The search for susceptibility genes in lumbar disc degeneration
Upload
khangminh22Category
view
3download
0
Utah State University Utah State University
DigitalCommons@USU DigitalCommons@USU
All Graduate Theses and Dissertations Graduate Studies
5-2012
Outcomes and Presurgical Correlates of Lumbar Fusion in Utah Outcomes and Presurgical Correlates of Lumbar Fusion in Utah
Workers' Compensation Patients: A Replication Study Workers' Compensation Patients: A Replication Study
Jessica M. Gundy Utah State University
Follow this and additional works at: https://digitalcommons.usu.edu/etd
Part of the Psychology Commons
Recommended Citation Recommended Citation Gundy, Jessica M., "Outcomes and Presurgical Correlates of Lumbar Fusion in Utah Workers' Compensation Patients: A Replication Study" (2012). All Graduate Theses and Dissertations. 1174. https://digitalcommons.usu.edu/etd/1174
This Dissertation is brought to you for free and open access by the Graduate Studies at DigitalCommons@USU. It has been accepted for inclusion in All Graduate Theses and Dissertations by an authorized administrator of DigitalCommons@USU. For more information, please contact [email protected].
OUTCOMES AND PRESURGICAL CORRELATES OF LUMBAR FUSION IN UTAH
WORKERS�’ COMPENSATION PATIENTS: A REPLICATION STUDY
by
Jessica M. Gundy
A dissertation submitted in partial fulfillment of the requirements for the degree
of
DOCTOR OF PHILOSOPHY
in
Psychology Approved: M. Scott DeBerard, Ph.D. Susan L. Crowley, Ph.D. Major Professor Committee Member Michael P. Twohig, Ph.D. JoAnn T. Tschanz, Ph.D. Committee Member Committee Member Edward M. Heath, Ph.D. Mark R. McLellan, Ph.D. Committee Member Vice President for Research and Dean of the School of Graduate Studies
UTAH STATE UNIVERSITY Logan, Utah
2012

ii
Copyright © Jessica M. Gundy 2012
All Rights Reserved

iii
ABSTRACT
Outcomes and Presurgical Correlates of Lumbar Fusion in Utah Workers�’
Compensation Patients: A Replication Study
by
Jessica M. Gundy, Doctor of Philosophy
Utah State University, 2012
Major Professor: M. Scott DeBerard, Ph.D. Department: Psychology
Lumbar fusion performed among injured workers has dramatically increased over
the past two decades, coinciding with the increased use of more advanced surgical
technology. Despite recent changes in how this surgery is performed, few outcome
studies have been conducted, particularly among workers compensation populations. In
prior studies, several biopsychosocial risk factors were found to be predictors of
functional outcomes of lumbar fusion. Considering the recent changes in lumbar fusion
surgery, there is a need to identify how patient outcomes have changed among injured
workers, and whether a biopsychosocial model continues to be predictive of outcomes.
The current study aimed to address multidimensional patient outcomes associated with
lumbar fusion and examine the relationship between presurgical biopsychosocial
variables and outcomes by testing the predictive efficacy of a multiple variable model.
Injured workers (N = 245) who underwent their first lumbar fusion between 1998
iv and 2007 were included in a retrospective-cohort study performed in two phases that
involved coding presurgical information documented in patient medical charts in the
Worker�’s Compensation Fund of Utah computer database (Phase 1) and administering a
telephone outcome survey with patients at least 2 years post-surgery (Phase 2). Of the
total sample, 45% (n = 110) of patients were contacted and completed follow-up outcome
surveys on several measures of patient satisfaction, quality of life, fusion status,
dysfunction level, disability status, pain, and general physical and mental health
functioning.
Results revealed injured workers reported a solid fusion rate of 89.0%, disability
rate of 28.7%, and a poor outcome rate of 57.1%. Multiple linear regression analyses
demonstrated an eight variable model was a statistically significant predictor of multiple
patient outcomes. Involvement of a nurse case manger, vocational rehabilitation, and
litigation at the time of fusion were the most prominent predictors across outcome
measures, while age and depression history showed modest prediction of outcomes. Prior
back operations, number of vertebral levels fused, and type of instrumentation showed no
statistically significant prediction of outcomes. Results were evaluated and compared to
prior lumber fusion studies on injured worker and fusion outcome literature, in general.
Specific implications for our findings and limitations associated with this study were
addressed.
(164 pages)
v
PUBLIC ABSTRACT
Outcomes and Presurgical Correlates of Lumbar Fusion in Utah Workers�’
Compensation Patients: A Replication Study
by
Jessica M. Gundy, Doctor of Philosophy
Utah State University, 2012
Over the past 2 decades, lumbar fusion surgeries performed in the United States
have increased dramatically, particularly for compensated workers. Costs for these
procedures have also risen substantially in the past decade, primarily due to the use of
more sophisticated surgical devices such as interbody fusion cages. While surgical
instrumentation and technology may improve the rates of solid bony vertebral fusion,
overall improvements in quality of life and pain outcomes related to this new technology
are still inconclusive.
In collaboration with the Workers Compensation Fund of Utah (WCFU) and Utah
State University (USU), a psychology professor, Dr. M. Scott DeBerard, and a USU
doctoral student, Jessica Gundy, proposed a study examining multiple outcomes of
lumbar fusion surgery in a sample of injured workers. The projects main purpose was to
evaluate several biological, social, and, psychological outcomes among injured workers
undergoing lumbar fusion in terms of quality of life, fusion rates, patient satisfaction, and

vi disability. Another important aim was to evaluate how outcomes have changed since the
advent of new spine surgical fusion technology.
Findings from our project show that over the past decade, overall fusion rates
have increased significantly. However, despite enhanced fusion rates, injured workers
who have undergone lumbar fusion in Utah demonstrated somewhat worse outcomes
than those documented a decade ago. Specifically, the present study demonstrated
significant increases in disability rates and reported decreases in functional capacity and
poor quality of life. While these findings do not support the position that compensated
workers cannot benefit from lumbar fusion, they do highlight the importance of medical
providers and surgeons to use more discretion when recommending lumbar fusion as a
treatment option for injured workers. Further, there appear to be some strong incentives
for surgeons to perform lumbar fusion with surgical devices that do not have adequate
evidence to support their utility. These issues are imperative when considering both the
financial costs associated with these surgeries, as well as the human costs such as pain,
suffering, time away from family, job loss, and overall disability.
vii
ACKNOWLEDGMENTS
The process of completing this project was a long journey and I had invaluable
support, advice, and assistance along the way. I want to first express my overwhelming
gratitude to my advisor and mentor, Dr. Scott DeBerard, who believed in my ability to
take on this project. He taught me so much and I am grateful to have a mentor who will
have an enduring impact throughout my future career as a psychologist. I would also like
to thank my committee members, Drs. Michael Twohig, JoAnn Tschanz, Susan Crowley,
and Edward Heath, who all gave important input and encouragement to make this project
what it is. I also appreciate the Workers Compensation Fund of Utah for providing access
to our population of interest.
My lab partner and friend, Anthony Wheeler, was a valuable collaborator and
contributed to this project�’s integrity. Casey Nelson was also an asset who helped with
data entry. Thanks to Tyler Christensen for guiding me through the dissertation process. I
want to thank Kim Pratt and Michelle Woidneck for being my confidants over the last 4
years. I cannot imagine having this experience without you both. I will treasure going
through this extraordinary journey together. I am incredibly grateful to my parents who
continuously provided the love and support I needed to give me the strength to pursue a
doctorate. Joe, I will be forever thankful for the encouragement and love you gave me
throughout this journey. Finally, I thank the participants of this study for giving me their
time and energy to help bring awareness to better serve future patients. Talking about
pain and suffering is not easy and I am inspired by the courage of these individuals.
Jessica M. Gundy

viii
CONTENTS
Page ABSTRACT ................................................................................................................... iii PUBLIC ABSTRACT ................................................................................................... v ACKNOWLEDGMENTS ............................................................................................. vii LIST OF TABLES ......................................................................................................... x LIST OF FIGURES ....................................................................................................... xii CHAPTER I. INTRODUCTION AND STATEMENT OF THE PROBLEM ..................... 1 II. REVIEW OF LITERATURE ......................................................................... 8 Low Back Pain: General Prevalence and Workplace Prevalence ................... 8 Low Back Pain: Costs ..................................................................................... 9 Low Back Pain: Progression of Treatments Used .......................................... 10 Lumbar Fusion: Indications and Procedure .................................................... 11 Lumbar Fusion: Prevalence and Cost ............................................................. 13 Lumbar Fusion: Review of Outcome Measures ............................................. 14 Lumbar Fusion: Review of Outcomes Studies ............................................... 16 Lumbar Fusion: Review of Variables Predictive of Outcomes ...................... 19 Conclusions from the Literature Review ........................................................ 30 Research Purpose and Study Objectives ......................................................... 31 Research Questions ......................................................................................... 31 III. METHODS ..................................................................................................... 35 Population and Sample ................................................................................... 35 Study Design ................................................................................................... 37 Procedure ........................................................................................................ 37 Materials and Instrumentation ........................................................................ 39 Analysis........................................................................................................... 46 IV. RESULTS ....................................................................................................... 48 Descriptive Statistics ....................................................................................... 48
ix
Page
Response Rates and Bias Checks .................................................................... 52 Patient Outcomes ............................................................................................ 56 Intercorrelations of Outcome .......................................................................... 66 Correlations Between Patient Characteristics and Outcomes ......................... 68 Multivariate Prediction of Outcomes .............................................................. 69 Summary of Outcome Prediction .................................................................... 85 V. DISCUSSION ................................................................................................. 87 Descriptive Characteristics of Patient and Procedural Variables ................... 87 Multidimensional Outcomes of Fusion ........................................................... 89 Multivariate Prediction of Outcomes .............................................................. 93 Implications..................................................................................................... 98 Limitations and Future Research .................................................................... 102 REFERENCES .............................................................................................................. 105 APPENDICES ............................................................................................................... 119 Appendix A: Medical Records Review Instrument ...................................... 120 Appendix B: Letter of Information ............................................................... 125 Appendix C: Fusion Study Telephone Survey Cover Sheet ........................ 128 Appendix D: Telephone Outcome Script ..................................................... 130 Appendix E: Stauffer-Coventry Index, Global Perceived Effect, Verbal Numeric Rating Scale, and Patient Satisfaction Items ............ 132 Appendix F: Rolland-Morris Disability Questionnaire ............................... 135 Appendix G: Short Form Health Survey, Version 2, Standard Interview for SF-36 Health Survey ......................................................... 137 Appendix H: The Pain Catastrophizing Scale (PCAS) ................................. 142 CURRICULUM VITAE ................................................................................................ 144

x
LIST OF TABLES
Table Page 1. Descriptive Statistics of Patient Characteristics ................................................ 49 2. Descriptive Statistics of Patient Diagnosis and Surgical Variables ................... 51 3. Comparisons of Select Patient Variables for Patient Follow-up Versus Patients Lost to Follow-Up ................................................................................ 53 4. Correlations Between Patient and Procedural Variables ................................... 55 5. Fusion Status, Disability Status and Roland-Morris Disability Questionnaire Outcomes and Comparisons with Prior Study ................................................... 57 6. Patient Satisfaction and Quality of Life Related to Fusion Outcomes .............. 58 7. The Stauffer-Coventry Index Outcomes ............................................................ 61 8. Global Perceived Effect and Verbal Numeric Rating Scale .............................. 62 9. Pain Catastrophizing Scale (PCAS) Scores and Comparisons .......................... 63 10. SF-36(v.2) Multidimensional Health Outcomes and Comparisons ................... 65 11. Correlations Between Outcome Variables ......................................................... 67 12. Correlations of Prefusion Variables with Selected Outcome Variables ............ 70 13. Correlations of Prefusion Variables with Short-Form 36 Subscales and Composite Scales ............................................................................................... 71 14. Logistic Regression Model: Disability Classification ....................................... 74 15. Logistic Regression Equation Predicting Disability Status with Eight Prefusion Variables as Predictors ...................................................................... 74 16. Simultaneous-Entry Multiple Regression Model Predicting the RDQ Total Score ......................................................................................................... 75 17. Simultaneous-Entry Multiple Regression Model Predicting the SF-36 Physical Component Summary Score ................................................................ 77

xi Table Page 18. Simultaneous-Entry Multiple Regression Model Predicting the SF-36 Mental Component Summary Score .................................................................. 77 19. Simultaneous-Entry Multiple Regression Model Predicting the SF-36 Physical Functioning Subscale .......................................................................... 78 20. Simultaneous-Entry Multiple Regression Model Predicting the SF-36 Role-Physical Subscale ...................................................................................... 79 21. Simultaneous-Entry Multiple Regression Model Predicting the SF-36 Bodily Pain Scale ............................................................................................... 79 22. Simultaneous-Entry Multiple Regression Model Predicting the SF-36 General Health Subscale .................................................................................... 80 23. Simultaneous-Entry Multiple Regression Model Predicting the SF-36 Vitality Subscale ................................................................................................ 80 24. Simultaneous-Entry Multiple Regression Model Predicting the SF-36 Social Functioning Subscale .............................................................................. 81 25. Simultaneous-Entry Multiple Regression Model Predicting the SF-36 Role-Emotional Subscale ................................................................................... 81 26. Simultaneous Entry Multiple Regression Model Predicting the SF-36 Mental Health Subscale ..................................................................................... 82

xii
LIST OF FIGURES Figure Page 1. A summary of patient and outcome variables.................................................... 32 2. Process of patient selection and follow-up participation ................................... 36 3. Research questions and associated analyses ...................................................... 47 4. Short Form-36 subscale and summary scores for fusion patients, back pain/sciatica sample, and general population ..................................................... 66
CHAPTER I
INTRODUCTION AND STATEMENT OF THE PROBLEM
Low back pain (LBP) represents one of the most complex and costly public health
concerns for society. LBP is the most prevalent type of pain reported by adults (Deyo,
Mirza, & Martin, 2006) and is the fifth most common reason for physician visits in the
US (Hart, Deyo, & Cherkin, 1995). A recent national survey indicated that annually more
than 50% of working-age adults experience LBP and 15% to 20% of those people seek
medical help every year (Hurwitz & Shekelle, 2006). Further, a North American
epidemiology review indicated point prevalence rates of LBP range from 13.7% to 28.7%
(Loney & Stratford, 1999).
High LBP prevalence rates are particularly concerning for work-place
populations. An estimated 5.6 million cases of work-related back pain were documented
in 1995 (Murphy & Volinn, 1999), with projections that 60% to 80% of the adult
population will experience at least one episode of LBP during their active work life
(Nordin, Andersson, & Pope, 1997). Further, LBP represents approximately16% of all
workplace compensation claims and is the most common reason for workers to file
compensation claims in the US (Hadler, Carey, & Garrett, 1995). Such a high prevalence
has had a dramatic influence on costs related to LBP for general and workplace
populations.
The economic impact of LBP can be understood in terms of the total costs that the
disease has incurred compared to the expense if the problem did not exist (Dagenais,
Caro, & Haldeman, 2008). This incorporates both direct health care costs and indirect

2 tangential costs related to loss of employment and decreased productivity (Mantyselka,
Kumpusalo, Ahonen, & Takala, 2002). The total cost of LBP in the US exceeds $100
billion per year with indirect expenses, such as lost wages and decreased productivity,
accounting for almost two thirds of total costs (Katz, 2006). LBP has had a significant
impact on the workers�’ compensation system, which covers approximately 127 million
U.S. workers (Green-McKenzie, 2004). Workers�’ compensation is a system of state and
federal laws that provides benefits for employees who are injured on the job. The
compensation amount is based on any monetary loss associated with the specific injury
that usually includes medical bills, hospital bills, wage replacement, rehabilitation,
medications, and additional related expenses. In 1994, it was projected more than $11
billion was paid annually in the US for workers�’ compensation benefits for work-related
LBP (Webster & Snook, 1994). For workers�’ compensation claims, LBP injury accounts
for 33% to 41% of the total costs, but only accounts for 10% to 19% of all compensation
claims filed (Hadler et al., 1995; Nachemson, 1992).
In 1994, the U.S. Department of Health and Human Services implemented
evidence-based guidelines for the treatment of lumbar and thoracic pain (Bigos et al.,
1994). The guidelines stressed the need to shift attention away from focusing care
exclusively on conventional treatments to address acute and chronic LBP and move
toward helping patients improve activity tolerance. Acute LBP is typically defined as
pain that persist less than 6 weeks with symptoms often ranging from muscle ache and
limited flexibility (Kinkade, 2007). However, some acute pain syndromes can become
more serious. LBP is often considered chronic if it persists for more than 7-12 weeks
3 (Andersson, 1999). Recently, The American College of Physicians (ACP) and the
American Pain Society (APS) issued a comprehensive joint clinical practice guideline for
the diagnosis and treatment of acute and chronic LBP (Chou et al., 2007). These
guidelines offer recommendations related to how to categorize the type of LBP patients
experience, when and what type of diagnostic imaging tests to perform, what medications
to prescribe based on patients pain and functional impairment, and the usefulness of
nonpharmacological therapy. Although these guidelines are intended to assist clinicians
with patient management and to promote the use of conservative treatments, there has
been little done to translate these guidelines for managing workplace LBP. Further,
despite most of these guidelines advocating conservative nonsurgical care as first line
approaches, increasing numbers of patients are having spine surgery.
Internationally, the US has the highest rate of back surgery (Ehrlich, 2003). There
are many types of LBP surgery used today (discectomy, foraminotomy, laminectomy,
fusion, fusion). Typically, a first line spine surgery will involve a less invasive procedure.
For example, discectomy is considered a less invasive surgical treatment for herniated
discs of the lumbar spine that involves removing part of the damaged disc to relieve the
pressure on the nerve tissue causing the pain (Spangler, 1982). While this procedure is
often effective in reducing pain, long-term follow-up studies suggest that a significant
number of patients have poor outcomes (DeBerard, LaCaille, Spielmans, Colledge, &
Parlin, 2009; Loupasis et al., 1999). Such patients, particularly those with spinal
instability, will turn to lumbar fusion surgery as a next possible solution.
The underlying principle for lumbar fusion surgery assumes that instability of

4 vertebral bodies is causing pressure on spinal nerves, which, in turn, causes LBP and
associated neurological symptoms (e.g., sciatica, reflex changes, muscle weakness)
(Herkowitz, 1995). Thus, by fusing the unstable vertebral bodies, and limiting their
movement, it is presumed the fusion will reduce pain, increase function, and quality of
life (An et al., 2003). Surgical implants (also known as instrumentation) are often used
for lumbar fusion surgeries to provide additional spinal stability while helping the fusion
solidify, thus improving the rates of successful spinal fusion. Examples of such implants
include pedicle screws and rods and interbody fusion cages (Deyo, Gray, Kreuter, Mirza,
& Martin, 2005).
Since 1992, lumbar fusion surgeries performed in the US have dramatically
increased when compared to other less invasive procedures such as lumbar discectomy
and laminectomy (Weinstein, Lurie, Olson, Bronner, & Fisher, 2006). Rates of lumbar
fusion surgery in the US have risen more than 250% over the past decade (Deyo &
Mirza, 2006), with more than 200,000 spinal fusion surgeries performed annually to
relieve discogenic back pain and instability (Starkweather, 2006). The prevalence of
fusion surgeries performed is even more concerning for compensated workers. In one
study, patients with work-place LBP injuries covered by workers�’ compensation were
1.37 times more likely to undergo surgery involving fusion than other patients with LBP
and almost twice as likely to have a subsequent reoperation within 3 years of the index
surgery (Taylor, Deyo, Ciol, & Kreuter, 1996).
In the past decade, overall costs for spinal fusion are estimated to have increased
more than 500%, from $75 million to $482 million. In 1992, lumbar fusion represented
5 14% of total spending for back surgery; by 2003, the number increased to 47%
(Weinstein et al., 2006). A recent study comparing current medical costs for compensated
lumbar fusion patients in Utah to costs identified in a prior similar study in the 1990s
revealed medical costs have risen approximately 174% (Wheeler, Gundy, & DeBerard, in
press). The high prevalence and cost increase is likely due, in part, to an introduction and
use of more sophisticated surgical devices in the early 1990s (e.g., interbody fusion
cages; Deyo et al., 2005).
However, while such surgical instrumentation and technology may improve the
rate of solid fusion, overall improvements in quality of life and pain outcomes related to
this new technology are still inconclusive (DeFrances & Hall, 2007; Deyo & Mirza,
2006). In fact, a recent study demonstrated no benefit in outcomes for patients who
underwent more complex and expensive fusion surgeries (Wilson-MacDonald et al.,
2008). Further, there is evidence that patients with LBP who receive workers�’
compensation have even poorer clinical fusion outcomes than other patients with back
problems (DeBerard, Masters, Colledge, & Holmes, 2003; Taylor et al., 1996). In Utah, a
study on lumbar fusion outcomes for compensated workers at 2-year postsurgical follow-
up found that 36.1% of fusion patients reported worse pain with 35.4% demonstrating
their overall quality of life was no better than before surgery (DeBerard, Masters,
Colledge, Schleusener, & Schlegel, 2001). Additional research has indicated that the use
of surgical implantation is associated with increased risk of complications and showed no
improvements in disability or reoperation rates versus noninstrumented fusion (Maghout-
Juratli, Franklin, Mirza, Wickizer, & Fulton-Kehoe, 2006). Although such studies have
6 started to address outcomes related to new surgical technology, research has been limited
to surgeries performed before 2001 when the use of interbody fusion cages was just
starting to climb.
Due to these considerable cost increases, amplified use of lumbar fusion surgery,
and poor clinical outcomes, there is an impetus to examine presurgical patient
characteristics that might predispose patients to differential outcomes. Presurgical
psychosocial predictors have been shown to be important in predicting surgical outcomes
for LBP patients (DeBerard et al., 2001; Keeley et al., 2008). DeBerard and colleagues
(2001) identified several presurgical psychosocial variables as correlates related to the
surgical outcomes of Utah workers who received lumbar fusion surgery. The study
showed that older age, lawyer involvement, increased number of prior low back
surgeries, low income, compensation, increased time of work disability, and depression
were all predictive of lumbar fusion outcomes. The study also found that a diagnostic
severity index based upon presurgical imaging studies (MRI, CT) did not predict fusion
outcomes indicating that presurgical psychosocial factors are more consistently predictive
of patient outcomes. In terms of work-related and compensation variables, another Utah
study showed that workers compensation claims involving a nurse case manager and
vocational rehabilitation prior to lumbar discectomy were more likely to have poorer
outcomes (DeBerard et al., 2009). However, no known studies to date have addressed
how these particular variables might impact lumbar fusion outcomes. Additionally,
research on LBP patients has shown that that anxiety, depression, fear avoidance beliefs
relating to work, and back-pain related stresses predicted impairment in subsequent
7 physical health-related quality of life and healthcare utilization (Keeley et al., 2008).
While such studies have had a significant impact on influencing evidence based
guidelines for surgical decisions regarding lumbar fusion, screening for psychosocial
variables that may identify LBP patients at risk for poorer outcomes is still not a common
procedure in clinics for work-place injury patients.
There is evidence of substantial increases in the prevalence and costs associated
with lumbar fusion surgery. Development of new surgical implant technology to facilitate
solid fusion is clearly associated with these increases. Despite advances in surgery
technology, it is unclear if outcomes associated with lumbar fusion have improved
significantly over time. Recent studies suggest a significant number of patients still
experience poor clinical outcomes following lumbar fusion. Lumbar fusion has been
studied less in workers�’ compensation patients, and while preliminary studies suggest a
substantial percent of poor outcomes in this population, additional outcome studies are
clearly needed, particularly given the increase in cost as a result of increased surgical
technology. There is also a clear need to further investigate how presurgical factors
influence lumbar fusion outcomes among worker�’s compensation patients. The current
study has three primary purposes: (a) to examine patient presurgical variables and
understand the interrelationships between such variables; (b) to characterize multiple
outcomes associated with lumbar spinal fusion surgery patients in terms of quality of life,
function, and health status variables, as well as fusion rates, patient satisfaction, and
disability; and (c) to explore the relationship of presurgical variables to outcomes and test
the predictive efficacy of a multiple variable predictive model.

8
CHAPTER II
REVIEW OF LITERATURE
The following literature review describes studies related to LBP, lumbar fusion
outcomes, workers compensation populations, and back pain related disability. The
primary purposes of this review were to: (a) describe estimated prevalence and costs of
LBP and lumbar fusion; (b) characterize contemporary indications and surgical
procedures for lumbar fusion; (c) describe patient outcomes associated with lumbar
fusion, particularly among injured workers; and (d) identify potential presurgical
biopsychosocial correlates of outcomes. Articles were primarily identified through the
Medline and PsychINFO computer databases using the following search terms: lumbar
fusion; patient outcomes; biopsychosocial; prediction, workers compensation. Based
upon this review, a comprehensive list of relevant presurgical biopsychosocial patient
variables and outcomes were proposed for purposes of this study. The study produced a
specific multivariate predictive model of surgical outcomes based on the number of
presurgical variables reviewed and analyzed.
Low Back Pain: General Prevalence and Workplace Prevalence
LBP is among the most significant socioeconomic and medical problems in our
society. In the US, LBP is known as one of the most common symptom for which people
seek medical care (Deyo et al., 2006) with point prevalence rates ranging from 14% to
28% (Loney & Stratford, 1999). A recent survey by (Deyo et al., 2006) showed
approximately one quarter of U.S. adults reported back pain during a 3-month period.
9 Hurwitz and Shekelle (2006) reported similar finding indicating, annually, more than
50% of working age adults experience LBP and 15% to 20% of those people seek
medical help.
LBP is shown to be responsible for approximately 16% of all workplace
compensation claims and is the most common reason for workers to file compensation
claims in the US (Hadler et al., 1995). In 1995, an estimated 5.6 million cases were
documented for work-related back-pain (Murphy & Volinn, 1999), with projections
suggesting 60% to 80% of the adult population will experience at least one episode of
LBP during their active work life (Nordin et al., 1997).
Low Back Pain: Costs
The expenditures associated with spinal problems and LBP remain a significant
economic burden as direct health care cost and indirect tangential costs continue to be on
the rise (Dagenais et al., 2008; Mantyselka et al., 2002; Martin et al., 2008). Direct costs
comprise expenditures related to physician services, medical devices, imaging and
diagnostic testing, medications, and hospital stay. To examine associated trends related to
back and neck pain, a recent study estimated health care expenditures in the US
comparing national data from 1997 to 2005 (Martin et al., 2008). The study found
inflation-adjusted health care expenditures for spine problems increased from $4,695 in
1997 per person to $6,096 in 2005 yielding an estimated $85.9 billion in total direct costs
in 2005. While outpatient visits accounted for the largest proportion of total cost ($30.8
billion), the greatest increase was observed for medications expenditures ($7.3 billion in
10 1997 to $19.8 billion in 2005). The authors concluded other increases may be related to
imaging and diagnostic tests, spinal injections, and increased use of spinal fusion surgery
and instrumentation.
Indirect tangential costs associated with LBP are also largely responsible for the
significant increases in expenditures (Dagenais et al., 2008; Mantyselka et al., 2002).
Indirect costs are related to estimated loss of productivity and wage replacement benefits
that are often provided by the workers compensation system. Annually, approximately
149 million lost work days resulted from work related LBP injuries with annual
productivity losses estimated at $28 billion (Maetzel & Li, 2002). Workers�’
compensation is a system of state and federal laws that provides benefits for employees
who are injured on the job and covers approximately 127 million U.S. workers (Green-
McKenzie, 2004). In addition to compensation costs, workers�’ compensation is often
responsible for medical related costs. Compensation costs typically include all wage
replacement and the final impairment settlement related to the work-place injury. In
1994, it was projected that more than $11 billion was paid annually in the U.S. for
workers�’ compensation benefits for work-related LBP (Webster & Snook, 1994). For
workers�’ compensation claims, LBP injury accounts for 33% to 41% of the total costs,
but only accounts for 10% to 19% of all compensation claims filed (Hadler et al., 1995;
Nachemson, 1992).
Low Back Pain: Progression of Treatments Used
Over the past two decades, there is significant progress in the development of

11 treatment guidelines for health care professionals concerning the progression, indications,
and interventions for LBP (Bigos et al., 1994; Chou et al., 2007; van Tulder et al., 2006).
Most recently, the ACP and the APS established evidence-based guidelines for the
management of LBP with recommendations regarding diagnostic testing, patient
education, and pharmacological interventions (Chou et al., 2007). Typically, acute,
nonspecific LBP has no serious underlying pathology and there is evidence to suggest
that conservative care, such as acetaminophen, nonsteroidal anti-inflammatory drugs,
skeletal muscle relaxants, physical activity, heat therapy, physical therapy, and patient
education, are considered appropriate lines of treatment (Kinkade, 2007). However, if
specific �“red flags�” or indicators of latent spinal pathology are present, a more thorough
evaluation will be deemed necessary. Imaging studies (i.e., MRI, x-ray, CT) and various
subjective physical tests and indicators (i.e., supine straight leg raising, reflexes, back
pain with radiation, focal weakness) are often utilized to determine lumbar instability and
the extent of �“mechanical�” LBP (Jarvik & Deyo, 2002; Jensen et al., 1994). Typically,
surgery is not considered until LBP is recognized as chronic, which is indicated by pain
that persists for more than 7 to 12 weeks (Andersson, 1999). If conservative care has
failed, a first line surgery (i.e., discectomy, foraminotomy, and laminectomy) will likely
be considered before lumbar fusion (Esses & Huler, 1992; Hestbaek, Leboeuf-Yde, &
Manniche, 2003).
Lumbar Fusion: Indications and Procedure
Indications for using lumbar fusion are influenced by the reality that some
12 patients do not achieve adequate relief of their LBP after conservative care or first-line
surgeries (Esses & Huler, 1992; Hestbaek et al., 2003). If pain persists and there is
evidence of instability of spinal segments, then lumbar fusion is often a next surgical
option. Spinal fusion was first described by Hibbs (1911) as an operation that involves
fusing the �“spinous processes, laminae and intervertebral articulations�” to prevent further
progression of curvature of the spine in a patient with spinal tuberculosis. In later years,
spinal fusion was adopted in the treatment of additional spinal conditions, such as LBP
with sciatica pain and other conditions caused by lumbar instability due to structural
defects or to regressive degeneration of the lumbar spine (Herkowitz, 1995). The
rationale behind lumbar fusion is to prevent motion between unstable vertebral bodies by
fusing and limiting their movement, thus, decreasing or eliminating the back pain created
by the motion (An et al., 2003). Lumbar spinal conditions that are currently associated
with lumbar fusion include, but are not limited to, degenerative disk disease, herniated
lumbar disc, spondylolisthesis, spinal stenosis, deformity, distal extension of previous
fusions, fracture, and trauma (Waddell & Turk, 2001). There is criticism that the
diagnostic indications for lumbar fusion surgery are poorly defined and outcomes vary
with different underlying pathologies (Glassman et al., 2009). Due to the high variability
in patient selection for lumbar fusion, there is a lack of consensus regarding well-defined
indications for the procedure.
There are a variety of different surgical techniques, which can be used to achieve
lumbar fusion; however, all methods involve adding a bone graft to an area of the spine
to encourage a biological response, which causes a bony fusion graft to grow between the

13 two vertebral bodies (Cotler & Cotler, 1990). Lumbar fusion surgeries are typically
performed using either posterior lumbar interbody fusion (PLIF), or anterior lumbar
interbody fusion (ALIF). However, more recently there is a trend to combine surgeries
from both the posterior and the anterior approach thus creating a �“circumferential�” or
�“360 degree fusion,�” which purportedly maximizes spinal stability immediately following
surgery and ultimately increases the chance of solid fusion (Fritzell, Hagg, Wessberg, &
Nordwall, 2001). Surgeons often rely on the addition of surgical implants (also known as
instrumentation), such as pedicle rods and screws and interbody fusion cages, which are
used in addition to the bone graft to further stabilize the spine. Such methods have been
introduced at a rapid rate. While recent reviews conclude these devices improve fusion
success rates (Burkus, Gornet, Schuler, Kleeman, &. Zdeblick, 2009), outcome data
regarding pain, disability and psychosocial functioning remains unclear (Maghout-Juratli
et al., 2006).
Lumbar Fusion: Prevalence and Cost
Lumbar fusions performed in the US have dramatically increased since 1992
(Deyo & Mirza, 2006; Starkweather, 2006; Weinstein et al., 2006). In 1991, the total
number of lumbar fusions performed annually was estimated to be 46,500 (Taylor, Deyo,
& Cherkin, 1994). One decade later, a study reported there were 200,000 fusion surgeries
performed annually to relieve discogenic low back pain and instability (Starkweather,
2006). Deyo and Mirza (2006) estimated that the rates of lumbar fusion surgery in the US
have climbed more than 250% over the past decade with rates rising most rapidly among
14 patients over age 60. Such dramatic increases in lumbar fusion rates have been linked to
technological advances in fusion techniques (i.e., new spinal implantation devices;
Maghout-Juratli et al., 2006). High prevalence rates of lumbar fusion surgeries performed
are even more substantial for workers compensation patients. Taylor and colleagues
(1996) reported that patients with work-place LBP injuries covered by workers�’
compensation were 1.37 times more likely to undergo surgery involving fusion than other
patients with LBP and almost twice as likely to have a subsequent reoperation within 3
years of the index surgery. In the 1990s, DeBerard and colleagues (2003) found average
compensation and medical costs for compensated lumbar fusion patients in Utah to be
$30,103 and $27,218, respectively. Recently, this study was replicated in a similar cohort
of Utah workers and found that medical costs increased 174%, while compensation costs
increased relative to the pace of inflation (Wheeler et al., in press). When considering the
drastic increase in lumbar fusions and associated costs, particularly among injured
workers, there is a clear need to examine patient outcomes associated with these
procedures.
Lumbar Fusion: Review of Outcome Measures
Treatment outcomes are often difficult to assess due to the subjective nature of an
individual�’s experience of LBP. Recently, an emphasis has been placed on how exactly to
measure a �“successful�” surgical outcome (Mannion & Elfering, 2006). In the past,
outcomes for lumbar spinal fusion surgery have typically been determined based on
radiographic evidence (e.g., X rays) to assess whether or not the patient achieves a solid

