A cross-sectional study of postpartum depressive symptoms and infant weight outcomes: Do well-child...
11
A Cross-sectional Study of Postpartum Depressive Symptoms and Infant Weight Outcomes: Do Well-Child Visits make a Difference? Rada K Dagher 1 and Taryn W Morrissey 2 1 Department of Health Services Administration, University of Maryland, College Park, Maryland, USA 2 Department of Public Administration and Policy, School of Public Affairs, American University, USA * Corresponding author: Rada K. Dagher, Ph.D., M.P.H., Assistant Professor, School of Public Health, University of Maryland, 3310B School of Public Health Building, College Park, Maryland 20742, USA, Tel: 301-405-1210; Fax: 301-405-2542; E-mail: [email protected] Rec date: Jul 21, 2014, Acc date: Feb 05, 2015, Pub date: Feb 12, 2015 Abstract Background: Maternal postpartum depression affects 10% to 20% of new mothers, but little research has examined its relationship with weight outcomes during infancy and whether clinical interventions can mitigate this relationship. This study investigated the associations of postpartum depressive symptoms with infants’ weight-for-length z-scores, obesity, and overweight at 9 months of age; and whether the number of well-child visits moderated these associations. Methods: We used data from the Early Childhood Longitudinal Study-Birth Cohort (ECLS-B), a nationally representative sample of approximately 10,700 children born in the U.S. in 2001. Results: At 9 months postpartum, 6% of the mothers were considered severely depressed, and 18.2% either moderately or severely depressed, on the Center for Epidemiologic Studies Depression Scale. Approximately 15% of the infants were obese and 29% were overweight (at or above the 95th or 85th percentiles for weight and length, respectively). Higher maternal depression scores were associated with lower odds of obesity (OR=0.997, 95% CI: 0.970-0.994) and overweight (OR=0.990, 95% CI: 0.981-0.999) among their infants, and higher numbers of well-child-visits were associated with even lower odds of child overweight among mothers with higher depression scores (OR=0.996, 95% CI: 0.993-0.999). Depressive scores had no associations with infants’ continuous weight-for-length z-scores. Conclusion: While the causal directions and mechanisms remain unclear, findings suggest that well-child visits may provide an opportunity to address mothers’ depressive symptoms and establish healthy habits among their children. Keywords: Maternal depression; Infant obesity and overweight; Well-child visits Introduction Childhood obesity and overweight are significant public health problems in the United States (U.S.). Although the obesity rate among very young children has decreased in recent years, in 2011-2012, 22.8% of 2 to 5 year old U.S. children were overweight and 8.4% were considered obese [1]. In addition, 15.2% of 9 months old U.S. children were at-risk for obesity and 16.7% were considered obese [2]. Childhood obesity is associated with negative health outcomes including atherosclerotic plaque [3], development of insulin resistance and type 2 diabetes [3], and high prevalence of high blood pressure, high plasma triglycerides, low HDL cholesterol levels, asthma, shortness of breath, and obstructive sleep apnea [4,5]. Moreover, childhood obesity has psychological consequences among children including stigmatization, eating disturbances, and depression [6,7]. Maternal postpartum depression is also an important public health issue, not only for women themselves but also for their children and families. Postpartum depression is prevalent among 10% to 20% of new mothers [8] and has been shown to negatively affect mothers’ quality of life [9], their close and intimate relationships [10,11], and may have negative effects on children’s emotional and cognitive development [12,13], maternal-infant interactions [14,15], and maternal self-efficacy in the first few years of a child’s life [16]. Postpartum depression typically begins within four weeks after childbirth but may start as late as 3, 6, or 9 months postpartum [17]. Symptoms can be severe and persistent, usually lasting for months [18]. Maternal postpartum depression may play a role in children’s weight outcomes during early childhood. The postpartum period is an important time for the infant to develop a secure attachment to the mother, which contributes to healthy development [19]. Household production theory maintains that families “produce” child outcomes, such as physical health, through parental resources or a lack thereof [20], including maternal postpartum depression. The literature on failure to thrive and studies in a number of developing countries have shown significant associations between maternal depression and infant growth delays [21]; however, studies on maternal depression and child obesity-the other end of the growth spectrum- are limited. Depressed mothers may be less likely to breastfeed, contributing to greater reliance on formula or cow’s milk and bottle-feeding, which is associated with poorer self-regulation and weight gain in infancy [22]. Families with depressed mothers may also have difficulty establishing and maintaining healthy eating habits and mealtime and bedtime routines [23,24]. Moreover, the stress from living with a mother facing depressive symptoms may lead to metabolic abnormalities contributing to weight gain [25] or to weight loss [26]. The established associations between maternal depression and impaired mother-infant relationships [15] may also play a role in infant weight gain or loss. The findings from the few studies conducted in this area of research show conflicting results. Three studies found that exposure to maternal depression or depressive symptoms during the early childhood period was associated with a higher probability of being overweight and being obese among infants aged 6-24 months living in low-income families in Brazil [27], with higher overall adiposity among 3-year-olds in a prospective sample in Boston [28], and with higher likelihood of being overweight for children who were 12, 24, and 36 months from 10 states in the U.S. [29]. Conversely, two other studies found that maternal depression was associated with slower Dagher and Morrissey, J Womens Health, Issues Care 2015, 4:2 http://dx.doi.org/10.4172/2325-9795.1000179 Journal of Women’s Health, Issues & Care Research Article A SCITECHNOL JOURNAL All articles published in Journal of Women’s Health, Issues & Care are the property of SciTechnol and is protected by copyright laws. Copyright © 2015, SciTechnol, All Rights Reserved.
Transcript of A cross-sectional study of postpartum depressive symptoms and infant weight outcomes: Do well-child...

A Cross-sectional Study ofPostpartum Depressive Symptomsand Infant Weight Outcomes: DoWell-Child Visits make aDifference?Rada K Dagher1 and Taryn W Morrissey2
1Department of Health Services Administration, University of Maryland, CollegePark, Maryland, USA2Department of Public Administration and Policy, School of Public Affairs,American University, USA*Corresponding author: Rada K. Dagher, Ph.D., M.P.H., Assistant Professor,School of Public Health, University of Maryland, 3310B School of Public HealthBuilding, College Park, Maryland 20742, USA, Tel: 301-405-1210; Fax:301-405-2542; E-mail: [email protected] date: Jul 21, 2014, Acc date: Feb 05, 2015, Pub date: Feb 12, 2015
Abstract
Background: Maternal postpartum depression affects 10% to20% of new mothers, but little research has examined itsrelationship with weight outcomes during infancy and whetherclinical interventions can mitigate this relationship. This studyinvestigated the associations of postpartum depressivesymptoms with infants’ weight-for-length z-scores, obesity, andoverweight at 9 months of age; and whether the number ofwell-child visits moderated these associations.
Methods: We used data from the Early Childhood LongitudinalStudy-Birth Cohort (ECLS-B), a nationally representativesample of approximately 10,700 children born in the U.S. in2001.
Results: At 9 months postpartum, 6% of the mothers wereconsidered severely depressed, and 18.2% either moderatelyor severely depressed, on the Center for Epidemiologic StudiesDepression Scale. Approximately 15% of the infants wereobese and 29% were overweight (at or above the 95th or 85thpercentiles for weight and length, respectively). Highermaternal depression scores were associated with lower odds ofobesity (OR=0.997, 95% CI: 0.970-0.994) and overweight(OR=0.990, 95% CI: 0.981-0.999) among their infants, andhigher numbers of well-child-visits were associated with evenlower odds of child overweight among mothers with higherdepression scores (OR=0.996, 95% CI: 0.993-0.999).Depressive scores had no associations with infants’ continuousweight-for-length z-scores.
Conclusion: While the causal directions and mechanismsremain unclear, findings suggest that well-child visits mayprovide an opportunity to address mothers’ depressivesymptoms and establish healthy habits among their children.
Keywords: Maternal depression; Infant obesity andoverweight; Well-child visits
IntroductionChildhood obesity and overweight are significant public health
problems in the United States (U.S.). Although the obesity rate amongvery young children has decreased in recent years, in 2011-2012, 22.8%of 2 to 5 year old U.S. children were overweight and 8.4% wereconsidered obese [1]. In addition, 15.2% of 9 months old U.S. childrenwere at-risk for obesity and 16.7% were considered obese [2].Childhood obesity is associated with negative health outcomesincluding atherosclerotic plaque [3], development of insulin resistanceand type 2 diabetes [3], and high prevalence of high blood pressure,high plasma triglycerides, low HDL cholesterol levels, asthma,shortness of breath, and obstructive sleep apnea [4,5]. Moreover,childhood obesity has psychological consequences among childrenincluding stigmatization, eating disturbances, and depression [6,7].
