
A stage of change approach to reducing occupational ill health
7
A stage of change approach to reducing occupational ill health Z. Whysall ⁎ , C. Haslam, R. Haslam Health and Safety Ergonomics Unit, Department of Human Sciences, Loughborough University, Loughborough, Leicestershire, LE11 3TU, UK Available online 14 August 2006 Abstract Objective. Interventions targeted by stage of change have been shown to improve the efficacy of public health promotion initiatives in areas such as smoking cessation, alcohol reduction, and mammography screening. Targeted interventions are designed to tackle the key attitudes, beliefs, and intentions that underpin an individual's health-related behavior. Work-related ill health is an increasingly serious issue, the most common cause of which in both the UK and the US is musculoskeletal disorders. This study examined whether the stage approach could be applied to workplace interventions aimed at improving occupational health. Method. A total of 24 multi-component occupational interventions aimed at reducing musculoskeletal disorders were monitored over a period of 4–6 months. In half of these cases, approaches were targeted according to workers' stage of change. Results. Targeted interventions were found to be significantly more effective in promoting risk awareness and desired behavior change among workers. Significant reductions were also found in self-reported musculoskeletal discomfort among workers having received targeted interventions. No significant differences were found in self-reported musculoskeletal discomfort among workers following standard interventions. Conclusion. Stage-matched approaches may offer scope for substantially improving the efficacy of occupational health and safety interventions by increasing the uptake, implementation, and maintenance of risk-reducing measures. © 2006 Elsevier Inc. All rights reserved. Keywords: Occupational health; Workplace interventions; Stages of change; Behavior change; Musculoskeletal disorders Introduction Musculoskeletal disorders (MSDs) are the most common form of occupational ill health, leading to 11.8 million lost working days a year in the UK, accounting for 30–60% of absenteeism costs (HSC, 2004). MSDs accounted for 34% of injuries and illnesses in the U.S. involving days away from work in 2002 (BLS, 2004), although this may be an underestimate (Silverstein et al., 1998). While WHO (1988) and HSE (2002) recommended that interventions combine ergonomics improvements with activities aimed at modifying workers' behavior, in practice, interventions focus on the physical aspects of work (Whysall et al., 2004). The Stage of Change Model (Prochaska and DiClemente, 1982) may offer a way to improve interventions (Dejoy, 1996; Haslam and Haslam, 2000; Prochaska et al., 2001). Used with behaviors such as drinking, smoking, and exercise, the model assumes that behavior change involves movement through stages: (i) precontemplation (resistance to recognizing or modifying problem behavior), (ii) contemplation (thinking about changing, but not ready to act), (iii) preparation (intending to change in the next 30 days and/or having made plans to do so), (iv) action (changed behavior, no longer than 6 months ago), and (v) maintenance (changed over 6 months ago, working to consolidate gains made and avoid relapse). Stage determines receptiveness to (and the effec- tiveness of) health education. Individuals in the precontem- plative stage require information about the health risk associated with their current behavior while those in later stages need practical advice on how to change. Stage-matched interventions increase the likelihood that individuals will quit smoking, reduce alcohol intake, or attend mammography screening (e.g. Prochaska et al., 1993; Rakowski et al., 1998). Attempts to apply the model to occupational health are limited. Urlings et al. (1990) explored the feasibility of adopting the approach to promote standing aids in the Dutch furniture industry but did not evaluate the implementation. Whysall et al. (in press) developed a tool for assessing worker stage of change, found to have high levels of reliability. This Preventive Medicine 43 (2006) 422 – 428 www.elsevier.com/locate/ypmed ⁎ Corresponding author. Fax: +44 1509 223940. E-mail address: [email protected] (Z. Whysall). 0091-7435/$ - see front matter © 2006 Elsevier Inc. All rights reserved. doi:10.1016/j.ypmed.2006.07.004
-
Upload
nottinghamtrent -
Category
Documents
-
view
0 -
download
0
Transcript of A stage of change approach to reducing occupational ill health
(2006) 422–428www.elsevier.com/locate/ypmed
Preventive Medicine 43
A stage of change approach to reducing occupational ill health
Z. Whysall ⁎, C. Haslam, R. Haslam
Health and Safety Ergonomics Unit, Department of Human Sciences, Loughborough University, Loughborough, Leicestershire, LE11 3TU, UK
Available online 14 August 2006
Abstract
Objective. Interventions targeted by stage of change have been shown to improve the efficacy of public health promotion initiatives in areassuch as smoking cessation, alcohol reduction, and mammography screening. Targeted interventions are designed to tackle the key attitudes,beliefs, and intentions that underpin an individual's health-related behavior. Work-related ill health is an increasingly serious issue, the mostcommon cause of which in both the UK and the US is musculoskeletal disorders. This study examined whether the stage approach could beapplied to workplace interventions aimed at improving occupational health.
Method. A total of 24 multi-component occupational interventions aimed at reducing musculoskeletal disorders were monitored over a periodof 4–6 months. In half of these cases, approaches were targeted according to workers' stage of change.
Results. Targeted interventions were found to be significantly more effective in promoting risk awareness and desired behavior change amongworkers. Significant reductions were also found in self-reported musculoskeletal discomfort among workers having received targetedinterventions. No significant differences were found in self-reported musculoskeletal discomfort among workers following standard interventions.
Conclusion. Stage-matched approaches may offer scope for substantially improving the efficacy of occupational health and safetyinterventions by increasing the uptake, implementation, and maintenance of risk-reducing measures.© 2006 Elsevier Inc. All rights reserved.
