
A multivariate approach linking reported side effects of clinical antidepressant and antipsychotic...
12
A multivariate approach linking reported side effects of clinical antidepressant and antipsychotic trials to in vitro binding affinities Johanna Michl a , Christian Scharinger b , Miriam Zauner b , Siegfried Kasper b , Michael Freissmuth c , Harald H. Sitte c , Gerhard F. Ecker a,n , Lukas Pezawas b a Department of Pharmaceutical Chemistry, University of Vienna, Vienna, Austria b Department of Psychiatry and Psychotherapy, Medical University Vienna, Vienna, Austria c Department of Pharmacology, Medical University Vienna, Vienna, Austria Received 28 February 2014; received in revised form 23 June 2014; accepted 26 June 2014 KEYWORDS Schizophrenia; Depressive disorder; Antidepressive agents; Antipsychotic agents; Clinical pharmacol- ogy; Adverse effects Abstract The vast majority of approved antidepressants and antipsychotics exhibit a complex pharma- cology. The mechanistic understanding of how these psychotropic medications are related to adverse drug reactions (ADRs) is crucial for the development of novel drug candidates and patient adherence. This study aims to associate in vitro assessed binding affinity profiles (39 compounds, 24 molecular drug targets) and ADRs (n = 22) reported in clinical trials of antidepressants and antipsychotics (n459.000 patients) by the use of robust multivariate statistics. Orthogonal projection to latent structures (O-PLS) regression models with reasonable predictability were found for several frequent ADRs such as nausea, diarrhea, hypotension, dizziness, headache, insomnia, sedation, sleepiness, increased sweating, and weight gain. Results of the present study support many well-known pharmacological principles such as the association of hypotension and dizziness with α 1 -receptor or sedation with H 1 -receptor antagonism. Moreover, the analyses revealed novel or hardly investigated mechanisms for www.elsevier.com/locate/euroneuro http://dx.doi.org/10.1016/j.euroneuro.2014.06.013 0924-977X/& 2014 Published by Elsevier B.V. Abbreviations: 5-HT, 5-hydroxy tryptamine (serotonin); 5-HTT, serotonin transporter; AAP, atypical antipsychotics; ACH, acetylcholine; ADR, adverse drug reaction; AP, antipsychotic; CDSR, cochrane database of systematic reviews; CTZ, chemotrigger zone; DAT, dopamine transporter; EMA, european medicines agency; EPMS, extrapyramidal motor symptoms; FDA, food and drug administration; GI, gastrointestinal; K i , inhibition constant; MAO, monoamine oxidase; MDD, major depressive disorder; NDRI, norepinephrine-dopamine re-uptake inhibitor; NET, norepinephrine transporter; O-PLS, orthogonal projection to latent structures; PDSP, psychoactive drugs screening program; p 1 , principal component 1; pK i , negative common logarithm of K i ; PRESS, prediction error sum of squares; SARI, serotonin antagonist and re-uptake inhibitor; SD, standard deviation; SNRI, serotonin norepinephrine re-uptake inhibitor; SSRI, selective serotonin re-uptake inhibitor; TAP, typical antipsychotic; TCA, tricyclic antidepressant; TeCA, tetracyclic antidepressant n Corresponding author. Tel.: + 43 1 4277 55110; fax: + 43 1 4277 855110. E-mail address: [email protected] (G.F. Ecker). European Neuropsychopharmacology (]]]]) ], ]]]–]]] Please cite this article as: Michl, J., et al., A multivariate approach linking reported side effects of clinical antidepressant and antipsychotic trials to in.... European Neuropsychopharmacology (2014), http://dx.doi.org/10.1016/j.euroneuro.2014.06.013
-
Upload
independent -
Category
Documents
-
view
5 -
download
0
Transcript of A multivariate approach linking reported side effects of clinical antidepressant and antipsychotic...

A multivariate approach linking reported sideeffects of clinical antidepressant andantipsychotic trials to in vitrobinding affinities
Johanna Michla, Christian Scharingerb, Miriam Zaunerb,Siegfried Kasperb, Michael Freissmuthc, Harald H. Sittec,Gerhard F. Eckera,n, Lukas Pezawasb
aDepartment of Pharmaceutical Chemistry, University of Vienna, Vienna, AustriabDepartment of Psychiatry and Psychotherapy, Medical University Vienna, Vienna, AustriacDepartment of Pharmacology, Medical University Vienna, Vienna, Austria
Received 28 February 2014; received in revised form 23 June 2014; accepted 26 June 2014
KEYWORDSSchizophrenia;Depressive disorder;Antidepressiveagents;Antipsychotic agents;Clinical pharmacol-ogy;Adverse effects
AbstractThe vast majority of approved antidepressants and antipsychotics exhibit a complex pharma-cology. The mechanistic understanding of how these psychotropic medications are related toadverse drug reactions (ADRs) is crucial for the development of novel drug candidates andpatient adherence. This study aims to associate in vitro assessed binding affinity profiles (39compounds, 24 molecular drug targets) and ADRs (n=22) reported in clinical trials ofantidepressants and antipsychotics (n459.000 patients) by the use of robust multivariatestatistics. Orthogonal projection to latent structures (O-PLS) regression models with reasonablepredictability were found for several frequent ADRs such as nausea, diarrhea, hypotension,dizziness, headache, insomnia, sedation, sleepiness, increased sweating, and weight gain.Results of the present study support many well-known pharmacological principles such as theassociation of hypotension and dizziness with α1-receptor or sedation with H1-receptorantagonism. Moreover, the analyses revealed novel or hardly investigated mechanisms for
www.elsevier.com/locate/euroneuro
http://dx.doi.org/10.1016/j.euroneuro.2014.06.0130924-977X/& 2014 Published by Elsevier B.V.
Abbreviations: 5-HT, 5-hydroxy tryptamine (serotonin); 5-HTT, serotonin transporter; AAP, atypical antipsychotics; ACH, acetylcholine;ADR, adverse drug reaction; AP, antipsychotic; CDSR, cochrane database of systematic reviews; CTZ, chemotrigger zone; DAT, dopaminetransporter; EMA, european medicines agency; EPMS, extrapyramidal motor symptoms; FDA, food and drug administration;GI, gastrointestinal; Ki, inhibition constant; MAO, monoamine oxidase; MDD, major depressive disorder; NDRI, norepinephrine-dopaminere-uptake inhibitor; NET, norepinephrine transporter; O-PLS, orthogonal projection to latent structures; PDSP, psychoactive drugs screeningprogram; p1, principal component 1; pKi, negative common logarithm of Ki; PRESS, prediction error sum of squares; SARI, serotoninantagonist and re-uptake inhibitor; SD, standard deviation; SNRI, serotonin norepinephrine re-uptake inhibitor; SSRI, selective serotoninre-uptake inhibitor; TAP, typical antipsychotic; TCA, tricyclic antidepressant; TeCA, tetracyclic antidepressant
nCorresponding author. Tel.: +43 1 4277 55110; fax: +43 1 4277 855110.E-mail address: [email protected] (G.F. Ecker).
European Neuropsychopharmacology (]]]]) ], ]]]–]]]
Please cite this article as: Michl, J., et al., A multivariate approach linking reported side effects of clinical antidepressant andantipsychotic trials to in.... European Neuropsychopharmacology (2014), http://dx.doi.org/10.1016/j.euroneuro.2014.06.013

common ADRs including the potential involvement of 5-HT6-antagonism in weight gain,muscarinic receptor antagonism in dizziness, or 5-HT7-antagonism in sedation. To summarize,the presented study underlines the feasibility and value of a multivariate data mining approachin psychopharmacological development of antidepressants and antipsychotics.& 2014 Published by Elsevier B.V.
1. Introduction
The development of more effective treatments of majorneuropsychiatric disorders such as major depressive disor-der (MDD) or schizophrenia is urgently needed due to theirleading and unchanged role as contributors to global diseaseburden over the past two decades (Vos et al., 2012). Despitethe doubtless beneficial effects of currently available anti-depressants (ADs) and antipsychotics (APs), reported med-ication discontinuation rates are much higher thanacceptable. Patient adherence is severely affected byadverse drug reactions (ADRs) (Insel, 2012), which are alsoan important factor leading to the attrition of clinical trialsduring drug development (Lounkine et al., 2012). Well-studied ADRs among many others include weight gain,sedation, extrapyramidal motor symptoms (EPMS), sexualdysfunction, and QT-interval prolongation (Castro et al.,2013). In contrast to other medical fields, pharmacologicaldevelopment in psychiatry is challenged by its unknownetiology and lack of biological meaningful diagnostic cate-gories (Insel, 2012). Hence, ADs and APs have not beenengineered based on prior knowledge of molecular path-ways, but were identified by serendipity within the class ofanti-histaminergic drugs (Lopez-Munoz and Alamo, 2009).Therefore, it is not surprising that numerous available ADsand APs target a broad spectrum of membrane proteinscomprising receptors, transporters, and ion channels thatresult in complex pharmacological actions (Roth et al.,2004).