Maternal postpartum depression is also an important public healthissue, not only for women themselves but also for their children andfamilies. Postpartum depression is prevalent among 10% to 20% ofnew mothers [8] and has been shown to negatively affect mothers’quality of life [9], their close and intimate relationships [10,11], andmay have negative effects on children’s emotional and cognitivedevelopment [12,13], maternal-infant interactions [14,15], andmaternal self-efficacy in the first few years of a child’s life [16].Postpartum depression typically begins within four weeks afterchildbirth but may start as late as 3, 6, or 9 months postpartum [17].Symptoms can be severe and persistent, usually lasting for months[18].
Maternal postpartum depression may play a role in children’sweight outcomes during early childhood. The postpartum period is animportant time for the infant to develop a secure attachment to themother, which contributes to healthy development [19]. Householdproduction theory maintains that families “produce” child outcomes,such as physical health, through parental resources or a lack thereof[20], including maternal postpartum depression. The literature onfailure to thrive and studies in a number of developing countries haveshown significant associations between maternal depression and infantgrowth delays [21]; however, studies on maternal depression and childobesity-the other end of the growth spectrum- are limited. Depressedmothers may be less likely to breastfeed, contributing to greaterreliance on formula or cow’s milk and bottle-feeding, which isassociated with poorer self-regulation and weight gain in infancy [22].Families with depressed mothers may also have difficulty establishingand maintaining healthy eating habits and mealtime and bedtimeroutines [23,24]. Moreover, the stress from living with a mother facingdepressive symptoms may lead to metabolic abnormalitiescontributing to weight gain [25] or to weight loss [26]. The establishedassociations between maternal depression and impaired mother-infantrelationships [15] may also play a role in infant weight gain or loss.
The findings from the few studies conducted in this area of researchshow conflicting results. Three studies found that exposure tomaternal depression or depressive symptoms during the earlychildhood period was associated with a higher probability of beingoverweight and being obese among infants aged 6-24 months living inlow-income families in Brazil [27], with higher overall adiposityamong 3-year-olds in a prospective sample in Boston [28], and withhigher likelihood of being overweight for children who were 12, 24,and 36 months from 10 states in the U.S. [29]. Conversely, two otherstudies found that maternal depression was associated with slower
Dagher and Morrissey, J Womens Health, Issues Care 2015, 4:2http://dx.doi.org/10.4172/2325-9795.1000179 Journal of Women’s
Health, Issues & Care
Research Article A SCITECHNOL JOURNAL
All articles published in Journal of Women’s Health, Issues & Care are the property of SciTechnol and is protected bycopyright laws. Copyright © 2015, SciTechnol, All Rights Reserved.

weight gain from 0 to 4 months among infants from NortheastEngland [30], and being exposed to chronic maternal depression wasassociated with lower risk for overweight among Latina infants in SanFrancisco in the first two years of life [26]. A cohort study spanningfive European countries (Belgium, Germany, Italy, Poland, Spain)found no associations between postpartum depression and infants’ z-scores for weight-for-length or other anthropometric indices ininfants’ first two years of life [31]. These contradictory results may beexplained by the diverse samples studied in different countries, studydesign differences and in some instances small sample sizes.
Depressed mothers report less positive parenting practices inrelation to health promotion and disease prevention activities thatcould affect child health and weight. These include lower rates of well-child-care visits and up-to-date vaccinations [32], lower likelihood ofpositive enrichment activity with their children such as reading,singing, and story-telling [33,34], less healthy infant sleep practices[24,34], fewer rules regarding mealtimes [24], and a lower likelihood ofbreastfeeding [34,35]. Despite these established associations and thefact that mothers remain the primary decision-makers for theirchildren’s health behaviors and health services use [31], little is knownon how mothers’ parental practices affect the relationship betweenmaternal depression and children’s weight outcomes, especially thelikelihood of obesity or overweight among children.
If maternal postpartum depression does indeed influence children’sweight outcomes, the clinical and preventive strategies for mitigatingthese effects are important to understand. Well-child visits during thefirst year of a child’s life have been shown in a number of studies topresent a good opportunity for screening mothers for postpartumdepression and ensuring appropriate treatment and follow-up [36].Importantly, most preventive health care for children under two yearsof age is usually administered during these visits, including theadministration of vaccines, anthropomorphic measurements,nutritional guidance, developmental assessments, and screening testsamong others [37]. The American Academy of Pediatrics recommendsa minimum of seven well-child visits during a child’s first year of life[38]. During well-child visits, pediatricians have the opportunity todiscuss nutrition and physical activity with parents and screenchildren for underweight, overweight and obesity as well as addressmothers’ maternal depressive symptoms; thus, well-child visits maymitigate the negative impacts of maternal depression on children’sweight outcomes.
This study addresses these gaps in the literature by investigating therelationship between postpartum maternal depressive symptoms andtheir infants’ weight-for-length z-scores, obesity, and overweightoutcomes at 9 months of age using a nationally representative sampleof U.S. infants. In addition, we test the moderating effect of well-childvisits in the relationship between maternal depressive symptoms andeach of these weight outcomes. We hypothesize that postpartumdepressive symptoms are associated with higher weight-for-length z-scores and an increased likelihood of obesity and overweight amongtheir infants. Further, we hypothesize that associations betweenpostpartum depressive symptoms and poorer infant weight outcomes(higher z-scores, obesity, and overweight) are weaker among infantswho received higher numbers of well-child visits.
Materials and Methods
SampleThis study uses data from the Early Childhood Longitudinal Study-
Birth Cohort (ECLS-B), a comprehensive, longitudinal study of anational sample of approximately 10,700 children born in the U.S. in20011. The ECLS-B over-sampled Asian and American-Indianchildren, twins, and low and very low birth weight children. This studyuses the data collected on these children at 9 months of age (wave 1,collected in 2001-2002). Data were collected using parent surveys,direct child assessments, and observations of the home and childcareenvironments at the 9 months wave. This secondary data analysisreceived exemption by our university Institutional Review Boards.
MeasuresMeasures of infants’ weight-for-length z-scores, obesity, and
overweight serve as dependent variables. Anthropometric measures ofinfants’ weight and length were collected in the lab at 9 months bytrained data collectors. Child length was measured using a measuremat and child weight was measured by subtracting the weight of themother when standing on a SECA weight scale alone from her weightwhen carrying the child. Each physical measurement was obtainedtwice to minimize error. If the two measures were more than 5% apart,a third measurement was taken. The two closest measurements werethen averaged together. Infants’ weight-for-length z-scores and thebinary measures of obesity (at or above the 95th percentile) andoverweight (at or above the 85th percentile) standardized by age andsex, were calculated using Centers for Disease Control (CDC)standards [39].
Our independent variable of maternal depressive symptoms at 9months was measured using a modified version of the Center forEpidemiologic Studies Depression Scale [40]. Consistent with otherresearch using the modified 12-item CES-D, we considered those whoscored 10 or higher on the CES-D scale as experiencing moderate orsevere depressive symptoms and those who scored higher than 15 asexperiencing severe depressive symptoms [34]. However, we usecontinuous depression scores as an independent variable, as we lackclinical diagnoses of depression. Respondents (mostly biologicalmothers) reported the number of well-baby check-ups the child hadreceived since he/she was born, which served as our independent andmoderating variable.
Based on a priori causal assumptions, several covariates that couldconfound the relationship between maternal depressive symptoms andinfant weight outcomes were included as control variables in theregression models. These covariates included child age (in months),child sex (reference=male), child race/ethnicity (Black; Hispanic;multiracial; versus White), household size, birthweight (moderatelylow; very low; versus normal), child health (fair/poor; good; versusexcellent/very good), maternal age (in years), maternal employment(full-time; part-time; looking for work; versus unemployed), mother’smarital status (married versus not), maternal education (high schoolgraduate; college graduate or higher; versus below high schooleducation), household income (four categories of income versus$0-25,000), child’s health insurance status (reference=uninsured),child’s residence (suburban; urban; versus rural), whether the childwas ever breastfed or not, and mothers’ pre-pregnancy weight (in
1 The reported sample sizes are rounded to the nearest 50, per NCES regulations regarding disclosure of restricted-use data.
