







Bahasa
Halaman
Hukum


STUDY OF THE ANATOMICAL POSITION OF THE APPENDIX IN NORMAL POPULATION AND IN INFLAMED CASES
by
Dr Thyagaraj. J
Dissertation Submitted to the Rajiv Gandhi University Of Health Sciences, Karnataka, Bangalore
In partial fulfillment of the requirements for the degree of
Master of Surgery in
General Surgery
Under the guidance of Professor & H.O.D Dr T.K. Lakshmikanth
Department of Surgery Bangalore Medical College
Bangalore
2005
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES
DECLARATION BY THE CANDIDATE
I hereby declare that this dissertation/thesis entitled “STUDY OF ANATOMICAL
POSITION OF THE APPENDIX IN NORMAL POPULATION AND IN
INFLAMED CASES" is a bonafide and genuine research work carried out by me under
the guidance of Dr T.K. Lakshmikanth, M.S., Professor and Head of the Department
of surgery, Bangalore Medical College, Bangalore.
Signature of the CandidateName Dr. Thyagaraj. J
Date: Place: Bangalore
II
CERTIFICATE BY THE GUIDE
This is to certify that the dissertation entitled “STUDY OF ANATOMICAL
POSITION OF THE APPENDIX IN NORMAL POPULATION AND IN
INFLAMED CASES" is a bonafide research work done by Dr. Thyagaraj. J in partial
fulfillment of the requirement for the degree of Master in Surgery
Date : Place: Bangalore. Signature of the Guide
Dr. T.K. Lakshmikanth M.S., Professor & Head of The Department of Surgery Bangalore Medical College Bangalore.
ENDORSEMENT BY THE HOD, PRINCIPAL/HEAD OF THE
INSTITUTION
This is to certify that the dissertation entitled “STUDY OF ANATOMICAL
POSITION OF THE APPENDIX IN NORMAL POPULATION AND IN
INFLAMED CASES" is a bonafide research work done by Dr. Thyagaraj. J under the
guidance of Dr T.K. Lakshmikanth, M.S., Professor and Head of the Department of
surgery, Bangalore Medical College, Bangalore.
Seal & Signature of the HOD Name: Dr T.K. Lakshmikanth
Seal & Signature of the Principal Name Date: Place: Bangalore
Date : Place: Date : Place: Bangalore.
III
COPYRIGHT
Declaration by the Candidate I hereby declare that the Rajiv Gandhi University of Health Sciences, Karnataka shall
have the rights to preserve, use and disseminate this dissertation / thesis in print or
electronic format for academic / research purpose.
Date : Place: Bangalore.
Signature of the Candidate Name: Dr. Thyagaraj. J
IV
ACKNOWLEDGMENT
The writing of dissertation brings a trying time. During this period, one
enters a seemingly endless tunnel of references, discussions, corrections and statistical
data. It would be very easy to give in to despair but for the support of god, my teachers
and colleagues.
I wish to express my profound gratitude to my guide, Dr. T.K.
LAKSHMIKANTH, Professor and Head of the Department of Surgery, BMC. Bangalore.
His vast experience, patients-first attitude and enduring patience with my inexperience,
saw me through to the completion of this dissertation work. With wholehearted gratitude,
I wish to acknowledge my unrepayable debt to him.
I also wish to thank Dr. Shivaswamy, with a deep sense of gratitude for his
support and able guidance.
I am grateful to Dr. Sheshasayi, Assistant Professor Department of general
surgery for his sustaining support, encouragement and able guidance
I am grateful to Dr. Suresh Chandu and Dr. Jayaraj Ravikar, for their
constant support and encouragement at every stage.
I wish to express my profound gratitude to Dr. Beemappa Havanur.
Incharge Head of the Department of forensic medicine for his generous support and
guidance during every stage of this work
My hearty thanks to Mrs. Padmaja, Statistician Department of community
medicine Bangalore Medical College, Bangalore, For simplifying the intricacies of this
dissertation’s statistical work.
V
My sincere thanks to all the post graduate colleagues in the Department of
General Surgery and Forensic Medicine for their wholehearted support and help
I am grateful to my ´PATIENTS` for their co-operation in the present
study. I am also grateful for the ´cadavers` used in the present study without which this
dissertation would not have been possible.
In the end, with all humility, I thank God, Almighty for his grace in seeing
through to the completion of my dissertation work.
Date:
Place: Bangalore Signature of the Candidate Name Dr. Thyagaraj
VI

LIST OF ABBREVIATIONS USED
(in alphabetical order)
VII
ABSTRACT
Background & Objectives The most common position of the appendix is a subject
of controversy also the relation of the position of appendix and clinical picture and course
of the appendix is a subject of controversy. The objective is to study the various positions
of the appendix in normal population, and the position of the appendix in inflamed cases,
and the relation of the position to the clinical presentation and management of
appendicitis.
Methods All patients undergoing appendectomy in Bowring and Lady Curzon
hospitals and Victoria hospital May 2003 to August 2005 were included in the clinical
group. In normal population group, all cadavers undergoing autopsy from June 2003 to
July 2005, at Bowring and Lady Curzon hospitals mortuary were included.
Results There were a total of 150 cases, 50 in clinical group, and 100 in autopsy group.
The commonest position of the appendix is Retro-caecal (32.6%), Followed by Post-ileal
(26.6%), Pelvic (21.3%), Para-caecal (8%), Sub-caecal (5.3%) and Pre-ileal (4%). There
was no statistically significant difference in the position of the appendix in the clinical
and autopsy group. Certain positions like fixed retro-caecal, pelvic and post-ileal
presented more often atypically. Only 3 of 29 (10.3%) cases with typical presentation had
complications whereas 11 of the 21 cases (52.4%) with atypical presentation had
complications.
VIII
Interpretation & Conclusion There is no increased predisposition for any of the
position of the appendix to get inflamed. Complications were more common in cases
fixed retro-caecal, post-ileal and pelvic appendix. The patients with the above positions
presented more often atypically than typically and with subtle signs and symptoms
leading to delayed diagnosis and increased complications.
Keywords: Vermiform appendix; Anatomical position of Vermiform appendix; Appendicitis; Retrocaecal appendicitis; Pelvic appendicitis.
IX
TABLE OF CONTENTS 1. Introduction Page No. 1 2. Objectives Page No. 4 3. Review of Literature Page No. 5 4. Methodology Page No. 54 5. Results Page No. 60 6. Discussion Page No. 72 7. Conclusion Page No. 82 8. Summary Page No. 86 9. Bibliography Page No. 88 10. Annexures Page No. 98
X
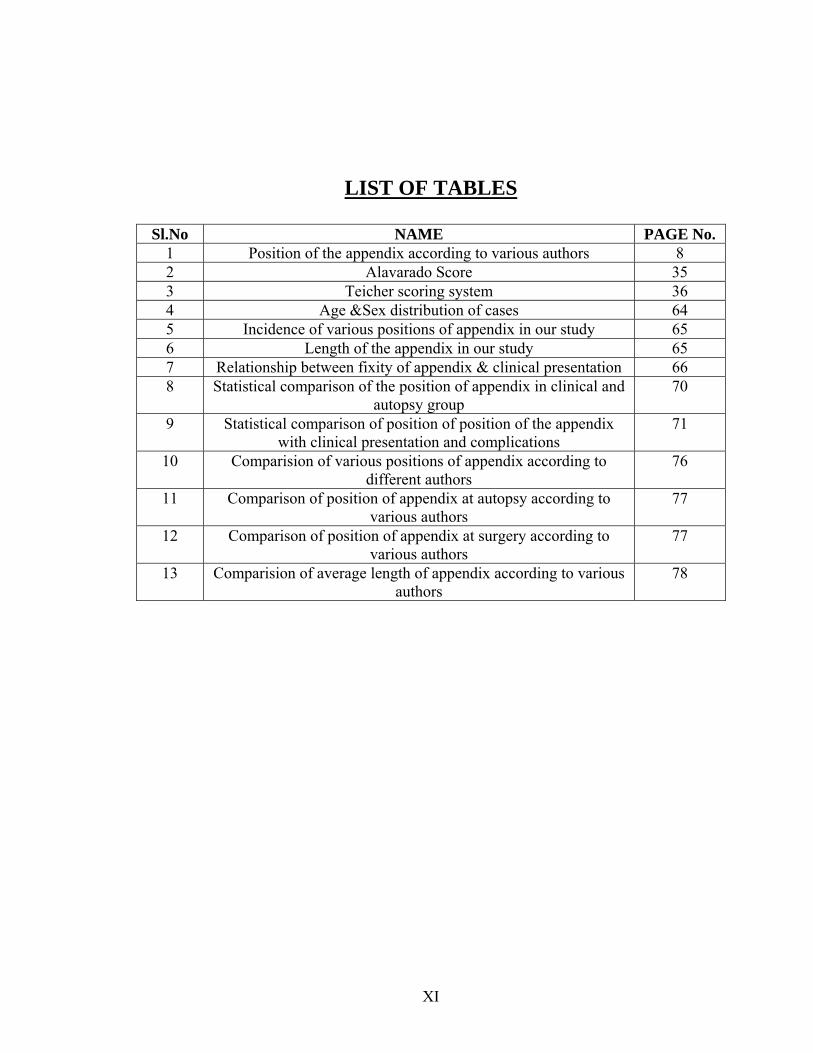
LIST OF TABLES
Sl.No NAME PAGE No. 1 Position of the appendix according to various authors 8 2 Alavarado Score 35 3 Teicher scoring system 36 4 Age &Sex distribution of cases 64 5 Incidence of various positions of appendix in our study 65 6 Length of the appendix in our study 65 7 Relationship between fixity of appendix & clinical presentation 66 8 Statistical comparison of the position of appendix in clinical and
autopsy group 70
9 Statistical comparison of position of position of the appendix with clinical presentation and complications
71
10 Comparision of various positions of appendix according to different authors
76
11 Comparison of position of appendix at autopsy according to various authors
77
12 Comparison of position of appendix at surgery according to various authors
77
13 Comparision of average length of appendix according to various authors
78
XI
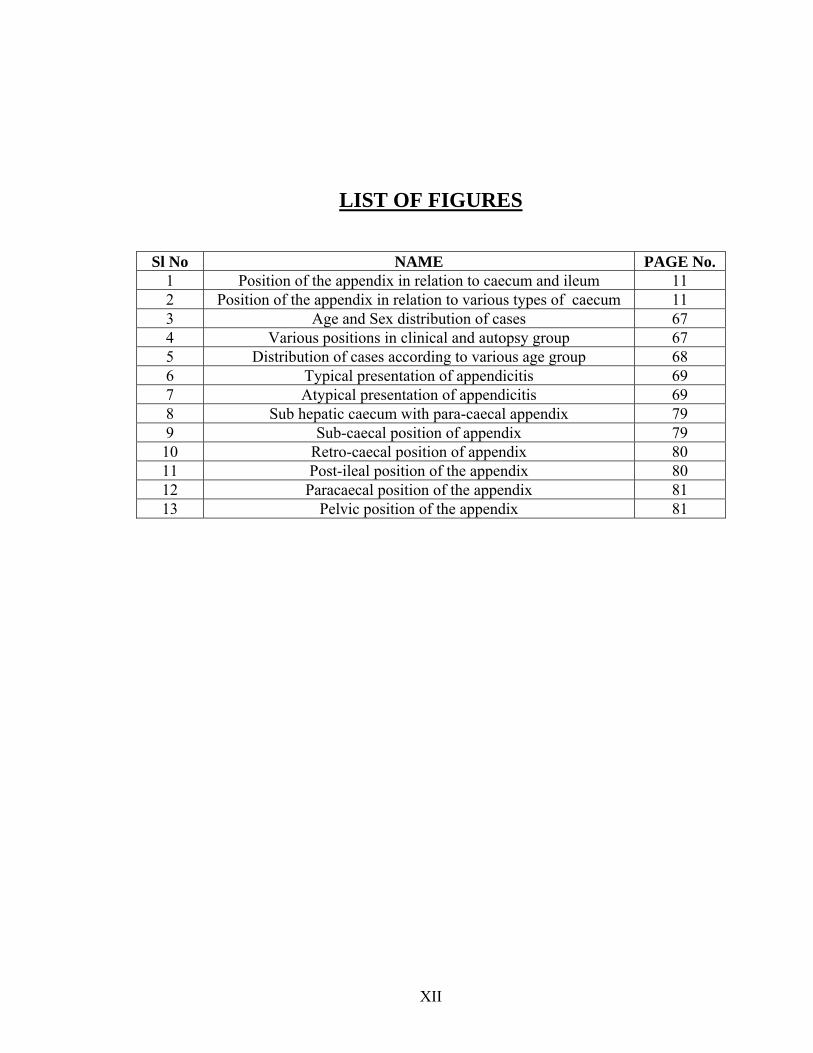
LIST OF FIGURES
Sl No NAME PAGE No. 1 Position of the appendix in relation to caecum and ileum 11 2 Position of the appendix in relation to various types of caecum 11 3 Age and Sex distribution of cases 67 4 Various positions in clinical and autopsy group 67 5 Distribution of cases according to various age group 68 6 Typical presentation of appendicitis 69 7 Atypical presentation of appendicitis 69 8 Sub hepatic caecum with para-caecal appendix 79 9 Sub-caecal position of appendix 79 10 Retro-caecal position of appendix 80 11 Post-ileal position of the appendix 80 12 Paracaecal position of the appendix 81 13 Pelvic position of the appendix 81
XII
INTRODUCTION
Appendicitis is a common sometimes confusing, and treacherous cause of
acute abdomen at all ages. The appendix is regarded as a vestigial organ, useless to man,
with no known important function, but can be a real nuisance at times, when it may
become the seat of infection. The diagnosis of appendicitis can be difficult, occasionally
taxing the skills of the most experienced clinician. The delays in the diagnosis arise from
errors either from the patient or physicians.
Anatomy is rightly called the father of surgery; this is made more evident
in case of appendix as the variations in the positions of the appendix will lead to varied
clinical presentation.
The most common position of the appendix is variously described by
many authors Wakeley et- al as retrocaecal (65.3%) (1), Collins et-al as pelvic (78.5%) (2)
and Pickens G et-al as postileal (3). Guidry SP et al have concluded that anatomic
variations of the location of appendix are often responsible for delays in the diagnosis of
appendicitis (4). Poole GV has stated that the paucity of symptoms and signs, in patients
with hidden appendix, is responsible for the delayed diagnosis of appendicitis before
perforation (5).
1
With the advent of laparoscopic appendectomy, there is a controversy as
to which is the better approach, as most of the appendices can be removed with a small
incision by the open approach. Karl A Zucker et-al have opined that the laparoscopic
appendectomy would be preferred approach in case of retrocaecal appendix, as the
incision required in open approach is longer with its associated morbidity, which can be
reduced by laparoscopic approach, also other abdominal viscera can be evaluated (tubes
& ovaries) as diagnosis of appendix is by excluding other pelvic pathology. Left sided
appendicitis may be confusing and is better evaluated by laparoscopy (6).
Varshney et-al have concluded that the retrocaecal position of the
appendix is less prone to infection (7), whereas Collins et-al have described higher
incidence of perforation and serious complications in acute appendicitis (8), other studies
one prospective (9) and two retrospective studies have established that the retrocaecal
position of the appendix does not alter the clinical course of acute appendicitis (10,11).
Appendicitis in different positions may mimic various other diseases, like
in Retro-colic =colitis, Post-ileal = Ureteric colic, Pelvic = enteric ileal perforation,
Pelvic inflammatory disease, Torsion of ovarian cyst, Ruptured tubal gestation, Sub-
hepatic = Hepatitis, Biliary colic.
From the above information it is evident that there are lots of
controversies regarding the various positions of appendix and also clinical presentation of
appendicitis, in relation to different positions. Hence there is a need for the study of the
2
various positions of appendix in the normal population and in patients with appendicitis
and also the clinical picture and complication in the various positions.
Our study is performed in clinical cases representing the inflamed
appendix group and the autopsy group, which represents the normal appendix group, in
the inflamed group the relation between the various positions of the appendix, and the
clinical presentation and complications is studied.
3
OBJECTIVES OF THE STUDY
To study the various positions of the appendix in normal population, as determined,
by the position in cadavers (100 cases) and the position of the appendix in inflamed
cases, as determined by the position of the appendix at laparotomy in clinical cases,
and the relation of the position to the clinical presentation and management of
appendicitis.
REVIEW OF LITERATURE
ANATOMY (12, 13, 14, 15)
4
Anatomy is the father of surgery Development (12) : - During the early stages of development, the midgut is attached to
the dorsal wall of the body by means of a short dorsal mesenterium. Because the
midgut grows considerably faster than does the rest of the embryonal body, it experiences
various regular movements & rotations, which can be divided into three phases.
Phase I: - (Physiologic umbilical hernia) During 6th week of gestation, the midgut
undergoes considerable elongation, resulting in a hairpin bend loop. As the embryonal
cavity does not have enough room to accommodate the intestinal loops, the loop extends
to the extra embryonic coelom. Around the axis of the superior mesenteric artery the
intestinal loop rotates 90 degrees anticlockwise.
Phase II: - (closure of physiological umbilical hernia) During 10th week of gestation the
intestinal loops relocate into the embryonal cavity, with an additional 180 degrees
counter clockwise rotation. The bud like complex of the caecum is now located on the
right side of the upper abdominal cavity directly below the liver. With the elongation of
the transeverse colon the caecum is pushed in a caudal direction (descensus) & caecum
finally lies in the right iliac fossa.
Phase III: -At about 12th week of gestation the mesenterium of the ascending &
descending colon is pushed against the dorsal body wall and fuses completely with the
parietal peritoneum
Development of the appendix (12) : - At about 6th week of gestation a small diverticulum
appears on the caudal limb of the midgut loop and this later differentiates into caecum
5
and appendix. According to Borman the increasing accumulation of meconium with in
the colon is the cause of the increase in diameter of this section of the intestine, because
of a mucosal fold the distal part cannot be filled completely with meconium so the
growth is not stimulated there and the vermiform appendix borders against the caecum as
a thin structure. Post-partum the caecum exhibits increased growth laterally resulting in
the dislocation of the vermiform appendix in the medial direction
Normal variations in the peritoneal fixation of appendix (12)
1 - Intra-peritoneal
2 - Intra-peritoneal retro-caecal with in paracaecal fossa
3 - Extra-peritoneal retro-caecal, para-caecal fossa present
4 - Extra-peritoneal retro-caecal, para-caecal fossa absent
5 - Extra-peritoneal retro-caecal, lying anterior to the right kidney & associated with sub-hepatic caecum.
Anatomy of the appendix (12,13,14)
Vermiform appendix is a narrow worm shaped part of the intestine, which arises from the
postero-medial part of the caecum 2cm or less below the ileo-colic junction, all taenia
start at the base of the appendix. The canal of the appendix is small and open into the
caecum by an orifice lying below & a little beyond the ileo-caecal opening, the orifice is
guarded by a mucosal fold (Gerlach valve) lumen may be partly or wholly obliterated in
the later part of the life. The length of the appendix varies from 2 – 35 cms the average
being 9 cms. It is longer in children than the adult life; its position may vary.
6
Sir Frederich Treaves has described the following positions of the appendix, making the
vermiform appendix as pointer and caecum as the dial of the clock as follows (14,16).
Para-colic or Para-caecal or 11 O’ clock position - Appendix is directed upwards &
to the right and lies on the right side of the caecum. In this position it may lie either
behind the peritoneum or may partially project into the peritoneal cavity & may lie in
front of the right kidney.
Retro-caecal or Retro-colic or12 O’ clock position - Appendix lies either behind the
caecum or the ascending colon and may be intraperitoneal or lie behind the peritoneum.
Splenic or 2 O’ clock position - Appendix is directed towards the spleen and may pass
either in front of the ileum (Pre-ileal) or behind the terminal part of the ileum (Post-ileal)
Promonteric or 3 O’ clock position - Appendix is directed transversely inwards
towards the sacral promontory.
Pelvic or 4 O’ clock position - Appendix hangs over the brim of the pelvis and projects
into the pelvic cavity
Midinguinal or 6 O’ clock position: – Appendix passes downward towards the middle
of the inguinal ligament (Sub-caecal position).
In 1901 Holmes reported, a case in which the proximal portion of the appendix
was situated extra-peritoneally and its distal portion was free (17). In 1904, Briggs cited a
case of girl aged 20 years in whom tip of the appendix was both retro-caecal and extra
peritoneal (17). In 1905 Kelly and Hurdon described a case of buried retro-caecal
appendix operated upon by Follis (17). Kelly cited a case operated on by Finney in 1898
7
in which a retro-caecal appendix was not only retro peritoneal but also lay with the tip
buried in the substance of the psoas muscle (17).
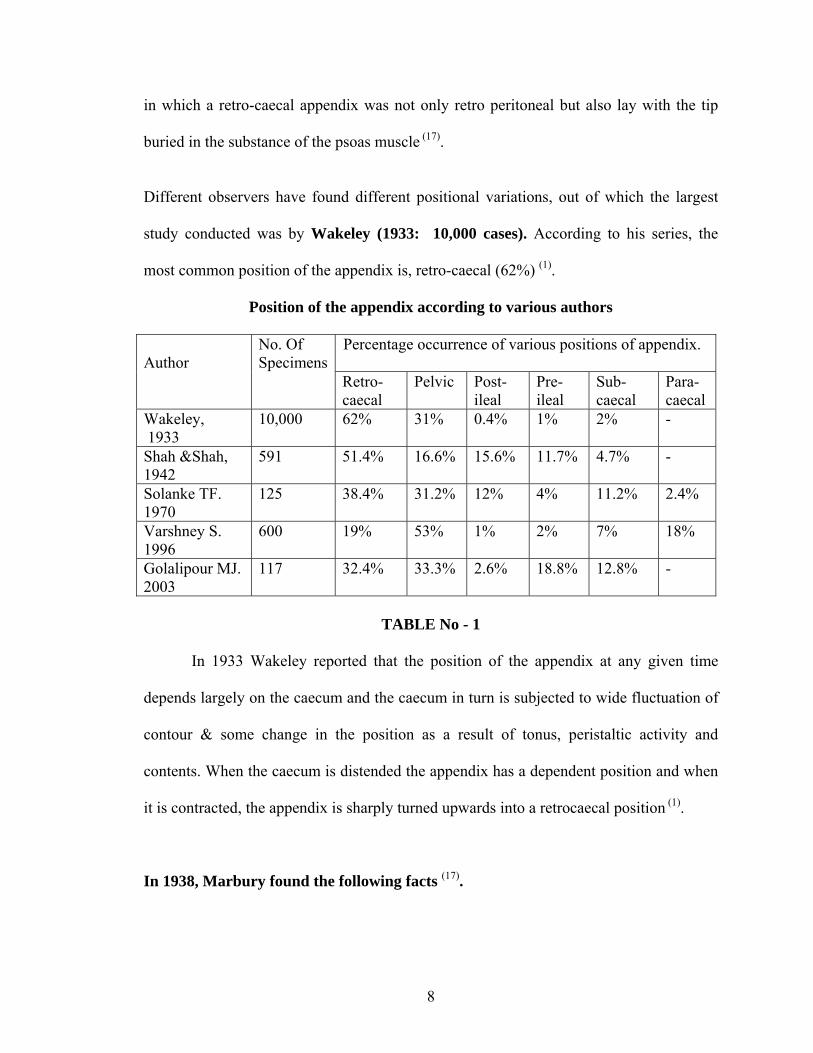
Different observers have found different positional variations, out of which the largest
study conducted was by Wakeley (1933: 10,000 cases). According to his series, the
most common position of the appendix is, retro-caecal (62%) (1).
Position of the appendix according to various authors
Percentage occurrence of various positions of appendix.
Author
No. Of Specimens
Retro- caecal
Pelvic Post- ileal
Pre- ileal
Sub- caecal
Para-caecal
Wakeley, 1933
10,000 62% 31% 0.4% 1% 2% -
Shah &Shah, 1942
591 51.4% 16.6% 15.6% 11.7% 4.7% -
Solanke TF. 1970
125 38.4% 31.2% 12% 4% 11.2% 2.4%
Varshney S. 1996
600 19% 53% 1% 2% 7% 18%
Golalipour MJ. 2003
117 32.4% 33.3% 2.6% 18.8% 12.8% -
TABLE No - 1
In 1933 Wakeley reported that the position of the appendix at any given time
depends largely on the caecum and the caecum in turn is subjected to wide fluctuation of
contour & some change in the position as a result of tonus, peristaltic activity and
contents. When the caecum is distended the appendix has a dependent position and when
it is contracted, the appendix is sharply turned upwards into a retrocaecal position (1).
In 1938, Marbury found the following facts (17).
8
1. The relative position of the appendix in the body, and its relation to the
peritoneum is governed by embryological factors. In th 4th month the caecum
leaves its position on the left side of abdomen; ascends with its mesenteric
attachment rotates to right iliac fossa, however the ascent and rotation may
cease at any point and hence appendix may be found anywhere along the
course followed by the caecum.
2. If the meso appendix is short, the appendix will be situated either in the
retrocaecal or retrocolic positon.
3. Appendix may be attached to the posterior parietal peritoneum at any time
during the descent of the colon, if descent is arrested early, tip of the appendix
may be found in the region of the gallbladder, if not the appendix may attain
retrocaecal position or may even be free in the peritoneal cavity.
Variations from the typical origin of the appendix from the caecum and the various forms
of the caecum as described by Treaves (16).
Type I - Foetal type: (2%) The caecum is conical in shape & appendix arises from the
apex.
Type II - Quadrilateral: (3%) Appendix arises from between the two bulging sacculi Type III - Usual / Adult type: (90%) appendix arises dorso-medial aspect of the
caecum
Type IV - (4%) In this appendix originates at the ileo-caecal angle
In 1936 Nicholson has shown that deformities of the appendix are, responsible for
the ill health and poor development of children, and are predisposing causes of the
disease. He also stated that the predisposition to acute appendicitis is familial (18,19).
9
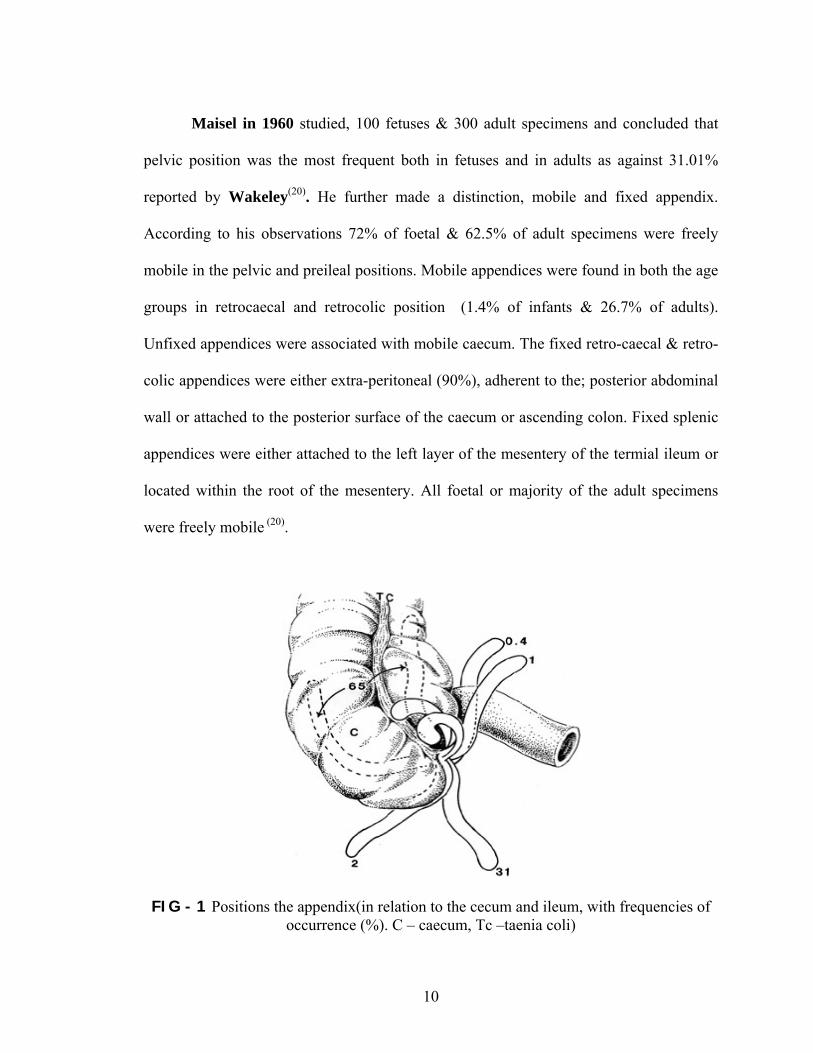
Maisel in 1960 studied, 100 fetuses & 300 adult specimens and concluded that
pelvic position was the most frequent both in fetuses and in adults as against 31.01%
reported by Wakeley(20). He further made a distinction, mobile and fixed appendix.
According to his observations 72% of foetal & 62.5% of adult specimens were freely
mobile in the pelvic and preileal positions. Mobile appendices were found in both the age
groups in retrocaecal and retrocolic position (1.4% of infants & 26.7% of adults).
Unfixed appendices were associated with mobile caecum. The fixed retro-caecal & retro-
colic appendices were either extra-peritoneal (90%), adherent to the; posterior abdominal
wall or attached to the posterior surface of the caecum or ascending colon. Fixed splenic
appendices were either attached to the left layer of the mesentery of the termial ileum or
located within the root of the mesentery. All foetal or majority of the adult specimens
were freely mobile (20).
