







Bahasa
Halaman
Hukum


REVIEW ARTICLE
S. N. Papageorgiou
I. Konstantinidis
K. Papadopoulou
A. J€ager
C. Bourauel
A systematic review and
meta-analysis of experimental
clinical evidence on initial aligning
archwires and archwire sequences
Authors' affiliations:S. N. Papageorgiou, C. Bourauel,
Department of Oral Technology, School of
Dentistry, University of Bonn, Bonn,
Germany
S. N. Papageorgiou, K. Papadopoulou,
A. J€ager, Department of Orthodontics,
School of Dentistry, University of Bonn,
Bonn, Germany
I. Konstantinidis, Mount Sinai School of
Medicine, New York, NY, USA
Correspondence to:S. N. Papageorgiou
Department of Orthodontics
School of Dentistry
University of Bonn
Welschnonnenstraße 17
D-53111 Bonn
Germany
E-mail: [email protected]
Papageorgiou S. N., Konstantinidis I., Papadopoulou K., J€ager A.,
Bourauel C. A systematic review and meta-analysis of experimental
clinical evidence on initial aligning archwires and archwire sequences
Orthod Craniofac Res 2014. © 2014 John Wiley & Sons A/S. Published by
John Wiley & Sons Ltd
Abstract
The aim of the study was to assess treatment effects and potential side
effects of different archwires used on patients receiving orthodontic
therapy. Electronic and manual unrestricted searches were conducted in
19 databases including MEDLINE, Cochrane Library, and Google Scholar
until April 2012 to identify randomized controlled trials (RCTs) and quasi-
RCTs. After duplicate study selection, data extraction, risk of bias assess-
ment with the Cochrane risk of bias tool, and narrative analysis, mean
differences (MDs) with confidence intervals (CIs) of similar studies were
pooled using a random-effects model and evaluated with GRADE. A total
of 16 RCTs were included assessing different archwire characteristics on
1108 patients. Regarding initial archwires, meta-analysis of two trials
found slightly greater irregularity correction with an austenitic-active
nickel-titanium (NiTi) compared with an martensitic-stabilized NiTi arch-
wire (corresponding to MD: 1.11 mm, 95% CI: �0.38 to 2.61). Regarding
archwire sequences, meta-analysis of two trials found it took patient trea-
ted with a sequence of martensitic-active copper-nickel-titanium (CuNiTi)
slightly longer to reach the working archwire (MD: 0.54 months, 95% CI:
�0.87 to 1.95) compared with a martensitic-stabilized NiTi sequence.
However, patients treated with a sequence of martensitic-active CuNiTi
archwires reported general greater pain intensity on the Likert scale 4 h
and 1 day after placement of each archwire, compared with a martens-
itic-stabilized NiTi sequence. Although confidence in effect estimates ran-
ged from moderate to high, meta-analyses could be performed only for
limited comparisons, while inconsistency might pose a threat to some of
them. At this point, there is insufficient data to make recommendations
about the majority of initial archwires or for a specific archwire sequence.
Key words: aligning archwire; alignment; archwire sequence; bracket;
fixed orthodontic treatment; initial archwire; orthodontic archwire
Date:Accepted 30 April 2014
DOI: 10.1111/ocr.12048
© 2014 John Wiley & Sons A/S.
Published by John Wiley & Sons Ltd

IntroductionRationale
Developments in the last decades regarding
orthodontic archwires used during fixed appli-
ance treatment include the introduction of vari-
ous archwires from NiTi alloys, multistranded
archwires and esthetic coated or uncoated arch-
wires.
Developments of orthodontic archwires based
on NiTi alloys using a recent classification
(1) and in chronological order include 1) the
martensitic-stabilized (Mstab) – conventional –
NiTi, 2) the austenitic-active (Aact) – known as
superelastic – NiTi, 3) the martensitic-active
(Mact) – heat-activated – NiTi or copper-nickel-
titanium (CuNiTi), and 4) the graded Mact NiTi
archwires. The in vitro beneficial properties of
the last three categories of NiTi archwires have
been previously documented (1–4), but have not
been confirmed clinically (5–7). Retrieval analy-
ses indicated that intra-oral aging (8) may alter
the physical properties of the NiTi archwires (9,
10), the bracket (11) or ligation modules (12).
Multistranded stainless steel (SS) archwires
have been developed to fulfill the requirements
of an ideal archwire (1) and have been proposed
as an economical alternative to NiTi archwires
(13, 14), as they are equally efficient (15) and
produce low force and moment levels (16). Vari-
ous attempts at the development of an esthetic
archwire have been made (17–19). Recently,
shape memory polymeric archwires were devel-
oped (20, 21), in which moieties in the material
act as molecular switches upon irradiation with
UV light of k < 260 nm (22).
Archwire sequences used in clinical practice
vary greatly, with first coming the use of a NiTi
archwire followed by beta titanium or SS arch-
wires and a mean number of four to five arch-
wires per sequence being a popular choice
among orthodontists (23, 24). In general, the
orthodontist strives to use archwires with greater
stiffness and smaller range moving from the
aligning phase to the working and finally the fin-
ishing phase. Investigating a specific archwire
sequence is based on the need to establish a
standard way of reaching the working archwire,
which will be clinically effective and biologically
sound (25, 26).
Previous systematic reviews have attempted to
summarize evidence regarding initial aligning
archwires (27) or specific sequences of archwires
(28). However, inclusion of observational studies,
limited literature search, and exclusion of gray
literature may limit the value and validity of a
systematic review/meta-analysis (29, 30). Also,
most knowledge syntheses focus on a single
archwire characteristic, although it is not agreed
whether it is the bracket, the archwire, or their
interaction that mainly influences the mechani-
cal behavior of the bracket–archwire complex
(31, 32). Therefore, investigation of the bracket–
archwire complex may be more appropriate. As
earlier reviews included trials up to 2008 or
2009, an update was decided.
Objectives
This systematic review aims to critically appraise
existing evidence from randomized controlled
trials (RCTs) and quasi-RCTs regarding the effec-
tiveness, efficiency, and potential side effects of
the various archwires used during fixed appli-
ance orthodontic treatment.
MethodsProtocol
This review’s protocol was made a priori based
on the guidelines of the PRISMA statement (33),
its extension for abstracts (34), and the Cochrane
Handbook for Systematic Reviews of Interven-
tions 5.1.0 (35).
Eligibility criteria
Type of studies
Randomized controlled trials (RCTs) and quasi-
RCTs (36) of parallel or split-mouth design.
Split-mouth trials were eligible, if no carryover
effect was possible and clustering (or pairing) of
teeth was taken statistically into account (37–
39). When trial reports used the word ‘random’
once, but no further information was given, the
2 | Orthod Craniofac Res 2014
Papageorgiou et al. Systematic review on initial archwires and archwire sequences

authors were contacted to clarify whether true
randomization had taken place.
Type of participants
Humans of any age or sex.
Intervention
Placement of initial archwire and/or of the
following archwire sequence in the frame of
orthodontic therapy with fixed orthodontic
appliances to correct existing malocclusion. In
order for a study to be included, all of the
patient’s teeth of one or both jaws (excluding
third and possibly second molars) were required
to have received treatment with fixed orthodon-
tic appliances and archwire(s).
Comparison
Comparable patients for age, sex, and malocclu-
sion receiving therapy with another combination
of archwire and bracket (no untreated control
groups). Trials were excluded, if the comparison
group did not differ from the experimental
group in at least one from the following charac-
teristics: 1) archwire material, 2) archwire cross-
section shape, or 3) archwire cross-section size.
Primary outcome
Tooth alignment as measured by 2-D or 3-D
(intertooth) contact point differences or reduc-
tion in Little’s Irregularity Index (LII) (40). Alter-
natively, the outcome of orthodontic treatment
was included and measured in Peer Assessment
Rating (PAR) scores (41), the Index of Outcome,
Complexity and Need (ICON) (42), or any other
valid measuring method of malocclusion sever-
ity. Both overall correction of the dental arch
and correction of the labial/buccal segments
were included.
Secondary outcomes
1) Time to misalignment correction (where not
defined, a final cutoff value of 2 mm irregularity
was deemed adequate), 2) time to proceed to the
next archwire in the sequence, 3) time to reach
the working archwire, 4) treatment duration, 5)
number of appointments, 6) space closure
of extraction sites, 7) dental/skeletal changes,
8) patient-reported pain intensity measurement
by visual analog scale (VAS) (43), Likert scale (LS)
(44), or other valid scale, 9) clinician-prescribed
or self-prescribed analgesics use, 10) bracket fail-
ure (only for identical groups regarding bonding
systems used), 11) archwire fracture, 12) External
Apical Root Resorption (EARR), and 13) post-
treatment stability and relapse.
Studies were excluded if: 1) different arch
forms or bendings of identical archwires were
compared (i.e., preformed vs. computer-aided
bended archwires, etc.) or 2) patients had previ-
ous active treatment or relevant medical history.
Information sources, search, study selection, and data
collection process
Systematic searches for RCTs and quasi-RCTs
(completed or ongoing) were conducted. A total
of 19 general, open-access, regional, or gray
literature databases were searched from their
inception up to April 2012, including MEDLINE,
Cochrane Library, Google Scholar, and Clinical
Trials (Table S1). There was no language, publi-
cation year, or publication status (i.e., unpub-
lished articles) restriction. Translations of papers
were arranged where necessary.
The reference and citation lists of all included
trials and relevant reviews were scanned for
additional entries. Manual updates of journals
and databases were made weekly up to July
2012. Corresponding authors of registered trials,
conference abstracts, and posters were inquired
on their current status.
One author (SNP) screened all titles and
abstracts obtained from the database searches.
Two authors (SNP and KP) reviewed unblinded
(45) the full text of potentially relevant studies
and completed pre-defined data extraction
forms. Corresponding authors were contacted
for clarifications [with open-ended questions to
avoid overly positive answers (35)], missed trials,
and further data.
Risk of bias in individual or across studies
Two authors (SNP and KP) independently
assessed the risk of bias of the included studies
Orthod Craniofac Res 2014 | 3
Papageorgiou et al. Systematic review on initial archwires and archwire sequences

using the Cochrane Collaboration’s tool for
assessing risk of bias (46), guided by the Cochra-
ne Handbook for Systematic Reviews of Inter-
ventions (35). Each RCT was assigned an overall
risk of bias in terms of high risk (‘high’ for ≥2key domains), unclear risk (‘unclear’ for ≥2 key
domains), and low risk for the remaining. The
exact definitions used for each of the domains
were pre-specified in the protocol (available on
request).
The quality of evidence and strength of recom-
mendations for each meta-analysis outcome
were ultimately assessed according to the
GRADE approach (Grades of Recommendation,
Assessment, Development, and Evaluation) (47).
Disagreements concerning study selection,
data extraction, or risk of bias were settled by a
third author (IK), and agreement was assessed
using the unweighted j coefficient (48). The two
authors were calibrated before the actual proce-
dures by pilot running the search results of a
previous systematic review (49) regarding all
duplicate procedures, until almost perfect agree-
ment (j > 0.8) was reached both between
authors and with the results of that review.
Summary measures, synthesis of results, and additional
analyses
Data were considered suitable for pooling if sim-
ilar interventions were used in the same way
and similar outcomes were reported. A random-
effects model as proposed by DerSimonian and
Laird (50) was chosen, because the observed
effect was expected to differ across studies due
to differences in the sample (i.e., patient’s den-
tal/skeletal age) and implementation (i.e., treat-
ment with/without extractions or different
mechanics used). In case of meta-analyses with
three or more trials, 95% prediction intervals
(PIs) (51, 52) were calculated to predict treat-
ment effects in a new trial. Although all 95% PIs
were calculated, only PIs for significant meta-
analyses are provided here (the remainder being
available on request).
The extent and impact of between-study heter-
ogeneity were assessed by inspecting the forest
plots and by calculating the tau-squared and the
I2 statistic, respectively. When heterogeneity was
present (I2 between 25% and 75%), possible
sources of heterogeneity were sought with strati-
fication by bracket/archwire or treatment char-
acteristics. When heterogeneity was >75%, data
were not pooled. If a sufficient number of trials
were identified (n > 7), analyses were planned
for ‘small-study effects’ and publication bias.
All analyses were carried on the basis of inten-
tion-to-treat (worst-case analysis) when possible.
Experimental groups were defined by character-
istics of the bracket–archwire complex, as listed
in the inclusion criteria section. For example, a
possible comparison could be a trial arm of con-
ventionally ligated (CL) metallic 0.022″ brackets
with a 0.016″ Mact CuNiTi initial archwire versus
a trial arm of self-ligating (SL) ceramic 0.022″
brackets with a 0.014″ Mstab NiTi archwire. When
two or more arms were classified, the same (for
example two different brands of brackets
identical to all characteristics), fixed-effect meta-
analysis was used to merge them, prior to com-
parison with the group that differed. For trials
providing before-and-after data for two groups
but no increments, a modest pre-/post-correla-
tion of 0.25 was used (after sensitivity analyses
with 0.25, 0.50, and 0.75). Split-mouth trials were
meta-analyzed separately from parallel trials,
identifying differences in effect size due to
design and pooled only if similar (39), as data
for the ‘inverse variance method’ were often
unavailable.
Mean differences (MD) or standardized mean
differences (SMD) for continuous outcomes and
their corresponding 95% confidence intervals
(CIs) were calculated. When possible, explor-
atory stratified analyses according to the
bracket/archwire characteristics used to define
the groups were performed with pre-specified
subgroup analyses (SG): (i.e., SL vs. CL brackets;
metallic vs. ceramic brackets). Robustness of
the results was a priori to be checked according
to 1) severity of the initial malocclusion and
2) the inclusion of extractions in the treatment
plan. A priori sensitivity analyses for each
outcome were planned based on the improve-
ment of the GRADE classification. RevMan ver-
sion 5.1 (Nordic Cochrane Centre, Cochrane
4 | Orthod Craniofac Res 2014
Papageorgiou et al. Systematic review on initial archwires and archwire sequences
Collaboration, Copenhagen, Denmark) was used
to carry out the meta-analyses for comparable
trials and outcomes, and Stata version 10 (Stata-
Corp LP, College Station, TX, USA) was used for
calculating Cohen’s j and 95% PIs. Significance
(a) was set at 0.05, except for a 0.10 used for the
heterogeneity tests (53).
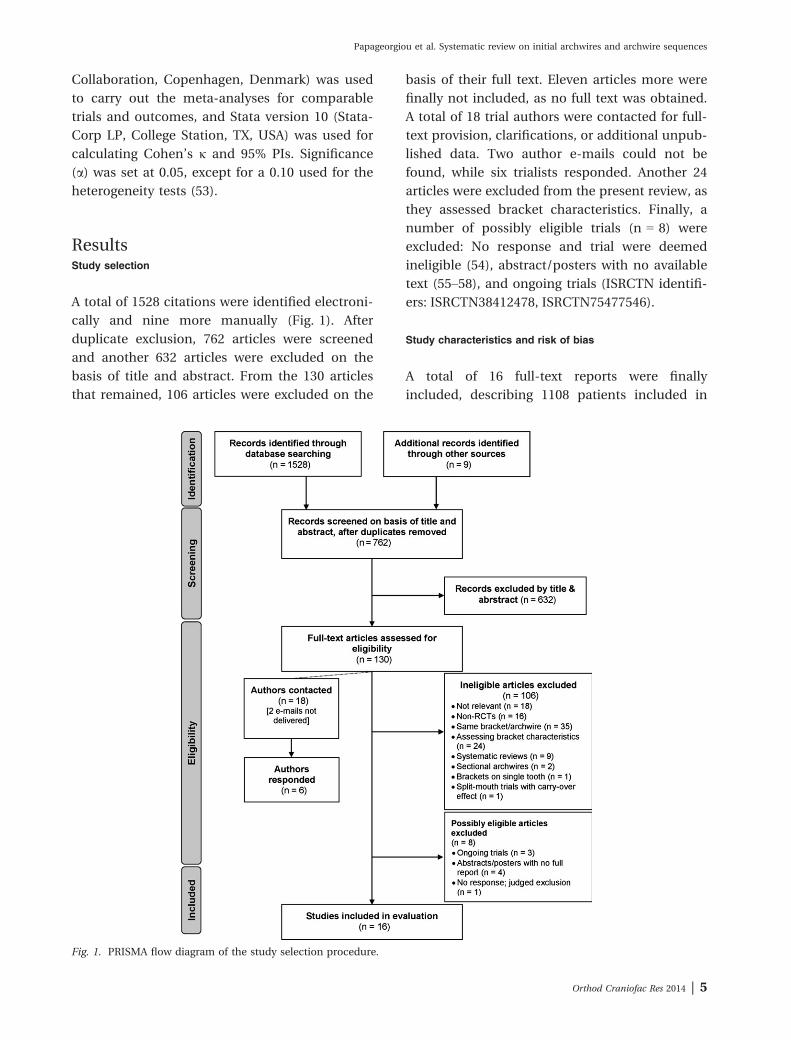
ResultsStudy selection
A total of 1528 citations were identified electroni-
cally and nine more manually (Fig. 1). After
duplicate exclusion, 762 articles were screened
and another 632 articles were excluded on the
basis of title and abstract. From the 130 articles
that remained, 106 articles were excluded on the
basis of their full text. Eleven articles more were
finally not included, as no full text was obtained.