Over the past years, there has been an ongoing debateamong scientists with regard to the benefits and harms ofselective versus non-selective (Roth et al., 2004) as well asunimodal versus multimodal (Nutt, 2009) medications andtheir impact on observed efficacy and tolerability of psy-chopharmacological drug treatment. A major argument infavor of selectivity has been the broad clinical use ofunimodal psychotropic medications such as selective sero-tonin re-uptake inhibitors (SSRIs) that demonstrated a morefavorable side effect profile than older non-selective tri-cyclic antidepressants (TCAs) or early multimodal medica-tions such as trazodone (Bauer et al., 2013; Grunze et al.,2013; Nutt, 2009). Considering the limitations of availablemeta-analyses (Huf et al., 2011) it has been suggested thatincreased selectivity has not lead to an overall improvedantidepressive efficacy (Bauer et al., 2013), but instead ledto a more acceptable side effect profile (Baghai et al.,2012). On the other hand, several non-selective medicationsincluding second-generation APs have been found to provideacceptable treatment efficacy without jeopardizing drugtolerability (Hasan et al., 2013). Given these counter-intuitive results with respect to drug selectivity, it becomesapparent that further research is urgently needed that
facilitates the understanding on how receptor profiles ofpsychopharmacological medications translate into clinicallyobserved ADRs. Ideally, inferences should be made fromclinical trials investigating the occurrence of ADRs duringthe application of highly selective drugs that bind to singledrug targets. However, most psychopharmacological com-pounds licensed for medical use are not selective and bindto a variety of drug targets. Therefore, inferences on therelationship between a specific receptor system and aspecific ADR are difficult to extrapolate from a singlecompound. Hence, complimentary evidence stems fromnumerous drug safety studies in animals that inferredundesired drug effects from occupancy research to humans,a conclusion that has been criticized in the past.
Recently, alternative approaches have been developedincluding computational strategies that utilize informationon the chemical structure of investigational drugs in orderto predict ADRs (Bender et al., 2007; Lounkine et al., 2012).While such strategies are definitely novel and promote theunderstanding of drug structure-ADR relationships, metho-dological limitations exist including a restriction to singledrug- (or off-) targets as well as the qualitative nature ofthese techniques. Since ADRs are likely to result from drugactions on multiple protein targets interacting with avariety of signaling pathways, a quantitative multivariateapproach applied to large data sets may be more suitableand might be capable to detect associations that areotherwise impossible to deconvolute.
To demonstrate the feasibility and clinical plausibility ofsuch a quantitative multivariate data analysis strategy, weperformed an orthogonal projections to latent structures(O-PLS) analysis with the goal to associate binding affinityprofiles of 39 antidepressants and antipsychotics licensedfor medical use with high-quality ARDs data compiled fromclinical trials comprising more than 59,000 patients. Both,binding and clinical data were extracted from publiclyavailable databases. Our unprecedented approach verifiedsome associations that had previously been suspected or lessappreciated, e.g., a prominent role of 5HT6-receptor block-age in triggering weight gain or a surprisingly large numberof targets linked to sedation.
2. Experimental procedures
2.1. Data sources
Biological activities (Ki values) were retrieved from the openlyaccessible PDSP database (Psychoactive Drug Screening Program,http://pdsp.med.unc.edu). Reported side effect frequencies wereextracted from the publically available Cochrane Database ofSystematic Reviews (http://www.thecochranelibrary.com).
J. Michl et al.2
Please cite this article as: Michl, J., et al., A multivariate approach linking reported side effects of clinical antidepressant andantipsychotic trials to in.... European Neuropsychopharmacology (2014), http://dx.doi.org/10.1016/j.euroneuro.2014.06.013

2.2. Data selection
2.2.1. Binding affinity dataThe following inclusion criteria were applied to PDSP data: (1) psy-chotropic medications had been licensed for clinical use by theFood and Drug Administration (FDA) or European Medicines Agency(EMA), (2) psychotropic medications showed significant bindingactivities (Kio10 mM) for at least two different receptor systems.In case of the availability of binding affinity data from multiplesources, human data were preferred over animal data and averaged(86.4% human vs. 13.6% non-human). Average binding affinities foradrenergic receptors were determined regardless of receptor sub-types. A maximum Ki of 10 mM was used as cut-off for low-affinityinteractions. Fifty-two compounds fulfilled the above mentionedinclusion criteria and were further used for the selection of clinicaltrials (see Supplementary material, Table S1).
2.2.2. Clinical dataThe following inclusion criteria were applied to reported side effectfrequencies in the Cochrane Database of Systematic Reviews:(1) systematic reviews investigating side effect frequencies of theabove-defined 52 compounds (n=71); (2) reviews were excludedthat investigated combination therapy or dose finding studies. Inaddition, we included exclusively oral psychotropic medicationsthereby discarding clinical trials of depot antipsychotics (n=22).This procedure resulted in 49 systematic reviews comprisingrandomized and placebo- (39%) or active reference-controlled(61%) clinical trials that were considered eligible for this study;included reviews contained ADRs frequency data for 39 differentpsychotropic medications (19 antidepressants and 20 antipsycho-tics) in more than 59,000 patients (Table S2). The weighted average(based on the number of study participants) ADR frequency (in %) ofall included studies was extracted for each substance resulting in avector consisting of mean ADRs (column) for different medications(rows). Data of side effect terms were merged in case of high inter-correlations, typically applying to terms that are clinically indis-tinguishable or at least very similar (e.g. agitation and anxiety,dizziness and vertigo/faintness, nausea and vomiting, sleepinessand drowsiness, abnormal vision and blurred vision). The completematrix is shown in the Supplementary material, Table S3.
2.2.3. Data reductionThe above mentioned selection process resulted in 39 psychotropicmedications with available binding affinity profiles for 31 drugtargets in total and 69 reported side effects. In order to guaranteestatistical robustness, drug targets were excluded from furtheranalysis, if the pertinent Ki values were not available for more thanhalf of the 39 included psychotropic medications (n=7). Applicationof these criteria resulted in an array of drug targets including threemonoamine transporters (serotonin transporter (5-HTT), norepi-nephrine transporter (NET), and dopamine transporter (DAT)), 20Gprotein-coupled receptors (5-HT1A, 5-HT1B, 5-HT1D, 5-HT2A, 5-HT2C,5-HT6, 5-HT7; α1, α2, β1; M1, M2, M3, M4, M5; D1, D2, D3, D4; H1), andone ligand-gated ion channel receptor (5-HT3). Average bindingaffinities (Ki values) were converted to their negative commonlogarithm (pKi values). The resulting binding affinity data matrix isshown in Table S4. In an analogous manner, ADR frequenciesreported in clinical trials were only included if based on a sampleof more than 50 study participants. Moreover, specific side effectswere excluded, if data were available for less than 15 compounds.Hence, the following side effects were considered in this study:agitation, akathisia, constipation, diarrhea, dizziness, dry mouth,dystonia, fatigue, gastrointestinal symptoms, headache, hypoten-sion, insomnia, sexual dysfunction, nausea, increased salivation,sedation, sleepiness, increased sweating, tremor, urination disor-ders, abnormal vision, and weight gain. Table S5 displays the ADRprofile matrix.
2.3. Statistics
2.3.1. Orthogonal projections to latent structures (O-PLS)O-PLS regression analysis was used for associating clinical endpoints(ADR frequencies) with receptor binding profiles of ADs and APs.Briefly, similar to its predecessor partial least squares (PLS) regres-sion, O-PLS is a method for relating two data matrices, X and Ywithin a linear multivariate model. The O-PLS method (Trygg andWold, 2002) is designed to handle systematic variation in X that isnot subject to linear correlation with Y (Y-orthogonal variation).The systematic variation in X is divided into two parts, one that islinearly related (and therefore predictive) to Y, and one that isorthogonal to Y. Removal of Y-orthogonal variation usually facil-itates better interpretation of the model, but does not affect itspredictive power (Trygg and Wold, 2002).
2.3.2. Data matricesThe selection process outlined above resulted in an m-by-n X matrixcomprising binding affinities (pKi values) of 39 compounds assessedon 24 drug targets. Elements of the m-by-1 Y matrix representreported frequencies of a specific side effect for the includedcompounds. A separate O-PLS model was calculated for eachspecific side effect (n=22). The dimensions of the X and Y matricesemployed for each side effect were variable ranging from 15(dystonia) to 34 rows (dry mouth) depending on the availability ofreported ADRs.
2.3.3. Statistical modelingSIMCA-P+ (Version 12.0, Umetrics, Umea, Sweden) was used forcalculating the O-PLS models. All X variables were centered but notscaled. The goodness-of-fit of the model was determined by thesquared correlation coefficient (R2) and the goodness-of-predictionby the 7-fold cross-validated R2 (Q2; Eq. (1)).
Q 2 ¼ðSD#PRESSÞ
SDSD¼ Σðxi#μÞ2 ð1Þ
Eq. (1): Equation for Q2, the fraction of Y that can be predictedby a component, as estimated by cross-validation [PRESS, predic-tion error sum of squares; SD, standard deviation].
A value of one represents either a complete explanation of thedependent variable by the regression model (R2) or a perfect match ofpredicted and observed values in leave-n-out cross validation runs. Q2
is typically lower than R2 and a large difference between these twoparameters might indicate chance correlations. A negative Q2 impliesthat the model is not predictive at all. The most suitable number ofcomponents for each O-PLS model was estimated by cross-validation.For each O-PLS model loadings and variable importance plots wereconstructed to study whether binding affinities correlated positivelyor negatively, significantly or non-significantly, with Y variables(frequency of ADR).
