
“What do you want me to tell?” The inferential texture of Alice ...
Cognitive Therapy and Research, Vol. 28, No. 4, August 2004 ( C© 2004), pp. 487–509
Adaptive Inferential Feedback, DepressogenicInferences, and Depressed Mood: A Laboratory Studyof the Expanded Hopelessness Theory of Depression
Roseanne DeFronzo Dobkin,1,6 Catherine Panzarella,2 Jennifer Fernandez,3
Lauren B. Alloy,4 and Michele Cascardi5
Cross-sectional and prospective research indicates that inferential feedback, a subtypeof social support that addresses the cause, meaning, and consequences of negative lifeevents, impacts depressed mood, depressogenic inferences, and depressive disorders.However, inferential feedback has not been manipulated in any prior study makingit difficult to determine if it plays a causal role in depression. The current studyrepresents the first controlled test of the role of adaptive inferential feedback in thereduction of depressive symptoms and depressogenic cognitive inferences. Individualswho received adaptive inferential feedback following a stressful life event demon-strated the greatest decreases in dysphoria and depressogenic inferences followingthe receipt of feedback compared to individuals who received other types of socialsupport. Moreover, decreases in dysphoria were partially mediated by decreases indepressogenic inferences. The role of adaptive inferential feedback as a clinical toolin prevention and intervention programs is emphasized.
KEY WORDS: social support; adaptive inferential feedback; depression; inferential style.
It has been suggested that the promise of social support research is thatnaturally occurring support relations can help to prevent and decrease distress andreduce the need for formal psychological intervention (Lakey & Drew, 1997; Lakey& Lutz, 1996). Although it is well documented that social support exerts a salubriousimpact on depression (e.g., Barnett & Gotlib, 1988; Cohen & Wills, 1985; Roberts& Gotlib, 1997), broad definitions of social support and vague mechanisms of actionfor the effect of social support on depression has made it difficult to develop specific
1Department of Psychiatry, UMDNJ/Robert Wood Johnson Medical School, Piscataway, New Jersey.2City of Philadelphia, Office of Behavioral Health, Philadelphia, Pennsylvania.3Department of Psychology, Drexel University, Philadelphia, Pennsylvania.4Department of Psychology, Temple University, Philadelphia, Pennsylvania.5Independent Consultant.6Correspondence should be directed to Roseanne DeFronzo Dobkin, PhD, Department of Psychiatry,UMDNJ/Robert Wood Johnson Medical School, 675 Hoes Lane, Room D-317, Piscataway, New Jersey08855; e-mail: [email protected].
487
0147-5916/04/0800-0487/0 C© 2004 Springer Science+Business Media, Inc.

488 DeFronzo Dobkin, Panzarella, Fernandez, Alloy, and Cascardi
social support interventions that could be incorporated into mental health programsto enhance their efficacy.
Recently, a subtype of social support, “inferential feedback,” that addressesthe cause, meaning, and consequences of negative life events, was proposed andoperationally defined within the context of an Expanded Hopelessness Theory ofdepression (Panzarella & Alloy, 1995; Panzarella, Alloy, & Whitehouse, 2004).Moreover, three precise mechanisms through which inferential feedback mayinfluence the development of depression were supported in longitudinal (Panzarellaet al., 2004) and cross-sectional studies (DeFronzo, Panzarella, & Butler, 2001).Specifically, adaptive inferential feedback has been found to be associated withthe experience of fewer and less severe negative life events, the formulation offewer depressogenic inferences in response to stressors and a decreased abilityto maintain a negative inferential style over time. However, because adaptiveinferential feedback had not been manipulated in any of these studies, it was notpossible to determine if it plays a causal role in depression. The current studyrepresents the first controlled test of the role of adaptive inferential feedback in thereduction of depressive symptoms and depressogenic cognitive inferences. Evidenceof a causal relationship will lend further support to the Expanded HopelessnessTheory and its implications for harnessing adaptive inferential feedback as partof intervention and prevention programs. Preliminary research regarding the Ex-panded Hopelessness Theory of depression, the concept of adaptive inferentialfeedback, and the three mechanisms by which adaptive inferential feedback mayameliorate depressed mood and negative cognitions are described in detail below.
EXPANDED HOPELESSNESS THEORY OF DEPRESSION
The Expanded Hopelessness Theory of depression (Panzarella et al., 2004;Panzarella & Alloy, 1995) elaborates on the possibility that social processes, inaddition to cognitive processes and stress, contribute to vulnerability to depression(see Abramson, Metalsky, & Alloy, 1989, for a description of Hopelessness Theory).In the Expanded Hopelessness Theory, a subtype of social support, inferential feed-back (that exists along an adaptive to maladaptive continuum), was identified andthe specific mechanisms through which inferential feedback may impact depressivesymptoms and diagnoses were tested.
Adaptive inferential feedback (AIF) occurs when a supporter attributes thecause of a negative event to unstable, specific factors instead of stable, global factors.Adaptive inferential feedback also occurs when the supporter suggests that theevent neither implies negative consequences nor negative characteristics about theperson. AIF directly modifies maladaptive thinking by providing alternatives todepression-inducing inferences, thereby decreasing the likelihood that an individualwill become hopeless in the face of a negative life event. In other words, adaptiveinferential feedback reduces hopelessness and depression by countering depresso-genic inferences for negative life events.
For example, a woman might make the following statement to a friend follow-ing a relationship break-up: “I will never find a good partner. I must be unlovable.”
A Lab Test of the EHT of Depression 489
The friend could respond by saying, “Having problems in one relationship doesnot make you unlovable and does not mean that you will not have a successfulrelationship in the future. You are a warm, caring person.”
The friend’s response would be considered adaptive inferential feedback. Thefriend has suggested that the cause of the breakup is unstable (e.g., problemsin one relationship) and that this one bad relationship does not imply negativeconsequences for the future (e.g., will have a successful relationship in the future)or negative characteristics about the self (e.g., does not mean that she is unlovable).The provision of these alternative, adaptive inferences helps to counter the devel-opment of hopelessness and symptoms of depression, which are the hypothesizedresults of maladaptive, depressogenic inferences. Alternatively, if the friend hadprovided feedback that supported the woman’s depressogenic inferences (e.g., “It’simpossible to find a partner these days”) this would be considered maladaptiveinferential feedback.
It is also important to mention that the friend could have provided positivesocial support that is not adaptive inferential feedback. For example, the friendcould have stated, “Forget about him. We will go out to dinner tonight and youwon’t even think about him.” This type of support may be beneficial as the friendis offering to keep her company and focus her attention on other areas of her life.However, unlike adaptive inferential feedback, this type of support does not directlycounter depressogenic cognitions through the provision of alternative, adaptiveinferences. In addition, whereas “constructive criticism” and “corrective feedback”might be considered “adaptive” in certain situations, especially where behaviorchange might be required to alter outcomes, these types of social exchanges do notmeet the theoretical definition of adaptive inferential feedback and their discussionis beyond the scope of the current paper. “Adaptive” in the context of the ExpandedHopelessness Theory of depression refers to the reduction of immediate risk forhopelessness and depressive symptoms by altering or weakening depressogenicinferences, not to behavior changes that might directly alter future circumstancesor to other possible mechanisms for reducing depressive affect.
Panzarella and Alloy (1995) proposed three mechanisms by which inferentialfeedback may impact the onset and maintenance of depression in general andhopelessness depression in particular (Fig. 1). First, social support in general maydecrease the number and severity of stressful events that an individual experiences.For example, a mother may be struggling to find childcare. Yet, this event maynot be perceived as stressful if the mother has friends who offer to baby-sit.Second, individuals who consistently attribute the cause of negative life events tostable/global factors and infer that the event implies negative consequences aboutthe future and negative characteristics about the self have been described as having adepressogenic inferential style (Abramson, Metalsky, & Alloy, 1989). This cognitivestyle is a risk factor for depression as it increases the likelihood that an individualwill make negative inferences when confronted with a stressful situation. However,adaptive inferential feedback may buffer against the development of depressionby decreasing a person’s likelihood of maintaining a depressogenic inferential styleover time. The more that a person’s negative thoughts are challenged and adaptiveinferences are provided, the less likely he or she will be to think in a persistently