A total of 18 trial authors were contacted for full-
text provision, clarifications, or additional unpub-
lished data. Two author e-mails could not be
found, while six trialists responded. Another 24
articles were excluded from the present review, as
they assessed bracket characteristics. Finally, a
number of possibly eligible trials (n = 8) were
excluded: No response and trial were deemed
ineligible (54), abstract/posters with no available
text (55–58), and ongoing trials (ISRCTN identifi-
ers: ISRCTN38412478, ISRCTN75477546).
Study characteristics and risk of bias
A total of 16 full-text reports were finally
included, describing 1108 patients included in
Fig. 1. PRISMA flow diagram of the study selection procedure.
Orthod Craniofac Res 2014 | 5
Papageorgiou et al. Systematic review on initial archwires and archwire sequences

16 RCTs published between 1990 and 2012. All
trial reports were in English, except for one in
Chinese (59). The bracket and archwire products
used in the included trials are provided sepa-
rately in Table S2. The kappa score for the selec-
tion of studies, the data extraction, and the risk
of bias assessment were 0.870, 0.916, and 0.921,
respectively, indicating an almost perfect level of
inter-reviewer agreement (48).
Trial characteristics and risk of bias assess-
ment for each of the 16 trials, based on pub-
lished data and author communication, are
given in Table 1, Table S3, Table 2, Table S4,
and Table 3, respectively. One split-mouth trial
(60) was included, which used appropriate statis-
tical methods (Wilcoxon signed-rank test). Only
three trials (61–63) provided a CONSORT flow-
chart with complete patient data.
Trials on initial archwires
A total of 13 trials with 863 patients were
included, assessing various factors: cross-section
of archwires (64), N+ implantation of archwires
(60, 65), and archwire materials (61–63, 66–71).
The association of archwire cross-section size
with reported pain intensity during the first
7 days after initial archwire placement was
investigated by Erdinc� and Dinc�er (64), who
reported significantly less pain and lower analge-
sic use in the 0.016″ group compared with the
0.014″ group. The method of N+ ion implanta-
tion of b-Ti or NiTi archwires, to alter surface
roughness and presumably facilitate easier slid-
ing, was investigated in two trials (60, 65) that
did not find a significant improvement.
Mact NiTi archwires
The use of an initial Mact NiTi compared with a
Mstab NiTi archwire was assessed in two trials
that reported no significant difference on allevia-
tion of tooth irregularity (69) or time to align the
anterior teeth (62).
The use of an initial Mact NiTi compared with
an Aact NiTi archwire was assessed in three tri-
als, two of which found no difference in tooth
alignment (69, 70). In the third trial (72),
patients treated with a Mact NiTi initial archwire
were reported to have lower pain intensity (VAS)
at the second, third, and fourth day after arch-
wire insertion. Treatment efficacy between
patients treated with Mact NiTi compared with a
multistranded SS initial archwires was assessed
on the basis of 3-D contact point movement by
two trials (66, 70) that found no significant dif-
ference, while issues of sample adequacy and
existing bias may reduce validity of the results.
Aact NiTi archwires
As stated above, significant differences in pain
intensity or analgesic use were found after an
initial Aact NiTi or a Mact NiTi archwire (72).
The use of an initial Aact NiTi archwire was
compared with a Mstab NiTi archwire in terms of
3-D contact point movement (61, 70), LII reduc-
tion (69), and pain intensity (67). The SMD was
used to pool contact point movement, and LII
reductions from two trials were pooled, while
data from the third one were unavailable.
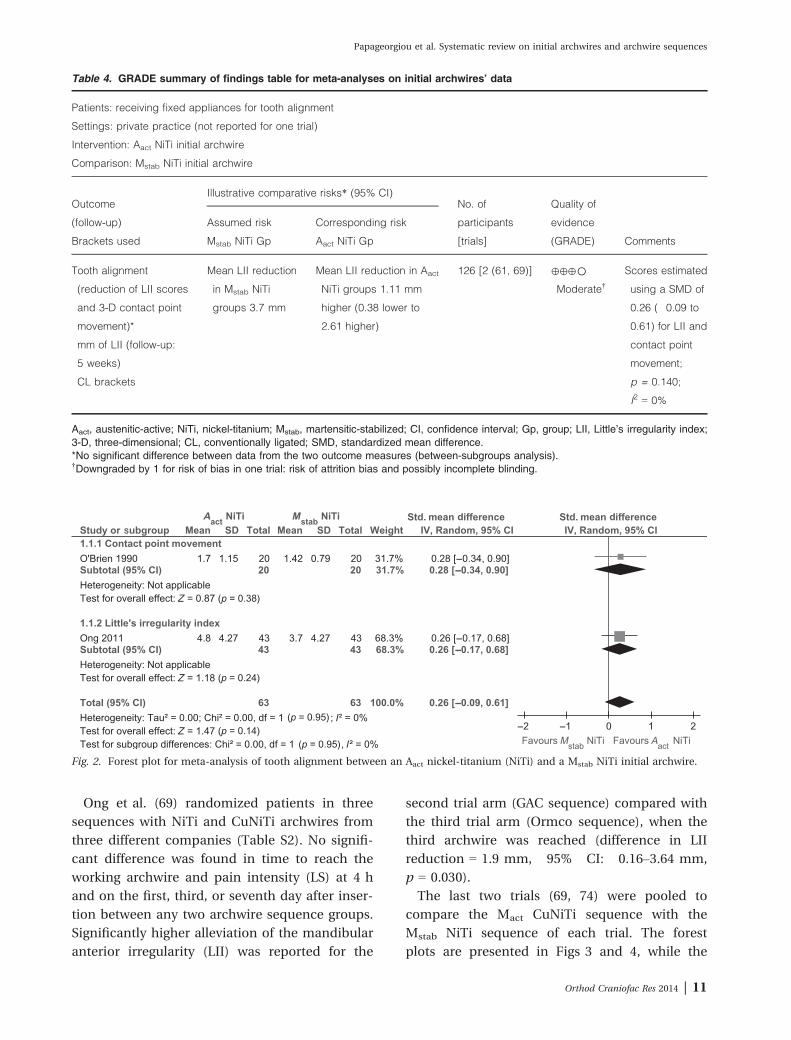
Meta-analysis showed that use of Aact NiTi initial
archwires was associated with a small and statis-
tically nonsignificant benefit in irregularity alle-
viation compared with Mstab NiTi initial
archwires (Table 4; Fig. 2), with evidence being
classified according to GRADE as ‘moderate’.
Finally, pain intensity and analgesic use differed
significantly between groups only at the fourth
day, with the Aact NiTi group reporting less pain.
Pain after engagement of an initial Aact NiTi
archwire was compared in a trial to a multi-
stranded SS archwire (68), without finding signif-
icant differences. Regarding the comparison of
alignment efficiency, the results were contradic-
tory, with one trial finding no difference in LII
reduction (69) and one trial finding significantly
higher 3-D contact point movement of the ante-
rior segment for the Aact NiTi compared with the
multistranded SS archwires (71).
Multistranded archwires
As stated above for each type of NiTi archwire,
no differences were found between multistran-
ded SS archwires compared with Aact NiTi arch-
wires in terms of intertooth contact point
movement (70, 71) or patient pain intensity (68).
Moreover, no difference was found between
6 | Orthod Craniofac Res 2014
Papageorgiou et al. Systematic review on initial archwires and archwire sequences
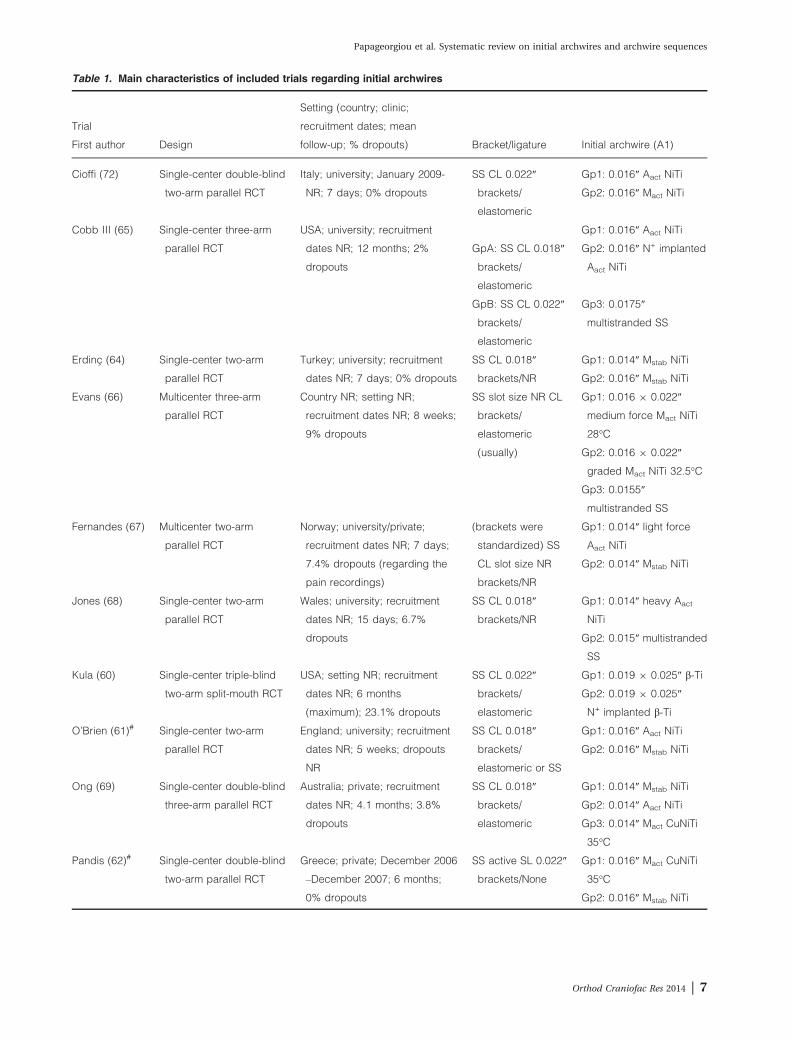
Table 1. Main characteristics of included trials regarding initial archwires
Trial
First author Design
Setting (country; clinic;
recruitment dates; mean
follow-up; % dropouts) Bracket/ligature Initial archwire (A1)
Cioffi (72) Single-center double-blind
two-arm parallel RCT
Italy; university; January 2009-
NR; 7 days; 0% dropouts
SS CL 0.022″
brackets/
elastomeric
Gp1: 0.016″ Aact NiTi
Gp2: 0.016″ Mact NiTi
Cobb III (65) Single-center three-arm
parallel RCT
USA; university; recruitment
dates NR; 12 months; 2%
dropouts
Gp1: 0.016″ Aact NiTi
GpA: SS CL 0.018″
brackets/
elastomeric
Gp2: 0.016″ N+ implanted
Aact NiTi
GpB: SS CL 0.022″
brackets/
elastomeric
Gp3: 0.0175″
multistranded SS
Erdinc� (64) Single-center two-arm
parallel RCT
Turkey; university; recruitment
dates NR; 7 days; 0% dropouts
SS CL 0.018″
brackets/NR
Gp1: 0.014″ Mstab NiTi
Gp2: 0.016″ Mstab NiTi
Evans (66) Multicenter three-arm
parallel RCT
Country NR; setting NR;
recruitment dates NR; 8 weeks;
9% dropouts
SS slot size NR CL
brackets/
elastomeric
(usually)
Gp1: 0.016 9 0.022″
medium force Mact NiTi
28°C
Gp2: 0.016 9 0.022″
graded Mact NiTi 32.5°C
Gp3: 0.0155″
multistranded SS
Fernandes (67) Multicenter two-arm
parallel RCT
Norway; university/private;
recruitment dates NR; 7 days;
7.4% dropouts (regarding the
pain recordings)
(brackets were
standardized) SS
CL slot size NR
brackets/NR
Gp1: 0.014″ light force
Aact NiTi
Gp2: 0.014″ Mstab NiTi
Jones (68) Single-center two-arm
parallel RCT
Wales; university; recruitment
dates NR; 15 days; 6.7%
dropouts
SS CL 0.018″
brackets/NR
Gp1: 0.014″ heavy Aact
NiTi
Gp2: 0.015″ multistranded
SS
Kula (60) Single-center triple-blind
two-arm split-mouth RCT
USA; setting NR; recruitment
dates NR; 6 months
(maximum); 23.1% dropouts
SS CL 0.022″
brackets/
elastomeric
Gp1: 0.019 9 0.025″ b-Ti
Gp2: 0.019 9 0.025″
N+ implanted b-Ti
O’Brien (61)# Single-center two-arm
parallel RCT
England; university; recruitment
dates NR; 5 weeks; dropouts
NR
SS CL 0.018″
brackets/
elastomeric or SS
Gp1: 0.016″ Aact NiTi
Gp2: 0.016″ Mstab NiTi
Ong (69) Single-center double-blind
three-arm parallel RCT
Australia; private; recruitment
dates NR; 4.1 months; 3.8%
dropouts
SS CL 0.018″
brackets/
elastomeric
Gp1: 0.014″ Mstab NiTi
Gp2: 0.014″ Aact NiTi
Gp3: 0.014″ Mact CuNiTi
35°C
Pandis (62)# Single-center double-blind
two-arm parallel RCT
Greece; private; December 2006
–December 2007; 6 months;
0% dropouts
SS active SL 0.022″
brackets/None
Gp1: 0.016″ Mact CuNiTi
35°C
Gp2: 0.016″ Mstab NiTi
Orthod Craniofac Res 2014 | 7
Papageorgiou et al. Systematic review on initial archwires and archwire sequences

multistranded SS archwires compared with Mact
NiTi archwires in terms of intertooth contact
point movement (66, 70). In contrast, multistran-
ded Aact NiTi archwires were reported to be sig-
nificantly more efficient in terms of 3-D contact
point movement than its single-stranded ana-
logs.
Trials on archwire sequences
Four trials (59, 69, 73, 74) investigated archwire
sequences used on 364 patients with SS CL
brackets. AlQabandi et al. (73) compared a
sequence of round SS archwires with progres-
sively greater cross-section with a sequence of a
rectangular Mact CuNiTi archwire, followed by a
rectangular SS archwire and found no significant
difference in treatment effects.