FIG - 1 Positions the appendix(in relation to the cecum and ileum, with frequencies of occurrence (%). C – caecum, Tc –taenia coli)
10
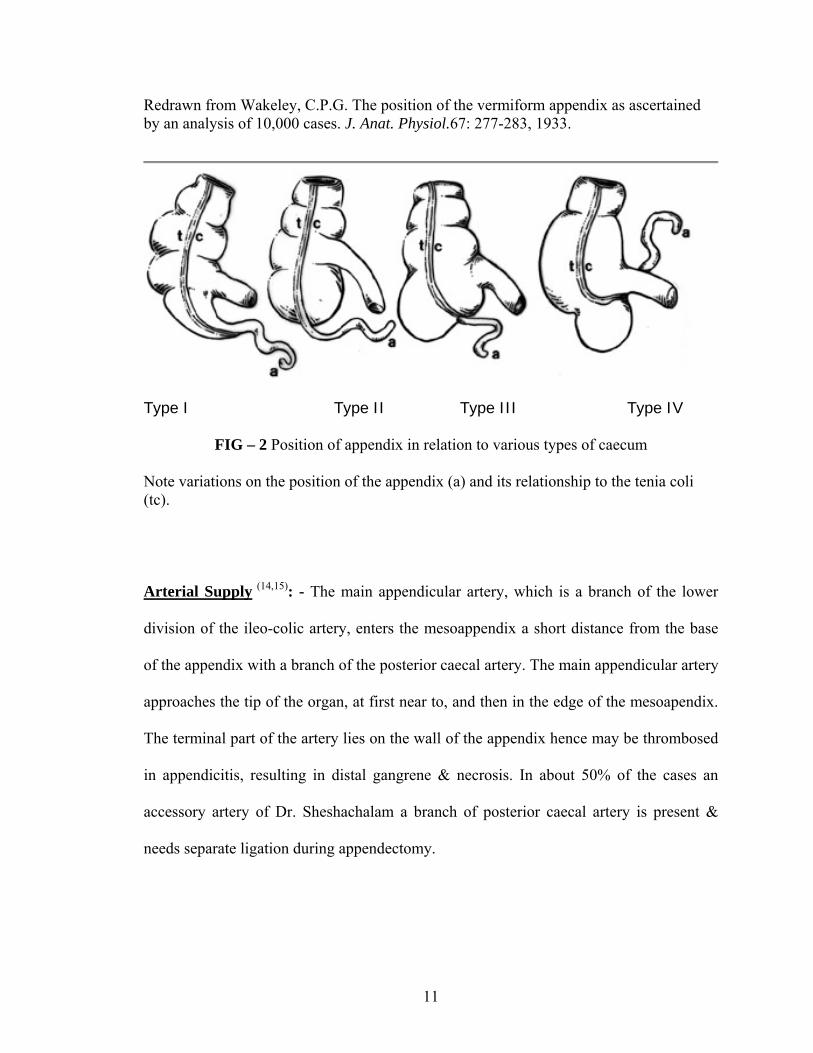
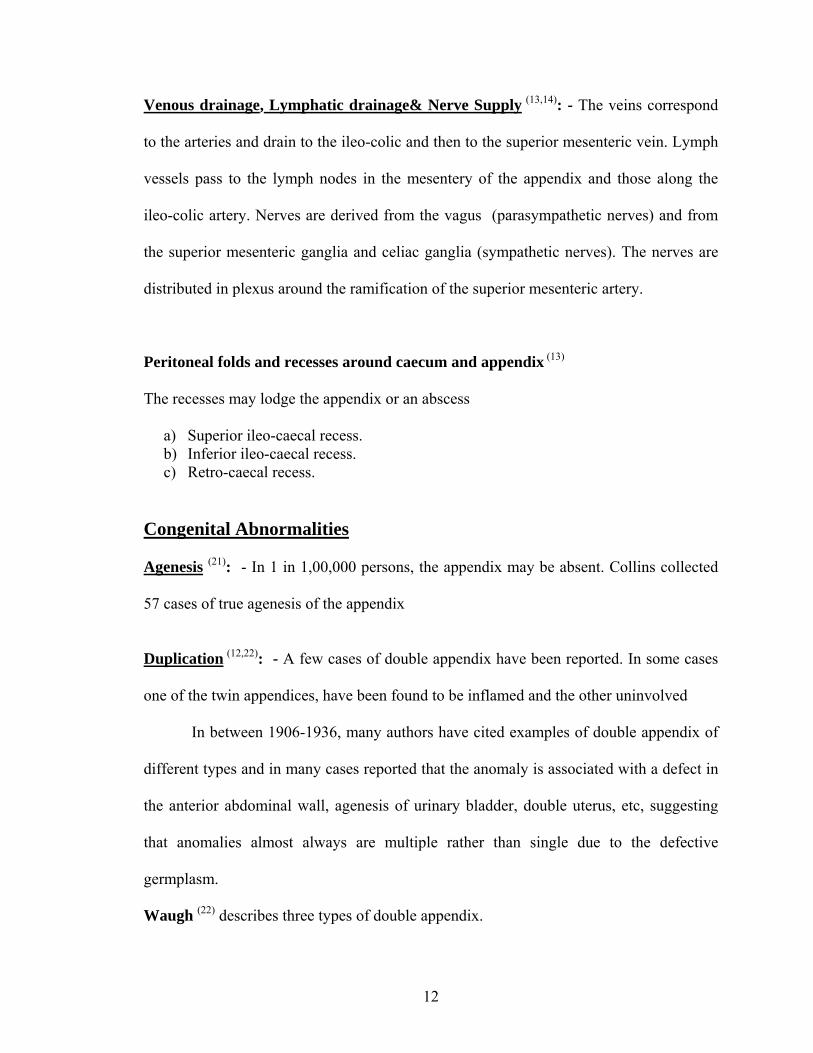
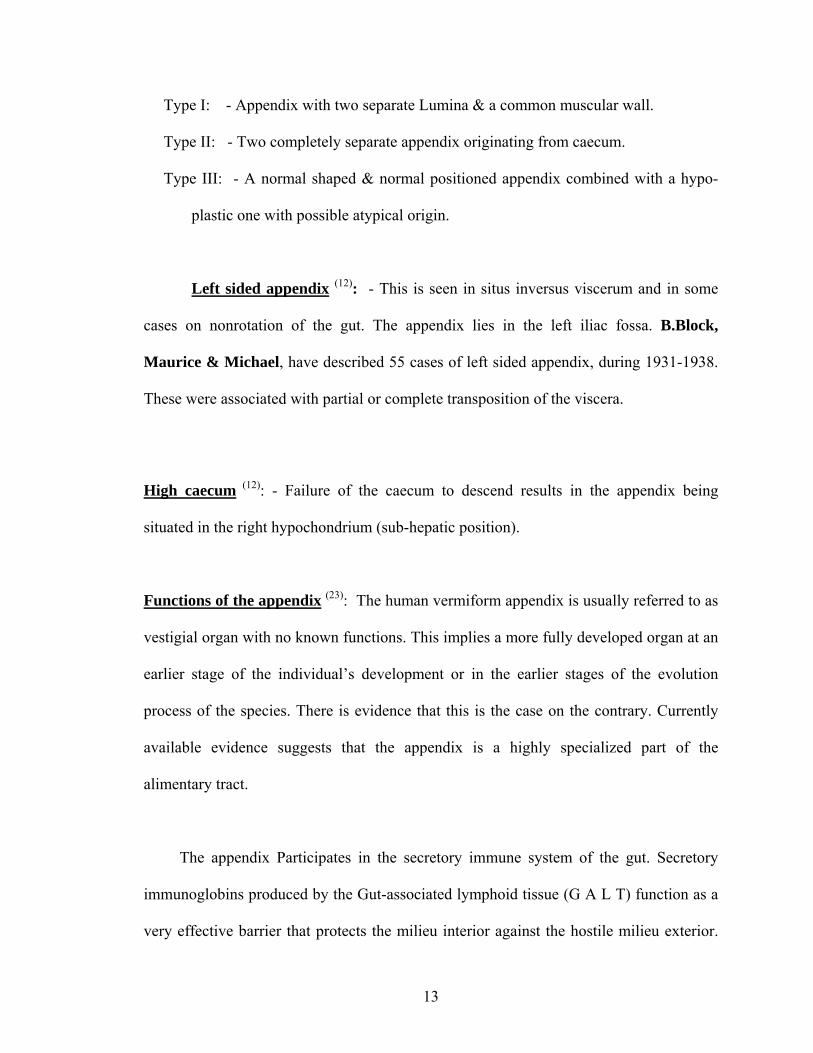
Redrawn from Wakeley, C.P.G. The position of the vermiform appendix as ascertained by an analysis of 10,000 cases. J. Anat. Physiol.67: 277-283, 1933.
Type I Type II Type III Type IV
FIG – 2 Position of appendix in relation to various types of caecum
Note variations on the position of the appendix (a) and its relationship to the tenia coli (tc). Arterial Supply (14,15): - The main appendicular artery, which is a branch of the lower
division of the ileo-colic artery, enters the mesoappendix a short distance from the base
of the appendix with a branch of the posterior caecal artery. The main appendicular artery
approaches the tip of the organ, at first near to, and then in the edge of the mesoapendix.
The terminal part of the artery lies on the wall of the appendix hence may be thrombosed
in appendicitis, resulting in distal gangrene & necrosis. In about 50% of the cases an
accessory artery of Dr. Sheshachalam a branch of posterior caecal artery is present &
needs separate ligation during appendectomy.
11
Venous drainage, Lymphatic drainage& Nerve Supply (13,14): - The veins correspond
to the arteries and drain to the ileo-colic and then to the superior mesenteric vein. Lymph
vessels pass to the lymph nodes in the mesentery of the appendix and those along the
ileo-colic artery. Nerves are derived from the vagus (parasympathetic nerves) and from
the superior mesenteric ganglia and celiac ganglia (sympathetic nerves). The nerves are
distributed in plexus around the ramification of the superior mesenteric artery.
Peritoneal folds and recesses around caecum and appendix (13)
The recesses may lodge the appendix or an abscess
a) Superior ileo-caecal recess. b) Inferior ileo-caecal recess. c) Retro-caecal recess.
Congenital Abnormalities Agenesis (21): - In 1 in 1,00,000 persons, the appendix may be absent. Collins collected
57 cases of true agenesis of the appendix
Duplication (12,22): - A few cases of double appendix have been reported. In some cases
one of the twin appendices, have been found to be inflamed and the other uninvolved
In between 1906-1936, many authors have cited examples of double appendix of
different types and in many cases reported that the anomaly is associated with a defect in
the anterior abdominal wall, agenesis of urinary bladder, double uterus, etc, suggesting
that anomalies almost always are multiple rather than single due to the defective
germplasm.
Waugh (22) describes three types of double appendix.
12
Type I: - Appendix with two separate Lumina & a common muscular wall. Type II: - Two completely separate appendix originating from caecum. Type III: - A normal shaped & normal positioned appendix combined with a hypo-
plastic one with possible atypical origin.
Left sided appendix (12): - This is seen in situs inversus viscerum and in some
cases on nonrotation of the gut. The appendix lies in the left iliac fossa. B.Block,
Maurice & Michael, have described 55 cases of left sided appendix, during 1931-1938.
These were associated with partial or complete transposition of the viscera.
High caecum (12): - Failure of the caecum to descend results in the appendix being
situated in the right hypochondrium (sub-hepatic position).
Functions of the appendix (23): The human vermiform appendix is usually referred to as
vestigial organ with no known functions. This implies a more fully developed organ at an
earlier stage of the individual’s development or in the earlier stages of the evolution
process of the species. There is evidence that this is the case on the contrary. Currently
available evidence suggests that the appendix is a highly specialized part of the
alimentary tract.
The appendix Participates in the secretory immune system of the gut. Secretory
immunoglobins produced by the Gut-associated lymphoid tissue (G A L T) function as a
very effective barrier that protects the milieu interior against the hostile milieu exterior.
13
Though the appendix is an integral part of the G A L T, Mediated Secretory globulin
immune mechanism, it is not indispensable. Removal of the appendix produces no
detectable defect in the functioning of the immunoglobin system. Thus the human
appendix is a useful, though not indispensable immunologic organ.
HISTORICAL ASPECTS (24, 25, 26) Those who cannot remember the past are condemned to repeat it
- santayana. The existence of the appendix was known even when the pyramids were being built
because certain Coptic jars containing bowel, inscribed with references to the WORM
OF THE BOWEL, and the hermetic books of Thoth and Books of the Dead, contain
statements which probably refer to the appendix (24).
Berengas Da Corpi (1954) gave the first full account of the appendix and
appendicular perforation (24). Andreas Vesalius (1534) Professor of anatomy at Ponda,
has given a detailed description of the normal appendix in his treatise on Defabrica
14
alumini Corporis (24). Morgagni, in his Adversaria Anatomica, has devoted some
portion of his work to the appendix, to describe its size, size, and its relations to other
structures (25). Verhgen (1710) coined the word Appendix. Liberkuhn, in 1739,
published a classic paper on the appendix in which he described, for the first time, crypts
in the mucosa, which bear his name (24). In 1735, on December 6th, Claudius amyad
performed the first appendectomy (26). In 1755, Heister recognized that the appendix
might be the site of acute primary inflammation (24). In 1842, Wyes Killer gave a
presentation entitled Observations in the inflammatory conditions of caecal appendix (24).
In 1886, Fitz Professor of medicine at Harvard published his classic monograph on
25 patients with perforating diseases of the Vermiform appendix, with special reference
to early diagnosis and treatment. He gave a lucid & logical description of the clinical
features & described, in detail, the pathologic changes in the disease. He was the first to
use the term appendicitis. He also suggested that, appendectomy would be essential for
cure (24).
Mc Burney in New York, in 1899 gave a lucid description, of the clinical features of
acute appendicitis and pioneered the removal of the acutely inflamed appendix before
perforation occurred and also devised the muscle – splitting incision (grid iron), named
after him (25). The teaching of Murphy at Chicago further popularized the early
intervention (24).
In 1901 Homes described, a case in which the proximal portion of the appendix was
situated extra-peritoneally. In 1904, Briggs cited a case of girl aged 20 years in whom tip
of the appendix was both retrocaecal and extra peritoneal. In 1905 Kelly and Hurdon
15
described a case of buried retrocaecal appendix operated upon by Follis. Kelly cited a
case operated on by Finney in 1898 in which a retro-caecal appendix was not only retro-
peritoneal but also lay with the tip buried in the substance of the psoas muscle. In 1915,
Strauss, found 22 extra-peritoneal appendices in 1651 autopsies. In 1910, Albert
Oschner, in chicgao, and James Sherren in London, advocated conservative line of
management in late cases. In 1928, Small, reported 7 cases of retroperitoneal appendices
operated upon by him over a period of 25 years. In 1932 Donald C Collins reviewing
literature on the length and position of appendix from 1861 to 1929 has cited the longest
appendix which measures 33 cms reported by Graver (1890) and the shortest 0.5 cms
reported by Huntington (1903) (2).
INCIDENCE OF APPENDICITIS Acute appendicitis is the most common cause of acute surgical abdomen and
appendectomy is the commonest emergency operation being performed. The lifetime
rate of appendectomy is 12% for men and 25% for women, with approximately 7% of
all people undergoing appendectomy for acute appendicitis (30,31). Over a 10-year
period from 1987 – 1997, the overall rate of appendectomy rate decreased parallel to
the decrease in incidental appendectomy (32).
Age Incidence (28): - While all ages are susceptible, the second and third decades are
the most frequently affected, while it is relatively less common at the extremes of age.
16
Sex incidence (28): - There is no particular predilection for either sex in acute
appendicitis till puberty. Among teenagers and young adults, the male to female ratio
is 3: 2. After the age of 25, the excess of male incidence decreases gradually until the
sex ratio is equal
Geo-graphic distribution (26): Appendicitis is most frezuently observed in North
America, British Isles, Australia, New Zealand, and among white South Africans. It is
rare in most of Asia, Central Africa, and among Eskimos. When people from these
areas migrate to the Weatern world or change to a Western diet, appendicitis becomes
prevalent, suggesting that the distribution of disease is determined environmentally
rather than genetically.
CLASSIFICATION OF APPENDICITIS (23,33)
1. Acute appendicitis
2. Recurrent appendicitis
-Recurrent acute appendicitis
-Recurrent sub-acute appendicitis
3. Chronic Appendicitis
Classification of Acute Appendicitis (33)
Depending on the gross and microscopic picture of the inflamed appendix:
17
1. Acute focal appendicitis: The appendix is grossly normal, but the microscopic
sections studied show scattered foci of inflammatory infiltrate with in the wall:
mucosal ulcers may be present.
2. Acute suppurative appendicitis: The appendix is grossly inflamed, oedematous
and injected, with peritoneal exudates. Microscopic sections show diffuse
inflammation.
3. Acute gangrenous appendicitis: Vascular thrombosis is present in addition to
signs of inflammation but with no gross perforation.
4. Acute Appendicitis with perforation: There is severe inflammation of the
appendix, with the disruption of the wall and exit of appendiceal contents into the
peritoneal cavity
5. Acute appendicitis with Peri-appendiceal abscess: This is secondary to
perforation with an attempt at localization of the inflammatory process by the
adjacent structures
Chronic appendicitis (34):
Divergence of opinion exists regarding the entity of chronic appendicitis, as a
cause of recurrent pain in the right iliac fossa. This always requires investigation to
exclude inflammatory bowel disease and gynecological disorders in females.
Relief of pain follows appendectomy in a proportion of these patients. The
appendix is usually long, fibrotic and contains faecolith. Histological examination shows
chronic inflammation.
18

ETIOLOGY AND PATHOGENESIS
ETIOLOGY: The following etiological factors are important but for the most part they
are purely contributory.
Race & Diet (26): Appendicitis is particularly common in highly civilized, European,
American and Australian countries, while it is less common in Asians, Africans and
Polynesians. It is possible that the rise of appendicitis amongst the highly civilized races
is due to departure from a simple diet, rich in cellulose, to one relatively rich in meat.
Familial susceptibility (18): This is unusual, but generally well-accepted fact, could be
accounted for by, an inherited malformation or mal-position of organs, which predisposes
to infection and similar diet consumption amongst the family members.
Bacterial factors (34): Any specific bacteria or protozoa do not cause acute appendicitis.
Culture from inflamed appendices showed normal bowel flora, Suggesting secondary
invasion of the damaged tissue from the lumen of the bowel. Though appendicitis has
been reported with salmonella and shigella enterocololitis, is probably due to obstruction
by hyper-plastic lymphatic follicles in the appendix
OBSTRUCTION: Wilkie (1914), Wangensteen et al (1937 and 1940) and Peiper et al
(1983) have documented appendicitis following obstruction of the appendix in
experimental animals. Wangensteen et al showed that combined obstruction and bacterial
19
invasion resulted in acute appendicitis whereas obstruction of a bacteria free lumen
resulted in mucocoele.
The obstruction may be
1. In the lumen: Faecoliths, parasites, (Pin worms, Ascaris, taenia) foreign bodies
(rare cause) – vegetables & fruit seeds, inspissated barium, pins, lead shot, bones,
eggshells, glass, teeth, nails, dice, the bulb of thermometer or others.
2. In the wall: lymphatic hyperplasia, stricture, tumors, carcinoid, appendix,
appendicular metastases, especially from breast carcinoma.
3. Outside the wall: Adhesions and kinks, congenital and post-inflammatory
strangulation in a hernial sac, carcinoma of the caecum and ascending colon.
i. FAECOLITH: Faecal material is commonly present in normal and inflamed
appendix. Faecolith is ovoid about 1-2 cm in length. Unlike ordinary faeces, a true
faecolith shows a well- ordered lamination on section.
Composition: Inspissated faecal material, calcium and magnesium phosphates and
carbonates, bacteria and epithelial debris and rarely, a foreign body may be incorporated.
Significance: In 10% of the cases of appendicitis, a faecolith was demonstrated by plain
radiograph of the abdomen. Radiological demonstration of a stone is an absolute
indication for appendectomy, irrespective of the signs or symptoms.
20
ii. LYMPHATIC HYPERPLASIA: The amount of lymphatic tissue in the appendix
parallels the incidence of acute appendicitis, the peak for both occurring in the early
teens. Hyper-plastic follicles may partially obstruct the lumen, setting the stage for the
development of appendicitis. Hyperplasia of the lymphoid tissue may be a response to
acute respiratory or other diseases producing a generalized reaction of the lymphoid
tissue. The lymphatic follicles of the appendix also respond to infection in the gut
iii. PARASITES (25): Pinworms and Ascaris are the commonest parasites reported to
cause obstruction of the appendix.
PATHOGENESIS (33)
The primary pathogenic event in acute appendicitis was thought to be intra-luminal
obstruction
ROLE OF LUMINAL OBSTRUCTION:
The events that follow obstruction of the appendix depend upon interaction amongst
four factors, - the contents in the lumen, the degree of obstruction, the continued
secretion by the appendiceal mucosa and the inelastic character of the appendiceal serosa.
The sequence of events following the occlusion of lumen is probably as follows. –
A closed loop obstruction is produced by the proximal block and continuing normal
secretion of the appendiceal mucosa, very rapidly, resulting in distension. The luminal
capacity of normal appendix is only about 0.1 to 0.2 ml. As little as 0.5 ml, distal to a
block, raises the intraluminal pressure to about 60 cm of water.
21
The human being is one of the few animals with an appendix capable of
secreting at pressures high enough to lead to gangrene and perforation. Progressive
mucous accumulation raises the intra luminal pressure; virulent bacteria convert the
accumulating mucus to pus. Continued secretion, combined with relative inelasticity of
the serosa, leads to further rise in the pressure within the lumen; obstruction of the
Lymphatic drainage ensues, leading to oedema of the appendix; diapedisis of the bacteria
begins and mucosal ulcers appear. This is the stage of acute focal appendicitis.
The bacterial invasion spreads through the walls of the appendix. This stage is called
acute suppurative appendicitis. The inflamed serosa of the appendix comes in contact
with the parietal peritoneum, as a result of which somatic pain arises. This is perceived as
classic shift and localization of pain in the right lower quadrant.
These pathologic processes continue, resulting in venous thrombosis and then to
compromise the arterial blood supply. The area of the appendix with the poorest blood
supply undergoes gangrene, with the appearance of ellipsoidal infarcts. The development
of gangrenous appendicitis is the first stage of complicated appendicitis. Morbidity
increases, as these infarcts functionally act as perforations. They permit the escape of
bacteria from the lumen of the appendix and contamination of the peritoneal cavity.
Secretion from the viable portions of the appendiceal mucosa, Continued high
intraluminal pressure finally leads to perforation through a gangrenous infarct, spilling
out accumulating pus. Perforated appendicitis now increases the morbidity and mortality.
22
Fortunately, in most cases, the obstruction that initially led to appendicitis blocks
continued spillage of faeces from the caecum through the perforated appendix.
If appendicitis has not progressed too rapidly, inflammatory adhesions form
between the loops of the bowel, peritoneum and omentum to hide the appendix.
Perforation in such cases leads to localized peritonitis. A peri-appendiceal abscess forms
eventually, if untreated.
This sequence is not inevitable. Some episodes of acute appendicitis apparently
subside spontaneously. Many patients, found at operation to have acute appendicitis, give
a of previous similar, but less severe, attacks of right lower quadrant pain.
Pathological examination of the appendices removed from these patients often
reveals thickening and scarring, suggesting old, healed, acute inflammation. Presumably,
obstruction of the lumen, when due to lymphoid hyperplasia or soft faecolith, can be
spontaneously relieved, allowing subsidence of appendiceal inflammation and attendant
symptoms.
CLINICAL DIAGNOSIS
The diagnosis of acute appendicitis is the classic example of the application of
clinical skills by the surgeon. Recently, algorithms and symptoms ranking systems, to
improve clinical examination, have been reported, but these aids have not really
improved the overall accuracy of preoperative diagnosis.
Sequence of events (26): The sequence of events in acute appendicitis is usually
characteristic and follows like this; it begins with diffuse abdominal pain, followed by
23
anorexia nausea and vomiting. Later, the pain shifts to the right side of the abdomen,
accompanied by a slight rise in the body temperature. Pain is present in all cases of
appendicitis, except in those with transeverse myelitis or similar disability.
Typical pain (26): This consists of an initial diffuse, central not very severe, visceral pain,
followed by somatic pain that is more severe and well localized to the right lower
quadrant.
Visceral pain(26) : This is steady, sometimes intermittent, cramping, and usually lasts 4-
6hrs (ranging from 1 –12 hrs). It is mild to moderately severe. The pain is felt around the
umbilicus. In the epigastrium or it may be generalized. It is due to the distension of the
appendix and irritation of the visceral peritoneum and hence is vague. This pain is
constant in non-obstructive and colicky in obstructive cases.
Somatic pain (26): Pain shifts to the point where the inflamed appendix irritates the
parietal peritoneum, which is highly sensitive. This pain is steady and very severe,
aggravated by motion or coughing and is usually located in the right lower quadrant.
The classic pain sequence in case of appendicitis is found in 55% of patients, but may
also occur in one fourth of the patients with other intra abdominal conditions.
Variations in the anatomical position of the appendix may account for variations in the
principal focus of the somatic pain. Long appendix with the tip located in the left iliac
fossa may cause pain in that area. A retrocaecal appendix may cause pain principally in
the flank or back. A pelvic appendix mainly causes pain in the suprabic area. While
24
postileal appendix may cause testicular pain, presumably from irritation of the spermatic
cord or ureters (23,29).
Anorexia, nausea and vomiting (29): About 95% of the patients have anorexia, nausea or
vomiting. Patient vomits only once or twice, a few hours after the onset of pain, but
anorexia persists even though nausea subsides.
Change in the Bowel and bladder habits (23,29): Patients may give history of obstipation
before the onset of abdominal pain and may feel that defecation will relieve their
abdominal pain. Diarrhea occurs in some patients especially in children. These symptoms
are probably due to proximity to the ileum, as in the postileal and preileal position of
the appendix or due to proximity to the rectum as in cases of pelvic position of the
appendix. Patients with pelvic appendicitis may have dysuria, and hematuria usually
microscopic. In retro-caecal appendicitis, urinary frequency may result from direct
irritation of the ureter.
Pain due to perforation: The pain of acute appendicitis was believed to be relieved
immediately after perforation. This older concept, which attributed this to sudden
decrease in pressure in the appendix, is disagreed upon in the present, as in most patients,
pain continues or increases in severity after perforation. In addition, the patient becomes
more ill with the distension of the abdomen beginning to develop because of supervening
diffuse peritonitis.
25
PHYSICAL EXAMINATION (23,26,29)
Appearance and Posture: Patient is usually flushed and in obvious pain.The patients
prefer to lie supine, with the thighs, particularly the right, drawn up because any motion
increases the pain due to irritation of the parietal peritoneum.
Temperature: Rarely rises above 38° C in uncomplicated appendicitis. Temperatures
above 38° C should always suggest the presence of perforation and peritonitis or abscess
formation. Normal temperature is sometimes present in advanced appendicitis, Children
usually present with higher temperatures, but very high pyrexia suggests some other
diagnosis like pyelitis or respiratory tract. Infection.
Pulse rate: Is normal or slightly elevated, especially in complicated appendicitis.
Tenderness: There cannot be acute appendicitis with out tenderness, which may be mild
and diffuse in early stages of the disease, later on localizing according to the position of
the appendix, In pelvic position suprapubic region is the site of maximum tenderness, in
retrocaecal position maximum tenderness is present posteriorly, extending toward, but
rarely as high as, the costo-vertebral angle (23).
Muscle guarding and rigidity: Muscle guarding and rigidity indicate the severity of the
inflammatory process. Especially in younger patients, early in the disease, resistance felt
is because of voluntary guarding. As the peritoneal irritation progresses, muscle spasm
increases guarding.
26
Cutaneous hyper-aesthesia (25): Over the area supplied by the spinal nerves T10, T11 &
T12 on the right side is frequent, but not constant, component of acute appendicitis. In
patients with obvious appendicitis, this sign is evident, but in some early cases, this may
be the first positive sign.
Rovsing’s sign: Pain in the right iliac fossa when pressure is exerted in the left iliac
fossa, is a manifestation of referred, rebound tenderness. It also indicates the site of
peritoneal irritation.
Psoas sign: The test is performed with the patient lying on the left side. The examiner
slowly extends the right thigh of the patient, thus stretching the ilio-psoas muscle. The
test is positive if extension produces pain. This indicates localized psoas muscle irritation
by the inflamed retrocaecal appendix (35).
Baldwin’s test: This test is, positive in retrocaecal appendicitis. While maintaining
fingertip pressure over the right flank, the patient is asked to lift the right lower limb off
the bed, keeping the knees extended. This test is positive if the patients complains of pain
or drops the limb with an expression of agony on the face (35).
Obturator sign: With the patient in supine position, passive internal rotation of the
flexed, right thigh, causes hypo-gastric or adductor pain. If positive, it indicates inflamed
pelvic appendix irritating the obturator internus muscle (35).
27
Mc Burney’s sign: Fingertip pressure is applied over the Mc Burney’s point. Patient
complains of pain on pressure. It is a predictive sign in early or sub-acute appendicitis.
Shifting tenderness: This sign is useful in the diagnosis of appendicitis in pregnant
women. Locate the tenderest spot & mark it on the skin. Then request the patient to turn
to the left side and wait for a full minute, should the tenderness be of uterine origin, like
concealed accidental hemorrhage or necrosis of a uterine fibroid, it will shift with the
uterus, whereas in appendicitis the position will remain constant.
Rectal examination: It is indicated primarily to exclude lesions such as ovarian cyst or
tubal pathology in females and to elicit tenderness in cases of pelvic appendicitis. In
about 1 in 3 patients with inflamed appendix, in or adjacent to the pelvis, the presence of
mass, or tenderness specifically localized to the right side may be elicited. In a few
subjects whose inflamed appendix lies entirely within the pelvis, tenderness on rectal
examination may be the only positive physical sign.
Diagnostic variability: Considering the range of possible presentations, the lack of
diagnostic accuracy comes as no surprise.
Gilmore et al (36) reported that senior consultants could accurately diagnose
appendicitis in 80% of the cases, while junior consultants may be wrong 50% of the time.
De Dombal and Leaper (37), who also said that young women were more commonly
misdiagnosed than any other age group, confirmed this. Pieper et al (38) found that 6 –
28
30% of patients do not have appendicitis on laparotomy, of which 4-13% of patients have
some other concurrent surgical disease, but almost 25% are negative laparotomies.
In women of reproductive age, this figure is as high as 45%, No other segment in
general surgery compares to this level of misdiagnosis (36,39).
Appendicitis is a disease with protean manifestations. The position of vermiform
appendix is not constant and there are suggestions that it could change with movement of
caecum (40).
Many presentations of appendicitis are atypical because of an atypical position of
the appendix, the patient’s age or the presence of associated conditions such as
pregnancy.
Retro-caecal or Post- ileal: These differ from the classical variety, since the inflamed
appendix is shielded from the anterior abdominal wall by the caecum and the ileum, there
is less of discomfort, and guarding may be absent (9)
In retro -caecal position patient may present with features of upper urinary tract
infection due to the proximity of the ureters and kidneys. Kao CT et al have described a
case of ruptured retro-caecal appendicitis presenting as peri-nephric abscess (41).
Harsha WT, and others believe that retro-caecal position of the appendix
whether fixed by the inflammatory process or during the development is felt by some
29
clinicians to present an enigmatic and challenging clinical problem when appendicitis
develops (42).
Collins argued: Acute retro-caecal appendicitis is largely responsible for the
atypical symptoms in cases of acute appendicitis that deceive the incautitious clinicians,
and cause many deaths. In his review of 751 cases of retro-caecal appendicitis he
emphasized the frequently bizarre nature of early signs and symptoms. Only 18.9% of his
patients presented with classic signs and symptoms of appendicitis (43).
Pelvic appendicitis: The pain is localized to the left in a number of patients. The urge to
defecate or urinate is prominent, and tenderness may be elicited on pelvic examination.
It may also present as prostatitis, in males, due to the extension of inflammation to the
prostate. In females it may present with, features of pelvic inflammatory disease (pelvic
adnexal mass, cervical motion tenderness (44).
An appendico-vesical fistula may develop, which presents as recurrent attacks of
cystitis, which is refractory to usual antibiotic treatment. Five cases of appendiceal-
ureteral fistulas have also been described (44).
In children acute appendicitis may very rarely present as acute urinary retention
Hoffmann has given the hypothesis that the prostatic urethra may become obstructed
either by the inflammatory mass, or the abscess itself, by sympathetic mechanism
leading, to sphincter spasm or as a result of prostatic congestion (44).
Appendicitis in infants and children (45): It is difficult to diagnose for obvious reasons.
Increased irritability may be the only symptom (45). The incidence of perforation is the
30
highest in children below 2 years of age. Harrington et al reported a perforation rate of
90% in infants (46).
Appendicitis in elderly: In elderly it is difficult to diagnose because of unclear
symptoms (47) and refusal by the treating physician to consider the diagnosis.
Appendicitis in pregnancy: The disease is no different in pregnant women than it is in
non-pregnant women, but diagnostic difficulty and delay and the severity and
complications add to its significance (48). Appendicitis is more prone to occur in the first 6
months (74%) (49). During this period, symptoms such as anorexia, nausea, vomiting and
abdominal pain may be attributed to the pregnancy. Physical findings of localized
tenderness, rebound tenderness, and muscle guarding are not altered by cephalad of
caecum by the enlarging uterus; caecal displacement, progressively cephalad after the
initial 6 months, tends to localize pain and tenderness to the upper quadrant and flank.
When inflammation extends to the parietal peritoneum (50). Stretched abdominal
musculature alters the reflex responses, and there is inability to examine the abdomen
satisfactorily. All of these contribute to the diagnostic dilemma (51).
Complications of acute appendicitis (23,26,29)
I. Perforation and its consequences
II. Abscess formation and its complications
- Appendico - cutaneous fistula.
- Appendico – vesical fistula. (In cases of pelvic appendicitis)
31
III. Diffuse peritonitis. (Usually seen in intraperitoneal position of the appendix)
- Due to contamination of the peritoneal cavity before defensive adhesion
formation.
- Secondary rupture of intra abdominal abscesses that were produced by
ruptured appendicitis. Perforation: A Serious complication of appendicitis, that results from a delay in
diagnosis and surgical treatment. Reports in the literature suggest an occurrence of
appendiceal perforation as high as 32% (52) and a startling frequency in children
(conservative estimates of 30-42% (53), with the extremes as high as 50-83% being
reported (54)).
62% of patients with perforation had been symptomatic for more than 24 hrs, in
contrast to 33% of those without perforation. This explains that delay in seeking medical
attention, is, probably, the most important factor leading to perforation. Scher reported
that the mean duration of symptoms was 2.5 days for those with perforation, compared to
1 to 5 days for those without perforation, he also reported that 30.6% of perforated cases
got operated after 24 hours as compared to 15.4% of non-perforated cases (52).
Perforation should be suspected when the duration of symptoms exceeds 24 hrs,
the temperature is more than 38º C and WBC count greater than 15,000 cells/cu.mm.
These are uncommon findings in non-perforated appendicitis.
A history of diffuse abdominal pain following symptoms confined to right lower
quadrant, accompanied by signs of diffuse peritonitis on physical examination indicates
that perforation has occurred.
32
If the perforation has been walled off into an appendicular abscess, a tender mass
can often be palpated in the right lower quadrant. If discomfort makes palpation of the
right lower quadrant difficult, it is helpful to examine the patient under anesthesia before
the incision is made. In retro-caecal appendicitis the abscess is usually outside the
peritoneal cavity and does not contaminate the peritoneum, hence it can be drained
extraperitoneally
.