Citation: Dagher RK, Morrissey TW (2015) A Cross-sectional Study of Postpartum Depressive Symptoms and Infant Weight Outcomes: Do Well-Child Visitsmake a Difference?. J Womens Health, Issues Care 4:2.
doi:http://dx.doi.org/10.4172/2325-9795.1000179
Volume 4 • Issue 2 • 1000179 • Page 2 of 11 •
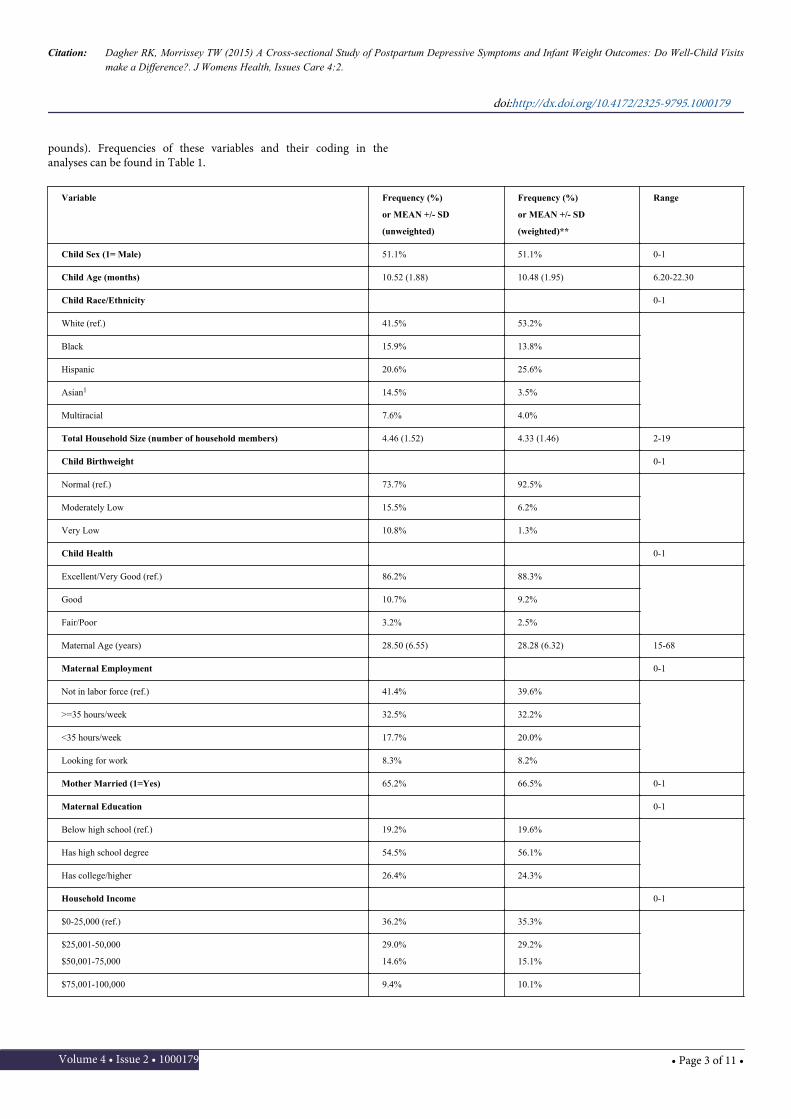
pounds). Frequencies of these variables and their coding in theanalyses can be found in Table 1.
Variable Frequency (%)
or MEAN +/- SD
(unweighted)
Frequency (%)
or MEAN +/- SD
(weighted)**
Range
Child Sex (1= Male) 51.1% 51.1% 0-1
Child Age (months) 10.52 (1.88) 10.48 (1.95) 6.20-22.30
Child Race/Ethnicity 0-1
White (ref.) 41.5% 53.2%
Black 15.9% 13.8%
Hispanic 20.6% 25.6%
Asian1 14.5% 3.5%
Multiracial 7.6% 4.0%
Total Household Size (number of household members) 4.46 (1.52) 4.33 (1.46) 2-19
Child Birthweight 0-1
Normal (ref.) 73.7% 92.5%
Moderately Low 15.5% 6.2%
Very Low 10.8% 1.3%
Child Health 0-1
Excellent/Very Good (ref.) 86.2% 88.3%
Good 10.7% 9.2%
Fair/Poor 3.2% 2.5%
Maternal Age (years) 28.50 (6.55) 28.28 (6.32) 15-68
Maternal Employment 0-1
Not in labor force (ref.) 41.4% 39.6%
>=35 hours/week 32.5% 32.2%
<35 hours/week 17.7% 20.0%
Looking for work 8.3% 8.2%
Mother Married (1=Yes) 65.2% 66.5% 0-1
Maternal Education 0-1
Below high school (ref.) 19.2% 19.6%
Has high school degree 54.5% 56.1%
Has college/higher 26.4% 24.3%
Household Income 0-1
$0-25,000 (ref.) 36.2% 35.3%
$25,001-50,000
$50,001-75,000
29.0%
14.6%
29.2%
15.1%
$75,001-100,000 9.4% 10.1%
Citation: Dagher RK, Morrissey TW (2015) A Cross-sectional Study of Postpartum Depressive Symptoms and Infant Weight Outcomes: Do Well-Child Visitsmake a Difference?. J Womens Health, Issues Care 4:2.
doi:http://dx.doi.org/10.4172/2325-9795.1000179
Volume 4 • Issue 2 • 1000179 • Page 3 of 11 •
>$100,000 10.7% 10.3%
Child has Health Insurance (1=Yes)
Child Residence 96.5% 95.9% 0-1
Rural area (ref.) 15.0% 14.4%
Suburban area 12.3% 12.0%
Urban Area 72.7% 73.5%
Child was Breastfed (1=Yes) 67.5% 69.5% 0-1
Maternal Pre-pregnancy Weight (Kg) 65.85(16.39) 66.60 (15.87) 34-180
Maternal depression score at 9 months postpartum 5.23(5.58) 4.91(5.45) 0-36
Mothers meeting threshold for severe depression (>15) 6.0% 5.5% 0-1
Mothers meeting threshold for moderate/severe depression (>9) 18.2% 16.1% 0-1
Child weight-for-length z-scores 0.27(1.84) 0.36(1.94) -47.34- -17.07
Child is obese (weight-for-length => 95th percentile) 15.0% 17.0% 0-1
Child overweight (weight-for-length => 85th percentile) 29.0% 32.0% 0-1
Number of well-child visits up to 9 months old 5.64(2.72) 5.40(2.37) 0-20
*Sample size was rounded to the nearest 50, in accordance with NCES regulations. **Frequencies and means using sampling weights. 1Includes Asian/Native Hawaiian/PacificIslander/American Indian/Alaska Native
Table 1: Sample Characteristics (N=10,700)*
Statistical analysesAnalyses were conducted using Stata software (v.11.2; Stata
Corporation, College Station, Texas, USA). Using multiple linearregression, main effects associations between the main independentvariables (maternal depressive symptoms and well-child visits) andinfants’ weight-for-length z-scores were first tested, without thecontrol variables or the interaction effects (Model 1)2. Next, anadjusted model, including the main effects and control variables, wastested (Model 2). Finally, the moderating effect of well-child visits onmaternal depression scores was tested in the adjusted model [41] usingan interaction term (Model 3). These series of analyses were repeatedfor the binary dependent variables of infant obesity and infantoverweight status, using logistic regression analyses.