15 fusion. Other common surgical outcomes include post-operative complications (e.g.,
pseudarthrosis or nonfusion, infection, bone donor site pain) and reoperation rates
(Champain, Mazel, Skalli, & Mitulescu, 2007). However, over the last decade,
researchers have demonstrated quite modest correlations of these common surgical
outcomes with patient-oriented outcomes such as pain levels, quality of life, and
disability. Thus, most current spine researchers would agree that it is prudent to utilize a
multidimensional approach to assess patient outcome based not only on fusion success
but also patient-health status and quality of life (Glassman et al., 2009). This is consistent
with the World Health Organization (WHO) definition of health acknowledged in 1948
as �“a state of complete physical, mental, and social well-being and not merely the
absence of disease or infirmity�” (WHO, 1948, p. 100). In 1998, a standardized set of
measures for assessing LBP outcome data was recommended to allow for improved
comparisons between studies and produce quality systematic reviews (Deyo et al., 1998).
This review was revised in 2000 to include five domains specific to the assessment of
self-reported LBP including pain, back specific function, work disability, generic health
status, and patient satisfaction (Bombardier, 2000). In the treatment of degenerative spine
disorders, the Short Form Health Survey (SF-36v2; Ware, Snow, Kosinski, & Gandek,
2000) and the Oswestry Disability Index (ODI; Fairbank & Pynsent, 2000) are the most
commonly used self-report measures (Glassman et al., 2009). Other commonly used
measures identified in the literature include the Roland and Morris Disability Scale
(RMDS; Roland & Morris, 1983a, 1983b), and Visual Analog Scale or Verbal Numeric
Rating Scale (VAS/VNRS; Von Korff, Jensen, & Karoly, 2000).
16
Lumbar Fusion: Review of Outcomes Studies
In 1992, Turner and colleagues published a review that included 47 published
lumbar fusion studies from 1966 to 1991. The review indicated that patients undergoing
lumbar fusion had satisfactory outcomes ranging from 16% to 95%, with a mean of 68%.
The study also indicated high complication rates associated with lumbar fusion surgery
and confirmed there were no randomized control trials comparing lumbar spinal fusion
with any other technique. The variability in reported success rates in this review was
indicative of the need for more outcome research addressing the effectiveness of lumbar
fusion for LBP when compared to surgery without fusion and nonsurgical treatments. To
date, lumbar fusion is shown to be very beneficial for fractures, infections, progressive
deformity, and instability with spondylolisthesis (Carragee, Lincoln, Parmar, & Alamin,
2006; Moller & Hedlund, 2000; Swan et al., 2006). For example, Moller and Hedlund
conducted a prospective randomized study comparing spinal fusion surgery and an
exercise program for patients with spondylolisthesis (a condition where one vertebral
segment slips forward on another). The ODI was used as a responsive outcome measure
that addresses the impact of back pain on daily functioning and disability. The patients
who underwent surgery reported greater benefits at two years in terms of ODI scores
compared with those who engaged in the exercise program. While lumbar fusion shows
encouraging results for specific diagnoses indicative of LBP (e.g., spondylolisthesis,
vertebral fracture), there is inconclusive evidence that fusion surgery effectively
alleviates pain for persistent nonradicular LBP with common degenerative changes (e.g.,
degenerative disc disease; Chou et al., 2009; Nguyen, Randolph, Talmage, Succop, &
17 Travis, 2011).
There is criticism the majority of randomized control trials on surgery for less
specific diagnostic categories for LBP compare surgical techniques (e.g., instrumentation
vs. noninstrumentation; PLIF vs. 360 degree fusion) rather than comparing lumbar fusion
to nonoperative care (Don & Carragee, 2008). The few studies focused on this issue have
found little, if any, supportive evidence in favor of lumbar fusion for broad diagnoses of
LBP. Four known randomized studies looked at differences between nonoperative
treatments versus lumbar fusion for chronic LBP (Brox et al., 2006; Brox et al., 2003;
Fairbank et al., 2005; Fritzell et al., 2001). Fritzell and colleauges published a rigorous
trial for LBP, which concluded lumbar fusion in patients with severe chronic LBP is
more effective in reducing pain and disability than �“usual�” nonoperative treatment. While
the study supported the indication for using lumbar fusion over nonoperative care, the
control group was given an unstructured, heterogeneous therapy that was mostly physical
therapy, however was also supplemented with other forms of treatment, including
education, treatment aimed at pain relief (i.e., acupuncture, injections), cognitive and
functional training, and/or coping strategies. To address this concern, Fairbank and
colleagues compared lumbar fusion surgery (n = 176) with an intensive rehabilitation
program (n = 173) for patients with chronic LBP. The difference between the treatment
groups for outcomes related to functional disability was only marginally statistically
significant with the surgery group demonstrating only modest improvements in functional
disability. However, this study was limited due to high dropout rates for both the surgical
group (22%) and the nonsurgical group (16%). In another study, Brox and colleagues
18 (2003) published a randomized control trial comparing lumbar fusion to cognitive
intervention/exercise for treatment of 64 patients with chronic LBP. At 1 year follow-up,
no differences were found for pain improvement or functional disability between the two
groups. Further, both the surgical and nonoperative treatment groups improved
significantly compared to pretreatment conditions. A later study found similar results, in
a sample of 60 patients with low back pain lasting longer than one year after previous
surgery for disc herniation who were randomized to either lumbar fusion or cognitive
intervention with exercise group (Brox et al., 2006). Results indicated no differences
were found in functional disability between the two interventions indicating a success
rate of 50% in the fusion group and 48% in the cognitive intervention/exercise group.
While the Brox and colleagues (2003, 2006) studies suggest that fusion may not be more
effective than a structured cognitive and exercise rehabilitation program, it is important to
interpret their findings with caution based on small sample sizes.
In addition to comprehensive evidence with regards to general LBP populations,
there is evidence that fusion patients who receive workers�’ compensation have even
poorer clinical outcomes than uncompensated patients (Carreon, Glassman, Kantamneni,
Mugavin, & Djurasovic, 2010; DeBerard et al., 2003; Maghout-Juratli et al., 2006; Taylor
et al., 1996). For example, in a retrospective population-based cohort study on lumbar
fusion outcomes for compensated workers in Utah, DeBerard and colleagues (2001)
found that 36% of fusion patients reported worse pain, with 35% demonstrating their
overall quality of life was no better than before surgery at 2-year postsurgical follow-up.
A recent retrospective population-based cohort study found between 1994 and 2001,
19 1,950 compensated workers who underwent lumbar fusion had an overall disability rate
of 63.9 %, a reoperation rate of 22.1%, and a complication rate of 11.8 % at 2 years post-
surgery. While the literature review identified convincing evidence of positive fusion
outcomes for specific, well-defined diagnoses indicative of LBP, convincing evidence is
lacking for positive outcomes in the absence of conclusive diagnoses and a limited
amount of research has compared surgical versus nonsurgical treatment of LBP.
Lumbar Fusion: Review of Variables Predictive of Outcomes
Based on the previous review, there are a considerable number of patients who do
not do well following lumbar fusion, particularly for workers compensation populations.
Previous research has attempted to identify specific presurgical characteristics that may
account for some of the variability in surgical outcomes. The following section will
review several low back and lumbar fusion studies that have identified a number of
presurgical variables shown to have some correlations with LBP and surgical outcome.
Demographic Variables
Despite the potential benefits of lumbar fusion surgery, age is often indicated as a
strong risk factor for surgical outcomes. While there is a small body of research
suggesting older age is related to poor lumbar fusion outcomes (Chen, Baba, Kamitani,
Furusawa, & Immure, 1994; DeBerard et al., 2001, 2003; Kim, Lenke, Bridwell, Kim &
Steger-May, 2005), the majority of the literature regarding lumbar surgeries in older
patients focuses on the risk of perioperative (during the procedure) complications (Benz,
Ibrahim, Afshar, & Garfin, 2001; Deyo, Cherkin, Loeser, Bigos, & Ciol, 1992;
20 Kalbarczyk, Lukes, & Seiler, 1998;). For example, Deyo and colleagues found in a
sample of 27,111 Medicare patients, the rates of complications and mortality rates
doubled in patients who had spinal fusion surgery when compared to other surgeries. In
another study, results showed that older age was associated with a higher rate of
pseudoarthrosis (also known as nonfusion), with 46% of patients over age 55 and only
12% under age 55 demonstrating pseudoarthrosis (Kim et al., 2005). Additionally,
DeBerard and colleagues (2001) found that after age 25, each 5-year increase in age
resulted in a 119% increase in postfusion disability. While most of these studies indicate
age as a predictive factor for poor outcomes, there is criticism that the literature regarding
lumbar fusion in older patients focuses more on the prevalence of complications rather
than differences in clinical outcomes between older and younger patients (Glassman,
Polly, Bono, Burkus, & Dimar, 2008). To address the need for more evidence for older
populations, Glassman and colleagues recently compared instrumented lumbar fusion
outcomes of 50 patients older than 65 and 174 patients younger than 65 in a randomized
control study. For both groups, results showed statistically significant improvements from
baseline in all health-related quality of life measures used at 6-month, 1-year, and 2-year
postoperative follow-up. Further, older patients�’ back and leg pain related symptoms
improved more than younger patients at all-time intervals (reaching significance at 6-
months follow-up). Results also showed that 94.7% of older patients indicated fusion
compared to 87.7% of younger patients. Such findings indicate older patients undergoing
lumbar fusion with instrumentation may show symptomatic improvement at rates similar
to those in younger patients.

21 Although the literature remains mixed on the issue of gender, studies have shown
a relationship between gender and patient outcome and satisfaction after spinal surgery
(Airaksinen, Herno, Turunen, Saari, & Suomlainen, 1997; Iversen, Daltroy, Fossel, &
Katz, 1998; Katz et al., 1994; Shabat et al., 2005). One study found gender influences the
satisfaction rate of lumbar surgery with 57% of women reporting satisfactory results
compared to 77% of men (Shabat et al., 2005). In another outcome study for lumbar
surgery, participants who were younger and male reported more improvements in
physical functioning and ability to walk after surgery (Iversen et al., 1998). One possible
explanation for such differences may be women have a greater ability to discriminate
among pain intensities, report lower pain thresholds, and higher pain ratings when
compared to men (Bush, Harkins, Harrington, & Price, 1993; Ellermeier & Westphal,
1995; Feine, Bushnell, Miron, & Duncun, 1991). This is supported by laboratory research
indicating a clear sex-linked biological element in pain perception (Berkley, 1997).
Several studies have indicated that chronic LBP is associated with education
level. Evidence suggests that patients with higher levels of education tend to have a
decreased risk of developing low back pain (Barnes, Smith, Gatchel, & Mayer, 1989;
Bigos et al., 1991; Kwon et al., 2006). This relationship is, at least in part, due to the fact
that people with less education tend to have more physically intensive jobs that are
related to higher incidences of chronic LBP (Damkot, Pope, Lord, & Frymoyer, 1984). In
2001, the National Research Council published a review that indicated a positive
relationship between low back disorders and heavy physical work. However, there is
contradictory evidence regarding the relationship between the physical demands of work
22 and low back pain by evidence suggesting sedentary workers may also suffer from low-
back pain. Such findings have caused some to question whether physical demands cause
low back pain, or whether they worsen an underlying condition (Snook, 2004).
Compensation and Litigation Variables
The LBP literature has extensive research identifying specific work related factors
including compensation and litigation, as predictor variables for future pain and
disability. There is evidence that filing worker�’s compensation claims is strongly linked
with a poor prognosis of chronic pain and disability in patients with back related injuries
(Damkot et al., 1984; Rasmussen, Leboeuf-Yde, Hestbæk, & Manniche, 2008). Other
studies have found more than two thirds of workers who filed compensation claims for
back pain and returned to work experienced subsequent episodes of back-pain-related
sick leave (Baldwin, Johnson, & Butler, 1996). In a recent study, 1,831 U.S. workers who
filed workers�’ compensation claims for back pain between 1999 and 2002 found that
30% of workers experienced multiple episodes of sick leave at 1-year follow-up (Cote,
Baldwin, Johnson, Frank, & Butler, 2008). In addition, workers who did not go on sick-
leave and/or return to work in a short amount of time reported significantly better health
outcomes than workers who experienced multiple episodes of sick leave or no return to
work.
Work-related factors, such as worker�’s compensation, disability claims, work
status, and the duration of sick leave, have also been identified as predictors of surgical
outcome (DeBerard et al., 2001; Hodges, Humphreys, Eck, Covington, & Harrom, 2001;
Mannion & Elfering, 2006). A meta-analysis including data from more than 20,000

23 patients found that compensated patients were four times more likely to have
unsatisfactory outcome after surgery when compared to noncompensated patients (Harris,
Mulford, Solomon, van Gelder, & Young, 2005). In another study, Greenough, Peterson,
Hadlow, and Fraser (1998) found that workers�’ compensation patients who underwent
lumbar fusion surgery had significant increases in pain and psychological disturbances, as
well as, lower rates of returning to work when compared to noncompensated patients.
Further, no differences were found in fusion rates, frequency of physician consultations,
or level of functioning.
The role of the legal system also plays an important role in back surgery
outcomes. Several studies demonstrate the relationship between compensation claims
involving litigation and increased rate of disability and pain (Bernard, 1993; Greenough
et al., 1998; Greenough, Taylor, & Fraser, 1994; Junge, Dvorak, & Ahrens, 1995). For
lumbar fusion specifically, retrospective studies show involvement of a lawyer in
compensation claims is a predictor of a various negative outcomes after lumbar fusion
(DeBerard et al., 2001, 2003; LaCaille, DeBerard, Masters, Colledge, & Bacon, 2005).
One study indicated compensation claims involving a lawyer revealed a 376% increase in
the probability patients would remain disabled two years following lumbar fusion
compared to claims not involving a lawyer (DeBerard et al., 2001). Specific mechanism
related to the association between compensation and poor outcome are proposed to
include, but are not limited to, the effect of patients blaming others for their injury,
secondary gain (i.e., medication and/or money), and the role of exposure to a complex
and adversarial system (i.e., legal and insurance systems; Harris, 2007).
24
Perceived higher-risk surgery cases are often referred to nurse case managers and
or vocational rehabilitation to help manage patient�’s medical treatments and facilitate
return to work. Despite such proactive measures, studies have shown an association of
assigning nurse case managers and vocational rehabilitation with worse patient outcomes
for discectomy patients (DeBerard et al., 2009); however, the association of referral to
nurse case manager and utilization of vocational rehabilitation on fusion outcomes
remains unknown. While these findings seem counterintuitive, as the intention of
providing nurse case managers and vocational rehabilitation are to reduce risk and lower
costs, patients referred to such services are often at higher risk from the outset. These
findings lend support for further evaluation of these services in terms of lumbar fusion
patient outcomes in workers compensation populations.
Health-Related Variables
While studies have indicated individuals with LBP have an increased risk of
relying on substances for pain relief such as alcohol or pain medication (e.g., Frymoyer,
1992; Stevenson, Weber, Smith, Dumas, & Albert, 2001), there is still a lack of evidence
suggesting their impact on back surgery outcomes (Block & Callewart, 1999; Turner et
al., 1992). Conversely, the literature indicates nicotine use is responsible for significant
increases in LBP (Battie et al., 1990; Bigos et al., 1991, 1994), as well as negatively
impacting fusion rates (An, Simpson, Glover, & Stephany, 1995; Silcox et al., 1995;
Wing, Fisher, O�’Connell & Wing, 2000). Evidence supports smoking may potentially act
as a bone toxin by disrupting the ability for normal bone formation and growth, thus,
inhibiting fusion to take place (Andersen et al., 2001). One study indicated smokers who

25 underwent spinal fusion showed an increased rate of pseudoarthrosis (fusion failure) by
47% when compared to nonsmokers (An et al., 1995). More recently, a study compared
the clinical outcomes and fusion status at 2-year post surgical follow-up of 188 cigarette
smokers and 169 nonsmokers who underwent lumbar fusion. Rates for nonunion were
14% for nonsmoking patients and 27% for smoking patients; however, patients that quit
smoking between 1 and 6 months after surgery had a nonunion rate of 18% (Glassman et
al., 2000). Such findings indicate smoking may be both a predictor variable, as well as a
mediating variable for fusion outcomes. In addition to increased pseudoarthrosis risk,
there is empirical support that smoking also affects clinical outcomes independent of
fusion success. In one study, nonsmoking patients with successful fusion had superior
physical pain scores (significant at 12- and 24-months postoperative) and mental ability
scores (significant at 6- and 12- months postoperative) when compared to smoking
patients with successful fusion (Harvinder, Thomas, Foley, Safdar, & Fengyu, 2001).
Such results question whether the negative effect on fusion rate is related to smoking
itself or to others factors associated with smoking.
Obesity is well documented as an independent predictor for low back pain (Deyo
& Bass, 1989). While a few studies have addressed the effect of obesity on clinical
outcomes of a variety of spine surgeries (Andreshak, An, Hall, & Stein, 1997; Gepstein et
al., 2004), most of the emphasis was on perioperative complications with little outcome
data on patient-based, health-related quality of life measures. Recently, one study looked
at clinical outcomes and complication rates of patients undergoing lumbar spinal fusion
by comparing health related outcome measures and numerical rating scales of back and
26 leg pain of obese patients to nonobese patients (Djurasovic, Bratcher, Glassman, Dimar,
& Carreon, 2008). Despite the fact that overall complication rates were lower in the
nonobese group (17.4%) compared to the obese group (28.4%), improvement levels did
not differ significantly with both groups showing significant improvement in back and
leg pain after surgery. Similarly, quality of life and disability scores showed significant
improvement after surgery in both obese and nonobese groups. Such findings suggest that
obese patients who meet acceptable criteria and indications for lumbar fusion may
achieve similar benefits as nonobese patients.
Research on LBP patients has shown that psychological factors such as anxiety,
depression, fear avoidance relating to work, and back-pain-related stresses predict
impairment in subsequent physical health-related quality of life and healthcare utilization
(Keeley et al., 2008). While some studies demonstrate psychological distress is not
predictive of post-operative improvement in patients who underwent lumbar fusion
(Tandon, Campbell, & Ross, 1999), the majority of the literature suggests presurgical
psychological characteristics do play an important role in surgical outcome (DeBerard et
al., 2001; LaCaille et al., 2005). One study examined whether three aspects of
psychological distress (depression, anxiety, and hostility) predict several surgical
outcomes (employment status, subjective pain change ratings, and changes in functional
abilities; Trief, Grant, & Fredrickson, 2000). Results indicated inability to return to work
and failure to report improvement in pain and functional abilities were significantly
predicted by presurgical anxiety and depression. Due to the probable impact
psychological variables may have on fusion outcomes, there are additional concerns that
27 patients who are clinically depressed preoperatively will likely have an increase in
depressive symptoms postoperatively leading to continued negative effects on surgery
outcomes (Block, Gatchel, Deardorff, & Guyer, 2003). Thus, by screening patients prior
to surgery, patients have the option to treat their depression prior to surgery.
Back-Related Physiological and Surgical Procedural Variables
Although there are advances with regards to proper diagnosis, there is criticism
about the frequency of nonspecific and subjective diagnoses used in outcome studies
evaluating the effectiveness of lumbar fusion (Franklin, Haug, Heyer, McKeefrey &
Picciano, 1994; Glassman et al., 2009; Turner et al., 1992). Diagnoses are often grouped
into broad categories such as chronic LBP (Fairbank et al., 2005; Fritzell et al., 2001) or
degenerative disc disease (Dimar, Glassman, Burkus, & Carreon, 2006; Sasso, Kitchel, &
Dawson, 2004). Such a lack in specificity for diagnosis limits the ability to compare
effectively the benefit of surgical versus nonsurgical treatment, one surgical technique
versus another, or the potential added benefit of a surgical implant. In a recent study,
Glassman and colleagues found fusion outcome improvements are not equal among
diagnostic subgroups. Specifically, the study indicated the most substantial improvement
in fusion outcomes were for patients with spondylolisthesis and scoliosis, followed by the
diagnosis of disc pathology, postdiscectomy revision, instability, stenosis, and adjacent
level degeneration. The least improvement for patients after surgery was seen in patients
with pseudoarthrosis of a prior fusion.
Recent evidence based guidelines suggest patients with LBP should undergo

28 diagnostic imaging such as x-ray, magnetic resonance imaging (MRI), or computed
tomography (CT), only if there is a strong indication nerve damage or a specific cause of
the low back pain would show up on the test and that positive results would potentially
lead to surgery or epidural steroid injection for suspected (Chou et al., 2007). There is
criticism the identification of abnormalities with early MRI leads to increase costs of care
and increased number of spine operations without any predictive value for outcomes. For
example, studies have indicated MRIs or CT for individual without low back pain
commonly present with images of disk herniations, disk bulges, and disk degeneration
(Boden, Davis, Dina, Patronas, & Wiesel, 1990; Jarvik, Hollingworth, Heagerty, Haynor,
& Deyo, 2001). These findings are often nonspecific and there is no compelling evidence
routine imaging affects treatment decisions or improves outcomes (Chou et al., 2007).
Some evidence exists combining various diagnostic criteria with results of objective
imaging studies (MRI, CT, discography) is a more reliable predictor of surgical outcome
than diagnosis alone (Boos, Marchesi, & Aebi, 1991; Hasenbring, Marienfeld,
Kuhlendahl, & Soyka, 1994; Lacroix et al., 1990). However, more recent finding suggest
that, for patients undergoing lumbar fusion, a surgical diagnostic severity score based on
presurgical imaging indicated no predictive power for either disability status, global
outcome, or physical or social functioning (DeBerard et al., 2001).
A considerable amount of research has been directed toward examining different
aspects of surgical history and procedural variables in relation to predicting lumbar fusion
outcomes. Multiple-levels spinal fusion is shown to be predictive of clinical outcomes
(Franklin et al., 1994; Glassman et al., 1998; Narayan, Haid, Subach, & Rodts, 2002;
29 Turner et al., 1992). In one study, successful fusion rates in 457 patients were correlated
with the number of fusion levels indicating fusion rates declined significantly in relation
to each additional level fused. However, recently, Glassman and colleagues (2006)
compared patients who underwent either a single-level fusion (n = 324) or a two-level
fusions indicating no significant differences between the two groups with both groups
revealing significant improvement from preoperative to postoperative outcome at 1- and
2-year follow-up. Several studies also shown a history of prior back surgeries is a
predictor of poorer outcomes (DeBerard et al., 2001; Franklin et al., 1994).
Recently, research has started to address the influence new surgical implants (i.e.,
interbody fusion cages) have on lumbar fusion outcomes (Maghout-Juratli et al., 2006).
Interbody fusion cages were developed and introduced to provide better mechanical
strength in addition to bone on bone fusion. However, whether interbody fusion cages
provide better functional outcomes than bone only fusion or pedicle screw and rod
fixation remains unclear. For example, a recent study examining interbody fusion cage
outcomes reported poor quality of life and continued functional impairment, with 38% of
patients totally disabled at approximately 2-years follow-up (LaCaille et al., 2005). These
findings are similar to previous outcome research on surgeries that did not use such
sophisticated technology (DeBerard et al., 2001; Turner et al., 1994). Further, the use of
interbody fusion cages have also been associated with increased post-operative
complication risk compared to bone-only fusions (Maghout-Juratli et al., 2007).
30
Conclusions from the Literature Review
Despite the several demographic, occupational, health, psychological, and
surgical variables associated with lumbar fusion outcomes, only a few studies have
addressed the predictive nature of multiple variables on lumbar fusion outcomes. The
biopsychosocial model suggests biological, psychological, and social factors are
interrelated in their role of human functioning for any given state of health or illness
(Gatchel & Bell, 2000; Taylor, 1999). This model remains distinct from the biomedical
approach that suggests illness has a single underlying pathophysiological cause that is
independent from psychological and social factors (Wright, 2005). Such a model could
only be supported if the removal of the pathology resulted in a return to health. For LBP,
this is clearly not the case. There is evidence that lumbar spine pathology is often present
in people who experience no symptoms associated with the pathology (Boden et al.,
1990; Jarvik et al., 2001). Conversely, lumbar fusion patients who do have pathology
often have limited functional recovery after surgical repair of the pathology (DeBerard et
al., 2001; Franklin et al., 2004). Further, there is evidence to suggest presurgical
diagnosis and the severity of lumbar spinal pathology are not predictive of lumbar fusion
outcomes (DeBerard et al., 2001; Turner et al., 1992). Such evidence supports the
justification for viewing low back pain from a perspective that combines physical,
mental, and social well-being, as well as broadens the focus not to simply �“cure�” disease,
but also to promote health. The current study will use the biopsychosocial model as a
foundation when considering multiple types of predictors for outcomes as well as
conceptualize and assess outcomes in a multidimensional fashion.

31
The current study replicates the methods of DeBerard and colleagues (2001) and
LaCaille and colleagues (2005) studies that examined predictors of lumbar fusion surgery
outcomes and expands on these early finding by including additional variables affiliated
with more recent lumbar fusion literature and advancements in surgical technology. The
factors to be used in the model were identified from the variables currently reviewed and
include: age at the time of the procedure, gender, level of education, BMI, litigation
status, time between injury and surgery, previous history of depression, presurgical
psychological evaluation, smoking history, prior history of back surgery, pain medication
use, pain severity (1-10), diagnosis, type of surgery, instrumentation use, and number of
levels fused (see Figure 1).
Research Purpose and Study Objectives
The current study has three primary objectives: (a) to examine patient presurgical
variables and understand the interrelationships between such variables; (b) to characterize
multiple outcomes associated with lumbar fusion patients in terms of quality of life,
function, and health status variables, as well as fusion rates, patient satisfaction, and
disability; and (c) to explore the relationship of presurgical variables to outcomes and test
the predictive efficacy of a multiple variable predictive model.
Research Questions
This study addressed the following research questions related to objective 1.
1. What are the patient characteristics of this sample in terms of the presurgical

32
PREDICTIVE VARIABLES PATIENT OUTCOME VARIABLES
DEMOGRAPHIC VARIABLES *Age at injury Income Level *Education Level Gender Ethnicity Marital Status Child Care Responsibility PHYSIOLOGICAL VARIABLES *Obesity Status Diagnosis Physical Exam Data Pain Severity (1-10) TREATMENT VARIABLES *Number of Levels Fused Diagnosis *Number of Prior Back Operations Type of Procedure *Instrumentation Type HEALTH VARIABLES *Smoking at Time of Fusion General Health Problems Alcohol Use *Amount of Pain Before Fusion Use of Pain Meds Prior to Fusion WORK/COMPENSATION VARIABLES *Lawyer Involvement Total Compensation Costs *History of Prior Claims Time Between Date of Injury and Fusion Employed at Time of Fusion Occupation Title *Case Manager Assigned *Vocational Rehabilitation Assigned PSYCHOLOGICAL VARIABLES *History of Depression *Presurgical Psychological Evaluation
FUSION RATE % based on chart and self-report DISABILITY Current Work/Disability Status Roland-Morris Disability Scale STAUFFER-COVENTRY INDEX Good, Fair, and Poor Outcome Categories PATIENT SATISFACITON Global Perceived Effect Current Pain Level on 11-Point Scale (VNRS) Back Pain Following Surgery Quality of Life Following Fusion Have Fusion Again Pain Better or Worse than Expected How Satisfied if Back Condition Continued ROLAND-MORRIS DISABILITY QUESTIONNAIRE Level of Dysfunction Score HEALTH & MENTAL HEALTH Back Procedures 2 years post-Fusion (from med chart and survey) Pain Catastrophizing Scale
Total Score Rumination Magnification Helplessness
Short-Form Health Survey Physical Health Component Score Mental Health Component Score Physical Functioning Role Functioning Social Functioning General Mental Health Current Health Perceptions Pain
*Identifies variables considered for prediction analyses.
Figure 1. A summary of patient and outcome variables.
33
psychosocial variables of interest?
2. What are the intercorrelations among presurgical predictor variables of
interest?
This study addressed the following research question related to objective 2.
3. What is the percentage of solid fusion in the population sample of interest?
4. What percentage of the subject sample is still work-disabled following
surgery?
5. What is the level of postsurgical back pain disability among participants and is
it consistent with existing back pain patient norms and previous workers
compensation populations?
6. What is the percentage breakdown for patient satisfaction variables?
7. What is the percentage breakdown of good, fair, and poor outcomes (i.e.,
based upon pain reduction, return to work, physical functioning, medication
usage) for the patient sample?
8. What is the subjective pain level reported my fusion patients?
9. What are the mean values for mental health and overall health indices (i.e.,
physical functioning, role functioning, social functioning, general mental
health, current health perceptions, and pain perception) and are these
consistent with existing patient, nonpatient, and worker�’s compensation
population norms?
10. What are the interrelationships among the outcome variables?
This study addressed the following research question related to objective 3.

34
11. What are the intercorrelations among presurgical predictor variables of
interest and outcomes?
12. Is a multiple-variable presurgical model predictive of determined patient
outcomes?

35
CHAPTER III
METHODS
Population and Sample
All adults insured through Workers�’ Compensation Fund of Utah (WCFU) who
were at least 2 years post lumbar fusion surgery were eligible for inclusion in this study.
The 2-year follow-up was used in accordance with the suggested minimum follow-up
period indicated by editors of Spine, a major medical subspecialty journal (Nachemson &
LaRocca, 1987). Participants were excluded if their condition was related to a fracture of
the spine at the time of the surgery. WCFU gave signed authorization to review patient
files and initiate telephone contact. The WCFU computer database was used to identify
all patients who had undergone lumbar fusion surgery from 1998 to 2007. The final
sample size was determined based on the original sample extracted from the database and
number of participants contacted at follow-up for gathering outcome data.
Figure 2 identifies the process of patient selection and follow-up participation. A
total of 286 medical charts of patients who had undergone lumbar fusion were available
for review via the WCFU database. However, due to inclusion criteria, several patients
were ineligible for participation, yielding a total sample of 245 injured workers who were
included for medical chart review (see Phase 1 below). Patient�’s primary diagnosis given
by the operating surgeon according to the operative report included disc herniation
(39.2%), degenerative disc disease (30.2%), spondylolisthesis (13.5%), spinal stenosis
(7.8%), radiculopathy (3.3%), and other (5.7%). While previous retrospective studies

36
Figure 2. Process of patient selection and follow-up participation.
indicate an approximate outcome follow-up rate for back surgery patients of 50%
(DeBerard et al., 2001; LaCaille et al., 2005), our sample obtained outcome data for 110
patients who were contacted by telephone and agreed to participate in the telephone
interview portion of the study (see Phase 2 below), yielding an overall response rate of
45%. The author and one other graduate student conducted all 110 of the interviews. Of
the remaining 135 patients who did not participate, 20 were contacted but declined to
participate, 7 were deceased, and the remaining 108 were unavailable or relocated to an
unknown destination.
Due to the nature of the statistical analyses related to presurgical patient
characteristics and procedural variables, these will be thoroughly addressed in the results
section. The specific differences between patients available for follow-up and patients
Lumbar fusion patients identified in WCFU database
n = 286
Excluded patients Fractured spine: n = 14
Not index surgery: n = 27
Eligible patients n = 245
Patients not available for follow-up Could not reach: n = 106
Contacted but refused: n = 20 Deceased: n = 9
Patients Available for follow-up n = 110

37 lost to follow-up will also be addressed. Because the target population for the current
study is specifically injured workers receiving compensation from WCF, it is intended
the findings from the current review will generalize to similar populations of injured
workers across the US.
Study Design
This study was a retrospective-cohort design. Phase 1 involved gathering
presurgical information documented in patient medical charts and in the WCFU computer
database. Phase 1 was followed by mailing participants a letter describing the study and
notification that they would be contacted for a 20-minute telephone survey. Phase 2
consisted of a telephone survey.
Procedure
Phase 1
Phase 1 began with identifying the specific number of participants that met
researcher established inclusion/exclusion criteria. This was followed by a medical chart
and WCFU document review for each participant. The purpose of this chart review was
to code information regarding the treatment, clinical, and relevant biopsychosocial status
of the participant prior to the intervention. Reviews were conducted onsite at the WCFU
in Salt Lake City. A specific medical chart review coding instrument was completed for
each participant (see Appendix A). To ensure interrater reliability of the medical chart
review, another graduate student independently reviewed 5% of the medical charts.

38 Interrater reliability was determined by dividing the total number of agreements by the
total number of ratings for each item on the medical chart that was coded. Interrater
reliability for this review was .95.
Phase 2
Phase 2 involved contacting each participant identified in Phase 1 for a telephone
interview. The most recent address and phone number for each participant identified in
the medical chart and recorded on the medical chart review coding instrument was used.
Participants were given notification in the form of a letter (see Appendix B) that provided
a detailed description about the study. This letter ensured patient confidentiality.
Participants were encouraged to participate by offering a $10 incentive that was sent out
following completion of the telephone survey via check. A self-addressed stamped
postcard was included with the letter so participants could provide updated phone
numbers or addresses. Participant were asked to send postcards back even if their address
and/or phone number were unchanged. Other methods of obtaining contact information
were used (e.g., internet searches, directory assistance) if participants were not reached at
the address or telephone number listed in the WCFU database. Later, all participants with
correct phone numbers were contacted to complete the survey.
Detailed records for phone calling were kept for each participant (see Appendix
C). In cases where postcards were not returned, verbal consent was obtained through
telephone contact. A written script (see Appendix D) adapted from DeBerard (1998) was
used for initial participant telephone contacts. Follow-up concerning the letter with
regards to confidentiality and participation incentives were emphasized for the

39 participants contacted. The assessment measures (described below) used in the telephone
interview was administered at the initial time of contact unless participants requested to
not participate or to participate at a later scheduled time. Two graduate students
performed all of the outcome surveys over the phone. Both students were well trained to
conduct standardized telephone interviews by the supervisor of the current project. While
the interview was intended to last from 20 to 30 minutes based on the content of the
outcome survey, the amount of time with each participant varied considerably, ranging
from 20 to 75 minutes. Several participants in this study are socially isolated, lonely, and
suffer from chronic pain. Further, many have not had good experiences dealing with the
workers compensation system. These contextual variables were important when
determining how to interact with the patient during the interview, while also maintaining
a systematic approach to data collection. This required interviewers to be well trained in
advanced clinical skills so they could interact with participants from a supportive, calm
and respectful stance. To ensure interrater reliability, for 10% of the outcome surveys
another graduate student listened on a separate line and independently coded patient
responses. Interrater reliability was determined by dividing the total number of
agreements by the total number of ratings for each item on the outcome survey. Interrater
reliability for this review was .97
Materials and Instrumentation
There is strong evidence to suggest presurgical diagnosis and the severity of
lumbar spinal pathology are not predictive of lumbar fusion outcomes (DeBerard et al.,
40 2001; Turner et al., 1992). This supports the notion to view LBP from a perspective that
combines physical, mental, and social well-being and to use the biopsychosocial model as
a foundation to conceptualize and assess outcomes in a multidimensional fashion. To
select specific outcome measures a review was conducted on outcome measures used in
larger-scale fusion and low back surgery studies. The list of potential outcome measures
was determined by selecting the most comprehensive and feasible measure from a
number of possibilities. Measures were also selected that allowed for comparisons of the
present study findings directly to other published studies. Final selection was determined
by ensuring each measure was published widely and evidence for psychometric reliability
and/or validity was available.
Medical Chart Review Instrument
The medical chart review instrument discussed earlier in Phase 1 of the study (see
Appendix A) was adapted from a previous instrument used for gathering information
from the WCFU database in earlier research (e.g., DeBerard et al., 2001; LaCaille et al.,
2005). This instrument consisted of several biopsychosocial variables of interest related
to low back pain and surgery outcomes discussed previously in the literature review.
Modifications to the instrument were made relevant to the purposes of this study. For
example, an adjustment was made to include more specific diagnoses, additional surgical
procedures, and types of instrumentation to address a lack of such reports in previous
studies. Psychological variables including whether or not presurgical psychological
evaluations were given, and if psychotropic medication or therapy was utilized prior to
surgery, were also added to the measure.
41 Telephone Survey Instruments
Following the telephone script (see Appendix D), participants were asked using
various assessments measures on their level of satisfaction with their workers
compensation claim, surgical outcome, level of dysfunction and disability status, and
basic demographic information. Any information not attained in the medical chart review
was obtained at that time.
Fusion Outcomes
Although the review of the postsurgical medical records at WCFU may have
documentation on whether solid fusion was achieved, participants were asked to confirm
the status of the fusion if not obtained in chart review.
Patient Satisfaction
Patient satisfaction was determined using five close-ended questions used in
previous research on spinal surgery outcomes (DeBerard et al., 2001; LaCaille et al.,
2005) that are specific to their lumbar fusion procedure (see Appendix E items 5, 6, 7, 17,
and 19). The items included addressed patient satisfaction related to back/leg pain
improvement, quality of life improvement as a result of lumbar fusion, and satisfaction
with back condition at time of follow-up. These items used a response format ranging
from a 3- to 7-point scale.
Stauffer-Coventry Index
The Stauffer-Coventry Index (SCI; Stauffer & Coventry, 1972) is a measure that
has been used in previous research assessing outcomes following lumbar fusion surgery

