10 10 tips ampuh mengobati penyakit flu secara cepat - klinik kosasih
HipertensiHipertensi secarasecara KlinikKlinik
Edwin Edwin Setiabudi,dr.SpPDSetiabudi,dr.SpPD


JNC VII : Classification of hypertension
Systolic Diastolic
Normal
Prehypertension
Stage 1 hypertension
Stage 2 hypertension
< 120
120-139
140-159
≥160
< 80
80-89
90-99
≥100
and
or
or
or
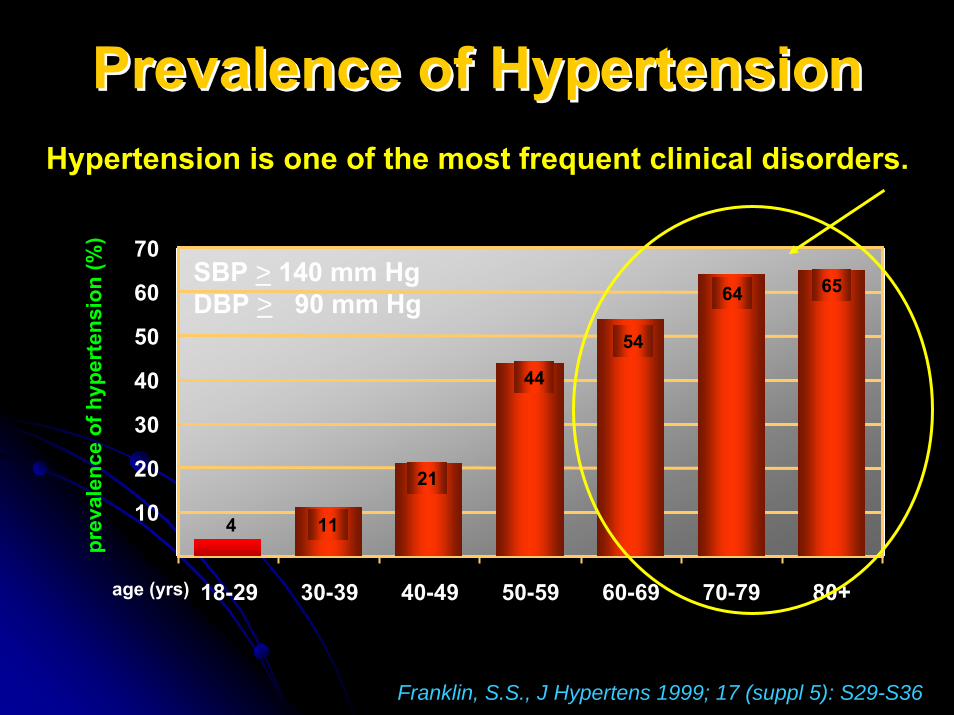
Franklin, S.S., J Hypertens 1999; 17 (suppl 5): S29-S36
Hypertension is one of the most frequent clinical disorders.
