2005 Evaluation of the Sandyford Initiative Having Your Voice Heard – Interim Report Contents
107
Evaluation of the Sandyford Initiative Having Your Voice Heard – Interim Report April 2002 Louise Lawson Mhairi Mackenzie Jane Mackinnon Mulu Ayana Jon Shute Health Promotion Policy Unit Department of Public Health University of Glasgow
-
Upload
manchester -
Category
Documents
-
view
0 -
download
0
Transcript of 2005 Evaluation of the Sandyford Initiative Having Your Voice Heard – Interim Report Contents
Evaluation of the Sandyford Initiative
Having Your Voice Heard –
Interim Report April 2002
Louise Lawson Mhairi Mackenzie Jane Mackinnon Mulu Ayana Jon Shute Health Promotion Policy Unit Department of Public Health University of Glasgow

2
Contents

3

4
Chapter One - Background to the study and introduction to
the Sandyford Initiative
During recent years there has been a shift in thinking and policy regarding the health
of the population. It has become widely acknowledged that in order to improve the
health and well being of individuals there is a need not only to improve and
modernise services, but it is also vital to tackle the wider determinants of health. This
was taken on board by The Public Health White Paper ‘Towards a Healthier
Scotland’ (1999) which highlights the need for public health policies to tackle these
wider determinants of health that affect quality of life. In order to work towards this it
also states the importance of the role of Health Boards in protecting and improving
the health of their population and in demonstrating clear reductions in health
inequalities. This move towards a focus on inequalities is reinforced in The White
Paper ‘Designed to Care – Renewing the NHS in Scotland’ (1997). This also aims to
refocus health care provision in order to create a shift towards patient centred care,
emphasising the role of primary care and the need for improving health and reducing
health inequalities.
In line with this shift in policy, work has been carried out by The Family Planning and
Sexual Health Directorate of the Greater Glasgow Primary Care Trust to develop a
social model of care. This model is based on one first tested and evaluated in
Castlemilk, a large and deprived housing estate situated on the outskirts of Glasgow.
This model involves a holistic approach to women’s contraception and reproductive
health as well as encouraging health promotion, referral to other statutory and
voluntary agencies and a client driven approach to health care.
In addition to these developments within the family planning services there was an
acknowledgement by the Genitourinary Medicine (GUM) services within Glasgow
that there was a need for strategic change. This was based on the need within
Glasgow to provide a highly accessible service to the population which would not
only fulfil clinical needs, but would also have a focus on health promotion in order to
improve knowledge of sexual health in those who used the service.
The third service that was in place in Glasgow was the Centre for Women’s Health,
which had a history of multi-agency working since it began in 1993. This was
5
providing a well-used service that was built on a more holistic approach to the health
of its users. Following a review of these three services alongside the implementation
of a multi-agency sexual health strategy led by Greater Glasgow Health Board a
decision was reached to merge these three services and form the Sandyford
Initiative.
The Sandyford Initiative is the development of a collaborative and integrated sexual
health service that encompasses the principals of the social model of health, which
opened in July 2000 in Sandyford Place, Glasgow. It brings together Family Planning
and Sexual Health, Genitourinary Medicine and the Centre for Women’s Health,
alongside the Steve Retson Project and the Routes Out of Prostitution Social
Inclusion Partnership Intervention Team. The inception of the Initiative was due to the
desire for the three core services to further develop a social and holistic model of
health care. In addition to the services provided within these main clinics and centres
the Sandyford Initiative also incorporates the delivery of community-based services.
Following the opening of the Sandyford Initiative a series of work was carried out to
look at the integration of management structures. This included a staff consultation
exercise by Greater Glasgow Primary Care Trust (April 2001). Following this the
Sandyford Initiative now has a single directorship for all services, and four Associate
Directors support this position.
Overall Aim and Strategic Objectives of the Sandyford
Initiative
The overall aim of the Initiative is to implement a citywide initiative to enhance the
promotion of sexual, reproductive and women’s health and the quality of health care
using a social model of health.
The strategic objectives of the Initiative are:
� Maximising the integration of clinical and social aspects of health in each of the
three main services
� Creating an innovative model of barrier free health which builds on existing
collaboration between the three services

6
� Implementing ways of working to address unmet needs of current and potential
service users
� Pro-actively informing policy development in different organisations to promote
sexual, reproductive and women’s health (see Sandyford Initiative Development
Plan)
There are currently five different services provided within the three main branches of
the Sandyford Initiative. Although the services are outlined separately for the
purposes of this introduction, the delivery of these services is an integrated process
in which the three branches work closely together. In addition to the three main
services the Sandyford Initiative also runs individual projects such as Roots Out of
Prostitution, which aim to reach individual communities with specific sexual and
social health needs.
Family Planning
This service aims to provide a welcoming environment for individuals to come and
receive family planning support. It is based on the holistic approach to women’s
contraception and reproductive health first developed in Castlemilk. The service also
actively encourages health promotion and a more patient-centred approach to health
care. The centre provides appointments and a drop-in service at a range of times
with the aim of increasing the accessibility of the service.
The Place
Within the family planning services this drop-in centre provides a service dedicated to
young people aged between 12 and 25. It aims to encourage young people,
particularly those who may not otherwise visit their doctor, to come and get help and
advice in a non-threatening and confidential environment. It provides a range of
services including clinical, nursing and counselling input together with support
services. The place also provides young people with a wide range of information
covering many aspects of life that may affect their health and well being, such as
sexual health, substance misuse and problems at home or in schools and the
workplace.
7
Genito-urinary Medicine
The GUM clinic provides a sexual health service to individuals on both an
appointment and drop-in basis. The service has been designed to provide a more
approachable and accessible service in order to encourage an increase in the
number of people accessing sexual health services in Glasgow. Within the centre
users receive their care from doctors, nursing staff and health care workers. Health
promotion plays an important part in the running of this service with information to
improve the knowledge of users and to give them greater control over their own
sexual health in future.
Steve Retson project
This specialist branch of the GUM service, the Steve Retson Project, provides a
range of services for gay men and men who have sex with men. As with the GUM
clinic this service provides information, testing and treatment of sexually transmitted
infections. It also provides a support system for those using the service and advice
on living a healthy life. The Steve Retson Project has its own website which provides
a range of information about the service and life in Glasgow. This can be found at
http://www.steveretsonproject.org.uk .
Centre for Women’s Health
This centre aims to provide direct services to women, training and education to staff
in statutory and voluntary agencies and informs policy and decision making agendas
that impact on the lives and health of women (Scott et al, 2000). The Centre for
Women’s Health runs a strict women-only policy in order to provide a safe and non-
threatening environment for women attending the service. Women can be seen
individually by counsellors at the centre. The centre also provides a range of support
groups and focus groups in which women can discuss issues that are of importance
to them, whether they are health related or concern other aspects of their life. This
provides a mutually supportive environment for women with a wide range of issues
such as abuse or domestic violence.
Discussions are currently underway at the Sandyford Initiative around making
counselling services a core stream of the work at the initiative. These discussions are
presently at a very early stage and will develop during 2002.
8
Together, these services provided by the Sandyford Initiative aim to improve the
health and well being of individuals by encompassing the social model of health. This
model and its applications are explored in chapter two.

9
Chapter Two - Literature Review
Towards Developing a Social Model of Health Care
In the Interim Report of the Evaluation of the Sandyford Initiative (Mackenzie,
Lawson and Mackinnon 2001) we conducted a literature view exploring the social
model of health in the context of health care. In the following report we summarise
some of the key issues arising from that review, and further develop the idea of a
social model of health care by incorporating new ideas including sections on
women’s health, and lay health beliefs. This review then has the following thematic
approach:
� Revisiting the social model of health
� Lay and professional health perspectives
� Women’s health
� Development of the social model of health care – structure, process and
outcome
Methodological constraints
The information contained in this review is from the theoretical literature and
published research studies. However, there are relatively few studies which have
been undertaken with health service users, and much of the available data relates to
findings from studies undertaken with health professionals, particularly doctors.
Social model of health
In the Interim Report of the Sandyford Initiative we summarised the key aspects of
the social model of health and illustrated this through the various models that have
been reproduced in theoretical and policy literature about health promotion
(Whitehead 1995, Labonte 1998 and Evans and Stoddart 1994). Generally, the
social model proposes a holistic approach and a multi-causal model where people
are more than bodies. A healthy life suggests not only a healthy body but also a
healthy mind and a safe environment – health becomes a concept that embraces all
the dimensions of human existence (Hughes, 2000). The only social model
developed to date that includes the health care system is that by Evans and Stoddart
(1994).

10
In terms of health care, it has been argued that the social model of health is
ideologically opposed to the biomedical model. The biomedical model can be seen
as that offered by a service dominated by a specialised profession, providing medical
solutions to medically interpreted problems. The social model, by contrast, seeks to
lessen medical domination, places greater emphasis on holistic health care, and
proposed non-medical treatment to clinical problems as well as emphasising
preventive health.
In the context of the Sandyford Initiative, the social model of health care has been
coined to define a model of health care delivery that recognises two main issues.
Firstly, the detection and management of health problems should take into account
social and economic determinants of health. Secondly, the provision and practice of
health care should reflect the social needs of the user although the quality of care
depends not only on the quality of the interaction between user and professional but
also on the organisational environment in which care is delivered (Laughlin et al
2001). Thus the social model is concerned not only with health consciousness
raising but also with the creation of a service framework that allows medical problems
to be tackled by social solutions (Craddock and Reid 1993).
Broader perspectives
The social model recognises that people are complex beings and that a wide range
of factors impact on their health and feelings, from age and gender, to life
circumstances and wider economic and environmental influences. Whereas the
medical model focuses on the ailment or disease, the social model aims to treat the
person as an individual. This means taking into account the factors in a person’s life
that might affect their health. It also needs to be acknowledged that the process of
treating the whole person is not always relevant or appropriate depending on the
individuals’ reasons for accessing a service. This aspect perhaps needs further
exploration.
There is a wide literature on the ways in which poverty and socio-economic
disadvantage affects health (for example Whitehead 1995). In the way that we can
see a connection between life circumstances and health, there is the awareness that
many health problems have a social or economic root cause. In the context of HIV,
for instance, many biomedical scientists have come to recognise the importance of
social and cultural factors in explaining the epidemic (Doyal 2000). Mental health

11
problems can also be the result of women’s unequal position in society (Doyal 2000).
In the following section we use gender as an example to show how being female in
society can determine health status, and how a social model is more appropriate in
the context of women’s health care than the biomedical model, or in the context of
men’s health care.
Women’s health
Gender is a determinant of health; not only through the biological distinction of sex,
but also because of socio-economic differences associated with gender (Hills et al
2002). Thus women as a group not only experience different types of health issues
than men, they also experience the same health issues differently than men. Women
are more likely to be living on lower incomes, to be employed in lower paying and
less stable jobs, and to be encouraged by societal gender expectations to be the
primary givers of support to others, even if this is detrimental to their own needs and
health (Graham 1998, Janzen 1998). Also, women are confronted by barriers to the
health care system. Poverty and lack of childcare or transportation are examples of
barriers faced by women (Broom 1998).
In recent years a large body of work has demonstrated the interrelationship between
gender inequalities and both mental and physical health (Annandale and Hunt 2000,
Doyal 2000). As well as looking at life expectancy they have looked at more
qualitative dimensions of wellbeing, and have shown that many of the health
problems women face are not related in any direct way to their specific biological
characteristics. Rather they reflect the discrimination and disadvantage that many
continue to experience as they carry out gendered activities making up their daily
lives. Anxiety and depression, for instance, are more common among females than
males yet there is no evidence that women are constitutionally more susceptible to
these problems than men (Busfield, 1996).
As previously discussed, the traditional model of health, based on a biomedical
model, gives primacy to biological factors over psychological and societal factors. A
New York survey found that women were more than twice as likely as men to change
doctors because they were dissatisfied and because they felt patronised or ‘talked
down’ to (Broom 1998). Australian studies suggest that doctors often do not respond
appropriately to women’s psychological problems or physical assault by partners
(cited in Broom 1998). As an alternative to this biological reductionist view, the
women’s health movement has adopted a ‘holistic approach’ that involved a
12
fundamentally different vision of health and illness. Such a client-centred type of
healthcare based on a social model can prevent health problems from being unjustly
attributed to either medical or psychological causes, and treatment being exclusively
or unnecessarily sought in the medical or psychotherapeutic sphere. This calls for
major changes in the training, attitude and beliefs of healthcare providers and for a
restructuring of existing, segregated health care services.
Lay and professional health perspectives
Another perspective we consider is the meshing of lay and professional beliefs and
the relevance of lay beliefs to the social model of health care. Research from
different social science perspectives has explored the complexity of lay models of
health (for example Blaxter 1990, Calnan 1987). Given that doctors are trained
within the framework of a more unified medical perspective and that differences exist
between patients’ models of health and those held by medical profession, then this
has wider implications in terms of communication and understanding. Differences in
ways of conceptualising health can potentially result in difficulties in reaching a
shared understanding within the consultation with GPs and patients speaking a
fundamentally different language (Ogden 2001). Although often at variance with
medical models of disease, patients’ explanatory models of illness and causes of
illness have been shown to be plausible, rational and sophisticated (Blaxter 1983,
O’Flynn 2000).
A study by Ogden et al (2001) operationalised some of the constructs identified in the
qualitative literature as a means to compare patients’ and GPs’ models of health. The
results from this study suggest that doctors and patients not only have different
models for specific health problems such as depression and obesity, but may also
have very different ways of conceptualising health. Such a difference could
potentially result in difficulties in reaching a shared understanding within the
consultation with GPs and patients speaking a fundamentally different language.
This emphasises the need of the importance of communication and partnership in a
doctor-patient consultation. It has been suggested therefore that the key to
successful doctor-patient partnerships is to recognise that patients are experts too
(Balint 1957, Coulter 1999). The doctor should be well informed about diagnostic
techniques, the causes of disease, prognosis, treatment options and preventive
strategies, but only the patient knows his or her experience of illness, social
circumstances, habits, behaviour, attitudes to risk, values and preferences. Both

13
types of knowledge are needed to manage health problems successfully (Coulter
1999).
Developing a social model of health care
In the Interim Report of the Sandyford Initiative Evaluation (2001) we started to
explore some of the key factors that were seen as important in developing a social
model of health care. We have already described some of the key theoretical
concepts: holistic and multi-causal models, recognising the wider health
determinants, factors such as gender, disadvantage and discrimination, the
importance of lay knowledge. These are all important aspects that must underpin a
social model of health care delivery and must be at the heart of it. These might be
described as the ‘intangible’ aspects in the model.
As well as acknowledging these wider issues, we started to unpack some of the more
‘tangible’ aspects of the model that can be incorporated into a social model of health
care framework. These include aspects such as organisational structure and
physical layout, providing support and a comfortable environment, a wide range of
staff and accessible information. We previously identified four factors – which were
not discrete but closely inter-woven – patient-centred care, access, understanding
culture/ideology and health promotion (Mackenzie, Lawson and Mackinnon 2001).
While still relevant we would like to propose a social model of health care using a
different themed approach based around structure (organisation and environment),
process (patient centred care, communication, decision-making, time, inter-personal
skills) and outcome (health, user involvement) into which we will incorporate the
previous factors. These separate themes are inter-linked and access can be said to
underpin them all. These themes mesh well with the Sandyford Initiative’s definition
of the social model of health care which states that the provision and practice of
health care should reflect the social needs of the user, although the quality of care
depends not only on the quality of the interaction between user and professional
(process) but also on the organisational environment in which care is delivered
(structure).
Structure - Organisation and Environment
Campbell and colleagues (2000) in defining quality of care identified structure as the
organisational factors that define the health system under which care is provided.
Two domains of structure were identified: physical characteristics and staff
14
characteristics. The physical characteristics relate to resources and environmental
organisation whereas staff characteristics relate to the mix of staff, including non-
medical personnel.
Previously we introduced the notion of space, place and boundaries. In the context
of women’s health centres, buildings and their occupants were sometimes referred to
as ‘home’ incorporating images of family, security, safety and being welcomed. A
gender delimited space was welcomed by some, particularly women who had been
subject to abuse by men (Broom 1997). Young people expressed the need for
privacy and respect in a safe environment (West 2000). The spatial boundaries of
social relationships, of open communication and non-hierarchical encounters were
regarded as equally important as the physical spaces to people’s experience of care.
Craddock and Reid (1993) in discussing the implementation of a well woman clinic in
Glasgow discuss structure and organisation in a typical clinic (based on a biomedical
model) as institutional, lacking in ornamentation, badly designed waiting areas,
separate areas for each part of consultation process, official areas and marked
territories. The Women’s Health Movement has seen a move towards non-
hierarchical environments, breaking down the boundaries with less bureaucracy.
This approach was reflected in the Ballantay Project (a well woman clinic) in Glasgow
that introduced various innovations to break down the bureaucratic format. It
‘domesticated’ the waiting areas, provided more literature and information and
altered physical layout. Certain organisational aspects of the clinic service were
altered leaving less reliance on the doctor such as the setting up of non-medical and
counselling services and self-help groups.
Location of premises, availability of outreach services, car parking facilities or
situation close to public transport routes can predict access to services. Similarly the
availability of childcare facilities, and appointments, sessions or classes to meet
individual needs (to fit with working patterns, home/family commitments) can greatly
enhance people’s opportunities to access services. Language interpreters and
facilities for disabled people, such as the availability of personal assistants, are also
important considerations.
Process
In terms of process, we are concerned with the ways users interact with health
workers. However, process factors directly relate to structure and whether the

