35070298.pdf - International Atomic Energy Agency
131
NAHRES-72 Vienna, 2002 CO-ORDINATED RESEARCH PROJECT ON ISTOPIC AND COMPLEMENTARY TOOLS FOR THE STUDY OF MICRONUTRIENT STATUS AND INTERACTIONS IN DEVELOPING COUNTRY POPULATIONS EXPOSED TO MULTIPLE NUTRITIONAL DEFICIENCES Report on the First Research Co-ordination Meeting IAEA Headquarters, Vienna, 24-28 June 2002 INTERNATIONAL ATOMIC ENERGY AGENCY
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of 35070298.pdf - International Atomic Energy Agency

NAHRES-72
Vienna, 2002
CO-ORDINATED RESEARCH PROJECT
ON
ISTOPIC AND COMPLEMENTARY TOOLS FOR THE STUDY OF MICRONUTRIENT STATUS AND INTERACTIONS IN DEVELOPING COUNTRY POPULATIONS EXPOSED TO
MULTIPLE NUTRITIONAL DEFICIENCES
Report on the First Research Co-ordination Meeting
IAEA Headquarters, Vienna, 24-28 June 2002
INTERNATIONAL ATOMIC ENERGY AGENCY

EDITORIAL NOTE This report is not a formal publication of the International Atomic Energy Agency (IAEA). Although all rights are reserved by the IAEA the report may nevertheless be freely reviewed, abstracted, reproduced and translated, in part or in whole with appropriate citation – but not for sale nor for use in conjunction with commercial purposes. The views expressed in this report do not necessarily reflect those of the IAEA or of governments of the Member States or organizations under whose auspices the work described herein was carried out. The use in this report of particular designations of countries or territories does not imply any judgment by the IAEA as to the legal status of such countries or territories, of their authorities and institutions or of the delimitation of their boundaries. The mention of specific companies or of their products or brand names does not imply any endorsement or recommendation on the part of the IAEA. Some of the reports in the NAHRES series are recorded in the IAEA’s International Nuclear Information System (INIS).

ISOTOPIC AND COMPLEMENTARY TOOLS FOR THE STUDY OF MICRONUTRIENT STATUS AND INTERACTIONS IN DEVELOPING COUNTRY POPULATIONS EXPOSED TO
MULTIPLE NUTRITIONAL DEFICIENCES
Report on the First Research Co-ordination Meeting
IAEA Headquarters, Vienna, 24-28 June 2002
NAHRES-72, IAEA, Vienna (2002)
A report prepared by the
Section of Nutritional and Health-Related Environmental Studies Division of Human Health
Department of Nuclear Sciences and Applications International Atomic Energy Agency P.O. Box 100, A-1400 Vienna, Austria
Single copies of this report are available cost-free on request from the above address


CONTENTS
PART I: SUMMARY REPORT………………………………………………………1 PART II: HIGHLIGHTS AND ACHIEVEMENTS………………………………….9 PART III: COUNTRY REPORTS
STABLE ISOTOPE STUDIES ON IRON BIO-AVAILABILITY IN YOUNG INDIAN WOMEN: EFFECTS OF NUTRITIONAL STATUS, INTERACTIONS AND ETHNICITY S. MUTHAYYA, S.K. AGGARWAL, T. WALCZYK, A.V. KURPAD R. HURRELL….………………………………………………………………………..23
MASS SPECTROMETRY FOR DETERMINING ISOTOPE RATIOS OF IRON (Fe) S.K.AGGARWAL………………………………………………………………………..31 ESTIMATING BIO-AVAILABILITY OF ZINC AND IRON FROM HOME-AVAILABLE COMPLEMENTARY FOODS IN PAKISTAN: A STUDY IN YOUNG INFANTS USING STABLE ISOTOPES ZULFIQAR A. BHUTTA, RAHAT NAZ, LENA DAVIDSON, THOMAS WALCZYK, IQTIDAR KHAN…………………………………………………..39
EVALUATION OF BIOAVAILABILITY OF FOOD FORTIFICANTS USING STABLE ISOTOPIC METHODS DAVID C. HILMERS, STEVEN A. ABRAMS………………..……………………………51
INTERACTION BETWEEN MICRONUTRIENTS, THEIR IMPACT ON BIOAVAILABILITY AND SIGNIFICANCE IN NUTRITION INTERVENTION CHANDRANI E. LIYANAGE…………………………….………………………………59 EVALUATION OF THE NEWLY PROPOSED VITAMIN A SUPPLEMENTATION REGIMEN FOR POSTPARTUM MOTHERS USING STABLE CARBON ISOTOPES SAMUEL NEWTON, SHERRY A. TANUMIHARDJO, BRUNO DE BENOIST…………….…..67
EFFECT OF THE MOST COMMON SPICES AND HERBS IN TYPICAL NORTHEASTER THAI DIET ON HUMAN IRON ABSORPTION EMORN WASANTWISUT, S. TUNTIPOPIPAT, P.WINICHAGOON S. CHAROENKIATKUL, R. KONGKACHUICHAI…………….……………………………85

EFFECT OF ZINC AND FAT INTAKE ON ABSORPTION AND CONVERSION OF INGESTED β-CAROTENE TO VITAMIN A IN LACTATING INDONESIAN WOMEN MUHILAL, DEWI PERMAESIH, ABDULLAH FIRMANSAH, CLIVE WEST, HANS VERHOEF…..………………………………………………….….95
ASSESSMENT OF NATURAL VARIATION OF IRON AND ZINC ISOTOPE RATIOS DURING AN IRON INTERVENTION STUDY IN LACTATING WOMEN OF BANGLADESH J.A. HOOGEWERFF, M.A.WAHED, K.E. ISLAM, B. TEURCHER, S.K. ROY, M.A. MALEK…………………………………………………………...…107
PART IV: APPENDICES Appendix 1: Agenda of the Meeting………………………………………………..115
Appendix 2: List of Participants……………………………………………….…...119

PART I: SUMMARY REPORT


FIRST RESEARCH CO-ORDINATION MEETING OF THE THEMATIC CO-ORDINATED RESEARCH PROJECT ON “ISOTOPIC AND COMPLEMENTARY TOOLS FOR THE STUDY OF MICRONUTRIENT STATUS AND INTERACTIONS IN DEVELOPING COUNTRY POPULATIONS EXPOSED TO MULTIPLE MICRONUTRIENT DEFICIENCIES”
SUMMARY REPORT
Section of Nutritional and Health-Related Environmental Studies, Division of Human Health, Department of Nuclear Sciences and Applications, International Atomic Energy Agency, P.O. Box 100, A-1400 Vienna, Austria
INTRODUCTION From a global perspective and in spite of decades of nutrition programmes, micronutrients deficiency is at alarming proportions in many developing societies today. It affects millions of people worldwide, and includes consequences that potentially compromise morbidity, mortality, cognitive development, and growth, reproductive and work capacity. Recent estimates by the WHO are that deficiencies of iron (Fe), iodine (I), and vitamin A continue to influence the health of 2000 million, 740 million, and 250 million persons respectively. In addition to these three micronutrients, the possible negative consequences of deficiencies of zinc (Zn), copper (Cu) and selenium (Se) are now also being increasingly recognized as important health concerns. As a result of the increasing recognition of the co-existence of multiple micronutrient deficiencies in developing countries, United Nations Agencies have urged that supplementation, fortification and dietary modification/diversification programmes are designed to combat multiple micronutrient deficiencies simultaneously. Fortificant levels for fortification, like supplementation, must be carefully selected to minimize risk of antagonistic nutrient interactions and to take into account the toxic threshold level for normal individuals. Possible antagonistic interactions that may interfere with the utilisation of trace elements in the supplements or fortificants per se, and/or with the utilization of elements intrinsic to the food or the meal include those between Cu-Zn, Cu-Fe, Fe-Zn, Mn-Fe, Ca-Zn. Stable isotope techniques play an important role in quantifying the optimal levels and the bioavailability of micronutrient supplements and fortificants for a range of indigenous meals consumed in developing countries, especially those containing potent absorption inhibitors. This Capacity building CRP or Thermatic CRP (T-CRP) addresses the need to develop effective strategies to combat micro-nutrient malnutrition in developing countries using isotopic and nuclear methods, the focus being primarily on the known incidence of Fe, I, vitamin A deficiencies in humans and the potential for deficiencies of other trace minerals (e.g. Zn, Cu, Se) due to inadequate intakes, and the possible interactions between nutrients (e.g. nutrient affecting the availability of another nutrient). This CRP aims to bring in several issues concerning micronutrient malnutrition under one project to enable participants to choose an area that best suits their country’s public health problems. In addition, this CRP is aimed at the creation of a high educational level degree (e.g. PhD) from each participating center, and establishing a foundation for developing leadership skills among young nutrition professionals.
1

This CRP is based on the recommendations of two Consultants meetings (NAHRES 57, 1999) and (NAHRES 55, 2000). The first Research Co-ordination Meeting (RCM) of the IAEA-Thematic Co-ordinated Research Project on “Isotopic and complementary tools for the study of micronutrient status and interactions in developing country populations exposed to multiple nutritional deficiencies” was held at the IAEA Headquarters in Vienna from 24-28 June 2002. This report summarizes the main activities of this first RCM. Participating countries are: Ghana, United Kingdom, United States of America, India, Indonesia, The Netherlands, Pakistan, Bangladesh, Sri Lanka, Thailand, Switzerland and Austria. THE OVERALL OBJECTIVE • To devise approaches for sustainable focus on micronutrient malnutrition in populations
by evaluating micro-nutrient interactions (Fe, folic acid, Zn, Vitamin A, I, Se, Cu, among others) using isotopic and complementary tools for assessing micronutrient status.
• To support capacity building in the area of food and nutrition in developing countries.
SPECIFIC PROGRAMME OBJECTIVES • To measure nutrient bio-availability from fortified or natural foods eaten in meals, and to
evaluate the status of different micronutrients in target populations and help evaluate interventions undertaken to improve micronutrient status.
• To assist large scale physiologically oriented studies investigating Fe and Zn deficiency in target populations in field studies; instruments for making isotopic measurements have considerably improved so that larger numbers of samples can be analysed with adequate precision using isotopic (e.g. stable isotopes) and related techniques (e.g. ICP-MS and TIMS).
• To evaluate nutritional interventions at the national, regional or international level that have potential wide spread application, for which evidence of efficacy and safety needs to be established before wide-spread use can be recommended.
• To promote post-graduate level research and training in developing countries leading to the award of higher degrees in the area of food and nutrition. This is accomplished by giving an opportunity to the participating countries to structure a research proposal that is relevant to their problem in the micronutrient area.
EXPECTED RESEARCH OUTPUTS • Harmonization of the protocols and procedures for sampling and analysis. • Determination of micronutrient deficiency levels in target populations. • Understanding mechanisms of interactions between nutrients.
2

EXPECTED ACADEMIC OUTPUTS • Creation of at least one PhD from each participating centre, and establishing a foundation
for developing leadership skills among young nutrition professionals. • Publication of scientific papers in peer reviewed journals by the PhD scholar. • Presentation of the results of the IAEA study at various national and international
professional/scientific congresses. • Increased collaboration between the scientists from the developed and developing
countries in the field of medical research. PROJECT HIGHLIGHTS Individual TCRP project was presented by the Chief Scientific Investigator followed by comments of the consultants and general discussion. Highlights of the TCRP projects including comments are presented below: Ghana “Evaluation of the Newly Proposed Vitamin A Supplementation Regimen for Postpartum Mothers using Stable Carbon Isotopes”. The collaborating institutes included the Kintampo Health Research Center, Ghana; University of Wisconsin, Madison, USA and the World Health Organization. The project aims to evaluate changes in vitamin A status after administration of 400,000 IU versus 200,000 IU using the modified relative dose response (MRDR) test and to determine in parallel, vitamin A body pool and reserves using the C13-retinol isotope dilution test. Comments: Suggestion was made for the investigators to provide the basis for small sample size. India “Stable Isotope Studies on Iron Bio-availability in Young Indian Women. Effects of Nutritional Status, Interactions and Ethnicity”. The collaborating Institutions are St-John’s Medical College, Bangalore, India and Bhabha Atomic Research Center, Mumbai, India and Laboratory of Human Nutrition, Swiss Federal Institute of Technology, Zurich, Switzerland. The project aims to assess by means of stable isotope technique, the response of young Indian women of different iron status to the effect of enhancers and inhibitors of dietary iron absorption; and to identify differences in iron absorption due to ethnical differences using stable isotope technique. Comments: Suggestions were made to redefine the population group (slum dwellers versus lower middle class) and to consider prioritizing the objectives as well as downsizing the proposal. Bangladesh The project “Assessment of Natural Variation of Iron and Zinc Isotope Ratios During an Iron Intervention Study in Lactating Women of Bangladesh” represents collaboration between ICDDR,B Center for Health and Population Research, Dhaka, Bangladesh; Institute of Nutrition and Food Science, Dhaka University, Bangladesh and Institute of Food Research,
3

Norwich, United Kingdom. The project aims to assess the usefulness of iron and zinc isotopic variation in biological samples as a novel status indicator in lactating women. Comments: The project should focus on non-intervention malnourished women and to increase sample size. The protocol needs to be reviewed with bi-lateral consultations between the Contract and Agreement Holders. Indonesia “Effect of Zinc and Fat Intake on Absorption and Conversion of Ingested B-carotene to Vitamin A in Lactating Indonesian Women”. The collaborating institutions are the Nutrition Research and Development Centre, Bogor, Indonesia and Wageningen University, The Netherlands. The objective is to evaluate the effect of dietary fat and/or zinc on the bioefficacy of ingested beta-carotene in lactating Indonesian women. Comments: Suggestions were made to narrow postpartum range, to observe changes of status during the run-in period (fat 40 mg/day, zinc 10 mg/day) and to consider a shorter period of adjustment using a standardized diet. Pakistan “Estimating Bio-availability of Zinc and Iron from Home-Available Complementary Foods in Pakistan: a Study in Young Infants using Stable Isotopes”. The collaborating institutes include The Aga Khan University, Karachi, Pakistan and the Laboratory of Human Nutrition, Swiss Federal Institute of Technology, Zurich, Switzerland. The project aims to compare the bio-availability of iron and zinc from a standardized home-available weaning diet (khitchri) and micronutrient supplement using stable isotope techniques. Comments: The form of supplements (ferrous sulfate-unstable, the use of tablets versus syrup) should be reviewed; the method of feeding labeled complementary food to infants; baseline iron absorption in supplemented versus non-supplemented infants; and to control the variable of “contact time” (time spent with mothers/caretakers) between groups. Sri Lanka “Interaction between micronutrients, their impact on bioavailability and significance in nutrition intervention”. The collaborating institutes include Faculty of Medicine, University of Ruhuna, Sri Lanka and USDA/ARS Children’s Nutrition Research Centre, Houston, Texas, USA. The project aims to study possible interactions between iron and zinc that may interfere with utilization by a double-blind randomized controlled trial using stable isotope techniques. Comments: Suggestions were made on the issues concerning sustainability of the micronutrient supplementation program; difficulties on the preparation of isotopically labeled elemental iron used as fortificant in wheat flour; adjusting the project towards impact of micronutrient supplementation; focusing “iron and zinc” in the supplement; including cross-sectional study on zinc and selenium status; and to include zinc-protoporphyrin as status indicator.
4

Thailand “Effect of the Most Common Spices and Herbs in Typical Northeastern Thai Diet on Human Iron Absorption”. The collaborating institutes are the Institute of Nutrition, Mahidol University and the Laboratory of Human Nutrition, Swiss Federal Institute of Technology, Zurich, Switzerland. The project aims to identify relevant spices and herbs commonly used in Thai habitual diets; to characterize the selected spices and herbs regarding their content of inhibitors and enhancers of iron absorption; and to determine the effect of the selected spices and herbs on human iron absorption using stable isotope techniques. Comments: Suggestions were made to consider the population prevalence of H. pylori infection for subject selection; complete the analytical profile of herbs and spices; seasonal variation and a possibility to include in vitro test prior to in vivo study.
RECOMMENDATIONS: • Project teams should review their protocols according to the recommendations issued
from the meeting and send the updated version to NAHRES. • IAEA should procure isotopes in “bulk” from a reliable source. • Resource mobilization: mechanism to link TCRP to obtain additional support from other
sources such as Regional TC, Ellison Medical Foundation-International Nutrition Foundation Fellowship Program, International funding bodies etc. should be explored.
• Participants are encouraged to cooperate on a bilateral and/or multilateral basis, especially if their research interests are closely related. The co-operation may take any form including exchange of sampling and analytical methodologies, expertise, data, and samples for comparative and/or complementary analyses (e.g. to increase the number of analytes).
• Participants are requested to acknowledge the contribution of the IAEA quoting the CRP in their publications and circulate these amongst the participants.
• Video-conferencing as a complementary tool to RCM (every 6-8 months) should be explored.
NEXT RCM The next RCM is planned for 2004. Location will be decided later.
5

6
PART II: HIGHLIGHTS
AND ACHIEVEMENTS
7

8

TITLE EVALUATION OF THE NEWLY PROPOSED VITAMIN A SUPPLEMENTATION REGIMEN FOR POSTPARTUM MOTHERS USING STABLE CARBON ISOTOPES
CSI SAMUEL NEWTON
INSTITUTE: Kintampo Health Research Center, Health Research Unit, Ministry of Health, PO Box 200, Kintampo, Brong Ahafo Region, Ghana
SCIENTIFIC BACKGROUND Vitamin A deficiency is a major public health program in many developing countries and has even been identified in the lower socioeconomic groups in the United States. Because serum retinol concentrations are homeostatically controlled and can be depressed by infection, other indicators of vitamin A status have been developed. To this end, we will apply two sensitive indicators of vitamin A status, the modified relative dose response (MRDR) test and the 13C2-retinol isotope dilution assay to a program in Ghana designed to improve total body reserves of vitamin A in lactating women.
SCIENTIFIC OBJECTIVES • To determine the length of time mothers are protected against depletion after receiving
either 400,000 IU of vitamin A in two doses of 200,000 IU 24 hours apart or one dose of 200,000 IU. The modified relative dose response (MRDR) test will be used at monthly intervals for 5 months post-dosing to assess changes in vitamin A status.
• To determine the degree of dilution in the vitamin A body pool after dosing women with either 200,000 or 400,000 IU of vitamin A using stable 13C2-retinol as a tracer.
• To determine the difference in total vitamin A body reserves of women who received either 200,000 or 400,000 IU of vitamin A using the 13C2-retinol isotope dilution (13C2-RID) test.
OUTPUT SINCE ACCEPTANCE OF PROPOSAL • We have prepared the 3,4-didehydroretinyl acetate for the baseline determination and will
continue synthesis for the follow-up intervention. • The synthesis procedure for the labeled retinol has been worked out and we will be able to
synthesize the necessary labeled retinol in the next year. • We have identified a BSc candidate who will continue towards their MSc leading onto a
Ph.D. in the future. • We have prepared a larger grant based upon the proposed studies and will continue to look
for supplemental money. • Ghana has received ethical approval for the first study. • Our entire team of senior investigators was able to attend the first RCM meeting.
9

PROGRAMME OF WORK FOR 2002/2003 • We will begin the baseline MRDR assessment beginning in September 2002 which is part
of the larger WHO funded Vitamin A supplementation trial. • We will synthesize the labeled retinol at UW-Madison. • We will seek ethical approval for the stable isotope studies. • We will contact the University of Ghana to ensure admission to the MSc program.
EXPECTED OUTPUT FOR 2002 • We will finish the baseline assessment using the MRDR. • The labeled retinol will be synthesized. • Ethical approval will be completed.
APPROACH OF WORK FOR 2003 • The analytical procedures will be worked out in the USA laboratory. • The isotope will be delivered to Ghana and the second objective will be started and
completed and the samples will be hand carried to USA. • The households for objective 3 will be determined.
PROGRAMME OF WORK FOR 2003 • The samples for the MRDR will be completed at Noguchi Memorial Institute for Medical
Research of the University of Ghana and the isotope samples will be analyzed at UW-Madison.
SUPPLEMENTARY PROJECTS • We will continue to seek external funds to work out the methods for the isotope studies to
be performed in infants and children in at-risk populations. SUMMARY Thus, we plan to use stable carbon methods to answer important public health questions concerning vitamin A in the next few years. We look forward to aiding vitamin A supplementation programs through evaluation of outcomes.
10

TITLE: ASSESSMENT OF NATURAL VARIATION OF IRON AND ZINC ISOTOPE RATIOS DURING AN IRON INTERVENTION STUDY IN LACTATING WOMEN OF BANGLADESH.
CSI: M A WAHED
INSTITUTE: ICDDR,B, Centre for Health and Population Research Dhaka-1212, Bangladesh SCIENTIFIC BACKGROUND: The natural isotopic variation of Fe and Zn isotopes in human tissues might be influenced by the nutritional status of the individuals. It has been documented that the population of Bangladesh, particularly children and woman of childbearing age, are subject to systematic Fe and Zn deficiency. SCIENTIFIC OBJECTIVE: To assess if the of natural variation of iron and zinc isotope ratios during an iron intervention study in lactating women (6 to 9 months post partum) of Bangladesh reflects the expected change in Fe and Zn status. OUTPUT • Representatives of both the CHI and the AHI attended the first RCM. • Refinement of the initial proposal as discussed in the first T-CRP RCM. • The Ph.D. candidate has been identified and evaluated. • Provisions have been made for the obtainment of the Ph.D. at Dhaka University. • The protocol for the Research Review Comm. and Ethical Review Comm. (RRC/ERC) is
short of being finalized. PROGRAM OF WORK JUNE 2002 –DEC 2003 • Finalize protocol and submit to RRC/ERC • Initial training of the Ph.D. candidate in basic isotope methods, volunteer management
and sampling methods, data recording on volunteers and diet during early autumn of 2002 (One to two months at the AHI).
• Recruitment of volunteers and additional staff and procurement of consumables, supplies and equipment.
• Dietary data collection (habitual Fe and Zn intake) • Selection of suitable Fe (and possibly Zn) supplement • Visit of AHI staff to CHI to fine tune the project in the field. • Perform the intervention study • Determine relevant parameters for Fe and Zn status in Bangladesh • Prepare sample in Bangladesh for isotope analysis at the AHI • Perform final sample preparation for isotopic ratio analysis and measurement of Fe and Zn
isotope ratios at the AHI (6 months during summer/autumn 2003) • Initial data analysis, draft report for 2nd RCM and make suggestions for continuation of
the project.
11

EXPECTED OUTPUT FOR FIRST 18 MONTHS • Preliminary assessment of the variation of Fe and Zn isotope ratios in the volunteers due
to the intervention study. • An assessment of the variation of Fe and Zn isotopes in the Bangladeshi diet. • Training of the Ph.D. candidate. • Suggestions for continuing/supplementary research • Report for 2nd RCM
BUDGET Main problem is the procurement of the UV705 Digester (9000 USD) with the present allocation of 6000 USD to the CHI. An advance on the budget, or additional funds could solve this problem.
OTHER PROBLEMS ARE • Agreement on the funding for the totally 9 months visit of the Ph.D. student to the AHI. • Agreement on the funding for the visit of two scientists from the AHI for a short period to
the CHI. • Costs of relevant Labtests at the CHI.
12

TITLE: ESTIMATING BIO-AVAILABILITY OF ZINC AND IRON FROM HOME- AVAILABLE COMPLEMENTARY FOODS IN PAKISTAN: A STUDY IN YOUNG INFANTS USING STABLE ISOTOPES
CSI: DR ZULFIQAR A. BHUTTA
INSTITUTE: The Aga Khan University, Karachi, Pakistan
SCIENTIFIC BACKGROUND: Studies of infant growth patterns in Pakistan reveal that the growth faltering starts after 5-6 months of age, and usually parallels the transition from exclusive or predominant breastfeeding to mixed feeding with home available complementary foods. Micronutrient deficiencies it is possible to improve the dietary quality and diversification of complementary foods but it is unclear to programs if micronutrient supplementation is the most efficient way of addressing the public problem of micronutrient deficiencies. This protocol will be nested within the larger cluster randomized project on a complementary feeding intervention in a community setting in Pakistan
SCIENTIFIC OBJECTIVES: • To develop and validate a simple minimally-invasive protocol in a phased fashion, using
stable isotopes for the estimation of bioavailability of iron and zinc in ambulatory young children receiving home available diets and complementary foods.
• To compare the bioavailability of iron and zinc from a standardized home-available weaning diet (khitchri) and micronutrient supplement extrinsically labeled with stable-isotopes (58Fe, 57Fe, 68Zn and 67Zn).
OUTPUT SINCE ACCEPTANCE OF PROPOSAL: • Given the need to identify additional sources of funding, the mother project was submitted
for funding to the Micronutrient Initiative who have agreed to review it for the second round. Revisions have been submitted and a funding decision will be expected within the next two months.
• In the event of failure to secure funds from the aforementioned source, the proposal will be submitted for funding to the WHO or other agencies such as the Thrasher Fund or the Nestle Nutrition Foundation.
• The principal investigator has paid a site visit to the Laboratory for Human Nutrition in Zurich and the collaborator at the latter institution paid a visit to Karachi in February 2002 and assessed the field site.
• Presently they collaborators have worked together to further modify the isotopic protocol and to streamline a work schedule as indicated below
13

PROGRAMME OF WORK FOR 2002/2003 The following is the proposed plan of activities for the next 12-18 months: 1. The collaborators will review and revise the protocol for stable isotope work in
accordance with the recommendations and feedback at the CRP. 2. This will consist of the following principal alterations to the stable isotope protocol
a. The zinc bioavailability studies will be deferred until Phase 2 of the project and the
first Phase will focus on iron bioavailability work b. The isotope requirement for the Pakistan project for 57Fe and 58Fe will be estimated
and these procured in bulk through IAEA. This information will be conveyed to IAEA within the next 8 weeks.
c. The stable isotope analytical component of the project will be prepared by Dr Lena Davidsson at the Laboratory for Food Sciences in Zurich and submitted to IAEA.
3. The main complementary feeding project preparatory work i.e. preparation of nutrition
education messages, development of the micronutrient supplement (iron and zinc) and field protocols will be undertaken within the next 6 months.
4. We anticipate starting the actual recruitment of the birth cohort in September 2002 with initiation of complementary feeding after about six months i.e. by March 2003.
5. Thus the first series of field-based studies on assessing iron bioavailability will take place in Karachi around June 2003.
6. The first laboratory-based analysis of stable isotope on the first four patients studied will take place in Zurich between August-October 2003.
EXPECTED OUTPUT FOR 2002 • Revised work plan and protocol for the iron bioavailability stable isotope work (Phase 1) • Completion of main complementary feeding protocol and project funding • Development of field operation and work manuals • Procurement plan for stable isotopes (57Fe and 58Fe)
APPROACH & PROGRAMME OF WORK FOR 2003 • Continued surveillance of the birth cohort and recruitment for stable isotope
bioavailability studies. • Initiation of Phase 1 iron bioavailability studies as per protocol June 2003 (at an average 9
months of age) • Analysis of the data from the first four sets of blood samples (for assessment of 57Fe and
58Fe enrichment of RBCs) at Zurich (with the PhD student in attendance)
14

TITLE: EFFECT OF ZINC AND FAT INTAKE ON ABSORPTION AND CONVERSION OF INGESTED ß-CAROTENE TO VITAMIN A IN LACTATING INDONESIAN WOMEN
CSI: MUHILAL
INSTITUTE: Nutrition Research and Development Centre, Ministry of Health, Jalan Dr Sumeru 63, Bogor 16122, Indonesia
SCIENTIFIC BACKGROUND Plant foods are the major source of vitamin A for most of the world’s poor population, but low bioefficacy of provitamin A carotenoids from these foods severely limits the supply of vitamin A. Enhancement of this bioefficacy is required to increase the efficacy and effectiveness of dietary interventions aimed at controlling vitamin A deficiency disorders in developing countries.
STUDY OBJECTIVES The project proposed aims at quantifying the change in bioefficacy of ingested β-carotene that can be achieved by simultaneous consumption of dietary fat and/or zinc in lactating Indonesian women, and to examine the mechanisms involved. We hypothesize that increased dietary fat intake increases the bioavailability of β-carotene ingested, and that an improved zinc intake/status increases either the bioavailability of β-carotene or its bioconversion into vitamin A or both.
OUTPUT SINCE ACCEPTANCE OF THE PROPOSAL • Established contact between collaborating partners (by mail) • Prepared a preliminary proposal • Participated in the Research Coordination Meeting (Vienna, 24-28 June 2002).
PROGRAMME OF WORK FOR 2002/2003 • Preparation of a full proposal • Visit by researchers from Wageningen University to Indonesia to finalise proposal and for
discussions with counterpart institutions. • Application for TC funds from the IAEA. • Submission of proposal(s) to funding agencies to obtain complementary money
(additionally to funds requested from IAEA). • Visit by PhD candidate for a 6-months period to The Netherlands to prepare a detailed
protocol and make other preparations for the study (first phase of a ‘sandwich’ PhD).
15

EXPECTED OUTPUT FOR 2002 • Full proposals developed and submitted to IAEA (to both Division of Nuclear Application
and Division of Technical Cooperation), the Netherlands Foundation for the Advancement of Tropical Research (NWO/WOTRO).
APPROACH AND PROGRAMME OF WORK FOR 2003 • To train the PhD candidate in a 6-months period in The Netherlands (including course
work, development of a detailed protocol and preparations for the study) (1 April - 30 September).
• To request and obtain scientific and ethical clearence in Indonesia and The Netherlands. • To prepare for a pilot study in Indonesia (1 October - 31 December).
16

TITLE: INTERACTION BETWEEN MICRONUTRIENTS, THEIR IMPACT ON BIOAVAILABILITY AND SIGNIFICANCE IN NUTRITION INTERVENTION.
CSI: CHANDRANI E. LIYANAGE
INSTITUTE: Nuclear Medicine Unit, Faculty of Medicine, University of Ruhuna, Sri Lanka
SCIENTIFIC BACKGROUND Micronutrient deficiencies are of greatest public health significance in SLanka, and as such investigating an effective programme for the prevention is urgently required. Scientific objectives: • To study possible interactions between micronutrients (iron and zinc) that may interfere
with utilization by a double blind randomized control trial. • To determine the bioavailability of iron and zinc using stable isotope methodology. • To study iron and zinc status in patients diagnosed as having endemic goitre. • To assess the selenium status among the preadolescents.
OUTPUT SINCE ACCEPTANCE OF THE PROPOSAL: • Literature survey done on epidemiology of micronutrient deficiencies in Sri Lanka and in
other countries, absorption & utilization and interaction of micronutrients, and use of stable isotope methodology in the determination of the absorption of micronutrients.
• Detailed research proposal has been developed and, ethical clearance obtained from the Faculty of Medicine, University of Ruhuna to conduct the proposed studies.
• Preparation of the micronutrient supplements for the randomization trial is in the process, at a private drug company after obtaining approval from the Drug Regulation Authority, Sri Lanka.
PROGRAMME OF WORK FOR 2002/2003 • Carry out sampling for the efficacy study from the preadolescents attending schools in the
Galle District. • Get the manufacturing of micronutrient supplements completed by end of July 2002. • Start the efficacy study and collect baseline information from the study subjects, and carry
out a 24 hour dietary recall in them • Assess growth in them by anthropometry; collect information on school performance by
conducting information processing tests; on morbidity and appetite and, on susceptibility to infections etc.
• Obtain a blood sample to determine the initial status of iron, zinc in them. • Start micronutrient supplementation to the study subjects and visit them at every 2 weeks,
to collect information (in 4 above). • After 4 weeks of supplementation, a sub sample will be selected for the bioavailability
study, and this will be conducted in collaboration with the Bayer College group.
17

