







Bahasa
Halaman
Hukum

ORIGINAL PAPER
VEP asymmetry with ophthalmological and MRI findingsin two achiasmatic children
Jelka Brecelj Æ Branka Stirn-Kranjc ÆNuska Pecaric-Meglic Æ Miha Skrbec
Received: 5 July 2006 / Accepted: 6 December 2006 / Published online: 13 January 2007� Springer Science+Business Media B.V. 2007
Abstract Achiasmia is a rarely diagnosed visual
pathway maldevelopment where all or the major-
ity of nasal retinal fibres fail to decussate at the
optic chiasm. It has been identified by neuroi-
maging and also by visual evoked potential
(VEP) asymmetry. VEP asymmetry has not been
defined consistently in previous studies. The aim
was to study VEP asymmetry to flash stimulation
in two children with maldevelopment of the optic
chiasm in comparison to control children. Both
children had congenital nystagmus, optic nerve
hypoplasia with a bilateral small double ring,
bitemporal visual field defect and normal colour
vision. In child 1 visual acuity in both eyes was
0.1, in child 2 it was 0.2. MRI showed reduced
chiasmal size in child 1, while in child 2 it was
combined with other midline abnormalities. VEP
to monocular flash stimulation showed in both
children distinctive occipital distribution, which
was not observed in control children. The N2
wave was distributed asymmetrically over the
ipsilateral hemisphere to the stimulated eye,
while the P2 wave was distributed over both
hemispheres. The P2 wave was however better
defined over the ipsilateral hemisphere. Flash
VEP occipital distribution remained similar in
child 1, who was followed from 10 months to
9 years. These cases of achiasmia demonstrate a
distinctive VEP asymmetry in the distribution of
the flash VEP N2 wave, as well as the expected
structural defect determined by neuroimaging.
Keywords Achiasmia � Bitemporal visual field
defect � Nystagmus � Optic nerve hypoplasia �Optic chiasm � Septo-optic dysplasia � Visual
evoked potentials
Introduction
In the visual pathway optic nerve fibres from the
nasal part of each retina decussate at the optic
chiasm and project to the contralateral hemi-
sphere. A congenital visual pathway maldevelop-
ment, in which optic nerve fibres from the nasal
half of each retina fail to decussate, was first
detected by visual evoked potentials (VEP).
Apkarian et al. [1] demonstrated in two children
that optic nerve fibres from the nasal retina did
not cross at the chiasm, but projected to the
ipsilateral instead of the contralateral visual
cortex. This achiasmatic condition was confirmed
by MRI and reported as the non-decussating
retinal-fugal fibre syndrome. In further studies, a
J. Brecelj (&) � B. Stirn-KranjcUnit for Visual Electrophysiology, Eye Clinic,University Medical Centre, 1525 Ljubljana, Sloveniae-mail: [email protected]
N. Pecaric-Meglic � M. SkrbecClinical Institute for Radiology, University MedicalCentre, Ljubljana, Slovenia
123
Doc Ophthalmol (2007) 114:53–65
DOI 10.1007/s10633-006-9037-6

small number of children with absence or defi-
ciency of optic nerve fibres that cross over at the
optic chiasm, have also been presented [2–9].
Ophthalmological findings in achiasmia and
chiasmal hypoplasia were shown to be associated
with congenital nystagmus. See-saw, rotatory or
purely horizontal nystagmus were noted. Visual
fields were normal or abnormal, but bitemporal
hemianopia was not reported. Optic discs ap-
peared normal or hypoplastic. MRI findings
showed complete achiasmia as an isolated devel-
opmental abnormality, or were found together
with other midline abnormalities (a review in [7]).
Electrophysiological features that distin-
guished absent or reduced chiasmal decussation
had not been reported consistently in previous
studies. Apkarian et al. [1, 2] found ipsilateral
asymmetric occipital distribution to onset stimu-
lation in two achiasmatic children and to flash
stimulation in one of them. It was demonstrated
that the peak of the potential distribution was
lateralized over the left hemisphere following left
eye stimulation and shifted to the right hemi-
sphere following right eye stimulation. Leitch
et al. [3] reported that the main positivity was
recorded over the contralateral visual cortex to
flash stimulation in a child with no chiasm.
Thompson et al. [4] described a crossed asymme-
try occipital distribution to flash stimulation in
five children with achiasmia or chiasmal hypopla-
sia. A waveform, which was shown from one
child, was described as a negative peak at 80–
100 ms at the channel ipsilateral to the stimulated
eye and a positive peak at the channel contralat-
eral to the stimulated eye. Jansonius et al. [5]
showed that a positive wave around 150–200 ms
was lateralised over the hemisphere on the side of
the stimulated eye to flash stimulation in one
achiasmatic child. Korff et al. [6] reported ipsi-
lateral asymmetry to flash and pattern onset
stimulation in one achiasmatic child. Sami et al.
[7] reported crossed contralateral positvity to
flash stimulation in a review of nine achiasmatic
children, while they presented waveforms in only
two of them. In a recent study, VEP crossed
asymmetry was reported to the left eye flash
stimulation, while to the right eye stimulation was
VEP attenuated and prolonged in a child
with achiasmia and optic nerve hypoplasia [8].
A number of these studies showed that recording
differential potentials between hemispheric chan-
nels was helpful in demonstrating abnormal optic
pathway decussation in achiasmia and chiasmal
hypoplasia [1, 2, 4, 6–8]. Some studies did not
define components or their polarities within VEP
asymmetries [6–9].
So far in literature, a small number of VEP
waveforms in children with achiasmia or chiasmal
hypoplasia have been reported, unfortunately
there is no consistency in the reporting of asym-
metrical occipital distributions. This gives us a
good reason to present two more children with
achiasmia in which VEP asymmetry was studied
to flash stimulation and compared to control
children. Ophthalmological and electrophysiolog-
ical follow-up and MRI findings were also stud-
ied. Both children were defined as achiasmatic
according to Sami et al. [7], who described
achiasmia as an absence or relative lack of
crossing fibres at the optic chiasm.
Subjects and methods
The study was approved by the Slovene Research
and Medical Ethics Committee. Two boys were
referred in infancy because of congenital nystag-
mus, both of whom had a normal neurological
and psychomotor development and attend regular
school. Electrophysiological features were also
studied in 16 control children (mean 5 years;
range 4–7.6 years).
