







Bahasa
Halaman
Hukum

J Oral Maxillofac Surg70:e43-e50, 2012
Effect of Drilling Dimension on ImplantPlacement Torque and Early
Osseointegration Stages: An ExperimentalStudy in Dogs
Felipe E. Campos, DDS,* Julio B. Gomes, DDS,†
Charles Marin, DDS, PhD,‡ Hellen S. Teixeira, DDS,§
Marcelo Suzuki, DDS,¶ Lukasz Witek, MSc,�Darceny Zanetta-Barbosa, DDS, PhD,# and
Paulo G. Coelho, DDS, PhD**
Purpose: Primary stability has been regarded as a key factor to ensure uneventful osseointegration ofdental implants. Such stability is often achieved by placing implants in undersized drilled bone. Thepresent study evaluated the effect of drilling dimensions in insertion torque and early implant osseointe-gration stages in a beagle dog model.
Materials and Methods: Six beagle dogs were acquired and subjected to bilateral surgeries in the radii1 and 3 weeks before death. During surgery, 3 implants, 4 mm in diameter by 10 mm in length, wereplaced in bone sites drilled to 3.2 mm, 3.5 mm, and 3.8 mm in diameter. The insertion torque wasrecorded for all samples. After death, the implants in bone were nondecalcified processed and morpho-logically and morphometrically (bone-to-implant contact and bone area fraction occupancy) evaluated.Statistical analyses were performed using the Kruskal-Wallis test followed by Dunn’s post hoc test formultiple comparisons at the 95% level of significance.
Results: The insertion torque levels obtained were inversely proportional to the drilling dimension,with a significant difference detected between the 3.2-mm and 3.8-mm groups (P � .003). Despite asignificant increase in the bone-to-implant contact over time in vivo for all groups (P � .007), no effectfor the drilling dimension was observed. Additionally, no effect of the drilling dimension and time wasobserved for the bone area fraction occupancy parameter (P � .31). The initial healing pathways differedbetween implants placed in bone drilled to different dimensions.
Conclusions: Although different degrees of torque were observed with different drilling dimensionsand these resulted in different healing patterns, no differences in the histometrically evaluated parame-ters were observed.© 2012 American Association of Oral and Maxillofacial Surgeons
J Oral Maxillofac Surg 70:e43-e50, 2012*Department of Oral and Maxillofacial Surgery, Universidade Fed-
eral de Uberlandia, Minas Gerias, Brazil.
†Department of Oral and Maxillofacial Surgery, Universidade
Federal de Uberlandia, Minas Gerias, Brazil.
‡Department of Oral and Maxillofacial Surgery, Universidade
Federal de Santa Catarina, Florianopolis, Brazil.
§Department of Biomaterials and Biomimetics, New York Uni-
versity, New York, NY.
¶Department of Prosthodontics, Tufts University School of Den-
tal Medicine, Boston, MA.
�Department of Biomaterials and Biomimetics, New York Univer-
sity, New York, NY.
#Department of Oral and Maxillofacial Surgery, Universidade
Federal de Uberlandia, Minas Gerias, Brazil.
**Department of Biomaterials and Biomimetics, New York Uni-
versity, New York, NY.
Address correspondence and reprint requests to Lukasz Witek:
Department Biomaterials and Biomimetics, New York University,
345 East 24th Street, Room 813S, New York, NY 10010; e-mail:
© 2012 American Association of Oral and Maxillofacial Surgeons
0278-2391/12/7001-0$36.00/0
doi:10.1016/j.joms.2011.08.006
e43

csm
iithichamdtfftms
e44 DRILLING DIMENSION EFFECT ON TORQUE AND OSSEOINTEGRATION
The use of dental implants to replace missing teethhas become one of the most successful treatmentmodalities in dental practice. Despite the predictabil-ity of the conventional protocol involving 2 surgicalstages established by Brånemark et al,1,2 the quest fordecreased treatment periods between device place-ment and its subsequent functional loading has fos-tered implant engineering design modifications at dif-ferent length scales.3 Of special interest is thehallenge of immediate/early functional loading ofingle implant crowns that, unlike multiple units, lackutual or cross-arch stabilization,4,5 resulting in de-
creased primary stability that is strongly influenced bythe combination of implant design, loading condi-tions, surgical technique, and bone density and qual-ity.6
From a clinical perspective, the consensus is thatimplant stability immediately and early after place-ment is desirable, because the relative motion be-tween implant and bone could risk osseointegra-tion.2,7,8 Thus, implant and surgical drilling techniqueinterplay that provides high degrees of implant pri-mary stability, low levels of compressive stress imme-diately after placement, and low degrees of micromo-tion have been regarded as potential benefits in thequest for atemporal implant stability during the earlystages of osseointegration. Considering that implantstability is influenced by the interplay between im-plant design and the surrounding bone, it has beensuggested that a high peak insertion torque is desir-able for improved implant stability during osseointe-gration,9–11 especially because these studies haveshown that high insertion torque values prevent ad-verse micromovement under loading greater than 100�m. In contrast, several studies have suggested thathigh insertion torque values do not necessarily trans-late into high degrees of primary stability.12–14
Although changing the design parameters are in-sightful from a purely engineering standpoint, it mustbe considered that bone is a dynamic tissue that willrespond to surgical procedure stimulation and/or theinteraction between the implant macrogeometry andits associated drilling dimensions.15
The ideal condition of implant atemporal stabilityduring the early healing periods has been questioned,because several biomechanical and histologic studieshave shown that even if implant primary stability isrendered during placement, owing to the initial re-modeling and subsequent bone apposition, a decreasein implant stability is likely to be observed before thebridging of the old bone and implant surface rendersthe system with secondary stability.16 –18 Such arationale has led to the presumption that if oste-oclastic activity undermines primary stability be-
fore new bone formation prevents implant micro-motion, a stability decrease will take place earlyafter implantation.19
It is common practice to use “underdimensioned”drilling dimensions in an attempt to increase the pri-mary stability.9 However, although greater degrees ofnsertion torque levels can be achieved by placingmplants in sites of undersized dimensions, the host-o-implant early response can be affected, becauseigh degrees of bone mechanical strain can evolve
mmediately after placement. Although the ever-in-reasing number of published studies on this topicas shed light on different aspects of implant designnd primary stability, the complexity of the possibleultivariable interaction, including different implant
esigns, drilling dimension and implant geometry in-erplay, and timetables for the initiation of implantunction has not yet provided an informed platformor implant/prosthetic system design rationale. Thus,he present study evaluated the effect of drilling di-ensions on insertion torque and early implant os-
eointegration stages in a beagle dog model.