• In the bioavailability study group, an initial blood sample and, another sample after 14 days of introducing the stable isotopes will be collected for the stable isotope counting.
• The AHI will visit the project and make available the stable isotopes. • The CRPF will be visiting the Bayer College for the training on stable isotope
methodology. • In the efficacy study, the supplementation trial will be carried out for a period of 12
months. • At the end of 12 months, the growth will be assessed, a blood sample will be collected to
determine the status of iron and zinc and information (in 4 above) will be obtained.
EXPECTED OUTPUT FOR 2002 • To get the micronutrient supplements (capsules) made. • To start the efficacy trial that will be completed in 12 month’s time. • If the Expert visit is made in 2002, bioavailability study would be done and collected the
samples to be taken to AHI for analysis. • To analyse the blood samples collected at base line of the efficacy study, for iron and zinc
status.
APPROACH FOR 2003: • To complete the trial of the efficacy study and assess the impact of the study. • To conduct the bioavailability study if not done in 2002.
PROGRAMME OF WORK FOR 2003: • Supplementation to be continued for a period of 12 months in the efficacy study, and the
blood samples be obtained to determine the levels of iron and zinc. • Statistical analysis would be done to assess the impact of supplementation • CRPF visiting the AHI for the training in stable isotope technology
18

TITLE: EFFECT OF THE MOST COMMON SPICES AND HERBS IN TYPICAL NORTHEASTERN THAI DIET ON HUMAN IRON ABSORPTION
CSI: EMORN WASANTWISUT
INSTITUTE: Institute of Nutrition, Mahidol University, Phutthamonthon 4 Road, Salaya, Phutthamonthon, Nakhon Pathom 73170, THAILAND
SCIENTIFIC BACKGROUND Iron deficiency anaemia is highly prevalent among rural population of Northeast Thailand. The habitual diets are plant-based. Several herbal vegetables and spices such as lead tree leaves, ivy gourd, Thai basil, chilli peppers etc are consumed in a substantial in common Northeast dishes. High contents of phytate and polyphenol compounds including tannin in these herbs and spices may profoundly influence iron bioavailability in the northeast population.
SCIENTIFIC OBJECTIVES • To identify relevant spices and herbs commonly used in Thai habitual diets. • To characterize the selected spices and herbs based on vitamin C, phytate, polyphenol and
tannin contents as well as iron dialisability (in vitro). • To determine the effect of individual spices and herbs as selected by objectives 1 and 2 on
dietary non-heme iron absorption in vivo by stable isotope erythrocyte incorporation technique.
OUTPUT SINCE ACCEPTANCE OF PROPOSAL • Formation of a research investigator team. • Review of scientific data relating to effect of polyphenols and phytate on non-heme iron
absorption. • Compilation of information on food consumption pattern in the upper and lower regions
of Northeast Thailand. • A list of popular dishes with spices and herbs in both regions. • Identify PhD fellow: Miss Siriporn Tuntipopipat. • Discussion with project collaborators from ETH Human Nutrition Laboratory on the
overall design with an emphasis on the in vivo studies.
PROGRAM OF WORK FOR 2002/2003 (18M, SECOND RCM) • To identify popular dishes in habitual northeast diets. • To collect data on frequency of consumption of identified popular dishes in a group of
villages per study area by food frequency questionnaire. • Based on the above information, a list of common spices and herbs in the popular dishes
will be identified. • To quantify the amount of consumption of spices and herbs per dish by a double portion
technique.
19

• To estimate average serving size of individual spices and herbs. • To collect food specimens of spices and herbs in both dry and rainy seasons for further
chemical analysis including ascorbic acid, phytate, tannin and polyphenol contents.
EXPECTED OUTPUT FOR 2002 • Short lists of popular dishes in the upper and lower regions of northeast Thailand. • Frequency of consumption of the popular dishes. • Amount of consumption of common spices and herbs in the popular dishes in the rainy
season. • Estimated serving size of common spices and herbs. • Food samples of spices and herbs in the rainy season.
APPROACH FOR 2003 • To obtain similar data for the “dry” season of the frequency and amount of consumption
of common spices and herbs. • To calculate the average serving size of spices and herbs in both dry and rainy seasons. • To collect food specimens of spices and herbs in both seasons and analyse for nutrient and
non-nutrient contents including ascorbic acid, phytate, tannin and polyphenols.
PROGRAM OF WORK FOR 2003 • Complete field data collection on consumption pattern of common spices and herbs. • Collect food specimens of spices and herbs. • Chemical analysis of nutrient and non-nutrient contents via standard methods.
20

PART III: COUNTRY REPORTS

22

STABLE ISOTOPE STUDIES ON IRON BIO-AVAILABILITY IN YOUNG INDIAN WOMEN: EFFECTS OF NUTRITIONAL STATUS, INTERACTIONS, AND ETHNICITY.
S. MUTHAYYA, PHD1, S.K. AGGARWAL, PHD2, T. WALCZYK, PHD3, A.V.KURPAD, MD, PHD1, R. HURRELL, PHD3
1Division of Nutrition, Department of Physiology, St. John’s Medical College, Sarjapur Road, Bangalore 560 034, India. 2Mass Spectrometry Section, Fuel Chemistry Division, Bhabha Atomic Research Centre, Trombay, Mumbai – 400 085, India. 3Laboratory of Human Nutrition, Institute of Food Sciences, Swiss Federal Institute of Technology (ETH) Zurich, Seestrasse 72, CH-8803 Ruschlikon, Switzerland.
1. BACKGROUND Iron is an essential micronutrient. As an integral part of hemoglobin, it is essential for the transport of oxygen in blood to the tissues. It is an important component of cytochromes and other tissue enzymes that are critical for cellular respiration and of myoglobin that helps maintain oxygen reserve in the muscle. It is also involved in the normal functioning of the immune function, and in the synthesis of steroid hormones and bile acids. There are serious functional consequences to iron deficiency and iron deficiency anemia (IDA) in the human body. The deleterious effects include increased morbidity, preterm delivery, low birth weight, delayed cognitive development, lowered cellular immunity and reduced physical work capacity [1-4]. However, iron deficiency and IDA remain the world’s most common deficiency disease in the 21st century. Recent estimates of people affected with iron deficiency and IDA are 3.5 billion [5]. Iron deficiency anemia is most prevalent and severe in women and children because of their greater physiological need for iron. In India, the prevalence of IDA is high at 40-88 per cent in pregnant women and 50-60 per cent in adolescent girls [6]. Sixteen percent of all maternal deaths in India are attributable to anemia [7]. Deficiency of iron may arise from inadequate intake, impaired absorption or utilization, and blood loss, such as from parasitic infections. Until such a time when sanitary conditions are markedly improved in India, deworming is the only alternative available for control of parasitic infestations. Some studies have shown that iron supplements along with anti-parasitics produce a much greater response in hemoglobin (Hb) levels than iron alone [8] while others have shown that iron supplementation alone raised Hb levels significantly and that the addition of any anti-parasitics did not produce any further effect [9,10]. Country wise data indicates that iron intakes are not very low in the South Asian region [11]. Recent population data for mean iron intakes of Indian women is at 23 mg/day [12]. Regulation of iron in the human body is achieved by control of iron absorption from the intestinal tract since it has no mechanisms to control iron losses. Absorption is increased during deficiency and as body stores increase, the amount of iron absorbed tends to decrease to match losses [13,14]. The extent to which iron is absorbed also depends on the sources and content of iron in a meal and concurrently consumed enhancers or inhibitors of iron absorption. However, it is not known how the body regulates iron absorption in the presence of absorption inhibitors in iron deficient and iron replete individuals. There is also no data on the effect of absorption enhancers in further increasing mineral absorption that is up regulated in an iron deficient state.
23

Dietary iron exists in two chemical forms: heme iron present in flesh foods and non-heme iron found predominantly in plant foods such as cereals, pulses or beans, vegetables, fruits, nuts, dairy products and eggs and in smaller amounts in some animal foods. Heme iron is highly bioavailable (15 – 35%) and is affected only minimally by the composition of meals and gastrointestinal secretions. Non-heme, however, is less available for absorption by the human body (2 - 20%). Its absorption is also subject to the effects of enhancers and inhibitors and the iron status of the individual [15,16]. Cereals, vegetables and pulses (which contain non-heme iron) constitute the regular diet of most Indians. Their intake of more expensive foods such as milk and milk products, fruits and animal products is limited. Though their dietary iron intake, which is primarily non-heme iron, may be close to requirement levels, prevalence of IDA is still among the highest in the world. Such a situation, which appears to be present in many South Asian countries, clearly warrants strategies for improvement of dietary iron absorbed as a long term solution rather than addition of iron to the diet using supplementation or fortification. Of the dietary constituents that can enhance non-heme absorption, ascorbic acid in its natural form (from fruits and vegetables) is important in the South Asian context. It is an effective enhancer both in its natural form and when added as a free compound [17,18]. The enhancing effect is dose related [18]. When ascorbic acid is added to a meal, iron complexes with ascorbic acid in the stomach and passes into the intestine as an iron-ascorbate complex. This complex is not influenced by the ligands that normally bind iron in the duodenum and inhibit absorption [19]. The consumption of ascorbic acid has been shown to be low in poor Indian households [6]. In a randomized experiment on anemic young vegetarian Indian women, 100 g of guava fruit providing 200 mg of ascorbic acid but no iron was included in the meal at both lunch and dinner for one month. This resulted in an increase in Hb levels of 2.2 g/dl while a control group showed no change [20]. A more recent study showed a rise in Hb level of 1.5 g/dl in young Indian women who consumed goose berry juice which contained 40 mg of ascorbic acid, three times a week for a total of 6 months [21]. Many studies have offered data to support the enhancing effect of meat, particularly of cysteine-containing peptides on iron absorption [22,23]. A study of iron absorption from a simple Latin American diet found that 75 g of ground beef improved iron bioavailability as much as 50 mg of ascorbic acid [24]. The effects of these enhancers depend on the amount and /or type of inhibitors in the meal [25]. In recent years, the effects of Na2EDTA as an iron absorption enhancer have been studied. Na2EDTA was found to be as good an enhancer of iron absorption as ascorbic acid when tested in an iron fortified breakfast consumed by Peruvian school children using stable isotopes, 57Fe and 58Fe [26]. The overcoming effect of iron absorption enhancers on inhibitors to enhance iron availability in iron deficient individuals requires meticulous study. Equally, understanding the role of inhibitors of iron absorption will also help in devising methods to improve absorption. Phytic acid present in cereal products, legumes, nuts and seeds is the major factor responsible for low bio-availability of iron in plant based diets. The dose dependent inhibitory of phytate on iron absorption has been demonstrated by adding varying amounts of sodium phytate to bread rolls [27]. Polyphenolic compounds such as phenolic acids, flavonoids and their polymerisation products found in tea, coffee, cocoa and some vegetables have been shown to inhibit iron absorption [28]. The effects of different polyphenol-containing beverages on iron absorption from a bread meal estimated in adult human subjects from the erythrocyte incorporation of radio-Fe showed that herb teas, as well as black tea, coffee and cocoa can be potent inhibitors of iron absorption [29]. Iron absorption from a vegetarian Indian diet low in ascorbic acid was only 2-5% when accompanied by a beverage such as tea [30,31]. A recent study by Samman et al [32] assessed the effect of
24

phenolic-rich extracts obtained from green tea or rosemary on non-heme iron absorption using radio isotopes 55Fe and 59Fe. These investigators found iron absorption to decrease from 12.1% to 8.9% in the presence of green tea and from 7.5% to 6.4% in the presence of rosemary extract. Food processes including soaking, germination and fermentation were, under optimal conditions, demonstrated to completely reduce the phytate content of cereals and vegetables [33]. The need for iron varies markedly during each trimester of pregnancy. Following a decrease during the first trimester, iron requirements increase thereafter through the remainder of pregnancy. Studies with radioactive and stable isotope of iron show that the overall pattern in iron absorption was remarkably similar, i.e. with a progressive rise in absorption as pregnancy advanced [34]. Median iron absorption measured longitudinally in 12 healthy women from a mixed meal using radio labelled iron was 0.7%, 4.5%, 13.5% in the first, second and third trimesters respectively [35]. The relatively low values of iron absorption were reportedly due to several iron absorption inhibitors. In another study conducted by the same author, median iron absorbed during early pregnancy was 3 times greater when a hamburger meal was eaten [36]. In developing country pregnant women, the effects of both high and low amounts of enhancers and inhibitors added to standard diets will provide new insights to developing strategies for improved iron status. It would also be interesting to study ethnic differences in iron bio-availability in apparently healthy non-anemic individuals of comparable nutritional status, diet preferences and other factors. Our current knowledge on the effect of dietary inhibitors and enhancers on mineral and trace element absorption is largely derived from studies conducted in North America and Europe in white populations. Although it is widely assumed it is largely unknown if these findings can be simply extrapolated to other ethnic groups and vice versa. Differences in genotype may affect mineral and trace element metabolism as may differences in general nutritional status or infections. Use of stable isotopes offers a unique opportunity to meet the need for evidence based dietary guidelines for minerals. They provide physiological information regarding nutrient metabolism that is otherwise unobtainable [37]. To date, very few isotope studies have been performed in developing countries. Enriched stable isotopes used as tracers have proven to be the only safe and reliable tools for the study of absorption and metabolism of minerals in humans. Unlike radioisotopes, they can be used in high-risk population groups such as infants, children and women without ethical considerations. Inorganic nutrient metabolism, traditionally, was investigated by the chemical balance technique which is both time and labour intensive with low precision because of inherent methodological problems. It compares the intake of a mineral with its total excretion not taking into account that the faeces contains minerals from both food and endogenous origins. By using isotopic tracers, the metabolic fate of minerals in a particular food or meal can be followed by analysis of the isotope. The use of isotopes to label food minerals allows studies of absorption from single foods and total diets, allowing the systematic study of many factors that influence absorption [38]. Studies of erythrocyte incorporation of stable iron isotopes are currently widely used for studying iron bio-availability [39] with thermal ionisation mass spectrometers (TIMS) providing the most accurate and precise isotope ratio measurements.
25

2. DETAILED STUDY OBJECTIVES AND STUDY PLAN: 2.1. Objectives:
• To better understand the etiology of iron deficiency in women of reproductive age in the Bangalore region, South India
• To identify the most relevant sources of inhibitors of iron absorption (phytic acid and polyphenolic compounds) and enhancers (ascorbic acid, animal protein) in the diet of undernourished women in this region
• To evaluate by means of stable isotope techniques if subjects of different iron status respond in the same way to inhibitors and enhancers of iron absorption in the diet (phytic acid, polyphenolic compounds, ascorbic acid, animal protein).
• To identify by means of stable isotope techniques if the maternal body is able to upregulate iron absorption over the course of pregnancy even at elevated levels of absorption inhibitors in the diet
• To assess the relevance of ethnic differences on the effect of inhibitors and enhancers on dietary iron absorption by means of stable isotope techniques.
2.2. Detailed study plan for the entire duration of the project
2.2.1. Survey on iron (Fe) status, diet and infection in the Bangalore region, South India Identify and study 150 anemic women, between 18 and 35 years of age, from two slum settlements situated in urban Bangalore. Measures • demographic details and anthropometry • three day weighed food records, food frequency questionnaire • Fe status measurements: hemoglobin, serum ferritin, C-reactive protein and serum
transferrin receptors • intestinal parasites Outcome • prevalence of Fe deficiency and Fe deficiency anemia in the region/studied population
group • relevance of infection to the etiology of Fe deficiency and Fe deficiency anemia in the
region/studied population group 2.2.2. Fe content and enhancers/inhibitors of Fe absorption in the South Indian diet Based on the outcomes of the survey, the most relevant foods in the South Indian diet regarding Fe nutrition will be selected. Foods will be analyzed for Fe content, known enhancers of Fe absorption (ascorbic acid) and known inhibitors of Fe absorption (phytic acid and polyphenolic compounds). Meat sources in the diet and mean meat intake will be estimated. Data from food composition data bases will also be used.
26

Outcome • most relevant Fe sources in the South Indian diet • most relevant foods in the local diet that are high in enhancers and inhibitors of Fe
absorption • identification of the test meals to be evaluated in the following Fe absorption studies by
means of stable isotope techniques. Test meals will be identified by Fe content, frequency of consumption and enhancers/inhibitors of Fe absorption.
2.2.3. Influence of Fe status on the effect of Fe absorption inhibitors/enhancers in the diet Fe absorption from two different test meals high and low in enhancers/inhibitors of Fe absorption will be compared by using the double label erythrocyte incorporation technique (57Fe and 58Fe). Test meals will be labeled differently and administered to the same subject on consecutive days for direct comparison. Fe absorption from the test meals will be determined from the fraction of label incorporated into the erythrocytes 14 days after test meal administration. All iron isotopic analysis will be performed by Dr S.K. Aggarwal, Head, Mass Spectrometry Section, Fuel Chemistry Division, Bhabha Atomic Research Centre, Trombay, Mumbai, India. All studies will be performed in parallel in anemic and non-anemic, non-iron deficient subjects to evaluate the influence of Fe status on the effect of absorption inhibitors/enhancers. Alternatively, a longitudinal study design can be chosen in which test meal administration is repeated in anemic subjects after Fe repletion. All subjects will be screened for hemoglobin, serum ferritin, serum transferrin receptors, intestinal parasites, C-reactive proteins, malaria, VDRL, hepatitis-B and HIV. Four comparisons will be performed in 10 women of reproductive age per subject group: • Comparison A: test meal of low vs. test meal of high phytic acid content • Comparison C: test meal of low vs. test meal of high ascorbic acid content 2.2.4. The effect of pregnancy on the effect of enhancers/inhibitors of Fe absorption in the diet Fe absorption from test meals high in enhancers/inhibitors of Fe absorption will be compared longitudinally during pregnancy by using the double label erythrocyte incorporation technique. Test meals will be labeled with 57Fe and an intravenous dose of 58Fe will be given shortly after test meal intake as the reference. Iron absorption from the test meal will be determined in the same subject in the first, second and third trimester. Three different test meals will be evaluated in groups of 10 subjects each. All subjects will be screened for hemoglobin, serum ferritin, serum transferrin receptors, intestinal parasites, C-reactive proteins, VDRL, malaria, hepatitis-B and HIV. • Group A: test meal low in phytic acid/ascorbic acid (control) • Group B: test meal high in phytic acid, low in ascorbic acid • Group C: test meal low in phytic acid, high in ascorbic acid
27

2.2.5.The effect of ethnic differences on the effect of enhancers/inhibitors of Fe absorption in the diet To identify if ethnic differences exist in Fe absorption, absorption studies will be performed in parallel in India and Switzerland in apparently healthy, non-anemic subjects of comparable Fe status. Factors with a potential influence on Fe absorption/metabolism will be considered as far as possible in the exclusion criteria (infection, gender, intestinal parasites, Malaria, Vit A status, vegetarianism etc.). Iron absorption will be determined by the double isotope erythrocyte incorporation technique using 57Fe and 58Fe to label the Fe in the test meals. Differently labeled test meals (high vs. low in phytic acid) will be fed to each subject. Twenty subjects in each country will participate in the study. This study will be combined with comparison A as outlined in part C. All subjects will be screened for hemoglobin, serum ferritin, serum transferrin receptors, intestinal parasites, C-reactive proteins, malaria, VDRL, hepatitis-B and HIV.
3. WORK DONE SO FAR: In order to carry out the survey on iron status, diet and infection in the Bangalore region, which is described in the detailed study plan under section A, a typical crowded slum settlement with a total of 800 houses was identified in Bangalore and a house-to-house survey was conducted. Information on family composition and demographic details were obtained in 513 of the 800 homes visited. The remaining houses were found locked during the time of survey. There was roughly one woman between the ages 18-35 years in every household (511 in 513 homes) visited. The mean age of these 511 women was 25.4 years. Twenty-nine percent of them were illiterate, 6% had upto 5 years of schooling, 23% had studied 8 years at school and the remaining 42% had been educated for upto 10 years or more. Sixty percent of the women were housewives. A great majority of the women (97%) were non-vegetarian. Thirty seven of the women were pregnant at the time of survey. Mean family size was 5.8 persons. Seventy percent of the households lived in single room structures. Overall crowding could be expressed as a mean of 4.7 people / room in this slum. One hundred and fifty women will be chosen randomly from the slum in whom the detailed iron survey will be carried during the next phase.
28

REFERENCES [1] SCHOLL TO, HEDIGER ML, FISCHER RL, SHEARER JW. Anemia vs iron deficiency: increased risk of preterm delivery in a prospective study. Am J Clin Nutr 1992; 55:985-988. [2] KANDOI A, BHATIA BD, OANDEY S, SEN PC, SATYA K. Cellular immunity status in anaemia in pregnancy. Indian J Med Res 1991; 94:11-15. [3] BAYNES RD AND BOTHWELL TH. Iron deficiency. Ann Rev Nutr 1990; 10:133- 148. [4] POLLITT E. Iron deficiency and cognitive function. Ann Rev Nutr 1993; 13: 21-37. [5] ACC/SCN 2000. Report on the world situation. Geneva: ACC/SCN. [6] SESHADRI S. A data base on iron deficiency anaemia (IDA) in India: Prevalence, aetiology, consequences and strategies for control. Prepared for Task Force on Micronutrient Malnutrition Control, Department of Women and Child Development, Ministry of Human Resources Development. New Delhi, 1996. [7] World Health Organisation. Prevention and management of severe anaemia in pregnancy: Report of a technical working group. Geneva: WHO, 1993. [8] GOPALDAS T, RAGHAVAN R AND KANANI S. Nutritional impact of anti- parasitic drugs, prophylactic Vitamin A and iron-folic acid on underprivileged school girls in India. Nut Res 1983; 3: 831-844. [9] SOOD SK, RAMACHANDRAN K, MATHUR M, GUPTA K, RAMALINGASWAMI V, SWARNABAI C, PONNIAH J, MATHAN VI AND BAKER SJ. WHO sponsored collaborative studies on nutritional anaemia in India: The effects of supplemental oral iron administration to pregnant women. Q J Med 1975; XLIV: 241-258. [10] SESHADRI S, HIRODE K, NAIK P, SHAH A AND GUPTA N. An effective intervention to reduce the prevalence of anaemia in children. Ind J Med Res 1984; 80: 164-173. [11] SESHADRI S. Nutritional anaemia in South Asia. In: Malnutrition in South Asia: A regional profile, UNICEF, 1997. [12] NNMB -National Nutrition Monitoring Bureau. 2000. Special Report. Technical report no: 20, Hyderabad, India. [13] MAGNUSSON B, BJORN-RASMUSSEN E, HALLBERG L AND ROSSANDER L. Iron absorption in relation to iron status. Model proposed to express results of food iron absorption measurements. Scand J Haematol 1981; 27: 201-208. [14] TAYLOR P, MARTINEZ-TORRES C, LEETS I, RAMIREZ J, GARCIA-CASAL MN AND LAYRISSE M. Relationships among iron absorption, percent saturation of plasma transferrin and serum ferritin concentration in humans J Nutr 1988; 118: 1110- 1115. [15] BOTHWELL TH, BAYNES RD, MACFARLANE BJ, MACPHAIL AP. Nutritional iron requirements and food iron absorption. J Int Med 1989; 226:357-365. [16] CRAIG WJ. Iron status of vegetarians. Am J Clin Nutr 1994; 59(suppl): 1233S- 1237S. [17] BALLOT D, BAYNES RD, BOTHWELL TH, GILLOOLY M, MACFARLANE BJ, MACPHAIL AP, LYONS G, DERMAN DP, BEZWODA WR, TORRANCE JD, et al. The effects of fruit juices and fruits on the absorption of iron from a rice meal. Br J Nutr 1987; 57: 331-43. [18] COOK JD AND MANSEN ER. Vitamin C, the common cold, and iron absorption. Am J Clin Nutr 1977; 30: 235-241. [19] HURRELL R. 1984. Bioavailability of different iron compounds used to fortify
29

formulas and cereals: technological problems. In: Iron nutrition in infancy and childhood. Ed. A. Stekel. New York: Vervey/Raven Press Ltd. 193-208. [20] Seshadri et al. Unpublished data. [21] GOPALDAS T Iron-deficiency anemia in young working women can be reduced by increasing the consumption of cereal-based fermented foods or goose berry juice at the work place. Food Nutr Bull (Japan) 2002; 23(1): 94-105. [22] TAYLOR PG, MARTINEZ-TORRES C, ROMANO EL AND LAYRISSE M. The effect of cysteine-containing peptides released during meat digestion on iron absorption in humans. Am J Clin Nutr 1986; 43: 68-71. [23] MARTINEZ-TORRES C AND LAYRISSE M. Effect of amino acids on iron absorption from a staple vegetable food. Blood 1970; 35: 669-682. [24] HALLBERG L AND ROSSANDER L. Improvement of iron nutrition in developing countries: Comparison of adding meat, soy protein, ascorbic acid, citric acid and ferrous sulphate on iron absorption from a simple Latin American type of meal. Am J Clin Nutr 1984; 39: 577-583. [25] MONSEN ER, HALLBERG L, LAYRISSE M, HEGSTED DM, COOK JD et al. Estimation of available dietary iron. Am J Clin Nutr 1978; 31: 134-141. [26] DAVIDSSON L, WALCZYK T, ZAVALETA N, HURRELL R. Improving iron absorption from a Peruvian school breakfast meal by adding ascorbic acid or Na2EDTA. Am J Clin Nutr 2001; 73: 283-287. [27] HALLBERG L, BRUNE M, ROSANDER L. Iron absorption in man: ascorbic acid and dose-dependent inhibition by phytate. Am J Clin Nutr 1989; 49: 140-144. [28] HURRELL RF. Bio-availability of iron. Eur J Clin Nutr 1997; 51 (suppl 1): S4-S8. [29] HURRELL RF, REDDY M AND COOK JD. Inhibition of non-haem iron absorption in man by polyphenolic-containing beverages. Br J Nutr 1999; 81: 289-295. [30] NARASINGA RAO BS. Bio-availability of dietary iron. Proc Nutr Soc India 1983; 28: 1-6. [31] CHRISTIAN P AND SESHADRI S. Counteracting the inhibitory effect of tea on the in-vitro availability of iron from cereal meals. J Sci Food Agric 49 431-436, 1989. [32] SAMMAN S, SANDSTROM B, TOFT MB, BUKHAVE K, JENSEN M, SORENSEN SS AND HANSEN M. Green tea or rosemary extract added to foods reduces nonheme-iron absorption. Am J Clin Nutr 2001; 73: 607-612. [33] SANDBERG AS. The effect of food processing on phytate hydrolysis and availability of iron and zinc. Adv Exp Med Biol 1991; 289: 499-508. [34] BOTHWELL TH. Iron requirements in pregnancy and strategies to meet them. Am J Clin Nutr 2000; 72: 257S-264S. [35] SVANBERG B, ARVIDSSON B, BJORN-RASMUSSEN E, HALLBERG L, ROSSANDER L AND SWOLIN B. Dietary iron absorption in pregnancy - a longitudinal study with repeated measurements of non-haem iron absorption from whole diet. Acta Obstet Gynecol Scand Suppl 1975; 48: 43-68. [36] SVANBERG B. Iron absorption in early pregnancy - a study of the absorption of non- haem iron and ferrous iron in early pregnancy. Acta Obstet Gynecol Scand Suppl (Sweden), 1975; 48: 69-85. [37] ABRAMS SA. Using stable isotopes to assess mineral absorption and utilization by children Am J Clin Nutr 1999; 70: 955-964. [38] SANDSTROM B, FAIRWEATHER-TAIT S, HURRELL R AND VAN DOKKUM W. Methods for studying mineral and trace element absorption in humans using stable isotopes. Nut Res Rev 1993; 6: 71-95. [39] JANGHORBANI N, TING BTG AND FOMON SJ. Erythrocyte incorporation of ingested stable isotope of iron (58Fe). Am J Hematol 1986; 21: 277-288.
30

MASS SPECTROMETRY FOR DETERMINING ISOTOPE RATIOS OF IRON (FE)
S.K.AGGARWAL,
Mass Spectrometry Section, FCD, BARC, Mumbai 400 085, India
1. INTRODUCTION Stable isotope tracers are very useful for the study of micronutrient status and interactions in humans. In particular, these are invaluable in assessing the nutritional status of infants, children, pregnant women and nursing mothers since these subjects are of prime importance. The use of stable isotopes has many advantages when compared to the previously used radioactive isotopes which are not ethically acceptable for the large majority of healthy human volunteers. Since the stable isotopes do not emit any radiation, their use in humans is safe and non-invasive and does not lead to exposure to any kind of radiations. Further, since there is no problem of radioactive decay of these isotopes, the measurements can be done comfortably after the collection of samples and if desired, the measurements can be repeated. It is also possible to study the interactions between different elements by using stable isotope tracers of more than one element simultaneously due to complete elimination of radiation hazard to individual. The presence/absence of these stable isotope tracers can be measured in biological samples e.g. blood of individuals using suitable isotope ratio mass spectrometric technique. Change in the atom ratio of the stable isotope tracer with respect to those already present in the body (endogenous) can be used to study the absorption etc. of the element of interest. A number of inorganic mass spectrometric techniques are available and have been used for the determination of atom ratios of different isotopes of an element [1]. These include Thermal Ionisation Mass Spectrometry (TIMS), Inductively Coupled Plasma Mass Spectrometry (ICP-MS), Gas Chromatography – Mass Spectrometry (GC-MS), Fast Atom Bombardment Mass Spectrometry (FABMS), Resonance Ionisation Mass Spectrometry (RIMS) etc. Amongst these, TIMS is considered as a “GOLD STANDARD” and provides the best possible data on isotope ratios in terms of precision and accuracy. This is particularly important since small changes in the isotope ratios brought out by administering small amounts of the stable isotope tracers to humans (oral/intravenous) have to be determined. One of the limitations to the use of stable isotope tracers is the restricted availability of the enriched stable isotopes from a few commercial suppliers, in addition to the high cost of these stable isotope tracers. Also the cost of mass spectrometric analysis is quite high since the instrumentation and expertise are not available in many countries. However, mass spectrometry provides much better precision and accuracy compared to neutron activation analysis used previously for determining the stable isotope tracer. In the present T-CRP, stable isotope tracers 57Fe and 58Fe, which are the two least abundant natural isotopes of Fe, will be used to provide answers to some of the questions concerning Iron Deficiency Anemia (IDA) in India and Thermal Ionisation Mass Spectrometry will be used for isotope ratio measurements. In particular, using the stable isotopes, the following points would be addresses during the present study.
31

• If subjects of same Fe status respond in the same way to inhibitors (phytic acid) and enhancers (ascorbic acid) of Fe absorption in the diet
• If the maternal body is able to upregulate Fe absorption over the course of pregnancy even at elevated levels of absorption inhibitors in the diet
• If there is any relevance of ethnic differences on the effect of inhibitors and enhancers on Fe dietary absorption.
2. SCIENTIFIC BACKGROUND Iron (Fe) has four naturally occurring isotopes: 54Fe (5.8%), 56Fe (91.7%), 57Fe (2.1%) and 58Fe(0.33%). Artifical radioactive isotopes which are convenient to use for biological studies are 55Fe (T1/2 = 2.7 yr), 59Fe (T1/2 = 45.1 days), 60Fe (T1/2 = 105 yrs). Amongst these, 55Fe and 59Fe can be easily prepared and have been used. Fe can exist in different oxidation states ranging from +2 to +6, but in biological systems, the most commonly encountered oxidation states are +2 (ferrous), +3 (ferric) and +4 (ferryl). Fe is the oxygen carrying component of the blood and is the main determinant of how much oxygen reaches and is used by all body tissues including brain, muscle, heart and liver. The average Fe content of a healthy adult is about 4 grams. About two-thirds of the iron in the body is present in blood mainly as hemoglobin and approximately 3% as myoglobin. The majority of the remainder is stored Fe found in liver, spleen, bone marrow and muscle in the form of ferritin or hemosiderin. It has been demonstrated using food tagged with radioactive 59Fe that persons who are iron-deficient tend to absorb iron more efficiently and in greater quantities than normal subjects. Healthy subjects normally absorb only 5 to 10% of the Fe in their foods whereas Fe-deficient subjects may absorb twice this amount. Hence from a diet consisting of 15 mg of Fe, 0.75 to 1.5 mg of Fe would be absorbed in a normal subject whereas 3 mg can be absorbed in an Fe-deficient subject. Similarly, Fe absorption is generally increased during growth and pregnancy. The availability of Fe in foodstuffs is quite variable. Fe in food exists in two main forms: (i) heme iron found in meat as part of hemoglobin and myoglobin and (ii) nonheme iron naturally present in cereals, vegetables and other foods. Heme and nonheme Fe are absorbed by different pathways with different degrees of efficiency depending upon the chemical form, other dietary constituents and level of Fe stores in the individual. It is generally agreed that between 20 to 30% of heme Fe is absorbed and this is a constant figure and is relatively unaffected by other dietary or physiological variables such as body Fe stores. On the other hand, nonheme Fe absorption can be enhanced or inhibited by a large number of dietary variables. As an example, the presence of phytates, phosphates and polyphenols in food inhibit the absorption of nonheme Fe due to the formation of large insoluble polymers. On the other hand, the presence of ligands such as ascorbic acid (vitamin C), citric acid, fructose, amino acids and peptides form soluble complexes with Fe, thus preventing precipitation and polymerization and thereby promoting absorption of nonheme Fe. Iron competes with Ca, Mn and Zn for absorption in the intestine and excess intake of any one of these minerals could produce a deficiency of others. Acute Fe poisoning is not uncommon. Since there is no defined upper limit to Fe absorption, chronic Fe overload may be produced by high oral intake over a prolonged period e.g. “bronze diabetes” was observed in South Africa some years ago in people consuming large quantities of local beer that was brewed in Fe pots.
32

