
Returns to regionalism : an evaluation of nontraditional gains from regional trade agreements

16
Assessing Fit of Nontraditional AssistiveTechnologies
ADRIANE B. RANDOLPHKennesaw State UniversityandMELODY M. MOORE JACKSONGeorgia Institute of Technology
There is a variety of brain-based interface methods which depend on measuring small changes inbrain signals or properties. These methods have typically been used for nontraditional assistivetechnology applications. Non-traditional assistive technology is generally targeted for users withsevere motor disabilities which may last long-term due to illness or injury or short-term due tosituational disabilities. Control of a nontraditional assistive technology can vary widely acrossusers depending upon many factors ranging from health to experience. Unfortunately, there isno systematic method for assessing usability of nontraditional assistive technologies to achievethe best control. The current methods to accommodate users through trial-and-error result in theloss of valuable time and resources as users sometimes have diminishing abilities or suffer fromterminal illnesses. This work describes a methodology for objectively measuring an individual’sability to control a specific nontraditional assistive technology, thus expediting the technology-fitprocess.
Categories and Subject Descriptors: H.5.2 [Information Interfaces and Presentation]: UserInterfaces—Evaluation/methodology
General Terms: Human Factors, Design, Performance
Additional Key Words and Phrases: user profiles, individual characteristics, brain-based inter-faces, brain-computer interface, direct-brain interface, galvanic skin response, functional near-infrared, assistive technology
ACM Reference Format:Randolph, A. B. and Moore Jackson, M. M. 2010. Assessing fit of nontraditional assistive technolo-gies. ACM Trans. Access. Comput. 2, 4, Article 16 (June 2010), 31 pages.DOI = 10.1145/1786774.1786777. http://doi.acm.org/10.1145/1786774.1786777.
Authors’ addresses: A. B. Randolph, School of Accountancy-Business Information Systems, Ken-nesaw State University, 1000 Chastain Road MD0402, Kennesaw, GA 30144; email: [email protected]; M. M. Moore Jackson, College of Computing, Georgia Institute of Technology, TSRB85 5th Street, NW, Atlanta, GA 30308; email: [email protected] to make digital or hard copies of part or all of this work for personal or classroom useis granted without fee provided that copies are not made or distributed for profit or direct com-mercial advantage and that copies show this notice on the first page or initial screen of a displayalong with the full citation. Copyrights for components of this work owned by others than ACMmust be honored. Abstracting with credit is permitted. To copy otherwise, to republish, to poston servers, to redistribute to lists, or to use any component of this work in other works requiresprior specific permission and/or a fee. Permissions may be requested from the Publications Dept.,ACM, Inc., 2 Penn Plaza, Suite 701, New York, NY 10121-0701 USA, fax +1 (212) 869-0481, [email protected]© 2010 ACM 1936-7228/2010/06-ART16 $10.00 DOI: 10.1145/1786774.1786777.
http://doi.acm.org/10.1145/1786774.1786777.
ACM Transactions on Accessible Computing, Vol. 2, No. 4, Article 16, Pub. date: June 2010.

16: 2 · A. B. Randolph and M. M. Moore Jackson
1. INTRODUCTION
Traditional computer applications and assistive technology devices requiremuscle movement for input, such as needed to manipulate a mouse and key-board or a sip-and-puff switch. However, brain-based interface methods, suchas electroencephalograms and functional near-infrared images of blood vol-ume, may be used for nontraditional assistive technology (NTAT) applications[Birbaumer 2006; Mason et al. 2005; Pfurtscheller et al. 2008; Wolpaw et al.2002]. These nontraditional interfaces are also known as brain-computer in-terfaces (BCIs), direct-brain interfaces (DBIs), and brain-machine interfaces(BMIS) [Serruya et al. 2002; Wolpaw et al. 2002].
Brain-based interface technology has been demonstrated in assistive tech-nologies generally targeting users with severe motor disabilities as a result ofdisease, illness, or injury and nondisabled users with situational disabilitiesinduced by their environment, such as with jet pilots and astronauts subjectedto extreme forces, soldiers in hostile territory, and even video gamers [Brittet al. 2006; Gao et al. 2003; Iturrate et al. 2009; Nijholt et al. 2009, 2008; Trejoet al. 2006]. Nontraditional assistive technologies provide these users with ca-pabilities for communication and control of environmental, navigational, andprosthetic devices. As a result, people who might not otherwise have an out-let can interact with their friends and family members and take more proac-tive roles in their environment. Thus, severely disabled users who are ableto control NTATs can experience a significant improvement in their quality oflife [Moore 2003]. However, everyone does not experience equal success withNTAT interfaces; one person may be able to control a particular NTAT withgreat reliability whereas another person cannot control it at all.
We define the match between an individual and technology as his or herindividual-technology fit (ITF), and this fit can be reflected by the individ-ual’s control of that technology. More people would be able to effectively utilizeNTATs if we understood more about the factors that affect control of these sys-tems. Currently, there exists a disparity in goals among researchers and assis-tive technology practitioners investigating brain-based interfaces. Researcherstend to focus more on characteristics of the technology being developed, andpractitioners focus more on characteristics of the user. The result is that avail-able NTATs are often matched to users through trial and error based on thespecialized knowledge of the attending team. Unfortunately, this unsystematicapproach can waste valuable time and resources as users sometimes have di-minishing abilities or suffer from terminal illnesses which preclude them fromenjoying the full benefits of the provided system. A methodology that explainscontrol of available NTATs based on individual characteristics can greatly ex-pedite the technology fit process [Randolph 2008].
This work examines an important consideration for NTAT interface design:describing characteristics of an individual user and his or her fit with a specifictechnology. Characteristics are a person’s demographic traits, physiologicaltraits, and experience. Individuals vary in their characteristics across manydimensions. It is necessary to develop paradigms and heuristics that link indi-vidual characteristics to available technologies to determine which approach is
ACM Transactions on Accessible Computing, Vol. 2, No. 4, Article 16, Pub. date: June 2010.

Assessing Fit of Nontraditional Assistive Technologies · 16: 3
likely to be most effective [Allison et al. 2010; Guger et al. 2009]. Then, assis-tive technology practitioners may better incorporate information about theirusers to refine their design efforts, and research teams may refer these usersto other targeted groups specializing in the most appropriate technology. Withbetter means for explaining control of various NTATs, we make better use ofthe time and resources expended in offering impactful solutions to a sensitiveuser population. Further, we help advance the field of nontraditional inter-faces for use by all persons by understanding the overall concept of individual-technology fit.
Existing models for understanding how to match people with various tech-nologies include the Human Activity Assistive Technology (HAAT) model[Cook and Hussey 2002], the keystroke-level model (KLM) [Card et al. 1980],the three-state model [Buxton 1990], the Matching Person and Technology(MPT) model [Scherer 1998], and the Institute of Medicine Model [Brandtand Pope 1997]; however, these models are seen as technology-specific andhave not been applied to the more nontraditional technology associated withbrain-based interfaces. In the BCI field, Kennedy and Adams [2003] proposedmatching users to interfaces but did so based solely on the person’s functionalcapabilities. None of these models are intended to uncover the significant usercharacteristics necessary for an effective pairing with various NTATs. There-fore, this work proposes that: significant individual user characteristics maybe identified and modeled in a way that matches with features of nontradi-tional assistive technologies to explain control.
The following sections describe a methodology for understanding control ofNTATs according to individual user characteristics. First, this work providesbackground on both direct and indirect brain-based interfaces and existingtechniques for capturing information about users for system personalizationand performance enhancement. Then, this work describes a study that ex-plores individual-technology fit with two NTATs.
2. CONTINUUM OF ASSISTIVE TECHNOLOGY CONTROL
Approximately one out of five people in the United States has a disability [U.S.Census Bureau 2009], which is a long-lasting impairment prohibiting certainfunctions [World Health Organization 1980]. A disability is classified accord-ing to six categories: sensory, physical, mental, self-care, difficulty going out-side the home, and employment disability [Waldrop and Stern 2003]. Motordisabilities can be understood along a continuum ranging from the retentionof fine motor control by nondisabled individuals to the loss of all voluntarymovement and speech, termed being locked-in.
More than half a million people worldwide are considered to be locked intotheir own bodies [National Organization for Rare Disorders 2000]. A personmay become locked-in due to conditions such as amyotrophic lateral sclerosis(ALS—also known as Lou Gehrig’s disease), spinal cord injury, or brain-stemstroke. Approximately 30,000 people have ALS in the United States at anygiven time [ALS Association 2007]. Although they have lost the ability for un-aided control of their environment, locked-in persons are generally cognitively
ACM Transactions on Accessible Computing, Vol. 2, No. 4, Article 16, Pub. date: June 2010.

16: 4 · A. B. Randolph and M. M. Moore Jackson
Fig. 1. A continuum of motor disabilities and control interfaces. Figure adapted from Moore et al.[2005].
intact, but this state may deteriorate over time [Aluniello 1999]. Figure 1 il-lustrates this continuum of motor disabilities and the input devices most com-monly used at each stage. It is helpful to understand the functional capabilitiesof users with respect to the technology being used [Price and Sears 2009].
Figure 1 also lists various technical options that aid persons with motor dis-abilities and help improve their quality of life. However, more work is neededto make the interfaces less obtrusive for users and the people with whom theyinteract. A way to achieve this goal is by better matching the related technolo-gies to users based on individual characteristics. In particular for people withsevere motor disabilities, it would be advantageous to know which NTATs aremost effective based on a profile of their individual characteristics. If theseindividual characteristics were indicators of a person’s capabilities for controlof NTATs, they could be linked to features of the technology to explain controland ultimately improve nontraditional interface design.
3. NONTRADITIONAL ASSISTIVE TECHNOLOGY
A nontraditional assistive technology (NTAT) is the resulting system whenelectrophysiological and psychophysiological measures, such as electroen-cephalograms (EEGs) and functional near-infrared (fNIR) images of blood vol-ume, are used for non-muscularly-controlled assistive technology applications.A direct-brain interface is a type of nontraditional interface that specificallyutilizes measures of brain activity as input from sensors placed over areasof the brain. Similarly, an indirect-brain interface also utilizes measures ofbrain activity as input, but that brain activity is reflected in other resultingphysiological functions and not measured directly from the brain. Evolvingfrom medical diagnostic systems, nontraditional interfaces are now also in-vestigated in the assistive technology and human-computer interaction (HCI)fields. Traditionally, the targeted users are locked-in, but people who havemotor disabilities (e.g., people with severe cerebral palsy) or who experiencesituational disabilities (e.g., jet pilots, military combat personnel) may alsofind these NTATs useful.
Research in the field of nontraditional interfaces spans several disci-plines including computer science, electrical engineering, cognitive psychology,ACM Transactions on Accessible Computing, Vol. 2, No. 4, Article 16, Pub. date: June 2010.

