2. DKA IDI
31
Emergency in Diabetes Management : “From Bedside to Clinical Practice Sony Wibisono M Diabetes and Nutrition Centre - dr. Sutomo Hospital Faculty of Medicine Airlangga University Surabaya,11 April 2012
Transcript of 2. DKA IDI
Emergency in Diabetes Management :
“From Bedside to Clinical Practice
Sony Wibisono MDiabetes and Nutrition Centre - dr. Sutomo
Hospital Faculty of Medicine Airlangga University
Surabaya,11 April 2012
Topic of Presentation1. Why should we decrease blood
sugar in hospital hyperglycemia
2. Emergency in diabetes3. Treatment Emergency in
diabetes4. Insulin treatment in hospital

What evidence exists that in-hospital hyperglycemia is associated with adverse
outcomes?BG > 110 mg/dL with or without DM pts AMI : ↑mortality and CHF.FBG >126 mg/dL , RBG >200 mg/dL : 18 x in-hospital mortality, ↑ LOS (9 vs. 4.5 days).
Cardiac surgery suffer ↑ mortality, Deep-wound infections, > overall infection Critical illness conventional tx , > mortality, sepsis, ARF, and neuropathy
Poor outcome in patients with CVA: BG 110 - 126 mg/dl < 121 - 144 mg/dL < 140 mg/dLPregnancy complicated
ACE Position Statement on Inpatient Diabetes and Metabolic Control, Endocr Pract. 2004;10(No. 1)

Does reduction of hyperglycemia improve outcomes?
Reduces morbidity and mortality in acutely ill patients
• Intensive iv insulin inf (>110 mg/dL): mortality ↓ 34% (prospective trial)• Cardiac surgery pts : first 3 postop days : ↓ mortality of 57% and 50%• Long term survival rates AMI improved by 28% at 3.4 years. If normoglycemia • Deep sternal wound infection in cardiac surgery pts directly - ↑ BG postoperation
• ↓ 66%—to a rate equal to that seen in the non diabetic population• ↓ sepsis (46%), ARF (41%), transfusions (50%), and polyneuropathy (44%)• LOS ↓ 1 day each 50 mg/dL, ↓ average 3-day post op• Savings of more than $680/patientACE Position Statement on Inpatient Diabetes and Metabolic Control, Endocr Pract. 2004;10(No. 1)

To what extent does the impact of metabolic regulation extend beyond merely glycemic
regulation?
• Beneficial effects insulin– Inhibits lipolysis; ↑ FFA → poor outcomes, cardiac arrhythmias.
– Inhibits inflammatory GF (activator protein 1 and early growth response gene-1)
– Stimulates e-NOs, ↑ nitric oxide, → arterial vasodilation, other beneficial effects on oxidation and inflammation.
– Euglycemia/ near euglycemia, inhibit proinflammatory cytokines, adhesion molecules, and chemokines

What methods for such regulation should be used?
• Insulin, intravenous as a continuous or subcutaneous
• Indications for iv insulin therapy, but are not limited to:• Critical illness• Prolonged NPO (nothing by mouth) status in patients who are insulin deficient
• Peri operative period• After organ transplantation• Total par enteral nutrition therapy• Elevated glucose exacerbated by high-dose glucocorticoid therapy• Stroke• Labor and delivery• As a ose-finding strategy prior to conversion to subcutaneous (SQ) insulin therapy
• Other illnesses requiring prompt glucose control

Emergency in Diabetes1. Hypoglycemia2. Lacto acidosis3. Diabetic Keto Acidosis4. Hyperglycemia Hyperosmolar
State