490 DeFronzo Dobkin, Panzarella, Fernandez, Alloy, and Cascardi
Fig. 1. The Expanded Hopelessness Theory of depression.
negative way. Third, adaptive inferential feedback may decrease the likelihood thatan individual will make depressogenic inferences in certain situations, regardlessof inferential style. Even if people generally attribute the cause of negative lifeevents to stable and global factors, they may make more adaptive inferences incertain situations when provided with adaptive inferential feedback. For example,an employee with a cognitive vulnerability in the achievement domain may con-sistently attribute “average” performance reviews at work to lack of intelligence.Adaptive inferential feedback from a coworker following a particular evaluation,which suggests that the supervisor set unrealistic performance standards that allemployees had problems meeting, might lead the employee to make healthierinferences about this particular evaluation, even though the employee tends to makedepressogenic inferences about job performance in general. Conversely, a personwho does not have a depressogenic inferential style may still be more vulnerable todepressive reactions in response to a particular event when inferential feedback isnegative.
Evidence for the Expanded Hopelessness Theory
Panzarella and Alloy (1995) initially tested the Expanded Hopelessness Theoryin a prospective/longitudinal study. College undergraduates, classified as eitherhigh or low risk for the development of depression, based on the presence orabsence of a depressogenic inferential style and dysfunctional attitudes, werefollowed for nine months. The students had no depressive disorders at the start of

A Lab Test of the EHT of Depression 491
the study. Every 6 weeks, the students completed self-report measures of stress,cognitions, and depressive symptoms. In addition, students were interviewed at6-week intervals by trained clinical researchers to assess onsets/offsets and severityof any depressive symptoms and diagnoses that developed, as well as to pinpointonset/offset dates of stressful life events and cognitions such as hopelessness. Every12 weeks (every other assessment), participants completed measures of adaptiveinferential feedback.
Panzarella and Alloy (1995) found evidence consistent with the three pro-posed mechanisms of inferential feedback on hopelessness, depressive symptoms,and depressive disorders. In support of the first mechanism, adaptive inferentialfeedback was associated with fewer and less severe negative life events. Moreover,inferential feedback predicted changes in stressful events over time, whereas stressdid not predict changes in inferential feedback over time. In support of the secondmechanism, a depressogenic inferential style was associated with less adaptiveinferential feedback and inferential feedback predicted change in inferential styleover time, controlling for negative life events. Consistent with the third mechanism,individuals who received adaptive inferential feedback made more adaptive infer-ences for actual negative life events that occurred recently than those who did notreceive adaptive feedback, regardless of inferential style. Inferential feedback alsoexplained variance in ensuing hopelessness, depressive symptoms, and diagnoses ofdepressive disorders after controlling for negative inferential styles, suggesting thatthe effect of inferential feedback was not merely reflective of inferential style (withself-reported social support, it is not possible to determine the extent to which socialfactors vs. subjective interpretation of them influence reporting).
Additional studies have also shown that the receipt of adaptive inferentialfeedback is associated with lower risk for depression, hopelessness, and dysfunc-tional attitudes (e.g., Alloy et al., 2001; Crossfield, Alloy, Gibb, & Abramson,2002; DeFronzo & Panzarella, 1999, 2000; DeFronzo, Panzarella, & Butler, 2001).Moreover, inferential feedback has been found to explain depressive symptomsover and above other known contributors such as global perceptions of socialsupport, unmet support needs, depressogenic inferential style, and stressful lifeevents (e.g., Panzarella et al., 2004). Thus, inferential feedback appears to be apromising construct to examine as it exerts an impact on depressive symptoms overand above that which can be explained by other social-cognitive factors.
CURRENT STUDY
Although the initial tests of the Expanded Hopelessness Theory appear promis-ing, preliminary empirical evidence derived from studies of naturally occurringevents and social support do not allow for the experimental control required to infera causal link between inferential feedback, depressogenic inferences, and depressivesymptoms. Adaptive inferential feedback has not been manipulated in any previousstudy, making it difficult to isolate its role in the prevention or alleviation ofdepressive symptoms. If a causal relationship between adaptive inferential feedbackand depressed mood and depressogenic inferences emerges in a laboratory setting

492 DeFronzo Dobkin, Panzarella, Fernandez, Alloy, and Cascardi
that utilizes natural supporters, adaptive inferential feedback training may holdpromise as an intervention tool.
Thus, social support (adaptive inferential feedback vs. other types of socialsupport vs. no support) was manipulated in the current study and feelings ofdysphoria and inferences following the receipt of social support after a stressfulevent were the dependent variables. Inferential style, baseline depressive symptoms,expectations for performance on an academic task, the quality of the relationshipbetween the support provider and support recipient, and the type of inferentialfeedback received in response to a recent negative life event were also measuredas these variables could potentially influence feelings of dysphoria, inferences,and the impact of social support in the laboratory setting (Alloy et al., 1999;Follette & Jacobson, 1987; Metalsky, Abramson, Seligman, Semmel, & Peterson,1982; Sarason, Sarason, & Gurung, 1997). Rather than use confederates, naturalsupporters were trained to provide differing types of social support in order toduplicate as closely as possible a real-life support exchange in the context of alaboratory paradigm. Because, by definition, social support usually occurs in thenatural social environment, it is not clear if the results of laboratory studies thatutilize confederates who are strangers to provide feedback can be generalized tounderstand individuals’ reactions to feedback from significant others.
Hypothesis 1. It was expected that individuals who received adaptive inferen-tial feedback would show the greatest decrease in dysphoria from Time 1(poststressor) to Time 2 (postsupport), compared to those who received gen-eral/nonspecific social support without an adaptive inferential feedback compo-nent or no social support.
Hypothesis 2. It was expected that individuals who received adaptive inferentialfeedback would experience the greatest decrease in depressogenic inferencesfrom Time 1 (poststressor) to Time 2 (postsupport), compared to those whoreceived general/nonspecific social support without an adaptive inferential feed-back component or no social support.
Hypothesis 3. It was expected that the change in dysphoria (from Time 1 to Time 2)would be partially mediated by the change in inferences (from Time 1 to Time 2)following the receipt of social support.
METHOD
Participants
One hundred sixty-three undergraduate students completed preliminary studyquestionnaires. One hundred fifty of these people returned to complete the secondphase of the study with a partner. The target member of each pair (the supportrecipient; 30 men, 137 women) was an undergraduate student from a diverse urbanuniversity. The partners (support providers; 48 men, 99 women) were either under-graduate students or friends or relatives that were not currently attending college.Individuals received either course credit or monetary compensation ($10.00) forparticipating in the study.