LABORATORY INVESTIGATIONS AND SCORING (23,25,26,28)
Laboratory is a good servant but poor master
-Boyd.
This is very much true of acute appendicitis, as only laboratory investigations, with out
any clinical grounds, does not establish diagnosis.
I.Total WBC count and differential count (55).
Moderate leukocytosis, ranging from about 10,000 – 18,000 cells/cu.mm, with
neutrophilia, is the common picture in acute appendicitis.
With normal total & differential counts, the diagnosis of acute appendicitis is still
a possibility. If WBC count is > 18,000 cells/cu.mm and shift to the left is extreme,
perforated appendicitis or an acute inflammatory disease of greater magnitude than
33
appendicitis is more probable. Leukocytosis is usual, but by no means inevitable, and
seldom diagnostic (Fowler).
II Scoring systems
Scoring systems based on clinical and laboratory findings have been introduced.
Ramirez and Deus used Bayesian probability to produce a rationalized model of clinical
decision-making (56).
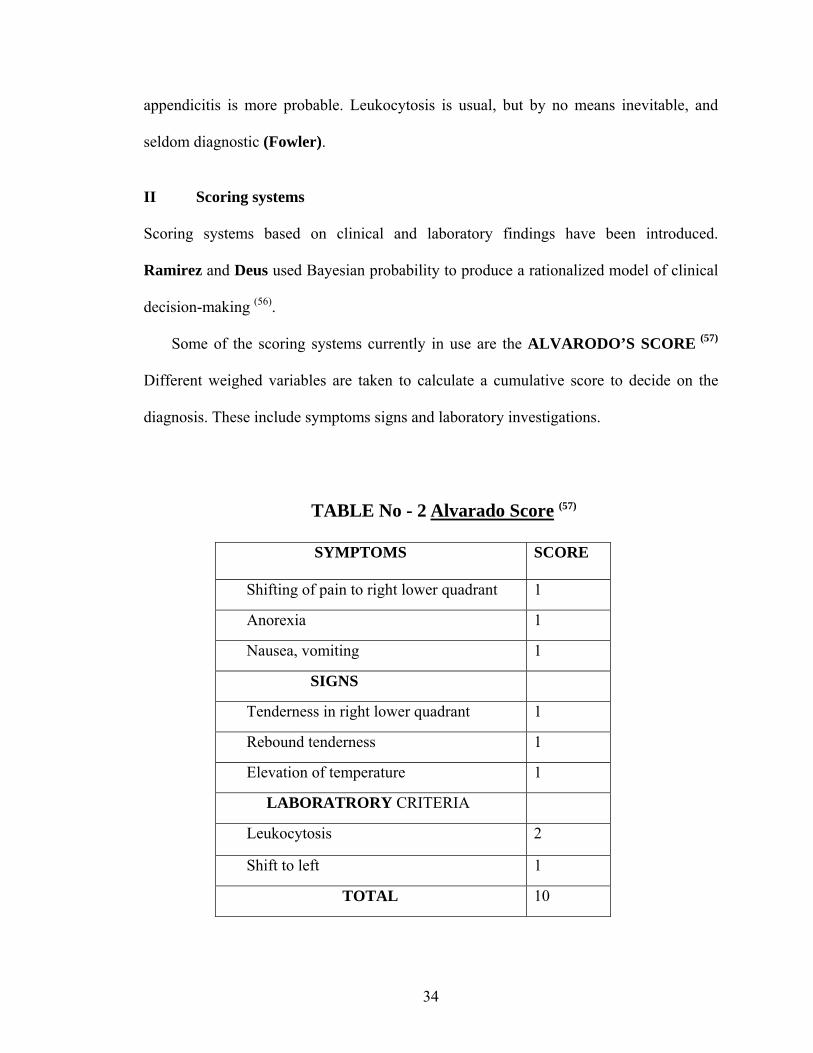
Some of the scoring systems currently in use are the ALVARODO’S SCORE (57)
Different weighed variables are taken to calculate a cumulative score to decide on the
diagnosis. These include symptoms signs and laboratory investigations.
TABLE No - 2 Alvarado Score (57)
SYMPTOMS SCORE
Shifting of pain to right lower quadrant 1
Anorexia 1
Nausea, vomiting 1
SIGNS
Tenderness in right lower quadrant 1
Rebound tenderness 1
Elevation of temperature 1
LABORATRORY CRITERIA
Leukocytosis 2
Shift to left 1
TOTAL 10
34
Fenyo G and Kang et al (58) used the Alvarado score as a determinant factor for surgical
intervention and found a score of less than or equal to 6 to be clinically dubious and more
than or equal to 7 to be typical.
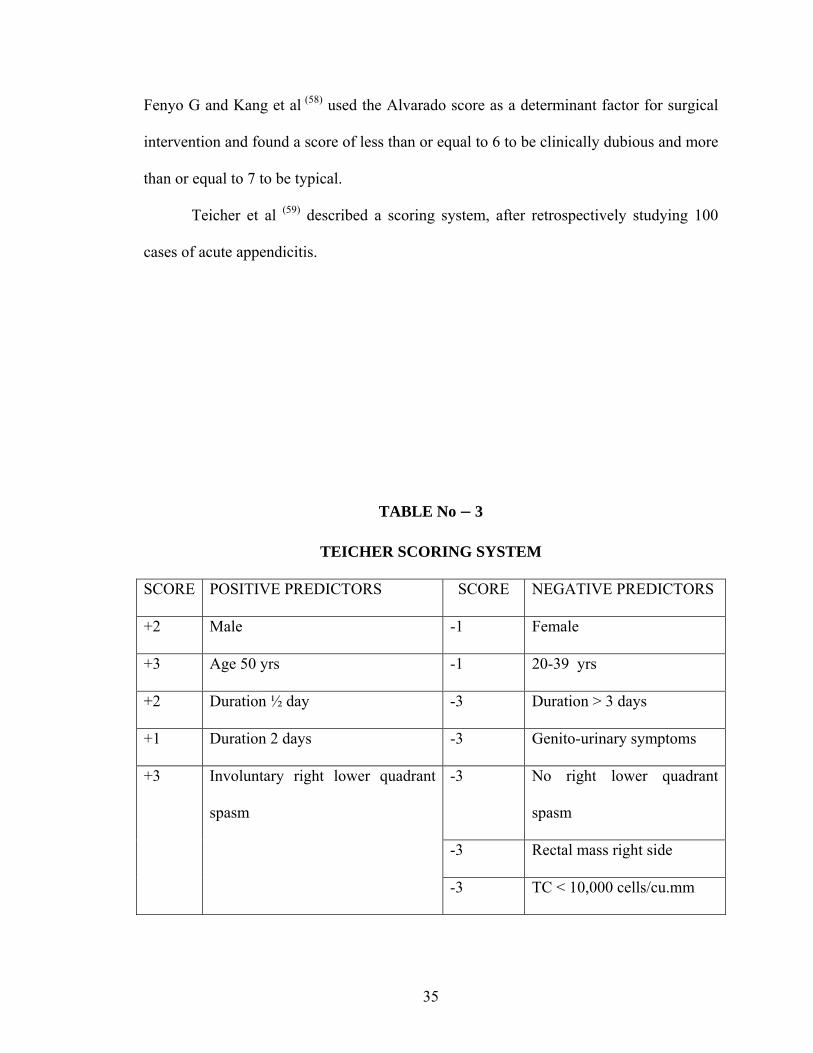
Teicher et al (59) described a scoring system, after retrospectively studying 100
cases of acute appendicitis.
TABLE No – 3
TEICHER SCORING SYSTEM
SCORE POSITIVE PREDICTORS SCORE NEGATIVE PREDICTORS
+2 Male -1 Female
+3 Age 50 yrs -1 20-39 yrs
+2 Duration ½ day -3 Duration > 3 days
+1 Duration 2 days -3 Genito-urinary symptoms
-3 No right lower quadrant
spasm
-3 Rectal mass right side
+3 Involuntary right lower quadrant
spasm
-3 TC < 10,000 cells/cu.mm
35
A score greater than 3 was taken as a positive predictor of acute appendicitis. This system
if applied would have prevented negative laparotomies in 38% of the patients and 5%
would have been kept for observation.
Scoring systems help augment the clinical decision making with considerable
economy of resources and have a favorable cost benefit ratio.
IMAGING MODALITIES
I. Plain Radiography.
Plain radiography has been used for the diagnosis of the acute abdomen since
1906 (60). However there is no single sign that is pathognomonic of acute appendicitis
in a plain film. Brooks et al (60) in 1975 described several signs in a case of acute
appendicitis.
1. Presence of appendicolith.
2. Sentinel loop in right iliac fossa.
3. Dilated caecum.
4. Widening and blurring of pre-peritoneal fat line.
5. Haziness of right lower quadrant.
36
6. Scoliosis, concave to the right.
7. Right lower quadrant mass indenting the caecum.
8. Blurring of the right psoas outline.
9. Gas in the appendix (rare).
However, plain radiograph lacks specificity, with similar findings being found in normal
patients as well as in other conditions. It is relatively contraindicated in certain conditions
e.g. in pregnant patients. The low diagnostic yield (8% sensitivity) adds to its
unattractiveness as a diagnostic aid (61).
II. Barium meal follow through: (rarely done)
Schisgall et al (62) in 1983 reported an accuracy of 95% in the diagnosis of acute
appendicitis in children by barium meal follow through examination. This involved a
slightly higher (0.2 rad) radiation exposure as compared to a barium enema.
The signs of acute appendicitis are:
1. Non visualization of the appendix
2. Mass effect on the caecum.
III. Barium enema: (rarely done)
Barium enema examination is based on the rationale that the lumen of the normal
appendix can be demonstrated with barium enema, and appendiceal luminal obstruction
37
represents acute appendicitis, with extrinsic pressure effects (reverse 3 sign) on the
caecum.
Rajagopal et al (63) found the following signs highly suggestive of appendicitis on
barium enema examination:
1. Persistent non-visualization of the appendix.
2. Partial Visualization (Beheaded appendix)
3. Pressure effect on the caecum (Reverse 3 sign)
4. Irritability of the caecum and terminal ileum on fluoroscopy.
However, Persistent non-visualization of the appendix is a finding in 5- 10% of normal
individuals and may occur due to a faecolith (64).
The advantage of barium is that it does not require specialized equipment. It can
also diagnose certain conditions, which may mimic acute appendicitis like colonic
carcinoma, terminal ileitis and ischaemic colitis (64).
Fedyshin et al found the procedure cumbersome and that it entails exposure to
ionizing radiation, as its great drawbacks (65).
IV Ultrasound:
In the clinical management of suspected acute appendicitis, graded compression
ultrasonography is the examination of choice. It is mainly used to exclude the other
causes of abdominal pain, which mimic appendicitis like calculi, ruptured tubal gestation,
and other pelvic causes.
38
Currently the diagnostic criteria used for the diagnosis of acute appendicitis by
ultrasound are (After Jeffrey) (66)
1. Blind ending, immobile, non compressible, a peristaltic, tubular structure.
Measuring the diatance from the echogenic mucosa to the outer oedematous wall
that shows few echoes assesses mural thickness.
2. Cannot be displaced on pressure.
3. Bull’s eye or target lesion visualized in the transeverse plane with diameter >
6mm.
4. Faecolith in the lumen.
5. Peri-appendiceal collection.
6. Hypo or hyper – peristaltic loops in the right iliac fosssa.
7. Sonographic Mc Burney’s sign of maximum tenderness by the probe. This sign is
lost in appendicular perforation.
8. Miscellaneous signs: Cockade around target lesion. Tubular structure > 50 mm in
length.
Chesbrough et al have reported an increased diagnostic yield of ultrasound by self-
localization of the site of maximum tenderness (67).
Poor results have been reported in the diagnosis of appendicular perforation.
Puylaert et al (68) stated the following reasons:
1. Loss of localizing rebound tenderness.
2. Decompression of the target lesion and decrease in the diameter.
3. Ileus with dilated bowel loops with in the right iliac fossa.
39
The low sensitivity in the group with perforated appendicitis is not necessarily worrying,
as the need for an operation was obvious.
V. Colour Doppler: Colour Doppler Examination is based on the principle that
acute inflammation of the appendix is associated with increased blood flow to
the region. Quillin et al (69), in 1994, imaged 100 children concurrently with
Colour Doppler and gray scale ultrasonography, and found sensitivity of 87%
and a specificity of 97%, with an accuracy of 93%, using colour doppler,
compared to an accuracy of 90% by gray scale ultrasonography. A finding of
increased vascularity was considered positive for appendicitis and a
hyperemic right lower quadrant mass was suggestive of an abscess.
VI. Computed Tomographic scanning: Useful, Especially in the obese and
distended patients, where ileus makes visualization by ultrasound a problem
(70,71). It has been shown to be more accurate in advanced appendicitis in the
diagnosis of perforation (72), While diagnostic accuracy in early appendicitis is
still suspect.
In a study of 38 patients, Gale et al (72) found that C.T had a sensitivity of 92% and a
specificity of 79%. They described the common findings in acute appendicitis on C.T as:
1. Peri-caecal inflammation. (68%)
2. Abscess formation. (55%)
3. Calcified appendicolith. (23%)
40
4. Abnormal appendix. (18%)
Balthazar et al (70) analyzed 100 consecutive cases with both, ultrasound and C.T, and
found the accuracy to be 93% as contrasted to 84% by ultrasound. The sensitivity of C.T
was found to be 96%. C.T was found to be more useful in detecting location, nature and
extent of the disease process (70). Normal C.T does not rule out acute appendicitis without
peri- appendiceal inflammation (70,71).
VII Diagnostic Peritoneal Aspiration Cytology / Lavage:
Evans et al (73) in 1975 have investigated peritoneal lavage, as a diagnostic modality for
non-traumatic acute abdomen, and, Hoffman et al (74) confirmed its utility in 1988.
Complications reported were 2 cases of colonic perforation during the procedure. This
procedure is also contraindicated in the presence of a sub-umbilical midline scar.
Performance of this procedure was found to be difficult in the presence of paralytic ileus
or obesity. Caldwell et al (75) reported that a negative result does not definitely rule out
significant intra abdominal pathology. However leukocyte rich pus in the peritoneal
aspirate of a young male is diagnostic of acute appendicitis.
VIII. Miscellaneous Investigations
1. Urine analysis: The presence of haematuria or pyuria in acute appendicitis has been
demonstrated. Graham et al (76) found microscopic haematuria and pyuria in 9 patients of
41
62 positive appendectomies. An appendiceal tip being close to the ureter or the bladder
can cause haematuria and pyuria.
2. Phospho-lipase A2 levels: Group II phospholipase A2, in the serum is an acute phase
reactant. Gronroos et al (77) prospectively studied 186 patients, also using CRP and
leukocyte count. Whereas leukocyte count was the investigation of choice in acute
uncomplicated appendicitis, C-reactive protein and phospho-lipase A2 correlated better
with protracted inflammation and appendicular perforation. Increased phospholipase A2
values did not unequivocally indicate diagnosis but when all the values were normal,
appendicitis could be excluded with 100% certainty.
3. Creactive protein levels: C reactive protein is basically an acute phase reactant which
has been shown by Gronroos et al (77) to stay persistently elevated in cases of acute
appendicitis, unlike the total leukocyte count which progressively decreases with time.
Combined sequential assessment of CPR and total count has been proposed in the
subgroup of patients who have been kept for observation. Eriksson et al (78), in a study
of 227 patients, found that CRP had a sensitivity of 87% and a specificity of 50%.
4. Interleukin – 6 levels (IL-6) Assessment of IL-6 levels has been found to correlate
well with acute appendicitis, although specificity is uncertain (77).
5. Radio- isotope scanning: After a report in 1985 that there was a rapid accumulation of
radioisotope labeled leukocytes at the sites of infection, radioisotope studies, for the
diagnosis of acute appendicitis, were attempted.
42
This involved withdrawing 30 –90 ml of patient’s blood, separating of the leukocytes by
differential sedimentation and labeling them with radioisotope, usually Technetium 99 or
Indium 111. Scanning was done 2hrs after injection of the mixture.
Navvaro et al (79) used Indium 111 and found a sensitivity of 93% with an overall
accuracy rate of 91%.
It is however, unreliable in women, as gynecological conditions may mimic the scan
appearance of appendicitis.
6. Diagnostic laparoscopy: Kelling et al introduced diagnostic laparoscopy as early as
1902, but its use in acute abdomen was reported only as late as 1970 (25).
Diehl et al (80), Deutsh et al (81), Leape et al (82), highlighted its utility at
laparotomy in reducing the negative laparotomy rates for appendicitis. The negative
appendectomy rates reduced from 30% to 1-2% (61).
Hoffman (61) summed up the signs of acute appendicitis on laparoscopy.
1. Partial or complete visualization of inflamed appendix.
2. Pus in the right iliac fossa.
3. Omentum adherent to structure of the right iliac fossa.
4. Inflammation of the peri-caecal tissues.
The advantage of laparoscopy is positive visualization and the exclusion of the
differential diagnosis such as salphingitis, terminal ileitis, ectopic pregnancy,
endometriosis, ruptured corpus-luteal cysts, tumour infiltrates, Para ovarian cysts and
mittelschemerz syndrome.
Disadvantage: It cannot be done in obesity, previous laparotomy, sub- umbilical scar,
and abdominal distension due to ileus, pregnancy and ascites.
43
7. Abdominal thermography: Steele et al (83) measured the abdominal skin temperature
in patients undergoing emergency appendectomy and found to be significantly elevated
over the normal controls.
It is becoming very clear that the negative appendectomy rate of 20-25% accepted by
most surgeons is too high to justify, in the presence of modern systems of diagnosis. A
myriad of evolving modalities are available, which can reduce the negative laparotomy
rate to 1-2%.
TREATMENT (23,25,26,28,84)
The one and the only answer to the treatment of appendicitis and its
complications, is surgery, and the only dilemma it carries with it is, the timing of surgical
intervention.
There is a general agreement on the timing of the operation for three categories of
appendicitis already mentioned – acute appendicitis without rupture, ruptured appendix
with local peritonitis or phlegmon formation, and ruptured appendix with spreading
peritonitis, when appendectomy should be performed immediately.
There has been a difference of opinion, however, concerning the optimal timing
of operation for ruptured appendicitis with frank peritoneal abscess formation. A.T
Oschner advocated expectant treatment in 1901. If progression occurs, the abscess is
drained. If the patient improves, conservative treatment is continued. With these
measures, the majority of appendiceal abscesses resolve satisfactorily, although many
44
days of hospitalization are required. An elective appendectomy 6 weeks to 3 months later
is strongly advised, since the recurrence rate is very high.
Prompt surgery for all categories of appendicitis is especially important in
children, since expectant treatment of ruptured appendicitis has been less successful than
in adults.
NON – OPERATIVE therapy may be appropriate if (26) –
1. The patient is moribund with advanced peritonitis
2. The attack has already resolved.
3. An appendix mass has formed without evidence of generalized peritonitis
Preoperative preparation: All patients, but especially those in whom perforation and
peritonitis are suspected, should receive intensive pre-operative preparation, this rarely
requires more than 3-4hrs and often can be accomplished in an hour or less. Patients with
a palpable peri-appendiceal mass may in selected cases, be managed initially, without an
operation.
Fluid replacement with Ringer’s lactate solution and 5% dextrose in water is given as
rapidly as possible with the objective of establishing a good urinary output. Naso-gastric
suction is helpful in all the cases, particularly in those with peritonitis.
Antibiotics: These are administered preoperatively to help control any local or
generalized sepsis that may be present, and to reduce the incidence of post-operative
wound infection. These are especially useful in patients who have gangrenous or
perforated appendicitis.
45
Examination under anesthesia: With the patient under the effect of anesthesia, the
abdomen should be carefully and systematically palpated once more. On occasion, such
examination will show the gallbladder to be the real cause of the patient’s symptoms.
Incisions (26,28,84): There are a number of choices for an incision, each of which has its
advantages and disadvantages. The incision should be one that gives sufficient exposure,
Permits the needed exposure with least amount of tissue injury, and allows easy
extension, should it become necessary. Also to be considered is the likelihood of
complications directly attributable to the incision, such as dehiscence, incisional hernia,
denervation of the skin and muscle, and scar given by the incision itself.
There are a few standard incisions that may be applied to appendectomy,
transverse incision of Elliot-Rockey-Davis (so called Rockey- Davis), McArthur,
McBurney’s grid iron incision, with or without the medial Harrington-Weir-Fowler
extension (so called Weirs extension), or vertical Rutherford-Morrison extension,
Lanz incision, vertical right paramedian or pararectus (Battle) incision and midline
vertical incision.
The McBurney’s incision is undoubtedly the most popular, but it is the
Transverse or Rockey-Davis incision that meets the criteria for an appropriate incision
most closely. It is particularly useful in retro-caecal appendices & in those patients who
are obese.
46
Transverse or Rockey-Davis incision (84): It is centered on the midclavicular-
midinguinal line, usually made at the level 1-2 cm inferior to the umbilicus, depending on
the size of the patient’s abdomen and the location of maximum tenderness. The length of
the incision should be 1-2 cm longer than the width of the surgeon’s hand.
This approach gives rapid access to the right lower portion of abdomen. If the incision is
appropriately placed (i.e not too low), The exposure of the caecum and the appendix is
excellent. This incision produces minimal trauma to the muscle and other tissues and is
easily extended medially by further incising the rectus sheath and rarely, the rectus
muscle itself, converting it into a proper transverse abdominal incision.
However, there is a theoretical objection to transverse incision. The medial end of the
incision is relatively close to the midline, so that is localized pus is present and spillage
occurs, there is a danger of dissemination.
McArthur-McBurney’s incision (26,28,84): It is the time tested, muscle splitting incision
that probably is most widely used today for appendectomy. Its advantage, like that of
Rockey-Davis incision, is that the separation of the muscles in line with their fibers
produces a wound that does not entirely depend on sutures for establishment of tissue
continuity.
Nevertheless, a post-operative hernia can occur with both the incisions. The
McBurney’s incision provides good exposure when the appendix lies free in the
peritoneal cavity. However, if the appendix is in different positions such as retrocaecal,
exposure can be cumbersome. This incision can be extended medially by partially
47
transecting the rectus sheath as described by Weir, but produces a hockey stick type of
skin incision. Perhaps the greatest disadvantage of McBurney’s incision is that it follows
an oblique course in the right lower quadrant, cutting across the skin lines. The scar
widens with time thus producing a cosmetic result that is less than optimal.
The incision (7-10 cms) in length, lies at right angles to the line joining the
anterior superior iliac spine and the umbilicus, centered at the Mc Burney’s point i.e., at
the junction of the lateral and middle thirds of that line.
External oblique aponeurosis is split in the line of its fibers and the underlying muscles
split, to expose the transversalis fascia and peritoneum. Both these are picked up as one
layer and are incised. If more access us required in a medial direction, the incision is
extended as described by Weir. Under desperate circumstances, a Gridiron incision can
be extended vertically by dividing the oblique muscles at right angles to its fibers. This
method destroys the rationale of this incision, but is occasionally required to expose a
retro-caecal appendix.
The Lanz incision (28): This is a minor modification of the Gridiron incision. The skin
incision is made more or less transversely and curves so that it lies in the inter-spinous
crease. Thereafter, the muscles are divided as in a classic Gridiron approach. The method
has a definitive cosmetic value in producing an almost invisible scar, but difficulties are
encountered if the incision is to be enlarged.
48
Other incisions: Although some surgeons continue to use vertical, right paramedian
incision or a pararectus (Battle)(84) incision, neither of these provides good access to the
appendix as that achieved through either the Rockey-Davis or the Mc Burney’s incision.
The Battle incision is particularly susceptible to disruption, either acutely as dehiscence
or subsequently as a ventral hernia. It is likely to denervate substantial segments of the
rectus muscle as well as to interrupt its blood supply and exposure given is also not ideal.
ROUTINE APPENDECTONY (26,84)
After the incision is deepened through the fat and Scarpa’s fascia, the aponeurosis of the
External oblique muscle is exposed and incised in the line of the fibers. The fibers of
Internal oblique muscle, which are now exposed, are muscular and having normally
distinct fibers, which are now separated, followed by the separation of the fibers of
Transversus abdominis, which laterally becomes aponeurotic. The peritoneum is picked
up and incised in the line of incision. The caecum and the appendix are drawn out into the
wound, and the appendix is delivered. The mesoappendix is serially clipped with an
artery forceps, divided and subsequently ligated. Approximately 5mm distal to the base
of the appendix, the organ is crushed and the forceps is applied 7-8 mm distally. A silk
ligature is applied to the crushed area and the organ transected. The exposed mucous
membrane is then swabbed with a cauterizing agent either electrocautery or absolute
alcohol (this helps in sealing off the mucosa). The stump is invaginated (buried). Some
surgeons do not advocate burying of the stump, if the appendix is oedematous and turgid.
49
Wound closure: After removal, the operated area is irrigated ( in gangrenous or
perforated appendix) each fascial and muscular layer is closed with an absorbable suture
material. Skin is closed with non-absorbable sutures.
Advantages of invagination of the ligated stump: Better control of hemorrhage from
the stump, doubly secure closure of the caecal wall, less chance of peritoneal
contamination due to burial of infected stump and reduced risk of post-operative
adhesions by minimizing the extent of exposed, raw surface.
Disadvantages of invagination of the ligated stump: Internal abscess formation,
intussusceptions of the caecum following stump invagination, peritonitis resulting from
rupture of an intramural abscess, high incidence of adhesions following rupture of
intramural abscess.
Retrograde appendectomy (26,84): It is the retrograde removal of the appendix by
dividing the appendix at the base and thereafter dissecting till the tip. It is indicated if the
exposure of the appendix is difficult either because it is excessively long, or it occupies
the retrocaecal position, or if the appendix is densely adherent and inflamed distally.
Appendectomy-en –passant (Incidental appendectomy) (23) This is the removal of
normal appendix during the course of abdominal operation for other conditions. This
practice is readily rationalized when the appendix appears to be diseased, as in carcinoid
50
involvement. It seems to be reasonable at exploratory laparotomy for crohn’s disease,
when the appendix and caecum are not involved in the inflammatory process, because of
the recurrence rate and chronicity of the primary process and its tendency to stimulate
appendicitis. It should not be done in the face of other inflammatory intra-peritoneal
disease.
COMPLICATIONS OF APPENDECTOMY (23,26) :
Early complications:
1. Paralytic ileus invariably accompanies generalized peritonitis.
2. Sepsis – Local wound abscess, pelvic abscess, and subphrenic abscess.
3. Rupture of the stump or caecal wall. This is very rare, but occurs when a portion
of the stump or the caecal wall gives way in the first few days after
appendectomy.
4. Hemorrhage: Sudden abdominal pain and shock at any time during the first 72 hrs
after surgery means either leakage from the stump or a slipped arterial ligature,
both of which are now rare.
Late complications:
1. Intestinal obstruction due to local adhesive bands.
2. Incisional hernia.
51
LAPAROSCOPIC APPENDECTOMY (84,85,86)
This is the latest procedure introduced by Kurt Semm (85) in 1982. Advantages and
disadvantages of this procedure are weighed against those of conventional
appendectomy.
Advantages:
1. It is diagnostic as well as therapeutic tool.
2. It is minimally invasive surgery.
3. Less postoperative pain.
4. Hospital stay is minimized.
5. Fewer post operative adhesions.
6. Superior cosmetic results.
7. Early return to normal activities.
8. If the appendix is found normal, other organs can be visualized.
9. This is the procedure of choice in obese patients.
10. The incision is the same even in case of difficult appendectomies like in
retrocaecal appendix.
Disadvantages:
1. It is expensive compared to conventional method.
2. Expertise in technique is needed.
3. Procedure is not useful if perforation or peritonitis is present.
4. Operative time required is more compared to open appendectomy.
52
5. Setting up of instruments and team is difficult for emergency appendectomy.
In summary, laparoscopic appendectomy is a safe alternative to open appendectomy.
METHODOLOGY
For inflamed (clinical) cases
Materials for this study was obtained from patients admitted to Bowring and Lady curzon
Hospitals and Victoria Hospital attached to Bangalore medical college, Bangalore, from
May 2003 to August 2005 with a diagnosis of appendicitis. All cases were subjected to
clinical assessment using signs, symptoms and laboratory criteria, and also the position of
the appendix, which were recorded in the proforma. All patient were subjected to
ultrasound examination by a qualified radiologist to exclude any other associated
pathology and also to confirm the diagnosis in doubtful cases.
After admission to ward detailed history was taken regarding presenting complaints, their
duration severity, sequence of onset of symptoms, mode of onset, progression, change in
the pattern at the time of presentation and any atypical symptoms, Enquiry was made into
53
family history suggestive of appendicitis, menstrual and obstetric history and past history
of appendicitis.
A careful and detailed abdominal examination of each patient made including local
temperature, guarding / rigidity site of maximum tenderness any swelling or mass
formation, rebound tenderness, Rovsing’s sign, Poas sign, Obturator sign, Baldwin’s sign
and also per rectal examination is made to look for pelvic tenderness or mass formation.
Surgery was done either under general anesthesia or spinal anesthesia. Abdomen was
opened with Lanz or Mc Burney’s, or right lower Para median incision. At surgery the
Position of the appendix was first identified before disturbing the structures and the
position of the appendix identified and recorded together with the length of the appendix
and also weather it was fixed or freely mobile in the peritoneal cavity, peri-appendiceal
collection, presence of perforation or other complications of appendicitis. Also a note was
made of the status surrounding organs. After completion of the appendectomy the
specimen was subjected to histopathological examination by the qualified pathologist
only those cases, which were proved as, appendicitis by the histopathology were included
in the study. Those with normal appendix on histopathology were excluded from the
study.
For normal population (autopsy cases)
Materials for this study were obtained from all the fresh cadavers undergoing autopsy in
the Bowring and Lady curzon Hospitals mortuary attached to Bangalore medical college
Bangalore, from June 2003 to July 2005. These cases represented the position of the
appendix in normal population. The cases, which were included, were fresh cadavers
54

with intact torso, and those who have died because of some non-abdominal cause. All
cases were opened in a classical fashion and after opening the abdomen the position of
the appendix were noted before disturbing any of the structures, the length of the
appendix and also weather it is fixed or freely mobile in the peritoneal cavity is noted and
recorded as in the proforma.
Those cases, which were decomposed, and those in which the torso was mutilated as in
railway accidents were excluded from the study. The cases, in which only the extremities
were disrupted, were included in the study.
PROFORMA
For clinical cases (representing inflamed cases)
Serial No. Age: Sex
Name: Ward: Unit:
I.P.No. Occupation:
Address:
Date of admission:
Date of operation:
Date of discharge:
I. Presenting complaints:
a) Pain : Duration :
55
Nature : Typical /Atypical
Radiation :
b) Vomiting: Duration: Frequency:
Projectile / Regurgitated / bile stained / Not bile stained /
Pain relief after vomiting / contents of vomitus.
c) Fever: Duration: Intermittant / continuous
Associated with chills & rigors.
d) Diarrhoea / Constipation / Tenesmus / Blood & mucous.
e) Urinary complaints: Duration: Frequency:
Dysuria / Burning / Haematuria / Radiation of pain.
f) Any other complaints:
II. Family history
III. Past history: Number of similar attacks in the past:
Previous hospitalization & follow-up:
IV. Menstrual history: Regular / Irregular Spotting
______/_____days
Deliveries:
V. Per - Abdomen
Inspection : Normal / Fullness
Visible scar Pointing test : Umbilicus / RIF Palpation:
Site of maximum tenderness: RIF / Flank / Mc Burney’s point.
56
Rebound tenderness
Rovsing’s sign Psoas sign:
Local temperature Baldwin’s sign:
Mass: Obturator sign:
P.R : Tenderness - Yes / No Mass : Yess / No
VI. Investigations :
Hb:_____gm% TC: DC: ESR:
Urine : Albumin_____ , Sugar______ , Microscopy______
Ultrasound Abdomen:
RIF : APPENDIX - Length
- Diameter
- Mass / Abscess
- Appendicolith
- Probe tenderness
Pelvis:
Other findings:
VII. SURGERY:
Date: Time: Emergency/Elective
Preoperative diagnosis:
Postoperative diagnosis:
Incision:
57
Type of anaessthesia:
Operative findings: - Position: Preileal / Postileal / Retrocaecal /
Paracaecal / Subcaecal / Pelvic / Promonteric
- Length
- Appearance
- Intraperitoneal / Extraperitoneal
- Fixed / Mobile
Caecum:
Ileum:
Other organs:
PROFORMA
For autopsy cases (representing normal population)
Serial No: Age : Sex:
Name P.M. No.