Emergency in Diabetes1. Hypoglycemia2. Lacto acidosis3. Diabetic Keto Acidosis4. Hyperglycemia Hyperosmolar
State
*******
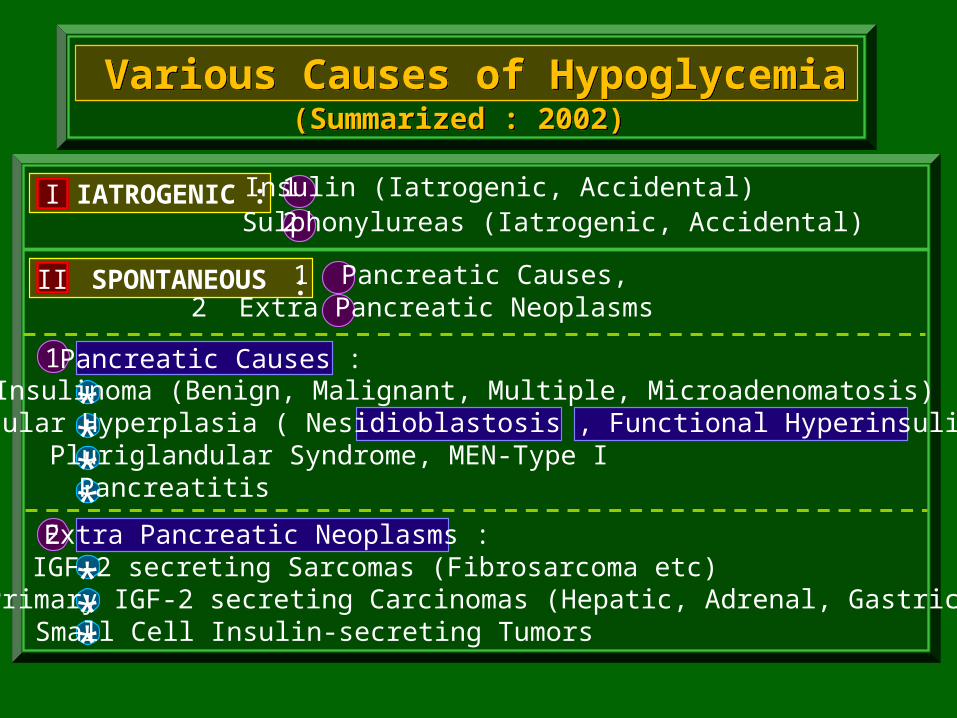
I IATROGENIC : 1 Insulin (Iatrogenic, Accidental)2 Sulphonylureas (Iatrogenic, Accidental)
II SPONTANEOUS :1 Pancreatic Causes,2 Extra Pancreatic Neoplasms
1 Pancreatic Causes :Insulinoma (Benign, Malignant, Multiple, Microadenomatosis)
Insular Hyperplasia ( Nesidioblastosis , Functional Hyperinsulinism )Pluriglandular Syndrome, MEN-Type IPancreatitis
2 Extra Pancreatic Neoplasms :IGF-2 secreting Sarcomas (Fibrosarcoma etc)
Primary IGF-2 secreting Carcinomas (Hepatic, Adrenal, Gastric)Small Cell Insulin-secreting Tumors
Various Causes of Hypoglycemia(Summarized : 2002)

Classification, Pathogenesis, and Treatment(Clinical Experience : Tjokroprawiro 2000,2002)
Hypoglycemia in Clinical Pratice
Non-DiabetogenicDiabetogenic
OHA-Induced
Honey Moon Period
- Very High C-peptide- Diabetic Diet- No Refined Cbh.- D-5% infusion
Insulin Induced
D-10% Infusion
Non-Honey Moon
- Normal C-peptide- Refined Cbh is allowed- D-10% infusion
DNA Mutation
- High C-peptide- D-5% infusion- Diabetic Diet
Hypertrophic
Insulinoma
- Very High C-Peptide- D-5% infusion- Diabetic Diet- CT-Scan etc.
Non-Pancreatic
(Hepatogenic-Nephrogenic)- D-10% infusion
- Refined Cbh is allowed
Pancreatic
R/ MedicalR/ Surgical
IGF-2 secretingTumors
or
R/ Surgical

