1 Strength training is as effective as stretching for improving ...
52
1 Strength training is as effective as stretching for improving range of motion: A systematic 1 review and meta-analysis. 2 3 José Afonso, Ph.D. 1* , Rodrigo Ramirez-Campillo, Ph.D. 2,3 , João Moscão 4 , Tiago Rocha, 4 M.Sc. 5 , Rodrigo Zacca, Ph.D. 1,6,7 , Alexandre Martins, B.Sc. 1 , André A. Milheiro, M.Sc. 1 , 5 João Ferreira, B.Sc. 8 , Hugo Sarmento, Ph.D. 9 , Filipe Manuel Clemente, Ph.D. 10,11 6 7 1 Centre for Research, Education, Innovation and Intervention in Sport, Faculty of Sport of the University of Porto. 8 Rua Dr. Plácido Costa, 91, 4200-450 Porto, Portugal. 9 2 Department of Physical Activity Sciences. Universidad de Los Lagos. Lord Cochrane 1046, Osorno, Chile. 10 3 Centro de Investigación en Fisiología del Ejercicio. Facultad de Ciencias. Universidad Mayor. San Pio X, 2422, 11 Providencia, Santiago, Chile. 12 4 REP Exercise Institute. Rua Manuel Francisco 75-A 2º C 2645-558 Alcabideche, Portugal. 13 5 Polytechnic of Leiria, Rua General Norton de Matos, Apartado 4133, 2411-901 Leiria, Portugal. 14 6 Porto Biomechanics Laboratory (LABIOMEP), University of Porto, Rua Dr. Plácido Costa, 91, 4200-450 Porto, 15 Portugal. 16 7 Coordination for the Improvement of Higher Educational Personnel Foundation (CAPES), Ministry of Education 17 of Brazil, Brasília, Brazil. 18 8 Superior Institute of Engineering of Porto, Polytechnic Institute of Porto. Rua Dr. António Bernardino de 19 Almeida, 431, 4249-015 Porto, Portugal. 20 9 Faculty of Sport Sciences and Physical Education, University of Coimbra, 3040-256, Coimbra, Portugal. 21 10 Escola Superior Desporto e Lazer, Instituto Politécnico de Viana do Castelo, Rua Escola Industrial e Comercial 22 de Nun’Álvares, 4900-347, Viana do Castelo, Portugal. 23 11 Instituto de Telecomunicações, Department of Covilhã, 1049-001, Lisboa, Portugal. 24 25 *Corresponding author: José Afonso | [email protected]. 26 27 28
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of 1 Strength training is as effective as stretching for improving ...

1
Strength training is as effective as stretching for improving range of motion: A systematic 1
review and meta-analysis. 2
3
José Afonso, Ph.D. 1*, Rodrigo Ramirez-Campillo, Ph.D. 2,3, João Moscão4, Tiago Rocha, 4
M.Sc. 5, Rodrigo Zacca, Ph.D. 1,6,7, Alexandre Martins, B.Sc. 1, André A. Milheiro, M.Sc.1, 5
João Ferreira, B.Sc. 8, Hugo Sarmento, Ph.D. 9, Filipe Manuel Clemente, Ph.D. 10,11 6
7 1 Centre for Research, Education, Innovation and Intervention in Sport, Faculty of Sport of the University of Porto. 8
Rua Dr. Plácido Costa, 91, 4200-450 Porto, Portugal. 9 2 Department of Physical Activity Sciences. Universidad de Los Lagos. Lord Cochrane 1046, Osorno, Chile. 10 3 Centro de Investigación en Fisiología del Ejercicio. Facultad de Ciencias. Universidad Mayor. San Pio X, 2422, 11
Providencia, Santiago, Chile. 12 4 REP Exercise Institute. Rua Manuel Francisco 75-A 2º C 2645-558 Alcabideche, Portugal. 13 5 Polytechnic of Leiria, Rua General Norton de Matos, Apartado 4133, 2411-901 Leiria, Portugal. 14 6 Porto Biomechanics Laboratory (LABIOMEP), University of Porto, Rua Dr. Plácido Costa, 91, 4200-450 Porto, 15
Portugal. 16 7 Coordination for the Improvement of Higher Educational Personnel Foundation (CAPES), Ministry of Education 17
of Brazil, Brasília, Brazil. 18 8 Superior Institute of Engineering of Porto, Polytechnic Institute of Porto. Rua Dr. António Bernardino de 19
Almeida, 431, 4249-015 Porto, Portugal. 20 9 Faculty of Sport Sciences and Physical Education, University of Coimbra, 3040-256, Coimbra, Portugal. 21 10 Escola Superior Desporto e Lazer, Instituto Politécnico de Viana do Castelo, Rua Escola Industrial e Comercial 22
de Nun’Álvares, 4900-347, Viana do Castelo, Portugal. 23 11 Instituto de Telecomunicações, Department of Covilhã, 1049-001, Lisboa, Portugal. 24
25
*Corresponding author: José Afonso | [email protected]. 26
27
28
2
29
Summary box 30
What is already known? 31
• Stretching is effective for improving in range of motion (ROM), but promising findings 32
have suggested that strength training also generates ROM gains. 33
34
What are the new findings? 35
• Strength training seems to be as effective as stretching in generating ROM gains. 36
• In contradiction with existing guidelines, stretching is not strictly necessary for improving 37
ROM, as strength may provide an equally valid alternative. 38
• These findings were consistent across studies, regardless of the characteristics of the 39
population and of the specificities of strength training and stretching programs. 40
41
42

3
43
ABSTRACT 44
Background: Range of motion (ROM) is an important feature of sports performance and 45
health. Stretching is usually prescribed to improve promote ROM gains, but evidence has 46
suggested that strength training (ST) also improves ROM. However, it is unclear if its efficacy 47
is comparable to stretching. Objective: To perform a systematic review and meta-analysis of 48
randomized controlled trials (RCTs) assessing the effects of ST and stretching on ROM. 49
Protocol: INPLASY: 10.37766/inplasy2020.9.0098. Data sources: Cochrane Library, 50
EBSCO, PubMed, Scielo, Scopus, and Web of Science were consulted in early October 2020, 51
followed by search within reference lists and consultation of four experts. No constraints on 52
language or year. Eligibility criteria (PICOS): (P) humans of any sex, age, health or training 53
status; (I) ST interventions; (C) stretching interventions (O) ROM; (S) supervised RCTs. Data 54
extraction and synthesis: Independently conducted by multiple authors. Quality of evidence 55
assessed using GRADE; risk-of-bias assessed with RoB 2. Results: Eleven articles (n = 452 56
participants) were included. Pooled data showed no differences between ST and stretching on 57
ROM (ES = -0×22; 95% CI = -0×55 to 0×12; p = 0×206). Sub-group analyses based on RoB, 58
active vs. passive ROM, and specific movement-per-joint analyses for hip flexion and knee 59
extension showed no between-protocol differences in ROM gains. Conclusion: ST and 60
stretching were not different in improving ROM, regardless of the diversity of protocols and 61
populations. Barring specific contra-indications, people who do not respond well or do not 62
adhere to stretching protocols can change to ST programs, and vice-versa. 63
64
KEYWORDS: systematic review; meta-analysis; strength training; flexibility; stretching; 65
range of motion. 66
67

4
68

5
69
Introduction 70
Improving range of motion (ROM) is a core goal for the general population,[1] as well 71
as in clinical contexts,[2] such as when treating acute respiratory failure,[3] plexiform 72
neurofibromas,[4] and total hip replacement.[5] Unsurprisingly, ROM gains are also relevant 73
in different sports,[6] such as basketball, baseball and rowing,[7-9] among others. ROM is 74
improved through increased stretch tolerance, augmented fascicle length and changes in 75
pennation angle,[10] as well as reduced tonic reflex activity.[11] Stretching is usually 76
prescribed to increase ROM in sports,[12, 13] clinical settings such as chronic low back 77
pain,[14] rheumatoid arthritis,[15] and exercise performance in general.[16] Stretching 78
techniques include static (active or passive), dynamic, or proprioceptive neuromuscular 79
facilitation (PNF), all of which can improve ROM.[1, 17-20] 80
However, reduced ROM and muscle weakness are deeply associated.[21-23] Therefore, 81
although strength training (ST) primarily addresses muscle weakness through methods such as 82
resistance training or similar protocols, it has been shown to increase ROM in athletic 83
populations,[24, 25] as well as in healthy elderly people[26] and women with chronic 84
nonspecific neck pain.[27] ST focused on concentric and eccentric contractions has been 85
shown to increase fascicle length. [28-30] Better agonist-antagonist co-activation[31], 86
reciprocal inhibition,[32] and adjusted stretch-shortening cycles[33] may also explain why ST 87
is a suitable method for improving ROM. 88
Nevertheless, studies comparing the effects of ST and stretching in ROM have 89
presented conflicting evidence,[34, 35] and many have small sample sizes.[36, 37] Developing 90
a systematic review and meta-analysis (SRMA) may help summarize this conflicting evidence 91
and increase statistical power, thus providing clearer guidance for interventions.[38] Therefore, 92

6
the aim of this SRMA was to compare the effects of supervised and randomized ST versus 93
stretching protocols on ROM in participants of any health and training status. 94
95
96
METHODS 97
Protocol and registration 98
The methods and protocol registration were preregistered prior to conducting the 99
review: INPLASY, no.202090098, DOI: 10.37766/inplasy2020.9.0098. 100
101
Eligibility criteria 102
Articles were eligible for inclusion if published in peer-reviewed journals, with no 103
restrictions in language or publication date. The Preferred Reporting Items for Systematic 104
Reviews and Meta-Analyses (PRISMA) guidelines were adopted.[39] Participants, 105
interventions, comparators, outcomes, and study design (P.I.C.O.S.) were established as 106
follows: (i) participants with no restriction regarding health, sex, age, or training status; (ii) ST 107
interventions supervised by a certified professional, using resistance training or similar 108
protocols; (iii) comparators were supervised groups performing any form of stretching (iv) 109
outcomes were ROM assessed in any joint; (v) randomized controlled trials (RCTs). RCTs 110
reduce bias and better balance participant features between the groups,[38] and are important 111
for the advancement of sports science.[40] There were no limitations regarding intervention 112
length. 113
Reviews, letters to editors, trial registrations, proposals for protocols, editorials, book 114
chapters, and conference abstracts were excluded. Exclusion criteria based on P.I.C.O.S.: (i) 115
research with non-human animals; (ii) non-ST protocols or ST interventions combined with 116
other methods (e.g., endurance); unsupervised interventions; (iii) stretching or ST + stretching 117

7
interventions combined with other training methods (e.g., endurance); protocols without 118
stretching; unsupervised interventions; (iv) studies not reporting ROM; (v) non-randomized 119
interventions. 120
121
Information sources and search 122
Six databases were used to search and retrieve the articles in early October 2020: 123
Cochrane Library, EBSCO, PubMed (including MEDLINE), Scielo, Scopus, and Web of 124
Science (Core Collection). Boolean operators were applied to search the article title, abstract 125
and/or keywords: (“strength training” OR “resistance training” OR “weight training” OR 126
“plyometric*” OR “calisthenics”) AND (“flexibility” OR “stretching”) AND “range of 127
motion” AND “random*”. Specificities of each search engine: (i) in Cochrane Library, items 128
were limited to trials, including articles but excluding protocols, reviews, editorials and similar 129
publications; (ii) in EBSCO, the search was limited to articles in scientific, peer-reviewed 130
journals (iii) in PubMed, the search was limited to title or abstract; publications were limited 131
to RCTs and clinical trials, excluding books and documents, meta-analyses, reviews and 132
systematic reviews; (iv) in Scielo, Scopus and Web of Science, the publication type was limited 133
to article; and (v) in Web of Science, “topic” is the term used to refer to title, abstract and 134
keywords. 135
An additional search within the reference lists of the included records was conducted. 136
The list of articles and inclusion criteria were then sent to four experts to suggest additional 137
references. The search strategy and consulted databases were not provided in this process to 138
avoid biasing the experts’ searches. More detailed information is available as supplementary 139
material. 140
141
Search strategy 142

8
Here, we provide the specific example of search conducted in PubMed: 143
((("strength training"[Title/Abstract] OR "resistance training"[Title/Abstract] OR 144
"weight training"[Title/Abstract] OR "plyometric*"[Title/Abstract] OR 145
"calisthenics"[Title/Abstract]) AND (“flexibility”[Title/Abstract] OR 146
“stretching”[Title/Abstract])) AND (“range of motion”[Title/Abstract])) AND 147
(“random*”[Title/Abstract]). 148
After this search, the filters RCT and Clinical Trial were applied. 149
150
Study selection 151
J.A. and F.M.C. each conducted the initial search and selection stages independently, 152
and then compared result to ensure accuracy. J.F. and T.R. independently reviewed the process 153
to detect potential errors. When necessary, re-analysis was conducted until a consensus was 154
achieved. 155
156
Data collection process 157
J.A., F.M.C., A.A.M. and J.F. extracted data, while J.M., T.R., R.Z. and A.M. 158
independently revised the process. Data for the meta-analysis was extracted by JA and 159
independently verified by A.A.M. and R.R.C. Data is available for sharing. 160
161
Data items 162
Data items: (i) Population: subjects, health status, sex/gender, age, training status, 163
selection of subjects; (ii) Intervention and comparators: study length in weeks, weekly 164
frequency of the sessions, weekly training volume in minutes, session duration in minutes, 165
number of exercises per session, number of sets and repetitions per exercise, load (e.g., % 166
1RM), full vs. partial ROM, supervision ratio; in the comparators, modality of stretching 167
applied was also considered; adherence rates were considered a posteriori; (iii) ROM testing: 168

