KNEE OA
45
KNEE OSTEOARTHRITIS Nama : Anasti Putri Paramatasari NIM : 030.10.028 Pembimbing : dr. Gatot, Sp. OT Selasa, 12 Januari 2015 Kepaniteraan Klinik Bagian Ilmu Bedah Sub Departement Orthopedic Rumah Sakit Umum Bekasi Periode 5 Januari – 14 Maret 2015
-
Upload
anasti-putri-paramatasari -
Category
Documents
-
view
20 -
download
4
description
please, use it wisely..
Transcript of KNEE OA
KNEE OSTEOARTHRITISNama : Anasti Putri Paramatasari
NIM : 030.10.028
Pembimbing : dr. Gatot, Sp. OT
Selasa, 12 Januari 2015
Kepaniteraan Klinik Bagian Ilmu BedahSub Departement Orthopedic
Rumah Sakit Umum BekasiPeriode 5 Januari – 14 Maret 2015
TOPIK BAHASAN

TOPIK BAHASAN
Knee OA
Definisi
Prevalensi dan
Insidensi
Etiologi dan Klasifikasi
Faktor Resiko
Pathogenesis dan
Pathology
Manifestasi Klinis
Pemeriksaan Penunjang
Diagnosis
Diagnosis Banding
Terapi
Prognosis
DEFINISI
DEFINISI
Degenerative joint disease Osteoarthrosis Degenerative arthritis Senescent arthritis Hypertrophic arthritis Ialah gangguan pada satu atau lebih sendi yang
dicetuskan oleh perburukan dari articular cartilage dan ditandai oleh: degenerasi kartilago yang progresif, hipertrofi dan remodelling dari subchondral bone, dan inflamasi sekunder pada membran synovial.1
1. Salter RB. Textbook of Disorders and Injuries of the Muskuloskeletal System. Degenerative Disoreders of Joints and Related Tissues. 3rd ed. Philadelaphia, PA: Mosby; 1999; p. 213-23.
PREVALENSI DAN INSIDENSI
PREVALENSI DAN INSIDENSI
Data di US selama tahun 2005, OA mengenai 13,9% individu dewasa berusia lebih dari 25 tahun dan 33,6% (12,4 juta individu) berusia lebih dari 65 tahun.2
Insidensi rates dari symptomatic radiographic OA pada individu dewasa berusia ≥ 26 tahun: Hand OA = 100 per 100,000 individu per tahun Hip OA = 88 per 100,000 individu per tahun Knee OA = 240 per 100,000 individu per tahun.3
Insidensi rates dari OA meningkat sejelan dengan usia, dan menetap sekitar usia 80 tahun.4
Wanita memiliki rates yang lebih tinggi dibandingkan pria, terutama pada usia lebih dari 50 tahun.4
2. Lawrence RC, Felson DT, Helmick CG, et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part II. Arthritis Rheum. 2008;58(1):26-35.3. Oliveria SA, Felson DT, Reed JI, et al. Incidence of symptomatic hand, hip and knee osteoarthritis among patients in health maintenance organization. Arthritis Rheum. 1995;38(8):134-1141. 4. Buckwalter JA, Saltzman C, Brown T. The impact of osteoarthritis. Clin Orthoped Rei Res. 200:427S:S6-S15.
ETIOLOGI DAN KLASIFIKASI
ETIOLOGI DAN KLASIFIKASI
• Kelainan degenerative pada sendi yang mengenai banyak sendi tanpa diketahui adanya abnormalitas sebelumnya.1
Primary
• Didahului adanya luka, deformitas atau penyakit yang dapat mencetuskan initial cartilage lesion yang berkembang menjadi progressive secondary degenerative joint disease.1
Secondary
1. Salter RB. Textbook of Disorders and Injuries of the Muskuloskeletal System. Degenerative Disoreders of Joints and Related Tissues. 3rd ed. Philadelaphia, PA: Mosby; 1999; p. 213-23.
ETIOLOGI DAN KLASIFIKASI (2)
Keadaan yang dapat menginisiasi proses degenerasi yang progresif pada 2nd type of OA:1
Congenital abnormalities of joints : congenital dislocation of the hip, clubfeet.
Infections of joints : septic (pyogenic) arthritis, tuberculous arthritis. Nonspesific inflammatory disorders of joints : rheumatoid arthritis,
ankylosing spondylitis. Metabolic arthritis : gout, ochronosis. Repeated hemarthrosis : hemophilia Injury : (a) Major trauma‒intra-articular fractures; (b) Minor trauma‒
occupational stresses. Acquired incongruity of joint surfaces : avascular necrosis, slipped
epiphysis. Extra-articular deformities with malaginment of joints : genu
valgus, genu varus. Joints instability : lax ligaments, subluxation. Iatrogenic damage to cartilage : continues compression of joint
surfaces during treatment.
1. Salter RB. Textbook of Disorders and Injuries of the Muskuloskeletal System. Degenerative Disoreders of Joints and Related Tissues. 3rd ed. Philadelaphia, PA: Mosby; 1999; p. 213-23.
FAKTOR RESIKO
FAKTOR RESIKO5,7-10
• Gender : wanita ↑ resiko• Usia: resiko meningkat seiring dengan usia,
sekitar usia 75 tahun.• Ras : Asian ↓resiko• Genetik
Non-modifable
• Massa tubuh berlebih• Cedera sendi (akibat olahraga, trauma,
perkerjaan)• Nyeri lutut• Hand OA• Pekerjaan (mechanical stress: hard labor, heavy
lifting, knee bending, repetitive motion).
