
CSS Trauma Kepala Luq
32
Disusun oleh : M. Luqman Hasan Preseptor : Dr. Arief Guntara, Sp. B SMF BEDAH RSUD AL IHSAN BANDUNG HEAD TRAUMA ATLS (Advance Trauma Life Support)
-
Upload
luqmanhasans -
Category
Documents
-
view
238 -
download
0
Transcript of CSS Trauma Kepala Luq

8/13/2019 CSS Trauma Kepala Luq
http://slidepdf.com/reader/full/css-trauma-kepala-luq 1/32
Disusun oleh :M . L u q m a n H a s a n
Preseptor :
Dr. Arief Guntara, Sp. B
SMF BEDAH RSUD AL IHSAN BANDUNG
HEAD TRAUMA
ATLS(Advance Trauma Life Support)
8/13/2019 CSS Trauma Kepala Luq
http://slidepdf.com/reader/full/css-trauma-kepala-luq 2/32
8/13/2019 CSS Trauma Kepala Luq
http://slidepdf.com/reader/full/css-trauma-kepala-luq 3/32
Informasi penting yang harus didapat ketikaterdapat pasien dengan head injury
1.Usia dan mekanisme injury2. Status respirasi dan Cardiovaskular
3. Neurological examination (Level kesadaran, reaksipupil, dan kelemahan ekstremitas
4. Tipe non Cerebral injury5. Hasil dari studi diagnosis (Rontgen kepala, CT
scan)
8/13/2019 CSS Trauma Kepala Luq
http://slidepdf.com/reader/full/css-trauma-kepala-luq 4/32
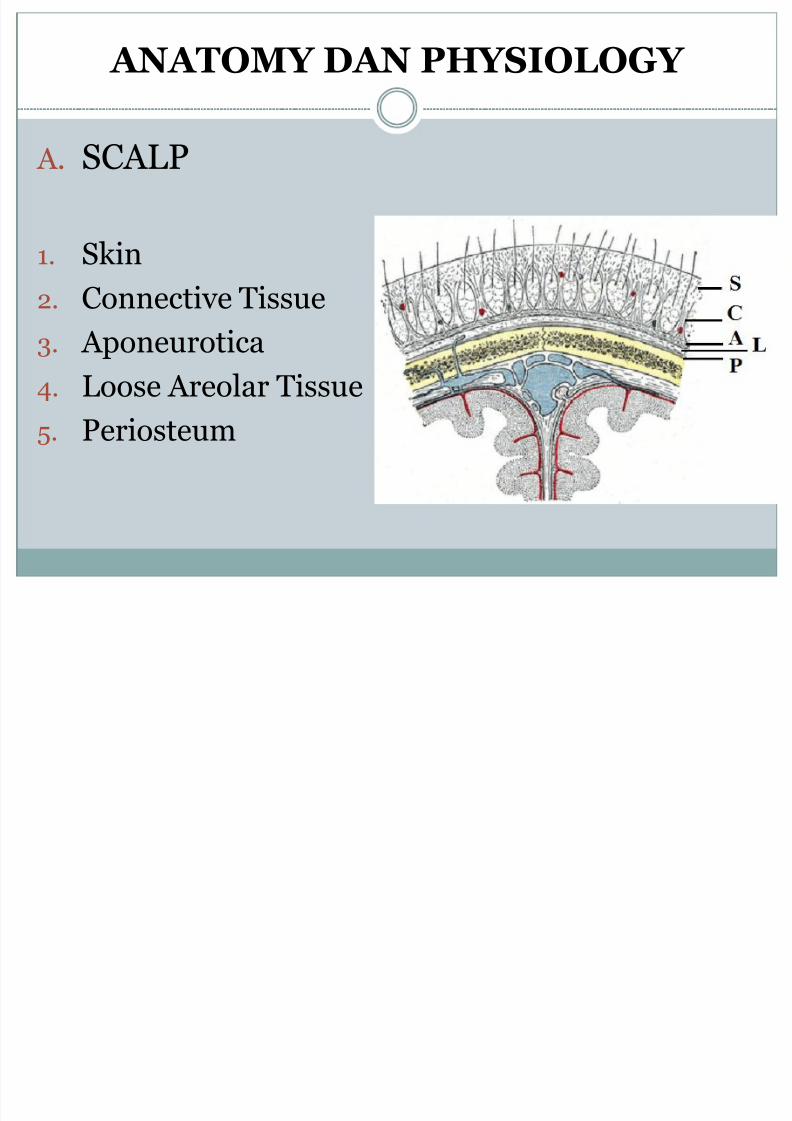
ANATOMY DAN PHYSIOLOGY