3. EXPERIMENTAL Meals labeled with enriched 57Fe isotope will be administered followed by an intravenous administration of enriched 58Fe. The amount of tracer to be given orally is normally much higher than that administered by I.V. mainly due to the poor absorption of Fe. The actual amount of isotope to be given orally/I.V. depends upon the body Fe pool and the precision of isotope ratio measurements. Higher is the precision, smaller is the dose to be given of the stable isotope. The Fe isotope ratios are determined in blood samples collected 14 days after the administration of stable isotope tracers since it takes nearly 14 days for these tracers to get incorporated into RBCs/erythrocytes. The blood samples collected from these subjects will be treated and the fraction containing Fe after suitable digestion, separation and purification procedure will be used for mass spectrometric analysis. This would allow to obtain dynamic picture of relevant processes such as the intestinal absorption or the main excretion path ways. It will be possible to know the kinetics in blood plasma and of the renal elimination process. Efficient separation of Fe from Ni will be required since 58Ni (68 atom%) is the most abundant isotope of Ni which would interfere at 58Fe tracer. There are a number of mass spectrometric techniques which have been tried and discussed in literature for carrying out Fe isotope ratio measurements [2-13]. The following Section would present a brief introduction to these different mass spectrometric techniques.
4. MASS SPECTROMETRIC METHODS The various mass spectrometers which can be used for isotope ratio measurements of Fe can be broadly classified into two categories viz. (i) General purpose organic mass spectrometers and (ii) Dedicated inorganic mass spectrometers. The general purpose organic mass spectrometers are more commonly available in biomedical laboratories and have been tried in the past. However, these do not provide the high level of precision and accuracy desirable when carrying out studies on bio-availability of trace elements using expensive enriched stable isotope tracers. Dedicated inorganic mass spectrometers are more commonly used for these studies. 4.1. Direct Probe Mass Spectrometry [2] The isotope ratios of Fe in blood serum were measured by preparing volatile chelate [Fe(acac)3] of Fe using the β-diketone (2,4-pentane dione). A solid probe sample inlet along with a Finningan Model 3300 quadrupole mass spectrometer was employed. Ions of interest were 252, 254, 255 and 256 corresponding to different isotopes of Fe in the two-ligand fragment Fe(acac)2 + of the chelate. The relative abundance of different isotopes of Fe was determined by measuring the ion currents and integrating them over time. Discrepancies were observed between the experimentally determined and theoretically calculated ion abundance ratios.
33

4.2. Fast Atom Bombardment Mass Spectrometry [3,4] FABMS also known as particle-induced desorption mass spectrometry is attractive as it requires little or no sample preparation and may be performed with a conventional high resolution mass spectrometer. A few µL of the sample solution is placed on the probe tip (SS, Cu, Au) and is dried in a stream of air. A beam of high energy Xe atoms (7-8 keV) is used to desorb ions from the surface of the sample. Since the process of ion formation is not selective, different molecular species are produced from a complex matrix such as plasma and urine. The interference from metal hydride ions, which is variable over the course of the experiment, has been reported using this technique. FABMS with a high resolution mass spectrometer (MS 80 RFA, Kratos Analytical) at a resolution of 3000 was used for determining Fe stable isotope enrichments in standards and in ashed fecal samples from Fe bioavailability studies. Solvent extraction with diethyl ether was used to isolate Fe from isobaric interfering Ni present in the ashed fecal sample. A sensitivity of about 5 µg was reported, with the volatility and high ionization potential (7.9 eV) of Fe limiting the measurement reproducibility from 1 to 6% RSD. A subsequent study by the same authors for the quantitative determination of Fe in food reported a slope of 1.25 when comparing the measured 54Fe/56Fe atom ratios against the theoretical ratios. 4.3. Resonance Ionisation Mass Spectrometry [5] Resonance ionization mass spectrometry for Fe was carried out using one-wavelength, two photon ionization scheme with UV light at 283.6 nm. The UV photons were obtained by using a Nd-YAG (10 Hz, 350-mJ pulses at 532 nm) pumped dye laser (Rhodamine 6G) with frequency doubling (3 mJ pulse energy in the wavelength region 279-289 nm). Fe atoms were thermally vaporized from a filament heated to 1250K. A magnetic sector mass spectrometer equipped with a detector system capable of measuring the pulsed ion currents produced in the experiment was used. The RIMS technique has the potential to provide elemental selectivity and thus eliminates isobaric interferences from 54Cr (2.4%) at 54Fe and from 58Ni (68%) at 58Fe. Also, the ionization efficiency of RIMS is much better for Fe than that with TIMS, though the precision and accuracy are poor in RIMS. The concentration of Fe was determined in two reference materials (i) the human serum (SRM 909) and (ii) Trace elements in water (SRM 1643b) at levels of 1.94 ppm and 99.2 ppb, respectively. The precision and accuracy of the measurements was reported to be 2-3%. 4.4. Inductively Coupled Plasma Mass Spectrometry [6,7]
Inductively coupled plasma mass spectrometry is a useful multielement determination technique and has the advantages of lower cost, less sample preparation, much faster throughputs and ease of operation. There are different types of ICP-MS instruments available commercially and these include quadrupole based as well as double focusing magnetic sector based single collector and multiple collector mass spectrometers. In the case of Fe, the isotope ratio measurements by quadrupole based ICP-MS has problems due to isobaric interferences from molecular species 40Ar14N+ and 40Ar16O+ at m/z values of 54 and 56, which overlap with 54Fe and 56Fe. These isobaric interferences are quite severe since Ar is used as a plasma gas and the sample is usually dissolved in HNO3 and this provides a source of both O and N When Fe isotope ratios are to determined, the sample can
34

be dissolved in HCl instead of HNO3 thereby reducing the formation of Ar-N molecular species. The quadrupole based ICP-MS instrument is useful only when spiked solutions, not including 56Fe measurements, are to be analysed. Though the isotopes of Fe can be resolved from these molecular interferences by using high resolution double focusing mass spectrometers, accurate isotope ratio measurements of Fe are possible only if these molecular interferences are eliminated or reduced to manageable proportions. Other atomic isobaric interferences from 54Cr and 58Ni have also to be corrected at 54Fe and 58Fe, respectively. This can be achieved by monitoring 52Cr and 60Ni and using the 52Cr/54Cr and 60Ni/58Ni ratios of natural Cr and Ni, respectively. Also to find out mass dependent discrimination among different isotopes in the Fe mass region, the factor derived by measuring isotope ratios of Cu has been used. It may be noted that ICP-MS has advantage of higher ionization efficiency of Fe compared to that in TIMS. Sample introduction by electrothermal vaporization has also been tried instead of the normal nebuliser-spray chamber to reduce the level of polyatomic isobaric interferences. This was done during the measurement of Fe isotope ratios in blood to assess the fractional absorption of Fe during pregnancy in women, after administering 54Fe (5mg) and 57Fe (200 µg) as oral and I.V. tracers, respectively. 4.5. Thermal Ionisation Mass Spectrometry Thermal ionization mass spectrometry provides the best possible precision and accuracy in isotope ratio measurements and is considered as a “GOLD STANDARD”. However, the technique demands extensive clean up of the sample and also isotope fractionation effects during mass spectrometric analysis must be taken into account. The isotope fractionation effects lead to variable systematic error and must be corrected to realize the full potential of present generation TIMS instruments. The TIMS instruments are based on an extended geometry magnetic sector analyzer with a Multi Faraday cup collector system to eliminate the time-dependent fluctuations in the ion current among different isotopes. TIMS with a quadrupole analyzer was used as a rapid analysis method for Fe nutritional tracer studies since the variations in the Fe isotope ratios extended over a wide range. However, the quadrupole based TIMS is of only limited use. Due to the high ionization potential of Fe, special sample loading techniques are to be used. In one of the studies, 10-15 µg of Fe as FeCl3 was loaded onto the two side filaments of a triple filament (high purity zone refined Re), was evaporated to dryness and then reduced in hydrogen atmosphere to a mixture of iron and iron oxides. In another study, the use of silica-gel and phosphoric acid as ionization enhancing agent to improve the emission of Fe+ ions was reported. A single filament Re assembly using boric acid instead of phosphoric acid has also been used. Recently, a single filament assembly pre-loaded with an Al2O3 slurry has also been used. In this study, the sample containing about 4 µg of Fe was loaded after adding an Al2O3 slurry. The Fe sample loading was followed by 1 M H3PO4 and silica gel. The Al2O3 slurry emitter was reported to produce long lasting and more stable ion beams and high ion currents as compared to the boric acid-silica gel technique. The isotope ratios of Fe have recently been measured by using negative ions in magnetic sector field TIMS using FeF4
- ion [8,9]. MAT-262 TIMS equipped with a multi collector system was used for simultaneous data acquisition of different Fe isotopes. Barium fluoride coated rhenium filament of a double filament assembly together with silver fluoride was used to enhance the formation of FeF4
- ions. In this study, because of the high enrichment of the
35

isotopically enriched tracers (57Fe and 58Fe) used and also due to the incorporation of low amounts of these tracers into the red blood cells, natural 54Fe/56Fe isotope ratio was used to carry out internal normalization of the data obtained to eliminate the variable isotope fractionation effects. A variety of approaches can be used to correct for isotope fractionation effects in TIMS [10]. These include external normalization to Fe standards, internal normalization (applicable only when one invariant isotope ratio is available) and double spike method. Recently, the total evaporation and ion current integration has also been tried for some of the elements with a view to minimizing the isotope fractionation effects. Amongst these, the external normalization approach is empirical and is based on the pre-determination of isotope fractionation factor by analyzing isotopic reference materials prepared by gravimetric mixing of the enriched isotopes. This approach is still the most commonly used but leads to variation in isotope ratios due to practical problems in strictly reproducing the different parameters from one filament loading to the next, particularly when analyzing unknown samples. The double spike approach is applicable only to those elements e.g. Fe which have four or more isotopes. Generally, this approach requires two mass spectrometric analyses: one of the unspiked aliquot of the unknown sample and the other of the mixture of the unknown sample and the double spike. The isobaric interferences from 54Cr and 58Ni are also observed in TIMS and can be accounted for. This can be achieved by monitoring 52Cr and 60Ni and using the natural 52Cr/54Cr and 60Ni/58Ni atom ratios to subtract the contributions of 54Cr and 58Ni at 54Fe and 58Fe, respectively, during the mass spectrometric analysis of Fe isotope ratios. In addition, there is no memory effect observed with TIMS in contrast to the gas source mass spectrometry. 5. FE ISOTOPIC REFERENCE STANDARD: Since the relative abundances of the isotopes of Fe in terrestrial samples are expected to vary according to thermodynamic and kinetic effects leading to fractionation [11], natural sample of Fe cannot be used as an isotopic reference material. The Fe isotopic reference standard IRMM-14 is commercially available and has been certified by the Institute for Reference Materials and Measurements (IRMM), European Commission, Joint Research Centre, Belgium. This reference material should be used to validate the mass spectrometric methodology employed for Fe isotope ratio measurements in unknown samples of biological, geological or any other origin.
36

REFERENCES [1] AGGARWAL S.K., KINTER M., FITZGERALD R.L., HEROLD D.A., Mass spectrometry of trace elements in biological samples, Critical Rev. in Clin. Lab. Sci. 31 (1994) 35-87. [2] MILLER D.D., VAN CAMPEN D., A method for the detection and assay of iron stable isotope tracers in blood serum, Am. J. Clin. Nutr. 32 (1979) 2354-2361. [3] EAGLES J., FAIRWEATHER-TAIT S.J., SELF R., Stable isotope ratio mass spectrometry for iron bioavailability studies, Anal. Chem. 57 (1985) 469-471. [4] SELF R., FAIRWEATHER-TAIT S.J., EAGLES J., A double stable isotope labeling method for iron bioavailability studies using fast atom bombardment mass spectrometry, Anal. Proc. 22 (1985) 194-195. [5] FASSETT J.D., POWELL L.J., MOORE L.J., Determination of iron in serum and water by resonance ionization isotope dilution mass spectrometry, Anal. Chem. 56 (1984) 2228-2233. [6] WHITTAKER P.G., LIND T., WILLIAMS J.G., GRAY A.L., Inductively coupled plasma mass spectrometric determination of the absorption of iron in normal women, Analyst 114 (1989) 675-678. [7] WHITTAKER P.G., BARRETT J.F.R., WILLIAMS J.G., Precise determination of iron isotope ratios in whole blood using inductively coupled plasma mass spectrometry, J. Anal. At. Spectrom. 7 (1992) 109-113. [8] WALCZYK T., Iron isotope ratio measurements by negative thermal ionization mass spectrometry, Int. J. Mass Spectrom. Ion Proc. 161 (1996) 217-227. [9] DAVIDSSON L., WALCZYK T., ZAVALETA N., HURRELL R.F., Improving iron absorption from a Peruvian school breakfast meal by adding ascorbic acid or Na2EDTA, Am. J. Clin. Nutr. 73 (2001) 283-287. [10] JOHNSON C.M., BEARD B.L., Correction of instrumentally produced mass fractionation during isotopic analysis of Fe by thermal ionization mass spectrometry, Int. J. Mass Spectrom. 193 (1999) 87-99. [11] ZHU X.K., O’NIONS R.K., GUO Y., REYNOLDS B.C., Secular variation of iron isotopes in North Atlantic deep water, Science 287 (2000) 2000-2002. [12] BELSHAW N.S., ZHU X.K., GUO Y., O’NIONS R.K., High precision measurement of iron isotopes by plasma source mass spectrometry, Int. J. Mass Spectrom. 197 (2000) 191-195. [13] JACKSON G.S., WEAVER C., ELMORE D., Use of accelerator mass spectrometry for studies in nutrition, Nutrition Res. Rev. 14 (2001) 317-334.
37

38

ESTIMATING BIO-AVAILABILITY OF ZINC AND IRON FROM HOME-AVAILABLE COMPLEMENTARY FOODS IN PAKISTAN: A STUDY IN YOUNG INFANTS USING STABLE ISOTOPES
ZULFIQAR A. BHUTTA1, RAHAT NAZ, LENA DAVIDSSON2, THOMAS WALCZYK3, IQTIDAR KHAN1
1Department of Paediatrics, The Aga Khan University, Karachi, Pakistan, Laboratory of Human Nutrition, 2Institute of Food Sciences, Zurich, Switzerland
Abstract Although the widespread prevalence of malnutrition in south Asia is well recognized, the extent and severity of micronutrient deficiencies is less well appreciated [1]. Although significant iron deficiency is almost ubiquitous, and iron deficiency anemia is widespread [2] the extent and severity of vitamin A [3, 4] and zinc deficiency is less well appreciated [5, 6]. While poor maternal nutrition and inappropriate early breastfeeding practices underlie some of the problem, a major cause of widespread micronutrient malnutrition is the poor state of complementary feeding. Studies of infant growth patterns in Pakistan reveal that the growth faltering starts after 5-6 months of age, and usually parallels the transition from exclusive or predominant breastfeeding to mixed feeding with home available complementary foods [7]. While the recent global recommendations of exclusive breastfeeding for six months in developing countries are clearly appropriate [8], the optimal approach in order to provide adequate micronutrients is uncertain.
1. SCIENTIFIC BACKGROUND AND SCOPE OF THE PROJECT Despite relatively low concentrations, bioavailability of iron, zinc and vitamin A from breast milk is good [9, 10] and therefore exclusive breastfeeding for at least 4-6 months after birth is entirely appropriate for micronutrient requirements. However, thereafter once complementary feeding is initiated, the most appropriate strategy for providing sufficient intake of micronutrients is uncertain. Most diets used for complementary feeding in young infants in South Asia are plant and cereal-based, with relatively high phytate content [11, 12, 13]. Available information from studies of bioavailability of iron and zinc from such traditional diets indicate that the absorption may be significantly reduced [8]. Much of this data derives from either theoretical estimation of micronutrient content and calculations based on food-composition tables, some of which have been lately shown to be over estimates. Additionally, some of the assumptions of conversion of provitamin A carotenoids to the active retinol have been seriously questioned [14, 15, 16, 17] with several folds lowering of “bioavailable” vitamin A values [18]. Others have indicated that despite low bioavailability of vitamin A from green leafy vegetables, cooking in an appropriate amount and type of fat may greatly increase absorption [19]. Such information on micronutrient bioavailability is vital to the planning of appropriate intervention strategies. These findings and limitations are of great public health importance as they determine the need for either micronutrient supplementation or fortification in preference to entirely food-based approaches. If established cultural practices indicate the intake of diets which limit the absorption of essential micronutrients, then a combined strategy of dietary modification and supplementation may be appropriate. Alternatively, governments may consider investing in large-scale food-fortification programs targeting foods used for feeding mothers, infants and pre-school children. Given the practical difficulties in assuring a regular supply and intake of a micronutrient supplement, many public health workers prefer the latter approach as a more
39

logical, practical and holistic strategy in developing countries. In recent years considerable thought has been given to alternative dietary strategies for improving micronutrient intake such as increasing maternal vitamin A intake [20], improving iron absorption [21, 22], reducing phytate content and increasing zinc bioavailability [23, 24]. However, it is imperative that these public health nutrition decisions are based on solid bedrock of scientific evidence of micronutrient status and bioavailability [25]. A major limitation of appropriate methods for investigating bioavailability of micronutrients in developing countries, has been the lack of non-invasive alternative methods of investigation. Much of the available information is either based on animal studies or complex metabolic balance studies in adults [26, 27]. Moreover, few studies of micronutrient bioavailability from either foods or supplements, have been conducted in actual domiciliary settings, which thus limits their applicability and relevance to the field situation. However, recently available techniques for measuring micronutrients bioavailability using stable isotopes [28-35] may allow these critical estimates, necessary for planning interventions. To illustrate, preliminary data from a recent study of zinc absorption in India indicates a much lower fractional absorption of zinc from weaning foods compared with milk [36]. We propose to evaluate micronutrient bioavailability in a village-based cohort in Pakistan employing stable isotopes.
2. OBJECTIVES: • To use a simple minimally-invasive protocol employing stable isotopes for the estimation
of bioavailability of iron and zinc in ambulatory young children receiving home available diets and complementary foods.
• To assess the effect of concomitant administration of two different concentrations of ascorbic acid on the bioavailability of iron.
• In Phase 1 of the study assess the bioavailability of iron using 57Fe and 58Fe to label the standard weaning diet (khitchri) with the addition of defined amounts of vitamin C.
• In a subsequent Phase 2 of the project, to compare the bioavailability of iron and zinc from a standardized home-available weaning diet (khitchri) and micronutrient supplement extrinsically labeled with stable-isotopes (58Fe, 57Fe, 68Zn and 67Zn).
3. STUDY METHODOLOGY Infants already recruited from the community intervention study of complementary feeding strategies will be eligible for these field-based studies of micronutrient bioavailability (Figure 1). These studies will be performed in a subset of 20 children from group A representing the population with the individual education intervention alone and the combined intervention of nutrition education and micronutrient supplementation, respectively. Informed written consent will be obtained from all parents taking part in this sub-study and the infants (age 9 months) will be randomly identified at inclusion in the study. This particular time point has been deliberately chosen to minimize the biological variability in the cohort of infants due to growth and coincidental morbidity (ies).
40

FIGURE 1: SAMPLE FRAME
Birth Cohort of a Bilal Colony near Karachi (2002-3) n=750
Group A Group B Group C n=250* n=250 n=250*
Exclusive Breastfeeding for 5-6 months
Exclusive breastfeeding for 5-6 months
Exclusive breastfeeding for 5-6 months
IMCI care IMCI care IMCI care EPI vaccinations EPI vaccinations EPI vaccinations
Growth Monitoring Growth monitoring Growth monitoring
Nutrition Education Daily micronutrient supplement Nutrition Education
Daily micronutrient supplement
The mothers and infants from the control group A will be selected for the stable isotope bioavailability study, and invited to participate in the study. Infants will be admitted to the metabolic research unit for bioavailability studies. These will be performed in the metabolic study unit at the Nutrition Research Laboratory of the Aga Khan University. Following full explanation, a written informed and understood consent the mother-infant pairs will be admitted for 4-5 days and the studies performed under standardized conditions with full monitoring. Only infants already well established on complementary foods will be enrolled in the study.
41

4. RESEARCH DESIGN AND METHODS The complementary feeding study protocol has been reviewed and approved by the Ethical Review Committee (ERC) at the Aga Khan University Medical Center. Revisions to the stable isotope Bioavailability study protocol made in June 2002 have been conveyed to the ERC and further clearance sought. A favorable decision and clearance is expected within the next two weeks 4.1. Infants Apparently healthy children (at approximately 9 months of age; max 10 kg body weight) will be recruited from the population in an urban community of Bilal Colony in Karachi. Only infants who have received complementary feeds for at least 4 weeks will be enrolled in the study. Parents will be informed about the aims and procedures of the study and informed and understood consent will be obtained from at least one parent volunteering for the study. As indicated above, in Phase 1 of the project (between 2002-2003) we will only estimate iron bioavailability and these studies will be conducted in the Nutrition Research Laboratory under close supervision. For this Phase of the study, mothers and infants will be admitted to the metabolic ward at AKU for the duration of the study (5 days). In Phase 2 of the project (between 2004-2005) we will also undertake zinc bioavailability studies as well and develop a composite protocol for assessing iron and zinc bioavailability using stable isotopes. Twenty mother/infant pairs will be recruited for the study. Sample size calculations are based on our previous experience with studies of Fe absorption in infants and children, using paired observations in 10 children per group [37-41]. Before enrollment in the study, all infants will be fed Khitchri during for 2 days under similar conditions as during the Fe absorption study to ensure acceptability. 4.2. Phase 1 (Iron Bioavailability Studies) 2002-2003 4.2.1. Test meals Khitchri, a traditional Pakistani complementary food, based on rice and lentils will be used in both studies. Each test meal will consist of 50 g regular Khitchri, made from a standard recipe of rice, lentils and oil as per standard formulation [42, 43]. Standardized Khitchri will be prepared freshly in the Nutrition Laboratory kitchen, refrigerated as required and used over 24 hours. The native Fe content of the test meal will include 0.25mg Fe added as 58Fe or 57Fe, which will increase the total Fe content to about 0.5mg per test meal. 4.2.2. Iron absorption Fe absorption will be measured by a double stable isotope technique developed at the Institute for Food Sciences Human Nutrition Laboratory [37, 41] based on the incorporation of stable Fe isotopes into erythrocytes 14 days after administration of labeled test meals. The following protocol will be used in Phase 1
42

A test meal of Regular Khitchri (50g) labeled with 0.25mg 57Fe plus added ascorbic acid or 58Fe with no ascorbic acid added, followed by intake of water (60g). The test meal will be prepared under standardized conditions and administered 4 times (two test meals/day on Day 1-2 and two between day 3-4) under standardized conditions. The test meals will thus be labeled with a total dose of 1.0 mg 57Fe or 58Fe. 57FeSO4 or 58FeSO4 will be prepared from highly enriched 57Fe or 58Fe metal dissolved in 0.1 MH2SO4 [37] and individual doses will be filled into Teflon containers, purged with argon and refrigerated until used. The isotopic composition of the Fe labels will be determined by negative thermal ionization mass spectrometry (NTI-MS) using FeF4 molecular ions [41] and a magnetic sector field instrument (MAT 262, Finnigan MAT, Bremen, Germany). A similar approach will be used to prepare the 57Zn and 58ZnSO4 respectively for Phase 2 of the project. On Day 1 a baseline blood sample (2ml) will be drawn from the antecubital vein for Fe status indices (Hb, ferritin and circulating transferrin receptor) and isotopic composition. All labeled test meals will be served 2 hrs after the last breast-feeding on days 1-4. Water (60g) will be given to the infants as a drink after intake of labeled test meals to minimize the variation in the total volume of food and fluid consumed with the meals. No additional food or fluid will be given for 3h following intake of each labeled test meal. A blood sample (2ml) will be drawn from the antecubital vein 14 days after intake of the last test meal (Day 18). Blood samples will be analyzed for their isotopic composition by thermal ionization mass spectrometry (TIMS). Body weight will be measured at the time of blood sampling. Thus the Phase 1 study protocol can be summarized as follows Group A. Study 1 (10 infants). These infants will receive the following diet Days 1-2: Test meal a) khitchri labeled with 58Fe Days 3-4: Test meal b) khitchri labeled with 57Fe PLUS added vitamin C at molar ratio 1:1 relative to Fe Group B. Study 2 (10 infants). These infants will receive the following Days 1-2: Test meal a) khitchri labeled with 58Fe Days 3-4; Test meal b) khitchri labeled with 57Fe PLUS added vitamin C at molar ratio 2:1 relative to Fe 4.2.3. Blood analysis Stable isotope composition of Fe will be measured by thermal ionization mass spectrometry (TIMS) according to the method of Walczyk [41]. Whole blood samples will be mineralized using an HNO3/H2O2 mixture and microwave digestion (MLS 1200, MLS, Leutkirch, Switzerland). Sample Fe will be separate from the matrix by anion-exchange chromatography following a solvent/solvent extraction step into diethyl ether [41, 44]. All isotopic analysis will be performed by NTI-MS using a magnetic sector field mass spectrometer (MAT 262) equipped with a multi-collector system for simultaneous ion beam detection, using the recently developed NTI-technique for Fe [41]. Fe separated from the samples will be loaded on BaF2 coated rhenium-filaments of a double filament ion source together with AgF to promote the formation of negatively charged FeF4 ions.
43
4.2.4. Iron status Anthropometry (body weight and length) will be measured on Days 1 and 18, Blood samples will be aliquoted for the analysis of Hb and plasma will be separated, aliquoted and frozen for later analysis of Hb and plasma will be separated, aliquoted and frozen for later analysis of ferritin, circulating transferring receptor and C-reactive protein. Hb will be measured using standard methods on a Coulter Counter. Plasma ferritin will be estimated using the Immulite methods and circulating transferring receptor will be assessed by ELISA kits (Ramco Laboratories, Houston, Texas) and C-reactive by nephelometry (TdX systems, USA). The laboratory at the Aga Khan University employs an extensive external quality control system using Bio-Rad Laboratory Systems. 4.2.5. Calculation of Fe absorption Based on the shift of the Fe isotopes ratios in the blood samples and the amount of Fe circulating in the body, the amount of 57Fe or 58Fe label present in the blood 14 days after administration will be calculated, following the principles of isotope dilution and considering that the Fe labels are not mono-isotopic [41]. Circulating Fe will be calculated based on blood volume and Hb concentration. Blood volume calculations will be based on body weight [45]. For calculation of fractional absorption, 90% incorporation of the absorbed Fe into red blood cells will be assumed. Because of the high enrichment of the isotopically enriched labels and the low amounts of label incorporated into the red blood cells, the 54Fe/56Fe isotope ratio in the blood can be expected to remain unchanged within the reproducibility of the isotopic analysis after incorporation of the labels. Therefore, it will be possible to normalize the data for the natural isotope ratio 54Fe/56Fe to correct for mass dependent isotopic fractionation effects [46]. 4.3. Phase 2 (Iron and Zinc Bioavailability Studies) 2004-2005 4.3.1. Zinc bioavailability study The infants will receive an oral dose of 1 mg 67Zn (elemental zinc) mixed with the total daily diet for 24 hours (i.e. in three to four divided doses. The administration of test meal and the stable isotope dose (in four divided doses) will be as regular khitchri (50g) labeled with 0.25mg 57Zn followed by intake of water (60g) (Figure 2). Each test meal will be administered 4 times (four test meals/day on Day 1-2) under standardized conditions All stool specimens will be collected for 72 hours in specially prepared trace-element free disposable diapers, and similarly the urinary samples will be collected. The 72 hours metabolic study will terminate with the appearance of the stool marker (carmine red) given at the initiation of the protocol. The amounts of respective isotopes in the stool specimens will be measured by fast-atom bombardment mass spectroscopy and the fractional absorption of zinc will be estimated [47-49].
44

FIGURE 2: SUGGESTED PROTOCOL FOR MEASUREMENT OF IRON BIOAVAILABILITY AT 7 TO 9 MONTHS OF AGE (PHASE 1)
Birth Cohort (consented to participate)
N = 250 in each treatment group
Groups A (nutrition education alone) and Group C (supplemented as well) Interventions to start from 6 months of age
sub-selected for initial bio-availability study at 8 months
~ 6 months 9 months
Supplementation
Blood sampling Blood samples for RBC uptake of 57Fe Day 1 Day 18
Phase 1 (Iron bioavailability on two dose regimen of vitamin C) Group A 57FeSO4 or 58FeSO4 absorption with vitamin C 1:1 molar ratio with Fe) Days 1-2: Test meal a) khitchri labeled with 58Fe Days 3-4: Test meal b) khitchri labeled with 57Fe with added vitamin C at molar ratio 1:1 relative to Fe Group B 57FeSO4 or 58FeSO4 absorption with vitamin C 1:1 molar ratio with Fe) Days 1-2: Test meal a) khitchri labeled with 58Fe Days 3-4: Test meal b) khitchri labeled with 57Fe with added vitamin C at molar ratio 2:1 relative to Fe
45

4.4. Staff Exchange and training in mass-spectroscopic analysis of stable isotopes in Zurich
Although mass spectroscopic facilities are available in Karachi at the HEJ Institute of Chemistry, the experience in measurements of stable isotopes of zinc and iron is extremely limited. It is anticipated therefore that a 2-3 month period of training at the Laboratory of Human Nutrition, Institute of Food Sciences, Zurich, Switzerland, will be undertaken in the fall of the year 2003 to learn the necessary mass spectroscopic techniques. This will be followed by the establishing the protocol in Karachi with external validation of samples in Zurich.
46

