Multiplex Screening for Interacting Compounds in Paediatric ...

Aetiology of acute paediatric gastroenteritis inBulgaria during summer months: prevalence of viralinfections
Zornitsa Mladenova,1 Andrej Steyer,2 Adela Fratnik Steyer,3
Balasubramanian Ganesh,43 Petar Petrov,5 Tanja Tchervenjakova6
and Miren Iturriza-Gomara7
Correspondence
Zornitsa Mladenova
Received 27 November 2014
Accepted 28 December 2014
1 (former) Department of Virology, National Centre of Infectious and Parasitic Diseases, Sofia, Bulgaria
2University of Ljubljana, Faculty of Medicine, Institute of Microbiology and Immunology, Ljubljana,Slovenia
3Blood Transfusion Centre of Slovenia, Ljubljana, Slovenia
4Division of Virology, National Institute of Cholera and Enteric Diseases, Kolkata, India
5Infectious Ward, University Hospital ‘St Anna’, Sofia, Bulgaria
6Infectious Wards 1 and 2, Specialized Hospital for Infectious and Parasitic Diseases ‘Prof. IvanKirov’, Sofia, Bulgaria
7Institute of Infection and Global Health, University of Liverpool, Liverpool, UK
Paediatric acute gastroenteritis is a global public health problem. Comprehensive laboratory
investigation for viral, bacterial and parasitic agents is helpful for improving management of acute
gastroenteritis in health care settings and for monitoring and controlling the spread of these
infections. Our study aimed to investigate the role of various pathogens in infantile diarrhoea in
Bulgaria outside the classical winter epidemics of rotavirus and norovirus. Stool samples from 115
hospitalized children aged 0–3 years collected during summer months were tested for presence
of 14 infectious agents – group A rotavirus, astrovirus, Giardia, Cryptosporidium and Entamoeba
using ELISAs; norovirus by real-time RT-PCR; picobirnavirus and sapovirus by RT-PCR;
adenovirus using PCR, and Salmonella, Shigella, Escherichia coli, Yersinia and Campylobacter
using standard bacterial cultures. Infectious origin was established in a total of 92 cases and 23
samples remained negative. A single pathogen was found in 67 stools, of which rotaviruses were
the most prevalent (56.7 %), followed by noroviruses (19.4 %), enteric adenoviruses (7.5 %),
astroviruses (6.0 %), bacteria and parasites (4.5 % each) and sapoviruses (1.4 %). Rotavirus
predominant genotypes were G4P[8] (46.3 %) and G2P[4] (21.4 %); for astroviruses, type 1a was
the most common, while the GII.4/2006b variant was the most prevalent among noroviruses.
Bacteria were observed in five cases, with Salmonella sp. as the most prevalent, while parasites
were found in ten stool samples, with Giardia intestinalis in five cases. The results demonstrated
high morbidity associated with viral infections and that rotavirus and norovirus remain the most
common pathogens associated with severe gastroenteritis during summer months in Bulgaria, a
country with a temperate climate, and significant molecular diversity among circulating virus
strains.
INTRODUCTION
Paediatric acute gastroenteritis (AGE) is a global publichealth problem accounting for 1.5 billion diarrhoealepisodes and 3 million deaths each year. A broad spectrumof enteric pathogens can cause acute infantile diarrhoea(Hilmarsdottir et al., 2012; Gonzalez et al., 2011; Tam et al.,2012). The main bacterial and protozoan organisms isolated
3Present address: Laboratory Division, National Institute of Epidemiology,Chennai, India.
Abbreviations: AdV, adenovirus; AGE, acute gastroenteritis; AstV,astrovirus; NoV, norovirus; PBV, picobirnavirus; RdRp, RNA-dependentRNA polymerase; RV, rotavirus; SaV, sapovirus.
The GenBank/EMBL/DDBJ accession numbers for the nucleotidesequences of Bulgarian Nov, SaV and AstV are KP123636–KP123644and KP162248–KP162261.
Journal of Medical Microbiology (2015), 64, 272–282 DOI 10.1099/jmm.0.000018
272 000018 G 2015 The Authors Printed in Great Britain

from stool samples of children less than 5 years of age arediarrhoeagenic Escherichia coli, Salmonella spp., Shigellaspp., Yersinia spp. and Campylobacter spp., and Giardiaintestinalis, Entamoeba histolytica and Cryptosporidium spp.,respectively. In addition, the representatives of four viralfamilies – rotaviruses (RVs) (Reoviridae), noroviruses (NoVs)and sapoviruses (SaVs) (Caliciviridae), human astroviruses(AstVs) (Astroviridae) and adenoviruses (AdVs) subgenus F(Adenoviridae) – are commonly detected in childhood viralgastroenteritis (Gonzalez et al., 2011; Tam et al., 2012).
Human RV group A is considered the leading cause of AGEin children less than 5 years, and is responsible for over 140million diarrhoeal episodes yearly worldwide. RV is a non-enveloped virus with a genome of 11 double-stranded RNAsegments and triple-layered capsid with two surface pro-teins: VP7 (glycoprotein, G) and VP4 (protease-sensitiveprotein, P). RVs are highly divergent and, to date, 27 G and35 P types have been described (Matthijnssens et al., 2011).NoVs affect individuals of all ages, and are the most commoncause of sporadic cases and outbreaks of gastroenteritis(Tam et al., 2012; Ahmed et al., 2014), while SaVs lead torelatively mild gastroenteritis in small outbreaks andsporadic cases. These viruses are non-enveloped, with anicosahedral capsid that surrounds a positive-sense single-stranded RNA genome with three overlapping ORFsencoding the non-structural (ORF1) and structural (ORF2and ORF3) viral proteins. Based on their genetic hetero-geneity, NoVs are currently classified in six genogroups (GI–GVI), with GI (nine genotypes) and GII (22 genotypes)containing the majority of the strains associated with humandisease (Green, 2013). Phylogenetically, SaVs can be dividedinto five genetic clusters, GI–GV, based on their capsid-coding region, and except for GIII, all other genotypes infecthumans (Hansman et al., 2007). AstVs and enteric AdVs(types 40 and 41) are much less often identified as cause ofacute diarrhoea in children under the age of 5 years. Theincidence of AstV infections ranges from 2–9 % in developedcountries up to 26 % in developing countries. Eight AstVgenotypes and 17 lineages have been identified (Martellaet al., 2014), with genotype 1 being the predominant type inmost parts of the world (Mendez & Arias, 2007). AmongAdVs, subgroup F has been detected in AGE cases mostfrequently, but other subgenera such as A (type 31) and C(type 2) have also been implicated in infantile diarrhoea.Moreover, some other viral agents such as picobirnaviruses(PBVs, Picobirnaviridae), Aichi virus and parechoviruses(Picornaviridae), human bocaviruses (Parvoviridae) andtoroviruses (Coronaviridae) have also been reported inassociation with human gastroenteritis (Guarino et al., 2008).
In Bulgaria, all hospitalized cases of infectious AGE arenotifiable in the National Notifiable Disease SurveillanceSystem (www.ncipd.org). Infectious diarrhoea is defined asthe presence of three or more defecations per day withstools with changed consistency, colour, smell andpathological impurities (mucus/blood), and when one ormore of the following criteria are met: fever, vomiting,abdominal cramps, epidemiological background (recent
travel history, consumption of food/drinks, attendance atwater sources, etc.). Indications for hospital admission arepatient’s age (infants and toddlers ,1 year old, adults .60years old) and health conditions (moderate to severe clinicalconditions, prematurity, additional acute/chronic disease).The investigation of enteropathogenic bacteria, Salmonellaspp., Shigella spp., diarrhoeagenic E. coli, Yersinia spp. andCampylobacter spp. are obligatory, as well as for RVA inchildren ,9 years of age (since June 2011).
