
Alleviating Poverty in the Philippines Through Entrepreneurship
Upload
johnshopkinsCategory
view
0download
0
The Gerontologist Copyright 2003 by The Gerontological Society of AmericaVol. 43, No. 3, 335–344
A Comparison of Assistive Technology andPersonal Care in Alleviating Disability andUnmet Need
Emily M. Agree, PhD,1 and Vicki A. Freedman, PhD2
Purpose: The authors examine differences in reportsof residual disability and unmet need by type of long-term care arrangement (assistive technology orpersonal care). Design and Methods: This studycompares three specific dimensions of residualdifficulty (pain, fatigue, and time intensity) andreports of unmet need across care arrangements.Samples from the U. S. 1994–1995 National HealthInterview Survey Phase 2 Disability Supplementsinclude adults with limitations in bathing, transferring,walking, and getting outside. Results: Even whendifferences in underlying disability are accounted for,assistive technology (AT) confers no additional benefitin the three dimensions of residual difficulty analyzedhere. AT users equally or more often report that tasksare tiring, time consuming, or painful, even when theyuse assistance. Though this would appear to indicateunmet needs for care, fewer AT users report a desirefor hands-on personal care. Implications: Thoughdisability alleviation by technology is no better onspecific dimensions of difficulty, technology usersreport less unmet need for personal care. Designingappropriate and cost-effective home care for adultswith disabilities requires a better understanding of theways in which technology users may differ from
others and the circumstances under which technologycan be most effective.
Key Words: Long-term care, Effectiveness,Activities of daily living
Designing appropriate and cost-effective homecare for adults with disabilities is a priority in agingsocieties. The number of older adults with disabil-ities is large and continues to grow, despite re-ductions in disability rates over the past two decades(Schoeni, Freedman, & Wallace, 2001). Currently,approximately 15% of the adult U. S. population, or40 million people, are limited in activities as a resultof a chronic health condition (Kaye, LaPlante, Carl-son, & Wenger, 1996). The vast majority of adultswith disabilities live in the community, and faci-litating their ability to live independently is anincreasingly important public health concern.
More than 75% of older adults with disabilitiesuse some kind of assistive device, most often to assistwith mobility (Russell, Hendershot, LeClere, Howie,& Adler, 1997), and the number has been growingover time (Manton, Corder, & Stallard, 1993;Russell et al., 1997). Devices are used both indepen-dently and in conjunction with personal caregivingservices. However, the relative advantages of assis-tive technology and personal care are not wellunderstood, in part because most studies evaluateone or the other, but rarely the two together.
Most research on assistive technology evaluatesthe efficacy and costs of specific devices (e.g., Chen,Mann, Tomita, & Burford, 1998; Gitlin & Levine,1992; Kohn, LeBlanc, & Mortola, 1994; Mann,Hurren, Charvat, & Tomita, 1996; Sanford, Arch, &Megrew, 1995; Steinfeld & Shea, 1995), or it broadlyexamines the use of any assistive devices (Mantonet al., 1993; Norburn et al., 1995; Zimmer & Chap-pell, 1994) or the number of devices used (Hartke,Prohaska, & Furner, 1998; Heide et al., 1993; Mann,Hurren, & Tomita, 1993). Studies of assistivetechnology emphasize the extent to which the
Prior versions of this article were presented in Syracuse, NY, at theCenter for Policy Research Seminar Series in Aging, Labor, and PublicFinance in October 2000 and in Washington, DC, at the AnnualMeetings of the Population Association of America in March 2001. Weacknowledge the able assistance of Jonas Marainen and Hakan Aykan inpreparing the data and the tables, and Mary Alice Ernish forbibliographic assistance. We also thank Donna Strobino, Douglas Wolf,and Timothy Smeeding for their helpful comments. This work wassupported by Grant R01-AG15135 from The National Institute onAging.
Address correspondence to Emily M. Agree, PhD, Department ofPopulation and Family Health Sciences, Johns Hopkins BloombergSchool of Public Health, 615 North Wolfe Street, Room E4014,Baltimore, MD 21205. E-mail: [email protected]
1Department of Population and Family Health Sciences, Johns Hop-kins Bloomberg School of Public Health, Baltimore, MD.
2Polisher Research Institute, Madlyn and Leonard Abramson Centerfor Jewish Life (formerly PhiladelphiaGeriatricCenter),NorthWales, PA.
Vol. 43, No. 3, 2003 335
by guest on March 27, 2016
http://gerontologist.oxfordjournals.org/D
ownloaded from

acceptability and effectiveness of home-based tech-nologies vary, depending on the training provided(Gitlin & Levine, 1992), the amount of stigmaperceived by the user (Arras, 1995), and how muchthe introduction of assistive technologies transformsthe home from a personal space to a health caredelivery location (Tamm, 1999). Similarly, popula-tion-based efforts to understand the effectiveness ofpersonal care arrangements often altogether excludea consideration of self-care through assistive tech-nology (Allen & Mor, 1997; Desai, Lentzner, &Weeks, 2001; Tennstedt, McKinlay, & Kasten,1994). These studies instead focus on the trade-offsbetween formal and informal care or on the extent towhich formal care can defer institutionalization(Soldo & Freedman, 1994).
