
A high physical symptom count reduces the effectiveness of treatment for depression, independently...
7
A high physical symptom count reduces the effectiveness of treatment for depression, independently of chronic medical conditions Klaas M.L. Huijbregts a, b, c, ⁎, Fransina J. de Jong d , Harm W.J. van Marwijk c , Aartjan T.F. Beekman e , Herman J. Adèr f , Christina M. van der Feltz-Cornelis a, g, h a Netherlands Institute of Mental Health and Addiction (Trimbos Institute), Utrecht, The Netherlands b GGZinGeest, partner of VU University Medical Center, Amsterdam, The Netherlands c Department of General Practice and the EMGO + Institute for Health and Care Research, VU University Medical Center, Amsterdam, The Netherlands d Dimence GGZ, Deventer, the Netherlands e Department of Psychiatry and the EMGO + Institute for Health and Care Research, VU University Medical Center, Amsterdam, The Netherlands f Johannes van Kessel Advising, Huizen, The Netherlands g Department of Tranzo, University of Tilburg, Tilburg, The Netherlands h Top Clinical Centre for Body, Mind and Health, GGz Breburg, Tilburg, The Netherlands abstract article info Article history: Received 1 October 2012 Received in revised form 9 January 2013 Accepted 10 January 2013 Keywords: Depression Collaborative care Primary care Concomitant physical symptoms Somatization Aim: To assess to what extent a high physical symptom count influences the effect of treatment for major depres- sive disorder (MDD), and whether or not actual comorbid medical conditions explain this relationship. Method: Secondary data-analysis on a cluster-randomized trial in primary care, comparing the effectiveness of collaborative care with care as usual (CAU). MDD was measured using the PHQ-9. The Physical Symptoms Ques- tionnaire (PSQ) was filled out at baseline by 115 patients (77.2% of those who entered the trial). Multilevel logis- tic regression models were used to test whether a high physical symptom count predicted lack of response to treatment, adding interaction terms to test differential effects on collaborative care versus CAU. Results: A high physical symptom count negatively influenced the effect of both collaborative care and care as usual (no interaction). Specifically, a high physical symptom count predicted lack of response in both conditions at 3 (odds ratio = 6.8), 6 (OR = 4.1), and 9 months follow-up (OR = 6.4). This was not explained by chronic physical illness. Conclusion: In this RCT, patients with MDD accompanied by a high physical symptom count benefited less from treatment for MDD in primary care, regardless of the type of treatment (either collaborative care or CAU). This was not explained by the presence of comorbid medical conditions. Further research is needed to improve treat- ment for MDD accompanied by a high physical symptom count, although collaborative care for depression is still more effective than CAU for this group of patients. Trial registration: Dutch trial register ISRCTN15266438. © 2013 Elsevier Inc. All rights reserved. Introduction Patients under treatment for Major Depressive Disorder (MDD) often report concomitant physical symptoms. Indeed, 70% report phys- ical instead of psychological symptoms during their first visit to a gener- al practitioner (GP) for what later turns out to be MDD [1]. Moreover, epidemiological data indicate that MDD frequently co-occurs with both somatoform disorders [2] and chronic medical conditions [3]. However, there has not been much research into the topic of the possi- ble influence of concomitant physical symptoms – particularly if the effect of these symptoms is assessed after a correction for the effect of chronic medical conditions – on the effectiveness of treatment for MDD [4]. This is an important issue because there is ample room for improve- ment in terms of response and remission percentages for MDD in every- day care, even though efficacious treatments are available [5,6]. In the usual care arm in the large IMPACT-trial, assessing the effectiveness of collaborative care in primary care, only 16.7% of the participating pa- tients achieved remission after 6 months [7]. One of the reasons why treatment for MDD appears to be suboptimal in everyday care may well be the high co-occurrence with physical symptoms. In the primary care setting, for instance, GPs are faced with competing demands, as physical symptoms and psychological symptoms are often presented simultaneously in the short time span of a consultation [8]. This may interfere with effective treatment for MDD. Studies into the possible influence of persistent physical symptoms on the outcome of MDD have so far focused almost exclusively on pain [9]. A systematic review [4] and a recent study in primary care [10], however, showed that studies should also look at the wider Journal of Psychosomatic Research 74 (2013) 179–185 ⁎ Corresponding author at: GGZinGeest, Polikliniek Psychosomatiek, Osdorpplein 880, 1068 TD Amsterdam, The Netherlands. Tel.: +31 20 788 4571. E-mail address: [email protected] (K.M.L. Huijbregts). 0022-3999/$ – see front matter © 2013 Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/j.jpsychores.2013.01.004 Contents lists available at SciVerse ScienceDirect Journal of Psychosomatic Research
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of A high physical symptom count reduces the effectiveness of treatment for depression, independently...

Journal of Psychosomatic Research 74 (2013) 179–185
Contents lists available at SciVerse ScienceDirect
Journal of Psychosomatic Research
A high physical symptom count reduces the effectiveness of treatment for depression,independently of chronic medical conditions
Klaas M.L. Huijbregts a,b,c,⁎, Fransina J. de Jong d, Harm W.J. van Marwijk c, Aartjan T.F. Beekman e,Herman J. Adèr f, Christina M. van der Feltz-Cornelis a,g,h
a Netherlands Institute of Mental Health and Addiction (Trimbos Institute), Utrecht, The Netherlandsb GGZinGeest, partner of VU University Medical Center, Amsterdam, The Netherlandsc Department of General Practice and the EMGO+ Institute for Health and Care Research, VU University Medical Center, Amsterdam, The Netherlandsd Dimence GGZ, Deventer, the Netherlandse Department of Psychiatry and the EMGO+ Institute for Health and Care Research, VU University Medical Center, Amsterdam, The Netherlandsf Johannes van Kessel Advising, Huizen, The Netherlandsg Department of Tranzo, University of Tilburg, Tilburg, The Netherlandsh Top Clinical Centre for Body, Mind and Health, GGz Breburg, Tilburg, The Netherlands
⁎ Corresponding author at: GGZinGeest, Polikliniek Psy1068 TD Amsterdam, The Netherlands. Tel.: +31 20 788
E-mail address: [email protected] (K.M.L. H
0022-3999/$ – see front matter © 2013 Elsevier Inc. Allhttp://dx.doi.org/10.1016/j.jpsychores.2013.01.004
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 1 October 2012Received in revised form 9 January 2013Accepted 10 January 2013Keywords:DepressionCollaborative carePrimary careConcomitant physical symptomsSomatization
Aim: To assess towhat extent a highphysical symptomcount influences the effect of treatment formajor depres-sive disorder (MDD), and whether or not actual comorbid medical conditions explain this relationship.Method: Secondary data-analysis on a cluster-randomized trial in primary care, comparing the effectiveness ofcollaborative care with care as usual (CAU).MDDwasmeasured using the PHQ-9. The Physical Symptoms Ques-tionnaire (PSQ)was filled out at baseline by 115 patients (77.2% of thosewho entered the trial). Multilevel logis-tic regression models were used to test whether a high physical symptom count predicted lack of response totreatment, adding interaction terms to test differential effects on collaborative care versus CAU.Results: A high physical symptom count negatively influenced the effect of both collaborative care and care as usual(no interaction). Specifically, a highphysical symptomcount predicted lack of response in both conditions at 3 (oddsratio=6.8), 6 (OR=4.1), and 9 months follow-up (OR=6.4). This was not explained by chronic physical illness.