Ji et al. (59) similarly compared a sequence of
four progressively larger round Mstab NiTi arch-
wires, followed by two rectangular SS archwires
and a sequence of 0.016″ Mact round NiTi, fol-
lowed by a rectangular Mact NiTi and a rectangu-
lar SS archwire. No significant difference was
found in treatment duration or bracket failure
between the groups, while significantly more
archwire fractures were observed in the first
(Mstab NiTi) group. Nevertheless, caution is
advised due to the lack of sample size calculation,
the unclear risk of bias, and the lack of complete
reporting that precluded direct assessment.
Mandall et al. (74) randomized patients in
three sequences including various NiTi, CuNiTi,
and SS archwires, which are all manufactured by
the same company (Table S2). Assessed out-
comes included time/appointments to reach the
working archwire, pain intensity (LS) after arch-
wire insertion, and EARR of the maxillary central
incisor. No significant difference was found
among groups for any outcome in the maxillary
arch. In the mandibular arch, however, signifi-
cantly less time to reach the working archwire
and significantly lower pain intensity (LS) at 4 h,
the first and the seventh day after insertion were
reported for the archwire sequence ‘round and
then rectangular Mstab NiTi’ (Gp1) compared
with the sequence ‘round Mstab NiTi and then
round SS’ (Gp2). Also, significantly lower pain
intensity (LS) at the first, third, and seventh day
after insertion was reported for the ‘round then
rectangular Mstab NiTi’ sequence compared with
the sequence ‘rectangular Mact CuNiTi.’
Table 1. (continued)
Trial
First author Design
Setting (country; clinic;
recruitment dates; mean
follow-up; % dropouts) Bracket/ligature Initial archwire (A1)
Quintao (70) Single-center four-arm
parallel RCT
Brazil; university; recruitment
dates NR; 8 weeks; dropouts
NR
SS CL 0.022″
brackets/NR
Gp1: 0.016″ light force
Aact NiTi
Gp2: 0.016″ Mact NiTi
Gp3: 0.0155″
multistranded SS
Gp4: 0.014″ SS
Sebastian (63) Single-center double-blind
two-arm parallel RCT
India; university; recruitment
dates NR; 12 weeks; 0%
dropouts
SS CL 0.022″
brackets/
elastomeric
(usually) and SS
Gp1: 0.016″ multistranded
Aact NiTi
Gp2: 0.016″ Aact NiTi
West (71) Single-center two-arm
parallel RCT
Ireland; setting NR; recruitment
dates NR; 6 weeks; dropouts
NR
SS CL slot NR
brackets/NR
Gp1: 0.014″ Aact NiTi
Gp2: 0.0155″
multistranded SS
A1, first archwire; RCT, randomized controlled trial; NR, not reported; SS, stainless steel; CL, conventionally ligated; Gp, group;Aact, austenitic-active; NiTi, nickel-titanium; Mact, martensitic-active; Mstab, martensitic-stabilized; b-Ti, beta titanium; SL, self-ligating;#including data from author communication.
8 | Orthod Craniofac Res 2014
Papageorgiou et al. Systematic review on initial archwires and archwire sequences
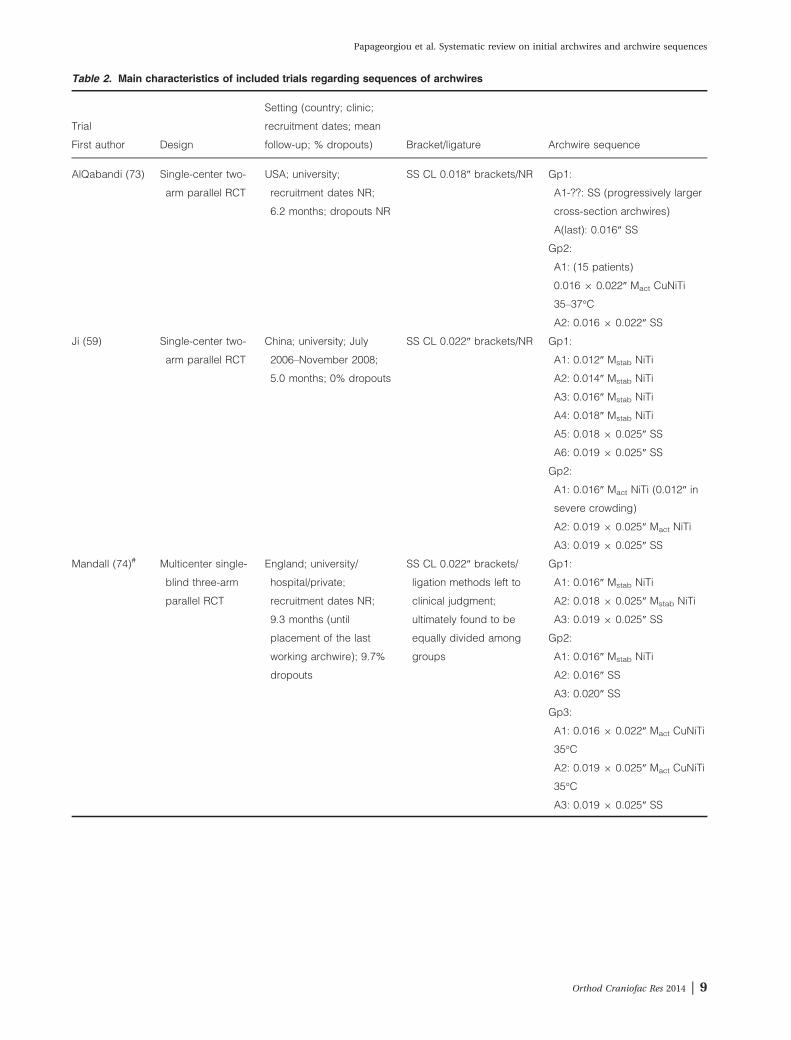
Table 2. Main characteristics of included trials regarding sequences of archwires
Trial
First author Design
Setting (country; clinic;
recruitment dates; mean
follow-up; % dropouts) Bracket/ligature Archwire sequence
AlQabandi (73) Single-center two-
arm parallel RCT
USA; university;
recruitment dates NR;
6.2 months; dropouts NR
SS CL 0.018″ brackets/NR Gp1:
A1-??: SS (progressively larger
cross-section archwires)
A(last): 0.016″ SS
Gp2:
A1: (15 patients)
0.016 9 0.022″ Mact CuNiTi
35–37°C
A2: 0.016 9 0.022″ SS
Ji (59) Single-center two-
arm parallel RCT
China; university; July
2006–November 2008;
5.0 months; 0% dropouts
SS CL 0.022″ brackets/NR Gp1:
A1: 0.012″ Mstab NiTi
A2: 0.014″ Mstab NiTi
A3: 0.016″ Mstab NiTi
A4: 0.018″ Mstab NiTi
A5: 0.018 9 0.025″ SS
A6: 0.019 9 0.025″ SS
Gp2:
A1: 0.016″ Mact NiTi (0.012″ in
severe crowding)
A2: 0.019 9 0.025″ Mact NiTi
A3: 0.019 9 0.025″ SS
Mandall (74)# Multicenter single-
blind three-arm
parallel RCT
England; university/
hospital/private;
recruitment dates NR;
9.3 months (until
placement of the last
working archwire); 9.7%
dropouts
SS CL 0.022″ brackets/
ligation methods left to
clinical judgment;
ultimately found to be
equally divided among
groups
Gp1:
A1: 0.016″ Mstab NiTi
A2: 0.018 9 0.025″ Mstab NiTi
A3: 0.019 9 0.025″ SS
Gp2:
A1: 0.016″ Mstab NiTi
A2: 0.016″ SS
A3: 0.020″ SS
Gp3:
A1: 0.016 9 0.022″ Mact CuNiTi
35°C
A2: 0.019 9 0.025″ Mact CuNiTi
35°C
A3: 0.019 9 0.025″ SS
Orthod Craniofac Res 2014 | 9
Papageorgiou et al. Systematic review on initial archwires and archwire sequences
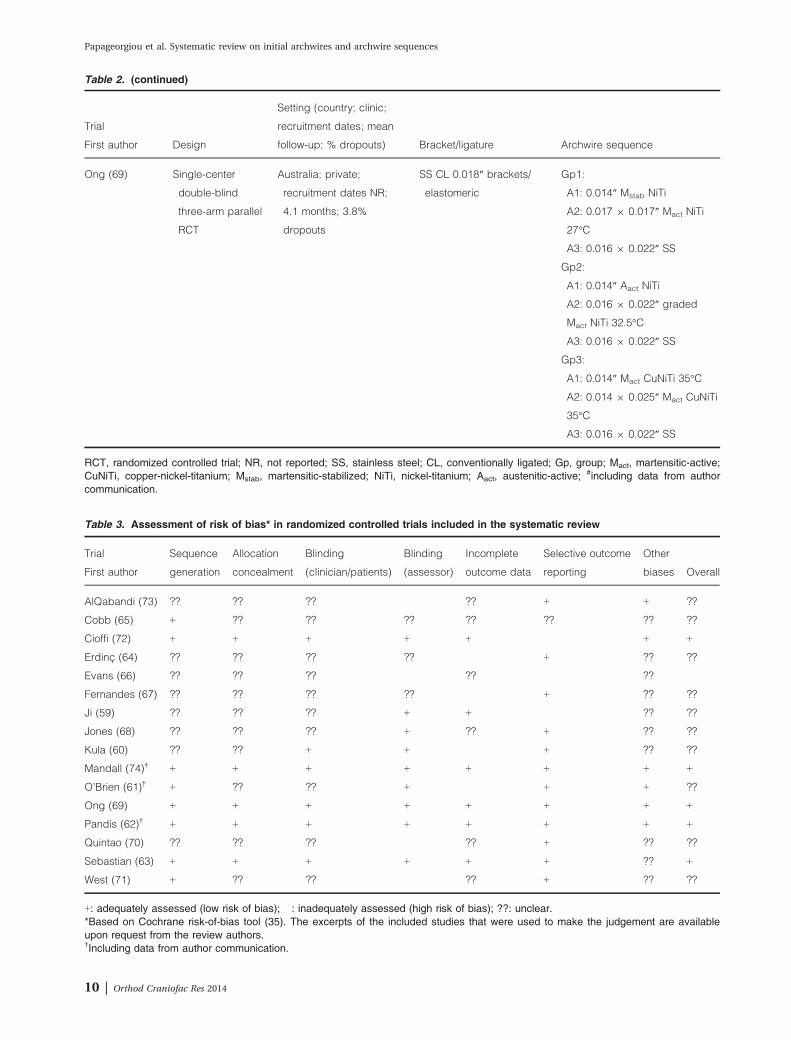
Table 2. (continued)
Trial
First author Design
Setting (country; clinic;
recruitment dates; mean
follow-up; % dropouts) Bracket/ligature Archwire sequence
Ong (69) Single-center
double-blind
three-arm parallel
RCT
Australia; private;
recruitment dates NR;
4.1 months; 3.8%
dropouts
SS CL 0.018″ brackets/
elastomeric
Gp1:
A1: 0.014″ Mstab NiTi
A2: 0.017 9 0.017″ Mact NiTi
27°C
A3: 0.016 9 0.022″ SS
Gp2:
A1: 0.014″ Aact NiTi
A2: 0.016 9 0.022″ graded
Mact NiTi 32.5°C
A3: 0.016 9 0.022″ SS
Gp3:
A1: 0.014″ Mact CuNiTi 35°C
A2: 0.014 9 0.025″ Mact CuNiTi
35°C
A3: 0.016 9 0.022″ SS
RCT, randomized controlled trial; NR, not reported; SS, stainless steel; CL, conventionally ligated; Gp, group; Mact, martensitic-active;CuNiTi, copper-nickel-titanium; Mstab, martensitic-stabilized; NiTi, nickel-titanium; Aact, austenitic-active; #including data from authorcommunication.
Table 3. Assessment of risk of bias* in randomized controlled trials included in the systematic review
Trial
First author
Sequence
generation
Allocation
concealment
Blinding
(clinician/patients)
Blinding
(assessor)
Incomplete
outcome data
Selective outcome
reporting
Other
biases Overall
AlQabandi (73) ?? ?? ?? � ?? + + ??
Cobb (65) + ?? ?? ?? ?? ?? ?? ??
Cioffi (72) + + + + + � + +
Erdinc� (64) ?? ?? ?? ?? � + ?? ??
Evans (66) ?? ?? ?? � ?? � ?? �Fernandes (67) ?? ?? ?? ?? � + ?? ??
Ji (59) ?? ?? ?? + + � ?? ??
Jones (68) ?? ?? ?? + ?? + ?? ??
Kula (60) ?? ?? + + � + ?? ??
Mandall (74)† + + + + + + + +
O’Brien (61)† + ?? ?? + � + + ??
Ong (69) + + + + + + + +
Pandis (62)† + + + + + + + +
Quintao (70) ?? ?? ?? � ?? + ?? ??
Sebastian (63) + + + + + + ?? +
West (71) + ?? ?? � ?? + ?? ??
+: adequately assessed (low risk of bias); �: inadequately assessed (high risk of bias); ??: unclear.*Based on Cochrane risk-of-bias tool (35). The excerpts of the included studies that were used to make the judgement are availableupon request from the review authors.†Including data from author communication.
10 | Orthod Craniofac Res 2014
Papageorgiou et al. Systematic review on initial archwires and archwire sequences
Ong et al. (69) randomized patients in three
sequences with NiTi and CuNiTi archwires from
three different companies (Table S2). No signifi-
cant difference was found in time to reach the
working archwire and pain intensity (LS) at 4 h
and on the first, third, or seventh day after inser-
tion between any two archwire sequence groups.
Significantly higher alleviation of the mandibular
anterior irregularity (LII) was reported for the
second trial arm (GAC sequence) compared with
the third trial arm (Ormco sequence), when the
third archwire was reached (difference in LII
reduction = 1.9 mm, 95% CI: 0.16–3.64 mm,
p = 0.030).
The last two trials (69, 74) were pooled to
compare the Mact CuNiTi sequence with the
Mstab NiTi sequence of each trial. The forest
plots are presented in Figs 3 and 4, while the
Table 4. GRADE summary of findings table for meta-analyses on initial archwires’ data
Patients: receiving fixed appliances for tooth alignment
Settings: private practice (not reported for one trial)
Intervention: Aact NiTi initial archwire
Comparison: Mstab NiTi initial archwire
Outcome
(follow-up)
Brackets used
Illustrative comparative risks* (95% CI)No. of
participants
[trials]
Quality of
evidence
(GRADE) Comments
Assumed risk Corresponding risk
Mstab NiTi Gp Aact NiTi Gp
Tooth alignment
(reduction of LII scores
and 3-D contact point
movement)*
mm of LII (follow-up:
5 weeks)
CL brackets
Mean LII reduction
in Mstab NiTi
groups 3.7 mm
Mean LII reduction in Aact
NiTi groups 1.11 mm
higher (0.38 lower to
2.61 higher)
126 [2 (61, 69)] ⊕⊕⊕○Moderate†
Scores estimated
using a SMD of
0.26 (�0.09 to
0.61) for LII and
contact point
movement;
p = 0.140;
I2 = 0%
Aact, austenitic-active; NiTi, nickel-titanium; Mstab, martensitic-stabilized; CI, confidence interval; Gp, group; LII, Little’s irregularity index;3-D, three-dimensional; CL, conventionally ligated; SMD, standardized mean difference.*No significant difference between data from the two outcome measures (between-subgroups analysis).†Downgraded by 1 for risk of bias in one trial: risk of attrition bias and possibly incomplete blinding.
Fig. 2. Forest plot for meta-analysis of tooth alignment between an Aact nickel-titanium (NiTi) and a Mstab NiTi initial archwire.