Assessing Fit of Nontraditional Assistive Technologies · 16: 5
neuroscience, and information systems all working to discover the most ap-propriate alternatives for users with severe motor disabilities. Although non-traditional interfaces have yielded working applications for humans based onnonmuscular input for control, they currently only reach an approximate in-formation transfer rate of 68 bits/minute (i.e., 9 characters/minute is possiblewith a predictive program) and trade off speed and accuracy for the number ofchoices possible [Gao et al. 2003; Pfurtscheller et al. 2008]. Despite this perfor-mance, these systems lend great hope to people who otherwise may not haveanother outlet.
There are several approaches to recording the signals which serve as in-put to nontraditional interfaces although it is not yet clear which approachworks best for a particular person for control. This work focuses on nonin-vasive techniques that involve sensors placed on the skin’s surface for signalacquisition instead of surgically implanted devices. The most common of theseapproaches is the use of EEGs to measure electrical activity of the brain col-lected from scalp electrodes. Another approach includes the use of functionalmagnetic resonance imaging (fMRI) as a noninvasive method for measuringoxygenated blood volume using a powerful, magnetized probe that can re-flect activity throughout the brain. Other approaches include galvanic skinresponse (GSR) for measuring skin conductance and fNIR for also measuringoxygenated blood volume in the brain but using near-infrared light reflections.The following describes in greater detail the two nontraditional interface ap-proaches used in this work: fNIR and GSR.
3.1 Functional Near-Infrared Imaging
In addition to the more widely examined electrical brain activity recorded di-rectly by EEGs, researchers are beginning to explore another process of thebrain, oxygenation of blood, as input to indirect-brain interfaces [Coyle et al.2007; Stenger 2005; Weiskopf et al. 2004]. Oxygenation of blood is a reflectionof vascular activity that has a three- to seven-second delay and only indirectlyreflects brain activity. Near-infrared spectroscopy (NIRS) is a process used tomeasure changes in oxygenated blood volume on the surface of the brain re-sulting in what is called fNIR imaging. A device such as Archinoetic’s OpticalTomographic Imaging Spectrometer (OTIS) [Nishimura et al. 2006] illustratedin Figure 2 may be used for fNIR sensing. In this process, near-infrared lightis used to noninvasively penetrate the scalp and skull and is absorbed by oxy-gen carriers within the bloodstream, or hemoglobin. The person on the rightof Figure 2 shows how the sensor may be placed on the surface of the head todetect blood volume in different areas of the brain. Different functions suchas counting or moving a finger alter the amount of oxygen being absorbed at agiven time [Kleinschmidt et al. 1996] and may allow a nontraditional interfaceto be controlled.
3.2 Galvanic Skin Response
Similar to an interface based on fNIR, galvanic skin response (GSR) also re-flects brain activity in an indirect manner. Although GSR is controlled by the
ACM Transactions on Accessible Computing, Vol. 2, No. 4, Article 16, Pub. date: June 2010.

16: 6 · A. B. Randolph and M. M. Moore Jackson
Fig. 2. The OTIS fNIR device and sensor placement. Photo on left used with permission fromNishimura et al. [2006]. Photo on right taken by Stanley Leary and used with permission.
Fig. 3. Example configuration for GSR electrodes. Modified from Michael Gasperi’s Web site(http://www.extremenxt.com/gsr.jpg).
Autonomic Nervous System (ANS) [Leslie and Millenson 1996] which does notinclude the spinal cord and brain [Martini et al. 2001], it is a measure takennoninvasively of the electrical conductivity of the skin whose levels may varyaccording to human emotional and mental states. Although the electrodes maybe placed anywhere, a typical configuration for a GSR device (commonly knownas a polygraph system) includes two electrodes placed on the index and middlefingers, areas of the skin with the most active sweat glands, as illustrated inFigure 3. The device sends an imperceptibly small amount of electrical currentthrough the electrodes to measure the momentary amount of skin conductivitycreated in response to various stimuli or the person’s own imagery. Galvanicskin response has been used to control a computer application [Moore and Dua2004].
4. NONTRADITIONAL ASSISTIVE TECHNOLOGY DESIGN
Researchers have explored the design of NTATs from a system perspectiveand not from an individual perspective [Mason and Birch 2003]. AlthoughNTATs have largely been studied in laboratory settings, there is little workthat provides general characterizations of the electrophysiology and how it re-lates to the users generating the phenomenon for control purposes. In addition,there is currently no formal usability method for assessing what NTAT is mostappropriate for a user. For example, current BCI community practices and un-derlying technical infrastructures do not easily allow for a comprehensive setACM Transactions on Accessible Computing, Vol. 2, No. 4, Article 16, Pub. date: June 2010.

Assessing Fit of Nontraditional Assistive Technologies · 16: 7
of tests to determine the most appropriate means for signal control by a userwho is locked-in. Therefore, users often only benefit from the approach offeredby their attending team which may not be the optimal choice.
4.1 User Profiling
Research on profiling and ways to more effectively incorporate informationabout the system user were proposed to help overcome problems of ineffec-tive interfaces. User profiling is a way to allow information filtering based ona user’s personal characteristics and is often used interchangeably with theterm user modeling [Hanani et al. 2001]. It has been described as taking acontent-centered approach by capturing information about a person’s habitsand taking a user-centered approach that focuses on particular user traits orcharacteristics. User-centered profiling, as Jameson [2001] describes it, takesinto account both current state and long-term characteristics of the user com-bined with environmental context. Current state characteristics include as-pects of the user’s current cognitive or psychological state such as current levelof emotional arousal. Longer-term characteristics include: objective personalcharacteristics; level of knowledge of particular topics; level of interest in par-ticular topics; and perceptual and motor skills and limitations. This work in-corporates user-centered profiling.
4.2 Individual Characteristics
Individual characteristics are the distinguishing factors between people andinclude their demographic, physiological, and cognitive differences. Littleis known about which individual characteristics best match with particularNTATs although there are numerous assessments of human capabilities rang-ing from functional limitations to the amount of system training received.
Table I lists and provides justifications for a proposed set of characteristicsaffecting NTAT control. This list is based on a review of related literature anddiscussions with researchers in the fields of brain-based interfaces and assis-tive technology concerning observed or plausible electrophysiological effects.It represents an initial list of categories and characteristics to explore andmore may be considered in future studies. Although characteristics such asage change over time and vision may degrade for locked-in users [Allison et al.2008; Kubler et al. 2009], these characteristics generally remain constant formore than a few days and may be considered more stable. In addition, thereare more dynamic characteristics of an individual such as the amount of sleepand recent intake of caffeine that may significantly affect control [Guger et al.2009]. These dynamic or momentary characteristics can vary so much overa short period of time that it is difficult to use them as stable constructs, sotheir potential effects are noted through the use of a session questionnaire forfurther consideration.
5. EXPERIMENTAL DESIGN
The NTAT user profiling process was developed as an approach for derivingcomprehensive user profiles that may be used to explain individuals’ control
ACM Transactions on Accessible Computing, Vol. 2, No. 4, Article 16, Pub. date: June 2010.

16: 8 · A. B. Randolph and M. M. Moore Jackson
Table I. Proposed Individual Characteristics to Test
Category Attribute Justification for InclusionDemographicTrait
Sex There are a number of physiological and spatial reference dif-ferences based on sex. For example, sex may be a key factorfor GSR-based control since skin conductivity is based on theamount of sweat; although women have more sweat glandsthan men, men’s sweat glands are more active [Medline Plus2009].
Age Age moderates various physiological differences. For exam-ple, older people (age 52 +/- 10 years) have lower increases inlocalized levels of oxygenated blood [Hock et al. 1995].
Handedness Human handedness relates to location of the language cen-ter in the brain where this center is generally located in theleft, front hemisphere but sometimes found on the right forleft-handed individuals [Annett 1985, 2001]. A common pro-tocol for fNIR recordings is to place the sensor over the lefthemisphere Broca’s area for language production [Nishimuraet al. 2006].
PhysiologicalTrait
Athleticism Athletes’ cardiovascular systems respond differently fromthe average population and from people with limited mo-tor functions, such as people with quadriplegia [Patil et al.1993]. This difference may affect control with a system basedon vascular responsiveness.
SmokingExperience
Limited exposure to nicotine has been shown to increaseparietal activity [Giessinga et al. 2005] and people classi-fied as smokers have increased cerebral blood flow velocity[Terborg et al. 2002].
Paralysis Studies have shown that the strength of electrical signalsfrom sensorimotor cortex activity weakens as physical abilitydeclines [Tran et al. 2004].
Hair Color Collaborators using fNIR technology have shared anecdotalevidence of difficulty calibrating their systems with individ-uals with darker hair color.
Skin Color Collaborators using fNIR technology have shared anecdotalevidence of difficulty calibrating their systems with individ-uals with darker skin color.
Hair Texture Collaborators using fNIR technology have shared anecdotalevidence of difficulty calibrating their systems with individ-uals with thicker hair.
AffectiveDrugs
Some drugs and vitamins are known to affect mental per-formance and alertness. For example, antihistamines, anti-depressants, and antianxiety drugs may make a person lessalert [White and Rumbold 1988] whereas some recreationaldrugs and vitamins may help increase performance intelli-gence [Chang et al. 2009].
RegularCaffeineConsumption
Caffeine makes a person more alert and increases reactiontime [Rogers and Dernoncourt 1998], increases blood pres-sure and blood flow [Hartley et al. 2004; Lane and Williams2007], and has been used to stimulate patients during exper-iments.
RegularAlcoholConsumption
Regular consumption of alcohol acts as a blood thinner[Mukamal et al. 2005].
SustainedHead Injury
Traumatic brain injuries often impact cognitive function[Schretlen and Shapiro 2003].
ACM Transactions on Accessible Computing, Vol. 2, No. 4, Article 16, Pub. date: June 2010.

