated nega-tively with HIV-1 plasma viral load (pVL). CD8 T cellsexpressing CD27 and CD28 correlated positively withCD4 T cell count and negatively with HIV-1 pVL(Fig. 3). CD28 MFI on CD8 T cells and its subsets corre-lated negatively with activated CD8 T cells expressingCD38 and HLA-DR
T Cell Subset Classification Based on CD27 CD28Expression
We next divided the T cell subsets in HIV-1 infectedsubjects and study control to discern HIV-1 inducedchanges in T cell differentiation and maturation (10).
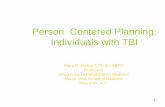
FIG. 1. Schematic model of T cell differentiation subsets based on expression pattern of CD45RA, CCR7, CD27, and CD28. A: CCR7 and CD45RAexpression divides CD4 and CD8 T cells into N (CD45RAþCCR7þ), CM (CD45RA�CCR7þ), EM (CD45RA�CCR7�), and TEMRA(CD45RAþCCR7�). These subsets are further subdivided on basis of expression of co-stimulatory molecules CD27 and CD28. N and CM cells arepredominantly CD45RAþCCR7þ. TEMRA subset is divided into pE1 (CD27þCD28þ), pE2 (CD27þCD28�), and E (CD27�CD28�). EM populationis divided into EM1 (CD27þCD28þ), EM2 (CD27þCD28�), EM3 (CD27�CD28�), and EM4 (CD27�CD28þ). B: Representative example of subsetdetermination for CD8 T cells. C: Representative example of subset determination for CD4 T cells.
ALTERED T-CELL DIFFERENTIATION IN HIV INFECTION 45
Cytometry Part B: Clinical Cytometry

Figure 1B shows the results of CD27 and CD28 stainingwithin the CD8þ N, CM, EM, and TEMRA populationsas defined in Figure 1A.
In contrast to what was observed by Romero and col-leagues, in healthy control subjects, we could discern asubstantial proportion on CD27�CD28� naı̈ve (39%)and central memory (60%) CD8 T cells, although therewere large interindividual variation in these subsets.CD4 T cell compartment, however, showed a high levelof CD27 and CD28 expression, leading to an absence ofthese atypical subsets (Figs. 4A and 4B).
Increased Proportion Of Intermediate DifferentiatedSubsets in HIV-1 Infected Subjects
HIV-1 infected therapy naı̈ve study subjects showed auniform depletion of CD28 expressing T cell subsets,with a resultant accumulation of intermediate TEMRA,naı̈ve, CM, and EM CD8 T cell subsets (lacking CD28expression, CD27þCD28�) (% CD28� TEMRA CD8 Tcells: healthy controls, 12%; HIV-1 infected subjects,27.1%; p ¼ 0.006, % CD28� naı̈ve CD8 T cells: healthycontrols, 3.11%; HIV-1 infected subjects, 6.42%; p ¼
0.04, % CD28� CM CD8 T cells: healthy controls,6.99%; HIV-1 infected subjects, 22.2%; p < 0.001, %CD28� EM CD8 T cells: healthy controls, 10.3%; HIV-1infected subjects, 41.1%; p < 0.001). There was con-comitant decrease in early CD27þCD28þ expressingCD8 T cell subsets, with these differences being statisti-cally significant for CD27þCD28þ TEMRA, and EM cells(Fig. 4A). Of note, late differentiation subsets(CD27�CD28�) were substantially raised only in theEM CD8 T cell subset, whereas other subsets onlyshowed slight increase of these fully differentiated celltypes.
