







Bahasa
Halaman
Hukum


Musculoskeletal side effects
of aromatase inhibitors
treatment in women with
breast cancer
Author: Maria Rodríguez Sanz
DOCTORAL THESIS UPF YEAR 2016
Supervisors: Dr. Natalia Garcia Giralt and Dr. Xavier Nogués Solán
Tutor: Dr. Josep Mª Antó Boqué
Musculoskeletal research group
Inflammatory and Cardiovascular Research Program
Hospital del Mar Medical Research Institute (IMIM)

iii
To my family and friends,


v
ACKNOWLEDGMENTS
First of all, I woul” like to a“knowle”ge my PhD supervisors, Dr. Natalia
Gar“ia Giralt an” Dr. Xavier Nogués Solan for giving me the opportunity to
join their laboratory an” for their ex“ellent gui”an“e. I woul” also like to
thank my “olleagues at the URFOA: Laura De Ugarte, Guy Yoskovitz, Sergi
Ariño, Laura Tio, Anna Martín, Marta Pine”a, Enrique Caro, Ivan Valle”or,
Selene Luna, Anabela Areias...
Gra“ias a Laura ”e Ugarte Corbalán (The Prin“ess), por “ompartir “a”a
minuto ”el “amino, ”es”e el primer hasta el último ”ía. Contigo las
”ifi“ulta”es han si”o menos ”ifí“iles, aunque las “ajas ”e kleenex se a“aben
antes. Las ané“”otas que “ompartimos son innumerables y jamás las
olvi”aré. Deseo que se “umplan to”as tus metas profesionales para el
futuro: ingeniera ”e biomateriales, ”iseña”ora ”e mo”a, “oreβgrafa,
”ete“tive priva”o por las no“hes, mo”elo, fisioterapeuta ”e juga”ores ”e
alto ren”imiento, jui“y girl en Hawaï... (seguro que alguna se me olvi”a). Eso
sí, por favor, ¡bajo ningún “on“epto te hagas pastelera, ni ”ejes que yo lo
sea!. Creo que la etapa que ahora llega será maravillosa, pero hasta nueva
or”en, ya sabes: ¡uñitas, me“hitas y más uñitas!.

Gra“ias a Guy Yoskovitz (alias Dios) por enseñarnos tantas “osas “on tu
pa“ien“ia infinita. Gra“ias por haberme he“ho, no sβlo “reer en otras formas
”e “on“ebir la familia, sino a”emás presumir ”e haber teni”o “omo
“ompañero a un pa”re maravilloso e inmejorable. Gra“ias in“luso por tus
listas ”e análisis esta”ísti“os pen”ientes que pare“ían repro”u“irse por
biparti“iβn. ¡Nene, nene! Te e“hamos mu“hísimo ”e menos.
Gra“ias a Sergi Ariño (“atalán ”e origen pero “ubano ”e alma), por tanta
risa. Pare“e que los enanitos nos están ”an”o un respiro a ambos ¿no?.
Finalmente el Papa Noel ”e la esquina “umpliβ “on su trabajo. Bueno, o eso, o
están pillan”o “arrerilla para la venganza más gran”e ”e la historia XD. EL
humor ”e URFOA se que”β “ojo “uan”o te fuiste, pero me alegro mu“ho ”e
que vayas ha“ién”ote un hue“o en la farán”ula.
Gra“ias a Anna Martín, ¡por esas inye““iones ”e energía fresquísima!. Por tu
alegría ”esbor”ante “a”a vez que entras por la puerta. ¡Hello!. No sé si en tu
trajín ”e ir y venir te habrás lleva”o mu“ho ”e URFOA, pero si estoy segura
”e que has apren”i”o algo muy importante: en el siglo XV antes ”e Cristo ya
había gente en el mun”o. Espero seguir vién”ote mu“ho tiempo más.
Gra“ias a las más re“ientes aunque fuga“es in“orpora“iones: Enrique Caro,
Marta Pine”a e Iván Valle”or. Aunque hay personas a las que “uesta mu“ho
reemplazar , to”os vosotros habéis supera”o las expe“tativas. Marta
Pine”a, mi su“esora, te ”eseo mu“ha suerte en tu nueva etapa. A ti también
Enrique Caro. A”miro tu toleran“ia y tus ganas ”e lu“har por un mun”o
mejor. También te ”oy las gra“ias por ha“erme ver que existen personas
igual (¡¡¡¡¡ o mu“hísimo más!!! XD) ”e ”espista”as que yo (jeje). A ti, Iván
Valle”or, gra“ias por to”as las “ari“aturas en papel y por to”os los buenos

vii
momentos ”e telenovela. Re“uer”a: Respon”e al nombre ”e Soraya .
Gra“ias a Aina, que está lejos, pero apren”ien”o mu“hísimo. Me alegro ”e
que estés vivien”o miles ”e experien“ias. Espero que tú también nos e“hes
mu“ho ”e menos a nosotros y al “ajβn ”e Guy. ¡¡¡¡Vuelve algún ”ia!!!
Gra“ias a Lara ”e Llobet por reapare“er, y por juntarte “on to”os nosotros.
Eres una más ”e nuestra pequeña familia.
Gra“ias a mis amigos fuera ”e URFOA: Carmen, Virginia, Moki, Quique, Osqui,
Canu, Esti, Alain, Simone, Ali“ia, Naty... A to”os: gra“ias por formar parte ”e
mi vi”a. Mis logros también tienen una parte ”e “a”a uno ”e vosotros. Sé
que nos que”an mu“hísimas aventuras juntos, así que... ¡Nos vemos el fin ”e
semana! :D
Gra“ias a Jor”an, por millones ”e “osas que no “abrían en estas páginas. Has
si”o uno ”e los pilares más importantes ”urante to”o este pro“eso. Espero
que sigamos apren”ien”o el uno ”el otro por mu“hísimo más tiempo.
Y por último y más importante, gra“ias a mis pa”res, que me han brin”a”o
to”o el apoyo físi“o y mental ne“esario para llevar a”elante esta exigente
etapa ”e mi vi”a. Sin ellos, ver”a”eramente no habría si”o posible.


ix
ABSTRACT
The intro”u“tion of aromatase inhibitors (AI) therapy for the treatment of
postmenopausal women with hormone re“eptor-positive breast “an“er has
le” to a signifi“ant improvement of patient survival. However, AI-asso“iate”
si”e effe“ts, whose etiology is still unexplaine”, “ompromise quality of life
an” lea” to non-“omplian“e, representing a signifi“ant bur”en. In this thesis,
we fo“us on mus“uloskeletal symptoms, essentially joint pain an” bone
mineral ”ensity loss with the asso“iate” in“rease in fra“ture risk. In a “ontext
of every”ay “lini“al pra“ti“e, we ”es“ribe the evolution of these out“omes
”uring AI therapy. A signifi“ant in“rease in the intensity of joint pain has
been ”ete“te”. Patients also experien“e an a““elerate” bone mineral ”ensity
loss whi“h is ”imme” by oral bisphosphonates. Our resear“h lea”s us to state
that the geneti“ ba“kgroun” of the in”ivi”ual is essential in this setting. Thus,
polymorphi“ variants in genes involve” in steroi” an” vitamin D metaboli“
pathways may “ontribute to the onset an”/or intensity of these un”esirable
symptoms. Furthermore, bone is raise” for the first time as a potential
steroi”ogeni“ tissue. The results are promising an” reveal new insights into
the fun“tioning of these mus“uloskeletal events.


xi
RESUMEN
La terapia “on inhibi”ores ”e aromatasa (IA) para el tratamiento ”el “án“er
”e mama positivo para re“eptor ”e estrβgenos en mujeres
postmenopáusi“as ha pro”u“i”o un aumento signifi“ativo ”e la
superviven“ia. No obstante, los efe“tos se“un”arios aso“ia”os a este
tratamiento, “uya etiología es to”avía ”es“ono“i”a, “omprometen la “ali”a”
”e vi”a ”e las pa“ientes y ”isminuyen la a”heren“ia al tratamiento,
representan”o un gran in“onveniente. Esta tesis se enfo“a en los síntomas
mus“uloesqueléti“os, espe“ífi“amente el ”olor arti“ular y la pér”i”a ”e
”ensi”a” mineral βsea “on el “onse“uente aumento ”el riesgo ”e fra“tura. Se
”es“ribe la evolu“iβn ”e estos síntomas ”urante la terapia “on IA en la
prá“ti“a “líni“a habitual. Se ha ”ete“ta”o un aumento en la intensi”a” ”el
”olor arti“ular. A”emás las pa“ientes experimentan una pér”i”a a“elera”a ”e
la ”ensi”a” mineral βsea, que pue”e ser atenua”a “on bifosfonatos orales.
Nuestros estu”ios nos permiten afirmar que el “omponente genéti“o ”el
in”ivi”uo es esen“ial en este “ontexto. Así, variantes polimβrfi“as en genes
involu“ra”os en las vías metabβli“as ”e los estrβgenos y la vitamina D pue”en
“ontribuir a la apari“iβn y/o intensi”a” ”e estos efe“tos a”versos. A”emás, el
hueso se plantea por primera vez “omo un teji”o esteroi”ogéni“o poten“ial.
Los resulta”os son promete”ores y revelan nuevos “ono“imientos a“er“a ”el
fun“ionamiento ”e estas manifesta“iones mus“uloesqueléti“as.


xiii
PREFACE
The work presente” in this ”o“toral thesis was “arrie” out in the
Inflammatory an” Car”iovas“ular Disor”ers Program of Hospital ”el Mar
Me”i“al Resear“h Institute (IMIM) in Bar“elona, Spain, un”er the supervision of
Dr. Natalia Gar“ia Giralt an” Dr. Xavier Nogués Solán.
The “ontent of this thesis provi”es novel insights on the “ausal me“hanisms
un”erlying the si”e effe“ts asso“iate” to AI treatment in postmenopausal
women with breast “an“er. The results presente” here illustrate an important
role for the geneti“ ba“kgroun” in the onset an”/or intensity of joint pain
an” bone mineral ”ensity loss asso“iate” to this me”i“ation.


xv
CONTENTS
V ACKNOWLEDGEMENTS
IX ABSTRACT
XI RESUMEN
XIII PREFACE
XV GLOSSARY
1 CHAPTER 1- INTRODUCTION 3 1. BREAST CANCER
4 1.1. BREAST CANCER EPIDEMIOLOGY
6 2. BREAST CANCER CLASSIFICATION
6 2.1. RECEPTOR STATUS
6 2.1.1 Human epi”ermal growth fa“tor re“eptor-2 (HER2)
7 2.2.1. Hormonal re“eptors
9 3. RISK FACTORS FOR BREAST CANCER
9 3.1. GENETIC RISK FACTORS
9 3.1.1. High penetran“e genes
9 3.1.2. Low penetran“e genes
10 3.2. HORMONAL RISK FACTORS
10 3.2.1. Repro”u“tive fa“tors
11 3.2.2. Other hormonal fa“tors

xvi
12 3.3. NON-HORMONAL RISK FACTORS
12 3.3.1. Age
12 3.3.2. Geographi“al variation an” Ethni“ity
13 3.3.3. Ra”iation
13 3.3.4. Previous benign ”isease
14 3.3.5. Lifestyle an” ”ietary fa“tors
15 4. ESTROGENS AND BREAST CANCER
15 4.1. STEROID BIOSYNTHESIS
15 4.1.1. Cholesterol transport
16 4.1.2. Cyto“hrome P450 an” HSDs
17 4.1.3. Steroi”ogenesis
19 4.2. STEROIDOGENIC TISSUES AND REGULATION
22 4.3. STEROIDS IN POSTMENOPAUSAL WOMEN
24 4.4. STEROID MECHANISMS OF BREAST CARCINOGENESIS
24 4.4.1. ER signalling.
25 4.4.2. Pro”u“ts of estrogen metabolism
27 5. BREAST CANCER THERAPIES
28 5.1. SURGERY
28 5.2. RADIOTHERAPY
28 5.3. CHEMOTHERAPY
29 5.4. BIOLOGICAL THERAPY
29 5.5. ENDOCRINE THERAPY
29 5.5.1. Surgi“al Oophore“tomy
30 5.5.2. LH-RH (Luteinizing Hormone-Releasing Hormone) Analogues
30 5.5.3. Sele“tive estrogen re“eptor mo”ulators (SERMs) an”
”ownregulators (SERDs)
32 5.5.4. Aromatase Inhibitors (AI)
36 6. SECONDARY EFFECTS OF AI THERAPY
36 6.1. CARDIOVASCULAR RISK AND LIPID METABOLISM
37 6.2. MUSCULOESKELETAL EFFECTS
38 6.2.2. Etiology of AIA
40 6.2.3. AIA signifi“an“e: a”heren“e, treatment effi“a“y an” mortality
41 6.2.4. AIA management

xvii
42 6.3. OSTEOPOROSIS AND RISK OF FRACTURE
44 6.3.1. Bone stru“ture
46 6.3.2. Bone matrix
47 6.3.3. Osteoblasts
47 6.3.4. Osteo“ytes
48 6.3.5. Osteo“lasts
48 6.3.6. Bone remo”elling
50 6.3.7. Mole“ular effe“ts of estrogen ”efi“ien“y on remo”elling
52 6.3.8. Aromatase inhibitor in”u“e” bone loss (AIBL) an” fra“ture risk.
54 7. AIBL MANAGEMENT
54 7.1. LIFESTYLE INTERVENTIONS
54 7.2. BONE LOSS SCREENING AND MONITORING
56 7.3. PHARMACOLOGICAL THERAPY: BISPHOSPHONATES (BP)
56 7.3.1. Me“hanism of a“tion
58 7.3.2. Clini“al role of BP
58 7.4. FARMACOLOGICAL THERAPY: DENOSUMAB
59 7.5. THE ROLE OF BONE MICROARCHITECTURE IN FRACTURE RISK:
TRABECULAR BONE SCORE (TBS)
63 8. VITAMIN D AND AI ADVERSE EFFECTS
63 8.1. SYNTHESIS OF VITAMIN D
66 8.2. EFFECTS OF VITAMIN D ON AIA
67 8.3. EFFECTS OF VITAMIN D ON AIBL
69 9. GENETIC STUDY OF COMPLEX TRAITS
70 9.1. GENETIC BASIS OF AIA
71 9.2. GENETIC BASIS OF AIBL
73 CHAPTER 2- RESULTS 75 Manuscript 1. Geneti“ ”eterminants of aromatase inhibitor-relate”
arthralgia: the B-ABLE “ohort stu”y
89 Manuscript 2. AI-relate” BMD variation in a“tual pra“ti“e “on”itions: a
prospe“tive “ohort stu”y
xviii
101 Manuscript 3. CYP11A1 expression in bone is asso“iate” with aromatase
inhibitor-relate” bone loss
115 Manuscript 4. Evolu“iβn ”e la DMO ”urante el tratamiento “on inhibi”ores ”e
aromatasa y su rela“iβn “on el gen CYP11A1: estu”io prospe“tivo ”e la
“ohorte B-ABLE
125 Manuscript 5. TBS an” BMD at the en” of AI-therapy: a prospe“tive stu”y of
the B-ABLE “ohort
135 CHAPTER 3- DISCUSSION 138 JOINT PAIN IN THE B-ABLE COHORT
141 BMD EVOLUTION IN THE B-ABLE COHORT
146 EFFECTS OF BP ON BMD EVOLUTION
148 BONE MICROARCHITECTURE: A POSSIBLE ROLE FOR TBS
150 HIGH VARIABILITY IN THE STUDIED OUTCOMES
155 INTERINDIVIDUAL DIFFERENCES IN SEX STEROID LEVELS: A POSSIBLE
UNDERLYING MECHANISM FOR VARIATION IN AI SECONDARY EFFECTS
158 THE ROLE OF LOCAL ESTROGEN SYNTHESIS
159 P450SCC IN BONE: FURTHER UNKNOWN FUNCTIONS?
160 VITAMIN D ACTIVATION AND AI SECONDARY EFFECTS
161 THE CHALLENGES AHEAD OF THE STUDY
162 I”entifi“ation of “ausal sequen“e variants
163 Sex steroi” hormone levels in AI-treate” women
164 Bio“hemi“al assessment of bone remo”elling an” “artilage ”egra”ation
”uring AI treatment
167 CHAPTER 4- CONCLUSSIONS
169 CONCLUSSIONS
171 BIBLIOGRAPHY

xix
GLOSSARY
Abbreviation Meaning
17 HSDs 17 -hy”roxysteroi” ”ehy”rogenases enzymes
3 HSD 3 -hy”roxysteroi” ”ehy”rogenase
ACTH A”reno“orti“otropi“ hormone
AI Aromatase inhibitors
AIA AI-relate” arthralgia
AIBL Aromatase inhibitor in”u“e” bone loss
ASCO Ameri“an So“iety of Clini“al On“ology
ATAC Arimi”ex, Tamoxifen, Alone or in Combination trial
BMD Bone mineral ”ensity
BMI Bo”y mass in”ex
BMU Basi“ multi“ellular unit
BP Bisphosphonates
BTM Bone turnover markers
COMT Cate“hol-O-methyltransferase enzyme
CV Coeffi“ient of variation
CYPs Cyto“hrome P450s
DBP Vitamin D bin”ing protein
DHC Dehy”ro“holesterol
DHEA Dehy”roepian”rosterone
DHEA-S Dehy”roepian”rosterone-sulphate
DHT Dihy”rotestosterone
DXA Dual-energy X-ray absorptiometry

xx
ECM Extra“ellular matrix
ER Estrogen re“eptor
FGF Fibroblast growth fa“tor
FN Femoral ne“k
FSH Folli“ular stimulating hormone
GnRH Gona”otrophin releasing hormone
GWAS Genome wi”e asso“iation stu”y
HER-2 Human epi”ermal growth fa“tor re“eptor-2
HRT Hormone repla“ement therapy
HSDs Hy”roxysteroi” ”ehy”rogenases
IGF Insulin growth fa“tor
IL Interleukin
INF-ɣ Interferon gamma
IOM Institute of me”i“ine
LBD Ligan” bin”ing ”omain
LH Luteinizing hormone
LH-RH Luteinizing hormone-Releasing Hormone
LRP5 Low-”ensity lipoprotein re“eptor-relate” protein 5 gene
LS Lumbar spine
M-CSF Ma“rophage “olony stimulating fa“tor
NAD Ni“otinami”e a”enine ”inu“leoti”e phosphate
NADPH Ni“otinami”e a”enine ”inu“leoti”e phosphate
NCI National Can“er Institute
OPG Osteoprotegerin
P450“17 17 -hy”roxylase/17,20-Lyase
P450s““ Cholesterol si”e-“hain “leavage enzyme
PPI Inorgani“ pyrophosphate
PR Progesterone re“eptor
PTH Parathyroi” hormone
RANK-L Re“eptor a“tivator of nu“lear fa“tor-κ
RCT Ran”omize” “ontrol trial
xxi
SEER Surveillan“e, Epi”emiology, an” En” Results
SERDs Sele“tive estrogen re“eptor ”ownregulators
SERMs Sele“tive estrogen re“eptor mo”ulators
SNPs Single nu“leoti”e polymorphisms
SRD5 5 -re”u“tase enzymes
StAR Steroi”ogeni“ a“ute regulatory protein
SULT Sulfotransferase enzymes
TBS Trabe“ular bone s“ore
TCL1A T-“ell leukaemia 1A gene
TGF- Transforming growth fa“tor beta
TNF- Tumour ne“rosis fa“tor alpha
VAS Visual analogi“ s“ale
VDR Vitamin D re“eptor
VitD2 Vitamin D2
VitD3 Vitamin D3

1
Chapter1
Dios no juega a los ”a”os “on el Universo
Albert Einstein
INTRODUCTION

3
INTRODUCTION
1. BREAST CANCER
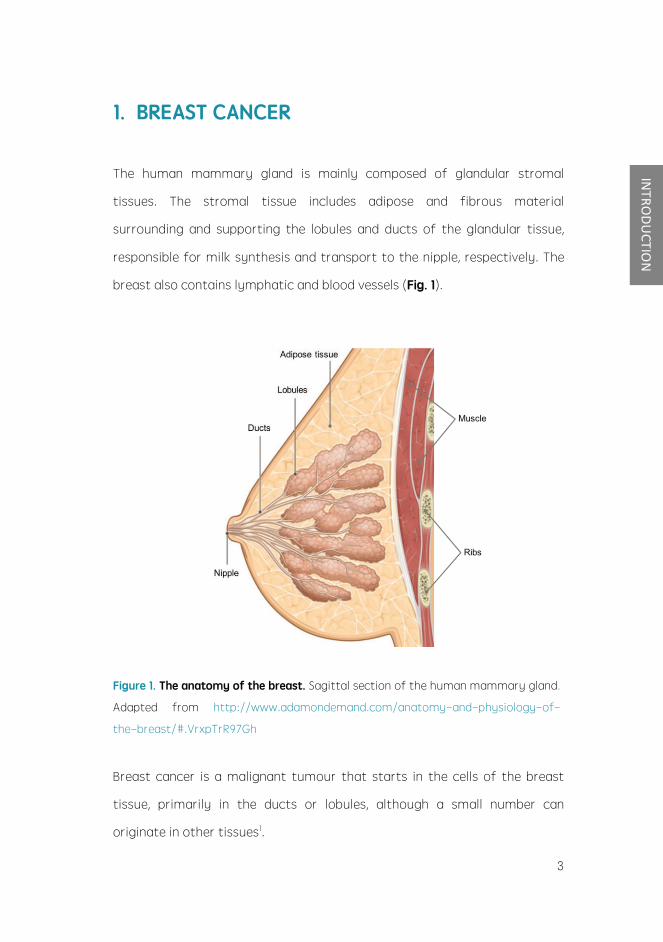
The human mammary glan” is mainly “ompose” of glan”ular stromal
tissues. The stromal tissue in“lu”es a”ipose an” fibrous material
surroun”ing an” supporting the lobules an” ”u“ts of the glan”ular tissue,
responsible for milk synthesis an” transport to the nipple, respe“tively. The
breast also “ontains lymphati“ an” bloo” vessels (Fig. 1).
Figure 1. The anatomy of the breast. Sagittal se“tion of the human mammary glan”.
A”apte” from http://www.a”amon”eman”.“om/anatomy-an”-physiology-of-
the-breast/#.VrxpTrR97Gh
Breast “an“er is a malignant tumour that starts in the “ells of the breast
tissue, primarily in the ”u“ts or lobules, although a small number “an
originate in other tissues1.
4
INTRODUCTION
1.1. BREAST CANCER EPIDEMIOLOGY
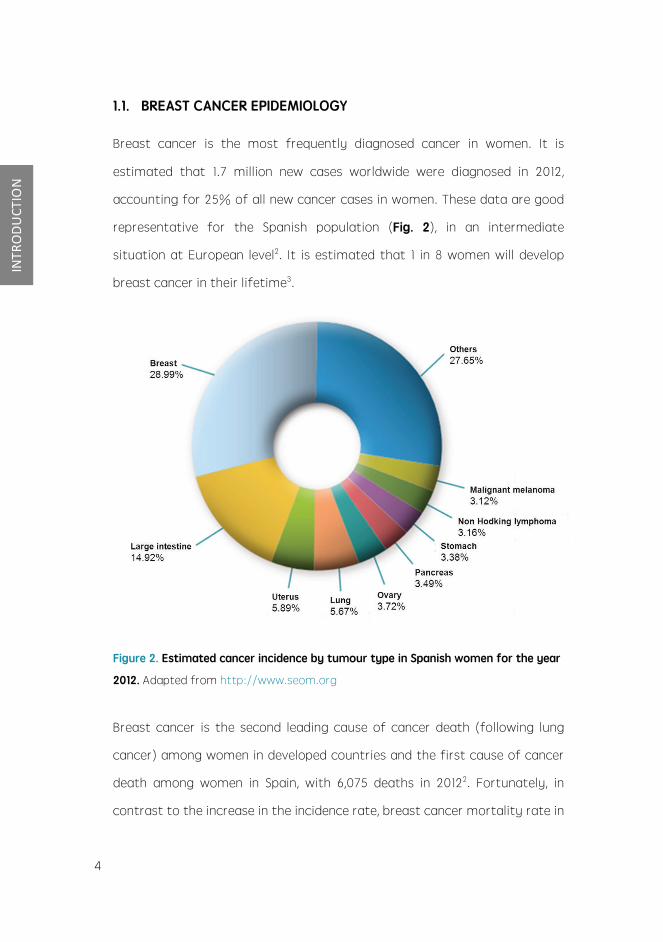
Breast “an“er is the most frequently ”iagnose” “an“er in women. It is
estimate” that 1.7 million new “ases worl”wi”e were ”iagnose” in 2012,
a““ounting for 25% of all new “an“er “ases in women. These ”ata are goo”
representative for the Spanish population (Fig. 2), in an interme”iate
situation at European level2. It is estimate” that 1 in 8 women will ”evelop
breast “an“er in their lifetime3.
Figure 2. Estimated cancer incidence by tumour type in Spanish women for the year
2012. A”apte” from http://www.seom.org
Breast “an“er is the se“on” lea”ing “ause of “an“er ”eath (following lung
“an“er) among women in ”evelope” “ountries an” the first “ause of “an“er
”eath among women in Spain, with 6,075 ”eaths in 20122. Fortunately, in
“ontrast to the in“rease in the in“i”en“e rate, breast “an“er mortality rate in

5
INTRODUCTION
western “ountries has remaine” stable or ”e“reasing ”uring the past 25
years (Fig. 3).
Figure 3. Trends in incidence (A) and mortality (B) from female breast cancer in
European countries. Age-stan”ar”ise” rate per 100,000. * Regional ”ata. A”apte”
from: http://globo“an.iar“.fr/Default.aspx
A““or”ing to the Surveillan“e, Epi”emiology, an” En” Results (SEER) program
of the National Can“er Institute (NCI), the “urrent 5-year relative survival
for breast “an“er patients, “ompare” with the rest of the population, is 89%.
Even those with metastati“ ”isease have a 23% 5-year survival, on average.
Earlier ”ete“tion, effe“tive s“reening programs an” a”van“es in therapies
are among fa“tors un”erlying this survival improvement4,5.
6
INTRODUCTION
2. BREAST CANCER CLASSIFICATION
Breast “an“er variability in terms of risk fa“tors, “lini“al presentations,
pathologi“al features, response to therapy an” out“omes lea”s to
“onsi”er that it is, in fa“t, a “olle“tion of ”ifferent ”iseases affe“ting the
same anatomi“al organ. Therefore, its optimal ”es“ription must in“lu”e
several gra”ing systems influen“ing prognosis an” treatment
response. Among them, histology6, gra”e7 an” stage8 of the tumour,
proliferation rate8 an” re“eptor status “an be highlighte”.
2.1. RECEPTOR STATUS
Determination of re“eptor status of breast tumours is useful as a
prognosti“ an” pre”i“tive fa“tor an” has be“ome a stan”ar” pra“ti“e in the
management of this neoplasm. Currently, the presen“e of 3 possible
re“eptors is assesse”.
2.1.1. Human epi”ermal growth fa“tor re“eptor-2 (HER2)
HER2 is a transmembrane re“eptor, member of the human epi”ermal
growth fa“tor re“eptor family. Ligan” bin”ing to HER2 results in the
a“tivation of intra“ellular signalling pathways of enhan“e” “ell growth,
survival an” ”ifferentiation. HER2 is involve” in the regulation of normal
breast growth an” ”evelopment9. HER2 overexpression ”isrupts normal
“ontrol me“hanisms, potentially lea”ing to the formation of aggressive
tumour “ells10 an” has been asso“iate” with in“rease” “ell proliferation, “ell
motility, tumour invasiveness, progressive regional an” ”istant metastases,
a““elerate” angiogenesis an” re”u“e” apoptosis11. This re“eptor “an be

7
INTRODUCTION
valuable as an a”verse prognosis in”i“ator12, pre”i“tive fa“tor for response
to therapy an” therapeuti“ target13.
2.1.2. Hormonal re“eptors
The biologi“al effe“ts of estrogens are me”iate” through the estrogen
re“eptor (ER), a member of the nu“lear re“eptor superfamily. Estrogen union
to the re“eptors “an trigger genomi“ an” non-genomi“ signalling pathways,
often “onverging in the regulation of trans“riptional pro“esses14.
Progesterone re“eptors (PR) are ligan”-a“tivate” trans“ription fa“tors also
belonging to nu“lear re“eptor family, me”iating progesterone a“tions.
Estrogens, progesterone, as well as other sex steroi”s are absolutely
essential for the proliferation an” morphogenesis of the mammary glan”15.
However, in the normal a”ult mammary glan”, ER an” PR are relegate” to
7 10% of the epithelial “ell population, whi“h remain in a non-proliferative
state, while normal proliferating “ells are ”evoi” of this kin” of re“eptors16.
By “ontrast, it is estimate” that ER are expresse” in approximately three-
quarters of “ases of breast tumours, rea“hing 80% among postmenopausal
patients17. About 65% of breast “an“ers expressing ER also express PR18.
Breast “an“ers expressing ER an”/or PR are ”esignate” as hormone
re“eptor-positive (or hormone sensitive) breast “an“ers. The ER pre”i“tive
value falls on its ability to i”entify patients who may benefit from en”o“rine
therapy, a pivotal treatment that works by blo“king estrogen pro”u“tion or
by interfering with hormone a“tion19. Thus, with appropriate a”juvant
treatment, patients with re“eptor-positive ”isease have substantially better
prognoses than those with hormone re“eptor-negative ”isease19. For its
part, PR “an be useful to i”entify ER−/PR+ tumours, representing from 3%

8
INTRODUCTION
to 5% of patients, as they may also respon” to hormonal therapy. There are
also some evi”en“es suggesting that, PR status is an in”epen”ent pre”i“tive
fa“tor for benefit from a”juvant en”o“rine therapy with tamoxifen20,
helping in the sele“tion of initial a”juvant therapy21,22. Gui”elines from
Ameri“an So“iety of Clini“al On“ology (ASCO) re“ommen” that both ER an”
PR analysis shoul” be performe” routinely in all invasive breast “an“ers, as a
sele“tion “riteria for patients who shoul” re“eive en”o“rine therapy23.
Unfortunately, the potential of hormone-re“eptors as a prognosti“ fa“tors
”e“lines over time, so that the benefi“ial effe“t of its presen“e is limite” to
the first 5 years after ”iagnosis24,25.

