3D Bioprinting and Its Application to Military Medicine
10
MILITARY MEDICINE, 185, 9/10:e1510, 2020 3D Bioprinting and Its Application to Military Medicine Jordan F. Betz, PhD*†; Vincent B. Ho, MD, MBA†; Joel D. Gaston, PhD*† ABSTRACT Introduction Traditionally, tissue engineering techniques have largely focused on 2D cell culture models—monolayers of immortalized or primary cells growing on tissue culture plastic. Although these techniques have proven useful in research, they often lack physiological validity, because of the absence of fundamental tissue properties, such as multicellular organization, specialized extracellular matrix structures, and molecular or force gradients essential to proper physiological function. More recent advances in 3D cell culture methods have facilitated the development of more complex physiological models and tissue constructs; however, these often rely on self-organization of cells (bottom-up design), and the range of tissue construct size and complexity generated by these methods remains relatively limited. By borrowing from advances in the additive manufacturing field, 3D bioprinting techniques are enabling top-down design and fabrication of cellular constructs with controlled sizing, spacing, and chemical functionality. The high degree of control over engineered tissue architecture, previously unavailable to researchers, enables the generation of more complex, physiologically relevant 3D tissue constructs. Three main 3D bioprinting techniques are reviewed—extrusion, droplet-based, and laser-assisted bioprinting techniques are among the more robust 3D bioprinting techniques, each with its own strengths and weaknesses. High complexity tissue constructs created through 3D bioprinting are opening up new avenues in tissue engineering, regenerative medicine, and physiological model systems for researchers in the military medicine community. Materials and Methods Recent primary literature and reviews were selected to provide a broad overview of the field of 3D bioprinting and illustrate techniques and examples of 3D bioprinting relevant to military medicine. References were selected to illustrate specific examples of advances and potential military medicine applications in the 3D bioprinting field, rather than to serve as a comprehensive review. Results Three classes of 3D bioprinting techniques were reviewed: extrusion, droplet-based, and laser-assisted bioprinting. Advantages, disadvantages, important considerations, and constraints of each technique were discussed. Examples from the primary literature were given to illustrate the techniques. Relevant applications of 3D bioprinting to military medicine, namely tissue engineering/regenerative medicine and new models of physiological systems, are discussed in the context of advancing military medicine. Conclusions 3D bioprinting is a rapidly evolving field that provides researchers the ability to build tissue constructs that are more complex and physiologically relevant than traditional 2D culture methods. Advances in bioprinting techniques, bioink formulation, and cell culture methods are being translated into new paradigms in tissue engineering and physiological system modeling, advancing the state of the art, and increasing construct availability to the military medicine research community. INTRODUCTION The speedy recovery of service members from their wounds and injuries remains a priority of military medicine. The ability to grow or restore tissues in vitro continues to be * Geneva Foundation, 917 Pacific Ave, Tacoma, WA 98402 † Department of Radiology and Radiological Sciences, Uniformed Ser- vices University of the Health Sciences, 4301 Jones Bridge Road, Bethesda, MD 20814 The information or content and conclusions do not necessarily represent the official position or policy of, nor should any official endorsement be inferred on the part of, USU, the Department of Defense, or the U.S. Government. doi:10.1093/milmed/usaa121 © The Author(s) 2020. Published by Oxford University Press on behalf of the Association of Military Surgeons of the United States. All rights reserved. For permissions, please e-mail: [email protected]. challenging with modest success. Innovations in the field have had notable advancements for service members, particularly for skin, connective, and musculoskeletal tissues. Most in vitro regenerative medicine research has been conducted using 2D cell culturing techniques, producing a single layer of cells rather than the 3D structures observed in vivo. Two-dimensional culture systems fail to recapitulate the complex signaling and architecture of the native 3D tissue environment; this failure is a factor in the modest success of regenerative medicine. There has been a move toward 3D culture techniques, including building complex tissue using multiple cell types, by embedding cells within a hydrogel scaffold, or culturing cells as spheroids. 1– 3 Three- dimensional cell cultures more closely approximate normal human physiological conditions through a broader range of cell-cell interactions (e.g. physical and chemical signaling e1510 MILITARY MEDICINE, Vol. 185, September/October 2020 Downloaded from https://academic.oup.com/milmed/article/185/9-10/e1510/5854784 by guest on 26 June 2022
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of 3D Bioprinting and Its Application to Military Medicine

MILITARY MEDICINE, 185, 9/10:e1510, 2020
3D Bioprinting and Its Application to Military Medicine
Jordan F. Betz, PhD*†; Vincent B. Ho, MD, MBA†; Joel D. Gaston, PhD*†
ABSTRACTIntroductionTraditionally, tissue engineering techniques have largely focused on 2D cell culture models—monolayers of immortalizedor primary cells growing on tissue culture plastic. Although these techniques have proven useful in research, they oftenlack physiological validity, because of the absence of fundamental tissue properties, such as multicellular organization,specialized extracellular matrix structures, and molecular or force gradients essential to proper physiological function.More recent advances in 3D cell culture methods have facilitated the development of more complex physiological modelsand tissue constructs; however, these often rely on self-organization of cells (bottom-up design), and the range of tissueconstruct size and complexity generated by these methods remains relatively limited. By borrowing from advances inthe additive manufacturing field, 3D bioprinting techniques are enabling top-down design and fabrication of cellularconstructs with controlled sizing, spacing, and chemical functionality. The high degree of control over engineered tissuearchitecture, previously unavailable to researchers, enables the generation of more complex, physiologically relevant3D tissue constructs. Three main 3D bioprinting techniques are reviewed—extrusion, droplet-based, and laser-assistedbioprinting techniques are among the more robust 3D bioprinting techniques, each with its own strengths and weaknesses.High complexity tissue constructs created through 3D bioprinting are opening up new avenues in tissue engineering,regenerative medicine, and physiological model systems for researchers in the military medicine community.
Materials and MethodsRecent primary literature and reviews were selected to provide a broad overview of the field of 3D bioprinting andillustrate techniques and examples of 3D bioprinting relevant to military medicine. References were selected to illustratespecific examples of advances and potential military medicine applications in the 3D bioprinting field, rather than toserve as a comprehensive review.
ResultsThree classes of 3D bioprinting techniques were reviewed: extrusion, droplet-based, and laser-assisted bioprinting.Advantages, disadvantages, important considerations, and constraints of each technique were discussed. Examples fromthe primary literature were given to illustrate the techniques. Relevant applications of 3D bioprinting to military medicine,namely tissue engineering/regenerative medicine and new models of physiological systems, are discussed in the contextof advancing military medicine.
Conclusions3D bioprinting is a rapidly evolving field that provides researchers the ability to build tissue constructs that are morecomplex and physiologically relevant than traditional 2D culture methods. Advances in bioprinting techniques, bioinkformulation, and cell culture methods are being translated into new paradigms in tissue engineering and physiologicalsystem modeling, advancing the state of the art, and increasing construct availability to the military medicine researchcommunity.