A Lab Test of the EHT of Depression 493
Individuals who expressed suicidal ideation by endorsing answer choices #2 or#3 on item 9 of the Beck Depression Inventory (BDI; 2 = I would like to kill myself,3 = I would kill myself if I had the chance) or received a score >25 on the BDI wereexcluded from participation in the study, as it was judged unethical to expose theseindividuals to a negative mood induction. Three individuals scored >25 on the BDI.In these cases, a risk assessment was conducted and an appropriate referral wasmade.
Materials
Target participants completed a 35-item cognitive abilities test that containedlogic, math, analogy, and vocabulary problems that were selected from various“intelligence tests,” which were posted on the Internet Majon online IQ tests;Seriously entertaining IQ tests. Twenty-five of the questions on the test weredifficult, but solvable with ambiguous answer choices. Ten questions that could besolved with greater ease were also included. Failure feedback received on similartypes of cognitive abilities tests has been found to negatively impact mood (e.g.,Chartier & Ranieri, 1989; Doherty & Schlenker, 1995; Houston, 1995; Mehlman &Synder, 1985; Stiensmeier-Pelster, 1989).
Consistent with previous findings, pilot testing on a separate sample of 19individuals indicated that participants reported significantly more dysphoria, asassessed by the Multiple Affect Adjective Checklist (Zuckerman & Lubin, 1965),after taking this cognitive abilities test and receiving false feedback about theirperformance (Time 1, M = 16.53, SD = 6.19) than they did prior to the cognitiveabilities test (Time 0, M = 11.79, SD = 5.96), t(18) = 5.15, p < .01.
Measures
Adaptive Inferential Feedback Questionnaire (AIFQ; Panzarella & Alloy, 1995)
The AIFQ (α = .90 in current sample) is a four-question scale that examinesthe extent to which members of an individual’s social network support or refute anindividual’s depressogenic inferences about a negative life event. The AIFQ targetsthe following dimensions: the globality and stability of the cause of the negative lifeevent, future consequences, and meaning about the self. All items are rated on a 5-point scale. For example, respondents are asked to rate “What did person 1, person2, and person 3 indicate to you about whether the cause of this stressor has to dowith this particular circumstance or if it will lead to problems in other areas of yourlife” (e.g., 5 = completely unlikely to lead to problems in other areas of my life; 3 =somewhat unlikely to lead to problems in other areas of my life; 0 = completely likelyto lead to problems in other areas of my life; see Fig. 2 for additional examples). Atotal inferential feedback score is comprised by calculating an average score for thetype of feedback received, on each dimension, and then adding across dimensions.High scores are indicative of adaptive inferential feedback whereas low scores areindicative of maladaptive inferential feedback. In the current study, the AIFQ was

494 DeFronzo Dobkin, Panzarella, Fernandez, Alloy, and Cascardi
Fig. 2. Examples of questions from the Adaptive Inferential Feedback Questionnaire.
used to assess the type of inferential feedback that individuals had recently receivedfrom members of their natural support network in response to a negative lifeevent.

A Lab Test of the EHT of Depression 495
Cognitive Style Questionnaire (CSQ; Alloy et al., 2000)
The CSQ (α = .93 in current sample) is a measure of inferential style, derivedfrom a revised version of the Attributional Style Questionnaire (ASQ; Peterson& Villanova, 1988; Seligman, Abramson, Semmel, & von Baeyer, 1979), which istailored specifically for use with college students (Alloy et al., 2000). The CSQcontains 12 positive and 12 negative hypothetical events and requires respondentsto write down their perception of the cause of the event presented, allowing forthe assessment of a depressogenic inferential style. Individuals rate the cause thatthey provided for the hypothetical event on the following attributional dimensionson a scale ranging from 1 to 7: internal/external, stable/unstable, global/specific.Individuals also rate the extent to which they believe that future negative conse-quences will result from the hypothetical events, as well as the degree to whichthey believe that the event implies negative meaning about the self. The compositescore for attributions for negative events, which is thought to be most representativeof an individual’s general inferential style, was used in the current study (Alloyet al., 1999). The internality dimension was not included in the CSQ negative eventscomposite score to be consistent with the Inference Questionnaire composite, whichis described below.
Expectation Questionnaire (DeFronzo, Panzarella, & Alloy, 2000)
The Expectation Questionnaire was designed for descriptive purposes for thecurrent study in order to assess participants’ expectations for their performanceon the cognitive abilities test on a scale ranging from the 1st to 100th percentile(five percentile point intervals; α = .61). The scale consisted of three questionswhich included, “In which percentile bracket do you hope to score on this test?”;“A score in which percentile bracket would make you happy?”; “A score in whichpercentile bracket would make you unhappy?” Each percentile bracket was codedwith a number ranging from 1 (1st–5th percentile) to 20 (95th–100th percentile) suchthat higher code numbers represent higher expectations.
Beck Depression Inventory (BDI; Beck, Rush, Shaw, & Emery, 1979)
The BDI (α = .81 in current sample) is a 21-item self-report questionnaire thatmeasures cognitive, motivational, somatic, and affective symptoms of depression, aswell as the severity of each symptom, on a scale ranging from 0 to 3 (Beck et al.,1979). It has been found to be a reliable and valid measure of depressive symptomswith both psychiatric and normal patients (Beck et al., 1988).
Relationship Questionnaire (DeFronzo & Cascardi, 2000)
Participants were asked the following three questions for descriptive purposes(α = .66): “Please describe your relationship to your partner in this study?” (1 =acquaintance, 2 = friend, 3 = best friend, 4 = family member); “How long have youknown your partner in this study?” (1 = less than 1 week, 2 = less than 1 month,3 = less than 6 months, 4 = less than 1 year, 5 = less than 5˜years, 6 = more than5˜years); “How comfortable are you discussing your thoughts and feelings with your

496 DeFronzo Dobkin, Panzarella, Fernandez, Alloy, and Cascardi
partner in this study?” (0 = very uncomfortable, 3 = somewhat comfortable, 5 = verycomfortable).
Multiple Affect Adjective Checklist (MAACL; Zuckerman & Lubin, 1965)
The depression subscale score of the MAACL was used to assess dysphoria inthe current study (α = .80 in current sample). The MAACL depression subscalehas demonstrated sensitivity to fluctuations in mood states following natural (e.g.,midterm exams) and laboratory stresses (e.g., Abela & Seligman, 2000; Alloy,Abramson, & Viscusi, 1981; Alloy & Clements, 1992; Follette & Jacobson, 1987;Houston, 1995; Metalsky et al., 1982; Metalsky, Halberstadt, & Abramson, 1987;Sacks & Bugental, 1987). It has been recommended for use in laboratory experi-ments that induce stress reactions and require a before and after measure of affect(Zuckerman & Lubin, 1965).
Inference Questionnaire (IQ; Alloy & Abramson, 1999)
The IQ is an 11-item measure that assesses the inferences that individuals makefor recent negative life events that have been experienced on the following dimen-sions: causality, consequences, characteristics about the self, and controllability ofthe event. For example, participants are asked to rate if the cause of the negativelife event will cause similar problems in the future, on a scale ranging from 0 to 4(e.g., 0 = will never again cause similar problems in the future, 4 = will always causesimilar problems in the future). A 4-item composite that consists of items pertainingto stability, globality, negative consequences, and negative meaning about the selfwas used in the current study and in a previous study (Panzarella & Alloy, 1995),given that these are the four types of inferences that adaptive inferential feedbackdirectly targets (α = .82 in current sample).
Adaptive Inferential Feedback Questionniare 2
A modified version of the AIFQ (AIFQ2) that contained three questions aboutsocial feedback (α = .74) was also used in the current study. Participants were askedto rate if the feedback received from their partner made them feel “better, worse,or the same” about their performance on the cognitive abilities test and the degreeto which they felt supported and understood by their study partners.
Procedure
All individuals participated in the experiment with a partner (e.g., friend, class-mate, family member). Target participants were randomly assigned to receive eitheradaptive inferential feedback (N = 52), general/nonspecific social support that didnot contain an adaptive inferential feedback component (N = 49), or no socialsupport following the academic failure experience (N = 46). Group compositionwas equivalent regarding potential confounding variables such as cognitive style,relationship quality, baseline depressive symptoms, type of social support recentlyreceived, and expectations for the academic task, as indicated in Table I.
At least one day prior to the lab study, target participants completed measuresof inferential style, and the amount of inferential feedback that was received in

