







Bahasa
Halaman
Hukum


www.elsevier.com/locate/clae
Available online at www.sciencedirect.com
Contact Lens & Anterior Eye 31 (2008) 57–64
Review
Polymeric hydrogels for novel contact lens-based ophthalmic drug
delivery systems: A review
Li Xinming a,*, Cui Yingde a,1, Andrew W. Lloyd b,2, Sergey V. Mikhalovsky b,3,Susan R. Sandeman b,4, Carol A. Howel b,4, Liao Liewen c,5
a Department of Chemistry and Chemical Engineering, Zhongkai University of Agriculture and Technology, No. 24 Dongsha Street,
Fangzhi Road, Haizhu District, Guangzhou 510225, Guangdong, PR Chinab School of Pharmacy and Biomolecular Science, University of Brighton, Moulsecoomb, Brighton BN2 4GJ, UK
c School of Materials Science and Engineering, Northwestern Polytechnical University, No. 127 Youyixi Road, Xi’an 710072, Shanxi, PR China
Abstract
Only about 5% of drugs administrated by eye drops are bioavailable, and currently eye drops account for more than 90% of all ophthalmic
formulations. The bioavailability of ophthalmic drugs can be improved by a soft contact lens-based ophthalmic drug delivery system. Several
polymeric hydrogels have been investigated for soft contact lens-based ophthalmic drug delivery systems: (i) polymeric hydrogels for
conventional contact lens to absorb and release ophthalmic drugs; (ii) polymeric hydrogels for piggyback contact lens combining with a drug
plate or drug solution; (iii) surface-modified polymeric hydrogels to immobilize drugs on the surface of contact lenses; (iv) polymeric
hydrogels for inclusion of drugs in a colloidal structure dispersed in the lens; (v) ion ligand-containing polymeric hydrogels; (vi) molecularly
imprinted polymeric hydrogels which provide the contact lens with a high affinity and selectivity for a given drug. Polymeric hydrogels for
these contact lens-based ophthalmic drug delivery systems, their advantages and drawbacks are critically analyzed in this review.
# 2007 British Contact Lens Association. Published by Elsevier Ltd. All rights reserved.
Keywords: Hydrogels; Contact lens; Ophthalmic drug delivery system
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 58
2. Polymeric hydrogels for conventional contact lens to absorb and release ophthalmic drugs. . . . . . . . . . . . . . . . . . . . . . . . . 58
3. Polymeric hydrogels for piggyback contact lens combining with a drug plate or drug solution . . . . . . . . . . . . . . . . . . . . . . 59
4. Surface-modified polymeric hydrogels to immobilize drugs on the surface of contact lenses. . . . . . . . . . . . . . . . . . . . . . . . 59
5. Polymeric hydrogels for inclusion of drugs in a colloidal structure dispersed in the lens . . . . . . . . . . . . . . . . . . . . . . . . . . 60
6. Ion ligand-containing polymeric hydrogels . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60
7. Molecularly imprinted polymeric hydrogels . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 62
8. Perspectives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 62
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63
* Corresponding author. Tel.: +86 20 8901 3955; fax: +86 20 3428 0984.
E-mail addresses: [email protected] (L. Xinming), [email protected] (C. Yingde), [email protected] (A.W. Lloyd),
[email protected] (S.V. Mikhalovsky), [email protected] (S.R. Sandeman), [email protected] (C.A. Howel),
[email protected] (L. Liewen).1 Tel.: +86 20 8900 3002; fax: +86 20 3428 0984.2 Tel.: +44 1273 642049; fax: +44 1273 642031.3 Tel.: +44 1273 642034; fax: +44 1273 679333.4 Tel.: +44 1273 642015.5 Tel.: +86 130 2201 5152.
1367-0484/$ – see front matter # 2007 British Contact Lens Association. Published by Elsevier Ltd. All rights reserved.
doi:10.1016/j.clae.2007.09.002

L. Xinming et al. / Contact Lens & Anterior Eye 31 (2008) 57–6458
1. Introduction
The success of the therapy of eye ailments with
ophthalmic drugs strongly depends on achieving sufficient
drug concentration on the cornea for a sufficient period of
time, but the typical delivery of drugs by eye drops which
currently account for more than 90% of all ophthalmic
formulations is very inefficient and in some instances leads
to serious side effects [1–3]. Upon instillation in the eye, the
drug mixes with the fluid present in the tear film and has a
short residence time of approximately 2 min in the film.
