
A Population-Based Survey of Lumbar Surgery Beliefs in the United States
10
© 2014 by National Association of Orthopaedic Nurses Orthopaedic Nursing • July/August 2014 • Volume 33 • Number 4 207 RESEARCH A Population-Based Survey of Lumbar Surgery Beliefs in the United States Merrill R. Landers ▼ Emilio Puentedura ▼ Adriaan Louw ▼ Amanda McCauley ▼ Zak Rasmussen ▼ Tim Bungum INTRODUCTION: Studies have shown that lumbar surgery (LS) outcomes may be influenced by perception. However, the perceptions of the general population regarding LS are not known. Therefore, the purpose of this study was to in- vestigate the general population’s perceptions regarding LS. SUBJECTS: This study included 262 participants (mean age: 46.1 years; 125 males and 137 females) from the Las Vegas (NV) metropolitan area. METHODS: A questionnaire was developed by an expert panel and was assessed for face and content validity. After revision and establishment of test–retest reliability, partici- pants were surveyed at 12 randomly selected grocery stores in Las Vegas. The questionnaire assessed demographics, personal and family medical history, and 11 items pertaining to perceptions of LS. RESULTS: The participants had a somewhat uncertain expectation about the potential success of LS; however, approximately two-thirds believed that LS is unsuccessful to the point that they would not be able to return to their previous level of activity after LS. Of the questions dealing with success of LS, the neutral response had the greatest frequency suggesting a lack of knowledge or uncertainty about LS. More than half of the respondents were fearful of LS and anticipated a protracted recovery accompanied by undesired side effects. Three quarters of the respondents agreed that they would try all other means of treatment before opting for LS, yet 39% said that they would undergo LS if they had severe lower back pain (LBP). CONCLUSIONS: The general population has an uncertain view of LS outcomes and anticipates postoperative side effects and a protracted recovery; these views may explain why a majority of participants expressed fear of LS and why most would only opt for LS as a last resort. This uncer- tainty and anticipation of poor outcomes may be a strong contributor to preoperative fear and anxiety, which could deleteriously influence postoperative outcomes. lifetime (Deyo, Mirza, & Martin, 2006; Long et al., 1996; Waddell & Burton, 2005). Epidemiological data show that the prevalence of LBP remains at epidemic propor- tions and is a debilitating and costly problem (Buchbinder, Jolley, & Wyatt, 2001; Waddell & Burton, 2005). With failed conservative care, worsening symp- toms, and increased disability, patients will often con- sider lumbar surgery (LS) to alleviate their pain and in- crease function (Friedly, Chan, & Deyo, 2007; Ostelo, de Vet, Waddell, et al., 2003). Lumbar surgery is prevalent in the United States; rates are at least 40% higher than that in any other country and more than five times higher than that in England (Deyo et al., 2006; Lurie, Birkmeyer, & Weinstein, 2003; Ostelo, de Vet, Waddell, et al., 2003; Weinstein, Lurie, Olson, Bronner, & Fisher, 2006). Success rates of LS have been good in some studies and mediocre in others (Deyo, Gray, Kreuter, Mirza, & Martin, 2005; Deyo & Mirza, 2006; Deyo, Nachemson, & Mirza, 2004; Martin et al., 2007; Ostelo, de Vet, Waddell, et al., 2003). A review of lumbar disc surgery has shown that surgical interventions have between 60% and 90% success rates whereas 10%–40% of patients have unsatis- factory or poor outcomes, which include persistent pain, loss of movement, and low level of function (Dolan, Greenfield, Nelson, & Nelson, 2000; McGregor, Dore, Morris, Morris, & Jamrozik, 2011; Morris, Morris, McGregor, Dore, & Jamrozik, 2011; Ostelo, de Vet, Merrill R. Landers, PT, DPT, PhD, OCS, Chair and Associate Professor, Department of Physical Therapy, University of Nevada Las Vegas. Emilio Puentedura, PT, DPT, PhD, GDMT, OCS, FAAOMPT, Associate Professor, Department of Physical Therapy, University of Nevada Las Vegas. Adriaan Louw, PT, MAppSc, GCRM, CSMT, PhD, Chief Executive Officer and Senior Faculty, International Spine and Pain Institute, Story City, Iowa. Amanda McCauley, DPT, Physical Therapist, Department of Physical Therapy, University of Nevada Las Vegas. Zak Rasmussen, DPT, Physical Therapist, Department of Physical Therapy, University of Nevada Las Vegas. Tim Bungum, DrPH, Associate Professor, Department of Occupational and Environmental Health, School of Community Health Sciences, University of Nevada, Las Vegas. The authors have disclosed no conflicts of interest. DOI: 10.1097/NOR.0000000000000064 Introduction Low back pain (LBP) is the most widely reported muscu- loskeletal disorder in the world, and it is reported that 70%–80% of all people will develop LBP during their Copyright © 2014 by National Association of Orthopaedic Nurses. Unauthorized reproduction of this article is prohibited.
Transcript of A Population-Based Survey of Lumbar Surgery Beliefs in the United States
© 2014 by National Association of Orthopaedic Nurses Orthopaedic Nursing • July/August 2014 • Volume 33 • Number 4 207
RESEARCH
A Population-Based Survey of Lumbar Surgery Beliefs in the United States
Merrill R. Landers ▼ Emilio Puentedura ▼ Adriaan Louw ▼ Amanda McCauley ▼ Zak Rasmussen ▼ Tim Bungum
INTRODUCTION: Studies have shown that lumbar surgery (LS) outcomes may be infl uenced by perception. However, the perceptions of the general population regarding LS are not known. Therefore, the purpose of this study was to in-vestigate the general population’s perceptions regarding LS. SUBJECTS: This study included 262 participants (mean age: 46.1 years; 125 males and 137 females) from the Las Vegas (NV) metropolitan area. METHODS: A questionnaire was developed by an expert panel and was assessed for face and content validity. After revision and establishment of test–retest reliability, partici-pants were surveyed at 12 randomly selected grocery stores in Las Vegas. The questionnaire assessed demographics, personal and family medical history, and 11 items pertaining to perceptions of LS. RESULTS: The participants had a somewhat uncertain expectation about the potential success of LS; however, approximately two-thirds believed that LS is unsuccessful to the point that they would not be able to return to their previous level of activity after LS. Of the questions dealing with success of LS, the neutral response had the greatest frequency suggesting a lack of knowledge or uncertainty about LS. More than half of the respondents were fearful of LS and anticipated a protracted recovery accompanied by undesired side effects. Three quarters of the respondents agreed that they would try all other means of treatment before opting for LS, yet 39% said that they would undergo LS if they had severe lower back pain (LBP). CONCLUSIONS: The general population has an uncertain view of LS outcomes and anticipates postoperative side effects and a protracted recovery; these views may explain why a majority of participants expressed fear of LS and why most would only opt for LS as a last resort. This uncer-tainty and anticipation of poor outcomes may be a strong contributor to preoperative fear and anxiety, which could deleteriously infl uence postoperative outcomes.
lifetime ( Deyo, Mirza, & Martin, 2006 ; Long et al., 1996 ; Waddell & Burton, 2005 ). Epidemiological data show that the prevalence of LBP remains at epidemic propor-tions and is a debilitating and costly problem ( Buchbinder, Jolley, & Wyatt, 2001 ; Waddell & Burton, 2005 ). With failed conservative care, worsening symp-toms, and increased disability, patients will often con-sider lumbar surgery (LS) to alleviate their pain and in-crease function ( Friedly, Chan, & Deyo, 2007 ; Ostelo, de Vet, Waddell, et al., 2003 ). Lumbar surgery is prevalent in the United States; rates are at least 40% higher than that in any other country and more than fi ve times higher than that in England ( Deyo et al., 2006 ; Lurie, Birkmeyer, & Weinstein, 2003 ; Ostelo, de Vet, Waddell, et al., 2003 ; Weinstein, Lurie, Olson, Bronner, & Fisher, 2006 ).
Success rates of LS have been good in some studies and mediocre in others ( Deyo, Gray, Kreuter, Mirza, & Martin, 2005 ; Deyo & Mirza, 2006 ; Deyo, Nachemson, & Mirza, 2004 ; Martin et al., 2007 ; Ostelo, de Vet, Waddell, et al., 2003 ). A review of lumbar disc surgery has shown that surgical interventions have between 60% and 90% success rates whereas 10%–40% of patients have unsatis-factory or poor outcomes, which include persistent pain, loss of movement, and low level of function ( Dolan, Greenfi eld, Nelson, & Nelson, 2000 ; McGregor, Dore, Morris, Morris, & Jamrozik, 2011 ; Morris, Morris, McGregor, Dore, & Jamrozik, 2011 ; Ostelo, de Vet,
Merrill R. Landers, PT, DPT, PhD, OCS , Chair and Associate Professor, Department of Physical Therapy, University of Nevada Las Vegas.
Emilio Puentedura, PT, DPT, PhD, GDMT, OCS, FAAOMPT , Associate Professor, Department of Physical Therapy, University of Nevada Las Vegas.