A. SCALP
1. Skin
2. Connective Tissue
3. Aponeurotica
4. Loose Areolar Tissue
5. Periosteum
8/13/2019 CSS Trauma Kepala Luq
http://slidepdf.com/reader/full/css-trauma-kepala-luq 5/32
8/13/2019 CSS Trauma Kepala Luq
http://slidepdf.com/reader/full/css-trauma-kepala-luq 6/32
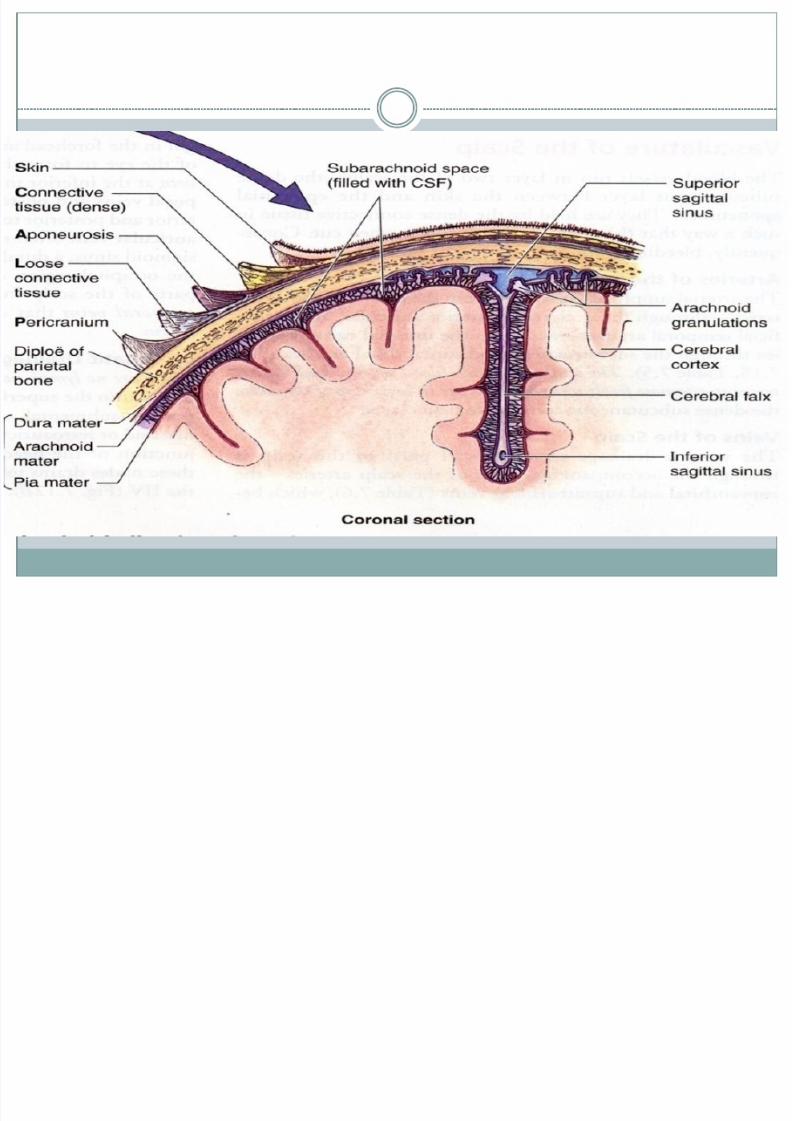
B. SkullTerdiri dari calvarium dan base
C. MeningensTersusun dari :
Duramater : lapisan luar fibrous yang kuat, tebalsubdural space
Arachnoidmater : lapisan tengah yang tipissubarachnoid space
Piamater : lapisan dalam yang tipis bervaskular
D. BrainE. Cerebrospinal Fluid
Diproduksi oleh choroid plexus, dikeluarkan ke dalam ventrikel otak, dan bersirkulasi melalui subarachnoid space

8/13/2019 CSS Trauma Kepala Luq
http://slidepdf.com/reader/full/css-trauma-kepala-luq 7/32
G. Consciousness
Alteration of consciousness is the hallmark of brain injury
H. Intracranial Pressure
Monroe-Kellie Hypothesis
K ICP ~ V CSF + V BI + V Br
K : ConstancyICP : Intracranial Pressure V : volumeCSF : Cerebrospinal fluidBl : Blood
Br : Brain
8/13/2019 CSS Trauma Kepala Luq
http://slidepdf.com/reader/full/css-trauma-kepala-luq 8/32
ASSESMENT OF HEAD INJURY
A. History