REFERENCES [1] GILLESPIE S (Ed), Malnutrition in South Asia: a regional profile. UNICEF.ROSA Publication Number 5, 1997 [2] BHUTTA ZA. Iron and Zinc intake from complementary foods: some issues from Pakistan. Pediatrics 2000;106:1295-1297. [3] BLOEM MW, DE PEE S, DARNTON-HILL I. Vitamin A deficiency in India, Bangladesh and Nepal. In Gillespie S (Ed), Malnutrition in South Asia: a regional profile. UNICEF.ROSA Publication Number 5, 1997;pp125-44 [4] BHUTTA ZA. Is vitamin A deficiency a public health problem in Pakistan? Position Paper, Nutrition Division, Planning Commission, Government of Pakistan, Islamabad, May 1999. [5] BHUTTA ZA. The role of zinc in health and disease. J Pak Med Assoc 1997;47:68- 73. [6] BAHL R, BHANDARI N, HAMBIDGE KM, BHAN MK. Plasma zinc as a predictor of diarrheal and respiratory morbidity in children in an urban setting. Am J Clin Nutr 1998;68:(Suppl 2):414S-417S. [7] JALIL F, KARLBERG J, HANSON LA, LINDBLAD BS. Growth disturbance in an urban area of Lahore, Pakistan, related to feeding patterns, infections and age, sex, socioeconomic factors and seasons. Acta Paediatr 1989; Suppl 350:44-54. [8] WORLD HEALTH ORGANIZATION. Complementary feeding of young children in developing countries: a review of current scientific knowledge. World Health Organization, Geneva, 1998, WHO/NUT/98.1. [9] ABRAMS SA, WEN J, STUFF JE. Absorption of calcium, zinc, and iron from breast milk by five to seven month old infants. Pediatr Res 1997;41:814. [10] HEMALATHA P, BHASKARAM P, KUMAR PA, KHAN MM, ISLAM MA. Zinc status of breastfed and formula-fed infants of different gestational ages. J Trop Pediatr 1997 ;43:52-4. [11] FERGUSON EL, GIBSON RS, THOMPSON LU OUNPUU S. Dietary calcium, phytate, and zinc intakes and the calcium phytate, and zinc molar ratios of the diets of a selected group of east African children. Am J Clin Nutr 1989;50:1450-6. [12] WISE A. Phytate and zinc bioavailability. Int J Food Sci Nutr 1995;46:53-63. [13] OBERLAEAS D, HARLAND B. Phytate content of foods: effect on dietary zinc bioavailability. J of the American Dietetic Association. 1981;79:433-436. [14] DE PEE S, BLOEM MW, GORSTEIN J ET AL. Reappraisal of the role of vegetables in the vitamin A status of mothers in Central Java, Indonesia. Am J Clin Nutr 1998l68(5):1068-74. [15] DE PEE S, BLOEM MW, SATOTO, YIP R, SUKATON A, TJIONG R, SHIRMPTON R, MUHILAL, KODYAT B. Impact of a social marketing campaign promoting dark-green leafy vegetables and eggs in central Java, Indonesia. Int J Vitam Nutr Res 1998;68:389-98. [16] DE PEE S, WEST CE, PERMAESIH D ET AL. Orange fruit is more effective than are dark-green, leafy vegetables in increasing serum concentrations of retinol and beta-carotene in school children in Indonesia. Am J Clin Nutr 1998; 68:1058-67. [17] DE PEE S, WEST CE. Dietary carotenoids and their role in combating vitamin A deficiency: a review of the literature. Eur J Clin Nutr 1996;50 (Suppl 3):S38-S53. [18] HULSHOF PJM, CHAO X, BOVENKAMP P, WEST CE. Green leafy vegetables contain less provitamin A than reported in food tables. Eur J Clin Nutr 1996;50:S80. [19] JAYARAJAN P, REDDY V, MOHANRAM M. Effect of dietary fat on absorption of beta-carotene from green leafy vegetables in children. Indian J Med Res 1980;71:53-
47

56. [20] MANORAMA R, BRAHMAM GN, RUKMINI C. Red palm oil as a source of beta- carotene for combating vitamin A deficiency. Plant Foods Hum Nutr 1996 ;49:75-82. [21] FAIRWEATHER-TAT SJ, WHARF SG, FOX TE. Zinc absorption in infants fed iron-fortified weaning food. Am J Clin Nutr 1995;62:785-9. [22] LAYRISSE M, CASAL MNG. Strategies for the prevention of iron deficiency through foods in the household. Nutr Rev 1997;55:233-239. [23] GIBSON RS, DONOVAN UM, HEALTH AL. Dietary strategies to improve the iron and zinc nutriture of young women following a vegetarian diet. Plant foods Hums Nutr 1997;51:1-16. [24] GIBSON RS, YEUDALL F, DROST N, MTITIMUNI B, CULLINAN T. Dietary interventions to prevent zinc deficiency. Am J. Clin Nutr 1998;68:484S-7S. [25] WASTNEY ME, HENKIN RI. Calculation of zinc absorption in Humans using tracers by fecal monitoring and a compartmental approach. J. Nutr 1989;119:1438-1443. [26] KNUDSEN E, JENSEN M, SOLGAARD P, SORENSEN SS, SANDSTROM B. Zinc absorption estimated by fecal monitoring of zinc stable isotopes validated by comparison with whole-body retention of zinc radioisotopes. J. Nutr 1995;125:1274- 1282. [27] KNUDSEN E, SANDSTROM B, SOLGAARD P. Zinc, copper and magnesium absorption from a fibre-rich diet. J Trace Elem Med Biol 1996;10:68-76. [28] AGGETT PJ. Iron, copper, and zinc absorption and turnover: the use of stable isotopes. Eur J Pediatr 1997;156:S29-S34. [29] VAN DEN HEUVEL EG, MUYS T, PELLEGROM H, BRUYNTJES JP, VAN DOKKUM W, SPANHAAK S, SCHAAFSMA G. A new method to measure iron absorption from the enrichment of 57Fe and 58Fe in young erythroid cells. Clin Chem 1998;44:649-54. [30] ZLOTKIN SH, LAY DM, KJARSGAARD J, LONGLEY T. Determination of iron absorption using erythrocyte iron incorporation of two stable isotopes of iron (57Fe and 58Fe) in very low birth weight Premature infants. J Pediatr Gastroenterol Nutr 1995;21:190-9 [31] JACKSON MJ, JONES DA, EDWARDS RHT. Zinc homeostatis in man: studies using a new stable isotope-dilution technique. Br J. of Nutr 1984;51:199-208. [32] JACKSON MJ. Stable isotope metabolic studies of zinc nutrition in slum-dwelling lactating women in the Amazon valley. Br J Nutr 1988;59:193-203. [33] KALTWASSER JP, HANSEN C, OEBIKE Y, WERNER E. Assessment of iron availability using stable 54Fe. Eur J Clin Invest 1991;21:436-42. [34] EHRENKRANZ RA, ACKERMAN BA, NELLI CM, JANGHORBANI M. Determination with stable isotopes of the dietary bioavailability of zinc in premature infants. Am J Clin Nutr 1984;40:72-81. [35] FRIEL JK, NAAKE VL, MILLER LV, FENNESSEY PV, HAMBIDGE KM. The analysis of stable isotopes in urine to determine the fractional absorption of zinc. Am J Clin Nutr 1992;55:473-7. [36] JALLA S, SAZAWAL S, HAMBIDGE KM, PATTERSON K, MENON VP, PADMA P, BLACK RE. Bioavailability of zinc in children in developing countries. FASEB 1999. Abstract. [37] KASTENMEYER P, DAVIDSSON L, GALAN P ET AL. A double stable isotope technique for measuring iron absorption in infants. Br J Nutr 1994;71:411-424. [38] DAVIDSSON L, GALAN P, KASTENMEYER P ET AL. Iron bioavailability studied in infants: the influence of phytic acid and ascorbic acid in infant formulas based on soy isolate. Pediatr Res 1994;36:816-22.
48

[39] DAVIDSSON L, MACKENZIE J, KASTENMEYER P ET AL. Dietary fiber in weaning cereals: a study of the effect on stool characteristics and absorption of energy nitrogen and minerals in healthy infants. J Peditar Gastroenterol Nutr 1996;22:167- 180. [40] DAVIDSSON L, WALCYCK T, MORRIS A, HURRELL RF. The influence of ascorbic acid on iron absorption by Jamaican children from an iron fortified chocolate- flavored milk drink. Am J Clin Nutr 1998;67:873-77. [41] WALCYCK T, DAVIDSSON L, ZAVALETA N, HURREL RF. Stable isotope labels as a tool to determine iron absorption by Peruvian school children from a breakfast meal. Fresenius J Anal Chem 1997;359:445-49. [42] BHUTTA ZA, MOLLA AM, ISANI Z, BADRUDDIN S, HENDRICKS K, SNYDER JD. Dietary management of persistent diarrhoea: Comparison of a traditional rice-lentil based diet with soy formula. Pediatrics 1991; 88: 1010-18. [43] BHUTTA Z A, MOLLA A M, ISSANI Z, BADRUDDIN S, HENDRICKS K, SNYDER J D. Nutrient absorption and weight gain in persistent diarrhoea: Comparison of a traditional rice-lentil-yogurt-milk diet with soy formula. J Pediatr Gastroenterol Nutr 1994;18:45-52. [44] BEER B, HEUMANN KG. Trace analysis of U, Th and other heavy metals in high purity aluminum with isotope dilution mass spectrometry. Fresenius J Anal Chem 1992;343:741-45. [45] LINDERKAMP O, VERSMOLD HT, RIEGEL KP, BETKE K. Estimation and prediction of blood volume in infants and children. Eur J Pediatr 1977;125:227-34. [46] TAYLOR PDP, MAECK R, DE BIEVRE P. Determination of the absolute isotopic composition and atomic weight of a reference sample of natural iron. Int J Mass Spectrom Ion Proc 1992;121:111-25. [47] HAMBIDGE MK, KREBS FN, MILLER L. Evaluation of zinc metabolism with use of stable-isotope techniques: implications for the assessment of zinc status. Am J Clin Nutr 1998;68:410-3. [48] AGGETT PJ. Iron, copper, and zinc absorption and turnover; the use of stable isotopes. Eur J Pediatr 1997;156:S29-S34. [49] DAVIDSSON L, MAKENZIE J, KASTENMAYER P, AGGETT PJ, HURRELL RF. Zinc and calcium apparent absorption from and infant cereal a stable isotope study in healthy infants. Br J Nutr 1996;75:291-300.
49

50

EVALUATION OF BIOAVAILABILITY OF FOOD FORTIFICANTS USING STABLE ISOTOPIC METHODS
DAVID C. HILMERS, MD, EE, MPH, STEVEN A. ABRAMS, MD
Baylor College of Medicine, Children’s Nutrition Research Center, Houston, Texas 77030, USA
Abstract
Because of the complex biochemical processes affecting the bioavailability of micronutrients, it is critical to understand regional factors that affect the design of a nutritional supplementation strategy. These factors include the prevalence of multiple micronutrient deficiencies, the presence of inhibitors in indigenous foods, interactions among co-fortificants, and coexisting medical diseases affecting absorptive capacity. Each of these can lessen the bioavailability, and thus the effectiveness, of supplements. Stable isotopic studies can help determine the fate of ingested micronutrients; therefore, they can evaluate the efficacy of fortification programs, provide evidence of poor bioavailability, and point to potential remedies. This has been the focus of several recent investigations by the Baylor Stable Isotope Laboratory and a proposed project in Sri Lanka. In Indonesia an efficacy study evaluated the current program of iron fortification of flour and the proposed addition of zinc. Three groups of 30 children ages 4 to 8 were given supplemented flour (iron only, iron plus zinc sulfate, iron plus zinc oxide). Each group exhibited iron absorption of greater than 10%, but concomitant zinc administration decreased iron bioavailability. This decrease was only statistically significant for zinc sulfate, however. Zinc absorption exceeded 20% in both the zinc oxide and zinc sulfate groups. In Peru four groups of one-year old children were given supplemented rolls containing iron, iron plus vitamin A, iron plus zinc, and iron plus zinc plus vitamin A. Isotopic analysis demonstrated that iron absorption was significantly better with the addition of vitamin A, marginally worse when zinc was included, and nearly equivalent when the three supplements were given in combination. Another recent study in Peru demonstrated the efficacy of a beverage fortified with multiple micronutrients in school age children. This investigation showed that balanced micronutrient supplementation resulted in iron and zinc absorption of greater than 10% and 20% respectively. Iron absorption was not significantly affected by consumption of the beverage with a meal. These studies demonstrate the power and flexibility of stable isotopic methods in the evaluation and design of micronutrient supplementation programs.
1. SCIENTIFIC BACKGROUND AND SCOPE. Heretofore, there has been little data available on the prevalence of micronutrient deficiencies in Sri Lanka. Cross-sectional data obtained in adolescent girls indicated iron deficiency in greater than 50% of this cohort and vitamin A deficiency in 21%1. Another study demonstrated 46% of pregnant or post-partum women had low serum retinol and 45% had low serum zinc levels.2 Little other prevalence data is available, but these statistics, coupled with the predominately plant-based diet, are strongly suggestive of widespread multiple micronutrient deficiencies in Sri Lanka. Currently, there is only a very limited program of micronutrient supplementation. This includes a pre-cooked food supplement enriched with a variety of micronutrients for infants age 6-12 months and iron/folate supplements for pregnant women. Little is known about the impact of planned staple fortification on the health of the general population. The broad-based objectives of this collaboration will be to target prevalent micronutrient deficiencies, identify food products for fortification, and to find efficacious supplements. The bioavailability of these products and the antagonistic/synergistic effects of various micronutrient combinations will be analyzed. National capacity-building will be
51

accomplished through the development of local expertise in the investigation of the efficacy of the supplementation and fortification program by the use of stable isotopic methods.
2. METHODS AND RESULTS Several previous studies performed by the Baylor group are illustrative of the stable isotopic methods that will be used in the Sri Lanka investigations. The results of each study are combined in this section for clarity. 2.1. Indonesia. Co-fortification of flour with iron and zinc.3
The government of Indonesia currently fortifies flour with iron at 60 ppm and is considering zinc as an additional fortificant. However, little extant data existed as to the efficacy of the current iron supplementation program, the effectiveness of zinc supplementation, and potential interaction between the two micronutrients when combined. Three groups of 30 children each were studied. Each child was 4-8 years old, had no recent illnesses, and was above the 3rd percentile for both weight and height. The children consumed 25 grams of flour fortified with iron, iron plus zinc oxide, or iron plus zinc sulfate. Iron labeling was accomplished with 1.5 mg (60 ppm) of 58Fe in the form of iron sulfate, and either zinc oxide or zinc sulfate was labeled with 1.5 mg (60 ppm) of 67Zn. After an overnight fast, blood was drawn for hemoglobin, ferritin, and transferrin receptors; the labeled flour was consumed by each group; and an IV infusion of 70Zn was completed. Urine samples were collected at 48 and 72 hours to determine the zinc isotope ratios and blood was collected at 14 days to measure the incorporation of labeled iron into erythrocytes. Tables 1-3 show the effects of fortification on iron absorption. It can be seen that iron absorption exceeds 10% in all groups, but there was a significant decrease in iron absorption when Zn SO4 was added. Mean zinc absorption was greater than 20% and was similar in both the zinc sulfate and zinc oxide groups.
TABLE 1: IRON ABSORPTION BY GROUP
Group N Mean +/- std dev (%) Range
Fe 29 15.9 +/- 6.8 1.2 – 35.2 Fe & Zn Ox 28 14.0 +/- 8.0 1.6 – 33.4 Fe & Zn SO4 29 11.5 +/- 4.9 1.2 – 35.2
ANOVA p=0.068
52

TABLE 2: BETWEEN GROUP DIFFERENCES IN IRON ABSORPTION
Groups Mean difference % p-value Fe +/- Zn Ox 1.88 0.32 Fe +/- Zn SO4 4.36 0.021 Zn Ox +/- Zn S04 2.48 0.19
Fisher’s PLSD
TABLE 3: ZINC ABSORPTION
Group N Mean +/- std dev (%) Zinc oxide 28 24.1 +/- 8.2 Zinc sulfate 29 23.7 +/- 11.2
ANOVA p=0.70 2.2. Peru Bioavailability of iron and zinc from a fortified beverage.4
We conducted a bioavailability study of a proprietary micronutrient-fortified beverage in Lima, Peru in November, 2001. Previously, a successful blinded, placebo-controlled efficacy study was performed in Botswana in children ages 5-11 in two schools on the outskirts of Gaborone from February to April, 2001.5,6 Table 4 shows the nutritional content of the beverage:
TABLE 4 NUTRITIONAL CONTENT OF BEVERAGE PER 240 ML SERVING
Nutrient Chemical Form Amount/Serving % US RDA Children 9 – 13 y***
100 kcal per 240 mL Vitamin A β-Carotene 2400 µg 33* Vitamin B2 riboflavin 0.40 mg 44 Niacin niacin 2.7 mg 23 Vitamin B6 pyridoxine HCl 0.5 mg 50 Folic Acid folic acid 140 µg 47 Vitamin B12 cyanocobalamin 1.0 µg 55 Vitamin C ascorbic acid 60 mg 133 Vitamin E dl-α-tocopherol acetate 7.5 mg 31** Calcium tricalcium phosphate 120 mg 9
Iron ferrous bisglycinate. chelate 7.0 mg 88
Iodine potassium iodide 60 µg 50 Zinc zinc gluconate 3.75 mg 47
53

Thirty-eight children, ages 6.0-9.9 yr, were recruited from a lower income peri-urban community in Lima, Peru. They received one 240 mL serving daily of the fortified beverage for 28 days. On days 15 and 16 each received two drinks, one labeled with 58Fe (as bisglycinate) and 70Zn (as zinc gluconate) with bread, butter, and milk, the other labeled with 57Fe and 67Zn without a meal. A 2 mg IV infusion of 68Zn was accomplished on day 15. Zinc absorption was calculated from the relative fractional urinary excretion of the oral and IV isotopes 72 hrs later. Iron absorption was calculated from the red blood cell incorporation of the iron isotopes on day 28. Consumption of the beverage led to similar zinc absorption with and without a meal (24.5±10.7% vs 22.8±7.6 %, p 0.21). Fractional iron absorption was adequate and slightly lower with the meal (9.8 ±6.7% vs 11.6 ±6.9%, p = 0.04). The total iron absorption of 0.69 mg/d meets most of the age-specific requirements for iron. From this study it was determined that zinc and iron were well absorbed from the beverage. The meal did not affect zinc absorption, and minimally influenced that of iron, and thus it could be demonstrated that adequate absorption of these essential nutrients occurred when the beverage was given in combination with a meal. 2.2.1. Peru. Interactions between Vitamin A, iron, and zinc.7
The final study using stable isotopes that will be described here is another investigation performed in Peru that examined the nutrient interactions occurring when flour is fortified with vitamin A, iron, and zinc. We measured Fe and Zn absorption in a cohort of 1-yr-old Peruvian children (N=54) from a low-income urban area who had been randomized to receive a daily weaning meal for 6 months based on milk and wheat flour fortified with one of four combinations of micronutrients: iron alone, iron with Zn, iron with vitamin A, or iron, zinc, and vitamin A. On day 1 of the investigation
58Fe-sulfate and
70Zn-sulfate were mixed with
porridge (fortified flour, sugar, oil, and milk) and 57Fe was given apart from the meal in orange juice with ascorbic acid as a reference dose.
67Zn was given intravenously. Iron
absorption was determined from red blood cell incorporation at 14 days and zinc absorption from the relative recovery of the oral vs intravenous tracer at 72-96 hrs after dosing. Samples were analyzed by thermal ionization mass spectrometry following preparation using ion exchange columns. We found that there was a lower percentage of Zn absorption in Zn supplemented children, 28.1% ± 8.9 vs 37.3 ± 14.5, p = 0.01 (Figure 1)
54

FIGURE 1: ZINC ABSORPTION
Zinc supplemented group
.
p = 0.01
Perc
ent A
bsor
ptio
n
Addition of a 4 mg zinc supplement decreases fractional zinc absorption. Data are Mean ± SE.
0
10
20
30
40
No Zinc supplementation
.
Iron absorption was significantly greater in children receiving vitamin A than iron alone with the reference dose, (57Fe: 30.1% ± 17.4 vs 19.5 ± 11.7, p = 0.008), and also with the meal (58Fe: 10.4% ±5.9 vs 7.6 ± 3.9, p = 0.04). See Figure 2. Iron absorption (57Fe) was decreased by zinc supplementation when iron plus zinc was compared to iron alone (25. 9% ± 16.8 vs 15.9 ± 8.7, p = 0.05). However, combined iron, zinc, and vitamin A supplementation showed comparable absorption with the reference dose (57Fe: 25.5% ± 12.3) as iron alone (57Fe, 21.7% ± 12.9, p = 0.44). (Figure 3)
55

FIGURE 2: IRON ABSORPTION COMPARISON
p
IronVitamin A +Iron
IronZinc +Iron
IronVitamin A +Iron
IronZinc +Iron
Reference Dose
.
With Porridge
0
5
10
15
Perc
ent 5
8Fe
abso
rptio
nPe
rcen
t 57 F
e ab
sorp
tion
Perc
ent 5
8 Fe
abso
rptio
n
Vitamin A added to iron supplementation increases its absorption whereas zinc tends to decrease the iron absorption. Values shown are for pairwise comparisons only and do not include subjects who received all three micronutrients (iron, zinc and vitamin A). Data are Mean ± SE.
P = 0.04
P = 0.16
P = 0.12P = 0.26
0
10
20
30
40
50
56

FIGURE 3: IRON ABSORPTION WITH VITAMIN A, IRON, AND ZINC SUPPLEMENTATION
R efe ren ce D ose
.
57Fe 58Fe
p = 0.44
p = 0.40
W ith P o rrid ge
Per
cent
Ab
sorp
tion
W h e n z in c a nd v ita min A a r e a d d e d to a n ir o n s u p p le me n t, ir o n a b s o rp tio n is s im ila r to th a t w h ic h o c c ur s w h en th e ir o n is g iv e n a lo n e . D a ta a r e Me a n ± SD .
0
10
20
30
40Fe/Zn/Vitamin AFe alone
These data indicate that 6 mo of Zn supplementation leads to decreased fractional Zn absorption likely related to improved Zn status. Vitamin A enhances Fe absorption and co-supplementation of Fe with Zn and vitamin A leads to similar Fe absorption as providing Fe alone.
3. PLANS FOR FUTURE WORK
These studies demonstrate how stable isotopic methods can be used to answer specific research questions about food fortification programs. Detailed laboratory and statistical methods for analysis of stable isotope studies can be found in reference 8. Similar types of research questions as those mentioned here can be addressed as part of the Sri Lanka studies. Representative objectives of this contract include: • Possible antagonistic interactions between copper, iron, vitamin A, zinc, and iodine that
may occur among healthy school children. • The bioavailability of copper and iodine. • The zinc and iron status of patients diagnosed with endemic goiter. • Bioavailability of iron in iron supplements. • The relative efficiency of absorption of different combinations of iron, zinc, vitamin A,
and vitamin C. In addition, training of Sri Lanka technical personnel will be done in the Baylor College of Medicine laboratories. This research will be the subject of a PhD dissertation by a doctoral candidate from Sri Lanka.
57

REFERENCES [1] MUDALIGE R, NESTAL P. Prevalence of anaemia in Sri Lanka. The Cey J Med Sci 1996;39: 9-16 [2] DE SILVA L.D.R., Atukorala TMS. Micronutrient status of plantation workers in Sri Lanka during pregnancy and post partum. J Obs Gynae res. 1996;22: 239-246. [3] HERMAN S, GRIFFIN O.J, SUWARTI S, ERNAWATI F, PERMAESIH D, PAMBUDI D, ABRAMS S.A. Co-fortification of iron fortified flour with zinc sulfate, but not zinc oxide, decreases iron absorption in Indonesian children. In press AJCN. [4] MISHAN A, ABRAMS S.A, HILMERS D.C. Evaluation of iron and zinc bioavailability from a new vitamin and mineral fortified beverage. Abstract submitted to American College of Nutrition Annual Meeting. [5] ABRAMS S.A, MUSHI A, HILMERS D.C, GRIFFIN I.J, DAVILA P, ALLEN L. A multi-nutrient-fortified beverage enhances the nutritional status of children in Botswana. Submitted for publication in Pediatrics. [6] HILMERS D.C., MUSHI A, GRIFFIN I.J., ALLEN L.H., HICKS P.D., ABRAMS S.A. A trial of amulti-nutrient fortified beverage in Botswana children. Pediatr Res 2002;51:210A. [7] ABRAMS S.A., ZAVALETA N, LONNERDAL B. Absorption of iron (Fe) and zinc (Zn) by 1-yr-old Peruvian children consuming a diet based on wheat flour fortified with Fe with or without Zn and/or vitamin A. Pediatr Res 2002;51:189A. [8] ABRAMS S.A. Using stable isotopes to assess mineral absorption and utilization by children. Am J Clin Nutr 1999;70:955-64.
58

INTERACTION BETWEEN MICRONUTRIENTS, THEIR IMPACT ON BIOAVAILABILITY AND SIGNIFICANCE IN NUTRITION INTERVENTION.
CHANDRANI E. LIYANAGE, M.SC., PH. D.
Nuclear Medicine Unit, Faculty of Medicine, University of Ruhuna, PO. Box 70, Galle. Sri Lanka
Abstract Micronutrient malnutriation is a serious problem in Sri Lanka; the deficiencies of greatest public health significance are iron, iodine and vitamin A. In addition, zinc deficiency also has beeen reported in some age groups. A presence of competitive antagonism has been highlighted between micronutrients and as such, an investigation will be carried out to determine the possible antagonistic interactions between iron and zinc by linear regression analysis. It has also been planned to study the coexisting micronutrient deficiencies (iron and zinc) and their impact on preexisting deficiency of iodine. Further, it is aimed to decide on a suitable micronutrient combination and study the impact of it by supplementing several combinations on healthy subjects. Data on zinc status of the Sri Lankan population are not adequate at present and, the selenium status is not known yet. As such, zinc and selenium status assessments will be carried out in the present programme. The present study programme therefore, would fill in the gaps in the existing knowledge on micronutrient malnutrition and, be beneficial for the people in Sri Lanka.
1. SCIENTIFIC BACKGROUND AND SCOPE Micronutrient malnutrition is a serious threat to the health and productivity of more than 2000 million people worldwide, even though it is highly preventable. The three micro nutrient deficiencies of greatest public health significance in Sri Lanka are those of iron, iodine and vitamin A and these have been given much emphasis in the national health policy. An island wide research programme 1994-95 revealed 45% among preschoolers, 58% among children between 5-11 years, 36% among adolescents, 45% of non-pregnant women and 39% of pregnant women were anaemic1. A cross sectional study on adolescent girls indicated a depletion of iron status in 54% and very low serum Vitamin A in 21%2 and as such, the need for interventions during adolescence has been highlighted. In another study on micronutrient status among plantation workers during pregnancy and post partum, it was noted 46.2% were having low serum vitamin A levels (< 20µg/dl) and 45.2% were with low serum zinc levels (< 8µmol/l) at 10-26 weeks of gestation3. There is a national programme on supplementation of micronutrients (iron and folate) but is being done only among pregnant women. Efficacy of this intervention has been studied and found to be not very satisfactory4,5. A supplementary pre-cooked food (Thriposha) that is enriched with iron, vitamin A, and some other micronutrients is also distributed to pregnant women and children from six months to one year of age; the efficacy of which has not yet been studied, nor the impact of interactions between micronutrients. As such, in order to embark on an effective micronutrient supplementation programme in the country it is a necessity to study the above aspects. In Sri Lanka, staple diet is plant based and, intake of the food of animal origin is often low. As a result, they often contain high levels of certain inhibitors (e.g., phytate, polyphenols), which are known to affect the bioavailability of calcium, iron, and/or zinc by forming
59

insoluble complexes in the gastrointestinal tract6,7. The extent to which these inhibitors influence the bioavailability of iron has been studied in our laboratory in the commonly used foods including weaning foods8,9, however, the influence on the other essential inorganic nutrients such as copper, manganese, selenium, chromium, iodine and magnesium are not well established and require further studies. Recently, it has been emphasized that consumption of predominantly plant based diets leads to multiple micronutrient deficiencies, notably iron, zinc, vitamin A, riboflavin, vitamin B12, and possibly selenium and iodine and such co-existing micronutrient deficiencies can induce interactions (e.g., vitamin A-zinc, vitamin A-iron, iodine-iron), which may exacerbate pre-existing deficiency states10,11,12. Of the dietary factors affecting bioavailability, a presence of possible competitive antagonism between ions (copper-zinc, copper-iron, iron-zinc, iron-iodine, zinc-iodine)13,14,15 may interfere with utilization of trace elements especially when high doses of supplements are consumed. There has been increasing recognition of the co-existence of multiple micro nutrient deficiencies in the developing countries and supplementation levels and fortification programmes have to be carefully designed to combat their deficiencies, minimizing risk of antagonistic nutrient interactions. Combining multiple micronutrients in a single delivery mechanism has been suggested as cost effective way to achieve multiple benefits16,17. Although on paper prevention and treatment of micronutrient deficiency is simple, achieving these goals in practical is not easy. Some have questioned the effectiveness of nutrients combined within a supplement because of possible interactions of the nutrients of the supplement as well as those intrinsic to the food or interference in their absorption18,19. Preventing and correcting micronutrient deficiency among children and adolescents in the country is urgent because of its negative consequences and the fact that adolescent girls are an important target group because they are future mothers. As such, in the proposed study programme it is also aimed at preparing a combined multiple Micronutrients supplement, which is effective and efficacious in combating the micronutrient malnutrition in them.
2. AIMS & OBJECTIVES: To study possible antagonistic interaction between zinc and iron that may interfere with utilization (during digestion, absorption, and transportation) by a randomized placebo controlled trial. Possible interactions between micronutrients have been proposed and it is important to establish the relationships among the micronutrients of which deficiencies are mostly seen in our population. Assessment of the existence of competitive antagonism between ions by a randomized control trial. To study iron and zinc status in patients diagnosed as having endemic goiter. Patients diagnosed with endemic goiter will be investigated for the Ferrous and Zinc status, to find out any relationship between Iodine and Zinc, Iodine and Ferrous in metabolism.
60

To determine the bioavailability of zinc and iron (in vivo) from food using stable isotope methodology. To assess the status of zinc and selenium in different age groups of the population in Southern Sri Lanka. To study interaction in multiple micro nutrient supplements: relative efficiency of absorption of combinations (iron+zinc+vit A+vit C, iron+zinc+vit C, iron+vit A+vit C) of micro nutrient supplements and the impact of interaction by double blind placebo controlled efficacy study.
3. METHODOLOGY 3.1. Protocol 1 Intervention group
Age adolescents 14-18 yrs Design randomized control study Sample healthy schoolgirls of 14-18 years (sample size 1584), 198
in each supplement group Baseline Information nutritional status will be assessed by anthropometry
(weight, height, BMI) dietary survey will be conducted by 24 hour dietary recall. Data on morbidity, appetite, school performance, and susceptibility to infection will be obtained. initial status of the following indices will be determined; Indices Serum Zinc Serum zinc portophyrin Serum Ferritin Hb%
Supplementation with Mineral Capsules of different combinations
1. Ferrous 60 mg + Zinc 13.1 mg 2. Ferrous 60 mg 3. Zinc 13.1 mg 4. Placebo
Duration of Supplementation
five days per week / 16 weeks
Collection of Blood samples
before and after supplementation (status of the above indices will be determined after the supplementation as well)
61

3.2. Protocol 2 Intervention group
Age adults (male & female) Design cross sectional study by simple random sampling Sample size selected from patients attending the surgical clinics of the
Teaching Hospital having low urinary iodine, Data collection: a blood sample will be drawn and, determined the following Indices Serum Zinc
Serum Ferritin Zinc portopophyrin Seum Thyroxine Serum TSH Hb%
3.3. Protocol 3
Sample adolescents of 14-18 years (about 20) Design double isotopic study, Baylor College group to decide Setting: Faculty of Medicine, Galle, Sri Lanka Baseline information height and weight
Dietary recall Collection of samples
at baseline and after 14 days of introducing the isotopes
Analysis of samples at Baylor College by the CRPF 3.4. Protocol 4
Intervention group adolescents and adults Design: cross sectional prevalence study Sample size to be worked out Baseline information height and weight
Infections Collection of samples for determine the levels of serum zinc and selenium
62

3.5. Protocol 5 Intervention group
Age adolescents of 14-18 yrs Design double blind placebo controlled efficacy study Sample healthy schoolgirls of 14-18 years, equal proportions from both rural &
urban areas, by random sampling Baseline Information nutritional status will be assessed by anthropometry (weight, height,
BMI) dietary survey will be conducted using a food frequency questionnaire initial status of the following indices will be determined; Indices: Serum Zinc Serum Retinol Serum Ferritin Hb%
Supplementation with micronutrient capsules of different combinations
1. Zinc 13.1 mg + Ferrous 60mg + Vitamin A 500 IU + Vitamin C 30mg 2. Zinc 13.1 mg + Ferrous 60mg + Vitamin C 30mg 3. Ferrous 60mg + Vitamin A 500IU + Vitamin C 30mg 4. Ferrous 60 mg 5. Zinc 13.1 mg 6. Placebo capsule
Duration of Supplementation
five days per week / 16 weeks
Collection of Blood samples
before and after supplementation
Indices Serum Zinc Serum Ferritin Vitamin A Hb%
63