Currently, there are no published data on the aetiology ofpaediatric acute diarrhoea in Bulgaria and, in the absenceof routine screening, the incidence of virus infections otherthan RV remains largely unknown.
Increased morbidity associated with AGE of unknownaetiology during summer months has been observed inBulgaria since 2007 (www.ncipd.org). In order to invest-igate the spectrum of diarrhoeal enteropathogens (six viral,five bacterial and three parasitic) and to assess molecularepidemiology of the main viral agents, we conducted astudy including 115 children with AGE symptoms aged 0–3years, hospitalized in the infectious wards of twometropolitan hospitals in the summer of 2009.
METHODS
Patients and samples. Our study was conducted at two
metropolitan hospitals: the Specialized Hospital for Infectious and
Parasitic Diseases ‘Prof. Ivan Kirov’ and the University Multi-Profiled
Hospital for Active Treatment ‘St Anna’, Sofia, Bulgaria. These
hospitals have the only paediatric infectious wards that serve the child
population in Sofia city and region of approximately 40 000–42 000
children aged 0–5 years (data of the National Statistic Institute for
2013).
A total of 115 children hospitalized with AGE between June and
September 2009 were randomly selected and enrolled in the study.
The children were between 40 days and 3 years old, and the
male : female ratio was 1 : 1. The study population represented 10 %
of all children ,3 years old admitted to both hospitals with AGE for
the entire period of the study.
The criteria for hospital admission of children with AGE were
presence of diarrhoea (three or more watery or loose stools in the
preceding 24 h) and/or vomiting (two or more episodes in 24 h) and/
or fever (.37 uC) and clinical evidence of grade II–III dehydration
(.5 % body weight loss, abnormal skin turgor and elasticity, sunken
eyes and/or fontanelles, changes in pulse/heart and respiratory rate,
mental changes such as lethargy or irritability, decreased urine
volume). Children with prolonged diarrhoea (.1 week) and those
who received antibiotic therapy before admission were excluded from
the study. On admission all patients were clinically examined and the
patient’s history including nutritional and epidemiological informa-
tion was documented.
One stool sample was collected from each child and was divided into
three portions: one for bacterial testing, the second for viral and
protozoan detection and the third portion was stored at 270 uC for
molecular-based investigation.
Laboratory tests and analysis. Bacterial pathogens such as
Salmonella spp., Shigella spp., diarrhoeagenic E. coli, Yersinia spp.
and Campylobacter spp. were detected using standard bacterial
Aetiology of acute infantile diarrhoea in Bulgaria
http://jmm.sgmjournals.org 273

cultures. Presence of group A RVs, AstVs, G. intestinalis, Crypto-
sporidium parvum and Cryptosporidium hominis, and Entamoeba
histolytica and Entamoeba dispar were examined using antigen-detec-
tion immunoenzyme commercial tests RIDASCREEN (R-Biopharm).
All stools were prepared as 20 % stool suspension in 1 ml PBS and
viral RNA/DNA was extracted by PureLink Viral RNA/DNA Mini kit
(Invitrogen) according to manufacturer’s instructions. Extracted
RNA/DNA was eluted in 50 ml, and 20 ml of eluent was reverse-
transcribed using random hexamers (Invitrogen). RV-positive samples
were characterized by semi-nested PCR with primers toward VP7 and
VP4 genome segments of group A RVs according to European
Rotavirus Detection and Characterization Methods v4 (http://www.
eurorota.net/docs.php; Iturriza-Gomara et al., 2011). Previously
described oligonucleotide primer sets Mon340/Mon348, targeting the
ORF1a (Belliot et al., 1997), and Mon269/Mon270, targeting ORF2
(Noel et al., 1995), were used to obtain initial PCR products for
sequencing and genotyping of the AstV strains detected. Real-time RT-
PCR for NoV genogroups I and II detection was performed with
primers COG1F-COG1R and COG2F-COG2R and FAM-BHQ-
labelled fluorescent probe mixture of RING1(a)-TP and RING1(b)-
TP, and RING2-TP, respectively, using Opticon 2 real-time cycler (Bio-
Rad) (Kageyama et al., 2003). In addition, a total of eight PCR products
of NoVs GI (two strains) and GII (six strains) were obtained after
amplification by primer sets toward the capsid-coding region (Kojima
et al., 2002). The presence of SaV and of AdV group F was detected by
PCRs using primer pairs SR80-JV33 and AdenoF-AdenoR, and
protocols described previously (Vinje et al., 2000; Tiemessen & Nel,
1996). In addition, extracted RNAs were tested for the presence of PBV
genogroups I and II, as described elsewhere (Bhattacharya et al., 2006).
A detailed genetic characterization of a total of 16 viral strains (seven
AstVs, two NoVs GI, six NoVs GII and one SaV) was performed by
direct sequencing, using ABI PRISM BigDye Terminator Cycle
Sequencing Reaction kit (Applied Biosystems). The sequences obtained
were edited manually and aligned using the BLAST program. The
nucleotide comparisons were done by BioEdit and MEGA4 software,
and phylogenetic trees were reconstructed using the neighbour-joining
method and bootstrap 100 through the MEGA4 program (Tamura et
al., 2007). Nucleotide sequences of Bulgarian NoV, SaV and AstV
strains obtained in the present study have been deposited in GenBank
under the accession numbers KP123636–KP123644 and KP162248–
KP162261.
RESULTS
Infectious origin of AGE was established in 92 of 115 cases(80 %) and 23 (20 %) samples remained negative after alldiagnostic tests were performed. A single pathogen wasfound in 67 stools, of which RVs were the most prevalent(38; 56.7 %), followed by NoVs (13; 19.4 %), enteric AdVs(5; 7.5 %), AstVs (4; 6 %), bacteria (3; 4.5 %), parasites (3;4.5 %) and SaVs (1; 1.5 %). Double and triple infectionswere detected in 19 (16.5 %) and six (5.2 %) of samples,respectively, mostly combinations of RV or NoV with otherpathogens (Table 1). PBVs genogroups I and II were notdetected in the stool specimens tested.
Diarrhoea severity was recorded from all children enrolledin the study. The mean duration of diarrhoea was shortestin viral infections (3.3±0.48 days) and longest in bacterialinfections (9.8±1.6 days). Vomiting of .3 episodes/day21
was commonly registered among patients with NoVs(90 %) and RVs (76 %), while high temperatures .38 uCwere mostly associated with bacterial AGE (92 %). Upper
respiratory tract infections were most common in RV(37 %) and enteric AdV (32 %) groups, whereas mucoid/bloody stools and abdominal cramps were found in themajority of patients (81 %) with bacterial infection. Nodifferences were found on the severity of disease betweenmixed viral–bacterial infections and bacterial alone. Allpatients fully recovered and were discharged.
Overall, RVs were found in a total of 56 samples (48.7 %),among which genotypes G1P[8] (3; 5.4 %), G2P[4] (12;21.4 %), G4P[8] (26; 46.3 %) and G9P[8] (7; 12 %) weredetected most frequently. Unusual G–P combinations suchas as G12P[8] and G4P[6] (1; 1.8 % each) were alsoidentified. Co-infections with two RV strains, G4P[8] andG3P[8], were observed in two stool samples and four RVstrains remained partly genotyped (Table 2).