Modifiable
5. Jordan JM, Helmick Cg, renner JB, et al. Prevalence of knee symptoms and radiographic and symptomatic knee osteoarthititis in African Ameriicans and Caucasians: The Jhonston County Osteoarthitis Project. J Rheumatol. 2007;34(1):172-80..7. Felson DT. Risk Factors of osteoarthritis. Clin Orthoped Rel Res. 2004;427S:S16-S21.8. Rossignol M, Leclerc A, Allaeret FA, et al. Primary osteoarthritis of hip, knee and hand in relation to occupational exposure. Occup Environ Med. 2005;62:772-777.9. Cooper C, Snow S, McAlindon TE, et al. Risk factors for the incidence and progression of radiographic knee ostoarthrits. Arthritis Rheum. 2000;43(5):995-1000.10. Blogojevic M, Jinks C, Jeffrey A, et al. Risk factors for onset of osteoarthritis of the knee in older adults: a systematic review and metanalysis. Osteoarthritis Cartilage. 2010;18(1):24-33.
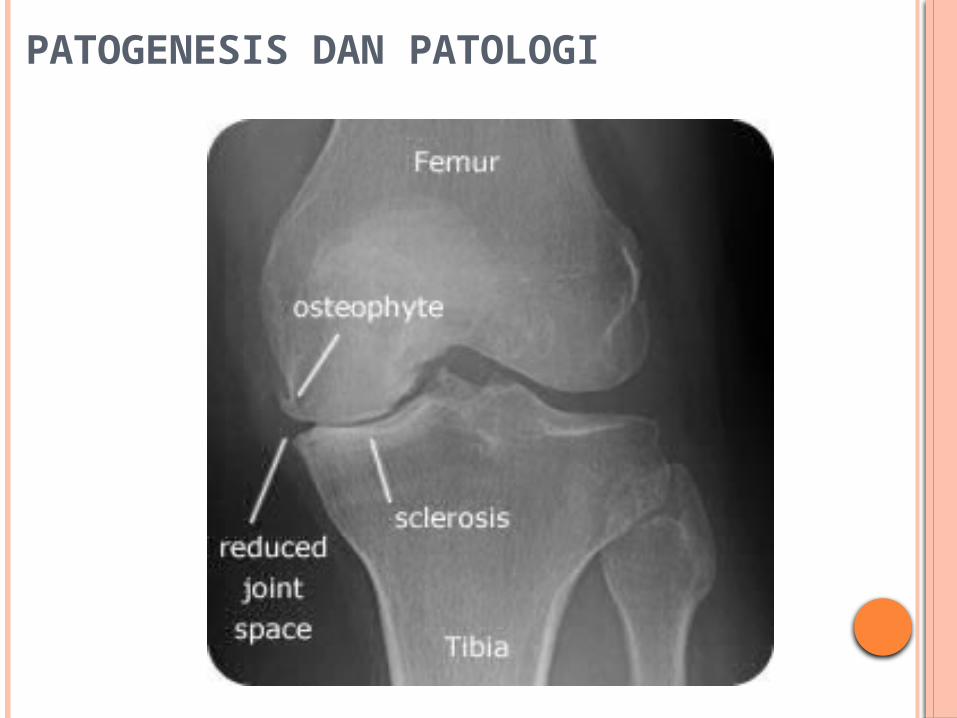
PATOGENESIS DAN PATOLOGI
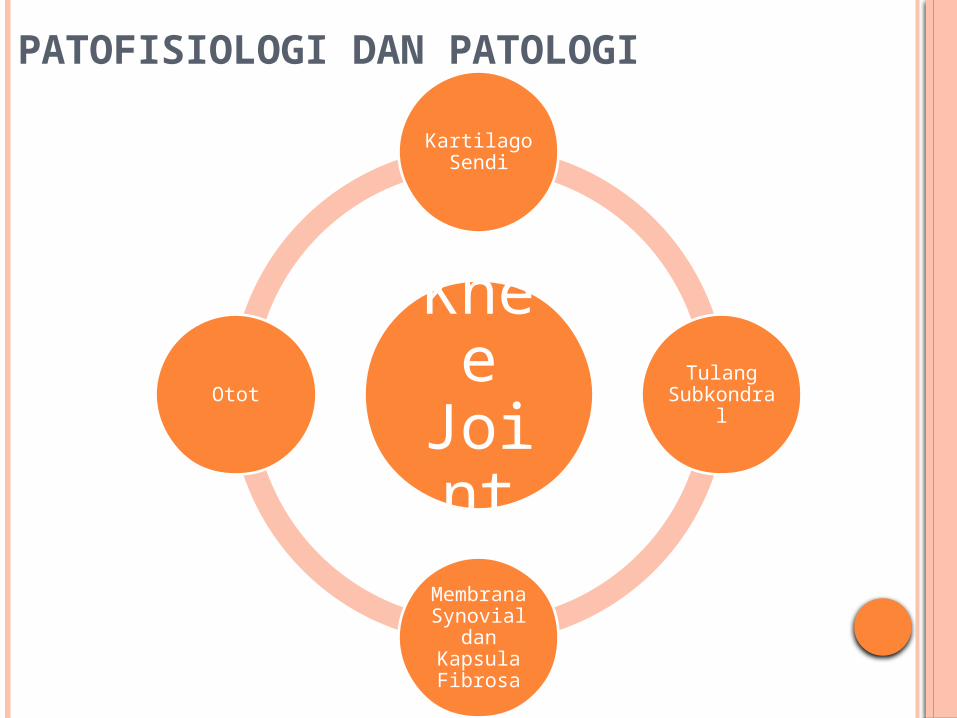