PETUNJUK PRAKTIS TERAPI HIPOGLIKEMIA DENGAN RUMUS 3-2-1
PETUNJUK PRAKTIS TERAPI HIPOGLIKEMIA DENGAN RUMUS 3-2-1
Kadar GlukosaTerapi Hipoglikemia Dengan Rumus 3-2-1Glukosa mg/dl (Askandar Tjokroprawiro, 1996)1 Flakon = 25 ml
40% (10 gram)
30 mg/dl :Injeksi Intravena Dekstrosa 40%, bolus 3 FlakonRumus - 3
30-60 mg/dl :Injeksi Intravena Dekstrosa 40%, bolus 2 FlakonRumus - 2
60-100*) mg/dl :Injeksi Intravena Dekstrosa 40%, bolus 1 FlakonRumus - 1

Emergency in Diabetes1. Hypoglycemia2. Lacto acidosis3. Diabetic Keto Acidosis4. Hyperglycemia Hyperosmolar
State

Tx : Kausal
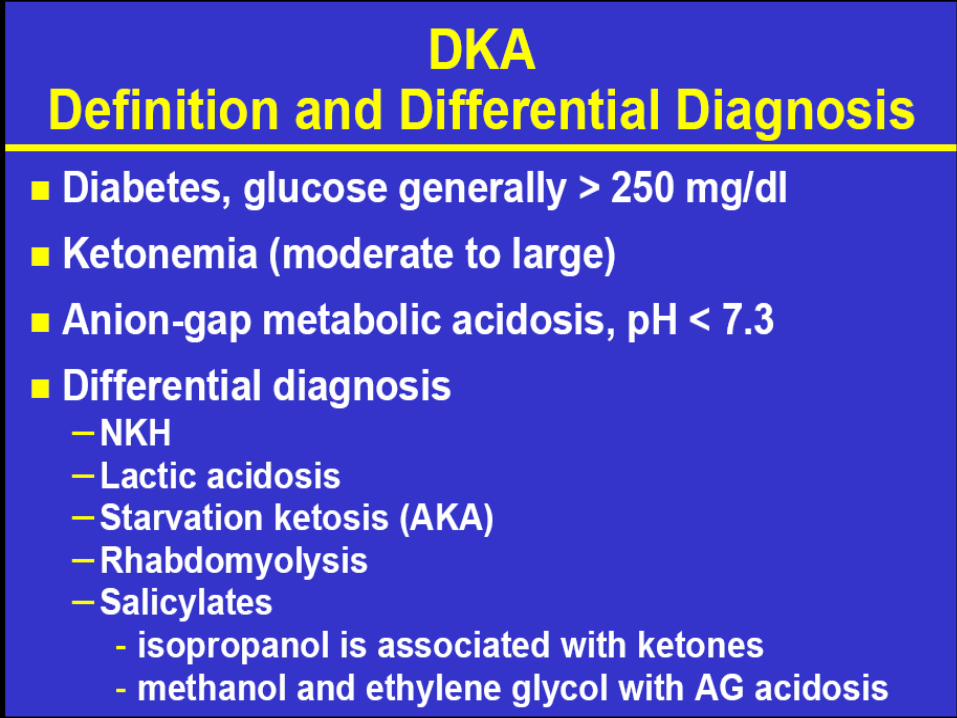
Dx : Hiperglikemia plus Anion Gap > 20 mEq(K + Na) - (Cl + CO2) > 20 mEq atau
(Na) - (Cl + CO2) > 15 mEq
KOMA ASIDOSIS ASAM LAKTAT (KAAL)(Tipe A dan Tipe B)
(Summarized : Tjokroprawiro 1991-1998)
ASAM LAKTAT + H2O + O2 B i k a r b o n a t
Terganggu
Infeksi, Shock, Peny. Kardiovaskuler/AngiopatiLFT-RFT , DM + Biguanide, Gg. Oksigenasi : PPOM, dll
KAAL - Tipe A
(Primer : Hipoksia)1. Semua jenis shock2. Decomp. Cordis3. Asfiksia4. Intoksikasi CO
KAAL - Tipe B
Kelainan Sistemik1. DM
2. Neoplasia3. RFT/LFT terganggu4. Konvulsi
Obat1. Biguanide2. Salisilat
3. Alkohol (Metanol, Etanol)4. Glukosa-Alkohol (Sorbitol, dll)