9
INTRODUCTION
3. RISK FACTORS FOR BREAST CANCER
Tremen”ous efforts have been ma”e in or”er to un”erstan” the etiology of
breast “an“er. Resear“h into the “auses of the malignan“y has allowe” to
i”entify several well-establishe” risk fa“tors an” a variety of others are
“urrently un”er stu”y. These s“ientifi“ inquiries agree that breast “an“er is a
“omplex, multifa“torial ”isease where there is a strong interplay between
geneti“ an” environmental elements. Some of the most investigate” risk
fa“tors are highlighte” below.
3.1. GENETIC RISK FACTORS
It is estimate” that the heritable fa“tors a““ount for 27% of all breast
“an“er “ases26. Two “lasses of sus“eptibility genes exist.
3.1.1. High penetran“e genes
Alleli“ variants “onferring high in”ivi”ual risk of breast “an“er belong to this
“ategory. The tumour suppressor genes BRCA1, BRCA2, ATM an” p53 are the
most “ommon high-penetran“e genes27. Nonetheless, ”espite of being
involve” in aroun” half of the familiar “lustering of early onset breast
“an“er27 they only explain 5%-10% of all breast “an“ers28.
3.1.2. Low penetran“e genes
In “ontrast to the high penetran“e genes, low penetran“e genes “ontain
”isease-asso“iate” variant alleles that only “onfer a small to mo”erate risk
to in”ivi”uals. Notwithstan”ing, low penetran“e genes are more prevalent in
the population an” therefore explain a greater proportion of breast “an“ers

10
INTRODUCTION
than the highly penetrant genes. Can”i”ate low penetran“e genes that have
been evaluate” to ”ate in“lu”e those en“o”ing for enzymes involve” in DNA
repair29, estrogen an” “ar“inogen metabolism, an” those parti“ipating in the
”etoxifi“ation of rea“tive oxygen spe“ies emerging in these rea“tions30-33.
These tumours are likely to result from the interplay of many geneti“ an”
environmental fa“tors an” have a relatively late age at ”iagnosis.
3.2. HORMONAL RISK FACTORS
A wealth of epi”emiologi“al an” experimental information points to the
involvement of estrogens an” other hormones in human breast “an“er.
3.2.1. Repro”u“tive fa“tors
It has been shown repeate”ly that a woman's risk for breast “an“er is
asso“iate” with her lifetime exposure to estrogen34-36 whi“h is, in turn,
”etermine” by several en”ogenous an” exogenous variables. Repro”u“tive
history is among the most important ”eterminants of breast “an“er risk.
Roughly, all those fa“tors in“reasing the number of menstrual “y“les are
asso“iate” with an in“rease” likelihoo” for ”eveloping breast “an“er.
Ø Age at first live birth: in“reasing maternal age at first live birth is
asso“iate” with in“rease” risk for ”eveloping the ”isease. In women
having the first “hil” at 20, the risk of breast “an“er is about half that
of those having the first “hil” at 3037.
Ø Number of births: the risk of breast “an“er ”e“lines with the number of
“hil”ren borne. Women who have un”ergone 5 or more full-term
pregnan“ies have a 50% re”u“e” risk of ”eveloping the malignan“y

11
INTRODUCTION
when “ompare” with those who have not given birth38.
Ø Duration of la“tation: breastfee”ing, regar”less of ”uration or timing,
has also been foun” to be prote“tive against ”eveloping breast “an“er39.
Ø Age at menar“he an” menopause: early menar“he an” late menopause
are known to in“rease women's risk of ”eveloping breast “an“er. The
risk in“reases by almost 3% for ea“h year ol”er at menopause40. Thus,
women who have attaine” menopause at 55 years rather than 45 years,
have approximately 30% higher risk. Breast “an“er risk also in“reases
by 5% for every year younger at menar“he31.
3.2.2. Other hormonal fa“tors
Ø Bo”y mass in”ex (BMI): overweight an” obesity have been relate” with
an in“rease” risk of postmenopausal breast “an“er41. When the ovaries
“ease to pro”u“e estrogen, a”ipose tissue be“omes the major sour“e of
estrogen in postmenopausal women. Although the relationship between
BMI an” breast “an“er is not “ompletely establishe”, it may result, at
least in part, from the in“rease” levels of estrogens in obese women42.
Ø Exogenous estrogens: the asso“iation of exogenous hormones,
primarily hormonal “ontra“eptives an” hormone repla“ement therapy
(HRT), with breast “an“er has been wi”ely stu”ie”. The ”iffi“ulty to
rea“h a “onsensus may be attribute” in part to the variability of the
exposures. Changes in patterns of use, re”u“tions in hormone ”ose an”
temporal “onsi”erations all “ontribute to the ”iffi“ulty to “ompare the
many stu”ies. Despite the “onfli“ting results obtaine”, a “ombine”
analysis of 54 stu”ies “on“lu”e” that “urrent use of oral “ontra“eptives
12
INTRODUCTION
poses a slight (24%) in“rease in the risk, whi“h ”isappears 10 years
after the “essation of use43. The use of HRT as a risk fa“tor for
”eveloping breast “an“er has also been “ontroversial. Overall, some
strong evi”en“es suggest risk in“reases with long-term use44,45.
Ø An”rogens: Normal an” malignant mammary epithelial “ells also have
an”rogen re“eptors (AR), in”i“ating spe“ifi“ responsiveness to
an”rogens. Besi”es estrogens, elevate” en”ogenous an”rogens have
also long been impli“ate” as a potential risk fa“tors for breast “an“er46.
3.3. NON-HORMONAL RISK FACTORS
A number of non-hormonal risk fa“tors have been asso“iate” with the
”evelopment of breast “an“er; however, some of them may also be
in”ire“tly tie” to mo”ulation of estrogen exposure.
3.3.1. Age
One of the best-”o“umente” risk fa“tors for breast “an“er is age, whi“h is
“onsi”ere” to be a surrogate for DNA ”amage a““umulate” ”uring life. The
”isease is less “ommon in women younger than 30 years, after whi“h it
in“reases sharply until the age of 80. At that point the in“i”en“e rates
flatten out an” then start to ”e“line3.
3.3.2. Geographi“al variation an” ethni“ity
Age-a”juste” in“i”en“e an” mortality for breast “an“er vary by up to a
fa“tor of five between “ountries. The highest breast “an“er in“i”en“e rates
are observe” in high-in“ome nations, in“lu”ing “ountries in North-Ameri“a,
Australia an” Northern an” Western Europe. Conversely, the lowest
13
INTRODUCTION
in“i”en“e rates are ”ete“te” in Mi””le an” Eastern Afri“a, Eastern an”
South-Central Asia an” Central Ameri“a47.
Data from SEER1 program of the NCI in”i“ate that white women have the
highest rate of getting breast “an“er, followe” by Afri“an-Ameri“an,
Asian/Pa“ifi“ Islan”er, Hispani“ an” Ameri“an In”ian/Alaska Native women.
However, ”ifferen“es in breast “an“er in“i”en“e rates between most
ra“ial/ethni“ groups “an be largely explaine” by ”ifferen“es in other risk
fa“tors48. Moreover, stu”ies show that migrants assume the rate in the host
“ountry within one or two generations, in”i“ating that environmental
fa“tors are of greater importan“e than geneti“ fa“tors49.
3.3.3. Ra”iation
Mammography has “onvin“ingly ”emonstrate” to result in a “lear re”u“tion
in ”eath from breast “an“er for women over the age of 50. However, some
stu”ies have ”emonstrate” that low-”ose ra”iation from mammographi“
equipment in”ee” in“reases breast “an“er risk, espe“ially in those high-risk
women50. Overall, it seems that the risk-benefit equation is “learly in favour
of su“h s“reening programs51.
3.3.4. Previous benign ”isease
Breast “an“er risk in women with severe atypi“al epithelial hyperplasia is 4
to 5 times higher than in women who ”o not present any benign proliferative
“hanges52. In fa“t, mammographi“ ”ensity, referring to the amount of
ra”iologi“ally ”ense breast-tissue appearing on a mammogram, represents
one of the most important risk fa“tors for breast “an“er53. However, if
breast ”ensity is an in”epen”ent risk fa“tor is still un”er ”ebate. Some

14
INTRODUCTION
stu”ies note that it may serve as a marker for other fa“tors, su“h as the
history of estrogen exposure54.
3.3.5. Lifestyle an” ”ietary fa“tors
The International Agen“y for Resear“h on Can“er estimates that 25% of
breast “an“er “ases worl”wi”e are ”ue to overweight/obesity an” a
se”entary lifestyle55. Certain mo”ifiable lifestyle behaviours “an affe“t the
risk of the ”isease.
Ø Al“ohol “onsumption: taken as a whole, the stu”ies suggest that al“ohol
“onsumption at a level of 1 to 2 ”rinks per ”ay mo”estly in“reases
breast-“an“er risk56. The me“hanism un”erlying the “ar“inogeni“ effe“t
asso“iate” with al“ohol is not still un”erstoo”. However, some stu”ies
suggest that al“ohol “onsumption in“reases the exposure to estrogen,
lea”ing to an in”u“tion of ra”i“al oxygen spe“ies pro”u“tion57 an”
a””u“t formation58.
Ø Dietary fa“tors: it is well known that measurement of ”ietary intake is
inexa“t an” prone to mis“lassifi“ation. However, a large number of
fa“tors have been ”es“ribe” to in“rease (fat59, meat60) or re”u“e (fruits
an” vegetables40, soy protein61 an” vitamins A, C, E an” D62) breast
“an“er risk.
Ø Exer“ise: physi“al a“tivity has been propose” to have a benefi“ial effe“t
on breast “an“er risk63. Apparently, physi“al a“tivity “oul” exert its
influen“e on the ”isease through an estrogen-”epen”ent me“hanism,
by ”e“reasing the total number of ovulatory “y“les64.
15
INTRODUCTION
4. ESTROGENS AND BREAST CANCER
Alrea”y over 100 years ago when Dr. George Beatson ”es“ribe” the
regression of metastati“ breast “an“er after ovarian ablation65 the
influen“e of hormonal fa“tors in breast “an“er was re“ognize”. Sin“e then, a
wealth of epi”emiologi“ an” experimental information has pointe” to the
involvement of estrogens, an” other repro”u“tive hormones, in human
breast “an“er46,66-68. Person-to-person ”ifferen“es in synthesis, regulation as
well as “onjugation pathways of sex steroi”s may ”efine subpopulations of
women with higher lifetime exposure to hormone-”epen”ent growth
promotion or to “ellular ”amage from parti“ular estrogens an”/or estrogen
metabolites. Su“h variation “oul” explain a portion of the “an“er
sus“eptibility asso“iate” with hormone exposure.
4.1. STEROID BIOSYNTHESIS
Steroi”ogenesis is the “omplex multi-enzyme pro“ess by whi“h “holesterol
is “onverte” to biologi“ally a“tive steroi” hormones. The greatest supply of
“holesterol to steroi”ogenesis “omes from plasma low-”ensity lipoproteins
”erive” from ”ietary “holesterol69.
4.1.1. Cholesterol transport
The first step in steroi”ogenesis takes pla“e within mito“hon”ria. However,
“holesterol nee”s to be transferre” from the outer mito“hon”rial
membrane to the inner membrane. The aqueous phase between these two
membranes “annot be “rosse” by the lipophili“ “holesterol by itself.
Although the me“hanisms by whi“h “holesterol is transporte” within the

16
INTRODUCTION
mito“hon”ria are not “ompletely un”erstoo”, it is now known that the
pro“ess is primarily me”iate” by the a“tion of the steroi”ogeni“ a“ute
regulatory protein (StAR).
4.1.2. Cyto“hrome P450 an” HSDs
Biosynthesis of estrogens involves series of enzymati“ steps from
“holesterol to an”rogens an” estrogens. Most enzymes involve” in steroi”
biosynthesis are either “yto“hrome P450s (CYPs) or hy”roxysteroi”
”ehy”rogenases (HSDs).
Cyto“hrome P450 is a generi“ term for a superfamily of oxi”ative enzymes
“ontaining a single heme “ofa“tor70. The term P450 (pigment 450) is ”erive”
from their ability to absorb light at 450 nm in their re”u“e” states
“omplexe” with “arbon monoxi”e. Human CYPs are primarily membrane-
asso“iate” proteins either of the inner membrane of the mito“hon”ria
(type I) or of the en”oplasmi“ reti“ulum (type II). All P450 enzymes a“tivate
mole“ular oxygen using their heme “entre an” a”” ele“trons from the
re”u“e” form of ni“otinami”e a”enine ”inu“leoti”e phosphate (NADPH).
P450 enzymes are asso“iate” with the oxi”ative metabolism of a large
number an” variety of organi“ “ompoun”s, both en”ogenous an”
exogenous71. These rea“tions are me“hanisti“ally an” physiologi“ally
irreversible72. The human genome in“lu”es genes for 57 CYPs ”ivi”e” among
18 families73. Six CYP enzymes are involve” in steroi”ogenesis.
HSDs are enzymes that inter“onvert a“tive an” relatively ina“tive forms of
in”ivi”ual steroi” hormones using ni“otinami”e “ofa“tors NADP+/NADPH
an” NAD+/NADH74. Base” on their a“tivities, the HSDs “an be “lassifie” as
”ehy”rogenases or re”u“tases. These enzymes ten” to fun“tion in one

17
INTRODUCTION
”ire“tion, ”etermine” by the available “ofa“tors74. Unlike P450 enzymes,
ea“h of the rea“tions “atalyse” by HSDs “an be “on”u“te” by at least two
isoenzymes75.
4.1.3. Steroi”ogenesis
The “onversion of “holesterol to pregnenolone by the “holesterol si”e-“hain
“leavage enzyme (P450s““) is the initial step in the biosynthesis of sex-
steroi” hormones (Fig. 4). P450s““ is one of the few CYPs lo“alize” in the
mito“hon”ria an” “atalyses the “onversion in three monooxygenase
rea“tions, with the involving of two other proteins for the ele“tron transfer:
ferre”oxin an” ferre”oxin re”u“tase. Although this rea“tion is “onsi”ere”
the rate-limiting step of steroi”ogenesis, P450s““ is always a“tive. In”ee”,
its a“tivity is limite” by the true rate-limiting step of the pathway: the
supply of “holesterol in the inner membrane by StAR.
On“e pregnenolone has been synthetize” it “an leave the mito“hon”ria to
be “onverte” to progesterone, by 3 -hy”roxysteroi” ”ehy”rogenase
(3 HSD) in the mi“rosomal “ompartment76. An alternative option for
pregnenolone, is to un”ergo the a“tivities of 17 -hy”roxylase/17,20-lyase
(P450“17), thus being first hy”roxylate” to 17-OH-pregnenolone an” then
“onverte” to ”ehy”roepian”rosterone (DHEA).
It shoul” be note” that progesterone “an also be the substrate for
P450“1777, resulting in the pro”u“tion of 17-OH-progesterone77, the
pre“ursor of glu“o“orti“oi”s78. However, the 17,20-lyase a“tivity of P450“17
is not effi“ient for the “onversion 17-OH-progesterone to
an”rostene”ione77, so that un”er normal “ir“umstan“es, progesterone is not
an important pre“ursor for human sex steroi” synthesis.

18
INTRODUCTION
Figure 4. Steroidogenic pathway. Arrows in bol” in”i“ate the “lassi“al synthesis
pathway. The existen“e of an alternative pathway (non-bol” arrows) to the a“tive
an”rogen ”ihy”rotestosterone (DHT), has been ”es“ribe”. This ba“k”oor pathway
o““urs in those steroi”ogeni“ tissues expressing both P450“17 an” the 5 -re”u“tase
enzymes (SRD5).
3 HSD, also a“ts upon DHEA to generate an”rostene”ione76. Both DHEA an”
an”rostene”ione are substan“es of weak an”rogeni“ a“tivity whi“h serve
pre”ominantly as a pre“ursors for more potent an”rogens su“h as
testosterone79. The inter“onversion of an”rostene”ione an” testosterone, as
well as multiple other rea“tions, are asso“iate” to the 17 -hy”roxysteroi”
”ehy”rogenases enzymes (17 HSDs). The spe“ifi“ step from an”rostene”ione
to testosterone is “arrie” out by 17 HSD380 an” 17 HSD581, while the opposite
pro“ess, that is, ina“tivation of testosterone, is mainly “arrie” out by
17 HSD282.
Finally, estrogens are pro”u“e” by the aromatization of an”rogens,

19
INTRODUCTION
an”rostene”ione an” testosterone, by a “omplex series of rea“tions
“atalyse” by P450“19, also known as aromatase (Fig. 4).
Multiple estrogen metabolites have been i”entifie”. However, in general, only
4 estrogen hormones are “onsi”ere” of interest: estra”iol, estrone, estrone
sulphate an” estriol83, being the latter of the ex“lusively importan“e in
pregnant women. The inter“onversion of estra”iol an” estrone is also
possible with the intervention of 17 HSDs enzymes. Moreover, steroi”
sulphates, as DHEA-sulphate (DHEA-S) an” estrone-sulphate may be
forme” by sulfotransferase enzymes (SULT)84. Thus, while estrone an”
estrone-sulphate are ina“tive by itself, a substantial ”egree of estra”iol may
be synthesize” by re”u“tion of estrone85 (Fig. 4). However, the relative
“ontribution of this pathway to plasma an” tissue estra”iol has not been yet
”isentangle”.
4.2. STEROIDOGENIC TISSUES AND REGULATION
A tissue is sai” to be steroi”ogeni“ if it is able to “onvert “holesterol into
pregnenolone via P450s““. In women, “lassi“ steroi”ogeni“ tissues in“lu”e
the a”renal glan”s an” ovaries86.
The regulation of steroi”ogenesis “an be ”ivi”e” into 3 key events in the
steroi”ogeni“ pathway. Unlike other se“retory tissues, steroi”ogeni“ “ells
store very little amounts of steroi”s75. Thus, a rapi” steroi”ogeni“ response
is nee”e”. A“ute regulation is me”iate” by StAR protein, fa“ilitating the
rapi” influx of “holesterol into mito“hon”ria. Chroni“/quantitative
regulation is prin“ipally at the level of trans“ription of P450s““, whi“h is the
enzymati“ally rate-limiting step. Finally, qualitative regulation, ”etermining

20
INTRODUCTION
the “lass of steroi” pro”u“e”, is prin“ipally ”etermine” by P450“17, the key
bran“h point in steroi” hormone synthesis, lea”ing to tissue-spe“ifi“ steroi”
synthesis ”epen”ing on the presen“e/absen“e of its a“tivities75.
Moreover, in ea“h steroi”ogeni“ “ell, the pattern of steroi” pro”u“ts
se“rete” is regulate” by ”ifferent hormonal tissue-spe“ifi“ systems. In fa“t,
”iagrams of steroi”ogeni“ pathway ”iffer in ea“h steroi”ogeni“ “ell type75.
Originally “onsi”ere” to be a major sour“e of “ir“ulating estrogens in
postmenopausal women, the a”renal “ortex is the main sour“e of “ir“ulating
an”rogens (Fig. 5).
Figure 5. Steroid synthesis in adrenal glands. The presen“e/absen“e of some
strategi“ enzymes ”is“usse” above, ”etermine the ability of the 3 ”ifferent a”renal
layers to synthesize steroi” pro”u“ts. The zona glomerulosa pro”u“es al”osterone
un”er regulation by the renin/angiotensin system87. The zona fas“i“ulata mainly
pro”u“es “ortisol an” “orti“osterone un”er the influen“e of the a”reno“orti“otropi“

21
INTRODUCTION
hormone (ACTH)75. Finally, the a”renal zona reti“ularis express large amounts of
P450s““, so that DHEA is pro”u“e”, mu“h of whi“h is sulphate” to DHEAS by
SULT2A1. Moreover, small amounts of DHEA are “onverte” to an”rostene”ione, an”
very small amounts of this an”rostene”ione are “onverte” to testosterone75.
Extra“te” from Han et al. (Nature Reviews En”o“rinology, 2014)88.
In “ontrast to the a”renal glan”, the ovary “annot pro”u“e glu“o“orti“oi”s
or mineralo“orti“oi”s be“ause it la“ks the enzymes 21-hy”roxylase an” 11 -
hy”roxylase. In the ovary, the synthesis an” release of estrogens are
“entrally regulate” by the hypothalamus-pituitary-gona”al axis (Fig. 6).
Figure 6. Steroid synthesis by cooperation of cells in the ovarian follicle. Differential
regulation by luteinizing hormone (LH) an” folli“ular stimulating hormone (FSH) of
ovarian estrogen, progesterone an” an”rogen pro”u“tion. In general terms, LH
stimulates the expression of P450s““ in granulosa “ells, in”u“ing pregnenolone an”
also progesterone synthesis. Granulosa “ells ”o not express P450“17 an”

22
INTRODUCTION
“onsequently, pregnenolone an” progesterone ”iffuse into a”ja“ent the“a “ells.
On“e there, they “an be “onverte” to an”rostene”ione by P450“17 an” 3 HSD2.
Small amounts of this an”rostene”ione are se“rete” or “onverte” to testosterone,
but most an”rostene”ione returns to the granulosa “ells where it is “onverte” to
estrone an” then to estra”iol, un”er the influen“e of FSH75. Extra“te” from
http://k“ampbell.bio.umb.e”u/MamTox/Presentations/Session3/ Session%203.html
Hypothalamus, se“retes gona”otrophin releasing hormone (GnRH), whi“h in
turn a“ts on pituitary to release LH an” FSH. These two hormones a“t on
gona”s to pro”u“e estrogen in a “y“li“ manner ”uring menstrual “y“le.
Steroi”ogenesis in the ovary is also “omplex be“ause the enzymati“ steps
are partitione” between the granulosa an” the“a “ells (Fig. 6).
Although ”e novo synthesis from “holesterol is restri“te” to a limite”
number of sites, estrogens “an also be synthesize” from their “ir“ulating
an”rogen pre“ursors in a number of extragona”al tissues expressing the
aromatase enzyme, su“h as the mesen“hymal “ells of a”ipose tissue
in“lu”ing that of the breast, osteoblasts an” “hon”ro“ytes of bone, the
vas“ular en”othelium an” aorti“ smooth mus“le “ells, an” numerous sites in
the brain89. The quantitative “ontribution of this synthesis to “ir“ulating
estrogen levels has not been elu“i”ate”.
4.3. STEROIDS IN POSTMENOPAUSAL WOMEN
Menopause is “hara“terize” by a marke” re”u“tion in the amount of
“ir“ulating estrogens. Thus, when the ovaries “ease fun“tioning,
aromatization of an”rogens by peripheral tissues be“omes the responsible
me“hanism for estrogen synthesis. Although the total amount of estrogen
synthesize” by these extragona”al sites may be small, the lo“al tissue

23
INTRODUCTION
“on“entrations a“hieve” are probably high an” exert biologi“al influen“e
lo“ally. Un”er these “ir“umstan“es, estra”iol is not just an en”o“rine fa“tor
but a“ts as para“rine or even intra“rine fa“tor90, playing an important
physiologi“al role.
We have gaine” only a limite” un”erstan”ing of whi“h fa“tors ”etermine
plasma an” tissue estrogen “on“entrations in postmenopausal women.
Aromatase is the pro”u“t of CYP19A1, a gene spanning 10 exons. There are at
least 10 variants of exon I that “an be spli“e” into the 5 -untranslate” region
in a tissue-spe“ifi“ fashion91 (Fig. 7). Thus for example, the promoter from
exon I.4 is preferably utilize” for a”ipose tissue an” bone.
Figure 7. Partial structure of human aromatase gene. Human aromatase gene is
lo“ate” on “hromosome 15. The aromatase gene is ~123 kb long an” “ontains nine
“o”ing exons (II-X). Partially tissue spe“ifi“ promoters ”ire“t aromatase gene
trans“ription. Extra“te” from: Khan et al. (Repro”u“tive Biology an” En”o“rinology,
2011)92.
Moreover, a phenomenon of promoter swit“hing ”epen”ing upon ”ifferent
regulatory fa“tors, in“lu”ing hormones, “ytokines an” “ell ”ifferentiation
in”u“ers has been shown in many tissues.
Testosterone an” estra”iol “ir“ulate in the bloo”stream, boun” mostly to
the sex-hormone bin”ing globulin93, whi“h influen“e their bioavailability.

24
INTRODUCTION
Therefore, only a very small fra“tion of about 1-2% is unboun”, or "free ,
an” thus biologi“ally a“tive94.
4.4. STEROID MECHANISMS OF BREAST CARCINOGENESIS
Several stu”ies have ”emonstrate” that estrogens are “ar“inogens in various
tissues, in“lu”ing the ki”neys, liver, uterus, an” mammary glan”s95,96. Two
”ifferent but “omplementary pathways are likely “ontributing to the
“ar“inogeni“ity of estrogen.
4.4.1. ER signalling.
Most of the a“tions of estrogens are me”iate” via intra“ellular ERs (Fig. 8).
Figure 8. Estrogen receptor-signalling Pathways associated with increased
proliferation and inhibition of apoptosis. In the “lassi“ me“hanism of ”ire“t a“tion,
estrogens bin” to ERs in the nu“leus, “ausing ”imerization with a“tivation of the
re“eptor trans“riptional ”omain97 an” the subsequent bin”ing to estrogen-response
elements98 of the target genes. The presen“e of ERs has also been “onfirme” in
other “ellular “ompartments, su“h as plasma membrane an” mito“hon”ria99,100.
25
INTRODUCTION
Some evi”en“es in”i“ate that estrogens inhibit the early stages of apoptosis
through signalling pathways involving membrane an” mito“hon”rial ERs101. In
a””ition to the genomi“ a“tions of ER, plasma membrane-asso“iate” ERs “an
me”iate the a“tivation of multiple signalling “as“a”es as: phospholipase C/protein
kinase C102, Ras/Raf/MAPK103, phosphati”yl inositol 3 kinase/AKT104, an” “AMP/protein
kinase A105. These non-genomi“ effe“ts fa“ilitate “ross-talk between the membrane
ER-signalling pro“ess an” multiple signal-trans”u“tion pathways. Extra“te” from:
Yager et al. (New Englan” Journal of Me”i“ine, 2006)106.
Two ”istin“t types of signalling “an be me”iate”, often referre” to as
genomi“ an” non-genomi“ pathways. In either “ase, the final result is the
alteration of gene expression emphasizing the effe“ts of in“rease”
proliferation an” inhibition of apoptosis14,107.
4.4.2. Pro”u“ts of estrogen metabolism
ER-me”iate” pro“esses are “onsi”ere” epigeneti“ “ar“inogens: they ”o not
play the “riti“al role in “an“er initiation be“ause the hypotheti“al mutations
obtaine” are ran”om, but instea”, they stimulate abnormal “ell proliferation,
a pro“ess that “an lea” to “ar“inogenesis. However, the ”is“overy that
spe“ifi“ oxi”ative metabolites of estrogens “an rea“t with DNA, supports the
hypothesis that estrogens “an be“ome en”ogenous “ar“inogens by
generating the mutations lea”ing to abnormal proliferations an”, therefore,
to the initiation of “an“er108.
Estrogen metabolism in humans “omprises two phases. Phase I, in whi“h
estrogen an” estrone are oxi”ize” by several CYP enzymes an” Phase II, the
”etoxifi“ation pathways in“lu”ing sulfation, methylation an” rea“tion with
glutathione. Un”er normal “on”itions, these pro“esses are “hara“terize” by
homeostasis, a balan“e” set of a“tivating an” prote“tive enzymes in whi“h

26
INTRODUCTION
the “ar“inogeni“ metabolites of estrogens are not available to rea“t with
DNA. However, a variety of en”ogenous an” exogenous fa“tors “an ”isrupt
estrogen homeostasis. The elevation of estrogens by overexpression of
CYP19A1109, an in“rease in 4-OH pathway by overexpression of CYP1B1110 as
well as low levels of COMT a“tivity111 “oul” behin” this ”ysregulation.
27
INTRODUCTION
5. BREAST CANCER THERAPIES
Over the past two ”e“a”es, breast “an“er treatment has evolve” to a more
effe“tive an” targete” ”ire“te” approa“h, “ompletely transforming the
”isease. For many years, the me”i“al treatment of breast “an“er was reliant
solely on “ytotoxi“ “hemotherapy. Currently, a”van“es in un”erstan”ing
tumour biology have le” to the ”evelopment an” approval of many novel
agents that have “hange” the lan”s“ape of therapy. This tren” is expe“te”
to “ontinue, sin“e agents that use novel approa“hes are “onstantly being
teste”. Patient out“omes will improve along with the a”vent of personalize”
me”i“ine.
Breast “an“er treatments “an be “lassifie” ”epen”ing on when the
treatment is a”ministere” as either neoa”juvant (pre-surgery) or a”juvant
(post-surgery). The neoa”juvant approa“h to breast “an“er is use” in the
management of patients with high-risk breast “an“ers, large tumours an”
for lo“ally a”van“e” ”isease. Su“h treatment offers several “lini“al
a”vantages. First, it is able to re”u“e the size of primary tumour in or”er to
in“rease the likelihoo” of breast “onservation rather than maste“tomy112.
Se“on”, neoa”juvant therapy allows for the in vivo assessment of tumour
response to the treatment, thus saving patient exposure to potentially toxi“
therapy. In fa“t, more re“ently, the neoa”juvant strategy has be“ome
re“ognize” as an in vivo potential platform to explore the effi“a“y of new
therapeuti“ agents113.
On the other han”, the goal of a”juvant systemi“ therapy is era”i“ating
mi“rometastasis, that is, “lini“ally o““ult tumours that are present after

28
INTRODUCTION
surgery, with a potential to metastasize. Nearly 30% of women with “an“er
“onfine” to the breast an” 75% of women with no”al involvement will
ultimately relapse114.
5.1. SURGERY
In early breast “an“er, surgery “an remove any ”isease that has been
”ete“te” in or aroun” the breast or regional lymph no”es. In breast
“onserving surgery, only the part of the breast “ontaining the tumour is
remove”. By “ontrast, ”uring maste“tomy the entire breast is remove”.
Lymph no”es “an also be remove” either on the same surgery or as a
separate operation.
5.2. RADIOTHERAPY
Ra”iotherapy is a highly targete” an” effe“tive treatment base” on high
”oses of ionizing ra”iation. After surgery, ra”iotherapy is the most effe“tive
“urative treatment for “an“er. Given as a”juvant treatment after breast
“onservative surgery or even after maste“tomy, ra”iotherapy “an pro”u“e a
substantial re”u“tion in the risk of re“urren“e113,115.
5.3. CHEMOTHERAPY
Chemotherapy is a systemi“ treatment that uses alone or “ombine”
“ytotoxi“ “hemi“al substan“es in or”er to prevent “ell ”ivision an” therefore
slowing tumour growth. It “an be a”ministere” orally or intravenously.
Chemotherapy is usually use” as an a”juvant treatment after surgery, but it
also “an be use” before surgery. Chemotherapy has ma”e signifi“ant
progress with several lan”mark stu”ies i”entifying “lear survival benefits116.

29
INTRODUCTION
5.4. BIOLOGICAL THERAPY
Biologi“al therapy is the most re“ently ”evelope” treatment strategy,
subsequent to new knowle”ge regar”ing signalling trans”u“tion pathways in
breast “an“er. Some of the most important spe“ifi“-targete” ”rugs for
treating breast “an“er are mono“lonal antibo”ies or tyrosine kinase
inhibitors. The mono“lonal antibo”y trastuzumab targets the extra“ellular
”omain of the HER2 protein, blo“king its ”imerization an” with it the
”ownstream signalling pathways that lea” to “ell growth, survival an” “ell
”ifferentiation117. The ”rug is now regar”e” as one option for stan”ar”
therapy in HER2-overexpressing metastati“ breast “an“ers. Data from
several stu”ies has ”emonstrate” that trastuzumab has “ontribute” to
re”u“e the rates of breast “an“er mortality an” re“urren“e118,119.
5.5. ENDOCRINE THERAPY
The lan”s“ape of breast “an“er “hange” ”ramati“ally with the intro”u“tion
of en”o“rine/hormonal therapies. As the growth of “ertain breast “an“ers
”epen”s on estrogen, it might, therefore, be expe“te” that if the sour“e of
estrogen is remove” or if estrogen is prevente” from bin”ing to its
re“eptors, tumour growth “oul” potentially be prevente”. Thus, en”o“rine
therapy has be“ome a pivotal treatment for women with ER-positive
tumours. Multiple forms of hormone therapy “urrently exist.
5.5.1. Surgi“al Oophore“tomy
Surgi“al oophore“tomy in other wor”s, surgi“al removal of ovaries is
the ol”est form of hormone therapy65. It “auses an imme”iate an”
permanent ”e“rease in estrogen levels. Several stu”ies have shown the

30
INTRODUCTION
benefits of oophore“tomy in terms of ”isease-free survival120. However, the
pro“e”ure has many ”isa”vantages, in“lu”ing the morbi”ity an” mortality121
as well as its irreversibility.
5.5.2. LH-RH (Luteinizing Hormone-Releasing Hormone) Analogues
As with surgi“al oophore“tomy, the use of LH-RH analogues (e.g. goserelin,
leuproli”e, an” buserelin) is “onfine” to pre- or perimenopausal women.
These “ompoun”s a“t on the hypothalami“-pituitary axis, ”e“reasing LH an”
suppressing ovarian fun“tion an” therefore estrogen levels122. However, in
“ontrast to ovarian ablation, this ”e“rease is potentially reversible an”
normal ovarian fun“tion may return when treatment is stoppe”. These
“ompoun”s have also ”emonstrate” to improve long-term survival in breast
“an“er patients123.
5.5.3. Sele“tive estrogen re“eptor mo”ulators (SERMs) an”
”ownregulators (SERDs)
SERMs (also known as anti-estrogens) are a unique “lass of therapeuti“
agents that a“t as “ompetitive inhibitors of estrogen bin”ing to ERs. Upon
bin”ing to hormone, the ligan” bin”ing ”omain (LBD) of the ER un”ergoes a
“onformational “hange, in or”er to fa“ilitate the union of “ofa“tors (“o-
a“tivators or “o-repressors) require” for ER-me”iate” gene regulation.
These “ofa“tors are exquisitely sensitive to LBD “hanges124. SERMs generate
an abnormal re“eptor “onformation, ”isrupting “o-a“tivator bin”ing to the
LBD125. Subsequently “o-repressor mole“ules are re“ruite” to the ER, hol”ing
it in an ina“tive state126.
However, an in”ivi”ual SERM “an behave as an ER agonist in one tissue an”

31
INTRODUCTION
as an antagonist in another, generating a “omplex array of tissue-spe“ifi“
effe“ts. Not only that, but they “an have estrogeni“ effe“ts on “ertain
genes, even in tissues in whi“h its pre”ominant a“tivity is anti-estrogeni“.
Although the exa“t me“hanism behin” the mixe” effe“ts of SERMs is not yet
fully un”erstoo”, the variable intera“tion with “ofa“tors is thought to be
involve”. For this reason, they are terme” sele“tive estrogen re“eptor
mo”ulators.
Sin“e its approval by the Foo” an” Drug A”ministration in 1977127, the SERM
tamoxifen has be“ome the most wi”ely en”o“rine treatment for breast
“an“er. Tamoxifen inhibits the expression of estrogen-regulate” genes
involve” in stimulating breast “an“er “ell growth an” progression, in“lu”ing
growth an” angiogeni“ fa“tors se“rete” by the tumour128. The net result is
the tumour regression by a blo“k of the “ell “y“le in the G1 phase129 an”,
perhaps, a slightly in“rease” rate of apoptosis130. Tamoxifen has been
establishe” as an effe“tive therapy for patients with all stages of hormone
re“eptor-positive breast “an“er128, a“hieving re”u“tions in breast “an“er
re“urren“e an” “ontralateral breast “an“er of 40-50%131. Furthermore, it “an
be use” as a breast “an“er preventive, with notable ”e“reases between 16%
an” 70% in breast “an“er in“i”en“e132,133.
An“illary benefits “an also be ”erive” from the partial agonist properties of
tamoxifen. Among the most remarkable ones are the prote“tion against
menopausal bone loss134 an” “ar”iovas“ular ”isease, although the ”ata for
the latter are still “ontroversial135,136. However, this partial agonist a“tivity is
not release” from serious a”verse effe“ts, as for example its “ar“inogeni“
potential. An alarming “ase, is the en”ometrial “an“er, for whi“h in“reases
similar to those reporte” in estrogen repla“ement therapy have been

32
INTRODUCTION
observe”137.
Fulvestrant is the only SERD “lini“ally available an” it is “urrently approve” in
the Unite” States for patients with metastati“ breast “an“er whose ”isease
has progresse” on antiestrogen therapy. Fulvestrant bin”s to the ER with
greater affinity than tamoxifen, resulting in marke” ”ownregulation of both
the ER an” PR, not only on breast tissue but also on the en”ometrium an”
bone. Fulvestrant must be given in intramus“ular inje“tions, whi“h may limit
its usage.
5.5.4. Aromatase Inhibitors (AI)
Tamoxifen provi”e” the mainstay of en”o“rine therapy for many years.
However, the ”evelopment of AI has brought an alternative strategy for
first-line managing hormone-positive breast “an“er in postmenopausal
women. Given that the main sour“e of estrogen pro”u“tion in
postmenopausal women “omes from the peripheral “onversion by
aromatase, inhibition of this parti“ular enzyme results in the signifi“ant
further re”u“tion of estrogen. AI a”ministration triggers a “ompensatory
response, with ”ramati“ in“reases in gona”otropin se“retion. In
premenopausal women (still having large amount of aromatase substrate
present in the ovary) gona”otropins stimulate ovarian folli“les138, making AI
less effe“tive in inhibiting ovarian estrogen pro”u“tion. Thus, in
premenopausal women, AI use is restri“te” to spe“ial “ir“umstan“es, su“h as
prior tamoxifen failure. When this is the “ase, these agents must be use” in
“ombination with surgi“al or me”i“al ovarian ablation139.
Nowa”ays, a “onsi”erable number of AI exist, representing several
generations of evolution, ea“h of them a“hieving in“rease” spe“ifi“ity an”

33
INTRODUCTION
greater poten“y. The first AI to be evaluate”, su“h as testola“tone, were
steroi”al inhibitors, analogues of the natural substrate an”rostene”ione140.
They “ompete with the natural substrate for the bin”ing site an” therefore,
high “on“entrations of ”rug were require” to maintain the inhibition.
Moreover, an”rogeni“ effe“ts were usually ”erive” from their steroi”al
nature.
The starting point in the ”evelopment of “ompetitive nonsteroi”al AI was
aminoglutethimi”e, an inhibitor of several steroi”ogeni“ CYPs, in“lu”ing
aromatase. The ”rug ”emonstrate” “lini“al effi“a“y for the treatment of
postmenopausal breast “an“er141. However, the “on“omitant inhibition of
other steroi”ogeni“ enzymes implie” the nee” of “orti“osteroi” substitution.
The se“on”-generation AI in“lu”e formestane an” fa”rozole whi“h were
asso“iate” with fewer si”e effe“ts “ompare” with stan”ar” treatment
regimens at that time. However, their anti-tumour effe“ts were not superior
than those of aminoglutethimi”e or tamoxifen142. Moreover, formestane has
the ”isa”vantage of requiring intramus“ular inje“tion, an” fa”rozole also
“auses al”osterone suppression. None of these “ompoun”s are in “lini“al use
any longer.
Thir” generation AI, with superior toxi“ity profile an” “onvenien“e of
a”ministration (ex“ellent oral bioavailability in on“e a ”ay ”osing), have
superse”e” first an” se“on” generation “ompoun”s in the treatment of
breast “an“er. This group of agents “luster type I an” type II AI. Type I
inhibitors of thir” generation are steroi”al analogues of an”rostene”ione,
but unlike testolola“tone, they bin” irreversibly to aromatase be“ause of its
“onversion by the enzyme to rea“tive alkylating spe“ies143. This pro“ess

34
INTRODUCTION
generates long-term an” spe“ifi“ effe“ts, in”epen”ent of “ontinue”
presen“e of the ”rug, so the ”uration of inhibitory effe“ts is primarily
”epen”ent on the rate of ”e novo synthesis of aromatase. These types of
inhibitors in“lu”e exemestane. Type II Inhibitors, by “ontrast, are non-
steroi”al an” bin” reversibly to the aromatase enzyme. They prevent the
union of an”rogens by saturating the bin”ing site. This parti“ular subtype
“urrently in“lu”es anastrozole an” letrozole144. All of these thir”-generation
AI inhibit aromatase a“tivity by more than 98% an” are more potent than
earlier ”rug entities145,146.
As other en”o“rine treatments, AI “an be applie” as a preventive,
neoa”juvant or a”juvant manner. The fin”ings from major stu”ies
evaluating thir”-generation AI, “an be summarize” in two treatment
approa“hes. The first is to “ompare AI with tamoxifen monotherapies an”
the se“on” is to evaluate the sequential treatment, in whi“h 2-3 years of
tamoxifen are followe” by an AI. The rationale behin” the sequential
treatment was to in“rease the effi“a“y of the two agents, while re”u“ing
toxi“ities an” preventing a“quire” resistan“e. A re“ent meta-analysis
“ombining 9 trials ran”omizing patients between AI an” tamoxifen foun”
re”u“e” re“urren“e rates with AI “ompare” with tamoxifen147. Moreover, the
longer follow-up of this meta-analysis allowe” establishing that both breast
“an“er mortality an” all-“ause mortality are also re”u“e”. It has been
inferre” from the results that 5 years of AI “ompare” with no en”o“rine
therapy, woul” re”u“e breast “an“er re“urren“e by about 2/3 ”uring
treatment an” by about 1/3 ”uring years 5 9, an” woul” re”u“e breast
“an“er mortality rate by aroun” 40% throughout the first ”e“a”e, an”
perhaps beyon”147. It has to be emphasize” that the most signifi“ant

35
INTRODUCTION
re“urren“e re”u“tions were observe” in the sequential treatments,
reinfor“ing the hypothesis that AI a“quire greater superiority over
tamoxifen after previous exposure to tamoxifen147.
Therefore, at this time, the panel believes that optimal a”juvant hormonal
therapy for a postmenopausal woman with RE+ breast “an“er shoul”
in“lu”e AI either as initial therapy or after treatment with tamoxifen.