Keywords: Occupational health; Workplace interventions; Stages of change; Behavior change; Musculoskeletal disorders
Introduction
Musculoskeletal disorders (MSDs) are the most commonform of occupational ill health, leading to 11.8 million lostworking days a year in the UK, accounting for 30–60% ofabsenteeism costs (HSC, 2004). MSDs accounted for 34% ofinjuries and illnesses in the U.S. involving days away fromwork in 2002 (BLS, 2004), although this may be anunderestimate (Silverstein et al., 1998). While WHO (1988)and HSE (2002) recommended that interventions combineergonomics improvements with activities aimed at modifyingworkers' behavior, in practice, interventions focus on thephysical aspects of work (Whysall et al., 2004).
The Stage of Change Model (Prochaska and DiClemente,1982) may offer a way to improve interventions (Dejoy,1996; Haslam and Haslam, 2000; Prochaska et al., 2001).Used with behaviors such as drinking, smoking, and exercise,the model assumes that behavior change involves movement
⁎ Corresponding author. Fax: +44 1509 223940.E-mail address: [email protected] (Z. Whysall).
0091-7435/$ - see front matter © 2006 Elsevier Inc. All rights reserved.doi:10.1016/j.ypmed.2006.07.004
through stages: (i) precontemplation (resistance to recognizingor modifying problem behavior), (ii) contemplation (thinkingabout changing, but not ready to act), (iii) preparation(intending to change in the next 30 days and/or havingmade plans to do so), (iv) action (changed behavior, no longerthan 6 months ago), and (v) maintenance (changed over6 months ago, working to consolidate gains made and avoidrelapse). Stage determines receptiveness to (and the effec-tiveness of) health education. Individuals in the precontem-plative stage require information about the health riskassociated with their current behavior while those in laterstages need practical advice on how to change. Stage-matchedinterventions increase the likelihood that individuals will quitsmoking, reduce alcohol intake, or attend mammographyscreening (e.g. Prochaska et al., 1993; Rakowski et al., 1998).Attempts to apply the model to occupational health arelimited. Urlings et al. (1990) explored the feasibility ofadopting the approach to promote standing aids in the Dutchfurniture industry but did not evaluate the implementation.Whysall et al. (in press) developed a tool for assessing workerstage of change, found to have high levels of reliability. This

423Z. Whysall et al. / Preventive Medicine 43 (2006) 422–428
study used the tool to determine if interventions targeted bystage of change are more effective in reducing MSDs thanstandard approaches.
Method
Sample
Recruitment was achieved through a press release from the UniversityPublicityOffice, inviting organizations intending to tackleMSDs to participate inthe study. If they met the basic criteria (i.e. organizations within high-riskindustries for MSDs), respondents were selected on a first come first serve basis.A number of interventions within different departments of the same organizationwere recruited, providing comparable cases, and 16 different organizations wereinvolved. A questionnaire was administered to all workers involved in theinterventions, where feasible. In large organizations where interventions wereintroduced organization-wide, the questionnaire was administered to a sample ofthe workforce, determined by the access given by the employer. No employees
Table 1Intervention details
Tailored/standard Intervention details
1 Standard Monthly safety ‘toolbox talks’, health screening for new stamonthly safety improvement team meetings (employee reprereporting system, improved staff facilities (canteen, showersmanual handling of damaged stock).
2 Tailored Job rotation, introduction of powered wire cutters, tool bintroduction of ergonomics issues board on shopfloor (proviactions).
3 Standard Extensive changes to remove the most physically arduous asperiods, management training in health and safety, imprmanagement commitment to implementing actions required
4 Tailored Production process altered to enable tasks to be undertakenassessment procedure (incorporating MSD risks), accident re
5 Standard Interactive, individual web-based training package available fareas for risks, and the types of changes that should be impl
6 Tailored As above.7 Standard Risk assessments, manual handling training for all workers,
height, placement of equipment, chairs adjusted for each indivreorganization of storage areas for improved accessibility, au
8 Tailored Health and safety focus groups with employees, introduction oredesign of sorting frames, redesign of sack frames to preve
9 Standard Risk assessments of all workstations, new curved, adjustable dand foot rests where desired.
10 Tailored Health and safety focus groups with employees, introduction oredesign of sorting frames, risk assessments of delivery rout
11 Standard As above.12 Tailored Introduction of self-service terminal and drop boxes to reduce
trolleys to improve maneuverability, reorganization of equipidentify problems.
13 Standard Moving and handling training, reorganization of storage, ass14 Tailored Installation of automatic doors, replacement of delivery trolle
to back up to loading bay, enforcement of mail bag weight l15 Standard All work areas assessed for MSD risks using a package to c
performing the tasks, rotation of tasks based on recommenda16 Tailored Training in manual handling, health screening, improved sto17 Standard Reduction of baggage weights permitted.18 Tailored Training in manual handling, health screening, improved sto19 Standard Reduction of baggage weights permitted, training in manual20 Tailored Reduction of baggage weights permitted.21 Standard Training in moving and handling, reorganization of storage22 Tailored Training regarding the potential effects of MSDs and work-r23 Standard Training in manual handling, health screening, improved sto24 Standard Moving and handling training, reorganization of storage area
declined participation, resulting in a total of 384workers pre-implementation and304 post-implementation.