NoV genogroups I and II were detected in 15 (13 %) and18 (15.7 %) samples, respectively, using real-time RT-PCR.Five GI and six GII NoV-positive samples were selectedbased on their different collection points for performingconventional RT-PCR followed by sequencing. Of these,amplicons of two GI isolates and all six GII NoVs weresuccessfully obtained. Part of the ORF2, the capsid-codingfragment of viral genome, of the two GI Bulgarian NoVswas sequenced, and the phylogenetic analysis allowed theirclustering into genotype GI.4 (Fig. 1). The GI NoV strains
Table 1. Viral, bacterial and parasitic agents detected in single,double and triple infections in 115 sporadic AGE cases inchildren aged 0–3 years old
Single infections
Total 67
Rotavirus group A 38
Norovirus 13
Astrovirus 4
Adenovirus 5
Sapovirus 1
Salmonella spp. 3
Cryptosporidium parvum 1
G. intestinalis 1
Entamoeba histolytica 1
Double infections
Total 19
Rotavirus+norovirus 9
Rotavirus+adenovirus 3
Rotavirus+E. coli 1
Norovirus+astrovirus 2
Norovirus+G. intestinalis 4
Triple infections
Total 6
Rotavirus+norovirus+adenovirus 2
Rotavirus+norovirus+Cryptosporidium 1
Rotavirus+adenovirus+Cryptosporidium 1
Rotavirus+astrovirus+Shigella flexneri 1
Norovirus+astrovirus+Entamoeba
histolytica
1
Z. Mladenova and others
274 Journal of Medical Microbiology 64

BG629/2009 and BG675/2009 had nucleotide (nt) andamino acid (aa) sequence homology of 91 and 95 %,respectively. The strain BG629/2009 was 98–99 % nt similarto several NoV isolates from oysters in Taiwan in 2009(GQ401126-129), while isolate BG675/2009 resembled theUS strain Hu/GI.4/1643/2008/US (GQ413970) and NoVsdetected in a water-borne outbreak in Sweden (Nenonenet al., 2012).
Among the GII NoVs investigated in the present study, allstrains but one belonged to genotype GII.4. A single strain,BG638/2009, was closely related to the GII.3 NoV strains(Fig. 2). Phylogenetic analysis of the capsid-coding regionshowed that it had 96–97 % nt homology with the GII.3strain Hu/5017.34/2003/JPN (EU187437), detected in Japanin 2003–2004, and the recombinant Hu/GII.3/CBNU1/2006/KOR (GU980585) from an outbreak in South Korea3 years later. The genetic analysis of part of the ORF1 gene ofBG638/2009 revealed it was GIIb genotype. All five GII.4NoVs (BG672/2009, BG703/2009, BG737/2009, BG746/2009and BG752/2009) represented the pandemic GII.4 DenHaag2006b variant (EF126965) according to the capsid gene,and displayed 98–99 % nt and 99–100 % aa inter-strainsimilarity.
A single SaV strain was detected in the present study(prevalence of 0.9 %). The sequence and phylogeneticanalyses of partial RNA-dependent RNA polymerase(RdRp) gene revealed that Bulgarian strain BG697/2009shared closest match (95 % nt identity) to SaV strainsdetected in Turkey in 2007 (GQ253120), in India in 2007(AB447416) and in different parts of the world during thepast decade (Fig. 3). The BG679/2009 strain showed also90–93 % nt homology to other strains included in the GIIgenetic cluster –, Ehime-1107 (DQ058829) and SW278(DQ125333), which were described as inter-genogrouprecombinant SaV strains (Hansman et al., 2007).
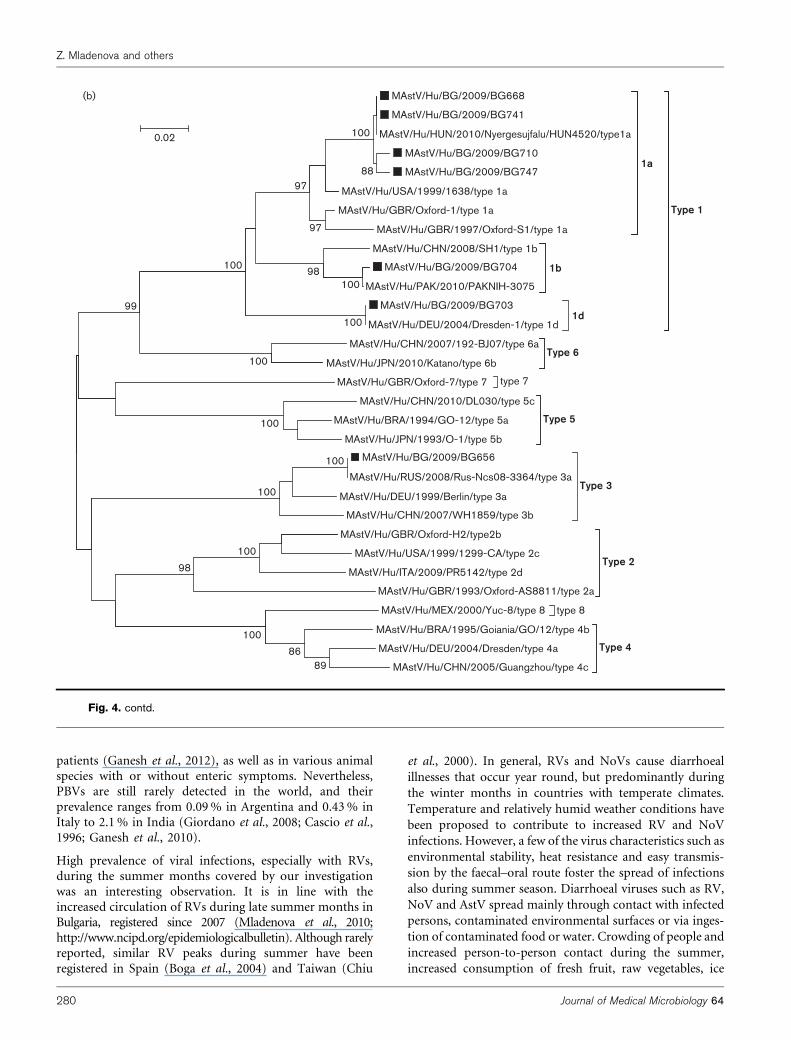
Seven of eight AstV strains detected in this study wereanalysed by sequencing of fragments of ORF1a (nt 1248–1467; 219 nt length) and ORF2 (nt 4579–4959; 380 ntlength) genes (Fig. 4a, b). Phylogenetic analysis of BulgarianAstV strains revealed that four of the strains (BG668, BG710,
BG741, BG747) aligned (99–100 % homology) with a type1a strain, MAstV/Hu/HUN/ 2010/Nyergesujfalu/HUN4520(HQ398856), that was detected in 2010 (1 year later) andwas responsible for a single outbreak in a nursery inHungary. The ORF1a and ORF2 sequences of the BulgarianAstV BG703 were found to be 99 and 100 % similar at nt andaa levels to the strain MAstV/Hu/DEU/2004/Dresden-1(AY720892), which belongs to the type 1d. The geneticanalysis of AstV BG704 showed that it closely matchedunassigned isolates from India V1182 (AB325804) andKorea (clones from KS106205 to KS106208; AF361030 toAF361033) in ORF1a, while the ORF2 part was 99 % nt and100 % aa similar to several Pakistani type 1 strains (referencestrain PAKNIH-3075; KC896126). In addition, BG strainBG656 clustered in a common branch with strain MAstV/Hu/PAK/2008/PAK_NIH_VS_908, a type 3/5 recombinantfrom Pakistan, and type 5 Chinese AstV DL030 (JQ103408)according to the ORF1a sequence, but it was 100 % nt and aasimilar to the type 3a strain isolated in Russia in 2008, Rus-Nsc08-3364, based on the ORF2 sequence.
