






Bahasa
Halaman
Hukum

Priority setting and implementation in acentralized health system: a case study ofKerman province in IranAkram Khayatzadeh-Mahani,1,2,3* Marianna Fotaki4 and Gillian Harvey4
1Research Center for Modeling in Health, Kerman University of Medical Sciences, Kerman, Iran, 2Research Center for Health ServicesManagement, Kerman University of Medical Sciences, Kerman, Iran, 3School of Management and Medical Informatics, Kerman Universityof Medical Sciences, Kerman, Iran and 4Manchester Business School, The University of Manchester, UK
*Corresponding author. Research Center for Modeling in Health, Kerman University of Medical Sciences, Jahad Blvd, Kerman 7619813159,Iran. E-mail: [email protected]. Tel: þ98-913-397-3153
Accepted 6 June 2012
The question of how priority setting processes work remains topical, contentious
and political in every health system across the globe. It is particularly acute in
the context of developing countries because of the mismatch between needs and
resources, which is often compounded by an underdeveloped capacity for
decision making and weak institutional infrastructures. Yet there is limited
research into how the process of setting and implementing health priorities
works in developing countries. This study aims to address this gap by examining
how a national priority setting programme works in the centralized health
system of Iran and what factors influence its implementation at the meso and
micro levels. We used a qualitative case study approach, incorporating mixed
methods: in-depth interviews at three levels and a textual analysis of policy
documents.
The data analysis showed that the process of priority setting is non-systematic,
there is little transparency as to how specific priorities are decided, and the
decisions made are separated from their implementation. This is due to the
highly centralized system, whereby health priorities are set at the macro level
without involving meso or micro local levels or any representative of the public.
Furthermore, the two main benefit packages are decided by different bodies
(Ministry of Health and Medical Education and Ministry of Welfare and Social
Security) and there is no co-ordination between them. The process is also
heavily influenced by political pressure exerted by various groups, mostly
medical professionals who attempt to control priority setting in accordance with
their interests. Finally, there are many weaknesses in the implementation of
priorities, resulting in a growing gap between rural and urban areas in terms of
access to health services.
Keywords Health care priority setting, benefit package, implementation, Iran
Published by Oxford University Press in association with The London School of Hygiene and Tropical Medicine
� The Author 2012; all rights reserved.
Health Policy and Planning 2012;1–15
doi:10.1093/heapol/czs082
1
Health Policy and Planning Advance Access published September 22, 2012 at U
niversity of Manchester on O
ctober 23, 2012http://heapol.oxfordjournals.org/
Dow
nloaded from

KEY MESSAGES
� The processes of setting and implementing health priorities should be integrated to enhance their feasibility of service
provision.
� The decision making team on health priorities should include representation from a range of stakeholders, in particular
policy implementers and the public.
� The health priority setting decision-making process should be based on transparent criteria, in order to provide a rationale
behind the decisions made to providers and the public alike.
� Health policy makers should always be aware of the political environment they work in, since decision making on health
priorities is as much a political as it is a technical process.
IntroductionAll health systems across the world need to prioritize health
services. Among the key reasons are the scarcity of resources,
with the demand for services outstripping the available
resources (Bate et al. 2007), and concerns about equity in the
distribution of and access to services (Hoedemaekers and
Dekkers 2003). Health care priority setting is of particular
importance in developing countries, where a mismatch between
needs and resources is often compounded by an underdevel-
oped capacity for decision making, and weak institutional
infrastructures (Baltussen et al. 2006). Priority setting in
developing countries is perceived to be difficult and full of
uncertainties, due to the lack of reliable evidence, analytical
methods for identifying priority options and coherent processes
for decision making (Kapiriri et al. 2003). This gives rise to a
proliferation of approaches to priority setting and has provoked
an ongoing debate about the best way to conduct this process.
The most recent debate is how to make the process more
explicit (transparent), based on defendable evidence, rather
than an implicit, informal process supported by heuristics or
intuition (Mitton and Donaldson 2004; Rosen 2006). Needs
assessment and health economics evaluation methods therefore
constitute the main technical approaches to setting health
priorities (Donaldson and Mooney 1991).
While there is a wealth of literature describing priority setting
processes at the macro (national) level in many health systems,
this mostly focuses on developed countries (for example, Ham
1997; Busse 1999; Calltorp 1999; Rissanen and Hakkinen 1999;
Stepan and Sommersguter-Reichmann 1999; Pedersen et al.
2005; Sabik and Lie 2008). Most of the studies on priority
setting focus on evaluating the fairness of the process using the
Accountability for Reasonableness (also known as A4R) frame-
work (Daniels and Sabin 2002). Most importantly, while there
is a growing body of knowledge on the decision makers’
perspectives on the priority setting process (e.g. Gibson et al.
2004; Mitton and Prout 2004), we have only a very limited
understanding from the implementers’ perspectives (Kinnunen
et al. 1998; Mshana et al. 2007). Because of the limited research
on health priority setting in developing nations (Hrabac et al.
2000; Gonzalez-Pier et al. 2006; Kapiriri et al. 2007), there is a
distinct lack of evidence about how priorities are decided and
implemented at all levels of the system.
This research aims to address these gaps by examining how a
macro-level priority setting programme works in a centralized
health care system, and what factors influence its
implementation at the meso and micro levels, using Iran as a
case study. The national-level decision making bodies in the
Iranian health system, such as the Ministry of Health
and Medical Education (MOHME) and the Ministry of
Welfare and Social Security (MOWSS), are not new, but there
is a paucity of information available about the priority setting
processes they use and the factors governing their decisions. In
other words, the rationale behind health priority decisions
has not been made explicit or publicly discussed. Moreover,
despite the introduction of new technical priority setting tools
into the Iranian health system, such as Burden of Disease
(BOD), it is unclear how those tools are understood and applied
in practice. Alongside the lack of detailed information about the
process of priority setting, there is an equal knowledge gap in
terms of how priorities are implemented at a service delivery
level. In addressing these knowledge gaps, the research
presented in this paper sought to answer two specific research
questions:
(1) How does a macro-level health care priority setting process
work in practice in the centralized health system of Iran?
(2) What factors influence the process of priority setting and
implementation in this system?
Qualitative methodologies were chosen as the most suitable
means for our investigation, because of the type of research
questions addressed (what and how health priorities are set
and put in practice), the novelty of the research topic in this
specific context and the complexity of the phenomenon under
investigation (Creswell 2009). The study is one of the rare
empirical examples exploring the perceptions of policy makers
at the macro level, key decision makers at the meso (provincial/
regional) level, and health authorities at the micro (local/
district) level of the health system with regards to the national
priority setting process and its implementation.
By providing empirical evidence in an area that has not been
previously investigated, research makes a contribution to
knowledge, through three distinct ways. First, it identifies
factors influencing the process of setting and implementing
priorities in a specific context, namely the centralized health
system of Iran. Second, it evaluates how the system of priority
setting works at various levels by examining the views of both
policy makers and policy implementers. Third, it explores the
priority setting programme from two perspectives, namely, the
process (how benefit packages underpinning priority setting are
developed at the macro level of a health system), and the
2 HEALTH POLICY AND PLANNING
at University of M
anchester on October 23, 2012
http://heapol.oxfordjournals.org/D
ownloaded from

outcomes (how the benefit packages are implemented at the
meso and micro levels of a health system).
In the remainder of the paper we describe the context and
methods before presenting the findings of the study. We then
discuss these and a put forward a number of policy implications
resulting from the study.
Context
Iran has a population of nearly 75 million, with 72% living in
urban areas and 28% in rural parts (Statistical Centre of Iran
2010). The country is administratively divided into 30 provinces
(Ostans); each province, in turn, is split into a number of
districts (Shahrestans or sub-province), and each district includes
a number of urban centres (cities/towns) and villages. Up to
95% of the rural population has access to the primary health
care (PHC) services (Aghajanian et al. 2007). As far as
secondary and tertiary care are concerned, the broad population
coverage by various health insurance schemes in Iran has
improved access to health services for over 92% of the
population (Russell 2005; World Bank 2007).
In the period following the 1979 Islamic revolution, the
Iranian government focused on PHC development, especially in
rural areas. This has led to success in improving several health
indicators such as decreased child and maternal mortality rates,
and increased life expectancy at birth (Mehryar 2004).
However, according to the World Health Organization (WHO),
Iran was ranked 93rd among 191 countries in terms of the
population’s health status, and 112th with respect to the fair
financial contribution index (FFCI) (WHO 2000). The poor
performance of the Iranian health system measured by the
FFCI index is due to many households lacking any type of
health insurance or financial protection against the costs of
illness. Accordingly, there is a high rate of out-of-pocket (OOP)
payment among Iranian households as revealed by the World
Bank report (2007). Almost 50% of health expenditures in Iran
are OOP (Ibrahimipour et al. 2011). Another challenge facing
the Iranian health system is the change in the burden of
disease pattern towards non-communicable diseases and acci-
dents, which is similar to many other health systems world-
wide. A recent study of the BOD in Iran revealed a high
percentage of cardiovascular disorders, cancers, mental health
disorders, traffic accidents and injuries (Naghavi 2006). All of
these challenges suggest that the issue of how priorities are set
and implemented in the Iranian health system is an important
and timely issue to study.
