







Bahasa
Halaman
Hukum


Neuropsychologia 66 (2015) 55–66
Contents lists available at ScienceDirect
Neuropsychologia
http://d0028-39
n CorrE-m
journal homepage: www.elsevier.com/locate/neuropsychologia
Interaction of memory systems during acquisition of tool knowledgeand skills in Parkinson's disease
Shumita Roy a,n, Norman W. Park a, Eric A. Roy b,c, Quincy J. Almeida c
a Department of Psychology, York University, 4700 Keele Street, Toronto, Ontario, Canada M3J 1P3b Department of Kinesiology, University of Waterloo, Waterloo, Ontario, Canadac Sun Life Financial Movement Disorders Research and Rehabilitation Centre, Wilfrid Laurier University, Waterloo, Ontario, Canada
a r t i c l e i n f o
Article history:Received 18 August 2014Received in revised form30 October 2014Accepted 6 November 2014Available online 11 November 2014
Keywords:Memory systemsDeclarative memoryProcedural memorySkilled tool useMotor skill learningParkinson's disease
x.doi.org/10.1016/j.neuropsychologia.2014.11.032/& 2014 Elsevier Ltd. All rights reserved.
esponding author. Tel.: +1 416 736 2100×221ail addresses: [email protected] (S. Roy), npar
a b s t r a c t
Previous research suggests that different aspects of tool knowledge are mediated by different memorysystems. It is believed that tool attributes (e.g., function, color) are represented as declarative memorywhile skill learning is supported by procedural memory. It has been proposed that other aspects (e.g.,skilled tool use) may rely on an interaction of both declarative and procedural memory. However, thespecific form of procedural memory underlying skilled tool use and the nature of interaction betweendeclarative and procedural memory systems remain unclear. In the current study, individuals withParkinson's disease (PD) and healthy controls were trained over 2 sessions, 3 weeks apart, to use a set ofnovel complex tools. They were also tested on their ability to recall tool attributes as well as their abilityto demonstrate grasp and use of the tools to command. Results showed that, compared to controls,participants with PD showed intact motor skill acquisition and tool use to command within sessions, butfailed to retain performance across sessions. In contrast, people with PD showed equivalent recall of toolattributes and tool grasping relative to controls, both within and across sessions. Current findings de-monstrate that the frontal-striatal network, compromised in PD, mediates long-term retention of motorskills. Intact initial skill learning raises the possibility of compensation from declarative memory forfrontal-striatal dysfunction. Lastly, skilled tool use appears to rely on both memory systems which mayreflect a cooperative interaction between the two systems. Current findings regarding memory re-presentations of tool knowledge and skill learning may have important implications for delivery of re-habilitation programs for individuals with PD.
& 2014 Elsevier Ltd. All rights reserved.
1. Introduction
Frey (2007) defines tools as “manipulable objects that are usedto transform an actor's motor output into predictable mechanicalactions for purposes of attaining specific goals”. Tools can be fur-ther classified as being either simple tools, which amplify themovement of the upper limbs (e.g., using a stick to extend reach),or complex tools, which are manufactured to provide a mechanicaladvantage in performing a task (e.g., cutting paper with scissors;Frey, 2007; Heilman, 2002). As humans, we rely on complex toolsto perform many activities of daily living (ADLs; e.g., using a fork toeat) as well as instrumental activities of daily living (IADLs; e.g.,using cooking utensils to prepare a meal). In addition, we have aremarkable adaptive ability to learn how to use novel tools toperform new tasks. Thus, the ability to use both familiar and novelcomplex tools is essential for continued independent living.
05
59; fax: þ1 416 736 [email protected] (N.W. Park).
Studies have shown that the inability to perform ADLs and IADLscan have a substantial negative impact on a person's quality of lifeas they are not able to function independently (Foundas et al.,1995). However, our understanding of the cognitive processesunderlying complex tool use, including how we acquire tool-re-lated knowledge and skills, is still incomplete.
