DEPRESI ANAK
43
DEPRESI PADA ANAK Clinical Guideline sarka ade
-
Upload
fauzan-keren -
Category
Documents
-
view
238 -
download
5
Transcript of DEPRESI ANAK
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 1/43
DEPRESI PADA ANAK
Clinical Guideline
sarka ade
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 2/43
Intro Context Key priorities and recommendations Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
PETUNJUK KLINIK
• Direkomendasi untuk praktek yang baik yang
didasarkan pada bukti (evidence based).
• Pedoman untuk standar yan kesehatan yang lebihbaik dalam mengimplementasikan pedoman klinis
• Lembaga- Komisi Kesehatan akan memonitor
kepatuhan dengan panduan.
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 3/43
Intro Context Key priorities and recommendations Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
Alasan Pedoman:
• Profesional yang terlibat dengan pengasuhan anak-
anak dan orang muda harus lebih mampu
mengidentifikasi tanda-tanda depresi.• Sekitar 75% dari kasus mungkin tidak terdeteksi
Kenapa?
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 4/43
Intro Context Key priorities and recommendations Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
DEPRESI TIDAK TERDETEKSI?
• Pasien:
– Gejala tidak dikenali
– Salah mengerti keparahan n konsekuensinya – Terbatasnya akses yan kes
– Stigma gangguan jiwa
– Kepatuhan yg kurang
• Tenaga Kesehatan
– Edukasi yg kurang ttg gg jiwa
– Waktu konsults yg tidak cukup
– Ide/teori yg sdh terbentuk sebelumnya
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 5/43
Intro Context Key priorities and recommendations Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
What this guideline covers
• Best practice advice on the care of children andyoung people aged 5 –18 years with depression
• Recommendations for healthcare and other professionals who have a role to play in ensuringchildren and young people and their families andcarers get appropriate care and support, in both
primary and secondary care
• A clinical description of depression based on ICD-10
5
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 6/43
Intro Context Key priorities and recommendations Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
• Praktik terbaik nasihat tentang perawatan anak-anak
dan orang muda berusia 5 -18 tahun dengan depresi
Rekomendasi untuk kesehatan dan profesional lain
yang memiliki peran dalam memastikan anak-anak
dan orang muda dan keluarga mereka dan wali
mendapatkan perawatan yang tepat dan dukungan,
baik dalam perawatan primer dan sekunder
Penjelasan depresi klinis berdasarkan ICD-10
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 7/43Intro Context Key priorities and recommendations Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
Prevalence
• Pada setiap, waktu satu perkiraan jumlah anak danremaja yang menderita depresi:1 dari 100 anak-anak
1 dari 33 anak muda Angka Prevalensi melebihi angka pengobatan:sekitar 25% dari anak-anak dan orang muda dengandepresi terdeteksi dan diobatiBunuh diri adalah:3 penyebab utama kematian di 15-24-year-olds6 penyebab utama kematian di 5-14-year-olds