Ophthalmological examination
Child 1 was presented for ophthalmological eval-
uation at 9 months and child 2 at 2 months of age.
Both had complete eye examinations and had
been followed-up for over 7 years. Visual acuity
tests for near and distance (Jaeger, L. Hyvarinnen
system, Teller Acuity Cards, Cambridge Acuity
cards, standard optotypes), refractive error
(retinoscopy, ultrasound biometric measure-
ments, Retinomax and Humphrey automated
refractometers), contrast sensitivity testing
(Vision Optotech), colour vision (Ishihara tables,
Farnsworth 15 hue) and visual fields (Goldmann
perimetry, automated Octopus G2 top) were
54 Doc Ophthalmol (2007) 114:53–65
123

evaluated. Ocular fundus morphology was vali-
dated by fundus digital image analysis.
Electrophysiological examination
Both were followed, child 1 from 10 months till
9 years and child 2 from 2 months till 7 years.
Child 1 was recorded at 10 months, 5, 6 and
9 years to binocular and monocular flash stimu-
lation, while child 2 was recorded at 2 and
9 months only to binocular flash stimulation and
at 6 and 7 years to binocular and monocular flash
stimulation. Flash VEP, which was tested from
child 2 at 2 and 9 months only to binocular
stimulation, was found abnormal for age and
reported as suspected for visual pathway dysfunc-
tion. In both children were simultaneously re-
corded also electroretinograms (ERG) to flash
stimulation with skin electrodes and without pupil
dilatation. Flash ERG were normal for age at all
recordings from both children [10].
VEP were recorded from three electrodes
applied to the posterior scalp according to Kriss
and co-workers [11], who introduced this montage
in paediatric electrophysiology: the midline elec-
trode was placed at Oz (International 10–20
system, 10% of the nasion-to-inion separation),
while the electrode over the right hemisphere
(O2’) and the electrode over the left hemisphere
(O1’) were placed to either side of the midline
electrode (halfway between Oz and the mastoid,
approximately 4 cm). VEP electrodes were refer-
red to Fz. ERG were recorded by skin electrodes
(disposable Nicolet electrodes) attached to the
lower eyelid and referred to Fz [10, 11].
ERG and VEP activity (Espion Diagnosys
LLC, Littleton, MA) was recorded to white
flashes elicited with a Grass PS33 plus (Astro-
Med Inc, West Wanwick, Rhode Island, USA)
flash stimulator (intensity setting 4) which was
hand held at a distance of 20 cm. The flash
intensity was 455 cd s/m2 (calibrated with inte-
grating photometer International Light IL1700,
Newburyport, Massachusetts, USA). The stimu-
lation rate of flash was 3 Hz. The analysis time
was 300 ms (with a 10 ms pre-stimulus interval).
The band pass was 0.3–300 Hz. Each time 100
responses were averaged and repeated at least
twice.
VEP recordings were analysed to monocular
stimulation. Amplitudes (peak to peak) and laten-
cies were measured at channels O2’ (right hemi-
sphere), O1’ (left hemisphere) and O1’-O2’
(channel which showed the difference in potentials
between the left and right hemisphere). A negative
wave (N2) and a positive wave (P2) were analysed
in control children and in children with achiasmia.
The nomenclature used was according to ISCEV
standards [12] and for evaluation of peak latencies
and polarities of waves in children was considered
a review [13] and our normative data.
MRI examination
Magnetic resonance images were obtained with a
1.5 T system (General Electric, Signa Horizon) in
both children. In child 1 Spin Echo (SE) T1-
weighted images (TR/TE 460/15 ms, 5.0 mm slice
thkickness (thk), 1.5 mm interslice space (sp)) and
Fast Spin Echo (FSE) T2-weighted images (TR/
TE 3000/82.5 ms, 5.0 mm thk, 1.5 mm sp) in the
axial plane, FSE T2-weighted coronal images
through the anterior visual pathways (TR/TE
4800/88.6 ms, 3.0 mm thk, 1.5 mm sp) and SE
T1-weighted images (TR/TE 420/18 ms, 3.0 mm
thk, 0.3 mm sp) in the oblique axial, coronal and
sagittal planes through the anterior visual path-
ways were performed. In child 2 3-D spoiled
gradient echo sequences (3DSPGR: TR/TE 30/6
ms) with reconstructions (1.4 mm thk, 0.0 mm sp)
in the sagittal, coronal and oblique axial planes
through the anterior visual pathways, FSE T2
weighted images (TR/TE 4000/98.2 ms, 3.0 mm
thk, 0.1 mm sp) in the axial and coronal planes and
Fluid-Attenuated Inversion Recovery (FLAIR:
TR/TE/TI 8777/133/2193 ms, 5.0 mm thk, 0.5 mm
sp) in the axial plane were performed.