ResultsTable 1 presents the maternal and infant characteristics of the
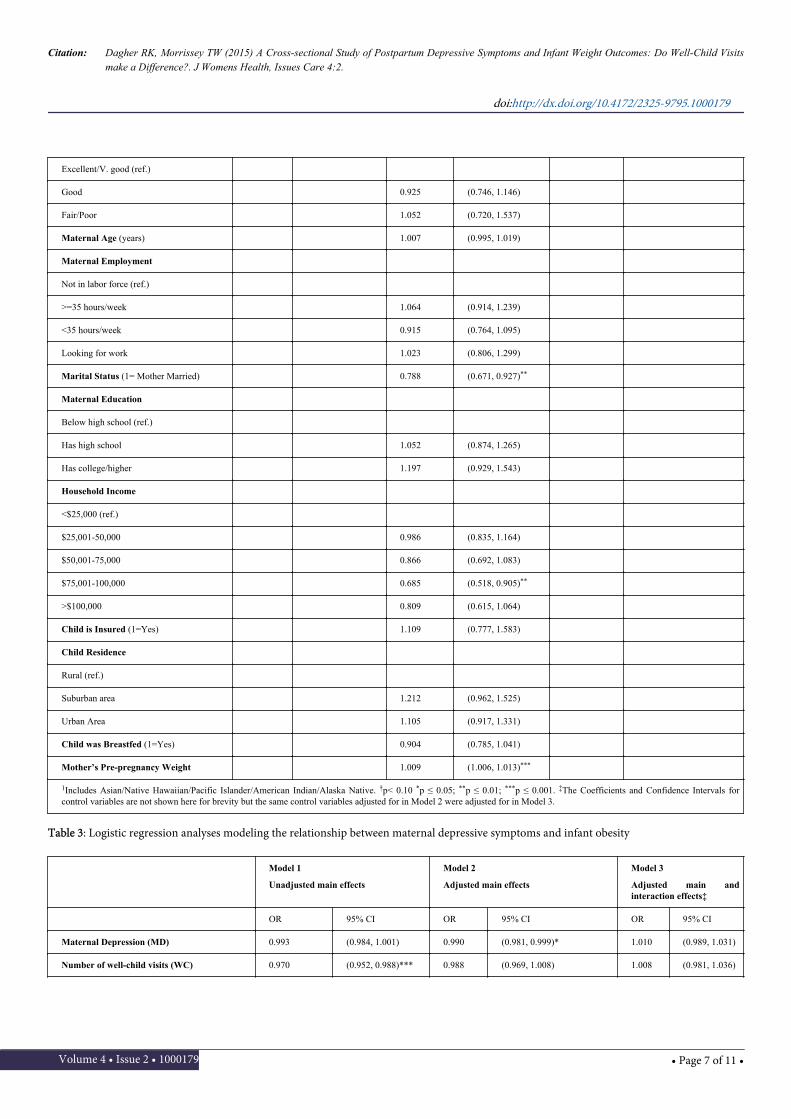
sample. The average maternal depression score was 5.23 (SD: 5.58,Range: 0-36); 6% of the mothers met the threshold for being severelydepressed (i.e. >15) and 18.2% met the threshold for being moderatelyor severely depressed (i.e. >9). Approximately 15% of the infants wereobese (had a weight-for-length at or greater than the 95th percentile)and 29% were overweight (had a weight-for-length at or greater thanthe 85th percentile). The average number of well-child visits up to 9months of age in this sample was 5.64 (SD: 2.72; Range: 0-20).
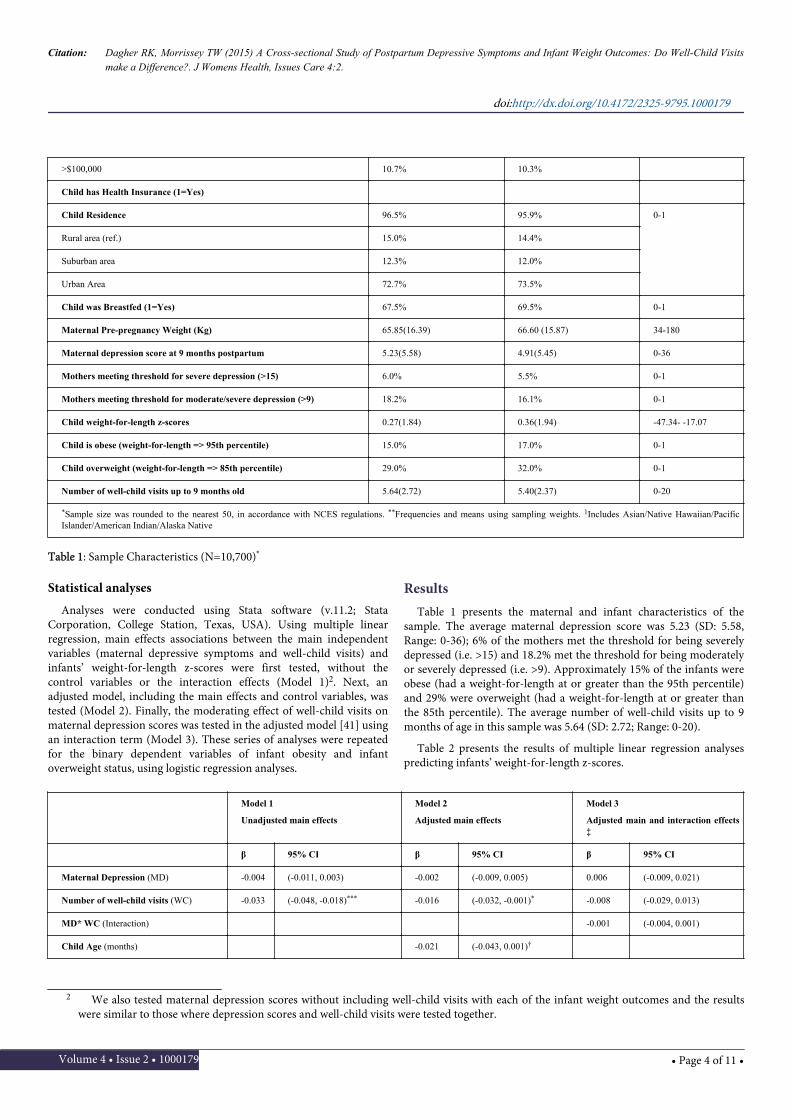
Table 2 presents the results of multiple linear regression analysespredicting infants’ weight-for-length z-scores.
Model 1
Unadjusted main effects
Model 2
Adjusted main effects
Model 3
Adjusted main and interaction effects‡
β 95% CI β 95% CI β 95% CI
Maternal Depression (MD) -0.004 (-0.011, 0.003) -0.002 (-0.009, 0.005) 0.006 (-0.009, 0.021)
Number of well-child visits (WC) -0.033 (-0.048, -0.018)*** -0.016 (-0.032, -0.001)* -0.008 (-0.029, 0.013)
MD* WC (Interaction) -0.001 (-0.004, 0.001)
Child Age (months) -0.021 (-0.043, 0.001)†
2 We also tested maternal depression scores without including well-child visits with each of the infant weight outcomes and the resultswere similar to those where depression scores and well-child visits were tested together.
Citation: Dagher RK, Morrissey TW (2015) A Cross-sectional Study of Postpartum Depressive Symptoms and Infant Weight Outcomes: Do Well-Child Visitsmake a Difference?. J Womens Health, Issues Care 4:2.
doi:http://dx.doi.org/10.4172/2325-9795.1000179
Volume 4 • Issue 2 • 1000179 • Page 4 of 11 •
Child Sex (1= Male) 0.169 (0.091, 0.247)***
Child Race/Ethnicity
White (ref.)
Black -0.085 (-0.216, 0.047)
Hispanic 0.231 (0.113, 0.348)***
Asian1 -0.006 (-0.134, 0.122)
Multiracial 0.074 (-0.074, 0.223)
Household Size -0.013 (-0.041, 0.014)
Birthweight
Normal (ref.)
Moderately Low -0.272 (-0.384, -0.160)***
Very Low -0.413 (-0.549, -0.276)***
Child Health
Excellent/V. good (ref.)
Good -0.183 (-0.313, -0.052)**
Fair/Poor -0.062 (-0.299, 0.176)
Maternal Age 0.006 (-0.002, 0.013)
Maternal Employment
Not in labor force (ref.)
>=35 hours/week 0.024 (-0.072, 0.120)
<35 hours/week -0.056 (-0.166, 0.055)
Looking for work -0.078 (-0.231, 0.076)
Marital Status (1= Mother Married) -0.147 (-0.251, -0.042)**
Maternal Education
Below high school (ref.)
Has high school degree -0.126 (-0.245, -0.008)*
Has college/higher -0.072 (-0.232, 0.088)
Household Income
$0-25,000 (ref.)
$25,001-50,000 0.029 (-0.078, 0.136)
$50,001-75,000 0.051 (-0.088, 0.191)
$75,001-100,000 -0.010 (-0.175, 0.156)
>$100,000 0.083 (-0.086, 0.252)
Child is Insured (1=Yes) -0.002 (-0.223, 0.219)
Child Residence
Rural area (ref.)
Citation: Dagher RK, Morrissey TW (2015) A Cross-sectional Study of Postpartum Depressive Symptoms and Infant Weight Outcomes: Do Well-Child Visitsmake a Difference?. J Womens Health, Issues Care 4:2.
doi:http://dx.doi.org/10.4172/2325-9795.1000179
Volume 4 • Issue 2 • 1000179 • Page 5 of 11 •
Suburban area 0.161 (0.015, 0.308)*
Urban Area 0.148 (0.034, 0.262)*
Child was Breastfed (1=Yes) 0.007 (-0.082, 0.097)
Mother’s Pre-pregnancy Weight 0.007 (0.005, 0.009)***
1 Includes Asian/Native Hawaiian/Pacific Islander/American Indian/Alaska Native
‡The Coefficients and Confidence Intervals for control variables are not shown here for brevity but the same control variables adjusted for in Model 2 were adjusted for in Model 3.