0
10
20
30
40
50
60
70
18-29 30-39 40-49 50-59 60-69 70-79 80+
SBP > 140 mm Hg DBP > 90 mm Hg
age (yrs)
prev
alen
ce o
f hyp
erte
nsio
n (%
)
4 11
21
44
54
64 65
Prevalence of HypertensionPrevalence of HypertensionPrevalence of Hypertension
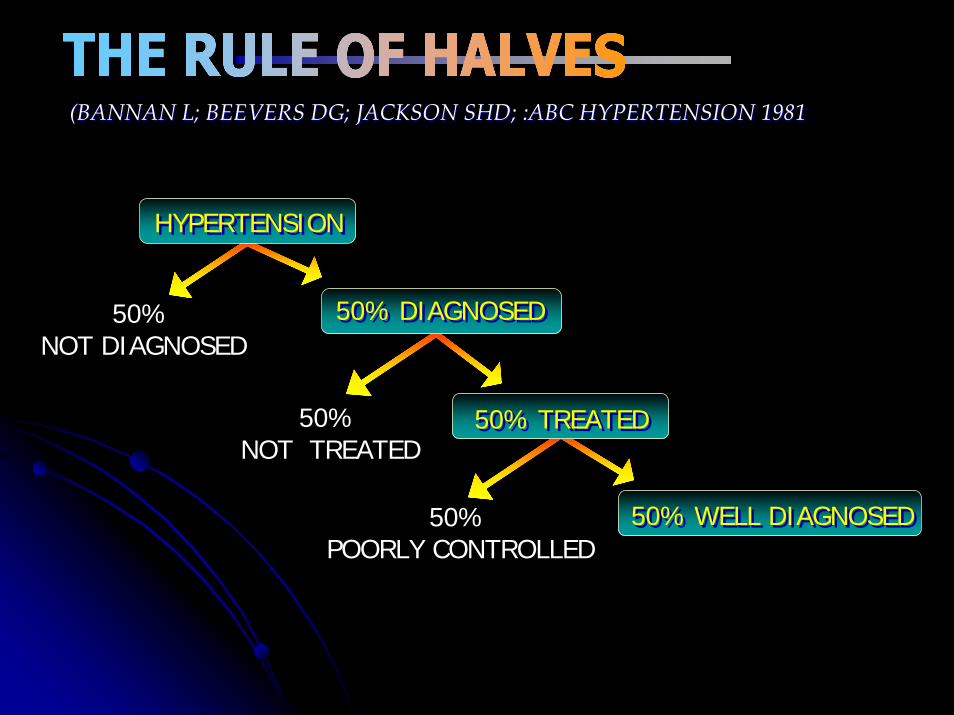
(BANNAN L; BEEVERS DG; JACKSON SHD; :ABC HYPERTENSION 1981(BANNAN L; BEEVERS DG; JACKSON SHD; :ABC HYPERTENSION 1981
HYPERTENSIONHYPERTENSION
50% DIAGNOSED50% DIAGNOSED
50% TREATED50% TREATED
50% WELL DIAGNOSED50% WELL DIAGNOSED
50% NOT DIAGNOSED
50% NOT TREATED
50% POORLY CONTROLLED
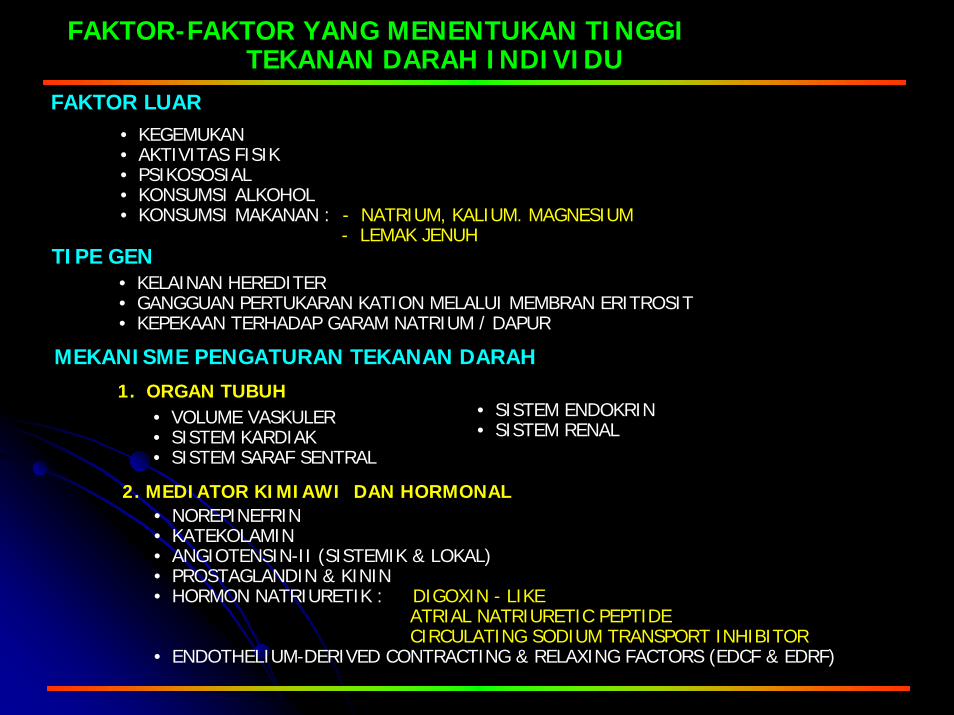
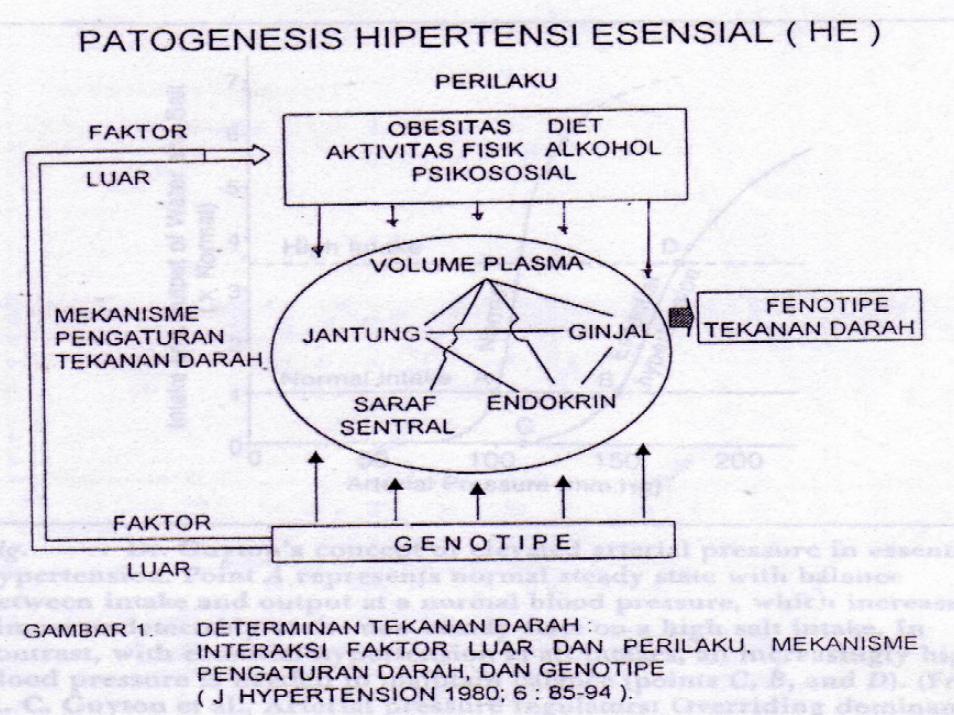
• KEGEMUKAN• AKTIVITAS FISIK• PSIKOSOSIAL• KONSUMSI ALKOHOL• KONSUMSI MAKANAN : - NATRIUM, KALIUM. MAGNESIUM
- LEMAK JENUH
FAKTOR-FAKTOR YANG MENENTUKAN TINGGI TEKANAN DARAH INDIVIDU
FAKTOR LUAR
TIPE GEN• KELAINAN HEREDITER• GANGGUAN PERTUKARAN KATION MELALUI MEMBRAN ERITROSIT• KEPEKAAN TERHADAP GARAM NATRIUM / DAPUR
