262591-overview#showall -...
29
http://emedicine.medscape.com/article/262591-overview#showall Diagnosis kehamilan memerlukan pendekatan multifaset menggunakan 3 alat diagnostik utama. Ini adalah sejarah dan pemeriksaan fisik, evaluasi laboratorium, dan ultrasonografi. Saat ini, dokter mungkin akan menggunakan semua alat-alat untuk mendiagnosis kehamilan pada awal kehamilan dan untuk membantu menyingkirkan patologi lainnya. Diagnosis kehamilan secara tradisional dibuat berdasarkan riwayat dan pemeriksaan fisik temuan. Aspek-aspek penting dari riwayat menstruasi harus diperoleh. Wanita itu harus menjelaskan pola menstruasi, termasuk tanggal menstruasi terakhir, durasi, aliran, dan frekuensi. Item yang dapat membingungkan diagnosis awal kehamilan adalah periode terakhir menstruasi atipikal, penggunaan kontrasepsi, dan riwayat menstruasi tidak teratur. Selain itu, sebanyak 25% wanita mengalami perdarahan selama trimester pertama mereka, lebih rumit penilaian. [1] Waspada untuk naik human chorionic gonadotropin (hCG) tingkat, rahim kosong diamati pada sonogram, sakit perut, dan pendarahan vagina karena ini mungkin menandakan kehamilan ektopik. [2, 3] kehamilan ektopik adalah penyebab utama dari trimester pertama kematian ibu dan harus didiagnosis dini, sebelum pecah kehamilan atau pasien menjadi tidak stabil (lihat gambar di bawah). [4] Diagnosis kehamilan. Sonogram menunjukkan massa kompleks dalam adneksa (berlabel EP). Hal ditemukan kehamilan ektopik pada saat operasi. Faktor-faktor sejarah lain yang terkait dengan kehamilan ektopik meliputi manipulasi sebelum tuba, penyakit radang panggul, kehamilan ektopik sebelumnya, penyakit tuba, penggunaan alat kontrasepsi dalam rahim untuk kontrasepsi, terapi kesuburan, dan ligasi tuba. [3, 5, 6] Lihat Kehamilan Ektopik untuk deskripsi lengkap dan detail. Presentasi klasik kehamilan adalah wanita dengan menstruasi frekuensi biasa yang datang dengan amenore, mual, muntah, malaise umum, dan nyeri payudara. Pada pemeriksaan fisik, orang dapat menemukan rahim yang membesar setelah pemeriksaan bimanual, perubahan payudara, dan pelunakan dan pembesaran leher rahim (Hegar tanda; diamati sekitar 6 minggu). The Chadwick Tanda adalah perubahan warna kebiruan serviks dari kongesti vena dan dapat diamati oleh 8-10 minggu. Rahim yang gravid dapat teraba rendah di perut jika kehamilan telah berkembang cukup jauh, biasanya dengan 12 minggu.
Transcript of 262591-overview#showall -...
http://emedicine.medscape.com/article/262591-overview#showall
Diagnosis kehamilan memerlukan pendekatan multifaset menggunakan 3 alat diagnostik
utama. Ini adalah sejarah dan pemeriksaan fisik, evaluasi laboratorium, dan ultrasonografi.
Saat ini, dokter mungkin akan menggunakan semua alat-alat untuk mendiagnosis kehamilan
pada awal kehamilan dan untuk membantu menyingkirkan patologi lainnya.
Diagnosis kehamilan secara tradisional dibuat berdasarkan riwayat dan pemeriksaan fisik
temuan. Aspek-aspek penting dari riwayat menstruasi harus diperoleh. Wanita itu harus
menjelaskan pola menstruasi, termasuk tanggal menstruasi terakhir, durasi, aliran, dan
frekuensi. Item yang dapat membingungkan diagnosis awal kehamilan adalah periode
terakhir menstruasi atipikal, penggunaan kontrasepsi, dan riwayat menstruasi tidak teratur.
Selain itu, sebanyak 25% wanita mengalami perdarahan selama trimester pertama mereka,
lebih rumit penilaian. [1]
Waspada untuk naik human chorionic gonadotropin (hCG) tingkat, rahim kosong diamati
pada sonogram, sakit perut, dan pendarahan vagina karena ini mungkin menandakan
kehamilan ektopik. [2, 3] kehamilan ektopik adalah penyebab utama dari trimester pertama
kematian ibu dan harus didiagnosis dini, sebelum pecah kehamilan atau pasien menjadi tidak
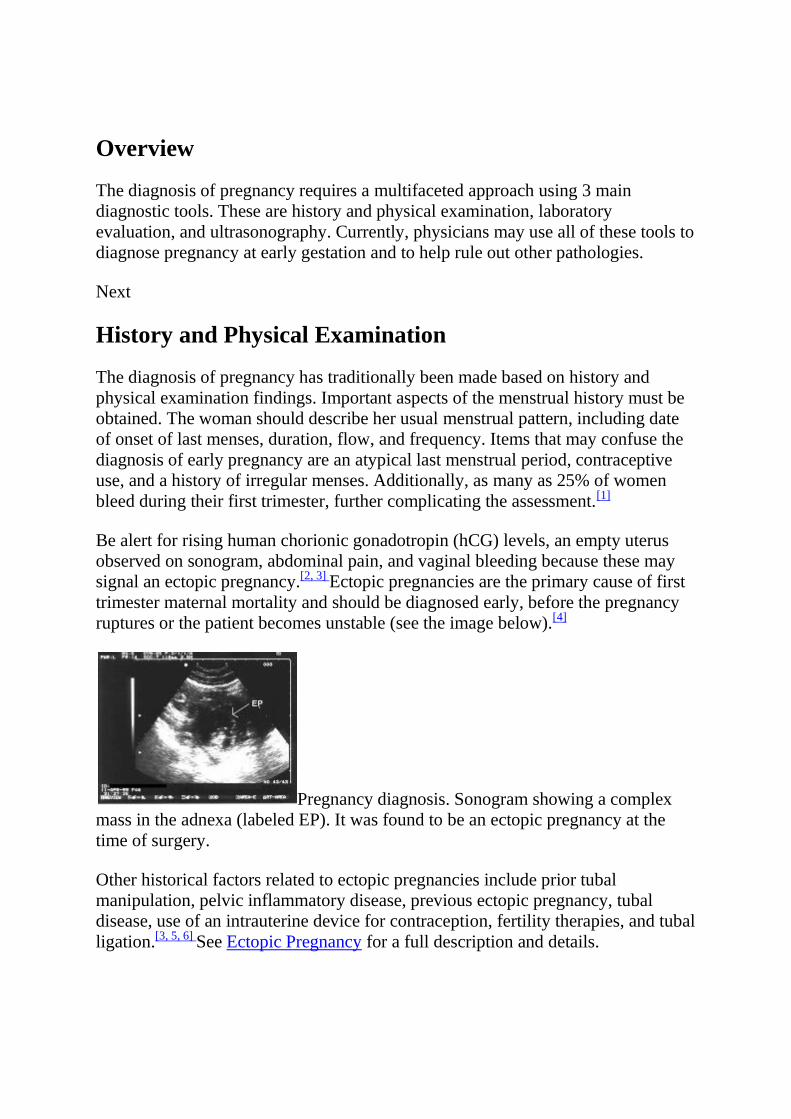
stabil (lihat gambar di bawah). [4]
Diagnosis kehamilan. Sonogram menunjukkan massa kompleks dalam adneksa (berlabel EP).
Hal ditemukan kehamilan ektopik pada saat operasi.
Faktor-faktor sejarah lain yang terkait dengan kehamilan ektopik meliputi manipulasi
sebelum tuba, penyakit radang panggul, kehamilan ektopik sebelumnya, penyakit tuba,
penggunaan alat kontrasepsi dalam rahim untuk kontrasepsi, terapi kesuburan, dan ligasi
tuba. [3, 5, 6] Lihat Kehamilan Ektopik untuk deskripsi lengkap dan detail.
Presentasi klasik kehamilan adalah wanita dengan menstruasi frekuensi biasa yang datang
dengan amenore, mual, muntah, malaise umum, dan nyeri payudara.
Pada pemeriksaan fisik, orang dapat menemukan rahim yang membesar setelah pemeriksaan
bimanual, perubahan payudara, dan pelunakan dan pembesaran leher rahim (Hegar tanda;
diamati sekitar 6 minggu). The Chadwick Tanda adalah perubahan warna kebiruan serviks
dari kongesti vena dan dapat diamati oleh 8-10 minggu. Rahim yang gravid dapat teraba
rendah di perut jika kehamilan telah berkembang cukup jauh, biasanya dengan 12 minggu.
Saat ini, melalui penggunaan tes kimia dan ultrasonografi, dokter mampu membuat diagnosis
kehamilan sebelum banyak tanda-tanda fisik dan gejala yang jelas. [7]
Beberapa hormon dapat diukur dan dimonitor untuk membantu dalam diagnosis kehamilan.
Tes yang paling umum digunakan adalah untuk subunit beta hCG. Hormon lain yang telah
digunakan termasuk progesteron dan faktor kehamilan awal.
The sitotrofoblas dan sinsitiotrofoblas masing-masing mengeluarkan berbagai hormon yang
termasuk, tetapi tidak terbatas pada, hormon corticotropin-releasing hormone gonadotropin-
releasing, thyrotropin-releasing hormone, somatostatin, corticotropin, chorionic thyrotropin
manusia, manusia plasenta laktogen, inhibin / aktivin, mengubah faktor pertumbuhan beta-,
pertumbuhan insulin faktor 1 dan 2, faktor epidermal pertumbuhan, kehamilan spesifik beta-1
glikoprotein, plasenta protein 5, dan kehamilan terkait plasma protein-A. Sampai saat ini,
tidak ada tes layak secara komersial yang menggunakan hormon ini telah dibuat tersedia
untuk membantu diagnosis kehamilan.
Chorionic gonadotropin beta-manusia
hCG merupakan glikoprotein mirip dengan struktur follicle-stimulating hormone (FSH),
luteinizing hormone (LH), dan thyrotropin. hCG terdiri dari alpha dan beta subunit. Alpha
subunit hCG mirip dengan subunit alfa FSH, LH, dan thyrotropin. Subunit beta hCG bebas
berbeda dari yang lain dalam hal ini memiliki sebuah tailpiece asam amino 30-di ujung
COOH. Subunit beta gratis terdegradasi oleh enzim makrofag dalam ginjal untuk membuat
sebuah fragmen inti beta subunit, yang terutama terdeteksi dalam sampel urin.
