
Reliabilities, validities, and cutoff scores of the Depression Hopelessness Suicide Screening Form...
18
http://cjb.sagepub.com/ Behavior Criminal Justice and http://cjb.sagepub.com/content/38/8/779 The online version of this article can be found at: DOI: 10.1177/0093854811409004 2011 38: 779 originally published online 10 June 2011 Criminal Justice and Behavior Daryl G. Kroner, Tamara Kang, Jeremy F. Mills, Andrew J.R. Harris and Michelle M. Green Screening Form Among Women Offenders Reliabilities, Validities, and Cutoff Scores of the Depression Hopelessness Suicide Published by: http://www.sagepublications.com On behalf of: International Association for Correctional and Forensic Psychology can be found at: Criminal Justice and Behavior Additional services and information for http://cjb.sagepub.com/cgi/alerts Email Alerts: http://cjb.sagepub.com/subscriptions Subscriptions: http://www.sagepub.com/journalsReprints.nav Reprints: http://www.sagepub.com/journalsPermissions.nav Permissions: http://cjb.sagepub.com/content/38/8/779.refs.html Citations: What is This? - Jun 10, 2011 OnlineFirst Version of Record - Jun 23, 2011 Version of Record >> at SOUTHERN IL UNIV CARBONDALE on July 26, 2012 cjb.sagepub.com Downloaded from
Transcript of Reliabilities, validities, and cutoff scores of the Depression Hopelessness Suicide Screening Form...

http://cjb.sagepub.com/Behavior
Criminal Justice and
http://cjb.sagepub.com/content/38/8/779The online version of this article can be found at:
DOI: 10.1177/0093854811409004
2011 38: 779 originally published online 10 June 2011Criminal Justice and BehaviorDaryl G. Kroner, Tamara Kang, Jeremy F. Mills, Andrew J.R. Harris and Michelle M. Green
Screening Form Among Women OffendersReliabilities, Validities, and Cutoff Scores of the Depression Hopelessness Suicide
Published by:
http://www.sagepublications.com
On behalf of:
International Association for Correctional and Forensic Psychology
can be found at:Criminal Justice and BehaviorAdditional services and information for
http://cjb.sagepub.com/cgi/alertsEmail Alerts:
http://cjb.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
http://cjb.sagepub.com/content/38/8/779.refs.htmlCitations:
What is This?
- Jun 10, 2011 OnlineFirst Version of Record
- Jun 23, 2011Version of Record >>
at SOUTHERN IL UNIV CARBONDALE on July 26, 2012cjb.sagepub.comDownloaded from
779
CRIMINAL JUSTICE AND BEHAVIOR, Vol. 38 No. 8, August 2011 779-795DOI: 10.1177/0093854811409004© 2011 International Association for Correctional and Forensic Psychology
AUTHORS’ NOTE: Gratefully acknowledged are Caroline Page and Iliana Lilova for their assistance with the study. Correspondence concerning this article should be addressed to Daryl G. Kroner, Southern Illinois University Carbondale; email: [email protected].
RELIABILITIES, VALIDITIES, AND CUTOFF SCORES OF THE DEPRESSION HOPELESSNESS SUICIDE SCREENING FORM AMONG WOMEN OFFENDERSDARYL G. KRONERTAMARA KANGSouthern Illinois University Carbondale
JEREMY F. MILLSCarleton University
ANDREW J. R. HARRISMICHELLE M. GREENCorrectional Service Canada
Depression and hopelessness can be associated with negative outcomes among offenders, such as reduced treatment impact, institutional misconduct, suicide risk, and health care costs. This study evaluated the reliability and validity of the Depression Hopelessness Suicide Screening Form (DHS) among women offenders. The DHS Depression and Hopelessness scales showed good internal consistency and test–retest reliability. Convergent and discriminant validities were supported through the relationship of the DHS with other established scales of depression, mood, suicidal intentions, and psychological distress. Optimal and conservative cutoff scores for the DHS Depression and Hopelessness scales were evaluated against criteria from a DSM-IV-based interview. Discussion centers on the importance of gender-based norms when assessing women offenders.
Keywords: women offenders; gender-sensitive assessment; depression; hopelessness; offender cutoff scores
An overview of the offender literature would suggest that the assessment of depression and hopelessness is often considered a lower priority, especially when compared to the
factors that typically predict institutional behavior and recidivism outcomes. Yet depression and hopelessness can be associated with a host of negative consequences, such as self-harm or suicide behaviors and reduced treatment impact and have indirect consequence of co-occurring disorders, resulting in increased health care costs.
Depression’s association with suicide-related thoughts and behaviors is well established across varied populations (Dieserud, Roysamb, Ekeberg, & Kraft, 2001; Konick & Gutierrez, 2005; Rudd, Joiner, & Rajab, 1996). Among 1,900 offenders in the Canadian federal correctional system, lifetime depressive disorders ranged from 21.5% (stringent criteria) to 29.8% (wide criteria ignoring severity and exclusions) of the sample (Motiuk & Porporino, 1992). Hopelessness, defined as “a system of negative expectancies concerning himself and his future life” (Beck, Weissman, Lester, & Trexler, 1974, p. 861), is also key in the assessment of suicide risk (Dieserud et al., 2001; Dixon, Heppner, & Rudd, 1994; Konick & Gutierrez, 2005; Rudd et al., 1996). Although some suicidal protocols ignore the
at SOUTHERN IL UNIV CARBONDALE on July 26, 2012cjb.sagepub.comDownloaded from

780 CRIMINAL JUSTICE AND BEHAVIOR
measurement of depression and hopelessness (Correia, 2000), these two areas are essential to suicide risk assessment.
In efforts to treat offenders, depression and hopelessness can be factors in how receptive and responsive offenders are to interventions. In a multisite study, depression was shown to be a more powerful factor among programs for women as compared to programs for males (Staton-Tindall et al., 2007). The treatment engagement measures of counselor rap-port and willingness to participate in treatment were the outcome variables. Depression was more strongly related to these two treatment engagement variables for programs designed for women than those designed for men.
Not only can there be a direct link between depression and related criminal justice out-comes, but indirect consequences of depression can exasperate the impact of negative out-comes. Individuals who suffer from depression often suffer from other disorders, typically substance abuse, and specific personality disorders, such as borderline personality disorder. In a recent meta-analysis, examining the co-occurrence of depression and personality disor-ders, a personality disorder doubled the risk of a poor outcome for depression (Newton-Howes, Tryer, & Johnson, 2006). In a review of the costs of depression, Panzarino (1998) argued that high-frequency users of medical services have higher rates of depression and are more likely to have a co-occurring disorder with depression. This same relationship appears to hold with offenders. Depression, as measured by self-report, was associated with chronic ill health, but not with length of sentence served (Murdoch, Morris, & Holmes, 2008).
Rates of mental health symptoms and diagnosis generally differ between women and men. For example, women typically have higher rates of affective disorders, whereas men have higher rates of antisocial related disorders (Dohrenwend et al., 1992; Khan, Jacobson, Gardner, Prescott, & Kendler, 2005; Piccinelli & Wilkinson, 2000). A multicountry, multi-method study that examined common mental health disorders found that being a woman increased the likelihood of a mental disorder (Patel, Araya, Lima, Ludermir, & Todd, 1999). When specific disorders such as depression are considered, women not only have higher rates than men but also have higher rates of comorbidity (Afifi, 2007). Similar to the different rates of comorbidity, how depression interacts with social supports differs between women and men. In a two-wave, opposite-sex twin pair study, lack of global sup-port predicted future depression in women but not in men (Kendler, Myers, & Prescott, 2005). Also, when the types of support were examined, lack of support from the co-twin, other relatives, parents, and spouse was more strongly related with future likelihood of depression for women than for men. Thus, not only are rates of disorder likely to differ, but the etiological pathway of a disorder is likely to differ between females and males.
As in the population at large, evidence suggests that female offenders are more likely to experience depression than are male offenders (Ng et al., 2010). Also, unique factors among women contribute to criminal justice outcomes. These unique factors have emerged from the literature suggesting that women have different pathways to crime. These path-ways include victimization and abuse, mental health, dysfunctional relationships, self-esteem, self-efficacy, and parental distress (Salisbury, Van Voorhis, & Spiropoulos, 2009). Female-centered instruments to measure these areas are called gender-responsive instru-ments. Within the mental health domain, the use of two gender-responsive instruments of current depression or anxiety and current psychosis resulted in better predictions of the number of institutional misconducts over 6- and 12-month periods (Wright, Salisbury, & Van Voorhis, 2007). The gender-responsiveness psychosis scale was the strongest predictor
at SOUTHERN IL UNIV CARBONDALE on July 26, 2012cjb.sagepub.comDownloaded from

Kroner et al. /DHS AMONG WOMEN OFFENDERS 781
of misconducts (r = .26, 6 months; r = .31, 12 months), stronger than the gender-neutral predictor scale of history of mental illness (r = .12, 6 months; r = .19, 12 months). Given the different negative affect levels between female and male offenders and the potential different pathways to crime, it is expected that the guidelines for interpreting results with women offenders would benefit from the use of women-based norms and the development of gender-specific cutoff scores.