Assessing Fit of Nontraditional Assistive Technologies · 16: 9
Table I. Proposed Individual Characteristics to Test (Cont.)
Category Attribute Justification for InclusionHandDexterity
Degree of motor engagement has been linked to control ofBCIs based on sensorimotor signals [Randolph et al. 2006].
Play(ed) Sports Long-term engagement in exercise improves cardiovascu-lar function and memory in adults [Hill et al. 1993].
Experience Prior Electro-physiologically-based Training
The amount of hours of training with particular BCIs af-fects a person’s ability to control electrical signals suchas those from sensorimotor cortex activity [Wolpaw et al.2002]. It is possible that training with a brain-based as-sistive technology increases kinetic intelligence [Gardner1993] and thus will improve overall control with anynontraditional assistive technology.
17-24. VideoGameExperience:action/first-person shooter,adventure,puzzle,real-timestrategy,rhythm,role-playing,simulation,and sportsgames
High-speed interactive video game players versus non-high-speed interactive video game players experiencechanges in their visual attention [Green and Bavelier2003], a key factor for visually-evoked potentials (VEPs)recorded through EEG. It is possible that experience withparticular types of video games will also impact control ofother NTATs but is unknown although some anecdotal ev-idence has been found [Allison et al. 2008].
Computer Use A person’s self-reported assessment of his or her aptitudefor using basic computer applications was found to affectIS performance [Goodhue 1995].
ActingExperience
There is an acting method pioneered by KonstantinStanislavski called “Method Acting” where actors learn toexpress their character’s emotions based on recollection ofactual emotions felt in the past .....[WordNet].
MeditationExperience
By using techniques such as the Transcendental Methodfor meditation, people are trained to focus their minds andproduce calm states [Yogi 2005].
Years ofEducation
Cognitive functions, such as perceptual speed, are posi-tively affected by years of education [Bennett et al. 2003].
of nontraditional assistive technologies. This study investigated individual-technology fit of the proposed characteristics with the fNIR and GSR NTATs.The BioGauges Method was used to measure and characterize the capabilitiesof a user with an NTAT [Randolph et al. 2005a, 2007, 2005b]. It assesses auser’s range, reliability, and granularity of control with an NTAT based onvery basic tasks.
In this study, in addition to nondisabled participants, it was necessary togain participants who had severe motor disabilities and who represented awide range of ages such as found in the target population for nontraditionalinterfaces. The timeframe for explanation covered the person’s initial state inusing the technology because user needs change over time [Hanani et al. 2001].This work focused on the person’s initial use of the technology and not his or
ACM Transactions on Accessible Computing, Vol. 2, No. 4, Article 16, Pub. date: June 2010.

16: 10 · A. B. Randolph and M. M. Moore Jackson
her intention for future use. In addition, some individuals never express theability for control of particular nontraditional interfaces. Although traininghas been cited as needing great consideration when analyzing a person’s abilityto use a nontraditional interface [Ron-Angevin et al. 2009; Wolpaw et al. 2002],studies have varied in their reported inclusion of all subjects and their successrates [Moore Jackson et al. 2006] and have not shown that training gives amarked advantage when initial abilities vary [Tan et al. 2009]. Thus, trainingeffects were not considered here.
5.1 Participants
The study included 38 adult participants (33 nondisabled and 5 with varyingmotor disabilities due to ALS). Although participants had a range of prior ex-perience using an NTAT (logging zero to over eleven hours), all were noviceswith the fNIR and GSR technologies. Overall, the ages ranged from 21 to 67with an average of 39 years (13 females and 25 males). Participants includedundergraduate students, graduate students, trade workers, and workingprofessionals.
Participants were self-reported to be cognitively intact and those individualswith ALS were observed to possess a range of motor disabilities not includingtotal loss of sight or hearing. The range of motor disabilities included oneperson who still had upper body movement but used a wheelchair and fourwho were dependent on others to operate their wheelchairs. Of those fourdependent wheelchair operators, one still relied on very slight vocalization tocommunicate, two utilized computerized, assistive communication devices inconjunction with eye movement, and one was able to communicate using aslight muscular reflex felt in his wrist but were otherwise considered to belocked-in.
All participants were recruited via word of mouth to participate in the study.The study consisted of one session per person and lasted two hours. Sessionswith nondisabled participants were conducted in a laboratory setting. Ses-sions with participants with severe motor disabilities were conducted in theirhomes with steps taken to provide a controlled atmosphere similar to the labsetting by requesting a quiet environment away from directly streaming sun-light which could affect the fNIR readings. Participants each attempted 72trials per technology across a single session totaling 5,360 trials in the overallstudy (2,716 total fNIR trials and 2,644 total GSR trials).
5.2 Apparatus
The approaches for signal collection selected for this work were GSR1 andfNIR2 to enable cross-comparisons between results because the associatedtransducers produced continuous output. In addition, these approaches wereportable and relatively easy to operate due to their related hardware andnoninvasive nature. The complete system setup with GSR is illustrated in
1Lafayette Instrument Company’s DataLab 2000 system (www.lafayetteinstrument.com).2Archinoetics’ OTISTM system (www.archinoetics.com).
ACM Transactions on Accessible Computing, Vol. 2, No. 4, Article 16, Pub. date: June 2010.

Assessing Fit of Nontraditional Assistive Technologies · 16: 11
Fig. 4. Complete experimental system setup with GSR.
Figure 4. A standard laptop was used to run the BioGauges system shown onthe left-most laptop and a separate laptop was used to run the electrophysio-logical recording software for fNIR and GSR shown on the right-most laptop.
5.3 Capturing Individual Characteristics
Individual characteristics may be used to populate an NTAT user profile whichis a representation of the most salient features of a user for explaining controlof nontraditional assistive technologies in a concise representation. A type ofNTAT user profile was first outlined in the work conducted by Davis et al.[2003] to indicate communication topics for use with a brain-based interface.Although the attributes differ slightly when used for explanation of controlof a nontraditional interface technology, the process for populating the valuesremains the same. This previous work revealed that when initially settingup user profiles, as for a conversational system for a user with severe motordisabilities, an explicit approach should be implemented [Moore et al. 2004],which requires active user involvement to provide the information [Hananiet al. 2001].
A questionnaire format was found appropriate for explicitly obtaining thesample NTAT user profile values illustrated in Table II. A questionnaire wasdevised specifically for this study to obtain the values for each property of theNTAT user profile while keeping in mind temporary influences (e.g., possi-ble sleep deprivation, biological rhythms, illness) and vasoactive agents (e.g.,stimulants such as caffeine) which could significantly affect the control by par-ticipants [Alluisi and Morgan 1976; Liu et al. 2004]. The questionnaire under-went pilot testing with two nondisabled users and a researcher experienced inworking with people with ALS to ensure content validity.
5.4 Measuring Control
After completing the questionnaires about the participant’s individual charac-teristics and momentary influences, the researcher verified correct positioning
ACM Transactions on Accessible Computing, Vol. 2, No. 4, Article 16, Pub. date: June 2010.

16: 12 · A. B. Randolph and M. M. Moore Jackson
Table II. Sample Nontraditional Assistive Technology User Profile for OneLocked-In Participant
Category Attribute-Value PairDemographic Traits Sex = male
Age = 45Handedness = right
Physiological Traits Athleticism = lowSmoking Experience = noParalysis = 7 yearsHair Color = brownSkin Color = whiteHair Texture = curlyAffective Drugs = yesRegular Caffeine = noRegular Alcohol = noHead Injury = noHand Dexterity = yesPlay(ed) Sports = yes
Experience Prior Electrophys. Training = 14+ hoursVideo Game Experience (action/first-person shooter,adventure, puzzle, real-time strategy, rhythm,role-playing, simulation, and sports games) = noneComputer Use = extensivelyActing Experience = noMeditation Experience = yesYears of Education = 16
of the electrophysiological sensor and calibrated the recording system. ForGSR, the sensors were always cleaned with an alcohol-based gel and thenplaced on the pads of the index and middle fingers of the right hand and se-cured by Velcro. Then the DataLab 2000 software provided an end-to-end cal-ibration of the recording system. For fNIR, the OTISTM Pucklink software’sSignal Quality Assessment tool was used to verify correct sensor placementover the Broca’s area by when it achieved an accurate heart rate and a heart-beat signal-to-noise ratio greater than 2.0. Actual heart rate was taken by theparticipant or researcher feeling for the pulse over a thirty second period or byusing a pulse oximeter.
Next, the BioGauges system was calibrated according to the low and highvalues that each person was able to achieve at that moment. Detrending, aprocess for obtaining a moving average of values, was not incorporated intothe BioGauges system because it was important to reduce biases for control.For GSR, participants were asked to relax for a low value and then think ofsomething exciting that raised their temperature for a high value. Participantswere asked to devise their own imagery since different things excite differentpeople but to try to vary the images since people habituate over time; whatis exciting at one time may no longer be exciting in the future. For fNIR,participants were asked to think of a nonsensical, droning sound created byrepeating “la-la” slowly in their heads for a low value and then to think ofcounting rapidly but clearly enunciating each number in their heads for a highvalue. Participants then used this imagery to attempt control of each of theNTATs.ACM Transactions on Accessible Computing, Vol. 2, No. 4, Article 16, Pub. date: June 2010.

Assessing Fit of Nontraditional Assistive Technologies · 16: 13
Fig. 5. BioGauges interface for the attain task.
Fig. 6. Pucklink interface for use with fNIR brain-based assistive technology with translatingcomponent for the BioGauges interface.
Participants were tested with each of the NTATs in random order and thetrials within each session were also randomly ordered. An objective outcomemeasure of control was taken after each trial using the BioGauges method-ology and toolset. For this study, control was indicated by the proportion oftotal trials in which a person was able to successfully move a cursor and mo-mentarily acquire a bounded target within an allotted timeframe. This studyincorporated a bounded attain task to test spatial control using an fNIR and aGSR-based brain-based interface with continuous output. The bounded attaintask is illustrated in Figure 5 and shows what the participant saw on his orher computer screen.
Figure 6 shows what the researcher saw on her computer screen while moni-toring the electrophysiological phenomenon used to control the interface. Here,sample blood oxygenation readings appeared as the lines at the top of thegraph on the operator’s screen.
In this study, after the system provided a warning signal a cursor was pre-sented as a square that always started in the middle of the screen. Therewere four possible targets presented randomly along a one-dimensional track
ACM Transactions on Accessible Computing, Vol. 2, No. 4, Article 16, Pub. date: June 2010.