Subunit beta-hCG hadir dalam lapisan syncytial dari blastomere. Hyperglycosylated hCG
adalah bentuk hCG diproduksi oleh sel sitotrofoblas invasif di awal kehamilan dan
implantasi. hCG messenger RNA terdeteksi dalam blastomer dari 6 hingga embrio 8-sel pada
2 hari tetapi tidak dapat diisolasi dalam media kultur sampai 6 hari. Deteksi dalam serum ibu
dan urin jelas hanya setelah implantasi dan komunikasi vaskular telah dibentuk dengan
desidua oleh sinsitiotrofoblas 8-10 hari setelah pembuahan.
hCG hadir dalam sirkulasi maternal baik sebagai utuh dimer, alpha atau beta subunit, dan
bentuk terdegradasi, atau inti beta fragmen. Utuh dan bebas subunit beta awalnya bentuk
dominan dari hCG, dengan fragmen inti beta muncul sebagai bentuk dominan di minggu
kelima setelah pembuahan. Selain itu, utuh dan bebas subunit beta memiliki paling
variabilitas sehari-hari dan secara sementara tidak terdeteksi bahkan 10 hari setelah deteksi
kehamilan. [8] Secara optimal, tes yang digunakan untuk deteksi awal kehamilan harus
mampu mengenali semua bentuk hCG utuh, termasuk subunit beta gratis dan fragmen inti
beta.
Saat ini, 4 tes hCG utama yang digunakan: (1) radioimmunoassay, (2) uji
immunoradiometric, (3) enzim-Linked Immunosorbent Assay (ELISA), dan (4) fluoroimuno.
Tes ini sangat spesifik untuk hCG dengan antibodi yang ditujukan terhadap 2 atau lebih
isotop pada molekul hCG yang utuh. Waktu deteksi terkait dengan sensitivitas uji yang
digunakan. Kebanyakan tes kehamilan saat ini memiliki kepekaan terhadap sekitar 25 mIU /
mL. Perangkat Urine harus dirumuskan untuk mendeteksi hCG hyperglycosylated, yang
merupakan molekul kunci pada awal kehamilan.
Karakteristik masing-masing tes hCG terdaftar sebagai berikut:
radioimmunoassay
Sensitivitas - 5 mIU / mL
Waktu untuk menyelesaikan - 4 jam
Usia Postconception ketika pertama kali positif - 10-18 hari
Usia kehamilan saat pertama positif - 3-4 minggu
Assay immunoradiometric (lebih sensitif)
Sensitivitas - 150 mIU / mL
Waktu untuk menyelesaikan - 30 menit
Usia Postconception ketika pertama kali positif - 18-22 hari
Usia kehamilan saat pertama positif - 4 minggu
Assay immunoradiometric (kurang sensitif)
Sensitivitas - 1500 mIU / mL
Waktu untuk menyelesaikan - 2 menit
Usia Postconception ketika pertama kali positif - 25-28 hari
Usia kehamilan saat pertama positif - 5 minggu
Enzim-Linked Immunosorbent Assay (lebih sensitif)
Sensitivitas - 25 mIU / mL
Waktu untuk menyelesaikan - 80 menit
Usia Postconception ketika pertama kali positif - 14-17 hari
Usia kehamilan saat pertama positif - 3,5 minggu
Enzim-Linked Immunosorbent Assay (kurang sensitif)
Sensitivitas - Kurang dari 50 mIU / mL
Waktu untuk menyelesaikan - 5-15 menit
Usia Postconception ketika pertama kali positif - 18-22 hari
Usia kehamilan saat pertama positif - 4 minggu
fluoroimuno
Sensitivitas - 1 mIU / mL
Waktu untuk menyelesaikan - 2-3 jam
Usia Postconception ketika pertama kali positif - 14-17 hari
Usia kehamilan saat pertama positif - 3,5 minggu
Dimer hCG dan kedua alpha dan beta subunit diproduksi di kelenjar hipofisis perempuan
hamil dan dilepaskan dalam hubungan dengan LH. Meskipun tingkat yang jauh lebih tinggi
pada wanita pascamenopause (110 pg / mL vs 10 pg / mL), mereka masih di bawah
sensitivitas alat tes klinis yang paling sensitif (sekitar 1 mIU / mL) yang digunakan dalam
pemantauan kehamilan.
Pemantauan hCG Serial
hCG dapat dideteksi dalam serum sekitar 5% dari pasien 8 hari setelah pembuahan dan di
lebih dari 98% dari pasien hari 11. Pada kehamilan 4 minggu (18-22 d postconception), dimer
dan beta subunit hCG dua kali lipat waktu adalah sekitar 2,2 hari (standar deviasi ± 0,8 d) dan
jatuh ke 3,5 hari (standar deviasi ± 1,2 d) dengan usia kehamilan 9 minggu. tingkat puncak
pada 10-12 minggu kehamilan dan kemudian mulai menurun dengan cepat sampai yang lain,
kenaikan lebih bertahap dimulai pada 22 minggu kehamilan, yang berlanjut sampai jangka
panjang.
Tingkat awal kenaikan, diukur dengan seri pengujian hCG kuantitatif, penting dalam
pemantauan kehamilan rumit awal yang belum didokumentasikan sebagai layak dan / atau
intrauterine. Kegagalan untuk mencapai tingkat proyeksi kenaikan mungkin menyarankan
kehamilan ektopik atau aborsi spontan. hCG dua kali lipat kali tunduk pada fluktuasi hCG
utuh selama awal kehamilan, sehingga penafsiran nilai-nilai ini harus memperhitungkan tes
yang digunakan dan gambaran klinis.
Dalam satu studi, 200 perempuan yang menerima diagnosis kehamilan ektopik dengan hCG
seri dievaluasi. Tidak mengejutkan, kenaikan nilai hCG pada wanita dengan kehamilan
ektopik lebih lambat dibandingkan dengan kehamilan yang layak dan penurunan nilai hCG
pada wanita dengan kehamilan ektopik lebih lambat dibandingkan mereka yang
menyelesaikan aborsi spontan. Namun, 20,8% dari wanita dengan kehamilan ektopik
disajikan dengan kenaikan hCG nilai sama dengan kenaikan minimal untuk wanita dengan
kehamilan yang layak, dan 8% wanita disajikan dengan penurunan nilai hCG mirip dengan
wanita dengan abortus spontan selesai. [9] Beberapa penelitian lebih seperti ini menunjukkan
bahwa pola tunggal hCG tidak ada untuk awal kehamilan normal, jadi hati-hati harus diambil
dalam menafsirkan nilai-nilai hCG serial dalam evaluasi awal kehamilan.
Di sisi lain, tingkat abnormal tinggi atau kenaikan dipercepat dapat meminta penyelidikan
kemungkinan kehamilan mola, kehamilan multipel, atau kelainan kromosom.
Salah hasil hCG positif
Seperti kebanyakan tes, hasil tes hCG dapat berupa palsu negatif atau positif. Prevalensi hasil
serum hCG positif palsu rendah, dengan perkiraan mulai 0,01-2%. Hasil serum hCG positif
palsu biasanya karena gangguan oleh zat non-hCG atau deteksi hipofisis hCG. Beberapa
contoh zat non-hCG yang dapat menyebabkan hasil positif palsu termasuk LH manusia,
antibodi immunoglobulin antianimal, faktor rheumatoid, antibodi heterofil, dan protein yang
mengikat. Kebanyakan hasil positif palsu yang ditandai dengan kadar serum yang umumnya
kurang dari 1000 mIU / mL dan biasanya kurang dari 150 mIU / mL. Konsentrasi serum rata-
rata untuk pasien dengan hasil positif palsu dilaporkan kepada Food and Drug Administration
(FDA) 1985-2001 adalah 75 mIU / mL. Juga, perhatikan bahwa hanya 2 (0,74%) dari 271
penentuan hCG terpisah sera murni di kedua database FDA dan literatur yang lebih besar dari
1000 mIU / mL.
Beberapa metode yang tersedia untuk membantu mendeteksi hasil serum hCG positif palsu.
Langkah pertama adalah untuk memeriksa kadar hCG urin. Free beta-hCG subunit
selanjutnya terdegradasi dalam ginjal inti fragmen beta subunit yang memiliki kurang dari
setengah berat molekul beta subunit gratis. Beberapa zat yang dapat menyebabkan serum
positif palsu hasil memiliki berat molekul yang lebih tinggi agar tidak mudah disaring
melalui glomeruli ginjal; Oleh karena itu, mereka tidak menghasilkan hasil hCG urin positif.
Langkah-langkah lain untuk memverifikasi atau menyangkal hasil serum hCG positif
termasuk pengujian ulang spesimen yang sama, pengujian spesimen baru, melakukan
pengukuran serial untuk mencari kenaikan, melakukan pengenceran serial untuk mencari
linearitas, dan pengujian menggunakan metode yang berbeda.
Lima sumber potensial hasil hCG positif di luar kehamilan dijelaskan sebagai berikut: [10,
11]
phantom hCG
Disebabkan oleh antibodi heterophilic yang mengikat penangkapan dan diberi label antibodi
bersama-sama tanpa hCG hadir
Hasil produksi antibodi dari paparan hewan yang digunakan untuk memproduksi antibodi
yang digunakan dalam uji
Mengesampingkan dengan uji urine sensitif, karena antibodi ini tidak menyeberang ke urin
pituitary hCG
Dirangsang oleh hormon gonadotropin-releasing; ditekan dengan gonadotropin-releasing
hormone agonis dan estrogen / progestin terapi
Dapat dideteksi pada wanita menopause karena meningkatnya sekresi GnRH (Snyder et al
mengusulkan bahwa wanita menopause harus memiliki cutoff yang lebih tinggi untuk hCG
negatif 14 IU / L [12])
Didiagnosis dengan pemberian pil kontrasepsi oral, yang harus menekan kadar hCG
Administrasi eksogen hCG
Digunakan oleh beberapa pusat untuk membantu dalam penurunan berat badan dengan
pemberian intramuskular atau lisan
Tes hCG Ulangi harus negatif jika administrasi eksogen dihentikan selama setidaknya 24 jam
Neoplasma trofoblas - Terdiri dari kehamilan, kehamilan neoplasia trofoblas (GTN), dan
plasenta tumor trofoblas situs (PSTTs)
Gestational neoplasia trofoblas
Diam - Constant, rendahnya tingkat hCG tanpa bukti keganasan primer atau metastasis;
negara premalignant; tahan terhadap kemoterapi dan operasi; ikuti dengan kadar hCG sering
dan jika ditemukan akan meningkat, pertimbangkan aktif kehamilan neoplasia trofoblas
Aktif - sitotrofoblas Invasif menghasilkan hCG hyperglycosylated hanya ditemukan di awal
kehamilan dan invasif neoplasia trofoblas gestasional; dengan demikian, hyperglycosylated
hCG atau invasif antigen trofoblas dapat diukur untuk memerintah pada penyakit aktif

Plasenta tumor trofoblas situs - Didiagnosis dengan tingkat rendah hCG dalam kombinasi
dengan lesi intramiometrial pada pencitraan
Neoplasma Nontrophoblastic - Bisa disekresikan oleh kanker yang berbeda, (misalnya, testis,
kandung kemih, rahim, paru-paru, hati, pankreas, perut)
Hasil hCG negatif palsu
Hasil tes hCG negatif palsu biasanya melibatkan urin dan karena sifat kualitatif tes. Alasan
untuk hasil tes negatif dapat mencakup konsentrasi hCG di bawah ambang sensitivitas tes
khusus yang digunakan, salah perhitungan dalam terjadinya menstruasi tidak terjawab, atau
tertunda menstruasi dari kerugian awal kehamilan. Ovulasi tertunda atau implantasi tertunda
alasan lain untuk konsentrasi hCG rendah pada saat pengujian, yang menghasilkan hasil
negatif palsu.
