Toilet Training for Individuals with ASD
30
ToiletTraining for Individuals with ASD Presented by Laura O’Rourke, MS, BCBA
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of Toilet Training for Individuals with ASD

Toilet Training for Individuals with ASD
Presented by Laura O’Rourke, MS, BCBA

Description
Ê In this presentation, participants will learn how to effectively identify readiness skills associated with successful toilet training of individuals with ASD, how to set up and monitor a toilet training program, and how to trouble shoot different challenges that may occur along the way. This training will be geared toward toilet training younger children, but is also applicable to older learners into adulthood wanting to establish more independent toileting skills.

Agenda
Ê Definitions
Ê Toilet training: Definition, Readiness & Implications
Ê Planning the toilet training program
Ê Initiating the toilet training program
Ê Monitoring the toilet training program
Ê Fading the toilet training program
Ê Troubleshooting

What does ‘Toilet Trained’ Mean?
Ê Child is able to remain dry for a period of 1 month without accidents (excludes night training).
Ê Without reminders, child is able to: (1) Communicate a need to go to the bathroom, (2) Walk independently to the bathroom, (3) Pull down pants and underwear, (4) Urinates and or passes a bowel movement in the toilet, (5) Wipes self clean, and (6) Pulls up underwear and pants.

Why is Toilet Training Important Ê Anderson (2011) Questionnaire:
Ê Featured adult individuals with developmental disabilities in the South Sound area. Ê Questionnaire looked at the most common needs of adult residents in local agencies.
Ê Support for Challenging Behaviors Ê Dressing Ê Medication Administration
Ê Making Appointments Ê Arranging Transportation Ê TOILETING Ê Grooming
Ê Preparing Meals Ê Selecting/Communication/Engagement in Community Ê Feeding
Ê THE MORE INDEPENDENT THE INDIVIDUAL AS AN ADULT, THE MORE ACCES TO SERVICES WILL BE AVAILABLE TO THEM.
Typical Toilet Training Readiness
Ê Children typically begin to show readiness for toilet training from 12-‐30 months (American Academy of Pediatrics) as seen by:
Ê Stay dry for up to 2 hours at a time.
Ê Imitates motor actions.
Ê Refuse/say ‘no’ (verbally or non-‐verbally).
Ê Can request
Ê Sit for 3-‐5 minutes.
Ê Pull up and down underwear/pants.
Ê Shows discomfort with being soiled
Ê Has preferred items or reinforcers.
Ê Interest in cleaning up.

Set the Stage for Success!
Ê Use Incentives! What will your child do anything for?
Ê Make items readily available (everything in one room).
Ê Let your child pick out special soap or towels, underwear!
Ê Provide child access to special activities geared to increase sitting (books, game, etc.).
Ê Identify behavior cues child has for when they need to go. Model and teach cues to child through books, videos, etc.
Ê Get a baseline.

Diapers, Pull Ups or Underwear, oh my!
Ê Using absorbent diapers has shown to increase amount of incontinence in children (Tarbox, Williams, & Friman, 2004; Oorsouw et. al, 2009).
Ê Consider using underwear (make sure you have lots of changes).
Ê If this is too much, consider wearing underwear under the diaper, or using a modified approach such as a cloth diaper or nighttime ‘underwear’.

Establishing a ‘Baseline’
Ê PRIOR TO STARTING TOILET TRAINING INTERVENTION: Ê Record for 3-‐5 days. Ê Record every hour for 6-‐8 hours. Ê Record any urinary and bowel accidents which occur at
hourly checks. Ê Record fluid intake times and amounts. Ê Change diaper immediately if wet/soiled (if in between
hourly checks, record time of accident as well).
Ê Optional: if concerned about diet, constipation, or diarrhea are evident, may want to also record food intake.

Baseline Data Sheet Example
* OPWDD Targeting the Big 3-‐ Toilet Training by Dr. Helen Yoo 2012

Baseline Data Sheet Example
*OPWDD Targeting the Big 3-‐ Toilet Training by Dr. Helen Yoo 2012