6
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 8/43Intro Context Key priorities and recommendations Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
Symptoms• Key symptoms
– persistent sadness, or low or irritable mood
– loss of interests and/or pleasure
– fatigue or low energy• Associated symptoms – poor or increased sleep
– low self-confidence
– poor concentration or indecisiveness
– poor or increased appetite
– suicidal thoughts or acts
– guilt or self-blame
– agitation or slowing of movement
7
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 9/43Intro Context Key priorities and recommendations Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
Recommendations identified as key
priorities• Assessment and coordination of care
• Treatment considerations in all settings
• Step 1: Detection and risk profiling
• Step 2: Recognition
• Step 3: Mild depression
• Steps 4 and 5: Moderate to severe depression
8
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 10/43Intro Context Key priorities and recommendations Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
• Pengkajian dan koordinasi perawatan
Pengobatan pertimbangan dalam semua pengaturan
Langkah 1: Deteksi dan profil risikoLangkah 2: Pengakuan
Langkah 3: depresi ringan
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 11/43Intro Context Key priorities and recommendations Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
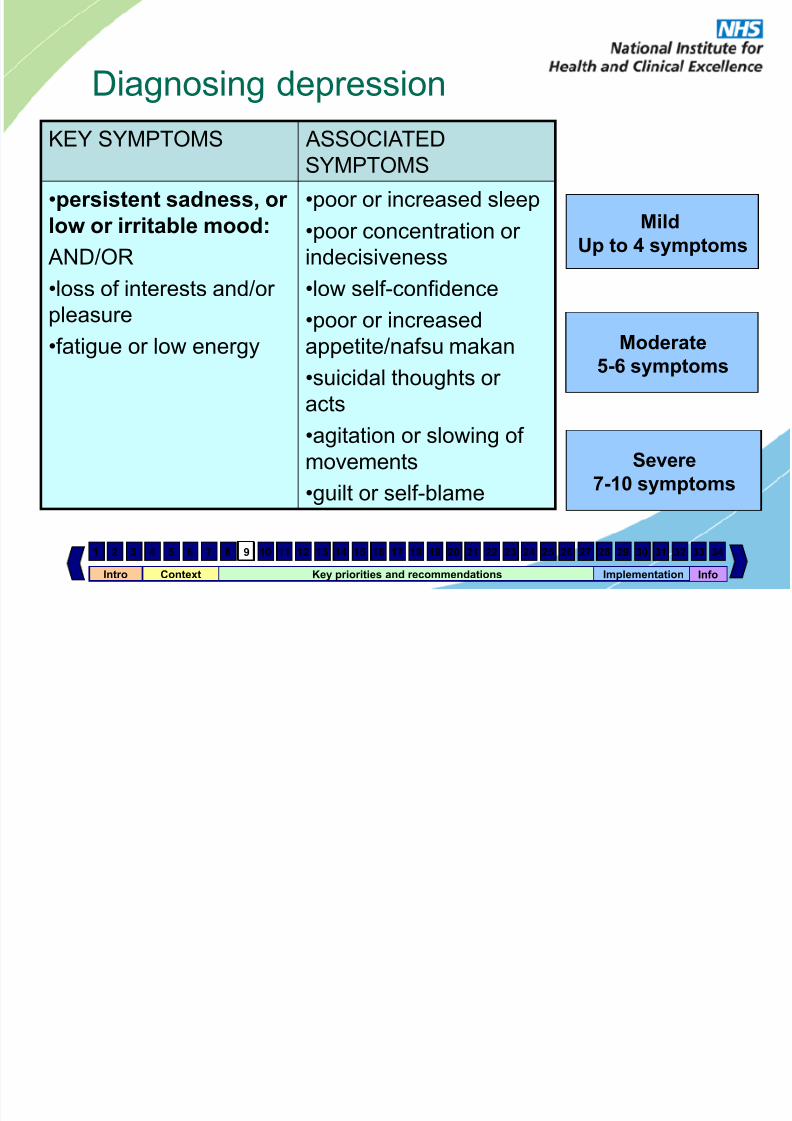
Diagnosing depression
KEY SYMPTOMS ASSOCIATEDSYMPTOMS
•persistent sadness, or
low or irritable mood:
AND/OR
•loss of interests and/or
pleasure
•fatigue or low energy
•poor or increased sleep
•poor concentration or
indecisiveness
•low self-confidence
•poor or increased
appetite/nafsu makan
•suicidal thoughts or
acts•agitation or slowing of
movements
•guilt or self-blame
9
Mild
Up to 4 symptoms
Moderate
5-6 symptoms
Severe
7-10 symptoms
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 12/43Intro Context Key priorities and recommendations Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
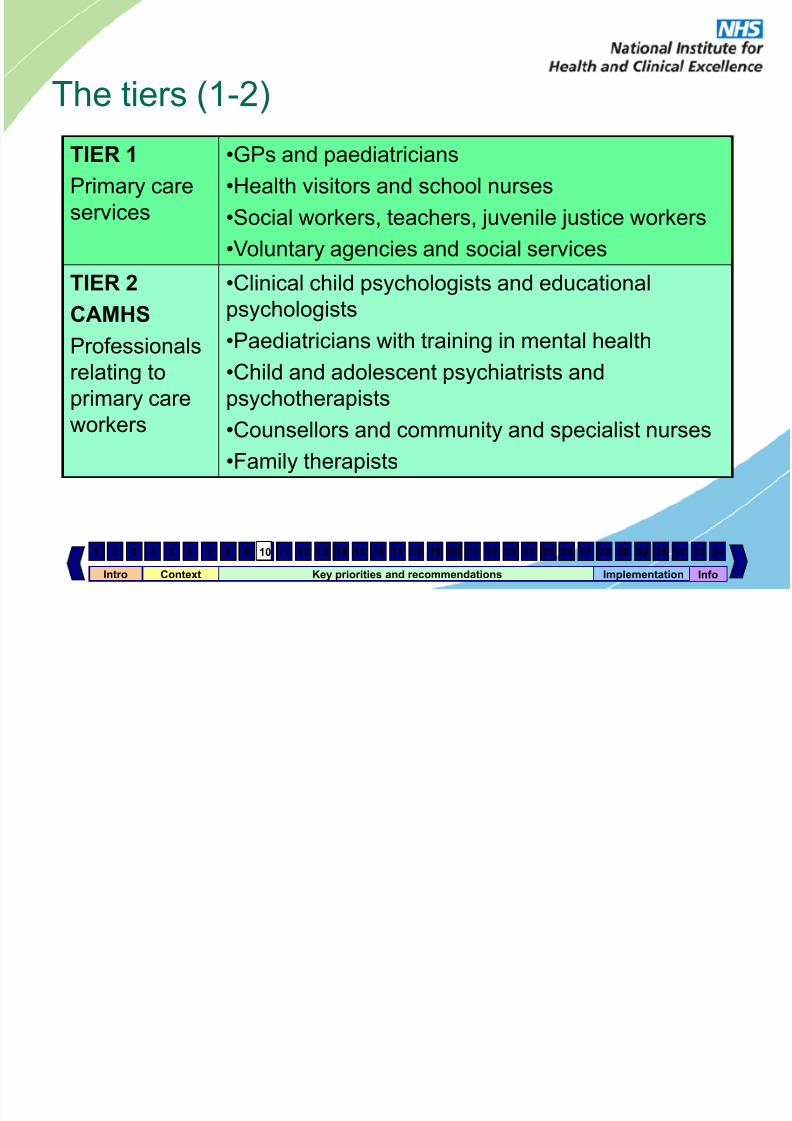
The tiers (1-2)
TIER 1
Primary care
services
•GPs and paediatricians
•Health visitors and school nurses
•Social workers, teachers, juvenile justice workers
•Voluntary agencies and social services
TIER 2
CAMHS
Professionals
relating to
primary care
workers
•Clinical child psychologists and educationalpsychologists
•Paediatricians with training in mental health
•Child and adolescent psychiatrists and
psychotherapists
•Counsellors and community and specialist nurses
•Family therapists
10
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 13/43Intro Context Key priorities and recommendations Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
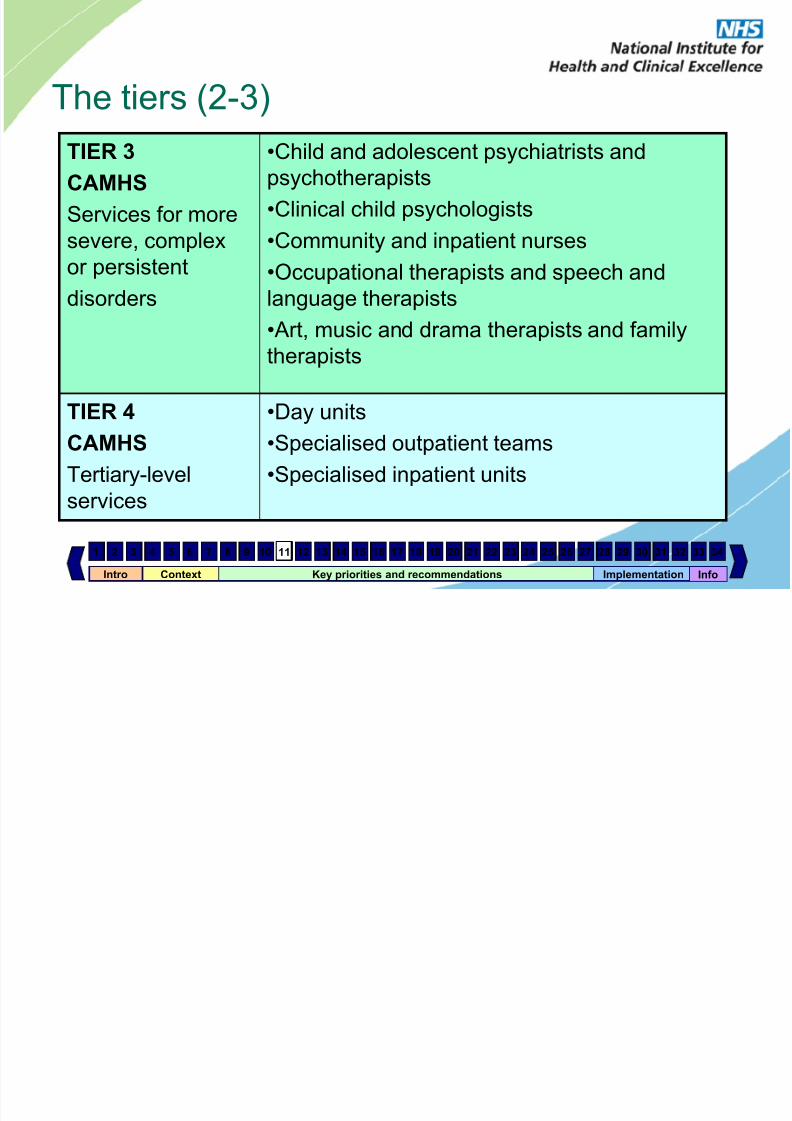
The tiers (2-3)
TIER 3
CAMHS
Services for more
severe, complex
or persistentdisorders
•Child and adolescent psychiatrists and
psychotherapists
•Clinical child psychologists
•Community and inpatient nurses