4. ANALYSIS • The correlation among the initial micronutrient status and the dietary intake and
anthropometrical measurements (linear height, weight and BMI) will be assessed. • The correlation between the initial micronutrient status and after the supplementation
programme will be assessed using RIA and chemical methods. • The impact of iron and/or zinc with iodine in iodine deficient people will be assessed • Bioavailabiliy of copper and iodine will be assed by using stable isotope methodology in
humans. • The prevalence of zinc and selenium deficiency states will be assessed.
5. STATISTICAL ANALYSIS • Differences between groups in concentrations of biochemical indicators of the start of the
study will be tested by analysis of variance. • Differences in concentrations between group at baseline and at the end of supplementation
will be tested by analysis of variance. • Chi-squared test will be employed to compare the prevalence. • The association between the rate of improvement of micro nutrient status and possible
interactions will be studied by using the multiple linear regressions with appropriate modifications.
• Differences in supplement effect (baseline compared with end results) as a within-subject factor. A significant p value for the within-subject factor will indicate a change over time on the combined values of the six groups and will be further investigated by using paired t test for each group.
6. ETHICAL CONSIDERATION • Informed written consent will be obtained from each of the participants’ parent/guardian
who are selected for the study. • At any time during the study, participants will have a right to leave the study. Doing so
will not affect their subsequent care. • Blood samples of 5 ml (volume needed for the nutrient assessment) will be drawn under
sterile techniques by the investigator before and after the supplementation. • Confidentiality will be ensured for all information collected in the study, only group data
will be published, and no personnel data will be exposed. • The risks and benefits will be explained to each individual before referring for possible
treatment. • Those study subjects request any treatment, will also be referred for possible treatment
and followed up. • An incidental finding of any illness will be referred for relevant care.
64

7. TIME FRAME FOR THE FIRST YEAR STARTING FROM 15TH DECEMBER 2001.
Task D J F M A M J J A S O N 1.Literature survey 2.Formulate Objectives 3.Designing and planning 4.Preparation of micronutrients 5.Initiating the investigation 01(objective 01) 6.Analysis of baseline samples 7.Report Writing
65

REFERENCES [1] MUDALIGE R, NESTAL P. Prevalence of anaemia in Sri Lanka. The Cey J Med Sci 1996;39: 09-16 [2] LANEROLLE P, Atukorala TMS Iron and vitamin A status of adolescent school girls in an urban and a rural area of Sri Lanka. Cey J Med Sci 1998;41(2): 35-45 [3] DE SILVA L.DDR, Atukorala TMS Micronutrient status of plantation workers in Sri Lanka during pregnancy and post partum. J Obs Gynae Res 1996;22: 239-246 [4] ATHUKORALA T.M.S, DE SILVA R.S. Evaluation of effectiveness of iron-folate supplementation and antihelminthic therapy against anaemia in pregnancy,: a study in the plantation sector of Sri Lanka. Am J Clin Nutr 1994;60: 286-292 [5] GOONEWARDENA I.M.R, LIYANAGE C. SEEKKUGE J. Antenatal iron status and its correlation to haemoglobin levels in pregnant women attending an antenatal clinic Cey Med J 1995;40(2): 67-69 [6] ADAMS C, RAHOY V, KERBS N, WESTCOTT J, LEI S, HAMBIDGE M. The effect of low phytic and corn mutants on zinc absorption. San Diego, FASEB J, A510,2000 [7] FAIRWEATHER TAIT S, HURREL R. Bioavailability of minerals and trace elements. Nutr Res Rev 1996;9: 295-324 [8] LIYANAGE K.D.C.E., THABREW M.I., Goonaratne C Iron deficiency anaemia in children aged 09-24 months from a rural area of south of Sri Lanka. Sri Lanka Dental Journal 1995;18: 14-17 [9] LIYANAGE C. Iron availability of low cost weaning foods in Sri Lanka; An in-vitro study using 59fe as the tracer Asia Pacific Food Analysis Network Conference. [10] UDOMKESMALLE E, DHANAMITTA S, SIRISAHA S et al Effect of vitamin A and zinc supplementation on the nutrition of children in north east Thailand. Am J Clin Nutr 1992;56: 50-57 [11] BLOEM M.W. Interdependence of vitamin A and iron: an important association for programmes of anaemia control. Proc Nutr Soc 1995;54: 501-508 [12] HETZEL B.S. The prevention and control of iodine deficiency disorders. United Nations ACC/SCN state of the art seris Nutrition Policy Discussion paper no 03, 1998. [13] SOLOMONS N.W. Competitive interaction of iron and zinc in the diet; consequences for human nutrition. J Nutr 1986;116: 927-935 [14] SOLOMONS N.W. Competitive interaction of iron and zinc in the diet; consequences for human nutrition. J Nutr 1986;116: 927-935 [15] FISCHER P.W.F, GIROUX Z, C’abbe MR. Effect of zinc supplementation on copper status in adult men. Am J Clin Nutr 1984;40: 743-746 [16] MILNE D.B., CANFIELD W.K., MAHALLO J.R., SANDSTEAD H.H. Effect of oral folic acid supplements on zinc, copper, and iron absorption and excretion. Am J Clin Nutr 1984;39: 535-539 [17] NILSON A, Piza J Food fortification: a tool for fighting hidden hunger. Food Nutr Bull 1998;19: 49-60 [18] YARDIK M.K., KENNEY M.A., WINTERFELDT E.A. Iron copper and zinc status: response to supplementation with zinc or zinc and iron in adult females. Am J Clin Nutr 1989;49: 145-150 [19] ARGIRATOS, SAMMAN. The effect of calcium carbonate and calcium citrate on the absorption of zinc in health female subjects. Eur J Nutr 1994;45: 198-204
66

EVALUATION OF THE NEWLY PROPOSED VITAMIN A SUPPLEMENTATION REGIMEN FOR POSTPARTUM MOTHERS USING STABLE CARBON ISOTOPES
SHERRY A. TANUMIHARDJO1, SAMUEL NEWTON2 AND PAUL ARTHUR (DECEASED MARCH 2002)
1UW-Madison, Dept. of Nutritional Sciences, 1415 Linden Dr., Madison, WI 53713, USA 2Kintampo Health Research Center, Health Research Unit, Ministry of Health, PO Box 200, Kintampo, Brong Ahafo Region, Ghana
Abstract The long-term goal of this project is to establish public health programs to improve the health of women and children globally by determining safe and effective methods to improve vitamin A status. By improving the vitamin A status of mothers and infants, mortality and morbidity of children will be reduced. The specific aims of this proposal are: • To determine the length of time mothers are protected against depletion after receiving either
400,000 IU of vitamin A in two doses of 200,000 IU 24 hours apart or one dose of 200,000 IU. The modified relative dose response (MRDR) test will be used at monthly intervals for 5 months post dosing to assess changes in vitamin A status.
• To determine the degree of dilution in the vitamin A body pool after dosing women with either 200,000 or 400,000 IU of vitamin A using stable 13C2-retinol as a tracer.
• To determine the difference in total vitamin A body reserves of women who received either 200,000 or 400,000 IU of vitamin A using the 13C2-retinol isotope dilution (13C2-RID) test.
This proposal addresses the following hypothesis: In women who are given 400,000 IU of vitamin A, the length of protection from vitamin A depletion is increased but not doubled. A 400,000 IU dose dilutes the vitamin A pool more than 200,000 IU but not by 2:1 and a 400,000 IU dose increases the total body reserves of vitamin A over 200,000 IU but not by 2:1.
1. SCIENTIFIC BACKGROUND AND SCOPE OF THE PROJECT The vitamin A statuses of under-privileged women and children in both the underdeveloped world [1-4] and the United States [5,6] are compromised for many reasons. For women, low dietary intakes and increased requirements during pregnancy and lactation are the main reasons for vitamin A inadequacy and both of these are exacerbated by low social and economic status and living in a poor environment. For children, inadequate dietary intake and multiple childhood infections can result in depleted vitamin A liver reserves, and an increased risk of morbidity has been associated with mild vitamin A deficiency [7]. During acute infection, retinol is excreted in significant amounts in the urine [8, 10], enhancing total vitamin A requirements. This proposal will address the need for assessment of vitamin A status in response to intervention trials aimed at improving the health of women and children. Assessing vitamin A status is important in determining which population groups are at risk of deficiency, depletion, and excess or toxicity. Dietary surveys are inappropriate for determining vitamin A status because multiple factors affect the absorption and utilization of pro-vitamin A carotenoids and pre-formed vitamin A [11, 12]. Biochemical assessment of vitamin A status is not straightforward. Serum concentrations of vitamin A (retinol) are
67

homeostatically controlled and do not begin to decline until liver reserves are dangerously low [13]. Also, in times of infection, serum concentrations are transiently reduced due to the acute phase response [14]. In a healthy individual, the liver contains approximately 80-90% of the total body reserves of vitamin A mostly in the form of retinyl esters. A liver reserve of > 0.070 �mol retinol/g liver has been defined as adequate for humans. The reported range of liver reserves in well-nourished healthy American adults is 0.44-0.74 �mol retinol/g [13]. However, liver biopsies of humans are only justifiable in certain instances. Therefore indirect methods to determine liver reserves are needed. Minimally invasive methods to accurately determine vitamin A liver reserves in a population with the smallest sample size possible are still under development [15]. Biochemical assessment techniques that are currently used include the relative dose response (RDR) test, the modified relative dose response (MRDR) test [16], and the deuterated retinol dilution (DRD) assay [17, 18]. The RDR and MRDR tests operate on the same principle. As liver reserves become depleted, apo-retinol binding protein (RBP) accumulates in the liver. A challenge dose of either retinyl ester in the RDR or dehydroretinyl acetate in the MRDR is administered and the response of the retinol or dehydroretinol-holo-RBP complex is measured in the serum 5 h after dosing. The major difference in practice is that 2 blood samples are needed for the RDR (before and after) and only one for the MRDR (post-dosing). However, the dose response tests lack utility in defining the actual liver reserve of vitamin A and will only distinguish between a moderately inadequate and adequate through toxic vitamin A status. The deuterated retinol dilution (DRD) assay has been successfully applied in several population groups, but large doses of vitamin A (70-140 �mol in adults) have been used and the gas chromatography-mass spectrometer (GC-MS) analysis is not very sensitive [17,18]. Using electron capture negative chemical ionization for detection improved the sensitivity of the MS. However, the retinol needed to be derivatized and a relatively large dose (35 �mol) of deuterated retinyl acetate was administered to adults [19]. Nevertheless, stable isotope methods are helping investigators answer important questions about carotenoid bioavailability and vitamin A equivalence [20-23]. In intervention studies with children, 10.5-17.5 �mol was administered, but two enrichments of the isotope, i.e. d4- and d8-retinol, were used to differentiate the first dose from the second in the GC-MS analysis [21,22]. To improve the stable isotope methods, we developed an isotope dilution assay by synthesizing retinyl acetate with 4-13C’s incorporated into the isoprene backbone of the molecule [24]. Instead of using conventional GC-MS, we used gas chromatography-combustion-isotope ratio mass spectrometry (GCCIRMS) for analysis [25]. Small physiological doses can be used and the GCCIRMS is much more sensitive than conventional GC-MS [26]. The new isotope dilution method was developed to determine the total body reserves (TBR) of vitamin A in rats, and was found to do so with “textbook” accuracy [27]. The method holds considerable promise for use in determining TBR in human population groups and in being sensitive to changes in liver concentration of vitamin A [28]. This proposal outlines how we will use the 13C2-retinol isotope dilution (13C-RID) test to answer important public health questions.
68

2. METHODS In 1993, the WHO proposed a regimen to extend supplementation to young infants (below 6 months of age). This regimen took advantage of the high reported contact with the Expanded Program of Immunization (EPI) to provide three doses of 25,000 IU vitamin A before 6 months of age, at the time of DPT/Polio immunizations, together with a 200,000 IU postpartum dose to the mother within 6-8 weeks of delivery. This regimen is well tolerated, safe, and does not interfere with the immune response to DPT and polio [29]. The efficacy of this regimen was evaluated in a WHO-coordinated multi-center study, carried out in Ghana, India, and Peru (1995-1997). About 10,000 mother-infant pairs were recruited and divided into two groups. Group 1, breast-feeding mothers received 200,000 IU vitamin A while their infants received three 25,000 IU doses at the time of their DPT/Polio immunizations. Group 2 received placebos that looked identical to the supplements given to Group 1. The groups were comparable at baseline. At six months, there was a small, but statistically significant improvement in the vitamin A status of the children who received vitamin A compared with those who received the placebo. However, the regimen was not adequate for improving the vitamin A status of the children beyond 6 months of age. In the newly proposed postpartum and infant regimens, the amount of supplemental vitamin A to be administered is doubled. One of the efficacy trial study sites is Ghana, at the same location that the earlier WHO multi-center trial was carried out. In the new trial, the proposed regimen (two postpartum doses of 200,000 IU to the mother, plus three doses of 50,000 IU to the young infant) will be compared with the previous regimen (200,000 IU postpartum, plus three doses of 25,000 IU to the young infant). The Ghana main trial began early in 2002. We propose to evaluate the difference in total body reserves of vitamin A using the 13C-retinol isotope dilution test in women as an add on to the main trial, which has the data collection infrastructure already in place. The women in the on-going Ghana trial are individually randomized following double blind-placebo controlled procedures. Mothers in Group 1 (Intervention Group) receive TWO oral doses of 200,000 IU vitamin A, given on their registration day and 24 hours later. Mothers in Group 2 (Control Group) receive a single oral dose of 200,000 IU vitamin A on registration day and a placebo 24 hours later. This trial is currently being evaluated using the modified relative dose response test and breast milk retinol concentrations. The mothers are visited at home about 7 to 10 days after delivery, and recruited into the trial using the established procedures at the Kintampo Health Research Centre. This involves a meeting of the potential trial subjects together with their heads of household or other elder(s), and soliciting their agreement to participate in the trial after reading to them a prepared information sheet written in the local language. This explains the purpose of the study, the study procedures, the obligations of the investigators, and what will be required of participants if they agree to participate. Opportunity is given for questions and for checking that the information provided has been understood. Mothers are then asked to indicate their consent to participate by appending their signature or other personal mark to a prepared declaration. After this, the mothers are issued with a study ID card bearing their ID details, including their unique study IDs.
69

AIM 1 To determine the length of time mothers are protected against depletion after receiving either 400,000 IU of vitamin A in two doses of 200,000 IU 24 hours apart or one dose of 200,000 IU using the modified relative dose response (MRDR) test at monthly intervals for 5 months post dosing. In the first year of this proposal, we will perform the MRDR test in the women at monthly intervals for 5 months after receiving their vitamin A doses. This will allow the newly formed research team to work together with an assay that they are all familiar with. At the same time more 13C2-retinol will be synthesized (FIGURE 1) at UW-Madison for subsequent utilization at the field site. We will also set up and establish the analysis for the 13C-RID studies at UW-Madison.
70

O COOEt
CH 2 OH
CHO
O
*COOEt
*CH 2 OH
*CH 2 OCOCH 3
LiAlH 4
1 2 NaH
LiAlH 4
(EtO) 2 PO- CH - 2 CO 2Et
EtO 2
(EtO) 2 PO 13 CH 2
13 CO 2 Et
EtO 2
NaH
Acetone
MnO 2
(CH 3 CO) 2 O
OH -
2
3
3 4
4
5
5 6
6 7
7
8
* Denotes 13C
*
*
*
FIGURE 1: Organic synthesis of 14,15-13C2-retinyl acetate
71

Synthesis of 3,4-didehydroretinyl acetate for the MRDR test [30] In support of the use of the modified relative dose response test globally, 3,4-didehydroretinyl acetate is synthesized twice per year at UW-Madison. Therefore, the 3,4-didehydroretinyl acetate needed for completion of AIM 1 is readily available. In this process, all-trans retinoic acid is methylated with diazomethane to protect it from subsequent reactions (~99% yield). The methyl retinoate is then oxidized to 4=oxo-methyl retinoate and purified on 8% deactivated alumina (50% yield). Subsequently, 4=oxo-methyl retinoate is reduced with sodium borohydride to 4-hydroxy methyl retinoate (~99% yield) and crystallized from hexane. 4-hydroxy-methyl retinoate is dehydrated to make 3,4-didehydro-methyl retinoate (80% yield) which is subsequently reduced with lithium aluminum hydride to 3,4-didehydroretinol. Finally, the dehydroretinol is acetylated with acetic anhydride to result in 3,4-didehydroretinyl acetate with an overall yield of approximately 25-30%. This synthesis has been refined and yields have been doubled over the last decade. Assessment of length of protection from both the 200,000 to 400,000 IU doses The MRDR test will involve giving a single oral dose of 8.8 µmol of 3,4-didehydroretinyl acetate and taking a single venous blood sample (7 mL) 5 hours after dosing. After baseline MRDR tests on all of the women, four groups of 25 women will be randomly assigned to a follow-up assessment and each group will be invited back once. Based on data in children [1, 31], 200,000 IU was protective for at least one month. Therefore we propose that the second assessments be done in months 2, 3, 4 and 5. TABLE 1 represents the sampling and n at each time point.
TABLE 1- STUDY DESIGN FOR AIM 1 Month after dosing 0 2 3 4 5
Number enrolled from each group 100 25 25 25 25
The total number of women to be enrolled in this study is 200. MRDR tests will be performed on all women at the outset and then on 50 of the same women (25 from each group) at monthly intervals after that starting 2 months after dosing. Women will be selected at the time of their first MRDR test and will be invited back at randomly selected times. The assays will be done at the Noguchi Memorial Institute for Medical Research (NMIMR) in Ghana. As this procedure is the same as at baseline, the consent form will be reread to the women at the second MRDR test.
72

AIM 2: To determine the degree of dilution of the retinol body pool after dosing women with either 200,000 or 400,000 IU of vitamin A. Dilution of the retinol pool with 200,000 IU and 400,000 IU doses After a 10 mL baseline blood sample, a 5 mg dose of 13C2-retinyl acetate will be administered to 20 women one week prior to administering the high dose postpartum capsules. A second blood sample will be collected before giving the high dose to determine the enrichment of the serum retinol pool with 13C2-retinol. After allowing the high doses to equilibrate for three weeks with the body pool of retinol, a follow up blood sample will be drawn. This will provide information on the degree of dilution of the labeled retinol for the two separate dose levels. Prepared serum samples will be frozen and shipped or hand carried to the US. Thus, a total of 3 blood samples will be needed from each of these 20 women over a one-month period. These women will be contacted before their enrollment into the main study cohort. They will be asked to sign a consent form that is different from the main trial as the procedure is slightly different from the main trial. The dosing and blood draw schedule is outlined in TABLE 2.
TABLE 2 – STUDY DESIGN FOR AIM 2 Blood sample and time of collection
Baseline serum sample at time 0
Enrichment determined 1 week after dosing with 13C2-
retinol
Dilution of enrichment at 3 weeks after dose
Dosage Test dose with 5 mg 13C2-retinyl acetate
High dose capsules: 400,000 and 200,000 IU vitamin A No dose
Number of women 10 women from each group Same 20 women Same 20 women
73

AIM 3 To determine the difference in total vitamin A body reserves of women who received either 200,000 or 400,000 IU of vitamin A using the 13C2-retinol isotope dilution (13C2-RID) test. Isotope dilution studies to determine total body reserves After equilibration of the high dose supplements (about one month), isotope dilution testing will begin in a third study. This study will include 5 groups of 10 women. A baseline blood sample will be drawn from the first group of 10 women at time zero. Immediately afterwards, a single 2 mg dose of 13C2-retinyl acetate will be administered. After three weeks a second blood sample will be drawn. No baseline blood samples will be needed for the women selected to give blood in the subsequent 4 months as the 10 baseline women will provide the baseline measure for all 5 groups. The basis for this is that we found only a 0.2% CV in the baseline measure in Malawi women (n = 8) which means that taking a baseline blood sample for all women in a study where the same source of supplemental vitamin A is given is not necessary. Thus, each woman in months 2 through 5 will only have one blood sample taken 3 weeks after administration of the 13C2-retinyl acetate. Serum samples will be frozen and shipped or hand carried to US. Ten women per month is a sufficient sample size for each dose level (TABLE 3).
TABLE 3 – STUDY DESIGN FOR AIM 3 Time after high dose vitamin A supplementation
One month Two months
Three months Four months Five
months
Baseline measure one month after high dose
Dose with 13C2-retinyl acetate (RA)
Dose with 13C2-RA
Dose with 13C2-RA
Dose with 13C2-RA
Dose with 13C2-RA
Blood sample 3 wk after 13C2-RA
3 wk after 13C2-RA
3 wk after 13C2-RA
3 wk after 13C2-RA
3 wk after 13C2-RA
n = 10 Same 10 as baseline 10 10 10 10
Thus, 100 women will be enrolled in this evaluation of total body reserves (50 from group one and 50 from group 2). We anticipate that the women who received the 400,000 IU dose will have higher body stores of vitamin A but not by 2:1 due to overwhelming the body with vitamin A. These women will be enrolled into this study after their initial screening into the trial. They will be asked to sign a consent form that is similar to AIM 3 as the procedure is the same as AIM 3.
74

3. RESULTS Current status of research using the 13C-retinol isotope dilution assay: Successful synthesis of 14,15-13C2-retinyl acetate 10,11,14,15-13C4-retinyl acetate was synthesized [24] for use in rat and pilot human experiments [27, 28] using a modification of Bergen et al. [38]. Briefly, C18-tetraene ketone was synthesized from β-ionone, a commercially available precursor. Using a modified Whittig-Horner procedure, C-18 tetraene ketone was reacted with the carbanion of 13C2-labeled triethylphosphonoacetate to add 2-13C’s to the backbone of the retinol moiety. The resulting ethyl ester was reduced to the alcohol and esterified to 13C2-retinyl acetate with acetic anhydride. The synthetic vitamin was purified carefully on 8%-water-deactivated alumina using relatively innocuous, highly volatile, organic solvents, e.g. hexanes and diethyl ether. The resulting preparation was characterized using UV-VIS spectroscopy, TLC and HPLC. For long-term storage, the 14,15-13C2-retinyl acetate is stored dissolved in corn oil at –80oC. Thus, we have 0.5 g of >96% all-trans-13C2-retinyl acetate available to begin our proposed studies. From these valuable experiments in the rat and human, it was apparent that our GCCIRMS method was so sensitive that the 4-13C’s are not required. Therefore, we reduced the cost by using only 2-13C’s in the backbone of the retinol moiety in the 14 and 15 positions (FIGURE 1). Not only did this modification decrease the costs associated with the synthesis, it led to increased yields due to the nature of the synthesis. Rat experiment The proposed methodology, based on the rodent model has been published [27]. In summary, the 13C4-retinyl acetate isotope dilution assay was very good at determining the vitamin A status of rats over a very broad range of liver reserves of vitamin A (2-10 fold difference) (FIGURE 2) while serum retinol did not detect a difference. The relationship of the calculated vs. measured total body reserves (TBR) of retinol was indeed linear (r = 0.98, P < 0.0001). Thus, the assay will be able to estimate the TBR of retinol in groups of women with a 2-fold difference in supplementation.
75
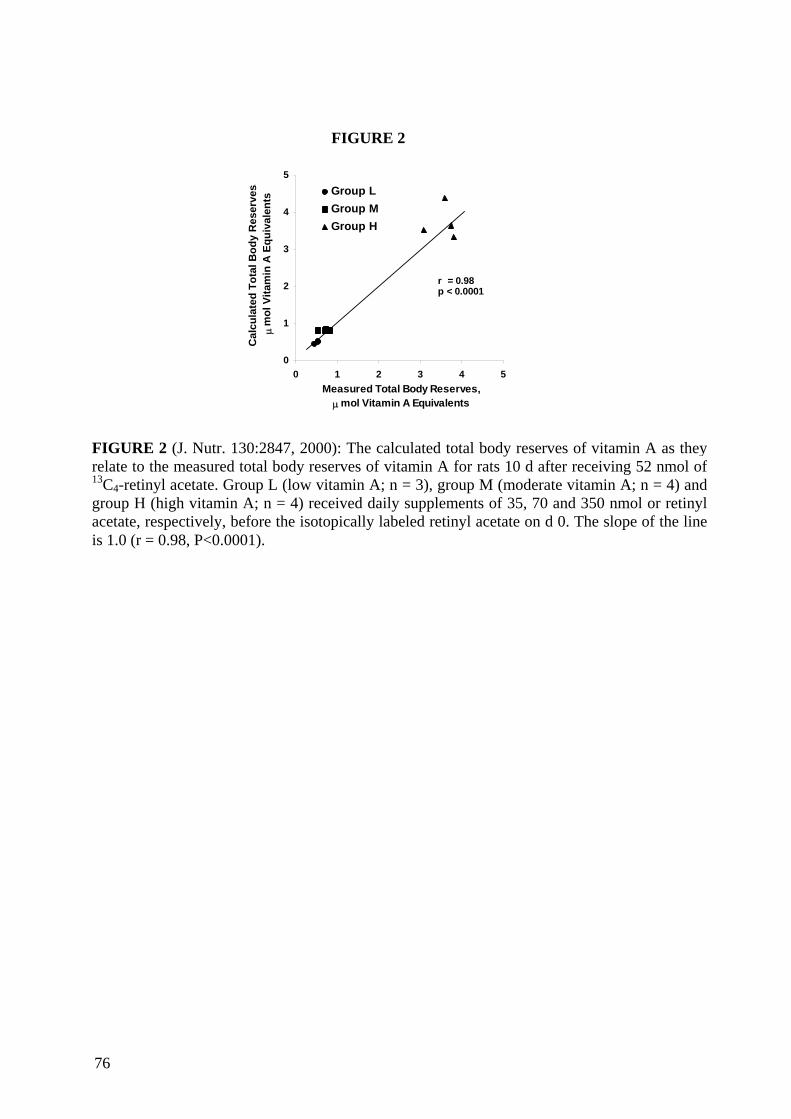
0
1
2
3
4
5
0 1 2 3 4 5Measured Total Body Reserves,
µ mol Vitamin A Equivalents
Cal
cula
ted
Tota
l Bod
y R
eser
ves,
µm
ol V
itam
in A
Equ
ival
ents
Group LGroup MGroup H
r = 0.98p < 0.0001
FIGURE 2
FIGURE 2 (J. Nutr. 130:2847, 2000): The calculated total body reserves of vitamin A as theyrelate to the measured total body reserves of vitamin A for rats 10 d after receiving 52 nmol of13C4-retinyl acetate. Group L (low vitamin A; n = 3), group M (moderate vitamin A; n = 4) andgroup H (high vitamin A; n = 4) received daily supplements of 35, 70 and 350 nmol or retinylacetate, respectively, before the isotopically labeled retinyl acetate on d 0. The slope of the lineis 1.0 (r = 0.98, P<0.0001).
76

Human Pilot Study 1 [28] Application of the 13C-RID test to humans After a baseline blood sample (10 mL) was taken, a healthy adult female ingested a 17.5 �mol dose of 13C4-retinyl acetate dissolved in corn oil, which was one-half the amount that was used in the deuterated isotope dilution assay in human adults (35 �mol d4-retinol) [19]. Thereafter, blood samples were obtained on days 2, 4, 8, 16, 24, 32, 64, 128 and 256. Two-mL serum samples were extracted and purified on two reversed-phase HPLC systems before injection into the GCCIRMS system as described below. In the human volunteer, the synthetic labeled retinol was absorbed very well and the enrichment of the serum retinol with 13C4-retinol began to plateau in as little as 8 days (FIGURE 3). In humans the observed mean serum to liver ratio of labeled retinol to unlabeled retinol was found to be 0.8 using the deuterated retinol assay and larger doses of d4-retinol [32]. Using this value for the serum to liver ratio of the 13C/12C and equation {1} [33], the calculated liver reserves for this female from the day 24 data was 0.32 �mol/g. Because the subject continued to consume vitamin A during the equilibration period, the calculated liver reserves should also be corrected for both the loss of labeled vitamin A due to turnover in the liver and because of the replacement by absorbed unlabeled dietary vitamin A over time. The half-life of vitamin A turnover in the liver has been determined to be 140 d [34,35]. Thus, this correction [e-kt] is equal to 0.89 where k = 0.69/140 and t is the time [24 days] since the dose which changes the calculated liver reserve to 0.29 �mol/g, which is a normal value for a healthy American not taking supplements. {1} (Fa X a) + (Fb X b) = (Fc X c) Where: a refers to the amount of dose absorbed and stored; determined experimentally to be 0.5 of that administered [36,37] b is baseline reserves of vitamin A c = a + b = total post dose reserves of vitamin A R F = _______ and R is 13C/12C
R+1 The Fa for the dose is 0.200 because 4 out of 20 of the C atoms are labeled with 13C. Fb is determined before dosing and Fc is determined after dosing with 13C4-retinyl acetate. FIGURE 3 illustrates the change in atom % excess with time in the retinol. At 256 days, the retinol was still highly enriched with 13C, being approximately 0.11 atom % over baseline. That value is 50 to 100 times the SD of the assay. The retinol will continue was monitored until the 13C/12C reached a value within 0.01 atom % of natural abundance. Samples were collected at 1.2, 2, 3 and 4 y. The 13C in the retinol did not return to baseline until 4 years post-dosing. The data will be mathematically modeled. Parameters of interest that can be calculated from the plasma retinol pool size and the fractional transfer coefficients include: fractional absorption of vitamin A, vitamin A absorption efficiency, vitamin A disposal rate, and total traced mass of vitamin A (vitamin A stores). This analysis will be very useful in application to the proposed studies.
77

Human Pilot Study 2 Baseline 13C/12C characteristics of a group of adult women from Malawi Looking ahead to the utilization of the 13C-RID test as a measure of vitamin A status in developing countries, baseline 13C enrichment information was collected from a group of adult women (n = 8) in Malawi. The mean 13C/12C + SD was 0.010931 + 0.000019. This represents a CV of a mere 0.2% in the baseline measure. The implication of this is that when the test is applied in a survey study of the vitamin A status of groups, the baseline measure need not be obtained in all individuals. Therefore, we could essentially have an estimate of total body reserves of vitamin A in one blood sample for the majority of people enrolled. The timing of this blood sample is yet to be determined, but with appropriate estimates others have indicated that 3 d may be a useful indicator of TBR with the DRD test [19,21]. In our human pilot study, the ratio at 8 d compared closely to that at 24 d. Because we are proposing to use lower doses than that administered previously, the equilibration time may be shortened. In applying the test to monitor changes in TBR of vitamin A in intervention studies, baseline measures will be needed to reestablish 13C enrichment because the GCCIRMS is so sensitive that the 13C from the pre-intervention assessment will still be measurable. However, we will not have to administer retinol with a different enrichment as has been done with conventional GC-MS [21-23], because the GCCIRMS measures a ratio of 13C to 12C and not just a mass-to-mass comparison. We hypothesize that the sensitivity of the test is so great that small numbers of subjects will be needed for evaluation of intervention studies. FIGURE 3
0
0 .2
0 .4
0 .6
0 .8
1
1 .2
1 .4
1 .6
0 1 0 0 2 0 0 3 0 0T im e a f te r d o s in g (d a y s )
Ato
m %
exc
ess
Distribution phase
Pseudo-equilibrium Turnover
Figure 3: The atom % excess over time in a female human volunteer followed for 256 days after ingesting 17.5 µmol of 13C4-retinyl acetate. The precision of GCCIRMS is 0.001 atom % excess
78

4. PLANS FOR FUTURE WORK Sub-study to AIM 3: Determination of limits of detection of the analytical method and investigation of ways to compensate for this discrepancy. After analyzing the samples from the women, we propose to look at factors that could limit the use of the 13C-RID test globally: venipuncture and sample volume. In studies in Ghana [39], one mL finger prick samples are easily obtained. This usually leads to samples of 250-500 �L of serum, which provides 0.05 and 0.1 µg of retinol from children with a mean retinol concentration of 20 µg/dL serum. Although we were able to easily analyze 0.1 µg retinol previously [27] and current specifications of new GCCIRMS systems are 12 ng of retinol (Finnigan, personal communication), this does not account for chromatographic losses from the purification of small amounts of retinol from serum. Using surplus serum from the adult women studies, we will look at ways to spike small sample volumes with highly purified, well-characterized retinol. We will HPLC purify retinol using the methods developed for the analysis of the samples. This retinol will be analyzed by GCCIRMS to get the accurate baseline enrichment of the retinol with 13C, which we expect to be ~1%. We will then add exactly 1.00 µg retinol to two different volumes of serum, i.e. 250 and 500 µL of the women’s serum at the same time as internal standard is added. Thus, we will prepare 20 samples total, 10 each at 250 and 500 µL. The expected relationship is illustrated in FIGURE 4. Ultimately, this gives us masses of 1.075 and 1.15 µg, respectively for the spiked samples assuming the average women has a serum retinol concentration of 30 µg/dL. We will be able to calculate Fb for the serum using equation {1} (Fa X a) + (Fb X b) = (Fc X c). Then Fb becomes Fc for calculation of total body stores.
79

Association
0
100
200
300
400
500
600
700
800
1
Enric
hmen
ts (r
aw v
alue
s)
FIGURE 4: The expected relationshipcharacterized retinol to the undiluted sam SUMMARY: Thus, we plan to use stable carbon mconcerning vitamin A in the next fsupplementation programs through eval
80
FIGURE 4
s of diluted sam ples
2 3
Range of sam ples
of the 500 µL (_ _ _ ) and 250 µL (- - -) spiked with
ples (___) from the women’s study.
ethods to answer important public health questions ew years. We look forward to aiding vitamin A uation of outcomes.