Attempts to measure outcomes that reflect theeffectiveness of interventions for disability are rela-tively new and differ depending on whether the goalis to evaluate rehabilitation services specifically ormore general effects on the ability to live indepen-dently (Andresen, Lollar, & Meyers, 2000). A recentnational study examined the effectiveness of assistivetechnology in terms of its impact on hours of per-sonal care for older adults with disabilities, assumingthat the decision to use devices is independent of theacquisition of caregivers (Allen, Foster, & Berg,2001). This study found that those who use assistivetechnology also use fewer hours of personal care.Two additional small-scale experiments have evalu-ated the effectiveness of interventions to increase theuse of assistive devices (Mann, Ottenbacher, Fraas,Tomita, & Granger, 1999) and environmental modi-fications for dementia (Gitlin, Corcoran, Winter,Boyce, & Hauck, 2001). Although sample sizes weresmall, both studies suggested that increased use oftechnology may slow functional declines, lowerhealth care costs, and increase efficacy among somecaregivers. However, none of these studies directlycompare the effect of assistive technology andpersonal care on functional health. Two other na-tionally representative studies have evaluated therelative effectiveness of assistive technology and per-sonal care in terms of reported reduction of disability(Agree, 1999; Verbrugge, Rennert, & Madans, 1997).Both studies found that the use of assistive tech-nology was associated with greater reduction ofoverall levels of difficulty in either activities of dailyliving (ADLs) or mobility impairments when com-pared with personal care. Though each used distinctmeasures and different data sets, these studies bothrelied on broad judgments about levels of difficultywith tasks to determine effectiveness.
In sum, much of the prior research on this topiceither has failed to directly compare outcomesrelated to assistive technology and personal care,begging the question as to when and whether each ismost appropriately used (Allen et al., 2001; Gitlinet al., 2001; Mann et al., 1999), or has relied onglobal assessments of residual difficulty that do not
offer insight into the mechanisms by which differentcare arrangements alleviate needs (Agree, 1999;Verbrugge et al., 1997).
The purpose of this study is to further investigatethe relative effectiveness of assistive technology andpersonal care in alleviating disability among adultswith difficulty in ADLs. Using nationally represen-tative disability survey data, we compare threedimensions of disability for which both underlyingand residual difficulty can be assessed—pain, fatigue,and time intensity—across different combinations ofassistive technology and personal care use. We alsoexamine reports of the need for hands-on assistanceacross care arrangements.
Framework
The conceptual framework of the disablementprocess (e.g., Pope & Tarlov, 1991; Verbrugge &Jette, 1994) gives us some foundation for under-standing how different care arrangements mayalleviate different dimensions of disability. In thisframework, disability is socially defined, being theproduct of the individual’s functional capacity, thedemands of the physical and social environment,and his or her own expectations about daily life.Verbrugge and Jette (1994) make the additional im-portant distinction between underlying difficulty—the level of difficulty without help or specialequipment—and residual difficulty—that is, withwhatever assistance is generally used.
Both underlying and residual disability encompassvarious levels of difficulty. At one extreme, anindividual may be completely unable to carry out anactivity without assistance; alternatively, an individ-ual may be able to carry out an activity withoutassistance but with some or a lot of difficulty. Themost commonly reported dimensions of difficulty inthis context are pain and fatigue (Albrecht &Devlieger, 1999); tasks that are time consuming tocarry out (or more time consuming than under usualor optimally functioning circumstances) may also beidentified as being difficult. Closely related to residualdifficulty is the concept of unmet need, that is,whether an individual thinks he or she requires moreassistance.
The disabling effects of an impairment can bereduced or potentially eliminated in a number ofways (see Figure 1). Individuals may compensate fortheir disability by using personal care, they may altertheir ability to carry out the task (through rehabil-itation or device use), or they may alter the demandsof the environment (through, e.g., a home modifica-tion). Each of these approaches may be adopted inisolation or may be combined into a more complexcare arrangement. Compensation, because it in-volves the cooperation of one or more helpers,creates a state of dependency. In contrast, assistivetechnologies and related environmental modifica-tions enhance independence either by expanding the
336 The Gerontologist
by guest on March 27, 2016
http://gerontologist.oxfordjournals.org/D
ownloaded from

capacity of the individual or reducing the demandsof the environment.
In this article we hypothesize that differentapproaches to bridging disability may alleviatedifficulty in different ways. We expect that assistivedevices may alleviate difficulty by minimizing thepain associated with a task, whereas personal caremay lessen the time and energy necessary to accom-plish a task. Because devices increase an individual’scapacity for self-care, we expect devices to be moreeffective than personal care in reducing unmet need.
Methods
Data
Data are from the 1994 and 1995 Phase 2Disability Supplements to the U. S. National HealthInterview Survey, hereafter referred to as the NHIS-D2 (National Center for Health Statistics, 1998a,1998b). These data provide detailed information onthe use of assistive devices and environmentalmodifications for limitations in ADLs.
The U. S. NHIS is a nationally representativehealth survey of approximately 48,000 households(122,000 persons) conducted annually by the U. S.National Center for Health Statistics. The surveyconsists of a core questionnaire that collects healthinformation and demographic background on everyperson in the household. Each year supplementalsurveys on specific health topics are included. In 1994and 1995, a supplement on disability was adminis-tered in two phases over approximately 3 years.Phase 1, administered at the same time as the NHIScore interview, collected basic measures of impair-ment and functional health from a designated in-dividual about all household members.