•Occupational therapists and speech andlanguage therapists
• Art, music and drama therapists and family
therapists
TIER 4CAMHS
Tertiary-level
services
•Day units•Specialised outpatient teams
•Specialised inpatient units
11
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 14/43Intro Context Key priorities and recommendations Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
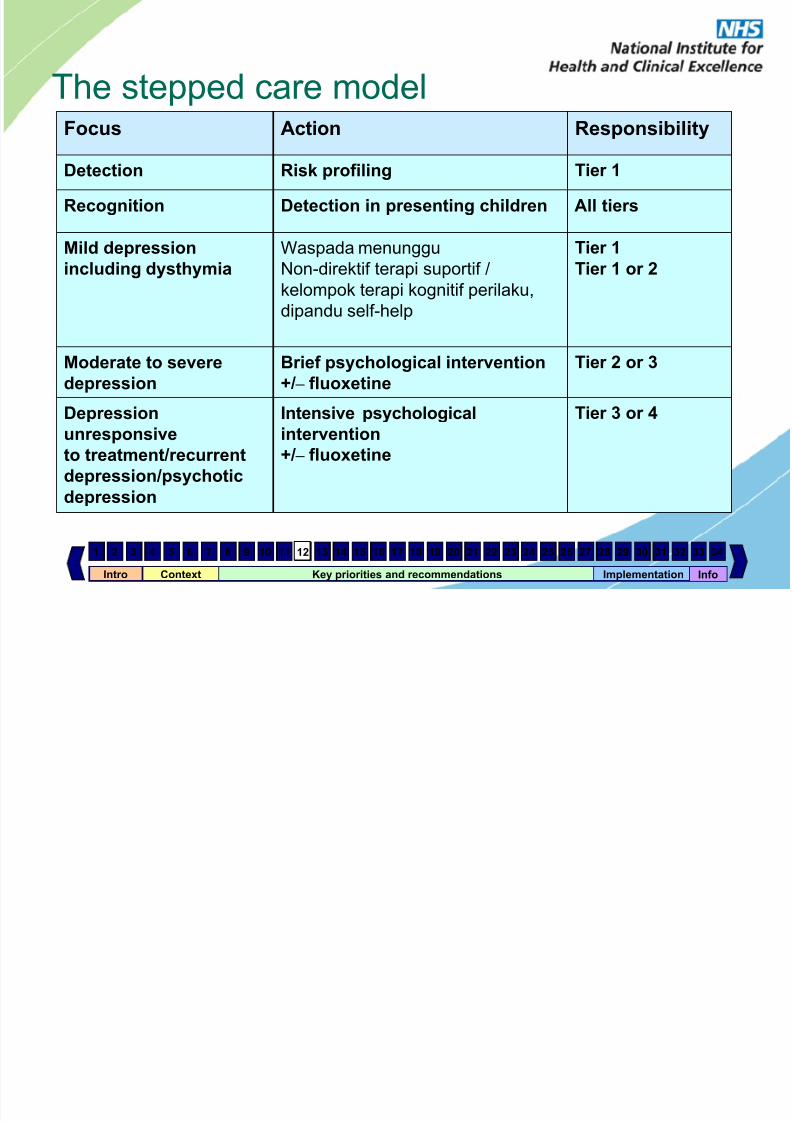
The stepped care modelFocus Action Responsibility
Detection Risk profiling Tier 1Recognition Detection in presenting children All tiers
Mild depression
including dysthymia
Waspada menunggu
Non-direktif terapi suportif /kelompok terapi kognitif perilaku,
dipandu self-help
Tier 1Tier
1 or 2
Moderate to severe
depression
Brief psychological intervention
+/ – fluoxetine
Tier 2 or 3
Depressionunresponsive
to treatment/recurrent
depression/psychotic
depression
Intensive psychologicalintervention
+/ – fluoxetine
Tier 3 or 4
12
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 15/43Intro Context Key priorities and recommendations Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
Step 1: detecting depression• Profesional di perawatan primer, sekolah dan
masyarakat perlu:sadar akan faktor risiko
terlibat 'mendengar aktif' dan 'teknik percakapan'mendeteksi gejalamemberikan dukungan yang sesuaitahu kapan untuk merujuk
13
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 16/43Intro Context Key priorities and recommendations Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
Assessing and coordinating care
• Perawatan harus bersifat komprehensif dan holistik
dan mempertimbangkan:
penyalahgunaan narkoba dan alkohol
pengalaman bullying atau penyalahgunaan
orangtua depresi
risiko merugikan diri sendiri dan bunuh diri
penggunaan bahan self-help dan metode
masalah kerahasiaan
14
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 17/43
Intro Context Key priorities and recommendations Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
Step 2: recognising depression• Untuk meningkatkan kemampuan mereka untuk
mengenali CAMHS depresi profesional harus dilatihterutama dalam:
• penggunaan kuesioner laporan diri dan instrumen
• pewawancara berbasisskrining untuk gangguan mood dan ketrampilandalam penilaian non-verbal suasana hati pada anak-
anak muda• Sejarah keluarga dan dinamika keluarga
15
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 18/43
Intro Context Key priorities and recommendations Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
Indications that management can remain at
tier 1• Exposure to a single undesirable event in the
absence of other risk factors for depression
• Exposure to a recent undesirable life event in the
presence of two or more other risk factors with no evidence of depression and/or self-harm
• Exposure to a recent undesirable life event in thecontext of multiple-risk histories for depression in oneor more family members (parents or children)providing that there is no evidence of depressionand/or self-harm in the child/young person
• Mild depression without comorbidity
16