Setidaknya 1 laporan kasus dalam literatur adalah penting ketika mempertimbangkan hasil tes
hCG urine negatif palsu. Seorang wanita 37-tahun datang ke unit gawat darurat di syok
hipovolemik 13 minggu setelah periode menstruasi terakhirnya. Dia memiliki dilatasi dan
kuretase untuk kehamilan intrauterin 8 minggu sebelum presentasi. Dua sampel yang berbeda
menghasilkan urin kualitatif hasil tes kehamilan negatif. Hasil pengujian hCG urine ketiga
lemah positif, dan, pada waktu itu, tingkat serum hCG nya 22.430 mIU / mL. Dia didiagnosis
dengan kehamilan ektopik interstitial dan menjalani operasi, di mana sekitar 2000 mL darah
bebas ditemukan dalam rongga peritoneal nya. Kehamilan interstisial membuat kurang dari
3% dari kehamilan tuba, tetapi mereka dapat hadir dalam hubungannya dengan hasil tes
kehamilan urin negatif.
progesteron
Mengukur serum progesteron dapat menjadi tambahan yang berguna untuk mengevaluasi
awal kehamilan normal. Progesteron serum merupakan cerminan dari produksi progesteron
oleh korpus luteum, yang dirangsang oleh kehamilan yang layak. Pengukuran serum
progesteron murah dan dipercaya bisa memprediksi kehamilan prognosis. Saat ini,
radioimmunoassays dan fluoroimmunoassays yang tersedia yang dapat diselesaikan dalam 3-
4 jam. Sebuah dipstick ELISA yang dapat menentukan tingkat serum progesteron kurang dari
15 ng / mL juga di pasar. ELISA membantu sebagai alat skrining untuk populasi berisiko
karena tingkat progesteron yang lebih besar dari 15 ng / ml membuat kehamilan ektopik
mungkin. [13]
Layak kehamilan intrauterin dapat didiagnosis dengan sensitivitas 97,5% jika kadar serum
progesteron lebih besar dari 25 ng / mL (> 79,5 nmol / L). Sebaliknya, menemukan kadar
serum progesteron kurang dari 5 ng / mL (<15,9 nmol / L) dapat membantu dalam diagnosis
kehamilan nonviable dengan sensitivitas 100%. Menemukan tingkat progesteron serum
kurang dari 5 ng / mL memungkinkan evaluasi diagnostik rahim pada pasien yang stabil,
bahkan jika kehamilan ektopik tidak dapat dibedakan dari aborsi spontan intrauterin
sebelumnya. Dalam hal tingkat serum progesteron adalah 5-25 ng / mL, pengujian lebih
lanjut dengan menggunakan AS, tes hormon tambahan, atau pemeriksaan serial dijamin
untuk menetapkan kelangsungan hidup kehamilan. Algoritma menggunakan serum
progesteron yang tersedia untuk evaluasi dan pengelolaan pasien dengan awal kehamilan
normal.
Faktor awal kehamilan
Faktor kehamilan awal (EPF) assay mungkin berguna di masa depan. EPF adalah protein
imunosupresif buruk didefinisikan yang telah diisolasi dalam serum ibu tak lama setelah
pembuahan dan merupakan penanda yang tersedia awal untuk menunjukkan pembuahan. Hal
ini terdeteksi dalam serum 36-48 jam setelah pembuahan, puncak di awal trimester pertama,
dan hampir tidak terdeteksi pada jangka panjang. EPF juga muncul dalam waktu 48 jam dari
sukses in vitro transfer embrio fertilisasi. EPF tidak dapat dideteksi 24 jam setelah
melahirkan atau penghentian kehamilan ektopik atau intrauterine. EPF juga terdeteksi di
banyak kehamilan ektopik dan aborsi spontan, menunjukkan bahwa ketidakmampuan untuk
mengidentifikasi EPF selama kehamilan bentara prognosis buruk.
EPF telah membatasi aplikasi klinis saat ini karena molekul sulit untuk mengisolasi. Deteksi
EPF saat bergantung pada alat tes yang kompleks dan berat disebut tes inhibisi roset. EPF
mungkin memainkan peran yang lebih menonjol di masa depan sebagai diagnosis konsepsi
sebelum implantasi memaparkan strategi baru untuk kontrasepsi, sangat akurat kencan, dan
studi genetik maju.
Tes kehamilan di rumah
Setidaknya 25 tes kehamilan di rumah yang berbeda saat ini dipasarkan di Amerika Serikat.
[14] Tes ini sekarang menggunakan uji immunometric modern. Sebagian besar tes
mengklaim "99% akurasi" atau beberapa pernyataan serupa pada kemasan atau produk insert.
Sebagian besar tes sekarang juga mengiklankan bahwa mereka dapat digunakan "sedini hari
periode menstruasi tidak terjawab." Beberapa tes kehamilan di rumah benar-benar
menginstruksikan bahwa mereka dapat digunakan 3-4 hari sebelum masa haid.
Klaim akurasi yang berasal dari pedoman FDA yang mengacu pada kemampuan tes untuk
mengidentifikasi sekitar 100 sampel urine hamil dilengkapi dengan hCG utuh dari jumlah
yang sama dari sampel urin tidak dilengkapi dengan hCG. 99% Pernyataan -accuracy luas

dibuat untuk tes dengan sensitivitas untuk konsentrasi hCG mulai dari 25 mIU / mL (cukup
sensitif) tes dengan sensitivitas dari 100 mIU / mL (kurang sensitif). 99% Pernyataan -
accuracy mengacu pada pedoman FDA menyesatkan dalam hal ini memiliki bantalan pada
kemampuan tes kehamilan di rumah untuk mendeteksi dini kehamilan.
Tes kehamilan yang paling sering digunakan pada minggu setelah periode menstruasi tidak
terjawab (keempat selesai minggu kehamilan). Nilai hCG urin sangat bervariasi pada saat ini
dan dapat berkisar dari 12 mIU / mL untuk lebih dari 2500 mIU / mL. Variabilitas ini terus
berlanjut ke minggu kelima, ketika nilai-nilai telah terbukti berkisar dari 13 mIU / mL untuk
lebih dari 6000 mIU / mL. Kedua minggu memiliki persentase nilai hCG urin yang berada di
bawah sensitivitas deteksi untuk tes kehamilan di rumah umum (kisaran 25-100 mIU / mL).
Beberapa studi telah menguji tes kehamilan di rumah yang berbeda untuk sensitivitas dan
akurasi klaim.
Satu studi yang diuji 18 tes kehamilan di rumah yang berbeda pada 5 konsentrasi yang
berbeda hCG (0, 12,5, 25, 50, dan 100 mIU / mL). Tidak ada perbedaan dalam sensitivitas
terdeteksi antara tes yang telah lama membaca kali (biasanya sekitar 5 menit) dibandingkan
dengan mereka dengan waktu membaca pendek (1 menit). Jelas hasil positif hanya ditemukan
pada 44% dari merek ketika diuji pada konsentrasi hCG tertinggi (100 mIU / mL).
Sensitivitas meningkat menjadi 83% dari merek diuji pada 100 mIU / mL ketika garis samar
dilihat juga dianggap sebagai hasil yang positif. Uji sensitivitas juga meningkat ketika
membaca kali diperpanjang sampai 10 menit. Secara keseluruhan, akurasi 100% hanya
dicapai dalam semua 18 merek diuji ketika konsentrasi hCG tertinggi (100 mIU / ml)
digunakan, waktu membaca diperpanjang digunakan, dan samar-samar hasil dilihat
dimasukkan sebagai positif.
Studi lain dievaluasi 7 tes kehamilan di rumah dan menemukan bahwa meskipun klaim,
deteksi kehamilan pada hari terlambat haid bervariasi 16-95%, dan beberapa perangkat yang
rusak (didefinisikan sebagai perangkat gagal untuk menghasilkan sebuah band di jendela
control) .
Penelitian lain menemukan bahwa tes kehamilan di rumah dengan bacaan digital dapat
menawarkan manfaat yang signifikan atas tes nondigital tradisional.
Keterbatasan tes ini harus dipahami sehingga deteksi kehamilan tidak tertunda secara
signifikan. Deteksi awal kehamilan memungkinkan untuk dimulainya pemeriksaan
kehamilan, perubahan pengobatan potensial, perubahan gaya hidup untuk mempromosikan
kehamilan yang sehat (diet yang tepat, menghindari alkohol, tembakau, dan obat-obatan
tertentu), atau penghentian kehamilan awal jika diinginkan.
Nilai hCG serum infertilitas
Nilai hCG serum untuk diagnosis awal kehamilan pada pasien yang menjalani in-vitro
fertilisasi mentransfer embrio (IVF-ET) telah dipelajari. [15] Tingkat Serum hCG 14 hari
setelah transfer embrio berkorelasi dengan hasil kehamilan. Dalam sebuah studi dari 111
pasien dengan kadar hCG kuantitatif positif 14 hari setelah transfer embrio, hasil kehamilan
berikut yang diamati:
Tingkat <300 mIU / mL, angka kehamilan yang sedang berlangsung adalah 9%
Tingkat 300-600 mIU / mL, angka kehamilan yang sedang berlangsung adalah 50%
Tingkat> 600 mIU / mL, tingkat kehamilan ganda adalah 100%
Oleh karena itu, pada populasi tertentu, hasil uji kuantitatif dapat digunakan untuk memandu
konseling dan evaluasi lebih lanjut
Dengan munculnya ultrasonografi transvaginal (TVUS), diagnosis kehamilan dapat dibuat
lebih awal daripada yang mungkin dengan ultrasonografi transabdominal (tau). AS telah lama
digunakan dalam kehamilan rumit untuk kencan dan sebagai pemeriksaan skrining untuk
anomali janin. AS tidak biasanya digunakan untuk mendiagnosis kehamilan kecuali pasien
mengalami perdarahan vagina atau sakit perut di awal kehamilan atau berisiko tinggi pasien
obstetri. TVUS adalah cara yang paling akurat untuk mengkonfirmasi kehamilan intrauterin
dan usia kehamilan selama awal trimester pertama.