Materials and Methods
Thirty-six, commercially pure grade 2, threaded en-dosseous implants, 4 mm in diameter and 10 mm inlength (Colosso, Emfils, Itu, Brazil), with a grit-blastedand acid-etched surface, were used. For the laboratoryin vivo model, 6 adult male beagle dogs approxi-mately 1.5 years old were acquired after the approvalof the Ethics Committee for Animal Research at Uni-versidade Federal de Uberlandia, Brazil.
Before general anesthesia, intramuscular atropinesulfate (0.044 mg/kg) and xylazine chlorate (8 mg/kg)were administered. A 15 mg/kg ketamine chloratedose was then used to achieve general anesthesia.
The surgical site was the central region of theradius diaphysis. After hair shaving, skin exposure,and antiseptic cleaning with iodine solution at thesurgical and surrounding area, an �5-cm length inci-sion to access the periosteum was performed and aflap reflected for bone exposure.
Three implants were placed along the radius fromproximal to distal in an alternated distribution, withstarting drilling dimension (3.2-, 3.5-, and 3.8-mm finaldrill diameter) interchanged in every radius to mini-mize bias from the different implantation sites (sites 1to 3 from proximal to distal). Therefore, the 36 im-plants of the drilling technique, remaining in vivo foreither 1 or 3 weeks (right and left radii providedsamples that remained in vivo for 1 and 3 weeks,respectively), were allocated to sites 1 to 3 in an equaldistribution. This approach resulted in balanced sur-gical procedures that allowed the comparison of thesame number of implant surfaces per time in vivo,
limb, surgical site (1 through 3), and animal. The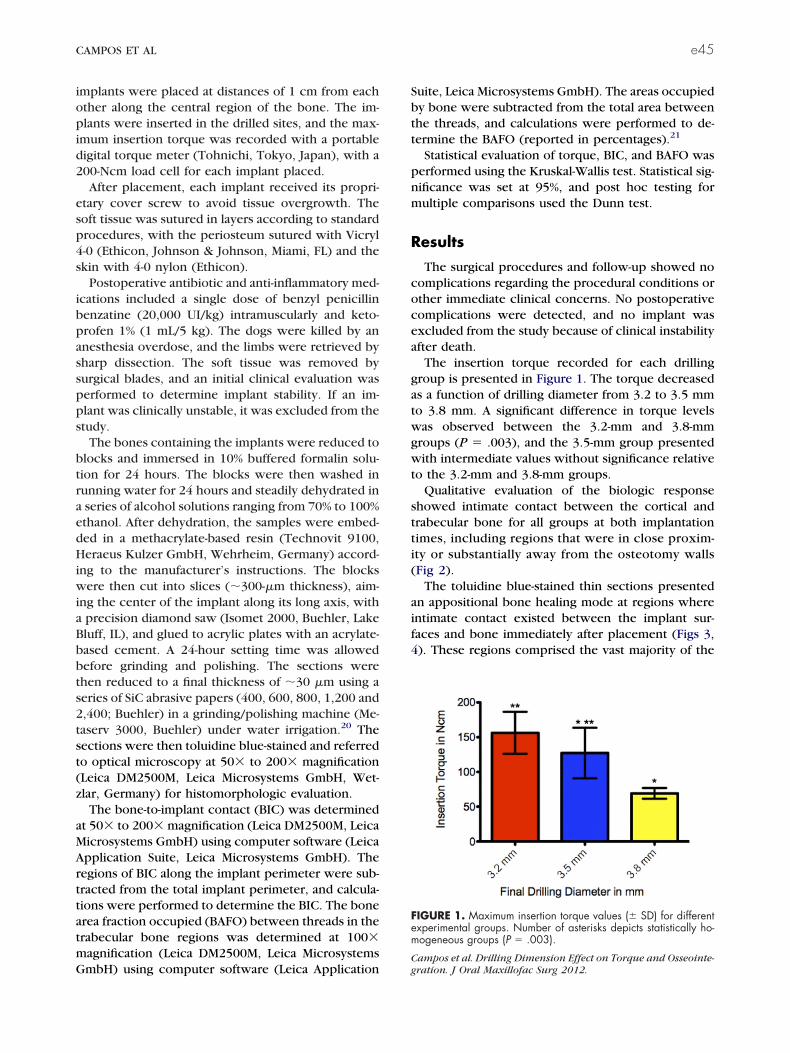
s2t
CAMPOS ET AL e45
implants were placed at distances of 1 cm from eachother along the central region of the bone. The im-plants were inserted in the drilled sites, and the max-imum insertion torque was recorded with a portabledigital torque meter (Tohnichi, Tokyo, Japan), with a200-Ncm load cell for each implant placed.