Conclusion: In this RCT, patients with MDD accompanied by a high physical symptom count benefited less fromtreatment for MDD in primary care, regardless of the type of treatment (either collaborative care or CAU). Thiswas not explained by the presence of comorbidmedical conditions. Further research is needed to improve treat-ment forMDD accompanied by a high physical symptom count, although collaborative care for depression is stillmore effective than CAU for this group of patients. Trial registration: Dutch trial register ISRCTN15266438.© 2013 Elsevier Inc. All rights reserved.
Introduction
Patients under treatment for Major Depressive Disorder (MDD)often report concomitant physical symptoms. Indeed, 70% report phys-ical instead of psychological symptoms during their first visit to a gener-al practitioner (GP) for what later turns out to be MDD [1]. Moreover,epidemiological data indicate that MDD frequently co-occurs withboth somatoform disorders [2] and chronic medical conditions [3].However, there has not been much research into the topic of the possi-ble influence of concomitant physical symptoms – particularly if theeffect of these symptoms is assessed after a correction for the effect of
chosomatiek, Osdorpplein 880,4571.uijbregts).
rights reserved.
chronic medical conditions – on the effectiveness of treatment forMDD [4].
This is an important issue because there is ample room for improve-ment in terms of response and remission percentages forMDD in every-day care, even though efficacious treatments are available [5,6]. In theusual care arm in the large IMPACT-trial, assessing the effectiveness ofcollaborative care in primary care, only 16.7% of the participating pa-tients achieved remission after 6 months [7]. One of the reasons whytreatment for MDD appears to be suboptimal in everyday care maywell be the high co-occurrence with physical symptoms. In the primarycare setting, for instance, GPs are faced with competing demands, asphysical symptoms and psychological symptoms are often presentedsimultaneously in the short time span of a consultation [8]. This mayinterfere with effective treatment for MDD.
Studies into the possible influence of persistent physical symptomson the outcome of MDD have so far focused almost exclusively onpain [9]. A systematic review [4] and a recent study in primary care[10], however, showed that studies should also look at the wider

180 K.M.L. Huijbregts et al. / Journal of Psychosomatic Research 74 (2013) 179–185
spectrum of physical symptoms, such as fatigue, indigestion, dizziness,and fainting [11]. Such physical symptoms in patients with MDD maybe due to a chronic medical condition, may be considered a symptomdimension of the depression, or may remain medically unexplained.Concomitant physical symptoms might well be a relevant factor incourse and treatment of MDD, regardless of their origin, but up untilnowwe are not aware of any empirical research that assesses the inde-pendent contribution of accompanying physical symptoms on the out-come of MDD after a correction for chronic medical conditions [4].Physical symptoms are often operationalized by measuring them on ascale, but evidently this does not clarify to what extent an effect ofsuch symptoms is due to underlying somatic pathology. Crombez andcolleagues have called this ‘the unbearable lightness of somatisation’[12].
A good opportunity to test the assumption that concomitant physicalsymptoms, interfere with treatment of MDD, even after a correction forchronic medical comorbidity, would be a pre-planned secondary data-analysis on a trial assessing the effectiveness of enhanced treatmentfor MDD in primary care. A correction for chronic medical conditionsdoes not imply that physical symptoms are indeed unexplained (to bereasonably sure of that all symptomswould have to be assessed at base-line by amedical doctor), but it does shed light on the independent con-tribution of these symptoms regardless of the underlying pathology.Forthermore, if it is true that concomitant physical symptomsnegativelyinfluence the effect of treatment forMDD, thismight be less pronouncedwhen patients are treated in an enhanced care arrangement, where aspecialized nurse (care manager) operates next to the GP (as thismight reduce the burden of competing demands). If a care manager isavailable to address psychosocial issues, this may enhance effectivenessof treatment for MDD even when concomitant physical symptoms arepresent. An example of a form of enhanced care for MDD that incorpo-rates these elements is collaborative care [7,13,14].
We tested the assumption that concomitant physical symptoms in-fluence the effectiveness of treatment for MDD in a recently completedRCT that evaluated the effectiveness of collaborative care in primarycare in The Netherlands [14]. Given the fact that most patients reportphysical symptoms when suffering from MDD, we decided to look atthe group with a relatively high physical symptom count. The physicalsymptom count was measured at baseline (before the start of treat-ment) and the outcome in terms of depression severity was determinedat follow-up. We hypothesized (i) that a high physical symptom countat baseline has a generic negative effect on the lack of response to treat-ment for MDD at follow-up, (ii) that this effect may be stronger in CAUthan in collaborative care, and (iii) that this effect is independent of thepresence of chronic physical illness. Thus, if hypothesis iii holds true, thisimplies that the results regarding hypothesis i and ii still hold truewhenthe model is corrected for chronic physical illnesses.
Methods
Design and patients
We conducted a pre-planned secondary analysis of data from acluster-randomized trial assessing the effectiveness of collaborativecare for MDD in primary care in The Netherlands [14]. The design ofthe study has been described in more detail elsewhere, but is summa-rized below [14]. The study protocol was approved by the MedicalEthics Committee (METC) of the VU University Medical Center (pro-tocol number 2006/158). The trial was registered in the Dutch trialregister: ISRCTN15266438.