The CD4 T cell subsets also exhibited decrease inearly CD27þCD28þ subsets, although this differencereached statistical significance only for early EM CD4 Tcells (p ¼ 0.024). However in comparison to CD8 T cell
Table 1Patient Cohort Characteristics
S. No. Age SexCD4
(cells/ll)Viral load(copies/ml)
HAARTduration
1 48 M 288 456,000 Naı̈ve2 27 M 565 2,240 Naı̈ve3 32 M 88 4,37,000 Naı̈ve4 32 F 934 50 Naı̈ve5 23 M 448 26,900 Naı̈ve6 43 F 630 50 13 months7 35 M 687 221 12 months8 46 M 616 1,561 11 months9 35 F 626 1,720 Naı̈ve
10 35 M 325 15,000 Naı̈ve11 36 F 690 91 16 months12 40 M 268 5,94,000 Naı̈ve13 30 F 261 2,140 Naı̈ve14 55 M 221 10,60,000 Naı̈ve15 30 F 225 43,500 Naı̈ve16 23 F 225 74,700 Naı̈ve17 37 M 333 71 13 months18 35 F 303 93,800 Naı̈ve19 35 M 42 3,68,000 Naı̈ve20 29 M 200 53,100 Naı̈ve21 40 M 38 7,50,000 Naı̈ve22 53 F 279 5,57,000 Naı̈ve23 38 F 1251 324 Naı̈ve24 30 F 558 249 13 months25 22 F 608 734 Naı̈ve26 34 F 567 59 11 months27 22 F 593 5,060 Naı̈ve28 43 M 716 1,650 Naı̈ve29 25 M 358 17,600 Naı̈ve30 30 M 305 53,000 Naı̈ve31 27 M 140 44,000 Naı̈ve32 50 M 297 7,700 Naı̈ve33 35 M 425 50 14 months34 38 F 526 16,500 Naı̈ve35 46 F 796 50 11 months36 38 M 130 42,500 Naı̈ve37 28 M 526 70,400 Naı̈ve38 30 M 50 22,900 Naı̈ve39 32 M 398 17,890 Naı̈ve
FIG. 2. Expression of CD27 and CD28 on T cells. A: Percentage of CD27-expressing and CD28-expressing CD4 and CD8 T cells in HAART-naı̈veand HAART-treated subjects in comparison to HIV-1 uninfected controls. B: Mean fluorescence intensity (MFI) of CD27 and CD28 on CD4 and CD8T cells. *Level of significance (P < 0.05); **Level of significance (P < 0.01).
46 MOJUMDAR ET AL.
Cytometry Part B: Clinical Cytometry

subsets from HIV-1 infected subjects, CD4 T cell subsetsshowed a marked increase in late differentiated T cellsubsets (CD27�CD28�), with these differences beingstatistically significant for late differentiated TEMRA, CM,and EM CD4 T cells (Fig. 4B). Overall, least perturba-tions were observed in the naı̈ve CD4 T cell compart-ment in terms of CD27 and CD28 expression, with
almost all cells expressing both the co-stimulatorymolecules.
HAART treatment resulted in a decrease in the lateand intermediate CD8 T cell subsets, and thesedecreases were significant for intermediate TEMRA, CMand EM subsets, associated with an increase in earlyCD27þCD28þ expressing TEMRA, naı̈ve, and CM CD8
FIG. 3. Association of CD27 and CD28 expression profile on selected CD4 and CD8 T cell subsets with HIV-1 disease progression markers(n ¼ 30). *Level of significance (P < 0.05); **Level of significance (P < 0.01). Only statistically significant associations depicted here.
ALTERED T-CELL DIFFERENTIATION IN HIV INFECTION 47
Cytometry Part B: Clinical Cytometry

T cells (Fig. 4A). HAART generated changes in intermedi-
ate and late differentiated T cell subsets were less appa-
rent in the CD4 T cell compartment, with only naı̈ve
CD4 T cells showing a significant decrease in
CD27þCD28� population in the HAART-treated subjects
compared to HAART-naı̈ve subjects (Fig. 4B).
Intermediate and Late Differentiated Subsets Associatedwith Disease Progression
We observed significant positive association of earlydifferentiation subsets in TEMRA and naı̈ve CD4 andCD8 T cells, and early EM, and CM CD4 T cells withCD4 T cell counts (Fig. 5). Most early differentiation
FIG. 4. Expression of co-stimulatory molecules on T cell subsets. Frequencies of CD27þCD28þ, CD27�CD28�, CD27�CD28þ, CD27þCD28�in N, EM, CM, and TEMRA in (A) CD4þ and (B) CD8þ T cells in HAART naı̈ve subjects (open circles), HAART treated subjects (filled triangles), anduninfected controls (open squares). *Level of significance (P < 0.05); **Level of significance (P < 0.01).