3. Results
3.1. Descriptive statistics
3.1.1. Binding affinities of studied ADs and APsWe compiled information on binding affinity data (pKivalues) of 39 psychoactive compounds comprising severaldrug classes. This comprehensive list highlights specific andwell-known profiles, in which psychotropic medicationsdiffer in both, qualitative and quantitative traits (TableS4, Figure 1a). The heat map representation (Figure 1a)shows comprehensively the fact that the vast majority ofpsychotropic medications are likely to interact with manytargets when administered at clinically relevant doses. Even
3Linking clinically reported side effects to in vitro binding profiles
Please cite this article as: Michl, J., et al., A multivariate approach linking reported side effects of clinical antidepressant andantipsychotic trials to in.... European Neuropsychopharmacology (2014), http://dx.doi.org/10.1016/j.euroneuro.2014.06.013

SSRIs, which are thought to be the most selective class ofpsychoactive medications, show quite unique binding pro-files. (1) Citalopram shows mild anti-histaminergic proper-ties, which do not occur in its S-enantiomer escitalopram,the most selective SSRI. (2) Highest 5-HTT affinity is foundin paroxetine, in addition to anti-muscarinergic andNET-inhibiting properties. (3) Sertraline with its relativelyhigh DAT. (4) Fluoxetine with significantly high NETas well as5-HT2C-receptor affinity reflect known differences of SSRIbinding profiles that might eventually be transferred to aclinical level. Similarly, binding profiles of SNRIs are asexpected exhibiting a strong and balanced NET and 5-HTTinhibition for milnacipran followed by duloxetine, andrather low NET inhibition for venlafaxine. Bupropriondisplays low DAT-inhibition compared to NET-inhibition.Mirtazapine and its precursor mianserin have beenfound to exhibit α-antagonistic, anti-serotonergic and
anti-histaminergic properties as anticipated. SARIs such astrazodone and nefazodone are displaying 5-HT antagonistaction at 5-HT2A and 5-HT2C-receptors, 5-HTT re-uptakeinhibition as well as α2-antagonism. In addition, bindingprofiles highlight subtle differences between these psycho-tropic medications such as low 5-HTT inhibition for trazo-done and a moderate NET-inhibition for nefazodone. Incontrast, tricyclic antidepressants (TCAs) included in thisstudy exhibit a potent NET and 5-HTT-inhibition as well ashigh affinities for M1, α1 and H1-receptors, which areresponsible for accompanying ADRs.
Most antipsychotics can easily be distinguished within thistable due to their complex and numerous affinities atvarious receptor systems. Differences between typical(TAP) and most atypical (AAP) antipsychotics can also beseen such as lower D2 and higher 5-HT2A binding affinity forAAPs compared to TAPs. It is noteworthy that atypicality is
Citalopram SSRI Escitalopram SSRI Fluoxetine SSRI Fluvoxamine SSRI Paroxetine SSRI Sertraline SSRI Duloxetine SNRI Milnacipran SNRI Venlafaxine SNRI Bupropion NDRIMianserin NaSSAMirtazapine NaSSANefazodone SARI Trazodone SARI Amitriptyline TCAClomipramine TCADothiepin TCAImipramine TCAMaprotiline TeCA
AAP AmisulprideAripiprazole AAP Olanzapine AAP Quetiapine AAP Risperidone AAP Sertindole AAPZiprasidone AAP Clozapine AAPZotepine AAP Chlorpromazine TAPFluphenazine TAP Haloperidol TAP Loxapine TAP Molindone TAP Penfluridol TAP Perphenazine TAP Pimozide TAPSulpiride TAP Thioridazine TAP Trifluoperazine TAP
5-H
TT
NET
D
AT
5-H
T 1A
5-H
T 1B
5-H
T 1D
5-H
T 2A
5-H
T 2C
5-H
T 35-
HT 6
5-H
T 7α 1 α 2 β 1 M
1M
2M
3M
4M
5D
1D
2D
3D
4H
1
a gita
tion
akat
hisi
aco
nstip
atio
n di
arrh
ea
dizz
ines
s dr
y m
outh
dy
ston
iafa
tigue
gast
roin
test
inal
sym
ptom
s he
adac
he
hypo
tens
ion
inso
mni
a se
xual
dys
func
tion
naus
ea
incr
ease
d sa
livat
ion
seda
tion
slee
pine
ss
incr
ease
d sw
eatin
gtre
mor
ur
inat
ion
diso
rder
s ab
norm
al v
isio
n w
eigh
t gai
n
Figure 1 Heat maps displaying binding affinities (pKi values) (a) and adverse drug reaction (ADR) (%) profiles (b) for 39 psychotropicmedications comprising different drug classes (SSRI, selective serotonin re-uptake inhibitor; SNRI, serotonin-norepinephrinere-uptake inhibitor; NDRI, norepinephrine-dopamine re-uptake inhibitor; NaSSA, noradrenergic and specific serotonergic anti-depressant; SARI, serotonin antagonist and re-uptake inhibitor; TeCA, tetracyclic antidepressant; TCA, tricyclic antidepressant; AAP,atypical antipsychotic; TAP, typical antipsychotic). Binding affinities (in pKi values) range from 5 (inactive, black) to 9.68 (highlyactive, white), whereas ADR frequencies (in %) range from 0% (no occurrence, black) to 67.9% (very frequent, white). Bindingaffinity profiles were extracted from the Psychoactive Drugs Screening Program (PDSP) database and side effect frequencies arebased on clinical trial data extracted from the Cochrane Database of Systematic Reviews (CDSR).
J. Michl et al.4
Please cite this article as: Michl, J., et al., A multivariate approach linking reported side effects of clinical antidepressant andantipsychotic trials to in.... European Neuropsychopharmacology (2014), http://dx.doi.org/10.1016/j.euroneuro.2014.06.013

defined by the frequency of EPMS and hyperprolactinaemia,but not by a specific mechanism of action. Currently knownmechanisms include muscarinergic antagonism, partial5-HT1A-receptor agonism as well as antagonistic actions atseveral 5-HT sub-receptors. Similar to TCAs, TAPs and to alesser degree AAPs are frequently accompanied by ADRs.This can also be derived from their binding affinity profiles:5-HT2C, M3 and H1 receptor antagonism leads frequently tometabolic ADRs, and M1, H1, and α1-receptor antagonismleads to sedation and cognitive malfunctioning.
3.1.2. Adverse drug reactions (ADRs) in clinical trialsADRs were organized in an analogous way for the identicalset of psychotropic medications as presented for bindingprofiles (Table S5, Figure 1b). Many well-known ADRs thatare related to specific drug classes can easily be derivedfrom this ‘real-world’ data matrix. Headache and nauseaare frequently reported under SSRI treatment. In accor-dance to differing receptor profiles of several SSRIs, certainADRs occur more frequently such as fatigue, dry mouth, andconstipation for paroxetine, or a relatively broad spectrumof ADRs for fluvoxamine, which might be related to studiesof its initial short-release formulation. Sexual dysfunctionhas been reported as expected with most SSRIs as well asvenlafaxine and basically no other class of antidepressants.SNRIs differ only slightly from the ADR patterns seen in SSRIswith marginally higher number of dry mouth, dizziness, andurination problems as well as agitation for venlafaxine, andabnormal vision for milnacipran. Mirtazapine and mianserinshowed in accordance with their H1-antagonistic action anincrease in excessive daytime sleepiness reports. Well-studied TCAs such as clomipramine showed the expectedhigher frequency of typical TCA-related side effects com-pared to newer antidepressants. Similarly, but more strik-ing, are the differences in ADRs between TAPs and AAPswhich is clearly in favor of AAPs for basically all ADRs withthe exception of older compounds such as clozapine andzotepine. Clearly, akathisia and dystonia are more prevalentin TAPs in line with their D2-antagonistic properties. How-ever, reports of sedation and sleepiness occurring under AAPtreatment including zotepine, clozapine, olanzapine; andquetiapine; surpassed several of older and typically high-potent TAPs.
3.2. Quantitative statistics
3.2.1. O-PLS model qualityHeat maps shown in Figure 1 allow for the visual detectionof obvious associations between binding profiles and ADRs asdetailed above. However, in most instances, inferences aredifficult to make due to the complexity of relationshipsbetween binding profiles and individual ADRs. Accordingly,O-PLS regression was used to link binding affinities of these39 psychotropic medications for the array of selectedtargets to the clinically reported ADRs frequencies(Figure 2). Model quality of 22 calculated O-PLS modelsfor each specific ADR varied substantially (Figure S1): e.g.,the O-PLS model for sedation resulted in an R2 value of 0.97and a Q2 value of 0.77. However, other regression modelshad negative Q2 values e.g. abnormal vision, akathisia,
agitation, dystonia, increased salivation, tremor, urinationdisorders and sexual dysfunction. The lack of predictivepower of these models indicated that the O-PLS analysis didnot support the presence of any link between the availableset of binding affinity profiles and reported ADRs. Thenumber of observations and components as well as R2X,R2Y, and Q2Y values for each model are provided in theSupplementary material Table S6. Only O-PLS models(n=10) with reasonable quality (R240.2, Q240.01) werefurther investigated including the following ADRs: nausea,diarrhea, hypotension, dizziness, headache, insomnia, seda-tion, daytime sleepiness, increased sweating, and weightgain. Loadings plots for the predictive component of thesemodels are shown in Figure 3 and reflect statistical sig-nificant associations between receptor binding profiles andADRs. Furthermore, variable importance values reflectingthe adverse and beneficial effects of antagonistic action atcommon drug targets are shown in Table 1 and Figure S2.
drug targets
com
poun
ds
side effect
O-PLS
drug targets
load
ings
(39, 24) (39, 1)
Figure 2 Statistical approach for relating binding affinityprofiles to clinically reported adverse drug reactions (ADRs).Elements of the X matrix represent binding affinities (pKivalues) for 39 psychotropic medications comprising 24 drugtargets. Elements of the Y vector represent frequencies of asingle ADR reported in clinical trials of these 39 psychotropicmedications. For each specific ADR (n=22) a separate ortho-gonal projection to latent structures (O-PLS) model was calcu-lated. Principal component 1 (p[1]) loadings plots were used tointerpret the relationship between drug target interactions andADR frequencies. Positive p[1] loadings indicate that bindingaffinities correlate positively with the Y variable (frequency ofADR), whereas negative p[1] loadings indicate a negativecorrelation. p[1] loadings close to zero demonstrate theabsence of any correlation between binding affinities and ADRfrequencies.