Only about 5% of the drug is absorbed into the cornea and
the remaining either gets absorbed in the conjunctiva or
flows through the upper and the lower canaliculi into the
lacrimal sac [4,5]. The drug containing tear fluid is carried
from the lacrimal sac into the nasolacrimal duct. The
nasolacrimal duct empties into the nasal cavity, where the
drug is then absorbed into the bloodstream. This absorption
leads to drug wastage, and more importantly, the presence of
certain drugs in the bloodstream leads to undesirable side
effects. Furthermore, the application of ophthalmic drugs by
eye drops results in a rapid variation in the drug delivery
rates to the cornea and this limits the efficacy of the
therapeutic system [6,7]. In addition, dosage through eye
drops is inconsistent and difficult to regulate, as most of the
drug is released in an initial burst of concentration [8,9]. To
increase the residence time of the drug in the eye, thereby
reducing wastage and minimizing side effects, a number of
researchers have proposed using contact lenses for
ophthalmic drug delivery. It has been shown that in the
presence of a lens, ophthalmic drugs have a much longer
residence time in the post-lens tear film, compared with
2 min in the case of topical application as eye drops [10–13].
The longer residence time will result in higher drug flux
through the cornea and reduce the drug inflow into the
nasolacrimal sac, thus reducing drug absorption into the
bloodstream. Several methods have been proposed to make
ophthalmic drugs deliverable by soft contact lens. In this
review, the advantages and drawbacks of polymeric
hydrogels for novel contact lens-based ophthalmic drug
delivery systems are critically analyzed.
2. Polymeric hydrogels for conventional contact lens
to absorb and release ophthalmic drugs
Conventional soft contact lenses have the ability to absorb
a number of drugs when the lenses are pre-soaked in the drug
solution, subsequently releasing them into the post-lens
lacrimal fluid. As an alternative, one can also insert
conventional soft contact lenses into eyes then apply eye
drops. By this means, drugs can be absorbed and released by
the soft contact lens, minimizing clearance and sorption
through the conjunctiva [13–16]. Several polymeric hydro-
gels have been investigated as a conventional soft contact
lens-based ophthalmic drug delivery system. Poly-hydro-
xyethylmethacrylate (pHEMA) hydrogels which are widely
used for preparing soft contact lenses, have been investigated
for delivery of several ophthalmic drugs [17,18]. To enhance
the potential of pHEMA hydrogels as an effective biomaterial
for contact lens-based ophthalmic drug delivery system, 4-
vinylpyridine (VP) and N-(3-aminopropyl)methacrylamide
(APMA) were incorporated into the network [19]. The
incorporated monomers did not change the viscoelastic
properties of the contact lens or the state of water within the
contact lens, but remarkably increased the amount of
ibuprofen (up to 10-fold) and diclofenac (up to 20-fold)
loaded. Dried loaded pHEMA–APMA and pHEMA–VP
hydrogels quickly swelled in water; but ionic/hydrophobic
interactions limited the drugs released to be below 10%. By