42 (DeBerard et al., 2001; LaCaille et al., 2005; Turner et al., 1992). Items are highly face
valid The measure consists of four multiple response self-report questions regarding pain
reduction, return to work, limitations of physical activities, and medication usage. The
questions are highly face valid and responses reflect three subscales that categorize good,
fair, and poor outcomes: Good outcomes are determined by 76% to 100% relief in leg
and back pain, return to previous work status, minimal or no restriction of physical
activities, occasional mild analgesics or no analgesics; Fair outcome are determined by
26% to 75% relief of leg and back pain, return to lighter work, moderate restrictions of
physical activities, regular use of nonnarcotic analgesics; and Poor outcome are
determined 0% to 25% relief of leg and back pain, no return to work after surgery, severe
restrictions of physical activities, occasional or regular use of narcotic analgesics (see
Appendix E items 1-4).
Global Perceived Effect
The Global Perceived Effect (GPE; Beurskens, de Vet, Köke, van der Heijden, &
Knipschild, 1996) is a one-item response (see Appendix E, item 22) that provides a
subjective report of the patient�’s level of improvement. The patient is asked: �“Compared
to when this episode first started, how would you describe your back these days?�” The
response is based on a 4-point Likert scale (1-complete relief of pain, 2-more than 50%
relief, 3-no change, 4-increase of pain). Intraclass correlation coefficient values of 0.90 to
0.99 indicate excellent test-retest reliability of the GPE for chronic LBP patients
(Kampera et al., 2010)
43 Verbal Numeric Rating Scale
The Verbal Numeric Rating Scale (VNRS) was used to evaluate patients�’
perceived level of pain at the time of the telephone interview as well as an average rating
of their pain over the past week (see Appendix E, items 20 and 21). The patient was
asked to verbally rate their pain from 0 to 10 (an 11-point scale), where 0 represents �“no
pain�” and 10 represents �“the worst pain imaginable.�” The VNRS has been widely used
clinically for the assessment of pain (Jensen, Karoly, O�’Riordan, Bland, & Burns, 1989;
Kaplan, Metzger, & Jablecki, 1983). The VNRS shows strong test-retest reliability with
Pearson coefficient as high as .99 (Gallasch, Alexandre, & Amick, 2007).
Disability Status
During the telephone survey, disability status was assessed by asking participants
whether or not they currently receive total disability for their back condition (see
Appendix E, item 10). This was also verified by medical chart review. Scales for physical
functioning and daily activities were also considered factors determining disability.
Roland-Morris Disability Questionnaire
The Roland-Morris Disability Questionnaire (RDQ; Roland & Morris, 1983a,
1983b) is a 24-item self-report health status instrument intended to assess level of
dysfunction in patients with LBP (see Appendix F). Participants are asked to provide a
�“yes�” or �“no�” response to each question. To score the measure, the total number of �“yes�”
responses is calculated. Higher scores indicate more physical dysfunction severity with a
cut-off score of 14 or higher representative of a poor outcome (Roland & Morris, 1983a,
44 1983b). RDQ shows strong psychometric properties, with evidence of internal
consistency and responsiveness (Kopec & Esdaile, 1995). The internal consistency for
the RDQ is high (r = .91; Roland & Morris, 1983a, 1983b) and the measure is considered
valid and sensitive to change over time for groups of patients with low back pain (Klein
& Eek, 1990).
Short Form Health Survey-36, Version 2
The Short Form Health Survey (SF-36v2; Ware et al., 2000) is a 36-item general
health survey that assesses eight dimensions of health-related quality of life. The eight
dimensions assessed by this measure include (a) physical functioning: extent to which
health interferes with performance of behavioral activities (e.g., sports, climbing stairs,
and walking); (b) role physical: extent to which health interferes with usual daily
activities (work, housework, or school; (c) bodily pain: intensity of bodily pain during
last month and extent to which it interferes with normal work; (d) general health: current
evaluation of personal health; (e) vitality: degree to which a person has vigor and energy
versus worn out and tired; (f) social functioning: extent to which health interferes with
normal social activities; (g) role emotional: degree to which emotional problems resulted
in problems with work or daily function; and (h) mental health: degree to which a person
feels nervous and depressed. The eight subscales may also be aggregated into Mental
Health (MCS) and Physical Health (PCS) Component Summary scales (Ware &
Kosinski, 2001). These summary scales are responsible for 80% to 85% of the variance in
the eight SF-36 scales and allow researchers to perform statistical analyses on two
higher-order constructs (MCS/PCS) rather than separate analyses for each of the eight
45 SF-36 subscales (Appendix G). Norm based scoring for all scales has a general
population mean of 50 and standard deviation of 10. To date, several studies have yielded
content, concurrent, criterion, construct, and predictive evidence of validity for the SF-36
(Ware et al., 2000). For the general population, reliability coefficients range from .83 to
.95 for the eight scales, and two summary scores (MCS and PCS) using both internal
consistency and test�–retest methods (Ware, Kosinski, & Keller, 1994; Ware et al., 2000).
Further, in the treatment of degenerative spine disorders, the SF-36v2 is among the most
commonly used self-report measures (Glassman et al., 2009).
Pain Catastrophizing Scale
The Pain Catastrophizing Scale (PCAS; Sullivan, Bishop, & Pivik, 1995) is a 13-
item self-report instrument that asks patients to reflect on a pain experience and then to
provide ratings as to how often they dwell on pain-related thoughts and feelings (see
Appendix H). The items are scored on a 5-point Likert scale with scoring ranging from
�“not at all�” (score = 0) to �“always�” (score = 4). The total score ranges from 0 to 52 and
high scores indicate that more catastrophic thoughts or feelings are experienced. The
PCAS comprises one general construct and three empirically derived subscales, namely
magnification (items 6, 7 and 13), rumination (items 8, 9, 10 and 11) and helplessness
(items 1, 2, 3, 4, 5 and 12). For community and outpatient pain samples, psychometric
studies have shown adequate internal consistency and Cronbach�’s alpha coefficients ( )
for the total and subscale scores. In the community sample, the for the total score was
.95, while for the rumination, magnification, and helplessness subscale scores were .95,
.88, and .91, In the outpatient sample, the for the total score was, .92. The for the
46 rumination, magnification, and helplessness subscales were .85, .75, and .86 (Osman et
al., 2000). Studies also support the PCAS as a useful measure in differentiating pain
clinic patients with community-based samples (Sullivan et al., 1995; Osman et al., 2000).
Analysis
Data collected were analyzed using the Statistical Packages for Social Sciences
(PASW, Version 18.0). The analyses addressed three primary objectives for a sample of
worker�’s compensation patients who have undergone lumbar fusion including () to
examine patient presurgical variables and understand the interrelationships between such
variables; (b) to characterize multiple outcomes associated with lumbar fusion patients in
terms of quality of life, function, and health status variables, as well as fusion rates,
patient satisfaction, and disability; and (c) to explore the relationship of presurgical
variables to outcomes and test the predictive efficacy of a multiple variable predictive
model. Descriptive statistics including percentages, means, and standard deviation were
used to characterize the sample in relation to the specific variables. Intercorrelations
between the variables were assessed using Pearson correlation coefficients. The first and
second research objectives were addressed by calculating the descriptive statistics and the
intercorrelations among the presurgical predictor variables of interest and multiple
outcomes associated with lumbar spinal fusion surgery. The third objective was
addressed by using a series of logistic and multiple linear regression analyses to test the
strength of a multivariate predictive model of patient outcomes. Specific research
questions and their corresponding data analyses are summarized in Figure 3.
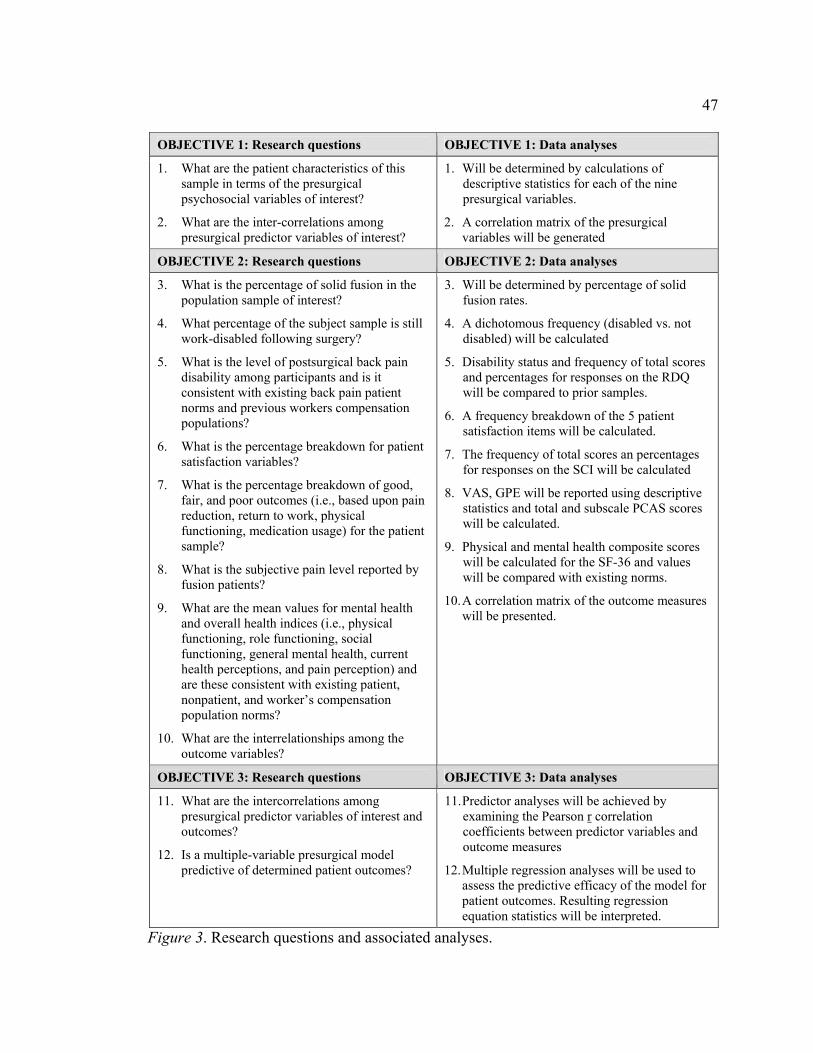
47
OBJECTIVE 1: Research questions OBJECTIVE 1: Data analyses
1. What are the patient characteristics of this sample in terms of the presurgical psychosocial variables of interest?
2. What are the inter-correlations among presurgical predictor variables of interest?
1. Will be determined by calculations of descriptive statistics for each of the nine presurgical variables.
2. A correlation matrix of the presurgical variables will be generated
OBJECTIVE 2: Research questions OBJECTIVE 2: Data analyses
3. What is the percentage of solid fusion in the population sample of interest?
4. What percentage of the subject sample is still work-disabled following surgery?
5. What is the level of postsurgical back pain disability among participants and is it consistent with existing back pain patient norms and previous workers compensation populations?
6. What is the percentage breakdown for patient satisfaction variables?
7. What is the percentage breakdown of good, fair, and poor outcomes (i.e., based upon pain reduction, return to work, physical functioning, medication usage) for the patient sample?
8. What is the subjective pain level reported by fusion patients?
9. What are the mean values for mental health and overall health indices (i.e., physical functioning, role functioning, social functioning, general mental health, current health perceptions, and pain perception) and are these consistent with existing patient, nonpatient, and worker�’s compensation population norms?
10. What are the interrelationships among the outcome variables?
3. Will be determined by percentage of solid fusion rates.
4. A dichotomous frequency (disabled vs. not disabled) will be calculated
5. Disability status and frequency of total scores and percentages for responses on the RDQ will be compared to prior samples.
6. A frequency breakdown of the 5 patient satisfaction items will be calculated.
7. The frequency of total scores an percentages for responses on the SCI will be calculated
8. VAS, GPE will be reported using descriptive statistics and total and subscale PCAS scores will be calculated.
9. Physical and mental health composite scores will be calculated for the SF-36 and values will be compared with existing norms.
10. A correlation matrix of the outcome measures will be presented.
OBJECTIVE 3: Research questions OBJECTIVE 3: Data analyses
11. What are the intercorrelations among presurgical predictor variables of interest and outcomes?
12. Is a multiple-variable presurgical model predictive of determined patient outcomes?
11. Predictor analyses will be achieved by examining the Pearson r correlation coefficients between predictor variables and outcome measures
12. Multiple regression analyses will be used to assess the predictive efficacy of the model for patient outcomes. Resulting regression equation statistics will be interpreted.
Figure 3. Research questions and associated analyses.
48
CHAPTER IV
RESULTS
The results of this study are organized according to the following sections: (a)
descriptive statistics and intercorrelations of patient and procedural variables; (b)
response rates and bias checks; (c) patient outcomes; (d) intercorrelations of outcomes (e)
intercorrelations between patient characteristics and outcomes; and (h) prediction of
outcomes. Each research questions and their subsequent statistical analysis in the study
will be addressed as outlined in Figure 3.
Descriptive Statistics
To address the first objective of this study, it was important to comprehensively
identify specific patient and procedural variables for injured workers who had undergone
lumbar fusion (see research question 1). Based on the information gathered from patient
medical charts and surgical reports, descriptive statistics were performed for the entire
sample (N = 245).
Table 1 includes patient characteristics for the following variables: gender, age,
ethnicity, education, average weekly income, body mass index, smoking history,
depression history, case manager involvement, vocational rehabilitation assignment,
litigation involvement, total compensation/medical costs incurred, and number of prior
compensation claims. Results indicated that 81.6% of patients were male and 18.4%
female. The average age of patients at the time of their lumbar fusion was 40.0 years (SD
= 10.7). Ethnicity data revealed that patients were 94.9% White, 4.7% Hispanic, and .4%
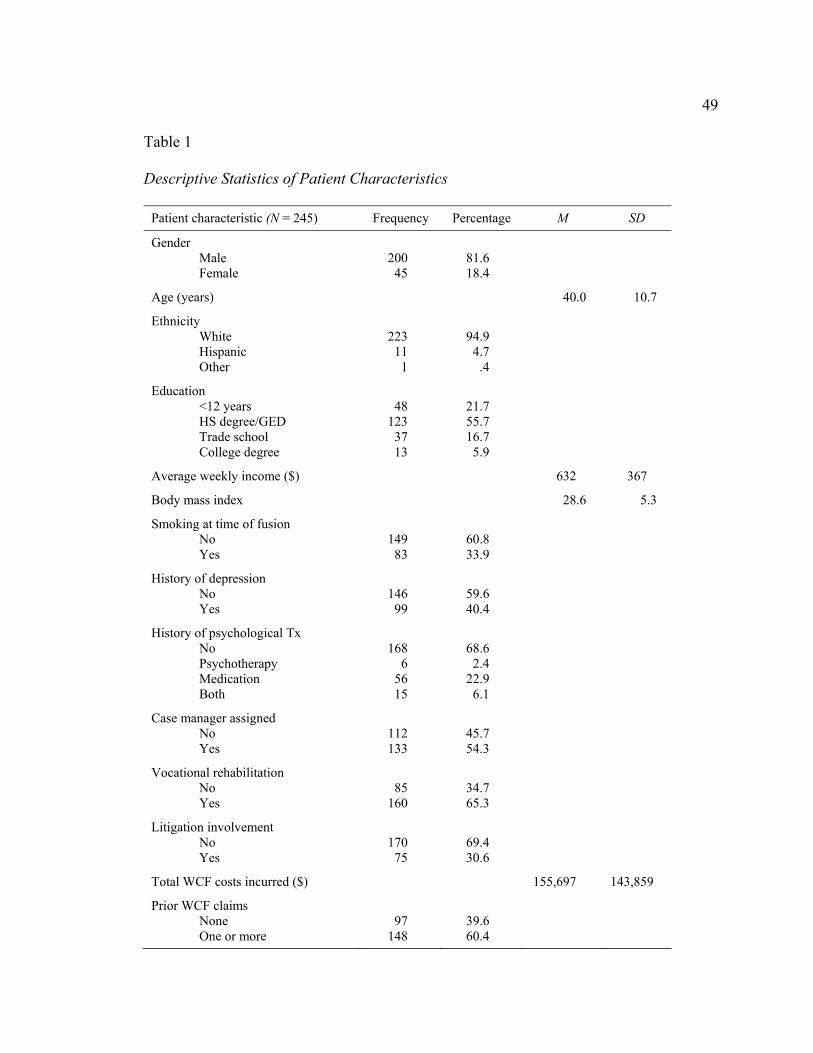
49 Table 1
Descriptive Statistics of Patient Characteristics
Patient characteristic (N = 245) Frequency Percentage M SD
Gender Male Female
200 45
81.6 18.4
Age (years) 40.0 10.7
Ethnicity White Hispanic Other
223 11
1
94.9 4.7
.4
Education <12 years HS degree/GED Trade school College degree
48
123 37 13
21.7 55.7 16.7 5.9
Average weekly income ($) 632 367
Body mass index 28.6 5.3
Smoking at time of fusion No Yes
149
83
60.8 33.9
History of depression No Yes
146 99
59.6 40.4
History of psychological Tx No Psychotherapy Medication Both
168
6 56 15
68.6 2.4
22.9 6.1
Case manager assigned No Yes
112 133
45.7 54.3
Vocational rehabilitation No Yes
85
160
34.7 65.3
Litigation involvement No Yes
170 75
69.4 30.6
Total WCF costs incurred ($) 155,697 143,859
Prior WCF claims None One or more
97
148
39.6 60.4
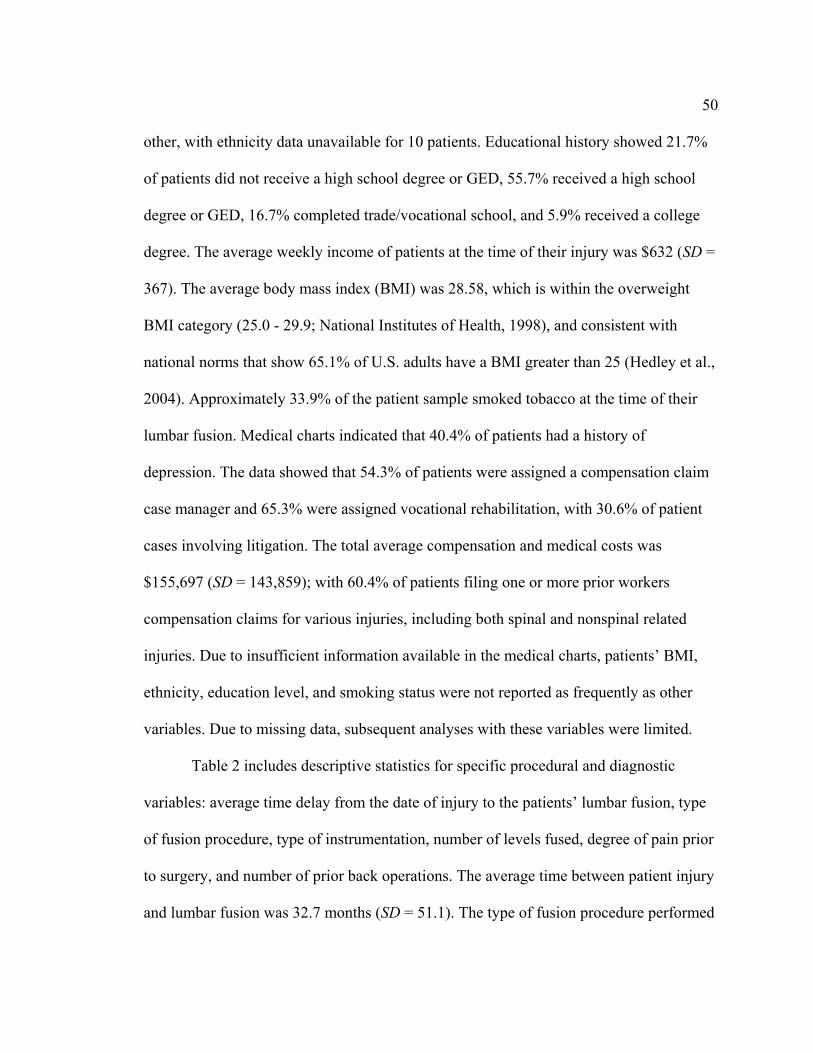
50 other, with ethnicity data unavailable for 10 patients. Educational history showed 21.7%
of patients did not receive a high school degree or GED, 55.7% received a high school
degree or GED, 16.7% completed trade/vocational school, and 5.9% received a college
degree. The average weekly income of patients at the time of their injury was $632 (SD =
367). The average body mass index (BMI) was 28.58, which is within the overweight
BMI category (25.0 - 29.9; National Institutes of Health, 1998), and consistent with
national norms that show 65.1% of U.S. adults have a BMI greater than 25 (Hedley et al.,
2004). Approximately 33.9% of the patient sample smoked tobacco at the time of their
lumbar fusion. Medical charts indicated that 40.4% of patients had a history of
depression. The data showed that 54.3% of patients were assigned a compensation claim
case manager and 65.3% were assigned vocational rehabilitation, with 30.6% of patient
cases involving litigation. The total average compensation and medical costs was
$155,697 (SD = 143,859); with 60.4% of patients filing one or more prior workers
compensation claims for various injuries, including both spinal and nonspinal related
injuries. Due to insufficient information available in the medical charts, patients�’ BMI,
ethnicity, education level, and smoking status were not reported as frequently as other
variables. Due to missing data, subsequent analyses with these variables were limited.
Table 2 includes descriptive statistics for specific procedural and diagnostic
variables: average time delay from the date of injury to the patients�’ lumbar fusion, type
of fusion procedure, type of instrumentation, number of levels fused, degree of pain prior
to surgery, and number of prior back operations. The average time between patient injury
and lumbar fusion was 32.7 months (SD = 51.1). The type of fusion procedure performed
51 Table 2 Descriptive Statistics of Patient Diagnosis and Surgical Variables
for injured workers was posterior lumbar interbody fusion (76.7%), anterior lumbar
interbody fusion (10.6%), and 360-degree posterior/anterior interbody fusion (12.2%).
Surgical reports indicated 59.6% of patients had one vertebral level fused, 37.6% had two
vertebral levels fused, and 2.9% had three or more vertebral levels fused. At the time of
surgery, 4.0% of patients reported mild pain, 59.0% reported moderate pain, and 39.3%
reported severe pain. According to patient medical charts, 45.7% of patients had one or
more back surgeries prior to the fusion.
Variable Frequency % M SD
Time between injury and fusion (months) 32.7 51.1
Type of fusion procedure Posterior lumbar interbody Anterior lumbar interbody Posterior/anterior interbody
188 26 20
76.7 10.6 12.2
Type of instrumentation None Pedicle screws Fusion cages Cages plus screws
3
107 29
106
1.2
43.7 11.8 43.3
Number of levels fused One Two Three or more
146 92
7
59.6 37.6 2.9
Degree of pain prior to surgery Mild Moderate Severe
4
138 92
1.7
59.0 39.3
Number of prior back surgeries None One Two Three or more
133 82 24
6
54.3 33.5 9.8 2.4

52
Response Rates and Bias Checks
As previously discussed, the medical chart review (Phase 1) included a total
sample size of 245 injured workers who underwent their first lumbar fusion surgery. Of
the 245 patients, a total of 110 were contacted by telephone and agreed to participate in
the telephone interview portion of the study (Phase 2), yielding an overall response rate
of 45%. The author and one other graduate student conducted all 110 of the interviews.
To evaluate differential bias between patients who completed the outcome survey
(responders) and patients lost to follow-up (nonresponders), specific sociodemographic
and medical characteristics were compared using univariate t tests and chi-squared tests
(see Table 3). Analyses revealed alpha values between .00 and .95 with effect sizes
ranging from -.19 to .48. Both age and BMI showed statistically significant differences
between responders and nonresponders; with moderate Cohen�’s d effect size values of
.48 and .39, respectively. Further, while the data showed that vocational rehabilitation
and a history of prior back surgeries were statistically significantly different between
responders and nonresponders, Phi and Cramer�’s V effect sizes of -.19 and .23 indicating
only weak associations. There were no statistically significant differences between
responders and nonresponders for months between date of the fusion surgery and initial
date of attempted contact during Phase 2. While there were some statistically significant
differences for a small number of patient variables (i.e., age, BMI, and vocational
rehabilitation), it was determined that controlling for these differences would not change
significant findings for the sample. In general, responders and nonresponders are still
considered statistically equivalent on a number of important patient characteristics. Thus,

53 Table 3 Comparisons of Select Patient Variables for Patient Follow-up Versus Patients Lost to Follow-Up
Patient variables
Means or proportion (%)
Effect size
Cohen�’s da, Phib or Cramer�’s Vc
Responders (n = 110)
Nonesponders (n = 135)
t or chi-square p value
Age 42.75 37.75 .001 .48
Smoking at time of fusion 30.7 39.7 .16 -.09
Body mass index 29.66 27.60 .01 .39
History of depression 36.4 43.7 .24 -.07
Case manager assigned 50.0 57.8 .22 -.08
Vocational rehabilitation 55.5 73.3 .001 -.19
Litigation involvement 26.4 34.1 .19 -.08
Type of instrumentation None Pedicle screws Fusion cages Cages plus screws
.9
48.2 7.3
43.6
1.5
40.0 15.6 43.0
.20 .14
Number of levels fused One Two Three or more
59.1 39.1 1.8
60.0 36.3 3.7
.64 .06
Prior back surgery None One Two Three or more
45.5 35.5 13.6 5.5
61.5 31.9 6.7 0.0
.01 .23
Prior wcf claims None One or more
40.9 59.1
38.5 61.5
.70 -.02
Degree of pain prior to surgery Mild Moderate Severe
1.9
57.9 40.2
1.6
59.8 38.6
.95 .02
Months between surgery and follow-up attempt
78.69 76.69 .58 .07
a Cohen�’s d is defined as the difference between two means divided by a standard deviation for the data. b Phi is defined as the square root of the chi-square statistic divided by the sample size. c Cramer�’s V is the effect size for a greater than 2 x 2 contingency table.
54 it can be assumed that the following data is generalizeable to other similar workers
compensation populations. To address research question 2, intercorrelations among a set
of patient variables were calculated and are presented in a correlation matrix (see Table
4). The 13 variables in the matrix are part of the original set of predictors that were
considered for regression analyses and include age at time of fusion, education level,
body mass index, smoking at time of fusion, history of depression, history of
psychological treatment, case manager, vocational rehabilitation, litigation involvement,
perceived pain prior to surgery, prior back operations, and prior WCF claims.
Results revealed correlation coefficients that ranged between -.26 to .66 and 15
were statistically significant at or below an alpha level of .05. The BMI of patients at the
time of surgery was positively correlated with patient�’s age (r = .18, p < .05) and
education level (r = .16, p < .05). Smoking was negatively correlated with educational
level (r = .24, p < .01) and positively correlated with BMI; thus, indicating that patients
who smoked at the time of surgery were more likely to have a higher BMI and less
education. History of depression was positively correlated with a history of psychological
treatment (r = .66, p < .01). Patients with a case a manager assigned were more likely to
be older (r = .14, p < .05) and smoke (r =14, p < .05). Vocational rehabilitation
involvement was negatively correlated with education level and positively correlated with
smoking (r = .19, p < .01) and being assigned a case manager (r = .35, p < .01). Litigation
involvement was positively correlated with a history of depression (r = .26, p < .01) and
psychological treatment (r = .18, p < .01). The number of prior back surgeries was
negatively correlated to age (r = .15, p < .05), while the number of workers compensation

Ta
ble
4 C
orre
latio
ns B
etw
een
Patie
nt a
nd P
roce
dura
l Var
iabl
es
Var
iabl
e
Var
iabl
e
1 2
3 4
5 6
7 8
9 10
11
12
1.
Age
at t
ime
of fu
sion
--
-
2.
Educ
atio
n le
vel
.125
--
-
3.
Bod
y m
ass i
ndex
.1
78*
.160
* --
-
4.
Smok
ing
at ti
me
of fu
sion
-.0
38
-.235
**
.215
**
---
5.
His
tory
of d
epre
ssio
n -.0
63
-.073
.0
86
.001
--
-
6.
His
tory
of p
sych
olog
ical
Tx
-.063
.0
14
.067
-.0
22
.661
**
---
7.
Cas
e m
anag
er a
ssig
ned
.138
* .0
04
.105
.1
42*
.121
.0
74
---
8.
Voc
atio
nal r
ehab
ilita
tion
.0
72
-.145
* .0
20
.195
**
.076
.0
87
.347
**
---
9.
Litig
atio
n in
volv
emen
t .0
58
-.098
.0
03
.112
.2
65**
.1
80**
-.0
13
.075
--
-
10.
Perc
eive
d pa
in p
rior t
o su
rger
y .0
17
-.090
.0
19
.119
.0
05
.028
.1
08
.025
.0
62
---
11.
Num
ber o
f prio
r bac
k op
erat
ions
-.1
51*
.127
-.0
19
-.016
.0
02
.086
-.0
68
-.108
.0
54
-.043
--
-
12.
Num
ber o
f WC
F cl
aim
s -.0
15
.118
.0
04
.078
.0
54
.063
.1
28*
.199
**
-.042
-.0
13
-.026
--
-
13.
Type
of i
nstru
men
tatio
n -.1
12
-.126
-.0
20
.109
.0
77
.103
-.0
79
-.022
-.0
63
.045
-.0
21
---
N =
245
.
* p
.05.
**
p
.01.
55

56 claims was positively correlated with case manager assignment (r = .13, p < .05) and
vocational rehabilitation (r = .20, p < .01). With the exception of the strong relationship
between a history of depression and psychological treatment, the magnitude of these
intercorrelations were fairly modest which likely minimizes problems due to
multicollinearity.
Patient Outcomes
To achieve the second objective of this study, lumbar fusion patient outcomes
were calculated and presented in the following sequence: (a) fusion rate, disability status
and functional impairment; (b) patient satisfaction and quality of life; (c) categorization
of outcome; (d) subjective pain levels; (e) general physical and mental health functioning.
The results of these analyses addressed research questions 3 through 9, with specific
questions highlighted in the appropriate sections.
Fusion Rates, Disability Status, and Functional Impairment
Table 5 includes the current study�’s fusion rates, work-disability status, and back-
specific functional impairment following lumbar fusion and compares these rates to a
prior fusion study with Utah workers compensation patients (DeBerard et al., 2001).
Injured workers were considered disabled only if their back condition related to
the lumbar fusion procedure was the primary cause of inability to work. To address
research question 3, at the time of follow-up, injured workers reported solid fusion rates
of 89%, compared to 71.9% in the prior study. Research questions 4 and 5 were
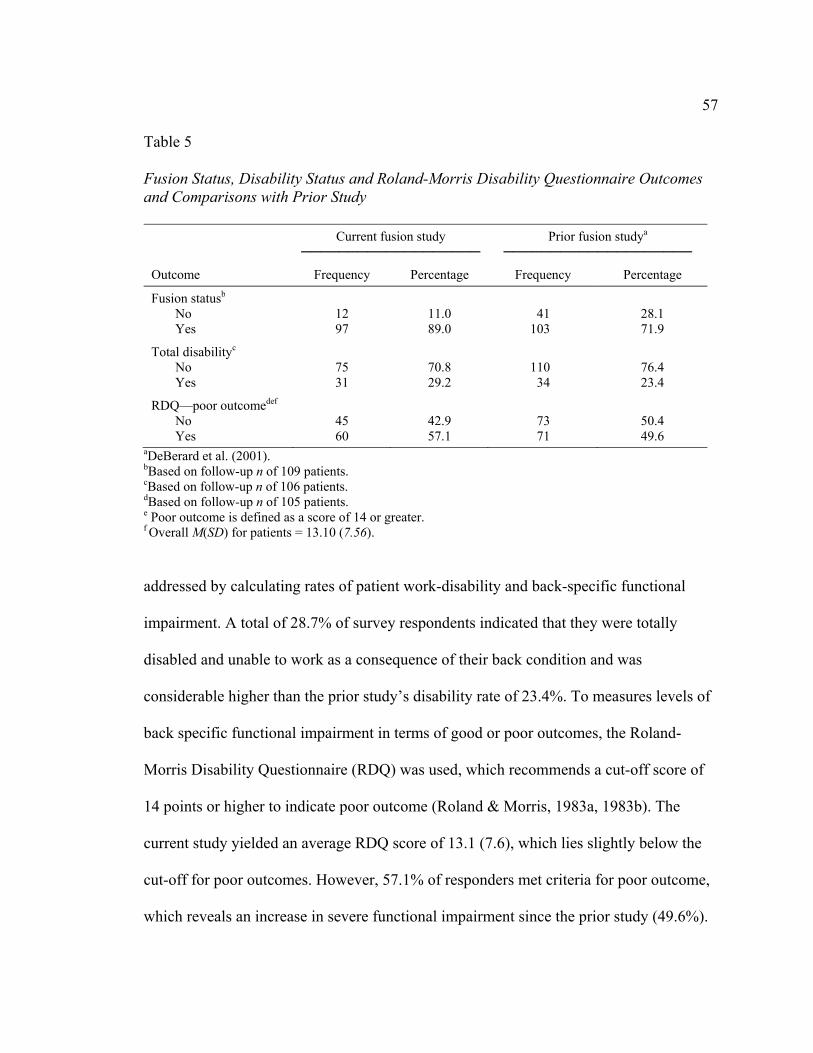
57 Table 5 Fusion Status, Disability Status and Roland-Morris Disability Questionnaire Outcomes and Comparisons with Prior Study
Current fusion study
Prior fusion studya
Outcome Frequency Percentage Frequency Percentage
Fusion statusb
No Yes
12 97
11.0 89.0
41
103
28.1 71.9
Total disabilityc
No Yes
75 31
70.8 29.2
110 34
76.4 23.4
RDQ�—poor outcomedef No Yes
45 60
42.9 57.1
73 71
50.4 49.6
aDeBerard et al. (2001). bBased on follow-up n of 109 patients. cBased on follow-up n of 106 patients. dBased on follow-up n of 105 patients. e Poor outcome is defined as a score of 14 or greater. f Overall M(SD) for patients = 13.10 (7.56).
addressed by calculating rates of patient work-disability and back-specific functional
impairment. A total of 28.7% of survey respondents indicated that they were totally
disabled and unable to work as a consequence of their back condition and was
considerable higher than the prior study�’s disability rate of 23.4%. To measures levels of
back specific functional impairment in terms of good or poor outcomes, the Roland-
Morris Disability Questionnaire (RDQ) was used, which recommends a cut-off score of
14 points or higher to indicate poor outcome (Roland & Morris, 1983a, 1983b). The
current study yielded an average RDQ score of 13.1 (7.6), which lies slightly below the
cut-off for poor outcomes. However, 57.1% of responders met criteria for poor outcome,
which reveals an increase in severe functional impairment since the prior study (49.6%).
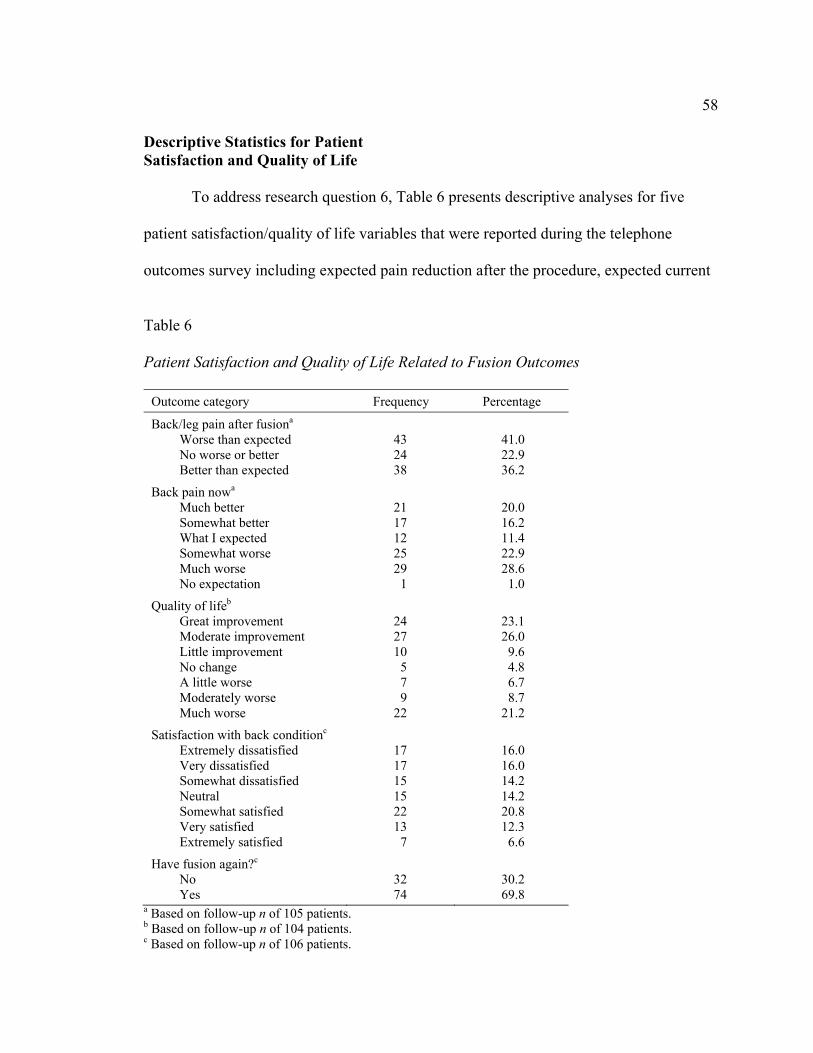
58 Descriptive Statistics for Patient Satisfaction and Quality of Life
To address research question 6, Table 6 presents descriptive analyses for five
patient satisfaction/quality of life variables that were reported during the telephone
outcomes survey including expected pain reduction after the procedure, expected current
Table 6
Patient Satisfaction and Quality of Life Related to Fusion Outcomes
Outcome category Frequency Percentage
Back/leg pain after fusiona
Worse than expected No worse or better Better than expected
43 24 38
41.0 22.9 36.2
Back pain nowa
Much better Somewhat better What I expected Somewhat worse Much worse No expectation
21 17 12 25 29
1
20.0 16.2 11.4 22.9 28.6 1.0
Quality of lifeb
Great improvement Moderate improvement Little improvement No change A little worse Moderately worse Much worse
24 27 10
5 7 9
22
23.1 26.0 9.6 4.8 6.7 8.7
21.2
Satisfaction with back conditionc
Extremely dissatisfied Very dissatisfied Somewhat dissatisfied Neutral Somewhat satisfied Very satisfied Extremely satisfied
17 17 15 15 22 13
7
16.0 16.0 14.2 14.2 20.8 12.3 6.6
Have fusion again?c
No Yes
32 74
30.2 69.8
a Based on follow-up n of 105 patients. b Based on follow-up n of 104 patients. c Based on follow-up n of 106 patients.

