90 ISSN 2252-541 85 HUBUNGAN INTERPROFESIONAL ...
39
JST Kesehatan, Januari 2017, Vol. 7 No. 1 : 85 – 90 ISSN 2252-541 85 HUBUNGAN INTERPROFESIONAL KOLABORASI DENGAN PELAKSANAAN CATATAN PERKEMBANGAN PASIEN TERINTEGRASI DI RSUD. PROF. DR. H.M. ANWAR MAKKATUTU KABUPATEN BANTAENG The Relationship between Interprofesional Collaboration and the Integrated Record of Patient Progress at Prof. dr. H.M. Anwar Makkatutu Local Public Hospital in Bantaeng Yani Lestari 1 , Ariyanti Saleh 2 , Syahrir A. Pasinringi 3 1 RSUD. Prof. Dr. H.M. AnwarMakkatutu Kabupaten Bantaeng (Email: [email protected]) 2 Dosen Program Studi Ilmu Keperawatan Universitas Hasanuddin, Makassar (Email: [email protected]) 3 Dosen Program Studi Ilmu Keperawatan Universitas Hasanuddin, Makassar (Email: [email protected]) ABSTRAK Model rekam medik terintegrasi merupakan standar penilaian mutu rumah sakit, sehingga setiap rumah sakit diharapkan dapat mengembangkan model ini demi terpenuhinya standar mutu pelayanan kesehatan. Penelitian ini bertujuan menganalisis Hubungan Interprofesional Koloborasi terhadap pelaksanaan catatan perkembangan pasien terintegrasi di Ruang Rawat inap RSUD. Prof. Dr. H.M. Anwar Makkatutu Kabupaten Bantaeng. Penelitian ini menggunakan metode kuantitatif dengan pendekatan cross sectional study. Jumlah sampel sebanyak 81 orang dengan berbagai profesi di ruang perawatan bedah, anak, interna, neuro dan obgin RSUD. Prof. Dr. H.M. Anwar Makkatutu Kabupaten Bantaeng. Pengumpulan data dilakukan melalui pengisian kusioner dan observasi untuk memperoleh data sosial demografi dan penilaian pelaksanaan IPC serta catatan perkembangan pasien terintegrasi. Hasil penelitian dengan analisis uji chi-Square dan uji spearman correlation yang menunjukkan pelaksanaan kolaborasi interprofesional berjalan baik dalam pengisian catatan perkembangan pasien terintegrasi dengan kekuatan korelasi kuat dan arah kekuatan positif dilihat dari aspek kerjasama yaitu 98,6% (p=0,000) dengan nilai korelasi r=0,635,aspek kemitraan 97,2% (p=0,000) nilai korelasi r=0,590, aspek koordinasi 98,6% (p=0,000) nilai korelasi r=0,686 dan aspek pengambilan keputusan bersama 95,9% (p=0,001) dengan nilai r=0,531. Kata kunci: IPC, Interprofessional Collaboration, Catatan perkembambangan pasien terintegrasi ABSTRACT A model of integrated medical record is a standard hospital quality ratings, so that every hospital is expected to develop this model by fulfillment of quality standards of health care.This study aims to analyze the relationship between Interprofesional collaboration and the integrated record of patient progress in the patient rooms of Prof. Dr. H.M. Anwar Makkatutu Local Public Hospital in Bantaeng. The Research used the quantitative method with the cross sectional study approach. It involved 81 sample of 81 from various professions in the surgical treatment, pediatric, internal medicine, neurologi and Obstetrics and gynocology rooms of Prof. Dr. H.M. Anwar Makkatutu Local Public Hospital in Bantaeng.The data about social demography conditions were collected with questionnaires and observations. There was also and assessment of IPC and the integrated record of patient progress. The results of chi- square analysis and Spearman correlation test showed that the Interprofesional Collaboration has been well Implemented in the integrated record of patient progress, with a strong correlation and positive strength direction, in terms of collaboration aspect (98.6%, p = 0.000, r=0,635), partnership aspect (97.2%, p= 0.000, r=0,590), coordination aspect (98.6%, p = 0.000, r=0.686), and shared decision-making aspect (95.9%, p = 0.001, r=0.531). Keywords: IPC, interprofessional Collaboration, integrated record of patient improvement
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of 90 ISSN 2252-541 85 HUBUNGAN INTERPROFESIONAL ...

JST Kesehatan, Januari 2017, Vol. 7 No. 1 : 85 – 90 ISSN 2252-541
85
HUBUNGAN INTERPROFESIONAL KOLABORASI DENGAN PELAKSANAAN CATATANPERKEMBANGAN PASIEN TERINTEGRASI DI RSUD. PROF. DR. H.M. ANWAR
MAKKATUTU KABUPATEN BANTAENG
The Relationship between Interprofesional Collaboration and the Integrated Record of Patient Progress atProf. dr. H.M. Anwar Makkatutu Local Public Hospital in Bantaeng
Yani Lestari1, Ariyanti Saleh2, Syahrir A. Pasinringi3
1RSUD. Prof. Dr. H.M. AnwarMakkatutu Kabupaten Bantaeng (Email: [email protected])2Dosen Program Studi Ilmu Keperawatan Universitas Hasanuddin, Makassar (Email: [email protected])
3Dosen Program Studi Ilmu Keperawatan Universitas Hasanuddin, Makassar (Email: [email protected])
ABSTRAK
Model rekam medik terintegrasi merupakan standar penilaian mutu rumah sakit, sehingga setiap rumah sakit diharapkandapat mengembangkan model ini demi terpenuhinya standar mutu pelayanan kesehatan. Penelitian ini bertujuanmenganalisis Hubungan Interprofesional Koloborasi terhadap pelaksanaan catatan perkembangan pasien terintegrasi diRuang Rawat inap RSUD. Prof. Dr. H.M. Anwar Makkatutu Kabupaten Bantaeng. Penelitian ini menggunakan metodekuantitatif dengan pendekatan cross sectional study. Jumlah sampel sebanyak 81 orang dengan berbagai profesi diruang perawatan bedah, anak, interna, neuro dan obgin RSUD. Prof. Dr. H.M. Anwar Makkatutu Kabupaten Bantaeng.Pengumpulan data dilakukan melalui pengisian kusioner dan observasi untuk memperoleh data sosial demografi danpenilaian pelaksanaan IPC serta catatan perkembangan pasien terintegrasi. Hasil penelitian dengan analisis uji chi-Squaredan uji spearman correlation yang menunjukkan pelaksanaan kolaborasi interprofesional berjalan baik dalam pengisiancatatan perkembangan pasien terintegrasi dengan kekuatan korelasi kuat dan arah kekuatan positif dilihat dari aspekkerjasama yaitu 98,6% (p=0,000) dengan nilai korelasi r=0,635,aspek kemitraan 97,2% (p=0,000) nilai korelasir=0,590, aspek koordinasi 98,6% (p=0,000) nilai korelasi r=0,686 dan aspek pengambilan keputusan bersama 95,9%(p=0,001) dengan nilai r=0,531.
Kata kunci: IPC, Interprofessional Collaboration, Catatan perkembambangan pasien terintegrasi
ABSTRACT
A model of integrated medical record is a standard hospital quality ratings, so that every hospital is expected to developthis model by fulfillment of quality standards of health care.This study aims to analyze the relationship betweenInterprofesional collaboration and the integrated record of patient progress in the patient rooms of Prof. Dr. H.M.Anwar Makkatutu Local Public Hospital in Bantaeng. The Research used the quantitative method with the crosssectional study approach. It involved 81 sample of 81 from various professions in the surgical treatment, pediatric,internal medicine, neurologi and Obstetrics and gynocology rooms of Prof. Dr. H.M. Anwar Makkatutu Local PublicHospital in Bantaeng.The data about social demography conditions were collected with questionnaires andobservations. There was also and assessment of IPC and the integrated record of patient progress. The results of chi-square analysis and Spearman correlation test showed that the Interprofesional Collaboration has been wellImplemented in the integrated record of patient progress, with a strong correlation and positive strength direction, interms of collaboration aspect (98.6%, p = 0.000, r=0,635), partnership aspect (97.2%, p= 0.000, r=0,590), coordinationaspect (98.6%, p = 0.000, r=0.686), and shared decision-making aspect (95.9%, p = 0.001, r=0.531).
Keywords: IPC, interprofessional Collaboration, integrated record of patient improvement

Yani Lestari ISSN 2252-541
86
PENDAHULUANRumah sakit merupakan sarana
penyelenggaraan pembangunan kesehatan.Pelayanan kesehatan yang bermutu merupakantanggung jawab pemberi pelayanan kesehatansecara komperhensif, baik itu dari dokter, perawat,nutrisionist, terapi, dan profesi kesehatan lainnya(Pohan, 2015). Perkembangan ilmu pengetahuandan teknologi, serta perkembangan masyarakatyang semakin kritis, menyebabkan rumah sakitharus melakukan berbagai inovasi dalam rangkamenghasilkan pelayanan bermutu bagi pasien.Salah satu indikator penilaian akreditasi yangmencerminkan mutu pelayanan kesehatan adalahrekam medik (KARS, 2012).
Pomey (2010), menemukan fakta bahwaakreditasi bermanfaat dalam memulai peningkatanmutu berkelanjutan, kepemimpinan dalampeningkatan mutu, dan memberi kesempatankepada staf untuk mengembangkan berbagaipeluang yang dapat menunjang terlaksananyabeberapa program yang menjadi kreteria penilaianstandar akreditasi rumah sakit seperti halnyadengan penggunaan rekam medik secaraterintegrasi. Sesuai dengan penelitian yangdilakukan oleh Mishra (2015), yangmenyimpulkan bahwa sistem pencatatan rekammedis yang tidak terintegrasi dapat menyebabkanantara unit satu dengan lainnya tidak efisien dalampengerjaanya karena data yang diinput dibuatberulang mulai dari admission, poliklinik danpelaporan di rekam medis. Sedangkan sistemrekam medis secara terintegrasi dapat memberikankesempatan bagi tenaga profesional gunamembuat keputusan korektif dan keputusan klinisdalam rangka menganalisis dan mempertahankankondisi pasien.
Melihat berbagai kenyataan yang adaperlu dilakukan inovasi dalam pencatatan rekammedik, sehingga bisa berdampak pada mutupelayanan kesehatan. Berdasarkan KomiteAkreditasi Rumah Sakit di Indonesia yangmengacu kepada standar JCI, model rekam medikterintegrasi merupakan standar penilaian muturumah sakit, sehingga setiap rumah sakitdiharapkan dapat mengembangkan model ini demiterpenuhinya standar mutu pelayanan kesehatan.Salah satu bagian dari status pasien terintegrasiadalah pelaksanaan catatan perkembangan pasiensecara terintegrasi.
Praktek residensi di RSUD Prof. Dr. H.M.Anwar Makkatutu Kabupaten Bantaeng 2015diperoleh bahwa salah satu penyebab tidakoptimalnya pelaksanaan MPKP adalah belumterlaksananya sistem pencatatan perkembanganpasien secara terintegrasi yang merupakan bentukdari pelaksanaan praktek koloborasiinterprofesional yang merupakan salah satu bagianpenilaian akreditasi. Berdasarkan data awal yangdiperoleh dari Kabid Keperawatanmengemukakan bahwa pelaksanaaninterprofesional kolaborasi dan implementasicatatan perkembangan pasien terintegrasidilaksanakan mulai bulan maret 2016 sejalandengan penggunaan status pasien terintegrasi.
Berdasarkan uraian diatas penilititertarik untuk melakukan penelitian tentang“Hubungan Interprofesional Kolaborasi DenganPelaksanaan Catatan Perkembangan PasienTerintegrasi Di RSUD. Prof. Dr. H.M. AnwarMakkatutu Bantaeng”.
BAHAN DAN METODELokasi dan Desain Penelitian
Penelitian ini dilaksanakan di RSUD.Prof. Dr. H.M. Anwar Makkatutu Bantaeng.Penelitian ini menggunakan jenis penelitian noneksperimental, dengan pendekatan kuantitatif,deskriptif korelasi dan desain cross sectional.Populasi dan Sampel
Populasi dalam penelitian ini adalahsemua pemberi pelayanan kesehatan yangmemberikan pelayanan kesehatan pada pasien diruang perawatan RSUD Prof. Dr. H.M. AnwarMakkatutu Bantaeng. Sampel adalah Petugaskesehatan yaitu profesi dokter, perawat/bidan,nutrisionis, dan fisioterafi di ruang perawataninterna, perawatan bedah, saraf, anak dan obginyang terdiri 81 orang. Pengambilan sampelmenggunakan pendekatan proportionate stratifiedrandom sampling.Teknik Pengumpulan Data
Data primer diperoleh dengan carapengisian kuesioner dan observasi. Data sekunderdiperoleh dari instansi terkait yaitu RSUD Prof.Dr. H.M. Anwar Makkatutu BantaengAnalisis dan Penyajian data
Analisa data dilakukan dengan programSPSS 21 for Windows dan uji statistik denganmenggunakan uji univariat dengan frekuensi, ujibivariat chi-square, dan uji spearmen correlation.