Household members who were identified asdisabled in Phase 1, using a broad definition of dis-
ability (the presence of any impairment, functionallimitation, or disability), were interviewed in person7–17 months later to obtain more detailed informa-tion (Phase 2). Separate questionnaires were admin-istered to children (under 18) and adults (age 18 andolder). Response rates were approximately 95% forthe core and 87% for the supplements.
Sample Selection
To examine the effectiveness of care arrangementsin alleviating disability, we focus on the adultpopulation with underlying limitations in ADLs—those who report that they have difficulty carryingout an activity by themselves and without specialequipment. This definition includes both personscurrently using some form of care as well asa substantial number who report difficulty but makeuse of no personal care or assistive devices.
Because assistive devices tend to be task specific inresponse to disabling conditions (Agree & Freed-man, 2000), analyses are conducted separately forsamples reporting underlying difficulty with each offour daily activities: bathing or showering (n ¼3,493), getting in or out of bed or chairs (n¼ 3,834),walking (n¼ 7,051), and getting outside (n¼ 3,542).Although respondents also were asked about diffi-culty with dressing, eating, and getting to or usingthe toilet, sample sizes were too small, and the use ofassistive technology too rare in the case of dressingand eating, to analyze care arrangements for theseactivities. Respondents with multiple ADL difficul-ties may be in more than one sample.
Measures of Assistive Technology andPersonal Care
Questions are asked about assistive technologyin the ADL assessment section of the NHIS-D2
Figure 1. Alleviating underlying disability through personal care and assistive technology.
Vol. 43, No. 3, 2003 337
by guest on March 27, 2016
http://gerontologist.oxfordjournals.org/D
ownloaded from

instrument. For each ADL, participants who answerthat they use a special device or piece of equipmentto perform a task are asked to name the type oftechnology that they use. Interviewers use a checklistto simplify the recording of answers. For the fouractivities we analyze here, the specific equipmentincludes hand bars or rails, and bath stools, seats,or chairs (bathing); canes, walkers, special cushions,lift chairs, a hospital bed, and a trapeze or sling(transferring); and canes, walkers, crutches, andwheelchairs (getting around indoors and goingoutside). An analysis of specific items was not pos-sible because devices other than canes and walkerswere not mentioned frequently enough to allowseparate analyses. Grouping all assistive technologiesfor a given activity together also allowed us to in-clude sample persons who reported using specialequipment without providing a specific type.
Respondents also were asked in the same sectionwhether they received hands-on help from anotherperson with that activity. For each ADL, informationwas obtained on the type and amount of personalcare provided to the respondent. On the basis of thisinformation, we classified respondents into fourgroups: no care, assistive technology only, hands-on personal care only, and both personal care andassistive technology.
Level of Underlying Difficulty
Comparing the effectiveness of care arrangementsrequires some ability to control for the differentialselection of these arrangements based on the severityof underlying disability. For each activity, respon-dents were classified as having some difficulty, a lotof difficulty, or being completely unable to carry outthe activity without assistance. We also present anal-yses for all respondents and for the subgroupreporting a lot of underlying difficulty with a giventask.
Measures of Effectiveness
The NHIS-D2 provides task-specific measures ofresidual difficulty and unmet need. The surveyincluded information on three explicit dimensionsof residual difficulty. For each activity, respondents(with the exception of those who were completelyunable to perform the task) were asked to assesswhether the activity is ‘‘very tiring,’’ ‘‘takes a longtime,’’ or is ‘‘very painful’’ under two circumstances:first, if it is performed without personal care orassistive technology, and second, when it is per-formed with the assistance of personal care ordevices (if used). This information was used toclassify whether respondents’ difficulty with anactivity was ‘‘eliminated’’ when using personal careor assistive technology or whether they reportresidual difficulty even when using assistance. In
addition, all respondents who reported underlyingdifficulty with a given task were asked whether theyneeded (more) hands-on help with that activity,which was used to derive a measure of unmet need.
Limitations of the Data
Although the NHIS-D is a rich source of in-formation on the health and care arrangements ofpersons with disabilities in the United States, thereare some limitations of the data that merit attentionhere. First, as already noted, the NHIS-D2 excludesthe most severely disabled (those who report thatthey are unable to perform a task without assistance)from the questions about specific dimensions ofunderlying and residual difficulty, thus limiting ourconclusions to a more moderately disabled popula-tion for those particular analyses. Second, the sen-sitivity of a disability measure to clinically detectabledifferences in functional status is an important factorin comparing across types of care (Cohen &Marino,2000). In this study, the dichotomous indicators foreach specific dimension of difficulty made it possibleto examine effectiveness only in terms of completeelimination of difficulty. We are therefore limited inour ability to examine more refined gradations ofeffectiveness in disability reduction as has been donein previous studies (Agree, 1999; Verbrugge et al.,1997). Finally, the cross-sectional nature of the datamake it impossible to assess the role that the timingof acquisition of assistive technology and personalcare plays in the effectiveness of such arrangements.
As already noted, prior research has indicated thatassistive technologies may be more effective thanpersonal care in alleviating disability. Consequently,we expect in the following analyses to find that,when we control for the level of underlying need,those who use assistive devices are less likely thanthose using personal care to report (a) residualdifficulty on all dimensions of disability and (b)unmet need for personal care.
Methods
Because the NHIS-D2 is not a simple randomsample but instead has a complex design withgeographic clustering, statistical tests have beenadjusted to take into account the complex surveydesign. All estimates are weighted with analyticweights normed to the appropriate sample size.Results discussed in the text are statistically signifi-cant at the p , .05 level unless otherwise noted.