Address
Date of postmortem:
Position of the appendix
- Retro-caecal
- Para-caecal
- Sub-caecal
58
- Pelvic
- Promonteric
- Post-ileal
- Pre-ileal
Length of the appendix
Intra-peritoneal / Extra-peritoneal
RESULTS
The total numbers of cases studied are 150; of this 50 are clinical group,
which were biopsy positive; hence these represent the inflamed appendices. The other
100 are of autopsy group, the cause of death of these cases being non-abdominal cause,
so that these represent the normal population.
Among the 50 cases two cases presented with generalized peritonitis (Case
No –25) & (Case No – 31) the position of appendix in these cases was Post-ileal and
Para-caecal respectively. Two cases (Case No – 26) & (Case No – 49) had previously
presented with appendicular mass hence these were managed conservatively and
subsequently underwent interval appendectomy. All the other cases presented as acute
appendicitis, which were either operated on emergency basis or electively, depending
upon the severity of inflammation. Totally 15 cases (30%) were operated on an
emergency basis and the rest as elective cases (70%).
59
In our series appendicitis was more common during the 3rd decade
(48%), followed by the 2nd decade (32%). Appendicitis is slightly more common in
males, M : F ratio is 2.8 : 1 in our series.
All the patients with acute appendicitis had pain and most of the patients
had pain in the right iliac fossa. Even though many of the patients presented with atypical
symptoms 21 of the 50 cases (42%) The site of maximum pain was in the right iliac fossa
in 41 of 50 cases. Only 9 cases had maximal pain at a site other than right iliac fossa.
Anorexia was seen in 76% of the cases, while nausea is less constant is
seen in 46% of the cases. Vomiting is rarely seen (28%) and is usually few episodes.
Tenderness in the right iliac fossa is a constant feature in all the cases of
appendicitis. The site of maximum tenderness was in the right iliac fossa in 40 of 50
cases even though few had tenderness at other sites leading to difficulty in the diagnosis.
Only 10 cases had maximal tenderness at a site other than right iliac fossa.
Leukocytosis or neutrophilia was present in 36 of the 50 cases, with an
accuracy of 72%.
Of the 15 cases, which were operated on an emergency basis, 6 (40%)
were complicated by perforation, abscess or gangrene, whereas among the 35 elective
cases only 8 were complicated (22.8%).
60

There was a preponderance of young patients in our study in the clinical
group 40 of 50 cases (80%) were in the 10-29 yrs age group and in the autopsy group 43
of the 100 cases (43%) were in the same age group.
The position of the appendix at laparotomy was variable with the most
common position being retro-caecal (36%). At autopsy also the retro-caecal position of
the appendix is the most common position (31%).
There length of the appendix is also quite variable, the smallest in our
series being 3cm and the longest being 18cm and the average of 8.70cm. In our study
females had a slightly longer appendix with an average of 9.10cm, and the males had
smaller appendix with an average length of 8.55cm.
The position of the appendix influences the clinical presentation of the
appendicitis with the retro-caecal position (44.4% of cases), post-ileal position (54.5% of
cases), and the Pelvic position (60% of cases) in all the other positions (9.09% of cases)
presenting with atypical symptoms.
In case of retro-caecal position 88.8% of the fixed retro-caecal cases,
which had got fixed, either because of the adhesions or the extra-peritoneal fixation of the
appendix during development presented atypically and none of the cases with mobile
appendix presented atypically. These patients presented with flank pain & tenderness and
also symptoms of the upper urinary tract infection
61
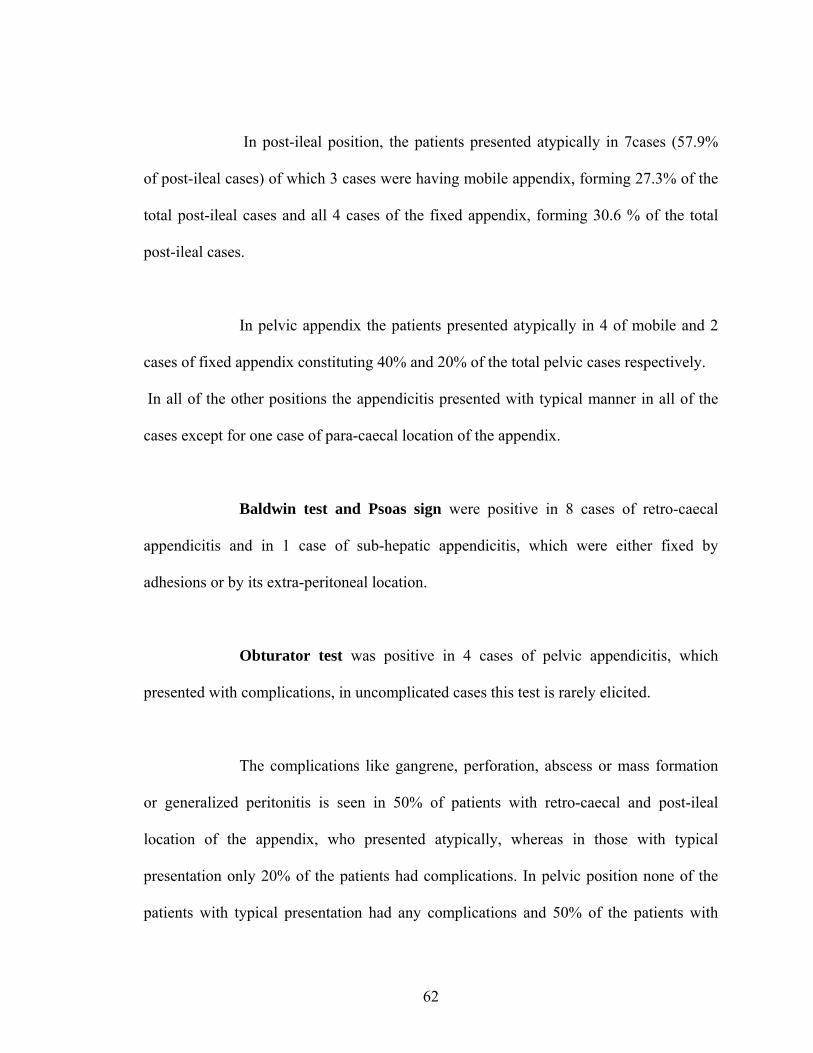
In post-ileal position, the patients presented atypically in 7cases (57.9%
of post-ileal cases) of which 3 cases were having mobile appendix, forming 27.3% of the
total post-ileal cases and all 4 cases of the fixed appendix, forming 30.6 % of the total
post-ileal cases.
In pelvic appendix the patients presented atypically in 4 of mobile and 2
cases of fixed appendix constituting 40% and 20% of the total pelvic cases respectively.
In all of the other positions the appendicitis presented with typical manner in all of the
cases except for one case of para-caecal location of the appendix.
Baldwin test and Psoas sign were positive in 8 cases of retro-caecal
appendicitis and in 1 case of sub-hepatic appendicitis, which were either fixed by
adhesions or by its extra-peritoneal location.
Obturator test was positive in 4 cases of pelvic appendicitis, which
presented with complications, in uncomplicated cases this test is rarely elicited.
The complications like gangrene, perforation, abscess or mass formation
or generalized peritonitis is seen in 50% of patients with retro-caecal and post-ileal
location of the appendix, who presented atypically, whereas in those with typical
presentation only 20% of the patients had complications. In pelvic position none of the
patients with typical presentation had any complications and 50% of the patients with
62
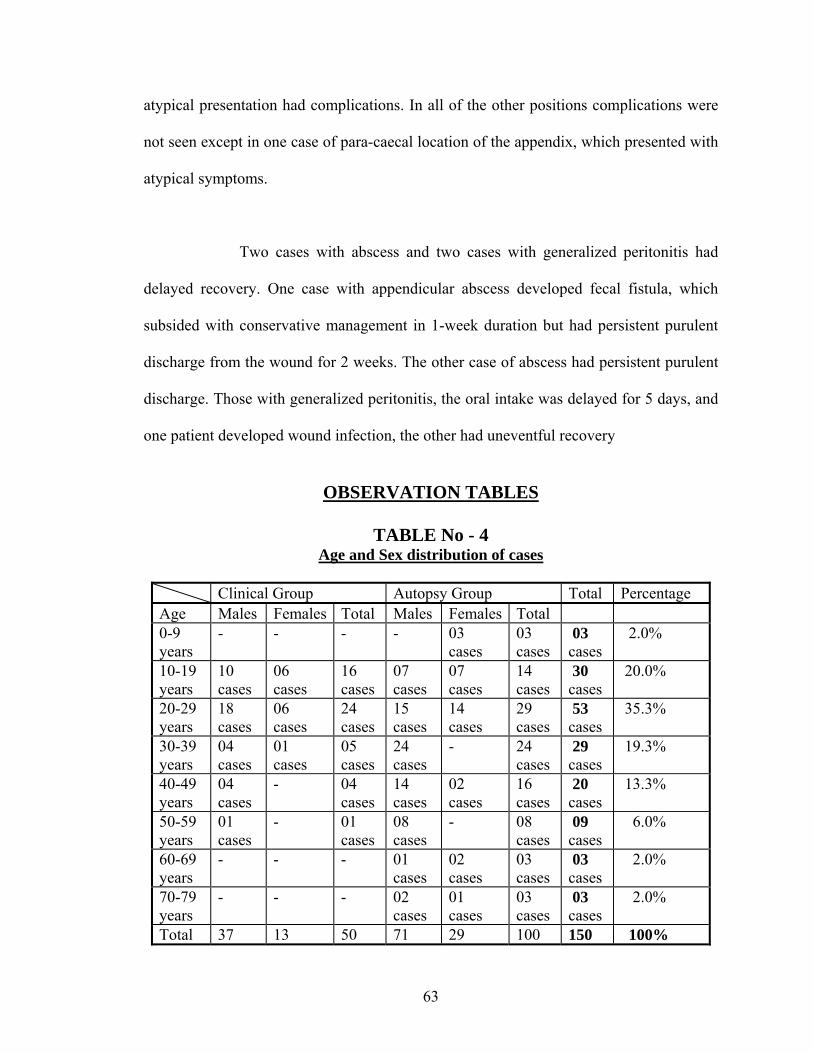
atypical presentation had complications. In all of the other positions complications were
not seen except in one case of para-caecal location of the appendix, which presented with
atypical symptoms.
Two cases with abscess and two cases with generalized peritonitis had
delayed recovery. One case with appendicular abscess developed fecal fistula, which
subsided with conservative management in 1-week duration but had persistent purulent
discharge from the wound for 2 weeks. The other case of abscess had persistent purulent
discharge. Those with generalized peritonitis, the oral intake was delayed for 5 days, and
one patient developed wound infection, the other had uneventful recovery
OBSERVATION TABLES
TABLE No - 4
Age and Sex distribution of cases
Clinical Group Autopsy Group Total Percentage Age Males Females Total Males Females Total 0-9 years
- - - - 03 cases
03 cases
03 cases
2.0%
10-19 years
10 cases
06 cases
16 cases
07 cases
07 cases
14 cases
30 cases
20.0%
20-29 years
18 cases
06 cases
24 cases
15 cases
14 cases
29 cases
53 cases
35.3%
30-39 years
04 cases
01 cases
05 cases
24 cases
- 24 cases
29 cases
19.3%
40-49 years
04 cases
- 04 cases
14 cases
02 cases
16 cases
20 cases
13.3%
50-59 years
01 cases
- 01 cases
08 cases
- 08 cases
09 cases
6.0%
60-69 years
- - - 01 cases
02 cases
03 cases
03 cases
2.0%
70-79 years
- - - 02 cases
01 cases
03 cases
03 cases
2.0%
Total 37 13 50 71 29 100 150 100%
63
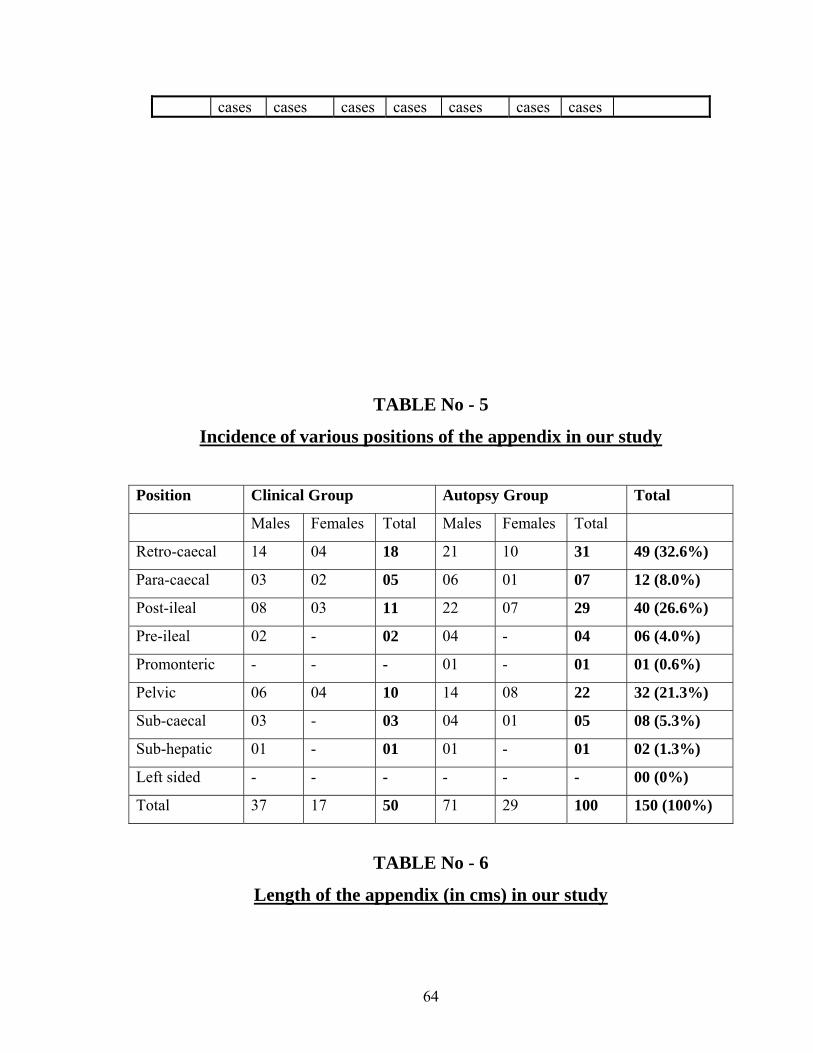
cases cases cases cases cases cases cases
TABLE No - 5
Incidence of various positions of the appendix in our study
Position Clinical Group Autopsy Group Total
Males Females Total Males Females Total
Retro-caecal 14 04 18 21 10 31 49 (32.6%)
Para-caecal 03 02 05 06 01 07 12 (8.0%)
Post-ileal 08 03 11 22 07 29 40 (26.6%)
Pre-ileal 02 - 02 04 - 04 06 (4.0%)
Promonteric - - - 01 - 01 01 (0.6%)
Pelvic 06 04 10 14 08 22 32 (21.3%)
Sub-caecal 03 - 03 04 01 05 08 (5.3%)
Sub-hepatic 01 - 01 01 - 01 02 (1.3%)
Left sided - - - - - - 00 (0%)
Total 37 17 50 71 29 100 150 (100%)
TABLE No - 6
Length of the appendix (in cms) in our study
64
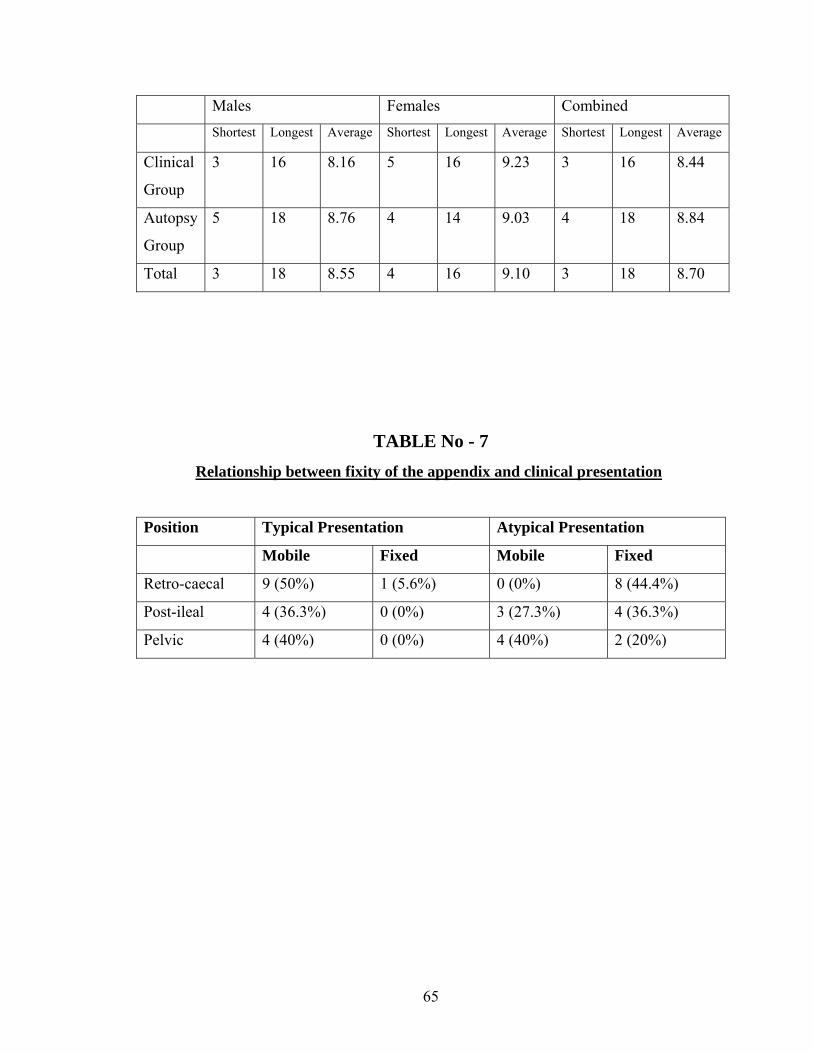
Males Females Combined
Shortest Longest Average Shortest Longest Average Shortest Longest Average
Clinical
Group
3 16 8.16 5 16 9.23 3 16 8.44
Autopsy
Group
5 18 8.76 4 14 9.03 4 18 8.84
Total 3 18 8.55 4 16 9.10 3 18 8.70
TABLE No - 7
Relationship between fixity of the appendix and clinical presentation
Position Typical Presentation Atypical Presentation
Mobile Fixed Mobile Fixed
Retro-caecal 9 (50%) 1 (5.6%) 0 (0%) 8 (44.4%)
Post-ileal 4 (36.3%) 0 (0%) 3 (27.3%) 4 (36.3%)
Pelvic 4 (40%) 0 (0%) 4 (40%) 2 (20%)
65
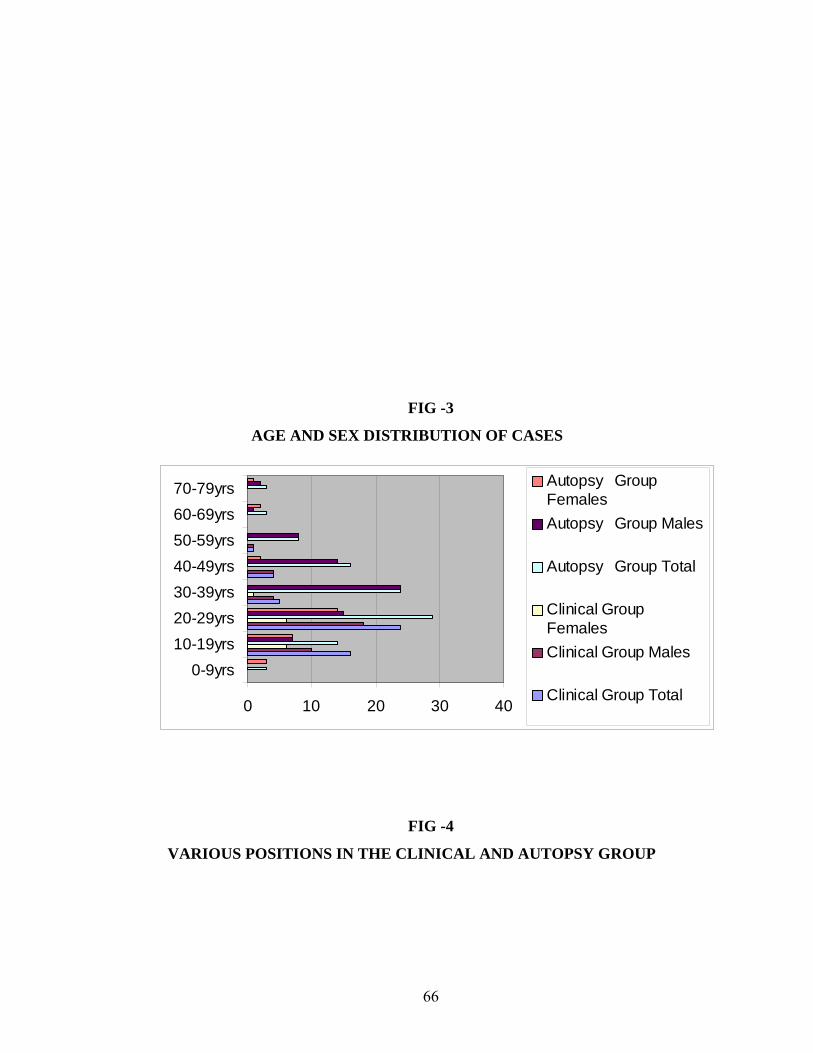
FIG -3
AGE AND SEX DISTRIBUTION OF CASES
0 10 20 30 40
0-9yrs10-19yrs20-29yrs30-39yrs40-49yrs50-59yrs60-69yrs70-79yrs Autopsy Group
FemalesAutopsy Group Males
Autopsy Group Total
Clinical GroupFemalesClinical Group Males
Clinical Group Total
FIG -4
VARIOUS POSITIONS IN THE CLINICAL AND AUTOPSY GROUP
66
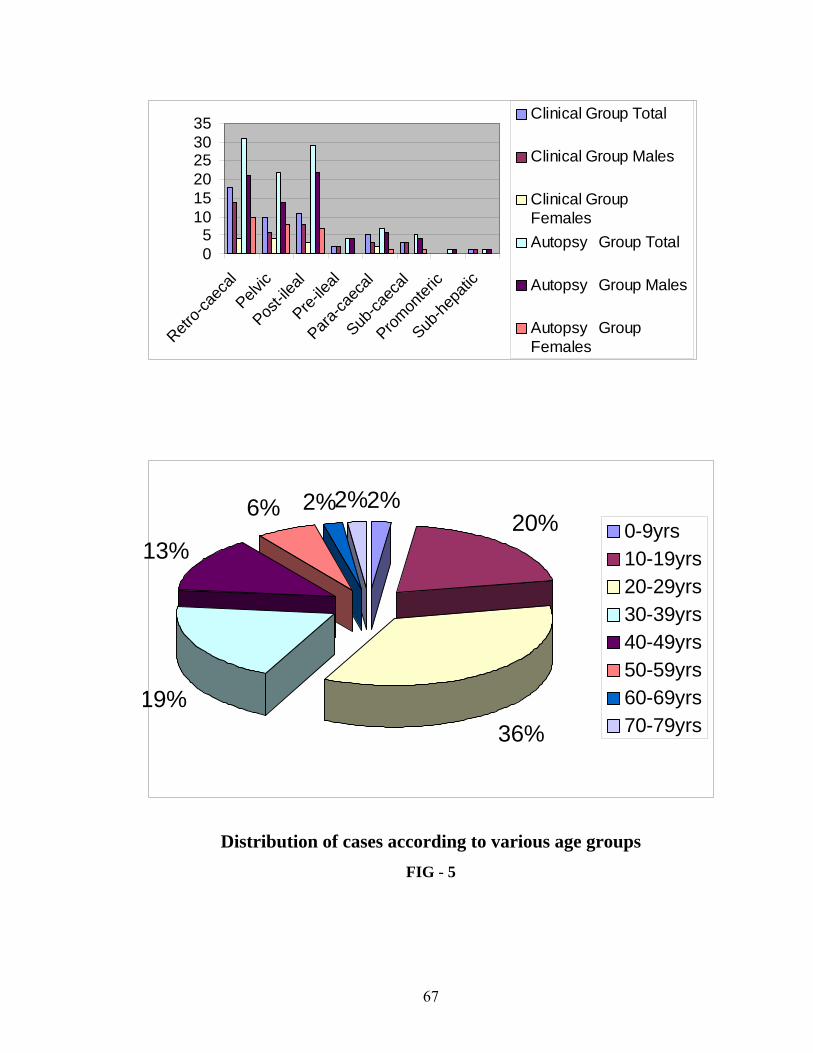
05
101520253035
Retro-c
aeca
l
Pelvic
Post-il
eal
Pre-ile
al
Para-ca
ecal
Sub-ca
ecal
Promon
teric
Sub-he
patic
Clinical Group Total
Clinical Group Males
Clinical GroupFemalesAutopsy Group Total
Autopsy Group Males
Autopsy GroupFemales
Distribution of cases according to various age groups
2%20%
36%19%
13%
6% 2%2%0-9yrs10-19yrs20-29yrs30-39yrs40-49yrs50-59yrs60-69yrs70-79yrs
FIG - 5
67
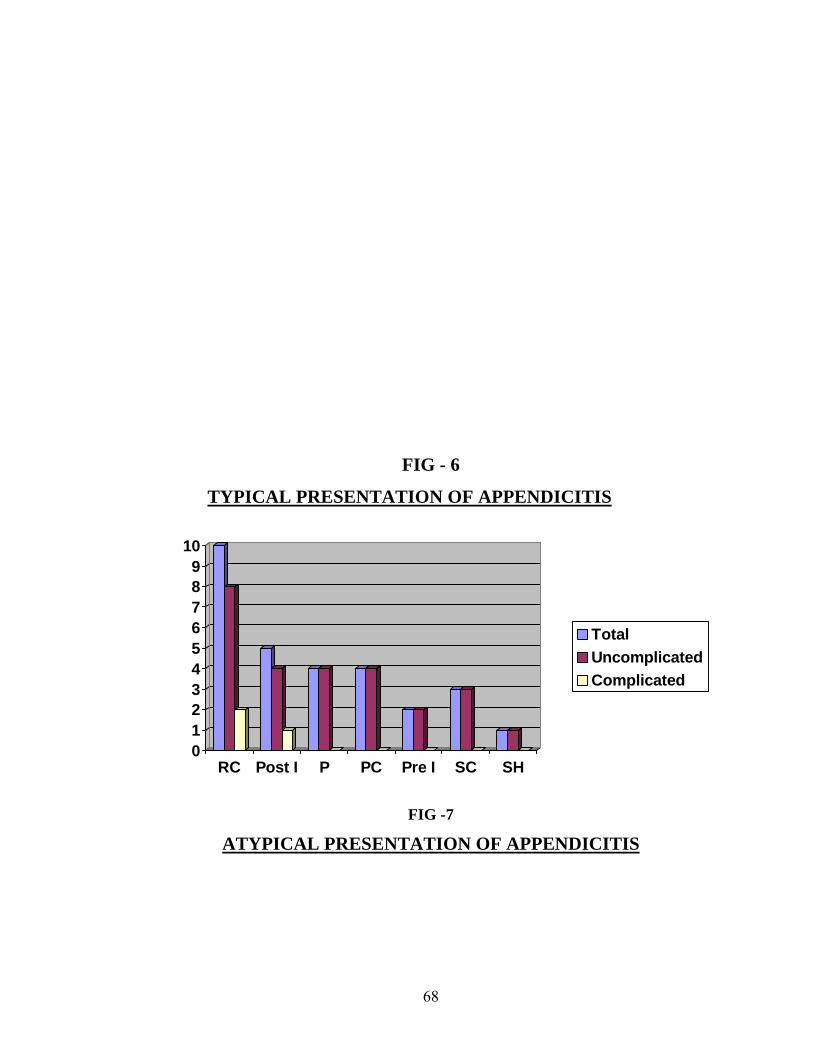
FIG - 6
TYPICAL PRESENTAT APPENDICITISION OF
0123456789
10
RC Post I P PC Pre I SC SH
TotalUncomplicatedComplicated
FIG -7
ATYPICAL PRESENT OF APPENDICITISATION
68
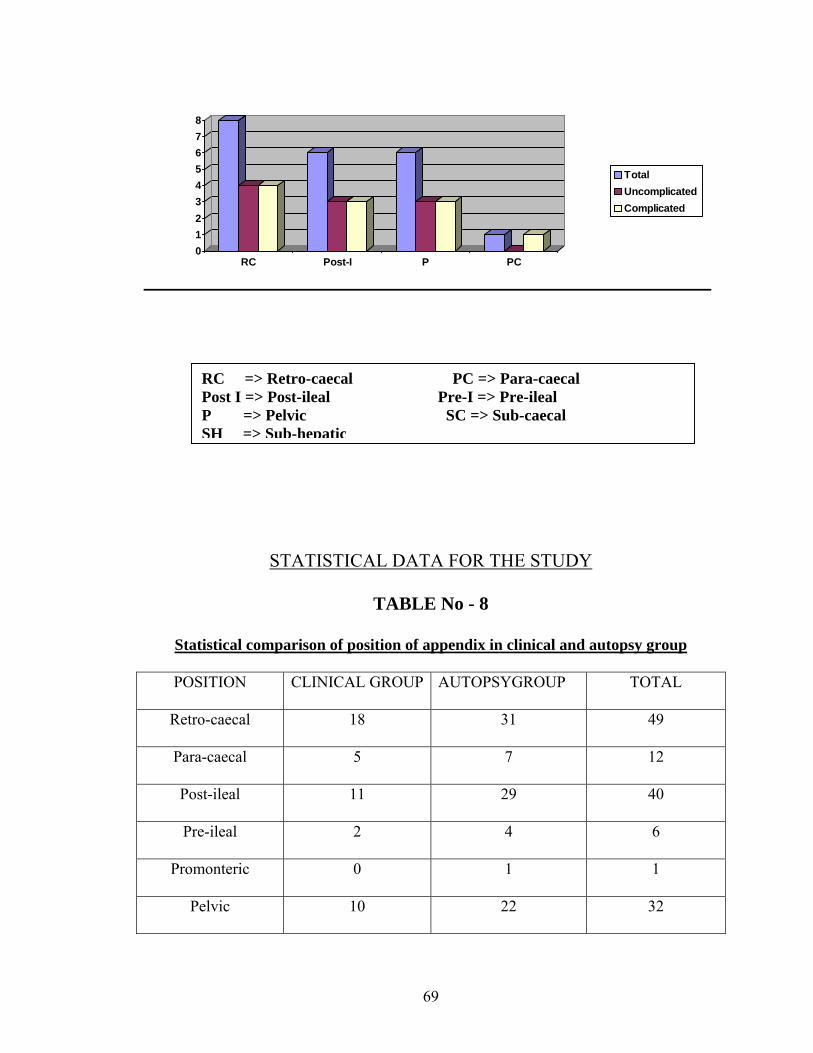
012345678
RC Post-I P PC
TotalUncomplicatedComplicated
Sta
PO
Retr
Par
Po
Pr
Prom
P
RC => Retro-caecal PC => Para-caecal Post I => Post-ileal Pre-I => Pre-ileal P => Pelvic SC => Sub-caecal SH => Sub-hepatic
STATISTICAL DATA FOR THE STUDY
TABLE No - 8
tistical comparison of position of appendix in clinical and autopsy group
SITION CLINICAL GROUP AUTOPSYGROUP TOTAL
o-caecal 18 31 49
a-caecal 5 7 12
st-ileal 11 29 40
e-ileal 2 4 6
onteric 0 1 1
elvic 10 22 32
69
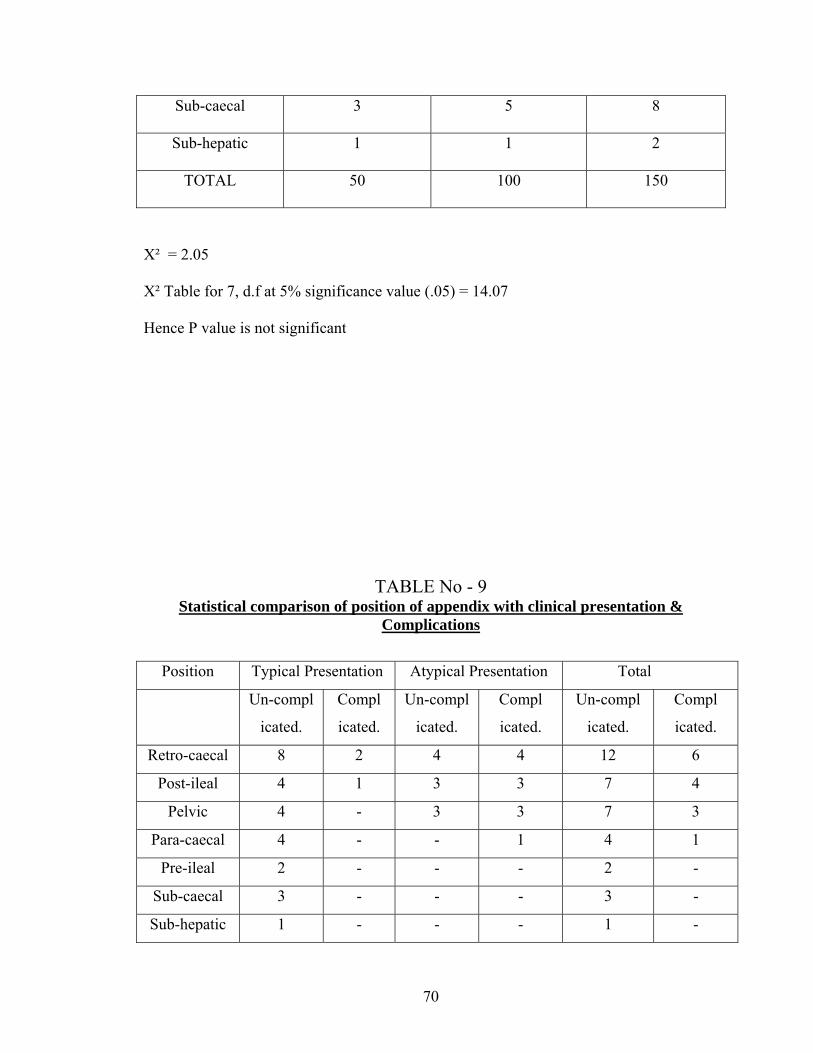
Sub-caecal 3 5 8
Sub-hepatic 1 1 2
TOTAL 50 100 150
Χ² = 2.05
Χ² Table for 7, d.f at 5% significance value (.05) = 14.07
Hence P value is not significant
TABLE No - 9 Statistical comparison of position of appendix with clinical presentation &
Complications
Position Typical Presentation Atypical Presentation Total
Un-compl
icated.