59 pain level, improved quality of life, satisfaction with back condition, and whether they
would repeat the fusion. In relation to pain outcome expectations after the fusion, the first
satisfaction item asked patients if their pain following fusion was �“worse than expected,�”
�“no worse or better than expected,�” or �“better than expected,�” which generated rates of
41.0%, 22.9%, and 36.2%. In relation to current pain outcome expectations, the second
satisfaction item asked patients to rate on a 6-point scale whether their �“back pain was
better or worse than expected at this point.�” As determined by this item, 36.2% of patient
felt their current back pain was somewhat or much better than they expected, while
51.0% indicated their current back pain was somewhat or much worse than they
expected. The third satisfaction item asked patients if their quality of life was better or
worse as a result of their fusion. Fifty-nine percent of respondents indicating their quality
of life improved after surgery, while the remaining individuals reported either no change
(4.8%) or worse quality of life (36.6%). The fourth satisfaction item refers to patients�’
overall satisfaction with their back condition as it is right now. Approximately 46.2% of
patients felt either somewhat, very, or extremely satisfied, 39.7% felt either somewhat,
very, or extremely dissatisfied, and 14.2% felt neither satisfied nor dissatisfied. The fifth
satisfaction item asked patients if they would, retrospectively, have the lumbar fusion
procedure again. About one third (30.2%) of the patient sample felt that they would not
choose to have the fusion surgery again if they could go back in time.
Outcome Categorization
To address research question 7, the Stauffer-Coventry Index (SCI; Stauffer &
Coventry, 1972) self-report instrument was used to gain information about patient
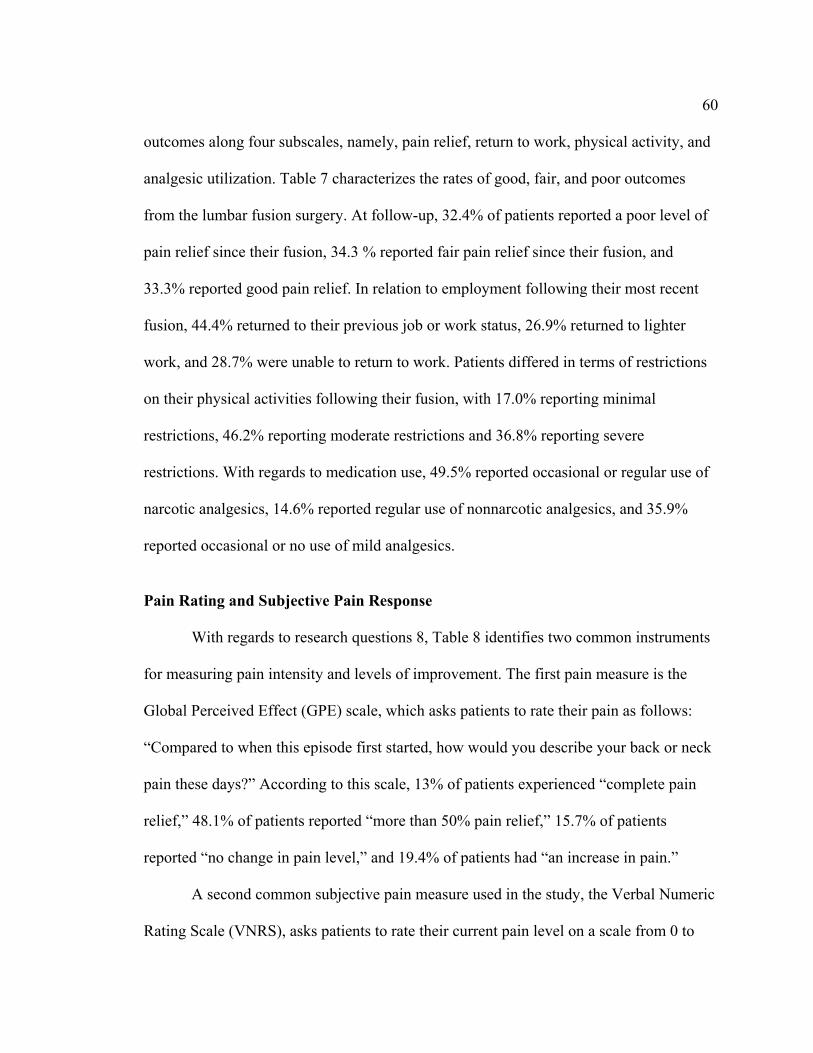
60 outcomes along four subscales, namely, pain relief, return to work, physical activity, and
analgesic utilization. Table 7 characterizes the rates of good, fair, and poor outcomes
from the lumbar fusion surgery. At follow-up, 32.4% of patients reported a poor level of
pain relief since their fusion, 34.3 % reported fair pain relief since their fusion, and
33.3% reported good pain relief. In relation to employment following their most recent
fusion, 44.4% returned to their previous job or work status, 26.9% returned to lighter
work, and 28.7% were unable to return to work. Patients differed in terms of restrictions
on their physical activities following their fusion, with 17.0% reporting minimal
restrictions, 46.2% reporting moderate restrictions and 36.8% reporting severe
restrictions. With regards to medication use, 49.5% reported occasional or regular use of
narcotic analgesics, 14.6% reported regular use of nonnarcotic analgesics, and 35.9%
reported occasional or no use of mild analgesics.
Pain Rating and Subjective Pain Response
With regards to research questions 8, Table 8 identifies two common instruments
for measuring pain intensity and levels of improvement. The first pain measure is the
Global Perceived Effect (GPE) scale, which asks patients to rate their pain as follows:
�“Compared to when this episode first started, how would you describe your back or neck
pain these days?�” According to this scale, 13% of patients experienced �“complete pain
relief,�” 48.1% of patients reported �“more than 50% pain relief,�” 15.7% of patients
reported �“no change in pain level,�” and 19.4% of patients had �“an increase in pain.�”
A second common subjective pain measure used in the study, the Verbal Numeric
Rating Scale (VNRS), asks patients to rate their current pain level on a scale from 0 to
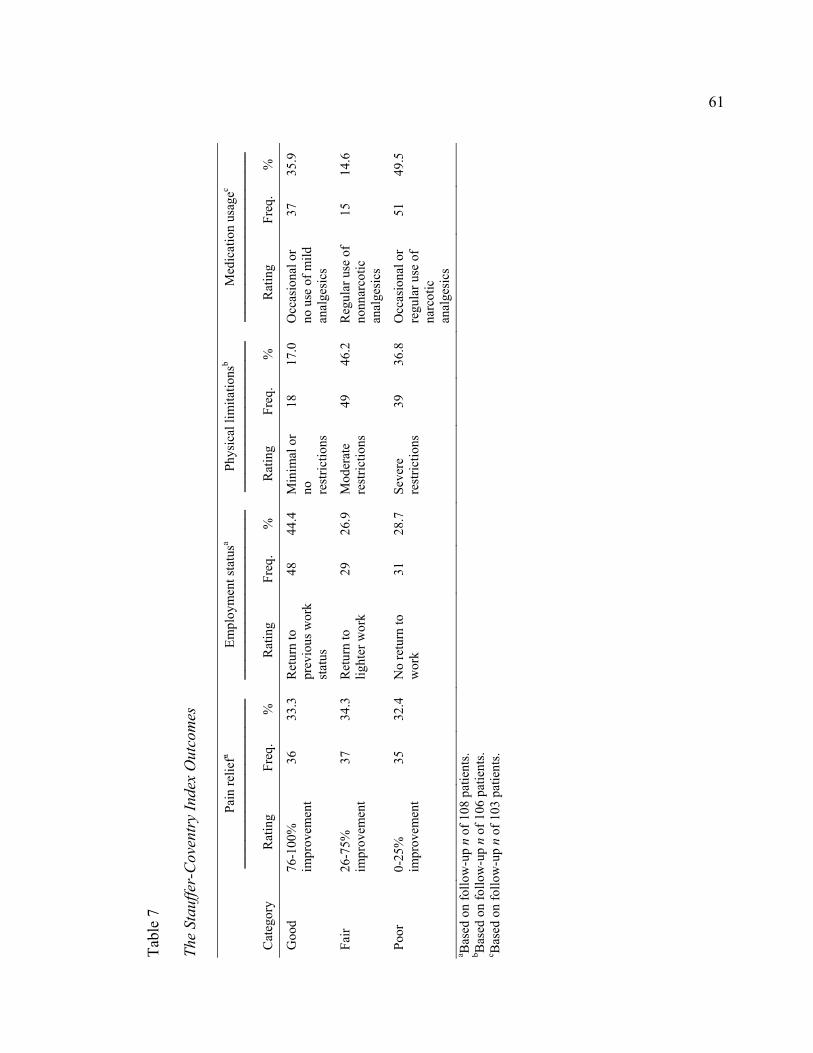
Ta
ble
7 Th
e St
auffe
r-C
oven
try
Inde
x O
utco
mes
Pa
in re
liefa
Em
ploy
men
t sta
tusa
Ph
ysic
al li
mita
tions
b
M
edic
atio
n us
agec
Cat
egor
y R
atin
g Fr
eq.
%
Rat
ing
Freq
. %
R
atin
g Fr
eq.
%
Rat
ing
Freq
. %
Goo
d 76
-100
%
impr
ovem
ent
36
33.3
R
etur
n to
pr
evio
us w
ork
stat
us
48
44.4
M
inim
al o
r no
re
stric
tions
18
17.0
O
ccas
iona
l or
no u
se o
f mild
an
alge
sics
37
35.9
Fair
26-7
5%
impr
ovem
ent
37
34.3
R
etur
n to
lig
hter
wor
k 29
26
.9
Mod
erat
e re
stric
tions
49
46
.2
Reg
ular
use
of
nonn
arco
tic
anal
gesi
cs
15
14.6
Poor
0-
25%
im
prov
emen
t 35
32
.4
No
retu
rn to
w
ork
31
28.7
Se
vere
re
stric
tions
39
36
.8
Occ
asio
nal o
r re
gula
r use
of
narc
otic
an
alge
sics
51
49.5
a Bas
ed o
n fo
llow
-up
n of
108
pat
ient
s. b B
ased
on
follo
w-u
p n
of 1
06 p
atie
nts.
c Bas
ed o
n fo
llow
-up
n of
103
pat
ient
s.
61
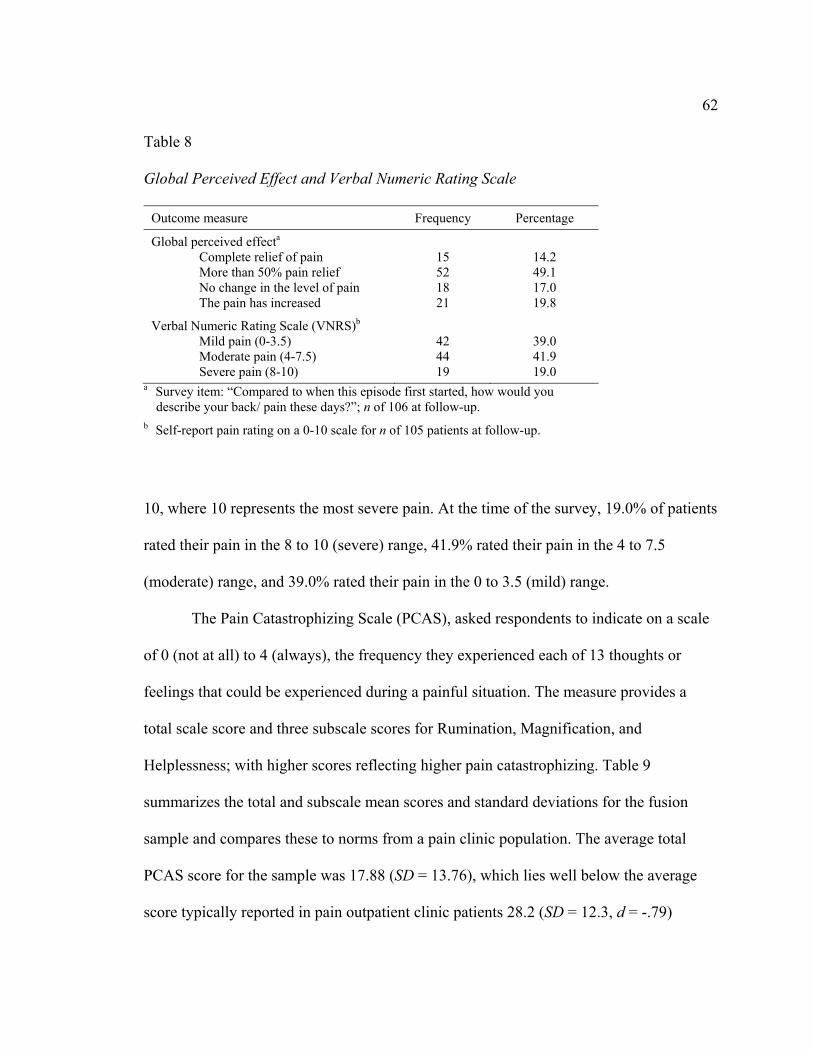
62 Table 8 Global Perceived Effect and Verbal Numeric Rating Scale
Outcome measure Frequency Percentage
Global perceived effecta Complete relief of pain More than 50% pain relief No change in the level of pain The pain has increased
15 52 18 21
14.2 49.1 17.0 19.8
Verbal Numeric Rating Scale (VNRS)b Mild pain (0-3.5) Moderate pain (4-7.5) Severe pain (8-10)
42 44 19
39.0 41.9 19.0
a Survey item: �“Compared to when this episode first started, how would you describe your back/ pain these days?�”; n of 106 at follow-up.
b Self-report pain rating on a 0-10 scale for n of 105 patients at follow-up. 10, where 10 represents the most severe pain. At the time of the survey, 19.0% of patients
rated their pain in the 8 to 10 (severe) range, 41.9% rated their pain in the 4 to 7.5
(moderate) range, and 39.0% rated their pain in the 0 to 3.5 (mild) range.
The Pain Catastrophizing Scale (PCAS), asked respondents to indicate on a scale
of 0 (not at all) to 4 (always), the frequency they experienced each of 13 thoughts or
feelings that could be experienced during a painful situation. The measure provides a
total scale score and three subscale scores for Rumination, Magnification, and
Helplessness; with higher scores reflecting higher pain catastrophizing. Table 9
summarizes the total and subscale mean scores and standard deviations for the fusion
sample and compares these to norms from a pain clinic population. The average total
PCAS score for the sample was 17.88 (SD = 13.76), which lies well below the average
score typically reported in pain outpatient clinic patients 28.2 (SD = 12.3, d = -.79)
63 Table 9
Pain Catastrophizing Scale (PCAS) Scores and Comparisons
Scale
Fusion patients
Pain clinic patientsa
Effect size
M SD M SD Cohen�’s d
Total score 17.88 13.76 28.2 12.3 -.79
Rumination 7.01 5.20 10.1 4.3 -.65
Magnification 3.12 2.92 4.8 2.8 -.59
Helplessness 7.74 6.63 13.3 6.1 -.87
Note. Based on n of 102 at follow-up. a Patients undergoing evaluation and treatment at a multidisciplinary pain clinic.
(Sullivan et al., 1995). Fusion patients also showed lower average scores for the
rumination (M = 7.01, SD =5.20), magnification (M = 3.12, SD = 2.92), and helplessness
(M = 7.74, SD = 6.63) subscales when compared to pain clinic patients with moderate to
large effect sizes of -.65, -.59, and -.87, respectively. These data indicate fusion patients
showed considerably lower levels of pain catastrophization than what is commonly found
in chronic pain patients.
General Physical and Mental Health Functioning
To address research question 9, Version 2.0 of the Short-Form Health Survey (SF-
36v2; Ware et al., 2000) was used to reflect various aspects of health and mental health
from the perspective of the patient. The SF-36v2 groups items into eight subscales
[physical functioning (PF), role-physical functioning (RP), bodily pain (BP), general
health (GH), vitality (VT), social functioning (SF), role-emotional functioning RE), and
64 mental health (MH)] that are then combined to form the physical and mental component
summary scores (PCS and MCS). Normative data allows for interpretation of the SF-
36v2 subscales and summary measure scores in our sample by comparing them with the
distribution of scores for other individuals. Scores are understood as variation from
expected or typical scores called norms. The scores of the current sample were compared
to existing normative data drawn from the general U.S. adult population (N = 6742) and a
sample of outpatient pain/sciatica patients (N = 481; Ware et al., 2000). Norm based
scoring was used with the fusion sample, which has a general population mean of 50 and
standard deviation of 10. Patient characteristics and response rates are summarized in
Table 10. The data shows that the current fusion sample demonstrated considerably lower
average subscale than the norms obtained from the general population ranging from small
(-.33) to large (-1.14) effect sizes. The highest effect sizes were noted on scales
associated with physical health, pain, and functional limitations associated with physical
health. Fusion patients also scored consistently lower than the back pain/sciatica norm
reference group with effect sizes between -.16 and -.81. Related trends were observed
with the largest effect sizes observed for physical health related scales. These
comparisons are also presented on a graph in Figure 4. Both scores for the PCS (M =
37.4, SD = 11.9) and MCS (M = 45.9, SD = 13.9) in the current fusion sample were lower
than both normative populations. While the PCS scale revealed large effect sizes when
compared to the general (-1.51) and back/sciatica pain population (-.72), the MCS
revealed only modest effect sizes of -.33 and -.16. Overall these data suggest that injured
workers who have undergone lumbar fusion, reported poorer physical health outcomes

Ta
ble
10
SF-3
6(v.
2) M
ultid
imen
sion
al H
ealth
Out
com
es a
nd C
ompa
riso
ns
Fu
sion
sam
ple
G
ener
al p
opul
atio
na G
ener
al
popu
latio
n ef
fect
Siz
eb
Bac
k pa
in/s
ciat
icac
B
ack
pain
/sci
atic
a ef
fect
size
b SF
-36
subs
cale
M
SD
M
SD
M
SD
Phys
ical
func
tioni
ng
36.8
12
.9
50.0
10.0
-1
.14
46.6
11
.3
-.81
Rol
e fu
nctio
ning
37
.7
14.2
50
.010
.0
-1.0
1 46
.4
11.4
-.6
8
Bod
ily p
ain
38.9
11
.5
50.0
10.0
-1
.03
44.6
9.
3 -.5
5
Gen
eral
hea
lth
43.9
10
.9
50.0
10.0
-.5
8 46
.5
10.6
-.2
4
Vita
lity
42.9
12
.7
50.0
10.0
-.6
1 46
.5
10.2
-.3
1
Soci
al fu
nctio
ning
40
.8
15.7
50
.010
.0
-.70
46.9
11
.2
-.45
Rol
e-em
otio
nal f
unct
ioni
ng
41.9
14
.2
50.0
10.0
-.6
6 47
.6
11.3
-.4
4
Men
tal h
ealth
func
tioni
ng
45.6
13
.3
50.0
10.0
-.3
7 47
.6
10.9
-.1
6
Phys
ical
com
pone
nt su
mm
ary
37.4
11
.9
50.0
10.0
-1
.15
45.6
10
.8
-.72
Men
tal c
ompo
nent
sum
mar
y 45
.9
13.9
50
.010
.0
-.33
47.9
11
.0
-.16
Not
e. S
core
s ran
ge fr
om 0
-100
. A h
igh
scor
e in
dica
tes b
ette
r hea
lth st
atus
. Bas
ed o
n n
of 1
05 a
t fol
low
-up.
a G
ener
al U
.S. a
dult
popu
latio
n; N
= 6
742
(War
e et
al.,
200
0).
b Ef
fect
size
repr
esen
ts C
ohen
�’s d
.
c N
orm
s for
sam
ple
com
orbi
d co
nditi
on: b
ack
pain
/sci
atic
a (in
last
6 m
onth
s) w
ith h
yper
tens
ion;
N =
481
.
65
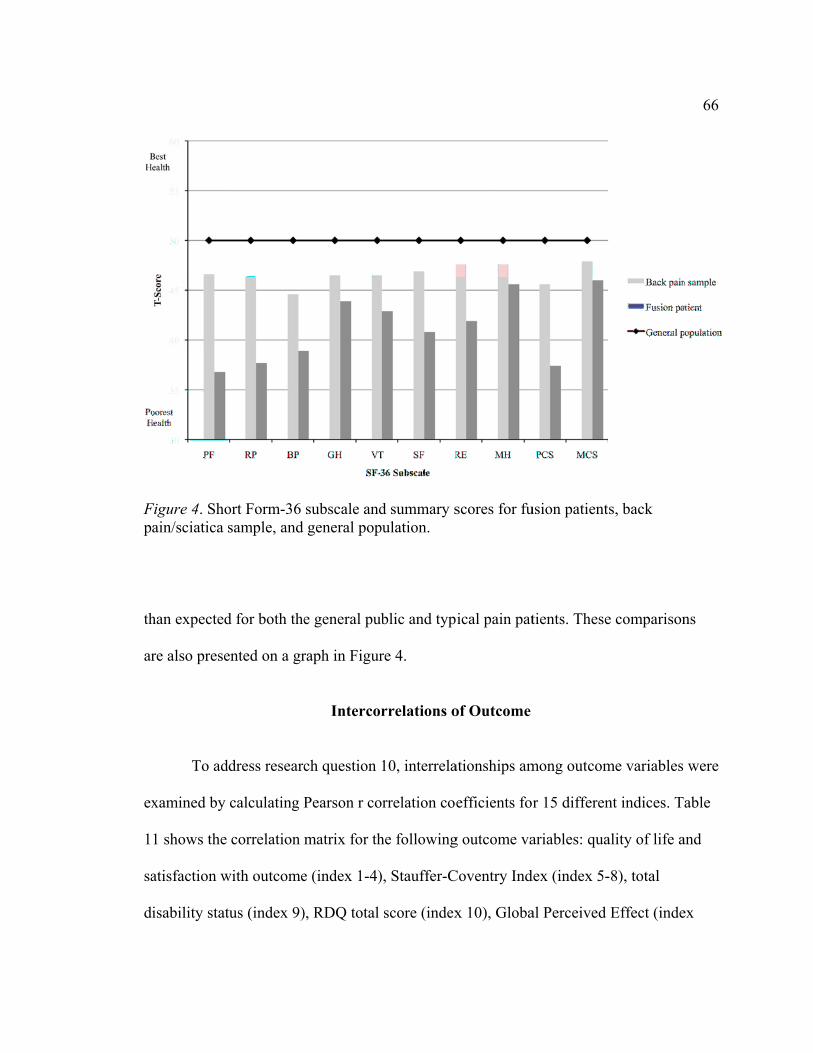
Fp
th
ar
ex
1
sa
d
Figure 4. Shoain/sciatica s
han expected
re also prese
To ad
xamined by
1 shows the
atisfaction w
isability stat
ort Form-36 sample, and
d for both the
ented on a gr
ddress researc
calculating P
correlation m
with outcome
tus (index 9)
subscale andgeneral pop
e general pu
raph in Figur
Interco
ch question
Pearson r co
matrix for th
e (index 1-4)
), RDQ total
d summary spulation.
ublic and typ
re 4.
rrelations o
10, interrela
orrelation coe
he following
), Stauffer-C
score (index
scores for fu
ical pain pat
of Outcome
ationships am
efficients fo
g outcome va
Coventry Ind
x 10), Globa
usion patient
tients. These
mong outcom
r 15 differen
ariables: qua
dex (index 5-
al Perceived
s, back
e comparison
me variables
nt indices. T
ality of life a
-8), total
Effect (inde
66
ns
were
able
and
ex

