
a systematic review of prevalence, risk factors, and clinica
39
Vol.:(0123456789) 1 3 International Archives of Occupational and Environmental Health https://doi.org/10.1007/s00420-019-01467-8 REVIEW Musculoskeletal disorders and complaints in professional musicians: a systematic review of prevalence, risk factors, and clinical treatment effects Gabriele Rotter 1,2,3 · Katharina Noeres 1 · Isabel Fernholz 2,3,4 · Stefan N. Willich 1,3 · Alexander Schmidt 2,3,5 · Anne Berghöfer 1,3 Received: 6 December 2018 / Accepted: 19 July 2019 © The Author(s) 2019 Abstract Purpose Musicians’ practice and performance routines reportedly lead to musculoskeletal complaints and disorders (MCD) that impact their wellbeing and performance abilities. This systematic review aims to assess the prevalence, risk factors, prevention and effectiveness of treatments for MCD in professional musicians and consider the methodological quality of the included studies. Methods A systematic literature search was performed in December 2017 using electronic databases and supplemented by a hand search. Case–control studies, cohort studies, cross-sectional studies, interventional studies and case reports inves- tigating the prevalence, risk factors, prevention or treatment effects of MCD in professional musicians or music students (age ≥ 16 years) were included. Quality assessments of the included studies were performed using an adapted version of the “Study Quality Assessment Tools” from the National Heart, Lung, and Blood Institute. Results One case–control study, 6 cohort studies, 62 cross-sectional studies, 12 interventional studies and 28 case reports were included and assessed for methodological quality. The study designs, terminology, and outcomes were heterogeneous, as the analyses mostly did not control for major confounders, and the definition of exposure was often vague. Therefore, evidence that being a professional musician is a risk factor for MCD as well as the causal relationship between these factors remains low despite the fact that a large number of studies have been performed. Conclusions Studies with high internal and external validity regarding the prevalence, risk factors and effectiveness of the prevention or treatment of MCD in professional musicians are still missing. Further high-quality observational and inter- ventional studies are required. Keywords Musicians’ medicine · Occupational medicine · Playing-related musculoskeletal disorders · Prevalence · Incidence · Systematic review Electronic supplementary material The online version of this article (https://doi.org/10.1007/s00420-019-01467-8) contains supplementary material, which is available to authorized users. * Gabriele Rotter [email protected] 1 Institute for Social Medicine, Epidemiology and Health Economics, Charité - Universitätsmedizin Berlin, Luisenstrasse 57, 10117 Berlin, Germany 2 Kurt-Singer-Institute for Music Physiology and Musicians’ Health, Hanns Eisler School of Music Berlin and University of the Arts Berlin, Charlottenstrasse 55, 10117 Berlin, Germany 3 Berlin Center for Musicians’ Medicine, Charité - Universitätsmedizin Berlin, Luisenstrasse 13, 10117 Berlin, Germany 4 Department of Psychiatry and Psychotherapy, Charité - Universitätsmedizin Berlin, Charitéplatz 1, 10117 Berlin, Germany 5 Department of Audiology and Phoniatrics, Charité - Universitätsmedizin Berlin, Luisenstrasse 13, 10117 Berlin, Germany
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of a systematic review of prevalence, risk factors, and clinica

Vol.:(0123456789)1 3
International Archives of Occupational and Environmental Health https://doi.org/10.1007/s00420-019-01467-8
REVIEW
Musculoskeletal disorders and complaints in professional musicians: a systematic review of prevalence, risk factors, and clinical treatment effects
Gabriele Rotter1,2,3 · Katharina Noeres1 · Isabel Fernholz2,3,4 · Stefan N. Willich1,3 · Alexander Schmidt2,3,5 · Anne Berghöfer1,3
Received: 6 December 2018 / Accepted: 19 July 2019 © The Author(s) 2019
AbstractPurpose Musicians’ practice and performance routines reportedly lead to musculoskeletal complaints and disorders (MCD) that impact their wellbeing and performance abilities. This systematic review aims to assess the prevalence, risk factors, prevention and effectiveness of treatments for MCD in professional musicians and consider the methodological quality of the included studies.Methods A systematic literature search was performed in December 2017 using electronic databases and supplemented by a hand search. Case–control studies, cohort studies, cross-sectional studies, interventional studies and case reports inves-tigating the prevalence, risk factors, prevention or treatment effects of MCD in professional musicians or music students (age ≥ 16 years) were included. Quality assessments of the included studies were performed using an adapted version of the “Study Quality Assessment Tools” from the National Heart, Lung, and Blood Institute.Results One case–control study, 6 cohort studies, 62 cross-sectional studies, 12 interventional studies and 28 case reports were included and assessed for methodological quality. The study designs, terminology, and outcomes were heterogeneous, as the analyses mostly did not control for major confounders, and the definition of exposure was often vague. Therefore, evidence that being a professional musician is a risk factor for MCD as well as the causal relationship between these factors remains low despite the fact that a large number of studies have been performed.Conclusions Studies with high internal and external validity regarding the prevalence, risk factors and effectiveness of the prevention or treatment of MCD in professional musicians are still missing. Further high-quality observational and inter-ventional studies are required.
Keywords Musicians’ medicine · Occupational medicine · Playing-related musculoskeletal disorders · Prevalence · Incidence · Systematic review
Electronic supplementary material The online version of this article (https ://doi.org/10.1007/s0042 0-019-01467 -8) contains supplementary material, which is available to authorized users.
* Gabriele Rotter [email protected]
1 Institute for Social Medicine, Epidemiology and Health Economics, Charité - Universitätsmedizin Berlin, Luisenstrasse 57, 10117 Berlin, Germany
2 Kurt-Singer-Institute for Music Physiology and Musicians’ Health, Hanns Eisler School of Music Berlin and University of the Arts Berlin, Charlottenstrasse 55, 10117 Berlin, Germany
3 Berlin Center for Musicians’ Medicine, Charité - Universitätsmedizin Berlin, Luisenstrasse 13, 10117 Berlin, Germany
4 Department of Psychiatry and Psychotherapy, Charité - Universitätsmedizin Berlin, Charitéplatz 1, 10117 Berlin, Germany
5 Department of Audiology and Phoniatrics, Charité - Universitätsmedizin Berlin, Luisenstrasse 13, 10117 Berlin, Germany

International Archives of Occupational and Environmental Health
1 3
Introduction
To a great extent, professional musicians rely on their physical and mental health to guarantee their vocational and artistic positions, meet high audience demands or succeed in competitive settings. Even minor complaints may impair the precision of motion sequences and musi-cal technique, thus creating a major threat to the artist’s existence.
The discipline of musicians’ medicine dates back to the 18th century (Ramazzini 1705). In the 1920s, Kurt Singer first systematically described symptoms of musi-cians’ vocational diseases and their treatment (Singer and Lakond 1932; Harman 1993). Currently, musicians’ medi-cine is dedicated to the prevention, diagnosis and therapy of health problems which may arise or have arisen as a result of making music or which have an effect on making music (Spahn et al. 2011).
In clinical practice, musculoskeletal and mental prob-lems, especially performance anxiety, are very common amongst professional musicians (Fishbein et al. 1988). Up to now, several narrative and systematic reviews exist that provide data on a wide range of playing-related symptoms and diseases, with broadly varying prevalence rates (Har-man 1982; Zaza 1998; Milan 1996; Zuskin et al. 2005). The varying prevalence rates may mainly be caused by the lack of a precise definition of playing-related symptoms and diseases as well as a lack of coordinated research.
Reviews of publications including patients with mus-culoskeletal complaints and disorders (MCD) used dif-ferent definitions of musculoskeletal disorders or simply referenced “overuse syndrome” (Hoppmann and Patrone 1989; Bejjani et al. 1996). In 1998, Zaza (1998) introduced the term “playing-related musculoskeletal disorders” (PRMD), which aggregated the various musculoskeletal disorders while assuming a common etiological factor. The prevalence of PRMD in musicians was thus deemed to be comparable to vocation-related musculoskeletal disorders in other professions.
The most recent systematic review by Bragge et al. (2006) furthered the use of PRMD as an aggregate term for overuse syndrome, repetitive strain injuries or cumula-tive trauma disorders. The review reported a prevalence ranging between 26 and 93%. Further systematic reviews added only limited information, as they did not use pre-defined review protocols or used a narrow search strategy (Wu 2007; Moraes and Antunes 2012). Furthermore, pre-vious reviews did not focus on the methodological quality of the included studies.
Since various musculoskeletal disorders were inconsist-ently summarized under the term PRMD and the methodo-logical quality of included publications was not assessed
in previous reviews, we aimed to perform a comprehensive systematic review including published literature without language restrictions, based on an elaborated study proto-col, to assess the prevalence, risk factors, prevention and effectiveness of MCD treatment in professional musicians, including the assessment of the methodological quality of the included studies.
Methods
The research methods and reporting of this study followed the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines (Liberati et al. 2009; Moher et al. 2009) and the recommendations of the Cochrane Collaboration (Green and Higgins 2011). Prior to conducting the review, a study protocol was prepared by all of the review authors, placing special emphasis on study selection, data extraction and quality assessment.
Criteria for considering studies for the current review
Types of studies
Observational studies (case–control studies, cohort studies, cross-sectional studies), intervention studies (controlled clinical trials and pre–post intervention studies without a control group), case reports and case series reporting clinical interventions published in peer-reviewed journals without language or publication date restrictions were included in this review. Studies published in non-peer-reviewed journals, theses, and gray literature were excluded.
Types of participants
Participants in the included studies were male or female professional musicians of all musical genres, including music teachers, instrument teachers and music students in higher education institutions (for example, universities, colleges, conservatories). Studies examining mixed profes-sional populations (amateur, semi-professional/professional) or mixed artistic populations (musicians, actors, dancers) were included only if results were reported for the respective subgroups. When the professional status of the participants was not clearly defined in the publication, a consensus of the reviewing authors was obtained. For studies involving high school music students, participants had to be of at least 16 years of age (defined in this review as “adult”) to be included. Publications on mixed populations (children, ado-lescents, adults) were included only if results were reported for the respective subgroups. The included studies investi-gated MCD that was potentially caused by or thought to be

International Archives of Occupational and Environmental Health
1 3
related to practicing or performing music. This also included dental and jaw diseases, myofascial pain syndromes, cra-niomandibular dysfunctions, shoulder belt compression syndromes (like thoracic outlet syndrome and congestion syndrome of the upper thoracic aperture) and percussion hemoglobinuria. Studies lacking relevant information on the different types of participants were excluded.
Types of interventions
Studies investigating the effectiveness or efficacy of any type of clinical intervention, including interventions using complementary and integrated medicine in the defined study population, were considered.
Types of comparisons
A control group comparison was not required to meet the eligibility criteria.
Types of outcome measures
Studies were considered if the primary outcomes included the prevalence, incidence or other information about the prevalence of MCD or risk factors for MCD or clinical treat-ment effects due to an intervention (preventive, therapeutic or rehabilitative). Studies providing only non-clinical treat-ment effects or validating methods of measurements were not included.
Data sources and searches
The electronic databases MEDLINE and EMBASE via OvidSP and via EbscoHost CINAHL, PsycArticles, Psy-cInfo and ERIC were searched between January 6th, 2015 and December 7th, 2017, with no limit on the publication date.
Hand searches were performed as follows: the scientific journal Medical Problems of Performing Artists (MPPA, until volume 24, issue 4 December 2009, after in MED-LINE) between February 13th and 27th, 2015 and actual-ized on December 7th, 2017 as well as the German jour-nal Fachzeitschrift Musikphysiologie und Musikermedizin (FMM, years 1994–1999 were excluded, because online access was not available), the official scientific publica-tion of the German Association for Music Physiology and Musicians’ Medicine (DGfMM), between February 28th and March 8th 2015 and actualized on December 7th, 2017. Reference lists of seven identified systematic reviews (Zaza 1998; Bragge et al. 2006; Wu 2007; Baadjou et al. 2016; Jacukowicz 2016; Kok et al. 2016; Vervainioti and Alexo-poulos 2015) were searched for further studies. The search strategy followed three guidelines: the study population,
investigated MCD and study design. The search strategy is shown in Appendix 1.
Data collection and analyses
Study selection
The titles and abstracts of the identified studies were screened for eligibility by two authors (KN, GR). Studies not meeting the inclusion criteria were excluded. The remaining studies were evaluated for inclusion via full-text reviews by two of the four authors (KN, GR, AS, AB). During the full-text review, a predefined checklist form was completed as reported in “Assessment of study quality and dealing with missing data”. For articles not published in English or Ger-man, a translated summary was examined for eligibility cri-teria. Discrepancies in the study selection between authors were resolved in a consensus conference.
Data extraction
Data extraction was performed by two of the four authors (KN, GR, AS, AB) using standardized data extraction forms as reported below. Discrepancies in the data extraction between the reviewing authors were resolved by discussion and consensus.
Assessment of study quality and dealing with missing data
Depending on the study design, the quality of studies can be assessed using various checklists or scores. A standard assessment tool is the Study Quality Assessment Tool of the National Heart, Lung, and Blood Institute (NHLBI). It provides a thorough assessment of the quality of studies in all medical disciplines. It can be applied to observational studies such as intervention studies and seemed appropriate to be extended by a scoring system for comparison purposes in this review.
To apply comparable quality assessment tools to all of the included study designs, the reviewing authors developed a modified version of the “Study Quality Assessment Tool” from the National Heart, Lung, and Blood Institute. The “Quality Assessment of Observational Cohort and Cross-Sectional Studies,” “Quality Assessment of Before-After (Pre–Post) Studies With No Control Group” and the “Qual-ity Assessment of Controlled Intervention Studies” (NHLBI) were adapted by adding items to the quality assessment tools about the Critical Appraisal Skills Program (CASP), the “CASP-Checklists” (CASP 2013) and the “Methodology Checklists” of the Scottish Intercollegiate Guidelines Net-work (SIGN). The instructions for application were prede-fined and adapted in a consensus by all authors. A scoring system was implemented in which one point was given for

International Archives of Occupational and Environmental Health
1 3
each item on the form that was fulfilled by the study and one point was subtracted for each item that was not fulfilled. If an item was not applicable to a study, zero points were given. If a study did not report on the requested item, one point was subtracted for that item. The total score was calculated by add-ing the individual points without weighting for single items. The total number of possible points varied for each evaluation instrument depending on the type of study. Case–control stud-ies could reach a maximum of 14 points, cohort studies and cross-sectional studies could reach a maximum of 16 points, controlled intervention studies could reach a maximum of 18 points and pre–post studies without a control group could reach a maximum of 15 points (Appendix 2). Total scores were not comparable across different types of study designs. The described modified quality assessment tools were used for the quality assessments of the individual studies by two of the four authors (KN, GR, AS, AB). Disagreements over study quality assessment and scoring were resolved by discussion and consensus. If multiple publications were produced from one study, only one quality assessment was performed based on the publication we considered to be the most comprehen-sive and with the highest methodological quality.
Data synthesis
The extracted information included the (1) authors, (2) date of publication, (3) population(s) studied, (4) number of par-ticipants, (5) exposure or interventions relevant to the review questions, (6) randomization status; (7) outcomes and (8) results. If these data were not provided, they were marked as missing. The results of individual studies were reported as frequencies in percentages, effect sizes, mean values with standard deviations or standard errors, significance values, odds ratios and confidence intervals. With the exception of percentages, no calculations were made based on the values provided. If a study did not provide quantitative data in num-bers, the narratively described results were used.
Results
Overview of selected studies
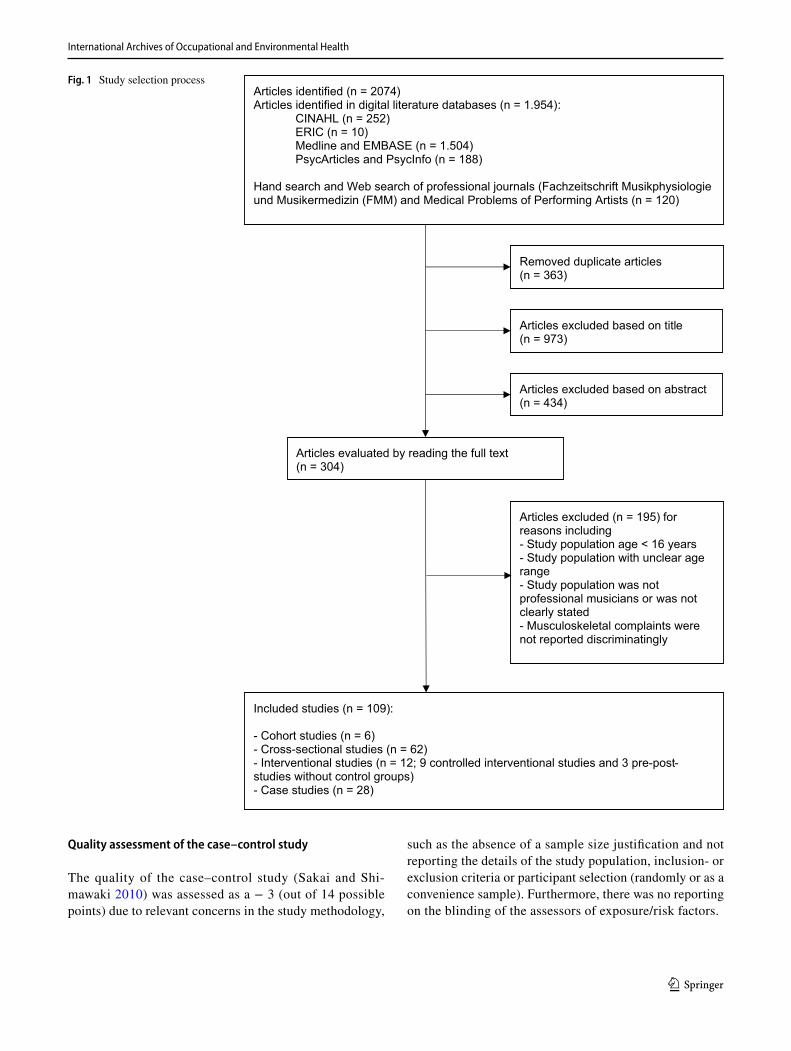
The search strategy identified 2074 articles. Figure 1 depicts the results of the individual steps of the selection process. In total, 109 articles were included in the study, 28 of which were case studies and 81 of which were articles for qual-ity assessment. The 81 articles assessed for methodological quality included 1 case–control study, 6 cohort studies, 62 cross-sectional studies, and 12 interventional studies (9 con-trolled intervention studies and 3 pre–post studies without control groups).
The characteristics of the included studies are shown in Tables 1 through 6. Across all study types, we found that the different terms used and the definitions of outcome parameters significantly limited the comparability of the included studies. In the “outcomes” columns in Tables 1 through 5, the individual terms used by the studies are cited. Even the abbreviation “PRMD” is used and defined heterogeneously.
The term “PRMD” as “performance-related mus-culoskeletal disorders” was used in seven publications (Ackermann et al. 2002b, 2011, 2012; Chan et al. 2013; Chan et al. 2014; Khalsa and Cope 2006; Khalsa et al. 2009). Among these, two intervention studies defined performance-related musculoskeletal disorders according to Zaza and Farewell as “any pain, weakness, numbness, tingling or any other symptoms that interfere with your ability to play your instrument at the level you are accus-tomed to. This definition does not include transient aches or pains” (Ackermann et al. 2002b; Chan et al. 2014; Zaza and Farewell 1997). One study defined the same term as “a musculoskeletal disorder was considered performance-related if the injury occurred during or immediately after playing and the musician specified that playing the instru-ment was the main contributor to their injury“(Chan et al. 2013). The term “PRMD” as “performance-related muscu-loskeletal pain disorders” was applied in three other pub-lications (Kenny and Ackermann 2015; Ackermann et al. 2012; Kenny et al. 2016) that used the definition based on Zaza and Farewell (Zaza and Farewell 1997), as mentioned above. The term “PRMD” as “playing-related musculo-skeletal disorders” was used in ten studies (Steinmetz et al. 2012; Arnason et al. 2014; Kim et al. 2012; Kaufman-Cohen and Ratzon 2011; Mishra et al. 2013; Kochem and Silva 2017; Monaco et al. 2012; Sousa et al. 2016; de Greef et al. 2003; Rickert et al. 2012). The definitions within the studies were heterogeneous; for example, in one study (Rickert et al. 2012), the term “PRMD” was used without further definition but was used synonymously with “injury” without the specific association that the PRMD was related to playing an instrument. A broad variety of additional terms were applied, sometimes only in one or a few studies (see Tables 1 through 5).
Case–control study
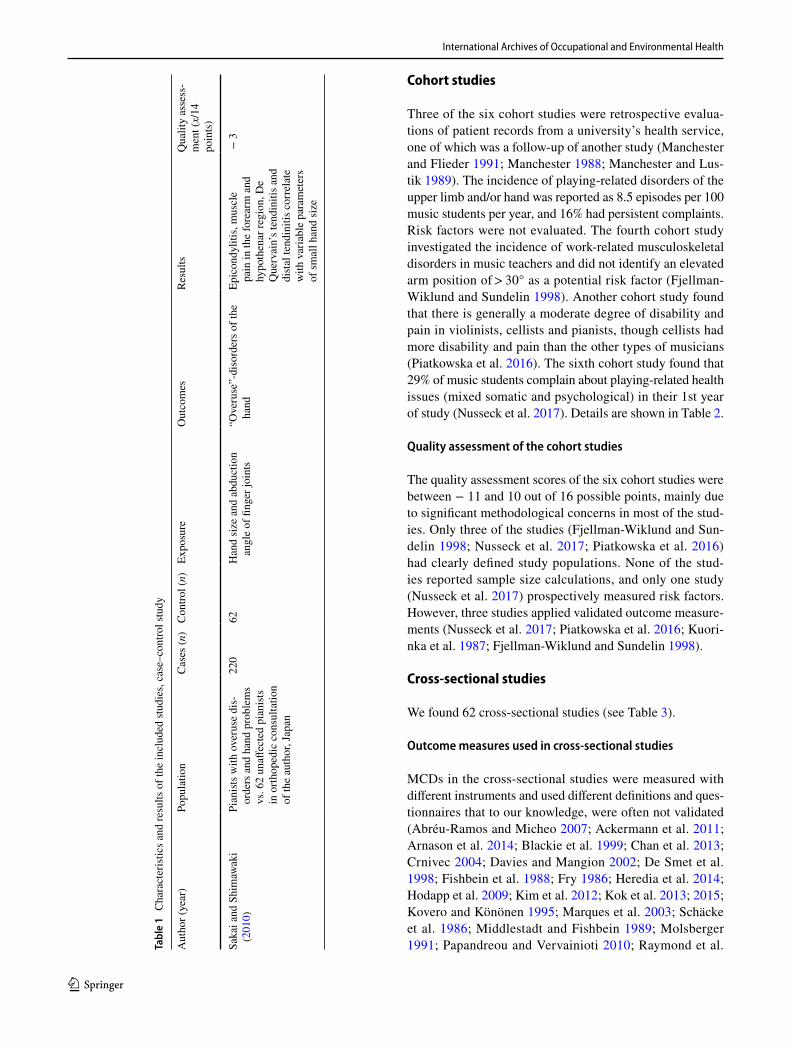
The included case–control study (Sakai and Shimawaki 2010) investigated the indices of hand and movement angles in 220 pianists in Japan with overuse disorders and 62 unaf-fected pianists as controls. The authors reported that epicon-dylitis, muscle pain in the forearm and hypothenar region, De Quervain’s tendinitis and distal tendinitis were correlated with variable parameters of small hand size (Table 1).
International Archives of Occupational and Environmental Health
1 3
Quality assessment of the case–control study
The quality of the case–control study (Sakai and Shi-mawaki 2010) was assessed as a − 3 (out of 14 possible points) due to relevant concerns in the study methodology,
such as the absence of a sample size justification and not reporting the details of the study population, inclusion- or exclusion criteria or participant selection (randomly or as a convenience sample). Furthermore, there was no reporting on the blinding of the assessors of exposure/risk factors.
Fig. 1 Study selection process
Included studies (n = 109):
- Cohort studies (n = 6)- Cross-sectional studies (n = 62)- Interventional studies (n = 12; 9 controlled interventional studies and 3 pre-post-studies without control groups)- Case studies (n = 28)
Articles excluded (n = 195) for reasons including- Study population age < 16 years - Study population with unclear age range - Study population was notprofessional musicians or was not clearly stated- Musculoskeletal complaints were not reported discriminatingly
Articles identified (n = 2074)Articles identified in digital literature databases (n = 1.954):
CINAHL (n = 252)ERIC (n = 10)Medline and EMBASE (n = 1.504)PsycArticles and PsycInfo (n = 188)
Hand search and Web search of professional journals (Fachzeitschrift Musikphysiologie und Musikermedizin (FMM) and Medical Problems of Performing Artists (n = 120)
Removed duplicate articles (n = 363)
Articles evaluated by reading the full text (n = 304)
Articles excluded based on title(n = 973)
Articles excluded based on abstract (n = 434)
International Archives of Occupational and Environmental Health
1 3
Cohort studies
Three of the six cohort studies were retrospective evalua-tions of patient records from a university’s health service, one of which was a follow-up of another study (Manchester and Flieder 1991; Manchester 1988; Manchester and Lus-tik 1989). The incidence of playing-related disorders of the upper limb and/or hand was reported as 8.5 episodes per 100 music students per year, and 16% had persistent complaints. Risk factors were not evaluated. The fourth cohort study investigated the incidence of work-related musculoskeletal disorders in music teachers and did not identify an elevated arm position of > 30° as a potential risk factor (Fjellman-Wiklund and Sundelin 1998). Another cohort study found that there is generally a moderate degree of disability and pain in violinists, cellists and pianists, though cellists had more disability and pain than the other types of musicians (Piatkowska et al. 2016). The sixth cohort study found that 29% of music students complain about playing-related health issues (mixed somatic and psychological) in their 1st year of study (Nusseck et al. 2017). Details are shown in Table 2.
Quality assessment of the cohort studies
The quality assessment scores of the six cohort studies were between − 11 and 10 out of 16 possible points, mainly due to significant methodological concerns in most of the stud-ies. Only three of the studies (Fjellman-Wiklund and Sun-delin 1998; Nusseck et al. 2017; Piatkowska et al. 2016) had clearly defined study populations. None of the stud-ies reported sample size calculations, and only one study (Nusseck et al. 2017) prospectively measured risk factors. However, three studies applied validated outcome measure-ments (Nusseck et al. 2017; Piatkowska et al. 2016; Kuori-nka et al. 1987; Fjellman-Wiklund and Sundelin 1998).
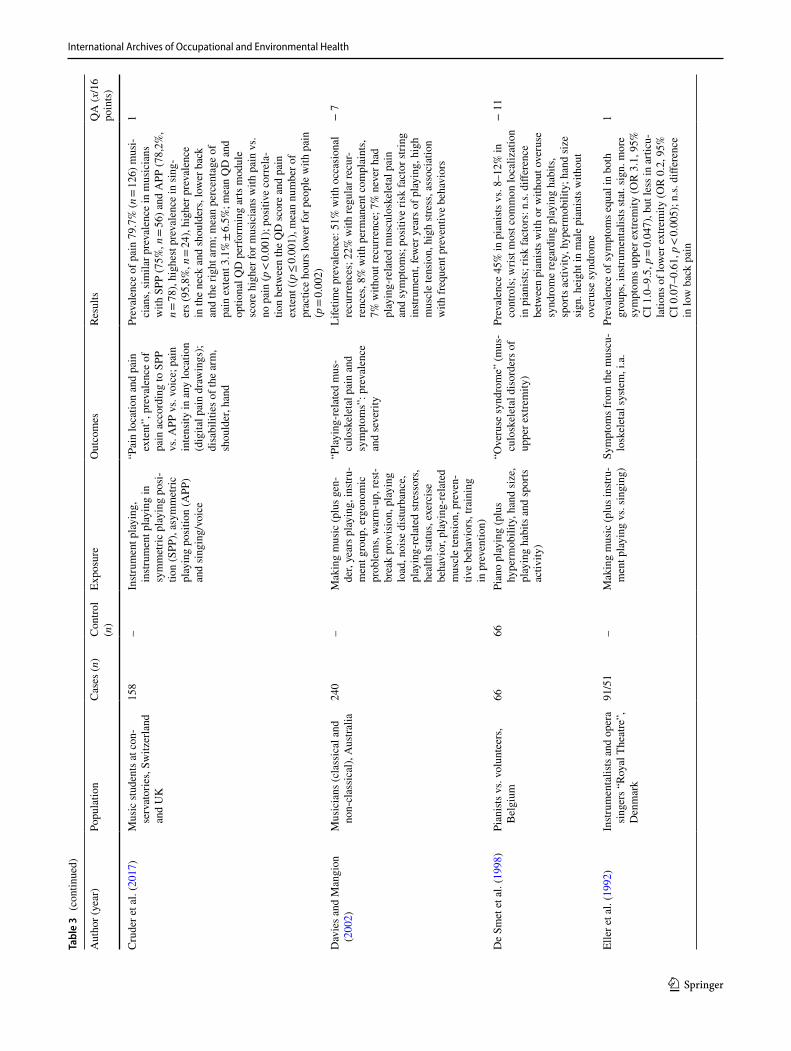
Cross‑sectional studies
We found 62 cross-sectional studies (see Table 3).
Outcome measures used in cross‑sectional studies
MCDs in the cross-sectional studies were measured with different instruments and used different definitions and ques-tionnaires that to our knowledge, were often not validated (Abréu-Ramos and Micheo 2007; Ackermann et al. 2011; Arnason et al. 2014; Blackie et al. 1999; Chan et al. 2013; Crnivec 2004; Davies and Mangion 2002; De Smet et al. 1998; Fishbein et al. 1988; Fry 1986; Heredia et al. 2014; Hodapp et al. 2009; Kim et al. 2012; Kok et al. 2013; 2015; Kovero and Könönen 1995; Marques et al. 2003; Schäcke et al. 1986; Middlestadt and Fishbein 1989; Molsberger 1991; Papandreou and Vervainioti 2010; Raymond et al. Ta
ble
1 C
hara
cter
istic
s and
resu
lts o
f the
incl
uded
stud
ies,
case
–con
trol s
tudy
Aut
hor (
year
)Po
pula
tion
Cas
es (n
)C
ontro
l (n)
Expo
sure
Out
com
esRe
sults
Qua
lity
asse
ss-
men
t (x/
14
poin
ts)
Saka
i and
Shi
maw
aki
(201
0)Pi
anist
s with
ove
ruse
dis
-or
ders
and
han
d pr
oble
ms
vs. 6
2 un
affec
ted
pian
ists
in o
rthop
edic
con
sulta
tion
of th
e au
thor
, Jap
an
220
62H
and
size
and
abd
uctio
n an
gle
of fi
nger
join
ts“O
veru
se”-
diso
rder
s of t
he
hand
Epic
ondy
litis
, mus
cle
pain
in th
e fo
rear
m a
nd
hypo
then
ar re
gion
, De
Que
rvai
n’s t
endi
nitis
and
di
stal
tend
initi
s cor
rela
te
with
var
iabl
e pa
ram
eter
s of
smal
l han
d si
ze
− 3