5Linking clinically reported side effects to in vitro binding profiles
Please cite this article as: Michl, J., et al., A multivariate approach linking reported side effects of clinical antidepressant andantipsychotic trials to in.... European Neuropsychopharmacology (2014), http://dx.doi.org/10.1016/j.euroneuro.2014.06.013
-0.6
-0.4
-0.2
0.0
0.2
0.4
0.6
-0.4
-0.2
0.0
0.2
0.4
0.6
-0.5
0.0
0.5
1.0
-0.5
0.0
0.5
1.0
-1.0
-0.5
0.0
0.5
-1.0
-0.5
0.0
0.5
1.0
-1.0
-0.5
0.0
0.5
1.0
-1.0
-0.5
0.0
0.5
1.0
-0.5
0.0
0.5
1.0
-0.4
-0.2
0.0
0.2
0.4
0.6
5-H
TTN
ETD
AT 1A 1B 1D 2A 2C 3 6 7 1 2 1 1 2 3 4 5 1 2 3 4H
15-HT α M D 5-
HTT
NET
DAT 1A 1B 1D 2A 2C 3 6 7 1 2 1 1 2 3 4 5 1 2 3 4H
1
5-HT α M D 5-H
TTN
ETD
AT 1A 1B 1D 2A 2C 3 6 7 1 2 1 1 2 3 4 5 1 2 3 4H
1
5-HT α M D
5-H
TTN
ETD
AT 1A 1B 1D 2A 2C 3 6 7 1 2 1 1 2 3 4 5 1 2 3 4H
1
5-HT α M D 5-H
TTN
ETD
AT 1A 1B 1D 2A 2C 3 6 7 1 2 1 1 2 3 4 5 1 2 3 4H
15-HT α M D 5-
HTT
NET
DAT 1A 1B 1D 2A 2C 3 6 7 1 2 1 1 2 3 4 5 1 2 3 4H
1
5-HT α M D
5-H
TTN
ETD
AT 1A 1B 1D 2A 2C 3 6 7 1 2 1 1 2 3 4 5 1 2 3 4H
1
5-HT α M D 5-H
TTN
ETD
AT 1A 1B 1D 2A 2C 3 6 7 1 2 1 1 2 3 4 5 1 2 3 4H
15-HT α M D
5-H
TTN
ETD
AT 1A 1B 1D 2A 2C 3 6 7 1 2 1 1 2 3 4 5 1 2 3 4H
1
5-HT α M D 5-H
TTN
ETD
AT 1A 1B 1D 2A 2C 3 6 7 1 2 1 1 2 3 4 5 1 2 3 4H
1
5-HT α M D
p[1]
load
ings
p[1]
load
ings
p[1]
load
ings
p[1]
load
ings
p[1]
load
ings
p[1]
load
ings
p[1]
load
ings
p[1]
load
ings
p[1]
load
ings
p[1]
load
ings
noisnetopyhaesuanaeohrraid
ainmosniehcadaehssenizzid
ssenipeelsnoitades
weight gainincreased sweating
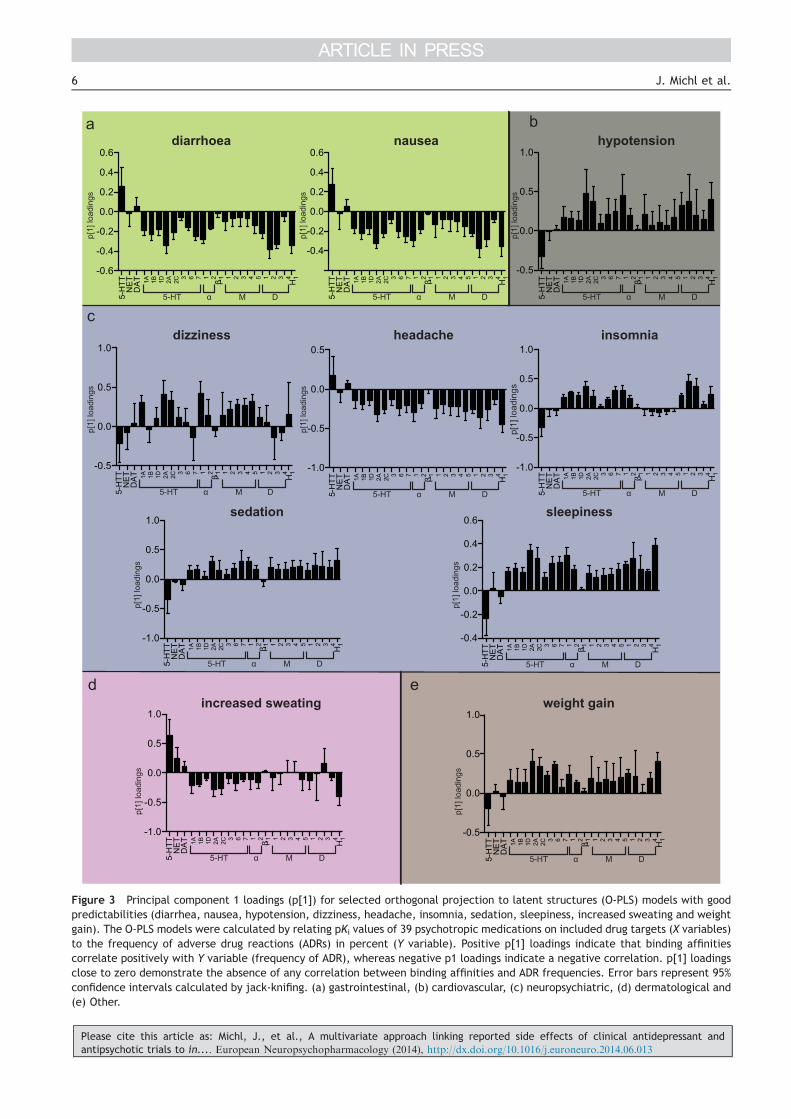
Figure 3 Principal component 1 loadings (p[1]) for selected orthogonal projection to latent structures (O-PLS) models with goodpredictabilities (diarrhea, nausea, hypotension, dizziness, headache, insomnia, sedation, sleepiness, increased sweating and weightgain). The O-PLS models were calculated by relating pKi values of 39 psychotropic medications on included drug targets (X variables)to the frequency of adverse drug reactions (ADRs) in percent (Y variable). Positive p[1] loadings indicate that binding affinitiescorrelate positively with Y variable (frequency of ADR), whereas negative p1 loadings indicate a negative correlation. p[1] loadingsclose to zero demonstrate the absence of any correlation between binding affinities and ADR frequencies. Error bars represent 95%confidence intervals calculated by jack-knifing. (a) gastrointestinal, (b) cardiovascular, (c) neuropsychiatric, (d) dermatological and(e) Other.
J. Michl et al.6
Please cite this article as: Michl, J., et al., A multivariate approach linking reported side effects of clinical antidepressant andantipsychotic trials to in.... European Neuropsychopharmacology (2014), http://dx.doi.org/10.1016/j.euroneuro.2014.06.013

Results of associations of receptor binding profiles andindividual ADRs with sufficient model quality will be sum-marized in the following paragraphs:
Gastrointestinal ADRs (Figure 3a). Results of nausea anddiarrhea associations have been grossly identical and willtherefore be reported together. O-PLS analysis showed that5-HTT re-uptake inhibition appears to be the main reasonfor nausea and diarrhea within the array of studied recep-tors and transporters. Interestingly, inhibition of the over-whelming majority of all other receptors and transportersresulted in opposing effects. Highest negative correlationswere seen for H1-, 5-HT2A-, or D2-receptors indicating areduced chance to suffer from nausea and diarrhea, whenthese systems are blocked.
Cardiovascular ADRs (Figure 3b). Antagonism of α1-recep-tors has been associated with reports of hypotension asexpected. It is noteworthy, that 5-HT2A-, 5-HT2C-, D1-, D2-,and H1-receptors have also been found to correlate withhypotension. Interestingly, our analyses showed a reducedchance of hypotension, when 5-HTT inhibition has beenpresent.
Neuropsychiatric ADRs (Figure 3c). Reports of dizzinessare predominantly correlated with antagonism at α1-,5-HT2A-, 5-HT2C-, and muscarinergic receptors reflect a
variety of reasons for dizziness such as orthostatic hypoten-sion and vestibular suppression among others. Headachewas associated with 5-HTT and DAT inhibition. Interestingly,blockage of many receptors appeared to confer a protectiveeffect, most notably H1-receptor inhibition. Reported ADRsfrequencies for insomnia showed maximal correlations withD2- and D3- receptor antagonism. Sedation and excessivedaytime sleepiness have been unsurprisingly correlated withsimilar targets due to their inherent relationship with thefunctionality of the arousal system. Antagonistic action atserotonergic, adrenergic, muscarinergic, dopaminergic, andhistaminergic receptors showed to increase sedation andsleepiness. Interestingly, only β1-antagonism has been unre-lated. In contrast, inhibition of 5-HT and to a lower degreedopamine re-uptake demonstrated to reduce the likelihoodof reporting sedation and sleepiness in investigated clinicaltrials. Furthermore, our analyses reflected the similaritybetween sleepiness and insomnia, which are known to beco-occurring symptoms of many sleep disorders (hypo-vigilance during the day and hyper-vigilance at night).Therefore, we found similar associations for insomniareports with histaminergic, dopaminergic, adrenergic, andserotonergic receptor antagonism. In is noteworthy thatmuscarinergic, β1, 5-HT3, DAT, and NET antagonism was
Table 1 Adverse and beneficial effects of antagonistic action at common drug targets of antidepressants and antipsychotics.Variable importance values are displayed (Figure S2) with values greater than one in the O-PLS analysis. (+) indicates thatinhibition of the target is positively correlated to any specific adverse drug reaction (ADR) and possibly causal, whereas (#)stands for a negative correlation with the ADR putatively reflecting protective properties. (+ +) and (# #) denote variableimportance values higher than 1.5.