48 MOJUMDAR ET AL.
Cytometry Part B: Clinical Cytometry

subsets correlated negatively with HIV-1 pVL.CD27�CD28� and CD27þCD28� T cell subsets corre-lated negatively with CD4 T cell counts and positivelywith HIV-1 pVL (Fig. 5).
Increased Replicative Senescence Associated withHIV-1 Infection
HIV-1 infection is associated with replicative senes-cence and has been correlated with expression of CD57on T cell subsets. We observed a higher percentage ofCD57 expressing CD4 T cells in infected subjects com-pared to study controls (median percentage of CD4 Tcells expressing CD57: HIV-1 infected subjects, 7.14%;uninfected controls, 4.64%; p ¼ 0.016). CD57 express-ing CD8 T cells were also expanded in HIV-1 infectedsubjects compared to controls, although this increasewas not statistically significant. Further to this, weobserved a higher percentage of CD57 expressing CD4T cell subsets in HIV-1 infected subjects compared touninfected controls, with this difference being signifi-cant for CD4 TEMRA cells (p ¼ 0.009), and CD4 EM
cells (p ¼ 0.006). Similarly, CD8 T cell subsets express-ing CD57 were also expanded, with this increase statisti-cally significant for all CD8 T cell subsets.
As there was large interindividual variation in CD57expression levels, we compared the CD57 expressingpercentage of cells and CD57 MFI on the various differ-entiation subsets in HIV-1 uninfected controls and HIV-1infected subjects with advanced HIV-1 disease (CD4 Tcell counts below 200 cells/ll). Here we observed a sig-nificant increase in CD57 MFI on early differentiatedCD8 EM cells (EM1, CD27þCD28þ) and also on inter-mediate differentiated (EM2, CD27þCD28�) and late dif-ferentiated EM cells (EM3, CD27�CD28�). Significantincrease in CD57 MFI was also observed on intermediatedifferentiated CM CD8 T cells lacking CD28(CD45RA�CCR7þCD27þCD28�), and most CD8TEMRA subsets; late subset (E, CD27�CD28�), interme-diate subset (pE2, CD27þCD28�), and early differentia-tion subset (pE1, CD27þCD28þ) (Figs. 6A and 6B).Similar increase in CD57 expression was observed inCD4 T cell subsets also, although significance was
FIG. 5. Association of selected CD4 and CD8 T cell differentiation subsets with HIV-1 disease progression markers. *Level of significance(P < 0.05); **Level of significance (P < 0.01). Only statistically significant associations depicted here.
ALTERED T-CELL DIFFERENTIATION IN HIV INFECTION 49
Cytometry Part B: Clinical Cytometry

achieved for CD57 MFI on naı̈ve and CM cells lackingCD27 (CD45RA�CCR7þCD27�CD28þ) and TEMRAcells lacking CD27 (CD45RAþCCR7�CD27�CD28þ).HAART resulted in a decrease of CD57 expression on
almost all subsets, although statistical significance wasobserved only for EM1 (CD27þCD28þ) and TEMRA E(CD27�CD28�) CD8 T cell subsets and EM3(CD27�CD28�) CD4 T cell subset.
FIG. 6. CD57 expression on T cell subsets CD57. MFI on subsets of N, EM, CM, and TEMRA in (A) CD8þ and (B) CD4þ T cells. HAART naı̈ve sub-jects with CD4 T cell counts less than 200 cells/lL (open circles), uninfected controls (open squares). *Level of significance (P < 0.05); **Level ofsignificance (P < 0.01).
50 MOJUMDAR ET AL.
Cytometry Part B: Clinical Cytometry

DISCUSSION
The present study aimed at characterizing the effectof HIV-1 infection on T cell differentiation and resultantimmunosenescence in a group of HIV-1 infected Indiansubjects. We comparatively analyzed T cell subsets (gen-erated by use of CD45RA, CCR7, CD27, and CD28) inHIV-1 infected versus uninfected control subjects. Fur-ther, CD57 expression on these subsets was utilized asan immunosenescence marker to identify late stage sub-sets lacking proliferative capabilities.