Ta
ble
11
Cor
rela
tions
Bet
wee
n O
utco
me
Vari
able
s
V
aria
ble
Var
iabl
e 1a
2 3
4a5a
6a7a
8a9a
10a
11a
12a
13
14
15
1a --
-
2 .5
1**
---
3 .5
2**
.39**
--
-
4a .6
2**
.32**
.6
8**
---
5a .6
2**
.43**
.4
7**
.62**
--
-
6a .3
5**
.18
.29**
.3
0**
.34**
--
-
7a .5
6**
.25**
.4
8**
.48**
.5
9**
.46**
--
-
8a .3
7**
.23*
.31**
.2
8**
.54**
.2
6**
.34**
--
-
9a .4
5**
.18
.38**
.3
7**
.49**
.5
3**
.49**
.4
6**
---
10a
.64**
.3
6**
.60**
.6
9**
.68**
.4
7**
.75**
.4
5**
.54**
--
-
11a
.60**
.3
9**
.64**
.6
9**
.65**
.3
4**
.56**
.3
8**
.47**
.6
4**
---
12a
.62**
.3
1**
.53**
.6
1**
.57**
.4
2**
.59**
.3
3**
.51**
.6
7**
.58**
--
-
13
.52**
.3
2**
.51**
.5
6**
.64**
.6
0**
.71**
.4
7**
.61**
.8
4**
.60**
.6
3**
---
14
.54**
.3
5**
.36**
.3
4**
.29**
.1
6 .4
0**
.28**
.2
9**
.51**
.3
2**
.43**
.3
3**
---
15
.20*
.29**
.1
2 .1
8 .2
6**
.14
.19*
.06
.10
.25*
.22*
.23*
.28**
.1
9 --
- N
ote.
1=q
ualit
y of
life
cha
ngea ; 2
=ret
rosp
ectiv
ely,
wou
ld re
peat
fusi
on (n
o=1:
yes
=2);
3=sa
tisfa
ctio
n w
ith c
urre
nt b
ack
cond
ition
; 4=b
ack/
leg
pain
cha
ngea ;
5=SC
I: pa
in re
lief (
%)a ; 6
=SC
I: em
ploy
men
t sta
tusa ; 7
=SC
I: ph
ysic
al li
mita
tions
; 8=S
CI:
med
icat
ion
usag
ea ; 9=d
isab
ility
stat
us (n
o=1;
yes
=2)a ; 1
0=R
DQ
to
tal s
core
a ; 11=
Glo
bal P
erce
ived
Eff
ecta ; 1
2= V
NR
Sa ; 13=
SF-
36: P
hysi
cal C
ompo
nent
Sum
mar
y; 1
4= S
F-36
: Men
tal C
ompo
nent
Sum
mar
y; 1
5=Fu
sion
St
atus
. a
Rev
erse
cod
ed so
hig
her s
core
s ref
lect
bet
ter f
unct
ioni
ng/o
utco
me.
* p
.05,
** p
.0
1, N
=11
0.
67
68 11), Verbal Numeric Rating Scale (index 12), and the Short Form Health Survey (MCS
and PCS) (index 13-14), and fusion status (index 15). In order to allow for transparent
understanding of the interrelationships, 10 of the outcome indices were reverse coded to
reflect higher reflect better functioning/outcome. The analysis yielded 96/105 significant
correlations coefficients that ranged between .06 and .85. Moderate to large
intercorrelations were observed within various categories of outcome measures. For
instance, intercorrelations were between .34 and .59 for items on the SCI and between .32
and .68 on patient satisfaction/quality of life variables. The intercorrelation was moderate
(r = .33) between MCS and PCS scores. The intercorrelation between GPE and VRNS
was significant (r = 60), and both GPE and VRNS were significantly correlated with all
other outcome variables with coefficients between .31 and .69. Similarly, disability status
was significantly correlated with physical status and functional limitation measures,
though it was not linked to patient satisfaction items. The RDQ total score had the
strongest intercorrelations that ranged from .25 (SCI: pain relief) to .84 (SF-36: PCS).
Fusion status demonstrated the weakest intercorrelations yielding only mild to no
statistically significant relationships with outcome measures. As a whole, the correlation
matrix indicates consistent overlap among outcome variables in a direction that would be
expected. However, the extent of these relationships does not denote excessive overlap to
warrant a combination of any of the outcome variables.
Correlations Between Patient Characteristics and Outcomes
To address the third and final objective of the current study, intercorrelations
69 between patient presurgical variables and outcomes were examined (research question
11) in order to test predictive efficacy of a presurgical multiple variable model of lumbar
fusion outcomes. Tables 12 and 13 display statistically significant relationships between
patient demographic factors and functional outcomes after surgery. Involvement of a
nurse case management and assignment to vocational rehabilitation were significantly
related to worse outcomes in terms of pain relief, return to work, physical restrictions,
disability status, functional severity (RDQ score), SF-36 PCS scales and several SF-36
subscales. Litigation involvement was significantly related to return to work, disability
status, functional severity, both SF-36 MCS and SF-36 PCS scales, and several SF-36
subscales. Patients with a history of depression showed a significant relationship with
higher disability status, lower SF-36 MCS and SF-36 subscales scores. There were no
significant relationships between prior back surgeries, pain severity at time of fusion,
levels fused, and type of instrumentation with any of the outcome variables. Finally, the
time between surgery and follow-up showed no significant relationships with any of the
outcome variables; therefore, this variable was not included as a covariate in any of the
subsequent multivariate analyses. Based on the Pearson correlations, depression history,
nurse case management, vocational rehabilitation, and litigation involvement, are the
predictors that consistently account for variation in outcomes.
Multivariate Prediction of Outcomes
The following section addresses research question 12 by testing the predictive
efficacy of a presurgical multiple variable model for lumbar fusion outcomes. Due to the
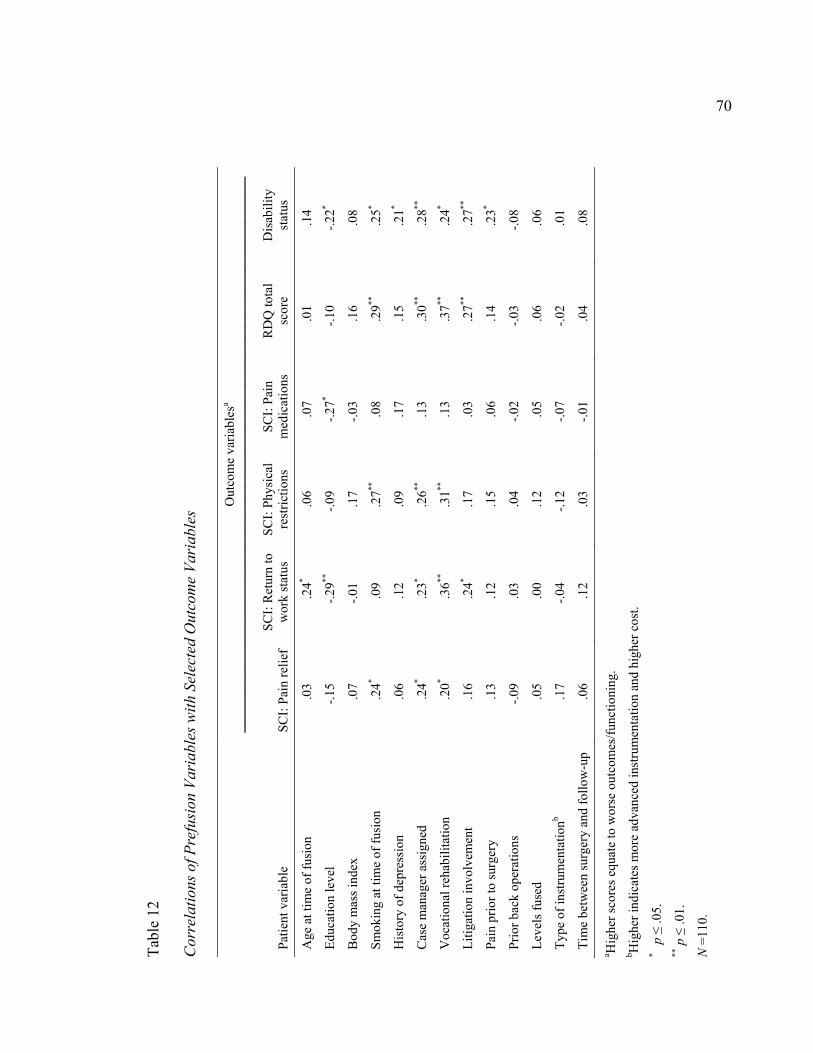
Ta
ble
12
Cor
rela
tions
of P
refu
sion
Var
iabl
es w
ith S
elec
ted
Out
com
e Va
riab
les
O
utco
me
varia
bles
a
Patie
nt v
aria
ble
SCI:
Pain
relie
f SC
I: R
etur
n to
w
ork
stat
us
SCI:
Phys
ical
re
stric
tions
SC
I: Pa
in
med
icat
ions
R
DQ
tota
l sc
ore
Dis
abili
ty
stat
us
Age
at t
ime
of fu
sion
.0
3 .2
4* .0
6 .0
7 .0
1 .1
4
Educ
atio
n le
vel
-.15
-.29**
-.0
9 -.2
7* -.1
0 -.2
2*
Bod
y m
ass i
ndex
.0
7 -.0
1 .1
7 -.0
3 .1
6 .0
8
Smok
ing
at ti
me
of fu
sion
.2
4* .0
9 .2
7**
.08
.29**
.2
5*
His
tory
of d
epre
ssio
n .0
6 .1
2 .0
9 .1
7 .1
5 .2
1*
Cas
e m
anag
er a
ssig
ned
.24*
.23*
.26**
.1
3 .3
0**
.28**
Voc
atio
nal r
ehab
ilita
tion
.2
0* .3
6**
.31**
.1
3 .3
7**
.24*
Litig
atio
n in
volv
emen
t .1
6 .2
4* .1
7 .0
3 .2
7**
.27**
Pain
prio
r to
surg
ery
.13
.12
.15
.06
.14
.23*
Prio
r bac
k op
erat
ions
-.0
9 .0
3 .0
4 -.0
2 -.0
3 -.0
8
Leve
ls fu
sed
.05
.00
.12
.05
.06
.06
Type
of i
nstru
men
tatio
nb .1
7 -.0
4 -.1
2 -.0
7 -.0
2 .0
1
Tim
e be
twee
n su
rger
y an
d fo
llow
-up
.06
.12
.03
-.01
.04
.08
a Hig
her s
core
s equ
ate
to w
orse
out
com
es/fu
nctio
ning
. b H
ighe
r ind
icat
es m
ore
adva
nced
inst
rum
enta
tion
and
high
er c
ost.
* p
.05.
**
p
.01.
N =
110.
70
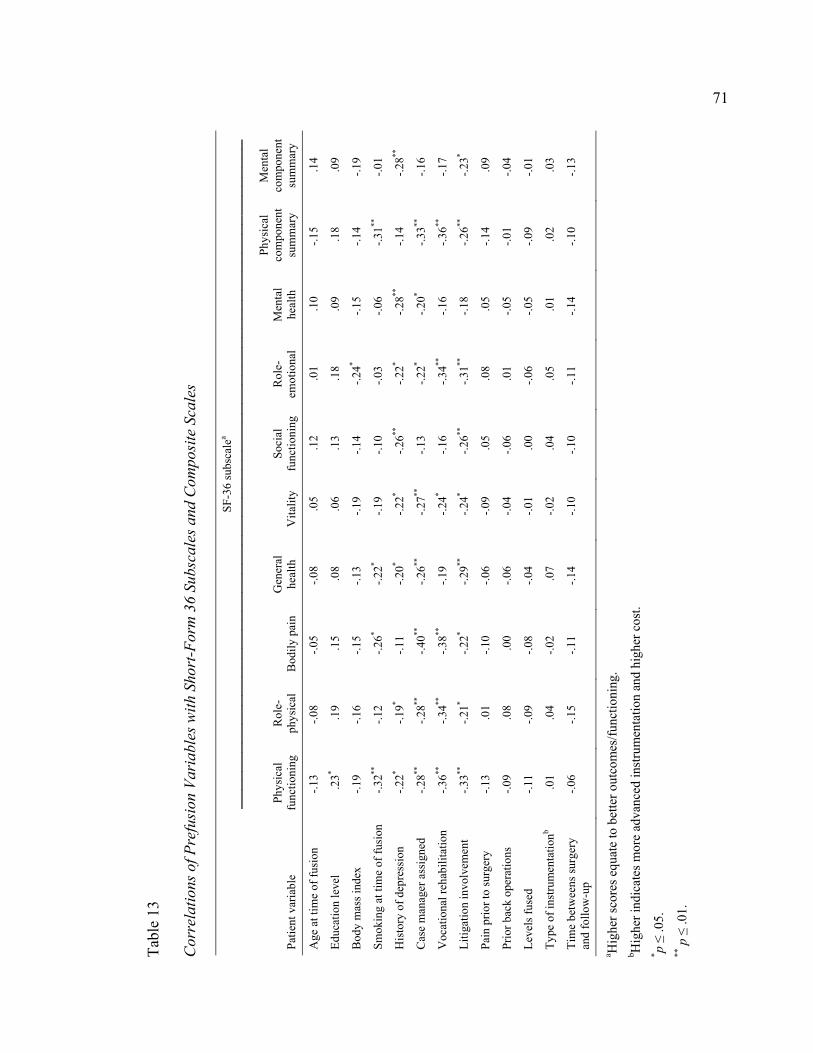
Ta
ble
13
Cor
rela
tions
of P
refu
sion
Var
iabl
es w
ith S
hort
-For
m 3
6 Su
bsca
les a
nd C
ompo
site
Sca
les
SF
-36
subs
cale
a
Patie
nt v
aria
ble
Phys
ical
fu
nctio
ning
R
ole-
phys
ical
B
odily
pai
n G
ener
al
heal
th
Vita
lity
Soci
al
func
tioni
ng
Rol
e-em
otio
nal
Men
tal
heal
th
Phys
ical
co
mpo
nent
su
mm
ary
Men
tal
com
pone
nt
sum
mar
y
Age
at t
ime
of fu
sion
-.1
3 -.0
8 -.0
5 -.0
8 .0
5 .1
2 .0
1 .1
0 -.1
5 .1
4
Educ
atio
n le
vel
.23*
.19
.15
.08
.06
.13
.18
.09
.18
.09
Bod
y m
ass i
ndex
-.1
9 -.1
6 -.1
5 -.1
3 -.1
9 -.1
4 -.2
4* -.1
5 -.1
4 -.1
9
Smok
ing
at ti
me
of fu
sion
-.3
2**
-.12
-.26*
-.22*
-.19
-.10
-.03
-.06
-.31**
-.0
1
His
tory
of d
epre
ssio
n -.2
2* -.1
9* -.1
1 -.2
0* -.2
2* -.2
6**
-.22*
-.28**
-.1
4 -.2
8**
Cas
e m
anag
er a
ssig
ned
-.28**
-.2
8**
-.40**
-.2
6**
-.27**
-.1
3 -.2
2* -.2
0* -.3
3**
-.16
Voc
atio
nal r
ehab
ilita
tion
-.3
6**
-.34**
-.3
8**
-.19
-.24*
-.16
-.34**
-.1
6 -.3
6**
-.17
Litig
atio
n in
volv
emen
t -.3
3**
-.21*
-.22*
-.29**
-.2
4* -.2
6**
-.31**
-.1
8 -.2
6**
-.23*
Pain
prio
r to
surg
ery
-.13
.01
-.10
-.06
-.09
.05
.08
.05
-.14
.09
Prio
r bac
k op
erat
ions
-.0
9 .0
8 .0
0 -.0
6 -.0
4 -.0
6 .0
1 -.0
5 -.0
1 -.0
4
Leve
ls fu
sed
-.11
-.09
-.08
-.04
-.01
.00
-.06
-.05
-.09
-.01
Type
of i
nstru
men
tatio
nb .0
1 .0
4 -.0
2 .0
7 -.0
2 .0
4 .0
5 .0
1 .0
2 .0
3
Tim
e be
twee
ns su
rger
y an
d fo
llow
-up
-.06
-.15
-.11
-.14
-.10
-.10
-.11
-.14
-.10
-.13
a Hig
her s
core
s equ
ate
to b
ette
r out
com
es/fu
nctio
ning
. b H
ighe
r ind
icat
es m
ore
adva
nced
inst
rum
enta
tion
and
high
er c
ost.
* p .0
5.
** p
.0
1.
71
72 nature of this study, it was necessary to identify one multivariate predictive model to use
for all logistic and multiple regression analyses. It was important that this model included
a limited number of presurgical variables with the strongest evidence of predictability
based on previous research. Because fewer participants were recruited for telephone
interviews, we decreased the number of predictors used in the multiple regression
analyses to eight patient variables. This number was based on the conventional standard
of approximately one predictor per 10-15 observations (Stevens, 2009).
Several important factors were considered when determining the inclusion of
specific independent variables in the model. First, final predictors were included only if
there was a theoretical rational based on research with similar worker�’s compensation
populations and suggestions from the lumbar fusion outcome and low back pain
literature. Thus, it was essential that the final eight-variable model include demographic,
occupational, health, psychological, and surgical variables representative of the
biopsychosocial perspective. Second, issues of multicollinearity were addressed by
dropping one of two variables that were highly correlated. In this case, psychological
treatment was dropped from consideration due to a high positive correlation with
depression. Based on these factors, the final eight-variable model included the following
predictors: age at time of fusion, smoking at time of fusion, history of depression, case
manager assigned, vocational rehabilitation, litigation involvement, number of vertebral
levels fused, and instrumentation use.
Multivariate Prediction of Disability Status
Using the eight-variable model, the first regression analysis involved predicting
73 disability status. Because disability status was reported as a dichotomous variable
(yes/no), logistic regression analysis was most appropriate to determine the importance of
predictor variables in the model. Alternate analysis, such as a multiple linear regression,
is only suitable if the outcome variable is continuous and assumptions about linearity are
met. Logistic regression is used when the dependent variable has a binomial distribution
of scores and does not assume a linear relationship between the independent and
dependent variables.
The logistic regression indicated that the model fit significantly improved (chi-
square = 22.79, p .001) with the addition of the eight predictor variables. As shown in
Table 14, the classification table counts the correct and incorrect estimates for the model.
The columns depict the two predicted values of the dependent variable, and the rows are
the two observed values of the dependent variable. Here, the model predicts 41.9% of
disabled cases and 93.3% of nondisabled cases, yielding an overall rate of 78.3% that
were correctly predicted. Table 15 lists the unstandardized regression coefficient ( ), the
Wald statistic and its significance (p), the odds ratio (Exp ), and the confidence limits on
the odds ratio. The Wald statistic is the squared ratio of the unstandardized logistic
coefficient and its standard error. The odds ratio is the predicted change in odds for 1 unit
increase in the corresponding independent variable. In this case, odds ratios greater than 1
corresponds with an increase in likelihood of patient disability, while odds ratios less than
1 correspond with a decrease in the likelihood. Consequently, odds ratios close or equal
to 1 indicate that changes in the independent variable do not increase or decrease the
likelihood of disability status. As observed in Table 15, case management and litigation
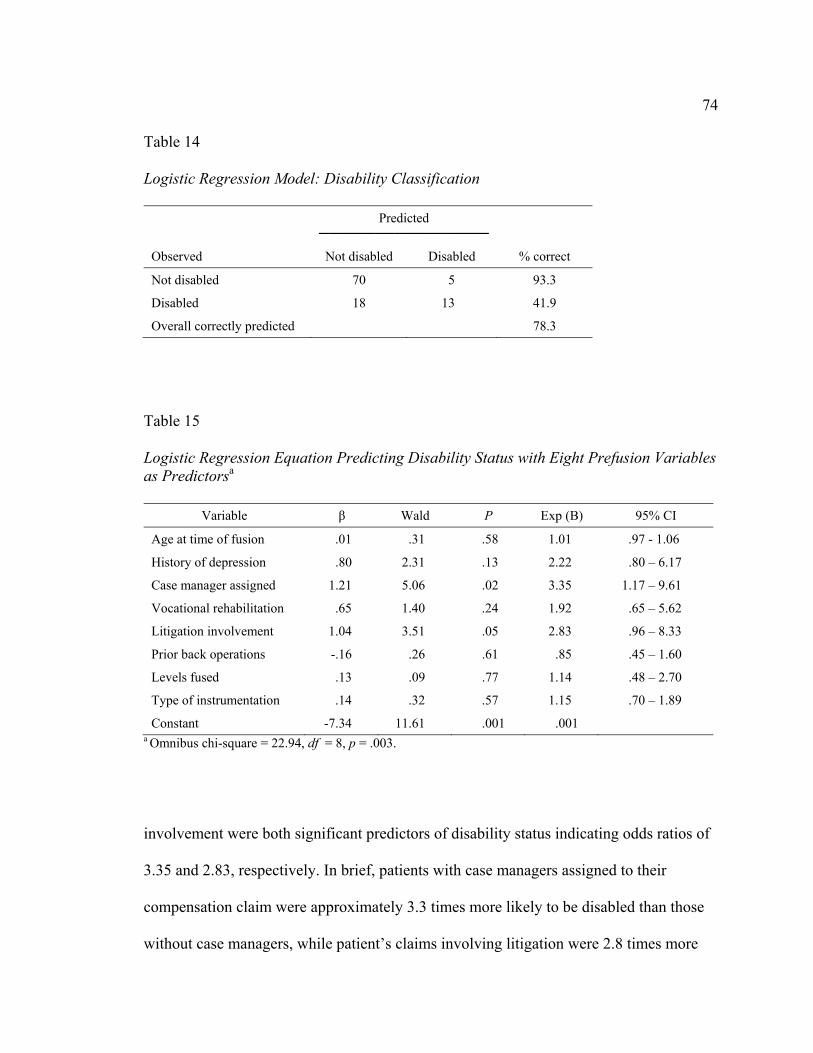
74 Table 14 Logistic Regression Model: Disability Classification
Predicted
Observed Not disabled Disabled % correct
Not disabled 70 5 93.3
Disabled 18 13 41.9
Overall correctly predicted 78.3
Table 15 Logistic Regression Equation Predicting Disability Status with Eight Prefusion Variables as Predictorsa
Variable Wald P Exp (B) 95% CI
Age at time of fusion .01 .31 .58 1.01 .97 - 1.06
History of depression .80 2.31 .13 2.22 .80 �– 6.17
Case manager assigned 1.21 5.06 .02 3.35 1.17 �– 9.61
Vocational rehabilitation .65 1.40 .24 1.92 .65 �– 5.62
Litigation involvement 1.04 3.51 .05 2.83 .96 �– 8.33
Prior back operations -.16 .26 .61 .85 .45 �– 1.60
Levels fused .13 .09 .77 1.14 .48 �– 2.70
Type of instrumentation .14 .32 .57 1.15 .70 �– 1.89
Constant -7.34 11.61 .001 .001 a Omnibus chi-square = 22.94, df = 8, p = .003.
involvement were both significant predictors of disability status indicating odds ratios of
3.35 and 2.83, respectively. In brief, patients with case managers assigned to their
compensation claim were approximately 3.3 times more likely to be disabled than those
without case managers, while patient�’s claims involving litigation were 2.8 times more
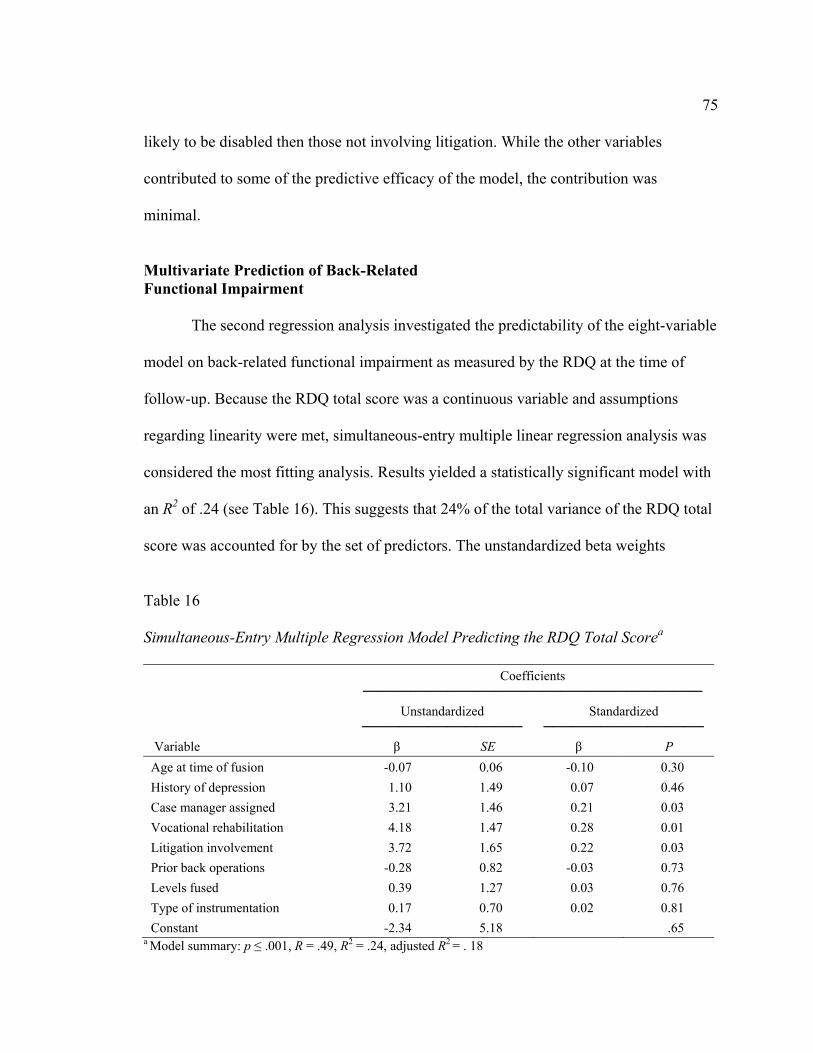
75 likely to be disabled then those not involving litigation. While the other variables
contributed to some of the predictive efficacy of the model, the contribution was
minimal.
Multivariate Prediction of Back-Related Functional Impairment
The second regression analysis investigated the predictability of the eight-variable
model on back-related functional impairment as measured by the RDQ at the time of
follow-up. Because the RDQ total score was a continuous variable and assumptions
regarding linearity were met, simultaneous-entry multiple linear regression analysis was
considered the most fitting analysis. Results yielded a statistically significant model with
an R2 of .24 (see Table 16). This suggests that 24% of the total variance of the RDQ total
score was accounted for by the set of predictors. The unstandardized beta weights
Table 16 Simultaneous-Entry Multiple Regression Model Predicting the RDQ Total Scorea
Coefficients
Variable
Unstandardized
Standardized
SE P Age at time of fusion -0.07 0.06 -0.10 0.30 History of depression 1.10 1.49 0.07 0.46 Case manager assigned 3.21 1.46 0.21 0.03 Vocational rehabilitation 4.18 1.47 0.28 0.01 Litigation involvement 3.72 1.65 0.22 0.03 Prior back operations -0.28 0.82 -0.03 0.73 Levels fused 0.39 1.27 0.03 0.76 Type of instrumentation 0.17 0.70 0.02 0.81 Constant -2.34 5.18 .65
a Model summary: p .001, R = .49, R2 = .24, adjusted R2 = . 18
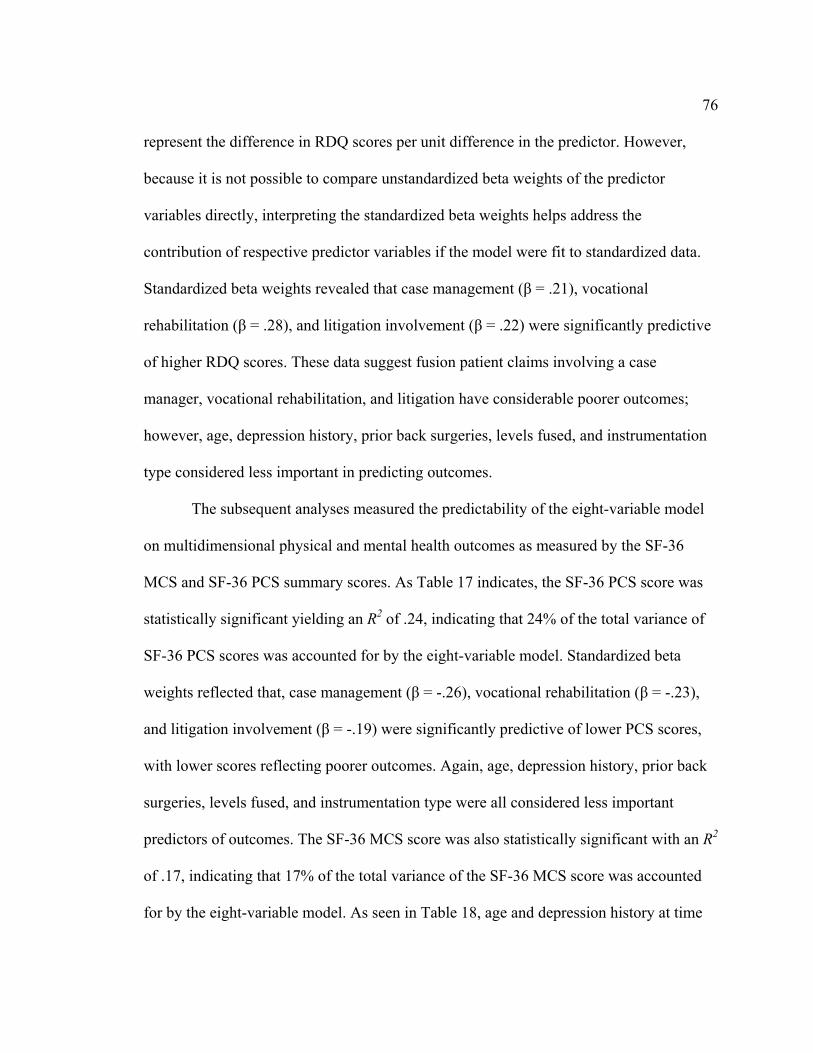
76 represent the difference in RDQ scores per unit difference in the predictor. However,
because it is not possible to compare unstandardized beta weights of the predictor
variables directly, interpreting the standardized beta weights helps address the
contribution of respective predictor variables if the model were fit to standardized data.
Standardized beta weights revealed that case management ( = .21), vocational
rehabilitation ( = .28), and litigation involvement ( = .22) were significantly predictive
of higher RDQ scores. These data suggest fusion patient claims involving a case
manager, vocational rehabilitation, and litigation have considerable poorer outcomes;
however, age, depression history, prior back surgeries, levels fused, and instrumentation
type considered less important in predicting outcomes.
The subsequent analyses measured the predictability of the eight-variable model
on multidimensional physical and mental health outcomes as measured by the SF-36
MCS and SF-36 PCS summary scores. As Table 17 indicates, the SF-36 PCS score was
statistically significant yielding an R2 of .24, indicating that 24% of the total variance of
SF-36 PCS scores was accounted for by the eight-variable model. Standardized beta
weights reflected that, case management ( = -.26), vocational rehabilitation ( = -.23),
and litigation involvement ( = -.19) were significantly predictive of lower PCS scores,
with lower scores reflecting poorer outcomes. Again, age, depression history, prior back
surgeries, levels fused, and instrumentation type were all considered less important
predictors of outcomes. The SF-36 MCS score was also statistically significant with an R2
of .17, indicating that 17% of the total variance of the SF-36 MCS score was accounted
for by the eight-variable model. As seen in Table 18, age and depression history at time
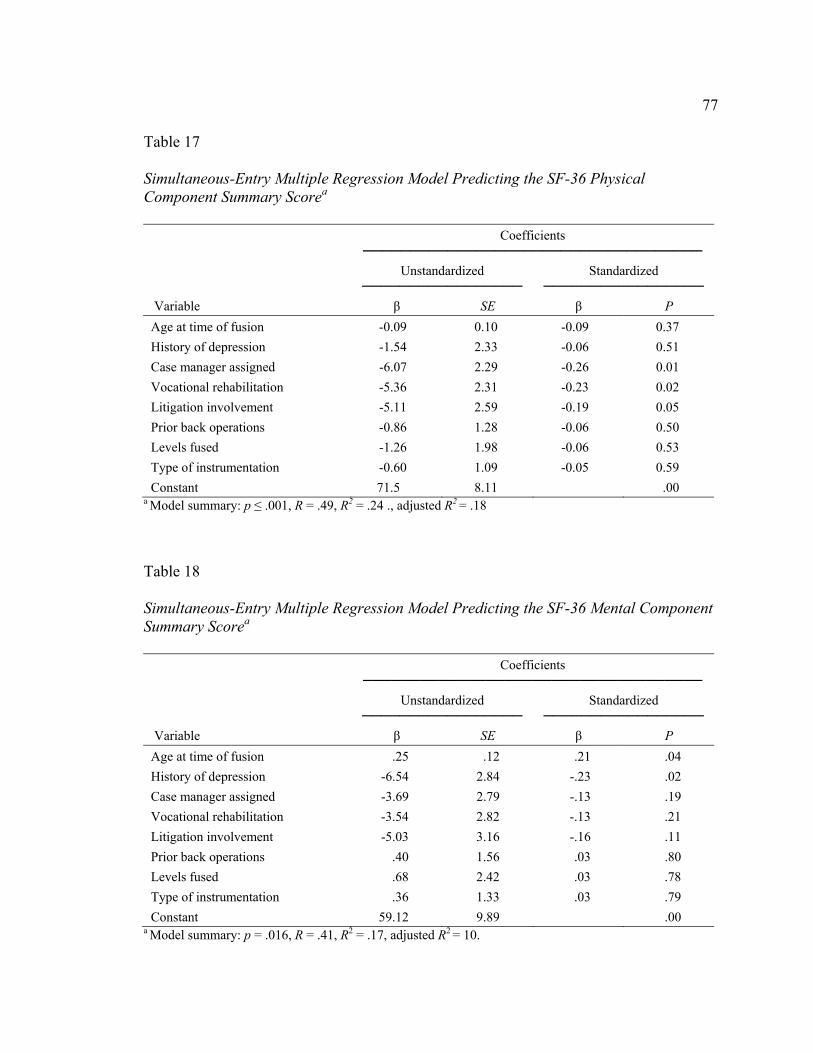
77 Table 17 Simultaneous-Entry Multiple Regression Model Predicting the SF-36 Physical Component Summary Scorea
Coefficients
Variable
Unstandardized
Standardized
SE P Age at time of fusion -0.09 0.10 -0.09 0.37 History of depression -1.54 2.33 -0.06 0.51 Case manager assigned -6.07 2.29 -0.26 0.01 Vocational rehabilitation -5.36 2.31 -0.23 0.02 Litigation involvement -5.11 2.59 -0.19 0.05 Prior back operations -0.86 1.28 -0.06 0.50 Levels fused -1.26 1.98 -0.06 0.53 Type of instrumentation -0.60 1.09 -0.05 0.59 Constant 71.5 8.11 .00
a Model summary: p .001, R = .49, R2 = .24 ., adjusted R2 = .18
Table 18 Simultaneous-Entry Multiple Regression Model Predicting the SF-36 Mental Component Summary Scorea
Coefficients
Variable
Unstandardized
Standardized
SE P Age at time of fusion .25 .12 .21 .04 History of depression -6.54 2.84 -.23 .02 Case manager assigned -3.69 2.79 -.13 .19 Vocational rehabilitation -3.54 2.82 -.13 .21 Litigation involvement -5.03 3.16 -.16 .11 Prior back operations .40 1.56 .03 .80 Levels fused .68 2.42 .03 .78 Type of instrumentation .36 1.33 .03 .79 Constant 59.12 9.89 .00
a Model summary: p = .016, R = .41, R2 = .17, adjusted R2 = 10.

78 of fusion were both considered statistically significant with standardized beta weights of
.21 and -.23. While the other variables within the model contributed to the models
statically significance as a whole, when taken individually, these variables did not reach a
statistically significant level. These data suggest that older patients who have no history
of depression are more likely to have higher mental health functioning.
Based on the significant predictability of the eight-variable model for the SF-36
PCS and SF-36 MCS scores, it was necessary to gather more comprehensive data related
to patient functioning. Thus, the following subsequent simultaneous-entry multiple linear
regression analyses were performed for the eight SF-36 subscales. Tables 19 through 26
include all pertinent information with respect to these final analyses. This final step will
conclude the results section of the current study.
Table 19 Simultaneous-Entry Multiple Regression Model Predicting the SF-36 Physical Functioning Subscalea
Coefficients
Variable
Unstandardized
Standardized
SE P Age at time of fusion -.09 .11 -.08 .39 History of depression -3.20 2.47 -.12 .20 Case manager assigned -5.22 2.43 -.20 .03 Vocational rehabilitation -6.18 2.45 -.24 .01 Litigation involvement -6.67 2.75 -.23 .02 Prior back operations -1.89 1.36 -.13 .17 Levels fused -1.61 2.11 -.07 .45 Type of instrumentation -.72 1.16 -.06 .53 Constant 77.00 8.60 .00
a Model summary: p .001, R = .52, R2 = .27, adjusted R2 = .21.

79 Table 20
Simultaneous-Entry Multiple Regression Model Predicting the SF-36 Role-Physical Subscalea
Coefficients
Variable
Unstandardized
Standardized
SE P Age at time of fusion .03 .12 .02 .81 History of depression -4.28 2.86 -.15 .14 Case manager assigned -5.07 2.81 -.18 .07 Vocational rehabilitation -7.14 2.84 -.25 .01 Litigation involvement -4.15 3.18 -.13 .19 Prior back operations 1.19 1.57 .07 .45 Levels fused -1.15 2.44 -.04 .64 Type of instrumentation .10 1.34 .01 .94 Constant 66.55 9.96 .00
a Model summary: p = .005, R = 45., R2 = 20., adjusted R2 = 13. Table 21 Simultaneous-Entry Multiple Regression Model Predicting the SF-36 Bodily Pain Scalea
Coefficients
Variable
Unstandardized
Standardized
SE P Age at time of fusion .03 .10 .03 .72 History of depression -.80 2.22 -.03 .72 Case manager assigned -7.46 2.18 -.33 .00 Vocational rehabilitation -5.84 2.20 -.25 .01 Litigation involvement -4.49 2.46 -.17 .07 Prior back operations -.50 1.22 -.04 .69 Levels fused -1.06 1.89 -.05 .58 Type of instrumentation -1.01 1.04 -.09 .33 Constant 69.31 7.72 .00
a Model summary: p .001, R = .52, R2 = .27, adjusted R2 = .21.

80 Table 22 Simultaneous-Entry Multiple Regression Model Predicting the SF-36 General Health Subscalea
Coefficients
Variable
Unstandardized
Standardized
SE P Age at time of fusion -0.04 0.10 -0.04 0.70 History of depression -2.66 2.23 -0.12 0.24 Case manager assigned -5.34 2.19 -0.25 0.02 Vocational rehabilitation -1.33 2.21 -0.06 0.55 Litigation involvement -5.47 2.48 -0.22 0.03 Prior back operations -0.97 1.23 -0.08 0.43 Levels fused -0.09 1.90 0.00 0.96 Type of instrumentation 0.29 1.05 0.03 0.78 Constant 66.17 7.77 .00
a Model summary: p = .016, R = .42, R2 = .17, adjusted R2 = .11. Table 23 Simultaneous-Entry Multiple Regression Model Predicting the SF-36 Vitality Subscalea
Coefficients
Variable
Unstandardized
Standardized
SE P Age at time of fusion .13 .11 .11 .26 History of depression -4.29 2.59 -.16 .10 Case manager assigned -6.09 2.55 -.24 .02 Vocational rehabilitation -3.93 2.57 -.15 .13 Litigation involvement -4.92 2.88 -.17 .09 Prior back operations -.41 1.42 -.03 .77 Levels fused .67 2.21 .03 .76 Type of instrumentation -.71 1.22 -.06 .56 Constant 66.33 9.01 .00
a Model summary: p = .009, R = .43 , R2 = .19, adjusted R2 = .12.
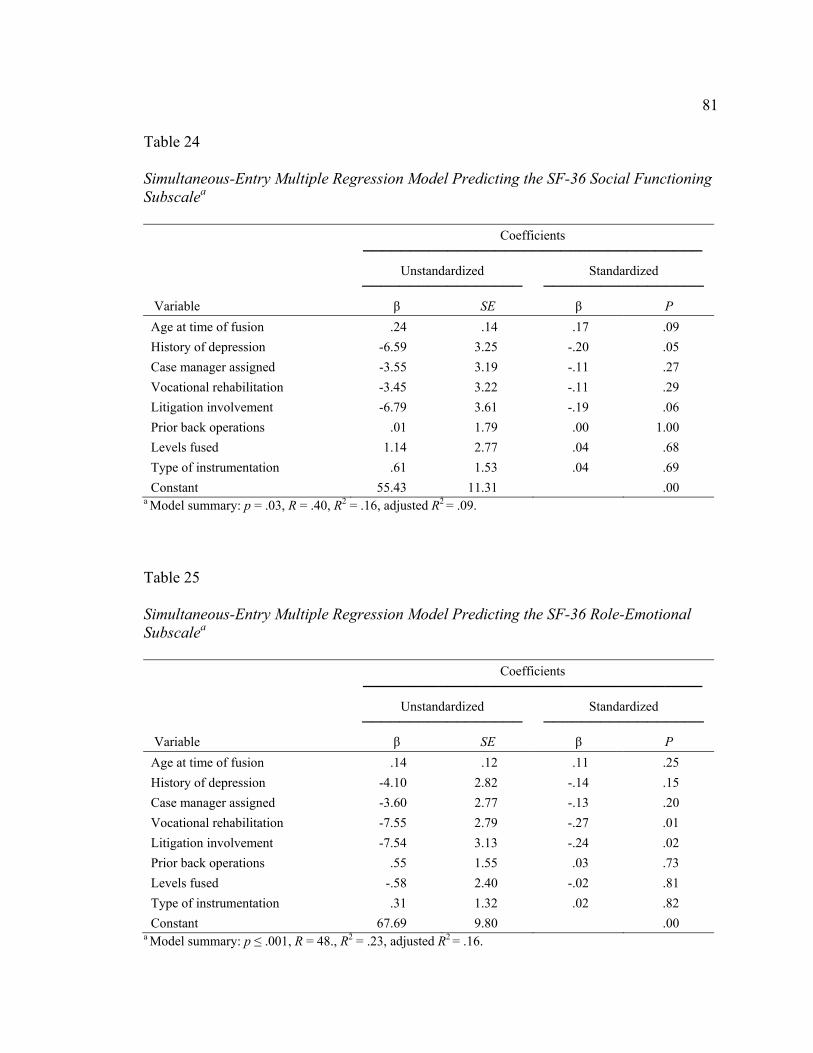
81 Table 24 Simultaneous-Entry Multiple Regression Model Predicting the SF-36 Social Functioning Subscalea
Coefficients
Variable
Unstandardized
Standardized
SE P Age at time of fusion .24 .14 .17 .09 History of depression -6.59 3.25 -.20 .05 Case manager assigned -3.55 3.19 -.11 .27 Vocational rehabilitation -3.45 3.22 -.11 .29 Litigation involvement -6.79 3.61 -.19 .06 Prior back operations .01 1.79 .00 1.00 Levels fused 1.14 2.77 .04 .68 Type of instrumentation .61 1.53 .04 .69 Constant 55.43 11.31 .00
a Model summary: p = .03, R = .40, R2 = .16, adjusted R2 = .09. Table 25 Simultaneous-Entry Multiple Regression Model Predicting the SF-36 Role-Emotional Subscalea
Coefficients
Variable
Unstandardized
Standardized
SE P Age at time of fusion .14 .12 .11 .25 History of depression -4.10 2.82 -.14 .15 Case manager assigned -3.60 2.77 -.13 .20 Vocational rehabilitation -7.55 2.79 -.27 .01 Litigation involvement -7.54 3.13 -.24 .02 Prior back operations .55 1.55 .03 .73 Levels fused -.58 2.40 -.02 .81 Type of instrumentation .31 1.32 .02 .82 Constant 67.69 9.80 .00
a Model summary: p .001, R = 48., R2 = .23, adjusted R2 = .16.
82
Table 26 Simultaneous Entry Multiple Regression Model Predicting the SF-36 Mental Health Subscalea
Coefficients
Variable
Unstandardized
Standardized
SE P Age at time of fusion .17 .12 .15 .15 History of depression -6.92 2.77 -.25 .01 Case manager assigned -4.89 2.72 -.18 .08 Vocational rehabilitation -2.67 2.74 -.10 .33 Litigation involvement -2.76 3.07 -.09 .37 Prior back operations -.20 1.52 -.01 .90 Levels fused -.31 2.36 -.01 .90 Type of instrumentation -.04 1.30 .00 .98 Constant 63.43 9.63 .00
a Model summary: p = .03, R = .40, R2 = .16, adjusted R2 = .09.
For the physical functioning (PF) subscale, the model was statistically significant
with an R2 of .27, demonstrating the eight-variable model accounted for 27% of the total
variance of PF scores. Standardized beta weights reflected that, case management (
= -.20), vocational rehabilitation ( = -.24), and litigation involvement ( = -.23) were
significantly predictive of lower PF scores. This indicates that claims involving a case
manager, vocational rehabilitation, and litigation are more likely to reflect poorer
physical health. Age, depression history, prior back surgeries, levels fused, and
instrumentation type were all considered less important predictors of outcomes; however,
these variables still contributed to the overall variance of the model.

83
For the role-physical (RP) subscale, the model was statistically significant with an
R2 of .20, indicating that the model accounted for 20% of the total variance of RP scores.
The RP scale refers to patients�’ role limitations, such as work, parenting, or being active,
due to physical problems. Standardized beta weights indicated that only case
management ( = -.18), and vocational rehabilitation ( = -.25) were significantly
predictive of lower RP scores, with depression history ( = -.15) and litigation
involvement ( = -.13) next in line for highest predictability among variables.
The bodily pain (BP) subscale was also statistically significant with an R2 of .27,
indicating the eight-variable model accounted for 27% of the total variance of the BP
score. Standardized beta weights reflected case management ( = -.33) had the highest
significant predictability, with vocational rehabilitation ( = -.25), and litigation
involvement ( = -.17) also showing significant predictability of lower BP scores. While
the other variables within the model contributed to the models statistical significance as a
whole, when taken individually, these variables did not reach a statistically significant
level. These data suggest that patients reporting higher levels of bodily pain were more
likely to have claims that involved litigation, case management, and vocational
rehabilitation prior to their fusion procedure.
The general health (GH) subscale also showed a more modest statistically
significant model (p = .016) with an R2 of .17, demonstrating the eight-variable model
accounted for 17% of the total variance of GH scores. Standardized beta weights
reflected that, case management ( = -.25) and litigation involvement ( = -.22) were
significantly predictive of lower GH scores. This indicates that claims involving a case

84 manager and litigation are more likely to reflect poorer general health. Age, depression
history, vocational rehabilitation, prior back surgeries, levels fused, and instrumentation
type were all considered less important predictors of outcomes; however, these variables
still contributed to the overall variance of the model.
For the vitality (VT) subscale, the model was statistically significant with an R2 of
.19, which indicated the eight-variable model accounted for 19% of the total variance of
VT scores.
Standardized beta weights showed case management ( = -.24) and litigation
involvement ( = -.17) were significantly predictive of lower VT scores. The VT scale
refers to the patient�’s presence of energy, and enthusiasm with the absence of fatigue and
exhaustion. Thus, this analysis indicates that patients whose claim involved a case
manager and litigation prior to their fusion are more likely to experience low energy and
�“aliveness.�” While the other variables in the model were not significant predictors, they
still contributed to the overall variance of the model.
The social functioning (SF) subscale score was also statistically significant with
an R2 of .16, indicating that 16% of the total variance of the SF score was accounted for
by the eight-variable model. While standardized beta weights indicated that a history of
depression ( = -.20) was the only predictor variable in the model that reached
statistically significance, both litigation involvement ( = -.19) and age ( = -.17) at the
time of fusion approached significance. These data suggest that patients who had a
history of depression prior to their fusion are more likely experience limitations in
interpersonal behavior and prosocial activities.