Bacterial pathogens were found in five diarrhoeal cases(4.3 %), with Salmonella species being the most common(2.6 %). Strains of Salmonella enteridis groups OC and ODwere identified in two and one faecal samples, respectively.Enterohaemorrhagic E. coli strain O157 and Shigella flexneristrains were detected as co-pathogens in single samples(0.9 % each). Parasites were found in ten stool samples(8.7 %) with G. intestinalis in five samples (4.3 %),Cryptosporidium spp. in three samples (2.6 %) andEntamoeba spp. in two samples (1.7 %).
DISCUSSION
Our study indicates a significant number of cases of AGEwith infectious aetiology (80 %) during the 4 month studyperiod. Viral, bacterial and parasitic pathogens accountedfor 83.7 (77/92), 3.3 (3/92) and 3.3 % (3/92), alone, and9.8 % (9/92), as co-infections, of all gastroenteritis hospi-talizations among children less than 3 years of age. Anincidence rate of infectious diarrhoea ranging between 39and 86 % has been reported in several countries in Europeand the rest of the world (Tam et al., 2012; Levidiotou et al.,2009; Colomba et al., 2006; Olesen et al., 2005; Boga et al.,2004; Youssef et al., 2000; Sethi et al., 1989), which is inaccordance with our results. However, most of the studiespublished were focused on viral infections alone (Shojaet al., 2014; Sanchez-Fauquier et al., 2011; Jakab et al.,2009; Fabiana et al., 2007; Oh et al., 2003; Chikhi-Brachetet al., 2002), where virus-positive rates varied from 39 % inFrance to 62 % in Turkey (Chikhi-Brachet et al., 2002;Akhter et al., 2014). The difference in the viral prevalenceseen in the literature might reflect the discrepancies of thestudies conducted based on geographical [number ofhospital(s) included, region(s) and general populationcovered], temporal [year(s)/season(s) investigated] orpopulation features (sample size, age of the patients, in/outpatient or hospitalized cases, sporadic alone or mixed
Table 2. RV G–P combinations detected among 56 RV-positive samples
RV G–P genotype Number of cases
G1P[8] 3
G2P[4] 12
G4P[6] 1
G4P[8] 26
G9P[8] 7
G12P[8] 1
G–mixedP[8] 2
G/P partly or fully untypable 4
Total 56
Aetiology of acute infantile diarrhoea in Bulgaria
http://jmm.sgmjournals.org 275

sporadic and outbreak cases), as well as the testing methodsused and number of virus targets included for detection.The high burden of infectious diarrhoea cases in our studymight be due to the improved clinical assessment of AGEcases (consent for acute infectious intestinal infections ofthe Bulgarian Society of Infectious Diseases/2009, http://www.bsid-bg.org/index.php/consensi/acute-int-infections)and the use of diagnostic methods with better diagnosticefficacy such as RT-PCR for NoV, AstV and SaV screening.
On the other hand, 20 % of the samples remained negativein all diagnostic tests performed. Although the diagnostictests used in our study are highly sensitive and specific, theproportion of false-negative cases with infectious origin isunknown because of some limitations of our investigation.It must be noted that detection of other diarrhoeal-relatedpathogens such as picornaviruses or Clostridium difficile,which affect mainly children less than 5 years of age, wasnot performed. Also, it could not be ruled out that a fewspecimens with viral aetiology might have been counted asfalse-negative in the molecular methods used because ofthe limited sensitivity of this type of diagnostic in sampleswith low viral load or with presence of strain variants. Theuse of molecular methods for the detection of bacterialpathogens in recent years has also resulted in increasedsensitivity of detection, particularly for fastidious bacterialpathogens such as Campylobacter (Tam et al., 2012).
Our study has shown that viral AGE was characterized bywatery stools without mucus/blood and shorter duration ofdiarrhoea. In contrast, bloody/mucoid stools, abdominalpain and higher temperature were common features inpatients with bacterial disease. Dehydration and upperrespiratory tract infections were described more oftenamong virus-infected children than in those with bacterialillness. Bacterial disease caused by Salmonella spp. wasmore severe and characterized by prolonged duration (8–12 days), bloody stools, abdominal cramps and high fever(39–40 uC).
Our findings clearly demonstrated that viral infectionswere the predominant cause of severe diarrhoea requiringhospital admission in summer months. Overall, viruseswere found as a sole pathogen in 53 % of the samplestested, while bacteria and parasites were detected in 13 % inboth single and mixed infections. Data from our neighbour-ing countries Turkey, Greece and Albania (Akhter et al.,2014; Levidiotou et al., 2009; Fabiana et al., 2007) and alsofrom Hungary, Spain and France (Jakab et al., 2009; Bogaet al., 2004; Chikhi-Brachet et al., 2002) are concordant withour findings. Most data for Bulgaria are limited to theaetiology of bacterial and parasitic gastroenteritis (Parmakovaet al., 2012, 2013; http://www.ncipd.org/epidemiologicalbulletin).Parmakova et al. (2012) described the aetiology of bacterialAGE in the country for all age groups for the period
Hu/GI.4/BG629/2009/BG
OysterGI/BFDA-GI-07/2009/TAW
Hu//GII.4/Beijing/55169/2008/CHN
80
97
Hu//GI/Jeju-50/2007/KOR
Hu/GI/2005/8086/Chelyabinsk/RUS
Hu/NLV/Valetta/95/Malta
Hu/GI.4/BG675/2009/BG
GI.4
99
100
Hu/GI.4/1643/2008/US
Hu/GI/7/JPN
Hu/NLV/Chiba 407/1987/JP94
Hu/NLV/Thistlehall/90/UK
Norwalk/GI.1
Southhampton/GI.2
NLV/Boxer/2001/US/GI.8
NLV/VA98115/1998/GI.3
DSV395/GI.387
88100
NLV/Winchester/94/UK/GI.7
SzUG1/GI.5
BS5/GER/GI.6100
Lordsdale GII.4 – outgroup
20
Fig. 1. Phylogenetic tree of NoV GI sequences reconstructed using the partial N-terminal capsid region. Bulgarian GI NoVs aremarked with &. The Lordsdale virus with GII.4 genotype was used as outgroup strain.
Z. Mladenova and others
276 Journal of Medical Microbiology 64

2007–2011, and showed that prevalence varied from year toyear, with predominance of salmonellosis (12–21 %),shigellosis (9–11 %) and E. coli illnesses (7–11 %), andmarked seasonality in the summer and autumn (May toOctober) could be seen. The low incidence of bacterial andprotozoal infections observed in our study is in agreementwith data from many European countries, such as Greece(Levidiotou et al., 2009), Italy (Colomba et al., 2006), Spain(Boga et al., 2004) and Denmark (Olesen et al., 2005), andclearly demonstrates the successful implementation ofEurope-wide control strategies in livestock production andthe food industry.
Our investigation has shown that RVs were responsible forthe majority of the viral gastroenteritis (62 % from allmono-infections; 38/61), but NoV, AstV, enteric AdV andSaV also contributed to diarrhoea-associated morbidity(38 %). RV surveillance in Bulgaria started in 2005 and
since then it has allowed us to evaluate the incidence of RVinfections and the prevalence of circulating genotypes. Inour previous investigation of RV diarrhoea cases in childrenand adults, which covered a period from 2005 to 2008, anaverage detection rate of 32.4 % (27–43 %) has beenestablished (Mladenova et al., 2010).