PATOFISIOLOGI DAN PATOLOGI
Knee
Joint
Kartilago Sendi
Tulang Subkondra
l
Membrana Synovial
dan Kapsula Fibrosa
Otot
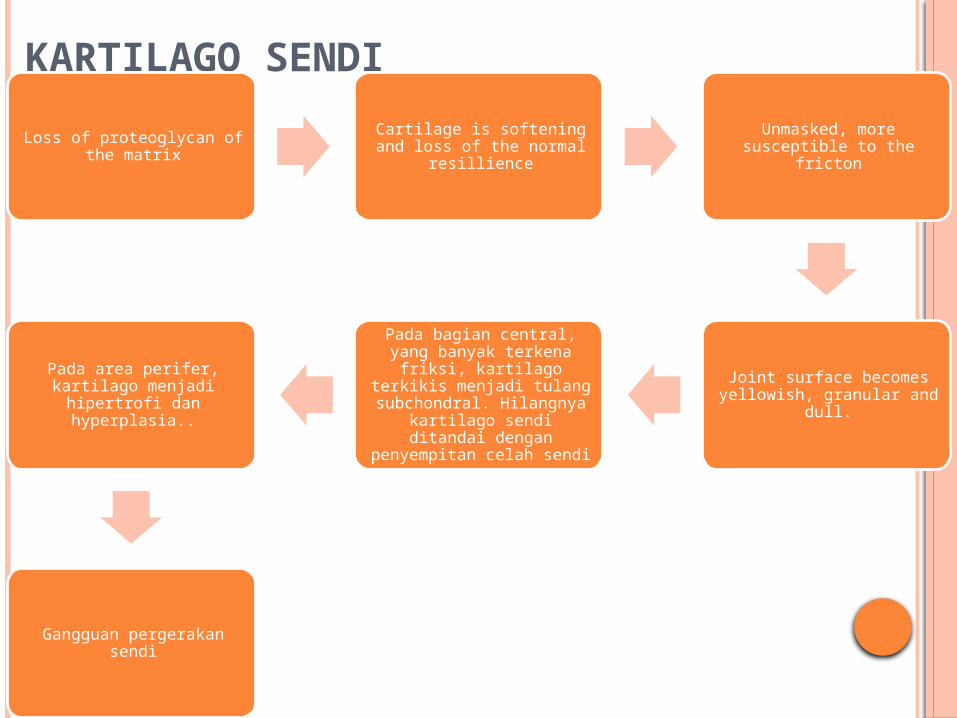
KARTILAGO SENDI
Loss of proteoglycan of the matrix
Cartilage is softening and loss of the normal resillience
Unmasked, more susceptible to the fricton
Joint surface becomes yellowish, granular and dull.
Pada bagian central, yang banyak terkena friksi,
kartilago terkikis menjadi tulang subchondral.
Hilangnya kartilago sendi ditandai dengan
penyempitan celah sendi
Pada area perifer, kartilago menjadi hipertrofi dan
hyperplasia..
Gangguan pergerakan sendi
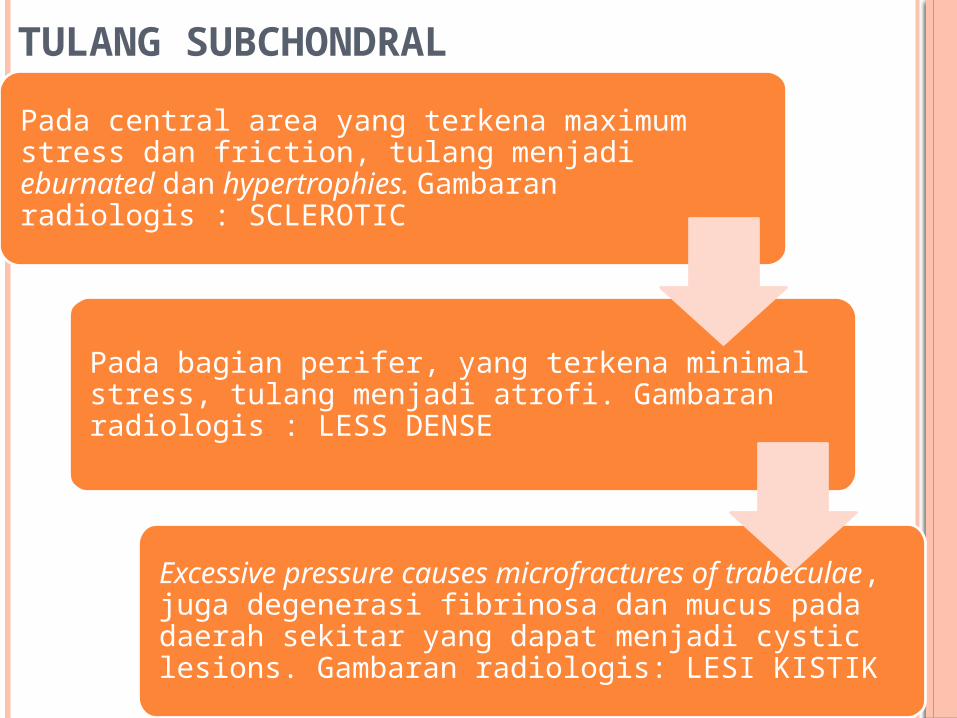
TULANG SUBCHONDRAL
Pada central area yang terkena maximum stress dan friction, tulang menjadi eburnated dan hypertrophies. Gambaran radiologis : SCLEROTIC
Pada bagian perifer, yang terkena minimal stress, tulang menjadi atrofi. Gambaran radiologis : LESS DENSE