16: 14 · A. B. Randolph and M. M. Moore Jackson
represented as the horizontal bar in Figure 5. The one-dimensional track wascalibrated to the participants’ low and high values generated and partitionedinto five bins: center, far left, mid-left, mid-right, and far right. In addition,the two edges of the one-dimensional track were infinite meaning that it waspossible for the participant to exceed the range of initial calibration visuallyrepresented by the horizontal bar. The participant attempted to activate thesystem and move the cursor to attain a target presented to the right or left.The target was represented by a nonfilled rectangle. A new trial started oncethe participant attained the target by momentarily placing the cursor com-pletely within the target boundary lines or the system timed out. The partici-pant had twenty seconds to attempt to attain the target before system timeout.
At the end of the session, each participant then completed an exit question-naire. The participants with ALS completed all of the related pre and postquestionnaires via email within a few days outside of the prescribed sessiontime. Four of the five participants with ALS were able to complete the ques-tionnaires on their own using assistive technology. The fifth participant withALS completed the questionnaires with the help of a family member who inti-mately knew his history and experience.
5.5 Understanding Individual-Technology Fit
For this study, control was the observable evidence of fit between individualcharacteristics and the fNIR or GSR technology tested. Again, a higher valueof control indicated a better match and a lower value of control indicated apoorer match. Table III details the predicted exploratory relationships thateach individual characteristic would have with control based on extrapolationfrom the justifications provided in Table I. Exploratory relationships were alsodescribed for these characteristics and are included below. These hypothe-ses serve as a theoretical basis for understanding the observed phenomenonwithin this study.
5.6 Analysis
Results were aggregated into an overall average success value for each NTATper person where success was the proportion of successfully completed trialsout of the total number of trials attempted. The chance of achieving successand hitting the desired target was 1/7 = .143 because although there were fourpossible targets, there were five bins including the center bin where the cursoralways started and then two infinite edges totaling seven possible results forcursor placement. All targets were weighted equally.
As is common with many behavioral science studies and especially com-mon within the BCI literature due to the time-intensive requirements ofgathering electrophysiological data, this exploratory study included a statis-tically small number of people with just 38 sampled, including 5 with dis-abilities [Birbaumer et al. 1999; Donchin et al. 2000; Hoffmann et al. 2008].Based on the data, both standard regression and nonparametric tests were se-lected as analysis techniques for this study. First, nonparametric testing withchi-square for independence and Mann-Whitney U revealed if there were anyACM Transactions on Accessible Computing, Vol. 2, No. 4, Article 16, Pub. date: June 2010.

Assessing Fit of Nontraditional Assistive Technologies · 16: 15
Table III. Hypothesized Relationships of Individual Characteristics with Control of fNIR andGSR Technologies
Category No. DependentVariable
fNIRControl
GSRControl
Value Set
DemographicTrait
1. Sex Males >
FemalesMales >
FemalesCategorical(1=male,0=female), self-reported variable
2. Age Decreaseswith age
Decreaseswith age
Continuous, self-reported variable
3. Handedness Right-handers >
Left-handers
No effectantici-pated
Categorical(1=right, 0=left),self-reportedvariable
PhysiologicalTrait
4. Athleticism Increasesas moreathletic
Increasesas moreathletic
Scaled (7-pointsof athletic iden-tity ranging from1=sedentary to7=trainedathlete), self-reported variable
5. SmokingExperience
Smokers >
Non-smokers
Smokers> Non-smokers
Categorical(1=yes, 0=no),self-reportedvariable
6. Paralysis Decreaseswithincreasedyears ofparalysis
Decreaseswithincreasedyears ofparalysis
Continuous(years withparalysis),self-reportedvariable
7. Hair Color Decreaseswith darkerhair
No effectantici-pated
Scaled(1=Blond/None,2=Brown,3=Black,4=Gray),Observed
8. Skin Color Decreaseswithdarker skinpigmenta-tion
No effectantici-pated
Scaled (1=White,2=LightBrown,3=Medium-Brown,4=DarkBrown),Observed
9. Hair Texture Decreasesas hairgets morecurly/dense
No effectantici-pated
Scaled (1=None,2=Straight,3=Curly),Observed
10. Affective Drugs Decreaseswithuse of drugsthat affectalertness
Decreaseswith useof drugsthat affectalertness
Categorical(1=yes, 0=no),self-reportedvariable
11. Regular CaffeineConsumption
Increaseswithregular useof caffeine
Increaseswithregularuse ofcaffeine
Categorical(1=yes, 0=no),self-reportedvariable
ACM Transactions on Accessible Computing, Vol. 2, No. 4, Article 16, Pub. date: June 2010.

16: 16 · A. B. Randolph and M. M. Moore Jackson
Table III. Hypothesized Relationships of Individual Characteristics with Control of fNIR andGSR Technologies (Cont.)
12. Regular AlcoholConsumption
Increaseswithregular con-sumption ofalcohol
Increaseswithregularconsump-tion ofalcohol
Categorical(1=yes, 0=no),self-reportedvariable
13. Sustained HeadInjury
Decreaseswith injury
No effectantici-pated
Categorical(1=yes, 0=no),self-reportedvariable
14. Hand Dexterity Increaseswithdexterity
Increaseswithdexterity
Categorical(1=yes, 0=no),self-reportedvariable
15. Play(ed) Sports Increaseswith sportsplayed
Increaseswithsportsplayed
Categorical(1=yes, 0=no),self-reportedvariable
Experience 16. Prior Electro-physiologically-based Training
Increaseswith moretraining
Increaseswith moretraining
Scaled (Approx.Hours: 0, 2, 7,14), self-reportedvariable
17. Action/First-Person VideoGame Experience(e.g., Quake)
Unknowneffect
Unknowneffect
Categorical(1=none, 2=some,3=extensive),self-reportedvariable
18. Adventure VideoGame Experience(e.g., Myst)
Unknowneffect
Unknowneffect
Categorical(1=none, 2=some,3=extensive),self-reportedvariable
19. Puzzle VideoGame Experience(e.g., Tetris)
Unknowneffect
Unknowneffect
Categorical(1=none, 2=some,3=extensive),self-reportedvariable
20. Real-TimeStrategy VideoGame Experience(e.g., StarCraft)
Unknowneffect
Unknowneffect
Categorical(1=none, 2=some,3=extensive),self-reportedvariable
21. Rhythm VideoGameExperience (e.g.,Dance DanceRevolution)
Unknowneffect
Unknowneffect
Categorical(1=none, 2=some,3=extensive),self-reportedvariable
22. Role-PlayingVideo GameExperience (e.g.,Final Fantasy)
Unknowneffect
Unknowneffect
Categorical(1=none, 2=some,3=extensive),self-reportedvariable
ACM Transactions on Accessible Computing, Vol. 2, No. 4, Article 16, Pub. date: June 2010.

Assessing Fit of Nontraditional Assistive Technologies · 16: 17
Table III. Hypothesized Relationships of Individual Characteristics with Control of fNIR and GSRTechnologies (Cont.)
23. Simulation VideoGame Experience(e.g., GranTurismo)
Unknowneffect
Unknowneffect
Categorical(1=none, 2=some,3=extensive),self-reportedvariable
24. Sports VideoGame Experience(e.g., Madden)
Unknowneffect
Unknowneffect
Categorical(1=none, 2=some,3=extensive),self-reportedvariable
25. Computer Use No effectanticipated
No effectanticipated
Scaled (1=HardlyEver, 2=A Little,3=Extensively),self-reportedvariable
26. ActingExperience
No effectanticipated
Actors >
Non-actorsCategorical(1=yes, 0=no),self-reportedvariable
27. MeditationExperience
Meditators> Non-meditators
Meditators< Non-meditators
Categorical(1=yes, 0=no),self-reportedvariable
28. Years ofEducation
Increaseswitheducation
Decreaseswitheducation
Continuous,inferred
differences between nondisabled participants and participants with motor dis-abilities. Then, regression was run to discover which variables had significantimpact on control of each NTAT tested by testing for main effects. SpearmanRank Order was used to determine correlations between independent vari-ables. The variables for handedness and head injury were thrown out becausethere were only four people who displayed being left-handed and one personwho had sustained a head injury; five was needed as a minimum for compar-ative statistical analysis. This reduced the number of variables analyzed totwenty-six.
6. RESULTS AND DISCUSSION SUCCESS
6.1 Success
For brain-based interfaces, an accuracy of 70% has generally been assumedas the baseline level for effective communication and control [Kubler et al.2009], however we may consider values greater than chance as an indicationof some level of useful control [Sellers et al. 2006]. In the previous section, wecalculated the chance of hitting a target as .143. On a 95% confidence interval,.330 was calculated as the upper bound of the range for chance [Lowry 2008].Thus, the success values needed to be greater than .330 to fall beyond the 95%confidence interval and be considered significantly greater than chance at the.05 level. Here, the overall average fNIR success was .466 and the overallaverage success for GSR was .354. Because these average success values were
ACM Transactions on Accessible Computing, Vol. 2, No. 4, Article 16, Pub. date: June 2010.
16: 18 · A. B. Randolph and M. M. Moore Jackson
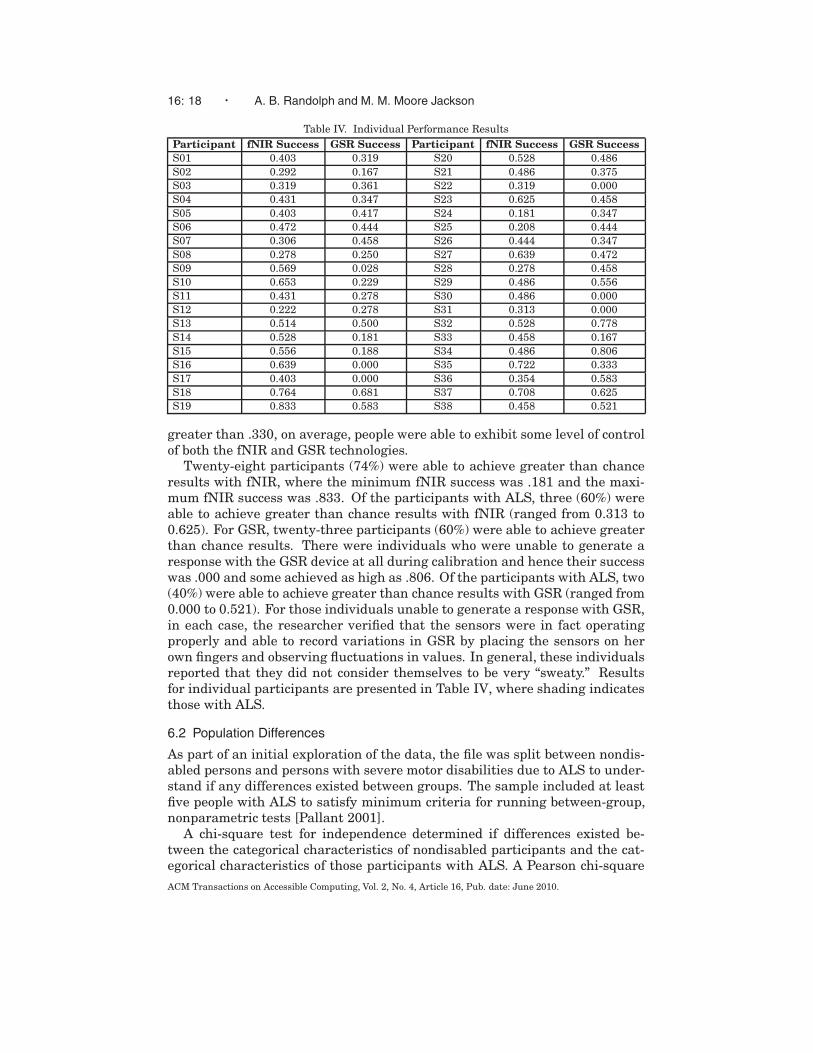
Table IV. Individual Performance ResultsParticipant fNIR Success GSR Success Participant fNIR Success GSR SuccessS01 0.403 0.319 S20 0.528 0.486S02 0.292 0.167 S21 0.486 0.375S03 0.319 0.361 S22 0.319 0.000S04 0.431 0.347 S23 0.625 0.458S05 0.403 0.417 S24 0.181 0.347S06 0.472 0.444 S25 0.208 0.444S07 0.306 0.458 S26 0.444 0.347S08 0.278 0.250 S27 0.639 0.472S09 0.569 0.028 S28 0.278 0.458S10 0.653 0.229 S29 0.486 0.556S11 0.431 0.278 S30 0.486 0.000S12 0.222 0.278 S31 0.313 0.000S13 0.514 0.500 S32 0.528 0.778S14 0.528 0.181 S33 0.458 0.167S15 0.556 0.188 S34 0.486 0.806S16 0.639 0.000 S35 0.722 0.333S17 0.403 0.000 S36 0.354 0.583S18 0.764 0.681 S37 0.708 0.625S19 0.833 0.583 S38 0.458 0.521
greater than .330, on average, people were able to exhibit some level of controlof both the fNIR and GSR technologies.
Twenty-eight participants (74%) were able to achieve greater than chanceresults with fNIR, where the minimum fNIR success was .181 and the maxi-mum fNIR success was .833. Of the participants with ALS, three (60%) wereable to achieve greater than chance results with fNIR (ranged from 0.313 to0.625). For GSR, twenty-three participants (60%) were able to achieve greaterthan chance results. There were individuals who were unable to generate aresponse with the GSR device at all during calibration and hence their successwas .000 and some achieved as high as .806. Of the participants with ALS, two(40%) were able to achieve greater than chance results with GSR (ranged from0.000 to 0.521). For those individuals unable to generate a response with GSR,in each case, the researcher verified that the sensors were in fact operatingproperly and able to record variations in GSR by placing the sensors on herown fingers and observing fluctuations in values. In general, these individualsreported that they did not consider themselves to be very “sweaty.” Resultsfor individual participants are presented in Table IV, where shading indicatesthose with ALS.
6.2 Population Differences
As part of an initial exploration of the data, the file was split between nondis-abled persons and persons with severe motor disabilities due to ALS to under-stand if any differences existed between groups. The sample included at leastfive people with ALS to satisfy minimum criteria for running between-group,nonparametric tests [Pallant 2001].
A chi-square test for independence determined if differences existed be-tween the categorical characteristics of nondisabled participants and the cat-egorical characteristics of those participants with ALS. A Pearson chi-squareACM Transactions on Accessible Computing, Vol. 2, No. 4, Article 16, Pub. date: June 2010.