The organization and structure of the Iranianhealth system
Planning and policy making are decided at the central level in
Iran, and are then devolved via the meso level to the micro
levels for implementation. The implementation of centrally
developed plans is supervised by the macro level. For many
years and until recently there was no official centre for policy
making. The only body for planning and decision making was
the Management and Planning Organization (MPO) based at
the macro level under direct supervision of the president.
However, in 2007, a centre called the ‘Health Policy Unit’ was
launched within the MOHME to devise policies and provide the
evidence underpinning these policies, supported by the
establishment of a dedicated research centre (Khayatzadeh-
Mahani 2010).
There are many providers and purchasers, including the
public sector, the private sector, non-government organizations
(NGOs) and various health insurance organizations, which play
a role in the provision and financing of health care, but the
health system is managed primarily by the government. The
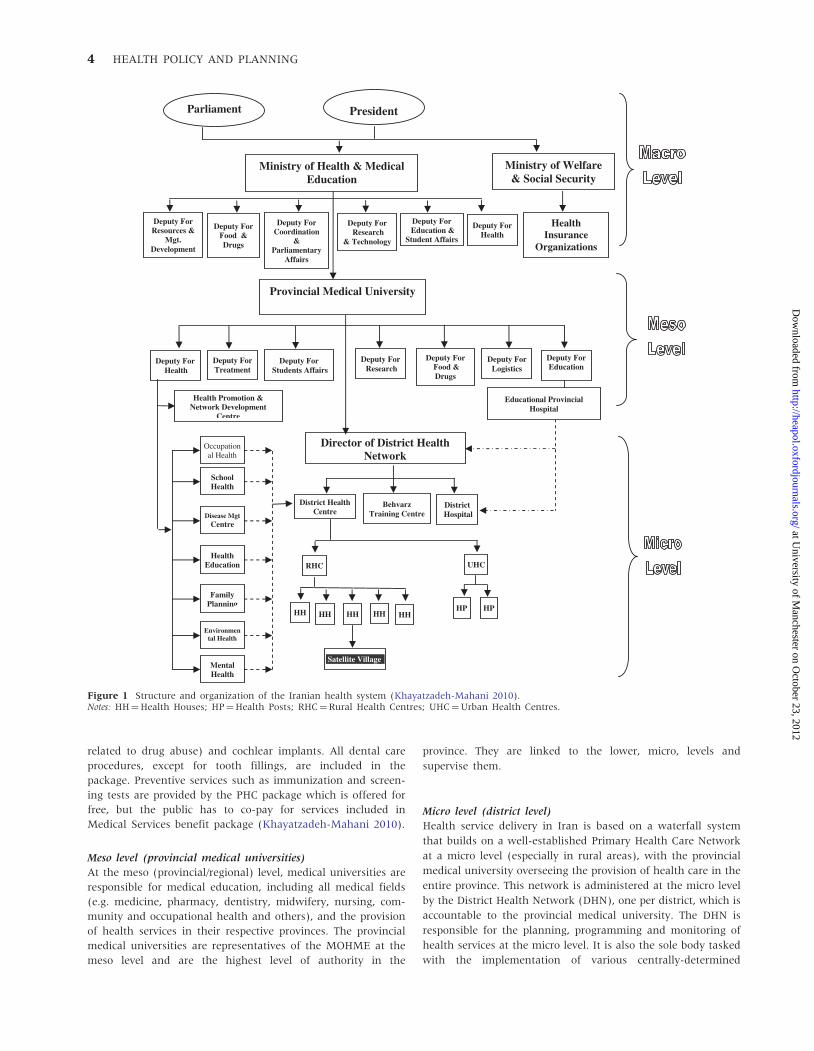
structure of the public health system of Iran spans through
three levels, as presented in Figure 1: macro (national), meso
(provincial or regional) and micro (local or district).
Macro level
The MOHME and the MOWSS1 are the main organizations at
the national level responsible for providing and financing
health services in Iran. The respective ministers are accountable
to both the parliament and the government (that is the cabinet
or president, see Figure 1), but are also members of the cabinet
and are proposed and appointed by the president, subject to
approval by the parliament (Schieber and Klingen 1999; WHO
2004). The MOHME is the ultimate decision maker on matters
concerning the Iranian health system. It is responsible for the
provision of health care services, medical education, supervision
and regulation, as well as policy making, production and
distribution of pharmaceuticals, and research and development.
It also regulates the provision of private health services and
the health services provided by the NGOs. The PHC benefit
package is developed and financed by the MOHME at the
macro level.
The MOWSS, on the other hand, develops and finances the
Medical Services benefit package via health insurance organ-
izations. The MOWSS comprises four major health insurance
organizations, all of which are controlled by the government:
(1) the Social Security Organization (SSO) for formal sector
employees and the self-employed and their dependants; (2) the
Medical Services Insurance Organization (MSIO) for govern-
ment employees, rural households, the self-employed and
others, such as students; (3) the Armed Forces Medical
Services Organization, for members of the military and their
dependants; and (4) the Imam Khomeini Relief Committee,
which covers the poor. These four organizations come under the
jurisdiction of the High Council for Health Insurance (HCHI),
made up of ministers from seven ministries and headed by the
Minister of Health. HCHI is responsible for inclusion or
exclusion of services, and sets the fee schedule for providers’
payments. All health insurance schemes use the same fee
schedule. Some major banks (e.g. Melli Bank) and companies
(e.g. Oil Company) also have specific benefit packages for their
own employees. Private insurance is supplementary to these
public programmes.
The Medical Services benefit package provides a comprehen-
sive set of curative services, including hospitalization, diagnostic
tests and pharmaceuticals, for which the public has to co-pay.
People who have health insurance coverage can visit any
specialist directly and use the secondary and tertiary level of
health services without going through the referral system. All
curative services are potentially included in this package. A few
services are excluded, which are cosmetic surgeries, transplants
(e.g. heart, liver, and fingers), infertility services, joint replace-
ments, non-accidental injuries (e.g. knife stabbing or problems
HEALTH CARE PRIORITY SETTING AND IMPLEMENTATION 3
at University of M
anchester on October 23, 2012
http://heapol.oxfordjournals.org/D
ownloaded from
related to drug abuse) and cochlear implants. All dental care
procedures, except for tooth fillings, are included in the
package. Preventive services such as immunization and screen-
ing tests are provided by the PHC package which is offered for
free, but the public has to co-pay for services included in
Medical Services benefit package (Khayatzadeh-Mahani 2010).
Meso level (provincial medical universities)
At the meso (provincial/regional) level, medical universities are
responsible for medical education, including all medical fields
(e.g. medicine, pharmacy, dentistry, midwifery, nursing, com-
munity and occupational health and others), and the provision
of health services in their respective provinces. The provincial
medical universities are representatives of the MOHME at the
meso level and are the highest level of authority in the
province. They are linked to the lower, micro, levels and
supervise them.
Micro level (district level)
Health service delivery in Iran is based on a waterfall system
that builds on a well-established Primary Health Care Network
at a micro level (especially in rural areas), with the provincial
medical university overseeing the provision of health care in the
entire province. This network is administered at the micro level
by the District Health Network (DHN), one per district, which is
accountable to the provincial medical university. The DHN is
responsible for the planning, programming and monitoring of
health services at the micro level. It is also the sole body tasked
with the implementation of various centrally-determined
Figure 1 Structure and organization of the Iranian health system (Khayatzadeh-Mahani 2010).Notes: HH¼Health Houses; HP¼Health Posts; RHC¼Rural Health Centres; UHC¼Urban Health Centres.
4 HEALTH POLICY AND PLANNING
at University of M
anchester on October 23, 2012
http://heapol.oxfordjournals.org/D
ownloaded from

packages of health services, mainly the PHC package and the
Medical Services benefit package.
Each DHN is composed of three main parts: the district
health centre (DHC), the district hospital and a Behvarz training
centre. Each DHC, in turn, comprises different health facilities
identified as (1) Health Houses whose responsibility is to
implement the PHC programmes (with a Behvarz, who is a
community health worker, delivering the PHC benefit package
for rural residents), (2) Health Posts (similar to Health Houses,
providing the PHC benefit package for urban residents), and
(3) Urban and Rural Health Centres (UHC and RHC). All these
facilities work under the supervision of a DHN Director who is
the representative of the provincial medical university chancel-
lor at the micro level (Shadpour 2000).
MethodsData collection
This study adopted a qualitative research stance and a case
study methodology in order to gain a depth of understanding
about the priority setting programme in the context of the
Iranian centralized health system (Ritchie and Lewis 2005).
Two main approaches to data collection were employed:
(1) face-to-face in-depth interviews conducted at three levels
of the health system: macro, meso and micro; and (2) docu-
mentary analysis of key policy texts. The interviews constituted
the main data source, supported by a review of relevant
documentation. Thematic analysis of the data was carried out
to identify emerging categories and sub-categories, as described
in more detail below.