A Lab Test of the EHT of Depression 497
Table I. Check on Random Assignment
Variable F df p
Recent Adaptive Feedback (AIFQ) 0.845 2, 65 .43Depressive Symptoms (BDI) 0.245 2, 123 .78Cognitive Style (CSQ) 2.39 2, 123 .10Nature of Relationship with Partner (RQ) 1.38 2, 122 .26Length of Relationship with Partner (RQ) 1.59 2, 122 .21Comfort Level with Partner (RQ) 1.09 2, 122 .34Expected Score (EQ) 2.27 2, 123 .11“Happy” Score (EQ) 2.98 2, 123 .06“Unhappy” Score (EQ) 1.70 2, 123 .19
response to a recent negative life event (Time 0). On the day of the experiment,target participants reported to the lab with a partner. Individuals were informedthat the study was being conducted to determine the relationship between anindividual’s personality and his or her performance on a test of intelligence andproblem solving that predicts professional success. Target participants and partnerswere separated upon entry into the lab, and told that they needed to completeseparate tasks for parts of the study but would participate in activities togetherduring other parts of the study.
Target participants first completed measures of mood (MAACL, BDI, Time 0).They were then read a standard script that explained the nature and purpose of thecognitive abilities test that they were about to complete (e.g., scores above the 75thpercentile predict professional success). Participants were next asked to complete ameasure of their expectations for their performance on the cognitive abilities test(Time 0), target.
The participants were then given 30 min to complete the test. The examinerthen “scored” the exam in a separate room and informed the participant that he/shereceived a score 19 percentile points lower than would make him/her unhappy asindicated by the Expectation Questionnaire. Scores 19 points below expectationshave been assigned to individuals in other laboratory tests of the HopelessnessTheory of depression (Houston, 1995), as 19 is a fairly large, yet uncommonnumber. Because a standard number was subtracted from all participants’ percentilescore that would make them unhappy, individuals should have been “equally”disappointed in their scores. Participants were then asked to complete measuresof mood (MAACL) and inferences about the task (Time 1).
While the participants were completing the cognitive abilities test, the partnersin the adaptive inferential feedback and general/nonspecific social support groups(e.g., active support conditions) were informed that they would soon be asking thetarget participants to discuss their thoughts and feelings about their performance onan intelligence test that predicts professional success. These partners were trainedto offer either adaptive inferential feedback or general/nonspecific social supportin response to the target participants’ comments. As part of this 30-min training,a series of worksheets were completed and role-plays were conducted in order tohelp the partners naturally generate statements tailored to the support condition towhich they were assigned and to refrain from offering the type of social support thatwas being provided in the alternative active condition. The partners were informedof the deception that was being utilized in the study, but were encouraged to come

498 DeFronzo Dobkin, Panzarella, Fernandez, Alloy, and Cascardi
across as genuine as possible, and not to tell the participants about the deception orto exacerbate the participants’ distress. All partners agreed to these guidelines. Thepartners in the no social support condition were provided with magazines to readduring the support training portion of the experiment.
The target participants and partners were reunited after the cognitive abilitiestest and social support training had been completed in the active social supportconditions and were given 2 min to discuss the experience with the cognitive abilitiestest. The research assistant left the room during this time and the conversationbetween participants and partners was tape-recorded. Individuals in the no socialsupport condition remained separated from their partners until debriefing. They satalone for the same 2-min period of time that social support was exchanged in theother two conditions.
After the 2-min social support manipulation, target participants were informedthat they would be completing a general informational interview with anotherresearcher. This statement was made so that participants were not aware that thesocial support was the last active phase of the study. The partners then left the roomand the participants sat alone for 5 min waiting to complete the “next interview.”(The individuals in the no social support condition sat alone for 7 min since theydid not receive the 2-min support intervention.) Target participants were thenasked to complete measures of mood (MAACL) inferences about the task and toindicate how helpful they felt the social support was, and how comfortable they felttalking with their partner in the study (Time 2). Participants and partners were thenreunited and debriefed.
Following the lab interaction, coders blind to condition reviewed all tapes todetermine the quantity and type of social support offered. At minimum, all partnerswere required to make at least one support statement consistent with their assignedcondition for the case to be retained. In order to isolate the construct of adaptiveinferential feedback (AIF), cases from the nonspecific condition were also excludedif any AIF had been exchanged during the 2-min interaction. Although partners inthe AIF condition were discouraged from offering nonspecific support, they werenot excluded for doing so as long as greater than 50% of the support offered wascoded as AIF. This allowance was made as it is difficult and artificial to removeall components of nonspecific support (e.g., empathy, reflective listening) from anatural dialogue. Nine AIF and 12 nonspecific cases were eliminated due to theprovision of insufficient or unspecified support. Included in the final analysis were43 adaptive inferential feedback, 37 general/nonspecific, and 46 control cases.
Throughout the remainder of the paper, Time 0 refers to baseline, Time 1 refersto postacademic stressor, and Time 2 refers to postsupport.
RESULTS
Overview of Social Support Manipulation
The majority of target participants completed the second part of the study witha friend (52.3%) or a best friend (28.1%). An overwhelming majority (92.3%) ofthe participants felt comfortable with their partners; 86.5% of the participants knew

A Lab Test of the EHT of Depression 499
their partner for at least 1 month, whereas approximately 50% of the participantsknew their partner for at least 1 year.
The number and type of social support statements offered by partners in eachgroup were determined by the ratings completed by two coders blind to conditionafter their review of the transcriptions of the 2-min audiotaped interactions. In-terrater reliability was 100% for social support condition and 94% for number ofsupport statements offered. Partners in the adaptive inferential feedback conditionoffered significantly more adaptive inferential feedback statements than partnersin the general support condition, t(78) = 9.63, p < .01, while partners assignedto the general support condition offered significantly more nonspecific supportstatements than those in the adaptive inferential feedback group, t(78) = 10.57,p < .01. Partners in the nonspecific group offered more support statements thatwere consistent with their assigned condition than those in the adaptive inferentialfeedback group, t(78) = 6.29, p < .01. However, partners in the adaptive inferentialfeedback condition offered significantly more total, t(78) = 2.73, p <.01, and uniquesupport statements (e.g., did not repeat the exact same words verbatim), t(78) =2.98, p < .01, than those in the general/nonspecific condition, despite equivalenttraining procedures. It is important to note that covarying these variables (numberof total and unique support statements) out of subsequent analyses yielded nosignificant effects, indicating that they were not confounds in the analyses reportedbelow.
Participants who received adaptive inferential feedback reported that they feltsignificantly “better” about their experience with the cognitive abilities test, afterspeaking with their partner, than individuals who received nonspecific support,t(77) = 2.10, p = .04. Participants who received adaptive inferential feedback alsoreported feeling more supported, t(78) = 2.83, p < .01, and understood by theirpartners, t(78) = 3.5, p < .01, than those who received nonspecific support. Means,standard deviations, and ranges regarding group comparisons for all variablesassociated with the social support manipulation can be found in Table II.
Manipulation Check of the Cognitive Abilities Test (Academic Stressor)
A 3 (Group; adaptive inferential feedback, nonspecific support, no support)by 2 (Time; Time 0, Time 1) Repeated Measures ANOVA was conducted toexamine the impact of the academic stressor on dysphoric mood. As expected, therewas a significant main effect of time on mood such that all participants reportedsignificantly more dysphoric mood following the academic failure experience than
Table II. Overview of Social Support Manipulation
Adaptive feedback Nonspecific support
Variable Mean SD Range Mean SD Range
Total no. of support statements 11.47 7.01 1–35 7.97 3.61 2–17No. of nonspecific 1.51 1.60 0–7 7.97 3.61 2–17No. of adaptive feedback 9.95 6.28 1–34 0.00 0.00 0Total no. of unique statements 8.88 4.48 1–19 6.38 2.63 2–15% Consistent with condition 87.56 12.00 57–100 100.00 0.00 0