Drug.target
Diarrhea Nausea Hypotension Dizziness Headache Insomnia Sedation Sleepiness Increasedsweating
Weightgain
5-HTT + + # # # # + + #NET +DAT +5-HT1A # +5-HT1B +5-HT1D5-HT2A # # # + + + + + + # + +5-HT2C # + + # + +5-HT3 +5-HT6 + # + +5-HT7 # # + + +α1 # + + + + + + + +α2β1M1 + # #M2 + #M3 + + +M4 + #M5 + + + # +D1 # + #D2 # # # # + + # + + + + +D3 # # # + + + + +D4 +H1 # # # # # # + + + + # # + +
7Linking clinically reported side effects to in vitro binding profiles
Please cite this article as: Michl, J., et al., A multivariate approach linking reported side effects of clinical antidepressant andantipsychotic trials to in.... European Neuropsychopharmacology (2014), http://dx.doi.org/10.1016/j.euroneuro.2014.06.013

unrelated to insomnia in our study. Moreover, we also foundthat 5-HTT inhibition reduced the risk of insomnia reports ininvestigated clinical trials.
Dermatological ADRs (Figure 3d). Reports of increasedsweating are mainly correlated with 5-HTT and NET inhibi-tion. On the other hand, blockage of various 5-HT receptorsas well as H1-receptor antagonism conferred a reducedchance to report increased sweating.
Metabolic ADRs (Figure 3e). In addition to well knowncandidates such as 5-HT2c, M3, H1 receptors, we found avariety of other antagonistic receptor interactions to belinked to weight gain. 5-HT2A and 5-HT6 showed thestrongest effects in the loading plots. A few targets showeda lack of association with weight gain such as NET, DAT, β1,and D3. Conversely, 5-HT re-uptake inhibition has beenlinked to decreased reporting of weight gain.
4. Discussion
The present study supports the idea that in vitro bindingaffinity profiles can be utilized to gain insights into putativemechanisms of ADRs occurring in clinical psychopharmaco-logical trials. While many findings are well-known, severalreported associations are novel and of potential interest forfuture pharmacological experiments. Our strategy of asso-ciating binding affinity profiles with ADRs has proven tobe robust and feasible and constitutes a useful strategyfor psychopharmacological research (Kroeze et al., 2003;Selent et al., 2010).
The present study was able to link the majority ofcommon and important ADRs observed in clinical trials ofADs and APs to in vitro binding affinity profiles. 5-HTTinhibition has been identified to be the main contributor ofnausea and diarrhea. Nausea is frequently observed at thebeginning of SSRI treatment (Tuerke et al., 2012). However,the exact mechanism of SSRIs-induced nausea is stillunclear. Interestingly, 5-HT3-antagonism, which is effectivein chemotherapy-induced nausea has shown little effect onAD-induced nausea (Leatherman et al., 1999), which is inline with our results. Moreover, presented data indicatepossible anti-emetic effects of 5-HT7-receptor antagonismin AD-induced nausea, which has not previously beenpublished to our best knowledge. In addition, this studyprovides human evidence of an anti-emetic effect of 5-HT2A-antagonism rendering animal work (Wolff and Leander,2000). Furthermore, our analysis was able to detect D2- andH1-mediated anti-emetic effects, which are therapeuticallyexploited by drugs such as metoclopramide and betahisti-dine. Diarrhea was highly associated with 5-HTT inhibitionin our study. This is not surprising, given the high concen-tration of 5-HTTs in the GI tract and the prominent role of5-HT signaling in GI mobility (Gershon, 2004). Interestingly,5-HT2A- and H1-receptor antagonisms have been found to bemore protective against psychotropic medication-induceddiarrhea than muscarinergic receptor antagonism, whichcannot be anticipated from current understanding of GIphysiology.
The present study further reflected the importance ofα1-receptor antagonism in orthostatic hypotension and con-secutive dizziness. However, orthostatic hypotension isknown to result from a much broader range of molecular
mechanisms. This is underlined by the fact that severalinvestiged psychotropic medications do not exhibit a sig-nificant α1-receptor affinity but still induce hypotensionsuch as sulpiride (Figure 1). In addition to α1-recpetorantagonism, dizziness was predominately associated withmuscarinergic and serotonergic antagonism in our study.Acetylcholine (ACH) is the primary neurotransmitter investibulocerebellar pathways, which may account foreffects of muscarinic antagonists in motion sickness andreported dizziness during ACE-inhibitor treatment (Jones,2010). Interestingly, M3-antagonism has been linked todizziness (Zinner et al., 2005) similar to our results. More-over, this study revealed a link between 5-HT2A-antagonismand dizziness in line with reports of dizziness duringketanserin treatment (Nagatomo et al., 2004). In additionto 5-HTT inhibition, we also observed an associationbetween DAT inhibition and headache. This finding supportsrecent migraine models postulating ictal dopamine releaseas trigger for headache, which is based on accompanyingdopaminergic symptoms such as yawning, nausea, postdro-mal somnolence, euphoria, and polyuria (Barbanti et al.,2013). Interestingly, the analysis revealed a negative corre-lation between H1 and M1 antagonism and headache,indicating that these receptor interactions have protectiveeffects. While the implication of histamine in pain and itspotential to trigger headaches has been reported before(Haas et al., 2008), the relationship of M1 antagonism andheadache deserves further attention.
At least five neurotransmitters (histamine, dopamine,norepinephrine, 5-HT, and ACH) relevant for our study areknown to modulate neuronal arousal (Sehgal and Mignot,2011). Mirroring this complex regulation, we have identifiedseveral mechanisms that are associated with sleepiness,sedation, and insomnia. It is noteworthy that hypovigilanceduring the day and hypervigilance at night are typicallyfeatures of sleep disorders and are caused by the samemolecular mechanisms. H1- and α1-antagonism were asso-ciated with sedation and sleepiness in this study reflectingits use in hypnotic drugs or frequent reports of these ADRs inclinical trials (Mitchell and Weinshenker, 2010). Insomnia inrestless leg syndrome is treated by dopamine agonists suchas pramipexole (Montplaisir et al., 2006). Caffeine-inducedarousal is thought to be mediated by D2-receptors, whichare coupled with purine receptors (Ferre, 2010). Hence, ourfindings of increased insomnia due to dopaminergic antag-onism are supported by previous studies. Sleep symptomssuch as insomnia occurring during a depressive episode arealso affected by 5-HT and are reduced in MDD patients underchronic SSRIs treatment. Recent research suggests that 5-HT2A-receptor antagonism (e.g. ritanserin) might be effective instaying asleep but not falling asleep (Vanover and Davis, 2010).We have observed a linkage between 5-HT2A antagonism andsedation, which is in line with pharmacological trials ofnelotanserin (Al-Shamma et al., 2010). 5-HT7-mediated effectson sleepiness or sedation are further highlighted by our study.Although 5-HT7-dependent regulation of sleep as well as itspharmacological exploitation (Lopez-Rodriguez et al., 2003)have been suggested before, available human evidence is verylimited. Furthermore, we found a linkage between 5-HT2Cantagonism and sleepiness. The role of the 5-HT2C receptor inpromoting sleep has previously been proposed for drugs such asmelatonin and agomelatin (Mitchell and Weinshenker, 2010).
J. Michl et al.8
Please cite this article as: Michl, J., et al., A multivariate approach linking reported side effects of clinical antidepressant andantipsychotic trials to in.... European Neuropsychopharmacology (2014), http://dx.doi.org/10.1016/j.euroneuro.2014.06.013

Antidepressant-induced sweating is commonly related tonoradrenergic stimulation (Stahl et al., 2005). Surprisingly,in this study increased sweating has mainly been attributedto 5-HTT inhibition and only to a lesser degree to NETinhibition. It is noteworthy that medication-inducedchanges of thermoregulation are poorly understood andlikely result from altered hypothalamic 5-HT signaling,which is in line with our findings (Ghaleiha et al., 2012).Apart from well-studied candidates such as 5-HT2C-, M3-, H1-receptors (Kroeze et al., 2003; Silvestre and Prous, 2005),we report further molecular targets to be potentially linkedto weight gain such as 5-HT2A and specifically 5-HT6. It isgenerally accepted that 5-HT-ergic neurotransmissionimpinges on food intake. This is also substantiated by theclinical efficacy of fluoxetine in the treatment of bulimia.However, the specific post-synaptic effector sites are stillunder debate: 5-HT6-receptor antagonists have beenobserved to reduce food intake in rodents (Halford et al.,2007). In rats, this has been linked to an action at 5-HT6-receptors expressed in the paraventricular nucleus of thehypothalamus and/or the nucleus tractus solitarii but not atthe arcuate nucleus (Garfield et al., 2014). Surprisingly, ourobservations suggest that blockage of 5-HT6-receptors is asso-ciated with weight gain in patients. At present, it is obviouslyimpossible to resolve this discrepancy. It is worth noting,though, that there are large interspecies differences in thedistribution of 5-HT6-receptors (Hirst et al., 2003). This suggeststhat murine data cannot be readily extrapolated to thesituation in people. Furthermore, several paradigms thatexamined rodent feeding behavior focused on short termhypohagic responses to 5-HT6-receptor antagonists (see e.g.,(Garfield et al., 2014)). Long term exposure to 5-HT6-receptoragonist, however, causes a hypophagic response in rats (Fisaset al., 2006). This observation predicts that long-term treat-ment with 5-HT6-receptor antagonists results in hyperphagiaand weight gain, which – in fact – emerged from our analysis.Furthermore, the human 5-HT6-receptor has a high constitutiveactivity, while the rat receptor is silent under basal conditions(Fisas et al., 2006). The high basal activity of the unligandedhuman receptor ought to augment effects resulting fromantagonist occupancy. Last but not least it is important to notethat our analyses included depressive and schizophrenicpatients and not humans suffering from obesity. Moreover,acute depression and psychosis are frequently associated withunderweight due to lack of appetite and malnutrition (Suzukiet al., 2014). Hence, our finding of 5-HT6-related weight gainmight indicate important differences between psychiatric andobesity patient populations. Furthermore, 5-HT2A antagonismwas identified as a major contributor to weight gain. The roleof 5-HT2A in obesity has previously been proposed based on anassociation between genetic variability within the 5-HT2Areceptor gene and food as well as alcohol intake in obesepatients (Aubert et al., 2000). Finally, we found that NET and5-HTT inhibition are either not linked to or even protectiveagainst weight gain. This is in line with SNRI studies thatresulted in the licensing as anti-obesity drugs (e.g. sibutra-mine). Notably, other mechanisms such as peripheralincreased lipogenesis and decreased insulin sensitivity(Sacher et al., 2008) are also thought to be involved inantipsychotic-induced metabolic side effects.