After placement, each implant received its propri-etary cover screw to avoid tissue overgrowth. Thesoft tissue was sutured in layers according to standardprocedures, with the periosteum sutured with Vicryl4-0 (Ethicon, Johnson & Johnson, Miami, FL) and theskin with 4-0 nylon (Ethicon).
Postoperative antibiotic and anti-inflammatory med-ications included a single dose of benzyl penicillinbenzatine (20,000 UI/kg) intramuscularly and keto-profen 1% (1 mL/5 kg). The dogs were killed by ananesthesia overdose, and the limbs were retrieved bysharp dissection. The soft tissue was removed bysurgical blades, and an initial clinical evaluation wasperformed to determine implant stability. If an im-plant was clinically unstable, it was excluded from thestudy.
The bones containing the implants were reduced toblocks and immersed in 10% buffered formalin solu-tion for 24 hours. The blocks were then washed inrunning water for 24 hours and steadily dehydrated ina series of alcohol solutions ranging from 70% to 100%ethanol. After dehydration, the samples were embed-ded in a methacrylate-based resin (Technovit 9100,Heraeus Kulzer GmbH, Wehrheim, Germany) accord-ing to the manufacturer’s instructions. The blockswere then cut into slices (�300-�m thickness), aim-ing the center of the implant along its long axis, witha precision diamond saw (Isomet 2000, Buehler, LakeBluff, IL), and glued to acrylic plates with an acrylate-based cement. A 24-hour setting time was allowedbefore grinding and polishing. The sections werethen reduced to a final thickness of �30 �m using aeries of SiC abrasive papers (400, 600, 800, 1,200 and,400; Buehler) in a grinding/polishing machine (Me-aserv 3000, Buehler) under water irrigation.20 The
sections were then toluidine blue-stained and referredto optical microscopy at 50� to 200� magnification(Leica DM2500M, Leica Microsystems GmbH, Wet-zlar, Germany) for histomorphologic evaluation.
The bone-to-implant contact (BIC) was determinedat 50� to 200� magnification (Leica DM2500M, LeicaMicrosystems GmbH) using computer software (LeicaApplication Suite, Leica Microsystems GmbH). Theregions of BIC along the implant perimeter were sub-tracted from the total implant perimeter, and calcula-tions were performed to determine the BIC. The bonearea fraction occupied (BAFO) between threads in thetrabecular bone regions was determined at 100�magnification (Leica DM2500M, Leica Microsystems
GmbH) using computer software (Leica ApplicationSuite, Leica Microsystems GmbH). The areas occupiedby bone were subtracted from the total area betweenthe threads, and calculations were performed to de-termine the BAFO (reported in percentages).21
Statistical evaluation of torque, BIC, and BAFO wasperformed using the Kruskal-Wallis test. Statistical sig-nificance was set at 95%, and post hoc testing formultiple comparisons used the Dunn test.
Results
The surgical procedures and follow-up showed nocomplications regarding the procedural conditions orother immediate clinical concerns. No postoperativecomplications were detected, and no implant wasexcluded from the study because of clinical instabilityafter death.