International Archives of Occupational and Environmental Health
1 3
Tabl
e 2
Cha
ract
erist
ics a
nd re
sults
of t
he in
clud
ed st
udie
s, co
hort
studi
es
Aut
hor (
year
)Po
pula
tion
Cas
es (n
)C
ontro
l (n)
Expo
sure
Out
com
esRe
sults
QA
(x/1
4 po
ints
)
Fjel
lman
-Wik
lund
and
Su
ndel
in (1
998)
Mus
ic te
ache
rs, S
wed
en61
–W
orki
ng a
s a m
usic
te
ache
r (pl
us a
rm p
osi-
tion)
“WM
SD’s
” (w
ork-
rela
ted
mus
culo
skel
etal
dis
or-
ders
) and
dis
com
fort,
m
odifi
ed v
ersi
on o
f N
ordi
c Q
uesti
onna
ire
Initi
al 1
2-m
onth
pre
va-
lenc
e 80
%, a
fter 8
yea
rs
at 9
2%, c
ompl
aint
s m
ostly
in sh
ould
ers,
neck
and
low
er b
ack;
cu
mul
ativ
e “i
ncid
ence
s”
0.45
for s
houl
der,
0.33
fo
r low
er b
ack,
0.3
2 fo
r nec
k; c
orre
latio
n be
twee
n fr
eque
ncy
of
arm
lift
and
disc
om-
fort
> 30
°, Pe
arso
n´s
prod
uct-m
omen
t cor
rela
-tio
n co
effici
ent =
0.46
− 2
Man
ches
ter (
1988
)M
usic
stud
ents
who
co
nsul
ted
the
auth
or’s
stu
dent
hea
lth se
rvic
e du
e to
pla
ying
-rel
ated
m
uscu
losk
elet
al d
isor
-de
rs o
f the
upp
er li
mb,
U
SA
132
–In
strum
ent p
layi
ng (p
lus
gend
er, i
nstru
men
t gr
oup)
“Upp
er e
xtre
mity
pro
b-le
ms b
roug
ht b
y pl
ayin
g an
instr
umen
t”, e
spe-
cial
ly h
and
diso
rder
s
“Inc
iden
ce”
of h
and
diso
rder
s 8.5
per
100
m
usic
stud
ents
per
ye
ar (m
: 5.7
, f: 1
1.5)
, ke
yboa
rd in
strum
ents
: 13
.2, s
tring
s: 9
.6, w
ind
instr
umen
ts: 3
.9)
− 1
1
Man
ches
ter a
nd L
ustik
(1
989)
Mus
ic st
uden
ts w
ho
cons
ulte
d th
e au
thor
’s
stude
nt h
ealth
serv
ice
due
to p
layi
ng re
-rel
ated
m
uscu
losk
elet
al d
isor
-de
rs o
f the
upp
er li
mb,
U
SA
49–
Stud
ying
mus
ic“P
erfo
rman
ce-r
elat
ed
hand
pro
blem
s”50
% o
f fol
low
-up
patie
nts
wer
e sy
mpt
om-f
ree,
34%
ha
d a
com
plai
nt re
duc-
tion,
16%
had
per
siste
nt
com
plai
nts
− 8
Man
ches
ter a
nd F
liede
r (1
991)
Mus
ic st
uden
ts w
ho
cons
ulte
d th
e au
thor
’s
stude
nt h
ealth
serv
ice
due
to p
layi
ng re
-rel
ated
m
uscu
losk
elet
al d
isor
-de
rs o
f the
upp
er li
mb,
U
SA
114
–St
udyi
ng m
usic
(plu
s gen
-de
r, in
strum
ent g
roup
)“P
erfo
rman
ce-r
elat
ed
hand
pro
blem
s”“I
ncid
ence
” of
han
d pr
oble
ms 8
.5 (r
ange
8–
9.5)
per
100
mus
ic
stude
nts p
er y
ear (
m:
rang
e 4.
9–7.
2, f:
rang
e 9.
5–12
.1, p
< 0.
04, f
or
keyb
oard
instr
umen
ts
and
strin
gs h
ighe
r tha
n fo
r win
d in
strum
ents
, p <
0.01
)
− 1
1

International Archives of Occupational and Environmental Health
1 3
f fem
ale,
m m
ale,
ND
I Nec
k D
isab
ility
Inde
x, st
at. s
ign.
stat
istic
ally
sign
ifica
nt, Q
A qu
ality
ass
essm
ent,
VAS
visu
al a
nalo
g sc
ale
Tabl
e 2
(con
tinue
d)
Aut
hor (
year
)Po
pula
tion
Cas
es (n
)C
ontro
l (n)
Expo
sure
Out
com
esRe
sults
QA
(x/1
4 po
ints
)
Nus
seck
et a
l. (2
017)
Mus
ic st
uden
ts, 5
uni
vers
i-tie
s of m
usic
, Ger
man
y28
8–
Stud
ying
mus
ic, p
re-
vent
ive
activ
ities
and
he
alth
-rel
ated
cou
rses
at
univ
ersi
ties
“Pla
ying
-rel
ated
hea
lth
prob
lem
s” (m
ixed
so
mat
ic a
nd p
sych
olog
i-ca
l)
No
diffe
renc
es b
etw
een
the
univ
ersi
ties,
prev
a-le
nce
durin
g “c
ours
e of
stu
dy”:
29%
in 1
st ye
ar,
42%
in 2
nd y
ear,
amon
g stu
dent
s with
com
plai
nts
som
atic
com
plai
nts 7
5%
1st y
ear,
64%
2nd
yea
r, 66
% 3
rd y
ear,
65%
4th
ye
ar; r
isk/
prev
entiv
e fa
c-to
rs: 4
1% st
uden
ts w
ith-
out c
ompl
aint
s and
73%
of
stud
ents
with
com
-pl
aint
s atte
nd p
reve
n-tiv
e co
urse
s in
1st y
ear
(Chi
2 (285
) = 23
.615
, p <
0.00
1), 8
4% st
uden
ts
with
out c
ompl
aint
s an
d 68
% st
uden
ts w
ith
com
plai
nts a
ttend
pre
-ve
ntiv
e co
urse
s in
2nd
year
(Chi
2 (134
) = 4.
822,
p =
0.02
8), n
o st
at. s
ing.
di
ffere
nce
3rd
year
70%
vs
. 85%
, or 4
th y
ear 7
7%
vs. 7
7%, h
igh
drop
out
be
twee
n ye
ars
10
Piat
kow
ska
et a
l. (2
016)
Mus
ic st
uden
ts, P
olan
d45
(15
viol
in,
15 c
ello
, 15
pia
no)
–In
strum
ent p
layi
ng: 1
. gr
oup
viol
in, 2
. gro
up
cello
, 3. g
roup
pia
no
“Cer
vica
l pai
n” b
y VA
S (0
–10
cm),
disa
bilit
y by
N
DI (
inte
r alia
)
Mod
erat
e de
gree
of d
is-
abili
ty a
nd p
ain
in a
ll th
e gr
oups
, mor
e di
sabi
lity
and
pain
in th
e ce
llists
, sl
ight
ly lo
wer
in th
e vi
olin
ists a
nd th
e lo
wes
t in
the
pian
ists,
pain
stat
. si
gn. l
ower
(p =
0.04
) 12
wee
ks a
fter b
asel
ine
in p
iani
sts c
ompa
red
to
celli
sts
1

International Archives of Occupational and Environmental Health
1 3
Tabl
e 3
Cha
ract
erist
ics a
nd re
sults
of t
he in
clud
ed st
udie
s, cr
oss-
sect
iona
l stu
dies
Aut
hor (
year
)Po
pula
tion
Cas
es (n
)C
ontro
l (n
)Ex
posu
reO
utco
mes
Resu
ltsQ
A (x
/16
poin
ts)
Abr
éu-R
amos
and
M
iche
o (2
007)
Orc
hestr
a m
usic
ians
“P
uerto
Ric
o Sy
mph
ony
Orc
hestr
a”, P
uerto
Ric
o
75–
Instr
umen
t pla
ying
(plu
s in
strum
ent g
roup
, gen
-de
r, ag
e)
“MSK
Ps”
(mus
culo
skel
etal
pr
oble
ms)
that
affe
ct
play
ing
Life
time
prev
alen
ce M
SKPs
81%
(fem
ale
87,5
% v
s. m
ale
97.7
%);
mos
t com
mon
ba
ck p
ain
(75%
); m
ost c
omm
on in
low
er
strin
gs (9
3%) a
nd p
ercu
ssio
nists
(100
%),
in y
oung
er (2
2–29
yea
rs, 8
3%) a
nd o
lder
(5
0–61
yea
rs, 9
1%) p
opul
atio
ns; f
emal
e se
x, a
ge, i
nstru
men
t pla
yed
are
risk
fact
ors
− 3
Ack
erm
ann
and
Ada
ms
(200
3)V
iolin
ists a
nd v
iolis
ts
(stu
dent
s and
orc
hestr
a m
usic
ians
), A
ustra
lia
32–
Instr
umen
t pla
ying
(plu
s an
thro
pom
etric
mea
s-ur
emen
ts [l
engt
h an
d RO
M])
“Per
form
ance
-rel
ated
pa
in”:
pai
n in
diff
eren
t bo
dy si
tes r
elat
ed to
pl
ayin
g
Life
time
prev
alen
ce “
Perfo
rman
ce-r
elat
ed
pain
” 88
%, m
ost c
omm
on le
ft up
per
extre
mity
(69%
), th
orac
ic sp
ine
(63%
), rig
ht u
pper
ext
rem
ity (5
3%) a
nd c
ervi
cal
spin
e (4
4%);
4 gr
eate
r RO
M o
f the
left
hand
com
pare
d w
ith th
e rig
ht; l
eft h
and
anth
ropo
met
rics a
re n
ot re
late
d to
pai
n bu
t ant
hrop
omet
rics o
f the
righ
t arm
se
ems t
o be
a ri
sk fa
ctor
− 5
Ack
erm
ann
et a
l. (2
011)
Col
legi
ate
flute
pla
yers
, “S
ydne
y C
onse
rvat
oriu
m
of M
usic
”, A
ustra
lia
20–
Flut
e pl
ayin
g“P
RM
Ds”
(per
form
ance
-re
late
d m
uscu
losk
elet
al
diso
rder
s): p
reva
lenc
e an
d ch
arac
teris
tics
Life
time
prev
alen
ce o
f 43
diffe
rent
PR
MD
s 95
%, (
37%
lasti
ng <
3 m
onth
s, 63
%,
lasti
ng fo
r > 3
mon
ths)
, mos
t com
mon
lo
catio
n: u
pper
ext
rem
ity; m
ost c
omm
on
sym
ptom
: pai
n
− 9
Am
orim
and
Jorg
e (2
016)
Vio
linist
s (pr
ofes
sion
al
and
stude
nts i
n hi
gher
ed
ucat
ion
train
ing)
, Po
rtuga
l
93–
Vio
lin p
layi
ng“T
MD
” (te
mpo
rom
andi
bu-
lar d
isor
der)
in re
latio
n to
MPA
leve
l, in
strum
ent
prac
tice
time,
chi
nres
t ty
pe, g
ende
r and
age
Prev
alen
ce T
MD
58%
(n =
50),
slig
htly
hi
gher
in fe
mal
es (5
5% v
s. 53
%),
youn
ger p
laye
rs a
ged ≤
30 y
rs. (
61%
vs.
55%
), m
usic
ians
with
< 20
-yea
r exp
eri-
ence
(55%
vs.
52%
), pr
actic
e < 22
h/w
eek
(54%
vs.
53%
) ove
r the
tailp
iece
chi
nres
t m
odel
(57%
vs.
50%
in D
resd
en c
hinr
est
and
44%
oth
er m
odel
s); r
isk
fact
or:
asso
ciat
ion
betw
een
the
prev
alen
ce o
f TM
D a
nd h
igh
MPA
leve
ls (p
< 0.
001)
, th
e m
ost a
nxio
us v
iolin
ists 6
tim
es (9
5%
CI 2
.51–
15.3
3; p
< 0.
001)
mor
e lik
ely
to
repo
rt TM
D sy
mpt
oms v
s. le
ast a
nxio
us
viol
inist
s
3
Arn
ason
et a
l. (2
014)
Mus
ic st
uden
ts (c
lass
ical
vs
. rhy
thm
ic m
usic
), Ic
elan
d
74–
Instr
umen
t pla
ying
(plu
s cl
assi
cal v
s. rh
ythm
ic
mus
ic, i
nstru
men
t gro
up,
gend
er)
“PR
MD
” (p
layi
ng-r
elat
ed
mus
culo
skel
etal
dis
-or
der)
: pre
vale
nce
and
seve
rity
of m
uscu
losk
el-
etal
dis
orde
rs
Life
time
prev
alen
ce P
RM
D 6
2% (7
0%
clas
sica
l vs.
39%
rhyt
hmic
mus
ic; 6
1%
in fe
mal
e, 3
9% in
mal
e, n
.s. d
iffer
ence
s be
twee
n in
strum
ent g
roup
s); p
reva
lenc
e PR
MD
last
7 da
ys 4
0% (n
.s. d
iffer
ence
s cl
assi
cal v
s. rh
ythm
ic m
usic
)
− 7

International Archives of Occupational and Environmental Health
1 3
Tabl
e 3
(con
tinue
d)
Aut
hor (
year
)Po
pula
tion
Cas
es (n
)C
ontro
l (n
)Ex
posu
reO
utco
mes
Resu
ltsQ
A (x
/16
poin
ts)
Bar
ton
et a
l. (2
008)
Mus
ic st
uden
ts, U
SA97
–In
strum
ent p
layi
ng (p
lus
gend
er, i
nstru
men
t gr
oup)
“Phy
sica
l sym
ptom
s”, d
is-
abili
ties b
y D
ASH
; pai
n in
any
loca
tion
Ave
rage
DA
SH sc
ore
per p
erso
n 6.
62/1
00
(SD
8.6
9; ra
nge
0.0–
45.0
) f 8
.58,
m
4.67
); str
ings
hig
her m
ean
DA
SH sc
ore
than
bra
ss (m
ean
diffe
renc
e = 7.
98,
p < 0.
01) a
nd w
oodw
inds
(mea
n di
ffer-
ence
= 6.
50, p
< 0.
01);
65%
cur
rent
pai
n,
(sta
t. si
gn. m
ore
f, si
gn d
iff. b
etw
een
instr
umen
t gro
ups)
− 5
Ber
que
et a
l. (2
016)
Perm
anen
tly e
mpl
oyed
cl
assi
cal o
rche
stra
mus
i-ci
ans f
rom
3 o
rche
stras
, Sc
otla
nd
101
–In
strum
ent p
layi
ng (p
lus
gend
er, a
ge, i
nstru
men
t gr
oup,
pla
ying
pro
fes-
sion
ally
in a
n or
ches
tra)
“PR
MPs
” (p
layi
ng-
rela
ted
mus
culo
skel
etal
pr
oble
ms)
, pai
n in
tens
ity
and
pain
inte
rfere
nce
on
func
tion
and
psyc
hoso
cial
va
riabl
es b
y M
uscu
lo-
skel
etal
Pai
n In
tens
ity
and
Inte
rfere
nce
Que
s-tio
nnai
re fo
r Mus
icia
ns
(MPI
IQM
)
Prev
alen
ce P
RM
Ps: l
ifetim
e 77
.2%
, 12
mon
ths 4
5.5%
, poi
nt p
reva
lenc
e 36
.6%
, am
ong
PRM
P 43
% p
ain
in ≥
3 lo
catio
ns, m
ost c
omm
only
the
right
up
per l
imb,
nec
k, le
ft fo
rear
m a
nd e
lbow
, va
riatio
ns b
etw
een
instr
umen
t gro
up;
mea
n pa
in in
tens
ity in
mus
icia
ns w
ith
PRM
P 12
.4 ±
7.63
(out
of 4
0), m
ean
pain
inte
rfere
nce
scor
e 15
.2 ±
12.3
9 (o
ut
of 5
0), i
ncre
asin
g w
ith th
e nu
mbe
r of
repo
rted
pain
loca
tions
(p =
0.04
4); m
ean
age
in m
usic
ians
with
PR
MP
alm
ost 5
yr
s. ol
der v
s. no
n-PR
MP
(p =
0.02
9),
aver
age
num
ber o
f yea
rs o
f pla
ying
pro
-fe
ssio
nally
in a
n or
ches
tra w
ith m
usic
ians
w
ith P
RM
P ha
ving
alm
ost 5
yrs
. mor
e vs
. non
-PR
MP
(p =
0.04
6)
3
Bla
ckie
et a
l. (1
999)
Pian
o stu
dent
s, U
SA16
–Pi
ano
play
ing
Play
ing-
rela
ted
“inj
urie
s”/
over
use:
inci
denc
e, i.
a.Pr
eval
ence
93%
, 27
play
ing-
rela
ted
inju
ries
repo
rted
(66%
in h
and
and
wris
t, am
ong
them
21%
pai
n or
dis
com
fort
impa
irs
activ
ities
oth
er th
an p
iano
)
− 5
Cha
n et
al.
(201
3)O
rche
stra
mus
icia
ns
(sym
phon
y or
ches
tra),
Aus
tralia
83–
Instr
umen
t pla
ying
Mus
culo
skel
etal
“in
jurie
s”
incl
. “PR
MD
s” (p
erfo
r-m
ance
-rel
ated
mus
culo
-sk
elet
al d
isor
ders
), i.a
.
99 c
onsu
ltatio
ns (8
3 in
divi
dual
s) a
mon
g th
em 6
6% o
f inj
urie
s cla
ssifi
ed P
RM
Ds
(26%
acu
te, 4
6% c
hron
ic re
curr
ing,
28%
ch
roni
c; 9
3% c
urre
ntly
affe
ct p
layi
ng,
94%
pre
vent
able
); m
ost c
omm
on lo
ca-
tions
shou
lder
(22%
), ne
ck (1
8%),
uppe
r ba
ck (1
8%),
hand
(8%
)
− 1
1
Crn
ivec
(200
4)O
rche
stra
mus
icia
ns
“Slo
vene
Phi
lhar
mon
ic
Orc
hestr
a” v
s. m
arke
t-in
g-w
orke
rs “
Phili
p M
orris
Ent
erpr
ise”
, Sl
oven
ia
7028
Instr
umen
t pla
ying
“Per
form
ance
-rel
ated
mus
-cu
losk
elet
al d
isor
ders
”,
i.a.
Mus
culo
skel
etal
dis
orde
rs m
ost c
omm
on
heal
th im
pairm
ent o
f mus
icia
ns, a
lmos
t 6
times
hig
her t
han
cont
rol g
roup
(147
vs.
25),
mos
t hig
h in
dou
ble
bass
and
cel
lo
play
ers
− 9
International Archives of Occupational and Environmental Health
1 3
Tabl
e 3
(con
tinue
d)
Aut
hor (
year
)Po
pula
tion
Cas
es (n
)C
ontro
l (n
)Ex
posu
reO
utco
mes
Resu
ltsQ
A (x
/16
poin
ts)
Cru
der e
t al.
(201
7)M
usic
stud
ents
at c
on-
serv
ator
ies,
Switz
erla
nd
and
UK
158
–In
strum
ent p
layi
ng,
instr
umen
t pla
ying
in
sym
met
ric p
layi
ng p
osi-
tion
(SPP
), as
ymm
etric
pl
ayin
g po
sitio
n (A
PP)
and
sing
ing/
voic
e
“Pai
n lo
catio
n an
d pa
in
exte
nt”,
pre
vale
nce
of
pain
acc
ordi
ng to
SPP
vs
. APP
vs.
voic
e; p
ain
inte
nsity
in a
ny lo
catio
n (d
igita
l pai
n dr
awin
gs);
disa
bilit
ies o
f the
arm
, sh
ould
er, h
and
Prev
alen
ce o
f pai
n 79
.7%
(n =
126)
mus
i-ci
ans,
sim
ilar p
reva
lenc
e in
mus
icia
ns
with
SPP
(75%
, n =
56) a
nd A
PP (7
8,2%
, n =
78),
high
est p
reva
lenc
e in
sing
-er
s (95
,8%
, n =
24),
high
er p
reva
lenc
e in
the
neck
and
shou
lder
s, lo
wer
bac
k an
d th
e rig
ht a
rm; m
ean
perc
enta
ge o
f pa
in e
xten
t 3.1
% ±
6.5%
; mea
n Q
D a
nd
optio
nal Q
D p
erfo
rmin
g ar
ts m
odul
e sc
ore
high
er fo
r mus
icia
ns w
ith p
ain
vs.
no p
ain
(p <
0.00
1); p
ositi
ve c
orre
la-
tion
betw
een
the
QD
scor
e an
d pa
in
exte
nt ((
p ≤ 0.
001)
, mea
n nu
mbe
r of
prac
tice
hour
s low
er fo
r peo
ple
with
pai
n (p
= 0.
002)
1
Dav
ies a
nd M
angi
on
(200
2)M
usic
ians
(cla
ssic
al a
nd
non-
clas
sica
l), A
ustra
lia24
0–
Mak
ing
mus
ic (p
lus g
en-
der,
year
s pla
ying
, ins
tru-
men
t gro
up, e
rgon
omic
pr
oble
ms,
war
m-u
p, re
st-br
eak
prov
isio
n, p
layi
ng
load
, noi
se d
istur
banc
e,
play
ing-
rela
ted
stres
sors
, he
alth
stat
us, e
xerc
ise
beha
vior
, pla
ying
-rel
ated
m
uscl
e te
nsio
n, p
reve
n-tiv
e be
havi
ors,
train
ing
in p
reve
ntio
n)
“Pla
ying
-rel
ated
mus
-cu
losk
elet
al p
ain
and
sym
ptom
s”: p
reva
lenc
e an
d se
verit
y
Life
time
prev
alen
ce: 5
1% w
ith o
ccas
iona
l re
curr
ence
s; 2
2% w
ith re
gula
r rec
ur-
renc
es, 8
% w
ith p
erm
anen
t com
plai
nts,
7% w
ithou
t rec
urre
nce;
7%
nev
er h
ad
play
ing-
rela
ted
mus
culo
skel
etal
pai
n an
d sy
mpt
oms;
pos
itive
risk
fact
or st
ring
instr
umen
t, fe
wer
yea
rs o
f pla
ying
, hig
h m
uscl
e te
nsio
n, h
igh
stres
s, as
soci
atio
n w
ith fr
eque
nt p
reve
ntiv
e be
havi
ors
− 7
De
Smet
et a
l. (1
998)
Pian
ists v
s. vo
lunt
eers
, B
elgi
um66
66Pi
ano
play
ing
(plu
s hy
perm
obili
ty, h
and
size
, pl
ayin
g ha
bits
and
spor
ts
activ
ity)
“Ove
ruse
synd
rom
e” (m
us-
culo
skel
etal
dis
orde
rs o
f up
per e
xtre
mity
)
Prev
alen
ce 4
5% in
pia
nists
vs.
8–12
% in
co
ntro
ls; w
rist m
ost c
omm
on lo
caliz
atio
n in
pia
nists
; ris
k fa
ctor
s: n
.s. d
iffer
ence
be
twee
n pi
anist
s with
or w
ithou
t ove
ruse
sy
ndro
me
rega
rdin
g pl
ayin
g ha
bits
, sp
orts
act
ivity
, hyp
erm
obili
ty; h
and
size
si
gn. h
eigh
t in
mal
e pi
anist
s with
out
over
use
synd
rom
e
− 1
1
Elle
r et a
l. (1
992)
Instr
umen
talis
ts a
nd o
pera
si
nger
s “Ro
yal T
heat
re”,
D
enm
ark
91/5
1–
Mak
ing
mus
ic (p
lus i
nstru
-m
ent p
layi
ng v
s. si
ngin
g)Sy
mpt
oms f
rom
the
mus
cu-
losk
elet
al sy
stem
, i.a
.Pr
eval
ence
of s
ympt
oms e
qual
in b
oth
grou
ps, i
nstru
men
talis
ts st
at. s
ign.
mor
e sy
mpt
oms u
pper
ext
rem
ity (O
R 3
.1, 9
5%
CI 1
.0–9
.5, p
= 0.
047)
, but
less
in a
rticu
-la
tions
of l
ower
ext
rem
ity (O
R 0
.2, 9
5%
CI 0
.07–
0.61
, p <
0.00
5); n
.s. d
iffer
ence
in
low
bac
k pa
in
1