Compl
icated.
Un-compl
icated.
Compl
icated.
Un-compl
icated.
Compl
icated.
Retro-caecal 8 2 4 4 12 6
Post-ileal 4 1 3 3 7 4
Pelvic 4 - 3 3 7 3
Para-caecal 4 - - 1 4 1
Pre-ileal 2 - - - 2 -
Sub-caecal 3 - - - 3 -
Sub-hepatic 1 - - - 1 -
70

Total 26 3 10 11 36 14
The level of significance was calculated using ANOVA table (Analysis of variance)
F1 = 6.21
F2 = 14.09
Ftable for (6,6) d.f = 0.233
Ftable for (1,6) d.f = 0.0043
The value of F1 & F2 is greater than the Ftable value; hence the value is significant; hence
the difference in the complications and clinical presentation with regard to position is
significant.
DISCUSSION
Although surgeons have been confronting acute appendicitis as a clinical entity
for over a hundred years, an accurate preoperative diagnosis remains a challenge because
of the various other conditions, which mimic appendicitis. The problem is further
compounded by the variations in the position of the appendix and the associated varied
clinical picture of the appendicitis.
In our study two groups were taken the autopsy group, which represented the
normal population, and the clinical group, which represented the inflamed cases. In the
71
clinical group the cases were evaluated with clinical features at presentation, the position
of the appendix at laparotomy and also the associated complications. All cases in the
clinical group were confirmed by histo-pathology.
Our study found appendicitis to be more common in the third decade followed by
the second decade 48% and 32% respectively. The average mean age of presentation is
25.1 years. Lewis et al (39) (1975) in their study found that the 2nd and 3rd decades to be
the most common age groups for acute appendicitis.
The total no of male patients in the clinical group were 37 and the total no of female
patients were 13 Male to female ratio is 2.8 : 1. Men outnumbered women in our study,
men are believed to suffer from appendicitis more often because, probably the male is
being subjected to more stress and strain, as highlighted by Boyd (1961). Addis et al &
Korner et al, have reported a slight male preponderance (with male to female ratio of 1.2
to 1.3 : 1) (30,31)
Anorexia was seen in 76% of the cases, while nausea was present in 46%
of the cases. Vomiting is rarely seen (28%) and is usually few episodes. Lewis et al (39),
in his analysis, found anorexia, nausea or vomiting to be present in 66% of the cases.
Fever is uncommonly encountered among patients in our study, being
present in 46% of our patients; the fever was usually mild degree except in cases of
abscess and generalized peritonitis. Berry et al (87) in 1984 have in their analysis; found
that temperature elevation is rarely more than 10 C (1.80 F). Changes of greater
72
magnitude indicate that the complication has occurred or some other diagnosis should be
considered.
The various positions in the clinical group, representing the inflamed appendix and the
Autopsy group representing the normal appendix, were compared with Chi square test,
the P-value was >0.1. Hence the difference observed was not significant, indicating that
there is no increased predisposition of any position to get inflamed.
The position of the appendix and its relation to the clinical presentation and
course of acute appendicitis has been a subject of controversy with various authors giving
various results and conclusions.
Varshney et-al (7), have come to the conclusion that the retro-caecal position is
less prone to infection, by comparing the incidence of retro-caecal appendix in operated
cases with the previous autopsy studies. He hypothesized that the retro-caecal position of
the appendix is advantageous because, gravity aided drainage of the appendicular lumen,
may reduce the episodes of luminal obstruction, which reduce the incidence of
appendicitis. Shen GK, et-al (9), Williamson WA, et-al (10), has established that the retro-
caecal position does not alter the clinical course of appendicitis.
The theory of Varshney et-al (7) is not acceptable, as many of the autopsy studies do not
accept that the retro-caecal position, as the most common position (Maisel et-al (20),
Peterson et-al, describe pelvic position to be the most common).
73
In our study there is an increased incidence in the complications in those with
typical presentation, than those with atypical presentation, In case of retro-caecal position
20% with typical & 50% with atypical presentation, in post-ileal position 25% with
typical & 50% with atypical presentation, and in pelvic position 0% with typical & 50%
with atypical presentation, had complications. In all the other positions the number of
complications are very less. The difference obtained is significant as; the P value is <0.05
as obtained by the ANOVA table.
In case of retro-caecal position, the fixed appendix is associated with more
complications (55%) as opposed to (12%) of cases with mobile appendix. The difference
obtained is significant (P<0.001 obtained from chi square test). In other positions the
obtained for fixity and complications is not significant (P > 0.05), But the difference in
complications in relation to typical or atypical is significant as obtained by ANOVA table
described above.
Varshney et-al (7) have described that advanced appendicitis (perforation or gangrene) is
more common in those with retro-caecal appendicitis. They have given the explanation
that some early cases may have been misdiagnosed, as urinary tract infection, leading to
delay in the diagnosis, and increased incidence of complications.
74
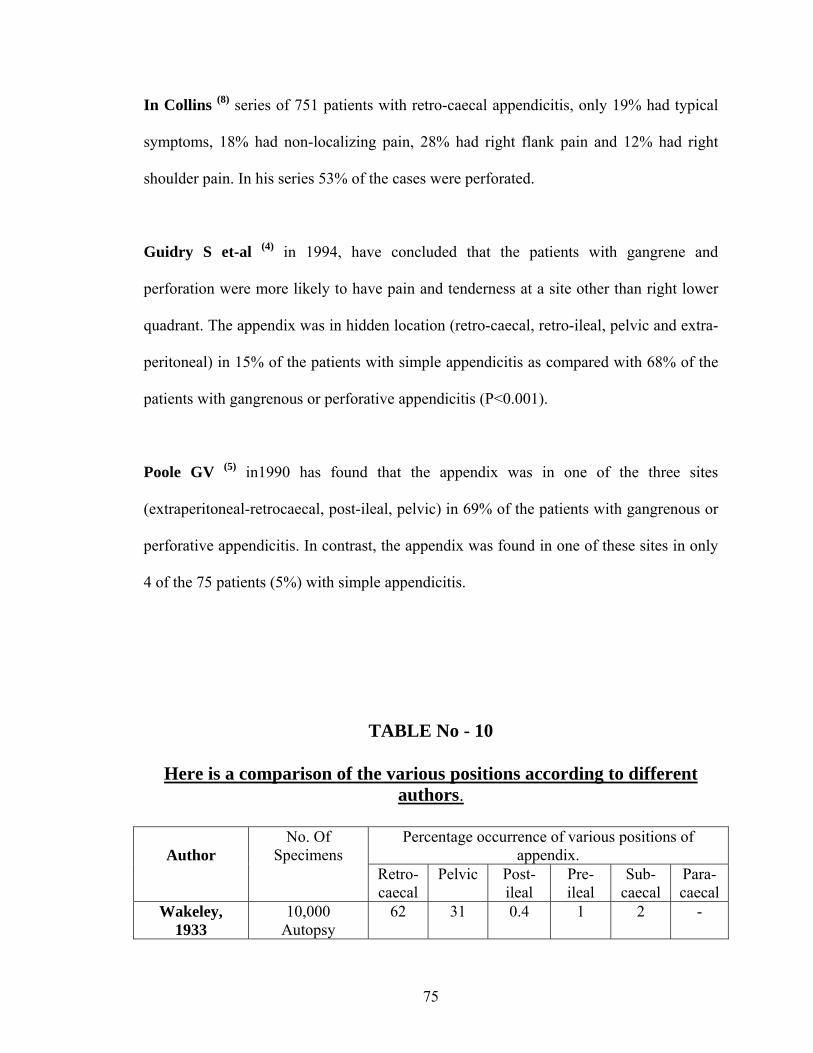
In Collins (8) series of 751 patients with retro-caecal appendicitis, only 19% had typical
symptoms, 18% had non-localizing pain, 28% had right flank pain and 12% had right
shoulder pain. In his series 53% of the cases were perforated.
Guidry S et-al (4) in 1994, have concluded that the patients with gangrene and
perforation were more likely to have pain and tenderness at a site other than right lower
quadrant. The appendix was in hidden location (retro-caecal, retro-ileal, pelvic and extra-
peritoneal) in 15% of the patients with simple appendicitis as compared with 68% of the
patients with gangrenous or perforative appendicitis (P<0.001).
Poole GV (5) in1990 has found that the appendix was in one of the three sites
(extraperitoneal-retrocaecal, post-ileal, pelvic) in 69% of the patients with gangrenous or
perforative appendicitis. In contrast, the appendix was found in one of these sites in only
4 of the 75 patients (5%) with simple appendicitis.
TABLE No - 10
Here is a comparison of the various positions according to different authors.
Percentage occurrence of various positions of
appendix.
Author No. Of
Specimens Retro- caecal
Pelvic Post- ileal
Pre- ileal
Sub- caecal
Para-caecal
Wakeley, 1933
10,000 Autopsy
62 31 0.4 1 2 -
75
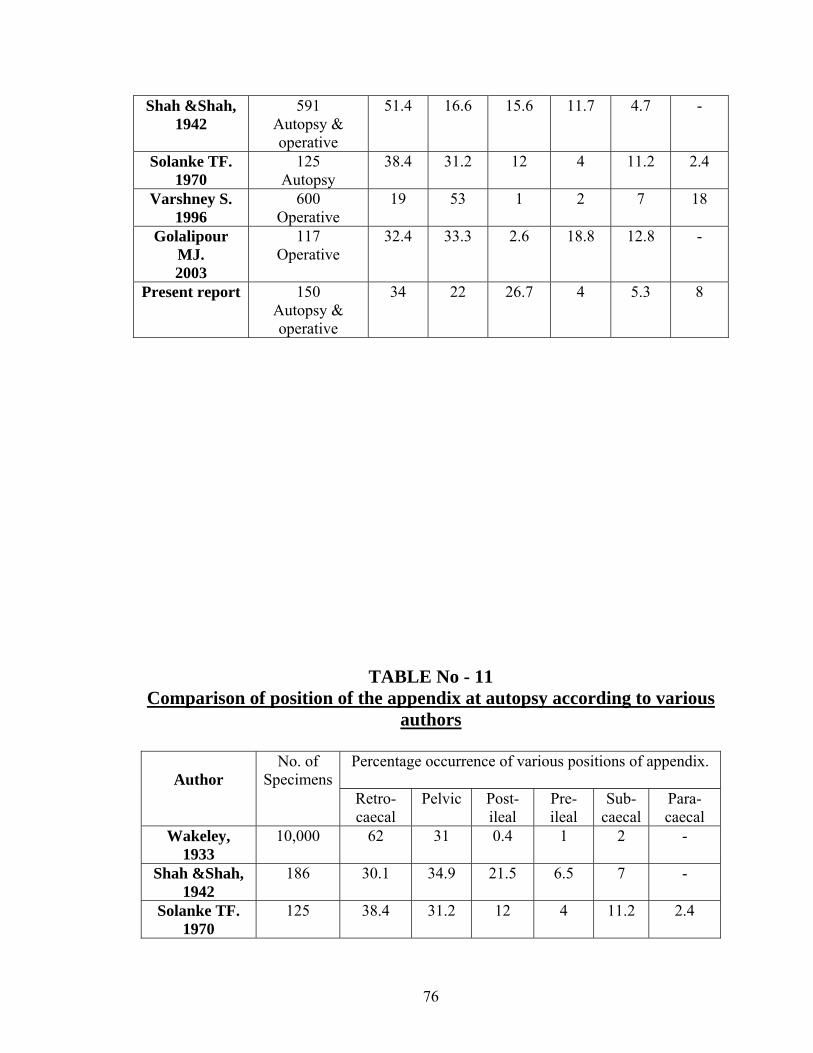
Shah &Shah, 1942
591 Autopsy & operative
51.4 16.6 15.6 11.7 4.7 -
Solanke TF. 1970
125 Autopsy
38.4 31.2 12 4 11.2 2.4
Varshney S. 1996
600 Operative
19 53 1 2 7 18
Golalipour MJ. 2003
117 Operative
32.4 33.3 2.6 18.8 12.8 -
Present report
150 Autopsy & operative
34 22 26.7 4 5.3 8
TABLE No - 11 Comparison of position of the appendix at autopsy according to various
authors
Percentage occurrence of various positions of appendix.
Author
No. of Specimens
Retro- caecal
Pelvic Post- ileal
Pre- ileal
Sub- caecal
Para-caecal
Wakeley, 1933
10,000 62 31 0.4 1 2 -
Shah &Shah, 1942
186 30.1 34.9 21.5 6.5 7 -
Solanke TF. 1970
125 38.4 31.2 12 4 11.2 2.4
76
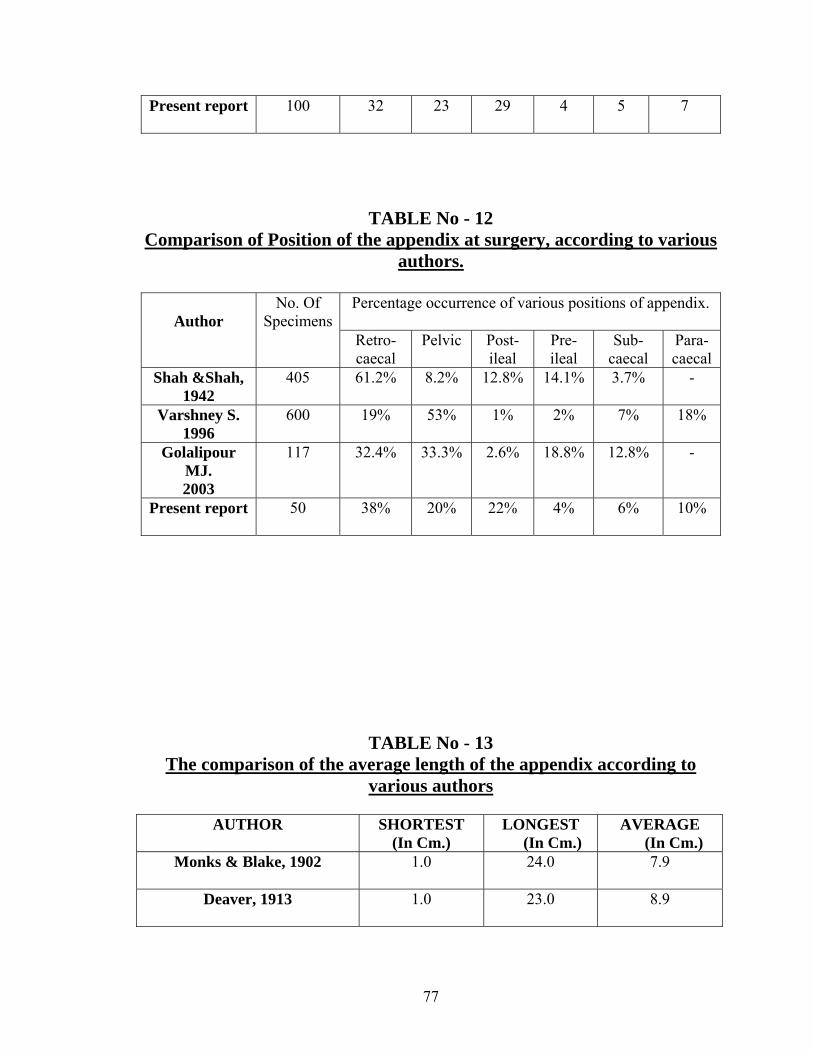
Present report
100 32 23 29 4 5 7
TABLE No - 12 Comparison of Position of the appendix at surgery, according to various
authors.
Percentage occurrence of various positions of appendix.
Author
No. Of Specimens
Retro- caecal
Pelvic Post- ileal
Pre- ileal
Sub- caecal
Para-caecal
Shah &Shah, 1942
405 61.2% 8.2% 12.8% 14.1% 3.7% -
Varshney S. 1996
600 19% 53% 1% 2% 7% 18%
Golalipour MJ. 2003
117 32.4% 33.3% 2.6% 18.8% 12.8% -
Present report
50 38% 20% 22% 4% 6% 10%
TABLE No - 13 The comparison of the average length of the appendix according to
various authors
AUTHOR SHORTEST (In Cm.)
LONGEST (In Cm.)
AVERAGE (In Cm.)
Monks & Blake, 1902 1.0 24.0 7.9
Deaver, 1913 1.0 23.0 8.9
77
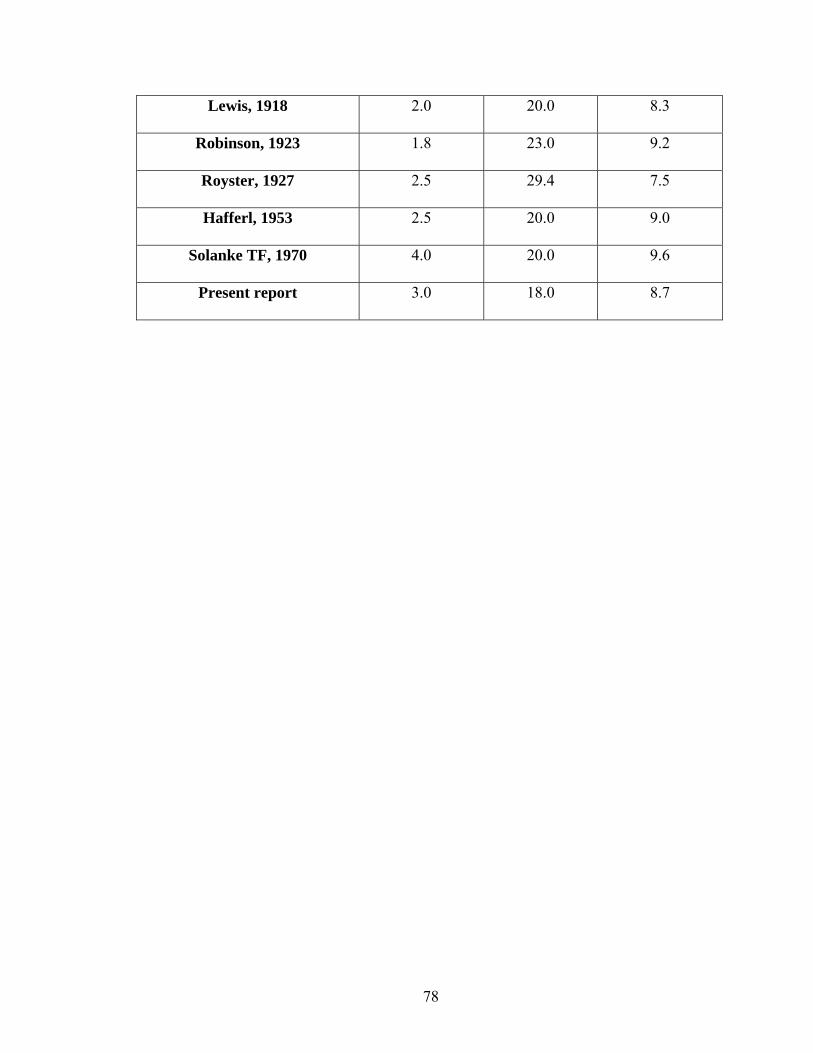
Lewis, 1918 2.0 20.0 8.3
Robinson, 1923 1.8 23.0 9.2
Royster, 1927 2.5 29.4 7.5
Hafferl, 1953 2.5 20.0 9.0
Solanke TF, 1970 4.0 20.0 9.6
Present report 3.0 18.0 8.7
78
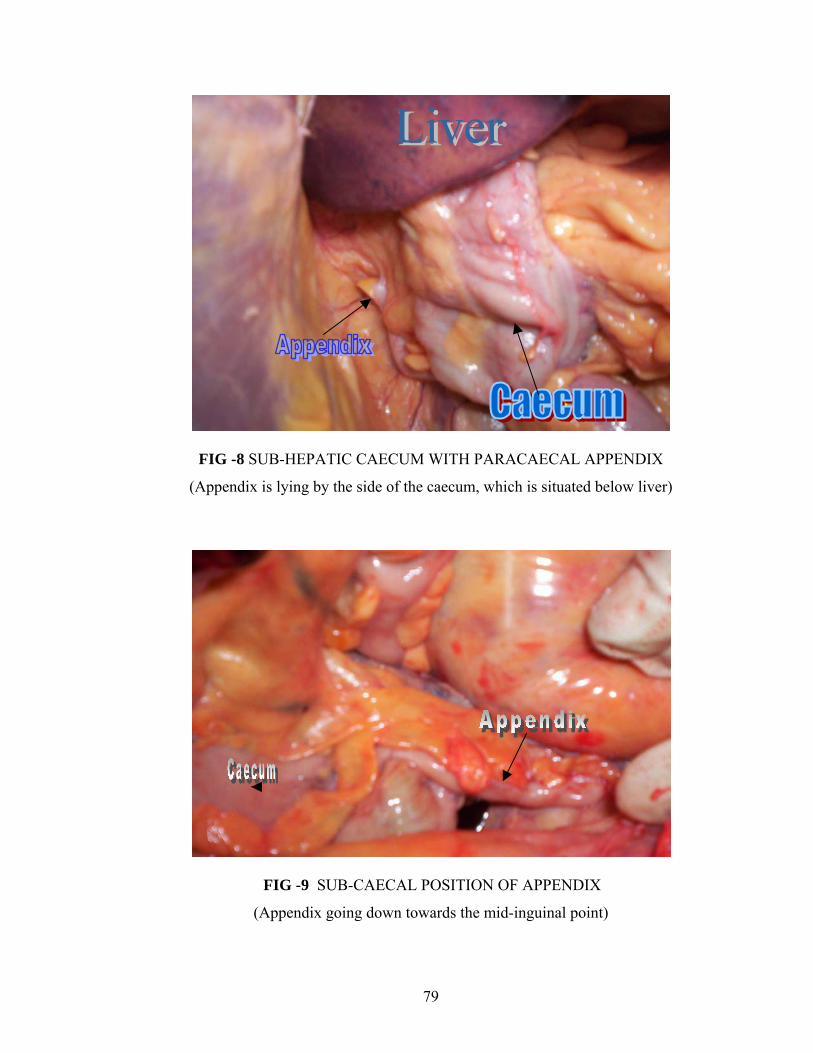
FIG -8 SUB-HEPATIC CAECUM WITH PARACAECAL APPENDIX
(Appendix is lying by the side of the caecum, which is situated below liver)
FIG -9 SUB-CAECAL POSITION OF APPENDIX
(Appendix going down towards the mid-inguinal point)
79
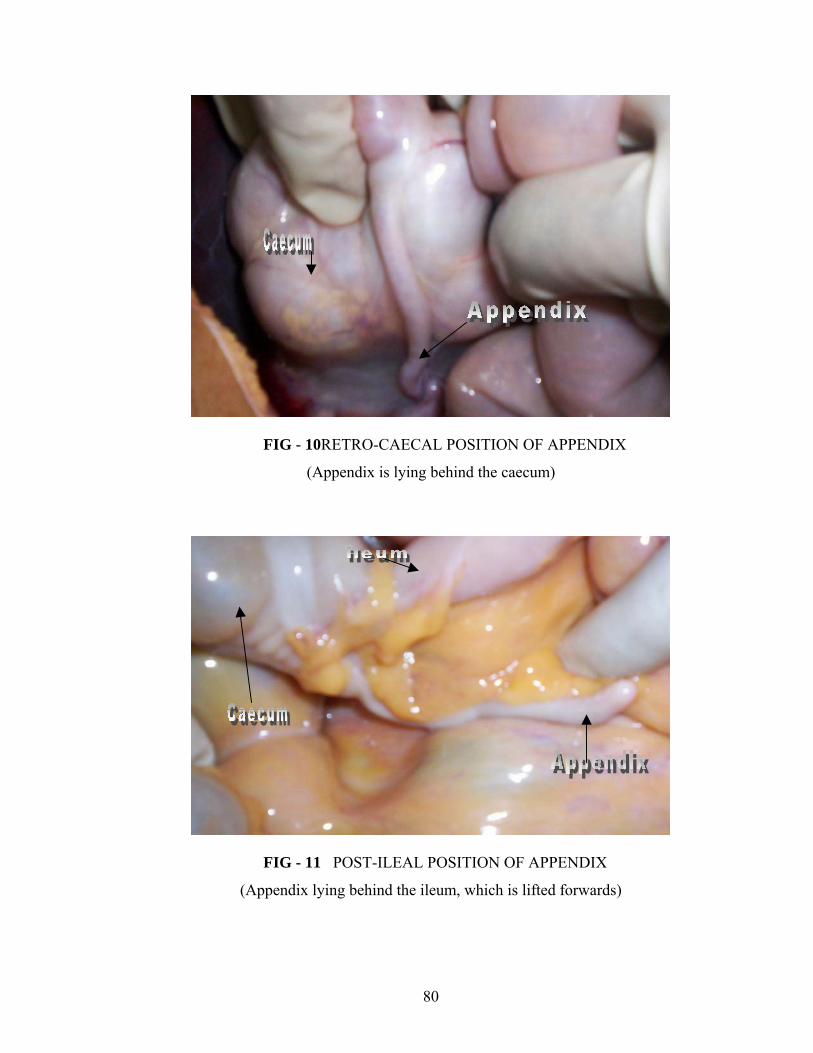
FIG - 10RETRO-CAECAL POSITION OF APPENDIX
(Appendix is lying behind the caecum)
FIG - 11 POST-ILEAL POSITION OF APPENDIX
(Appendix lying behind the ileum, which is lifted forwards)
80
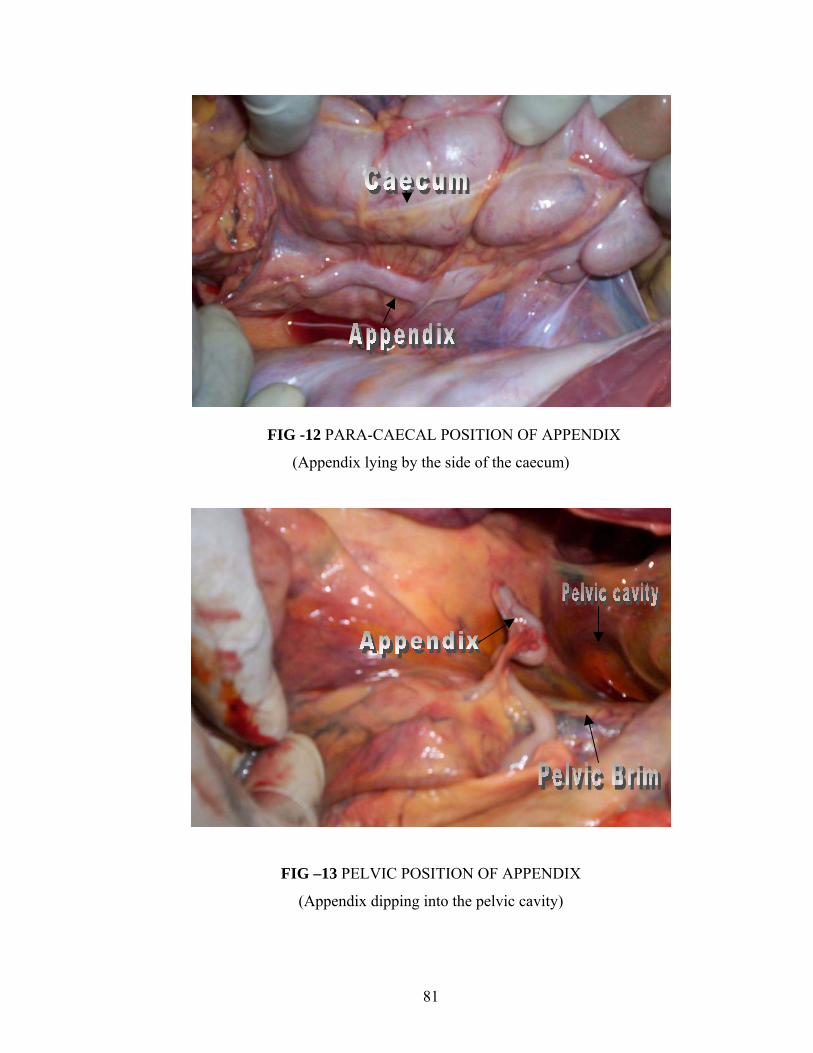
FIG -12 PARA-CAECAL POSITION OF APPENDIX
(Appendix lying by the side of the caecum)
FIG –13 PELVIC POSITION OF APPENDIX
(Appendix dipping into the pelvic cavity)
81
CONCLUSIONS
This study was conducted from May 2003 to August 2005, for a period of 28 months in
Bowring and Lady Curzon hospitals and Victoria hospital attached to Bangalore
Medical College, Bangalore, for clinical group. For autopsy group the study was
conducted from June 2003 to July 2005, for a period of 26 months at Bowring and Lady
Curzon hospitals mortuary. There were 50 cases in the clinical group, which were
biopsy positive for appendicitis, and 100 cases in the autopsy group.
The following conclusions were drawn from the present study
Appendicitis is commonest during the 3rd decade (48%), followed by the 2nd
decade (32%)
Appendicitis is slightly more common in males, M : F ratio is 2.8 : 1.
Pain occurred in all patients. Typical pain (58% of cases) is more common than
atypical pain (42% of cases) in acute appendicitis. Site of pain varies with
position of the appendix. In pelvic appendix patients had supra-pubic pain, in
retro-caecal appendix patient had pain in the right lumbar region or right flank, in
sub- hepatic position the patients had pain in the right hypochondriac region.
Atypical pain was more common in cases of fixed retro-caecal appendix and in
cases of pelvic appendicitis.
82
Patients with post-ileal and pelvic appendix had some sort of bowel disturbance
(constipation or diarrhea)
Patients with retro-caecal appendix had symptoms of upper urinary tract infection,
due to irritation of the adjacent ureter and pelvic appendix had symptoms of lower
urinary tract infection, due to irritation of the adjacent bladder.
Anorexia(76% of cases) is the most commonly seen in appendicitis, nausea(46%
of cases) and vomiting(28% of cases) are seen less commonly .
Incidence and severity of vomiting is more in patients with complicated
appendicitis (50%) as compared to simple acute appendicitis (19.4%). Vomiting
usually does not relieve pain.
Tenderness was present in all cases of acute appendicitis. Site of tenderness may
vary and depends on the position of the appendix. In retro-caecal position
tenderness may be present in the right flank or in the right lumbar region more so
if the appendix is fixed either by the adhesions or because of its extra-peritoneal
location (in these cases tenderness will be more in this region rather than right liac
fosasa). In case of pelvic position tenderness may be present in the suprapubic
region or the patient may have rectal tenderness. In sub-hepatic position patient
may have tenderness in the right hypochondriac region.