contrast, once the water-swollen hydrogels were transferred to
pH 5.8 or 8.0 phosphate buffers or NaCl solutions, the release
was prompted by competition with ions in the media. The
remaining hydrophobic interactions and the high polymeric
density of the pHEMA hydrogels contributed to sustaining the
release process for at least 24 h for ibuprofen and almost 1
week for diclofenac. This release rate was also independent of
the salt content and pH in the physiological range of values,
which enables the design of hydrogel-based delivery systems
with predictable release rates.
Researchers have also been investigating the copolymer
hydrogels of N,N-dimethylacrylamide (DMAAM) and 2-(N-
ethylperfluorooctanesulfonamido)ethyl acrylate (FOSA) for
potential application of contact lens-based drug delivery
systems [20]. Since hydrogels of poly(DMAAM) exhibit
rather low mechanical strength, FOSA, a hydrophobic
monomer, can be incorporated into the networks to modify
the glass transition temperature and water sorption and
desorption kinetics of the hydrogels by changing the
structure, location, or concentration of the hydrophobic
group. When pheniramine maleate (PM) was used as a
model drug, it was found that copolymerizing FOSA with
DMAAM-based hydrogels decreased (i) the media penetra-
tion velocity through the hydrogels, (ii) the change in
hydrogels volume during swelling, (iii) the equilibrium
media content in the hydrogels, and (iv) the drug diffusion
rate through the hydrogels. The pH of the aqueous media
into which the drug substance diffused had a much less
dramatic effect on the hydrogels, but it was found that
increasing the media pH slightly slowed the diffusion of the
drug substance by decreasing the swelling ability of the
hydrogels. Copolymer hydrogels of HEMA and acrylic acid
(AA) were also investigated as a contact lens-based
ophthalmic drug delivery system [21]. Soft contact lenses
based on commercially available silicon-containing hydro-
gels and poly-vinyl alcohol (PVA) hydrogels were also
examined for delivery of ophthalmic drugs [22–26]. Results
showed that the ability of conventional soft contact lenses to
be a drug reservoir strongly depends on the water content
and thickness of the lens, the molecular weight of the drug,
the concentration of the drug loading solution, the solubility
of the drugs in the gel matrix, and the time the lens remains
L. Xinming et al. / Contact Lens & Anterior Eye 31 (2008) 57–64 59
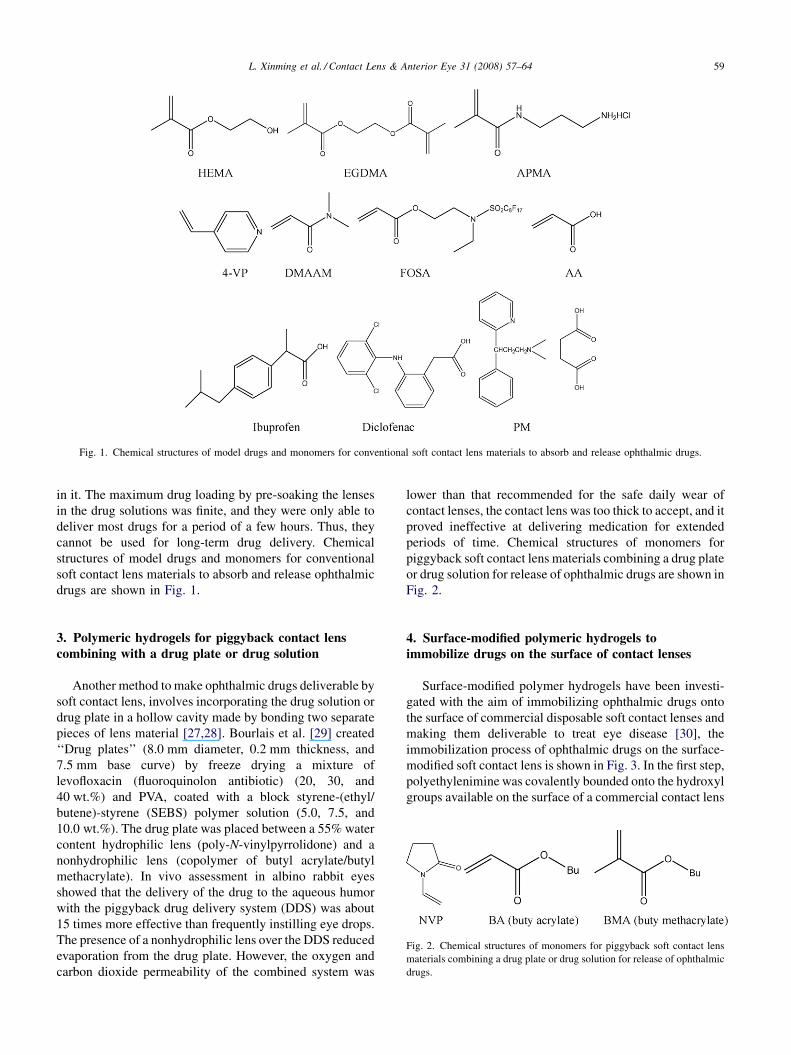
Fig. 1. Chemical structures of model drugs and monomers for conventional soft contact lens materials to absorb and release ophthalmic drugs.
in it. The maximum drug loading by pre-soaking the lenses
in the drug solutions was finite, and they were only able to
deliver most drugs for a period of a few hours. Thus, they
cannot be used for long-term drug delivery. Chemical
structures of model drugs and monomers for conventional
soft contact lens materials to absorb and release ophthalmic
drugs are shown in Fig. 1.
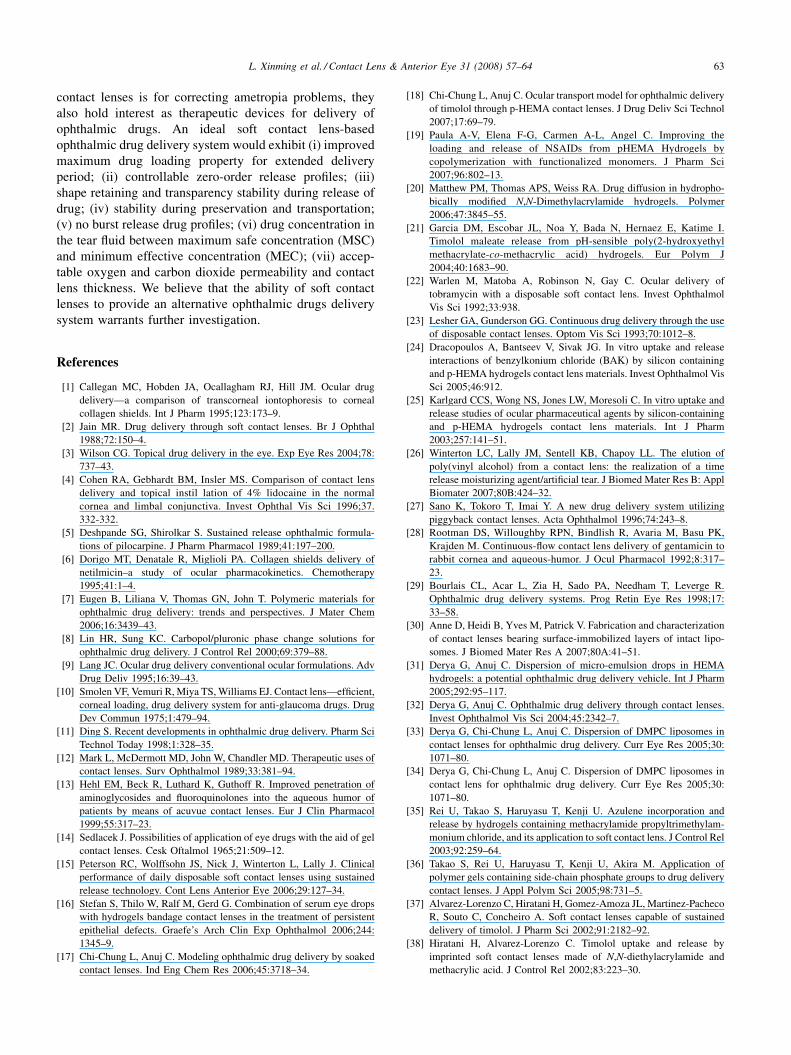
Fig. 2. Chemical structures of monomers for piggyback soft contact lens
materials combining a drug plate or drug solution for release of ophthalmic
drugs.