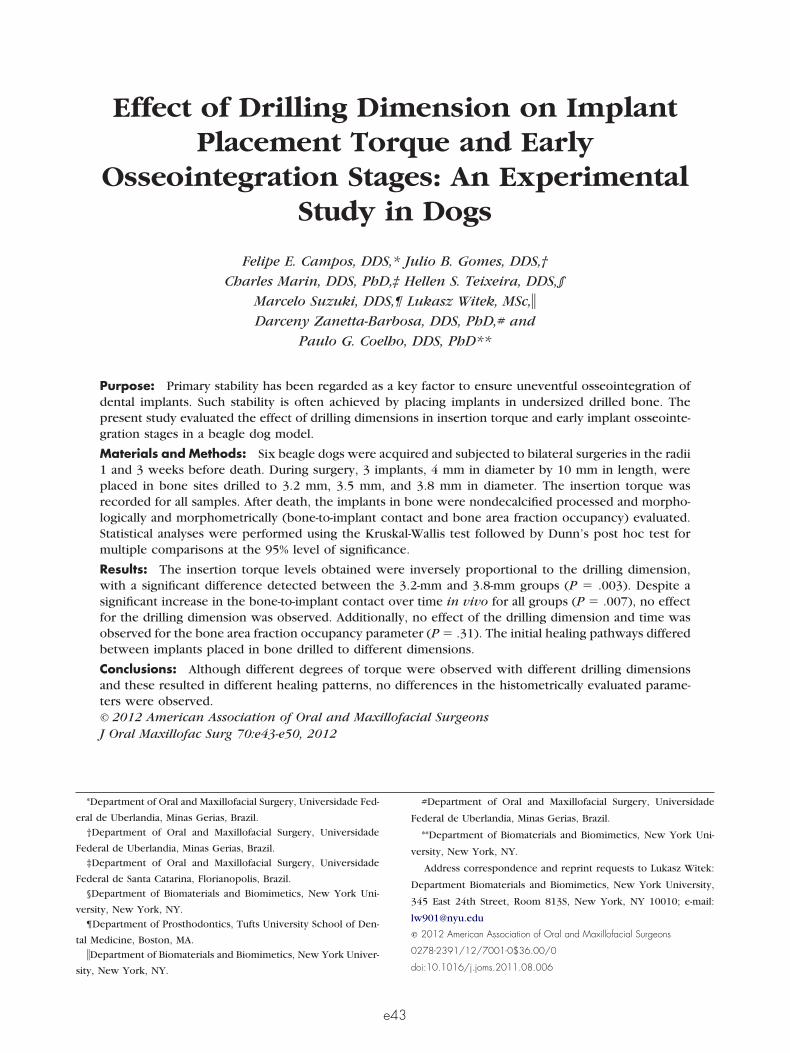
The insertion torque recorded for each drillinggroup is presented in Figure 1. The torque decreasedas a function of drilling diameter from 3.2 to 3.5 mmto 3.8 mm. A significant difference in torque levelswas observed between the 3.2-mm and 3.8-mmgroups (P � .003), and the 3.5-mm group presentedwith intermediate values without significance relativeto the 3.2-mm and 3.8-mm groups.
Qualitative evaluation of the biologic responseshowed intimate contact between the cortical andtrabecular bone for all groups at both implantationtimes, including regions that were in close proxim-ity or substantially away from the osteotomy walls(Fig 2).
The toluidine blue-stained thin sections presentedan appositional bone healing mode at regions whereintimate contact existed between the implant sur-faces and bone immediately after placement (Figs 3,4). These regions comprised the vast majority of the
FIGURE 1. Maximum insertion torque values (� SD) for differentexperimental groups. Number of asterisks depicts statistically ho-mogeneous groups (P � .003).
Campos et al. Drilling Dimension Effect on Torque and Osseointe-
gration. J Oral Maxillofac Surg 2012.
aua
egratio
e46 DRILLING DIMENSION EFFECT ON TORQUE AND OSSEOINTEGRATION
perimeter of implants placed into the 3.2-mm and3.5-mm drilling sites, and the outer aspects of thethreads of implants placed into 3.8-mm drilling sites.In contrast to implants placed into the 3.2-mm and3.5-mm drilling sites, the initial healing pattern ob-served in proximity of the implant inner thread diam-eter and drilled walls (forming healing chambers)when implants were placed into 3.8-mm drilling sitesfollowed an intramembranous-type healing mode(Figs 3, 4).
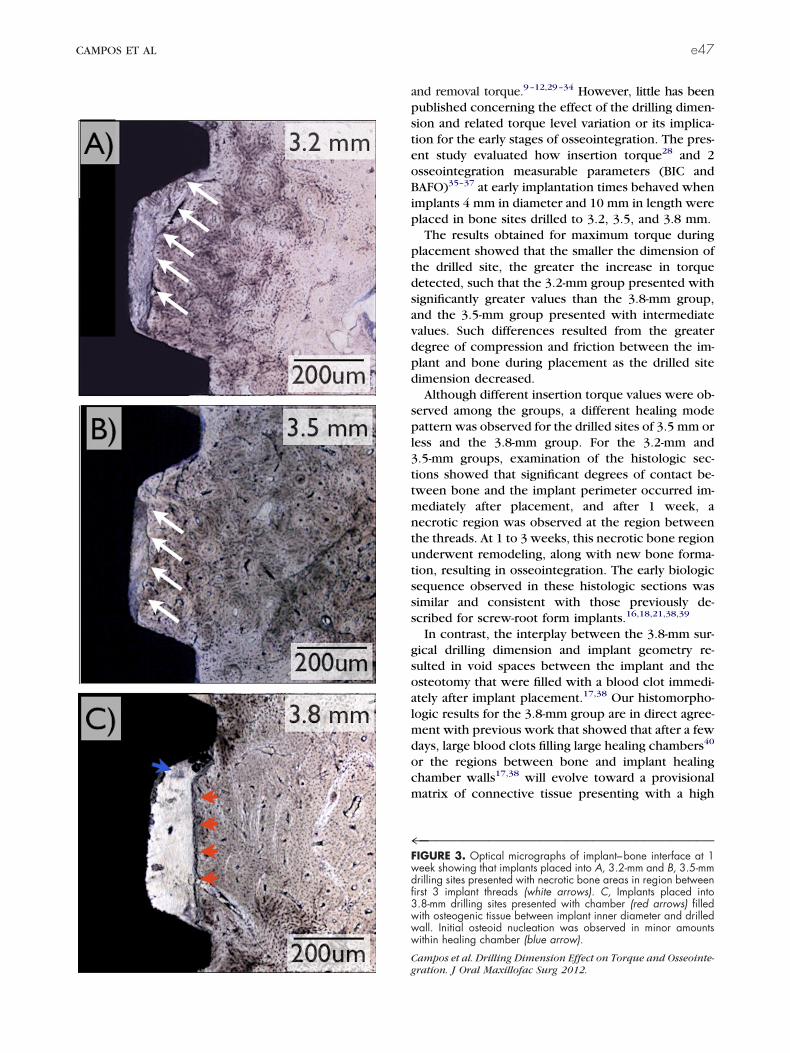
Temporal morphologic changes were observed forthe different experimental groups. At 1 week, im-plants placed into 3.2-mm and 3.5-mm drilling sitespresented extensive necrotic bone areas in the regionbetween the first 3 implant threads (Figs 3A, 3B).These necrotic regions evolved to remodeling sitesthat were present along with newly formed bone at 3weeks implantation time (Figs 4A, 4B).