Adriaan Louw, PT, MAppSc, GCRM, CSMT , PhD, Chief Executive Offi cer and Senior Faculty, International Spine and Pain Institute, Story City, Iowa.
Amanda McCauley, DPT , Physical Therapist, Department of Physical Therapy, University of Nevada Las Vegas.
Zak Rasmussen, DPT , Physical Therapist, Department of Physical Therapy, University of Nevada Las Vegas.
Tim Bungum, DrPH , Associate Professor, Department of Occupational and Environmental Health, School of Community Health Sciences, University of Nevada, Las Vegas.
The authors have disclosed no confl icts of interest.
DOI: 10.1097/NOR.0000000000000064
Introduction Low back pain (LBP) is the most widely reported muscu-loskeletal disorder in the world, and it is reported that 70%–80% of all people will develop LBP during their
Copyright © 2014 by National Association of Orthopaedic Nurses. Unauthorized reproduction of this article is prohibited.
ONJ625_LR 207ONJ625_LR 207 7/19/14 3:04 AM7/19/14 3:04 AM

208 Orthopaedic Nursing • July/August 2014 • Volume 33 • Number 4 © 2014 by National Association of Orthopaedic Nurses
Vlaeyen, et al., 2003 ; Ostelo, de Vet, Waddell, et al., 2003 ). For instrumented lumbar spinal fusion, several studies indicate that the success rate (based on func-tional outcomes and pain measurement) is approxi-mately 50%; thus, half of the patients still report sig-nifi cant pain and disability following the surgery ( Button, Gupta, Barrett, Cammack, & Benson, 2005 ; Deyo et al., 2004, 2005 ; Fenton, Mirza, Lahad, Stern, & Deyo, 2007 ; Martin et al., 2007 ). Even newer technolo-gies aimed at improving lumbar fusion outcomes, such as lumbar arthroplasty, have shown failure rates around 20% ( David, 2007 ; McAfee et al., 2006 ; Siepe, Mayer, Wiechert, & Korge, 2006 ). Based on the current data on outcomes related to various forms of LS, many patients report poor outcomes and these poor outcomes might infl uence others to have negative perceptions of LS. Furthermore, the expectation of poor outcomes preop-eratively could negatively infl uence postoperative out-comes as has been shown in many studies on LS ( Davidson, Noonan, Dvorak, Zhang, & Fisher, 2010 ; Gepstein, Arinzon, Adunsky, & Folman, 2006 ; Toyone, Tanaka, Kato, Kaneyama, & Otsuka, 2005 ).
It is well established that the preoperative surgical environment is associated with stress and anxiety ( Galaal, Deane, Sangal, & Lopes, 2007 ; Rosen, Svensson, & Nilsson, 2008 ; Salzwedel et al., 2008 ) and several stud-ies have shown that heightened anxiety in the preopera-tive period is associated with increased postoperative pain ( Muglali & Komerik, 2008 ; O’Conner-Von, 2008 ; Rice, Glasper, Keeton, & Spargo, 2008 ; Rosen et al., 2008 ; Salzwedel et al., 2008 ; Wang, Shen, Lu, & Yang, 2008 ). More specifi c to LS, it has been shown that preop-erative expectations ( Yee, Adjei, Do, Ford, & Finkelstein, 2008 ), preoperative stress levels ( Starkweather, Witek-Janusek, Nockels, Peterson, & Mathews, 2006 ), and higher anxiety are associated with poor surgical out-comes ( Trief, Grant, & Fredrickson, 2000 ). Because un-satisfactory LS outcomes may cause negative public per-ceptions of LS, which in turn may deleteriously effect postoperative outcomes, there is a need to examine the public’s perception of LS. To date, no published studies are available on the general population’s beliefs regard-ing LS in the United States. The primary purpose of this study was to gain some understanding on the views and beliefs of the general public regarding LS. A secondary purpose was to explore whether these views and beliefs were differentially affected by the following variables: age, gender, race/ethnicity, socioeconomic status, and history of LBP.
Methods Q UESTIONNAIRE D EVELOPMENT AND V ALIDATION Because no previous study of this kind could be located, a Lumbar Surgery Questionnaire (LSQ) was developed (see the Appendix). The LSQ was developed on the basis of the objectives of the study and previous question-naires sampling the general population’s beliefs regard-ing LBP ( Buchbinder et al., 2001 ; Gross et al., 2006 ; Schmidt et al., 2007 ; Urquhart et al., 2008 ). To establish face and content validity, the provisional LSQ was sent to an expert panel that included three orthopaedic
physical therapists who specialize in LBP treatment, three spine surgeons, two surgical assistants/nurses, two researchers specializing in questionnaire design, and two pain scientists. Each had a background in the assessment and treatment of patients with LBP. The panel members were provided with a checklist where they rated question clarity, content validity, and the con-struct validity of the questionnaire. A 70% agreement among experts for each item was considered satisfac-tory to proceed ( Powell, 2003 ).
Next, a small pilot study (n = 12) was conducted to assess test-retest reliability. The initial LSQ was distrib-uted to a convenience sample of community members and 2 weeks later the same sample responded to the sur-vey. During statistical analysis of the initial question-naire, a few questions were found to be problematic. These questions were reworded or fi ltered out and the two-step testing process was repeated with another set of 12 members of the general population. Statistical analysis of the questions in the revised version found intraclass correlation coeffi cient values ranging from 0.739 to 0.976.
The fi nal LSQ (see the Appendix) included a demo-graphic section (age, gender, race, ethnicity, work sta-tus, educational background, and income), items re-garding personal and immediate family history of LBP (also LS and general orthopaedic surgery), and a section that assessed LS beliefs. A 5-point Likert scale with the following anchors was used to gauge answers to these 11 questions about LS: 1 = “totally agree,” 2 = “agree,” 3 = “neutral,” 4 = “disagree,” and 5 = “totally disagree.”
D ATA C OLLECTION
Subjects Systematic sampling techniques (1 of every 3) were used to recruit shoppers (over the age of 18 years) at grocery stores in the Las Vegas metropolitan area. Subjects provided verbal consent before taking the sur-vey. Those who completed the questionnaire were of-fered a soft drink for their participation.
Locations Grocery stores were selected as the best location to eas-ily access a sample of convenience of the general public ( Aday, 1996 ; Grimmer & Bialocerkowski, 2005 ). Two major national grocery chains in the Las Vegas metro-politan area, including Henderson, agreed to allow re-searchers to have access to their patrons. To ensure a demographically representative sample of the commu-nity, all stores from these two chains in the Las Vegas area were divided into six sections of the metropolitan area corresponding to zip codes. Two stores from each of the six city regions were then randomly selected.
Results R ESPONDENTS In all, 262 participants completed the LSQ. The mean age of the sample was 46.1 ± 16.9 years (range, 18–85 years), with 91.5% of the respondents being Nevada
Copyright © 2014 by National Association of Orthopaedic Nurses. Unauthorized reproduction of this article is prohibited.
ONJ625_LR 208ONJ625_LR 208 7/19/14 3:04 AM7/19/14 3:04 AM
© 2014 by National Association of Orthopaedic Nurses Orthopaedic Nursing • July/August 2014 • Volume 33 • Number 4 209
residents (4.2% from neighboring states and the re-mainder from other states). Demographics are pre-sented in Table 1 .
O VERALL F INDINGS The overall fi ndings of the survey suggest that the gen-eral population had a somewhat positive expectation
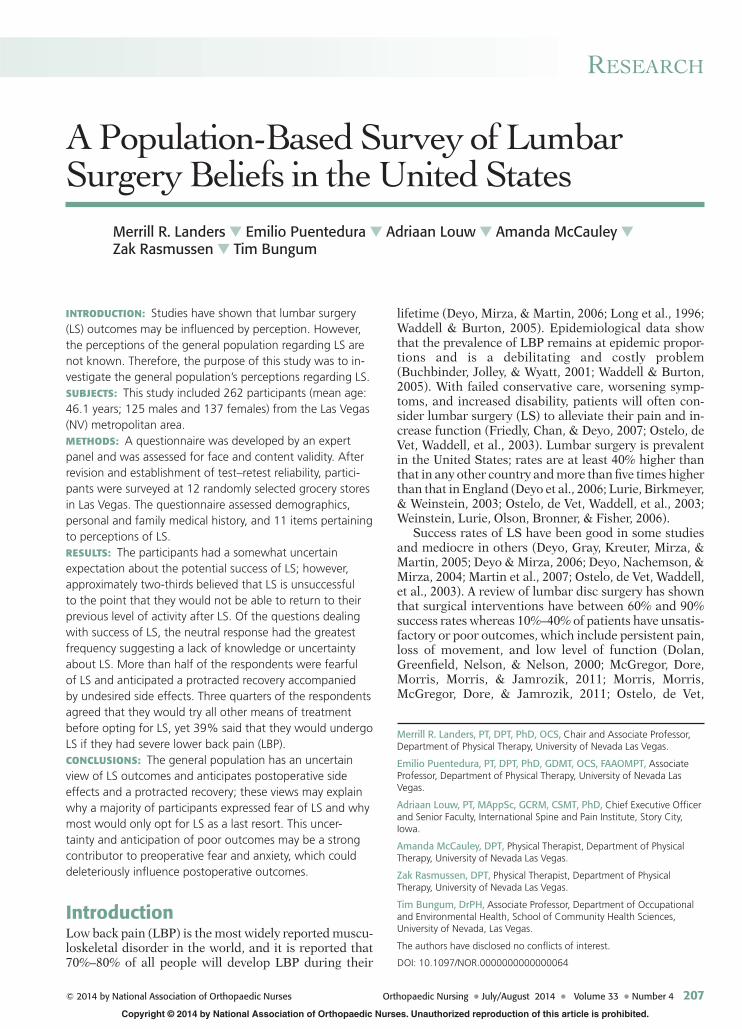
about the potential success of LS in that more respond-ents had a favorable impression compared with those with a negative impression; however, most of the re-spondents would be afraid to have LS and would try any or all other treatments before having LS (see Figures 1 and 2 ). In addition, a majority of respondents antici-pated side effects and a protracted recovery from LS. Of the questions dealing with success or outcomes of LS, the neutral response had the greatest frequency suggest-ing a lack of knowledge or uncertainty about LS (see Figure 1 ).