Eighteen primary care centers (with a total of 82GPs)were random-ly assigned to either collaborative care (CC) or care as usual (CAU) by anindependent statistician using a computer algorithm for cluster alloca-tion [15]. GPs in primary care centers randomized to the CC conditionreceived training in the collaborative care model, the use of a web-based tracking system, and cooperation with a consultant psychiatrist.
Patients of the respective practices could enter the trial in twoways: ei-ther by screening or after identification by their GP. Screeningwas doneas follows: all patients who had consulted their GP during the past6 months received the PHQ-9 [16] by mail, regardless of the reasonfor prior consultation. The reason for this broad approach is that litera-ture suggests that patients suffering from Major Depressive Disorder(MDD) are more likely to report miscellaneous physical symptoms totheir GP instead of the core symptoms of MDD [1,8].
After informed consent patients were asked to return the question-naire regardless of whether or not they still had any symptoms. At themoment of screening, patients were unaware of their allocation. Inclu-sion criteria were age >17 years, PHQ-9 score ≥10 and a classificationof MDD according to the MINI neuropsychiatric interview [17], whichwas administered by telephone. Exclusion criteriawere suicidality, psy-chosis, dementia drug or alcohol dependence, being already under spe-cialtymental health treatment, or insufficient knowledge of Dutch tofillin the most important questionnaires. Suicidality was evaluated if pa-tients scored at least 2 on item 9 of the PHQ-9 (thoughts that youwere better off dead or of hurting yourself in some way). In thesecases an assessment of the risk was made with section C of the MINIneuropsychiatric interview (a high risk is defined as actual plans or aprior suicide attempt combined with current suicidal thoughts). Apatient's GP was informed when the suicide risk based on the MINI washigh. The GP assessed whether or not immediate treatment was neces-sary. If this was not the case a patient could still be included in the trial.
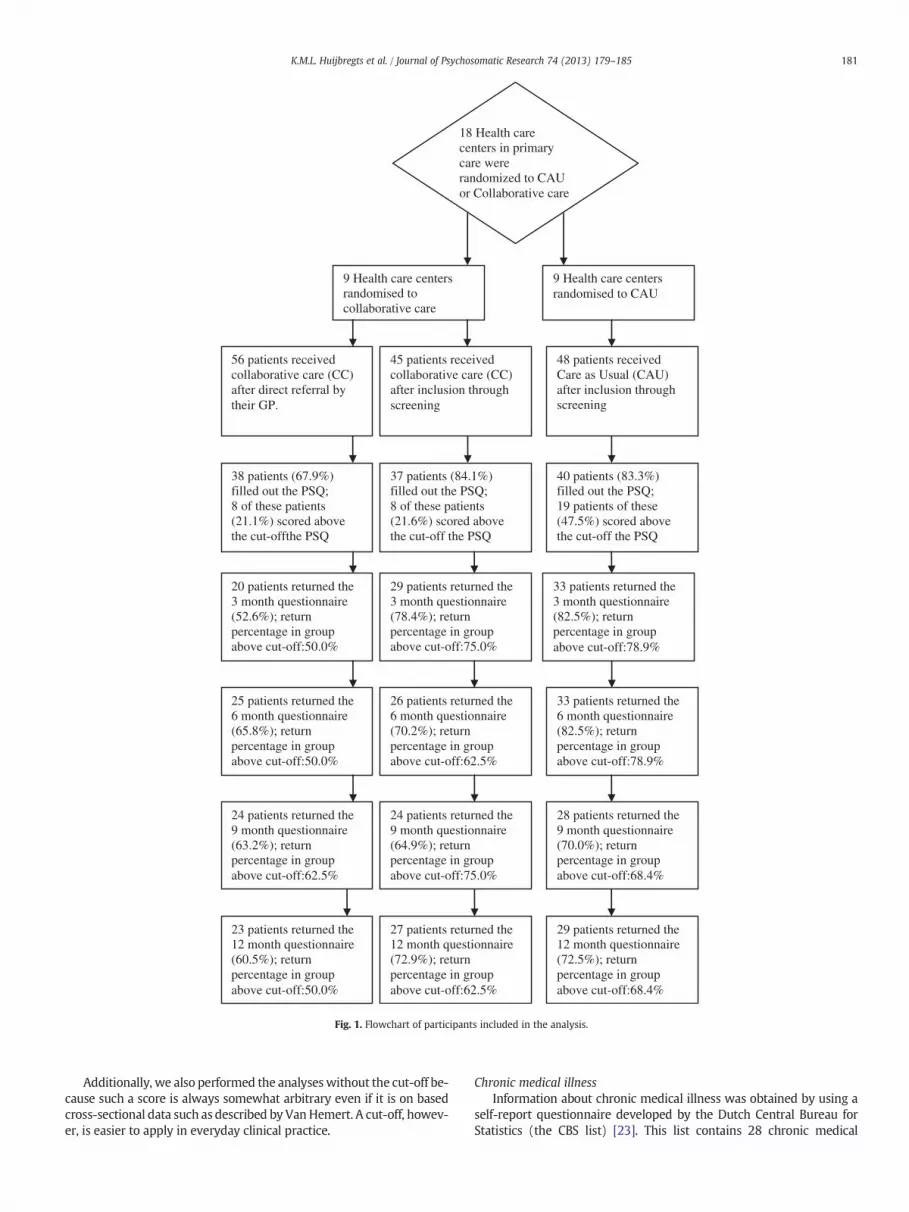
The trial flowchart describing the randomization procedure and thepercentages of patients who returned the follow-up-questionnaire atthree, six, nine, and twelve months is presented in Fig. 1. The patientswho received collaborative care after identification by their GP weretreated as a separate group in theflowchart (to provide insight in the in-clusion process), but we will present results for the collaborative caregroup as a whole.
The collaborative care intervention is described in more detail else-where [14]. Briefly, a GP, a depression care manager (for instance a spe-cialized nurse), and a consultant psychiatrist operate as a team toprovide optimized primary care for MDD based on a stepped care algo-rithm. Usual care could be any form of care that was available to a pa-tient. The results of the trial were described elsewhere, and showed abetter outcome in terms of treatment response for collaborative carecompared to CAU [18].
Study oversightThis study was part of the Netherlands Depression Initiative [19,20],
a national initiative aimed to improve depression treatment. The studywas supervised by a steering committee and a supervisory board thatmet 4 times a year.