INTRODUCTIONThe speedy recovery of service members from their woundsand injuries remains a priority of military medicine. Theability to grow or restore tissues in vitro continues to be
*Geneva Foundation, 917 Pacific Ave, Tacoma, WA 98402†Department of Radiology and Radiological Sciences, Uniformed Ser-
vices University of the Health Sciences, 4301 Jones Bridge Road, Bethesda,MD 20814
The information or content and conclusions do not necessarily representthe official position or policy of, nor should any official endorsement beinferred on the part of, USU, the Department of Defense, or the U.S.Government.
doi:10.1093/milmed/usaa121© The Author(s) 2020. Published by Oxford University Press on behalf of
the Association of Military Surgeons of the United States. All rights reserved.For permissions, please e-mail: [email protected].
challenging with modest success. Innovations in the field havehad notable advancements for service members, particularlyfor skin, connective, and musculoskeletal tissues.
Most in vitro regenerative medicine research has beenconducted using 2D cell culturing techniques, producing asingle layer of cells rather than the 3D structures observed invivo. Two-dimensional culture systems fail to recapitulatethe complex signaling and architecture of the native 3Dtissue environment; this failure is a factor in the modestsuccess of regenerative medicine. There has been a movetoward 3D culture techniques, including building complextissue using multiple cell types, by embedding cells within ahydrogel scaffold, or culturing cells as spheroids.1–3 Three-dimensional cell cultures more closely approximate normalhuman physiological conditions through a broader range ofcell-cell interactions (e.g. physical and chemical signaling
e1510 MILITARY MEDICINE, Vol. 185, September/October 2020
Dow
nloaded from https://academ
ic.oup.com/m
ilmed/article/185/9-10/e1510/5854784 by guest on 26 June 2022

Military Medical Applications of 3D Bioprinting
stimuli) than traditional 2D techniques. By providing theseadditional stimuli or allowing cellular self-organization,researchers have been able to develop new in vitro modelsof tissues and/or diseases that more accurately reflect humanphysiology.4–6
Better control over the 3D cellular microenvironmentallows for the development of advanced models to investigatespecific cell interactions and complex models of humandisease. The use of tissue biofabrication enables consistent,reproducible methods to build tissue and organ specificmodels inclusive of extracellular matrix (ECM), cells, andgrowth factor signaling. Biofabrication has two distinctapplications: (1) as a research tool for scientific investigationand (2) actual fabrication of replacement tissue or tissueproducts for direct application (e.g. transplant) into patients.In the first case, tissue models, whether representative ofhealthy (e.g. “organ-on-chip” models) or diseased tissue(e.g. cancer), are valuable tools for the identification ofbiomarkers, in vitro drug testing, and investigation of diseaseconditions.7,8 In the second application, biofabricated tissueproducts are constructed for in vivo human-use, appliedto replace damaged tissue or dramatically increase woundhealing. Perhaps the most common application of this lattercategory is the use of skin to cover burn wounds or assplit thickness autografts.9,10 The use of 3D bioprintingcan provide the reproducibility and precision necessary tofabricate 3D tissue architecture required to meet both of theseapplications.
3D PRINTING (ADDITIVE MANUFACTURING)3D printing is an additive manufacturing process in which acomplex structure is created through the deposition of sequen-tial 2-dimensional (2D) layers of material to produce a 3Dobject. A moveable print head traces the desired pattern inthe X-Y direction at each level, with the third dimension (Z)coming from the vertical movement of the stage or print headover time. Using this method, complex shapes can be designedand fabricated beyond the limitations of traditional machiningtools. The additive manufacturing techniques developed for3D printing have moved beyond traditional engineering mate-rials and are being adapted to fabricate 3D cellular microen-vironments.
3D BIOPRINTINGBorrowing techniques from the 3D printing industry, researchersin the field of bioprinting have developed methods to constructcomplex biological structures and develop models of differenttissues and organs. This article will provide a brief overviewof printable “bioinks” and the main techniques for bioprinting,highlighting the various benefits and limitations for eachmethod.
BIOINKS: A BRIEF OVERVIEWA bioink is a biomaterial with physical, chemical, andmechanical properties that allow it to be printed into a 3Dstructure. Though it can be as simple as a suspension of cellsor spheroids (cell aggregates consisting of one or multiplecell types), the majority of current bioinks are derived fromsynthetic and natural polymers.
Biopolymer hydrogels, attributable to their chemical struc-ture and intrinsic ionic charges, sequester water and pro-vide structural support for cells similar to that of the nativeECM surrounding cells in most human tissues. Commonlyemployed biopolymers, such as alginate, hyaluronic acid, orcollagen have been heavily characterized and are readily avail-able from commercial sources. More comprehensive reviewsincluding specific material properties of these hydrogels areavailable in the literature.11,12
Hydrogel engineering offers several mechanisms for gela-tion, including thermal, chemical cross-linking, or ultraviolentcuring. Hydrogel gelation kinetics can vary widely, dependingon the material and cross-linking method employed; theseparameters must be taken into account when designing a 3Dbioprinted construct. For some applications, cell-free hydrogelscaffolds may be sufficient to achieve the required functionand mechanical properties. Many hydrogels can be loadedwith cells before printing, or can be seeded with cells afterprinting and gelation. When cells are included in the hydrogel,more stringent processing conditions are required to ensurecell viability; bioinks are typically kept at or near body temper-ature and more cell-friendly gelation conditions and crosslink-ers are employed.
The wide range of biopolymers that can be induced toform a hydrogel also allows for modification of chemical andphysical properties to promote cell proliferation, differentia-tion, or maintenance of a desired cell phenotype. Additionalgrowth factors or signaling molecules can be covalentlybound to many of these biopolymers or dispersed through-out, allowing additional flexibility in creating a specificmicroenvironment.
A number of synthetic polymers, derived from biologicalor petrochemical feedstocks, can also be used for bioprinting.These polymers inherently lack protein motifs that promotecell adhesion and spreading, so they are often employed inconjunction with materials that allow for cell attachment.Thermoplastics like poly(ε-caprolactone), poly(L-lactic acid),and poly(lactic-co-glycolic acid) are typically used for struc-tural or mechanical support, as seen in bone and osteochondraltissue engineering. These polymers can be mixed withother nonbiological materials, such as hydroxyapatite orgraphene,13,14 to improve the mechanical properties of theprinted construct and influence the behavior of cells seededonto these scaffolds. Other synthetic polymers, such as thePluronic family of polymers, are fluid at low temperatures(<10◦C) and form hydrogels at higher temperatures. These
MILITARY MEDICINE, Vol. 185, September/October 2020 e1511
Dow
nloaded from https://academ
ic.oup.com/m
ilmed/article/185/9-10/e1510/5854784 by guest on 26 June 2022

Military Medical Applications of 3D Bioprinting
can be effective as fugitive (sacrificial) inks and selectivelyeliminated from the bioprinted construct at a desired time,creating channels or pores for improved nutrient flux.15
METHODS FOR 3D BIOPRINTING
Extrusion Bioprinting
Extrusion systems are popular for bioprinting, functioningby dispensing bioink using pneumatic pressure, a plunger,or a mechanical screw (Fig. 1). Several systems are commer-cially available, spanning a range of materials, build volumes,and spatial resolutions. Extrusion 3D bioprinters are capableof printing a wide variety of materials, including syntheticbiocompatible polymers (e.g. poly(lactic-co-glycolic acid)),biopolymers (e.g. collagen), and dense suspensions of cells.Biocompatible synthetic polymers are melted by heat or dis-solved in a solvent, extruded into the desired pattern, and thensolidified by cooling or solvent evaporation. These processingconditions are typically too harsh for cell survival, so extrudedparts are used to form more rigid and robust acellular scaffoldsthat can later be modified or seeded with cells, often seenin bone and osteochondral tissue engineering applications.Natural biopolymers and biocompatible polymers are typi-cally extruded as bioink hydrogels.16–18 By altering the degreeand type of cross-linking, the mechanical properties of thehydrogel can be tuned to fit specific extrusion parameters,such as printing pressure. Hydrogel bioinks can also be loadedwith cells, providing a method to directly print cells with asurrounding support matrix.
