Acute concentration of hydroxyproline in different methods of strength training
7
I.J. Fitness (2010) 6, Issue 1, pp.17 -23 Acute concentration of hydroxyproline in different methods of strength training Antonio de Carvalho Nogueira', Juan C. Colado 2 , Januário Gomes Mouráo e Lima 3 , Rodrigo Gomes de Souza Vale', Xavier García-Massó 5 and Estélio Henrique Martín Dantas 6 1.4.6Laboratoryof Biological Sciences of the human motor (UCB - Rio de Janeiro Brazil). Email: [email protected] 2.50epartment of Physical Education and Sports, University of Valencia, Valencia, Spain. 3LaboratoryofMorphology (UNISUAM RiodeJaneiro Brazil). Abstract. This research was designed to measure the levels 01hydroxyproline (HP) in urine alter the application of two diflerent methods of strength training. Thirty fit, healthy men were randomly divided into two groups: exercise (EG) and control (CG). 80th groups provided urine samples priorto training, although only the EG performed 1 repetition maximum (RM); 5RM and 30RM tests. Alter this, the EG performed three series of 5RM. Alter two hours, urine samples were collected lrom the EG. Sixteen days later, the same pl;.ocedure took place using a 30RM protocol. The HP levels in urine were quantified colorimetrically using a spectrophotometer. Statistically signilicant diflerences in HP values were found only lor the the 5RM training method (e. = -22%, P < 0.05). Itwas concluded that damage to the conjunctive tissue only took place with 5RM training, thus confirming that one way 01avoiding stagnation in the adaptation 01subjects with certain experience 01strength training is to use more intense methods .. However, in such training protocols, the recovery time between sessions should be greater due to the resulting increase in tissue damage. Keywords: Urine, Resistance exercise, Conjunctivetissue, Damage. Introduction Conjunctive tissue is present in numerous body structures, such as the tendons, epimysium and perimysium located in the muscles. With the latter, the consecutive and parallel structures of the tissue distribute the effort produced by muscle contraction (Brown et al., 1999). The connective tissue can be damaged when physical exercise is performed at intensities larger than usual (Brown et al., 1997). This damage can be measured by assessing collagen metabolismo Hydroxyproline is generated by the hydroxylation of proline, a reaction that takes place during the catabolism of collagen. As a result, the measurement ofhydroxyproline in the blood or urine is often used as an indicator of collagen degradation (Brown et al., 1997; Murguria et al., 1998; Virtanen et al., 1993). In the event of an injury, sufficient time must be allowed to rest and to ensure the total recovery from the damage caused to the conjunctive tissue. If this is not tbe case, the injury could worsen as the tissue adaptation process is hindered (Tofas et al., 2008). This makes it necessary to identify the acute phy'siological stress that is involved in each specific kind oftraining, as we can then prescribe longer rest periods between training sessions, and thus avoid excessive exercise and favour recovery from injury (Avery and Bailey, 2005). In addition, identification of the physiological stress that can be caused by different strength training methods would also allow us to identify the best metbods according to tbe pbysical condition and goals of the person exercising. This would favour the prescription of more © 2010 Fitness Society of India
Transcript of Acute concentration of hydroxyproline in different methods of strength training

I.J. Fitness (2010)6, Issue 1, pp.17 -23
Acute concentration of hydroxyproline in differentmethods of strength training
Antonio de Carvalho Nogueira', Juan C. Colado2, Januário Gomes Mouráo e Lima3
,
Rodrigo Gomes de Souza Vale', Xavier García-Massó5and Estélio Henrique Martín Dantas6
1.4.6Laboratoryof Biological Sciences of the human motor (UCB - Rio de Janeiro Brazil).Email: [email protected] of Physical Education and Sports, University of Valencia, Valencia, Spain.3LaboratoryofMorphology (UNISUAM RiodeJaneiro Brazil).
