
Midwifery & Women's Health Nurse Practitioner Certification ...

Midwifery 28 (2012) e874–e879
Contents lists available at SciVerse ScienceDirect
Midwifery
0266-61
doi:10.1
n Corr
E-m
e.turkst
p.scuffh
journal homepage: www.elsevier.com/midw
A non-randomised trial investigating the cost-effectiveness of MidwiferyGroup Practice compared with standard maternity care arrangementsin one Australian hospital
Jocelyn Toohill, MMid, Grad Dip Educ, Grad Cert Hlth Mgmt (Lecturer)a,n, Erika Turkstra,PhD (Senior Lecturer)b, Jenny Gamble, PhD (Associate Professor, Deputy Head of School)a,Paul A. Scuffham, PhD (Professor)c
a School of Nursing and Midwifery, Research Centre for Clinical and Community Practice Innovation, Griffith University, University Drive,
Meadowbrook 4131, Australiab Health Technology Assessment, School of Medicine Griffith University, University Drive, Meadowbrook 4131, Australiac Health Economics, School of Medicine Griffith University, University Drive, Meadowbrook 4131, Australia
a r t i c l e i n f o
Article history:
Received 9 December 2010
Received in revised form
10 October 2011
Accepted 31 October 2011
Keywords:
Midwifery Group Practice
Birth centre
Cost-effectiveness
Continuity of carer
38/$ - see front matter & 2011 Elsevier Ltd. A
016/j.midw.2011.10.012
esponding author.
ail addresses: [email protected], jtoohil
[email protected] (E. Turkstra), j.gamble@gri
[email protected] (P.A. Scuffham).
a b s t r a c t
Objective: to compare cost-effectiveness of two models of maternity service delivery: Midwifery Group
Practice (MGP) at a birth centre and standard care (SC).
Design: a prospective non-randomised trial.
Setting: an Australian metropolitan hospital.
Method: women at 36 weeks gestation were approached in the birth centre or hospital antenatal clinics
between March and December 2008. Of 170 consecutive women who met birth centre eligibility
criteria, 70% (n¼119) were recruited to the study. Women (MGP n¼52 or standard care n¼50) were
followed through to 6 weeks postpartum. Publically funded care costs were collected from women’s
diaries, handheld pregnancy health records, medical records and the hospital accounting system. Main
outcome measures: health-care costs to the hospital and government.
Analysis: generalised linear models with covariates of age, nulliparity, private health insurance (yes/no)
and household income category.
Findings: women receiving MGP care were less likely to experience induction of labour, required fewer
antenatal visits, received more postnatal care, and neonates were less likely to be admitted to special care
nursery than those receiving standard care. Statistically significant lower costs were found for women
and babies receiving MGP care compared with women receiving standard care during pregnancy, labour
and birth and postpartum to 6 weeks. MGP resulted in lower costs for the hospital ($AUD4,696 vs.
$AUD5,521 po0.001) and the government ($AUD4,722 vs. $AUD5,641 po0.001). When baby costs were
excluded MGP care remained statistically significantly cheaper than standard care.
Conclusion: for women at low-risk of birth complications, Midwifery Group Practice was cost effective,
and women experienced fewer obstetric interventions compared with standard maternity care. The
evidence suggests Midwifery Group Practice is safe and economically viable.
& 2011 Elsevier Ltd. All rights reserved.
Introduction
Midwifery service delivery models have a philosophy to providecontinuity of woman-centred care. However implementation ofthese models is inconsistent within countries, and throughout theworld. Variations include diversity in setting, midwife to woman
ll rights reserved.
[email protected] (J. Toohill),
ffith.edu.au (J. Gamble),
ratio, duration and number of visits, length of hospital stay, gestationat booking and duration of care after birth. Consequently the mostcost-effective model is unknown (Henderson and Petrou, 2008).
In Australia, team midwifery incorporating antenatal care in a
community setting (Homer et al., 2001) and Midwifery Group
Practice in a stand-alone unit have been found to be cost effective
(Tracy and Hartz, 2006). A comparison of birth centre care alongside
a tertiary level conventional delivery suite found no difference in
costs (Byrne et al., 2000). However, rostered team midwifery in
a stand-alone birth centre showed slightly higher birth costs
compared with public hospital birth (Senate Community Affairs

J. Toohill et al. / Midwifery 28 (2012) e874–e879 e875
References Committee, 1999). No study in Australia or internation-ally that we could find, has specifically investigated salaried Mid-wifery Group Practice (MGP) within a birth centre offering homeantenatal and postnatal visiting compared with standard care.