15
structures are in place to enable meaningful interactions between users and staff.
Much of the literature in this area focuses on the concepts of patient centred care,
decision-making strategies and communication. The main focus is on interactions
between user (or patient) and doctor, with little available information about
interactions with other personnel, including non-medical personnel, in the system
(e.g. receptionists, nurse, counsellor). However, ease of accessing the service in the
first instance (for example through a receptionist) may be an important consideration
for some and be an important predictor of whether they continue to use a service.
Patient-centred care
A key element of process is the interaction between user and health care worker. In
our previous report we discussed some of the components of a ‘patient-centred
approach’ to health care. Although the patient-centred model of doctor consultation is
widely advocated, its use in practice is probably rather limited (Little et al 2001). The
model encompasses five principal domains: exploring the illness experience or
expectations, the whole person, finding common ground, health promotion and
enhancing the doctor-patient relationship. In an observational study by Little et al
(2001) to identify patient preferences for patient centred care, the study provided
empirical evidence that there are at least three important and distinct domains of
patient-centredness: communication, partnership and health promotion.
Treating the ‘whole person’
In terms of exploring the illness experience and treating the ‘whole person’ (cited as
principal domains of patient-centredness) there is little data about how this can be
achieved during a consultation and whether people expect, or want, to share this
information about themselves. The notion of treating the whole person might be
more relevant to certain types of treatment or in certain settings such as women’s
health centres, services for gay/bisexual men and counselling? Some of these
issues were explored in the Interim Report under ‘Understanding culture/ideology’
(Mackenzie, Lawson and Mackinnon 2001).
Social research with HIV positive people in Australia suggests an alternative
approach in which doctors and patients are seen as agents operating in clinical
space that is wider than the consultation (Hurley 2002). The consultation is a key
element in the constitution of clinical space, but it is not definitive of it. HIV positive
people in Australia rely heavily on specialist HIV general practitioners for information
about their pharmaceutical treatments, but they distinguish between information and

16
wider perspectives on living with HIV. Their negotiation of decisions about treatment
occurs in a framework of self-care. Patients may pre-empt the consultation at
different times and on different issues. For example, decisions about adherence,
drug holidays, and the use of recreational drugs seem to be made in the context of
mostly well informed self care practices than on the basis of a clinical consultation
alone.
Communication
In her comprehensive review of health outcomes, Stewart (1995) concluded that four
key dimensions of communication were related to positive patient or user outcomes
(emotional health, symptom, resolution, function and physiological health):
� Provision of clear information
� Questions from the patient or user
� Willingness to share (discuss) decisions
� Agreement between patient and doctor about the problem and the plan
Communication also has relevance in terms of the knowledge that the patient or user
brings to the consultation; the recognition that patients or users are also experts and
that lay knowledge is valid needs to be accepted. Both professional and lay
knowledge are needed to manage illness successfully (Coulter 1999).
Partnership and Decision-making
There is a wide literature on the different types of decision-making in a consultation
(Guadagnoli 1998). For many decades, the dominant approach to making decisions
about treatment in the medical encounter has been one of paternalism. In recent
years this notion has been challenged by doctors, patients, medical ethicists and
researchers who advocate more of a partnership relationship between doctors and
patients. In broad terms, three models of doctor-patient interaction have been
described – paternalism, informed choice and shared decision-making. (Elwyn et al
1999). ‘Shared decision making’ describes the middle ground, but exactly how the
principle of ‘involving’ patients or users resonates with practice has not been
explored (Guadagnoli 1998, Elwyn 1999).
A qualitative study by Elwyn et al (1999) explored the views of general practice
registrars about involving patients in decision-making and to assess the feasibility of
using the shared decision-making. The barriers to sharing decisions included a lack
of available information, the nature of the decision with different decision-making
17
approaches required depending on individual circumstances, and issues around time
and timing. However, although not all patients or users will want to take control, it is
still important that their concerns, desires and values be incorporated into decisions
about their health care (Guadgnoli 1998).
Time
In order to fully endorse a social model approach to health care, there needs to be
the time and willingness for this to happen which can be against the capacity of the
system. In a typical eight minute consultation how feasible is it to determine patient’s
or user’s preferences and sensitivities and provide full and unbiased information?
(Coulter 1999). Lack of time was cited as a barrier to sharing decisions by general
practice registrars (Elwyn 1999) although it was agreed that ‘sharing a decision is a
process not an event’.
Time is especially important for certain groups. Having an extended time frame is
important for those whose first language is not English (Peberdy, 1997). For
disabled people, particularly those with communication difficulties, time may be
required. For people with emotional difficulties, time may again be required to get
through the issues in a consultation.
The importance of inter-personal relationships
We previously discussed the importance of inter-personal relationships (Mackenzie,
Lawson and Mackinnon 2001). Examples were provided of the value and importance
of staff who were understanding, listening, non-judgemental, helpful and supportive.
The importance of time to allow communication (both listening and speaking), trust,
compassion, understanding, confidence and care to be displayed were seen as
important ingredients of the collaborative relationship between service users and
health care providers in women’s health centres (for example West 2000).
An Australian qualitative study involving interviews with lay people about their
experiences with medical practitioners over their lifetime (in Lupton, 1996) found that
communication was a major factor when participants were discussing notions of a
‘good’ or ‘bad’ doctor. The majority of participants considered the inter-personal
features of doctors most important, over and above their medical knowledge or
expertise, particularly their ability to ‘listen’ and ‘communicate’, their willingness to
‘spend time with you’ and ‘talk things over’. According to the participants, trust is built
largely on communication, on a doctor having the ability to ‘draw out’ a patient as well

18
as the interest to go beyond the symptoms to the patient’s emotions and personal
relations. In this study there was resentment about doctors who did not treat
individuals as ‘real people’. This has resonance with the social model ideal of
treating the whole person and seeking to understand the wider issues in a person’s
life.
Consistency of care
An ethnographic study of patients with human immunodeficiency virus/acquired
immunodeficiency syndrome (HIV/AIDS) in Lothian found that people wanted to see
the same general practitioner, and that the GP-patient relationship was valuable for
being familiar and ongoing. As with people with HIV/AIDS, different aspects of care
are likely to be important to people depending on the problem they need to deal with
and the context of their life circumstances (Adam and Guthrie 2001).
Outcome
Outcomes are consequences of care and may be influenced by structure as well as
process, indirectly or directly. In adopting a social model of health care, there is an
emphasis on non-medical solutions where relevant and appropriate. Little has been
written about health outcomes in a social model context. Perhaps the best examples
are from women’s experiences of using women’s health centres. However, we can
pose some questions that might be relevant to the concept of a social model of
health care. To what extent did the user feel that he or she was treated as an
individual? To what extent did the user have a say on the best treatment route? Was
it a partnership approach based on shared decision making? Did the health worker
seek to find out if broader issues in the person’s life had any effect on the reason for
attendance? If so, was this reflected in the course of treatment offered?
User involvement is also an important outcome and has been identified as having
two purposes. Firstly, to contribute to the development of services that are sensitive
to the needs of users and secondly, to contribute to the empowerment of users both
in respect of their control over the services they receive and their lives more
generally (Truman and Raine 2001). User involvement is also a key part of the
process of health care.
Conclusions
In the Interim Report we discussed some of the issues raised by Scott et al (2001). It
was noted that tensions could arise in treating the varied and competing needs of

19
clients, such as in a rape case where there could be competing pressures to provide
both medical care and counselling support. A further issue was the feasibility of
implementing all domains in practice, and whether a targeted approach could be
used for particular patient or user groups. Further work is required therefore to
explore issues around the ‘appropriateness’ of adopting a social model of health care
in different environments and for different circumstances.
We have only just started to further develop some of the issues associated with a
social model of health care and there is further research required in this area,
particularly around what users expect from health care delivery and how they would
like to experience a social model of health care. The Sandyford Initiative Evaluation
findings (Users’ Voices) will make a valuable contribution to the model, particularly in
relation to expectations and experiences of health care, and ways of experiencing a
social model approach to health care. It would also be of interest to explore health
workers’ perspectives in relation to adopting a social model; by this the wider
personnel operating in a health care system and not just doctors. Thus, this is the
starting point for developing a social model of health care, and there is the potential
to undertake a more detailed exploration of all factors that will contribute towards it.

20
Chapter 3 - Aims and Methodology
The Sandyford Initiative Evaluation Framework
This investigation of users’ views is being conducted within a wider evaluation
framework for the Sandyford Initiative. It will be used by the service in addition to two
other pieces of work that have already been undertaken. The first of these is a
before-and-after patient satisfaction survey. The baseline survey was carried out at
the Family Planning Centre in Claremont Terrace, prior to the opening of Sandyford
and was followed up one year later in all the clinics within the Sandyford initiative.
This survey collected quantitative data including information about accessibility,
facilities, attitudes of staff, and the quality of service delivered. The second piece of
work was a process evaluation carried out with the aim of collecting baseline
information from key staff involved in the restructuring of services. In-depth semi-
structured interviews were conducted to gather individual perceptions and
experiences of the development and potential of the initiative including barriers to
taking a progressive approach to health care delivery. In addition to these pieces of
work there have been a number of workstreams developed around the counselling
services at the Sandyford Initiative. These have taken place in 2001 and are
continuing into 2002.
In addition to these pieces of work there have been ongoing user involvement studies
at the Sandyford Initiative, most recently during the week of Valentine’s Day 2002.
The services within the Initiative also contribute to the collection of information with
ongoing monitoring, evaluations and use of comments sheets to collect the views of
service users.
Aims of the current study
This evaluation will complement data already collected to give a further perspective
to the Sandyford evaluation framework. The main aim of this piece of work is to elicit
users’ views of the Sandyford Initiative and to add to the information presented in
Evaluation of the Sandyford Initiative, Having Your Voice Heard- Interim Report
(Mackenzie et al, 2001). The objectives of this study are:

21
� To describe users’ experiences of the more ‘intangible’ social model of health
within the Initiative
� To ascertain users’ views of good practice in terms of user involvement in service
planning and delivery.
The aim was to collect the views and personal perceptions of the social model of
health from the various user groups at the Sandyford Initiative. The study included
users from each of five services within Sandyford; the Centre for Women’s Health,
Family Planning, Genitourinary Medicine, The Place for young people and the Steve
Retson Project.
Interview Schedule Design
From a review of the literature and through discussion with Health Board leads, key
issues which could inform the development of the interview schedule were identified
in Spring 2001. The key issues arising were organised into themes for the purposes
of this study. The idea of the social model of health is included throughout the
interview, with particular reference to perceptions of staff attitudes, satisfaction with
the holistic nature of care and accessing users’ voices. The issues of access also
emerged from the literature review as a key issue when developing new services.
This interview included a number of access issues such as geographical access,
telephone access and factors which may affect people’s ability to attend the service
such as childcare and expenses. Access was also investigated in terms of the
degree of cultural sensitivity and appropriateness of language.
Users’ views on the surroundings and relationships with care givers are highlighted
as important issues in the literature review and are incorporated in this interview by
asking service users to give their views of the surroundings, both in the waiting areas
and consulting rooms, and similarly to give their perceptions of staff attitudes towards
them. It was hoped that this would also highlight any areas which could be seen by
individuals as potential barriers to receiving appropriate care or returning to a service
in the future.
As highlighted in the literature, one of the important aspects of the social model of
health is consulting with service-users with the aim of involving them in the
improvement of both their own health and well-being, and also to contribute to the
22
development of services. For this reason it was important to gather views and
perceptions on individual care. However, it was also important to seek the views of
service users on how best to collect the views of Sandyford users’ in future and how
to access those not currently aware of the services available.
A total of six key themes were included in the semi-structured interview schedule
(see Interim report, Mackenzie et al, 2001). From the results the Having Your Voice
Heard study conducted in Spring 2001 these six key themes were modified and
further developed. The purpose of this was to incorporate issues that participants
raised during previous interviews and to further describe individual perceptions of the
social model of health and expectations of health care. From this information a
modified version of the semi-structured interview schedule was designed and the
following seven key themes included.
Box 1: Key themes included in interview schedule
1. History of service use
2. Access Issues: including how individuals feel about getting to and contacting
the service, and any barriers to attendance
3. Satisfaction with surroundings: general feelings about the centre, privacy,
comfort and facilities
4. Satisfaction with health care: individual perceptions of the staff, how they
were treated during a visit, e.g. sensitivity, confidentiality, respect and
professionalism by reception and health care staff; how individuals feel about
the care they received at the Sandyford initiative, e.g. time for explanations
and discussion during consultations; communication amongst staff about an
individuals care; extent to which an individuals own views of care were taken
on board
5. Individual needs: ability to discuss aspects of life which may affect an
individual’s health, if this was encouraged, and if it is perceived to be an
important or relevant part of an individual’s care.
6. Health promotion: how information or care/treatment received has improved
knowledge of services, helped individuals to access services, helped improve
knowledge of own health and given individuals greater control of own health.
7. Expectations of the Sandyford Initiative: how it may differ from other health

23
care services; do experiences at the Sandyford meet with individual
expectations of the initiative; any additional services or improvements
highlighted by users.
A full copy of the interview schedule can be seen in Appendix 1.
Sampling
Interviews were conducted with a sample of individuals from each of the five
services. The original aim was to contact and arrange interviews with participants
from the study in Spring 2001 who had consented to take part in this follow-up study.
However, researchers were unable to make contact with any of these individuals.
Subsequently the modified aim was to obtain a sample of five clients from each of the
clinics and to conduct a focus group with one of the existing support groups within
the CWH. Sampling was purposive and was carried out over a six week period.
Researchers aimed to recruit individuals who had visited the Sandyford Initiative on
more than one occasion in order to give a broader perspective of users’ views of the
services. At the end of this period a cut-off was imposed in order to complete the
study on schedule.
A variety of methods were used to approach potential participants depending on the
nature of the individual clinics:
� In the Centre for Women’s Health counsellors employed by the centre
identified and approached three suitable participants from individual
counselling sessions or from support groups. The researcher also
approached two participants directly and the potential participants for a focus
group.
� At the Steve Retson Project individuals were approached informally in the
clinic waiting room by a ‘host helper’ who briefly explained the purpose of the
study using materials provided, and identified those who were willing to take
part.

24
� In the GUM, The Place and Family Planning individuals were approached
directly by the researchers in the waiting areas.
It is recognised that in the instances where individuals were identified by staff from
the centre this may have introduced some bias. However, this was largely reduced
by the fact that staff did approach all service users for recruitment. They did not
exclude any individual unless there was a specific reason not to do so (for example,
where individuals receiving counselling were felt to be particularly vulnerable).
Consent
Before any interview was conducted full written consent was obtained from all
individuals. A small amount of socio-demographic information about each of the
service users was also collected at this stage. This included age and service
attended. The interview consent form can be seen in Appendix 2. A copy of the
consent form with the contact details of the researcher who carried out the interview
was given to each participant. This was in order to give them the opportunity to
contact their researcher, to withdraw from the study or to put forward any queries
they may have had about the study.
Interviews
Each of the centres provided a room within which interviews could be carried out in
privacy. All of the interviews except one were conducted with the individual service
user alone. Two young women attending The Place requested to be interviewed
together. The interviews were all taped and later transcribed for analysis. All
interviews were confidential and the results anonymised. For the purposes of this
investigation the interviews were analysed thematically, and emerging key themes
identified by service.
Interview Data
Table 1 provides a summary of the numbers of individuals approached for interviews
along with the numbers who consented and those who declined to take part in the
study.

25
26
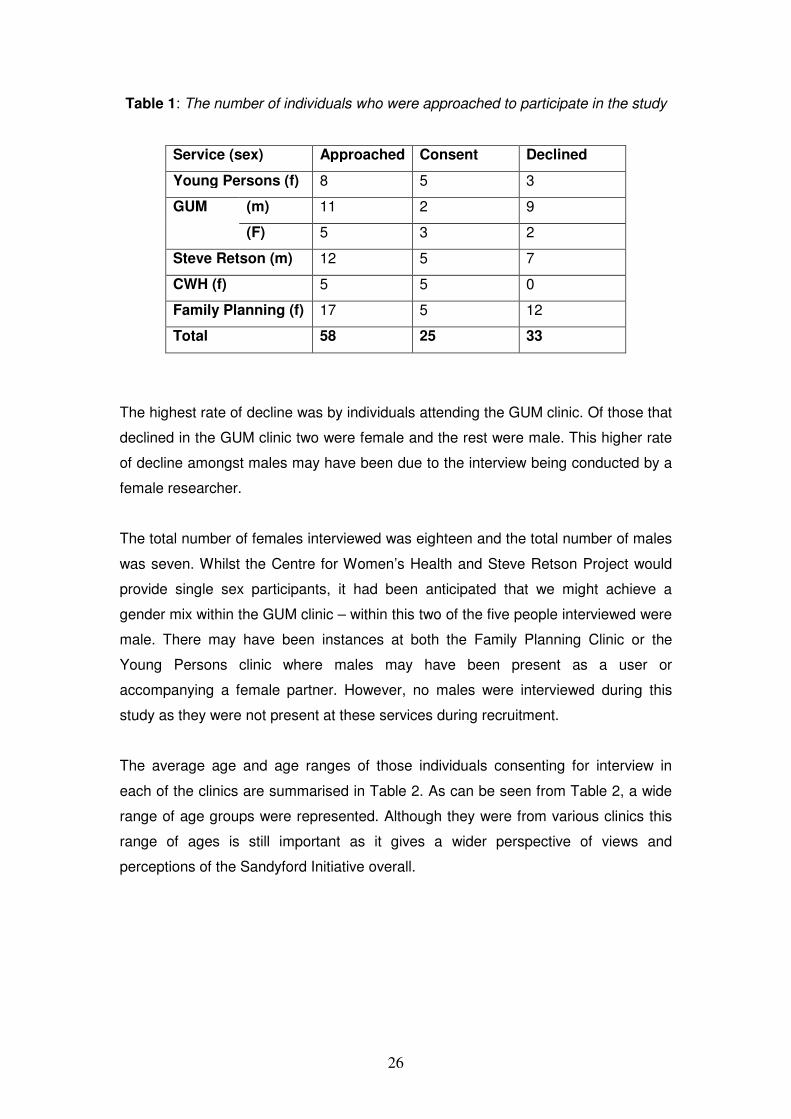
Table 1: The number of individuals who were approached to participate in the study
Service (sex) Approached Consent Declined
Young Persons (f) 8 5 3
GUM (m) 11 2 9
(F) 5 3 2
Steve Retson (m) 12 5 7
CWH (f) 5 5 0
Family Planning (f) 17 5 12
Total 58 25 33
The highest rate of decline was by individuals attending the GUM clinic. Of those that
declined in the GUM clinic two were female and the rest were male. This higher rate
of decline amongst males may have been due to the interview being conducted by a
female researcher.
The total number of females interviewed was eighteen and the total number of males
was seven. Whilst the Centre for Women’s Health and Steve Retson Project would
provide single sex participants, it had been anticipated that we might achieve a
gender mix within the GUM clinic – within this two of the five people interviewed were
male. There may have been instances at both the Family Planning Clinic or the
Young Persons clinic where males may have been present as a user or
accompanying a female partner. However, no males were interviewed during this
study as they were not present at these services during recruitment.
The average age and age ranges of those individuals consenting for interview in
each of the clinics are summarised in Table 2. As can be seen from Table 2, a wide
range of age groups were represented. Although they were from various clinics this
range of ages is still important as it gives a wider perspective of views and
perceptions of the Sandyford Initiative overall.