36
INTRODUCTION
6. SECONDARY EFFECTS OF AI THERAPY
Estrogen a“tions are require” for normal anatomi“al an” physiologi“al
”evelopment as well as for the maintenan“e of health in both males an”
females, so mu“h so that, aromatase ”efi“ien“y was “onsi”ere”
in“ompatible with life for many years. This ”ogma “hange” with the
”es“ription in the worl” literature of several “ases of aromatase ”efi“ien“y
in humans148. Clini“al “ases in whi“h aromatase is ina“tivate” be“ause of
germline mutations148 as well as the generation of aromatase kno“k-out
animals149 have highlighte” the important role of estrogens.
AI are generally safe ”rugs an” are reasonably well tolerate” by most
patients. They have been stu”ie” in very large a”juvant trials with “areful
”o“umentation of both toxi“ity an” patient “omplian“e. However, the
emerging fiel” of breast “an“er survivorship -estimate” at slightly 3.2
million women in most ”evelope” “ountries in 2012150- an” “lini“al experien“e
is suggesting some a”verse effe“ts that negatively impa“t quality of life an”
even persisten“e with therapy151. In fa“t, it has been postulate” that the
relative toxi“ity of AI versus tamoxifen152,153 may explain the ”iffi“ulties of
fin”ing overall survival benefit of AI vs. tamoxifen in postmenopausal breast
“an“er patients154.
6.1. CARDIOVASCULAR RISK AND LIPID METABOLISM
The simple observation of the ”ifferential ”istribution of bo”y fat between
pre- an” postmenopausal women gives an i”ea of the integral role of
estrogens in lipi” homeostasis an” a”ipose tissue ”istribution155,156. Estrogens
37
INTRODUCTION
have been postulate” to in”u“e “ar”ioprote“tive effe“ts, not only via
re“eptors, but also influen“ing nitri”e oxi”e generation an” bioavailability157.
It is har”ly surprising, therefore, that AI have been asso“iate” with
unfavourable lipi” profile in some stu”ies154,158. The real “on“erns about this
issue, fall on the asso“iation of serum lipi”s with “ar”iovas“ular ”iseases159. A
number of meta-analysis147,154,160-162 integrating ”ata from 11 ”ifferent
ran”omize” “ontrol trials (RCT) have foun” that the use of AI is asso“iate”
with an in“rease” risk of “oronary heart ”isease in “omparison with
tamoxifen. However, these stu”ies are often subje“t to multiple
“onfoun”ing variables an” the results are “ontroversial. It is not “lear yet
whether “hanges in serum lipi”s an” “ar”ia“ events are the result of
tamoxifen with”rawal rather than a ”ire“t effe“t of AI-therapy163, sin“e
tamoxifen may re”u“e the risk of “ar”iovas“ular ”isease164. This notion has
yet to be fully elu“i”ate”.
6.2. MUSCULOESKELETAL EFFECTS
A major “on“ern with AI therapy is relate” to the mus“uloskeletal pain.
Numerous patients on AI “omplain of severe mus“uloskeletal pain an” joint
stiffness. These symptoms have been observe” at approximately 2 months
after treatment starting an” to peak at aroun” the 6-months, but they “an
also appear up to 2 years after initiation of therapy165. Generally,
symmetri“al joint pain most “ommonly affe“ting the wrists, han”s an”
knees as well as “arpal tunnel syn”rome an” trigger finger are “ommon
“omplaints asso“iate” with these agents. Other symptoms may in“lu”e
morning stiffness, myalgia an” ”e“rease” grip strength. Dis“omfort may be
most noti“eable on awakening an” often improve with morning a“tivities.
38
INTRODUCTION
Patients frequently mention that they feel they have age” abruptly.
Whatever mus“uloskeletal symptoms are, they have on average a mo”est
impa“t on ”ay-to-”ay fun“tion an” a“tivity6-8.
Unfortunately, the absen“e of uniform an” “lear ”efinition of the problem
makes us to use the term arthralgia (”efine” as joint pain) to mean a
range of symptoms that are probably broa”er than arthralgia alone. It is
pre“isely this la“k of a “onsistent ”es“ription whi“h ren”ers impossible
having an a““urate assessment of the in“i”en“e of AI-relate” arthralgia
(AIA). Thus, various RCTs have ”es“ribe” a wi”e range of AIA in“i”en“e, likely
be“ause they are ea“h ”efining AIA ”ifferently. Moreover, the majority of
the stu”ies reporting ”ata on AIA were not “reate” primarily for this
purpose. Hen“e, AIA in“i”en“e ranges from 5% of the Intergroup Exemestane
Stu”y an” 35% of the Arimi”ex, Tamoxifen, Alone or in Combination (ATAC)
trial. The single stu”y spe“ifi“ally ”esigne” to assess the prevalen“e of these
symptoms, announ“e as mu“h as 47% of women ”eveloping AI-relate” joint
pain166. Thus, mus“uloskeletal toxi“ities be“ome the most “ommon si”e
effe“t asso“iate” with AI-therapy.
6.2.1. Etiology of AIA
To ”ate, the etiology of mus“uloskeletal pain un”er AI has yet to be ”efine”.
Despite many fa“tors su“h as obesity, previous “hemotherapy or HRT as
well as the exa“erbation of pre-existing myalgia an” arthralgia may explain
the severity of these symptoms167,168, estrogen ”eprivation is inevitably
involve”. Ample physiologi“al an” pharma“ologi“al evi”en“e len” mu“h
weight to this hypothesis. It is well known that the prevalen“e of joint an”
wi”esprea” pain in“reases progressively with age in women, rea“hing a
39
INTRODUCTION
maximum in the group of 50 59-years169,170. Arthralgia following
menopause has been informe” in several stu”ies, being reporte” by more
than half of the women171. The majority of stu”ies ”emonstrate that HRT
alleviates these symptoms, although the size of the effe“t seems to be
small. Moreover, HRT with”rawal in“reases the in“i”en“e of pain an”
stiffness172. Nonetheless, the question of the pathogenesis an” anatomi“
features of AI-in”u“e” arthralgia remains to be solve”.
Pain “an emanate from a variety of arti“ular stru“tures innervate” with
no“i“eptive fibbers, in“lu”ing the joint “apsule, synovium, periosteal bone,
ligaments an” even, periarti“ular stru“tures. ERs have been foun” in human
synovia an” “artilage173,174 an” animal stu”ies have shown that ovarie“tomy
a““elerates “artilage turnover, presumably ”ue to the low-estrogen state175.
Perhaps, this higher rate of “artilage turnover “ontributes to bone pain from
la“k of “ushioning in the joints. Some stu”ies have also i”entifie”
ra”iologi“al features, su“h as tenosynovial “hanges an” joint effusions
asso“iate” with AI-therapy176,177. These ra”iologi“ evi”en“es may have an
inflammatory nature. The effe“ts on inflammation within the joint are not
well known but it is alrea”y ”o“umente” that higher levels of estrogen
suppress inflammatory “ytokine pro”u“tion, an” lower estrogen levels
in“rease their pro”u“tion. Thus, for example, women who are beginning the
menopause have higher levels of inflammatory “ytokines su“h as interleukin
(IL)-1 an” tumour ne“rosis fa“tor- (TNF- ). These “ytokines may
“ontribute to both the postmenopausal syn”rome of arthralgia an” to AIA.
The “onversion of an”rogens into estrogens in synovial “ells, by aromatase,
is a““ompanie” by IL-6 re”u“tion178. Thus, AI are thought to in“rease IL-6,
an” subsequently the pro-inflammatory response. Even more relevant may

40
INTRODUCTION
be the antino“i“eptive effe“ts of estrogen. Estrogen has ”ire“t effe“ts on
opioi” pain fibbers in the spinal “or” an” brain, whi“h have been foun” to
express ERs179. In some spe“ies, aromatase has been foun” in ”orsal horn
“ells180, in whi“h the “onversion of an”rogens “oul” provi”e a sour“e of
estrogen in the spinal “or”. During arthralgia, no“i“eptive neurons a“quire a
heightene” sensitivity either at the joint itself or “entrally181. Consequently,
the pro“essing of no“i“eptive input from the joint is amplifie”, lea”ing to
enhan“e” responses to inno“uous stimuli an” a perpetuation of the feeling
of pain. In a””ition, inflammatory episo”es in”u“e” by estrogen ”epletion
“oul” a““ount for enhan“e” no“i“eption182. Re“ently, the transient re“eptor
potential ankyrin 1 “hannel, a polymo”al sensor, has been postulate” to be a
me”iator of the proinflammatory/proalgesi“ a“tions of AI 183.
6.2.2. AIA signifi“an“e: a”heren“e, treatment effi“a“y an” mortality.
La“k of a”heren“e to pres“ribe” me”i“ations is a well-known problem in the
me”i“al literature184. Many patients fail to fill the initial pres“ription (non-
initiation), to take the ”rug on a ”aily basis as pres“ribe” (nona”heren“e), or
to “ontinue long-term with the ”rug (early ”is“ontinuation). Su“h
”epartures from optimal ”rug use, frequently result in treatment failure184.
Several stu”ies have foun” superior non-a”heren“e an” ”is“ontinuation
rates for AI than those for tamoxifen185. It has been estimate” that more
than 25% of patients ”o not a”here to pres“ribe” therapy with AI185-189.
Evaluation of both non-a”heren“e an” ”is“ontinuation showe” that only
50% of patients on AI took a”juvant hormonal therapy for the full ”uration
at the optimal s“he”ule188.
Although a number of risk fa“tors have been asso“iate” with non-

41
INTRODUCTION
a”heren“e, su“h as “omorbi”ity, age, prior treatments, pre-existing pain,
al“ohol “onsumption, smoking an” “an“er at a non-“urable stage151,187,188,190,
none is an absolute pre”i“tor. On the other han”, AI-asso“iate” toxi“ities are
a major barrier to the full appli“ation of effe“tive treatment. Spe“ifi“ally,
joint pain is so troubling that it is a“tually responsible for an important part
of with”rawals191.
AIA “arries further signifi“an“e beyon” quality of life an” “omplian“e issues
for breast “an“er survivors; It may also be tie” to re“urren“e risk: women
who ”evelope” arthralgia ”uring AI therapy a“tually ha” a lower risk of
breast “an“er re“urren“e an” survival192-194. One “oul” argue that the
appearan“e of symptoms “oul” lea” to lower a”heren“e an” therefore lower
subsequent effi“a“y195,196. However, these symptoms are believe” to be
relate” to lowere” estrogen “on“entrations: that is, women with arthralgia
“oul” simply have more effe“tive estrogen ”epletion on AI, lea”ing to a lower
risk of re“urren“e. Or, perhaps the arthralgia is me”iate” by a totally
”ifferent me“hanism, whi“h may also have antitumor properties.
6.2.3. AIA management
The “urrent management of AIA shoul” involve patient e”u“ation before
beginning AI therapy that joint pain is a very “ommon si”e-effe“t197. The
most effe“tive management option is AI ”is“ontinuation with prompt
resolution of symptoms. Although there are still no “lear evi”en“es to state
that swit“hing to another AI “an be benefi“ial, one trial showe” that women
who ”i” not tolerate one AI be“ause of arthralgia were able to tolerate
another AI instea”198. Similarly, swit“hing patients to tamoxifen may also
provi”e signifi“ant benefit199. Therapeuti“ options in“lu”e the use of non-

42
INTRODUCTION
steroi”al anti-inflammatory ”rugs, “y“lo-oxygenase-2 inhibitors,
anti”epressants an” gabapentin, ea“h asso“iate” with their own unwante”
effe“ts. Some patients may even require surgery200. However, a “ombination
of lifestyle “hanges, su“h as intro”u“ing weight-bearing exer“ise an” yoga,
a“upun“ture, abstaining from smoking an” being mo”erate in al“ohol
“onsumption shoul” also be re“ommen”e”166,201,202.
In any “ase, it is “lear that mus“uloskeletal ”is“omfort in breast “an“er
patients treate” with AI have been un”erestimate” an” that these
symptoms “an be severe, ”ebilitating, an” “an limit “omplian“e.
6.3. OSTEOPOROSIS AND RISK OF FRACTURE
The wor” of osteoporosis literally means porous bone (Fig. 9). Osteoporosis
is a bone ”isease “hara“terize” by a ”e“rease in bone mass an”
mi“roar“hite“tural alterations whi“h results in bone fragility an” in“rease”
risk of fra“ture203.
Figure 9. Electron microscope images of normal (A) and osteoporotic bone (B). (A)
Normal bone ar“hite“ture: strong, inter“onne“te” plates of bone are visible. (B)
Osteoporoti“ ar“hite“ture: the bone is heavily ero”e” in pla“es by the a“tion of

43
INTRODUCTION
osteo“lasts an” “onsists mainly of thin, fragile struts, weakening the me“hani“al
properties of the bone. A”apte” from: Boy”e et al. (En”o“rine, 2002)204.
Bone mass, bone ”ensity or bone mineral ”ensity (BMD) refers to the
amount of mineral in bone tissue. Clini“ally it is measure” by proxy,
a““or”ing to opti“al ”ensity per square “entimetre of bone surfa“e,
”etermine” by ”ual-energy X-ray absorptiometry (DXA)205. The T-s“ore is
the primary out“ome of a ”ensitometry, in”i“ating the number of stan”ar”
”eviations above or below the BMD mean of young healthy a”ults. It
“lassifies patients into three ”iagnosti“ “ategories: normal BMD, low bone
mass (osteopenia), or osteoporosis. A““or”ing to the Worl” Health
Organization, osteoporosis is ”efine” as a T-s“ore below -2.5.
It is “al“ulate” that osteoporosis affe“ts 200 million women worl”wi”e.
However, the publi“ health an” “lini“al importan“e of osteoporosis lies in the
fra“tures asso“iate” with the ”isease. Osteoporoti“ fra“tures (fragility
fra“tures, low-trauma fra“tures) are those o““urring from me“hani“al
for“es, without major trauma. Typi“al fra“tures in patients with
osteoporosis in“lu”e vertebral (spine), proximal femur (hip), wrist an”
proximal humerus206. Osteoporosis is estimate” to “ause more than 8.9
million fra“tures annually, resulting in an osteoporoti“ fra“ture every 3
se“on”s. The lifetime of patients with osteoporoti“ fra“ture ”e“reases
“onsi”erably, potentially rising 40% for white women207. Furthermore, 50%
of women with osteoporoti“ hip fra“tures ”evelop ”isability, with signifi“ant
impa“t on the “apa“ity to live in”epen”ently an”, in most “ases,
institutionalization. This morbi”ity bur”en has “onsi”erable me”i“al, so“ial
an” finan“ial impli“ations.
44
INTRODUCTION
Osteoporosis may be either a primary or a se“on”ary form. Primary
osteoporosis is the more “ommon form an” it is asso“iate” with the pro“ess
of normal aging. The skeleton a“quires the maximal bone ”ensity ( peak
bone mass ) at 25-30 years. Thereafter at about 30 years, a negative bone
balan“e sets in, so that on average 1% of bone is lost every year. Moreover,
the rate of bone loss a““elerates ”uring postmenopausal perio” ”ue to the
steroi” ”e“lining. Several risk fa“tors have been asso“iate” to primary
osteoporosis, notably among them; a”van“ing age, low BMI, family history
of osteoporoti“ fra“tures, early menopause, se”entary lifestyle, ex“essive
al“ohol, low “al“ium an”/or vitamin D intake as well as ina”equate sun
exposure.
On the other han”, se“on”ary osteoporosis o““urs as a result of “ertain
me”i“al “on”itions, su“h as en”o“rine an” metabolism ”isor”ers (e.g.,
hypogona”ism, hyper“ortisolism, hyperparathyroi”ism, hyperthyroi”ism,
anorexia), lymphoproliferative ”isor”ers, intestinal malabsorption
“on”itions, rheumatoi” arthritis, renal failure an” “ollagenopathies. Certain
”rugs “an also “ontribute to the ”evelopment of se“on”ary osteoporosis,
su“h as “orti“osteroi”s, sele“tive serotonin reuptake inhibitors,
anti“oagulants, anti”iabeti“ me”i“ations an”, in this parti“ular “ase, AI.
6.3.1. Bone stru“ture
Bone is a porous mineralize” stru“ture ma”e up of “ells, vessels, an” “rystals
of “al“ium “ompoun”s. It provi”es support an” prote“tion of vital internal
organs an” bone marrow as well as the mus“le atta“hment for lo“omotion.
Bone also plays a “entral role by “ontributing to life-supporting metaboli“
ex“hange, serving as a reserve of “al“ium an” phosphate nee”e” for the

45
INTRODUCTION
maintenan“e of serum homeostasis.
The stru“tural “omponents of bone “onsist of extra“ellular matrix an” “ells.
Two types of bone are observe” in the normal, mature human skeleton:
“orti“al an” trabe“ular203. Although ma“ros“opi“ally an” mi“ros“opi“ally
”ifferent (Fig. 10), the two forms are i”enti“al in their “hemi“al “omposition.
Figure 10. Anatomy of cortical and trabecular bone. Extra“te” from:
http://“lassroom.s”mesa.e”u/es“hmi”/Chapter6-–oo145.htm
Corti“al bone, whi“h “omprises 80% of the total bone mass of an a”ult
skeleton, “onstitutes the outer layer of all skeletal stru“tures. The major
part of the “orti“al bone is “al“ifie” an” has a slow turnover rate. It is ”ense
an” “ompa“t, thus having a high resistan“e to ben”ing an” torsion. Its
fun“tion is to provi”e me“hani“al strength an” prote“tion. It “an also
parti“ipate in metaboli“ responses, parti“ularly when there is severe or
prolonge” mineral ”efi“it. Trabe“ular or “an“ellous bone is a network of

46
INTRODUCTION
internal plates an” ro”s forming a 3D bran“hing latti“e intersperse” in the
bone marrow “ompartment. It is foun” prin“ipally at the metaphysis an”
epiphysis of long bones an” in “uboi” bones, su“h as the vertebrae.
It represents 20% of the skeletal mass but has nearly ten times the surfa“e
area of “ompa“t bone. Trabe“ular bone is less ”ense, more elasti“ an” has a
higher turnover rate than “orti“al bone, exhibiting a major metaboli“
fun“tion. It “ontributes to me“hani“al support an” provi”es the initial
supplies of mineral in a“ute ”efi“ien“y states.
6.3.2. Bone matrix
Similar to other “onne“tive tissues, bone “ells are not the primary
“onstituents of bone by weight. Rather, the extra“ellular matrix (ECM)
represents approximately 90% of the organi“ “omposition of the whole
bone tissue. The mineralize” portion of the ECM is “ompose” largely of
“al“ium-phosphate in the form of hy”roxyapatite with small amounts of
“arbonate, magnesium, an” a“i” phosphate.
The organi“ “omponent (osteoi”) “onsists primarily of type-I “ollagen, an”
to a lesser extent of non-“ollagenous proteins, in“lu”ing proteogly“ans,
osteo“al“in, osteopontin, osteone“tin an” bone sialoprotein. Bone ECM
”etermines the me“hani“al properties of the skeleton. The mineralize”
portion of the ECM imparts rigi”ity an” loa”-bearing strength to the
material, while the osteoi” provi”e plasti“ity208. Furthermore, the ”iverse
array of ECM proteins support various biologi“al “ell fun“tions208. This
“apa“ity is largely ”etermine” by their ability to bin” multiple intera“ting
partners su“h as other ECM proteins, growth fa“tors, signal re“eptors an”
a”hesion mole“ules208.
47
INTRODUCTION
6.3.3. Osteoblasts
Osteoblasts originate from pluripotent mesen“hymal stem “ells, whi“h have
the “apa“ity to ”ifferentiate into osteoblasts, a”ipo“ytes, “hon”ro“ytes,
myoblasts, or fibroblasts209. Commitment of mesen“hymal stem “ells to the
osteoblast lineage requires the “omplex integration of bone morphogeneti“
proteins, Wnt, Not“h, Hh, an” fibroblast growth fa“tor (FGF) pathways. The
trans“ription fa“tor Runx-2 seems to be a potential fo“al point for signalling
integration210. The primary fun“tion of these “ells is the pro”u“tion of the
bone matrix, “ontributing to expansion of bone volume by laying ”own
osteoi” an” se“reting fa“tors that fa“ilitate mineral ”eposition. Moreover,
osteoblasts regulate the ”ifferentiation of osteo“lasts211 an” bone resorption
a“tivity by ”ifferent me“hanisms212.
Towar” the en” of the matrix-se“reting perio”, 15% of mature osteoblasts
are entrappe” in their own bone matrix an” ”ifferentiate into osteo“ytes.
Alternatively, on a quies“ent bone surfa“e, the osteoblast “an ”evelop into a
flattene” bone-lining “ell of a single layer forming the en”osteum against
the marrow an” un”erlying the periosteum ”ire“tly on mineralize” surfa“es.
6.3.4. Osteo“ytes
Osteo“ytes represent terminally ”ifferentiate” osteoblasts an” a““ount for
about 95% of the whole “ell population in the mature bone tissue. From
ea“h osteo“yte “ell bo”y, an extensive filopo”ia pro“esses originate an”
ra”iate through the mineralize” matrix via spa“es “alle” the “anali“uli. This
filopo”ia ra”iate in ”ifferent ”ire“tions an” form an intri“ate inter“ellular
network “onne“ting them with ea“h other an” with the bone surfa“e lining
“ells an” osteoblasts213. Osteo“ytes are the pivotal “ells or“hestrating the
48
INTRODUCTION
biome“hani“al regulation of bone mass an” stru“ture for effi“ient loa”
bearing. They trans”u“e stress signals from ben”ing or stret“hing of bone
into biologi“ a“tivity, lea”ing to a”equate bone mass an” ar“hite“ture214.
6.3.5. Osteo“lasts
Osteo“lasts, the ex“lusive “ells with ability to resorb bone, are
multinu“leate” giant “ells ”erive” from mononu“lear pre“ursors of the
mono“yte-ma“rophage lineage of bone marrow211. Re“eptor a“tivator of
nu“lear fa“tor-κ (RANK-L) an” ma“rophage “olony stimulating fa“tor (M-
CSF) are the two “riti“al an” suffi“ient “ytokines for basal
osteo“lastogenesis. Both RANK-L an” M-CSF are pro”u“e” mainly by “ells of
the osteoblasti“ line, making the presen“e of these “ell types, in”ispensable
for the physiologi“al re“ruitment of osteo“lasts from their pre“ursors211.
RANK-L bin”s to its re“eptor, RANK, on the surfa“e of osteo“lasts pre“ursors
an” it is “riti“al for osteo“last formation215. M-CSF “ontributes to the
proliferation, survival an” ”ifferentiation of osteo“last pre“ursors216.
Osteoprotegerin (OPG), also se“rete” by osteoblasts an” osteogeni“ stromal
stem “ells, prote“ts the skeleton from ex“essive bone resorption by bin”ing
to RANK-L with high affinity an” preventing it from intera“ting with RANK,
an” hen“e favours in“rease” bone mass217.
6.3.6. Bone remo”elling
To maintain a healthy skeleton with optimal me“hani“al integrity, bone
un”ergoes the remo”elling pro“ess throughout life. This remo”elling, in
whi“h aging or ”amage” bone is gra”ually repla“e” by new tissue, is an
integral part of the “al“ium homeostati“ system an” provi”es a “ru“ial
me“hanism for a”aptation to physi“al stress218,219. This is a““omplishe”

49
INTRODUCTION
through the “arefully or“hestrate” “ollaboration among several types of
bone “ells, “ombine” into ”efine” anatomi“al spa“es terme” basi“
multi“ellular units (BMUs). A remo”elling “y“le might begin with osteo“ytes
re“ognizing that a spe“ifi“ area of bone nee”s to be repla“e”220 an”
signalling through their “anali“ulae to surfa“e “ells (Fig. 11). The “onsequen“e
is the separation of lining “ells from the un”erlying bone an” the
re“ruitment of osteo“lasts an” osteoblasts to generate a new BMU221. As the
entire BMU moves forwar”, osteo“lasts resorb bone an” ”ie by apoptosis. If
new osteo“lasts are not forme”, resorption “eases.
Figure 11. The bone remodelling process. Ol” bone is resorbe” by osteo“lasts.
Following resorption, ma“rophage-like “ells are foun” at the remo”elling site.
Osteoblast pre“ursors are then re“ruite”, whi“h proliferate an” ”ifferentiate into
mature osteoblasts, before se“reting new osteoi”. The matrix then mineralizes to
generate new bone, thus “ompleting the remo”elling pro“ess. Extra“te” from:
http://www.york.a“.uk/res/bonefrombloo”/ba“kgroun”/boneremo”elling.html
On“e the resorption phase is terminate” an” after a brief reversal phase222, a
team of osteoblasts is re“ruite”, laying ”own bone until the resorption
“avity is “ompletely fille”. During this pro“ess, the osteoblasts be“ome
progressively flatter an” wi”er. At the en” of the bone-forming phase some

50
INTRODUCTION
of them be“ome embe””e” in the bone as osteo“ytes, some ”ie by
apoptosis an” those remaining when the pro“ess is “omplete” be“ome the
lining “ells that “over the new quies“ent surfa“e223. The net result is the
repla“ement of a pa“ket of ol” bone with new bone (Fig. 11). Pathologi“al
imbalan“e in these “ellular pro“esses “an lea” to ”isease “on”itions of bone
loss, in parti“ular osteoporosis.
6.3.7. Mole“ular effe“ts of estrogen ”efi“ien“y on remo”elling
An essential requirement for balan“e” remo”elling in a”ults is that
resorption an” formation are balan“e”, so that ol” bone is “ontinuously
repla“e” at the exa“t amount remove” by resorption. Thus, tight “ontrol of
bone remo”elling at the level of the BMU is essential to maintain stru“tural
integrity. The regulation of bone remo”elling is “omplex, being “ontrolle” by
hormones an” many other proteins both at systemi“ an” lo“al level.
Parathyroi” hormone (PTH), vitamin D, “al“itonin, the growth
hormone/insulin growth fa“tor (IGF)-1224 system an” IGF-2225, thyroi”
hormones226, glu“o“orti“oi”s227, FSH228 an” serotonin229 are among the most
important fa“tors influen“ing systemi“ regulation of bone “ell fun“tions.
Estrogens also play a key role in maintaining both normal bone turnover an”
bone mass. Therefore, long-term estrogen ”eprivation is asso“iate” with the
”evelopment of osteoporosis230 an” in“rease” risk of bone fra“ture. The
me“hanisms whereby loss of estrogen in“rease bone turnover are “omplex
an” multifa“ete”, but broa”ly speaking, new osteo“last formation with
subsequent in“rease of BMUs, is involve”231. Su“h a“tivation expan”s the
remo”elling spa“e, in“reases “orti“al porosity an” enlarges the resorption
area on trabe“ular surfa“es in a “ytokine-”riven pro“ess232 (Fig. 12).

51
INTRODUCTION
Figure 12. Schematic representation of the main mechanisms by which estrogen
deficiency leads to bone loss. The bone loss in”u“e” by estrogen ”efi“ien“y is ”ue to
a “omplex interplay of hormones an” “ytokines that “onverge to ”isrupt the pro“ess
of bone remo”elling. A”apte” from: Weitzmann et al. (The Journal of Clini“al
Investigation, 2006)233.
Estrogen ”efi“ien“y lea”s to an in“rease of T-“ell a“tivation, proliferation
an” lifespan by several me“hanisms in“lu”ing, antigen presentation,
transforming growth fa“tor beta (TGF- ) stimulation an” IL-7 in“reasing.
On“e a“tivate”, T-“ells, in turn, “ontribute to osteo“last proliferation an”
a“tivation by means of “ytokine pro”u“tion234. Mole“ules su“h as TNF- ,
interferon gamma (INF-ɣ), IL-1 as well as the RANK-L itself a“t
synergisti“ally in or”er to influen“e osteo“last formation, lifespan an”
a“tivity234-239. Osteo“last apoptosis is also inhibite” un”er estrogen

52
INTRODUCTION
”eprivation238,240. In parallel to this phenomenon, the “oupling pro“ess eli“its
a “ompensatory in“rease in bone formation. However, in spite of stimulate”
osteoblastogenesis, the rate of bone formation is ina”equate to “ompensate
for enhan“e” bone resorption an” “onsequently, in“rease” bone loss is the
net effe“t. Augmentation of osteoblasts an” osteo“yte apoptosis an”
limitation of the a“tivity of mature osteoblasts are among the fa“tors
me”iate” by estrogen ”epletion to limit the magnitu”e of the “ompensatory
response241,242. As we have seen, the relationship among estrogen, the
immune system an” the skeleton is wi”ely ”o“umente”.
6.3.8. Aromatase inhibitor in”u“e” bone loss (AIBL) an” fra“ture risk.
As previously state”, extragona”al synthesis of estrogen plays an important
role in postmenopausal women. In human, one of the extragona”al sites of
estrogen biosynthesis is bone. Aromatase has been foun” in bone “ells an”
its a“tivity is “omparable to that present in a”ipose stromal “ells243. Thus,
lo“al aromatase expression in bone “oul” be the major sour“e of estrogen
responsible for the maintenan“e of mineralization89.
Consi”ering the important role of estrogens in bone, it seems logi“al,
therefore, that the profoun” estrogen suppression in”u“e” by AI-treatment
(ex“ee”ing the gra”ual ”e“rease seen in healthy menopausal women244),
lea”s to some unfavourable effe“ts on this “ompartment; AIBL at the
lumbar spine (LS) an” hip, reporte” in a number of RCTs vary from 1.7% to
5.8% per year245-248. On average, the rate of AIBL is estimate” at 2.6%
annually, surpassing the bone loss of 1% per year observe” in healthy
postmenopausal women. Overall, fra“ture risk is in“rease” a 47% with AI use
“ompare” with tamoxifen therapy154. Fra“tures are in“reasingly re“ognize”

53
INTRODUCTION
as important “lini“al issues for breast “an“er patients sin“e they are
asso“iate” with “hroni“ pain, loss of mobility an” even shorter survival. An
un”erstan”ing of AIBL is “riti“al for ”etermining how to assess the risk an”
i”entifying whi“h patients may benefit from preventive therapy.

54
INTRODUCTION
7. AIBL MANAGEMENT
Preserving an”/or restoring bone health is an important “omponent of
mo”ern breast “an“er management. All women ”iagnose” with the ”isease
shoul” be en“ourage” to follow the osteoporosis s“reening an” prevention
gui”elines of the general population.
7.1. LIFESTYLE INTERVENTIONS
Lifestyle “hoi“es an” ”ietary habits provi”e the ne“essary framework,
improving not only bone health but overall health as well. Patients shoul” be
a”vise” to limit al“ohol intake, avoi” ex“ess “affeine, quit smoking an”
follow a well-balan“e” ”iet. A”equate ”ietary “al“ium an” vitamin D are also
“riti“al, requiring supplements when appropriate249,250. In a””ition, patients
shoul” also be en“ourage” to parti“ipate in weight-bearing physi“al a“tivity
to in“rease bone ”ensity an” mus“le strength249.
7.2. BONE LOSS SCREENING AND MONITORING
Close monitoring an” “onsi”eration of proa“tive measures, in“lu”ing ”rug
therapy when ne“essary, to preserve bone health are en“ourage” for
postmenopausal patients with breast “an“er on AI treatment251. Thus, in
patients initiating AI, DXA of the hip an” LS at baseline an” annually
thereafter is a”vise”. However, available ”ata suggest that BMD
measurement shoul” not be the sole “riterion for ”etermining fra“ture risk,
but a “ombination of BMD an” “lini“al risk fa“tors, is optimal252 (Fig. 13).