Publicly funded midwifery models are becoming more prevalent,albeit slowly, in response to consumer demand, research evidence,and government reviews and inquiries (Senate Community AffairsReferences Committee, 1999; Maternity Coalition, 2002; Hatemet al., 2008; Department of Health and Ageing, 2009). In 2005, areview of maternity services in the Australian state of Queenslandcalled ‘Rebirthing’ echoed findings of previous state/territory andnational reviews and recommended improving women’s access tocontinuity of care and carer (Hirst, 2005). A priority area for actionwas addressing the widespread poor quality of post birth care.Consequently, in 2006 a birth centre was established at the GoldCoast Hospital (GCH), which has around 3,500 births/year. The birthcentre was staffed by midwives working within a Midwifery GroupPractice, founded on primary health-care principles (Thorogood,2010). This study compares costs and maternal and newborn out-comes of MGP within the Gold Coast Birth Centre with standardcare at the same publicly funded hospital sharing one set of clinicalguidelines.
Midwifery Group Practice (MGP)
Three full-time midwives with a personal caseload of 40women per year work in each Midwifery Group Practice (MGP).Two MGPs operate within the birth centre with a total combinedcaseload of 240 women annually. Midwives are not rostered toshifts, but within each group practice provide backup for eachother through an on-call arrangement. This arrangement ensureswomen have their primary midwife or a known midwife available24 hrs a day from booking until 6 weeks postpartum.
Most women in MGP give birth in the centre and are usuallyhome within 4 hrs of birth. Home-based care for pregnancy, earlylabour and postnatal care to 6 weeks postpartum is a feature ofMGP. MGP spans the same geographic area as that of postnatalhome visiting as part of standard care. Postnatal home careincludes mother and baby physical and psychosocial health checks,promotion and support of breast feeding, early parenting andgeneral health education, and linking families to appropriateagencies according to their needs. A dedicated obstetrician isattached to each MGP and women attend that consultant’s antena-tal clinic should complications arise. If women birth in the hospitalbirth suite or operating theatre, continuity of care is maintained byher MGP midwife until 6 weeks postpartum. Women in this modelexperience 75% attendance of their primary midwife or 92%attendance of a MGP midwife for labour and birth (Toohill, 2008).
Standard care
In standard care, women have the option of attending ageneral practitioner, a hospital midwife at a community outreachcentre, a hospital midwife clinic or an obstetric clinic at thehospital for pregnancy check-ups. Routine visits are scheduled inthe outpatient obstetric clinic at 36 and 41 weeks gestation.Intrapartum and postnatal care is provided by rostered midwiferyand medical staff, with optional postnatal home visiting for up to7 days postpartum. Services following discharge are provided bycommunity child health nurses and general practitioners.
Method
A non-randomised pilot study following the TREND statement(Des Jarlais et al., 2004) was designed to assess the costs and
outcomes of MGP and standard care. A total study sample of 100‘low obstetric risk’ woman, who met birth centre eligibility criteria,was required for the study. Women self-selected for their model ofcare; but access to MGP was limited due to capacity. Women’shealth records were reviewed to determine if they met theeligibility criteria for the study prior to seeking consent. Thisincluded meeting the birth centre eligibility criteria, living withinthe defined geographic catchment area, and commencing care atthe Gold Coast Hospital prior to 24 weeks gestation. Eligibilitycriteria were determined against a ‘well woman’ health checklistand meeting suitability for midwifery care (Australian College ofMidwives, 2008). The groups were not matched for baselinedemographics. Recruitment occurred at the woman’s 36 weekantenatal appointment. Women were provided with verbal andwritten information prior to consenting to participate in the study.
Measures and data collection procedures
At recruitment, women completed baseline demographicinformation and were provided with a diary to record whereand with whom maternity visits occurred. At 6 weeks post birthwomen returned their diary of care in a post paid envelope to theresearch assistant.
Costs were collected from two perspectives: the hospitalperspective and the federal government perspective in Australiandollars. The latter included costs for mother and baby primarycare visits (antenatal and postnatal) with general practitioners.Using the medical record number for the mother and baby, thehospital Decision Support Services team provided all hospitalcosts attributed to the woman and her baby by applying standardhospital processes in determining hospital costs. This processinvolves medical coders reviewing the medical record and align-ing episodes of care and procedures to Australian-Refined Diag-nostic-Related Groupings (Department of Health and Ageing,2006). Any costs not attached directly to the maternity episodewere not used. All costs to the hospital from 36 weeks gestationto 6 weeks postpartum were included. Regardless of change torisk status or intended place of birth (birth centre or birth suite),women’s costs were analysed by intended mode of care.