At 1 week, the implants placed into the 3.8-mmdrilling sites presented a chamber filled with osteo-genic tissue between the implant inner diameter andthe drilled wall (Fig 3C). Initial osteoid nucleation wasobserved in minor amounts within the healing cham-ber (Fig 3C). Primary engagement by the threads’outer region without extensive necrotic bone areaswas observed (Fig 3C). At 3 weeks, extensive wovenbone formation was observed at the drilled bonewalls and implant surface and within the healingchamber volume (Fig 4C).
Statistical assessment of BIC showed significantlygreater values for all groups at 3 weeks relative to 1week (P � .07; Fig 5A) for all groups. Within thedifferent implantation times, no significant differ-ences were observed between experimental groups.
FIGURE 2. Merged micrographs of implant perimeter represenassessment.
Campos et al. Drilling Dimension Effect on Torque and Osseoint
The BAFO results showed a temporal increase from 1 m
to 3 weeks for all groups (Fig 5B); however, no sig-nificant differences were detected within the experi-mental groups at the different times in vivo and be-tween experimental groups within the times in vivo(P � .31).
Discussion
During the past 40 years, dental implant therapyprotocols substantially deviating from the classic2-stage protocol22 have been suggested, typically un-der the rationale of implant design modifications thatwould improve the odds of implant temporal stabilityduring the initial stages of healing.23–27 From a litera-ture review of early implant stability in which theclinical, histologic, and biomechanical componentswere considered, Raghavendra et al19 established anempirical implant stability chart. This stability charthas been widely accepted, not only because highdegrees of primary stability are often achieved, butalso because of the support that numerous histology-based studies have provided concerning the potentialmechanical stability loss given interfacial remodelingfollowed by bone apposition that finally results insecondary stability.
Primary stability assessment of implants and its re-lated clinical implication has been a challenge, be-cause it is not only dependent on insertion torque andhost bone density, but also on implant geometry,surgical drilling dimensions, and surface characteris-tics.28 During the past 5 years, the biomechanicalspects of implant primary stability have been studiedsing different methods such as resonance frequencynalysis, implant stability quotient, histologic
of 1 implant in bone used for morphologic and morphometric
n. J Oral Maxillofac Surg 2012.
tative
easurements, contact endoscopy, insertion torque,
psteoB
3www
Cg
CAMPOS ET AL e47
and removal torque.9–12,29–34 However, little has beenublished concerning the effect of the drilling dimen-ion and related torque level variation or its implica-ion for the early stages of osseointegration. The pres-nt study evaluated how insertion torque28 and 2sseointegration measurable parameters (BIC andAFO)35–37 at early implantation times behaved when
implants 4 mm in diameter and 10 mm in length wereplaced in bone sites drilled to 3.2, 3.5, and 3.8 mm.
The results obtained for maximum torque duringplacement showed that the smaller the dimension ofthe drilled site, the greater the increase in torquedetected, such that the 3.2-mm group presented withsignificantly greater values than the 3.8-mm group,and the 3.5-mm group presented with intermediatevalues. Such differences resulted from the greaterdegree of compression and friction between the im-plant and bone during placement as the drilled sitedimension decreased.