3. Polymeric hydrogels for piggyback contact lens
combining with a drug plate or drug solution
Another method to make ophthalmic drugs deliverable by
soft contact lens, involves incorporating the drug solution or
drug plate in a hollow cavity made by bonding two separate
pieces of lens material [27,28]. Bourlais et al. [29] created
‘‘Drug plates’’ (8.0 mm diameter, 0.2 mm thickness, and
7.5 mm base curve) by freeze drying a mixture of
levofloxacin (fluoroquinolon antibiotic) (20, 30, and
40 wt.%) and PVA, coated with a block styrene-(ethyl/
butene)-styrene (SEBS) polymer solution (5.0, 7.5, and
10.0 wt.%). The drug plate was placed between a 55% water
content hydrophilic lens (poly-N-vinylpyrrolidone) and a
nonhydrophilic lens (copolymer of butyl acrylate/butyl
methacrylate). In vivo assessment in albino rabbit eyes
showed that the delivery of the drug to the aqueous humor
with the piggyback drug delivery system (DDS) was about
15 times more effective than frequently instilling eye drops.
The presence of a nonhydrophilic lens over the DDS reduced
evaporation from the drug plate. However, the oxygen and
carbon dioxide permeability of the combined system was
lower than that recommended for the safe daily wear of
contact lenses, the contact lens was too thick to accept, and it
proved ineffective at delivering medication for extended
periods of time. Chemical structures of monomers for
piggyback soft contact lens materials combining a drug plate
or drug solution for release of ophthalmic drugs are shown in
Fig. 2.
4. Surface-modified polymeric hydrogels to
immobilize drugs on the surface of contact lenses
Surface-modified polymer hydrogels have been investi-
gated with the aim of immobilizing ophthalmic drugs onto
the surface of commercial disposable soft contact lenses and
making them deliverable to treat eye disease [30], the
immobilization process of ophthalmic drugs on the surface-
modified soft contact lens is shown in Fig. 3. In the first step,
polyethylenimine was covalently bounded onto the hydroxyl
groups available on the surface of a commercial contact lens

L. Xinming et al. / Contact Lens & Anterior Eye 31 (2008) 57–6460
Fig. 3. Immobilization of ophthalmic drugs on the surface-modified soft
contact lens.
(Hioxifilcon B), followed by NHS–PEG–biotin molecules
being bonded onto the surface amine groups by carbodii-
mide chemistry. Neutravidin was then bonded onto the
PEG–biotin layer, and liposomes containing PEG-biotiny-
lated lipids were docked onto the surface-immobilized
Neutravidin. Consecutive addition of further Neutravidin
and liposome layers enabled fabrication of multilayers.
Multilayers of liposomes were also produced by exposing
contact lenses coated with Neutravidin to liposome
aggregates produced by the addition of free biotin in
solution. The release kinetics of a fluorescent dye
demonstrated that intact liposomes had been immobilized
onto the contact lens surface, with the stability showing
temperature dependence. The surface-bonded liposomes can
be stored up to 1 month at 48 8C with little release of their
content. The multilayer scheme utilized provides strong
interfacial bonding, consisting of either covalent bonding or
biotin/avidin affinity between the individual layers, thus
minimizing the risk of liposome detaching from contact lens
surfaces. The drawbacks of this method include the risk of
the liposomes detaching from contact lens surface, and the
multilayer scheme of the liposomes decreases the oxygen
permeability, although the risk of the liposomes detaching
from the surface can be decreased. The release rate of
ophthalmic drugs from liposomes was found to display a
behavior indicative of diffusion control, thus the release
profile is difficult to regulate.