Excessive pressure causes microfractures of trabeculae, juga degenerasi fibrinosa dan mucus pada daerah sekitar yang dapat menjadi cystic lesions. Gambaran radiologis: LESI KISTIK
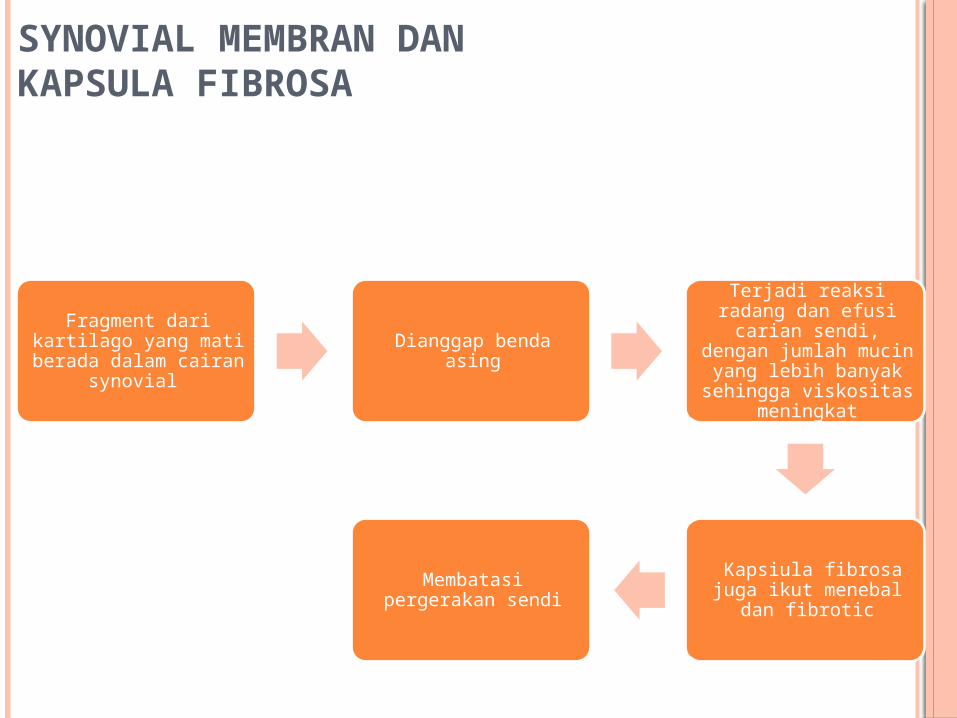
SYNOVIAL MEMBRAN DAN KAPSULA FIBROSA
Fragment dari kartilago yang mati berada dalam cairan
synovial
Dianggap benda asing
Terjadi reaksi radang dan efusi carian sendi, dengan jumlah mucin
yang lebih banyak sehingga viskositas
meningkat
Kapsiula fibrosa juga ikut menebal dan
fibrotic
Membatasi pergerakan sendi
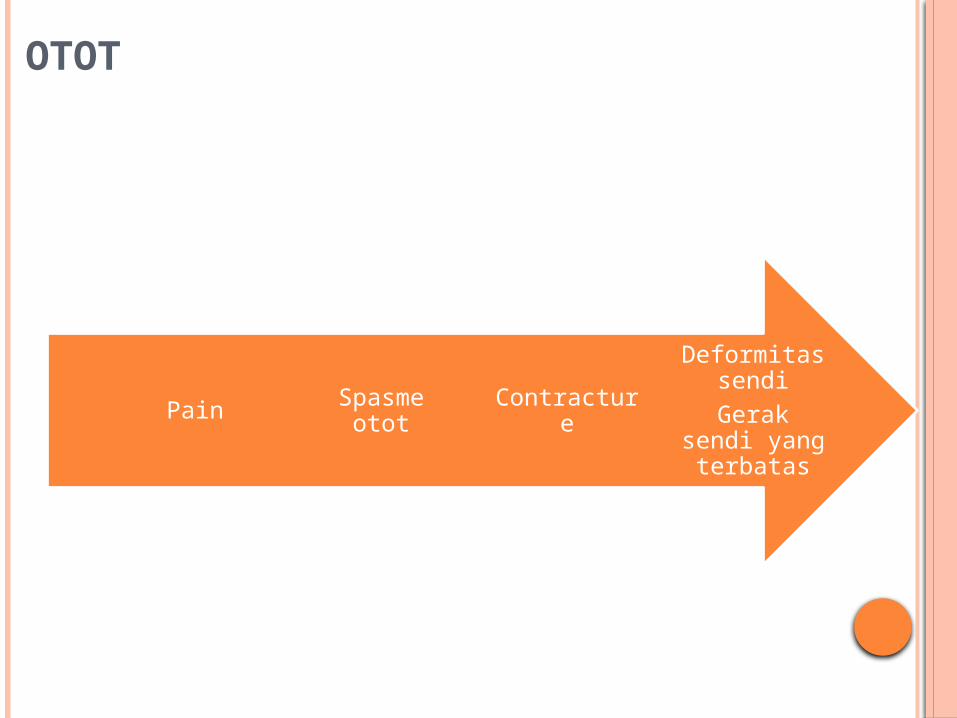
OTOT
Deformitas sendi
Gerak sendi yang
terbatas
ContractureSpasme ototPain
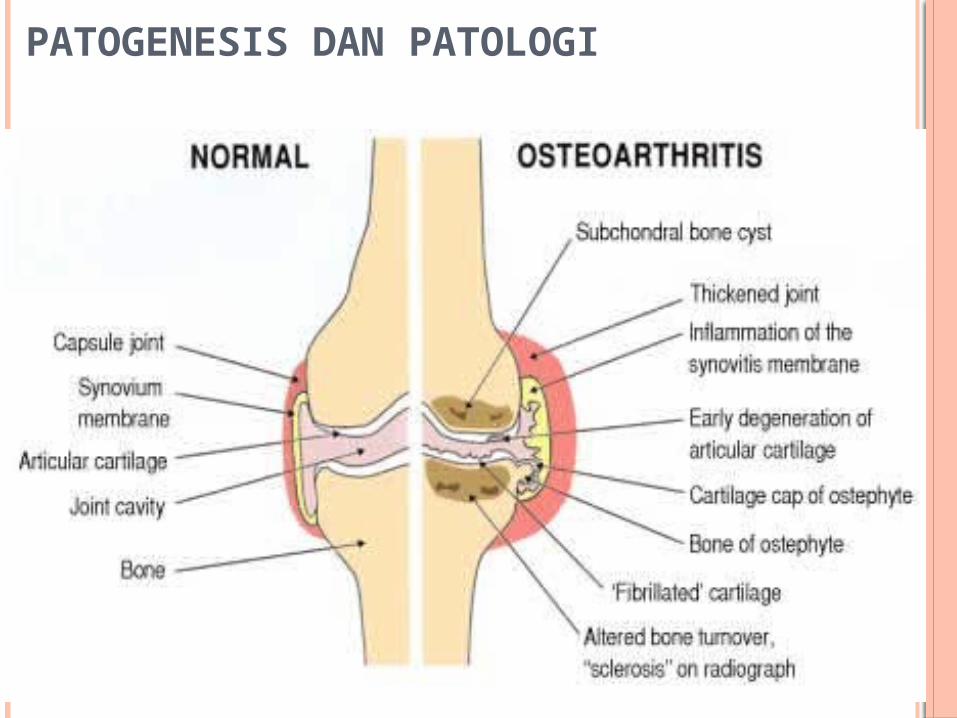
PATOGENESIS DAN PATOLOGI
PATOGENESIS DAN PATOLOGI

MANIFESTASI KLINIS
GEJALA
Nyeri Tumpul sampai dnegan nyeri yang terasa sangat
berat Dicetuskan dengan pergerakan sendi (friction
effect) dan berkurang saat istirahat. Resting pain dapat dirasakan, hal ini
berhubungan dengan hiperemia pada tulang subchondral.