Research assistants cross-checked visits, admission, birth anddischarge dates against the women’s diaries, medical records andhospital activity system. The first author identified any costoutliers in the data and a research assistant checked accuracyagainst care received. Decision Support Services were alerted ifcare and cost did not align, with women removed from the studyif gross inaccuracies were confirmed.
The number of general practitioner visits was extracted fromeach woman’s diary or pregnancy handheld record (PHHR).The PHHR is a comprehensive booklet that the woman carriesthroughout pregnancy to provide her with maternity informationand ownership of her care, and a space for her to record her birthplan. It is used by care providers to document the woman’s healthand obstetric history and care provided throughout pregnancy.Each general practitioner visit was costed using Medicare BenefitsSchedule item number 16,500 (Department of Health and Ageing,2008) (Schedule July 2008, $AUD38.65 per visit).
Ethics approval was granted from the hospital and universityhuman research ethics committees.
Data analysis
All statistical analyses were performed using SPSS (version17.0). For baseline characteristics, Pearson w2 tests were used forcategorical data and Student’s t-tests were used for continuousdata to assess differences in baseline characteristics betweenMGP and SC. For all outcomes, data were analysed using

J. Toohill et al. / Midwifery 28 (2012) e874–e879e876
generalised linear models (univariate analysis of variance forcontinuous data and logistic models for categorical data) withcovariates of age, nulliparity, private health insurance (yes/no),and household income category. These covariates were includedas they may impact on outcomes. Statistical significance wasdetermined using p-value o0.05.
Findings
A research midwife randomly attended birth centre or hospi-tal antenatal clinics at an average of 1–2 4 hrs clinics per week torecruit participants. Between March and December 2008, 170consecutive women who met birth centre eligibility criteria(MGP n¼70, SC n¼100) were approached for participation inthe study. A non-randomised sample of 119 women (70%) wererecruited to the study at 36 weeks gestation (MGP n¼58 orstandard care n¼61). Seventeen women were not included inthe final analysis (Fig. 1) for the following reasons: consent notcompleted (n¼2) did not give birth at GCH (n¼2), withdrewconsent at follow-up (n¼11), and other (n¼2). This resulted in102 women remaining in the study (MGP n¼52; SC n¼50).Standard Care consisted of women receiving antenatal care witha GP n¼29 (58%), obstetric clinic n¼10 (20%) or midwives clinicn¼11 (22%). Participant characteristics were similar across thetwo groups except women accessing MGP were more likely tohave higher family income (p¼0.003) and private health insur-ance (po0.001) (Table 1).
There were significant differences in the outcomes for womenand their babies between the two models of service delivery.Women receiving standard care had more antenatal visits(p¼0.001), but fewer postnatal visits consistent with a reducedperiod of postnatal care in that model (po0.001) (Table 1). Fewerwomen in MGP used pharmacologic pain relief in labour comparedto women receiving standard care (pethidine, p¼0.058, epiduralp¼0.001 and nitrous oxide po0.001) with epidural use threetimes higher in standard care (Table 2). Additionally womenreceiving standard care were more likely to have labour induced(p¼0.026), and less likely to experience an operative vaginal birth(p¼0.024) (Table 2). More women receiving standard care experi-enced a caesarean section (n¼7) compared with MGP (n¼3) butthis difference was not statistically significant (p¼0.51).
Newborns to mothers receiving standard care were admitted tospecial care nursery four times more frequently compared to MGP(p¼0.028) (Table 2), and stayed in the nursery longer (SC¼42.3 hrs;MGP¼23.6 hrs; p¼0.026). There was no difference between groupsfor duration of stay in the birthing environment (MGP¼9.6 hrs;SC¼12.4 hrs; p¼0.164). However women using MGP went homeearlier (MGP¼18.0 hrs; SC¼53.1 hrs; po0.001), significantly redu-cing postnatal bed occupancy rates. There was insufficient data todraw statistically significant conclusions on breast-feeding out-comes and this may have been due to lower reporting of thisoutcome in the women’s records. The available data indicated thatwomen in MGP were more likely to fully breast feed following birth(MGP n¼47, 92%; SC n¼38, 78%; p¼0.230), on discharge (MGPn¼45, 88%; SC n¼38, 76%; p¼0.065) and at 6 weeks postnatal(MGP n¼27, 82%; SC n¼13, 59%; p¼0.332). Only 55 womenreported on feeding patterns at 6 weeks (MGP n¼33, SC n¼22).Postnatal readmissions were low (MGP n¼1; SC n¼3) with mean-ingful statistical analysis not able to be determined. Twenty-threeper cent of women required transfer from MGP to collaborativeobstetric care (n¼6, 11.5% in pregnancy, n¼6, 11.5% during labour,none postpartum) with continuity of midwifery care continued andcosts attributed to booked model of care.