Abstract. This research was designed to measure the levels 01hydroxyproline (HP) in urine alter theapplication of two diflerent methods of strength training. Thirty fit, healthy men were randomly dividedinto two groups: exercise (EG) and control (CG). 80th groups provided urine samples priorto training,although only the EG performed 1 repetition maximum (RM); 5RM and 30RM tests. Alter this, the EGperformed three series of 5RM. Alter two hours, urine samples were collected lrom the EG. Sixteendays later, the same pl;.ocedure took place using a 30RM protocol. The HP levels in urine werequantified colorimetrically using a spectrophotometer. Statistically signilicant diflerences in HP valueswere found only lor the the 5RM training method (e.= -22%, P< 0.05). It was concluded that damage tothe conjunctive tissue only too k place with 5RM training, thus confirming that one way 01 avoidingstagnation in the adaptation 01 subjects with certain experience 01 strength training is to use moreintense methods .. However, in such training protocols, the recovery time between sessions should begreater due to the resulting increase in tissue damage.
Keywords: Urine, Resistance exercise, Conjunctivetissue, Damage.
IntroductionConjunctive tissue is present in numerous body structures, such as the tendons, epimysium andperimysium located in the muscles. With the latter, the consecutive and parallel structures ofthe tissue distribute the effort produced by muscle contraction (Brown et al., 1999). Theconnective tissue can be damaged when physical exercise is performed at intensities larger thanusual (Brown et al., 1997). This damage can be measured by assessing collagen metabolismoHydroxyproline is generated by the hydroxylation of proline, a reaction that takes place duringthe catabolism of collagen. As a result, the measurement ofhydroxyproline in the blood or urineis often used as an indicator of collagen degradation (Brown et al., 1997; Murguria et al., 1998;Virtanen et al., 1993). In the event of an injury, sufficient time must be allowed to rest and toensure the total recovery from the damage caused to the conjunctive tissue. If this is not tbecase, the injury could worsen as the tissue adaptation process is hindered (Tofas et al., 2008).This makes it necessary to identify the acute phy'siological stress that is involved in eachspecific kind oftraining, as we can then prescribe longer rest periods between training sessions,and thus avoid excessive exercise and favour recovery from injury (Avery and Bailey, 2005). Inaddition, identification of the physiological stress that can be caused by different strengthtraining methods would also allow us to identify the best metbods according to tbe pbysicalcondition and goals of the person exercising. This would favour the prescription of more
© 2010 Fitness Society of India

18 A C Nogueira, J C. Colado, J G Mourao e Lima, R G S Vale, X Garcia-Massó and E H M Dantas
precise and safer training prograrnmes (Colado and Chulvi, 2008).
Numerous studies have analysed the acute response to different strength training methods withregard to hormone levels (Kraemer and Ratamess, 2005) and the irnmune response (Simonson,2001). However, only one study has analysed post-exercise hydroxyproline modifications, yetit failed to compare the stress caused on the conjunctive tissue by different strength trainingmethods (Tofas et al., 2008). Therefore, our study measures hydroxyproline levels in urine afterthe application of two different strength training methods to young, fit, male subjects. Wehypothesized that the method involving greater than normal muscle tension levels would causegreater damage to the conjunctive tissue. If this were to be the case, our study would offerimportant insights into research measuring hydroxyproline levels as a biomarker ofthe damagethat strength training inf1icts on the conjunctive tissue (Tofas et al., 2008). This is because ourstudy would provide objective evidence favouring cautious prescription of this kind ofexercise, not only with respect to the recovery time between workouts but also with regard tothe criteria to be used for defining the appropriate protocols for the periodic altemation betweendifferent training methods.