Joint crepitus Articular gelling
Kekakuan sendi setelah fase istirahat.
1. Salter RB. Textbook of Disorders and Injuries of the Muskuloskeletal System. Degenerative Disoreders of Joints and Related Tissues. 3rd ed. Philadelaphia, PA: Mosby; 1999; p. 213-23.
PEMERIKSAAN FISIK
• Swelling of the joint, karena ada moderate effusion, dan sedikit penebalan synovial. Edema akan semakin jelas karena adanya atrofi dari otot sekitar.
• Heberden’s nodes pada DIP. Biasanya terdapat pada primary type, lebih banyak pada wanita.
Look
• Teraba kaku.Feel• Gerak aktif dan pasif lebih terbatas. Hal ini dapat
diakibatkan karena adanya kekakuan maupun rasa sakit. • Krepitasi saat sendi digerakkan.Move
1. Salter RB. Textbook of Disorders and Injuries of the Muskuloskeletal System. Degenerative Disoreders of Joints and Related Tissues. 3rd ed. Philadelaphia, PA: Mosby; 1999; p. 213-23.
PEMERIKSAAN PENUNJANG
PEMERIKSAAN PENUNJANG
o Pemeriksaan Laboratorium• Darah : LED mungkin↑, namun jarang menunjukkan
adanya penyakit sistemik.• Cairan sendi : ↑ mucin
o Radiographic• Menunjukkan perubahan pada sendi yang
berkorelasi dengan proses patologis yang terjadi, seperti:a. Penyempitan celah sendi.b. Subchondral sclerosis dan cyst,c. Pembentukan osteophyte,d. Joint remodelling dan incongruity.
1. Salter RB. Textbook of Disorders and Injuries of the Muskuloskeletal System. Degenerative Disoreders of Joints and Related Tissues. 3rd ed. Philadelaphia, PA: Mosby; 1999; p. 213-23.
DIAGNOSIS
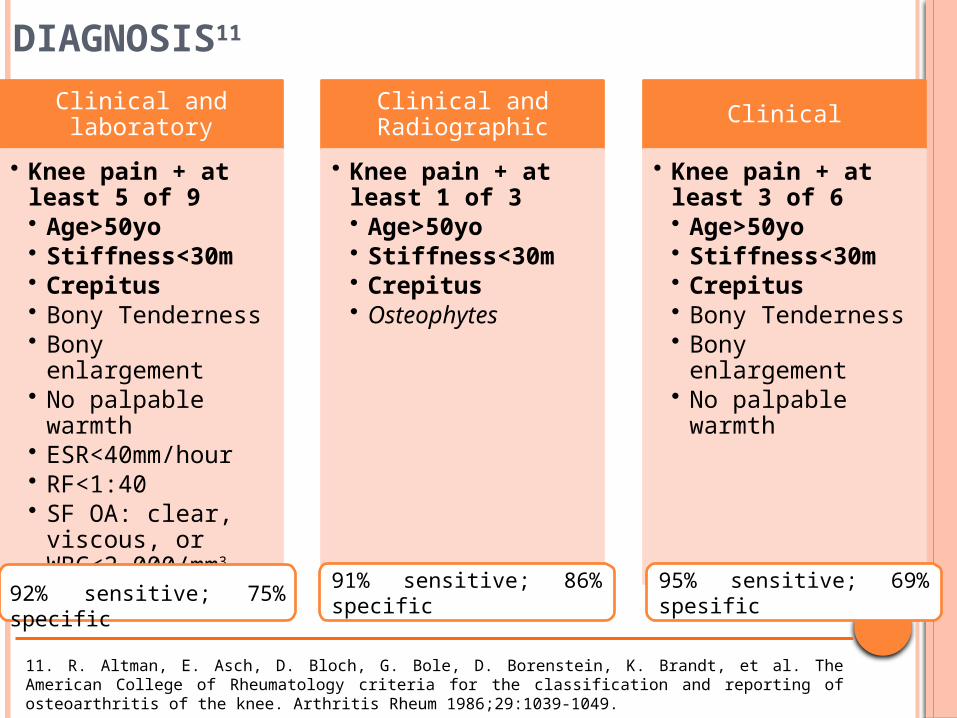
DIAGNOSIS11
Clinical and laboratory
• Knee pain + at least 5 of 9• Age>50yo• Stiffness<30m• Crepitus• Bony Tenderness• Bony enlargement• No palpable
warmth• ESR<40mm/hour• RF<1:40• SF OA: clear,
viscous, or WBC<2,000/mm3
Clinical and Radiographic
• Knee pain + at least 1 of 3• Age>50yo• Stiffness<30m• Crepitus• Osteophytes
Clinical
• Knee pain + at least 3 of 6• Age>50yo• Stiffness<30m• Crepitus• Bony Tenderness• Bony enlargement• No palpable
warmth
92% sensitive; 75% specific
91% sensitive; 86% specific
95% sensitive; 69% spesific
11. R. Altman, E. Asch, D. Bloch, G. Bole, D. Borenstein, K. Brandt, et al. The American College of Rheumatology criteria for the classification and reporting of osteoarthritis of the knee. Arthritis Rheum 1986;29:1039-1049.