500 DeFronzo Dobkin, Panzarella, Fernandez, Alloy, and Cascardi
Table III. Means, Standard Deviations, and Change Scores of Dysphoria and Depressogenic InferencesAcross Social Support Groups and Time Points
Dysphoria Inferences
Social support group Time 1 Time 2 Change Time 1 Time 2 Change
No support(Control)
19.28 (6.07) 18.27 (6.07) 1.01 2.76 (2.94) 2.48 (2.67) 0.28
General/nonspecific 17.64 (5.62) 17.11 (5.65) 0.53 2.41 (2.44) 2.05 (2.51) 0.36Inferential feedback 20.38 (5.67) 17.66 (5.12) 2.72 2.77 (2.93) 1.93 (2.19) 0.84
they endorsed prior to the stressor, F(1, 123) = 77.37, p < .01. There was no maineffect of group, F(2, 123) = 2.33, p = .11, and the groups were not differentiallyimpacted by the academic stressor as indicated by the nonsignificant Group by Timeinteraction, F(2, 123) = 2.09, p = .13.
Hypothesis 1
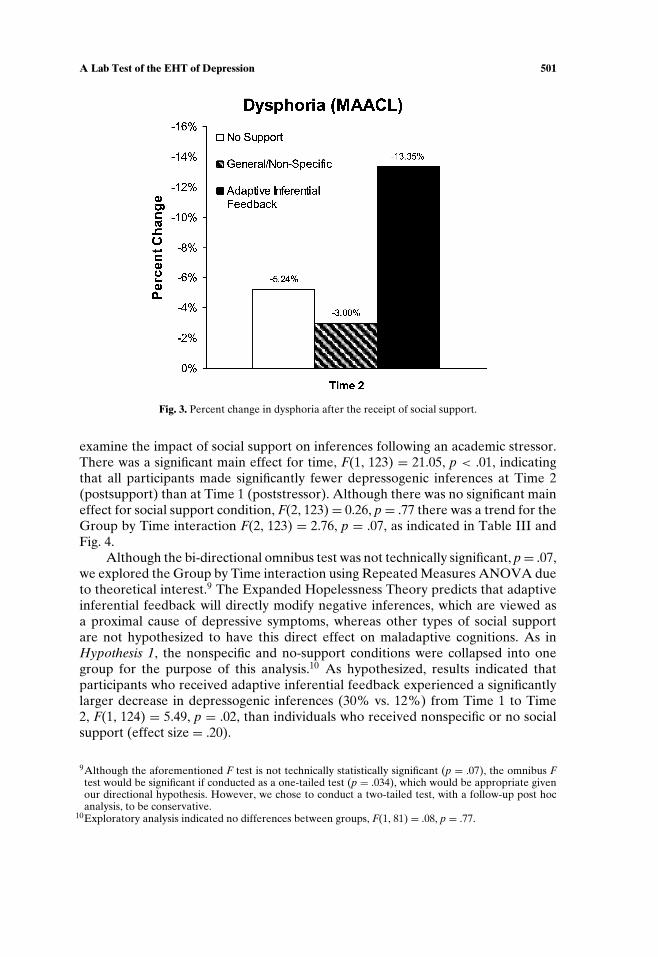
A 3 (Group; adaptive inferential feedback, nonspecific support, no support)by 2 (Time; Time 1, Time 2) Repeated Measures Analysis of Covariance wasconducted to examine differences in dysphoria between time points and socialsupport conditions, controlling for baseline mood (MAACL Time 0). There wasa significant main effect of time, F(1, 122) = 14.41, p < .01, which indicated that allindividuals were significantly less distressed postsupport (Time 2) than they werepoststressor (Time 1). Although no main effect for group, F(2, 122) = 1.72, p =.18, was observed, the time by social support group interaction term was statisticallysignificant, F(2, 122) = 3.91, p = .02, indicating that the individuals in the variousgroups were differentially impacted by the receipt of social support, as indicated inTable III and Fig. 3.
A Repeated Measures Analysis of Covariance was conducted to examine thesource of the Group by Time interaction. The nonspecific support and no-supportconditions were collapsed into one group for the purpose of this analysis.7 Asexpected, the Time by Group interaction term was statistically significant when com-paring the adaptive inferential feedback group to the nonspecific and no-supportconditions, F(1, 123) = 7.54, p < .01. Inspection of means showed that individualswho received adaptive inferential feedback demonstrated a larger reduction (13%vs. 4%) in dysphoric mood from poststressor (Time 1) to postsupport (Time 2) thanindividuals who received nonspecific or no social support (effect size = .34).8
Hypothesis 2
A 3 (Group; adaptive inferential feedback, nonspecific support, no support)by 2 (Time; Time 1, Time 2) Repeated Measures ANOVA was conducted to
7Exploratory analysis indicated no difference between the nonspecific and no-support conditions,F(1, 80) = 0.32, p = .52.
8Effect size was calculated by subtracting the change score in nonspecific/no-support group from thechange score in adaptive feedback group and dividing by the pooled standard deviation across socialsupport groups and time points in both Hypotheses 1 and 2 (Hopkins, 2000).
A Lab Test of the EHT of Depression 501
Fig. 3. Percent change in dysphoria after the receipt of social support.
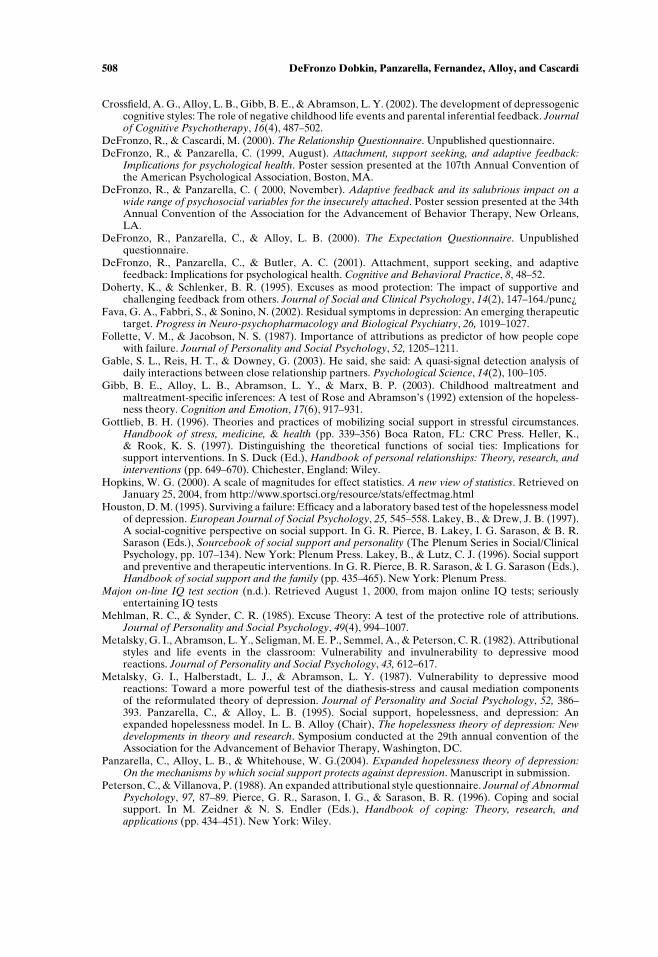
examine the impact of social support on inferences following an academic stressor.There was a significant main effect for time, F(1, 123) = 21.05, p < .01, indicatingthat all participants made significantly fewer depressogenic inferences at Time 2(postsupport) than at Time 1 (poststressor). Although there was no significant maineffect for social support condition, F(2, 123) = 0.26, p = .77 there was a trend for theGroup by Time interaction F(2, 123) = 2.76, p = .07, as indicated in Table III andFig. 4.
Although the bi-directional omnibus test was not technically significant, p = .07,we explored the Group by Time interaction using Repeated Measures ANOVA dueto theoretical interest.9 The Expanded Hopelessness Theory predicts that adaptiveinferential feedback will directly modify negative inferences, which are viewed asa proximal cause of depressive symptoms, whereas other types of social supportare not hypothesized to have this direct effect on maladaptive cognitions. As inHypothesis 1, the nonspecific and no-support conditions were collapsed into onegroup for the purpose of this analysis.10 As hypothesized, results indicated thatparticipants who received adaptive inferential feedback experienced a significantlylarger decrease in depressogenic inferences (30% vs. 12%) from Time 1 to Time2, F(1, 124) = 5.49, p = .02, than individuals who received nonspecific or no socialsupport (effect size = .20).
9Although the aforementioned F test is not technically statistically significant (p = .07), the omnibus Ftest would be significant if conducted as a one-tailed test (p = .034), which would be appropriate givenour directional hypothesis. However, we chose to conduct a two-tailed test, with a follow-up post hocanalysis, to be conservative.
10Exploratory analysis indicated no differences between groups, F(1, 81) = .08, p = .77.