Mechanisme Injury (venticular crash or not)
Patient’s condition immediatly after inciden
B. Initial Assessment
Airway
Breathing
Circulary Control
8/13/2019 CSS Trauma Kepala Luq
http://slidepdf.com/reader/full/css-trauma-kepala-luq 9/32
C. Assessment of Vital Signs
1. Never presume brain injury is the cause ofhypotension
Although bleeding from scalp may cause ofhemorrhagic shock (especially child), intracranial
bleeding can’t cause shock. Hipotension occure dueto terminal process of brain damage, because of
medulary center failure.
8/13/2019 CSS Trauma Kepala Luq
http://slidepdf.com/reader/full/css-trauma-kepala-luq 10/32
2. Cushing response
Progressive hypertension associated with
bradycardia and diminished respiratory rate
3. Hypertension in combination with hyperthermia
Reflect central autonomic dysfunction caused brain injury
8/13/2019 CSS Trauma Kepala Luq
http://slidepdf.com/reader/full/css-trauma-kepala-luq 11/32
D. AVPU + Minineurologic Examination
Alert
Response to Vocal stimuliResponse to Pain stimuli
Unresponsive
8/13/2019 CSS Trauma Kepala Luq
http://slidepdf.com/reader/full/css-trauma-kepala-luq 12/32
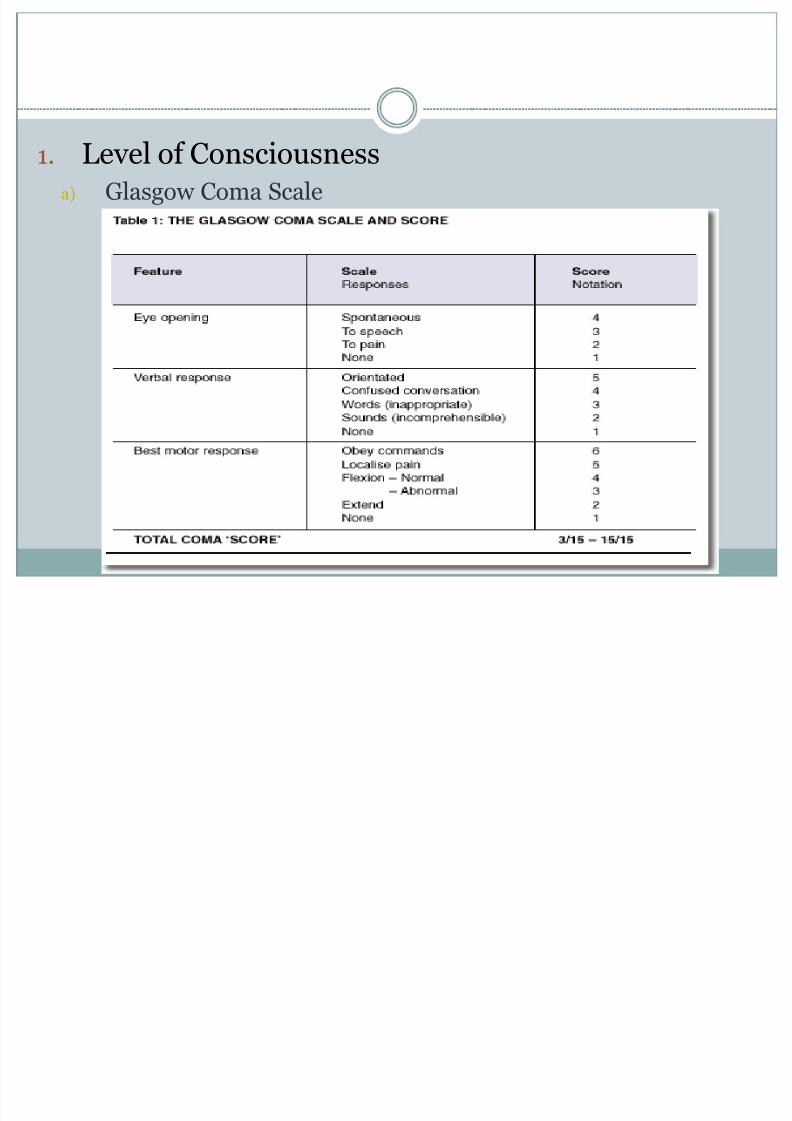