Procedure
Twenty-four interventions were monitored within a variety of organiza-tions and industry sectors. Interventions varied, consisting of multiplecomponents, including redesign of the workplace or work processes, theintroduction of new tools (e.g. assistive lifting devices, ergonomic tools),job rotation, manual handling training, health monitoring, and theimplementation of safety improvement teams (see Table 1). Questionnaireswere distributed to workers prior to and 4–6 months following theimplementation of interventions. Interventions were allocated to either the‘stage-matched’ or ‘standard’ condition alternately, in the order that theywere recruited, to avoid biasing selection. Where interventions wereimplemented in different departments of the same organization, comparablecases were allocated to the standard and stage-matched conditions. Elevenwere targeted interventions, and 13 were ‘standard’ interventions. A slightlylarger proportion of standard interventions resulted, due to inability to tailor
ff, health and safety inductions, return to work interviews following absence,sentatives and management), reduction in shift length, introduction of near miss, staff room), resurfacing of yard, stock rotation system (reducing the need for
alancer, low impact hammers, advice regarding improved working postures,ding information on MSDs symptoms, minutes from safety meetings, intended
pects of production, increased availability of equipment (e.g. FLTs), longer restoved risk-assessment procedure (emphasis on identifying risks for MSDs),by risk assessments.at operative's own pace, raised stacking table, health screening, improved risk-porting system, workshop for senior managers on the risks of MSDs.or employees' ongoing use, educating employees about how to assess their ownemented to help to reduce the risks.
foot and wrist rests provided where desired, workstation adjustments (e.g. tableidual and labeled), trolley for transporting mail sacks, space under desks cleared,tomatic staplers, job rotation, blinds replaced to reduce glare.f ergonomically designed trolleys to remove weight of delivery from the person,nt overfilling, risk assessments of delivery routes.esks, monitor risers, new adjustable chairs, reorganization of workstations, wrist
f ergonomically designed trolleys to remove weight of delivery from the person,es, and consequent reorganization of routes.
handling of books by staff at issue desk, foot rests where desired, maintenance ofment storage to ease access, refresher training in manual handling and how to
istive lifting devices, job rotation.y with motorized vehicle, removal of obstacles in delivery area enabling vehiclesimits around the organization.alculate scores for MSD risk for each task based on video footage of workerstions generated, ergonomic redesign of production line, light weight tools.rage of products on vehicles, mobile ramps to facilitate delivery.
rage of products on vehicles, mobile ramps to facilitate delivery.handling, return to work interviews following absence, health screening.
areas, assistive lifting devices, adjustable wheeled stool for teachers.elated risks of MSDs.rage of products on vehicles, mobile ramps to facilitate delivery.s, assistive lifting devices, job rotation, adjustable wheeled stool for teachers.

424 Z. Whysall et al. / Preventive Medicine 43 (2006) 422–428
one case, owing to a narrow time window between being granted accessand implementation.
Employee stage was determined using a standard staging algorithmbased on their responses in the stage of change tool. A stage of changeprofile was generated for each workforce, and tailored interventions weretargeted according to the stage within which the majority of employeesresided. Support for this approach is provided by evidence that stage profiletends to be relatively homogeneous within an organization, while differingsignificantly between organizations (Whysall et al., in press). With each ofthe interventions that were to be tailored, feedback was provided regardingthe specific advice and information relevant to the stage of change of theworkers within each of these organizations. Leaflets and PowerPointpresentations containing this information were provided to organizations tofacilitate the communication of these messages. Following this advice, stage-matched information was provided to employees (in the form of leaflets andCD-ROMs). A standard framework was used for targeting information tostage (Velicer et al., 1998; Ferguson and Chandler, 2005) and is summarizedin Table 2. Where workers were in the precontemplative stage, emphasiswas placed on the use of strong messages about the detrimental effects ofMSDs while workers in preparation received practical advice and skillstraining. In standard interventions, organizations carried out their interven-tions as they planned. As pre- and post-intervention surveys were carried outin both conditions, workers in both two conditions received the sameamount of contact with researchers. Details of case studies are shown inTable 3.
Research instruments
The questionnaire comprised of 3 sections: demographic characteristics andbackground information, stage of change, and musculoskeletal pain/discomfort.A tool shown to have high levels of reliability in assessing stage of change inrelation to MSDs (Whysall et al., in press) was used. This tool is based upon the
Table 2Stage-matched approaches
Key beliefs Key messages to convey
1. Precontemplation (not considering changing)No need to change—MSDs notconsidered a significant risk
Raising awareness of risks, risk severitypotential detrimental effects on health a
2. Contemplation (thinking about changing)Risks acknowledged—contemplatingneed to make changes
Highlight the efficacy of interventions acan be gained from taking action (e.g. rinjury prevention)
3. Preparation (strong intention to change)Intention to make changes in near futureand/or concrete plans for thespecific steps to be taken
Types of changes that can be effective iFor managers—most effective approach(e.g. value of taking a systems approach
4. Action (actually engaged in changing behavior)Engaged in change efforts Ongoing advice and support
Skills trainingPerformance feedback
5. Maintenance (working to prevent relapse or consolidate gains made)Working to consolidate and maintainthe changes/improvements
Emphasize need for continual efforts toContinually changing risksNeed for ongoing vigilance
traditional method of assessing of stage (DiClemente et al., 1991). Question itemsare shown in Table 4.