Material and Methods
Subjects: The sample consisted of 30 male volunteers (19 ± 0.5 years, 174 ± 4 cm, 72.6 ± 4.8kg, Body Mass Index ::s 25 kg/m2
). A power analysis based on preliminary data established thatwith a sample size ono subjects, the statistical power of our study was approximately 70%. Thesubjects completed the PAR-Q questionnaire. They were aH found to be healthy individualswith no kind of cardiovascular or osteomuscular pathology. AlI subjects were familiar withstrength training and the devices used, as they had been performing this type of exercise for atleast the previous six months. Specifically, their normal training schedule included at leastthree weekly training sessions at 50-75% of 1 maximum reRetition (RM) with an effortperception near to the volitional muscular failure using training methods that prioritised localmuscular endurance and muscle hypertrophy. The subjects were randomly divided into twoequal groups: the exercise grOUP(EG) and the control grOUP(CG), baseline levels to which theprocess was not applied. AH subjects signed an informed consent formo The study was approvedby the Human Research Ethics Cornmittee at the University of Castelo Branco (Brazil) inagreement with the 1975 Declaration of Helsinki. During the preliminary tests and trainingsessions the subjects were told not to alter their sleep pattems or diet.
Experimental Approach to the Problem: A randomized controlled repeated measure was used.Subjects in the exercise group were subjected to two different protocols for strength training: 3sets x 5RM or 3 sets x 30RM, on the leg press machines at 45° (LP) and horizontal bench presswith bar (HBP) (Fitness equipment, Franklin Park, IL. )). The main aim ofthe 5RM training wasto promote structural adaptations and to produce an increase ofmaximum strength; in contrast,the 30RM training protocol was used to improved muscle endurance. Thus, we would be able tocompare two very different training methods and their effects on connective tissue.
Hydroxyproline levels in urine were measured two hours after each workout using highperformance liquid chromatography (HPLC).
Assessment o/ 1 Repetition Maximum (lRM): The assessment of lRM of the EG wereperformed on three different days. On the first day, after taking anthropometric measurementsoftotal body weight and stature ofthe 30 subjects? the EG performed the lRM test on the leg

Hydroxyproline and Strength Training 19
press machines at 45° (LP) and on the horizontal bench press with bar (HBP) (Fitnessequipment, Franklin Park, IL.). Volunteers for each exercise sequence were selected randomly.In order to ensure the reproducibility ofthe loads, the EG had a recovery period of24 hours aftereach maximum load evaluation (total ofthree). The lRM was defined the best value found overthe three test days, allowing for a maximum difference of 5%. The recovery intervals betweenthe series and exercises were three minutes long (Kraemer and Ratamess, 2004). No physicalactivity was allowed during the recovery intervals between the different evaluation sessions. Inorder to ensure the validity of the measurements obtained, the following strategies wereadopted: standardised and precise information about the whole process was always provided,the subjects were instructed on the correct techniques to use when carrying out the exercises,the evaluators were properly trained and were responsible for both the correct performance ofthe exercises, and the quality ofthe evaluation tests at all times.Assessment of5 Repetition Maximum (5RM): The 5RM ofthe EG were also performed on theLP and HBP (Fitness equipment, Franklin Park, IL.), and in three different days. Volunteers foreach exercise sequence were selected randomly. In order to ensure the reproducibility of theloads, the EG had a recovery period of24 hours after each maximum 5RM load session (total ofthree). The 5RM was defined as the best value found over the three test days, allowing amaximum difference of 5%. The recovery intervals between the series and exercises were threeminutes long (Kraemer and Ratamess, 2004). No physical activity was allowed during therecovery intervals between the different evaluation sessions. In order to ensure the validity ofthe measurements obtained, we implemented the strategies described for lRM assessment(seeabove).Pre-training Urine Sample: Thirty-six hours after the 5RM tests for the EG, the CG and EGgroups fasted for 12 hours (during the night). Immediately after the fasting period, theyeliminated the initial urine and hydrated themselves with pure water. Participants then had aperiod of two hours to collect their urine in containers we had provided. These urine sampleswere immediately placed in ice and taken to the laboratory for analysis. High performanceliquid chromatography (HPLC) was used to estimate the concentration of hydroxyproline.Hydroxyproline was quantified colorimetrically (reagent: Ninhydrin) using a spectrophotometer(Micronal model B 295). The hydroxyproline values were expressed inmi11igramsper 24 hours(mg/24h), with reference values that oscillated between 15 and 43 mg/24h for adults over 21years of age (Wyngaarden and Smith, 1984).Training with 5RM: The EG underwent training in the afternoon of the day the urinesample was taken. Before starting the training protocol, a specific warm-up took place forboth the HBP and LP exercises. Warm-up consisted of a series of five repetitions with60% of the weight obtained for 5RM. The three 5RM series of the respective exerciseswere then performed, always in the same order (HBP and LP). Protocols were designed sothat there was no reduction in total training volume. The recovery intervals between theseries and exercises were three minutes long (Kraemer and Ratamess, 2004). The rhythmof the exercise was contro11ed by using a metronome (Casio HS-30W®). Three secondswere given for each complete movement, including the concentric and eccentric phases,giving a total of 15 seconds for the 5RM. A professional strength trainer supervised theubjects in order to ensure that the subjects performed a11the repetitions according to theprotocol. The ubjects caITÍed out the training session at maximum voluntary effort inea h ene.