Many countries in the world have reported that RVs are aleading cause of paediatric AGE, accounting for 27–51 % ofall diarrhoea cases in children under 5 years of age (Parasharet al., 2006; Soriano-Gabarro et al., 2006). The RV prevalenceobserved in this study is higher than previously found inBulgaria and in many other studies globally. However, ourstudy only included children less than 3 years of age, in whomthe first and usually most severe RV infections requiringhospital admission occur. Thus, the introduction of an RVvaccine in the national immunization programme coulddecrease significantly the RV morbidity in Bulgaria.
Hu/GII.4/BG703/2009
Hu/GII.4/BG746/2009
Hu/GII.4/BG672/2009
Hu/GII.4/BG737/2009
Hu/GII.4/BG752/2009
Hu/DenHaag89/2006/NL
Hu/Duan/Beijing/2006/CHN
2006b90
Hu/Hokkaido2/2006/JP
Hu/NSW696T/2006/AUS
Hu/Lanzhou/35666/2002/CHN
Hu/Chiba/04-1050/2005/JP
Hu/Farmington Hills/2002/USA
Hu/Hunter504D/040/2004/AUS
Hu/Hong Kong/CU050140/2005/CHN
Hu/Toronto/SK/2005/CANGII.4
Hu/0317/2004/NL
Hu/Aomori2/2006/JP
Hu/NZ327/2006/NZL
Hu/Yerseke38/2006/NL
Hu/New Orleans1805/2009/USA
Hu/GII.4/Apeldoorn317/2007/NL
Hu/OC08086/2008/JP
Grimsby/1996/UK
Hu/OC07138/2007/JP
85
Hu/NLV/Camberwell/1994/AUS
Hu/Kaiso/030556/2003/JP
Bristol/B463/UK
Lordsdale/UK
Hu/GII.3/BG638/2009
99
Hu/5017.34/2003/JPN
Hu/GII.3/CBNU1/2006/KOR
GII.3
90
99
0.05
Fig. 2. Phylogenetic tree of NoV GII.4 and GII.3 sequences reconstructed using the partial N-terminal capsid region. BulgarianGII NoVs are marked with &.
Aetiology of acute infantile diarrhoea in Bulgaria
http://jmm.sgmjournals.org 277

The present study was designed to investigate the role of
viral agents such as NoV, SaV, AstV, AdV and PBV in
childhood diarrhoea and their epidemiology features. In
the only previous investigation in Bulgaria, our research
group has reported 46.8 % (220/470) diarrhoea cases with
viral aetiology among hospitalized children aged 25 days–
12 years in a retrospective 5 month (December 2006–April
2007) survey (Mladenova et al., 2008). In that study, NoVs
were found in 12.1 % of cases, and a great diversity of
genotypes (GII.3, GII.4/2002, GII.4/2006a, GII.4/2006b,
GII.9 and GII.Karachi) was observed. In the present study,
NoVs were the second major viral agent of acute infantile
diarrhoea registered, and genotype diversity was detected
again, along with the first detection of NoV GI genotype in
Bulgaria. Both GI NoV strains identified belonged to
different lineages in the GI.4 cluster, which might indicate
a different source of infection. In addition, the globally
spread NoV GII.4 variant DenHaag2006b was also detected
among five patients who were residents of different locations
in Sofia city or Sofia region and were admitted to hospitalbecause of severe gastroenteritis symptoms. All theseBulgarian GII.4/DenHaag2006b strains were identical insequence analysis, which strongly suggests an outbreak(s)with a common but unrecognized source of infection.
A single possible recombinant, NoV BG638/2009, withGII.b polymerase and GII.3 capsid genome fragments, wasalso identified. Detection of NoVs that have recombinantcharacteristics has been recently reported (Giammancoet al., 2012; Rimoldi et al., 2011). These data confirm thatrecombination is an important genetic mechanism forsurvival and continuous evolution of viruses. Moreover,additional genetic mechanisms such as point mutationscan generate great strain diversity among NoVs. Thesegenetic mechanisms contribute to the emergence of newstrains or variants with increased stability in the envir-onment and fitness, and could be a potential obstacle fordiagnostics of viral infections, as well as have an influence onthe phylogenetic classification and future vaccine designs.
Hu/Bristol/98/UK
Hu/Mc2/TH/2002/THA
Hu/V1716/07/IND
85
85
Hu/GII.1/VIG-481/PA/BRA/2003
Hu/GII.1/VIG-336/PA/BRA/2003
Hu/BG697/2009
Hu/Afyon/65/2007/TRY
GII94
80100 GII cluster
Hu/A141/CHN
Hu/Karlsruhe/1386/2002/DEU
Hu/London/29845/92/UK
100
Hu/Hou7-1181
Hu/Ehime1107/2002/JP
Hu/SW278/2004/SE
GIV100
Hu/Parkville/UK
HuCV/Houston/27/90/USAGI
Hu/Sapporo/82/JP100
100
Hu/Manchester/UKGI
Hu/NongKhai-24/THA
Hu/Ehime475/2004/JPGV
100
GIIIPo/Cowden/USA
0.05
Fig. 3. Phylogenetic tree of SaV sequences reconstructed with the partial RdRp-coding region. The Bulgarian SaV is markedwith &. Genotypes according to the capsid-coding sequences are noted with square brackets, while the GII cluster involvingSaV strains based on the sequencing of the RdRp-coding region are depicted with a round bracket. Porcine GIII SaV is used asoutgroup strain.
Z. Mladenova and others
278 Journal of Medical Microbiology 64

SaVs were detected only in 0.9 % of samples included inthis study. This detection rate is similar to other reportsfrom Europe where the detection level varies between 0.6 %in Italy and 2.0–2.4 % in the UK and The Netherlands(Rimoldi et al., 2011; Amar et al., 2007; de Wit et al., 2001).The first detection of a SaV strain in Bulgaria revealed thatits polymerase-coding region sequence was closely relatedto SaVs clustering in the GII genogroup and also to inter-genogroup recombinant strains with the GII RdRp/GIV-capsid region. However, if the Bulgarian strain is a possiblerecombinant or a typical GII SaV, further investi-gations of its capsid-coding genome fragment are needed.
AstVs were detected in 8.7 % (8/92), which is in accordancewith our previous data for lower frequency of theseinfections in hospitalized children (0.2 %; Mladenova et al.,2008). Genotyping of AstV strains by sequence analysis wascarried out for the first time in Bulgaria, and it revealed theexistence of a diverse AstV population. Four of the eightBulgarian AstVs that were identified as genotype 1a,BG668/2009, BG710/2009, BG741/2009 and BG747/2009
shared high nt and aa inter-strain identity and likelyrepresent a single AstV strain and source of infection.These four isolates together with the isolate BG703/2009,which belongs to genotype 1d, represent classical AstVswith ORF1a and ORF2 of the same type. In contrast, theother two AstV isolates, BG656/2009 and BG704/2009,each detected in a single sporadic gastroenteritis case, arepossible recombinants as the ORF1a and ORF2 parts of thegenes belonged to different phylogenetic clusters. In arecent paper by Martella et al. (2014), a great lineagediversification in ORF2 due to point mutations, recomb-ination and rearrangements events has been observed, butgenetic analysis of ORF1 and ORF2 in parallel will betterclarify the AstV diversity.