IPC, Interprofessional Collaboration, Catatan perkembambangan pasien terintegrasi ISSN 2252-541
87
HASILAnalisa Univariat
Tabel 1 menunjukkan bahwa sebagianbesar responden terdiri dari dewasa awal 56 orang(69,1%), mayoritas perempuan yaitu 62 orang(76,5%). Berdasarkan lama kerja respondensebagian besar responden >3 tahun yaitu 60 orang(74,1%). Responden berdasarkan pendidikanterbanyak adalah D3 yaitu sebanyak 43 orang(43,1%), berdasarkan profesi responden perawat50 orang (61,7%), bidan 13 orang (13,0%), dokter7 orang (8,6%), Fisioterapist 5 orang (6,2%),nutrisionist 6 orang (7,4%). Pada masing-masingvariabel memperlihatkan hasil bahwa mayoritasresponden dengan kerjasama yang baik yaitusebanyak 73 orang (90,1%), kemitraan 72responden (88,9%) responden yang memilikikoordinasi baik sebanyak 71 orang (87,7%),dalam pengambilan keputusan bersama rata-rataresponden memiliki data yang baik yaitu 91,4%atau 74 orang, dan pelaksanaan catatanperkembangan pasien terintegrasi sebesar 91,4%atau sebesar 74 responden.
Tabel 1. Distribusi Frekuensi KarakteristikResponden Tenaga Kesehatan Berdasarkan Umur,Jenis Kelamin, Pendidikan, Lama Kerja, DanJenis Profesi Di RSUD. Prof. Dr. H.M. AnwarMakkatutu Kabupaten Bantaeng (N=81)
Tabel 2 memperlihatkan bahwa mayoritasresponden dengan kerjasama yang baik yaitu
sebanyak 73 orang (90,1%) dan 8 orang dengankerjasama kurang (9,9%). Sebanyak 72 (88,9%)responden memiliki kemitraan yang baik, dankurang 9 orang (11,1%). Responden dengankoordinasi baik sebanyak 71 orang (87,7%)selebihnya kurang (12,3%) atau 10 responden.Dalam pengambilan keputusan bersama rata-rataresponden memiliki data yang baik yaitu 91,4%atau 74 orang, sedangkan yang kurang sebesar8,6% atau sebanyak 7 orang dan pelaksanaancatatan perkembangan pasien terintegrasi yanglengkap sebesar 91,4% atau 74 responden.
Tabel 2. Distribusi Responden BerdasarkanVariabel Kolaborasi Interprofesional meliputiKerjasama, Kemitraan, Koordinasi, PengambilanKeputusan Bersama di RSUD Prof. Dr. H.M.Anwar Makkatutu Bantaeng
Analisa BivariatTabel 3 menunjukkan nilai p=0,000,
(p<0,05) yang berarti ada hubungan antarakerjasama dengan pelaksanaan catatanperkembangan pasien terintegrasi. Nilai korelasir=0,635 menunjukkan kekuatan korelasi kuatdengan arah korelasi yang positif yang berartisemakin baik kerjasama dalam kolaborasiinterprofesional maka semakin baik pulapelaksanaan catatan perkembangan pasienterintegrasi.
Tabel 3. Hubungan Kolaborasi InterprofesionalAspek Kerjasama, Kemitraan, Koordinasi,Pengambilan keputusan bersama DenganPelaksanaan Catatan Perkembangan PasienTerintegrasi
KarakteristikJumlah
n %
Umur Remaja akhir (17-25 thn)Dewasa awal (26-35)Dewasa akhir (36-45 thn) Lansiaawal (46-55 thn)
1056123
12,369,114,83,7
Jenis Kelamin Laki-lakiPerempuan
1962
23,576,5
Pendidikan D3S1S2NersSpesialis
43121
187
43,114,81,2
22,28,6
Lama kerja < 3 thn
> 3 thn
2160
25,974,1
Profesi tenagaKesehatan
Dokter
Perawat
BidanNutrisionistFisioterafist
7501365
8,661,716,07,46,2
Sumber : Data primer 2016
Variabel PenelitianJumlah
n = 81 %Kerjasama
Baik 73 90,1Kurang 8 9,9
KemitraanBaik 72 88,9Kurang 9 1,1
KoordinasiBaik 71 87,7Kurang 10 12,3
Pengambilan KeputusanBersama
Baik 74 91,4Kurang 7 8,6
Catatan perkembanganTerintegrasi
Lengkap 74 91,4Tidak Lengkap 7 8,6
Sumber : Data Primer 2016
Yani Lestari ISSN 2252-541
88
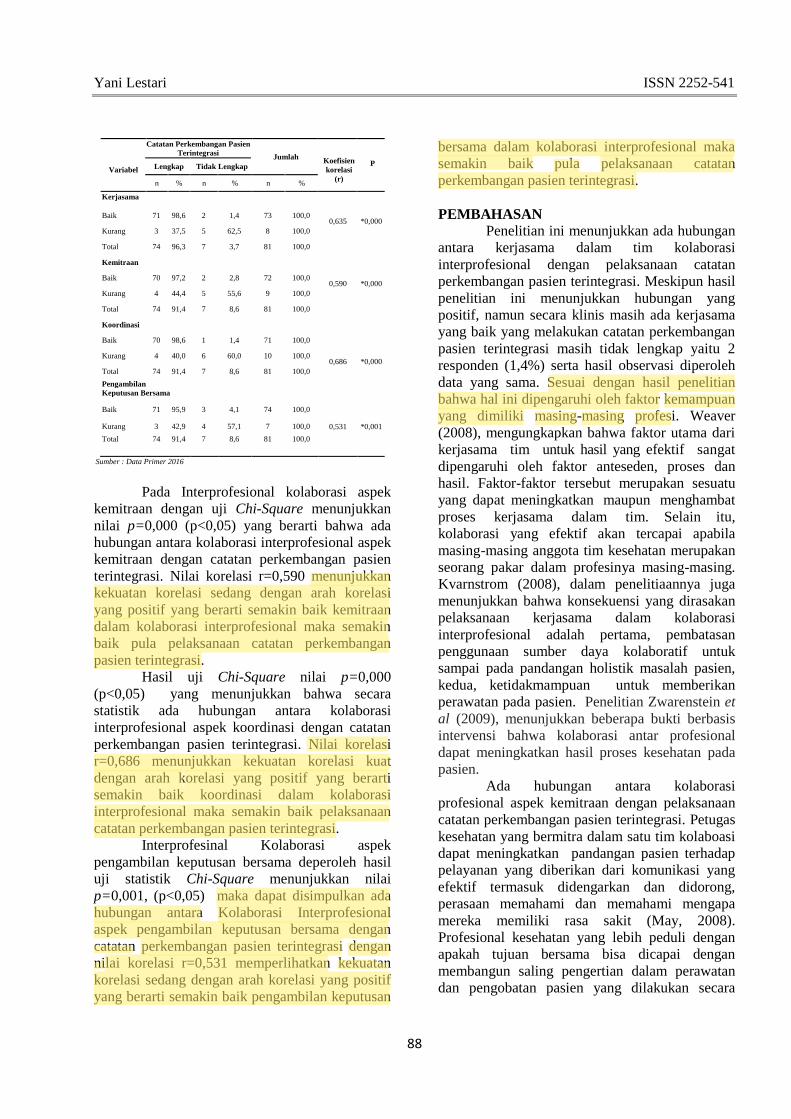
Pada Interprofesional kolaborasi aspekkemitraan dengan uji Chi-Square menunjukkannilai p=0,000 (p<0,05) yang berarti bahwa adahubungan antara kolaborasi interprofesional aspekkemitraan dengan catatan perkembangan pasienterintegrasi. Nilai korelasi r=0,590 menunjukkankekuatan korelasi sedang dengan arah korelasiyang positif yang berarti semakin baik kemitraandalam kolaborasi interprofesional maka semakinbaik pula pelaksanaan catatan perkembanganpasien terintegrasi.
Hasil uji Chi-Square nilai p=0,000(p<0,05) yang menunjukkan bahwa secarastatistik ada hubungan antara kolaborasiinterprofesional aspek koordinasi dengan catatanperkembangan pasien terintegrasi. Nilai korelasir=0,686 menunjukkan kekuatan korelasi kuatdengan arah korelasi yang positif yang berartisemakin baik koordinasi dalam kolaborasiinterprofesional maka semakin baik pelaksanaancatatan perkembangan pasien terintegrasi.
Interprofesinal Kolaborasi aspekpengambilan keputusan bersama deperoleh hasiluji statistik Chi-Square menunjukkan nilaip=0,001, (p<0,05) maka dapat disimpulkan adahubungan antara Kolaborasi Interprofesionalaspek pengambilan keputusan bersama dengancatatan perkembangan pasien terintegrasi dengannilai korelasi r=0,531 memperlihatkan kekuatankorelasi sedang dengan arah korelasi yang positifyang berarti semakin baik pengambilan keputusan
bersama dalam kolaborasi interprofesional makasemakin baik pula pelaksanaan catatanperkembangan pasien terintegrasi.
PEMBAHASANPenelitian ini menunjukkan ada hubungan
antara kerjasama dalam tim kolaborasiinterprofesional dengan pelaksanaan catatanperkembangan pasien terintegrasi. Meskipun hasilpenelitian ini menunjukkan hubungan yangpositif, namun secara klinis masih ada kerjasamayang baik yang melakukan catatan perkembanganpasien terintegrasi masih tidak lengkap yaitu 2responden (1,4%) serta hasil observasi diperolehdata yang sama. Sesuai dengan hasil penelitianbahwa hal ini dipengaruhi oleh faktor kemampuanyang dimiliki masing-masing profesi. Weaver(2008), mengungkapkan bahwa faktor utama darikerjasama tim untuk hasil yang efektif sangatdipengaruhi oleh faktor anteseden, proses danhasil. Faktor-faktor tersebut merupakan sesuatuyang dapat meningkatkan maupun menghambatproses kerjasama dalam tim. Selain itu,kolaborasi yang efektif akan tercapai apabilamasing-masing anggota tim kesehatan merupakanseorang pakar dalam profesinya masing-masing.Kvarnstrom (2008), dalam penelitiaannya jugamenunjukkan bahwa konsekuensi yang dirasakanpelaksanaan kerjasama dalam kolaborasiinterprofesional adalah pertama, pembatasanpenggunaan sumber daya kolaboratif untuksampai pada pandangan holistik masalah pasien,kedua, ketidakmampuan untuk memberikanperawatan pada pasien. Penelitian Zwarenstein etal (2009), menunjukkan beberapa bukti berbasisintervensi bahwa kolaborasi antar profesionaldapat meningkatkan hasil proses kesehatan padapasien.
Ada hubungan antara kolaborasiprofesional aspek kemitraan dengan pelaksanaancatatan perkembangan pasien terintegrasi. Petugaskesehatan yang bermitra dalam satu tim kolaboasidapat meningkatkan pandangan pasien terhadappelayanan yang diberikan dari komunikasi yangefektif termasuk didengarkan dan didorong,perasaan memahami dan memahami mengapamereka memiliki rasa sakit (May, 2008).Profesional kesehatan yang lebih peduli denganapakah tujuan bersama bisa dicapai denganmembangun saling pengertian dalam perawatandan pengobatan pasien yang dilakukan secara
Variabel
Catatan Perkembangan PasienTerintegrasi Jumlah Koefisien
korelasi(r)
Lengkap Tidak Lengkap P
n % n % n %
Kerjasama
Baik 71 98,6 2 1,4 73 100,00,635 *0,000
Kurang 3 37,5 5 62,5 8 100,0
Total 74 96,3 7 3,7 81 100,0
Kemitraan
Baik 70 97,2 2 2,8 72 100,00,590 *0,000
Kurang 4 44,4 5 55,6 9 100,0
Total 74 91,4 7 8,6 81 100,0
Koordinasi
0,686 *0,000
Baik 70 98,6 1 1,4 71 100,0
Kurang 4 40,0 6 60,0 10 100,0
Total 74 91,4 7 8,6 81 100,0
PengambilanKeputusan Bersama
Baik 71 95,9 3 4,1 74 100,0
0,531 *0,001Kurang 3 42,9 4 57,1 7 100,0
Total 74 91,4 7 8,6 81 100,0
Sumber : Data Primer 2016

IPC, Interprofessional Collaboration, Catatan perkembambangan pasien terintegrasi ISSN 2252-541
89
bersama-sama (Jeffrey & Foster, 2012). Dalampenelitiannya Merrigan et al (2016), di rumahsakit anak Philadelphia menunjukkan bahwakemitraan dalam kolaborasi antar profesi untukmembantu rancangan, menilai, dan memajukanperawatan dalam pelayanan kepada pasien dankeluarga. Penelitian Igumbor et al (2014),menunjukkan kemampuan bermitra dokter danpetugas kesehatan lainnya untuk secara efektifmempertahankan hasil pengobatan dan perawatanpasien dan berpotensi memberikan kontribusiuntuk pengobatan pasien HIV dengan mekanismedukungan yang relevan. Demikian pula penelitianBond et al (2012), menyimpulkan bahwakemitraan dalam kolaborasi memiliki potensiuntuk meningkatkan akses, kualitas, dan efisiensidalam perawatan kesehatan. Kemitraan lebihtersebut harus dikembangkan dan dievaluasisecara mendalam, dan pelajaran yang dapat secaraluas dibagi untuk memandu para pembuatkebijakan.
Secara statistik diketahui ada hubunganantara kolaborasi interprofesional aspekkoordinasi dengan pelaksanaan catatanperkembangan pasien terintegrasi. Kebutuhanmengkoordinasikan berasal dari berbagaispesialisasi. Aspek spesialisasi pengetahuan yangberbeda ini, membutuhkan penggabungan, berupatransfer informasi secara medis dan sosialsehingga pelayanan yang diberikan kepada pasienlebih komprehensif (Morris & Boussebbaas,2010). Sesuai dengan penelitian Perry & Robben(2012), menyatakan bahwa dari hasil wawancarabanyak peserta wawancara yang mengungkapkanbahwa terjadi peningkatan kolaborasi antara paraprofesional dengan disiplin lain. Hu (2014), dalampenelitiannya yang menggunakan pendekatanmulti metode untuk menganalisis dampak daripelayanan pasien secara terintegrasi dilayanansosial dengan melibatkan berbagai profesi,diperoleh hasil bahwa koordinasi dengan berbagaitim kesehatan lain dalam hal pelayanan terhadappasien dapat meningkatkan perbaikan dalamfungsi fisik dan meningkatkan kepuasan pasiendari 82% menjadi 85%.
Hasil penelitian menunjukkan bahwasecara statistik ada hubungan antara pengambilankeputusan bersama dengan pelaksanaan catatanperkembangan pasien terintegrasi (p=0,001). Nilaikorelasi r=0,531 menunjukkan kekuatan korelasisedang dengan arah korelasi yang positif yang
berarti semakin baik pengambilan keputusanbersama dalam kolaborasi interprofesional makasemakin baik pelaksanaan catatan perkembanganpasien terintegrasi. Pengambilan keputusan dalamhal pengisian lembar catatan perkembanganpasien terintegrasi menunjukkan paling banyakpada kategori baik (95,9%). PenelitianWahyuningsih (2013), menunjukkan bahwapengambilan keputusan memiliki pengaruh positifterhadap kinerja para petugas kesehatan. Hal inidapat dilihat pula pada hasil lembar observasibahwa lebih dari separuh petugas kesehatan dalampengisian lembar terintegrasi berada dalamkategori lengkap. Penelitian Dominick et al(2012), menyimpulkan bahwa pengambilankeputusan bersama dalam kolaborasiinterprofesional dalam hal perawatan pasien yangtertuang dalam dokumentasi terintegrasimemerlukan waktu agak lama, kurangnyainformasi berpusat pada pasien yang menjaditantangan struktural penting untuk pengambilankeputusan bersama. Menurut penelitianMoisoglou et al (2014), bahwa perawat dandokter tidak memiliki pandangan yang samamengenai efektivitas komunikasi dan peran dalamproses pengambilan keputusan dari pasien perawatperawatan.
KESIMPULAN DAN SARANPenelitian ini menyimpulkan secara
statistik maupun secara klinik terdapat hubunganinterprofesional kolaborasi baik dari aspekkerjasama, kemitraan, koordinasi maupunpengambilan keputusan bersama denganpelaksanaan catatan perkembangan pasien secaraterintegrasi. Perlu pengembangan modelinterprofesional kolaborasi yang baku di RSUDProf. Dr. H.M. Anwar Makkatutu KabupatenBantaeng dan adanya kebijakan-kebijakan rumahsakit yang mendukung pelaksanaan IPC yangdapat meningkatkan kemampuan tenaga kesehatandalam hal skill dan sikap yang mampuberkolaborasi sehingga pelaksanaan IPC dapatlebih baik.Menyajikan efektifitas sistem teknologiinformasi dalam melakukan pencatatan sertapendokumentasian perkembangan pasienterintegrasi menggunakan sistem komputerisasisebagai sarana komunikasi antar tim kesehatankhususnya keperawatan dalam pemberian asuhankeperawatan secara komprehensif dan profesional.Dibuatkan sistem pengembangan Sumber Daya

Yani Lestari ISSN 2252-541
90
Manusia (SDM) dengan melakukan berbagaiprogram pelatihan berkesinambungan danpendidikan terkait IPC dan pelaksanaan catatanperkembangan pasien terintegrasi kepada seluruhtenaga kesehatan yang terlibat. Meningkatkankerjasama perawat, dokter maupun tenagakesehatan lainnya dalam kegiatan formal daninformal untuk menjalin keakraban dankomunikasi yang efektif.Penelitian terkaitinterprofesional kolaborasi dan pelaksanaancatatan perkembangan terintegrasi masih jarangdilakukan, diharapkan ke depan penelitian dengantopik ini akan lebih banyak.
DAFTAR PUSTAKABond C., Alison B., & David K. (2012).
Prescribing And Partnership With Patients:British Journal Of Clinical Pharmacology.DOI:10.1111/j.1365-2125.2012.04330.x
Dominick L., Suepattra G., May R., Caroline T.,& Glyn E. (2012) Authoritarian PhysiciansAndPatients’ Fear Of BeingLabeled‘Difficult’ Among Key ObstaclesToShared Decision Making: Health Affairs DOI10.1377.2011.0576.
Hu X. (2014). The Effect of Breast Cancer HealthEducation on Knowledge, Attitudes, andPractice: Community Health Center. JournalCancer Education. 29:375-381 DOI10.1007/s13187-014-0622-1.
Igumbor J., Pascoe S., Rajap S., Townsend W., &Sargent J. (2014). A South African Public-Private Partnership HIV Treatment Model:Viability and SuccessFactors
Jeffrey J. & Foster N. (2012). A QualitativeInvestigationof Physical Therapists’Experiences And Feelings OfManagingpatients With Nonspecific LowBack Pain. Physical Therapy
Kvarnstrom S. (2008). Difficulties InCollaboration: A Critical Incident Study OfInterprofessional Healthcare Teamwork:Journal Of Interprofessional Care. 22(2):191 – 203.
Komisi Akreditasi Rumah Sakit. (2012). PanduanPenyusunan Dokumen Akreditasi. 2012
May S. (2008). Patient Satisfaction WithManagement Ofback Pain Main. Part 2: An
Explorative, Qualitative Stud Into Patients’Satisfaction With Physiotherapy.Physiotherapy 87,10–20.
Moisoglou I., Gikopolou D., Lazakidou A., &Prezerakos P. (2014). The Assessment OfNurses’ Work Environment: The Case of aGreek General Hospital. Hemodialysis Unit,General Hospital of Lamia: Greece.
Merrigan K., Elizabeth A., & Steinmiller. (2016).Kids Care: A Behavioral Model ToStrengthen Patient And Familypartnerships:Family Matters.
Mishra D. (2015). Understanding SecurityFailures of Two Autenthication and KeyAgreement Schemes for Telecare MedicineInformation System. Springer ScienceBusiness Media: New York.
Morris F. & Boussebbaas. (2010). CoordinationOf Physicians' Operational Activities: AContingency Perspective.doi.10.1108/01443571111111919.
Pohan I. (2015). Jaminan mutu LayananKesehatan : Dasar-dasar Pengertian danPenerapan. EGC: Jakarta.
Pomey. (2010). Does Accreditation StimulateChange? A Study of Impact of theAccreditation Process on Canadian HealthCare Organizations. Licensee BioMedCentral Ltd.
Perry & Robben. (2012). Impact OfInterprofessional Education OnCollaboration Attitudes, Skills, And BehaviorAmong Primary Care Professionals. IssueJournal Of Continuing Education In TheHealth Professions 32 (3) 196–204.
Wahyuningsih. (2013). Kepercayaan DanPengambilan Keputusan Terhadap KinerjaPerawat. 2nd International Seminar onQuality and Affordable Education (ISQAE2013).
Weaver T. (2008). Enhancing MultipleDisciplinary Teamwork. Nursing Outlook,56(3), pp.108-114.e2.
Zwarenstein M., Goldman J., & Reeves S. (2009).Interprofessional collaboration:effects ofpractice-based interventions on professionalpractice and healt care outcomes.doi:10.1002/14651858.CD000072.
Prosiding Seminar Nasional Unimus (Volume 1, 2018)
e-ISSN: 2654-3257 p-ISSN: 2654-3168
Peningkatkan Komunikasi dalam Pelaksanaan Interprofessional
Collaboration melalui Catatan Perkembangan Pasien Terintegrasi Improving Communication in The Implementation of Interprofessional Collaboration with
Universitas Diponegoro Semarang
Mahasiswa Magister Keperawatan ([email protected])1, Dosen Kepemimpinan dan
Manajemen Keperawatan2
Abstrak
Latar Belakang : IPC adalah kemitraan antara tenaga kesehatan dengan latar belakang
profesi yang berbeda dan bekerja sama untuk memecahkan masalah kesehatan dan
menyediakan pelayanan kesehatan. Namun kenyataannya di beberapa rumah sakit besar di
Indonesia masih belum tampak kolaborasi tim. Salah satu faktor yang menghambat
pelaksanaan kolaborasi interprofesi adalah karena buruknya komunikasi antar profesi.
Tujuan : Memberikan gambaran upaya dalam peningkatan komunikasi dalam pelaksanaan
interprofessional Collaboration
Metode : Metode yang digunakan pada makalah ini menggunakan studi literature review.
Literatur yang digunakan didapatkan dari Science Direct, Google Scholarrodan Jurnal
Kedokteran Indonesia dari tahun 2004 sampai tahun 2017. Pencarian literatur dilakukan
dengan kata kunci transformasional leadership, Interprofessional Collaboration (IPC),
Komunikasi dan catatan perkembangan pasien terintegrasi.
Hasil dan Pembahasan : Upaya yang dilakukan untuk meningkatkan komunikasi dalam
pelaksanaan interprofessional collaboration adalah dengan menggunakan catatan
perkembangan pasien terintegrasi (CPPT). Metode pencatatan terintegrasi ini diharapkan
dapat meningkatkan komunikasi efektif antar profesi, pencatatan dilakukan lebih optimal,
meminimalkan mis komunikasi, dan meningkatkan keselamatan pasien yang berdampak
kepada mutu pelayanan.
Kesimpulan : Peningkatan komunikasi dalam praktek interprofessional collaboration dapat
ditingkatkan dengan penerapan catatan perkembangan pasien terintegrasi
Kata kunci :Transformasional Leadership, Interprofessional Collaboration (IPC),
Komunikasi Dan Catatan Perkembangan Pasien Terintegrasi.
Abstract
Background : IPC is a partnership between health workers from different background to
collaborate solving health problem together and providing health service. But in reality, in
few big hospitals in Indonesia, there is no good team cooperation shown. One obstacle of
inter-profession collaboration practice is because of the lack of communication between the
profession.
Goals :To give big picture of how to improve communication in inter-profession
collaboration practice.
Method :Method used in this paper is literature review study. Literatures used are from
Science Direct, Google Scholarro and Indonesia Medical Journal from 2004 until 2017.
Literature search is done with keywords as follow, transformational leadership,
Interprofessional Collaboration (IPC), communication, and integrated patient development
notes.
Result and Study : Efforts made to develop communication in Interprofessional
Collaboration practice is by using integrated patient development notes (CPPT). This method
Integrated Patient Development Notes
Imaningtyas Ridar1, Agus Santoso
2
~ 144 ~
http://prosiding.unimus.ac.id