A GE Subjects were categorized into three groups on the basis of their age: 40 years or less ( n = 99); 41–60 years ( n = 105), and 61 years or more ( n = 57). Of the 11 questions, only two of them had a signifi cant difference in the re-sponse ratio for the three age groups using chi-square analyses: “would you be afraid to get LS?” ( p = .04) and “after LS, I would be afraid to return to work” ( p = .005). For the “would you be afraid to get LS?” question, 62.6% of the ≤ 40 years group would be afraid, whereas only 55.7% and 45.6% would be afraid in the 41 to 60 years and > 61 years groups, respectively. For the “after LS, I would be afraid to return to work” question, 49.5% of respondents in the ≤ 40 years group would be afraid, whereas only 33.9% and 28.1% of the 41 to 60 years and > 61 years groups, respectively, would be afraid.
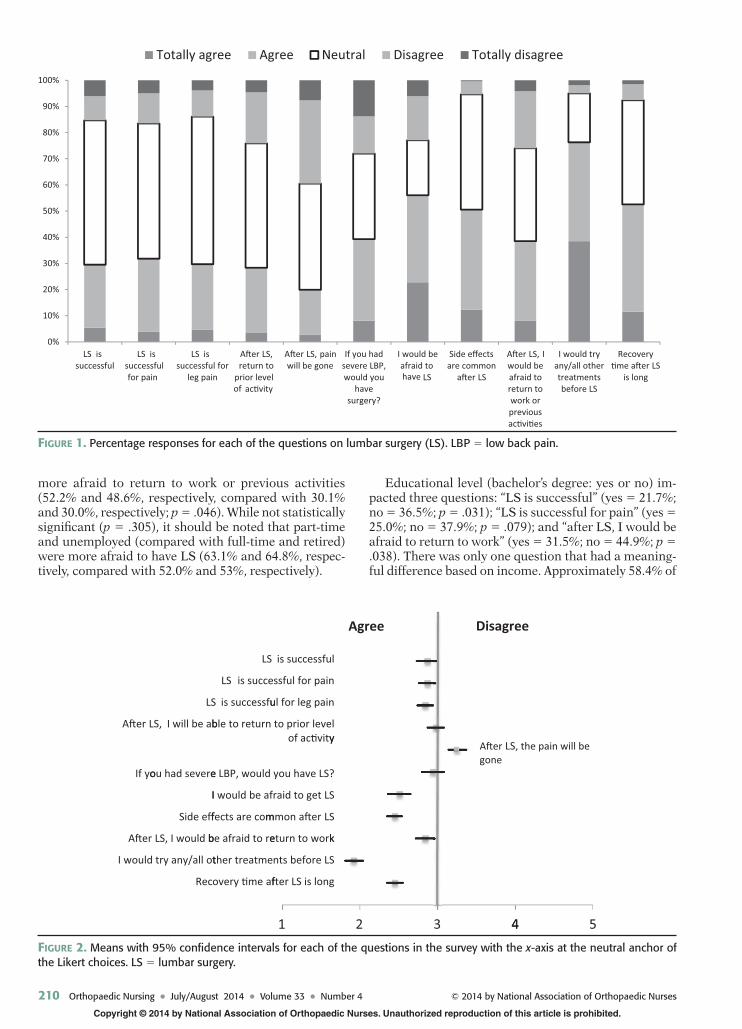
G ENDER Response frequencies reveal that, in general, women have a more negative outlook about LS than do men. Of the 11 questions, women had a slightly more negative outlook than men regarding LS on all but one question (see Figure 3 ).
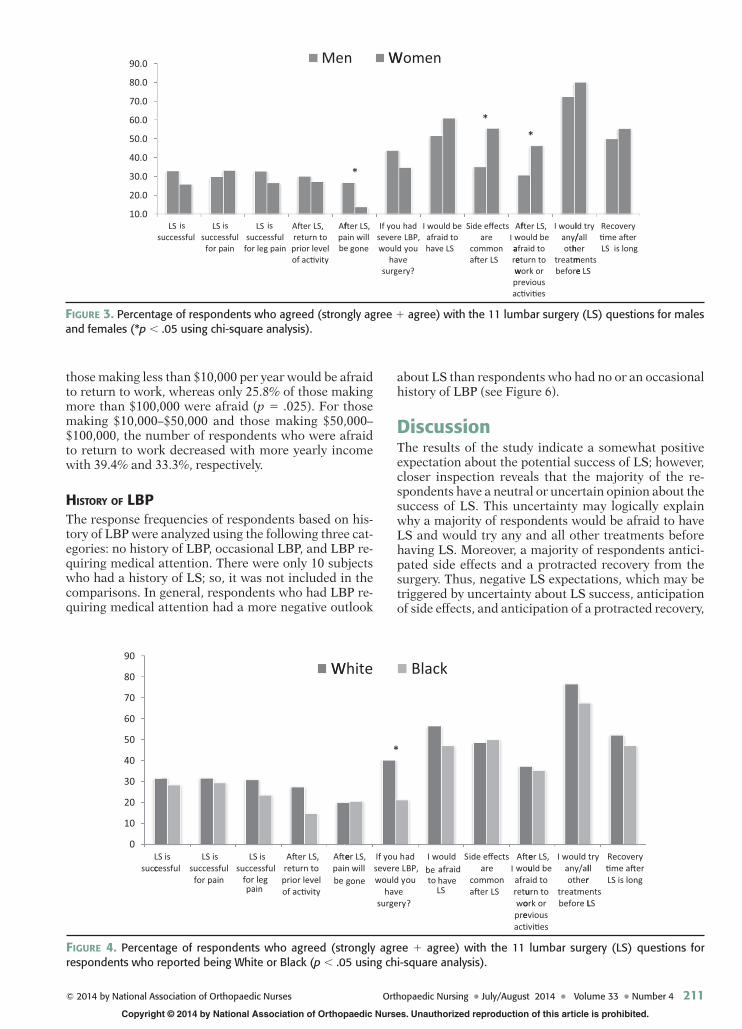
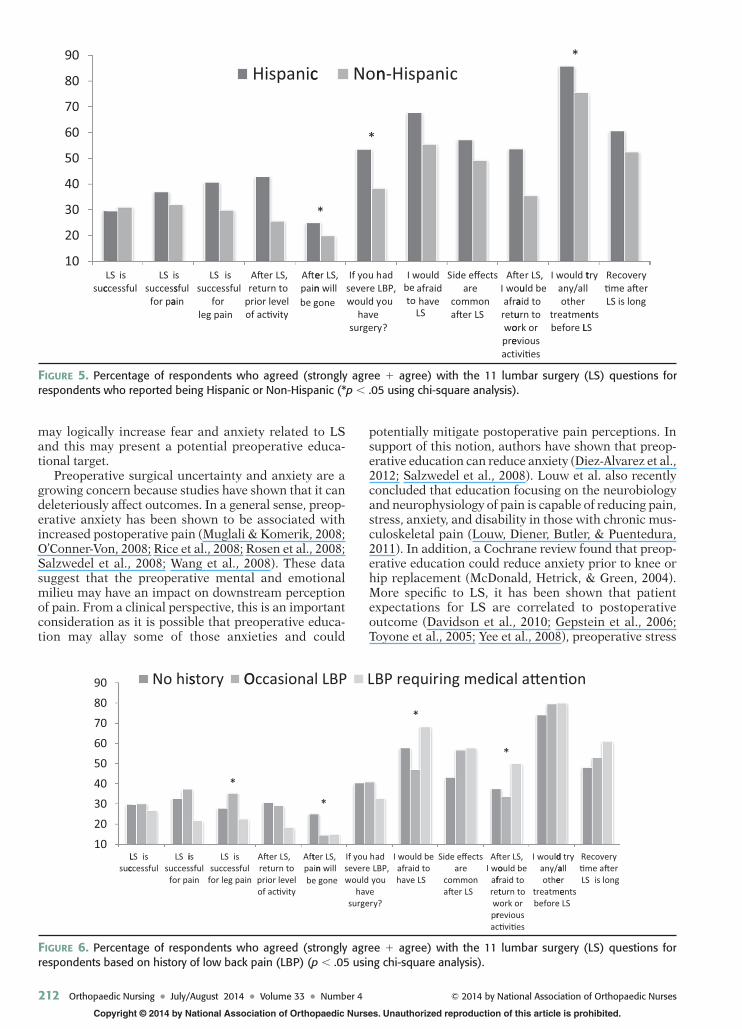
R ACE AND E THNICITY Because there were too few respondents who reported being Asian, Native Hawaiian, American Indian, two or more races, and some other race (see Table 1 ), only White and Black responses were cross-tabulated and analyzed with chi-square analyses. While there were no signifi cant trends in the data suggesting a difference in overall opinion when comparing Whites and Blacks, there was one question that stood out with Whites hav-ing a more positive outlook on LS: “would you get LS?” (White = 40.3%; Black = 21.2%; p = 0.044) (see Figure 4 ). Although the question “after LS, I would return to prior level of activity” (White = 27.4%; Black = 14.7%) was not statistically signifi cant ( p = .294), a lower per-centage of Blacks agreed with this statement. Hispanics had a generally more positive outlook about LS regard-ing pain outcomes and would be more inclined to have LS than non-Hispanics; however, Hispanics reported being more fearful, anticipated more side effects, and would be more afraid to return to work (see Figure 5 ).