Orthod Craniofac Res 2014 | 11
Papageorgiou et al. Systematic review on initial archwires and archwire sequences
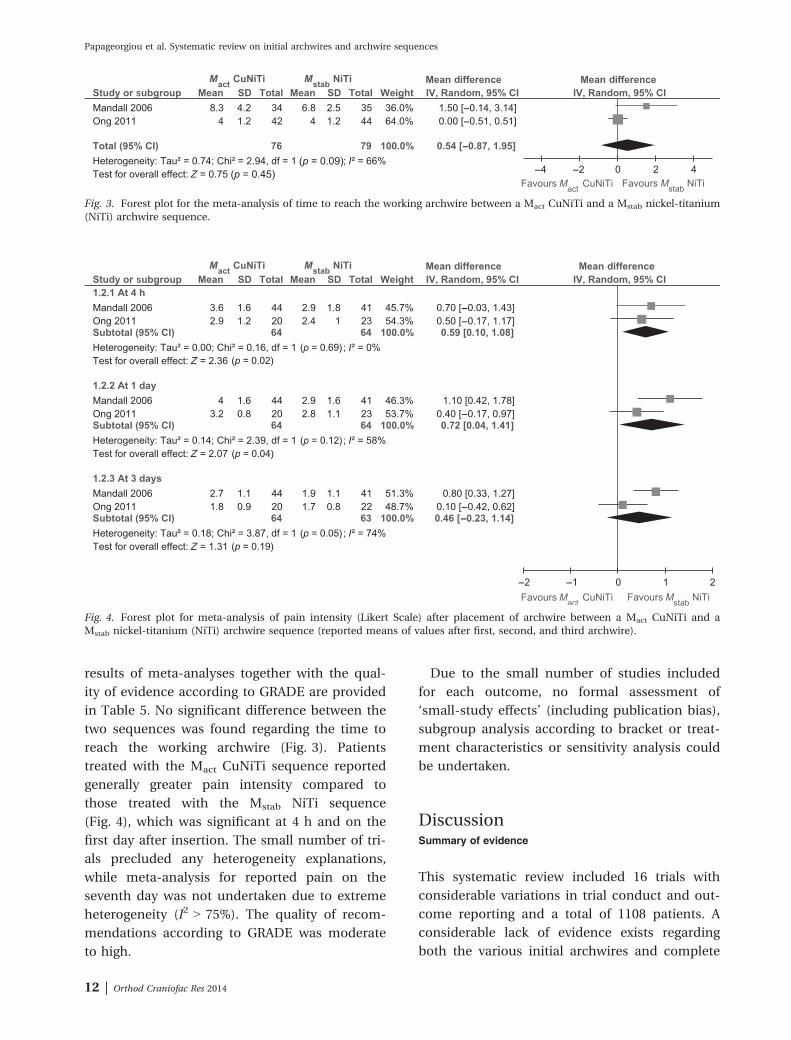
results of meta-analyses together with the qual-
ity of evidence according to GRADE are provided
in Table 5. No significant difference between the
two sequences was found regarding the time to
reach the working archwire (Fig. 3). Patients
treated with the Mact CuNiTi sequence reported
generally greater pain intensity compared to
those treated with the Mstab NiTi sequence
(Fig. 4), which was significant at 4 h and on the
first day after insertion. The small number of tri-
als precluded any heterogeneity explanations,
while meta-analysis for reported pain on the
seventh day was not undertaken due to extreme
heterogeneity (I2 > 75%). The quality of recom-
mendations according to GRADE was moderate
to high.
Due to the small number of studies included
for each outcome, no formal assessment of
‘small-study effects’ (including publication bias),
subgroup analysis according to bracket or treat-
ment characteristics or sensitivity analysis could
be undertaken.
DiscussionSummary of evidence
This systematic review included 16 trials with
considerable variations in trial conduct and out-
come reporting and a total of 1108 patients. A
considerable lack of evidence exists regarding
both the various initial archwires and complete
Fig. 3. Forest plot for the meta-analysis of time to reach the working archwire between a Mact CuNiTi and a Mstab nickel-titanium
(NiTi) archwire sequence.
Fig. 4. Forest plot for meta-analysis of pain intensity (Likert Scale) after placement of archwire between a Mact CuNiTi and a
Mstab nickel-titanium (NiTi) archwire sequence (reported means of values after first, second, and third archwire).
12 | Orthod Craniofac Res 2014
Papageorgiou et al. Systematic review on initial archwires and archwire sequences
archwire sequences that are commercially avail-
able.
Orthodontic mechanotherapy has been based
on the incremental variation of archwire
dimension or archwire material (and modulus
of elasticity) (75). The effect of the size and
shape of the archwire’s cross-section could not
be assessed in this review. Various authors
have reported a correlation between frictional
behavior and vertical wire dimension (76–78),
with friction increasing as vertical wire dimen-
sion becomes greater. Conversely, an increased
clearance between wire and bracket results in
reduced friction, as well as in diminished con-
trol during tooth movement (79). Regarding the
cross-section shape, even an artificially induced
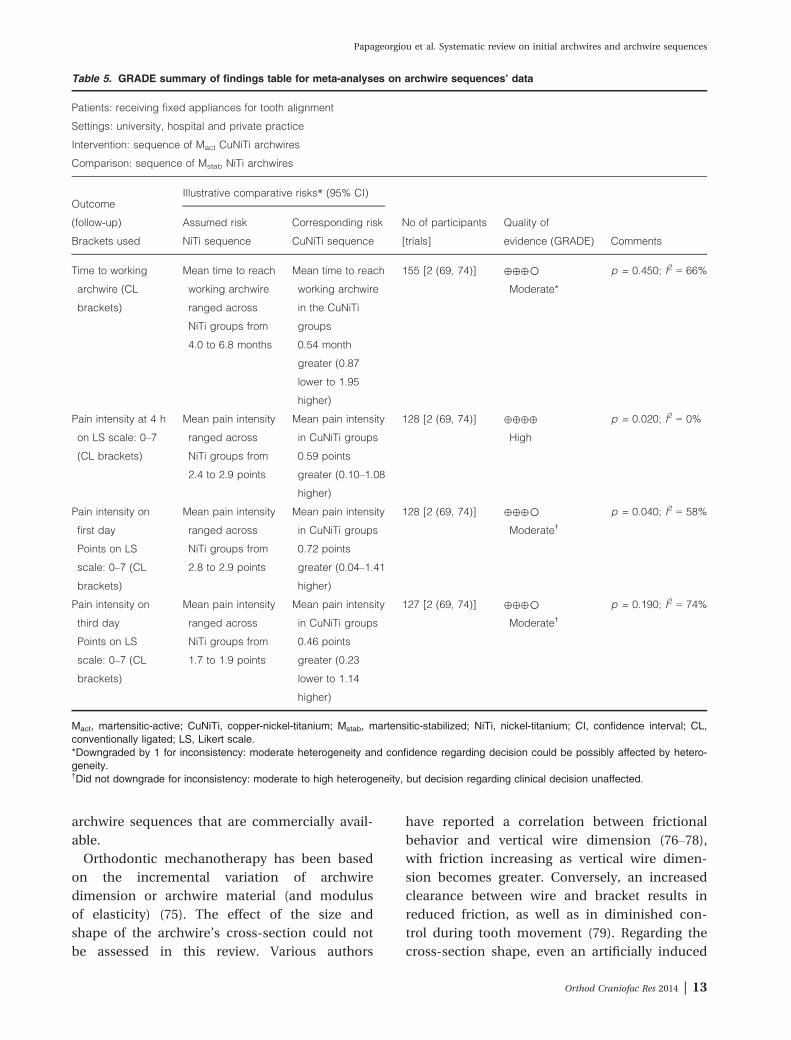
Table 5. GRADE summary of findings table for meta-analyses on archwire sequences’ data
Patients: receiving fixed appliances for tooth alignment
Settings: university, hospital and private practice
Intervention: sequence of Mact CuNiTi archwires
Comparison: sequence of Mstab NiTi archwires
Outcome
(follow-up)
Brackets used
Illustrative comparative risks* (95% CI)
No of participants
[trials]
Quality of
evidence (GRADE) Comments
Assumed risk Corresponding risk
NiTi sequence CuNiTi sequence
Time to working
archwire (CL
brackets)
Mean time to reach
working archwire
ranged across
NiTi groups from
4.0 to 6.8 months
Mean time to reach
working archwire
in the CuNiTi
groups
0.54 month
greater (0.87
lower to 1.95
higher)
155 [2 (69, 74)] ⊕⊕⊕○Moderate*
p = 0.450; I2 = 66%
Pain intensity at 4 h
on LS scale: 0–7
(CL brackets)
Mean pain intensity
ranged across
NiTi groups from
2.4 to 2.9 points
Mean pain intensity
in CuNiTi groups
0.59 points
greater (0.10–1.08
higher)
128 [2 (69, 74)] ⊕⊕⊕⊕
High
p = 0.020; I2 = 0%
Pain intensity on
first day
Points on LS
scale: 0–7 (CL
brackets)
Mean pain intensity
ranged across
NiTi groups from
2.8 to 2.9 points
Mean pain intensity
in CuNiTi groups
0.72 points
greater (0.04–1.41
higher)
128 [2 (69, 74)] ⊕⊕⊕○Moderate†
p = 0.040; I2 = 58%
Pain intensity on
third day
Points on LS
scale: 0–7 (CL
brackets)
Mean pain intensity
ranged across
NiTi groups from
1.7 to 1.9 points
Mean pain intensity
in CuNiTi groups
0.46 points
greater (0.23
lower to 1.14
higher)
127 [2 (69, 74)] ⊕⊕⊕○Moderate†
p = 0.190; I2 = 74%
Mact, martensitic-active; CuNiTi, copper-nickel-titanium; Mstab, martensitic-stabilized; NiTi, nickel-titanium; CI, confidence interval; CL,conventionally ligated; LS, Likert scale.*Downgraded by 1 for inconsistency: moderate heterogeneity and confidence regarding decision could be possibly affected by hetero-geneity.†Did not downgrade for inconsistency: moderate to high heterogeneity, but decision regarding clinical decision unaffected.
Orthod Craniofac Res 2014 | 13
Papageorgiou et al. Systematic review on initial archwires and archwire sequences

beveling of rectangular archwires can reduce
friction (80).
Ion implantation of b-Ti or NiTi archwires was
assessed independently by two trials with no sig-
nificant effect found. These investigations are
based on in vitro data showing that altering of
the surface roughness of the archwire may
reduce corrosion, friction and possibly enable
faster sliding of the archwire (81–83). However,
this may hold true only when both opposing
surfaces have been ion implanted (60). Also, NiTi
archwires are subject to surface alterations by
intra-oral conditions and/or bracket engagement
(10), which could modify their performance. The
idea that surface roughness and friction reduc-
tion is crucial to efficient mechanics also forms
the basis of using metal or silica inserts or
glazed slot bases in ceramic brackets (84).
Although current evidence suggests that the clin-
ical role of friction may have been overestimated
(85), further research under non-simplified con-
ditions and in collaboration with biomedical
engineers is recommended (86).
A wide variety of NiTi-based archwires is
available, which have been studied extensively
in vitro (5, 7, 15, 83, 87–89). Factors of archwires
that must be taken into account are their bio-
compatibility (90) and intra-oral aging (8, 91),
followed by an increased risk of fracture (9),
especially when planning longer appointment
intervals, although the actual causes remain
unclear (92).
Limited data preclude firm conclusions on the
use of Mact NiTi archwires. Pandis et al. (62)
reported no significant advantage in alleviation
of mandibular anterior tooth irregularity com-
pared with Mstab NiTi, while Cioffi et al. (72)
reported lower pain intensity at the second,
third, and fourth day after placement compared
with Aact NiTi. Both studies provide evidence
that would be rated as ‘high quality’ by the
GRADE approach; nevertheless, additional stud-
ies are needed.
Meta-analysis of two trials found that Aact
NiTi was slightly more effective in tooth align-
ment than Mstab NiTi, although not to a signifi-
cant extent. However, this difference must be
verified by subsequent large studies, as the
small number of trials or differences in trial
conduct and outcomes reported could have
affected this estimate. Nevertheless, many of the
included trials reported that considerable wire
deflections are needed for the superelastic
plateau of Aact archwires to be clinically useful
(93). Also, recent observational evidence indi-
cates that the bracket prescription may possibly
affect the clinical performance of Aact NiTi arch-
wires (94).
No clear conclusions can be made for the use
of multistranded archwires due to the diverse
comparisons between single- and multistranded
archwires and serious methodological issues. In
the trial of Sebastian et al. (63), a significant
advantage of the multistranded Aact NiTi arch-
wire was reported compared with its single-
stranded analog with the provided evidence
rated as ‘high quality’.
Many different esthetic archwire coatings
have been used to improve the frictional and
esthetic characteristics of orthodontic archwires
(95), with a number of issues identified. For
example, epoxy resin-coated Aact NiTi archwires
have been reported to produce lower loading
and unloading force values than uncoated arch-
wires of the same nominal dimensions for CL
brackets and even more with SL brackets (96).
Also, retrieved specimens presented increased
surface roughness, deterioration of esthetics,
and reduction of unloading force values, the
latter being observed for CL and not SL brack-
ets (18). On the other hand, certain coatings of
archwires may prevent or minimize archwire
corrosion of orthodontic archwires intra-orally
(97).
The use of an archwire sequence of Mact CuNiTi
was found to be associated with greater pain
intensity compared with a sequence of Mstab NiTi
at 4 h and 1 day after archwire insertion. This
issue should not be taken lightly, as post-
insertion pain is more intense and lasts longer
than post-extraction pain (98). Orthodontic pain
may be influenced by numerous factors (99),
which may lead to poor patient compliance or
treatment discontinuation (100, 101) and are
believed to be associated with the amount of
force applied to the tooth (102). Also, the two
14 | Orthod Craniofac Res 2014
Papageorgiou et al. Systematic review on initial archwires and archwire sequences

identified and pooled trials of archwire sequences
differed in some aspects. Mandall et al. (74) used
sequences from a single company, while Ong
et al. (69) from three different companies. Arch-
wire change in Mandall et al. was made when the
archwire was passive, while in Ong et al. when
the archwire could be completely engaged.
Finally, Ong et al. used brackets of smaller slot
size than Mandall et al. (0.018″ vs. 0.022″), result-
ing in reduced slot-wire play and potentially
more efficient treatment, although this has not
yet been empirically proven (103).
Strengths and limitations
The conduct and reporting of this review was
based on standard guidelines (33–35). Apart
from published articles, unpublished/ongoing
trials were inquired upon and additional data
were provided after communication with trial-
ists. Blinding is not always possible, and when
not, it is inappropriate to describe all such stud-
ies as of ‘low quality’ (35). Unclear classifica-
tions were not resolved by exclusion of the trial,
but included, reported, and will be improved in
a following update (planned in 5–6 years). Sensi-
tivity analyses took into account sources of
unclear or high risk of bias. Methodological ade-
quacy of included trials was assessed in terms of
within-study risk of bias, sample size calcula-
tions, assessment of the method error, and
appropriateness of statistics used [as for exam-
ple in split-mouth trials (39)]. Between-study
heterogeneity was both tested and included in
the random-effects model, while the 95% PIs
were calculated, because robust conclusions
from random-effects meta-analyses mandate
their use (52). Finally, the GRADE approach was
used to evaluate the across studies evidence
provided by the meta-analyses (47). However,
the major limitation of this review is the lack of
substantial high-level evidence for many of the
interventions and outcomes assessed. Secondly,
the lack of consistent reporting across studies,
missing data due to non-response of trialists,
and inability to examine publication bias and
other reporting biases may have increased the
risk of bias.
Conclusions
There is insufficient data at present to make rec-
ommendations for the use of any available arch-
wire type regarding effectiveness, efficacy,
treatment outcome, or potential side effects. The
meta-analyses conducted are limited by the
small number of trials and methodological issues
and must therefore be subsequently confirmed.
Regarding initial archwires, meta-analysis of
two trials indicates that in CL brackets, use of an
austenitic-active NiTi initial archwire was not
significantly more effective in tooth alignment
than a martensitic-stabilized NiTi archwire
(moderate evidence quality).