Prosiding Seminar Nasional Unimus (Volume 1, 2018)
e-ISSN: 2654-3257 p-ISSN: 2654-3168
is expected to develop effective communication between profession, notes recording is done
more optimal, minimalize miss communication, and develop patient safety which has impact
to service quality.
Summary :communication development in interprofessional collaboration practice can be
done with the use of integrated patient development notes.
Keywords :Transformational Leadership, Interprofessional Collaboration (IPC),
Communication And Integrated Patient Development Notes
PENDAHULUAN
Menurut UU nomor 44 tahun 2009 pasal 1 ayat 1 tentang rumah sakit, pengertian
rumah sakit adalah institusi yang memberikan pelayanan kesehatan paripurna yang
menyediakan pelayanan melalui rawat jalan, rawat inap dan gawat darurat. Pelayanan
kesehatan yang paripurna menurut UU nomor 44 tahun 2009 pasal 1 ayat 3 adalah pelayanan
yang meliputi pelayanan promotif, preventif, kuratif dan rehabilitatif.
Pelayanan kesehatan yang diberikan di rumah sakitdilakukan oleh berbagai profesi
tenaga kesehatan. Berbagai profesi yang terlibat dalam pelayanan kesehatan terdiri dari
tenaga medis, tenaga psikologi klinis, tenaga keperawatan, tenaga kebidanan, tenaga
kefarmasian, tenaga gizi, tenaga keterapian fisik, tenaga keteknisian medis dan teknik
biomedika (UU Nomor 36 tahun 2014). Pelayanan kesehatan di rumah sakit merupakan
pelayanan dari berbagai profesi kesehatan yang berkolaborasi untuk mengoptimalkan
pelayanan kesehatan (Sitorus, 2006).Institute of Medicine (IOM) dan World Health
Organization (WHO) meminta tenaga kesehatan profesional untuk bekerja sama dalam
Interprofessional Collaboration (IPC) untuk meningkatkan pelayanan kesehatan (IOM, 2010).
Kolaborasi Interprofesi atau Interprofessional Collaboration (IPC) adalah kemitraan
antara orang dengan latar belakang profesi yang berbeda dan bekerja sama untuk
memecahkan masalah kesehatan dan menyediakan pelayanan kesehatan (Morgan et al, 2015).
Menurut WHO, IPC terjadi saat berbagai profesi kesehatan bekerja sama dengan pasien,
keluarga dan komunitas untuk menyediakan pelayanan komprehensif dan berkualitas tinggi
(WHO, 2010). IPC dimaksudkan untuk mencapai tujuan dan memberi manfaat bersama bagi
semua yang terlibat (Green and Johnson, 2015).
Tenaga kesehatan harus melakukan praktek kolaborasi dengan baik dan tidak
melaksanakan pelayanan kesehatan sendiri-sendiri (Orchar et al, 2005 dan Fatalina, 2015).
Dampak dari kolaborasi yang buruk adalah tingginya kesalahan dalam pembuatan resep di
Indonesia (sebanyak 98,69%) akibat dari kesalahan dalam penulisan resep dokter, apoteker
yang tidak tepat dalam penyiapan obat dan pemberian informasi mengenai obat tersebut
(Easton, 2009). Selain itu menurut National Prescribing Service Australia menyebutkan
bahwa 6% kasus yang terjadi di rumah sakit disebabkan karena efek samping obat dan
kesalahan selama perawatan. Hal ini muncul karena buruknya kolaborasi antar profesi
kesehatan (Perwitasari, 2010). WHO (2009) menjelaskan bahwa 70-80% kesalahan yang
terjadi di pelayanan kesehatan diakibatkan oleh buruknya komunikasi dan kurangnya
pemahaman anggota tim. Kolaborasi tim yang baik dapat mengurangi masalah patient safety
(WHO, 2009).
Kurangnya penerapan kolaborasi interprofesi sesuai dengan penelitian yang dilakukan
oleh Fatalina (2015) yang berjudul Persepsi dan Penerimaan Interprofessional Collaborative
Practice di Bidang Maternitas pada Tenaga Kesehatan. Penelitian tersebut dilakukan di RSUP
Dr. Sardjito. Penelitian tersebut mengatakan bahwa belum terlaksana kolaborasi interprofesi
dan masih dilaksanakannya stereotyping kolaborasi tradisional yang beranggapan bahwa
~ 145 ~
http://prosiding.unimus.ac.id
Prosiding Seminar Nasional Unimus (Volume 1, 2018)
e-ISSN: 2654-3257 p-ISSN: 2654-3168
dokter adalah leader dan decision making dan pelaksana adalah perawat, bidan dan farmasi.
Selain itu masih kurangnya komunikasi yang terjalin antar anggota profesi.
Salah satu faktor yang menghambat pelaksanaan kolaborasi interprofesi adalah karena
buruknya komunikasi antar profesi (Setiadi, 2017). Komunikasi adalah aspek terpenting
dalam kolaborasi antar profesi. Tanpa komunikasi yang efektif maka perawatan pasien akan
menjadi kehilangan arah dan berdasar pada stereotype semata (Cross-Sudworth, 2007).
Komunikasi dalam pelaksanaan IPC juga merupakan unsur penting dalam peningkatan
kualitas perawatan dan keselamatan pasien (Reni, A 2010).
Menurut The American Nurses Association (ANA, 2010), komunikasi menjadi
standar dalam praktek keperawatan profesional. Komunikasi interprofesi menjasi kompetensi
inti dalam praktek kolaborasi interprofesi. Untuk melakukan kolaborasi yang baik dibutuhkan
komunikasi secara efektif dengan tim kesehatan lain, sehingga dapat melakukan tindakan
pelayanan kesehatan yang aman dan efektif. Hal ini juga diatur dalam Permenkes
1691/MENKES/PER/VIII/2011 yang menyebutkan bahwa salah satu dari sasaran
keselamatan pasien adalah komunikasi yang efektif.
Berdasarkan latar belakang tersebut, penulis ingin mengetahui mengenai gambaran
upaya yang dilakukan untuk meningkatkan komunikasi dalam kolaborasi interprofesi.
METODE
Metode yang digunakan pada makalah ini menggunakan studi literature review.
Literatur yang digunakan didapatkan dari Science Direct,Google Scholardan Jurnal
Kedokteran Indonesia. Sumber yang diambil dari tahun 2006 sampai tahun 2015. Pencarian
literatur dilakukan dengan kata kunci transformasional leadership, Interprofessional
Collaboration (IPC), Komunikasi dan catatan perkembangan pasien terintegrasi.
HASIL DAN PEMBAHASAN
A. Peran transformasional leadership
Beberapa penelitian menyebutkan bahwa faktor yang mempengaruhi komunikasi
dalam pelaksanaan kolaborasi interprofesi adalah kepemimpinan, pengetahuan
(Kesrianti, 2014) dan lama bekerja (Hilda, 2017).
Kepemimpinan transformasional memiliki peran dalam peningkatan komunikasi.
Kepemimpinan transformasional memberikan inspirasi, motivasi untuk mencapai tujuan
dan merubah sikap, perilaku dan nilai-nilai dasar bawahannya untuk melakukan
perubahan (Suryo, 2010). Kepemimpinan transformasional yang dimiliki para tenaga
kesehatan berfokus pada membangun hubungan dan komunikasi dengan orang lain dan
menciptakan perubahan dengan menekankan nilai-nilai(To, Tse & Ashkanasy,
2015).Kepemimpinan transformasional mendukung sejauh mana anggota melibatkan diri
dalam komunikasi dua arah seperti mendengar, memotivasi dan melibatkan orang lain
dalam pengambilan keputusan (Ratih, 2008).
Pemerintah memiliki peran penting dalam peningkatan komunikasi antar profesi
kesehatan. Pemerintah mengeluarkan Permenkes 1691/MENKES/PER/VIII/2011 yang
menjelaskan tentang keselamatan pasien rumah sakit. Pada Permenkes
1691/MENKES/PER/VIII/2011 pasal 7 ayat 2 dijelaskan bahwa salah satu standar
keselamatan pasien adalah komunikasi staf kesehatan untuk mencapai keselamatan
pasien.
Komisi Akreditasi Rumah Sakit pada tahun 2017 juga mengatur tentang komunikasi
dan pertukaran informasi antar profesi kesehatan. Komunikasi dan informasi penting
selama pelaksanaan proses asuhan dikomunikasikan dengan menggunakan catatan
perkembangan pasien terintegrasi (CPPT).
~ 146 ~
http://prosiding.unimus.ac.id

Prosiding Seminar Nasional Unimus (Volume 1, 2018)
e-ISSN: 2654-3257 p-ISSN: 2654-3168
B. Komisi Akreditasi Rumah Sakit
Komisi Akreditasi Rumah Sakit (KARS, 2017) di standar MKE (Manajemen
Komunikasi dan Edukasi) 5 mengatur tentang manajemen komunikasi dan edukasi antar
profesi kesehatan. Standar MKE 5 menjelaskan bahwa informasi asuhan pasien dan hasil
asuhan harus dikomunikasikan antar profesi kesehatan selama bekerja dalam shift.
Komunikasi antar profesi kesehatan penting untuk berjalannya proses asuhan.
Komunikasi dan informasi antar profesi kesehatan dituangkan dalam catatan
perkembangan pasien terintegrasi (CPPT).
C. Catatan Perkembangan PasienTerintegrasi
Sarana komunikasi antar profesi kesehatan adalah dokumentasi.
Pendokumentasian merupakan bukti pelayanan kesehatan yang berupa pencatatan,
pelaporan dan penyimpanan kegiatan dalam pengelolaan klien (Klehr, 2009).
Salah satu tanda kurangnya komunikasi antar profesi adalah masih digunakannya
dokumentasi dalam catatan yang terpisah antar anggota profesi. Catatan yang terpisah
kurang menggambarkan respon pasien dalam kegiatan antar profesi kesehatan (Iyer,
2004). Penelitian yang dilakukan oleh Mishra (2015) menunjukkan bahwa sistem
pendokumentasian yang tidak terintegrasi menyebabkan ketidak efisienan karena data
yang diinput berulang dalam pelaporan di rekam medis.
Untuk meningkatkan kualitas komunikasi antar profesi, digunakan catatan
profesional kesehatan menjadi satu yang disebut catatan perkembangan pasien
terintegrasi.Catatan Perkembangan Pasien Terintegrasi adalah dokumentasi antar profesi
pemberi asuhan keperawatan mengenai perkembangan pasien dalam bentuk terintegrasi
dalam rekam medis pasien (KARS, 2017). Rencana perawatan yang terintegrasi dan
tunggal lebih terukur dan lebih baik daripada rencana perawatan yang terpisah. Rencana
perawatan pasien harus mencerminkan sasaran perawatan yang khas untuk masing-
masing individu sehingga penilaian dan rencana ulang dapat dilakukan (Iyer, 2004).
Paradigma pasien saat ini mulai berubah dengan memusatkan pada perhatian pada
pasien (Patient Centered Care). Pelayanan patient centered care ini di terapkan dalam
bentuk catatan perkembangan pasien terintegrasi (CPPT) yang dikerjakan oleh para
profesional pemberi asuhan keperawatan interprofesi (Komisi Akreditasi Rumah Sakit,
2017).
Dengan adanya catatan terintegrasi mewajibkan setiap profesi melakukan
pencatatan pada dokumen yang sama. Metode pencatatan terintegrasi ini diharapkan
dapat meningkatkan komunikasi efektif antar profesi, pencatatan dilakukan lebih
optimal, meminimalkan mis komunikasi, dan meningkatkan keselamatan pasien yang
berdampak kepada mutu pelayanan (Frelita, 2011).
Terdapat hubungan antara peningkatan komunikasi kolaborasi interprofesi
dengan pelaksanaan catatan perkembangan pasien terintegrasi. Interprofesi kesehatan
memiliki spesialisasi pengetahuan yang berbeda. Catatan perkembangan pasien
terintegrasi memfasilitasi transfer informasi antar petugas kesehatan sehingga pelayanan
yang diberikan kepada pasien lebih komprehensif dan terarah (Morris & Boussebbas,
2010). Penelitian yang dilakukan oleh Perry & Robben (2012) menyatakan bahwa
dengan adanya catatan perkembangan pasien terintegrasi meningkatkan kolaborasi antar
profesi kesehatan. Penelitian lain yang dilakukan Lestari (2017) juga menunjukkan
terdapat korelasi kuat antara komunikasi antar profesi kesehatan dengan pelaksanaan
catatan perkembangan pasien terintegrasi.
Penelitian yang dilakukan oleh Lasmani (2014) mengenai evaluasi implementasi
catatan terintegrasi di RSUP Dr Sardjito menyebutkan bahwa catatan terintegrasi tidak
~ 147 ~
http://prosiding.unimus.ac.id