1. Level of Consciousnessa) Glasgow Coma Scale

8/13/2019 CSS Trauma Kepala Luq
http://slidepdf.com/reader/full/css-trauma-kepala-luq 13/32
b) Patient Catagorization
1. Coma ( GSC <8 )
Define as : Having no eye opening (E=1)
No ability to follow comands (M=1 to 5)No word verbalization (V= 1 to 2)
2. Head injury severity
Severe = less than or equale to eightModerate = GCS 9 to 12
Minor = GCS 13 to 15
8/13/2019 CSS Trauma Kepala Luq
http://slidepdf.com/reader/full/css-trauma-kepala-luq 14/32
2. Assessment of pupillary function
A difference in pupil diameters more than 1 mm is abnormal
3. Lateralized extremity weaknessSuggest an intracranial mass lesion
8/13/2019 CSS Trauma Kepala Luq
http://slidepdf.com/reader/full/css-trauma-kepala-luq 15/32
Special Assessment
1. Skull rontgenograms
2. Computed tomography
3. Other testLumbar puncture, electroencephalogram
8/13/2019 CSS Trauma Kepala Luq
http://slidepdf.com/reader/full/css-trauma-kepala-luq 16/32
SPECIFIC TYPES OF HEAD INJURY
Head injury include (1) skull fracture, (2) diffuse brain injury, and (3) focal injury.
Pathophysiology, severity, need for urgenttreatment , and outcome are different in eachgroup.