MEKANISME PENGATURAN TEKANAN DARAH1. ORGAN TUBUH
• VOLUME VASKULER• SISTEM KARDIAK• SISTEM SARAF SENTRAL
• SISTEM ENDOKRIN• SISTEM RENAL
2. MEDIATOR KIMIAWI DAN HORMONAL• NOREPINEFRIN• KATEKOLAMIN• ANGIOTENSIN-II (SISTEMIK & LOKAL)• PROSTAGLANDIN & KININ• HORMON NATRIURETIK : DIGOXIN - LIKE
ATRIAL NATRIURETIC PEPTIDECIRCULATING SODIUM TRANSPORT INHIBITOR
• ENDOTHELIUM-DERIVED CONTRACTING & RELAXING FACTORS (EDCF & EDRF)

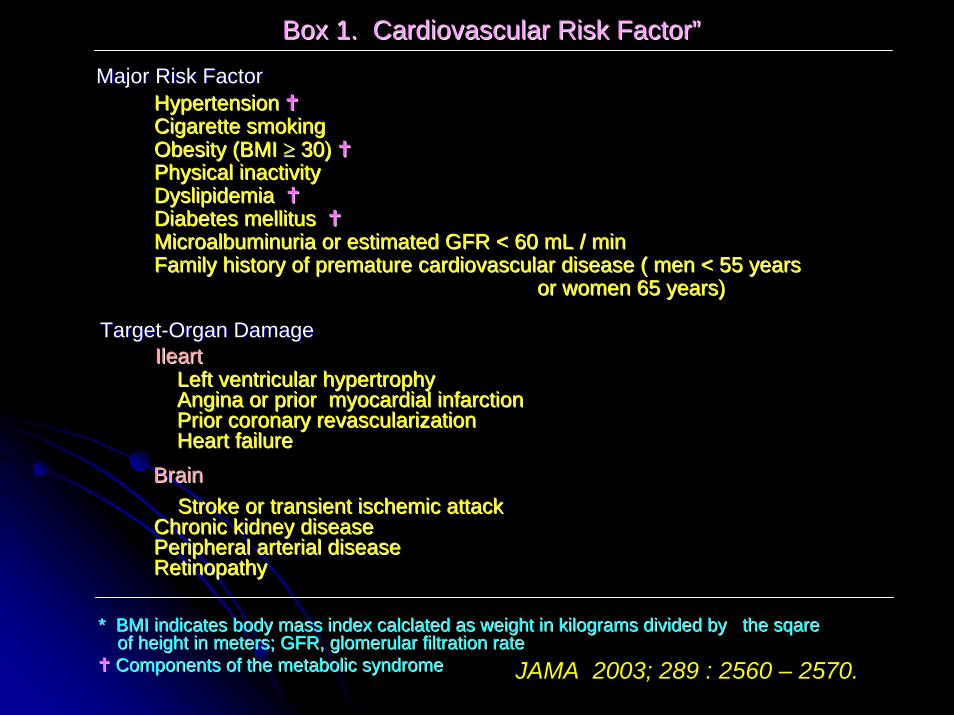
Box 1. Cardiovascular Risk FactorBox 1. Cardiovascular Risk Factor””
Major Risk FactorMajor Risk FactorHypertension Hypertension Cigarette smokingCigarette smokingObesity (BMI Obesity (BMI ≥≥ 30) 30) Physical inactivityPhysical inactivityDyslipidemiaDyslipidemiaDiabetes mellitus Diabetes mellitus MicroalbuminuriaMicroalbuminuria or estimated GFR < 60 or estimated GFR < 60 mLmL / min/ minFamily history of premature cardiovascular disease ( men < 55 yeFamily history of premature cardiovascular disease ( men < 55 years ars
or women 65 years)or women 65 years)
TargetTarget--Organ DamageOrgan DamageIleartIleart
Left ventricular hypertrophyLeft ventricular hypertrophyAngina or prior myocardial infarctionAngina or prior myocardial infarctionPrior coronary revascularization Prior coronary revascularization Heart failureHeart failure
BrainBrainStroke or transient ischemic attackStroke or transient ischemic attack
Chronic kidney diseaseChronic kidney diseasePeripheral arterial diseasePeripheral arterial diseaseRetinopathyRetinopathy
* BMI indicates body mass index * BMI indicates body mass index calclatedcalclated as weight in kilograms divided by the as weight in kilograms divided by the sqaresqareof height in meters; GFR, of height in meters; GFR, glomerularglomerular filtration ratefiltration rateComponents of the metabolic syndromeComponents of the metabolic syndrome JAMA 2003; 289 : 2560 – 2570.