REFERENCES [1] TANUMIHARDJO, S.A., PERMAESIH, D., MUHERDIYANTINGSIH, RUSTAN, E., RUSMIL, K., FATAH, A.C., WILBUR, S., MUHILAL, KARYADI, D. and OLSON, J.A, Vitamin A status of Indonesian children infected with Ascaris lumbricoides after dosing with vitamin A supplements and albendazole. J. Nutr. 126 (1996) 451-457. [2] TANUMIHARDJO, S.A., MUHERDIYANTINGSIH, PERMAESIH, D., DAHRO, A.M., MUHILAL, KARYADI, D. and OLSON, J.A, Assessment of the vitamin A status in lactating and in nonlactating, nonpregnant Indonesian women by use of the modified relative dose response (MRDR) assay. Am. J. Clin. Nutr. 60 (1994) 142- 147. [3] TANUMIHARDJO, S.A., SUHARNO, D., PERMAESIH, D., MUHERDIYANTINGSIH, DAHRO, A.M., MUHILAL, KARYADI, D. and OLSON, J.A. Application of the modified relative dose response test to pregnant Indonesian women for assessing vitamin A status. Eur. J. Clin. Nutr. 49 (1995) 897-903. [4] TANUMIHARDJO, S.A., CHENG, J.C., PERMAESIH, D., MUHERDIYANTINGSIH, RUSTAN, E., MUHILAL, KARYADI, D. and OLSON, J.A. Refinement of the modified-relative-dose-response test as a method for assessing vitamin A status in a field setting: experience with Indonesian children. Am. J. Clin. Nutr. 64 (1996) 966-971. [5] SPANNAUS-MARTIN, D.J., COOK, L.R., TANUMIHARDJO, S.A., DUITSMAN, P.K. and OLSON, J.A. Vitamin A and vitamin E statuses of preschool children of socioeconomically disadvantaged families living in the midwestern United States. Eur. J. Clin. Nutr. 51 (1997) 864-869. [6] DUITSMAN, P.K, COOK, L.R., TANUMIHARDJO, S.A. and OLSON, J.A. The vitamin A statuses of pregnant women from disadvantaged socioeconomic backgrounds in urban Iowa. Nutr. Res. 15 (1995) 1263-1276. [7] SOMMER, A., KATZ, J. and TARWOTJO, I. Increased risk of respiratory disease and diarrhea in children with preexisting mild vitamin A deficiency. Am. J. Clin. Nutr. 40 (1984) 1090-1095. [8] STEPHENSEN, C.B., ALVAREZ, J.O., KOHATSU, J., HARDMEIER, R., KENNEDY JR., J.I. and GAMMON JR., R.B. Vitamin A is excreted in the urine during acute infection. Am. J. Clin. Nutr. 60 (1994) 388-392. [9] ALVAREZ, J.O., SALAZAR-LINDO, E., KOHATSU, J., MIRANDA, P. and STEPHENSEN, C.B. Urinary excretion of retinol in children with acute diarrhea. Am. J. Clin. Nutr. 61 (1995) 1273-1276. [10] MITRA, A.K., ALVAREZ, J.O., GUAY-WOODFORD, L., FUCHS, G.J., WAHED, M.A. and STEPHENSEN, C.B. Urinary retinol excretion and kidney function in children with shigellosis. Am. J. Clin. Nutr. 68 (1998) 1095-1103. [11] DE PEE, S. and WEST C.E. Dietary carotenoids and their role in combating vitamin A deficiency: a review of the literature. Eur. J. Clin. Nutr. 50 (1996) S38-53. [12] TANUMIHARDJO, S.A. Factors influencing the conversion of carotenoids to retinol: Bioavailability to bioconversion to bioefficacy. Int. J. Vitam. Nutr. Res. 72 (2002) 40- 45. [13] UNDERWOOD, B.A. “Vitamin A in animal and human nutrition.” The Retinoids, Vol. 1 (SPORN, M.B., ROBERTS, A.B. and GOODMAN, D.S., Eds.), Academic Press, Orlando (1984) 282-392. [14] WILLUMSEN, J.F., SIMMANK, K., FILTEAU, S.M., WAGSTAFF, L.A. and TOMKINS, A.M. Toxic damage to the respiratory epithelium induces acute phase changes in vitamin A metabolism without depleting retinol stores of South African
81

children. J. Nutr. 127 (1997) 1339-1343. [15] TANUMIHARDJO, S.A. Assessing vitamin A status: Past, present and future. J. Nutr. (2002) in press. [16] TANUMIHARDJO, S.A., PERMAESIH, D., DAHRO, A.M., RUSTAN, E., MUHILAL, KARYADI, D. and OLSON, J.A. Comparison of vitamin A assessment techniques in children from two Indonesian villages. Am. J. Clin. Nutr. 60 (1994) 136-141. [17] HASKELL, M.J., ISLAM, M.A., HANDELMAN, G.J., PEERSON, J.M., JONES, A.D., WAHED, M.A., MAHALANABIS, D. and BROWN, K.H. Plasma kinetics of an oral dose of 2H4-retinyl acetate in human subjects with estimated low or high total body stores of vitamin A. Am. J. Clin. Nutr. 68 (1998) 90-95. [18] FURR, H.C., AMEDEE-MANESME, O., CLIFFORD, A.J., BERGEN, H.R., III, JONES, A.D. and OLSON, J.A. Vitamin A concentrations in liver determined by isotope dilution assay with tetra-deuterated vitamin A and by biopsy in generally healthy adult humans. Am. J. Clin. Nutr. 49 (1989) 713-716. [19] RIBAYA-MERCADO, J.D., MAZARIEGOS, M., TANG, G., ROMERO-ABAL, M.E., MENA, I., SOLOMONS, N.W. and RUSSELL, R.M. Assessment of total body stores of vitamin A in Guatemalan elderly by the deuterated-retinol-dilution method. Am. J. Clin. Nutr. 69 (1999) 278-284. [20] TANG, G., QIN, J., DOLNIKOWSKI, G.G. and RUSSELL, R.M. Vitamin A equivalence of β-carotene in a woman as determined by a stable isotope reference method. Eur. J. Clin. Nutr. 39 (2000) 7-11. [21] RIBAYA-MERCADO, J.D., SOLON, F.S., SOLON, M.A., CABAL-BARZA, M.A. PERFECTO, C.S., TANG, G., SOLON, J.A., FJELD, C.R. and RUSSELL, R.M., Bioconversion of plant carotenoids to vitamin A in Filipino school-aged children varies inversely with vitamin A status. Am. J. Clin. Nutr. 72 (2000) 455-465. [22] TANG, G., GU, X., HU, S., XU, Q., QIN, J., DOLNIKOWSKI, G.G., FJELD, C.R., GAO, X., RUSSELL, R.M. and YIN, S. Green and yellow vegetables can maintain body stores of vitamin A in Chinese children. Am J. Clin. Nutr. 70 (1999) 1069-1076. [23] VAN LIESHOUT, M., WEST, C.E., MUHILAL, PERMAESIH, D., WANG, T., XU, X., VAN BREEMAN, R.B., CREEMERS, A.F.L., VERHOEVEN, M.A. and LUGTENBURG, J. Bioefficacy of β-carotene dissolved in oil studied in children in Indonesia. Am. J. Clin. Nutr. 73 (2001) 949-958. [24] TANUMIHARDJO, S.A. Synthesis of 10,11,14,15-13C4- and 14,15-13C2-retinyl acetate. J. Labelled Cpd Radiopharm. 44 (2001) 365-372. [25] GOODMAN, K.J. and BRENNA, J.T. High-precision gas chromatography- combustion isotope ratio mass spectrometry at low signal levels. J. Chromatography 689 (1995) 63-68. [26] PARKER, R.S., BRENNA, J.T., SWANSON, J.E., GOODMAN, K.J. and MARMOR, B. Assessing metabolism of beta-[13C]carotene using high-precision isotope ratio mass spectrometry. Methods in Enzymol. 282 (1997) 130-140. [27] TANUMIHARDJO, S.A. Vitamin A status assessment in rats using 13C4-retinyl acetate and gas chromatography-combustion isotope ratio mass spectrometry (GCCIRMS). J. Nutr. 130 (2000) 2844-2849. [28] TANUMIHARDJO, S.A. Application of 13C4-retinyl acetate and gas chromatography- combustion isotope ratio mass spectrometry to vitamin A assessment in the human. FASEB J. 15 (2001) A256; Abstract 228.5. [29] HALSEY, N.A., CLEMENTS, J., SOMMER, A. et al. Combining Vitamin A distribution with EPI contacts. Report of an IVACG Task Force. Washington, D.C. International Life Sciences Institute. [30] TANUMIHARDJO, S.A., BARUA, A.B. and OLSON, J.A. Use of 3,4-
82

didehydroretinol to assess vitamin A status in rats. Int. J. Vitam. Nutr. Res. 57 (1987) 127-132. [31] TANUMIHARDJO, S.A. Can lack of improvement in indicators of vitamin A status be explained by little or no change in overall vitamin A status? J. Nutr. 131 (2001) 3316-3318. [32] HASKELL, M.J., HANDELMAN, G.J., PEERSON, J.M., JONES, A.D., RABBI, M.A., AWAL, M.A. WAHED, M.A., MAHALANABIS, D. and BROWN, K.H. Assessment of vitamin A status by the deuterated-retinol-dilution technique and comparison with hepatic vitamin A concentration in Bangladeshi surgical patients. Am. J. Clin. Nutr. 66 (1997) 67-74. [33] GOODMAN, K.J. and BRENNA, J.T. High sensitivity tracer detection using high- precision gas chromatography-combustion isotope ratio mass spectrometry and highly enriched [U-13C]-labeled precursors. Anal. Chem. 64 (1992) 1088-1095. [34] SAUBERLICH, H.E., HODGES, H.E., WALLACE, D.L., KOLDER, H., CANHAM, J.E., HOOD, J., RAICA JR., N. and LOWRY, L.K. Vitamin A metabolism and requirements in the human studied with the use of labelled retinol. Vitam. Horm. 32 (1974) 251-275. [35] OLSON, J.A. The recommended dietary intakes of vitamin A in humans. Am. J. Clin. Nutr. 45 (1987) 704-716. [36] HUGHES, D.R., RIETZ, P., VETTER, W. and PITT, G.A.J. A method for the estimation of the vitamin A status of rats. Int. J. Nutr. Res. 46 (1976) 231-234. [37] BAUSCH, J. and RIETZ, P. Method for the assessment of vitamin A liver stores. Acta Vitaminol. Enzymol. 31 (1977) 99-112. [38] BERGEN, H.R., FURR, H.C. and OLSON, J.A. Synthesis of Tri-, Tetra-, and Penta- deuterated forms of vitamin A. J. Labelled Cpd. Radiopharm. 25 (1988) 11-21. [39] FILTEAU, S.M., MORRIS, S.S., RAYNES, J.G., ARTHUR, P., ROSS, D.A., KIRKWOOD, B.R., TOMKINS, A.M. and GYAPONG, J.O. Vitamin A supplementation, morbidity, and serum acute-phase proteins in young Ghanaian children. Am. J. Clin. Nutr. 62 (1995) 434-438.
83

84

EFFECT OF THE MOST COMMON SPICES AND HERBS IN TYPICAL NORTHEASTERN THAI DIET ON HUMAN IRON ABSORPTION
1WASANTWISUT E, 2TUNTIPOPIPAT S, 1WINICHAGOON P, 1SUNGPUAG 1P, CHAROENKIATKUL S, 1KONGKACHUICHAI R, 2WALCZYKT, 2HURRELL R. 1Institute of Nutrition, Mahidol University (INMU), Phuttamonthon 4Rd. Salaya, Phuttamonthon District Nakhon Pathom 73170, Thailand 2Laboratory for Human Nutrition, Swiss Federal Institute of Technology (ETH), Seestrasse 72, Zürich, Switzerland Abstract The prevalence of iron deficiency anemia in rural Northeast (NE) region is one of the highest in Thailand. The typical NE diets are plant-based. Non-heme iron is the major form in plant source. The bioavailability of non-heme iron depends largely on the presence of enhancers e. g. ascorbic acid, animal protein, organic acid and inhibitors e. g. polyphenolic compounds including tannin, phytate in the food matrix of composite meals. The habitual NE Thai dishes consist of a variety of chili dips usually consumed with substantial amount of vegetables and spices. High contents of iron inhibitors such as phytate and polyphenolic compounds including tannin in these herbs and spices may profoundly influence iron bioavailability in the northeast population. However, this inhibitory effect can partially be compensated in vivo by their effect on increasing gastric emptying time and enhancing gastric acid secretion. Although spices and herbs are used in abundance in the developing world and are likely to affect iron absorption in these regions, no systematic investigations in humans have been performed to date. The objective of this study is to evaluate the impact of the most common herbs and spices in typical Northeast diets on human iron absorption by stable isotope techniques. A series of studies will be conducted beginning with the identification of relevant spices and herbs commonly used in Thai habitual diets by 24 hours recall together with food frequency of consumption of popular local dishes. Later, the amount of spices/herbs per serving in popular dishes will be quantified by weighing method followed by the selection of spices/herbs. Food specimens collected in dry and rainy season will be analyzed individually for ascorbic acid, phytate, polyphenol and tannin contents. The three most relevant spices/herbs in the diet will be studied individually. First, the iron absorption from a basic test meal (plain white rice) with and without added spice/herb will be determined in vivo by stable isotope erythrocyte incorporation technique. In parallel, the effect of the spice/herb on gastric emptying will be studied by stable isotope techniques using 13C-octanoicacid.Later,the effect of selected spices / herbs on iron absorption from popular northeast composite meal (mixture of spices and herbs) will be examined. Test meals will be served either with or without added spices/herbs.Data from this study can be used to effectively plan a food-based program to address iron deficiency problem in northeast Thailand.
1. SCIENTIFIC BACKGROUND OF THE PROJECT The prevalence of iron deficiency anemia in Thailand ranges from 25-30% in pregnant women and from 15-20% in women of reproductive age [1-3]. Prevalence is also high among infants and children. Study in two districts in rural northeast Thailand showed the anemia prevalence of 32% (n=293) and 72% (n=100) among infants aged 4-6 months. Among the underfives, the survey by the Ministry of Public Health in 1996-97 reported the anemia prevalence of 25.2% [4]. Among the school-aged children, the routine surveillance system reported the anemia prevalence of 12%, but several small-scale research projects have reported the range of 25-50% [4].
85
To reduce such a high prevalence of IDA, all vital intervention strategies should be considered and used in conjunction with each other, when appropriate. Such strategies include: 1) Food-based approaches including dietary diversification, the fortification of staple foods
and commonly used condiments with high bioavailable iron fortificants, multi-nutrient fortification;
2) Supplementation of vulnerable groups such as pregnant women, infants and young children;
3) Control and treatment of malaria and helminthic infections and 4) nutrition education. 4) Nutrition Education To date, iron supplementation has been the main strategy to overcome iron deficiency focusing primarily on all pregnant women. Iron supplementation program has also been available for school children, but limited to those having access to hospitals. The national iron supplementation program for pregnant women in Thailand resulted in a significant decline of the prevalence of anemia in this group [1,2] However, food-based approaches are preferable for addressing the problem in population groups other than pregnant women, e.g. in infants, children and women of childbearing age. For the design and the evaluation of food-based strategies including indigenous foods and fortified vehicles, identification of the main factors influencing iron bioavailability is crucial. Non-heme iron is the major form of iron in habitual diets of Southeast Asians as meat intake is usually low. Contrary to heme-iron which is present in meat and meat products, the bioavailability of non-heme iron depends largely on the presence of enhancers e. g. ascorbic acid [5 - 21], animal protein [12, 22 - 27], organic acid [5, 28-30] and inhibitors e.g. polyphenolic compounds including tannin [11-12, 23,31 - 40], phytate [10, 14,41 - 46] in the food matrix of composite meals. In Thailand, the staple - food are plant sources rather than animal products. Typical Thai dishes consist of variety of chili dips usually consumed with raw or blanching vegetables, curry dishes, spicy soups, stir-fried vegetables etc. Spices and herbal vegetables are common ingredients in these dishes. The dietary iron in vegetables is non-heme which is poorly available due to the presence of phytate and tannin. Tuntawiroon et al [14a] reported a high content of tannin in a popular Thai vegetable, Yod Kratin (leaves of lead tree, Leucaena glauca) which strongly inhibited non-heme iron absorption in humans. The inhibitory iron absorption effect was tannin dose-dependent while ascorbic acid only partly counteracted this inhibitory effect. No systematic survey on the phytate and tannin contents of Thai vegetables has been conducted up to now. However, Suttikomon and Kongkachuichai [45] began to analyze vitamin C, phytate and tannin contents in commonly consumed Thai vegetables for both raw and cooked items. Phytate contents were high in cauliflower, mung-bean sprout, wax gourd and pumpkin. High tannin levels were found in leafy vegetables, especially ivy gourd. Food preparation such as cooking, boiling and stir-frying markedly reduced vitamin C and phytate contents but had little effect on tannin levels [45]. Spices and herbal vegetables are used in all kinds of Thai dishes and often in substantial amounts. These ingredients are commonly rich in polyphenolic compounds [32,45]. Polyphenols are natural antioxidants, antimutagens, and scavengers of free radicals with implications in the prevention of pathologies such as cancer and cardiovascular diseases. Epidemiological studies have shown a correlation between an increased consumption of
86

phenolic antioxidants and a reduced risk of cardiovascular disease [47-49] and certain types of cancer [49-50]. On the other hand, polyphenolic compounds are well known inhibitors of dietary iron absorption [11,12,32,35,36,37]. Polyphenols can bind soluble iron in the intestinal tract making the iron unavailable for the human body. This effect has been demonstrated in the past in vivo and in vitro e.g. for beverages containing polyphenolic compounds such as black tea, herb teas and red wine [38, 51]. The effect of spices and herbs on iron absorption has been evaluated in vitro at the Laboratory for Human Nutrition, ETH Zurich, Switzerland. Iron dialisability of test meals (cooked white rice, 15g dry rice) prepared with and without spices/herbs (0.5 g) was compared after in vitro digestion. All spices and herbs under investigation (anise, cinnamon, clover, galanga, ginger, laurel, oregano, pimento, rosemary and tumeric) reduced iron dialisability substantially. Reductions relative to the control test meal ranged from 40% for rosemary to 95% for clover at an added amount of 0.5 g spice/herb per test meal. Reduction of iron dialisability was found to be dose dependent. The addition of 0.2g tumeric per test meal reduced iron dialisability by 60% versus 72% for 0.4g tumeric, 95% for 0.9g tumeric and 93% for 1.8 g tumeric in the same test meal. Recently, the effect of purified phenolic-rich extracts in green tea and rosemary on nonheme iron absorption were evaluated in vivo by Samman et al. [38]. The study showed that the presence of phenolic-rich extracts resulted in decreased nonheme-iron absorption in human. Iron absorption decreased from 12.1 ± 4.5 % to 8.9 ± 5.2 % in the presence of 37 mg / meal of green tea extract and from 7.5 ± 4.0 % to 6.4 ± 4.7 % in the presence of 32 mg / meal of rosemary extract. However, an inhibitory effect of spices and herbs could partially be compensated in vivo by their effect on gastrointestinal function. Spices were found to increase gastric emptying time in humans [52-54] and to increase gastric acid secretion in the rat model [55-56]. Both may have an enhancing effect on iron absorption. Although spices and herbs are used in abundance in the developing world and are likely to affect iron absorption in these regions, no systematic investigations in humans have been performed to date. It is recognized that the prevalence of iron deficiency anemia in rural Northeast region is one of the highest in Thailand [4]. Habitual diets are plant-based and several herbs and spices such as lead tree-top leaves, ivy gourd, onion-young green, Thai basil, fennel leaves, mint leaves, chili pepper, garlic, shallot bulbs, and lemon-grass etc. are consumed in substantial amounts in common northeast dishes. High contents of polyphenolic compounds including tannin in these herbs and spices may profoundly influence iron bioavailability in the northeast population. Therefore, to effectively plan a food-based program to address iron deficiency, the knowledge concerning the effect of the most common spices and herbs on iron absorption from typical northeast diet is essential.
2. SCIENTIFIC SCOPE OF THE PROJECT 2.1. General Objective
To evaluate the impact of the most common herbs and spices in typical Northeast diets on human iron absorption in vivo and in vitro
87

2.2. Specific Objectives (4 year Ph. D. program) • To identify relevant spices and herbs commonly used in Thai habitual diets
A survey will be conducted in Northeastern Thailand on the use of spices and herbs in the local diet. Most common spices and herbs will be identified by 24 hours recall together with a food frequency questionnaire on consumption patterns of popular local dishes. Later, the amount of spices/herbs per serving in popular dishes will be quantified by weighing.
• To characterize the selected spices and herbs based on vitamin C, phytate, polyphenol and tannin content Most relevant spices and herbs in the local diets will be collected and analyzed individually for ascorbic acid, phytate, polyphenol and tannin contents. Differences in consumption patterns between dry and rainy season will be considered. The candidates of spices and herbs for closer investigation will be selected based on contents of enhancers and inhibitors of iron absorption and their effect on iron dialisability.
• To determine the effect of individual spices and herbs as selected by objectives 1 and 2 on dietary non-heme iron absorption in vivo by stable isotope erythrocyte incorporation technique.
A series of studies will be conducted to determine the effect of spices and herbs in vivo by stable isotope techniques. The three most relevant spices/herbs in the diet will be studied individually. Iron absorption from a basic test meal (plain white rice) with and without added spice/herb will be determined. In parallel, the effect of the spice/herb on gastric emptying will be studied by stable isotope techniques using 13C-octanoic acid [57].
In a series of studies, the effect of selected spices / herbs on iron absorption from popular northeast composite diet will be examined. Test meals will be typical for the Thai diet and will be prepared according to local recipes (mixture of spices and herbs) and extrinsically labeled with stable isotopes. Test meals will be served either with or without added spices/herbs.
In all absorption studies, stable isotope techniques (13C-urea breath tests) will be used to exclude subjects with H. pylori infection which may affect gastric acid juice excretion [58].
3. METHOD The protocol for the field survey to identify relevant spices and herbs in habitual diets in the Northeast of Thailand is described in the next section of the first year work plan. Iron absorption will be determined in vivo using stable isotope techniques initially developed for iron absorption studies in infants [59] and recently made applicable to studies in adults by novel mass spectrometric techniques [60]. Native iron in the test meals will be labeled extrinsically with 57Fe and 58Fe, respectively (testmeal A and testmeal B). Test meals will be fed after fasting for 12 hours. Test meals will be fed to each subject for breakfast on two consecutive days. A paired study design will be used, i.e., each volunteer will act as her own
88

control in each study. Iron absorption will be based on erythrocyte incorporation of stable isotopes 14 days after intake of labeled test meals. On day 1, a venous blood sample will be drawn after an overnight fast for determination of iron status parameters (hemoglobin, ferritin, transferrin receptor). Body weight and height will be measured and the first labeled test meal (test meal A) will be served. On the following day, the second test meal (test meal B) will be fed under strictly standardized conditions and close supervision of the investigators. No intake of food and fluids will be allowed for 3 hours after test meal intake. Otherwise, diet remains unrestricted. A second venous blood sample will be drawn 14 days after intake of the second test meal (day 16). Young, non-pregnant women of childbearing age will be recruited for the study (n=10). Subjects with genetic defects in hemoglobin synthesis such as thalassemia will be excluded from the study. Each isotopically enriched blood sample will be analyzed in duplicate for its iron isotopic composition under chemical blank monitoring. Whole blood samples will be mineralized using a HNO3/H2O2 mixture and microwave digestion followed by separation of sample iron by anion-exchange chromatography and a solvent/solvent extraction step into diethylether [61]. All isotope analysis will be performed by NTI-MS using magnetic sector field mass spectrometry equipped with a multi-collector system for simultaneous ion beam detection [60]. Iron separated from the sample will be loaded on BaF2 coated rhenium filaments of a double-filament ion source together with AgF to promote the formation of negatively charged FeF-
4 ions. Because of the high enrichment of the isotopically enriched labels and the low amounts of isotopic label incorporated into the red blood cells, data will be normalized for the natural 56Fe/54Fe isotope ratio [66] to correct for mass dependent fractionation effects in the ion source. Based on the shift of the Fe isotope ratios in the blood samples and the amount of Fe circulating in the body, the amounts of 57Fe and 58Fe isotopic label present in the blood 14 days after test meal administrations will be calculated based on the principles of isotope dilution and considering that the Fe isotopic labels are not mono-isotopic [60]. Circulating Fe will be calculated based on blood volume and Hb concentration [59]. Blood volume calculations will be based on height and weight [63]. For calculations of fractional iron absorption, 80% incorporation of the absorbed Fe into red blood cells will be assumed. The effect of the spices/ herbs on gastric emptying will be studied by stable isotope techniques using 13C-octanoic acid. In all absorption studies, stable isotope techniques (13C-urea breath tests) will be used to exclude subjects with H. pylori infection that may affect gastric acid juice excretion. Food samples will be analyzed for iron and calcium by atomic absorption spectroscopy (Spectr AA-20, Varian techtron, Australia). The phytate content will be determined by the method of AOAC 1995 [64]. Ascorbic acid will be analysed by microfluorometric method [64]. Nonheme-iron and heme iron will be determined by the method described earlier [65,66]. Polyphenol content will be determined by Folin-Ciocalteau method [67] and tannin content will be quantitated as previously described [32].
89
4. DETAILED WORK PLAN FOR FIRST YEAR Phase 1: Survey on the use of spices and herbs in Northeast (NE) Thailand. Aim - To Identify relevant spices and herbs commonly used in popular dishes in Northeast (NE) Thailand Workplan: Month 1-3: • To compile the existing information on food consumption pattern in NE region from
previous research studies.
Expected Output • Short lists of popular dishes • Ranking of commonly consumed spices and vegetable herbs in habitual local diets based
on frequency of consumption Month 4 – 12: • Verify frequency and amount of consumption of listed spices and herbs in common dishes
in upper and lower • Northeast region by weighing record, in both dry and rainy seasons. Activities 1) Study areas: 2 provinces will be selected as representatives for upper and lower part of NE
Thailand (Thailand map)
i Ubon Ratchathani province as a representative of lower NE region ii Khonkhaen province as a representative of upper NE region
2) Data collection
i Frequent consumption of initially identified popular dishes will be verified by food frequency questionnaire (FFQ)
ii 20-30 villages in each province will be selected for interview using FFQ. Data on frequently consumed dishes, ingredients in each recipe and serving size per meal among different age groups will be obtained.
iii Based on the above information, a list of popular dishes and spices/herbs will be identified. Local dishes that are consumed less frequently and in small quantities will be excluded.
iv Based on the selected dishes in 2.3, amount of consumption of spices and herbs per dish will be quantified by double portion technique in 10 representative households. The average serving size of individual spices and herbs in common NE dishes will be calculated.
v Sampling of spices and herbs specimens will be performed according to the protocol previously described [68] for nutrients and non-nutrient analyses including ascorbic acid, phytate, tannin and total polyphenol contents.
90