The spatial resolution of extrusion printed constructs isfundamentally governed by the physical and chemical proper-ties of the material being extruded. The minimum bioink linewidth is largely determined by the diameter of the extrusionnozzle (100 μm to >1 mm); the actual line width dependson parameters such as bioink flow rate and print head speed.After extrusion, the material gelation speed and viscosity (howquickly the resulting material spreads before it gels) deter-mines the spatial resolution of constructs. This is particularlyrelevant in the Z-direction, as the thickness of the gelled bioinkdetermines the layer height for extruded constructs.
Bioinks used in extrusion are often not robust enough tosupport themselves and the weight of additional printed layerswhen first extruded. Recently, several support media havebeen developed to counteract this, bracing the extruded bioinkas it gels and increases in strength. These support media,consisting of small particles of protein or polysaccharide,behave as a solid unless undergoing shear stress.19–22 As theneedle of the extrusion printer passes through the media, thebehavior changes to that of a fluid, moving out of the wayof the needle and the newly extruded bioink, flowing backinto place once the needle moves out of the way. These newsupport media have expanded the shape and complexity oftissue constructs that can be printed with bioinks that havelower viscosities or long gelation times.
Advantages of Extrusion Bioprinting
Extrusion-based 3D bioprinting systems have several advan-tages over other bioprinting methods, including scalability,bioink variety, and high cell density deposition. Extrusionreadily lends itself to mass production and scaling; once thebioink and toolpath are defined, the process can be scaledup simply by the addition of more printheads.23 Bioinks witha wide variety of physical characteristics can be printed byextrusion, ranging from cell spheroids to decellularized ECMhydrogels. Extrusion printing is currently the only viablemethod to bioprint extremely high density bioinks. As typicalhuman tissue consists of densely packed cells, printing cellsat high density will be necessary for any constructs fabricatedfor in vivo use.24
Disadvantages of Extrusion Bioprinting
Notable disadvantages of extrusion 3D bioprinting includeslow fabrication speeds, lower cell viability, and limited reso-lution. Extrusion systems tend to be slow, with linear printingspeeds restricted by the viscosity and gelation kinetics of theprinted material. Because each layer is typically extruded as acontinuous filament or series of filaments, the serial nature ofthis process can result in long build times for each layer. Longbuild times can affect cell viability, especially without cellularaccess to nutrients during the printing process. Cell viabilityis also affected by the physical forces experienced duringthe extrusion process. The cells are subject to shear forcesas they are extruded, resulting in lower viability than otherbioprinting methods.18 The magnitude of the shear forces islargely dependent on the extrusion tip diameter and polymerviscosity; optimization of printing parameters can mitigateadverse effects experienced by the cells.
Applications of Extrusion Bioprinting to MilitaryMedicine
Extrusion bioprinting has several published examples of tis-sues and models relevant to military medicine. Musculoskele-tal injuries are common in the young, high-demand militarypopulation.25,26 In addition to the bone examples mentionedin section Bioinks: A Brief Overview, another important siteof musculoskeletal injury is the meniscus.13,14 Some extrusionbioprinted models of the meniscus use thermoplastics forincreased mechanical support, whereas others seed constructswith mesenchymal stem cells for differentiation into chon-drocytes responsible for meniscal remodeling.27,28 However,these soft, hydrogel-based tissue constructs do not have thesame mechanical properties as native tissue and can wear outprematurely.29,30
Volumetric muscle loss as a result of trauma is frequentlyobserved in the military population, and was a factor inover 90% of muscle-related medical retirements from thearmed services during Operation Iraqi Freedom and Opera-tion Enduring Freedom.31,32 Bioprinted muscle has largelyfocused on the heart and musculoskeletal system; bioprinted
e1512 MILITARY MEDICINE, Vol. 185, September/October 2020
Dow
nloaded from https://academ
ic.oup.com/m
ilmed/article/185/9-10/e1510/5854784 by guest on 26 June 2022
Military Medical Applications of 3D Bioprinting
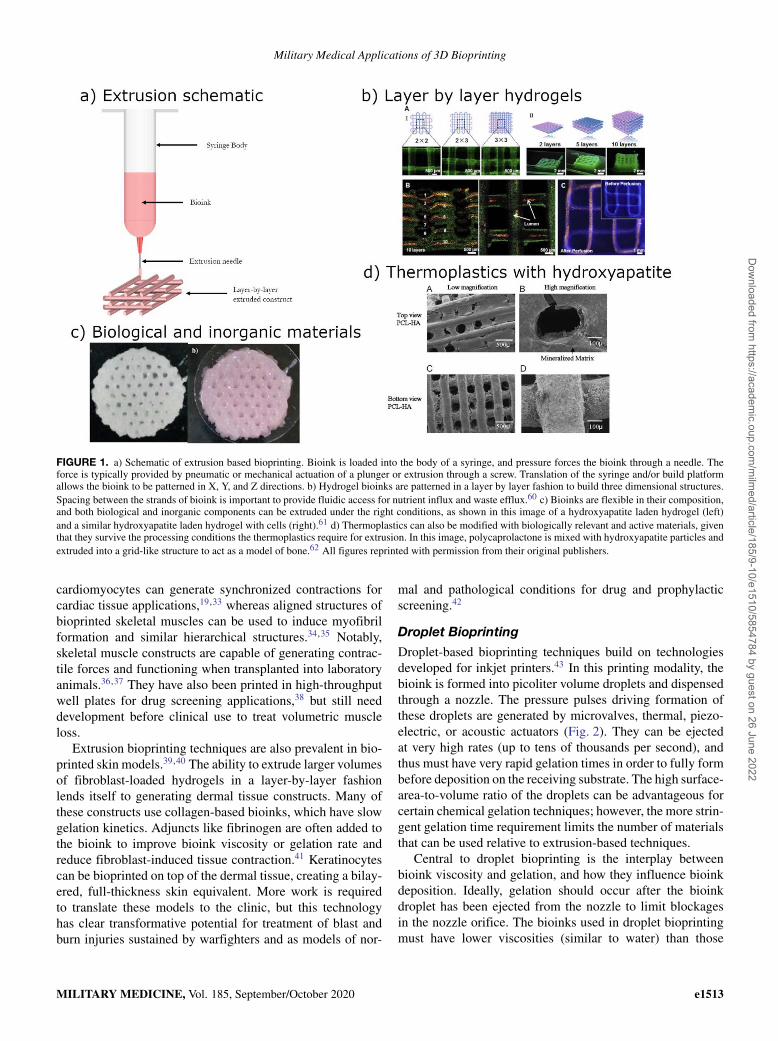
FIGURE 1. a) Schematic of extrusion based bioprinting. Bioink is loaded into the body of a syringe, and pressure forces the bioink through a needle. Theforce is typically provided by pneumatic or mechanical actuation of a plunger or extrusion through a screw. Translation of the syringe and/or build platformallows the bioink to be patterned in X, Y, and Z directions. b) Hydrogel bioinks are patterned in a layer by layer fashion to build three dimensional structures.Spacing between the strands of bioink is important to provide fluidic access for nutrient influx and waste efflux.60 c) Bioinks are flexible in their composition,and both biological and inorganic components can be extruded under the right conditions, as shown in this image of a hydroxyapatite laden hydrogel (left)and a similar hydroxyapatite laden hydrogel with cells (right).61 d) Thermoplastics can also be modified with biologically relevant and active materials, giventhat they survive the processing conditions the thermoplastics require for extrusion. In this image, polycaprolactone is mixed with hydroxyapatite particles andextruded into a grid-like structure to act as a model of bone.62 All figures reprinted with permission from their original publishers.