9
joints and actions, body positions (e.g., standing, supine), mode of testing (i.e., active, passive, 169
both), pre-testing warm-up, timing (e.g., pre- and post-intervention, intermediate assessments), 170
results considered for a given test (e.g., average of three measures), data reliability, number of 171
testers and instructions provided during testing; (iv) Outcomes: changes in ROM for 172
intervention and comparator groups; (vi) funding and conflicts of interest. 173
174
Risk of bias in individual studies 175
Risk of bias (RoB) in individual studies was assessed using the Cochrane risk-of-bias 176
tool for randomized trials (RoB 2).[41] J.A. and A.M. independently completed RoB analysis, 177
which was reviewed by F.M.C. Where inconsistencies emerged, the original articles were re-178
analyzed until a consensus was achieved. 179
180
Summary measures 181
Meta-analysis was conducted when ≥3 studies were available.[42] Pre- and post-182
intervention means and standard deviations (SDs) for dependent variables were used after 183
being converted to Hedges’s g effect size (ES).[42] When means and SDs were not available, 184
they were calculated from 95% confidence intervals (CIs) or standard error of mean (SEM), 185
using Cochrane’s RevMan Calculator for Microsoft Excel.[43] When ROM data from different 186
groups (e.g. men and women) or different joints (e.g. knee and ankle) was pooled, weighted 187
formulas were applied.[38] 188
189
Synthesis of results 190
The inverse variance random-effects model for meta-analyses was used to allocate a 191
proportionate weight to trials based on the size of their individual standard errors,[44] and 192
accounting for heterogeneity across studies.[45] The ESs were presented alongside 95% CIs 193

10
and interpreted using the following thresholds:[46] <0×2, trivial; 0×2–0×6, small; >0×6–1×2, 194
moderate; >1×2–2×0, large; >2×0–4×0, very large; >4×0, extremely large. Heterogeneity was 195
assessed using the I2 statistic, with values of <25%, 25-75%, and >75% considered to represent 196
low, moderate, and high levels of heterogeneity, respectively.[47] 197
198
Risk of bias across studies 199
Publication bias was explored using the extended Egger’s test,[48] with p<0×05 200
implying bias. To adjust for publication bias, a sensitivity analysis was conducted using the 201
trim and fill method,[49] with L0 as the default estimator for the number of missing studies.[50] 202
203
Moderator analyses 204
Using a random-effects model and independent computed single factor analysis, 205
potential sources of heterogeneity likely to influence the effects of training interventions were 206
selected, including i) ROM type (i.e., passive vs active), ii) studies RoB in randomization and 207
iii) studies RoB in measurement of the outcome.[51] These analyses were decided post-208
protocol registration. 209
210
All analyses were carried out using the Comprehensive Meta-Analysis program 211
(version 2; Biostat, Englewood, NJ, USA). Statistical significance was set at p≤0×05. Data for 212
the meta-analysis was extracted by JA and independently verified by A.A.M. and R.R.C. 213
214
Quality and confidence in findings 215
Although not planned in the registered protocol, we decided to abide by the Grading of 216
Recommendations Assessment, Development, and Evaluation (GRADE),[52] which addresses 217
five dimensions that can downgrade studies when assessing the quality of evidence in RCTs. 218

11
RoB, inconsistency (through heterogeneity measures), and publication bias were addressed 219
above and were considered a priori. Directness was guaranteed by design, as no surrogates 220
were used for any of the pre-defined P.I.C.O. dimensions. Imprecision was assessed on the 221
basis of 95% CIs. 222
223
224
RESULTS 225
Study selection 226
Initial search returned 194 results (52 in Cochrane Library, 11 in EBSCO, 11 in 227
PubMed, 9 in Scielo, 88 in Scopus, and 23 in Web of Science). After removal of duplicates, 228
121 records remained. Screening the titles and abstracts for eligibility criteria resulted in the 229
exclusion of 106 articles: 26 were not original research articles (e.g., trial registrations, 230
reviews), 24 were out of scope, 48 did not have the required intervention or comparators, five 231
did not assess ROM, two were non-randomized and one was unsupervised. Fifteen articles 232
were eligible for full-text analysis. One article did not have the required intervention,[53] and 233
two did not have the needed comparators.[54, 55] In one article, the ST and stretching groups 234
performed a 20-30 minutes warm-up following an unspecified protocol.[56] In another, the 235
intervention and comparator were unsupervised[57], and in one the stretching group was 236
unsupervised[58]. Finally, in one article, 75% of the training sessions were unsupervised.[59] 237
Therefore, eight articles were included at this stage.[24, 34-37, 60-62] 238
A manual search within the reference lists of the included articles revealed five 239
additional potentially fitting articles. Two lacked the intervention group required[63, 64] and 240
two were non-randomized.[65, 66] One article met the inclusion criteria.[67] Four experts 241
revised the inclusion criteria and the list of articles and suggested eight articles based on their 242
titles and abstracts. Six were excluded: interventions were multicomponent;[68, 69] 243

12
comparators performed no exercise;[70, 71] out of scope;[72] and unsupervised stretching 244
group.[73] Two articles were included,[74, 75] increasing the list to eleven articles,[24, 34-37, 245
60-62, 67, 74, 75] with 452 participants eligible for meta-analysis (Figure 1). 246
247
248

13
249
250
Figure 1. Flowchart describing the study selection process. 251
252
253
Records identified through database search
(n = 194)
Records after duplicates removed (n = 121)
Records screened (n = 121)
Records excluded (n = 106)
Full-text articles assessed for eligibility (n = 15)
Full-text articles excluded, with reasons (n = 7)
• 3 articles did not have the required intervention and/or comparators.
• 3 had at least one group of interest performing the intervention unsupervised.
• 1 had an undisclosed warm-up protocol that was longer than the intervention.
Studies included in qualitative synthesis (n = 8+1+2 = 11)
Studies included in quantitative synthesis (n = 11)
Additional records fitting inclusion criteria identified after search within the reference
lists of the included articles (n = 1)
Additional records fitting inclusion criteria recommended by four external experts from two countries and three different institutions
(n = 2)
14
254
Study characteristics and results 255
The data items can be found in Table 1. The study of Wyon, Smith [62] required 256
consultation of a previous paper[76] to provide essential information. Samples ranged from 257
27[37] to 124 subjects,[34] including: trained participants,[24, 36, 61, 62] healthy sedentary 258
participants,[35, 60, 67] sedentary and trained participants,[75] workers with chronic neck 259
pain,[37] participants with fibromyalgia,[74] and elderly participants with difficulties in at least 260
one of four tasks: transferring, bathing, toileting, and walking.[34] Seven articles included only 261
women[36, 62, 67, 74] or predominantly women,[34, 35, 37] three investigated only men[24, 262
75] or predominantly men,[60] and one article had a balanced mixture of men and women.[61] 263
Interventions lasted between five[60] and 16 weeks[67]. Minimum weekly training frequency 264
was two sessions[37, 74] and maximum was five.[62] Six articles provided insufficient 265
information concerning session duration.[35, 36, 61, 62, 67, 75] Ten articles vaguely defined 266
training load for the ST and stretching groups,[24, 34, 37, 60, 61, 74, 75] or for stretching 267
groups.[35, 36, 67] Six articles did not report on using partial or full ROM during ST 268
exercises.[24, 34, 36, 37, 61, 67] Different stretching modalities were implemented: static 269
active,[35, 37, 60, 67, 74, 75] dynamic,[34, 36] dynamic with a 10-second hold,[24] static 270
active in one group and static passive in another,[62] and a combination of dynamic, static 271
active, and PNF.[61] 272
Hip joint ROM was assessed in seven articles,[24, 34, 36, 60-62, 67] knee ROM in 273
five,[34-36, 60, 75] shoulder ROM in four,[34, 36, 60, 74] elbow and trunk ROM in two,[34, 274
36] and cervical spine[37] and the ankle joint ROM in one article.[34] In one article, active 275
ROM (AROM) was tested for the trunk, while passive ROM (PROM) was tested for the other 276
joints.[34] In one article, PROM was tested for goniometric assessments and AROM for hip 277
flexion.[36] In another, AROM was assessed for the shoulder and PROM for the hip and 278

15
knee.[60] Three articles only assessed PROM[35, 61, 75] and four AROM,[24, 37, 67, 74] 279
while one assessed both for the same joint.[62] 280
281
282

16
Table 1. Characteristics of included randomized trials. 283 Article Population and common
program features Strength training group Comparator group(s)* ROM testing Qualitative
results for ROM Task-Specific
Resistance Training to Improve the Ability of
Activities of Daily Living–Impaired Older Adults to Rise from a Bed and
from a Chair.[34]
Subjects: 161. Health status: Elderly people
dependent on help for performing at least one of four
tasks: transferring, bathing, toileting and walking.
Gender: ST: 84% women; STRE: 88% women.
Age: ST: 82·0±6·4; STRE: 82·4±6·3.
Training status: Not participating in regular
strenuous exercise. Selection of subjects: Seven
congregate housing facilities. Length (weeks): 12. Weekly sessions: 3.
Adherence: average 81% of the sessions.
Funding: National Institute on Aging (NIA) Claude Pepper Older Adults Independence
Center (Grant AG0 8808 and NIA Grant AG10542), the Department of Veterans Affairs Rehabilitation
Research and Development, and the AARP-Andrus
Foundation. Conflicts of interest: N/A.
n = 81 (60 completed). Weekly volume (minutes):
180. Session duration in
minutes: 60. No. exercises per session:
16. No. sets and repetitions:
1*7-8 based on maximum target of 9 (bed-rise tasks). 1*5 based on maximum target of 6
(chair-rise tasks). Load: Unclear. Loads were incremented if
subjects were not feeling challenged enough.
Full or partial ROM: N/A.
Supervision ratio: 1:1.
STRE n = 80 (64 completed). Weekly volume (minutes): 180.
Session duration in minutes: 60. No. exercises per session: N/A. No. sets and repetitions: N/A. Stretching modality: Dynamic.
Load: Low-intensity, but without a specified criterion.
Full or partial ROM: N/A. Supervision ratio: One supervisor per group, but group size was N/A.
Joints and actions: Elbow (extension), shoulder
(abduction), hip (flexion and abduction), knee (flexion and
extension), ankle (dorsiflexion) and trunk
(flexion, extension, lateral flexion).
Positions: Supine (elbow, shoulder, hip, knee and
ankle); standing (lumbar spine).
Mode: Active for trunk, passive for the other joints.
Warm-up: N/A. Timing: Baseline, 6 weeks,
12 weeks. Results considered in the
tests: N/A. Data reliability: ICCs of 0·65
to 0·86 for trunk measures. Unreported for other
measures. No. testers: N/A.
Instructions during testing: N/A.
The ST group had significant
improvements in all ROM
measures, except hip flexion and
abduction.
The STRE group had no significant change in any of the ROM values.
Stretching versus strength training
in lengthened position in
subjects with tight hamstring
Subjects: 45 undergraduate students.
Health status: 30º knee extension deficit with the hip
at 90º when in supine position. No injuries in the
n = 15. Weekly volume (minutes):
N/A. Session duration in
minutes: N/A.
STRE n = 15. Weekly volume (minutes): N/A.
Session duration in minutes: N/A. No. exercises per session: 1.
No. sets and repetitions: 4*30’’. Stretching modality: Static.
Joints and actions: Knee (extension).
Positions: Sitting. Mode: Passive.
Warm-up: Yes, but unclear with regard to specifications.
None of the groups
experienced significant
improvements in ROM.