20 A C Nogueíra, J C. Colado, J G Mourao e Lima, R G S Vale, X García-Massó and E H M Dantas
Post-training urine sample with 5RM: Two hours after the EG training session, the second urinesample was taken. The same procedure, as described for the pre-training, was followed. Itshould be emphasized that, for the second urine samples, the EG group was hydrated during therecovery intervals between the series.Tests, Training and Urine Samples for ]()RM: Sixteen days later, the EG performed the 30RMtest on the LP and HBP (Fitness equipment, Franklin Park, IL.). Volunteers for each exercisesequence were selected randomly. In order to ensure the reproducibility ofthe loads, the EG hada recovery period of 24 hours after each 30RM load session (total of three). The 30RM wasdefined as the best value found over the three test days, allowing a maximum difference of 5%.The recovery intervals between the series and exercises were three minutes long (Kraemer andRatamess, 2004). No physical activity was allowed during the recovery intervals bctween thedifferent evaluation sessions. In arder to ensure the validity ofthe measurements obtained, weimplemented the strategies described for lRM and 5RM assessments (see aboye).Thirty-six hours after training, the EG fasted for 12hours, hydrated and provided urine samplesin the two hours after hydration. During the following aftemoon, the EG performed a specificwarm-up with 60% of the weight identified for the 30RM test. The EG then performed three30RM series with the HBP and LP, respectively. The recovery intervals between series andexercises were three minutes long (Kraemer and Ratamess, 2004), and the time of musculartension for each complete movement, inc1uding the concentric and eccentric phases, was threeseconds. Two hours after the 30RM training session and hydration, urine samples of bothgroups were taken for analysis in the laboratory.
Statistical Analyses: Initially, we only estimated descriptive statistics for the data. Once thenormality and homogeneity ofthe data were confirmed, inferential statistics were obtained bypaired-samples t-student test and analysis ofvariance (ANOVA) with repeated measures withthe post hoc test of the least significant difference (LSD). The data was processed usingStatistica® 5.5 software (Statsoft®, USA). Statistical significance was set at 5%.
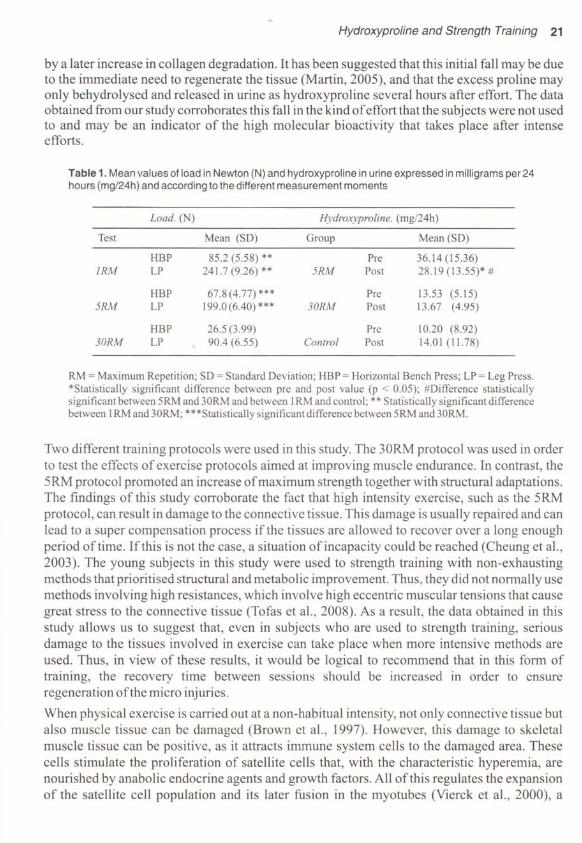
ResultsTable 1 shows the means and standard deviations (between brackets) of the loads, and themeans and standard deviations ofHP concentration after each of the training condi tions. For theload test ofthe EG, no significant differences (p> 0.05) were found between the values ofthelRM testand of5RM. However, both were significantly different from the 30RM test (p < 0.01and p < 0.05, respectively). With respect to the levels of HP, no significant differences werefound in the EG after applying the 30RM training method (p > 0.05). In contrast, the HP valuewas significantly decreased after applying the 5RM training (22% lower than rest, p < 0.05) Inthe CG, we observed an intra-c1ass correlation coefficient of 0.91, and no significantdifferences between any ofthe measurements.