International Archives of Occupational and Environmental Health
1 3
Tabl
e 3
(con
tinue
d)
Aut
hor (
year
)Po
pula
tion
Cas
es (n
)C
ontro
l (n
)Ex
posu
reO
utco
mes
Resu
ltsQ
A (x
/16
poin
ts)
Engq
uist
et a
l. (2
004)
Orc
hestr
a m
usic
ians
vs.
acto
rs, S
wed
en10
310
6In
strum
ent p
layi
ng (p
lus
instr
umen
t gro
up, g
en-
der,
age)
“Mus
culo
skel
etal
pai
n”:
prev
alen
ce a
nd in
tens
ity,
VAS
(0–2
0)
Poin
t pre
vale
nce
pain
61%
vs.7
1% (O
R
0.6)
; 12-
mon
th p
reva
lenc
e ch
roni
c pa
in
47%
vs.
51%
(OR
1);
neck
and
shou
lder
m
ost c
omm
on, s
tring
s mos
t ofte
n; n
o gr
oup
diffe
renc
e re
gard
ing
inte
nsity
of
pain
or r
isk
fact
or g
ende
r
− 5
Gas
enze
r et a
l. (2
017)
Orc
hestr
a m
usic
ians
, 132
G
erm
an c
ultu
ral o
rche
s-tra
s, G
erm
any
740
–M
akin
g m
usic
“Chr
onic
pai
n”: p
reva
-le
nce;
deg
ree
of im
pair-
men
t, pa
in lo
catio
ns p
er
instr
umen
t gro
up, i
.a.
Prev
alen
ce 6
6% (n
= 49
0) c
urre
nt o
r rec
ur-
ring
pain
, 64%
(n =
470)
con
tinuo
us p
ain
or p
ain >
3 m
onth
s, m
ost f
requ
ent i
n ba
ck
(70%
), sh
ould
ers (
68%
), ne
ck (6
4%),
hand
s and
wris
ts (4
0%);
27%
pai
n w
ith
high
deg
ree
of im
pairm
ent (
Kor
ff sc
ale)
; ris
k fa
ctor
hig
h str
ings
hig
hest
rate
in
chro
nic
shou
lder
pai
n i.a
.; m
ean
pain
m
axim
al in
tens
ity 6
.0 (S
D ±
2.4)
− 5
Fjel
lman
n-W
iklu
nd
et a
l. (2
003)
Mus
ic te
ache
rs, S
wed
en20
8–
Empl
oyed
mus
ic te
ache
rs
(plu
s Phy
sica
l act
iv-
ity d
urin
g le
isur
e tim
e, p
erce
ived
hea
lth,
phys
ical
wor
k en
viro
n-m
ent,
psyc
hoso
cial
wor
k en
viro
nmen
t)
“Mus
culo
skel
etal
dis
com
-fo
rt in
the
neck
–sho
ulde
r re
gion
”: p
reva
lenc
e, S
NQ
12-m
onth
pre
vale
nce
82%
, mos
t com
mon
ne
ck (5
9%),
shou
lder
(55%
), lo
wer
bac
k (4
5%);
risk
fact
or fe
mal
e st
at. s
ign.
mor
e sy
mpt
oms i
n ne
ck, s
houl
der,
uppe
r bac
k;
in fe
mal
e: st
rong
est r
isk
fact
ors a
ssoc
i-at
ed w
ith n
eck–
shou
lder
dis
com
fort:
hi
gh p
sych
olog
ical
dem
ands
(OR
6.0
, CI
1.1–
32.4
), te
achi
ng m
any
scho
ols (
OR
4.
8, C
I 1.0
–24.
4); i
n m
ale:
lifti
ng (O
R
8.7,
CI 2
.1–3
4.8)
, pla
ying
the
guita
r (O
R
6.0,
CI 1
.5–2
3.6)
, low
soci
al su
ppor
t (O
R
3.1,
CI 1
.0–9
.7)
5
Fotia
dis e
t al.
(201
3)O
rche
stra
mus
icia
ns
(sym
phon
ic o
rche
stra)
“A
then
s and
The
ssa-
loni
ki S
tate
Sym
phon
y O
rche
stra”
, Gre
ece
147
–In
strum
ent p
layi
ng (p
lus
gend
er, a
ge, i
nstru
men
t gr
oup,
dai
ly in
strum
ent
prac
tice)
“Mus
culo
skel
etal
dis
or-
ders
”: p
reva
lenc
eLi
fetim
e pr
eval
ence
82%
, 66%
with
con
-si
dera
ble
influ
ence
on
perfo
rmin
g ab
ility
; ris
k fa
ctor
s: n
eck/
shou
lder
in fe
mal
e st
at.
sign
. mor
e fr
eque
nt; s
houl
der i
n str
ing
instr
umen
talis
ts st
at. s
ign.
Mor
e fr
eque
nt
than
in b
rass
/woo
dwin
d in
strum
enta
lists
; w
rist/h
and
in m
usic
ians
> 60
yea
rs. s
tat.
sign
. mor
e fr
eque
nt, h
ours
of p
ract
ice
per d
ay is
a c
riter
ion
for o
ccur
renc
e of
m
uscu
losk
elet
al d
isor
ders
1
Fry
(198
6)O
rche
stra
mus
icia
ns, A
us-
tralia
, USA
, Eng
land
485
–In
strum
ent p
layi
ng“O
veru
se sy
ndro
me”
: pai
n an
d pr
eval
ence
with
se
verit
y
Prev
alen
ce 6
4%, m
ost c
omm
on lo
caliz
a-tio
n ha
nd/w
rist (
41%
), ne
ck (3
8%),
shou
lder
(35%
) and
LW
S (2
6%)
− 9

International Archives of Occupational and Environmental Health
1 3
Tabl
e 3
(con
tinue
d)
Aut
hor (
year
)Po
pula
tion
Cas
es (n
)C
ontro
l (n
)Ex
posu
reO
utco
mes
Resu
ltsQ
A (x
/16
poin
ts)
Goh
l et a
l. (2
006)
Uni
vers
ity p
iani
sts “
Bel
-m
ont U
nive
rsity
Sch
ool
of M
usic
” an
d “V
an-
derb
ilt U
nive
rsity
Bla
ir Sc
hool
of M
usic
”, U
SA
19–
Pian
o stu
dies
“Med
ian
and
ulna
r neu
-ro
path
ies”
in e
ither
upp
er
extre
mity
Prev
alen
ce 1
6% e
lect
rodi
agno
stic
evid
ence
of
ear
ly m
edia
n ne
urop
athy
at o
r dist
al to
th
e w
rist,
no fu
rther
sign
s of n
euro
path
y
− 1
Hei
kkilä
et a
l. (2
012)
Orc
hestr
a m
usic
ians
“S
info
nia
Laht
i” a
nd
“The
Fin
nish
Rad
io
Sym
phon
y O
rche
stra”
, Fi
nlan
d
73–
Instr
umen
t pla
ying
(plu
s in
strum
ent g
roup
, age
, ge
nder
, stre
ss, n
ight
br
uxis
m, d
ay b
ruxi
sm,
slee
p di
sturb
ance
s, ph
ysic
al e
xerc
ise)
“Sym
ptom
s of T
MD
s and
fa
cial
pai
n”1-
mon
th p
reva
lenc
e 56
%; n
o di
ffere
nce
in in
strum
ent g
roup
s; ri
sk fa
ctor
s: sl
eep
distu
rban
ces a
nd n
ight
bru
xism
seem
to
incr
ease
TM
D’s
, TM
Ds d
imin
ish
with
ag
e
3
Her
edia
et a
l. (2
014)
Pop-
mus
icia
ns “
Orq
uest
a B
uena
Vist
a So
cial
Clu
b an
d Su
ppor
ting
Ban
ds”,
K
uba
36–
Mak
ing
mus
ic“M
uscu
losk
elet
al c
ondi
-tio
ns”
12-m
onth
pre
vale
nce
37%
− 9
Hod
app
et a
l. (2
009)
Orc
hestr
a m
usic
ians
(o
pera
and
sym
phon
ic
orch
estra
vs.
amat
eur
orch
estra
), G
erm
any
122
28In
strum
ent p
layi
ng (p
lus
prof
essi
onal
vs.
amat
eur
mus
icia
ns, w
ork
com
-pl
exity
, wor
king
con
di-
tions
, sco
pe o
f act
ion,
so
cial
stre
ssor
s, nu
mbe
r of
per
form
ance
s and
re
hear
sals
, i.a
.)
“Bod
ily c
ompl
aint
s”
incl
udin
g m
uscu
losk
el-
etal
com
plai
nts,
i.a.
Prev
alen
ce m
uscu
losk
elet
al c
ompl
aint
s m
ore
in p
rofe
ssio
nal m
usic
ians
than
in
amat
eurs
(M 5
.24,
SD
4.7
6 vs
. M 2
.71,
SD
= 2.
21; p
< 0.
001)
; ris
k fa
ctor
s wor
k str
esso
rs a
nd n
umbe
r of p
erfo
rman
ces
corr
elat
e po
s. w
ith m
uscu
losk
elet
al
com
plai
nts
− 5
Kau
fman
-Coh
en a
nd
Rat
zon
(201
1)O
rche
stra
mus
icia
ns
(stri
ng a
nd w
ind
play
-er
s), I
srae
l
59–
Instr
umen
t pla
ying
(plu
s bi
omec
hani
cal,
envi
ron-
men
tal,
psyc
hoso
cial
an
d pe
rson
al ri
sk fa
ctor
s, in
divi
dual
pla
ying
cha
r-ac
teris
tics)
“PR
MD
” (p
layi
ng-
rela
ted
mus
culo
skel
etal
di
sord
ers)
: mus
culo
skel
-et
al p
ain
and
func
tiona
l im
pairm
ent d
urin
g la
st ye
ars,
seve
rity,
SN
Q,
DA
SH, R
ULA
12-m
onth
pre
vale
nce
PRM
PD m
in. 1
bod
y re
gion
83%
, > 1
body
regi
on 7
3%; b
iom
e-ch
anic
al a
nd p
ostu
ral l
oadi
ng, i
nstru
men
t w
eigh
t, ris
k fa
ctor
s per
ceiv
ed p
hysi
cal
envi
ronm
ent,
aver
age
play
ing
hour
s per
w
eek,
gen
der a
nd w
arm
-up’
s cor
rela
te
with
PR
MD
s
5
Kim
et a
l. (2
012)
Trad
ition
al K
orea
n str
ing
instr
umen
t pla
yers
, K
orea
86–
Instr
umen
t pla
ying
(plu
s ty
pe o
f ins
trum
ent,
age,
he
ight
, wei
ght,
BM
I, ye
ars o
f car
eer,
gend
er,
prac
tice
habi
ts, e
xerc
ise
inte
nsity
, hob
by st
yles
, dr
inki
ng a
nd sm
okin
g ha
bits
, stre
tchi
ng)
“PR
MD
s” (p
layi
ng-r
elat
ed
mus
culo
skel
etal
dis
or-
ders
): m
uscu
losk
elet
al
diso
rder
s
Prev
alen
ce e
ach >
50%
in fo
rear
m, n
eck,
ba
ck, s
houl
der,
uppe
r arm
, wris
t and
kn
ee; r
isk
fact
ors:
var
ious
stat
. sig
n. c
or-
rela
tions
bet
wee
n de
mog
raph
ic v
aria
bles
an
d m
uscu
losk
elet
al d
isor
ders
dep
endi
ng
on ty
pe o
f ins
trum
ent
− 7

International Archives of Occupational and Environmental Health
1 3
Tabl
e 3
(con
tinue
d)
Aut
hor (
year
)Po
pula
tion
Cas
es (n
)C
ontro
l (n
)Ex
posu
reO
utco
mes
Resu
ltsQ
A (x
/16
poin
ts)
Ack
erm
ann
et a
l. (2
012)
Orc
hestr
a m
usic
ians
, A
ustra
lia37
7–
Instr
umen
t pla
ying
(plu
s in
strum
ent g
roup
)“P
RM
Ds”
(per
form
ance
-re
late
d m
uscu
losk
elet
al
diso
rder
s, pe
rform
ance
-re
late
d m
uscu
losk
elet
al
pain
dis
orde
rs),
mus
culo
-sk
elet
al d
isor
ders
Life
time
prev
alen
ce 8
4%, p
oint
pre
vale
nce
50%
, mos
t com
mon
loca
lizat
ion:
low
er
back
(14.
1%),
uppe
r bac
k (1
1.7%
) and
sh
ould
er/u
pper
arm
(11.
1%);
loca
lizat
ion
varie
s acc
ordi
ng to
instr
umen
t gro
up
1
Ken
ny a
nd A
cker
man
n (2
015)
Instr
umen
t pla
ying
(plu
s ge
nder
, age
, dep
ress
ion,
pe
rform
ance
anx
iety
, so
cial
pho
bia)
Life
time
prev
alen
ce 8
4%, p
oint
pre
vale
nce
50%
, ris
k fa
ctor
: fem
ale,
pos
itive
cor
rela
-tio
n be
twee
n pe
rform
ance
anx
iety
and
in
tens
ity o
f PR
MD
and
bet
wee
n de
pres
-si
on a
nd in
tens
ity P
RM
DK
enny
et a
l. (2
016)
Orc
hestr
a m
usic
ians
, A
ustra
lia37
8–
Instr
umen
t pla
ying
in
diffe
rent
orc
hestr
a ty
pes:
pi
t, st
age
and
com
bine
d st
age
and
pit
“PR
MD
s” (p
erfo
rman
ce-
rela
ted
mus
culo
skel
etal
di
sord
ers)
, “ph
ysic
al a
nd
men
tal h
ealth
indi
cato
rs”,
VA
S pa
in, i
.a.
Life
time
prev
alen
ce p
ain
or in
jurie
s cau
sed
by p
layi
ng 8
1–95
%, l
ifetim
e pr
eval
ence
pa
in o
r inj
urie
s int
erfe
ring
with
pla
ying
85
–90%
, poi
nt p
reva
lenc
e pa
in o
r inj
ury
46–5
6%, n
.s. d
iffer
ence
bet
wee
n 3
type
s of
orc
hestr
as re
gard
ing
lifet
ime
or p
oint
pr
eval
ence
of P
RM
D; 4
2% p
it, 2
3% st
age
and
28%
stag
e/pi
t mus
icia
ns h
ad ti
me
off
wor
k du
e to
phy
sica
l pai
n or
inju
ry la
st 18
mon
ths,
n.s.
diffe
renc
e in
num
ber o
f da
ys ta
ken
− 1
Koc
hem
and
Silv
a (2
017)
Vio
linist
s, B
razi
l10
6–
Instr
umen
t pla
ying
“PR
MD
s” (p
layi
ng-r
elat
ed
mus
culo
skel
etal
dis
or-
ders
): pr
eval
ence
by
SNQ
la
st 12
mon
ths a
nd la
st 7
days
, ass
ocia
ted
fact
ors,
disa
bilit
ies b
y D
ASH
12-m
onth
pre
vale
nce:
87%
, 1-w
eek
prev
alen
ce 7
7%, p
reva
lenc
e of
PR
MD
s re
spon
sibl
e fo
r the
tem
pora
ry in
ter-
rupt
ion
of m
usic
al a
ctiv
ity: 8
%; m
ost
freq
uent
ly a
ffect
ed in
bot
h tim
e pe
riods
ne
ck, t
hora
cic
area
, rig
ht a
nd le
ft sh
oul-
ders
, lef
t wris
t/han
dPr
eval
ence
> 50
% fo
r dys
func
tiona
l upp
er
limbs
acc
ordi
ng to
the
DA
SH o
ptio
nal
mod
ule;
mea
n D
ASH
scor
e 10
.6 p
oint
s (S
D 8
.6),
optio
nal D
ASH
mus
ic m
odul
e m
ean
scor
e of
17.
6 po
ints
(19.
8)R
isk
fact
ors:
wom
en m
ore
likel
y PR
MD
s (O
R 4
.4, C
I 1.9
–10.
0, p
< 0.
001)
; old
er
mus
icia
ns m
ore
likel
y pa
in in
last
7 da
ys
(OR
3.3
, CI 5
.1–1
0.97
; p =
0.04
) and
hi
gher
scor
es o
n D
ASH
(OR
1.8
, CI
1.1–
3.1;
p =
0.01
); al
so a
ssoc
iate
d w
ith
PRM
D: b
ody
mas
s ind
ex, p
ract
ice
hour
s pe
r wee
k, fi
nal D
ASH
scor
e, i.
a.
3

International Archives of Occupational and Environmental Health
1 3
Tabl
e 3
(con
tinue
d)
Aut
hor (
year
)Po
pula
tion
Cas
es (n
)C
ontro
l (n
)Ex
posu
reO
utco
mes
Resu
ltsQ
A (x
/16
poin
ts)
Kok
et a
l. (2
015)
Mus
ic st
uden
ts v
s. m
edic
al
stude
nts,
Net
herla
nds
8349
4St
udyi
ng m
usic
(plu
s in
strum
ent g
roup
)“C
AN
S” (c
ompl
aint
s of
arm
, nec
k, a
nd/o
r sh
ould
er n
ot c
ause
d by
a
syste
mic
dis
ease
or a
cute
tra
uma)
and
gen
der
Poin
t pre
vale
nce
in m
usic
stud
ents
vs
. med
ical
stud
ents
(47%
vs.
18%
, p <
0.00
1), 1
2-m
onth
pre
vale
nce
in m
usic
stu
dent
s vs.
med
ical
stud
ents
(81%
vs
42%
, p <
0.00
1), c
hron
ic C
AN
S in
mus
ic
stude
nts v
s. m
edic
al st
uden
ts (3
6% v
s. 10
%, p
< 0.
001)
; mus
ic st
uden
ts: m
ore
com
plai
nts p
er a
nato
mic
loca
lizat
ion
and
mor
e lo
caliz
atio
ns, m
usic
stud
ents
m
ore
seve
re in
fluen
ce o
f CA
NS
on d
aily
fu
nctio
ning
(5.0
vs.
3.1,
p <
0.00
1); m
ost
com
mon
nec
k in
46%
mus
ic st
uden
ts
and
27%
med
ical
stud
ents
(p =
0.00
1);
risk
fact
or: h
ighe
r pre
vale
nce
of C
AN
S in
fem
ale
mus
ic st
uden
ts v
s. m
ale
mus
ic
stude
nts (
84%
vs.
71%
, p =
0.21
2), h
ighe
r pr
eval
ence
of C
AN
S in
bac
helo
r’s st
u-de
nts v
s. m
aste
r’s st
uden
ts (8
5% v
s. 55
%,
p = 0.
018)
− 1
Kok
et a
l. (2
013)
“Mus
culo
skel
etal
com
-pl
aint
s”Po
int p
reva
lenc
e in
mus
ic st
uden
ts
vs. m
edic
al st
uden
ts (6
3% v
s. 43
%,
p = 0.
001,
OR
2.2
5);
12-m
onth
pre
vale
nce
in m
usic
stud
ents
vs
. med
ical
stud
ents
(89%
vs.
78%
, p =
0.01
9, O
R 2
.33)
; in
tota
l mor
e co
m-
plai
nts i
n up
per b
ody
half
− 1
Kov
ero
and
Kön
önen
(1
995)
Vio
linist
s and
vio
lists
“H
elsi
nki P
hilh
arm
onic
O
rche
stra”
vs.
patie
nts
of In
stitu
te o
f Den
tistry
, U
nive
rsity
of H
elsi
ki,
Finl
and
2626
Prof
essi
onal
pla
ying
vi
olin
e or
vio
la, w
eekl
y pl
ayin
g tim
e
“Sig
ns a
nd sy
mpt
oms o
f TM
D”
or ra
diol
ogic
al
abno
rmal
ities
in th
e te
m-
poro
man
dibu
lar c
ondy
les
Freq
uenc
y of
tem
poro
man
dibu
lar p
ain
27%
(mus
icia
ns);
mus
icia
ns h
ave
mor
e si
gns (
but n
ot sy
mpt
oms o
r rad
iolo
gica
l ab
norm
aliti
es) o
f TM
D th
an c
ontro
ls;
pos.
corr
elat
ion
betw
een
wee
kly
play
ing
time
and
sym
ptom
s of T
MD
, i.a
.
− 7
Leav
er e
t al.
(201
1)O
rche
stra
mus
icia
ns
(sym
phon
ic o
rche
stra)
, En
glan
d
243
–In
strum
ent p
layi
ng (p
lus
phys
ical
act
iviti
es a
t w
ork,
psy
chos
ocia
l fac
-to
rs o
f wor
king
env
iron-
men
t, pe
rform
ance
anx
i-et
y, in
strum
ent g
roup
, m
enta
l hea
lth, s
mok
ing,
ag
e, g
ende
r)
“Mus
culo
skel
etal
pai
n”:
prev
alen
ce a
nd im
pact
, re
latio
n to
pla
ying
con
di-
tions
, inc
ludi
ng in
stru-
men
t cat
egor
y, i.
a.
12-m
onth
pre
vale
nce
of re
gion
al p
ain
86%
, im
pairi
ng p
ain
41%
, 1-m
onth
pre
vale
nce
of re
gion
al p
ain
71%
; ris
k fa
ctor
s: p
osi-
tive
corr
elat
ion
with
hig
h so
mat
izin
gsc
ores
(OR
2.5
) and
fem
ale
gend
er; n
o co
rrel
atio
n w
ith p
erfo
rman
ce a
nxie
ty;
varia
tion
of d
isor
ders
acc
ordi
ng to
instr
u-m
ent g
roup
5

International Archives of Occupational and Environmental Health
1 3
Tabl
e 3
(con
tinue
d)
Aut
hor (
year
)Po
pula
tion
Cas
es (n
)C
ontro
l (n
)Ex
posu
reO
utco
mes
Resu
ltsQ
A (x
/16
poin
ts)
Lim
a et
al.
(201
5)O
rche
stra
viol
inist
s, B
elo
Hor
izon
te, B
razi
l18
/33
–In
strum
ent p
layi
ng“F
unct
iona
l dis
orde
rs o
f th
e m
uscu
losk
elet
al sy
s-te
ms”
; VA
S pa
in, B
PSF
Prev
alen
ce o
f mus
cula
r pai
n 78
%(n
= 14
) of
mus
cula
r fat
igue
33%
(n =
6), p
reva
-le
nce
of re
porte
d di
agno
ses b
y pa
rtici
-pa
nts (
n = 15
resp
onde
nts)
: ten
dini
tis in
th
e up
per e
xtre
mity
28%
(n =
5), p
ain
cerv
ical
spin
e 17
% (n
= 3)
, bac
k pa
in
17%
(n =
3) i.
a., V
AS
pain
(0–1
0): a
ver-
age
5.6;
Pre
vale
nce
acco
rdin
g to
Wis
con-
sin’
s Pai
n In
vent
ory
(sho
rt fo
rm) p
ain
in:
lum
bar s
pine
24%
(n =
8); s
houl
ders
21%
(n
= 7)
, for
earm
s and
han
ds 1
8% (n
= 6)
; ce
rvic
al sp
ine
12%
(n =
4); l
egs a
nd fe
et
6% (n
= 2)
; and
hea
dach
es 6
% (n
= 2)
; pr
eval
ence
of p
ain
inte
rferin
g w
ith w
ork
(sca
le o
f 0–1
0): a
vera
ge ra
ting
of 7
.1
(med
ian
8.0)
− 9
Logu
e et
al.
(200
5)C
ello
stud
ents
“B
elm
ont
Uni
vers
ity S
choo
l of
Mus
ic”
and
“Van
derb
ilt
Uni
vers
ity B
lair
Scho
ol
of M
usic
”, U
SA
14–
Cel
lo st
udie
s“M
edia
n an
d ul
nar n
eu-
ropa
thie
s”: p
reva
lenc
e,
eith
er u
pper
ext
rem
ity,
phys
ical
exa
min
atio
n,
EMG
No
evid
ence
of m
edia
n or
uln
ar n
euro
path
y1
Mar
ques
et a
l. (2
003)
Gui
taris
ts (p
artic
ipan
ts o
f cl
asse
s abo
ut p
reve
ntio
n of
ove
ruse
), Sp
ain
64_
Gui
tar p
layi
ng, c
lass
i-ca
l gui
tar v
s. fla
men
co
guita
r
“Ove
ruse
synd
rom
e”:
prev
alen
cePo
int p
reva
lenc
e 75
%, c
lass
ic g
uita
rists
vs.
flam
enco
gui
taris
ts: 6
6% v
s. 88
%−
5
Fish
bein
et a
l. (1
988)
Orc
hestr
a m
usic
ians
, USA
2212
–In
strum
ent p
layi
ng“M
uscu
losk
elet
al p
rob-
lem
”, i.
a.Pr
eval
ence
(all
loca
lizat
ions
) 82%
, mos
t co
mm
on lo
caliz
atio
ns: s
houl
der (
20%
), ne
ck (2
2%) a
nd lo
wer
bac
k (2
2%)
− 7
Mid
dles
tadt
and
Fis
h-be
in (1
988)
Instr
umen
t pla
ying
(plu
s pe
rcei
ved
occu
patio
nal
stres
s)
Ris
k fa
ctor
: sig
nific
ant r
elat
ions
hip
betw
een
num
ber o
f mus
culo
skel
etal
pr
oble
ms a
nd p
erce
ived
occ
upat
iona
l str
ess
Mid
dles
tadt
(199
0)O
rche
stra
mus
icia
ns, U
SA22
12–
Instr
umen
t pla
ying
(plu
s ge
nder
)“M
uscu
losk
elet
al p
rob-
lem
”, i.
a.Pr
eval
ence
(all
loca
lizat
ions
) 82%
, pre
va-
lenc
e of
seve
re re
porte
d m
uscu
losk
elet
al
diso
rder
s: 5
9% (r
isk
fact
or fe
mal
e vs
. m
ale
70%
vs.
54%
)
− 7
Mid
dles
tadt
and
Fis
h-be
in (1
989)
Orc
hestr
a m
usic
ians
: su
bgro
up st
ring
play
ers,
USA
1378
–In
strum
ent p
layi
ng (p
lus
instr
umen
t gro
up)
Prev
alen
ce o
f sev
ere
repo
rted
mus
culo
-sk
elet
al p
robl
ems:
66%
in st
ring
play
ers
(com
pare
d to
woo
dwin
d pl
ayer
s with
48
% a
nd b
rass
pla
yers
with
32%
), m
ost
com
mon
shou
lder
, nec
k an
d lo
wer
bac
k;
risk
fact
or st
ing
play
ing:
pre
vale
nce
stat
. si
gn. h
ighe
r in
fem
ales
vs.
mal
es

International Archives of Occupational and Environmental Health
1 3
Tabl
e 3
(con
tinue
d)
Aut
hor (
year
)Po
pula
tion
Cas
es (n
)C
ontro
l (n
)Ex
posu
reO
utco
mes
Resu
ltsQ
A (x
/16
poin
ts)
Mill
er e
t al.
(200
2)M
usic
stud
ents
“Ro
yal
Nor
ther
n C
olle
ge o
f M
usic
” (s
tring
pla
y-er
s, ke
yboa
rd p
laye
rs)
vs. n
onm
usic
ians
from
va
rious
hos
pita
l dep
art-
men
ts, E
ngla
nd
9264
Instr
umen
t pla
ying
(plu
s pr
evio
us in
jury
, yea
rs
at c
olle
ge, i
nstru
men
t gr
oup,
yea
rs p
layi
ng a
n in
strum
ent,
dura
tion
of
prac
tice
perio
ds, a
ge,
gend
er, v
ario
us a
nthr
o-po
met
ric p
aram
eter
s, i.a
.
“Upp
er li
mb
pain
and
dy
sfun
ctio
n”, a
nato
mic
al
abno
rmal
ities
Prev
alen
ce: m
usic
stud
ents
five
tim
es m
ore
likel
y fo
r upp
er li
mb
pain
; ris
k fa
ctor
pr
evio
us in
jurie
s, ye
ars a
t col
lege
, ins
tru-
men
t gro
up, y
ears
stud
ying
instr
umen
t an
d pr
actic
e pe
riod
stat
. sig
n. c
orre
-la
te w
ith u
pper
lim
b pa
in; a
nato
mic
al
abno
rmal
ities
(and
var
iatio
ns) 7
2% v
s. 59
% (n
.s.)
− 5
Mis
hra
et a
l. (2
013)
Indi
an ta
bla
play
ers,
Indi
a85
–Ta
bla
play
ing
(fold
ed-k
nee
sitti
ng p
ostu
re)
“PR
MD
s” (p
layi
ng-
rela
ted
mus
culo
skel
etal
di
sord
ers)
: pre
vale
nce
by
NM
Q
Prev
alen
ce in
low
bac
k 73
%, r
ight
shou
lder
60
%, n
eck
54%
, lef
t sho
ulde
r 51%
, upp
er
back
45%
, rig
ht k
nee
45%
, lef
t kne
e 46
%,
VAS
scor
es (n
o sc
ale
repo
rted)
for i
nten
-si
ty o
f dis
com
fort
in d
iffer
ent b
ody
parts
3.
42 (l
ow b
ack)
to 1
.63
(rig
ht k
nee)
− 7
Mol
sber
ger (
1991
)O
rche
stra
mus
icia
ns
“Deu
tsch
e O
per B
erlin
” an
d “D
üsse
ldor
fer S
ym-
phon
iker
”, G
erm
any
100
–In
strum
ent p
layi
ng“D
isor
ders
of t
he lo
com
o-to
r app
arat
us”,
i.a.
Prev
alen
ce 7
5%, m
ost c
omm
on: n
eck
35%
, oth
er p
arts
of s
pina
l col
umn
16%
; av
erag
e di
seas
e du
ratio
n 61
.3 m
onth
s, pr
eval
ence
of i
mpa
iring
dis
orde
rs: 4
5%.
− 7
Mon
aco
et a
l. (2
012)
Orc
hestr
a m
usic
ians
“Te
a-tro
del
l’ O
pera
”, It
alia
65–
Instr
umen
t pla
ying
“PR
MD
s” (p
layi
ng-r
elat
ed
mus
culo
skel
etal
dis
or-
ders
), D
ASH
Prev
alen
ce m
uscu
losk
elet
al d
isor
ders
in
dai
ly li
fe (d
efine
d as
≥ 15
poi
nts i
n D
ASH
i) 28
%, p
reva
lenc
e co
mpl
aint
s du
ring
play
ing
51%
(DA
SH a
dditi
onal
m
odul
e)
− 9
Moo
re e
t al.
(200
8)M
usic
stud
ents
(upp
er
strin
g pl
ayer
s) v
s. co
ntro
l gr
oup,
USA
1018
Instr
umen
t pla
ying
(plu
s ye
ars i
nstru
men
t pla
yed,
w
eekl
y pl
ayin
g tim
e, re
st tim
e, sh
ould
er a
sses
s-m
ent d
ata)
“Pre
disp
osin
g fa
ctor
s for
sh
ould
er im
ping
emen
t sy
ndro
me”
(Sig
ns a
nd
sym
ptom
s of s
houl
der
impi
ngem
ent)
Prev
alen
ce o
f pai
n w
hile
pla
ying
70%
, m
ost c
omm
on sh
ould
ers (
left
50%
, rig
ht
30%
) and
nec
k (le
ft 40
%, r
ight
20%
). 30
% sh
ould
er im
ping
emen
t vs.
0% in
co
ntro
ls (s
tat.
sign
. cor
rela
tion)
; ris
k fa
ctor
s: n
.s. c
orre
latio
n w
ith y
ears
instr
u-m
ent p
laye
d, w
eekl
y pl
ayin
g tim
e, re
st tim
e, sh
ould
er a
sses
smen
t dat
a)
− 1
Nav
ia A
lvar
ez e
t al.
(200
7)O
rche
stra
mus
icia
ns,
Spai
n48
–In
strum
ent p
layi
ng“N
eck
pain
synd
rom
e”:
prev
alen
ceLi
fetim
e pr
eval
ence
nec
k pa
in 6
9%,
12-m
onth
pre
vale
nce
63%
; pre
vale
nce
last
7 da
ys 2
7%; l
ifetim
e pr
eval
ence
tin
glin
g in
upp
er e
xtre
mity
44%
, life
time
prev
alen
ce lo
ss o
f sen
satio
n or
forc
e 40
%; m
ost i
mpo
rtant
risk
fact
or: l
abor
str
ess,
no c
lear
rela
tion
betw
een
instr
u-m
ent p
laye
d an
d th
e ye
ars o
f pro
fess
iona
l ac
tivity
, nei
ther
with
the
sex
or a
ge
− 9