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 19/43
Intro Context Key priorities and recommendations Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
• Paparan peristiwa tunggal yang tidak diinginkan tanpa adanya
faktor risiko lain untuk depresi
Paparan peristiwa kehidupan baru-baru ini tidak diinginkan di
hadapan dua atau lebih faktor risiko lain tanpa bukti depresi dan/ atau membahayakan diri
Paparan peristiwa kehidupan baru-baru ini yang tidak diinginkan
dalam konteks sejarah multi-risiko depresi pada satu atau lebih
anggota keluarga (orang tua atau anak-anak) menyediakan
bahwa tidak ada bukti depresi dan / atau membahayakan diripada anak / orang muda
Depresi ringan tanpa komorbiditas (gg lain yg menyertai )
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 20/43
Intro Context Key priorities and recommendations Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
Step 3: mild depression• Treatment includes:
– up to 4 weeks ‘watchful waiting’
– non-directive supportive therapy
– group CBT
– guided self-help
– no use of antidepressants at this stage
17
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 21/43
Intro Context Key priorities and recommendations Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
Criteria for referral to tier 2 or 3 CAMHS
• Depression with two or more other risk factors for depression
• Depression with multiple-risk histories in another family member
• Mild depression and no response to interventions in tier 1 after
2 –3 months• Moderate or severe depression (including psychotic depression)
• Recurrence after recovery from previous moderate or severe
depression
• Unexplained self-neglect of at least 1 month’s duration that
could be harmful to physical health
• Active suicidal ideas or plans
• Young person or parent/carer requests referral
18
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 22/43
Intro Context Key priorities and recommendations Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
• Depresi dengan dua atau lebih faktor risiko lain untuk
depresi
Depresi dengan sejarah beberapa-risiko anggota
keluarga yang lain
Depresi ringan dan tidak ada respon terhadap
intervensi dalam 1 tier setelah 2-3 bulan
Sedang atau berat depresi (termasuk depresi
psikotik)Kambuh setelah sembuh dari depresi sedang atau
berat sebelumnya
Dijelaskan pengabaian diri durasi minimal 1 bulan
yang bisa ber bahaya bagi kesehatan f isik Aktif ide atau rencana bunuh diri
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 23/43
Intro Context Key priorities and recommendations Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
Steps 4 and 5: moderate or severe
depression• General recommendations
– Approach tailored to needs of family
– Family’s preferences to be taken into account
• E.g. when too depressed• Does not want family involved
– May require change of approach especially if symptoms deteriorate
• Treatment starts with review by multidisciplinary team
• First line of treatment is specific psychological
therapy for about 3 months – Individual cognitive behavioural therapy
– Interpersonal therapy