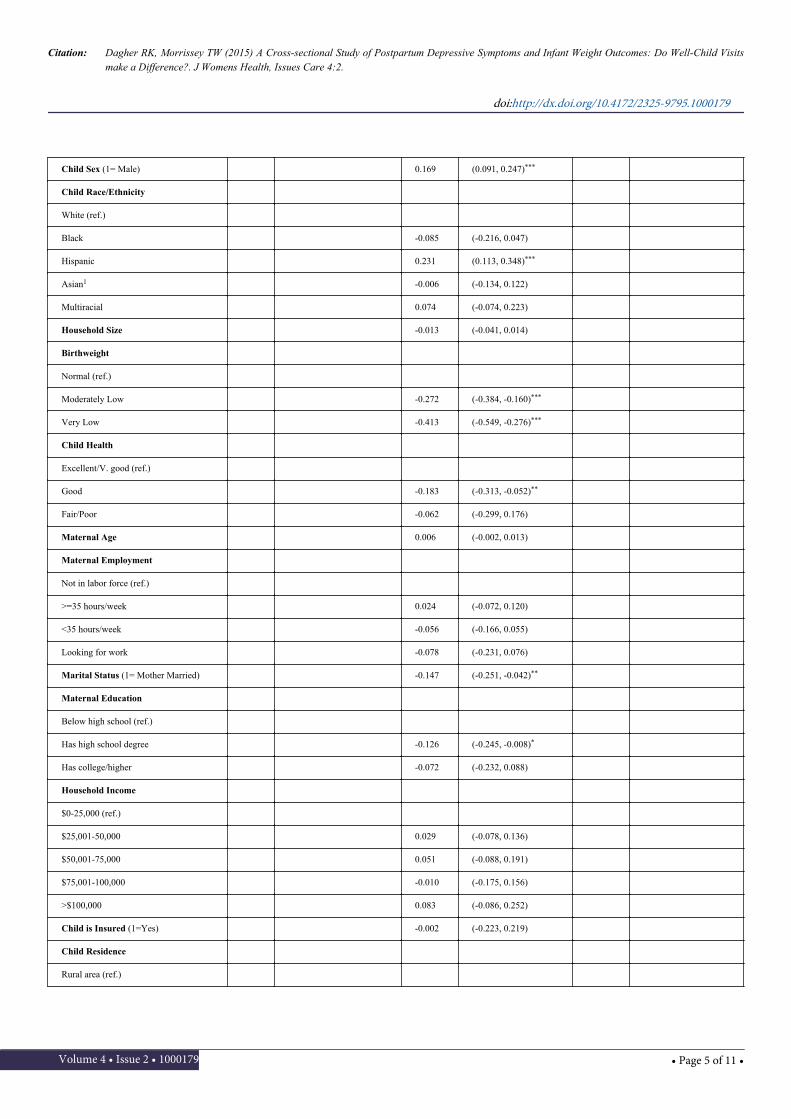
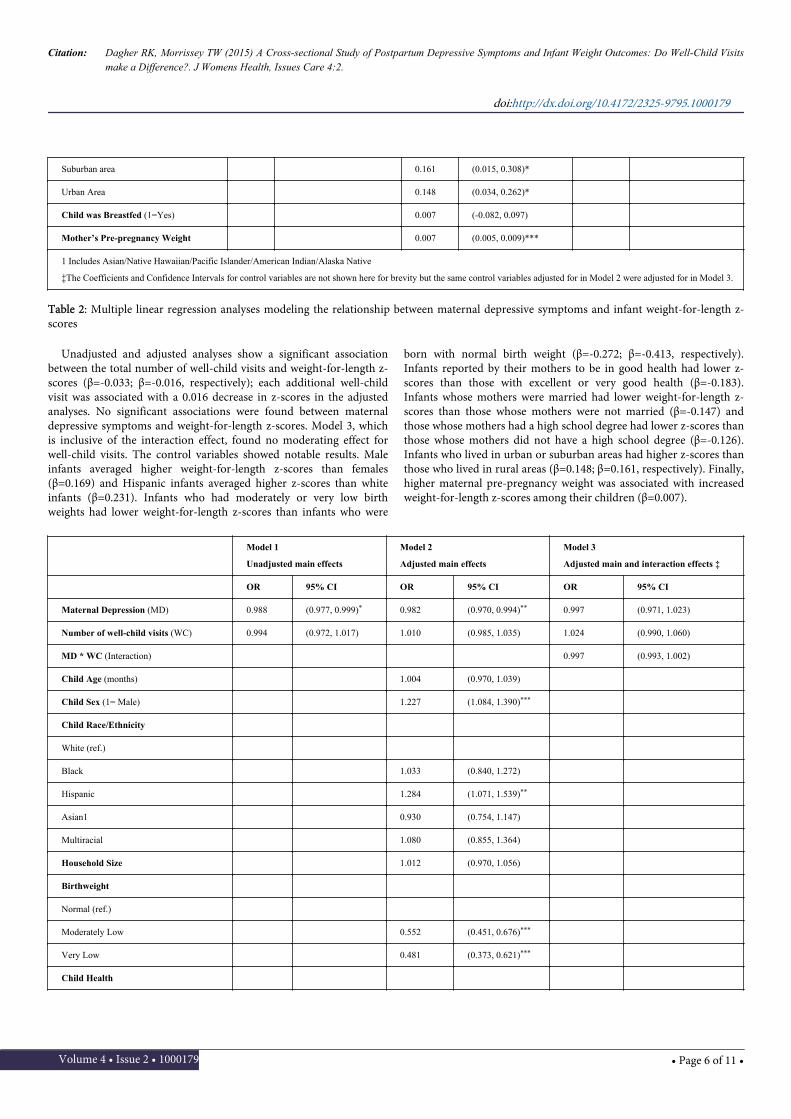
Table 2: Multiple linear regression analyses modeling the relationship between maternal depressive symptoms and infant weight-for-length z-scores
Unadjusted and adjusted analyses show a significant associationbetween the total number of well-child visits and weight-for-length z-scores (β=-0.033; β=-0.016, respectively); each additional well-childvisit was associated with a 0.016 decrease in z-scores in the adjustedanalyses. No significant associations were found between maternaldepressive symptoms and weight-for-length z-scores. Model 3, whichis inclusive of the interaction effect, found no moderating effect forwell-child visits. The control variables showed notable results. Maleinfants averaged higher weight-for-length z-scores than females(β=0.169) and Hispanic infants averaged higher z-scores than whiteinfants (β=0.231). Infants who had moderately or very low birthweights had lower weight-for-length z-scores than infants who were
born with normal birth weight (β=-0.272; β=-0.413, respectively).Infants reported by their mothers to be in good health had lower z-scores than those with excellent or very good health (β=-0.183).Infants whose mothers were married had lower weight-for-length z-scores than those whose mothers were not married (β=-0.147) andthose whose mothers had a high school degree had lower z-scores thanthose whose mothers did not have a high school degree (β=-0.126).Infants who lived in urban or suburban areas had higher z-scores thanthose who lived in rural areas (β=0.148; β=0.161, respectively). Finally,higher maternal pre-pregnancy weight was associated with increasedweight-for-length z-scores among their children (β=0.007).
Model 1
Unadjusted main effects
Model 2
Adjusted main effects
Model 3
Adjusted main and interaction effects ‡
OR 95% CI OR 95% CI OR 95% CI
Maternal Depression (MD) 0.988 (0.977, 0.999)* 0.982 (0.970, 0.994)** 0.997 (0.971, 1.023)
Number of well-child visits (WC) 0.994 (0.972, 1.017) 1.010 (0.985, 1.035) 1.024 (0.990, 1.060)
MD * WC (Interaction) 0.997 (0.993, 1.002)
Child Age (months) 1.004 (0.970, 1.039)
Child Sex (1= Male) 1.227 (1.084, 1.390)***
Child Race/Ethnicity
White (ref.)
Black 1.033 (0.840, 1.272)
Hispanic 1.284 (1.071, 1.539)**
Asian1 0.930 (0.754, 1.147)
Multiracial 1.080 (0.855, 1.364)
Household Size 1.012 (0.970, 1.056)
Birthweight
Normal (ref.)
Moderately Low 0.552 (0.451, 0.676)***
Very Low 0.481 (0.373, 0.621)***
Child Health
Citation: Dagher RK, Morrissey TW (2015) A Cross-sectional Study of Postpartum Depressive Symptoms and Infant Weight Outcomes: Do Well-Child Visitsmake a Difference?. J Womens Health, Issues Care 4:2.
doi:http://dx.doi.org/10.4172/2325-9795.1000179
Volume 4 • Issue 2 • 1000179 • Page 6 of 11 •
Excellent/V. good (ref.)
Good 0.925 (0.746, 1.146)
Fair/Poor 1.052 (0.720, 1.537)
Maternal Age (years) 1.007 (0.995, 1.019)
Maternal Employment
Not in labor force (ref.)