Results
Ophthalmological findings
Both children studied and followed up had
horizontal nystagmus of low frequency and
amplitude with a vertical component, but no
signs of a see-saw nystagmus, and also both had a
very mild convergent concomitant alternate stra-
bismus. Their anterior eye segments and optic
Doc Ophthalmol (2007) 114:53–65 55
123
media were normal and there was no evident
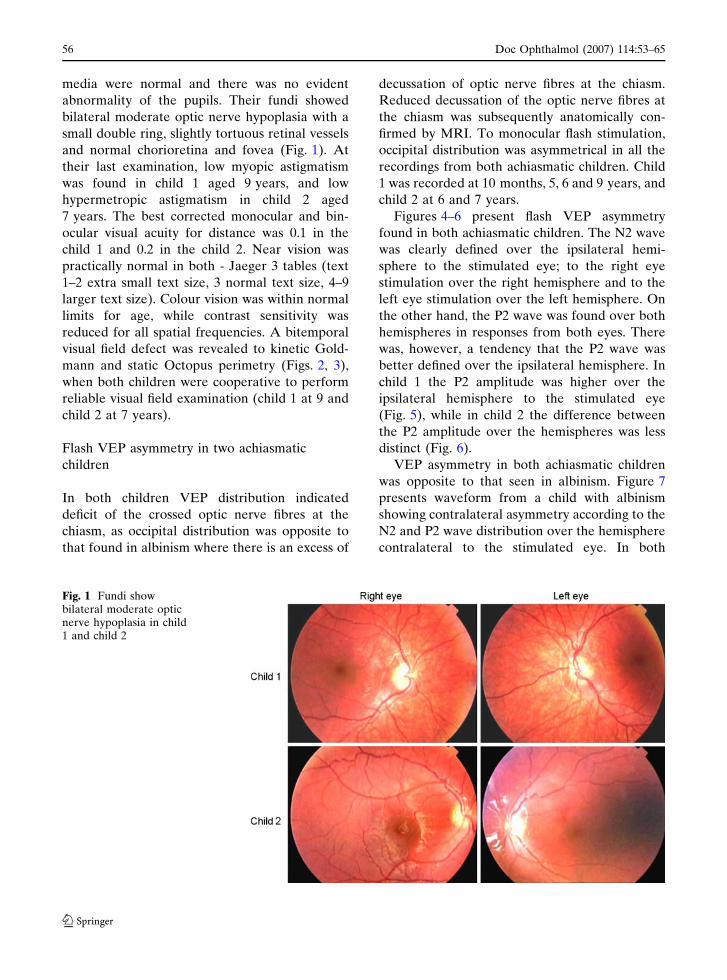
abnormality of the pupils. Their fundi showed
bilateral moderate optic nerve hypoplasia with a
small double ring, slightly tortuous retinal vessels
and normal chorioretina and fovea (Fig. 1). At
their last examination, low myopic astigmatism
was found in child 1 aged 9 years, and low
hypermetropic astigmatism in child 2 aged
7 years. The best corrected monocular and bin-
ocular visual acuity for distance was 0.1 in the
child 1 and 0.2 in the child 2. Near vision was
practically normal in both - Jaeger 3 tables (text
1–2 extra small text size, 3 normal text size, 4–9
larger text size). Colour vision was within normal
limits for age, while contrast sensitivity was
reduced for all spatial frequencies. A bitemporal
visual field defect was revealed to kinetic Gold-
mann and static Octopus perimetry (Figs. 2, 3),
when both children were cooperative to perform
reliable visual field examination (child 1 at 9 and
child 2 at 7 years).
Flash VEP asymmetry in two achiasmatic
children
In both children VEP distribution indicated
deficit of the crossed optic nerve fibres at the
chiasm, as occipital distribution was opposite to
that found in albinism where there is an excess of
decussation of optic nerve fibres at the chiasm.
Reduced decussation of the optic nerve fibres at
the chiasm was subsequently anatomically con-
firmed by MRI. To monocular flash stimulation,
occipital distribution was asymmetrical in all the
recordings from both achiasmatic children. Child
1 was recorded at 10 months, 5, 6 and 9 years, and
child 2 at 6 and 7 years.
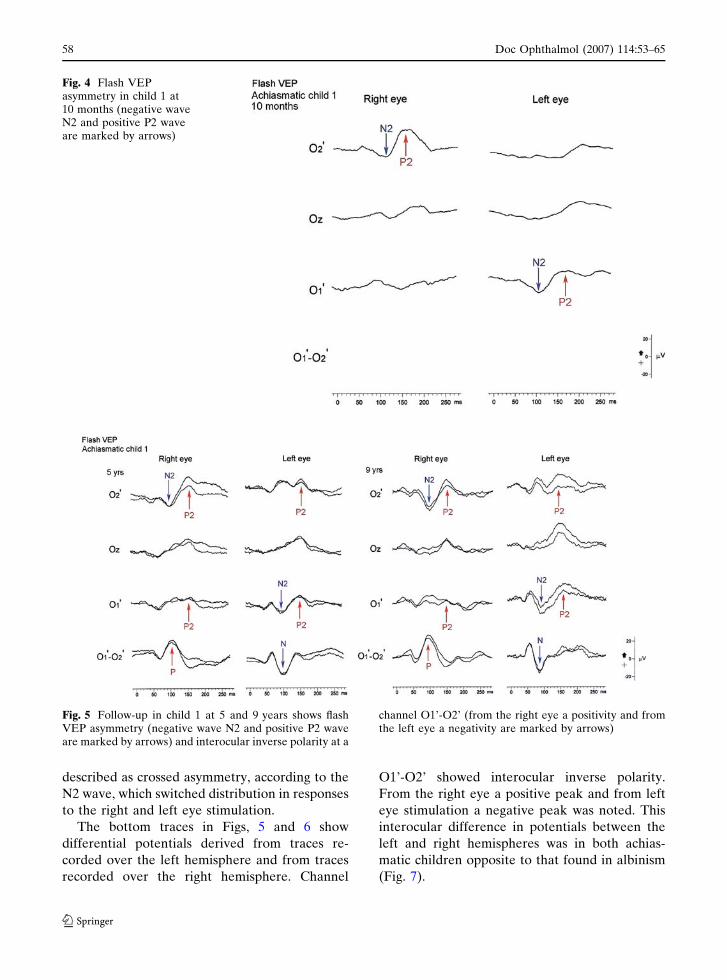
Figures 4–6 present flash VEP asymmetry
found in both achiasmatic children. The N2 wave
was clearly defined over the ipsilateral hemi-
sphere to the stimulated eye; to the right eye
stimulation over the right hemisphere and to the
left eye stimulation over the left hemisphere. On
the other hand, the P2 wave was found over both
hemispheres in responses from both eyes. There
was, however, a tendency that the P2 wave was
better defined over the ipsilateral hemisphere. In
child 1 the P2 amplitude was higher over the
ipsilateral hemisphere to the stimulated eye
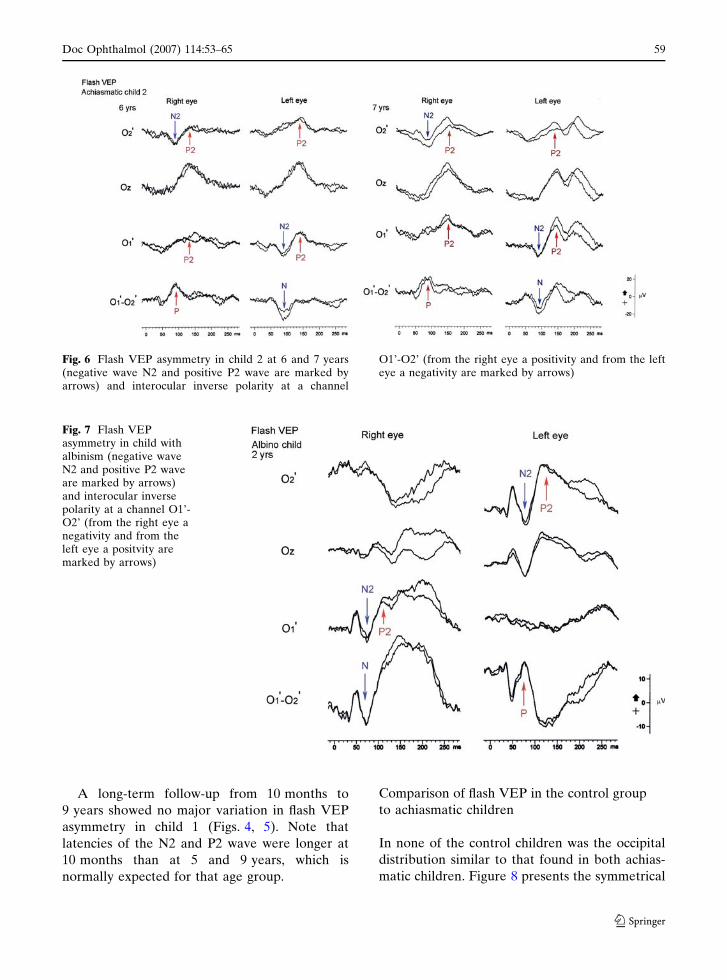
(Fig. 5), while in child 2 the difference between
the P2 amplitude over the hemispheres was less
distinct (Fig. 6).