Regarding archwire sequences, meta-analysis
of two trials indicates that in CL brackets, a
sequence of martensitic-active CuNiTi archwires
compared with a sequence of martensitic-stabi-
lized NiTi archwires:
• Has no effect on time needed to reach the
working archwire (moderate evidence), and
• Results in greater patient-reported pain inten-
sity, which was statistically significant 4 h and
1 day after placement of each archwire (mod-
erate to high evidence).
The clinical effects of orthodontic archwires
should be evaluated in parallel RCTs, reported
according to the CONSORT statement and with
detailed intervention and outcome data to justify
their use.
Clinical relevance
Regarding initial archwires, superelastic NiTi arch-
wire was not more effective in tooth alignment
compared with conventional NiTi. Regarding
sequences of archwires, use of a heat-activated
NiTi archwire sequence was associated with
greater pain intensity 4 h and 1 day after inser-
tion of each archwire, but did not differ in terms
of effectiveness from a conventional NiTi archwire
sequence. Further studies are needed to justify
the clinical superiority of any type of archwire
used during orthodontic treatment over another.
Orthod Craniofac Res 2014 | 15
Papageorgiou et al. Systematic review on initial archwires and archwire sequences

Acknowledgements: We thank the following authors for
providing missing articles, clarifications, and/or addi-
tional data: Bondemark L. (Malm€o University, Malm€o,
Sweden), Cioffi I. (University of Naples Federico II,
Naples, Italy), Kula K. (Indiana University, Indianapolis,
Ind), Mandall N.A. (Tameside General Hospital, Ashton
under Lyne, UK, O’Brien K. (University of Manchester,
Manchester, UK). and Pandis N. (Private Practice, Corfu,
Greece) for providing individual patient data.
Conflict of interest
The authors report no commercial, proprietary,
or financial interest in the products or compa-
nies described in this article.
Literature search update
An update of the systematic literature search
was undertaken after acceptance of the paper on
April first, 2014 in four databases (Cochrane
Library, MEDLINE, Scopus, and ISI Web of
Knowledge) using the same search strategies as
listed in Table S1. After study selection, two
additional eligible studies were identified (Gravi-
na MA, Brunharo IH, Fraga MR, Artese F, Cam-
pos MJ, Vitral RW et al. Clinical evaluation of
dental alignment and leveling with three
different types of orthodontic wires. Dental Press
J Orthod 2013;18:31–7 & Sandhu SS, Sandhu J. A
randomized clinical trial investigating pain asso-
ciated with superelastic nickel-titanium and
multistranded stainless steel archwires during
the initial leveling and aligning phase of ortho-
dontic treatment. J Orthod 2013;40:276–85) and
it was judged that they would not overly influ-
ence the review’s conclusions. They are planned
to be incorporated in a future update of the sys-
tematic review.
References1. Kusy RP. A review of contemporary
archwires: their properties and
characteristics. Angle Orthod
1997;67:197–207.
2. Andreasen GF, Brady PR. A use
hypothesis for 55 Nitinol wire for
orthodontics. Angle Orthod
1972;42:172–7.
3. Pandis N, Bourauel CP. Nickel-
titanium (NiTi) arch wires: the clin-
ical significance of super elasticity.
Semin Orthod 2010;16:249–57.
4. Petoumeno E, Kislyuk M,
Hoederath H, Keilig L, Bourauel C,
J€ager A. Corrosion susceptibility
and nickel release of nickel
titanium wires during clinical
application. J Orofac Orthop
2008;69:411–23.
5. Schumacher HA, Bourauel C, Dre-
scher D. The deactivation behavior
and effectiveness of different
orthodontic leveling arches–a
dynamic analysis of the force sys-
tems. Fortschr Kieferorthop
1992;53:273–85.
6. Drescher D, Bourauel C, Sonne-
born W, Schmuth GP. The long-
term fracture resistance of ortho-
dontic nickel-titanium wires.
Schweiz Monatsschr Zahnmed
1994;104:578–84.
7. Plietsch R, Bourauel C, Drescher
D, Nellen B. A computer-con-
trolled flexing test for determining
the elastic parameters of highly
flexible orthodontic wires. Fortschr
Kieferorthop 1994;55:84–95.
8. Eliades T, Bourauel C. Intraoral
aging of orthodontic materials: the
picture we miss and its clinical rel-
evance. Am J Orthod Dentofacial
Orthop 2005;127:403–12.
9. Eliades T, Eliades G, Athanasiou
AE, Bradley TG. Surface character-
ization of retrieved NiTi orthodon-
tic archwires. Eur J Orthod
2000;22:317–26.
10. Bourauel C, Scharold W, J€ager A,
Eliades T. Fatigue failure of as-
received and retrieved NiTi ortho-
dontic archwires. Dent Mater
2008;24:1095–101.
11. Pandis N, Bourauel C, Eliades T.
Changes in the stiffness of the
ligating mechanism in retrieved
active self-ligating brackets. Am J
Orthod Dentofacial Orthop
2007;132:834–7.
12. Eliades T, Eliades G, Watts DC.
Structural conformation of in vitro
and in vivo aged orthodontic elas-
tomeric modules. Eur J Orthod
1999;21:649–58.
13. Kusy RP, Dilley GJ. Elastic prop-
erty ratios of a triple-stranded
stainless steel arch wire. Am J
Orthod 1984;86:177–88.
14. Taneja P, Duncanson MG Jr,
Khajotia SS, Nanda RS. Deactiva-
tion force-deflection behavior of
multistranded stainless steel wires.
Am J Orthod Dentofacial Orthop
2003;124:61–8.
15. Quintao CCA, Cal-Neto JP, Mene-
zes LM, Elia CN. Force-deflection
properties of initial orthodontic
archwires. World J Orthod
2009;10:29–32.
16. Fuck LM, Drescher D. Force
systems in the initial phase of
orthodontic treatment – a
comparison of different leveling
arch wires. J Orofac Orthop
2006;67:6–18.
17. Cacciafesta V, Sfondrini MF, Lena
A, Scribante A, Vallittu PK, Lassila
LV. Force levels of fiber-reinforced
composites and orthodontic stain-
less steel wires: a 3-point bending
test. Am J Orthod Dentofacial
Orthop 2008;133:410–3.
16 | Orthod Craniofac Res 2014
Papageorgiou et al. Systematic review on initial archwires and archwire sequences

18. Elayyan F, Silikas N, Bearn D. Ex
vivo surface and mechanical
properties of coated orthodontic
archwires. Eur J Orthod
2008;30:661–7.
19. Goldberg AJ, Liebler SA, Burstone
CJ. Viscoelastic properties of
an aesthetic translucent ortho-
dontic wire. Eur J Orthod
2011;33:673–8.
20. Jung YC, Cho JW. Application of
shape memory polyurethane in
orthodontic. J Mater Sci Mater
Med 2010;21:2881–6.
21. Lendlein A, Kelch S. Shape-
memory polymers. Angew Chem
Int Ed Engl 2002;41:2035–57.
22. Shahinpoor M, Schneider HJ.
Intelligent Materials. : Cambridge:
Royal Society of Chemistry; 2007.
pp. 311–2.
23. Keim RG, Gottlieb EL, Nelson AH,
Vogels DS 3rd. 2008 JCO study of
orthodontic diagnosis and treat-
ment procedures, part 1: results
and trends. J Clin Orthod
2008;42:625–40.
24. Banks P, Elton V, Jones Y, Rice P,
Derwent S, Odondi L. The use of
fixed appliances in the UK: a
survey of specialist orthodontists.
J Orthod 2010;37:43–55.
25. Burstone CJ, Koenig HA. Force
systems from an ideal arch. Am J
Orthod 1974;65:270–89.
26. Waters NE. A rationale for the
selection of orthodontic wires. Eur
J Orthod 1992;14:240–5.
27. Riley M, Bearn DR. A systematic
review of clinical trials of aligning
archwires. J Orthod 2009;36:42–51.
28. Wang Y, Jian F, Lai W, Zhao Z,
Yang Z, Liao Z, et al. Initial arch
wires for alignment of crooked
teeth with fixed orthodontic
braces. Cochrane Database Syst
Rev 2010;4:CD007859.
29. Papageorgiou SN, Papadopoulos
MA, Athanasiou AE. Evaluation of
methodology and quality charac-
teristics of systematic reviews in
orthodontics. Orthod Craniofac Res
2011;14:116–37.
30. Papageorgiou SN, Papadopoulos
MA, Athanasiou AE. Reporting
characteristics of meta-analyses in
orthodontics: methodological
assessment and statistical recom-
mendations. Eur J Orthod
2014;36:74–85.
31. Miles PG. Author’s response. Am J
Orthod Dentofacial Orthop
2008;133:5.
32. Pandis N, Eliades T, Partowi S,
Bourauel C. Moments generated
during simulated rotational correc-
tion with self-ligating and conven-
tional brackets. Angle Orthod
2008;78:1030–4.
33. Liberati A, Altman DG, Tetzlaff J,
Mulrow C, Gøtzsche PC, Ioannidis
JP, et al. The PRISMA statement
for reporting systematic reviews
and meta-analyses of studies that
evaluate health care interventions:
explanation and elaboration. J Clin
Epidemiol 2009;62:e1–34.
34. Beller EM, Glasziou PP, Altman
DG, Hopewell S, Bastian H, Chal-
mers I, et al. PRISMA for
Abstracts: reporting systematic
reviews in journal and conference
abstracts. PLoS Med 2013;10:
e1001419.
35. Higgins JPT, Green S, editors.
Cochrane Handbook for Systematic
Reviews of Interventions Version
5.1.0 (updated March 2011). Avail-
able from: http://www.cochra-
ne-handbook.org.
36. Cochrane Renal Group Editorial
Team. How to Write a Protocol.
Available from: http://www.coch-
rane-renal.org/docs/how to write a
protocol.pdf.
37. Glenny AM, Harrison JE. How
to..interpret the orthodontic litera-
ture. J Orthod 2003;30:159–64.
38. Machin D, Day S, Green S, editors.
Textbook of Clinical Trials, 2nd
edn. Chichester: Wiley & Sons;
2007. pp. 246.
39. Lesaffre E, Philstrom B, Needle-
man I, Worthington H. The design
and analysis of split-mouth stud-
ies: what statisticians and clini-
cians should know. Stat Med
2009;28:3470–82.
40. Little RM. The irregularity index: a
quantitative score of mandibular
anterior alignment. Am J Orthod
1975;68:554–63.
41. Richmond S, Shaw WC, O’Brien
KD, Buchanan IB, Jones R, Ste-
phens CD, et al. The development
of the PAR Index (Peer Assessment
Rating): reliability and validity. Eur
J Orthod 1992;14:125–39.
42. Daniels C, Richmond S. The devel-
opment of the index of complex-
ity, outcome and need (ICON).
J Orthod 2000;27:149–62.
43. Chapman CR, Casey KL, Dubner
R, Foley KM, Gracely RH, Reading
AE. Pain measurement: an over-
view. Pain 1985;22:1–31.
44. Likert R. A technique for the mea-
surement of attitudes. Arch Psychol
1931;140:44–53.
45. Moher D, Cook DJ, Jadad AR, Tug-
well P, Moher M, Jones A, et al.
Assessing the quality of reports of
randomized trials: implication for
the conduct of meta-analyses.
Health Technol Assess 1999;3:1–98.
46. Higgins JP, Altman DG, Gøtzsche
PC, J€uni P, Moher D, Oxman AD,
et al. The Cochrane Collabora-
tion’s tool for assessing risk of bias
in randomised trials. BMJ
2011;343:d5928.
47. Guyatt GH, Oxman AD, Sch€une-
mann HJ, Tugwell P, Knottnerus A.
GRADE guidelines: a new series of
articles in the Journal of Clinical
Epidemiology. J Clin Epidemiol
2011;64:380–2.
48. Cohen J. A coefficient of agree-
ment for nominal scales. Educ
Psychol Meas 1960;20:37–46.
49. Papageorgiou SN, Zogakis IP,
Papadopoulos MA. Failure rates
and associated risk factors of
orthodontic miniscrew implants: a
meta-analysis. Am J Orthod Dento-
facial Orthop 2012;142:577–95.e7
50. DerSimonian R, Laird N. Meta-
analysis in clinical trials. Control
Clin Trials 1986;7:177–88.
51. Higgins JP, Thompson SG, Spiegel-
halter DJ. A re-evaluation of ran-
dom effects meta-analysis. J R Stat
Soc Ser A Stat Soc 2009;172:137–59.
52. Graham PL, Moran JL. Robust
meta-analytic conclusions mandate
the provision of prediction intervals
in meta-analysis summaries. J Clin
Epidemiol 2012;65:503–10.
53. Ioannidis JP. Interpretation of tests
of heterogeneity and bias in meta-
analysis. J Eval Clin Pract
2008;14:951–7.
54. Dalstra M, Melsen B. Does the
transition temperature of Cu-NiTi
archwires affect the amount of
tooth movement during align-
ment? Orthod Craniofac Res
2004;7:21–5.
55. Bernhold M, Bondemark L. Super-
elastic nickel-titanium heat-acti-
Orthod Craniofac Res 2014 | 17
Papageorgiou et al. Systematic review on initial archwires and archwire sequences
vated archwires for tooth move-
ment – a prospective randomized
study of apical root resorption
[abstract]. Swed Dent J
2001;25:177.
56. Bloom KL, Bhatia SN. Comparison
of copper NiTi and Nitinol arch-
wires in initial alignment [abstract].
Eur J Orthod 1998;20:614.
57. Chekay BA, Killiany DM, Purcell
MV, Frost RA. Apical root resorp-
tion: a comparison of wire materi-
als [abstract]. J Dent Res
1999;78:202.
58. Patel S, Levinkind M, Lee RT. Pain
reported during alignment using
various nickel titanium wires
[abstract]. Eur J Orthod
1998;20:636.
59. Ji L, He H, Zhong XL, Huang DY.
Evaluation of heat-activated and
common nickel-titanium wire for
orthodontic treatment. J Clin
Rehabil Tissue Eng Res
2010;14:2929–32.
60. Kula K, Phillips C, Gibilaro A, Prof-
fit WR. Effect of ion implantation
of TMA archwires on the rate of
orthodontic sliding space closure.
Am J Orthod Dentofacial Orthop
1998;114:577–80.
61. O’Brien K, Lewis D, Shaw W,
Combe E. A clinical trial of align-
ing archwires. Eur J Orthod
1990;12:380–4.
62. Pandis N, Polychronopoulou A,
Eliades T. Alleviation of mandibu-
lar anterior crowding with copper-
nickel-titanium vs nickel-titanium
wires: a double-blind randomized
control trial. Am J Orthod Dentofa-
cial Orthop 2009;136:152.e1–7.
63. Sebastian B. Alignment efficiency
of superelastic coaxial nickel-tita-
nium vs superelastic single-
stranded nickel-titanium in reliev-
ing mandibular anterior crowding.
Angle Orthod 2012;82:703–8.
64. Erdinc� AM, Dincer B. Perception
of pain during orthodontic treat-
ment with fixed appliances. Eur J
Orthod 2004;26:79–85.
65. Cobb NW 3rd, Kula KS, Phillips C,
Proffit WR. Efficiency of multi-
strand steel, superelastic Ni-Ti and
ion-implanted Ni-Ti archwires for
initial alignment. Clin Orthod Res
1998;1:12–9.
66. Evans TJ, Jones ML, Newcombe
RG. Clinical comparison and
performance perspective of three
aligning arch wires. Am J Orthod
Dentofacial Orthop 1998;114:32–9.
67. Fernandes LM, Ogaard B, Skogl-
und L. Pain and discomfort experi-
enced after placement of a
conventional or a superelastic NiTi
aligning archwire. A randomized
clinical trial. J Orofac Orthop
1998;59:331–9.