5. Polymeric hydrogels for inclusion of drugs in acolloidal structure dispersed in the lens
Researchers have been dispersing micro-emulsion drops
of ophthalmic drugs into soft contact lenses to treat eye
ailments [31–34]. First, ophthalmic drug formulations have
been encapsulated in dimyristoyl phosphatidylcholine
(DMPC) liposomes, and the drug-laden liposomes were
dispersed in the lens material. If the nanoparticle size and
loading are sufficiently low (the exact value depends on the
refractive index mismatch between the gel and the particles),
the particle-loaded lens remains transparent. Upon insertion
into the eye, the drug will diffuse from the particles, travel
through the lens matrix, and enter the pre-lens (the film
between the air and the lens) and the post-lens (the film
between the cornea and the lens) tear films. The p-HEMA
hydrogels matrix has been synthesized by bulk or solution-
free radical polymerization of HEMA monomers in the
presence of a cross-linker such as ethylene glycol-di-
methacrylate (EGDMA). Addition of drug-laden micro-
emulsion drops in the polymerizing medium results in
particle dispersion in the hydrogels matrix. In the presence
of a lens, drug molecules have a much longer residence time
in the post-lens tear film than the residence time of 2 min
that is the case with topical application of drugs as eye drops.
This longer residence time would presumably result in
higher drug flux through the cornea and reduce the drug
absorption into the blood stream through the conjunctiva or
the nasolacrimal duct. In addition, as a result of the slow
diffusion of the drug molecules through the particles and the
lens matrix, drug-laden contact lenses could provide
continuous drug release for extended periods. However, it
was found that the transparency of micro-emulsion-loaded
contact lenses decreased with increasing micro-emulsion
loading, and the system was unstable during preservation
and transportation because the loaded drugs diffused into the
gel matrix. Another drawback of this type of ophthalmic
drug delivery by nanoparticle-laden gels is the decaying
release rate.
6. Ion ligand-containing polymeric hydrogels
Ion ligand-containing polymer hydrogels have been
synthesized for a contact lens-based ophthalmic drug
delivery system. Ionized ophthalmic drugs were bound in
the soft contact lenses through ion ligands, and released into
tear fluid by ion exchange. Hydrogels containing cationic
functional groups in their side chain were investigated by
copolymerization of methacrylamide propyltrimethylam-
monium chloride (MAPTAC) and HEMA (chemical
structures of the model drug and monomers for cationic
ion ligand-containing soft contact lens materials are shown
in Fig. 4), and their capability to store the anionic drug based
on ion-exchange reaction was examined. It is expected that
the incorporated anionic drug would be released under
physiological conditions [35]. A size change in the
hydrogels was found before and after drug release (size
change during drug release of ion ligand-containing
polymeric hydrogels for soft contact lens-based ophthalmic
drug delivery systems is schematically illustrated in Fig. 5);
however, the addition of an anionic monomer such as
methacrylic acid (MAA) or 2-methacryloxyethyl acid
phosphate (MOEP) to the above-mentioned composition
was effective in preventing the size change.

L. Xinming et al. / Contact Lens & Anterior Eye 31 (2008) 57–64 61
Fig. 4. Chemical structures of the model drug and monomers for cationic ion ligand-containing soft contact lens materials.
Fig. 5. Size change during drug release of ion ligand-containing polymeric hydrogels for soft contact lens-based ophthalmic drug delivery systems.
Hydrogels that contain phosphate groups in side chains
were also studied for their usefulness in drug delivery soft
contact lenses (SCL) [36]. Naphazoline, a model drug
containing a cationic group, was incorporated into SCL via
its phosphate groups and was released over a period of about
14 h (chemical structures of the model drug and the
hydrogels are shown in Fig. 6). For the SCL, the naphazoline
Fig. 6. Chemical structures of the model drug and poly(HEMA-co-MOEP-co-M
drawbacks include the size change of the contact lens that may occur before and aft
drug concentration cannot exceed the ion concentration in the tear fluid, because
content was equivalent to the phosphate group content. It has
been suggested that drug delivery SCL can be designed to
contain the required amount of a drug through the choice of
the ionic group acting as the ligand, and amide groups and
phosphate groups must be introduced into the polymer in
equimolar amounts to give the necessary polymer–drug
interaction.
Am) hydrogels. For ion ligand-containing polymeric hydrogels, the main
er drug release as a result of drug concentration change, and the incorporated
the release of drugs relies on ion exchange.