Measures
High physical symptom countPhysical symptoms were measured using the validated Physical
Symptoms Questionnaire [21] which participants filled out at baseline.It measures 51 physical symptoms, such as chest pain, headache, dizzi-ness, seizures, intolerance to certain types of food, and shortness ofbreath. Symptoms are measured on a scale that ranges between0 (not present in the past week) and 3 (often present in the pastweek) and are added up. When a patient scores 2 or higher on an item,this is counted as a physical symptom. The verbal anchor for 1 is ‘some-times present in the last week’, the anchor for 2 is ‘regularly present inthe past week’.
According to Van Hemert and colleagues a score of 15 symptoms orhigher is the average for severe physical symptoms in men sufferingfrom anxiety or depression, and the same holds for a score of 17 symp-toms or higher for women [22]. We applied these means as cut-offscores for men and women in order to identify patients who were suf-fering from a high physical symptom count.
18 Health care centers in primary care wererandomized to CAU or Collaborative care
9 Health care centers randomised to collaborative care
9 Health care centers randomised to CAU
56 patients received collaborative care (CC) after direct referral by their GP.
45 patients received collaborative care (CC) after inclusion through screening
48 patients received Care as Usual (CAU) after inclusion through screening
40 patients (83.3%) filled out the PSQ;19 patients of these (47.5%) scored above the cut-off the PSQ
37 patients (84.1%) filled out the PSQ;8 of these patients (21.6%) scored above the cut-off the PSQ
38 patients (67.9%) filled out the PSQ; 8 of these patients (21.1%) scored above the cut-offthe PSQ
33 patients returned the 3 month questionnaire (82.5%); return percentage in group above cut-off:78.9%
29 patients returned the 3 month questionnaire(78.4%); return percentage in group above cut-off:75.0%
20 patients returned the 3 month questionnaire(52.6%); return percentage in group above cut-off:50.0%
25 patients returned the 6 month questionnaire (65.8%); return percentage in group above cut-off:50.0%
26 patients returned the 6 month questionnaire (70.2%); return percentage in group above cut-off:62.5%
33 patients returned the 6 month questionnaire (82.5%); return percentage in group above cut-off:78.9%
24 patients returned the 9 month questionnaire (63.2%); return percentage in group above cut-off:62.5%
24 patients returned the 9 month questionnaire (64.9%); return percentage in group above cut-off:75.0%
28 patients returned the 9 month questionnaire (70.0%); return percentage in group above cut-off:68.4%
23 patients returned the 12 month questionnaire (60.5%); return percentage in group above cut-off:50.0%
27 patients returned the 12 month questionnaire (72.9%); return percentage in group above cut-off:62.5%
29 patients returned the 12 month questionnaire (72.5%); return percentage in group above cut-off:68.4%
Fig. 1. Flowchart of participants included in the analysis.
181K.M.L. Huijbregts et al. / Journal of Psychosomatic Research 74 (2013) 179–185
Additionally, we also performed the analyseswithout the cut-off be-cause such a score is always somewhat arbitrary even if it is on basedcross-sectional data such as described by VanHemert. A cut-off, howev-er, is easier to apply in everyday clinical practice.
Chronic medical illnessInformation about chronic medical illness was obtained by using a
self-report questionnaire developed by the Dutch Central Bureau forStatistics (the CBS list) [23]. This list contains 28 chronic medical

Table 1Baseline characteristics, treatment (N=115).
PSQ bcut-off(N=80)
PSQ ≥cut-off(N=35)
P-value⁎
Mean age (sd) 48.1 (11.9) 52.1 (16.7) .207Gender (% male) 23.8% 28.6% .584Living alone (%) 48.8% 42.9% .560Non Dutch origin (%) 25.0% 21.2% .668PHQ-9 at baseline (sd) 14.8 (4.9) 16.2 (5.5) .171CC (%) 78.6% 21.4% .00⁎
CAU (%) 52.5% 47.5% .00⁎
CC=collaborative care. There are significantly more patients who score above the PSQcut-off in the CAU-group. We controlled for this variable (condition) in the modeldisplayed in Table 2.⁎ Statistically significant (Pb0.05), chi square test for dichotomous variables and T-test
for continuous variables.
182 K.M.L. Huijbregts et al. / Journal of Psychosomatic Research 74 (2013) 179–185
conditions, such as cancer, COPD, high blood pressure, and diabetes. Al-though an assessment of themedical status by amedical doctor at base-line – as opposed to our method of self-report – might have beenpreferable, results from a large cohort-study suggest that patients'self-reports on chronic diseases are fairly accurate [24]. This was alsofound by the National Center for Health Statistics in the USA, particular-ly for well known chronic conditions such as diabetes and high bloodpressure [25].
Outcome measured with the PHQ-9The primary outcome measure was treatment response in terms of
at least 50% reduction in depression severity between baseline andfollow-up after 3, 6, 9, and 12 months of treatment. This was measuredwith the PHQ-9 [16], the depression subscale of the self-report PatientHealth Questionnaire (PHQ) [26]. The PHQ-9 consists of 9 items refer-ring to the DSM IV criteria for MDD. Each item is scored from 0 (not atall) to 3 (nearly every day). The total-score thus varies between 0 and27. Given the fact that patients had to have a PHQ-9 baseline score ofat least 10 to be included and that the mean baseline score was around15 [18], a 50% reduction of the PHQ-9-score in our sample implies thatmost of these patients improved at least 5 points on this questionnaire.A reduction of at least 5 points implies a clinically significant improve-ment [16].
Statistical analyses
We applied multilevel logistic regression analysis (MLA) to deter-mine the association of a high physical symptom count measured atbaselinewith the dichotomous outcomemeasure response to treatment(a 50% reduction of the PHQ-9-score between baseline and follow-up).The PHQ-9 was administered 3, 6, 9, and 12 months after baseline. Weused MLA since randomization had been done at the level of healthcare center. The levels used in theMLA-modelswere: health care center,GP, patient and occasion (number of days between baseline and com-pletion of the follow-up questionnaire at three months). The analyseswere conducted using MLwiN 2.0 multilevel software [27]. Additionallypropensity scores were added to the model in order to correct for thepossibility of selection bias due to the cluster randomization [28]. Thisis a commonly applied procedure in cluster randomized studies [28].