Musculoskeletal discomfort was measured using a body map and discomfortintensity ratings (Corlett, 1995; Corlett and Bishop, 1976). Workers were askedwhether they had experienced pain/discomfort in the previous 7 days and toidentify the area/s in which pain was experienced. Participants were asked to ratethe discomfort severity for each body area identified on a scale of 1–7 (1—minimal discomfort, 7—extreme discomfort). A 7-day period was selected aslonger reporting periods introduce recall bias (Marshall et al., 1995).
Analysis
Descriptive statistics were used to identify the distribution of stage of changeand workers' reported pain/discomfort. Chi-square tests were used to identifysignificant differences in stage of change before and after the implementation,and Wilcoxon signed ranks tests to identify significant differences in pain/discomfort ratings.
Results: standard interventions
Prior to the implementation of interventions, the mean age ofworkers in the standard condition (N=187) was 39 years (SD11.5 years) and the mean number of hours worked per week was34 (SD 13.4 h). Following implementation, the mean age in thestandard condition (N=162) was 40 years (SD 10.9 years) andthe mean number of hours worked per week was 38 (SD 8.8 h).Examination of the baseline data for missing respondentsrevealed that they were not significantly different from the restof the sample (mean age 39 years, SD 11.9 years; mean number
Materials/approaches
, susceptibility,nd lifestyle
Graphic informationProbability of illness/injurySignificance of injury/illnessCase studies of sufferers
nd the benefits thateduced fatigue,
Information regarding the benefits of changeCase studies/statistics documenting success cases(e.g. reduced absence, improved morale)
n reducing MSDs Practical advice on range of approacheses to implementation, worker participation)
Skills trainingReduction of barriers to implementation of changesDevelopment of specific and realistic plans of action
ParticipationFeedbackAssistance with tools/equipment
prevent relapse Reinforcement of need to assess and maintainlow levels of riskOngoing relationship with advisorsEstablishment of systems for ongoingmonitoring and evaluation
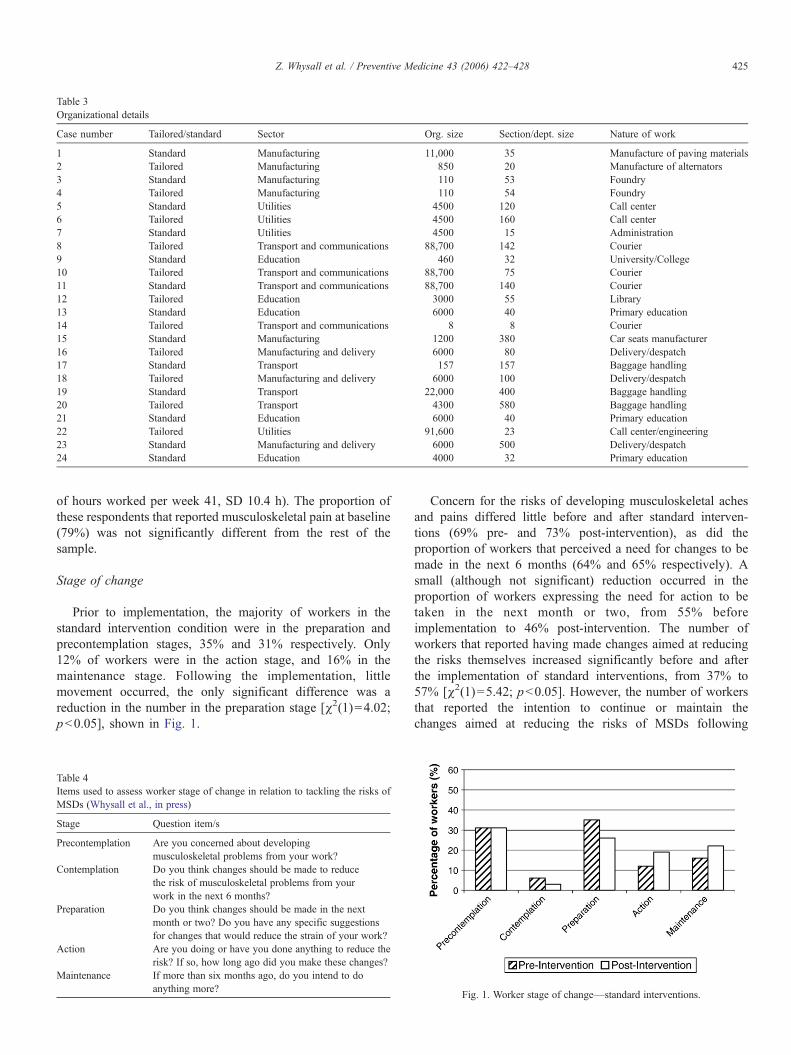
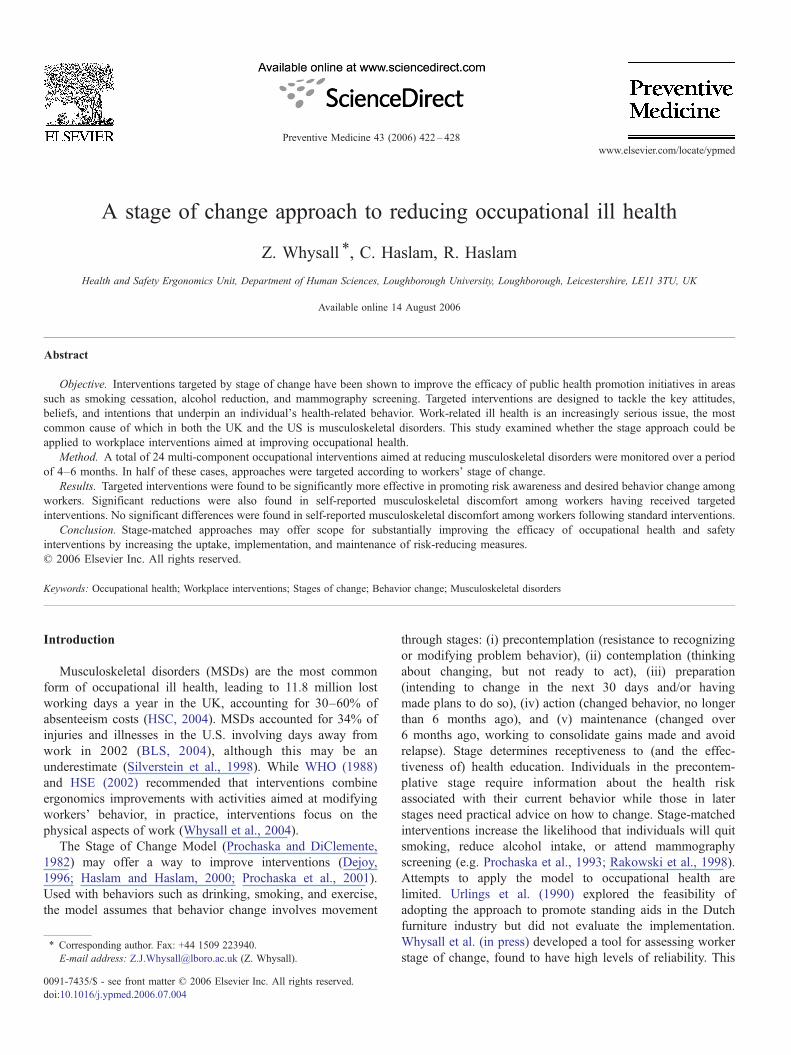
Table 3Organizational details
Case number Tailored/standard Sector Org. size Section/dept. size Nature of work
1 Standard Manufacturing 11,000 35 Manufacture of paving materials2 Tailored Manufacturing 850 20 Manufacture of alternators3 Standard Manufacturing 110 53 Foundry4 Tailored Manufacturing 110 54 Foundry5 Standard Utilities 4500 120 Call center6 Tailored Utilities 4500 160 Call center7 Standard Utilities 4500 15 Administration8 Tailored Transport and communications 88,700 142 Courier9 Standard Education 460 32 University/College10 Tailored Transport and communications 88,700 75 Courier11 Standard Transport and communications 88,700 140 Courier12 Tailored Education 