8/13/2019 CSS Trauma Kepala Luq
http://slidepdf.com/reader/full/css-trauma-kepala-luq 17/32
A. Skull Fractures1. Linear, nondepressed fractures
Seen on roentgen as lucent line
2. Depressed skull fractures
8/13/2019 CSS Trauma Kepala Luq
http://slidepdf.com/reader/full/css-trauma-kepala-luq 18/32
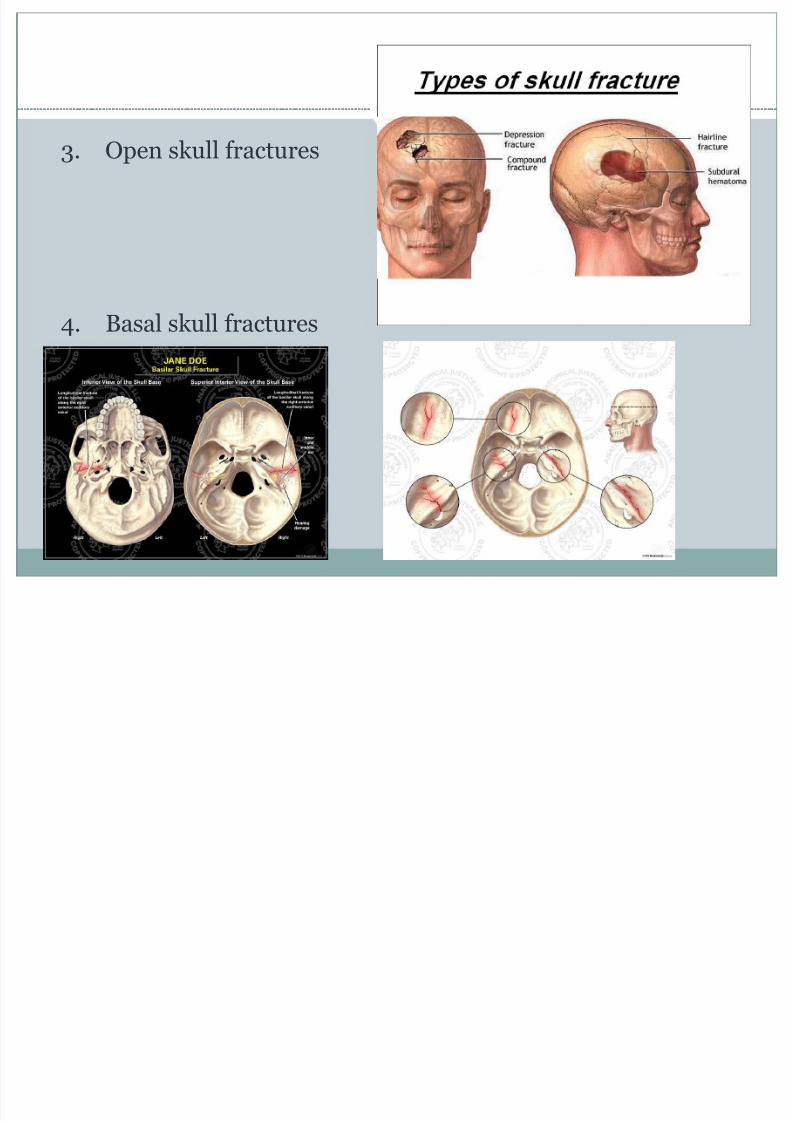
3. Open skull fractures
4. Basal skull fractures
8/13/2019 CSS Trauma Kepala Luq
http://slidepdf.com/reader/full/css-trauma-kepala-luq 19/32
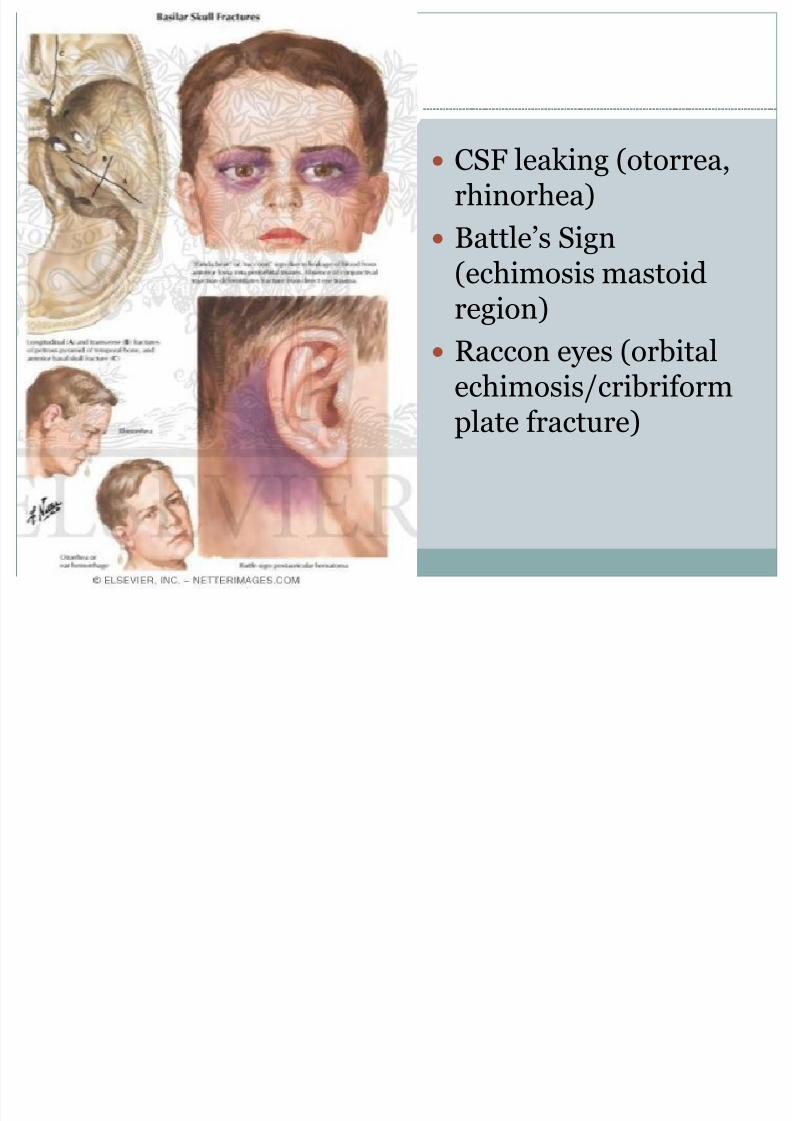
CSF leaking (otorrea,rhinorhea)
Battle’s Sign
(echimosis mastoidregion)
Raccon eyes (orbitalechimosis/cribriform
plate fracture)
8/13/2019 CSS Trauma Kepala Luq
http://slidepdf.com/reader/full/css-trauma-kepala-luq 20/32
B. Diffuse Brain Injury
Produced when rapid head motion (acceleration ordeceleration) cause widespread interuption of brain
function in most area of the brain.1. Concussion
Brain injury accompanied by loss neurologic function, maycause temporary confusion or amnesia or loss of consciousness
2. Diffuse axonal injuryBrain-stem injury, closed head injury
Characterized by prolong coma, last days to weeks.

8/13/2019 CSS Trauma Kepala Luq
http://slidepdf.com/reader/full/css-trauma-kepala-luq 21/32
C. Focal Injuries
1. Contusion
Patiens sustaining cerebral contusion should be admitted tothe hospital for observation, because delayed edema orswelling around contusion may cause neurologic deterioration
8/13/2019 CSS Trauma Kepala Luq
http://slidepdf.com/reader/full/css-trauma-kepala-luq 22/32
2. Intracranial Hemorrhages
Meningeal hemorrhagea) Acute epidural hemorrhage
bleeding from dural artery, usually middle meningeal artery
relative rare (0,5% in unselected head injury)
Sign and symptoms
1. Loss consciousness, followed by lucid interval (the lucidperiod may not be return to full consciousness)
2. Secondary depression of consciousness3. Development of hemiparesis on the opposite side

8/13/2019 CSS Trauma Kepala Luq
http://slidepdf.com/reader/full/css-trauma-kepala-luq 23/32
b) Acute subdural hematoma
Much more common than epidural hematomas(30% of severe head injuries).
Rupture of bridging veins between cerebral cortexand dura.