Prosiding Seminar Nasional Unimus (Volume 1, 2018)
e-ISSN: 2654-3257 p-ISSN: 2654-3168
terisi lengkapsebanyak 14,6%. Alasan mengenai tidak terisinya catatan terintegrasi
adalah karena keterbatasan waktu dan tenaga petugas kesehatan, dokter merasa bahwa
kolom yang disediakan terlalu kecil dan sempit sehingga dokter merasa lebih pas
menggunakan format sebelumnya yang tidak terintegrasi.Selain itu dokter merasa format
yang ditulis belum sesuai dan berbeda dengan format sebelumnya.
Mengatasi hal tersebut, pihak rumah sakit menyepakati bahwa format catatan
terintegrasi lebih diperlebar. Selain itu, pihak RSUP Dr. Sardjito akan mengoptimalkan
proses sosialisasi tentang panduan rekam medis menurut standar WHO, peraturan
kementerian kesehatan dan kebijakan internal RSUP Dr. Sardjito kepada seluruh profesi
kesehatan terkait. Dalam sosialisasi tersebut, petugas kesehatan diharapkan langsung
melakukan dokumentasi setelah melakukan proses asuhan keperawatan sehingga dapat
mengefisienkan waktu. Sosialisasi tersebut juga menekankan antar profesi kesehatan
agar memiliki kesadaran profesi untuk mendokumentasikan dalam catatan terintegrasi
sesuai dengan tanggung gugat dan tanggung jawab (Lasmani, 2014). Menurut
Notoatmodjo, seseorang mengadopsi perilaku baru dibutukan pengetahuan, kesadaran
dan sikap positif agar perilaku baru tersebut dapat bersifat langgeng (Notoatmodjo,
2007).
KESIMPULAN
Peningkatan komunikasi secara efektif dengan tim kesehatan lain dibutuhkan dalam
pelaksanaan Interprofessional Collaboration sehingga petugas kesehatan dapat melakukan
tindakan pelayanan kesehatan yang aman dan efektif. Upaya yang dilakukan untuk
meningkatkan komunikasi antar profesi adalah dengan catatan perkembangan pasien
terintegrasi.
Menurut Komite Akreditasi Rumah Sakit, Catatan Perkembangan Pasien Terintegrasi
adalah dokumentasi antar profesi pemberi asuhan keperawatan mengenai perkembangan
pasien dalam bentuk terintegrasi dalam rekam medis pasien. Rencana perawatan yang
terintegrasi dan tunggal lebih terukur dan lebih baik daripada rencana perawatan yang
terpisah. Rencana perawatan pasien harus mencerminkan sasaran perawatan yang khas untuk
masing-masing individu sehingga penilaian dan rencana ulang dapat dilakukan. Komisi
Akreditasi Rumah Sakit juga mengatur catatan perkembangan pasien terintegrasi dalam
standar MKE (Manajemen Komunikasi dan Edukasi) 5.
REFERENSI
Cross-Sudworth F. 2007. Maternity linkworkers: a Cinderella service? RCM
Midwives10(7):325–327.
Easton K, Margon T. 2009. Medication Errors in Outpatients of A Government Hospital in
Yogyakarta Indonesia. 1(1) : 8 – 10
Fatalina Femi, Sunartini, Widyandana, Sedyowinarso Mariyono. 2015. Persepsi dan
penerimaan Interprofessional Collaborative Practice Bidang Maternitas pada tenaga
kesehatan. Universitas Gadjah Mada : Fakultas Kedokteran. Jurnal Kedokteran Indonesia.
Frelita, G., Situmorang, T.J., & Silitonga, D.S. 2011. Joint Commission International
Accreditation Standards for Hospitals, 4 th ed. Oakbrook Terrace, Illinois 60181 U.S.A.
Institute of Medicine, 2010. The future of nursing: leading change, advancing health.
Retrieved from.http://iom.nationalacademies.org/Reports/2010/The-Future-of-Nursing-
Leading-Change-Advancing-Health.aspx.
Iyer Patricia W, & Nancy H Camp. 2004. Dokumentasi Keperawatan. Jakarta: EGC.
Klehr, J, dkk. 2009. Menggambarkan dokemuntasi pada catatan sistem elektronik rekam
medis yang memberikan catatan elektronik kesehatan.
Komisi Akreditasi Rumah Sakit. 2017. Standar Nasional Akreditasi Rumah Sakit Edisi 1.
~ 148 ~
http://prosiding.unimus.ac.id
Prosiding Seminar Nasional Unimus (Volume 1, 2018)
e-ISSN: 2654-3257 p-ISSN: 2654-3168
Lasmani, Patricia., Haryanti, Fitri., Lazuardi, Lutfan. 2014. Evaluasi Implementasi Rekam
Medis Terintegrasi di Instalasi Rawat Inap RSUP Dr. Sardjito Yogyakarta.Jurnal
Manajemen Pelayanan Kesehatan, Vol. 17, No. 1 Maret 2014
Lestari, Yani., Saleh, Ariyanti., Pasinringi, Syahrir. 2017. Hubungan Interprofessional
Kolaborasi dengan Pelaksanaan Catatan Perkembangan Pasien Terintegrasi di RSUD
Prof Dr H.M Anwar Makkatutu Kabupaten Bantaeng. JST Kesehatan, Januari 2017, Vol.
7 No. 1 : 85 – 90.
Morgan, S., Pullon, S., McKinlay, E., 2015. Observation of interprofessional collaborative
practice in primary care teams: an integrative literature review. Int. J. Nurs. Stud. 52 (7),
1217–1230.
Morris F & Boussebbass. 2010. Coordination of Physicians Operational Activities : A
Contingency Perspective.
Notoatmodjo,S. 2007. Promosi Kesehatan dan Ilmu Perilaku. Yogyakarta : Reneka Cipta.
Orchar, CA, Curran , V, Kabene, S. 2005. Creating a culture for Interdiciplinnary
Collaboration Profesional Practice. Med. Educ
Pohan I. (2015). Jaminan mutu Layanan Kesehatan : Dasar-dasar Pengertian dan
Penerapan.Jakarta : EGC
Perry & Robben. 2012. Impact of Interprofessional Education On Collaboration Attitudes,
Skills and Behavior Among Primary Care Professionals. Journal Of Continuing Education
In The Health Professions 32 (3) 196 – 204.
Ratih, Agnes. 2008. Hubungan Komunikasi Antar Pribadi dengan Peningkatan Kinerja
Karyawan PT Asa Globalindo Pratama. Universitas Pembangunan Nasional : FISIP.
Reni, Arya; Yudianto, Kurniawan; Somantri, Irman. 2010. Efektifitas Pelaksanaan Komu-
nikasi dalam Kolaborasi Antara Perawat dan Dokter di Ruang Rawat Inap Rumah Sakit
Umum Sumedang. Jurnal unpad.ac.id/mku/article. Vol. 12, No. 1 Maret 2010– September
2010 Hal 36,
Rokhmah, Noor Ariyani. 2017. Komunikasi Efektif dalam Praktek Kolaborasi Interprofesi
sebagai Upaya Meningkatkan Kualitas Pelayanan. Universitas Diponegoro. Journal of
Health Studies, Vol 1 No 1 Maret 2017 : 65 – 71.
Setiadi, Adji dkk. 2017. Factors contributing to interprofessional collaboration in Indonesia
health centres : A focus group study. Journal of Interprofessional Education & Practice 8
(2017) 69-74
Sitorus, R. 2006. Model Praktik Keperawatan Professional di Rumah Sakit. Jakarta : EGC
To, M., Tse, H., & Ashkanasy, N. (2015). A multilevel model of transformational leadership,
affect, and creative process behavior in work teams. The Leadership Quarterly, 26, 543–
556.
Undang-Undang Republik Indonesia Nomor 44 tahun 2009 tentang Rumah Sakit.
Undang-Undang Republik Indonesia Nomor 36 tahun 2014 tentang Tenaga Kesehatan.
World Health Organisation (WHO), 2010. Framework for Action on Interprofessional
Education and Collaborative Practice. World Health Organisation, Geneva.
World Health Organisation (WHO), 2009. Human Factors in Patient Safety Review of topics
and Tools.World Health Organisation, Geneva.
~ 149 ~
http://prosiding.unimus.ac.id

32 Puput Risti Kusumaningrum, Edi Dharmana, Madya Sulisno, 2018. JNKI, Vol. 6, No. 1, Tahun 2018, 33-42
The Implementation of Integrated Patient Progress Notes in Interprofessional Collaborative Practice
Puput Risti Kusumaningrum1, Edi Dharmana2, Madya Sulisno3
1STIKes Muhammadiyah Klaten, Mahasiswa Magister Keperawatan FK UNDIP2Fakultas Kedokteran Universitas Diponegoro Semarang.
3Departemen Ilmu Keperawatan, Fakultas Kedokteran, UNDIP, Semarang.E-mail: [email protected]
AbstrakInterprofessional Collaborative Practice (IPCP) adalah bentuk kolaborasi dan komunikasi di antara profesi kesehatan dalam pendekatan terkoordinasi untuk berbagai pengambilan keputusan tentang masalah kesehatan untuk memastikan bahwa perawatan yang diberikan dapat diandalkan dan berkelanjutan. Implementasi IPCP membutuhkan media pendukung, yaitu, dengan mengintegrasikan catatan perkembangan pasien ke dalam yang terintegrasi. Oleh karena itu, petugas kesehatan dapat berkolaborasi dengan menggunakan catatan perkembangan pasien terintegrasi ini. Penelitian ini bertujuan untuk mengeksplorasi dokumentasi implementasi catatan perkembangan pasien terintegrasi di IPCP oleh dokter, perawat, apoteker, ahli gizi, dan fi sioterapis di ruang rawat inap Rumah Sakit UGM, Yogyakarta. Penelitian ini menggunakan desain kualitatif dengan pendekatan fenomenologis hermeneutik. Sampel direkrut menggunakan purposive sampling, yang melibatkan 14 peserta utama. Data dikumpulkan melalui wawancara mendalam dengan wawancara semi terstruktur dan dianalisis menggunakan teknik analisis isi. Hasil mengidentifi kasi 4 tema terkait, termasuk: (1) pemahaman, (2) kepatuhan, (3) media penggerak IPCP, (4) beban kerja, sikap, perilaku dan kebijakan (sosialisasi) yang menghambat implementasi IPCP. Studi ini menyimpulkan bahwa mendokumentasikan catatan perkembangan pasien terintegrasi dapat mendorong praktik kolaboratif untuk mengoptimalkan layanan terintegrasi.
Kata Kunci: Catatan Perkembangan Pasien, Praktik Kolaboratif Interprofesional, Ilmu Multidisiplin
AbstractInterprofessional Collaborative Practice (IPCP) is a form of collaboration and communication among the health professions in a coordinated approach to various decision-making on health issues to ensure that the care provided is reliable and sustainable. The implementation of IPCP requires supporting media, i.e., by integrating the patient progress notes into the integrated one. Therefore, the health workers can collaborate by the use of this integrated patient progress note. This study aimed to explore the documentation implementation of integrated patient progress notes in IPCP by doctors, nurses, pharmacists, nutritionists, and physiotherapists in the inpatient wards of UGM Hospital, Yogyakarta. This study used a qualitative design with a hermeneutic phenomenological approach. The samples were recruited using purposive sampling, involving 14 main participants. The data were collected through in-depth interviews with semistructured interviews and analyzed using the content analysis technique. The results identifi ed 4 related themes, including: (1) the understanding, (2) the compliance, (3) the driving media of IPCP, (4) the workloads, attitudes, behaviors and policies (socialization) which inhibited the implementation of IPCP.
ISSN 2354-7642 (Print), ISSN 2503-1856 (Online)Jurnal Ners dan Kebidanan IndonesiaTersedia online pada: http://ejournal.almaata.ac.id/index.php/JNKI
INDONESIAN JOURNAL OF NURSINGAND MIDWIFERY

The Implementation of Integrated Patient Progress Notes in Interprofessional Collaborative Practice 33
This study concluded that documenting the integrated patient development record could foster collaborative practices to optimize the integrated services.
Keywords: Patient Development Record, Interprofessional Collaborative Practice, Multidisciplinary Science
Article info:Article submitted on July 04, 2017Articles revised on August 06, 2017 Articles received on September 26, 2017DOI: http://dx.doi.org/10.21927/jnki.2018.6(1).32-41
INTRODUCTION Interprofessional Collaborative Practice
( IPCP) is a form of co l laborat ion and communication among the health professions in a coordinated approach to various decision-making on health issues to ensure that the care provided is reliable and sustainable (1)(2).
IPCP is very important in making collective decisions and improving effectiveness and effi ciency in the delivery of service to patients. In this matter, each health profession involved should have a sense of trust, totality, tolerance, fairness, and togethernessso that the service provided can be optimal (3). This is in line with Doughertyet al. (2005) who argued that collaboration could decrease mortality risk and increased patient satisfaction (4).
Barriers in interprofessional collaboration can be a major cause of medical errors, nursing errors or adverse events (5). The Institute of Medicine (2000) reported the patient mortality rate in hospitals reached to 44,000 to 98,000 patients each year. In 2010, The Center for Medicare and Medicaid reported 13.5% of patients experienced adverse events, and the costs they had to spend to resolve the problems reached $ 4.4 billion (US Department of Health and Human Services, 2010). In 2011, the Joint Commission Sentinel Event Statistic received 1,243 reports; 60% of them were due to problems in collaboration (6).
IPCP has not ye t been opt ima l ly implemented so far. One of the issues emerging
is because many health professions still use a type of medical recordwhich is separated with care records and other health profession records used to document the condition of the patient (7)(8). The written records do not describe detail information about the patient’s responses and what the patient feels. Even, some health professionals may not read the record since it is writtenon separate sheets (7)(9)(10).
The 2012 hospital accreditation guideline states caregiver professionals should implement an integrated patient care, which includes a dynamic care process and involvement of many healthcare practitioners such as nurses, doctors, midwives, nutritionists, pharmacists, therapists, and many others. This integrated care may also involve otherwork units and services described in the care record (11). Dealing with this issue, it is essential to optimize the implementation of IPCP among the health professions. Therefore, the care record can be written more optimally since all health professions write in the same sheet, and thus minimize miscommunication, reduce the number of adverse events, and in the end, it can improve patient safety and give impacts on improving the quality of services (12)(13).
MATERIALS AND METHODSThis study used a qualitative design with
a phenomenological approach. The population included medical specialists, nurses, pharmacists, nutritionists and physiotherapists in UGM Hospital

34 Puput Risti Kusumaningrum, Edi Dharmana, Madya Sulisno, 2018. JNKI, Vol. 6, No. 1, Tahun 2018, 33-42
Yogyakarta.The samples were recruited using a nonprobability sampling with purposive sampling technique (14)(15). Fourteen participants were recruited based on the inclusion criteria, which included (1) having work experience of ≥ 1 year, (2) obtaining a degree of education of either medical specialist, nurse (at least DIII), pharmacist (pharmacist profession), nutritionist (bachelor), and physiotherapist (at least DIII), and (3) expressing a voluntary participation as evidenced by signing an informed consent prior to the study. Meanwhile, the exclusion criteria were the health professions who were on leave, refused to participate, or could not continue the interviews due to illness, and expressed refusal to have next interview sessions.
The data were analyzed using a content analysis technique, which included transcribing the interviews, determining meaning units to search for relationships between words, sentences or paragraphs, and performing data abstractions to form several themes.
RESULTS AND DISCUSSIONThe participants involved in this study
were 14, consisting of three medical specialists, three nurses, twopharmacists, three nutritionists, and three physiotherapists.This study revealed four themes, describing the implementation of integrated patient progress notes (IPPN) in the implementation of IPCP. The followings are the resulted themes.
Adequate understanding of the caregiver professional is importantin the implementation of integrated patient progress note (IPPN) documentation in IPCP by the role of each health professionUnderstanding of IPPN
The participants revealed thatintegrated patient progress note is such a form of communication among the health professions
which is written on the similar sheet and provides information on the progress of the patient until the patient discharge from the hospital. It is then not necessary for the health workers to go through different forms used for the patient monitoring. As a result, the health professional can manage the patient comprehensively to provide patient-centered care.A total of 10 health professions stated this accordingly, as follow:
“…it is information about the progress of the patient which is writtenon the same sheet” (P01)“…there is no need to fl ip back the paper because the information is completed.” (P04)“…it is a note or evidence that we (health professional) monitorthe patient on a day-to-day basis.” (P05)“…the note is written on the same sheet for all health professions that are patient-oriented.” (P06)“…it is more completed, and provides integrated patient progress note; more comprehensive.” (P07)“…it is an integrated record in which the health professions are patient-centered.” (P14).
The Caregiver Professionals
All participants indicated that all medical or paramedical professions taking care of or handling the patients write and read the IPPN.
“...all professions can write and read on the same sheet, i.e., IPPN.” (P02) “...thereis medical or paramedical personnel.” (P05)“… all health professions taking care of the patient write on the same sheet.” (P08)“…it is written by all health professions on the same sheet.” (P13).
The Implementation
In implementing the documentation of integrated patient progress notes, all health
The Implementation of Integrated Patient Progress Notes in Interprofessional Collaborative Practice 35
professions work together, discuss and coordinate each other in decision making; all health professions also have an equal position.The following statements were presented by the participants:
“In writing the note, we coordinate each other in making the decisions. We also discuss it with each other.” (P05)“In the implementation, we have discussions with all teams involved, and we workcollaboratively.” (P07)“The patient management can be performed more quickly since all health personnel cooperates with each other.” (P09).
The Role of the Health Professions
The participants stated that the fulfi llment of IPPN requires the roles of each health profession according to their respective disciplines so that collaborative practices can be created, and thus will accelerate healing and reduce the adverse events. The following statements were presented by the participants.
“… the doctor in charge of patient mainly functions to coordinate the patient problems; the others give some inputs.” (P10)“…the doctor in charge of thepatient will establish themedical diagnosis, g i v e t h e t h e r a p y, a n d m a k e adecisionregarding the treatment given to the patient as well as make a decision on the patient’s discharge from thehospital.” (P09).“The nu rses have a r o l e as acommunicatorbetween health professions, and between patients and health professions.” (P07) “My role as a physiotherapist is to educate patients to develop their self-reliance.”(P03)“I think the role of a nutritionist is to performnutritional care to patients, provide food, and give nutrition education.” (P11)
“The role of a nutritionist includes nutritional assessment, nutritional calculations, and provide adiet to the patient.” (P02)
“The physiotherapist works in the scope of the motion problem and body function.” (P04)
The understanding of the health profession about IPPN documentation in the implementation of IPCP, in general,is suitable with the concept that IPPN is information about the development of patient care which is written in the same sheet by multiple disciplines. Therefore, it provides an ease for the caregivers to access information on patient progress. This integration requires each profession to perform their duties and authority professionally (11).
In implementing IPPN, the health professionals need to cooperate, discuss, and coordinate each other in making decisions. All health professions have anequal position so that the principle of collaboration can be created. This is in line witha study by Yani Lestariet al (2017) which indicated that interprofessional collaboration was well implemented in the writing of IPPN. The study indicated a strong and positive correlation in the aspect of cooperation, partnership, and decision making. Thus, better implementation of IPCP will result in better IPPN.
The health professions playing their respective fi elds of science willadvanceIPCP among the health professions, where the focus is on the patient or patient-centered care, sustainable and integrated in accordance with the concept of integrated care.
Patient-centered care requires integrated documentation that demands each profession to make a record of the patientin the same document. This method is expected to optimize IPCP among health professions. Furthermore, the fulfi llment of the record can be more optimal since all health professions write on the same