S OCIOECONOMIC S TATUS Employment status (i.e., full-time, part-time, unem-ployed, retired) did not appear to affect the opinion of the respondents for most of the questions. Part-time and unemployed (compared with full-time and retired) were
Copyright © 2014 by National Association of Orthopaedic Nurses. Unauthorized reproduction of this article is prohibited.
T ABLE 1. R ESPONDENT D EMOGRAPHIC S TATISTICS Variable n (%)
Gender
Male 124 (47.3%)
Female 136 (51.9%)
Missing 2 (0.8%)
Race
White 180 (68.7%)
Black 34 (13.0%)
Asian 5 (1.9%)
Native Hawaiian 5 (1.9%)
American Indian 9 (3.4%)
Two or more 13 (5.0%)
Some other race 9 (3.4%)
Missing 7 (2.7%)
Ethnicity
Hispanic/Latino 28 (10.7%)
Non-Hispanic/Latino 200 (76.3%)
Other 23 (8.8%)
Missing 11 (4.2%)
Employment
Full-time 123 (46.9%)
Part-time 46 (17.6%)
Unemployed 37 (14.1%)
Disabled 11 (4.2%)
Retired 40 (15.3%)
Student 4 (1.5%)
Missing 1 (0.4%)
4-year college degree
Yes 124 (47.3%)
No 138 (52.7%)
Income
$100,000 + 31 (11.8%)
$50,000–100,000 75 (28.6%)
$10,000–50,000 109 (41.6%)
< $10,000 36 (13.7%)
Missing 11 (4.2%)
Personal history of low back pain
No history 104 (39.7%)
Occasional 83 (31.7%)
LBP requiring medical attention 60 (22.9%)
Low back surgery 11 (4.2%)
Note . LBP = low back pain.
ONJ625_LR 209ONJ625_LR 209 7/19/14 3:04 AM7/19/14 3:04 AM
210 Orthopaedic Nursing • July/August 2014 • Volume 33 • Number 4 © 2014 by National Association of Orthopaedic Nurses
more afraid to return to work or previous activities (52.2% and 48.6%, respectively, compared with 30.1% and 30.0%, respectively; p = .046). While not statistically signifi cant ( p = .305), it should be noted that part-time and unemployed (compared with full-time and retired) were more afraid to have LS (63.1% and 64.8%, respec-tively, compared with 52.0% and 53%, respectively).
Educational level (bachelor’s degree: yes or no) im-pacted three questions: “LS is successful” (yes = 21.7%; no = 36.5%; p = .031); “LS is successful for pain” (yes = 25.0%; no = 37.9%; p = .079); and “after LS, I would be afraid to return to work” (yes = 31.5%; no = 44.9%; p = .038). There was only one question that had a meaning-ful difference based on income. Approximately 58.4% of
Copyright © 2014 by National Association of Orthopaedic Nurses. Unauthorized reproduction of this article is prohibited.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
LS issuccessful
LS issuccessful for pain
LS issuccessful for
leg pain
A�er LS,return to
prior level of ac�vity
A�er LS, painwill be gone
If you hadsevere LBP,would you
havesurgery?
I would beafraid to have LS
Side effectsare common
a�er LS
A�er LS, Iwould beafraid toreturn towork orpreviousac�vi�es
I would tryany/all othertreatmentsbefore LS
Recovery�me a�er LS
is long
Totally agree Agree Neutral Disagree Totally disagree
FIGURE 1. Percentage responses for each of the questions on lumbar surgery (LS). LBP = low back pain.
A�er
If yo
A�er
I would
LS
LS, I will be ab
ou had severe
I
Side eff
LS, I would b
try any/all ot
Rec
LS
LS is succe
is successfu
ble to return
e LBP, would
I would be af
fects are com
be afraid to re
ther treatme
overy �me af
1
is successful
ssful for pain
ul for leg pain
to prior levelof ac�vity
you have LS?
raid to get LS
mmon a�er LS
eturn to work
nts before LS
fter LS is long
2
y
k
Agree
3 4
Disagree
A�er LSgone
4
, the pain will
5
be
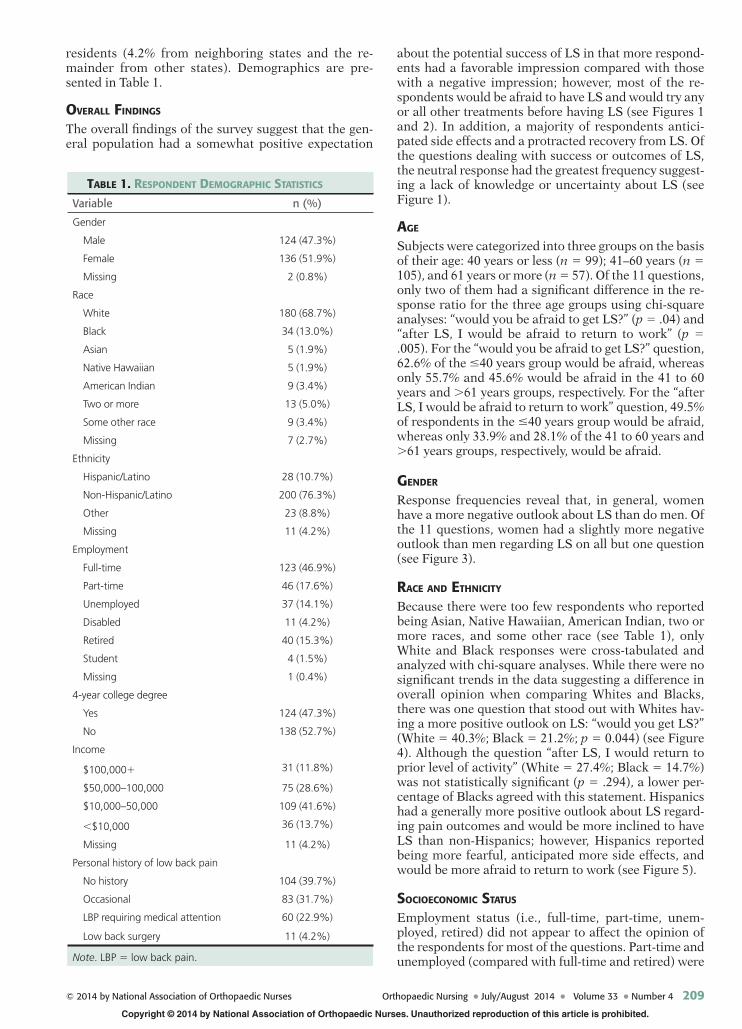
F IGURE 2. Means with 95% confi dence intervals for each of the questions in the survey with the x -axis at the neutral anchor of the Likert choices. LS = lumbar surgery.
ONJ625_LR 210ONJ625_LR 210 7/19/14 3:04 AM7/19/14 3:04 AM
© 2014 by National Association of Orthopaedic Nurses Orthopaedic Nursing • July/August 2014 • Volume 33 • Number 4 211
those making less than $10,000 per year would be afraid to return to work, whereas only 25.8% of those making more than $100,000 were afraid ( p = .025). For those making $10,000–$50,000 and those making $50,000–$100,000, the number of respondents who were afraid to return to work decreased with more yearly income with 39.4% and 33.3%, respectively.