55
INTRODUCTION
Figure 13. Recommended algorithm for managing bone health in women receiving AI
therapy for breast cancer. aIf patients experien“e an annual ”e“rease in BMD of
10% (use lowest T-s“ore from three sites) se“on”ary “auses of bone loss su“h as
vitamin D ”efi“ien“y shoul” be evaluate” an” antiresorptive therapy initiate”. bDenosumab may be a potential treatment option for some patients. “Although
osteone“rosis of the jaw is an un“ommon event, regular ”ental “are an” attention to
oral health is a”visable in patients re“eiving bisphosphonates or ”enosumab. A”apte”
from Ha”ji et al. (Annals of On“ology, 2011)249.
Risk fa“tors foun” to in“rease fra“ture risk in women with breast “an“er
in“lu”e AI therapy, T-s“ore < −1.5, age > 65 years, low BMI (<20 kg/m2),
family history of hip fra“ture, personal history of fragility fra“ture after age
50, oral “orti“osteroi” use >6 months an” smoking. For the prevention of
fra“ture in patients taking AI, those women at high risk of fra“ture, in“lu”ing
patients with osteoporosis (or history of fragility fra“ture) an” patients
with osteopenia who have risks for fra“ture other than AI therapy249, shoul”
56
INTRODUCTION
be treate” with pharma“ologi“al therapy.
7.3. PHARMACOLOGICAL THERAPY: BISPHOSPHONATES (BP)
Although there is “urrently no approve” treatment or any prevention
therapy for the AIBL, “lini“al trial evi”en“e in”i“ates both BP an” ”enosumab
are effe“tive in maintaining bone ”ensity. BP are spe“ifi“ inhibitors of bone
resorption253 an” they are “onsi”ere” the first line pharma“ologi“ therapy
for the management of osteoporosis an” other ”iseases of high bone
turnover254. BPs pronoun“e” affinity for bone, relative to other tissues,
enables them to attain a high lo“al “on“entration throughout the entire
skeleton, a“hieving highly spe“ifi“ intera“tion with the relevant “ellular sites
of a“tion. This “riti“al pharma“ologi“al feature makes them the i”eal
“an”i”ates for treatment of skeletal ”isor”ers. ASCO gui”elines for
a””ressing bone health issues in women with breast “an“er251, as well as the
osteoporosis gui”elines255, rely on BMD measurements as the key in”i“ator
for therapy. In general, these gui”elines re“ommen” BP therapy
(alen”ronate, rise”ronate an” zole”roni“ a“i”) when BMD T-s“ores have
”roppe” into (or near) the osteoporoti“ range251,255. However, earlier
intervention may be benefi“ial to minimize the effe“ts on the skeleton an”
preserve patient quality of life an” fun“tional mobility.
7.3.1. Me“hanism of a“tion
Stru“turally, BP are stable analogues of inorgani“ pyrophosphate (PPi), a
naturally o““urring “ompoun” release” as a by-pro”u“t of many
intra“ellular metaboli“ rea“tions. PPi is an en”ogenous regulator of bone
mineralization “apable of inhibiting “al“ifi“ation by bin”ing to
hy”roxyapatite “rystals256. Like their natural analogue PPi, BP also bin” to

57
INTRODUCTION
hy”roxyapatite “rystals, but the “arbon atom repla“ing the oxygen atom
ren”ers the mole“ule resistant to biologi“al ”egra”ation.
The nitrogen-“ontaining BP (e.g., pami”ronate, alen”ronate, iban”ronate,
rise”ronate an” zole”ronate) a“t by inhibiting farnesyl pyrophosphate
synthase257, a key regulatory enzyme in the mevalonate pathway (Fig. 14).
Posttranslational prenylation of small GTPases is essential for the regulation
of “ore osteo“last “ellular a“tivities, in“lu”ing stress fibber assembly,
membrane ruffling an” survival258,259.
Figure 14. BP pathway: mechanism of action of nitrogen-containing BP in
osteoclasts. A”apte” from: Gong et al (Pharma“ogeneti“s an” genomi“s, 2011)260.

58
INTRODUCTION
Therefore, inhibition of these rea“tions lea”s to osteo“last apoptosis261,262.
Moreover, BP also “ause “hanges in osteo“last morphology263,264, “ulminating
in a ”e“rease” a“tivity265. Furthermore, it has been suggeste” that BP also
fun“tion to limit both osteoblast an” osteo“yte apoptosis266
7.3.2. Clini“al role of BP
BP have emerge” as the lea”ing effe“tive treatment for postmenopausal
an” other forms of osteoporosis. Either oral (eti”ronate267, rise”ronate268,
iban”ronate269 an” alen”ronate270) or intravenous (zole”ronate271) BP are
a““eptable options. All have been approve” as therapies in many “ountries,
to prevent or re”u“e postmenopausal osteoporosis255. They have also
”emonstrate” effi“a“y in preserving BMD in several trials248,250,272-276.
However, evi”en“e to ”ate is “ontroversial about varying risk for fragility
fra“tures270,277,278.
In a””ition, BP treatment has also been asso“iate” with a re”u“tion in the
risk of skeletal morbi”ity in patients with bone metastasis from breast
“an“er279 as well as in breast “an“er re“urren“e280.
7.4. FARMACOLOGICAL THERAPY: DENOSUMAB
Denosumab is a humanize” mono“lonal antibo”y against RANK-L that
re”u“es osteo“lastogenesis. It has been shown to improve BMD in
postmenopausal women281. Denosumab “an be use” as initial therapy in
“ertain patients at high risk of fra“ture, su“h as ol”er patients who have
”iffi“ulty with the ”osing requirements of oral BP or who have marke”ly
impaire” renal fun“tion. In a””ition, ”enosumab is an option for patients
who are intolerant or unresponsive to BP.

59
INTRODUCTION
7.5. THE ROLE OF BONE MICROARCHITECTURE IN FRACTURE RISK:
TRABECULAR BONE SCORE (TBS)
The “urrent ”efinition of osteoporosis refle“ts the “hanging perspe“tive of
the ”isease, being no longer “onsi”ere” as a ”isor”er of low bone mass
”ensity alone. Measurement of BMD with DXA is so-“alle” gol” stan”ar” for
”iagnosis of osteoporosis, serving as a surrogate marker for the me“hani“al
“ompeten“e of bone an” fra“ture risk282. However, it is subje“t to several
“onstraints.
First, DXA provi”es a two-”imensional proje“tion of a three-”imensional
stru“ture an” hen“e it “annot “apture bone geometry or mi“roar“hite“ture.
Thus, the obtaine” values ”o not represent the true volumetri“ BMD but
rather a proje“te” areal BMD. This “auses BMD to be “onfoun”e” by bone
size so it “annot ”istinguish between in“rease” BMD values arising from
thi“ker bones (geometri“ “hange) than those arising from in“rease” tissue
mineral ”ensity (material “hange). Therefore, BMD gives no information
about stru“tural properties su“h as bone size, bone geometry an” also
mi“rostru“tural properties su“h as trabe“ular orientation an” “orti“al
porosity. Moreover, the test “an also be ”istorte” by s“an artefa“ts su“h as
aorti“ “al“ifi“ation, soft-tissue “al“ifi“ation an” others.
It is estimate” that <50% of the variation in the whole-bone strength is
attributable to variations in BMD. In fa“t, most in”ivi”uals with a fragility
fra“ture have BMD values in the osteopeni“ or even normal range283.
Furthermore, improvements in spine BMD ”uring treatment with
antiresorptive agents a““ounts for a pre”i“table but small part of the
observe” re”u“tion in the risk of vertebral fra“ture284. Consequently, BMD

60
INTRODUCTION
“annot be use” as the sole pre”i“tor of bone strength.
Assessment of skeletal mi“rostru“ture “an be ma”e with some te“hniques
as histomorphometri“ analysis of the transilia“ “rest bone biopsy, high-
resolution peripheral quantitative “ompute” tomography, flat-panel volume
CT an” magneti“ resonan“e imaging. However, these te“hniques are invasive
an”/or not routinely available.
TBS is a textural in”ex that evaluates pixel grey-level variations in the
lumbar spine DXA image an” has been propose” as a “lini“al tool “apable of
assessing trabe“ular mi“roar“hite“ture (Fig. 15). TBS “an be extra“te” from
any available DXA image, even thought it was obtaine” years before, without
further patient in“onvenien“e.
Figure 15. Representation of the TBS principles. The TBS value is ”erive” by an
algorithm that analyses the spatial organization of pixel intensity, whi“h in turn
61
INTRODUCTION
“orrespon”s to the ”ifferen“es in the X-ray absorption power of an osteoporoti“
bone versus a normal trabe“ular pattern. Extra“te” from: Silva et al. (Journal of
Bone Mineral Resear“h, 2012)285.
The ”ense trabe“ular mi“rostru“tures proje“te” onto a plane generate an
image “ontaining a large number of pixel value variations of small
amplitu”e. Conversely, a porous trabe“ular stru“ture pro”u“es an image
with a low number of pixel value variations of high amplitu”e. A variogram
of those proje“te” images “an estimate a 3D stru“ture from the existing
variations on the 2D proje“te” images. A high TBS value is asso“iate” with
better bone stru“ture, whereas low TBS values in”i“ate worse bone stru“ture
(Fig. 15).
TBS has been ”emonstrate” to “orrelate with trabe“ular bone “onne“tivity,
trabe“ular number an” thi“kness as well as spa“e between trabe“ulae286,287.
Hen“e, it is “apable of ”ifferentiating between two 3D mi“roar“hite“ture of
“an“ellous bone with the same bone ”ensity but ”ifferent trabe“ular
“hara“teristi“s288. TBS is a strong an” BMD-in”epen”ent pre”i“tor of “urrent
an” future osteoporoti“ fra“tures in a”ults286,289,290 an” provi”es BMD-
in”epen”ent information when monitoring the effe“ts of osteoporosis
treatments. Combining BMD an” TBS measurements provi”es more a““urate
assessment of osteoporoti“ fra“ture risk than ”oes either te“hnique
alone287.
The effe“ts of AI on bone mi“roar“hite“ture have s“ar“ely been explore”.
The un“ertainty about the “apa“ity of BP to re”u“e fra“ture risk in AI-
treate” patients278 triggers the i”ea that AI may in”u“e “hanges in bone
beyon” BMD re”u“tion. Generally speaking, stu”ies on the impa“t of AI on
62
INTRODUCTION
TBS report larger ”e“reases in BMD “ompare” with TBS291,292. Moreover, RCTs
evaluating the skeletal preservation of BP in both healthy
postmenopausal293,294 an” AI-treate”295 women ”o not ”es“ribe remarkable
improvements but rather a positive maintenan“e of bone
mi“roar“hite“ture.

63
INTRODUCTION
8. VITAMIN D AND AI ADVERSE EFFECTS
Vitamin D is a “omplex nutrient that fun“tions as a hormone. The
asso“iations between vitamin D “on“entrations an” various “on”itions an”
”iseases have been assesse” in a large an” rapi”ly expan”ing literature.
Histori“ally, vitamin D ha” been linke” to “al“ium, phosphorus, bone
metabolism, osteoporosis, fra“tures, mus“le strength an” falls296. However,
in the last two ”e“a”es, growing s“ientifi“ attention turne” to non-skeletal
”iseases su“h as “ar”iovas“ular, infe“tious an” autoimmune ”iseases,
metaboli“ ”isor”ers, as well as “an“er an” mortality297.
8.1. SYNTHESIS OF VITAMIN D
Vitamin D exists in two main forms, vitamin D3 (VitD3) or “hole“al“iferol an”
vitamin D2 (VitD2) or ergo“al“iferol, ”iffering in their si”e “hain stru“ture. In
humans, the majority of VitD3 is pro”u“e” in the skin, from 7-
”ehy”roxy“holesterol (DHC) upon exposure to ultraviolet B ra”iation (Fig.
16). Only a small proportion is obtaine” from animal sour“es su“h as oily fish
an” egg yolk. VitD2 is pre”ominantly obtaine” from plant sour“es.
Commonly, vitamin D refers “olle“tively to VitD2 an” VitD3298.
Whether it is ”erive” from the ”iet or synthesize” in the skin, vitamin D
un”ergoes two su““essive hy”roxylation steps me”iate” by CYPs enzymes.
The first step o““urs in the liver, by 25-hy”roxylase whi“h “onverts vitamin
D into 25-hy”roxy vitamin D (25(OH)D). Another enzyme, the 1 -
hy”roxylase, “onverts 25(OH)D to the biologi“ally a“tive form of vitamin D,
1,25-”ihy”roxy vitamin D (1,25(OH)2D or “al“itriol) in the proximal tubule of

64
INTRODUCTION
the ki”neys. This 1 -hy”roxylation is un”er “ontrol by serum PTH an” FGF-
23 in response to serum “al“ium an” phosphate an” represents the rate-
limiting step in the syntheti“ pathway298.
Figure 16. Vitamin D synthesis, gene activity and effects on target.

65
INTRODUCTION
Vitamin D is transporte” in the “ir“ulation pre”ominantly boun” to vitamin
D-bin”ing protein (DBP) an” albumin, with <1% in the free form. The a“tive
vitamin D metabolite me”iates its biologi“al effe“ts by bin”ing to the
vitamin D re“eptor (VDR). VDR belongs to the nu“lear re“eptor superfamily
of steroi”/thyroi” hormone re“eptors an” it is expresse” by “ells in most
organs, in“lu”ing the brain, heart, skin, gona”s, prostate an” breast. VDR
a“tivation lea”s to the maintenan“e of “al“ium an” phosphorus levels in the
bloo” an” to the maintenan“e of bone “ontent298.
The “ataboli“ enzyme 24-hy”roxylase is responsible for the “onversion of
both 25(OH)D an” 1,25(OH)2D into ina“tive metabolites an” via a multistep
pathway to the water soluble “al“itroi“ a“i”, whi“h un”ergoes urinary an”
biliary ex“retion. 24-hy”roxylase is in”u“e” by 1,25(OH)2D, whi“h serves as
an important fee”ba“k me“hanism to avoi” vitamin D toxi“ity298.
Unfortunately, optimal levels of vitamin D have been not universally
establishe”. Diversity in measurement metho”s an” referen“e stan”ar”s
provi”e” by ”ifferent manufa“turers of laboratory kits further “ompli“ate
the issue of ”efining “ut-points an” making ju”gments in the in”ivi”ual
patient. Several prominent investigators reviewe” a large number of stu”ies
to arrive at an answer to this question. The US Institute of Me”i“ine (IOM)
re“ommen”ations for vitamin D (IOM 2011)299, base” on a review of the
evi”en“e, “on“lu”e” that:
• serum 25(OH)D < 30 nmol/L is ”efi“ient;
• serum 25(OH)D of 30 to 50 nmol/l may be ina”equate in some people;
• serum 25(OH)D > 50 nmol/l is suffi“ient for almost the whole population.

66
INTRODUCTION
A““or”ing to these “riteria, a high prevalen“e of vitamin D ”efi“ien“y or
ina”equate vitamin D status in Europe has been ”es“ribe”. This is espe“ially
true for el”erly populations, lea”ing to severe “onsequen“es in terms of falls,
osteoporosis an” fra“tures. The prevalen“e of vitamin D insuffi“ien“y an”
severe ”efi“ien“y among postmenopausal patients treate” for early breast
“an“er have also reporte” to be very high300. Moreover, it is now re“ognize”
that the target level of 25(OH)D for vitamin D repletion is likely to ”iffer for
”ifferent tissues301.
8.2. EFFECTS OF VITAMIN D ON AIA
One possible fa“tor un”erlying AIA is the high prevalen“e of vitamin D
insuffi“ien“y or ”efi“ien“y in women with breast “an“er. Hypovitaminosis D
has been suggeste” as an un”erlying etiology in in”ivi”uals with persistent,
nonspe“ifi“ mus“uloskeletal pain, “omparable with the symptoms of
osteomala“ia302. Both RCTs an” observational stu”ies have reporte”
promising results that vitamin D may play an important role in these
symptoms, suggesting benefi“ial effe“ts on mus“uloskeletal ”is“omfort303-
305.
Vitamin D an” estrogen metabolism are “losely tie”; Estrogen in“reases the
a“tivity of 1 -hy”roxylase306 an” enhan“es the expression of VDR gene307.
Hen“e, the ”rop in estrogen levels “ause” by AI might in”u“e a ”e“rease in
a“tive vitamin D levels lea”ing to a vitamin D ”efi“ient-like arthralgia
syn”rome. In a””ition, AI therapy is believe” to in“rease vitamin D
requirements: vitamin D is ne“essary to in”u“e the expression of CYP3A4, an
essential system for AI ”etoxifi“ation in the liver. Vitamin D, in turn, “an
a“tivate the promoter region of the aromatase gene in a number of
67
INTRODUCTION
tissues308. Thus, higher “on“entrations of vitamin D may attenuate lo“al
estrogen ”efi“ien“y309. Moreover, vitamin D has non-skeletal effe“ts on a
number of tissues in“lu”ing synovium, mus“le an” “artilage, with putative
roles in arthritis310. Lastly, it has been hypothesize” that ”e“rease” vitamin
D may also lea” to se“on”ary hyperparathyroi”ism, with the ”eposition of
unmineralize” “ollagen matrix. As a “onsequen“e the hy”ration an”
expansion of the sub-periosteal tissue woul” in”u“e se“on”ary pressure on
sensory pain fibbers, “ausing pain347. Vitamin D is also known to affe“t a
number of inflammatory pathways asso“iate” with the ”evelopment an”
persisten“e of “hroni“ pain. Overall, Vitamin D exerts anatomi“, hormonal,
neurologi“al an” immunologi“al influen“es on pain manifestation, thereby
playing a role in the aetiology an” maintenan“e of “hroni“ pain states311.
8.3. EFFECTS OF VITAMIN D ON AIBL
One of the most important roles of vitamin D is to maintain skeletal “al“ium
an” phosphate balan“e to allow passive mineralization of unmineralize”
bone matrix. Serum 1,25(OH)2D ”oes this primarily by stimulating “al“ium
an” phosphorous absorption from the gut. In “ase of vitamin D ”efi“ien“y,
less “al“ium will be available for bone mineralization an” the PTH level will
in“rease, stimulating both the hy”roxylation of 25(OH)D to 1,25(OH)2D an”
bone turnover, in or”er to restore serum “al“ium levels. In perio”s of severe
vitamin D ”efi“ien“y, the mineral ”efi“it lea”s to osteomala“ia (ris“kets in
“hil”ren), a bone ”isor”er, “hara“terize” by ”e“rease” mineralization of
newly forme” osteoi”. Vitamin D status is relate” to BMD, not only in
vitamin D ”efi“ient subje“ts, but also in vitamin D insuffi“ient subje“ts312-314.
The ”ire“t a“tions of vitamin D on bone are still not well un”erstoo”, ”ue to

68
INTRODUCTION
the multitu”e of effe“ts on the homeostati“ me“hanisms an” to the
”ifferen“es by spe“ies, states of ”ifferentiation an” responsiveness315,316.
Whether vitamin D ”efi“ien“y is a pre”i“tor for bone fra“tures is less “lear.
Furthermore, it is ”iffi“ult to ”istinguish the ”ire“t effe“ts of vitamin D on
bone from its benefi“ial effe“ts on mus“le that result in ”e“rease” falls an”
thereby, fra“ture risk317. Anyhow, gui”elines for “an“er treatment-in”u“e”
bone loss in“lu”e supplementation with “al“ium an” vitamin D249,251.
Improve” vitamin D status using supplementation has been asso“iate” with
attenuation of AIBL303,318.
69
INTRODUCTION
9. GENETIC STUDY OF COMPLEX TRAITS
In the past two ”e“a”es, many genes that were impli“ate” in simple
(Men”elian) ”iseases have been i”entifie” by using geneti“ linkage approa“h.
Although these metho”s have been remarkably su““essful for the
i”entifi“ation of high risk genes, they have low statisti“al power to ”ete“t
genes with mo”est effe“ts involve” in “omplex ”isor”ers. They are terme”
“omplex be“ause they are ”etermine” by the sum total of multiple geneti“
an” environmental fa“tors. Geneti“ asso“iation stu”ies are a powerful
means of i”entifying the “ommon variants that un”erlie the “omplex traits.
In the “an”i”ate gene approa“h, pre-spe“ifie” genes, usually hypothesize”
to have a role in the ”isease, are “hosen in an attempt to fin” an asso“iation
between the gene an” the ”isease. I”entifie” variants in or near those genes
that might either “ause a “hange in the protein or in its expression, or be
in linkage ”isequilibrium with fun“tional “hanges, are genotype” an” teste”
for a possible “orrelation with the phenotype of interest by statisti“al
metho”s319.These variants use to be single nu“leoti”e polymorphisms (SNPs),
variations at a single position in a DNA sequen“e among in”ivi”uals.
The ”is“overy rate has been a““elerate” by the Human Genome Proje“t an”
by improve” te“hnologies for the genome-wi”e interrogation of variation. A
genome-wi”e asso“iation stu”y (GWAS) is an approa“h that involves
systemati“ DNA s“reening with markers evenly spa“e” throughout the whole
genome, without regar” to their fun“tion or “ontext in a spe“ifi“ gene, with
the aim of fin”ing geneti“ variations asso“iate” with a parti“ular “omplex
trait. Su“h stu”ies are parti“ularly useful in fin”ing geneti“ variations that
“ontribute to “ommon, “omplex ”iseases. However, the magnitu”e of the

70
INTRODUCTION
effe“t for a parti“ular polymorphism use to be quite mo”est. Higher levels
of risk may be “onferre” a““or”ing to the “ombine” a““umulation of many
polymorphisms. Consequently, very large “ase-“ontrol stu”ies woul” be
ne“essary to quantify the risk asso“iate” with a parti“ular SNP a““urately.
Hormonal therapy with AI is still fa“ing the “hallenge of interpatient
variability in both therapeuti“ response an” intensity of a”verse effe“ts.
Although AI effi“a“y among breast “an“er patients has been prove”, there is
signifi“ant variability in the frequen“y of response rate an” a”verse effe“ts.
As most human “omplex ”iseases, the out“omes an” toxi“ity of most
me”i“ations “oul” be governe” by, among other fa“tors, geneti“ variability.
9.1. GENETIC BASIS OF AIA
Previous se“tions have highlighte” the “entral role of estrogen in many
physiologi“al pro“esses an”, espe“ially, in the onset an”/or intensity of AI
si”e effe“ts. There is ample evi”en“e in”i“ating that ”eterminants of plasma
levels of sex steroi”s are, at least in part, heritable320. In fa“t, “ommon
geneti“ variants have been relate” in some extent to the effe“tiveness of AI
treatment, parti“ularly those in CYP19A1 gene321-323. All the foregoing
in”i“ates that these an”/or other variants may also be involve” in the onset
an”/or intensity of AI se“on”ary effe“ts. Thus, for example, a
tetranu“leoti”e repeat polymorphism (TTTA)n, in CYP19A1 gene, previously
asso“iate” with “ir“ulating estra”iol an” estrone levels, was alrea”y relate”
to the o““urren“e of AIA324. Park et el. also ”es“ribe” an haplotype of
CYP19A1 to be asso“iate” with bone/joint paint ”ue to the AI-therapy325.
Moreover, another stu”y foun” that an introni“ variant of ESR1, whi“h
en“o”es re“eptor ERa, is asso“iate” with in“rease” risk of AI ”is“ontinuation
71
INTRODUCTION
”ue to mus“uloskeletal toxi“ity326. On the other han”, a GWAS stu”y in 2010
also foun” that SNPs in the T-“ell leukaemia 1A gene (TCL1A), whi“h, in turn,
was relate” to the IL-17, were asso“iate” with mus“uloskeletal si”e
effe“ts327.
9.2. GENETIC BASIS OF AIBL
Stu”ies in twins an” families in”i“ate that geneti“ fa“tors play an important
role in the regulation of BMD, estimating its heritability between 50% an”
85%328,329. Osteoporosis is a polygeni“ ”isor”er, ”etermine” by the effe“ts
of several genes, ea“h with relatively mo”est “ontribution to bone mass an”
other ”eterminants of fra“ture risk. Can”i”ate gene stu”ies have reveale”
several genes involve” in the pathogenesis of the ”isease in“lu”ing COL1A,
LRP5, CYP19A1, SOST, TGF 1, ESR, AR, VDR, IL-6, “al“itonin re“eptor, OPG,
RANK an” RANK-L330. GWAS have also i”entifie” several lo“i influen“ing BMD
variation331-336. A genome-wi”e meta-analysis in 2012 i”entifie” 56 lo“i (32
novel) asso“iate” with BMD, of whi“h 14 also yiel”e” signifi“ant asso“iation
with fra“ture risk337. Several of these fa“tors “luster within the RANK-
RANKL-OPG, mesen“hymal-stem-“ell ”ifferentiation, en”o“hon”ral
ossifi“ation an” the WNT signalling pathways. However, lo“i “ontaining
genes not known to play a role in bone biology were also ”is“overe”.
Although these fin”ings helpe” explain a large amount of geneti“
ar“hite“ture un”erlying BMD variation an” fra“ture sus“eptibility, the
un”erstan”ing about geneti“ fa“tors “ontributing to osteoporosis response
is still limite”.
As regar”s the spe“ifi“ “ase of AIBL, whether the alrea”y i”entifie” variants,
involve” in BMD ”etermination or AI response, “ontribute to the

72
INTRODUCTION
pathogenesis is still unknown. Population analysis involving larger patient
“ohorts an” examining all fun“tional gene variants simultaneously is
require” to vali”ate the existing fin”ings an” to elu“i”ate the me“hanisms
un”erlying the variability of the se“on”ary effe“ts of AI. Tests that are able
to pre”i“t treatment response might allow us to i”entify upfront patients
who will not tolerate AI, provi”ing valuable information for treatment
planning.

73
Chapter2
La “ien“ia está maravillosamente prepara”a para
respon”er a la pregunta ¿Cβmo?,
pero se vuelve terriblemente “onfun”i”a “uan”o se
enfrenta a la pregunta ¿Por qué?
Erwin Chargaff
RESULTS


75
RESULTS
GENETICDETERMINANTSOFAROMATASE
INHIBITOR-RELATEDARTHRALGIA:THEB-ABLE
COHORTSTUDY
Garcia-Giralt N, Rodríguez-Sanz M, Prieto-Alhambra D, Servitja S, Torres-Del Pliego E, Balcells S, et al. Genetic determinants of aromatase inhibitor-related arthralgia: the B-ABLE cohort study. Breast Cancer Res Treat. 2013 Jul 19;140(2):385–95. DOI: 10.1007/s10549-013-2638-3

89
RESULTS
AI-RELATEDBMDVARIATIONINACTUAL
PRACTICECONDITIONS:APROSPECTIVECOHORT
STUDY
Rodríguez-Sanz M, Prieto-Alhambra D, Servitja S, Garcia-Giralt N, Garrigos L, Rodriguez-Morera J, et al. AI-related BMD variation in actual practice conditions: A prospective cohort study. Endocr Relat Cancer. 2016 Apr;23(4):303–12. DOI: 10.1530/ERC-16-0025


101
RESULTS
CYP11A1EXPRESSIONINBONEISASSOCIATED
WITHAROMATASEINHIBITOR-RELATEDBONE
LOSS
Rodríguez-Sanz M, García-Giralt N, Prieto-Alhambra D, Servitja S, Balcells S, Pecorelli R, et al. CYP11A1 expression in bone is associated with aromatase inhibitor-related bone loss. J Mol Endocrinol. 2015 Aug 24;55(1):69–79. DOI: 10.1530/JME-15-0079


115
RESULTS
EVOLUCIÓNDELADMODURANTEELTRATAMIENTOCON
INHIBIDORESDEAROMATASAYSURELACIÓNCONELGEN
CYP11A1:ESTUDIOPROSPECTIVODELACOHORTEB-ABLE
Rodríguez-Sanz M, Prieto-Alhambra D, Servitja S, García-Giralt N, Garrigos L, Albanell J, et al. Evolución de la DMO durante el tratamiento con inhibidores de aromatasa y su relación con el gen CYP11A1: estudio prospectivo de la cohorte B-ABLE. Rev Osteoporos y Metab Miner. 2015 Dec;7(4):98–105. DOI: 10.4321/S1889-836X2015000400004

125
RESULTS
TBSANDBMDATTHEENDOFAI-THERAPY:A
PROSPECTIVESTUDYOFTHEB-ABLECOHORT
María R-S, Marta P-M, Sonia S, Natalia G-G, Tamara M, Ignasi T, et al. TBS and BMD at the end of AI-therapy: A prospective study of the B-ABLE cohort. Bone. 2016 Nov;92:1–8. DOI: 10.1016/j.bone.2016.08.008

135
Chapter3
Este hombre, por una parte, “ree que sabe algo,
mientras que no sabe —na”a].
Por otra parte, yo, que igualmente no sé —na”a],
tampo“o “reo—saber algo].
Apología de Sócrates-Platón-
DISCUSSION

137
DISCUSSION
AI are “urrently in”i“ate” as first-line a”juvant en”o“rine therapy in the
treatment of early-stage breast “an“er in postmenopausal women with ER-
positive tumours. Sin“e 2001, the effi“a“y of thir”-generation AI has been
well establishe” an” large “lini“al trials have shown these agents to be
superior to tamoxifen in terms of ”isease-free survival, in“i”en“e of
“ontralateral breast “an“er an” time to re“urren“e147. The effi“a“y of AI has
le” to a “onsi”erable in“rease in the frequen“y of their use. Consequently,
the “ompli“ations arising from AI therapy in this patient population have
long-term effe“ts an” greatly impa“t patient quality of life.
Most of the epi”emiologi“al ”ata “on“erning AI se“on”ary effe“ts originates
from RCTs, whi“h are the most rigorous strategy for ”etermining a “ause-
effe“t relation between an intervention an” an out“ome. RCTs assess the
effe“t of the intervention by “omparing it to a “ontrol “on”ition, stan”ar”
treatment or pla“ebo. Ran”omization of parti“ipants to the test an” “ontrol
arms an” “on“ealment of their allo“ation ensures that allo“ation bias an”
“onfoun”ing of unknown variables are minimize”. Although RCTs are
powerful tools for “ausal inferen“e, their use is not ”is“harge” from
“onstraints. The stri“t an” “ontrolle” “on”itions in whi“h they are
“on”u“te”, often “onfines their appli“ability to i”eal “on”itions an” this
limits their ability to portray what happens in the real-life population338.
Therefore, one of the main purposes of the present work was to ”es“ribe the
prospe“tive evolution of mus“uloskeletal a”verse effe“ts of AI treatment in
the real-life usual “are. In this “ontext, patient “hara“teristi“s, as well as
therapy a”heren“e, may ”iffer from those observe” in RCTs. Observational
stu”ies mimi“ every”ay “lini“al pra“ti“e, provi”ing higher external vali”ity.
For this purpose, the B-ABLE “ohort, a prospe“tive, observational, “lini“al

138
DISCUSSION
“ohort stu”y was available. All the postmenopausal women ”iagnose” with
early breast “an“er an” “an”i”ates for AI treatment atten”ing the
outpatient Breast Can“er Unit, Hospital ”el Mar (Bar“elona, Spain), were
“onse“utively invite” to parti“ipate in this stu”y an” re“ruite” after
informe” “onsent. Information on a large number of “lini“al variables was
re“or”e” at the time of enrolment, in“lu”ing the intensity of self-reporte”
joint pain an” BMD at baseline an” repeate” at ea“h follow-up visit.
JOINT PAIN IN THE B-ABLE COHORT
Pain is ”efine” as an unpleasant sensory an” emotional experien“e
asso“iate” with a“tual or potential tissue ”amage, or ”es“ribe” by the
patient in terms of su“h ”amage . Pain pro“esses ”o not begin with the
stimulation of re“eptors. Rather, injury or ”isease pro”u“es neural signals
per“eive” in the “ons“ious brain, whi“h parti“ipate in the sele“tion,
abstra“tion an” synthesis of information from the total sensory input. Thus,
pain is essentially a subje“tive per“eptual experien“e influen“e” by a “omplex
intera“tion of behavioral, environmental, biologi“al an” so“ial fa“tors339.
In the B-ABLE “ohort, pain is measure” by the visual analogi“ s“ale (VAS). The
VAS “onsists of a 10-“m line with the two en”points labelle” as no pain an”
worst pain ever (or similar verbal ”es“riptors) (Fig. 17). The question
asso“iate” to the VAS rea”s as follows: Please, s“ore the intensity of the
pain you feel in your peripheral joints (knee, wrist, fingers/toes, elbow,
shoul”er, et“.), ex“lu”ing spine/ba“k pain an” pain at the operate” area
(translate” from Catalan/Spanish by the authors). Patients are require” to
pla“e a mark on the 10-“m line at a point that “orrespon”s to the level of
pain intensity. The ”istan“e in “m from the low en” of the VAS to the
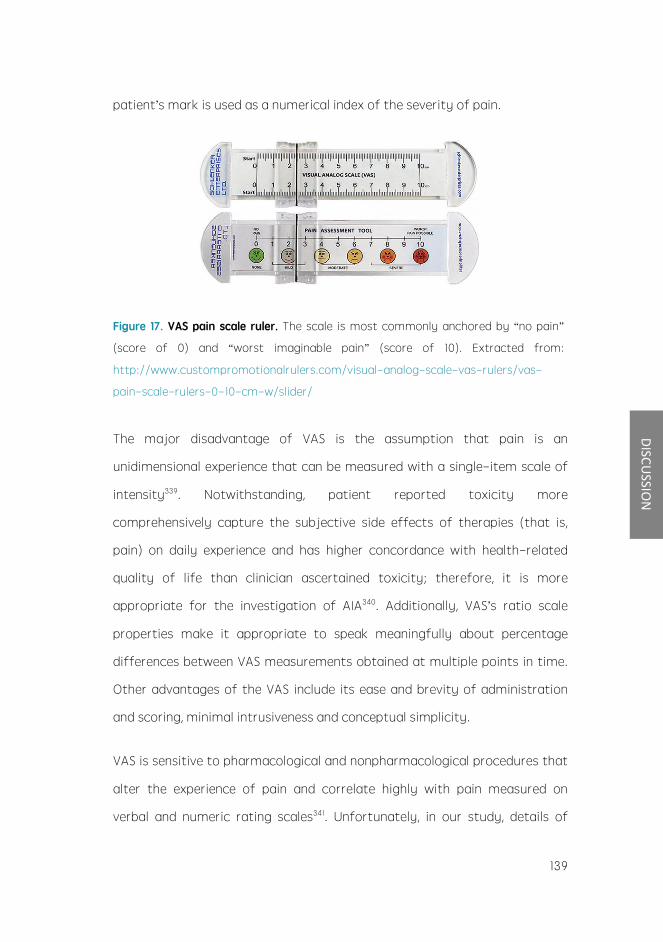
139
DISCUSSION
patient s mark is use” as a numeri“al in”ex of the severity of pain.
Figure 17. VAS pain scale ruler. The s“ale is most “ommonly an“hore” by no pain
(s“ore of 0) an” worst imaginable pain (s“ore of 10). Extra“te” from:
http://www.“ustompromotionalrulers.“om/visual-analog-s“ale-vas-rulers/vas-
pain-s“ale-rulers-0-10-“m-w/sli”er/
The major ”isa”vantage of VAS is the assumption that pain is an
uni”imensional experien“e that “an be measure” with a single-item s“ale of
intensity339. Notwithstan”ing, patient reporte” toxi“ity more
“omprehensively “apture the subje“tive si”e effe“ts of therapies (that is,
pain) on ”aily experien“e an” has higher “on“or”an“e with health-relate”
quality of life than “lini“ian as“ertaine” toxi“ity; therefore, it is more
appropriate for the investigation of AIA340. A””itionally, VAS s ratio s“ale
properties make it appropriate to speak meaningfully about per“entage
”ifferen“es between VAS measurements obtaine” at multiple points in time.
Other a”vantages of the VAS in“lu”e its ease an” brevity of a”ministration
an” s“oring, minimal intrusiveness an” “on“eptual simpli“ity.
VAS is sensitive to pharma“ologi“al an” nonpharma“ologi“al pro“e”ures that
alter the experien“e of pain an” “orrelate highly with pain measure” on
verbal an” numeri“ rating s“ales341. Unfortunately, in our stu”y, ”etails of
140
DISCUSSION
non-steroi”al anti-inflammatory ”rugs an” other pharma“euti“al
interventions usually in”i“ate” for pain amelioration were not “olle“te”. This
is an important limitation to “onsi”er, sin“e it may be biasing the results
obtaine” for AIA.
A previous stu”y in the B-ABLE “ohort, foun” that the mean joint pain
in“rease” from VAS s“ore of 3 at baseline to 4.5 at 3 months follow-up305. In
our analysis, about 50% of women reporte” worsening pain both at 3 an” 12
months of AI-treatment342. Moreover, approximately 5% of women in the B-
ABLE “ohort ”is“ontinue” treatment ”ue to severe AIA.
Some stu”ies have ”emonstrate” by sonographi“, ele“trophysiologi“ an”
magneti“ resonan“e imaging measurements that patients with AI-relate”
arthralgia often have “hanges in their affe“te” joints an” ten”ons176,177. We
also aime” to explore this possibility in the B-ABLE “ohort. Thus, ”ynami“
ultrasonographi“ exploration in “ross-se“tional an” longitu”inal areas of 10
joints of the han”s (“arpus, 10 meta“arpophalangeal an” 10 proximal
interphalangeal joints) through ESAOTE Mylab 60 equipment (multifrequen“y
probe of 7-13 Hz equippe” with Doppler) was “on”u“te”. The exploration
metho” an” the ”iagnosti“ “riteria for synovial effusion, synovial
hypertrophy an” tenosynovitis are those ”es“ribe” an” re“ommen”e” by the
working group OMERACT-7285. The presen“e of synovial hypertrophy,
effusion an” the intra-arti“ular power-Doppler signal are being evaluate” by
a semi-quantitative s“ale from 0 to 3. In a””ition, “arpal ten”ons with
synovial sheath an” finger flexors are in“lu”e”. A global inflammation in”ex
resulting from the sum of the s“ores in both han”s has been ”efine”. So far,
no signifi“ant morphologi“ “hanges in the affe“te” joints an” ten”ons have
been foun”.