36 Puput Risti Kusumaningrum, Edi Dharmana, Madya Sulisno, 2018. JNKI, Vol. 6, No. 1, Tahun 2018, 33-42
document. This will minimize miscommunication, lower the rate of adverse events, and in the end, improve patient safety and the quality of service (13)(16). Compliance with the Integrated Patient Progress Note Implementation Requires Availability of Infrastructure and Facilities, Motivation, Evaluation and Feedback Monitoring System and Role of Case Manager.Level of Compliance
Participants revealed that the fulfi llment of patient progress note was integrated with SOAP format for medical specialists, nurses, pharmacists. Meanwhile, the physiotherapists documented the progress note with ADIME (nutritionist). They all write the date, time, signature and name. They write what they do and do what they have written. If the note is incorrectly written, they would cross it and put their initials. They also use standard abbreviations in their writing. The followings are some statements presented by the participants.
“Once I am done with the patient intervention, I immediately write it on the IPPN using ADIME format.” (P01)“After finishing a procedure to the patient, I then write it on the IPPN by writing the date, hour, and profession. Next to it, there is a column to writeaSOAP. I just put my signature and name there.” (P03)“If there is incorrect writing, I should cross it and put an initial. I should not erase it.” (P05)“If you write the abbreviated word, you shou ld use the s tandard abbreviation….” (P08).
Facilities and Infrastructures
Participants mentioned that the facilities and infrastructures are readily available as stated by some participants below:
“Yes, we are all well facilitated. There are IPPN forms which are always available in accordance withthe hospital accreditation procedure. There are also pens in the nurse station for each of us, so we don’t need to share the pen with others.” (P03)“The hospital has provided the facilities well. There are NIC/NOC books in the ward, so if we forget things, we can open the book. There is also a HER, even though it is not yet optimal in the inpatient ward. The IPPN sheets are also always available.” (P05)“Such facilities available are the IPPN sheets. They are easily accessible and never run out of the stock.” (P07).
Motivation (Reward and Punishment) Results of interviews revealed that forms of
motivation (reward&punishment) were manifested in compliments and warnings. The rewards in the form of money or punishment in the form of apay cuthave not been implemented, as stated by some participants below:
“Rewards in the form of money are not yet implemented.” (P01)“It is the commitment from us. Therefore, though there are no rewards and punishment, the program can run well.” (P03)“... The reward is not in the form of money. It is like when you are doing good, you will be given compliments. On the other hand, when you are doing something wrong, you will be given a warning.” (P08)“The money reward is not yet available. The punishment in the form of money cut is not available either.” (P13) .
Monitoring, Evaluation and Feedback System
Participants stated that the monitoring, evaluation and feedback system had been implemented such as through CMRR (Close Medical Record Review). Some participants stated the following:

The Implementation of Integrated Patient Progress Notes in Interprofessional Collaborative Practice 37
“I have attended the CMRR. It is such an activity where one representative of each health profession is to do an evaluation, including the IPPN.” (P01)“…through the medical record review, we canevaluate the completeness of IPPN.” (P02)“To my knowledge, usually there is an integrated medical records audit including IPPN especially in the face of accreditation.” (P07).
The Role of Case Manager
Participants revealed that the roles of acase managerare as facilitator, collaborator, performing monitoring and evaluation, as well as providing feedback. There were three case managers at the study site who carried out the task in accordance withtheir roles.
“There is already a case manager, who performs the evaluation and also supervision to the ward.” (P02)“There is a case manager. He is the one who checks whether there is a professional who is not yet visiting. He also does the supervision and gives a reminder.” (P04)“Here, there is also a case managerwho acts as a collaborator between health workers, and between patients and health workers.” (P09)
The compliance of the health profession in documenting the IPPN in the implementation of IPCP requires facilities and infrastructure, monitoring system, evaluation and feedback, motivation and role of case manager. This study also shows that the procedure of writing IPPN documentation has been appropriately carried out. An understanding of IPPN writing by medical specialists, nurses, pharmacists and physiotherapists using SOAP and nutritionists using ADIME indicates that this understanding is important so that the patient planning can be clearer and more directional, more communicative
and more collaborative; the interventions are clear and thus minimizeoverlapping events (17). This is congruent with a study by Patriciaet al. (2014) which found that integrated medical record makes the services more integrated, the patients are givenmore attention,andthe collaboration can be better (18).
The documentation of IPPN can be optimally implemented if there are adequate supporting facilities. The availability of such facilities and infrastructure as the documentation form/sheet, room for fi lling the IPPN, NIC/NOC books, pens for nurses in the wards are very important to motivate health professionsto carry out documentation according to the hospital standard (19).
Motivation related to reward and punishment in documenting IPPN in this study has not been structured and not yet applied. The fundamental principle of motivation is the power that drives the individual to do something to meet the need at a particular time (20). This is related to the need for such a system for IPPN documentation so that the compliance can be increased and the program runs optimally. Improving IPPN documentation can be done through monitoring and evaluation since regular and periodic monitoringand evaluation can result in some feedbacks submitted to the health profession for optimal improvement. Once the compliance behavior is developed, there will emerge positive cultureson the basis of awareness of the health professions that IPPN documentation is important to do in accordance with the standard (21).
The roleof case managers is very essential in developing positive cultures. One of the roles of case managers in implementing IPPN documentation is to monitor the fi lling of the records by the health professions of doctors, nurses, pharmacists, nutritionists,and physiotherapists. According to KARS (2015), a case manager is a hospital professional who conducts the patient service management, coordinates with the
38 Puput Risti Kusumaningrum, Edi Dharmana, Madya Sulisno, 2018. JNKI, Vol. 6, No. 1, Tahun 2018, 33-42
health professions and patient-family to meet the needs of patients and their families through communications and available resourcesto deliver quality outcomes. Some roles that a case manager should play includes the function of assessment, utility, planning, facilities,and advocacy, service coordination, evaluation and follow-up of discharge planning. A case manager should be able to coordinate all disciplines that provide services to patients to produce satisfactory and patient-centered care (22)(23). A study conducted by Miculincher, et al (2007) reported that lack of commitment of the head nurse in carrying out his duty as case manager causes 46% of non conducive services in the ward (24). Another study by Susan, K. Mc Greehan (2005) reported that out of the many number of multidisciplinary models to embrace multidisciplinary, the case manager model is the one which can be implemented (25).
IPPN as Driving Media in the Implementation of Interprofessional Collaborative Practice
Results of interviews with participants revealed that the IPPN is a medium which can be used as a drivein the implementation of the IPCP. The followings are some statements from the participants.
“It is possible to encourage the implementation of IPCP practices.” (P01)“I think it strongly supports the collaborative practice” (P06)“By reading the IPPN, there can raise the idea of a joint visite since there are things that should be discussed together for optimal results” (P08)“It can function as communication media between the health professions. The IPPN is the driving force for the implementation of IPCP.” (P11)
One of the media which can be used to facilitate the implementation of IPCP is the
IPPN. Documenting IPPN is a non-verbal communication among the health professionals and facilitate them to collaborate (26).
The statements of participants regarding the implementation of IPPN is in line with the theory that medical record documentation functions as a means of communication between health professions in providing services to patients. This communicationis inter-professional communication that aims to prevent the occurrence of misinformation, encourage interdisciplinary coordination, prevent repetitive information, and give assistance in the time management (27).
Workloads, Attitudes,and Behavior of Health Professions and Inappropriate Policy Can Threaten the Existing IPPN DocumentationWorkloads
Nine participants mentioned that the workload was an obstacle in documenting the IPPN. Some participants mentioned:
“It is really a diffi cult time when the polyclinic is full of the patients, as well as the inpatient wards. The work is just so overloaded.”(P04)“We sometimes forget to complete the IPPN due to a lot of work. Sometimes we are about to fi ll it, but then the patient calls us, or sometimes the doctor is visiting, and some other reasons. It’s a very high mobility” (P10)“Our wo rk load i s somet imes overloaded. I t is because one pharmacist should be responsible for two wards. Sometimes, the other wards or ICUs also contact us for collaboration with the pharmacists.” (P13)“As much as possible, I complete the IPPN. However, there will always be abusy time. Sometimes there are surgeries or consultation, and thus the record is not maximally fulfi lled.” (P09)

The Implementation of Integrated Patient Progress Notes in Interprofessional Collaborative Practice 39
“In addition to the IPPN, we should also write the nutritional care. Sometimes, I write the nutritional care in the nutrient installation, and the IPPN is not comprehensively written due to the busy work.” (P02).
Attitudes and Behaviors of the Health Personnel
The negative attitudes and behaviors of health professions that can inhibit the implementation of IPPN, among others are laziness, tiredness, differences in perception, forgetfulness and being in a rush. These are expressed by some patients as below:
“When there is information missing in the IPPN, probably it is because we forget or be in a hurry. There is no intention to do so.” (P06)“Sometimes I feel lazy since I have to fi ll the IPPN every day. So sometimes I don’t do it maximally.” (P11)“The inhibiting factor is the difference of perception. There is only one rep resen ta t i ve a t tend ing the socialization, so there can be adifferent perception. Sometimes we also forget NIC NOC, and we are sometimes too lazy to open the book.” (P07)“Sometimes we are doing it in a hurry, and thus the result is not appropriate with the existing standard.” (P11)
Policy (Socialization)
The results of interviews revealed that the socialization of IPPN conducted by hospital management still lackssince it has not reached all the health professions and has not been thoroughly carried out. The following statements are mentioned by the participants:
“What inhibits the program is because the policy of the hospital which only invites one representativeto be present at the socialization. There is also lack of training to improve the skills of the health professions.” (P04)
“IPPN is vigorously socialized before the accreditation; but when the accreditation is over, things go like usual.” (P05)“There is a lack of socialization through workshop/seminar/training. If there is socialization, unfortunately, only one representative, who is usually the head of theunit, is participating. After that, he/she will share the information with others, and this can lead to different perceptions.” (P08)
Based on the results of interviews with doctors, nurses, nutritionists, pharmacists,and physiotherapists, it was indicated that the workload, attitudes,and behaviors of health professions and inappropriate policies could be an obstacle if they are not fi xed immediately. A study by I Gusti AA showed that there was a relationship between knowledge, attitudes and workloadsand the completeness of documenting process (28). The health professions at UGM hospital, although they have high workload due to a large number of patients and have to share their focus to serve doctor’s visit in the inpatients and outpatients, had applied professional attitudes, i.e., prioritizing patient safety, working according to their competence, and being responsible. The health professions have played their roles regarding time allocation, roles of health professions, staff relations, adivision of authority, and joint decision making though they are not yet maximal. Un-optimal attitudes and behaviors in the documentation of IPPN were due to the workload and lack of human resources in the professions of pharmacists, nutritionists, and physiotherapists. As a result, they do not pay attention to the completeness of the document fi lling.
The po l i c ies wh ich i nh ib i t ed the implementation of IPPN include the limitation of representatives who participated in the program socialization and lack of training related to the documentation of IPPN, as well as the

40 Puput Risti Kusumaningrum, Edi Dharmana, Madya Sulisno, 2018. JNKI, Vol. 6, No. 1, Tahun 2018, 33-42
lack of SPO socialization. Every good quality management system is always based on SPO which is disseminated to all the competent parties who are to implement it. It is important for every health professionto understandand implementall patient services in accordance with the SPO, including the documentation of IPPN. SPO is a series of written and standardized work instructions on the process of organizing corporate administration, how and when to do and by whom it is implemented (28).
CONCLUSIONS AND SUGGESTIONS Conclusions
Results of the study indicated that the health professionshad performed the documentation of IPPN with a good understanding and worked in accordance with the role of each profession. Documenting IPPN should refl ect collaborative practices so that in the real practice, there will be communication, discussion, cooperation, and coordination in the joint decision making. Document ing IPPN can be a medium or tool in collaborative practice among the health professionals to better optimize the implementation of IPCP. The documentation of IPPN will be optimally implemented if they are equipped with adequate infrastructure, proper motivation, and transparent, continuous and sustainable monitoring and evaluation and feedback system, as well as the role of case manager that can facilitate and become acollaborator for all health professions. The implementation of IPPN by the health professions experienced several obstacles such as workload, attitudes,andbehaviors of the health profession that lead to negative behaviors. Furthermore, the policy related to the socialization of IPPN in the hospitalis not implemented optimally.
SuggestionThe support from hospital management is 1. badly needed. It is in the form of regular
mentoring and evaluation activitiesand providing facilities and infrastructures to support the successful documentation of IPPN. The hospital management is expected to 2. provide routine training/workshops/ seminars related to the documentation of IPPN to increase the knowledge and skill of the health personnel.The availability of reward and punishment 3. system can increase the motivation of health personnel in performing the documentation of IPPN in accordance with the standards set by the hospital.
ACKNOWLEDGMENTS The researchers would like to thank Prof.
dr. Edi Dharmana, M.Sc, Ph.D., Sp. Par (K) and Madya Sulisno, S.Kp., M. Kes as the supervisors who have provided guidance and inputs. The researchers also thanked the participants for their participation in this study.
REFERENCES Dimitriadou A. Interprofessional Collaboration 1. and Collaboration among Nursing Staff Members in Northern Greece. Int J Caring. 2008;1(3):140-146.Leticia San Martin-Rodriguez Marie-2. Dominique Beaulieu Danielle D’Amor Marcela Ferrada-Videla. The determinants of successful collaboration: A review of theoretical and empirical studies. J Interprof Care. 2005;1(May):132-147.Keith, K.M. & Skin DF. Effective collaboration 3. : The Key to Better Healthcare. Can J Nurs Leadership (CJNL). 2008; 21 (2): 51- 61. Dougherty MB, Larson E. A Review of 4. Instruments Measuring Nurse-Physician Co l labora t ion . JONA J Nurs Adm . 2005;35(5):244-253. World Health Organization. 5. World Health Statistics. 2010.

The Implementation of Integrated Patient Progress Notes in Interprofessional Collaborative Practice 41
Bleich S. Medical errors: Five Years After The 6. IOM Report. Issue Brief (Commonw Fund). 2005;(830):1-15. Huron Perth Healthcare Alliance. HPHA 7. Interprofessional Practice Model. 2011.Fewster-Thuente L and Velsor-Friedrich B. 8. Interdisciplinary Collaboration for Healthcare Professionals, Nurs. Admin. Q. 2008; 32(1): 40-48.Alligood, Martha Raile. Theoretical Nursing : 9. Development&Progress. 5th edition. 2012.Hariyati TS. Perencanaan Pengembangan 10. Dan Utilisasi Tenaga Keperawatan. Jakarta: Rajawali Pers. 2014.Pratama, Febrina Mega; Sugiyanto Z. KARS 11. Accreditation Readiness Review Section Of Communication And. 2010.JCI. Journal on Quality and Patient Safety, 12. Root Causes of Sentinel Events. 2006.Iyer Patricia W & NHC. 13. Dokumentasi Keperawatan. Jakarta : EGC; 2005.Basrowi & Suwandi. 14. Memahami Penelitian Kualitatif. Jakarta: Rineka Cipta; 2008.Sugiyono. 15. Memahami Penelitian Kualitatif. Jakarta: Alfabeta; 2010.JCI Accreditation Standards for Hospitals. 4th 16. Edition. Effective 1 January 2011 .Frelita G, Situmorang TJ, & Silitonga DS. 17. Joint Commission International Accreditation Standards for Hospitals 4 th ed., Oakbrook Terrace, Illinois 60181 U.S.A, 2011.Patricia Suti Lasmani dkk. Evaluation of 18. Integrated Medical Record Implementation Case Study in. 2014;17(1):3-8.Renta, Pagela Pascarel la. Evaluasi 19. Pelaksanaan Patient Centered Care di RS PKU Muhammadiyah Yogyakarta Unit 1. 2016.
Henki Idris Issakh & Zahrida Wiryawan. 20. Pengantar Manajemen. Edisi 2. In Media. Jakarta. 2015.Pourasghar, F., Kazemi, A., Malekafzali, h, 21. Ellenius, J., and Fors, U., (2008), What they fill in today, may not be useful tomorrow : Lesson Learned from Studying Medical records at the Woman Hospital in Tabriz, Iran, BMC public health, vol.8Komisi Akreditasi Rumah Sakit. Panduan 22. Penyusunan Dokumen Akreditasi. 2012.Komisi Akreditasi Rumah Sakit. Panduan 23. Pelaksanaan Dokter Penanggung Jawab Pelayanan (DPJP) dan Case Manajer. 2015Mikulincer, M. , & Shaver, P. R. Attachment 24. in Adulthood: Structure,Dynamics, AND Changer. New York : Guilford Publication. 2007.Susan K. McGeehan. Case Management 25. in Integrated Models Of Care.Manuscript submitted for publication. 2005.Klehr J, Hafner J, Spelz LM, Steen S, 26. Weaver K. Implementation of standardized nomenclature in the electronic medical record. Int J Nurs Terminol Classi f . 2009;20(4):169-180. doi:10.1111/j.1744-618X.2009.01132.x.Mastini , I Gusti AA Putr i . Hubungan 27. Pengetahuan, Sikap, dan Beban Kerja dengan kelengkapan Pendokumentasian Asuhan Keperawatan IRNA di Rumah Sakit Umum Pusat Sanglah Denpasar. 2013.Atmoko T. Standar Operasional Prosedur 28. (SOP) dan Jurnal Manajemen Pelayanan Kesehatan. 2011; 14(1): Akuntabilitas Kinerja Instansi Pemerintah. [Research]. 36-43. Universitas Diponegoro, Semarang. 2008

PENINGKATAN KOMUNIKASI DALAM PELAKSANAAN
INTERPROFESSIONAL COLLABORATION PADA PASIEN DI
RUMAH SAKIT
Muhaini Atmayana Purba / 181101131
ABSTRAK
Latar belakang : IPC adalah kemitraan antara tenaga kesehatan dengan latar belakang profesi
yang berbeda dan bekerja sama untuk memecahkan masalah kesehatan dan menyediakan
pelayanan kesehatan. Namun kenyataannya di beberapa rumah sakit besar di Indonesia masih
belum tampak kolaborasi tim. Salah satu faktor yang menghambat pelaksanaan kolaborasi
interprofesi adalah karena buruknya komunikasi antar profesi. Tujuan : Tujuan penulisan ini
yaitu mengidenifikasi peningkatan komunikasi dalam pelaksanaan interprofessional
collaboration pada pasien di rumah sakit. Metode : Metode yang digunakan merupakan
literatur review atau suatu perbandingan atau analisis antara satu jurnal dengan jurnal lainnya
dari berbagai sumber seperti referensi jurnal, buku teks dan e-book. Hasil : Upaya yang
dilakukan untuk meningkatkan komunikasi dalam pelaksanaan interprofessional collaboration
adalah dengan menggunakan catatan perkembangan pasien terintegrasi (CPPT). Metode
pencatatan terintegrasi ini diharapkan dapat meningkatkan komunikasi efektif antar profesi,
pencatatan dilakukan lebih optimal, meminimalkan mis komunikasi, dan meningkatkan
keselamatan pasien yang berdampak kepada mutu pelayanan. Kesimpulan : Peningkatan
komunikasi dalam praktek interprofessional collaboration dapat ditingkatkan dengan penerapan
catatan perkembangan pasien reintegrasi.
Kata Kunci : Peningkatan komunikasi, Interprofessional Collaboration (IPC), rumah sakit.
ABSTRACT
Background : IPC is a partnership between health workers with different professional
backgrounds and working together to solve health problems and provide health services. But the
reality is that in some large hospitals in Indonesia there is still no team collaboration. One factor
that hinders the implementation of interprofessional collaboration is due to poor communication
between professions. Purpose : The purpose of this paper is to identify improved
communication in the implementation of interprofessional collaboration in patients in hospitals.
Method : The method used is a literature review or a comparison or analysis of one journal with
other journals from various sources such as journal references, textbooks and e-books. Results :
Efforts made to improve communication in the implementation of interprofessional
collaboration were to use integrated patient development records (CPPT). This integrated
recording method is expected to improve effective communication between professions,
recording is carried out more optimally, minimizing mis communication, and increasing patient
safety which has an impact on service quality. Conclusion : Improved communication in
interprofessional collaboration practices can be improved by applying reintegration patient
progress notes.
Keywords : Improved communication, Interprofessional Collaboration (IPC), hospitals.