The determinant of focus to test the first hypothesis (that a highphysical symptom count might have a generic negative effect on theoutcome of treatment for MDD), was the dichotomized PSQ-score(cut-off score PSQ≥15 for men and PSQ≥17 for women). Additional-ly, a composite score was computed based on the first time point toachieve treatment remission or response. This composite score com-bines information on two outcome measures of the trial: response (areduction on the PHQ-9 of at least 50% compared to baseline) and re-mission (a PHQ-9 score lower than 5), assuming that remission is amore favorable outcome than response and that early response or re-mission is more favorable than later response or remission.
We also performed the logistic regression analyses without thecut-off (thus determining odds ratios per point on the PSQ) given thefact that such a score is always arbitrary up to a certain extent. Differ-ences between treatment groups on this score were also analyzedusing MultiLevel Analysis [29].
To explore whether or not the hypothetical effect of a high physicalsymptom count was differential for the treatment conditions (collabo-rative care or CAU) the interaction term ‘treatment condition timesphysical symptoms’ (cut-off score PSQ ≥15 for men and PSQ ≥17 forwomen) was tested for statistical significance (Pb .05).
The number of chronic physical conditions a patient reported atbaseline was added to the model as an independent variable to explorewhether or not the hypothetical effect of physical symptoms was inde-pendent of chronic medical comorbidity. Sixty-seven percent of the pa-tients in our sample reported at least one chronicmedical condition and22% of the patients reported three or more chronic medical conditions.
Additionally we also tested the above mentioned hypothesis by addingthe dichotomous variable ‘at least one chronic medical condition versusnone’ to themodel, thus comparing those patients without a known so-matic cause for at least some of their symptoms to those with a partialexplanation for their physical symptoms.
Results
Study population
A total of 149 patients participated in the trial: 101 in the collaborative care group(either selected through screening or through identification by the GP) and 48 in theCare as Usual group (CAU). Because we did not include a GP-identified CAU-group inthe trial, the number of patients receiving collaborative care is almost twice as largeas the number of patients receiving CAU. As mentioned in the Methods section andbelow in this section we corrected for this in the analyses.
For 115 patients (77.2% of thosewhoentered the trial) a baseline assessment based onthe PSQ could be made as to whether they scored below or above the cut-off for a highphysical symptomcount (PSQ≥15 formen and PSQ≥17 forwomen). 75 of these patientswere included in the collaborative care group (74.3% of the collaborative care patients inthe trial), compared to 40 in the CAU group (83.3%). These percentages did not deviate sig-nificantly from each other (P=.365). Therewas also no significant difference on a numberof other key variables between those who did and those who did not fill out the PSQ: age(P=.36), civil status (living alone or living together as a couple; P=.36), gender (P=.44),and the PHQ-9-score at baseline (P=.64). Therewas a differencewith regard to ethnicity:more patients who did not fill out the PSQ were not of Dutch origin (P=.02). This impliesthat it will be more difficult to generalize our results for this subgroup.
Patients who scored above the cut-off on the PSQ did not differ significantly from pa-tients who scored below this cut-off on key baseline variables such as age, civil status (liv-ing alone or living together as a couple), gender, and their PHQ-9-score. They did differhowever with respect to treatment condition. Patients who scored above the cut-off onthe PSQ were more likely to have received care as usual (CAU) than patients who scoredbelow the cut-off (P=.004). We therefore corrected the MLA-models for the variabletreatment condition. The baseline scores for all variables can be found in Table 1.
The available 115 patients were followed and included in the analysis. Follow-up datawere obtained on aminimumof 76 (66.1%) patients at T3 to amaximumof 84 (73.0%) pa-tients at T2, as shown in theflowchart. Therewas no evidence of selective non response tothe questionnaires. Only 4.3% of the patients did not return any of the follow-up question-naires. These patients were not included in the analyses. They were evenly distributedover both groups: the group scoring above the cut-off on the PSQ and the group scoringbelow the cut-off (P=.64).
Effect of physical symptoms on the effectiveness of collaborative care
Overall, a high physical symptom count did exert a negative effect on response for col-laborative care and care as usual, but the effect was the same for both conditions. Therewas no interaction effect, which in combination with a substantial main effect, showsthat collaborative careworks for these patients aswell (although lesswell than for patientsnot reporting a high physical symptom count, but this problem is also present for patientsin the CAU-group).
TheMLA revealed a generic negative effect of a physical symptom count (PSQ≥15 formen and PSQ≥17 for women, yes/no) on response to treatment (hypothesis i). This effectwas statistically significant (even after correction for treatment condition) after three (T1),six (T2), and nine months (T3), but not at after 12 months (T4). The outcome in terms ofodds ratios for response to treatment (a decrease of at least 50% on the PHQ-9 betweenbaseline and follow-up) is displayed in Table 2. Table 2 also provides columnswith respectto the results without the correction for chronic medical conditions, and with respect tothe results for the correction for the dichotomous variable ‘at least one chronic medicalcondition reported versus none’. As one can see when comparing columns one and two

Table 2Odds ratios for response to treatment for patients who had a PSQ-score above the cut-off for clinically significant physical symptoms.a
OR PSQ ≥cut-off (CI)Corrected for the number of chronicmedical conditions
OR PSQ ≥cut-off (CI)Corrected for at least one chronicmedical condition vs none
OR PSQ ≥cut-off (CI)Without correction for chronicmedical conditions
N
Three months (T1) 6.83 (1.27–36.81)⁎ 7.85 (1.35–45.74)⁎ 6.87 (1.27–37.04)⁎ 82Six months (T2) 4.10 (1.11–15.06)⁎ 4.60 (1.22–17.41)⁎ 4.83 (1.31–6.14)⁎ 84Nine months (T3) 6.38 (1.64–24.80)⁎ 4.76 (1.36–16.74)⁎ 5.06 (1.48–17.27)⁎ 76Twelve months (T4) 1.94 (.57–6.60) 1.96 (0.58–6.71) 1.93 (.57–6.55) 79
OR=odds ratio; CI=confidence interval.a All ORs corrected for treatment condition (CAU or CC); note that these ORs imply a negative effect: for instance the odds on response are 6.83 times lower for patients scoring
above the cut-off after 3 months of treatment (after a correction for the number of chronic medical conditions).⁎ Pb .05.
183K.M.L. Huijbregts et al. / Journal of Psychosomatic Research 74 (2013) 179–185
with column three, hypothesis iii is confirmed: the effect of a high physical symptom countis independent of both the presence and the number of chronic medical conditions.