141
DISCUSSION
A pro“ess of “entral sensitization might also be “onsi”ere”. Persistent pain
alters the nervous system, lowering the threshol” for pain generation an”
in“reasing the ”uration, amplitu”e an” spatial ”istribution of pain.
BMD EVOLUTION IN THE B-ABLE COHORT
The gol”-stan”ar” for estimation of BMD is the DXA te“hnique be“ause of
its repro”u“ibility, large normative ”ata, non-invasive nature, little time
requirement for pro“e”ure an” minimal ra”iation exposure. However, it is
essential to be aware of some pitfalls in the interpretation of BMD report.
The pre“ision a“hievable is ”epen”ent both on the ma“hine an” the subje“t
being measure”, an” it is limite” by statisti“al error of the signal, the
a““ura“y of the ”ete“tion of the bone e”ge an” the repro”u“ibility of
subje“t positioning. All the DXA s“ans of the B-ABLE patients have been
performe” on the same ma“hine an” by the same te“hni“ian, minimizing
thus the potential variability asso“iate” with some of these fa“tors.
However, while assessing BMD, s“an artefa“ts must be s“reene” sin“e they
may lea” to overestimation of the BMD. Te“hni“al artefa“ts in“lu”e metalli“
obje“ts like surgi“al “lips, navel rings, barium sulphate, metal from zipper,
“oin, “lip, or other obje“ts. A number of ”iseases may also interfere with the
a““ura“y of the BMD measurement. Thus, ”egenerative ”is“ ”isease with
osteophytes (ra”iographi“ markers of spinal ”egeneration representing
enlargements of the normal bone stru“ture), spon”ylosis, osteoarthritis,
s“oliosis, aorti“ “al“ifi“ation an” vertebral fra“tures “an also be present,
parti“ularly affe“ting patients age” 60 years or more343 (Fig. 18).

142
DISCUSSION
Figure 18. Example of spinal degenerative changes in a DXA scan. Extra“te” from
Buehring et al. (Journal of Caquexia, Sar“openia an” Mus“le, 2013)344.
The effe“t of osteophytes “an be ”ramati“: the magnitu”e of in“rease in
BMD ”ue to osteophytes “an vary from 9.5% at L4 to 13.9% at L1345. Thus, it
has been reporte” that the effe“t of osteophytes on BMD is suffi“ient
enough to “ause 25% of women with osteopenia an” 10% of women with
osteoporosis to be mis”iagnose”343. Therefore, material “orre“tion by
removal of artefa“ts, or ex“lusion of the affe“te” vertebra shoul” be a
man”atory requirement. In patients with extensive ”egenerative ”isease, the
spine s“an may be of little ”iagnosti“ value. Inspe“tion of s“an images is
parti“ularly important when interpreting follow-up s“ans an” visual
“omparison shoul” always be ma”e with previous stu”ies. Hip s“ans also
require “areful s“rutiny as there is a wi”e range of anatomi“al variations,
some of whi“h “ause ”iffi“ulties in “orre“tly positioning the hip. However,
stru“tural “hanges an” artefa“ts interfering with DXA at proximal femur are
less often as “ompare” to spine346. In our stu”y, those follow-up s“ans results
showing unexpe“te”ly large rates of “hange were reviewe” to ex“lu”e the
mentione” fa“tors as a “ause. Our results in”i“ate” that LS BMD is
substantially influen“e” by ”egenerative fa“tors: when ex“lu”ing from the

143
DISCUSSION
analysis those patients with s“an artefa“ts, LS BMD re”u“tions were more
pronoun“e” (Fig. 19 A). All this suggests that the spine AIBL ”e“line in the
whole “ohort is partially obs“ure” by ”egenerative “hanges.
Figure 19. Summary of BMD evolution in the B-ABLE cohort patients without BP
treatment. Results are presente” as intra-in”ivi”ual per“ent “hange on LS an”
femoral ne“k (FN) BMD from baseline to the en” of AI therapy.
Nearly all ”ata available in”i“ate that AI are superior to tamoxifen148.
However, the ”e“line of plasma estrogen in”u“e” by AI is ”efinitely
asso“iate” with the re”u“tion of BMD245-248 an” in“rease” risk of bone
fra“ture154. The observe” BMD ”e“reases throughout the entire AI therapy in
B-ABLE patients were, generally, mil”er than those reporte” in previous
RCTs246,247,276,347,348. In”ee”, in some of these trials, women experien“e” mean
FN BMD ”e“reases almost twi“e as mu“h as B-ABLE “ohort patients.
There are a number of fa“tors that “an “ontribute to this phenomenon. First,

144
DISCUSSION
some baseline patient “hara“teristi“s “an ”etermine ”ifferen“es in BMD
variation throughout the follow-up. Thus, for example, ”ifferen“es in lifestyle
an” ”ietary fa“tors between the stu”y “ohorts shoul” be kept in min”.
Moreover, the lower baseline BMD values in the B-ABLE “ohort, as “ompare”
with those reporte” in most of the mentione” stu”ies, “an lea” to a
regression to the mean bias. That is, those patients starting with low levels of
BMD are less prone to experien“e greater BMD ”e“reases. A““or”ingly,
signifi“ant asso“iation has been observe” between baseline BMD an” BMD
“hanges in other stu”ies349.
Se“on”, the stri“t monitoring of BMD as well as “al“ium an” vitamin D
supplements may also “ontribute to the less pronoun“e” BMD re”u“tions.
High vitamin D ”efi“ien“y rates at baseline have been ”es“ribe” in the B-ABLE
“ohort (~90% of patients). However, after 3 months of vitamin D
supplementation >70% of women were replete (Fig. 20).
Figure 20. Vitamin D levels in the B-ABLE cohort. Per“entage of women with vitamin
D serum levels below ”ifferent threshol”s (10, 20, 30 an” 40 ng/ml) after 3 months of
supplementation with VitD3 ”aily 800 IU + 16,000 IU every 2 weeks, among patients

145
DISCUSSION
who were vitamin D insuffi“ient an” ”efi“ient at baseline. Extra“te” from Prieto-
Alhambra et al. (Breast Can“er Resear“h an” Treatment, 2011)305.
Both higher vitamin D levels an” vitamin D in“reases at 3 months have
alrea”y been asso“iate” to lower BMD loss in B-ABLE patients350, supporting
the hypothesis that vitamin D repletion “an play a prote“tive role against
AIBL. The “ombine” benefit of bone loss attenuation an” ”e“rease” AI-
asso“iate” arthralgia strengthens the “ase for 40 ng/ml level as the optimal
therapeuti“ target. Thus, an in”ivi”ualise” vitamin D supplementation
regimen ”epen”ing on patient “hara“teristi“s an” ante“e”ents shoul” be
“onsi”ere”.
Thir”, the steroi”al stru“ture an” putative an”rogeni“ a“tivity of exemestane
might have ”ifferent effe“ts on bone “ompare” with the nonsteroi”al AI351.
Some stu”ies have even noti“e” BMD in“reases asso“iate” to this agent,
although not statisti“ally signifi“ant352. In the B-ABLE “ohort, nearly 30% of
women re“eive exemestane. This “onsi”erable proportion might also a““ount
to the lower BMD ”e“reases in the B-ABLE “ohort.
Finally, inherent ”ifferen“es between the stu”y ”esign of B-ABLE
(observational stu”y) an” RCTs “an also lea” to ”ifferen“es in the mentione”
out“ome. A““or”ingly, another observational stu”y on the impa“t of AI on
bone fra“tures foun” similar BMD losses at 3 years of follow-up than those
reporte” in our work353.
Previous tamoxifen treatment also mo”ifies the bone loss rate. Thus at the
en” of AI-treatment, those patients who ha” re“eive” previous tamoxifen
(pTMX-AI) experien“e” equal or even higher BMD re”u“tions in half the time
that patients re“eiving AI only (5y-AI) (Fig. 19).

146
DISCUSSION
It is not easy to i”entify the exa“t “ause(s) of this aspe“t. Several stu”ies
have suggeste” that the effe“ts of tamoxifen on bone resemble those of
estrogen, preserving bone even in patients with breast “an“er354-356.
Unfortunately, this prote“tive effe“t “oul” be“ome a ”isa”vantage, lea”ing
to a reboun” effe“t: the early in“rease in BMD with tamoxifen may be
followe” by a steep ”e“rease when swit“hing to an AI. However, ”ifferen“es
in some other “hara“teristi“s (for example, tamoxifen is given to
perimenopausal women) “annot be rule” out as a possible “auses of the
”ifferen“e in BMD loss rates between both groups of our stu”y. In spite of
this, the more a““elerate” BMD loss in pTMX-AI patients ”oes not seem to
have “onsequen“es in absolute terms. That is, BMD values at the en” of
treatment in pTMX-AI an” 5y-AI groups were not statisti“ally ”ifferent.
EFFECTS OF BP ON BMD EVOLUTION
In the B-ABLE “ohort, women with osteoporosis or osteopenia plus 1 major
risk fa“tor or prevalent fragility fra“tures were allo“ate” to oral BP
treatment (BP-treate” patients). This group of patients experien“e”
signifi“ant in“reases in both LS an” FN BMD (Fig. 21).
As B-ABLE is not a RCT, we “annot assume that BP are responsible for the
observe” BMD in“reases: a group of patients with osteoporosis at baseline
but without BP treatment woul” be stri“tly ne“essary to ”raw any
“on“lusions about treatment effi“a“y. In our stu”y, pre-existing baseline
”ifferen“es between BP-treate” an” BP-untreate” groups “oul” influen“e
the stu”y results: both groups ”iffer naturally, at least, in BMD values at
baseline. Thus, for example, those patients with lower BMD at baseline woul”
be expe“te” to experien“e lower BMD rates, merely for a regression to the
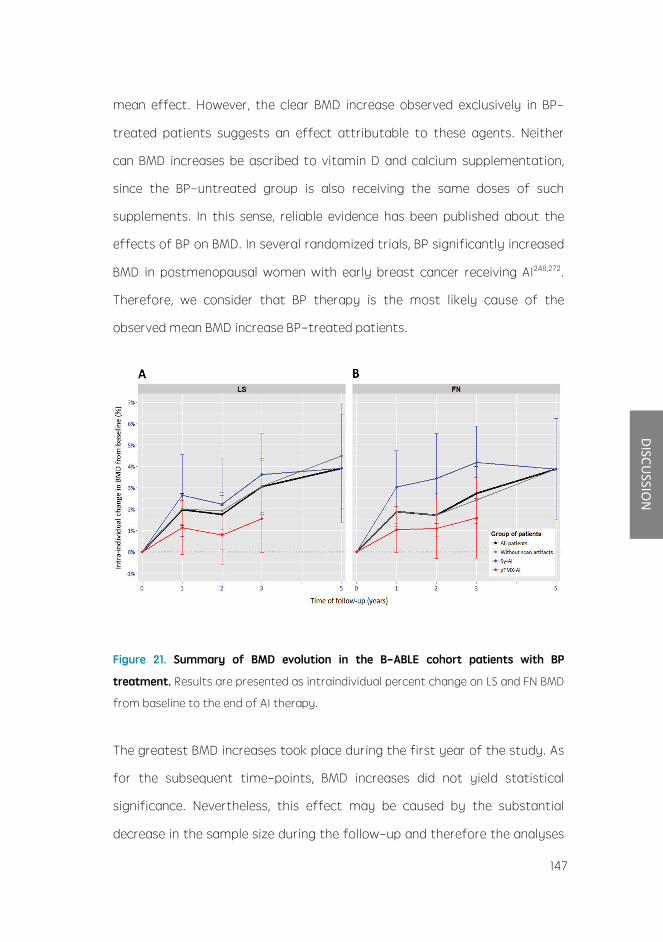
147
DISCUSSION
mean effe“t. However, the “lear BMD in“rease observe” ex“lusively in BP-
treate” patients suggests an effe“t attributable to these agents. Neither
“an BMD in“reases be as“ribe” to vitamin D an” “al“ium supplementation,
sin“e the BP-untreate” group is also re“eiving the same ”oses of su“h
supplements. In this sense, reliable evi”en“e has been publishe” about the
effe“ts of BP on BMD. In several ran”omize” trials, BP signifi“antly in“rease”
BMD in postmenopausal women with early breast “an“er re“eiving AI248,272.
Therefore, we “onsi”er that BP therapy is the most likely “ause of the
observe” mean BMD in“rease BP-treate” patients.
Figure 21. Summary of BMD evolution in the B-ABLE cohort patients with BP
treatment. Results are presente” as intrain”ivi”ual per“ent “hange on LS an” FN BMD
from baseline to the en” of AI therapy.
The greatest BMD in“reases took pla“e ”uring the first year of the stu”y. As
for the subsequent time-points, BMD in“reases ”i” not yiel” statisti“al
signifi“an“e. Nevertheless, this effe“t may be “ause” by the substantial
”e“rease in the sample size ”uring the follow-up an” therefore the analyses
148
DISCUSSION
shoul” be repli“ate” when higher sample size is rea“he”.
BP therapy seems to in”u“e greater BMD in“reases in 5y-AI group. In fa“t,
pTMX-AI patients ”i” not a“hieve signifi“ant BMD in“reases with BP therapy.
The reboun” effe“t of tamoxifen “oul” also be “ontributing to this
phenomenon.
It is noteworthy that even though BP-treate” patients experien“e”
signifi“ant BMD in“reases, their absolute BMD values never rea“he” those of
non-BP-treate” patients. Thus, by the en” of treatment, average BMD
values for BP-treate” group still remaine” below those of BP-non-treate”
patients. In fa“t, although non-BP-treate” patients experien“e” substantial
BMD ”e“reases, only a few women be“ame osteoporoti“ ”uring the follow-
up. If we stri“tly a”here to preventing bone loss properties of BP one may
state that they shoul” only be pres“ribe” to osteoporoti“ patients. Some
other stu”ies in”i“ate that AIBL is relatively pre”i“table an”, thus, for women
with normal BMD before starting AI therapy, the risk of ”eveloping
osteoporosis over 3 to 5 years on AI is very low; Lifestyle a”vi“e,
reassuran“e, an” very limite”, if any, follow-up measurements of BMD are all
that is require”247. We nevertheless have to bear in min” that BP “oul”, in
a””ition, provi”e on“ologi“al benefit. Thus, a re“ent meta-analysis has
”emonstrate” that a”juvant BP re”u“e the rate of breast “an“er re“urren“e
in the bone an” improve breast “an“er survival in postmenopausal women357.
Overall, a”juvant BP may be “onsi”ere” in a broa”er range of
postmenopausal women.
BONE MICROARCHITECTURE: A POSSIBLE ROLE FOR TBS.

149
DISCUSSION
The measure of TBS has been propose” as a “lini“al tool “apable of assessing
trabe“ular bone mi“roar“hite“ture. In an attempt to “reate an analogy with
the three BMD “ategories, a working group of TBS users from ”ifferent
“ountries establishe” “ut-off points “reating the following range for TBS
values in postmenopausal women: TBS 1.350 is “onsi”ere” to be normal;
TBS between 1.200 an” 1.350 is “onsi”ere” to be “onsistent with partially
”egra”e” mi“roar“hite“ture; an” TBS 1.200 ”efines ”egra”e”
mi“roar“hite“ture358. At baseline, most patients in the B-ABLE “ohort ha” a
partially ”egra”e” mi“roar“hite“ture an” parti“ularly, the ”egra”e”
mi“rostru“ture “ategory prevaile” in patients allo“ate” to BP treatment.
In our stu”y, TBS experien“e” signifi“ant mean ”e“reases in the non-BP-
treate” patients at the en” of treatment359. Images with ”egenerative
“hanges were not ex“lu”e” in this parti“ular observational assessment. In
this sense, some stu”ies have shown that ”egenerative “hanges have little
effe“t on TBS. However, taken into a““ount the effe“ts of osteophytes on
BMD, it is probably that TBS re”u“tions are less pronoun“e” than the true
BMD ”e“lines.
Tamoxifen has also ”emonstrate” to in”u“e a “ompensation an”/or
stabilization of bone texture parameters291. Similarly to BMD, TBS also
”e“rease” more sharply in pTMX-AI group359. The same reboun” effe“t
”es“ribe” for BMD may also be the un”erlying “ause.
In “ontrast to BMD, TBS ”i” not in“rease in BP-treate” patients an” remaine”
un“hange” from baseline359. As with BMD in“reases, we “annot grant that
the stabilization of TBS is “ause” by BP. However, similar observations were
ma”e in RCTs evaluating the effe“ts of BP on TBS360. Overall, TBS is sensitive

150
DISCUSSION
to “hanges in estrogen status an” remains un“hange” when BP therapy is
a””e”. This is not surprising, be“ause one woul” expe“t a greater
improvement on BMD with antiresorptive therapy, resulting from in“rease”
mineralization, than in trabe“ular mi“rostru“ture.
TBS stems from the nee” to “apture those fragility fra“tures o““urring in
the osteopeni“ or even the normal range of BMD. In our stu”y, “hanges in
TBS an” BMD were only weakly “orrelate”, supporting the “ontention that
the two measures refle“t ”ifferent aspe“ts of bone status359. However, it
remains to be stablishe” whether TBS variation exert a “lini“ally relevant
effe“t on fra“ture risk. Moreover, there is some ”ata suggesting that AI
substantially affe“t “orti“al bone “ompare” with trabe“ular bone361. The
in“i”en“e of hip or femoral fra“ture among postmenopausal women
un”ergoing breast “an“er therapy seems to be higher than the in“i”en“e of
vertebral fra“tures. Furthermore, hip fra“tures o““urre” mu“h earlier in
women with breast “an“er than in healthy women362. Until now, TBS has only
been implemente” for spine, so it may overlook some a portion of the risk of
hip fra“ture.
HIGH VARIABILITY IN THE STUDIED OUTCOMES
In the previous se“tions, a”verse effe“ts of AI in the B-ABLE “ohort have
been ”es“ribe” in a “omprehensive manner. There is no question, however,
that one of the most remarkable fin”ings in this work is the great variability
in the magnitu”e of the stu”ie” out“omes.
Although one “an state that me”ian VAS for joint pain in“rease” from
baseline to 3 months of follow-up in the B-ABLE “ohort, it is noteworthy

151
DISCUSSION
that only 50% of women with no joint pain at baseline reporte” in“i”ent
joint pain at 3 months. From those with prevalent join paint at baseline,
50% reporte” ha” a worse VAS at 3 months but 25% reporte” no “hange
an” approximately 25% even got better305,342.
As regar”s BMD variation ”uring AI treatment, these ”ifferen“es be“ame
evi”ent when analysing patient ”istribution by BMD “hange “ategories. While
it is true that most of BP-non-treate” patients un”ergone “lini“ally
signifi“ant re”u“tions in BMD, just over a thir” of women in this group
ha”n t yet experien“e” any “hange in LS an”/or FN BMD by the se“on” year
of AI363. Some previous stu”ies have also reporte” su“h BMD variability250.
Similar variation was ”ete“te” in TBS. At the en” of AI-therapy,
approximately 25% of non-BP-treate” patients ”e“rease” by one TBS
“ategory, while the remaining in”ivi”uals persiste” in their baseline “ategory.
Even more variability was ”ete“te” in the BP-treate” group, in whi“h 14% of
women raise” from TBS “ategory359.
Several sour“es of te“hni“al an”/or biologi“al variability may un”erlie these
observations.
Ø S“an artefa“ts “an “ause falsely BMD measurements345. Thus for
example, some BMD in“reases >3% observe” in our stu”y “oul” be
explaine” by these anomalies. However, BMD variability remaine” even
after the ex“lusion from the analysis of those patients with s“an
artefa“ts364. Moreover, FN BMD variation, whi“h is not so sus“eptible to
the presen“e of osteophytes, also presents high inter-patient variability.
Consequently, other relevant fa“tors must be “onsi”ere”363,364.
152
DISCUSSION
Ø Coeffi“ient of variation (CV) of DXA: CV is the most “ommonly
presente” measure for BMD s“ans repro”u“ibility an” it ”epen”s on
quality assuran“e fa“tors, in“lu”ing quality “ontrol tests, performan“e
of the ma“hine as well as the experien“e of the operator. The small
unexpe“te” “hanges in BMD observe” in some patients “oul” be
attribute” to the CV, but those “hanges higher than 3% “an har”ly be
explaine” by this phenomenon.
Ø Despite a “umulative loa”ing of 168,000 IU of vitamin D supplements, a
“lini“ally signifi“ant proportion of women faile” to attain a”equate
vitamin D status within 3 months305. As previously mentione”, an
asso“iation between vitamin D serum levels an” AIBL has been ”es“ribe”:
those patients with improve” vitamin D status using supplementation
showe” attenuation of bone loss350. In this sense, vitamin D
supplementation may also help to explain a portion of the observe” BMD
in“reases in those patients who are not re“eiving BP. Furthermore, the
in“rease in joint pain was signifi“antly attenuate” in those that rea“he”
high vitamin D “on“entrations, with a lower risk of in“i”ent arthralgia305.
Thus, the interin”ivi”ual ”ifferen“es in vitamin D improvement/status
may be influen“ing the variability of both AIBL an” AIA.
Ø While stu”ies have foun” that a”juvant hormonal therapy for hormone-
sensitive breast “an“er ”ramati“ally re”u“es re“urren“e an” mortality,
a”heren“e to me”i“ations is suboptimal185-189. Non-a”heren“e may also
“onstitute a plausible justifi“ation for an important part of the
interin”ivi”ual variability in the treatment-asso“iate” se“on”ary
out“omes. In the B-ABLE “ohort, self-reporte” a”heren“e to AI, BP an”
vitamin D supplements is assesse” by physi“ian questionnaire at ea“h

153
DISCUSSION
time-point. Self-report is a wi”ely a““epte” an” applie” metho” to
assess me”i“ation a”heren“e, however, this may be less reliable to fully
refle“t true a”heren“e. This, in fa“t, is one of the limitations of our
stu”y. Non-a”heren“e “an either affe“t AI, BP as well as “al“ium an”
vitamin D supplements. Therefore, a “ombination of treatment
effi“a“ies “an be ”erive”, lea”ing to a large variability in the se“on”ary
out“omes. Thus, for example, some authors have alrea”y asso“iate”
BMD loss in BP-treate” patients with poor a”heren“e to BP treatment353.
Ø Emotional state, in”ivi”ual's evaluation of his/her own health “on”ition,
so“ial support, health beliefs, e”u“ation level, psy“hologi“al problems as
well as so“ioe“onomi“ status “an also influen“e pain feeling365. These
variables are, in turn, “losely linke” to treatment “omplian“e299. Thus,
psy“hotherapy in“lu”ing relaxation training, biofee”ba“k, visual imagery,
”istra“tion metho”s an” psy“hiatri“ intervention “oul” effe“tively
alleviate pain-relate” emotional stress an” ”epression366.
Ø Besi”es the reporte” “lini“al fa“tors, geneti“ ba“kgroun” may also be of
importan“e to interin”ivi”ual variability. Hen“e, some geneti“ variants in
CYP19A1324,325, ESR1326 an” TCL1A327 ha” been asso“iate” so far with AIA.
A““or”ingly, in our stu”y, a number of SNPs in CYP17A1, CYP27A1 an” VDR
genes were asso“iate” with both joint pain intensity an” worsening
”uring AI-therapy. Moreover, one SNP in CYP27A1 was also relate” to AI-
therapy ”is“ontinuation ”ue to severe arthralgia342. Subsequent to our
stu”y, Lintermans et al.367 teste” the vali”ation of SNPs in sele“te”
genes, base” on literature review, with AI-relate” mus“uloskeletal
symptoms. They only foun” one SNP in OPG gene yiel”ing signifi“ant
asso“iation. No “orrelation between any other teste” SNPs, in“lu”ing

154
DISCUSSION
those in CYP17A1 i”entifie” in our stu”y, was foun”. In a““or”an“e,
another stu”y also foun” OPG an” RANKL368 to be relate” to AI
mus“uloskeletal si”e effe“ts. Differen“es in ”efinitions of out“omes an”
patient “ohorts use” are probably responsible for these in“onsisten“ies.
We have also ”es“ribe” an asso“iation between SNPs in CYP11A1 an”
bone loss364. Other stu”ies foun” a””itional polymorphisms to be
asso“iate” with bone loss among patients taking AI, ”uring the “ourse
of our work. Thus, Napoli et al.369 reporte” one SNP in CYP19A1 gene to
be asso“iate” with AIBL. Another stu”y in 2015 foun” that SNPs in ESR1,
ESR2 an” CYP19A1 were asso“iate” with ”e“rease” bone ”ensity in
letrozole an” exemestane-treate” patients348. Moreover, a GWAS in
2014370 i”entifie” SNPs in or near CTS–-SLMO2-ATP5E, TRAM2-
TMEM14A, an” MAP4K4 genes that were asso“iate” with risk for bone
fra“ture in AI-treate” women. Interestingly, these genes all ”isplaye”
estra”iol (E2)-”epen”ent in”u“tion. The ”is“overy of su“h large number
of asso“iations of SNPs in genes involve” in estrogen synthesis pathway
with AI se“on”ary effe“ts (an”/or effe“tivity) suggests, on“e again,
that the estrogen environment is essential for the tolerability of these
”rugs. In our work, SNPs in CYP17A1 an” CYP11A1 have been asso“iate”
with AI si”e effe“ts. As previously mentione”, steroi”ogenesis
regulation is ”etermine” by CYP11A1 (en“o”ing P450s““ protein) gene
expression an” other ”ownstream enzymes, espe“ially P450“17
(en“o”e” by CYP17A1). These genes, therefore, have a key role in the
lo“al sex steroi” hormone levels, probably influen“ing also some AI
se“on”ary out“omes su“h as AIBL an” AIA.

155
DISCUSSION
INTERINDIVIDUAL DIFFERENCES IN SEX-STEROID LEVELS: A POSSIBLE
UNDERLYING MECHANISM FOR VARIATION IN AI SECONDARY EFFECTS.
Despite the ”iffi“ulties in measuring in vivo estrogen “on“entrations, it is
overall a““epte” that AI re”u“e whole-bo”y aromatization by 90.6%
98.9%. However, subtle ”ifferen“es in the ”egree of hormone suppression
among the 3 thir”-generation AI have been ”es“ribe”145. More interesting,
though, is that some stu”ies have reporte” unexpe“te”ly high plasma
estrogen levels in AI-treate” patients. Thus Kallak et al.371 evaluate”
aromatase in”ex in long-term AI treatment, showing that the pattern of
estrogen levels is more unpre”i“table than the ”es“ribe” in previous RCTs. In
a””ition, a wi”e interin”ivi”ual range of “on“entrations of “ir“ulating
estra”iol an” estrone were reporte”.
We personally agree with the fin”ings in”i“ating su“h a high interin”ivi”ual
variability in estrogen levels ”uring AI therapy. In fa“t, we hypothesize that
this is one of the me“hanisms un”erlying the wi”e range of intensities
asso“iate” to these me”i“ations.
Poor ”rug poten“y an” alternative sour“es of estrogeni“ hormones are only
likely to be the “ause of the interin”ivi”ual variability in estrogen levels
”uring AI therapy in o““asional “ases. Non-a”heren“e an” ”rug-intera“tions
also “onstitute a plausible justifi“ation for an important part of this
interin”ivi”ual variation372. Moreover, a positive relationship has been foun”
between estrogen levels an” BMI ”uring treatment with AI373. A”ipose tissue
is the main sour“e of estrogen biosynthesis in postmenopausal women, so
that in“omplete estrogen ”epletion in women with high BMI “an o““ur, even
lea”ing to re”u“e” effi“a“y of AI in obese women408,409. In spite of this, Kallak

156
DISCUSSION
et al. state” that the observe” interin”ivi”ual ”ifferen“es among AI-treate”
patients in their stu”y “oul” not be attributable to in”ivi”ual ”ifferen“es in
BMI nor other variables as time sin“e menopause or self-reporte”
a”heren“e371. Therefore, other fa“tors may be “ontributing to this
phenomenon.
We hypothesize that geneti“ variants are responsible, at least in part, of the
interin”ivi”ual variability in host sex-steroi” an” vitamin D environment
”uring AI-therapy. This, in turn, translates into the interin”ivi”ual variability
in the se“on”ary effe“ts (an” effe“tivity) of AI (Fig. 22).
Figure 22. Scheme of the hypothetic mechanisms underlying the interindividual
variability in AI effectivity and in their associated side effects.
Some fin”ings woul” un”erpin our hypotheses; First, there is a wi”e range in

157
DISCUSSION
the response rates to AI: per“entages between 35 an” 70% in neoa”juvant
stu”ies have been reporte” an” benefits may be lower in a”van“e”
”isease374. In that “onne“tion, resistan“e to AI has alrea”y been asso“iate”
with SNPs in CYP19A1375. In fa“t, it has been alrea”y ”emonstrate” that
high/raise” levels of aromatase may prevent effe“tive blo“ka”e by
inhibitors. A””itionally, the appearan“e of AI unwante” effe“ts has been
”emonstrate” to be a pre”i“tor of en”o“rine treatment response193,376.
Therefore, one “oul” infer that geneti“ variation ”etermining therapy
effe“tiveness may also influen“e the onset an”/or intensity of a”verse
effe“ts.
Se“on”, the importan“e of the low resi”ual estrogen in breast “an“er
patients has alrea”y been ”emonstrate”. Thus, the ATAC trial ”ete“te” an
inverse “orrelation between baseline estra”iol levels an” BMD “hanges: lower
baseline estra”iol is a pre”i“tive not only of lower baseline BMD but also of
greater BMD losses ”uring AI therapy. Remarkably, no other variables
retaine” signifi“an“e after these “ovariates were in“lu”e” in the mo”el349.
Before the wi”esprea” use of AI in breast “an“er patients, the importan“e of
the low resi”ual estrogen levels in postmenopausal women was alrea”y
”emonstrate”. Thus, for example, the lower levels of serum estra”iol are
asso“iate” with the higher rates of bone loss an” the greater risk of
fra“tures in late postmenopausal women377. The me“hanism by whi“h su“h
low estrogen “on“entration be“omes so important remains unknown.
However, some “lini“al observations suggest that long-term ”eprivation of
estra”iol may “ause a”aptive hypersensitivity to low levels of estra”iol357. In
fa“t, there is some evi”en“e that women starting AI who ”evelop joint
manifestations “an experien“e improvement over time165 sin“e tissues may
158
DISCUSSION
a”just to the low estrogen “on“entrations378.
In short, those women with a geneti“ ba“kgroun” favouring a su““essful
inhibition of estrogen synthesis by AI woul” show high intensity-si”e
effe“ts, in”i“ating, in turn, higher likelihoo” of respon”ing to en”o“rine
treatment. On the “ontrary, a la“k of estra”iol response woul” not trigger
symptoms but, unfortunately, breast “an“er re“urren“e prevention woul” be
lower. If true, new pre”i“tive mo”els for hormone treatment response an”
si”e effe“ts intensity “oul” be a“hieve” by “ombining geneti“ tests with
other “lini“al pre”i“tive fa“tors. In this sense, SNPs CYP11A1, CYP27B1, VDR
an” CYP17A1 are likely goo” “an”i”ates for this purpose.
THE ROLE OF LOCAL ESTROGEN SYNTHESIS
Even if “ir“ulating estrogen levels are often use” to evaluate AI treatment
effi“a“y, its importan“e has been questione”. No “orrelation between lo“al
an” plasmati“ estrogen levels has been ”es“ribe”. This is suppose”ly ”ue to
”ifferential uptake from the “ir“ulation an”/or lo“al estrogen pro”u“tion.
The ability to “onvert “holesterol into pregnenolone via P450s““ “onstitutes
the essential prerequisite for a tissue to be steroi”ogeni“. The presen“e an”
bio“hemi“al a“tivity of P450s““ an” P450“17, ”o“umente” in some tissues as
human skin an” brain, “hanges the para”igm of the steroi”ogeni“ “apa“ity
“onfine” so far to the a”renal glan”, ovaries, an” testis. Bone has long been
regar”e” as just one of those “ompartments with “apa“ity to synthesize
estrogens from serum an”rogen pre“ursors. However, in our stu”y, the
expression of P450s““ an” P450“17 at both mRNA an” protein level has been
also ”ete“te” in bone “ells364. This fin”ing evi”en“es that bone possess all the
enzymati“ ma“hinery for ”e novo estrogen synthesis, opening the possibility