68. Jones M, Chan C. The pain and
discomfort experienced during
orthodontic treatment: a random-
ized controlled clinical trial of two
initial aligning arch wires. Am J
Orthod Dentofacial Orthop
1992;102:373–81.
69. Ong E, Ho C, Miles P. Alignment
efficiency and discomfort of three
orthodontic archwire sequences: a
randomized clinical trial. J Orthod
2011;38:32–9.
70. Quintao C, Jones M, Menezes L,
Koo D, Elias C. A prospective clini-
cal trial to compare the perfor-
mance of four initial orthodontic
archwires. Korean J Orthod
2005;35:381–7.
71. West AE, Jones ML, Newcombe
RG. Multiflex versus superelastic: a
randomized clinical trial of the
tooth alignment ability of initial
arch wires. Am J Orthod Dentofa-
cial Orthop 1995;108:464–71.
72. Cioffi I, Piccolo A, Tagliaferri R,
Paduano S, Galeotti A, Martina R.
Pain perception following first
orthodontic archwire placement–
thermoelastic vs superelastic
alloys: a randomized controlled
trial. Quintessence Int 2012;43:
61–9.
73. AlQabandi AK, Sadowsky C, BeG-
ole EA. A comparison of the effects
of rectangular and arch wires in
leveling the curve of Spee. Am J
Orthod Dentofacial Orthop
1999;116:522–9.
74. Mandall N, Lowe C, Worthington
H, Sandler J, Derwent S, Abdi-Osk-
ouei M, et al. Which orthodontic
archwire sequence? A randomized
clinical trial. Eur J Orthod
2006;28:561–6.
75. Burstone CJ. Variable-modulus
orthodontics. Am J Orthod
1981;80:1–16.
76. Drescher D, Bourauel C, Schum-
acher HA. Frictional forces
between bracket and arch wire.
Am J Orthod Dentofacial Orthop
1989;96:397–404.
77. Drescher D, Bourauel C, Schum-
acher HA. The loss of force by fric-
tion in arch-guided tooth
movement. Fortschr Kieferorthop
1990;51:99–105.
78. Schumacher HA, Bourauel C, Dre-
scher D. The effect of the ligature
on the friction between bracket
and arch. Fortschr Kieferorthop
1990;51:106–16.
79. Schumacher HA, Bourauel C, Dre-
scher D. The influence of bracket
design on frictional losses in the
bracket/arch wire system. J Orofac
Orthop 1999;60:335–47.
80. Schumacher HA, Bourauel C, Dre-
scher D. Frictional forces when
rectangular guiding arches with
varying edge bevel are employed.
J Orofac Orthop 1998;59:139–49.
81. Hartel A, Bourauel C, Drescher D,
Schmuth GP. The surface rough-
ness of orthodontic wires–a laser
optical and profilometric study.
Schweiz Monatsschr Zahnmed
1992;102:1195–202.
82. Kusy RP, Tobin EJ, Whitley JQ, Si-
oshansi P. Frictional coefficients of
ion-implanted alumina against
ion-implanted beta-titanium in the
low load, low velocity, single pass
regime. Dent Mater 1992;8:167–72.
83. Bourauel C, Fries T, Drescher D,
Plietsch R. Surface roughness of
orthodontic wires via atomic force
microscopy, laser specular reflec-
tance, and profilometry. Eur J Or-
thod 1998;20:79–92.
84. Jones SP, Amoah KG. Static fric-
tional resistances of polycrystalline
ceramic brackets with conven-
tional slots, glazed slots and metal
slot inserts. Aust Orthod J
2007;23:36–40.
85. Burrow SJ. Friction and resistance
to sliding in orthodontics: a critical
review. Am J Orthod Dentofacial
Orthop 2009;135:442–7.
86. Brantley WA, Eliades T. The role of
biomedical engineers in the design
and manufacture of customized
orthodontic appliances. In: Krish-
nan V, Davidovitch Z, editors.
Integrated Clinical Orthodontics.
Hoboken, NJ: Wiley-Blackwell
Publishing; 2012. pp. 366–78.
87. Widu F, Drescher D, Junker R,
Bourauel C. Corrosion and
18 | Orthod Craniofac Res 2014
Papageorgiou et al. Systematic review on initial archwires and archwire sequences

biocompatibility of orthodontic
wires. J Mater Sci Mater Med
1999;10:275–81.
88. van Aken CA, Pallav P, Kleverlaan
CJ, Kuitert RB, Prahl-Andersen B,
Feilzer AJ. Effect of long-term
repeated deflections on fatigue of
preloaded superelastic nickel-tita-
nium archwires. Am J Orthod Dento-
facial Orthop 2008;133:269–76.
89. Pakshir M, Bagheri T, Kazemi MR.
In vitro evaluation of the electro-
chemical behaviour of stainless
steel and Ni-Ti orthodontic arch-
wires at different temperatures.
Eur J Orthod 2013;35:407–13.
90. Petoumenou E, Arndt M, Keilig L,
Reimann S, Hoederath H, Eliades
T, et al. Nickel concentration in
the saliva of patients with nickel-
titanium orthodontic appliances.
Am J Orthod Dentofacial Orthop
2009;135:59–65.
91. Eliades T, Athanasiou AE. In vivo
aging of orthodontic alloys: impli-
cations for corrosion potential,
nickel release, and biocompatibil-
ity. Angle Orthod 2002;72:222–37.
92. Zinelis S, Eliades T, Pandis N, Eli-
ades G, Bourauel C. Why do
nickel-titanium archwires fracture
intraorally? Fractographic analysis
and failure mechanism of in-vivo
fractured wires. Am J Orthod
Dentofacial Orthop 2007;132:84–9.
93. Kayser D, Bourauel C, Braumann
B, J€ager A. Comparison of
mechanical properties of ortho-
dontic nickel-titanium wires. Bio-
med Tech (Berl) 2002;47:334–42.
94. Sandhu SS, Shetty VS, Mogra S,
Varghese J, Sandhu J, Sandhu JS.
Efficiency, behavior, and clinical
properties of superelastic NiTi ver-
sus multistranded stainless steel
wires. Angle Orthod 2012;82:915–
21.
95. Husmann P, Bourauel C, Wessing-
er M, J€ager A. The frictional behav-
ior of coated guiding archwires. J
Orofac Orthop 2002;63:199–211.
96. Elayyan F, Silikas N, Bearn D.
Mechanical properties of coated
superelastic archwires in conven-
tional and self-ligating orthodontic
brackets. Am J Orthod Dentofacial
Orthop 2010;137:213–7.
97. Neumann P, Bourauel C, J€ager A.
Corrosion and permanent fracture
resistance of coated and conven-
tional orthodontic wires. J Mater
Sci Mater Med 2002;13:141–7.
98. Jones ML, Chan C. Pain in the
early stages of orthodontic
treatment. J Clin Orthod
1992;26:311–3.
99. Oz AA, Arici N, Arici S. The clinical
and laboratory effects of bracket
type during canine distalization
with sliding mechanics. Angle Or-
thod 2012;82:326–32.
100. Patel V. Non-completion of active
orthodontic treatment. Br J Orthod
1992;19:47–54.
101. Sergl HG, Klages U, Zentner A.
Functional and social discomfort
during orthodontic treatment:
effects on compliance and predic-
tion of patients’ adaptation by
personality variables. Eur J Orthod
2000;22:307–15.
102. Dalili F. Pain perception at differ-
ent stages of orthodontic treat-
ment [thesis]. Kuopio: University
of Kuopio; 2009.
103. Papageorgiou SN, Konstantinidis I,
Papadopoulou K, J€ager A, Boura-
uel C. Clinical effects of pre-
adjusted edgewise orthodontic
brackets: a systematic review and
meta-analysis. Eur J Orthod 2013.
Doi: 10.1093/ejo/cjt064. [Epub
ahead of print].
Supporting Information
Additional Supporting Information may be
found in the online version of this article:
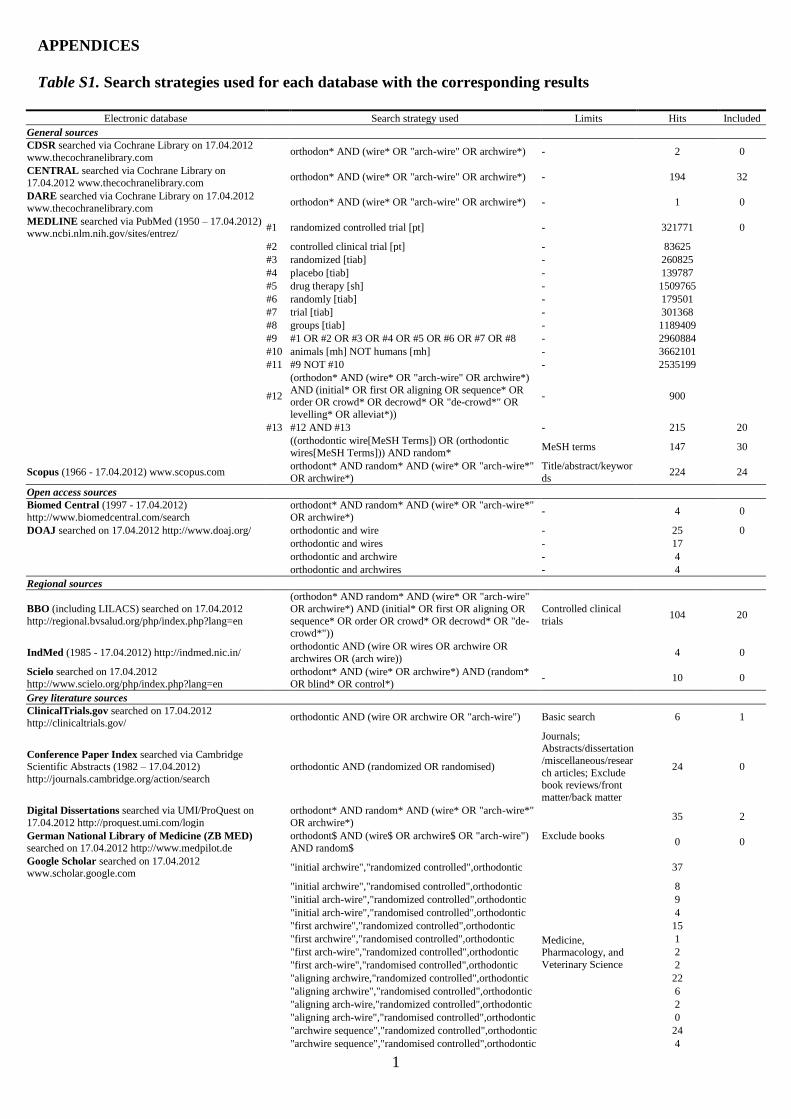
Table S1. Search strategies used for each data-
base with the corresponding results.
Table S2. Product names of brackets and arch-
wires used in the included trials.
Table S3. Supplementary trial characteristics
from Table 1.
Table S4. Supplementary trial characteristics
from Table 2.
Orthod Craniofac Res 2014 | 19
Papageorgiou et al. Systematic review on initial archwires and archwire sequences
1
APPENDICES
Table S1. Search strategies used for each database with the corresponding results
Electronic database Search strategy used Limits Hits Included
General sources
CDSR searched via Cochrane Library on 17.04.2012
www.thecochranelibrary.com orthodon* AND (wire* OR "arch-wire" OR archwire*) - 2 0
CENTRAL searched via Cochrane Library on
17.04.2012 www.thecochranelibrary.com orthodon* AND (wire* OR "arch-wire" OR archwire*) - 194 32
DARE searched via Cochrane Library on 17.04.2012
www.thecochranelibrary.com orthodon* AND (wire* OR "arch-wire" OR archwire*) - 1 0
MEDLINE searched via PubMed (1950 – 17.04.2012) www.ncbi.nlm.nih.gov/sites/entrez/
#1 randomized controlled trial [pt] - 321771 0
#2 controlled clinical trial [pt] - 83625
#3 randomized [tiab] - 260825
#4 placebo [tiab] - 139787
#5 drug therapy [sh] - 1509765
#6 randomly [tiab] - 179501
#7 trial [tiab] - 301368
#8 groups [tiab] - 1189409
#9 #1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 - 2960884
#10 animals [mh] NOT humans [mh] - 3662101
#11 #9 NOT #10 - 2535199
#12
(orthodon* AND (wire* OR "arch-wire" OR archwire*)
AND (initial* OR first OR aligning OR sequence* OR order OR crowd* OR decrowd* OR "de-crowd*" OR
levelling* OR alleviat*))
- 900
#13 #12 AND #13 - 215 20
((orthodontic wire[MeSH Terms]) OR (orthodontic
wires[MeSH Terms])) AND random* MeSH terms 147 30
Scopus (1966 - 17.04.2012) www.scopus.com orthodont* AND random* AND (wire* OR "arch-wire*"
OR archwire*)
Title/abstract/keywor
ds 224 24
Open access sources
Biomed Central (1997 - 17.04.2012)
http://www.biomedcentral.com/search
orthodont* AND random* AND (wire* OR "arch-wire*"
OR archwire*) - 4 0
DOAJ searched on 17.04.2012 http://www.doaj.org/ orthodontic and wire - 25 0
orthodontic and wires - 17
orthodontic and archwire - 4
orthodontic and archwires - 4
Regional sources