Although different insertion torque values were ob-served among the groups, a different healing modepattern was observed for the drilled sites of 3.5 mm orless and the 3.8-mm group. For the 3.2-mm and3.5-mm groups, examination of the histologic sec-tions showed that significant degrees of contact be-tween bone and the implant perimeter occurred im-mediately after placement, and after 1 week, anecrotic region was observed at the region betweenthe threads. At 1 to 3 weeks, this necrotic bone regionunderwent remodeling, along with new bone forma-tion, resulting in osseointegration. The early biologicsequence observed in these histologic sections wassimilar and consistent with those previously de-scribed for screw-root form implants.16,18,21,38,39
In contrast, the interplay between the 3.8-mm sur-gical drilling dimension and implant geometry re-sulted in void spaces between the implant and theosteotomy that were filled with a blood clot immedi-ately after implant placement.17,38 Our histomorpho-logic results for the 3.8-mm group are in direct agree-ment with previous work that showed that after a fewdays, large blood clots filling large healing chambers40
or the regions between bone and implant healingchamber walls17,38 will evolve toward a provisionalmatrix of connective tissue presenting with a high
4™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™FIGURE 3. Optical micrographs of implant–bone interface at 1week showing that implants placed into A, 3.2-mm and B, 3.5-mmdrilling sites presented with necrotic bone areas in region betweenfirst 3 implant threads (white arrows). C, Implants placed into.8-mm drilling sites presented with chamber (red arrows) filledith osteogenic tissue between implant inner diameter and drilledall. Initial osteoid nucleation was observed in minor amountsithin healing chamber (blue arrow).
ampos et al. Drilling Dimension Effect on Torque and Osseointe-
ration. J Oral Maxillofac Surg 2012.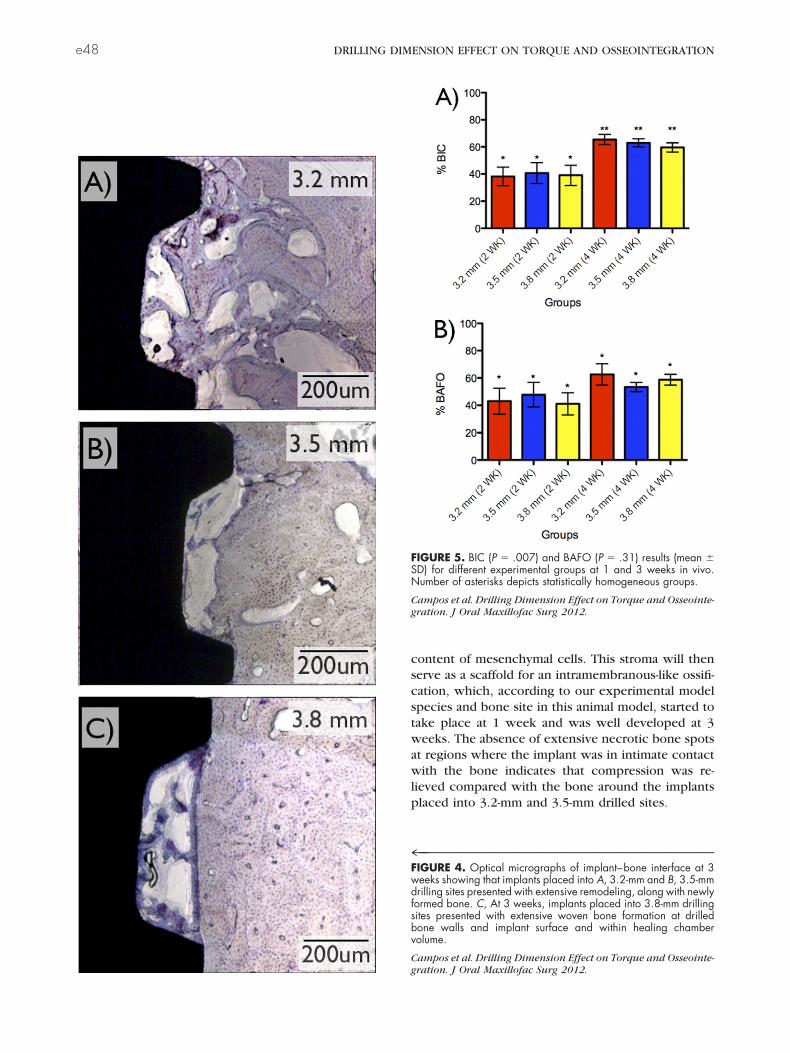
df
e48 DRILLING DIMENSION EFFECT ON TORQUE AND OSSEOINTEGRATION
content of mesenchymal cells. This stroma will thenserve as a scaffold for an intramembranous-like ossifi-cation, which, according to our experimental modelspecies and bone site in this animal model, started totake place at 1 week and was well developed at 3weeks. The absence of extensive necrotic bone spotsat regions where the implant was in intimate contactwith the bone indicates that compression was re-lieved compared with the bone around the implantsplaced into 3.2-mm and 3.5-mm drilled sites.
4™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™FIGURE 4. Optical micrographs of implant–bone interface at 3weeks showing that implants placed into A, 3.2-mm and B, 3.5-mmrilling sites presented with extensive remodeling, along with newlyormed bone. C, At 3 weeks, implants placed into 3.8-mm drillingsites presented with extensive woven bone formation at drilledbone walls and implant surface and within healing chambervolume.
Campos et al. Drilling Dimension Effect on Torque and Osseointe-
FIGURE 5. BIC (P � .007) and BAFO (P � .31) results (mean �SD) for different experimental groups at 1 and 3 weeks in vivo.Number of asterisks depicts statistically homogeneous groups.