Tenderness in the right lower quadrant and rebound tenderness were the most
common signs (76% & 52% respectively)
Tenderness at the Mc Burney’s point is present in only 4 patients (8%) In all the
other cases tenderness was either medial or lateral to the Mc Burney’s point.
83
Psoas sign and Baldwin test though not consistently positive in all the cases of
retro-caecal appendicitis, they are positive in cases most cases of fixed retro-
caecal appendix (8 of 9 cases).
Obturator test though not positive in all the cases of pelvic appendicitis is positive
in most of the complicated appendicitis. All 3 cases of complicated cases of pelvic
appendicitis had positive obturator test and only 2 of the 7 uncomplicated cases
had positive obturator test.
Rectal examination detects pelvic peritonitis or pelvic abscess in case of pelvic
appendicitis. Rectal tenderness was present in 8 of the 10 cases of pelvic
appendicitis and in two cases of generalized peritonitis
Patients with mobile appendix presented with typical signs and symptoms,
whereas those with fixed appendix either by inflammatory process or by its extra-
peritoneal location mostly presented with atypical signs and symptoms.
The signs and symptoms are subtle or atypical in case of retro-caecal fixed, post-
ileal, pelvic appendicitis, leading to increased risk of complications in cases of
appendicitis in these positions. P – value <0.01.
Moderate leukocytosis with polymorphonuclear predominance nearly always
accompanies acute appendicitis. A higher WBC count suggests complications.
Leukocytosis was present in 72% of the cases.
The most common position both at surgery and autopsy was Retro-caecal,
followed by Pelvic, Post-ileal, Para-caecal & Sub-caecal.
There is no predisposition for any of the position of appendix to develop
appendicitis
84
The length of the appendix is slightly more in females than males both in autopsy
group (9.03cms : 8.76cms) and in the clinical group (9.23cms : 8.16cms).
There is increased risk of complications in those with atypical presentation than
those with typical presentation. Only 3 of 29 (10.3%) cases with typical
presentation had complications whereas 11 of the 21 cases (52.4%) with atypical
presentation had complications.
The patients with appendicular abscess and generalized peritonitis who were
operated had delayed recovery; in other patients there was no difference in the
post-operative recovery of the patients whether they were complicated or
uncomplicated.
85
SUMMARY
This study was conducted from May 2003 to August 2005, for a period of 28 months in
Bowring and Lady Curzon hospitals and Victoria hospital attached to Bangalore
Medical College, Bangalore, for clinical group. For autopsy group the study was
conducted from June 2003 to July 2005, for a period of 26 months at Bowring and Lady
Curzon hospitals mortuary. There were 50 cases in the clinical group, which were
biopsy positive for appendicitis, and 100 cases in the autopsy group.
Appendicitis is commonest during the 3rd decade (48%), followed by the 2nd
decade (32%)
Appendicitis is slightly more common in males, M : F ratio is 2.8 : 1.
The most common position of the appendix in our study is the retro-caecal
position both in the clinical and autopsy group, but contrary to the study
conducted by wakeley et al the frequency of retro-caecal position is much less,
also the frequency of the postileal appendix is more.
There was no statistically significant difference in the position of the appendix in
clinical and autopsy group, suggesting that there is no predilection of any position
of the appendix to get inflamed.
The position of the appendix influences the clinical presentation of the appendix
even though most of the patients experience pain and tenderness in the right iliac
fossa, depending on the position of the appendix patients may experience
additional symptoms and signs, which frequently results in delayed diagnosis.
86
In retro-caecal appendicitis the patient may experience flank pain and tenderness
and symptoms of upper urinary tract infection because of proximity of the
appendix to the ureters, these features are more common if the appendix is fixed
either because of adhesions or because of its extra-peritoneal location. In pelvic
appendicitis patients will present with supra-pubic pain and other symptoms of
lower urinary tract infection, patients will usually present with subtle symptoms
and may occasionally have bowel disturbances; tenderness on digital rectal
examination is a constant feature. In post-ileal position patients will have subtle
signs and symptoms and may occasionally have bowel disturbances.
Patients with fixed retro-caecal, post-ileal, and pelvic position of the appendix;
diagnosis was delayed because of the atypical clinical presentation leading to
increased incidence of complications in patients with these positions of the
appendix.
The length of the appendix is slightly more in females than males both in autopsy
group and in the clinical group.
87
BIBILIOGRAPHY
1. Wakeley CPG. The position of vermiform appendix as ascertained by the
analysis of 10,000 cases J.Anat 1933; 67: 277-283.
2. Collins DC. 71,000 human appendix specimens: a final report, summarizing 40
years study. Am J Proctol 1963; 14:365-381.
3. Pickens G, Ellis H, The normal vermiform appendix at C.T visualization and
anatomical location. Clin. Anat, 1993; 6:9.
4. Guidry SP, Poole GV. The anatomy of appendicitis. Am Surg. 1994 Jan; 60(1):
68-71
5. Poole GV. Anatomic basis for delayed diagnosis of appendicitis. South Med J.
1990 Jul; 83(7): 771-773.
6. Karl A Zucker, Surgical Laparoscopy 2nd edition Lippincot Williams &
Wilkins, P: 229-236
7. Varshney S, Jhonson CD, Rangnekar GV. Retrocaecal appendix appears to be
less prone to infection. Br J Surg 1996; 83:223-224
8. Collins DC, Acute retro-caecal appendicitis. Arch Surg. 1938; 36:729-743.
9. Shen GK, Wong R, Daller J, Melcer S, Tsen A, Awry S, et-al. Does the
retrocaecal position of the vermiform appendix alter the clinical course of acute
appendicitis? Arch Surg. 1991; 126:569-570.
88
10. Williamson WA, Bush RD, William LF. Retrocaecal appendicitis. Am J Surg
1981; 141:507-509
11. Grunditz T, rayden CI, Janzon L Does the retrocaecal position influence the
course of acute appendicitis? Acta Chir Scand. 1983; 249 :707-710.
12. Volker Schumpelick, Bernhard dreuw, Kerstin Ophoff, Andreas Prescher,
APPENDIX AND CAECUM Embryology, Anatomy, and Surgical applications.
Surgical Clinics of North America, Feb 2000; 8(1): 295-318.
13. Williams Pl, Bannister LH,Berry MM, Collins P, Dyson M, Dussec JE, et-al
alimentary system In GRAY’S ANATOMY..36th edition, Churchill Livingstone,
New York. 1995, 1353-1354.
14. SAHANA’S HUMAN ANATOMY, Descriptive and Applied. Vol-II, Ankur
edition Ankur Publications (AP): Jul 1994,362-367.
15. Romanes, CUNNINGHAM’S TEXT BOOK OF ANATOMY 12th edition
OXFORD: 1981, 462-463.
16. Treaves F, Lectures on the anatomy of the intestinal canal and peritoneum in
man. Brit Med J, 1885; 1:527-530.
17. William B Marbury, Retrocaecal appendix. Ann Surg, 1938; 107 : 819.
18. Nicholson, Percy: Mechanical lesions of the Appendix in children as a basis for
appendicitis. Jour. Paediatrics, 1936 Nov; 9:647-654.
19. Downs TMK. Congenital malformations of Vermiform appendix: A Familial
Disease. Ann Surg, 1942; 115: 21-24.
89
20. Maisel H. The position of vermiform appendix in fetal and adult age groups.
Anat Rec 1960; 136: 385-389.
21. Collins DC, Agenesis of vermiform appendix. Am J Surg. 1951; 82:689.
22. Waugh TH. Appendix Vermiformis Duplex. Arch Surg 1941; 42: 311-320.
23. Gordon McHardy The appendix in Bockus Gastroenterology, 4th edition Vol-4
Saunders P: 2609-2624.
24. Collins DC, Historic phases of acute appendicitis, Ann Surg. 1931; 94:179-196.
25. Bernard M Jaffe and David H Berger, The Appendix in Schwartz’s Principles
of Surgery, 8th edition, Mc. Graw Hill.2005: 1119-1137.
26. Harold Ellis, L. Keith Nathanson. Appendix and Appendectomy in Maingot’s
ABDOMINAL OPERATIONS, Vol-II, 10th edition. APPLETON AND
LANGE: 1997; 1191-1227.
27. Charles M. Ferguson, - Acute appendicitis in – Oxford Textbook of Surgery,
Vol-2, 2nd edition, OXFORD, 2000, P: 1539-1543
28. R.C.G Russel, Norman S. Williams, Christopher J.K.Bulstrode, Bailey & Love’s
SHORT PRACTICE OF SURGERY, 24th edition. London: ARNOLD: 2004;
1203-1218.
90
29. Theodore R. Schrock. Acute Appendicitis in Sleisenger/ Fordtran
Gastrointestinal diseases Pathophysiology, Diagnosis and management, 4th
edition Vol-II, SAUNDERS: 1989; 1382-1389.
30. Addis DG, Shaffer N, Fowler BS, The epidemiology of acute appendicitis in
United States. Am J Epidemiol.1990; 132:910.
31. Korner H, Sondenna K, Soreide JA. Incidence of acute non-perforated and
perforated appendicitis: Age specific and sex specific analysis. World J Surg.
1997; 21:313.
32. Flum DR, Morris A, Koepsell T, Has misdiagnosis of appendicitis has decreased
over time? A population based analysis. JAMA 2001; 286:1748.
33. Stanley L, Robbins et-al, Basic pathology. WB Saunders International, 5th
edition, 1994, 519-520.
34. John Sheperd, The appendix in, ROB & SMITH’S CLINICAL SURGERY Butter
worth, London. 1960, Vol-10, 110-122.
35. D. Mike Hardin. Acute appendicitis: Review and update, American Family
Physician, 1999; Nov 60(7).
36. Gilmore OJA, Brownettt JP, Griffith PH. Appendicitis and mimicking
conditions; a prospective study. Lancet1975; ii: 421-424.
37. De Dombal FF, Laeper DJ, Horrocks JC. Human computer aided diagnosis of
abdominal pain; further report with emphasis on performance of clinicians. Br.
Med J 1974;i: 376-380.
91
38. Peiper R, Koger L, Nasman P. Acute appendicitis, a clinical study 1018 cases of
emergency appendectomy. Acta Chir Scand 1982; 148:51.
39. Lewis FR, Holcroft JW, Boey et-al. Appendicitis: a critical review of the
diagnosis and treatment in 1000 cases. Arch Surg 1975; 110: 677-684.
40. Buschaard K and Kjaeldgaard A. Investigation and analysis of position, length,
fixation and embryology of vermiform appendix. Acta Chir Scand 1973; 139 :
293.
41. Kao CT, Tsai JD, Lee HC, Wang NL, Shih SL, Lin CC, Right perinephric
abscess: a rare presentation of ruptured retro-caecal appendicitis. Pediatr
Nephrol 2002; 17:177-180.
42. Harsha WT, Retro-caecal appendix: its diagnosis and surgical approach. Surg
Gynecol Obstet 1942; 74:180-181.
43. Collins DC. Acute retro-caecal appendicitis, based on seven hundred and fifty
one instances. Arch Surg 1938; 76:729-43.
44. William G. Jones, Philip S. Barie. Urological manifestations of acute
appencicitis. J Urol 1988 Jun 139(6): 1325-1328.
45. Putnam TL, Gagliano, Emmens et al. Appendicitis in children. Surg Gyenecol
Obstet 1990; 170:527.
46. Harrison MW, Linda JJ et al. Acute appendicitis in children: factors affecting
morbidity. Am J Surg 1984; 147: 605.
47. Houratas ML, Guyton DP, Wu D. A reappraisal of acute appendicitis in the
elderly. Am J Surg 1990; 166: 291.
92
48. Sarason EL, Bauman S. Acute appendicitis in pregnancy: Difficulties in
diagnosis. Obstet Gynecol 1963; 22: 382-386.
49. Gomez A, Wood M. Acute appendicitis during pregnancy. Am J Surg 1979;
137:180-183.
50. Black WP. Acute appendicitis in pregnancy. Br Med J 1960; 1:1938-1941.
51. Cunningham FG, McCubbin JH. Appendicitis complicating pregnancy. Obstet
Gynecol 1975; 45:415-420.
52. Scher KS, Coil JA. Appendicitis: Factors that influence the frequency of
perforation. South Med J 1980; 73:1561-1563.
53. Savrin RA, Chatworthy HW, Appendiceal rupture. Paediatrics. 1979; 63:37-
43.
54. Stone HH, Sanders SL, Martin JDJr. Perforated appendicitis in children.
Surgery 1971; 69:673-679.
55. Doraiswamy NV. Leukocyte counts in the diagnosis and prognosis of acute
appendicitis in children, Br J Surg, 1979; 60: 782-784.
56. Ramirez JM and Deus J. Practical score to aid decision making in acute
appendicitis. Br J Surg 1994; 81:680-683.
57. Alavarodo. A practical score for the early diagnosis of appendicitis. Ann of Em
Med 1986; 15: 557-564.
93
58. Fenyo G. routine use of scoring system for decision-making in suspected acute
appendicitis in adults. Acta Chir Scand 1987; 153:545-551.
59. Teicher I, Lanada B, Cohen M, Kabicek S. Scoring system to aid in diagnosis
of appendicitis. Ann Surg 1983; 198:753-759.
60. Brooks DW, Vellein DR. Roentgenographic findings in acute appendicitis.
Surgery 1965; 57:377-384.
61. Hoffman J, Rasmussen O. Aids in the diagnosis of acute appendicitis. Br J Surg
1989; 76:774-79.
62. Schisgall RM. Use of Barium swallow, in the diagnosis of acute appendicitis
Am J Surg 1983; 146: 633-637.
63. Rajagopalan AE, Mason JH, Kennedy N, Pawlikowsky J. The value of Barium
enema in the diagnosis of acute appendicitis. Arch Surg 1977; 112:531-533.
64. Sakover RP, De fara et al. Frequency of visualization of normal appendix with
barium enema examination. AJR 1974; 121: 372-377.
65. Fedshin P, Kelvin FM, Rice RP. Non-specificity of barium enema findings in
acute appendicitis. AJR 1984; 143:99-102.
66. Jeffrey RB, Liang FC, Lewis FR. Acute appendicitis High resolution realtime
US findings. Radiology 1987; 163:11-14.
67. Chesbrough RM, Burkhand TK, Barbara ZN. Self-localization in US of
appendicitis: an addition to graded compression. Radiology 1993; 187:349-357.
94
68. Pulyert JBCM et al. Acute appendicitis: Visualization using graded
compression. Radiology 1986; 158:355-360.
69. Quillin SP, Seigel MJ. Appendicitis in children-Colour Doppler sonography.
Radiology 1992; 184:745-747.
70. Balthazaar EJ, Megibow AJ, Holnick et al. C.T of appendicitis AJR 1986;
147:705-710.
71. Shafi MI, Tarr RW, Partain CL, James AE. Computer tomography and
Magnetic resonance imaging of acute abdomen. Surg Clin of North Am 1988;
68:233-235
72. Gale ME, Brinbaum S, Gerzof et al. CT appearance of appendicitis and its
complications. J Comput Assist Tomog 1985; 9:34-37.
73. Evans C, Rashid A, Rosenberg IL, An appraisal of peritoneal lavage in the
diagnosis of acute abdomen. Br J Surg 1975; 62:119-120.
74. Hoffman J. Peritoneal lavage as an aid in the diagnosis of acute peritonitis of
non-traumatic origin. Dig Dis 1988; 6:185-193.
75. Caldwell MTP, Watson RGK. Peritoneal aspiration cytology as a diagnostic aid
in acute appendicitis. Br J Surg 1994; 81 :276-278.
76. Graham JA. Urinary cell counts in appendicitis. Scott Med J 1965; 10:126.
77. Gronroos JM, Forstrom JJ, Irjala K. Phospholipase A2, CRP and white blood
cell count in the diagnosis of acute appendicitis. Clinical Chemistry 1994;
40:1757-1760.
95
78. Eriksson S, Granstrom L, Carlstrom A. The diagnostic value of repetitive pre-
operative analysis of C reactive protein and total leukocyte count in patients with
suspected acute appendicitis. Scand J Gastroenterology 1994; 29:1145-1149.
79. Navarro DN, Weber PM, Kant. Indium 111 leukocyte imaging in acute
appendicitis. AJR 1987; 148: 733-736.
80. Diehl JT, Eisental MS, Gilinov, Rao D. The role of peritoneoscopy in the
diagnosis of acute abdominal conditions. Cleve Clin Q 1981; 48: 325-330.
81. Deutsch AA, Zelikovsky A, Reiss R. Laparoscopy in the prevention of
appendectomy: a prospective study. Br J Surg 1982; 69 : 336-337.
82. Laepe LL, Ramenofsky ML. Laparoscopy in infants and children. J. paediatric
Surg 1977; 12:929-938.
83. Steele RJC. Abdominal Thermography in acute appendicitis. Scott Med J 1986;
31:229-230.
84. Thomas V. Berne, Adrian Ortega. Appendicitis and appendiceal abscess in
MASTERY OF SURGERY, Little, Brown and company 3rd edition. Vol-II;
1997: P-1407-1411.
85. Lori L Fritts, Rocco Orlando, Hartford Conn, Laparoscopic appendectomy:
A safety and cost effective analysis. Arch Surg.1993; 1(3): 208-212.
86. Nowzardan Y et- al Laparoscopic appendectomy for acute appendicitis;
indications and current use, J Laparoendose Surg, Oct 1991; 1(5) 247-257.
87. Berry J, Malt RA: Appendicitis near its centenary. Ann Surg1984; 200:567.
96
88. Thomas HJ, Jones PF. Active observation in acute abdominal pain. Am J Surg
1986; 152:522-525
89. Toriola F. Solanke. The position, length, and content of vermiform appendix in
Nigerians. Br J Surg 1970, Feb; 57(2): 100-102
90. Ajmani ML and Ajmani K The position length and arterial supply of vermiform
appendix Anat Anz 1983; 153(4): 693
91. Golalipur M.J. Arya B. Azarhoosh R. Jahanshahi.M. Anatomical Variations
of vermiform appendix in South-East Caspian Sea (Gorgoan-Iran). J Anat Soc
India (2003); 52(2) 141-143.
92. Shah MA. Shah M. The position of vermiform appendix. Ind Med Gaz, 1945;
80:494-495.
93. Tinkler LF. Tripple appendix verformis a unique case Br J Surg 1968; 55: 79
94. De Garis CF. Topography and Development of the Caecum-Appendix. Ann
Surg, 1941; 113(4): 540-548.
95. Ushiyama T, Nakajima R, Maeda T, Kawasaki T, Matsusue Y. Perforated
appendicitis causing thigh emphysema – a case report. J Orthop Surg (Hong
Kong) 2005; Apr 13(1): 93-95.
97
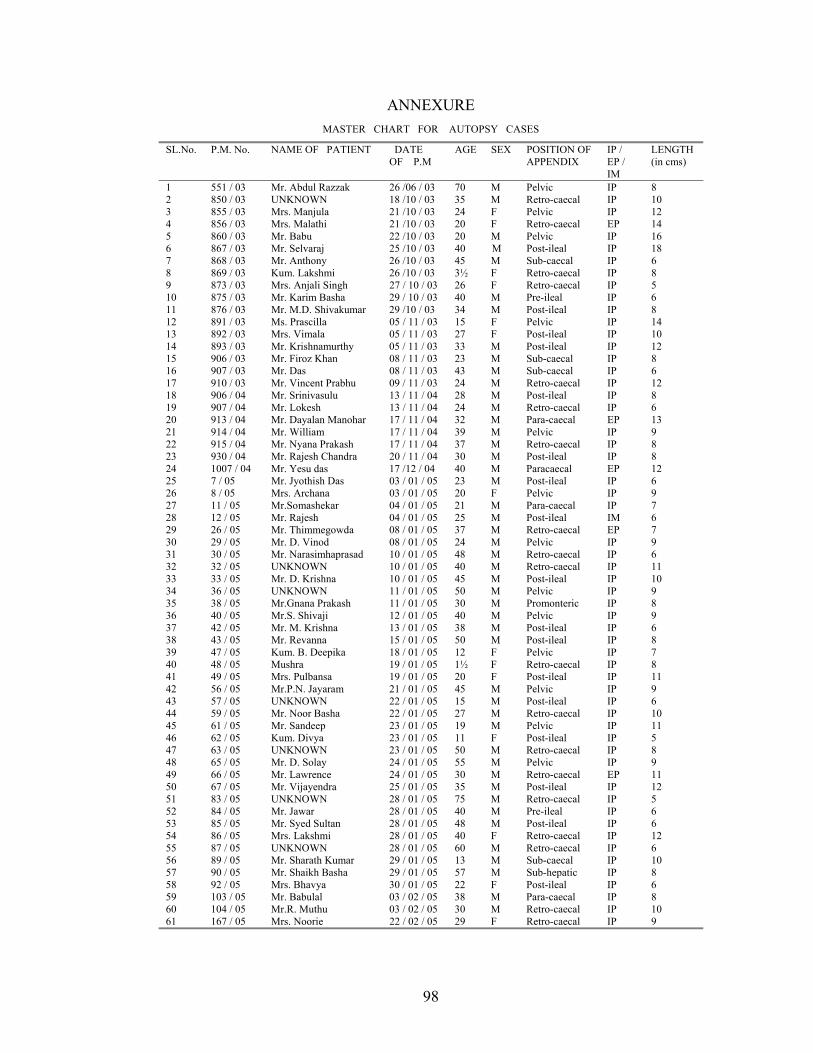
ANNEXURE MASTER CHART FOR AUTOPSY CASES
SL.No. P.M. No. NAME OF PATIENT DATE OF P.M
AGE SEX POSITION OF APPENDIX
IP / EP / IM
LENGTH (in cms)
1 551 / 03 Mr. Abdul Razzak 26 /06 / 03 70 M Pelvic IP 8 2 850 / 03 UNKNOWN 18 /10 / 03 35 M Retro-caecal IP 10 3 855 / 03 Mrs. Manjula 21 /10 / 03 24 F Pelvic IP 12 4 856 / 03 Mrs. Malathi 21 /10 / 03 20 F Retro-caecal EP 14 5 860 / 03 Mr. Babu 22 /10 / 03 20 M Pelvic IP 16 6 867 / 03 Mr. Selvaraj 25 /10 / 03 40 M Post-ileal IP 18 7 868 / 03 Mr. Anthony 26 /10 / 03 45 M Sub-caecal IP 6 8 869 / 03 Kum. Lakshmi 26 /10 / 03 3½ F Retro-caecal IP 8 9 873 / 03 Mrs. Anjali Singh 27 / 10 / 03 26 F Retro-caecal IP 5 10 875 / 03 Mr. Karim Basha 29 / 10 / 03 40 M Pre-ileal IP 6 11 876 / 03 Mr. M.D. Shivakumar 29 /10 / 03 34 M Post-ileal IP 8 12 891 / 03 Ms. Prascilla 05 / 11 / 03 15 F Pelvic IP 14 13 892 / 03 Mrs. Vimala 05 / 11 / 03 27 F Post-ileal IP 10 14 893 / 03 Mr. Krishnamurthy 05 / 11 / 03 33 M Post-ileal IP 12 15 906 / 03 Mr. Firoz Khan 08 / 11 / 03 23 M Sub-caecal IP 8 16 907 / 03 Mr. Das 08 / 11 / 03 43 M Sub-caecal IP 6 17 910 / 03 Mr. Vincent Prabhu 09 / 11 / 03 24 M Retro-caecal IP 12 18 906 / 04 Mr. Srinivasulu 13 / 11 / 04 28 M Post-ileal IP 8 19 907 / 04 Mr. Lokesh 13 / 11 / 04 24 M Retro-caecal IP 6 20 913 / 04 Mr. Dayalan Manohar 17 / 11 / 04 32 M Para-caecal EP 13 21 914 / 04 Mr. William 17 / 11 / 04 39 M Pelvic IP 9 22 915 / 04 Mr. Nyana Prakash 17 / 11 / 04 37 M Retro-caecal IP 8 23 930 / 04 Mr. Rajesh Chandra 20 / 11 / 04 30 M Post-ileal IP 8 24 1007 / 04 Mr. Yesu das 17 /12 / 04 40 M Paracaecal EP 12 25 7 / 05 Mr. Jyothish Das 03 / 01 / 05 23 M Post-ileal IP 6 26 8 / 05 Mrs. Archana 03 / 01 / 05 20 F Pelvic IP 9 27 11 / 05 Mr.Somashekar 04 / 01 / 05 21 M Para-caecal IP 7 28 12 / 05 Mr. Rajesh 04 / 01 / 05 25 M Post-ileal IM 6 29 26 / 05 Mr. Thimmegowda 08 / 01 / 05 37 M Retro-caecal EP 7 30 29 / 05 Mr. D. Vinod 08 / 01 / 05 24 M Pelvic IP 9 31 30 / 05 Mr. Narasimhaprasad 10 / 01 / 05 48 M Retro-caecal IP 6 32 32 / 05 UNKNOWN 10 / 01 / 05 40 M Retro-caecal IP 11 33 33 / 05 Mr. D. Krishna 10 / 01 / 05 45 M Post-ileal IP 10 34 36 / 05 UNKNOWN 11 / 01 / 05 50 M Pelvic IP 9 35 38 / 05 Mr.Gnana Prakash 11 / 01 / 05 30 M Promonteric IP 8 36 40 / 05 Mr.S. Shivaji 12 / 01 / 05 40 M Pelvic IP 9 37 42 / 05 Mr. M. Krishna 13 / 01 / 05 38 M Post-ileal IP 6 38 43 / 05 Mr. Revanna 15 / 01 / 05 50 M Post-ileal IP 8 39 47 / 05 Kum. B. Deepika 18 / 01 / 05 12 F Pelvic IP 7 40 48 / 05 Mushra 19 / 01 / 05 1½ F Retro-caecal IP 8 41 49 / 05 Mrs. Pulbansa 19 / 01 / 05 20 F Post-ileal IP 11 42 56 / 05 Mr.P.N. Jayaram 21 / 01 / 05 45 M Pelvic IP 9 43 57 / 05 UNKNOWN 22 / 01 / 05 15 M Post-ileal IP 6 44 59 / 05 Mr. Noor Basha 22 / 01 / 05 27 M Retro-caecal IP 10 45 61 / 05 Mr. Sandeep 23 / 01 / 05 19 M Pelvic IP 11 46 62 / 05 Kum. Divya 23 / 01 / 05 11 F Post-ileal IP 5 47 63 / 05 UNKNOWN 23 / 01 / 05 50 M Retro-caecal IP 8 48 65 / 05 Mr. D. Solay 24 / 01 / 05 55 M Pelvic IP 9 49 66 / 05 Mr. Lawrence 24 / 01 / 05 30 M Retro-caecal EP 11 50 67 / 05 Mr. Vijayendra 25 / 01 / 05 35 M Post-ileal IP 12 51 83 / 05 UNKNOWN 28 / 01 / 05 75 M Retro-caecal IP 5 52 84 / 05 Mr. Jawar 28 / 01 / 05 40 M Pre-ileal IP 6 53 85 / 05 Mr. Syed Sultan 28 / 01 / 05 48 M Post-ileal IP 6 54 86 / 05 Mrs. Lakshmi 28 / 01 / 05 40 F Retro-caecal IP 12 55 87 / 05 UNKNOWN 28 / 01 / 05 60 M Retro-caecal IP 6 56 89 / 05 Mr. Sharath Kumar 29 / 01 / 05 13 M Sub-caecal IP 10 57 90 / 05 Mr. Shaikh Basha 29 / 01 / 05 57 M Sub-hepatic IP 8 58 92 / 05 Mrs. Bhavya 30 / 01 / 05 22 F Post-ileal IP 6 59 103 / 05 Mr. Babulal 03 / 02 / 05 38 M Para-caecal IP 8 60 104 / 05 Mr.R. Muthu 03 / 02 / 05 30 M Retro-caecal IP 10 61 167 / 05 Mrs. Noorie 22 / 02 / 05 29 F Retro-caecal IP 9
98
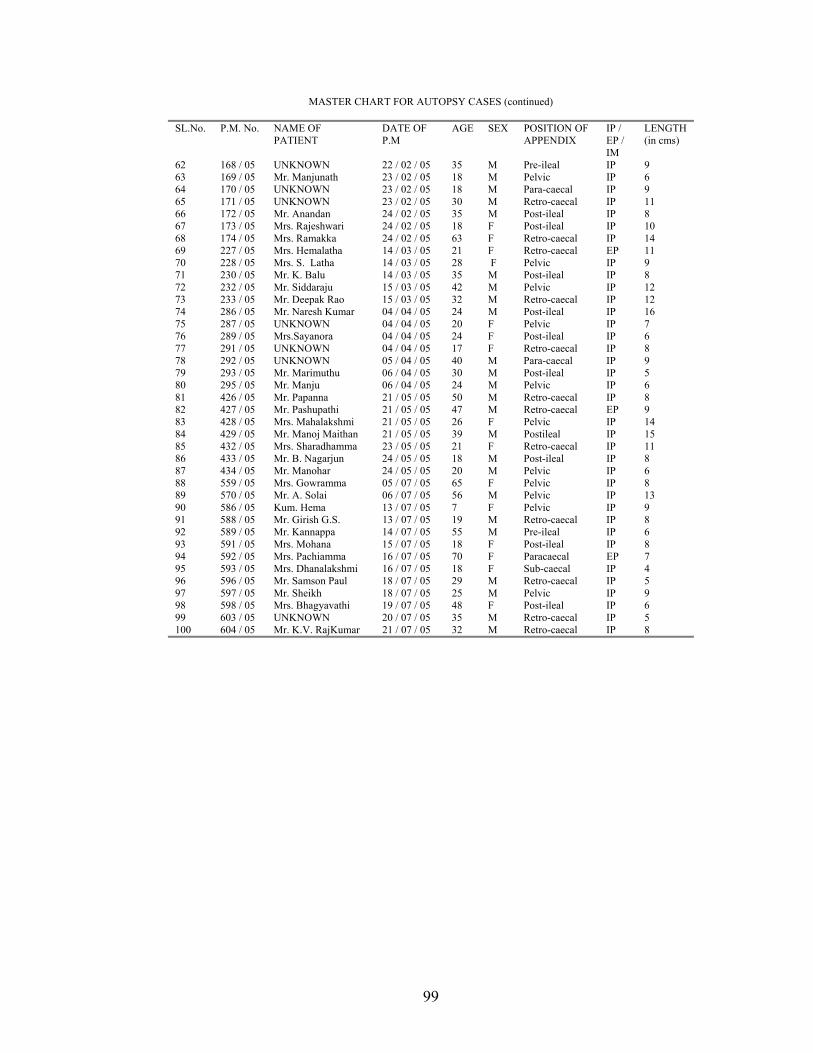
MASTER CHART FOR AUTOPSY CASES (continued)
SL.No. P.M. No. NAME OF PATIENT
DATE OF P.M
AGE SEX POSITION OF APPENDIX
IP / EP / IM
LENGTH (in cms)
62 168 / 05 UNKNOWN 22 / 02 / 05 35 M Pre-ileal IP 9 63 169 / 05 Mr. Manjunath 23 / 02 / 05 18 M Pelvic IP 6 64 170 / 05 UNKNOWN 23 / 02 / 05 18 M Para-caecal IP 9 65 171 / 05 UNKNOWN 23 / 02 / 05 30 M Retro-caecal IP 11 66 172 / 05 Mr. Anandan 24 / 02 / 05 35 M Post-ileal IP 8 67 173 / 05 Mrs. Rajeshwari 24 / 02 / 05 18 F Post-ileal IP 10 68 174 / 05 Mrs. Ramakka 24 / 02 / 05 63 F Retro-caecal IP 14 69 227 / 05 Mrs. Hemalatha 14 / 03 / 05 21 F Retro-caecal EP 11 70 228 / 05 Mrs. S. Latha 14 / 03 / 05 28 F Pelvic IP 9 71 230 / 05 Mr. K. Balu 14 / 03 / 05 35 M Post-ileal IP 8 72 232 / 05 Mr. Siddaraju 15 / 03 / 05 42 M Pelvic IP 12 73 233 / 05 Mr. Deepak Rao 15 / 03 / 05 32 M Retro-caecal IP 12 74 286 / 05 Mr. Naresh Kumar 04 / 04 / 05 24 M Post-ileal IP 16 75 287 / 05 UNKNOWN 04 / 04 / 05 20 F Pelvic IP 7 76 289 / 05 Mrs.Sayanora 04 / 04 / 05 24 F Post-ileal IP 6 77 291 / 05 UNKNOWN 04 / 04 / 05 17 F Retro-caecal IP 8 78 292 / 05 UNKNOWN 05 / 04 / 05 40 M Para-caecal IP 9 79 293 / 05 Mr. Marimuthu 06 / 04 / 05 30 M Post-ileal IP 5 80 295 / 05 Mr. Manju 06 / 04 / 05 24 M Pelvic IP 6 81 426 / 05 Mr. Papanna 21 / 05 / 05 50 M Retro-caecal IP 8 82 427 / 05 Mr. Pashupathi 21 / 05 / 05 47 M Retro-caecal EP 9 83 428 / 05 Mrs. Mahalakshmi 21 / 05 / 05 26 F Pelvic IP 14 84 429 / 05 Mr. Manoj Maithan 21 / 05 / 05 39 M Postileal IP 15 85 432 / 05 Mrs. Sharadhamma 23 / 05 / 05 21 F Retro-caecal IP 11 86 433 / 05 Mr. B. Nagarjun 24 / 05 / 05 18 M Post-ileal IP 8 87 434 / 05 Mr. Manohar 24 / 05 / 05 20 M Pelvic IP 6 88 559 / 05 Mrs. Gowramma 05 / 07 / 05 65 F Pelvic IP 8 89 570 / 05 Mr. A. Solai 06 / 07 / 05 56 M Pelvic IP 13 90 586 / 05 Kum. Hema 13 / 07 / 05 7 F Pelvic IP 9 91 588 / 05 Mr. Girish G.S. 13 / 07 / 05 19 M Retro-caecal IP 8 92 589 / 05 Mr. Kannappa 14 / 07 / 05 55 M Pre-ileal IP 6 93 591 / 05 Mrs. Mohana 15 / 07 / 05 18 F Post-ileal IP 8 94 592 / 05 Mrs. Pachiamma 16 / 07 / 05 70 F Paracaecal EP 7 95 593 / 05 Mrs. Dhanalakshmi 16 / 07 / 05 18 F Sub-caecal IP 4 96 596 / 05 Mr. Samson Paul 18 / 07 / 05 29 M Retro-caecal IP 5 97 597 / 05 Mr. Sheikh 18 / 07 / 05 25 M Pelvic IP 9 98 598 / 05 Mrs. Bhagyavathi 19 / 07 / 05 48 F Post-ileal IP 6 99 603 / 05 UNKNOWN 20 / 07 / 05 35 M Retro-caecal IP 5 100 604 / 05 Mr. K.V. RajKumar 21 / 07 / 05 32 M Retro-caecal IP 8
99

100
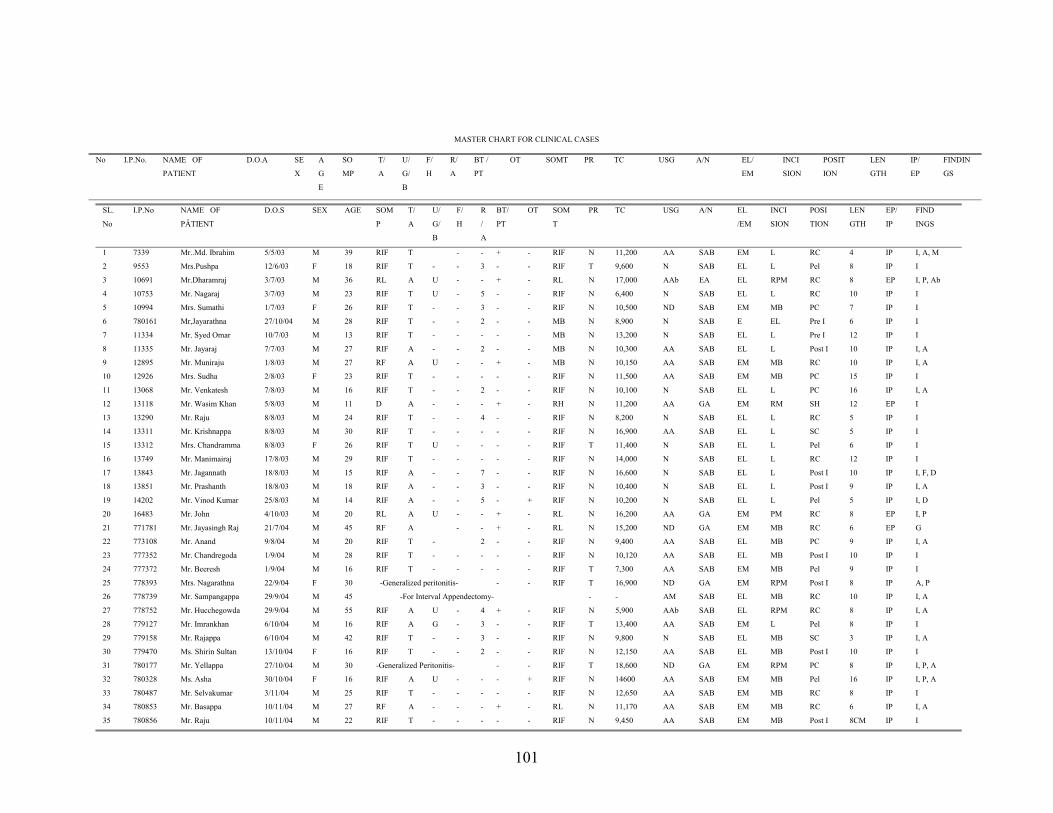
MASTER CHART FOR CLINICAL CASES
No I.P.No. NAME OF
PATIENT
D.O.A SE
X
A
G
E
SO
MP
T/
A
U/
G/
B
F/
H
R/
A
BT /
PT
OT SOMT PR TC USG A/N EL/
EM
INCI
SION
POSIT
ION
LEN
GTH
IP/
EP
FINDIN
GS
SL.