Sampling methods
Qualitative inquiries typically focus on small samples chosen
purposefully to get an in-depth understanding of the phenom-
enon under study (Patton 2002). Kerman province was selected
as the most accessible case for the principal researcher to
conduct the fieldwork (Hartley 2004), in order to explore the
implementation of nationally set health priorities. In conduct-
ing the case study, we were guided by a constructivist
methodology, hence were less concerned about the generaliz-
ability of the results and focused on providing a rich and
detailed description of the case under study (Stake 1995). The
selected province, however, shows similar demographic and
health indicators to that of the country (see Table 1), and as
such it is broadly representative of Iran.
In order to select the interviewees at the macro level, we
applied snowball sampling. We drew up an initial short-list of
potential participants using the organizational chart of the
MOHME and three previously conducted pilot interviews.
Snowball sampling was then followed in order to identify all
participants involved in the process of priority setting. At the
meso level, purposive methods were used. The focus at the
meso level was on provincial health authorities who were in
charge of transferring the centrally set health priorities from the
macro level to the micro levels. At the micro level, in order to
employ maximum variation as a sampling strategy, and to
represent diverse cases to describe the implementation process
(Creswell 2009), all ten District Health Networks affiliated to
the Kerman Medical University were included because of their
distinct socio-economic and cultural characteristics. In each
district, two main health authorities were then selected: the
District Health Centre Director responsible for implementing
the PHC benefit package, and the District Hospital Director in
charge of implementing the Medical Services benefit package.
Table 2 shows the location and number of interviewees from
macro to micro level.
All interviews took place in the interviewees’ work place as
agreed in advance. Permission to record the interview was sought
in all cases. All interviews were fully transcribed in Farsi, but were
analysed by the principal researcher in English. Ethical guidelines
were adhered to throughout the research. These included
obtaining official approval for the research (from the MOHME
and key decision makers at Kerman Medical University),
providing the research participants with a consent form and
information letter, and ensuring them of anonymity.
Notes were also taken at all of the interviews. The principal
researcher analysed the following documents: (1) the Third
Five-Year Development Plan of Iran (2000/2001–2004/2005);
(2) the Fourth Five-Year Development Plan (2005/2006–2009/
2010); (3) articles related to health in the Iranian Constitution
(e.g. Article 29); (4) the Iranian Budget Law (e.g. the Year
2007–08); (5) the Iranian National Health Insurance Act;
(6) BEHBAR and Family Medicine policies; and (7) documents
showing the results of important studies done by the MOHME,
such as the BOD study, the National Health Account study, and
the Demographic and Health Survey study. The data gathered
from these documents included extracts captured in such a way
as to record and preserve the original context (Patton 2002).
Data analysis
We used a qualitative thematic framework analysis, which is a
matrix-based analytical method (Ritchie et al. 2003; Bryman
2008), to analyse the interview data and excerpts from docu-
ments (Patton 2002). The data analysis took an a priori
thematic approach (Bryman 2008) in line with the analytical
framework method (Ritchie and Spencer 1994). An initial
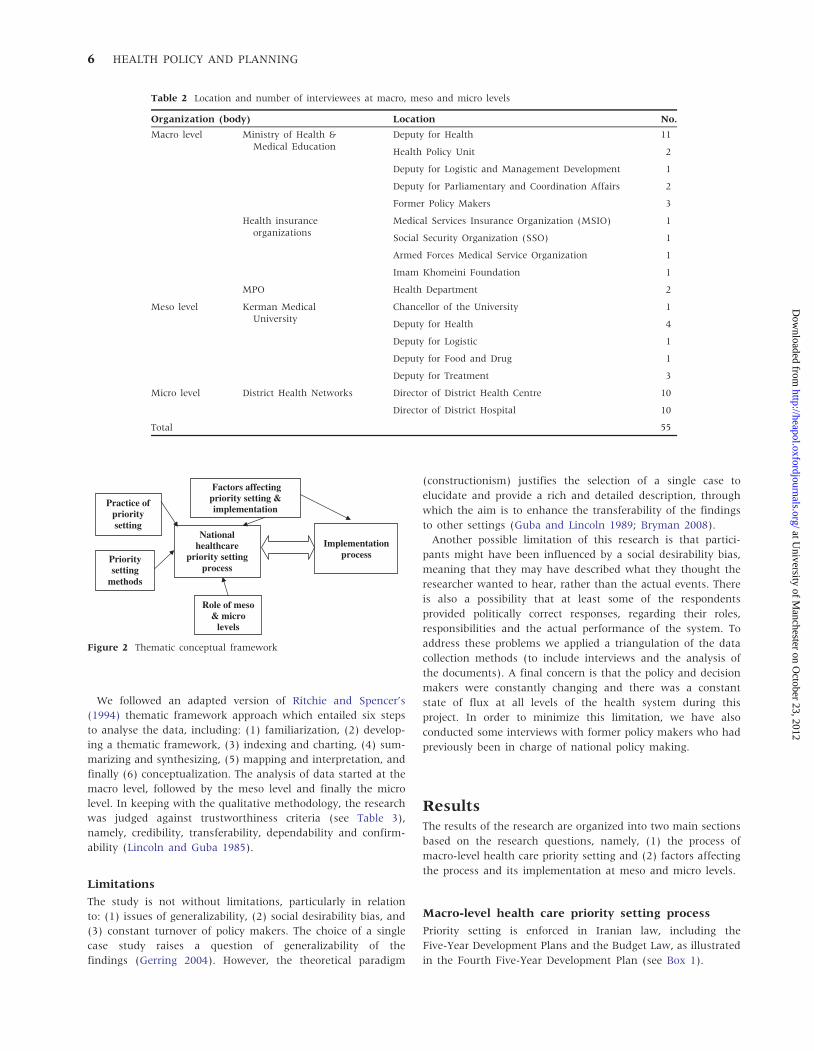
thematic conceptual framework (see Figure 2), based on the
research questions, was developed at a very early stage of the
analysis (Ritchie et al. 2003).
Table 1 Comparing selected demographic and health indicatorsbetween Kerman province and Iran as a whole in the year 2000
Indicator Kermana Irana,b
Population under 5 years (%) 8.9 8.0b
Population under 15 years (%) 35.3 28.7b
Population above 65 years (%) 5.3 5.5a
Access to improved drinking-water sources (%) 89 93a
Birth rate (births per 1000 population) 18.3 14.3b
Total fertility rate (average number ofchildren per woman)
2.4 2a
Adult literacy rate (%) 79.9 82.4a
Sources: aMOHME (2000), Population and health in the Islamic Republic of
Iran: Demographic and Health Survey.bWorld Health Statistics 2008 (WHO 2008).
HEALTH CARE PRIORITY SETTING AND IMPLEMENTATION 5
at University of M
anchester on October 23, 2012
http://heapol.oxfordjournals.org/D
ownloaded from
We followed an adapted version of Ritchie and Spencer’s
(1994) thematic framework approach which entailed six steps
to analyse the data, including: (1) familiarization, (2) develop-
ing a thematic framework, (3) indexing and charting, (4) sum-
marizing and synthesizing, (5) mapping and interpretation, and
finally (6) conceptualization. The analysis of data started at the
macro level, followed by the meso level and finally the micro
level. In keeping with the qualitative methodology, the research
was judged against trustworthiness criteria (see Table 3),
namely, credibility, transferability, dependability and confirm-
ability (Lincoln and Guba 1985).
Limitations
The study is not without limitations, particularly in relation
to: (1) issues of generalizability, (2) social desirability bias, and
(3) constant turnover of policy makers. The choice of a single
case study raises a question of generalizability of the
findings (Gerring 2004). However, the theoretical paradigm
(constructionism) justifies the selection of a single case to
elucidate and provide a rich and detailed description, through
which the aim is to enhance the transferability of the findings
to other settings (Guba and Lincoln 1989; Bryman 2008).
Another possible limitation of this research is that partici-
pants might have been influenced by a social desirability bias,
meaning that they may have described what they thought the
researcher wanted to hear, rather than the actual events. There
is also a possibility that at least some of the respondents
provided politically correct responses, regarding their roles,
responsibilities and the actual performance of the system. To
address these problems we applied a triangulation of the data
collection methods (to include interviews and the analysis of
the documents). A final concern is that the policy and decision
makers were constantly changing and there was a constant
state of flux at all levels of the health system during this
project. In order to minimize this limitation, we have also
conducted some interviews with former policy makers who had
previously been in charge of national policy making.
ResultsThe results of the research are organized into two main sections
based on the research questions, namely, (1) the process of
macro-level health care priority setting and (2) factors affecting
the process and its implementation at meso and micro levels.
Macro-level health care priority setting process
Priority setting is enforced in Iranian law, including the
Five-Year Development Plans and the Budget Law, as illustrated
in the Fourth Five-Year Development Plan (see Box 1).
Table 2 Location and number of interviewees at macro, meso and micro levels
Organization (body) Location No.