27
Table 2: Age (by sex) of individuals attending each of the clinics
Service (Sex of
interviewee)
Median Age Range
Young Persons (F) 17 15-22
GUM (M) 24 22-26
(F) 33 27-40
Steve Retson (M) 34 22-47
CWH (F) 48 28-54
Family Planning (F) 29 21-41
In order to try and gain a better understanding of users’ views of the service
researchers tried to recruit individuals who had been users of the Sandyford Initiative
for a range of timescales. Box 2 summarises the attendance profile of participants in
the study. Further details of service attendance at the Sandyford Initiative and
elsewhere prior to this are discussed in the individual service chapters.
28
Box 2: Summary of participant attendance at the Sandyford Initiative
Centre for Women’s Health
The six participants from the CWH had all attended the service on a number of
occasions. The time-span ranged from a few weeks to eighteen months.
Steve Retson Project
Three users of the SRP had attended for health checks between two and six times.
Two users had been attending counselling and had visited the SRP around twelve
times.
Genitourinary Medicine
One of the GUM users was attending the service for the first time, two users had
attended twice and the final two participants had attended the service on a number of
occasions.
The Place
Of the young women attending TP two were attending the service for the first time.
The three remaining participants had been attending the service for around one year
and had visited TP on a number of occasions.
Family Planning
All women attending FP had done so numerous times and had attended the service
at Claremont Terrace prior to the opening of the Sandyford Initiative. The longest
history of use was a woman who had been attending FP for seven years.
Chapters four to eight of this report now present the findings from each service and
discuss their implications. Common themes across services are summarised in
chapter nine along with a discussion of how the social model of health is being
applied and received by users of the Sandyford Initiative.

29
Chapter Four - Centre for Women’s Health
History of service use
Five women using counselling services at the Centre for Women’s Health
participated in interviews. Two of these were also attending a group. A further woman
was interviewed who was attending a group only; a modified schedule designed for
group purposes (which omitted the questions around experiences of a one-to-one
consultation/session) was used. Length of service use ranged from three counselling
sessions to eighteen months. The group user had attended five classes and was half
way through the course.
Respondents had found out about the Sandyford Initiative through a range of sources
– from GP and word-of-mouth to morning TV and victim support. Respondents varied
in terms of their use and experience of similar services. Some were or had been
receiving treatment from the GP, two had attended self-help groups previously and
others had attended counselling services in other venues.
Access and Environment
A range of approaches were used to contact the Centre initially – internet/email,
phone, calling in person and through a third person. Finding and getting to the Centre
was an issue for one respondent who was disabled and had to take two buses to
reach it. Others either lived locally or travelled long distances but felt that reaching
the Centre not an issue. In the previous evaluation, car parking close to Sandyford
was raised as being problematic. Some felt that the Sandyford Initiative was difficult
to find initially because it was not well sign posted.
The waiting time to get an initial appointment at the Centre varied from two weeks to
over four months and seemed to vary depending on the type of counselling
requested. The group respondent had waited four months before getting a place.
One respondent had phoned the Centre every Wednesday morning to try and get a
place on the waiting list:
30
The centre you have to phone on a Wednesday morning at 9
o’clock and I had to do that for three or four weeks before I got on
the waiting list, and that is just the way they run the system (CWH1)
One respondent felt very unhappy with the initial wait of between three and four
months to get an appointment:
I think it was the hardest thing I’ll tell you waiting all that time. I had
no one to talk to, discuss my problems, I was quite demented
(CWH4)
On making contact with the Centre all respondents found staff to be helpful and
friendly, although the length of time to secure an appointment was frustrating for
some. A similar picture was portrayed in the previous evaluation where there was
initial frustration at the length of time before a first appointment. The systems in place
to support women whilst waiting for an appointment, however, were regarded as
good. The phone back service (where a counsellor phones back and allows the user
to talk for half an hour) was experienced as reassuring for one woman. Another
woman had called into the Centre (without an appointment) on the advice of her GP
and was pleased that there was someone there to listen (the Listening Ear service).
Once in the system one respondent’s counsellor left to move jobs after several
counselling sessions. This meant that the user had to wait another lengthy period
(between five and six months) for an opening with another counsellor, during which
time she was severely depressed and felt that she had no one to speak to:
It is terrible you are left high and dry and I was just starting to open
up and then I was left with nobody you know and it was quite
devastating at times (CWH4)
For most users the availability and timing of appointments seemed adequate.
However, one respondent noted that because she was aware of the long waiting list,
time was quite precious, and therefore she felt she wasn’t able to take up too much
time. Issues were also raised around the timing of appointments to suit people’s
individual needs. One user, for instance, could only get an appointment late
afternoon. As she was disabled and had to take two buses to reach Sandyford, this
proved difficult for her as it meant that she would be arriving home when it was dark
31
and this posed a personal safety issue. Another had to change arrangements
because she got a new counsellor who worked on a different day. However, one
respondent felt that the staff aimed to work around the needs of the user:
They tend to try and work round you yourself, my first appointments
used to be 4 o’clock which meant I had to get a child minder for my
wee girl coming in from school, and I explained it to them and they
worked round it for me now (CWH5)
Environment
I was very anxious about coming but once I was in about five
minutes I settled (CWH5)
No respondents experienced any physical barriers to accessing services. There was
unanimous agreement from all respondents that the environment and surroundings
at the Centre were relaxing, friendly and comfortable. Respondents used adjectives
such as ‘safe’, ‘calm’ and ‘private’ to explain how they felt about the overall ethos of
the Centre. This relates well to findings in the previous evaluation where the majority
of respondents found the surroundings pleasant:
I call it the little house on the prairie (CWH2)
I think it’s very relaxing, it’s very private and the people in the place
make you feel so welcome you know (CWH4)
The warmth…quite big sofas, it’s lovely and clean, it’s private, it’s
not noisy, it’s not people bashing about the place, it’s not like you
know when you go to the doctors you walk in you smell the doctor
don’t you, you smell the hospital, it’s like walking into somebody’s
nice wee lounge (CHW5)
The privacy of the waiting area was also regarded as a key feature of the Centre and
was compared to the waiting areas in doctors’ surgeries - “I imagined like sitting in a
big doctor’s waiting room you know with people, [but] it is so pleasant, so private you
know” (CWH5). Although the seating area was described by one respondent as

32
being quite small, another noted that it was always relatively quiet so you were never
in a situation where you were crammed in with lots of other people. In relation to the
Centre’s place within the Sandyford Initiative, another respondent was pleased that
there were no big signs or notices saying where the service was, as this was viewed
negatively in terms of the stigma associated with attending such services. This is an
interesting contrast to users’ experiences of other services at Sandyford and the
desire for clearer sign posting.
Some respondents also noted that they felt safe in view of the fact that it was a
women only space:
I feel very safe in the surroundings. The fact that there are no men
around is a great idea to make you feel safe (CWH1)
Perceptions of care and support
General perceptions of staff at all levels at the Centre were regarded in a very
positive light. Unlike findings from the previous evaluation, none of the respondents
had experienced any negative encounters with staff:
Very friendly, they go out of their way and they can’t help you
enough (CWH4)
The receptionist sort of showed me where everything was and just
sort of said mull about and make yourself feel at home, so basically
I did (CWH3)
Users’ perceptions of the care they received frequently related to their expectations
of previous experiences of care in other settings. Most felt that the Centre for
Women’s Health offered something different from more medical approaches offered
by GPs. Indeed some of the women had already been to see their GP in relation to
the reason they were attending the Centre:
[been] trying to get on the system for such a long time. I had a
previous traumatic experience which the health service did not give
counselling for and I had a couple of interviews with doctors but it
33
was not to give me support or counselling it was to give me medical
treatment…(CWH1)
Time is a crucial element of the care that users receive at the Centre. Some
comparisons were made with the time allowed for a consultation with a GP and the
time given in other settings. As well as having a one-hour counselling session, there
was a feeling that staff in the Centre took the time to listen, it wasn’t a case of being
rushed in and out:
They have got more time for you and you are not getting a
prescription, they understand you, it’s private and confidential, it’s
comfortable, other women (CWH2)
She listens and in a lot of major problems you don’t have people
who will listen to you and she listens, she takes time, she is like
your best friend (CWH5)
Although being ‘given time’ was seen as a positive feature of the Centre, some
respondents felt that a one hour session was often not long enough to get through
everything. Others mentioned that one hour was a good balance as your needs for
counselling varied from week to week:
Yes you would like more time because you are in such a waiting list
and there are so many people here, at the moment I am here once
a fortnight because the second one is for a group, so if you are cut
short that week, you think I am not going to see her for two weeks
(CWH2)
‘Being believed’ was also raised as an issue. This was in relation to the way one
woman had been treated previously in other services; as she did not present with a
recognisable medical complaint she had the impression that her concern was not
valid. Some respondents felt that most doctors do not fully believe or understand you
if you have a mental health problem, and they can be dismissive of such concerns:
When you go in whether you have got a sore leg or a sore knee
you always go and get a wee bit of paper, that’s your cure the wee
bit of paper and you go to the chemist. When you come here they
34
are so understanding, for about the first six months every time I
came in here I was in tears and you can just feel the warmth. You
don’t have to have a bandage, they understand your mental health
problems…(CWH2)
I mean you go to your doctor and you are only allowed about ten
minutes there, you can’t speak about everything, about how you
are feeling and when I got this counsellor I thought it was great she
believed me (CWH2)
It’s so cold in a GPs and you are just a number, you are in and out.
Here they make you feel special and you feel that even if you are
the lowest of the low, I have seen some very depressed people out
there, they make you feel very warm and caring (CWH5)
The Centre was also seen to be more open and non-judgmental than other services.
Respondents felt that this applied to all staff at the Centre, not just the counsellors:
It’s a far more open atmosphere, it appeared less judgemental than
other places, everyone seems nice and they are not interested why
you are here if you know what I mean, it’s just kind of you’re
welcome here and it doesn’t really matter why and no-one seems to
be nosey or anything (CWH3)
[compared to experiences of using other services] it is more
welcoming and it is accepted that you have got a right to be here,
and they are not really trying to shove you back out the door
(CWH3)
A concern was expressed in relation to confidentiality. Although one respondent felt
assured that she was being treated in the strictest confidence, because she was
revealing so much about herself then she was slightly concerned that this information
was open to others, even if this meant the counsellor’s supervisor or the wider
system:
35
That was the only thing that worried me, the confidentiality, she has
to talk to someone and the boss but other than that she’s told me
it’s confidential (CWH4)
Another respondent felt that it was reassurance of the confidential nature of the
service that enabled her to be completely at ease and open with her counsellor:
I think the confidentiality thing you know, that clinches it for you
(CWH5)
Three respondents used a group at the Centre. In relation to expectations of the
group, one respondent felt the group was not meeting her needs. She had expected
the group to be practical rather than supportive:
It’s not what I expected, I thought it would be totally different, I
thought it would be more to do with how to cope if you have got low
self-esteem and how to go about it, but this class is not like that.
We just talk about our problems and it is not really telling you how
to cope (CWH6)
Despite these comments, the user had still enjoyed attending the class and enjoyed
certain aspects such as the social interaction aspect and hearing about the ways
other people have coped to overcome situations in their lives. Other respondents
who used the group found it beneficial, for instance through the sharing of
experiences and mutual support:
What is good you realise going to this class, we have all got
problems you know you think you are the only person in the world
that has got a problem because you’re looking outside, it is a
fabulous thing. I hope they do more classes like self-esteem,
confidence building, assertiveness (CWH4)
36
Wider issues
There was recognition that a range of issues – relationships, work, children, money -
are brought into the counselling session at the Centre and that time was required to
discuss some of these issues. This was contrary to the service offered by most GPs:
…he’s a pretty young doctor I’ve had him two years now and he
knows what I have went through from the beginning and he has
sometimes spent twenty minutes with me and I am embarrassed
because he has got a big load of people waiting and he won’t rush
you out the door, but then other doctors when I don’t see him they
have got me in and out in two minutes…but [anyway] he wouldn’t
have time for all these issues that you could get to talk to in a place
like this (CWH4)
The Centre for Women’s Health has a history of adopting a social and holistic model
of health. At the same time one of the aims of most types of counselling is to take
into account the wider things happening in a person’s life. Furthermore, the
Counsellor Service in the Centre is underpinned by a feminist analysis and
understanding of women’s position in society. From this perspective, therefore, taking
into account the woman’s ‘whole person’ should be an intrinsic part of the service
offered. In this section of the interview we aimed to understand whether respondents
felt able to discuss the wider issues in their lives, and to what extent they felt this was
an important or relevant part of their health care.
One respondent was aware that there were many things happening which were
affecting the way she felt, yet at the same time saw this as being quite separate to
the actual counselling session – if she discussed these things (“junk”) then there was
less time for the counselling:
Time is of the essence you know sometimes I have a lot of things
that I feel I have to off load which doesn’t leave any time for her to
instigate any form of counselling (CWH1)
I feel that I need to off load junk before I get down to the nitty gritty,
whereas I sometimes get the impression that [the counsellor] would
37
prefer that I left that at home and got on with the initial [counselling]
(CWH1)
Another respondent recognised the importance of the wider perspective and saw this
as an important part of her care, yet felt at the same time that the counsellor kept her
focused and prevented her from going off too much off course:
Yes I rabble on about work quite a lot and stuff like that and she is
quite open and sort of discusses anything. If she feels like you’re
going off on a tangent she will sort of hem you in again but you can
talk about anything, yes (CWH3)
I think most of the concentration is on the reason why you are here
but without constantly checking on other things as I go along then it
would be pointless (CWH3)
It seem that on the whole a flexible approach is adopted. One respondent spoke
about having the choice to discuss things. You are not under any pressure to give
everything about yourself, and what you choose to give will depend on the way you
are feeling, yet there is the freedom to discuss wider issues if you choose:
I think just opening up and being honest about how you are feeling,
for me it works to speak about everything…you are not under any
pressure when you come here and if I only wanted to speak about
one thing then that’s fine. As I said with me I have spoke about
everything that has happened in my life (CWH2)
Because I felt comfortable I could talk about personal issues that I
might not talk about to my doctor, you know something for women
as well (CWH4)
It does vary, how you feel yourself and have they got time (CWH2)

38
Closure
In relation to the notion that the Centre is a safe place where people can feel
completely open and relaxed, the issue was raised of moving on and extending this
feeling once outside the Centre. The respondents who had been in counselling long-
term (some were coming to the end) talked about the procedures in place for moving
on and viewed them positively whilst acknowledging that it could be a difficult
process. Most respondents were also actively engaged in the process of deciding
the best route of moving on:
If I unload, if it’s a day that you speak about everything, before if I
went to the doctors I would get medication and I would think put this
key in the door I don’t want to go in here I am so depressed. I can
look at it now, looking through different eyes, it’s just totally
changed my life and I hope that when I do become a lot better I will
still come up here (CWH2)
Information and Empowerment
The wider environment of the Centre for Women’s Health (and the Sandyford
Initiative) provides information about other groups, classes and services that relate to
women’s health needs and wider health needs. Most users were aware of things
happening from the posters, information and resources in the centre. However, few
of the users had accessed the services that were advertised, although their
awareness had been raised about availability.
[in terms of accessing services] for me personally no because I
have already got the information of where to go, but I think for
others coming without the background that I have, I think they do
supply as much information as possible related to women’s health
and wellbeing (CWH1)
One respondent raised the fact that she would like to know more about the
Sandyford Initiative and felt that there was a lack in terms of promoting classes:
39
I don’t really know much about the centre because I haven’t really
used it before, I have only really used the library but I would like to
know more things that go on in the centre (CWH6)
The library was seen as an excellent resource by one respondent:
They do go out of their way to try their best to try and accommodate
you. There are so many interesting books, you wouldn’t get them in
the library or if you did you wouldn’t see them, what I like is what
they have got under headings and I can go straight to that heading
(CWH4)
In discussing how users’ experiences at the Centre had changed the way they felt
about themselves and their health, some agreed that they had moved forward since
attending services there:
I am a bit more confident, not 100%, but I am a bit more
confident…when I came here I could say how I was feeling, why I
was upset and there was somebody there to listen, they believed
what I was saying, what was going on in my life and it has made a
big difference to me… (CWH2)
It is always better pouring it out to someone else anyway instead of
keeping it to yourself so in that sense it has been quite cathartic
(CWH3)
Other respondents were less clear, or felt that it was too early to tell:
Well I don’t think I am progressing but she thinks I am and other
people think that I am, but I have to see it myself, but I probably am
because a year ago I would never even be sitting here I was crying
all the time so I probably am (CWH4)
I think I still feel the same but I like coming to the group and quite
enjoy it (CWH6)
40
One respondent felt that her experience at the Centre had made a very positive
impact on her life:
Fantastic, I mean I’ve been ill for three years and the last six
months I’m a brand new person… I feel like I am a person again,
where I used to run after everybody else it has made me take stock
of my life, to know that I am an individual (CWH5)
Summary
Findings from the interviews compared well with those in the previous evaluation of
the Sandyford Initiative, although we managed to delve further into some of the
issues raised. The majority of respondents had positive experiences of using the
Centre for Women’s Health and most felt that this had helped them move on in some
aspects of their lives. Some respondents had experienced previous negative
encounters when seeking help, for instance not being taken seriously or believed, or
feeling that they were dismissed because they had a mental health problem which
could not be medically labelled. In view of this, experiences at the Centre for
Women’s health were viewed in a new light. Positive features were identified as the
safe, private, relaxing and comfortable environment, treatment by staff in terms of
respect and a non-judgemental approach, and having the time to be listened to. The
Centre adopts a holistic approach to health and most felt that they could discuss the
wider things happening in their lives, yet there was no pressure to do so.
Some of the key issues raised include:
� Centre for Women’s Health is seen as a service in its own right. It is unclear
whether people regard the Service as being within the Sandyford Initiative or
as part of the Sandyford Initiative.
� The length of wait to see a counsellor was problematic for some users; some
had been on the waiting list for several months which was particularly difficult
in times of crisis.
� One respondent expressed a concern regarding assurances about
confidentiality.
� Provision of information prior to attending a group (re. aims and content)
could be beneficial for some, as one user felt that the group she was
attending did not live up to her expectations.