Emergency in Diabetes1. Hypoglycemia2. Lacto acidosis3. Diabetic Keto Acidosis4. Hyperglycemia Hyperosmolar
State

↑Growth Hormone↑Glucagon↑Cortisol
↑Catecholamine
Absolute def Insulin
Relative Insulin def
↑ Lipolisis
↑ FFA LIVER
↑ KETOGENESIS
KETOACIDOSIS
Glucose unitilization ↓
↑ proteolysis
Triacylglycerol
↓ protein sintesis
↑ gluconeogenic substrate
↑ gluconeogenesis
Abscent or minimalketogenesis
Hyperlipidemia
Hyperglycemia
Glucosuria(osmotic diuresis)Loss water and electrolytes
Dehidration
Impaired renal function
Hyperosmolarity HHS
DKA
Stress, infection and/or insuf insulin intake
↓ fluid intake
↑ glycogenolisis
HHS

(Krentz et al 1997, Marshall et al 1997, Tjokroprawiro 1991-1998)
HYPERGLYCEMIA HYPEROSMOLAR STATE (HHS)
(Krentz et al 1997, Marshall et al 1997, Tjokroprawiro 1991-1998)
Pathogenesis Diagnosis Therapy
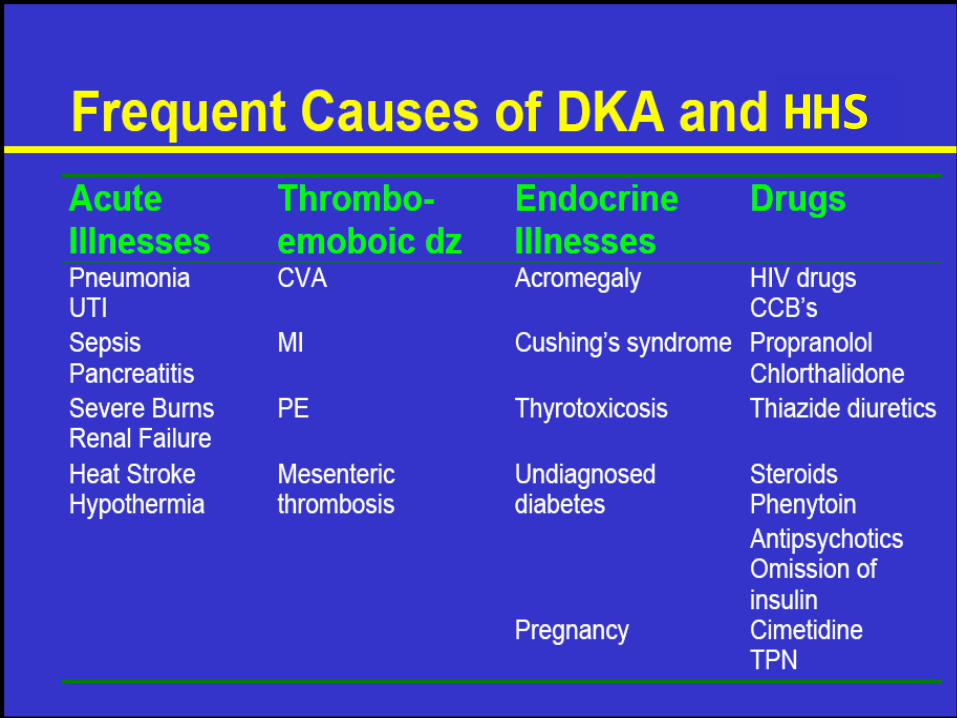
Precipitating Factors :
1Thiazide2Glucose Drinks3Infection4Corticosteroid5Beta Blocker6Phenytoin7Cimetidine8Chlorpromazine
Pathophysiology
Grossly Elevated GlucagonRelative Insulin Deficiency
Sufficient Insulin to inhibit lipolysis
TETRALOGY HHS : 1H + 3 NO
Tetralogy + 5 = PENTALOGY HHS (Definite Dx)
Glucose (mg/dl) Ureum (mg/dl)
18 6Osm/l = 2x (Na + K) + +5
Supporting Findings :1(pH > 7.30)2Neurological Sign 3Prerenal uremia4Mental Impairment 5Severe Dehydration6More than 60 years old
+
+
Clinical Dx (Suspect):
1IH: Glycemia > 800 mg/dl 2NO: DM History or 3NO: Kussmaul , 4NO: Ketonuria or
(Tetralogy HHS)
+ +
1 Tx DKAPlasma Na <150 mEq/l
Normal Saline
Hypotonic Saline
b Plasma Na >150 mEq/l
2 a

Comparison of DKA to HHS
Am Fam Physician 2005;71:1723-30.