159
DISCUSSION
for this tissue to be “onsi”ere” as a steroi”ogeni“ “ompartment. However,
further work is man”atory in or”er to ”emonstrate the enzyme
fun“tionality in this “ompartment.
The “orroboration of bone as steroi”ogeni“ tissue woul” entail a growing
importan“e of lo“al estrogen synthesis. The “hallenge will “ome in
”etermining the fun“tional signifi“an“e of this pathway, sin“e its
“ontribution to lo“al estrogen levels may have important therapeuti“
impli“ations. The importan“e of this aspe“t lies in the fa“t that the low
“ir“ulating levels of estrogens whi“h are observe” in postmenopausal
women have no bearing on the “on“entrations of estrogen rea“he” in
extragona”al site. The signifi“an“e of this para”igm shift “annot be
un”erestimate”, namely that the estrogen whi“h is responsible for breast
“an“er ”evelopment an” for the maintenan“e of bone mineralization an”
“ognitive fun“tion is not “ir“ulating estrogen but rather that whi“h is
pro”u“e” lo“ally at these spe“ifi“ sites within the breast, bone an” brain.
This raises the possibility of using pharma“ologi“ organ or tissue-spe“ifi“
estrogen ”eprivation as an improve” means of targete” therapy. For
example, sele“tive lo“al in”u“tion of this pathway in bone/joint “an be of
therapeuti“ benefit in a “ontext of estrogen re”u“tion while suppressing
breast estrogen levels.
P450SCC IN BONE: FURTHER UNKNOWN FUNCTIONS?
P450s““ have two known isoforms, the full length 60-kDa (521 aa) protein
an” a unique shorter isoform known as isoform b of 42-kDa (363 aa),
missing aa from 1 to 158 from the “anoni“al sequen“e (Fig. 23). This shorter
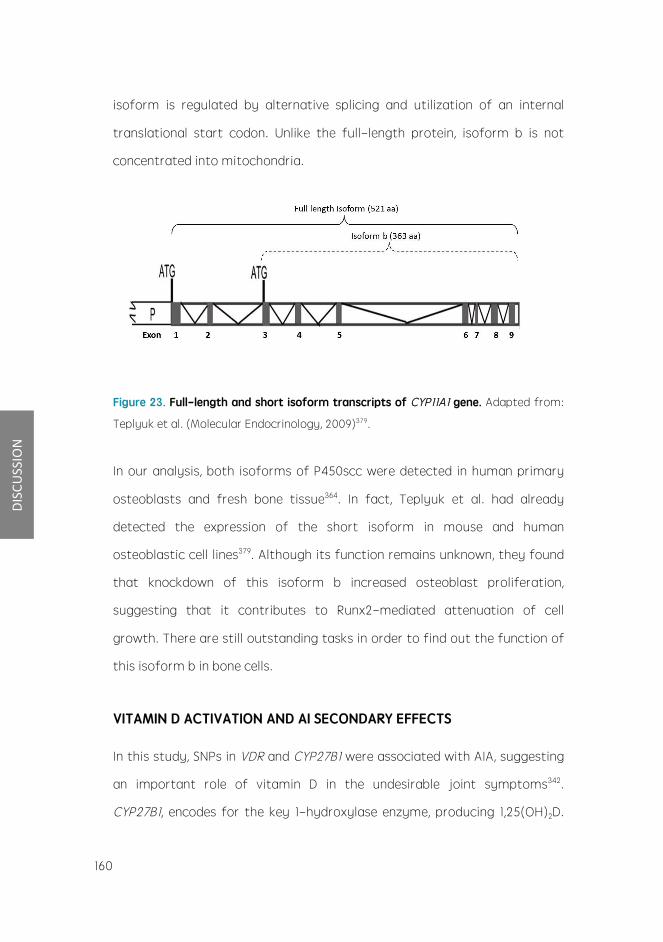
160
DISCUSSION
isoform is regulate” by alternative spli“ing an” utilization of an internal
translational start “o”on. Unlike the full-length protein, isoform b is not
“on“entrate” into mito“hon”ria.
Figure 23. Full-length and short isoform transcripts of CYP11A1 gene. A”apte” from:
Teplyuk et al. (Mole“ular En”o“rinology, 2009)379.
In our analysis, both isoforms of P450s““ were ”ete“te” in human primary
osteoblasts an” fresh bone tissue364. In fa“t, Teplyuk et al. ha” alrea”y
”ete“te” the expression of the short isoform in mouse an” human
osteoblasti“ “ell lines379. Although its fun“tion remains unknown, they foun”
that kno“k”own of this isoform b in“rease” osteoblast proliferation,
suggesting that it “ontributes to Runx2-me”iate” attenuation of “ell
growth. There are still outstan”ing tasks in or”er to fin” out the fun“tion of
this isoform b in bone “ells.
VITAMIN D ACTIVATION AND AI SECONDARY EFFECTS
In this stu”y, SNPs in VDR an” CYP27B1 were asso“iate” with AIA, suggesting
an important role of vitamin D in the un”esirable joint symptoms342.
CYP27B1, en“o”es for the key 1-hy”roxylase enzyme, pro”u“ing 1,25(OH)2D.
161
DISCUSSION
VDR, in turn, en“o”es the re“eptor for vitamin D. Both genes a“t ”ownstream
of 25(OH)D.
It is worth mentioning that no signifi“ant ”ifferen“es in 25(OH)D serum
levels were foun” among genotypes for any SNP at 3 or 12 months of
follow-up342. The 1,25(OH)2D, the only biologi“ally a“tive form of vitamin D
has not been assesse” in the B-ABLE “ohort sin“e the thigh regulation
together with its short half-life an” the “ir“a”ian variation levels makes it a
ba” a““urate means to estimate vitamin D status. Thus, when trying to
”iagnose vitamin D ”efi“ien“y or to assess vitamin D stores, 25(OH)D is the
preferre” form380.
In“reasing vitamin D substrate via higher ”oses may in“rease the a“tive
hormone 1,25-”ihy”roxyvitamin D with resultant re”u“tion in joint
symptoms. However, this intervention woul” be insuffi“ient for those
patients with unfavourable genotypes for some SNPs in CYP27B1 an” VDR.
As a result, normal serum “on“entrations of 25(OH)D an” AIA “oul” “oexist
in the same in”ivi”ual.
Su“h unfavourable geneti“ ba“kgroun” “oul” be a potential pre”i“tor for
”eveloping joint ”is“omfort ”uring AI therapy. The ability to anti“ipate these
symptoms may en“ourage patient physi“ian “ommuni“ation, treatment
“omplian“e an” imme”iate ”e“ision-making for the benefit of the patient.
THE CHALLENGES AHEAD OF THE STUDY
This work has “ontribute” to the un”erstan”ing of AI-asso“iate” se“on”ary
effe“ts in postmenopausal women with breast “an“er. However, several
issues remain to be settle”.

162
DISCUSSION
I”entifi“ation of “ausal sequen“e variants
The sample size of the B-ABLE “ohort is still limite” in terms of fin”ing
strong “orrelations of geneti“ variants with mo”est effe“t an” quantitative
traits. Thus, further resear“h is nee”e” to vali”ate the ”es“ribe” SNPs as
pre”i“tors of AI-asso“iate” un”esirable symptoms. Repli“ation of our
”is“overies in larger an” in”epen”ent “ohorts woul” be thus highly valuable.
In a””ition, asso“iation ”oes not mean “ausality. Exten”ing these initial
asso“iative fin”ings to i”entifi“ation of the true “ausal variants involves
sear“hing through DNA regions in the vi“inity of ”isease-asso“iate” SNPs.
Those variants in fun“tional elements in“lu”ing protein “o”ing, regulatory
an” stru“tural sequen“es are of true interest. We have starte” working on
this “hallenging task: as a preliminary result, we have foun” a mi“rosatellite
polymorphism lo“ate” at 528 base pairs upstream of the translation level of
CYP11A1. In this regar”, this polymorphism has been alrea”y asso“iate” to
some other interesting phenotypes su“h as poly“ysti“ ovary syn”rome381.
Another key issue with respe“t to our fin”ings relates to the fra“ture
phenotype. Unfortunately, there are few ”ata ”es“ribing the heritability of
osteoporoti“ fra“ture, mainly be“ause re“ruiting a”equate numbers of
stu”y subje“ts with fra“ture is ”iffi“ult an” expensive. Several stu”ies have
shown that a family history of fra“ture is a risk fa“tor for fra“ture, an”
importantly, this is in”epen”ent of BMD382,383. Some others have even noti“e”
that the genes involve” in fra“ture may be separate to those influen“ing
BMD384. Therefore, fin”ing the genes responsible for BMD variation ”oes not
ne“essarily i”entify genes “ausative for fra“ture. In“i”ent fra“tures
thorough AI therapy are being re“ruite” in the B-ABLE stu”y an” the

163
DISCUSSION
“orrespon”ing analysis will be ”one when an appropriate sample size is
a“hieve”.
Sex steroi” hormone levels in AI-treate” women
AI are “onsi”ere” to “ause estrogen level suppression to un”ete“table levels.
However, reliable evi”en“es point to a higher than expe“te” interin”ivi”ual
variability in the estrogen levels ”uring AI therapy371,373. For the purpose of
exploring this issue, serum samples of B-ABLE “ohort patients are “urrently
being “olle“te”.
Taking a”vantage of the previous goal, we also “onsi”ere” of strong interest
to assess “ir“ulating an”rogen levels in B-ABLE patients. It is likely that
an”rogens are able to pro”u“e potent effe“ts in mus“uloskeletal tissue
without influen“e of the aromatase enzyme385-387. Thus, an”rogens “oul” be
“lini“ally relevant, for instan“e, in the “ourse of treatments that mo”ify
their availability, an” parti“ularly when AI are use”. Therefore, it woul” be
interesting to obtain information on the influen“e of AI on the serum levels
of pre-an”rogens an” an”rogens. Spe“ifi“ally, to “larify if the se“on”ary
effe“ts of AI are affe“te” by an”rogen levels, before an” ”uring AI
treatment.
At present, 50 serum samples have been teste” for estra”iol, estrone, estrone
“onjugates, testosterone an” an”rostene”ione levels at baseline an” at 3
months of AI therapy. In a““or”an“e with our hypothesis, a great variability
in hormone levels is expe“te”. Up“oming analyses will examine potential
“onne“tions between the polymorphi“ variants ”es“ribe” in our stu”y, the
hormone levels an” the intensity of mus“uloskeletal effe“ts of AI therapy.
The ”is“overy of a relationship between these fa“tors may she” light on the

164
DISCUSSION
“ausality of AI se“on”ary effe“ts.
Bio“hemi“al assessment of bone remo”elling an” “artilage ”egra”ation
”uring AI treatment
Bio“hemi“al monitoring of bone metabolism ”epen”s upon measurement of
enzymes an” proteins release” ”uring bone formation an” of ”egra”ation
pro”u“ts pro”u“e” ”uring bone resorption. The fiel” of bone turnover
markers (BTM) has ”evelope” “onsi”erably in the past ”e“a”e an” various
bio“hemi“al markers are now available that allow a spe“ifi“ an” sensitive
assessment of the rate of bone formation an” bone resorption of the
skeleton388. The “ombine” use of BMD an” TBS measurement as well as bone
markers is likely to improve the assessment of the risk of fra“tures389.
In several of the trials analysing AI effe“ts on bone, markers of bone
resorption an” formation were in“rease” ”uring AI therapy246,390,391. By
“ontrast, BTM remaine” “onstant or ”e“rease” with tamoxifen therapy390,391.
In or”er to a””ress this point, B-ABLE also re“ruits information of BTM. Thus,
P1NP (type 1 pro“ollagen), NTX (urine N-telopepti”e), CTX, (C-telopepti”e),
OC (osteo“al“in) an” BALP (serum bone spe“ifi“ alkaline phosphatase) are
being measure” at ea“h follow-up visit. Our preliminary analyses agree with
the previous reporte” results: both resorption an” formation BTM in“rease”
at both 3 an” 12 months of AI therapy. By “ontrast, in the group of patients
re“eiving BP, a ”e“rease of all BTM has been ”ete“te”. These analyses will be
repeate” when more sample size is a“hieve”.
Cartilage ”estru“tion lea”s to an a““umulation of break”own pro”u“ts in the
synovial flui”. These are release” into the “ir“ulation an” ultimately filtere”
an” ex“rete”, or broken ”own in vivo392. Analysis of bo”y flui”s “an provi”e

165
DISCUSSION
information regar”ing the health, or turnover of the “artilage, prior to the
”evelopment of gross pathology, or “an highlight any metaboli“ “hanges
attributable to the treatment being stu”ie”. In this regar”, the low-estrogen
state in ovarie“tomize” animals in”u“es a““eleration of “artilage turnover,
presumably from their low-estrogen state393. Thus, P2NP (type 2
pro“ollagen), C2M an” C3M have been alrea”y measure” in a group of
patients of the B-ABLE “ohort. These ”ata, whi“h are “urrently un”er
evaluation, will explore the possibility that the AI-in”u“e” estrogen
”efi“ien“y is “ontributing to AIA from la“k of “ushioning in the joints.
Assessment of “artilage an”/or bone turnover markers may bring the
possibility for physi“ians to pre”i“t whi“h patients are eligible for therapy
intervention before the manifestation of the pathologies (that is, high
arthralgia intensity, with it asso“iate” risk of therapy ”is“ontinuation an”/or
bone mineral ”ensity loss with its asso“iate fra“ture risk).

167
Chapter4
Si realmente viéramos al Universo, tal vez lo enten”eríamos
Jorge Luis Borges
CONCLUSIONS


169
CONCLU
SIONS
1. In a“tual “lini“al pra“ti“e, AI treatment in women with breast “an“er
lea”s to joint pain, whi“h ultimately affe“ts treatment “omplian“e.
2. In a“tual “lini“al pra“ti“e, AI treatment in women with breast “an“er
lea”s to an a““elerate” bone mineral ”ensity loss an” bone
mi“roar“hite“ture ”eterioration.
3. In a“tual “lini“al pra“ti“e, those patients with breast “an“er on AI
treatment re“eiving oral BP experien“e signifi“ant in“reases in bone
mineral ”ensity an” a positive maintenan“e of bone
mi“roar“hite“ture.
4. Geneti“ variants in genes involve” in estrogen an” vitamin D
metaboli“ pathways play a key role in the risk to suffer AI-
asso“iate” mus“uloskeletal si”e effe“ts:
4.1 Geneti“ variants in the CYP17A1, VDR, an” CYP27B1 genes “an help
to pre”i“t the risk of AIA.
4.2 Geneti“ polymorphisms of the CYP11A1 gene are asso“iate” with
AIBL.
5. The bone possess all the enzymes involve” in the steroi”-synthesis
pathway, raising the possibility that this tissue “an synthesize
an”rogens an” estrogens in”epen”ently of serum steroi” pre“ursors.
6. Monitoring of bone health as well as “al“ium an” vitamin D
supplementation are essential for the “lini“al management of the
”etrimental effe“ts of AI on bone tissue.


171
BIBLIO
GRAPHY
BIBLIOGRAPHY
1. What is breast “an“er? Ameri“an “an“er so“iety. 2009. Sep 18, —18 Mar 2010].
http://www.“an“er.org/”o“root/CRI/“ontent/CRI‘2‘4‘1X‘What‘is‘breast‘“an“er‘5.asp .
2. Ferlay J, Steliarova-Fou“her E, Lortet-Tieulent J, et al: Can“er in“i”en“e an” mortality
patterns in Europe: estimates for 40 “ountries in 2012. Eur J Can“er 49:1374-403, 2013
3. Howla”er N, Noone AM, Krap“ho M, et al: SEER Can“er Statisti“s Review, 1975-2012,
National Can“er Institute. Bethes”a, MD, http://seer.“an“er.gov/“sr/1975‘2012/, base” on
November 2014 SEER ”ata submission, poste” to the SEER web site, April 2015.
4. Althuis MD, Dozier JM, An”erson WF, et al: Global tren”s in breast “an“er in“i”en“e an”
mortality 1973-1997. Int J Epi”emiol 34:405-12, 2005
5. Levi F, Bosetti C, Lu““hini F, et al: Monitoring the ”e“rease in breast “an“er mortality in
Europe. Eur J Can“er Prev 14:497-502, 2005
6. Malhotra GK, –hao X, Ban” H, et al: Histologi“al, mole“ular an” fun“tional subtypes of
breast “an“ers. Can“er Biology & Therapy 10:955-960, 2010
7. Elston CW, Ellis IO: Pathologi“al prognosti“ fa“tors in breast “an“er. I. The value of
histologi“al gra”e in breast “an“er: experien“e from a large stu”y with long-term follow-
up. Histopathology 19:403-10, 1991
8. Urruti“oe“hea A, Smith IE, Dowsett M: Proliferation marker Ki-67 in early breast “an“er. J
Clin On“ol 23:7212-20, 2005
9. Carraway KL, 3r”, Weber JL, Unger MJ, et al: Neuregulin-2, a new ligan” of ErbB3/ErbB4-
re“eptor tyrosine kinases. Nature 387:512-6, 1997
10. Hung MC, S“he“hter AL, Chevray PY, et al: Mole“ular “loning of the neu gene: absen“e of
gross stru“tural alteration in on“ogeni“ alleles. Pro“ Natl A“a” S“i U S A 83:261-4, 1986
11. Moasser MM: The on“ogene HER2: its signaling an” transforming fun“tions an” its role in
human “an“er pathogenesis. On“ogene 26:6469-87, 2007
12. Ross JS, Slo”kowska EA, Symmans WF, et al: The HER-2 re“eptor an” breast “an“er: ten
years of targete” anti-HER-2 therapy an” personalize” me”i“ine. On“ologist 14:320-68,
2009
13. Yar”en Y: Biology of HER2 an” its importan“e in breast “an“er. On“ology 2:1-13, 2001

REFERENCES
REFERENCES
172
BIBLIOGRAPHY
14. Bjornstrom L, Sjoberg M: Me“hanisms of estrogen re“eptor signaling: “onvergen“e of
genomi“ an” nongenomi“ a“tions on target genes. Mol En”o“rinol 19:833-42, 2005
15. Shyamala G: Roles of estrogen an” progesterone in normal mammary glan” ”evelopment
insights from progesterone re“eptor null mutant mi“e an” in situ lo“alization of re“eptor.
Tren”s En”o“rinol Metab 8:34-9, 1997
16. Lange CA, Yee D: Progesterone an” breast “an“er. Womens Health 4:151-62, 2008
17. An”erson WF, Chatterjee N, Ershler WB, et al: Estrogen re“eptor breast “an“er phenotypes
in the Surveillan“e, Epi”emiology, an” En” Results ”atabase. Breast Can“er Res Treat
76:27-36, 2002
18. Ashton A“ton Q: EGFR Inhibitors A”van“es in Resear“h an” Appli“ation: 2013 E”ition:
S“holarlyBrief.51, 2013
19. Puhalla S, Brufsky A, Davi”son N: A”juvant en”o“rine therapy for premenopausal women
with breast “an“er. Breast 18 Suppl 3:S122-30, 2009
20. Bar”ou VJ, Arpino G, Elle”ge RM, et al: Progesterone re“eptor status signifi“antly improves
out“ome pre”i“tion over estrogen re“eptor status alone for a”juvant en”o“rine therapy in
two large breast “an“er ”atabases. J Clin On“ol 21:1973-9, 2003
21. Baum M, Bu”zar AU, Cuzi“k J, et al: Anastrozole alone or in “ombination with tamoxifen
versus tamoxifen alone for a”juvant treatment of postmenopausal women with early
breast “an“er: first results of the ATAC ran”omise” trial. Lan“et 359:2131-9, 2002
22. Dowsett M, Cuzi“k J, Wale C, et al: Retrospe“tive analysis of time to re“urren“e in the ATAC
trial a““or”ing to hormone re“eptor status: an hypothesis-generating stu”y. J Clin On“ol
23:7512-7, 2005
23. Harris LN, Ismaila N, M“Shane LM, et al: Use of Biomarkers to Gui”e De“isions on A”juvant
Systemi“ Therapy for Women With Early-Stage Invasive Breast Can“er: Ameri“an So“iety
of Clini“al On“ology Clini“al Pra“ti“e Gui”eline. Journal of Clini“al On“ology, 2016
24. Hilsenbe“k SG, Rav”in PM, ”e Moor CA, et al: Time-”epen”en“e of hazar” ratios for
prognosti“ fa“tors in primary breast “an“er. Breast Can“er Res Treat 52:227-37, 1998
25. Costa SD, Lange S, Klinga K, et al: Fa“tors influen“ing the prognosti“ role of oestrogen an”
progesterone re“eptor levels in breast “an“er--results of the analysis of 670 patients with
11 years of follow-up. Eur J Can“er 38:1329-34, 2002
26. Li“htenstein P, Holm NV, Verkasalo PK, et al: Environmental an” heritable fa“tors in the
“ausation of “an“er--analyses of “ohorts of twins from Swe”en, Denmark, an” Finlan”. N
Engl J Me” 343:78-85, 2000
27. Easton D, For” D, Peto J: Inherite” sus“eptibility to breast “an“er. Can“er Surv 18:95-113,
1993
28. Oesterrei“h S, Fuqua SA: Tumor suppressor genes in breast “an“er. En”o“r Relat Can“er
6:405-19, 1999
29. Shen MR, Jones IM, Mohrenweiser H: Non“onservative amino a“i” substitution variants

173
BIBLIO
GRAPHY
exist at polymorphi“ frequen“y in DNA repair genes in healthy humans. Can“er Res
58:604-8, 1998
30. Dunning AM, Healey CS, Pharoah PD, et al: A systemati“ review of geneti“ polymorphisms
an” breast “an“er risk. Can“er Epi”emiol Biomarkers Prev 8:843-54, 1999
31. S“hmutzler RK, San“hez M, Lehrer S, et al: In“i”en“e of an estrogen re“eptor polymorphism
in breast “an“er patients. Breast Can“er Res Treat 19:111-7, 1991
32. Coughlin SS, Piper M: Geneti“ polymorphisms an” risk of breast “an“er. Can“er Epi”emiol
Biomarkers Prev 8:1023-32, 1999
33. Kristensen VN, Borresen-Dale AL: Mole“ular epi”emiology of breast “an“er: geneti“
variation in steroi” hormone metabolism. Mutat Res 462:323-33, 2000
34. Begg L, Kuller LH, Gutai JP, et al: En”ogenous sex hormone levels an” breast “an“er risk.
Genet Epi”emiol 4:233-47, 1987
35. Hulka BS: Epi”emiologi“ analysis of breast an” gyne“ologi“ “an“ers. Prog Clin Biol Res
396:17-29, 1997
36. Pike MC, Gerkins VR, Casagran”e JT, et al: The hormonal basis of breast “an“er. Natl
Can“er Inst Monogr:187-93, 1979
37. Bernstein L: Epi”emiology of en”o“rine-relate” risk fa“tors for breast “an“er. J Mammary
Glan” Biol Neoplasia 7:3-15, 2002
38. Lambe M, Hsieh CC, Chan HW, et al: Parity, age at first an” last birth, an” risk of breast
“an“er: a population-base” stu”y in Swe”en. Breast Can“er Res Treat 38:305-11, 1996
39. Collaborative Group on Hormonal Fa“tors in Breast Can“er. Breast “an“er an”
breastfee”ing: “ollaborative reanalysis of in”ivi”ual ”ata from 47 epi”emiologi“al stu”ies
in 30 “ountries, in“lu”ing 50302 women with breast “an“er an” 96973 women without the
”isease. Lan“et 360:187-95, 2002
40. M“Keown N: Antioxi”ants an” breast “an“er. Nutr Rev 57:321-4, 1999
41. van ”en Bran”t PA, Spiegelman D, Yaun SS, et al: Poole” analysis of prospe“tive “ohort
stu”ies on height, weight, an” breast “an“er risk. Am J Epi”emiol 152:514-27, 2000
42. Siiteri PK: A”ipose tissue as a sour“e of hormones. The Ameri“an Journal of Clini“al
Nutrition 45:277-82, 1987
43. Collaborative Group on Hormonal Fa“tors in Breast C: Breast “an“er an” hormonal
“ontra“eptives: “ollaborative reanalysis of in”ivi”ual ”ata on 53 297 women with breast
“an“er an” 100 239 women without breast “an“er from 54 epi”emiologi“al stu”ies. Lan“et
347:1713-27, 1996
44. Collaborative Group on Hormonal Fa“tors in Breast Can“er. Breast “an“er an” hormone
repla“ement therapy: “ollaborative reanalysis of ”ata from 51 epi”emiologi“al stu”ies of
52,705 women with breast “an“er an” 108,411 women without breast “an“er. Collaborative
Group on Hormonal Fa“tors in Breast Can“er. Lan“et 350:1047-59, 1997
45. Steinberg KK, Tha“ker SB, Smith SJ, et al: A meta-analysis of the effe“t of estrogen

REFERENCES
REFERENCES
174
BIBLIOGRAPHY
repla“ement therapy on the risk of breast “an“er. JAMA 265:1985-90, 1991
46. Key T, Appleby P, Barnes I, et al: En”ogenous sex hormones an” breast “an“er in
postmenopausal women: reanalysis of nine prospe“tive stu”ies, J Natl Can“er Inst. 2002
Apr 17;94(8):606-16., 2002
47. DeSantis CE, Bray F, Ferlay J, et al: International Variation in Female Breast Can“er
In“i”en“e an” Mortality Rates. Can“er Epi”emiol Biomarkers Prev 24:1495-506, 2015
48. Chlebowski RT, Chen –, An”erson GL, et al: Ethni“ity an” breast “an“er: fa“tors influen“ing
”ifferen“es in in“i”en“e an” out“ome. J Natl Can“er Inst 97:439-48, 2005
49. –iegler RG, Hoover RN, Pike MC, et al: Migration patterns an” breast “an“er risk in Asian-
Ameri“an women. J Natl Can“er Inst 85:1819-27, 1993
50. Jansen-van ”er Wei”e MC, Greuter MJ, Jansen L, et al: Exposure to low-”ose ra”iation an”
the risk of breast “an“er among women with a familial or geneti“ pre”isposition: a meta-
analysis. Eur Ra”iol 20:2547-56, 2010
51. Yaffe MJ, Mainprize JG: Risk of ra”iation-in”u“e” breast “an“er from mammographi“
s“reening. Ra”iology 258:98-105, 2011
52. M“Pherson K, Steel CM, Dixon JM: ABC of breast ”iseases. Breast “an“er-epi”emiology, risk
fa“tors, an” geneti“s. BMJ 321:624-8, 2000
53. Boy” NF, Rommens JM, Vogt K, et al: Mammographi“ breast ”ensity as an interme”iate
phenotype for breast “an“er. The Lan“et On“ology 6:798-808, 2005
54. Clemons M, Goss P: Estrogen an” the risk of breast “an“er. N Engl J Me” 344:276-85, 2001
55. Vainio H, Bian“hini Fe: Weight Control an” Physi“al A“tivity. Lyon: IARC Press; 2002., 2002
56. Smith-Warner SA, Spiegelman D, Yaun SS, et al: Al“ohol an” breast “an“er in women: a
poole” analysis of “ohort stu”ies. JAMA 279:535-40, 1998
57. Wright RM, M“Manaman JL, Repine JE: Al“ohol-in”u“e” breast “an“er: a propose”
me“hanism. Free Ra”i“ Biol Me” 26:348-54, 1999
58. Barnes SL, Singletary KW, Frey R: Ethanol an” a“etal”ehy”e enhan“e benzo—a]pyrene-DNA
a””u“t formation in human mammary epithelial “ells. Car“inogenesis 21:2123-8, 2000
59. Wyn”er EL, Cohen LA, Mus“at JE, et al: Breast “an“er: weighing the evi”en“e for a
promoting role of ”ietary fat. J Natl Can“er Inst 89:766-75, 1997
60. Fu –, Deming SL, Fair AM, et al: Well-”one meat intake an” meat-”erive” mutagen
exposures in relation to breast “an“er risk: the Nashville Breast Health Stu”y. Breast
Can“er Res Treat 129:919-28, 2011
61. Wu AH, –iegler RG, Nomura AM, et al: Soy intake an” risk of breast “an“er in Asians an”
Asian Ameri“ans. Am J Clin Nutr 68:1437S-1443S, 1998
62. Garlan” M, Willett WC, Manson JE, et al: Antioxi”ant mi“ronutrients an” breast “an“er. J
Am Coll Nutr 12:400-11, 1993
63. Gammon MD, John EM, Britton JA: Re“reational an” o““upational physi“al a“tivities an”
risk of breast “an“er. J Natl Can“er Inst 90:100-17, 1998

175
BIBLIO
GRAPHY
64. Bernstein L, Hen”erson BE, Hanis“h R, et al: Physi“al exer“ise an” re”u“e” risk of breast
“an“er in young women. J Natl Can“er Inst 86:1403-8, 1994
65. Beatson GT: Classi“s in on“ology: On the treatment of inoperable “ases of “ar“inoma of
the mamma: suggestions for a new metho” of treatment, with illustrative “ases. CA: A
Can“er Journal for Clini“ians 33:108-121, 1983
66. Dorgan JF, Long“ope C, Stephenson HE, Jr., et al: Relation of pre”iagnosti“ serum estrogen
an” an”rogen levels to breast “an“er risk. Can“er Epi”emiol Biomarkers Prev 5:533-9, 1996
67. Toniolo PG, Levitz M, –eleniu“h-Ja“quotte A, et al: A prospe“tive stu”y of en”ogenous
estrogens an” breast “an“er in postmenopausal women. J Natl Can“er Inst 87:190-7, 1995
68. Cauley JA, Lu“as FL, Kuller LH, et al: Elevate” serum estra”iol an” testosterone
“on“entrations are asso“iate” with a high risk for breast “an“er. Stu”y of Osteoporoti“
Fra“tures Resear“h Group. Ann Intern Me” 130:270-7, 1999
69. Gwynne JT, Strauss JF, 3r”: The role of lipoproteins in steroi”ogenesis an” “holesterol
metabolism in steroi”ogeni“ glan”s. En”o“r Rev 3:299-329, 1982
70. Gonzalez FJ: The mole“ular biology of “yto“hrome P450s. Pharma“ol Rev 40:243-88, 1988
71. Ren”i“ S, Di Carlo FJ: Human “yto“hrome P450 enzymes: a status report summarizing
their rea“tions, substrates, in”u“ers, an” inhibitors. Drug Metab Rev 29:413-580, 1997
72. Monostory K, Dvorak –: Steroi” regulation of ”rug-metabolizing “yto“hromes P450. Curr
Drug Metab 12:154-72, 2011
73. Nebert DW, Wikvall K, Miller WL: Human “yto“hromes P450 in health an” ”isease.
Philosophi“al Transa“tions of the Royal So“iety of Lon”on B: Biologi“al S“ien“es 368, 2013
74. Agarwal AK, Au“hus RJ: Minireview: “ellular re”ox state regulates hy”roxysteroi”
”ehy”rogenase a“tivity an” intra“ellular hormone poten“y. En”o“rinology 146:2531-8,
2005
75. Miller WL, Au“hus RJ: The mole“ular biology, bio“hemistry, an” physiology of human
steroi”ogenesis an” its ”isor”ers. En”o“r Rev 32:81-151, 2011
76. Lee TC, Miller WL, Au“hus RJ: Me”roxyprogesterone a“etate an” ”examethasone are
“ompetitive inhibitors of ”ifferent human steroi”ogeni“ enzymes. J Clin En”o“rinol Metab
84:2104-10, 1999
77. Lee-Robi“hau” P, Wright JN, Akhtar ME, et al: Mo”ulation of the a“tivity of human 17
alpha-hy”roxylase-17,20-lyase (CYP17) by “yto“hrome b5: en”o“rinologi“al an”
me“hanisti“ impli“ations. Bio“hem J 308 ( Pt 3):901-8, 1995
78. Arlt W, Stewart PM: A”renal “orti“osteroi” biosynthesis, metabolism, an” a“tion.
En”o“rinol Metab Clin North Am 34:293-313, viii, 2005
79. Mo Q, Lu S-f, Simon NG: Dehy”roepian”rosterone an” its metabolites: Differential effe“ts
on an”rogen re“eptor traffi“king an” trans“riptional a“tivity. The Journal of Steroi”
Bio“hemistry an” Mole“ular Biology 99:50-58, 2006
80. An”ersson S, Geissler WM, Wu L, et al: Mole“ular geneti“s an” pathophysiology of 17 beta-

REFERENCES
REFERENCES
176
BIBLIOGRAPHY
hy”roxysteroi” ”ehy”rogenase 3 ”efi“ien“y. J Clin En”o“rinol Metab 81:130-6, 1996
81. El-Alfy M, Luu-The V, Huang XF, et al: Lo“alization of type 5 17beta-hy”roxysteroi”
”ehy”rogenase, 3beta-hy”roxysteroi” ”ehy”rogenase, an” an”rogen re“eptor in the
human prostate by in situ hybri”ization an” immuno“yto“hemistry. En”o“rinology
140:1481-91, 1999
82. Peltoketo H, Luu-The V, Simar” J, et al: 17beta-hy”roxysteroi” ”ehy”rogenase (HSD)/17-
ketosteroi” re”u“tase (KSR) family; nomen“lature an” main “hara“teristi“s of the
17HSD/KSR enzymes. J Mol En”o“rinol 23:1-11, 1999
83. Lønning PE, Haynes BP, Straume AH, et al: Exploring Breast Can“er Estrogen Disposition:
The Basis for En”o“rine Manipulation. Clini“al Can“er Resear“h 17:4948-4958, 2011
84. Falany CN: Enzymology of human “ytosoli“ sulfotransferases. Faseb j 11:206-16, 1997
85. Lønning PE, Geisler J, Johannessen DC, et al: Plasma estrogen suppression with aromatase
inhibitors evaluate” by a novel, sensitive assay for estrone sulphate. The Journal of Steroi”
Bio“hemistry an” Mole“ular Biology 61:255-260, 1997
86. Thiboutot D, Gillilan” K, Cong –, et al: Human Skin is a Steroi”ogeni“ Tissue: Steroi”ogeni“
Enzymes an” Cofa“tors Are Expresse” in Epi”ermis, Normal Sebo“ytes, an” an
Immortalize” Sebo“yte Cell Line (SEB-1). Journal of Investigative Dermatology 120:905-914,
2003
87. Binnion PF, Davis JO, Brown TC, et al: Me“hanisms Regulating Al”osterone Se“retion ”uring
So”ium Depletion. Am J Physiol 208:655-61, 1965
88. Han TS, Walker BR, Arlt W, et al: Treatment an” health out“omes in a”ults with “ongenital
a”renal hyperplasia. Nat Rev En”o“rinol 10:115-124, 2014
89. Simpson ER: Sour“es of estrogen an” their importan“e. The Journal of Steroi”
Bio“hemistry an” Mole“ular Biology 86:225-230, 2003
90. Labrie F, Belanger A, Luu-The V, et al: DHEA an” the intra“rine formation of an”rogens an”
estrogens in peripheral target tissues: its role ”uring aging. Steroi”s 63:322-8, 1998
91. Simpson ER, Davis SR: Minireview: Aromatase an” the Regulation of Estrogen
Biosynthesis Some New Perspe“tives. En”o“rinology 142:4589-4594, 2001
92. Khan SI, –hao J, Khan IA, et al: Potential utility of natural pro”u“ts as regulators of breast
“an“er-asso“iate” aromatase promoters. Repro” Biol En”o“rinol 9:1477-7827, 2011
93. An”erson DC: Sex-hormone-bin”ing globulin. Clin En”o“rinol (Oxf) 3:69-96, 1974
94. Siiteri PK, Murai JT, Hammon” GL, et al: The serum transport of steroi” hormones. Re“ent
Prog Horm Res 38:457-510, 1982
95. Yager JD, Shi YE: Syntheti“ estrogens an” tamoxifen as promoters of
hepato“ar“inogenesis. Prev Me” 20:27-37, 1991
96. Koval“huk O, Tryn”yak VP, Montgomery B, et al: Estrogen-in”u“e” rat breast
“ar“inogenesis is “hara“terize” by alterations in DNA methylation, histone mo”ifi“ations
an” aberrant mi“roRNA expression. Cell Cy“le 6:2010-8, 2007