3000 55 Library13 Standard Education 6000 40 Primary education14 Tailored Transport and communications 8 8 Courier15 Standard Manufacturing 1200 380 Car seats manufacturer16 Tailored Manufacturing and delivery 6000 80 Delivery/despatch17 Standard Transport 157 157 Baggage handling18 Tailored Manufacturing and delivery 6000 100 Delivery/despatch19 Standard Transport 22,000 400 Baggage handling20 Tailored Transport 4300 580 Baggage handling21 Standard Education 6000 40 Primary education22 Tailored Utilities 91,600 23 Call center/engineering23 Standard Manufacturing and delivery 6000 500 Delivery/despatch24 Standard Education 4000 32 Primary education
425Z. Whysall et al. / Preventive Medicine 43 (2006) 422–428
of hours worked per week 41, SD 10.4 h). The proportion ofthese respondents that reported musculoskeletal pain at baseline(79%) was not significantly different from the rest of thesample.
Stage of change
Prior to implementation, the majority of workers in thestandard intervention condition were in the preparation andprecontemplation stages, 35% and 31% respectively. Only12% of workers were in the action stage, and 16% in themaintenance stage. Following the implementation, littlemovement occurred, the only significant difference was areduction in the number in the preparation stage [χ2(1)=4.02;p<0.05], shown in Fig. 1.
Table 4Items used to assess worker stage of change in relation to tackling the risks ofMSDs (Whysall et al., in press)
Stage Question item/s
Precontemplation Are you concerned about developingmusculoskeletal problems from your work?
Contemplation Do you think changes should be made to reducethe risk of musculoskeletal problems from yourwork in the next 6 months?
Preparation Do you think changes should be made in the nextmonth or two? Do you have any specific suggestionsfor changes that would reduce the strain of your work?
Action Are you doing or have you done anything to reduce therisk? If so, how long ago did you make these changes?
Maintenance If more than six months ago, do you intend to doanything more?
Concern for the risks of developing musculoskeletal achesand pains differed little before and after standard interven-tions (69% pre- and 73% post-intervention), as did theproportion of workers that perceived a need for changes to bemade in the next 6 months (64% and 65% respectively). Asmall (although not significant) reduction occurred in theproportion of workers expressing the need for action to betaken in the next month or two, from 55% beforeimplementation to 46% post-intervention. The number ofworkers that reported having made changes aimed at reducingthe risks themselves increased significantly before and afterthe implementation of standard interventions, from 37% to57% [χ2(1)=5.42; p<0.05]. However, the number of workersthat reported the intention to continue or maintain thechanges aimed at reducing the risks of MSDs following
Fig. 1. Worker stage of change—standard interventions.