TREATMENT DKA & HHS
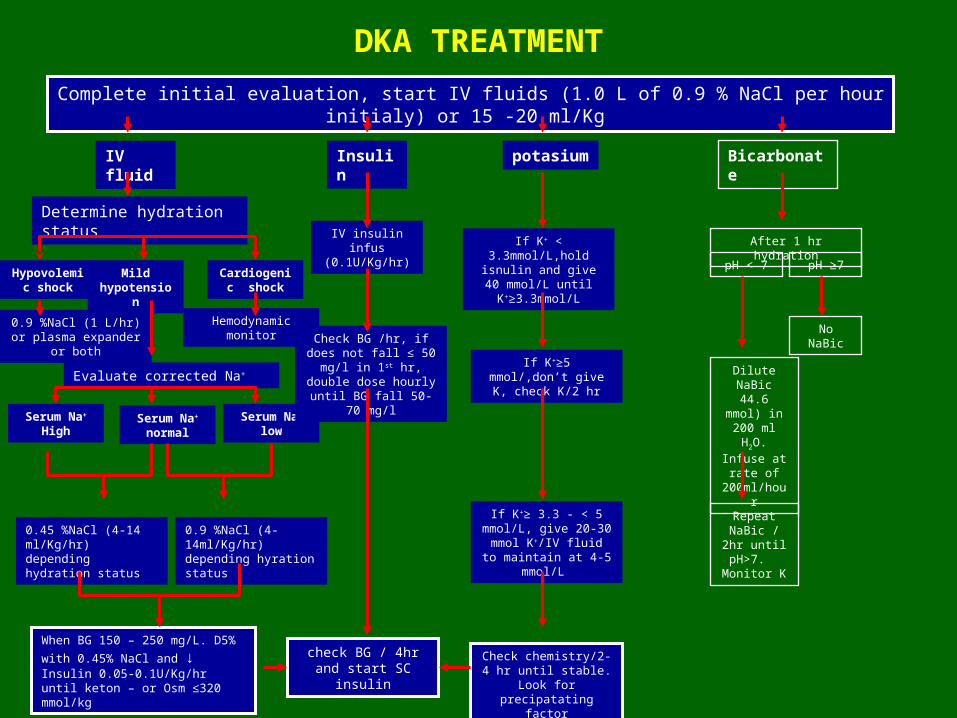
Complete initial evaluation, start IV fluids (1.0 L of 0.9 % NaCl per hour initialy) or 15 -20 ml/Kg
IV fluid
Insulin
Bicarbonate
potasium
Determine hydration status
Hypovolemic shock
Mild hypotensio
n
Cardiogenic shock
0.9 %NaCl (1 L/hr) or plasma expander
or both
Evaluate corrected Na+
Hemodynamic monitor
Serum Na+
lowSerum Na+ normal
Serum Na+
High
0.9 %NaCl (4-14ml/Kg/hr) depending hyration status
0.45 %NaCl (4-14 ml/Kg/hr) depending hydration status
When BG 150 – 250 mg/L. D5% with 0.45% NaCl and ↓ Insulin 0.05-0.1U/Kg/hr until keton – or Osm ≤320 mmol/kg
IV insulin infus
(0.1U/Kg/hr)
Check BG /hr, if does not fall ≤ 50 mg/l in 1st hr,
double dose hourly until BG fall 50-
70 mg/l
check BG / 4hr and start SC
insulin
If K+ < 3.3mmol/L,hold isnulin and give 40 mmol/L until K+≥3.3mmol/L
If K+≥5 mmol/,don’t give K, check K/2 hr
If K+≥ 3.3 - < 5 mmol/L, give 20-30 mmol K+/IV fluid
to maintain at 4-5 mmol/L
Check chemistry/2-4 hr until stable.
Look for precipatating
factor
Dilute NaBic 44.6
mmol) in 200 ml H2O.
Infuse at rate of
200ml/hour
After 1 hr hydrationpH < 7 pH ≥7
Repeat NaBic /
2hr until pH>7.
Monitor K
No NaBic
DKA TREATMENT
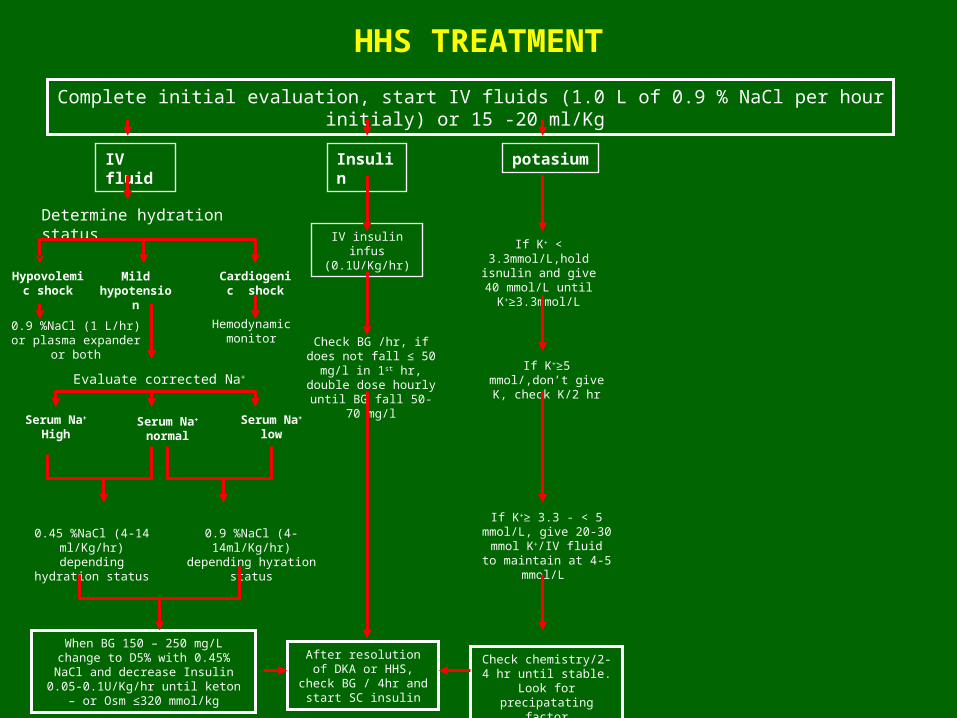
Complete initial evaluation, start IV fluids (1.0 L of 0.9 % NaCl per hour initialy) or 15 -20 ml/Kg
IV fluid
Insulin
potasium
Determine hydration status
Hypovolemic shock
Mild hypotensio
n
Cardiogenic shock
0.9 %NaCl (1 L/hr) or plasma expander
or both
Evaluate corrected Na+
Hemodynamic monitor
Serum Na+
lowSerum Na+ normal
Serum Na+
High
0.9 %NaCl (4-14ml/Kg/hr)
depending hyration status
0.45 %NaCl (4-14 ml/Kg/hr) depending
hydration status
When BG 150 – 250 mg/L change to D5% with 0.45% NaCl and decrease Insulin
0.05-0.1U/Kg/hr until keton – or Osm ≤320 mmol/kg
IV insulin infus
(0.1U/Kg/hr)
Check BG /hr, if does not fall ≤ 50 mg/l in 1st hr,
double dose hourly until BG fall 50-
70 mg/l
After resolution of DKA or HHS,
check BG / 4hr and start SC insulin
If K+ < 3.3mmol/L,hold isnulin and give 40 mmol/L until K+≥3.3mmol/L
If K+≥5 mmol/,don’t give K, check K/2 hr
If K+≥ 3.3 - < 5 mmol/L, give 20-30 mmol K+/IV fluid
to maintain at 4-5 mmol/L
Check chemistry/2-4 hr until stable.
Look for precipatating
factor
HHS TREATMENT