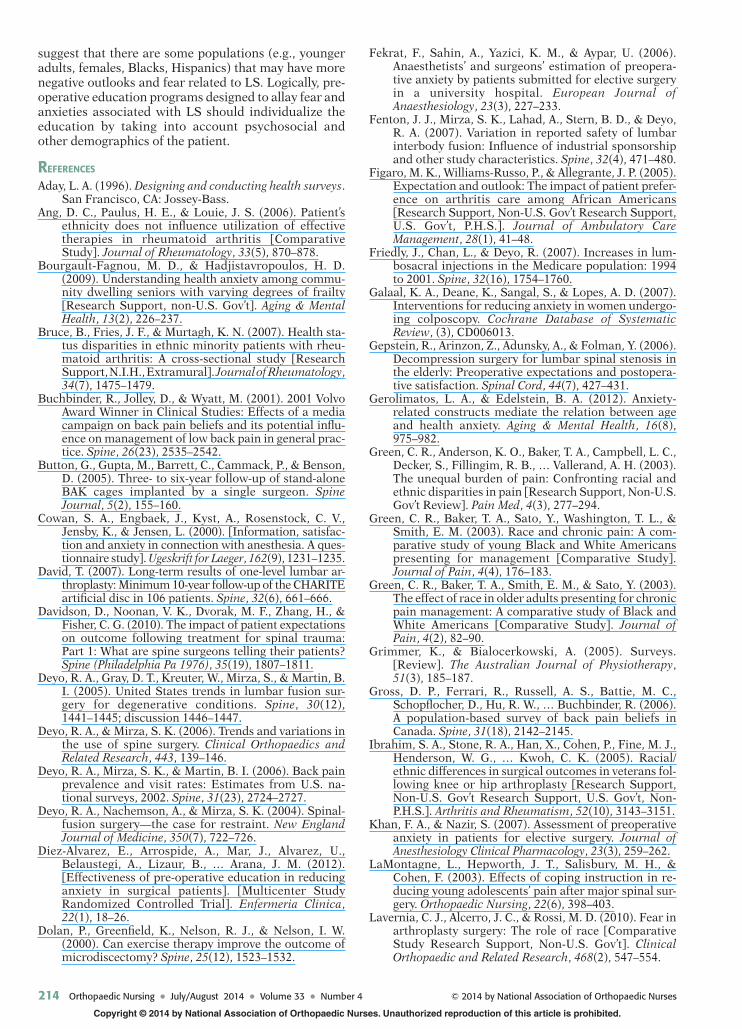
H ISTORY OF LBP The response frequencies of respondents based on his-tory of LBP were analyzed using the following three cat-egories: no history of LBP, occasional LBP, and LBP re-quiring medical attention. There were only 10 subjects who had a history of LS; so, it was not included in the comparisons. In general, respondents who had LBP re-quiring medical attention had a more negative outlook
about LS than respondents who had no or an occasional history of LBP (see Figure 6 ).
Discussion The results of the study indicate a somewhat positive expectation about the potential success of LS; however, closer inspection reveals that the majority of the re-spondents have a neutral or uncertain opinion about the success of LS. This uncertainty may logically explain why a majority of respondents would be afraid to have LS and would try any and all other treatments before having LS. Moreover, a majority of respondents antici-pated side effects and a protracted recovery from the surgery. Thus, negative LS expectations, which may be triggered by uncertainty about LS success, anticipation of side effects, and anticipation of a protracted recovery,
Copyright © 2014 by National Association of Orthopaedic Nurses. Unauthorized reproduction of this article is prohibited.
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
90.0
suLS is
ccessfulLS
succefor p
isssfulain
LS issuccessfu
for leg pailn
A�er LS,return toprior levelof ac�vity
Afpa
Men
fter LS,in will
be gone
If youseverewould
havsurge
W
*
had LBP, youery?
I would beafraid tohave LS
Women
Side effectsare
commona�er LS
Afwarewpac�vi�es
*
fter LS, I ould beafraid toeturn towork orrevious
I woulany/oth
treatmbefore
*
ld try/all
hermentse LS
Recovery�me a�eLS is long
r
FIGURE 3. Percentage of respondents who agreed (strongly agree + agree) with the 11 lumbar surgery (LS) questions for males and females (*p < .05 using chi-square analysis).
0
10
20
30
40
50
60
70
80
90
LS is LS issucccessful
successf
for paiul
n
LS is successful
for leg pain
A�er LS,return toprior levelof ac�vity
A�epain
g
W
er LS,will
be one
If you hsevere Lwould y
havesurgery
White
*
adBP,ou
?
I would be afraid to have
LS
S
Black
ide effectsare
commona�er LS
A�ewouafrretuwopreact
er LS, I uld be
aid tourn toork oreviousivi�es
I would any/alother
treatmebefore L
tryllrnts
LS
Recovery�me a�erLS is long
F IGURE 4. Percentage of respondents who agreed (strongly agree + agree) with the 11 lumbar surgery (LS) questions for respondents who reported being White or Black ( p < .05 using chi-square analysis).
ONJ625_LR 211ONJ625_LR 211 7/19/14 3:04 AM7/19/14 3:04 AM
212 Orthopaedic Nursing • July/August 2014 • Volume 33 • Number 4 © 2014 by National Association of Orthopaedic Nurses
may logically increase fear and anxiety related to LS and this may present a potential preoperative educa-tional target.
Preoperative surgical uncertainty and anxiety are a growing concern because studies have shown that it can deleteriously affect outcomes. In a general sense, preop-erative anxiety has been shown to be associated with increased postoperative pain ( Muglali & Komerik, 2008 ; O’Conner-Von, 2008 ; Rice et al., 2008 ; Rosen et al., 2008 ; Salzwedel et al., 2008 ; Wang et al., 2008 ). These data suggest that the preoperative mental and emotional milieu may have an impact on downstream perception of pain. From a clinical perspective, this is an important consideration as it is possible that preoperative educa-tion may allay some of those anxieties and could
potentially mitigate postoperative pain perceptions. In support of this notion, authors have shown that preop-erative education can reduce anxiety ( Diez-Alvarez et al., 2012 ; Salzwedel et al., 2008 ). Louw et al. also recently concluded that education focusing on the neurobiology and neurophysiology of pain is capable of reducing pain, stress, anxiety, and disability in those with chronic mus-culoskeletal pain ( Louw, Diener, Butler, & Puentedura, 2011 ). In addition, a Cochrane review found that preop-erative education could reduce anxiety prior to knee or hip replacement ( McDonald, Hetrick, & Green, 2004 ). More specifi c to LS, it has been shown that patient expectations for LS are correlated to postoperative outcome ( Davidson et al., 2010 ; Gepstein et al., 2006 ; Toyone et al., 2005 ; Yee et al., 2008 ), preoperative stress
Copyright © 2014 by National Association of Orthopaedic Nurses. Unauthorized reproduction of this article is prohibited.
10
20
30
40
50
60
70
80
90
LSsuc
isccessful
LS isuccess
for pa
ssful
ain
LS issuccessful
forleg pain
A�er LS,return to
prior levelof ac�vity
A�epain
g
Hispanic
er LS,n will
be one
If you hsevere LBP,would y
havesurgery
c Non
*
*
ad
ou
?
I wouldbe afraidto have
LS
S
n-Hispani
ide effectsare
commona�er LS
A�ewouafra
retuwopreact
c
r LS,I uld be
aid tourn toork oreviousivi�es
I would tany/alother
treatmenbefore L
*
tryl
ntsLS
Recovery�me a�erLS is long
FIGURE 5. Percentage of respondents who agreed (strongly agree + agree) with the 11 lumbar surgery (LS) questions for respondents who reported being Hispanic or Non-Hispanic (*p < .05 using chi-square analysis).
10
20
30
40
50
60
70
80
90
Lsuc
LS isccessful
LS isucces
for pa
No his
issfulin
LS issuccessful
for leg pain
story O
*
A�er LS,return toprior levelof ac�vity
Aftpain
Occasiona
ter LS,n will
be gone
If you hseverewould
havesurger
l LBP L
*
adLBP,you
y?
I would beafraid tohave LS
BP requir
*
Side effectsare
commona�er LS
A�woafretwprac
ing medi
er LS,I ould be
fraid toturn toork or
revious�vi�es
I wouldany/aothe
treatmebefore
ical a�en
*
d tryallerentsLS
Recovery�me a�erLS is long
�on
F IGURE 6. Percentage of respondents who agreed (strongly agree + agree) with the 11 lumbar surgery (LS) questions for respondents based on history of low back pain (LBP) ( p < .05 using chi-square analysis).
ONJ625_LR 212ONJ625_LR 212 7/19/14 3:04 AM7/19/14 3:04 AM

© 2014 by National Association of Orthopaedic Nurses Orthopaedic Nursing • July/August 2014 • Volume 33 • Number 4 213
( Starkweather et al., 2006 ), anxiety, and fear ( LaMontagne, Hepworth, Salisbury, & Cohen, 2003 ; Louw, Louw, & Crous, 2009 ; Trief et al., 2000 ; Walters & Coad, 2006 ). Indeed, the fact that a majority of the respondents in the present study are afraid to have LS and would exhaust all alternative treatment options highlights the importance that fear, stress, anxiety, and surgical expectations may have on LS outcomes.