Latar Belakang
Menurut UU nomor 44 tahun
2009 pasal 1 ayat 1 tentang rumah sakit,
pengertian rumah sakit adalah institusi
yang memberikan pelayanan kesehatan
paripurna yang menyediakan pelayanan
melalui rawat jalan, rawat inap dan
gawat darurat. Pelayanan kesehatan
yang paripurna menurut UU nomor 44
tahun 2009 pasal 1 ayat 3 adalah
pelayanan yang meliputi pelayanan
promotif, preventif, kuratif dan
rehabilitatif.
Pelayanan kesehatan yang
diberikan di rumah sakitdilakukan oleh
berbagai profesi tenaga kesehatan.
Berbagai profesi yang terlibat dalam
pelayanan kesehatan terdiri dari tenaga
medis, tenaga psikologi klinis, tenaga
keperawatan, tenaga kebidanan, tenaga
kefarmasian, tenaga gizi, tenaga
keterapian fisik, tenaga keteknisian
medis dan teknik biomedika (UU
Nomor 36 tahun 2014). Pelayanan
kesehatan di rumah sakit merupakan
pelayanan dari berbagai profesi
kesehatan yang berkolaborasi untuk
mengoptimalkan pelayanan kesehatan
(Sitorus, 2006).Institute of Medicine
(IOM) dan World Health Organization
(WHO) meminta tenaga kesehatan
profesional untuk bekerja sama dalam
Interprofessional Collaboration (IPC)
untuk meningkatkan pelayanan
kesehatan (IOM, 2010).
Kolaborasi Interprofesi atau
Interprofessional Collaboration (IPC)
adalah kemitraan antara orang dengan
latar belakang profesi yang berbeda dan
bekerja sama untuk memecahkan
masalah kesehatan dan menyediakan
pelayanan kesehatan (Morgan et al,
2015).
Menurut WHO, IPC terjadi saat
berbagai profesi kesehatan bekerja sama
dengan pasien, keluarga dan komunitas
untuk menyediakan pelayanan
komprehensif dan berkualitas tinggi
(WHO, 2010). IPC dimaksudkan untuk
mencapai tujuan dan memberi manfaat
bersama bagi semua yang terlibat
(Green and Johnson, 2015).
Tenaga kesehatan harus
melakukan praktek kolaborasi dengan
baik dan tidak melaksanakan pelayanan
kesehatan sendiri-sendiri (Orchar et al,
2005 dan Fatalina, 2015).
Dampak dari kolaborasi yang
buruk adalah tingginya kesalahan dalam
pembuatan resep di Indonesia (sebanyak
98,69%) akibat dari kesalahan dalam
penulisan resep dokter, apoteker yang
tidak tepat dalam penyiapan obat dan
pemberian informasi mengenai obat

tersebut (Easton, 2009). Selain itu
menurut National Prescribing Service
Australia menyebutkan bahwa 6% kasus
yang terjadi di rumah sakit disebabkan
karena efek samping obat dan kesalahan
selama perawatan. Hal ini muncul
karena buruknya kolaborasi antar
profesi kesehatan (Perwitasari, 2010).
WHO (2009) menjelaskan bahwa 70-
80% kesalahan yang terjadi di
pelayanan kesehatan diakibatkan oleh
buruknya komunikasi dan kurangnya
pemahaman anggota tim. Kolaborasi
tim yang baik dapat mengurangi
masalah patient Safety (WHO, 2009).
Kurangnya penerapan kolaborasi
interprofesi sesuai dengan penelitian
yang dilakukan oleh Fatalina (2015)
yang berjudul Persepsi dan Penerimaan
Interprofessional Collaborative Practice
di Bidang Maternitas pada Tenaga
Kesehatan. Penelitian tersebut
dilakukan di RSUP Dr. Sardjito.
Penelitian tersebut mengatakan bahwa
belum terlaksana kolaborasi interprofesi
dan masih dilaksanakannya stereotyping
kolaborasi tradisional yang beranggapan
bahwa dokter adalah leader dan
decision making dan pelaksana adalah
perawat, bidan dan farmasi.
Selain itu masih kurangnya
komunikasi yang terjalin antar anggota
profesi. Salah satu faktor yang
menghambat pelaksanaan kolaborasi
interprofesi adalah karena buruknya
komunikasi antar profesi (Setiadi,
2017). Komunikasi adalah aspek
terpenting dalam kolaborasi antar
profesi. Tanpa komunikasi yang efektif
maka perawatan pasien akan menjadi
kehilangan arah dan berdasar pada
stereotype semata (Cross-Sudworth,
2007).
Komunikasi dalam pelaksanaan
IPC juga merupakan unsur penting
dalam peningkatan kualitas perawatan
dan keselamatan pasien (Reni, A 2010).
Menurut The American Nurses
Association (ANA, 2010), komunikasi
menjadi standar dalam praktek
keperawatan profesional. Komunikasi
interprofesi menjasi kompetensi inti
dalam praktek kolaborasi interprofesi.
Untuk melakukan kolaborasi yang baik
dibutuhkan komunikasi secara efektif
dengan tim kesehatan lain, sehingga
dapat melakukan tindakan pelayanan
kesehatan yang aman dan efektif. Hal
ini juga diatur dalam Permenkes
1691/MENKES/PER/VIII/2011 yang
menyebutkan bahwa salah satu dari
sasaran keselamatan pasien adalah
komunikasi yang efektif.

Berdasarkan latar belakang
tersebut, penulis ingin mengetahui
mengenai gambaran upaya yang
dilakukan untuk meningkatkan
komunikasi dalam kolaborasi
interprofesi.
Tujuan
Tujuan penulisan ini yaitu
mengidenifikasi peningkatan
komunikasi dalam pelaksanaan
interprofessional collaboration pada
pasien di rumah sakit.
Metode
Metode yang digunakan
merupakan literatur review atau suatu
perbandingan atau analisis antara satu
jurnal dengan jurnal lainnya dari
berbagai sumber seperti referensi jurnal,
buku teks dan e-book.
Hasil & Pembahasan
Komisi Akreditasi Rumah Sakit
(KARS, 2017) di standar MKE
(Manajemen Komunikasi dan Edukasi)
5 mengatur tentang manajemen
komunikasi dan edukasi antar profesi
kesehatan. Standar MKE 5 menjelaskan
bahwa informasi asuhan pasien dan
hasil asuhan harus dikomunikasikan
antar profesi kesehatan selama bekerja
dalam shift. Komunikasi antar profesi
kesehatan penting untuk berjalannya
proses asuhan. Komunikasi dan
informasi antar profesi kesehatan
dituangkan dalam catatan
perkembangan pasien terintegrasi
(CPPT).
Sarana komunikasi antar profesi
kesehatan adalah dokumentasi.
Pendokumentasian merupakan bukti
pelayanan kesehatan yang berupa
pencatatan, pelaporan dan penyimpanan
kegiatan dalam pengelolaan klien
(Klehr, 2009). Salah satu tanda
kurangnya komunikasi antar profesi
adalah masih digunakannya
dokumentasi dalam catatan yang
terpisah antar anggota profesi. Catatan
yang terpisah kurang menggambarkan
respon pasien dalam kegiatan antar
profesi kesehatan (Iyer, 2004).
Penelitian yang dilakukan oleh Mishra
(2015) menunjukkan bahwa sistem
pendokumentasian yang tidak
terintegrasi menyebabkan ketidak
efisienan karena data yang diinput
berulang dalam pelaporan di rekam
medis. Untuk meningkatkan kualitas
komunikasi antar profesi, digunakan
catatan profesional kesehatan menjadi
satu yang disebut catatan perkembangan
pasien terintegrasi. Catatan
Perkembangan Pasien Terintegrasi
adalah dokumentasi antar profesi
pemberi asuhan keperawatan mengenai

perkembangan pasien dalam bentuk
reintegrasi dalam rekam medis pasien
(KARS, 2017). Rencana perawatan
yang terintegrasi dan tunggal lebih
terukur dan lebih baik daripada rencana
perawatan yang terpisah. Rencana
perawatan pasien harus mencerminkan
sasaran perawatan yang khas untuk
masing-masing individu sehingga
penilaian dan rencana ulang dapat
dilakukan (Iyer, 2004).
Paradigma pasien saat ini mulai
berubah dengan memusatkan pada
perhatian pada pasien (Patient Centered
Care). Pelayanan patient centered care
ini di terapkan dalam bentuk catatan
perkembangan pasien terintegrasi
(CPPT) yang dikerjakan oleh para
profesional pemberi asuhan
keperawatan interprofesi (Komisi
Akreditasi Rumah Sakit, 2017). Dengan
adanya catatan terintegrasi mewajibkan
setiap profesi melakukan pencatatan
pada dokumen yang sama. Metode
pencatatan terintegrasi ini diharapkan
dapat meningkatkan komunikasi efektif
antar profesi, pencatatan dilakukan
lebih optimal, meminimalkan mis
komunikasi, dan meningkatkan
keselamatan pasien yang berdampak
kepada mutu pelayanan (Frelita, 2011).
Terdapat hubungan antara peningkatan
komunikasi kolaborasi interprofesi
dengan pelaksanaan catatan
perkembangan pasien terintegrasi.
Interprofesi kesehatan memiliki
spesialisasi pengetahuan yang berbeda.
Catatan perkembangan pasien
terintegrasi memfasilitasi transfer
informasi antar petugas kesehatan
sehingga pelayanan yang diberikan
kepada pasien lebih komprehensif dan
terarah (Morris & Boussebbas, 2010).
Penelitian yang dilakukan oleh Perry &
Robben (2012) menyatakan bahwa
dengan adanya catatan perkembangan
pasien terintegrasi meningkatkan
kolaborasi antar profesi kesehatan.
Penelitian lain yang dilakukan Lestari
(2017) juga menunjukkan terdapat
korelasi kuat antara komunikasi antar
profesi kesehatan dengan pelaksanaan
catatan perkembangan pasien
terintegrasi.
Kesimpulan & Saran
Peningkatan komunikasi secara
efektif dengan tim kesehatan lain
dibutuhkan dalam pelaksanaan
Interprofessional Collaboration
sehingga petugas kesehatan dapat
melakukan tindakan pelayanan
kesehatan yang aman dan efektif. Upaya
yang dilakukan untuk meningkatkan

komunikasi antar profesi adalah dengan
catatan perkembangan pasien
terintegrasi.
Menurut Komite Akreditasi
Rumah Sakit, Catatan Perkembangan
Pasien Terintegrasi adalah dokumentasi
antar profesi pemberi asuhan
keperawatan mengenai perkembangan
pasien dalam bentuk terintegrasi dalam
rekam medis pasien. Rencana
perawatan yang terintegrasi dan tunggal
lebih terukur dan lebih baik daripada
rencana perawatan yang terpisah.
Rencana perawatan pasien harus
mencerminkan sasaran perawatan yang
khas untuk masing-masing individu
sehingga penilaian dan rencana ulang
dapat dilakukan. Komisi
Akreditasi Rumah Sakit juga
mengatur catatan perkembangan pasien
terintegrasi dalam standar MKE
(Manajemen Komunikasi dan Edukasi)
5.
Daftar Pustaka
Cahyono, Suharjo. (2008) Membangun
Budaya Keselamatan Pasien
dalam Praktik Kedokteran.
Yogyakarta : Kanisius
Easton K, Margon T. 2009. Medication
Errors in Outpatients of A
Government Hospital in
Yogyakarta Indonesia. 1(1) : 8 –
10
Fatalina Femi, Sunartini, Widyandana,
Sedyowinarso Mariyono. 2015.
Persepsi dan penerimaan
Interprofessional Collaborative
Practice Bidang Maternitas pada
tenaga kesehatan. Universitas
Gadjah Mada : Fakultas
Kedokteran. Jurnal Kedokteran
Indonesia
Iskandar, Heru, Halimi Maksum, dan
Nafisah. (2014). Faktor Penyebab
Penurunan Pelaporan Insiden
Keselamatan Pasien Rumah Sakit.
Malang : Fakultas Kedokteran
Universitas Brawijaya Malang,
2014 Nugroho, SriH.P.,
Sujianto,U. Supervisi Kepala
Ruang Model Proctor Untuk
Meningkatkan Pelaksanaan
Keselamatan Pasien. Jurnal
Keperawatan Indonesia.20,
(1):56-64
Iyer Patricia W, & Nancy H Camp.
2004. Dokumentasi Keperawatan.
Jakarta: EGC.
Klehr, J, dkk. 2009. Menggambarkan
dokemuntasi pada catatan sistem
elektronik rekam medis yang
memberikan catatan elektronik
kesehatan.
Lestari, Yani., Saleh, Ariyanti.,
Pasinringi, Syahrir. 2017.
Hubungan Interprofessional
Kolaborasi dengan Pelaksanaan
Catatan Perkembangan Pasien
Terintegrasi di RSUD Prof Dr
H.M Anwar Makkatutu
Kabupaten Bantaeng. JST
Kesehatan, Januari 2017, Vol. 7
No. 1 : 85 – 90.
Morgan, S., Pullon, S., McKinlay, E.,
2015. Observation of
interprofessional collaborative
practice in primary care teams:
an integrative literature review.
Int. J. Nurs. Stud. 52 (7), 1217–
1230.
Morris F & Boussebbass. 2010.
Coordination of Physicians
Operational Activities : A
Contingency Perspective.
Notoatmodjo, S. (2003). Pendidikan
dan Perilaku Kesehatan. Jakarta :
PT. Rineka Cipta.
Pohan I. (2015). Jaminan mutu Layanan
Kesehatan : Dasar-dasar
Pengertian dan
Penerapan.Jakarta : EGC
Perry & Robben. 2012. Impact of
Interprofessional Education On
Collaboration Attitudes, Skills
and Behavior Among Primary
Care Professionals. Journal Of
Continuing Education In The
Health Professions 32 (3) 196 –
204.
Rahayu, Sri. (2011). Pengembangan
Program Patient Safety
Berdasarkan Awareness dan
Komitmen Individu. RSUD Ibnu
Sina Kabupaten Gresik
Rachmawati, Alifa Rizqia, dkk. (2017).
ANALISIS PELAKSANAAN
TUJUH LANGKAH MENUJU
KESELAMATAN PASIEN DI
RUMAH SAKIT ISLAM
SULTAN AGUNG
SEMARANG. JURNAL
KESEHATAN MASYARAKAT
(e-Journal) Volume 5, Nomor 1
(ISSN: 2356-3346)
R.H, Simamora. (2019). Buku Ajar
Pelaksanaan Identifikasi Pasien.
Uwais Inspirasi Indonesia
R.H, Simamora. (2019). Documentation
Of Patient Identification Into The
Electronic System To Improve
The Quality Of Nursing Services.
International Jurnal Of Sciensific
& Technology
R.H, Simamora. (2019). The Influence
Of Training Handover Based
SBAR Communication For
Improving Patients Safety. Indian

Journal Of Public Health
Research & Deveropment.
Undang-Undang Republik Indonesia
Nomor 44 tahun 2009 tentang
Rumah Sakit.
Undang-Undang Republik Indonesia
Nomor 36 tahun 2014 tentang
Tenaga Kesehatan.
Widajat, Rochmanadji. (2009). Being a
Great and Sustainable Hospital.
Jakarta : PT Gramedia Pustaka
Utama
World Health Organisation (WHO),
2010. Framework for Action on
Interprofessional Education and
Collaborative Practice. World
Health Organisation, Geneva.
World Health Organisation
(WHO), 2009. Human Factors in
Patient Safety Review of topics
and Tools.World Health
Organisation, Geneva.