cardiomyocytes can generate synchronized contractions forcardiac tissue applications,19,33 whereas aligned structures ofbioprinted skeletal muscles can be used to induce myofibrilformation and similar hierarchical structures.34,35 Notably,skeletal muscle constructs are capable of generating contrac-tile forces and functioning when transplanted into laboratoryanimals.36,37 They have also been printed in high-throughputwell plates for drug screening applications,38 but still needdevelopment before clinical use to treat volumetric muscleloss.
Extrusion bioprinting techniques are also prevalent in bio-printed skin models.39,40 The ability to extrude larger volumesof fibroblast-loaded hydrogels in a layer-by-layer fashionlends itself to generating dermal tissue constructs. Many ofthese constructs use collagen-based bioinks, which have slowgelation kinetics. Adjuncts like fibrinogen are often added tothe bioink to improve bioink viscosity or gelation rate andreduce fibroblast-induced tissue contraction.41 Keratinocytescan be bioprinted on top of the dermal tissue, creating a bilay-ered, full-thickness skin equivalent. More work is requiredto translate these models to the clinic, but this technologyhas clear transformative potential for treatment of blast andburn injuries sustained by warfighters and as models of nor-
mal and pathological conditions for drug and prophylacticscreening.42
Droplet Bioprinting
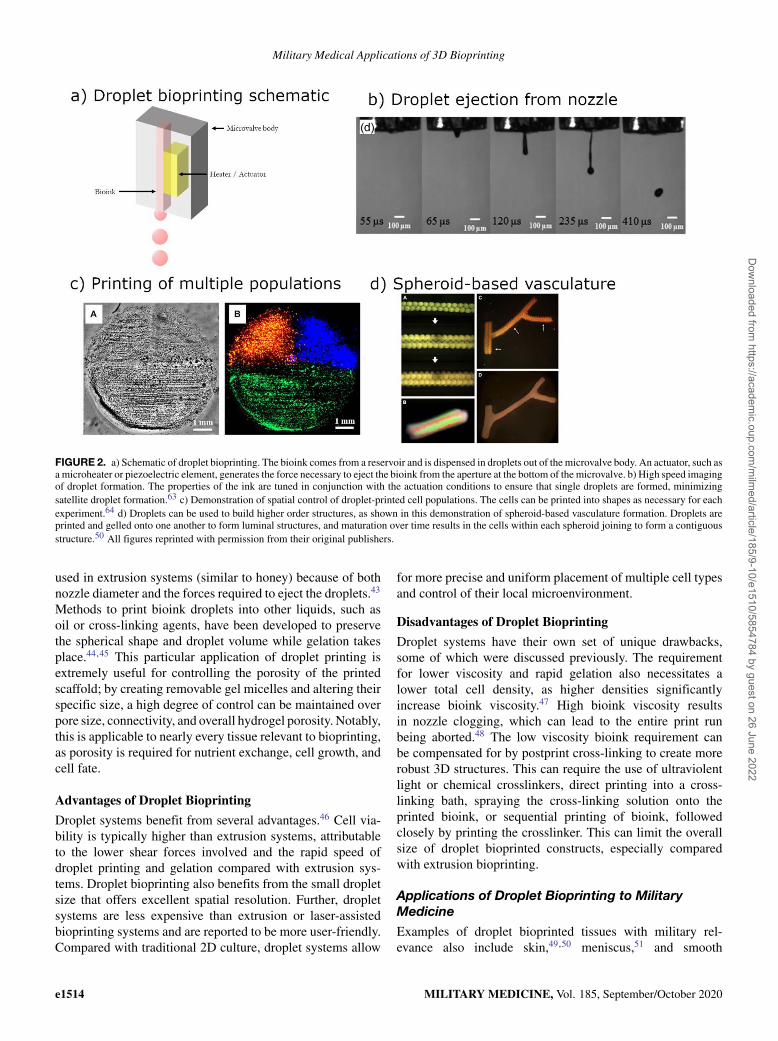
Droplet-based bioprinting techniques build on technologiesdeveloped for inkjet printers.43 In this printing modality, thebioink is formed into picoliter volume droplets and dispensedthrough a nozzle. The pressure pulses driving formation ofthese droplets are generated by microvalves, thermal, piezo-electric, or acoustic actuators (Fig. 2). They can be ejectedat very high rates (up to tens of thousands per second), andthus must have very rapid gelation times in order to fully formbefore deposition on the receiving substrate. The high surface-area-to-volume ratio of the droplets can be advantageous forcertain chemical gelation techniques; however, the more strin-gent gelation time requirement limits the number of materialsthat can be used relative to extrusion-based techniques.
Central to droplet bioprinting is the interplay betweenbioink viscosity and gelation, and how they influence bioinkdeposition. Ideally, gelation should occur after the bioinkdroplet has been ejected from the nozzle to limit blockagesin the nozzle orifice. The bioinks used in droplet bioprintingmust have lower viscosities (similar to water) than those
MILITARY MEDICINE, Vol. 185, September/October 2020 e1513
Dow
nloaded from https://academ
ic.oup.com/m
ilmed/article/185/9-10/e1510/5854784 by guest on 26 June 2022
Military Medical Applications of 3D Bioprinting
FIGURE 2. a) Schematic of droplet bioprinting. The bioink comes from a reservoir and is dispensed in droplets out of the microvalve body. An actuator, such asa microheater or piezoelectric element, generates the force necessary to eject the bioink from the aperture at the bottom of the microvalve. b) High speed imagingof droplet formation. The properties of the ink are tuned in conjunction with the actuation conditions to ensure that single droplets are formed, minimizingsatellite droplet formation.63 c) Demonstration of spatial control of droplet-printed cell populations. The cells can be printed into shapes as necessary for eachexperiment.64 d) Droplets can be used to build higher order structures, as shown in this demonstration of spheroid-based vasculature formation. Droplets areprinted and gelled onto one another to form luminal structures, and maturation over time results in the cells within each spheroid joining to form a contiguousstructure.50 All figures reprinted with permission from their original publishers.
used in extrusion systems (similar to honey) because of bothnozzle diameter and the forces required to eject the droplets.43
Methods to print bioink droplets into other liquids, such asoil or cross-linking agents, have been developed to preservethe spherical shape and droplet volume while gelation takesplace.44,45 This particular application of droplet printing isextremely useful for controlling the porosity of the printedscaffold; by creating removable gel micelles and altering theirspecific size, a high degree of control can be maintained overpore size, connectivity, and overall hydrogel porosity. Notably,this is applicable to nearly every tissue relevant to bioprinting,as porosity is required for nutrient exchange, cell growth, andcell fate.