REFERENCES [1] Nutrition Division, Ministry of Public Health. The Third National Nutrition Survey, 1986 Bangkok Thailand (1995) [2] Nutrition Division, Ministry of Public Health. The Fourth National Nutrition Survey, 1996/97. Bangkok Thailand (1999) [3] Nutrition Division, Ministry of Public Health. (series of reports) Surveillance of anemia among pregnant women and school Children (Monograph, Thai), 1988-1999 [4] WINICHAGOON P. Prevention and control of anemia: Thailand experiences. J.Nutr. 132 (2002) 862-866 [5] GILLOOLY M, BOTHWELL T.H., TORRANCE J.D., MACPHAIL A.P., DERMAN D.P., BENZODA W.R., MILLS W, CHARLTON R.W. The effects of organic acids, phytates and polyphenols on absorption of iron from vegetables. Br J Nutr 49: (1983) 331-42 [6] HAZELL T, JOHNSON I.R. In vitro estimation of iron availability from a range of plant foods: influence of phytate, ascorbate,and citrate.Br J Nutr 57 (1987a.) 223-33. [7] HAZELL T, JOHNSON I.T. Effects of food processing and fruit juices on in vitro estimated iron availability from cereals, vegetables and fruits. J Sci Food Agric 38 (1987b) 73-82 [8] DYCK K.V., TAS S,, ROBBERRECHT H, DEELSTRA H. The influence of different food components on the in vitro availability of iron, Zinc, and calcium from a composed meal. Int J Food Sci & Nutr 47 (1996) 499-506 [9] COOK J.D., REDDY M.B. Effect of ascorbic acid intake on nonheme iron absorption from a complete diet. Am J Clin Nutr 73 (2001) 93-8. [10] HALLBERG L, BRUNE M, ROSSANDER L. Iron absorption in man: ascorbic and dose-dependent inhibition by phytate. Am Jclin Nutr 49 (1989) 104-14. [11] SIEGENBERG D, BAYNES R.D., BOTHWELL T.H., MACFARLANE B.J., LAMPARELLI R.D., CAR N.G., MACPHAIL P., SCHMIDT U., TAL A., MAYET F. Ascorbic acid prevents the dose-dependent inhibitory effects of polyphenols and phytates on nonheme iron absorption. Am J Clin Nutr 53 (1991) 537-41 [12] LYNCH S.R. Interaction of iron with other nutrients. Nutr Rev 55 (1997) (4):102-10 [13] HALLBERG L, BRUNE M, ROSSANDER L. Effect of ascorbic acid on iron absorption from different types of meals studies with ascorbic acid rich foods and synthetic acid given in different amounts with different meals. Hum Nutr Applied Nutr A40 (1986) 97-113 [14] TUNTAWIROON M, SRITONGKUL N, ROSSANDER-HULTEN L, PLEEHACHINDA R. Rice and iron absorption in man. Eu J Clin Nutr 44 (1990) 489- 97 [15] TUNTAWIROON M, SRITONGKUL N, BRUNE M, ROSSANDER-HULTEN L, PLEEHACHINDA R, SUWANIK R, HALLBERG L. Dose –dependent inhibitory effect of phenolic compounds in foods on non-heme iron absorption in men. Am J Clin Nutr 53 (1991), 554-7 [16] FAIRWEATHER-TAIT S, FOX T, WHARF SG, EAGLES J. The bioavailability of iron in different weaning foods and the enhancing effect of a fruit drink containing ascorbic acid. Pediatr Res 37 (1995) 389-94 [17] DAVIDSSON L, WALCZYK T, MORRIS A, HURRELL R.F. Influence of ascorbic ascorbic acid on iron absorption from an iron-fortified, chocolate-flavoured milk drink in Jamaican children. Am J Clin Nutr 67(5)(1998) 873-7 [18] DAVIDSSON L, DIMITRIOU T, WALCZYK T, HURRELL R.F. Iron absorption from experimental infant formulas based on pea (Pisum sativum) – protein isolate: the
91

effect of phytic acid and ascorbic acid. Br J Nutr 85(1) (2001) 59-63 [19] DAVIDSSON L, WALCZYK T, ZAVALETA N, HURRELL R.F. Improving iron absorption from a Peruvian school breakfast meal by adding ascorbic acid or Na2EDTA. Am Society Clin Nutr 73(2)(2001) 283-7 [20] ZLOTKIN S, ARTHUR P, ANTWI K.Y, YEUNG G. Treatment of anemia with microencapsulated ferrous fumarate plus ascorbic acid supplied as sprinkles to complementary (weaning) foods. Am J Clin Nutr 74(6)(2001) 791-5 [21] COOK J.D, MONSEN E.R. Vitamin C, the common cold, and iron absorption. Am J Clin Nutr 30(1977) 235-41 [22] GERHOFF S.N. Vitamin C (ascorbic acid): new roles, new requirements? Nutr Rev 51(11)(1993) 313-26 [23] KIM Y, CARPENTER C.E, MAHONEY A.W. Gastric acid production, iron status and dietary phytate alter enhancement by meat of iron absorption in rats. J Nutr 123(1993) 940-6 [24] MONSEN E.R. Iron nutrition and absorption: dietary factors which impact iron bioavailability. J Am Diet Assoc 88: (1988) 786-90 [25] REDDY M.B, COOK J.D. Assessment of dietary determinants of nonheme iron absorption in humans and rats. Am J Clin Nutr 54 (1991) 723-8 [26] HALLBERG L, ROSSANDER L. Improvement of iron nutrition in developing countries: comparison of adding meat, soy protein, ascorbic acid, citric acid and ferrous sulfate on iron absorption from a simple Latin American-type of meal. Am J Clin Nutr 39 (1984) 577-83 [27] GARCIA-CASAL M.N, MARTINEZ-TORRES C, LEETS I, TROPPER E, RAMIREZ J, LAYRISSE M. Heat treatment on heme iron and iron-containing proteins in meat: iron absorption in humans from diets containing cooked meat fractions. J Nutr Biochem 7 (1996) 49-54 [28] ENGELMANN M.D, DAVIDSON L, SANDSTROM B, WALCZYK T, HURRELL R.F, MICHAELSEN K.F. The influence of meat on nonheme iron absorption in infants. Pediatric Research 43(6) (1998) 768-73 [29] ALLEN L.H, AHLUWALIA N. Improving iron status through diet. John Snow, Inc, Arlington, VA, 1997 [30] BALLOT D, BAYNES R.D, BOTHWELL T.H, GILLOOLY M, MACFARLANE B.J, MACPHAIL A.P, LYONS G, DERMAN D.P, BEZWODA W.R, TORRANCE J.D, BOTHWELL J.E. The effect of fruti juices and fruits on the absorption of iron from a rice meal. Br J Nutr 57 (1987) 331-43 [31] GARCIA-CASAL M.N; LAYRISSE M; SOLANO L; BARON M.A; ARGUELLO F; LLOVERA D; RAMIREZ J; LEETS I; TROPPER E. Vitamin A and beta-carotene can improve nonheme iron absorption from rice, wheat and corn by humans. J Nutr 128 (3) (1998) 646-50 [32] NARASINGA RAO BS, PRABHAVATHI T. Tannin content of foods commonly consumed in India and its influence on ionizable iron. J Sci Food Agric 33 (1982) 89- 96 [33] BRUNE M, ROSSANDER L, HALLBERG L. Iron absorption and phenolic compounds: importance of different phenolic structures. Eu J Clin Nutr 43 (1989) 547-58 [34] GARCIA-LOPEZ J.S, ERDMAN J.W, SHERMAN A.R. Iron retention by rats from casein-legume test meals: effect of tannin level and previous diet. J Nutr 120(1990) 760-6 [35] BRAVO L. Polyphenols: chemistry, dietary sources, metabolism, and nutritional significance. Nutr Rev 56(11)(1998) 317-33 Bagepalli X, Narasinga R, Prabhavathi T. Tannin content of foods commonly consumed in India and its influence on ionisable
92
iron. J Sci Food Agric 33(1982) 89-96 [36] ROZO M.P, VALEZ J, GARCIA L.A. Effect of polyphenols of coffee pulp on iron absorption. Arch Latinoam Nutr 35(2)(1985) 287-96 [37] HURRELL R.F, REDDY M, COOD J.D. Inhibition of nonheme iron absorption in man by polyphenolic-containing beverages. Br J Nutr 81(4)(1998) 289-95 [38] LAYRISSE M, GARCIA-CASAL M.N, SOLANO L, BARON M.A, ARGUELLE F, LOVERA D, et al. Iron bioavailability in humans from breadfasts enriched with iron bio-glycine chelate, phytates and polyphenols. J Nutr 130(2000) 1295-9 [39] SAMMAN S, TOFT M, BUKHAVE K, JENSEN M, HANSEN M. Green tea or rosemary extract added to foods reduces nonheme iron absorption. Am J Clin Nutr 73(2001) 607-12 [40] BROODS S.P.J, LAMPI B.J. Problems associated with measuring phytate in infant cereals. J Agric Food Chem 49 (2001) 564-9 [41] TORRE M, RODRIGUEZ A, SAURA-CALIXTO F. Effects of dietary fiber and phytic acid on mineral bioavailability. Crit Rev Food Sci 1 (1991) 1-22 [42] BOTHWELL T.H, BAYNES R.D, MACFAVLANE B.J, MACPHAIL A.P. Nutritional iron requirements and food iron absorption. J Internal Med 226 (1989) 357-65 [43] RAVINDRAN V, RAVINDRAN G, SIVALOGAN S. Total and phytate phosphorus contents of various foods and feedstuffs of plant origin. Food Chem 50(1994) 133-6 [44] REDDY M.B, HURRELL R.F, JUILLERAT M.A, COOD J.D. The influence of different protein sources on phytate inhibition of nonheme iron absorption in humans. Am J Clin Nutr 63(2)(1996) 203-7 [45] SANDBERG A.S, BRUNE M, CARLSSON N.G, HALLBERG L, SKOGLUND E, ROSSANDER-HULTHEN L. Inositol phosphates with different numbers of phosphate groups influence iron absorption in humans. Am J Clin Nutr 70(2)(1999) 240-6 [46] SUTTIKOMON W. AND KONGKACHUICHAI R. Effect of blanching, boiling and sir-frying on total iron, vitamin C, phytate and tannin contents in Thai vegetables. M.Sc.Thesis in Food and Nutrition for Development, Faculty of Graduate Studies, Mahidol University (2002). [47] BRUNE M, HALLBERG L, SKANBERG A-B. Determination of iron-binding phenolic groups in foods. J Food Sci 56 (1991) 131-7. [48] HERTOG M.G.L, FESKENS E.J.M,HOLLMAN P.C.H, et al. Dietary antioxidant flavonoids and risk of coronary heart disease: the Zutphen Elderly Study. Lancet 342 (1993) 1007-11 [49] HERTOG M.G.L, SWEETNAM P.M, FEHILY A.M, et al., Antioxidant flavonols and ischemic heart disease in a Welsh population of men: the Caerphilly Study. Am J Clin Nutr 65 (1995) 1489-94 [50] HERTOG M.G.L, KROMHOUT D, ARAVANIS C, et al., Flavonoid intake and long- term risk of coronary heart disease and cancer in the Seven Countries Study. Arch Intern Med 155 (1995) 381-6 [51] HERTOG M.G.L, FESKENS E.J.M, HOLLMAN P.C.H, et al. Dietary flavonoid and cancer risk in the Zutphen Elderly Study. Nutr Cancer.22 (1994) 175-84 [52] COOK J.D, REDDY M.R, HURRELL R.F. The effect of red and white wines on nonheme-iron absorption in humans. Am J Clin Nutr. 61 (1995) 800-4. [53] JENSEN-JAROLIM E, GAJDZIK L, HABERL I, KRAFT D et al. Hot spices influence permeability of human intestinal epithelial monolayers. J Nutr .128 (1998) 577-81. [54] KOCHHAR K.P, BIJLANI R.L, SACHDEVA U et al. Gastro-intestinal effects of Indian spice mixture (Garam Masala). Trop. Gastroenterol. 170 (1999) 170-4.
93

[55] MYERS B.M, SMITH J.L, GRAHAM D.Y. Effect of red pepper and black pepper on the stomach. Am J Gastroenterol. 82 (1987) 211-14. [56] PLATEL K, SRINIVASAN K. Influence of dietary spices and their active principles on pancreatic digestive enzymes in albino rats. Nahrung. 44(2000) 42-6. [57] VASUDEVAN K, VEMBAR S, VEERARAGHAVAN K, HARANATH P.S. Influence of intragastric perfusion of aqueous spice extracts on acid secretion in anesthetized albino rats. Indian J. Gastroenterol. 19 (2000) 53-6. [58] WEAVER L.T. Stable isotope breath tests. Nutrition 47 ( 1998 ) 706-12 [59] ROLAND M, LAMBERT I, GORMALLY S, et al. Carbon 13-labeled urea breath test for diagnosis of Helicobacter pyroli infection in children. J Pediatr 131 ( 1997 ) 815- 20 [60] KASTENMAYER P, DAVIDSSON L, GALAN P, CHEROUVRIER F, HERCBERG S. AND HURRELL R.F. A double stable isotope technique for measuring iron absorption in infants Br. J. Nutr. 71(1994) 411-24. [61] WALCZYK T. Iron isotope ratio measurements by negative thermal ionization mass spectrometry. Int. J. Mass. Spectrom. Ion Processess 161(1997) 217-27. [62] WALCZYK T, DAVIDSSON L, ZAVALETA N. AND HURRELL R.F. Stable isotope labels as a tool to determine iron absorption by Peruvian school children from a breakfast meal. Fresenius J. Anal. Chem. 359(1997) 445-9. [63] TAYLOR P.D.P., MAECK R. AND DEBIEVRE P. Determination of absolute isotopic composition and atomic weight ofa reference sample of natural iron. Tnt. J. Mass Spectrom Ion Processess 121 (1992) 111-25. [64] BROWN E, HOPPER JR. J., HODGES JR. J. L., et al., Red cell, plasma and blood volume in health women measured by radio chromium cell-labelling and hematocrit. J. Clin. Invest. 41(1962) 2182-2190. [65] AOAC (2000). Official methods of analysis of the Associstion of Official Analytical Chemists (W. Horwitz, Ed), 17th edn.,Methods:96.22, 986.11. Association of Official Analytical Chemists, Washinton, DC, USA. [66] RHEE K.S., ZIPRIN Y.A. Modification of the Schricker nonheme iron method to minimize pigment effects for red meats. J Food Sci 52 (1987) 1174-6. [67] CLARK E.M, MAHONEY A.W, CARPENTER C.E. Heme and total iron inready to eat chicken. J Agric Food Chem 45 (1997) 124 - 6. [68] SINGLETON, V.L, ROSSI J.A.J. Colorimetry of total phenolics with phosphomolybdic-phosphotungstic acid reagents. Am.J.Enol. Vitic. 16 (1965) 144-58. [69] GREENFIELD AND SOUTHGATE, Food Composition Data, Production, Management and use, Elsevier Applied Science, London (1992)
94

EFFECT OF ZINC AND FAT INTAKE ON ABSORPTION AND CONVERSION OF INGESTED ß-CAROTENE TO VITAMIN A IN LACTATING INDONESIAN WOMEN
1MUHILAL, PHD, 2ABDULLAH FIRMANSAH, MD, 3CLIVE E WEST, PHD DSC, 1DEWI PERMAESIH, MSC, 3HANS VERHOEF, PHD
1Nutrition Research and Development Centre, Ministry of Health, Jalan Dr Sumeru 63, BOGOR 16122, Indonesia 2 Padjadjaran University, Bandung, Jalan Dipati Ukur 35, Bandung 40184, Indonesia 3 Division of Human Nutrition and Epidemiology, Wageningen University, P.O. Box 8129, 6700 EV Wageningen, The Netherlands
ABSTRACT
When sufficiently severe to cause night blindness, vitamin A deficiency may also lead to anemia, morbidity from infectious diseases, and maternal and infant death. Interventions to increase the supply of vitamin A to lactating women may also improve vitamin A status of their breastfeeding children. Plant foods are the major source of vitamin A for most of the world’s poor population, but low bioefficacy of provitamin A carotenoids from these foods severely limits the supply of vitamin A. We propose two randomised controlled trials to determine the extent to which bioefficacy of ingested ß-carotene may be increased by zinc supplementation or other measures to increase zinc intake. For this purpose, we intend to use a stable isotope technique that we have developed and that may be the best method available to estimate the bioavailability and bioefficacy of dietary carotenoids. A pilot study will be conducted to assess the time from initiation of a controlled diet with fixed content of carotenoids and retinol, and with medium-level intakes of zinc (10 mg/d) and fat (40 g/d), until new homeostatic levels are achieved of concentrations in serum and breastmilk of retinol and carotenoids. We subsequently will carry out two randomised controlled trials, both with a parallel design and two experimental treatments, in lactating women who have received the controlled diet described above for a period sufficient in duration to have achieved stable concentrations in serum and breastmilk of retinol and carotenoids. Of these women, 40 will be randomly allocated to either continue receiving medium of fat (40 g/d) or high intakes of fat (80 g/d) for a period of three weeks. Another 40 lactating women will be randomly allocated to daily supplements of zinc (as sulphate) providing either continued medium intakes (10 mg/d) or in high intakes (30 mg/d), also for a period of three weeks. In addition, all women will daily consume capsules containing 60 µg 13C10-β-carotene and 60 µg 13C10-retinol. Blood samples will be collected from each woman by venipuncture (<5 mL) when starting the controlled diet, at randomisation, and the end of the 3-wk intervention period. Concentrations of retinol and carotenoids in serum and breastmilk will be measured using high performance liquid chromatography (HPLC). The degree of isotopic enrichment in serum retinol with 13C5-retinol and 13C10-retinol, and β-carotene with 13C10-β-carotene will be measured using reversed phase HPLC coupled with mass spectrometry (Van Breemen 1998, Wang 2000). Data analysis will be carried out using the CarRet PIE mathematical model (Van Lieshout 2001ab). Differences between groups in the isotopic enrichment of retinol and β-carotene indicate differences in the bioefficacy of β-carotene consumed simultaneously with a low-fat diet or with a normal-fat diet, and with supplements of zinc or its placebo. The stable isotope method will be extended to enable measurement of concentrations and degree of isotopic enrichment of retinol and β-carotene in breast milk.
95

1. SCIENTIFIC BACKGROUND AND SCOPE OF THE PROJECT Vitamin A deficiency is widespread in developing countries (Mason et al. 2001). When sufficiently severe to cause night blindness, it may also lead to anemia, morbidity from infectious diseases, and maternal and infant death (Christian et al. 1998, 2000, 2001). Vitamin A is essential for immune function and vision. Randomised controlled trials have shown that supplementation of children <5 years of age in developing countries may improve linear growth (Villamor et al. 2000), leads to reduced morbidity from common childhood infections such as respiratory and diarrhoeal diseases (Sommer and West 1996), measles (West 2000), malaria (Shankar et al. 1999), and a reduction of risk of all-cause mortality by 23% (Beaton 1993, Sommer and West 1996). Vitamin A transfer from mother-to-child occurs in two ways: via the placenta during gestation and via breast milk during lactation (Underwood 1994, Stoltzfus and Underwood 1995). While transfer of vitamin A during gestation is limited (as is evident from the absent or low vitamin A stores in neonates), transfer via breastmilk is quantitatively more important, with 60 times more vitamin A being transferred via breastmilk during 6 months of lactation than via the placenta during nine months of gestation (Stoltzfus and Underwood 1995). Adequate maternal vitamin A status is important because retinol concentrations in breastmilk are associated with vitamin A intake and status during the third trimester of pregnancy (Ortega et al. 1997) and lactation (De Pee et al. 1995). This indicates that interventions to increase the supply of vitamin A to lactating women may also improve vitamin A status of their breastfeeding children. Vitamin A is supplied by animal products (including breast milk) as preformed vitamin A (retinol), and by both animal products and plant foods as provitamin A carotenoids (ß-carotene, α-carotene and ß-cryptoxanthin). Plant foods are the major source of vitamin A in the diet of most of the world’s poor population (IVACG 1999). Red palm oil, dark-green leafy vegetables, yellow and orange fruits, and red and orange roots and tubers, such as carrots and red/yellow sweet potato are particularly rich in provitamin A carotenoids (FAO/WHO 1988), but staple foods are relatively poor sources. There is mounting evidence that low bioefficacy of provitamin A carotenoids severely limits the supply of vitamin A from plant foods (Castenmiller et al. 1999). This largely explains the low effectiveness (i.e. impact under field conditions) observed of food-based interventions to improve vitamin A status. Several factors that determine the bioefficacy of provitamin A carotenoids (De Pee and West 1996, Castenmiller and West 1998, Van het Hof et al. 2000) are listed in the mnemonic 'SLAMENGHI': Species of carotenoid, molecular Linkage; Amount of carotenoids consumed in a meal; Matrix in which the carotenoid is incorporated; Effectors of absorption and bioconversion; Nutrient status of the host; Genetic factors; Host related factors; and mathematical Interactions between the other factors. Regarding these factors, most attention has so far been paid to the matrix of plants. Thus it appears that carotenoids in dark-green leafy vegetables are trapped in chloroplasts, which makes them largely unavailable for absorption from the intestine, thereby reducing bioefficacy. We showed earlier that various food processing techniques aimed at disrupting the food matrix can improve absorption of ß-carotene (Castenmiller et al. 1999). We have developed a stable isotope technique that may be the best method available to estimate the bioavailability and bioefficacy of dietary carotenoids (Solomons and Russell 2001, Van Lieshout et al. 2001b). Formulation and evaluation of appropriate policies and programs for controlling vitamin A deficiency can be improved by extending this technique to quantify the effect of several SLAMENGHI factors on bioefficacy of ß-carotene in food. We
96

propose to assess the effect of two other important factors influencing bioefficacy of β-carotene, namely fat intake and zinc intake/status of the host. Both vitamin A and carotenoids are fat-soluble. Several studies have indicated that absorption of ß-carotene is markedly increased (up to 50%) by concomitant intake of dietary fat (Jayarajan 1980, Dimitrov 1988, Jalal et al. 1998). Some populations in developing countries consume diets containing very low amounts of fat. Thus, to develop guidelines for food-based approaches for controlling vitamin A deficiency, it is necessary to estimate accurately the potential of increasing bioefficacy of carotenoids by increasing fat content of food. Approximately 61% of people in developing countries are at risk of low dietary zinc intake (Brown and Wuehler 2000). In a study conducted in Indonesia, it was found that zinc deficiency as assessed by plasma zinc concentration <10.7 µmol/L occurred in 25% of mothers and 17% of children studied (Dijkhuizen 2001a). Evidence accumulating from studies in animals (Smith et al. 1973, Christian and West 1998) and humans (Christian and West 1998, Rahman et al. 2001, 2002, Dijkhuizen et al. 2001b,c) indicate that carotenoids and zinc supplements may act synergistically in improving vitamin A status. We recently showed that zinc supplementation in pregnant women consuming ß-carotene in the last two trimesters of pregnancy substantially increased vitamin A status of both mothers (including retinol concentrations of breast milk) and their infants until at least 6 months after consumption of the last supplement (Dijkhuizen 2001b). There is now evidence that zinc regulates retinol absorption, transport of retinol though synthesis of retinol-binding protein, and synthesis of enzymes regulating retinol function (Cristian and West 1998). Additionally, zinc is required for the enzymatic cleavage of absorbed ß-carotene into vitamin A and other fundamental activities such as gene expression (Bondi and Sklan 1984, Olson 2000). Thus bioefficacy of provitamin A carotenoids from plant foods may possibly be increased by zinc supplementation or other measures to increase zinc intake. Our stable isotope technique has the additional advantage that the degree of isotopic enrichment of retinol and β-carotene can be measured in breast milk. This can be used to estimate the proportion of carotenoids and retinol ingested by mothers that is transferred through breast milk to their infants. We earlier adaptated the LC-MS methods for measurement of the degree of isotopic enrichment of retinol and β–carotene in serum to that in feces (Van Lieshout et al. 2001c). Based on this experience, we expect that some modifications of the LC-MS technique will be required to enable such measurements in breast milk.
2. OBJECTIVES The aim of the proposed project is to quantify the change in bioefficacy of ingested β-carotene that can be achieved by simultaneous consumption of dietary fat and/or zinc in lactating Indonesian women, and to examine the mechanisms involved. We hypothesize that increased dietary fat intake increases the bioavailability of β-carotene ingested, and that an improved zinc intake/status increases either the bioavailability of β-carotene or its bioconversion into vitamin A or both.
97

3. METHODS Lactating women will be identified through community census and antenatal clinics. Women will be invited for study and be medically examined to determine whether they are eligible for study. Eligibility criteria are: 2-13 months post-partum, free of symptoms of infectious disease in both mother and child, free of symptoms or signs of vitamin A deficiency, body mass index <18.5 kg m-2, no signs of genetic defects or mental retardation in both mother and child, informed consent given. To improve compliance during follow-up, consideration will be given to also obtain informed consent from the husband. 3.1. Pilot study To plan for a randomised controlled trial, we will conduct a study to assess the time from initiation of a controlled diet with fixed content of carotenoids, retinol, zinc and fat until new homeostatic levels are achieved of concentrations in serum and breastmilk of retinol and carotenoids. For this purpose, women (n=20) will be supervised to consume three daily meals based exclusively on plant foods with low dietary carotenoid concentrations. In addition, they will receive supplements so that their intake of vitamin A is 100% of the US recommended daily allowance (700 retinol activity equivalents, of which 50% is provided as β-carotene in oil and 50% as supplements of retinyl palmitate), and medium-level intakes of fat (40 g/d) and zinc (daily supplements of 10 mg zinc as sulphate) are relatively high. This diet will be maintained for 12 weeks. In this period, capillary blood samples (≤1 mL) will be collected daily. Breastmilk samples will be collected at baseline and at subsequent 2-weekly intervals until the end of the observation period (12 weeks after baseline). Serum will be separated and stored at −20 °C until biochemical analysis. Concentrations in serum or breastmilk of retinol and carotenoids are the outcomes of primary interest and will be measured using high performance liquid chromatography (HPLC). Analysis of repeated measures will be used to model changes in these outcomes occurring over time, and to determine the time until concentrations have stabilised. 3.2. Intervention study We subsequently will carry out two randomised controlled trials, each with a parallel design and two experimental treatments. Eligible women will be identified using similar methods as in the pilot study, except that blood samples (<5 mL) will be collected by venipuncture. Of these, 100 women will be supervised to consume a controlled diet as foreseen in the pilot study. After a pre-determined period on this diet (tentatively: 5 weeks, but exact period will be determined on the basis of the results of the pilot study), we will conduct another medical examinination and collect samples of blood by venipuncture (<5 mL) and breastmilk. After eligibility for further study has been established (same criteria as above), 80 women will randomised to enter the experimental phase. The period before randomisation will serve to stabilise concentrations in serum and breastmilk of retinol and carotenoids. Subjects being lost-to-follow have the potential to undermine a crucial aspect of design of randomised controlled trials, namely that potential confounding factors are equally distributed over the experimental groups so that effects measured can be attributed exclusively to the intervention. Most cases of women being lost to follow-up are likely to occur in the first few weeks following that start of the trial. Hence, the period before randomisation will also serve to minimize the number of cases of loss to follow-
98

up that may occur after randomisation, or to exclude those with poor compliance to treatments administered, thereby maintaining the integrity of the trial. The design of the intervetion study is shown in the figure below. In the experimental phase, 40 women will be randomly allocated to either continue receiving medium of fat (40 g/d) or high intakes of fat (80 g/d). Another 40 women will be randomly allocated to daily supplements of zinc (as sulphate) providing either continued medium intakes (10 mg/d) or in high intakes (30 mg/d). Both participating women and field staff will be blinded to treatments with zinc and placebo. The experimental treatment phase will last three weeks. Throughout the study period, all meals will be prepared, and consumption of all meals and supplements supervised, by field staff. In addition, all women will be supervised to consume capsules (2 capsules/d, 7 d/wk) each containing 30 µg 13C10-β-carotene and 30 µg 13C10-retinol (Lugtenburg et al. 1999). Methods for synthesis of labeled retinol and β-carotene have been described elsewhere (Lugtenburg et al. 1999, Van Lieshout et al. 2001a,b). These compounds are now commercially available. The compounds are subject to purity criteria as laid down in Codex Alimentarius and the European Pharmacopoeia (1993). Methods of analysis of the degree of isotopic enrichment of retinol and β-carotene in serum have been described earlier (Van Breemen et al. 1998, Wang et al. 2000). These methods will be adapted to enable measurement of the degree of isotopic enrichment of retinol and β-carotene in breast milk. A third and last blood sample will be collected from each woman by venipuncture (<5 mL) at the end of the 3-wk intervention period. Concentrations of retinol and carotenoids in serum and breastmilk will be measured using high performance liquid chromatography (HPLC). The degree of isotopic enrichment in serum retinol with 13C5-retinol and 13C10-retinol, and β-carotene with 13C10-β-carotene will be measured using reversed phase HPLC coupled with mass spectrometry (Van Breemen et al. 1998, Wang et al. 2000).
Medium intakes of fat (40 g/d) and zinc (10 mg/d)
Controlled diet (providing 100% of RDA vitamin A*)to stabilise serum concentrations of retinol and carotenoids
* Plant foods with low carotenoid concentrations plus vitamin A supplements (100%of RDA, with 50% as retinol and 50% as ß-carotene)
0 87654321
→ Time, weeks
High-fat (80 g/d)
Medium-fat (40 g/d)R
High-zinc supplement (30 mg/d)
Medium-zinc supplement (10 g/d)R
[13C10] β-carotene (60 µg/d) plus[13C10] retinol (60 µg /d)
Design of the intervention study (n=80)
Randomisation
99

The β-carotene and retinol at plateau isotopic enrichment (CarRet PIE) mathematical model used for the quantification of the bioavailability and bioefficacy of β-carotene has been described in earlier papers from our group (Van Lieshout et al. 2001a,b). Differences between groups in the isotopic enrichment of retinol and β-carotene indicate differences in the bioefficacy of β-carotene consumed simultaneously with a low-fat diet or with a normal-fat diet, and with supplements of zinc or its placebo. The stable isotope method will be extended to enable measurement of concentrations and degree of isotopic enrichment of retinol and β-carotene in breast milk. 3.3. Ethical issues Principles as contained in the revised Helskinki declaration of the World Medical Association will be used as ethical guidelines. Stable isotopes emit no radiation that can be used safely in human studies. Scientific and ethical clearance will be obtained through procedures and from institutions indicated by the Indonesian government. All women will be treated immediately and free of charge for common sicknesses that may occur throughout the study period, and after having completed the study will receive chemotherapy for extant worm infestations.
4. RESULTS The Nutrition Research and Development Centre in Bogor, Indonesia, and the Division of Human Nutrition and Epidemiology, Wageningen University, have jointly completed a series of studies in Indonesia to determine bioavailability and bioconversion of ß-carotene from vegetables, fruit and cooking oil. The initial studies measured concentrations of retinol/ß-carotene in serum and breast milk in randomised controlled trials. These studies provided effect estimates of dietary interventions and supplementation on vitamin A status, as well as indirect estimates of bioavailability of dietary carotenoids (De Pee et al. 1995, 1998). The results indicate that bioefficacy of provitamin A carotenoids from plants is only 20-50% of previously estimated values, and that bioefficacy is too low to supply vitamin A in adequate amounts through plant-based diets (De Pee et al. 1998, Khan et al. 1998, Van Lieshout et al. 2001b, West and Eilander 2001). The amount of vitamin A or carotenoids supplying 1 µg of retinol has been defined as one retinol equivalent, or RE. Thus 1 µg of ingested retinol corresponds to 1 RE. In 1988, the FAO/WHO recommended that ingestion of 6 µg of ß-carotene or 12 µg of other provitamin A carotenoids from a diet of mixed plant foods is required to produce 1 µg of retinol (FAO/WHO 1988). However, corresponding estimates from subsequent studies in Indonesia and Vietnam indicate values of 26 µg ingested ß-carotene from dark green leafy vegetables or 12 µg ingested ß-carotene from orange fruits (De Pee et al. 1998, Khan et al. 1998). These estimates corroborate findings from a study in China, which found that 27 µg ß-carotene from green and yellow vegetables was required to produce 1 µg retinol (Tang 1999). Based on these studies it can be estimated that as much as 21 µg ß-carotene in a mixed diet (4:1 vegetables to fruit intake) has the same vitamin A activity as 1 µg retinol, which is markedly more that the previous estimate of 6 µg ß-carotene by FAO/WHO (1988). Based on these findings, the authorative US Institute of Medicine (IOM 2001) recently revised its dietary intake recommendations, and conservatively doubled the estimated amount of β-carotene in a mixed diet having the same vitamin A activity as 1 µg retinol to 12 µg.
100

We subsequently conducted studies using stable isotopes techniques to estimate bioefficacy of provitamin A carotenoids directly. This involves a two-step process (West and Eilander 2001). The first step concerns a comparison of the bioefficacy of ß-carotene in oil with that of retinol in oil. For this purpose, we developed and tested a technique that is based on reach plateau isotopic enrichment of β-carotene and retinol, each specifically labeled with ten 13C atoms (Van Lieshout et al. 2001a,b). These studies have provided the most reliable estimates so far, and showed that 2.6 µg β-carotene in oil has the same vitamin A activity as 1 µg retinol in oil. By contrast, previous estimates by FAO/WHO (1967, 1988) and the US IOM (2001) were 2 µg and 3.3 µg β-carotene. For the second step – the relative bioavailability of ß-carotene in food compared with that of ß-carotene in oil – there is still a paucity of data. Recent studies using our stable isotope technique (Van Lieshout et al. 2001b) confirmed our earlier reports of the low bioefficacy of ß-carotene in dark green leafy vegetables compared with orange fruit, and that was based on findings from randomised controlled trials (De Pee et al. 1998). The data on the first and second step can be used to re-evaluate recommendations on the bioefficacy of carotenoids in food by national and international organizations as part of their guidelines on recommended dietary allowances. In addition, these new data have important implications for estimations of the effective vitamin A intake of populations in various regions of the world. Based on existing FAO food balance sheets and the older FAO/WHO conversion rates (6:1), all populations in the world should be able to meet their vitamin A requirements from existing dietary sources (FAO/WHO 1988), which contradicts findings of widespread vitamin A deficiency in developing countries (Mason et al. 2001). This discrepancy seems largely resolved when recalculating the supply of vitamin A with revised estimates of carotenoid bioefficacy. Such an analysis shows that populations in Asia, South America and Africa do not meet their recommended daily allowances (West and Eilander 2001), and confirms that low bioefficacy of carotenoids from plant foods is a crucial determinant of vitamin status in developing countries.
5. PLANS FOR FUTURE WORK 5.1. April-September 2002:
• Preparations in Wageningen: • Background reading, and learning techniques. • PhD fellow will also attend conferences and courses. • Preparation for first study. 5.2. Oct 2002-Mar 2003 • Preparation of the first study in Indonesia.
101

6. COLLABORATING PARTNERS The table below gives an overview of the scientists and the institutions involved in the proposed project, and their responsibilities. These institutions have a history of successful collaboration forms the basis for the current proposal and that resulted in a PhD thesis entitled: ‘Bioavailability and bioefficacy of ß-carotene measured using 13C-labeled ß-carotene and retinol: studies in Indonesian children’.
Researcher/institution Responsibility
Muhilal, A Firmansah (field investigator; PhD candidate), D Permaesih Nutrition Research and Development Centre, Bogor, Indonesia
Design, implementation and supervision of field work, biochemical analyses (non-nuclear)
CE West, H Verhoef Division of Human Nutrition and Epidemiology, Wageningen University, The Netherlands
Overall academic responsibility, support in aspects of design, data analysis, interpretation of results, biochemical analyses (non-nuclear)
J Lugtenburg Leiden Institute of Chemistry, Leiden University, The Netherlands
Synthesis of labelled compounds
R van Breemen Dept of Medicinal Chemistry and Pharmacognosy, College of Pharmacy, University of Chicago, USA
Biochemical analysis of labelled compounds
6.1. The Division of Human Nutrition and Epidemiology, Wageningen University The Dvision has a track record in implementing PhD projects in Indonesia (eight PhD projects in Indonesia have been completed or are on-going) and a range of other developing countries (projects have been completed or are on-going in Bangladesh, Benin, Burkina Faso, China, Ecuador, Ethiopia, Guatemala, Kenya, Malawi, Singapore, South Africa, Sudan, Tanzania and Vietnam). These projects have contributed to >300 publications relevant to developing countries. It has 45-70 PhD students at any point in time, of whom approximately one-third comes from from developing countries. Of those from developing countries who obtained their PhD degree in the past, 89% is at present still work in developing countries, and 84% are still working in their own country. The Division puts high value on local capacity building, and has done so in the past by providing laboratory support, organising and conducting national and regional courses, sustained support of post-docs, and stimulation of South-to-South collaboration within the network of its collaborating partners and ex-PhD students.
102