Results
Assistive device use is quite common amongpersons who have underlying difficulty with the fouractivities considered here. Between 16% (of personswith underlying difficulty transferring) and 39% (of
338 The Gerontologist
by guest on March 27, 2016
http://gerontologist.oxfordjournals.org/D
ownloaded from

those who have underlying difficulty walking) useassistive technology alone to accommodate theirdifficulty (see Table 1). An additional 13–33% useassistive technology in combination with personalcare. Taken together, 29–64% use one or moredevices, with devices dominating most clearly inbasic mobility activities (walking and going outside).
Those with underlying difficulty bathing orgetting outside are slightly older on average (67 vs.63 years). However, the distributions by sex,minority status, and education are similar acrossthe samples, with a majority of people being female;approximately 16–17% are non-White, approxi-mately 7% are Hispanic, and the majority have atleast completed high school (;55%).
Table 2 shows the distribution of the severity ofunderlying disability stratified by the type of careused for each of the four ADLs. This table confirmsthat the combination of care adopted is clearlyrelated to the overall amount of underlying difficultywith the task. Those who use no care of any kind arethe least disabled, with between 66% and 79%reporting some underlying difficulty and 1–7%reporting they are completely unable to carry outthe activity without assistance (11–20% report somedifficulty and 48–60% report being completely un-able to carry out the activity).
Among those who do use some type of assistance,those who use assistive devices alone report moremoderate levels of underlying difficulty comparedwith those who use hands-on help (alone or incombination with assistive technology). Only 13–21% of those who use technology by itself state thatthey would be unable to perform the task withoutassistance, compared with 26–43% of those depend-ing on personal care alone. As already noted, those
who rely on both personal care and assistive tech-nology report the greatest amount of difficulty, with51–59% reporting that they would be completelyunable to perform the task without assistance.
Figure 2 shows for those with underlying difficultyin each of the four activities the proportion who alsoreport underlying difficulty on three specific dimen-sions: whether the activity is very tiring, very painful,or takes a long time. The top panel shows estimatesfor all levels of difficulty, and the bottom panel islimited to those reporting a lot of underlyingdifficulty. For example, 63% of those with difficultybathing say that they find the activity to be tiringwhen they do not have help or equipment. We findthat substantial proportions of persons who reportunderlying difficulty with a given task find theactivity very tiring, time consuming, or very painfulwhen they do not have hands-on help or useequipment (47–76%, depending on the specific task).Not surprisingly, the proportions reporting underly-ing difficulty on each of the specific dimensions areconsistently higher among those who report a lot ofunderlying difficulty on the task, ranging 59–88% onaverage for all activities.
We also investigated (not shown) whether theproportion who reported underlying difficulty oneach of the three specific dimensions varied acrosscare arrangements. We found that those using bothpersonal care and assistive technology were generallymore likely than those using either one alone toreport that a task is very tiring, takes a long time, oris very painful when carried out without assistance.When we stratified by the level of underlyingdifficulty, we found a much weaker relationship be-tween care arrangement and specific dimensions ofunderlying difficulty.
Table 1. Care Arrangements and Sample Characteristics
CharacteristicBathing
(n ¼ 3,493)Transferring(n ¼ 3,834)
Walking(n ¼ 7,051)
Getting Outside(n ¼ 3,542)
Care arrangement (%)
No care 25.8 50.1 40.0 23.3AT only 20.5 15.9 39.2 31.0Personal care only 24.6 20.6 6.3 13.1Personal care and AT 29.2 13.4 14.5 32.7Total 100.0 100.0 100.0 100.0
Age (mean; years) 67.7 62.6 63.8 66.9
% Female 63.5 61.2 60.4 64.2% Non-White 16.5 16.2 16.7 17.9% Hispanic 6.7 7.1 6.7 6.8
Education (%)
Primary only (0–7) 17.5 14.5 14.7 17.1Some HS (8–11) 27.6 27.4 28.6 28.6HS graduate (12) 32.6 33.5 33.4 32.5Some college (13þ) 22.3 24.7 23.2 21.8Total 100.0 100.0 100.0 100.0
Note: AT¼ assistive technology; HS¼ high school.
Vol. 43, No. 3, 2003 339
by guest on March 27, 2016
http://gerontologist.oxfordjournals.org/D
ownloaded from

We next examine reports of residual difficulty,using the same three dimensions (whether the task istiring, time consuming, or painful) and controllingagain for the level of underlying difficulty. As shownin the top panel of Table 3, among persons withunderlying difficulty, those who use assistive tech-nology alone report residual difficulty more oftenthan those using personal care (with or withoutdevices). This relationship is significant, however,only for two dimensions (whether the task is tiring ortime consuming) and three of the tasks (bathing,transferring, and going outside). For example,among those who report underlying difficulty withbathing, 75% of assistive technology users reportthat the task is very tiring when they use theirequipment, compared with only 55% of those whouse personal care alone (p , .05). Pain varies theleast across care arrangements and is not significantlyrelated to the type of care for any of the activities.
The same general pattern is evident when theinvestigation is restricted to those with more severeactivity limitations (bottom panel of Table 3),although the differences are statistically significantonly for bathing. For many activities and dimensionsof difficulty, especially pain, care arrangements arenot significantly related to residual difficulty. How-ever, in those cases in which a significant associationis found, it is opposite to the expected direction—
assistive technology users more often report thata task is tiring or takes a long time even when theyuse assistance.