Based on the above review, a single cutoff score is likely to be inappropriate for both female and male offenders. Inappropriate cutoff scores can result in overclassification or underclassification of the target construct or domain. Two common strategies may result in overclassification among women offenders. First, if women have a lower base rate of an outcome variable, a predictive instrument may unnecessarily classify women into a high category. That is, the instrument’s cutoff scores may indicate a threshold for an event, when that condition or future event is unlikely to occur. This type of overclassification can occur when male-derived cutoff scores are used for security level classification. Typically, com-pared to their male counterparts, women offenders have a lower rate of institutional mis-conducts and their offenses are less severe (Harer & Langan, 2001). In this situation, using a cutoff score from a male-derived instrument will overclassify women offenders. That is, too many women will be placed in a high level of security, when such a placement is not warranted. Cutoff scores developed on male offenders have classified women offenders to higher security both in New Zealand (Collie & Polascheck, 2003) and in the U.S. federal system (Harer & Langan, 2001). The second situation of overclassification may result from increased instrument scores not because of reasons directly related to crime-related needs but because of past traumatic experiences. Increased scores can be a result of past traumatic experiences, which may not typify a male experience. Whether because of base rate or instrumentation, overclassification results in a misuse of correctional resources, placing women in more restrictive environments than necessary.
The Depression Hopelessness Suicide Screening Form (DHS; Mills & Kroner, 2003) was developed to screen for depression and hopelessness as well as gather information on suicide risk factors such as history of suicide attempts, previous diagnosis for depression, family members who have committed suicide, and suicidal ideation. In addition to screen-ing for these risk factors, the DHS was also developed to overcome some drawbacks of the more commonly used depression inventories. For example, items that referenced guilt were not included in the DHS because they may have ambiguous meaning within a criminal justice context. The source of guilt can be of either a legal factual nature (guilty of a crime) or an affective nature (feeling guilty without a direct cause).
The purpose of this study was threefold. First, we wanted to report reliability and valid-ity information on the DHS among female offenders. Validity was examined via conver-gent and discriminant validities with established measures of affective functioning. In addition, the efficacy of the DHS critical items was examined. Second, because of the potential of misclassification with female offenders, optimal cutoff scores were developed. Sensitivity, specificity, positive predictive power, and negative predictive power were examined for two methods of deriving cutoff scores. To further facilitate a gender-based interpretation, suggestions for content interpretation of the depression and hopelessness scales were made. Third, because it was expected that the depression and hopelessness scales would be correlated, the optimal cutoff score for each scale was compared for both depression and hopelessness outcomes.
at SOUTHERN IL UNIV CARBONDALE on July 26, 2012cjb.sagepub.comDownloaded from
782 CRIMINAL JUSTICE AND BEHAVIOR
METHOD
PARTICIPANTS
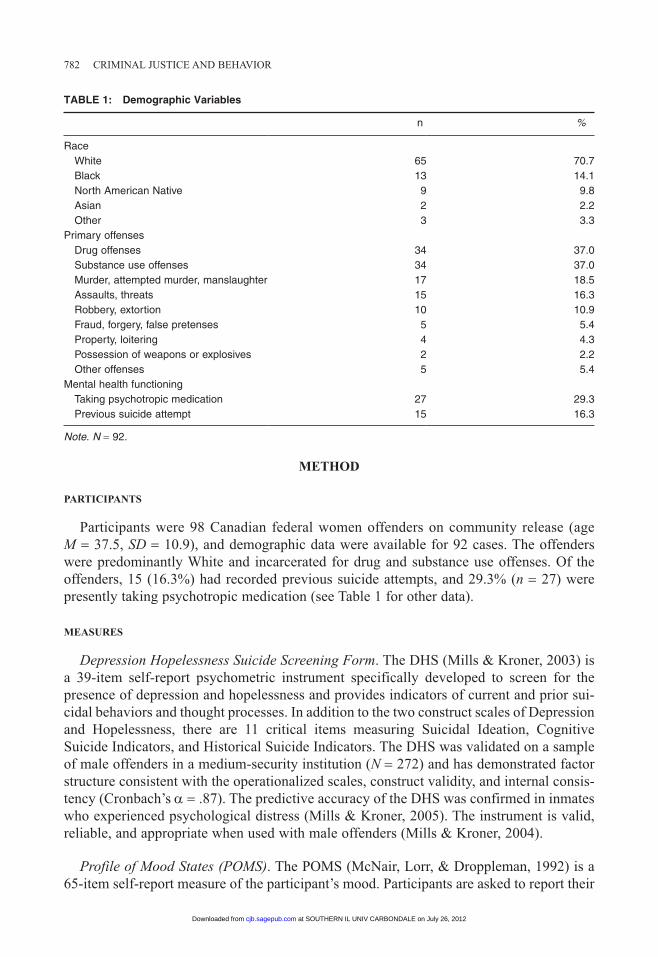
Participants were 98 Canadian federal women offenders on community release (age M = 37.5, SD = 10.9), and demographic data were available for 92 cases. The offenders were predominantly White and incarcerated for drug and substance use offenses. Of the offenders, 15 (16.3%) had recorded previous suicide attempts, and 29.3% (n = 27) were presently taking psychotropic medication (see Table 1 for other data).
MEASURES
Depression Hopelessness Suicide Screening Form. The DHS (Mills & Kroner, 2003) is a 39-item self-report psychometric instrument specifically developed to screen for the presence of depression and hopelessness and provides indicators of current and prior sui-cidal behaviors and thought processes. In addition to the two construct scales of Depression and Hopelessness, there are 11 critical items measuring Suicidal Ideation, Cognitive Suicide Indicators, and Historical Suicide Indicators. The DHS was validated on a sample of male offenders in a medium-security institution (N = 272) and has demonstrated factor structure consistent with the operationalized scales, construct validity, and internal consis-tency (Cronbach’s a = .87). The predictive accuracy of the DHS was confirmed in inmates who experienced psychological distress (Mills & Kroner, 2005). The instrument is valid, reliable, and appropriate when used with male offenders (Mills & Kroner, 2004).
Profile of Mood States (POMS). The POMS (McNair, Lorr, & Droppleman, 1992) is a 65-item self-report measure of the participant’s mood. Participants are asked to report their
TABLE 1: Demographic Variables
n %
RaceWhite 65 70.7Black 13 14.1North American Native 9 9.8Asian 2 2.2Other 3 3.3
Primary offensesDrug offenses 34 37.0Substance use offenses 34 37.0Murder, attempted murder, manslaughter 17 18.5Assaults, threats 15 16.3Robbery, extortion 10 10.9Fraud, forgery, false pretenses 5 5.4Property, loitering 4 4.3Possession of weapons or explosives 2 2.2Other offenses 5 5.4
Mental health functioningTaking psychotropic medication 27 29.3Previous suicide attempt 15 16.3
Note. N = 92.
at SOUTHERN IL UNIV CARBONDALE on July 26, 2012cjb.sagepub.comDownloaded from
Kroner et al. /DHS AMONG WOMEN OFFENDERS 783
mood for three different time periods: For the present study participants reported their mood during the past week. Six mood factors are identified and measured by the POMS: Tension–Anxiety, Depression–Dejection, Anger–Hostility, Vigor–Activity, Fatigue–Inertia, and Confusion–Bewilderment. Among women cancer patients, Cronbach’s alpha for the POMS scales ranged from .33 (Depression–Dejection) to .78 (Vigor–Activity; Hack et al., 2010). McNair et al. (1992) provided evidence of concurrent and predictive validities for the POMS. The POMS was validated on a standardized sample of adults (N = 564; Nyenhuis & Yamamoto, 1999) and has been examined in a sample of 1,350 offenders, including female and male offenders (Samuelson, Carmody, Kabat-Zinn, & Bratt, 2007).