Am Fam Physician 2005;71:1723-30.
Strength of Recommendations*
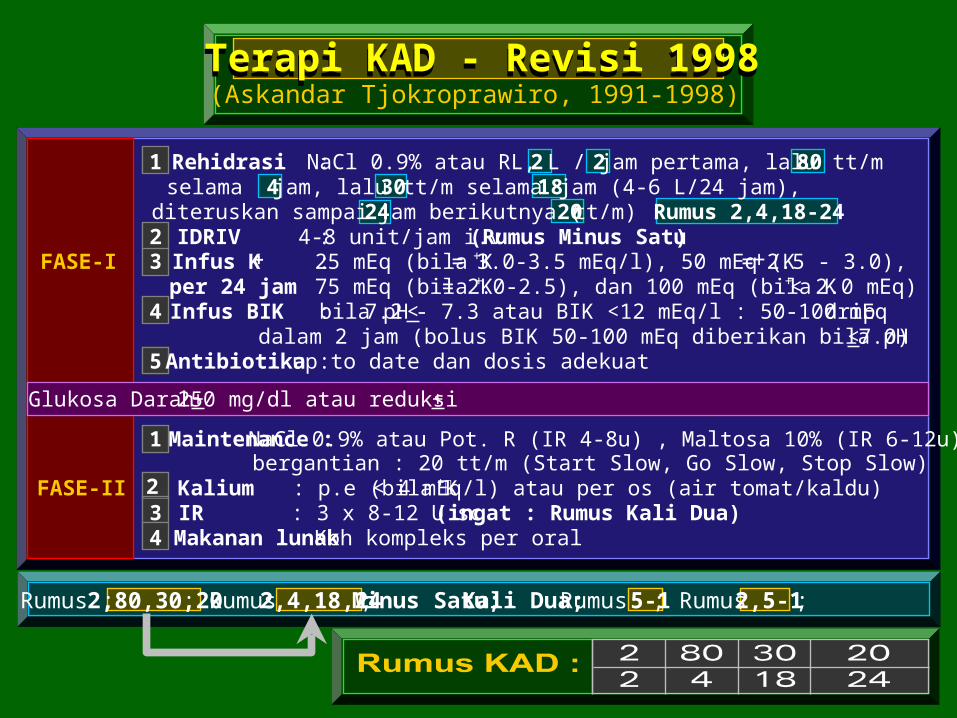
(Askandar Tjokroprawiro, 1991-1998)Terapi KAD - Revisi 1998Terapi KAD - Revisi 1998
1 Rehidrasi :NaCl 0.9% atau RL, 2 L / 2 jam pertama, lalu 80 tt/mselama 4 jam, lalu 30 tt/m selama 18 jam (4-6 L/24 jam),
diteruskan sampai 24 jam berikutnya ( 20 tt/m) : Rumus 2,4,18-242 IDRIV :4-8 unit/jam i.v (Rumus Minus Satu)
FASE-I 3 Infus K+ :25 mEq (bila K+ = 3.0-3.5 mEq/l), 50 mEq (K+ = 2.5 - 3.0),per 24 jam 75 mEq (bila K+ = 2.0-2.5), dan 100 mEq (bila K+ < 2.0 mEq)
4 Infus BIK :bila pH < 7.2 - 7.3 atau BIK <12 mEq/l : 50-100 mEq dripdalam 2 jam (bolus BIK 50-100 mEq diberikan bila pH < 7.0)
5Antibiotika :up to date dan dosis adekuat
Glukosa Darah + 250 mg/dl atau reduksi +
1 Maintenance : NaCl 0.9% atau Pot. R (IR 4-8u) , Maltosa 10% (IR 6-12u) bergantian : 20 tt/m (Start Slow, Go Slow, Stop Slow)
FASE-II 2 Kalium : p.e (bila K+< 4 mEq/l) atau per os (air tomat/kaldu)3 IR : 3 x 8-12 U sc (ingat : Rumus Kali Dua)4 Makanan lunak Kbh kompleks per oral
Rumus : 2,80,30,20 ; Rumus 2,4,18,24 ; Minus Satu; Kali Dua; Rumus 5-1 ; Rumus 2,5-1 ;

