A multicentre comparative study of serum lipids and apolipoproteins in long-term users of DMPA and a...
15
Contraception 47:177-191,1993 A MULTICENTRE COMPARATIVE STUDY OF SERUM LIPIDS AND APOLIPOPROTEINS IN LONG-TERM USERS OF DMPA AND A CONTROL GROUP OF IUD USERS WORLD HEALTH ORGANIZATION Task Force on Long-Acting Systemic Agents for Fertility Regulation Special Programme of Research, Development and Research Training in Human Reproduction Rachanee Kongsayreepong, Supawat Chutivongse Chulalongkom Hospital Medical School, Bangkok, Thailand P. George, S. Joyce and J.M. McCone The Princess Margaret Hospital, Christchurch, New Zealand J. Garza-Flores, V. Valles de Bourges, D.L. de La Cruz and G. Perez-Palacios Department of Reproductive Biology, National Institute of Nutrition, Mexico City, Mexico M. Rosseneu and W. De Keersgieter Clinical Chemistry Laboratory, Algemeen Ziekenhuis Sint Jan, Brugge, Belgium C. d’Arcangues, E.M. Belsey, N. Carlson, P. Hall, and F. Schlagenhaft Special Programme of Research, Development and Research Training in Human Reproduction, World Health Organization, Geneva, Switzerland Address for correspondence: Catherine d’Arcangues, Special Programme of Research, Development and Research Training in Human Reproduction, World Health Organization, 1211 Geneva 27, Switzerland Submitted for publication April 29, 1992 Accepted for publication December 8, 1992 Copyright 0 1993 Butterworth-Heinemann
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of A multicentre comparative study of serum lipids and apolipoproteins in long-term users of DMPA and a...

Contraception 47:177-191,1993
A MULTICENTRE COMPARATIVE STUDY OF SERUM LIPIDS AND APOLIPOPROTEINS IN LONG-TERM USERS OF DMPA
AND A CONTROL GROUP OF IUD USERS
WORLD HEALTH ORGANIZATION
Task Force on Long-Acting Systemic Agents for Fertility Regulation Special Programme of Research, Development and Research
Training in Human Reproduction
Rachanee Kongsayreepong, Supawat Chutivongse Chulalongkom Hospital Medical School, Bangkok, Thailand
P. George, S. Joyce and J.M. McCone The Princess Margaret Hospital, Christchurch, New Zealand
J. Garza-Flores, V. Valles de Bourges, D.L. de La Cruz and G. Perez-Palacios Department of Reproductive Biology, National Institute of Nutrition, Mexico City, Mexico
M. Rosseneu and W. De Keersgieter Clinical Chemistry Laboratory, Algemeen Ziekenhuis Sint Jan, Brugge, Belgium
C. d’Arcangues, E.M. Belsey, N. Carlson, P. Hall, and F. Schlagenhaft Special Programme of Research, Development and Research Training in Human Reproduction, World Health Organization, Geneva, Switzerland
Address for correspondence:
Catherine d’Arcangues, Special Programme of Research, Development and Research Training in Human Reproduction, World Health Organization, 1211 Geneva 27, Switzerland
Submitted for publication April 29, 1992 Accepted for publication December 8, 1992
Copyright 0 1993 Butterworth-Heinemann

178 Contraception
ABSTRACT
A clinical trial was conducted in three centres to assess the effects of long-term use of the injectable contraceptive depot-medroxyprogesterone acetate (DMPA) on lipid metabolism. Fifty women who had used DMPA at a dose of 150 mg every three months for 3 to 9 years were recruited in Bangkok, Christchurch and Mexico City. They were compared to a control group of 120 IUD users. Total cholesterol, LDL-cholesterol, HDL-cholesterol, total triglycerides, apolipoproteins AI, AI1 and B were measured throughout one injection interval.
Significant findings differed between centres. Compared to their own centre controls, DMPA users in Bangkok had higher LDL-cholesterol levels; those in Christchurch had lower HDL-cholesterol, apolipoprotein (apo) AI and apo AI/B ratio and higher apo B levels; those in Mexico City had a lower apo AI/B ratio. Further changes were observed during the injection interval, some of which were correlated to changes in serum MPA levels.
It is concluded that long-term use of DMPA induces moderate changes in lipid metabolism which are unfavourable in terms of risk for atherosclerosis. This should be borne in mind when weighing the overall risks and benefits of this contraceptive method for a potential user.
INTRODUCTION
Depot-medroxyprogesterone acetate (DMPA) is a progestogen-only injectable contraceptive used widely throughout the world by approximately 10 million women. A review of its safety as a contraceptive, carried out by WHO in 1982 (l), pointed out that limited data are available on its effect on lipid metabolism, particularly with long-term use. Subsequent studies have given contradictory results, possibly because of the various clinical trial designs, methodologies used and populations studied.
At the contraceptive dose of 150 mg DMPA every 3 months over one year, Tankeyoon et al. (2) observed in 16 women a progressive fall in total cholesterol, significant at 9 and 12 months of use, and a significant decrease in total triglycerides, as early as 2 months after the first injection. Under the same conditions, Amatayakul et al. (3) observed no change in total cholesterol, total triglycerides or phospholipids in 12 Thai women, nor did Fajumi (4) studying 63 Nigerian women, some of whom had used DMPA for 30 months. By contrast, in a cross-sectional study of 157 DMPA users compared to 162 controls, Liew et al. (5) found that, with prolonged use of up to 5 years, there was a gradual increase in total cholesterol but no consistent change in triglycerides.