Advantages of Droplet Bioprinting
Droplet systems benefit from several advantages.46 Cell via-bility is typically higher than extrusion systems, attributableto the lower shear forces involved and the rapid speed ofdroplet printing and gelation compared with extrusion sys-tems. Droplet bioprinting also benefits from the small dropletsize that offers excellent spatial resolution. Further, dropletsystems are less expensive than extrusion or laser-assistedbioprinting systems and are reported to be more user-friendly.Compared with traditional 2D culture, droplet systems allow
for more precise and uniform placement of multiple cell typesand control of their local microenvironment.
Disadvantages of Droplet Bioprinting
Droplet systems have their own set of unique drawbacks,some of which were discussed previously. The requirementfor lower viscosity and rapid gelation also necessitates alower total cell density, as higher densities significantlyincrease bioink viscosity.47 High bioink viscosity resultsin nozzle clogging, which can lead to the entire print runbeing aborted.48 The low viscosity bioink requirement canbe compensated for by postprint cross-linking to create morerobust 3D structures. This can require the use of ultraviolentlight or chemical crosslinkers, direct printing into a cross-linking bath, spraying the cross-linking solution onto theprinted bioink, or sequential printing of bioink, followedclosely by printing the crosslinker. This can limit the overallsize of droplet bioprinted constructs, especially comparedwith extrusion bioprinting.
Applications of Droplet Bioprinting to MilitaryMedicine
Examples of droplet bioprinted tissues with military rel-evance also include skin,49,50 meniscus,51 and smooth
e1514 MILITARY MEDICINE, Vol. 185, September/October 2020
Dow
nloaded from https://academ
ic.oup.com/m
ilmed/article/185/9-10/e1510/5854784 by guest on 26 June 2022

Military Medical Applications of 3D Bioprinting
muscle.52 Many of these tissue models use gelatin, alginate, orcollagen-based bioinks that can readily be dispensed throughinkjet print heads. Given the smaller volumetric throughputof droplet systems as compared with extrusion, as well asthe inability to print thermoplastic support materials withdroplet bioprinting, bone and skeletal muscle droplet printinglag behind other areas. However, combining both droplet andextrusion has been demonstrated as well, using extrusion tocreate larger bulk hydrogels and depositing cells with higherspatial resolution using droplet bioprinting,53 overcominglimitations of individual bioprinting modalities.
One area of military medical relevance where dropletbioprinting may have advantages in spatial resolution isprinting vasculature. Vasculature is essential to producinglarger cell-laden tissues by transporting nutrients and signal-ing molecules while removing waste products.15 Diffusionof nutrients and waste currently limits the fabrication oftissues to a few 100 μm. Without adequate nutrient supply andwaste removal, bioprinted tissue constructs become necrotic.Creating functional vasculature represents the single largestbarrier to the translation of 3D bioprinted tissue constructsinto useful clinical solutions for tissue regeneration.8,11,54
Using droplet printing techniques with support media enablesinkjet bioprinting to create complex vascular structures withlumens and bifurcations.55,56 Although the resolution ofdroplet bioprinting does not currently allow the printing offunctional microvasculature at the arteriole or capillary sizescale, advances in bioprinting techniques continue to expandthe limits of what is possible.
Laser Bioprinting
Laser-induced forward transfer (also called Biological LaserPrinting or BioLP) bioprinting methods use focused laserpulses to transfer materials from a support “target” to a“receiving” substrate.57,58 The support target, typically aquartz or glass slide, is coated with ∼100 nm of a laserabsorptive metal or metal oxide layer. An aqueous bioinksolution (cells or other bioactive components) is spread ontop of the absorptive layer, and a laser beam is focused tothe interface of the target substrate and the absorptive metal.Once pulsed, the laser causes the thermal volatilization ofa picoliter volume of bioink near the interface, causing thecreation of a microbubble (Fig. 3). The creation and expansionof this microbubble causes ejection of a microliter volumebioink droplet toward the receiving substrate. Deposition ofthe droplet onto the receiving substrate at a specific location isachieved through the use of computer-controlled translationstages; the stages are aligned such that the droplet lands inthe specific location. Notably, this entire process does notresult in loss of viability or DNA damage to either bacteria ormammalian cells.59–61
Advantages of Laser Bioprinting
BioLP has several advantages primarily because of the noz-zleless approach and application of a laser as the driving force
for the print. The lack of a traditional printing nozzle meansthat bioinks with higher viscosity can be printed, as there is noconcern about clogging. Furthermore, bioinks with differentmaterial properties or cellular compositions can easily bechanged by simply switching the support target. The use ofa laser to drive the deposition of microliter sized dropletsreadily lends this technique to very high precision printing.Depending on laser frequency and target translation speed,hundreds of droplets can be printed in a single second. Celldensity of the printed bioinks can also easily be tuned suchthat each individual laser pulse results in the deposition of asingle cell on the receiving substrate.
Disadvantages of Laser Bioprinting
There are some significant drawbacks to BioLP, mainlybecause of system complexity. Like other bioprintingmethods, BioLP must be set up in an aseptic environmentto ensure sterility of the final product. However, unlike otherbioprinting techniques, this can cause significant operationalissues, attributable to the need for translation stages andlaser alignment. As such, the price of the overall printer andsetup increases drastically as the build volume increases. Thedroplet nature of BioLP also limits the volume of materialdeposited; although hundreds of individual cells can be printedper minute, they are deposited in microliter volumes. Thisresults in poor overall volume deposition over time, andrequires maintenance of the receiving substrate environment.Finally, the target substrate must be prepared and maintainedbefore printing. To maintain bioink properties and cellviability, the material must be printed just after preparation asit is subject to rapid evaporation. This requires the creation ofa humid environment surrounding the target substrate, whichfurther increases system complexity and cost. Comparedwith 2D culture, BioLP enables very precise positioning ofmultiple cell types and ECM components, while also offeringunprecedented control over 3D interactions between cells.
Applications of Laser Bioprinting to MilitaryMedicine
BioLP has printing applications for a variety of militaryrelevant tissues, most notably skin and bone. The high-resolution patterning possible with BioLP has been employedto print multilayered skin constructs, including keratinocytesand fibroblasts, as a treatment method for burn therapy. Theprinted tissue was successfully grafted onto mice and devel-oped small blood vessels, indicating partial vascularization ofthe biofabricated tissue.62 BioLP has been used for in situ boneprinting, another area of great military interest. Researchersused BioLP to print specific patterns (ring or disk geometries)of osteoconducive mesenchymal stem cells directly to boneinjury in a mouse model.63 Significant increases in boneformation and wound repair were observed up to two monthsafter printing, particularly in the center of the bone defect.Additional experiments aimed at BioLP printing of bone
MILITARY MEDICINE, Vol. 185, September/October 2020 e1515
Dow
nloaded from https://academ
ic.oup.com/m
ilmed/article/185/9-10/e1510/5854784 by guest on 26 June 2022

Military Medical Applications of 3D Bioprinting
FIGURE 3. a) Biological laser printing schematic. Cells are placed onto a glass slide (the “ribbon”) with an energy absorbing layer. A laser pulse hits thisenergy absorbing layer, causing cells to be ejected from the surface of the glass slide. These ejected cells follow a ballistic trajectory towards their target.Translation of the slide or target and adjustment of the distance between the ribbon controls the XYZ position of the ejected cell. b) Fluorescent cells printedusing biological laser printing show that they can be deposited in different positions and across multiple layers.65 c) Laser printing can be used to create customsurface functionalities, such as these arrays of regularly spaced hydroxyapatite clusters.66 d) Biological laser printing maintains high spatial fidelity, as shownin this annular pattern of two cell populations.67 All figures reprinted with permission from their original publishers.
biomaterials, such as hydroxyapatite, has also demonstratedmarked success in generating bone tissue in vitro.64 Utilizationof this technology for rapid in situ treatment of traumaticbone injuries suffered on the battlefield or fabricate bioactivebone inserts for surgical engraftment may allow for quickerrecovery and return to duty.