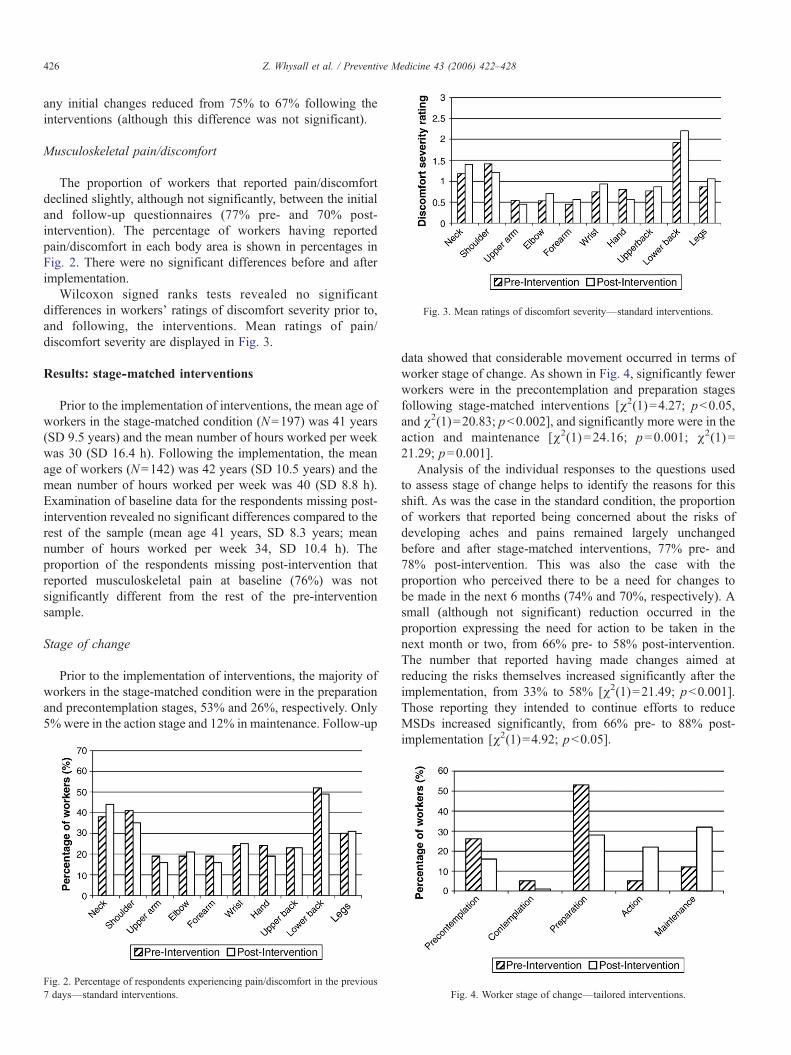
Fig. 3. Mean ratings of discomfort severity—standard interventions.
426 Z. Whysall et al. / Preventive Medicine 43 (2006) 422–428
any initial changes reduced from 75% to 67% following theinterventions (although this difference was not significant).
Musculoskeletal pain/discomfort
The proportion of workers that reported pain/discomfortdeclined slightly, although not significantly, between the initialand follow-up questionnaires (77% pre- and 70% post-intervention). The percentage of workers having reportedpain/discomfort in each body area is shown in percentages inFig. 2. There were no significant differences before and afterimplementation.
Wilcoxon signed ranks tests revealed no significantdifferences in workers' ratings of discomfort severity prior to,and following, the interventions. Mean ratings of pain/discomfort severity are displayed in Fig. 3.
Results: stage-matched interventions
Prior to the implementation of interventions, the mean age ofworkers in the stage-matched condition (N=197) was 41 years(SD 9.5 years) and the mean number of hours worked per weekwas 30 (SD 16.4 h). Following the implementation, the meanage of workers (N=142) was 42 years (SD 10.5 years) and themean number of hours worked per week was 40 (SD 8.8 h).Examination of baseline data for the respondents missing post-intervention revealed no significant differences compared to therest of the sample (mean age 41 years, SD 8.3 years; meannumber of hours worked per week 34, SD 10.4 h). Theproportion of the respondents missing post-intervention thatreported musculoskeletal pain at baseline (76%) was notsignificantly different from the rest of the pre-interventionsample.
Stage of change
Prior to the implementation of interventions, the majority ofworkers in the stage-matched condition were in the preparationand precontemplation stages, 53% and 26%, respectively. Only5% were in the action stage and 12% in maintenance. Follow-up
Fig. 2. Percentage of respondents experiencing pain/discomfort in the previous7 days—standard interventions.
data showed that considerable movement occurred in terms ofworker stage of change. As shown in Fig. 4, significantly fewerworkers were in the precontemplation and preparation stagesfollowing stage-matched interventions [χ2(1)=4.27; p<0.05,and χ2(1)=20.83; p<0.002], and significantly more were in theaction and maintenance [χ2(1)=24.16; p=0.001; χ2(1)=21.29; p=0.001].
Analysis of the individual responses to the questions usedto assess stage of change helps to identify the reasons for thisshift. As was the case in the standard condition, the proportionof workers that reported being concerned about the risks ofdeveloping aches and pains remained largely unchangedbefore and after stage-matched interventions, 77% pre- and78% post-intervention. This was also the case with theproportion who perceived there to be a need for changes tobe made in the next 6 months (74% and 70%, respectively). Asmall (although not significant) reduction occurred in theproportion expressing the need for action to be taken in thenext month or two, from 66% pre- to 58% post-intervention.The number that reported having made changes aimed atreducing the risks themselves increased significantly after theimplementation, from 33% to 58% [χ2(1)=21.49; p<0.001].Those reporting they intended to continue efforts to reduceMSDs increased significantly, from 66% pre- to 88% post-implementation [χ2(1)=4.92; p<0.05].