PBVs were not detected in our investigation. These viruseswere first detected in 1988 in stool samples of children andrats (Pereira et al., 1988), and since then have beenrecognized as a putative infectious agent or opportunisticpathogen in children and adults with/without diarrhoea,immunocompromised persons and kidney-transplant
MAstV/Hu/BG/2009/BG703
MAstV/Hu/DEU/2004/Dresden-1/1d
98
Hu/China/Beijing/180/2005/CHN
Hu/China/Beijing/291/2007/CHN/rb 1b/1d
MAstV/Hu/DEU/1999/Berlin/3a
MAstV/Hu/RUS/2008/Rus-Nsc08-3364/3a
100
MAstV/Hu/GBR/Oxford-H2/2b
MAstV/Hu/DEU/2004/Dresden/4a
MAstV/Hu/PAK/2008/PAK_NIH_VS908/rb 3/5
MAstV/Hu/BG/2009/BG65694
MAstV/Hu/CHN/2010/DL030/5
MAstV/Hu/GBR/Oxford-1/1a
MAstV/Hu/BRA/1995/Goiania/GO/12/4b
MAstV/Hu/BG/2009/BG66898
MAstV/Hu/BG/2009/BG710
MAstV/Hu/HUN/2010/Nyergesujfalu/HUN4520/1a
MAstV/Hu/BG/2009/BG741
MAstV/Hu/BG/2009/BG747
97
100
MAstV/Hu/BRA/1994/GO-12/5a
MAstV/Sewage/VEN/2007/GuRIV/8
MAstV/Hu/MEX/2000/Yuc-8/8
MAstV/Hu/KOR/KS106207
MAstV/Hu/BG/2009/BG704
MAstVHu/IND/2004/V1182
MAstV/Hu/KOR/KS106208
MAstV/Hu/GBR/Oxford-7/7
90
83
MAstV/Hu/JPN/2010/Katano/6b
MAstV/Hu/CHN/2007/192-BJ07/6a83
0.02
(a)
Fig. 4. Phylogenetic tree of AstV sequences reconstructed with the RdRp-coding (a) and partial capsid-coding (b) regions.Bulgarian AstVs are marked with &. Genotypes according to the capsid-coding region are noted at the end of the isolatenames.
Aetiology of acute infantile diarrhoea in Bulgaria
http://jmm.sgmjournals.org 279
patients (Ganesh et al., 2012), as well as in various animalspecies with or without enteric symptoms. Nevertheless,PBVs are still rarely detected in the world, and theirprevalence ranges from 0.09 % in Argentina and 0.43 % inItaly to 2.1 % in India (Giordano et al., 2008; Cascio et al.,1996; Ganesh et al., 2010).
High prevalence of viral infections, especially with RVs,during the summer months covered by our investigationwas an interesting observation. It is in line with theincreased circulation of RVs during late summer months inBulgaria, registered since 2007 (Mladenova et al., 2010;http://www.ncipd.org/epidemiologicalbulletin). Although rarelyreported, similar RV peaks during summer have beenregistered in Spain (Boga et al., 2004) and Taiwan (Chiu
et al., 2000). In general, RVs and NoVs cause diarrhoeal
illnesses that occur year round, but predominantly during
the winter months in countries with temperate climates.
Temperature and relatively humid weather conditions have
been proposed to contribute to increased RV and NoV
infections. However, a few of the virus characteristics such as
environmental stability, heat resistance and easy transmis-
sion by the faecal–oral route foster the spread of infections
also during summer season. Diarrhoeal viruses such as RV,
NoV and AstV spread mainly through contact with infected
persons, contaminated environmental surfaces or via inges-
tion of contaminated food or water. Crowding of people and
increased person-to-person contact during the summer,
increased consumption of fresh fruit, raw vegetables, ice
MAstV/Hu/BG/2009/BG668(b)
MAstV/Hu/BG/2009/BG741
MAstV/Hu/HUN/2010/Nyergesujfalu/HUN4520/type1a
MAstV/Hu/BG/2009/BG710
MAstV/Hu/BG/2009/BG7471a
97
88
100
MAstV/Hu/USA/1999/1638/type 1a
MAstV/Hu/GBR/Oxford-1/type 1a
MAstV/Hu/GBR/1997/Oxford-S1/type 1a
MAstV/Hu/CHN/2008/SH1/type 1b
MAstV/Hu/BG/2009/BG704 1b
Type 1
98100
97
MAstV/Hu/PAK/2010/PAKNIH-3075
MAstV/Hu/BG/2009/BG703
MAstV/Hu/DEU/2004/Dresden-1/type 1d1d
MAstV/Hu/CHN/2007/192-BJ07/type 6a
MAstV/Hu/JPN/2010/Katano/type 6bType 6
100
100
99
100
type 7MAstV/Hu/GBR/Oxford-7/type 7
MAstV/Hu/CHN/2010/DL030/type 5c
MAstV/Hu/BRA/1994/GO-12/type 5a
MAstV/Hu/JPN/1993/O-1/type 5b
Type 5100
MAstV/Hu/BG/2009/BG656
MAstV/Hu/RUS/2008/Rus-Ncs08-3364/type 3a
MAstV/Hu/DEU/1999/Berlin/type 3a
MAstV/Hu/CHN/2007/WH1859/type 3b
Type 3
MAstV/Hu/GBR/Oxford-H2/type2b
100
100
MAstV/Hu/USA/1999/1299-CA/type 2c
MAstV/Hu/ITA/2009/PR5142/type 2d
MAstV/Hu/GBR/1993/Oxford-AS8811/type 2a
Type 2
type 8MAstV/Hu/MEX/2000/Yuc-8/type 8
100
98
MAstV/Hu/BRA/1995/Goiania/GO/12/type 4b
MAstV/Hu/DEU/2004/Dresden/type 4a
MAstV/Hu/CHN/2005/Guangzhou/type 4c
Type 4
89
86
100
0.02
Fig. 4. contd.
Z. Mladenova and others
280 Journal of Medical Microbiology 64

cream and sea food (mainly bivalves), attendance at recre-ational water sources or emergence of a new virus variant inthe susceptible child population may potentially be factorsthat favour the spread of virus gastroenteritis agents duringthe summer months. However, to date, we do not have adefinitive explanation for the seasonality of viral infectionsor for the differences seen in seasonal patterns betweendifferent parts of the world.
CONCLUSION
In summary, our study is, we believe, the first systematicinvestigation of the aetiology spectrum of AGE in a smallcohort of children under 3 years of age in Bulgaria, coveringdetection of 14 diarrhoeal infectious pathogens, the mostcommon viral (six), bacterial (five) and parasitic (three)agents. Infectious origin was established in 80 % of thesamples tested. Of them, viruses were detected in 75 % of thepositive samples, which confirms their leading role ascausative agents of acute childhood diarrhoea. Our studyalso revealed high morbidity associated with viral infectionsduring summer months and a significant genetic diversityamongst these pathogens, ruling out that the high prevalenceof RV or NoV was due to outbreaks. Overall, 20 % of thestool samples investigated for viral, bacterial and parasiticpathogens remained negative in all diagnostic tests per-formed. Widening of routine laboratory diagnostics towardother bacterial or viral (Clostridium difficile, entero/parecho-viruses) or new emerging viral agents (Aichi virus, bocavirus,torovirus) and the inclusion of molecular methods for theinvestigation of bacterial pathogens, in particular those thatare challenging to culture, will help improve AGE manage-ment in health care settings in Bulgaria.