– Shorter-term family therapy
19
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 24/43
Intro Context Key priorities and recommendations Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
• Rekomendasi Umum
Pendekatan yang disesuaikan dengan kebutuhan
keluarga
Keluarga preferensi untuk diperhitungkan
Misalnya bila terlalu tertekan
Tidak mau terlibat keluarga
Mungkin memerlukan perubahan pendekatan
terutama jika gejala memburukPengobatan dimulai dengan review oleh tim
multidisipliner
Baris pertama pengobatan adalah terapi psikologis
khusus untuk sekitar 3 bulan Masin -masin tera i erilaku ko nitif
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 25/43
Intro Context Key priorities and recommendations Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
Steps 4 and 5: moderate or severe
depression – if unresponsive
• If there is no response after 4-6 sessions – Multidisciplinary review
– Alternative psychological therapy that has not been tried
– Offer fluoxetine in combination with psychological treatment to
young people (12 –18) and cautiously consider it in younger children
(5 –11)
• If still no response after further 6 sessions – A further multidisciplinary review
– Systemic family therapy of at least 15 fortnightly sessions
– Individual child psychotherapy (30 weekly sessions)
20
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 26/43
Intro Context Key priorities and recommendations Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
• Jika tidak ada respon setelah 4-6 sesi
Multidisiplin tinjauan
Alternatif terapi psikologis yang belum pernah dicoba
Penawaran fluoxetine dalam kombinasi dengan
pengobatan psikologis kepada orang-orang muda
(12-18) dan hati-hati mempertimbangkan itu pada
anak-anak muda (5-11)
Jika masih tidak ada respon setelah lebih 6 sesiSuatu tinjauan multidisiplin lebih lanjut
Keluarga terapi sistemik minimal 15 sesi dua minggu
Individu anak psikoterapi (30 sesi mingguan)
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 27/43
Intro Context Key priorities and recommendations Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
Referral criteria for tier 4 services• High recurrent risk of acts of self-harm or suicide
• Significant ongoing self-neglect (such as poor personal hygiene or significant reduction in eating
that could be harmful to physical health)
• Intensity of assessment/treatment and/or level of supervision that is not available in tiers 2 or 3
21
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 28/43
Intro Context Key priorities and recommendations Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
• Tinggi berulang risiko tindakan merugikan diri atau
bunuh diri
Signifikan yang sedang berlangsung pengabaian diri
(seperti kebersihan yang rendah atau penurunan
yang signifikan dalam makan yang dapat berbahaya
bagi kesehatan fisik)
Intensitas penilaian / pengobatan dan / atau tingkat
pengawasan yang tidak tersedia di tingkatan 2 atau 3
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 29/43
Intro Context Key priorities and recommendations Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