Kremer et al. (6) monitored the HDL-cholesterol (HDL-C) levels of 23 one-year users of DMPA, over one injection period. HDL-C was significantly lower than in an IUD control group and did not vary during the injection interval. More recently, Barnes et al. (7) also measured the effect of one-year use of DMPA in contraceptive dose in 17

Contraception 179
women: total cholesterol and LDL-cholesterol (LDL-C) had decreased significantly while HDL-C levels were unchanged. Deslypere et al. (8) found that 15 Belgian women who had used DMPA for contraception for an average period of 7 years continuously had reduced HDL-C and apolipoprotein AI (apo AI) levels when compared to controls, but no difference in total C, LDL-C and apolipoprotein B (apo B).
In view of these various findings, this study was undertaken to evaluate the effects of DMPA after several years of use for contraception, in different populations worldwide.
MATERIAL AND METHODS
Desien of the study
Women recruited in the study were healthy, informed volunteers, aged between 25 and 40 years old inclusive, who had been using DMPA for contraception at a dose of 150 mg every 3 months, continuously for several years, preferably for a minimum of 4 years and a maximum of 6 years.
They were compared to a control group of healthy women volunteers, in the same age group, who were using a non-hormone releasing IUD or barrier methods for contraception. Other recruitment criteria for these control subjects were that: they should be at least 6 months postpartum or post-abortion, having had one normal cycle since delivery or abortion; they should not be lactating and should have stopped lactating at least 6 months before admission into the study; they should not have used any oral hormonal contraceptive for 6 months or injectable hormonal contraceptive for 12 months before admission into the study.
Women were not included in this study if they had any of the following conditions: hypertension, diabetes, history of thromboembolism, recent or severe past liver disease, suspected malignancy, abnormal Papanicolaou smear. Women who were receiving treatment for lipid disorders in the form of a restricted diet and/or drug therapy and those who were receiving long-term treatment for a chronic disorder were also excluded.
DMPA users had blood samples drawn during one DMPA injection interval on the following days: day of injection, 2, 4, 8 weeks later and on the day of the next injection, i.e., 13 weeks later. Control subjects had two blood samples taken, two weeks apart.
The study was conducted in three centres, in Bangkok (Thailand), Christchurch (New Zealand) and Mexico City.
180
Laboratorv orocedures
Contraception
1.
2.
3.
4.
5.
Each blood sample was assayed for the following:
Total cholesterol, determined by an enzymatic method (9).
HDL-C, using precipitation by addition of phosphotungstate and magnesium ions
(10).
LDL-C, using precipitation by addition of polyvinyl sulphate (11).
Total triglycerides, determined by an enzymatic calorimetric method (12).
Apolipoproteins AI, AI1 and B by electroimmunoassay (13,14).
The cholesterol assays and the triglycerides assay were performed with reagents from Boehringer Mannheim, Federal Republic of Germany. Apofilms and reagents from Sebia, France, were used for the apolipoprotein assays.
All the laboratories participated in a lipid standardization programme conducted by the clinical chemistry reference laboratory of Algemeen Ziekenhuis Sint Jan in Brugge, Belgium. After an initial workshop in Brugge, to review the methodology of each assay, several months were spent setting up the assays in each laboratory and instituting internal and external quality control monitoring.
The interlaboratory coefficients of variation measured through regular external quality control exercises varied between 2.4 and 3.3 % for total cholesterol, 3.2 and 11.1% for HDL-C, 7.1 to 8.9% for LDL-C, and 4.8 and 5.8% for triglycerides. It should be noted that the samples used for these exercises were lyophilized specimens and that few of them were fully satisfactory for HDL-C and LDL-C assays. The centres noted consistently a much greater reproducibility in their measurements on fresh serum specimens. With internal quality controls, coefficients of variation varied between 0.3 and 3.0% for total cholesterol, 1.0 and 2.5% for HDL-C, 0.6 to 2.4 for LDL-C, 0.8 and 6.4% for triglycerides, 5.7 and 19% for apo B, 4.7 and 14% for apo AI, and 8.4 and 10% for apo AII.
In addition, serum haemoglobin and fasting glucose were measured on admission in all subjects. Medroxyprogesterone acetate levels were measured in the serum samples of DMPA users, by radioimmunoassay performed at the WHO Collaborating Centre for Research in Human Reproduction, Karolinska Institute, Stockholm, Sweden (15).
Statistical orocedures
Either the t-test or analysis of variance was used to determine the significance of differences in individual characteristics on admission between the DMPA users and
Contraception 181
controls within each centre, and between the three centres within each group. Comparisons between groups and centres with respect to Serum lipid levels on admission were made by means of analysis of covariance, with number of alcoholic drinks per week, number of cigarettes smoked per day, and Quetelet index as the covariates. Changes in serum MPA and lipid levels in the DMPA users, over the 13-week injection interval, were analyzed by repeated measures analysis of variance.