17
muscles: A randomized controlled trial.[35]
lower limbs and no lower back pain.
Gender: 39 women, 6 men. Age: 21·33±1·76 years (ST); 22·60±1·84 years (STRE).
Training status: No participation in ST or STRE
programs in the previous year. Selection of subjects:
announcements posted at the University.
Length (weeks): 8. Weekly sessions: 3. Adherence: N/A. Funding: N/A.
Conflicts of interest: N/A.
No. exercises per session: 1.
No. sets and repetitions: 3*12.
Load: 60% of 1RM. Full or partial ROM:
Partial. Supervision ratio: N/A.
Load: Unclear. Full or partial ROM: Full.
Supervision ratio: N/A.
Timing: Baseline, 1-week post-protocol.
Results considered in the tests: mean of three
measures. Data reliability: High. No. testers: 1 (blinded).
Instructions during testing: N/A.
Group-based exercise at
workplace: short-term effects of
neck and shoulder resistance
training in video display unit
workers with work-related chronic neck pain – a pilot randomized
trial.[37]
Subjects: 35 video display unit workers, 27 completed
the program. Health status: chronic neck
pain. Gender: 27 women, 8 men. Age: 43 (41-45) in ST; 42
(38·5-44) in STRE. Training status: N/A.
Selection of subjects: intranet form.
Length (weeks): 7. Weekly sessions: 2.
Adherence: average 85% of the sessions in ST and 86% in
STRE. Funding: Under
“disclosures”, the authors stated “none”.
Conflicts of interest: Under “disclosures”, the authors
stated “none”.
n = 14. Weekly volume (minutes):
90. Session duration in
minutes: 45. No. exercises per session:
10. No. sets and repetitions:
2-3*8-20. Isometric contractions up to 30’’.
Load: free-weights with a maximum of 75% MVC
and elastic bands of unspecified load.
Full or partial ROM: N/A.
Supervision ratio: ~1:8.
STRE n = 13. Weekly volume (minutes): 90.
Session duration in minutes: 45. No. exercises per session: 11.
No. sets and repetitions: 10*10’’. Stretching modality: Static.
Load: N/A. Full or partial ROM: N/A.
Supervision ratio: ~1:8.
Joints and actions: Cervical spine (flexion, extension, lateral flexion, rotation).
Positions: Sitting (flexion, extension, lateral flexion) and
supine position (rotation). Mode: Active.
Warm-up: N/A. Timing: Baseline, 1-week
post-protocol. Results considered in the
tests: N/A. Data reliability: N/A.
No. testers: 1 (blinded). Instructions during testing:
N/A.
Significant improvements in both groups for
all ROM measurements.
No differences
between the two groups.
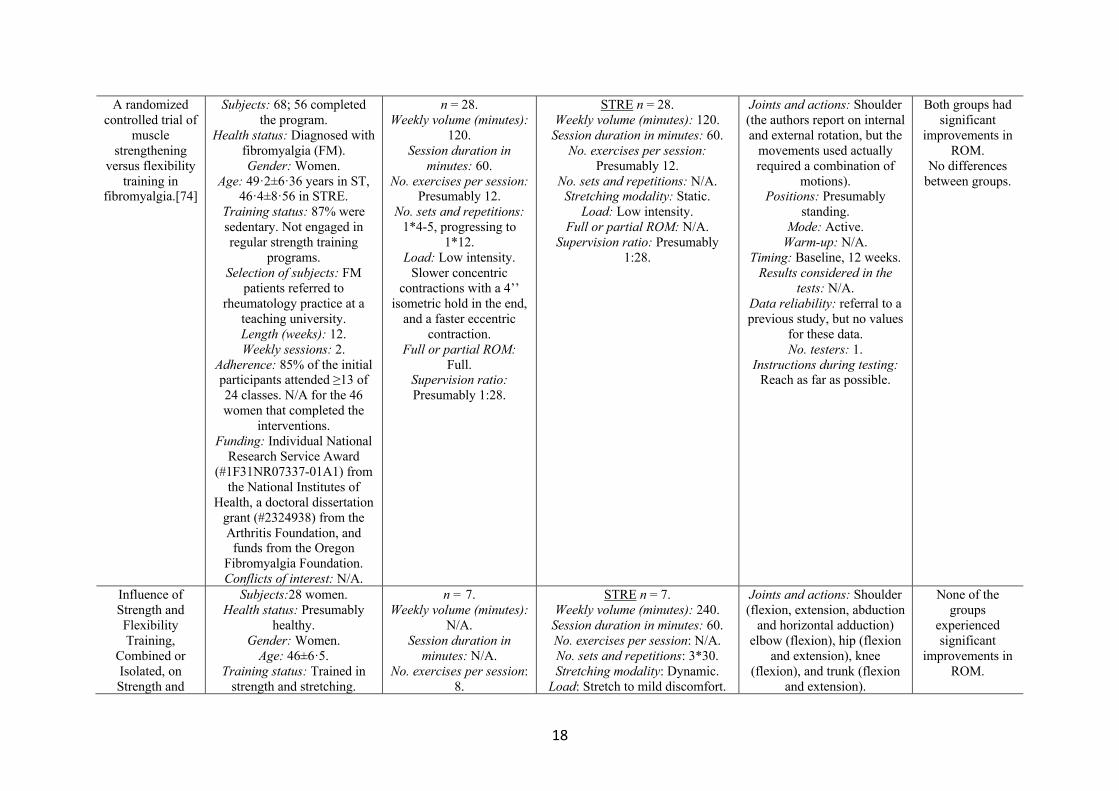
18
A randomized controlled trial of
muscle strengthening
versus flexibility training in
fibromyalgia.[74]
Subjects: 68; 56 completed the program.
Health status: Diagnosed with fibromyalgia (FM). Gender: Women.
Age: 49·2±6·36 years in ST, 46·4±8·56 in STRE.
Training status: 87% were sedentary. Not engaged in regular strength training
programs. Selection of subjects: FM
patients referred to rheumatology practice at a
teaching university. Length (weeks): 12. Weekly sessions: 2.
Adherence: 85% of the initial participants attended ≥13 of 24 classes. N/A for the 46 women that completed the
interventions. Funding: Individual National
Research Service Award (#1F31NR07337-01A1) from
the National Institutes of Health, a doctoral dissertation
grant (#2324938) from the Arthritis Foundation, and funds from the Oregon
Fibromyalgia Foundation. Conflicts of interest: N/A.
n = 28. Weekly volume (minutes):
120. Session duration in
minutes: 60. No. exercises per session:
Presumably 12. No. sets and repetitions:
1*4-5, progressing to 1*12.
Load: Low intensity. Slower concentric
contractions with a 4’’ isometric hold in the end,
and a faster eccentric contraction.
Full or partial ROM: Full.
Supervision ratio: Presumably 1:28.
STRE n = 28. Weekly volume (minutes): 120.
Session duration in minutes: 60. No. exercises per session:
Presumably 12. No. sets and repetitions: N/A.
Stretching modality: Static. Load: Low intensity.
Full or partial ROM: N/A. Supervision ratio: Presumably
1:28.
Joints and actions: Shoulder (the authors report on internal and external rotation, but the
movements used actually required a combination of
motions). Positions: Presumably
standing. Mode: Active.
Warm-up: N/A. Timing: Baseline, 12 weeks.
Results considered in the tests: N/A.
Data reliability: referral to a previous study, but no values
for these data. No. testers: 1.
Instructions during testing: Reach as far as possible.
Both groups had significant
improvements in ROM.
No differences between groups.
Influence of Strength and Flexibility Training,
Combined or Isolated, on Strength and
Subjects:28 women. Health status: Presumably
healthy. Gender: Women.
Age: 46±6·5. Training status: Trained in
strength and stretching.
n = 7. Weekly volume (minutes):
N/A. Session duration in
minutes: N/A. No. exercises per session:
8.
STRE n = 7. Weekly volume (minutes): 240.
Session duration in minutes: 60. No. exercises per session: N/A. No. sets and repetitions: 3*30. Stretching modality: Dynamic.
Load: Stretch to mild discomfort.
Joints and actions: Shoulder (flexion, extension, abduction
and horizontal adduction) elbow (flexion), hip (flexion
and extension), knee (flexion), and trunk (flexion
and extension).
None of the groups
experienced significant
improvements in ROM.

19
Flexibility Gains.[36]
Selection of subjects: Volunteers that would refrain
from exercise outside the intervention.
Length (weeks):12. Weekly sessions: 4. Not
explicit; 48 sessions over 12 weeks.
Adherence: Minimum was 44 of the 48 sessions.
Funding: N/A. Conflicts of interest: N/A.
No. sets and repetitions: 3*8-12 during the 1st
month; 3*6-10RM in the 2nd month; 3*10-15RM in
the 3rd month. Load: 6-15RM,
depending on the month. Full or partial ROM:
N/A. Supervision ratio: N/A.
Full or partial ROM: Full. Supervision ratio: N/A.
STRE + ST n = 7.
Completion of both protocols. Unknown duration.
ST + STRE n = 7.
Completion of both protocols in reverse order. Unknown duration.
Positions: Supine (shoulder flexion, abduction, horizontal
adduction, elbow and hip flexion), prone (shoulder and
hip extension, and knee flexion) and upright (trunk flexion and extension) for goniometric evaluations. Sitting for sit-and-reach.
Mode: Passive for goniometry. Active for sit-
and-reach. Warm-up: 5- minute walking
on treadmill at mild to moderate intensity and four
stretching exercises. Timing: Baseline, 12 weeks.
Results considered in the tests: Best of 3 trials.
Data reliability: Very high. No. testers: 1.
Instructions during testing: N/A.
Effects of Flexibility and
Strength Interventions on Optimal Lengths
of Hamstring Muscle-Tendon
Units.[61]
Subjects: 40 college students. Health status: No history of
lower extremity injury in the 2 years prior to the study.
Gender: 20 men, 20 women.
Age: 18–24 years. Training status: participating
in exercise 2–3 times per week.
Selection of subjects: college students.
Length (weeks): 8. Weekly sessions: 3. Adherence: N/A.
n = 20. Weekly volume (minutes):
N/A. Session duration in
minutes: N/A No. exercises per session:
4. No. sets and repetitions:
2-4*8-15. For one exercise, 2*50-60’’.
Load: N/A. Full or partial ROM:
N/A. Supervision ratio: N/A.
STRE n = 20. Weekly volume (minutes): N/A.
Session duration in minutes: N/A. No. exercises per session: 4.
No. sets and repetitions: 2*15 for dynamic stretching, 2*40-60’’ for static stretching, 3*50’’ for PNF
and 3*40-50’’ for foam roll. Stretching modality: active static,
dynamic and PNF. Load: N/A.
Full or partial ROM: N/A. Supervision ratio: N/A.
Joints and actions: Hip (flexion).
Positions: Supine. Mode: Passive.
Warm-up: Six-minute warm-up including jogging and
jumping. Timing: Baseline, 8 weeks. Results considered in the tests: Mean of three trials.
Data reliability: Very high. No. testers: N/A.
Instructions during testing: N/A.
Men and women in both groups significantly
improved ROM.
No differences between groups.
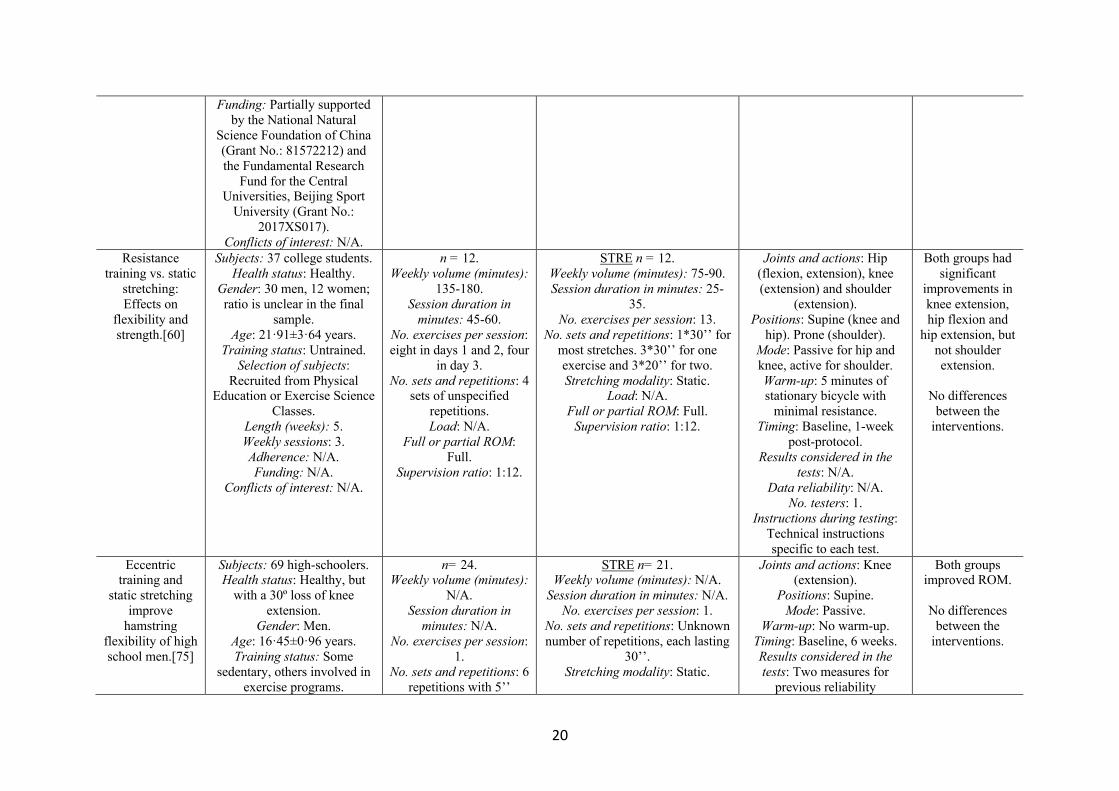
20
Funding: Partially supported by the National Natural
Science Foundation of China (Grant No.: 81572212) and the Fundamental Research
Fund for the Central Universities, Beijing Sport
University (Grant No.: 2017XS017).
Conflicts of interest: N/A. Resistance
training vs. static stretching: Effects on
flexibility and strength.[60]
Subjects: 37 college students. Health status: Healthy.
Gender: 30 men, 12 women; ratio is unclear in the final
sample. Age: 21·91±3·64 years.
Training status: Untrained. Selection of subjects:
Recruited from Physical Education or Exercise Science
Classes. Length (weeks): 5. Weekly sessions: 3. Adherence: N/A. Funding: N/A.
Conflicts of interest: N/A.
n = 12. Weekly volume (minutes):
135-180. Session duration in
minutes: 45-60. No. exercises per session: eight in days 1 and 2, four
in day 3. No. sets and repetitions: 4
sets of unspecified repetitions. Load: N/A.
Full or partial ROM: Full.
Supervision ratio: 1:12.
STRE n = 12. Weekly volume (minutes): 75-90. Session duration in minutes: 25-
35. No. exercises per session: 13.
No. sets and repetitions: 1*30’’ for most stretches. 3*30’’ for one exercise and 3*20’’ for two. Stretching modality: Static.
Load: N/A. Full or partial ROM: Full.
Supervision ratio: 1:12.
Joints and actions: Hip (flexion, extension), knee (extension) and shoulder
(extension). Positions: Supine (knee and
hip). Prone (shoulder). Mode: Passive for hip and knee, active for shoulder. Warm-up: 5 minutes of stationary bicycle with
minimal resistance. Timing: Baseline, 1-week
post-protocol. Results considered in the
tests: N/A. Data reliability: N/A.
No. testers: 1. Instructions during testing:
Technical instructions specific to each test.
Both groups had significant
improvements in knee extension, hip flexion and
hip extension, but not shoulder extension.
No differences
between the interventions.
Eccentric training and
static stretching improve
hamstring flexibility of high school men.[75]
Subjects: 69 high-schoolers. Health status: Healthy, but
with a 30º loss of knee extension.
Gender: Men. Age: 16·45±0·96 years. Training status: Some
sedentary, others involved in exercise programs.
n= 24. Weekly volume (minutes):
N/A. Session duration in
minutes: N/A. No. exercises per session:
1. No. sets and repetitions: 6
repetitions with 5’’
STRE n= 21. Weekly volume (minutes): N/A.
Session duration in minutes: N/A. No. exercises per session: 1.
No. sets and repetitions: Unknown number of repetitions, each lasting
30’’. Stretching modality: Static.
Joints and actions: Knee (extension).
Positions: Supine. Mode: Passive.
Warm-up: No warm-up. Timing: Baseline, 6 weeks. Results considered in the tests: Two measures for
previous reliability
Both groups improved ROM.
No differences
between the interventions.