41
� More classes for self-esteem, assertiveness, confidence building, anxiety and
depression, and the provision of alternative therapies such as aromatherapy
and homeopathy, were raised as suggested ways of improving services at the
Centre.
� Some felt that services at the Centre were not well promoted and that more
people could benefit from them, yet it was acknowledged that there was
unlikely to be the capacity to meet this need.
42
Chapter Five – Family Planning
History of Service Use
Of the five women interviewed, three were attending the Family Planning Clinic whilst
two were attending one of the specialist clinics1 within Family Planning Clinic
(Colposcopy, Medical Gynaecology). The length of time these women had been
using the services ranged from three visits in the space of a month to eight years
(which includes the services which were available previously at Claremont Terrace).
Four of the women had previously used the service at Claremont Terrace whilst one
woman had been referred to the Sandyford Initiative by her GP. Only one woman
had used services other than Family Planning within the Sandyford Initiative, the
Genito-Urinary Medicine Clinic.
Some of the women had decided to use the services at the Sandyford (and
previously those at Claremont Terrace) because of negative encounters with health
professionals elsewhere:
You know the reason why I came here was I didn’t particularly want
to discuss this with my own doctor because she is patronising and
you know I am not going to be patronised by a doctor. (FP 2)
For one woman in particular, previous experiences had been particularly worrying:
They must think everybody has got a mammy at home who knows
the ins and outs of everything you know, but that isn’t the case with
me, every time I left, I was worried about the worst case scenario
which was thinking that I had cervical cancer. (FP 1)
A couple of the women chose to use the services offered at the Sandyford Initiative
because they believed they were being seen by experts in the area of family
planning:
1There are five specialist Family Planning clinics: Colposcopy, Medical Gynaecology,
Psychosexual, Vasectomy and Menopause.
43
[Although] I have a good doctor now – this is what they do. This is
what they are most knowledgeable with and the important thing is
to come for guidance here all the time. (FP 2)
Access to the Sandyford Initiative
Physical Access
In general those interviewed reported little difficulty in accessing the service choosing
either to walk or drive to the clinic, although one person mentioned that parking could
be a problem:
The only problem is parking here. I was half an hour late recently
because I couldn’t get parked and I tried to get parked and just
zoom in and get it like car wars (laughs) access isn’t so good for
parking. (FP 3)
One woman felt that the signposting at the entrance was a bit confusing:
It’s a bit confusing because when you come in the first place you go
to, is it the meeting place for the young people? I think that is really
confusing, there should probably be a central reception to guide
you” (FP 3)
Facilities/services
A fundamental aspect of employing a social model of health care is to ensure that the
facilities and services provided meet the needs of individuals. One woman felt that
the clinic provided a service that was more easily accessible than other services:
Well I think it is positive in that, I think that you know when young
people come in they get free condoms and you get advice. I don’t
know how much they use that younger people but, yes I think there
is a lot less sort of red tape involved in going through a GP for the
same information. (FP 4)
44
Childcare was only an issue for two of those interviewed although this did not hinder
attending appointments as alternative arrangements were made. However neither of
these women was aware that a crèche facility was available to them at the Sandyford
Initiative.
One woman raised the issue of patients being offered the choice of non-medical
treatments, although these had not been offered to her:
It is quite common for a lot of women to have menstrual problems
when they are having emotional problems. The two are quite
closely linked and especially if everything looks normal, you know,
and a person is continuing to have physical problems, well, yes,
why not have a counsellor. (FP 3)
Availability and Length of Appointments
None of the interviewees had any difficulties in making appointments to be seen at a
clinic and all reported that they arranged this by phoning the clinic in advance.
I always make a telephone call. They are fine, they are all fine.
(FP2)
Most of these women were satisfied with how quickly they were taken for their
appointment. One woman had noticed a difference between daytime and evening
appointments, having experienced a longer wait in the evenings. Another commented
that she expected to wait if she used the drop-in clinic and that she usually made a
fixed appointment for this reason. However one woman had been kept waiting for a
fixed appointment on a number of occasions:
I don’t mind waiting like five, ten minutes, but I get annoyed when it
is like an hour or an hour and half sometimes. I just think, why
have they made these appointments? (FP 4)
One woman had been kept waiting during an appointment which she found
disturbing:
I had waited at least twenty to thirty minutes and I thought, have
they forgotten about me? (FP 3)

45
There was general satisfaction with the length of their consultations:
I don’t feel you are rushed out, they are usually quite quick, but…I
go in wanting to be in and out anyway. (FP 4)
All these women felt able to ask staff questions, although one woman commented
that she was aware that the staff’s time was limited:
…and where you can ask a question and you feel, I had better not
ask another one, you know. But I do anyway, I remember to, but
some people might not. (FP 3)
Only one woman reported feeling rushed and she felt that this was due to her arriving
late for an appointment.
Satisfaction with Surroundings
It is recognised that the environment of a clinic should be comfortable and make
people feel at ease. The women interviewed provided for the most part positive
comments about the surroundings at the clinic. The atmosphere was felt to be
welcoming yet professional:
Yes I think its trying to be a bit more informal for a start, so it is
more user friendly, people want to come, it is trying to have a kind
of relaxed, obviously professional environment. (FP3)
One woman compared the surroundings favourably to those of a previous experience
elsewhere:
It’s a lot calmer. I was flung in a visit room like this in the (hospital);
there was probably about 14 chairs and it was full, crammed full.
(FP 1)
Most of the women interviewed felt that they had enough privacy, although one
woman did feel that this wasn’t always the case:

46
Yes I mean they do shout, because they have got to shout. The
only thing where you would say, I hope she doesn’t shout my
details across the middle of the room, but that’s all. (FP 2)
When asked to consider issues around safety none of these women felt these to be
relevant to them.
Perceptions of patient-centred care
The expectations of women using the service are important in gauging whether the
social model of health care used is one that women appreciate or want. Most of the
women interviewed expected a professional service and in the main felt they
received this at the Family Planning Clinic.
I mean it provides a very useful service, very professional and that’s
what it should be. (FP 2)
Providing a service that was pleasant and welcoming was also viewed by these
women as being important and again something which they felt was provided:
I would expect to sort of get, I don’t know, a sort of friendly service,
making people comfortable and they always do that. (FP 4)
One woman had firm expectations about confidentiality:
Confidentiality, that’s the biggest thing I think and you get that here,
you definitely get that here. (FP 5)
However, one woman described how when having a smear, her request to see her
cervix was met with discomfort by the health professional treating her, something that
the interviewee was surprised at given the type of service she was using:
I asked if I could see my cervix and I actually thought they would be
able to let me see my cervix, but she said, ‘oh no we can’t do that’,
and seemed a bit flustered. And I thought that was a bit unusual
47
because especially in a place like this I thought they would be
prepared for that. (FP 3)
One woman reported negative past experiences in services provided out with the
Sandyford Initiative. However she described her experiences at the clinic as being
completely different and positive and comments on how her expectations of what a
Family Planning of service should offer have altered:
Came here and it is just day and night … I just feel as if I have got
more control…I now realise that this isn’t the way people are
treated. (FP 1)
Perceptions of Staff Attitudes
The approach taken by staff will very much determine whether women feel
comfortable and able to talk to them. All the women provided a very positive account
of the staff they encountered at the Sandyford Initiative. The reception staff were
described as friendly and pleasant. Within consultations staff were also considered to
be friendly as well as helpful and professional:
She asked me before the treatment and after the treatment, was
there anything that you want to ask me. And basically she had
covered every angle, so therefore I didn’t have to ask her anything
so she had done her job most efficiently. (FP 1)
Those interviewed felt that they were treated with respect:
Yes they are never nasty to you or make you feel uncomfortable or
anything. (FP 5)
Staff were also described as being discreet:
I feel much more comfortable coming here, you know, no questions
asked, you just kind of feel, get your smear test or whatever. For
me that’s quite comforting. (FP 4)
All those interviewed commented on how the staff made them feel comfortable:
48
...they make you feel at ease, very comfortable. (FP 5)
A couple of the women who had had bad experiences in the past commented on the
staff’s ability to address their anxieties:
Because the very first time I ever came in they made me feel totally
at ease, because they are picking up on your body language, they
know that you are anxious about this, you know. (FP 1)
The Consultation
Most women reported that the health professional they consulted with had introduced
his/herself. However one woman could not say with certainty whether they had or
not. However for all the women, the health professional’s manner was more
important to them:
No, but I know her from the last time I was here and she
remembers how anxious I was. Her name is not important, just that
she dos her job efficiently. (FP 1)
There were mixed views regarding the issue of continuity of care. The importance of
seeing the same person was felt by two participants to be unimportant whilst it was
felt to be important but generally unfeasible by one woman:
Because it’s unrealistic you never see the same person twice, so
you don’t build in the sense that you build a relationship with your
doctor, you don’t build a relationship here because I haven’t seen
the anybody twice. Em, because it’s routine I don’t mind (FP 2)
Yet the same person believed that it would be important to know the member of staff
if a less routine, more serious problem was being dealt with:
…But I think if I had something wrong, like say for instance that I
had something that was wrong then I would want to get to know the
person that was dealing with me. (FP 2)

49
Two of the women had seen the same person on more than one occasion, although
this was believed to be a chance occurrence. However for one of these women it
was felt to be important:
The first time I came in it was the colposcopy thing which was
obviously my main concern. It was the lady who dealt with me
today and it was good to see her face again, because I think that it
is pretty tough sometimes. (FP 1)
Most women felt that the staff took time to explain things and answer their questions.
… they do explain it. (FP 5)
The one exception to this was one woman who felt that the explanations she got
were inadequate and that assumptions were made about what she understood, when
in fact she felt she did not understand why things were happening:
…what is polycystic, you know. I was a bit panicky to ask at the
previous appointment, but I did ask her … and she pointed it out,
what the ovaries look like as they are, but it was nice for her to
explain all that to me, but I didn’t know what to ask. (FP 3)
Information
Providing information and an opportunity to ask questions and be a part of the
decision making process is one way of ensuring a patient-centred approach is
applied. Most women felt that they got enough information and that things were
explained to them:
The pill that I am taking…there was a few years ago a lot in the
press about it and again we would have a long conversation
explaining the pros and cons of being on that particular type of pill.
So I always felt that when I needed information I got it and I got
very objective information. (FP 2)
However this experience was not one shared by another of those interviewed:
50
I mean I was asking about polycystic ovaries because they were
suspecting that, and she said, ‘oh your scan looks normal’. What’s
normal? What does that look like? And she tried to explain to me a
little about that later. But initially when they said we will give you a
scan because it might be this, she didn’t really explain what that
was and I thought, my God what is that, you know. (FP 3)
Holistic Approach
In order to employ a social model of health, it is essential for staff to provide patients
with the opportunity to discuss issues that are relevant in the wider context of their
lives. These women differed in their opinions as to whether staff should take this
more holistic approach to health. One woman felt that this would have been useful
for her:
I know they are not here to treat you for that but it would be a lot
easier if there were people like this. (FP 1)
For most women discussing social issues that might impact on their health had not
arisen within consultations and some felt that this was not why they used the service:
It has never really come up. I wouldn’t have thought of bringing it
up. If there were things in my life, if I was having a problem, I would
normally go to my doctor. (FP 4)
Another woman felt that the opportunity to discuss matters was there if she wanted to
take it:
I am not one to start discussing my sexual relationships…but I
would probably be happy doing that here than anywhere else
because they are not going to be judgemental. (FP 2)
However, one woman described how only the clinical aspects of her care had been
dealt with (not only at Sandyford but also prior to her referral) something she was
clearly unhappy about:
51
Yes it is sad in a way because obviously what triggered it was
emotional and they never really touched on that, especially now
that they have checked everything and everything is fine.
Obviously it was emotional and your emotions will cause your
hormones to rise up and down and cause upset in lots of different
body systems but you know, they never even asked me. (FP 3)
One of the positive things that some of women talked about was the personalised
approach taken by the staff towards their care:
They are more educated, they treat you as an individual, they have
got time to talk to you. They are reading your body language from
the minute you come in the door and they are putting you at ease.
(FP 1)
Feelings about own Health
A few women felt a greater sense of control over their own health as a result of their
experiences at the Sandyford. This was largely to do with knowing what was
happening and being aware of the options available:
Yes a bit. There was a thing I was talking to her about today,
something I have been wondering about for a while and now I know
that upstairs, [there’s] somewhere you can actually go and find out.
(FP 5)
Most of those interviewed did not feel that they had a greater knowledge of their
condition as a result of using the Family Planning clinic. For a couple of women this
was because their appointments were routine visits to collect the pill. However one
woman searched for further information elsewhere about her condition in order to
provide her with what she felt was sufficient information to ask the ‘right’ questions:
I was a bit, not in shock, but I was kind of taken aback and I didn’t
really know what to ask and then I went and I did some research to
tell me what to ask by the time I went back. (FP 3)

52
Satisfaction with Services and Treatment
All the women interviewed expressed high satisfaction with the service provided:
…And especially getting the scan, it was really quick, I thought I
would have to wait months to get a scan, months to get a result, but
it was really quick. I got the scan, I got the result, I got the follow up,
it was all very quick. I thought that excellent. (FP 3)
However despite one woman’s bad experience whilst having a smear at the
Sandyford, this did not discourage her from using the service again:
The person who is going to be with the doctor had seen what the
first person had done so they would naturally know what state I was
likely to be in for that one and the second one was completely
different, but she was just spot on. She knew what she was doing.
(FP 2)
Recommendations for Improving the Service
On the whole, those interviewed were happy with the current service. When asked
about any changes they might recommend making to the current service, most felt
that the service was fine as it was:
I don’t think I would improve anything. It is pretty good the way it is.
(FP 5)
However a couple of women suggested a few improvements. One woman felt the
issue of long waiting times needed to be addressed. Another felt that the services
offered at Sandyford should be advertised more widely:
So they need to get their information out there, about times,
appointment times and drop-in clinics. But not just here, if you don’t
know this exists, how are you going to find out? It needs to be
hospitals and doctor and GPs and health centres. (FP 3)
53
This woman also felt that the medical staff should provide more unprompted
information:
…Doctors I think could be aware that patients would like to know
more and they should be more willing to come up with information
even without having to ask. A lot of the times people are afraid to
ask, because they don’t know what to ask. (FP 3)
Most of the women stated that there were no other services they would like to see
provided by the Sandyford Initiative in addition to those currently provided. Only one
woman said she would like to see alternative therapies:
The complimentary therapy that would be good because people are
interested in that, people would take than on board. (FP 3)
Summary
The general satisfaction reported here reflects those of the findings in the previous
evaluation of the Sandyford Initiative (2001). It is clear that the aspects that most
women appreciate are very much a part of the patient-centred approach taken by the
Sandyford Initiative. In the main, the respondents felt able to access the services
available to them and most women felt happy with the length and availability of
appointments. These women were very complimentary about the surroundings
describing them as friendly and relaxed but also professional. Participants had clear
expectations of the service; that it was professional, welcoming and confidential and
these were largely met. As with the findings of the previous evaluation, the
participants were positive about the staff and their professionalism. Furthermore the
women made many references to the ability of the staff to make people feel at ease.
Most participants felt that the staff provided enough information, explained things well
and took time to answer questions. Being informed of what was happening in their
treatment and being aware of available options led to some of the women to feel a
greater sense of control over their own health. These findings reflect those of the
previous evaluation where respondents for the most part did not feel the need to
raise social issues that may have impacted on their health, but felt that they had the
opportunity to do so. Nevertheless it is clear that most participants did not see this