(Askandar Tjokroprawiro, 1991-1998)Terapi HHS - Revisi 1998
1 Rehidrasi :NaCl 0.9% atau RL, 2 L / 2 jam pertama, lalu 80 tt/mselama 4 jam, lalu 30 tt/m selama 18 jam (4-6 L/24 jam),
diteruskan sampai 24 jam berikutnya ( 20 tt/m) : Rumus 2,4,18-242 IDRIV :4-8 unit/jam i.v (Rumus Minus Satu)
FASE-I 3 Infus K+ :25 mEq (bila K+ = 3.0-3.5 mEq/l), 50 mEq (K+ = 2.5 - 3.0),per 24 jam 75 mEq (bila K+ = 2.0-2.5), dan 100 mEq (bila K+ < 2.0 mEq)
4 :Antibiotikaup to date dan dosis adekuat
Glukosa Darah + 250 mg/dl atau reduksi +
1 Maintenance : NaCl 0.9% atau Pot. R (IR 4-8u) , Maltosa 10% (IR 6-12u) bergantian : 20 tt/m (Start Slow, Go Slow, Stop Slow)
FASE-II 2 Kalium : p.e (bila K+< 4 mEq/l) atau per os (air tomat/kaldu)3 IR : 3 x 8-12 U sc (ingat : Rumus Kali Dua)4 Makanan lunak Kbh kompleks per oral
Rumus : 2,80,30,20 ; Rumus 2,4,18,24 ; Minus Satu; Kali Dua; Rumus 5-1 ; Rumus 2,5-1 ;