21
Selection of subjects: Volunteers with tight
hamstrings. Length (weeks): 6.
Weekly sessions: 3 for STRE. N/A for ST.
Adherence: N/A for ST. STRE: subjects missing >4
sessions were excluded. Funding: N/A.
Conflicts of interest: N/A.
isometric hold between each.
Load: N/A. Full or partial ROM:
Full. Supervision ratio:
Description suggests a 1:1 ratio.
Load: Stretch until a gentle stretch was felt on the posterior thigh.
Full or partial ROM: Full. Supervision ratio: Description
suggests a 1:1 ratio.
calculations, but unclear for the groups’ evaluation.
Data reliability: Very high. No. testers: 2 (1 blinded).
Instructions during testing: N/A.
Effects of flexibility
combined with plyometric
exercises vs. isolated
plyometric or flexibility mode
in adolescent men
hurdlers.[24]
Subjects: 34 trained hurdlers. Health status: No lower extremity injury in the
previous 30 days. Gender: Men.
Age: 15±0·7 years. Training status: ≥3 years of experience in hurdle racing.
Selection of subjects: Recruited from three athletic
teams. Length (weeks): 12. Weekly sessions: 4. Adherence: N/A.
Funding: No funding. Conflicts of interest: No
conflicts of interest.
n= 9. Weekly volume (minutes):
320. Session duration in
minutes: 80. No. exercises per session:
4. No. sets and repetitions:
3*30’’. Load: Evolved from low to hard intensity, but no criteria were provided. Full or partial ROM:
N/A. Supervision ratio: N/A.
STRE n = 8. Weekly volume (minutes): 320.
Session duration in minutes: 80. No. exercises per session: 7.
No. sets and repetitions: 5*10’’. Stretching modality: Dynamic with
10’’ static hold. Load: Evolved from low to hard
intensity, but no criteria were provided.
Full or partial ROM: N/A. Supervision ratio: N/A.
STRE+ ST n = 9.
Weekly volume (minutes): 320. Session duration in minutes: 80. No. exercises per session: 11 (4
plyometric; 7 flexibility). No. sets and repetitions: 3*30’’ for plyometrics, 5*10’’ for stretching. Stretching modality: Dynamic with
10’’ static hold. Load: Evolved from low to hard
intensity, but no criteria were provided.
Full or partial ROM: N/A. Supervision ratio: N/A.
Joints and actions: Hip (flexion and extension).
Positions: Supine. Mode: Active.
Warm-up: N/A. Timing: Baseline, 12 weeks.
Results considered in the tests: Best of 3 attempts.
Data reliability: Referral to a previous study, but no values
for these data. No. testers: 2.
Instructions during testing: N/A.
All interventions had significant
improvements in ROM.
No differences
between the interventions.

22
The influence of strength,
flexibility, and simultaneous training on
flexibility and strength
gains.[67]
Subjects: 80 women. Health status: Healthy.
Gender: Women. Age: 35±2·0 (ST), 34±1·2
(STRE), 35±1·8 (ST + STRE), 34±2·1 (non-
exercise). Training status: Sedentary.
Selection of subjects: Volunteers that were
sedentary ≥12 months. Length (weeks): 16. Weekly sessions: 3.
Adherence: Minimum was 46 of the 48 sessions.
Funding: N/A. Conflicts of interest: N/A.
n = 20. Weekly volume (minutes):
N/A. Session duration in
minutes: N/A. No. exercises per session:
8. No. sets and repetitions: 3*8-12 in the 1st and 4th months; 3*6-10 in 2nd month; 3*10-15 in 3rd
month. Load: 8-12RM (1st and
4th months); 6-10RM (2nd month); 10-15RM (3rd
month). Full or partial ROM:
N/A. Supervision ratio: N/A.
STRE n = 20. Weekly volume (minutes): N/A.
Session duration in minutes: N/A. No. exercises per session: N/A. No. sets and repetitions: 4*15-
60’’. Duration of each set started at 15’’ and progressed to 60’’ during
the intervention. Stretching modality: Static.
Load: Performed at the point of mild discomfort.
Full or partial ROM: N/A. Supervision ratio: N/A.
ST + STRE n = 20.
STRE protocol followed by the ST protocol.
Joints and actions: Hip (flexion) and knee
(extension) combined. Positions: Sitting.
Mode: Active. Warm-up: 4 stretching
exercises (2*10’’). Timing: Baseline, 16 weeks.
Results considered in the tests: Maximum of 3
attempts. Data reliability: Very high.
No. testers: 1. Instructions during testing:
N/A.
The interventions significantly
improved ROM.
No differences between the
interventions.
A comparison of strength and
stretch interventions on
active and passive ranges of
movement in dancers: a
randomized control trial.[62]
Subjects: 39 dance students, 35 completed.
Health status: N/A. Gender: Women (39).
Age: 17±0·49 years (ST group); 17±0·56 years (low-intensity STRE); 17±0·56 years (moderate to high
intensity STRE). Training status: Moderately
trained dance students. Selection of subjects:
Recruited from dance college. Length (weeks): 6. Weekly sessions: 5. Adherence: N/A. Funding: N/A.
Conflicts of interest: N/A.
n = 11. Weekly volume (minutes):
N/A. Session duration in
minutes: N/A. No. exercises per session:
1. No. sets and repetitions: 3*5, increasing to 3*10
during the program. Each repetition included a 3’’
isometric hold. Load: Unclear, but using
body weight. Full or partial ROM:
Partial (final 10º). Supervision ratio: N/A.
Low-intensity STRE n = 13. Weekly volume (minutes): N/A.
Session duration in minutes: N/A. No. exercises per session: 5.
No. sets and repetitions: N/A, but 1’ for each stretch.
Stretching modality: Active static. Load: 3/10 perceived exertion.
Full or partial ROM: N/A. Supervision ratio: N/A.
Moderate-intensity or high-
intensity STRE n = 11. Weekly volume (minutes): N/A.
Session duration in minutes: N/A. No. exercises per session: 5.
No. sets and repetitions: N/A. Stretching modality: Passive.
Load: 8/10 perceived exertion. Full or partial ROM: N/A.
Joints and actions: Hip (flexion).
Positions: Standing. Mode: Active and passive. Warm-up: 10 minutes of
cardiovascular exercise and lower limb stretches.
Timing: Baseline, 6 weeks. Results considered in the
tests: N/A. Data reliability: N/A.
No. testers: N/A. Instructions during testing:
Positioning cues for ensuring proper posture.
The three groups significantly
improved passive ROM, without
differences between the
groups.
The moderate-to-high intensity
STRE group did not improve in
active ROM. The two other
interventions did.

23
Supervision ratio: N/A. Legend: N/A – Information not available. ST – Strength training. STRE - Stretching. ROM – Range of motion. MVC – Maximum voluntary contraction. PNF – 284 Proprioceptive neuromuscular facilitation. * Non-exercise groups are not considered in this column. 285 286
287

24
288
289
In seven articles,[24, 37, 60, 61, 67, 74] ST and stretching groups significantly 290
improved ROM, and the differences between the groups were non-significant. In one article, 291
the ST group had significant improvements in 8 of 10 ROM measures, while dynamic 292
stretching did not lead to improvement in any of the groups.[34] In another article, the three 293
groups significantly improved PROM, without between-group differences; the ST and the 294
static active stretching groups also significantly improved AROM.[62] In two articles, none of 295
the groups improved ROM.[35, 36] 296
297
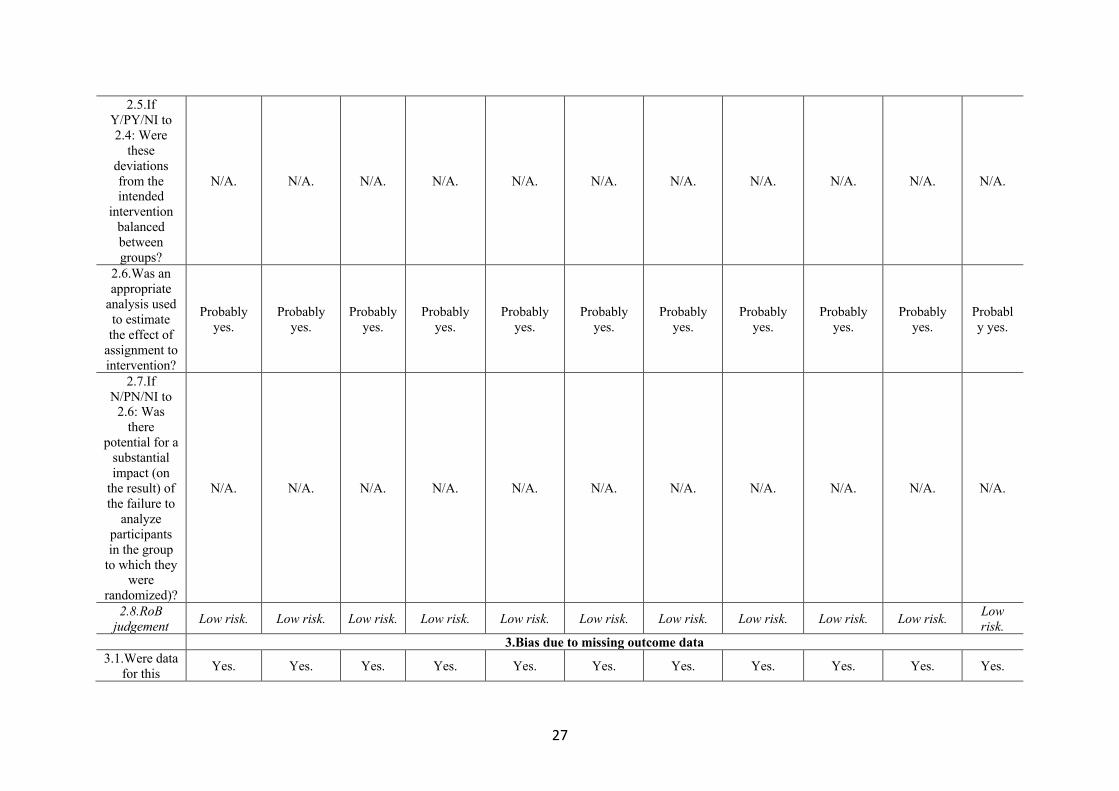
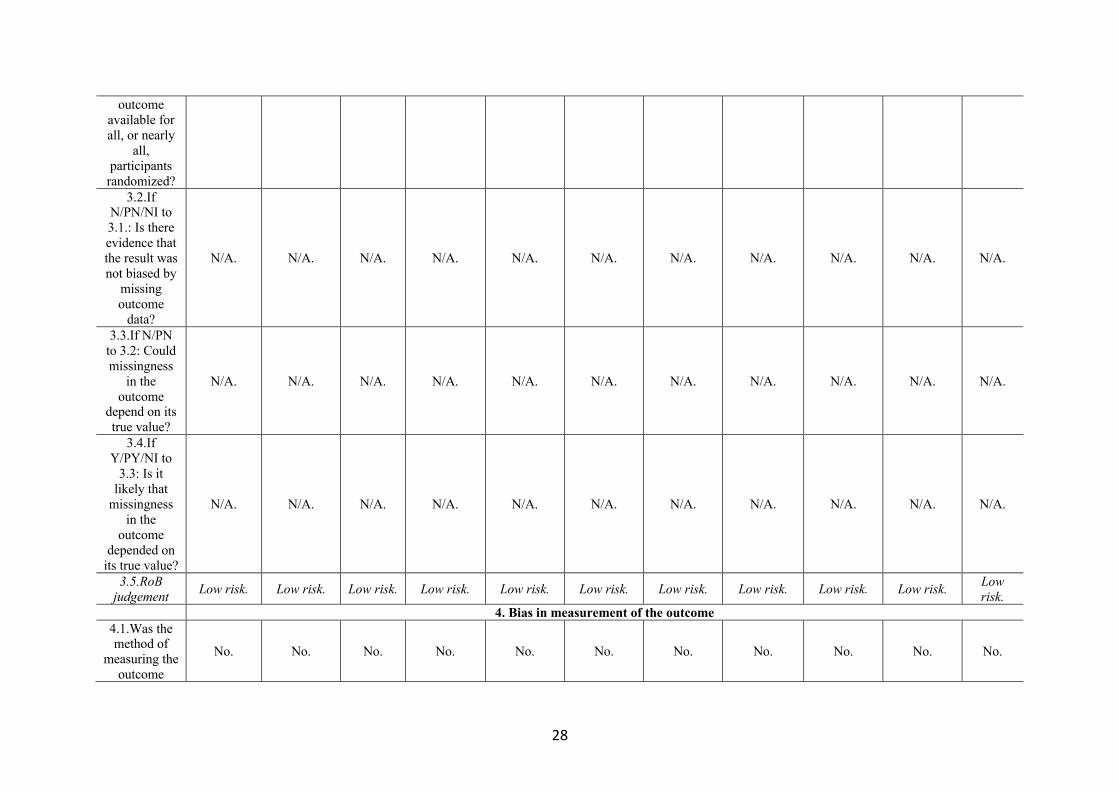
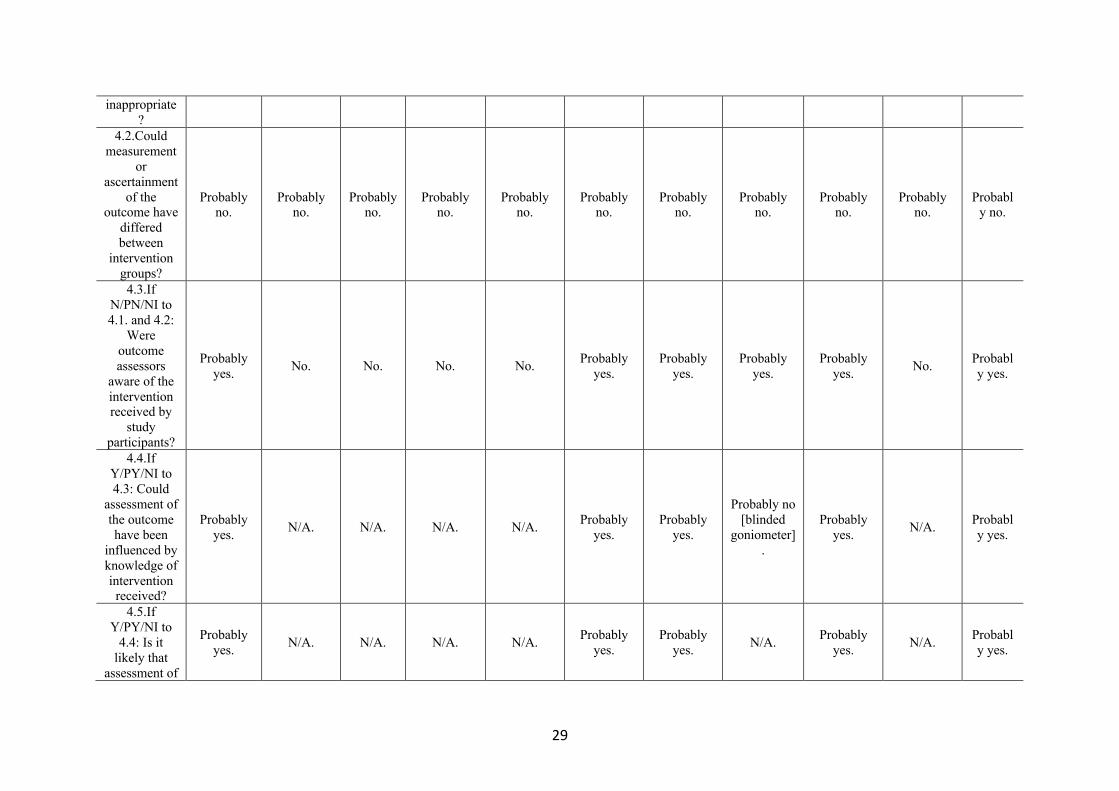
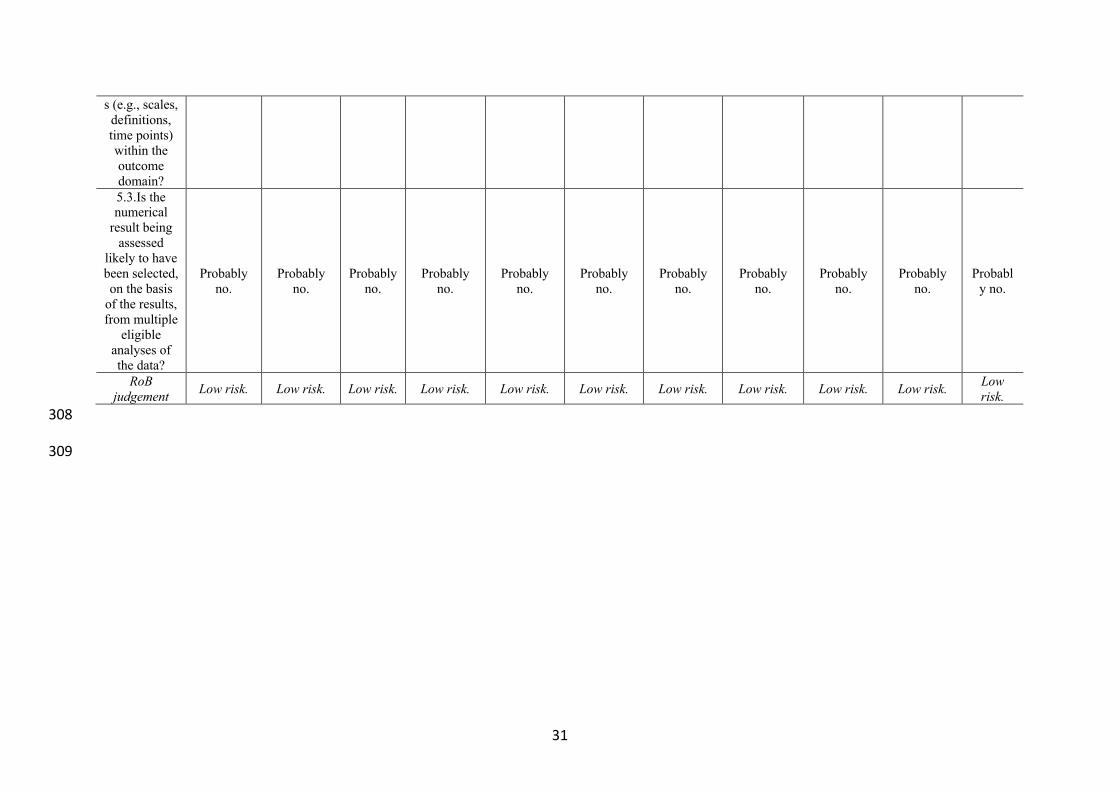
Risk of bias within studies 298
Table 2 presents assessments of RoB. Bias arising from the randomization process was 299
low in four articles,[34, 36, 62, 74] moderate in one,[37] and high in six.[24, 35, 60, 61, 67, 300
75] Bias due to deviations from intended interventions, missing outcome data, and selection of 301
the reported results was low. Bias in measurement of the outcome was low in six articles,[35-302
37, 67, 74, 75] but high in five.[24, 34, 60-62] 303
304
305
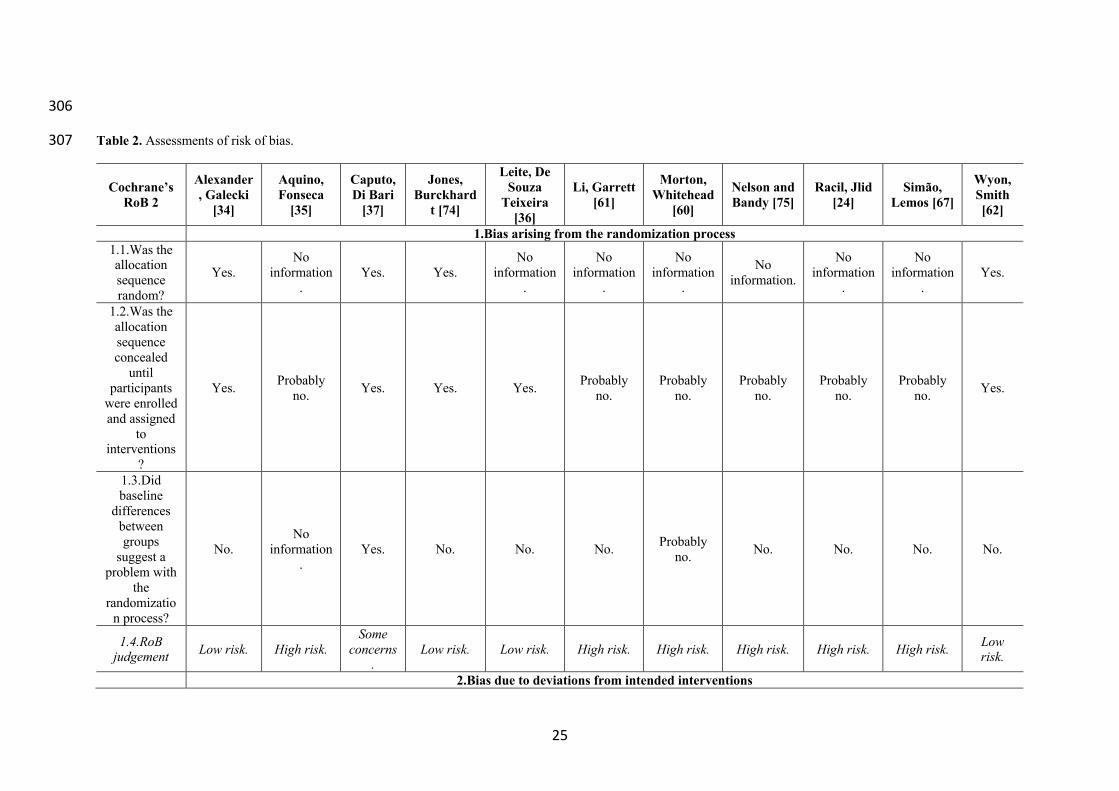
25
306
Table 2. Assessments of risk of bias. 307
Cochrane’s RoB 2
Alexander, Galecki
[34]
Aquino, Fonseca
[35]
Caputo, Di Bari
[37]
Jones, Burckhard
t [74]
Leite, De Souza
Teixeira [36]
Li, Garrett [61]
Morton, Whitehead
[60]
Nelson and Bandy [75]
Racil, Jlid [24]
Simão, Lemos [67]
Wyon, Smith [62]
1.Bias arising from the randomization process 1.1.Was the allocation sequence random?
Yes. No
information.
Yes. Yes. No
information.
No information
.
No information
.
No information.
No information
.
No information
. Yes.
1.2.Was the allocation sequence concealed
until participants
were enrolled and assigned
to interventions
?
Yes. Probably no. Yes. Yes. Yes. Probably
no. Probably
no. Probably
no. Probably
no. Probably
no. Yes.
1.3.Did baseline
differences between groups
suggest a problem with
the randomizatio
n process?
No. No
information.
Yes. No. No. No. Probably no. No. No. No. No.
1.4.RoB judgement Low risk. High risk.
Some concerns
. Low risk. Low risk. High risk. High risk. High risk. High risk. High risk. Low
risk.
2.Bias due to deviations from intended interventions