54
as part of the consultation process but something additional. That women do not
expect this to be part of the process suggests that the social model of health is
perhaps not being adopted in its fullest extent.
Even though women were mainly positive about the service, some aspects were
criticised. While some of the points relate to the experiences of one particular
participant they raise some general concerns about the overall social model of health
care and ‘patient-centred approach’ taken by the Sandyford Initiative:
• The lack of opportunity to see a counsellor - raises concerns about why one
user was unable to access support when counselling services are available
within the Sandyford Initiative.
• Not providing adequate explanations - despite asking questions she left the
consultations confused. This experience illustrates the importance of taking
time to explain and make sure patients are aware of what is happening
particularly in less routine consultations where decisions are harder to make
and outcomes are more serious.
• Only having the clinical aspects of care dealt with - leaving her feeling that her
emotional health was not considered nor was she asked about her views
about what the problem was. Again this experience clearly illustrates that in
order to embrace a social model of health that all aspects of a patient’s needs
must be explored and not just the physical. Furthermore, this example
emphasises how crucial it is to listen to patients.
Other issues
• Waiting times for fixed appointments need to be addressed.
• Privacy could be compromised in an open waiting area.
• Parking close to the initiative was raised as being problematic.
Suggested improvements
• Provision of more unprompted information from staff during consultations
• Provision of complementary therapies
55
Chapter Six – Genitourinary Medicine
History of Service Use
All five participants from the GUM service were interviewed individually. Two of the
participants had previously used the same service at the Royal Infirmary and had
since visited the GUM clinic at the Sandyford Initiative on a number of occasions.
Two participants were visiting the GUM for the second time. One of these users had
previously been using the Family Planning (FP) services at the Sandyford, and at
Claremont Terrace before that, for several years. She had heard about the GUM
clinic through the FP service. The final participant was visiting the Sandyford Initiative
for the first time and had previously used the Brownlee Centre at Gartnavel General
Hospital.
When asked to think about previous experiences of using health services and their
resulting expectations of the Sandyford initiative users did not express any real
expectations of the Sandyford Initiative other than thinking it would be more relaxed:
Not really. I mean I didn't, I just kind of assumed that it would be
relatively laid back and relaxed and, you know, that was based on
my experience at FP and everything. So, it was fine. (GUM1)
The only potential barrier to attendance highlighted by one of the users was the
potentially long waiting times at the drop-in services. However, having used these
services this young woman simply commented, “I know I have to come really early if
I'm coming to one of the drop in sessions, but that's just par for the course then”
(GUM1). A second user (GUM3) highlighted the same problem with the drop-in
service. She now just attends the GUM with an appointment. Users did not report any
barriers that had previously prevented them attending services at the Sandyford
Initiative. The participant who had previously been to the Brownlee Centre
commented:
I found the service in general much better at the Sandyford…I have
got a lot of good things to say. (GUM4)
56
Access to the Sandyford Initiative
Three of the five users of the GUM service had walked to the centre and access was
not a problem. One user had travelled by bus, which she found relatively easy,
compared to travelling by bus to the Royal Infirmary. This woman reported being
particularly satisfied with access to the centre. Having rescheduled an appointment
from the previous week there was no record of her appointment on arrival at the
centre, but she was still seen very quickly by a doctor:
So they saw me, which was quite good, I mean they could have
said I had to come back but the doctor saw me and I was attended
to. (GUM 2)
This same participant also suffers from Rheumatoid Arthritis (RA) but did not have
any problems accessing the centre and could use the lift whenever necessary. The
final participant had travelled to the GUM by car. Although this woman lived thirty
miles away and had to arrange childcare she did not find these to be barriers to
attending the GUM. She had not needed to use the crèche facilities at the Sandyford
Initiative, as visits were times during her child’s nursery hours. One access issue
highlighted by only one respondent was difficulty in contacting the GUM by telephone
as the line was “constantly engaged” (GUM3).
Satisfaction with surroundings
In relation to the responses given by users in the evaluation of 2001, all of the
participants in 2002 also found the general atmosphere at the GUM to be very
relaxed. This was stated by a number of the users:
I think the surroundings are fine I think they are really good, the
staff are very good, it’s very relaxed, very welcoming. (GUM5)
A second user described the GUM:
I don’t feel like I am in a hospital I feel more like I am somewhere
else. (GUM6)

57
Another of the users felt the service was very friendly and found it to be “much more
approachable than the one down in Glasgow Royal” (GUM3). The décor, reading
materials and the water machine were also highlighted by a number of the
participants as contributing to a more pleasant atmosphere. One of the key issues
highlighted was the level of privacy in the GUM. All users were satisfied at the high
level of privacy in the waiting areas and within their consultations. The presence of
separate male and female waiting areas and the attitudes of the GUM staff were both
raised as a key issue by all of the respondents:
…they seem to be very respectful that people do feel a bit
uncomfortable. Like you've got the male reception and female
reception, they address you only by your first name and you can
give another name if you want to, so – they're pretty considerate.
(GUM1)
One of the users (GUM2) had attended the GUM prior to the separation of the male
and female booking-in and waiting areas and felt that the system now provided much
more privacy for service users. Another user stated:
I think the fact that the male and the female [waiting areas] are kind
of screened off. I mean it doesn't bother me but I can understand
why it would make some people feel more comfortable, that's a
good thing. (GUM1)
Satisfaction with health care
The following responses relate to the experiences of care that the users have had at
the GUM. When participants were asked to consider the way they had been treated
by staff at the centre the responses were unanimously positive. Although the
responses by participants in the 2001 study were also mostly positive there were
some issues raised in relation to reception at the waiting area and confusion as to
whether a consultation had ended or not. Responses in 2002 suggest a more
positive overall view of the GUM by service users.
One respondent described how she had been treated:
58
I'd say really, really well. You know, they're very sympathetic and
non-judgemental… (GUM1)
All of the other users felt they were treated with respect and made to feel very
comfortable. Participants were also satisfied that appropriate language had been
used and everything well explained. This was of particular importance for one user
whose first language was not English (GUM4). Another of the users felt that
explanations were given when requested:
Yeah, I mean obviously if they do come up with something they
explain it, I usually ask if I don't understand what they're saying.
(GUM3)
When asked to describe their experiences during consultations, again responses
were positive. One particular issue highlighted was in relation to an examination:
I mean I had one, you know, especially when it was for an internal
examination, the one I had, I mean she was really good, you know,
it was very, very laid back and relaxed and that was fine. (GUM1)
The participant who suffered from RA was also positive about the way staff
responded to her needs:
Because I've got rheumatoid arthritis and sometimes I need to get a
lift here if I'm bad and they're dead good, you know, they know I've
got this illness and that…But aye, that doctor there, she's
absolutely brilliant – they've all been brilliant, they're dead nice! I've
never felt uncomfortable or anything with any of them. (GUM2)
One less positive experience highlighted was in relation to a visit to FP:
Yeah, they're quite friendly towards you and they make you feel a
bit more at ease…I've never had any problems. Apart from once in
the Family Planning Clinic when they put me in a room and forgot
about me, and about ¾ of an hour later they eventually
remembered about me. (GUM3)
59
More positive feelings were extended to the amount of time participants had during
their consultations with all respondents feeling they had enough time and had
“…never felt pushed for time” (GUM1). This is a continuation of the positive
responses given by users in 2001 in relation to the length of time they were given in
consultations. Another user expressed his satisfaction about the consultation:
Yes they are quite good at explaining exactly what’s been
happening. There’s always plenty time. (GUM5)
Participants were also satisfied that they were given plenty of opportunity to ask any
questions they had. One particular example given by the woman with RA is:
Because I've asked that doctor a lot of questions about me and my
husband and that – and she just gave me the answers I was
looking for. Like my husband came here last year with me thinking
– because I've got this, you know, maybe it's him, and he's fine, it's
only because my resistance is low because of the rheumatoid,
that's when this flares up. You know, and she's explained
everything there, she's showed us everything. (GUM2)
Users were also asked to describe the extent to which they felt their own views about
their care had been asked for and taken on board. Two of the users felt that they
were given plenty of opportunity to ask questions, but on this visit had not felt it
necessary or appropriate to express their own views. Both of these users were
satisfied with this level of interaction:
Yes they listened to what I said, I had a question for the reason for
coming here and I got what I was looking for…I felt that if I had any
questions they would be answered. (GUM4)
And the second participant commented:
I don’t know if they have asked my views but they certainly have
asked me questions round the reason why I am here. (GUM5)
Although this level of interaction with user GUM5 may not be considered as applying
the social model of health, he went on to explain that he had attended the GUM for a
60
very simple problem. For this reason the participant did not feel it would have been
appropriate to discuss further issues regarding his life on that visit. Similar views
were expressed by some of the participants of the 2001 evaluation. It is this balance
between accessing individual needs and respecting an individuals’ right to privacy
that the services provided by a centre like the Sandyford Initiative are working
towards.
A further two of the participants were also satisfied that their own views had been
considered and that staff had made them feel comfortable:
As I say, they're usually quite good at making you feeling at ease,
so I've never had a problem with that. (GUM3)
Another of the participants compared her experience of having her views listened to
at the GUM service to a visit to FP:
I remember I went to FP and I'd enquired about something…I kind
of got the impression that they were sort of discouraging me from
going ahead with it, but when I came to the GUM they were very
much, well, yeah, let's just do it. So, but that didn't come over as
sort of feeling very negative about it, I think it just maybe sometimes
happens.
The participant attending the GUM who has RA was also very satisfied that her own
views about her care and lifestyle were asked for. This will be discussed further in the
following section. All participants reported being happy with the outcome of their
consultations and did not feel there was any stage of their visit at which they could
have been treated with more sensitivity or respect.
Individual needs
The aim of this section of the interview was to see whether users felt able to discuss
things happening in their lives that might affect their health or the way they were
feeling. There were mixed responses to the question. Three of the users had not
discussed any other issues, but simply because it had not been appropriate to do so
for them. However, they did all comment that they felt they would be able to discuss
61
other issues with the staff that they had seen at the GUM. One of the users did not
feel this was the right place to discuss the wider issues that may impact on his
health:
I wouldn’t feel that this would be the place to sit and talk about
things…I thought the purpose of the Sandyford Initiative was for the
Family Planning Clinic and testing for STDs. If I wanted to talk
about other problems then I feel I would go somewhere else.
(GUM4)
Two of the participants had discussed other aspects of their lives with their health
workers, and had felt encouraged to do so due to their personal circumstances. One
woman stated:
Oh aye, there's nothing I can't say to them. I do it about my RA
which they always ask me about. I think if you were like stressed
and all that I think you could say because a lot of these things may
be like part of what you've got, do you know what I mean…they
would take it on board, aye, definitely. (GUM2)
Another woman had also discussed aspects of her home life during her consultation
(GUM3) and had received information about the services available at Centre for
Women’s Health (CWH). Although she would like to use the service she feels unable
to do so at the moment as she lives near Stirling. These last two users of the GUM
feel that the ability to discuss specific needs with their health workers was an
important and relevant part of their care and had been “very helpful” (GUM3).
Another of the users felt that it was a relevant part of care at times:
Well I think it is important to a degree but I suppose it just depends
on sort of why you're there, really. I mean there was one instance
when I came to the GUM and the interviewer asked me if anyone
had forced me to have sex, and I was quite taken aback. But I
thought well that's really good that they do, they acknowledge that.
(GUM1)
This participant was clearly not expecting to be asked questions like these. However
when she was she felt that it was important. As this woman and other users did not
62
express any real expectations of the service, through consultations like these staff
are asking different questions and raising wider issues about an individuals’ life and
health. This application of the social model of health will help to raise the
expectations of individuals and the type and level of service they can expect from a
centre like the Sandyford Initiative and health services in general.
The woman who had been advised about the services at the CWH felt that these
types of discussion were both important and relevant “…because a lot of it can be a
side kick from what's happened and in my case it has been – they have been quite
emotionally good when it comes down to being like that…and they listen to you as
well and offer you advice” (GUM3).
One user felt he could discuss other things but “I don’t want to keep them busy with
problems that I should be going to somewhere else [with]” (GUM4).
Health promotion
Three of the users of the GUM found that visiting the centre had improved both their
knowledge about their own health and also the other services available at the
Sandyford Initiative. These users all felt this had helped them to manage their own
health better. One participant commented on the leaflets available:
Well there are a lot of leaflets, they're all quite helpful the leaflets to
read. Obviously when you come the first time you don't know what
you're coming to and a lot of the leaflets explain what you're here
for and I found that quite good. (GUM2)
Another comment regarding the leaflets was:
Yeah, the leaflets, they always give you if there's something wrong,
then somebody comes in with a leaflet…and again, it's quite good,
they explain what it is and how to treat it and things. (GUM3)
The two male users of the GUM did not feel that visiting the service had improved
their knowledge. However, this was not presented as a criticism by either user and
was simply because they had found out the information for themselves prior to
63
attending the service. One of the participants did make an important statement about
the affect of his visit:
It’s made me feel more confident, I mean it’s up to me to not come
back in a sense, but I would feel no hesitation to coming back if I
should. (GUM4)
Expectations of the Sandyford Initiative
The final section of the interview asked users to consider how the Sandyford Initiative
differed from other health services and clinics they had attended prior to coming to
GUM and how this met with any expectation they may have had about the centre.
Three of the users compared their experience at the Sandyford to their own GP. One
of these participants had only visited a GP in this country and one occasion so felt
that “I haven’t got much to compare with, but yes it seems to be professional, but so
does my GP” (GUM5).
At the start of the interviews the participants had been asked to think about their
expectations of a service like the Sandyford Initiative compared to previous
experiences of health care settings. None of the users had any real expectations
other than thinking that the service would be more relaxed than the more traditional
settings. In these cases the experience of the users had met with their expectations
and users felt that the Sandyford Initiative offered a different type of service to their
own GP, for instance:
…because I certainly feel more comfortable coming here than going
to my GP about sort of sexual health issues. And with the fact that
it's specialist and you know, it makes a real difference…I think that
sort of specialist training and expertise is really needed for
something like sexual health. (GUM1)
Another user had negative perceptions of the views of some GPs:
It's a bit more personal; GPs tend to refer you to something like this
anyway because GPs don't want to know. In some case they do
and some cases they don't. The last one did and was quite happy

64
to take swabs and things, but it takes longer. Whereas if you come
here you get a result virtually straight away…So that's the good
thing about it, I'd rather know straight away than having to wait.
(GUM3)
Similar views were expressed in the 2001 evaluation when users preferred the
Sandyford Initiative to other sexual health services and their own GPs. One of the
participants in the current study compared his experience at the GUM to attending a
similar service at the Brownlee Centre at Gartnavel General Hospital. His experience
at the Sandyford Initiative was more positive than at Brownlee:
There are much more leaflets everywhere here than there was at
Brownlee, nice colourful information and stuff, and this place is
closer to the centre of town its more convenient for me to get to…I
also feel the speed of the results was much faster here as well so I
liked it here a lot more. (GUM4)
The final issue that participants were asked to consider was if there were any other
services or general improvements they would like to see at GUM and the Sandyford
Initiative in general. Two of the participants felt there were no improvements that
could be made. One user raised the issue of waiting times at the drop-in sessions:
Well I mean it's only just sort of like logistical, like it's a shame that
waiting times are so long…and this is like the drop in session,
which is unfortunate…On the grand scale of things it's quite low
down on my list [of] priorities. The services are very successful.
(GUM1)
One of the users felt that it would be good to have “…a few more magazines or
books, a bit more diverse” as the ones there at the moment were “not very
interesting” (GUM4). Other than these comments the only other issue raised was one
of advertising and PR for the Sandyford Initiative and the GUM services:
I don’t know about PR, you know, just making you aware that its
here because I was kind of told by friends and the yellow pages.
Maybe there could be more advertising at the university? (GUM5)
65
Summary
The overall picture emerging from the interviews conducted with the five users of the
GUM service is a positive one. This compares well with the results of the previous
evaluation of users views of the Sandyford Initiative conducted in 2001, and users
are still expressing a high level of satisfaction with and confidence in the service
provided.
Although initially the participants from GUM did not express any real expectations of
the service, they all found it to be a very relaxed place to be. One user had previously
attended sexual health services at the Brownlee centre at Gartnavel General Hospital
and the GUJ service at the Sandyford Initiative compared favourably with his
experience there.
No problems regarding access were raised by respondents. All found the centre
accessible, including one woman who has RA, and another who travels around thirty
miles to the centre. The surroundings within the centre were found to be relaxed and
welcoming and far more approachable than services based in hospitals such as the
Glasgow Royal Infirmary. Users who participated in the 2001 evaluation reported
similar satisfaction with their surroundings. Participants of both studies have also
expressed satisfaction with the high level of privacy in the GUM, both at the reception
area and within the consultations. The separate male and female waiting areas was
raised as an important factor in this privacy and also as an acknowledgement to the
GUM service sensitivity towards individuals who visit the service.
Whilst responses in the 2001 evaluation were positive regarding satisfaction with
health care in GUM, participants in 2002 were unanimously positive regarding the
care they have received. Staff were described as sensitive and non-judgemental and
individuals felt they were treated with respect and made to feel comfortable.
Participants felt they had plenty time within consultations and were able to ask any
questions they wanted to, in addition to which any explanations were clear and
understandable to users.
In relation to health promotion respondents reported a greater increase in knowledge
of services and health issues than they had done in 2001. Although some of the
66
participants were unsure what the Sandyford Initiative was and what services were
included, they had never had any cause to visit the other services and received all
the care they needed within the GUM. However, two of the participants were aware
of other services. one had become aware of the GUM service through attending FP,
and one was told about the CWH whilst attending the GUM. In these instances a
more holistic approach to health care was appropriate and where other services were
required they were provided.
Two users who did not feel attending the GUM had improved their knowledge of their
sexual health felt this was not a fault of the service, but simply that they had found
information for themselves prior to attending the service. One important issue
highlighted by one of these users was the increased confidence he now felt in
relation to his sexual health and attending the GUM. His visit had raised his
expectations of the service he could receive.
In relation to increasing the expectations of service users and acknowledging
individual needs a number of points were raised by the participants at the GUM:
• In comparison to their own GP services, the Sandyford Initiative had met with
their expectations and their experience had been more comfortable and
relaxed than visiting a GP.
• The provision of a specialist service was a key issue that service users felt
was better than a GP service
• The Sandyford Initiative was also preferred to other settings in hospitals such
as the Glasgow Royal Infirmary and Gartnavel Hospital.
• All users felt able to discuss individual needs, although not all felt they had
needed to. Some felt this was not the appropriate service to do that.
• Where users had discussed individual needs they were satisfied that staff had
responded to them well and they had received the advice and help they had
needed.
Suggestions for improvements
• Two of the participants at GUM felt there were no improvements to be made
to the service.