Unresponsive depression
• Reassess if no response
• Offer more intensive psychological treatments
– alternative psychological therapy which has not been tried – systemic family therapy
– individual child psychotherapy
• Consider combining with SSRIs
22
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 30/43
Intro Context Key priorities and recommendations Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
• Menilai kembali jika tidak ada respon
Psikologis menawarkan perawatan yang lebih intensif
alternatif terapi psikologis yang belum pernah dicoba
keluarga terapi sistemik
psikoterapi individu anak
Pertimbangkan menggabungkan dengan SSRI
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 31/43
Intro Context Key priorities and recommendations Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
The limited place for
antidepressants
• Should only be prescribed following assessment by apsychiatrist
• Should only be offered in combination with psychologicaltreatments
• First-line treatment is fluoxetine*
• Do NOT use: tricyclic antidepressants, paroxetine,venlafaxine, St John’s wort
• Monitor for agitation, hostility, suicidal ideation and self-
harm and advise urgent contact with prescribing doctor if detected
* Fluoxetine does not have a UK Marketing Authorisation for use in children and adolescents under the ageof 18 at the time of publication (Sept 2005)
23
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 32/43
Intro Context Key priorities and recommendations Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
The limited place for
antidepressants
• Sertraline or citalopram* as second-line treatment
• Consider adding atypical antipsychotic if psychotic
depression
• Continue for 6 months if remission, then phase out over 6 –12 weeks
• Issues: – Discussion, consent and written advice important
– Pre- and post-prescribing monitoring – Continuation of medication post recovery
* Sertraline and citalopram do not have a UK Marketing Authorisation for use in children
and adolescents under the age of 18 at the time of publication (Sept 2005)
24
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 33/43
Intro Context Key priorities and recommendations Implementation1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
Discharge to primary care• Inform primary care professional within 2 weeks of
discharge and provide contact details if symptomsrecur
• Review for 12 months after first remission (< 2symptoms for 8 weeks)
• Consider follow-up psychological treatment if secondepisode to prevent relapse
• Review for 24 months if recurrent depression inremission
• Re-refer early if signs of relapse
25
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 34/43
Intro Context Key priorities and recommendations Implementation1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info28 29 30 31 32 33 34
• Menginformasikan perawatan primer profesional
dalam 2 minggu debit dan memberikan rincian kontak
jika gejala kambuh
Review selama 12 bulan setelah remisi pertama (<2
gejala selama 8 minggu)