26
(effect of assignment to intervention) 2.1.Were
participants aware of their
assigned intervention during the
trial?
Yes. Yes. Yes. Yes. Yes. Yes. Yes. Yes. Yes. Yes. Yes.
2.2.Were carers and
people delivering the interventions
aware of participants’
assigned intervention during the
trial?
Yes. Yes. Yes. Yes. Yes. Yes. Yes. Yes. Yes. Yes. Yes.
2.3.If Y/PY/NI to 2.1 or 2.2: Were there deviations from the intended
intervention because of
the trial context?
Probably no.
Probably no.
Probably no.
Probably no.
Probably no.
Probably no.
Probably no.
Probably no.
Probably no.
Probably no.
Probably no.
2.4.If Y/PY to 2.3: Were
these deviations
likely to have affected the outcome?
N/A. N/A. N/A. N/A. N/A. N/A. N/A. N/A. N/A. N/A. N/A.
27
2.5.If Y/PY/NI to 2.4: Were
these deviations from the intended
intervention balanced between groups?
N/A. N/A. N/A. N/A. N/A. N/A. N/A. N/A. N/A. N/A. N/A.
2.6.Was an appropriate
analysis used to estimate the effect of
assignment to intervention?
Probably yes.
Probably yes.
Probably yes.
Probably yes.
Probably yes.
Probably yes.
Probably yes.
Probably yes.
Probably yes.
Probably yes.
Probably yes.
2.7.If N/PN/NI to
2.6: Was there
potential for a substantial impact (on
the result) of the failure to
analyze participants in the group
to which they were
randomized)?
N/A. N/A. N/A. N/A. N/A. N/A. N/A. N/A. N/A. N/A. N/A.
2.8.RoB judgement Low risk. Low risk. Low risk. Low risk. Low risk. Low risk. Low risk. Low risk. Low risk. Low risk. Low
risk. 3.Bias due to missing outcome data
3.1.Were data for this Yes. Yes. Yes. Yes. Yes. Yes. Yes. Yes. Yes. Yes. Yes.
28
outcome available for all, or nearly
all, participants randomized?
3.2.If N/PN/NI to 3.1.: Is there evidence that the result was not biased by
missing outcome
data?
N/A. N/A. N/A. N/A. N/A. N/A. N/A. N/A. N/A. N/A. N/A.
3.3.If N/PN to 3.2: Could missingness
in the outcome
depend on its true value?
N/A. N/A. N/A. N/A. N/A. N/A. N/A. N/A. N/A. N/A. N/A.
3.4.If Y/PY/NI to
3.3: Is it likely that
missingness in the
outcome depended on
its true value?
N/A. N/A. N/A. N/A. N/A. N/A. N/A. N/A. N/A. N/A. N/A.
3.5.RoB judgement Low risk. Low risk. Low risk. Low risk. Low risk. Low risk. Low risk. Low risk. Low risk. Low risk. Low
risk. 4. Bias in measurement of the outcome
4.1.Was the method of
measuring the outcome
No. No. No. No. No. No. No. No. No. No. No.
29
inappropriate?
4.2.Could measurement
or ascertainment
of the outcome have
differed between
intervention groups?
Probably no.
Probably no.
Probably no.
Probably no.
Probably no.
Probably no.
Probably no.
Probably no.
Probably no.
Probably no.
Probably no.
4.3.If N/PN/NI to 4.1. and 4.2:
Were outcome assessors
aware of the intervention received by
study participants?
Probably yes. No. No. No. No. Probably
yes. Probably
yes. Probably
yes. Probably
yes. No. Probably yes.
4.4.If Y/PY/NI to 4.3: Could
assessment of the outcome have been
influenced by knowledge of intervention received?
Probably yes. N/A. N/A. N/A. N/A. Probably
yes. Probably
yes.
Probably no [blinded
goniometer].
Probably yes. N/A. Probabl
y yes.
4.5.If Y/PY/NI to
4.4: Is it likely that
assessment of
Probably yes. N/A. N/A. N/A. N/A. Probably
yes. Probably
yes. N/A. Probably yes. N/A. Probabl
y yes.