No
I.P.No NAME OF
PÂTIENT
D.O.S SEX AGE SOM
P
T/
A
U/
G/
B
F/
H
R
/
A
BT/
PT
OT SOM
T
PR TC USG A/N EL
/EM
INCI
SION
POSI
TION
LEN
GTH
EP/
IP
FIND
INGS
1 7339 Mr..Md. Ibrahim 5/5/03 M 39 RIF T - - + - RIF N 11,200 AA SAB EM L RC 4 IP I, A, M
2
9553 Mrs.Pushpa 12/6/03 F 18 RIF T - - 3 - - RIF T 9,600 N SAB EL L Pel 8 IP I
3 10691 Mr.Dharamraj 3/7/03 M 36 RL A U - - + - RL N 17,000 AAb EA EL RPM RC 8 EP I, P, Ab
4 10753 Mr. Nagaraj 3/7/03 M 23 RIF T U - 5 - - RIF N 6,400 N SAB EL L RC 10 IP I
5 10994 Mrs. Sumathi 1/7/03 F 26 RIF T - - 3 - - RIF N 10,500 ND SAB EM MB PC 7 IP I
6 780161 Mr,Jayarathna 27/10/04 M 28 RIF T - - 2 - - MB N 8,900 N SAB E EL Pre I 6 IP I
7 11334 Mr. Syed Omar 10/7/03 M 13 RIF T - - - - - MB N 13,200 N SAB EL L Pre I 12 IP I
8 11335 Mr. Jayaraj 7/7/03 M 27 RIF A - - 2 - - MB N 10,300 AA SAB EL L Post I 10 IP I, A
9 12895 Mr. Muniraju 1/8/03 M 27 RF A U - - + - MB N 10,150 AA SAB EM MB RC 10 IP I, A
10 12926 Mrs. Sudha 2/8/03 F 23 RIF T - - - - - RIF N 11,500 AA SAB EM MB PC 15 IP I
11 13068 Mr. Venkatesh 7/8/03 M 16 RIF T - - 2 - - RIF N 10,100 N SAB EL L PC 16 IP I, A
12 13118 Mr. Wasim Khan 5/8/03 M 11 D A - - - + - RH N 11,200 AA GA EM RM SH 12 EP I
13 13290 Mr. Raju 8/8/03 M 24 RIF T - - 4 - - RIF N 8,200 N SAB EL L RC 5 IP I
14 13311 Mr. Krishnappa 8/8/03 M 30 RIF T - - - - - RIF N 16,900 AA SAB EL L SC 5 IP I
15 13312 Mrs. Chandramma 8/8/03 F 26 RIF T U - - - - RIF T 11,400 N SAB EL L Pel 6 IP I
16 13749 Mr. Manimairaj 17/8/03 M 29 RIF T - - - - - RIF N 14,000 N SAB EL L RC 12 IP I
17 13843 Mr. Jagannath 18/8/03 M 15 RIF A - - 7 - - RIF N 16,600 N SAB EL L Post I 10 IP I, F, D
18 13851 Mr. Prashanth 18/8/03 M 18 RIF A - - 3 - - RIF N 10,400 N SAB EL L Post I 9 IP I, A
19 14202 Mr. Vinod Kumar 25/8/03 M 14 RIF A - - 5 - + RIF N 10,200 N SAB EL L Pel 5 IP I, D
20 16483 Mr. John 4/10/03 M 20 RL A U - - + - RL N 16,200 AA GA EM PM RC 8 EP I, P
21 771781 Mr. Jayasingh Raj 21/7/04 M 45 RF A - - + - RL N 15,200 ND GA EM MB RC 6 EP G
22 773108 Mr. Anand 9/8/04 M 20 RIF T - 2 - - RIF N 9,400 AA SAB EL MB PC 9 IP I, A
23 777352 Mr. Chandregoda 1/9/04 M 28 RIF T - - - - - RIF N 10,120 AA SAB EL MB Post I 10 IP I
24 777372 Mr. Beeresh 1/9/04 M 16 RIF T - - - - - RIF T 7,300 AA SAB EM MB Pel 9 IP I
25 778393 Mrs. Nagarathna 22/9/04 F 30 -Generalized peritonitis- - - RIF T 16,900 ND GA EM RPM Post I 8 IP A, P
26 778739 Mr. Sampangappa 29/9/04 M 45 -For Interval Appendectomy- - - AM SAB EL MB RC 10 IP I, A
27 778752 Mr. Hucchegowda 29/9/04 M 55 RIF A U - 4 + - RIF N 5,900 AAb SAB EL RPM RC 8 IP I, A
28 779127 Mr. Imrankhan 6/10/04 M 16 RIF A G - 3 - - RIF T 13,400 AA SAB EM L Pel 8 IP I
29 779158 Mr. Rajappa 6/10/04 M 42 RIF T - - 3 - - RIF N 9,800 N SAB EL MB SC 3 IP I, A
30 779470 Ms. Shirin Sultan 13/10/04 F 16 RIF T - - 2 - - RIF N 12,150 AA SAB EL MB Post I 10 IP I
31 780177 Mr. Yellappa 27/10/04 M 30 -Generalized Peritonitis- - - RIF T 18,600 ND GA EM RPM PC 8 IP I, P, A
32 780328 Ms. Asha 30/10/04 F 16 RIF A U - - - + RIF N 14600 AA SAB EM MB Pel 16 IP I, P, A
33 780487 Mr. Selvakumar 3/11/04 M 25 RIF T - - - - - RIF N 12,650 AA SAB EM MB RC 8 IP I
34 780853 Mr. Basappa 10/11/04 M 27 RF A - - - + - RL N 11,170 AA SAB EM MB RC 6 IP I, A
35 780856 Mr. Raju 10/11/04 M 22 RIF T - - - - - RIF N 9,450 AA SAB EM MB Post I 8CM IP I
101
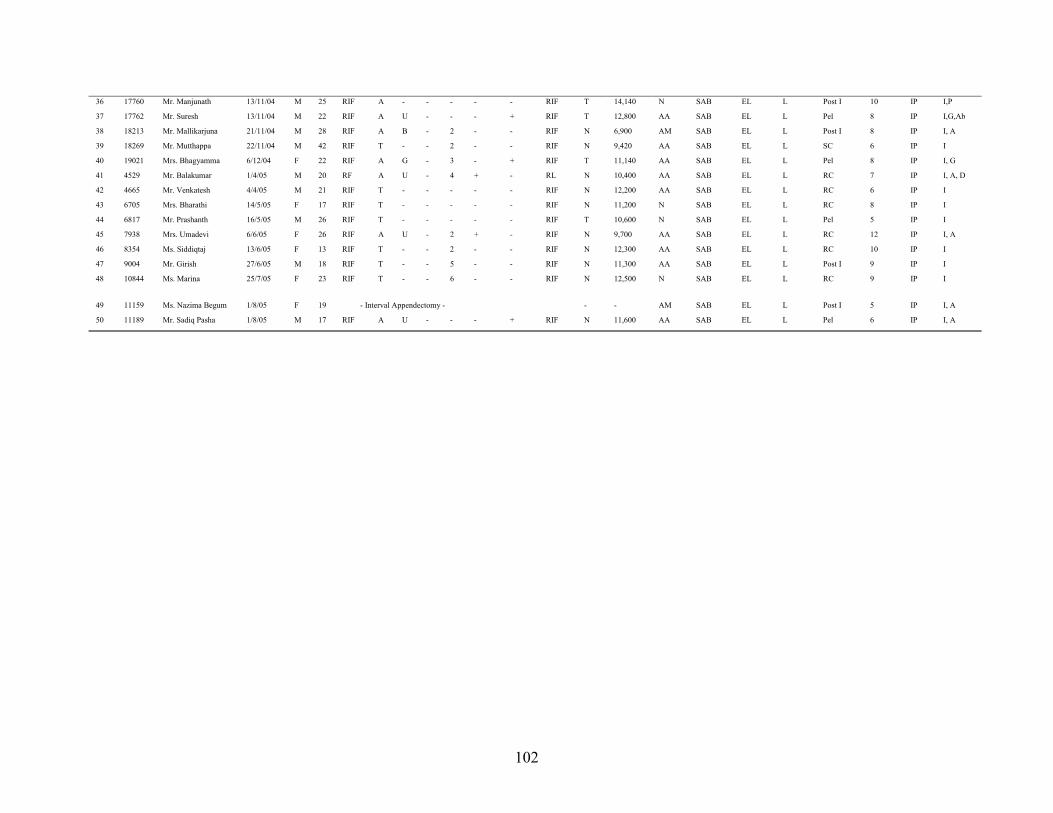
36 17760 Mr. Manjunath 13/11/04 M 25 RIF A - - - - - RIF T 14,140 N SAB EL L Post I 10 IP I,P
37
17762 Mr. Suresh 13/11/04 M 22 RIF A U - - - + RIF T 12,800 AA SAB EL L Pel 8 IP I,G,Ab
38 18213 Mr. Mallikarjuna 21/11/04 M 28 RIF A B - 2 - - RIF N 6,900 AM SAB EL L Post I 8 IP I, A
39 18269 Mr. Mutthappa 22/11/04 M 42 RIF T - - 2 - - RIF N 9,420 AA SAB EL L SC 6 IP I
40 19021 Mrs. Bhagyamma 6/12/04 F 22 RIF A G - 3 - + RIF T 11,140 AA SAB EL L Pel 8 IP I, G
41 4529 Mr. Balakumar 1/4/05 M 20 RF A U - 4 + - RL N 10,400 AA SAB EL L RC 7 IP I, A, D
42 4665 Mr. Venkatesh 4/4/05 M 21 RIF T - - - - - RIF N 12,200 AA SAB EL L RC 6 IP I
43 6705 Mrs. Bharathi 14/5/05 F 17 RIF T - - - - - RIF N 11,200 N SAB EL L RC 8 IP I
44 6817 Mr. Prashanth 16/5/05 M 26 RIF T - - - - - RIF T 10,600 N SAB EL L Pel 5 IP I
45 7938 Mrs. Umadevi 6/6/05 F 26 RIF A U - 2 + - RIF N 9,700 AA SAB EL L RC 12 IP I, A
46 8354 Ms. Siddiqtaj 13/6/05 F 13 RIF T - - 2 - - RIF N 12,300 AA SAB EL L RC 10 IP I
47 9004 Mr. Girish 27/6/05 M 18 RIF T - - 5 - - RIF N 11,300 AA SAB EL L Post I 9 IP I
48
10844 Ms. Marina 25/7/05 F 23 RIF T - - 6 - - RIF N 12,500 N SAB EL L RC 9 IP I
49 11159 Ms. Nazima Begum 1/8/05 F 19 - Interval Appendectomy - - - AM SAB EL L Post I 5 IP I, A
50 11189 Mr. Sadiq Pasha 1/8/05 M 17 RIF A U - - - + RIF N 11,600 AA SAB EL L Pel 6 IP I, A
102
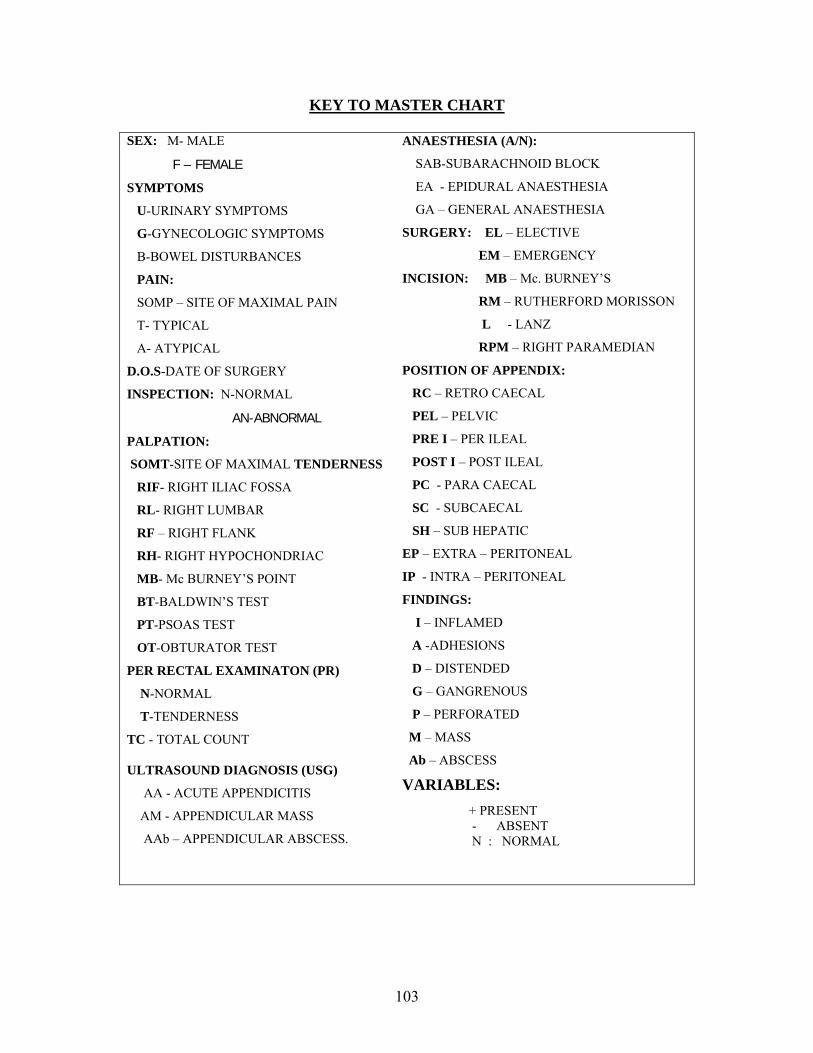
KEY TO MASTER CHART
SEX: M- MALE
F – FEMALE
SYMPTOMS
U-URINARY SYMPTOMS
G-GYNECOLOGIC SYMPTOMS
B-BOWEL DISTURBANCES
PAIN:
SOMP – SITE OF MAXIMAL PAIN
T- TYPICAL
A- ATYPICAL
D.O.S-DATE OF SURGERY
INSPECTION: N-NORMAL
AN-ABNORMAL
PALPATION:
SOMT-SITE OF MAXIMAL TENDERNESS
RIF- RIGHT ILIAC FOSSA
RL- RIGHT LUMBAR
RF – RIGHT FLANK
RH- RIGHT HYPOCHONDRIAC
MB- Mc BURNEY’S POINT
BT-BALDWIN’S TEST
PT-PSOAS TEST
OT-OBTURATOR TEST
PER RECTAL EXAMINATON (PR)
N-NORMAL
T-TENDERNESS
TC - TOTAL COUNT
ULTRASOUND DIAGNOSIS (USG)
AA - ACUTE APPENDICITIS
AM - APPENDICULAR MASS
AAb – APPENDICULAR ABSCESS.
ANAESTHESIA (A/N):
SAB-SUBARACHNOID BLOCK
EA - EPIDURAL ANAESTHESIA
GA – GENERAL ANAESTHESIA
SURGERY: EL – ELECTIVE
EM – EMERGENCY
INCISION: MB – Mc. BURNEY’S
RM – RUTHERFORD MORISSON
L - LANZ
RPM – RIGHT PARAMEDIAN
POSITION OF APPENDIX:
RC – RETRO CAECAL
PEL – PELVIC
PRE I – PER ILEAL
POST I – POST ILEAL
PC - PARA CAECAL
SC - SUBCAECAL
SH – SUB HEPATIC
EP – EXTRA – PERITONEAL
IP - INTRA – PERITONEAL
FINDINGS:
I – INFLAMED
A -ADHESIONS
D – DISTENDED
G – GANGRENOUS
P – PERFORATED
M – MASS
Ab – ABSCESS
VARIABLES: + PRESENT - ABSENT N : NORMAL
103


105
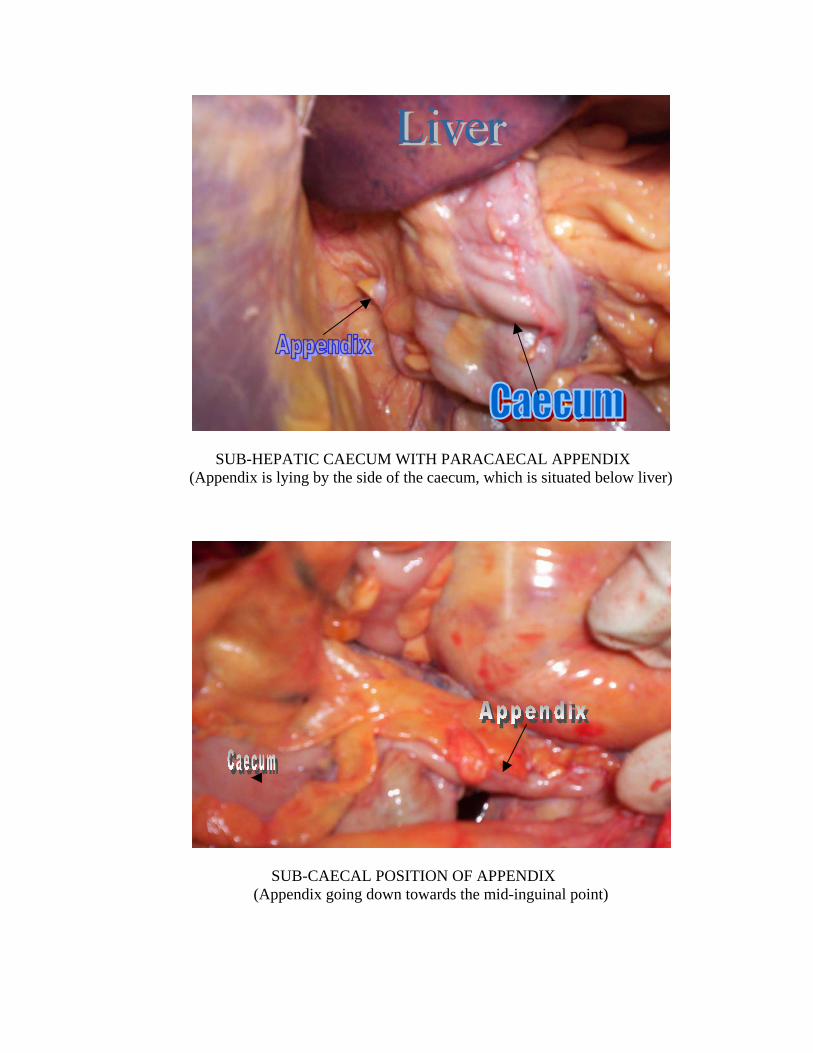
SUB-HEPATIC CAECUM WITH PARACAECAL APPENDIX
(Appendix is lying by the side of the caecum, which is situated below liver)
SUB-CAECAL POSITION OF APPENDIX
(Appendix going down towards the mid-inguinal point)
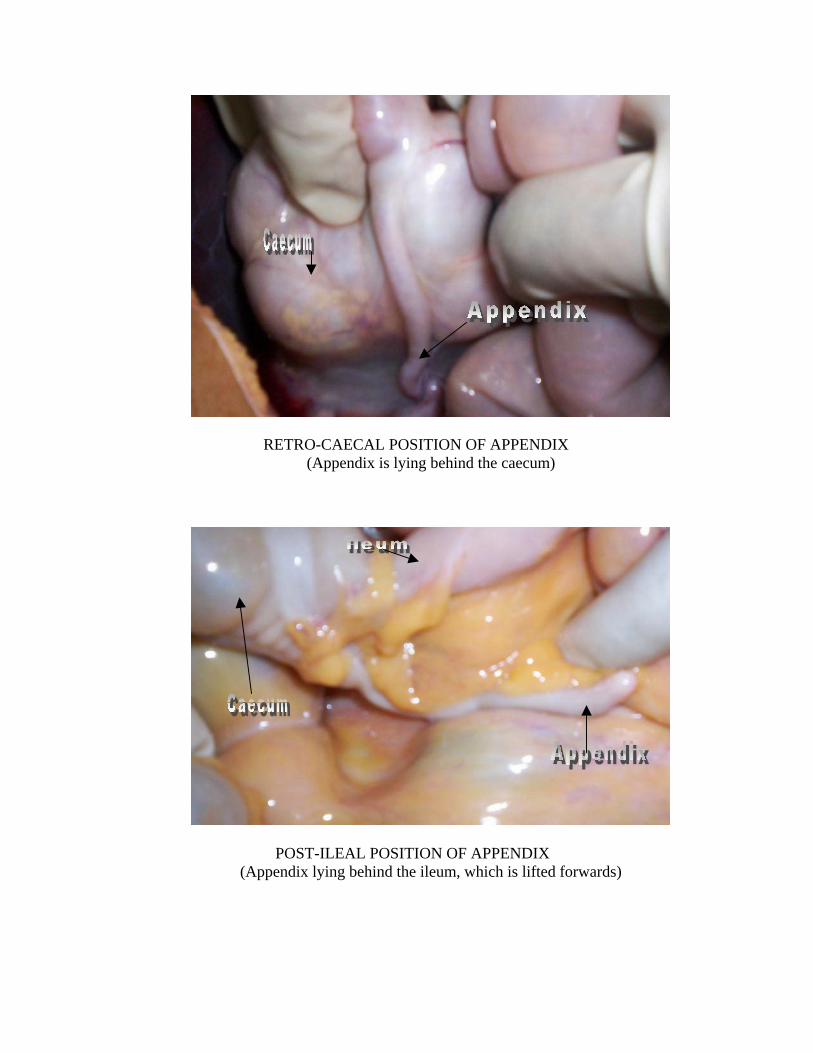
RETRO-CAECAL POSITION OF APPENDIX
(Appendix is lying behind the caecum)
POST-ILEAL POSITION OF APPENDIX
(Appendix lying behind the ileum, which is lifted forwards)
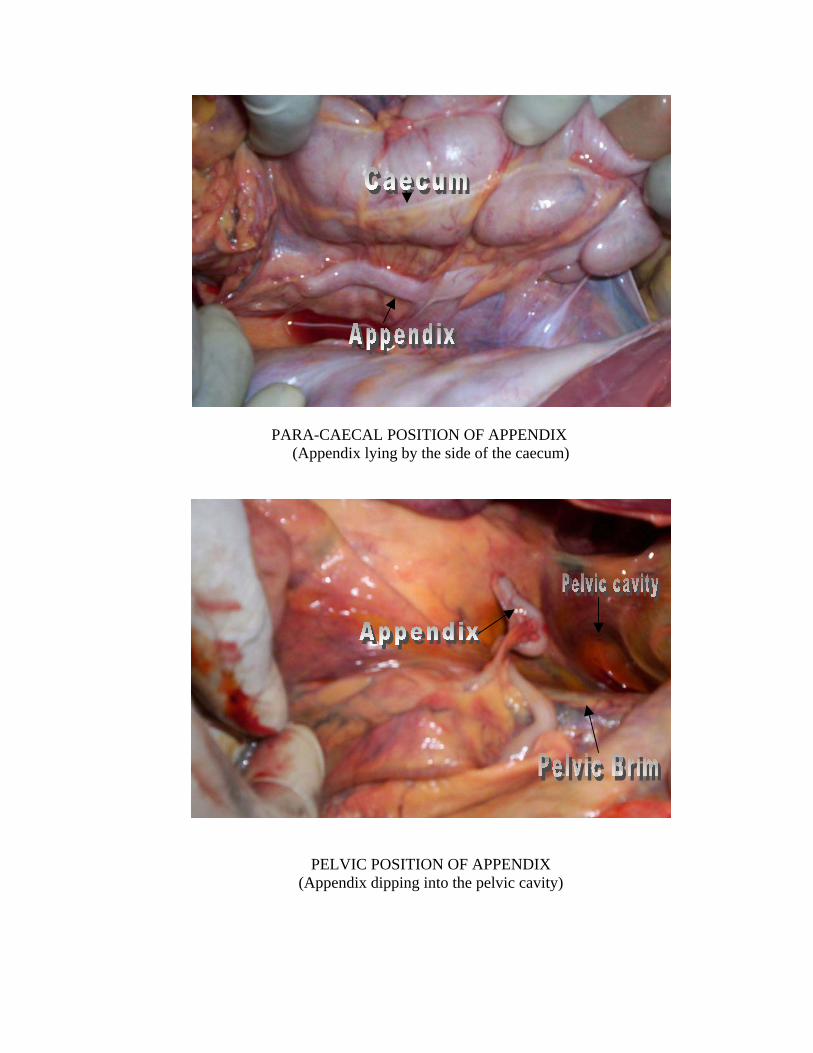
PARA-CAECAL POSITION OF APPENDIX
(Appendix lying by the side of the caecum)
PELVIC POSITION OF APPENDIX (Appendix dipping into the pelvic cavity)
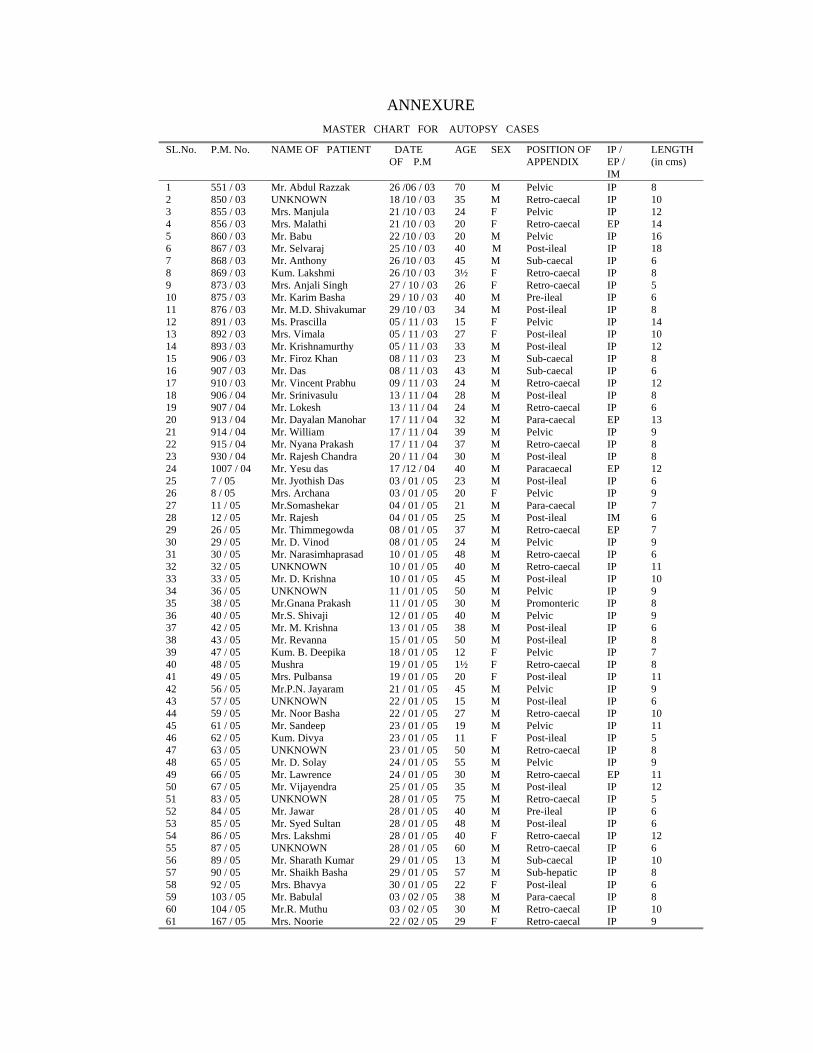
ANNEXURE MASTER CHART FOR AUTOPSY CASES
SL.No. P.M. No. NAME OF PATIENT DATE OF P.M
AGE SEX POSITION OF APPENDIX
IP / EP / IM
LENGTH (in cms)
1 551 / 03 Mr. Abdul Razzak 26 /06 / 03 70 M Pelvic IP 8 2 850 / 03 UNKNOWN 18 /10 / 03 35 M Retro-caecal IP 10 3 855 / 03 Mrs. Manjula 21 /10 / 03 24 F Pelvic IP 12 4 856 / 03 Mrs. Malathi 21 /10 / 03 20 F Retro-caecal EP 14 5 860 / 03 Mr. Babu 22 /10 / 03 20 M Pelvic IP 16 6 867 / 03 Mr. Selvaraj 25 /10 / 03 40 M Post-ileal IP 18 7 868 / 03 Mr. Anthony 26 /10 / 03 45 M Sub-caecal IP 6 8 869 / 03 Kum. Lakshmi 26 /10 / 03 3½ F Retro-caecal IP 8 9 873 / 03 Mrs. Anjali Singh 27 / 10 / 03 26 F Retro-caecal IP 5 10 875 / 03 Mr. Karim Basha 29 / 10 / 03 40 M Pre-ileal IP 6 11 876 / 03 Mr. M.D. Shivakumar 29 /10 / 03 34 M Post-ileal IP 8 12 891 / 03 Ms. Prascilla 05 / 11 / 03 15 F Pelvic IP 14 13 892 / 03 Mrs. Vimala 05 / 11 / 03 27 F Post-ileal IP 10 14 893 / 03 Mr. Krishnamurthy 05 / 11 / 03 33 M Post-ileal IP 12 15 906 / 03 Mr. Firoz Khan 08 / 11 / 03 23 M Sub-caecal IP 8 16 907 / 03 Mr. Das 08 / 11 / 03 43 M Sub-caecal IP 6 17 910 / 03 Mr. Vincent Prabhu 09 / 11 / 03 24 M Retro-caecal IP 12 18 906 / 04 Mr. Srinivasulu 13 / 11 / 04 28 M Post-ileal IP 8 19 907 / 04 Mr. Lokesh 13 / 11 / 04 24 M Retro-caecal IP 6 20 913 / 04 Mr. Dayalan Manohar 17 / 11 / 04 32 M Para-caecal EP 13 21 914 / 04 Mr. William 17 / 11 / 04 39 M Pelvic IP 9 22 915 / 04 Mr. Nyana Prakash 17 / 11 / 04 37 M Retro-caecal IP 8 23 930 / 04 Mr. Rajesh Chandra 20 / 11 / 04 30 M Post-ileal IP 8 24 1007 / 04 Mr. Yesu das 17 /12 / 04 40 M Paracaecal EP 12 25 7 / 05 Mr. Jyothish Das 03 / 01 / 05 23 M Post-ileal IP 6 26 8 / 05 Mrs. Archana 03 / 01 / 05 20 F Pelvic IP 9 27 11 / 05 Mr.Somashekar 04 / 01 / 05 21 M Para-caecal IP 7 28 12 / 05 Mr. Rajesh 04 / 01 / 05 25 M Post-ileal IM 6 29 26 / 05 Mr. Thimmegowda 08 / 01 / 05 37 M Retro-caecal EP 7 30 29 / 05 Mr. D. Vinod 08 / 01 / 05 24 M Pelvic IP 9 31 30 / 05 Mr. Narasimhaprasad 10 / 01 / 05 48 M Retro-caecal IP 6 32 32 / 05 UNKNOWN 10 / 01 / 05 40 M Retro-caecal IP 11 33 33 / 05 Mr. D. Krishna 10 / 01 / 05 45 M Post-ileal IP 10 34 36 / 05 UNKNOWN 11 / 01 / 05 50 M Pelvic IP 9 35 38 / 05 Mr.Gnana Prakash 11 / 01 / 05 30 M Promonteric IP 8 36 40 / 05 Mr.S. Shivaji 12 / 01 / 05 40 M Pelvic IP 9 37 42 / 05 Mr. M. Krishna 13 / 01 / 05 38 M Post-ileal IP 6 38 43 / 05 Mr. Revanna 15 / 01 / 05 50 M Post-ileal IP 8 39 47 / 05 Kum. B. Deepika 18 / 01 / 05 12 F Pelvic IP 7 40 48 / 05 Mushra 19 / 01 / 05 1½ F Retro-caecal IP 8 41 49 / 05 Mrs. Pulbansa 19 / 01 / 05 20 F Post-ileal IP 11 42 56 / 05 Mr.P.N. Jayaram 21 / 01 / 05 45 M Pelvic IP 9 43 57 / 05 UNKNOWN 22 / 01 / 05 15 M Post-ileal IP 6 44 59 / 05 Mr. Noor Basha 22 / 01 / 05 27 M Retro-caecal IP 10 45 61 / 05 Mr. Sandeep 23 / 01 / 05 19 M Pelvic IP 11 46 62 / 05 Kum. Divya 23 / 01 / 05 11 F Post-ileal IP 5 47 63 / 05 UNKNOWN 23 / 01 / 05 50 M Retro-caecal IP 8 48 65 / 05 Mr. D. Solay 24 / 01 / 05 55 M Pelvic IP 9 49 66 / 05 Mr. Lawrence 24 / 01 / 05 30 M Retro-caecal EP 11 50 67 / 05 Mr. Vijayendra 25 / 01 / 05 35 M Post-ileal IP 12 51 83 / 05 UNKNOWN 28 / 01 / 05 75 M Retro-caecal IP 5 52 84 / 05 Mr. Jawar 28 / 01 / 05 40 M Pre-ileal IP 6 53 85 / 05 Mr. Syed Sultan 28 / 01 / 05 48 M Post-ileal IP 6 54 86 / 05 Mrs. Lakshmi 28 / 01 / 05 40 F Retro-caecal IP 12 55 87 / 05 UNKNOWN 28 / 01 / 05 60 M Retro-caecal IP 6 56 89 / 05 Mr. Sharath Kumar 29 / 01 / 05 13 M Sub-caecal IP 10 57 90 / 05 Mr. Shaikh Basha 29 / 01 / 05 57 M Sub-hepatic IP 8 58 92 / 05 Mrs. Bhavya 30 / 01 / 05 22 F Post-ileal IP 6 59 103 / 05 Mr. Babulal 03 / 02 / 05 38 M Para-caecal IP 8 60 104 / 05 Mr.R. Muthu 03 / 02 / 05 30 M Retro-caecal IP 10 61 167 / 05 Mrs. Noorie 22 / 02 / 05 29 F Retro-caecal IP 9