A breakdown of care showed that antenatal costs across thetwo models were the same, labour costs were statistically higher
in standard care, with postnatal costs statistically higher in MGP.When compared overall there was a statistically significant lowercost associated with MGP compared to standard care (MGP$4,696 vs. SC $5,521, po0.001) based on the hospital costingsystem and when assessed against Federal government healthfunding arrangements (MGP $4,722 vs. SC $5,641, po0.001)(Table 3). After removing newborn costs, standard care remainedmore expensive (MGP $4,418 vs. SC $4,871, po0.001).
Discussion
For pregnant women at low-risk of birth complications, careprovided through a Midwifery Group Practice model of servicedelivery was less costly and women experienced fewer birthinterventions compared to a similar group of women receivingstandard maternity care. There was no mortality and no signifi-cant morbidity for women or babies between the two groups. Thisis consistent with existing published research showing continuityof midwifery care to be safe for women and babies, and satisfyingfor women (Hatem et al., 2008). Adopting a primary health modelof care, providing women with home-based visiting across thecontinuum, and increasing postnatal care provided better out-comes. Women entered spontaneous labour more often, werehome earlier, babies were admitted to nursery less often, andthere were fewer unplanned presentations to hospital.
Methods used to determine cost-effectiveness of midwiferymodels of service delivery vary (Henderson and Petrou, 2008).This is particularly so where there is a birth centre separate tothat of a hospital birth suite and where antenatal and postnatalhome visits are provided.
Difficulties in establishing comparative costs of midwiferymodels stem from different reporting and payment methods, skillmix complements, contexts of care (team or caseload, birth centreor freestanding centre, hospital or community care). Generally,hospital administrators compare cost centre reports to determinehow budgets are running. With a birth centre operating alongsidea main birth suite, cost centre reports do not provide a compar-ison of cost-effectiveness due to the different activities, skill mixand context of care. Therefore, this study used the hospital’saccounting system to track women’s care and costs. This studycommenced comparison from 36 weeks gestation as this was atime when all women were reviewed at the hospital regardless ofmodel of service delivery. Consistent with a previous study, wefound that community or home antenatal visits through MGPwere cost effective and women required less visits overall thanwomen in SC (Young et al., 1997).
Compared with other studies, it has been suggested thatsalaried midwifery models in the UK NHS require a mediancaseload of 39 women per midwife per year (Young et al.,1997), and in the USA that transfer rates from a free standingbirth centre to obstetric care must remain below 62% (Stone andWalker, 1995) to be cost neutral. In our study, midwives werepaid an annual salary under the state industrial award to care for40 women per year across the maternity continuum (QueenslandIndustrial Relations Commission, 2006, p. 27), and there was a23% transfer from birth centre to collaborative obstetric care withMGP continuity. The cost findings indicated that the lowerhospital resource use and improved clinical outcomes in theMGP model provided savings to support home visiting through-out pregnancy and up to 6 weeks following birth.