International Archives of Occupational and Environmental Health
1 3
Tabl
e 3
(con
tinue
d)
Aut
hor (
year
)Po
pula
tion
Cas
es (n
)C
ontro
l (n
)Ex
posu
reO
utco
mes
Resu
ltsQ
A (x
/16
poin
ts)
Nym
an e
t al.
(200
7)O
rche
stra
mus
icia
ns,
Swed
en23
5–
Instr
umen
t pla
ying
with
el
evat
ed a
rm p
ositi
on
and
daily
pla
ying
tim
e
“Nec
k–sh
ould
er p
ain”
Poin
t pre
vale
nce
26%
in w
hole
pop
ulat
ion;
ris
k fa
ctor
s: n
eutra
l arm
pos
ition
, < 2
h pe
r wor
kday
’: 9%
vs.
‘neu
tral a
rm p
osi-
tion,
> 3
h pe
r wor
kday
’: 19
%; ‘
elev
ated
ar
m p
ositi
on, <
2 h
per w
orkd
ay”:
30
% v
s. “e
leva
ted
arm
pos
ition
, > 3
h pe
r wor
kday
”: 3
5%; h
ighe
r odd
s for
su
bjec
ts w
ith n
eck/
shou
lder
pai
n in
the
grou
ps “
elev
ated
arm
pos
ition
, < 2
h pe
r w
orkd
ay”
[OR
4.1
5 (1
.30–
13.2
2)],
and
“ele
vate
d ar
m p
ositi
on, >
3 h
per w
ork-
day”
[OR
5.3
5 (1
.96–
14.6
2)] c
ompa
red
to th
e gr
oup
“neu
tral a
rm p
ositi
on, <
2 h
per w
orkd
ay”
5
Paar
up e
t al.
(201
1)O
rche
stra
mus
icia
ns
(sym
phon
ic o
rche
stra)
vs
. rep
rese
ntat
ive
sam
ple
from
the
Dan
ish
wor
k-fo
rce
from
The
Dan
ish
Wor
king
Env
iron-
men
t C
ohor
t, D
enm
ark
342
5436
Instr
umen
t pla
ying
(plu
s in
strum
ent g
roup
, ge
nder
)
“Per
ceiv
ed m
uscu
losk
elet
al
sym
ptom
s”: p
reva
lenc
e12
-mon
th p
reva
lenc
e fo
r dis
orde
rs in
min
. 1
regi
on: f
emal
e 97
% a
nd m
ale:
83%
(O
R 6
.5),
risk
fact
or: w
oodw
ind
play
ers
stat
. sig
n. lo
wer
risk
than
upp
er st
ring
play
ers;
sym
ptom
s mor
e fr
eque
nt a
nd
laste
d lo
nger
in m
usic
ians
than
in g
ener
al
wor
kfor
ce
3
Papa
ndre
ou a
nd V
erva
i-ni
oti (
2010
)Pe
rcus
sion
ists (
in a
ctiv
e m
usic
al a
ctiv
ity a
nd
stude
nts)
, Gre
ece
30–
Instr
umen
t pla
ying
(plu
s ag
e, m
ain
mus
ical
act
iv-
ity [s
tude
nt, o
rche
stra
mus
icia
ns, m
usic
te
ache
r, so
list],
pra
ctic
e ho
urs)
“Mus
culo
skel
etal
dis
or-
ders
”Pr
eval
ence
32%
in u
pper
ext
rem
ities
, 20%
in
ver
tebr
al c
olum
n−
3
Ray
mon
d et
al.
(201
2)C
lass
ical
orc
hestr
a m
usi-
cian
s, U
SA32
–In
strum
ent p
layi
ng“O
ccup
atio
nal i
njur
y an
d ill
ness
”, i.
a. m
uscu
losk
el-
etal
dis
orde
rs
Life
time
prev
alen
ce: p
ain
or st
iffne
ss in
sh
ould
ers 9
4%, p
ain
or st
iffne
ss in
nec
k 91
%, n
umbn
ess a
nd ti
nglin
g in
han
d or
ar
ms 8
1%, l
ow b
ack
pain
63%
; Life
time
prev
alen
ce o
f dia
gnos
ed m
ost c
omm
on
diso
rder
s: te
ndin
itis 4
7%, m
uscu
losk
ele-
tal d
isor
der 2
2%, c
arpa
l tun
nel s
yndr
ome
16%
− 7
Rein
et a
l. (2
010)
Org
anist
s and
pia
nists
vs.
cont
rols
with
no
wor
k-re
late
d in
crea
sed
use
of
thei
r fee
t, G
erm
any
30/3
030
Instr
umen
t pla
ying
“Wor
k-re
late
d in
fluen
ces
on fu
nctio
nal a
nkle
st
abili
ty”
Org
anist
s hav
e ne
ither
incr
ease
d fu
nctio
nal
ankl
e st
abili
ty n
or in
crea
sed
ROM
of
thei
r ank
le jo
ints
in c
ompa
rison
to c
on-
trols
; Pia
nists
hav
e in
crea
sed
flexi
on o
f th
e an
kle
join
t on
both
side
s in
com
pari-
son
to o
rgan
ists a
nd o
n th
e rig
ht si
de in
co
mpa
rison
to c
ontro
ls
− 3
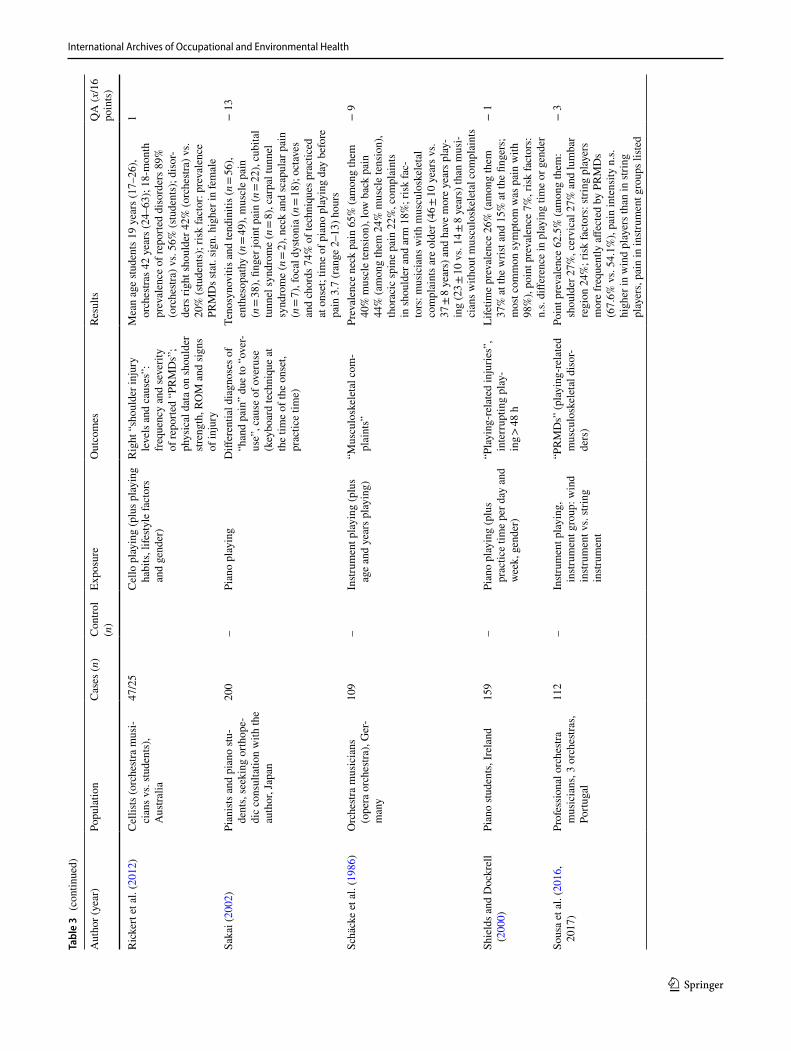
International Archives of Occupational and Environmental Health
1 3
Tabl
e 3
(con
tinue
d)
Aut
hor (
year
)Po
pula
tion
Cas
es (n
)C
ontro
l (n
)Ex
posu
reO
utco
mes
Resu
ltsQ
A (x
/16
poin
ts)
Ric
kert
et a
l. (2
012)
Cel
lists
(orc
hestr
a m
usi-
cian
s vs.
stude
nts)
, A
ustra
lia
47/2
5C
ello
pla
ying
(plu
s pla
ying
ha
bits
, life
style
fact
ors
and
gend
er)
Rig
ht “
shou
lder
inju
ry
leve
ls a
nd c
ause
s”:
freq
uenc
y an
d se
verit
y of
repo
rted
“PR
MD
s”;
phys
ical
dat
a on
shou
lder
str
engt
h, R
OM
and
sign
s of
inju
ry
Mea
n ag
e stu
dent
s 19
year
s (17
–26)
, or
ches
tras 4
2 ye
ars (
24–6
3); 1
8-m
onth
pr
eval
ence
of r
epor
ted
diso
rder
s 89%
(o
rche
stra)
vs.
56%
(stu
dent
s); d
isor
-de
rs ri
ght s
houl
der 4
2% (o
rche
stra)
vs.
20%
(stu
dent
s); r
isk
fact
or: p
reva
lenc
e PR
MD
s sta
t. si
gn. h
ighe
r in
fem
ale
1
Saka
i (20
02)
Pian
ists a
nd p
iano
stu-
dent
s, se
ekin
g or
thop
e-di
c co
nsul
tatio
n w
ith th
e au
thor
, Jap
an
200
–Pi
ano
play
ing
Diff
eren
tial d
iagn
oses
of
“han
d pa
in”
due
to “
over
-us
e”, c
ause
of o
veru
se
(key
boar
d te
chni
que
at
the
time
of th
e on
set,
prac
tice
time)
Teno
syno
vitis
and
tend
initi
s (n =
56),
enth
esop
athy
(n =
49),
mus
cle
pain
(n
= 38
), fin
ger j
oint
pai
n (n
= 22
), cu
bita
l tu
nnel
synd
rom
e (n
= 8)
, car
pal t
unne
l sy
ndro
me
(n =
2), n
eck
and
scap
ular
pai
n (n
= 7)
, foc
al d
ysto
nia
(n =
18);
octa
ves
and
chor
ds 7
4% o
f tec
hniq
ues p
ract
iced
at
ons
et; t
ime
of p
iano
pla
ying
day
bef
ore
pain
3.7
(ran
ge 2
–13)
hou
rs
− 1
3
Schä
cke
et a
l. (1
986)
Orc
hestr
a m
usic
ians
(o
pera
orc
hestr
a), G
er-
man
y
109
–In
strum
ent p
layi
ng (p
lus
age
and
year
s pla
ying
)“M
uscu
losk
elet
al c
om-
plai
nts”
Prev
alen
ce n
eck
pain
65%
(am
ong
them
40
% m
uscl
e te
nsio
n), l
ow b
ack
pain
44
% (a
mon
g th
em 2
4% m
uscl
e te
nsio
n),
thor
acic
spin
e pa
in 2
2%, c
ompl
aint
s in
shou
lder
and
arm
18%
; ris
k fa
c-to
rs: m
usic
ians
with
mus
culo
skel
etal
co
mpl
aint
s are
old
er (4
6 ± 10
yea
rs v
s. 37
± 8
year
s) a
nd h
ave
mor
e ye
ars p
lay-
ing
(23 ±
10 v
s. 14
± 8
year
s) th
an m
usi-
cian
s with
out m
uscu
losk
elet
al c
ompl
aint
s
− 9
Shie
lds a
nd D
ockr
ell
(200
0)Pi
ano
stude
nts,
Irel
and
159
–Pi
ano
play
ing
(plu
s pr
actic
e tim
e pe
r day
and
w
eek,
gen
der)
“Pla
ying
-rel
ated
inju
ries”
, in
terr
uptin
g pl
ay-
ing >
48 h
Life
time
prev
alen
ce 2
6% (a
mon
g th
em
37%
at t
he w
rist a
nd 1
5% a
t the
fing
ers;
m
ost c
omm
on sy
mpt
om w
as p
ain
with
98
%),
poin
t pre
vale
nce
7%, r
isk
fact
ors:
n.
s. di
ffere
nce
in p
layi
ng ti
me
or g
ende
r
− 1
Sous
a et
al.
(201
6,
2017
)Pr
ofes
sion
al o
rche
stra
mus
icia
ns, 3
orc
hestr
as,
Portu
gal
112
–In
strum
ent p
layi
ng,
instr
umen
t gro
up: w
ind
instr
umen
t vs.
strin
g in
strum
ent
“PR
MD
s” (p
layi
ng-r
elat
ed
mus
culo
skel
etal
dis
or-
ders
)
Poin
t pre
vale
nce
62.5
% (a
mon
g th
em:
shou
lder
27%
, cer
vica
l 27%
and
lum
bar
regi
on 2
4%; r
isk
fact
ors:
strin
g pl
ayer
s m
ore
freq
uent
ly a
ffect
ed b
y PR
MD
s (6
7.6%
vs.
54.1
%),
pain
inte
nsity
n.s.
hi
gher
in w
ind
play
ers t
han
in st
ring
play
ers,
pain
in in
strum
ent g
roup
s list
ed
− 3
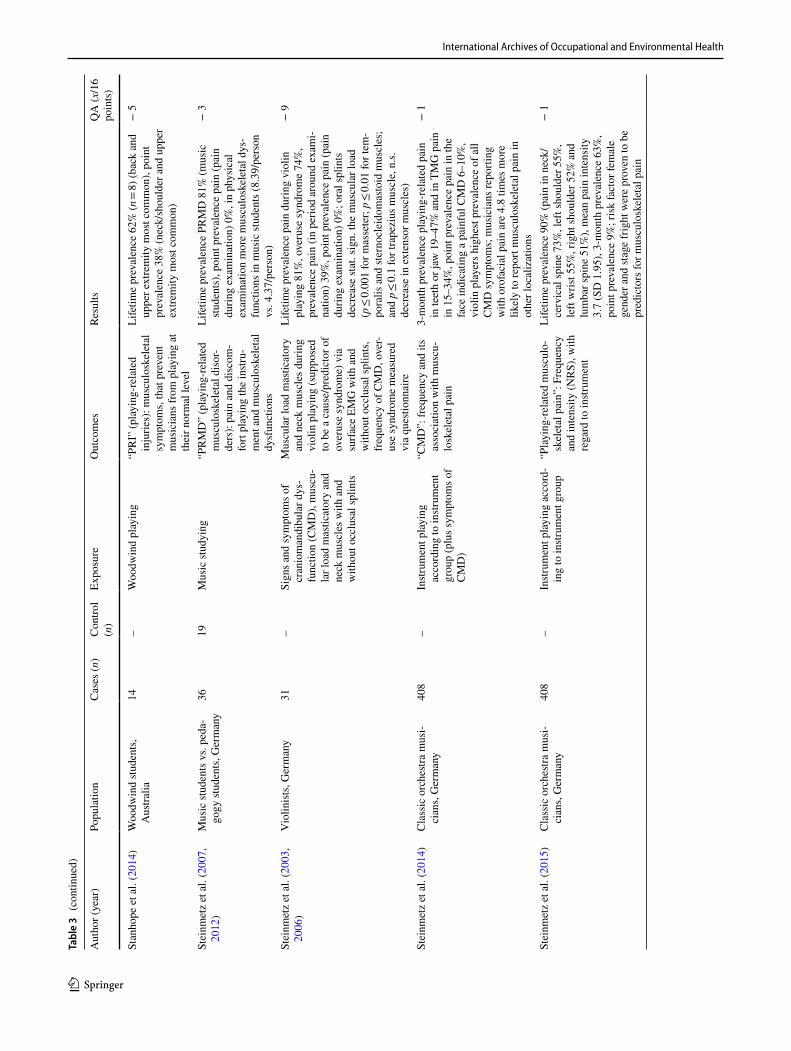
International Archives of Occupational and Environmental Health
1 3
Tabl
e 3
(con
tinue
d)
Aut
hor (
year
)Po
pula
tion
Cas
es (n
)C
ontro
l (n
)Ex
posu
reO
utco
mes
Resu
ltsQ
A (x
/16
poin
ts)
Stan
hope
et a
l. (2
014)
Woo
dwin
d stu
dent
s, A
ustra
lia14
–W
oodw
ind
play
ing
“PR
I” (p
layi
ng-r
elat
ed
inju
ries)
: mus
culo
skel
etal
sy
mpt
oms,
that
pre
vent
m
usic
ians
from
pla
ying
at
thei
r nor
mal
leve
l
Life
time
prev
alen
ce 6
2% (n
= 8)
(bac
k an
d up
per e
xtre
mity
mos
t com
mon
), po
int
prev
alen
ce 3
8% (n
eck/
shou
lder
and
upp
er
extre
mity
mos
t com
mon
)
− 5
Stei
nmet
z et
al.
(200
7,
2012
)M
usic
stud
ents
vs.
peda
-go
gy st
uden
ts, G
erm
any
3619
Mus
ic st
udyi
ng“P
RM
D”
(pla
ying
-rel
ated
m
uscu
losk
elet
al d
isor
-de
rs):
pain
and
dis
com
-fo
rt pl
ayin
g th
e in
stru-
men
t and
mus
culo
skel
etal
dy
sfun
ctio
ns
Life
time
prev
alen
ce P
RM
D 8
1% (m
usic
stu
dent
s), p
oint
pre
vale
nce
pain
(pai
n du
ring
exam
inat
ion)
0%
, in
phys
ical
ex
amin
atio
n m
ore
mus
culo
skel
etal
dys
-fu
nctio
ns in
mus
ic st
uden
ts (8
.39/
pers
on
vs. 4
.37/
pers
on)
− 3
Stei
nmet
z et
al.
(200
3,
2006
)V
iolin
ists,
Ger
man
y31
–Si
gns a
nd sy
mpt
oms o
f cr
anio
man
dibu
lar d
ys-
func
tion
(CM
D),
mus
cu-
lar l
oad
mas
ticat
ory
and
neck
mus
cles
with
and
w
ithou
t occ
lusa
l spl
ints
Mus
cula
r loa
d m
astic
ator
y an
d ne
ck m
uscl
es d
urin
g vi
olin
pla
ying
(sup
pose
d to
be
a ca
use/
pred
icto
r of
over
use
synd
rom
e) v
ia
surfa
ce E
MG
with
and
w
ithou
t occ
lusa
l spl
ints
, fr
eque
ncy
of C
MD
, ove
r-us
e sy
ndro
me
mea
sure
d vi
a qu
estio
nnai
re
Life
time
prev
alen
ce p
ain
durin
g vi
olin
pl
ayin
g 81
%, o
veru
se sy
ndro
me
74%
, pr
eval
ence
pai
n (in
per
iod
arou
nd e
xam
i-na
tion)
39%
, poi
nt p
reva
lenc
e pa
in (p
ain
durin
g ex
amin
atio
n) 0
%; o
ral s
plin
ts
decr
ease
stat
. sig
n. th
e m
uscu
lar l
oad
(p ≤
0.00
1 fo
r mas
sete
r; p ≤
0.01
for t
em-
pora
lis a
nd st
erno
clei
dom
asto
id m
uscl
es;
and
p ≤ 0.
1 fo
r tra
pezi
us m
uscl
e, n
.s.
decr
ease
in e
xten
sor m
uscl
es)
− 9
Stei
nmet
z et
al.
(201
4)C
lass
ic o
rche
stra
mus
i-ci
ans,
Ger
man
y40
8–
Instr
umen
t pla
ying
ac
cord
ing
to in
strum
ent
grou
p (p
lus s
ympt
oms o
f C
MD
)
“CM
D”:
freq
uenc
y an
d its
as
soci
atio
n w
ith m
uscu
-lo
skel
etal
pai
n
3-m
onth
pre
vale
nce
play
ing-
rela
ted
pain
in
teet
h or
jaw
19–
47%
and
in T
MG
pai
n in
15–
34%
, poi
nt p
reva
lenc
e pa
in in
the
face
indi
catin
g a
pain
ful C
MD
6–1
0%,
viol
in p
laye
rs h
ighe
st pr
eval
ence
of a
ll C
MD
sym
ptom
s; m
usic
ians
repo
rting
w
ith o
rofa
cial
pai
n ar
e 4.
8 tim
es m
ore
likel
y to
repo
rt m
uscu
losk
elet
al p
ain
in
othe
r loc
aliz
atio
ns
− 1
Stei
nmet
z et
al.
(201
5)C
lass
ic o
rche
stra
mus
i-ci
ans,
Ger
man
y40
8–
Instr
umen
t pla
ying
acc
ord-
ing
to in
strum
ent g
roup
“Pla
ying
-rel
ated
mus
culo
-sk
elet
al p
ain”
: Fre
quen
cy
and
inte
nsity
(NR
S), w
ith
rega
rd to
instr
umen
t
Life
time
prev
alen
ce 9
0% (p
ain
in n
eck/
cerv
ical
spin
e 73
%, l
eft s
houl
der 5
5%,
left
wris
t 55%
, rig
ht sh
ould
er 5
2% a
nd
lum
bar s
pine
51%
), m
ean
pain
inte
nsity
3.
7 (S
D 1
.95)
, 3-m
onth
pre
vale
nce
63%
, po
int p
reva
lenc
e 9%
; ris
k fa
ctor
fem
ale
gend
er a
nd st
age
frig
ht w
ere
prov
en to
be
pred
icto
rs fo
r mus
culo
skel
etal
pai
n
− 1
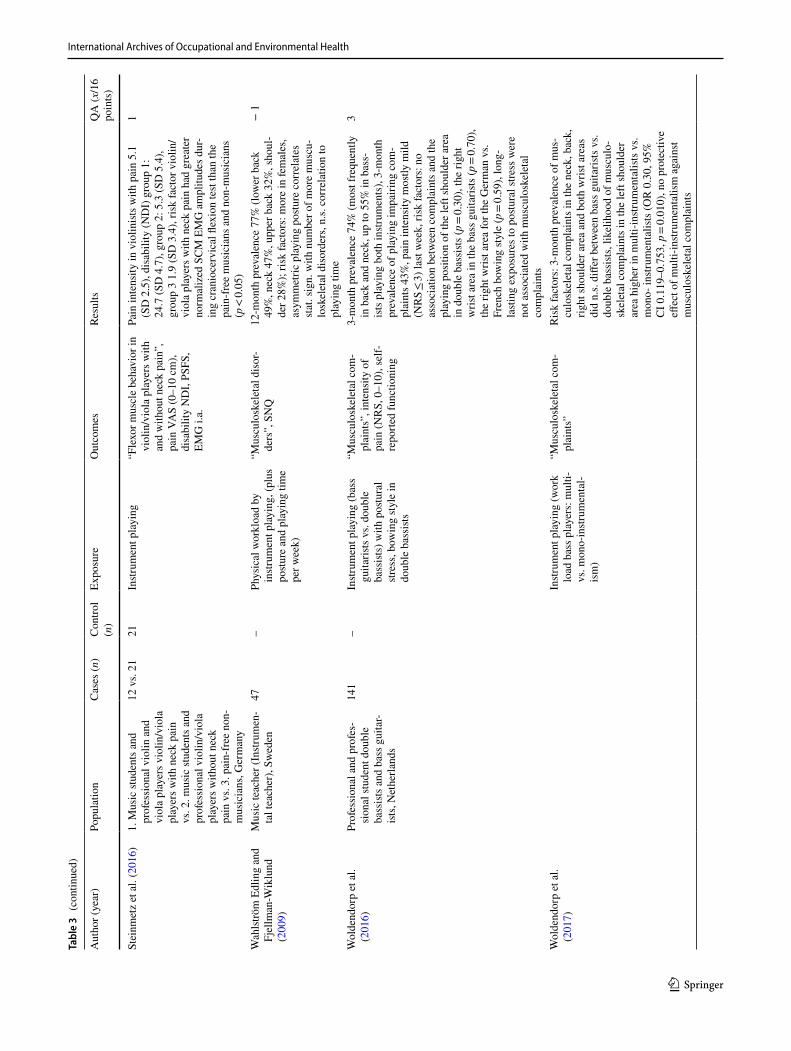
International Archives of Occupational and Environmental Health
1 3
Tabl
e 3
(con
tinue
d)
Aut
hor (
year
)Po
pula
tion
Cas
es (n
)C
ontro
l (n
)Ex
posu
reO
utco
mes
Resu
ltsQ
A (x
/16
poin
ts)
Stei
nmet
z et
al.
(201
6)1.
Mus
ic st
uden
ts a
nd
prof
essi
onal
vio
lin a
nd
viol
a pl
ayer
s vio
lin/v
iola
pl
ayer
s with
nec
k pa
in
vs. 2
. mus
ic st
uden
ts a
nd
prof
essi
onal
vio
lin/v
iola
pl
ayer
s with
out n
eck
pain
vs.
3. p
ain-
free
non
-m
usic
ians
, Ger
man
y
12 v
s. 21
21In
strum
ent p
layi
ng“F
lexo
r mus
cle
beha
vior
in
viol
in/v
iola
pla
yers
with
an
d w
ithou
t nec
k pa
in”,
pa
in V
AS
(0–1
0 cm
), di
sabi
lity
ND
I, PS
FS,
EMG
i.a.
Pain
inte
nsity
in v
iolin
ists w
ith p
ain
5.1
(SD
2.5
), di
sabi
lity
(ND
I) g
roup
1:
24.7
(SD
4.7
), gr
oup
2: 5
.3 (S
D 5
.4),
grou
p 3
1.9
(SD
3.4
), ris
k fa
ctor
vio
lin/
viol
a pl
ayer
s with
nec
k pa
in h
ad g
reat
er
norm
aliz
ed S
CM
EM
G a
mpl
itude
s dur
-in
g cr
anio
cerv
ical
flex
ion
test
than
the
pain
-fre
e m
usic
ians
and
non
-mus
icia
ns
(p <
0.05
)
1
Wah
lströ
m E
dlin
g an
d Fj
ellm
an-W
iklu
nd
(200
9)
Mus
ic te
ache
r (In
strum
en-
tal t
each
er),
Swed
en47
–Ph
ysic
al w
orkl
oad
by
instr
umen
t pla
ying
, (pl
us
postu
re a
nd p
layi
ng ti
me
per w
eek)
“Mus
culo
skel
etal
dis
or-
ders
”, S
NQ
12-m
onth
pre
vale
nce
77%
(low
er b
ack
49%
, nec
k 47
%, u
pper
bac
k 32
%, s
houl
-de
r 28%
); ris
k fa
ctor
s: m
ore
in fe
mal
es,
asym
met
ric p
layi
ng p
ostu
re c
orre
late
s st
at. s
ign.
with
num
ber o
f mor
e m
uscu
-lo
skel
etal
dis
orde
rs, n
.s. c
orre
latio
n to
pl
ayin
g tim
e
− 1
Wol
dend
orp
et a
l. (2
016)
Prof
essi
onal
and
pro
fes-
sion
al st
uden
t dou
ble
bass
ists a
nd b
ass g
uita
r-ist
s, N
ethe
rland
s
141
–In
strum
ent p
layi
ng (b
ass
guita
rists
vs.
doub
le
bass
ists)
with
pos
tura
l str
ess,
bow
ing
style
in
doub
le b
assi
sts
“Mus
culo
skel
etal
com
-pl
aint
s”, i
nten
sity
of
pain
(NR
S, 0
–10)
, sel
f-re
porte
d fu
nctio
ning
3-m
onth
pre
vale
nce
74%
(mos
t fre
quen
tly
in b
ack
and
neck
, up
to 5
5% in
bas
s-ist
s pla
ying
bot
h in
strum
ents
), 3-
mon
th
prev
alen
ce o
f pla
ying
impa
iring
com
-pl
aint
s 43%
, pai
n in
tens
ity m
ostly
mild
(N
RS
≤ 3)
last
wee
k, ri
sk fa
ctor
s: n
o as
soci
atio
n be
twee
n co
mpl
aint
s and
the
play
ing
posi
tion
of th
e le
ft sh
ould
er a
rea
in d
oubl
e ba
ssist
s (p =
0.30
), th
e rig
ht
wris
t are
a in
the
bass
gui
taris
ts (p
= 0.
70),
the
right
wris
t are
a fo
r the
Ger
man
vs.
Fren
ch b
owin
g sty
le (p
= 0.
59),
long
-la
sting
exp
osur
es to
pos
tura
l stre
ss w
ere
not a
ssoc
iate
d w
ith m
uscu
losk
elet
al
com
plai
nts
3
Wol
dend
orp
et a
l. (2
017)
Instr
umen
t pla
ying
(wor
k lo
ad b
ass p
laye
rs: m
ulti-
vs. m
ono-
instr
umen
tal-
ism
)
“Mus
culo
skel
etal
com
-pl
aint
s”R
isk
fact
ors:
3-m
onth
pre
vale
nce
of m
us-
culo
skel
etal
com
plai
nts i
n th
e ne
ck, b
ack,
rig
ht sh
ould
er a
rea
and
both
wris
t are
as
did
n.s.
diffe
r bet
wee
n ba
ss g
uita
rists
vs.
doub
le b
assi
sts, l
ikel
ihoo
d of
mus
culo
-sk
elet
al c
ompl
aint
s in
the
left
shou
lder
ar
ea h
ighe
r in
mul
ti-in
strum
enta
lists
vs.
mon
o- in
strum
enta
lists
(OR
0.3
0, 9
5%
CI 0
.119
–0.7
53, p
= 0.
010)
, no
prot
ectiv
e eff
ect o
f mul
ti-in
strum
enta
lism
aga
inst
mus
culo
skel
etal
com
plai
nts
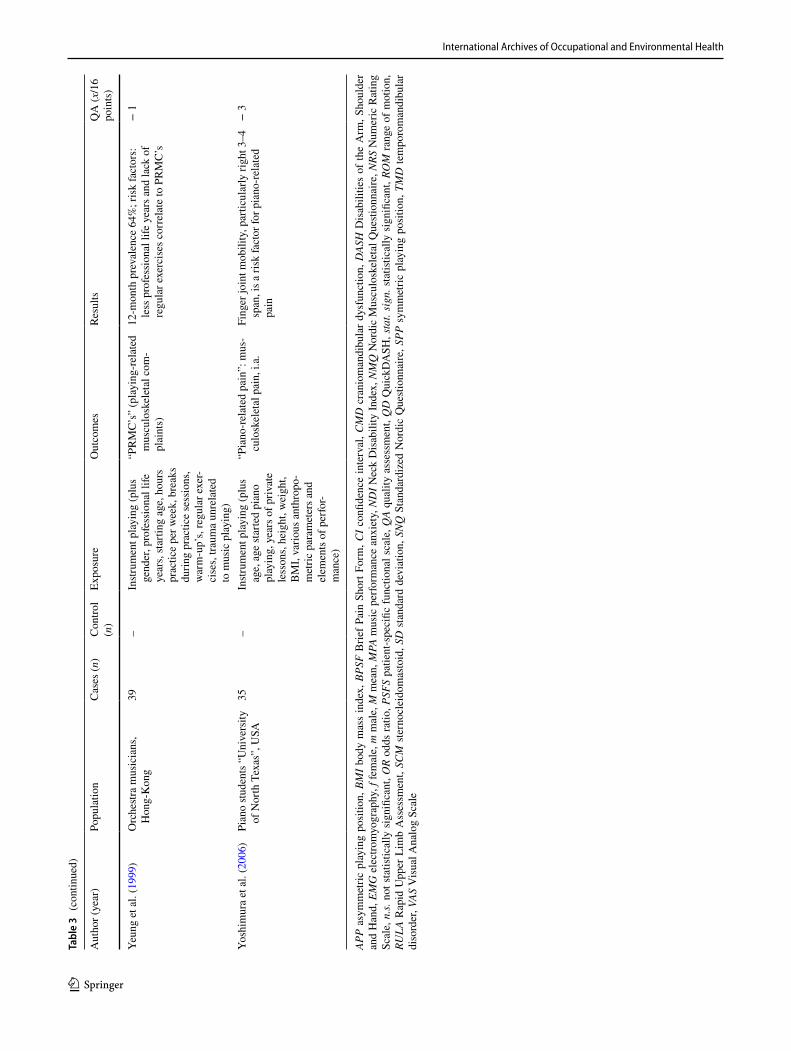
International Archives of Occupational and Environmental Health
1 3
Tabl
e 3
(con
tinue
d)
Aut
hor (
year
)Po
pula
tion
Cas
es (n
)C
ontro
l (n
)Ex
posu
reO
utco
mes
Resu
ltsQ
A (x
/16
poin
ts)
Yeun
g et
al.
(199
9)O
rche
stra
mus
icia
ns,
Hon
g-K
ong
39–
Instr
umen
t pla
ying
(plu
s ge
nder
, pro
fess
iona
l life
ye
ars,
star
ting
age,
hou
rs
prac
tice
per w
eek,
bre
aks
durin
g pr
actic
e se
ssio
ns,
war
m-u
p’s,
regu
lar e
xer-
cise
s, tra
uma
unre
late
d to
mus
ic p
layi
ng)
“PR
MC
’s”
(pla
ying
-rel
ated
m
uscu
losk
elet
al c
om-
plai
nts)
12-m
onth
pre
vale
nce
64%
; ris
k fa
ctor
s:
less
pro
fess
iona
l life
yea
rs a
nd la
ck o
f re
gula
r exe
rcis
es c
orre
late
to P
RM
C’s
− 1
Yosh
imur
a et
al.
(200
6)Pi
ano
stude
nts “
Uni
vers
ity
of N
orth
Tex
as”,
USA
35–
Instr
umen
t pla
ying
(plu
s ag
e, a
ge st
arte
d pi
ano
play
ing,
yea
rs o
f priv
ate
less
ons,
heig
ht, w
eigh
t, B
MI,
vario
us a
nthr
opo-
met
ric p
aram
eter
s and
el
emen
ts o
f per
for-
man
ce)
“Pia
no-r
elat
ed p
ain”
: mus
-cu
losk
elet
al p
ain,
i.a.
Fing
er jo
int m
obili
ty, p
artic
ular
ly ri
ght 3
–4
span
, is a
risk
fact
or fo
r pia
no-r
elat
ed
pain
− 3
APP
asym
met
ric p
layi
ng p
ositi
on, B
MI b
ody
mas
s in
dex,
BPS
F B
rief P
ain
Shor
t For
m, C
I con
fiden
ce in
terv
al, C
MD
cra
niom
andi
bula
r dys
func
tion,
DAS
H D
isab
ilitie
s of
the
Arm
, Sho
ulde
r an
d H
and,
EM
G e
lect
rom
yogr
aphy
, f fe
mal
e, m
mal
e, M
mea
n, M
PA m
usic
per
form
ance
anx
iety
, ND
I Nec
k D
isab
ility
Inde
x, N
MQ
Nor
dic
Mus
culo
skel
etal
Que
stion
naire
, NRS
Num
eric
Rat
ing
Scal
e, n
.s. n
ot s
tatis
tical
ly s
igni
fican
t, O
R od
ds ra
tio, P
SFS
patie
nt-s
peci
fic fu
nctio
nal s
cale
, QA
qual
ity a
sses
smen
t, Q
D Q
uick
DA
SH, s
tat.
sign
. sta
tistic
ally
sig
nific
ant,
ROM
rang
e of
mot
ion,
RU
LA R
apid
Upp
er L
imb
Ass
essm
ent,
SCM
ste
rnoc
leid
omas
toid
, SD
sta
ndar
d de
viat
ion,
SN
Q S
tand
ardi
zed
Nor
dic
Que
stion
naire
, SPP
sym
met
ric p
layi
ng p
ositi
on, T
MD
tem
poro
man
dibu
lar
diso
rder
, VAS
Vis
ual A
nalo
g Sc
ale