VEP asymmetry in both achiasmatic children
was opposite to that seen in albinism. Figure 7
presents waveform from a child with albinism
showing contralateral asymmetry according to the
N2 and P2 wave distribution over the hemisphere
contralateral to the stimulated eye. In both
Fig. 1 Fundi showbilateral moderate opticnerve hypoplasia in child1 and child 2
56 Doc Ophthalmol (2007) 114:53–65
123

achiasmatic children ipsilateral asymmetry was
seen according to the lateralization of the N2
wave over the ipsilateral hemisphere to the
stimulated eye. In addition the P2 wave was
better defined over the ipsilateral hemisphere. On
the other hand, the asymmetry could be also
Fig. 2 Bitemporal visualfield defect is shown byGoldmann and Octopusperimetry in child 1 at9 years of age
Fig. 3 Bitemporal visualfield defect is shown byGoldmann and Octopusperimetry in child 2 at7 years of age
Doc Ophthalmol (2007) 114:53–65 57
123
described as crossed asymmetry, according to the
N2 wave, which switched distribution in responses
to the right and left eye stimulation.
The bottom traces in Figs, 5 and 6 show
differential potentials derived from traces re-
corded over the left hemisphere and from traces
recorded over the right hemisphere. Channel
O1’-O2’ showed interocular inverse polarity.
From the right eye a positive peak and from left
eye stimulation a negative peak was noted. This
interocular difference in potentials between the
left and right hemispheres was in both achias-
matic children opposite to that found in albinism
(Fig. 7).
Fig. 4 Flash VEPasymmetry in child 1 at10 months (negative waveN2 and positive P2 waveare marked by arrows)
Fig. 5 Follow-up in child 1 at 5 and 9 years shows flashVEP asymmetry (negative wave N2 and positive P2 waveare marked by arrows) and interocular inverse polarity at a
channel O1’-O2’ (from the right eye a positivity and fromthe left eye a negativity are marked by arrows)
58 Doc Ophthalmol (2007) 114:53–65
123
A long-term follow-up from 10 months to
9 years showed no major variation in flash VEP
asymmetry in child 1 (Figs. 4, 5). Note that
latencies of the N2 and P2 wave were longer at
10 months than at 5 and 9 years, which is
normally expected for that age group.
Comparison of flash VEP in the control group
to achiasmatic children
In none of the control children was the occipital
distribution similar to that found in both achias-
matic children. Figure 8 presents the symmetrical
Fig. 6 Flash VEP asymmetry in child 2 at 6 and 7 years(negative wave N2 and positive P2 wave are marked byarrows) and interocular inverse polarity at a channel
O1’-O2’ (from the right eye a positivity and from the lefteye a negativity are marked by arrows)
Fig. 7 Flash VEPasymmetry in child withalbinism (negative waveN2 and positive P2 waveare marked by arrows)and interocular inversepolarity at a channel O1’-O2’ (from the right eye anegativity and from theleft eye a positvity aremarked by arrows)
Doc Ophthalmol (2007) 114:53–65 59
123

occipital distribution of the N2 and P2 wave to the
right and left eye stimulation in a control child.
Such symmetrical occipital distribution appeared
in some control children. In others, asymmetrical
occipital distribution was also seen as attenuation
of the N2 and P2 wave over the same hemisphere
to the right and left eye stimulation. The bottom
trace in Fig. 8 shows differential potentials
derived from traces recorded over the left hemi-
sphere and from traces recorded over the right
hemisphere in a control child. In none of the
control children a positive peak was found to the
right eye stimulation and a negative peak to the
left eye stimulation as was evident in both
achiasmatic children.
Figure 9 compares the N2 and P2 wave ampli-
tude and latency data for both achiasmatic
children from 5 recordings (for child 1 at 5, 6
and 9 years for child 2 at 6 and 7 years) and for
age-matched controls. Latency and amplitude
values of the P2 wave were similar over both
hemispheres to right and left eye stimulation in
both the control and achiasmatic children. There
was a difference in the N2 amplitude, but not in
the N2 latency, between the two groups. The N2
amplitude was similar over both hemispheres to
stimulation of both eyes in controls, while the N2
amplitude was obtained over the right hemi-
sphere to the right eye stimulation and over the
left hemisphere to the left eye stimulation in both
achiasmatic children.