Campos et al. Drilling Dimension Effect on Torque and Osseointe-gration. J Oral Maxillofac Surg 2012.
gration. J Oral Maxillofac Surg 2012.

CAMPOS ET AL e49
No differences were observed in BIC and BAFOamong the experimental groups at 1 and 3 weeks invivo, and overall increases were observed for allgroups over time (significant for BIC and not signifi-cant for BAFO). Although different physical relation-ships were achieved between the implant and bonefor the different groups, where intimate contact wasachieved for implants placed into the 3.2-mm and3.5-mm drilled sites and healing chambers formedaround implants placed into 3.8-mm drilled sites, thenecrotic bone regions decreased both BIC and BAFOto levels comparable to the void spaces comprised bythe healing chambers present at 1 week. Throughdifferent ossointegration pathways, where remodel-ing and new bone formation was the chief pathwayfor implants placed into the 3.2-mm and 3.5-mmdrilled sites, and intramembranous-like ossificationoccurred around implants placed into 3.8-mm drilledsites, these numbers increased for all experimentalgroups over time in a comparable fashion.
From a theoretical standpoint, one might considerthat the temporal stability of these implant systemswill follow different pathways. Although smaller dril-ling dimensions might increase primary stability, agreater amount of a necrotic “dieback” and interfacialremodeling will take place, potentially decreasing im-plant stability over time until secondary stability hasbeen achieved through new bone formation betweenthe implant surface and pristine bone. In contrast,although lower degrees of primary stability can beachieved through larger drilling dimensions, the com-pressive strain release could minimize the amount ofnecrotic “dieback” and remodeling at the regions,rendering primary stability to the implant, along withrapid woven bone filling in the healing chambersmight increase the speed of secondary stabilityachievement. From an implant design perspective, itis apparent that multifactorial studies addressing mac-rogeometric and surgical drilling dimension variationshould be addressed to determine what combination/circumstance would result in the greatest degrees ofstability over time. Finally, it should be stressed thatextrapolating healing data from animal models to hu-man healing is, at present, a challenge owing to thelack of controlled experiments in both models forcross-reference in the literature and should be care-fully performed.
References1. Brånemark PI, Adell R, Breine U, et al: Intra-osseous anchorage
of dental prostheses. I. Experimental studies. Scand J PlastReconstr Surg 3:81, 1969
2. Brånemark PI, Hansson BO, Adell R, et al: Osseointegratedimplants in the treatment of the edentulous jaw: Experiencefrom a 10-year period. Scand J Plast Reconstr Surg Suppl 16:1,
19773. Coelho PG, Granjeiro JM, Romanos GE, et al: Basic researchmethods and current trends of dental implant surfaces.J Biomed Mater Res B Appl Biomater 88:579, 2009
4. Atieh MA, Atieh AH, Payne AG, et al: Immediate loading withsingle implant crowns: A systematic review and meta-analysis.Int J Prosthodont 22:378, 2009
5. Schnitman PA. Wöhrle PS, Rubenstein JE, et al: Ten-year resultsfor Brånemark implants immediately loaded with fixed pros-theses at implant placement. Int J Oral Maxillofac Implants12:495, 1997
6. Javed F, Romanos GE: The role of primary stability for success-ful immediate-loading of dental implants: A literature review. JDent 38:612, 2010
7. Albrektsson T, Sennerby L, Wennerberg A: State of the art oforal implants. Periodontol 2000 47:15, 2008
8. Lemons JE: Biomaterials, biomechanics, tissue healing, andimmediate-function dental implants. J Oral Implantol 30:318,2004
9. O’Sullivan D, Sennerby L, Meredith N: Measurements compar-ing the initial stability of five designs of dental implants: Ahuman cadaver study. Clin Implant Dent Relat Res 2:85, 2000
10. Trisi P, Perfetti G, Baldoni E, et al: Implant micromotion isrelated to peak insertion torque and bone density. Clin OralImplants Res 20:467, 2009
11. Ottoni JM, Oliveira ZF, Mansini R, et al: Correlation betweenplacement torque and survival of single-tooth implants. IntJ Oral Maxillofac Implants 20:769, 2005
12. Akkocaoglu M, Cehreli MC, Tekdemir I, et al: Primary stabilityof simultaneously placed dental implants in extraoral donorgraft sites: A human cadaver study. J Oral Maxillofac Surg65:400, 2007
13. Akkocaoglu M, Uysal S, Tekdemir I, et al: Implant design andintraosseous stability of immediately placed implants: A humancadaver study. Clin Oral Implants Res 16:202, 2005
14. Akça K, Kökat AM, Cömert A, et al: Torque-fitting and reso-nance frequency analyses of implants in conventional socketsversus controlled bone defects in vitro. Int J Oral MaxillofacSurg 39:169, 2010