Assumptions that midwives on annualised salaries increasecosts of maternity care are not borne out in this study. Impor-tantly, cost must be assessed in context of the overall package ofcare. While MGP postnatal homecare to 6 weeks following birth
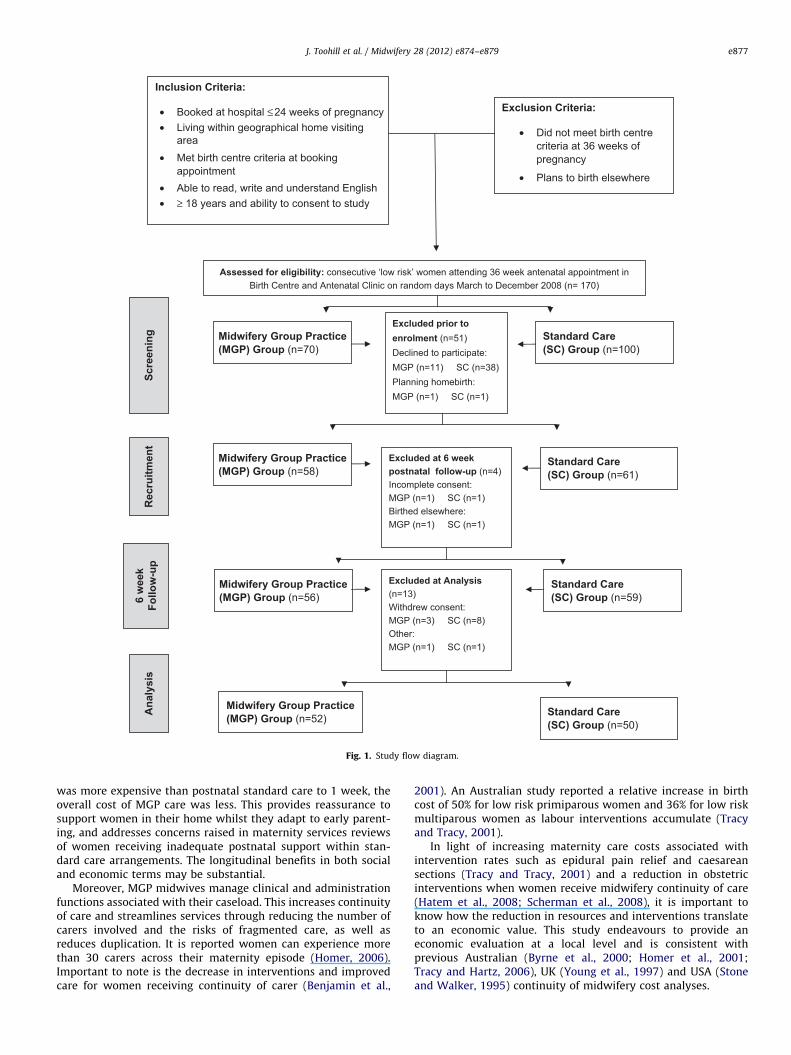
Assessed for eligibility: consecutive ‘low risk’ women attending 36 week antenatal appointment inBirth Centre and Antenatal Clinic on random days March to December 2008 (n= 170)
Inclusion Criteria:
• Booked at hospital ≤24 weeks of pregnancy • Living within geographical home visiting
area• Met birth centre criteria at booking
appointment• Able to read, write and understand English• ≥ 18 years and ability to consent to study
Exclusion Criteria:
• Did not meet birth centrecriteria at 36 weeks ofpregnancy
• Plans to birth elsewhere
Midwifery Group Practice(MGP) Group (n=70)
Standard Care(SC) Group (n=100)
Excluded prior toenrolment (n=51)Declined to participate:MGP (n=11) SC (n=38)Planning homebirth:MGP (n=1) SC (n=1)
Midwifery Group Practice(MGP) Group (n=58)
Standard Care(SC) Group (n=61)
Midwifery Group Practice(MGP) Group (n=52)
Scre
enin
gR
ecru
itmen
t
Midwifery Group Practice(MGP) Group (n=56)
Excluded at 6 weekpostnatal follow-up (n=4)Incomplete consent:MGP (n=1) SC (n=1)Birthed elsewhere:MGP (n=1) SC (n=1)
Standard Care(SC) Group (n=59)6
wee
kFo
llow
-up
Excluded at Analysis(n=13)Withdrew consent:MGP (n=3) SC (n=8)Other:MGP (n=1) SC (n=1)
Ana
lysi
s
Standard Care(SC) Group (n=50)
Fig. 1. Study flow diagram.
J. Toohill et al. / Midwifery 28 (2012) e874–e879 e877
was more expensive than postnatal standard care to 1 week, theoverall cost of MGP care was less. This provides reassurance tosupport women in their home whilst they adapt to early parent-ing, and addresses concerns raised in maternity services reviewsof women receiving inadequate postnatal support within stan-dard care arrangements. The longitudinal benefits in both socialand economic terms may be substantial.
Moreover, MGP midwives manage clinical and administrationfunctions associated with their caseload. This increases continuityof care and streamlines services through reducing the number ofcarers involved and the risks of fragmented care, as well asreduces duplication. It is reported women can experience morethan 30 carers across their maternity episode (Homer, 2006).Important to note is the decrease in interventions and improvedcare for women receiving continuity of carer (Benjamin et al.,
2001). An Australian study reported a relative increase in birthcost of 50% for low risk primiparous women and 36% for low riskmultiparous women as labour interventions accumulate (Tracyand Tracy, 2001).
In light of increasing maternity care costs associated withintervention rates such as epidural pain relief and caesareansections (Tracy and Tracy, 2001) and a reduction in obstetricinterventions when women receive midwifery continuity of care(Hatem et al., 2008; Scherman et al., 2008), it is important toknow how the reduction in resources and interventions translateto an economic value. This study endeavours to provide aneconomic evaluation at a local level and is consistent withprevious Australian (Byrne et al., 2000; Homer et al., 2001;Tracy and Hartz, 2006), UK (Young et al., 1997) and USA (Stoneand Walker, 1995) continuity of midwifery cost analyses.