Macro level Ministry of Health &Medical Education
Deputy for Health 11
Health Policy Unit 2
Deputy for Logistic and Management Development 1
Deputy for Parliamentary and Coordination Affairs 2
Former Policy Makers 3
Health insuranceorganizations
Medical Services Insurance Organization (MSIO) 1
Social Security Organization (SSO) 1
Armed Forces Medical Service Organization 1
Imam Khomeini Foundation 1
MPO Health Department 2
Meso level Kerman MedicalUniversity
Chancellor of the University 1
Deputy for Health 4
Deputy for Logistic 1
Deputy for Food and Drug 1
Deputy for Treatment 3
Micro level District Health Networks Director of District Health Centre 10
Director of District Hospital 10
Total 55
National healthcare
priority setting process
Implementation process
Factors affecting priority setting & implementation
Practice of priority setting
Priority setting
methods
Role of meso & micro
levels
Figure 2 Thematic conceptual framework
6 HEALTH POLICY AND PLANNING
at University of M
anchester on October 23, 2012
http://heapol.oxfordjournals.org/D
ownloaded from

The analysis of interview data from all levels confirmed that
the Iranian health system practises a centralized process in
terms of health care priority setting. In exploring the current
process of health care priority setting in practice, macro-level
respondents were able to describe these processes, including the
methods and procedures used to set priorities. Although
decisions on health priorities are taken at the macro level, the
meso- and micro-level participants delineated their important
roles in this process, as is explained in more detail below.
Different packages of health services
One of the emerging findings of this research was the
distinction, made by the macro-level participants, between
various health services (for example, public health care,
curative and diagnostic services, health technologies, and
drugs) and the various bodies responsible for setting priorities
and financing them, although the services may be still delivered
by the MOHME. As can be seen from the following table there
are four packages of health services available to the Iranian
population, which are financed by various bodies (see Table 4).
The main point made by almost all participants at the three
levels (macro, meso and micro) was a lack of co-ordination
between the different bodies in charge of setting and providing
various packages of health services. This was believed to have led
to a discontinuity of care in the public sector, which is worsened
by the lack of an effective referral system and gate keeping. The
recommendation offered was to integrate the separate packages
into a single, all-embracing package covering all sorts of services
including primary, secondary and tertiary care.
Ma11:2 ‘‘There are various decision making bodies which are
not linked together and each makes decisions in isolation. For
instance, the Ministry of Health and Medical Education sets policies
in isolation from the Ministry of Welfare and Social Security
and vice versa. So, it is no surprise to see that many poor rural
people, seeking medical treatments, are left unattended in towns
since policy making for preventive care is separated from curative
care.’’
Ma4: ‘‘. . . I remember that we at the Ministry of Health and
Medical Education were in long discussions with the health
insurance organizations in order to convince them to cover breast
cancer screening service. Our efforts, however, were unsuccessful.
Their argument was that this is a preventive service and should be
included into the PHC benefit package. This clearly shows that the
approach of health insurance organizations in this country is
treatment-oriented.’’
Another interesting set of findings concerned the structure of
current benefit packages. Almost all participants believed that
the two main benefit packages available to the Iranian
Box 1 Excerpts from Iran’s Fourth Five-Year Development Plan (Government of Iran 2004)
Article 91
The following measures shall be taken in order to increase effectiveness of the health service delivery system in the country
and to enhance and develop the universal health insurance system: A) All the commercial and non-commercial insurance
companies are permitted to render the basic and supplementary health services solely by observing the laws and regulations
of the High Council for Health Insurance; B) The High Council for Health Insurance shall initiate the required means of
establishing the family-physician-based health insurance and referral system; C) In order to expand equity in utilization of
health services, the basic rural health insurance services shall be defined and executed equal to their urban counterparts.
Article 96
Government is bound to increase gradually the population health insurance coverage and financial supports which are the
concerns of the Article twenty nine (29) of the Constitution of the Islamic Republic of Iran. The resources for this purpose
are the general revenues and the income derived from public participation, through insurance, protective and supportive
activities. In doing so, the following measures should be taken into account: A) To increase the social insurance coverage,
with due consideration of the rural inhabitants, tribal population and urban employees who have not been covered so far; B)
Complete population coverage (one hundred percent) by the public insurance for the basic medical services; C) To provide
special insurance for women who are head of households and for unprotected individuals, given priority to orphans.
Table 3 Strategies adopted to ensure trustworthiness
Criteria Strategy
Credibility Six main strategies were adopted to increase the credibility of this research including: (1) prolonged engagement, (2) fact-findingvisits, (3) peer debriefing, (4) triangulation, (5) member checks and (6) referential adequacy.
Transferability (1) Thick descriptions and (2) purposive sampling were the principal methods employed to enhance the transferability of thestudy findings.
Dependability Three tactics, namely (1) detailed documentation, (2) data checks and (3) an external auditor, were adopted to increase thedependability of the research.
Confirmability An external auditor, a final year PhD student, whose research was on the health system of a developing country, was used inorder to enhance the confirmability of the research. He reviewed the whole project and looked for relationships between theresearch questions and the findings, and consistency throughout the entire work.
HEALTH CARE PRIORITY SETTING AND IMPLEMENTATION 7
at University of M
anchester on October 23, 2012
http://heapol.oxfordjournals.org/D
ownloaded from

population (the PHC benefit package and the Medical Services
benefit package) are very wide, with a plethora of services and
interventions included. This was deemed to be the result of a
‘no exclusion’ policy. According to this policy, no formal and
explicit exclusion is allowed, although as the data illustrate,
exclusion happens informally, mostly in the form of rationing
of services. There was also a widely held belief that policy
makers were trying to avoid the possibility of public unrest
caused by the exclusion of services from the benefit packages,
and they reacted typically by rationing the excluded services
(for example, by offering it only in certain health facilities
or by certain health professionals) or even by lifting the ban
completely.
Macro-level participants made a distinction between priority
setting and rationing. It was acknowledged that rationing is
necessary alongside priority setting. However, rationing also
appears to occur instead of exclusion, apparently to avoid
problems caused by the explicit elimination of services, as the
following comments illustrate.
Ma23: ‘‘In the year 2002, the high council for health insurance
decided to include 13 items of drugs into the Medical Services
benefit package. In the meantime, it was decided to exclude
vitamins with the rationale that vitamins are not essential drugs
and are not usually included in the benefit packages of other
countries. The decision on exclusion led to an unrest in the country.
Thereafter, it was decided to place a limit by which vitamins could
only be offered in some specific hospitals.’’
Ma7: ‘‘I remember that the Beta HCG test was one of the services
covered by the health insurance organizations which could be
prescribed by all medical doctors including GPs. Recently, however,
only specialist physicians can prescribe it in order to reduce the
amount of prescriptions.’’
Another finding with respect to the exclusion of services was
that although there is no formal process of exclusion in
developing the current benefit packages, exclusion does happen
informally. For example, if a medical procedure or a drug is not
used or prescribed for a certain period of time, it can become
informally excluded.
Ma16: ‘‘Nowadays nobody uses Amoxicillin as physicians prescribe
Sephexin instead. So Amoxicillin will be gradually taken out of the
benefit package.’’
A further issue of concern, expressed mostly by micro-level
interviewees, was the vagueness of services and interventions
covered by the benefit packages, which was believed to lead to
personal interpretation and a degree of discretion at the micro
level as well as manipulation of priorities at the macro level.
Mi17: ‘‘. . . A few years ago the Ministry of Health allocated us
little funds to implement some interventions towards elderly care.
Unfortunately, they did not tell us what exactly to do. We were
confused at first what to do with this little money, but finally
decided to develop some brochures and flyers about elderly healthy
eating and distribute them across the city.’’
Mi4: ‘‘. . . The benefit package, for instance, indicates that it covers
X-surgery. But it does not specify in detail which procedures are
exactly covered. This leaves room for insurance organizations to
avoid reimbursing hospitals for some procedures used during a
surgery and this is a very common phenomenon in this country.’’
The centralized process was also criticized by micro-level
participants for setting priorities which were not feasible.
Participants at meso and micro levels revealed a further concern
about the centralized priority setting process at the macro level,
which does not provide them with a rationale behind the
inclusion of health services and interventions. Another issue of
concern expressed by micro-level participants was a lack of
transparency in the process of centralized priority setting.
Mi19: ‘‘A couple of years ago the family medicine policy was
enforced and we had to implement it across the rural parts. Some
GPs were assigned for our rural health facilities as gate keepers. At
the same time, the health ministry sent us several circulars and
booklets containing the clinical guidelines that the GP has to follow
as well as the duties of the family medicine team, including the
GP, and the list of medicines that the GP was allowed to prescribe.
We faced resistance from the GPs in, accepting the nationally
developed clinical guidelines and the list of medicines. I believe they
had a valid point to ask why we should perform the guidelines and
prescribe certain medicines that we don’t know who has decided
them and how and why.’’
Priority setting methods
The analysis of the data highlighted several technical and
non-technical methods, which are currently applied in setting
priorities in the Iranian health system. The two main
non-technical methods described were bargaining and the
historically-based approach. Bargaining was referred to by the
majority of respondents as the most common informal proced-
ure. The historically-based approach, on the other hand, was
considered the dominant perspective in allocating resources.