ACKNOWLEDGEMENTS
This study was supported in part by R-Biopharm (Darmstadt,
Germany), who provided all the ELISA commercial kits used, and by
the EuroRotaNet project led by Dr Iturriza-Gomara, University of
Liverpool, Liverpool, UK. We thank Maria Georgieva, NCIPD-Sofia,
for her contribution to the present investigations. We are also grateful
to all staff members of the infectious wards of the Specialized Hospital
for Infectious and Parasitic Diseases ‘Prof. Ivan Kirov’ and University
Hospital ‘St Anna’, Sofia, Bulgaria, M. Tiholova, N. Naidenova, L.
Andonova, A. Mangurov, A. Nikolova, Z. Georgieva, M. Rusenova, N.
Todorova, L. Panchev and E. Badalanova, for collecting the stool
samples for this work. The authors declare no conflict of interest.
REFERENCES
Ahmed, S. M., Hall, A. J., Robinson, A. E., Verhoef, L., Premkumar, P.,Parashar, U. D., Koopmans, M. & Lopman, B. A. (2014). Global
prevalence of norovirus in cases of gastroenteritis: a systematic review
and meta-analysis. Lancet Infect Dis 14, 725–730.
Akhter, S., Turegun, B., Kiyan, M., Gerceker, D., Guriz, H. & Sahin, F.(2014). [Investigation of seven different RNA viruses associated with
gastroenteritis in children under five years old]. Mikrobiyol Bul 48,
233–241 (in Turkish).
Amar, C. F., East, C. L., Gray, J., Iturriza-Gomara, M., Maclure, E. A. &McLauchlin, J. (2007). Detection by PCR of eight groups of entericpathogens in 4,627 faecal samples: re-examination of the English case-control Infectious Intestinal Disease Study (1993–1996). Eur J ClinMicrobiol Infect Dis 26, 311–323.
Belliot, G., Laveran, H. & Monroe, S. S. (1997). Detection and geneticdifferentiation of human astroviruses: phylogenetic grouping variesby coding region. Arch Virol 142, 1323–1334.
Bhattacharya, R., Sahoo, G. C., Nayak, M. K., Saha, D. R., Sur, D.,Naik, T. N., Bhattacharya, S. K. & Krishnan, T. (2006). Molecularepidemiology of human picobirnaviruses among children of a slumcommunity in Kolkata, India. Infect Genet Evol 6, 453–458.
Boga, J. A., Melon, S., Nicieza, I., De Diego, I., Villar, M., Parra, F. &De Ona, M. (2004). Etiology of sporadic cases of pediatric acutegastroenteritis in Asturias, Spain, and genotyping and characteriza-tion of norovirus strains involved. J Clin Microbiol 42, 2668–2674.
Cascio, A., Bosco, M., Vizzi, E., Giammanco, A., Ferraro, D. & Arista,S. (1996). Identification of picobirnavirus from faeces of Italianchildren suffering from acute diarrhea. Eur J Epidemiol 12, 545–547.
Chikhi-Brachet, R., Bon, F., Toubiana, L., Pothier, P., Nicolas, J. C.,Flahault, A. & Kohli, E. (2002). Virus diversity in a winter epidemic ofacute diarrhea in France. J Clin Microbiol 40, 4266–4272.
Chiu, T. F., Lee, C. N., Lee, P. I., Kao, C. L., Lin, H. C., Lu, C. Y., Tseng,H. Y., Hsu, H. L., Lee, C. Y. & Huang, L. M. (2000). Rotavirusgastroenteritis in children: 5-year experience in a medical center.J Microbiol Immunol Infect 33, 181–186.
Colomba, C., De Grazia, S., Giammanco, G. M., Saporito, L.,Scarlata, F., Titone, L. & Arista, S. (2006). Viral gastroenteritis inchildren hospitalised in Sicily, Italy. Eur J Clin Microbiol Infect Dis 25,570–575.
de Wit, M. A., Koopmans, M. P., Kortbeek, L. M., van Leeuwen, N. J.,Vinje, J. & van Duynhoven, Y. T. (2001). Etiology of gastroenteritis insentinel general practices in The Netherlands. Clin Infect Dis 33, 280–288.
Fabiana, A., Donia, D., Gabrieli, R., Petrinca, A. R., Cenko, F., Bebeci,D., Altan, A. M., Buonomo, E. & Divizia, M. (2007). Influence of entericviruses on gastroenteritis in Albania: epidemiological and molecularanalysis. J Med Virol 79, 1844–1849.
Ganesh, B., Nataraju, S. M., Rajendran, K., Ramamurthy, T.,Kanungo, S., Manna, B., Nagashima, S., Sur, D., Kobayashi, N. &Krishnan, T. (2010). Detection of closely related picobirnavirusesamong diarrhoeic children in Kolkata: evidence of zoonoses? InfectGenet Evol 10, 511–516.
Ganesh, B., Banyai, K., Martella, V., Jakab, F., Masachessi, G. &Kobayashi, N. (2012). Picobirnavirus infections: viral persistence andzoonotic potential. Rev Med Virol 22, 245–256.
Giammanco, G. M., Rotolo, V., Medici, M. C., Tummolo, F., Bonura,F., Chezzi, C., Martella, V. & De Grazia, S. (2012). Recombinantnorovirus GII.g/GII.12 gastroenteritis in children. Infect Genet Evol12, 169–174.
Giordano, M. O., Masachessi, G., Martinez, L. C., Barril, P. A.,Ferreyra, L. J., Isa, M. B. & Nates, S. V. (2008). Two instances of largegenome profile picobirnavirus occurrence in Argentinian infants withdiarrhea over a 26-year period (1977–2002). J Infect 56, 371–375.
Gonzalez, G. G., Liprandi, F. & Ludert, J. E. (2011). Molecularepidemiology of enteric viruses in children with sporadic gastro-enteritis in Valencia, Venezuela. J Med Virol 83, 1972–1982.
Green, K. Y. (2013). Caliciviridae: the noroviruses. In Field’s Virology,6th edn, pp. 582–608. Edited by D. M. Knipe & P. M. Howley.Philadelphia: Lippincott Williams and Wilkins.
Guarino, A., Albano, F., Ashkenazi, S., Gendrel, D., Hoekstra, J. H.,Shamir, R., Szajewska, H., European Society for Paediatric
Aetiology of acute infantile diarrhoea in Bulgaria
http://jmm.sgmjournals.org 281

Gastroenterology, Hepatology, and Nutrition & European Societyfor Paediatric Infectious Diseases (2008). European Society forPaediatric Gastroenterology, Hepatology, and Nutrition/EuropeanSociety for Paediatric Infectious Diseases evidence-based guidelinesfor the management of acute gastroenteritis in children in Europe.J Pediatr Gastroenterol Nutr 46 (Suppl. 2), S81–S122.
Hansman, G. S., Oka, T., Sakon, N. & Takeda, N. (2007). Antigenicdiversity of human sapoviruses. Emerg Infect Dis 13, 1519–1525.
Hilmarsdottir, I., Baldvinsdottir, G. E., Harðardottir, H., Briem, H. &Sigurðsson, S. I. (2012). Enteropathogens in acute diarrhea: a generalpractice-based study in a Nordic country. Eur J Clin Microbiol InfectDis 31, 1501–1509.
Iturriza-Gomara, M., Dallman, T., Banyai, K., Bottiger, B., Buesa, J.,Diedrich, S., Fiore, L., Johansen, K., Koopmans, M. & other authors(2011). Rotavirus genotypes co-circulating in Europe between 2006and 2009 as determined by EuroRotaNet, a pan-European collab-orative strain surveillance network. Epidemiol Infect 139, 895–909.