In contrast to the model of naı̈ve and central memoryT cell differentiation put forward by Romero et al., weobserved in our HIV-1 uninfected control subjects, na-ı̈ve, and central memory T cells in intermediate and latedifferentiation stages, as characterized by CM and N cellslacking either CD27 or CD28 or both. Rate of back-ground latent infections like tuberculosis, parasitic infec-tions, etc., is high in India, a developing nation with alarge rural population base. Chronic antigenic stimuli aswell as the pro-inflammatory cytokine milieu, resultingfrom these infections can lead to loss of CD27 andCD28 antigen expression (23,24) and can explain thepresence of these atypical differentiation phenotypes inHIV-1 uninfected individuals.
According to the expression of CD27 and CD28, anti-gen experienced T cells can be positioned along a linearputative model of differentiation: early (CD27þCD28þ),intermediate (CD27�CD28þCD4þ or CD27þCD28�CD8þ), and late (CD27�CD28�) differentiated subsets(25,26). However, HIV-1 infection is associated with per-sistent and continuous replication, chronic activation,and constant T cell turnover, all of which suggest termi-nal differentiation of T cell subsets in HIV-1 infectedsubjects (6,27). In our HIV-1 infected study subjects,however, we observed an over-representation of inter-mediate (CD27þCD28�) differentiated cells in N, EM,CM, and TEMRA CD8 T cells subsets. Late differentiatedT cell subsets were observed only in EM compartmentof CD8 T cells. This represents a maturation block insettings of HIV infection, thus leading to accumulationof incompletely differentiated CD8 T cells and havebeen reported by others (28–30). Previous studies haveassociated the intermediate differentiation phenotypewith a reduced functionality, notably a lesser cytolyticand cytokine secretory ability and a decreased prolifera-tive capacity (28,31–33). This skewed maturation, favor-ing a less effective intermediate differentiationphenotype, is likely a pathogenic strategy utilized by thevirus, whereby CD8 T cells are prevented from achiev-ing full effector functions. Such abnormal CD8 T cellmaturation, in turn may lead to a dearth of effectiveimmune responses to clear the virus, thus establishingdisease chronicity.
As we studied bulk CD8 T cells rather than HIV-1 spe-cific CD8 T cell population, our results highlight therole of HIV-1 replication induced immune activation onbystander T cell dysfunction as well (13). Further, reacti-vation of latent CMV, EBV, and other co-viral infections
may also provide a plethora of specific antigenic stimuliwithin the CD8þ memory compartment (34). In addi-tion to chronic immune activation and antigen presence,HIV-1 infection is also associated with alteration of cyto-kine secretion profile. T cells from HIV-1 infected indi-viduals have reduced IL-2 secretion capacity, with thisdefect reported in both CD4 (35) and CD8 T cell com-partments (36). A study by Nomura et al. has linked IL-2secretion defect and skewed T cell differentiation inHIV-1 infected individuals, with a direct correlationbetween IL-2 levels and CD28 expression (37). Thus,progressive HIV-1 disease, characterized by reduction inIL-2 levels, can result in the presence of pre-terminallydifferentiated CD8 T cell population in HIV-1 infection.
CD4 T cell subsets, on the other hand, showed statis-tically significant increase in late differentiated subsets.Accumulation of intermediate differentiation subsets wasless apparent in the CD4 T cell compartment comparedto CD8 T cell subsets. This is in contrast to studyreported by Yue et al., who show a comparative accu-mulation of pre-terminally differentiated cell populationin the HIV-specific CD4 T cell compartment (38). Theterminally differentiated CD4 TEMRA, CM, and EM Tcells represent IL2 deficient, single cytokine secreting(IFN-c), nonproliferative cells without protective func-tion and thus their increase in HIV-1 infected subjectsmay reflect loss of immune control (39,40).
Along with an increase in intermediate stage T cells inHIV-1 infected individuals, we also observed atypicalsubsets with loss of CD27 while still expressing CD28 inCD8 T cell subset and vice versa for CD4 T cell subset.This can be a result of transient or definitive downregu-lation of CD27 or could represent a transitory subsetappearing during the expansion phase of secondaryimmune response (10). These atypical subsets exhibitHIV-1 induced T cell maturational defects and explainHIV-1 associated functional impairments (28,30). CD28�cells have reduced divisional potential and delayed cellcycle kinetics, and CD4þCD28� cells are resistant toapoptotic signals. Taken together, CD28� cells have thecharacteristics of an aged immune system (41).