RESULTS
Subjects participatine and characteristics on admission
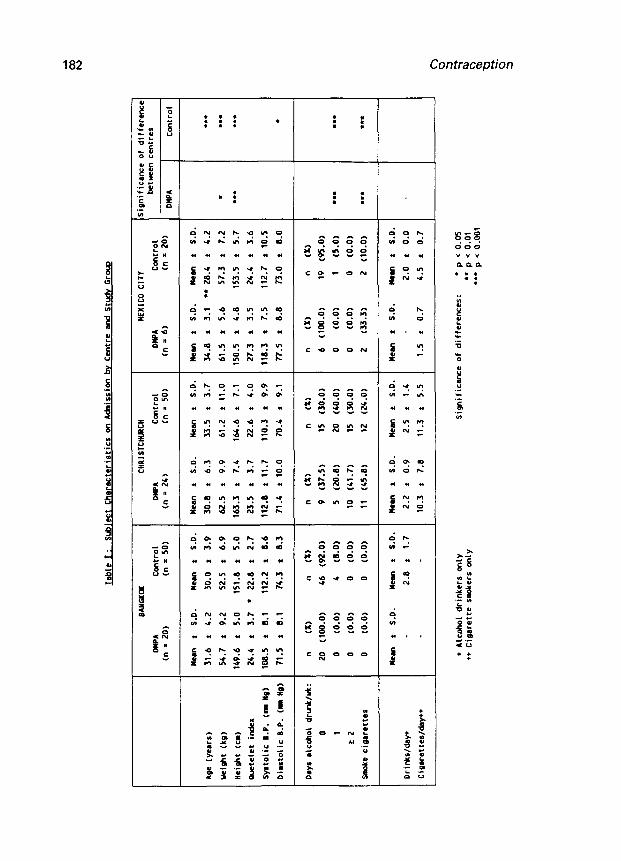
A total of 50 DMPA users and 120 controls were recruited to the study. There were significant differences between groups within two of the centres, and between centres within each group (Table I).
In Bangkok, 20 DMPA users who had used DMPA for a median time of 56 months (range 47-70 months) and 50 controls were admitted. The two groups were similar in age but the DMPA users were heavier and shorter, and thus, had a significantly higher Quetelet index than the controls.
In Christchurch, 24 DMPA users who had used DMPA for a median time of 60 months (range 45-118 months) and 50 controls were admitted. Both groups were similar with respect to weight, height, Quetelet index and blood pressure. The DMPA users were approximately 3 years younger than the controls and were almost twice as likely to smoke cigarettes, but these differences were not statistically significant.
In Mexico City, 6 DMPA users who had used DMPA for a median time of 53 months (range 48-75 months) and 20 controls were recruited. The DMPA users were significantly older than the controls, by more than 6 years.
There were a number of differences between the subjects recruited in the three centres . The DMPA usefs in Christchurch and Mexico City were heavier and more likely to smoke cigarettes than those admitted in Bangkok. The DMPA users in Christchurch were also taller and more likely to drink alcohol than those of the other centres. Control subjects in Christchurch were older than those in Bangkok or Mexico City.
LiDid measurements on admiSSiOn
Serum lipid levels were measured on admission in DMPA users and compared to the average of both measurements obtained in controls. After adjusting for alcohol drinking, smoking and Quetelet index, there were some significant differences in serum lipid levels between the study groups in each centre, but these were not consistent between centres (Table II).
Tabl
e I:
su
bjec
t Ch
arac
teri
stic
s 00
A&
issi
m bv
Ce
ntre
en
d St
udy
G~OL
Q
BAYG
XoX
cHRI
STcl
lwxn
HE
XlCO
CI
TY
Sign
ific
ance
of
di
ffer
mc
DWA
ccll
tro1
Dl
lPA
Cont
rol
DMPA
c0
ntro
1 be
twee
n cm
tres
(n =
20)
(n =
SD)
(ll =
26)
(n =
SD)
(I-I
= 6)
01
=
20)
DMPA
Co
ntro
l
Mem
t S.
D.
Meu,
t
S.D.
Me
can
t S.
D.
Mesn
t
S.D.
Il
ean
f S.
D.
Mean
t
S.D.
Age
(yea
rs)
31.6
t
b.2
3D.D
f
3.9
30.1
1 f
6.3
33.5
t
3.7
34.0
t
3.1
l * 28
.4
t 4.
2 l *.
ueio
ht (k
g)
54.7
t
9.2
52.5
t
6.9
62.5
t
9.9
61.2
t
11.0
61
.5
t 5.
6 57
.3
t 7.
2 l
. . .
Heig
ht (c
m)
149.
6 t
5.0
151.
0 f
5.0
163.
3 t
7.4
164.
6 t
7.1
150.
5 t
4.0
153.
5 s
5.7
l **
t.t
Were
let
inde
x 24
.4
t 3.
7 l
22.a
f
2.7
23.5
t
3.7
22.6
t
4.0
27.3
t
3.5
24.4
t
3.6
Syst
olic
B.
P. (I
tl
g)
ma.5
*
a.1
112.
2 t
a.6
112.
0 *
11.7
11
0.3
t 9.
9 11
0.3
* 7.
5 11
2.7
t 10
.5
Dias
toli
c B.
P. (I
I tl
g)
71.5
*
a.1
74.3
t
a.3
71.4
t
10.0
70
.4
t 9.
1 77
.5
t a.
a 73
.0
t a.
0 l
Days
al
coho
l dr
mk/&
: n
(X)
" (X
) "
(X)
" (X
) "
(X)
" w
D 20
(1
00.0
) 46
(9
2.0)
9
(37.