DiscussionUsually, it is possible to observe an increase in HP levels from 24 hours to 9 days after effort(Brown et al., 1997). However, although immediate post-effort measurement is notrecommendcd (Brown et al., 1997), sorne studies (Vietanen et al., 1993; Mouzopoulos et al.,2007) have been ab1e to quantify an initial acute fall in the amount of collagen degradedimmediately after effort involving high-intensity activjties. This decrease was usually followed .
Hydroxyproline and Strength Training 21
by a later increase in collagen degradation. It has been suggested that this initial fall may be dueto the immediate need to regenerate the tissue (Martin, 2005), and that the excess proline mayonly behydrolysed and released in urine as hydroxyproline several hours after effort. The dataobtained from our study corroborates this fall in the kind of effort that the subjects were not usedto and may be an indicator of the high molecular bioactivity that takes place after intenseefforts.
Table 1. Mean values 01load in Newton (N) and hydroxyproline in urine expressed in milligrams per 24hours (mgl24h) and according lo lhe differenl measuremenl momenls
Load. (N) Hydroxyproline. (rng/24h)
Test Mean (SD) Group Mean (SD)
HBP 85.2 (5.58) ** Pre 36.14 (15.36)IRM LP 241.7 (9.26) ** 5RM Post 28.19 (13.55)* #
HBP 67.8(4.77)*** Pre 13.53 (5.15)5RM LP 199.0(6.40) *** 30RM Post 13.67 (4.lJ5)
HBP 26.5 (3.99) Pre 10.20 (8.92)30RM LP 90.4 (6.55) Control Post 14.01 (11.78)
RM = Maxirnurn Repetition; SD = Standard Deviation; HBP = Horizontal Bench Press; LP = Leg Press.*Statistically significant difference between pre and post value (p < 0.05); #Difference statisticallysignificant between 5RM and 30RM and between 1RM and control; ** Statistically significant differencebetween lRM and 30RM; ***Statistically significant difference between 5RM and 30RM.