502 DeFronzo Dobkin, Panzarella, Fernandez, Alloy, and Cascardi
Fig. 4. Percent change in inferences after the receipt of social support.
Hypothesis 3
We tested Hypothesis 3 by conducting a mediational analysis to determinewhether the differential rate of change in dysphoria that occurred between socialsupport groups, from Time 1 to Time 2, was mediated by a change in inferences thatoccurred during this same time interval, based on criteria established by Baron andKenny (1986). When the inference change score (from Time 1 to Time 2) was en-tered as a covariate into the Repeated Measures design described under Hypothesis1, the Inference change score × Time interaction was statistically significant, F(1,121) = 18.36, p < .01, and the Social support group × Time interaction, was reducedin significance, F(2, 121) = 2.29, p = .11. Thus, consistent with the hypothesized roleof depressogenic inferences in the Expanded Hopelessness Theory of depression,the change in dysphoric mood (from Time 1 to Time 2) was partially mediated bythe change in inferences (from Time 1 to Time 2).
DISCUSSION
The current study provided the first controlled test of the relationship betweenadaptive inferential feedback, dysphoria, and depressogenic inferences. This study isalso unique in that an objective measure of received social support (e.g., audiotaped

A Lab Test of the EHT of Depression 503
support exchanges) was obtained. This is in contrast to most social support studiesto date, which have relied solely on subjective self-report measures, that may bebiased by factors such as the support recipient’s interpretation of the communicatedmessage (Gable, Reis, & Downey, 2003; Pierce et al., 1996).
Overall, results indicated that individuals who received adaptive inferentialfeedback following an academic failure experience, felt significantly “better,” moreunderstood, and more supported than individuals who received general/nonspecifictypes of support that did not include an adaptive inferential feedback component.Moreover, participants who received adaptive inferential feedback demonstrateda significantly greater decrease in depressogenic inferences and dysphoria post-support than those who received general/nonspecific types of support or no socialsupport. Thus, it may be possible to infer that the adaptive inferential componentof the social support interaction, as opposed to other types or components of socialsupport (e.g., social contact, empathy, reflective listening, companionship, offeringof tangible or material assistance, etc.) may be responsible for the observed changein mood and inferences.
However, it is important to note that individuals in the adaptive inferentialfeedback group received more total and unique social support than individualsin the general/nonspecific condition. Thus, one possible alternative explanationfor the aforementioned results is that the greater number of overall supportstatements that were offered and presented in more diverse ways, as opposedto the type of support, is responsible for the significant impact on mood andinferences.
Although this potential confound needs to be considered, it does not appearto be the most plausible explanation for the study results. First, the total numberof support statements provided and the number of unique statements offered werenot significant covariates when entered into core statistical tests. Second, statisti-cal tests indicated that the adaptive inferential feedback and general/nonspecificsupport conditions were qualitatively different, as significantly greater amountsof general/nonspecific support were offered in the general/nonspecific conditionand significantly greater amounts of adaptive inferential feedback were offered inthe adaptive feedback condition. Thus, each support condition may represent aunique construct and comparing the total number of support statements offeredwithin each qualitatively different condition may not be as meaningful as makingcomparisons across similar groups. Third, on average, partners in the adaptiveinferential feedback condition made two more support statements than partnersin the general/nonspecific group during the course of the interaction. When inter-preted from this perspective, partners in the general/nonspecific support conditionexchanged, on average, eight more support statements with the target participantthan partners in the control/no support condition, who had no contact with andthus exchanged no social support with the target participant. Yet, despite thisaverage difference of eight support statements, individuals in the general supportand no support groups demonstrated comparable changes in mood and inferencesfrom Time 1 to Time 2, as indicated by exploratory analyses. Thus, it does notseem likely that the quantity of support received is the primary mechanism ofchange in the current study. Moreover, research indicates that the quality of social

504 DeFronzo Dobkin, Panzarella, Fernandez, Alloy, and Cascardi
support, as opposed to the quantity, is the factor that is essential for well-being (e.g.Turner-Cobb, 2000; Vander Voort, 1999).
Challenges and Limitations
Duplication of a Stressful Event and Support Exchange in a Lab Setting
A major challenge was to duplicate as closely as possible a plausible real-lifestressor (e.g., academic failure) and the opportunity for social feedback about thestressor. A second challenge was to maintain a high degree of control while alsoallowing for social interaction between actual friends or family members that wasnot completely scripted.
The academic stressor utilized in this study did have the intended temporary,negative impact on mood as evidenced by statistical tests. In addition, duringthe debriefing, the overwhelming majority of the participants reported that theybelieved that the test was real as it resembled past achievement tests that they hadcompleted. Because the majority of participants came to the study with partnersthat they knew well and felt comfortable with, the social support manipulation wassomewhat analogous to a real-life support-seeking situation.
Additionally, after a 30-min structured training period, the majority of partnerswere able to adequately implement their respective social support interventions.Seventy-eight percent of the partners in the active support conditions met therigorous inclusion criteria (more than 50% of statements coded as AIF in theadaptive feedback group or no adaptive feedback statements in the nonspecificgroup). The average percentage of social support statements offered across bothactive groups, which were consistent with the assigned support condition, rangedfrom 88 to 100%. Moreover, the results of statistical tests indicated that theconditions were significantly different, as significantly more adaptive feedback wasoffered in the adaptive inferential feedback condition and significantly more generalsupport without an adaptive inferential feedback component was offered in thenonspecific condition.
Yet, there were some limitations associated with the use of natural supporters.First, different types of social support likely co-occur in natural interactions. On thebasis of the responses on a training exercise, approximately 60% of the partnersnaturally offered both adaptive inferential feedback and other types of nonspecificsupport when speaking with a distressed friend pretraining. Thus, the largestproblem encountered with the use of natural supporters (in 15% of the cases)was that it was difficult for some of the partners to refrain from offering adaptivefeedback and nonspecific support concurrently. In particular, it was especiallydifficult for partners in the nonspecific condition to refrain from challenging themaladaptive statements and validating the adaptive comments generated by thetarget participants during the conversation, despite the fact that they were trainednot to do so. For example, the participant statement of, “I’m so stupid because I didso bad on this test” was commonly followed by a partner response of, “You’re notstupid. You are smart,” leading to the exclusion of the general/nonspecific case fromthe study. Second, a more minor problem occurred when a small number of partners

A Lab Test of the EHT of Depression 505
(n = 4) did not make any support statements, and simply listened to the participantspeak. Third, since natural supporters were used, the intervention was limited to 2min in order to minimize the chances that support statements inconsistent with theassigned condition would be offered. It is possible that target participants were notgiven sufficient time in this laboratory paradigm to fully reformulate their cognitionsbased on social feedback, as the effects of adaptive inferential feedback were weakerfor changes in participants’ inferences than for dysphoria. A longer interventionmay have resulted in larger effect sizes.
External Validity
It is important to note that individuals may have reacted differently to stressand social support in the lab than they would have in response to a real-life stressor.For example, the academic failure in the lab study may not have affected individualsin the same way as failing a test in a class, the loss of a job, or a relationship breakup.Given that the lab stressor was mild, future research will be needed to determine ifadaptive inferential feedback is able to exert its buffering effect in the face of a moresevere stressor, perhaps when it is more difficult to believe the feedback received.As the majority of the support providers in the current study were classified as“friends” and not “romantic partners,” future research should also explore if theimpact of adaptive inferential feedback is moderated by the closeness or type ofrelationship.
Moreover, college students are representative of a nonclinical sample. Thus, theeffects of adaptive feedback on diagnoses or symptoms of depression could not bedirectly tested in this study. It was only possible to investigate the effects of adaptiveinferential feedback on temporary dysphoric mood reactions. In addition, requiringparticipants to have a partner may have introduced a selection bias into the studydesign, as individuals who are a part of a social network may react differently tosocial support than those who chronically lack social contact. Additional bias mayhave been introduced by the exclusion criteria. For example, if highly sociotropicor intelligent or motivated persons responded better to the brief training, the finalsample may have overrepresented certain types of partners.
Theoretical and Clinical Implications
This preliminary evidence of a causal relationship between adaptive inferentialfeedback, and depressogenic inferences and dysphoria provides additional supportfor the hypothesized role of adaptive inferential feedback in the Expanded Hope-lessness Theory of depression. Moreover, these results help to advance the socialsupport and depression literature, that has been consistently criticized for being“atheoretical,” through the provision of initial empirical evidence for a comprehen-sive theory that explains an etiological role that an operationally defined subtypeof social support plays in the onset and maintenance of depressive symptoms (e.g.,Roberts & Gotlib, 1997; Sarason, Sarason, & Pierce, 1990; Turner, 1999). The resultsof this study also speak to the importance of continuing to operationally definesubtypes of social support, such as adaptive inferential feedback, so that the specific