Assessing Fit of Nontraditional Assistive Technologies · 16: 19
Table V. Summary of Results of Tests for Differences Between Non-disabled Participants and Participants with Severe Motor Disabilities
Variable Z-value/Pearson p-valueChi-Square Value
Technology Ran First 2.073 .150fNIR Success −.368 .738GSR Success −1.363 .187Sex .086 .770Age −1.427 .159Athleticism −2.288 .021*Smoking Experience 2.056 .152Paralysis −6.064 p < .001*Hair Color 6.855 .077Skin Color 2.695 .441Hair Texture 1.085 .581Affective Drugs 14.528 p < .001*Regular Caffeine Consumption 2.699 .100Regular Alcohol Consumption 2.657 .103Hand Dexterity .001 .979Play(ed) Sports .010 .922Prior Training −.663 .615First-Person Shooter Games 3.573 .168Adventure Games 2.159 .340Puzzle Games .359 .836Strategy Games 1.303 .521Rhythm Games 2.056 .358Role-Playing Games 3.359 .187Simulation Games 2.795 .247Sports Games .722 .697Computer Use 7.206 .027*Acting Experience .494 .482Meditation Experience 25.498 p < .001*Years of Education −.941 .376
value with significance greater than .05 indicated that there did not appear tobe a difference between populations for that characteristic. A Mann-WhitneyU test determined if differences existed between the continuous/scaled charac-teristics of nondisabled participants and the continuous/scaled characteristicsof those participants with ALS. A Z-value with an exact significance greaterthan .05 indicated that there did not appear to be a difference between popu-lations for that characteristic. Table V presents a summary of the chi-squareand Mann-Whitney U tests for differences between the participants with andwithout disabilities. An asterisk indicates which values significantly differedacross groups at the level of p ≤ .05.
The results show that there was a significant difference in values (where p ≤.05) between nondisabled participants and participants with disabilities foronly five of the twenty-six total characteristics (less than twenty percent): useof affective drugs, meditation experience, computer use, level of athleticism,and years with paralysis. In addition, a chi-square test indicated that theorder in which the NTAT was presented to participants did not matter to theresults because the Pearson chi-square p-value was .150.
ACM Transactions on Accessible Computing, Vol. 2, No. 4, Article 16, Pub. date: June 2010.

16: 20 · A. B. Randolph and M. M. Moore Jackson
A significant difference in means was anticipated for the paralysis and ath-leticism variables because of the general limited mobility of people who haveALS and both variables assessed current states. There was a difference inmeans of 8.60 between nondisabled participants and participants with disabil-ities for paralysis, which was significant at the p ≤ .001 level. There was adifference in means of 1.79 between nondisabled participants and participantswith disabilities for athleticism, which was significant at the p = .021 level.Both variables represented current states of motor ability whereas the vari-able for play(ed) sports represented the person’s previous athletic ability forthose individuals with paralysis. Therefore, it made sense that the differencein the proportion of people who play(ed) sports to those who do/did not playsports between nondisabled participants (27:6) and participants with disabili-ties (4:1) was not observed to be significantly different with p = .922.
Further, people with ALS are often prescribed a cocktail of drugs to assisttheir immune systems and various other needs; these drugs often affect alert-ness levels, so the difference in proportion of people who did take affectivedrugs to those who did not take affective drugs between nondisabled partici-pants (3:30) and participants with disabilities (4:1) was expected to be signifi-cant (p ≤ .001).
The statistically significant differences observed in overall frequency of com-puter use between nondisabled participants (75.8%) and participants with dis-abilities (20%) at the p = .027 level may be due to some remaining confoundwith the survey question. Although mobility may be distinctly limited for peo-ple with ALS and they may have responded that they engaged in little to nocomputer use, the person may have previously used computers extensively andthus still been very computer literate; this is the crux of the computer usevariable.
There was no variation for meditation experience for people with ALS; theyall reported that they engaged in regular meditation which is perhaps a nec-essary coping mechanism when locked-in, thus explaining the significant dif-ference observed in the proportion of meditators to non-meditators betweennondisabled participants (2:31) and participants with disabilities (5:0) at thep ≤ .001 level. In addition, a Mann-Whitney U test revealed that there wasno significant difference observed between the mean fNIR and GSR successvalues for nondisabled participants (difference in means of .03012) and par-ticipants with disabilities (difference in means of .1825) because the p-valueswere .738 and .187 respectively.
Given these results, and the exploratory nature of this study, we proceedby combining the results of the two groups of participants. At the same time,we note that additional research, with a larger number of participants, wouldbe necessary to formally confirm that the characteristics of the two groups arecomparable. In addition, it is important to acknowledge that before consider-ing the possibility of substituting one group of participants for another it isnecessary to confirm not only that basic characteristics (e.g., age, hair color,education) are comparable but that the relationships between these charac-teristics and both performance and preferences are similar for the two groupsof individuals. While it is possible for research involving individuals without
ACM Transactions on Accessible Computing, Vol. 2, No. 4, Article 16, Pub. date: June 2010.

Assessing Fit of Nontraditional Assistive Technologies · 16: 21
Table VI. Summary of Regression Results
Individual Characteristic fNIR R2 fNIR fNIR GSR R2 GSR GSRValue Beta p-value Value Beta p-value
Sex .063 .251 .128 .176 .420 .009*Age .208 −.456 .004* .253 −.503 .001*Athleticism .009 .093 .578 .017 .131 .434Smoking Experience .001 −.031 .855 .000 −.012 .942Paralysis .000 .005 .976 .023 −.151 .356Hair Color .005 −.074 .659 .134 −.367 .024*Skin Color .002 −.043 .797 .149 −.386 .017*Hair Texture .070 .264 .109 .131 −.362 .026*Affective Drugs .024 −.154 .356 .041 −.203 .222Regular Caffeine Consumption .127 −.356 .028* .003 .057 .734Regular Alcohol Consumption .009 −.093 .580 .126 .355 .029*Hand Dexterity .003 .058 .728 .057 .238 .150Play(ed) Sports .009 .097 .564 .066 .258 .118Prior Training .029 .171 .305 .009 −.096 .565First-Person Shooter Games .062 .249 .132 .117 .342 .035*Adventure Games .057 .239 .149 .027 .163 .327Puzzle Games .046 .213 .198 .032 .178 .285Strategy Games .023 .152 .363 .178 .422 .008*Rhythm Games .030 .174 .297 .008 .089 .595Role-Playing Games .050 .224 .177 .205 .453 .004*Simulation Games .043 .206 .214 .135 .368 .023*Sports Games .049 .221 .183 .095 .308 .060Computer Use .014 .120 .474 .021 .146 .382Acting Experience .013 .115 .492 .066 −.256 .120Meditation Experience .002 −.040 .813 .218 −.467 .003*Years of Education .124 .352 .030* .001 −.030 .858
disabilities to provide valuable insights, such insights would need to be vali-dated with disabled users.
6.3 Fit of Individual Characteristics
Because the majority of individual characteristics were not found to be statisti-cally different, the data were combined for further analysis of participants’ re-sults. Regression was performed with each individual characteristic and fNIRsuccess and then again with GSR success. Table VI provides a summary ofthe twenty-six regressions for both technologies listed per individual charac-teristic. Table VI shows the R-square value which tells how much variancein success is explained by the characteristic, the Beta coefficient is reportedbecause this is a standardized value that allows cross-comparisons between co-efficient values independent of scale, and the p-value is the significance level.The individual characteristics that appear to have a significant relationshipwith control (p-value ≤ .05) are indicated with an asterisk.
For fNIR, there are three individual characteristics that appear to have asignificant relationship with control at p-value ≤ .05. These characteristicsshould be highly considered when deciding if a person is a good candidate foran fNIR device and are explained as follows.
(1) Age. There is a negative correlation with age which indicates that youngerpeople have better success than older people controlling an fNIR device.
ACM Transactions on Accessible Computing, Vol. 2, No. 4, Article 16, Pub. date: June 2010.