MRI findings
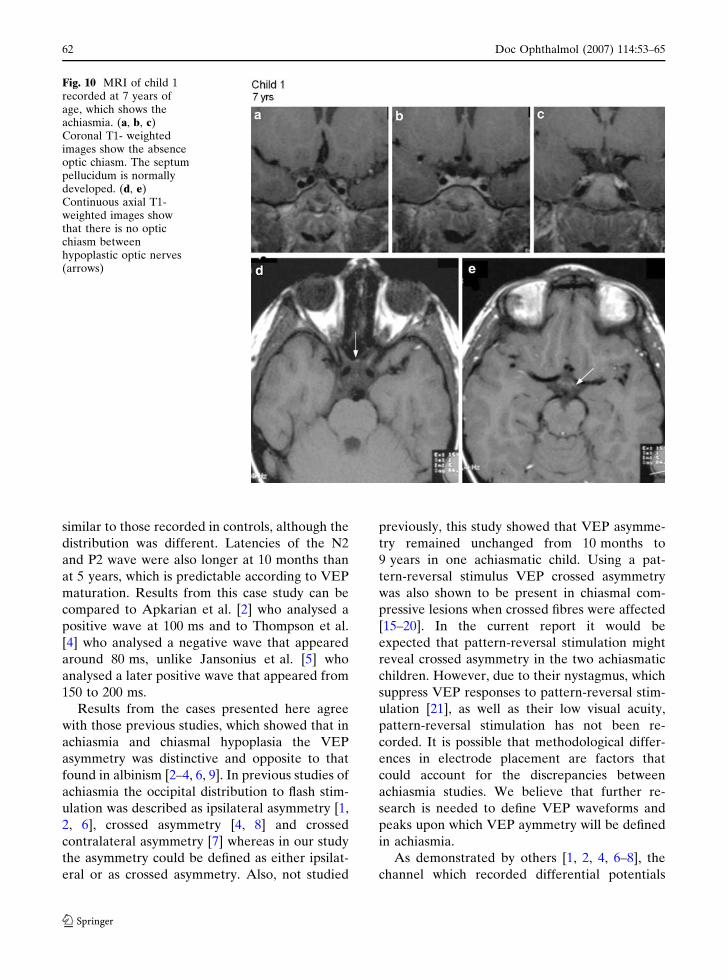
In child 1 MRI examination was performed at age
seven years. Images showed absence of the optic
chiasm. Both posterior parts of the optic nerves
were hypoplastic, the right more than the left, and
they continued posteriorly into the hypoplastic
optic tracts. Pituitary gland, septum pellucidum,
and other brain structures were normal (Fig. 10).
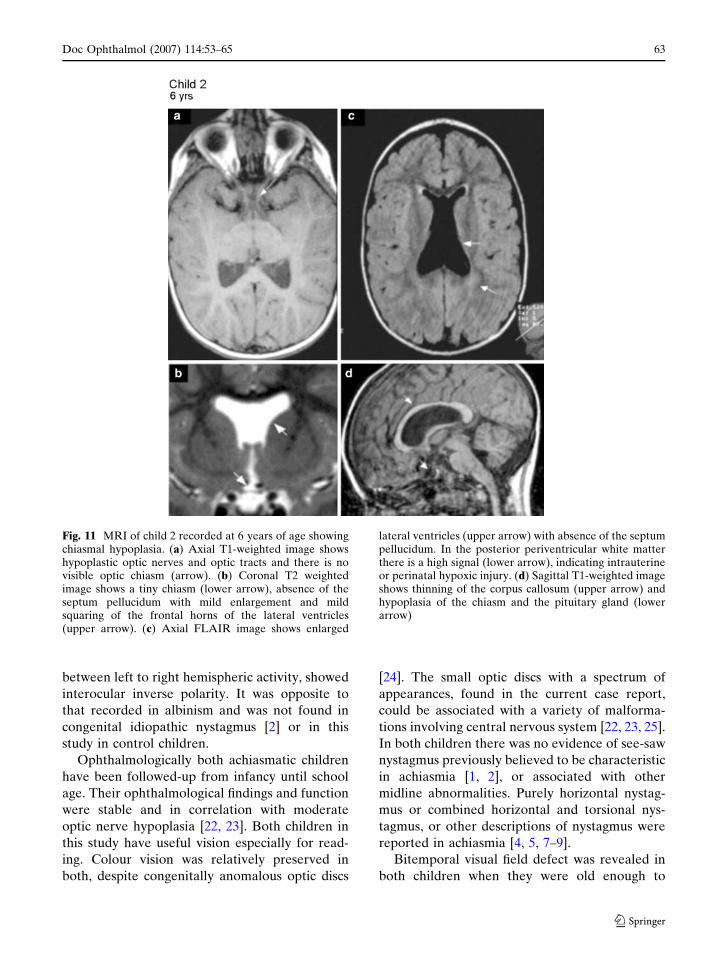
In child 2 MRI was performed at age six years.
Images showed hypoplasia in optic nerves, chiasm
and tracts, especially the chiasm. The infundibu-
lum and pituitary gland were very small, hypo-
plastic. The septum pellucidum was absent and
corpus callosum was thinner. Both lateral ventri-
cles were enlarged and periventricular white
matter was diminished with high signal changes
on FLAIR images, indicating possible mild peri-
ventricular leucomalacia after intrauterine or
perinatal hypoxic injury (Fig. 11).