Outlook and Future Directions
Although thorough treatment of the nuances of 3D bioprintingis beyond the scope of this manuscript, there are engineering,materials, medical, and regulatory challenges worth highlight-ing that must be addressed before these technologies canprogress to the clinic.7,65 On the engineering front, print-ing speed and feature size have previously been inverselycorrelated: parts with smaller features and finer spatial res-olution take longer to print. Newer technologies, such asstereolithographic bioprinting, are beginning to address theseshortcomings.66–69 However, these technologies have theirown limitations (e.g. materials and cell types) that must beaddressed through additional innovation or combination withother bioprinting modalities. Bioinks are currently limitedin complexity, cell compatibility, and printability. ECM innative tissue has multiple protein components, as well asmechanical and chemical gradients. The challenge of creating
bioinks that can recapitulate mechanical and chemical cues,maintain cell viability, while remaining printable will requireefforts from chemists, biologists, and engineers. In paral-lel with improvements in bioprinting processes and bioinks,researchers, and clinicians must determine what constitutesfunctional biofabricated tissue. For instance, innervation is anactive area of research in bioprinting, but is currently lackingin most bioprinted tissue constructs and will be needed forcomplete restoration of tissue function. Balancing the rightamount of top-down bioprinting design with the self-assemblyand repair capabilities of the host and printed cells will beessential to expediting viable clinical solutions. Finally, theregulatory framework and manufacturing infrastructure willneed to be developed for mass production of 3D bioprintedtissues. Tissue and bioink material consistency, safety, andefficacy will need to be addressed for widespread adoptionand approval of bioprinted tissues.
CONCLUSIONS3D bioprinting technologies are rapidly evolving. Currentresearch focuses on advancing the speed, spatial resolution,and diversity of materials and cell types printed by thesetechniques. In application, 3D bioprinting, through computeraided design, provides the reproducibility necessary to
e1516 MILITARY MEDICINE, Vol. 185, September/October 2020
Dow
nloaded from https://academ
ic.oup.com/m
ilmed/article/185/9-10/e1510/5854784 by guest on 26 June 2022
Military Medical Applications of 3D Bioprinting
ensure reliable tissue fabrication. Bioprinting is breakingground in translational regenerative medicine applications andenabling new models of tissues for basic and applied research.Extrusion-based 3D bioprinting allows for the printing oflarger structures at lower spatial resolutions with a widevariety of biomaterials, from hydrogels to thermoplastics.Droplet-based 3D bioprinting has better spatial resolution thanextrusion techniques, but has a narrower range of materialsthat can be printed, because of the fact that the printer headsrequire a lower viscosity ink. Laser-assisted bioprinting offersextremely high precision and cell viability, but the systemsare expensive and complex, and do not build structures aslarge as those from extrusion and droplet bioprinting. 3Dbioprinting has direct application to military medicine basicresearch, such as investigation of environmental exposures,drug discovery, and modeling of injuries such as blastinjury. This technology also promises to fast track tailoredtissue solutions in regenerative medicine for treatment of thewounded warriors such as skin in burn patients, and potentiallymuscle and/or nerve loss frequent in extremity injuries.
FUNDINGThis article was funded under award HU0001-17-2-0013. TheUniformed Services University of the Health Sciences (USU),4301 Jones Bridge Rd, Bethesda, Maryland 2081-4799 is theawarding and administering office of this award.
REFERENCES1. Rossi G, Manfrin A, Lutolf MP: Progress and potential in
organoid research. Nat Rev Genet 2018; 19(11): 671. doi: 10.1038/s41576-018-0051-9.
2. Duval K, Grover H, Han L-H, et al: Modeling physiological events in 2Dvs. 3D cell culture. Physiology 2017; 32(4): 266–77. doi: 10.1152/phys-iol.00036.2016.
3. Knight E, Przyborski S: Advances in 3D cell culture technologiesenabling tissue-like structures to be created in vitro. J Anat 2015; 227(6):746–56. doi: 10.1111/joa.12257.
4. Eglen RM, Reisine T: Human iPS cell-derived patient tissues and3D cell culture part 2: spheroids, organoids, and disease model-ing. SLAS Technol Transl Life Sci Innov 2019; 24(1): 18–27. doi:10.1177/2472630318803275.
5. Saliba J, Daou A, Damiati S, Saliba J, El-Sabban M, Mhanna R: Devel-opment of microplatforms to mimic the in vivo architecture of CNSand PNS physiology and their diseases. Genes. 2018; 9(6): 285. doi:10.3390/genes9060285.
6. Torras N, García-Díaz M, Fernández-Majada V, Martínez E: Mimickingepithelial tissues in three-dimensional cell culture models. Front BioengBiotechnol 2018; 6. doi: 10.3389/fbioe.2018.00197.
7. Derakhshanfar S, Mbeleck R, Xu K, Zhang X, Zhong W, Xing M:3D bioprinting for biomedical devices and tissue engineering: a reviewof recent trends and advances. Bioact Mater 2018; 3(2): 144–56. doi:10.1016/j.bioactmat.2017.11.008.
8. Heinrich MA, Liu W, Jimenez A, et al: 3D bioprinting: frombenches to translational applications. Small 2019; 15(23): 1805510. doi:10.1002/smll.201805510.
9. Hickerson WL, Compton C, Fletchall S, Smith LR: Cultured epidermalautografts and allodermis combination for permanent burn wound cov-erage. Burns 1994; 20: S52–6. doi: 10.1016/0305-4179(94)90091-4.
10. Min JH, Yun IS, Lew DH, Roh TS, Lee WJ: The use of Matriderm andautologous skin graft in the treatment of full thickness skin defects. ArchPlast Surg 2014; 41(4): 330–6. doi: 10.5999/aps.2014.41.4.330.
11. Hospodiuk M, Dey M, Sosnoski D, Ozbolat IT: The bioink: a compre-hensive review on bioprintable materials. Biotechnol Adv 2017; 35(2):217–39. doi: 10.1016/j.biotechadv.2016.12.006.
12. Panwar A, Tan LP: Current status of bioinks for micro-extrusion-based 3D bioprinting. Molecules 2016; 21(6): 685. doi:10.3390/molecules21060685.
13. Bittner SM, Smith BT, Diaz-Gomez L, et al: Fabrication and mechanicalcharacterization of 3D printed vertical uniform and gradient scaffoldsfor bone and osteochondral tissue engineering. Acta Biomater 2019; 90:37–48. doi: 10.1016/j.actbio.2019.03.041.
14. Wang W, Caetano G, Ambler WS, et al: Enhancing the hydrophilicityand cell attachment of 3D printed PCL/Graphene scaffolds for bone tis-sue engineering. Materials 2016; 9(12): 992. doi: 10.3390/ma9120992.