506 DeFronzo Dobkin, Panzarella, Fernandez, Alloy, and Cascardi
causal mechanisms by which different types of social support impact depression canbe more clearly tested. The understanding of these causal mechanisms may help toenhance theoretical development in the social support and depression literature andcould possibly lead to more specific and targeted therapeutic interventions.
Although the results of this study need to be replicated in both controlled andnaturalistic settings, this preliminary empirical evidence for a causal relationship be-tween adaptive inferential feedback, dysphoric mood, and depressogenic inferencessuggests that it may be important to explore the inclusion of an adaptive inferentialfeedback training component in primary and secondary prevention programs, aswell as in mental health and medical intervention programs. An adaptive inferentialfeedback training component may be especially important to incorporate intoprograms that target children and young adults, as inferential style tends to becomemore stable over time and the cognitive style and inferences of younger individualsmay be especially amenable to change (e.g., Abramson et al., 2002; Gibb, Alloy,Abramson, & Marx, 2003).
It has been proposed that naturally occurring types of social support, such asadaptive inferential feedback, are more effective in the prevention and reduction ofpsychological distress than more formalized support interventions such as attendingsupport groups (Gottlieb, 1996; Lakey & Lutz, 1996). Although more than halfof the partners in the current study naturally offered some adaptive feedbackprior to their participation in this study, as evidenced by their responses onpreliminary training questionnaires, adaptive feedback statements comprised a verysmall percentage of the overall number of support statements generated pretraining.Thus, it may be important to identify strategies for bolstering adaptive feedback inthe natural environment, given that our data suggests that inferential feedback maybe causally related to depressed mood.
For example, it might be helpful for therapists to provide adaptive inferentialfeedback training to a friend, family member, or significant other of a depressedclient (see DeFronzo, Panzarella, & Butler, 2001). Adaptive inferential feedbacktraining may offer the partner a very specific skill that can consistently be applied assituations arise on a daily basis, that mirrors the cognitive therapy for depressionthat is received in the office. The partner could be trained to recognize depres-sogenic inferences such as, “I’m so stupid for making a mistake at work” and tooffer nondepressogenic alternatives such as, “Everyone makes mistakes at worksometimes.”
Recent research suggests that social-cognitive factors, such as adaptive in-ferential feedback, may be important elements to incorporate into the combinedpharmacological and psychotherapeutic intervention approaches that need to beutilized with treatment refractory patients (Thase, Friedman, & Howland, 2001).Moreover, dysfunctional attributions, which adaptive inferential feedback targets,are a common residual symptom of depression among patients in remission thatare associated with poor long-term outcomes (Fava, Fabbri, & Sonino, 2002). Thus,the results of the current study may help to translate social support research intoeffective clinical interventions, which may decrease the need and length of formalpsychological treatment over time (Heller & Rook, 1997; Lakey & Drew, 1997;Lakey & Lutz, 1996).