Beck Depression Inventory–2nd Edition (BDI-II). The BDI-II (Beck, Steer, & Brown, 1996) is a 21-item self-report questionnaire developed to measure the severity of depres-sion, each question being scored on a scale of 0 to 3. Total scores ranging from 0 to 13 represent “minimal” depression, total scores from 14 to 19 are “mild” depression, total scores from 20 to 28 are “moderate” depression, and total scores from 29 to 63 represent “severe” depression (Beck, Steer, & Brown, 1996). The questionnaire asks participants to report how they have been feeling for the past 2 weeks. Questions include items relating to symptoms of depression such as hopelessness and irritability as well as physical symptoms such as fatigue. The BDI-II was validated on a sample of 117 incarcerated young adult offenders aged 18 to 21 in the United Kingdom. The BDI-II had a high level of internal consistency (Cronbach’s a = .90). Furthermore, the study found convergent validity, which was evident from the significant correlation between the BDI-II and BHS (r = .55, p < .001; Palmer & Binks, 2008). Boothby and Durham (1999) confirmed that women and younger offenders report higher scores on the BDI-II, which supported the view that mild and severe depression are more evident among women offenders. Perry and Gilbody (2009) estab-lished that the BDI-II had better predictive validity (area under the curve [AUC] = .75) than other related instruments when predicting actual self-harm behavior for their women offender sample with a 4-year follow-up.
Beck Hopelessness Scale (BHS). The BHS (Beck & Steer, 1988) is a 20-item self-report, true–false questionnaire designed to measure three major aspects of hopelessness: feelings about the future, loss of motivation, and expectations. The possible range of scores is 0 to 20. The BHS was validated on a sample of 544 university students and has demonstrated good internal consistency (Cronbach’s a = .88). The BHS has been used in a sample of 105 female offenders, with a correlation of .47 with suicide attempts (Chapman, Specht, & Cellucci, 2005).
Brief Symptom Inventory (BSI). The BSI (Derogatis, 1993) is a 53-item self-report, multi-dimensional measure of psychological distress. The scale was designed to test psychopathol-ogy. The test is based on nine primary symptom dimensions: Somatization, Obsessive Compulsiveness, Interpersonal Sensitivity, Depression, Anxiety, Hostility, Phobic Anxiety, Paranoid Ideation, and Psychoticism. The items are scored on a 5-point scale from 0 (not at all distressed) to 4 (extremely distressed). The BSI was validated on a sample of 200 people that represented community, clinical, and forensic populations (Kellett, Beail, Newman, & Frankish, 2003). All forensic participants demonstrated moderate to good Cronbach’s alpha and split-half alpha (a = .52 to .78). Among women offenders, the BSI scale’s correlations with distress ranged from .37 to .54 (Warren, Hurt, Loper, & Chauhan, 2004).
at SOUTHERN IL UNIV CARBONDALE on July 26, 2012cjb.sagepub.comDownloaded from
784 CRIMINAL JUSTICE AND BEHAVIOR
Beck Scale for Suicide Ideation (BSS). The BSS (Beck & Steer, 1991) is a 20-item scale designed to quantify aspects of suicidal intent and ideation. It is used to assess negative expectancies about the immediate and long-term future. The BSS is scored based on the response of the participant. If the response indicates hopelessness, a score of 1 is recorded, and if the participant indicates nonhopelessness, then a score of 0 is recorded, for a possible total of 20. A score of 14 or higher is severe hopelessness (Palmer & Connelly, 2005). The BSS was validated on 314 university students and demonstrated good internal consistency (Cronbach’s a = .81). The measure is reliable and is appropriate for measuring severity of suicide ideation in college students (Chioqueta & Stiles, 2006). The BSS has been used in a sample of 123 adult male prison inmates from a Category B local prison in England (Palmer & Connelly, 2005).
Structured Clinical Interview for DSM-IV Axis-I Disorders, Clinician Version (SCID-I). The SCID-I (First, Spitzer, Gibbon, & Williams, 1997) is a semistructured interview from which DSM diagnosis can be made. Two construct outcome measures were taken from the SCID-I. First was the diagnosis of Dysthymia, which incorporates multiple items scored via the guide. Dysthymia measures mild depression, and for the purposes of this article is labeled Mild Depression (1 = mild depression, 0 = absence). The second measure was a single hopelessness item from the SCID interview and is labeled Hopelessness (1 = hope-lessness, 0 = absence).
PROCEDURE
Offenders were approached to participate in a study examining emotional functioning in incarcerated women offenders. Data were collected by two women researchers, one at each of two Canadian federal women’s institutions between July 2007 and August 2008. One institution was primarily French speaking, which resulted in approximately one-third of the cases gathered in French. The researchers gathering the SCID-I data were blind to the self-report results from the DHS, POMS, BDI-II, BHS, BSI, and BSS.
STATISTICAL ANALYSIS
Three categories of analyses were conducted. The first category of analysis included basic reliabilities and convergent and discriminant validities. The second category of analyses examined optimal cutoff scores of the DHS Depression and Hopelessness scales. The SCID-I derived measures of mild depression and hopelessness served as the construct outcome criteria. Overall classification accuracy was assessed using receiver operating characteristic (ROC) curves. Sensitivity refers to the DHS correctly identifying those with either mild depression or hopelessness. Specificity refers to the DHS correctly identifying those without mild depression or hopelessness. Both the sensitivity and specificity of the DHS scales are needed to assess overall accuracy. Two strategies were used to determine cutoff scores. First is a statistical optimal point that equally considers the sensitivity and specificity parameters (Steadman, Scott, Osher, Agnese, & Robbins, 2005), which is calcu-lated with Youden’s index (Bewick, Cheek, & Ball, 2004; Perkins & Schisterman, 2006). Second, for a more conservative approach to the development of a cutoff score, the DHS’s sensitivity was emphasized over specificity (Ogloff, Roesch, & Hart, 1993; Reddon, Vander Veen, & Munchua, 2001). Maximal negative predictive power (NPP) was used to
at SOUTHERN IL UNIV CARBONDALE on July 26, 2012cjb.sagepub.comDownloaded from
Kroner et al. /DHS AMONG WOMEN OFFENDERS 785
derive the most conservative cutoff score. These two strategies incorporate the full range of the DHS’s continuous scores.
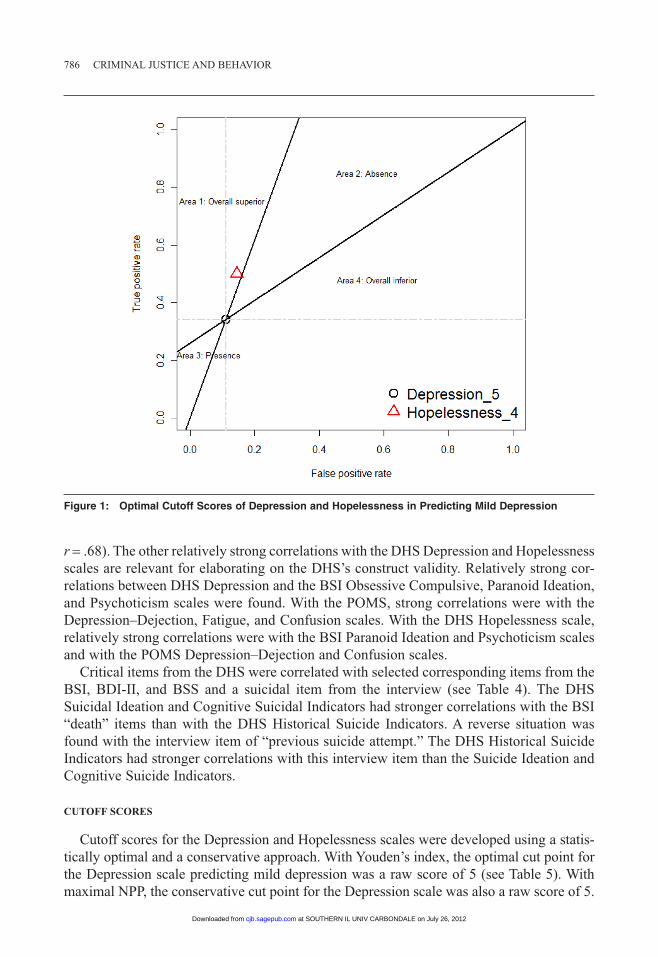
Using cutoff scores and not the full range of the DHS’s continuous scores, the third category of analyses compared the DHS Depression and Hopelessness scales’ optimal cut-off scores. Given that the two scales are strongly correlated, we wanted to determine if the Depression scale’s optimal cutoff score was better at detecting mild depression than the Hopelessness optimal cutoff score and if the Hopelessness optimal cutoff score was better at detecting hopelessness than the Depression optimal cutoff score. The benefit of these analyses is that specific cutoff scores for each scale are used, as compared to the full range of scores used by ROC curve analyses. By using a positive likelihood ratio and a negative likelihood ratio, the use of specific cutoff scores (i.e., a Depression cutoff score and a Hopelessness cutoff score) can directly translate into clinical use. A positive likelihood ratio indicates how many times more likely the participants with the target condition are to have a positive result than participants without the target condition. A negative likelihood ratio indicates how many times less likely the participants with the target condition are to have a negative result than participants without the target condition (Kondratovich, 2008). This comparison can be visually demonstrated in a likelihood graph. With the false positive rate on the x-axis and the true positive rate on the y-axis, the first test score (i.e., Depression) plotted is used as a reference for dividing the graph into four areas (Biggerstaff, 2000; see Figure 1). The first test score produces two solid lines: One line represents the positive likelihood ratio, passing through (0, 0) the bottom left of the graph; the second line repre-sents the negative likelihood ratio, passing through (1, 1) the top right of the graph. The second test score (i.e., Hopelessness cutoff score), the test of comparison, then falls into one of the four areas. Each area represents (Area 1) overall superior classification, (Area 2) better at detecting the absence of the condition (i.e., depression), (Area 3) better at detecting the presence of the condition, and (Area 4) overall inferiority classification (see Figure 1). The graph, with two reference points (D = one scale’s cutoff score, о = the other scale’s cutoff score; Figure 1), assists in comparing the abilities of two scales (Kondratovich, 2008). All cutoff score analyses were conducted in R.