TVUS memiliki beberapa keunggulan dibandingkan tau selama awal kehamilan. TVUS dapat
membantu mendeteksi tanda-tanda kehamilan intrauterin sekitar 1 minggu lebih awal dari
Taus. Pasien tidak perlu memiliki kandung kemih penuh dan tidak diperlukan untuk bertahan
tekanan tidak nyaman pada dinding perut dari probe eksternal. TVUS juga lebih baik bagi
pasien yang mengalami obesitas atau mereka yang menjaga selama tau. Salah satu kelemahan
adalah bahwa beberapa pasien cemas tentang probe transvaginal dan mungkin keberatan
dengan penyisipan.
Probe vagina biasanya frekuensi yang lebih tinggi (5-8 MHz) dari probe perut (3-5 MHz).
Frekuensi yang lebih tinggi memungkinkan untuk resolusi yang lebih baik dari gambar, tetapi
penetrasi kurang dari sinyal. Juga, praktek diperlukan untuk sosialisasi dengan orientasi pada
monitor AS saat melakukan TVUS.

Struktur awal diidentifikasi adalah (GS). GS dapat dilihat pada gambar TVUS oleh
kehamilan 4-5 minggu dan tumbuh pada tingkat 1 mm / d di awal kehamilan. Dengan usia
kehamilan 5,5-6 minggu, tanda double-desidua dapat dilihat, yang merupakan GS dikelilingi
oleh desidua menebal. Hadirnya GS dini dapat menjadi bingung dengan koleksi kecil cairan
atau darah atau pseudo GS dari kehamilan ektopik. Karena itu, diagnosis kehamilan
intrauterin tidak harus dilakukan atas dasar visualisasi GS saja.
The yolk sac dapat dikenali oleh 4-5 minggu kehamilan dan terlihat sampai sekitar 10 minggu
kehamilan. The yolk sac adalah bola kecil dengan pusat hypoechoic dan terletak di dalam GS
(lihat gambar di bawah).
Diagnosis kehamilan. Panah menunjuk ke
Diagnosis kehamilan. Panah menunjuk ke kantung kuning telur seperti yang terlihat dalam
kantung kehamilan (GS). The yolk sac biasanya diidentifikasi sebelum GS lebih besar dari 10
mm. Demikian juga, jika kantung kuning telur lebih besar dari 7 mm tanpa tanda-tanda tiang
janin berkembang, kemungkinan kehamilan normal meningkat.
Mengamati GS yang lebih besar 10 mm tanpa kantung yolk jarang, dan jika hal ini diamati,
kemungkinan besar merupakan kehamilan abnormal (lihat gambar di bawah).
Diagnosis kehamilan. Ini adalah kantung kehamilan (GS
Diagnosis kehamilan. Ini adalah kantung kehamilan (GS) yang berukuran sekitar 2 X 3 cm,
tanpa bukti kantung kuning telur. Ketika GS lebih besar dari 10 mm dan tidak ada yolk sac
diidentifikasi, kehamilan normal mungkin. Situasi ini khusus disebut sebagai blighted ovum
atau kehamilan anembryonic.
Demikian pula, yolk sac lebih besar dari 7 mm tanpa bukti tiang janin berkembang
menunjukkan kehamilan nonviable. Diagnosis kehamilan intrauterin dapat dibuat setelah
kuning telur hadir, yang juga tidak termasuk kehamilan ektopik, kecuali dalam contoh langka
kehamilan heterotopic. Sebuah kehamilan heterotopic, kehamilan intrauterine, dan kehamilan
ektopik selama kehamilan sama sekali dianggap sangat langka tapi sekarang telah
ditunjukkan untuk hadir di sebanyak 1 di 3000 kehamilan.
Tiang janin atau embrio yang pertama kali terlihat pada gambar TVUS pada usia kehamilan
sekitar 5-6 minggu. Ini harus selalu dilihat oleh TVUS ketika GS lebih besar dari 18 mm atau
tau ketika GS lebih besar dari 2,5 cm. Tiang janin adalah struktur hyperechoic linear yang
tumbuh di sekitar 1 mm / d.
Gerakan jantung kadang-kadang dapat diidentifikasi dalam 2 sampai 3 mm embrio tapi
hampir selalu hadir ketika embrio tumbuh sampai 5 mm atau lebih. Pada usia kehamilan 5-6
minggu, denyut jantung janin berkisar 100-115 denyut per menit. Detak jantung terus akan
meningkat menjadi rata-rata 140 denyut per menit dengan usia kehamilan 9 minggu.
Ultrasonografi menjadi lebih berguna untuk diagnosis awal kehamilan dan untuk
mengidentifikasi kehamilan normal bila digunakan dalam hubungannya dengan menilai kadar
hCG kuantitatif. Identifikasi struktur kehamilan dengan ultrasonografi berkorelasi dengan
tingkat tertentu hCG, disebut tingkat diskriminatif. Tingkat diskriminatif adalah tingkat hCG
di mana struktur tersebut harus selalu diidentifikasi.
GS telah diidentifikasi oleh TVUS dengan kadar hCG serendah 300 mIU / mL, dan operator
TVUS paling berpengalaman harus memvisualisasikan GS ketika tingkat sekitar 1000 mIU /
mL. Tingkat diskriminatif untuk GS adalah sekitar 3600 mIU / mL, dan jika tidak terlihat
pada saat ini, patologi lainnya harus disingkirkan. Banyak menggunakan tingkat yang lebih
konservatif diskriminatif untuk GS, 2000 mIU / mL oleh TVUS dan 3600 mIU / ml dengan
Taus, dan akan mulai untuk menyingkirkan patologi jika GS tidak terlihat. Adneksa harus
dipindai untuk kehamilan ektopik, dan sonogram dan kadar hCG harus diikuti sampai
diagnosis dibuat. Selain itu, sebuah studi menunjukkan bahwa kehamilan intrauterin layak
memiliki GS diidentifikasi oleh Taus untuk tingkat hCG yang lebih besar dari 6500 mIU /
mL.
Kegunaan evaluasi TVUS saat hCG kurang dari 1000 mIU / mL telah diperdebatkan. Satu
studi menunjukkan bahwa informasi berharga masih dapat mengumpulkan pada wanita yang
datang untuk muncul TVUS dengan tingkat hCG kurang dari 1000 mIU / mL. Dalam
penelitian ini, sekitar 13% dari kehamilan intrauterin normal dan 39% dari kehamilan ektopik
diidentifikasi oleh TVUS. Ultrasonografi tidak boleh ditunda murni atas dasar kadar hCG.
[16]
Struktur lain juga diantisipasi dalam korelasi dengan tingkat hCG tertentu. The yolk sac (lihat
gambar di bawah) umumnya diamati dengan tingkat hCG dari sekitar 2500 mIU / mL,
meskipun mungkin tidak dapat diidentifikasi sampai tingkat yang jauh lebih tinggi. Tiang
embrio biasanya menjadi jelas pada tingkat sekitar 5000 mIU / mL, dan detak jantung janin
dapat dilihat pada sebagian besar kehamilan normal ketika tingkat hCG mencapai 10.000
mIU / mL.
Diagnosis kehamilan dapat dibuat dengan beberapa metode. Wanita Normocyclic yang hadir
dengan amenore dan sejarah yang khas dan temuan pemeriksaan fisik memiliki presentasi
klasik dan dapat didiagnosis dengan kehamilan intrauterin layak jika mereka maju dengan
tepat. Saat ini, sebagian besar wanita yang didiagnosis dengan kehamilan setelah siklus
menstruasi tidak terjawab dan urin positif atau temuan hCG serum. Kehamilan didiagnosis
sebagai layak dengan pemeriksaan serial dan pengembangan kehamilan normal, hasil yang
normal setelah berpacaran ultrasonografi, atau temuan positif dari nada jantung janin
menggunakan studi Doppler.
Wanita yang dianggap berisiko tinggi atau mereka yang hadir dengan sakit perut atau
perdarahan vagina pada kehamilan awal lebih mungkin untuk dievaluasi dengan
ultrasonografi dan tes hormon tambahan. Sejumlah kombinasi yang berbeda dapat membantu
dalam diagnosis kehamilan intrauterin layak. Dokter harus memastikan apa yang paling tepat
pada saat presentasi pasien.
Untuk sumber daya pendidikan pasien sangat baik, kunjungi eMedicineHealth itu Kehamilan
Center. Juga, lihat pasien artikel pendidikan eMedicineHealth Home Pregnancy Test,
Kehamilan ektopik, Birth Control Ikhtisar, dan Kelahiran Metode Kontrol
1. Paspulati RM, Bhatt S, Nour SG. Sonographic evaluation of first-trimester
bleeding. Radiol Clin North Am. Mar 2004;42(2):297-314. [Medline].
2. Dart RG. Role of pelvic ultrasonography in evaluation of symptomatic first-trimester
pregnancy. Ann Emerg Med. Mar 1999;33(3):310-20. [Medline].
3. Seeber BE, Barnhart KT. Suspected ectopic pregnancy. Obstet Gynecol. February
2006;107(2):399-413.[Medline].
4. Female Sterilization: Risk of Ectopic Pregnancy After Tubal Sterilization Fact Sheet.
Atlanta, GA: Centers for Disease Control and Prevention; 2008. [Full Text].
5. Speroff L, Fritz MA. Clinical Gynecologic Endocrinology and Infertility. 7th
ed.
Philadelphia, PA: Lippincott Williams & Wilkins; 2005.
6. Berek JS, Adashi EY, Hillard PA. Novak's Gynecology. 14th. Baltimore, MD:
Lippincott Williams & Wilkins; 2006.
7. Paul M, Schaff E, Nichols M. The roles of clinical assessment, human chorionic
gonadotropin assays, and ultrasonography in medical abortion practice. Am J Obstet
Gynecol. Aug 2000;183(2 Suppl):S34-43.[Medline].
8. McChesney R, Wilcox AJ, O'Connor JF, et al. Intact HCG, free HCG beta subunit
and HCG beta core fragment: longitudinal patterns in urine during early
pregnancy. Hum Reprod. Apr 2005;20(4):928-35.[Medline].