67
• The length of wait at the drop-in sessions was raised as an issue. However,
users acknowledged that this was just a symptom of a busy service rather
than a fault of the system.
• A wider variety of reading materials in the waiting rooms for users was
suggested.
• Improved advertising of the services available at the Sandyford Initiative.
68
Chapter Seven - The Place (Young Persons’ Service)
History of Service Use
Of the five users who participated in the study two were attending the service for the
first time. Of these one had heard about the service through her sister and the other
through a friend who had previously attended The Place (TP). The three remaining
users had all been using the service for around one year and had made a number of
visits. One user had previously used the services provided at Claremont Terrace and
two had been to their own GP to talk about family planning. The final two users had
not previously used any other similar services prior to attending the Sandyford
initiative.
When asked to think about previous experiences of using health services and their
resulting expectations of the Sandyford initiative two users did not have any per-
existing expectations of the service. The remaining three users all used their GPs as
the points of comparison on which their expectations were based. Two young women
had high expectations of The Place due to the fact that it is perceived to provide a
more specialist service than their own GP. As one user explained:
I would expect them to be quite sort of gender sensitive, you know,
in a way that you should but might not expect your GP to be. I think,
yeah, definitely, you know, to be quite gender sensitive and morally,
I don't know, non-judgemental I suppose. (TP3)
Another user expected TP to be more approachable than her GP service:
I think you feel a bit more comfortable because you know it's a
place especially for [young people] and that they're that used to
hearing it all the time, it's not new to them. So that's how I think I felt
a bit more relaxed than when I was going to my doctor. (TP2)
The final user of TP voiced concerns around attending her GP due to her age and
how she perceived this might affect her patient confidentiality while she was under
the legal age for sexual consent:
69
Because your GP has got the right to tell your parents or whatever.
So if you end up there and say you're pregnant, they've got to say
something to them. (TP1)
Access to the Sandyford Initiative
Three of the interviewees had reached the Sandyford Initiative by bus and two had
walked. Those who had reached the centre by bus felt it was “quite far out” (TP1)
from their homes and they “didn’t know this end of town” (TP5) but were happy to
travel there due to the level of service they received. One user had got lost on the
way and had phoned the centre to get further directions.
None of the users had had any problems contacting the centre by telephone when
they needed to. One of the users had found the telephone help line very useful and
had used it on a number of occasions for queries she felt did not warrant the time she
would use up in a consultation:
…what I've done is I've 'phoned and I've said "Is there a nurse
there and could I ask just a quick question" or ask about a service
or whatever. And they've been great, they just put you through to
the medical folk and that's good, you know. (TP3)
One of the users felt that the Sandyford initiative was more accessible for sexual
health advice than other health services:
I prefer to go somewhere like the Sandyford because I just feel that
they know, kind of know, what they're doing a bit better. So when it
comes to kind of looking after particularly like female health, or for
sexual health then I do prefer to go somewhere like the Sandyford
because I just feel…they take it a bit more seriously as well.
The only access problem raised by a user of TP was in relation to the Family
Planning service:
The reason I have come into the drop in is because it is quite hard
to get an appointment soon, there is quite a long wait. (TP3)
70
On attending Family Planning she had also been told, “…if you're under 25 just pop
across and go to The Place and that would be quicker”.
None of the users of TP had experienced any other barriers to attending the
Sandyford Initiative.
Satisfaction with surroundings
When users were questioned on their views of the environment and surroundings at
the Sandyford Initiative the majority of responses in 2002 were good, as found
previously in 2001. In relation to the actual surroundings users described them as
being “very nice” (TP1) and “brilliant” (TP4).
In relation to the privacy of a visit the general responses were again positive. All
users felt that privacy in the consultation was good:
Aye, your privacy's really good, it's just you and the lassie. (TP1)
Only one user had a slight concern over privacy in the waiting area:
I don't think you get enough privacy to fill in the forms. I think there
should be a wee booth for you to fill in the forms.
The other four users were quite satisfied with privacy. As one user explained, “…it's
not bad, I think they do their best. I think it is really difficult to have absolute privacy”
(TP3). She related her experience to when she had accompanied a friend to the
GUM service and liked the system where “…you get a number and then you actually
go round yourself and they take details and stuff. I thought that was quite
impressive”.
Overall users of TP were happy with the surroundings:
It's good, it's quite relaxed, well it's as relaxed as it's ever going to
be in those kind of circumstances. It's bright and it's airy and it's
really got quite a nice sort of atmosphere. (TP3)
71
Satisfaction with health care
The following responses relate to the experiences of care that the users have had at
the Sandyford Initiative. In relation to first contact with members of staff users were
overall quite happy with the way they were treated, although one user felt that “it
depends on which doctor you see” (TP1). Another participant described one incident
that had made her feel uncomfortable on arrival at TP:
…it's like when you go to the front desk…and I was in for a
pregnancy test and you know how you've got to do the urine
sample in the wee bottle? Well this woman shouted it out in front of
everybody and I was quite embarrassed – "Right, just go and get a
urine sample from the toilet"! (TP2)
However, this appeared to be an isolated incident as the same young woman, who
had attended TP on a number of occasions, described overall that she was “…happy
I had been treated with respect” (TP2). This relatively positive overall response was
similar to that given by respondents in 2001. Another interviewee was very satisfied
with the system on arrival at TP:
I mean when I first came I didn't have to like say what I was there
for, just my name and I didn't have to tell her or loads of different
people why you're here. (TP5)
Users were also satisfied that staff spoke to them in simple terms and explained
everything well.
They're always very careful so that I understand what's going on.
They tell you as much as you need to know, they don't kind of over
do it. (TP3)
One of the younger users was very happy with the way staff spoke to her on the
same level:
They make it as if you can understand your position in the, they talk
in the same language as you…they don’t talk with loads of medical
terms. (TP5)

72
Another of the users was a medical student and felt that she was “… was treated with
respect and the language was fine” (TP4).
The experience of users during the consultation with staff was also viewed positively.
All users felt they had been treated with respect and made to feel comfortable. As
one user highlighted:
I can't remember going and being uncomfortable or more
uncomfortable than you would be anyway, that goes for any kind of
consultation. I think the staff generally have been great. (TP3)
As with participants in the 2001 evaluation, users also felt they had been given plenty
of time in their consultation to discuss everything they wanted to and ask any
questions:
Aye, because they always ask you at the end, are there any
questions you'd like to ask? or, do you need anything? (TP2)
Users were also asked to describe the extent to which they felt their own views about
their care had been asked for and taken on board. The response was that they had
where it had been appropriate:
My own views? Yeah, I think so; I think they've been quite sensitive.
(TP3)
One of the users also described a positive experience within her consultation:
She did know what she was talking about and she didn't try to make
you do anything you didn't want to. Yeah, she let me know the good
points and the bad points of everything, she didn't just kind of steer
me towards one thing. She let you make up your own mind. (TP5)
Participants from TP were all satisfied with the outcome of their consultations. One
user who had only gone along for contraception stated:
73
I was happy to get the pill there and then, I didn’t even need a
prescription. (TP4)
It is evident from these comments by users that the overall level of satisfaction with
care in TP was high. One user described how she felt after the consultation:
I couldn’t have been treated with any more sensitivity…you don't
feel embarrassed by it, it makes you feel more, I suppose
comfortable. They don't treat you as if it's anything to be
embarrassed about. (TP5)
Individual needs
The aim of this section of the interview was to see whether users felt able to discuss
things happening in their lives that might affect their health or the way they were
feeling. All of the users from TP felt that they would be able to discuss any such
problems because “they don’t make it just like rushing in, you can talk about anything
else that could affect you” (TP5). Other users would be happy to discuss things in
future if they needed to:
If I had any other sort of problem I would definitely come back.
(TP4)
The general consensus from the users of TP who participated in this study was that
being able to talk about these other issues in your life was an important part of your
care.
I think if you want to bring things up, you know, that are relevant to
your health and the reason that you're there or whatever to put
things in a better context and that kind of, you know, if it is sort of
important and, yeah, you should be able to bring that up. (TP3)
Another of the users felt that it was an important part of your care but was unsure
where it was best to place this type of service. She was relating her experience of her
and her mother seeing a counsellor through her school:

74
They’ll have my mum in one session and then me in another and try
and work things out so they can see it from the point of view. When
you come in here they're not – I'm not really sure but I think it's
good for people who can't get that elsewhere. (TP1)
Although this young woman had been able to access the counselling services
through her school she was aware that this not be available to other younger people.
However, she was also unsure whether a centre like the Sandyford Initiative that
provides sexual health services, would be a place she would come with her mother
for counselling. This is the type of preference that is likely to vary between individuals
and a centre such as The Place is just one medium for providing this type of service.
This is likely to be a personal preference whether an individual would want to come
to Sandyford or see a counsellor elsewhere. The final user of TP felt that being able
to discuss any other difficulties with staff at the Sandyford was an important part of
the care package:
I think, well, if there's not really anybody you can talk to in your
family or your friends or anything, then it's quite good that you can
come here. You can even come here just to talk about it and I think
that's quite good, suppose you've got a problem you can get it off
your chest without telling somebody like a sister or a brother, you
know. (TP2)
Health promotion
Users were also asked to think about how any information and care they had
received at TP had improved their knowledge of services available to them and
helped them understand their own health better. All users agreed that they had been
given plenty of information. This was a similar response to that given by participants
in the 2001 evaluation who felt they had received useful information on services and
health issues. One user in the current study described how her level of knowledge
had increased:
I am more aware of my health. I'm much better aware of the
services, of the kind of things that are available to me. (TP3)
75
Another user described her experience within the consultation:
It was all very straight forward but she went through everything to
make sure I understood. (TP4)
Another user raised the point that once you’ve been to the Sandyford Initiative once
you are much more likely to go back in future with any problems as you know what is
available and how you will be treated:
But I think once they've been a few times, you are more likely to
actually go and get things sorted out. I think I'm a little bit more
aware of what's kind of going on and I am much more likely to go in
because I think once you've been in a few times you realise it's not
really that scary and everyone's very nice and they don't think
you're stupid. (TP3)
Expectations of the Sandyford Initiative
The final section of the interview asked users to consider how the Sandyford Initiative
differed from other health services and clinics they had attended prior to coming to
TP and how this met with any expectation they may have had about the centre.
Users were generally happier with the service they received at the Sandyford
Initiative. This was the case in relation to the general atmosphere and also the more
specialist treatment they could offer.
I think it's got a better atmosphere and I think the, I think the
reception staff are definitely better than when you go to your GP's
office. But yeah, I think it is a more relaxed kind of atmosphere.
And I think for the sort of things that I go for…that's where their
skills lie, that's where their kind of specialist. I just feel that they are
more specifically kind of tailored for that because they have more
experience and they're more likely to pick things up (TP3)
This more specialised care was also highlighted with particular reference to the
needs of the younger users:
76
I think it's just the people – young people do things more but they
don't make a big thing about them. But if you went to your GP he'd
be shocked. But because a lot of people come in and they're used
to, you know, young people, and it takes a big weight off your
shoulders. (TP1)
Another of the users who had previously had a physical examination at both her own
GP and TP felt that staff at TP were more experienced and made her feel more at
ease:
I think they're just better practised. You know, whenever I've had
examinations and stuff I've felt more comfortable and I've generally
– it's been a lot more comfortable because they're just, they kind of
do it the whole time. (TP3)
The general feeling amongst users was that TP was better to go to than their own
GP, “…this is far better, it's much more easy to come here than to go to your doctor
about it” (TP4). Users of TP in 2001 had also described their feelings of being more
relaxed and feeling more comfortable at the TP than at their own GP.
The final issue that participants were asked to consider was if there were any other
services or general improvements they would like to see at TP and the Sandyford
Initiative in general. The two main issues raised were waiting times and the
availability of other services around Glasgow. Two users felt there were no changes
they would make to the current service:
No, I think they've got everything that you would ever need to come
for. (TP5)
One of the users raised the issue accessing minority ethnic groups at the Sandyford
Initiative:
I've always been impressed with their kind of attitude towards
ethnic minorities as well, that come in. It's just good, the fact that
they've got, everything's kind of printed in different languages.
(TP3)
77
As raised earlier in this chapter the issue of waiting times was more in relation to the
family planning service. Although users had sometimes had a longer wait at TP drop-
in service than they would have liked, it was accepted that this was just the nature of
a very busy drop-in service. As all users were happy with the care they had received
this was not raised as a major issue for users of TP.
In relation to further services, two of the users expressed an interest in seeing the
same kind of services provided in other parts of Glasgow as TP is providing an
important service for younger people:
I think they should do this in a couple of more places like maybe in
Shawlands or like other parts throughout Glasgow that's more easy
for other people to get to. (TP2)
Other than this users felt satisfied with the care they had received at TP. As one
participant highlighted:
The staff are really good, they make you comfortable, they don’t
make judgements of you. Like, I'm sure I'm not the only person that
has come here and thought you're going to get treated, they're
going to make you feel really bad. But they don't, they probably see
it every day but I mean they don't make it as if it's another case,
sort of thing. It's a very personal treatment. (TP5)
Summary
Summary
The young women using TP all responded positively to most of the questions.
Participants were very satisfied with the service provided by TP. Some of the key
issues raised by the young women were:
• Access had been simple and the availability of a telephone help line service
had been very useful on a number of occasions.
• The service was seen by users to be more accessible than other sexual
health services.
78
• There can be a longer wait at the drop-in service, but users realised this was
just as it was a busy service.
• Participants liked the surroundings and described the centre as relaxed,
bright and having a nice atmosphere. Privacy was felt to be high most of the
time, although one user felt she would like more privacy to complete forms at
the reception area.
• Overall, participants were happy with the health care they received at TP. The
‘checking-in’ system was preferred by some users as it did not mean having
to tell a number of staff why they were attending TP.
• Participants felt staff treated them with respect, made them feel comfortable
and were non-judgemental. Users were given plenty of time in consultations
and felt encourage to ask any questions they wanted.
• Participants were asked for their own views on their care and felt staff were
sensitive to these. One user discussed how staff had not pushed her towards
any decisions, but let her make up her own mind with the support and advice
she needed.
• Users felt they were given plenty of information and it had increased their
knowledge of their health and the services available to them at the Sandyford
Initiative. Staff took the time during consultations to make sure their clients
understood everything well.
• One participant felt that visiting TP meant that she was far more likely to seek
help in future due to the service she had received there.
When asked about their individual needs participants felt they had been able to
discuss them with staff where appropriate, and all felt they would be able to if they
needed advice. Participants also felt that this was an important part of their care
package. Previous experiences of health care services had left some users with no
high expectations of TP, whilst others expected a more relaxed and specialist
service. Some of the younger women who were under the legal age for sexual
consent also had higher expectations of the level of confidentiality they would receive
at TP. All users seemed to have their expectation met, and expectations appeared to
have been raised by experiences at TP. Users were generally much happier with the
service at TP than their own GP on a number of levels.
Suggested improvements
Users raised a small number of issues for improvement:

79
• Two service users felt there were no improvements to be made at TP.
• One user raised the issue of having difficulties getting appointments at FP,
and some under-25’s being sent across to TP. This has implications for TP
staffing levels for an already very busy service.
• Two users also discussed the possibility of developing other similar service
around Glasgow, in different parts of the city where more young people may
be able to get to.
Overall in relation to the evaluation of users views in 2001, the participants
interviewed in 2002 were more vocal in their responses. The poorer response in
2001 was raised as a key issue for consideration in this follow-up study. The
responses that were given in this second part of the evaluation may have been
longer for a number of reasons:
• The individuals being interviewed were more confident and vocal than those
interviewed in 2001.
• During the interview the researcher was less ‘prescriptive’ with the
questioning and used examples relating to experiences to explain questions
further. The examples used were dependent on the individual respondent, for
instance school or work, exam pressures, problems with parents or problems
with money for those who may be living away from home.
• Another reason may have been the presence of a friend at the time of
interview for the younger women who participated. Two friends were
interviewed together, and one of the younger women who was interviewed
wanted her friend to stay with her. The presence of a friend seemed to
increase the confidence of these young women in answering questions.
These may be important considerations for any further user involvement work that
takes place involving younger clients at the Sandyford Initiative.

80
Chapter Eight - Steve Retson Project
History of service use
In contrast to the first interim report, all interviewees had prior experience of sexual
health clinics – either outside Glasgow or at the Steve Retson Project (SRP) when
based at the Sandyford Initiative and other venues.
Previous use of services other than SRP
Three respondents had previous experience of sexual health services other than the
SRP: two had taken tests at clinics in Glasgow (Brownlee Centre and Ruchill clinic);
the third had regularly attended a variety of clinics over a number of years whilst
living in England. The remaining participants had only visited their GP prior to
attending the SRP.
Use of Sexual Health Services at other venues
Three respondents had used the SRP at different locations (either Royal Infirmary or
the Gay and Lesbian Centre).
Number of visits
This varied according to which aspect of the service had been used: those using it for
discrete check-ups, testing and/or follow-ups had visited between two and six times;
two respondents were currently receiving weekly counselling sessions and had
therefore visited over a dozen times.
Reasons for attendance
A variety of reasons were cited, ranging from routine health checks and treatment of
specific complaints to the desire for simple reassurance.
[I] initially came here because my ex partner had a bit of worry
about an STD, so I came along to support him more than anything
else but I thought I may as well get everything checked out myself
[SR1]
Two respondents had also sought out the project’s counselling service for help with
life crises.
81
I have a rather robust health generally….so I tend only to come to
the Steve Retson when I have things I want resolved, such as piece
of mind [SR5]
I had a sexual health problem that I wanted to have checked out. I
had that done and there was some follow up testing needed, and
also I had a personal crisis last year and wanted a counsellor [SR3]
Whilst all interviewees openly criticised aspects of their GP visits (see below), only
one mentioned this as a factor in their initial choice to attend the SRP:
I went to the doctor, he examined me and then he put me on a
waiting list for the genitourinary unit at the hospital. I was on that for
ages, not getting very far and then I bumped into someone who told
me about Steve Retson, so I came along that following week…..I
went along, really out of desperation because I was in some pain at
the time! [SR2]
Awareness of service
Two respondents had seen the service advertised in local gay bars (the SRP
distributes promotional materials and free condoms), others had had it recommended
to them or had become aware of it through attending with a partner.
Initial expectations
Although all interviewees who expressed an opinion seemed to have difficulties
answering this question, expectations seemed to centre on the fact that the project
was solely for gay men:
I thought it would be a bit more focused on specific gay men’s or
gay women’s, well gay men’s health issues, but apart from that I
didn’t know that to expect [SR2]
I didn’t have any particular expectations no, well I guess I did, I
thought it would be tailored to be more specific because it was a
gay men’s health clinic, and I guess I felt slightly less embarrassed
about going [SR4]