>=35 hours/week 1.064 (0.914, 1.239)
<35 hours/week 0.915 (0.764, 1.095)
Looking for work 1.023 (0.806, 1.299)
Marital Status (1= Mother Married) 0.788 (0.671, 0.927)**
Maternal Education
Below high school (ref.)
Has high school 1.052 (0.874, 1.265)
Has college/higher 1.197 (0.929, 1.543)
Household Income
<$25,000 (ref.)
$25,001-50,000 0.986 (0.835, 1.164)
$50,001-75,000 0.866 (0.692, 1.083)
$75,001-100,000 0.685 (0.518, 0.905)**
>$100,000 0.809 (0.615, 1.064)
Child is Insured (1=Yes) 1.109 (0.777, 1.583)
Child Residence
Rural (ref.)
Suburban area 1.212 (0.962, 1.525)
Urban Area 1.105 (0.917, 1.331)
Child was Breastfed (1=Yes) 0.904 (0.785, 1.041)
Mother’s Pre-pregnancy Weight 1.009 (1.006, 1.013)***
1Includes Asian/Native Hawaiian/Pacific Islander/American Indian/Alaska Native. †p< 0.10 *p ≤ 0.05; **p ≤ 0.01; ***p ≤ 0.001. ‡The Coefficients and Confidence Intervals forcontrol variables are not shown here for brevity but the same control variables adjusted for in Model 2 were adjusted for in Model 3.
Table 3: Logistic regression analyses modeling the relationship between maternal depressive symptoms and infant obesity
Model 1
Unadjusted main effects
Model 2
Adjusted main effects
Model 3
Adjusted main andinteraction effects‡
OR 95% CI OR 95% CI OR 95% CI
Maternal Depression (MD) 0.993 (0.984, 1.001) 0.990 (0.981, 0.999)* 1.010 (0.989, 1.031)
Number of well-child visits (WC) 0.970 (0.952, 0.988)*** 0.988 (0.969, 1.008) 1.008 (0.981, 1.036)
Citation: Dagher RK, Morrissey TW (2015) A Cross-sectional Study of Postpartum Depressive Symptoms and Infant Weight Outcomes: Do Well-Child Visitsmake a Difference?. J Womens Health, Issues Care 4:2.
doi:http://dx.doi.org/10.4172/2325-9795.1000179
Volume 4 • Issue 2 • 1000179 • Page 7 of 11 •
MD* WC (Interaction) 0.996 (0.993,0.999)*
Child Age (months) 0.985 (0.958, 1.012)
Child Sex (1= Male) 1.236 (1.122, 1.362)***
Child Race/Ethnicity
White (ref.)
Black 0.977 (0.829, 1.150)
Hispanic 1.196 (1.036, 1.382)*
Asian1 0.921 (0.785, 1.081)
Multiracial 1.014 (0.844, 1.219)
Household Size 1.008 (0.975, 1.043)
Birthweight
Normal (ref.)
Moderately Low 0.626 (0.540, 0.725)***
Very Low 0.525 (0.435, 0.634)***
Child Health
Excellent/V. good (ref.)
Good 0.826 (0.697, 0.978)*
Fair/Poor 1.061 (0.789, 1.427)
Maternal Age (years) 1.002 (0.993, 1.012)
Maternal Employment
Not in labor force (ref.)
>=35 hours/week 1.090 (0.967, 1.227)
<35 hours/week 0.997 (0.868, 1.144)
Looking for work 0.906 (0.747, 1.099)
Marital Status (1= Mother Married) 0.782 (0.687, 0.889)***
Maternal Education
Below high school (ref.)
Has high school 0.944 (0.816, 1.093)
Has college/higher 1.089 (0.894, 1.328)
Household Income
<$25,000 (ref.)
$25,001-50,000 1.019 (0.893, 1.164)
$50,001-75,000 0.899 (0.754, 1.072)
$75,001-100,000 0.950 (0.772, 1.169)
>$100,000 1.051 (0.853, 1.296)
Child is Insured (1= Yes) 0.959 (0.731, 1.258)
Citation: Dagher RK, Morrissey TW (2015) A Cross-sectional Study of Postpartum Depressive Symptoms and Infant Weight Outcomes: Do Well-Child Visitsmake a Difference?. J Womens Health, Issues Care 4:2.
doi:http://dx.doi.org/10.4172/2325-9795.1000179
Volume 4 • Issue 2 • 1000179 • Page 8 of 11 •

Child Residence
Rural (ref.)
Suburban area 1.172 (0.978, 1.404)†
Urban Area 1.082 (0.938, 1.250)
Child was Breastfed (1= Yes) 0.888 (0.795, 0.992)*
Mother’s Pre-pregnancy Weight 1.008 (1.005, 1.011)***
1Includes Asian/Native Hawaiian/Pacific Islander/American Indian/Alaska Native. †p< 0.10; *p ≤ 0.05; **p ≤ 0.01; ***p ≤ 0.001. ‡ The Coefficients and Confidence Intervals forcontrol variables are not shown here for brevity but the same control variables adjusted for in Model 2 were adjusted for in Model 3
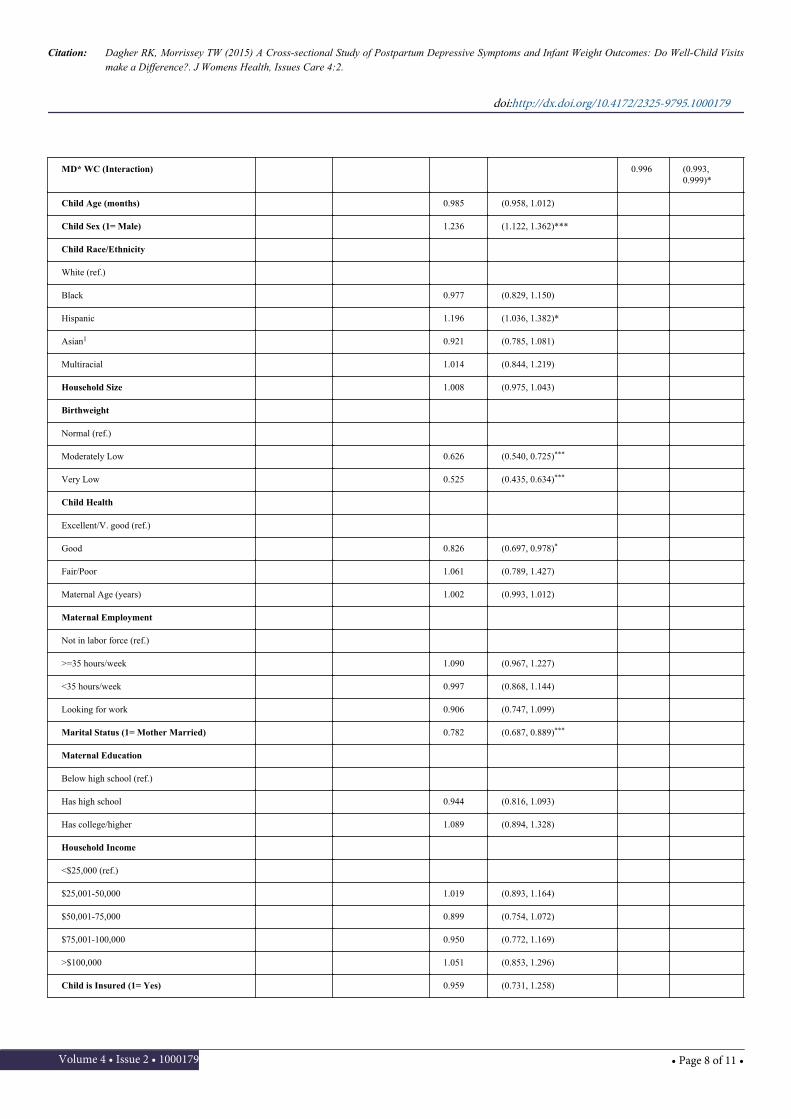
Table 4: Logistic regression analyses modeling the relationship between maternal depressive symptoms and infant overweight
DiscussionThis study investigated associations between mothers’ postpartum
depressive symptoms and their infants’ weight outcomes using a large,national dataset. Importantly, this study examined whether receipt ofthe recommended number of well-child visits mitigates the expectedrelationship between maternal depressive symptoms and infants’weight outcomes. In general, findings indicate that maternaldepressive symptoms, as measured at 9 months, are associated with avery small decrease in the likelihood of obesity and overweight amongtheir infants. Further, there is some evidence that more well-childvisits are associated with lower weight-for-length z-scores and lowerodds of overweight among infants of mothers with higher depressionscores. There are two primary explanations for these results.