Complete initial evaluation, start IV fluids (1.0 L of 0.9 % NaCl per hour initialy) or 15 -20 ml/Kg
Insulin
potasium
IV insulin bolus
(0.1U/Kg/hr)
Check BG /hr, if does not fall ≤ 50 mg/l in 1st hr,
double dose hourly until BG fall 50-
70 mg/l
After resolution of DKA or HHS,
check BG / 4hr and start SC insulin
If K+ < 3.3mmol/L,hold isnulin and give 40 mmol/L until K+≥3.3mmol/L
If K+≥5 mmol/,don’t give K, check K/2 hr
If K+≥ 3.3 - < 5 mmol/L, give 20-30 mmol K+/IV fluid
to maintain at 4-5 mmol/L
Check chemistry/2-4 hr until stable.
Look for precipatating
factor
IV insulin infus
(0.1U/Kg/hr)



REGULASI CEPAT DENGAN INSULIN
(Pengalaman Klinik : Askandar Tjokroprawiro, 1993, 1994, 1996)
Dapat dibagi menjadi :1. R.C. Intravena
2. R.C. Subkutan
Perlu diketahui, bahwa pada pelaksanaan RC (Regulasi Cepat), perlu diingat beberapa rumus antara lain :
1. Rumus Minus-Satu
2. Rumus Kali-Dua

2 00 - 300 1x 3 x 43 00 - 400 2x 3 x 64 00 - 500 3x 3 x 85 00 - 600 4x 3 x 106 00 - 700 5x 3 x 12
Rumus Minus Satu Rumus Kali Dua
6 Minus 1 = 5 6 Kali 2 = 12
Glukosa Awal Dosis Insulin Dosis RumatanSebelum R-C (mg/dl) Intravena a 4 U/jam Insulin Subkutan (unit)
Regulasi Cepat Intravena (RCI)(Tjokroprawiro 1987, 1993, 1994, 1995, 1996, 1997, 1998)
(Contoh : Kasus Glukosa Darah 650 mg/dl)Hiperglikemia >200 mg/dl

THANK YOU FOR YOUR ATTENTION