85
For the role-emotional (RE) subscale results yielded a statistically significant
model with an R2 of .23 (see Table 16). The RE scale refers to patients�’ role limitations,
such as work, parenting, or being active, due to emotional problems. This suggests that
23% of the total variance of the RE score was accounted for by the set of predictors.
Standardized beta weights revealed vocational rehabilitation ( = .28) and litigation
involvement ( = .22) were significantly predictive of lower RE scores. These data
suggest that fusion patient claims involving vocational rehabilitation and litigation prior
to fusion have considerable lower functioning due to emotional problems. Age,
depression history, vocational rehabilitation, prior back surgeries, levels fused, and
instrumentation type were considered less important in predicting outcomes.
Finally, the model for the mental health (MH) subscale score was also modestly
statistically significant with an R2 of .16, indicating that 16% of the total variance of the
MH score was accounted for by the eight-variable model. However, history of depression
was the only statistically significant predictor with a standardized beta weight of -.25;
with case management approaching significance at -.18. While the other variables within
the model contributed to the model�’s statistical significance as a whole, when taken
individually, these variables did not reach a statistically significant level. These data
suggest that patients who had a history of depression at the time of their fusion were more
likely to have lower mental health functioning at the time of follow-up.
Summary of Outcome Prediction
In brief, all logistic (disability status) and multiple linear regression analyses
86 (RDQ scores, SF-36 PCS, SF-36MCS, and eight SF-36 subscales) demonstrated the eight
variable multivariate predictive model was statistically significant. Involvement of a
nurse case manager, vocational rehabilitation, and litigation at the time of fusion were the
most prominent predictors across the various outcome measures. Age and depression
history at the time of fusion were also predictive of some outcomes, but these were
limited to outcome variables associated with mental health functioning. Interestingly,
none of the diagnostic or surgical variables (prior back operations, levels fused, and type
of instrumentation) were statistically significant predictors on their own in any of the
regression analyses. Frequency of statistical significance across the different predictor for
all analyses are as follows: age at the time of fusion (1/12), case manager (8/12),
vocational rehabilitation (7/12), depression history (3/12), lawyer involvement (7/12),
number of prior back (0/12), and number of levels fused, (0/12) and type of
instrumentation (0/12.). Finally, the statistical significance between zero order
correlations and outcomes is extremely similar to the significant variables among the
multiple regression models.
87
CHAPTER V
DISCUSSION
The current study addressed the three following research objectives: (1) to
examine patient presurgical variables and understand the interrelationships between such
variables; (2) to characterize multiple patient outcomes associated with lumbar fusion in
terms of quality of life, function, and health status variables, as well as fusion rates,
patient satisfaction, and disability; and (3) to explore the relationship of presurgical
variables to outcomes and test the predictive efficacy of a multiple variable predictive
model. Each objective was successfully evaluated during the course of the medical chart
review, follow-up telephone outcome survey, and examination of the data. As previously
indicated, the methods for the current investigation were adapted from an earlier study on
Utah workers�’ compensation patients who received fusion from 1990 to 1995 (DeBerard
et al., 2001). Thus, the discussion will largely focus on comparisons to the prior Utah
study, as well as, interpret empirical findings in accordance with the lumbar fusion
outcome literature. Specific implications for our findings, as well as limitations
associated with this study will be addressed.
Descriptive Characteristics of Patient and Procedural Variables
A major objective of this study was to focus on how presurgical patient and
procedural variable are related to outcomes; thus, it was important to thoroughly describe
several demographic, occupational, health, and surgical variables that are associated with
lumbar fusion outcomes and back pain patients, in general. These data also serve as

88 quality comparisons to other studies evaluating outcomes in workers compensation
patients who have undergone lumbar fusion as a result of a workplace injury.
Results for the current study indicated injured workers were predominately White
males with an average age of 40 at the time of their lumbar fusion. These figures are
consistent with prior studies on workers compensation fusion patients in Utah (DeBerard
et al., 2001); Washington State (Maghout-Juratli et al., 2006), and Ohio (Nguyen et al.,
2011); however, less comparable to fusion studies on general populations reporting more
balanced gender and ethnicity ratios (Brox et al., 2003, 2006; Fritzell et al., 2001).
Education level and weekly income were also similar to prior studies on compensated
workers, which generally reflect lower education and income (DeBerard et al., 2001;
Maghout-Juratli et al., 2006). For the current study, patient BMI and smoking rates at the
time of surgery were moderately lower, while depression history were considerable
higher when compared to rates of depression in prior studies on Utah workers (DeBerard
et al., 2009; LaCaille et al., 2005). This may, in part, be due to the conservative approach
those studies used when identifying positive cases of depression. The current study,
focused on depression history as a predictor and did not require patients to have a
diagnosis of depression at the time of surgery.
In terms of diagnostic and procedural variables, back related diagnoses for this
study were very similar to other workers compensation fusion studies (see DeBerard et
al., 2001, Maghout-Juratli et al., 2006, Ngyuen et al., 2011) with the most common
diagnoses including degenerative disc disease (30%), disc herniation (40%), and
radiculopathy (3%). Interestingly, it is well known in the literature that lumbar fusion is a
89 controversial operation for degenerative disc disease (Glassman et al., 2009). In fact,
recent evidence suggests that fusion is no more effective than nonsurgical conservative
approaches for return to work status of compensation workers with degenerative disc
disease, radiculopathy, or disc herniation (Nguyen et al., 2011). Despite similarities in
demographics and diagnosis, our study differed considerable from the prior Utah study
(DeBerard et al., 2001) when it came to utilization of surgical devices. The current
sample utilized fusion cages in 55% of cases compared to zero patients in the prior study.
This is an important comparison, as the intention behind using more advanced surgical
technology is to improve outcomes. While surgical instrumentation is shown to improve
the rate of solid fusion, evidence suggests it does not improve disability rates when
compared to fusion without instrumentation (DeFrances & Hall, 2007; Deyo & Mirza,
2006), and multidimensional outcome data regarding the benefit of these devices remains
unclear (Maghout-Juratli et al., 2006). Such finding will be highlighted in the following
portion of the discussion related to patient outcomes
Multidimensional Outcomes of Fusion
Based on the medical chart review, 245 injured workers met the criteria to
participate in the telephone outcome survey; however, only 110 patients were available
via phone for the follow-up phase of the study; yielding a follow-up rate of only 46%.
Follow-up data and information gathered in patient medical charts indicated 89% of
patients established a solid fusion after at least two years postsurgical follow-up. This
number is considerably higher than the prior Utah (DeBerard et al., 2001) and
90 Washington State (Maghout-Juratli et al., 2006) studies, which report fusion rates of 71%
and 75%, respectively. Despite higher fusion rates, disability rates increased from 23% in
the prior Utah study to 28% in the current study. Another study found that 84% of
patients using fusion cages established a solid fusion; yet, 38% were considered totally
disabled as a consequence of their back condition at follow-up (LaCaille et al., 2005).
Projective medical costs from 2001 to 2011 have risen approximately 174% for
compensated lumbar fusion patients in Utah (Wheeler et al., in press); a rise that is
strongly tied to the increase in use of more sophisticated surgical devices (e.g., interbody
fusion cages; Deyo et al., 2005). Consistent findings within the literature reporting high
fusion rates and poor functional outcomes associated with the use of fusion cages on
workers compensation patients are very concerning, particularly when considering the
costs associated these devices.
Descriptive Statistics for Patient Satisfaction and Quality of Life
Our finding indicated that on average, approximately 50% of injured Utah
workers were unsatisfied with their fusion surgery, and 50% reported that their back pain
after fusion was considerable worse than they expected. In terms of quality of life, 59%
of the current sample reported an improved quality of life since their fusion surgery.
Compared to the prior Utah study, these satisfaction and quality life rates were nearly
identical. In our study, 70% of patients reported they would have the fusion again; while
only 62% would in the prior study. These similarities in patient outcomes seem partly due
to similarities of the two samples.
91 Outcome Categorization
As measured by the Stauffer-Coventry Index, 68% of the current patient sample
reported good to fair pain relief compared to 75% in the prior Utah (2001) study. In both
the current and prior studies, approximately 70% patients reported minimal to moderate
physical activity restrictions. The most notable difference in outcome categorization
between the two studies was for medication use, with 50% of current study patients and
only 25% of the prior study patients reporting occasional to regular use of narcotic
medication. This increase is likely due to the dramatic rise in prescription medication use
over the past twenty years. Among patients with back-related disorders, from 1997 to
2004, there was a 108% increase in opioid prescriptions for pain with a 423% increase in
cost expenditures associated with such medications (Martin et al., 2008). For the current
study, patients�’ narcotic use is slightly higher than national norms of low back pain
patients, which were approximately 45% in 2006 (Fingerhut, 2006). While there is no
evidence suggesting that narcotic analgesic use prior to lumbar fusion predicts outcomes,
a primary risk factors of increased narcotic use includes work related back injury (Rhee,
Taitel, Walker, & Lau, 2007). There is also strong evidence that long-term treatment of
pain with narcotic medication is known to have a significant negative impact on quality
of life, concentration, pain sensitivity, libido, work ability, exercise, social functioning,
and sleep (Deyo, Mirza, Turner, & Martin, 2009; Rhee et al., 2007). While the current
study did not evaluate duration of medication use, this may be an important variable to
address in future research.

92 Pain Rating and Subjective Pain Response
At the time of follow-up, approximately 40% of patients had either no change or
an increase in pain after their lumbar fusion with more the 60% reporting current levels
of pain as moderate to severe. Within the literature there is considerable focus on the
psychosomatic aspects of chronic pain among working populations where pain is often
considered exasperated by workers due to psychological distress rather than objective
physical damage (Hadler, Tait, & Chibnall, 2007). Interestingly, our study reported
minimal pain catastrophizing rates on the PCAS; and considerable lower than what is
typically reported in pain clinic patients (Sullivan et al., 1995). This finding may indicate
that fusion patients receiving compensation do not tend to overestimate or inflate their
pain levels; however, this conclusion warrants further exploration.
General Physical and Mental Health Functioning
In the treatment of degenerative spine disorders, the 36-item Short Form Health
Survey (Ware et al., 2000) is among the most commonly used self-report measures
(Glassman et al., 2009). As expected, the present study�’s SF-36 scores revealed that the
greatest areas of impairment were associated with physical functioning, role functioning,
and bodily pain, while the areas of least impairment were related to mental health
functioning. Fusion patient also revealed much poorer outcomes than the general
population and the back pain/sciatica sample norms for the SF-36 MCS, SF-36 PCS and
all SF-36 subscales. While there is substantial evidence suggesting poorer health related
outcomes of lumbar fusion workers�’ compensation populations (DeBerard et al., 2001;

93 Maghout-Juratli et al., 2006; Trief, Ploutz-Snyder, & Fredrickson, 2006), most studies
have not directly compared outcomes to noncompensated patients. A recent study,
however, compared clinical outcomes of 60 lumbar fusion patients receiving workers�’
compensation to 58 fusion patients not receiving workers�’ compensation who were
identified and matched on several patient variables, including SF-36 PCS and SF-36
MCS scores (Carreon et al., 2010). At 2 years after operation, patients not receiving
workers�’ compensation had a significantly greater SF-36 PCS score compared to those
receiving workers�’ compensation; no differences were found between SF-36 MCS scores.
Further, only 16% of workers�’ compensation patients achieved a SF-36 PCS score that
represented a clinically important difference compared to 40% of those not receiving
workers�’ compensation. There is a need for additional comparison studies to identify
barriers associated with the workers compensation system that limit improvement of
clinical outcomes in patients.
Multivariate Prediction of Outcomes
The present study showed that multidimensional patient outcomes were predicted
based on presurgical variables. The most consistent predictors of poorer outcomes were
case manager involvement, vocational rehabilitation, and litigation involvement.
Depression history also showed some predictability, specifically for outcomes associated
with mental health and social functioning. Older age, which in prior research has shown
some risk for poor lumbar fusion outcomes (Carreon, Puno, Dimar, Glassman, &
Johnson, 2003; DeBerard et al., 2001), actually predicted higher mental health
94 functioning. Interestingly, none of the back related or surgical variables (i.e., prior back
surgeries, vertebral levels fused, and type of instrumentation) were predictive of
outcomes.
Case Manager and Vocational Rehabilitations as Predictors
In our study 42% of workers assigned a nurse case manager prior to fusion were
disabled at least 2-years postsurgery follow-up, while only 16% not assigned a case
manager were considered disabled. Disability among patients referred to vocational
rehabilitation was 39%, compared to only 17% of patients not referred. Until our study,
the association of nurse case manager assignments and referral to vocational
rehabilitation on multidimensional fusion outcomes was unknown. Past research has
shown these variables to be associated with worse patient outcomes for discectomy
patients (DeBerard et al., 2009); and most recently, a study evaluating only return to
work status among compensated fusion patients showed that patients with more
rehabilitative and vocational therapy were less likely to return to work compared to those
with no therapy (Ngyuen et al., 2011). Higher risk surgery cases are often referred to
nurse case managers and vocational rehabilitation to help manage patient�’s medical
treatments and facilitate return to work after surgery. While such preventative measures
are often costly and time intensive, there is an assumption these programs are worth the
higher expenditures based on perceived future benefits in terms of patient outcome and
disability status. There is considerable need to further evaluate services to determine
whether or not they benefit injured workers enough to be considered necessary.
95 Litigation Involvement as a Predictor
Involvement of litigation in patients�’ claim prior to lumbar fusion was found to be
a significant predictor of several multidimensional outcomes in this study, including
higher rates of disability, worse back related functional impairment, poor general health
and physical functioning, role limitation due to emotional distress, and lower vitality. In
fact, patient whose claims involved litigation were 280% more likely to be disabled than
those without litigation. The literature supports the relationship between the role of the
legal system and its impact on back surgery patient outcome with several studies
indicating compensation claims involving litigation result in increased rates of disability
and pain (Bernard, 1993; Greenough et al., 1994, 1998; Junge et al., 1995). Prior lumbar
fusion studies, in particular, show that the legal representative of injured workers is a
predictor of various negative outcomes after lumbar fusion (DeBerard et al., 2001, 2003;
LaCaille et al., 2005; Ngyuen et al., 2011). DeBerard and colleagues (2001) showed
patients with claims involving a lawyer were 376% more likely to be disabled 2 years
following lumbar fusion when compared to claims that did not involve a lawyer.
Although this is slightly more than the current sample, it is clear that litigation
involvement remains a problematic issue when considering patient outcome. Variables
noted by the literature possible influencing the relationship between litigation and poor
outcome include the effect of patients blaming others for their injury, secondary gain
(i.e., medication and/or money), and dealing with a complicated adversarial system (i.e.,
legal and insurance systems; Hadler, 2005; Harris, 2007). Further, injured workers who
hire attorneys are typically trying to prove their functional impairment to workers

96 compensation fund in order to receive disability status and compensation for their injury.
It is important to acknowledge this does not necessarily indicate patients are malingering;
however, this outcome may be associated with complexities between the psychosomatic
link of pain sensitivity and consequence of financial motivation and/or contextual
variables.
Age as Predictor
While prior studies on fusion patients have indicated that older age is a predictor
for poor outcomes (Carreon et al., 2003), our study did not show this relationship.
Actually, results indicated older patients have higher mental health functioning as
measured by the SF-36 MCS scale. There is criticism that past findings indicating age as
a predictive factor for poor outcomes are partially explained by their emphasis on
perioperative complications and older patients undergoing reoperation for failed fusion
rather than outcome differences for varying age groups (Glassman et al., 2008). While
rates of healing of vertebral bodies are lower in older aged patients (Boos et al., 1991);
fusion cages have dramatically increased the rate of fusion in older populations, thus ,
associated complications with nonfusion are being seen less in elderly populations
(Glassman et al., 2008). This is supported by recent research, which indicates older
patients who undergo lumbar fusion with instrumentation show symptomatic progress in
terms of quality of life comparable to those in younger patients (Glassman et al., 2008).
In fact, older patients had more complications, but complications did not worsen
outcomes.

97 Depression as a Predictor
Depression history was a significant predictor for poor outcomes on the SF 36
MCS, Mental Health, and Social Functioning scales; however, was not predictive of any
disability or back related functional outcomes. Research supports the notion that
psychological issues, such as anxiety, depression, fear avoidance beliefs relating to work,
and back-pain related stress, among low back pain patients predicts impairment in
subsequent physical health-related quality of life measures and healthcare utilization
(Keeley et al., 2008). However, the evidence is mixed on how psychological distress
predicts post-operative improvement in patients who have undergone lumbar fusion
(DeBerard et al., 2001; LaCaille et al., 2005; Tandon et al., 1999; Trief et al., 2000).
When considering the relationship between depression and spine surgery outcomes,
Block and colleagues (2003) suggested the importance of surgeons to identify whether an
individual is experiencing a reactive depression to their injury or if they have a pre-injury
history of depression. Typically, patients with reactive depression are more likely to
adjust to their condition with time; however, chronic back pain patients with a history of
depression before the onset of pain have a greater risk for poor spine surgery outcomes
(Block et al., 2003). Unfortunately, the current study did not specify if the onset of
depression was prior to the back injury. Also, prior workers compensation studies on
lumbar fusion outcomes have relied on identifying depression from physician
documentation of a diagnosis of depression in the patient�’s medical chart at the time of
fusion (DeBerarad et al, 2001; Maghout-Juratli et al., 2006; Trief et al., 2006). Thus, it is
unclear if a depression diagnosis was met prior to injury. This contextual variable may
98 play an important role in depressions varied predictability of lumbar fusion outcomes.
Back-Related Physiological and Procedural Variables as Predictors
Perhaps the most interesting finding is there were no significant interrelationship
between methods of assessing presurgical clinical severity, including pain severity,
number of vertebral levels fused, and history of prior back operations, with patients
outcomes. For pain severity, the finding were consistent with the prior Utah study
(DeBerard et al., 2001) indicating no predictive power of a surgical diagnostic severity
score for disability status, global outcome, or physical or social functioning. While prior
studies have shown that multiple-level spinal fusion and a history of prior back surgeries
is shown to be predictive of fusion outcomes (Franklin et al., 1994; Glassman et al.,
1998; Narayan et al., 2002; Turner et al., 1992); most of these studies focused specifically
on fusion rates, rather than multidimensional health-related outcomes. Further, although
this study supports evidence suggesting more advanced surgical technology improves
fusion rates (Maghout-Juratli et al., 2006), the data also indicate diagnostic severity has
no relationship with multidimensional outcome data.
Implications
Several implications can be drawn from the current findings. Perhaps the most
important implication is, over the past decade, injured workers who have undergone
lumbar fusion in Utah have shown an increase in disability rates, functional impairment,
and poor quality of life despite the improvement in solid fusion rates. Our findings, along
99 with the dramatic rise among workers compensation populations receiving lumbar fusion,
specify the need for providers and surgeons to use more discretion when recommending
lumbar fusion as a treatment option for injured workers without exploring alternative
options. This is imperative when considering both the financial the cost associated with
these surgeries, as well as the human costs such as pain, suffering, time away from
family, job loss, lost activities, and inconveniences associated with being disabled. The
data from this study do not, however, support the position that compensated workers
cannot benefit from lumbar fusion, as several presurgical variables were predictive of
patients outcomes.
When considering a biopsychosocial perspective, a second implication is based on
findings indicating psychological factors (i.e., depression history) and social factors (i.e.,
nurse case manager, vocational rehabilitation, lawyer involvement) were highly effective
in predicting long-term multidimensional patient outcomes for lumbar fusion. However,
biological variables such as pain severity, number of vertebral levels identified for
surgery, and prior back operations showed no relationship to outcomes. Such finding
underscore the importance of moving away from the traditional medical model of treating
low back pain, which suggests pain has a single underlying pathophysiological cause
independent from psychological and social factors (Wright, 2005). The literature supports
the notion that lumbar fusion patients who do have pathology also have limited functional
recovery after surgical repair of the pathology (DeBerard et al., 2001; Franklin et al.,
2004). Further, many researchers argue that a spinal fusion is appropriate only for a small
number of conditions, such as spinal instability, spinal fracture, or scoliosis. In fact,

100 recent evidence suggests lumbar fusion is no more effective than a nonsurgical control
group for return to work rates for patients with a diagnosis of disc degeneration, disc
herniation, and/or radiculopathy (Ngyuen et al., 2011). Our data indicate 73% of the
diagnoses for injured workers were disc degeneration, disc herniation, and radiculopathy.
This issue emphasizes a fundamental concern that patients, surgeons, and providers are
relying on lumbar fusion for conditions that are not indicative of the procedures utility.
Another implication is how to address the dramatic increase in use of fusion cages
since the prior 2001 Utah lumbar fusion study (DeBerard et al., 2001). Many argue
financial incentives are the reason for higher rates of lumbar fusion, which coincide with
a rise in use of advanced surgical technology (Lieberman, 2004). The market for spinal
instrumentation is estimated to be $2 billion a year, with a 20% annual growth rate.
Reimbursement for lumbar fusion procedures is more favorable than reimbursement for
most other back procedures performed by orthopedic surgeons due to elaborate spinal
devices used and the longer length of surgery (Waldman & Armstrong, 2010). Further,
several surgeons incomes are largely determined by their consulting and royalty
arrangements with surgical device manufacturers. This offers surgeons strong incentives
to perform lumbar fusion with surgical devises that do not have adequate evidence to
support their utility.
Although recommendations for systematic selection of patients based on risk
factors are deemed necessary, our study clearly indicates such practices are not occurring
with compensated Utah workers. Consequently, another important implication is how we
can move forward in applying our understanding of predicting patient outcomes to better
101 serve the patient. To do this, we need to consider the amount of control patients and
providers have in addressing these issues before moving forward with surgical
procedures. This is a systematic issue within the workers compensation system, which
needs to improve their efforts in evaluating what is working and not working in terms of
patient outcomes. For example, the paradoxical finding that nurse case manager
involvement and referral to vocational rehabilitation results in poorer outcomes, indicates
a further need to determine whether or not injured workers benefit enough to justify the
use of such services. Because the indications for an invasive and expensive procedure,
like lumbar fusion, is variable based on diagnosis, our study represents a clear need to
shift investigative efforts to determine how to better serve injured workers who may or
may not be good candidates for lumbar fusion surgery.
A final implication of our study is the importance of understanding outcomes
from a broad multidimensional perspective that includes pain, back specific function,
work disability, generic health status, and patient satisfaction. Our finding showed the
majority of injured workers had higher expectations of benefiting from their lumbar
fusion compared to the reality of their outcome. When patients are in significant pain
after an injury, surgeon and provider recommendations for how to proceed will likely be
interpreted as the best intervention to achieve successful outcome. However, how
outcome is determined, may be operationally defined very differently across patients (i.e.,
quality of life, pain reduction); surgeons (i.e., solid fusion); and the workers
compensation system (i.e., disability status). This is particularly important when
comparing new finding to past studies evaluating lumbar fusion outcomes.
102
Limitations and Future Research
Several limitations were noted for the current study. One important limitation is
the low follow-up rate of only 46%. This was unfortunate, in that prior studies have
reported at least a 50% follow-up rate (DeBerard et al., 2001; LaCaille et al., 2005).
Several variables may play a role as to why the rate of nonresponders has increased. The
clearest difference between workers who responded to the survey and who did not
respond was age, where responders were on average five years older than nonresponders.
In the past decade, society�’s reliability on landlines has dramatically declined with more
people using wireless devices as their primary mode of communication, particularly
among younger adults (Blumberg & Luke, 2009). As the percentage of cell phone use
increases, health researchers have reported more difficulty collecting telephone survey
data due to higher costs (i.e., cell phone minutes) and tendency to screen calls (Krisberg,
2009). Also, because our study included workers who had fusion surgery between 1998
and 2007, it is possible that contact information for injured workers who had landlines
and switched over to cell phones did not have information updated in the WCFU
database, particularly if their claim was closed.
Another limitation was the inclusion of data from only one state�’s perspective of
the workers�’ compensation system. Because this was a relatively homogenous sample of
injured workers from Utah, the generalizability of findings may be limited to other
workers compensation populations. Weinstein and colleagues (2006) indicates rates of
lumbar fusion performed within the US varies considerable based on geographic region
due to financial incentives to surgical intervention, and differences in clinical training and

103 hospital environments. Also, other workers compensation systems may provide different
incentives for returning to work, which, in turn, may mediate outcomes.
An additional limitation is although multidimensional patient outcomes were
collected prospectively, the study design was retrospective, which limits the probability
that patient variables were reported consistently in the database. For example, variables
such as socioeconomic status, educational level, smoking history, body mass index, were
not considered in the multivariate regression analyses due to poor documentation in
patient medical charts or missing data. Further, the predictive value of depression history
should be interpreted with caution, as the current study did not specify if the onset of
depression was prior to or after the initial back injury. In fact, to date, no known studies
have evaluated depression history prior to injury as a predictor of outcomes; thus, further
research is clearly needed to address this issue.
Lastly, there was also a limitation in how we dealt with interrater reliability when
conducting the outcome surveys. Interrater reliability was determined by having another
graduate student listen to the outcome survey on a separate line and independently code
patient responses for 10% of the surveys. Because the interviewer was aware that another
observer was coding their interviews, this might have influenced the way they
interviewed the participants. Further, the interviewer�’s style of interviewing may have
biased the responses.
When considering these limitations, there are several recommendations for future
research in the area of lumbar fusion outcome research for injured workers. Due to the
high costs associated with lumbar fusion and the potential for less costly nonsurgical

104 approaches to be equally effective, randomized controlled trials comparing lumbar fusion
to alternative nonsurgical approaches are clearly needed among workers compensation
populations. Also, because of the inherent difficulties associated with using randomized
designs when comparing fusion outcomes between compensated versus noncompensated
patients, there is a need for increased use of matched case control studies to evaluate
these differences more systematically. Future studies on lumbar fusion within workers
compensation populations will need to use more experimental designs with larger patient
samples to provide more details regarding presurgical patient variables. There is also a
pressing need for systematic prospective outcomes data to be collected among patients
within the workers compensation system. This could be done by using electronic
prospective outcomes databases often implemented in other health care setting (e.g.,
hospitals, physician practices, and insurance carriers), which would allow for a greater
opportunity to understand factors that influence patient outcomes.
105
REFERENCES
Airaksinen, O., Herno, A., Turunen, V., Saari, T., & Suomlainen, O. (1997). Surgical outcome of 438 patients treated surgically for lumbar spinal stenosis. Spine, 22, 2278-2282.
An, H. S., Boden, S. D., Kang, J., Sandhu, H. S., Abdu, W., & Weinstein, J. (2003). Emerging techniques for treatment for degenerative lumbar disc disease. Spine, 28, S24-S25.
An, H. S., Simpson, J. M., Glover, J. M., & Stephany, J. (1995). Comparison between allograft plus demineralized bone matrix versus autograft in anterior cervical fusion: A prospective multicenter study. Spine, 20, 2211-16.
Andersson, G. (1999). Epidemiological features of chronic low-back pain. The Lancet, 354, 581-585.
Andersen, T., Christensen, F. B., Laursen, M., Hoy, K., Hansen, E. S., & Bunger, C. (2001). Smoking as a predictor of negative outcome in lumbar spinal fusion. Spine, 26, 2623-2628.
Andreshak, T. G., An, H. S., Hall, J., & Stein, B. (1997). Lumbar spine surgery in the obese patient. Journal of Spinal Disorders, 10, 376-379.
Baldwin, M. L., Johnson, W. J., & Butler, R. J. (1996). The error of using returns-to-work to measure the outcomes of health care. American Journal of Industrial Medicine, 29, 632-641
Barnes, D., Smith, D., Gatchel, R. J., & Mayer, T. (1989). Psychosocioeconomic predictors of treatment success/failure in chronic low back pain patients. Spine, 14, 427-430.
Battie, M., Bigos, S., Fisher, L., Spengler, D. M., Hansson, T. H., Nachemson, A. L., & Wortley, M. D. (1990). The role of spinal flexibility in back pain complaints within industry, a prospective study. Spine, 15, 768-773.
Benz, R. J., Ibrahim, Z. G., Afshar, P., & Garfin, S. R. (2001). Predicting complications in elderly patients undergoing lumbar decompression. Clinical Orthopedics, 384, 116 121.
Berkley, K. J. (1997). Sex differences in pain. Behavioral and Brain Sciences, 20, 371-380.
Bernard, T. N. (1993). Repeat lumbar spine surgery: Factors influencing outcome. Spine, 18, 2196-2200.
106 Beurskens, A. J., de Vet, H. C. W., Köke, A. J. A., van der Heijden, G. J. M. G., &
Knipschild, P. G. (1995). Measuring the functional status of patients with low back pain: Assessment of the quality of four disease specific questionnaires. Spine, 20, 1017-1028.
Bigos, S. J., Battie, M. C., Spengler, D. M., Fisher, L. D., Fordyce, W. E., Hansson, T. H., �… Wortley, M. D. (1991). A prospective study of work perceptions and psychosocial factors affecting the report of back injury. Spine, 16, 1-6.
Bigos, S., Bowyer, O., Braen, G., Brown, K., Deyo, R., Haldeman, S., �… Weinstein, J. (1994). Acute Low Back Problems in Adults. Clinical Practice Guideline No. 14. AHCPR Publication No. 95-0642. Rockville, MD: Agency for Health Care Policy and Research, Public Health Service, U.S. Department of Health and Human Services.
Block, A. R., & Callewart, C. (1999). Surgery for chronic spine pain: Procedures for patient selection and outcome enhancement. In A. R. Block, E. F. Kremer, & E. Fernandez (Eds.), Handbook of pain syndromes: Biopsychosocial perspectives (pp. 191-212). Mahwah, NJ: Erlbaum.
Block, A. R., Gatchel, R. J., Deardorff, W., & Guyer, R. D. (2003). The psychology of spine surgery. Washington, DC: American Psychological Association.
Blumberg, S. J., & Luke, J. V. (2009). Reevaluating the need for concern regarding noncoverage bias in landline surveys. American Journal of Public Health, 99, 1806-1810.
Boden, S. D., Davis, D. O., Dina, T. S., Patronas, N. J., & Wiesel, S. W. (1990). Abnormal magnetic-resonance scans of the lumbar spine in asymptomatic subjects: a prospective investigation. Journal of Bone & Joint Surgery, 72, 403-408.
Bombardier, C. (2000). Outcome assessments in the evaluation of treatment of spinal disorders: Summary and general recommendations. Spine, 25, 3100-3103.
Boos, N., Marchesi, D., & Aebi, M. (1991). Treatment of spondylolysis and spondylolysthesis with Cotrel-Dubousset instrumentation: A preliminary report. Journal of Spinal Disorders, 4, 472-479.
Brox, J. I., Reikeras, O., Nygaard, O., Sorensen, R., Indahl, A., Holm, I., �… Friis, A. (2006). Lumbar instrumented fusion compared with cognitive intervention and exercises in patients with chronic back pain after previous surgery for disc herniation: A prospective randomized controlled study. Pain, 122, 145-155.

107 Brox, J., Sorensen, R., Friis, A., Nygaard, O., Indahl, A., Keller, A., �… Reikerås, O.
(2003). Randomized clinical trial of lumbar instrumented fusion and cognitive intervention and exercises in patients with chronic low back pain and disc degeneration. Spine, 28, 1913-1921.l
Burkus, J. K., Gornet, M. D., Schuler, T. C., Kleeman, T. J., & Zdeblick, T. A. (2009). Six-year outcomes of anterior lumbar interbody arthrodesis with use of interbody fusion cages and recombinant human bone morphogenetic protein. The Journal of Bone and Joint Surgery, 91, 1181-1189.
Bush, F. M., Harkins, S. W., Harrington, W. G., & Price, D. D. (1993). Analysis of gender effects on pain perception and symptom presentation in temporomandibular joint pain. Pain, 53, 78-80.
Carragee, E. J., Lincoln, T., Parmar, V. S., & Alamin, T. (2006). A gold standard evaluation of the �‘discogenic pain�’ diagnosis as determined by provocative discography. Spine, 31, 2115-2123.
Carreon, L. Y., Glassman, S. D., Kantamneni, N. R., Mugavin, M. O., & Djurasovic, M. (2010). Clinical outcomes after posterolateral lumbar fusion in workers�’ compensation patients: A case-control study. Spine, 35, 1812-1817.
Carreon, L. Y., Puno, R. M., Dimar, J. R., Glassman, S. D., & Johnson, J. R. (2003). Perioperative complications of posterior lumbar decompression and arthrodesis in older adults. The Journal of Bone and Joint Surgery, 85, 2089-2092.
Champain, S., Mazel, C., Skalli, W., & Mitulescu, A. (2007). Quantitative analysis in outcome assessment of instrumented lumbosacral arthrodesis. European Spine Journal, 16, 1241-1249.
Chen, Q., Baba, H., Kamitani, K., Furusawa N., & Imura, S. (1994). Postoperative bone re-growth in lumbar spinal stenosis: A multivariate analysis of 48 patients. Spine, 21, 2144-2149.
Chou, R., Qaseem, A., Snow, V., Casey, D., Cross, J. T., Shekelle, P., �… Owens, M. D. (2007). Diagnosis and treatment of low back pain: A joint clinical practice guideline from the American College of Physicians and the American Pain Society. Annals of Internal Medicine, 147, 478-491.
Chou, R., Loeser, J. D., Owens, D. K., Rosenquist, R.W., Atlas, S. J., Baisden, J., �…Wall, E. (2009). Interventional therapies, surgery, and interdisciplinary rehabilitation for low back pain: an evidence-based clinical practice guideline from the American Pain Society. Spine, 34, 1066-77.