More recently there was a shift to implementing economic
evaluation methods. Two commonly applied technical methods
Table 4 Type of packages and bodies responsible for priority setting and funding in Iran
Type of package Responsibility for priority setting and funding
Primary Health Care (PHC) benefit package Ministry of Health & Medical Education (MOHME)
Medical Services benefit package (secondary/hospital care) Ministry of Welfare & Social Security
The Supplementary Package (mostly providing health technologies, new medicalprocedures and drugs)
MOHME and the private health sector
Special Diseases Package (expensive medical treatments subsidized by the government) MOHME
8 HEALTH POLICY AND PLANNING
at University of M
anchester on October 23, 2012
http://heapol.oxfordjournals.org/D
ownloaded from

were BOD methodology and expert panels. The former is
employed to set priorities among different diseases, while the
latter is the most commonly used approach in setting priorities
among health services and interventions to be included into the
benefit packages. The results of the BOD study are not
reportedly employed in setting priorities for the Medical
Services benefit package; there does, however, seem to be
some (non-systematic) application of BOD data in the PHC
benefit package. However, there was a view expressed that
burden of risk factors should be measured instead of burden of
disease, with the directing of scarce resources towards high
burdened risk factors. This means that many diseases and
health problems that share the same risk factors could be
tackled simultaneously.
The data also revealed that expert panels, which decide on
priorities of the benefit packages based on a host of technical
and non-technical criteria such as systematic review (if any),
cost, international priorities (such as pandemics) and bargain-
ing, comprise, predominantly, of medical professionals acting as
policy makers in this instance. It also emerged that although
the principle of equity is an implicit influential criterion in
setting priorities in the main benefit packages, in practice (i.e.
during the implementation of priorities) the principle of
personal choice plays a greater role. In the Medical Services
benefit package, the most influential criterion on the deter-
mination of priorities was deemed to be cost (i.e. budget
impact). The analysis of documents and interview data revealed
that urban residents exercise a great deal of choice in Iran
compared with their rural counterparts whose choice has been
limited by state policies. Family Medicine and the BEHBAR
(rural health insurance for all rural residents) are the two state
policies, which have limited rural households access to second-
ary and tertiary care through a referral system, although they
aimed to improve rural access to basic health services.
Role of meso and micro levels in the macro-levelpriority setting process
The data analysis revealed that the meso level (the provincial
medical universities) report regularly on health indicators of
their provinces to the MOHME, which is supposed to set
priorities at the national level based on that evidence.
Nevertheless, there is also a degree of discretion allowed at
the meso level. The establishment of the Board of Trustees at
each provincial medical university, for example, has granted the
meso levels some managerial and financial responsibilities as
the following excerpt from the Fourth Five-Year Development
Plan (Article 49) shows:
‘Each provincial medical university should establish a Board
of Trustees and there should be a direct transfer of global
budgets from the government (MPO) to medical univer-
sities, which the Board of Trustees could then use their
discretion to allocate resources as needed’.
However, analysis of the interviews suggests a degree of
dissatisfaction with the level of discretion afforded to the meso
level, as policy implementers in the region are still required to
obtain authorization from the MOHME for many decisions. For
instance, in relation to the issue of resources, especially human
resources, it was highlighted that the meso level is not allowed
to hire personnel without the permission of the macro level.
Moving to the micro level, participants believed that the
health information produced at this level forms the basis for
macro-level priority setting. There was a general feeling among
respondents that they played a vital role in priority setting, with
a prevailing view that macro-level priorities are based on the
local data.
Mi10: ‘‘The Ministry of Health and Kerman Medical University
ask for health information and health indicators frequently and I
am sure they use those data in policy making. For instance, we
send them health information on all types of mortalities such as
maternal and child mortality as well as disease prevalence and
incidence rates. Definitely in the BOD study, our information is
used.’’
Factors affecting the setting and implementationof national health priorities
A host of factors influencing the process of setting and
implementing priorities were identified. Overall, three main
factors related to priority setting were: (1) the nature of decision
making, (2) political pressure and (3) policy makers’ behaviour,
as is discussed below. Regarding the implementation of
priorities, the most influential factors were: (1) the status and
the clout of health professionals implementing priorities,
(2) the private sector and (3) rural–urban disparities.
Factors influencing the process of setting priorities
The reactive nature of the decision making process was seen to
be the main factor impacting on the way health priorities were
set. It was suggested that reactive decision making (in response
to emergencies and not planned in advance), along with the
non-sustainability in decision making, lack of transparency and
non-systematic decision making have all contributed to weak
outcomes of the health priority setting process.
Ma8: ‘‘. . . Decision making for priority setting in Iran looks like a
crisis management. It responds to the daily problems which occur
and makes temporary decisions to sort them out.’’
Mi18: ‘‘. . . We don’t really know why they [policy makers] have
changed the procedures for child growth monitoring. They keep adding
paperwork for which we can’t see the point to fill them up.’’
Political pressure emerged as another key factor influencing
the process of setting health priorities. It was deemed to be
induced by different means, such as changes in the cabinet and
parliament, as can be seen in the following statement.
Ma21: ‘‘Change of some cabinet members such as president, health
minister, finance minister, or environment minister affects the
health system greatly. For instance, change of the finance minister
might affect GNP allocated to the health sector, which directly
affects priority setting because if more resources are allocated to the
health system, we can include more services into the publicly
funded benefit packages.’’
Other influences could also be discerned, such as the impact of
national and international trends, the policies of international
HEALTH CARE PRIORITY SETTING AND IMPLEMENTATION 9
at University of M
anchester on October 23, 2012
http://heapol.oxfordjournals.org/D
ownloaded from

organizations, group pressure applied by pharmaceutical com-
panies and companies importing new health technologies and
drugs, the medical profession, and the media.
Regarding the policy makers’ behaviour, factors identified
were personal interests, ethical viewpoints (e.g. libertarian or
egalitarian) and perceptions about priority setting (whether
they perceive it to be an important issue and what their specific
views are about it), as is reflected in the following statement.
Ma19: ‘‘. . . Many years ago, I was in the office of one of policy
makers and I could hear what he speaks on the phone. He was
basically saying that it is not important for me whether a medicine
is expensive or not, or if it is produced in Iran or abroad. What
matters for me is that this medicine should be available for patients
who need it. He actually had a very liberal point of view. I can
provide you with many examples like this.’’
Factors influencing the implementation of priorities
The three most influential factors affecting the implementation
of priorities related to the policy implementers’ political ‘clout’,
the power of the private sector, and rural–urban disparities.
While policy makers appeared to have the most influence on
the process of setting national priorities, policy implementers
including health personnel (responsible for implementing
the PHC benefit package) and physicians (who implement the
Medical Services benefit package) at the micro-level were the
most influential groups in putting those priorities into practice.
The study revealed an asymmetry in the amount of discretion
exercised by these two groups of policy implementers when
translating priorities into practice. Whilst health personnel
responsible for the PHC benefit package appeared to lack any
type of freedom, physicians enjoyed a high degree of discretion
when implementing the Medical Services benefit package. This
lack of autonomy for PHC personnel is typically compounded
by workload pressures, poor in-service training, lax supervision,
staff and resource shortages. The result is often a relatively low
standard of service delivery at the local level.
Me3: ‘‘. . . Every day you ask a Behvarz, with a high school
education, to perform a new service or intervention and you do not
tell her what to exclude. So, she excludes services on her own
decision. Even though she does not exclude any services, she
performs the service with a low quality.’’
Mi13: ‘‘. . . A few years ago, the ministry people decided to add the
blood pressure and diabetes screening intervention into the PHC
package. So, our Behvarzs had to perform this service for the whole
population over 35. Almost at the same time, another service was
added namely the national newborn screening programme for
congenital hypothyroidism, to be performed by Behvarz for all
newborns in 3–5 days of birth. Apart from these, there is a lot of
paperwork that a Behvarz has to do. We keep asking the same
Behvarz to do all these tasks with the same salary. Many times I
feel very uncomfortable to let them know of a newly added service
when I can’t add a new staff or can’t spare resources.’’
The private sector also appeared to wield considerable influ-
ence over the way national health priorities were put into
practice. In Iran, the public has a choice to seek all types of
health services (primary, secondary and tertiary) from either the
public or the private sector, based on, predominantly, their
ability and willingness to pay. This, however, is mainly induced
by the physicians practising in the private sector who encourage
utilization of services, mostly covered by the Supplementary
Package, including new medicines, new medical procedures, and
expensive diagnostic services such as Magnetic Resonance
Imaging (MRI) and Computed Tomography (CT)-scans.
Reasons for this behaviour that were put forward included a
lack of proper control by the public sector, a lack of support from
the government, the low rate of tariffs and easy access to high
medical technologies. There is a considerable difference in terms
of health service tariffs (service charge) between the private and
the public sectors, with the latter much lower than the former. It
was argued that, over the last few years, this gap has led to
under-staffing in the public sector, affecting the quality of
services, because the majority of physicians and health staff
prefer to work in the private sector where they can earn more.