REFERENCES [1] BEATON, G.H., MARTORELL, R., ARONSON, K.J., ET AL. Effectiveness of vitamin A supplementation in the control of young child morbidity and mortality in developing countries. ACC/SCN State-of-the-art-series: Nutrition policy discussion paper 13. Toronto: University of Toronto (1993). [2] BONDI, A., SKLAN, D. Vitamin A and carotene in animal nutrition, Prog. Food Nutr. Sci. 8 (1984)165-91. [3] BROWN, K.H., WUEHLER, S.E. (EDS.). Zinc and human health: results of recent trials and implications for program interventions and research. Ottawa, Canada: The Micronutrient Initiative, 2000. [4] CASTENMILLER, J.J., WEST, C.E. Bioavailability and bioconversion of carotenoids, Annu. Rev. Nutr. 18 (1998)19-38. [5] CASTENMILLER, J.J., WEST, C.E., LINSSEN, J.P., VAN HET HOF, K.H., VORAGEN, A.G. Food matrix of spinach is a limiting factor in determining the bioavailability of ß-carotene but to a lesser extent of lutein, J. Nutr. 129 (1999) 349- 355. [6] CHRISTIAN, P., WEST, K.P. Interactions between zinc and vitamin A: an update, Am. J. Clin. Nutr. 68 (1998) 435S-441S. [7] CHRISTIAN, P., WEST, K.P., KHATRY, S.K., ET AL. Night blindness of pregnancy in rural Nepal--nutritional and health risks. Int J Epidemiol 27 (1998) 231-237. [8] CHRISTIAN, P., WEST, K.P., KHATRY, S.K., ET AL. Night blindness during pregnancy and subsequent mortality among women in Nepal: effects of vitamin A and beta-carotene supplementation. Am J Epidemiol 152 (2000) 542-547. [9] CHRISTIAN, P., WEST, K.P., KHATRY, S.K., ET AL. Maternal night blindness increases risk of mortality in the first 6 months of life among infants in Nepal. J Nutr 131 (2001) 1510-1512. [10] DE PEE, S., WEST, C.E., MUHILAL, KARYADI, D., HAUTVAST, J.G. Lack of improvement in vitamin A status with increased consumption of dark-green leafy vegetables, Lancet 346 (1995) 75-81. [11] DE PEE, S., WEST, C.E. Dietary carotenoids and their role in combating vitamin A deficiency: a review of the literature, Eur. J. Clin. Nutr. 50 (Suppl) (1996) S38-S53. [12] DE PEE, S., WEST, C.E., PERMAESIH, D., MARTUTI, S., MUHILAL, HAUTVAST, J.G. Orange fruit is more effective than are dark-green, leafy vegetables in increasing serum concentrations of retinol and ß-carotene in schoolchildren in Indonesia, Am. J. Clin. Nutr. 68 (1998) 1058-1067. [14] DIJKHUIZEN, M.A., WIERINGA, F.T., WEST, C.E., MUHERDIYANTININGSIH, MUHILAL. Concurrent micronutrient deficiencies in lactating mothers and their infants in Indonesia, Am. J. Clin. Nutr. 73 (2001a) 786-791. [15] DIJKHUIZEN, M.A., WIERINGA, F.T., WEST, C.E., ET AL. “Zinc enhances ß-carotene supplementation”, Vitamin A, iron and zinc deficiency in Indonesia: micronutrient interactions and effects of supplementation (DIJKHUIZEN, M.A, WIERINGA, F.T.). PhD Thesis, Wageningen University, Wageningen, The Netherlands (2001b)151-165. [16] DIJKHUIZEN, M.A., WIERINGA, F.T., WEST, C.E., MUHILAL. “ß-Carotene supplementation only improves vitamin A status when given in combination with zinc” [17] DIJKHUIZEN, M.A., WIERINGA, F.T. Vitamin A, iron and zinc deficiency in Indonesia: micronutrient interactions and effects of supplementation. PhD thesis. Wageningen University, Wageningen, The Netherlands (2001c).
103

[18] DIMITROV, N.V., MEYER, C., ULLREY, D.E., ET AL. Bioavailability of ß- carotene in humans. Am. J. Clin. Nutr. 48 (1988) 298-304. [19] European Pharmacopoeia. 2nd ed. Maisonneuve, Sainte-Ruffine-les-Metz, France, (1993). [20] FAO/WHO. Requirements of vitamin A, thiamine, riboflavin and niacin. FAO Food and Nutrition Series 8, UN Food and Agriculture Organization, Rome (1967). [21] FAO/WHO. Requirements of vitamin A, iron, folate and vitamin B12. FAO Food and Nutrition Series 23, UN Food and Agriculture Organization, Rome (1988). [22] IVACG. The bioavailability of dietary carotenoids: current concepts. International Life Sciences Institute, Washington, DC (1999). [23] IOM. Dietary reference intakes for vitamin A, vitamin K, arsenic, boron, chromium, copper, iodine, iron, manganese, molybdenum, nickel, silicon, vanadium, and zinc, 1st ed., Institute of Medicine, National Academy Press, Washington, D.C (2001). [24] JALAL, F., NESHEIM, M.C., AGUS, Z., ET AL. Serum retinol concentrations in children are affected by food sources of ß-carotene, fat intake, and anthelmintic drug treatment, Am. J. Clin. Nutr. 68 (1998) 623-629. [25] JAYARAJAN, P., REDDY, V., MOHANRAM, M. Effect of dietary fat absorption of beta-carotene from green leafy vegetables in children, Indian J. Med. Res. 71 (1980) 53-56. [26] KHAN, N.C., WEST, C.E., DE PEE, S., KHÔI, H.H. Comparison of effectiveness of carotenoids from dark-green leafy vegetables and yellow and orange fruits in improving vitamin A status of breastfeeding women in Vietnam. Report of the XIII International Vitamin A Consultative Group meeting. International Life Sciences Institute, Washington, DC (1998) (abstr). [27] LUGTENBURG, J., CREEMERS, A.F., VERHOEVEN, M.A., ET AL. Synthesis of 13C labeled carotenoids and retinoids, Pure Appl. Chem. 71 (1999) 2245-2251. [28] MASON, J.B., LOFTI, M., DALMIYA, N., SETHURAMAN, K., DEITCHLER, M. The Micronutrient report: current progress and trends in the control of vitamin A, iodine, and iron deficiencies. The Micronutrient Initiative, Ottawa, Canada (2001). [29] OLSON, J.A. The effect of iron and copper status and of dietary carbohydrates on the activity of rat intestinal ß-carotene 15,15'-dioxygenase, Br. J. Nutr. 84 (2000) 3-4. [30] ORTEGA, R.M., ANDRES, P., MARTINEZ, R.M., LOPEZ-SOBALER, A.M. Vitamin A status during the third trimester of pregnancy in Spanish women: influence on concentrations of vitamin A in breast milk. Am J Clin Nutr 66 (1997) 564-568. [31] RAHMAN, M.M., VERMUND, S., WAHED, M.A., ET AL. Simultaneous zinc and vitamin A supplementation in Bangladeshi children: randomised double blind controlled trial, Br. Med. J. 323 (2001) 314-318. [32] RAHMAN, M.M., WAHED, M.A., FUCHS, G.J., BAQUI, A.H., ALVAREZ, J.O. Synergistic effect of zinc and vitamin A on the biochemical indexes of vitamin A nutrition in children. Am J Clin Nutr 75 (2002) 92-98. [33] SHANKAR, A.H., GENTON, B., SEMBA, R.D. ET AL. Effect of vitamin A supplementation on morbidity due to Plasmodium falciparum in young children in Papua New Guinea: a randomised trial. Lancet 354 (1999) 203-209. [34] SMITH, J.C., MCDANIEL, E.G., FAN, F.F., HALSTED, J.A. Zinc: a trace element essential in vitamin A metabolism. Science 181 (1973) 954-955. [35] SOLOMONS, N.W., RUSSEL, R.M. Appropriate technology for vitamin A field research, Am. J. Clin. Nutr. 73 (2001) 849-50. [36] SOMMER, A,, WEST, K.P. (eds.) Vitamin A deficiency: health, survival and vision. Oxford University Press, New York, NY (1996). [37] STOLTZFUS, R.J., UNDERWOOD, B.A. Breast-milk vitamin A as an indicator of the vitamin A status of women and infants. Bull World Health Organ 73 (1995) 703-
104

711. [38] TANG, G., GU, X., HU, S., ET AL. Green and yellow vegetables can maintain body stores of vitamin A in Chinese children, Am. J. Clin, Nutr, 70 (1999) 1069-1076. [39] UNDERWOOD, B.A. Maternal vitamin A status and its importance in infancy and early childhood. Am J Clin Nutr 59(2 Suppl) (1994) 517S-522S. [40] VAN BREEMEN, R.B., NIKOLIC, D., ET AL. Development of a method for quantitation of retinol and retinyl palmitate in human serum using high-performance liquid chromatography-atmospheric pressure chemical ionization-mass spectrometr,. J. Chromatogr. 794 (1998) 245-251. [41] VAN HET HOF, K.H., WEST, C.E., WESTSTRATE, J.A., HAUTVAST, J.G. Dietary factors that affect the bioavailability of carotenoids. J Nutr 130 (2000) 503- 506. [42] VAN LIESHOUT, M., WEST, C.E., MUHILAL, ET AL. Bioefficacy of ß-carotene dissolved in oil studied in children in Indonesia, Am. J. Clin. Nutr. 73 (2001a) 949- 958. [43] VAN LIESHOUT, M., WEST, C.E., WANG, Y., ET AL. “Bioavailability and bioefficacy of ß-carotene measured using ß-carotene and retinol labeled with 13C, in Indonesian children”, Bioavailability and bioefficacy of ß-carotene measured using 13C-labeled ß-carotene and retinol: studies in Indonesian children (VAN LIESHOUT, M .) PhD Thesis, Wageningen University, Wageningen, The Netherlands (2001b). [44] VAN LIESHOUT, M., WEST, C.E., VAN DE BOVENKAMP, P., ET AL. “Extraction of carotenoids from feces enabling the bioavailability of ß-carotene in Indonesian children”, Bioavailability and bioefficacy of ß-carotene measured using 13C-labeled ß-carotene and retinol: studies in Indonesian children (VAN LIESHOUT, M.) PhD Thesis, Wageningen University, Wageningen, The Netherlands (2001c). [45] VILLAMOR, E., FAWZI, W.W. Vitamin A supplementation: implications for morbidity and mortality in children. J Infect Dis 182 (Suppl 1) (2000) S122-133. [46] WANG, Y., XU, X., VAN LIESHOUT, M., ET AL. A liquid chromatography-mass spectrometry method for the quantification of bioavailability and bioconversion of carotene to retinol in humans, Annal. Chem. 72 (2000) 4999-5003. [47] WEST, C.E. Vitamin A and measles. Nutr Rev 58(2 Pt 2) (2000) S46-S54. [48] WEST, C.E., EILANDER, A. Consequences of revised estimates of carotenoid bioefficacy for vitamin A intake in developing countries, J. Nutr. (2001) (accepted for publication). [49] WEST, C.E., EILANDER, A., VAN LIESHOUT, M. Consequences of revised estimates of carotenoid bioefficacy for the dietary control of vitamin A deficiency in developing countries’, J. Nutr. (2001) (accepted for publication). [50] WEST, K.P., KATZ, J., KHATRY, S.K., ET AL. Double blind, cluster randomised trial of low dose supplementation with vitamin A or beta carotene on mortality related to pregnancy in Nepal. The NNIPS-2 Study Group, B.M.J. 318 (1999) 570-575.
105

106

ASSESSMENT OF NATURAL VARIATION OF IRON AND ZINC ISOTOPE RATIOS DURING AN IRON INTERVENTION STUDY IN LACTATING WOMEN OF BANGLADESH.
J A HOOGEWERFF2, M A WAHED1, K E ISLAM1, B TEUCHER2 AND S K ROY1, M A MALEK3
1ICDDR,B: Centre for Health and Population Research, Dhaka-1212, Bangladesh 2 Institute of Food Research, Norwich, UK 3 Institute of Nutrition and Food Science, Dhaka University, Bangladesh
Abstract: A high proportion of people living in developing countries are deficient in Fe and Zn. Accurate markers for Fe status are available, but we lack effective markers to measure Zn status. Due to limitations of any single reliable method to determine zinc status, specific information on the prevalence of deficiency in particular settings is still lacking. State of art research indicates that the isotope ratios of Zn in human tissues are not in isotopic equilibrium. Differences in readings are expected to vary by up to 20‰ in human tissues. In this study, we will examine natural variations in Fe and Zn isotope ratios in biological samples to provide new tools to assess Fe and Zn status of individuals. During the first 18 months a pilot study will be conducted with 16 lactating women in Bangladesh. Specific objectives of this study are (a) to assess the variation in the natural isotopic composition of iron and zinc isotopes in human biological samples before and after a three-month iron supplementation period and (b) to determine the natural variation of Fe and Zn isotopes in Bangladesh diet. There will be two study groups: One malnourished and one well-nourished group. Each group will consist of mothers in two subgroups: (1) iron supplementation (2) no supplementation. Natural variation of Fe and Zn isotope will be determined in both well-nourished and malnourished women. Fe and Zn levels in blood, faeces, urine, hair and nails, will be determined. Hemoglobin, serum ferritin and serum transferrin receptor level will be measured to determine iron status. Subjects will be followed up at home weekly to ensure the continuity of supplementation. Blood, urine, stool, hair, and nail samples will be collected on in regular intervals from day 0 to 80 with special care to limit contamination, as Zn is especially prone to environmental contamination. Representative samples of Bangladeshi foods (meat, fish, vegetables, pulses, rice) will be collected from each of the two groups during supplementation period, taking the diets on two random days.
BACKGROUND AND SCOPE OF THE PROJECT: Nutritional deficiency is widely prevalent in most of the developing countries. Deficiency of trace elements in human particularly in children and mothers of child bearing age is of particular concern. The deficiency could be result of inadequate intake of minerals in the diet, decreased or impaired absorption. Iron absorption whether due to inadequate intake or decreased absorption is the leading cause of iron deficiency anemia. During pregnancy, iron supplementation is being commonly recommended because most women have limited iron stores to meet the demands. A high proportion of people living in developing countries are deficient in Fe and Zn. There exist good marker for Fe status (Transferrin, Ferritin, Transferrin Receptor and hemoglobin levels). Because a sensitive indicator for determining zinc status has not been established, the requirement and recommended dietary allowance has been formulated with uncertainties. There are no good markers of Zn status and the state of Zn body stores can only be assessed by stable isotope methods (“exchangeable Zn-pooled method”). State of the art research is indicating that the isotope ratios of Zn in human tissues are not in isotopic equilibrium. The differences can be up to 20‰ (relative to a common standard). Due
107

to kinetic effects in biochemical reactions the lighter and heavier isotopes of these elements become fractionated. The rates of transfer of the element in question between the different body compartments will depend on the whole body status of the element in question. It is therefore, hypothesized that an abnormal Zn status in one individual as compared to a healthy population might be reflected in the isotopic ratio in blood or urine. Iron deficiency is the most common micronutrient deficiency and effects more than 2 billion persons worldwide, leading to anemia in > 40% of women in developing world. Iron deficiency in women and is associated with pre-term births, low birth weight babies and cognitive delays in infant and child development (1,2). In Bangladesh, about 50% of pregnant women 48.7% of lactating mothers and 38.4% of non-lactating women were found to be anemic according to the respective cut off points established by INACG/WHO (3). According to a recent UNICEF estimate, anemia accounts for about 25% of all deaths among young women in Bangladesh (4). Women lose iron during menstruation, delivery post partum period. (5). Less intake of dietary iron, lower bio-availability and presence of inhibitor that hampers iron absorption in the diet are the three most important cause of iron deficiency among women and children. Zinc is another important trace element, essential for optimum human growth and development (6). Over the last 15 years, a considerable number of well-designed clinical studies examined the relationship of zinc and human health and established the effect of zinc deficiency on growth, morbidity and immunological function. A recently completed meta analysis of 25 clinical trial of the effect of zinc supplementation on children’s growth showed that zinc supplementation had highly significant impact on children’s height increment (7). Zinc supplementation has been proved to have preventive effect on diarrhoeal disease. A pooled analysis of 7 community based trials showed that zinc supplementation was associated with reduced prevalence and incidence of diarrhoea (8). It has also been shown to reduce diarrhoeal duration and faster recovery than control group in both acute and persistent diarrhoea (9,10). Zinc deficiency is thought to be highly prevalent among people of low-income countries (11, 12). However, due to the limitation of any single reliable method to determine zinc status, specific information on the prevalence of deficiency in particular settings are still in lacking. It is necessary to study whether the natural variation of Zn and Fe isotope ratios is related to the nutritional status of well nourished and malnourished women in Bangladesh before and after intervention food supplemented with Fe.
OVERALL OBJECTIVES: To test the natural variation in Fe and Zn isotopes ratios in either blood, stool and urine in a population.
SPECIFIC OBJECTIVES FOR YEAR ONE: • To do a pilot Fe intervention study with apparently healthy women as well as moderately
malnourished women of urban and peri-urban area of Bangladesh (total 16 women). • To study the variation in the natural isotopic composition of iron and zinc isotopes in
blood, stool, urine, hairs and nails during the pilot study. • To make some assessments of the natural variation of Fe and Zn isotopes in Bangladesh
diet.
108

MATERIALS AND METHODS: Study design Prospective follow up study with iron supplementation. Study subjects Sixteen lactating women aged between 20 and 40 living in urban and peri-urban area of Dhaka city, Bangladesh. Inclusion criteria • Women (mother) aged between 20-40. • BMI 21-24 for well nourished group. • BMI Less than 21 but not less than 18.5 for malnourished group. • Live in and around Dhaka city. • Without any acute or chronic illness. Study groups There will be two study groups: • Group A: eight well-nourished mothers • Group B: eight malnourished mothers. Iron intervention and absorption study For intervention study, each group of women will be randomly divided into two Subgroups (1) Fe supplementation (four women) (2) No supplementation (four women) Determination of natural variation of Fe and Zn isotopes Natural variation of Fe and Zn isotope will be determined in both well nourished and malnourished of women. In all the women Fe and Zn levels in feces, urine hair and nail, will be determined. To measure the iron status, hemoglobin, ferritin and serum transferrin receptor levels will be measured.
109

Supplementation Fe supplementation will be started from day 1 after collection of all the baseline samples on day 0. Supplementation will be continued for 80 days. Follow-up Subjects will be followed up at home on weekly interval to ensure the continuity of supplementation Samples to be collected Blood, urine, stool, hair, nail and diet. Special care will be taken to limit contamination, as especially Zn is prone to environmental contamination. Human samples Day 0: Blood, urine, stool, hair and nails. Days 5,10,30,60: Blood, urine and stool. Day 80: Blood, urine, stool, hair and nails. Diet A representative samples of Bangladeshi foods (meat, fish, vegetables, pulses, rice). Duplicate samples of diets from each of the two groups during eleven-week supplementation period taking the diets on two random days. Sample analysis Human ICDDR,B: • Sample digestion for isotopic samples. • Blood hemoglobin , serum ferritin, STfR and plasma zinc. IFR: • Purification of Fe and Zn from blood (whole blood erythrocytes), urine, feces, hair and
nails • High accuracy stable isotope analysis Diet: ICDDR,B • Sample digestion for isotopic analysis. • IFR • Purification of Fe and Zn from food digests • High accuracy stable isotope analysis
110

REFERENCES [1] GUPTA A AND CRUMBLISS AL. Treatment of iron deficiency anemia: are monomeric iron compounds suitable for parenteral administration? J Lab Clin Med 2000 Nov; 136(5): 371-8. [2] CALLEN BL. Program of care for young women with iron deficiency anemia: a pilot .J Community Health Nurs 2000 winter; 17 (4): 247-62. [3] WORLD HEALTH ORGANIZATION (1997). Indicators for assessing iron deficiency and straetegies for its prevention. (1993 workshop), the World Health Organization (WHO), the United Nations Children’s Fund (UNICEF), the United Nations University (UNU), Geneva, Switzerland, WHO(Draft). [4] UNICEF 1991. State of the world children. New York. [5] HERCBERG-S; GALAN-P. Nutritional anemia’s. Baillieres-Clin-Haematol, 1992 Jan; 5(1):143- 68. [6] SUSKIND RM, Nestle Nutrition Workshop Series; Vol 19:pp.157. [7] BROWN K. H., PEERSON J.M. ALLEN A.H. Effect of zinc supplementation on children’s growth: a meta analysis of intervention trials. Bibliotheca Nutrition et Dieta, 54; 76-83. [8] BHUTTA Z.A, BLACK R.E, BROWN K.H. MEEKS GARDNER, J GORE S et al. Prevention of diarrhea and pneumonia by zinc supplementation in children in developing countries: pooled analysis of randomized controlled trials. Zinc investigators Collaborative Group. Journal of Pediatrics, 1199; 135: 689-697. [9] ROY S.K. TOMKINS A.M., AKRAMUZZAMAN S.M. BEHRENS R.H. R.HAIDER, MAHALANBIS D. FUCHS G. Randomized controlled trail of zinc supplementation in malnourished Bangladeshi children with acute diarrhoea. Arch Dis Child 1997;77:196-200. [10] ROY S.K. TOMKINS A.M., MAHALANBIS D., AKRAMUZZAMAN S.M., HAIDER R., BEHRENS R.H. AND FUCHS G.J. Impact of zinc supplementation on persistent diarrhoea in malnourished Bangladeshi children. Acta Paediatr 1988;87:1235-9. [11] SHRIMPTON R. Zinc deficiency: it widespread but underrecognized? 1993, ACC/SCN News 9, 24-27 [12] GIBSON R.S. Zinc nutrition in developing countries. Nutrition Reviews, 7 151-173
111

112

PART IV: APPENDICES
113

114
APPENDIX 1: AGENDA OF THE MEETING
FIRST RESEARCH CO-ORDINATION MEETING (RCM) FOR THE THEMATIC CO-ORDINATED RESEARCH PROJECT (CRP) ON
“ISOTOPIC AND COMPLEMENTARY TOOLS FOR THE STUDY OF MICRONUTRIENT STATUS AND INTERACTIONS IN DEVELOPING COUNTRY POPULATIONS EXPOSED TO MULTIPLE NUTRITIONAL
DEFICIENCIES”
MONDAY, 25 MAY 2002
8.30-9.15 Registration at the VIC UN security office, IAEA Main Gate -1
9.00-9.15 Participants arrive at the meeting room
9.15-10.45 Opening session of the RCM meeting Welcome: Scientific Secretary Head, NAHRES Section (Dr. G.V. Iyengar) Brief self introductions by the participants Introduction to T-CRP concept by DIR-NAHU (Dr. Groth) Experiences from another T-CRP related to nuclear medicine By the Head of Nuclear Medicine Section, NAHU, (Dr. A. Padhy)
10.45-11.15 Coffee Break
11.15-12.30 Session-1: Administrative/procedural matters Introductory remarks to the RCM; presentation of the meeting agenda; adoption of the agenda (Dr. G.V. Iyengar) Election of a general chair, co-chair and rapporteur for the meeting Administration arrangements.
12.30-14.00 Lunch
14.00 – 17.30 Session-2 (presentations by consultants); Chair: Dr. B. de Benoist
14.00-14.45 Designing human nutrition studies at the University of Vienna (Prof. Ibrahim Elmadfa)
14.45-15.30 Capacity Building in Micronutrient Area; WHO perspectives, WHO, Geneva (Dr. B. de Benoist)
15.30-16.00 Coffee Break
16.00 Discussion with NAHRES & TC counterparts.
115

TUESDAY 25 JUNE 2002
09.00-12.30 Session 3: Chair: (presentations/CRP participants) Dr. Walczyk
09.00 - 10.30 Bangladesh (Dr. Abdul and Dr. Hoogewerff) (Assessment of natural variation of Fe and Zn isotope ratios during an Fe intervention in women in Bangladesh)
10.30 – 11.00 Coffee
11.00-12.30 Ghana (Dr. Newton and Dr. S. Tonumihardjo) (Evaluation of new WHO vitamin A supplementation regimen for post-partum mothers using stable carbon isotopes)
12.30 – 14.00 Lunch
14.00 – 17.30 Session 4 (presentations/CRP participants) Chair: Dr. Liyanage
14.00 – 15.30 Indonesia (Dr. Muhilal/Dr. Verhoef) (Effect of dietary fat intake and of zinc intake/status on bioefficacy of beta-carotene in children and lactating women in Indonesia)
15.30 – 16.00 Coffee
16.00 – 17.30 Pakistan (Dr. Bhutta and Dr. Weaver) (Estimating bio-availability of zinc, iron and vitamin A from home available complementary foods in Pakistan: a community based study in young infants using stable isotopes)
17:30 Reception at A-24
WEDNESDAY 26 JUNE 2002
09.00-12.30 Session 5 (presentations/CRP participants) Chair: Dr. Newton
09.00 - 10.30 India (Dr. Muthayya/Dr. Aggarwal) (Stable isotope studies on iron bio-availability in young Indian women: effects of nutritional status, interactions and ethnicity)
10.30 – 11.00 Coffee
11.00-12.30 Sri Lanka (Dr. Liyanage/Dr. Hilmers) (Interaction between micronutrients, their impact on bioavailability and significance in nutrition internvention) and (Evaluation mineral absorption and metabolism in nutritionally at-risk children using stable isotopes)
12.30 – 14.00 Lunch
116

14.00 – 17.30 Session 6 (presentations/CRP participants) Chair: Dr. Aggarwal
14.00 – 15.30 Thailand (Dr. Wasantwisut/Dr. Walczyk) (The effect of the most common spices and herbs in the Thai diet on human iorn absorption)
15.30 – 16.00 Coffee
16.00 – 17.30 UNU Cente for Post-Graduate Studies in Food and Nutrition at the CFTRI, Mysore, India (Dr. V. Prakash) Academic issues related to International Nutrition as addressed at the Johns Hopkins University, Baltimore, MD, USA (Dr. S. Sazawal)
17:30 Discussion with NAHRES & TC counterparts
THURSDAY 27 JUNE 2002
09.00-12.30 Session 7 Discussions, Chair: Dr. Prakash
09.00 - 10.30 Comments by consultants
10.30 – 11.00 Coffee
11.00- Comments by participants
12.30 – 14.00 Lunch
14.00 – 17.30 Session 8 Chair: Bhutta Country team work to prepare written input for the RCM report 14.00 – 15.30 Bangladesh, Brazil, Ghana, India Indonesia, Pakistan, Sri Lanka, Thailand
15.30 – 16.00 Coffee
16.00 – 17.30 Brief presentations of the country team work to the whole group (ca. 10 minutes each) Bangladesh, Brazil, Ghana, India, Indonesia, Pakistan, Sri Lanka, Thailand
FRIDAY 28 JUNE 2002
09.00-12.30 Session 9 (General chair, co-chair and Rapporteur)
09.00 - 10.30 Finalisation of the input to RCM report by country teams and consultants in consultation with the General Chair and co-chair
10.30 – 11.00 Coffee
11.00- - 12.30 Presentation of the overall outcome of the First RCM by the General Chair Closing of the meeting
117

118

APPENDIX 2: LIST OF PARTICIPANTS
LIST OF PARTICIPANTS Dr. Jurian Hoogewerff Mass Spectrometry Team Institute of Food Research Norwich Research Park Colney, Norwich NR4 7UA United Kingdom Tel.: +44 1 603 255028 Fax: +44 1603 255038 E-mail: [email protected] Dr. Sam Newton Kintampo Health Research Centre Health Research Unit Ministry of Health PO Box 200, Kintampo Brong Ahafo Region Ghana Tel.: + 233 61 27304 Fax: + 233 61 27304 E-mail: [email protected] Dr. Sherry Tanumihardjo Department of Nutritional Sciences University of Wisconsin Madison 1415 Linden Drive, Madison WI 53706 USA
Tel.: +1 608 2650792 Fax: +1 608 2625860 E-mail: [email protected] Dr. Suresh Kumar Aggarwal Bhabha Atomic Research Centre Fuel Chemistry Division Trombay, Mumbai 400 085 India Tel.: + 91 22 5505050 ext 2463 Fax: + 91 22 5505151 or 5519613 E-mail: [email protected]
119
Dr. Hans Verhoef Division of Human Nutrition and Epidemiology Wageningen University PO Box 8129, 6700 EV Wageningen The Netherlands Tel.: +31 317 484317 Fax: + 31 317 483342 E-mail: [email protected] Dr. Zulfiqar Bhutta Aga Khan University Stadium Road PO Box 3500 Department of Paediatrics Karachi 74800 Pakistan Tel.: +92 21 493 0051 Fax: + 92 21 493 4294 or 493 2095 E-mail: [email protected] Dr. Chandrani Liyanage Nuclear Medicine Unit Faculty of Medicine University of Ruhuna P.O. Box 70, Galle Sri Lanka Tel.: + 94 9 34801/34803 Fax: + 94 9 22314 E-mail: [email protected] Dr. David Hilmers Mineral Mass Spectrometry Laboratory USDA/ARS Children’s Nutrition Research Centre Department of Pediatrics Baylor College of Medicine 1100 Bates St., Room 7066 Houston TX 77030 USA Tel.: + 1 713 7987164 Fax: + 1 713 7987119 E-mail: [email protected]
120
Dr. Emorn Wasantwisut Mahidol University at Salaya Institute of Nutrition Department of Human Nutrition Phutthamonthon 4 Nakhon Pathom 73170 Thailand Tel.: + 66 2 800 2380 ext. 305 Fax: + 66 2 4419344 E-mail: [email protected] Dr. Thomas Walczyk Eidgenoessische Technische Hochschule Zuerich Laboratory of Human Nutrition Seestrasse 71 P.O. Box 474 CH-8803 Rueschlikon Switzerland Tel.: + 41 1 7045704 Fax: + 41 1 7045710 E-mail: [email protected] Dr. Wahed Mohamed Abdul Associate Scientist and Head Nutritional Biochemistry Lab Sciences Division International Centre for Diarrhoeal Disease Research GPO Box 128, Dhaka 1000 Bangladesh Tel.: +880 2 8811751-60 ext. 2313 Fax: +880 2 8823116 or 8812529 E-mail: [email protected]
121

Consultants Dr. Bruno de Benoist Medical Officer, Focal for Micronutrients Department of Nutrition for Health and Development World Health Organization CH-1211 Geneva 27 Switzerland Tel.: + 41 22 7913412 Fax: + 41 22 7914156 E-mail: [email protected] Dr. V. Prakash Director, United Nations University Center for Post Graduate Studies Director, Central Food Technological Research Institute Mysore 570 013 Karanataka India Tel.: + 91 821 517760 Fax: + 91 821 516308 E-mail : [email protected] or [email protected] Dr. Sunil Sazawal Department of International Health Johns Hopkins University 615 North Wolfe Street Rm 5031 Baltimore MD 21205-2179 USA Tel.: + 1 443 6215779 Fax: + 1 410 9557159 E-mail : [email protected] Prof. Dr. Ibrahim Elmadfa Director Institute of Nutritional Sciences University of Vienna Althanstrasse 14 (Pharmaziezentrum) A-1090 Vienna Austria Tel.: + 43 1 313368213 Fax: + 43 1 31336773 E-mail : [email protected]
122

Scientific Secretary Dr. G.V. Iyengar Head, Section of Nutritional and Health-Related Environmental Studies Division of Human Health Department of Nuclear Sciences and Appliances IAEA, PO Box 100 A-1400 Vienna Austria Tel.: +43 1 2600 21657 Fax: +43 1 26007 E-mail: [email protected] Dr. N. Mokhtar Section of Nutritional and Health-Related Environmental Studies Division of Human Health Department of Nuclear Sciences and Appliances IAEA, PO Box 100 A-1400 Vienna Austria Tel.: +43 1 2600 21680 Fax: +43 1 26007 E-mail: [email protected]
123