5)
15
(30.
0)
6 (1
00.0
) 19
(9
5.0)
1 0
(0.0
) 4
(a-0
) 5
(2o.
a)
20
(40.
0)
D (0
.0)
1 (5
.0)
l **
. . .
L2
0 (0
.0)
D (0
.0)
10
(Cl.
71
15
(30.
0)
D (0
.0)
D (0
.0)
Smok
e ci
gare
ttes
D
(0.0
) D
(O-0
) 11
(4
5.a)
12
(2
4.0)
2
(33.
3)
2 (1
0.0)
**
* l t.
Hem
t S.
D.
Mean
t
S.D.
Re
m f
S.D.
Me
an
t S.
D.
lean
t
S.D.
Me
w f
S.D.
Drin
ks/d
.sy+
2.
8 t
1.7
2.2
t 0.
9 2.
5 t
1.4
2.0
t 0.
0 -
Cigw
ette
s/&y
++
10.3
t
7.8
11.3
t
5.5
1.5
t 0.
7 4.
5 t
0.7
+ Al
cd10
1 dr
inke
rs on
ly
Sign
ific
ance
of
di
ffer
ence
s:
l p
(: 0.0
5 ++
Ci
gare
tte
smok
ers
only
l . p
( 0.
01
. . .
p .z
0.00
1

4.&
2 *
0.31
b.
43 t
0.
16
S.M
*
1.M
4.
a t
0.85
tl.%
*
0.31
0.
97 *
0.
3b
3.62
*
1.10
2.
91 *
0.
73
l
1.14
*
0.16
1.
27 I
0.
M
136.
0 t
19.9
12
7.4
t 26
.8
32.0
t
5.2
32.5
t
1.6
81.1
t 21
.3
74.6
t
IV.‘
4.22
f
0.93
3.
V4
f 0.
69
1.7b
I
0.3v
1.
M
t 0.
56
CH
OIS
TC
IUllC
”
Mlp
A
cont
rol
sim
. tn
= 2
4)
tn =
SO
) O
f It
en
f S
.D.
Mea
n t
I.D
. di
ff.
8.V
f
1.0
a.5
t 0.
6 l
‘.37
t 0.
71
4.19
t
0.62
5.‘&
*
I.16
5.
35 t
o.
Vb
0.97
t
0.52
0.
M
* 0.
62
3.62
t
1.04
3.
17 *
o.
V4
l.bb
t 0.
31
1.66
t
0.30
l
lbb.
5 *
33.0
20
6.1
t 34
.7
l *
*
51.1
t
16.0
54
.4
* 11
.4
lob.
9 t
35.5
7b
.b
, 17
.6
9.9
3.46
t
0.83
3.
67 f
0.
69
l.ba
1 0.
60
2.74
t
0.6s
l =
=
)IE
XIC
O Cl,”
OW
L C
cntr
o,
Sig
n.
tn *
6)
C”
- 20
1 “t
all
* s.
0.
“en.
5.
0.
d::f
.
v.5
t 0.
6 v.
3 L
0.7
5.07
f
0.74
6.
35 t
0.
w
b.3a
f
1.0s
4.
3v *
0.
72
1.M
t
0.67
1.
u t
0.M
2.w
*
0.92
2.
b4 *
0.
65
0.99
*
0.20
1.
17 t
0.
30
lM.7
t
15.0
11
2.1
* lb
.0
38.5
t
6.9
34.1
*
3.b
bb.3
f
12.3
60
.1
* 9.
6
2.85
t
0.34
3.
30 *
0.
44
*
1.63
*
0.34
1.
90 L
0.
44
iiwlf
icm
cc
of d
iffe
rem
bC
tYem
cm
tre,
P
1 W
A
. .
. .
.
. .
.
. . . . .
. . .
. . .
. . .
. . . .
Sig
nifi
canc
e of
dif
frrm
m:
l
p ‘
o.V
s l *
p <
0.0
1 l *
* p
‘ O
.Wl
184 Contraception
In Bangkok, DMPA users had a mean LDL-C level significantly higher by 24% over that of the controls. Other differences were not statistically significant but included 8% higher total cholesterol, 10% lower HDL-C, 6% higher apo AI, 9% higher apo B mean levels and a 7% higher apo AI/AI1 ratio.
In Christchurch, compared to controls, DMPA users had significant differences in lipid levels: 13% lower HDL-C, 18% lower apo AI, 39% higher apo B mean levels and 39% lower apo AI/B ratio. In addition, they had higher cholesterol and triglycerides and lower apo AI1 and AI/AI1 ratio but these differences were not significant.
In Mexico City, the only significant difference was a 14% lower apo AI/AI1 ratio in DMPA users. In addition, DMPA users also demonstrated 11% higher LDL-C, 15 % lower HDL-C, 13% higher apos AI1 and B mean levels and a 14% lower apo AI/B ratio over controls.
The differences between the study groups were marked between centres. Control subjects differed in total cholesterol, triglycerides, HDL-C and all three apolipoproteins. DMPA users differed in HDL-C and apolipoproteins.
Serum MPA levels in DMPA users durine one iniection interval
Serum MPA measurements in each centre are summarized in Table III. The geometric mean of the MPA levels measured on admission, just before the next DMPA injection, varied between centres: 3.16 nmol/l in Bangkok, 4.86 nmol/l in Christchurch and 1.07 nmol/l in Mexico City (p < 0.05).