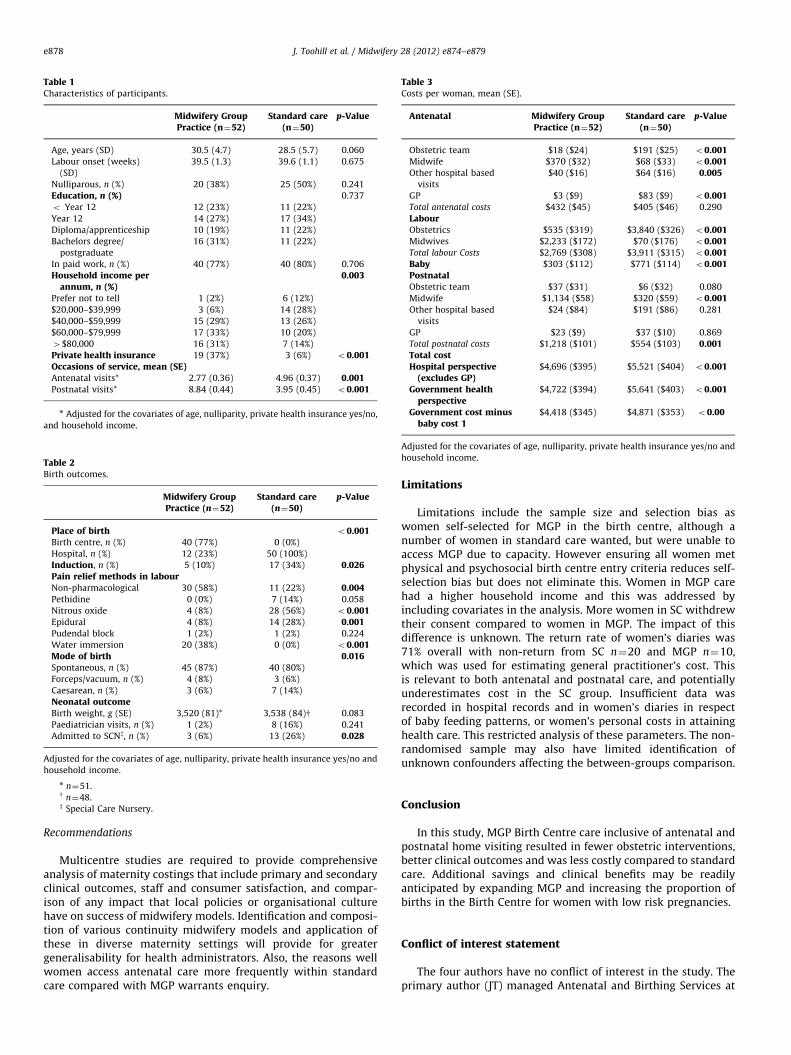
Table 1Characteristics of participants.
Midwifery GroupPractice (n¼52)
Standard care(n¼50)
p-Value
Age, years (SD) 30.5 (4.7) 28.5 (5.7) 0.060
Labour onset (weeks)
(SD)
39.5 (1.3) 39.6 (1.1) 0.675
Nulliparous, n (%) 20 (38%) 25 (50%) 0.241
Education, n (%) 0.737
o Year 12 12 (23%) 11 (22%)
Year 12 14 (27%) 17 (34%)
Diploma/apprenticeship 10 (19%) 11 (22%)
Bachelors degree/
postgraduate
16 (31%) 11 (22%)
In paid work, n (%) 40 (77%) 40 (80%) 0.706
Household income perannum, n (%)
0.003
Prefer not to tell 1 (2%) 6 (12%)
$20,000–$39,999 3 (6%) 14 (28%)
$40,000–$59,999 15 (29%) 13 (26%)
$60,000–$79,999 17 (33%) 10 (20%)
4$80,000 16 (31%) 7 (14%)
Private health insurance 19 (37%) 3 (6%) o0.001Occasions of service, mean (SE)Antenatal visits* 2.77 (0.36) 4.96 (0.37) 0.001Postnatal visits* 8.84 (0.44) 3.95 (0.45) o0.001
n Adjusted for the covariates of age, nulliparity, private health insurance yes/no,
and household income.
Table 2Birth outcomes.