The odds on response were significantly worse for the patientswith a high physicalsymptom count than for the patients without a high physical symptom count after3 months (6.83; 95% CI: 1.27 to 36.81), 6 months (4.05; CI: 1.10–14.92), and 9 months(6.38; CI: 1.64–24.80). Time to first response was also 4.3 months longer for the groupsuffering from a high physical symptom count. The logistic regression analyses withoutthe PSQ cut-off revealed significant ORs for lack of response (on the PHQ-9) per point(increase) on the PSQ at T1 and T3. Thus a high score on the PSQ implied worse oddsfor response. The OR per point (increase) at T1 was 1.12 (CI: 1.02–1.23), and at T3 itwas 1.10 (CI: 1.02–1.19). The results at T2 and T4 pointed in the direction of a negativeeffect of a higher PSQ score, but were non significant (P=.12 at T2; P=.06 at T4).
The more negative course of MDD for the group that scores above the cut-off for ahigh physical symptom count on the PSQ is also shown in Fig. 2.
However, no differential effect of a high physical symptom count could be demon-strated for one of the treatment conditions (hypothesis ii). There was no significant inter-action between treatment condition (either collaborative care or CAU) and a high physicalsymptom count (P at 3 months=.22; P at 6 months=.88; P at 9 months=.34; P at12 months=.94) with respect to the outcome measure response to treatment. Interac-tion was also not found in the logistic model without the cut-off on the PSQ.
Adding the number of chronic medical conditions to themodel did not have an effecton the outcome (hypothesis iii). When looking at the results as a whole, the conclusion isthat the correction for medical conditions did not influence the results, and that the effectof a high physical symptom count remained statistically significant after this correction.Furthermore the correction for chronic medical conditions (either the presence or thenumber) also did not influence the results for time to first treatment response.
As data were available on actual care given by the care managers in the collaborativecare arms of the trial, it was possible to explore the possibility that the negative effect of ahigh physical symptom countwas perhaps due to lower adherence to the protocol. In thatcase one would expect that it was less likely that care had been initiated when patientsscored above the cut-off on the PSQ and that these patients had received less sessions.We could not demonstrate this conclusively: 37.5% of the collaborative care patientswith a high physical symptom count did not go to a care manager at all (or only wentto the first appointment) as opposed to 20.3% of the collaborative care patients whoscore below the cut-off, but this difference was not significant (P=.154). The same was
Fig. 2. Negative effect of physical symptoms score PSQ on the course of depression for thewhole group (N=115).
true for the number of appointments with a care manager: patients with a high physicalsymptom count in the collaborative care groups received less sessions, on average 4.9(SD=3.8) appointments as opposed to 6.4 (SD=3.7) in the group of patients who scoredbelow the cut-off, but again this finding was not significant (P=.174).
Discussion
Ourhypothesis that a high physical symptomcountmight have a ge-neric negative effect on the outcome of treatment for MDD was con-firmed. Patients in the group scoring above the cut-off on the PSQresponded on average 4.3 months later than the others. Our second hy-pothesis was not confirmed: no differential effect for type of treatment(collaborative care or care as usual) could be demonstrated. Treatmentfor MDD in primary care thus appears to be less successful for all pa-tients (regardless of treatment condition) who have a high physicalsymptom count, but they can benefit from collaborative care anyway.The association with lack of response remained significant after 3, 6,and 9 months; and after the models were corrected for the presenceand the number of chronic medical illnesses (e.g. COPD or Diabetes).
Whether or not a chronic medical disorder is also present, does notseem to be relevant to the effect that scoring above the cut-off on thePSQhas on the course ofMDDand the outcomeof treatment for this dis-order. This is an important issue [12]: comorbidity of MDDwith chronicmedical illnesses is high [3], but so is comorbidity with somatoform dis-orders [2] where the underlying pathology is not explained (or whereunderlying pathology does not explain the severity of the symptoms).Minsky and colleagues report that the presence of 3 or more physicalsymptoms is a significant predictor of mental health service use [30],and that whether or not these symptoms are explained by a knownmedical disorder is not particularly relevant in that respect.
By asking patients at baseline about the medical conditions theywere suffering from, we were able to explore this issue. In our currentsample the distinction indeed appeared to be irrelevant when lookingat the relationship with the outcome of MDD. Replication in a studywhere the physical symptoms are assessed by amedical doctor at base-line is advisable, even though results from a large cohort-study suggestthat patients' self-reports on chronic diseases are fairly accurate [24].
Limitations
A first limitation of this study is the percentage of patients who didnot return a questionnaire at one or more of the time points of on aver-age 30.2% (ranging from27.0% at 6 months to 33.9% at 9 months). Therewas no evidence of selective non-response to the questionnaires at anyof the time points. Other studies with dropout percentages below 20%,have also found a negative association of concomitant physical symp-toms with MDD [4], which implies that there is little reason to doubtthefinding that a high physical symptomcount predicts amore negativecourse of MDD. More research seems necessary regarding the hypothe-sis that there might be interaction of a high physical symptom countwith the type of treatment that was provided (hypothesis ii). Our studymay have been underpowered to detect this.

184 K.M.L. Huijbregts et al. / Journal of Psychosomatic Research 74 (2013) 179–185
A second limitation could be that not all patients completed the PSQat baseline (77.2% did), as some patients found the questionnaires tootime consuming. It may, however, also (like the loss to follow-up)have influenced statistical power, and this might explain the lack of ef-fect of a high physical symptom count at T4. Asmentioned in the resultssection, there was no evidence for selective bias on most variables withrespect to patientswhodid andpatientswhodid notfill out the PSQ. Pa-tients of non Dutch origin were however more likely to have not filledout the PSQ. We presume that language problems may have been acause of this (the baseline questionnaires were time consuming, partic-ularly for patientswhohad language problems). Nevertheless, given theselectivity mentioned above, our results in this paper may not general-ize to the group of patients that is not of Dutch origin.
Finally, a third limitation of our current study, although it mainly re-fers to hypothesis iii as stated in the introduction (thehypothesis that theeffect of a high physical symptom count is independent of the presenceof an underlying chronic physical illness), might have been the absenceof the assessment of the concomitant physical symptoms by a medicaldoctor at baseline. The result is that it still remains somewhat unclearwhether or not the physical symptoms were medically explained ornot. By asking patients at baseline about the medical conditions theywere suffering from, we were able to explore this issue however. Inour current sample controlling for medical comorbidity appeared to beirrelevant when looking at the relationship of a high physical symptomcountwith the outcome ofMDD. Replication in a studywhere the phys-ical symptoms are assessed by a medical doctor at baseline is advisable,even though results from a large cohort-study suggest that patients'self-reports on chronic diseases are fairly accurate [24].