9. Silva C, Sammel MD, Zhou L, et al. Human chorionic gonadotropin profile for
women with ectopic pregnancy. Obstet Gynecol. Mar 2006;107(3):605-10. [Medline].

10. Olson TG, Barnes AA, King JK. Elevated hCG Outside of Pregnancy - Diagnostic
Considerations and Laboratory Evaluation. Obstet Gynecol Survey. Oct
2007;62(10):669-74. [Medline].
11. Valenzuela R, Iserson KV, Punguyire D. False-positive urine pregnancy tests -
clinicians as detectives. Pan Afr Med J. 2011;8:41. [Medline]. [Full Text].
12. Snyder JA, Haymond S, Parvin CA, et al. Diagnostic considerations in the
measurement of human chorionic gonadotropin in aging women. Clin Chem. Oct
2005;51(10):1830-5. [Medline].
13. Davies S, Byrn F, Cole LA. Human chorionic gonadotropin testing for early
pregnancy viability and complications. Clin Lab Med. Jun 2003;23(2):257-64,
vii. [Medline].
14. Cole LA. The utility of six over-the-counter (home) pregnancy tests. Clin Chem Lab
Med. Aug 2011;49(8):1317-22. [Medline].
15. Guth B, Hudelson J, Higbie J, et al. Predictive value of hCG level 14 days after
embryo transfer. J Assist Reprod Genet. Jan 1995;12(1):13-4. [Medline].
16. Dart RG, Kaplan B, Cox C. Transvaginal ultrasound in patients with low beta-human
chorionic gonadotropin values: how often is the study diagnostic?. Ann Emerg Med.
Aug 1997;30(2):135-40. [Medline].
17. Ankum WM, Van der Veen F, Hamerlynck JV, et al. Suspected ectopic pregnancy.
What to do when human chorionic gonadotropin levels are below the discriminatory
zone. J Reprod Med. Jul 1995;40(7):525-8.[Medline].
18. Barnhart K, Esposito M, Coutifaris C. An update on the medical treatment of ectopic
pregnancy. Obstet Gynecol Clin North Am. Sep 2000;27(3):653-67, viii. [Medline].
19. Barnhart KT, Sammel MD, Rinaudo PF, et al. Symptomatic patients with an early
viable intrauterine pregnancy: HCG curves redefined. Obstet Gynecol. Jul
2004;104(1):50-5. [Medline].
20. Barnhart KT, Simhan H, Kamelle SA. Diagnostic accuracy of ultrasound above and
below the beta-hCG discriminatory zone. Obstet Gynecol. Oct 1999;94(4):583-
7. [Medline].
21. Braunstein GD. False-positive serum human chorionic gonadotropin results: causes,
characteristics, and recognition. Am J Obstet Gynecol. Jul 2002;187(1):217-
24. [Medline].
22. Bree RL, Edwards M, Bohm-Velez M, et al. Transvaginal sonography in the
evaluation of normal early pregnancy: correlation with HCG level. AJR Am J
Roentgenol. Jul 1989;153(1):75-9. [Medline].
23. Cole LA, Khanlian SA, Sutton JM, et al. Accuracy of home pregnancy tests at the
time of missed menses.Am J Obstet Gynecol. Jan 2004;190(1):100-5. [Medline].
24. Cole LA, Sutton-Riley JM, Khanlian SA, et al. Sensitivity of over-the-counter
pregnancy tests: comparison of utility and marketing messages. J Am Pharm Assoc
(2003). Sep-Oct 2005;45(5):608-15. [Medline].
25. Goldstein SR, Snyder JR, Watson C, et al. Very early pregnancy detection with
endovaginal ultrasound.Obstet Gynecol. Aug 1988;72(2):200-4. [Medline].
26. Kim SW, Ha YR, Chung SP, et al. Ruptured interstitial pregnancy presenting with
negative beta-hCG and hypovolemic shock. Am J Emerg Med. Oct
2003;21(6):511. [Medline].
27. Klee GG. Interferences in hormone immunoassays. Clinics in Laboratory Medicine.
Mar 2004;24, Number 1.
28. Moore KL, Persaud TVN. The Developing Human: Clinically Oriented Embryology.
5th
ed. Philadelphia, Pa: WB Saunders; 1993:14-69.
29. Nyberg DA, Laing FC, Filly RA. Threatened abortion: sonographic distinction of
normal and abnormal gestation sacs. Radiology. Feb 1986;158(2):397-400. [Medline].
30. Nyberg DA, Mack LA, Harvey D, et al. Value of the yolk sac in evaluating early
pregnancies. J Ultrasound Med. Mar 1988;7(3):129-35. [Medline].
31. Romero R, Kadar N, Copel JA, et al. The value of serial human chorionic
gonadotropin testing as a diagnostic tool in ectopic pregnancy. Am J Obstet Gynecol.
Aug 1986;155(2):392-4. [Medline].
32. Timor-Tritsch IE, Yeh MN, Peisner DB, et al. The use of transvaginal
ultrasonography in the diagnosis of ectopic pregnancy. Am J Obstet Gynecol. Jul
1989;161(1):157-61. [Medline].
33. Tomlinson C, Marshall J, Ellis JE. Comparison of accuracy and certainty of results of
six home pregnancy tests available over-the-counter. Curr Med Res Opin. Jun
2008;24(6):1645-9. [Medline].
Overview
The diagnosis of pregnancy requires a multifaceted approach using 3 main
diagnostic tools. These are history and physical examination, laboratory
evaluation, and ultrasonography. Currently, physicians may use all of these tools to
diagnose pregnancy at early gestation and to help rule out other pathologies.
Next
History and Physical Examination
The diagnosis of pregnancy has traditionally been made based on history and
physical examination findings. Important aspects of the menstrual history must be
obtained. The woman should describe her usual menstrual pattern, including date
of onset of last menses, duration, flow, and frequency. Items that may confuse the
diagnosis of early pregnancy are an atypical last menstrual period, contraceptive
use, and a history of irregular menses. Additionally, as many as 25% of women
bleed during their first trimester, further complicating the assessment.[1]
Be alert for rising human chorionic gonadotropin (hCG) levels, an empty uterus
observed on sonogram, abdominal pain, and vaginal bleeding because these may
signal an ectopic pregnancy.[2, 3] Ectopic pregnancies are the primary cause of first
trimester maternal mortality and should be diagnosed early, before the pregnancy
ruptures or the patient becomes unstable (see the image below).[4]
Pregnancy diagnosis. Sonogram showing a complex
mass in the adnexa (labeled EP). It was found to be an ectopic pregnancy at the
time of surgery.
Other historical factors related to ectopic pregnancies include prior tubal
manipulation, pelvic inflammatory disease, previous ectopic pregnancy, tubal
disease, use of an intrauterine device for contraception, fertility therapies, and tubal
ligation.[3, 5, 6] See Ectopic Pregnancy for a full description and details.
The classic presentation of pregnancy is a woman with menses of regular
frequency who presents with amenorrhea, nausea, vomiting, generalized malaise,
and breast tenderness.
Upon physical examination, one may find an enlarged uterus after bimanual
examination, breast changes, and softening and enlargement of the cervix (Hegar
sign; observed at approximately 6 wk). The Chadwick sign is a bluish discoloration
of the cervix from venous congestion and can be observed by 8-10 weeks. A gravid
uterus may be palpable low in the abdomen if the pregnancy has progressed far
enough, usually by 12 weeks. Currently, through the use of chemical assays and
ultrasonography, physicians are capable of making the diagnosis of pregnancy
before many of the physical signs and symptoms are evident.[7]
Previous
Next
Laboratory Evaluation
Several hormones can be measured and monitored to aid in the diagnosis of
pregnancy. The most commonly used assays are for the beta subunit of hCG. Other
hormones that have been used include progesterone and early pregnancy factor.
The cytotrophoblast and syncytiotrophoblast each secrete a variety of hormones
that include, but are not limited to, corticotropin-releasing hormone, gonadotropin-
releasing hormone, thyrotropin-releasing hormone, somatostatin, corticotropin,
human chorionic thyrotropin, human placental lactogen, inhibin/activin,
transforming growth factor-beta, insulinlike growth factors 1 and 2, epidermal
growth factor, pregnancy-specific beta-1 glycoprotein, placental protein 5, and
pregnancy-associated plasma protein-A. To date, no commercially feasible tests
that use these hormones have been made available to aid in the diagnosis of
pregnancy.
Beta-human chorionic gonadotropin
hCG is a glycoprotein similar in structure to follicle-stimulating hormone (FSH),
luteinizing hormone (LH), and thyrotropin. hCG is composed of alpha and beta
subunits. The alpha subunit of hCG is similar to the alpha subunit of FSH, LH, and
thyrotropin. The free beta subunit of hCG differs from the others in that it has a
30–amino acid tailpiece at the COOH terminus. Free beta subunits are degraded by
macrophage enzymes in the kidney to make a beta subunit core fragment, which is
primarily detected in urine samples.
The beta-hCG subunit is present in the syncytial layer of the blastomere.
Hyperglycosylated hCG is a form of hCG produced by invasive cytotrophoblast
cells in early pregnancy and implantation. hCG messenger RNA is detectable in
the blastomeres of 6- to 8-cell embryos at 2 days but cannot be isolated in culture
medium until 6 days. Detection in maternal serum and urine is evident only after
implantation and vascular communication has been established with the decidua by
the syncytiotrophoblast 8-10 days after conception.
hCG is present in the maternal circulation as either an intact dimer, alpha or beta
subunit, and degraded form, or beta core fragment. Intact and free beta subunit are
initially the predominant forms of hCG, with the beta core fragment emerging as
the predominant form in the fifth week after conception. Additionally, intact and
free beta subunit have the most day-to-day variability and are transiently
undetectable even 10 days after detection of pregnancy.[8] Optimally, tests used for
early pregnancy detection should be able to recognize all forms of intact hCG,
including the free beta subunit and the beta core fragment.
Currently, 4 main hCG assays are used: (1) radioimmunoassay, (2)
immunoradiometric assay, (3) enzyme-linked immunosorbent assay (ELISA), and
(4) fluoroimmunoassay. These assays are highly specific for hCG with antibodies
directed against 2 or more isotopes on the intact hCG molecule. Time of detection
is related to the sensitivity of the assay being used. Most current pregnancy tests
have sensitivity to approximately 25 mIU/mL. Urine devices must be formulated to
detect hyperglycosylated hCG, which is the key molecule in early pregnancy.