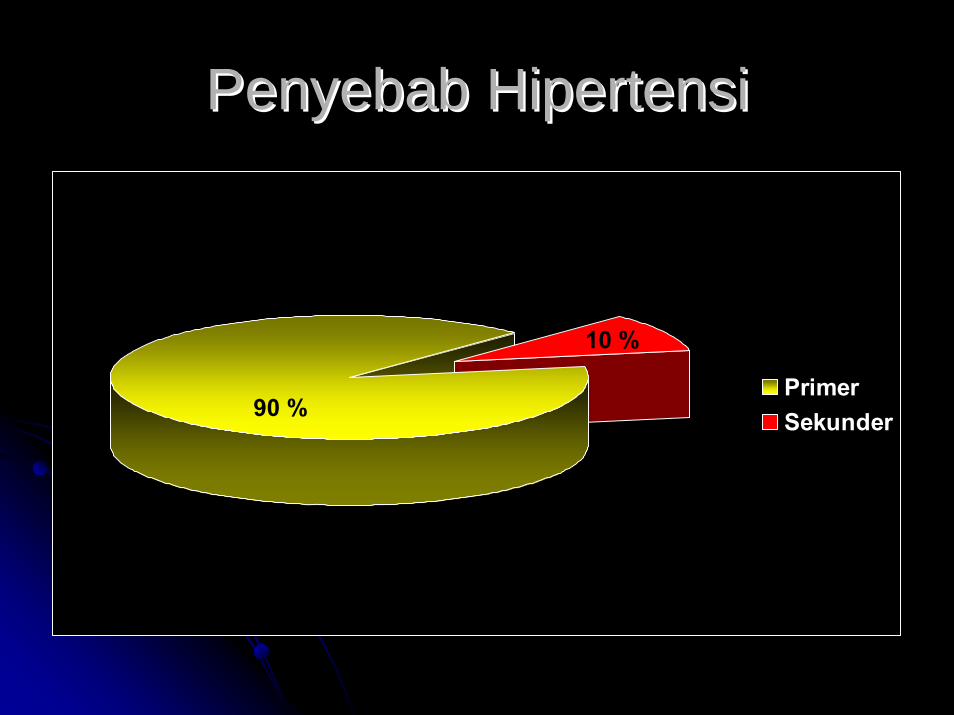
PenyebabPenyebab HipertensiHipertensi
PrimerSekunder90 %
10 %
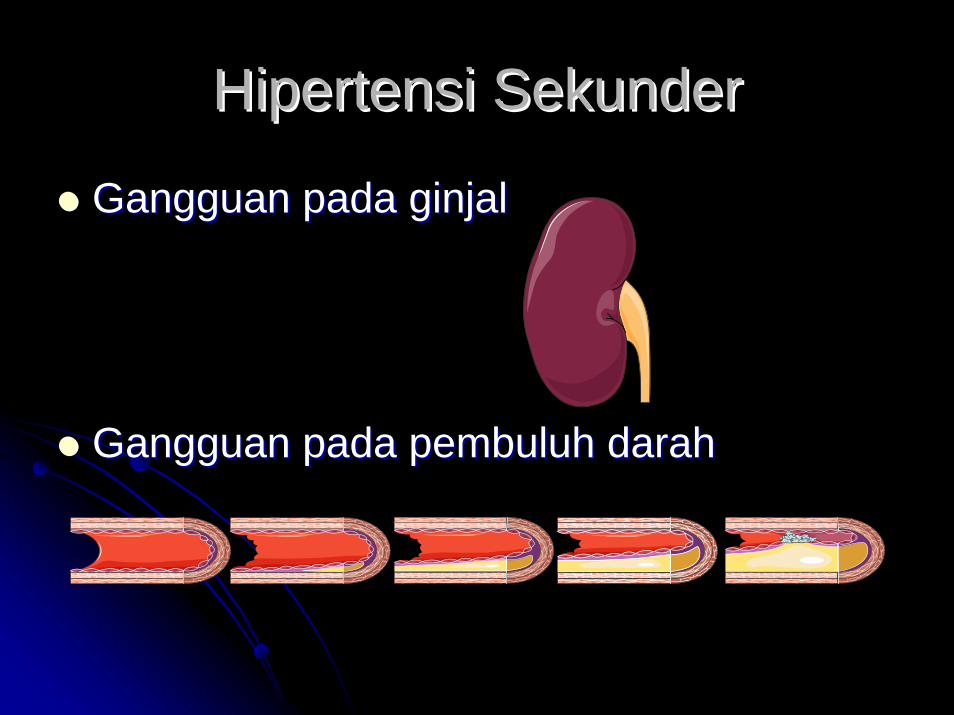
HipertensiHipertensi SekunderSekunder
GangguanGangguan padapada ginjalginjal
GangguanGangguan padapada pembuluhpembuluh darahdarah
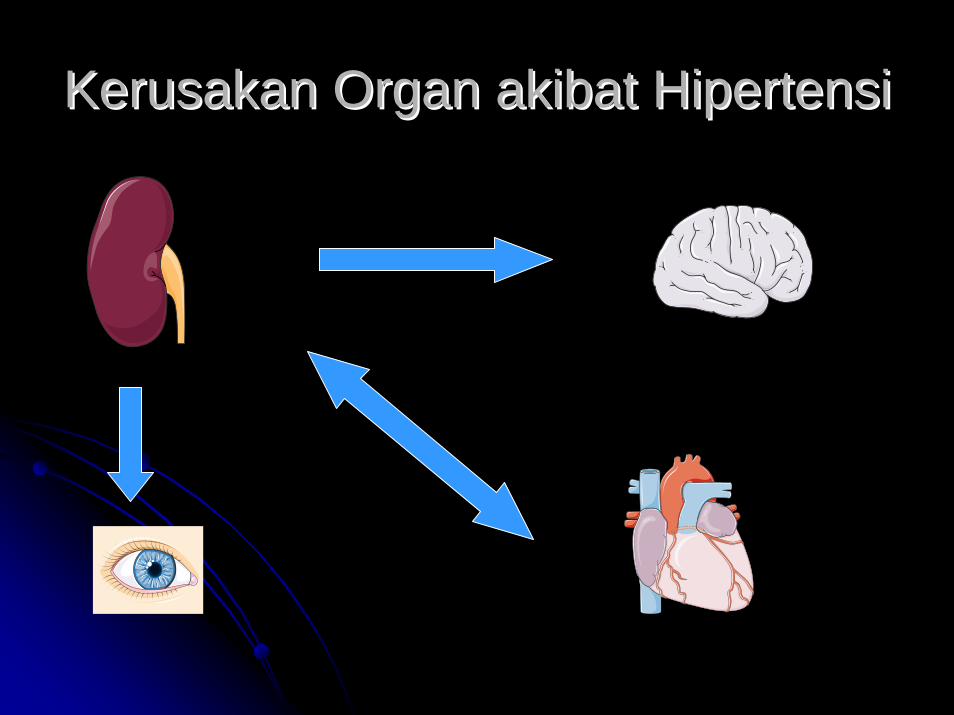
KerusakanKerusakan Organ Organ akibatakibat HipertensiHipertensi

TerapiTerapi NonNon--farmakologisfarmakologis
Diet yang Diet yang sehatsehat
KontrolKontrol beratberat badanbadan
KurangiKurangi garamgaram
NonNon--alkoholalkohol
Stop Stop merokokmerokok
OlahOlah ragaraga
55

Table 3. Lifestyle Modifications to Management Hypertension *Table 3. Lifestyle Modifications to Management Hypertension *
ModificationModification RecommendationRecommendation
Weight reductionWeight reduction
Approximate Systolic BPApproximate Systolic BPReduction, RangeReduction, Range
Adopt DASH eatingAdopt DASH eatingplanplan
Maintain normal body weight (BMI, 18.5Maintain normal body weight (BMI, 18.5--24.9)24.9) 55--20 mmHg/1020 mmHg/10--kg weight loss kg weight loss 23,24
Consume a diet rich in fruits, vegetables, andConsume a diet rich in fruits, vegetables, andlowlow--fat dairy products with a reducedfat dairy products with a reduced
content of saturated and total fat.content of saturated and total fat.