Initiating a Toilet Training Program
Ê Initiate when child is well.
Ê Initiate when child is calm.
Ê Initiate when child is not experiencing major transition or change.
Ê Initiate when the whole team is on board-‐ CONSISTENCY IS KEY.
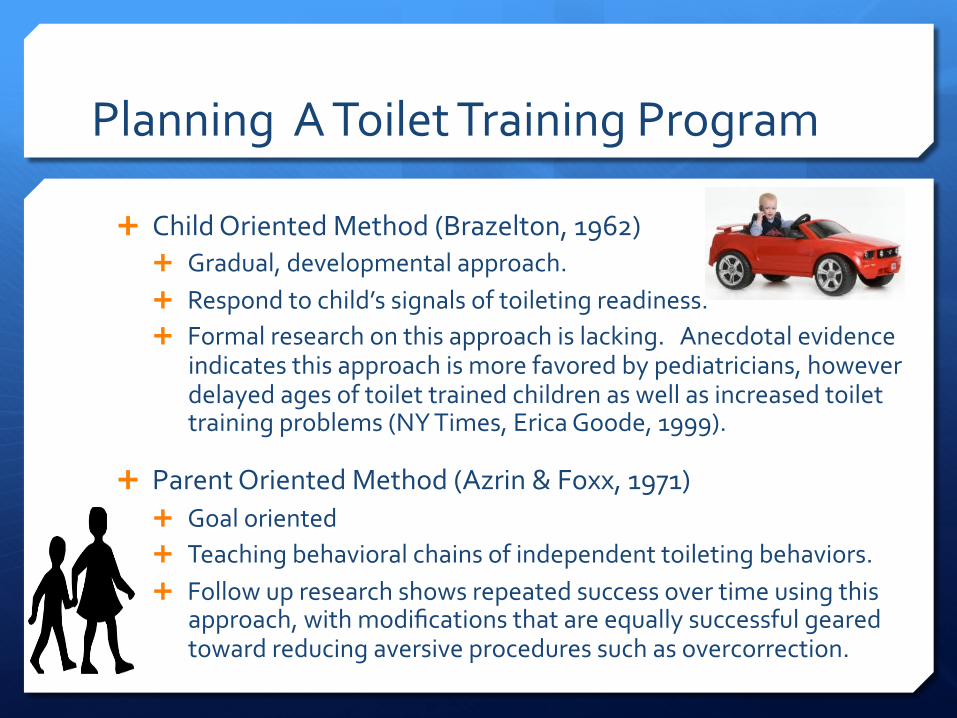
Planning A Toilet Training Program
Ê Child Oriented Method (Brazelton, 1962) Ê Gradual, developmental approach. Ê Respond to child’s signals of toileting readiness. Ê Formal research on this approach is lacking. Anecdotal evidence
indicates this approach is more favored by pediatricians, however delayed ages of toilet trained children as well as increased toilet training problems (NY Times, Erica Goode, 1999).
Ê Parent Oriented Method (Azrin & Foxx, 1971) Ê Goal oriented Ê Teaching behavioral chains of independent toileting behaviors. Ê Follow up research shows repeated success over time using this
approach, with modifications that are equally successful geared toward reducing aversive procedures such as overcorrection.

A Modified Caregiver Oriented Approach (Azrin & Foxx, 1971; LeBlanc et. al, 2005, Ardic & Cavkaytar, 2014)
1. Set aside one entire weekend (2-‐4 days) for toilet training.
2. Block out time for toilet training only (no phone calls, childcare, other children, cooking, chores, etc.)
3. Eliminate distractions.
4. Minimize interruptions.
5. Decide on a “word”. Consider age-‐appropriateness.
6. Gradual Fade Sit Schedule
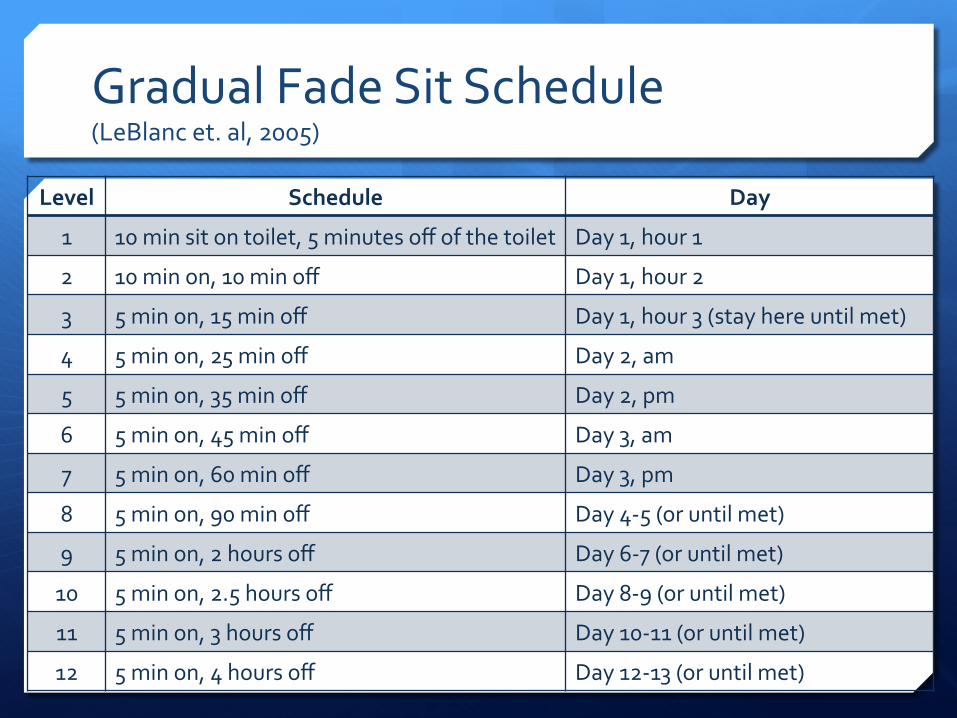
Gradual Fade Sit Schedule (LeBlanc et. al, 2005)
Level Schedule Day
1 10 min sit on toilet, 5 minutes off of the toilet Day 1, hour 1
2 10 min on, 10 min off Day 1, hour 2
3 5 min on, 15 min off Day 1, hour 3 (stay here until met)
4 5 min on, 25 min off Day 2, am
5 5 min on, 35 min off Day 2, pm
6 5 min on, 45 min off Day 3, am
7 5 min on, 60 min off Day 3, pm
8 5 min on, 90 min off Day 4-‐5 (or until met)
9 5 min on, 2 hours off Day 6-‐7 (or until met)
10 5 min on, 2.5 hours off Day 8-‐9 (or until met)
11 5 min on, 3 hours off Day 10-‐11 (or until met)
12 5 min on, 4 hours off Day 12-‐13 (or until met)
Increasing Fluid (LeBlanc et. al, 2005)
Ê 1st Hour: Prompt to drink liquid every 5 minutes
Ê 2nd Hour: Prompt to drink liquid every 10 minutes
Ê 3rd Hour: Every 15 minutes
Ê Rest of Day 1: Every 30 minutes