Although using a complex tool (e.g., a hammer) may seem ra-ther effortless, this act is supported by a complex set of cognitiveprocesses. For instance, there are multiple memory processes in-volved in both the acquisition and retrieval of different aspects oftool-related knowledge and skills (e.g., knowing the function ofthe tool, how to grasp it, how to manipulate it), and it has beenproposed that each of these aspects has a different memory re-presentation (Daprati and Sirigu, 2006). It has been argued thatmemory for tool-specific features (e.g., a tool's function) is re-presented within declarative memory (Warrington and Shallice,1984). In contrast, motor skills are believed to be primarily re-presented by procedural memory (Squire, 2009). Furthermore, ithas been proposed that some aspects of tool-related knowledgeand skills may rely on an interaction of both memory systems

S. Roy et al. / Neuropsychologia 66 (2015) 55–6656
(Negri et al., 2007; Roy and Park, 2010; Silveri and Ciccarelli, 2009).However, the specific memory representations of these differentaspects of tool-related knowledge and skills are still not well un-derstood. In addition, it is unclear how the declarative and pro-cedural memory systems may interact in mediating tool-relatedknowledge and skills.
In an earlier study, we systematically investigate the role ofdeclarative memory in acquiring novel tool knowledge and skillsin D.A., an individual with profound hippocampal amnesia (Royand Park, 2010). D.A. and a group of healthy controls were trainedto use a set of novel complex tools over three sessions. Participantswere tested on their ability to recall attributes of the tools (e.g.,function) as well as to demonstrate the appropriate manner of toolgrasping and use to command. Findings showed that D.A. learnedthe motor skills at the same rate as controls and retained theseskills over a 3-week delay. However, he was severely impaired inhis ability to recall tool attributes as well as demonstrate grasp andtool use to command. This pattern of results suggests that memoryfor tool attributes, tool grasping, and skilled tool use is at leastpartly dependent on declarative memory. In contrast, resultssuggest that motor skill learning associated with complex toolscritically relies on intact procedural memory. It was also proposedthat skilled tool use may rely on an interaction of both memorysystems. Although these findings shed light on the role of de-clarative memory in the acquisition of tool knowledge and skills,the specific type of procedural memory and its contributions havenot yet been directly investigated. Furthermore, possible interac-tion between the two memory systems with respect to mediatingskilled tool use is unclear. In the current study, we investigatedacquisition of tool-related knowledge and skills in an experimentsimilar to Roy and Park (2010) in a sample of individuals withParkinson's disease (PD) and healthy controls. It is well establishedthat motor procedural tasks depend on the striatal network, andpeople with PD have been shown to be impaired on tasks relyingon the striatum (Packard and Knowlton, 2002; Siegert et al., 2006).In contrast, declarative memory tends to be relatively intact in PD,at least in mild stages (Hay et al., 2002). If participants with PDhave impaired memory for certain aspects of tool knowledge andskills, it would suggest that these aspects rely on regions damagedin PD. Our findings may also provide insights into the interactionbetween declarative and procedural memory systems.
1.1. Human memory systems
Traditional theories have divided memory into two broad sys-tems: declarative memory and procedural memory (Squire, 2009).Declarative memory has been shown to rely on medial temporallobe structures and is believed to mediate recollection of facts andevents (Squire, 2009). In contrast, procedural memory mediatesthe formation of new skills and habits and is believed to rely on afrontal-striatal network (Squire, 2009, also see Doyon et al., 2009).Declarative memories can be acquired rapidly but tend to besensitive to interference and decay, whereas procedural memorytends to be resistant to both interference and decay (Gabrieli et al.,1993; Squire, 2009; but see Brashers-Krug et al., 1996). These twomemory systems have been considered to be functionally andanatomically dissociable (Cohen and Squire, 1980; also seeKnowlton et al., 1996). More recently, research has demonstratedthat the declarative and procedural memory systems may interactunder some circumstances (Packard and Goodman, 2013; Poldrackand Packard, 2003). For instance, there is evidence suggesting thatthe two memory systems interact in a cooperative manner whereboth systems are critically involved. There is also evidence show-ing that the two systems may interact in a competitive mannerwhere one system inhibits the other system (see Foerde andShohamy et al., 2011). In addition, it has been shown that one
system may compensate for the other in some situations (seeMoody et al., 2004). However, the characteristics of this interac-tion, as well as its limitations, are not well understood. In addition,much of the recent research regarding memory interactions hasbeen conducted with probabilistic classification learning, a com-puterized task involving learning of visual associations (Poldracket al., 2001). Therefore, the use of different types of memory tasksmay help to clarify the interaction between declarative and pro-cedural memory systems.