RESULTS
RELIABILITY ANALYSES, CONVERGENT AND DISCRIMINANT VALIDITIES, AND STATISTICAL PREDICTIONS
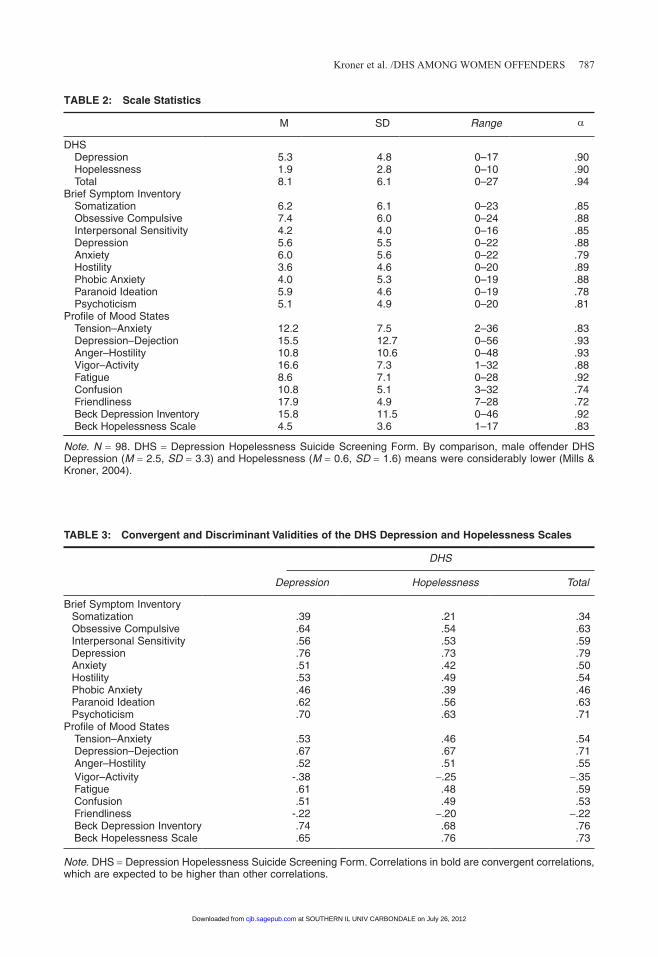
Scales means, ranges, and Cronbach’s alphas are presented in Table 2. The majority of alphas were fairly strong, with DHS Depression and the DHS Hopelessness scales having a Cronbach’s alpha of .90. A subsample of 38 offenders repeated the DHS after 2 weeks. Test–retest coefficients were .80 (Depression), .86 (Hopelessness), and .87 (Total).
The correlations between the DHS scales and the BSI, POMS, BHS, and BDI are in Table 3. In terms of convergent validity, the DHS Depression scale had stronger correla-tions with other depression specific scales (i.e., SSI Depression, r = .76; POMS Depression–Dejection, r = .67) as compared to noncorresponding scales (i.e., BSI Phobic Anxiety, r = .46; POMS Tension–Anxiety, r = .53). With the Beck scales, the corresponding DHS Depression (r = .74) and DHS Hopelessness correlations (r = .76) were stronger than the noncorre-sponding correlations (DHS Depression and BHS, r = .65; DHS Hopelessness and BDS,
at SOUTHERN IL UNIV CARBONDALE on July 26, 2012cjb.sagepub.comDownloaded from
786 CRIMINAL JUSTICE AND BEHAVIOR
Figure 1: Optimal Cutoff Scores of Depression and Hopelessness in Predicting Mild Depression
r = .68). The other relatively strong correlations with the DHS Depression and Hopelessness scales are relevant for elaborating on the DHS’s construct validity. Relatively strong cor-relations between DHS Depression and the BSI Obsessive Compulsive, Paranoid Ideation, and Psychoticism scales were found. With the POMS, strong correlations were with the Depression–Dejection, Fatigue, and Confusion scales. With the DHS Hopelessness scale, relatively strong correlations were with the BSI Paranoid Ideation and Psychoticism scales and with the POMS Depression–Dejection and Confusion scales.
Critical items from the DHS were correlated with selected corresponding items from the BSI, BDI-II, and BSS and a suicidal item from the interview (see Table 4). The DHS Suicidal Ideation and Cognitive Suicidal Indicators had stronger correlations with the BSI “death” items than with the DHS Historical Suicide Indicators. A reverse situation was found with the interview item of “previous suicide attempt.” The DHS Historical Suicide Indicators had stronger correlations with this interview item than the Suicide Ideation and Cognitive Suicide Indicators.
CUTOFF SCORES
Cutoff scores for the Depression and Hopelessness scales were developed using a statis-tically optimal and a conservative approach. With Youden’s index, the optimal cut point for the Depression scale predicting mild depression was a raw score of 5 (see Table 5). With maximal NPP, the conservative cut point for the Depression scale was also a raw score of 5.
at SOUTHERN IL UNIV CARBONDALE on July 26, 2012cjb.sagepub.comDownloaded from
Kroner et al. /DHS AMONG WOMEN OFFENDERS 787
TABLE 2: Scale Statistics
M SD Range a
DHSDepression 5.3 4.8 0–17 .90Hopelessness 1.9 2.8 0–10 .90Total 8.1 6.1 0–27 .94
Brief Symptom InventorySomatization 6.2 6.1 0–23 .85Obsessive Compulsive 7.4 6.0 0–24 .88Interpersonal Sensitivity 4.2 4.0 0–16 .85Depression 5.6 5.5 0–22 .88Anxiety 6.0 5.6 0–22 .79Hostility 3.6 4.6 0–20 .89Phobic Anxiety 4.0 5.3 0–19 .88Paranoid Ideation 5.9 4.6 0–19 .78Psychoticism 5.1 4.9 0–20 .81
Profile of Mood StatesTension–Anxiety 12.2 7.5 2–36 .83Depression–Dejection 15.5 12.7 0–56 .93Anger–Hostility 10.8 10.6 0–48 .93Vigor–Activity 16.6 7.3 1–32 .88Fatigue 8.6 7.1 0–28 .92Confusion 10.8 5.1 3–32 .74Friendliness 17.9 4.9 7–28 .72Beck Depression Inventory 15.8 11.5 0–46 .92Beck Hopelessness Scale 4.5 3.6 1–17 .83
Note. N = 98. DHS = Depression Hopelessness Suicide Screening Form. By comparison, male offender DHS Depression (M = 2.5, SD = 3.3) and Hopelessness (M = 0.6, SD = 1.6) means were considerably lower (Mills & Kroner, 2004).