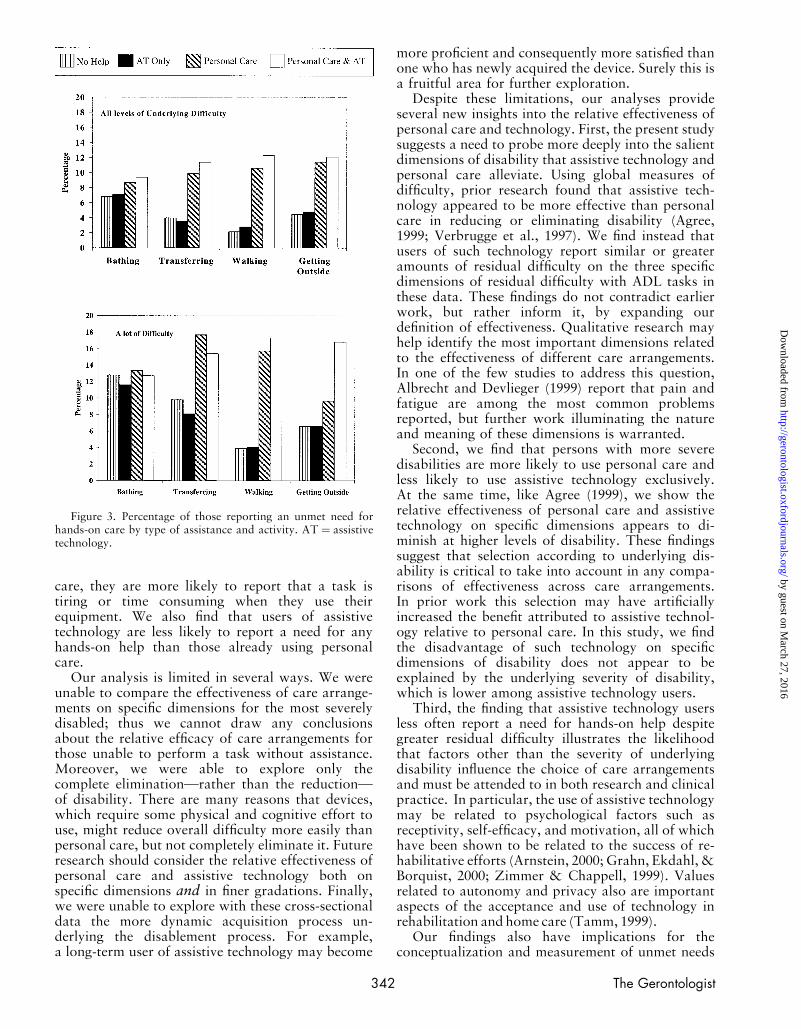
Figure 3 shows the proportion of people reportinga need for hands-on help by activity and level ofunderlying severity of disability. The proportionsshown here are consistent with those of other studies(e.g., Desai et al., 2001) and generally low in com-parison with the reports of residual difficulty shownin Table 3. The proportions reporting a need for(more) hands-on help are consistent across levels ofunderlying disability and types of care (the highestlevels are 12–18% reported by those with a lot ofunderlying difficulty and who use personal carealone).
However, those using assistive technology aloneare consistently less likely to state that they need anyhands-on help, at levels as low or lower than forthose who use no care. For bathing, levels of unmetneed are highest, but the differences across types ofcare are minimal and not significant (significancetests not shown). For the three mobility-relatedADLs, the differences between those who usepersonal care (either alone or in combination with
Table 2. Underlying Global Difficulty by Type of Assistanceand Activity
Type of Assistance
Activity NoneATOnly
PCOnly
PCand AT
Bathing (n ¼ 3,493)*
Some difficulty 71.1 46.9 34.3 17.0A lot of difficulty 23.4 32.4 22.5 23.8Completely unable 5.6 20.7 43.2 59.2Total 100.0 100.0 100.0 100.0
Transferring (n ¼ 3,834)*
Some difficulty 78.8 50.0 48.8 20.1A lot of difficulty 19.9 37.1 24.4 29.2Completely unable 1.3 13.0 26.8 50.7Total 100.0 100.0 100.0 100.0
Walking (n ¼ 7,051)*
Some difficulty 66.0 39.7 39.3 15.7A lot of difficulty 29.7 41.3 34.7 36.7Completely unable 4.2 19.1 26.0 47.6Total 100.0 100.0 100.0 100.0
Getting outside (n ¼ 3,542)*
Some difficulty 66.0 37.5 28.1 11.3A lot of difficulty 27.1 37.1 30.7 30.8Completely unable 6.9 25.4 41.3 58.0Total 100.0 100.0 100.0 100.0
Notes: Denominators are in parentheses. AT ¼ assistivetechnology; PC ¼ personal care.
*v2 test significant at p , .05.
Figure 2. Percentage of those with difficulty on each activityof daily living who report that a task is tiring, time consuming,or painful without assistance (those who are completely unableto perform an activity are not included).
340 The Gerontologist
by guest on March 27, 2016
http://gerontologist.oxfordjournals.org/D
ownloaded from

assistive technology) and those who do not (usingeither assistive devices alone or no care at all) aresubstantial and consistently significant across levelsof disability.