8/13/2019 CSS Trauma Kepala Luq
http://slidepdf.com/reader/full/css-trauma-kepala-luq 24/32
c) Subarachnoid hemorrhage
This type of hemorrhage results in bloody CSF andmeningeal irritation.
Patient usually complains : Headache
Photophobia
8/13/2019 CSS Trauma Kepala Luq
http://slidepdf.com/reader/full/css-trauma-kepala-luq 25/32
8/13/2019 CSS Trauma Kepala Luq
http://slidepdf.com/reader/full/css-trauma-kepala-luq 26/32
Brain Hemorrhages and laceration
1. Intracerebral hematomasNeurological deficits depend on these associated injuriesregion, and the size hemorrhage.
2. Impalement injuriesForeign bodies protuding from the skull, rontgen required todetermine the object’s single and depth of penetration
3. Bullet wounds
8/13/2019 CSS Trauma Kepala Luq
http://slidepdf.com/reader/full/css-trauma-kepala-luq 27/32
EMERGENCY MANAGEMENT
1. Maintenance of Cerebral Metabolic NeedsCerebral ischemia or hypoxia result insufficient substrat to
injured brain. The principal metabolic requirements of the brain are oxygen and glucose.
Delivery these substrate depends on their arterialconcentration and the blood flow to the brain.
Maintain arterial PO2 at greater than 80 mmHg.
2. Preventing / treating intracranial hypertension Fluid Control
Diuretics
Steroids (not recomended for treatment acute head injury)
8/13/2019 CSS Trauma Kepala Luq
http://slidepdf.com/reader/full/css-trauma-kepala-luq 28/32
Diuretics such manitol, cause diuresis by producingintravascular hyperosmolarity. Very effective inshrinking brain volume and lowering intracranialpressure.Doses : 1 g/kg , administred rapidly and intravenosly
Loop diuretics
Furosemide (40-80 mg IV for adults)
Urinary catheter is required

8/13/2019 CSS Trauma Kepala Luq
http://slidepdf.com/reader/full/css-trauma-kepala-luq 29/32
Other Manifestation of Head Injury
Seizures
10 mg of diazepam via an intravenous bolus, if has
another convulsion may be repeated once withcaution
Phenytoin 1 g IV at rate 50 mg/minute
Phenobarbital or anesthetic
Restlessness
Hyperthermia
8/13/2019 CSS Trauma Kepala Luq
http://slidepdf.com/reader/full/css-trauma-kepala-luq 30/32
Scalp Wounds
A. Blood LossCan be extensive, especially in children. General principles scalp
wound care include locating and stopping the bleeding.
B. Inspection of the Scalp Wound
Search for sign fracture or foreign material, also includes lookingfor CSF leaks.
C. Repairing the Scalp WoundIrrigate with saline, debris include hair, do not remove bone
fragment (because they may tamponading intracranial bleeding).
When possible , repair should be achived under sterile technique,as scalp wounds may become infected
8/13/2019 CSS Trauma Kepala Luq
http://slidepdf.com/reader/full/css-trauma-kepala-luq 31/32
Summary
A. Secure and maintain an open airwayB. Ventilate patient to maintain oxygenation
C. Treat shock, if present, and look for cause
D. Perform minineurologic examinationE. Establish an initial working diagnosis
F. Prevent secondary brain injury
G. Search for associated injuries
H. Obtain roentgenograms or CT scan, but only afterpatients stable
I. Consult neurosurgeon and consider transfer
8/13/2019 CSS Trauma Kepala Luq
http://slidepdf.com/reader/full/css-trauma-kepala-luq 32/32
مين اع ب ر ه مد اح
Thank You














![5.Css - Trauma Thoraks Tumpul[1]](https://static.fdokumen.com/doc/165x107/577cc5b21a28aba7119cf4f7/5css-trauma-thoraks-tumpul1.jpg)