Dietary sodiumDietary sodiumreductionreduction
Reduce dietary sodium intake to no more thanReduce dietary sodium intake to no more than100 100 mEqmEq/L (2.4 g sodium or 6 g sodium/L (2.4 g sodium or 6 g sodiumchloride)chloride)
8 8 –– 14 mmHg 14 mmHg 25,2725,27
Physical activityPhysical activity Engage in regular aerobic physical activityEngage in regular aerobic physical activitysuch as brisk walking (at least 30 minutessuch as brisk walking (at least 30 minutes
per day, most days of the week)per day, most days of the week)8 8 –– 14 mmHg 14 mmHg 28,2928,29
Moderation of alcoholModeration of alcoholconsumptionconsumption
Limit consumption to no more than 2 drinksLimit consumption to no more than 2 drinksper day (1 oz or 30 per day (1 oz or 30 mLmL ethanol [ ethanol [ egeg. 24 oz. 24 ozbeer, 10 oz wine, or 3 oz 80beer, 10 oz wine, or 3 oz 80--proofproofwhiskey]) in most men and no more thanwhiskey]) in most men and no more than 8 8 –– 14 mmHg 14 mmHg 3030
1 drink per day in women and1 drink per day in women andlighterlighter--weight persons.weight persons.
Abbreviations; BMI, body mass index calculated as weight in kiloAbbreviations; BMI, body mass index calculated as weight in kilograms divided by the square of height ingrams divided by the square of height inmeters; BP blood pressure; DASH, Dietary Approaches to Stopmeters; BP blood pressure; DASH, Dietary Approaches to Stop Hypertension.Hypertension.
* For overall cardiovascular risk reduction, stop smoking. The* For overall cardiovascular risk reduction, stop smoking. The effects of implementing these modifications are dose and time effects of implementing these modifications are dose and time dependent and could be higher for some individuals.dependent and could be higher for some individuals.
8 8 –– 14 mmHg 14 mmHg 25,2625,26
JAMA 2003; 289 : 2560 – 2570.

JNC 7 AlgorithmJNC 7 Algorithm
Not at goal BP (<140/90 mmHg) (<130/80 mmHg for diabetes or proteinuria
Drugs
Lifestyle
Stage 2 hypertension (SBP ≥160 or DBP ≥100)
Start 2 drugs, HCTZ +ACEI, or ARB, or BBL, or
CCB
Stage 1 hypertension(SBP 140–159 or DBP 90–99)
HCTZ May consider ACEI, ARB, BBL,
CCB,
Without other problems
Drug(s) for the problem ie.
Statin, Aspirin, Metformin etc.