Jakab, F., Varga, L., Nyul, Z., Walter, J., Berke, T., Mitchell, D. K.,Matson, D. O. & Szucs, G. (2009). Acute viral gastroenteritis amonghospitalized children between 2003 and 2005 in Baranya County,Hungary. J Clin Virol 44, 340–341.
Kageyama, T., Kojima, S., Shinohara, M., Uchida, K., Fukushi, S.,Hoshino, F. B., Takeda, N. & Katayama, K. (2003). Broadly reactiveand highly sensitive assay for Norwalk-like viruses based on real-timequantitative reverse transcription-PCR. J Clin Microbiol 41, 1548–1557.
Kojima, S., Kageyama, T., Fukushi, S., Hoshino, F. B., Shinohara, M.,Uchida, K., Natori, K., Takeda, N. & Katayama, K. (2002).Genogroup-specific PCR primers for detection of Norwalk-likeviruses. J Virol Methods 100, 107–114.
Levidiotou, S., Gartzonika, C., Papaventsis, D., Christaki, C., Priavali,E., Zotos, N., Kapsali, E. & Vrioni, G. (2009). Viral agents of acutegastroenteritis in hospitalized children in Greece. Clin Microbiol Infect15, 596–598.
Martella, V., Pinto, P., Tummolo, F., De Grazia, S., Giammanco, G. M.,Medici, M. C., Ganesh, B., L’Homme, Y., Farkas, T. & other authors(2014). Analysis of the ORF2 of human astroviruses reveals lineagediversification, recombination and rearrangement and provides thebasis for a novel sub-classification system. Arch Virol 159, 3185–3196.
Matthijnssens, J., Ciarlet, M., McDonald, S. M., Attoui, H., Banyai, K.,Brister, J. R., Buesa, J., Esona, M. D., Estes, M. K. & other authors(2011). Uniformity of rotavirus strain nomenclature proposed by theRotavirus Classification Working Group (RCWG). Arch Virol 156,1397–1413.
Mendez, E. & Arias, C. F. (2007). Astroviruses. In Fields Virology, 5thedn, pp. 982–984. Edited by D. M. Knipe, P. M. Howley & D. E.Griffin. Philadelphia: Lippincott Williams & Wilkins.
Mladenova, Z., Korsun, N., Geonova, T., Di Bartolo, I., Fiore, L. &Ruggeri, F. M. (2008). Viral agents detected in hospitalized pediatricgastroenteritis cases. Second Congress of Virology (Days of Virology inBulgaria), Sofia, 28–31 May, Proceeding and abstract book, pp. 191–198.
Mladenova, Z., Korsun, N., Geonova, T., Iturriza-Gomara, M. &Rotavirus Study Group (2010). Molecular epidemiology of rota-viruses in Bulgaria: annual shift of the predominant genotype. Eur JClin Microbiol Infect Dis 29, 555–562.
Nenonen, N. P., Hannoun, C., Larsson, C. U. & Bergstrom, T. (2012).Marked genomic diversity of norovirus genogroup I strains in awaterborne outbreak. Appl Environ Microbiol 78, 1846–1852.
Noel, J. S., Lee, T. W., Kurtz, J. B., Glass, R. I. & Monroe, S. S. (1995).Typing of human astroviruses from clinical isolates by enzyme
immunoassay and nucleotide sequencing. J Clin Microbiol 33, 797–801.
Oh, D. Y., Gaedicke, G. & Schreier, E. (2003). Viral agents of acutegastroenteritis in German children: prevalence and moleculardiversity. J Med Virol 71, 82–93.
Olesen, B., Neimann, J., Bottiger, B., Ethelberg, S., Schiellerup, P.,Jensen, C., Helms, M., Scheutz, F., Olsen, K. E. & other authors(2005). Etiology of diarrhea in young children in Denmark: a case-control study. J Clin Microbiol 43, 3636–3641.
Parashar, U. D., Gibson, C. J., Bresee, J. S. & Glass, R. I. (2006).Rotavirus and severe childhood diarrhea. Emerg Infect Dis 12, 304–306.
Parmakova, K., Asseva, G., Ivanova, K. & Petrov, P. (2012).[Surveillance of bacterial gastrointestinal infections in Bulgaria during2007–2011]. Medinfo 11, 36–38 (in Bulgarian).
Parmakova, K., Petrov, P., Asseva, G., Mladenova, Z. & Harizanov, R.(2013). [Gastrointestinal infections in childhood]. Medinfo 8, 1–4 (inBulgarian).
Pereira, H. G., Flewett, T. H., Candeias, J. A. & Barth, O. M. (1988). Avirus with a bisegmented double-stranded RNA genome in rat(Oryzomys nigripes) intestines. J Gen Virol 69, 2749–2754.
Rimoldi, S. G., Stefani, F., Pagani, C., Chenal, L. L., Zanchetta, N., DiBartolo, I., Lombardi, A., Ruggeri, F. M., Di Lillo, D. & other authors(2011). Epidemiological and clinical characteristics of pediatricgastroenteritis associated with new viral agents. Arch Virol 156,1583–1589.
Sanchez-Fauquier, A., Montero, V., Colomina, J., Gonzalez-Galan,V., Aznar, J., Aisa, M. L., Gutierrez, C., Sainz de Baranda, C. &Wilhelmi, I. (2011). Global study of viral diarrhea in hospitalizedchildren in Spain: results of structural surveillance of viralgastroenteritis net work (VIGESS-net) 2006–2008. J Clin Virol 52,353–358.
Sethi, S. K., Khuffash, F. A. & al-Nakib, W. (1989). Microbial etiologyof acute gastroenteritis in hospitalized children in Kuwait. PediatrInfect Dis J 8, 593–597.
Shoja, Z., Jalilvand, S., Mollaei-Kandelous, Y. & Validi, M. (2014).Epidemiology of viral gastroenteritis in Iran. Pediatr Infect Dis J 33,218–220.
Soriano-Gabarro, M., Mrukowicz, J., Vesikari, T. & Verstraeten, T.(2006). Burden of rotavirus disease in European Union countries.Pediatr Infect Dis J 25 (Suppl.), S7–S11.
Tam, C. C., O’Brien, S. J., Tompkins, D. S., Bolton, F. J., Berry, L.,Dodds, J., Choudhury, D., Halstead, F., Iturriza-Gomara, M. & otherauthors (2012). Changes in causes of acute gastroenteritis in theUnited Kingdom over 15 years: microbiologic findings from 2prospective, population-based studies of infectious intestinal disease.Clin Infect Dis 54, 1275–1286.
Tamura, K., Dudley, J., Nei, M. & Kumar, S. (2007). MEGA4:molecular evolutionary genetics analysis (MEGA) software version4.0. Mol Biol Evol 24, 1596–1599.
Tiemessen, C. T. & Nel, M. J. (1996). Detection and typing ofsubgroup F adenoviruses using the polymerase chain reaction. J VirolMethods 59, 73–82.
Vinje, J., Deijl, H., van der Heide, R., Lewis, D., Hedlund, K. O.,Svensson, L. & Koopmans, M. P. (2000). Molecular detection andepidemiology of Sapporo-like viruses. J Clin Microbiol 38, 530–536.
Youssef, M., Shurman, A., Bougnoux, M., Rawashdeh, M., Bretagne,S. & Strockbine, N. (2000). Bacterial, viral and parasitic entericpathogens associated with acute diarrhea in hospitalized childrenfrom northern Jordan. FEMS Immunol Med Microbiol 28, 257–263.
Z. Mladenova and others
282 Journal of Medical Microbiology 64
Copyright © 2022 FDOKUMEN