16: 22 · A. B. Randolph and M. M. Moore Jackson
This falls in line with the original exploratory relationship that localizedblood flow decreases with age and may explain this phenomenon. In ad-dition, there is often an inverse relationship found between successful useof technology and age which has been found true for certain BCIs [Allisonet al. 2010].
(2) Regular Caffeine Consumption. There is a negative correlation which in-dicates that non–caffeine consumers have better control of an fNIR device.This result is contrary to the exploratory relationships that regular caf-feine consumption has a positive effect on control. Perhaps regular con-sumers of caffeine are overstimulated and unable to concentrate at lengthon the benign tasks presented.
(3) Years of Education. There is a positive correlation which indicates thatas people spend more time in school, their control of an fNIR device in-creases, and this supports the original exploratory relationship about edu-cation and increased cognitive function.
Interestingly, hair color, skin color, and hair texture do not appear to havestrongly significant relationships with fNIR control. These characteristicswere thought to be among the more influential variables per anecdotal evi-dence from collaborators, but this study indicates that this is not the case. Per-haps there is more to consider in these anecdotal statements regarding types ofsensors used and variation in subjects observed. For example, a research teammay posit that darker-haired people are not good at operating an fNIR deviceif it observes a sample of one dark-haired person versus three light-haired in-dividuals and that one person does not perform well despite other individualdifferences to consider. In this example, anecdotal observation may become alocal rule and not be empirically supported. No definitive statements can bemade regarding a relationship with handedness because there were only fourpeople who were left-handers which precludes inter-group comparison. Fur-ther, characteristics related to physical abilities and sex also appear not tohave a relationship with control. This is encouraging for use of this technologyby people who are locked-in because there does not appear to be a dependencyon physical or motor ability for control. So, as a person progresses with ALS,he or she should be able to continue utilizing an fNIR device although thereappear to be trade-offs as age increases. Finally, despite wide statements thattraining should have a major role in successful control; here it was not foundto be statistically significant likely because participants did not have notableprior training with the fNIR technology. To fully test this relationship, moreparticipants should be included who have extensive training with the technolo-gies in question.
For GSR, there are twelve individual characteristics that appear to have asignificant relationship with control at p-value ≤ .05 and are as follows. Thesecharacteristics may be condensed into six variables and should be highly con-sidered when deciding if a person is a good candidate for being able to controla GSR device.
(1) Sex. There is a positive correlation with sex indicating that men per-form better than women at controlling GSR. This result supports the
ACM Transactions on Accessible Computing, Vol. 2, No. 4, Article 16, Pub. date: June 2010.

Assessing Fit of Nontraditional Assistive Technologies · 16: 23
proposed exploratory relationship about men sweating more thanwomen and thus having a better range of control.
(2) Age. There is a negative correlation with age which indicates thatyounger people have better success than older people with control-ling a GSR device. This falls in line with the original exploratoryrelationship that circulation slows with age affecting emission andabsorption of sweat.
(3.)–(5.) Hair color, Skin color, Hair texture. Contrary to the exploratory re-lationship, these individual characteristics all negatively correlatewith control indicating that as features lighten, control increases.Perhaps these features interact to reflect another characteristic thatmay be of consequence to GSR control, for example the amount ofoil present in the skin that may confound the system’s electrodes[Berardesca and Maibach 2003].
(6) Regular Alcohol Consumption. Regular alcohol consumption is pos-itively correlated with GSR control reflecting that alcohol promotesthinner blood and thus increases blood flow.
(7) Meditation. Meditation is negatively correlated with control indicat-ing that people who do not meditate regularly perform better con-trolling GSR. Although this may be contrary to some studies thatindicate individuals may learn to control their electrodermal activitythrough meditation .....[Blain et al. 2006], this supports the originalexploratory relationship and perhaps indicates that people who med-itate are calmer and have difficulty raising their excitement level,thus making control of a GSR device more difficult.
(8.)–(12.) FPS, Strategy, Role-Playing, and Simulation games. These gametypes all positively correlate with control. Further, these game typeswere found to highly correlate with each other. An average of thesevalues representing overall video game experience appears to be bet-ter to avoid multicollinearity issues in the future.
Overall, training again was not found to be statistically significant in itsrelation to GSR control with the same explanation holding as above for fNIR.Characteristics such as regular caffeine consumption and athleticism appearnot to have a significant effect on GSR control despite hypothesized rela-tionships perhaps due to the sample size. Meanwhile, the characteristics ofregular alcohol consumption and meditation experience appear to have coun-terintuitive results; such results in the field are deemed noteworthy and oftenencourage further investigation [Guger et al. 2009].
6.4 Summary of Results
Overall, from the experience of running thirty-eight participants with fNIR-and GSR-based interface technologies, it appears that there are significant re-lationships between different individual characteristics and control. The onlyshared result between fNIR and GSR control is the significantly observed in-verse relationship with age for both. As shown in Table V, age has the largest
ACM Transactions on Accessible Computing, Vol. 2, No. 4, Article 16, Pub. date: June 2010.

16: 24 · A. B. Randolph and M. M. Moore Jackson
Beta coefficient (−.456 for fNIR and −.503 for GSR) and R-Square (.208 forfNIR and .253 for GSR) values for both technologies indicating that age hasthe largest weight and explains the most variance of success with fNIR andGSR. Therefore, age should be given the most consideration when consideringa person’s match with either fNIR or GSR technologies because it appears thatyounger people have a better chance at success with both. To achieve successthat is significantly better than chance of .330, the person should be sixty-fiveyears or younger for fNIR and forty-three years or younger for GSR; this pivotpoint was calculated by taking the unstandardized coefficient (B1) for fNIR(−5.47 × 10−3) and for GSR (−8.27 × 10−3) and solving for X1 using the equa-tion: y = B0 + B1 X1, where y (dependent variable) was .330 and B0 (constant)was .681 for fNIR and .679 for GSR. The values for B1 and B0 come directlyfrom the resulting regression analysis.
In addition to younger age, increased success with fNIR appears to be re-lated to nonregular caffeine consumption and increased years of education.To achieve success that is significantly better than chance of .330, the personshould have 12 years or more of education calculated using a similar processto that for calculating the pivot point for age. Success with GSR appears toincrease for men, regular alcohol consumption, nonpractice of meditation, in-creased video game experience, and people with lighter hair colors. To achievesuccess that is significantly better than chance of .330, the person should havehair that is lighter than black (2.76) calculated using a similar process to thatfor calculating the pivot point for age.
These characteristics may be captured using an NTAT user profile. Oncecaptured within an NTAT user profile, to determine a person’s individual-technology fit with a similar fNIR or GSR technology, a checklist such as theNTAT checklist provided in Table VII may be used. An NTAT checklist laysout all of the discovered relationships with control for individual characteris-tics with a particular NTAT. In the table, a check or “x” indicates if individual-technology fit (ITF) is present or not for the technology with the particularcharacteristic expressed, and shading indicates that the characteristic has noobserved significant relationship with the technology.
Ideally, the person would have three checks for fNIR-ITF and six checks forGSR-ITF, representing an ideal fit profile for each NTAT. In deciding betweenthe two technologies for an individual, it may be possible to consider one tech-nology to be more appropriate than the other based on the characteristics thatare significant for one and not the other. For example, if an individual is fe-male, it appears that the GSR overall would not be a good fit but it is possiblethat she may have better success with the fNIR. This was the case for par-ticipant S09 who had 0.028 success with GSR but 0.569 success with fNIR.Likewise, a person who regularly consumes caffeine overall may not be a goodfit for fNIR but may have success with GSR. This was the case for partici-pant S03 who had 0.319 success with fNIR but 0.361 success with GSR. It isalso possible that these individuals would be unsuccessful with both technolo-gies. For example, a female participant S12 achieved 0.222 and 0.278 successwith fNIR and GSR respectively, and participant S02 who regularly consumedcaffeine achieved 0.292 and 0.167 success with fNIR and GSR respectively.
ACM Transactions on Accessible Computing, Vol. 2, No. 4, Article 16, Pub. date: June 2010.

Assessing Fit of Nontraditional Assistive Technologies · 16: 25
Table VII. Nontraditional Assistive Technology Checklist for fNIR and GSR Technologies
No. Individual Characteristic fNIR-ITF GSR-ITF1. The person is under the age of 43 ? ?2. The person is of age 43 to 64 ? x3. The person is 65 years or older x x4. The person is a male ?5. The person is a female x6. The person does not regularly consume caffeine ?7. The person does regularly consume caffeine x8. The person completed high school ?9. The person did not complete high school x10. The person does not regularly meditate ?11. The person does regularly meditate x12. The person plays/played video games ?13. The person does/did not play video games x14. The person regularly drinks alcohol ?15. The person does not regularly drink alcohol x16. The person has brown hair or lighter or no hair ?17. The person has black hair x
Fig. 7. Nontraditional assistive technology user profiling methodology.
A definitive rule for differentiating between NTATs would require furtherstudy with a larger sample size.
7. CONCLUSIONS
This work followed an exploratory design research approach by creating a newmethodology for matching individual characteristics with NTAT features todescribe usability. It proposed several characteristics of individuals to exam-ine based on a review of related literature on nontraditional interfaces, humanphysiology, and ongoing research with colleagues in the field of brain-based in-terfaces. The resulting NTAT user profiling is a helpful methodology to explainan individual’s control of fNIR or GSR technologies; by capturing his or herNTAT user profile and considering practical tradeoffs between the matches onparticular characteristics, we may determine an overall ITF. The steps of theNTAT user profiling methodology are shown in Figure 7.
An assistive technology practitioner may use a questionnaire that asksabout the person’s age, sex, regular caffeine consumption, experience playingvideo games, years of education, and meditation experience, and then observehair color. This would be a relatively short process with only seven questionsto ask the person. The eight total data points would then be compared againsta checklist to determine overall ITF. For fNIR, a younger adult who has gone
ACM Transactions on Accessible Computing, Vol. 2, No. 4, Article 16, Pub. date: June 2010.