Two different training protocols were used in this study. The 30RM protocol was used in orderto test the effects of exercise protocols aimed at improving muscle endurance. In contrast, the5RM protocol promoted an increase of maximum strength together with structural adaptations.The findings of this study corroborate the fact that high intensity exercise, such as the 5RMprotocol, can result in damage to the connective tissue. This damage is usually repaired and canlead to a super compensation process ifthe tissues are allowed to recover over a long enoughperiod oftime. Ifthis is not the case, a situation ofincapacity could be reached (Cheung et al.,2003). The young subjects in this study were used to strength training with non-exhaustingmcthods that prioritised struetural and metabolic improvement. Thus, they did not norrnally usemethods involving high resistances, which involve high eccentric muscular tensions that causegreat stress to the connective tissue (Tofas et al., 2008). As a result, the data obtained in thisstudy allows us to suggest that, even in subjects who are used to strength training, seriousdamage to the tissues involved in exercise can take place when more intensive methods areused. Thus, in view of these results, it would be logical to recommend that in this forrn oftraining, the recovery time between sessions should be increased in order to ensureregeneration ofthe micro injuries.When physical exercise is carried out at a non-habitual intensity, not only connective tissue butalso muscle tissue can be damaged (Brown et al., 1997). However, this damage to skeletalmuscle tissue can be positive, as it attracts immune system cells to the damaged area. Thesecells stimulate the proliferation of satellite cells that, with the characteristic hyperemia, arenourished by anabolic endocrine agents and growth factors. All ofthis regulates the expansionof the satellite cell population and its later fusion in the myotubes (Vierck et al., 2000), a
22 A e Nogueira, J C. Colado, J G Mourao e Urna, R G S Vale. X Garcia-Massó E Dantas
decisive factor in generating muscle hypertrophy. As there are studies that confirm that theextent of the damage to the connective tissue is directly related to that suffered by the muscle(Proske and Morgan, 2001), the data obtained in this study suggests that the use of highresistances and a limited number of repetitions may be a good way of increasing the musclemass of subjects. This improvement could also increase muscular strength (Kraemer andRatamess,2004).Although the Carpinel1i et al. (2004) research group does not consider it necessary todifferentiate between levels when establishing principIes for progression in the development ofmedium and long-term muscle conditioning programmes, the findings ofthis study confirm themethodological guidelines suggested by other researchers (Rhea et al., 2003; Kraemer andRatamess, 2004; Peterson et al., 2004). These researchers defend the need to differentiatebetween levels when establishing principIes for progression while carrying out medium andlong term muscle conditioning prograrnmers. Studies such as those ofDeschenes and Kraemer(Deschenes and Kraemer, 2002) have emphasized the fact that although there is great scope forimprovement in the initial mo~ths oftraining, the same does not happen afterwards. This is whysubjects wishing to continually improve their physiological and functional performance haveto use highly specific methods that are very different to those used in previous stages (Colado yChulvi, 2008; Colado et al., 2008). Our findings confirm that after several months oftraining,subjects need to change their training method in order to obtain the physiological stress that cancontinue favouring a process of adaptation. Specifically, we found that the physiologicalstress ofmethods habitually used by subjects (local muscular endurance with 30RM) does notresult in muscle damage. In contrast, muscle damage wasobserved when equally-experiencedsubjects used a method for maximum strength improvement (5RM). We recornmend thatcomplementary studies be carried out to take measurements after several days of effort, as wellas using a control group with little strength training experience. Also, intermediate protocolsmust be used to a better understand the hidroxiproline changes after metabolic, structural andneural training methods. Finally, hydroxyproline levels could be used to determine the optimalrest interval between workouts. We suggest that this should also be the focus offuture studiesaiming at developing optimal, long-term training protocols.
Practical Applications: The data obtained in this study suggest that damage to the conjunctivetissue only appeared with 5RM training. Therefore, these results suggest that one way ofavoiding stagnation in the adaptation of subjects with certain experience in strength training isto use a periodic training model. In such a model, methods with low-moderate resistances and amoderate-high number of repetitions are altemated with other methods involving highresistances and few repetitions. Apart from the hydroxyproline levels, the reduction ofmusclestrength can also determine the rest interval between workouts. This reduction remains forthree days post-training, and may reflect a combination ofthe effects offatigue and ofmuscledamage (Brown et al., 1997). Therefore, in methods involving high resistances and fewrepetitions, recovery time must be longer (three days), due to the significant tissue damage andstrength loss that these methods can cause in tbe post -exercise.