First, mothers’ postpartum depression interferes with parentingbehaviors related to their infants’ weight outcomes, such as feedingpractices, for which there is evidence [34,35], and this in turn affectstheir weight and growth. Contrary to our hypotheses, however, wefound that higher maternal depressive scores were associated with avery small decrease in the odds of obesity and overweight among theirinfants. It may be that, similar to research in international contexts[30] or in subpopulations in the U.S. [26], maternal depressioninterferes with a mothers’ ability to breastfeed, provide adequate foodor regular feeding practices and meal times for their young children.This in turn may lead to lower odds of being overweight or obese, butcould potentially lead to child underweight. Indeed, previous researchhas linked maternal depressive symptoms and children’s underweightin certain contexts [42,43] and to food insecurity in the U.S [44]. Inaddition, given the established association between maternaldepression and impaired mother-infant relationships [15] and theinfluence of maternal responsiveness on the infant’s capacity todevelop self-regulation [45], it may be that infants may lose weight inresponse to maternal depression. While an important public healthissue internationally, child underweight is much less common in theU.S. than overweight, with an estimated 3% of 2 to 5 year old childrenconsidered underweight (a BMI below the 5th percentile) in 2007-2010[46]. That is, although lower odds of overweight and lower obesity areoften viewed as positive, the children of depressed mothers may be atrisk for under nutrition. However, the receipt of well-child visitsstrengthened this relationship, such that more well-child visits wereassociated with lower odds of overweight. It may be that thismitigating effect occurs among the high end of the distribution, interms of children’s weight; that is, well-child visits provide anopportunity for assistance on feeding practices or other weight-related
issues, which decreases overweight among infants at risk. Theassociation between more well-child visits and lower weight-for-lengthz-scores and the moderating effects of well-child visits on therelationship between maternal depression scores and infants’overweight outcomes suggest that well-child visits may be a potentialtool for addressing child overweight. However, an alternativeexplanation is that well child visits could be a marker of more capableparents who can not only get their child to a well child visit more oftenbut may also make better choices around food, sleep, and otherhealthy practices. These potential explanations should be investigatedin future research.
A second explanation for the identified associations betweenmaternal depression, well-child visits, and infant weight is one ofselection. Indeed, some research finds no associations of maternaldepression with infant growth [47], weight outcomes of children atschool age [48], or with children’s BMI [49]. Our analyses control for arange of maternal, child, and household characteristics, but results aresubject to omitted variable bias in that several factors related tomaternal postpartum depressive symptoms, infants’ weight outcomes,and receipt of well-child visits are likely unmeasured and thusuncontrolled. For example, an infant with special needs or in need ofhealth care may see the doctor more often and potentially also be atrisk for experiencing maternal depression. Further, it may be thatfamilies with depressed mothers have different health care usepatterns. Previous research suggests that depressed mothers usepreventive care less often and visit emergency rooms more often thannon-depressed mothers [32].
Our numerous covariates involving demographic and maternalcharacteristics produced findings that add to the growing body ofliterature on health disparities relating to infant weight outcomes.Consistent with this literature [50], Hispanic infants were more likelyto be overweight and obese at 9 months than White infants and hadhigher weight-for-length z-scores. Infants living in lower-incomehouseholds and whose mothers were not married had higher z-scoresand higher odds of being obese than their counterparts in line withother studies [51]. Higher maternal pre-pregnancy weight wasassociated with increased length-for-weight z-scores and increasedodds of obesity and overweight among their infants [52]. Infants whowere breastfed had lower odds of overweight than those who were notas reported in the literature [53]. Additionally, the persisting effects oflow birth weight on infants’ weight outcomes at 9 months areapparent, such that these infants continue to be at the lower end of theweight distribution as evidenced by lower length-for-weight z-scoresand lower odds of obesity and overweight.
Citation: Dagher RK, Morrissey TW (2015) A Cross-sectional Study of Postpartum Depressive Symptoms and Infant Weight Outcomes: Do Well-Child Visitsmake a Difference?. J Womens Health, Issues Care 4:2.
doi:http://dx.doi.org/10.4172/2325-9795.1000179
Volume 4 • Issue 2 • 1000179 • Page 9 of 11 •

LimitationsAs with all research, this study has several limitations. First,
findings identified in this analysis are associations rather than causaleffects. For example, while maternal depression may change herfeeding behaviors and thus children’s weight, it is also possible thatchildren’s feeding problems could contribute to mothers’ depression.Second, our independent variable of maternal depressive symptomshas been found to be valid and reliable, but is not a clinical diagnosisof depression and is reported by mothers themselves. Third, we usemeasures of children’s weight-for-length at 9 months, which may bean imperfect measure of weight risk at this age, and approximatesBMI, which is a limited measure of adiposity at any age because it doesnot distinguish fat from muscle [54]. Further, we use the weight andheight standards recommended by the CDC; other studies may use theWorld Health Organization (WHO) standards, which are based on abroader sample of children [55]. Fourth, with the exception of infants’weight and length, our moderating and control variables are largelyreported by mothers; to the extent that depressive symptoms affect theresponses, these variables may be biased. Finally, mothers’ depressivesymptoms and their children’s weight outcomes were measured at thesame time (9 months); there may be a lagged effect of depression onchildren’s weight, such that positive associations between maternaldepression and child obesity and overweight emerge as children age.
ConclusionThis is one of the first studies to examine the moderating effects of
well-child visits on the association between mothers’ postpartumdepression and the concurrent weight outcomes of their infants usinga national U.S. sample. We find some evidence that mothers’depressive symptoms are associated with decreased odds of beingobese or overweight among their infants at 9 months of age, and thatreceipt of more well-child visits strengthens the latter negativerelationship. While the causal directions and mechanisms remainunclear, findings suggest that well-child visits may provide anopportunity to educate parents about healthy eating habits andaddressing mothers’ depressive symptoms, potentially benefiting theweight outcomes of children at risk for overweight. More research isneeded to clarify the causal relationship between maternal depressionand infants’ weight outcomes and to determine whether clinicalinterventions during well-child visits can help promote healthy weight.
Funding SupportThis project was supported by Grant Number R40MC23630 from
the Maternal and Child Health Bureau of the Health Services andResources Administration, U.S. Department of Health and HumanServices. Its contents are solely the responsibility of the authors and donot necessarily represent the official views of the Department ofHealth and Human Services.
AcknowledgmentsAuthors’ contributions: Rada K. Dagher contributed to the project’s
conception, secured the project funding as the Co-PrincipalInvestigator, conducted the statistical analyses, drafted the majority ofthe initial manuscript, and approved the final manuscript assubmitted. Taryn W. Morrissey led the conceptual design of the study,secured the project funding as the Principal Investigator, wrote thediscussion and conclusion sections, edited the manuscript, andapproved the final manuscript as submitted.
References1. Ogden CL, Carroll MD1, Kit BK2, Flegal KM1 (2014) Prevalence
of childhood and adult obesity in the United States, 2011-2012.JAMA 311: 806-814.
2. Moss BG, Yeaton WH (2011) Young children's weighttrajectories and associated risk factors: results from the EarlyChildhood Longitudinal Study-Birth Cohort. Am J HealthPromot 25: 190-198.
3. Stender SRS, Burghen GA, Mallare JT (2005) The prevention ofoverweight and Type 2 Diabetes in children and adolescents.Diabetes Spectr 18: 240-248.
4. Lauer RM, Clarke WR, Burns TL (1997) Obesity in childhood:the Muscatine Study. Zhonghua Min Guo Xiao Er Ke Yi Xue HuiZa Zhi 38: 432-437.
5. Waters EB, Baur LA (2003) Childhood obesity: modernity'sscourge. Med J Aust 178: 422-423.
6. McCabe MP, Ricciardelli LA (2003) Body image and strategies tolose weight and increase muscle among boys and girls. HealthPsychol 22: 39-46.
7. Ricciardelli LA, McCabe MP (2001) Children's body imageconcerns and eating disturbance: a review of the literature. ClinPsychol Rev 21: 325-344.
8. Chaudron LH (2003) Postpartum depression: what pediatriciansneed to know. Pediatr Rev 24: 154-161.
9. Beck CT (2002) Postpartum depression: a metasynthesis. QualHealth Res 12: 453-472.
10. O'Hara MW, Zekoski EM, Philipps LH, Wright EJ (1990)Controlled prospective study of postpartum mood disorders:comparison of childbearing and nonchildbearing women. JAbnorm Psychol 99: 3-15.
11. Zelkowitz P, Milet TH (1996) Postpartum psychiatric disorders:their relationship to psychological adjustment and maritalsatisfaction in the spouses. J Abnorm Psychol 105: 281-285.