30
the outcome was
influenced by knowledge of intervention received? 4.6.RoB
judgement High risk. Low risk. Low risk. Low risk. Low risk. High risk. High risk. Low risk. High risk. Low risk. High risk.
5.Bias in selection of the reported results 5.1.Were the
data that produced this
result analyzed in accordance with a pre-specified
analysis plan that was finalized before
unblinded outcome data
were available for
analysis?
Yes. Yes. Yes. Yes. Yes. Yes. Yes. Yes. Yes. Yes. Yes.
5.2.Is the numerical
result being assessed
likely to have been selected, on the basis
of the results, from multiple
eligible outcome
measurement
Probably no.
Probably no.
Probably no.
Probably no.
Probably no.
Probably no.
Probably no.
Probably no.
Probably no.
Probably no.
Probably no.
31
s (e.g., scales, definitions, time points) within the outcome domain? 5.3.Is the numerical
result being assessed
likely to have been selected, on the basis
of the results, from multiple
eligible analyses of the data?
Probably no.
Probably no.
Probably no.
Probably no.
Probably no.
Probably no.
Probably no.
Probably no.
Probably no.
Probably no.
Probably no.
RoB judgement Low risk. Low risk. Low risk. Low risk. Low risk. Low risk. Low risk. Low risk. Low risk. Low risk. Low
risk. 308
309
32
310
311
Synthesis of results 312
Comparisons were performed between ST and stretching groups, involving eleven 313
articles and 452 participants. Global effects on ROM were achieved pooling data from the 314
different joints. One article did not have the data required,[35] but the authors kindly supplied 315
it upon request. For another article,[36] we also requested data relative to the goniometric 316
evaluations, but obtained no response. Therefore, only data from the sit-and-reach test was 317
used. For one article,[37] means and SDs were obtained from 95% CIs, while in another SDs 318
were extracted from SEMs,[74] using Cochrane’s RevMan Calculator. 319
Of the five articles including both genders, four provided pooled data, with no 320
distinction between genders.[34, 35, 37, 60] One article presented data separated by gender, 321
without significant differences between men and women in response to interventions.[61] 322
Weighted formulas were applied sequentially for combining means and SDs of groups within 323
the same study.[38] Two studies presented the results separated by left and right lower limbs, 324
with both showing similar responses to the interventions;[24, 62] outcomes were combined 325
using the same weighted formulas for the means and SDs. Five articles only presented one 326
decimal place,[24, 34, 37, 61, 67] and so all values were rounded for uniformity. 327
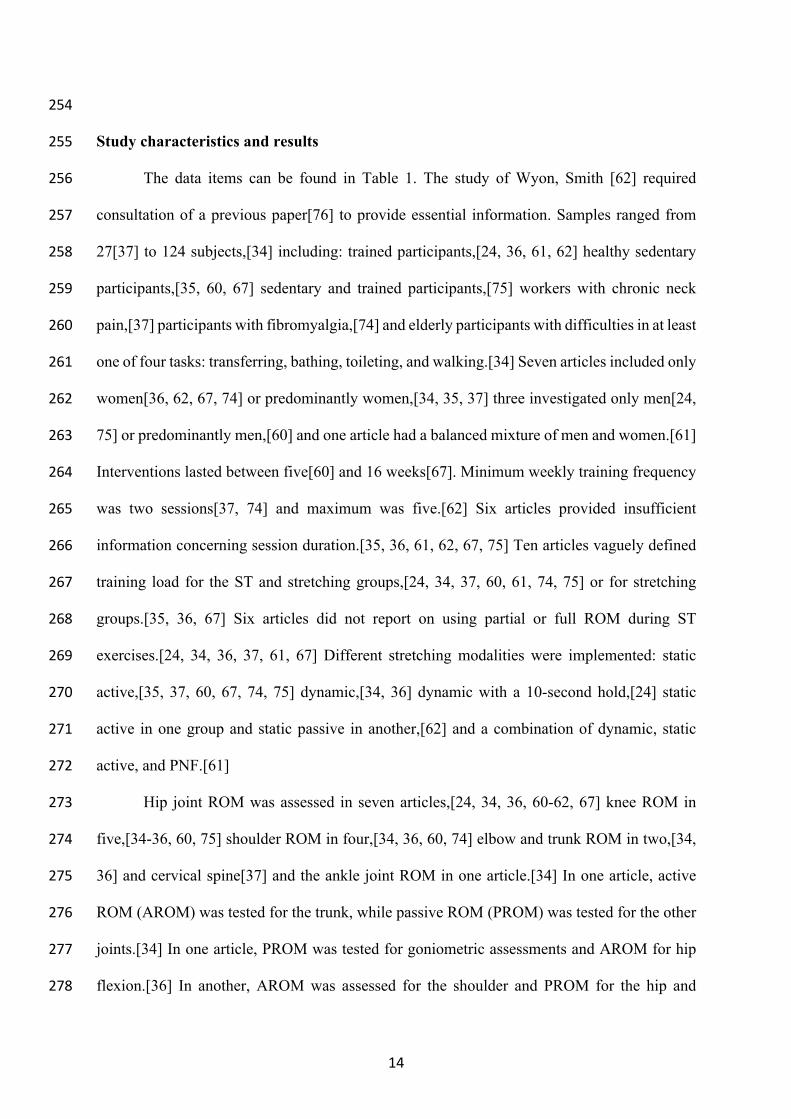
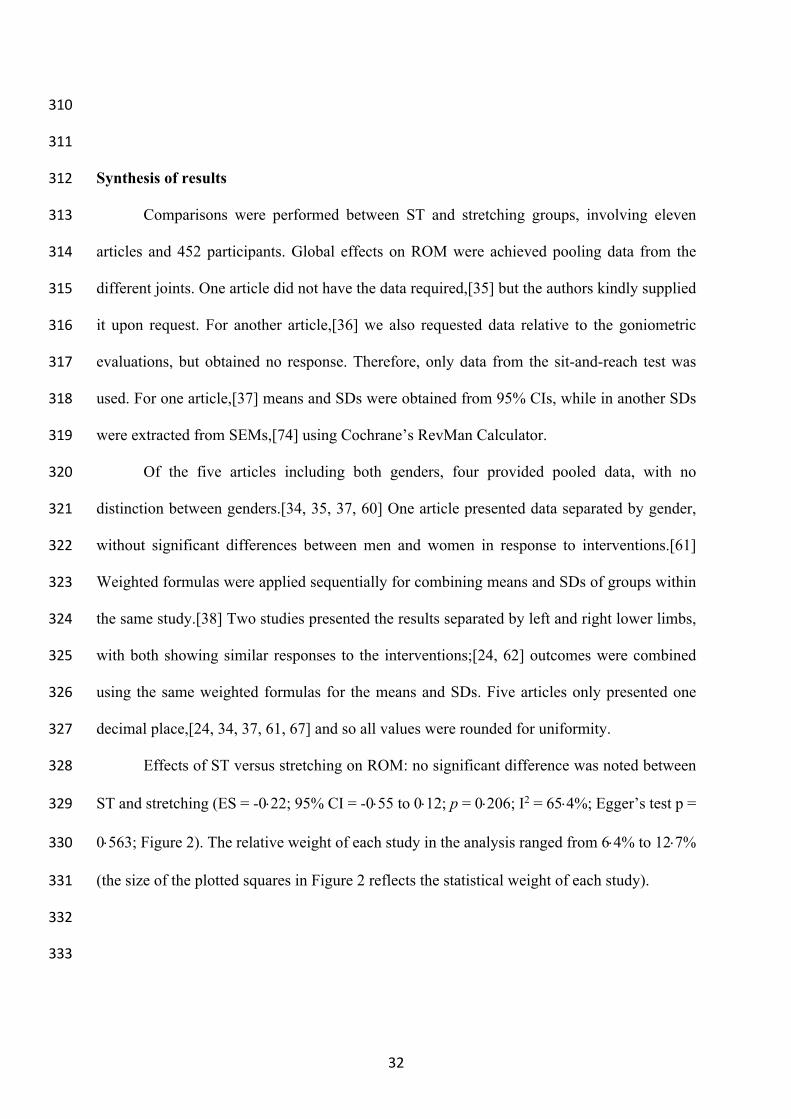
Effects of ST versus stretching on ROM: no significant difference was noted between 328
ST and stretching (ES = -0×22; 95% CI = -0×55 to 0×12; p = 0×206; I2 = 65×4%; Egger’s test p = 329
0×563; Figure 2). The relative weight of each study in the analysis ranged from 6×4% to 12×7% 330
(the size of the plotted squares in Figure 2 reflects the statistical weight of each study). 331
332
333

33
334
335
Figure 2. Forest plot of changes in ROM after participating in stretching-based compared to strength-based 336
training interventions. Values shown are effect sizes (Hedges’s g) with 95% confidence intervals (CI). The size 337
of the plotted squares reflects the statistical weight of the study. 338
339
Additional analysis 340
Effects of ST versus stretching on ROM, moderated by study RoB in randomization: No 341
significant sub-group differences in ROM changes (p = 0·256) was found when programs with 342
high RoB (6 studies; ES = -0·41; 95% CI = -1·02 to 0·20; within-group I2 = 77·5%) were 343
compared to programs with low RoB (4 studies; ES = -0·03; 95% CI = -0·29 to 0·23; within-344
group I2 = 0·0%) (Supplementary figure 1). 345
Effects of ST versus stretching on ROM, moderated by study RoB in measurement of 346
the outcome: No significant sub-group difference in ROM changes (p = 0·320) was found 347
when programs with high RoB (5 studies; ES = -0·04; 95% CI = -0·31 to 0·24; within-group 348
I2 = 8·0%) were compared to programs with low RoB (6 studies; ES = -0·37; 95% CI = -0·95 349
to 0·22; within-group I2 = 77·3%) (Supplementary figure 2). 350
Effects of ST versus stretching on ROM, moderated by ROM type (active vs. passive): 351
No significant sub-group difference in ROM changes (p = 0·642) was found after training 352
Study name Hedges's g and 95% CI
Hedges's g
Alexander et al. (2001) 0.045Aquino et al. (2010) 0.087Caputo et al. (2017) 0.220Jones et al. (2002) -0.282Leite et al. (2015) -0.229Li et al. (2020) -0.616Morton et al. (2011) 0.123Nelson & Bandy (2004) -0.101Racil et al. (2020) -0.000Simão et al. (2011) -1.922Wyon et al. (2013) 0.247
-0.215
-3.00 -1.50 0.00 1.50 3.00Favours stretching Favours strength
Stretching
(n) Strength
(n)
34
programs that assessed active (8 groups; ES = -0·15; 95% CI = -0·65 to 0·36; within-group I2 353
= 78·7%) compared to passive ROM (6 groups; ES = -0·01; 95% CI = -0·27 to 0·24; within-354
group I2 = 15·3%) (Supplementary figure 3). 355
Effects of ST versus stretching on hip flexion ROM: Seven studies provided data for hip 356
flexion ROM (pooled n = 294). There was no significant difference between ST and stretching 357
interventions (ES = -0·24; 95% CI = -0·82 to 0·34; p = 0·414; I2 = 80·5%; Egger’s test p = 358
0·626; Supplementary figure 4). The relative weight of each study in the analysis ranged from 359
12·0% to 17·4% (the size of the plotted squares in Figure 6 reflects the statistical weight of 360
each study). 361
Effects of ST versus stretching on hip flexion ROM, moderated by study RoB in 362
randomization: No significant sub-group difference in hip flexion ROM changes (p = 0·311) 363
was found when programs with high RoB in randomization (4 studies; ES = -0·46; 95% CI = 364
-1·51 to 0·58; within-group I2 = 86·9%) were compared to programs with low RoB in 365
randomization (3 studies; ES = 0·10; 95% CI = -0·20 to 0·40; within-group I2 = 0·0%) 366
(Supplementary figure 5). 367
Effects of ST versus stretching on hip flexion ROM, moderated by ROM type (active vs. 368
passive): No significant sub-group difference in hip flexion ROM changes (p = 0·466) was 369
found after the programs assessed active (4 groups; ES = -0·38; 95% CI = -1·53 to 0·76; within-370
group I2 = 87·1%) compared to passive ROM (4 groups; ES = 0·08; 95% CI = -0·37 to 0·52; 371
within-group I2 = 56·5%) (Supplementary figure 6). 372
Effects of ST versus stretching on knee extension ROM: Four studies provided data for 373
knee extension ROM (pooled n = 223). There was no significant difference between ST and 374
stretching interventions (ES = 0·25; 95% CI = -0·02 to 0·51; p = 0·066; I2 = 0·0%; Egger’s test 375
p = 0·021; Supplementary figure 7). After the application of the trim and fill method, the 376
adjusted values changed to ES = 0·33 (95% CI = 0·10 to 0·57), favoring ST. The relative 377

35
weight of each study in the analysis ranged from 11·3% to 54·2% (the size of the plotted 378
squares in Supplementary figure 7 reflects the statistical weight of each study). 379
One article behaved as an outlier in all comparisons (favoring stretching),[67] but after 380
sensitivity analysis the results remained unchanged (p>0·05), with all ST vs. stretching 381
comparisons remaining non-significant. 382
383
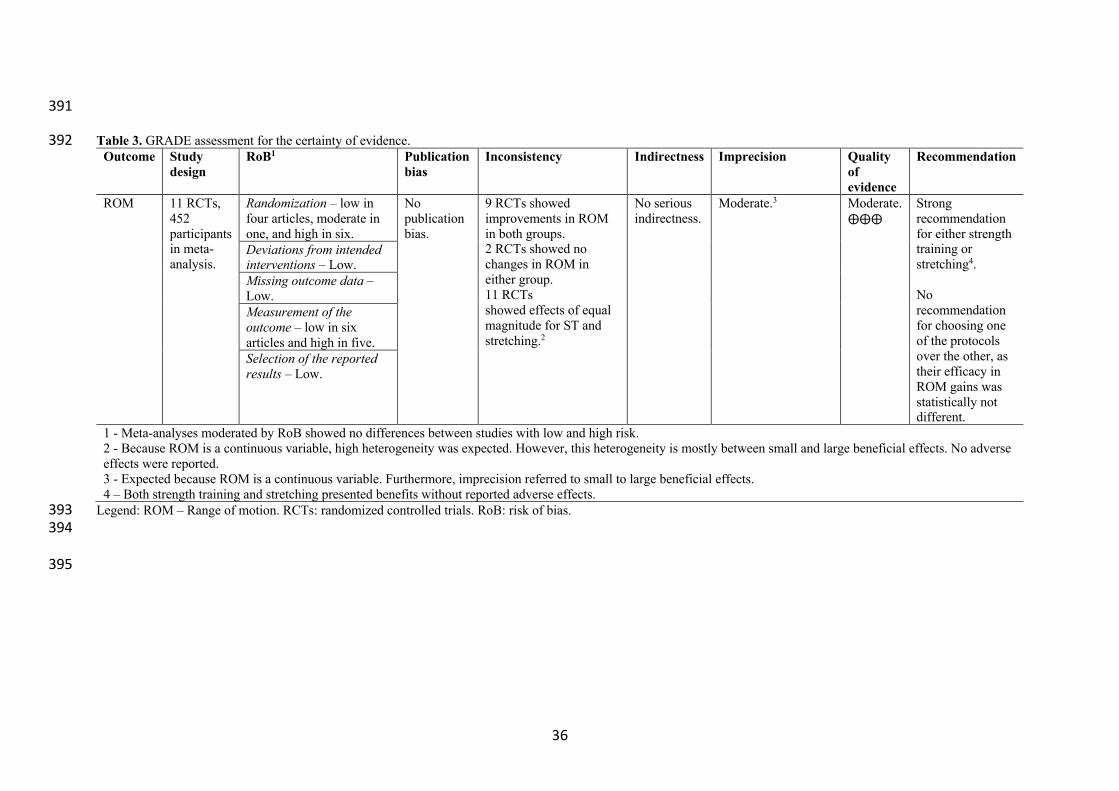
Confidence in cumulative evidence 384
Table 3 presents GRADE assessments. ROM is a continuous variable, and so a high 385
degree of heterogeneity was expected.[77] Imprecision was moderate, likely reflecting the fact 386
that ROM is a continuous variable. Overall, both ST and stretching consistently promoted 387
ROM gains, but no recommendation could be made favoring one protocol. 388
389
390
36
391
Table 3. GRADE assessment for the certainty of evidence. 392 Outcome Study
design RoB1 Publication
bias Inconsistency Indirectness Imprecision Quality
of evidence
Recommendation
ROM 11 RCTs, 452 participants in meta-analysis.
Randomization – low in four articles, moderate in one, and high in six.
No publication bias.
9 RCTs showed improvements in ROM in both groups. 2 RCTs showed no changes in ROM in either group. 11 RCTs showed effects of equal magnitude for ST and stretching.2
No serious indirectness.
Moderate.3 Moderate. ⨁⨁⨁
Strong recommendation for either strength training or stretching4. No recommendation for choosing one of the protocols over the other, as their efficacy in ROM gains was statistically not different.
Deviations from intended interventions – Low. Missing outcome data – Low. Measurement of the outcome – low in six articles and high in five. Selection of the reported results – Low.
1 - Meta-analyses moderated by RoB showed no differences between studies with low and high risk. 2 - Because ROM is a continuous variable, high heterogeneity was expected. However, this heterogeneity is mostly between small and large beneficial effects. No adverse effects were reported. 3 - Expected because ROM is a continuous variable. Furthermore, imprecision referred to small to large beneficial effects. 4 – Both strength training and stretching presented benefits without reported adverse effects.
Legend: ROM – Range of motion. RCTs: randomized controlled trials. RoB: risk of bias. 393 394
395
37
396
DISCUSSION 397
Summary of evidence 398
The aim of this SRMA was to compare the effects of supervised and randomized ST 399
compared to stretching protocols on ROM, in participants of any health and training status. 400
Qualitative synthesis showed that ST and stretching interventions were not statistically 401
different in improving ROM, regardless of the nature of the interventions and moderator 402
variables such as gender, health, or training status. Meta-analysis including 11 articles and 452 403
participants showed that ST and stretching interventions were not statistically different in 404
active and passive ROM changes, regardless of RoB in the randomization process, or in 405
measurement of the outcome. RoB was low for deviations from intended interventions, missing 406
outcome data, and selection of the reported results. No publication bias was detected. 407
High heterogeneity is expected in continuous variables,[77] such as ROM. However, 408
more research should be conducted to afford sub-group analysis according to characteristics of 409
the analyzed population, as well as protocol features. For example, insufficient reporting of 410
training volume and intensity meant it was impossible to establish effective dose-response 411
relationships, although a minimum of 5 weeks of intervention,[60] and two weekly sessions 412
were sufficient to improve ROM.[37, 74] Studies were not always clear with regard to the 413
intensity used in ST and stretching protocols. Assessment of stretching intensity is complex, 414
but a practical solution may be to apply scales of perceived exertion,[62] or the Stretching 415
Intensity Scale.[78] ST intensity may also moderate effects on ROM,[79] and ST with full vs 416
partial ROM may have distinct neuromuscular effects[70] and changes in fascicle length.[28] 417
Again, information was insufficient to discuss these factors, which could potentially explain 418
part of the heterogeneity of results. 419