16: 26 · A. B. Randolph and M. M. Moore Jackson
on to college and does not regularly consume caffeine should perform best.For GSR, a younger adult male with blond hair who does not regularly med-itate but does have extensive experience playing video games and regularlyconsumes alcohol should perform best. These serve as ideal NTAT user pro-files for fNIR and GSR. This work provides encouragement for more researchto further understand the differences between individuals and the impacts onnontraditional interface design.
This work is an important step toward better matching users with appropri-ate NTATs according to their characteristics, thus saving time and resourcesexpended. Although thirty-eight participants may sound small, this is themost extensive study to-date exploring fNIR and GSR devices for control pur-poses. The lack of significant difference between individuals with and withoutdisabilities on most of our measures (e.g., age, hair color, education) highlightsthe possibility of gaining valuable insights through studies involving individ-uals without disabilities. However, it is important to note that differences ineven a single characteristic could raise questions regarding the significance ofthese insights. For example, in the current study, meditation experience dif-fered between the two groups and also proved to be an important predictor ofsuccess. As highlighted above, it is also important to confirm not only thatbasic characteristics are comparable but that the relationships between thesecharacteristics and both performance and preferences are similar for the twogroups of individuals. Finally, while it is possible for research involving indi-viduals without disabilities to provide valuable insights, such insights wouldneed to be validated with disabled users.
8. LIMITATIONS AND FUTURE RESEARCH
There were some limitations to this study related to the control metrics. Par-ticipants attempted a difficult task to attain a bounded target instead of simplyactivating the system above or below a certain threshold to attain an infinitelylarge target area. Control should increase significantly with a thresholdedtask. Further, although detrending was not used in this study, participantsshould benefit from use of an interface that dynamically calibrates becausepeoples’ ranges sometimes shifted over the course of one task. However, thisstudy was not focused on understanding the interface designed but rather onunderstanding the underlying relationships of individual characteristics withcontrol.
A larger sample size would allow stronger conjectures by using parametricstatistics for data analysis. Unfortunately, achieving a larger sampling of par-ticipants with severe motor disabilities poses a definite challenge. Accordingto members of the ALS Association, although approximately thirty thousandpeople with ALS reside in the United States, many of them are unaware ofsupport networks available and do not have a technically savvy team to helpconnect them with resources. Furthermore, 2007 marked the first year that anational registry had been created for people with ALS. Therefore, it may benecessary to recruit participants with illnesses and conditions other than ALSthat result in motor disabilities. In addition, further investigation into theACM Transactions on Accessible Computing, Vol. 2, No. 4, Article 16, Pub. date: June 2010.

Assessing Fit of Nontraditional Assistive Technologies · 16: 27
effects of handedness on control may prove interesting because of differencesin cognitive development. Finally, more rigorous means for recording charac-teristics may be necessary for attributes such as hair color, skin color, and hairtexture as there may be confounds introduced through purely observationaldata.
This study focused on initial control but does not specifically address the po-tential long term effects of training with NTATs on control. It may be possiblethat training could supersede characteristics from a person’s NTAT user pro-file, but this correlation is presently unknown. A longitudinal, controlled studyis needed to isolate the effects of training on control with particular NTATs andmust include an analysis of type of training and amount.
Although we tested with a select set of NTATs, we may expand this method-ology to explain other types of continuous input technology, such as some EEG-based recordings. In addition to testing with different NTATs, different tasksmay be analyzed for their effect on control. Only one task was investigatedhere, but a study to replicate and extend this work may reveal a deeper cog-nitive relationship between the task and the type of NTAT. Similarly, environ-ment may also have a significant effect on control. Further investigation mayshow that use of NTATs in a laboratory setting is quite different than use in aperson’s home or a place with a great deal of distraction.
ACKNOWLEDGMENTS
The authors would like to thank Drs. Bruce Walker, Veda Storey, DetmarStraub, and Steven Mason for their field and design expertise.
REFERENCES
ALLISON, B., LUTH, T., VALBUENA, D., TEYMOURIAN, A., VOLOSYAK, I., AND GRAESER, A.2010. BCI demographics: How many (and what kinds of) people can use an SSVEP BCI? IEEETrans. Neur. Syst. Rehab. Engin.
ALLISON, B. Z., MCFARLAND, D. J., SCHALK, G., ZHENG, S. D., JACKSON, M. M., AND WOLPAW,J. R. 2008. Towards an independent brain–computer interface using steady state visual evokedpotentials. Clin. Neurophys. 119, 399–408.
ALLUISI, E. A. AND MORGAN, B. B. JR. 1976. Engineering psychology and human performance.Ann. Rev. Psych. 27, 305–330.
ALS ASSOCIATION. 2007. Facts You Should Know About ALS.ALUNIELLO, L. 1999. Unlocking locked-in syndrome. Brain Briefings ALS. 1–2, Society for
Neuroscience.ANNETT, M. 1985. Left, Right, Hand, and Brain: The Right Shift Theory. Erlbaum, Hillsdale, NJ.ANNETT, M. 2001. Handedness and Brain Asymmetry The Right Shift Theory. Psychology Press,
New York, NY.BENNETT, D. A., WILSON, R. S., SCHNEIDER, J. A., EVANS, D. A., LEON, C. F. M. D., ARNOLD,
S. E., BARNES, L. L., AND BIENIAS, J. L. 2003. Education modifies the relation of AD pathologyto level of cognitive function in older persons. Neurol. 60, 1909–1915.
BERARDESCA, E. AND MAIBACH, H. 2003. Ethnic skin: Overview of structure and function.J. Amer. Acad. Dermatol. 48, S139–S142.
BIRBAUMER, N. 2006. Brain–computer-interface research: Coming of age. Clin. Neurophys. 117,479–483.
BIRBAUMER, N., GHANAYIM, N., HINTERBERGER, T., IVERSEN, I., KOTCHOUBEY, B., KUBLER,A., PERELMOUTER, J., TAUB, E., AND FLOR, H. 1999. A spelling device for the paralyzed.Nature 398, 297–298.
ACM Transactions on Accessible Computing, Vol. 2, No. 4, Article 16, Pub. date: June 2010.

16: 28 · A. B. Randolph and M. M. Moore Jackson
BLAIN, S., MIHAILIDIS, A., AND CHAU, T. 2006. Conscious control of electrodermal activity: Thepotential of mental exercises. In Proceedings of the 28th Annual International Conference of theIEEE Engineering in Medicine and Biology Society (EMBS’06). 6561–6564.
BRANDT, E. N. AND POPE, A. M. 1997. Enabling America: Assessing the Role of RehabilitationScience and Engineering. National Academy Press, Washington, DC, 424.
BRITT, T. W., ADLER, A. B., AND CASTRO, C. A. 2006. Military Life: The Psychology of Serving inPeace and Combat. Greenwood Publishing Group.
BUXTON, W. 1990. A three-state model of graphical input. In Proceedings of the 3rd IFIP Interna-tional Conference on Human-Computer Interaction (INTERACT’90). D. Diaper, D. J. Gilmore, G.Cockton, and B. Shacketl Eds., North-Holland, Amsterdam, 449–456.
CARD, S. K., MORAN, T. P., AND NEWELL, A. 1980. The keystroke-level model for user perfor-mance with interactive systems. Comm. ACM 23, 396–410.
CHANG, N., KIM, E., KIM, K. N., KIM, H., KIM, S. Y., AND JEONG, B. S. 2009. Folate nutritionis related to neuropsychological functions in the elderly. Nutr. Resear. Pract. 3, 43–48.
COOK, A. M. AND HUSSEY, S. M. 2002. Assistive Technology: Principles and Practice. Mosby, Inc.,St. Louis, MO.
COYLE, S. M., WARD, T. E., AND MARKHAM, C. M. 2007. Brain–computer interface using asimplified functional near-infrared spectroscopy system. J. Neur. Engin. 4, 219–226.
DAVIS, A. B., MOORE, M. M., AND STOREY, V. 2003. Context aware communication for severelydisabled users. In Proceedings of the Conference on Universal Usability. ACM, 106–111.
DONCHIN, E., SPENCER, K. M., AND WIJESINGHE, R. 2000. The mental prosthesis: Assessingthe speed of a P300-based brain-computer interface. IEEE Trans. Rehab. Engin. 8, 174–179.
GAO, X., XU, D., CHENG, M., AND GAO, S. 2003. A BCI-based environmental controller for themotion-disabled. IEEE Trans. Neur. Syst. Rehab. Engin. 11, 137–140.
GARDNER, H. 1993. Frames of Mind: The Theory of Multiple Intelligences. Basic Books.GIESSINGA, C., THIELA, C. M., ROSLERC, F., AND FINK, G. R. 2005. The modulatory effects
of nicotine on parietal cortex activity in a cued target detection task depend on cue reliability.Neurosci. 137, 853–864.
GOODHUE, D. L. 1995. Understanding user evaluations of information systems. Manage. Sci. 41,1827–1844.
GREEN, C. S. AND BAVELIER, D. 2003. Action video game modifies visual selective attention.Nature 423, 534–537.
GUGER, C., DABAN, S., SELLERS, E., HOLZNER, C., KRAUSZ, G., CARABALONA, R., GRAMATICA,F., AND EDLINGER, G. 2009. How many people are able to control a P300-based brain–computerinterface (BCI)? Neurosci. Lett. 462, 94–98.
HANANI, U., SHAPIRA, B., AND SHOVAL, P. 2001. Information filtering: Overview of issues,research, and systems. User Model. User-Adapt. Interact. 11, 203–259.
HARTLEY, T. R., LOVALLO, W. R., AND WHITSETT, T. L. 2004. Cardiovascular effects of caffeinein men and women. Amer. J. Cardiol. 93, 1022–1026.
HILL, R. D., STORANDT, M., AND MALLEY, M. 1993. The impact of long-term exercise trainingon psychological function in older adults. J. Gerontol. 48, 12–17.
HOCK, C., MULLER-SPAHN, F., SCHUH-HOFER, S., HOFMANN, M., DIRNAGL, U., AND
VILLRINGER, A. 1995. Age dependency of changes in cerebral hemoglobin oxygenation dur-ing brain activation: A near-infrared spectroscopy study. J. Cerebral Blood Flow Metab. 15,1103–1108.
HOFFMANN, U., VESIN, J.-M., EBRAHIMI, T., AND DISERENS, K. 2008. An efficient P300-basedbrain–computer interface for disabled subjects. J. Neurosci. Meth. 167, 115–125.
ITURRATE, I., ANTELIS, J., MINGUEZ, J., AND KUEBLER, A. 2009. Non-invasive brain-actuatedwheelchair based on a P300 neurophysiological protocol and automated navigation. IEEE Trans.Robotics 25, 614–627.
JAMESON, A. 2001. Modeling both the context and the user. Pers. Ubiq. Comput. 5, 29–33.KENNEDY, P. R. AND ADAMS, K. D. 2003. A decision tree for brain-computer interface devices.
IEEE Trans. Neur. Syst. Rehab. Engin. 11, 148–150.
ACM Transactions on Accessible Computing, Vol. 2, No. 4, Article 16, Pub. date: June 2010.