Communication Training
Ê Communication training should be used prior to each visit to the bathroom. Ê Verbal request Ê Picture cue exchange Ê Signal or sign
Ê Praise for correct use of the communication cue.

Communication Training
Ê The same schedule should be used for toileting every time: 1. Enter bathroom 2. Pull pants down 3. Sit down 4. Pee/poop 5. Get toilet paper 6. Wipe 7. Pull up pants 8. Flush 9. Wash hands (this is a whole separate chain of skills) 10. Leave bathroom

What to Do While Sitting!
Ê Watch a moderately preferred video for Levels 1-‐2
Ê May use access to a moderately preferred activity to reinforce sitting behavior and/or relaxation.
What to Do With SUCCESS!
Ê Successful Urination/BM: Ê Immediate access to highly preferred toys, praise, food, drinks!
Ê Let them get up and leave the bathroom/toilet!
Ê Successful Initiation: Ê Praise and immediately go to the toilet.
Preferred items only if urination/BM follows the initiation.

What to Do With An Accident Ê Minimize Attention Approach (Ardic & Cavkaytar, 2014)
1. Provide minimal attention. 2. Change clothes immediately with as little socialization, eye contact,
talking, etc. as possible. 3. Remove any items child was playing with, say “you are not dry”. 4. No reinforcement for 10 minutes.
Ê Positive Practice Approach (LeBlanc et. al, 2005) 1. Say “no wet pants” in a firm voice. 2. Return to bathroom, sit for 1 minute. 3. If completes urination in toilet, continue on with normal schedule. 4. If no urination completion in toilet, stand up, pull up pants, return to the
accident location, and repeat this sequence 4 times.
Ê Do not punish. Avoid negative tones or making accidents ‘gross’ or otherwise negative. Do not mimic, joke, or express anger.

Monitoring the Program
Ê Alarms-‐ To use or not to use. Ê Use of alarms can help increase the success of the program as it
will help ‘catch’ all of the opportunities as they occur in real time.
Ê Wet Stop http://wetstop.com/
Ê Dry Easy Bed Wetting Alarm
Ê Potty Time Potty Watch
Ê Malem Ultimate Bed Wetting Alarm
Ê Chummie Premium Bed Wetting Alarm
Ê Check your DATA (yeah, you should still be doing that-‐ it helps). Ê Data that shows progress-‐ Keep it up!
Ê Data that shows no/slow progress-‐ Change it up!

Fading the Toilet Training Program Ê Once child has shown consistent periods of
dryness, allow periods where child wears underwear. Have them pick out special underwear of their own for increased success.
Ê Gradually reduce the reinforcers and praise. Ê Reduce from highly preferred-‐ moderate-‐ low-‐ none
items.
Ê Reduce praise from high-‐ medium-‐low-‐no praise.
Ê Gradually reduce the amount of prompts to go on a schedule as self-‐initiation increases.