One could argue that the physical symptoms as reported by thepatients in our sample might have been connected to the depression,as physical symptoms (e.g. fatigue, weight loss) are part of the diagnos-tic criteria for MDD. We presume that the use of the PSQ will have neu-tralized this problem to a large extent, as this questionnaire comprises55 physical symptoms. Furthermore patients had to score above apredefined cut-off of at least 15 symptoms. Nevertheless a follow-upstudy that replicated our results with an outcome measure that doesnot take physical symptomsof depression into account, would be an im-portant addition to our current findings. The PHQ-2 that includes onlythe core symptoms (depressed mood and loss of interest) of MDDmay be a good candidate for such an outcome measure.
Implications for research and clinical practice
Our analyses identify a group of patientswhose condition –MDDac-companied by a high physical symptom count according to a self reportquestionnaire – shows a substantially less favorable treatment response.Apparently the presence of such an amount of physical symptoms asexperienced by a patient and not necessarily the presence of a chronicmedical condition influences the outcome of treatment (both collabora-tive care and care as usual).
Such levels of physical symptoms perhaps point to deeper rootednegative cognitions that the patient is not aware of yet, or might beconsidered as anxiety equivalents with the subsequent avoidance be-havior, but such considerations remain speculative. In any case, thesepatients are frequent visitors to their GP and are generally high ser-vice utilizers [31,32]. Integrated treatment in primary care is there-fore a logical way forward.
Another possible explanation might be that these symptomsshould be considered expressions of MDD or comorbid anxiety condi-tions, i.e. mixed anxiety-depression, that often occur in primary careas well [33].
Althoughmore research into the specific characteristics of this groupis necessary, an important question for the future will be: how can weidentify and treat patients suffering from depression accompanied by ahigh level of physical symptoms successfully? Our results support theincreasing use in primary care of multidimensional symptom indicators
such as the PHQ-9 [16], PHQ-15 [34], and PSQ [21,22]. The PHQ-15 andthe PSQ were designed specifically to detect a high physical symptomcount in patients suffering from mental disorders.
Both collaborative care and care as usual for MDD are less effectivefor this group. The good news is that a high physical symptom countdoes not appear to be a contraindication for collaborative care (sincewe did not find interaction with type of treatment). Neverthelessthese symptoms do predict a more negative course of MDD, even if col-laborative care is applied. Our data on the actual care that was deliveredin the collaborative care arms of the trial suggest that patients sufferingfrom a high level of physical symptoms received less sessions (4.9 vs.6.4 on average) and that it was somewhat less likely that care hadbeen initiated. These results were not statistically significant however.Nevertheless it might be worthwhile to invest more time and energyto convince this group that treatment for depressionmight be beneficialfor them. After all, collaborative care is still more effective than care asusual for patients suffering from a high level of physical symptoms(but relatively less effective compared with the group that does notmeet these criteria).
Promising results in this respect, were found in previous research foran adapted version of the collaborative care model for patients whowere suffering from medically unexplained physical symptoms inwhich a consultant psychiatrist saw the patients together with the gen-eral practitioner in the primary care center [35]. This was not commonpractice in the collaborative care model in our current study, in whichthe consultant psychiatrist had a less proactive role: the psychiatristprovided consultation advice if a patient was not responding to treat-ment after a certain amount of time. Another option may be to add apsychosomatic physiotherapist to the collaborative care team. Thesephysiotherapists have been trained to recognize and influence the com-plex relationship betweenmotor function,mental function, and psycho-social context [36], which might be helpful in the treatment of patientswho suffer from both physical andmental problems. For patients suffer-ing from comorbid chronic somatoform disorders referral to a psycho-therapist or specialized mental health care may be worthwhile.Another treatment option for MDD patients with concomitant physicalsymptoms might be to add treatments effective for somatoform disor-ders such as cognitive-behavioral therapy and other evidence-basedtreatments [37]. In view of the negative influence on treatment re-sponse, research is warranted to improve the treatment model for pa-tients with MDD accompanied by a high physical symptom count inprimary care.
Funding
The study was funded by The Innovation fund health care insurers(Innovatiefonds zorgverzekeraars, formerly known as RVVZ) in theNetherlands.
References
[1] Simon GE, Vonkorff M, Piccinelli M, Fullerton C, Ormel J. An international study of therelation between somatic symptoms anddepression. N Engl JMed1999;341:1329–35.
[2] deWaalMW,Arnold IA, Eekhof JA, VanHemertAM. Somatoformdisorders in generalpractice: prevalence, functional impairment and comorbidity with anxiety anddepressive disorders. Br J Psychiatry 2004;184:470–6.
[3] Moussavi S, Chatterji S, Verdes E, Tandon A, Patel V, Ustun B. Depression, chronic dis-eases, and decrements in health: results from the World Health Surveys. Lancet2007;370:851–8.
[4] Huijbregts KM, van der Feltz-Cornelis CM, van Marwijk HW, de Jong FJ, van derWindt DA, Beekman AT. Negative association of concomitant physical symptomswith the course of major depressive disorder: a systematic review. J PsychosomRes Jun 2010;68:511–9.
[5] Gaynes BN, RushAJ, TrivediMH, et al. Primary versus specialty care outcomes for de-pressed outpatients managed withmeasurement-based care: results from STAR*D. JGen Intern Med 2008;23:551–60.
[6] Sobocki P. Health economics of depression, thesis. Stockholm: Department of Learn-ing, Informatics, Management and Ethics, Medical Management Centre, KarolinskaInstitutet. Stockholm Sweden, 2006.

185K.M.L. Huijbregts et al. / Journal of Psychosomatic Research 74 (2013) 179–185
[7] Unutzer J, KatonW, Callahan CM, et al. Collaborative caremanagement of late-life de-pression in the primary care setting: a randomized controlled trial. JAMA 2002;288:2836–45.
[8] Nutting PA, Rost K, Smith J, Werner JJ, Elliot C. Competing demands from physicalproblems: effect on initiating and completing depression care over 6 months. ArchFam Med 2000;9:1059–64.