38
Most studies showed ROM gains in ST and stretching interventions, although in two 420
studies neither group showed improvements.[35, 36] Though adherence rates were unreported 421
by Aquino, Fonseca [35], they were above 91.7% in Leite, De Souza Teixeira [36], thus 422
providing an unlikely explanation for these results. In the study of Aquino, Fonseca [35], the 423
participants increased their stretch tolerance, and the ST group changed the peak torque angle, 424
despite no ROM gains. The authors acknowledged that there was high variability in 425
measurement conditions (e.g., room temperature), which could have interfered with 426
calculations. Leite, De Souza Teixeira [36] suggested that the use of dynamic instead of static 427
stretching could explain the lack of ROM gains in the stretching and stretching + ST groups. 428
However, other studies using dynamic stretching have shown ROM gains.[24, 34] 429
Furthermore, Leite, De Souza Teixeira [36] provided no interpretation for the lack of ROM 430
gains in the ST group. 431
Globally, however, both ST and stretching were effective to improve ROM. Why would 432
ST improve ROM in a manner that is not statistically distinguishable from stretching? ST with 433
an eccentric focus demands the muscles to produce force on elongated positions, and a meta-434
analysis showed limited to moderate evidence that eccentric ST is associated with increases in 435
fascicle length.[80] Likewise, a recent study showed that 12 sessions of eccentric ST increased 436
fascicle length of the biceps femoris long head.[29] However, ST with an emphasis in 437
concentric training has been shown to increase fascicle length when full ROM was 438
required.[28] In a study with nine older adults, ST increased fascicle length in both the eccentric 439
and concentric groups, albeit more prominently in the former.[81] Conversely, changes in 440
pennation angle were superior in the concentric group (35% increase versus 5% increase). 441
Plyometric training can also increase plantar flexor tendon extensibility.[33] 442
One article showed significant reductions in pain associated with increases in 443
strength.[37] Thus, decreased pain sensitivity may be another mechanism through which ST 444

39
promotes ROM gains. An improved agonist-antagonist coactivation is another possible 445
mechanism promoting ROM gains, through better adjusted force ratios.[31, 62] Also, some 446
articles included in the meta-analysis assessed other outcomes in addition to ROM, and these 447
indicated that ST programs may have additional advantages when compared to stretching, such 448
as greater improvements in neck flexors endurance,[37] ten repetition maximum Bench Press 449
and Leg Press,[36, 67] and countermovement jump and 60-m sprint with hurdles,[24] which 450
may favor the choice of ST over stretching interventions. 451
452
453
Limitations 454
After protocol registration, we chose to improve upon the design, namely adding two 455
dimensions (directness and imprecision) that would provide a complete GRADE assessment. 456
Furthermore, subgroup analyses were not planned a priori. There is a risk of multiple subgroup 457
analyses generating a false statistical difference, merely to the number of analyses 458
conducted.[38] However, all analyses showed an absence of significant differences and 459
therefore provide a more complete understanding that the effects of ST or stretching on ROM 460
are consistent across conditions. Looking backwards, perhaps removing the filters used in the 461
initial searches could have provided a greater number of records. Notwithstanding, it would 462
also likely provide a huge number of non-relevant records, including opinion papers and 463
reviews. Moreover, consultation with four independent experts may hopefully have resolved 464
this shortcoming. 465
Due to the heterogeneity of populations analysed, sub-group analysis according to sex 466
or age group were not possible, and so it would be important to explore if these features interact 467
with the protocols in meaningful ways. And there was a predominance of studies with women, 468
meaning more research with men is advised. There was also a predominance of assessments of 469

40
hip joint ROM, followed by knee and shoulder, with the remaining joints receiving little to no 470
attention. In addition, dose-response relationships could not be addressed, mainly due to poor 471
reporting. 472
473
CONCLUSIONS 474
Overall, ST and stretching were not statistically different in ROM improvements, both 475
in short-term interventions[60] and in longer-term protocols,[67] suggesting that a combination 476
of neural and mechanical factors is at play. Therefore, if ROM gains are a desirable outcome, 477
both ST and stretching can be prescribed, in the absence of specific contraindications, 478
especially because studies did not report any adverse effects. People that do not respond well 479
or do not adhere to stretching protocols can change to ST programs, and vice-versa. 480
Furthermore, session duration may negatively impact adherence to an exercise program.[82] 481
Since ST generates ROM gains similar to those obtained with stretching, clinicians may 482
prescribe smaller, more time-effective programs when deemed convenient and appropriate, 483
thus eventually increasing patient adherence rates. 484
485
486
41
487
488
Declaration of interests: J.M. owns a company focused on Personal Trainer’s education but 489
made no attempt to bias the team in protocol design and search process and had no role in 490
extracting data for meta-analyses. The multiple cross-checks described in the methods 491
provided objectivity to data extraction and analysis. Additionally, J.M. had no financial 492
involvement in this manuscript. The other authors have no conflict of interest to declare. 493
494
Funding: No funding was used for conducting this meta-analysis. 495
496
497

42
498
Author’s contributions (following ICMJE recommendations) 499
Authors Substantial contributions to the conceptualization or design of the study; OR the
acquisition, analysis, or
interpretation of data
Drafting the manuscript; OR
revising the manuscript critically for important intellectual
content
Final approval
of the version to
be published
Agreement to be accountable for all
aspects of the work, and to ensure that issues
related to the accuracy or integrity of any part of
the work are appropriately
investigated and resolved José Afonso √ √ √ √
Rodrigo Ramirez-Campillo
√ √ √ √
João Moscão √ √ √ √ Tiago Rocha √ √ √ √
Rodrigo Zacca √ √ √ √ Alexandre Martins √ √ √ √ André A. Milheiro √ √ √ √
João Ferreira √ √ √ √ Hugo Sarmento √ √ √ √ Filipe Manuel
Clemente √ √ √ √
Acknowledgements Role Richard Inman Language editing and proof reading. Pedro Morouço Thorough pre-submission scientific review of the manuscript. Signed consent form
below. Daniel Moreira-
Gonçalves, Fábio Yuzo Nakamura plus
two experts who wished to remain
anonymous.
Review of inclusion criteria and included articles, and proposal of additional articles to be included in the systematic review and meta-analysis.
Signed consent forms below.
500
501

43
502
REFERENCES 503
1. ACSM. ACSM’s Guidelines for Exercise Testing and Prescription (10th Ed.): Wolters 504
Kluwer; 2018. 505
2. de Zoete RM, Armfield NR, McAuley JH, Chen K, Sterling M. Comparative 506
effectiveness of physical exercise interventions for chronic non-specific neck pain: a 507
systematic review with network meta-analysis of 40 randomised controlled trials. Br J Sports 508
Med. 2020 Nov 2. 509
3. Morris PE, Berry MJ, Files DC, Thompson JC, Hauser J, Flores L, et al. Standardized 510
Rehabilitation and Hospital Length of Stay Among Patients With Acute Respiratory Failure: 511
A Randomized Clinical Trial. Jama. 2016 Jun 28;315(24):2694-702. 512
4. Gross AM, Wolters PL, Dombi E, Baldwin A, Whitcomb P, Fisher MJ, et al. 513
Selumetinib in Children with Inoperable Plexiform Neurofibromas. N Engl J Med. 2020 Apr 514
9;382(15):1430-42. 515
5. Learmonth ID, Young C, Rorabeck C. The operation of the century: total hip 516
replacement. Lancet. 2007 Oct 27;370(9597):1508-19. 517
6. Pozzi F, Plummer HA, Shanley E, Thigpen CA, Bauer C, Wilson ML, et al. Preseason 518
shoulder range of motion screening and in-season risk of shoulder and elbow injuries in 519
overhead athletes: systematic review and meta-analysis. Br J Sports Med. 2020 520
Sep;54(17):1019-27. 521
7. Moreno-Pérez V, Del Coso J, Raya-González J, Nakamura FY, Castillo D. Effects of 522
basketball match-play on ankle dorsiflexion range of motion and vertical jump performance in 523
semi-professional players. J Sports Med Phys Fitness. 2020 Jan;60(1):110-8. 524
8. Downs J, Wasserberger K, Oliver GD. Influence of a Pre-throwing Protocol on Range 525
of Motion and Strength in Baseball Athletes. Int J Sports Med. 2020 Aug 26. 526
44
9. Li Y, Koldenhoven RM, Jiwan NC, Zhan J, Liu T. Trunk and shoulder kinematics of 527
rowing displayed by Olympic athletes. Sports Biomech. 2020 Jul 17:1-13. 528
10. Blazevich A, Cannavan D, Waugh CM, Miller SC, Thorlund JB, Aagaard P, et al. 529
Range of motion, neuromechanical, and architectural adaptations to plantar flexor stretch 530
training in humans. J Appl Physiol. 2014;117(5):452-62. 531
11. Guissard N, Duchateau J. Effect of static stretch training on neural and mechanical 532
properties of the human plantar-flexor muscles. Muscle Nerve. 2004 Feb;29(2):248-55. 533
12. Lima CD, Brown LE, Li Y, Herat N, Behm D. Periodized versus Non-periodized 534
Stretch Training on Gymnasts Flexibility and Performance. Int J Sports Med. 2019 535
Nov;40(12):779-88. 536
13. Behm DG, Kay AD, Trajano GS, Blazevich AJ. Mechanisms underlying performance 537
impairments following prolonged static stretching without a comprehensive warm-up. Eur J 538
Appl Physiol. 2020 Nov 11. 539
14. Deyo RA, Walsh NE, Martin DC, Schoenfeld LS, Ramamurthy S. A controlled trial of 540
transcutaneous electrical nerve stimulation (TENS) and exercise for chronic low back pain. N 541
Engl J Med. 1990 Jun 7;322(23):1627-34. 542
15. Lamb SE, Williamson EM, Heine PJ, Adams J, Dosanjh S, Dritsaki M, et al. Exercises 543
to improve function of the rheumatoid hand (SARAH): a randomised controlled trial. Lancet. 544
2015 Jan 31;385(9966):421-9. 545
16. Kokkonen J, Nelson AG, Eldredge C, Winchester JB. Chronic static stretching 546
improves exercise performance. Med Sci Sports Exerc. 2007;39(10):1825-31. 547
17. Santos C, Beltrão NB, Pirauá ALT, Durigan JLQ, Behm D, de Araújo RC. Static 548
Stretching Intensity Does Not Influence Acute Range of Motion, Passive Torque, and Muscle 549
Architecture. J Sport Rehabil. 2020;29(1):1-6. 550