82
The opinion of a frequent and longstanding user of sexual health clinics was more
definite:
Yes I did have some expectations without using words like
expectations so much, I knew what to expect - I was prepared for
the experience of going into a facility which was specifically for
sexual problems, or sexual health issues [SR3]
Access to the Sandyford Initiative
Comments relating to access were broadly very similar to those made in the first
interim report, with the majority of respondents praising the convenience of the both
the clinic location and timing of the weekly session. A small number of heavily
qualified criticisms were made regarding the making of appointments. Several
possible barriers to attending were highlighted.
Ease of making appointments
Generally, as experienced users of the service, all appointments were made by
telephone. Whilst this was described as the most ‘convenient’ method, views were
mixed as to the experience. Some respondents found it quick and friendly:
It is relatively quick, five minutes sometimes ten minutes,
depending how busy the reception is; how many appointments are
available. Yes they [staff taking calls] are very friendly and I have
never had any adverse reaction [SR5]
Others had difficulties getting through or had found aspects of the receptionist’s
manner problematic:
I telephoned and it was fairly easy, though when I called up I was a
bit confused because they asked for my patient number… They
didn’t seem very friendly on the phone, but when you come here,
everyone is really lovely. I made an appointment once more
recently and it was messed up….I probably had to wait just over a
week or so, but it’s fine [SR4]
83
It has been really difficult actually…I have got trouble keeping track
of numbers, so I expect to be able to get them from the phonebook
or the internet/ but I have noticed one of the phone numbers on the
website here is wrong, you know, and you ring it and it is just rather
embarrassing. [SR3]
The experience of telephoning contrasted with that of making an appointment in
person, which had been the initial (and very positive) contact of two interviewees:
I just came in it straight off the street….- I expected three or four
hours, but I was quite surprised it took about and hour and a half
two hours….I had forgotten I think it was my second appointment,
and they sent me a letter the next day to remind me you know
“Please come back” and that’s something my doctor doesn’t do,
you know you might wait like another month or so before they
actually get back in touch with you, but it was the next day that I got
the letter saying you know you missed this appointment please re
appoint. I thought that was quite good [SR1]
I actually came along on spec - I didn’t have an appointment, I just
turned up one Tuesday evening, explained the situation and I was
squeezed in and that was that - I mean I was very, very impressed
[SR2]
Timing of the clinic sessions
Virtually all of the participants described the Tuesday evening session as ‘fine’,
‘pretty ideal’ and being suitable for both the ‘nine-to-five person’ and shift workers.
When asked whether other times were preferable, one respondent gratefully stated
If it was available during the day then I certainly would make use of
it when I was free, but the fact its in the evening between half five
and half eight or whatever it is, is fine. It’s good that we have got it
at all quite frankly [SR2]
Only one small limitation was pointed out relating to the difficult of cancelling early
appointments:
84
The facility is not open until 5.30pm to the public…so, if something
comes up and I have to cancel a 5.30 appointment with the
counsellor or something, by the time I have contacted [him] to let
him know that I am not going to be there, the hour is wasted and
nobody else can take the appointment [SR3]
Ease of access
General approval was given to the central and therefore (at least for this group of
users), convenient location of the service. Four out of the five men described it as
being either ‘on the way’ to work or ‘near to’ home. Three out of the five had driven
and one walked. The only problem identified related to the proximity of early
appointments to rush hour:
It took me like about twenty minutes to get here [for a 5.30
appointment] because of the traffic. I can imagine that’s a big
problem for people with regards to parking the car and it’s that five
o’clock mark - the rush hour time. It’s a nightmare. [SR1]
Barriers to attendance
Despite the fact that several respondents admitted to a degree of embarrassment in
attending a sexual health service, their repeated attendance suggested that they
themselves had not been put off by this fact. When asked if there had been any
barriers to their attendance, two typical remarks were:
Not in the slightest [SR1]
No, nothing has every put me off I have always known it was here
and I have always felt perfectly able to come along and see
somebody [SR2]
A number of subtle and revealing obstacles to clinic attendance for the gay
community more generally were identified - both explicitly and implicitly - including
cultural and generational factors.

85
Glasgow isn’t as easy a place to be gay; everyone here is aware of
that and there are lots and lots more people here that are in the
closet, and it is really important for them to have a place like this
where they can come and find these services you know another
setting that is completely different, separate from their GP. No-one
who’s in the closet is going to see their GP [SR3]
There is always that uncomfortability when you first come along -
they know it’s a sexual thing you’re coming for. I think that’s actually
taboo anyway in the West Coast of Scotland, its very much so –
you know, we don’t talk about it; we don’t even indulge in those
things [SR1]
[I’ve been] around since the time of the aids coming to the fore and
all that, my generation are more than aware of the need to be safe
[but] you forget how time has gone on and there is a new
generation - the increase in sexually transmitted diseases, you
know, lack of contraception information, lack of people using it…
people should be educated, but if you keep people ignorant it is
going to be more of a strain on the National Health Service
eventually, because people are exposed to all those things without
protection [SR5]
Satisfaction with surroundings
A high degree of satisfaction was expressed regarding the general appearance and
atmosphere of the clinic. Words like ‘bright’ and ‘modern’ were used frequently and
attention drawn to the quality of promotional artwork. These comments, combined
with both the noted geniality of host helpers and availability of refreshments, were
seen as important factors in creating a relaxing and friendly environment that helped
reduce the intrinsic anxieties of attending a sexual health clinic.
Well here it is really nice its very luxurious with all the food and fruit
and stuff its great, and its great that they have someone who sort of
welcomes you and takes you to reception and stuff because I guess

86
it could be quite intimidating, showing up and not knowing the drill.
[SR4]
Privacy and space
Whilst virtually all respondents recognised that the waiting room/reception area was
fairly cramped, this was generally seen as a minor problem, if at all. One interviewee
did find the seating lay-out and lack of space compromised his desire for anonymity
but acknowledged that this was more of a comment on the size of the local gay
scene:
It’s to do with Glasgow being so small: every time I have been here
I have seen somebody I know and they haven’t necessarily been
people I have wanted to see, not because I have slept with them or
not because they are friends of mine or whatever, it’s simply that
my anonymity is comprised…you like to keep various areas of your
life, you know, private. [SR3]
The same respondent suggested a different seating arrangement (back to back rows
of seats as opposed to the existing ‘U’ shape) but was aware that this could not
counter the stated problem effectively.
Décor, comfort, atmosphere
These aspects of the reception and waiting areas attracted common praise. Far from
being incidental, they were seen as key to promoting a reassuring and soothing
environment for worried (and perhaps first time) service-users:
It was a very relaxed atmosphere when I came in that was one of
the things that first struck me, they had tea, coffee, conversation; it
was a very relaxed environment. [SR1]
It is very welcoming and modern, tastefully decorated, quite
fashionably decorated, you know, all the things that make it
appealing; makes you come in and relax. It does its feng shui
pretty well I’d say! [SR5}

87
Refreshments
Similarly, the availability of fruit, cakes and hot drinks was much appreciated:
Well I mean when you come in there is the prospect of various
things - you could be getting probed or getting results back, and
neither of those are particularly pleasant prospects so its really
nice, it puts you at ease and I appreciate it…. it [also] kind of gives
you something to do instead of sitting looking about and trying not
to catch anyone’s eye [SR4]
‘Welcome Host’
A key part of checking-in to the service involves being greeted by one of several
volunteer ‘hosts’, who direct users to the various parts of the service, serve
refreshments and are available for general support and conversation. Users
consistently described the host(s) as ‘very welcoming’, ‘great’, ‘friendly’ and ‘helpful’:
Who wants to go to something, especially when it is their first time,
walk in not know what to do? So it’s good to feel welcomed, and it
is good for somebody to be attentive to you, making sure you have
something to eat, something to drink, it just sets the scene, and
particularly for those who are nervous, or a bit jittery it puts them at
ease. I think we would still get a good service professionally if they
weren’t here but the fact they are here is a great benefit [SR2]
Participants were also mindful of the difficulty in being both friendly and appropriate,
given the nature of some users’ concerns:
You get seen, you get checked in, they have a nice system here,
with, I don’t know what you call them, the helpers. That is an
interesting one because there are always different ways at looking
at these things you know, and it is a difficult balance to strike in
terms of people being intrusive or people being helpful you know?
But the host helper idea is obviously there to help put people at
their ease, so even if it actually doesn’t always work, the fact that
it’s there is a statement that you know this is something we’re
looking to do, so that is a major plus point I think [SR3]

88
Satisfaction with health care
Participants were consistently very positive about the service in general, drawing
particular attention to the qualities of the staff and the general effort made to make
people feel at their ease (see also previous section):
I am happy with the service, more than happy and it is a great
peace of mind to know that it is there, it’s local, it’s discreet the
people are very friendly, very professional the doctors are
extremely approachable I couldn’t be happier with the service and
the treatment I have received. [SR5]
One participant attending counselling also drew attention both to the quality of the
service and to the difficulty of obtaining it more generally in Glasgow:
Counselling in Glasgow is actually quite hard to come by…[so] this
was a good resource to turn to. [SR3]
For a number of respondents, the prime criterion of service satisfaction was simply
‘did I get well because of the treatment provided?’:
[I am] very satisfied, I mean, any kind of disorder or problem has
been satisfactorily resolved, so as far as I am concerned the
decisions that they took were the right ones because I got well.
[SR2]
Whilst interviewees echoed the concerns expressed in the first interim report
regarding the appropriateness of the informality of staff for all service-users, none
had felt their treatment to be inappropriate. Moreover, each had confidence in the
ability of all staff – from host helpers to doctors – to tailor their approach to particular
clients. This included level of formality and directness, appropriate language use and
sensitivity to personal priorities regarding time and need for reassurance vs.
treatment.
The ability to tailor the service to individual circumstances was seen as key to striking
the correct balance between informality/putting people at ease and the desire to be
treated in a direct, professional manner; both considerations inspire confidence in the
service in different ways but may be mutually exclusive. The optimal mix of these

89
ingredients were summarised by one respondent [SR2] as ‘Professional, fast and
friendly’.
Professionalism
This was one of the more frequent comments from participants and generalised to all
roles (host, nurse, doctor, counsellor, health adviser): ‘because I rate the service as
professional, anybody who sees me, I just give them that benefit of the doubt you
know - that I am going to be seen professionally’ [SR2]. An experienced service user,
who was currently attending counselling session, rated the service as more
professional than it had been when offered at the Royal Infirmary (although he did
not rate the previous service as unprofessional).
Respect and putting at ease
Respondents felt they were accorded respect; an important consideration given the
traditionally perceived ‘Doctor-dominant’ power relation of the consultation setting:
The doctor was fine, made me feel very relaxed, explained
everything and he actually made the experience humorous up to a
point… I came in feeling a bit nervous, a bit apprehensive but I
came out feeling really relaxed and thought ‘that was such a laugh
in there [SR1]
One doctor I saw was really very, very chatty. Some people I know
would be put off by that [but]…I felt that was great and I also
appreciated the informality. [SR4]
The positive role of health workers was also highlighted:
The helpers and the health care workers are very adept at putting
people at ease, and that is very important I think…[especially] for
people who perhaps are having the trauma of being diagnosed HIV
positive. [SR5]
90
Sensitivity and confidentiality
Respondents felt that health-workers were sensitive to their anxieties and expressed
problems; they did not feel that they could have been dealt with more sensitively.
Confidentiality was an issue of general concern for a number of reasons. Firstly,
anonymity was felt to be vital given the stigma and embarrassment associated with
attending a sexual health clinic. The interaction of a small local gay scene and a
cramped reception area occasionally compromised the anonymity at least one
participant (see above). Secondly, several interviewees felt that their confidentiality
was better preserved by the SRP than at their regular GP practice, because their
visits to the former would not be recorded on their GP-held medical records. This was
felt to be important in the context of the requirement to disclose details of HIV testing
for insurance purposes. Finally, despite the fact that all of the men interviewed
trusted the service, one respondent felt that the use of actual names by waiting room
staff was problematic and for this reason, used a false name. This was articulated
with a more general concern about the long-term confidentiality and potential use of
data relating to sexuality and sexual health:
Names – [I have a problem with staff] using names: when I started
going to clinics they used numbers, you were called out by your
number but, you, know there is a balance between it being
impersonal and being clinical and making people more tense
because its an anonymous thing. I also gave a date of birth that
wasn’t mine and I remember both the alias’ DOB and mine,
because you know that laws can be changed, registers can be
suddenly implemented, governments change whatever, there is no
way of saying that this is going to be confidential for your lifetime.
[SR3]
Language use
The formality of language used by health workers was felt to be pitched at the correct
level and no respondents had experienced problems either understanding staff or
feeling patronised by them. Service-users had faith in the ability of doctors to tailor
their language use to the ‘level’ of the particular client, using formal and informal
terms as appropriate. No one had experienced use of judgmental language by staff.

91
[On language use] Oh very easy - it was like banter. He wouldn’t be
too serious about it but again that might be about his experience
with patients and how to read them. [SR1]
I think some guys will come along and they might not know the big
fancy words for it and as long as the nurses and doctors are able to
judge or match their description with theirs it should be ok. I have
noticed that some doctors are a bit more colloquial than others and
it is just knowing when to use which. [SR2]
I think they respond quite well and I think that is quite important
when you are dealing with such a vast cross section of public… its
fine using some of the jargon, whatever, that you would be aware of
and studying it, but if it’s a nineteen year old you know or younger,
all of that might be over their head. [SR3]
Consultation time
In contrast to their experience of attending GP practices, participants felt that a lot
more consultation time was available if necessary. This extra time was valued and
provided the opportunity to chat, express concerns and opinions and ask questions:
And again I feel more comfortable coming here than I do with my
own GP; again the local GP would be seeing, one would imagine, a
lot more people, and again its like ‘get them in, get them out’ and
you are not made to feel like that when you come here. Its not ‘oh
there’s a customer or client, in 5 minutes, do this, administer that,
do that, take a blood test and get them out, you are not made to
feel like that. You are important enough and he values what you are
saying to give you that time. [SR1]
The doctors - they have people to see so, there is a bit of a, you
know obviously they can’t spend forever and a day with you, which I
appreciate. So I think basically I would describe it in the main as a
no nonsense, professional and friendly service. [SR2]
92
One respondent, whilst not complaining of a lack of time, was aware of the pressure
staff were under in terms of numbers of appointments and therefore tried to keep his
consultation times to a minimum:
You get you know there is no sense of being hurried, there is no
sense of not being given anything you need. [SR3]
Participation
Another distinguishing feature of consultations at the SRP related to the opportunity
for active participation in health-care decisions. Whilst most respondents recognised
and deferred to the authority and knowledge of the health professional (doctor, nurse,
health adviser), they felt that they were able to ask questions, clarify concerns and
were helped to come to a decision regarding their health. Whilst the patient-doctor
dynamic varied according to the nature and complexity of the presenting concern2,
several respondents described a mutuality of approach and a model of listening,
enabling and supporting, as opposed to being very directive:
I suppose it is mutual but if anything I would say I was leading him
[the doctor]; it was at my prompt. I would ask certain questions, I
would say, you know, ‘and how do you think it will go, what will I
look for?’ So I felt as if the doctor has been happy to kind of advise
me. [SR1]
Well to be honest I don’t know what I’m wanting so I am very happy
for the doctors to say ‘just to say take this and go away’. It seems
that if I voiced an opinion that they would take it on board but I
haven’t. [SR4]
One participant made the point that the potential for participation was limited by
‘personality’ factors, with more confident, articulate or experienced users being able
to demand more of the health professional:
I think there is a good balance between practitioners and service-
user. Inevitably the situation boils down to personality: you go and
see a professional and the professional is going to know probably
2 Being more doctor-led in ‘simple’ cases like a repeat prescription.
93
better than yourself, otherwise you wouldn’t be asking, but then
again saying that, I come from a place whereby I have sixteen,
seventeen, eighteen years of using sexual health services so I can
speak from maybe a more informed view on my own behalf. [SR3]
Individual needs
The majority of respondents felt that they could speak about broader aspects of life
that were impacting on their health although very few of the men had actually done
this with doctors or health advisers. The major barrier to this was a very definite view
of professional boundaries: problems with relationships, finances, work etc, were felt
to relate to mental well-being and therefore the preserve of counsellors; physical
health problems were taken to traditionally defined health workers (doctors). Some
respondents felt encouraged to talk about their individual circumstances, although
opinions were mixed regarding the value of this:
That’s never come up [talking about individual circumstances] but I
would feel comfortable enough to do that. [SR1]
I don’t know because I have never done it, I know the limitations,
but I know that if I was to break down and say ‘listen I am having
problems with my boyfriend’ or something, I am sure they would be
receptive to that. [SR3]
If I arrived saying I couldn’t sleep and I was having pains in this part
or that part of my body whatever, you know, I would expect
someone saying ‘what kind of stresses have you been under
recently? Do you think this could be caused by such and such?’ –
by the fact you’ve just been fired or whatever, but then you know I
haven’t been presented with anything like that that would lead to
that kind of questioning but then again, you know, if I had things
that I particularly wanted to talk about in terms of my lifestyle and
stresses then I would see a counsellor to do this. [SR3]
Another user felt it helped to put him at his ease but was not important for his health:
94
Well certainly with the health advisor in my last visit, we talked
about relationships and things and I was quite happy with that. It
was relaxing for me but I don’t think it was important for my health.
[SR4]
One participant felt it approximated to a more holistic service:
Well I have [talked about my individual circumstances] but that has
been the counselling side. I haven’t done that with nurses or
doctors, because to be honest, that’s not what they are there for, it
really isn’t, I mean and it is not that I feel intimidated by doing it, I
just think, well you wouldn’t go to a pub and ask to buy a set of
curtains! I don’t want a jack-of-all-trades; I want a master of each
one. A doctor who is a bit of doctor, a bit of a nurse and a bit of a
counsellor and a bit of this and a bit of that, on the one hand it’s
very holistic, but on the other hand it could be he is spreading
himself far too thinly. I want my doctor to be a great doctor, who
knows a lot about other things, but who then refers me on to a great
therapist or a great urologist or whatever. So I think it is important
but I don’t’ think a holistic approach is from one person, I think a
holistic report comes from the whole centre and I think that is what
we are getting towards. So you come here it is not just individuals it
is the whole service. [SRP 2]
Two interviewees had been referred to counselling within the SRP by a health
adviser, one of whom had also been referred to a urologist and to another specialist
for a scan.
Health Promotion
This section of the interview aimed to assess the broader educational and reflective
impact of service-use. Respondents consistently reported knowledge gains from the
various information sources available. These gains, together with the nature of some
of the services offered within the SRP (e.g. counselling) had caused some to reflect
on aspects of their lifestyle and increased respondents’ sense of control over their
health.
95
Improved knowledge and source(s)
All participants felt that they had increased their knowledge of sexual health issues
and specific conditions by attending the clinic. This included an experienced user
who felt that risks had changed over the years. Some had deliberately sought out
information for themselves (or for friends) or had achieved learning through
treatment. Attention was consistently drawn to the quality and quantity of educational
literature available in the clinic:
Yes, I mean chlamydia, gonorrhoea, hepatitis ‘A’, HIV and urinary
tract infections, epididimitis, I mean I have only heard these
expressions and learned about them by coming here, so it has
increased my knowledge of medical terminology and medical
illnesses and what they are all about. So yes I have learned a lot
from that as well; from the leaflets and just from chatting really.
[SR2]
Doctors, but especially Health Advisers were also seen as important sources of
information:
A partner of mine has had herpes and I needed some information
about that and it was readily available here. So I think you know if
there is information, there are plenty of leaflets around. You know,
you can talk to the health advisors about risks which seem to have
changed since I have been visiting sexual health services. [SR3]
Altered perceptions of self regarding health
In common with the views reported in the first interim report, most participants
reported feeling that attending the clinic had increased their sense of control
regarding their health. Regular discussions with health advisers and counsellors had
also encouraged a degree of reflectivity regarding aspects of sexual lifestyle,
although this often occurred after the ‘problem’ event.
[I feel] more empowered…Sometimes you get a bit lax about your
sexual life style, you know, Friday, Saturday night – you’re a wee bit
pished, and you’re out and you think ‘he’s quite nice looking’. I
96
mean that happens, but coming into contact here, you kind of revisit
past experiences and think ‘I shouldn’t have done this, I shouldn’t
have done that’, and you are aware of your sexual health. [SR1]
You know in terms of feeling in control of your sexual sort of health I
think it offers you all the things that you need to do that, from
information, from accessories, from having people to talk to who are
around your own age. [SR3]
Well a combination of it [attending the service] and health problems
that I have been diagnosed with, I guess has changed my attitude
to sex a bit, yes. Also, I have been starting to feel like this is sort of
like coming to confession; the very fact that I have to say it out loud
makes me realise ‘Well! that was really fucking stupid’. [SR4]
Expectations and suggestions
Although many participants had few specific expectations of the service before using
it for the first time, all found key aspects of the service to be surprisingly good and
therefore in some sense, to exceed expectations. Many of the reasons for this have
been described above, yet another defining characteristic of the service (in contrast
to regular GP visits) was perceived to lie in its ability to personalise care and treat
people as individuals instead of minor elements of a service:
Again my ordinary doctor, the receptionists are so stand offish they
are so cold, so, you know, I’m just another client to them; here they
are a lot more kind of personal in the way they respond to you.
[SR1]
The overall service had raised expectation of what the NHS could offer more
generally, although participants were aware of the resource implications of doing this
combined with the institutional barriers (coldness, formality, treatment of symptoms
not people) associated with traditional models of service provision:
I was amazed, I just went right through the system from start to
finish. I was seen, I was examined, I was analysed, I was