BBO (including LILACS) searched on 17.04.2012
http://regional.bvsalud.org/php/index.php?lang=en
(orthodon* AND random* AND (wire* OR "arch-wire"
OR archwire*) AND (initial* OR first OR aligning OR
sequence* OR order OR crowd* OR decrowd* OR "de-crowd*"))
Controlled clinical
trials 104 20
IndMed (1985 - 17.04.2012) http://indmed.nic.in/ orthodontic AND (wire OR wires OR archwire OR
archwires OR (arch wire)) 4 0
Scielo searched on 17.04.2012
http://www.scielo.org/php/index.php?lang=en
orthodont* AND (wire* OR archwire*) AND (random*
OR blind* OR control*) - 10 0
Grey literature sources
ClinicalTrials.gov searched on 17.04.2012
http://clinicaltrials.gov/ orthodontic AND (wire OR archwire OR "arch-wire") Basic search 6 1
Conference Paper Index searched via Cambridge Scientific Abstracts (1982 – 17.04.2012)
http://journals.cambridge.org/action/search
orthodontic AND (randomized OR randomised)
Journals; Abstracts/dissertation
/miscellaneous/resear
ch articles; Exclude book reviews/front
matter/back matter
24 0
Digital Dissertations searched via UMI/ProQuest on
17.04.2012 http://proquest.umi.com/login
orthodont* AND random* AND (wire* OR "arch-wire*"
OR archwire*) 35 2
German National Library of Medicine (ZB MED) searched on 17.04.2012 http://www.medpilot.de
orthodont$ AND (wire$ OR archwire$ OR "arch-wire")
AND random$
Exclude books
0 0
Google Scholar searched on 17.04.2012 www.scholar.google.com
"initial archwire","randomized controlled",orthodontic
Medicine, Pharmacology, and
Veterinary Science
37
"initial archwire","randomised controlled",orthodontic 8
"initial arch-wire","randomized controlled",orthodontic 9
"initial arch-wire","randomised controlled",orthodontic 4
"first archwire","randomized controlled",orthodontic 15
"first archwire","randomised controlled",orthodontic 1
"first arch-wire","randomized controlled",orthodontic 2
"first arch-wire","randomised controlled",orthodontic 2
"aligning archwire,"randomized controlled",orthodontic 22
"aligning archwire","randomised controlled",orthodontic 6
"aligning arch-wire,"randomized controlled",orthodontic 2
"aligning arch-wire","randomised controlled",orthodontic 0
"archwire sequence","randomized controlled",orthodontic 24
"archwire sequence","randomised controlled",orthodontic 4
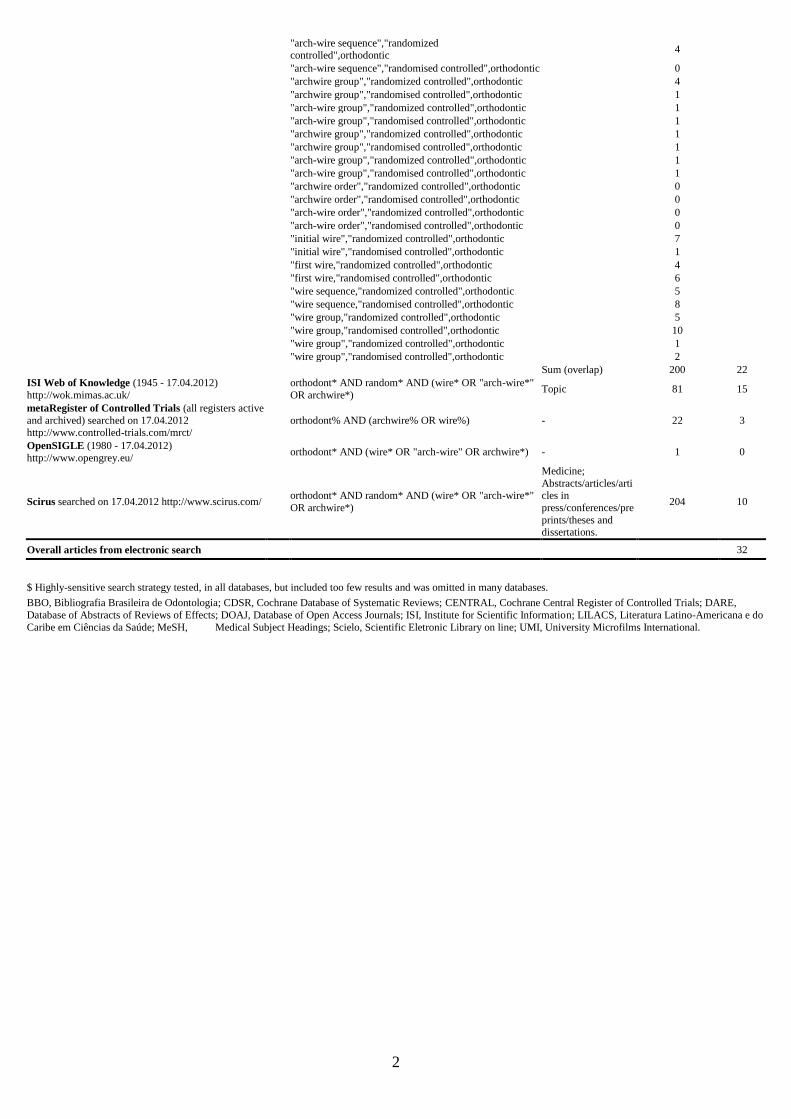
2
"arch-wire sequence","randomized controlled",orthodontic
4
"arch-wire sequence","randomised controlled",orthodontic 0
"archwire group","randomized controlled",orthodontic 4
"archwire group","randomised controlled",orthodontic 1
"arch-wire group","randomized controlled",orthodontic 1
"arch-wire group","randomised controlled",orthodontic 1
"archwire group","randomized controlled",orthodontic 1
"archwire group","randomised controlled",orthodontic 1
"arch-wire group","randomized controlled",orthodontic 1
"arch-wire group","randomised controlled",orthodontic 1
"archwire order","randomized controlled",orthodontic 0
"archwire order","randomised controlled",orthodontic 0
"arch-wire order","randomized controlled",orthodontic 0
"arch-wire order","randomised controlled",orthodontic 0
"initial wire","randomized controlled",orthodontic 7
"initial wire","randomised controlled",orthodontic 1
"first wire,"randomized controlled",orthodontic 4
"first wire,"randomised controlled",orthodontic 6
"wire sequence,"randomized controlled",orthodontic 5
"wire sequence,"randomised controlled",orthodontic 8
"wire group,"randomized controlled",orthodontic 5
"wire group,"randomised controlled",orthodontic 10
"wire group","randomized controlled",orthodontic 1
"wire group","randomised controlled",orthodontic 2
Sum (overlap) 200 22
ISI Web of Knowledge (1945 - 17.04.2012)
http://wok.mimas.ac.uk/
orthodont* AND random* AND (wire* OR "arch-wire*"
OR archwire*) Topic 81 15
metaRegister of Controlled Trials (all registers active
and archived) searched on 17.04.2012 http://www.controlled-trials.com/mrct/
orthodont% AND (archwire% OR wire%) - 22 3
OpenSIGLE (1980 - 17.04.2012)
http://www.opengrey.eu/ orthodont* AND (wire* OR "arch-wire" OR archwire*) - 1 0
Scirus searched on 17.04.2012 http://www.scirus.com/ orthodont* AND random* AND (wire* OR "arch-wire*"
OR archwire*)
Medicine;
Abstracts/articles/articles in
press/conferences/pre
prints/theses and dissertations.
204 10
Overall articles from electronic search 32
$ Highly-sensitive search strategy tested, in all databases, but included too few results and was omitted in many databases.
BBO, Bibliografia Brasileira de Odontologia; CDSR, Cochrane Database of Systematic Reviews; CENTRAL, Cochrane Central Register of Controlled Trials; DARE,
Database of Abstracts of Reviews of Effects; DOAJ, Database of Open Access Journals; ISI, Institute for Scientific Information; LILACS, Literatura Latino-Americana e do
Caribe em Ciências da Saúde; MeSH, Medical Subject Headings; Scielo, Scientific Eletronic Library on line; UMI, University Microfilms International.
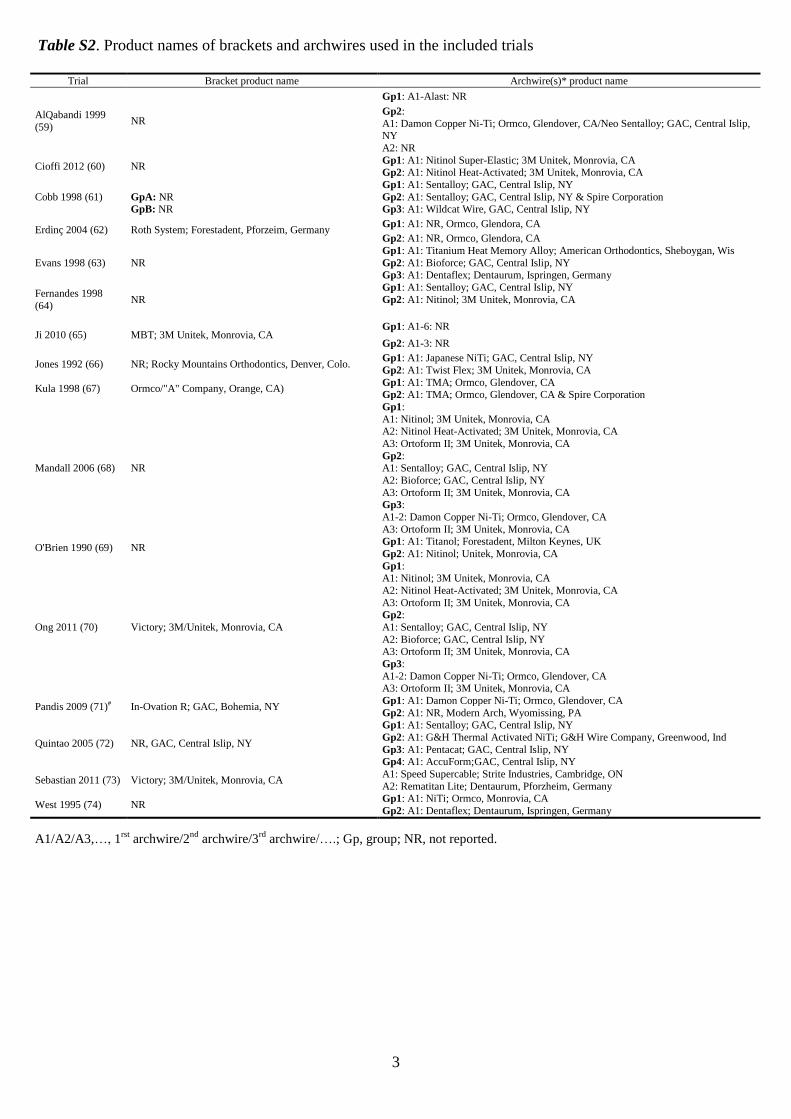
3
Table S2. Product names of brackets and archwires used in the included trials
Trial Bracket product name Archwire(s)* product name
AlQabandi 1999
(59) NR
Gp1: A1-Alast: NR
Gp2:
A1: Damon Copper Ni-Ti; Ormco, Glendover, CA/Neo Sentalloy; GAC, Central Islip, NY
A2: NR
Cioffi 2012 (60) NR Gp1: A1: Nitinol Super-Elastic; 3M Unitek, Monrovia, CA Gp2: A1: Nitinol Heat-Activated; 3M Unitek, Monrovia, CA
Cobb 1998 (61) Gp1: A1: Sentalloy; GAC, Central Islip, NY
GpA: NR Gp2: A1: Sentalloy; GAC, Central Islip, NY & Spire Corporation GpB: NR Gp3: A1: Wildcat Wire, GAC, Central Islip, NY
Erdinç 2004 (62) Roth System; Forestadent, Pforzeim, Germany Gp1: A1: NR, Ormco, Glendora, CA
Gp2: A1: NR, Ormco, Glendora, CA
Evans 1998 (63) NR
Gp1: A1: Titanium Heat Memory Alloy; American Orthodontics, Sheboygan, Wis
Gp2: A1: Bioforce; GAC, Central Islip, NY Gp3: A1: Dentaflex; Dentaurum, Ispringen, Germany
Fernandes 1998
(64) NR
Gp1: A1: Sentalloy; GAC, Central Islip, NY
Gp2: A1: Nitinol; 3M Unitek, Monrovia, CA
Ji 2010 (65) MBT; 3M Unitek, Monrovia, CA Gp1: A1-6: NR
Gp2: A1-3: NR
Jones 1992 (66) NR; Rocky Mountains Orthodontics, Denver, Colo. Gp1: A1: Japanese NiTi; GAC, Central Islip, NY
Gp2: A1: Twist Flex; 3M Unitek, Monrovia, CA
Kula 1998 (67) Ormco/"A" Company, Orange, CA) Gp1: A1: TMA; Ormco, Glendover, CA Gp2: A1: TMA; Ormco, Glendover, CA & Spire Corporation
Mandall 2006 (68) NR
Gp1:
A1: Nitinol; 3M Unitek, Monrovia, CA A2: Nitinol Heat-Activated; 3M Unitek, Monrovia, CA
A3: Ortoform II; 3M Unitek, Monrovia, CA
Gp2: A1: Sentalloy; GAC, Central Islip, NY
A2: Bioforce; GAC, Central Islip, NY
A3: Ortoform II; 3M Unitek, Monrovia, CA Gp3:
A1-2: Damon Copper Ni-Ti; Ormco, Glendover, CA
A3: Ortoform II; 3M Unitek, Monrovia, CA
O'Brien 1990 (69) NR Gp1: A1: Titanol; Forestadent, Milton Keynes, UK
Gp2: A1: Nitinol; Unitek, Monrovia, CA
Ong 2011 (70) Victory; 3M/Unitek, Monrovia, CA
Gp1: A1: Nitinol; 3M Unitek, Monrovia, CA
A2: Nitinol Heat-Activated; 3M Unitek, Monrovia, CA
A3: Ortoform II; 3M Unitek, Monrovia, CA Gp2:
A1: Sentalloy; GAC, Central Islip, NY
A2: Bioforce; GAC, Central Islip, NY A3: Ortoform II; 3M Unitek, Monrovia, CA
Gp3:
A1-2: Damon Copper Ni-Ti; Ormco, Glendover, CA A3: Ortoform II; 3M Unitek, Monrovia, CA
Pandis 2009 (71)# In-Ovation R; GAC, Bohemia, NY Gp1: A1: Damon Copper Ni-Ti; Ormco, Glendover, CA
Gp2: A1: NR, Modern Arch, Wyomissing, PA
Quintao 2005 (72) NR, GAC, Central Islip, NY
Gp1: A1: Sentalloy; GAC, Central Islip, NY
Gp2: A1: G&H Thermal Activated NiTi; G&H Wire Company, Greenwood, Ind
Gp3: A1: Pentacat; GAC, Central Islip, NY Gp4: A1: AccuForm;GAC, Central Islip, NY
Sebastian 2011 (73) Victory; 3M/Unitek, Monrovia, CA A1: Speed Supercable; Strite Industries, Cambridge, ON
A2: Rematitan Lite; Dentaurum, Pforzheim, Germany
West 1995 (74) NR Gp1: A1: NiTi; Ormco, Monrovia, CA
Gp2: A1: Dentaflex; Dentaurum, Ispringen, Germany
A1/A2/A3,…, 1rst
archwire/2nd
archwire/3rd
archwire/….; Gp, group; NR, not reported.
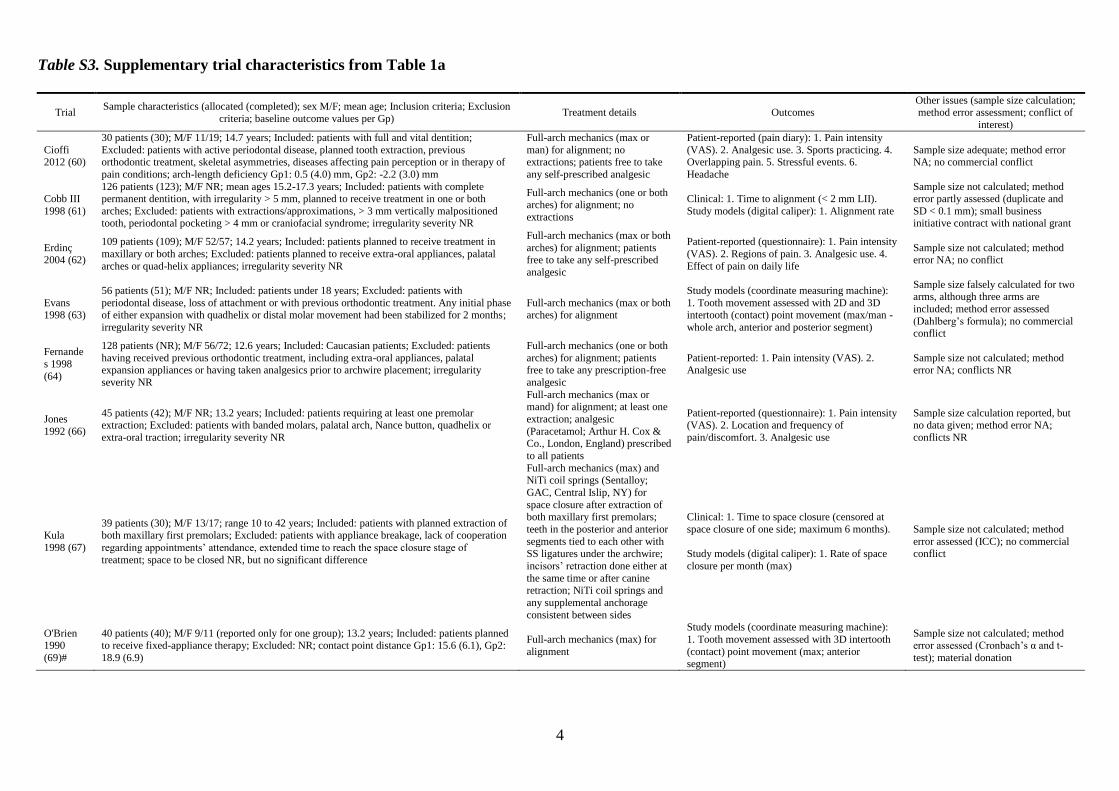
4
Table S3. Supplementary trial characteristics from Table 1a
Trial Sample characteristics (allocated (completed); sex M/F; mean age; Inclusion criteria; Exclusion
criteria; baseline outcome values per Gp) Treatment details Outcomes
Other issues (sample size calculation; method error assessment; conflict of
interest)
Cioffi 2012 (60)
30 patients (30); M/F 11/19; 14.7 years; Included: patients with full and vital dentition;
Excluded: patients with active periodontal disease, planned tooth extraction, previous orthodontic treatment, skeletal asymmetries, diseases affecting pain perception or in therapy of
pain conditions; arch-length deficiency Gp1: 0.5 (4.0) mm, Gp2: -2.2 (3.0) mm
Full-arch mechanics (max or
man) for alignment; no extractions; patients free to take
any self-prescribed analgesic
Patient-reported (pain diary): 1. Pain intensity
(VAS). 2. Analgesic use. 3. Sports practicing. 4. Overlapping pain. 5. Stressful events. 6.