TABLE 3: Convergent and Discriminant Validities of the DHS Depression and Hopelessness Scales
DHS
Depression Hopelessness Total
Brief Symptom InventorySomatization .39 .21 .34Obsessive Compulsive .64 .54 .63Interpersonal Sensitivity .56 .53 .59Depression .76 .73 .79Anxiety .51 .42 .50Hostility .53 .49 .54Phobic Anxiety .46 .39 .46Paranoid Ideation .62 .56 .63Psychoticism .70 .63 .71
Profile of Mood StatesTension–Anxiety .53 .46 .54Depression–Dejection .67 .67 .71Anger–Hostility .52 .51 .55Vigor–Activity -.38 -.25 -.35Fatigue .61 .48 .59Confusion .51 .49 .53Friendliness -.22 -.20 -.22Beck Depression Inventory .74 .68 .76Beck Hopelessness Scale .65 .76 .73
Note. DHS = Depression Hopelessness Suicide Screening Form. Correlations in bold are convergent correlations, which are expected to be higher than other correlations.
at SOUTHERN IL UNIV CARBONDALE on July 26, 2012cjb.sagepub.comDownloaded from

788 CRIMINAL JUSTICE AND BEHAVIOR
The sensitivity of the Depression scale in predicting mild depression was quite strong (.90). With Youden’s index, the optimal cut point for the Hopelessness scale in predicting hope-lessness was a raw score of 3 (see Table 6). With maximal NPP, the conservative cut point for the Hopelessness scale was also a raw score of 3. The Hopelessness scale’s sensitivity was weaker than the Depression scale in predicting mild depression, but the Hopelessness scale had relatively stronger specificity (.80 vs. .64) in predicting hopelessness.
In the present study, the DHS’s restriction of range and distributional characteristics likely contributed to the lack of differences between the optimal and conservative cutoff scores. The DHS items covered a broad range of serious depression and hopelessness areas, and therefore individual items are not likely to be in the midrange of endorsement (i.e., 30%–70%). If the items were in the endorsement midrange, the optimal and conservative cutoff scores would likely differ.
TABLE 4: Zero-Order Correlations Between the Critical Items From Corresponding Depression and Hopelessness Scales and the DHS
Suicide Ideation
Cognitive Suicide
Indicators Historical Suicide Indicators
#56 #62 #66 #67 #17 #35 #23 #29 #41 #47 #53
Brief Symptom Inventory“Death” item .47** .35** .19 .35** .29** .35** .24* .37** .12 .19 .10
Beck Depression Inventory“Suicide thoughts or wishes” .53** .42** .08 .61** .36** .56** .45** .41** .33** .39** .34**
Beck Suicide Inventory“No wish to live” .45** .80** .45** .59** .45** .55** .31** .38** .22* .35** .42**“Wish to die” .57** .64** .48** .63** .47** .69** .42** .45** .35** .46** .35**
InterviewPrevious suicide attempt .11 .16 .10 .32** .21* .29** .42** .50** .55** .62** .19
Note. DHS = Depression Hopelessness Suicide Screening Form. #56 = “Serious thoughts of suicide”; #62 = “Life is not worth living”; #66 = “I have a plan to hurt myself”; #67 = “I would rather be dead”; #17 = “Suicide is not an option for me”; #35 = “If circumstances get too bad, suicide is always an option”; #23 = “I have had serious thoughts of suicide in the past”; #29 = “I have intentionally hurt myself”; #41 = “In the past I have attempted sui-cide”; #47 = “I have attempted suicide more than once in the past”; #53 = “I have attempted suicide in the past two years.” The previous suicide attempt item came from the interview.*p < .05. **p < .01.
TABLE 5: Predictive Utility of Cutoff Scores for the DHS Depression, Hopelessness, and Total Scale Scores for the Mild Depression Criterion
DHS Cutoff Scores Sensitivity Specificity PPP NPP
Optimal Cutoff Score (Youden index)Depression (5) .90 .64 .40 .96Hopelessness (4) .47 .86 .47 .86Total (5) .90 .59 .36 .96
Maximal NPPDepression (5) .90 .64 .40 .96Hopelessness (2) .58 .71 .34 .86Total (5) .90 .59 .36 .96
Note. DHS = Depression Hopelessness Suicide Screening Form; PPP = positive predictive power; NPP = negative predictive power. The statistical predictions of mild depression, measured by the area under the curve, were .77 (95% CI = .67–.86) for the DHS Depression scale, .67 (95% CI = .59–.75) for the DHS Hopelessness scale, and .76 (95% CI = .65–.87) for the DHS total score.
at SOUTHERN IL UNIV CARBONDALE on July 26, 2012cjb.sagepub.comDownloaded from
Kroner et al. /DHS AMONG WOMEN OFFENDERS 789
COMPARISON OF DEPRESSION AND HOPELESSNESS CUTOFF SCORES
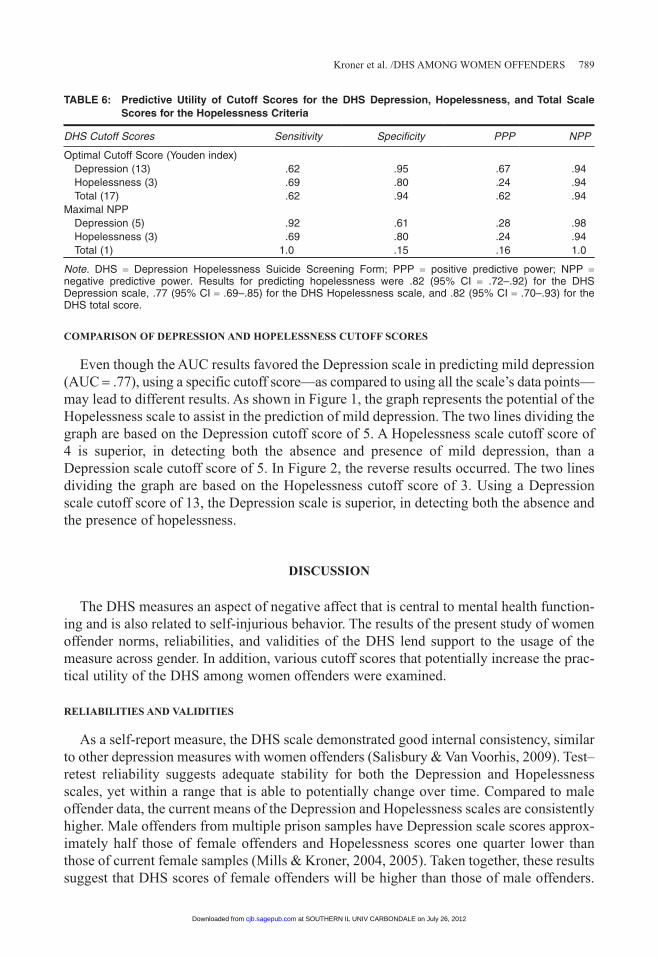
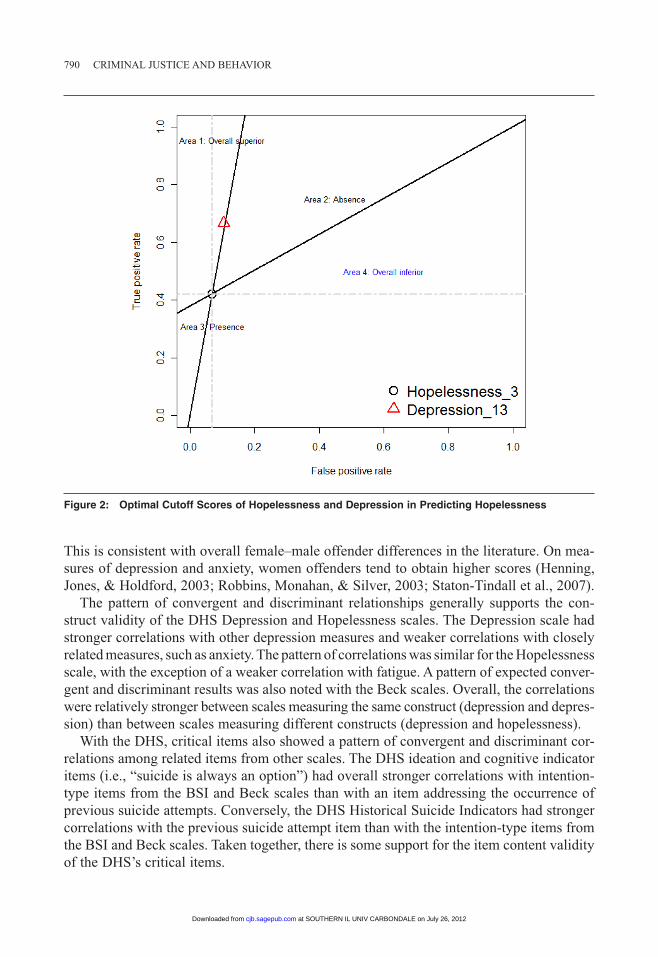
Even though the AUC results favored the Depression scale in predicting mild depression (AUC = .77), using a specific cutoff score—as compared to using all the scale’s data points—may lead to different results. As shown in Figure 1, the graph represents the potential of the Hopelessness scale to assist in the prediction of mild depression. The two lines dividing the graph are based on the Depression cutoff score of 5. A Hopelessness scale cutoff score of 4 is superior, in detecting both the absence and presence of mild depression, than a Depression scale cutoff score of 5. In Figure 2, the reverse results occurred. The two lines dividing the graph are based on the Hopelessness cutoff score of 3. Using a Depression scale cutoff score of 13, the Depression scale is superior, in detecting both the absence and the presence of hopelessness.