Fig. 8 Flash VEPdistribution of the N2 andP2 wave in a control child
60 Doc Ophthalmol (2007) 114:53–65
123
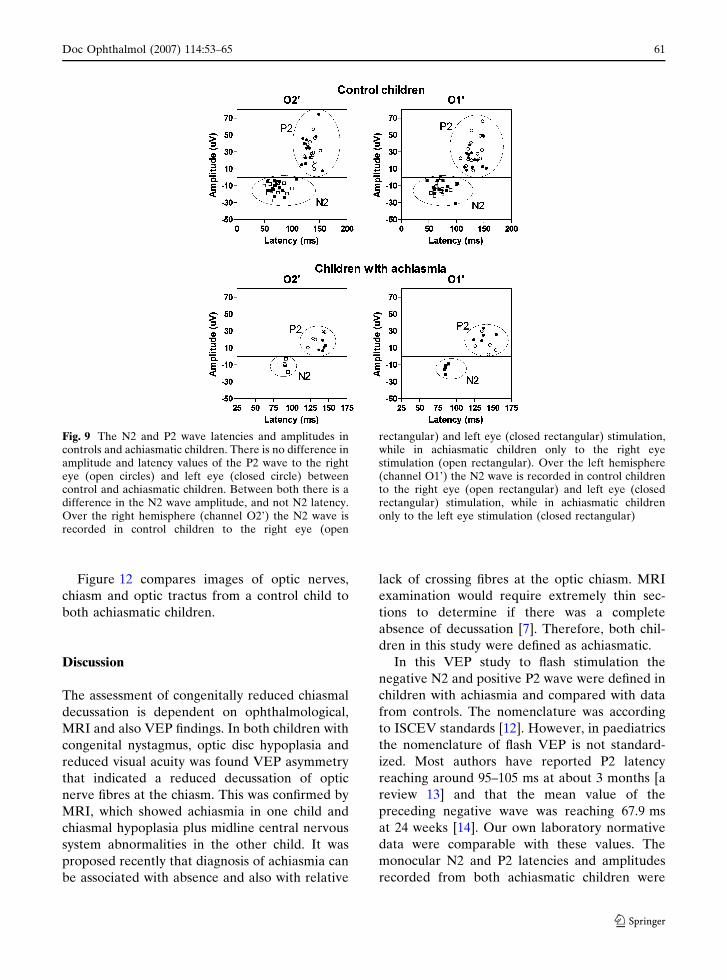
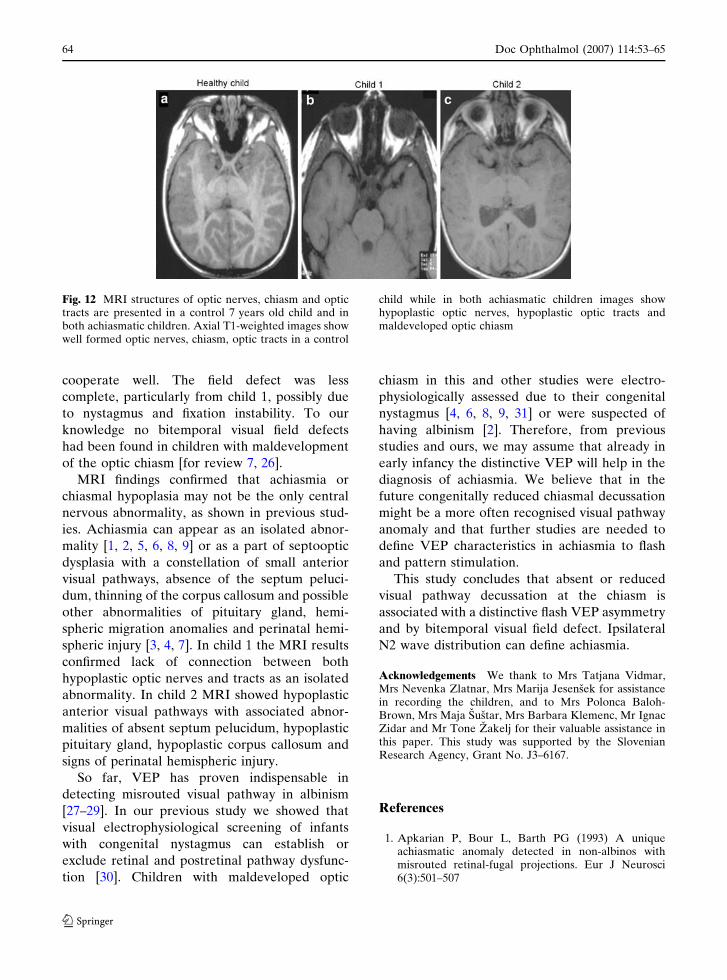
Figure 12 compares images of optic nerves,
chiasm and optic tractus from a control child to
both achiasmatic children.
Discussion
The assessment of congenitally reduced chiasmal
decussation is dependent on ophthalmological,
MRI and also VEP findings. In both children with
congenital nystagmus, optic disc hypoplasia and
reduced visual acuity was found VEP asymmetry
that indicated a reduced decussation of optic
nerve fibres at the chiasm. This was confirmed by
MRI, which showed achiasmia in one child and
chiasmal hypoplasia plus midline central nervous
system abnormalities in the other child. It was
proposed recently that diagnosis of achiasmia can
be associated with absence and also with relative
lack of crossing fibres at the optic chiasm. MRI
examination would require extremely thin sec-
tions to determine if there was a complete
absence of decussation [7]. Therefore, both chil-
dren in this study were defined as achiasmatic.
In this VEP study to flash stimulation the
negative N2 and positive P2 wave were defined in
children with achiasmia and compared with data
from controls. The nomenclature was according
to ISCEV standards [12]. However, in paediatrics
the nomenclature of flash VEP is not standard-
ized. Most authors have reported P2 latency
reaching around 95–105 ms at about 3 months [a
review 13] and that the mean value of the
preceding negative wave was reaching 67.9 ms
at 24 weeks [14]. Our own laboratory normative
data were comparable with these values. The
monocular N2 and P2 latencies and amplitudes
recorded from both achiasmatic children were
Fig. 9 The N2 and P2 wave latencies and amplitudes incontrols and achiasmatic children. There is no difference inamplitude and latency values of the P2 wave to the righteye (open circles) and left eye (closed circle) betweencontrol and achiasmatic children. Between both there is adifference in the N2 wave amplitude, and not N2 latency.Over the right hemisphere (channel O2’) the N2 wave isrecorded in control children to the right eye (open
rectangular) and left eye (closed rectangular) stimulation,while in achiasmatic children only to the right eyestimulation (open rectangular). Over the left hemisphere(channel O1’) the N2 wave is recorded in control childrento the right eye (open rectangular) and left eye (closedrectangular) stimulation, while in achiasmatic childrenonly to the left eye stimulation (closed rectangular)
Doc Ophthalmol (2007) 114:53–65 61
123
similar to those recorded in controls, although the
distribution was different. Latencies of the N2
and P2 wave were also longer at 10 months than
at 5 years, which is predictable according to VEP
maturation. Results from this case study can be
compared to Apkarian et al. [2] who analysed a
positive wave at 100 ms and to Thompson et al.
[4] who analysed a negative wave that appeared
around 80 ms, unlike Jansonius et al. [5] who
analysed a later positive wave that appeared from
150 to 200 ms.