The data analysis also revealed significant rural and urban
disparities in access to and utilization of health services, which is
partly linked to the activities of the private sector. The role of the
private health sector appeared to exacerbate the rural–urban
disparity as far as the implementation of national health
priorities is concerned. The private sector, which predominantly
operates in urban areas of Iran, increases the gap between rural
and urban regions in terms of access to and utilization of all types
of services (i.e. primary, secondary and tertiary) with the state
policies (i.e. Family Medicine and BEHBAR) intensifying this
divergence. It is interesting to note how perceived rural–urban
differences affect the implementation of benefit packages in
different regions: the provision of the PHC benefit package
services is the centre of attention in rural areas, while the Medical
Services benefit package is provided mainly in urban areas.
Me7: ‘‘. . . In the rural areas, a Behvarz performs actively all PHC
services for the whole population in her/his geographical area. For
instance, if a pregnant woman does not attend the health house to
receive the prenatal care, Behvarz visits that lady in her house. In
the urban areas, however, the PHC services are offered passively,
meaning that if the pregnant women do not refer themselves,
nobody will trace them. Apart from that, in towns pregnant
women do not usually seek services from health posts and urban
health centres. They prefer to receive the same care from the
gynaecologist because there is no limitation to visit a specialist in
this country. So, even for the very basic services, which a midwife
can perform more effectively, people visit a specialist physician.’’
DiscussionThe aim of the study was to investigate how a national priority
setting programme works in the centralized health system of
Iran and what factors influence its implementation at the meso
and micro levels. From the analysis of the findings, five key
themes emerge (as shown in Figure 3):
(1) The process of setting priorities is non-systematic, leading
to many shortfalls in developing the benefit packages;
(2) Health priorities are set at the macro level, by expert
panels, using a host of methods (e.g. cost, bargaining,
international priorities), without involving the local level
or any representatives of the public;
10 HEALTH POLICY AND PLANNING
at University of M
anchester on October 23, 2012
http://heapol.oxfordjournals.org/D
ownloaded from
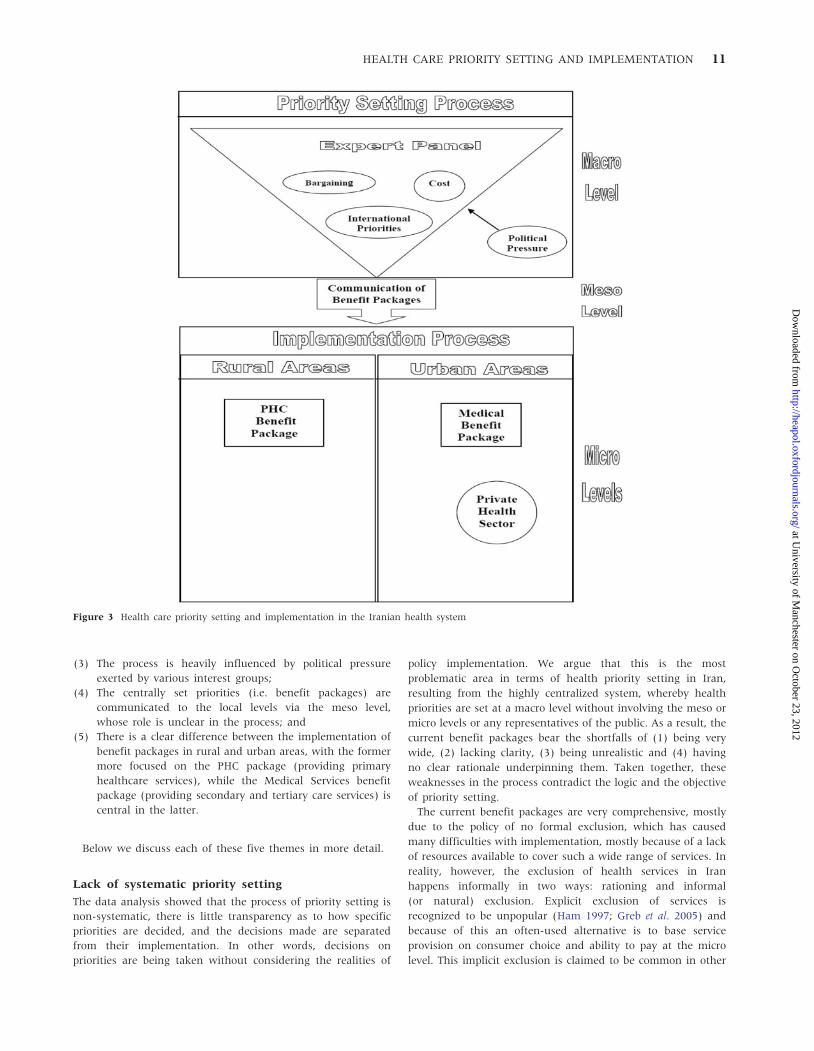
(3) The process is heavily influenced by political pressure
exerted by various interest groups;
(4) The centrally set priorities (i.e. benefit packages) are
communicated to the local levels via the meso level,
whose role is unclear in the process; and
(5) There is a clear difference between the implementation of
benefit packages in rural and urban areas, with the former
more focused on the PHC package (providing primary
healthcare services), while the Medical Services benefit
package (providing secondary and tertiary care services) is
central in the latter.
Below we discuss each of these five themes in more detail.
Lack of systematic priority setting
The data analysis showed that the process of priority setting is
non-systematic, there is little transparency as to how specific
priorities are decided, and the decisions made are separated
from their implementation. In other words, decisions on
priorities are being taken without considering the realities of
policy implementation. We argue that this is the most
problematic area in terms of health priority setting in Iran,
resulting from the highly centralized system, whereby health
priorities are set at a macro level without involving the meso or
micro levels or any representatives of the public. As a result, the
current benefit packages bear the shortfalls of (1) being very
wide, (2) lacking clarity, (3) being unrealistic and (4) having
no clear rationale underpinning them. Taken together, these
weaknesses in the process contradict the logic and the objective
of priority setting.
The current benefit packages are very comprehensive, mostly
due to the policy of no formal exclusion, which has caused
many difficulties with implementation, mostly because of a lack
of resources available to cover such a wide range of services. In
reality, however, the exclusion of health services in Iran
happens informally in two ways: rationing and informal
(or natural) exclusion. Explicit exclusion of services is
recognized to be unpopular (Ham 1997; Greb et al. 2005) and
because of this an often-used alternative is to base service
provision on consumer choice and ability to pay at the micro
level. This implicit exclusion is claimed to be common in other
Figure 3 Health care priority setting and implementation in the Iranian health system
HEALTH CARE PRIORITY SETTING AND IMPLEMENTATION 11
at University of M
anchester on October 23, 2012
http://heapol.oxfordjournals.org/D
ownloaded from

health systems, for example, the US, which has a strong private
insurance system, while most European policy makers are
against it for equity reasons (Greb et al. 2005). However, this is
not to say that exclusion does not occur by other implicit
means. For example, in the UK National Health Services (NHS),
exclusion is seen to occur at the point of access to health
services, with general practitioners (GPs) acting as gate-
keepers, for instance, by controlling access to secondary care
specialists (Coast 1996; Owen-Smith et al. 2010).
Another possible reason for including a plethora of services in
the Medical Services benefit package, provided by health insur-
ance organizations (i.e. the MOWSS), could be the payment
system by which hospitals are reimbursed (diagnosis-related
groups or DRGs). According to the DRG system, a fixed price is
paid for each episode of care. It is believed that one way for
providers to maintain their income under the DRG payment
system is to increase the number and range of services (Allen
2009).
Lack of clarity is another pitfall of the current benefit
packages available in Iran, which leads to either manipulation
of services at the macro level or individual interpretations of
priorities by the implementers at the micro level. Leese et al.
(2001), measuring the success of primary care organizations in
the British health system, found a similar situation, which they
attributed to the central decision making (Leese et al. 2001).
The benefit packages are also unrealistic and end up expres-
sing aspirational rather than actual policy, as is the case in
many other countries where there is an unwillingness to
exclude services explicitly for political reasons (Fotaki 2009).
Policy implementers in this research raised a general complaint
over the non-feasibility of many of the health interventions
(mostly those covered by the PHC package). This suggests that
the realities of implementation have not been taken into
account when the interventions were developed. It could also
be the result of decision making often carried out in a rush
without comprehensive advanced planning, which is a common
shortfall of decision making in Iran.
Lastly, the health care priority setting process in Iran does not
provide any rationale behind the prioritized services. This could
be one explanation for the shift of physicians towards the
private sector, and away from providing the services covered in
the benefit packages: the physicians may not be convinced
about why certain services (e.g. medicines) are included in (and
rarely excluded from) the benefit packages.
The two main benefit packages (the PHC benefit package and
the Medical Services benefit package) are decided by two
different bodies (MOHME and MOWSS, respectively) and there
is no co-ordination between the two, which has led to discon-
tinuity of care. We hypothesize that this might be due to the
autocratic government’s lack of willingness to make difficult
political decisions concerning the structure and governance of
the system and managing public expectations extending beyond
the declaration of intent as seen in other comparable cases
(Fotaki 2006; Fotaki 2009; O’Donnell 2010).