HCTZ, ACEI, ARB, BB, CCB as needed
With other problems
Increase dose or add more drugs until goal BP is achieved
Consult with hypertension specialist
Not at goal BP
Chobanian AV et al.2003;42:1206–52
< 140/90
Rendah garamOlahragaBBStop rokok
MulaiMulai thth/ / dg dg
ThiazideThiazide
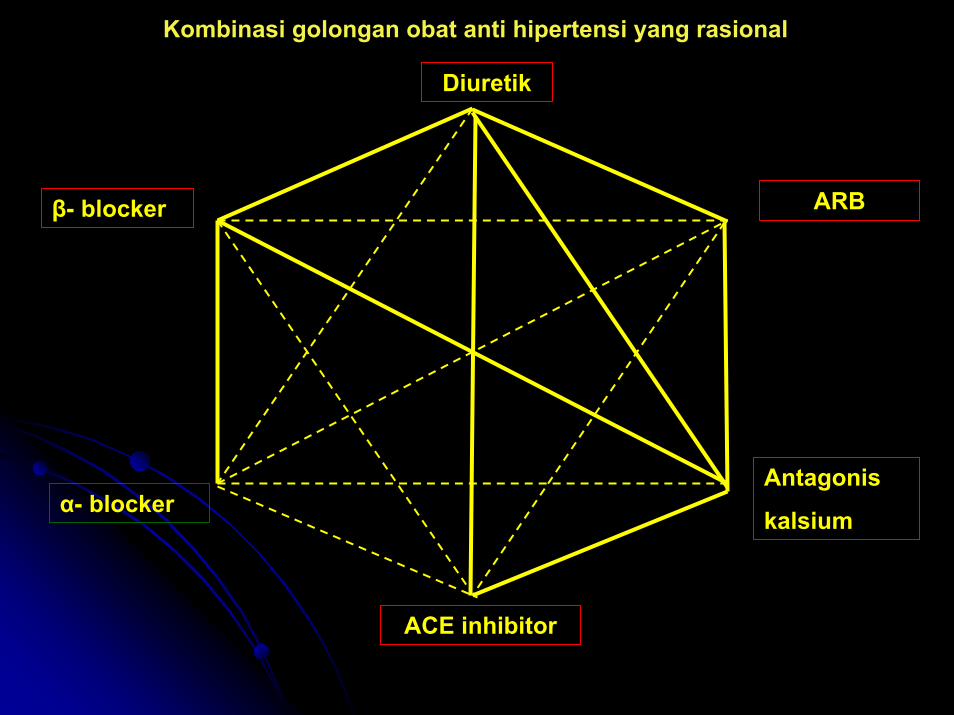
Diuretik
ARB
Antagonis
kalsium
ACE inhibitor
α- blocker
β- blocker
Kombinasi golongan obat anti hipertensi yang rasional

Box 3. Causes of Resistant HypertensionBox 3. Causes of Resistant HypertensionImproper blood pressure measurementImproper blood pressure measurementVolume overload and Volume overload and pseudotolerancepseudotolerance
Excess sodium intakeExcess sodium intakeVolume retention from kidney diseaseVolume retention from kidney diseaseInadequate diuretic therapyInadequate diuretic therapy
DrugDrug--induced or other causesinduced or other causes
NonadherenceNonadherenceInadequate dosesInadequate dosesInappropriate combinationsInappropriate combinationsNonsteroidalNonsteroidal antianti--inflammatory drugs; inflammatory drugs; cyclooxygenasecyclooxygenase 2 inhibitors2 inhibitorsCocaine, amphetamines, other illicit drugsCocaine, amphetamines, other illicit drugsSympathomimeticsSympathomimetics (decongestants, (decongestants, anorectiesanorecties))Oral contraceptivesOral contraceptivesAdrenal steroidsAdrenal steroidsCyclosporine and Cyclosporine and tacrolimustacrolimusErythropoietinErythropoietinLicorice (including some chewing tobacco)Licorice (including some chewing tobacco)Selected overSelected over--the counter dietary supplements and medicines the counter dietary supplements and medicines
((egeg, , ephedraephedra, ma , ma haunghaung, bitter orange), bitter orange)
Associated conditionsAssociated conditionsObesityObesityExcess alcohol intakeExcess alcohol intake
Identifiable causes of hypertension (see Box 2)Identifiable causes of hypertension (see Box 2)
JAMA 2003; 289 : 2560 – 2570.
Copyright © 2022 FDOKUMEN



![TUTORIAL KLINIK HIPERTENSI - rsud.patikab.go.id · Jantung Hipertrofi ventrikel kiri Angina atau infark miokardium Gagal jantung 2. ... Microsoft PowerPoint - HIPERTENSI.ppt [Read-Only]](https://static.fdokumen.com/doc/165x107/5b82b8527f8b9a315b8ba15a/tutorial-klinik-hipertensi-rsud-jantung-hipertrofi-ventrikel-kiri-angina.jpg)