A Lab Test of the EHT of Depression 507
ACKNOWLEDGMENTS
This article was based on a dissertation submitted to MCP HahnemannUniversity, under the direction of Catherine Panzarella. We thank other membersof the dissertation committee, Michele Cascardi, Pamela Geller, Julie Graham,James Herbert, and Michael Lowe, for their valuable assistance and feedback. Wealso thank Wayne Whitehouse for helping to facilitate data collection at TempleUniversity, Neil Rellosa and David Pan for assisting with participant recruitmentand audiotape transcription, and Michael Gara for providing thoughtful feedbackregarding previous versions of the manuscript.
REFERENCES
Abela, J. R. Z., & Seligman, M. E. P. (2000). The hopelessness theory of depression: A test of thediathesis-stress component in the interpersonal and achievement domains. Cognitive Therapy andResearch, 24(4), 361–378. Abramson, L. Y., Alloy, L. B., Hogan, M. E., Whitehouse, W. G.,Donovan, P., Rose, D. T., et al. (2002). Cognitive vulnerability to depression: Theory and evidence.In R. L. Leahy & E. T. Dowd (Eds.), Clinical advances in cognitive psychotherapy: Theory andapplication (pp. 75–92). New York: Springer.
Abramson, L. Y., Metalsky, G. I., & Alloy, L. B. (1989). Hopelessness depression: A theory basedsubtype of depression. Psychological Review, 96, 358–372.
Alloy, L. B., & Abramson, L. Y. (1999). The Temple-Wisconsin Cognitive Vulnerability to Depression(CVD) Project: Conceptual background, design, and methods. Journal of Cognitive Psychotherapy:An International Quarterly, 13, 227–262.
Alloy, L. B., Abramson, L. Y., Hogan, M. E., Whitehouse, W. G., Rose, D. T., Robinson, M. S., et al.(2000). The Temple-Wisconsin Cognitive Vulnerability to Depression Project: Lifetime history ofAxis I psychopathology in individuals at high and low cognitive risk for depression. Journal ofAbnormal Psychology, 109, 403–418.
Alloy, L. B., Abramson, L. Y., Tashman, N. A., Berrebbi, D. S., Hogan, M. E., Whitehouse, W. G., et al.(2001). Developmental origins of cognitive vulnerability to depression: Parenting, cognitive, andinferential feedback styles of the parents of individuals at high and low cognitive risk for depression.Cognitive Therapy and Research, 25(4), 397–423.
Alloy, L. B., Abramson, L. Y., & Viscusi, D. (1981). Induced mood and the illusion of control. Journal ofPersonality and Social Psychology, 41(6), 1129–1140.
Alloy, L. B., Abramson, L. Y., Whitehouse, W. G., Hogan, M. E., Tashman, N., Steinberg, D., et al.(1999). Depressogenic cognitive styles: Predictive validity, information processing and personalitycharacteristics, and developmental origins. Behaviour Research and Therapy, 37, 503–531.
Alloy, L. B., & Clements, C. M. (1992). Illusion of control: Invulnerability to negative affect anddepressive symptoms after laboratory and natural stressors. Journal of Abnormal Psychology,101(2), 234–245.
Barnett, P. A., & Gotlib, I. H. (1988). Psychosocial functioning and depression: Distinguishing amongantecedents, concomitants, and consequences. Psychological Bulletin, 104(1), 97–126.
Baron, R. M., & Kenny, D. A. (1986). The moderator–mediator variable distinction in social psycholog-ical research: Conceptual, strategic, and statistical considerations. Journal of Personality and SocialPsychology, 51, 1173–1182.
Beck, A. T., Rush, A. J., Shaw, B. F., & Emery, G. (1979). Cognitive therapy of depression. New York:Guilford Press.
Beck, A. T., Steer, R. A., & Garbin, M. G. (1988). Psychometric properties of the Beck DepressionInventory: Twenty five years of evaluation. Clinical Psychology Review, 8, 77–100.
Chartier, G. M., & Ranieri, D. J. (1989). Comparison of two mood induction procedures. CognitiveTherapy and Research, 13(3), 275–282.
Cohen, S., & Wills, T. A. (1985). Stress, social support, and the buffering hypothesis. PsychologicalBulletin, 98(2), 310–357.
508 DeFronzo Dobkin, Panzarella, Fernandez, Alloy, and Cascardi
Crossfield, A. G., Alloy, L. B., Gibb, B. E., & Abramson, L. Y. (2002). The development of depressogeniccognitive styles: The role of negative childhood life events and parental inferential feedback. Journalof Cognitive Psychotherapy, 16(4), 487–502.
DeFronzo, R., & Cascardi, M. (2000). The Relationship Questionnaire. Unpublished questionnaire.DeFronzo, R., & Panzarella, C. (1999, August). Attachment, support seeking, and adaptive feedback:
Implications for psychological health. Poster session presented at the 107th Annual Convention ofthe American Psychological Association, Boston, MA.
DeFronzo, R., & Panzarella, C. ( 2000, November). Adaptive feedback and its salubrious impact on awide range of psychosocial variables for the insecurely attached. Poster session presented at the 34thAnnual Convention of the Association for the Advancement of Behavior Therapy, New Orleans,LA.
DeFronzo, R., Panzarella, C., & Alloy, L. B. (2000). The Expectation Questionnaire. Unpublishedquestionnaire.
DeFronzo, R., Panzarella, C., & Butler, A. C. (2001). Attachment, support seeking, and adaptivefeedback: Implications for psychological health. Cognitive and Behavioral Practice, 8, 48–52.
Doherty, K., & Schlenker, B. R. (1995). Excuses as mood protection: The impact of supportive andchallenging feedback from others. Journal of Social and Clinical Psychology, 14(2), 147–164./punc¿
Fava, G. A., Fabbri, S., & Sonino, N. (2002). Residual symptoms in depression: An emerging therapeutictarget. Progress in Neuro-psychopharmacology and Biological Psychiatry, 26, 1019–1027.
Follette, V. M., & Jacobson, N. S. (1987). Importance of attributions as predictor of how people copewith failure. Journal of Personality and Social Psychology, 52, 1205–1211.
Gable, S. L., Reis, H. T., & Downey, G. (2003). He said, she said: A quasi-signal detection analysis ofdaily interactions between close relationship partners. Psychological Science, 14(2), 100–105.
Gibb, B. E., Alloy, L. B., Abramson, L. Y., & Marx, B. P. (2003). Childhood maltreatment andmaltreatment-specific inferences: A test of Rose and Abramson’s (1992) extension of the hopeless-ness theory. Cognition and Emotion, 17(6), 917–931.
Gottlieb, B. H. (1996). Theories and practices of mobilizing social support in stressful circumstances.Handbook of stress, medicine, & health (pp. 339–356) Boca Raton, FL: CRC Press. Heller, K.,& Rook, K. S. (1997). Distinguishing the theoretical functions of social ties: Implications forsupport interventions. In S. Duck (Ed.), Handbook of personal relationships: Theory, research, andinterventions (pp. 649–670). Chichester, England: Wiley.
Hopkins, W. G. (2000). A scale of magnitudes for effect statistics. A new view of statistics. Retrieved onJanuary 25, 2004, from http://www.sportsci.org/resource/stats/effectmag.html
Houston, D. M. (1995). Surviving a failure: Efficacy and a laboratory based test of the hopelessness modelof depression. European Journal of Social Psychology, 25, 545–558. Lakey, B., & Drew, J. B. (1997).A social-cognitive perspective on social support. In G. R. Pierce, B. Lakey, I. G. Sarason, & B. R.Sarason (Eds.), Sourcebook of social support and personality (The Plenum Series in Social/ClinicalPsychology, pp. 107–134). New York: Plenum Press. Lakey, B., & Lutz, C. J. (1996). Social supportand preventive and therapeutic interventions. In G. R. Pierce, B. R. Sarason, & I. G. Sarason (Eds.),Handbook of social support and the family (pp. 435–465). New York: Plenum Press.
Majon on-line IQ test section (n.d.). Retrieved August 1, 2000, from majon online IQ tests; seriouslyentertaining IQ tests
Mehlman, R. C., & Synder, C. R. (1985). Excuse Theory: A test of the protective role of attributions.Journal of Personality and Social Psychology, 49(4), 994–1007.
Metalsky, G. I., Abramson, L. Y., Seligman, M. E. P., Semmel, A., & Peterson, C. R. (1982). Attributionalstyles and life events in the classroom: Vulnerability and invulnerability to depressive moodreactions. Journal of Personality and Social Psychology, 43, 612–617.
Metalsky, G. I., Halberstadt, L. J., & Abramson, L. Y. (1987). Vulnerability to depressive moodreactions: Toward a more powerful test of the diathesis-stress and causal mediation componentsof the reformulated theory of depression. Journal of Personality and Social Psychology, 52, 386–393. Panzarella, C., & Alloy, L. B. (1995). Social support, hopelessness, and depression: Anexpanded hopelessness model. In L. B. Alloy (Chair), The hopelessness theory of depression: Newdevelopments in theory and research. Symposium conducted at the 29th annual convention of theAssociation for the Advancement of Behavior Therapy, Washington, DC.
Panzarella, C., Alloy, L. B., & Whitehouse, W. G.(2004). Expanded hopelessness theory of depression:On the mechanisms by which social support protects against depression. Manuscript in submission.
Peterson, C., & Villanova, P. (1988). An expanded attributional style questionnaire. Journal of AbnormalPsychology, 97, 87–89. Pierce, G. R., Sarason, I. G., & Sarason, B. R. (1996). Coping and socialsupport. In M. Zeidner & N. S. Endler (Eds.), Handbook of coping: Theory, research, andapplications (pp. 434–451). New York: Wiley.

A Lab Test of the EHT of Depression 509
Roberts, J. E., & Gotlib, I. H. (1997). Social support and personality in depression: Implications fromquantitative genetics. In G. R. Pierce, B. Lakey, I. G. Sarason, & B. R. Sarason (Eds.), Sourcebookof social support and personality (The Plenum Series in Social/Clinical Psychology, pp. 187–214).New York: Plenum Press.
Sacks, C. H., & Bugental, D. B. (1987). Attributions as moderators of affective and behavioral responsesto social failure. Journal of Personality and Social Psychology, 53, 939–947. Sarason, B. R., Sarason,I. G., & Gurung, R. A. R. (1997). Close personal relationships and health outcomes: A key to therole of social support. In S. Duck (Ed.), Handbook of personal relationships: Theory, research, andinterventions (pp. 547–573). Chichester, England: Wiley.
Sarason, B. R., Sarason, I. G., & Pierce, G. R. (1990). Social support: An interactional view. New York:Wiley.
Seligman, M. E. P., Abramson, L. Y., Semmel, A., & von Baeyer, C. (1979). Depressive attributionalstyle. Journal of Abnormal Psychology, 88, 242–247.
Seriously entertaining IQ tests. (n.d.). Retrieved on August 1, 2000, from majon online IQ tests; seriouslyentertaining IQ tests
Stiensmeier-Pelster, J. (1989). Attributional style and depressive mood reactions. Journal of Personality,57(3), 581–599.
Thase, M. E., Friedman, E. S., & Howland, R. H. (2001). Management of treatment-resistant depression:Psychotherapeutic perspectives. Journal of Clinical Psychiatry, 62(18), 18–24. Turner, R. J. (1999).Social support and coping. In A. V. Horwitz & T. L. Scheid (Eds.), A handbook for the study ofmental health. Social contexts, theories, and systems (pp. 198–210). New York: Cambridge UniversityPress.
Turner-Cobb, J. (2000). Social support and salivary cortisol in women with metastatic breast cancer.Psychosomatic Medicine, 62(3), 337–345.
Vander Voort, D. (1999). Quality of social support in mental and physical health. Current Psychology:Developmental, Learning, Personality, and Social, 18(2), 205–222.
Zuckerman, M., & Lubin, B. (1965). Multiple Affect Adjective Checklist. San Diego, CA: Educationaland Industrial Testing Service.

Copyright © 2022 FDOKUMEN




