Priority setting methods
The historically-based and bargaining methods that are cur-
rently applied in setting health priorities in Iran, which are also
the most commonly used approaches in all health systems
worldwide (Coast and Donovan 1996), are unlikely to maximize
health benefits within a given budget (Mitton and Donaldson
2004). In contrast, the BOD study, which is the main technical
health priority setting tool in Iran, and which uses local health
information (e.g. mortality and morbidity) (Murray and Lopez
1996), is believed to be a good method of setting priorities
among diseases. The missing loop in the Iranian health system
is the application of this evidence in developing the benefit
packages (i.e. setting priorities among health services and
interventions). One reason for the lack of uptake of the study
results could be that the BOD study conducted in Iran does not
prioritize among health interventions or risk factors. Moreover,
after establishing this study as a means of prioritizing among
the diseases, no follow-up studies were conducted to estimate
the cost-effectiveness of health interventions or their afford-
ability (Doherty 2010). In any case, our findings indicate that
the results of such studies are not utilized when deciding on
benefit packages, in turn suggesting a need to improve the
skills of policy makers in interpreting and applying sound
evidence.
Political pressure
Another key finding concerns the issue of political pressure
shaping the whole process. No matter how well the process is
managed by the application of sound technical methods,
political pressure (that is, the pressure imposed by various
interest groups) is crucial in determining what type of health
services, diseases or groups of people receive priority (Baltussen
and Niessen 2006; Dionne et al. 2008). In the Iranian health
system, power is predominantly in the hands of medical
professionals and pharmaceutical companies (Ibrahimipour
et al. 2011). Decisions on the inclusion (and rarely exclusion)
of services and interventions in the benefit packages are made
by expert panels, which are dominated by clinicians without
involving micro levels or any representatives of the public. The
current panel composition works against the main purpose of
holding expert panels, which is to assemble multidisciplinary
groups of experts to decide on priorities based on the evidence
available (Schmidt 2009). Mitton and Donaldson (2004) argue
that the composition should involve a mix of clinical personnel,
managers and lay participants. As such, the current situation is
far behind the classical pluralism concept proposed by Held
(2003) in which diverse and competing interest groups form
the basis for a democratic equilibrium. In such a governance
arrangement the distribution of power tends to be evened out.
However, in developing countries, a very small number of
groups exercise the majority of the power (Kimenyi and Mbaka
1993). Most policies are decided by small, elite groups within
the government or even outside it. This is more evident in a
centralized government, such as that of Iran, in which the
political power and the decision making process are dominated
by selected groups rather than broad representation.
Implementation at the meso and micro levels
The centrally set priorities (i.e. benefit packages) in the Iranian
health system are communicated to the micro levels via the
meso level, whose role is somewhat unclear in the process. It
could be seen to play a brokerage role between the top and
bottom levels of the health system but the key actors at the
12 HEALTH POLICY AND PLANNING
at University of M
anchester on October 23, 2012
http://heapol.oxfordjournals.org/D
ownloaded from

meso level lack any type of independent constituency or
political legitimacy. However, moving towards the micro level
and the point of service delivery, there is more diversity in
terms of the discretion allowed, although the extent of this
discretion varies with the status of those delivering the services.
Here, physicians, who primarily perform the Medical Services
benefit package, claim autonomy in the way they use their
clinical judgement in the allocation of resources to patients.
Physicians, particularly specialists, are mainly based in urban
areas. This explains why the Medical Services benefit package is
utilized and demanded more in the urban areas of Iran. This
may also explain the paradox whereby clinicians largely make
the decisions at a macro level, yet their colleagues in the field
do not necessarily follow the priorities set. Physicians can not
only influence the priority setting process, but they can also
jeopardize its implementation by shifting towards the private
sector when it suits them, and away from providing the services
covered in the benefit packages. In urban areas of Iran, it is
very common to see medical specialists (mostly the well-known
ones) refuse to contract with the health insurance organiza-
tions; meaning that they still offer services provided by the
Medical Services benefit package, but the public has to pay
the entire cost out-of-pocket as if the service is received from
the private sector. These physicians (mostly practising in the
private sector) also urge the public towards utilization of
services covered by the Supplementary Package, which are
mostly new medical technologies and new expensive medical
procedures and interventions. On the other hand, the health
staff (including GPs in rural areas) who implement the PHC
benefit package services, have a less secure professional status
and are accordingly given only limited control over the use of
their resources.
Rural–urban disparities
Unsurprisingly, the study revealed many weaknesses in the
implementation of priorities. Perhaps the most significant of
these is the growing gap between rural and urban areas in
terms of implementing benefit packages. One of the reasons for
this disparity could be the imperfect operation of the PHC
network, which has not been well extended to the urban areas.
There is, however, a strong private health sector, operating
predominantly in the urban areas, which intensifies this gap.
The PHC network, which is poorly established in the urban
areas, creates differences between rural and urban areas in
terms of health services provision and utilization. The urban
segment of the PHC network has remained underdeveloped,
mostly because of its poor referral system and gate keeping,
which does not facilitate the interface between various levels of
the PHC network (primary, secondary, tertiary; rural, district,
centre of province) and different levels of the health system
(micro, meso, macro). As a result, there is poor integration and
continuity of care and a real challenge in terms of controlling
unnecessary access to secondary and tertiary care.
An aspect of the rural–urban disparity in terms of benefit
package implementation could also be attributed to the strong
private health sector, which is poorly controlled by the govern-
ment. This leads to a high utilization of services and drugs not
covered by the Medical Services benefit package, especially
expensive diagnostic services, new health technologies and new
medical procedures. This is mainly because the private sector in
Iran is not involved in the provision of PHC services, but only
secondary and tertiary services. As a result, in urban areas,
there is a higher utilization of curative and diagnostic services
rather than the PHC services, which are used more in the rural
communities (Hosseinpoor et al. 2007).
ConclusionsThis research set out to examine how a macro-level priority
setting programme works in the centralized health system of
Iran, and what factors influence its implementation at the meso
and micro levels. The findings provide policy makers with a
number of practical recommendations to improve the process of
setting and implementing health priorities. Firstly, the process
of setting and implementing priorities should be integrated to
enhance the feasibility of provision of services. Secondly, the
decision making team should include representation from a
range of stakeholders, in particular policy implementers and the
public. Thirdly, the decision making process should be based on
transparent criteria, in order to provide a rationale behind the
decisions made to providers and the public alike. Fourthly,
decision makers should always be aware of the political
environment they work in, since decision making on health
priorities is as much a political as it is a technical process.
FundingThis work was supported financially by the Iranian Ministry of
Health and Medical Education.
Conflict of interestNone declared.
Endnotes1 In June 2011, the Iranian legislators passed a bill to merge the
MOWSS with two ministries of Labour and Social Affairs as wellas Cooperatives into the new Ministry of Cooperatives, Labour andSocial Security. Throughout this paper we use MOWSS as at thetime of the study it was the responsible national organization incharge of priority setting.
2 The abbreviations Ma, Me and Mi stand for macro, meso and micro,respectively; this code for the interviewees is used in order tomaintain the anonymity of the participants.
ReferencesAghajanian A, Mehryar AH, Ahmadnia S, Kezemipour A. 2007. Impact
of rural health development program in the Islamic Republic of
Iran on rural–urban disparities in health indicators. Eastern
Mediterranean Health Journal 13: 1466–75.
Allen P. 2009. Payment by results in the English NHS: the continuing
challenges. Public Money and Management 29: 161–6.
Baltussen R, Niessen L. 2006. Priority setting of health interventions:
The need for multi-criteria decision analysis. BMC Cost Effectiveness
and Resource Allocation 4: 1–9.
HEALTH CARE PRIORITY SETTING AND IMPLEMENTATION 13
at University of M
anchester on October 23, 2012
http://heapol.oxfordjournals.org/D
ownloaded from
Baltussen R, Stolk E, Chisholm D, Aikins M. 2006. Towards a multi-
criteria approach for priority setting: an application to Ghana.
Health Economics 15: 689–96.
Bate A, Donaldson C, Murtagh MJ. 2007. Managing to manage
healthcare resources in the English NHS? What can health
economics teach? What can health economics learn? Health Policy
84: 249–61.
Bryman A. 2008. Social Research Methods. Oxford: Oxford University Press.
Busse R. 1999. Priority setting and rationing in German health Care.
Health Policy 50: 71–90.
Calltorp J. 1999. Priority setting in health policy in Sweden and a
comparison with Norway. Health Policy 50: 1–22.
Coast J. 1996. Clarification and acceptance: a way forward in priority
setting. In: Coast J, Donovan J, Frankel S (eds). Priority Setting: The
Health Care Debate. Chichester, UK: John Wiley and Sons.
Coast J, Donovan J. 1996. Conflict, complexity and confusion: the
context for priority setting. In: Coast J, Donovan J, Frankel S (eds).
Priority Setting: The Health Care Debate. Chichester, UK: John Wiley
and Sons.
Creswell JW. 2009. Research Design: Qualitative, Quantitative, and Mixed
Methods Approaches. Thousand Oaks, CA: Sage.