L. Xinming et al. / Contact Lens & Anterior Eye 31 (2008) 57–6462
7. Molecularly imprinted polymeric hydrogels
Molecularly imprinted polymer hydrogels were recently
investigated biomaterials for contact lens-based ophthalmic
drug delivery systems. In general, the preparation of
molecularly imprinted polymers involves the self-assembly
of functional monomers and target molecules, followed by
polymerization with cross-linker in the presence of an inert
solvent as a porogen. Upon removal of the target molecules,
cavities that can recognize the spatial features and bonding
preferences of the target molecules are created, providing the
contact lens with a high affinity and selectivity for a given
drug. Although the polymerization is usually performed in an
organic solvent to give a macro-porous structure that allows
the target molecules access to the imprinted sites, one can
avoid the use of any solvent, taking advantage of the liquid
state of the monomers in preparation of molecular imprinted
polymer hydrogels. Molecularly imprinted polymer hydro-
gels have been prepared by dissolution of ethylene glycol
dimethacrylate (EGDMA, cross-linker) in HEMA with
methacrylic acid (MAA, functional monomer) or methyl
methacrylate (MMA, functional monomer) and with timolol
maleate (template, medicine for increasing the pressure in the
eye). Initiation of polymerization by addition of 2,2-azo-
bis(isobutyronitrile) (AIBN, initiator), resulting in a contact
lens and timolol release device [37]. Timolol release kinetics
in 0.9% NaCl, phosphate buffer (pH 7.4) and artificial
lacrimal fluid, and the timolol loading capacity at various pH
demonstrated that both water uptake and timolol release
exhibit Fickian kinetics. The incorporation of MAA as co-
monomer increases the timolol loading capacity to ther-
apeutically useful levels while retaining appropriate release
characteristics.
Another type of molecularly imprinted hydrogels were
prepared considering the preformation of complexes
between methacrylic acid (functional monomers), timolol
(target molecules), polymerization with N,N-diethylacryla-
mide (DEAAM), and ethylenglycol dimethacrylate
(EGDMA, cross-linker) by UV irradiation at room
temperature [38]. After polymerization, timolol molecules
were removed by washing. When the gels were immersed in
timolol solutions, the imprinted gels adsorbed greater
amount of timolol than the corresponding non-imprinted
ones. The imprinted contact lenses significantly improved
the affinity of the hydrogels for timolol. These results
indicate that adsorption sites capable of capturing the target
Fig. 7. Chemical structures of monomers for molecularly imprinted polymer
molecules were encoded effectively into the polymer
network by the molecularly imprinting technique and, in
consequence, improved the drug loading capacity of the
gels. Loaded imprinted contact lenses were able to prolong
timolol release in 0.9% NaCl aqueous solution for more than
24 h.
Other molecularly imprinted polymeric hydrogels inves-
tigated for contact lens-based ophthalmic drug delivery
systems include norfloxacin imprinted poly-HEMA [39];
timolol imprinted lenses prepared by UV irradiation of N,N-
diethylacrylamide (DEAAM), 2-hydroxyethylmethacrylate
(HEMA), 1-(tristrimethyl-siloxysilylpropyl)-methacrylate
(SiMA) and N,N-dimethylacrylamide (DMAAM) (50:50,
v/v), or methylmethacrylate (MMA) and DMAAM (50:50,
v/v) solutions, with functional monomer methacrylic acid
(MAA) and cross-linker ethyleneglycol dimethacrylate
(EGDMA) [40]; timolol imprinted lenses prepared by
copolymerization of N,N-diethylacrylamide (DEAAM,
main component of the matrix), methacrylic acid (MAA,
functional monomer) and ethylene glycol dimethacrylate
(EGDMA, cross-linker) [41]; timolol imprinted lenses
prepared from N,N-dimethylacrylamide (DMAAM) and
tris(trimethylsiloxy) sililpropyl methacrylate, methacrylic
acid (MAA, functional monomer), ethylene glycol dimetha-
crylate (EGDMA, cross-linker) [42]; natural receptor-based
poly(AA-co-AM-co-HEMA-co-PEG200DMA), poly(AM-
co-HEMA-co-PEG200DMA), poly(AA-co-AM-co-NVP-
co-HEMA-co-PEG200DMA), and poly(AA-co-HEMA-
co-PEG200DMA) [43]. Although all the results indicate
drug-loading capacity of contact lenses was improved by the
molecularly imprinting method, and the imprinted hydrogels
showed a higher affinity for template molecules are some
drawbacks. The maximum drug loading was limited by the
template molecules and functional monomers, and the
contact lenses deform on the release of drug. In addition, it is
difficult to regulate the release profile of drugs. Chemical
structures of some monomers for molecularly imprinted
polymeric hydrogels for contact lens-based ophthalmic drug
delivery systems are shown in Fig. 7.
8. Perspectives
Currently worldwide, approximately 100 million people
are estimated to be wearing contact lenses, and the number is
increasing exponentially [44]. Although the main use of
ic hydrogels for contact lens-based ophthalmic drug delivery systems.