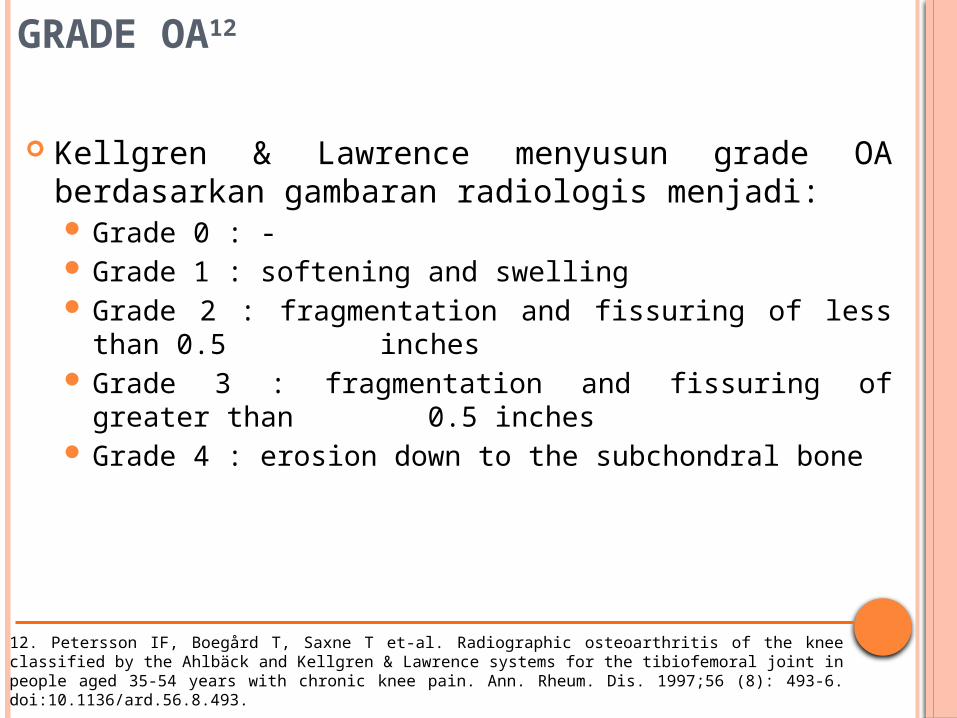
GRADE OA12
Kellgren & Lawrence menyusun grade OA berdasarkan gambaran radiologis menjadi: Grade 0 : - Grade 1 : softening and swelling Grade 2 : fragmentation and fissuring of less than 0.5
inches Grade 3 : fragmentation and fissuring of greater than
0.5 inches Grade 4 : erosion down to the subchondral bone
12. Petersson IF, Boegård T, Saxne T et-al. Radiographic osteoarthritis of the knee classified by the Ahlbäck and Kellgren & Lawrence systems for the tibiofemoral joint in people aged 35-54 years with chronic knee pain. Ann. Rheum. Dis. 1997;56 (8): 493-6. doi:10.1136/ard.56.8.493.
TATALAKSANA
PRINSIP TERAPI13,14
Non pharmacolog
ic
Pharmacologic
Mengurangi trasa sakit;
Meningkatkan status
fungsional
13. Zhang W, Moskowitz RW, Nuki G, Abramson S, Altman RD, Arden N, et al. OARSI recommendations for the management of hip and knee osteoarthritis, Part II: OARSI evidence-based, expert consensus guidelines. Osteoarthritis Cartilage. Feb 2008;16(2):137-62.14. Zhang W, Moskowitz RW, Nuki G, Abramson S, Altman RD, Arden N, et al. OARSI recommendations for the management of hip and knee osteoarthritis, part I: critical appraisal of existing treatment guidelines and systematic review of current research evidence. Osteoarthritis Cartilage. Sep 2007;15(9):981-1000.
NON-FARMAKOLOGIS14,15
Edukasi pasien Terapi panas dan dingin Penurunan berat badan Olahraga non weight bearing Terapi yang disesuaikan dengan aktivitas
14. Zhang W, Moskowitz RW, Nuki G, Abramson S, Altman RD, Arden N, et al. OARSI recommendations for the management of hip and knee osteoarthritis, part I: critical appraisal of existing treatment guidelines and systematic review of current research evidence. Osteoarthritis Cartilage. Sep 2007;15(9):981-1000.15. Felson DT, Zhang Y, Anthony JM, Naimark A, Anderson JJ. Weight loss reduces the risk for symptomatic knee osteoarthritis in women. The Framingham Study. Ann Intern Med. Apr 1 1992;116(7):535-9.
Tujuan dari terapi farmakologis
FARMAKOLOGIS
Untuk mengurangi morbiditas
Untuk mencegah komplikasi
Agen farmakologis yang digunakan dalam terapi OA antara lain: Acetaminophen Nonsteroidal anti-inflammatory drugs (NSAIDs), oral
and topical Intra-articular corticosteroids Intra-articular sodium hyaluronate Opioids Duloxetine Muscle relaxants Nutriceuticals (eg, glucosamine/chondroitin sulfate)
FARMAKOLOGIS
Untuk terapi OA lutut, American Collage of Rheumatology (ACR) merekomendasikan penggunaan salah satu diantara obat berikut:16: Acetaminophen Oral NSAIDs Topical NSAIDs Tramadol Intra-articular corticosteroid injections
Petunjuk praktek klinis dari American Academy of Orthopedic Surgeons (AAOS) merekomendasikan penggunaan farmakologis berikut untuk OA lutut simptomatis17: Oral NSAIDs Topical NSAIDs Tramadol
FARMAKOLOGIS (2)
16. Jordan JM, Helmick CG, Renner JB, Luta G, Dragomir AD, Woodard J, et al. Prevalence of knee symptoms and radiographic and symptomatic knee osteoarthritis in African Americans and Caucasians: the Johnston County Osteoarthritis Project. J Rheumatol. Jan 2007;34(1):172-80.17. American Academy of Orthopaedic Surgeons. Treatment of Osteoarthritis (OA) of the Knee. AAOS: American Academy of Orthopaedic Surgeons. Available at http://www.aaos.org/research/guidelines/GuidelineOAKnee.asp. Accessed July 8, 2013
TINDAKAN OPERATIF Indication:
To relieving pain et cause severe arthritis (e.g. OA grade III-IV) To correct deformity (e.g. moderate arthritis with moderate
contracture, valgus laxity, valrus laxity). Macam tindakan operative:
Arthroscopy: removal of meniscal tears and loose bodies; procedures include: debridement of loose articular cartilage with a microfracture technique
and cartilaginous implants in areas of eburnated subchondral bone.18
Osteotomy: principle underlying this procedure is to shift weight from the damaged cartilage on the medial aspect of the knee to the healthy lateral aspect of the knee.19
Arthroplasty: consists of the surgical removal of joint surface and the insertion of a metal and plastic prosthesis.20
Arthrodesis: union of bones on either side of the joint. This procedure relieves pain but prevents motion and puts more stress on surrounding joints20.