Our approach is not without limitations. While we havebeen able to reproduce many known mechanisms for ADRs
on a human as well as on an animal level, several ADRs (seeresults section) could not be significantly linked to in vitroreceptor- and transporter binding profiles. This lack ofassociation is not surprising and does not argue against thesensitivity of our approach. One reason for this failure is thefact that many reported symptoms such as fatigue andsexual dysfunction are frequent manifestations of thedisease itself rather than ADRs. Therefore, these symptomsare also reported to occur in placebo-treated controlgroups. Ideally ADR frequencies should be normalized to a‘baseline-frequency’. However, this was not possible sincethe majority of clinical trials included in this study werereference-controlled trials. Within this context it is impor-tant to note that reported Q2 values indicate the likelihoodthat such random correlations between drug target inter-action profiles and drug-unrelated symptoms can occur.Hence, results showing moderate or high Q2 values are verylikely to represent associations between drug targets and“true” ADRs. Another bias is the lack of standardizedreporting tools for ADRs in clinical trials. In most clinicaltrials, patients have to spontaneously report ADRs. Thisleads to considerably lower reports than when ADRs arecontinuously assessed using a questionnaire or scale duringeach study visit. For example, the occurrence of sexualdysfunction in males during SSRI treatment is known to bevery common (Perlis et al., 2009). However, patients areoften reluctant to report this symptom spontaneously. Onthe other hand, a rigorous assessment of certain ADRs maylead to over-estimation. For example, in trials comparingSSRIs to TCAs, reports of TCA-typical ADRs in the SSRI grouptend to be higher, since clinicians specifically focus on theassessment of their potential occurrence. Hence, it needs tobe mentioned that the measurement of in vitro bindingprofiles is possible with relatively high precision, whereasADR profiles are less precise.
Moreover, our model did not include all possible biologicalor pharmacological determinants that might affect theoccurrence of ADRs. The presence of active metaboliteshas not been considered within this study for e.g. effects ofquetiapine are thought to be mediated by the actions ofboth, quetiapine and its active metabolite norquetiapine.In contrast to quetiapine, norquetiapine has high affinity toNET, which may contribute to its broad spectrum of efficacy(Nyberg et al., 2013). Similarly, (2S, 3S)-hydroxybupropion,a major metabolite of bupropion, is believed to contributeto its antidepressant activity. Compared with bupropion,(2S, 3S)-hydroxybupropion produces similar or strongerinhibition of DA and NE uptake (Damaj et al., 2004).Furthermore, some ADRs may only occur under high-dosetreatment, whereas others occur even at low doses.In addition, certain ADRs are dependent on the durationof the drug treatment. For example, gastrointestinal symp-toms are more common during the initial phase of SSRItreatment, whereas sexual dysfunction or anticholinergicADRs also occur during chronic treatment. However, dose ortreatment duration were not separately analyzed in thisstudy due to the lack of specific information available in theCochrane reviews. Similarly, genetic susceptibility to ADRshas not been analyzed (Rabl et al., 2010).
Furthermore, this study did not consider interactionsbetween possible drug target combinations due to theastronomic number of possibilities. This is likely the reason
9Linking clinically reported side effects to in vitro binding profiles
Please cite this article as: Michl, J., et al., A multivariate approach linking reported side effects of clinical antidepressant andantipsychotic trials to in.... European Neuropsychopharmacology (2014), http://dx.doi.org/10.1016/j.euroneuro.2014.06.013

why we did for example not detect the protective effect of5-HT2A-receptor antagonism against extrapyramidal motorsymptoms, which only occurs in the presence of D2-receptorantagonism (Tauscher et al., 2002).
Due to above-mentioned reasons most models showedonly moderate predictive power. However, even modelswith low Q2 values can be plausible such as for constipation.Since diarrhea is frequently caused by SSRIs (Gartlehneret al., 2008), 5-HTT inhibition is likely protective againstconstipation. This relationship was well-preserved withinthis study despite a very low Q2 value.
ADRs provide a glimpse into the dynamics of humanmolecular biology that is otherwise inaccessible. This is inparticular true for the human brain and specifically mentaldisorders, which are difficult to study in animal experi-ments. Mining psychotropic medication-induced ADRs inpatient samples provides an ethically sound and informativeapproach to probe the molecular mechanisms of ADRsoccurring in patient populations, which lead frequently totreatment discontinuation.
In conclusion, this study provides compelling evidence fora multitude of associations between molecular targets andADRs that are observed in clinical trials of ADs and APs.While many mechanisms have been reported before, thisstudy was able to identify potential novel causes for ADRs,which should be considered in the development of futurepsychotropic medications, such as 5-HT6-receptor antagon-ism in weight gain, and 5-HT7-receptor antagonism insleepiness. Furthermore, the present study demonstratesthat many frequent ADRs such as hypotension, dizziness,sleepiness, insomnia and sedation are resulting from avariety of molecular mechanisms.
Role of funding source
Funding for this study was provided by the project program grantSFB35 of the Austrian Science Fund (FWF). The FWF had no furtherrole in study design; in the collection, analysis and interpretation ofdata; in the writing of the report; and in the decision to submit thepaper for publication.
Contributors
J. Michl, M. Zauner, C. Scharinger, H.H. Sitte, M. Freissmuth,L. Pezawas and G. F. Ecker participated in the research design.J. Michl and M. Zauner conducted experiments. J. Michl andG. F. Ecker performed data analysis. J. Michl wrote the first draftof the manuscript. All authors contributed to and have approvedthe final manuscript.
Conflict of interest
All authors declare that they have no conflicts of interest.
Acknowledgments
This study was funded by the project program grant SFB35 of theAustrian Science Fund (FWF).
Appendix A. Supplementary material
Supplementary data associated with this article can befound in the online version at http://dx.doi.org/10.1016/j.euroneuro.2014.06.013.
References
Al-Shamma, H.A., Anderson, C., Chuang, E., Luthringer, R., Grot-tick, A.J., Hauser, E., Morgan, M., Shanahan, W., Teegarden,B.R., Thomsen, W.J., Behan, D., 2010. Nelotanserin, a novelselective human 5-hydroxytryptamine2A inverse agonist for thetreatment of insomnia. J. Pharmacol. Exp. Ther. 332, 281–290.
Aubert, R., Betoulle, D., Herbeth, B., Siest, G., Fumeron, F., 2000.5-HT2A receptor gene polymorphism is associated with food andalcohol intake in obese people. Int. J. Obes. Relat. Metab.Disord. 24, 920–924.
Baghai, T.C., Blier, P., Baldwin, D.S., Bauer, M., Goodwin, G.M.,Fountoulakis, K.N., Kasper, S., Leonard, B.E., Malt, U.F., Stein,D.J., Versiani, M., Moller, H.J., 2012. Executive summary of thereport by the WPA section on pharmacopsychiatry on generaland comparative efficacy and effectiveness of antidepressants inthe acute treatment of depressive disorders. Eur. Arch. Psychia-try Clin. Neurosci. 262, 13–22.
Barbanti, P., Fofi, L., Aurilia, C., Egeo, G., 2013. Dopaminergicsymptoms in migraine. Neurol. Sci. 34 (Suppl 1), S67–S70.
Bauer, M., Pfennig, A., Severus, E., Whybrow, P.C., Angst, J.,Moller, H.J., 2013. World Federation of Societies of BiologicalPsychiatry (WFSBP) guidelines for biological treatment of uni-polar depressive disorders, part 1: update 2013 on the acute andcontinuation treatment of unipolar depressive disorders. WorldJ. Biol. Psychiatry 14, 334–385.
Bender, A., Scheiber, J., Glick, M., Davies, J.W., Azzaoui, K.,Hamon, J., Urban, L., Whitebread, S., Jenkins, J.L., 2007.Analysis of pharmacology data and the prediction of adversedrug reactions and off-target effects from chemical structure.ChemMedChem 2, 861–873.
Castro, V.M., Clements, C.C., Murphy, S.N., Gainer, V.S., Fava, M.,Weilburg, J.B., Erb, J.L., Churchill, S.E., Kohane, I.S., Iosifescu,D.V., Smoller, J.W., Perlis, R.H., 2013. QT interval and anti-depressant use: a cross sectional study of electronic healthrecords. Br. Med. J., 346.