International Archives of Occupational and Environmental Health
1 3
2012; Steinmetz and Möller 2007; Shields and Dockrell 2000; Sakai 2002).
Period of time investigated in cross‑sectional studies
The time period of the measured MCD varied substantially between studies, ranging from whole lifetimes, years play-ing an instrument, the previous 1, 3, 12 or 18 months, the last 7 days or current complaints. For some publications, we could not find a specification of the exact time frame used by the study, f.e. (Lima et al. 2015; Blackie et al. 1999; Crnivec 2004; De Smet et al. 1998; Eller et al. 1992; Fishbein et al. 1988; Fry 1986; Schäcke et al. 1986; Hodapp et al. 2009; Kim et al. 2012; Kovero and Könönen 1995; Middlestadt 1990; Middlestadt and Fishbein 1988, 1989; Molsberger 1991; Papandreou and Vervainioti 2010).
Prevalence reported in cross‑sectional studies
Due to substantial heterogeneity among the measured com-plaints, a comparison of prevalence and correlations to the MCD was not feasible. In the included studies, the preva-lence of MCDs ranged from point prevalence 0% in one small study (Logue et al. 2005) to 12-month prevalence 97% in a study of female orchestra musicians (Paarup et al. 2011). However, within the four studies that received a qual-ity assessment of 5, the 12-month prevalence ranged from 82 to 86% (Leaver et al. 2011; Kaufman-Cohen and Ratzon 2011; Fjellmann-Wiklund et al. 2003), with 26% of musi-cians reporting current complaints (Nyman et al. 2007).
Risk factors reported in cross‑sectional studies
The four studies with the best quality assessments reported playing with an elevated arm position as a risk factor for neck-shoulder pain (Nyman et al. 2007). Neck-shoulder dis-comfort in female music teachers was correlated with high psychological demands and teaching at multiple schools, whereas in male music teachers, it was associated with lift-ing, playing the guitar and low social support (Fjellmann-Wiklund et al. 2003). In symphony orchestras, MCD tended to be more frequent among women, in musicians experienc-ing low mood and in those with high somatizing scores. Only weak associations were observed with psychosocial work stressors and performance anxiety (Leaver et al. 2011). In musicians who play string instruments, the odds of wrist/hand pain were 2.9-fold higher than for those who play wind instruments (Leaver et al. 2011). In contrast, another study found that in classical musicians, string musicians showed higher PRMD scores than woodwind and brass players. Fur-thermore, the study found a correlation with biomechanical risk factors, perceived physical environment risk factors, instrument weight and average number of hours played per
week (Kaufman-Cohen and Ratzon 2011). However, cross-sectional studies have low validity for verifying risk factors such as exposure time, and the occurrence of outcomes can-not thus be properly measured.
Quality assessment of cross‑sectional studies
The quality scores of the 62 cross-sectional studies were between − 13 and 5 out of 16 possible points, with signifi-cant methodological concerns existing in the studies. Only one study (Nusseck et al. 2017) utilized a time frame that could reliably measure the association between the exposure and outcome, although several studies explicitly looked for risk or predicting factors. No studies reported the blinding of outcome measures. Sample size calculations were reported in only two of the studies (Kochem and Silva 2017; Kauf-man-Cohen and Ratzon 2011). Frequent concerns included the objectivity, reliability and validity of the outcome and exposure measurement tools. Often, no confounders were assessed, and only a few studies assessed at least some important confounders (Eller et al. 1992; Fjellmann-Wiklund et al. 2003; Leaver et al. 2011; Nyman et al. 2007; Kok et al. 2015; Nusseck et al. 2017; Piatkowska et al. 2016; Wolden-dorp et al. 2016, 2017).
Intervention studies
Study designs and methods of the interventional studies included
Three of the 12 intervention studies were performed using pre–post study designs without a control group (Table 4). One of these three studies compared two different inter-ventions, (strength vs. endurance training) stratified by instrument played, but further information on randomiza-tion was not provided (Ackermann et al. 2002b). The other nine interventions used controlled designs (Table 5). Seven of the 12 studies were randomized controlled trials. In one partially blind study, playing under the intervention or con-trol condition was randomized (Ackermann et al. 2002a). In one study with a three-armed design, participants in the two intervention groups were randomized, but the control group was recruited separately (Khalsa et al. 2009). In one non-randomized study, allocation of the nine eligible orches-tras followed geographical criteria; the six orchestras that were geographically closest to each other were selected as interventional orchestras, while the remaining three served as control orchestras (Brandfonbrener 1997). The second non-randomized study was a pilot study for a partially rand-omized trial that was conducted later. The pilot recruited its control group separately due to a low number of participants (Khalsa and Cope 2006; Khalsa et al. 2009). Two publi-cations about Tuina treatment appeared to be drawn from
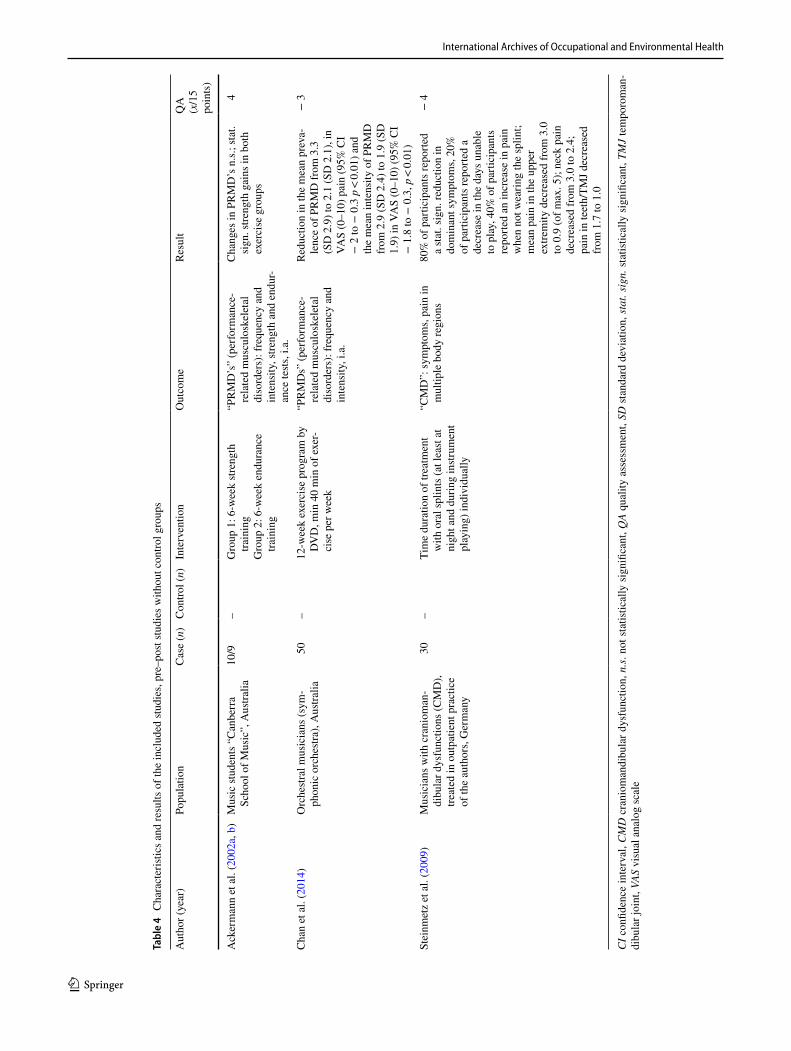
International Archives of Occupational and Environmental Health
1 3
Tabl
e 4
Cha
ract
erist
ics a
nd re
sults
of t
he in
clud
ed st
udie
s, pr
e–po
st stu
dies
with
out c
ontro
l gro
ups
CI c
onfid
ence
inte
rval
, CM
D c
rani
oman
dibu
lar d
ysfu
nctio
n, n
.s. n
ot st
atist
ical
ly s
igni
fican
t, Q
A qu
ality
ass
essm
ent,
SD st
anda
rd d
evia
tion,
stat
. sig
n. st
atist
ical
ly s
igni
fican
t, TM
J te
mpo
rom
an-
dibu
lar j
oint
, VAS
vis
ual a
nalo
g sc
ale
Aut
hor (
year
)Po
pula
tion
Cas
e (n
)C
ontro
l (n)
Inte
rven
tion
Out
com
eRe
sult
QA
(x
/15
poin
ts)
Ack
erm
ann
et a
l. (2
002a
, b)
Mus
ic st
uden
ts “
Can
berr
a Sc
hool
of M
usic
”, A
ustra
lia10
/9–
Gro
up 1
: 6-w
eek
stren
gth
train
ing
Gro
up 2
: 6-w
eek
endu
ranc
e tra
inin
g
“PR
MD
’s”
(per
form
ance
-re
late
d m
uscu
losk
elet
al
diso
rder
s): f
requ
ency
and
in
tens
ity, s
treng
th a
nd e
ndur
-an
ce te
sts, i
.a.
Cha
nges
in P
RM
D’s
n.s.
; sta
t. si
gn. s
treng
th g
ains
in b
oth
exer
cise
gro
ups
4
Cha
n et
al.
(201
4)O
rche
stral
mus
icia
ns (s
ym-
phon
ic o
rche
stra)
, Aus
tralia
50–
12-w
eek
exer
cise
pro
gram
by
DV
D, m
in 4
0 m
in o
f exe
r-ci
se p
er w
eek
“PR
MD
s” (p
erfo
rman
ce-
rela
ted
mus
culo
skel
etal
di
sord
ers)
: fre
quen
cy a
nd
inte
nsity
, i.a
.
Redu
ctio
n in
the
mea
n pr
eva-
lenc
e of
PR
MD
from
3.3
(S
D 2
.9) t
o 2.
1 (S
D 2
.1),
in
VAS
(0–1
0) p
ain
(95%
CI
− 2
to −
0.3
p <
0.01
) and
th
e m
ean
inte
nsity
of P
RM
D
from
2.9
(SD
2.4
) to
1.9
(SD
1.
9) in
VA
S (0
–10)
(95%
CI
− 1
.8 to
− 0
.3, p
< 0.
01)
− 3
Stei
nmet
z et
al.
(200
9)M
usic
ians
with
cra
niom
an-
dibu
lar d
ysfu
nctio
ns (C
MD
), tre
ated
in o
utpa
tient
pra
ctic
e of
the
auth
ors,
Ger
man
y
30–
Tim
e du
ratio
n of
trea
tmen
t w
ith o
ral s
plin
ts (a
t lea
st at
ni
ght a
nd d
urin
g in
strum
ent
play
ing)
indi
vidu
ally
“CM
D”:
sym
ptom
s, pa
in in
m
ultip
le b
ody
regi
ons
80%
of p
artic
ipan
ts re
porte
d a
stat
. sig
n. re
duct
ion
in
dom
inan
t sym
ptom
s, 20
%
of p
artic
ipan
ts re
porte
d a
decr
ease
in th
e da
ys u
nabl
e to
pla
y, 4
0% o
f par
ticip
ants
re
porte
d an
incr
ease
in p
ain
whe
n no
t wea
ring
the
splin
t; m
ean
pain
in th
e up
per
extre
mity
dec
reas
ed fr
om 3
.0
to 0
.9 (o
f max
. 5);
neck
pai
n de
crea
sed
from
3.0
to 2
.4;
pain
in te
eth/
TMJ d
ecre
ased
fro
m 1
.7 to
1.0
− 4
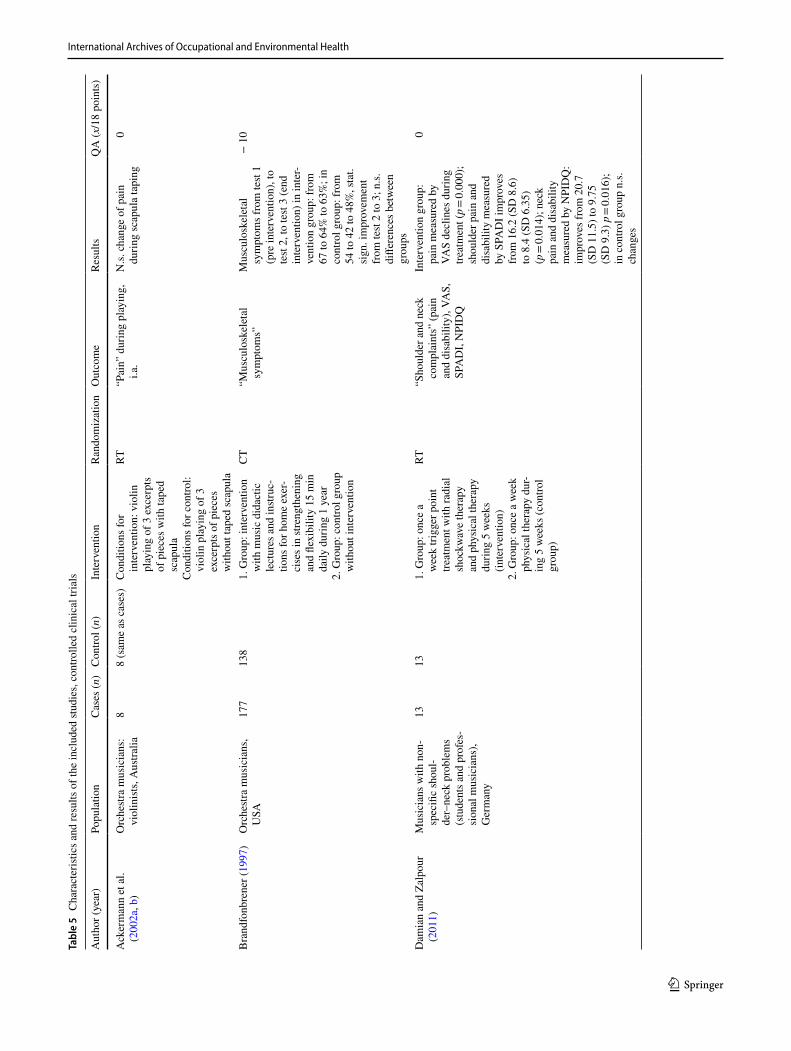
International Archives of Occupational and Environmental Health
1 3
Tabl
e 5
Cha
ract
erist
ics a
nd re
sults
of t
he in
clud
ed st
udie
s, co
ntro
lled
clin
ical
tria
ls
Aut
hor (
year
)Po
pula
tion
Cas
es (n
)C
ontro
l (n)
Inte
rven
tion
Ran
dom
izat
ion
Out
com
eRe
sults
QA
(x/1
8 po
ints
)
Ack
erm
ann
et a
l. (2
002a
, b)
Orc
hestr
a m
usic
ians
: vi
olin
ists,
Aus
tralia
88
(sam
e as
cas
es)
Con
ditio
ns fo
r in
terv
entio
n: v
iolin
pl
ayin
g of
3 e
xcer
pts
of p
iece
s with
tape
d sc
apul
aC
ondi
tions
for c
ontro
l: vi
olin
pla
ying
of 3
ex
cerp
ts o
f pie
ces
with
out t
aped
scap
ula
RT“P
ain”
dur
ing
play
ing,
i.a
.N
.s. c
hang
e of
pai
n du
ring
scap
ula
tapi
ng0
Bra
ndfo
nbre
ner (
1997
)O
rche
stra
mus
icia
ns,
USA
177
138
1. G
roup
: int
erve
ntio
n w
ith m
usic
did
actic
le
ctur
es a
nd in
struc
-tio
ns fo
r hom
e ex
er-
cise
s in
stren
gthe
ning
an
d fle
xibi
lity
15 m
in
daily
dur
ing
1 ye
ar2.
Gro
up: c
ontro
l gro
up
with
out i
nter
vent
ion
CT
“Mus
culo
skel
etal
sy
mpt
oms”
Mus
culo
skel
etal
sy
mpt
oms f
rom
test
1 (p
re in
terv
entio
n), t
o te
st 2,
to te
st 3
(end
in
terv
entio
n) in
inte
r-ve
ntio
n gr
oup:
from
67
to 6
4% to
63%
; in
cont
rol g
roup
: fro
m
54 to
42
to 4
8%, s
tat.
sign
. im
prov
emen
t fro
m te
st 2
to 3
; n.s.
di
ffere
nces
bet
wee
n gr
oups
− 1
0
Dam
ian
and
Zalp
our
(201
1)M
usic
ians
with
non
-sp
ecifi
c sh
oul-
der–
neck
pro
blem
s (s
tude
nts a
nd p
rofe
s-si
onal
mus
icia
ns),
Ger
man
y
1313
1. G
roup
: onc
e a
wee
k tri
gger
poi
nt
treat
men
t with
radi
al
shoc
kwav
e th
erap
y an
d ph
ysic
al th
erap
y du
ring
5 w
eeks
(in
terv
entio
n)2.
Gro
up: o
nce
a w
eek
phys
ical
ther
apy
dur-
ing
5 w
eeks
(con
trol
grou
p)
RT“S
houl
der a
nd n
eck
com
plai
nts”
(pai
n an
d di
sabi
lity)
, VA
S,
SPA
DI,
NPI
DQ
Inte
rven
tion
grou
p:
pain
mea
sure
d by
VA
S de
clin
es d
urin
g tre
atm
ent (
p = 0.
000)
; sh
ould
er p
ain
and
disa
bilit
y m
easu
red
by S
PAD
I im
prov
es
from
16.
2 (S
D 8
.6)
to 8
.4 (S
D 6
.35)
(p
= 0.
014)
; nec
k pa
in a
nd d
isab
ility
m
easu
red
by N
PID
Q:
impr
oves
from
20.
7 (S
D 1
1.5)
to 9
.75
(SD
9.3
) p =
0.01
6);
in c
ontro
l gro
up n
.s.
chan
ges
0
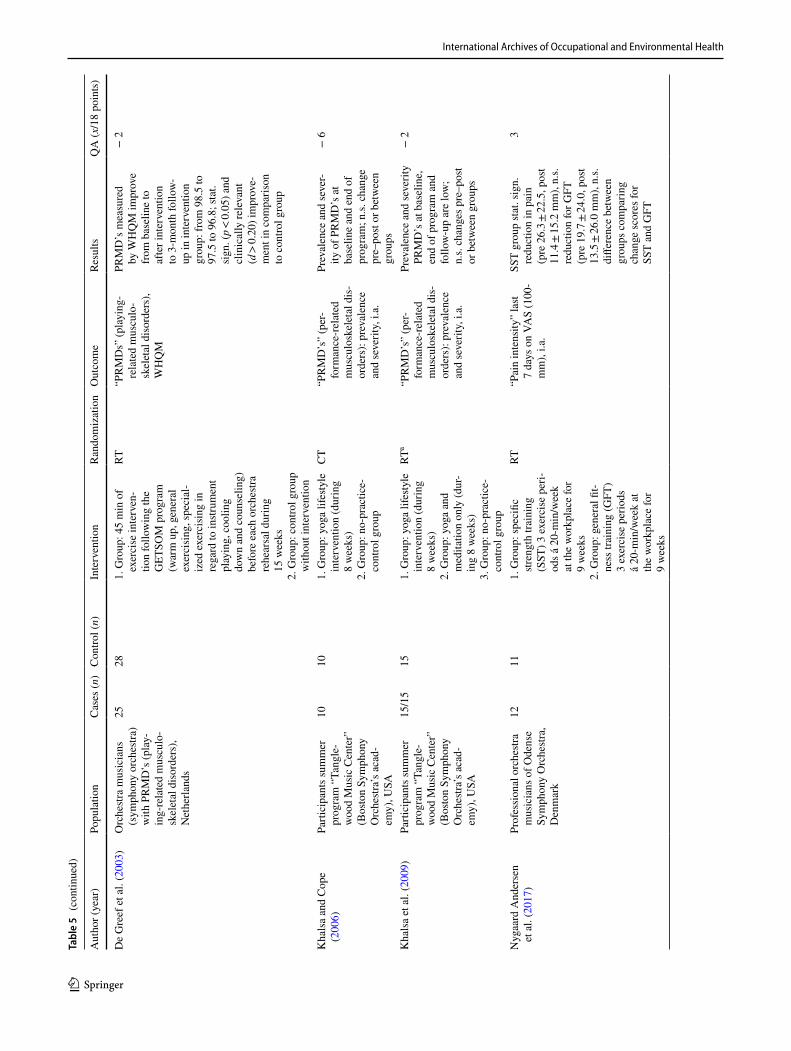
International Archives of Occupational and Environmental Health
1 3
Tabl
e 5
(con
tinue
d)
Aut
hor (
year
)Po
pula
tion
Cas
es (n
)C
ontro
l (n)
Inte
rven
tion
Ran
dom
izat
ion
Out
com
eRe
sults
QA
(x/1
8 po
ints
)
De
Gre
ef e
t al.
(200
3)O
rche
stra
mus
icia
ns
(sym
phon
y or
ches
tra)
with
PR
MD
’s (p
lay-
ing-
rela
ted
mus
culo
-sk
elet
al d
isor
ders
), N
ethe
rland
s
2528
1. G
roup
: 45
min
of
exer
cise
inte
rven
-tio
n fo
llow
ing
the
GET
SOM
pro
gram
(w
arm
up,
gen
eral
ex
erci
sing
, spe
cial
-iz
ed e
xerc
isin
g in
re
gard
to in
strum
ent
play
ing,
coo
ling
dow
n an
d co
unse
ling)
be
fore
eac
h or
ches
tra
rehe
arsa
l dur
ing
15 w
eeks
2. G
roup
: con
trol g
roup
w
ithou
t int
erve
ntio
n
RT“P
RM
Ds”
(pla
ying
-re
late
d m
uscu
lo-
skel
etal
dis
orde
rs),
WH
QM
PRM
D’s
mea
sure
d by
WH
QM
impr
ove
from
bas
elin
e to
af
ter i
nter
vent
ion
to 3
-mon
th fo
llow
-up
in in
terv
entio
n gr
oup:
from
98.
5 to
97
.5 to
96.
8; st
at.
sign
. (p <
0.05
) and
cl
inic
ally
rele
vant
(d
> 0.
20) i
mpr
ove-
men
t in
com
paris
on
to c
ontro
l gro
up
− 2
Kha
lsa
and
Cop
e (2
006)
Parti
cipa
nts s
umm
er
prog
ram
“Ta
ngle
-w
ood
Mus
ic C
ente
r”
(Bos
ton
Sym
phon
y O
rche
stra’
s aca
d-em
y), U
SA
1010
1. G
roup
: yog
a lif
esty
le
inte
rven
tion
(dur
ing
8 w
eeks
)2.
Gro
up: n
o-pr
actic
e-co
ntro
l gro
up
CT
“PR
MD
’s”
(per
-fo
rman
ce-r
elat
ed
mus
culo
skel
etal
dis
-or
ders
): pr
eval
ence
an
d se
verit
y, i.
a.
Prev
alen
ce a
nd se
ver-
ity o
f PR
MD
’s a
t ba
selin
e an
d en
d of
pr
ogra
m; n
.s. c
hang
e pr
e–po
st or
bet
wee
n gr
oups
− 6
Kha
lsa
et a
l. (2
009)
Parti
cipa
nts s
umm
er
prog
ram
“Ta
ngle
-w
ood
Mus
ic C
ente
r”
(Bos
ton
Sym
phon
y O
rche
stra’
s aca
d-em
y), U
SA
15/1
515
1. G
roup
: yog
a lif
esty
le
inte
rven
tion
(dur
ing
8 w
eeks
)2.
Gro
up: y
oga
and
med
itatio
n on
ly (d
ur-
ing
8 w
eeks
)3.
Gro
up: n
o-pr
actic
e-co
ntro
l gro
up
RTa
“PR
MD
’s”
(per
-fo
rman
ce-r
elat
ed
mus
culo
skel
etal
dis
-or
ders
): pr
eval
ence
an
d se
verit
y, i.
a.
Prev
alen
ce a
nd se
verit
y PR
MD
’s a
t bas
elin
e,
end
of p
rogr
am a
nd
follo
w-u
p ar
e lo
w;
n.s.
chan
ges p
re–p
ost
or b
etw
een
grou
ps
− 2
Nyg
aard
And
erse
n et
al.
(201
7)Pr
ofes
sion
al o
rche
stra
mus
icia
ns o
f Ode
nse
Sym
phon
y O
rche
stra,
D
enm
ark
1211
1. G
roup
: spe
cific
str
engt
h tra
inin
g (S
ST) 3
exe
rcis
e pe
ri-od
s á 2
0-m
in/w
eek
at th
e w
orkp
lace
for
9 w
eeks
2. G
roup
: gen
eral
fit-
ness
trai
ning
(GFT
) 3
exer
cise
per
iods
á
20-m
in/w
eek
at
the
wor
kpla
ce fo
r 9
wee
ks
RT“P
ain
inte
nsity
” la
st 7
days
on
VAS
(100
-m
m),
i.a.
SST
grou
p st
at. s
ign.
re
duct
ion
in p
ain
(pre
26.
3 ± 22
.5, p
ost
11.4
± 15
.2 m
m),
n.s.
redu
ctio
n fo
r GFT
(p
re 1
9.7 ±
24.0
, pos
t 13
.5 ±
26.0
mm
), n.
s. di
ffere
nce
betw
een
grou
ps c
ompa
ring
chan
ge sc
ores
for
SST
and
GFT
3
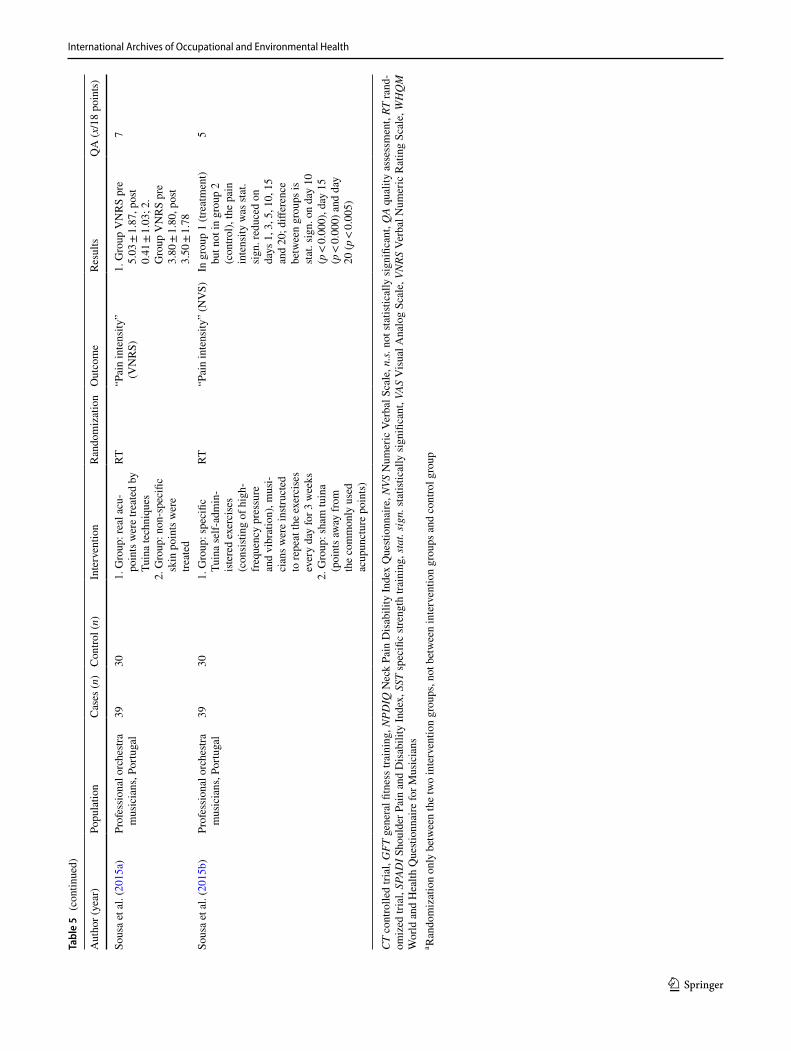
International Archives of Occupational and Environmental Health
1 3
Tabl
e 5
(con
tinue
d)
Aut
hor (
year
)Po
pula
tion
Cas
es (n
)C
ontro
l (n)
Inte
rven
tion
Ran
dom
izat
ion
Out
com
eRe
sults
QA
(x/1
8 po
ints
)
Sous
a et
al.
(201
5a)
Prof
essi
onal
orc
hestr
a m
usic
ians
, Por
tuga
l39
301.
Gro
up: r
eal a
cu-
poin
ts w
ere
treat
ed b
y Tu
ina
tech
niqu
es2.
Gro
up: n
on-s
peci
fic
skin
poi
nts w
ere
treat
ed
RT“P
ain
inte
nsity
” (V
NR
S)1.
Gro
up V
NR
S pr
e 5.
03 ±
1.87
, pos
t 0.
41 ±
1.03
; 2.
Gro
up V
NR
S pr
e 3.
80 ±
1.80
, pos
t 3.
50 ±
1.78
7
Sous
a et
al.
(201
5b)
Prof
essi
onal
orc
hestr
a m
usic
ians
, Por
tuga
l39
301.
Gro
up: s
peci
fic
Tuin
a se
lf-ad
min
-ist
ered
exe
rcis
es
(con
sisti
ng o
f hig
h-fr
eque
ncy
pres
sure
an
d vi
brat
ion)
, mus
i-ci
ans w
ere
instr
ucte
d to
repe
at th
e ex
erci
ses
ever
y da
y fo
r 3 w
eeks
2. G
roup
: sha
m tu
ina
(poi
nts a
way
from
th
e co
mm
only
use
d ac
upun
ctur
e po
ints
)
RT“P
ain
inte
nsity
” (N
VS)
In g
roup
1 (t
reat
men
t) bu
t not
in g
roup
2
(con
trol),
the
pain
in
tens
ity w
as st
at.
sign
. red
uced
on
days
1, 3
, 5, 1
0, 1
5 an
d 20
; diff
eren
ce
betw
een
grou
ps is
st
at. s
ign.
on
day
10
(p <
0.00
0), d
ay 1
5 (p
< 0.
000)
and
day
20
(p <
0.00
5)
5
CT
cont
rolle
d tri
al, G
FT g
ener
al fi
tnes
s tra
inin
g, N
PDIQ
Nec
k Pa
in D
isab
ility
Inde
x Q
uesti
onna
ire, N
VS N
umer
ic V
erba
l Sca
le, n
.s. n
ot st
atist
ical
ly si
gnifi
cant
, QA
qual
ity a
sses
smen
t, RT
rand
-om
ized
tria
l, SP
ADI S
houl
der P
ain
and
Dis
abili
ty In
dex,
SST
spec
ific
stren
gth
train
ing,
stat
. sig
n. st
atist
ical
ly si
gnifi
cant
, VAS
Vis
ual A
nalo
g Sc
ale,
VN
RS V
erba
l Num
eric
Rat
ing
Scal
e, W
HQ
M
Wor
ld a
nd H
ealth
Que
stion
naire
for M
usic
ians
a Ran
dom
izat
ion
only
bet
wee
n th
e tw
o in
terv
entio
n gr
oups
, not
bet
wee
n in
terv
entio
n gr
oups
and
con
trol g
roup