We correlated the CD4 and CD8 T cell differentiationsubsets with markers of HIV-1 disease progression andobserved a significant positive association of early differ-entiated cells (CD27þCD28þ) in all T cell subsets withCD4 T cell counts and negative association with viralload. T cell receptor activation results in the inductionof CD28 and CD27 expression on the surface of naive Tcells. It has been suggested that naive T cells may relyon heightened sensitivity to signals through these recep-tors to enter the cell cycle. Presence of early differenti-ated cells would thus indicate a cell population able toenter cell cycle and expand, thereby resulting in expan-sion of naı̈ve T cell population, explaining the positiveassociation of these cells with CD4 T cell counts (42).The intermediate and late differentiated subsets all corre-lated negatively with CD4 T cell counts and positivelywith HIV-1 pVL. The cells lacking expression of CD28and/or CD27 represent a cellular population with
ALTERED T-CELL DIFFERENTIATION IN HIV INFECTION 51
Cytometry Part B: Clinical Cytometry

limited cytokine secreting function and almost no prolif-erative ability and are thus less capable of clearing thevirus. Loss of CD28 expression on CD4 and CD8 T cellsis generally considered to be a feature of immunosenes-cence, and the frequency of CD28� T cells has beenshown to be a predictor of humoral incompetence tovaccination in the elderly (43).
We next investigated the T cell differentiation statusin subjects with history of successful highly active anti-retroviral therapy (HAART), resulting in CD4 T cellcount increase and HIV-1 viral load below detection lev-els. We observed a restoration in the proportion of earlystage N, EM, CM, and TEMRA cells, although theincrease in their levels was only partial (44). The medianHAART duration in our study population was only 13months, with some subjects having received HAART forless than a year. This can partly explain the lack of sig-nificant increase in the percentage of early differentiatedT cell subsets in treatment-receiving subjects, with onlya significant change being in the median level of expres-sion of CD27 and CD28 on the various T cell subsets.Primary HIV-1 infection leads to changes in T cell matu-ration and differentiation pathway. Accumulation of in-termediate and late stage cells occur early in the courseof HIV-1 infection and result in a subsequent irreversiblematurational block. Thus HAART may not be able tocause a complete reversal of the CD4 and CD8 T cellsinto normal differentiation phenotype. Initiation ofHAART during the first few months of HIV-1 infection,before the T cell alterations set in, may theoreticallyresult in complete restoration in the T cell differentia-tion phenotype to levels before HIV-1 infection (45) andwarrant further studies.
Replicative senescence as depicted by accumulationof end stage T cells is also a hallmark of ageing or immu-nosenescence. Immunosenescence has often been asso-ciated with increased expression of CD57 on T cellsubsets. We thus examined the level of CD57 expressingT cells in various differentiation compartments and alsothe association of CD57 expression level with diseaseprogression markers. We observed a marked increase ofCD57 on T cells subsets, with the increase most appa-rent in CD8 T cell compartment. CD8 EM cells showedmarked increase in CD57 expression, which representthe most differentiated T cell subpopulation. Also, CD57expression was noticeably high on intermediate stageCM subset and late stage TEMRA subset, thus highlight-ing their terminally differentiated status. Similar to CD8T cells, late, and intermediate differentiation stages inCD4 CM and TEMRA compartment had highest CD57expression, identifying these atypical subsets as termi-nally differentiated and associated with proliferativedefects. CD57 expression levels correlated negativelywith CD4 T cell counts and positively with HIV-1plasma viral load as has previously been reported.