Results from the cases presented here agree
with those previous studies, which showed that in
achiasmia and chiasmal hypoplasia the VEP
asymmetry was distinctive and opposite to that
found in albinism [2–4, 6, 9]. In previous studies of
achiasmia the occipital distribution to flash stim-
ulation was described as ipsilateral asymmetry [1,
2, 6], crossed asymmetry [4, 8] and crossed
contralateral asymmetry [7] whereas in our study
the asymmetry could be defined as either ipsilat-
eral or as crossed asymmetry. Also, not studied
previously, this study showed that VEP asymme-
try remained unchanged from 10 months to
9 years in one achiasmatic child. Using a pat-
tern-reversal stimulus VEP crossed asymmetry
was also shown to be present in chiasmal com-
pressive lesions when crossed fibres were affected
[15–20]. In the current report it would be
expected that pattern-reversal stimulation might
reveal crossed asymmetry in the two achiasmatic
children. However, due to their nystagmus, which
suppress VEP responses to pattern-reversal stim-
ulation [21], as well as their low visual acuity,
pattern-reversal stimulation has not been re-
corded. It is possible that methodological differ-
ences in electrode placement are factors that
could account for the discrepancies between
achiasmia studies. We believe that further re-
search is needed to define VEP waveforms and
peaks upon which VEP aymmetry will be defined
in achiasmia.
As demonstrated by others [1, 2, 4, 6–8], the
channel which recorded differential potentials
Fig. 10 MRI of child 1recorded at 7 years ofage, which shows theachiasmia. (a, b, c)Coronal T1- weightedimages show the absenceoptic chiasm. The septumpellucidum is normallydeveloped. (d, e)Continuous axial T1-weighted images showthat there is no opticchiasm betweenhypoplastic optic nerves(arrows)
62 Doc Ophthalmol (2007) 114:53–65
123
between left to right hemispheric activity, showed
interocular inverse polarity. It was opposite to
that recorded in albinism and was not found in
congenital idiopathic nystagmus [2] or in this
study in control children.
Ophthalmologically both achiasmatic children
have been followed-up from infancy until school
age. Their ophthalmological findings and function
were stable and in correlation with moderate
optic nerve hypoplasia [22, 23]. Both children in
this study have useful vision especially for read-
ing. Colour vision was relatively preserved in
both, despite congenitally anomalous optic discs
[24]. The small optic discs with a spectrum of
appearances, found in the current case report,
could be associated with a variety of malforma-
tions involving central nervous system [22, 23, 25].
In both children there was no evidence of see-saw
nystagmus previously believed to be characteristic
in achiasmia [1, 2], or associated with other
midline abnormalities. Purely horizontal nystag-
mus or combined horizontal and torsional nys-
tagmus, or other descriptions of nystagmus were
reported in achiasmia [4, 5, 7–9].
Bitemporal visual field defect was revealed in
both children when they were old enough to
Fig. 11 MRI of child 2 recorded at 6 years of age showingchiasmal hypoplasia. (a) Axial T1-weighted image showshypoplastic optic nerves and optic tracts and there is novisible optic chiasm (arrow). (b) Coronal T2 weightedimage shows a tiny chiasm (lower arrow), absence of theseptum pellucidum with mild enlargement and mildsquaring of the frontal horns of the lateral ventricles(upper arrow). (c) Axial FLAIR image shows enlarged
lateral ventricles (upper arrow) with absence of the septumpellucidum. In the posterior periventricular white matterthere is a high signal (lower arrow), indicating intrauterineor perinatal hypoxic injury. (d) Sagittal T1-weighted imageshows thinning of the corpus callosum (upper arrow) andhypoplasia of the chiasm and the pituitary gland (lowerarrow)
Doc Ophthalmol (2007) 114:53–65 63
123
cooperate well. The field defect was less
complete, particularly from child 1, possibly due
to nystagmus and fixation instability. To our
knowledge no bitemporal visual field defects
had been found in children with maldevelopment
of the optic chiasm [for review 7, 26].
MRI findings confirmed that achiasmia or
chiasmal hypoplasia may not be the only central
nervous abnormality, as shown in previous stud-
ies. Achiasmia can appear as an isolated abnor-
mality [1, 2, 5, 6, 8, 9] or as a part of septooptic
dysplasia with a constellation of small anterior
visual pathways, absence of the septum peluci-
dum, thinning of the corpus callosum and possible
other abnormalities of pituitary gland, hemi-
spheric migration anomalies and perinatal hemi-
spheric injury [3, 4, 7]. In child 1 the MRI results
confirmed lack of connection between both
hypoplastic optic nerves and tracts as an isolated
abnormality. In child 2 MRI showed hypoplastic
anterior visual pathways with associated abnor-
malities of absent septum pelucidum, hypoplastic
pituitary gland, hypoplastic corpus callosum and
signs of perinatal hemispheric injury.
So far, VEP has proven indispensable in
detecting misrouted visual pathway in albinism
[27–29]. In our previous study we showed that
visual electrophysiological screening of infants
with congenital nystagmus can establish or
exclude retinal and postretinal pathway dysfunc-
tion [30]. Children with maldeveloped optic
chiasm in this and other studies were electro-
physiologically assessed due to their congenital
nystagmus [4, 6, 8, 9, 31] or were suspected of
having albinism [2]. Therefore, from previous
studies and ours, we may assume that already in
early infancy the distinctive VEP will help in the
diagnosis of achiasmia. We believe that in the
future congenitally reduced chiasmal decussation
might be a more often recognised visual pathway
anomaly and that further studies are needed to
define VEP characteristics in achiasmia to flash
and pattern stimulation.
This study concludes that absent or reduced
visual pathway decussation at the chiasm is
associated with a distinctive flash VEP asymmetry
and by bitemporal visual field defect. Ipsilateral
N2 wave distribution can define achiasmia.
Acknowledgements We thank to Mrs Tatjana Vidmar,Mrs Nevenka Zlatnar, Mrs Marija Jesensek for assistancein recording the children, and to Mrs Polonca Baloh-Brown, Mrs Maja Sustar, Mrs Barbara Klemenc, Mr IgnacZidar and Mr Tone Zakelj for their valuable assistance inthis paper. This study was supported by the SlovenianResearch Agency, Grant No. J3–6167.