Our results suggest that exposure to healthcare for LBP may create a negative outlook about LS. Across al-most all of the opinion questions (see Figure 6 ), those with no or occasional history of LBP had more favorable view of LS than those who had LBP requiring medical attention. Perhaps, for some of the respondents, the medical treatment that they had received for their previ-ous episodes of LBP was not satisfactory and from that experience they developed a lack of confi dence about how LS could help. In light of this possibility, education for those with a history of treated LBP would seem espe-cially important.
For the most part, age did not appear to infl uence opinion on LS; however, younger respondents were more fearful of having LS and were more fearful about returning to work. These fi ndings are consistent with the work by Gerolimatos and Edelstein ( 2012 ), who found that young adults ( < 30 years) reported higher levels of health anxiety than older adults ( > 60 years). They further reported that anxiety sensitivity and intol-erance of uncertainty mediate the relation between age and health anxiety. This underscores the importance of education in the face of uncertainty in the preoperative LS milieu especially in younger adults. Bourgault-Fagnou and Hadjistavropoulos ( 2009 ) also reported lower levels of health anxiety in older adults than in younger adults, which suggests that age-related differ-ences in the severity of health anxiety need to be consid-ered with preoperative education. Perhaps younger adults simply believe that they have more to lose as a result of a poor surgical outcome.
Our results are consistent with fi ndings that show fe-males have more preoperative uncertainty and anxiety than males ( Cowan et al., 2000 ; Fekrat, Sahin, Yazici, & Aypar, 2006 ; Mackenzie, 1989 ; Perks, Chakravarti, & Manninen, 2009 ). Khan and Nazir ( 2007 ) found that fe-male patients were signifi cantly more anxious than male patients in the preoperative setting. They go on to suggest that females may need more preoperative psy-chological support. Perks et al. ( 2009 ) found a higher level of anxiety incidence in females and found that the most common preoperative anxieties were the wait, po-tential harm, and results of the surgery. This is consist-ent with the present study in that females had a gener-ally more negative outlook and reported a much higher fear of side effects and potential to return to work. Perks et al. ( 2009 ) further suggest that there is a need for educational intervention, particularly in patients with a high level of preoperative anxiety.
While there were no signifi cant trends across the questions, almost twice as many Whites as Blacks would have LS if they had severe back pain. This is consistent with the work by Lavernia et al., who found that Blacks had higher fear levels before joint arthroplasty com-pared with Whites ( Lavernia, Alcerro, & Rossi, 2010 ).
Blacks also generally have lower expectations of out-comes after knee arthroplasty and were less likely to be-lieve preoperatively that arthroplasty would help ( Figaro, Williams-Russo, & Allegrante, 2005 ). Moreover, they also reported that Blacks had poorer outcomes after the surgery. If Blacks indeed have poorer outcomes from or-thopaedic surgeries, it is possible that this belief could spread throughout the Black community and could in-fl uence others causing them to avoid or delay surgery. This notion may partially be supported by Skinner et al., who reported that Black men were less likely than White men to have a knee arthroplasty ( Skinner, Weinstein, Sporer, & Wennberg, 2003 ). Moreover, studies by Green et al. suggest that chronic pain affects Blacks more than White Americans before initial presentation for treat-ment ( Green, Anderson, et al., 2003 ; Green, Baker, Sato, Washington, & Smith, 2003 ; Green, Baker, Smith, & Sato, 2003 ). Hispanics, in the present study, were also more inclined to have LS than non-Hispanics; however, Hispanics reported being more fearful, anticipated more side effects, and would be more afraid to return to work. This is consistent with data that show that Hispanic pa-tients had worse rheumatoid arthritic symptoms than Whites and Blacks ( Ang, Paulus, & Louie, 2006 ; Bruce, Fries, & Murtagh, 2007 ; Yazici, Kautiainen, & Sokka, 2007 ). Anticipation of side effects among Hispanics is also consistent with data that have shown increased rates of postoperative orthopaedic infection ( Ibrahim et al., 2005 ). Taken together, these data, including results from the present study, offer evidence that the uncer-tainty and anxiety associated with orthopaedic surgeries such as LS may differentially affect populations on the basis of race and ethnicity.
In the present study, higher educational attainment correlated with increased skepticism. Because this skepticism could logically also affect postoperative out-comes, this should be an important educational consid-eration in preoperative counseling. In addition, those with higher income were not as likely to be afraid to return to work; not surprisingly, those in the lowest in-come bracket were more afraid about the return to work and this may refl ect the stability of their employ-ment and/or the fragility of their economic state. It is also possible that those in the lowest income brackets may have had more physically demanding work (e.g., manual labor, repetitive lifting) and the thought of re-turning to such work after a poor surgical outcome would indeed invoke some trepidation.
Conclusions While there were more people who had a favorable opinion or view of LS than those who have an unfavora-ble view, the majority of the respondents in our study were uncertain about the success of LS in terms of pain reduction and return to previous level of activity. This uncertainty may explain why more than half of the re-spondents would be afraid to have LS and why more than 70% would try any and all other treatments before having LS. Because fear and uncertainty have been shown to negatively infl uence postoperative outcomes, this may represent an important preoperative educational focus for those having LS. Our results also
Copyright © 2014 by National Association of Orthopaedic Nurses. Unauthorized reproduction of this article is prohibited.
ONJ625_LR 213ONJ625_LR 213 7/19/14 3:04 AM7/19/14 3:04 AM
214 Orthopaedic Nursing • July/August 2014 • Volume 33 • Number 4 © 2014 by National Association of Orthopaedic Nurses
suggest that there are some populations (e.g., younger adults, females, Blacks, Hispanics) that may have more negative outlooks and fear related to LS. Logically, pre-operative education programs designed to allay fear and anxieties associated with LS should individualize the education by taking into account psychosocial and other demographics of the patient.
R EFERENCES Aday , L. A. ( 1996 ). Designing and conducting health surveys .
San Francisco, CA : Jossey-Bass . Ang , D. C. , Paulus , H. E. , & Louie , J. S. ( 2006 ). Patient’s
ethnicity does not infl uence utilization of effective therapies in rheumatoid arthritis [Comparative Study] . Journal of Rheumatology , 33 ( 5 ), 870 – 878 .
Bourgault-Fagnou , M. D. , & Hadjistavropoulos , H. D. ( 2009 ). Understanding health anxiety among commu-nity dwelling seniors with varying degrees of frailty [Research Support, non-U.S. Gov’t] . Aging & Mental Health , 13 ( 2 ), 226 – 237 .
Bruce , B. , Fries , J. F. , & Murtagh , K. N. ( 2007 ). Health sta-tus disparities in ethnic minority patients with rheu-matoid arthritis: A cross-sectional study [Research Support, N.I.H., Extramural] . Journal of Rheumatology , 34 ( 7 ), 1475 – 1479 .
Buchbinder , R. , Jolley , D. , & Wyatt , M. ( 2001 ). 2001 Volvo Award Winner in Clinical Studies: Effects of a media campaign on back pain beliefs and its potential infl u-ence on management of low back pain in general prac-tice . Spine , 26 ( 23 ), 2535 – 2542 .
Button , G. , Gupta , M. , Barrett , C. , Cammack , P. , & Benson , D. ( 2005 ). Three- to six-year follow-up of stand-alone BAK cages implanted by a single surgeon . Spine Journal , 5 ( 2 ), 155 – 160 .
Cowan , S. A. , Engbaek , J. , Kyst , A. , Rosenstock , C. V. , Jensby , K. , & Jensen , L. ( 2000 ). [Information, satisfac-tion and anxiety in connection with anesthesia. A ques-tionnaire study] . Ugeskrift for Laeger , 162 ( 9 ), 1231 – 1235 .
David , T. ( 2007 ). Long-term results of one-level lumbar ar-throplasty: Minimum 10-year follow-up of the CHARITE artifi cial disc in 106 patients . Spine , 32 ( 6 ), 661 – 666 .
Davidson , D. , Noonan , V. K. , Dvorak , M. F. , Zhang , H. , & Fisher , C. G. ( 2010 ). The impact of patient expectations on outcome following treatment for spinal trauma: Part 1: What are spine surgeons telling their patients ? Spine (Philadelphia Pa 1976) , 35 ( 19 ), 1807 – 1811 .
Deyo , R. A. , Gray , D. T. , Kreuter , W. , Mirza , S. , & Martin , B. I. ( 2005 ). United States trends in lumbar fusion sur-gery for degenerative conditions . Spine , 30 ( 12 ), 1441 – 1445 ; discussion 1446–1447.
Deyo , R. A. , & Mirza , S. K. ( 2006 ). Trends and variations in the use of spine surgery . Clinical Orthopaedics and Related Research , 443 , 139 – 146 .
Deyo , R. A. , Mirza , S. K. , & Martin , B. I. ( 2006 ). Back pain prevalence and visit rates: Estimates from U.S. na-tional surveys, 2002 . Spine , 31 ( 23 ), 2724 – 2727 .
Deyo , R. A. , Nachemson , A. , & Mirza , S. K. ( 2004 ). Spinal-fusion surgery—the case for restraint . New England Journal of Medicine , 350 ( 7 ), 722 – 726 .