15. Coelho PG, Suzuki M, Guimaraes MV, et al: Early bone healingaround different implant bulk designs and surgical techniques:A study in dogs. Clin Implant Dent Relat Res 12:202, 2010
16. Abrahamsson I, Berglundh T, Linder E, et al: Early bone forma-tion adjacent to rough and turned endosseous implant surfaces:An experimental study in the dog. Clin Oral Implants Res15:381, 2004
17. Berglundh T, Abrahamsson I, Albouy JP, et al: Bone healing atimplants with a fluoride-modified surface: An experimentalstudy in dogs. Clin Oral Implants Res 18:147, 2007
18. Coelho PG, Suzuki M, Guimaraes MV, et al: Early bone healingaround different implant bulk designs and surgical techniques:A study in dogs. Clin Implant Dent Relat Res 12:202, 2009
19. Raghavendra S, Wood MC, Taylor TD: Early wound healingaround endosseous implants: A review of the literature. IntJ Oral Maxillofac Implants 20:425, 2005
20. Donath K, Breuner G: A method for the study of undecalcifiedbones and teeth with attached soft tissues: The Sage-Schliff(sawing and grinding) technique. J Oral Pathol 11:318, 1982
21. Leonard G, Coelho P, Polyzois I, et al: A study of the bonehealing kinetics of plateau versus screw root design titaniumdental implants. Clin Oral Implants Res 20:232, 2009
22. Brånemark PI: Osseointegration and its experimental back-ground. J Prosthet Dent 50:399, 1983
23. Albrektsson T, Wennerberg A: Oral implant surfaces: Part1—Review focusing on topographic and chemical propertiesof different surfaces and in vivo responses to them. Int JProsthodont 17:536, 2004
24. Albrektsson T, Wennerberg A: Oral implant surfaces: Part2—Review focusing on clinical knowledge of different sur-faces. Int J Prosthodont 17:544, 2004
25. Buser D, Broggini N, Wieland M, et al: Enhanced bone apposi-tion to a chemically modified SLA titanium surface. J Dent Res83:529, 2004
26. Butz F, Aita H, Wang CJ, et al: Harder and stiffer bone osseointe-
grated to roughened titanium. J Dent Res 85:560, 2006
e50 DRILLING DIMENSION EFFECT ON TORQUE AND OSSEOINTEGRATION
27. Coelho PG, Cardaropoli G, Suzuki M, et al: Early healing ofnanothickness bioceramic coatings on dental implants. An ex-perimental study in dogs. J Biomed Mater Res B Appl Biomater88B:387, 2008
28. Freitas AC Jr, Bonfante EA, Giro G, Janal MN, Coelho PG(2011). The effect of implant design on insertion torque andimmediate micromotion. Clinical Oral Implants Research. doi:10.1111/j.1600-0501.2010.02142.x
29. Engelke W, Decco OA, Rau MJ, et al: In vitro evaluation ofhorizontal implant micromovement in bone specimen withcontact endoscopy. Implant Dent 13:88, 2004
30. Gotfredsen K, Wennerberg A, Johansson C, et al: Anchorage ofTiO2-blasted, HA-coated, and machined implants: An experi-mental study with rabbits. J Biomed Mater Res 29:1223, 1995
31. Turkyilmaz I, Sennerby L, McGlumphy EA, et al: Biomechanicalaspects of primary implant stability: A human cadaver study.Clin Implant Dent Relat Res 11:113, 2009
32. da Cunha HA, Francischone CE, Filho HN, et al: A comparisonbetween cutting torque and resonance frequency in the assess-ment of primary stability and final torque capacity of standardand TiUnite single-tooth implants under immediate loading. IntJ Oral Maxillofac Implants 19:578, 2004
33. Niimi A, Ozeki K, Ueda M, et al: A comparative study ofremoval torque of endosseous implants in the fibula, iliac crest
and scapula of cadavers: Preliminary report. Clin Oral ImplantsRes 8:286, 199734. Cochran DL, Schenk RK, Lussi A, et al: Bone response tounloaded and loaded titanium implants with a sandblasted andacid-etched surface: A histometric study in the canine mandi-ble. J Biomed Mater Res 40:1, 1998
35. Marin C, Granato R, Suzuki M, et al: Biomechanical and histo-morphometric analysis of etched and non-etched resorbableblasting media processed implant surfaces: An experimentalstudy in dogs. J Mech Behav Biomed Mater 3:382, 2010
36. Marin C, Granato R, Suzuki M, et al: Histomorphologic andhistomorphometric evaluation of various endosseous implanthealing chamber configurations at early implantation times: Astudy in dogs. Clin Oral Implants Res 21:577, 2010
37. Giro G, Marin C, Granato R, et al: Effect of drilling technique onthe early integration of plateau root form endosteal implants:An experimental study in dogs. J Oral Maxillofac Surg 69:2158,2011
38. Berglundh T, Abrahamsson I, Lang NP, et al: De novo alveolarbone formation adjacent to endosseous implants. Clin OralImplants Res 14:251, 2003
39. Vignoletti F, Johansson C, Albrektsson T, et al: Early healing ofimplants placed into fresh extraction sockets: An experimentalstudy in the beagle dog. De novo bone formation. J ClinPeriodontol 36:265, 2009
40. Cardaropoli G, Wennström JL, Lekholm U: Peri-implant bone
alterations in relation to inter-unit distances. A 3-year retrospec-tive study. Clin Oral Implants Res 14:430, 2003Top Related
Copyright © 2022 FDOKUMEN