In Bangkok and Christchurch, serum MPA levels were significantly higher at 2, 4 and 8 weeks post-injection than pre-injection and they had returned to pre-injection levels by the 13th week. In Mexico City, they rose above the pre-injection level, only at the 2-week follow-up.
Lioid measurements in DMPA users durine one iniection interval
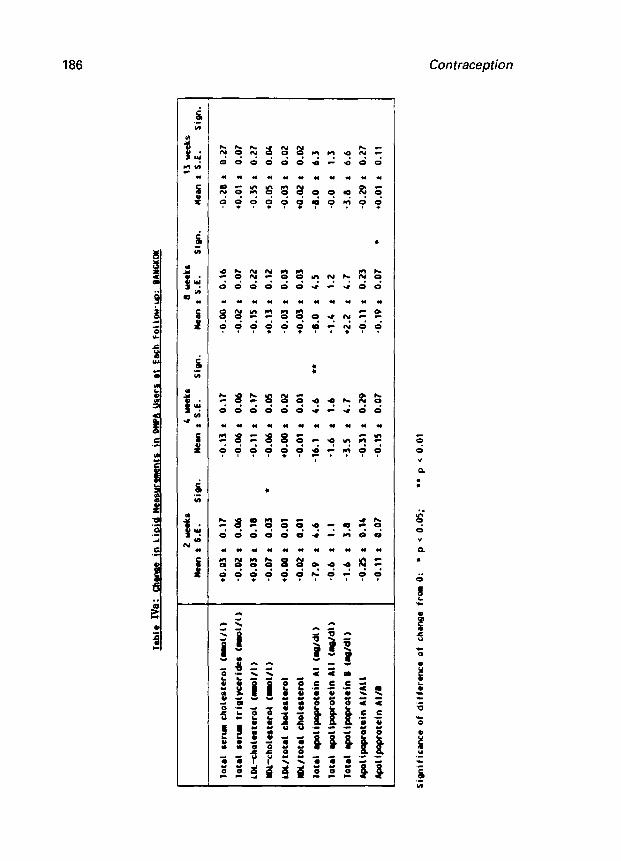
The changes in lipid levels observed over one 13-week injection interval in the DMPA users from Bangkok are summarized in Table IVa. Changes from pre-injection levels which reached statistical significance include a 6% decrease in HDL-C at 2 weeks, a 12% decrease in apo AI at 4 weeks and an 11% drop in the apo AI/B ratio at 8 weeks post-injection. There was no correlation between these changes and the variations in serum MPA levels measured during the injection interval in these women.
The same analysis for the data obtained in Christchurch is shown in Table IVb. Statistically significant changes from pre-injection levels include a 6% decrease in HDL- C, a 3 % rise in LDL-C/total cholesterol ratio and an 11% decrease in apo AI/B ratio at 2 weeks; a 5% decrease in total cholesterol and a 13% decrease in apo AI1 at 4 weeks; a 13% decrease in total triglycerides, a 17% decrease in apo AI1 and a 16% decrease in

Tab
lcII
I:
Ser
u W
A l
evel
s tm
olll
l ot
Ea
ch Vis
it nd
Chan
ats
in Ser
u MP
A at
Eac
h Fo
llow
-cc.
bv Ce
ntre
I
MN
GK
OK
cN
RIs
Yct
NB
cn
NE
XIc
o CI
TY
Ilen+
O
km
: ta
S.D
.)
Sign
. We
an+
Wean
t
t,, S.D
.)
Sign
. ue
an*
Mew
t t,
, S-D
.)
Sign
.
ADll
lSSI
af
3.16
(0
.17,
59.
68)
4.66
(2
.55,
9.
24)
1.07
(0
.37,
3.
08)
Zlae
kr
10.8
1 (6
.77,
17
.255
) l **
9.37
(5
.41,
16.
24)
l **
2.03
(0
.78,
5.
29)
4bme
km
8.28
(4
.68,
14.
64)
l *
8.09
(4
.45,
14.
71)
l **
1.65
(0
.70,
3.
91)
amek
r 6.
02
(3.4
3, lD.
56)
l
6.07
(3
.54,
10.
40)
l *
1.35
(0
.35,
5.
25)
13 wee
ks
3.23
<0
.81,
12.
79)
4.55
(2
.22.
9.
34)
1.25
(0
.42.
3-
R)
cn4n
GE Al:
Me
al
(95X
C.I
.)
Sign
. It
em
(95X
C.I
.)
Sig
n.
Item
(9
5X C
.I.,
Sifp
.
Zne
ekr
6.77
(+
5.59
. +7
.951
l **
+4.8
9 (e
3.64
. +6
.14)
l **
+1.1
7 (9
.13,
+2
.201
l
4unk
r l 4.26
(*
3.25
, 45
.28)
l ==
+J.b
2 (t
2.33
, 44
.90)
l **
l 0.68
(-
0.08
, l 1.44
1
8wek
I l l.91
t*
1.13
, l 2.70
) l **
+1.3
8 (*
0.23
. t2
.54)
l
l 0.57
(-
0.47
, l 1.62
)
13 neo
ks
-0.5
4 (-
1.43
. l 0.35
1 -0
.05
(-0.
99, l 0.90
1 *O
-26
(-0.