Nighttime Training
Ê Night dryness often takes several months or years after initial daytime dryness. This is expected.
Ê Once child routinely (7 days in a row) wakes up dry, begin nighttime training. Ê Have a change of bedding available. Ê Encourage going to the bathroom immediately before bed. Ê You may want to wake the child before you go to bed to have them
go once more for initial few weeks. Ê You may want to use a bed-‐wetting alarm.
Ê If child continues to have night time incontinence after age 6 or 7, seek medical guidance.

Troubleshooting
Ê Behavioral Ê Noise-‐ dryers, flushing Ê Tactile stimuli-‐ toilet paper, wipes, paper towels Ê Refusal to sit Ê Does not want to wipe Ê Masterbation/touching genitals Ê Digging Ê Smearing Ê Playing with water
Ê Rigidity and Predictability Ê Fear of where it all goes. Ê Unclear on what/how to do it. Ê Resistance to unfamiliar or different bathrooms (public, stalls, upstairs
vs. etc.)

When to Seek Medical Advice Ê Encopresis (chronic fecal soiling at age 4 or older).
Ê Enuresis (at least twice per month involuntary voiding during day or night in children over 5). Ê Boys are twice as likely as girls to have nocturnal
enuresis.
Ê Recurrent episodes of diarrhea lasting longer than 3 weeks.
Ê Frequent constipation or withholding (for longer than 3 weeks despite healthy diet).
*Tabbers et. al (2014), Issenman et. al (1999)

Recap Ê Take baseline.
Ê Get a Physical: Rule out medical conditions.
Ê Make a plan.
Ê Commit to the plan.
Ê Execute the plan. CONSISTENCY IS KEY! Track progress.
Ê Reinforce successes! Fade artificial reinforces gradually.
Ê Don’t give up.
Ê Seek medical assistance for concerns.

Last Thoughts (I promise…)
Ê Independence is key.
Ê Consider modesty.
Ê Self-‐Initiation is best. Ê If not possible, try to create a time based schedule the individual
can complete independently, and focus on increasing independent skills in the process (pants up/down, wiping, hand washing, etc.).

Resources Ê Toilet Training Caregiver Manual by NYS Office for People with Developmental Disabilities-‐
http://www.opwdd.ny.gov/opwdd_community_connections/autism_platform/behavior_management/targeting_the_big_3
Ê Toilet Training Information for Autism from The Children’s Guild Foundation-‐ http://www.kaleidahealth.org/services/pdfs/wchob/autism/ASD-‐Toilet-‐Training-‐6-‐12.pdf
Ê Little Friends Center for Autism-‐ http://www.theautismprogram.org/wp-‐content/uploads/tips-‐for-‐daily-‐life-‐toilet-‐training.pdf
Ê http://www.do2learn.com/picturecards/printcards/selselp_toileting.htm
Ê http://www.brighttots.com/Toilet_training_and_autism.html
Ê Ardic, A., Cavkaytar, A. (2014). Effectiveness of the modified intensive toilet training method on teaching toilet skills to children with autism. Education and Training in Autism and Developmental Disabilities. 49(2), 263-‐276.
Ê LeBlanc et. al (2005). Intensive Outpatient Behavioral Treatment of Primary Urinary Incontinence of Children with Autism. Focus on Autism and Other Developmental Disabilities. Summer 20(2).

Resources Ê American Academy of Pediatrics:
https://www2.aap.org/sections/scan/practicingsafety/module7.htm
Ê Anderson (2011). Current Trends in Occupational Therapy Services for Adults with Developmental Disabilities in Small Community Living Settings. Master’s Thesis. University of Puget Sound.
Ê Stadtler, Gorsky, Brazelton (1999). Toilet Training Methods, Clinical Interventions, and Recommendations. Pediatrics vol. 103 supplement 3.
Ê Azrin, Foxx (1974) Toilet Training in Less than a Day. New York, NY: Simon & Schuster.
Ê Brazelton, B. (1962). A Child Oriented Approach to Toilet Training. Pediatrics vol. 29 no. 1, 121-‐128.
Ê Isseman, R., Filmer, R., & Gorski, P. (1999). A Review of Bowel and Bladder Control Development in Children: How Gastrointestinal Conditions Relate to Problems in Toilet Training. Pediatrics vol. 103, no. 6.
Ê Tabbers, M.M. et al. (2014). Evaluation and Treatment of Functional Constipation in Infants and Children: Evidence-‐Based Recommendations from ESPGHAN and NASPGHAN. JPGN vol 58, no. 2.