International Archives of Occupational and Environmental Health
1 3
the same study population, reporting immediate effects and effects occurring after 3 weeks (Sousa et al. 2015a, b).
Duration of study interventions
The duration of the mostly physiotherapeutic interventions ranged from a single application given on 1 day with directly measured effects to interventions lasting 3, 5, 6, 8, 9, 12 and 15 weeks or interventions lasting up to 1 year. In one study, the treatment duration was individualized to each partici-pant; the median treatment duration was 27 months, with a standard deviation of 16.7 months (Steinmetz et al. 2009).
Study population of interventional studies
Five studies explicitly included participants with complaints to investigate the effectiveness of the interventions (Sousa et al. 2015a, b; Damian and Zalpour 2011; de Greef et al. 2003; Steinmetz et al. 2009). Six studies included both musi-cians with complaints and musicians without complaints and investigated the prevalence and intensity of complaints before and after the interventions (Nygaard Andersen et al. 2017; Ackermann et al. 2002b; Brandfonbrener 1997; Chan et al. 2014; Khalsa and Cope 2006; Khalsa et al. 2009) or during the interventions compared to control conditions (Ackermann et al. 2002b).
Used outcome parameters of interventional studies
The intervention studies did not reveal evidence that the interventions were effective. No statistically significant changes in MCD were found in violinists after scapula tap-ing, in musicians participating in yoga lifestyle interven-tions, or in orchestra musicians attending music didactic lectures and receiving instructions for home exercises or trigger point treatment with radial shockwave therapy com-bined with physical therapy or specific strength training in comparison to a control group (Ackermann et al. 2002a; Khalsa and Cope 2006; Khalsa et al. 2009; Brandfonbrener 1997; Damian and Zalpour 2011; Nygaard Andersen et al. 2017). However, two studies reported significant improve-ments within the treatment groups but not in the control group (Damian and Zalpour 2011; Nygaard Andersen et al. 2017). Tuina application and groningen exercise therapy did produce statistically significant reductions in pain in the treatment groups compared to the control groups (de Greef et al. 2003; Sousa et al. 2015a, b). Details are provided in Tables 4 and 5.
Quality assessment of interventional studies
Pre–post studies without control groups The quality assessment scores of the three studies in this category
were rated between − 3 and 4 out of 15 possible points. Overall, there were significant methodological concerns. None of the studies reported sample size calculations, suf-ficient blinding or the use of objective, reliable and vali-dated outcome measures. Inclusion and exclusion criteria were explicitly stated in only two studies (Ackermann et al. 2002b; Steinmetz et al. 2009). In one study, a group of participants received physiotherapy in addition to the examined intervention, but a subgroup analysis was not performed (Steinmetz et al. 2009).
Controlled clinical trials The quality assessment scores of the nine studies in this category ranged between − 10 and 7 out of 18 possible points. Overall, noticeable meth-odological concerns included not reporting on how blinding was conducted, not using reliable randomization procedures and not providing sample size calculations. Only one study (Ackermann and Adams 2003) reported an analysis or avoid-ance of additional treatments. Only a few studies reported an intention-to-treat-analysis or reported using all the par-ticipants in their assigned groups for the analyses (Sousa et al. 2015a, b; de Greef et al. 2003; Nygaard Andersen et al. 2017). In four studies, the outcome measurements were not considered to be objective, reliable and validated (Brandfon-brener 1997; de Greef et al. 2003; Khalsa et al. 2009; Khalsa and Cope 2006).
Case studies
There were 28 case studies included, most of which were retrospective single case reports (Table 6). Almost all case studies described improvements in the complaints following the respective treatments or associations between risk factors and special complaints. We were unable to identify subse-quent intervention studies to verify the treatment effects. The reported effects included surgical decompression procedures in nerve compression syndromes (Hoppmann 1997; Laha et al. 1978; Miliam and Basse 2009), surgical treatment in neurogenic thoracic outlet syndrome (Demaree et al. 2017), the use of individual orthotic or assistive devices (Ander-son 1990; Dommerholt 2010; Price and Watson 2011; Sakai 1992; Wilson 1989), conservative combined treat-ments (Lederman 1996; Patrone et al. 1989) partly involv-ing posture optimization (Manal et al. 2008; McFarland and Curl 1998; Potter and Jones 1993, 1995; Quarrier and Norris 2001) and physiotherapy with a special emphasis on mobilization of the radial and posterior interosseous nerves (Jepsen 2014), tensegrity massage and advice for positioning or leisure activities (Wilk et al. 2016). One report each exists for acupuncture (Molsberger and Molsberger 2012), EMG biofeedback (Levee et al. 1976), myofascial trigger point therapy (Dommerholt 2010) and the Feldenkrais method (Nelson 1989).

International Archives of Occupational and Environmental Health
1 3
Tabl
e 6
Cha
ract
erist
ics a
nd re
sults
of t
he in
clud
ed st
udie
s, ca
se st
udie
s
Aut
hor (
year
)D
escr
iptio
nRe
sults
And
erso
n (1
990)
Two
flaut
ists w
ith d
igita
l neu
ropa
thy
are
treat
ed w
ith in
divi
dual
orth
otic
de
vice
sRe
gres
sion
of s
ympt
oms w
ith tr
eatm
ent i
n bo
th c
ases
Bel
mar
sh a
nd Ja
rdin
(199
6)22
-yea
r-old
mal
e m
usic
stud
ent d
iagn
osed
with
uln
ar c
olla
tera
l lig
amen
t sp
rain
due
to o
veru
se a
fter c
hang
ing
the
prac
tice
tech
niqu
e is
trea
ted
with
oc
cupa
tiona
l the
rapy
Pain
subs
ided
sinc
e be
gin
of tr
eatm
ent
Ben
atar
(199
4)44
-yea
r-old
mal
e co
ncer
t flut
ist w
ith sn
appi
ng a
t the
littl
e fin
ger w
ith ra
dial
su
blux
atio
n of
the
conn
exus
inte
rtend
ineu
s of t
he m
etac
arpo
phal
ange
al
join
t rec
eive
s sur
gica
l app
roxi
mat
ion
of th
e co
nnex
us in
terte
ndin
eus
Impr
ovem
ent o
f com
plai
nts a
fter s
urge
ry
Dem
aree
et a
l. (2
017)
5 pr
ofes
sion
al fe
mal
e up
per s
tring
mus
icia
ns w
ith n
euro
geni
c th
orac
ic o
utle
t sy
ndro
me
(TO
S) u
nder
wen
t sur
gica
l tre
atm
ent,
all b
y fir
st rib
rese
ctio
n an
d sc
alen
ecto
my,
all
rece
ived
pos
tope
rativ
e ph
ysic
al th
erap
y:1.
34-
year
-old
vio
linist
with
TO
S sy
mpt
oms a
t the
righ
t sid
e in
the
last
2.6
year
s, w
eekl
y pl
ayin
g tim
e 40
h2.
36-
year
-old
vio
linist
with
TO
S sy
mpt
oms a
t the
righ
t sid
e in
the
last
2.8
year
s, w
eekl
y pl
ayin
g tim
e 60
h3.
42-
year
-old
vio
list w
ith T
OS
sym
ptom
s at t
he ri
ght s
ide
in th
e la
st 3.
2 ye
ars,
wee
kly
play
ing
time
50 h
4. 3
7-ye
ar-o
ld v
iolis
t with
TO
S sy
mpt
oms a
t the
left
side
in th
e la
st 1.
6 ye
ars,
wee
kly
play
ing
time
50 h
5. 2
9-ye
ar-o
ld v
iolin
ist w
ith T
OS
sym
ptom
s at t
he ri
ght s
ide
in th
e la
st 3.
8 ye
ars,
wee
kly
play
ing
time
50 h
All
mus
icia
ns w
ere
able
to re
turn
to th
eir m
usic
al c
aree
r fol
low
ing
treat
men
t. Th
e m
ean
posto
pera
tive
dura
tion
befo
re th
ey re
sum
ed th
eir m
usic
al c
aree
r w
as 5
mon
ths
Dom
mer
holt
(201
0)1.
19-
year
-old
mal
e m
usic
stud
ent (
bass
oon)
with
impa
iring
pai
n in
the
left
inde
x fin
ger d
urin
g th
e ba
ssoo
n pl
ayin
g du
e to
a m
ism
atch
bet
wee
n ha
nd
anth
ropo
met
ry a
nd si
ze o
f the
instr
umen
t rec
eive
s silo
pad™
pre
ssur
e se
nsiti
ve d
ots
2. 2
6-ye
ar-o
ld o
rgan
ist w
ith p
ersi
stent
pai
n in
the
right
wris
t and
thum
b is
tre
ated
with
myo
fasc
ial t
rigge
r poi
nt th
erap
y fo
r 4 m
onth
s
1. P
erfe
ct im
prov
emen
t of t
he c
ompl
aint
s whe
n pl
ayin
g w
ith S
ilopa
d™2.
App
roxi
mat
e pa
in re
lief a
fter 4
mon
ths
Hop
pman
n (1
997)
19-y
ear-o
ld fe
mal
e m
usic
stud
ent (
Fren
ch h
orn)
with
uln
ar n
erve
ent
rapm
ent
synd
rom
e at
the
left
elbo
w d
iagn
osed
due
to o
veru
se re
ceiv
es su
rger
y w
ith
ante
rior t
rans
posi
tion
of th
e ul
nar n
erve
at t
he e
lbow
Com
plet
e re
solu
tion
of sy
mpt
oms a
fter s
urge
ry
Jeps
en (2
014)
55-y
ear-o
ld m
ale
cont
raba
ssoo
nist
with
radi
al tu
nnel
synd
rom
e re
ceiv
es
phys
ioth
erap
y w
ith sp
ecia
l em
phas
is o
n th
e m
obili
zatio
n of
the
radi
al a
nd
poste
rior i
nter
osse
ous n
erve
s
Full
impr
ovem
ent o
f sym
ptom
s afte
r phy
siot
hera
py
Laha
et a
l. (1
978)
47-y
ear-o
ld m
ale
guita
rist w
ith p
rogr
essi
ve w
eakn
ess a
nd n
umbn
ess o
f the
rig
ht h
and
due
to n
erve
com
pres
sion
of t
he m
edia
n ne
rve
at th
e el
bow
with
a
tight
apo
neur
osis
of t
he b
icep
s ten
don
rece
ives
surg
ical
dec
ompr
essi
on
Full
impr
ovem
ent o
f sym
ptom
s afte
r sur
gery
Lede
rman
(199
6)1.
Mal
e do
uble
bas
sist
2. fe
mal
e vi
olin
ist 3
. mal
e pi
anist
4. f
emal
e m
usic
stu
dent
(obo
e), a
ll w
ith sh
ould
er p
ain
in c
onne
ctio
n w
ith in
strum
ent
play
ing
with
neu
ropa
thy
of th
e th
orac
ic lo
ngus
ner
ve a
re tr
eate
d w
ith a
co
mbi
natio
n of
pai
n m
edic
atio
n + av
oida
nce
of m
ovem
ents
, the
n re
-sta
rt w
ith n
orm
al m
ovem
ents
and
mus
cle
build
ing
1. N
o im
prov
emen
t2.
Impr
ovem
ent a
fter 1
0 m
onth
s3.
Som
e im
prov
emen
t4.
Impr
ovem
ent

International Archives of Occupational and Environmental Health
1 3
Tabl
e 6
(con
tinue
d)
Aut
hor (
year
)D
escr
iptio
nRe
sults
Leve
e et
al.
(197
6)52
-yea
r-old
mal
e m
usic
ian
(flut
e, c
larin
et, s
axop
hone
) with
incr
easi
ng
tight
ness
of m
uscl
es o
f the
lip,
mou
th, t
hroa
t and
face
is tr
eate
d w
ith 2
6 se
ssio
ns in
ele
ctro
myo
grap
hy b
iofe
edba
ck
Not
icea
ble
impr
ovem
ent i
n th
e sy
mpt
oms d
urin
g th
e co
urse
of t
he tr
eatm
ent,
no re
laps
e du
ring
the
6-m
onth
follo
w-u
p
Man
al e
t al.
(200
8)20
-yea
r-old
fem
ale
mus
ic st
uden
t (pi
ano,
vio
lin) w
ith p
ain
in th
e ne
ck a
nd
uppe
r sho
ulde
r reg
ion
and
as w
ell n
umbn
ess o
f the
thum
bs is
dia
gnos
ed
with
cer
vica
l rad
icul
opat
hy a
nd n
eura
l im
pairm
ent o
f the
thum
bs a
nd
treat
ed w
ith c
ompl
ex p
hysi
othe
rapy
and
occ
upat
iona
l the
rapy
as w
ell a
s le
arni
ng c
orre
ct p
ostu
re o
n th
e in
strum
ent a
nd a
ctiv
e pr
actic
e br
eaks
in 1
3 tre
atm
ent s
essi
ons
Not
icea
ble
impr
ovem
ent w
ith re
gard
to p
ain,
func
tion,
mob
ility
, i.a
.
McF
arla
nd a
nd C
url (
1998
)19
-yea
r-old
fem
ale
mus
icia
n (v
iolin
) with
shou
lder
pai
n on
bot
h si
des i
s di
agno
sed
with
rota
tor c
uff te
ndon
itis a
nd tr
eate
d w
ith ib
upro
fen,
phy
si-
othe
rapy
, col
d ap
plic
atio
n, m
ore
prac
tice
brea
ks p
ause
s and
pos
tura
l op
timiz
atio
n
Com
plai
nts r
educ
ed fr
om c
ontin
uous
to in
term
itten
t
Mili
am a
nd B
asse
(200
9)29
-yea
r-old
mal
e dr
umm
er w
ith a
nter
ior t
arsa
l tun
nel s
yndr
ome
rece
ives
su
rgic
al d
ecom
pres
sion
No
com
plai
nts a
t con
trols
afte
r 3 m
onth
s and
1 y
ear
Mol
sber
ger a
nd M
olsb
erge
r (20
12)
1. 5
7-ye
ar-o
ld m
ale
pian
ist w
ith p
ain
in th
e rig
ht tr
apez
ius m
uscl
e an
d rig
ht
elbo
w, s
ince
incr
ease
d pl
ayin
g lo
ad is
trea
ted
with
pla
ying
redu
ctio
n an
d 12
tim
es a
cupu
nctu
re2.
53-
year
-old
fem
ale
clar
inet
ist w
ith c
linic
al si
gns o
f sty
loid
itis u
lnae
and
rig
ht h
umer
al e
pico
ndyl
itis i
s tre
ated
with
8-ti
mes
acu
punc
ture
1. A
fter t
reat
men
t ret
urn
to fu
ll pl
ayin
g w
ithou
t com
plai
nts
2. C
ompl
ete
impr
ovem
ent o
f sym
ptom
s afte
r tre
atm
ent
Nel
son
(198
9)Fe
mal
e vi
olin
ist in
her
ear
ly 2
0 s w
ith n
eck
pain
is tr
eate
d w
ith a
t lea
st 11
Fe
lden
krai
s ses
sion
sIm
prov
emen
t of c
ompl
aint
s afte
r 7 se
ssio
ns
Nol
an a
nd E
aton
(198
9)28
-yea
r-old
orc
hestr
a m
usic
ian
(cel
lo) w
ith in
crea
sing
pla
ying
impa
iring
th
umb
pain
is d
iagn
osed
with
“ba
sal j
oint
laxi
ty”
and
rece
ives
ope
rativ
e vo
lar l
igam
ent r
econ
struc
tion
Retu
rn to
the
orch
estra
with
pai
n-fr
ee st
reng
th a
nd e
ndur
ance
Patro
ne e
t al.
(198
9)19
-yea
r-old
mus
ic st
uden
t (vi
olin
) with
dig
ital n
erve
com
pres
sion
synd
rom
e an
d hy
perm
obili
ty is
trea
ted
with
splin
t and
stre
ngth
exe
rcis
es2
wee
ks a
fter t
reat
men
t com
plet
e im
prov
emen
t of t
he sy
mpt
oms.
Afte
r 3
wee
ks, u
se o
f the
splin
t can
be
redu
ced
with
out t
he sy
mpt
oms r
etur
ning
Plan
as (1
982)
Mal
e tru
mpe
ter w
ith ru
ptur
e of
the
orbi
cula
ris o
ris re
ceiv
es su
rgic
al re
con-
struc
tion
Full
retu
rn o
f all
func
tions
and
skill
s afte
r sur
gery
Plan
as (1
988)
28-y
ear-o
ld m
ale
mus
ic st
uden
t (tru
mpe
t) w
ith ru
ptur
e of
the
orbi
cula
ris
oris
rece
ives
surg
ical
reco
nstru
ctio
n (a
nd se
cond
surg
ery
2 m
onth
s lat
er
due
to re
sidu
al fi
ndin
gs)
Goo
d fu
nctio
n of
the
orbi
cula
ris o
ris a
nd c
onte
nted
ness
of t
he p
atie
nt a
fter
surg
ery
Potte
r and
Jone
s (19
93)
Elite
mus
icia
n (S
cotti
sh g
reat
hig
hlan
d ba
gpip
e) w
ith n
umbn
ess a
nd ti
nglin
g in
the
med
ial a
rm a
nd m
edia
l han
d as
wel
l as p
ain
of ri
ght t
hena
r em
i-ne
nce
is d
iagn
osed
with
ove
ruse
synd
rom
e an
d tre
ated
with
alte
ratio
ns in
al
ignm
ent o
f the
instr
umen
t, pl
ayin
g te
chni
que
and
prac
tice
regi
men
Gra
dual
reso
lutio
n of
all
disc
omfo
rt an
d re
turn
to c
omfo
rtabl
e pl
ayin
g
Potte
r and
Jone
s (19
95)
22-y
ear-o
ld fe
mal
e vi
olin
ist w
ith b
ilate
ral s
houl
der p
ain
durin
g an
d af
ter
instr
umen
t pla
y is
dia
gnos
ed w
ith ro
tato
r cuff
tend
initi
s and
rece
ives
trea
t-m
ent w
ith re
st, a
nti-i
nflam
mat
ory
med
icat
ion
and
phys
ioth
erap
y
Sign
ifica
nt im
prov
emen
t of t
he sy
mpt
oms a
fter t
reat
men
t