[9] Bair MJ, Robinson RL, KatonW, Kroenke K. Depression and pain comorbidity: a liter-ature review. Arch Intern Med 2003;163:2433–45.
[10] Huijbregts KM, van Marwijk HW, de Jong FJ, Schreuders B, Beekman AT, van derFeltz-Cornelis CM. Adverse effects ofmultiple physical symptoms on the course of de-pressive and anxiety symptoms in primary care. Psychother Psychosom 2010;79:389–91.
[11] KroenkeK, Spitzer RL,Williams JB, et al. Physical symptoms in primary care. Predictorsof psychiatric disorders and functional impairment. Arch Fam Med 1994;3:774–9.
[12] CrombezG, Beirens S, CanDammeC, Eccleston J, Fontaine J. The unbearable lightnessof somatisation: a systematic review of the concept of somatisation in empiricalstudies of pain. Pain 2009;145:31–6.
[13] Katon W, Von Korff M, Lin E, et al. Collaborative management to achieve treatmentguidelines. Impact on depression in primary care. JAMA 1995;273:1026–31.
[14] IJff MA, Huijbregts KM, van Marwijk HW, et al. Cost-effectiveness of collaborativecare including PST and an antidepressant treatment algorithm for the treatment ofmajor depressive disorder in primary care; a randomised clinical trial. BMC HealthServ Res 2007;7.
[15] Van der Feltz-Cornelis CM, Ader HJ. Randomization in psychiatric intervention re-search in the general practice setting. Int J Methods Psychiatr Res 2000;9:134–42.
[16] Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severitymeasure. J Gen Intern Med 2001;16:606–13.
[17] SheehanDV, Lecrubier Y, Sheehan KH, et al. TheMini-International NeuropsychiatricInterview (M.I.N.I.): the development and validation of a structured diagnostic psy-chiatric interview for DSM-IV and ICD-10. J Clin Psychiatry 1998;59:22–33.
[18] Huijbregts KM, de Jong FJ, HWJv Marwijk, Beekman ATF, Adèr H, Hakkaart-Roijen L,et al. A target-driven collaborative care model for Major Depressive Disorder is effec-tive in primary care in The Netherlands. A randomized clinical trial from the Depres-sion Initiative. J AffectDisordOct 12 2012, http://dx.doi.org/10.1016/j.jad.2012.09.015[pii: S0165-0327(12)00643-X].
[19] Feltz-Cornelis CM. The depression initiative. Description of a collaborative caremodel for depression in the primary care setting in The Netherlands. Clin Neuro-psychiatry 2011;8:260–7.
[20] der Feltz-Cornelis CM Van. Towards integrated primary health care for depressivedisorder in The Netherlands. The Depression Initiative. Int J Integr Care1568-4156June 15 2009.
[21] Hemert AM. Lichamelijke Klachten Vragenlijst. Leiden: Leids Universitair MedischCentrum; 2003.
[22] Hemert AM, de Waal MW, Van Rood YR. Meetinstrumenten bij somatoformestoornissen. Tijdschr Psychiatr 2004;46:693–6.
[23] Hakkaart-Roijen L, Essink-Bot ML. Manual questionnaire illness and work [in Dutch:Handleiding Vragenlijst over Ziekte en Werk]. Rotterdam, The Netherlands: iMTA;1999.
[24] Kriegsman DM, Penninx BW, van Eijk JT, Boeke AJ, Deeg DJ. Self-reports and generalpractitioner information on the presence of chronic diseases in community dwellingelderly. A study on the accuracy of patients' self-reports and on determinants of in-accuracy. J Clin Epidemiol 1996;49:1407–17.
[25] National Center for Health Statistics. Vital and health statistics. Evaluation of nationalhealth interview survey diagnostic reporting. Series 2: data evaluation and methodsresearch, no. 120. Hyattsville, Maryland: U.S. Department of Health and Human Ser-vices; 1994.
[26] Spitzer RL, Kroenke K, Williams JB. Validation and utility of a self-report version ofPRIME-MD: the PHQ primary care study. Primary Care Evaluation of Mental Dis-orders. Patient Health Questionnaire. JAMA 1999;282:1737–44.
[27] Goldstein H, Rasbash J, Plewis I, et al. A users guide to MlwinN. Multilevel ModelsProject. London: University of London; 1998.
[28] Ader HJ, Mellenbergh GJ, Hand DJ. Advising on research methods: a consultant'scompanion. Huizen, The Netherlands: Johannes van Kessel Publishing; 2008.
[29] Ader H. A composite score that combines response and remission. Available fromwww.jvank.nl/Trimbos/Remres/Composite.pdf; 2012.
[30] Minsky S, Rebecca SE, Gara M, Escobar JI. Service use among patients with seriousmental illnesses who presented with physical symptoms at intake. Psychiatr Serv2011;62:146–51.
[31] Sheehan B, Bass C, Briggs R, Jacoby R. Somatization among older primary care at-tenders. Psychol Med 1996;33:867–77.
[32] Hiller W, Fichter MM. High utilizers of medical care: a crucial subgroup amongsomatizing patients. J Psychosom Res 2004;56:437–43.
[33] Fava M, Alpert JE, Carmin CN, et al. Clinical correlates and symptom patterns of anx-ious depression among patients with major depressive disorder in STAR*D. PsycholMed 2004;34:1299–308.
[34] Kroenke K, Spitzer RL, Williams JB. The PHQ-15: validity of a new measure for eval-uating the severity of somatic symptoms. Psychosom Med 2002;64:258–66.
[35] Van der Feltz-Cornelis CM, van Oppen P, Adèr H, van Dyck R. Randomised controlledtrial of a collaborative care model with psychiatric consultation for persistent medi-cally unexplained symptoms in general practice. Psychother Psychosom 2006;75:282–9.
[36] Mulders N, Boersma R, Ijntema R, Coppolse R. Competence profile for psychoso-matic physiotherapists [In Dutch: Beroepscompetentieprofiel Psychosomatischfysiotherapeut NFP]. In: de Gans Drukkerij, editor. Amersfoort, the Netherlands:Nederlandse Vereniging voor Fysiotherapie volgens de Psychosomatiek; 2009.
[37] Kroenke K. Efficacy of treatment for somatoform disorders: a review of randomizedclinical trials. Psychosom Med 2007;69:881–8.




