45
18. Iwata M, Yamamoto A, Matsuo S, Hatano G, Miyazaki M, Fukaya T, et al. Dynamic 551
stretching has sustained effects on range of motion and passive stiffness of the hamstring 552
muscles. J Sports Sci Med. 2019;18(1):13-20. 553
19. Lempke L, Wilkinson R, Murray C, Stanek J. The Effectiveness of PNF Versus Static 554
Stretching on Increasing Hip-Flexion Range of Motion. J Sport Rehabil. 2018;27(3):289-94. 555
20. Ford GS, Mazzone MA, Taylor K. The effect of 4 different durations of static hamstring 556
stretching on passive knee-extension range of motion. Journal of Sports Rehabilitation. 557
2005;14(2):95-107. 558
21. Frasson VB, Vaz MA, Morales AB, Torresan A, Telöken MA, Gusmão PDF, et al. Hip 559
muscle weakness and reduced joint range of motion in patients with femoroacetabular 560
impingement syndrome: a case-control study. Braz J Phys Ther. 2020 Jan-Feb;24(1):39-45. 561
22. Pettersson H, Boström C, Bringby F, Walle-Hansen R, Jacobsson LTH, Svenungsson 562
E, et al. Muscle endurance, strength, and active range of motion in patients with different 563
subphenotypes in systemic sclerosis: a cross-sectional cohort study. Scand J Rheumatol. 2019 564
2019/03/04;48(2):141-8. 565
23. Takeda H, Nakagawa T, Nakamura K, Engebretsen L. Prevention and management of 566
knee osteoarthritis and knee cartilage injury in sports. Br J Sports Med. 2011 Apr;45(4):304-9. 567
24. Racil G, Jlid MC, Bouzid MS, Sioud R, Khalifa R, Amri M, et al. Effects of flexibility 568
combined with plyometric exercises vs. isolated plyometric or flexibility mode in adolescent 569
male hurdlers. J Sports Med Phys Fitness. 2020;60(1):45-52. 570
25. Saraiva AR, Reis VM, Costa PB, Bentes CM, Costae Silva GV, Novaes JS. Chronic 571
Effects of different resistance training exercise orders on flexibility in elite judo athletes. 572
Journal of Human Kinetics. 2014;40(1):129-37. 573
46
26. Carneiro NH, Ribeiro AS, Nascimento MA, Gobbo LA, Schoenfeld BJ, Achour A, et 574
al. Effects of different resistance training frequencies on flexibility in older women. Clin Interv 575
Aging. 2015;10:531-8. 576
27. Ylinen J, Takala EP, Nykänen M, Häkkinen A, Mälkiä E, Pohjolainen T, et al. Active 577
neck muscle training in the treatment of chronic neck pain in women: a randomized controlled 578
trial. Jama. 2003 May 21;289(19):2509-16. 579
28. Valamatos MJ, Tavares F, Santos RM, Veloso AP, Mil-Homens P. Influence of full 580
range of motion vs. equalized partial range of motion training on muscle architecture and 581
mechanical properties. Eur J Appl Physiol. 2018 Sep;118(9):1969-83. 582
29. Marušič J, Vatovec R, Marković G, Šarabon N. Effects of eccentric training at long-583
muscle length on architectural and functional characteristics of the hamstrings. Scand J Med 584
Sci Sports. 2020 Jul 24. 585
30. Bourne MN, Duhig SJ, Timmins RG, Williams MD, Opar DA, Al Najjar A, et al. 586
Impact of the Nordic hamstring and hip extension exercises on hamstring architecture and 587
morphology: implications for injury prevention. Br J Sports Med. 2017 Mar;51(5):469-77. 588
31. de Boer MD, Morse CI, Thom JM, de Haan A, Narici MV. Changes in antagonist 589
muscles' coactivation in response to strength training in older women. J Gerontol A Biol Sci 590
Med Sci. 2007 Sep;62(9):1022-7. 591
32. Silva-Batista C, Mattos EC, Corcos DM, Wilson JM, Heckman CJ, Kanegusuku H, et 592
al. Resistance training with instability is more effective than resistance training in improving 593
spinal inhibitory mechanisms in Parkinson's disease. J Appl Physiol (1985). 2017 Jan 594
1;122(1):1-10. 595
33. Kubo K, Ishigaki T, Ikebukuro T. Effects of plyometric and isometric training on 596
muscle and tendon stiffness in vivo. Physiol Rep. 2017 Aug;5(15). 597

47
34. Alexander NB, Galecki AT, Grenier ML, Nyquist LV, Hofmeyer MR, Grunawalt JC, 598
et al. Task-specific resistance training to improve the ability of activities of daily living-599
impaired older adults to rise from a bed and from a chair. J Am Geriatr Soc. 2001;49(11):1418-600
27. 601
35. Aquino CF, Fonseca ST, Goncalves GG, Silva PL, Ocarino JM, Mancini MC. 602
Stretching versus strength training in lengthened position in subjects with tight hamstring 603
muscles: a randomized controlled trial. Man Ther. 2010 Feb;15(1):26-31. 604
36. Leite T, De Souza Teixeira A, Saavedra F, Leite RD, Rhea MR, Simão R. Influence of 605
strength and flexibility training, combined or isolated, on strength and flexibility gains. J 606
Strength Cond Res. 2015;29(4):1083-8. 607
37. Caputo GM, Di Bari M, Naranjo Orellana J. Group-based exercise at workplace: short-608
term effects of neck and shoulder resistance training in video display unit workers with work-609
related chronic neck pain-a pilot randomized trial. Clin Rheumatol. 2017 Oct;36(10):2325-33. 610
38. Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane 611
Handbook for Systematic Reviews of Interventions (2nd Ed.). Chichester (UK): John Wiley & 612
Sons; 2019. 613
39. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic 614
reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009 Jul 21;6(7):e1000097. 615
40. Bleakley C, MacAuley D. The quality of research in sports journals. British Journal of 616
Sports Medicine. 2002;36(2):124. 617
41. Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a 618
revised tool for assessing risk of bias in randomised trials. Bmj. 2019;366:l4898. 619
42. Skrede T, Steene-Johannessen J, Anderssen SA, Resaland GK, Ekelund U. The 620
prospective association between objectively measured sedentary time, moderate-to-vigorous 621
48
physical activity and cardiometabolic risk factors in youth: a systematic review and meta-622
analysis. Obes Rev. 2019 Jan;20(1):55-74. 623
43. Drahota A, Beller E. RevMan Calculator for Microsoft Excel [Computer software]: 624
Cochrane; 2020. 625
44. Deeks JJ, Higgins JP, Altman DG. Analysing data and undertaking meta-analyses. In: 626
Higgins JP, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions: 627
The Cochrane Collaboration The Cochrane Collaboration; 2008. p. 243-96. 628
45. Kontopantelis E, Springate DA, Reeves D. A re-analysis of the Cochrane Library data: 629
the dangers of unobserved heterogeneity in meta-analyses. PLoS One. 2013;8(7):e69930. 630
46. Hopkins WG, Marshall SW, Batterham AM, Hanin J. Progressive statistics for studies 631
in sports medicine and exercise science. Med Sci Sports Exerc. 2009 Jan;41(1):3-13. 632
47. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 633
2002 Jun 15;21(11):1539-58. 634
48. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a 635
simple, graphical test. Bmj. 1997 Sep 13;315(7109):629-34. 636
49. Duval S, Tweedie R. Trim and fill: A simple funnel-plot-based method of testing and 637
adjusting for publication bias in meta-analysis. Biometrics. 2000 Jun;56(2):455-63. 638
50. Shi L, Lin L. The trim-and-fill method for publication bias: practical guidelines and 639
recommendations based on a large database of meta-analyses. Medicine (Baltimore). 2019 640
Jun;98(23):e15987. 641
51. Shea BJ, Reeves BC, Wells G, Thuku M, Hamel C, Moran J, et al. AMSTAR 2: a 642
critical appraisal tool for systematic reviews that include randomised or non-randomised 643
studies of healthcare interventions, or both. Bmj. 2017 Sep 21;358:j4008. 644

49
52. Guyatt GH, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J, et al. GRADE guidelines: 645
1. Introduction-GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 646
2011 Apr;64(4):383-94. 647
53. Al-Wahab MGA, Salem EES, El-Hadidy EI, El-Barbary HM. Effect of plyometric 648
training on shoulder strength and active movements in children with Erb’s palsy. Int J 649
Pharmtech Res. 2016;9(4):25-33. 650
54. Fernandez-Fernandez J, Ellenbecker T, Sanz-Rivas D, Ulbricht A, Ferrauti A. Effects 651
of a 6-Week Junior Tennis Conditioning Program on Service Velocity. J Sports Sci Med. 2013 652
Jun;12(2):232-9. 653
55. de Resende-Neto AG, do Nascimento MA, de Sa CA, Ribeiro AS, Desantana JM, da 654
Silva-Grigoletto ME. Comparison between functional and traditional training exercises on joint 655
mobility, determinants of walking and muscle strength in older women. J Sports Med Phys 656
Fitness. 2019 Oct;59(10):1659-68. 657
56. Hajihosseini E, Norasteh A, Shamsi A, Daneshmandi H, Shahheidari S. Effects of 658
strengthening, stretching and comprehensive exercise program on the strength and range of 659
motion of the shoulder girdle muscles in upper crossed syndrome. Med Sport. 2016;69(1):24-660
40. 661
57. Fukuchi RK, Stefanyshyn DJ, Stirling L, Ferber R. Effects of strengthening and 662
stretching exercise programmes on kinematics and kinetics of running in older adults: A 663
randomised controlled trial. J Sports Sci. 2016;34(18):1774-81. 664
58. Häkkinen A, Kautiainen H, Hannonen P, Ylinen J. Strength training and stretching 665
versus stretching only in the treatment of patients with chronic neck pain: A randomized one-666
year follow-up study. Clin Rehabil. 2008;22(7):592-600. 667
59. Kalkman BM, Holmes G, Bar-On L, Maganaris CN, Barton GJ, Bass A, et al. 668
Resistance training combined with stretching increases tendon stiffness and is more effective 669

50
than stretching alone in children with cerebral palsy: A randomized controlled trial. Front 670
Pediatr. 2019;7:Article 333. 671
60. Morton SK, Whitehead JR, Brinkert RH, Caine DJ. Resistance training vs. static 672
stretching: Effects on flexibility and strength. J Strength Cond Res. 2011;25(12):3391-8. 673
61. Li S, Garrett WE, Best TM, Li H, Wan X, Liu H, et al. Effects of flexibility and strength 674
interventions on optimal lengths of hamstring muscle-tendon units. J Sci Med Sport. 675
2020;23(2):200-5. 676
62. Wyon MA, Smith A, Koutedakis Y. A comparison of strength and stretch interventions 677
on active and passive ranges of movement in dancers: A randomized controlled trial. J Strength 678
Cond Res. 2013;27(11):3053-9. 679
63. Girouard CK, Hurley BF. Does strength training inhibit gains in range of motion from 680
flexibility training in older adults? Med Sci Sports Exerc. 1995 Oct;27(10):1444-9. 681
64. Raab DM, Agre JC, McAdam M, Smith EL. Light resistance and stretching exercise in 682
elderly women: effect upon flexibility. Arch Phys Med Rehabil. 1988 Apr;69(4):268-72. 683
65. Klinge K, Magnusson SP, Simonsen EB, Aagaard P, Klausen K, Kjaer M. The effect 684
of strength and flexibility training on skeletal muscle electromyographic activity, stiffness, and 685
viscoelastic stress relaxation response. Am J Sports Med. 1997 Sep-Oct;25(5):710-6. 686
66. Nóbrega AC, Paula KC, Carvalho AC. Interaction between resistance training and 687
flexibility training in healthy young adults. J Strength Cond Res. 2005 Nov;19(4):842-6. 688
67. Simão R, Lemos A, Salles B, Leite T, Oliveira É, Rhea M, et al. The influence of 689
strength, flexibility, and simultaneous training on flexibility and strength gains. J Strength 690
Cond Res. 2011 May;25(5):1333-8. 691
68. Chen Y-H, Lin C-R, Liang W-A, Huang C-Y. Motor control integrated into muscle 692
strengthening exercises has more effects on scapular muscle activities and joint range of motion 693
51
before initiation of radiotherapy in oral cancer survivors with neck dissection: A randomized 694
controlled trial. PLoS ONE. 2020;15(8):e0237133-e. 695
69. Venkataraman K, Tai BC, Khoo EYH, Tavintharan S, Chandran K, Hwang SW, et al. 696
Short-term strength and balance training does not improve quality of life but improves 697
functional status in individuals with diabetic peripheral neuropathy: a randomised controlled 698
trial. Diabetologia. 2019 2019/12/01;62(12):2200-10. 699
70. Pallarés JG, Cava AM, Courel-Ibáñez J, González-Badillo JJ, Morán-Navarro R. Full 700
squat produces greater neuromuscular and functional adaptations and lower pain than partial 701
squats after prolonged resistance training. Eur J Sport Sci. 2020 Feb;20(1):115-24. 702
71. Çergel Y, Topuz O, Alkan H, Sarsan A, Sabir Akkoyunlu N. The effects of short-term 703
back extensor strength training in postmenopausal osteoporotic women with vertebral 704
fractures: comparison of supervised and home exercise program. Arch Osteoporos. 2019 Jul 705
27;14(1):82. 706
72. Albino ILR, Freitas CdlR, Teixeira AR, Gonçalves AK, Santos AMPVd, Bós ÂJG. 707
Influência do treinamento de força muscular e de flexibilidade articular sobre o equilíbrio 708
corporal em idosas. Rev Bras Geriatr Gerontol. 2012;15:17-25. 709
73. LeCheminant JD, Hinman T, Pratt KB, Earl N, Bailey BW, Thackeray R, et al. Effect 710
of resistance training on body composition, self-efficacy, depression, and activity in 711
postpartum women. Scand J Med Sci Sports. 2014 Apr;24(2):414-21. 712
74. Jones KD, Burckhardt CS, Clark SR, Bennett RM, Potempa KM. A randomized 713
controlled trial of muscle strengthening versus flexibility training in fibromyalgia. J 714
Rheumatol. 2002 May;29(5):1041-8. 715
75. Nelson RT, Bandy WD. Eccentric Training and Static Stretching Improve Hamstring 716
Flexibility of High School Males. J Athl Train. 2004;39(3):254-8. 717

52
76. Wyon MA, Felton L, Galloway S. A comparison of two stretching modalities on lower-718
limb range of motion measurements in recreational dancers. J Strength Cond Res. 2009 719
Oct;23(7):2144-8. 720
77. Guyatt GH, Oxman AD, Kunz R, Woodcock J, Brozek J, Helfand M, et al. GRADE 721
guidelines: 7. Rating the quality of evidence - inconsistency. J Clin Epidemiol. 2011 722
Dec;64(12):1294-302. 723
78. Freitas SR, Vaz JR, Gomes L, Silvestre R, Hilário E, Cordeiro N, et al. A New Tool to 724
Assess the Perception of Stretching Intensity. The Journal of Strength & Conditioning 725
Research. 2015;29(9). 726
79. Fatouros IG, Kambas A, Katrabasas I, Leontsini D, Chatzinikolaou A, Jamurtas AZ, et 727
al. Resistance training and detraining effects on flexibility performance in the elderly are 728
intensity-dependent. J Strength Cond Res. 2006;20(3):634-42. 729
80. Gérard R, Gojon L, Decleve P, Van Cant J. The Effects of Eccentric Training on Biceps 730
Femoris Architecture and Strength: A Systematic Review With Meta-Analysis. J Athl Train. 731
2020 May;55(5):501-14. 732
81. Reeves ND, Maganaris CN, Longo S, Narici MV. Differential adaptations to eccentric 733
versus conventional resistance training in older humans. Exp Physiol. 2009 Jul;94(7):825-33. 734
82. Medina-Mirapeix F, Escolar-Reina P, Gascón-Cánovas JJ, Montilla-Herrador J, 735
Jimeno-Serrano FJ, Collins SM. Predictive factors of adherence to frequency and duration 736
components in home exercise programs for neck and low back pain: an observational study. 737
BMC musculoskeletal disorders. 2009;10:Article 155. 738
739