DISCUSSION
The DHS measures an aspect of negative affect that is central to mental health function-ing and is also related to self-injurious behavior. The results of the present study of women offender norms, reliabilities, and validities of the DHS lend support to the usage of the measure across gender. In addition, various cutoff scores that potentially increase the prac-tical utility of the DHS among women offenders were examined.
RELIABILITIES AND VALIDITIES
As a self-report measure, the DHS scale demonstrated good internal consistency, similar to other depression measures with women offenders (Salisbury & Van Voorhis, 2009). Test–retest reliability suggests adequate stability for both the Depression and Hopelessness scales, yet within a range that is able to potentially change over time. Compared to male offender data, the current means of the Depression and Hopelessness scales are consistently higher. Male offenders from multiple prison samples have Depression scale scores approx-imately half those of female offenders and Hopelessness scores one quarter lower than those of current female samples (Mills & Kroner, 2004, 2005). Taken together, these results suggest that DHS scores of female offenders will be higher than those of male offenders.
TABLE 6: Predictive Utility of Cutoff Scores for the DHS Depression, Hopelessness, and Total Scale Scores for the Hopelessness Criteria
DHS Cutoff Scores Sensitivity Specificity PPP NPP
Optimal Cutoff Score (Youden index)Depression (13) .62 .95 .67 .94Hopelessness (3) .69 .80 .24 .94Total (17) .62 .94 .62 .94
Maximal NPPDepression (5) .92 .61 .28 .98Hopelessness (3) .69 .80 .24 .94Total (1) 1.0 .15 .16 1.0
Note. DHS = Depression Hopelessness Suicide Screening Form; PPP = positive predictive power; NPP = negative predictive power. Results for predicting hopelessness were .82 (95% CI = .72–.92) for the DHS Depression scale, .77 (95% CI = .69–.85) for the DHS Hopelessness scale, and .82 (95% CI = .70–.93) for the DHS total score.
at SOUTHERN IL UNIV CARBONDALE on July 26, 2012cjb.sagepub.comDownloaded from
790 CRIMINAL JUSTICE AND BEHAVIOR
This is consistent with overall female–male offender differences in the literature. On mea-sures of depression and anxiety, women offenders tend to obtain higher scores (Henning, Jones, & Holdford, 2003; Robbins, Monahan, & Silver, 2003; Staton-Tindall et al., 2007).
The pattern of convergent and discriminant relationships generally supports the con-struct validity of the DHS Depression and Hopelessness scales. The Depression scale had stronger correlations with other depression measures and weaker correlations with closely related measures, such as anxiety. The pattern of correlations was similar for the Hopelessness scale, with the exception of a weaker correlation with fatigue. A pattern of expected conver-gent and discriminant results was also noted with the Beck scales. Overall, the correlations were relatively stronger between scales measuring the same construct (depression and depres-sion) than between scales measuring different constructs (depression and hopelessness).
With the DHS, critical items also showed a pattern of convergent and discriminant cor-relations among related items from other scales. The DHS ideation and cognitive indicator items (i.e., “suicide is always an option”) had overall stronger correlations with intention-type items from the BSI and Beck scales than with an item addressing the occurrence of previous suicide attempts. Conversely, the DHS Historical Suicide Indicators had stronger correlations with the previous suicide attempt item than with the intention-type items from the BSI and Beck scales. Taken together, there is some support for the item content validity of the DHS’s critical items.
Figure 2: Optimal Cutoff Scores of Hopelessness and Depression in Predicting Hopelessness
at SOUTHERN IL UNIV CARBONDALE on July 26, 2012cjb.sagepub.comDownloaded from

Kroner et al. /DHS AMONG WOMEN OFFENDERS 791
DHS CUTOFF SCORES
The purpose of including specific cutoff scores is to produce DHS scores that are spe-cific to women offenders and to enable a direct clinical application of the present results. Comparing the current results with those of other female correctional samples can place the sensitivity and specificity rates within a broader context. Using a screening tool for general psychopathology, with Axis I and Axis II as predictive criteria, Ford, Trestman, Wiesbrock, and Zhang (2007) found optimal sensitivity rates between .54 and .63. With the DHS Depression scale (cutoff score = 5), the sensitivity rate was .90. This Depression cutoff score had a strong ability to detect those with mild depression. It appears that the DHS Depression content area covers a broad spectrum of the contributors to mild depression. The DHS Hopelessness scale (cutoff score = 3) had a sensitivity rate of .69, which is simi-lar to the Ford et al. sensitivity rates between .54 and .63. With regard to specificity, Ford et al.’s rates were between .79 and .94. With the DHS Depression scale, the rate was lower, at .64. Thus, the Depression scale detects mild depression well, but likely includes content of more serious forms of depression, which reduces the scale’s specificity. In addition, the current sample of women offenders may not have a high rate of more serious depression.
Although the full range of DHS Depression and Hopelessness scores shows convergent and discriminant validities, the application of specific cutoff scores for specific criteria in the lower range is not so clear. With specific cutoff scores, the Depression scale uniquely contributed to the prediction of hopelessness and the Hopelessness scale uniquely contrib-uted to the prediction of mild depression. It may be that the cutoff scores being at the lower end of the distribution may limit the prediction of narrowly defined outcomes. With more broadly defined criteria and greater severity, each scale may be better able to uniquely predict its respective outcomes.
Given that the optimal cutoff scores for male offenders were between 8 and 10 for the total DHS scores (Mills & Kroner, 2005), cutoff scores for the DHS among female offend-ers should be specific to them. The use of other, male-derived cutoff scores would mis-classify women offenders for mild depression and hopelessness. Also, the scale means are higher than those of male offenders. Drawing on the frequency argument in the gender-responsiveness literature (Van Voorhis, Wright, Salisbury, & Bauman, 2010), the different endorsement rates of depression and hopelessness would preclude a direct crossover application of male-derived DHS basic norms. Thus, in terms of differential endorsement rates, the present results provide some support for gender-specific interpretation guidelines (i.e., cutoff scores) for instruments used to assess women offenders.
In addition to endorsement rates, the consequences of depression and hopelessness may differ between female and male offenders. Benda (2005) found support for depression contributing to recidivism for women, but not for men. In predicting self-harm among women offenders, depression demonstrated stronger predictability than hopelessness (Perry & Gilbody, 2009), although others suggest that hopelessness may have a stronger role (Chapman et al., 2005). Wright et al. (2007) found current depression or anxiety to be predictive of prison misconduct among women at both 6-month and 12-month follow-up times. In addition to the direct consequences of depression and hopelessness, the interaction between depression or hopelessness and institutional characteristics may differ between female and male offenders. For example, Wolff and Shi (2009) found women to feel more safe in prison and experience less staff-on-offender victimization. Thus, the inability of
at SOUTHERN IL UNIV CARBONDALE on July 26, 2012cjb.sagepub.comDownloaded from

792 CRIMINAL JUSTICE AND BEHAVIOR
depression in the current study to predict major depression may be related to either the specific expression patterns of major depression among incarcerated women or an interac-tion between depression and characteristics of institutional confinement.
INTERPRETATION OF DHS RESULTS IN WOMEN
The above cutoff scores and convergent and discriminant validities may assist in deter-mining which scores are used for interpretation of the DHS among women offenders. To further facilitate the interpretation of the DHS, the following comments below, derived from the data in Table 3, may highlight a more gender-specific interpretation of the DHS scales:
With women offenders, elevated DHS Depression scores are associated with fatigue, being muddled, forgetfulness, feeling exhausted, sluggish, and tense. Elevated scores are associated with feeling alone, difficulties concentrating, and difficulty in trusting others.
With women offenders, elevated DHS Hopelessness scores are associated with difficulty in making decisions, feeling below others, and feeling that others dislike you. There is a pervasive feeling that something is wrong.