In conclusion, the present study was an attempt atidentifying HIV-1 associated T cell differentiation defectsin HIV-1 infected Indian population using four markersto classify the differentiation subsets. To the best of our
knowledge, this is the first study to report detailed phe-notypic classification of CD4 and CD8 differentiationsubsets in the Indian HIV-1 infected population. Weobserved increased accumulation of pre-terminally differ-entiated CD8þ N, CM, EM, and TEMRA cells lackingCD28 expression, while the CD4 compartment wasenriched in terminally differentiated cells lacking bothCD27 and CD28 expression. These cells lack prolifera-tive and functional capacities as has been reported byseveral previous studies, and thus drive HIV-1 associatedimmune dysfunction. Further, increased CD57 expres-sion also presents an aged immune system as a result ofchronic immune activation and constant antigenic pres-ence. In addition, HAART-generated viral replication inhi-bition does result in partial degree of phenotyperestoration associated with decrease in CD57 expressionand increase in CD4 T cell counts. With increasedefforts on vaccine efficacy studies targeting the IndianHIV-1 subtype C, an understanding of HIV-1 induced dif-ferentiation of CD4 and CD8 T cells and establishmentof memory T cells in this population will aid in the gen-eration of a successful cellular vaccine with ability toelicit sufficient long-lasting protective immunity.
LITERATURE CITED
1. Kalams SA, Walker BD. The critical need for CD4 help in maintain-ing effective cytotoxic T lymphocyte responses. J Exp Med 1998;188:2199–2204.
2. Alcami A, Koszinowski UH. Viral mechanisms of immune evasion.Immunol Today 2000;21:447–455.
3. Douek DC, McFarland RD, Keiser PH, Gage EA, Massey JM, HaynesBF, Polis MA, Haase AT, Feinberg MB, Sullivan JL, et al. Changes inthymic function with age and during the treatment of HIV infec-tion. Nature 1998;396:690–695.
4. Wolthers KC, Otto SA, Lens SM, Kolbach DN, van Lier RA, MiedemaF, Meyaard L. Increased expression of CD80. CD86 and CD70 on Tcells from HIV-infected individuals upon activation in vitro: Regula-tion by CD4þ T cells. Eur J Immunol 1996;26:1700–1706.
5. Appay V, Zaunders JJ, Papagno L, Sutton J, Jaramillo A, Waters A,Easterbrook P, Grey P, Smith D, McMichael AJ, et al. Characteriza-tion of CD4(þ) CTLs ex vivo. J Immunol 2002;168:5954–5958.
6. Hellerstein MK, Hoh RA, Hanley MB, Cesar D, Lee D, Neese RA,McCune JM. Subpopulations of long-lived and short-lived T cells inadvanced HIV-1 infection. J Clin Invest 2003;112:956–966.
7. Kaech SM, Wherry EJ, Ahmed R. Effector and memory T-cell differ-entiation: Implications for vaccine development. Nat Rev Immunol2002;2:251–262.
8. Rufer N, Zippelius A, Batard P, Pittet MJ, Kurth I, Corthesy P, Cerot-tini JC, Leyvraz S, Roosnek E, Nabholz M, et al. Ex vivo characteri-zation of human CD8þ T subsets with distinct replicative historyand partial effector functions. Blood 2003;102:1779–1787.
9. Okada R, Kondo T, Matsuki F, Takata H, Takiguchi M. Phenotypicclassification of human CD4þ T cell subsets and their differentia-tion. Int Immunol 2008;20:1189–1199.
10. Romero P, Zippelius A, Kurth I, Pittet MJ, Touvrey C, Iancu EM,Corthesy P, Devevre E, Speiser DE, Rufer N. Four functionally dis-tinct populations of human effector-memory CD8þ T lymphocytes.J Immunol 2007;178:4112–4119.
11. Koch S, Larbi A, Derhovanessian E, Ozcelik D, Naumova E, PawelecG. Multiparameter flow cytometric analysis of CD4 and CD8 T cellsubsets in young and old people. Immun Ageing 2008;5:6.
12. Marchetti G, Gazzola L, Trabattoni D, Bai F, Ancona G, Ferraris L,Meroni L, Galli M, Clerici M, Gori A, et al. Skewed T-cell maturationand function in HIV-infected patients failing CD4þ recovery uponlong-term virologically suppressive HAART. AIDS 2010;24:1455–1460.
13. van Baarle D, Kostense S, van Oers MH, Hamann D, Miedema F. Fail-ing immune control as a result of impaired CD8þ T-cell maturation:CD27 might provide a clue. Trends Immunol 2002;23:586–591.
14. Papagno L, Spina CA, Marchant A, Salio M, Rufer N, Little S, DongT, Chesney G, Waters A, Easterbrook P, et al. Immune activation
Cytometry Part B: Clinical Cytometry
52 MOJUMDAR ET AL.

and CD8þ T-cell differentiation towards senescence in HIV-1 infec-tion. PLoS Biol 2004;2:E20.