Characteristics of each hCG assay are listed as follows:
Radioimmunoassay
o Sensitivity - 5 mIU/mL
o Time to complete - 4 hours
o Postconception age when first positive - 10-18 days
o Gestational age when first positive - 3-4 weeks
Immunoradiometric assay (more sensitive)
o Sensitivity - 150 mIU/mL
o Time to complete - 30 minutes
o Postconception age when first positive - 18-22 days
o Gestational age when first positive - 4 weeks
Immunoradiometric assay (less sensitive)
o Sensitivity - 1500 mIU/mL
o Time to complete - 2 minutes
o Postconception age when first positive - 25-28 days
o Gestational age when first positive - 5 weeks
Enzyme-linked immunosorbent assay (more sensitive)
o Sensitivity - 25 mIU/mL
o Time to complete - 80 minutes
o Postconception age when first positive - 14-17 days
o Gestational age when first positive - 3.5 weeks
Enzyme-linked immunosorbent assay (less sensitive)
o Sensitivity - Less than 50 mIU/mL
o Time to complete - 5-15 minutes
o Postconception age when first positive - 18-22 days
o Gestational age when first positive - 4 weeks
Fluoroimmunoassay
o Sensitivity - 1 mIU/mL
o Time to complete - 2-3 hours
o Postconception age when first positive - 14-17 days
o Gestational age when first positive - 3.5 weeks
Dimeric hCG and both the alpha and beta subunits are produced in the pituitary
gland of nonpregnant females and are released in association with LH. Although
levels are much higher in postmenopausal women (110 pg/mL vs 10 pg/mL), they
are still below the sensitivity of the most sensitive clinical assays (approximately 1
mIU/mL) used in pregnancy monitoring.
Serial hCG monitoring
hCG is detectable in the serum of approximately 5% of patients 8 days after
conception and in more than 98% of patients by day 11. At 4 weeks' gestation (18-
22 d postconception), the dimer and beta subunit hCG doubling times are
approximately 2.2 days (standard deviation ± 0.8 d) and fall to 3.5 days (standard
deviation ± 1.2 d) by 9 weeks' gestation. levels peak at 10-12 weeks' gestation and
then begin to decline rapidly until another, more gradual rise begins at 22 weeks'
gestation, which continues until term.
The initial rate of rise, measured by serial quantitative hCG testing, is important in
the monitoring of early complicated pregnancies that have yet to be documented as
viable and/or intrauterine. Failure to achieve the projected rate of rise may suggest
an ectopic pregnancy or spontaneous abortion. hCG doubling times are subject to
fluctuations of intact hCG during early pregnancy, so interpretation of these values
must take into account the assays used and the clinical picture.
In one study, 200 women who received a diagnosis of ectopic pregnancy by serial
hCG were evaluated. Of no surprise, the rise in hCG values in women with ectopic
pregnancies was slower than those with viable pregnancies and the decline of hCG
values in women with ectopic pregnancies was slower than for those with
completed spontaneous abortion. However, 20.8% of women with ectopic
pregnancies presented with a rise in hCG values similar to the minimal rise for
women with a viable gestation, and 8% of women presented with a fall in hCG
values similar to women with a completed spontaneous abortion.[9] Several over
studies such as this one demonstrate that a single pattern of hCG does not exist for
abnormal early pregnancy, so caution must be taken in interpreting serial hCG
values in the evaluation of early pregnancy.
On the other hand, an abnormally high level or accelerated rise can prompt
investigation into the possibility of molar pregnancy, multiple gestations, or
chromosomal abnormalities.
False positive hCG results
As with most tests, hCG test results can be either falsely negative or positive. The
prevalence of false-positive serum hCG results is low, with estimates ranging from
0.01-2%. False-positive serum hCG results are usually due to interference by non-
hCG substances or the detection of pituitary hCG. Some examples of non-hCG
substances that can cause false-positive results include human LH, antianimal
immunoglobulin antibodies, rheumatoid factor, heterophile antibodies, and binding
proteins. Most false-positive results are characterized by serum levels that are
generally less than 1000 mIU/mL and usually less than 150 mIU/mL. The median
serum concentration for patients with false-positive results reported to the Food
and Drug Administration (FDA) from 1985-2001 is 75 mIU/mL. Also, note that
only 2 (0.74%) of 271 separate hCG determinations in undiluted sera in both the
FDA database and the literature were greater than 1000 mIU/mL.
Several methods are available to help detect false-positive serum hCG results. The
first step is to check urine hCG levels. The free beta-hCG subunit is further
degraded in the kidney to a beta subunit core fragment that has less than half the
molecular weight of the free beta subunit. Some of the substances that can cause
serum false-positive results have much higher molecular weights that are not easily
filtered through the renal glomeruli; therefore, they do not produce a positive urine
hCG result. Other steps to verify or disprove a positive serum hCG result include
retesting the same specimen, testing a new specimen, taking serial measurements
to look for a rise, performing serial dilutions to look for linearity, and testing using
a different method.
The five potential sources of positive hCG results outside of pregnancy are
described below:[10, 11]
Phantom hCG
o Caused by heterophilic antibodies that bind the capture and labeled
antibodies together without hCG being present
o Antibody production results from exposure to animals used to
produce antibodies used in assay
o Rule out with sensitive urine assay, as these antibodies do not cross
into urine
Pituitary hCG
o Stimulated by gonadotropin-releasing hormone; suppressed by
gonadotropin-releasing hormone agonist and estrogen/progestin
therapy
o Can be detected in postmenopausal women due to increased GnRH
secretion (Snyder et al propose that postmenopausal women should
have a higher cutoff for a negative hCG of 14 IU/L[12] )
o Diagnosed by administering oral contraceptive pills, which should
suppress hCG levels
Exogenous administration of hCG
o Used by some centers to aid in weight loss by intramuscular or oral
administration
o Repeat hCG assays should be negative if exogenous administration is
discontinued for at least 24 hours
Trophoblastic neoplasm - Consists of pregnancy, gestational trophoblastic
neoplasia (GTN), and placental site trophoblastic tumors (PSTTs)
o Gestational trophoblastic neoplasia
Quiescent - Constant, low levels of hCG without evidence of
primary or metastatic malignancy; premalignant state; resistant
to chemotherapy and surgery; follow with frequent hCG levels
and if found to be rising, consider active gestational
trophoblastic neoplasia
Active - Invasive cytotrophoblasts produce hyperglycosylated
hCG found only in early pregnancy and invasive gestational
trophoblastic neoplasia; thus, hyperglycosylated hCG or
invasive trophoblastic antigen can be measured to rule in active
disease
o Placental site trophoblastic tumors - Diagnosed with low-level hCG
in combination with intramyometrial lesions on imaging
Nontrophoblastic neoplasm - Can be secreted by different cancers, (eg,
testicular, bladder, uterine, lung, liver, pancreas, stomach)
False-negative hCG results
False-negative hCG test results usually involve urine and are due to the qualitative
nature of the test. Reasons for a negative test result may include an hCG
concentration below the sensitivity threshold of the specific test being used, a
miscalculation in the onset of the missed menses, or delayed menses from early
pregnancy loss. Delayed ovulation or delayed implantation are other reasons for
low hCG concentrations at the time of testing, which yields a false-negative result.
At least 1 case report in the literature is notable when considering false-negative
urine hCG test results. A 37-year-old woman presented to an emergency
department in hypovolemic shock 13 weeks after her last menstrual period. She
had a dilation and curettage for an intrauterine pregnancy 8 weeks before
presentation. Two different samples yielded negative qualitative urine pregnancy
test results. The third urine hCG test result was weakly positive, and, at that time,
her serum hCG level was 22,430 mIU/mL. She was diagnosed with an interstitial
ectopic pregnancy and underwent surgery, during which approximately 2000 mL
of free blood was found in her peritoneal cavity. Interstitial pregnancies make up
less than 3% of tubal pregnancies, but they can be present in conjunction with
negative urine pregnancy test results.
Progesterone
Measuring serum progesterone may be a useful adjunct for evaluating abnormal
early pregnancy. Serum progesterone is a reflection of progesterone production by
the corpus luteum, which is stimulated by a viable pregnancy. Measurement of
serum progesterone is inexpensive and can reliably predict pregnancy prognosis.
Currently, radioimmunoassays and fluoroimmunoassays are available that can be
completed in 3-4 hours. A dipstick ELISA that can determine a serum progesterone
level of less than 15 ng/mL is also on the market. ELISA is helpful as a screening
tool for at-risk populations because progesterone levels of greater than 15 ng/mL
make ectopic pregnancy unlikely.[13]
Viable intrauterine pregnancy can be diagnosed with 97.5% sensitivity if the serum
progesterone levels are greater than 25 ng/mL (>79.5 nmol/L). Conversely, finding
serum progesterone levels of less than 5 ng/mL (< 15.9 nmol/L) can aid in the
diagnosis of a nonviable pregnancy with 100% sensitivity. Finding serum
progesterone levels of less than 5 ng/mL allows diagnostic evaluation of the uterus
in a stable patient, even if an ectopic pregnancy cannot be distinguished from a
spontaneous intrauterine abortion beforehand. In the event that the serum
progesterone level is 5-25 ng/mL, further testing using US, additional hormonal
assays, or serial examinations is warranted to establish the viability of the
pregnancy. Algorithms using serum progesterone are available for the evaluation
and management of patients with abnormal early pregnancy.
Early pregnancy factor
The early pregnancy factor (EPF) assay may be useful in the future. EPF is a
poorly defined immunosuppressive protein that has been isolated in maternal
serum shortly after conception and is the earliest available marker to indicate
fertilization. It is detectable in the serum 36-48 hours after fertilization, peaks early
in the first trimester, and is almost undetectable at term. EPF also appears within
48 hours of successful in vitro fertilization embryo transfers. EPF cannot be
detected 24 hours after delivery or at the termination of an ectopic or intrauterine
pregnancy. EPF is also undetectable in many ectopic pregnancies and spontaneous
abortions, indicating that an inability to identify EPF during pregnancy heralds a
poor prognosis.
EPF has limited clinical applications at this time because the molecule is difficult
to isolate. Detection of EPF currently relies on a complex and unwieldy assay
termed the rosette inhibition test. EPF may play a more prominent role in the future
as the diagnosis of conception prior to implantation elucidates new strategies for
contraception, highly accurate dating, and advanced genetic studies.
Home pregnancy tests
At least 25 different home pregnancy tests are currently marketed in the United
States.[14] These tests now use the modern immunometric assay. Most of these tests
claim "99% accuracy" or some other similar statements on the packaging or
product insert. Most of the tests also now advertise that they can be used "as early
as the day of the missed menstrual period." Several home pregnancy tests actually
instruct that they may be used 3-4 days before the time of the missed period.