15. Kolesky DB, Homan KA, Skylar-Scott MA, Lewis JA: Three-dimensional bioprinting of thick vascularized tissues. Proc Natl AcadSci U S A 2016; 113(12): 3179–84. doi: 10.1073/pnas.1521342113.
16. Placone JK, Engler AJ: Recent advances in extrusion-based 3D printingfor biomedical applications. Adv Healthc Mater 2018; 7(8): 1701161.doi: 10.1002/adhm.201701161.
17. Ning L, Chen X: A brief review of extrusion-based tissue scaf-fold bio-printing. Biotechnol J 2017; 12(8): 1600671. doi: 10.1002/biot.201600671.
18. Ozbolat IT, Hospodiuk M: Current advances and future perspectivesin extrusion-based bioprinting. Biomaterials 2016; 76: 321–43. doi:10.1016/j.biomaterials.2015.10.076.
19. Noor N, Shapira A, Edri R, Gal I, Wertheim L, Dvir T: 3Dprinting of personalized thick and perfusable cardiac patches andhearts. Adv Sci Weinh Baden-Wurtt Ger 2019; 6(11): 1900344.doi: 10.1002/advs.201900344.
20. Senior JJ, Cooke ME, Grover LM, Smith AM: Fabrication of com-plex hydrogel structures using suspended layer additive manufac-turing (SLAM). Adv Funct Mater 2019; 29(49): 1904845. doi:10.1002/adfm.201904845.
21. Hinton TJ, Jallerat Q, Palchesko RN, et al: Three-dimensional printingof complex biological structures by freeform reversible embedding ofsuspended hydrogels. Sci Adv 2015; 1(9): e1500758. doi: 10.1126/sci-adv.1500758.
22. Lee A, Hudson AR, Shiwarski DJ, et al: 3D bioprinting of collagen torebuild components of the human heart. Science 2019; 365(6452): 482.doi: 10.1126/science.aav9051.
23. Skylar-Scott MA, Mueller J, Visser CW, Lewis JA: Voxelated soft mattervia multimaterial multinozzle 3D printing. Nature 2019; 575(7782):330–5. doi: 10.1038/s41586-019-1736-8.
24. Kang H-W, Lee SJ, Ko IK, Kengla C, Yoo JJ, Atala A: A 3D bioprintingsystem to produce human-scale tissue constructs with structural integrity.Nat Biotechnol 2016; 34(3): 312–9. doi: 10.1038/nbt.3413.
25. Jones JC, Burks R, Owens BD, Sturdivant RX, Svoboda SJ, CameronKL: Incidence and risk factors associated with meniscal injuries amongactive-duty US military service members. J Athl Train 2012; 47(1):67–73.
26. Baker BE, Peckham AC, Pupparo F, Sanborn JC: Review of meniscalinjury and associated sports. Am J Sports Med 1985; 13(1): 1–4. doi:10.1177/036354658501300101.
27. Roseti L, Cavallo C, Desando G, et al: Three-dimensional bioprintingof cartilage by the use of stem cells: a strategy to improve regeneration.Mater Basel Switz 2018; 11(9). doi: 10.3390/ma11091749.
28. Pereira H, Frias AM, Oliveira JM, Espregueira-Mendes J, Reis RL:Tissue engineering and regenerative medicine strategies in menis-cus lesions. Arthrosc J Arthrosc Relat Surg Off Publ ArthroscAssoc N Am Int Arthrosc Assoc 2011; 27(12): 1706–19. doi:10.1016/j.arthro.2011.08.283.
29. Daly AC, Freeman FE, Gonzalez-Fernandez T, Critchley SE, NultyJ, Kelly DJ: 3D bioprinting for cartilage and osteochondral tissue
MILITARY MEDICINE, Vol. 185, September/October 2020 e1517
Dow
nloaded from https://academ
ic.oup.com/m
ilmed/article/185/9-10/e1510/5854784 by guest on 26 June 2022

Military Medical Applications of 3D Bioprinting
engineering. Adv Healthc Mater 2017; 6(22): 1700298. doi: 10.1002/adhm.201700298.
30. You F, Eames BF, Chen X: Application of extrusion-based hydrogelbioprinting for cartilage tissue engineering. Int J Mol Sci 2017; 18(7):1597. doi: 10.3390/ijms18071597.
31. Cross JD, Ficke JR, Hsu JR, Masini BD, Wenke JC: Battle-field orthopaedic injuries cause the majority of long-term disabil-ities. J Am Acad Orthop Surg 2011; 19(Suppl 1): S1–7. doi:10.5435/00124635-201102001-00002.
32. Corona BT, Rivera JC, Owens JG, Wenke JC, Rathbone CR: Vol-umetric muscle loss leads to permanent disability following extrem-ity trauma. J Rehabil Res Dev 2015; 52(7): 785–92. doi: 10.1682/JRRD.2014.07.0165.
33. Wang Z, Lee SJ, Cheng H-J, Yoo JJ, Atala A: 3D bioprinted functionaland contractile cardiac tissue constructs. Acta Biomater 2018; 70: 48–56.doi: 10.1016/j.actbio.2018.02.007.
34. Popov A, Malferrari S, Kalaskar DM: 3D bioprinting for muscu-loskeletal applications. J 3D Print Med 2017; 1(3): 191–211. doi:10.2217/3dp-2017-0004.
35. García-Lizarribar A, Fernández-Garibay X, Velasco-Mallorquí F,Castaño AG, Samitier J, Ramon-Azcon J: Composite biomaterialsas long-lasting scaffolds for 3D bioprinting of highly alignedmuscle tissue. Macromol Biosci 2018; 18(10): e1800167. doi:10.1002/mabi.201800167.
36. Kim JH, Seol Y-J, Ko IK, et al: 3D bioprinted human skeletal muscleconstructs for muscle function restoration. Sci Rep 2018; 8(1): 12307.doi: 10.1038/s41598-018-29968-5.
37. Choi Y-J, Jun Y-J, Kim DY, et al: A 3D cell printed muscle construct withtissue-derived bioink for the treatment of volumetric muscle loss. Bioma-terials 2019; 206: 160–9. doi: 10.1016/j.biomaterials.2019.03.036.
38. Laternser S, Keller H, Leupin O, Rausch M, Graf-Hausner U, RimannM: A novel microplate 3D bioprinting platform for the engineering ofmuscle and tendon tissues. SLAS Technol 2018; 23(6): 599–613. doi:10.1177/2472630318776594.
39. Yan W-C, Davoodi P, Vijayavenkataraman S, et al: 3D bioprinting ofskin tissue: from pre-processing to final product evaluation. Adv DrugDeliv Rev 2018; 132: 270–95. doi: 10.1016/j.addr.2018.07.016.
40. Cubo N, Garcia M, Del Cañizo JF, Velasco D, Jorcano JL: 3D bioprintingof functional human skin: production and in vivo analysis. Biofabrication2016; 9(1): 015006. doi: 10.1088/1758-5090/9/1/015006.
41. Derr K, Zou J, Luo K, et al: Fully three-dimensional bioprinted skinequivalent constructs with validated morphology and barrier func-tion. Tissue Eng Part C Methods 2019; 25(6): 334–43. doi: 10.1089/ten.TEC.2018.0318.
42. Randall MJ, Jüngel A, Rimann M, Wuertz-Kozak K: Advances in thebiofabrication of 3D skin in vitro: healthy and pathological models. FrontBioeng Biotechnol 2018; 6: 154. doi: 10.3389/fbioe.2018.00154.