Pertimbangkan perawatan tindak lanjut psikologis jika
episode kedua untuk mencegah kambuh
Review selama 24 bulan jika berulang depresi dalamremisi
Re-lihat awal jika tanda-tanda kambuh
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 35/43
Intro Context Key priorities and recommendations Implementation1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info28 29 30 31 32 33 34
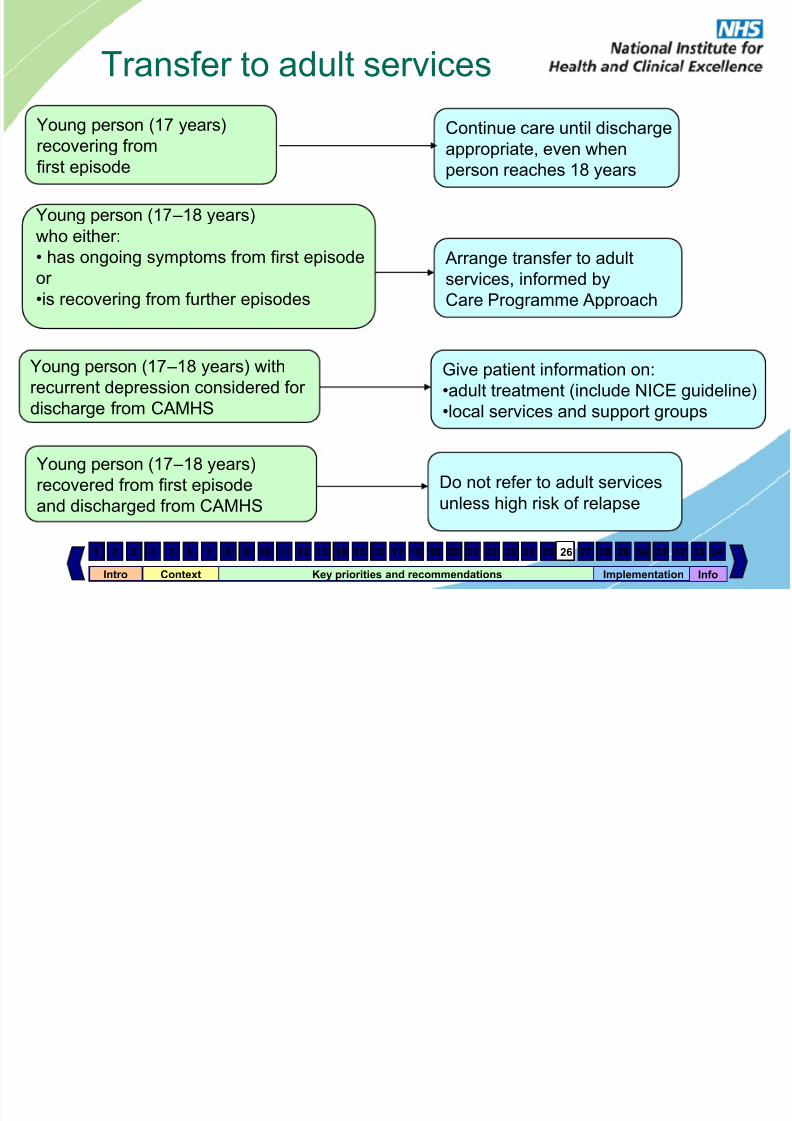
Transfer to adult services
Young person (17 years)
recovering fromfirst episode
Young person (17 –18 years)
who either:
• has ongoing symptoms from first episode
or •is recovering from further episodes
Young person (17 –18 years) with
recurrent depression considered for
discharge from CAMHS
Young person (17 –18 years)
recovered from first episode
and discharged from CAMHS
Continue care until discharge
appropriate, even whenperson reaches 18 years
Arrange transfer to adult
services, informed byCare Programme Approach
Give patient information on:
•adult treatment (include NICE guideline)
•local services and support groups
Do not refer to adult services
unless high risk of relapse
26
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 36/43
Intro Context Key priorities and recommendations Implementation1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info28 29 30 31 32 33 34
Other treatment options• Inpatient care when individual is at high risk of
suicide, serious self-harm or self-neglect, or when
required for intensive treatment or assessment
• Cautious use of electroconvulsive therapy for life-
threatening depression when other treatments have
failed – NOT recommended for children (5 –11 years)
27
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 37/43
Intro Context Key priorities and recommendations Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
Implementation issues for clinicians
• Diagnosis – Recognising and managing potential comorbidities and risk factors
in the wider social and educational context
– Providing care that is ethnically and culturally sensitive
• Treatment
– Knowing what psychological and drug treatments to offer and when – Applying the stepped care model in practice
– Treatment of parental depression
• Access to services
– Transition from CAMHS to adult mental health services
– Availability of services for parents
• Training
– Identifying and contributing to the training of other key workers
28
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 38/43
Intro Context Key priorities and recommendations Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
Implementation issues for managers
• Active dissemination of the guidance
• Carry out baseline assessment
• Development and implementation of an actionplan – what, when, how, who
• Ensuring CBT and specialist teams can be
accessed appropriately• Training of professionals in CBT
• Monitor and review
29
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 39/43
Intro Context Key priorities and recommendations Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
Organisation and planning
of services
CAMHS and PCTs should:
• consider introducing a primary mental health worker (or CAMHS link
worker) into each secondary school and secondary pupil referral unit as
part of tier 2 provision within the locality
• routinely monitor detection, referral and treatment rates of
children/young people with mental health problems from all ethnicgroups in local schools and primary care
• use information about these rates to plan services, and make it available
for local, regional and national comparison
Primary mental health workers (or CAMHS link workers) should:
• establish clear lines of communication between CAMHS and tiers 1 and
2, with named contact people in each tier/service
• develop systems for the collaborative planning of services for young
people with depression in tiers 1 and 2
30
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 40/43
Intro Context Key priorities and recommendations Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
Organisation and planning
of services All healthcare professionals should:
• routinely use, and record in the notes, appropriate outcome measures
(e.g. HoNOSCA or SDQ), for assessing and treating depression in
children/young people
• use this information from outcome measures to plan services, and make
it available for local, regional and national comparison
Commissioners and strategic health authorities should ensure that:
• inpatient treatment is available within reasonable travelling distance to
enable family involvement and maintain social links
• inpatient admission occurs within an appropriate time scale
• immediate inpatient admission can be offered if necessary
• inpatient services have a range of interventions available includingmedication, individual and group psychological therapies and family
support
• inpatient facilities are age appropriate and culturally enriching and can
provide suitable educational and recreational activities
31
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 41/43
Intro Context Key priorities and recommendations Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
Four implementation tools support this
guideline• Costing tools
– a local costing template
– a national costing report• implementation advice
• audit criteria
• this slide set
The tools are available on our website
www.nice.org.uk/implementation
32
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 42/43
Intro Context Key priorities and recommendations Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Info
28 29 30 31 32 33 34
Where is further information available?• Quick reference guide – summary of recommendations for health
professionals:
– www.nice.org.uk/cg028quickrefguide
• NICE guideline:
– www.nice.org.uk/cg028niceguideline • Full guideline – all of the evidence and rationale behind the
recommendations:
– www.rcpsych.ac.uk/publications
• Information for the public – plain English version for patients, carers and the
public:
– www.nice.org.uk/cg028publicinfo
33
7/30/2019 DEPRESI ANAK
http://slidepdf.com/reader/full/depresi-anak 43/43
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34
www.nice.org.uk
34