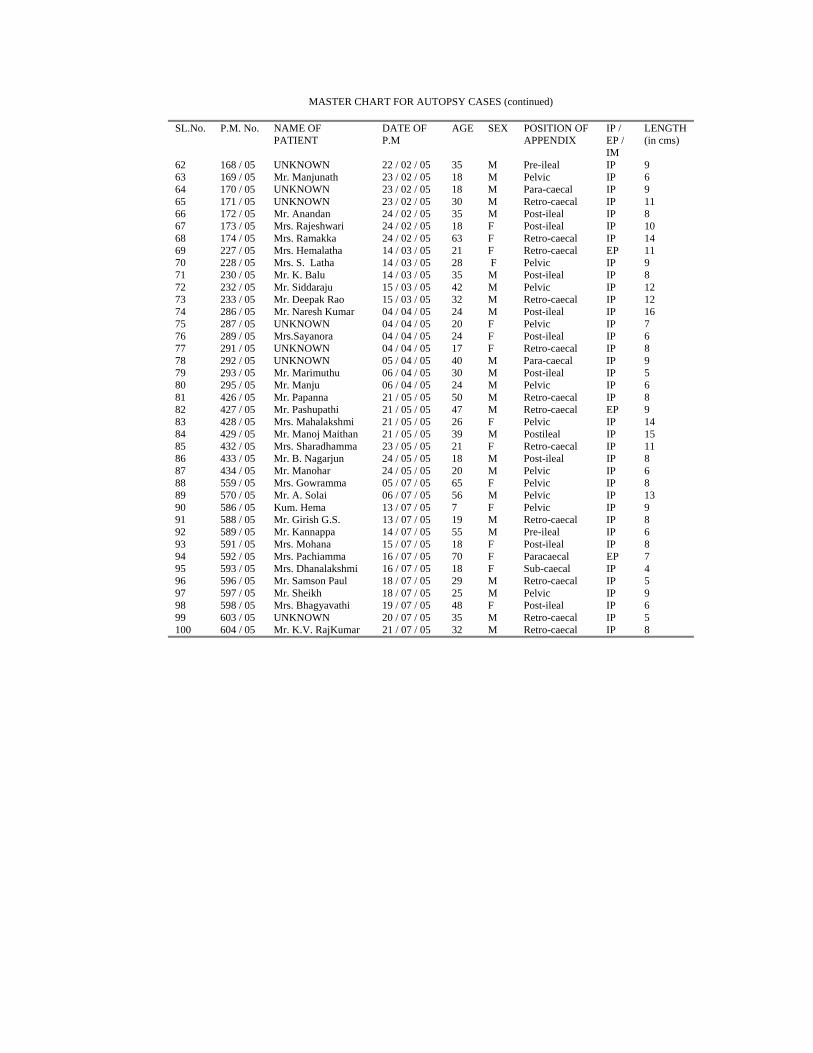
MASTER CHART FOR AUTOPSY CASES (continued)
SL.No. P.M. No. NAME OF PATIENT
DATE OF P.M
AGE SEX POSITION OF APPENDIX
IP / EP / IM
LENGTH (in cms)
62 168 / 05 UNKNOWN 22 / 02 / 05 35 M Pre-ileal IP 9 63 169 / 05 Mr. Manjunath 23 / 02 / 05 18 M Pelvic IP 6 64 170 / 05 UNKNOWN 23 / 02 / 05 18 M Para-caecal IP 9 65 171 / 05 UNKNOWN 23 / 02 / 05 30 M Retro-caecal IP 11 66 172 / 05 Mr. Anandan 24 / 02 / 05 35 M Post-ileal IP 8 67 173 / 05 Mrs. Rajeshwari 24 / 02 / 05 18 F Post-ileal IP 10 68 174 / 05 Mrs. Ramakka 24 / 02 / 05 63 F Retro-caecal IP 14 69 227 / 05 Mrs. Hemalatha 14 / 03 / 05 21 F Retro-caecal EP 11 70 228 / 05 Mrs. S. Latha 14 / 03 / 05 28 F Pelvic IP 9 71 230 / 05 Mr. K. Balu 14 / 03 / 05 35 M Post-ileal IP 8 72 232 / 05 Mr. Siddaraju 15 / 03 / 05 42 M Pelvic IP 12 73 233 / 05 Mr. Deepak Rao 15 / 03 / 05 32 M Retro-caecal IP 12 74 286 / 05 Mr. Naresh Kumar 04 / 04 / 05 24 M Post-ileal IP 16 75 287 / 05 UNKNOWN 04 / 04 / 05 20 F Pelvic IP 7 76 289 / 05 Mrs.Sayanora 04 / 04 / 05 24 F Post-ileal IP 6 77 291 / 05 UNKNOWN 04 / 04 / 05 17 F Retro-caecal IP 8 78 292 / 05 UNKNOWN 05 / 04 / 05 40 M Para-caecal IP 9 79 293 / 05 Mr. Marimuthu 06 / 04 / 05 30 M Post-ileal IP 5 80 295 / 05 Mr. Manju 06 / 04 / 05 24 M Pelvic IP 6 81 426 / 05 Mr. Papanna 21 / 05 / 05 50 M Retro-caecal IP 8 82 427 / 05 Mr. Pashupathi 21 / 05 / 05 47 M Retro-caecal EP 9 83 428 / 05 Mrs. Mahalakshmi 21 / 05 / 05 26 F Pelvic IP 14 84 429 / 05 Mr. Manoj Maithan 21 / 05 / 05 39 M Postileal IP 15 85 432 / 05 Mrs. Sharadhamma 23 / 05 / 05 21 F Retro-caecal IP 11 86 433 / 05 Mr. B. Nagarjun 24 / 05 / 05 18 M Post-ileal IP 8 87 434 / 05 Mr. Manohar 24 / 05 / 05 20 M Pelvic IP 6 88 559 / 05 Mrs. Gowramma 05 / 07 / 05 65 F Pelvic IP 8 89 570 / 05 Mr. A. Solai 06 / 07 / 05 56 M Pelvic IP 13 90 586 / 05 Kum. Hema 13 / 07 / 05 7 F Pelvic IP 9 91 588 / 05 Mr. Girish G.S. 13 / 07 / 05 19 M Retro-caecal IP 8 92 589 / 05 Mr. Kannappa 14 / 07 / 05 55 M Pre-ileal IP 6 93 591 / 05 Mrs. Mohana 15 / 07 / 05 18 F Post-ileal IP 8 94 592 / 05 Mrs. Pachiamma 16 / 07 / 05 70 F Paracaecal EP 7 95 593 / 05 Mrs. Dhanalakshmi 16 / 07 / 05 18 F Sub-caecal IP 4 96 596 / 05 Mr. Samson Paul 18 / 07 / 05 29 M Retro-caecal IP 5 97 597 / 05 Mr. Sheikh 18 / 07 / 05 25 M Pelvic IP 9 98 598 / 05 Mrs. Bhagyavathi 19 / 07 / 05 48 F Post-ileal IP 6 99 603 / 05 UNKNOWN 20 / 07 / 05 35 M Retro-caecal IP 5 100 604 / 05 Mr. K.V. RajKumar 21 / 07 / 05 32 M Retro-caecal IP 8

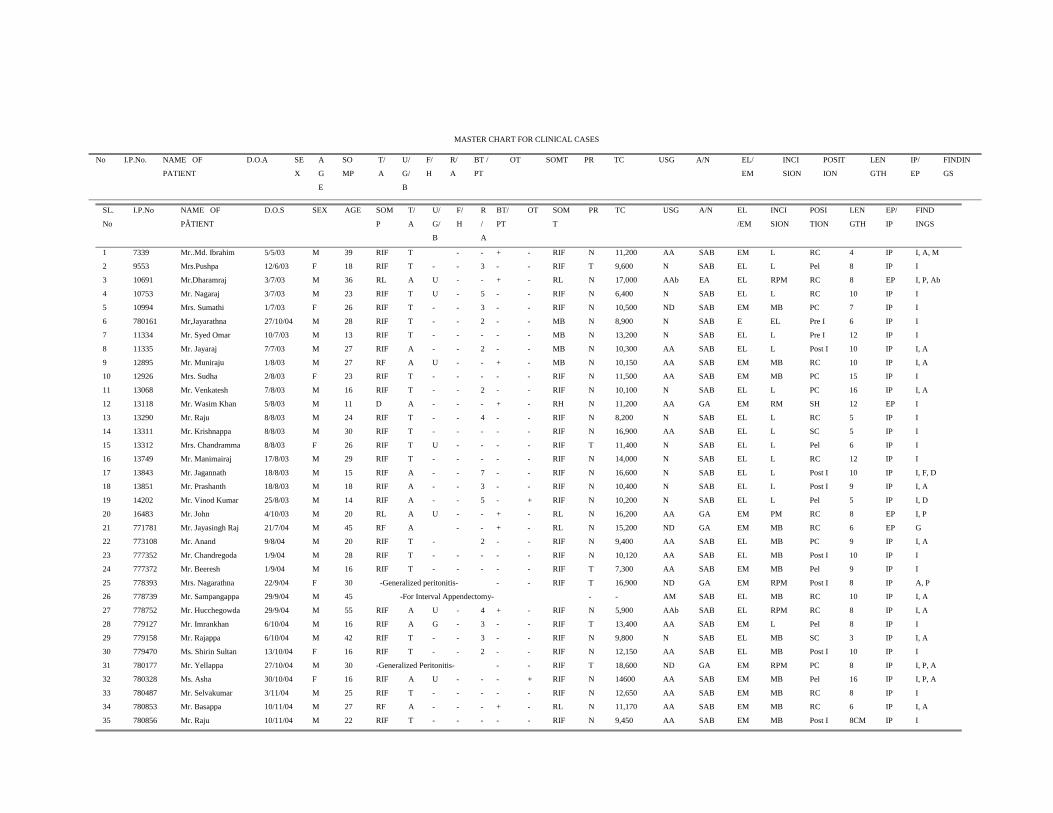
MASTER CHART FOR CLINICAL CASES
No I.P.No. NAME OF
PATIENT
D.O.A SE
X
A
G
E
SO
MP
T/
A
U/
G/
B
F/
H
R/
A
BT /
PT
OT SOMT PR TC USG A/N EL/
EM
INCI
SION
POSIT
ION
LEN
GTH
IP/
EP
FINDIN
GS
SL.
No
I.P.No NAME OF
PÂTIENT
D.O.S SEX AGE SOM
P
T/
A
U/
G/
B
F/
H
R
/
A
BT/
PT
OT SOM
T
PR TC USG A/N EL
/EM
INCI
SION
POSI
TION
LEN
GTH
EP/
IP
FIND
INGS
1 7339 Mr..Md. Ibrahim 5/5/03 M 39 RIF T - - + - RIF N 11,200 AA SAB EM L RC 4 IP I, A, M
2
9553 Mrs.Pushpa 12/6/03 F 18 RIF T - - 3 - - RIF T 9,600 N SAB EL L Pel 8 IP I
3 10691 Mr.Dharamraj 3/7/03 M 36 RL A U - - + - RL N 17,000 AAb EA EL RPM RC 8 EP I, P, Ab
4 10753 Mr. Nagaraj 3/7/03 M 23 RIF T U - 5 - - RIF N 6,400 N SAB EL L RC 10 IP I
5 10994 Mrs. Sumathi 1/7/03 F 26 RIF T - - 3 - - RIF N 10,500 ND SAB EM MB PC 7 IP I
6 780161 Mr,Jayarathna 27/10/04 M 28 RIF T - - 2 - - MB N 8,900 N SAB E EL Pre I 6 IP I
7 11334 Mr. Syed Omar 10/7/03 M 13 RIF T - - - - - MB N 13,200 N SAB EL L Pre I 12 IP I
8 11335 Mr. Jayaraj 7/7/03 M 27 RIF A - - 2 - - MB N 10,300 AA SAB EL L Post I 10 IP I, A
9 12895 Mr. Muniraju 1/8/03 M 27 RF A U - - + - MB N 10,150 AA SAB EM MB RC 10 IP I, A
10 12926 Mrs. Sudha 2/8/03 F 23 RIF T - - - - - RIF N 11,500 AA SAB EM MB PC 15 IP I
11 13068 Mr. Venkatesh 7/8/03 M 16 RIF T - - 2 - - RIF N 10,100 N SAB EL L PC 16 IP I, A
12 13118 Mr. Wasim Khan 5/8/03 M 11 D A - - - + - RH N 11,200 AA GA EM RM SH 12 EP I
13 13290 Mr. Raju 8/8/03 M 24 RIF T - - 4 - - RIF N 8,200 N SAB EL L RC 5 IP I
14 13311 Mr. Krishnappa 8/8/03 M 30 RIF T - - - - - RIF N 16,900 AA SAB EL L SC 5 IP I
15 13312 Mrs. Chandramma 8/8/03 F 26 RIF T U - - - - RIF T 11,400 N SAB EL L Pel 6 IP I
16 13749 Mr. Manimairaj 17/8/03 M 29 RIF T - - - - - RIF N 14,000 N SAB EL L RC 12 IP I
17 13843 Mr. Jagannath 18/8/03 M 15 RIF A - - 7 - - RIF N 16,600 N SAB EL L Post I 10 IP I, F, D
18 13851 Mr. Prashanth 18/8/03 M 18 RIF A - - 3 - - RIF N 10,400 N SAB EL L Post I 9 IP I, A
19 14202 Mr. Vinod Kumar 25/8/03 M 14 RIF A - - 5 - + RIF N 10,200 N SAB EL L Pel 5 IP I, D
20 16483 Mr. John 4/10/03 M 20 RL A U - - + - RL N 16,200 AA GA EM PM RC 8 EP I, P
21 771781 Mr. Jayasingh Raj 21/7/04 M 45 RF A - - + - RL N 15,200 ND GA EM MB RC 6 EP G
22 773108 Mr. Anand 9/8/04 M 20 RIF T - 2 - - RIF N 9,400 AA SAB EL MB PC 9 IP I, A
23 777352 Mr. Chandregoda 1/9/04 M 28 RIF T - - - - - RIF N 10,120 AA SAB EL MB Post I 10 IP I
24 777372 Mr. Beeresh 1/9/04 M 16 RIF T - - - - - RIF T 7,300 AA SAB EM MB Pel 9 IP I
25 778393 Mrs. Nagarathna 22/9/04 F 30 -Generalized peritonitis- - - RIF T 16,900 ND GA EM RPM Post I 8 IP A, P
26 778739 Mr. Sampangappa 29/9/04 M 45 -For Interval Appendectomy- - - AM SAB EL MB RC 10 IP I, A
27 778752 Mr. Hucchegowda 29/9/04 M 55 RIF A U - 4 + - RIF N 5,900 AAb SAB EL RPM RC 8 IP I, A
28 779127 Mr. Imrankhan 6/10/04 M 16 RIF A G - 3 - - RIF T 13,400 AA SAB EM L Pel 8 IP I
29 779158 Mr. Rajappa 6/10/04 M 42 RIF T - - 3 - - RIF N 9,800 N SAB EL MB SC 3 IP I, A
30 779470 Ms. Shirin Sultan 13/10/04 F 16 RIF T - - 2 - - RIF N 12,150 AA SAB EL MB Post I 10 IP I
31 780177 Mr. Yellappa 27/10/04 M 30 -Generalized Peritonitis- - - RIF T 18,600 ND GA EM RPM PC 8 IP I, P, A
32 780328 Ms. Asha 30/10/04 F 16 RIF A U - - - + RIF N 14600 AA SAB EM MB Pel 16 IP I, P, A
33 780487 Mr. Selvakumar 3/11/04 M 25 RIF T - - - - - RIF N 12,650 AA SAB EM MB RC 8 IP I
34 780853 Mr. Basappa 10/11/04 M 27 RF A - - - + - RL N 11,170 AA SAB EM MB RC 6 IP I, A
35 780856 Mr. Raju 10/11/04 M 22 RIF T - - - - - RIF N 9,450 AA SAB EM MB Post I 8CM IP I
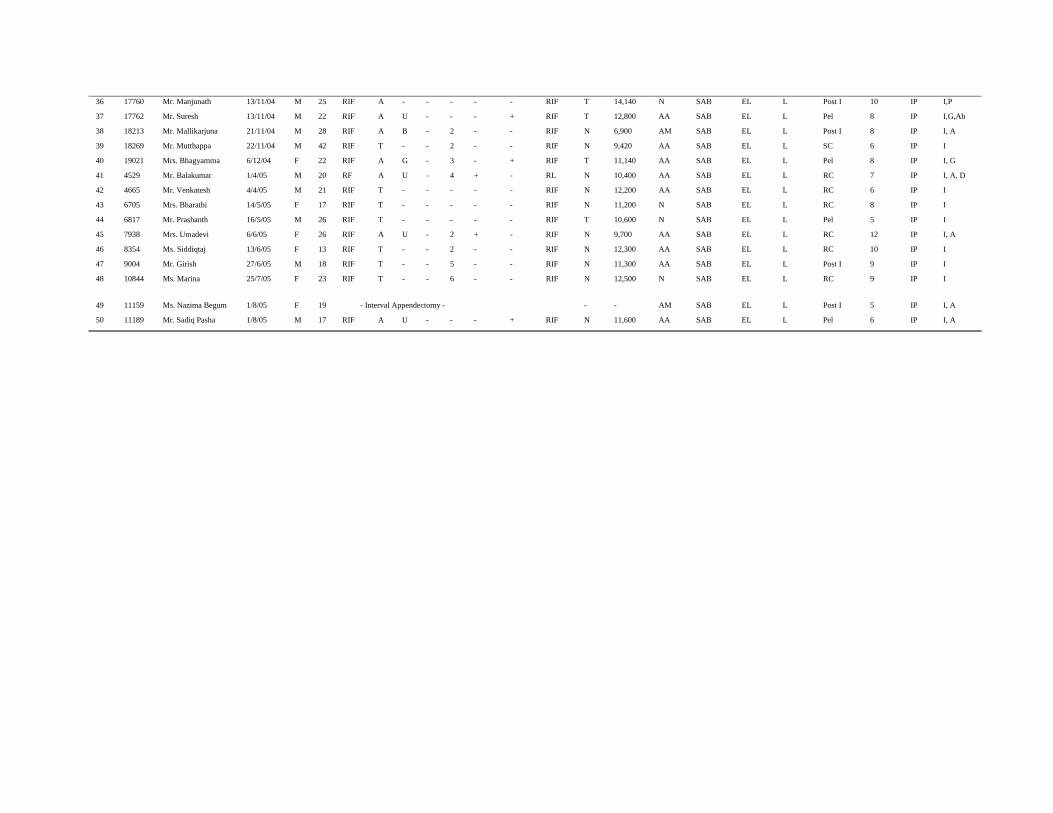
36 17760 Mr. Manjunath 13/11/04 M 25 RIF A - - - - - RIF T 14,140 N SAB EL L Post I 10 IP I,P
37
17762 Mr. Suresh 13/11/04 M 22 RIF A U - - - + RIF T 12,800 AA SAB EL L Pel 8 IP I,G,Ab
38 18213 Mr. Mallikarjuna 21/11/04 M 28 RIF A B - 2 - - RIF N 6,900 AM SAB EL L Post I 8 IP I, A
39 18269 Mr. Mutthappa 22/11/04 M 42 RIF T - - 2 - - RIF N 9,420 AA SAB EL L SC 6 IP I
40 19021 Mrs. Bhagyamma 6/12/04 F 22 RIF A G - 3 - + RIF T 11,140 AA SAB EL L Pel 8 IP I, G
41 4529 Mr. Balakumar 1/4/05 M 20 RF A U - 4 + - RL N 10,400 AA SAB EL L RC 7 IP I, A, D
42 4665 Mr. Venkatesh 4/4/05 M 21 RIF T - - - - - RIF N 12,200 AA SAB EL L RC 6 IP I
43 6705 Mrs. Bharathi 14/5/05 F 17 RIF T - - - - - RIF N 11,200 N SAB EL L RC 8 IP I
44 6817 Mr. Prashanth 16/5/05 M 26 RIF T - - - - - RIF T 10,600 N SAB EL L Pel 5 IP I
45 7938 Mrs. Umadevi 6/6/05 F 26 RIF A U - 2 + - RIF N 9,700 AA SAB EL L RC 12 IP I, A
46 8354 Ms. Siddiqtaj 13/6/05 F 13 RIF T - - 2 - - RIF N 12,300 AA SAB EL L RC 10 IP I
47 9004 Mr. Girish 27/6/05 M 18 RIF T - - 5 - - RIF N 11,300 AA SAB EL L Post I 9 IP I
48
10844 Ms. Marina 25/7/05 F 23 RIF T - - 6 - - RIF N 12,500 N SAB EL L RC 9 IP I
49 11159 Ms. Nazima Begum 1/8/05 F 19 - Interval Appendectomy - - - AM SAB EL L Post I 5 IP I, A
50 11189 Mr. Sadiq Pasha 1/8/05 M 17 RIF A U - - - + RIF N 11,600 AA SAB EL L Pel 6 IP I, A
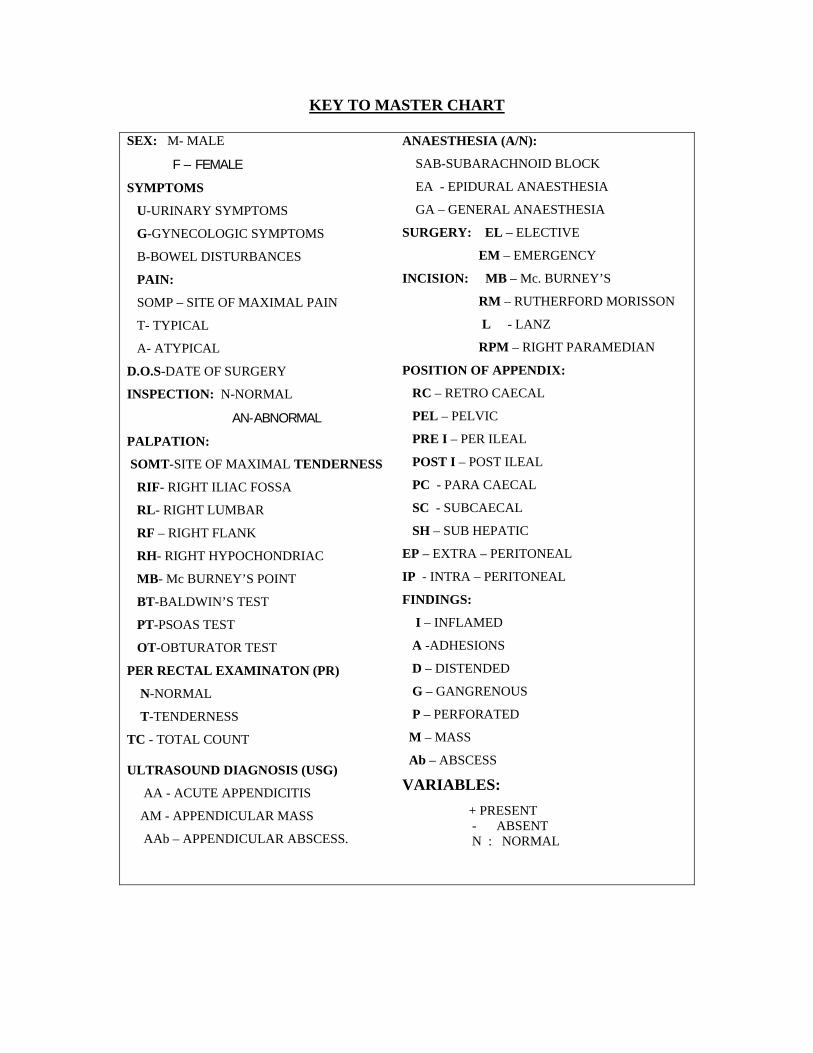
KEY TO MASTER CHART
SEX: M- MALE
F – FEMALE
SYMPTOMS
U-URINARY SYMPTOMS
G-GYNECOLOGIC SYMPTOMS
B-BOWEL DISTURBANCES
PAIN:
SOMP – SITE OF MAXIMAL PAIN
T- TYPICAL
A- ATYPICAL
D.O.S-DATE OF SURGERY
INSPECTION: N-NORMAL
AN-ABNORMAL
PALPATION:
SOMT-SITE OF MAXIMAL TENDERNESS
RIF- RIGHT ILIAC FOSSA
RL- RIGHT LUMBAR
RF – RIGHT FLANK
RH- RIGHT HYPOCHONDRIAC
MB- Mc BURNEY’S POINT
BT-BALDWIN’S TEST
PT-PSOAS TEST
OT-OBTURATOR TEST
PER RECTAL EXAMINATON (PR)
N-NORMAL
T-TENDERNESS
TC - TOTAL COUNT
ULTRASOUND DIAGNOSIS (USG)
AA - ACUTE APPENDICITIS
AM - APPENDICULAR MASS
AAb – APPENDICULAR ABSCESS.
ANAESTHESIA (A/N):
SAB-SUBARACHNOID BLOCK
EA - EPIDURAL ANAESTHESIA
GA – GENERAL ANAESTHESIA
SURGERY: EL – ELECTIVE
EM – EMERGENCY
INCISION: MB – Mc. BURNEY’S
RM – RUTHERFORD MORISSON
L - LANZ
RPM – RIGHT PARAMEDIAN
POSITION OF APPENDIX:
RC – RETRO CAECAL
PEL – PELVIC
PRE I – PER ILEAL
POST I – POST ILEAL
PC - PARA CAECAL
SC - SUBCAECAL
SH – SUB HEPATIC
EP – EXTRA – PERITONEAL
IP - INTRA – PERITONEAL
FINDINGS:
I – INFLAMED
A -ADHESIONS
D – DISTENDED
G – GANGRENOUS
P – PERFORATED
M – MASS
Ab – ABSCESS
VARIABLES: + PRESENT - ABSENT N : NORMAL

Top Related
Copyright © 2022 FDOKUMEN