Discussion
Facilitating the ability to live and work indepen-dently in the community is a central goal forgerontologists, policymakers, and public healthpractitioners. Although it is difficult to measureoptimal care arrangements for adults with disabil-ities (Jette & Keysor, 2002), the results presentedhere further our understanding of the relativeeffectiveness of assistive technology and personal
care in alleviating difficulty with daily activities.They also provide insights into the conceptualizationand measurement of unmet need.
Consistent with previous studies (Agree & Freed-man, 2000; Manton et al., 1993; Verbrugge et al.,1997), we find that assistive devices are the mostcommon means of managing day-to-day tasks forolder adults and that the extent to which assistivetechnology and personal care are used in combina-tion is closely related to the amount of difficultyreported. Unlike previous researchers, however, wecompare across care arrangements reports of re-sidual disability on specific dimensions such asfatigue, duration, and pain. We find that althoughadults with disabilities using only assistive technol-ogy tend to be less disabled than users of personal
Table 3. Residual Difficulty on Specific Dimensions by Global Level of Underlying Difficulty and Type of Assistance
Type of Assistance
Activity n AT Only PC Only PC and AT
All With Underlying Difficulty
Bathing
Very tiring* (695) 74.9 55.1 66.0Long time* (709) 83.0 49.4 62.8Very painful, ns (490) 70.2 62.5 67.0
Transferring
Very tiring* (694) 70.1 56.0 59.3Long time* (785) 76.2 57.0 57.3Very painful, ns (801) 82.4 79.1 76.9
Walking
Very tiring, ns (1877) 80.1 77.0 76.6Long time, ns (1892) 83.0 78.9 78.5Very painful, ns (1531) 82.1 79.7 83.0
Getting outside
Very tiring* (760) 86.7 78.2 77.2Long time* (766) 88.9 76.0 79.3Very painful, ns (617) 86.9 85.7 79.7
Those With a Lot of Underlying Difficulty
BathingVery tiring* (317) 76.3 60.2 70.3Long time* (332) 85.7 60.9 64.0Very painful, ns (222) 70.7 71.7 68.8
Transferring
Very tiring, ns (326) 75.1 68.6 66.5Long time, ns (350) 78.7 72.1 63.7Very painful, ns (336) 87.6 88.4 84.9
Walking
Very tiring, ns (1009) 85.4 87.1 82.7Long time, ns (1029) 87.2 86.6 85.8Very painful, ns (870) 85.1 87.0 86.1
Getting outside
Very tiring, ns (410) 90.7 87.2 84.3Long time, ns (419) 87.5 85.3 85.1Very painful, ns (346) 86.3 85.6 83.5
Notes: Reported information is for those who use some type of assistance. Respondents who report they are completely unableto perform an activity are not included. AT ¼ assistive technology; PC ¼ personal care; ns ¼ v2 test not significant (p . .10).
*v2 test significant at p , .05.
Vol. 43, No. 3, 2003 341
by guest on March 27, 2016
http://gerontologist.oxfordjournals.org/D
ownloaded from
care, they are more likely to report that a task istiring or time consuming when they use theirequipment. We also find that users of assistivetechnology are less likely to report a need for anyhands-on help than those already using personalcare.
Our analysis is limited in several ways. We wereunable to compare the effectiveness of care arrange-ments on specific dimensions for the most severelydisabled; thus we cannot draw any conclusionsabout the relative efficacy of care arrangements forthose unable to perform a task without assistance.Moreover, we were able to explore only thecomplete elimination—rather than the reduction—of disability. There are many reasons that devices,which require some physical and cognitive effort touse, might reduce overall difficulty more easily thanpersonal care, but not completely eliminate it. Futureresearch should consider the relative effectiveness ofpersonal care and assistive technology both onspecific dimensions and in finer gradations. Finally,we were unable to explore with these cross-sectionaldata the more dynamic acquisition process un-derlying the disablement process. For example,a long-term user of assistive technology may become
more proficient and consequently more satisfied thanone who has newly acquired the device. Surely this isa fruitful area for further exploration.
Despite these limitations, our analyses provideseveral new insights into the relative effectiveness ofpersonal care and technology. First, the present studysuggests a need to probe more deeply into the salientdimensions of disability that assistive technology andpersonal care alleviate. Using global measures ofdifficulty, prior research found that assistive tech-nology appeared to be more effective than personalcare in reducing or eliminating disability (Agree,1999; Verbrugge et al., 1997). We find instead thatusers of such technology report similar or greateramounts of residual difficulty on the three specificdimensions of residual difficulty with ADL tasks inthese data. These findings do not contradict earlierwork, but rather inform it, by expanding ourdefinition of effectiveness. Qualitative research mayhelp identify the most important dimensions relatedto the effectiveness of different care arrangements.In one of the few studies to address this question,Albrecht and Devlieger (1999) report that pain andfatigue are among the most common problemsreported, but further work illuminating the natureand meaning of these dimensions is warranted.
Second, we find that persons with more severedisabilities are more likely to use personal care andless likely to use assistive technology exclusively.At the same time, like Agree (1999), we show therelative effectiveness of personal care and assistivetechnology on specific dimensions appears to di-minish at higher levels of disability. These findingssuggest that selection according to underlying dis-ability is critical to take into account in any compa-risons of effectiveness across care arrangements.In prior work this selection may have artificiallyincreased the benefit attributed to assistive technol-ogy relative to personal care. In this study, we findthe disadvantage of such technology on specificdimensions of disability does not appear to beexplained by the underlying severity of disability,which is lower among assistive technology users.