OR I G I N A L R E S E A R C H
How to Optimize Integrated Patient Progress
Notes: A Multidisciplinary Focus Group Study in
IndonesiaThis article was published in the following Dove Press journal:
Journal of Multidisciplinary Healthcare
Hajjul Kamil 1
R Rachmah 1
Elly Wardani 1
Catrin Björvell 2
1Nursing Leadership and Management
Department, Faculty of Nursing,
Universitas Syiah Kuala, Banda Aceh,
Indonesia; 2Department of Neurobiology,
Care Sciences and Society, Karolinska
Institutet, Stockholm, Sweden
Introduction: Hospitals in Indonesia are obligated to implement Integrated Patient Progress
Notes (IPPNs), also known as the “Catatan Perkembangan Pasien Terintegrasi”. A progress
note contains the entire interaction between patients and health professionals, including
physicians, nurses, pharmacists, dietitians, and physiotherapists. However, since the first
launch in 2012, obstacles and problems in completing this integrated documentation remains
nationwide.
Aim: The objective of this investigation was to identify health professional’s perspectives on
obstacles and problems using IPPNs and facilitators that may optimize their use.
Methods: Five focus group discussions (FGDs) involving 37 participants took place. All
FGDs were recorded, translated, and transcribed verbatim. A thematic analysis was used to
interpret the data.
Results: The thematic analysis of the material revealed three main categories for each of the
two topics; Topic 1. Perceived problems hindering integrated documentation: lack of super-
vision, competence, workload; topic 2: perceived strategies to optimize integrated documen-
tation: organizational support, joint practices, integrating technology with IPPN.
Conclusion: The results indicate that health professionals see the importance of using
IPPNs but only if implemented with educational and organizational support and that the
use of an electronic patient record may be more effective than a paper record. To continue the
implementation of IPPNs, it is suggested that it is preceded by educational and organizational
support.
Keywords: integrated documentation, Indonesia, patient report, safety, service quality
IntroductionIntroducing care coordination as a health reformmeans essentializing communication and
increasing interactions between health professionals.Multiprofessional communication is
necessary to avoid or at least minimize misinformation, maintain coordination, and
improve caremanagement.1 It is acknowledged that proper documentation in the patient’s
health-care record has larger significance than simply recording the history. The patient’s
health-care record is themain communicationmediumbetween health-care professionals,
helping them to deliver a high quality of care. The importance of proper documentation in
the health-care setting has been noted for centuries. Florence Nightingale mentioned how
meticulous patient documentation is tightly linked to a high level of health-care quality.
A collection of data and information that Nightingale analyzed at that time provided
evidence linking cleanliness to the number of preventable deaths in health-care settings.2
Correspondence: Elly WardaniNursing Leadership and ManagementDepartment, Faculty of Nursing,Universitas Syiah Kuala, Banda Aceh,IndonesiaEmail [email protected]
Journal of Multidisciplinary Healthcare Dovepressopen access to scientific and medical research
Open Access Full Text Article
submit your manuscript | www.dovepress.com Journal of Multidisciplinary Healthcare 2020:13 1–8 1
http://doi.org/10.2147/JMDH.S229907
DovePress © 2020 Kamil et al. This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution – Non Commercial (unported, v3.0) License (http://creativecommons.org/licenses/by-nc/3.0/). By accessing the
work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. Forpermission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms (https://www.dovepress.com/terms.php).
Jo
urna
l of M
ultid
isci
plin
ary
Hea
lthca
re d
ownl
oade
d fr
om h
ttps:
//ww
w.d
ovep
ress
.com
/ by
165.
215.
209.
15 o
n 18
-Jan
-202
0F
or p
erso
nal u
se o
nly.
Powered by TCPDF (www.tcpdf.org)
1 / 1

Although the importance of health-care documentation
has been identified, communication problems across health-
care disciplines still exist. In 2005, Joint Commission
International3 reported that 90% of unanticipated events not
related to the patient’s illness that resulted in death or serious
physical or psychological injury to the patient were due to
breakdowns in communication between health-care
professionals.
It is difficult to deliver a high quality of care without
a transparent, uniform system of health-care documenta-
tion; hence, this is one of the hospital accreditation criteria
set out by the Hospital Accreditation Commission of
Indonesia (Komisi Akreditasi Rumah Sakit [KARS]).
Integrating health professionals’ patient progress notes
were viewed as a solution to bridge this information gap,
minimizing communication barriers between health-care
providers and hence decreasing unexpected or accidental
events.4 In response to this, KARS introduced the “Catatan
Perkembangan Pasien Terintegrasi”, referred to here as the
Integrated Patient Progress Note (IPPN). This was
a manifestation of a patient-centered care initiative aimed
at increasing the quality of documentation in general and
to minimize communication barriers between health-care
providers.
IPPNs required health professionals to document
patient progress notes on the same sheets in the same
part of the patient’s health record. The IPPNs contained
chronologic documentation of the entire interaction
between the patient and health professionals, including
physicians, nurses, pharmacists, dietitians, and phy-
siotherapists. KARS obligated all hospitals to implement
IPPNs in 2012. Efforts that have been made to optimize its
implementation include socialization programs through
training provided by KARS’s certified national surveyors,
benchmarking of provincial hospitals against national
health centers, or an assistance program whereby the sur-
veyors assisting hospitals with the introduction of IPPNs
and how to complete the form correctly.5,6 Despite all the
hard work, the implementation has been a dynamic pro-
cess involving multiple health-care teams.5,6 The aim of
IPPNs was to synchronize care between providers, but the
documentation still did not describe collaborative practices
among health professionals. In an audit by Noorkasiani
et al,7 the completion of the IPPN documentation was
shown to be poor. For example, it was found that only
60% of the nursing patient progress notes audited were
clear, accurate, and concise, contrary to the recommenda-
tion of the Indonesian Ministry of Health for 85%
accuracy.8 The most frequent mistakes were improper
method of error correction, which is supposed to be one
line crossed out and signed; nursing notes on patient pro-
gress were unclear and lacked information; the name and
signature of the provider were not written clearly; the date
and hour of completion of the patient progress note were
not recorded; the progress notes among the health provi-
ders were inconclusive. The progress notes from each
health professional were independent of and irrelevant to
other health professionals’ notes.9 These findings are con-
trary to the documentation procedures standardized by the
World Health Organization,10 whereby hospitals and
health professionals must provide comprehensive and
complete documentation.
Although these problems are known, less is known
about the factors that impede the ideal patient progress
documentation and solutions that would escalate the
implementation of IPPNs in Indonesia. To address this
gap, the aim of this study was to explore perspectives
and opinions on the problems hindering effective use of
IPPNs among health professionals as well as to identify
possible ways to optimize the completion of collaborative
patient progress notes.
MethodsThis qualitative study used focus group discussions (FGD)
to collect data and applied a thematic analysis as proposed
by Braun and Clarke11 to analyze the data. The study took
place in a large urban hospital in Indonesia with five-star
national accreditation. The hospital is a major referral
center and teaching hospital. To improve the hospital’s
quality of care and services, the hospital made their
debut toward international accreditation at the end of
2017, targeting Joint Commission International accredita-
tion by 2020.
ParticipantsIn order to cover as broad opinions as possible and be
able to create groups where the participants were comfor-
table with one another, a purposeful selection of partici-
pants was performed. Participants were selected from
lists provided by the human resource department. The
inclusion criterion was having one or more years of
work experience at the hospital. Potential participants
were called by phone and asked to take part in the
study. They were informed about the background and
aims of the study, and anonymity of participants. Thirty-
seven health professionals were selected: 8 dietitians, 8
Kamil et al Dovepress
submit your manuscript | www.dovepress.com
DovePressJournal of Multidisciplinary Healthcare 2020:132
Jo
urna
l of M
ultid
isci
plin
ary
Hea
lthca
re d
ownl
oade
d fr
om h
ttps:
//ww
w.d
ovep
ress
.com
/ by
165.
215.
209.
15 o
n 18
-Jan
-202
0F
or p
erso
nal u
se o
nly.
Powered by TCPDF (www.tcpdf.org)
1 / 1

doctors, 10 nurses, 6 pharmacists, and 5 physiotherapists.
The participating nurses came from intensive care, med-
ical, and surgical wards, and the participating doctors
were specialized in neurology, internal medicine, surgery,
and dermatology. Five participants were males and 32
were females; age groups were 25 to 35 years (n = 10),
35 to 45 years (n = 22), and 45 to 55 years (n = 5).
Educational backgrounds varied from diploma level to
specialist level. Most of the participants had
a bachelor’s degree (n = 27). More than half (n = 25) of
the participants had 5 to 10 years of work experience in
the hospital, and the rest (n = 12) had 10 years or more.
All participants were informed in detail about the study
and given assurance of full anonymity outside the focus
group before a consent form was signed.
Data CollectionKrueger13 describes focus groups as carefully planned
discussions used to obtain perceptions on a specific area
of interest in a permissive, non-threatening environment.
The purpose is to have group members influence each
other by responding to ideas and comments in the discus-
sion. This is considered an effective technique for explor-
ing the attitudes and needs of staff14 to generate
hypotheses for further investigation. The intent of focus
groups is not to infer or generalize but to determine the
range of and provide insights into how people perceive
a situation.13
Five FGDs were held each lasting 35 to 60 mins. Each
group consisted of one profession, with the purpose of
creating a permissive, non-threatening environment. The
FGDs took place during November and December 2018.
The location was selected for privacy, silence, and com-
fortable lighting. The seating design was a semi-circle
with the moderator (the principal author, HK) and the
assistant (EW) at the front so that everyone would be
visible to everybody else in the group. Each session was
initiated by the moderator explaining the aim of the FGD,
the purpose of audiotape recording, and the rule of full
anonymity outside the focus group. Two key topics were
used to initiate discussions: the experiences of using the
IPPN and ways to improve the use of IPPNs. Other than
the prepared questions, probing questions were also used
to make the session alive. The sessions were audio-
recorded and later transcribed verbatim by one of the
authors (RR). Informants names were not used in the
field notes or audiotape to establish confidentiality.
Ethical ConsiderationsApproval for this research study was obtained from the
university’s Ethics Committee (certificate number
113001180517) as well as the Research and
Development Center of the hospital where the study took
place.
Data AnalysisA thematic analysis as proposed by Braun and Clarke11
were used to analyze the data from the FGD. The stages
used were as follows: familiarization, initial coding, theme
identification and labeling, review, and comparison.
Despite these, the authors remained mindful of the possi-
bility that new information and concepts could arise.12 At
the initial stage, all the recorded discussions were tran-
scribed into Bahasa Indonesia. To build familiarity with
the texts, the transcripts were read and re-read by two of
the authors (HK and EW). Notes on early impressions
were taken during this time to organize and form preli-
minary ideas about possible codes.
When generating codes, HK and EW code the tran-
scripts separately using pens and highlighters. Both
focused on segment of the data that captured something
specific to the research question. HK and EW compared
the codes that they generated for each transcript, discussed
and modified them before moving on to the next text. New
codes and modifications of the existing ones were gener-
ated as the process evolved. The codes were examined and
collated into themes. Each theme was reviewed continu-
ously to ensure its robustness with the codes and the
dataset. Notes were taken on emerging patterns, and rela-
tionships were identified between constructs. These were
beneficial to create important notes for the data analysis
and to explain similar and contrasting viewpoints around
each theme.
At this stage, a third member of the research group
(RR) read the grouping of the data as well as codes,
themes and citations from focus group participants to
validate consistency with the raw data, established at ear-
lier phases. The results of the thematic analysis were then
translated into English in close cooperation with the lan-
guage center of the university. Two language experts
assisted the researchers during a back-translation proce-
dure to ensure the best semantic equivalent and accuracy
between Bahasa Indonesia and English. Lastly, the fourth
author (CB), with extensive experience in the method, then
examined all the findings. Careful consideration was given
Dovepress Kamil et al
Journal of Multidisciplinary Healthcare 2020:13 submit your manuscript | www.dovepress.com
DovePress3
Jo
urna
l of M
ultid
isci
plin
ary
Hea
lthca
re d
ownl
oade
d fr
om h
ttps:
//ww
w.d
ovep
ress
.com
/ by
165.
215.
209.
15 o
n 18
-Jan
-202
0F
or p
erso
nal u
se o
nly.
Powered by TCPDF (www.tcpdf.org)
1 / 1

to the possibility of new or emerging themes that might
emerge during the final check and a final agreement was
reached.
ResultsThirty-seven informants took part in five FGD sessions.
There was general agreement among the participants that
integrated documentation aimed to increase teamwork,
coordination, and ease the communication between team
members and that the IPPN helped the health professionals
to monitor patient progress because all professionals docu-
mented their notes on the same sheets. However, they
confirmed that they were still struggling to complete the
integrated notes to the expected level. There was extensive
understanding and acceptance of the pivotal role of inte-
grated notes to collaborate care documentation.
The thematic analysis of the material revealed three
main themes for each of the two topics that were discussed
in the focus groups. The themes were not mutually exclu-
sive because some of the statements could fit into more
than one theme.
Topic 1: Perceived problems hindering integrated
documentation:
Themes:
Lack of supervision
Competence
Workload
Topic 2: Perceived strategies to optimize integrated
documentation:
Themes:
Organizational support
Joint practices
Integrating technology with IPPN
Perceived Problems Hindering Integrated
DocumentationLack of Supervision
Minimal organizational support and supervision were per-
ceived as a barrier to the use of the IPPN. This issue arose
in all the professional groups under study. They expected
support from hospital management to ensure that the col-
laborative report maintained its function as
a communication medium among them. There was
a feeling of lack of attention from leaders on how to
maximize the function of the IPPN. A pharmacist said:
. . .we know that an integrated report is an advantage for
us, but I don’t see much attention is paid to this. We need
to know more about how to fill it correctly, and anything
related to it . . .. (Pharmacist 2)
This opinion was further expressed as:
. . . the integrated sheet is very important, we realize this.
I hope the top leadership would monitor and manage
continual supervision on documentation, not just leave it
to us . . .. (Doctor 5)
Competence
There was a consensus across the discussion groups that
there was no coherence in the patient progress notes pro-
vided by each professional. They felt that the flow of
patient care reports did not depict collaborative care.
A doctor said:
well, it is great to have the integrated report . . . I actually
expect a nice description to what we all have done to the
patients, but it does not seem to be there. To be honest, I rarely
look at other professional’s notes . . . somehow, the available
information is not updated on a regular basis. (Doctor 3)
Within the doctors’ group, there was an agreement that
other professionals’ patient documentation seemed less
meaningful. This perception was supported by the other
four groups of participants. The pharmacist group, for
example, realized that not all of their members had
a similar capability with regard to integrated patient doc-
umentation. As stated below, the root causes of this pro-
blem were the variability in educational attainment and
lack of training:
There are only a few clinical pharmacists [bachelor level]
working here, and we have a large number of assistant
pharmacists at diploma level . . . this gives us different
abilities to document our work on patients . . . I found
that our notes are not really meaningful in the integrated
documentation . . . the cover is the integrated report but in
the inside is just individual notes . . . it would be useful if
there is continuous learning or training on practices either
in-house or in the pre-clinical phase so that we know each
other better [each other’s work]. (Pharmacist 5)
The nurses’ group, in particular, saw the competence issue
much more intense than the other professionals. They
strongly elaborated on how mixed educational back-
grounds were an obstacle that contributed to making docu-
mented reports within the IPPN less informative. A nurse
expressed it as:
Kamil et al Dovepress
submit your manuscript | www.dovepress.com
DovePressJournal of Multidisciplinary Healthcare 2020:134
Jo
urna
l of M
ultid
isci
plin
ary
Hea
lthca
re d
ownl
oade
d fr
om h
ttps:
//ww
w.d
ovep
ress
.com
/ by
165.
215.
209.
15 o
n 18
-Jan
-202
0F
or p
erso
nal u
se o
nly.
Powered by TCPDF (www.tcpdf.org)
1 / 1