References
1. Apkarian P, Bour L, Barth PG (1993) A uniqueachiasmatic anomaly detected in non-albinos withmisrouted retinal-fugal projections. Eur J Neurosci6(3):501–507
Fig. 12 MRI structures of optic nerves, chiasm and optictracts are presented in a control 7 years old child and inboth achiasmatic children. Axial T1-weighted images showwell formed optic nerves, chiasm, optic tracts in a control
child while in both achiasmatic children images showhypoplastic optic nerves, hypoplastic optic tracts andmaldeveloped optic chiasm
64 Doc Ophthalmol (2007) 114:53–65
123
2. Apkarian P, Bour LJ, Barth PG, Wenninger-Prick L,Verbeeten B (1995) Non-decussating retinal-fugal fibresyndrome. An inborn achiasmatic malformationassociated with visuotopic misrouting, visual evokedpotential ipsilateral asymmetry and nystagmus. Brain118:1195–1216
3. Leitch RJ, Thompson D, Harris CM, Chong K,Russell-Eggitt I, Kriss A (1996) Achiasmia in a caseof midline craniofacial cleft with seesaw nystagmus. BrJ Ophthalmol 80:1023–1024
4. Thompson DA, Kriss A, Chong K, Harris C, Russell-Eggitt I, Shawkat F, Neville BGR, Aclimandos W,Taylor DSI (1999) Visual evoked potential evidence ofchiasmal hypoplasia. Ophthalmology 106:2354–2361
5. Jansonius NM, van der Vliet TAM, Cornelissen FW,Pott JWR, Kooijman AC (2001) A girl without achiasm: electrophysiologic and MRI evidence for theabsence of crossing optic nerve fibers in a girl with acongential nystagmus. J Neuroophthalmol 21(1):26–29
6. Korff CM, Apkarian P, Bour LJ, Meuli R, Verrey JD,Roulet Perez E (2003) Isolated absence of optic chiasmrevealed by congenital nystagmus, MRI and VEPs.Neuropediatrics 34:219–223
7. Sami DA, Saunders D, Thompson DA, Russell-EggittIM, Nischal KK, Jeffery G, Dattani M, Clement RA,Liassis A, Taylor DS (2005) The achiasmia spectrum:congenitally reduced chiasmal decussation. Br JOphthalmol 89:1311–1317
8. Pomeranz HD, Agadzi AK, Ekesten B (2006)Achiasmia and unilateral nerve hypoplasia in anotherwise healthy subject. Acta Ophthalmol Scand84:140–144
9. Brown MC, Southern CL, Anbarasu A, Kaye SB,Fisher AC, Hagan RP, Newman WD (2006)Congenital absence of optic chiasm: demonstration ofan uncrossed visual pathway using monocular flashvisual evoked potentials. Doc Ophthalmol 113(1):1–4
10. Brecelj J, Stirn-Kranjc B, Lenassi E, Likar K (2006)Recording ERG and VEP in infants and children.Ophthalmol Croat, in press
11. Kriss T, Jeffrey B, Taylor D (1992) Theelectroretinogram in infants and young children. JClin Neurophysiol 9:373–393
12. Odom JV, Bach M, Barber C, Brigell M, Marmor MF,Tormene AP, Holder GE, Vaegan (2004) Visualevoked potentials standard. Doc Ophthalmol108:115–123
13. Harden A (1982) Maturation of the visual evokedpotentials. In: Chiarenza GA, Papakostopoulos (eds)Clinical application of cerebral evoked potentials inpediatric medicine. Amsterdam: Excerpta Medica pp.41–59
14. Benavente I, Tamargo P, Tajada N, Yuste V, OlivanMJ (2005) Flash visually evoked potentials in thenewborn and their maturation during the first sixmonths of life. Doc Ophthalmol 110:255–263
15. Halliday AM, Halliday E, Kriss A, McDonald WI,Mushin J (1976) The pattern-evoked potential incompression of the anterior visual pathways. Brain99(2):357–374
16. Brecelj J, Denislic M, Skrbec M (1989) Visual evokedpotential abnormalities in chiasmal lesions. DocOphthalmol 73:139–148
17. Brecelj J, Strucl M, Skrbec M (1992) Visual evokedpotentials in compressive lesions of the optic chiasm.Neuro-ophthamol 12(4):207–214
18. Brecelj J (1992) A VEP study of the visual pathwayfunction in compressive lesions of the optic chiasm.Full-field versus half-field stimulation.Electroencephalogr Clin Neurophysiol 84(3):209–218
19. Halliday AM (1993) Evoked potentials in clinicaltesting, 2nd edition. Edinburgh: Churchill Livingstone
20. Brecelj J (1994) Electrodiagnostics of chiasmalcompressive lesions. Int J Psychophysiol 16:263–272
21. Hoffmann MB, Seufert PS, Bach M (2004) Simulatednystagmus suppresses pattern-reversal but not pattern-onset visual evoked potentials. Clin Neurophysiol115(11):2659–2665
22. Brodsky MC, Glasier CM (1993) Optic nervehypoplasia. Arch Ophthalmol 111:66–74
23. Hellstrom A, Wiklund LM, Svensson E (1999) Theclinical and morphologic spectrum of optic nervehypoplasia. J AAPOS 3(4):212–220
24. Brodsky MC (1994) Major review. Congenital opticdisk anomalies. Surv Ophthalmol 39(2):89–112
25. Fahnenhjelm TK, Wide K, Flodmark O, Ek U,Hellstrom A (2003) Posterior ocular malformationsin children: somatic, neuroradiologic and cognitiveaspects. Acta Paediatr 92(3):301–308
26. Victor JD, Apkarian P, Hirsch J, Conte MM, PackardM, Relkin NR, Kim KHS, Shapley RM (2000) Visualfunction and brain organization in non-decussatingretinal-fugal fibre syndrome. Cereb Cortex 10(1):2–22
27. Apkarian P, Reits D, Spekreijse H, Dorp van D (1983)A decisive electrophysiological test for humanalbinism. Electroencephalogr Clin Neurophysiol55(5):513–531
28. Kriss A, Russell-Eggitt I, Taylor D (1990) Childhoodalbinism. Visual electrophysiological features.Ophthalmol Paediatr Genet 11(3):185–192
29. Dorey SE, Neveu MM, Burton LC, Sloper JJ, HolderGE (2003) The clinical features of albinism and theircorrelation with visual evoked potentials. Br JOphthalmol 87:767–772
30. Brecelj J, Stirn-Kranjc B (2004) Visualelectrophysiological screening in diagnosing infantswith congenital nystagmus. Clin Neurophysiol115(2):461–470
31. Kriss A (1996) Nystagmus and pediatric visualelectrophysiology . In: Kimura J, Shibasaki H (eds)Recent advances in clinical neurophysiology.Amsterdam: Elsevier, pp. 480–487
Doc Ophthalmol (2007) 114:53–65 65
123
Top Related
Copyright © 2022 FDOKUMEN