Midwifery GroupPractice (n¼52)
Standard care(n¼50)
p-Value
Place of birth o0.001Birth centre, n (%) 40 (77%) 0 (0%)
Hospital, n (%) 12 (23%) 50 (100%)
Induction, n (%) 5 (10%) 17 (34%) 0.026Pain relief methods in labourNon-pharmacological 30 (58%) 11 (22%) 0.004Pethidine 0 (0%) 7 (14%) 0.058
Nitrous oxide 4 (8%) 28 (56%) o0.001Epidural 4 (8%) 14 (28%) 0.001Pudendal block 1 (2%) 1 (2%) 0.224
Water immersion 20 (38%) 0 (0%) o0.001Mode of birth 0.016Spontaneous, n (%) 45 (87%) 40 (80%)
Forceps/vacuum, n (%) 4 (8%) 3 (6%)
Caesarean, n (%) 3 (6%) 7 (14%)
Neonatal outcomeBirth weight, g (SE) 3,520 (81)* 3,538 (84)y 0.083
Paediatrician visits, n (%) 1 (2%) 8 (16%) 0.241
Admitted to SCNz, n (%) 3 (6%) 13 (26%) 0.028
Adjusted for the covariates of age, nulliparity, private health insurance yes/no and
household income.
n n¼51.y n¼48.z Special Care Nursery.
Table 3Costs per woman, mean (SE).
Antenatal Midwifery GroupPractice (n¼52)
Standard care(n¼50)
p-Value
Obstetric team $18 ($24) $191 ($25) o0.001Midwife $370 ($32) $68 ($33) o0.001Other hospital based
visits
$40 ($16) $64 ($16) 0.005
GP $3 ($9) $83 ($9) o0.001Total antenatal costs $432 ($45) $405 ($46) 0.290
LabourObstetrics $535 ($319) $3,840 ($326) o0.001Midwives $2,233 ($172) $70 ($176) o0.001Total labour Costs $2,769 ($308) $3,911 ($315) o0.001Baby $303 ($112) $771 ($114) o0.001PostnatalObstetric team $37 ($31) $6 ($32) 0.080
Midwife $1,134 ($58) $320 ($59) o0.001Other hospital based
visits
$24 ($84) $191 ($86) 0.281
GP $23 ($9) $37 ($10) 0.869
Total postnatal costs $1,218 ($101) $554 ($103) 0.001Total costHospital perspective
(excludes GP)$4,696 ($395) $5,521 ($404) o0.001
Government healthperspective
$4,722 ($394) $5,641 ($403) o0.001
Government cost minusbaby cost 1
$4,418 ($345) $4,871 ($353) o0.00
Adjusted for the covariates of age, nulliparity, private health insurance yes/no and
household income.
J. Toohill et al. / Midwifery 28 (2012) e874–e879e878
Recommendations
Multicentre studies are required to provide comprehensiveanalysis of maternity costings that include primary and secondaryclinical outcomes, staff and consumer satisfaction, and compar-ison of any impact that local policies or organisational culturehave on success of midwifery models. Identification and composi-tion of various continuity midwifery models and application ofthese in diverse maternity settings will provide for greatergeneralisability for health administrators. Also, the reasons wellwomen access antenatal care more frequently within standardcare compared with MGP warrants enquiry.
Limitations
Limitations include the sample size and selection bias aswomen self-selected for MGP in the birth centre, although anumber of women in standard care wanted, but were unable toaccess MGP due to capacity. However ensuring all women metphysical and psychosocial birth centre entry criteria reduces self-selection bias but does not eliminate this. Women in MGP carehad a higher household income and this was addressed byincluding covariates in the analysis. More women in SC withdrewtheir consent compared to women in MGP. The impact of thisdifference is unknown. The return rate of women’s diaries was71% overall with non-return from SC n¼20 and MGP n¼10,which was used for estimating general practitioner’s cost. Thisis relevant to both antenatal and postnatal care, and potentiallyunderestimates cost in the SC group. Insufficient data wasrecorded in hospital records and in women’s diaries in respectof baby feeding patterns, or women’s personal costs in attaininghealth care. This restricted analysis of these parameters. The non-randomised sample may also have limited identification ofunknown confounders affecting the between-groups comparison.
Conclusion
In this study, MGP Birth Centre care inclusive of antenatal andpostnatal home visiting resulted in fewer obstetric interventions,better clinical outcomes and was less costly compared to standardcare. Additional savings and clinical benefits may be readilyanticipated by expanding MGP and increasing the proportion ofbirths in the Birth Centre for women with low risk pregnancies.
Conflict of interest statement
The four authors have no conflict of interest in the study. Theprimary author (JT) managed Antenatal and Birthing Services at

J. Toohill et al. / Midwifery 28 (2012) e874–e879 e879
Gold Coast Hospital during the initial period of the study, fromFebruary to September 2008. Another author (JG) is a visitingscholar at Gold Coast Hospital. However these roles do notconflict with the study.