52. l 1.04
)
In Chr
istc
hurc
h, mul
yis
rest
rict
ed to s&
ject
s wh
o at
tend
ed for
all
4 fo
llow
-rpr
: Y
= 20
l Ge
omet
ric
m
Sign
ific
ance
of di
ffer
ence
fro
m aM
scio
n:
l p
( 0.
05
l * p ( 0.
01
l ** p
( 0.
001
Jebl
e I%
: C
hena
e in
Lio
id
ltee
rur-
ts
in W
A
Use
rs e
t E
ach
Follo
w-u
o:
BA
YGK
OK
Sim
ific
nce
of d
iffe
renc
e of
ch
enge
fro
m 0
: l
P (
0.
05;
l *
P ‘
0.
01
hote
l se
rm
chol
este
rol
(ml/l
)
lot8
1 8e
rtm
tri
glyc
erid
es
<ml/l
)
LDL-
chol
ater
ol
(mol
/l)
Y)L
-cho
lest
erol
(m
ot/f)
LOL/
tote
l ch
oles
tero
l
mL/
tote
l ch
oles
tero
l
Iote
l qo
lipop
rote
in
Al
(q/d
11
lota
L qo
l ip
opro
tein
A
l 1 t
qVdl
>
hote
l ep
olip
ofxo
tein
0
(Wdl
)
Apo
l ipa
pcor
cin
Al/A
l I
Apo
l ipo
pfot
ein
Al/B
2Mee
kr
4 w
eeks
8
met
a 13
w
eeks
M
en
t S
.E.
Sig
n.
Itee
n t
S.E
. S
ign.
ke
n r
S.E
. S
ign.
M
een
r S
.C.
Sig
n.
l 0.
03 t
0.
17
-0.1
3 t
0.17
-0
.00
t 0.
16
-0.2
8 f
0.27
-0.0
2 t
0.06
-0
.06
: 0.
06
-0.0
2 *
0.07
to
.01
t 0.
07
l 0.
03 t
0.
18
-0.1
1 t
0.17
-0
.15
t 0.
22
-0.3
5 t
0.27
-0.0
7 t
0.03
l
-0.0
6 *
0.05
l 0.
13
t 0.
12
+0.0
5 *
0.04
l o.
oo :
0.
01
l o.
oO *
0.
02
-0.0
3 t
0.03
-0
.03
* 0.
02
-0.0
2 :
0.01
-0
.01
t 0.
01
+0.0
3 t
0.03
to
.02
: 0.
02
-7.9
t
4.6
-16.
1 t
4.6
l *
-8
.0
t 4.
5 -6
.0
t 6.
3
-0.6
:
1.1
-1.6
t
1.6
-1.4
t
1.2
-0.0
t
1.3
-1.6
t
3.8
-3.5
t
4.7
+2.2
r
4.7
-3.8
a
6.6
-0.2
5 t
0.1c
-0
.31
* 0.
29
-0.1
1 t
0.23
-0
.29
r 0.
27
-0.1
1 i
0.07
-0
.15
t 0.
07
-0.1
9 t
0.07
l
to.0
1 f
0.11

Jabl
c l%
: Em
ma
in Lip
id Wca
sura
mmts
in
DWA
Us
ers at
Eac
h Fo
llow
-co:
CHR
ISTC
IWRC
H
lota
l sm
m ch
oles
tero
l (m
l/l)
Tota
L mr
u tr
igly
ceri
das <l
ol/l
)
LDL-
chol
rtrr
ol (r
ol/l
)
llD
1-&
0lrt
er0l
(m
l/l)
LD
l/to
taL
ch
olr
tero
l
IN/t
otal
ch
ol~s
taro
l
lota
l ap
olip
apro
teln
AI
(rp
/dl)
lota
l qm
lipo
prot
ein
All
(q/d
l)
Iota
l ap
oiip
apro
tein
B <W
dl)
Apol
lpo9
rote
in Al/
All
Apol
ipqr
otei
n AI
/I
2 ue
ets
4 mk
s 8 we
eks
13 wee
ks
Man
: I.
E.
Si9n
. Me
an :
S.E
. Si
gn.
Mean
* S.E
. Si
9n.
Mean
f S.E
. Si
gn.
-0.2
0 t
0.10
-0
.29 *
0.13
l
-0.1
7 t
0.14
-0
.06 *
0.13
-0.1
2 t
0.10
-0
.10 *
0.07
-0
.13 *
0.06
l
-0.0
4 *
0.09
-0.0
4 t
0.11
-0
.17 :
0.14
-0
.11 t
0.13
-0
.04 r
0.16
-0.0
9 t
0.Y
l
-0.0
8 t
0.05
-0
.10
t 0.
05
-0.0
7 t
0.06
l o.o
2 :
0.01
l
l O.O
l t
0.01
+
0.01
f
0.01
+
o.o
o
t 0.
02
-0.0
1 t
0.01
-0
.00 t
0.01
-0
.01 *
0.01
-0
.01 *
0.01
-0.9
*
5.1
-11.
4 f
1.5
-22.
0 *
11.0
-1
0.1
t 10
.6
-1.3
i
2.9
-6.6
t
2.9
l
-a.3
t
2.6
l *
4.5
t 2.
6
l i.z
t 4.
2 -2
.6
t 5.
2 -0
.4
t 7.