12. Beck CT (1998) The effects of postpartum depression on childdevelopment: a meta-analysis. Arch Psychiatr Nurs 12: 12-20.
13. Grace SL, Evindar A, Stewart DE (2003) The effect of postpartumdepression on child cognitive development and behavior: areview and critical analysis of the literature. Arch Womens MentHealth 6: 263-274.
14. Beck CT (1995) The effects of postpartum depression onmaternal-infant interaction: a meta-analysis. Nurs Res 44:298-304.
15. Righetti-Veltema M, Conne-Perréard E, Bousquet A, Manzano J(2002) Postpartum depression and mother-infant relationship at3 months old. J Affect Disord 70: 291-306.
16. Teti DM, Gelfand DM (1991) Behavioral competence amongmothers of infants in the first year: the mediational role ofmaternal self-efficacy. Child Dev 62: 918-929.
17. Goodman JH (2004) Postpartum depression beyond the earlypostpartum period. J Obstet Gynecol Neonatal Nurs 33: 410-420.
18. Cooper PJ, Murray L (1998) Postnatal depression. BMJ 316:1884-1886.
19. Duhn L (2010) The importance of touch in the development ofattachment. Adv Neonatal Care 10: 294-300.
20. Becker G (1991) A Treatise on the Family. Harvard UniversityPress, Cambridge, MA.
Citation: Dagher RK, Morrissey TW (2015) A Cross-sectional Study of Postpartum Depressive Symptoms and Infant Weight Outcomes: Do Well-Child Visitsmake a Difference?. J Womens Health, Issues Care 4:2.
doi:http://dx.doi.org/10.4172/2325-9795.1000179
Volume 4 • Issue 2 • 1000179 • Page 10 of 11 •
21. Stewart RC (2007) Maternal depression and infant growth: areview of recent evidence. Matern Child Nutr 3: 94-107.
22. Section on Breastfeeding (2012) Breastfeeding and the use ofhuman milk. Pediatrics 129: e827-841.
23. McLearn K, Minkovitz CS, Strobino D, Marks E, Hou W (2006)The timing of maternal depressive symptoms and mothers’parenting practices with young children: implications forpediatric practice. Pediatrics 118: e174-e182.
24. Morrissey TW (2014) Maternal depressive symptoms andweight-related parenting behaviors. Matern Child Health J 18:1328-1335.
25. Siervo M, Wells JC, Cizza G (2009) The contribution ofpsychosocial stress to the obesity epidemic: an evolutionaryapproach. Horm Metab Res 41: 261-270.
26. Wojcicki JM, Holbrook K, Lustig RH, Epel E, Caughey AB, et al.(2011) Chronic maternal depression is associated with reducedweight gain in latino infants from birth to 2 years of age. PLoSOne 6: e16737.
27. Surkan PJ, Kawachi I, Peterson KE (2008) Childhood overweightand maternal depressive symptoms. J Epidemiol CommunityHealth 62: e11.
28. Ertel KA, Koenen KC, Rich-Edwards JW, Gilman MW (2010)Antenatal and postpartum depression differentially affect earlychildhood weight and adiposity. Paediatr Perinat Epidemiol 24:179-189.
29. Wang L, Anderson JL, Dalton Iii WT, Wu T, Liu X, et al. (2013)Maternal depressive symptoms and the risk of overweight intheir children. Matern Child Health J 17: 940-948.
30. Wright CM, Parkinson KN, Drewett RF (2006) The influence ofmaternal socioeconomic and emotional factors on infant weightgain and weight faltering (failure to thrive): data from aprospective cohort. Arch Dis Child 91: 312-317.
31. Gross GJ, Howard M (2001) Mothers' decision-making processesregarding health care for their children. Public Health Nurs 18:157-168.
32. Minkovitz CS, Strobino D, Scharfstein D, Hou W, Miller T, et al.(2005) Maternal depressive symptoms and children's receipt ofhealth care in the first 3 years of life. Pediatrics 115: 306-314.
33. McLennan JD, Kotelchuck M (2000) Parental preventionpractices for young children in the context of maternaldepression. Pediatrics 105: 1090-1095.
34. Paulson JF, Dauber S, Leiferman JA (2006) Individual andcombined effects of postpartum depression in mothers andfathers on parenting behavior. Pediatrics 118: 659-668.
35. Taveras EM, Capra AM, Braveman PA, Jensvold NG, EscobarGJ, et al. (2003) Clinician support and psychosocial risk factorsassociated with breastfeeding discontinuation. Pediatrics 112:108-115.
36. Gjerdingen DK, Yawn BP (2007) Postpartum depressionscreening: importance, methods, barriers, and recommendationsfor practice. J Am Board Fam Med 20: 280-288.
37. Freed GL, Clark SJ, Pathman DE, Schectman R (1999) Influenceson the receipt of well-child visits in the first two years of life.Pediatrics 103: 864-869.
38. American Academy of Pediatrics, Committee on Practice,Ambulatory Medicine (2000) Recommendations for preventativepediatric health care. Pediatrics 105: 645-646.
39. Kuczmarski RJ, Ogden CL, Guo SS, Grummer-Strawn LM, FlegalKM, et al. (2002) 2000 CDC Growth Charts for the United States:methods and development. Vital Health Stat 11 : 1-190.
40. Radloff LS (1977) The CES-D: a self-report depression scale forresearch in the general population. Appl Psychol Meas 1:385-401.
41. Baron RM, Kenny DA (1986) The moderator-mediator variabledistinction in social psychological research: conceptual, strategic,and statistical considerations. J Pers Soc Psychol 51: 1173-1184.
42. Anoop S, Saravanan B, Joseph A, Cherian A, Jacob KS (2004)Maternal depression and low maternal intelligence as risk factorsfor malnutrition in children: a community based case-controlstudy from South India. Arch Dis Child 89: 325-329.
43. Rahman A, Iqbal Z, Bunn J, Lovel H, Harrington R (2004)Impact of maternal depression on infant nutritional status andillness: a cohort study. Arch Gen Psychiatry 61: 946-952.
44. Bronte-Tinkew J, Zaslow M, Capps R, Horowitz A, McNamaraM (2007) Food insecurity works through depression, parenting,and infant feeding to influence overweight and health intoddlers. J Nutr 137: 2160-2165.
45. Feldman R, Greenbaum CW, Yirmiya N (1999) Mother-infantaffect synchrony as an antecedent of the emergence of self-control. Dev Psychol 35: 223-231.
46. Fryar CD, Ogden CL (2012) Prevalence of Underweight amongChildren and Adolescents Aged 2 – 19 Years?: United States,1963 – 1965 through 2007 – 2010. National Center for HealthStatistics, Hyattsville, MD.
47. Grote V, Vik T, von Kries R, Luque V, Socha J, et al. (2010)Maternal postnatal depression and child growth: a Europeancohort study. BMC Pediatr 10: 14.
48. Ajslev TA, Andersen CS, Ingstrup KG, Nohr EA, Sørensen TI(2010) Maternal postpartum distress and childhood overweight.PLoS One 5: e11136.
49. Morrissey TW, Dagher RK2 (2014) A longitudinal analysis ofmaternal depressive symptoms and children's food consumptionand weight outcomes. Public Health Nutr 17: 2759-2768.
50. Strauss RS, Pollack HA (2001) Epidemic increase in childhoodoverweight, 1986-1998. JAMA 286: 2845-2848.
51. Strauss RS, Knight J (1999) Influence of the home environmenton the development of obesity in children. Pediatrics 103: e85.
52. Janjua NZ, Mahmood B, Islam MA, Goldenberg RL (2012)Maternal and Early Childhood Risk Factors for Overweight andObesity among Low-Income Predominantly Black Children atAge Five Years: A Prospective Cohort Study. J Obes 2012:457173.
53. Arenz S, Rückerl R, Koletzko B, von Kries R (2004) Breast-feeding and childhood obesity--a systematic review. Int J ObesRelat Metab Disord 28: 1247-1256.
54. Burkhauser RV, Cawley J (2008) Beyond BMI: the value of moreaccurate measures of fatness and obesity in social scienceresearch. J Health Econ 27: 519-529.
55. De Onis M, Garza C, Onyango AW, Martorell R (2006) WorldHealth Organization child growth standards. Acta Paediatr S450:1-101.
Citation: Dagher RK, Morrissey TW (2015) A Cross-sectional Study of Postpartum Depressive Symptoms and Infant Weight Outcomes: Do Well-Child Visitsmake a Difference?. J Womens Health, Issues Care 4:2.
doi:http://dx.doi.org/10.4172/2325-9795.1000179
Volume 4 • Issue 2 • 1000179 • Page 11 of 11 •