International Archives of Occupational and Environmental Health
1 3
Tabl
e 6
(con
tinue
d)
Aut
hor (
year
)D
escr
iptio
nRe
sults
Pric
e an
d W
atso
n (2
011)
Mal
e or
ches
tral t
rom
boni
st w
ith p
ostu
ral p
robl
ems a
nd p
ain
of th
e le
ft sh
ould
er, h
and
and
face
rece
ives
ove
r at l
east
9 m
onth
s a c
ompl
ex, n
ot
exac
tly d
efine
d tre
atm
ent i
nclu
ding
phy
siot
hera
py, A
lexa
nder
tech
niqu
e,
oste
opat
hy, t
hera
py b
y ne
urol
ogist
s, or
thop
edist
s, pl
astic
surg
eon,
rheu
ma-
tolo
gist,
orth
odon
tist a
nd d
entis
t and
use
s spe
cial
exp
edie
nt (“
Ergo
bone
”)
Rela
pse
afte
r ini
tial i
mpr
ovem
ent o
f sym
ptom
s
Qua
rrie
r and
Nor
ris (2
001)
1. fe
mal
e un
iver
sity
trom
bone
stud
ent w
ith in
crea
sing
dis
com
fort,
fatig
ue,
and
pain
in h
er le
ft ha
nd a
nd fo
rear
m w
ith e
xcee
ding
ly sm
all h
ands
re
ceiv
es a
n in
divi
dual
ly m
ade
spec
ial e
rgon
omic
splin
t2.
18-
year
-old
soph
omor
e in
a m
usic
con
serv
ator
y w
ho p
laye
d ba
ss tr
om-
bone
with
pro
gres
sive
pai
n of
the
left
hand
and
rela
tivel
y sm
all h
ands
re
ceiv
es in
itial
rest
treat
men
t, ph
ysio
ther
apy
and
mod
ifica
tion
of th
e in
strum
ent
1. D
ecre
ased
dis
com
fort
and
ultim
atel
y ce
ssat
ion
of p
ain
2. D
isap
pear
ance
of t
he sy
mpt
oms w
ithin
3–4
wee
ks
Rid
er (1
987)
34-y
ear-o
ld fe
mal
e or
ches
tra c
ellis
t with
per
form
ance
anx
iety
and
mus
cle
fatig
ue is
trea
ted
with
a c
ombi
natio
n of
mus
ic p
sych
othe
rapy
, bio
feed
back
, sy
stem
atic
des
ensi
tizat
ion
and
cogn
itive
restr
uctu
ring
over
8 se
ssio
ns
In th
e fo
llow
-up
redu
ctio
n of
the
shou
lder
pai
n, im
prov
ed p
erfo
rman
ce a
tti-
tude
s, se
lf-es
teem
and
per
form
ance
qua
lity
Saka
i (19
92)
1. 1
7-ye
ar-o
ld fe
mal
e pi
anist
with
late
ral e
pico
ndyl
itis a
fter i
ncre
ased
pl
ayin
g of
oct
aves
rece
ives
intra
-arti
cula
r inj
ectio
n of
ster
oids
and
loca
l an
esth
etic
s, fo
rear
m te
nnis
elb
ow su
ppor
t stra
p an
d str
etch
ing
exer
cise
s2.
22-
year
-old
pia
nist
with
pai
n in
the
right
wris
t due
to te
ndov
agin
itis
de Q
uerv
ain
afte
r rep
eate
d pr
actic
e of
oct
aves
and
wid
e-ex
tent
cho
rds
rece
ives
ster
oid
and
loca
l ane
sthe
tic in
ject
ion
in th
e fir
st co
mpa
rtmen
t
1. Im
prov
emen
t by
inje
ctio
n, n
ot w
earin
g th
e str
ap b
ecau
se o
f obs
truct
ion
of
play
ing,
impr
ovem
ent b
y str
etch
ing
exer
cise
s2.
Res
olvi
ng th
e pa
in
Stei
nmet
z et
al.
(200
8)44
-yea
r-old
mal
e vi
olin
ist w
ith p
ersi
stent
, per
form
ance
-impa
iring
left
side
ne
ck a
nd sh
ould
er p
ain
and
extre
me
exte
rnal
rota
tion
of v
iolin
and
shou
l-de
r firs
t uns
ucce
ssfu
lly re
ceiv
es m
anua
l the
rapy
and
phy
siot
hera
py a
nd is
th
en tr
eate
d w
ith a
mul
timod
al p
ain
ther
apy
prog
ram
, inc
ludi
ng m
anua
l th
erap
y an
d ch
ange
men
t of h
is p
atho
logi
cal m
ovem
ent p
atte
rns w
hile
pl
ayin
g th
e vi
olin
, wer
e re
solv
ed b
y te
achi
ng n
ew m
ovem
ent p
atte
rns
Reso
lutio
n of
the
pain
, the
mai
n sy
mpt
oms d
id n
ot re
cur a
fter s
ever
al m
onth
s of
follo
w-u
p
Wilk
et a
l. (2
016)
34-y
ear-o
ld m
ale
viol
inist
with
pai
n, si
nce
less
than
2 m
onth
s and
cra
mps
in
the
fore
arm
and
han
d m
uscl
es, r
ecei
ves 6
tens
egrit
y m
assa
ge se
ssio
ns,
45 m
in e
ach,
eve
ry 3
day
s dur
ing
15 d
ays p
lus a
dvic
e: e
xerc
ises
stre
tchi
ng,
impr
ovin
g po
sture
hab
its, a
ctiv
e fo
rms o
f lei
sure
. Afte
r the
end
of t
hera
py
the
patie
nt b
egan
regu
larly
exe
rcis
ing
at a
gym
Pain
on
VAS
decr
ease
d fro
m 8
(of 1
0) b
efor
e tre
atm
ent t
o 5
(of 1
0) a
fter t
he
third
trea
tmen
t, to
0 a
fter t
he si
xth
treat
men
t and
afte
r 6 m
onth
s
Wils
on (1
989)
24-y
ear-o
ld fe
mal
e cl
arin
etist
with
sym
ptom
s in
the
tem
poro
man
dibu
lar
join
t (pa
in, l
imite
d ex
curs
ion,
late
ral d
evia
tion
and
“cat
ch”
on th
e le
ft jo
int
upon
ope
ning
), si
nce
prac
ticin
g a
stac
cato
pas
sage
rece
ives
orth
odon
tic
treat
men
t and
bite
splin
t
Pain
-fre
e cl
arin
et p
layi
ng fo
r a p
erio
d of
2 y
ears

International Archives of Occupational and Environmental Health
1 3
Excluded studies
At the full-text level, 195 studies did not fulfill the inclusion criteria and were not included. Examples of the excluded studies are provided as follows. The study population included participants under 16 years of age (Vinci et al. 2015; Rodríguez-Romero et al. 2016; Stanek et al. 2017; Ioannou and Altenmüller 2015; Yasuda et al. 2016; Hag-berg et al. 2005; Rodriguez-Lozano 2008; Goodman and Staz 1989; Larsson et al. 1993; Mehrparvar et al. 2012), did not state the age range of participants (Zaza and Fare-well 1997; Lopez and Martinez 2013; Manchester and Park 1996; Kreutz et al. 2008; Revak 1989; Brandfonbrener 2000; Lee et al. 2012; Tubiana and Chamagne 1993; Williamon and Thompson 2006; Zetterberg et al. 1998) or provided insufficient information on the outcomes of interest when separated into age subgroups (Furuya et al. 2006; Dawson 2001). Further reasons for exclusion included that the pro-fessional status was not clearly specified (Pedrazzini et al. 2015; Takata et al. 2016; Mehrparvar et al. 2012; Brandfon-brener 2000, 2002; Tubiana and Chamagne 1993; Leder-man 2003), MCDs were not reported discriminatingly (Hiner et al. 1987; Spahn et al. 2001) or complaints were not clearly separated into non-musculoskeletal regions in the reported results (Kaneko et al. 2005).
Discussion
The study designs, terminology, and outcomes of the 109 studies included in this review were heterogeneous. The inclusion criteria were rarely mentioned throughout all study types, the analyses mostly did not check for major confound-ers, and the definition of exposure was often insufficient. In addition, the quality assessment of most studies included raised considerable methodological concerns. Therefore, sufficient statements cannot be provided for the prevalence, risk factors, prevention and effectiveness of treatment of MCD in professional musicians. Furthermore, a more pro-found differentiation, for example with regard to gender or the instrument played, is even less feasible.
In musicians´ medicine, we regularly observe that pro-fessional musicians suffer from MCD due to high physical and psychological work-related demands. The wide range in the prevalence of MCD, reported in the included studies may reflect the heterogeneous and often unclear definitions used to assess complaints in musicians. We assume that causality was already inferred due to the use of terms such as “PRMD” or by asking the study participants about com-plaints that were caused by or noticed while playing music. Thus, the basic assumption of causality was not questioned. In musicians´ medicine, we often lack validated assessment tools for MCD in relation to making music. However, some
tools do exist, such as the Disabilities of The Arm, Shoul-der and Hand (DASH) questionnaire (SooHoo et al. 2002; Hudak et al. 1996) with its optional sports/performing arts module.
From an epidemiological viewpoint, most of the included studies had only a small number of participants. Only one cross-sectional study (Fishbein et al. 1988; Middlestadt 1990; Middlestadt and Fishbein 1988) included a high number of participants (n = 2212). who were recruited from various US orchestras. Only this study was considered rep-resentative. However, even this study had considerable meth-odological shortcomings (see above).
The included studies had mostly a high risk of bias and little control of confounders. Some cross-sectional studies have been conducted on musicians in a single orchestra dur-ing a single rehearsal session. These studies likely suffered from a healthy-worker bias in addition to having little exter-nal validity or representativeness in the study results. When biographic data are gathered in cross-sectional studies, recall bias likely exists. Very few of the studies systemati-cally assessed confounders that may have influenced MCD independently of the treatment, such as other physical loads, increased physical activity, working in the house and garden, unilateral strain by special sport discipline, carrying toddlers or providing home care to relatives. Individual preventive activities, such as sports, physical training, and relaxation, were not included as possible confounders. Additionally, correlations between instrument-specific workload (e.g., daily playing time) and complaints were not assessed. To assess the risk factors for MCD in musicians’, observational cohort studies are needed that utilize a sufficient sample size, different instrument groups, workloads, or workplaces and account for physical activity and other risk factors. Clinical trials investigating conventional and complementary medi-cine approaches that differentiate between instrument groups are needed to assess effective therapy options for musicians.
Comparing our results to the literature we found seven systematic reviews about MCD in adult professional musi-cians (Zaza 1998; Bragge et al. 2006; Wu 2007; Baadjou et al. 2016; Jacukowicz 2016; Kok et al. 2016; Vervainioti and Alexopoulos 2015). The presented review is the first attempt to investigate the frequencies, risk factors and treat-ment options for MCD in musicians. Zaza (1998) reported that the prevalence of PRMD in adult classical musicians was comparable to that of work-related MCDs reported for other occupations. Due to the previously mentioned lack of evidence for the prevalence of PRMD, we are unable to draw a comparable conclusion. This finding is in line with another systematic review (Bragge et al. 2006) that concluded that the evidence did not provide sufficient information regarding the prevalence and risk factors associated with PRMDs in pianists due to common methodological limitations, includ-ing sampling/measurement biases, inadequate reporting of

International Archives of Occupational and Environmental Health
1 3
reliability/validity of the outcome measures, a lack of opera-tional definitions for PRMD and a lack of statistical signifi-cance testing. In her work on the occupational risk factors of MCD in musicians, Wu (2007) reported that the etiology of MCD is multifactorial in instrumental musicians; how-ever, she also pointed out that cross-sectional studies cannot investigate causality. This differs from our conclusion, since we could not identify studies that searched for risk factors using an appropriate study design. More recent systematic reviews also found methodological concerns (Baadjou et al. 2016; Jacukowicz 2016; Kok et al. 2016; Vervainioti and Alexopoulos 2015). In contrast to our review, the authors reported results from the subjects of each study. Baadjou et al. reported that previous musculoskeletal injuries, music performance anxiety, high levels of stress and being a female who plays a stringed instrument seem to be associated with more MCD (Baadjou et al. 2016). Kok et al. found a point prevalence of MCD in professional musicians ranging between 9 and 68%, a 12-month prevalence between 41 and 93% and a lifetime prevalence between 62 and 93%. Ten out of 12 studies show a higher prevalence of MCD among women (Kok et al. 2016). However, the authors used a dif-ferent scoring system to assess the quality of the included studies. In contrast to our assessment, the authors found that 13 out of 17 studies received high-quality scores (Kok et al. 2016). On the other hand, the results of the present study agree with the authors who reported that the current defini-tion of PRMD does not provide causality of the complaints. We further emphasize the importance of using adequate and validated instruments for measuring outcomes in future studies. Jacukowicz reported on the psychosocial aspects of work, such as long hours at work, work content, high job demands, low control/influence, and a lack of social sup-port were related to MCD (Jacukowicz 2016). Another sys-tematic review included professional musicians as well as active members of a classical orchestra who were of at least 16 years of age. The review proposed that further research should include seven categories of stressors that affect clas-sical instrumental musicians: public exposure, personal haz-ards, repertoire, competition, job context, injury/illness, and criticism (Vervainioti and Alexopoulos 2015).
Limitations and strengths
The presented systematic review is a comprehensive attempt to evaluate the quality of the available literature on the prevalence, risk factors, and effectiveness of prevention or treatment of MCD in professional musicians. Therefore, we included published observational studies (case–control studies, cohort studies and cross-sectional studies), inter-ventional studies (controlled clinical trials and pre–post intervention studies without control group), case reports and
case series reporting clinical interventions. Because the data were very heterogeneous, an assessment of publication bias, such as a funnel plot, was not feasible. The quality assess-ments of the included studies were performed according to the study protocol, and if a methodological procedure was not described in the assessed article, it was recorded as not done. This was very often the case, with very few procedures being explicitly described as not having been performed. This may have led to poorer evaluations of those studies that provided less detailed reporting or publications that were older than the current reporting guidelines. The real study method might have been underestimated based on the shortcomings of reporting. The authors were not contacted about the included studies, because several of the studies were performed more than 10 years ago. Regarding quality assessment and assessment of the bias risk of the original studies, a certain allowance for interpretation and discussion is generally required. Therefore, quality evaluations were each carried out by two people, and a consensus was drawn for each study after a detailed discussion. A limitation of the present review is that to allow for a quantitative estimation, the quality assessment instruments, which were modified by the authors, and the subsequent quantitative estimation were not validated previously. The term MCD comprises a large number of very different disorders. The aim of this review was to provide an overview of this research area as well as to search for clues about the causality between music making and diseases or disorders. Any restrictions to specified clini-cal diagnoses would, therefore, have been purely arbitrary and, given the conceptual uncertainty of numerous primary studies with many-sided overlaps, would have represented a random and, therefore, meaningless section of a complex, interwoven area.
Conclusions
The body of evidence regarding musculoskeletal disorders and complaints in professional musicians has grown sub-stantially, since the publication of earlier reviews. However, studies analyzing prevalence, risk factors and effectiveness of the prevention or treatment of MCD amongst professional musicians, using today’s methodological requirements, are still missing. To evaluate the extent of associations of practice and performance burden with MCD, prospective, long-term cohort studies that properly take into account the influencing factors are still needed. To evaluate the effective-ness of specific treatment options for specific instrumental groups, prospective randomized confirmatory intervention studies are necessary. The use of well-defined diagnostic criteria for MCD in musicians is needed to avoid bias when selecting study participants. Strict and consistent diagnostic criteria would help to avoid the large variation in results.

International Archives of Occupational and Environmental Health
1 3
Establishing and implementing a validated and reliable set of outcome measurements is necessary. If it is possible to optimize the methodology as proposed above, relevant risk factors for MCD in musicians may be identified more pre-cisely and allow for targeted prevention and intervention.
Acknowledgements We give our thanks to the native English-speaking editors at American Journal Experts for editing for proper English lan-guage, grammar, punctuation, spelling, and overall style (Certificate Verification Key: A58E-50C9-D188-34A7-40F4).
Author contributions Design of the study protocol: AB, KN, IF, SW. Performed the data search and study selection: KN, GR, AB, AS. Extracted and analyzed the data: KN, GR, AS, AB. Interpreted the data: AB, KN, GR, and AS. First draft of the manuscript: GR, KN. Revision of the paper and approval of the final version: GR, KN, IF, AS, AB, SW.
Compliance with ethical standards
Conflict of interest The authors declare that they have no competing interests.
Open Access This article is distributed under the terms of the Crea-tive Commons Attribution 4.0 International License (http://creat iveco mmons .org/licen ses/by/4.0/), which permits unrestricted use, distribu-tion, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Appendix 1: Search algorithms
MEDLINE and EMBASE via OvidSP
(musician$1 OR instrumentalist$1 OR orchestra OR sym-phony OR music student$1 OR pianist$1 OR harpsichord-ist$1 OR organist$1 OR string player$1 OR violinist$1 OR brass player$1 OR cellist$1 OR bassist$1 OR violist$1 1 OR harpist$1 OR woodwind$1 OR flute player$1 OR recorder player$1 OR oboist$1 OR clarinetist$1 OR bassoonist$1 OR hornist$1 OR saxophonist$1 OR brass player$1 OR trum-pet player$1 OR bugler$1 OR trombone player$1 OR tuba player$1 OR euphonium player$ OR percussionist$1 OR drummer$1)
AND(exp musculoskeletal diseases/ OR musculoskeletal dis-
ease/ OR exp pain/ OR exp cumulative trauma disorders/ OR cumulative trauma disorder/ OR exp “Sprains and Strains”/ OR musculoskeletal OR orthopedic OR pain OR cumulative trauma disorder$1 OR overuse OR repetive strain injur$ OR PRMD)
AND(Cross-sectional study/ OR cross-sectional studies/ OR
cohort studies/ OR cohort analysis/ OR case control studies/ OR case control study/ OR observational study/ OR case
reports/ OR case report/ OR intervention studies/ OR inter-vention study/ OR exp clinical trial/ OR randomized con-trolled trial/ OR systematic review/ OR risk factor/ OR risk factors/ OR therapy/ OR therapeutics/ OR exp clinical trials as topic/ OR exp “clinical trial (topic) “/ OR double-blind method/ OR double-blind procedure/ OR prevalence/ OR incidence/ OR cross-sectional stud$ OR cohort stud$ OR case-control-stud$ OR observational stud$ OR case report$1 OR intervention stud$ OR clinical trial$1 OR double-blind method OR randomized controlled trial$1 OR prevalence OR incidence OR systematic review$1 OR risk factor$1 OR treat$ OR therap$)
CINAHL via EbscoHost
(musician* OR instrumentalist* OR orchestra OR symphony OR music student* OR pianist* OR harpsichordist* OR organist* OR string player* OR violinist* OR brass player* OR cellist* OR bassist* OR violist OR harpist* OR wood-wind* OR flute player* OR recorder player OR oboist* OR clarinetist* OR bassoonist* OR hornist* OR saxophonist* OR brass player* OR trumpet player* OR bugler OR trom-bone player* OR tuba player* OR euphonium player* OR percussionist* OR drummer*)
AND((MH “Pain+”) OR (MH “Musculoskeletal Diseases+”)
OR (MH “Cumulative Trauma Disorders+”) OR muscu-loskeletal OR orthopedic OR pain OR cumulative trauma disorder* OR overuse OR repetive strain injur* OR PRMD)
AND((MH “Cross Sectional Studies”) OR (MH “Prospective
Studies+”) OR (MH “Case Control Studies+”) OR (MH “Nonexperimental Studies+”) OR (MH “Case Studies”) OR (MH “Experimental Studies+”) OR (MH “Systematic Review”) OR (MH “Risk Factors”) OR (MH “Clinical Tri-als+”) OR (MH “Double-Blind Studies”) OR (MH “Preva-lence”) OR (MH “Incidence”)OR Cross-sectional stud* OR cross-sectional stud* OR cohort stud* OR case-control stud* OR observational stud* OR case report* OR interven-tion stud* OR clinical trial* OR double-blind-method OR prevalence OR incidence OR randomized controlled trial* OR systematic review* OR risk factor* OR treatment* OR therap*)
PsycInfo + PsycArticles via EbscoHost
(musician* OR instrumentalist* OR orchestra OR sym-phony OR music student* OR pianist* OR harpsichordist* OR organist* OR string player* OR violinist* OR brass player* OR cellist* OR bassist* OR violist OR harpist* OR woodwind* OR flute player* OR recorder player OR oboist* OR clarinetist* OR bassoonist* OR hornist* OR saxophon-ist* OR brass player* OR trumpet player* OR bugler OR