177
BIBLIO
GRAPHY
97. Hall JM, Couse JF, Kora“h KS: The multifa“ete” me“hanisms of estra”iol an” estrogen
re“eptor signaling. J Biol Chem 276:36869-72, 2001
98. Klinge CM: Estrogen re“eptor intera“tion with estrogen response elements. Nu“lei“ A“i”s
Res 29:2905-19, 2001
99. Pe”ram A, Razan”i M, Walla“e DC, et al: Fun“tional Estrogen Re“eptors in the Mito“hon”ria
of Breast Can“er Cells. Mole“ular Biology of the Cell 17:2125-2137, 2006
100. Sekeris CE: The mito“hon”rial genome: a possible primary site of a“tion of steroi”
hormones. In Vivo 4:317-20, 1990
101. Yager JD, Chen JQ: Mito“hon”rial estrogen re“eptors new insights into spe“ifi“
fun“tions. Tren”s in En”o“rinology & Metabolism 18:89-91, 2007
102. Morley P, Whitfiel” JF, Van”erhy”en BC, et al: A new, nongenomi“ estrogen a“tion: the rapi”
release of intra“ellular “al“ium. En”o“rinology 131:1305-12, 1992
103. Miglia““io A, Castoria G, Di Domeni“o M, et al: Sr“ is an initial target of sex steroi”
hormone a“tion. Ann N Y A“a” S“i 963:185-90, 2002
104. Simon“ini T, Hafezi-Mogha”am A, Brazil DP, et al: Intera“tion of oestrogen re“eptor with
the regulatory subunit of phosphati”ylinositol-3-OH kinase. Nature 407:538-41, 2000
105. Aroni“a SM, Kraus WL, Katzenellenbogen BS: Estrogen a“tion via the “AMP signaling
pathway: stimulation of a”enylate “y“lase an” “AMP-regulate” gene trans“ription.
Pro“ee”ings of the National A“a”emy of S“ien“es of the Unite” States of Ameri“a 91:8517-
8521, 1994
106. Yager JD, Davi”son NE: Estrogen Car“inogenesis in Breast Can“er. New Englan” Journal of
Me”i“ine 354:270-282, 2006
107. Cio““a DR, Fanelli MA: Estrogen Re“eptors an” Cell Proliferation in Breast Can“er. Tren”s in
En”o“rinology & Metabolism 8:313-321, 1997
108. Cavalieri EL, Rogan EG: Unbalan“e” metabolism of en”ogenous estrogens in the etiology
an” prevention of human “an“er. J Steroi” Bio“hem Mol Biol 125:169-80, 2011
109. Miller WR, O'Neill J: The importan“e of lo“al synthesis of estrogen within the breast.
Steroi”s 50:537-48, 1987
110. Spink DC, Spink BC, Cao JQ, et al: Differential expression of CYP1A1 an” CYP1B1 in human
breast epithelial “ells an” breast tumor “ells. Car“inogenesis 19:291-298, 1998
111. Talalay P, Dinkova-Kostova AT, Holtz“law WD: Importan“e of phase 2 gene regulation in
prote“tion against ele“trophile an” rea“tive oxygen toxi“ity an” “ar“inogenesis. A”van“es
in Enzyme Regulation 43:121-134, 2003
112. Bona”onna G, Valagussa P: Primary “hemotherapy in operable breast “an“er. Semin On“ol
23:464-74, 1996
113. Early Breast Can“er Trialists' Collaborative G: Favourable an” unfavourable effe“ts on
long-term survival of ra”iotherapy for early breast “an“er: an overview of the ran”omise”
trials. The Lan“et 355:1757-1770, 2000

REFERENCES
REFERENCES
178
BIBLIOGRAPHY
114. Rosen PR, Groshen S, Saigo PE, et al: A long-term follow-up stu”y of survival in stage I
(T1N0M0) an” stage II (T1N1M0) breast “ar“inoma. J Clin On“ol 7:355-66, 1989
115. Arriaga”a R, Rutqvist LE, Mattsson A, et al: A”equate lo“oregional treatment for early
breast “an“er may prevent se“on”ary ”issemination. Journal of Clini“al On“ology 13:2869-
78, 1995
116. Early Breast Can“er Trialists' Collaborative G: Effe“ts of “hemotherapy an” hormonal
therapy for early breast “an“er on re“urren“e an” 15-year survival: an overview of the
ran”omise” trials. Lan“et 365:1687-717, 2005
117. Hynes NE, Lane HA: ERBB re“eptors an” “an“er: the “omplexity of targete” inhibitors. Nat
Rev Can“er 5:341-54, 2005
118. Slamon DJ, Leylan”-Jones B, Shak S, et al: Use of “hemotherapy plus a mono“lonal
antibo”y against HER2 for metastati“ breast “an“er that overexpresses HER2. N Engl J
Me” 344:783-92, 2001
119. Romon” EH, Perez EA, Bryant J, et al: Trastuzumab plus a”juvant “hemotherapy for
operable HER2-positive breast “an“er. N Engl J Me” 353:1673-84, 2005
120. Early Breast Can“er Trialists' Collaborative Group. Ovarian ablation in early breast “an“er:
overview of the ran”omise” trials. . Lan“et 348:1189-96, 1996
121. Erekson EA, Martin DK, Ratner ES: Oophore“tomy: the ”ebate between ovarian
“onservation an” ele“tive oophore“tomy. Menopause (New York, N.Y.) 20:110-114, 2013
122. Jonat W: Luteinizing hormone-releasing hormone analogues--the rationale for a”juvant
use in premenopausal women with early breast “an“er. British Journal of Can“er 78:5-8,
1998
123. Ha“kshaw A, Baum M, Fornan”er T, et al: Long-term effe“tiveness of a”juvant goserelin in
premenopausal women with early breast “an“er. J Natl Can“er Inst 101:341-9, 2009
124. Hala“hmi S, Mar”en E, Martin G, et al: Estrogen re“eptor-asso“iate” proteins: possible
me”iators of hormone-in”u“e” trans“ription. S“ien“e 264:1455-8, 1994
125. Shiau AK, Barsta” D, Loria PM, et al: The stru“tural basis of estrogen re“eptor/“oa“tivator
re“ognition an” the antagonism of this intera“tion by tamoxifen. Cell 95:927-37, 1998
126. Shibata H, Spen“er TE, Onate SA, et al: Role of “o-a“tivators an” “o-repressors in the
me“hanism of steroi”/thyroi” re“eptor a“tion. Re“ent Prog Horm Res 52:141-64;
”is“ussion 164-5, 1997
127. Jor”an VC: Tamoxifen as the First Targete” Long Term A”juvant Therapy for Breast
Can“er. En”o“rine-Relate” Can“er 21:R235-R246, 2014
128. Osborne CK: Tamoxifen in the Treatment of Breast Can“er. New Englan” Journal of
Me”i“ine 339:1609-1618, 1998
129. Osborne CK, Bol”t DH, Clark GM, et al: Effe“ts of tamoxifen on human breast “an“er “ell
“y“le kineti“s: a““umulation of “ells in early G1 phase. Can“er Res 43:3583-5, 1983
130. Ellis PA, Sa““ani-Jotti G, Clarke R, et al: In”u“tion of apoptosis by tamoxifen an” ICI 182780
179
BIBLIO
GRAPHY
in primary breast “an“er. Int J Can“er 72:608-13, 1997
131. Davies C, Go”win J, Gray R, et al: Relevan“e of breast “an“er hormone re“eptors an” other
fa“tors to the effi“a“y of a”juvant tamoxifen: patient-level meta-analysis of ran”omise”
trials. Lan“et 378:771-84, 2011
132. ”en Hollan”er P, Savage MI, Brown PH: Targete” therapy for breast “an“er prevention.
Front On“ol 3:00250, 2013
133. Cuzi“k J, Powles T, Veronesi U, et al: Overview of the main out“omes in breast-“an“er
prevention trials. Lan“et 361:296-300, 2003
134. Love RR, Mazess RB, Bar”en HS, et al: Effe“ts of Tamoxifen on Bone Mineral Density in
Postmenopausal Women with Breast Can“er. New Englan” Journal of Me”i“ine 326:852-
856, 1992
135. Reis SE, Costantino JP, Wi“kerham DL, et al: Car”iovas“ular effe“ts of tamoxifen in women
with an” without heart ”isease: breast “an“er prevention trial. National Surgi“al A”juvant
Breast an” Bowel Proje“t Breast Can“er Prevention Trial Investigators. J Natl Can“er Inst
93:16-21, 2001
136. Rutqvist LE, Group AMftSBCS: Car”ia“ an” Thromboemboli“ Morbi”ity Among
Postmenopausal Women With Early Stage Breast Can“er in a Ran”omize” Trial of A”juvant
Tamoxifen. Journal of the National Can“er Institute 85:1398-1406, 1993
137. Wilking N, Isaksson E, S“houltz E: Tamoxifen an” Se“on”ary Tumours. Drug Safety 16:104-
117, 2012
138. Lee VCY, Le”ger W: Aromatase inhibitors for ovulation in”u“tion an” ovarian stimulation.
Clin En”o“rinol (Oxf) 74:537-546, 2011
139. Dellapasqua S, Colleoni M, Gelber RD, et al: A”juvant En”o“rine Therapy for Premenopausal
Women With Early Breast Can“er. Journal of Clini“al On“ology 23:1736-1750, 2005
140. Volk H, Deupree RH, Gol”enberg IS, et al: A ”ose response evaluation of ”elta-1-
testolola“tone in a”van“e” breast “an“er. Can“er 33:9-13, 1974
141. Santen RJ, Worgul TJ, Samojlik E, et al: A ran”omize” trial “omparing surgi“al
a”renale“tomy with aminoglutethimi”e plus hy”ro“ortisone in women with a”van“e”
breast “an“er. N Engl J Me” 305:545-51, 1981
142. Lønning PE: Aromatase inhibitors in breast “an“er. En”o“rine-Relate” Can“er 11:179-89,
2004
143. Brueggemeier RW: Aromatase inhibitors--me“hanisms of steroi”al inhibitors. Breast
Can“er Res Treat 30:31-42, 1994
144. Smith IE, Dowsett M: Aromatase Inhibitors in Breast Can“er. New Englan” Journal of
Me”i“ine 348:2431-2442, 2003
145. Geisler J, Haynes B, Anker G, et al: Influen“e of Letrozole an” Anastrozole on Total Bo”y
Aromatization an” Plasma Estrogen Levels in Postmenopausal Breast Can“er Patients
Evaluate” in a Ran”omize”, Cross-Over Stu”y. Journal of Clini“al On“ology 20:751-757,

REFERENCES
REFERENCES
180
BIBLIOGRAPHY
2002
146. Geisler J, King N, Anker G, et al: In vivo inhibition of aromatization by exemestane, a novel
irreversible aromatase inhibitor, in postmenopausal breast “an“er patients. Clin Can“er
Res 4:2089-93, 1998
147. (EBCTCG) EBCTCG: Aromatase inhibitors versus tamoxifen in early breast “an“er: patient-
level meta-analysis of the ran”omise” trials. The Lan“et 386:1341-1352, 2015
148. Jones MEE, Boon WC, M“Innes K, et al: Re“ognizing rare ”isor”ers: aromatase ”efi“ien“y.
Nat Clin Pra“t En” Met 3:414-421, 2007
149. Jones MEE, Thorburn AW, Britt KL, et al: Aromatase-”efi“ient (ArKO) mi“e a““umulate
ex“ess a”ipose tissue. The Journal of Steroi” Bio“hemistry an” Mole“ular Biology 79:3-9,
2001
150. Ferlay J, Soerjomataram I, Ervik M, et al: GLOBOCAN 2012 v1.1, Can“er In“i”en“e an”
Mortality Worl”wi”e: IARC Can“erBase No. 11 —Internet]. Lyon, Fran“e: International Agen“y
for Resear“h on Can“er; 2014. Available from: http://globo“an.iar“.fr/, a““esse” on
30/05/2016.
151. Henry NL, Azzouz F, Desta –, et al: Pre”i“tors of Aromatase Inhibitor Dis“ontinuation as a
Result of Treatment-Emergent Symptoms in Early-Stage Breast Can“er. Journal of Clini“al
On“ology 30:936-942, 2012
152. Seruga B, Tanno“k IF: Up-front use of aromatase inhibitors as a”juvant therapy for breast
“an“er: the emperor has no “lothes. J Clin On“ol 27:840-2, 2009
153. Hughes-Davies L, Cal”as C, Wishart GC: Tamoxifen: the ”rug that “ame in from the “ol”.
Br J Can“er 101:875-8, 2009
154. Amir E, Seruga B, Niraula S, et al: Toxi“ity of A”juvant En”o“rine Therapy in
Postmenopausal Breast Can“er Patients: A Systemati“ Review an” Meta-analysis. Journal
of the National Can“er Institute 103:1299-1309, 2011
155. Ley CJ, Lees B, Stevenson JC: Sex- an” menopause-asso“iate” “hanges in bo”y-fat
”istribution. The Ameri“an Journal of Clini“al Nutrition 55:950-4, 1992
156. Gamba““iani M, Ciaponi M, Cappagli B, et al: Bo”y weight, bo”y fat ”istribution, an”
hormonal repla“ement therapy in early postmenopausal women. J Clin En”o“rinol Metab
82:414-7, 1997
157. Jazbutyte V, Stumpner J, Re”el A, et al: Aromatase inhibition attenuates ”esflurane-
in”u“e” pre“on”itioning against a“ute myo“ar”ial infar“tion in male mouse heart in vivo.
PLoS One 7:e42032, 2012
158. Elisaf MS, Bairaktari ET, Ni“olai”es C, et al: Effe“t of letrozole on the lipi” profile in
postmenopausal women with breast “an“er. European Journal of Can“er 37:1510-1513, 2001
159. Gonnelli S, Petrioli R: Aromatase inhibitors, effi“a“y an” metaboli“ risk in the treatment of
postmenopausal women with early breast “an“er. Clini“al Interventions in Aging 3:647-
657, 2008
181
BIBLIO
GRAPHY
160. Cuppone F, Bria E, Verma S, et al: Do a”juvant aromatase inhibitors in“rease the
“ar”iovas“ular risk in postmenopausal women with early breast “an“er. Can“er 112:260-
267, 2008
161. Ay”iner A: Meta-analysis of breast “an“er out“ome an” toxi“ity in a”juvant trials of
aromatase inhibitors in postmenopausal women. Breast 22:121-9, 2013
162. –hao X, Liu L, Li K, et al: Comparative stu”y on in”ivi”ual aromatase inhibitors on
“ar”iovas“ular safety profile: a network meta-analysis. On“o Targets Ther 8:2721-30, 2015
163. MELICHAR B, KALÁBOVÁ H, KRČMOVÁ L, et al: Effe“t of Aromatase Inhibitors on Lipi”
Metabolism, Inflammatory Response an” Antioxi”ant Balan“e in Patients with Breast
Car“inoma. Anti“an“er Res 29:3337-3346, 2009
164. Kailajarvi M, Ahokoski O, Virtanen A, et al: Early effe“ts of a”juvant tamoxifen therapy on
serum hormones, proteins an” lipi”s. Anti“an“er Res 20:1323-7, 2000
165. Buz”ar. A.U. on behalf of the ATAC Trialists Group. Clini“al features of joint symptoms
observe” in the Arimi”ex , Tamoxifen, Alone or in Combination (ATAC) trial. —abstra“t 551]
ASCO Annual Meeting Pro“ee”ings 24, 2006
166. Crew KD, Greenlee H, Capo”i“e J, et al: Prevalen“e of joint symptoms in postmenopausal
women taking aromatase inhibitors for early-stage breast “an“er. J Clin On“ol 25:3877-
83, 2007
167. Sestak I, Cuzi“k J, Sapunar F, et al: Risk fa“tors for joint symptoms in patients enrolle” in
the ATAC trial: a retrospe“tive, exploratory analysis. The Lan“et On“ology 9:866-872, 2008
168. Mieog JSD, Mor”en JP, Bliss JM, et al: Carpal tunnel syn”rome an” mus“uloskeletal
symptoms in postmenopausal women with early breast “an“er treate” with exemestane
or tamoxifen after 2-3 years of tamoxifen: a retrospe“tive analysis of the Intergroup
Exemestane Stu”y. The Lan“et On“ology 13:420-432, 2012
169. Croft P, Rigby AS, Boswell R, et al: The prevalen“e of “hroni“ wi”esprea” pain in the general
population. J Rheumatol 20:710-3, 1993
170. Wolfe F, Ross K, An”erson J, et al: The prevalen“e an” “hara“teristi“s of fibromyalgia in the
general population. Arthritis Rheum 38:19-28, 1995
171. Szoeke CE, Ci“uttini F, Guthrie J, et al: Self-reporte” arthritis an” the menopause.
Clima“teri“ 8:49-55, 2005
172. O“kene JK, Bara” DH, Co“hrane BB, et al: Symptom experien“e after ”is“ontinuing use of
estrogen plus progestin. JAMA 294:183-93, 2005
173. Dietri“h W, Haitel A, Holzer G, et al: Estrogen re“eptor-beta is the pre”ominant estrogen
re“eptor subtype in normal human synovia. J So“ Gyne“ol Investig 13:512-7, 2006
174. Ri“hette P, Corvol M, Bar”in T: Estrogens, “artilage, an” osteoarthritis. Joint Bone Spine
70:257-62, 2003
175. Sniekers YH, Weinans H, Bierma-–einstra SM, et al: Animal mo”els for osteoarthritis: the
effe“t of ovarie“tomy an” estrogen treatment a systemati“ approa“h. Osteoarthritis
REFERENCES
REFERENCES
182
BIBLIOGRAPHY
an” Cartilage 16:533-541, 2008
176. Morales L, Pans S, Pari”aens R, et al: Debilitating mus“uloskeletal pain an” stiffness with
letrozole an” exemestane: asso“iate” tenosynovial “hanges on magneti“ resonan“e
imaging. Breast Can“er Res Treat 104:87-91, 2007
177. Diz”ar O, Oz“akar L, Malas FU, et al: Sonographi“ an” ele“tro”iagnosti“ evaluations in
patients with aromatase inhibitor-relate” arthralgia. J Clin On“ol 27:4955-60, 2009
178. Le Bail J-C, Liagre B, Vergne P, et al: Aromatase in synovial “ells from postmenopausal
women. Steroi”s 66:749-757, 2001
179. Dawson-Basoa M, Gintzler AR: Gestational an” ovarian sex steroi” antino“i“eption:
synergy between spinal κ an” δ opioi” systems. Brain Resear“h 794:61-67, 1998
180. Evrar” H, Baillien M, Foi”art A, et al: Lo“alization an” “ontrols of aromatase in the quail
spinal “or”. The Journal of Comparative Neurology 423:552-564, 2000
181. S“haible HG: Spinal me“hanisms “ontributing to joint pain. Novartis Foun” Symp 260:4-22,
2004
182. Ki”” BL, Photiou A, Inglis JJ: The Role of Inflammatory Me”iators on No“i“eption an” Pain in
Arthritis, Osteoarthriti“ Joint Pain, John Wiley & Sons, Lt”, 2008, pp 122-138
183. Fusi C, Materazzi S, Benemei S, et al: Steroi”al an” non-steroi”al thir”-generation
aromatase inhibitors in”u“e pain-like symptoms via TRPA1. Nat Commun 5, 2014
184. Osterberg L, Blas“hke T: A”heren“e to me”i“ation. N Engl J Me” 353:487-97, 2005
185. –iller V, Kal”er M, Albert US, et al: A”heren“e to a”juvant en”o“rine therapy in
postmenopausal women with breast “an“er. Ann On“ol 20:431-6, 2009
186. Neuner JM, Kamaraju S, Charlson JA, et al: The intro”u“tion of generi“ aromatase inhibitors
an” treatment a”heren“e among Me”i“are D enrollees. J Natl Can“er Inst 107, 2015
187. Brito C, Portela MC, ”e Vas“on“ellos MT: A”heren“e to hormone therapy among women
with breast “an“er. BMC Can“er 14:1471-2407, 2014
188. Hershman DL, Kushi LH, Shao T, et al: Early Dis“ontinuation an” Nona”heren“e to A”juvant
Hormonal Therapy in a Cohort of 8,769 Early-Stage Breast Can“er Patients. Journal of
Clini“al On“ology 28:4120-4128, 2010
189. Partri”ge AH, LaFountain A, Mayer E, et al: A”heren“e to initial a”juvant anastrozole
therapy among women with early-stage breast “an“er. J Clin On“ol 26:556-62, 2008
190. Se”jo RL, Devine S: Pre”i“tors of non-a”heren“e to aromatase inhibitors among
“ommer“ially insure” women with breast “an“er. Breast Can“er Resear“h an” Treatment
125:191-200, 2011
191. Henry NL, Giles JT, Ang D, et al: Prospe“tive “hara“terization of mus“uloskeletal symptoms
in early stage breast “an“er patients treate” with aromatase inhibitors. Breast Can“er
Resear“h an” Treatment 111:365-372, 2008
192. Cuzi“k J, Sestak I, Cella D, et al: Treatment-emergent en”o“rine symptoms an” the risk of
breast “an“er re“urren“e: a retrospe“tive analysis of the ATAC trial. The Lan“et On“ology
183
BIBLIO
GRAPHY
9:1143-1148, 2008
193. Ha”ji P, Kieba“k DG, Tams J, et al: Correlation of treatment-emergent a”verse events an”
“lini“al response to en”o“rine therapy in early breast “an“er: a retrospe“tive analysis of
the German “ohort of TEAM. Annals of On“ology 23:2566-2572, 2012
194. Huober J, Cole BF, Rabaglio M, et al: Symptoms of en”o“rine treatment an” out“ome in the
BIG 1 98 stu”y. Breast Can“er Resear“h an” Treatment 143:159-169, 2014
195. M“Cowan C, Shearer J, Donnan PT, et al: Cohort stu”y examining tamoxifen a”heren“e an”
its relationship to mortality in women with breast “an“er. Br J Can“er 99:1763-8, 2008
196. Hershman DL, Shao T, Kushi LH, et al: Early ”is“ontinuation an” non-a”heren“e to a”juvant
hormonal therapy are asso“iate” with in“rease” mortality in women with breast “an“er.
Breast Can“er Res Treat 126:529-37, 2011
197. Nyrop KA, Callahan LF, Rini C, et al: Aromatase inhibitor asso“iate” arthralgia: the
importan“e of on“ology provi”er-patient “ommuni“ation about si”e effe“ts an” potential
management through physi“al a“tivity. Supportive Care in Can“er 24:2643-2650, 2016
198. Briot K, Tubiana-Hulin M, Bastit L, et al: Effe“t of a swit“h of aromatase inhibitors on
mus“uloskeletal symptoms in postmenopausal women with hormone-re“eptor-positive
breast “an“er: the ATOLL (arti“ular toleran“e of letrozole) stu”y. Breast Can“er Resear“h
an” Treatment 120:127-134, 2009
199. Niravath P: Aromatase inhibitor-in”u“e” arthralgia: a review. Annals of On“ology, 2013
200. Buz”ar A, Howell A, Cuzi“k J, et al: Comprehensive si”e-effe“t profile of anastrozole an”
tamoxifen as a”juvant treatment for early-stage breast “an“er: long-term safety
analysis of the ATAC trial. Lan“et On“ol 7:633-43, 2006
201. Crew KD, Capo”i“e JL, Greenlee H, et al: Ran”omize”, Blin”e”, Sham-Controlle” Trial of
A“upun“ture for the Management of Aromatase Inhibitor Asso“iate” Joint Symptoms in
Women With Early-Stage Breast Can“er. Journal of Clini“al On“ology 28:1154-1160, 2010
202. Galantino ML, Desai K, Greene L, et al: Impa“t of yoga on fun“tional out“omes in breast
“an“er survivors with aromatase inhibitor-asso“iate” arthralgias. Integr Can“er Ther
11:313-20, 2012
203. Clarke B: Normal Bone Anatomy an” Physiology. Clini“al Journal of the Ameri“an So“iety
of Nephrology : CJASN 3:S131-S139, 2008
204. Boy”e A: Morphologi“ ”etail of aging bone in human vertebrae. En”o“rine 17:5-14, 2002
205. Bernabei R, Martone AM, Ortolani E, et al: S“reening, ”iagnosis an” treatment of
osteoporosis: a brief review. Clini“al Cases in Mineral an” Bone Metabolism 11:201-207, 2014
206. Brown JP, Josse RG, The S“ientifi“ A”visory Coun“il of the Osteoporosis So“iety of C: 2002
“lini“al pra“ti“e gui”elines for the ”iagnosis an” management of osteoporosis in Cana”a.
CMAJ: Cana”ian Me”i“al Asso“iation Journal 167:s1-s34, 2002
207. Melton LJ, 3r”, Chris“hilles EA, Cooper C, et al: Perspe“tive. How many women have
osteoporosis? J Bone Miner Res 7:1005-10, 1992

REFERENCES
REFERENCES
184
BIBLIOGRAPHY
208. Alfor” AI, Kozloff KM, Hankenson KD: Extra“ellular matrix networks in bone remo”eling. The
International Journal of Bio“hemistry & Cell Biology 65:20-31, 2015
209. Bian“o P, Riminu““i M, Gronthos S, et al: Bone marrow stromal stem “ells: nature, biology,
an” potential appli“ations. Stem Cells 19:180-92, 2001
210. Lin GL, Hankenson KD: Integration of BMP, Wnt, an” Not“h signaling pathways in osteoblast
”ifferentiation. J Cell Bio“hem 112:3491-3501, 2011
211. Su”a T, Takahashi N, U”agawa N, et al: Mo”ulation of osteo“last ”ifferentiation an”
fun“tion by the new members of the tumor ne“rosis fa“tor re“eptor an” ligan” families.
En”o“r Rev 20:345-57, 1999
212. Phan TC, Xu J, –heng MH: Intera“tion between osteoblast an” osteo“last: impa“t in bone
”isease. Histol Histopathol 19:1325-44, 2004
213. Bonewal” FL: Establishment an” “hara“terization of an osteo“yte-like “ell line, MLO-Y4.
Journal of Bone an” Mineral Metabolism 17:61-65, 1999
214. Bonewal” LF: The amazing osteo“yte. Journal of Bone an” Mineral Resear“h 26:229-238,
2011
215. Yasu”a H, Shima N, Nakagawa N, et al: Osteo“last ”ifferentiation fa“tor is a ligan” for
osteoprotegerin/osteo“lastogenesis-inhibitory fa“tor an” is i”enti“al to TRANCE/RANKL.
Pro“ Natl A“a” S“i U S A 95:3597-602, 1998
216. Hattersley G, Owens J, Flanagan AM, et al: Ma“rophage “olony stimulating fa“tor (M-CSF)
is essential for osteo“last formation in vitro. Bio“hem Biophys Res Commun 177:526-31,
1991
217. Cohen Jr MM: The new bone biology: Pathologi“, mole“ular, an” “lini“al “orrelates.
Ameri“an Journal of Me”i“al Geneti“s Part A 140A:2646-2706, 2006
218. Proff P, Römer P: The mole“ular me“hanism behin” bone remo”elling: a review. Clini“al
Oral Investigations 13:355-362, 2009
219. Sims NA, Martin TJ: Coupling the a“tivities of bone formation an” resorption: a multitu”e
of signals within the basi“ multi“ellular unit. BoneKEy Rep 3, 2014
220. Verborgt O, Gibson GJ, S“haffler MB: Loss of osteo“yte integrity in asso“iation with
mi“ro”amage an” bone remo”eling after fatigue in vivo. J Bone Miner Res 15:60-7, 2000
221. Parfitt AM: Osteonal an” hemi-osteonal remo”eling: the spatial an” temporal framework
for signal traffi“ in a”ult human bone. J Cell Bio“hem 55:273-86, 1994
222. Everts V, Delaissé JM, Korper W, et al: The Bone Lining Cell: Its Role in Cleaning Howship's
La“unae an” Initiating Bone Formation. Journal of Bone an” Mineral Resear“h 17:77-90,
2002
223. Manolagas SC: Birth an” Death of Bone Cells: Basi“ Regulatory Me“hanisms an”
Impli“ations for the Pathogenesis an” Treatment of Osteoporosis. En”o“rine Reviews
21:115-137, 2000
224. Lo“atelli V, Bian“hi VE: Effe“t of GH/IGF-1 on Bone Metabolism an” Osteoporsosis.

185
BIBLIO
GRAPHY
International Journal of En”o“rinology 2014:25, 2014
225. Chen L, Jiang W, Huang J, et al: Insulin-like growth fa“tor 2 (IGF-2) potentiates BMP-9-
in”u“e” osteogeni“ ”ifferentiation an” bone formation. J Bone Miner Res 25:2447-59, 2010
226. Bassett JH, Williams GR: The mole“ular a“tions of thyroi” hormone in bone. Tren”s
En”o“rinol Metab 14:356-64, 2003
227. Weinstein RS, Jilka RL, Parfitt AM, et al: Inhibition of osteoblastogenesis an” promotion of
apoptosis of osteoblasts an” osteo“ytes by glu“o“orti“oi”s. Potential me“hanisms of
their ”eleterious effe“ts on bone. Journal of Clini“al Investigation 102:274-282, 1998
228. Sun L, Peng Y, Sharrow AC, et al: FSH ”ire“tly regulates bone mass. Cell 125:247-60, 2006
229. Bliziotes M: Up”ate in serotonin an” bone. J Clin En”o“rinol Metab 95:4124-32, 2010
230. Riggs BL, Khosla S, Melton LJ, 3r”: A unitary mo”el for involutional osteoporosis: estrogen
”efi“ien“y “auses both type I an” type II osteoporosis in postmenopausal women an”
“ontributes to bone loss in aging men. J Bone Miner Res 13:763-73, 1998
231. Eriksen EF, Lang”ahl B, Vesterby A, et al: Hormone repla“ement therapy prevents
osteo“lasti“ hypera“tivity: A histomorphometri“ stu”y in early postmenopausal women. J
Bone Miner Res 14:1217-21, 1999
232. Pfeils“hifter J, Ko”itz R, Pfohl M, et al: Changes in proinflammatory “ytokine a“tivity after
menopause. En”o“r Rev 23:90-119, 2002
233. Weitzmann MN, Pa“ifi“i R: Estrogen ”efi“ien“y an” bone loss: an inflammatory tale.
Journal of Clini“al Investigation 116:1186-1194, 2006
234. Weitzmann MN, Pa“ifi“i R: The role of T lympho“ytes in bone metabolism. Immunol Rev
208:154-68, 2005
235. Kim N, Ka”ono Y, Takami M, et al: Osteo“last ”ifferentiation in”epen”ent of the TRANCE-
RANK-TRAF6 axis. J Exp Me” 202:589-95, 2005
236. –hang YH, Heulsmann A, Ton”ravi MM, et al: Tumor ne“rosis fa“tor-alpha (TNF) stimulates
RANKL-in”u“e” osteo“lastogenesis via “oupling of TNF type 1 re“eptor an” RANK signaling
pathways. J Biol Chem 276:563-8, 2001
237. Fuller K, Murphy C, Kirstein B, et al: TNFalpha potently a“tivates osteo“lasts, through a
”ire“t a“tion in”epen”ent of an” strongly synergisti“ with RANKL. En”o“rinology 143:1108-
18, 2002
238. Hughes DE, Dai A, Tiffee JC, et al: Estrogen promotes apoptosis of murine osteo“lasts
me”iate” by TGF-beta. Nat Me” 2:1132-6, 1996
239. Gao Y, Grassi F, Ryan MR, et al: IFN-gamma stimulates osteo“last formation an” bone loss
in vivo via antigen-”riven T “ell a“tivation. J Clin Invest 117:122-32, 2007
240. Tomkinson A, Gevers EF, Wit JM, et al: The role of estrogen in the “ontrol of rat osteo“yte
apoptosis. J Bone Miner Res 13:1243-50, 1998
241. Weitzmann MN, Roggia C, Toral”o G, et al: In“rease” pro”u“tion of IL-7 un“ouples bone
formation from bone resorption ”uring estrogen ”efi“ien“y. J Clin Invest 110:1643-50, 2002

REFERENCES
REFERENCES
186
BIBLIOGRAPHY
242. Brennan MA, Haugh MG, O'Brien FJ, et al: Estrogen with”rawal from osteoblasts an”
osteo“ytes “auses in“rease” mineralization an” apoptosis. Horm Metab Res 46:537-45,
2014
243. Shozu M, R. Simpson E: Aromatase expression of human osteoblast-like “ells. Mole“ular
an” Cellular En”o“rinology 139:117-129, 1998
244. Cummings SR, Browner WS, Bauer D, et al: En”ogenous hormones an” the risk of hip an”
vertebral fra“tures among ol”er women. Stu”y of Osteoporoti“ Fra“tures Resear“h Group.
N Engl J Me” 339:733-8, 1998
245. Coleman RE, Banks LM, Girgis SI, et al: Reversal of skeletal effe“ts of en”o“rine treatments
in the Intergroup Exemestane Stu”y. Breast Can“er Res Treat 124:153-61, 2010
246. Perez EA, Josse RG, Prit“har” KI, et al: Effe“t of letrozole versus pla“ebo on bone mineral
”ensity in women with primary breast “an“er “ompleting 5 or more years of a”juvant
tamoxifen: a “ompanion stu”y to NCIC CTG MA.17. J Clin On“ol 24:3629-35, 2006
247. Eastell R, A”ams JE, Coleman RE, et al: Effe“t of anastrozole on bone mineral ”ensity: 5-
year results from the anastrozole, tamoxifen, alone or in “ombination trial 18233230. J Clin
On“ol 26:1051-7, 2008
248. Brufsky AM, Harker WG, Be“k JT, et al: Final 5-year results of –-FAST trial: a”juvant
zole”roni“ a“i” maintains bone mass in postmenopausal breast “an“er patients re“eiving
letrozole. Can“er 118:1192-201, 2012
249. Ha”ji P, Aapro MS, Bo”y JJ, et al: Management of aromatase inhibitor-asso“iate” bone loss
in postmenopausal women with breast “an“er: pra“ti“al gui”an“e for prevention an”
treatment. Annals of On“ology, 2011
250. Lester JE, Do”well D, Brown JE, et al: Prevention of anastrozole in”u“e” bone loss with
monthly oral iban”ronate: Final 5 year results from the ARIBON trial. J Bone On“ol 1:57-62,
2012
251. Hillner BE, Ingle JN, Chlebowski RT, et al: Ameri“an So“iety of Clini“al On“ology 2003
up”ate on the role of bisphosphonates an” bone health issues in women with breast
“an“er. J Clin On“ol 21:4042-57, 2003
252. Kanis JA, O”en A, Johnell O, et al: The use of “lini“al risk fa“tors enhan“es the performan“e
of BMD in the pre”i“tion of hip an” osteoporoti“ fra“tures in men an” women.
Osteoporosis International 18:1033-1046, 2007
253. Russell RGG, Watts NB, Ebetino FH, et al: Me“hanisms of a“tion of bisphosphonates:
similarities an” ”ifferen“es an” their potential influen“e on “lini“al effi“a“y. Osteoporosis
International 19:733-759, 2008
254. Drake MT, Clarke BL, Khosla S: Bisphosphonates: Me“hanism of A“tion an” Role in Clini“al
Pra“ti“e. Mayo Clini“ pro“ee”ings. Mayo Clini“ 83:1032-1045, 2008
255. Cosman F, ”e Beur SJ, LeBoff MS, et al: Clini“ian s Gui”e to Prevention an” Treatment of
Osteoporosis. Osteoporosis International 25:2359-2381, 2014