Acknowledgements
We appreciate support for this study provided by the ResearchCentre for Clinical and Community Practice Innovation at GriffithUniversity and a small grant from the Gold Coast HospitalFoundation. Personnel assisting data collection were Sandra Ryan& Natasha Pryde (Decision Support Services, Gold Coast Hospital),and research assistants Faith Hohaia, Cas McCulloch, Judy Batkin,Julie Fickel, Di Craig and Karen Milner. In addition, the commentsreceived from Prof Debra Creedy (School of Nursing, NationalUniversity of Singapore) on an earlier draft are greatly appre-ciated and have helped refine the presentation of this manuscript.
References
Australian College of Midwives, 2008. National Midwifery Guidelines for Con-sultation and Referral. 2nd edn. Australian Capital Territory. /http://midwives.rentsoft.biz/lib/pdf/ConsultationandReferralGuidelines2010.pdfS (lastaccessed 30 August 2010).
Benjamin, Y., Walsh, D., Taub, N., 2001. A comparison of partnership caseloadmidwifery care with conventional team midwifery care: labour and birthoutcomes. Midwifery 17, 234–240.
Byrne, J., Crowther, C., Moss, J., 2000. A randomised controlled trial comparingbirthing centre care with delivery suite care in Adelaide, Australia. Australianand New Zealand Journal of Obstetrics & Gynaecology 40, 268–274.
Department of Health and Ageing, 2006. Australian Refined Diagnosis RelatedGroups (AR-DRGs) AR-DRG V5.2. Australian Government (last accessed4 October 2010)/http://www.health.gov.au/internet/main/publishing.nsf/Content/health-casemixardrg1.htmS.
Department of Health and Ageing, MBS online July 2008 /http://www.health.gov.au/internet/mbsonline/publishing.nsf/Content/Medicare-Benefits-Schedule-MBS-1S (last accessed 4 October 2010).
Department of Health and Ageing, 2009. Report of the Maternity Services Review.Australian Government, Canberra.
Des Jarlais, D.C., Lyles, C., Crepaz, N., 2004. Improving the reporting quality of
nonrandomized evaluations of behavioral and public health interventions: theTREND statement. American Journal of Public Health 94 (3), 361–366 (last
accessed 29 September 2011).Hatem, M., Sandall, J., Devane, D., Soltani, H., Gates, S., 2008. Midwife-led versus
other models of care for childbearing women. Cochrane Database of Systema-tic Reviews 4. doi:10.1002/14651858.CD004667.pub2 art. no.: CD004667.
Henderson, J., Petrou, S., 2008. Economic Implications of home births and birth
centers: a structured review. Birth 35, 136–146.Hirst, C., 2005. Rebirthing—Report of the Review of Maternity Services in Queens-
land. Brisbane, Queensland Government Printer.Homer, C., Matha, D., Jordan, L., Wills, J., Davis, K., 2001. Community-based
continuity of midwifery care versus standard hospital care: a cost analysis.Australian Health Review 24, 85–93.
Homer, C., 2006. Challenging midwifery care, challenging midwives and challen-ging the system. Women & Birth 19, 79–83.
Maternity Coalition, 2002. Australian Maternity Action Plan. Birth Matters 6, 4–25.Queensland Industrial Relations Commission, 2006. Nurses (Queensland Health)
Certified Agreement (EB6) /http://www.health.qld.gov.au/eb/agreements/nurses.pdfS (last accessed 30 November 2010).
Scherman, S., Smith, J., Davidson, M., 2008. The first year of a midwifery-led modelof care in far north Queensland. Medical Journal of Australia 188, 85–88.
Senate Community Affairs References Committee, 1999. Rocking the Cradle. AReport Into Childbirth Procedures. Commonwealth Government, Canberra.
Stone, P., Walker, P., 1995. Cost-effectiveness analysis: birth center vs. hospitalcare. Nursing Economics 13, 299–308.
Thorogood, C., 2010. Challenges to women’s health. In: Pairman, S., Tracy, S.,
Thorogood, C., Pincombe, J. (Eds.), Midwifery Preparation for Practice. , Else-vier, Australia, pp. 128–161.
Toohill, J., 2008. Gold Coast Birth Centre—First 12 Month Review. QueenslandHealth, Australia.
Tracy, S., Tracy, M., 2001. Costing the cascade: estimating the cost of increasedobstetric intervention in childbirth using population data. BJOG—An Interna-tional Journal of Obstetrics and Gynaecology 110, 717–724.
Tracy, S., Hartz, D., 2006. The Quality Review of Ryde Midwifery Group Practice,September 2004 to October 2005: Final Report. Sydney, Northern Sydney and
Central Coast Health.Young, D., Lees, A., Twaddle, S., 1997. The costs to the NHS of maternity care:
midwife managed vs. shared. British Journal of Midwifery 5, 465–472.
Copyright © 2022 FDOKUMEN




