Although the present results support gender-specific norms of the DHS, there is some sup-port for the measurement of depression and hopelessness being equally valid between female and male offenders. The convergent and discriminant validities for the Depression and Hopelessness scales were in the expected direction, similar to what has been found with male offenders (Mills & Kroner, 2005). Also, the critical items demonstrated the expected convergent and discriminant validities. Even with adequate validities, having a closely related normative sample is a top priority. Normative samples are essential to a proper clinical interpretation (Nunnally & Bernstein, 1994). In choosing appropriate norms for interpretation, consideration should be given to context (i.e., community vs. maximum security), recency of the norms, and then basic demographics, such as gender, age, and race (Kroner, Mills, Gray, & Talbert, 2011).
The current study has its limitations. First, the expression of depressive symptoms may have skewed the self-report of depression and hopelessness toward overreporting. This may have contributed to a lack of relationship between the self-report measures of depres-sion and the diagnosis of major depression. Second, the two outcome criteria were different measurement models. The mild depression criteria involved a standardized rating scale that has been well researched, whereas the hopelessness criterion was one item. Typically single-item measures are subjected to reliability criticisms. Third, this study was of a cross-sectional design. Prediction is an important aspect of validity within criminal justice settings. The depression and hopelessness self-report measures were gathered at the same time as the criteria rating measures. The researchers who gathered the interview data were not aware of the self-report results, which limited potential contamination but precluded a truly predictive design. Research design issues may explain why with women offenders hope-lessness is less predictive of future self-harm (i.e., Perry & Gilbody, 2009) and relatively more predictive of women offender past history of self-harm (i.e., Chapman et al., 2005). Another limitation is that the DHS has not been used with nonoffender women, as to pro-vide comparisons with women offenders. In the application of measures to women offenders, Blanchette and Brown (2006) argue that measures developed on women offenders are optimal, with the development of specific cutoff scores for women offenders as an option.
at SOUTHERN IL UNIV CARBONDALE on July 26, 2012cjb.sagepub.comDownloaded from
Kroner et al. /DHS AMONG WOMEN OFFENDERS 793
Even with unique women cutoff scores, it should be noted that the basic reliabilities and validities are similar to those of male offenders.
CONCLUSIONS
Other areas of women offender assessment, such as risk assessment, have shown that gender-neutral instruments can work with women offenders (Blanchette & Motiuk, 2004; Folsom & Atkinson, 2007; Holtfreter & Cupp, 2007). But whole-scale application of instruments to a specific population will result in unwanted shortcomings. As with criminal justice risk assessment, aspects of the DHS basic validities for the Depression and Hopelessness scales function similarly among male offenders, but the interpretation and interpretation guidelines should be unique for female offenders.
REFERENCES
Afifi, M. (2007). Gender differences in mental health. Singapore Medical Journal, 48, 385-391.Beck, A. T., & Steer, R. A. (1988). Beck Hopelessness Scale manual. Orlando, FL: Psychological Corporation Harcourt
Brace Jovanovich.Beck, A. T., & Steer, R. A. (1991). Manual for Beck Scale for Suicide Ideation. San Antonio, TX: Psychological Corporation.Beck, A. T., Steer, R. A., & Brown, G. K. (1996). Beck Depression Inventory–Second Edition manual. San Antonio, TX:
Psychological Corporation.Beck, A. T., Weissman, A., Lester, D., & Trexler, L. (1974). The measurement of pessimism: The hopelessness scale. Journal
of Consulting and Clinical Psychology, 42, 861-865.Benda, B. B. (2005). Gender differences in life-course theory of recidivism: A survival analysis. International Journal of
Offender Therapy and Comparative Criminology, 49, 325-342.Bewick, V., Cheek, L., & Ball, J. (2004). Statistics review 13: Receiver operating characteristics curves. Critical Care, 8, 508-512.Biggerstaff, B. J. (2000). Comparing diagnostic tests: A simple graphic using likelihood ratios. Statistics in Medicine, 19,
649-663.Blanchette, K., & Brown, S. L. (2006). The assessment and treatment of women offenders: An integrative perspective.
New York, NY: John Wiley.Blanchette, K., & Motiuk, L. L. (2004). Taking down the straw man: A reply to Webster and Doob. Canadian Journal of
Criminology and Criminal Justice, 46, 621-630.Boothby, J. L., & Durham, T. W. (1999). Screening for depression in prisoners using Beck Depression Inventory. Criminal
Justice and Behavior, 26, 107-124.Chapman, A. L., Specht, M. W., & Cellucci, T. (2005). Factors associated with suicide attempts in female inmates: The
hegemony of hopelessness. Suicide and Life-Threatening Behavior, 35, 558-569.Chioqueta, A. P., & Stiles, T. C. (2006). Psychometric properties of the Beck Scale for Suicide Ideation: A Norwegian study.
Nord Journal of Psychiatry, 60, 400-404.Collie, R. M., & Polascheck, D. L. L. (2003). Sorting women’s risk: New Zealand women prisoners’ misconducts and inter-
nal security risk. New Zealand Journal of Psychology, 32, 101-109.Correia, K. M. (2000). Suicide assessment in a prison environment: A proposed protocol. Criminal Justice and Behavior, 27,
581-599.Derogatis, L. R. (1993). Brief Symptom Inventory: Administration scoring and procedures manual (3rd ed.). Minneapolis,
MN: National Computer Systems.Dieserud, G., Roysamb, E., Ekeberg, O., & Kraft, P. (2001). Toward an integrative model of suicide attempt: A cognitive
psychological approach. Suicide and Life-Threatening Behavior, 31, 153-168.Dixon, W. A., Heppner, P. P., & Rudd, M. D. (1994). Problem-solving appraisal, hopelessness, and suicide ideation:
Evidence for a mediational model. Journal of Counseling Psychology, 41, 91-98.Dohrenwend, B. P., Levav, I., Shrout, P. E., Schwartz, S., Naveh, G., Link, B. G., . . . & Stueve, A. (1992). Socioeconomic
status and psychiatric disorders: The causation-selection issue. Science, 255, 946-952.First, M. B., Spitzer, R. L., Gibbon, M., & Williams, J. B. W. (1997). Structured Clinical Interview for DSM-IV Axis-I
Disorders (SCID-I), Clinician Version. Washington, DC: American Psychiatric Press.
at SOUTHERN IL UNIV CARBONDALE on July 26, 2012cjb.sagepub.comDownloaded from

794 CRIMINAL JUSTICE AND BEHAVIOR
Folsom, J., & Atkinson, J. L. (2007). The generalizability of the LSI-R and the CAT to the prediction of recidivism in female offenders. Criminal Justice and Behavior, 34, 1044-1056.
Ford, J. D., Trestman, R. L., Wiesbrock, V., & Zhang, W. (2007). Development and validation of a brief mental health screen-ing instrument for newly incarcerated adults. Assessment, 14, 279-299.
Hack, T. F., Pickles, T., Ruether, D., Weir, L., Bultz, B. D., Mackey, J., & Degner, L. F. (2010). Predictors of distress and quality of life in patients undergoing cancer therapy: Impact of treatment type and decisional role. Psycho-Oncology, 19, 606-616. doi:10.1002/pon.1590
Harer, M. D., & Langan, N. P. (2001). Gender differences in predictors of prison violence: Assessing the predictive validity of a risk classification system. Crime & Delinquency, 47, 513-536.
Henning, K., Jones, A., & Holdford, R. (2003). Treatment needs of women arrested for domestic violence: A comparison with male offenders. Journal of Interpersonal Violence, 18, 839-856.
Holtfreter, K., & Cupp, R. (2007). Gender and risk assessment: The empirical status of the LSI-R for women. Journal of Contemporary Criminal Justice, 23, 363-382.
Kellett, S., Beail, N., Newman, D. W., & Frankish, P. (2003). Utility of the brief symptom inventory in the assessment of psychological distress. Journal of Applied Research in Intellectual Disabilities, 16, 127-134.
Kendler, K. S., Myers, J., & Prescott, C. A. (2005). Sex differences in the relationship between social support and risk for major depression: A longitudinal study of opposite-sex twin pairs. American Journal of Psychiatry, 162, 250-256.
Khan, A. A., Jacobson, K. C., Gardner, C. O., Prescott, C. A., & Kendler, K. S. (2005). Personality and comorbidity of com-mon psychiatric disorders. British Journal of Psychiatry, 186, 190-196.