Third, the finding that assistive technology usersless often report a need for hands-on help despitegreater residual difficulty illustrates the likelihoodthat factors other than the severity of underlyingdisability influence the choice of care arrangementsand must be attended to in both research and clinicalpractice. In particular, the use of assistive technologymay be related to psychological factors such asreceptivity, self-efficacy, and motivation, all of whichhave been shown to be related to the success of re-habilitative efforts (Arnstein, 2000; Grahn, Ekdahl, &Borquist, 2000; Zimmer & Chappell, 1999). Valuesrelated to autonomy and privacy also are importantaspects of the acceptance and use of technology inrehabilitation and home care (Tamm, 1999).
Our findings also have implications for theconceptualization and measurement of unmet needs
Figure 3. Percentage of those reporting an unmet need forhands-on care by type of assistance and activity. AT¼ assistivetechnology.
342 The Gerontologist
by guest on March 27, 2016
http://gerontologist.oxfordjournals.org/D
ownloaded from

for care. Studies of unmet need have traditionallyfocused on personal care (Allen et al., 2001; Gitlinet al., 2001; Mann et al., 1999), finding, as we didhere, quite low reported levels of unmet need, evenamong adults with severe disabilities. Such researchmay be missing a substantial amount of unmet needfor assistance, were the concept more broadlydefined to include needs for and use of assistivetechnology. Not only may there be unmet needs thatcan be better fulfilled by technology rather thanpersonal care, but the findings from this studysuggest that some proportion of the disabledpopulation may have unmet needs but would notreport a desire for personal care. Mann, Hurren, andTomita (1995) reported that persons with arthritisexpressed a need for additional devices, even de-scribing new technologies to be invented. Includingspecific questions about the need for additionaldevices to patient assessments and survey instru-ments would contribute a great deal to our under-standing of and interventions to reduce unmet needs.
In sum, indicators such as residual disability andunmet need do not in and of themselves allow us toidentify the reasons that a particular care arrange-ment is more or less satisfactory. They do, however,make it possible to uncover circumstances in whichtypes of care are less than optimal (Eldar, 2000). Tomeet the goal of facilitating the ability of adults tolive and work independently in the community, it isessential for future research to explore the role ofself-care more thoroughly. In particular, greaterattention should be paid to identification of thedifferent dimensions by which assistive technologyand personal care alleviate difficulty and enhanceindependence.
References
Agree, E. M. (1999). The influence of personal care and assistive technol-ogy on the measurement of disability. Social Science & Medicine, 48,427–443.
Agree, E. M., & Freedman, V. A. (2000). Incorporating assistive devices intocommunity-based long-term care: An analysis of the potential forsubstitution and supplementation. Journal of Aging and Health, 12,426–450.
Albrecht, G. L., & Devlieger, P. J. (1999). The disability paradox: Highquality of life against all odds. Social Science & Medicine, 48, 977–988.
Allen, S. M., Foster, A., & Berg, K. (2001). Receiving help at home: Theinterplay of human and technological assistance. Journal of Gerontol-ogy: Social Sciences, 56B, S374–S382.
Allen, S., & Mor, V. (1997). The prevalence and consequences of unmetneed—Contrasts between older and younger adults with disability.Medical Care, 35, 1132–1148.
Andresen, E. M., Lollar, D. J., & Meyers, A. R. (2000). Disability outcomesresearch: Why this supplement, on this topic, at this time? Archives ofPhysical Medicine and Rehabilitation, 81(Suppl. 2), S1–S4.
Arnstein, P. (2000). The mediation of disability by self-efficacy in differ-ent samples of chronic pain patients. Disability and Rehabilitation, 22,794–801.
Arras, J. (1995). Bringing the hospital home: Ethical and socialimplications of high tech home care. Baltimore: Johns HopkinsUniversity Press.
Chen, L. K., Mann, W. C., Tomita, M. R., & Burford, T. E. (1998). Anevaluation of reachers for use by older persons with disabilities. AssistiveTechnology, 10(2), 113–125.
Cohen, M. E., & Marino, R. J. (2000). The tools of disability outcomesresearch: Functional status measures. Archives of Physical Medicine andRehabilitation, 81(Suppl. 2), S21–S29.
Desai, M. M., Lentzner, H. R., & Weeks, J. D. (2001). Unmet need forpersonal assistance with activities of daily living among older adults. TheGerontologist, 41, 82–88.
Eldar, R. (2000). A conceptual proposal for the study of the qualityof rehabilitation care. Disability and Rehabilitation, 22(4): 163–169.
Gitlin, L. N., Corcoran, M., Winter, L., Boyce, A., & Hauck, W. W. (2001).A randomized, controlled trial of a home environmental intervention:Effect on efficacy and upset in caregivers and on daily function of personswith dementia. The Gerontologist, 41, 4–14.
Gitlin, L. N., & Levine, R. (1992). Prescribing adaptive devices to the elderly:Principles for treatment in the home. International Journal ofTechnology and Aging, 5(1), 107–118.
Grahn, B., Ekdahl, C., & Borquist, L. (2000). Motivation as a predictor ofchanges in quality of life and working ability in multidisciplinaryrehabilitation. Disability and Rehabilitation, 22(15), 639–654.
Hartke, R. J., Prohaska, T. R., & Furner, S. (1998). Older adults and assistivedevices: Use, multiple device use, and need. Journal of Aging and Health,10, 99–116.