Diez-Alvarez , E. , Arrospide , A. , Mar , J. , Alvarez , U. , Belaustegi , A. , Lizaur , B. , … Arana , J. M. ( 2012 ). [Effectiveness of pre-operative education in reducing anxiety in surgical patients]. [Multicenter Study Randomized Controlled Trial] . Enfermeria Clinica , 22 ( 1 ), 18 – 26 .
Dolan , P. , Greenfi eld , K. , Nelson , R. J. , & Nelson , I. W. ( 2000 ). Can exercise therapy improve the outcome of microdiscectomy ? Spine , 25 ( 12 ), 1523 – 1532 .
Fekrat , F. , Sahin , A. , Yazici , K. M. , & Aypar , U. ( 2006 ). Anaesthetists’ and surgeons’ estimation of preopera-tive anxiety by patients submitted for elective surgery in a university hospital . European Journal of Anaesthesiology , 23 ( 3 ), 227 – 233 .
Fenton , J. J. , Mirza , S. K. , Lahad , A. , Stern , B. D. , & Deyo , R. A. ( 2007 ). Variation in reported safety of lumbar interbody fusion: Infl uence of industrial sponsorship and other study characteristics . Spine , 32 ( 4 ), 471 – 480 .
Figaro , M. K. , Williams-Russo , P. , & Allegrante , J. P. ( 2005 ). Expectation and outlook: The impact of patient prefer-ence on arthritis care among African Americans [Research Support, Non-U.S. Gov’t Research Support, U.S. Gov’t, P.H.S.] . Journal of Ambulatory Care Management , 28 ( 1 ), 41 – 48 .
Friedly , J. , Chan , L. , & Deyo , R. ( 2007 ). Increases in lum-bosacral injections in the Medicare population: 1994 to 2001 . Spine , 32 ( 16 ), 1754 – 1760 .
Galaal , K. A. , Deane , K. , Sangal , S. , & Lopes , A. D. ( 2007 ). Interventions for reducing anxiety in women undergo-ing colposcopy . Cochrane Database of Systematic Review , ( 3 ), CD006013 .
Gepstein , R. , Arinzon , Z. , Adunsky , A. , & Folman , Y. ( 2006 ). Decompression surgery for lumbar spinal stenosis in the elderly: Preoperative expectations and postopera-tive satisfaction . Spinal Cord , 44 ( 7 ), 427 – 431 .
Gerolimatos , L. A. , & Edelstein , B. A. ( 2012 ). Anxiety-related constructs mediate the relation between age and health anxiety . Aging & Mental Health , 16 ( 8 ), 975 – 982 .
Green , C. R. , Anderson , K. O. , Baker , T. A. , Campbell , L. C. , Decker , S. , Fillingim , R. B. , … Vallerand , A. H. ( 2003 ). The unequal burden of pain: Confronting racial and ethnic disparities in pain [Research Support, Non-U.S. Gov’t Review] . Pain Med , 4 ( 3 ), 277 – 294 .
Green , C. R. , Baker , T. A. , Sato , Y. , Washington , T. L. , & Smith , E. M. ( 2003 ). Race and chronic pain: A com-parative study of young Black and White Americans presenting for management [Comparative Study] . Journal of Pain , 4 ( 4 ), 176 – 183 .
Green , C. R. , Baker , T. A. , Smith , E. M. , & Sato , Y. ( 2003 ). The effect of race in older adults presenting for chronic pain management: A comparative study of Black and White Americans [Comparative Study] . Journal of Pain , 4 ( 2 ), 82 – 90 .
Grimmer , K. , & Bialocerkowski , A. ( 2005 ). Surveys. [Review] . The Australian Journal of Physiotherapy , 51 ( 3 ), 185 – 187 .
Gross , D. P. , Ferrari , R. , Russell , A. S. , Battie , M. C. , Schopfl ocher , D. , Hu , R. W. , … Buchbinder , R. ( 2006 ). A population-based survey of back pain beliefs in Canada . Spine , 31 ( 18 ), 2142 – 2145 .
Ibrahim , S. A. , Stone , R. A. , Han , X. , Cohen , P. , Fine , M. J. , Henderson , W. G. , … Kwoh , C. K. ( 2005 ). Racial/ethnic differences in surgical outcomes in veterans fol-lowing knee or hip arthroplasty [Research Support, Non-U.S. Gov’t Research Support, U.S. Gov’t, Non-P.H.S.] . Arthritis and Rheumatism , 52 ( 10 ), 3143 – 3151 .
Khan , F. A. , & Nazir , S. ( 2007 ). Assessment of preoperative anxiety in patients for elective surgery . Journal of Anesthesiology Clinical Pharmacology , 23 ( 3 ), 259 – 262 .
LaMontagne , L. , Hepworth , J. T. , Salisbury , M. H. , & Cohen , F. ( 2003 ). Effects of coping instruction in re-ducing young adolescents’ pain after major spinal sur-gery . Orthopaedic Nursing , 22 ( 6 ), 398 – 403 .
Lavernia , C. J. , Alcerro , J. C. , & Rossi , M. D. ( 2010 ). Fear in arthroplasty surgery: The role of race [Comparative Study Research Support, Non-U.S. Gov’t] . Clinical Orthopaedic and Related Research , 468 ( 2 ), 547 – 554 .
Copyright © 2014 by National Association of Orthopaedic Nurses. Unauthorized reproduction of this article is prohibited.
ONJ625_LR 214ONJ625_LR 214 7/19/14 3:04 AM7/19/14 3:04 AM
© 2014 by National Association of Orthopaedic Nurses Orthopaedic Nursing • July/August 2014 • Volume 33 • Number 4 215
Long , D. M. , BenDebba , M. , Torgerson , W. S. , Boyd , R. J. , Dawson , E. G. , Hardy , R. W. , … Watts , C. ( 1996 ). Persistent back pain and sciatica in the United States: Patient characteristics . Journal of Spinal Disorders , 9 ( 1 ), 40 – 58 .
Louw , A. , Diener , I. , Butler , D. S. , & Puentedura , E. J. ( 2011 ). The effect of neuroscience education on pain, disability, anxiety, and stress in chronic musculoskel-etal pain [Review] . Archives of Physical Medicine and Rehabilitation , 92 ( 12 ), 2041 – 2056 .
Louw , A. , Louw , Q. , & Crous , L. C. C. ( 2009 ). Preoperative education for lumbar surgery for radiculopathy . South African Journal of Physiotherapy , 65 ( 2 ), 3 – 8 .
Lurie , J. D. , Birkmeyer , N. J. , & Weinstein , J. N. ( 2003 ). Rates of advanced spinal imaging and spine surgery . Spine , 28 ( 6 ), 616 – 620 .
Mackenzie , J. W. ( 1989 ). Daycase anaesthesia and anxiety. A study of anxiety profi les amongst patients attending a day bed unit . Anaesthesia , 44 ( 5 ), 437 – 440 .
Martin , B. I. , Mirza , S. K. , Comstock , B. A. , Gray , D. T. , Kreuter , W. , & Deyo , R. A. ( 2007 ). Are lumbar spine reoperation rates falling with greater use of fusion sur-gery and new surgical technology ? Spine , 32 ( 19 ), 2119 – 2126 .
McAfee , P. C. , Geisler , F. H. , Saiedy , S. S. , Moore , S. V. , Regan , J. J. , Guyer , R. D. , … Cunningham , B. ( 2006 ). Revisability of the CHARITE artifi cial disc replace-ment: Analysis of 688 patients enrolled in the U.S. IDE study of the CHARITE Artifi cial Disc . Spine , 31 ( 11 ), 1217 – 1226 .
McDonald , S. , Hetrick , S. , & Green , S. ( 2004 ). Pre-operative education for hip or knee replacement [Meta-Analysis Review] . Cochrane Database of Systematic Review , ( 1 ), CD003526 .
McGregor , A. H. , Dore , C. J. , Morris , T. P. , Morris , S. , & Jamrozik , K. ( 2011 ). ISSLS prize winner: Function After Spinal Treatment, Exercise, and Rehabilitation (FASTER): A factorial randomized trial to determine whether the functional outcome of spinal surgery can be improved. [Research Support, Non-U.S. Gov’t] . Spine , 36 ( 21 ), 1711 – 1720 .
Morris , S. , Morris , T. P. , McGregor , A. H. , Dore , C. J. , & Jamrozik , K. ( 2011 ). Function after spinal treatment, exercise, and rehabilitation: Cost-effectiveness analy-sis based on a randomized controlled trial [Research Support, Non-U.S. Gov’t] . Spine , 36 ( 21 ), 1807 – 1814 .
Muglali , M. , & Komerik , N. ( 2008 ). Factors related to pa-tients’ anxiety before and after oral surgery . Journal of Oral and Maxillofacial Surgery , 66 ( 5 ), 870 – 877 .
O’Conner-Von , S. ( 2008 ). Preparation of adolescents for outpatient surgery: Using an Internet program . AORN Journal , 87 ( 2 ), 374 – 398 .