L. Xinming et al. / Contact Lens & Anterior Eye 31 (2008) 57–64 63
contact lenses is for correcting ametropia problems, they
also hold interest as therapeutic devices for delivery of
ophthalmic drugs. An ideal soft contact lens-based
ophthalmic drug delivery system would exhibit (i) improved
maximum drug loading property for extended delivery
period; (ii) controllable zero-order release profiles; (iii)
shape retaining and transparency stability during release of
drug; (iv) stability during preservation and transportation;
(v) no burst release drug profiles; (vi) drug concentration in
the tear fluid between maximum safe concentration (MSC)
and minimum effective concentration (MEC); (vii) accep-
table oxygen and carbon dioxide permeability and contact
lens thickness. We believe that the ability of soft contact
lenses to provide an alternative ophthalmic drugs delivery
system warrants further investigation.
References
[1] Callegan MC, Hobden JA, Ocallagham RJ, Hill JM. Ocular drug
delivery—a comparison of transcorneal iontophoresis to corneal
collagen shields. Int J Pharm 1995;123:173–9.
[2] Jain MR. Drug delivery through soft contact lenses. Br J Ophthal
1988;72:150–4.
[3] Wilson CG. Topical drug delivery in the eye. Exp Eye Res 2004;78:
737–43.
[4] Cohen RA, Gebhardt BM, Insler MS. Comparison of contact lens
delivery and topical instil lation of 4% lidocaine in the normal
cornea and limbal conjunctiva. Invest Ophthal Vis Sci 1996;37.
332-332.
[5] Deshpande SG, Shirolkar S. Sustained release ophthalmic formula-
tions of pilocarpine. J Pharm Pharmacol 1989;41:197–200.
[6] Dorigo MT, Denatale R, Miglioli PA. Collagen shields delivery of
netilmicin–a study of ocular pharmacokinetics. Chemotherapy
1995;41:1–4.
[7] Eugen B, Liliana V, Thomas GN, John T. Polymeric materials for
ophthalmic drug delivery: trends and perspectives. J Mater Chem
2006;16:3439–43.
[8] Lin HR, Sung KC. Carbopol/pluronic phase change solutions for
ophthalmic drug delivery. J Control Rel 2000;69:379–88.
[9] Lang JC. Ocular drug delivery conventional ocular formulations. Adv
Drug Deliv 1995;16:39–43.
[10] Smolen VF, Vemuri R, Miya TS, Williams EJ. Contact lens—efficient,
corneal loading, drug delivery system for anti-glaucoma drugs. Drug
Dev Commun 1975;1:479–94.
[11] Ding S. Recent developments in ophthalmic drug delivery. Pharm Sci
Technol Today 1998;1:328–35.
[12] Mark L, McDermott MD, John W, Chandler MD. Therapeutic uses of
contact lenses. Surv Ophthalmol 1989;33:381–94.
[13] Hehl EM, Beck R, Luthard K, Guthoff R. Improved penetration of
aminoglycosides and fluoroquinolones into the aqueous humor of
patients by means of acuvue contact lenses. Eur J Clin Pharmacol
1999;55:317–23.
[14] Sedlacek J. Possibilities of application of eye drugs with the aid of gel
contact lenses. Cesk Oftalmol 1965;21:509–12.
[15] Peterson RC, Wolffsohn JS, Nick J, Winterton L, Lally J. Clinical
performance of daily disposable soft contact lenses using sustained
release technology. Cont Lens Anterior Eye 2006;29:127–34.
[16] Stefan S, Thilo W, Ralf M, Gerd G. Combination of serum eye drops
with hydrogels bandage contact lenses in the treatment of persistent
epithelial defects. Graefe’s Arch Clin Exp Ophthalmol 2006;244:
1345–9.
[17] Chi-Chung L, Anuj C. Modeling ophthalmic drug delivery by soaked
contact lenses. Ind Eng Chem Res 2006;45:3718–34.
[18] Chi-Chung L, Anuj C. Ocular transport model for ophthalmic delivery
of timolol through p-HEMA contact lenses. J Drug Deliv Sci Technol
2007;17:69–79.
[19] Paula A-V, Elena F-G, Carmen A-L, Angel C. Improving the
loading and release of NSAIDs from pHEMA Hydrogels by
copolymerization with functionalized monomers. J Pharm Sci
2007;96:802–13.
[20] Matthew PM, Thomas APS, Weiss RA. Drug diffusion in hydropho-
bically modified N,N-Dimethylacrylamide hydrogels. Polymer
2006;47:3845–55.
[21] Garcia DM, Escobar JL, Noa Y, Bada N, Hernaez E, Katime I.
Timolol maleate release from pH-sensible poly(2-hydroxyethyl
methacrylate-co-methacrylic acid) hydrogels. Eur Polym J
2004;40:1683–90.
[22] Warlen M, Matoba A, Robinson N, Gay C. Ocular delivery of
tobramycin with a disposable soft contact lens. Invest Ophthalmol
Vis Sci 1992;33:938.