18 Kirkley A, Birmingham TB, Litchfield RB, Giffin JR, Willits KR, Wong CJ, et al. A randomized trial of arthroscopic surgery for osteoarthritis of the knee. N Engl J Med. Sep 11 2008;359(11):1097-107.19. Pagenstert G, Knupp M, Valderrabano V, Hintermann B. Realignment surgery for valgus ankle osteoarthritis. Oper Orthop Traumatol. Mar 2009;21(1):77-87.20. Reichenbach S, Rutjes AW, Nüesch E, Trelle S, Jüni P. Joint lavage for osteoarthritis of the knee. Cochrane Database Syst Rev. May 12 2010;CD007320.
ARTHROSCOPY
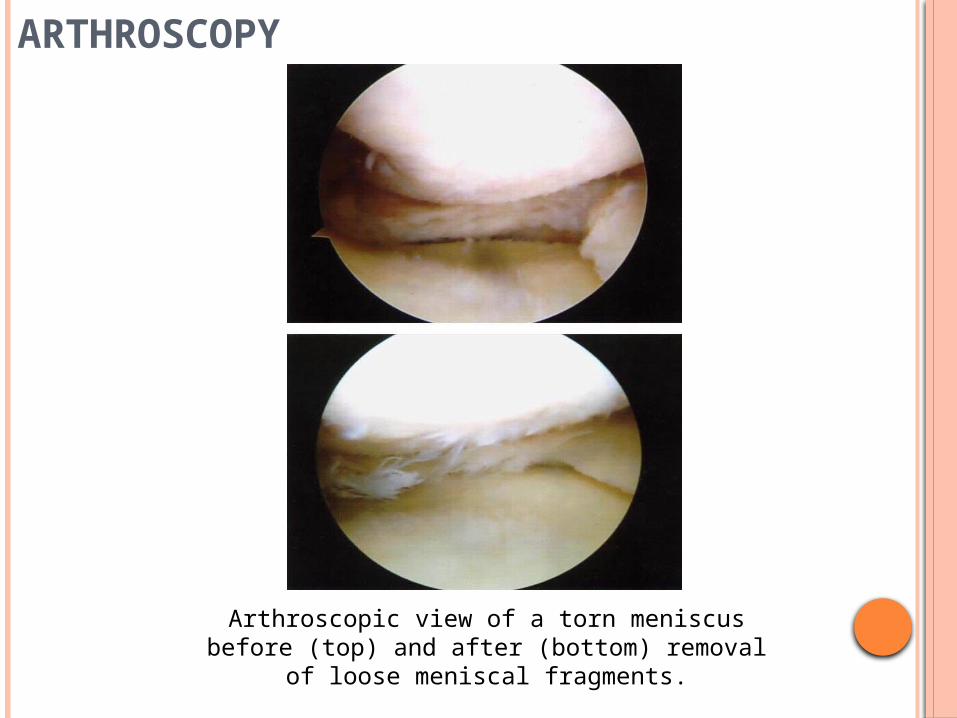
Arthroscopic view of a torn meniscus before (top) and after (bottom) removal of loose
meniscal fragments.

ARTHROPLASTY
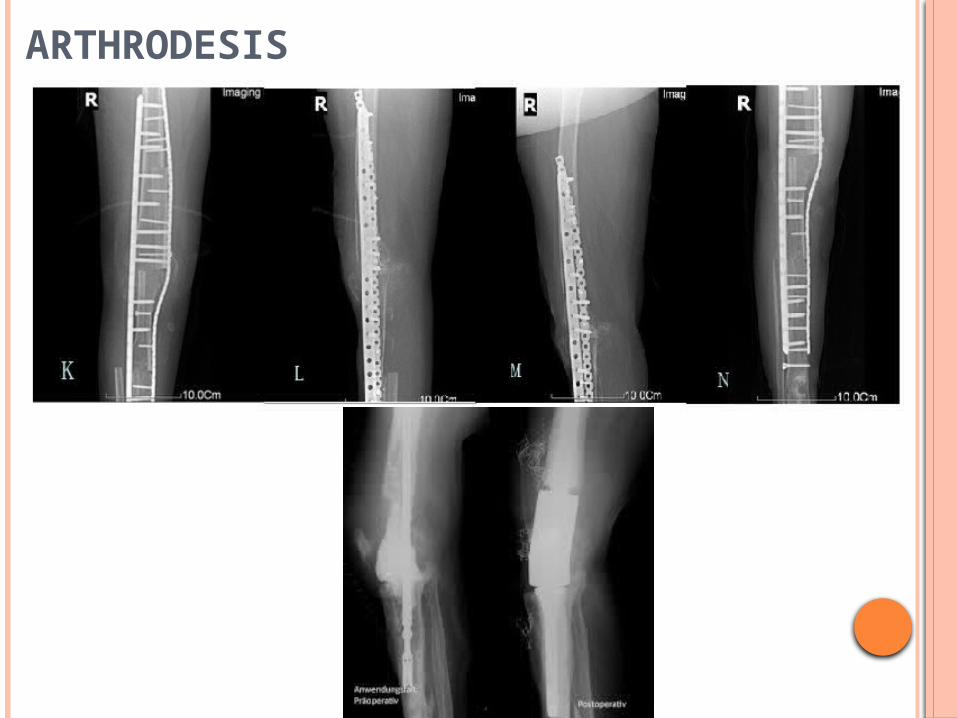
ARTHRODESIS
PROGNOSIS
PROGNOSIS
The prognosis in patients with osteoarthritis depends on the joints involved and on the severity of the condition.21
A systematic review found the following clinical features to be associated with more rapid progression of knee osteoarthritis21:
Older age Higher BMI Varus deformity Multiple involved joints
Patients with osteoarthritis who have undergone joint replacement have a good prognosis, with success rates for hip and knee arthroplasty generally exceeding 90%.21
21. Chapple CM, Nicholson H, Baxter GD, Abbott JH. Patient characteristics that predict progression of knee osteoarthritis: A systematic review of prognostic studies. Arthritis Care Res (Hoboken). Aug 2011;63(8):1115-25.