Damaj, M.I., Carroll, F.I., Eaton, J.B., Navarro, H.A., Blough, B.E.,Mirza, S., Lukas, R.J., Martin, B.R., 2004. Enantioselectiveeffects of hydroxy metabolites of bupropion on behavior andon function of monoamine transporters and nicotinic receptors.Mol. Pharmacol. 66, 675–682.
Ferre, S., 2010. Role of the central ascending neurotransmittersystems in the psychostimulant effects of caffeine. J. Alzhei-mers Dis. 20 (Suppl 1), S35–S49.
Fisas, A., Codony, X., Romero, G., Dordal, A., Giraldo, J., Merce,R., Holenz, J., Heal, D., Buschmann, H., Pauwels, P.J., 2006.Chronic 5-HT6 receptor modulation by E-6837 induces hypopha-gia and sustained weight loss in diet-induced obese rats. Br. J.Pharmacol. 148, 973–983.
Garfield, A.S., Burke, L.K., Shaw, J., Evans, M.L., Heisler, L.K.,2014. Distribution of cells responsive to 5-HT6 receptorantagonist-induced hypophagia. Behav. Brain Res. 266, 201–206.
Gartlehner, G., Gaynes, B.N., Hansen, R.A., Thieda, P., DeVeaugh-Geiss, A., Krebs, E.E., Moore, C.G., Morgan, L., Lohr, K.N.,2008. Comparative benefits and harms of second-generationantidepressants: background paper for the American College ofPhysicians. Ann. Intern. Med. 149, 734–750.
J. Michl et al.10
Please cite this article as: Michl, J., et al., A multivariate approach linking reported side effects of clinical antidepressant andantipsychotic trials to in.... European Neuropsychopharmacology (2014), http://dx.doi.org/10.1016/j.euroneuro.2014.06.013

Gershon, M.D., 2004. Review article: serotonin receptors andtransporters – roles in normal and abnormal gastrointestinalmotility. Aliment Pharmacol. Ther. 20 (Suppl 7), 3–14.
Ghaleiha, A., Jahangard, L., Sherafat, Z., Ahmadpanah, M., Brand,S., Holsboer-Trachsler, E., Bajoghli, H., Haghighi, M., 2012.Oxybutynin reduces sweating in depressed patients treated withsertraline: a double-blind, placebo-controlled, clinical study.Neuropsychiatr. Dis. Treat. 8, 407–412.
Grunze, H., Vieta, E., Goodwin, G.M., Bowden, C., Licht, R.W.,Moller, H.J., Kasper, S., Treatment, W.T.F., 2013. The WorldFederation of Societies of Biological Psychiatry (WFSBP) guide-lines for the biological treatment of bipolar disorders: update2012 on the long-term treatment of bipolar disorder. WorldJ. Biol. Psychiatry 14, 154–219.
Haas, H.L., Sergeeva, O.A., Selbach, O., 2008. Histamine in thenervous system. Physiol. Rev. 88, 1183–1241.
Halford, J.C., Harrold, J.A., Boyland, E.J., Lawton, C.L., Blundell,J.E., 2007. Serotonergic drugs: effects on appetite expressionand use for the treatment of obesity. Drugs 67, 27–55.
Hasan, A., Falkai, P., Wobrock, T., Lieberman, J., Glenthoj, B.,Gattaz, W.F., Thibaut, F., Moller, H.J., Guideli, W.T.F.T., 2013.World Federation of Societies of Biological Psychiatry (WFSBP)guidelines for biological treatment of schizophrenia, Part 2:update 2012 on the long-term treatment of schizophrenia andmanagement of antipsychotic-induced side effects. World J. Biol. Psychiatry 14, 2–44.
Hirst, W.D., Abrahamsen, B., Blaney, F.E., Calver, A.R., Aloj, L.,Price, G.W., Medhurst, A.D., 2003. Differences in the centralnervous system distribution and pharmacology of the mouse 5-hydroxytryptamine-6 receptor compared with rat and humanreceptors investigated by radioligand binding, site-directedmutagenesis, and molecular modeling. Mol. Pharmacol. 64,1295–1308.
Huf, W., Kalcher, K., Pail, G., Friedrich, M.E., Filzmoser, P., Kasper,S., 2011. Meta-analysis: fact or fiction? How to interpret meta-analyses. World J. Biol. Psychiatry 12, 188–200.
Insel, T.R., 2012. Next-generation treatments for mental disorders.Sci. Transl. Med. 4 (155ps119).
Jones, R.W., 2010. A review comparing the safety and tolerability ofmemantine with the acetylcholinesterase inhibitors. Int.J. Geriatr. Psychiatry 25, 547–553.
Kroeze, W.K., Hufeisen, S.J., Popadak, B.A., Renock, S., Steinberg,S.A., Ernsberger, P., Jayathilake, K., Meltzer, H.Y., Roth, B.L.,2003. HI-histamine receptor affinity predicts short-term weightgain for typical and atypical antipsychotic drugs. Neuropsycho-pharmacology 28, 519–526.
Leatherman, M.E., Bebchuk, J.M., Ekstrom, R.D., Heine, A.D.,Carson, S.W., Golden, R.N., 1999. The effects of serotonin(3) receptor blockade on the psychobiological response tointravenous clomipramine in healthy human subjects. Biol.Psychiatry 45, 238–240.
Lopez-Munoz, F., Alamo, C., 2009. Monoaminergic neurotransmis-sion: the history of the discovery of antidepressants from 1950suntil today. Curr. Pharm. Des. 15, 1563–1586.
Lopez-Rodriguez, M.L., Porras, E., Morcillo, M.J., Benhamu, B.,Soto, L.J., Lavandera, J.L., Ramos, J.A., Olivella, M., Campillo,M., Pardo, L., 2003. Optimization of the pharmacophore modelfor 5-HT7R antagonism. Design and synthesis of new naphtho-lactam and naphthosultam derivatives. J. Med. Chem. 46,5638–5650.
Lounkine, E., Keiser, M.J., Whitebread, S., Mikhailov, D., Hamon,J., Jenkins, J.L., Lavan, P., Weber, E., Doak, A.K., Cote, S.,Shoichet, B.K., Urban, L., 2012. Large-scale prediction andtesting of drug activity on side-effect targets. Nature 486,361–367.
Mitchell, H.A., Weinshenker, D., 2010. Good night and good luck:norepinephrine in sleep pharmacology. Biochem. Pharmacol. 79,801–809.
Montplaisir, J., Fantini, M.L., Desautels, A., Michaud, M., Petit, D.,Filipini, D., 2006. Long-term treatment with pramipexole inrestless legs syndrome. Eur. J. Neurol. 13, 1306–1311.
Nagatomo, T., Rashid, M., Abul Muntasir, H., Komiyama, T., 2004.Functions of 5-HT2A receptor and its antagonists in the cardi-ovascular system. Pharmacol. Ther. 104, 59–81.
Nutt, D.J., 2009. Beyond psychoanaleptics - can we improveantidepressant drug nomenclature? (vol 23, pg 343, 2009).J. Psychopharmacol. 23 861.
Nyberg, S., Jucaite, A., Takano, A., Kagedal, M., Cselenyi, Z.,Halldin, C., Farde, L., 2013. Norepinephrine transporter occu-pancy in the human brain after oral administration of quetiapineXR. Int. J. Neuropsychopharmacol. 16, 2235–2244.
Perlis, R.H., Laje, G., Smoller, J.W., Fava, M., Rush, A.J.,McMahon, F.J., 2009. Genetic and clinical predictors of sexualdysfunction in citalopram-treated depressed patients. Neurop-sychopharmacology 34, 1819–1828.
Rabl, U., Scharinger, C., Muller, M., Pezawas, L., 2010. Imaginggenetics: implications for research on variable antidepressantdrug response. Expert Rev. Clin. Pharmacol. 3, 471–489.
Roth, B.L., Sheffler, D.J., Kroeze, W.K., 2004. Magic shotgunsversus magic bullets: selectively non-selective drugs for mooddisorders and schizophrenia. Nat. Rev. Drug Discov. 3, 353–359.
Sacher, J., Mossaheb, N., Spindelegger, C., Klein, N., Geiss-Granadia, T., Sauermann, R., Lackner, E., Joukhadar, C., Muller,M., Kasper, S., 2008. Effects of olanzapine and ziprasidone onglucose tolerance in healthy volunteers. Neuropsychopharma-cology 33, 1633–1641.
Sehgal, A., Mignot, E., 2011. Genetics of sleep and sleep disorders.Cell 146, 194–207.
Selent, J., Bauer-Mehren, A., Lopez, L., Loza, M.I., Sanz, F., Pastor,M., 2010. A novel multilevel statistical method for the study ofthe relationships between multireceptorial binding affinityprofiles and in vivo endpoints. Mol. Pharmacol. 77, 149–158.
Silvestre, J.S., Prous, J., 2005. Research on adverse drug events. I.Muscarinic M3 receptor binding affinity could predict the risk ofantipsychotics to induce type 2 diabetes. Methods Find. Exp.Clin. Pharmacol. 27, 289–304.
Stahl, S.M., Grady, M.M., Moret, C., Briley, M., 2005. SNRIs: theirpharmacology, clinical efficacy, and tolerability in comparisonwith other classes of antidepressants. CNS Spectr. 10, 732–747.
Suzuki, Y., Sugai, T., Fukui, N., Watanabe, J., Ono, S., Tsuneyama,N., Saito, M., Someya, T., 2014. High prevalence of underweightand undernutrition in Japanese inpatients with schizophrenia.Psychiatry Clin. Neurosci. 68, 78–82.