The accuracy claims are derived from an FDA guideline that refers to the test's
ability to identify approximately 100 nonpregnant urine samples supplemented
with intact hCG from a similar number of urine samples not supplemented with
hCG. The broad 99%-accuracy statement is made for tests with sensitivities for
hCG concentrations ranging from 25 mIU/mL (fairly sensitive) to tests with
sensitivities of 100 mIU/mL (less sensitive). The 99%-accuracy statement in
reference to the FDA guideline is misleading in that it has no bearing on the ability
of the home pregnancy test to detect early pregnancy.
Home pregnancy tests are most commonly used in the week after the missed
menstrual period (fourth completed gestational week). Urine hCG values are
extremely variable at this time and can range from 12 mIU/mL to greater than
2500 mIU/mL. This variability continues into the fifth week, when values have
been shown to range from 13 mIU/mL to greater than 6000 mIU/mL. Both weeks
have a percentage of urine hCG values that is below the sensitivities of detection
for common home pregnancy tests (range 25-100 mIU/mL).
Several studies have tested different home pregnancy tests for sensitivity and
accuracy claims.
One study tested 18 different home pregnancy tests at 5 different hCG
concentrations (0, 12.5, 25, 50, and 100 mIU/mL). No difference in
sensitivity was detected between tests that had longer reading times (usually
approximately 5 min) compared with those with shorter reading times (1
min). Clearly positive results were only found in 44% of the brands when
tested at the highest hCG concentration (100 mIU/mL). The sensitivity was
improved to 83% of brands tested at 100 mIU/mL when a faintly discernible
line was also considered a positive result. Test sensitivity was also increased
when reading times were extended to 10 minutes. Overall, 100% accuracy
was only achieved in all 18 brands tested when the highest hCG
concentration (100 mIU/ml) was used, an extended reading time was used,
and faintly discernible results were included as positive.
Another study evaluated 7 home pregnancy tests and found that despite the
claims, the detection of pregnancy on the day of missed period varied from
16-95%, and some devices were faulty (defined as devices failing to yield a
band in the control window).
Other studies have found that home pregnancy tests with digital reading may
offer significant benefits over traditional nondigital tests.
The limitations of these tests must be understood so that pregnancy detection is not
significantly delayed. Early pregnancy detection allows for the commencement of
prenatal care, potential medication changes, lifestyle changes to promote a healthy
pregnancy (appropriate diet; avoidance of alcohol, tobacco, and certain
medications), or early pregnancy termination if desired.
Serum hCG values in infertility
Serum hCG values for the diagnosis of early pregnancy in patients undergoing in-
vitro fertilization–embryo transfer (IVF-ET) have been studied.[15]Serum hCG
levels 14 days after embryo transfer correlate with pregnancy outcome. In a study
of 111 patients with positive quantitative hCG levels 14 days after embryo transfer,
the following pregnancy outcomes were observed:
Levels < 300 mIU/mL, ongoing pregnancy rate was 9%
Levels 300-600 mIU/mL, ongoing pregnancy rate was 50%
Levels >600 mIU/mL, multiple pregnancy rate was 100%
Therefore, in this particular population, quantitative assay results can be used to
guide counseling and further evaluation.
Previous
Next
Ultrasonography
With the advent of transvaginal ultrasonography (TVUS), the diagnosis of
pregnancy can be made even earlier than is possible with transabdominal
ultrasonography (TAUS). US has long been used in uncomplicated pregnancies for
dating and as a screening examination for fetal anomalies. US is not typically used
to diagnose pregnancy unless the patient presents with vaginal bleeding or
abdominal pain early in gestation or is a high-risk obstetric patient. TVUS is the
most accurate means of confirming intrauterine pregnancy and gestational age
during the early first trimester.
TVUS has several advantages over TAUS during early pregnancy. TVUS can help
detect signs of intrauterine pregnancy approximately 1 week earlier than TAUS.
Patients are not required to have a full bladder and are not required to endure
uncomfortable pressure on the abdominal wall from the external probe. TVUS is
also better for patients who are obese or those who guard during TAUS. One
disadvantage is that some patients are anxious about the transvaginal probe and
may object to its insertion.
Vaginal probes are typically of higher frequency (5-8 MHz) than abdominal probes
(3-5 MHz). The higher frequency allows for better resolution of the image but less
penetration of the signal. Also, practice is necessary for familiarization with the
orientation on the US monitor when performing TVUS.
The earliest structure identified is the (GS). The GS can be seen on TVUS images
by 4-5 weeks' gestation and grows at a rate of 1 mm/d in early gestation. By 5.5-6
weeks' gestation, a double-decidual sign can be seen, which is the GS surrounded
by the thickened decidua. The presence of an early GS can be confused with a
small collection of fluid or blood or the pseudo GS of an ectopic pregnancy.
Because of this, the diagnosis of intrauterine pregnancy should not be made on the
basis of visualization of the GS alone.
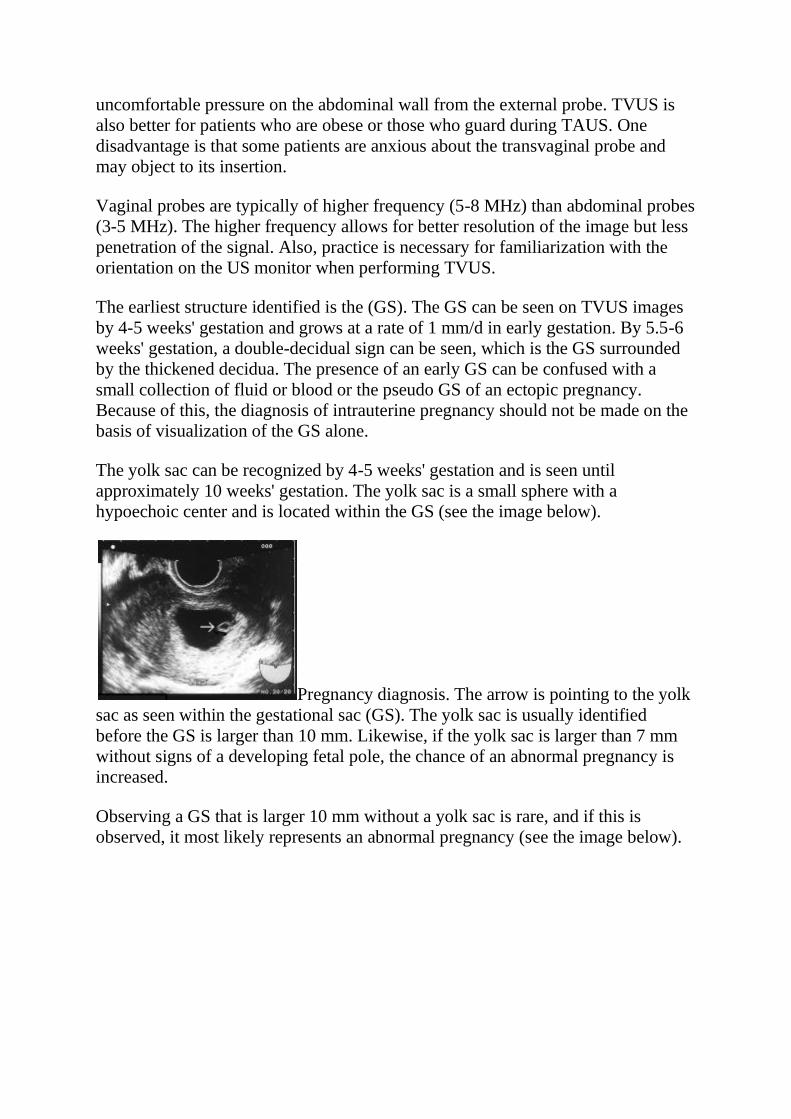
The yolk sac can be recognized by 4-5 weeks' gestation and is seen until
approximately 10 weeks' gestation. The yolk sac is a small sphere with a
hypoechoic center and is located within the GS (see the image below).
Pregnancy diagnosis. The arrow is pointing to the yolk
sac as seen within the gestational sac (GS). The yolk sac is usually identified
before the GS is larger than 10 mm. Likewise, if the yolk sac is larger than 7 mm
without signs of a developing fetal pole, the chance of an abnormal pregnancy is
increased.
Observing a GS that is larger 10 mm without a yolk sac is rare, and if this is
observed, it most likely represents an abnormal pregnancy (see the image below).
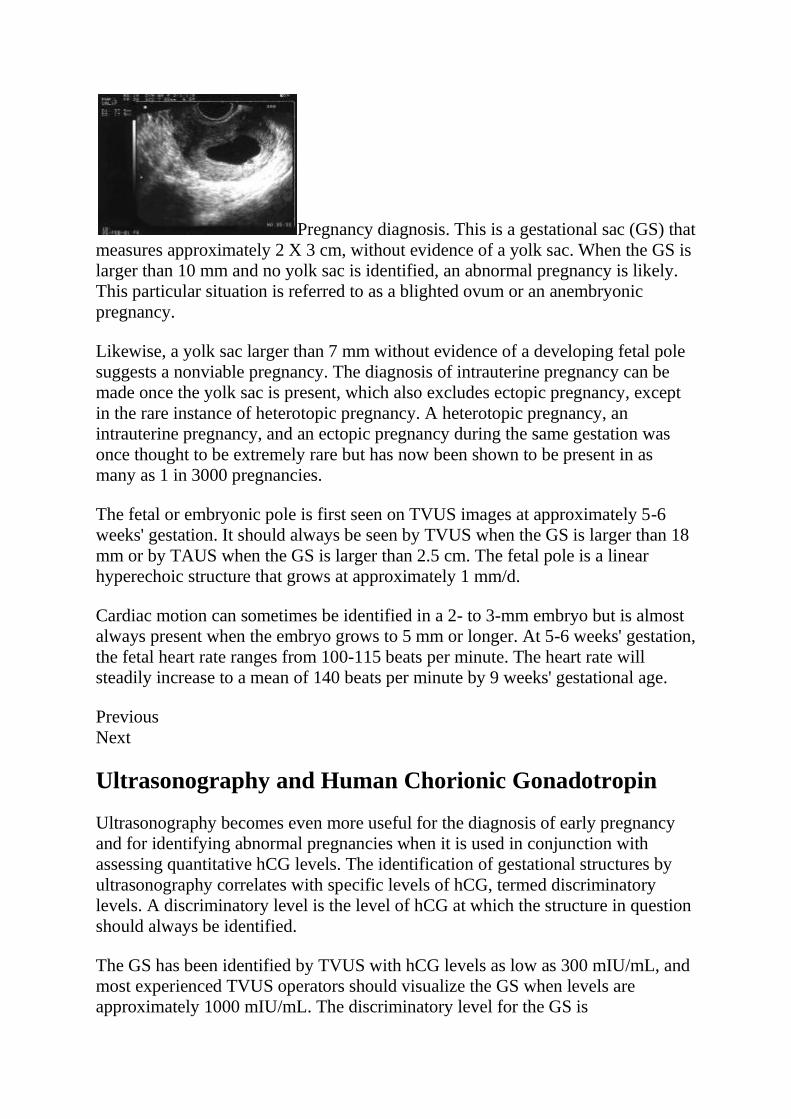
Pregnancy diagnosis. This is a gestational sac (GS) that
measures approximately 2 X 3 cm, without evidence of a yolk sac. When the GS is
larger than 10 mm and no yolk sac is identified, an abnormal pregnancy is likely.