4 l 7.
k
t 7.
0
-0.0
7 t
o-l
a
+o
.la
t
0.10
+0
.11 *
0.20
+o
.oi
t o.
za
-0.1
9 t
o.Oa
l
-0.1
4 t
0.11
-0
.20 t
0.13
l
-0.2
7 t
0.16
Anal
ysis
res
tric
ted to
sbj
rts
uho at
tend
ed for
alI
4 fo
llow
rps:
Y = 20
Si9n
ific
ancc
of di
ffer
ence
of ch
an9a
frc
m 0:
l p
( 0.
05;
l * p (
0.0
1

. .
Jebb
lc-
in -He
mu
ream
s in
WA
User
s at
Eec
h Fo
llow
-w:
MEXI
CO CIT
Y
2 ue
aks
4u
eekr
II
mks
13 u
eeks
km
t S.
E.
Sipn
. We
n t S.
E.
Sim.
Mm
n : S.
E.
sign
. ML
M t S.
E.
Sign
.
Tota
l l eru
ch
oles
tero
l (r
rl/l
) -0
.07 t
0.47
l 0.27
t 0.
28
l 0.33
t 0.
37
l O.JO
t
0.36
Tota
l sw
am tr
igty
ceri
br (m
l/O
-9.0
7 t
0.07
l O.M
t 0.
09
-0.0
1 t
0.21
-0
.03 t
0.23
LDl-
chol
eatc
rol (a
l/l)
ml-
cho
lnt~
rot
(ml/
l)
t.0l
ltot
ml chol
mero
l
lDL
Itot
r1 ch
oles
tero
l
Tota
L rp
olip
opro
tain
rl
(q/d
11
fob1
qm
lipq
rotr
in
All (W
dl)
Yota
l qm
llpo
prot
ein
I tg
/dl)
~ A
poli
popr
otri
n AI
/All
Apol
ipap
rotm
in Al/
6
-0.0
9 t
0.46
-0.0
6 t
0.04
-0.0
1 t
0.04
-0.0
2 t
0.02
+a.5
t
10.9
-4.2
i
2.5
-2.7
t
5.8
9.60
t
0.35
*O-1
6 *
0.16
+0.0
6 i
0.25
-0.0
2 t
0.03
-o.O
i! t
0.03
-0.9
3 t
0.01
a.0
t 10
.6
-b.3
t
0.7
+7.1
t
2.5
9.53
t
0.27
-9.0
3 f
0.19
. . .
l o.96
t 0.
25
-0.9
1 t
0.03
-0.9
3 t
0.03
-0.0
3 t
0.03
+1
.7
t 13
.9
-5.7
t
2.6
+0.2
t
3.1
+0.4
7 t
0.26
-9.0
1 t
0.20
+0.1
4 f
0.37
-0.0
6 :
0.06
-0.0
1 t
0.04
-0.0
3 t
0.03
-9.3
t 10
.0
-3.3
t
2.6
+1.9
t
3.5
+0.0
3 :
9.32
-0.1
8 t
0.13
simi
ficw
we
of dif
fere
nce of
chu
te fr
a 0:
l P
* 0.
05;
l * P s 9.
91
Contraception 189
the apo AI/B ratio at 8 weeks. The changes in apo AI1 and in the apo AI/B ratio observed at 8 weeks are correlated with the changes in serum MPA levels at 8 weeks (for apo AII: r = -0.59, p<O.O5; for the apo AI/B ratio: r = -0.63, p<O.Ol).
In Mexico City (Table IVc), only two measurements changed significantly during the injection interval, giving an 11% decrease in apo AI1 and an 11% increase in apo B, both seen 4 weeks post-injection. The change in apo AI1 is correlated with the change in serum MPA level at 4 weeks (r = -0.91, p<O.O5).
In all three centres, the lipid measurements returned to pre-injection levels by the thirteenth week.
DISCUSSION
This study of 50 DMPA users is one of the few multicentre clinical trials investigating the long-term effects of a progestogen-only injectable contraceptive. Although significant findings differ between centres, a pattern of lipid changes can be seen among DMPA users.
Before they receive their next injection, DMPA users have, compared to controls, an LDL-C mean level higher by 11 to 24 % , an HDL-C mean level lower by 10 to 15 % , an apo B mean level higher by 9 to 39 % , and a mean apo AI/B ratio lower by 3 to 39 % . Other findings such as a significant decrease in apo AI seen in Christchurch and a significant decrease in the apo AI/AI1 ratio observed in Mexico City, were not found in the other centres.
There were some differences in the characteristics of the women enrolled in the two study groups in each centre. In Bangkok, the DMPA users had a higher Quetelet index than the control subjects, in Mexico they were older by six years on average and in Christchurch they were almost twice as likely to smoke cigarettes. Yet, controlling for these factors, some of the lipid differences noted between the two study groups on admission remained statistically significant and attributable to DMPA use. In further support of an effect of DMPA, is the fact that the differences in lipid profile observed between DMPA-treated women and control subjects on admission are similar in three widely different populations, and that further lipid changes are observed over the DMPA injection interval, some of which are correlated to variations in MPA serum levels.