97
prescribed antibiotics there and then and then so I thought wow-
this is the business! So it was a huge contrast between the
conventional GP route and this specific route and I was very
impressed. A lot more personal and just very professional - going to
your GP, they see lots of people, you are just a number really, they
don’t have time to personalise it at all. [SR2]
Going to the GPs or whatever it’s just so faceless and kind of
minimal then you come here and get free medication and it is just
really pleasant surroundings and nice people. [SR4]
Suggestions for change were relatively minor in general (see ‘Access to service’
section, above) although one substantive comment was made regarding the
provision of a wider range of complementary treatments in the centre, in order to
strengthen its capacity to deliver a holistic service.
What about offering holistic treatments here like massage,
reflexology, therapies, face therapies, tai chi you know –
somewhere that people could go and, you know, maybe
hypnotherapy, acupuncture you know different things like a whole
range of services under one roof that people can come and pick
and choose and pay for, so the mind, body, spirit, everything can be
catered for. I think it would be holistic if I could see my doctor, my
nurse, my counsellor, my aromatherapist, my reflexologist I mean
everything, the whole caboodle situated in the one place. Yeah!
Like a huge big hypermarket of health! [SR2]
Summary
A clear and detailed picture has emerged from the five interviews of a valued,
modern and progressive service. Various barriers were identified that obstructed use
of ‘traditional’ sexual health services. These included:
• Institutional/service-culture barriers: NHS services perceived as rushed,
impersonal and involving long waiting times
98
• Cultural barriers: Sexual health still considered a taboo subject on the west coast
of Scotland; gay men ‘in the closet’ unlikely to go to GPs with sexual health
problems
• Generational barriers: ‘post-AIDS’ generation of young gay men not as sensitised
to sexual health issues as those first affected by the disease. Therefore less likely
to attend clinics for testing, check-ups, etc.
Although participants had overcome these barriers, it was clear that key
characteristics of the Steve Retson Project had helped them to do so. Furthermore,
their overwhelmingly positive views of the service ensured that they would both
continue to attend and recommend it to others. Key characteristics/good points
included:
• Good geographical and temporal accessibility of the service
• The availability of appointments ‘on spec’ and a brief wait for those made by
phone
• A physical environment conducive to relaxation and the minimisation of anxiety,
including bright, modern décor and refreshments.
• An informal, friendly and personalised service, incorporating a number of health
professionals tackling various dimensions of well-being (physical functioning,
lifestyle and mental health) under the same roof.
• The sense of there being enough time to express opinions, ask questions and
participate in treatment.
• The availability of health-promoting information from workers and literature
Whilst the opinions expressed by respondents is likely to be biased for a number of
reasons (articulate, middle-class, repeat users, working centrally and agreeing to
take part in the research), it is clear the SRP provides the kind of service
environment that is well placed to deliver a ‘social’ model of health.
Suggestions for change
• A larger waiting room with thought given to the seating arrangement, in order to
minimise unwanted encounters/improve anonymity. More sessions might also
achieve similar results, although this was not suggested.
• The option to withhold details such as name and date of birth (re: protection of
confidentiality).

99
• A more flexible system for cancelling early appointments in advance of the clinic
opening.
• Greater or more co-ordinated provision of alternative and complementary
therapies such as aromatherapy and reflexology.

100
Chapter Nine – Conclusions
As with the interim report the individual service chapters within this report present a
summary of the key findings that emerge from each service in turn. This final section
of the report pulls together the key themes and findings from the interviews with
participants across the five Sandyford Initiative services in relation to the experience
of a social model of health and, building of the interim report, considers the
usefulness of the current methodology as a means of assessing users’ views on an
ongoing basis. The decision to present the results by service as well as across the
Initiative as a whole is guided by the fact that whilst some findings are related to the
overall philosophy and organisation of the Initiativ, others are more service specific.
Whole System Issues
The following section looks at three separate themes emerging from the interviews
that have implications for the Sandyford Initiative as a whole. The first of these
concerns access issues and is discussed in relation to potential selection bias. The
second theme is the expectations that users have about health care and the third
relates to perceptions of the Sandyford as a cluster of services rather than a more
holistic service.
Access
The interim report discussed users’ views of the experience of accessing the
Sandyford Initiative. Once again, perceptions of ease of access were high with only
a small number of users finding it difficult to reach using public transport or finding
parking to be problematic. A small number of users did express the desire for
outreach services to be available in other areas of the city. The caveat that was
raised last year applies to the current findings – clearly those with major access
difficulties would not be those attending the service and therefore their views are not
represented. A detailed analysis of postcode information for all users would allow a
systematic assessment of whether the service is accessible to those in different
areas of the city and whether it provides an equitable service to those from more
socially deprived areas.
The earlier report discussed the perceived need for better signposting within the
Initiative and, whilst this is an issue that has been tackled by the service as a whole,
there is still a view that signposting is unclear. At the same time there would appear
101
to be a tension between those wishing clear unambiguous signposting of clinics and
those grateful for the lack of banners announcing the purpose of other services. The
main area where clarity would appear to be particularly appreciated is in
distinguishing between general Family Planning Clinics and The Place. The wish for
a front of house person was expressed again.
A final issue related to access is that of waiting times. Across the services there was
a degree of dissatisfaction either with the length of time spent on a waiting list before
being allocated a counsellor or with the time spent in waiting areas on the day of an
appointment. These voices of dissatisfaction were, however, tempered with an
acceptance of waiting as being part and parcel of receiving a good service.
Shaping expectations
As with the interim report, users’ expectations of receiving a social model of care and
perceptions of it having been delivered were variable. Those receiving counselling
services were far more likely to see their social world as being a legitimate domain
for health care and were generally happy that their needs were being addressed.
For those receiving more traditional types of service there was a greater likelihood of
users expressing uncertainty about the appropriateness of seeking advice about
social issues from medical and nursing staff. This is important from a number of
angles. Firstly, there was a view expressed that social problems are best disclosed
with a practitioner with whom one has an ongoing relationship and ensuring this type
of continuity of care is problematic with some of the Sandyford services. Secondly,
some participants appeared to view the discussion of personal social issues and
receiving professional care as being inimical to one another.
This relates to a final issue that should be strongly underlined in relation to the
findings on users’ expectations, namely, the role of services in shaping espectations.
Most users clearly expressed a view that they had previous negative experiences
with health services and that they were attracted either to the expertise and
professionalism or the holistic care offered by the Sandyford services. However, a
number of participants reflected that, whilst they felt that they had the opportunity to
ask questions and raise social issues, they didn’t know what to ask. This implies that
a service that operates a social model of care requires not only to provide space for
issues to emerge but to structure consultations in such a way that social issues are
102
seen by users to be integral components of the process of diagnosis and treatment.
The findings from the GUM clinic provide a good example of a user who, initially
surprised by a question concerning relationship issues, reflects on the legitimacy of
the question (p 61 of this report). Ways of supporting those services that provide
more traditional health care to positively shape users’ expectations should be
considered.
A holistic service (‘a huge big hypermarket of health’)
The interim evaluation found that, on the whole, users perceived the Sandyford
Initiative to be made up of disparate clinics with only those using the Centre for
Women’s Health tending to use more than one service. There was some evidence of
more users within the current group of participants moving between services. In the
last year a number of changes to the Initiative have been made that may in the future
lead to a greater sense of identity for the Initiative – the creation of a single Director
and the merging of counselling services. These may allow the development of a
range of joint service initiatives such as courses in self-esteem, aromatherapy and
other alternative treatments requested by some participants. Such integration should
also be encouraged as a means of providing support and a critical mass to the
shaping of users’ expectations as discussed above.
Accessing users’ views
An initial aim of this component of the evaluation was to use a longitudinal
methodology to assess changing perceptions of the delivery of a social model of
health within the Sandyford Initiative. This has proved to be problematic for two
reasons: firstly, the number of participants in the first round who gave consent to
being invited to take part in a second round of interviews was small; and, secondly,
none of those who gave consent were willing or available to be re-interviewed when
invited to do so.
It is perhaps unsurprising that, whilst many users are happy to give of their time on
one occasion when on the premises, they are less likely to make time for a repeat
interview when it might require more effort and planning. Initial consenters may also
have ceased contact with the Initiative.
We would argue, however, that the value of the second round of interviews is not
diminished by the fact that repeat participants were not available. Instead, the vast

103
majority of the interviewees were repeat users of the service and were, therefore,
able to reflect to a certain extent on changing expectations and experiences.
We would also argue that the approach of taking an annual snap-shot of users’ views
of the extent to which care conforms to a social model is a worthwhile exercise for
the Initiative as a whole. The interviews conducted as part of the current study have
allowed rich and detailed views to emerge and accessing the voices of a small
number of users in this manner (incorporating both repeat and new appointments)
may serve as a complement to other means of assessing views. This method need
not require the resources of external evaluation but might be incorporated within the
remit of the user involvement strategy.
In the initial round of interviews we struggled with three issues in accessing users’
views. In round two we have offered some means of resolving these. Firstly, in
services where there is a greater likelihood of stigmatisation it is helpful if the initial
contact with potential participants is by staff members. Secondly, in deconstructing
the language of the social model of health the notion of users’ expectations was a
helpful one. Finally, we suggest that the difficulty of encouraging younger people to
engage in discussions in this area may also be aided by conducting the interview in
the presence of a confidante.

104
References
Advanced searches were undertaken using BIDS databases (International
bibliography of social sciences) and Psychinfo dating from 1995 to 2001 (English
language)
Initially the words sexual and health and social were used. After the initial search,
sexual was replaced with reproductive and women. Many of the same articles were
identified but new ones also emerged. Using a range of these core articles as a
basis for the literature review, some key themes emerged and further searches were
undertaken using more specific terms, for example, youth and sexual health, ethnicity
and sexual health, empowerment and sexual health.
Further papers were located using references cited in papers during the primary
search. A range of relevant articles and books were also located by the researchers
using libraries at the Sandyford Initiative and the University of Glasgow, and again by
following up references cited in these.
Adam, R and Guthrie, B (2001) The death of the personal doctor, Journal of Health
Service Research and Policy, 6, 129-130
Annandale, E and Hunt, K (2000) Gender inequalities in health. Buckingham: Open
University Press
Balint, E (1969) The possibilities of patient centred medicine. Journal of the Royal
College of Practitioners 17, 269-276
Blaxter, M (1983) Causes of disease: women talking. Social Science and Medicine,
17, 59-69
Blaxter, M (1990) Health and Lifestyles. London: Routledge
Broom, D (1997) The best medicine: women using community health centres.
Australian and New Zealand Journal of Public Health 21, 275-280
105
Broom, D (1998) By women, for women: the continuing appeal of women’s health
centres. Women and Health 28 (1) 5-22
Busfield, J (1996) Men, women and madness: understanding gender and mental
disorder. London: Macmillan
Campbell, S., Rowland, M and Buetow, S (2000) Defining quality of care. Social
Science and Medicine 51, 1611-1625
Calnan, M (1987) Health and Illness: the lay perspective. London: Tavistock
publications
Coulter, A (1999) Paternalism or partnership?, British Medical Journal 319 (7212)
719-720
Craddock, C and Reid, M (1993) Structure and Struggle: implementing a social
model of a well woman clinic in Glasgow, Social Science and Medicine 36 (1) 67-76
Doyal, L (2000) Gender equity in health: debates and dilemmas, Social Science and
Medicine 51, 931-939
Elwyn, G., Edwards, A., Gwyn, R and Grol, R (1999) Towards a feasible model for
shared decision making: focus group study with general practice registrars. British
Medical Journal 319, 753-756
Evans, RG and Stoddart, GL (1994) Producing health, consuming health care. In RG
Evans, ML Barer and TR Marmor (eds) Why are some people healthy and others not.
New York: Walter de Gruyter
Graham, H (1998) Health at risk: poverty and national health strategies. In L Doyal
(ed) Women and health services (22-38), Open University Press
Greater Glasgow Primary Care Trust. Sandyford Initiative – Review of service
integration and management, April 2001.
Guadagnoli, E and Ward, P (1998) Patient participation in decision-making. Social
Science and Medicine 47 (3) 329-339
106
Hills, M and Mullett, J (2002) Women-centred care : working collaboratively to
develop gender inclusive health policy, Health Care for Women International 23: 84-
97
Hughes, W (2000) Medicalised Bodies in The Body, Culture and Society: an
introduction. Open University Press
Hurley, M (2002) Effect of patient-centredness and positive approach, BMJ 324,:543
Janzen, B (1998) Women, gender and health: a review of the recent literature.
Winnipeg: Prairie Women’s Health Centre of Excellence
Labonte, R (1998) A community development approach to health promotion: a
background paper on practice tensions, strategic models and accountability
requirements for health authority work on the broad determinants of health.
Edinburgh: Health Education Board for Scotland and the Research Unit in Health and
Behavioural Change, University of Edinburgh
Lupton, D (1996) Your life in their hands: trust in the medical encounter. In Health
and the sociology of emotions by V James and J Gabe (Eds), Blackwell Publishers
Laughlin, S, Nandwani, R, Ilett, R, Bigrigg, A (2001) The Sandyford Initiative: creating
added value to health and health care, Health Bulletin 59 (4) 238-243
Little, P., Everitt, H., Williamson, I., Warner, G et al (2001) Preferences of patients for
patient centred approach to consultation in primary care: observational study. British
Medical Journal 322, 468-472
Little, P., Everitt, H., Williamson, I., Warner, G et al (2001) Observational study of
effect of patient centredness and positive approach on outcomes of general practice
consultations, British Medical Journal 323, 908-911
Mackenzie, M, Lawson, L and Mackinnon, J (2001) Evaluation of the Sandyford
Initiaitve: having your voice heard – Interim Report

107
O’Flynn, N and Britten (2000) Menorrhagia in general practice – disease or illness,
Social Science and Medicine 50 (2000) 651-661
Ogden, J, Baig, S, Earnshaw, G, Elkington, H et al (2001) What is health? Where
GPs and patients’ worlds collide, Patient Education and Counselling 45 (2001) 265-
269
Peberdy, A (1997) Communicating across cultural boundaries, in M Sidell., L Jones,
J Katz and A Peberdy Eds (1997) Debates and Dilemmas in Promoting Health, Open
University
Stewart, M (1995) Effective physician-patient communication and health outcomes: a
review. Canadian Medical Association 152, 1423-1433
West, J (1999) (Not) talking about sex: youth, identity and sexuality. The
Sociological Review, 525-547
Whitehead, M (1995) Tackling health Inequalities: review of policy initiatives. In:
Benzeval, M., Judge, K, Whitehead, M (eds) Tackling Inequalities in Health, an
agenda for action. London: Kings Fund