International Archives of Occupational and Environmental Health
1 3
trombone player* OR tuba player* OR euphonium player* OR percussionist* OR drummer*)
AND((DE “Musculoskeletal Disorders” OR DE “Bone Dis-
orders” OR DE “Joint Disorders” OR DE “Muscular Dis-orders”) OR (DE “Pain” OR DE “Aphagia” OR DE “Back Pain” OR DE “Chronic Pain” OR DE “Headache” OR DE “Myofascial Pain” OR DE “Neuralgia” OR DE “Neuro-pathic Pain” OR DE “Somatoform Pain Disorder”) OR mus-culoskeletal OR orthopedic OR pain OR cumulative trauma disorder* OR overuse OR repetive strain injur* OR PRMD)
AND((DE “Cohort Analysis”) OR (DE “Case Report”) OR
(DE “Clinical Trials”) OR (DE “Risk Factors”) OR (DE “Alternative Medicine” OR DE “Medical Treatment (Gen-eral)” OR DE “Physical Treatment Methods” OR DE “Relaxation Therapy”) OR (DE “Treatment”) OR (DE “Clinical Trials”)OR Cross-sectional stud* OR cross-sec-tional stud* OR cohort stud* OR case-control stud* OR observational stud* OR case report* OR intervention stud* OR clinical trial* OR double-blind method OR prevalence OR incidence OR randomized controlled trial* OR system-atic review* OR risk factor* OR treatment* OR therap*)
ERIC via EbscoHost
(musician* OR instrumentalist* OR orchestra OR symphony OR music student* OR pianist* OR harpsichordist* OR organist* OR string player* OR violinist* OR brass player* OR cellist* OR bassist* OR violist OR harpist* OR wood-wind* OR flute player* OR recorder player OR oboist* OR clarinetist* OR bassoonist* OR hornist* OR saxophonist* OR brass player* OR trumpet player* OR bugler OR trom-bone player* OR tuba player* OR euphonium player* OR percussionist* OR drummer*)
AND(musculoskeletal OR orthopedic OR pain OR cumulative
trauma disorder* OR overuse OR repetive strain injur* OR PRMD)
AND((DE “Incidence”) OR Cross-sectional stud* OR cross-
sectional stud* OR cohort stud* OR case-control stud* OR observational stud* OR case report* OR intervention stud* OR clinical trial* OR double-blind method OR prevalence OR incidence OR randomized controlled trial* OR system-atic review* OR risk factor* OR treatment* OR therap*)
Appendix 2: Quality assessment tools
See online supplement.
References
Abréu-Ramos AM, Micheo WF (2007) Lifetime prevalence of upper-body musculoskeletal problems in a professional-level symphony orchestra: age, gender, and instrument-specific results. Med Probl Perform Artist 22(3):97–104
Ackermann B, Adams R (2003) Physical characteristics and pain pat-terns of skilled violinists. Med Probl Perform Artist 18(2):65–71
Ackermann B, Adams R, Marshall E (2002a) The effect of scapula taping on electromyographic activity and musical performance in professional violinists. Aust J Physiother 48(3):197–203
Ackermann B, Adams R, Marshall E (2002b) Strengh or endurance training for undergraduate music majors at university? Med Probl Perform Artists 17:33–41
Ackermann BJ, Kenny DT, Fortune J (2011) Incidence of injury and attitudes to injury management in skilled flute players. Work J Prev Assess Rehabil 40(3):255–259
Ackermann B, Driscoll T, Kenny DT (2012) Musculoskeletal pain and injury in professional orchestral musicians in Australia. Med Probl Perform Artist 27(4):181–187
Amorim MIT, Jorge AIL (2016) Association between temporoman-dibular disorders and music performance anxiety in violinists. Occup Med 66:558–563. https ://doi.org/10.1093/occme d/kqw08 0
Anderson JI (1990) Orthotic device for flutists’ digital nerve compres-sion. Med Probl Perform Artists 5(3):91–93
Arnason K, Arnason A, Briem K (2014) Playing-related musculo-skeletal disorders among Icelandic music students. Differences between students playing classical vs rhythmic music. Med Probl Perform Artists 29(2):74–79
Baadjou VA, Roussel NA, Verbunt JA, Smeets RJ, de Bie RA (2016) Systematic review: risk factors for musculoskeletal disorders in musicians. Occupational Medicine 66:614–622
Barton R et al (2008) Occupational performance issues and predictors of dysfunction in college instrumentalists. Med Probl Perform Artist 23:72–78
Bejjani FJ, Kaye GM, Benham M (1996) Musculoskeletal and neuro-muscular conditions of instrumental musicians. Arch Phys Med Rehabil 77(4):406–413
Belmarsh K, Jardin G (1996) Student paper. An overview of upper extremity cumulative trauma disorders in pianists. Work 7:121–127
Benatar N (1994) Radial subluxation of the connexus intertendineus at the MP joint of the little finger in musicians treated by connexus intertendineus proximalization. J Hand Surg Br 19:81–87
Berque P, Gray H, McFadyen A (2016) Playing-related musculoskeletal problems among professional orchestra musicians in Scotland. Med Probl Perform Artist 31:78–86. https ://doi.org/10.21091 /mppa.2016.2015
Blackie H, Stone R, Tiernan A (1999) An investigation of injury pre-vention among university piano students. Med Probl Perform Artist 14(3):141–149
Bragge P, Bialocerkowski A, McMeeken J (2006) A systematic review of prevalence and risk factors associated with playing-related musculoskeletal disorders in pianists. Occup Med 56(1):28–38. https ://doi.org/10.1093/occme d/kqi17 7
Brandfonbrener AG (1997) Orchestral injury prevention. Intervention study. Med Probl Perform Artists 12(1):9–14
Brandfonbrener A (2000) Joint laxity and arm pain in musicians. Med Probl Perform Artists 15(2):72–74
Brandfonbrener AG (2002) Joint laxity and arm pain in a large clinical sample of musicians. Med Probl Perform Artist 17(3):113–115
(CASP) CASP (2013) CASP checklists. http://www.casp-uk.net/casp-tools -check lists . Accessed 7 Dec 2017
International Archives of Occupational and Environmental Health
1 3
Chan C, Driscoll T, Ackermann B (2013) The usefulness of on-site physical therapy-led triage services for professional orchestral musicians—a national cohort study. BMC Musculoskelet Disord 14(98):98. https ://doi.org/10.1186/1471-2474-14-98
Chan C, Driscoll T, Ackermann B (2014) Exercise DVD effect on musculoskeletal disorders in professional orchestral musicians. Occup Med (Lond) 64(1):23–30. https ://doi.org/10.1093/occme d/kqt11 7
Crnivec R (2004) Assessment of health risks in musicians of the Slo-vene Philharmonic Orchestra, Ljubljana, Slovenia. Med Probl Perform Artists 19(3):140–145
Cruder C, Falla D, Mangili F, Azzimonti L, Araujo LS, Williamon A, Barbero M (2017) Profiling the location and extent of musicians’ pain using digital pain drawings. Pain Pract 18(1):53–66
Damian M, Zalpour C (2011) Trigger point treatment with radial shock waves in musicians with nonspecific shoulder-neck pain: data from a special physio outpatient clinic for musicians. Med Probl Perform Artist 26(4):211–217
Davies J, Mangion S (2002) Predictors of pain and other musculoskel-etal symptoms among professional instrumental musicians: eluci-dating specific effects. Med Probl Perform Artist 17(4):155–168
Dawson WJ (2001) Upper extremity overuse in instrumentalists. Med Probl Perform Artist 16(2):66–71
de Greef M, van Wijck R, Reynders K, Toussaint J, Hesseling R (2003) Impact of the Groningen Exercise Therapy for Symphony Orchestra Musicians program on perceived physical competence and playing-related musculoskeletal disorders of professional musicians. Med Probl Perform Artist 18(4):156–160
De Smet L, Ghyselen H, Lysens R (1998) Incidence of overuse syn-dromes of the upper limb in young pianists and its correlation with hand size, hypermobility and playing habits. Ann Hand Upper Limb Surg 17(4):309–313
Demaree CJ, Wang K, Lin PH (2017) Thoracic outlet syndrome affect-ing high-performance musicians playing bowed string instru-ments. Vascular 25:329–332
Dommerholt J (2010) Performing arts medicine—instrumentalist musi-cians: part III—case histories. J Bodyw Mov Ther 14(2):127–138. https ://doi.org/10.1016/j.jbmt.2009.02.005
Eller N, Skylv G, Ostri B, Dahlin E, Suadicani P, Gyntelberg F (1992) Health and lifestyle characteristics of professional singers and instrumentalists. Occup Med (Lond) 42(2):89–92
Engquist K, Orbaek P, Jakobsson K (2004) Musculoskeletal pain and impact on performance in orchestra musicians and actors. Med Probl Perform Artist 19:55–61
Fishbein M, Middlestadt SE, Ottani V, Straus S, Ellis A (1988) Medi-cal problems among ICSOM musicians: overview of a national survey. Med Probl Perform Artist 3(1):1–9
Fjellman-Wiklund A, Sundelin G (1998) Muscoloskeletal discomfort of music teachers: an eight-year perspective and psychosocial work factors. Int J Occup environ Health 4(2):89–98
Fjellmann-Wiklund A, Brulin C, Sundelin G (2003) Physical and psy-chosocial work-related risk factors associated with neck-shoulder discomfort in male and female music teachers. Med Probl Per-form Artist 18:33–41
Fotiadis DG, Fotiadou EG, Kokaridas DG, Mylonas AC (2013) Prev-alence of musculoskeletal disorders in professional symphony orchestra musicians in Greece: a pilot study concerning age, gender, and instrument-specific results. Med Probl Perform Art-ist 28:91–95
Fry HJH (1986) Incidence of overuse syndrome in the symphony orchestra. Med Probl Perform Artist 1:51–55
Furuya S, Nakahara H, Aoki T, Kinoshita H (2006) Prevalence and causal factors of playing-related musculoskeletal disorders of the upper extremity and trunk among Japanese pianists and piano students. Med Probl Perform Artist 21(3):112–117
Gasenzer ER, Klumpp MJ, Pieper D, Neugebauer EA (2017) The prevalence of chronic pain in orchestra musicians. Ger Med Sci. https ://doi.org/10.3205/00024 2
Gohl AP, Clayton SZ, Strickland K, Bufford YD, Halle JS, Greathouse DG (2006) Median and ulnar neuropathies in university pianists. Med Probl Perform Artist 21:17–24
Goodman G, Staz S (1989) Occupational therapy for musicians with upper extremity overuse syndrome: patient perceptions regarding effectiveness of treatment. Med Probl Perform Artists 4(1):9–14
Green S, Higgins J (2011) Chapter 2: preparing a Cochrane review. The Cochrane Collaboration. http://handb ook-5-1.cochr ane.org/. Accessed 7 Dec 2017
Hagberg M, Thiringer G, Brandstrom L (2005) Incidence of tinni-tus, impaired hearing and musculoskeletal disorders among students enroled in academic music education—a retrospective cohort study. Int Arch Occ Env Hea 78(7):575–583. https ://doi.org/10.1007/s0042 0-005-0621-y
Harman SE (1982) Occupational diseases of instrumental musicians, literature review. Md State Med J 31(6):39–42
Harman SE (1993) Odyssey: the history of performing arts medicine. Md Med J 42(3):251–253
Heredia L, Hinkamp D, Brodsky M, Llapur C (2014) Playing-related problems among musicians of the orquesta buena vista social club (r) and supporting bands. Med Probl Perform Artist 29(2):80–85
Hiner SL, Brandt KD, Katz BP, French RN, Beczkiewicz TJ (1987) Performance-related medical problems among premier violinists. Med Probl Perform Art 2(2):67–71
Hodapp V, Langendörfer F, Bongard S (2009) Arbeitsbedingungen, gesundheitliche Beschwerden und Aufführungsängste bei pro-fessionellen Orchestermusikern. Musikphysiologie und Musik-ermedizin 15(2):99–113
Hoppmann RA (1997) Ulnar nerve entrapment in a French horn player. Wien Klin Wochenschr 109(19):777–780
Hoppmann RA, Patrone NA (1989) A review of musculoskeletal problems in instrumental musicians. Semin Arthritis Rheum 19(2):117–126
Hudak PL, Amadio PC, Bombardier C (1996) Development of an upper extremity outcome measure: the DASH (disabilities of the arm, shoulder and hand) [corrected]. The Upper Extremity Collabo-rative Group (UECG). Am J Ind Med 29(6):602–608. https ://doi.org/10.1002/(sici)1097-0274(19960 6)29:6%3c602 :aid-ajim4 %3e3.0.co;2-l
Ioannou CI, Altenmüller E (2015) Approaches to and treatment strate-gies for playing-related pain problems among Czech instrumental music students. Med Probl Perform Artist 30(3):135–142
Jacukowicz A (2016) Psychosocial work aspects, stress and musculo-skeletal pain among musicians. A systematic review in search of correlates and predictors of playing-related pain. Work J Prev Assess Rehabil 54(3):657–668. https ://doi.org/10.3233/wor-16232 3
Jepsen JR (2014) Posterior interosseous neuropathy in the distal radial tunnel in a contrabassoon musician. Med Probl Perform Artist 29(1):23–26
Kaneko Y, Lianza S, Dawson WJ (2005) Pain as an incapacitating fac-tor in symphony orchestra musicians in São Paulo, Brazil. Med Probl Perform Artist 20(4):168–174
Kaufman-Cohen Y, Ratzon NZ (2011) Correlation between risk fac-tors and musculoskeletal disorders among classical musicians. Occup Med (Lond) 61(2):90–95. https ://doi.org/10.1093/occme d/kqq19 6
Kenny D, Ackermann B (2015) Performance-related musculoskel-etal pain, depression and music performance anxiety in profes-sional orchestral musicians: a population study. Psychol Music 43(1):43–60. https ://doi.org/10.1177/03057 35613 49395 3
International Archives of Occupational and Environmental Health
1 3
Kenny DT, Driscoll T, Ackermann BJ (2016) Is playing in the pit really the pits?: pain, strength, music performance anxiety, and workplace satisfaction in professional musicians in stage, pit, and combined stage/pit orchestras. Med Probl Perform Artist 31(1):1–7
Khalsa SBS, Cope S (2006) Effects of a yoga lifestyle intervention on performance-related characteristics of musicians: a preliminary study. Med Sci Monit 12(8):CR325–CR331
Khalsa SB, Shorter SM, Cope S, Wyshak G, Sklar E (2009) Yoga ameliorates performance anxiety and mood disturbance in young professional musicians. Appl Psychophysiol Biofeedback 34(4):279–289. https ://doi.org/10.1007/s1048 4-009-9103-4
Kim JY, Kim MS, Min SN, Cho YJ, Choi J (2012) Prevalence of play-ing-related musculoskeletal disorders in traditional Korean string instrument players. Med Probl Perform Art 27(4):212–218
Kochem FB, Silva JG (2017) Prevalence and associated factors of play-ing-related musculoskeletal disorders in Brazilian violin players. Med Probl Perform Artist 32(1):27–32
Kok LM, Vlieland TPMV, Fiocco M, Nelissen RGHH (2013) A com-parative study on the prevalence of musculoskeletal complaints among musicians and non-musicians. Bmc Musculoskelet 14(9):2. https ://doi.org/10.1186/1471-2474-14-9
Kok LM, Nelissen RGHH, Huisstede BMA (2015) Prevalence and consequences of arm, neck, and/or shoulder complaints among music academy students: a comparative study. Med Probl Per-form Artist 30(3):163–168
Kok LM, Huisstede BM, Voorn VM, Schoones JW, Nelissen RG (2016) The occurrence of musculoskeletal complaints among professional musicians: a systematic review. Int Arch Occ Env Hea 89(3):373–396
Kovero O, Könönen M (1995) Signs and symptoms of temporoman-dibular disorders and radiologically observed abnormalities in the condyles of the temporomandibular joints of professional violin and viola players. Acta Odontol Scand 53(2):81–84
Kreutz G, Ginsborg J, Williamon A (2008) Music students’ health problems and health-promoting behaviours. Med Probl Perform Artist 23(1):3–11
Kuorinka I, Jonsson B, Kilbom A, Vinterberg H, Biering-Sorensen F, Andersson G, Jorgensen K (1987) Standardised Nordic Ques-tionnaires for the analysis of musculoskeletal symptoms. Appl Ergon 18(3):233–237
Laha RK, Lunsford LD, Dujovny M (1978) Lacertus fibrosus compres-sion of the median nerve. J Neurosurg 48(5):838–841
Larsson L-G, Baum J, Mudholkar GS, Kollia GD (1993) Nature and impact of muscoloskeletal problems in a population of musi-cians. Med Probl Perform Artist 8:73–76
Leaver R, Harris EC, Palmer KT (2011) Musculoskeletal pain in elite professional musicians from British symphony orchestras. Occup Med (Lond) 61(8):549–555. https ://doi.org/10.1093/occme d/kqr12 9
Lederman RJ (1996) Long thoracic neuropathy in instrumental musi-cians: an often- unrecognized cause of shoulder pain. Med Probl Perform Artist 11(4):116–119
Lederman RJ (2003) Neuromuscular and musculoskeletal problems in instrumental musicians. Muscle Nerve 27(5):549–561. https ://doi.org/10.1002/mus.10380
Lee SH, Carey S, Dubey R, Matz R (2012) Intervention program in college instrumental musicians, with kinematics analysis of cello and flute playing: a combined program of yogic breathing and muscle strengthening-flexibility exercises. Med Probl Perform Art 27(2):85–94
Levee JR, Cohen MJ, Rickles WH (1976) Electromyographic biofeed-back for relief of tension in the facial and throat muscles of a woodwind musician. Biofeedb Self Regul 1(1):113–120
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, Ioan-nidis JP, Clarke M, Devereaux PJ, Kleijnen J, Moher D (2009)
The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med 6(7):e1000100. https ://doi.org/10.1371/journ al.pmed.10001 00
Lima RC, Magalhães Pinheiro TM, Dias EC, de Andrade EQ (2015) Development and prevention of work related disorders in a sample of Brazilian violinists. Work J Prev Assess Rehabil 51(2):273–280. https ://doi.org/10.3233/wor-14190 4
Logue EJ, Bluhm S, Johnson MC, Mazer R, Halle JS, Greathouse DG (2005) Median and ulnar neuropathies in university cellists. Med Probl Perform Artist 20(2):70–76
Lopez TM, Martinez JF (2013) Strategies to promote health and pre-vent musculoskeletal injuries in students from the high conserva-tory of music of Salamanca, Spain. Med Probl Perform Artists 28(2):100–106
Manal TJ, Hunter-Giordanoo AO, Fontenot M (2008) Performing Arts Special Interest Group Management of a music student with thoracic, shoulder, arm and hand pain. Orthop Phys Ther Pract 20(3):150–153
Manchester RA (1988) The incidence of hand problems in music stu-dents. Med Probl Perform Artist 3(1):15–18
Manchester R, Flieder D (1991) Further observations on the epide-miology of hand injuries in music students. Med Probl Perform Artist 6(1):11–14
Manchester RA, Lustik S (1989) The short-term outcome of hand prob-lems in music students. Med Probl Perform Artist 4(2):95–96
Manchester RA, Park S (1996) A case-control study of performance-related hand problems in music students. Med Probl Perform Artist 11(1):20–23
Marques DN, Rosset-Llobet J, Marques MFF, Gurgel IGD, Augusto LGS (2003) Flamenco guitar as a risk factor for overuse syn-drome. Med Probl Perform Artist 18(1):11–14
McFarland EG, Curl LA (1998) Shoulder problems in musicians. Md Med J 47:19–22
Mehrparvar AH, Mostaghaci M, Gerami RF (2012) Musculoskeletal disorders among Iranian instrumentalists. Med Probl Perform Artist 27(4):193–196
Middlestadt SE (1990) Medical problems of symphony orchestra musi-cians—from counting people with problems to evaluating inter-ventions. Revista Interamericana De Psicologia 24(2):159–172
Middlestadt SE, Fishbein M (1988) Health and occupational correlates of perceived occupational stress in symphony orchestra musi-cians. J Occup Med 30(9):687–692
Middlestadt SE, Fishbein M (1989) The prevalence of severe mus-culoskeletal problems among male and female symphony-orchestra string players. Med Probl Perform Artist 4(1):41–48
Milan KR (1996) Literature review of common injuries in the per-forming artist. Orthop Phys Ther Clin N Am 5(4):421–453
Miliam PB, Basse PN (2009) Anterior tarsal tunnel syndrome. [Danish] (Anterior tarsaltunnelsyndrom.). Ugeskrift for lae-ger 171(14):1194
Miller G, Peck F, Watson JS (2002) Pain disorders and variations in upper limb morphology in music students. Med Probl Perform Artist 17:169–172
Mishra W, De A, Gangopadhyay S, Chandra AM (2013) Playing-related musculoskeletal disorders among indian tabla players. Med Probl Perform Artist 28(2):107–111
Moher D, Liberati A, Tetzlaff J, Altman DG, Group P (2009) Pre-ferred reporting items for systematic reviews and meta-analy-ses: the PRISMA statement. PLoS Med 6(7):e1000097. https ://doi.org/10.1371/journ al.pmed.10000 97
Molsberger F (1991) Der Künstler als Patient. Wien Klin Wochen-schrift 103(8):236–241
Molsberger F, Molsberger A (2012) Acupuncture in treatment of musculoskeletal disorders of orchestra musicians. Work 41(1):5–13. https ://doi.org/10.3233/WOR-2012-1235
International Archives of Occupational and Environmental Health
1 3
Monaco E, Vicaro V, Catarinozzi E, Rossi M, Prestigiacomo C (2012) Patologie muscolo-scheletriche nei musicisti des “Tea-tro dell’Opera” di Roma. Giorno italiana di medicina del lavoro ed ergonomica 34(2):158–163
Moore M, DeHaan L, Ehrenberg T, Gross L, Magembe C (2008) Clini-cal assessment of shoulder impingement factors in violin and viola players. Med Probl Perform Artist 23:155–163
Moraes GFdS, Antunes AP (2012) Musculoskeletal disorders in professional violinists and violists. Systematic review. Acta Ortopedica Brasileira 20(1):43–47. https ://doi.org/10.1590/S1413 -78522 01200 01000 09
Navia Alvarez P, Arraez Aybar A, Alvarez Martinez P, Ardiaca Bur-gues L (2007) Incidence and risk factors for neck pain in Spanish orchestras musicians. Mapfre Med 18:27–35
Nelson SH (1989) Playing with the entire self: the Feldenkrais method and musicians. Semin Neurol 9(2):97–104. https ://doi.org/10.1055/s-2008-10413 10
(NHLBI) NHLaBI study quality assessment tools. https ://www.nhlbi .nih.gov/healt h-topic s/study -quali ty-asses sment -tools . Accessed 7 Dec 2017
Nolan WB, Eaton RG (1989) Thumb problems of professional musi-cians. Med Probl Perform Artist 4:20–22
Nusseck M, Mornell A, Voltmer E, Kötter T, Schmid B, Blum J, Türk-Espitalier A, Spahn C (2017) Gesundheit und Prävention-sverhalten von Musikstudierenden an verschiedenen deutschen Musikhochschulen. Fachzeitschrift Musikphysiologie und Musikermedizin 24(2):67–84
Nygaard Andersen L, Mann S, Juul-Kristensen B, SØgaard K (2017) Comparing the impact of specific strength training vs general fitness training on professional symphony orchestra musicians: a feasibility study. Med Probl Perform Artist 32(2):94–100. https ://doi.org/10.21091 /mppa.2017.2016
Nyman T, Wiktorin C, Mulder M, Johansson YL (2007) Work pos-tures and neck-shoulder pain among orchestra musicians. Am J Ind Med 50(5):370–376. https ://doi.org/10.1002/ajim.20454
Paarup HM, Baelum J, Holm JW, Manniche C, Wedderkopp N (2011) Prevalence and consequences of musculoskeletal symptoms in symphony orchestra musicians vary by gender: a cross-sectional study. BMC Musculoskelet Disord 12:223. https ://doi.org/10.1186/1471-2474-1112-1223, https ://doi.org/10.1186/1471-2474-12-223
Papandreou M, Vervainioti A (2010) Work-related musculoskeletal disorders among percussionists in Greece: a pilot study. Med Probl Perform Artist 25(3):116–119
Patrone NA, Hoppmann RA, Wahley J, Schmidt R (1989) Digital nerve compression in a violinist with benign hypermobility: a case study. Med Probl Perform Artist 4(2):91
Pedrazzini A, Martelli A, Tocco S (2015) Niccolo Paganini: the hands of a genius. Acta Bio Medica de l Ateneo Parmense 86(1):27–31
Piatkowska K, Wnuk B, Blicharska I, Rychlik M, Durmala J (2016) Cervical pain in young professional musicians—quality of life. Ortoped Traumatol Rehabil 18(1):21–29
Planas J (1982) Rupture of the orbicularis oris in trumpet players (Satchmo’s syndrome). Plast Reconstr Surg 69:690–693
Planas J (1988) Further experience with rupture of the orbicularis oris in trumpet players. Plast Reconstr Surg 81:975–977
Potter P, Jones IC (1993) Musculoskeletal symptoms associated with the great Highland bagpipe. Med Probl Perform Artist 8(3):81
Potter PJ, Jones IC (1995) Medical problems affecting musicians. Can Fam Physician 41:2121–2128
Price K, Watson AHD (2011) Postural problems of the left shoulder in an orchestral trombonist. Work 40(3):317–324. https ://doi.org/10.3233/WOR-2011-1238
Quarrier NF, Norris RN (2001) Adaptations for trombone performance: ergonomic interventions. Med Probl Perform Artist 16:77–80
Ramazzini B (1705) Of the diseases of musick masters, chaunters, and others of the like profession. In: Ramazzini B (ed) A treatise of the diseases of tradesmen. Andrew Bell, London, pp 221–225
Raymond DM 3rd, Romeo JH, Kumke KV (2012) A pilot study of occu-pational injury and illness experienced by classical musicians. Workplace Health Saf 60(1):19–24. https ://doi.org/10.3928/21650 799-20111 227-01
Rein S, Fabian T, Zwipp H, Heineck J, Weindel S (2010) The influence of profession on functional ankle stability in musicians. Med Probl Perform Artist 25:22–28
Revak JM (1989) Incidence of upper extremity discomfort among piano students. Am J Occup Ther 43(3):149–154
Rickert D, Barrett M, Halaki M, Driscoll T, Ackermann B (2012) A study of right shoulder injury in collegiate and professional orchestral cel-lists: an investigation using questionnaires and physical assessment. Med Probl Perform Artist 27(2):65–73
Rider MS (1987) Music therapy: therapy for debilitated musicians. Music Ther Perspect 4:40–43
Rodriguez-Lozano FJEA (2008) Bruxism related to violin playing. Med Probl Perform Artist 23(1):12–15
Rodríguez-Romero B, Pérez-Valiño C, Ageitos-Alonso B, Pértega-Díaz S (2016) Prevalence and associated factors for musculoskeletal pain and disability among Spanish music conservatory students. Med Probl Perform Artist 31(4):193–200. https ://doi.org/10.21091 /mppa.2016.4035
Sakai N (1992) Hand pain related to keyboard techniques in pianists. Med Probl Perform Artist 7(2):63–65
Sakai N (2002) Hand pain attributed to overuse among professional pianists—a study of 200 cases. Med Probl Perform Artist 17(4):178–180
Sakai N, Shimawaki S (2010) Measurement of a number of indices of hand and movement angles in pianists with overuse disorders. J Hand Surg Eur 35(6):494–498. https ://doi.org/10.1177/17531 93409 35240 5
Schäcke G, Kwiatkowski A, Wellstein F (1986) Muskel-Skelett-Beschw-erden bei Orchestermusikern. Fortschr Med 104(6):126–128
Shields N, Dockrell S (2000) The prevalence of injuries among pianists in music schools in Ireland. Med Probl Perform Artist 15(4):155–160
Singer K, Lakond W (1932) Diseases of the musical profession: a sys-tematic presentation of their causes, symptoms and methods of treatment. Greenberg, New York
SooHoo NF, McDonald AP, Seiler JG, McGillivary GR (2002) Evalua-tion of the construct validity of the DASH questionnaire by correla-tion to the SF-36. J Hand Surg Am 27(3):537–541
Sousa CM, Coimbra D, Machado J, Greten HJ (2015a) Effects of self-administered exercises based on Tuina techniques on musculoskel-etal disorders of professional orchestra musicians: a randomized controlled trial. J Integr Med 13(5):314–318
Sousa CM, Moreira L, Coimbra D, Machado J, Greten HJ (2015b) Immediate effects of Tuina techniques on working-related mus-culoskeletal disorder of professional orchestra musicians. J Integr Med 13(4):257–261
Sousa CM, Pereira Machado J, Johannes Greten H, Coimbra D (2016) Occupational diseases of professional orchestra musicians from Northern Portugal. Med Probl Perform Artist 31(1):8–12. https ://doi.org/10.21091 /mppa.2016.1002
Spahn C, Hildebrandt H, Seidenglanz K (2001) Effectiveness of a prophy-lactic course to prevent playing-related health problems of music students. Med Probl Perform Artist 16(1):24–31
Spahn C, Richter B, Altenmüller E (2011) Musikermedizin—eine Einfüh-rung. Musikermedizin: Diagnostik, Therapie und Prävention von musikerspezifischen Erkrankungen. Schattauer GmbH, Stuttgart, pp 1–5
Stanek JL, Komes KD, Murdock FA Jr (2017) A cross-sectional study of pain among U.S. college music students and faculty. Med
International Archives of Occupational and Environmental Health
1 3
Probl Perform Artists 32(1):20–26. https ://doi.org/10.21091 /mppa.2017.1005
Stanhope J, Milanese S, Grimmer K (2014) University woodwind students’ experiences with playing-related injuries and their management: a pilot study. J Pain Res 7:133–148. https ://doi.org/10.2147/JPR.S4962 0
Steinmetz A, Möller H (2007) Dysfunktionen des Bewegungssystems bei jungen Musikern. Musikphysiologie und Musikermedizin 14(1):12–16
Steinmetz A, Ridder PH, Reichelt A (2003) Craniomandibuläre Dys-funktionen als ein Einflussfaktor für die Entstehung von Über-lastungsbeschwerden bei Geigern. Musikphysiologie und Musik-ermedizin 10:203–209
Steinmetz A, Ridder PH, Reichelt A (2006) Craniomandibular dys-function and violin playing: Prevalence and theinfluence of oral splints on head and neck muscles in violinists. Med Probl Per-form Artist 21(4):183–189
Steinmetz A, Seidel W, Niemier K (2008) Shoulder pain and holding position of the violin—a case report. Med Probl Perform Artist 23:79–81
Steinmetz A, Ridder PH, Methfessel G, Muche B (2009) Professional musicians with craniomandibular dysfunctions treated with oral splints. Cranio 27(4):221–230. https ://doi.org/10.1179/crn.2009.033
Steinmetz A, Moller H, Seidel W, Rigotti T (2012) Playing-related mus-culoskeletal disorders in music students-associated musculoskeletal signs. Eur J Phys Rehabil Med 48(4):625–633
Steinmetz A, Zeh A, Delank KS, Peroz I (2014) Symptoms of cra-niomandibular dysfunction in professional orchestra musicians. Occup Med (Lond) 64:17–22. https ://doi.org/10.1093/occme d/kqt14 8
Steinmetz A, Scheffer I, Esmer E, Delank KS, Peroz I (2015) Fre-quency, severity and predictors of playing-related musculoskel-etal pain in professional orchestral musicians in Germany. Clin Rheumatol 34:965–973
Steinmetz A, Claus A, Hodges PW, Jull GA (2016) Neck muscle func-tion in violinists/violists with and without neck pain. Clin Rheu-matol 35:1045–1051
Takata K, Onuma K, Sukegawa K, Takaso M (2016) Osteochondritis dissecans of the fourth proximal interphalangeal joint in a Japanese drummer. Case Rep Plast Surg Hand Surg 3(1):83–85
Tubiana R, Chamagne P (1993) Occupational arm ailments in musicians. Bull Acad Natl Med 177(2):203–212 (discussion 206–212)
Vervainioti A, Alexopoulos EC (2015) Job-related stressors of classical instrumental musicians a systematic qualitative review. Med Probl Perform Artist 30(4):197–202
Vinci S, Smith A, Ranelli S (2015) Selected physical characteristics and playing-related musculoskeletal problems in adolescent string instrumentalists. Med Probl Perform Artist 30(3):143–151
Wahlström Edling C, Fjellman-Wiklund A (2009) Musculoskeletal Dis-orders and asymmetric playing postures of the upper extremity
and back in music teachers: a pilot study. Med Probl Perform Artist 24:113–118
Wilk I, Kurpas D, Andrzejewski W, Okreglicka-Forysiak E, Gworys B, Kassolik K (2016) The application of tensegrity massage in a professionally active musician—case report. Rehabil Nurs J 41(3):179–192
Williamon A, Thompson S (2006) Awareness and incidence of health problems among conservatoire students. Psychol Music 34(4):411–430
Wilson JS (1989) A dental appliance for a clarinettist experiencing tem-poromandibular-joint pain. Med Probl Perform Artist 4(3):118–121
Woldendorp KH, Boonstra AM, Tijsma A, Arendzen JH, Reneman MF (2016) No association between posture and musculoskeletal com-plaints in a professional bassist sample. Eur J Pain 20(3):399–407. https ://doi.org/10.1002/ejp.740
Woldendorp KH, Boonstra AM, Arendzen JH, Reneman MF (2017) Variation in occupational exposure associated with musculoskeletal complaints: a cross-sectional study among professional bassists. Int Arch Occup Environ Health 91:215–223
Wu SJ (2007) Occupational risk factors for musculoskeletal disorders in musicians: a systematic review. Med Probl Perform Artist 22(2):43–51
Yasuda E, Honda K, Hasegawa Y, Matsumura E, Fujiwara M, Hasegawa M, Kishimoto H (2016) Prevalence of temporomandibular disor-ders among junior high school students who play wind instruments. Int J Occup Med Environ Health 29(1):69–76
Yeung E, Chang W, Pan F, Sau P, Tsui M, Yu B, Zaza C (1999) A survey of playing-related musculoskeletal problems among pro-fessional orchestral musicians in Hong Kong. Med Probl Perform Artist 14:43–47
Yoshimura E, Paul PM, Aerts C, Chesky K (2006) Risk factors for piano-related pain among college students. Med Probl Perform Artist 21:118–125
Zaza C (1998) Playing-related musculoskeletal disorders in musi-cians: a systematic review of incidence and prevalence. CMAJ 158(8):1019–1025
Zaza C, Farewell VT (1997) Musicians’ playing-related musculoskel-etal disorders: an examination of risk factors. Am J Ind Med 32(3):292–300
Zetterberg C, Backlund H, Karkson J, Werner H, Olsson L (1998) Mus-culoskeletal problems among male and female music students. Med Probl Perform Artist 13(4):160–166
Zuskin E, Schachter EN, Kolcic I, Polasek O, Mustajbegovic J, Aru-mugam U (2005) Health problems in musicians—a review. Acta Dermatovenerol Croat 13(4):247–251
Publisher’s Note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.




