Headache
Sample size adequate; method error NA; no commercial conflict
Cobb III
1998 (61)
126 patients (123); M/F NR; mean ages 15.2-17.3 years; Included: patients with complete permanent dentition, with irregularity > 5 mm, planned to receive treatment in one or both
arches; Excluded: patients with extractions/approximations, > 3 mm vertically malpositioned tooth, periodontal pocketing > 4 mm or craniofacial syndrome; irregularity severity NR
Full-arch mechanics (one or both arches) for alignment; no
extractions
Clinical: 1. Time to alignment (< 2 mm LII).
Study models (digital caliper): 1. Alignment rate
Sample size not calculated; method error partly assessed (duplicate and
SD < 0.1 mm); small business initiative contract with national grant
Erdinç 2004 (62)
109 patients (109); M/F 52/57; 14.2 years; Included: patients planned to receive treatment in
maxillary or both arches; Excluded: patients planned to receive extra-oral appliances, palatal
arches or quad-helix appliances; irregularity severity NR
Full-arch mechanics (max or both
arches) for alignment; patients free to take any self-prescribed
analgesic
Patient-reported (questionnaire): 1. Pain intensity
(VAS). 2. Regions of pain. 3. Analgesic use. 4.
Effect of pain on daily life
Sample size not calculated; method error NA; no conflict
Evans 1998 (63)
56 patients (51); M/F NR; Included: patients under 18 years; Excluded: patients with
periodontal disease, loss of attachment or with previous orthodontic treatment. Any initial phase of either expansion with quadhelix or distal molar movement had been stabilized for 2 months;
irregularity severity NR
Full-arch mechanics (max or both arches) for alignment
Study models (coordinate measuring machine):
1. Tooth movement assessed with 2D and 3D intertooth (contact) point movement (max/man -
whole arch, anterior and posterior segment)
Sample size falsely calculated for two arms, although three arms are
included; method error assessed
(Dahlberg’s formula); no commercial conflict
Fernande
s 1998
(64)
128 patients (NR); M/F 56/72; 12.6 years; Included: Caucasian patients; Excluded: patients
having received previous orthodontic treatment, including extra-oral appliances, palatal expansion appliances or having taken analgesics prior to archwire placement; irregularity
severity NR
Full-arch mechanics (one or both
arches) for alignment; patients free to take any prescription-free
analgesic
Patient-reported: 1. Pain intensity (VAS). 2. Analgesic use
Sample size not calculated; method error NA; conflicts NR
Jones
1992 (66)
45 patients (42); M/F NR; 13.2 years; Included: patients requiring at least one premolar extraction; Excluded: patients with banded molars, palatal arch, Nance button, quadhelix or
extra-oral traction; irregularity severity NR
Full-arch mechanics (max or mand) for alignment; at least one
extraction; analgesic
(Paracetamol; Arthur H. Cox & Co., London, England) prescribed
to all patients
Patient-reported (questionnaire): 1. Pain intensity (VAS). 2. Location and frequency of
pain/discomfort. 3. Analgesic use
Sample size calculation reported, but no data given; method error NA;
conflicts NR
Kula
1998 (67)
39 patients (30); M/F 13/17; range 10 to 42 years; Included: patients with planned extraction of both maxillary first premolars; Excluded: patients with appliance breakage, lack of cooperation
regarding appointments’ attendance, extended time to reach the space closure stage of
treatment; space to be closed NR, but no significant difference
Full-arch mechanics (max) and NiTi coil springs (Sentalloy;
GAC, Central Islip, NY) for
space closure after extraction of both maxillary first premolars;
teeth in the posterior and anterior
segments tied to each other with
SS ligatures under the archwire;
incisors’ retraction done either at
the same time or after canine retraction; NiTi coil springs and
any supplemental anchorage
consistent between sides
Clinical: 1. Time to space closure (censored at
space closure of one side; maximum 6 months).
Study models (digital caliper): 1. Rate of space
closure per month (max)
Sample size not calculated; method
error assessed (ICC); no commercial
conflict
O'Brien 1990
(69)#
40 patients (40); M/F 9/11 (reported only for one group); 13.2 years; Included: patients planned to receive fixed-appliance therapy; Excluded: NR; contact point distance Gp1: 15.6 (6.1), Gp2:
18.9 (6.9)
Full-arch mechanics (max) for
alignment
Study models (coordinate measuring machine):
1. Tooth movement assessed with 3D intertooth
(contact) point movement (max; anterior segment)
Sample size not calculated; method error assessed (Cronbach’s α and t-
test); material donation
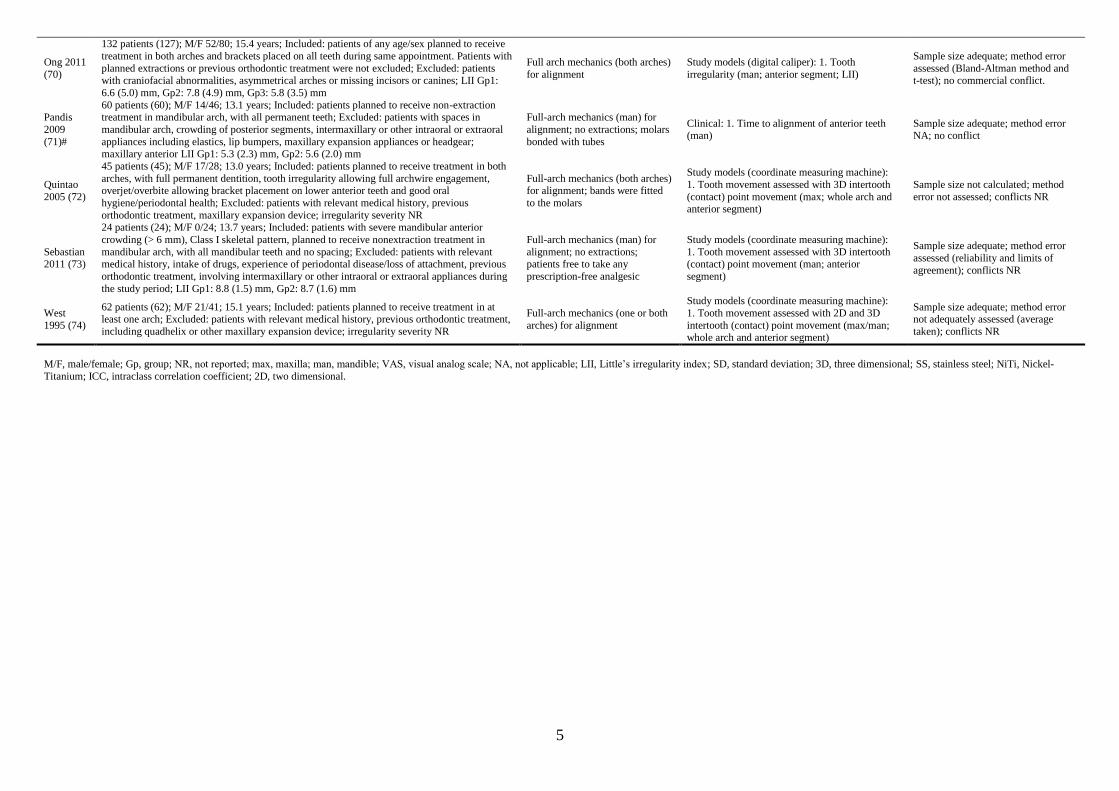
5
Ong 2011
(70)
132 patients (127); M/F 52/80; 15.4 years; Included: patients of any age/sex planned to receive
treatment in both arches and brackets placed on all teeth during same appointment. Patients with
planned extractions or previous orthodontic treatment were not excluded; Excluded: patients
with craniofacial abnormalities, asymmetrical arches or missing incisors or canines; LII Gp1:
6.6 (5.0) mm, Gp2: 7.8 (4.9) mm, Gp3: 5.8 (3.5) mm
Full arch mechanics (both arches)
for alignment
Study models (digital caliper): 1. Tooth
irregularity (man; anterior segment; LII)
Sample size adequate; method error
assessed (Bland-Altman method and
t-test); no commercial conflict.
Pandis
2009
(71)#
60 patients (60); M/F 14/46; 13.1 years; Included: patients planned to receive non-extraction treatment in mandibular arch, with all permanent teeth; Excluded: patients with spaces in
mandibular arch, crowding of posterior segments, intermaxillary or other intraoral or extraoral
appliances including elastics, lip bumpers, maxillary expansion appliances or headgear; maxillary anterior LII Gp1: 5.3 (2.3) mm, Gp2: 5.6 (2.0) mm
Full-arch mechanics (man) for
alignment; no extractions; molars
bonded with tubes
Clinical: 1. Time to alignment of anterior teeth (man)
Sample size adequate; method error NA; no conflict
Quintao
2005 (72)
45 patients (45); M/F 17/28; 13.0 years; Included: patients planned to receive treatment in both
arches, with full permanent dentition, tooth irregularity allowing full archwire engagement, overjet/overbite allowing bracket placement on lower anterior teeth and good oral
hygiene/periodontal health; Excluded: patients with relevant medical history, previous
orthodontic treatment, maxillary expansion device; irregularity severity NR
Full-arch mechanics (both arches) for alignment; bands were fitted
to the molars
Study models (coordinate measuring machine):
1. Tooth movement assessed with 3D intertooth
(contact) point movement (max; whole arch and anterior segment)
Sample size not calculated; method
error not assessed; conflicts NR
Sebastian 2011 (73)
24 patients (24); M/F 0/24; 13.7 years; Included: patients with severe mandibular anterior
crowding (> 6 mm), Class I skeletal pattern, planned to receive nonextraction treatment in
mandibular arch, with all mandibular teeth and no spacing; Excluded: patients with relevant medical history, intake of drugs, experience of periodontal disease/loss of attachment, previous
orthodontic treatment, involving intermaxillary or other intraoral or extraoral appliances during
the study period; LII Gp1: 8.8 (1.5) mm, Gp2: 8.7 (1.6) mm
Full-arch mechanics (man) for
alignment; no extractions; patients free to take any
prescription-free analgesic
Study models (coordinate measuring machine):
1. Tooth movement assessed with 3D intertooth (contact) point movement (man; anterior
segment)
Sample size adequate; method error
assessed (reliability and limits of
agreement); conflicts NR
West
1995 (74)
62 patients (62); M/F 21/41; 15.1 years; Included: patients planned to receive treatment in at least one arch; Excluded: patients with relevant medical history, previous orthodontic treatment,
including quadhelix or other maxillary expansion device; irregularity severity NR
Full-arch mechanics (one or both
arches) for alignment
Study models (coordinate measuring machine):
1. Tooth movement assessed with 2D and 3D
intertooth (contact) point movement (max/man; whole arch and anterior segment)
Sample size adequate; method error not adequately assessed (average
taken); conflicts NR
M/F, male/female; Gp, group; NR, not reported; max, maxilla; man, mandible; VAS, visual analog scale; NA, not applicable; LII, Little’s irregularity index; SD, standard deviation; 3D, three dimensional; SS, stainless steel; NiTi, Nickel-
Titanium; ICC, intraclass correlation coefficient; 2D, two dimensional.

6
Table S4. Supplementary trial characteristics from Table 1b
Trial Sample characteristics (allocated (completed); sex M/F; mean age;
Inclusion criteria; Exclusion criteria; baseline outcome values per Gp) Treatment details Outcomes
Other issues (sample size calculation; method error
assessment; conflict of interest)
AlQaban
di 1999
(59)
28 patients (28); M/F 14/14; 14.6 years; Included: patients with crowding
≤ 3 mm, moderate to deep curve of Spee, planned to receive non-extraction therapy on the mandibular arch; Excluded: NR; malocclusions
by group Class I/Class II Gp1: 17%/83%, Gp2: 19%/81%
Full-arch mechanics (man) for leveling the
curve of Spee; no
extractions; archwire not chinched
Study models: 1. Arch depth from the canines (man). 2. Intercanine width
(man). 3. Arch depth from the molars (man). 4. Depth of the curve of Spee. 5. Amount of crowding (man anterior segment)
Radiographic (cephalometric analysis with Björk’s superimposition): 1. Incisor angulation (man). 2. Change in axial inclination of the incisor
(man). 3. Distance of the center of rotation of the incisor (man)
Post-hoc sample calculation
showed that power probably inadequate; method error assessed
(t-test); material donation
Ji 2010
(65)
80 patients (80); M/F 40/40; 12-14 years; Included: patients with
complete permanent dentition and Class I malocclusion planned to
receive treatment with tooth extractions; Excluded: patients with
previous orthodontic or orthognathic treatment, TMJDs, history of
periodontal disease, CLP or any other defect of the tooth or bone tissues,
bad oral habits; irregularity severity NR
Full-arch mechanics
(arch NR) for alignment
Clinical: 1. Alignment duration. 2. Treatment duration. 3. Number of
appointments. 4. Bracket failures. 5. Archwire breakage
Sample size not calculated; method
error NA; no commercial conflict
Mandall 2006
(68)#
154 patients (129); M/F 62/92; 14.2 years; Included: patients under 18
years planned to receive therapy on both arches, with no extractions or
up to four premolar extractions; Excluded: patients wit pain from other dental or medical condition that could affect the reported discomfort,
planned to be treated with palatal arch, headgear or quadhelix at the same
visit that the initial archwire was placed; LII (man) Gp1: 6.5 (5.1) mm, Gp2: 5.7 (4.3) mm, Gp3: 6.1 (4.8)
Full-arch mechanics
(both arches); possible
premolar extractions; history of trauma,
central incisor filling or
history of EARR were recorded
Clinical: 1. Time to reach the working archwire. 2. Number of
appointments
Radiographic (periapical radiograph): 1. EARR of the central incisor
(max)
Patient-reported (questionnaire): 1. Pain intensity (LS).
Sample size adequate; method error assessed (ICC); no
commercial conflict
Ong 2011 (70)
132 patients (127); M/F 52/80; 15.4 years; Included: patients of any
age/sex planned to receive treatment on both arches and had brackets
placed on all the teeth at the same appointment. Patients with planned
extractions or previous orthodontic treatment not excluded; Excluded:
patients with craniofacial abnormalities, asymmetrical arches or missing incisors or canines; LII Gp1: 6.6 (5.0) mm, Gp2: 7.8 (4.9) mm, Gp3: 5.8
(3.5) mm
Full arch mechanics
(both arches) for
alignment
Clinical: 1. Time to reach the working archwire (man)
Study models (digital caliper): 1. Tooth irregularity (man; anterior
segment; LII). 2. Intercanine width (man)
Patient-reported (questionnaire): 1. Pain intensity (total and at archwire
change; LS)
Sample size adequate; method
error assessed (Bland-Altman method and t-test); no commercial
conflict
M/F, male/female; Gp, group; NR, not reported; man, mandible; TMJD, temporomandibular joint disorder; CLP, cleft lip palate; NA, not applicable; LII, Little’s irregularity index; EARR, external apical root resorption; max,
maxilla; LS, Likert scale; ICC, intraclass correlation coefficient.
Top Related
Copyright © 2022 FDOKUMEN