15. Appay V, Rowland-Jones SL. Premature ageing of the immune sys-tem: The cause of AIDS?. Trends Immunol 2002;23:580–585.
16. Cao W, Jamieson BD, Hultin LE, Hultin PM, Effros RB, Detels R. Pre-mature aging of T cells is associated with faster HIV-1 disease pro-gression. J Acquir Immune Defic Syndr 2009;50:137–147.
17. Pawelec G, Effros RB, Caruso C, Remarque E, Barnett Y, Solana R. Tcells and aging (update February 1999). Front Biosci 1999;4: D216–D269.
18. Brenchley JM, Karandikar NJ, Betts MR, Ambrozak DR, Hill BJ,Crotty LE, Casazza JP, Kuruppu J, Migueles SA, Connors M, et al.Expression of CD57 defines replicative senescence and antigen-induced apoptotic death of CD8þ T cells. Blood 2003;101:2711–2720.
19. Merino J, Martinez-Gonzalez MA, Rubio M, Inoges S, Sanchez-Ibar-rola A, Subira ML. Progressive decrease of CD8highþ CD28þCD57� cells with ageing. Clin Exp Immunol 1998;112:48–51.
20. Sadat-Sowti B, Debre P, Idziorek T, Guillon JM, Hadida F, Okzenhen-dler E, Katlama C, Mayaud C, Autran B. A lectin-binding soluble fac-tor released by CD8þCD57þ lymphocytes from AIDS patientsinhibits T cell cytotoxicity. Eur J Immunol 1991;21:737–741.
21. Interim proposal for a WHO Staging System for HIV infection andDisease. Weekly Epidemiol Rec 1990;65:221–224.
22. Sallusto F, Geginat J, Lanzavecchia A. Central memory and effectormemory T cell subsets: function, generation, and maintenance.Annu Rev Immunol 2004;22:745–763.
23. Choremi-Papadopoulou H, Viglis V, Gargalianos P, Kordossis T, Inio-taki-Theodoraki A, Kosmidis J. Downregulation of CD28 surfaceantigen on CD4þ and CD8þ T lymphocytes during HIV-1 infection.J Acquir Immune Defic Syndr 1994;7:245–253.
24. Hamann D, Roos MT, van Lier RA. Faces and phases of human CD8T-cell development. Immunol Today 1999;20:177–180.
25. Appay V, Almeida JR, Sauce D, Autran B, Papagno L. Acceleratedimmune senescence and HIV-1 infection. Exp Gerontol 2007;42:432–437.
26. Appay V, Rowland-Jones SL. The assessment of antigen-specificCD8þ T cells through the combination of MHC class I tetramer andintracellular staining. J Immunol Methods 2002;268:9–19.
27. Hazenberg MD, Otto SA, van Benthem BH, Roos MT, Coutinho RA,Lange JM, Hamann D, Prins M, Miedema F. Persistent immune acti-vation in HIV-1 infection is associated with progression to AIDS.AIDS 2003;17:1881–1888.
28. Appay V, Dunbar PR, Callan M, Klenerman P, Gillespie GM, PapagnoL, Ogg GS, King A, Lechner F, Spina CA, et al. Memory CD8þ Tcells vary in differentiation phenotype in different persistent virusinfections. Nat Med 2002;8:379–385.
29. Hoji A, Connolly NC, Buchanan WG, Rinaldo CR, Jr. CD27 andCD57 expression reveals atypical differentiation of human immuno-deficiency virus type 1-specific memory CD8þ T cells. Clin VaccineImmunol 2007;14:74–80.
30. van Baarle D, Kostense S, Hovenkamp E, Ogg G, Nanlohy N, CallanMF, Dukers NH, McMichael AJ, van Oers MH, Miedema F. Lack ofEpstein-Barr virus- and HIV-specific CD27�CD8þ T cells is associ-ated with progression to viral disease in HIV-infection. AIDS2002;16:2001–2011.