TERIMA KASIH
DAFTAR PUSTAKA
DAFTAR PUSTAKA
1. Salter RB. Textbook of Disorders and Injuries of the Muskuloskeletal System. Degenerative Disoreders of Joints and Related Tissues. 3rd ed. Philadelaphia, PA: Mosby; 1999; p. 213-23.
2. Lawrence RC, Felson DT, Helmick CG, et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part II. Arthritis Rheum. 2008;58(1):26-35.
3. Oliveria SA, Felson DT, Reed JI, et al. Incidence of symptomatic hand, hip and knee osteoarthritis among patients in health maintenance organization. Arthritis Rheum. 1995;38(8):134-1141.
4. Buckwalter JA, Saltzman C, Brown T. The impact of osteoarthritis. Clin Orthoped Rei Res. 200:427S:S6-S15.
5. Jordan JM, Helmick Cg, renner JB, et al. Prevalence of knee symptoms and radiographic and symptomatic knee osteoarthititis in African Ameriicans and Caucasians: The Jhonston County Osteoarthitis Project. J Rheumatol. 2007;34(1):172-80.
6. Felson DT, Zhang Y. An update on the epidemiology of knee and hip osteoarthritis with view to prevention. Arthritis Rheum. 1998:41(8):1343-55.
7. Felson DT. Risk Factors of osteoarthritis. Clin Orthoped Rel Res. 2004;427S:S16-S21.
8. Rossignol M, Leclerc A, Allaeret FA, et al. Primary osteoarthritis of hip, knee and hand in relation to occupational exposure. Occup Environ Med. 2005;62:772-777.
9. Cooper C, Snow S, McAlindon TE, et al. Risk factors for the incidence and progression of radiographic knee ostoarthrits. Arthritis Rheum. 2000;43(5):995-1000.
10. Blogojevic M, Jinks C, Jeffrey A, et al. Risk factors for onset of osteoarthritis of the knee in older adults: a systematic review and metanalysis. Osteoarthritis Cartilage. 2010;18(1):24-33.
11. R. Altman, E. Asch, D. Bloch, G. Bole, D. Borenstein, K. Brandt, et al. The American College of Rheumatology criteria for the classification and reporting of osteoarthritis of the knee. Arthritis Rheum 1986;29:1039--1049.
12. Petersson IF, Boegård T, Saxne T et-al. Radiographic osteoarthritis of the knee classified by the Ahlbäck and Kellgren & Lawrence systems for the tibiofemoral joint in people aged 35-54 years with chronic knee pain. Ann. Rheum. Dis. 1997;56 (8): 493-6. doi:10.1136/ard.56.8.493.
13. Zhang W, Moskowitz RW, Nuki G, Abramson S, Altman RD, Arden N, et al. OARSI recommendations for the management of hip and knee osteoarthritis, Part II: OARSI evidence-based, expert consensus guidelines. Osteoarthritis Cartilage. Feb 2008;16(2):137-62.
14. Zhang W, Moskowitz RW, Nuki G, Abramson S, Altman RD, Arden N, et al. OARSI recommendations for the management of hip and knee osteoarthritis, part I: critical appraisal of existing treatment guidelines and systematic review of current research evidence. Osteoarthritis Cartilage. Sep 2007;15(9):981-1000.
15. Felson DT, Zhang Y, Anthony JM, Naimark A, Anderson JJ. Weight loss reduces the risk for symptomatic knee osteoarthritis in women. The Framingham Study. Ann Intern Med. Apr 1 1992;116(7):535-9.
16. Jordan JM, Helmick CG, Renner JB, Luta G, Dragomir AD, Woodard J, et al. Prevalence of knee symptoms and radiographic and symptomatic knee osteoarthritis in African Americans and Caucasians: the Johnston County Osteoarthritis Project. J Rheumatol. Jan 2007;34(1):172-80.
17. American Academy of Orthopaedic Surgeons. Treatment of Osteoarthritis (OA) of the Knee. AAOS: American Academy of Orthopaedic Surgeons. Available at http://www.aaos.org/research/guidelines/GuidelineOAKnee.asp. Accessed July 8, 2013.
18. Kirkley A, Birmingham TB, Litchfield RB, Giffin JR, Willits KR, Wong CJ, et al. A randomized trial of arthroscopic surgery for osteoarthritis of the knee. N Engl J Med. Sep 11 2008;359(11):1097-107.
19. Pagenstert G, Knupp M, Valderrabano V, Hintermann B. Realignment surgery for valgus ankle osteoarthritis. Oper Orthop Traumatol. Mar 2009;21(1):77-87.
20. Reichenbach S, Rutjes AW, Nüesch E, Trelle S, Jüni P. Joint lavage for osteoarthritis of the knee. Cochrane Database Syst Rev. May 12 2010;CD007320.
21. Chapple CM, Nicholson H, Baxter GD, Abbott JH. Patient characteristics that predict progression of knee osteoarthritis: A systematic review of prognostic studies. Arthritis Care Res (Hoboken). Aug 2011;63(8):1115-25.
DAFTAR PUSTAKA (2)