Assessing Fit of Nontraditional Assistive Technologies · 16: 29
KLEINSCHMIDT, A., OBRIG, H., REQUARDT, M., MERBOLDT, K.-D., DIRNAGL, U., VILLRINGER,A., AND FRAHM, J. 1996. Simultaneous recording of cerebral blood oxygenation changes dur-ing human brain activation by magnetic resonance imaging and near-infrared spectroscopy.J. Cerebral Blood Flow Metab. 16, 817–826.
KUBLER, A., FURDEA, A., HALDER, S., HAMMER, E. M., NIJBOER, F., AND KOTCHOUBEY, B.2009. A brain-computer interface controlled auditory event-related potential (p300) spelling sys-tem for locked-in patients. Ann. N. Y. Acad. Sci. 1157, 90–100.
LANE, J. D. AND WILLIAMS, R. B. JR. 2007. Cardiovascular effects of caffeine and stress in regu-lar coffee drinkers. Psychophys. 24, 157–164.
LESLIE, J. C. AND MILLENSON, J. R. 1996. Principles of Behavioral Analysis. Taylor & Francis.LIU, T. T., BEHZADI, Y., RESTOM, K., ULUDAG, K., LU, K., BURACAS, G. T., DUBOWITZ, D. J.,
AND BUXTON, R. B. 2004. Caffeine alters the temporal dynamics of the visual BOLD response.Neuroimage 23, 1, 1402–1413.
LOWRY, R. 2008. Calculators. http://faculty.vassar.edu/lowry/polls/calcs.html.MARTINI, F., OBER, W. C., GARRISON, C. W., WELCH, K., AND HUTCHINGS, R. T. 2001. Funda-
mentals of Anatomy and Physiology. Prentice Hall.MASON, S. G. AND BIRCH, G. E. 2003. A general framework for brain-computer interface design.
IEEE Trans. Neur. Syst. Rehab. Engin. 11, 70–85.MASON, S. G., MOORE JACKSON, M. M., AND BIRCH, G. E. 2005. A general framework for char-
acterizing studies of brain interface technology. Ann. Biomed. Engin. 33, 1653–1670.MEDLINE PLUS. 2009. Sweating. In Medical Encyclopedia, U.S. National Library of Medicine,
Bethesda, MD.MOORE JACKSON, M. M., MASON, S. G., AND BIRCH, G. E. 2006. Analyzing trends in brain
interface technology: A method to compare studies. Ann. Biomed. Engin. 34, 859–877.MOORE, M. M. 2003. Real-world applications for brain-computer interface technology. IEEE
Trans. Neur. Syst. Rehab. Engin. 11, 162–165.MOORE, M. M. AND DUA, U. 2004. A galvanic skin response interface for people with severe motor
disabilities. In Proceedings of the 6th International ACM SIGACCESS Conference on Computersand Accessibility (ASSETS).
MOORE, M. M., STOREY, V. C., AND RANDOLPH, A. B. 2005. User profiles for facilitating con-versations with locked-in users. In Proceedings of the International Conference for InformationSystems (ICIS).
MOORE, M. M., STOREY, V., DAVIS, A. B., AND NAPIER, N. 2004. Deriving user profiles for aug-mentative communication. In Proceedings of the Americas Conference on Information Systems(AMCIS).
MUKAMAL, K. J., MASSARO, J. M., AULT, K. A., MITTLEMAN, M. A., SUTHERLAND, P. A.,LIPINSKA, I., LEVY, D., D’AGOSTINO, R. B., AND TOFLER, G. H. 2005. Alcohol consumptionand platelet activation and aggregation among women and men: The Framingham offspringstudy. Alcoholism: Clin. Exper. Resear. 29, 1906–1912.
NATIONAL ORGANIZATION FOR RARE DISORDERS (NORD) 2000. Locked-in syndrome. In RareDisease Database, Danbury, CT.
NIJHOLT, A., REUDERINK, B., AND BOS, D. O. 2009. Turning shortcomings into challenges:Brain-computer interfaces for games. In Intelligent Technologies for Interactive Entertainment.Springer, 153–168.
NIJHOLT, A., TAN, D., PFURTSCHELLER, G., BRUNNER, C., MILLAN, J. D. R., ALLISON, B.,GRAIMANN, B., POPESCU, F., BLANKERTZ, B., AND MULLER, K.-R. 2008. Brain-computer in-terfacing for intelligent systems. IEEE Intell. Syst. 23, 72–79.
NISHIMURA, E. M., DARLING, B. A., RAPOPORT, E. D., ZADRA, J. R., PROFFITT, D. R., DOWNS,T. H., AND DOWNS III, J. H. 2006. Functional near-infrared sensing for brain-computer inter-face control by a locked-in individual. In Proceedings of the 2nd Annual Augmented CognitionInternational Conference on Augmented Cognition.
PALLANT, J. 2001. SPSS Survival Manual: A Step by Step Guide to Data Analysis Using SPSS.Open University Press, Philadelphia, PA.
ACM Transactions on Accessible Computing, Vol. 2, No. 4, Article 16, Pub. date: June 2010.

16: 30 · A. B. Randolph and M. M. Moore Jackson
PATIL, R. D., KARVE, S. V., AND DICARLO, S. E. 1993. Integrated cardiovascular physiology:A laboratory exercise. Adv. Physiol. Educ. 10, 20–31.
PFURTSCHELLER, G., MULLER-PUTZ, G. R., SCHERER, R., AND NEUPER, C. 2008. Rehabilita-tion with brain-computer interface systems. IEEE Comput.
PRICE, K. J. AND SEARS, A. 2009. The development and evaluation of performance-based func-tional assessment: A methodology for the measurement of physical capabilities. ACM Trans.Access. Comput. 2.
RANDOLPH, A. B. 2008. An expert system for matching individual characteristics and features ofbrain-computer interface technologies with performance. In Proceedings of the SIGCHI Confer-ence Workshop on Brain-Computer Interfaces for HCI and Games. ACM.
RANDOLPH, A. B., KARMAKAR, S., AND JACKSON, M. M. 2006. Toward predicting control ofa brain-computer interface. In Proceedings of the International Conference on InformationSystems.
RANDOLPH, A. B., MCCAMPBELL, L. A., MASON, S. G., AND MOORE, M. M. 2005a. Methodologyfor characterizing biometric interface systems. In Proceedings of the 35th Annual Meeting of theSociety for Neuroscience, Poster.
RANDOLPH, A. B., MOORE JACKSON, M., MASON, S. G., AND MCCAMPBELL, L. A. 2005a.BioGauges for characterizing biometric interface systems. In Proceedings of the 3rd Interna-tional Meeting of Brain-Computer Interface Technology.
RANDOLPH, A. B., MOORE JACKSON, M., AND MASON, S. G. 2007. BioGauges: Toward more ob-jective evaluation of biometrically-based interfaces. In Proceedings of the 6th Annual Workshopon HCI Research in MIS Association for Information Systems (AIS).
ROGERS, P. J. AND DERNONCOURT, C. 1998. Regular caffeine consumption: A balance of adverseand beneficial effects for mood and psychomotor performance. Pharmacol. Biochem. Behav. 59,1039–1045.
RON-ANGEVIN, R., LOPEZ, M. A., AND PELAYO, F. 2009. The training issue in brain-computerinterface: A multi-Disciplinary field. In Bio-Inspired Systems: Computational and AmbientIntelligence. Springer, 666–673.
SCHERER, M. J. 1998. Matching Person & Technology Model. Institute for Matching Person andTechnology, Webster, NY.
SCHRETLEN, D. J. AND SHAPIRO, A. M. 2003. A quantitative review of the effects of traumaticbrain injury on cognitive functioning. Int. Rev. Psych. 15, 341–349.
SELLERS, E. W., KRUSIENSKI, D. J., MCFARLAND, D. J., VAUGHAN, T. M., AND WOLPAW, J. R.2006. A P300 event-related potential brain–computer interface (BCI): The effects of matrix sizeand inter stimulus interval on performance. Biol. Psych. 73, 242–252.
SERRUYA, M. D., HATSOPOULOS, N. G., PANINSKI, L., FELLOWS, M. R., AND DONOGHUE,J. P. 2002. Brain-machine interface: Instant neural control of a movement signal. Nature 416,141–142.
STENGER, B. 2005. Computer-aided brains. Scientific American Mind.TAN, L.-F., JANSARI, A., KENG, S.-L., AND GOH, S.-Y. 2009. Effect of mental training on BCI per-
formance. In Proceedings of the 13th International Conference on Human-Computer Interaction,Part II: Novel Interaction Methods and Techniques. Springer, 632–635.
TERBORG, C., BIRKNER, T., SCHACK, B., AND WITTE, O. W. 2002. Acute effects of cigarettesmoking on cerebral oxygenation and hemodynamics: A combined study with near-infrared spec-troscopy and transcranial doppler sonography. J. Neurol. Sci. 205, 71–75.
TRAN, Y., BOORD, P., MIDDLETON, J., AND CRAIG, A. 2004. Levels of brain wave activity (8-13Hz) in persons with spinal cord injury. Spin. Cord 42, 73–79.
TREJO, L. J., ROSIPAL, R., AND MATTHEWS, B. 2006. Brain–computer interfaces for 1-D and2-D cursor control: Designs using volitional control of the EEG spectrum or steady-state visualevoked potentials. IEEE Trans. Neur. Syst. Rehab. Engin. 14, 225–229.
U.S. CENSUS BUREAU 2009. Press Release: Americans with Disabilities Act.WALDROP, J. AND STERN, S. M. 2003. Disability status: 2000. In Census 2000 Brief. U.S. Census
Bureau, Washington, DC, 12.
ACM Transactions on Accessible Computing, Vol. 2, No. 4, Article 16, Pub. date: June 2010.

Assessing Fit of Nontraditional Assistive Technologies · 16: 31
WEISKOPF, N., MATHIAK, K., BOCK, S. W., SCHARNOWSKI, F., VEIT, R., GRODD, W., GOEBEL,R., AND BIRBAUMER, N. 2004. Principles of a brain-computer interface (BCI) based on real-timefunctional magnetic resonance imaging (fMRI). IEEE Trans. Biomed. Engin. 51, 966–970.
WHITE, J. M. AND RUMBOLD, G. R. 1988. Behavioral effects of histamine and its antagonists:A review. Psychopharmacol. 95, 1–14.
WOLPAW, J. R., BIRBAUMER, N., MCFARLAND, D. J., PFURTSCHELLER, G., AND VAUGHAN, T. M.2002. Brain-computer interfaces for communication and control. Clin. Neurophys. 113, 767–791.
WORDNET GLOSSARY. In Wordnet Search 3.0, G. A. Miller, Ed. Princeton University,Princeton, NJ.
WORLD HEALTH ORGANIZATION 1980. International Classification of Impairments, Disabilities,and Handicaps.
YOGI, M. M. 2005. The Transcendental Meditation (TM) Program. Maharishi Vedic EducationDevelopment Corporation.
Received August 2009; revised December 2009, February 2010; accepted February 2010
ACM Transactions on Accessible Computing, Vol. 2, No. 4, Article 16, Pub. date: June 2010.
Copyright © 2022 FDOKUMEN




