It has now been well demonstrated that LDL-C is a causative agent in the process of atherosclerosis while HDL-C and apolipoprotein AI are recognized as negative, and apolipoprotein B as positive risk indicators for this disorder. Decreases in the apo AI/B or the apo AI/AI1 ratio are also correlated to an increased risk of atherosclerosis. The overall picture which emerges from the findings of this study, with increases in LDL-C and apo B and decreases in HDL-C and apo AI, points to unfavourable changes in lipid metabolism in DMPA users. However, lipid metabolism is only one of the factors influencing atherosclerosis and previous studies (16,17) comparing the effects of MPA to those of other hormonal contraceptives on lipid metabolism have suggested that MPA

190 Contraception
is more beneficial in this respect. Thus, before a woman initiates DMPA use, possible effects on lipid metabolism must be taken into account in weighing the overall balance of risks and benefits of treatment. Her existing underlying risk for atherosclerosis should be assessed from clinical history and her lipid profile obtained in high risk cases.
The data presented here further emphasize regional differences that should be noted when comparing results from different centres. This factor complicates interpretation of data but cannot be ignored. In fact, the MPA levels measured in the three groups of contraceptive users reflect well-known ethnic differences in DMPA metabolism. Previous studies (18) have consistently shown that, for a same dose of DMPA, Mexican women have lower peak values and a longer half-life than Thai women. The data also show that measurable levels of MPA are found at the time of the next injection, with marked inter- individual variations. This confirms the findings of previous studies (19) that, at a dose of 150 mg, the duration of action of DMPA exceeds three months and there is a build-up of the drug with time.
Thus, work should continue to improve the formulation of DMPA in order to bring the dose necessary for effective contraception to the lowest dose possible, and thereby decrease its effect on lipid metabolism.
1.
2.
3.
4.
5.
6.
7.
REFERENCES
Facts about injectable contraceptives: Memorandum from a WHO meeting. Bull World Health Organization 1982; 60: 199-210.
Tankeyoon M, Dusitsin N, Pushyachinda V, Larsson-Cohn V. A study of glucose tolerance, serum transaminase and lipids in women using depot- medroxyprogesterone acetate and a combination type oral contraceptive. Contraception 1976; 14: 199-211.
Amatayakul K, Sivassomboon B, SingKamani R. Effects of medroxyprogesterone acetate on serum lipids, protein, glucose tolerance and liver function in Thai women. Contraception 1980; 21:283-97.
Fajumi J. Alterations in blood lipids and side-effects induced by depo-Provera in Nigerian women. Contraception 1983; 27: 161-75.
Liew DF, Ng CS, Yong YM, Ratnam SS. Long-term effects of depo-Provera on carbohydrate and lipid metabolism. Contraception 1985; 31:51&t.
Kremer J, de Bruijn HWA, Hindriks FR. Serum high density lipoprotein cholesterol levels in women using a contraceptive injection of depot- medroxyprogesterone acetate. Contraception 1980; 22:359-67.
Barnes RB, Roy S, Lobe RA. Comparison of lipid and androgen levels after conjugated estrogens or depo-medroxyprogesterone acetate treatment in postmenopausal women. Obstet Gynecol 1985; 66:216-9.
Contraception 191
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
Deslypere JP, Thiery M, Vermeulen A. Effect of long-term hormonal contraception on plasma lipid. Contraception 1985; 31:633-92.
Allain CC, Poon LS, Chan CSG. Enzymatic determination of total serum cholesterol. Clin Chem 1974; 20:470-5.
Grove TH. Effect of reagent pH on determination of high-density lipoprotein cholesterol by precipitation with sodium phosphotungstate/magnesium. Clin Chem 1979; 25:560-4.
Assmann G, Jabs HU, Kohnert U et al. LDL-cholesterol determination in blood serum following precipitation of LDL with polyvinyl sulfate. Clin Chim Acta 1984; 140:77-83.
Bucolo G, David H. Quantitative determination of serum triglycerides. Clin Chem 1973; 19:476-82.
Rosseneu M, Vercaemst R, Steinberg KK et al. Some considerations of methodology and standardization of apolipoprotein B immunoassays. Clin Chem 1983; 29~427-33.
Steinberg KK, Cooper GR, Rosseneu M. Evaluation and standardization of apolipoprotein AI immunoassays. Clin Chem 1983; 29:415-26.
Ahsan R, Sufi SB, Cekan S. Laboratory method manual for the radioimmunoassay of levonorgestrel, norethisterone and medroxyprogesterone acetate. WHO Collaborating Centre for Research and Reference Services in the Immunoassay of Hormones in Human Reproduction, Hammersmith Hospital, London. 1988; 60.
Silverstolpe G, Gustafson A, Samsioe G, Svanborg A. Lipid metabolism studies in oophorectomized women. Effects of three different progestogens. Acta Obstet Gynecol Scand Suppl 1979; 88:89-95.
Tikkanen MJ, Nikkiki EA, Kuusi T, Sipinen S. Different effects of two progestins on plasma high density lipoprotein (HDL2) and post-heparin plasma hepatic lipase activity. Atherosclerosis 1981; 40:365-9.
Hall PE. Long-acting injectable formulations. In: Dicfalusy E and Bygdeman M, eds. Fertility Regulation today and tomorrow. New York:Raven Press, Serono Symposia 1987: 119-41.
Garza-Flares J, De la Cruz DL, Valles de Bourges V et al. Long-term effects of depot-medroxyprogesterone acetate on lipoprotein metabolism. Contraception 1991: 44:61-71.