Heide, A. van der, Jacobs, J. W. G., Albada-Kuipers, G. A. van, Kraaimat,F. W., Geenen, R., & Bijlsma, J. W. J. (1993). Self-report functionaldisability scores and the use of devices: Two distinct aspects of physicalfunction in rheumatoid arthritis. Annals of Rheumatic Diseases, 52,497–502.
Jette, A. M., & Keysor, J. J. (2002). Uses of evidence in disability outcomesand effectiveness research. The Milbank Quarterly, 80, 325–345.
Kaye, S., LaPlante, M. P., Carlson, D., & Wenger, B. L. (1996). Trends indisability rates in the United States, 1970–1994 (National Institute onDisability and Rehabilitation Research Report). Washington, DC: U. S.Department of Health and Human Services.
Kohn, J. G., LeBlanc, M., & Mortola, P. (1994). Measuring quality andperformance of assistive technology. Assistive Technology, 6(2), 120–125.
Mann, W. C., Hurren, D., Charvat, B., & Tomita, M. (1996). The use ofphones by elders with disabilities: Problems, interventions, costs.Assistive Technology, 8, 23–33.
Mann, W. C., Hurren, D., & Tomita, M. (1993). Comparison of assistivedevice use and needs of home-based older persons with differentimpairments. American Journal of Occupational Therapy, 47, 980–987.
Mann, W. C., Hurren, D., & Tomita, M. (1995). Assistive devices used byhome-based elderly persons with arthritis. American Journal ofOccupational Therapy, 49, 810–820.
Mann, W. C., Ottenbacher, K. J., Fraas, L., Tomita, M., & Granger, C. V.(1999). Effectiveness of assistive technology and environmental inter-ventions in maintaining independence and reducing home care costs forfrail elderly: A randomized controlled trial. Archives of FamilyMedicine, 8, 210–217.
Manton, K., Corder, L., & Stallard, E. (1993). Changes in the use of personalassistance and special equipment from 1982 to 1989: Results from the1982 and 1989 NLTCS. The Gerontologist, 33, 168–176.
National Center for Health Statistics. (1998a). 1994 National HealthInterview Survey on Disability, Phase I and II [CD-ROM Series 10, No.8A]. Hyattsville, MD: U. S. Department of Health and Human Services.
National Center for Health Statistics. (1998b). 1995 National HealthInterview Survey on Disability, Phase I and II [CD-ROM Series 10, No.10A]. Hyattsville, MD: U. S. Department of Health and Human Services.
Norburn, J. E. K., Bernard, S., Konrad, T., Woomert, A., DeFriese, G.,Kalsbeek, W., et al. (1995). Self-care and assistance from others in copingwith functional status limitations among a national sample of olderadults. Journal of Gerontology: Social Sciences, 50B, S101–S109.
Pope, A. M., & Tarlov, A. (Eds.) (1991). Disability in America: Towarda national agenda for prevention. Washington, DC: National AcademyPress.
Russell, J. N., Hendershot, G. E., LeClere, F., Howie, L. J., & Adler, M.(1997). Trends and differential use of assistive technology devices:United States, 1994 (Advance Data No. 292). Washington, DC: NationalCenter for Health Statistics.
Sanford, J. A., Arch, M., & Megrew, M. B. (1995). An evaluation of grabbars to meet the needs of elderly people. Assistive Technology, 7, 36–47.
Schoeni, R., Freedman, V. A., & Wallace, R. (2001). Persistent, consistent,widespread, and robust? Another look at recent trends in old-agedisability. Journal of Gerontology: Social Sciences, 56B, S206–S218.
Soldo, B. J., & Freedman, V. A. (1994). Care of the elderly: Division of laboramong the family, the market, and the state. In S. Preston & L. G. Martin(Eds.), The demography of aging. Washington, DC: National AcademyPress.
Steinfeld, E., & Shea, S. M. (1995, November). Enabling home environ-ments: Strategies for aging in place. Paper presented at the 48th AnnualScientific Meeting of The Gerontological Society of America, LosAngeles, CA.
Tamm, M. (1999). What does a home mean and when does it cease to bea home? Home as a setting for rehabilitation and care. Disability andRehabilitation, 21, 49–55.
Vol. 43, No. 3, 2003 343
by guest on March 27, 2016
http://gerontologist.oxfordjournals.org/D
ownloaded from

Tennstedt, S., McKinlay, J., & Kasten, L. (1994). Unmet need amongdisabled elders: A problem in access to community long term care? SocialScience and Medicine, 38, 915–924.
Verbrugge, L. M., & Jette, A. M. (1994). The disablement process. SocialScience and Medicine, 38, 1–14.
Verbrugge, L., Rennert, C., & Madans, J. (1997). The great efficacy ofpersonal and equipment assistance in reducing disability. AmericanJournal of Public Health, 87, 384–392.
Zimmer, Z., & Chappell, N. (1994). Mobility restriction and the use of devicesamong seniors. Journal of Aging and Health, 6(2), 185–208.
Zimmer, Z., & Chappell, N. (1999). Receptivity to new technology amongolder adults. Disability and Rehabilitation, 21(5/6), 222–230.
Received April 25, 2002Accepted September 16, 2002Decision Editor: Laurence G. Branch, PhDDecision Editor:
344 The Gerontologist
by guest on March 27, 2016
http://gerontologist.oxfordjournals.org/D
ownloaded from
Copyright © 2022 FDOKUMEN




