It is so hard for some nurses to write integrated notes. We
have mostly diploma graduated nurses and some at bache-
lor level. Plus, the nurses graduated from multiple schools,
a mix of polytechnic, health higher education and univer-
sity . . . we are struggling to improve nurses critical think-
ing, but their confidence is not high enough to face other
professionals . . . how can we expect that the information
in there [the IPPN] would support other nurses or
a consultant physician in care delivery; we can’t guarantee
quality if looking at the nurses conditions here. I believe
they just write for administration purposes only . . . it is
true though. (Nurse 8)
The comments reflect the influence of the level of educa-
tion on documentation quality and teamwork ability.
Diverse educational backgrounds are seen as
a challenging factor to proper documentation, which also
lead to lack of competence in building mutual relation-
ships between professionals. Less opportunity to know and
engage with each other’s profession seemed to create
a wall between them.
Workload
The data revealed that the health professionals were in
agreement regarding the burden of responsibilities they
carry in their daily duties. This leads to workload issues.
There was a consensus about the extra burden of IPPNs.
However, among the five groups of informants’, phy-
siotherapist and dietitian felt it the most. The imbalance
number between the number of providers and the number
of patients was seen as an obstacle for proper patient
documentation, as a physiotherapist said:
. . . what we are doing is unbelievable. There are few
clinically certified providers, but we have to take care of
all units in the entire hospital . . . it is so hard to fill in the
integrated documentation while carrying a lot of work to
do with the patients. (Physiotherapist 2)
In line with the physiotherapist group, the dietitians ela-
borated similar views with regard to limited resources and
its impact on documentation. A dietitian explained:
. . . we always struggle to fulfill documentation demands . . .
we have loads of patients to visit while we have limited
resources, so we have to set aside a lot of time for docu-
mentation and do it at a later time . . . sometimes ending up
with no documentation because we are so busy. I know that
is wrong, but we can’t do anything so far . . .. (Dietitian 7)
Problems with understaffing were considered to promote
difficulties in completing the integrated documentation.
The time available and an increasing amount of work to
be finished were also viewed as affecting delayed docu-
mentation and the quality of written reports.
Perceived Strategies to Optimize the
Integrated DocumentationParticipants described several important steps to decrease
the perceived barriers.
Organizational Support
The notion of feeling safe and confident at work when the
hospital management board provides continued support for
the documentation procedure was strongly expressed by
all five groups of professionals. Supervision and regular
educational services were seen as pivotal factors for
improvement of the documentation. An informant said:
I believe that action is the result of education. It’s a lot
more comfortable to work if the hospital leadership com-
mits to continual education as well as supervision on
integrated documentation . . . it should be done on
a regular basis; if so, I am sure our performance would
be better. (Nurse 3)
This was supported by other health professionals:
We’ve been taught that integrated documentation is our
way to improve safety, both for patients and health provi-
ders . . . it feels nice if we do it right, of course we need
support for the learning process. (Physiotherapist 1)
They felt that the ability to provide quality documentation
would be a confidence booster at work. Informants’ com-
ments reflected the importance of educational interven-
tions to endorse the importance of improved integrated
documentation and best practices.
Joint Practices
Mutual respect, teamwork, and collaboration emerged as
an important collaborative practice. Informants, regardless
of their professional and educational background,
described the need to engage in a respectful collaborative
manner in order to pursue integrated care. The members of
all five groups consented that they required to work in
harmony. The need for this was stressed more strongly
among the nurses group than the others. The fact that they
are required to communicate with doctors and patients
around the clock made their strong wish for a more colla-
borative environment important. Seemingly, they felt that
the existing relationship was a social connection rather
than a professional one. A nurse explained:
Dovepress Kamil et al
Journal of Multidisciplinary Healthcare 2020:13 submit your manuscript | www.dovepress.com
DovePress5
Jo
urna
l of M
ultid
isci
plin
ary
Hea
lthca
re d
ownl
oade
d fr
om h
ttps:
//ww
w.d
ovep
ress
.com
/ by
165.
215.
209.
15 o
n 18
-Jan
-202
0F
or p
erso
nal u
se o
nly.
Powered by TCPDF (www.tcpdf.org)
1 / 1
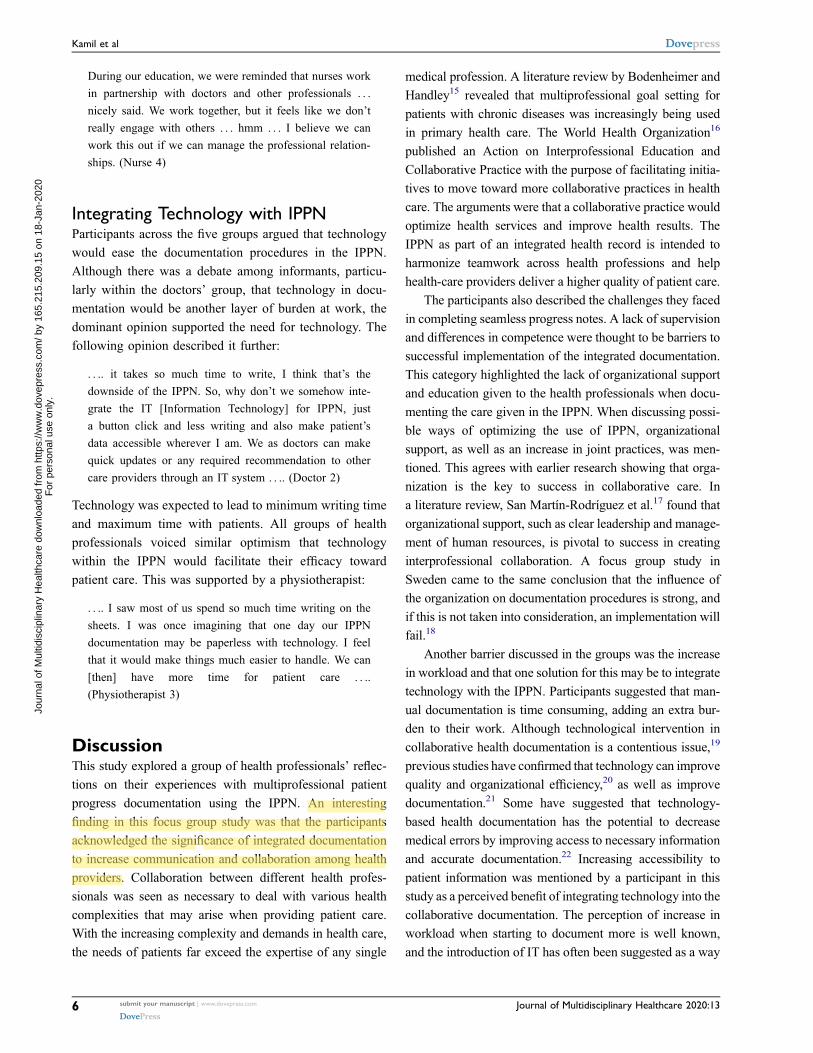
During our education, we were reminded that nurses work
in partnership with doctors and other professionals . . .
nicely said. We work together, but it feels like we don’t
really engage with others . . . hmm . . . I believe we can
work this out if we can manage the professional relation-
ships. (Nurse 4)
Integrating Technology with IPPNParticipants across the five groups argued that technology
would ease the documentation procedures in the IPPN.
Although there was a debate among informants, particu-
larly within the doctors’ group, that technology in docu-
mentation would be another layer of burden at work, the
dominant opinion supported the need for technology. The
following opinion described it further:
. . .. it takes so much time to write, I think that’s the
downside of the IPPN. So, why don’t we somehow inte-
grate the IT [Information Technology] for IPPN, just
a button click and less writing and also make patient’s
data accessible wherever I am. We as doctors can make
quick updates or any required recommendation to other
care providers through an IT system . . .. (Doctor 2)
Technology was expected to lead to minimum writing time
and maximum time with patients. All groups of health
professionals voiced similar optimism that technology
within the IPPN would facilitate their efficacy toward
patient care. This was supported by a physiotherapist:
. . .. I saw most of us spend so much time writing on the
sheets. I was once imagining that one day our IPPN
documentation may be paperless with technology. I feel
that it would make things much easier to handle. We can
[then] have more time for patient care . . ..
(Physiotherapist 3)
DiscussionThis study explored a group of health professionals’ reflec-
tions on their experiences with multiprofessional patient
progress documentation using the IPPN. An interesting
finding in this focus group study was that the participants
acknowledged the significance of integrated documentation
to increase communication and collaboration among health
providers. Collaboration between different health profes-
sionals was seen as necessary to deal with various health
complexities that may arise when providing patient care.
With the increasing complexity and demands in health care,
the needs of patients far exceed the expertise of any single
medical profession. A literature review by Bodenheimer and
Handley15 revealed that multiprofessional goal setting for
patients with chronic diseases was increasingly being used
in primary health care. The World Health Organization16
published an Action on Interprofessional Education and
Collaborative Practice with the purpose of facilitating initia-
tives to move toward more collaborative practices in health
care. The arguments were that a collaborative practice would
optimize health services and improve health results. The
IPPN as part of an integrated health record is intended to
harmonize teamwork across health professions and help
health-care providers deliver a higher quality of patient care.
The participants also described the challenges they faced
in completing seamless progress notes. A lack of supervision
and differences in competence were thought to be barriers to
successful implementation of the integrated documentation.
This category highlighted the lack of organizational support
and education given to the health professionals when docu-
menting the care given in the IPPN. When discussing possi-
ble ways of optimizing the use of IPPN, organizational
support, as well as an increase in joint practices, was men-
tioned. This agrees with earlier research showing that orga-
nization is the key to success in collaborative care. In
a literature review, San Martín-Rodríguez et al.17 found that
organizational support, such as clear leadership and manage-
ment of human resources, is pivotal to success in creating
interprofessional collaboration. A focus group study in
Sweden came to the same conclusion that the influence of
the organization on documentation procedures is strong, and
if this is not taken into consideration, an implementation will
fail.18
Another barrier discussed in the groups was the increase
in workload and that one solution for this may be to integrate
technology with the IPPN. Participants suggested that man-
ual documentation is time consuming, adding an extra bur-
den to their work. Although technological intervention in
collaborative health documentation is a contentious issue,19
previous studies have confirmed that technology can improve
quality and organizational efficiency,20 as well as improve
documentation.21 Some have suggested that technology-
based health documentation has the potential to decrease
medical errors by improving access to necessary information
and accurate documentation.22 Increasing accessibility to
patient information was mentioned by a participant in this
study as a perceived benefit of integrating technology into the
collaborative documentation. The perception of increase in
workload when starting to document more is well known,
and the introduction of IT has often been suggested as a way
Kamil et al Dovepress
submit your manuscript | www.dovepress.com
DovePressJournal of Multidisciplinary Healthcare 2020:136
Jo
urna
l of M
ultid
isci
plin
ary
Hea
lthca
re d
ownl
oade
d fr
om h
ttps:
//ww
w.d
ovep
ress
.com
/ by
165.
215.
209.
15 o
n 18
-Jan
-202
0F
or p
erso
nal u
se o
nly.
Powered by TCPDF (www.tcpdf.org)
1 / 1
to decrease workload and cut down in documentation time.
However, there are studies with inconclusive results regard-
ing the benefits of electronic health records when it comes to
saving time for the clinician. Still, there are other benefits to
electronic health records, such as improving workflow at one
point that may save time at another point.23
The strengths and limitations of the research should be
considered when interpreting the study findings.
A strength of this study is the diversity of participants
involved in the FGDs. Multiple professionals were
included from diverse health disciplines and with
a variety of expertise working in different hospital units.
This provided a broader perspective on the implementation
of the IPPN. However, this was somewhat reduced by
participants seeming a bit reluctant to expose their perso-
nal experience with the IPPN in favor of more generic,
group-centered answers. Their arguments mostly centered
around what was supposed to happen rather than on what
actually happened in real-life settings. Theoretical content
may have dominated their opinions, subjugating their real
experiences, resulting in a limitation to this study.
ConclusionsIntegrated care documentation is a relatively novel initia-
tive in Indonesia. This inaugural study has attempted to
identify health professionals’ perspectives of integrated
progress notes using the IPPN in a hospital setting in
Indonesia. The results indicate that health professionals
see the importance of using IPPNs but only if implemen-
ted with educational and organizational support and that
the use of an electronic patient record may be more effec-
tive than a paper record. To continue the implementation
of IPPNs, it is suggested that it is preceded by educational
and organizational support. Further research may be
needed to construct a questionnaire based on the findings
of this study and perform a survey of a large population of
health professionals in Indonesia.
AbbreviationsFGD, focus group discussion; IPPN, Integrated Patient
Progress Note.
Ethics Approval and InformedConsentEthical clearance for the research was issued by the
Faculty of Nursing, University of Syiah Kuala Ethics
Committee with certificate number: 113001180517, as
well as permission from the Research and Development
Center of the hospital where the study took place. Consent
for publication is available upon request.
Data Sharing StatementAll data generated or analyzed during this study are
included in this published article.
AcknowledgmentsOur thanks to all health professionals involved who con-
tributed their time and efforts in this study.
FundingThe research is part from Penelitian Unggulan Universitas
(University Excellent Research) funding scheme, grant
number: 276/UN11.2/PP/PNBP/SP3/2019, Universitas
Syiah Kuala.
DisclosureThe authors report no conflicts of interest in this work.
References1. Klehr J, Hafner J, Spelz LM, Steen S, Weaver K. Implementation of
standardized nomenclature in the electronic medical record.Int J Nurs Terminol Classif. 2009;20(4):169–180. doi:10.1111/j.1744-618X.2009.01132.x
2. Nightingale F. Notes on Hospitals. 3rd ed. London: Longman,Greene, Longman, Roberts and Green; 1863.
3. Joint Commission International (JCI). Patient Safety; Essentials forHealth Care. Oakbrook Terrace, IL: Joint Commission onAccreditation of Healthcare Organizations; 2005.
4. Frelita G, Situmorang TJ, Silitonga DS. Joint CommissionInternational Accreditation Standards for Hospitals. 4th ed.Oakbrook Terrace, IL: Joint Commission on Accreditation ofHealthcare Organizations; 2011.
5. Kemenkes RI, Komisi Akreditasi Rumah Sakit (KARS). StandarAkreditasi Rumah Sakit. Jakarta: Kementerian Kesehatan RepublikIndonesia; 2011. Indonesian.
6. Komisi Akreditasi Rumah Sakit (KARS). Standar NasionalAkreditasi Rumah Sakit, Edisi 1. Jakarta: Komisi Akreditasi RumahSakit; 2017. Indonesian.
7. Noorkasiani N, Gustina R, Maryam S. Faktor-Faktor yangBerhubungan dengan Kelengkapan Dokumentasi Keperawatan.Jurnal Keperawatan Indonesia. 2015;18(1):1–8. doi:10.7454/jki.v18i1.391
8. Siswanto L, Hariyati RrT RTS, Sukihananto S. Faktor-faktor yangberhubungan dengan kelengkapan pendokumentasian asuhankeperawatan. Jurnal Keperawatan Indonesia. 2013;16(2):77–84.doi:10.7454/jki.v16i2.5
9. Lasmani P, Haryanti F, Lazuardi L. Evaluasi implementasi rekammedis terintegrasi di instalasi rawat inap RSUP dr. SardjitoYogyakarta. Jurnal Manajemen Pelayanan Kesehatan. 2014;17(1):3–8.
10. World Health Organization. Guidelines for Medical Records andClinical Documentation. Geneva: World Health Organization; 2007.
11. Braun V, Clarke V. Using thematic analysis in psychology. Qual ResPsychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
Dovepress Kamil et al
Journal of Multidisciplinary Healthcare 2020:13 submit your manuscript | www.dovepress.com
DovePress7
Jo
urna
l of M
ultid
isci
plin
ary
Hea
lthca
re d
ownl
oade
d fr
om h
ttps:
//ww
w.d
ovep
ress
.com
/ by
165.
215.
209.
15 o
n 18
-Jan
-202
0F
or p
erso
nal u
se o
nly.
Powered by TCPDF (www.tcpdf.org)
1 / 1

12. King N. Using templates in the thematic analysis of text. In:Cassell C, Symon G, editors. Essential Guide to QualitativeMethods in Organizational Research. London: Sage; 2004. 256–270.
13. Krueger R. Focus Groups. A Practical Guide for Applied Research.2nd ed. Thousand Oaks, CA: Sage; 1994.
14. Kitzinger J. Qualitative research: introducing focus groups. BMJ.1995;311(7000):299–302. doi:10.1136/bmj.311.7000.299
15. Bodenheimer T, Handley MA. Goal-setting for behavior change inprimary care: an exploration and status report. Patient Educ Couns.2009;76:174–180. doi:10.1016/j.pec.2009.06.001
16. World Health Organization. Framework for Action onInterprofessional Education and Collaborative Practice. Geneva:World Health Organization; 2010.
17. San Martín-Rodríguez L, Beaulieu M-D, D’Amour D, Ferrada-Videla M. The determinants of successful collaboration: a review oftheoretical and empirical studies. J Interprof Care. 2005;19(suppl1):132–147. doi:10.1080/13561820500082677
18. Björvell C, Wredling R, Thorell-Ekstrand I. Prerequisites and con-sequences of nursing documentation in patient records as perceivedby a group of registered nurses. J Clin Nurs. 2003;12(2):206–214.doi:10.1046/j.1365-2702.2003.00723.x
19. Adler-Milstein J, DesRoches CM, Furukawa MF, et al. More thanhalf of US hospitals have at least a basic EHR, but stage 2 criteriaremain challenging for most. Health Aff. 2014;33(9):1664–1671.doi:10.1377/hlthaff.2014.0453
20. Buntin MB, Burke MF, Hoaglin MC, Blumenthal D. The benefits ofhealth information technology: a review of the recent literature showspredominantly positive results. Health Aff. 2011;30:464–471.doi:10.1377/hlthaff.2011.0178
21. Kruse CS, Mileski M, Vijaykumar AG, Viswanathan SV,Suskandla U, Chidambaram Y. Impact of electronic health recordson long-term care facilities: systematic review. JMIR Med Inform.2017;5(3):e35. doi:10.2196/medinform.7958
22. Schiff GD, Bates DW. Can electronic clinical documentation helpprevent diagnostic errors? N Engl J Med. 2010;362(12):1066–1069.doi:10.1056/NEJMp0911734
23. Baumann LA, Baker J, Elshaug AG. The impact of electronichealth record systems on clinical documentation times:a systematic review. Health Policy. 2018;122(8):827–836.doi:10.1016/j.healthpol.2018.05.014
Journal of Multidisciplinary Healthcare DovepressPublish your work in this journalThe Journal of Multidisciplinary Healthcare is an international, peer-reviewed open-access journal that aims to represent and publishresearch in healthcare areas delivered by practitioners of differentdisciplines. This includes studies and reviews conducted by multi-disciplinary teams as well as research which evaluates the results orconduct of such teams or healthcare processes in general. The journal
covers a very wide range of areas and welcomes submissions frompractitioners at all levels, from all over the world. The manuscriptmanagement system is completely online and includes a very quick andfair peer-review system. Visit http://www.dovepress.com/testimonials.php to read real quotes from published authors.
Submit your manuscript here: https://www.dovepress.com/journal-of-inflammation-research-journal
Kamil et al Dovepress
submit your manuscript | www.dovepress.com
DovePressJournal of Multidisciplinary Healthcare 2020:138
Jo
urna
l of M
ultid
isci
plin
ary
Hea
lthca
re d
ownl
oade
d fr
om h
ttps:
//ww
w.d
ovep
ress
.com
/ by
165.
215.
209.
15 o
n 18
-Jan
-202
0F
or p
erso
nal u
se o
nly.
Powered by TCPDF (www.tcpdf.org)
1 / 1
© 2020. This work is licensed underhttps://creativecommons.org/licenses/by-nc/3.0/ (the “License”).
Notwithstanding the ProQuest Terms and Conditions, you may use this contentin accordance with the terms of the License.