Ostelo , R. W. , de Vet , H. C. , Vlaeyen , J. W. , Kerckhoffs , M. R. , Berfelo , W. M. , Wolters , P. M. , & van den Brandt , P. A. ( 2003 ). Behavioral graded activity following fi rst-time lumbar disc surgery: 1-year results of a rand-omized clinical trial . Spine , 28 ( 16 ), 1757 – 1765 .
Ostelo , R. W. , de Vet , H. C. , Waddell , G. , Kerckhoffs , M. R. , Leffers , P. , & van Tulder , M. ( 2003 ). Rehabilitation fol-lowing fi rst-time lumbar disc surgery: A systematic review within the framework of the Cochrane collabo-ration . Spine , 28 ( 3 ), 209 – 218 .
Perks , A. , Chakravarti , S. , & Manninen , P. ( 2009 ). Preoperative anxiety in neurosurgical patients . Journal of Neurosurgical Anesthesiology , 21 ( 2 ), 127 – 130 .
Powell , C. ( 2003 ). The Delphi technique: Myths and reali-ties . Journal of Advanced Nursing , 41 ( 4 ), 376 – 382 .
Rice , M. , Glasper , A. , Keeton , D. , & Spargo , P. ( 2008 ). The effect of a preoperative education programme on peri-
operative anxiety in children: An observational study . Paediatric Anaesthesia , 18 ( 5 ), 426 – 430 .
Rosen , S. , Svensson , M. , & Nilsson , U. ( 2008 ). Calm or not calm: The question of anxiety in the perianesthesia pa-tient . Journal of Perianesthesia Nursing , 23 ( 4 ), 237 – 246 .
Salzwedel , C. , Petersen , C. , Blanc , I. , Koch , U. , Goetz , A. E. , & Schuster , M. ( 2008 ). The effect of detailed, video-assisted anesthesia risk education on patient anxiety and the duration of the preanesthetic interview: A ran-domized controlled trial . Anesthesia and Analgesia , 106 ( 1 ), 202 – 209 .
Schmidt , C. O. , Raspe , H. , Pfi ngsten , M. , Hasenbring , M. , Basler , H. D. , Eich , W. , … Kohlmann , T. ( 2007 ). Back pain in the German adult population: Prevalence, sever-ity, and sociodemographic correlates in a multiregional survey . Spine (Philadelphia Pa 1976) , 32 ( 18 ), 2005 – 2011 .
Siepe , C. J. , Mayer , H. M. , Wiechert , K. , & Korge , A. ( 2006 ). Clinical results of total lumbar disc replacement with ProDisc II: Three-year results for different indications . Spine , 31 ( 17 ), 1923 – 1932 .
Skinner , J. , Weinstein , J. N. , Sporer , S. M. , & Wennberg , J. E. ( 2003 ). Racial, ethnic, and geographic disparities in rates of knee arthroplasty among Medicare patients [Research Support, Non-U.S. Gov’t Research Support, U.S. Gov’t, P.H.S.] . New England Journal of Medicine , 349 ( 14 ), 1350 – 1359 .
Starkweather , A. R. , Witek-Janusek , L. , Nockels , R. P. , Peterson , J. , & Mathews , H. L. ( 2006 ). Immune func-tion, pain, and psychological stress in patients under-going spinal surgery . Spine (Philadelphia Pa 1976) , 31 ( 18 ), E641 – E647 .
Toyone , T. , Tanaka , T. , Kato , D. , Kaneyama , R. , & Otsuka , M. ( 2005 ). Patients’ expectations and satisfaction in lumbar spine surgery . Spine , 30 ( 23 ), 2689 – 2694 .
Trief , P. M. , Grant , W. , & Fredrickson , B. ( 2000 ). A prospec-tive study of psychological predictors of lumbar sur-gery outcome . Spine (Philadelphia Pa 1976) , 25 ( 20 ), 2616 – 2621 .
Urquhart , D. M. , Bell , R. J. , Cicuttini , F. M. , Cui , J. , Forbes , A. , & Davis , S. R. ( 2008 ). Negative beliefs about low back pain are associated with high pain intensity and high level disability in community-based women . BMC Musculoskeletal Disorders , 9 , 148 .
Waddell , G. , & Burton , A. K. ( 2005 ). Concepts of rehabilita-tion for the management of low back pain . Best Practice and Research Clinical Rheumatology , 19 ( 4 ), 655 – 670 .
Walters , M. , & Coad , J. ( 2006 ). Preparation of children for spinal surgery: An exploratory study . Paediatric Nursing , 18 ( 10 ), 27 – 29 .
Wang , Y. J. , Shen , J. , Lu , J. K. , & Yang , X. D. ( 2008 ). [Preoperative anxiety and depression in patients un-dergoing cardiac surgery and related infl uencing fac-tors] . Zhonghua Yi Xue Za Zhi , 88 ( 39 ), 2759 – 2762 .
Weinstein , J. N. , Lurie , J. D. , Olson , P. R. , Bronner , K. K. , & Fisher , E. S. ( 2006 ). United States’ trends and regional variations in lumbar spine surgery: 1992–2003 . Spine , 31 ( 23 ), 2707 – 2714 .
Yazici , Y. , Kautiainen , H. , & Sokka , T. ( 2007 ). Differences in clinical status measures in different ethnic/racial groups with early rheumatoid arthritis: Implications for interpretation of clinical trial data [Research Support, N.I.H., Extramural] . Journal of Rheumatology , 34 ( 2 ), 311 – 315 .
Yee , A. , Adjei , N. , Do , J. , Ford , M. , & Finkelstein , J. ( 2008 ). Do patient expectations of spinal surgery relate to functional outcome ? Clinical Orthopaedics and Related Research , 466 ( 5 ), 1154 – 1161 .
Copyright © 2014 by National Association of Orthopaedic Nurses. Unauthorized reproduction of this article is prohibited.
ONJ625_LR 215ONJ625_LR 215 7/19/14 3:04 AM7/19/14 3:04 AM

216 Orthopaedic Nursing • July/August 2014 • Volume 33 • Number 4 © 2014 by National Association of Orthopaedic Nurses
Appendix
LUMBAR SURGERY QUESTIONNAIRE Please read the following statements. On the 5-point scale provided, please mark with an X your answer in relation to you “totally agreeing,” “agreeing,” “neutral,” “disagreeing,” or “totally disagreeing” with the statement.
1. Lower back surgery is successful.
� Totally agree � Agree � Neutral � Disagree � Totally disagree
2. Lower back surgery is successful for treating pain in the lower back.
� Totally agree � Agree � Neutral � Disagree � Totally disagree
3. Lower back surgery is successful for treating symptoms into the leg (e.g., pain, numbness, weakness, tingling).
� Totally agree � Agree � Neutral � Disagree � Totally disagree
4. After lower back surgery, people are able to return to their prior level of activity.
� Totally agree � Agree � Neutral � Disagree � Totally disagree
5. Following lower back surgery you can expect the pain to be gone.
� Totally agree � Agree � Neutral � Disagree � Totally disagree
6. If you had severe low back pain, would you undergo lower back surgery?
� Totally agree � Agree � Neutral � Disagree � Totally disagree
7. I would be afraid to have lower back surgery.
� Totally agree � Agree � Neutral � Disagree � Totally disagree
8. Side effects are common after lower back surgery.
� Totally agree � Agree � Neutral � Disagree � Totally disagree
9. Following back surgery, I would be afraid to return to work or participate in previous physical activities?
� Totally agree � Agree � Neutral � Disagree � Totally disagree
10. I would rather try any/all other means of treatments (i.e., physical therapy, medication) before opting for lower back surgery
� Totally agree � Agree � Neutral � Disagree � Totally disagree
11. Recovery time after low back surgery is long.
� Totally agree � Agree � Neutral � Disagree � Totally disagree
Copyright © 2014 by National Association of Orthopaedic Nurses. Unauthorized reproduction of this article is prohibited.
National Offerings
May 16-19, 2015—NAON 35th Annual Congress. Care to be, Care to do, Care a calling. Nashville, TN.
Regional Offerings
August 22, 2014—Bone Up On Your Orthopaedic Skills Workshop. Provided by Swedish Hospital. Hosted by Denver NAON Chapter. Holiday Inn Denver East-Stapleton, 3333 Quebec St, Denver, CO 80207. For information, contact: Mary Jane Carroll, tel: (720) 373-5254 or [email protected].
September 23, 2014—NAON Orthopaedic Nursing Review Course. Provided by NAON. Hosted by Sanford Health. Sanford Health, 1711 S University Dr, Fargo, ND 58122-1511. For information, contact: Pam Friedrich, tel: 701-280-4804 or [email protected].
October 24, 2014—BONES 10th Anniversary at Hilton San Diego Mission Valley. Sponsored by University of San Diego Health System. For more information contact Chad Hutchison at 619-543-6177 or e-mail [email protected]. The link to register: http://health.ucsd.edu/medinfo/nursing/bones/Pages/default.aspx.
CALENDAR
ONJ625_LR 216ONJ625_LR 216 7/19/14 3:04 AM7/19/14 3:04 AM




