Kondratovich, M. V. (2008). Comparing two medical tests when results of reference standard are unavailable for those negative via both tests. Journal of Biopharmaceutical Statistics, 18, 145-166.
Konick, L. C., & Gutierrez, P. M. (2005). Testing a model of suicide ideation in college students. Suicide and Life-Threatening Behavior, 35, 181-192.
Kroner, D. G., Mills, J. F., Gray, A., & Talbert, K. (2011). Clinical assessment in correctional settings. In T. J. Fagan & R. K. Ax (Eds.), Correctional mental health: From theory to best practice (pp. 79-102). Thousand Oaks, CA: Sage.
McNair, D. M., Lorr, M., & Droppleman, L. F. (1992). Revised manual for the Profile of Mood States. San Diego, CA: Educational and Industrial Testing Services.
Mills, J. F., & Kroner, D. G. (2003). Depression, Hopelessness and Suicide Screening Form (DHS): User guide. Selby, Ontario: Authors.
Mills, J. F., & Kroner, D. G. (2004). A new instrument to screen for depression, hopelessness and suicide in offenders. Psychological Services, 1, 83-91.
Mills, J. F., & Kroner, D. G. (2005). Screening for suicide risk factors in prison inmates: Evaluating the efficiency of the Depression, Hopelessness and Suicide Screening Form (DHS). Legal and Criminological Psychology, 10, 1-12.
Motiuk, L. L., & Porporino, F. J. (1992). The prevalence, nature, and severity of mental health problems among federal male inmates in Canadian penitentiaries (Research Report No. R-24). Ottawa: Corrections Service Canada.
Murdoch, N., Morris, P., & Holmes, C. (2008). Depression in elderly life sentence prisoners. International Journal of Geriatric Psychiatry, 23, 957-962.
Newton-Howes, G., Tryer, P., & Johnson, T. (2006). Personality disorder and the outcome of depression: Meta-analysis of published studies. British Journal of Psychiatry, 188, 13-20.
Ng, I. Y. H., Shen, X., Sim, H., Sarri, R. C., Stoggregen, E., & Shook, J. J. (2010). Incarcerating juveniles in adult prisons as a factor in depression. Criminal Behaviour and Mental Health, 21, 21-34. doi:10.1002/cmb.783
Nunnally, J. C., & Bernstein, I. H. (1994). Psychometric theory (3rd ed.). New York, NY: McGraw-Hill.Nyenhuis, D. L., & Yamamoto, C. (1999). Adult and geriatric normative data and validation of the Profile of Mood States.
Journal of Clinical Psychology, 55, 79-86.Ogloff, J. R. P., Roesch, R., & Hart, S. D. (1993). Screening, assessment, and identification of services for mentally ill offend-
ers. In H. J. Steadman & J. J. Cocozza (Eds.), Mental illness in America (NCJ 151849; pp. 61-90). Washington, DC: U.S. Department of Health and Human Services.
Palmer, E. J., & Binks, C. (2008). Psychometric properties of the Beck Depression Inventory–II with incarcerated male offenders ages 18–21. Criminal Behaviour and Mental Health, 18, 232-242.
Palmer, E. J., & Connelly, R. (2005). Depression, hopelessness, and suicide ideation among vulnerable prisoners. Criminal Behaviour and Mental Health, 15, 164-170.
Panzarino, P. J., Jr. (1998). The costs of depression: Direct and indirect: Treatment versus nontreatment. Journal of Clinical Psychiatry, 59, 11-14.
Patel, V., Araya, R., Lima, M. S., Ludermir, A., & Todd, C. (1999). Women, poverty and common mental disorders in four restructuring societies. Social Science & Medicine, 49, 1461-1471.
Perkins, N. J., & Schisterman, E. F. (2006). The inconsistency of “optimal” cutpoints obtained by using two criteria based on the receiver operating characteristic curve. American Journal of Epidemiology, 163, 670-675.
Perry, A. E., & Gilbody, S. (2009). Detecting and predicting self-harm behaviour in prisoners: A prospective psychometric analysis of three instruments. Social Psychiatry and Epidemiology, 44, 853-861.
at SOUTHERN IL UNIV CARBONDALE on July 26, 2012cjb.sagepub.comDownloaded from
Kroner et al. /DHS AMONG WOMEN OFFENDERS 795
Piccinelli, M., & Wilkinson, G. (2000). Gender differences in depression. British Journal of Psychiatry, 177, 486-492.Reddon, J. R., Vander Veen, S., & Munchua, M. M. (2001). The hierarchical nexus of psychosocial adjustment and psycho-
pathology: Relationship of the Holden Psychological Screening Inventory (HPSI) with the Basic Personality Inventory (BPI) and the Differential Personality Inventory (DPI). In F. Columbus (Ed.), Advances in psychology research (Vol. 3, pp. 91-125). Huntington, NY: Nova Science.
Robbins, P. C., Monahan, J., & Silver, E. (2003). Mental disorder, violence, and gender. Law and Human Behavior, 27, 561-571.Rudd, M. D., Joiner, T., & Rajab, M. H. (1996). Relationships among suicide ideators, attempters, and multiple attempters
in a young-adult sample. Journal of Abnormal Psychology, 105, 541-550.Salisbury, E. J., & Van Voorhis, P. (2009). Gendered pathways: A qualitative investigation of women probationers’ paths to
incarceration. Criminal Justice and Behavior, 36, 541-566.Salisbury, E. J., Van Voorhis, P., & Spiropoulos, G. V. (2009). The predictive validity of a gender-responsive needs assess-
ment: An exploratory study. Crime & Delinquency, 55, 550-585.Samuelson, M., Carmody, J., Kabat-Zinn, J., & Bratt, M. A. (2007). Mindfulness-based stress reduction in Massachusetts
correctional facilities. The Prison Journal, 87, 254-268.Staton-Tindall, M., Garner, B. R., Morey, J. T., Leukefeld, C., Krietemeyer, J., Saum, C. A., & Oser, C. B. (2007). Gender
differences in treatment engagement among a sample of incarcerated substance abusers. Criminal Justice and Behavior, 34, 1143-1156.
Steadman, H. J., Scott, J. E., Osher, F., Agnese, T. K., & Robbins, P. C. (2005). Validation of the Brief Jail Mental Health Screen. Psychiatric Services, 56, 816-822.
Van Voorhis, P., Wright, E. M., Salisbury, E., & Bauman, A. (2010). Women’s risk factors and their contributions to exist-ing risk/needs assessment: The current status of a gender-responsive supplement. Criminal Justice and Behavior, 37, 261-288.
Warren, J. I., Hurt, S., Loper, A. B., & Chauhan, P. (2004). Exploring prison adjustment among female inmates-issues of measurement and prediction. Criminal Justice and Behavior, 31, 624-645.
Wolff, N., & Shi, J. (2009). Type, source, and patterns of physical victimization: A comparison of male and female inmates. The Prison Journal, 89, 172-191.
Wright, E. M., Salisbury, E. J., & Van Voorhis, P. (2007). Predicting the prison misconducts of women offenders: The importance of gender-responsive needs. Journal of Contemporary Criminal Justice, 23, 310-340.
Daryl G. Kroner, PhD, is an assistant professor in the Department of Criminology and Criminal Justice at Southern Illinois University Carbondale. His current projects include mental health assessment of female offenders, dynamic risk assessment during community supervision, evaluating community interventions, and treatment of offenders with mental illness.
Tamara Kang is a doctoral student in psychology at the University of Texas, El Paso. As a McNair Scholar student, she completed her undergraduate degree at Southern Illinois University Carbondale. Her research interests include affective functioning among women offenders.
Jeremy F. Mills, PhD, CPsych, is a psychologist with a practice in forensic, correctional, and counseling psychology in Kingston, Ontario, Canada. In addition, he serves as adjunct research professor in the Department of Psychology at Carleton University in Ottawa. He is a fellow of the American Psychological Association, and his research interests include violence risk assessment, violence risk communication, and the assessment of suicide risk.
Andrew J. R. Harris, PhD, CPsych, is a senior research manager at Correctional Service Canada National Headquarters. His clinical and research interests center around risk assessment for sexual offenders, with a particular emphasis on the assess-ment of dynamic risk of reoffense.
Michelle M. Green is a doctoral student in social/personality psychology at Brock University. She recently completed her master’s thesis exploring stress, social support, and health risk behaviors as mediators of the forgiveness–health relation.
at SOUTHERN IL UNIV CARBONDALE on July 26, 2012cjb.sagepub.comDownloaded from




