43. Gudapati H, Dey M, Ozbolat I: A comprehensive review on droplet-based bioprinting: past, present and future. Biomaterials 2016; 102:20–42. doi: 10.1016/j.biomaterials.2016.06.012.
44. Aqueous Two-Phase Emulsion Bioink-Enabled 3D Bioprinting ofPorous Hydrogels - Ying - 2018 - Advanced Materials - WileyOnline Library. https://onlinelibrary.wiley.com/doi/abs/10.1002/adma.201805460; accessed June 12, 2019.
45. Graham AD, Olof SN, Burke MJ, et al: High-resolution patternedcellular constructs by droplet-based 3D printing. Sci Rep 2017; 7(1):7004. doi: 10.1038/s41598-017-06358-x.
46. Ozbolat IT, Moncal KK, Gudapati H: Evaluation ofbioprinter technologies. Addit Manuf 2017; 13: 179–200. doi:10.1016/j.addma.2016.10.003.
47. Hölzl K, Lin S, Tytgat L, Vlierberghe SV, Gu L, Ovsianikov A: Bioinkproperties before, during and after 3D bioprinting. Biofabrication 2016;8(3): 032002. doi: 10.1088/1758-5090/8/3/032002.
48. Knowlton S, Anand S, Shah T, Tasoglu S: Bioprinting for neu-ral tissue engineering. Trends Neurosci 2018; 41(1): 31–46. doi:10.1016/j.tins.2017.11.001.
49. Lee V, Singh G, Trasatti JP, et al: Design and fabrication of humanskin by three-dimensional bioprinting. Tissue Eng Part C Methods 2013;20(6): 473–84. doi: 10.1089/ten.tec.2013.0335.
50. Lee W, Debasitis JC, Lee VK, et al: Multi-layered culture ofhuman skin fibroblasts and keratinocytes through three-dimensionalfreeform fabrication. Biomaterials 2009; 30(8): 1587–95. doi:10.1016/j.biomaterials.2008.12.009.
51. Filardo G, Petretta M, Cavallo C, et al: Patient-specific meniscus pro-totype based on 3D bioprinting of human cell-laden scaffold. BoneJoint Res 2019; 8(2): 101–6. doi: 10.1302/2046-3758.82.BJR-2018-0134.R1.
52. Moon S, Hasan SK, Song YS, et al: Layer by layer three-dimensional tis-sue epitaxy by cell-laden hydrogel droplets. Tissue Eng Part C Methods2009; 16(1): 157–66. doi: 10.1089/ten.tec.2009.0179.
53. Kim BS, Lee J-S, Gao G, Cho D-W: Direct 3D cell-printing ofhuman skin with functional transwell system. Biofabrication 2017; 9(2):025034. doi: 10.1088/1758-5090/aa71c8.
54. Bajaj P, Schweller RM, Khademhosseini A, West JL, Bashir R: 3D bio-fabrication strategies for tissue engineering and regenerative medicine.Annu Rev Biomed Eng 2014; 16: 247–76. doi: 10.1146/annurev-bio-eng-071813-105155.
55. Norotte C, Marga FS, Niklason LE, Forgacs G: Scaffold-free vasculartissue engineering using bioprinting. Biomaterials 2009; 30(30): 5910–7.doi: 10.1016/j.biomaterials.2009.06.034.
56. Christensen K, Xu C, Chai W, Zhang Z, Fu J, Huang Y: Freeform inkjetprinting of cellular structures with bifurcations. Biotechnol Bioeng 2015;112(5): 1047–55. doi: 10.1002/bit.25501.
57. Bohandy J, Kim BF, Adrian FJ: Metal deposition from a supported metalfilm using an excimer laser. J Appl Phys 1986; 60(4): 1538–9. doi:10.1063/1.337287.
58. Hopp B, Smausz T, Kresz N: et al: Survival and proliferative ability ofvarious living cell types after laser-induced forward transfer. Tissue Eng2005; 11(11-12): 1817–23.
59. Ringeisen BR, Chrisey DB, Piqué A, et al: Generation of meso-scopic patterns of viable Escherichia coli by ambient laser trans-fer. Biomaterials 2002; 23(1): 161–6. doi: 10.1016/S0142-9612(01)00091-6.
60. Ringeisen BR, Kim H, Barron JA, et al: Laser printing of pluripotentembryonal carcinoma cells. Tissue Eng 2004; 10(3–4): 483–91. doi:10.1089/107632704323061843.
61. Wu PK, Ringeisen BR: Development of human umbilical vein endothe-lial cell (HUVEC) and human umbilical vein smooth muscle cell(HUVSMC) branch/stem structures on hydrogel layers via biologi-cal laser printing (BioLP). Biofabrication 2010; 2(1): 014111. doi:10.1088/1758-5082/2/1/014111.
62. Michael S, Sorg H, Peck C-T, et al: Tissue engineered skin substitutescreated by laser-assisted bioprinting form skin-like structures in thedorsal skin fold chamber in mice. PLoS One 2013; 8(3): e57741. doi:10.1371/journal.pone.0057741.
63. Keriquel V, Oliveira H, Rémy M, et al: In situ printing of mesenchymalstromal cells, by laser-assisted bioprinting, for in vivo bone regenera-tion applications. Sci Rep 2017; 7(1): 1–10. doi: 10.1038/s41598-017-01914-x.
64. Catros S, Fricain J-C, Guillotin B, et al: Laser-assisted bioprint-ing for creating on-demand patterns of human osteoprogenitor cellsand nano-hydroxyapatite. Biofabrication 2011; 3(2): 025001. doi:10.1088/1758-5082/3/2/025001.
65. Zhang YS, Yue K, Aleman J, et al: 3D bioprinting for tissueand organ fabrication. Ann Biomed Eng 2017; 45(1): 148–63. doi:10.1007/s10439-016-1612-8.
e1518 MILITARY MEDICINE, Vol. 185, September/October 2020
Dow
nloaded from https://academ
ic.oup.com/m
ilmed/article/185/9-10/e1510/5854784 by guest on 26 June 2022

Military Medical Applications of 3D Bioprinting
66. Kelly BE, Bhattacharya I, Heidari H, Shusteff M, Spadaccini CM, TaylorHK: Volumetric additive manufacturing via tomographic reconstruction.Science 2019; 363(6431): 1075. doi: 10.1126/science.aau7114.
67. Xue D, Zhang J, Wang Y, Mei D: Digital light processing-based 3D print-ing of cell-seeding hydrogel scaffolds with regionally varied stiffness.ACS Biomater Sci Eng 2019; 5(9): 4825–33. doi: 10.1021/acsbiomate-rials.9b00696.
68. Grigoryan B, Paulsen SJ, Corbett DC, et al: Multivascular net-works and functional intravascular topologies within biocompati-ble hydrogels. Science 2019; 364(6439): 458. doi: 10.1126/science.aav9750.
69. Bernal PN, Delrot P, Loterie D, et al: Volumetric bioprinting of com-plex living-tissue constructs within seconds. Adv Mater 2019; 31(42):1904209. doi: 10.1002/adma.201904209.
MILITARY MEDICINE, Vol. 185, September/October 2020 e1519
Dow
nloaded from https://academ
ic.oup.com/m
ilmed/article/185/9-10/e1510/5854784 by guest on 26 June 2022