[23] Lesher GA, Gunderson GG. Continuous drug delivery through the use
of disposable contact lenses. Optom Vis Sci 1993;70:1012–8.
[24] Dracopoulos A, Bantseev V, Sivak JG. In vitro uptake and release
interactions of benzylkonium chloride (BAK) by silicon containing
and p-HEMA hydrogels contact lens materials. Invest Ophthalmol Vis
Sci 2005;46:912.
[25] Karlgard CCS, Wong NS, Jones LW, Moresoli C. In vitro uptake and
release studies of ocular pharmaceutical agents by silicon-containing
and p-HEMA hydrogels contact lens materials. Int J Pharm
2003;257:141–51.
[26] Winterton LC, Lally JM, Sentell KB, Chapoy LL. The elution of
poly(vinyl alcohol) from a contact lens: the realization of a time
release moisturizing agent/artificial tear. J Biomed Mater Res B: Appl
Biomater 2007;80B:424–32.
[27] Sano K, Tokoro T, Imai Y. A new drug delivery system utilizing
piggyback contact lenses. Acta Ophthalmol 1996;74:243–8.
[28] Rootman DS, Willoughby RPN, Bindlish R, Avaria M, Basu PK,
Krajden M. Continuous-flow contact lens delivery of gentamicin to
rabbit cornea and aqueous-humor. J Ocul Pharmacol 1992;8:317–
23.
[29] Bourlais CL, Acar L, Zia H, Sado PA, Needham T, Leverge R.
Ophthalmic drug delivery systems. Prog Retin Eye Res 1998;17:
33–58.
[30] Anne D, Heidi B, Yves M, Patrick V. Fabrication and characterization
of contact lenses bearing surface-immobilized layers of intact lipo-
somes. J Biomed Mater Res A 2007;80A:41–51.
[31] Derya G, Anuj C. Dispersion of micro-emulsion drops in HEMA
hydrogels: a potential ophthalmic drug delivery vehicle. Int J Pharm
2005;292:95–117.
[32] Derya G, Anuj C. Ophthalmic drug delivery through contact lenses.
Invest Ophthalmol Vis Sci 2004;45:2342–7.
[33] Derya G, Chi-Chung L, Anuj C. Dispersion of DMPC liposomes in
contact lenses for ophthalmic drug delivery. Curr Eye Res 2005;30:
1071–80.
[34] Derya G, Chi-Chung L, Anuj C. Dispersion of DMPC liposomes in
contact lens for ophthalmic drug delivery. Curr Eye Res 2005;30:
1071–80.
[35] Rei U, Takao S, Haruyasu T, Kenji U. Azulene incorporation and
release by hydrogels containing methacrylamide propyltrimethylam-
monium chloride, and its application to soft contact lens. J Control Rel
2003;92:259–64.
[36] Takao S, Rei U, Haruyasu T, Kenji U, Akira M. Application of
polymer gels containing side-chain phosphate groups to drug delivery
contact lenses. J Appl Polym Sci 2005;98:731–5.
[37] Alvarez-Lorenzo C, Hiratani H, Gomez-Amoza JL, Martinez-Pacheco
R, Souto C, Concheiro A. Soft contact lenses capable of sustained
delivery of timolol. J Pharm Sci 2002;91:2182–92.
[38] Hiratani H, Alvarez-Lorenzo C. Timolol uptake and release by
imprinted soft contact lenses made of N,N-diethylacrylamide and
methacrylic acid. J Control Rel 2002;83:223–30.

L. Xinming et al. / Contact Lens & Anterior Eye 31 (2008) 57–6464
[39] Carmen A-L, Fernando Y, Rafael B-I, Angel C. Imprinted soft contact
lenses as norfloxacin delivery systems. J Control Rel 2006;113:236–
44.
[40] Hiratani H, Alvarez-Lorenzo C. The nature of backbone monomers
determines the performance of imprinted soft contact lenses as timolol
drug delivery systems. Biomaterials 2004;25:1105–13.
[41] Hiratani H, Fujiwara A, Tamiya Y, Mizutani Y, Alvarez-Lorenzo C.
Ocular release of timolol from molecularly imprinted soft contact
lenses. Biomaterials 2005;26:1293–8.
[42] Hiratani H, Mizutani Y, Alvarez-Lorenzo C. Controlling drug release
from imprinted hydrogels by modifying the characteristics of the
imprinted cavities. Macromol Biosci 2005;5:728–33.
[43] Siddarth V, Stephen PS, Mark EB. Biomimetic hydrogels for enhanced
loading and extended release of ocular therapeutics. Biomaterials
2007;28:717–24.
[44] Alvarez-Lorenzo C, Hiratani H, Concheiro A. Contact lenses for drug
delivery: achieving sustained release with novel systems. Am J Drug
Deliv 2006;4:131–51.
Top Related
Copyright © 2022 FDOKUMEN