31. Appay V, Nixon DF, Donahoe SM, Gillespie GM, Dong T, King A,Ogg GS, Spiegel HM, Conlon C, Spina CA, et al. HIV-specific
CD8(þ) T cells produce antiviral cytokines but are impaired in cy-tolytic function. J Exp Med 2000;192:63–75.
32. Champagne P, Ogg GS, King AS, Knabenhans C, Ellefsen K, NobileM, Appay V, Rizzardi GP, Fleury S, Lipp M, et al. Skewed maturationof memory HIV-specific CD8 T lymphocytes. Nature 2001;410:106–111.
33. Mueller YM, De Rosa SC, Hutton JA, Witek J, Roederer M, AltmanJD, Katsikis PD. Increased CD95/Fas-induced apoptosis of HIV-spe-cific CD8(þ) T cells. Immunity 2001;15:871–882.
34. Doisne JM, Urrutia A, Lacabaratz-Porret C, Goujard C, Meyer L,Chaix ML, Sinet M, Venet A. CD8þ T cells specific for EBV, cyto-megalovirus, and influenza virus are activated during primary HIVinfection. J Immunol 2004;173:2410–2418.
35. Younes SA, Yassine-Diab B, Dumont AR, Boulassel MR, Grossman Z,Routy JP, Sekaly RP. HIV-1 viremia prevents the establishment ofinterleukin 2-producing HIV-specific memory CD4þ T cellsendowed with proliferative capacity. J Exp Med 2003;198:1909–1922.
36. Betts MR, Nason MC, West SM, De Rosa SC, Migueles SA, AbrahamJ, Lederman MM, Benito JM, Goepfert PA, Connors M, et al. HIVnonprogressors preferentially maintain highly functional HIV-spe-cific CD8þ T cells. Blood 2006;107:4781–4789.
37. Nomura LE, Emu B, Hoh R, Haaland P, Deeks SG, Martin JN,McCune JM, Nixon DF, Maecker HT. IL-2 production correlates witheffector cell differentiation in HIV-specific CD8þ T cells. AIDS ResTher 2006;3:18.
38. Yue FY, Kovacs CM, Dimayuga RC, Parks P, Ostrowski MA. HIV-1-specific memory CD4þ T cells are phenotypically less mature thancytomegalovirus-specific memory CD4þ T cells. J Immunol 2004;172:2476–2486.
39. Harari A, Vallelian F, Meylan PR, Pantaleo G. Functional heterogene-ity of memory CD4 T cell responses in different conditions ofantigen exposure and persistence. J Immunol 2005;174:1037–1045.
40. Harari A, Vallelian F, Pantaleo G. Phenotypic heterogeneity of anti-gen-specific CD4 T cells under different conditions of antigen per-sistence and antigen load. Eur J Immunol 2004;34:3525–3533.
41. Weyand CM, Brandes JC, Schmidt D, Fulbright JW, Goronzy JJ. Func-tional properties of CD4þ CD28� T cells in the aging immune sys-tem. Mech Ageing Dev 1998;102:131–147.
42. Luciano AA, Lederman MM, Valentin-Torres A, Bazdar DA, Sieg SF.Impaired induction of CD27 and CD28 predicts naive CD4 T cellproliferation defects in HIV disease. J Immunol 2007;179:3543–3549.
43. Goronzy JJ, Fulbright JW, Crowson CS, Poland GA, O’Fallon WM,Weyand CM. Value of immunological markers in predicting respon-siveness to influenza vaccination in elderly individuals. J Virol2001;75:12182–12187.
44. Burgers WA, Riou C, Mlotshwa M, Maenetje P, de Assis Rosa D,Brenchley J, Mlisana K, Douek DC, Koup R, Roederer M, et al. Asso-ciation of HIV-specific and total CD8þ T memory phenotypes insubtype C HIV-1 infection with viral set point. J Immunol2009;182:4751–4761.
45. Barbour JD, Ndhlovu LC, Xuan Tan Q, Ho T, Epling L, Bredt BM,Levy JA, Hecht FM, Sinclair E. High CD8þ T cell activation marksa less differentiated HIV-1 specific CD8þ T cell response that isnot altered by suppression of viral replication. PLoS One 2009;4:e4408.
Cytometry Part B: Clinical Cytometry
ALTERED T-CELL DIFFERENTIATION IN HIV INFECTION 53