This particular situation is referred to as a blighted ovum or an anembryonic
pregnancy.
Likewise, a yolk sac larger than 7 mm without evidence of a developing fetal pole
suggests a nonviable pregnancy. The diagnosis of intrauterine pregnancy can be
made once the yolk sac is present, which also excludes ectopic pregnancy, except
in the rare instance of heterotopic pregnancy. A heterotopic pregnancy, an
intrauterine pregnancy, and an ectopic pregnancy during the same gestation was
once thought to be extremely rare but has now been shown to be present in as
many as 1 in 3000 pregnancies.
The fetal or embryonic pole is first seen on TVUS images at approximately 5-6
weeks' gestation. It should always be seen by TVUS when the GS is larger than 18
mm or by TAUS when the GS is larger than 2.5 cm. The fetal pole is a linear
hyperechoic structure that grows at approximately 1 mm/d.
Cardiac motion can sometimes be identified in a 2- to 3-mm embryo but is almost
always present when the embryo grows to 5 mm or longer. At 5-6 weeks' gestation,
the fetal heart rate ranges from 100-115 beats per minute. The heart rate will
steadily increase to a mean of 140 beats per minute by 9 weeks' gestational age.
Previous
Next
Ultrasonography and Human Chorionic Gonadotropin
Ultrasonography becomes even more useful for the diagnosis of early pregnancy
and for identifying abnormal pregnancies when it is used in conjunction with
assessing quantitative hCG levels. The identification of gestational structures by
ultrasonography correlates with specific levels of hCG, termed discriminatory
levels. A discriminatory level is the level of hCG at which the structure in question
should always be identified.
The GS has been identified by TVUS with hCG levels as low as 300 mIU/mL, and
most experienced TVUS operators should visualize the GS when levels are
approximately 1000 mIU/mL. The discriminatory level for the GS is
approximately 3600 mIU/mL, and if it is not seen at this point, other pathology
must be excluded. Many use a more conservative discriminatory level for the GS,
at 2000 mIU/mL by TVUS and 3600 mIU/ml by TAUS, and will begin to rule out
pathology if the GS is not seen. The adnexa should be scanned for an ectopic
pregnancy, and sonograms and hCG levels should be followed until a diagnosis is
made. Furthermore, one study showed that all viable intrauterine pregnancies had a
GS identified by TAUS for hCG levels of greater than 6500 mIU/mL.
The usefulness of TVUS evaluation when the hCG is less than 1000 mIU/mL has
been debated. One study showed that valuable information can still be garnered in
women presenting for emergent TVUS with an hCG level of less than 1000
mIU/mL. In this study, approximately 13% of the abnormal intrauterine
pregnancies and 39% of the ectopic pregnancies were identified by TVUS.
Ultrasonography should not be delayed purely on the basis of hCG levels.[16]
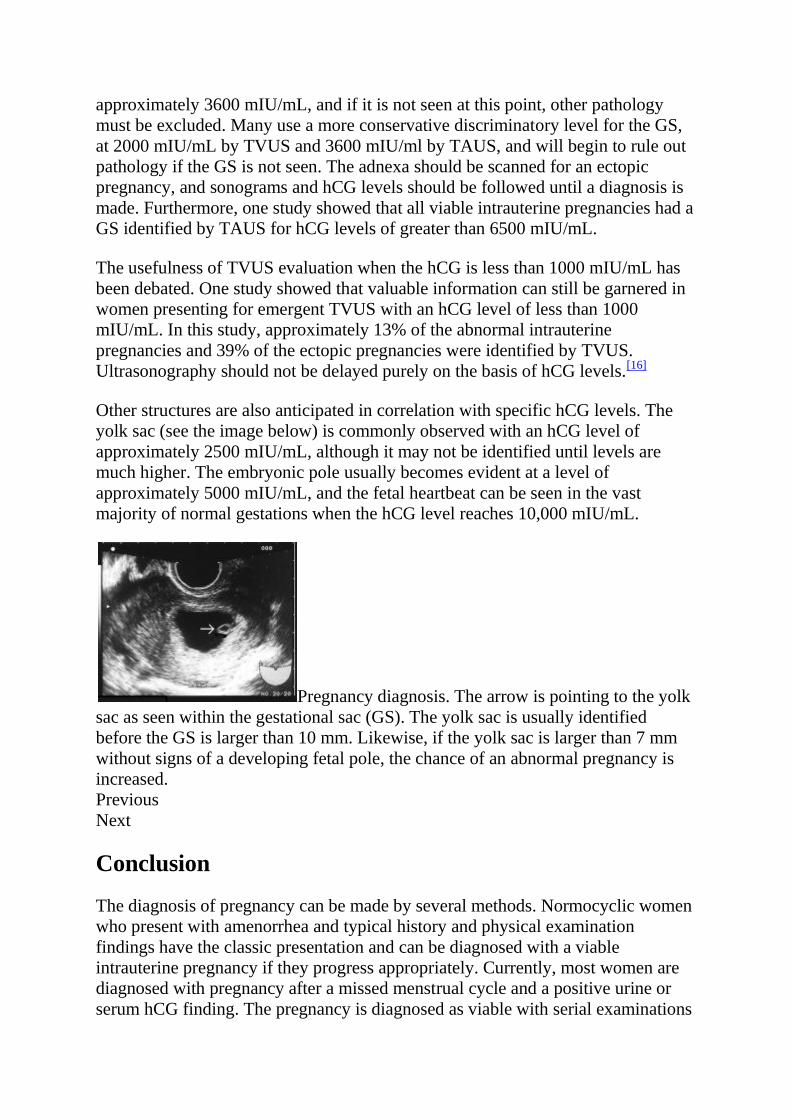
Other structures are also anticipated in correlation with specific hCG levels. The
yolk sac (see the image below) is commonly observed with an hCG level of
approximately 2500 mIU/mL, although it may not be identified until levels are
much higher. The embryonic pole usually becomes evident at a level of
approximately 5000 mIU/mL, and the fetal heartbeat can be seen in the vast
majority of normal gestations when the hCG level reaches 10,000 mIU/mL.
Pregnancy diagnosis. The arrow is pointing to the yolk
sac as seen within the gestational sac (GS). The yolk sac is usually identified
before the GS is larger than 10 mm. Likewise, if the yolk sac is larger than 7 mm
without signs of a developing fetal pole, the chance of an abnormal pregnancy is
increased.
Previous
Next
Conclusion
The diagnosis of pregnancy can be made by several methods. Normocyclic women
who present with amenorrhea and typical history and physical examination
findings have the classic presentation and can be diagnosed with a viable
intrauterine pregnancy if they progress appropriately. Currently, most women are
diagnosed with pregnancy after a missed menstrual cycle and a positive urine or
serum hCG finding. The pregnancy is diagnosed as viable with serial examinations
and normal pregnancy development, a normal result after dating ultrasonography,
or a positive finding of fetal heart tones using Doppler studies.
Women who are considered high-risk or those who present with abdominal pain or
vaginal bleeding in early gestation are more likely to be evaluated with
ultrasonography and additional hormonal assays. A number of different
combinations can aid in the diagnosis of a viable intrauterine pregnancy. The
physician must ascertain what is most appropriate at the time of patient
presentation.
For excellent patient education resources, visit eMedicineHealth's Pregnancy
Center. Also, see eMedicineHealth's patient education articles Home Pregnancy
Test, Ectopic Pregnancy, Birth Control Overview, and Birth Control Methods.
Previous
Contributor Information and Disclosures
Author
Andrea D Shields, MD, FACOG Chief of Obstetrics, Wright Patterson Medical
Center; Assistant Professor, Department of Obstetrics and Gynecology, Uniformed
Services University of the Health Sciences
Andrea D Shields, MD, FACOG is a member of the following medical
societies: Alpha Omega Alpha, American College of Obstetricians and
Gynecologists, American Institute of Ultrasound in Medicine, American Medical
Association, Association of Women Surgeons, and Society for Maternal-Fetal
Medicine
Disclosure: Nothing to disclose.
Specialty Editor Board
Bruce A Meyer, MD, MBA Executive Vice President for Health System Affairs,
Executive Director, Faculty Practice Plan, Professor, Department of Obstetrics and
Gynecology, University of Texas Southwestern Medical School
Bruce A Meyer, MD, MBA is a member of the following medical
societies: American College of Obstetricians and Gynecologists, American College
of Physician Executives, American Institute of Ultrasound in
Medicine, Association of Professors of Gynecology and Obstetrics, Massachusetts
Medical Society, Medical Group Management Association, and Society for
Maternal-Fetal Medicine
Disclosure: Nothing to disclose.
Francisco Talavera, PharmD, PhD Adjunct Assistant Professor, University of
Nebraska Medical Center College of Pharmacy; Editor-in-Chief, Medscape Drug
Reference
Disclosure: Medscape Salary Employment
Frederick B Gaupp, MD Consulting Staff, Department of Family Practice,
Hancock Medical Center
Frederick B Gaupp, MD is a member of the following medical societies: American
Academy of Family Physicians
Disclosure: Nothing to disclose.
Chief Editor
Christine Isaacs, MD Associate Professor, Department of Obstetrics and
Gynecology, Division Head, General Obstetrics and Gynecology, Medical Director
of Midwifery Services, Virginia Commonwealth University School of Medicine
Christine Isaacs, MD is a member of the following medical societies: American
College of Obstetricians and Gynecologists
Disclosure: Nothing to disclose.
Additional Contributors
The authors and editors of Medscape Reference gratefully acknowledge the
contributions of previous authors Randle L Likes, DO and Eric Rittenhouse, MD,
FACOG to the development and writing of this article.







![Kuretase [Dr. Endang]](https://static.fdokumen.com/doc/165x107/55cf989b550346d03398a0da/kuretase-dr-endang.jpg)