Tauscher, J., Kufferle, B., Asenbaum, S., Tauscher-Wisniewski, S.,Kasper, S., 2002. Striatal dopamine-2 receptor occupancy asmeasured with [123I]iodobenzamide and SPECT predicted theoccurrence of EPS in patients treated with atypical antipsycho-tics and haloperidol. Psychopharmacology 162, 42–49.
Trygg, J., Wold, S., 2002. Orthogonal projections to latent struc-tures (O-PLS). J. Chemom. 16, 119–128.
Tuerke, K.J., Limebeer, C.L., Fletcher, P.J., Parker, L.A., 2012.Double dissociation between regulation of conditioned disgustand taste avoidance by serotonin availability at the 5-HT3receptor in the posterior and anterior insular cortex. J. Neu-rosci. 32, 13709–13717.
Vanover, K.E., Davis, R.E., 2010. Role of 5-HT2A receptor antago-nists in the treatment of insomnia. Nat. Sci. Sleep 2, 139–150.
Vos, T., Flaxman, A.D., Naghavi, M., Lozano, R., Michaud, C.,Ezzati, M., Shibuya, K., Salomon, J.A., Abdalla, S., Aboyans, V.,Abraham, J., Ackerman, I., Aggarwal, R., Ahn, S.Y., Ali, M.K.,Alvarado, M., Anderson, H.R., Anderson, L.M., Andrews, K.G.,Atkinson, C., Baddour, L.M., Bahalim, A.N., Barker-Collo, S.,Barrero, L.H., Bartels, D.H., Basanez, M.G., Baxter, A., Bell,M.L., Benjamin, E.J., Bennett, D., Bernabe, E., Bhalla, K.,Bhandari, B., Bikbov, B., Bin Abdulhak, A., Birbeck, G., Black,J.A., Blencowe, H., Blore, J.D., Blyth, F., Bolliger, I.,
11Linking clinically reported side effects to in vitro binding profiles
Please cite this article as: Michl, J., et al., A multivariate approach linking reported side effects of clinical antidepressant andantipsychotic trials to in.... European Neuropsychopharmacology (2014), http://dx.doi.org/10.1016/j.euroneuro.2014.06.013

Bonaventure, L., Boufous, S., Bourne, R., Boussinesq, M.,Braithwaite, T., Brayne, C., Bridgett, L., Brooker, S., Brooks, P.,Brugha, T.S., Bryan-Hancock, C., Bucello, C., Buchbinder, R.,Buckle, G., Budke, C.M., Burch, M., Burney, P., Burstein, R.,Calabria, B., Campbell, B., Canter, C.E., Carabin, H., Carapetis,J., Carmona, L., Cella, C., Charlson, F., Chen, H., Cheng, A.T.,Chou, D., Chugh, S.S., Coffeng, L.E., Colan, S.D., Colquhoun, S.,Colson, K.E., Condon, J., Connor, M.D., Cooper, L.T., Corriere,M., Cortinovis, M., de Vaccaro, K.C., Couser, W., Cowie, B.C.,Criqui, M.H., Cross, M., Dabhadkar, K.C., Dahiya, M., Dahodwala,N., Damsere-Derry, J., Danaei, G., Davis, A., De Leo, D.,Degenhardt, L., Dellavalle, R., Delossantos, A., Denenberg, J.,Derrett, S., Des Jarlais, D.C., Dharmaratne, S.D., Dherani, M.,Diaz-Torne, C., Dolk, H., Dorsey, E.R., Driscoll, T., Duber, H.,Ebel, B., Edmond, K., Elbaz, A., Ali, S.E., Erskine, H., Erwin, P.J.,Espindola, P., Ewoigbokhan, S.E., Farzadfar, F., Feigin, V., Felson,D.T., Ferrari, A., Ferri, C.P., Fevre, E.M., Finucane, M.M., Flax-man, S., Flood, L., Foreman, K., Forouzanfar, M.H., Fowkes, F.G.,Franklin, R., Fransen, M., Freeman, M.K., Gabbe, B.J., Gabriel, S.E., Gakidou, E., Ganatra, H.A., Garcia, B., Gaspari, F., Gillum, R.F., Gmel, G., Gosselin, R., Grainger, R., Groeger, J., Guillemin,F., Gunnell, D., Gupta, R., Haagsma, J., Hagan, H., Halasa, Y.A.,Hall, W., Haring, D., Haro, J.M., Harrison, J.E., Havmoeller, R.,Hay, R.J., Higashi, H., Hill, C., Hoen, B., Hoffman, H., Hotez,P.J., Hoy, D., Huang, J.J., Ibeanusi, S.E., Jacobsen, K.H., James,S.L., Jarvis, D., Jasrasaria, R., Jayaraman, S., Johns, N., Jonas,J.B., Karthikeyan, G., Kassebaum, N., Kawakami, N., Keren, A.,Khoo, J.P., King, C.H., Knowlton, L.M., Kobusingye, O., Koran-teng, A., Krishnamurthi, R., Lalloo, R., Laslett, L.L., Lathlean, T.,Leasher, J.L., Lee, Y.Y., Leigh, J., Lim, S.S., Limb, E., Lin, J.K.,Lipnick, M., Lipshultz, S.E., Liu, W., Loane, M., Ohno, S.L., Lyons,R., Ma, J., Mabweijano, J., MacIntyre, M.F., Malekzadeh, R.,Mallinger, L., Manivannan, S., Marcenes, W., March, L., Margolis,D.J., Marks, G.B., Marks, R., Matsumori, A., Matzopoulos, R.,Mayosi, B.M., McAnulty, J.H., McDermott, M.M., McGill, N.,McGrath, J., Medina-Mora, M.E., Meltzer, M., Mensah, G.A.,Merriman, T.R., Meyer, A.C., Miglioli, V., Miller, M., Miller, T.R.,Mitchell, P.B., Mocumbi, A.O., Moffitt, T.E., Mokdad, A.A.,Monasta, M.N., Montico, M., Moradi-Lakeh, M., Moran, A.,
Morawska, L., Mori, R., Murdoch, M.E., Mwaniki, M.K., Naidoo,K., Nair, M.N., Naldi, L., Narayan, K.M., Nelson, P.K., Nelson,R.G., Nevitt, M.C., Newton, C.R., Nolte, S., Norman, P., Norman,R., O'Donnell, M., O'Hanlon, S., Olives, C., Omer, S.B., Ortblad,K., Osborne, R., Ozgediz, D., Page, A., Pahari, B., Pandian, J.D.,Rivero, A.P., Patten, S.B., Pearce, N., Padilla, R.P., Perez-Ruiz, F.,Perico, N., Pesudovs, K., Phillips, D., Phillips, M.R., Pierce, K.,Pion, S., Polanczyk, G.V., Polinder, S., Pope 3rd, C.A., Popova, S.,Porrini, E., Pourmalek, F., Prince, M., Pullan, R.L., Ramaiah, K.D.,Ranganathan, D., Razavi, H., Regan, M., Rehm, J.T., Rein, D.B.,Remuzzi, G., Richardson, K., Rivara, F.P., Roberts, T., Robinson,C., De Leon, F.R., Ronfani, L., Room, R., Rosenfeld, L.C.,Rushton, L., Sacco, R.L., Saha, S., Sampson, U., Sanchez-Riera,L., Sanman, E., Schwebel, D.C., Scott, J.G., Segui-Gomez, M.,Shahraz, S., Shepard, D.S., Shin, H., Shivakoti, R., Singh, D.,Singh, G.M., Singh, J.A., Singleton, J., Sleet, D.A., Sliwa, K.,Smith, E., Smith, J.L., Stapelberg, N.J., Steer, A., Steiner, T.,Stolk, W.A., Stovner, L.J., Sudfeld, C., Syed, S., Tamburlini, G.,Tavakkoli, M., Taylor, H.R., Taylor, J.A., Taylor, W.J., Thomas, B.,Thomson, W.M., Thurston, G.D., Tleyjeh, I.M., Tonelli, M.,Towbin, J.A., Truelsen, T., Tsilimbaris, M.K., Ubeda, C., Undur-raga, E.A., van der Werf, M.J., van Os, J., Vavilala, M.S.,Venketasubramanian, N., Wang, M., Wang, W., Watt, K., Weath-erall, D.J., Weinstock, M.A., Weintraub, R., Weisskopf, M.G.,Weissman, M.M., White, R.A., Whiteford, H., Wiersma, S.T.,Wilkinson, J.D., Williams, H.C., Williams, S.R., Witt, E., Wolfe,F., Woolf, A.D., Wulf, S., Yeh, P.H., Zaidi, A.K., Zheng, Z.J.,Zonies, D., Lopez, A.D., Murray, C.J., AlMazroa, M.A., Memish,Z.A., 2012. Years lived with disability (YLDs) for 1160 sequelae of289 diseases and injuries 1990-2010: a systematic analysis for theGlobal Burden of Disease Study 2010. Lancet 380, 2163–2196.
Wolff, M.C., Leander, J.D., 2000. A comparison of the behaviouraleffects of 5-HT2A and 5-HT2C receptor agonists in the pigeon.Behav. Pharmacol. 11, 355–364.
Zinner, N., Tuttle, J., Marks, L., 2005. Efficacy and tolerability ofdarifenacin, a muscarinic M3 selective receptor antagonist (M3SRA), compared with oxybutynin in the treatment of patientswith overactive bladder. World J. Urol. 23, 248–252.
J. Michl et al.12
Please cite this article as: Michl, J., et al., A multivariate approach linking reported side effects of clinical antidepressant andantipsychotic trials to in.... European Neuropsychopharmacology (2014), http://dx.doi.org/10.1016/j.euroneuro.2014.06.013




