Fig. 4. Worker stage of change—tailored interventions.
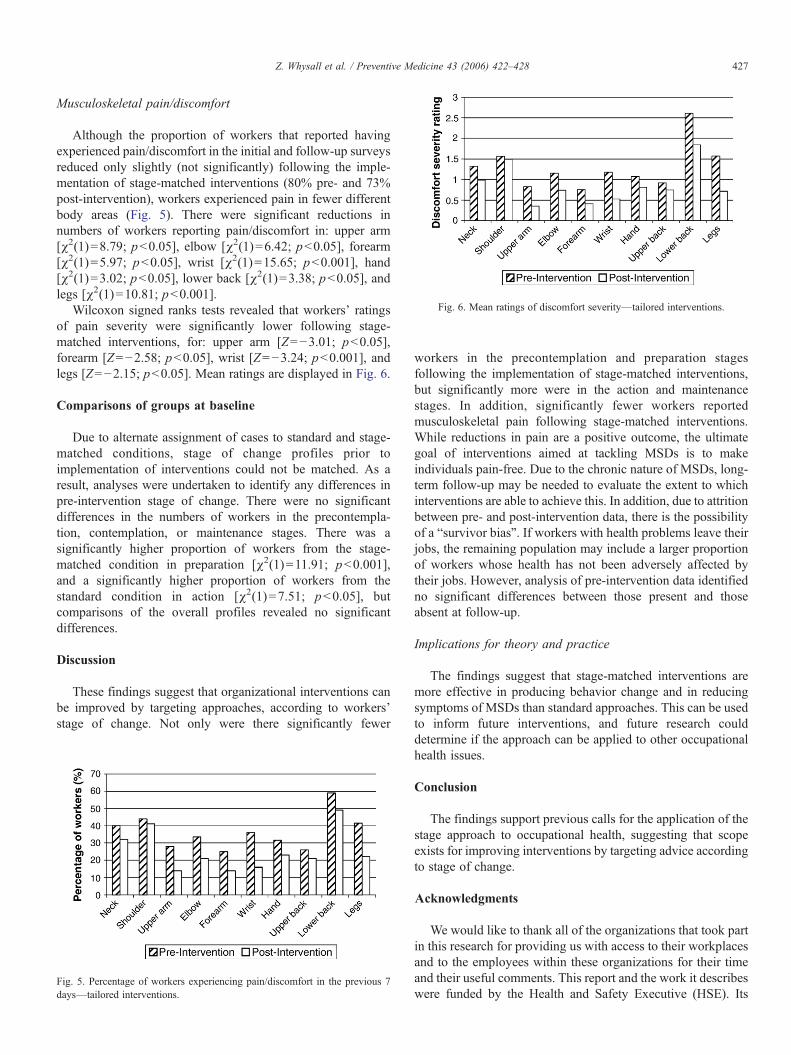
Fig. 6. Mean ratings of discomfort severity—tailored interventions.
427Z. Whysall et al. / Preventive Medicine 43 (2006) 422–428
Musculoskeletal pain/discomfort
Although the proportion of workers that reported havingexperienced pain/discomfort in the initial and follow-up surveysreduced only slightly (not significantly) following the imple-mentation of stage-matched interventions (80% pre- and 73%post-intervention), workers experienced pain in fewer differentbody areas (Fig. 5). There were significant reductions innumbers of workers reporting pain/discomfort in: upper arm[χ2(1)=8.79; p<0.05], elbow [χ2(1)=6.42; p<0.05], forearm[χ2(1)=5.97; p<0.05], wrist [χ2(1)=15.65; p<0.001], hand[χ2(1)=3.02; p<0.05], lower back [χ2(1)=3.38; p<0.05], andlegs [χ2(1)=10.81; p<0.001].
Wilcoxon signed ranks tests revealed that workers' ratingsof pain severity were significantly lower following stage-matched interventions, for: upper arm [Z=−3.01; p<0.05],forearm [Z=−2.58; p<0.05], wrist [Z=−3.24; p<0.001], andlegs [Z=−2.15; p<0.05]. Mean ratings are displayed in Fig. 6.
Comparisons of groups at baseline
Due to alternate assignment of cases to standard and stage-matched conditions, stage of change profiles prior toimplementation of interventions could not be matched. As aresult, analyses were undertaken to identify any differences inpre-intervention stage of change. There were no significantdifferences in the numbers of workers in the precontempla-tion, contemplation, or maintenance stages. There was asignificantly higher proportion of workers from the stage-matched condition in preparation [χ2(1)=11.91; p<0.001],and a significantly higher proportion of workers from thestandard condition in action [χ2(1)=7.51; p<0.05], butcomparisons of the overall profiles revealed no significantdifferences.