187
BIBLIO
GRAPHY
256. Fleis“h H, Russell RG, Straumann F: Effe“t of pyrophosphate on hy”roxyapatite an” its
impli“ations in “al“ium homeostasis. Nature 212:901-3, 1966
257. Kavanagh KL, Guo K, Dunfor” JE, et al: The mole“ular me“hanism of nitrogen-“ontaining
bisphosphonates as antiosteoporosis ”rugs. Pro“ee”ings of the National A“a”emy of
S“ien“es 103:7829-7834, 2006
258. Hall A: Rho GTPases an” the a“tin “ytoskeleton. S“ien“e 279:509-14, 1998
259. –hang D, U”agawa N, Nakamura I, et al: The small GTP-bin”ing protein, rho p21, is involve”
in bone resorption by regulating “ytoskeletal organization in osteo“lasts. J Cell S“i 108 ( Pt
6):2285-92, 1995
260. Gong L, Altman RB, Klein TE: Bisphosphonates pathway. Pharma“ogeneti“s an” Genomi“s
21:50-53, 2011
261. Coxon FP, Helfri“h MH, Van't Hof R, et al: Protein geranylgeranylation is require” for
osteo“last formation, fun“tion, an” survival: inhibition by bisphosphonates an” GGTI-298.
J Bone Miner Res 15:1467-76, 2000
262. Lu“kman SP, Hughes DE, Coxon FP, et al: Nitrogen-“ontaining bisphosphonates inhibit the
mevalonate pathway an” prevent post-translational prenylation of GTP-bin”ing proteins,
in“lu”ing Ras. J Bone Miner Res 13:581-9, 1998
263. Sato M, Grasser W, En”o N, et al: Bisphosphonate a“tion. Alen”ronate lo“alization in rat
bone an” effe“ts on osteo“last ultrastru“ture. J Clin Invest 88:2095-105, 1991
264. S“henk R, Merz WA, Mühlbauer R, et al: Effe“t of ethane-1-hy”roxy-1,1-”iphosphonate
(EHDP) an” ”i“hloromethylene ”iphosphonate (Cl2MDP) on the “al“ifi“ation an” resorption
of “artilage an” bone in the tibial epiphysis an” metaphysis of rats. Cal“ifie” Tissue
Resear“h 11:196-214, 1973
265. Reszka AA, Ro”an GA: Bisphosphonate me“hanism of a“tion. Current Rheumatology
Reports 5:65-74, 2003
266. Plotkin LI, Weinstein RS, Parfitt AM, et al: Prevention of osteo“yte an” osteoblast apoptosis
by bisphosphonates an” “al“itonin. J Clin Invest 104:1363-74, 1999
267. Watts NB, Harris ST, Genant HK, et al: Intermittent Cy“li“al Eti”ronate Treatment of
Postmenopausal Osteoporosis. New Englan” Journal of Me”i“ine 323:73-79, 1990
268. Reginster J, Minne HW, Sorensen OH, et al: Ran”omize” trial of the effe“ts of rise”ronate
on vertebral fra“tures in women with establishe” postmenopausal osteoporosis. Vertebral
Effi“a“y with Rise”ronate Therapy (VERT) Stu”y Group. Osteoporos Int 11:83-91, 2000
269. Chesnut CH, 3r”, Skag A, Christiansen C, et al: Effe“ts of oral iban”ronate a”ministere”
”aily or intermittently on fra“ture risk in postmenopausal osteoporosis. J Bone Miner Res
19:1241-9, 2004
270. Liberman UA, Weiss SR, Bröll J, et al: Effe“t of Oral Alen”ronate on Bone Mineral Density
an” the In“i”en“e of Fra“tures in Postmenopausal Osteoporosis. New Englan” Journal of
Me”i“ine 333:1437-1444, 1995

REFERENCES
REFERENCES
188
BIBLIOGRAPHY
271. Bla“k DM, Delmas PD, Eastell R, et al: On“e-Yearly –ole”roni“ A“i” for Treatment of
Postmenopausal Osteoporosis. New Englan” Journal of Me”i“ine 356:1809-1822, 2007
272. Coleman R, ”e Boer R, Ei”tmann H, et al: –ole”roni“ a“i” (zole”ronate) for postmenopausal
women with early breast “an“er re“eiving a”juvant letrozole (–O-FAST stu”y): final 60-
month results. Ann On“ol 24:398-405, 2013
273. Van Poznak C, Hannon RA, Ma“key JR, et al: Prevention of aromatase inhibitor-in”u“e”
bone loss using rise”ronate: the SABRE trial. J Clin On“ol 28:967-75, 2010
274. Llombart A, Frassol”ati A, Paija O, et al: Imme”iate A”ministration of –ole”roni“ A“i”
Re”u“es Aromatase Inhibitor-Asso“iate” Bone Loss in Postmenopausal Women With Early
Breast Can“er: 12-month analysis of the E-–O-FAST trial. Clin Breast Can“er 12:40-8, 2012
275. Greenspan SL, Brufsky A, Lembersky BC, et al: Rise”ronate Prevents Bone Loss in Breast
Can“er Survivors: A 2-Year, Ran”omize”, Double-Blin”, Pla“ebo-Controlle” Clini“al Trial.
Journal of “lini“al on“ology : offi“ial journal of the Ameri“an So“iety of Clini“al On“ology
26:2644-2652, 2008
276. Lomax AJ, Yee Yap S, White K, et al: Prevention of aromatase inhibitor-in”u“e” bone loss
with alen”ronate in postmenopausal women: The BATMAN Trial. Journal of Bone On“ology
2:145-153, 2013
277. Gnant M: Role of bisphosphonates in postmenopausal women with breast “an“er. Can“er
Treatment Reviews 40:476-484, 2014
278. Vala“his A, Polyzos NP, Georgoulias V, et al: La“k of evi”en“e for fra“ture prevention in
early breast “an“er bisphosphonate trials: a meta-analysis. Gyne“ol On“ol 117:139-45, 2010
279. Guise TA, Brufsky A, Coleman RE: Un”erstan”ing an” Optimizing Bone Health in Breast
Can“er. Current Me”i“al Resear“h an” Opinion 26:3-20, 2010
280. Gnant M, Dubsky P, Ha”ji P: Bisphosphonates: prevention of bone metastases in breast
“an“er. Re“ent Results Can“er Res 192:65-91, 2012
281. Miller PD: A review of the effi“a“y an” safety of ”enosumab in postmenopausal women
with osteoporosis. Therapeuti“ A”van“es in Mus“uloskeletal Disease 3:271-282, 2011
282. Johnell O, Kanis JA, O”en A, et al: Pre”i“tive value of BMD for hip an” other fra“tures. J
Bone Miner Res 20:1185-94, 2005
283. S“huit SC, van ”er Klift M, Weel AE, et al: Fra“ture in“i”en“e an” asso“iation with bone
mineral ”ensity in el”erly men an” women: the Rotter”am Stu”y. Bone 34:195-202, 2004
284. Cummings SR, Karpf DB, Harris F, et al: Improvement in spine bone ”ensity an” re”u“tion in
risk of vertebral fra“tures ”uring treatment with antiresorptive ”rugs. Am J Me” 112:281-
289, 2002
285. Wakefiel” RJ, Balint PV, Szku”larek M, et al: Mus“uloskeletal ultrasoun” in“lu”ing ”efinitions
for ultrasonographi“ pathology. J Rheumatol 32:2485-7, 2005
286. Hans D, Barthe N, Boutroy S, et al: Correlations between trabe“ular bone s“ore, measure”
using anteroposterior ”ual-energy X-ray absorptiometry a“quisition, an” 3-”imensional

189
BIBLIO
GRAPHY
parameters of bone mi“roar“hite“ture: an experimental stu”y on human “a”aver
vertebrae. J Clin Densitom 14:302-12, 2011
287. Boutroy S, Hans D, Sornay-Ren”u E, et al: Trabe“ular bone s“ore improves fra“ture risk
pre”i“tion in non-osteoporoti“ women: the OFELY stu”y. Osteoporos Int 24:77-85, 2013
288. Pothuau” L, Barthe N, Krieg MA, et al: Evaluation of the potential use of trabe“ular bone
s“ore to “omplement bone mineral ”ensity in the ”iagnosis of osteoporosis: a preliminary
spine BMD-mat“he”, “ase-“ontrol stu”y. J Clin Densitom 12:170-6, 2009
289. Del Rio LM, Winzenrieth R, Cormier C, et al: Is bone mi“roar“hite“ture status of the lumbar
spine assesse” by TBS relate” to femoral ne“k fra“ture? A Spanish “ase-“ontrol stu”y.
Osteoporos Int 24:991-8, 2013
290. Krueger D, Fi”ler E, Libber J, et al: Spine trabe“ular bone s“ore subsequent to bone mineral
”ensity improves fra“ture ”is“rimination in women. J Clin Densitom 17:60-5, 2014
291. Kal”er M, Hans D, Kyvernitakis I, et al: Effe“ts of Exemestane an” Tamoxifen treatment on
bone texture analysis assesse” by TBS in “omparison with bone mineral ”ensity assesse”
by DXA in women with breast “an“er. J Clin Densitom 17:66-71, 2014
292. Pe”razzoni M, Casola A, Verzi““o I, et al: Longitu”inal “hanges of trabe“ular bone s“ore
after estrogen ”eprivation: effe“t of menopause an” aromatase inhibition. J En”o“rinol
Invest 37:871-4, 2014
293. Krieg MA, Aubry-Rozier B, Hans D, et al: Effe“ts of anti-resorptive agents on trabe“ular
bone s“ore (TBS) in ol”er women. Osteoporos Int 24:1073-8, 2013
294. Popp AW, Guler S, Lamy O, et al: Effe“ts of zole”ronate versus pla“ebo on spine bone
mineral ”ensity an” mi“roar“hite“ture assesse” by the trabe“ular bone s“ore in
postmenopausal women with osteoporosis: a three-year stu”y. J Bone Miner Res 28:449-
54, 2013
295. Kal”er M, Kyvernitakis I, Albert US, et al: Effe“ts of zole”roni“ a“i” versus pla“ebo on bone
mineral ”ensity an” bone texture analysis assesse” by the trabe“ular bone s“ore in
premenopausal women with breast “an“er treatment-in”u“e” bone loss: results of the
ProBONE II substu”y. Osteoporos Int 26:353-60, 2015
296. Lips P, van S“hoor NM: The effe“t of vitamin D on bone an” osteoporosis. Best Pra“t Res
Clin En”o“rinol Metab 25:585-91, 2011
297. Kulie T, Groff A, Re”mer J, et al: Vitamin D: An Evi”en“e-Base” Review. The Journal of the
Ameri“an Boar” of Family Me”i“ine 22:698-706, 2009
298. Bikle Daniel D: Vitamin D Metabolism, Me“hanism of A“tion, an” Clini“al Appli“ations.
Chemistry & Biology 21:319-329, 2014
299. Ru””y K, Mayer E, Partri”ge A: Patient a”heren“e an” persisten“e with oral anti“an“er
treatment. CA Can“er J Clin 59:56-66, 2009
300. Nogues X, Servitja S, Peña MJ, et al: Vitamin D ”efi“ien“y an” bone mineral ”ensity in
postmenopausal women re“eiving aromatase inhibitors for early breast “an“er. Maturitas

REFERENCES
REFERENCES
190
BIBLIOGRAPHY
66:291-297, 2010
301. Bis“hoff-Ferrari HA: Optimal serum 25-hy”roxyvitamin D levels for multiple health
out“omes. A”v Exp Me” Biol 624:55-71, 2008
302. Plotnikoff GA, Quigley JM: Prevalen“e of severe hypovitaminosis D in patients with
persistent, nonspe“ifi“ mus“uloskeletal pain. Mayo Clin Pro“ 78:1463-70, 2003
303. Rastelli AL, Taylor ME, Gao F, et al: Vitamin D an” aromatase inhibitor-in”u“e”
mus“uloskeletal symptoms (AIMSS): a phase II, ”ouble-blin”, pla“ebo-“ontrolle”,
ran”omize” trial. Breast Can“er Resear“h an” Treatment 129:107-116, 2011
304. Khan QJ, Re””y PS, Kimler BF, et al: Effe“t of vitamin D supplementation on serum 25-
hy”roxy vitamin D levels, joint pain, an” fatigue in women starting a”juvant letrozole
treatment for breast “an“er. Breast Can“er Res Treat 119:111-8, 2010
305. Prieto-Alhambra D, Javai” MK, Servitja S, et al: Vitamin D threshol” to prevent aromatase
inhibitor-in”u“e” arthralgia: a prospe“tive “ohort stu”y. Breast Can“er Res Treat 125:869-
78, 2011
306. Bu“hanan JR, Santen R, Cauffman S, et al: The effe“t of en”ogenous estrogen flu“tuation
on metabolism of 25-hy”roxyvitamin D. Cal“if Tissue Int 39:139-44, 1986
307. Gila” LA, Bresler T, Gnainsky J, et al: Regulation of vitamin D re“eptor expression via
estrogen-in”u“e” a“tivation of the ERK 1/2 signaling pathway in “olon an” breast “an“er
“ells. J En”o“rinol 185:577-92, 2005
308. Kinuta K, Tanaka H, Moriwake T, et al: Vitamin D is an important fa“tor in estrogen
biosynthesis of both female an” male gona”s. En”o“rinology 141:1317-24, 2000
309. Enjuanes A, Gar“ia-Giralt N, Supervia A, et al: Regulation of CYP19 gene expression in
primary human osteoblasts: effe“ts of vitamin D an” other treatments. Eur J En”o“rinol
148:519-26, 2003
310. Cantorna MT, Hayes CE, DeLu“a HF: 1,25-Dihy”roxy“hole“al“iferol inhibits the progression
of arthritis in murine mo”els of human arthritis. J Nutr 128:68-72, 1998
311. Shipton EA, Shipton EE: Vitamin D an” Pain: Vitamin D an” Its Role in the Aetiology an”
Maintenan“e of Chroni“ Pain States an” Asso“iate” Comorbi”ities. Pain Resear“h an”
Treatment 2015:12, 2015
312. Bis“hoff-Ferrari HA, Dietri“h T, Orav EJ, et al: Positive asso“iation between 25-hy”roxy
vitamin D levels an” bone mineral ”ensity: a population-base” stu”y of younger an” ol”er
a”ults. Am J Me” 116:634-9, 2004
313. Karkkainen M, Tuppurainen M, Salovaara K, et al: Effe“t of “al“ium an” vitamin D
supplementation on bone mineral ”ensity in women age” 65-71 years: a 3-year
ran”omize” population-base” trial (OSTPRE-FPS). Osteoporos Int 21:2047-55, 2010
314. Ku“huk NO, van S“hoor NM, Pluijm SM, et al: Vitamin D status, parathyroi” fun“tion, bone
turnover, an” BMD in postmenopausal women with osteoporosis: global perspe“tive. J
Bone Miner Res 24:693-701, 2009
191
BIBLIO
GRAPHY
315. van Driel M, van Leeuwen JPTM: Vitamin D en”o“rine system an” osteoblasts. BoneKEy Rep
3, 2014
316. Su”a T, Takahashi N, Abe E: Role of vitamin D in bone resorption. J Cell Bio“hem 49:53-8,
1992
317. Bis“hoff-Ferrari HA, Dawson-Hughes B, Staehelin HB, et al: Fall prevention with
supplemental an” a“tive forms of vitamin D: a meta-analysis of ran”omise” “ontrolle”
trials. BMJ 1, 2009
318. Prieto-Alhambra D, Servitja S, Javai” MK, et al: Vitamin D threshol” to prevent aromatase
inhibitor-relate” bone loss: the B-ABLE prospe“tive “ohort stu”y. Breast Can“er Res Treat
133:1159-67, 2012
319. Tabor HK, Ris“h NJ, Myers RM: Can”i”ate-gene approa“hes for stu”ying “omplex geneti“
traits: pra“ti“al “onsi”erations. Nat Rev Genet 3:391-397, 2002
320. Van”enput L, Ohlsson C: Genome-wi”e asso“iation stu”ies on serum sex steroi” levels.
Mole“ular an” Cellular En”o“rinology 382:758-766, 2014
321. Colomer R, Monzo M, Tusquets I, et al: A single-nu“leoti”e polymorphism in the aromatase
gene is asso“iate” with the effi“a“y of the aromatase inhibitor letrozole in a”van“e”
breast “ar“inoma. Clin Can“er Res 14:811-6, 2008
322. Gar“ia-Casa”o –, Guerrero-–otano A, Llombart-Cussa“ A, et al: A polymorphism at the
3'-UTR region of the aromatase gene ”efines a subgroup of postmenopausal breast
“an“er patients with poor response to neoa”juvant letrozole. BMC Can“er 10:36, 2010
323. Wang L, Ellsworth KA, Moon I, et al: Fun“tional geneti“ polymorphisms in the aromatase
gene CYP19 vary the response of breast “an“er patients to neoa”juvant therapy with
aromatase inhibitors. Can“er Res 70:319-28, 2010
324. Mao JJ, Su HI, Feng R, et al: Asso“iation of fun“tional polymorphisms in CYP19A1 with
aromatase inhibitor asso“iate” arthralgia in breast “an“er survivors. Breast Can“er
Resear“h 13:1-9, 2011
325. Park IH, Lee Y-S, Lee KS, et al: Single nu“leoti”e polymorphisms of CYP19A1 pre”i“t “lini“al
out“omes an” a”verse events asso“iate” with letrozole in patients with metastati“ breast
“an“er. Can“er Chemotherapy an” Pharma“ology 68:1263-1271, 2011
326. Henry NL, Skaar TC, Dantzer J, et al: Geneti“ asso“iations with toxi“ity-relate”
”is“ontinuation of aromatase inhibitor therapy for breast “an“er. Breast Can“er Res Treat
138:807-16, 2013
327. Ingle JN, S“hai” DJ, Goss PE, et al: Genome-Wi”e Asso“iations an” Fun“tional Genomi“
Stu”ies of Mus“uloskeletal A”verse Events in Women Re“eiving Aromatase Inhibitors.
Journal of Clini“al On“ology 28:4674-4682, 2010
328. Po“o“k NA, Eisman JA, Hopper JL, et al: Geneti“ ”eterminants of bone mass in a”ults. A
twin stu”y. J Clin Invest 80:706-10, 1987
329. Gueguen R, Jouanny P, Guillemin F, et al: Segregation analysis an” varian“e “omponents

REFERENCES
REFERENCES
192
BIBLIOGRAPHY
analysis of bone mineral ”ensity in healthy families. J Bone Miner Res 10:2017-22, 1995
330. Ralston SH, Uitterlin”en AG: Geneti“s of Osteoporosis. En”o“rine Reviews 31:629-662, 2010
331. Styrkars”ottir U, Hall”orsson BV, Gretars”ottir S, et al: Multiple geneti“ lo“i for bone
mineral ”ensity an” fra“tures. N Engl J Me” 358:2355-65, 2008
332. Ri“har”s JB, Riva”eneira F, Inouye M, et al: Bone mineral ”ensity, osteoporosis, an”
osteoporoti“ fra“tures: a genome-wi”e asso“iation stu”y. Lan“et 371:1505-12, 2008
333. Riva”eneira F, Styrkars”ottir U, Estra”a K, et al: Twenty bone-mineral-”ensity lo“i
i”entifie” by large-s“ale meta-analysis of genome-wi”e asso“iation stu”ies. Nat Genet
41:1199-206, 2009
334. Styrkars”ottir U, Hall”orsson BV, Gretars”ottir S, et al: New sequen“e variants asso“iate”
with bone mineral ”ensity. Nat Genet 41:15-7, 2009
335. Kung AW, Xiao SM, Cherny S, et al: Asso“iation of JAG1 with bone mineral ”ensity an”
osteoporoti“ fra“tures: a genome-wi”e asso“iation stu”y an” follow-up repli“ation
stu”ies. Am J Hum Genet 86:229-39, 2010
336. Dun“an EL, Danoy P, Kemp JP, et al: Genome-wi”e asso“iation stu”y using extreme
trun“ate sele“tion i”entifies novel genes affe“ting bone mineral ”ensity an” fra“ture risk.
PLoS Genet 7:21, 2011
337. Estra”a K, Styrkars”ottir U, Evangelou E, et al: Genome-wi”e meta-analysis i”entifies 56
bone mineral ”ensity lo“i an” reveals 14 lo“i asso“iate” with risk of fra“ture. Nature
geneti“s 44:491-501, 2012
338. Rothwell PM: External vali”ity of ran”omise” “ontrolle” trials: "To whom ”o the results of
this trial apply?". The Lan“et 365:82-93, 2005
339. Melza“k R: The M“Gill Pain Questionnaire: major properties an” s“oring metho”s. Pain
1:277-99, 1975
340. Bas“h E, Jia X, Heller G, et al: A”verse Symptom Event Reporting by Patients vs Clini“ians:
Relationships With Clini“al Out“omes. JNCI Journal of the National Can“er Institute
101:1624-1632, 2009
341. Hawker GA, Mian S, Ken”zerska T, et al: Measures of a”ult pain: Visual Analog S“ale for Pain
(VAS Pain), Numeri“ Rating S“ale for Pain (NRS Pain), M“Gill Pain Questionnaire (MPQ),
Short-Form M“Gill Pain Questionnaire (SF-MPQ), Chroni“ Pain Gra”e S“ale (CPGS), Short
Form-36 Bo”ily Pain S“ale (SF-36 BPS), an” Measure of Intermittent an” Constant
Osteoarthritis Pain (ICOAP). Arthritis Care Res (Hoboken) 63 Suppl 11:S240-52, 2011
342. Gar“ia-Giralt N, Ro”riguez-Sanz M, Prieto-Alhambra D, et al: Geneti“ ”eterminants of
aromatase inhibitor-relate” arthralgia: the B-ABLE “ohort stu”y. Breast Can“er Res Treat
140:385-95, 2013
343. Liu G, Pea“o“k M, Eilam O, et al: Effe“t of osteoarthritis in the lumbar spine an” hip on
bone mineral ”ensity an” ”iagnosis of osteoporosis in el”erly men an” women. Osteoporos
Int 7:564-9, 1997

193
BIBLIO
GRAPHY
344. Buehring B, Krueger D, Binkley N: Effe“t of in“lu”ing histori“al height an” ra”ius BMD
measurement on sar“o-osteoporosis prevalen“e. J Ca“hexia Sar“openia Mus“le 4:47-54,
2013
345. Ran” T, Sei”l G, Kainberger F, et al: Impa“t of spinal ”egenerative “hanges on the
evaluation of bone mineral ”ensity with ”ual energy X-ray absorptiometry (DXA). Cal“if
Tissue Int 60:430-3, 1997
346. Prei”ler KW, White LS, Tashkin J, et al: Dual-energy X-ray absorptiometri“ ”ensitometry in
osteoarthritis of the hip. Influen“e of se“on”ary bone remo”eling of the femoral ne“k.
A“ta Ra”iol 38:539-42, 1997
347. Gnant M, Mlinerits“h B, S“hippinger W, et al: En”o“rine Therapy plus –ole”roni“ A“i” in
Premenopausal Breast Can“er. New Englan” Journal of Me”i“ine 360:679-691, 2009
348. Oesterrei“h S, Henry NL, Ki”well KM, et al: Asso“iations between geneti“ variants an” the
effe“t of letrozole an” exemestane on bone mass an” bone turnover. Breast Can“er
Resear“h an” Treatment 154:263-273, 2015
349. Eastell R, Hannon RA, Cuzi“k J, et al: Effe“t of an Aromatase Inhibitor on BMD an” Bone
Turnover Markers: 2-Year Results of the Anastrozole, Tamoxifen, Alone or in Combination
(ATAC) Trial (18233230). Journal of Bone an” Mineral Resear“h 21:1215-1223, 2006
350. Servitja S, Martos T, Ro”riguez Sanz M, et al: Skeletal a”verse effe“ts with aromatase
inhibitors in early breast “an“er: evi”en“e to ”ate an” “lini“al gui”an“e. Therapeuti“
A”van“es in Me”i“al On“ology 7:291-296, 2015
351. Goss PE, Ha”ji P, Subar M, et al: Effe“ts of steroi”al an” nonsteroi”al aromatase inhibitors
on markers of bone turnover in healthy postmenopausal women. Breast Can“er Resear“h
9:1-14, 2007
352. Lonning PE, Geisler J, Krag LE, et al: Effe“ts of exemestane a”ministere” for 2 years versus
pla“ebo on bone mineral ”ensity, bone biomarkers, an” plasma lipi”s in patients with
surgi“ally rese“te” early breast “an“er. J Clin On“ol 23:5126-37, 2005
353. Bouvar” B, Soulie P, Hoppe E, et al: Fra“ture in“i”en“e after 3 years of aromatase inhibitor
therapy. Ann On“ol 25:843-7, 2014
354. Fornan”er T, Rutqvist LE, Sjoberg HE, et al: Long-term a”juvant tamoxifen in early breast
“an“er: effe“t on bone mineral ”ensity in postmenopausal women. J Clin On“ol 8:1019-24,
1990
355. Turken S, Siris E, Sel”in D, et al: Effe“ts of tamoxifen on spinal bone ”ensity in women with
breast “an“er. J Natl Can“er Inst 81:1086-8, 1989
356. Ryan WG, Wolter J, Bag”a”e JD: Apparent benefi“ial effe“ts of tamoxifen on bone mineral
“ontent in patients with breast “an“er: Preliminary stu”y. Osteoporosis International
2:39-41, 1991
357. Song RX, Santen RJ, Kumar R, et al: A”aptive me“hanisms in”u“e” by long-term estrogen
”eprivation in breast “an“er “ells. Mol Cell En”o“rinol 193:29-42, 2002

REFERENCES
REFERENCES
194
BIBLIOGRAPHY
358. Cormier C, Lamy O, Poriau S: TBS in routine “linial pra“ti“e: proposals of use —Internet].
Plan-les-Outes, Switzerlan”: Me”imaps Group; Available
from:http://www.me”imapsgroup.“om/uploa”/MEDIMAPS-UK-WEB.p”f., 2012
359. María R-S, Marta P-M, Sonia S, et al: TBS an” BMD at the en” of AI-therapy: A prospe“tive
stu”y of the B-ABLE “ohort. Bone 92:1-8
360. Prasa” C, Greenspan SL, Vujevi“h KT, et al: Rise”ronate may preserve bone
mi“roar“hite“ture in breast “an“er survivors on aromatase inhibitors: A ran”omize”,
“ontrolle” “lini“al trial. Bone 90:123-126, 2016
361. Cheung AM, Tile L, Car”ew S, et al: Bone ”ensity an” stru“ture in healthy postmenopausal
women treate” with exemestane for the primary prevention of breast “an“er: a neste”
substu”y of the MAP.3 ran”omise” “ontrolle” trial. The Lan“et On“ology 13:275-284, 2012
362. Lee SJ, Kim KM, Brown JK, et al: Negative Impa“t of Aromatase Inhibitors on Proximal
Femoral Bone Mass an” Geometry in Postmenopausal Women with Breast Can“er. Cal“if
Tissue Int 97:551-9, 2015
363. Ro”riguez-Sanz M, Prieto-Alhambra D, Servitja S, et al: AI-relate” BMD variation in a“tual
pra“ti“e “on”itions: A prospe“tive “ohort stu”y. En”o“r Relat Can“er 23:303-12, 2016
364. Ro”riguez-Sanz M, Gar“ia-Giralt N, Prieto-Alhambra D, et al: CYP11A1 expression in bone is
asso“iate” with aromatase inhibitor-relate” bone loss. J Mol En”o“rinol 55:69-79, 2015
365. Thorne C: Management of arthralgias asso“iate” with aromatase inhibitor therapy.
Current On“ology 14:S11-S19, 2007
366. National Institutes of Health, Osteoporosis an” Relate” Bone Diseases, National Resour“e
Center. Osteoporosis: “oping with “hroni“ pain —Web page] Bethes”a: National Institutes of
Health; Mar, 2005. —Available at: http://“hfs.ky.gov/nr/r”onlyres/f26e7394-7“18-44e7-
8041-8b324”87b”ef/0/nihosteoporosis“opingwithpain.p”f; last entry: September 2016].
367. Lintermans A, Van Asten K, Jongen L, et al: Geneti“ variant in the osteoprotegerin gene is
asso“iate” with aromatase inhibitor-relate” mus“uloskeletal toxi“ity in breast “an“er
patients. European Journal of Can“er 56:31-36, 2016
368. Wang J, Lu K, Song Y, et al: RANKL an” OPG Polymorphisms Are Asso“iate” with Aromatase
Inhibitor-Relate” Mus“uloskeletal A”verse Events in Chinese Han Breast Can“er Patients.
PLoS One 10, 2015
369. Napoli N, Rastelli A, Ma C, et al: Geneti“ Polymorphism at Val(80) (rs700518) of the CYP19A1
Gene is Asso“iate” with Aromatase Inhibitor Asso“iate” Bone Loss in Women with ER (+)
Breast Can“er. Bone 55:309-314, 2013
370. Liu M, Goss PE, Ingle JN, et al: Aromatase Inhibitor-Asso“iate” Bone Fra“tures: A Case-
Cohort GWAS an” Fun“tional Genomi“s. Mole“ular En”o“rinology 28:1740-1751, 2014
371. Kunova“ Kallak T, Baumgart J, Stavreus Evers A, et al: Higher than expe“te” estra”iol levels
in aromatase inhibitor-treate”, postmenopausal breast “an“er patients. Clima“teri“
15:473-80, 2012
195
BIBLIO
GRAPHY
372. Brier MJ, Chambless D, Gross R, et al: Asso“iation between self-report a”heren“e measures
an” oestrogen suppression among breast “an“er survivors on aromatase inhibitors. Eur J
Can“er 51:1890-6, 2015
373. Folker” EJ, Dixon JM, Renshaw L, et al: Suppression of plasma estrogen levels by letrozole
an” anastrozole is relate” to bo”y mass in”ex in patients with breast “an“er. J Clin On“ol
30:2977-80, 2012
374. Mouri”sen H, Gershanovi“h M, Sun Y, et al: Phase III Stu”y of Letrozole Versus Tamoxifen as
First-Line Therapy of A”van“e” Breast Can“er in Postmenopausal Women: Analysis of
Survival an” Up”ate of Effi“a“y From the International Letrozole Breast Can“er Group.
Journal of Clini“al On“ology 21:2101-2109, 2003
375. Ha”fiel” KD, Newman WG: Pharma“ogeneti“s of aromatase inhibitors. Pharma“ogenomi“s
13:699-707, 2012
376. Fontein DB, Seynaeve C, Ha”ji P, et al: Spe“ifi“ a”verse events pre”i“t survival benefit in
patients treate” with tamoxifen or aromatase inhibitors: an international tamoxifen
exemestane a”juvant multinational trial analysis. J Clin On“ol 31:2257-64, 2013
377. Ettinger B, Pressman A, Sklarin P, et al: Asso“iations between low levels of serum estra”iol,
bone ”ensity, an” fra“tures among el”erly women: the stu”y of osteoporoti“ fra“tures. J
Clin En”o“rinol Metab 83:2239-43, 1998
378. Johnston SRD, Martin L-A, Hea” J, et al: Aromatase inhibitors: Combinations with
fulvestrant or signal trans”u“tion inhibitors as a strategy to over“ome en”o“rine
resistan“e. The Journal of Steroi” Bio“hemistry an” Mole“ular Biology 95:173-181, 2005
379. Teplyuk NM, –hang Y, Lou Y, et al: The Osteogeni“ Trans“ription Fa“tor Runx2 Controls
Genes Involve” in Sterol/Steroi” Metabolism, In“lu”ing Cyp11a1 in Osteoblasts. Mole“ular
En”o“rinology 23:849-861, 2009
380. Kennel KA, Drake MT, Hurley DL: Vitamin D Defi“ien“y in A”ults: When to Test an” How to
Treat. Mayo Clin Pro“ 85:752-758, 2010
381. Re””y KR, Deepika ML, Supriya K, et al: CYP11A1 mi“rosatellite (tttta)n polymorphism in
PCOS women from South In”ia. J Assist Repro” Genet 31:857-63, 2014
382. Torgerson DJ, Campbell MK, Thomas RE, et al: Pre”i“tion of perimenopausal fra“tures by
bone mineral ”ensity an” other risk fa“tors. J Bone Miner Res 11:293-7, 1996
383. Cummings SR, Nevitt MC, Browner WS, et al: Risk fa“tors for hip fra“ture in white women.
Stu”y of Osteoporoti“ Fra“tures Resear“h Group. N Engl J Me” 332:767-73, 1995
384. An”rew T, Antionia”es L, S“urrah KJ, et al: Risk of wrist fra“ture in women is heritable an”
is influen“e” by genes that are largely in”epen”ent of those influen“ing BMD. J Bone Miner
Res 20:67-74, 2005
385. Miki Y, Suzuki T, Hatori M, et al: Effe“ts of aromatase inhibitors on human osteoblast an”
osteoblast-like “ells: a possible an”rogeni“ bone prote“tive effe“ts in”u“e” by
exemestane. Bone 40:876-87, 2007

REFERENCES
REFERENCES
196
BIBLIOGRAPHY
386. Be“k DT, Yarrow JF, Beggs LA, et al: Influen“e of Aromatase Inhibition on the Bone-
Prote“tive Effe“ts of Testosterone. Journal of Bone an” Mineral Resear“h 29:2405-2413,
2014
387. Yarrow JF, Conover CF, Puran”are AV, et al: Supraphysiologi“al testosterone enanthate
a”ministration prevents bone loss an” augments bone strength in gona”e“tomize” male
an” female rats. Am J Physiol En”o“rinol Metab 295:9, 2008
388. Seibel MJ: Bio“hemi“al Markers of Bone Turnover Part I: Bio“hemistry an” Variability. The
Clini“al bio“hemist. Reviews / Australian Asso“iation of Clini“al Bio“hemists. 26:97-122,
2005
389. Unnanuntana A, Gla”ni“k BP, Donnelly E, et al: The Assessment of Fra“ture Risk. The
Journal of Bone an” Joint Surgery. Ameri“an volume. 92:743-753, 2010
390. Coleman RE, Banks LM, Girgis SI, et al: Skeletal effe“ts of exemestane on bone-mineral
”ensity, bone biomarkers, an” fra“ture in“i”en“e in postmenopausal women with early
breast “an“er parti“ipating in the Intergroup Exemestane Stu”y (IES): a ran”omise”
“ontrolle” stu”y. Lan“et On“ol 8:119-27, 2007
391. Eastell R, Hannon RA, Cuzi“k J, et al: Effe“t of an aromatase inhibitor on bm” an” bone
turnover markers: 2-year results of the Anastrozole, Tamoxifen, Alone or in Combination
(ATAC) trial (18233230). J Bone Miner Res 21:1215-23, 2006
392. Garvi“an ER, Vaughan-Thomas A, Innes JF, et al: Biomarkers of “artilage turnover. Part 1:
Markers of “ollagen ”egra”ation an” synthesis. Vet J 185:36-42, 2010
393. Din OS, Do”well D, Wakefiel” RJ, et al: Aromatase inhibitor-in”u“e” arthralgia in early
breast “an“er: what ”o we know an” how “an we fin” out more? Breast Can“er Res Treat
120:525-38, 2010

Top Related
Copyright © 2022 FDOKUMEN