Daniels N, Sabin J. 2002. Setting Limits Fairly: Can We Learn to Share Scarce
Resources? Oxford: Oxford University Press.
Dionne F, Mitton C, Smith N, Donaldson C. 2008. Decision maker views
on priority setting in the Vancouver Island Health Authority. BMC
Cost Effectiveness and Resource Allocation 6: 1–8.
Doherty J. 2010. Cost-effectiveness analysis for priority-setting in South
Africa – what are the possibilities? South African Medical Journal 100:
816–21.
Donaldson C, Mooney G. 1991. Needs assessment, priority setting, and
contracts for health care: an economic view. British Medical Journal
303: 1529–30.
Fotaki M. 2006. Users’ perceptions of health care reforms: quality of
care, patients’ rights and satisfaction with health insurance system
in four regions in the Russian Federation. Social Science & Medicine
63: 1637–47.
Fotaki M. 2009. Informal payments: a side effect of transition or a
mechanism for sustaining the illusion of ‘free’ healthcare? The
experience of four regions in the Russian Federation. Journal of
Social Policy 38: 649–70.
Gerring J. 2004. What is a case study and what is it good for? American
Political Science Review 98: 341–54.
Gibson J, Martin D, Singer P. 2004. Setting priorities in health care
organizations: criteria, processes, and parameters of success. BMC
Health Services Research 4: 1–8.
Gonzalez-Pier E, Gutierrez-Delgado C, Stevens G et al. 2006. Priority
setting for health interventions in Mexico’s system of social
protection in health. The Lancet 368: 1608–18.
Government of Iran. 2004. Fourth socioeconomic and cultural develop-
ment plan of the Islamic Republic of Iran. Tehran: Management
and Planning Organization of the Islamic Republic of Iran.
Greb S, Niebuhr D, Rothgang H, Wasem J. 2005. Criteria and procedures
for determining benefit packages in health care: a comparative
perspective. Health Policy 73: 78–91.
Guba E, Lincoln YS. 1989. Fourth Generation Evaluation. California: Sage.
Ham C. 1997. Priority setting in health care: learning from international
experience. Health Policy 42: 49–66.
Hartley J. 2004. Case study research. In: Cassell C, Symon G (eds).
Essential Guide to Qualitative Methods in Organizational Research. London:
Sage.
Held D. 2003. Models of Democracy. Oxford: Blackwell.
Hoedemaekers R, Dekkers W. 2003. Justice and solidarity in priority
setting in health care. Health Care Analysis 11: 325–43.
Hosseinpoor AR, Naghavi M, Alavian SM et al. 2007. Determinants of
seeking needed outpatient care in Iran: results from a national
health services utilization survey. Archives of Iranian Medicine 10:
439–45.
Hrabac B, Ljubic B, Bagaric I. 2000. Basic package of health entitlements
and solidarity in the Federation of Bosnia and Herzegovina.
Croatian Medical Journal 41: 287–93.
Ibrahimipour H, Maleki MR, Brown R et al. 2011. A qualitative study of
the difficulties in reaching sustainable universal health insurance
coverage in Iran. Health Policy and Planning 28: 485–95.
Kapiriri L, Norheim OF, Heggenhougen K. 2003. Using burden of
disease information for health planning in developing countries:
the experience from Uganda. Social Science and Medicine 56: 2433–24.
Kapiriri L, Norheim OF, Martin DK. 2007. Priority setting at the micro,
meso and macro levels in Canada, Norway and Uganda. Health
Policy 82: 78–94.
Khayatzadeh-Mahani A. 2010. Health care priority setting and imple-
mentation in a centralized health system: a case study of Iran. PhD
Thesis. The University of Manchester, UK.
Kimenyi M, Mbaka J. 1993. Rent seeking and institutional stability in
developing countries. Public Choice 77: 385–405.
Kinnune J, Lammintakanen J, Myllykangas M et al. 1998. Health care
priorities as a problem of local resource allocation. International
Journal of Health Planning and Management 13: 216–29.
Leese B, Baxter K, Goodwin N, Scott J, Mahon A. 2001. Measuring the
success of primary care organizations: is it possible? Journal of
Management in Medicine 15: 172–80.
Lincoln YS, Guba E. 1985. Naturalistic Inquiry. Newbury Park, CA: Sage.
Mehryar A. 2004. Primary health care and the rural poor in the Islamic
Republic of Iran. Scaling up Poverty Reduction. A Global Learning
Process Conference, Shanghai, China.
Mitton C, Donaldson C. 2004. Health care priority setting: principles
practice and challenges. BioMed Central 2: 1–8.
Mitton C, Prout S. 2004. Setting priorities in the south west of Western
Australia: where are we now? Australian Health Review 28: 301–10.
MOHME. 2000. Health Situation and Trend in the Islamic Republic of Iran.
[in Farsi] Tehran, Iran: Ministry of Health and Medical Education.
Mshana S, Shemilu H, Ndawi B et al. 2007. What do district health
planners in Tanzania think about improving priority setting
using ‘Accountability for Reasonableness’? BMC Health Services
Research 7: 1–5.
Murray CJL, Lopez AD. 1996. The Global Burden of Disease: A comprehensive
assessment of mortality and disability from diseases, injuries, and risk
factors in 1990 and projected to 2020. Boston, MA: Harvard School of
Public Health, for the World Health Organization and the World
Bank.
Naghavi M. 2006. Mortality profile for 23 provinces of Iran (2003) [in Farsi].
Tehran: Ministry of Health and Medical Education.
O’Donnell G. 2010. Democracy, Agency, and the State: Theory and Comparative
Intent. Oxford: Oxford University Press.
Owen-Smith A, Coast J, Donovan J. 2010. The desirability of being open
about health care rationing decisions: findings from a qualitative
study of patients and clinical professionals. Journal of Health Services
Research and Policy 15: 14–20.
Patton MQ. 2002. Qualitative Research and Evaluation Methods. Thousand
Oaks, CA: Sage.
Pedersen KM, Christiansen T, Bech M. 2005. The Danish health care
system: evolution – not revolution – in a decentralised system.
Health Economics 14: S41–S57.
14 HEALTH POLICY AND PLANNING
at University of M
anchester on October 23, 2012
http://heapol.oxfordjournals.org/D
ownloaded from

Rissanen P, Hakkinen U. 1999. Priority setting in Finnish healthcare.
Health Policy 50: 143–53.
Ritchie J, Lewis J. 2005. Qualitative Research Practice: A Guide for Social
Science Students and Researchers. London: Sage.
Ritchie J, Spencer L, O’Connor W. 2003. Carrying out qualitative
analysis. In: Ritchie J, Lewis J (eds). Qualitative Research Practice: A
Guide for Social Science Students and Researchers. Thousand Oaks, CA:
Sage.
Ritchie J, Spencer L. 1994. Qualitative data analysis for applied policy
research. In: Bryman A, Burgess RG (eds). Analyzing Qualitative
Data. London: Routledge.
Rosen P. 2006. Public dialogue on healthcare prioritization. Health Policy
79: 107–16.
Russell M. 2005. Applying DALY to assessing national health insur-
ance performance: the relationship between the national health
insurance expenditures and the burden of disease measures in
Iran. International Journal of Health Planning and Management 20:
89–98.
Sabik LM, Lie RK. 2008. Priority setting in health care: lessons from the
experiences of eight countries. International Journal for Equity in
Health 7: 1–13.
Schieber G, Klingen N. 1999. Health financing reform in Iran:
principles and possible next steps. Health Economic Congress,
Tehran, Iran.
Schmidt WP. 2009. Setting priorities in diarrheal disease research:
merits and pitfalls of expert opinion. Journal of Health Population 27:
313–15.
Shadpour K. 2000. Primary health care networks in the Islamic Republic
of Iran. Eastern Mediterranean Health Journal 6: 822–5.
Stake RE. 1995. The Art of Case Study Research. Newbury Park, CA: Sage.
Statistical Centre of Iran. 2010. Household survey on the characteristics of
employment and unemployment [in Farsi]. Tehran: Statistical Centre
of Iran Publications.
Stepan A, Sommersguter-Reichmann M. 1999. Priority setting in
Austria. Health Policy 50: 91–104.
World Bank. 2007. Islamic Republic of Iran: Health Sector Review.
Washington, DC: World Bank.
WHO. 2000. World Health Report 2000 – Health Systems: Improving
Performance. Geneva: World Health Organization.
WHO. 2004. Country cooperation strategy for World Health Organization
and Islamic Republic of Iran. Geneva: World Health Organization,
Online at: http://www.who.int/countryfocus/cooperation_strategy/
ccsbrief_irn_en.pdf, accessed 4 September 2012.
WHO. 2008. World Health Statistics: Demographic and Socioeconomic
Statistics. Geneva: World Health Statistics. Online at: http://
www.who.int/whosis/whostat/EN_WHS08_Full.pdf, accessed 4
September 2012.
HEALTH CARE PRIORITY SETTING AND IMPLEMENTATION 15
at University of M
anchester on October 23, 2012
http://heapol.oxfordjournals.org/D
ownloaded from
Top Related
Copyright © 2022 FDOKUMEN