Discussion
These findings suggest that organizational interventions canbe improved by targeting approaches, according to workers'stage of change. Not only were there significantly fewer
Fig. 5. Percentage of workers experiencing pain/discomfort in the previous 7days—tailored interventions.
workers in the precontemplation and preparation stagesfollowing the implementation of stage-matched interventions,but significantly more were in the action and maintenancestages. In addition, significantly fewer workers reportedmusculoskeletal pain following stage-matched interventions.While reductions in pain are a positive outcome, the ultimategoal of interventions aimed at tackling MSDs is to makeindividuals pain-free. Due to the chronic nature of MSDs, long-term follow-up may be needed to evaluate the extent to whichinterventions are able to achieve this. In addition, due to attritionbetween pre- and post-intervention data, there is the possibilityof a “survivor bias”. If workers with health problems leave theirjobs, the remaining population may include a larger proportionof workers whose health has not been adversely affected bytheir jobs. However, analysis of pre-intervention data identifiedno significant differences between those present and thoseabsent at follow-up.
Implications for theory and practice
The findings suggest that stage-matched interventions aremore effective in producing behavior change and in reducingsymptoms of MSDs than standard approaches. This can be usedto inform future interventions, and future research coulddetermine if the approach can be applied to other occupationalhealth issues.
Conclusion
The findings support previous calls for the application of thestage approach to occupational health, suggesting that scopeexists for improving interventions by targeting advice accordingto stage of change.
Acknowledgments
We would like to thank all of the organizations that took partin this research for providing us with access to their workplacesand to the employees within these organizations for their timeand their useful comments. This report and the work it describeswere funded by the Health and Safety Executive (HSE). Its

428 Z. Whysall et al. / Preventive Medicine 43 (2006) 422–428
contents, including any opinions and/or conclusions expressed,are those of the authors alone and do not necessarily reflect HSEpolicy.
References
Bureau of Labor Statistics, 2004. Lost-worktime injuries and illnesses:characteristics and resulting days away from work, 2002. US Departmentof Labor, Washington, DC.
Corlett, E.N., 1995. The evaluation of posture and its effects, In: Wilson, J.R.,Corlett, E.N. (Eds.), Evaluation of HumanWork, 2nd ed. Taylor and Francis,London, pp. 662–713.
Corlett, E.N., Bishop, R.P., 1976. A technique for measuring posturaldiscomfort. Ergonomics 9, 175–182.
Dejoy, D.M., 1996. Theoretical models of health behavior and workplace self-protective behavior. J. Saf. Res. 27, 61–72.
DiClemente, C.C., Prochaska, J.O., Fairhurst, S.K., Velicier, W.F., Velasquez,M.M., Rossi, J.S., 1991. The process of smoking cessation: an analysisof precontemplation, contemplation, and preparation stages of change.J. Consult. Clin. Psychol. 59, 295–304.
Ferguson, E., Chandler, S., 2005. A stage model of blood donor behaviour:assessing voluntary behaviour. J. Health Psychol. 10, 359–372.
Haslam, C., Haslam, R.A., 2000. A stage specific approach to improvingoccupational health and safety. Proceedings of the XIVth TriennialCongress of the International Ergonomics Association and 44thAnnual Meeting of the Human Factors and Ergonomics Society, vol. 6,pp. 253–255.
Health and Safety Executive, 2002. Upper limb disorders in the workplace. HSEBooks, Sudbury, UK.
Health and Safety Commission, 2004. Health and safety statistics highlights2003/04. HSE Books, Sudbury, UK.
Marshall, P.D., OConnor, M., Hodgkinson, J.P., 1995. The perceived relation-ship between neck symptoms and precedent injury. Injury 26 (1), 17–19.
Prochaska, J.O., DiClemente, C.C., 1982. Transtheoretical therapy: toward amore integrative model of change. Psychotherapy: Theory Research andPractice 19, 276–288.
Prochaska, J.O., DiClemente, C.C., Velicer, W.F., Rossi, J.S., 1993. Standar-dised, individualised, interactive, and personalised self-help programmes forsmoking cessation. Health Psychol. 12, 399–405.
Prochaska, J.M., Prochaska, J.O., Levesque, D.A., 2001. A transtheoreticalapproach to changing organizations. Adm. Policy Ment. Health 28 (4),247–261.
Rakowski, W., Ehrich, B., Goldstein, M.G., Rimer, B.K., Pearlman, D.N., Clark,M.A., Velicer, W.F., Woolverton, H., 1998. Increasing mammographyamong women aged 40–74 by use of a stage-matched, tailored intervention.Prev. Med. 27, 748–756.
Silverstein, B.A., Welp, E., Nelson, N., Kalat, J., 1998. Claims incidence ofwork-related disorders of the upper extremities: Washington state, 1987through 1995. Am. J. Public Health 88 (12), 1827–1833.
Urlings, I.J.M., Nijboer, I.D., Dul, J., 1990. A method for changing the attitudesand behavior of management and employees to stimulate the implementationof ergonomic improvements. Ergonomics 33 (5), 629–637.
Velicer, W.F, Prochaska, J.O., Fava, J.L., Norman, G.J., Redding, C.A., 1998.Smoking cessation and stress management: applications of the transtheoret-ical model of behavior change. Homeostasis 38, 216–233.
Whysall, Z., Haslam, R.A., Haslam, C., 2004. Reducing the risk of work-relatedmusculoskeletal disorders: processes, barriers, and outcomes of ergonomicsconsultancy. Appl. Ergon. 35 (4), 343–351.
Whysall, Z.J., Haslam, C., Haslam, R.A. in press. Developing the stage ofchange approach for the reduction of work-related musculoskeletaldisorders. J. Health Psychol.
World Health Organization, 1988. Health promotion for working popula-tions. Report of a WHO expert committee, Technical Report Series 765.Geneva: WHO.




