ReferencesAvery N.e. and Bailey A.J. (2005). Enzymic and non-enzymic cross-linking mechanisms in relalion lo lurnover ofcollagen: relevance lo agingand exercise. Scand J Med Sci Sports 15: 231-240.Brown S.J., Child R.B., Day S.H., and Donnelly A.E. (1997). Indices ofskelelal muscledamage and connective tissue

Hydroxyproline and Strength Training 23
breakdownfollowing eccentric musclecontractions. Eur JAppl Physiol75: 369-374.Brown S, Day S, and Donnelly A. (1999). Indirect evidence of human skeletal muscle damage and collagenbreakdown after eccentric muscle actions. J Sport Sci 17: 397-402.Carpinelli R.N., Ono R.M., and Winnet R.A. (2004). A critical analysis ofthe ACSM position stand on resistan cetraining.InsujJicient evidence to support recommended training protocols. lEPonline 7 (3): 1-60.Cheung K., Hume P., and Maxwell L. (2003). Delayed onset muscle soreness: treatment strategies and performancefactors. Sports Med 33: 145-164.Colado J. C. and Chulvi I. (2008). Criteria for the development of general neuromuscular conditioning programswithin the health area. In: Physical exercise for muscular conditioning in weight rooms: Scientific-medical bases forhealthy and safely performance. Rodriguez PL, ed. Madrid: Panamericana. pp 91-127.Colado J.C., Chulvi l., and Heredia J.R. (2008). Criteriafor the development ofmuscular conditioning programswith afunetiunal aim. In: Physical exercise for muscular conditioning in weight rooms: Scientijic-medical bases forhealthy and safely performance. Rodríguez PL, ed. Madrid: Panamericana, pp. 154-167.Deschenes M.R. and Kraemer W,J. (2002). Performance and physiologic adaptation to resistance training. Aro JPhys Med Rehabil81 (Suppl): 3-16.Kraemer W,J., and Ratamess N.A.(2004). Fundamental of resistance progression and exercise prescription. MedSci Sports Exerc 36: 674-688.Kraemer W.J., and Ratamess N.A.(2005). Hormonal responses and adaptations to resistance exercise and training.Sports Med35: 339-361.Martin R. The epithelial mitogom keratinocyte growth factor binds to collagens via the consensus sequen ce Olycine-Proline-Hydroxyproline. Avalaible in hnp://www.jbc.org.Accesson: 24/06/2005.Mouzopoulos O., Stamatakos M., Tzurbakis M., Tsembeli A., Manti c., Safio leas M. and Skandalakis P. (2007).Changes ofbone turnovermarkers after marathon runningover 245 km. IntJ Sports Med 28: 576-579.Murguria M.J., Vailas A., Mandelbaum B.,Nortun J., Hodgdon J., Ooforth H. and Riedy M. (1998). Elevated plasmahydroxyproline: apossible riskfactor associated whit connective tissue injuries during overuse. Aro J Sports Med 16:660-664.Peterson M.D., Rhea M.R. and Alvar B.A. (2004). Maximizing strength development in athletes: a meta-analysisi todetermine thedose-response relationship. J Strength Cond Res 18: 377-382.Proske U. and Morgan D.L. (2001). Muscle damage from eccentric exercise: mechanism, mechanical signs,adaptations and clinical applicatinns. J Physiol537: 333-345.Rhea M.R., Alvar B.A., Burken L.N. and Ball S.D. (2003). A meta-analysis to determine the dose responseforstrength development. Med Sci Sports Exerc 35: 456-464.Simonson S.R. (200 1). The immune response to resistance exercise. J Strength Cond Res 15: 378-384.Tofas T, Jamurtas A.Z., Fatouros l., Nikolaidis M.O., Koutedakis Y., Sinouris E.A., Papageorgakopoulou N. andTheocharis D.A. (2008). Plyometric exercise increases serum indices ofmuscle damage and collagen breakdown. JStrength Cond Res 22: 490-496.Vierck, J, O·Reilly, B, Hossner, K,Antonio, JA, Byrne, K, Bucci, L, and Dodson M. Satellite cell regulationfollowingmyotrauma caused by resistance exercise. Cell Biol Int 24: 263-272,2000.Virtanen P., Viitasalo J.T, Vuori J., Viiiiniinen K. and Takala TE. (1993). EjJect ofconcentric exercise on serummuscle and collagen markers. JAppl Physiol75: 1272-1277.Wyngaarden LB. and Smith L.H.( 1984). Treaty ofinternal medicine. Rio de Janeiro: Interamericano.