108 Cote, P., Baldwin, M., Johnson, W., Frank, J., & Butler, R. (2008). Patterns of sick-leave
and health outcomes in injured workers with back pain. European Spine Journal, 17, 484-493.
Cotler, J. M., & Cotler, H. B. (1990). Spinal fusion: Science and technique. New York, NY: Springer-Verlag.
Dagenais, S., Caro, J., & Haldeman, S. (2008). A systematic review of low back pain cost of illness studies in the United States and internationally. Spine, 8, 8-20.
Damkot, D. K., Pope, M. H., Lord, J., & Frymoyer, J. W. (1984). The relationship between work history, work environment, and low back pain in men. Spine, 9, 395-399.
DeBerard, M. S. (1998). Predicting lumbar fusion outcomes from presurgical patient variables: The Utah lumbar fusion outcome study (Unpublished doctoral dissertation). Utah State University, Logan, UT.
DeBerard, M. S., LaCaille, R. A., Spielmans, G. I., Colledge, A., & Parlin, M. A. (2009). Outcomes and presurgery correlates of lumbar discectomy in Utah Workers�’ Compensation patients. The Spine Journal, 9, 193-203.
DeBerard, M. S., Masters, K. S., Colledge, A. L., & Holmes, E. B. (2003). Presurgical biopsychosocial variables predict medical and compensation costs of lumbar fusion in Utah workers�’ compensation patients. The Spine Journal, 3, 420-429.
DeBerard, M. S., Masters, K. S., Colledge, A. L., Schleusener, R. L., & Schlegel, J. D. (2001). Outcomes of posterolateral lumbar fusion in Utah patients receiving workers�’ compensation: a retrospective cohort study. Spine, 26, 738.
DeFrances, C. J., & Hall, M.J. (2007). National Hospital Discharge Survey. Advance data (No. 371). Hyattsville, MD: National Center for Health Statistics.
Deyo, R. A., & Bass, J. E. (1989). Lifestyle and low-back pain. The influence of smoking and obesity. Spine, 14, 501-506.
Deyo, R. A., Battie, M., Beurskens, A. J., Bombardier, C., Croft, P., Koes, B., �… Waddel, G. (1998). Outcome measures for LBP research. A proposal for standardized use. Spine, 23, 2003-2013.
Deyo, R. A., Cherkin, D. C., Loeser, J. D., Bigos, S. J., & Ciol, M. A. (1992). Morbidity and mortality in association with operations on the lumbar spine: The influence of age, diagnosis, and procedure. Journal of Bone and Joint Surgery, 74, 536-543.
109 Deyo, R. A., Gray, D. T., Kreuter, W., Mirza, S., & Martin, B. I. (2005). United States
trends in lumbar fusion surgery for degenerative conditions. Spine, 30, 1441-1145.
Deyo, R. A., & Mirza, S. K. (2006). Trends and variations in the use of spine surgery. Clinical Orthopaedics and Related Research, 443, 139-146.
Deyo, R. A., Mirza, S. K., & Martin, B. I. (2006). Back pain prevalence and visit rates: estimates from U.S. national surveys, 2002. Spine, 31, 2724-2727.
Deyo, R. A., Mirza, S. K., Turner, J. A., & Martin, B. I. (2009). Overtreating chronic back pain: Time to back off? Journal of American Board Family Medicine, 22, 62-68.
Dimar, J. R., Glassman, S. D., Burkus, K. J., & Carreon, L. Y. (2006). Clinical outcomes and fusion success at 2 years of single-level instrumented posterolateral fusions with recombinant human bone morphogenetic protein-2/compression resistant matrix versus iliac crest bone graft. Spine, 31, 2534-2539.
Djurasovic, M., Bratcher, K. R., Glassman, S. D., Dimar, J. A., & Carreon, L. Y. (2008). The effect of obesity on clinical outcomes after lumbar fusion. Spine, 33, 1789-1792.
Don, A. S., & Carragee, E. (2008). A brief overview of evidence-informed management of chronic low back pain with surgery. The Spine Journal, 8, 258-265.
Ehrlich, G. E. (2003). Low back pain. Bulletin of the World Health Organization, 81, 671-676.
Ellermeier, W., & Westphal, W. (1995). Gender differences in pain ratings and pupil reactions to painful pressure stimuli. Pain, 61, 435-439.
Esses, S. I., & Huler, R. J. (1992). Indications for lumbar spine fusion in the adult: Newest knowledge of LBP. Clinical Orthopaedics and Related Research, 279, 87-100.
Fairbank, J., Frost, H., Wilson-MacDonald, J., Yu, L. M., Barker, K., & Collins, R. (2005). Randomized controlled trial to compare surgical stabilization of the lumbar spine with an intensive rehabilitation program for patients with chronic low back pain: the MRC spine stabilization trial. The Behavior Medical Journal, 330, 1233-1239.
Fairbank, J. C. T., & Pynsent, P. B. (2000). The Oswestry disability index. Spine, 25, 2940-2953.

110 Feine, J. S., Bushnell, M. C., Miron, D., & Duncan, G. H. (1991). Sex differences in the
perception of noxious heat stimuli. Pain, 44, 255-262.
Fingerhut, L. A. (2006). Increases in methadone related deaths: 1999-2004. Hyattsville, MD: National Center for Health Statistics.
Fritzell, P., Hagg, O., Wessberg, P., & Nordwall, A. (2001). Swedish lumbar spine study group: 2001 Volvo award winner in clinical studies: Lumbar fusion versus nonsurgical treatment for chronic low back pain. Spine, 26, 2521-2534.
Franklin, G. M., Haug, J., Heyer, N. J., McKeefrey, S. P., & Picciano, J. F. (1994). Outcome of lumbar fusion in Washington State workers�’ compensation. Spine, 19, 1897-1903.
Frymoyer, J. W. (1992). Predicting disability from low back pain. Clinical Orthopaedics & Related Research, 279, 101-109.
Gallasch, C. H., Alexandre, N. C., & Amick, I. B. (2007). Cross-cultural adaptation, reliability, and validity of the work role functioning questionnaire to Brazilian Portuguese. Journal of Occupational Rehabilitation, 17(4), 701-711.
Gatchel, R. J., & Bell, G. (2000).The biopsychosocial approach to spine care and research. Spine, 25, 2572.
Gepstein, R., Shabat, S., Arinzon, Z. H., Berner, Y., Catz, A., & Folman, Y. (2004). Does obesity affect the results of lumbar decompressive spinal surgery in the elderly? Clinical Orthopaedics & Related Research, 426, 138-144.
Glassman, S. D., Anagnost, S. C., Parker, A., Burke, D., Johnson, J. R., & Dimar, J. R. (2000). The effect of cigarette smoking and smoking cessation on spinal fusion. Spine, 25, 2608-2615.
Glassman, S. D., Carreon, L. Y., Djurasovic, M., Dimar, J. R., Johnson, J. R., Puno, R. M., & Campbell, M. J. (2009). Lumbar fusion outcomes stratified by specific diagnostic indication. The Spine Journal, 9, 13-21.
Glassman, S. D., Gornet, M. F., Branch, C., Polly, D., Peloza, J., Schwender, J. D., & Carreon, L. (2006). MOS Short Form 36 and Oswestry Disability Index outcomes in lumbar fusion: A multicenter experience. The Spine Journal, 6, 21-26.
Glassman, S. D., Minkow, R. E., Dimar, J. R., Puno, R. M., Raque, G. H., & Johnson, J. R. Z. (1998). Effect of prior lumbar discectomy on outcome of lumbar fusion: A prospective analysis using the SF-36 measure. Journal of Spinal Disorders, 11, 383-388.

111 Glassman, S., Polly, D., Bono, C., Burkus, K., & Dimar, J. (2008). Outcome of lumbar
fusion in patients over 65 years old. The Spine Journal, 8, 2-3.
Green-McKenzie, J. (2004). Workers�’ compensation costs: Still a challenge. Clinical Journal of Occupational & Environmental Medicine, 4, 395-398.
Greenough, C. G., Peterson, H. D., Hadlow, S., & Fraser, R. D. (1998). Instrumented post-lateral fusion: Results and comparisons with anterior lumbar fusion. Advances in Therapy, 8, 12-20.
Greenough, C. G., Taylor, L. J., & Fraser, R. D. (1994). Anterior lumbar fusion: Results, assessment techniques, and prognostic factors. European Spine Journal, 3, 225-230.
Hadler, N. M. (2005). Occupational Musculoskeletal Disorders, Third Edition. Philadelphia, PA: Lippincott, Williams & Wilkins.
Hadler, N. M., Carey, T. S., & Garrett, J. (1995). The influence of indemnification by workers�’ compensation insurance on recovery from acute backache: North Carolina back pain project. Spine, 20, 2710-2715.
Hadler, N. M., Tait, R. C., & Chibnall, J. T. (2007). Back pain in the workplace. Journal of the American Medical Association, 297, 1594-1596.
Harris, I. A. (2007). Personal injury compensation. ANZ Journal of Surgery, 77, 606-607.
Harris, I., Mulford, J., Solomon, M., van Gelder, J. M., & Young, J. (2005). Association between compensation status and outcome after surgery: A meta-analysis. Journal of the American Medical Association, 293, 1644-1652.
Hart, L. G., Deyo, R. A., & Cherkin D. C. (1995). Physician office visits for low back pain. Frequency, clinical evaluation, and treatment patterns from a U.S. national survey. Spine, 20, 11-19.
Harvinder, S., Thomas, Z., Foley, K., Safdar, K., & Fengyu, Z. (2001). Members spinal fusion and smoking: Is pseudarthrosis the cause for poorer clinical outcome? The Spine Journal, 2(Suppl. 1), 82-83.
Hasenbring, M., Marienfeld, G., Kuhlendahl, D., & Soyka, D. (1994). Risk factors of chronicity in lumbar disc patients. Spine, 19, 2759-2765.
Hedley, A. A., Ogden, C. L., Johnson, C. L., Carroll, M. D., Curtin, L. D., & Flegal, K. M. (2004). Brief report: Prevalence of overweight and obesity among US children, adolescents, and adults, 1999-2002. Journal of the American Medical Association, 291, 2847-2850.
112 Herkowitz, H. N. (1995). Spine update. Degenerative lumbar spondylolisthesis. Spine,
20, 1084-90.
Hestbaek, L., Leboeuf-Yde, C., & Manniche, C. (2003). Low back pain: What is the long-term course? A review of studies of general patient populations. European Spine Journal, 12, 149-165.
Hibbs, R. A. (1911). An operation for progressive spinal deformity. New York Medical Journal, 21, 1013-1016.
Hodges, S. D., Humphreys, S. C., Eck, J. C., Covington, L. A., & Harrom, H. (2001). Predicting factors of successful recovery from lumbar spine surgery among workers�’ compensation patients. Journal of the American Osteopathic Association, 101, 78-83.
Hurwitz, E. L., & Shekelle, P. G. (2006). Epidemiology of low back syndromes. In C. E. Morris (Ed.), Low back syndromes: Integrated clinical management (pp. 83-118). New York, NY: McGraw-Hill.
Iversen, M. D., Daltroy, L. H., Fossel, A. H., & Katz, J. N. (1998). The prognostic importance of patient pre-operative expectations of surgery for lumbar spinal stenosis. Patient Education & Counseling, 34, 169-178.
Jarvik, J. G., & Deyo, R. A. (2002). Diagnostic evaluation of low back pain with emphasis on imaging. Annals of Internal Medicine, 137, 586-597.
Jarvik, J. J., Hollingworth, W., Heagerty, P., Haynor, D. R., & Deyo, R. A. (2001). The longitudinal assessment of imaging and disability of the back (LAIDBack) study. Spine, 26, 1158-1166.
Jensen, M. C., Brant-Zawadzki, M. N., Obuchowski, N., Modic, M. T., Malkasian, D., & Ross, J. S. (1994). Magnetic resonance imaging of the lumbar spine in people without back pain. New England Journal of Medicine, 331, 69-73.
Jensen, M. P., Karoly, P., O�’Riordan, E. F., Bland, F., Jr., & Burns, R. S. (1989). The subjective experience of acute pain. An assessment of the utility of 10 indices. Clinical Journal of Pain, 5, 153-159.
Junge, A., Dvorak, J., & Ahrens, S. (1995). Predictors of bad and good outcomes of lumbar disc surgery: A prospective clinical study with recommendations for screening to avoid bad outcomes. Spine, 20, 460-468.
Kalbarczyk, A., Lukes, A., & Seiler, R. W. (1998). Surgical treatment of lumbar spinal stenosis in the elderly. Acta Neurochirurgica, 140, 637-641.

113 Kampera, S. J., Ostelob, W. J. G., Knolb, D. L., Mahera, C. G. Henrica , C. W., Vetb, L.,
& Hancock, M. G. (2010). Global Perceived Effect scales provided reliable assessments of health transition in people with musculoskeletal disorders, but ratings are strongly influenced by current status. Journal of Clinical Epidemiology, 63, 760-766.
Kaplan, R. M., Metzger, G., & Jablecki, C. (1983). Brief cognitive and relaxation training increases tolerance for a painful clinical electromyographic examination. Psychosomatic Medicine, 45, 155-162.
Katz, J. N. (2006). Lumbar disc disorders and low back pain: Socioeconomic factors and consequences. Journal of Bone and Joint Surgery, 88, S21-S24.
Katz, J. N., Wright, E. A., Guadagnoli, E., Liang, M. H., Karlson, E. W., & Cleary, P. D. (1994). Differences between men and women undergoing major orthopedic surgery for degenerative arthritis. Arthritis & Rheumatism, 37, 687-694.
Keeley P., Creed F., Tomenson B., Todd, C., Borglin, G., & Dickens, C. (2008). Psychosocial predictors of health-related quality of life and health service utilization in people with chronic low back pain. Pain, 135, 142-150.
Kim, Y. J., Lenke, L. G., Bridwell, K. H., Kim, K. L., & Steger-May, K. (2005). Pulmonary function in adolescent idiopathic scoliosis relative to the surgical procedure. Journal of Bone & Joint Surgery, 87, 1534-41
Kinkade, S. (2007). Evaluation and treatment of acute low back pain. American Journal of Family Physicians, 75, 1181-1188.
Klein, R.G., & Eek, B.C. (1990). Low-energy laser treatment and exercise for chronic low back pain: Double-blind controlled trial. Archives of Physical & Medical Rehabilitation, 71, 34-37.
Kopec, J., & Esdaile, J. (1995). Spine update: Functional disability scales for back pain. Spine. 20, 1943-1949.
Krisberg, L. (2009). Cell phone popularity a barrier for public health data collection: More Americans forgoing phone landlines. Nations Health, 39, 1-12.
Kwon, M. A., Shim, W. S., Kim, M. H. Gwak, M. S., Hahm, T. S., Kim, G. S., �… Kim, T. H. (2006). A correlation between low back pain and associated factors: A study involving 772 patients who had undergone general physical examination. Journal of Korean Medical Science, 21, 1086-1091.
LaCaille, R. A., DeBerard, M. S., Masters, K. S., Colledge, A. L., & Bacon, W. (2005). Biopsychosocial predictors and multidimensional outcomes of interbody cage lumbar fusion. The Spine Journal, 5, 71-78.
114 Lacroix, M. J., Powell, J., Lloyd, G. J., Doxey, N. C. S., Mitson, G. L., & Aldam, C. F.
(1990). Low back pain: Factors of value in predicting outcome. Spine, 16, 495-499.
Lieberman, I. H. (2004). Disc bulge bubble: Spine economics 101. Spine, 4, 609-613.
Loney, P. L., & Stratford, P. W. (1999). The prevalence of low back pain in adults: A methodological review of the literature. Physical Therapy, 79, 384-396.
Loupasis, G. A., Stamos, K., Katonis, P. G., Sapkas, G., Korres, D. S., & Hartofilakidis, G. (1999). Seven- to 20-year outcome of lumbar discectomy. Spine, 24, 2313-2317.
Maetzel, A., & Li, L. (2002). The economic burden of low back pain: A review of studies published between 1996 and 2001. Best Practices in Research Clinical Rheumatology, 16, 23-30.
Maghout-Juratli S., Franklin, G. M., Mirza, S. K., Wickizer, T. M., & Fulton-Kehoe, D. (2006). Lumbar fusion outcomes in Washington state workers�’ compensation. Spine, 31, 15-23.
Mannion, A. F., & Elfering, A. (2006). Predictors of surgical outcome and their assessment. European Spine Journal, 15, S93-108.
Mantyselka, P. T., Kumpusalo, E. A., Ahonen, R., & Takala, J. K. (2002). Direct and indirect costs of managing patients with musculoskeletal pain-challenge for health care. European Journal of Pain, 6, 141-148.
Martin, B. I., Deyo, R. A., Mirza, S. K., Turner, J., Comstock, B. A., Hollingworth, W., & Sullivan, S. D. (2008). Expenditures and health status among adults with back and neck problems. Journal of the American Medical Association, 299, 656-664.
Moller, H., & Hedlund, R. (2000). Surgery versus conservative management in adult isthmic spondylolisthesis: A prospective randomized study: Part 1. Spine, 25, 1711-1715.
Murphy, P. L., & Volinn, E. (1999). Is occupational low back pain on the rise? Spine, 24, 691-697.
Nachemson, A. L. (1992). Newest knowledge of low back pain. A critical look. Clinical Orthopaedics & Related Research, 279, 8-20.
Nachemson, A. L., & LaRocca, H. (1987). Editorial. Spine, 12, 427-429.

115 Narayan, P., Haid, R. W., Subach, B. R., & Rodts, G. E. (2002). Effect of spinal disease
on successful arthrodesis in lumbar pedicle screw fixation. Journal of Neurosurgery, 9, 468-472.
National Institutes of Health. (1998). Body mass index and health. Retrieved from http://www.cnpp.usda.gov/publications/nutritioninsights/insight16.pdf
National Research Council. (2001). Musculoskeletal disorders and the workplace: Low back and upper extremities. Washington, DC: National Academy Press.
Nguyen, T. H., Randolph, D. C., Talmage, J., Succop, P., & Travis, R. (2011). Long-term outcomes of lumbar fusion among workers�’ compensation subjects: A historical cohort study. Spine, 36, 320-331.
Nordin, M., Andersson, G. B. J., & Pope, M. H. (1997). Musculoskeletal disorders in the workplace: Principle and practice. New York, NY: Mosby.
Osman, A., Barrios, F. X., Gutierrez, P. M., Kopper, B. A., Merrifield, T., & Grittmann, L. (2000). The pain catastrophizing scale: Further psychometric evaluation with adult samples. Journal of Behavioral Medicine, 23, 351-365.
Rasmussen, C., Leboeuf-Yde, C., Hestbæk, L., & Manniche, C. (2008). Poor outcome in patients with spine-related leg or arm pain who are involved in compensation claims: A prospective study of patients in the secondary care sector. Scandinavian Journal of Rheumatology, 37, 462-468.
Rhee, Y., Taitel, M. S., Walker, D. R., & Lau, D. T. (2007). Narcotic drug use among patients with lower back pain in employer health plans: A retrospective analysis of risk factors and health care services. Clinical Therapeutics, 29, 2603-2612.
Roland, M., & Morris, R. (1983a). A study of the natural history of back pain. Part I: development of a reliable and sensitive measure of disability in low-back pain. Spine, 8, 141-144.
Roland, M., & Morris, R. (1983b). A study of the natural history of low-back pain. Part II: development of guidelines for trials of treatment in primary care. Spine, 8, 145-150.
Sasso, R. C., Kitchel, S. H., & Dawson, E. G. (2004). A prospective, randomized Controlled clinical trial of anterior lumbar interbody fusion using a titanium cylindrical threaded fusion device. Spine, 29, 113-121.
Shabat, S., Folman, Y., Arinzon, Z., Adunsky, A., Catz, A., & Gepstein, R. (2005). Gender differences as an influence on patients�’ satisfaction rates in spinal surgery of elderly patients. European Spine Journal, 14, 1027-1032.
116 Silcox, D. H., Daftari, T., Boden, S. D., Schimandle, J. H., Hutton, W. C., & Whitesides,
T. E. (1995). The effect of nicotine on spinal fusion. Spine, 20, 1549-1553.
Spangler, D. M. (1982). Lumbar discectomy: Results with limited disc excision and selected foraminotomy. Spine, 7, 604-607.
Snook, S. (2004). Work-related low back pain: Secondary intervention. Journal of Electromyography and Kinesiology, 14, 153-160.
Starkweather, A. R. (2006). Evaluation and management of low back pain: An algorithmic approach. The American Journal of Nurse Practitioners. 10, 9-16.
Stauffer, R. N., & Coventry, M. B. (1972). Anterior interbody lumbar spine fusion: Analysis of the Mayo Clinic series. The Journal of Bone and Joint Surgery, 54, 756-768.
Stevens, J. (2009). Applied multivariate statistics for the social sciences (5th ed.). Mahwah, NJ: Erlbaum.
Stevenson, J. M., Weber, C. L., Smith, J. T., Dumas, G. A., & Albert, W.A. (2001). A longitudinal study of low back pain in an industrial population. Spine, 26, 1370-1377.
Sullivan, M. J. L., Bishop, S., & Pivik, J. (1995). The Pain Catastrophizing Scale: Development and validation. Psychological Assessment, 7, 524-532.
Swan, J., Hurwitz, E., Malek, F., van den Haak, E., Cheng, I., Alamin, T., & Carragee, E. (2006). Surgical treatment for unstable low-grade isthmic spondylolisthesis in adults: a prospective controlled study of posterior instrumented fusion compared with combined anterior-posterior fusion. The Spine Journal, 6, 606-14.
Tandon, V., Campbell, F., & Ross, E. R. (1999). Posterior lumbar interbody fusion: Association between disability and psychological disturbance in noncompensation patients. Spine, 24, 1833-1838.
Taylor, S. E. (1999). Health psychology (4th ed). New York, NY: McGraw-Hill.
Tayler, V. M., Deyo, R. A., & Cherkin, D. C. (1994). Low back pain hospitalization. Recent U.S. trends and regional variations. Spine, 19, 1207-1212.
Taylor, V. M., Deyo, R. A., Ciol, M., & Kreuter, W. (1996). Surgical treatment of patients with back problems covered by workers compensation versus those with other sources of payment. Spine, 21, 2255-2259.
Trief, P. M., Grant, W., & Fredrickson, B. (2000). A prospective study of psychological predictors of lumbar surgery outcome. Spine, 25, 2616-2621.
117 Trief, P. M., Ploutz-Snyder, R., & Fredrickson, B. E. (2006). Emotional health predicts
pain and function after fusion: A prospective multi-center study. Spine, 31, 823-830.
Turner, J. A., Ersek, M., Herron, L., Haselkorn, J., Kent, D., Ciol, M. A., & Deyo, R. (1992). Patient outcomes after lumbar spinal fusions. The Journal of the American Medical Association, 268, 907-911.
van Tulder, M., Becker, A., Bekkering, T., Breen, A., del Real, M. T., Hutchinson, A., �… Malmivaara, A. (2006). European guidelines for the management of acute nonspecific LBP in primary care. European Spine Journal, 15, S169-91.
Von Korff, M., Jensen, M., & Karoly, M. (2000). Assessing global pain severity by self-report in clinical and health services research. Spine, 25, 3140-3151.
Waddell, G., & Turk, D. C. (2001). Clinical assessment of low back pain. In D. C. Turk & R. Melzack (Eds.), Handbook of pain assessment (2nd ed., pp. 431-453). New York, NY: Guilford.
Waldman, P., & Armstrong, D. (2010). Doctors getting rich with fusion surgery debunked by studies. Retrieved from http://www.bloomberg.com/news/2010-12-30/highest- paid-u-s-doctors-get-rich-with-fusion-surgery-debunked-by-studies.html
Ware, J. E., & Kosinski, M. (2001). SF-36 physical and mental health summary scales: A manual for users of version 1 (2nd ed.). Lincoln, RI: Quality Metric.
Ware, J. E., Kosinski, M., & Keller, S. K. (1994). SF-36 physical and mental health summary scales: A user’s manual. Boston, MA: The Health Institute.
Ware, J. E., Snow, K. K., Kosinski, M. A., & Gandek, M. S. (2000). SF-36 health survey: manual and interpretation guide (2nd ed.). Lincoln, RI: Quality Metric.
Webster, B. S., & Snook, S. H. (1994). The cost of 1989 workers�’ compensation low back pain claims. Spine, 19, 1111-1115.
Weinstein, J. N., Lurie, J. D., Olson, P. R., Bronner, K. K., & Fisher, E. S. (2006). United States�’ trends and regional variations in lumbar spine surgery: 1992-2003. Spine, 31, 2707-2714.
Wheeler, A. J., Gundy, J. M., & DeBerard, M. S. (In press). Predicting compensation and medical costs of lumbar fusion patients receiving workers�’ compensation in Utah using presurgical biopsychosocial variables. Spine.

118 Wilson-MacDonald, J., Fairbank, J., Frost H., Yu, L. M., Barker, K., Collins, R., �…
Campbell, H. (2008). The MRC spine stabilization trial: Surgical methods, outcomes, costs, and complications of surgical stabilization. Spine, 33, 2334-2340.
Wing, K. J., Fisher, C. G., Connell, J. X., & Wing, P. C. (2000). Stopping nicotine exposure before surgery: the effect on spinal fusion in a rabbit model. Spine , 25, 30-34.
World Health Organization. (1948). International classification of impairments, disabilities, and handicaps: A manual classification relating to the consequences of disease. Geneva, Switzerland: Author.
Wright, E. S. (2005). Biomedical models and healthcare systems: New model will be useful if it alters allocation of resources. British Medical Journal, 330, 419-419.

119
APPENDICES

120
Appendix A
Medical Records Review Instrument

121
Medical Records Review Instrument
DEMOGRAPHIC/COMPENSATION VARIABLES 1. Patient Name:
2. Address: 3. Phone Number (home):
4. Claim Number:
5. Gender 0=not reported 1= Male 2= Female
6. SSN:
7. Study Number:
8. Date of Birth:
9. Date of Injury:
10. Hire Date:
11. Months worked for employer prior to injury:
12. Marital Status At Time of Injury: 0=Not reported 1=Married 2=Divorced 3=Separated 4=In a significant relationship (i.e., boyfriend or girlfriend) 5=Single
13. Date of Index Lumbar Fusion Surgery:
14. Time interval between injury and fusion surgery? (Days):
15. Date WCFU File Created:
16. Patient’s Weekly Wage at Time of Injury: ______________________ 0=not reported
17. Case Manager Assigned? 0 = not reported 1 = no 2 = yes
18. Occupation At Time of Injury:
19. Child Care Responsibility: 0=Not reported 1=No 2=Yes Total # Dependents__________
20. Lawyer involvement in compensation case? (prior to surgery) 0=not reported 1=no 2=yes
21. Red Flags A. AGE (AG) - Claimant age over 50.................1=yes 2=no B. ALCOHO (AL) - History of Alcoholism................1=yes 2=no C. CREDIB (CR) - Questionable Validity.................1=yes 2=no D. CUMTRA (CT) - Cumulative Trauma...................1=yes 2=no E. DISVAL (DI) - Disputed Validity Settlement....1=yes 2=no F. DRUG (DR) - History of Drug Abuse...............1=yes 2=no G. EDUCAT (ED) - Education Level..........................1=yes 2=no H. EMPLOY (EF) - Employment Factors...................1=yes 2=no I. FNCOVER (FO) - Functional Overlay......................1=yes 2=no J. FRAUD (FR) - Fraud.............................................1=yes 2=no K. LEGAL (LG) - Claim Involves Litigation...........1=yes 2=no L. LIEN (LI) - Claim Involves Lienholder..........1=yes 2=no M. NESPEK (NE) - Language Barriers.......................1=yes 2=no N. OBESE (OB) - Obesity..........................................1=yes 2=no O. OFFCR (OF) - Claimant Officer/Partner...........1=yes 2=no P. OTHER (OT) - Other Factors...............................1=yes 2=no Q. OVRPAY (OP) - Compensation Overpayments....1=yes 2=no R. PIREF (PR) - Private Investigator Referred...1=yes 2=no S. PREEXI (PR) - Pre-Existing Condition................1=yes 2=no T. PRIORS (PS) - Claiman has prior claims.............1=yes 2=no U. PSYCH (PF) - Psychological Factors...................1=yes 2=no V. PTSD (PT) - Post-Traumatic Stress Dis...........1=yes 2=no W. SOCIAL (SF) - Social Factors................................1=yes 2=no Y. SUBSYM (SS) - CLMT has subjective sympt.......1=yes 2=no X. SYSDIS (SD) - Systemic Diseases......................... 1=yes 2=no
22. Description of Accident a. Accident Code________ b. Injury Type Code: c. ICD-9 Code__________ b. Narrative:_____________ ________________________________________________________________________________________________________

122 WORK/COMPENSATION VARIABLES 23. Date Last Worked:
28. Total Paid Temporary Comp: 40. Percent Physical Impairment Paid
Out:
24. History of prior industrial claim? (Generic) 0=not reported 1=no 2=yes Total Number_________________ Specific Code #�’s_______________ Type of Injury_______________
29. Total Paid Permanent Comp: 41. Expected Duration
30. Total Paid Comp: 42. Medical Stability Date:
25. History of prior industrial claim? (Low Back Pain) 0=not reported 1=no 2=yes Total Number__________________ Specific Codes #�’s______________
31. Total Paid Medical:
43. Return to Work 0=not reported 1=no 2=yes
32. Total Paid ALAE:
44. Return to Work Date
26. Vocational Rehabilitation following surgery? 0=not reported 1=no 2=yes
33. Total Paid Rehab 45. Time to Medical Stability From Date
Of Fusion (days):
34. Total Paid to Date
27. Modified Employment Available 0=not reported 1=no 2=yes
35. Total ALAE
36. Total MEDICAL:
37. Total REHAB:
WCFU Adjustor Name:
38. Total Comp
39. Grand Total Incurred:

123 PHYSICAL/HEALTH/SURGICAL VARIABLES 46. Physical Exam Data a. Height_____ b. Weight_____ c. Straight Leg Raise (30-70 degree raise produces radicular pain below knee) 0=Not Reported 1=Positive 2=None d. Femoral Tension Sign (Anterior thigh pain in a radicular pattern with flexion of knee and hip extension in a prone position) 0=Not Reported 1=Positive 2=None e. Depressed Patellar Reflexes 0=Not Reported 1=Positive 2=None f. Depressed Ankle Reflexes 0=Not Reported 1=Positive 2=None g. Back pain without radiation 0=Not Reported 1=Positive 2=None h. Radicular Pain 0=Not Reported 1=Positive 2=None 3=Left/Right to Thigh 4=Left/Right to Leg 5=Left/Right to Foot i. Motor Weakness (asymmetric) 0=Not Reported 1=Positive 2=None 3=Hip Flexors 4=Knee Extensors 5=Ankle Dorsoflexors 6=Great Toe Dorsoflexors 7=Ankle Plantar Flexors j If yes, does motor weakness correspond to nerve root placement? 0=Not Reported 1=Positive 2=Negative 9=Not Applicable k. Any Nonorganic signs present? 0=not reported 1=superficial or NonAnatomic Tenderness 2=Pain with Simulated Axial Loading or Rotation 3=Distraction (SLR different sitting v. supine) 4= Regional Disturbance (Nonanatomic sensory pr motor deficit) 5 = Overrreaction 47. Number of Prior Low Back Operations? 0=None
48. Patients’ Primary Surgical Diagnosis 0=Not Reported Options: (Washington Study, 2006) 1=Radiculopathy 2=Disc Herniation 3= Stenosis 4= Spondylolisthesis 5= Degenerative disc disease 6= Other_______________ Turner et al., 1992 (Meta Analysis) 1= Disc Herniation 2=Degenerative disc disease (internal disc derangement 3= Degenerative Scoliosis 4= Segmental Instability 5= Pseudoarthrosis 6= Spondylolisthesis 7= Spinal Stenosis
50.General Health Problems (List up to 5) 0=None reported 1=Diabetes 2=Heart Disease 3=Stroke 4=Arthritis 5=Asthma 7=Hypertension 8=Colitis 9=Psoriasis 10=Cancer history 11=Trauma history 12=Infectious history 13=Auto-immune history 14=Steroid usage 15=Other
51. Imaging Studies Conducted prior to surgery? 0=none reported 1=X-ray 2=CT 3=MRI 4=CT Myelogram 5=Discography 6=Other__________________________
49. Patients’ Secondary Surgical Diagnosis 0=Not Reported Options: (Washington Study, 2006) 1=Radiculopathy 2=Disc Herniation 3= Stenosis 4= Spondylolisthesis 5= Degenerative disc disease 6= Other_______________ Turner et al., 1992 (Meta-Analysis) 1= Disc Herniation 2=Degenerative disc disease (internal disc derangement 3= Degenerative Scoliosis 4= Segmental Instability 5= Pseudoarthrosis 6= Spondylolisthesis 7= Spinal Stenosis
52. Number of Levels Fused 0=not reported 1=One Level 2=Two Levels 3=Three or three plus 53. Type of Fusion 0=not reported 1=Posterolateral gutter fusion 2= Posterior lumbar interbody fusion (PLIF/TLIF) 3= Anterior lumbar interbody fusion (ALIF) 4= Anterior/posterior spinal fusion 5=Other_______________
58. Surgical Complications 0=Not reported 1=none 2=In hospital mortality 3=Deep infection 4=Superficial infection 5=Deep vein thrombosis/ thrombophlebitis 6=Pulmonary embolus 7=Dural Tear-CSF Leak 8=Nerve Root Injury 9=Operation at wrong level 10=Vascular injury 11=Failed back syndrome 12=other________________________________
54. Type of Instrumentation Used? 0=Not Reported 1=None 2= Pedicle screws and rods 3= Titanium Cages Type___________ 4= Both Screws and cages 5= Other _________
59. Additional Procedures Performed 60. Was Solid Arthrodesis Achieved? 0=Not Reported 1=No 2=Yes
55: If Yes, was instrumentation removed?
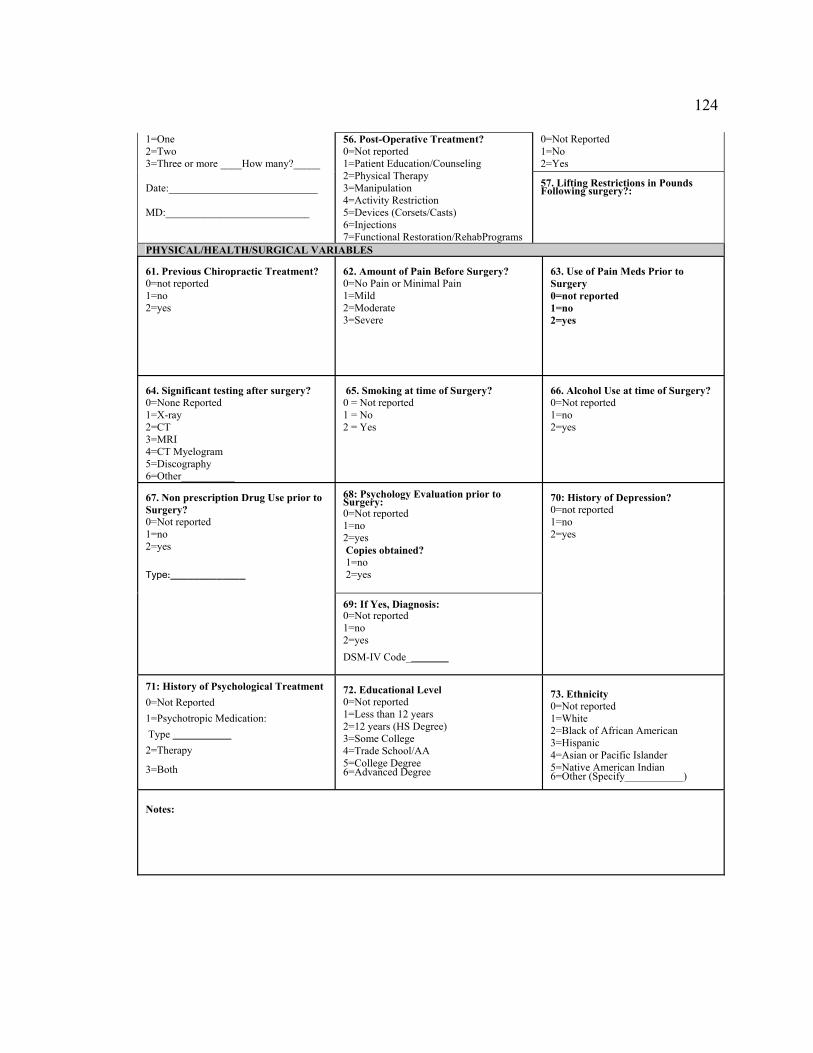
124 1=One 2=Two 3=Three or more ____How many?_____ Date:____________________________ MD:___________________________
56. Post-Operative Treatment? 0=Not reported 1=Patient Education/Counseling 2=Physical Therapy 3=Manipulation 4=Activity Restriction 5=Devices (Corsets/Casts) 6=Injections 7=Functional Restoration/RehabPrograms
0=Not Reported 1=No 2=Yes 57. Lifting Restrictions in Pounds Following surgery?:
PHYSICAL/HEALTH/SURGICAL VARIABLES 61. Previous Chiropractic Treatment? 0=not reported 1=no 2=yes
62. Amount of Pain Before Surgery? 0=No Pain or Minimal Pain 1=Mild 2=Moderate 3=Severe
63. Use of Pain Meds Prior to Surgery 0=not reported 1=no 2=yes
64. Significant testing after surgery? 0=None Reported 1=X-ray 2=CT 3=MRI 4=CT Myelogram 5=Discography 6=Other__________
65. Smoking at time of Surgery? 0 = Not reported 1 = No 2 = Yes
66. Alcohol Use at time of Surgery? 0=Not reported 1=no 2=yes
67. Non prescription Drug Use prior to Surgery? 0=Not reported 1=no 2=yes Type:_____________
68: Psychology Evaluation prior to Surgery: 0=Not reported 1=no 2=yes Copies obtained? 1=no 2=yes
70: History of Depression? 0=not reported 1=no 2=yes
69: If Yes, Diagnosis: 0=Not reported 1=no 2=yes DSM-IV Code________
71: History of Psychological Treatment 0=Not Reported 1=Psychotropic Medication: Type ___________ 2=Therapy 3=Both
72. Educational Level 0=Not reported 1=Less than 12 years 2=12 years (HS Degree) 3=Some College 4=Trade School/AA 5=College Degree 6=Advanced Degree
73. Ethnicity 0=Not reported 1=White 2=Black of African American 3=Hispanic 4=Asian or Pacific Islander 5=Native American Indian 6=Other (Specify___________)
Notes:

125
Appendix B
Letter of Information

126
Analysis of Utah Workers’ Compensation Patient Outcomes Following Lumbar Fusion
Department of Psychology 2810 Old Main Hill Logan, UT 84322-2810 Tel: (435) 797-1462 Date «FirstName» «LastName» «Address1» «City», «State» «PostalCode» Dear Participant: Professor Scott DeBerard, Ph.D. and graduate student Jessica Gundy, M.A. from the Department of Psychology at Utah State University (USU) are conducting a research study to evaluate outcomes following lumbar fusion. USU has established a research partnership with the Workers�’ Compensation Fund of Utah (WCFU) and with their permission, we obtained your name and address from their database. The research team at USU is very interested in hearing about your results from this spine treatment and sends this letter to inform you in advance of our request for a telephone interview. We hope to have approximately 250 participants in this study. To select participants for this study, information regarding your prior fusion procedure was collected from the WCFU database. Participants were selected based upon this review and the information is now stored in a confidential manner at USU. There is minimal risk involved in participating in this research study.
During the months of October through December of 2009, one of our interviewers from USU will call you about an outcome survey of patients who have undergone the lower back surgical procedure called lumbar/spinal fusion. The interview will be conducted over the telephone, at your convenience, and will take approximately 20 to 30 minutes. The interview will consist of primarily �‘yes/no�’ or rating-type questions and will be conducted from a private office to maintain privacy of the interviews. Your consent to participate in the study will be requested by the interviewer before the interview begins.
Participation in research is voluntary and you may withdraw at any time without consequence. We want to emphasize this research is being conducted independently from WCFU and that your participation in this research will in no way affect your compensation status or treatment now or at any time in the future. All patient data will be examined by USU and the WCFU in a combined summarized manner. Individual cases will not be revealed or examined by USU or the WCFU.
Study records that identify you will be kept confidential as required by law. Federal Privacy Regulations provide safeguards for privacy, security, and authorized access. Except when required by law, you will not be identified by name, social security

127 number, address, telephone number, or any other direct personal identifier in study records disclosed outside of USU. In the unlikely event that we learn that you are having serious thoughts of, or are engaging in behaviors related to harming yourself or others, we may need to report this to the appropriate authorities.
All of your responses will be strictly confidential. To maintain your confidentiality, all information will be kept in a locked file cabinet in a locked room at USU. Only the researchers will have access to this information. To protect your privacy, your name and identifying information will be replaced with a confidential ID number, which will be used in any datasets generated from this project. Your name and identifying information will be stored separately from these datasets in order to maximize your privacy.
We are interested in documenting outcomes following lumbar fusion and learning how to better predict lumbar fusion outcomes. We are hopeful that the information you provide may help future candidates for this procedure by predicting those patients who are most likely to benefit from this procedure. People who have been treated for back pain often report a mixture of both positive and negative results. Your unique experience, whether positive or negative, is very important to us.
If you have questions or concerns you may contact Dr. DeBerard (telephone contact and email address is below). If you are interested in receiving a summary of our study results, please notify us and we will send you a copy. We will be offering a $10.00 incentive to you that will be sent to you following completion of the telephone survey via check.
The Institutional Review Board for the protection of human participants at USU has approved this research study. If you have any pertinent questions or concerns about your rights or a research-related injury, you may contact the IRB Administrator at (435) 797-0567. If you have a concern or complaint about the research and you would like to contact someone other than the research team, you may contact the IRB Administrator to obtain information or to offer input.
To help us in contacting you, please fill in your name, address, phone number and the best time to contact you on the enclosed postcard and drop it in a mailbox. Returning the postcard does not imply that you are giving your consent to participate; consent will be asked of you at the time of your telephone interview. Your participation will be greatly appreciated since this is a very important study. If you have any questions, please do not hesitate to call me at (435) 797-1462. Sincerely, ________________________ ____________________________ Scott DeBerard, Ph.D. Jessica M. Gundy, M.A. Research Director Graduate Assistant Utah Lumbar Fusion Outcome Study Utah Lumbar Fusion Outcome Study [email protected] [email protected]

128
Appendix C
Fusion Study Telephone Survey Cover Sheet
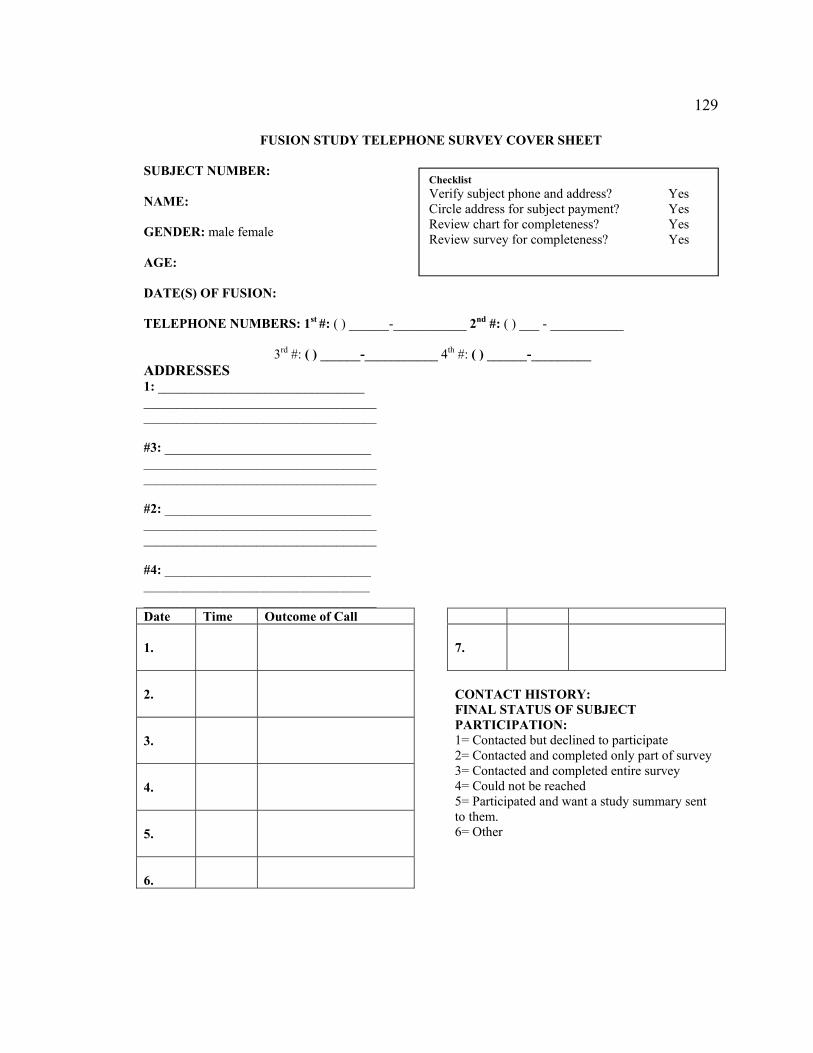
129
FUSION STUDY TELEPHONE SURVEY COVER SHEET
SUBJECT NUMBER: NAME: GENDER: male female AGE: DATE(S) OF FUSION: TELEPHONE NUMBERS: 1st #: ( ) ______-___________ 2nd #: ( ) ___ - ___________
3rd #: ( ) ______-___________ 4th #: ( ) ______-_________ ADDRESSES 1: _______________________________ ___________________________________ ___________________________________ #3: _______________________________ ___________________________________ ___________________________________ #2: _______________________________ ___________________________________ ___________________________________ #4: _______________________________ __________________________________ ___________________________________ Date Time Outcome of Call 1.
2.
3.
4.
5.
6.
7.
CONTACT HISTORY: FINAL STATUS OF SUBJECT PARTICIPATION: 1= Contacted but declined to participate 2= Contacted and completed only part of survey 3= Contacted and completed entire survey 4= Could not be reached 5= Participated and want a study summary sent to them. 6= Other
Checklist Verify subject phone and address? Yes Circle address for subject payment? Yes Review chart for completeness? Yes Review survey for completeness? Yes

130
Appendix D
Telephone Outcome Script
131
UTAH FUSION OUTCOME STUDY TELEPHONE INTERVIEW SCRIPT
Hello. Is this the_______________________residence? (If wrong number, then terminate). This is calling from Utah State University. We are conducting a study to learn more about people who have undergone spinal fusion to treat their back pain. Earlier this month a letter describing the study was sent to you? Did you receive it? If yes: (Proceed with the rest of the introduction). If no: I am sorry it did not reach you. The letter was to inform you of this call and the nature of the study. (Proceed to the introduction).
INTRODUCTION As the letter (or The letter indicated) indicated you were chosen for this study because you underwent a fusion procedure to treat your back pain through the Worker�’s Compensation Fund of Utah. Your opinion of how you have progressed since this procedure is critical to this study and results of the survey will be used to help others who are considering having a fusion. Your participation is voluntary and your treatment or compensation status will in no way be affected by your participation. For your participation in the survey we will be sending you $10 and if you wish we could also send you a brief report of the study findings. All of your answers will be kept confidential as provided by law and you may skip any questions you prefer not to answer. Okay? Please feel free to ask questions at any time during the survey. The survey will take about 20 to 30 minutes to complete. Would you be willing to participate?
Yes, verbal consent obtained: (Proceed with survey)
No, verbal consent not obtained: Would you prefer we call you back at a better time?
Yes: Date:
Day: Time:
No: Okay, thank you for your time. (Do not proceed with survey)

132
Appendix E
Stauffer-Coventry Index, Global Perceived Effect,
Verbal Numeric Rating Scale, and Patient Satisfaction Items

133
Stauffer-Coventry Index, Global Perceived Effect, Verbal Numeric Rating Scale, and Patient Satisfaction Items
Utah Lumbar Fusion Outcome Study Telephone Survey - General Questions
The next part of the survey will involve some general questions about how you have done since you had your fusion. Please respond to each question according to how you feel today. Okay? 1. Since yourfusion, how much pain relief have you experienced in your back and lower extremities? Please provide a percent rating from 0 to 100. _______________ Category Rating: 1=Good (76-100 % improvement) 2= Fair (26-75% improvement) 3= Poor (0-25% improvement)
2. With regard to your employment after fusion, which of the following best describes your status after treatment? 1=Return to previous work status following surgery 2=Return to lighter work following surgery 3=No return to work following surgery
3. With regard to your physical activities after fusion, which of the following best describes your status after treatment?: 1=Minimal or no restrictions of physical activities. 2=Moderate restrictions of physical activities 3=Severe restrictions of physical activities
4. With regard to your use of analgesic medications after fusion, which of the following best describes your usage: 1=Occasional mild analgesics or no analgesics 2=regular use of nonnarcotic analgesics 3=occasional or regular narcotic analgesics
5. With regard to your back/leg pain following fusion, which of the following is true: 1=Back or leg pain is worse than expected 2=Back or leg pain is no worse or better than expected 3=Back or leg pain is better than expected
6. Is your quality of life better or worse as a result of fusion? That is, is it: 1=A great improvement 2=A moderate improvement 3=A little improvement 4=No change 5=A little worse 6=Moderately worse 7=Much worse
7. Given what you know: If you could go back in time, would you choose to have the fusion again? 0=Undecided 1=No 2=Yes
8. What was your principal occupation/job title at the time of your injury?:
9. Are you currently working? 1. No 2. Yes, Full Time 3. Yes, Part Time 4. No answer
10. If not working, which of the following best describes why you are not employed?: 1. I am still disabled 2.I am not disabled & I want to work but cannot find a job. 3. I was laid off. 4. I am a student. 5. I am a homemaker. 6. I am retired 7. Other____________________ 8. No answer
11. How many days have you worked in the past 4 weeks?
12. How many hours a week do you usually work at your job?
13. Did you change jobs because of your back problem? 1=no 2=yes 3=not applicable 0=No answer
14. Do you currently retain an attorney because of you back/neck problems? 1=no 2=yes 0=No answer
15. Do smoke now? 1=no 2=yes 0=No answer 15.a. Ever Smoked? 1=yes/2=no
16. Have you had any back operations since your fusion? 1=No 2=No, but I�’m scheduled to 3=Yes Operation Types:
17. Overall, is your back or leg pain problem better than or worse than you expected it to be at this point? That is, is it? 1. Much better 2. Somewhat better 3.What I expected 4. Somewhat worse 5. Much worse 6. No expectations
18. What is the highest year in school you completed? 1. Less than High School 2. Some High School 3. High School Graduate/GED 4. Attended or graduated from technical school 5. Attended college but did not graduate 6. College graduate 7. Graduate Studies
19. If you had to spend the rest of your life with your back condition as it is right now, how would you feel about it? 1. Extremely dissatisfied 2. Very dissatisfied 3. Somewhat dissatisfied 4. Neutral 5. Somewhat satisfied 6. Very satisfied 7. Extremely satisfied
134
20. On a scale from zero to ten, where zero represents no pain and ten represents the worst pain imaginable, how would you rate your current pain level? #:_______
21. Now, using the same scale, how would you rate your level of pain on average over the past week? #:________
22. Compared to when this episode first started, how would you describe your back/neck these days? 1. Complete relief of pain 2. More than 50% pain relief 3. No change in the level of pain 4. The pain has increased

135
Appendix F
Rolland-Morris Disability Questionnaire

136
Disability Questionnaire
Now we are going to ask you more specific questions about your back.... “When your back hurts, you may find it difficult to do some of the things you normally do. The list I’m going to read you now contains some sentences people have used to describe themselves when they have back pain. As I read the list, think of yourself today. When I read a sentence that describes you today, please indicate so by telling me yes. If the sentence does not describe how you feel today, please indicate so by telling me no. Do you have any questions? Yes No
Items
1 2
1 2
1 2
1 2
1 2
1 2
1 2
1 2
1 2
1 2
1 2
1 2
1 2
1 2
1 2
1 2
1 2
1 2
1 2
1 2
1 2
1 2
1 2
1 2
1. I stay at home most of the time because of my back.
2. I change positions frequently to try and get my back comfortable.
3. I walk more slowly than usual because of my back.
4. Because of my back I am not doing any of the jobs I usually do around the house.
5. Because of my back, I use a handrail to get upstairs.
6. Because of my back, I lie down to rest more often.
7. Because of my back, I have to hold on something to get out of an easy chair.
8. Because of my back, I try to get other people to do things for me.
9. I get dressed more slowly than usual because of my back.
10. I only stand up for short periods of time because of my back.
11. Because of my back, I try to not bend or kneel down.
12. I find it difficult to get out of a chair because of my back.
13. My back is painful almost all of the time.
14. I find it difficult to turn over in bed because of my back.
15. My appetite is not very good because of my back pain.
16. I have trouble putting on my socks (or stockings) because of pain in my back.
17. I only walk short distances because of my back pain.
18. I sleep less well because of my back.
19. Because of my back pain, I get dressed with help from someone else.
20. I sit down for most of the day because of my back.
21. I avoid heavy jobs around the house because of my back.
22. Because of my back pain, I am more irritable and bad tempered with people than usual.
23. Because of my back, I go upstairs more slowly than usual.
24. I stay in bed most of the time because of my back.

137
Appendix G
Short Form Health Survey, Version 2,
Standard Interview for SF-36 Health Survey

StaShort Form
andard Interv
m Health Sur
view for SF-rvey, Version-36 Health S
n 2 Survey
138

139

140

141

142
Appendix H
The Pain Catastrophizing Scale (PCAS)

143
Pain Catastrophizing Questionnaire
Okay, everyone experiences painful situations at some point in their lives. Such experiences may include headaches, tooth pain, joint pain, or muscle pain. People are often exposed to situations that may cause pain such as illness, injury, dental procedures, or surgery. We are interested in the types of thoughts and feelings that you have when you are in pain. Listed below are thirteen statements describing different thoughts and feelings that may be associated with pain. Using the following scale, please indicate the degree to which you have these thoughts and feelings when you are experiencing pain. 0—not at all 1—to a slight degree 2—to a moderate degree 3—to a great degree 4—all the time
Ask yourself, when I�’m in pain�… I worry all the time about whether the pain will end.
I feel I can�’t go on.
It�’s terrible and I think it�’s never going to get any better.
It�’s awful and I feel that it overwhelms me.
I feel I can�’t stand it any more.
I become afraid that the pain will get worse.
I keep thinking of other painful events.
I anxiously want the pain to go away
I can�’t seem to keep it out of my mind.
I keep thinking about how much it hurts.
I keep thinking about how badly I want the pain to stop.
There�’s nothing I can do to reduce the intensity of the pain.
I wonder whether something serious may happen.

144
CURRICULUM VITAE
JESSICA M. GUNDY Utah State University, 2810 Old Main Hill Logan, UT 84322-2810 323-351-5050 [email protected] EDUCATION
Ph.D. Utah State University, Logan, UT 2012 Combined Clinical/Counseling/School Psychology (APA Accredited)
Doctoral Dissertation: Outcomes and Presurgical Predictor Correlates of Lumbar Fusion in Utah Workers�’ Compensation Patients Chair: M. Scott DeBerard, Ph.D.
M.A. California State University, Los Angeles, CA 2007 General Psychology
Master’s Thesis: An Investigation of Eating Attitudes and Prevalence of Eating Disorders Among Students in Culinary Arts School Chair: Brigitte K. Matthies, Ph.D.
B.A. University of Montana, Missoula, MT 2001 Professional Psychology �– with Honors HONORS & AWARDS 2010-2011 Dissertation Fellowship ($5,000) - Utah State University 2008; 2009; 2010 Graduate School Travel Award (3-$300) - Utah State University 2008; 2009 Departmental Travel Award (3-$300) - Utah State University 2007-2008 Presidential Fellowship ($12,000) - Utah State University 2006-2007 Graduate Equity Fellowship ($1500) - CSU, Los Angeles 2006 Emeriti Fellowship ($1000) - CSU, Los Angeles 2006 Travel Conference Award ($600) - CSU, Los Angeles 1999-2001 Western Undergraduate Exchange Scholarship, University of Montana 1998-2001 Deans Lists - University of Montana 1999-Present Psi Chi National Honors Society 2000-Present Golden Key National Honors Society PROFESSIONAL ASSOCIATIONS America Psychology Association (APA), Division 12; Division 38, Student Member Utah Psychological Association (UPA), Student Member Society of Behavioral Medicine (SBM), Member Association for Contextual and Behavioral Sciences (ACBS), Student Member

145
Association for Behavioral and Cognitive Therapies (ABCT), Student Member CLINICAL EXPERIENCE
10/10-Present Behavioral Health Therapist - Clinical Health Practicum Logan Regional Hospital Cancer Center - Logan, UT
Brief assessment and individual psychotherapy services for patients diagnosed with various types of cancer; consultation with families, medical providers, and personnel; treatment targets end of life issues, treatment compliance, support system development, persistent pain, and behavioral activation. Supervisor: M. Scott DeBerard, Ph.D.
09/10-Present Advanced Student Therapist�–Child/Adolescent Practicum
Avalon Hills Residential Eating Disorders Program - Adolescent -Petersboro, UT Psychodiagnostic assessments and report writing; individual therapy with adolescents focused on body image; family therapy; peer-supervision; multidisciplinary consultation. Supervisors: Tera Lensegrav-Benson, Ph.D.
01/10-Present Graduate Assistant Therapist - Clinical Assistantship
Avalon Hills Residential/ Intensive Outpatient Eating Disorders Program, Adult Facility - Paradise, UT Individual therapy for residential and intensive outpatient adult patients; family therapy; transition coordination for patients�’ outpatient treatment team; primary therapist for experiential groups including acceptance and commitment therapy (ACT), mindfulness, dialectical behavior therapy (DBT), and process group; collaboration with multidisciplinary treatment team. Supervisors: Tera Lensegrav-Benson, Ph.D.; Martin Toohill, Ph.D., Michael P. Twohig, Ph.D. (consultation supervisor)
08/09-07/10 Behavioral Health Consultant/Liaison - Clinical Health Practicum
Student Health and Wellness Center - Utah State University Behavioral health services within an integrated primary care setting including intake assessments, individual psychotherapy, behavioral consultation services, and collaboration with primary care providers; targeted behavioral issues including eating disorders, obesity, chronic pain, treatment adherence, substance abuse, PTSD, ADD/ADHD. Supervisor: M. Scott DeBerard, Ph.D.
06/09-12/09 Graduate Student Therapist �– Practicum in Psychology Avalon Hills Residential Eating Disorders Program - Adolescent Unit -Petersboro, UT and Adult Unit - Paradise, UT Co-led experiential groups including recovery maintenance, ACT, mindfulness, spirituality, DBT skills, and process group; treatment team collaboration and consultation. Supervisors: Tera Lensegrav-Benson, Ph.D., Martin Toohill, Ph.D.
146
08/08-05/09 Graduate Student Therapist - Counseling Practicum Counseling and Psychological Services - Utah State University Individual and group counseling for students presenting with a variety of behavioral health issues (e.g., trauma, eating disorders, anxiety/mood disorders, stress management, insomnia); co-led DBT skills group; crisis consultations; outreach services (veterans and body-image workshops); mental health screenings; clinical case presentations. Direct Clinical Hours: 141; Total Hours: 464 Supervisors: David Bush, Ph.D., Jodie Benabe-Matz, Intern
08/07-05/08 Therapist in Training - Integrative Clinical Practicum
Psychology Community Clinic - Utah State University Mental health services for children, adolescents, and adults in the community; intake assessments; individual and family psychotherapy services; parent-training; psychoeducational assessments (e.g., LD, ADHD); comprehensive psychological evaluations; classroom observations; treatment planning; clinical case presentations. Supervisors: Susan L. Crowley, Ph.D., Gretchen Gimpel Peacock, Ph.D.
RELATED APPLIED CLINICAL EXPERIENCE June 2010 Veterans Affair Training Videos - Acceptance and Commitment
Therapy (ACT) for Combat and Military Sexual Trauma. Project Coordinator: Robyn Walser Role played the client role for training videos with a therapist who is an
expert in delivering ACT to veterans struggling with post-traumatic stress.
Spring 2009; 2010 Body Image Fair Counseling and Psychological Services - Utah State University
Provided presentation and exhibits on topics including �“Men�’s issues with body image�” and the National Eating Disorder Association (NEDA) slogan, �“Be comfortable in your genes.�”
Spring 2009 Residential Housing Couples Workshop
Counseling and Psychological Services - Utah State University Co-led 60-min presentation on dating and relationship issues. (2 workshops)
November 2008 Veteran’s Day Mental Health Awareness Outreach
Counseling and Psychological Services - Utah State University Provided information at a university veterans event about mental health conditions typical in veteran populations (e.g., substance abuse, depression PTSD); offered resources to help male and female veterans coping with transition issues associated with military service.
Fall 2008 University Student Anxiety Screening/Awareness
Counseling and Psychological Services - Utah State University Conducted brief anxiety screenings for students. (3 hours)
147
02/07-07/07 Applied Behavioral Therapist Autism Spectrum Therapies - Culver City, CA Extensive training in the principles of applied behavioral analysis; direct therapy services in a paid therapist position for individuals with autism and their families; taught acquisition and maintenance of appropriate social and academic skills.
RESEARCH EXPERIENCE
2008-Present Research Assistant - Lumbar Fusion Outcome Project Utah State University �– Department of Psychology Supervisor: M. Scott DeBerard, Ph.D. Co-developed project; co-principle investigator on grant; conducted all patient medical chart reviews; administered standardized outcome surveys; managed outcome data collection and analysis in SPSS; manuscript writing and submissions; multiple paper and poster presentations at professional conferences.
2009-Present Research Project Coordinator – Eating Disorder Outcome Studies
Utah State University - Center for Clinical Studies & Avalon Hills Residential Treatment Program
Supervisor: Michael P. Twohig, Ph.D. Evaluated multidisciplinary intervention for patients in a residential eating disorder facility; involvement in writing Institutional Review Board proposal and revisions; assisted in grant writing and submission; intervention implementation; data analysis of pre-post assessment; currently developing multiple-baseline study on an exposure-based and ACT intervention.
2006-2007 Research Project Coordinator - Culinary Student Eating Behavior
Study California State University, Los Angeles �– Department of Psychology Supervisor: Brigitte K. Matthies, Ph.D. Designed and coordinated study on eating behavior and attitudes for students in culinary arts school; participant recruitment; data collection, management in SPSS, and analysis; report writing.
2006-2007 Research Assistant - Women’s Health Project Lab
California State University, Los Angeles �– Department of Psychology Supervisor: Fary M. Cachelin, Ph.D. Examined treatment barriers for ethnic minority populations struggling with eating disorders; evaluated parental factors and treatment modalities for obesity and weight related concern in children; data management in SPSS; data analysis; report writing; conference presentation.
2006-2007 Research Assistant - Pasadena Pain Rehabilitation Institute
Pasadena, CA Supervisor: Harold Gottlieb, Ph.D., Phillip Corrado, Ph.D. Evaluated clinical correlates of psychogenic pain and attachment style;

148
data collection; data interpretation; MMPI interpretation; report writing. 1999-2001 Research Assistant - Early Infant Development and Attachment Project
University of Montana, Missoula �– Department of Psychology Supervisor: Lynne S. Koester, Ph.D.
Data collection for studies of contingency responding by mothers to infants; videotaped observation coding of mother-infant interaction; data entry. Supervisor: Paul Silverman, Ph.D. Conducted child and parent interviews; evaluated children�’s emotional coping strategies and adjustment to parental discord; reliability coding; data entry.
PEER REVIEWED PUBLICATIONS Deberard, M. S., Wheeler, A. J., Gundy, J. M. & Grew, J. (in press) Presurgical biopsychosocial
variables predict medical, compensation, and aggregate costs of percutaneous or open lumbar discectomy in Utah Workers�’ Compensation Patients. The Spine Journal.
Crosby, J. M., Gundy, J. M., Armstrong, A., Nye, E., Bowman, A., & Twohig, M. P. (2010).
How well are we doing at reporting participant characteristics in our research? The Behavior Therapist. 33, 125-147.
Gundy, J. M., Woidneck, M. R., Pratt, K. M., Christian, A. W., & Twohig, M. P. (in press).
Acceptance and Commitment Therapy: The state of the evidence in the field of health psychology. Scientific Review of Mental Health Practice.
BOOK CHAPTERS DeBerard, M. S., Gundy, J. M., Pratt, K. M, & Wheeler, A. J. (in press). Carpal Tunnel and
Rotator Cuff Surgeries. In A. R. Block & D. B. Sarwer (Eds.) Presurgical Psychological Screening: Understanding Patients, Improving Outcomes.
MANUSCRIPTS UNDER REVIEW Woidneck, M. R., Pratt, K. M., Gundy, J. M., Nelson, C., & Twohig, M. P. A Review of the
Effectiveness of Acceptance and Commitment Therapy with Minority Populations. Professional Psychology: Research and Practice.
Wheeler, A. J., Gundy, J. M., Deberard, M. S. Using presurgical psychological variables to
predict compensation and medical costs of lumbar fusion patients receiving workers�’ compensation in Utah. Spine.
MANUSCRIPTS IN PREPARATION Gundy, J. M., Crosby, J. M., Field, C. & Twohig, M. P. Evaluating the acceptability of
exposure-based treatment for children and adolescents: Client and therapist perspectives.
1998-2001 Research Assistant - Interparental Conflict and Child Adjustment Study
University of Montana, Missoula - Department of Psychology

149
Gundy, J. M., Mitchell, P. R., Lensegrav-Benson, T., Quakenbush-Roberts, B., & Twohig, M. P.
Quality of life outcomes for residential treatment of eating disorders. Matthies, B., Gundy, J. M., & Cachelin, F. Duration of culinary arts school training is associated
with increased scores on measures of eating disorders behaviors. CONFERENCE PRESENTATIONS Mitchell, P. R., Gundy, J. M., Lensegrav-Benson, T., Quakenbush-Roberts, B., & Twohig, M. P.
(2010). Quality of life outcomes for residential treatment of eating disorders. Poster to be presented at the Annual Convention of the Association for Behavioral and Cognitive Therapies in San Francisco, CA.
Gundy, J. M., Wheeler, A. J., & DeBerard, M. S. (2010). Biopsychosocial predictors of return to
work status in a sample of lumbar fusion worker’s compensation patients. Focus paper presentation at the North American Spine Society (NASS) Annual Meeting in Orlando, FL.
Wheeler, A. J., Gundy, J. M., & DeBerard, M. S. (2010). Presurgical biopsychosocial variables predict medical and compensation costs in compensated lumbar fusion patients: A look at recent changes. Focus paper presentation at the North American Spine Society Annual Meeting in Orlando, FL.
Gundy, J. M., Wheeler, A. J., & DeBerard, M. S. (2010). Cost effectiveness of case manager and
vocational rehabilitation services in a sample of lumbar fusion worker’s compensation patients. Poster presented at the Society of Behavioral Medicine�’s Annual Meeting and Scientific Sessions in Seattle, WA.
Wheeler, A. J., Gundy, J. M., & DeBerard, M. S. (2010). Using presurgical psychological
variables to predict compensation and medical costs of lumbar fusion patients receiving workers’ compensation in Utah. Poster presented at the Society of Behavioral Medicine�’s Annual Meeting and Scientific Sessions in Seattle, WA.
Woidneck, M. R., Pratt, K. M., Gundy, J. M., Nelson, C., & Twohig, M. P. (2010). A Review of
the Effectiveness of Acceptance and Commitment Therapy with Minority Populations. Poster presented at the Association for Contextual Behavioral Science World Conference VIII in Reno, NV.
Crosby, J. M., Gundy, J. M., Nye, E., Bowman, A., & Twohig, M. P. (2009). How well are we
doing at reporting participant characteristics in our research? Poster presented at the Annual Convention of the Association for Behavioral and Cognitive Therapies in New York, NY.
DeBerard, M. S., Gundy, J. M., Doty, J., Grewe, J. R., & LaCaille, R. A. (2009). The use of
retrospective-cohort designs in behavioral medicine research. Poster presented at the Society of Behavioral Medicine�’s Annual Meeting and Scientific Sessions in Montreal Quebec, Canada.

150
Gundy, J. M., Matthies, B., Cachelin, F., Regan, P. & DeBerard, M. S. (2008). Duration of culinary arts school training is associated with increased scores on measures of eating disorders behaviors. Poster presented at the Society of Behavioral Medicine�’s Annual Meeting and Scientific Sessions in San Diego, CA.
DeBerard, M. S., LaCaille, R. A., Spielmans, G. I., Parlin, M. A., Gundy, J. M. & Grew, J.
(2008). Patient satisfaction with the Utah workers’ compensation system following lumbar discectomy: A validity study. Poster presented at the Annual Meeting for the Society of Behavioral Medicine in San Diego, CA.
Gundy, J. M. & Cachelin, F. (2006). Differences in perceptions of food amounts between
purging-type and nonpurging type eating disordered women. Poster presented at the Obesity Society�’s Annual Scientific Meeting in Boston, MA.
Kamman, T., Gundy, J. M., & Koester, L. (2000). Infant emotions during variations in maternal
availability: Correlations with types of maternal contingency. Poster presented at the University of Montana Conference on Undergraduate Research in Missoula, MT.
Kamman, T., Gundy, J. M., and Silverman, P. (1999). The relationship between regulation of
emotional complexity and the use of denial as a coping strategy in children. Poster Presented at the Western Psychological Association Conference in Irvine, CA.
GRANT ACTIVITY
2008-2010 Research Co-Principle Investigator (funded) Lumbar fusion outcomes in Utah Workers�’ Compensation Patients: A
replication study. Amount: $30,000 Funding Source: Workers�’ Compensation Fund of Utah Principal Investigator: M. Scott DeBerard
April 2010 Research Co-Investigator (not funded) The relationship between biopsychosocial risk factors, perceived
workplace safety, and sustained injuries among Utah workers. Amount: $30,000 total Funding Source: Utah Labor Commission Principal Investigator: M. Scott DeBerard
February 2010 Research Co-Investigator (not funded) Cognitive Behavioral Therapy as a treatment for workers compensation
lumbar fusion patients with neuropathic back pain. Amount: $50,000 Funding Source: North American Spine Society Principal Investigator: M. Scott DeBerard
PROFESSIONAL DEVELOPMENT TRAINING June 2010 ACT in Real Time: A workshop to Actively Refine your ACT Skills.
Presenters: Robyn Walser, Ph.D.; Mary Sawyer, Ph.D. ACBS World Conference VIII in Reno, NV.
151
June 2010 Enhancing Values Work in Psychotherapy: Practical Tools and Exercises. Presenters: Joanne Dahl, Ph.D., Jennifer Plumb, M.A. ACBS World Conference VIII in Reno, NV.
June 2010 ACT With Challenging Patients.
Presenter: Kirk Strosahl, Ph.D. ACBS World Conference VIII in Reno, NV.
April 2010 An Integrated Approach to Complex Psychological Trauma.
Presenter: John Briere, Ph.D. 16th Annual Utah State University Counseling & Psychological Services Conference
June 2009 Professional Ethics Workshop: Ethical and Legal Aspects of
Supervision. Presenter: Stephen Behnke, J.D., Ph.D. Utah Psychological Association & Utah State University
April 2009 Two-Day Experiential Workshop on Acceptance and Commitment
Therapy. Presenter: Steven C. Hayes, Ph.D Utah State University, Logan, UT
April 2009 An Introduction to Acceptance and Commitment Therapy.
Presenter: Steven C. Hayes, Ph.D 15th Annual Utah State University Counseling & Psychological Services Conference
January 2009 Ethics and Ethical Decision Making for Utah Psychologist.
Presenter: Stephen Behnke, J.D., Ph.D. Utah Psychological Association & Utah State University, Logan, UT
October 2008 Acceptance and Values-Based Multicultural Training to Increase
Multicultural Competency and Engagement in Faculty Members and Graduate Students. Presenters: Michael P. Twohig, Ph.D. & Melanie D. Rodriguez, Ph.D. Utah State University, Logan, UT
Fall 2008 Seminar: Acceptance and Commitment Therapy. (3 credit semester)
Instructor: Michael P. Twohig, Ph.D. Utah State University, Logan, UT
TEACHING EXPERIENCE
Fall 2009 Course Instructor - Utah State University
Developmental Psychology: Conception to Adolescence Taught one semester covering key information on the basic aspects of developmental psychology; organized and executed lectures, used relevant demonstrations; assistant with student research proposals;
152
constructed quizzes and tests; held regular office hours; mentored TA assigned to course.
Summer 2008 Course Instructor - Utah State University
General Psychology Taught one semester covering introductory topics in psychology; planned and carried out instruction using a variety of teaching methods including lecturing, learning activities, and discussion; constructed quizzes and tests; allocated final grades.
2008-2010 Guest Lectures/Seminars - Utah State University Introduction to Psychology: Lab Series (2 lecture) Topic: Acceptance and Commitment Therapy for Eating Disorders. School Psychology Graduate Course (1 lecture) Topic: Self-Injury: What School Psychologists Should Know. History and Systems in Psychology (4 seminars) Topic: Seminar leader for undergraduate students on various topics
2006-2007 Teachers Assistant - California State University, Los Angeles
Introduction to Psychology (Fall/Spring/Winter quarters) Professor: Gaithri Fernando, Ph.D.
Obtained materials needed for classes; proctored examinations; maintained regular office hours to meet with students; graded examinations, assignments, and papers; recorded grades.
2006-2007 Teachers Assistant - California State University, Los Angeles
Experimental Psychology (Fall/Winter/Spring quarters) Professor: Fary M. Cachelin, Ph.D. Led discussions and laboratory sections; provided assistance to students in developing final research projects; managed and graded student assignments and research activities; proctored tests.
Copyright © 2022 FDOKUMEN