1.2. Memory representations of tool-related knowledge and skills
1.2.1. Motor skill learningIt has been proposed that motor skill learning takes place over
three stages (Albouy et al., 2013; Doyon et al., 2009). First, there isan early learning phase in which rapid gains are made withinsession. It has been argued that this early stage is supported by anetwork of brain regions including the hippocampus, and bothcortico-striatal and cortico-cerebellar circuits (Albouy et al., 2013;Schendan et al., 2003). Second, there is a consolidation phaseduring which the motor skill becomes resistant to decay or in-terference. Consolidation of skills is believed to be critically de-pendent on the striatum (Doyon et al., 2009). Third, there is a slowlearning phase during which the motor skill continues to becomeautomatized and can be performed with very little attention. It hasbeen shown that the striatum, as well as motor and parietal cor-tices, are all involved in the slow learning phase (Doyon et al.,2009). Thus, regions from both declarative and procedural mem-ory systems are believed to be involved in motor skill learning.Furthermore, it has been suggested that the relative involvementof the two systems varies across the different stages of learning(e.g., greater striatal involvement during consolidation; Doyonet al., 2009).
The serial reaction time task (SRTT) is a commonly used taskbelieved to measure implicit skill learning (Nissen and Bullemer,1987). Studies have shown that people with PD are impaired onthe SRTT, indicating that the procedural memory system, involvingthe striatum, has a critical role in motor sequence learning (Siegertet al., 2006). However, there is currently a debate in the literatureregarding the role of the hippocampus and declarative memory inmotor skill learning. One position argues that motor sequencelearning is predominantly procedural and occurs independently ofany explicit awareness or declarative knowledge of what is learned(Song et al., 2007). A second position argues that there is a com-petitive interaction between the two memory systems duringearly stages of motor skill learning. According to this position, thehippocampus is heavily involved in early stages of skill learning,but gradually becomes deactivated as the striatum takes on agreater role in latter stages (see Albouy et al., 2013). A third po-sition argues that early stages of motor skill learning require acooperative interaction of both declarative and procedural mem-ory systems (see Penhune and Steele, 2012). Finally, it has beenproposed that there may be a compensatory relationship. Findingsfrom a recent study suggested that two participants with PD mayhave employed declarative memory to perform a striatally medi-ated motor sequence learning task (Gobel et al., 2013). This theoryof compensation would suggest that in cases of damage to theprocedural system (e.g., PD), the declarative system may be en-gaged to undertake functions typically mediated by the proceduralsystem. Overall, there is growing evidence to suggest that thedeclarative system has a role in motor skill learning, but the pre-cise role of declarative memory and its interaction with proceduralmemory is still unclear.

S. Roy et al. / Neuropsychologia 66 (2015) 55–66 57
1.2.2. Skilled tool useSkilled tool use (i.e., intentional demonstration of a tool's use)
is similar to motor skill learning in that they both involve motorexpression of a skill; however, there are some key differences.During motor skill learning, the learner typically has access toexternal supports (e.g., trainer, manual) to scaffold skill develop-ment. In contrast, during skilled tool use, the learner must recreatethe training context independently and demonstrate the motorskill previously acquired during training. As with motor skill ac-quisition, there are mixed views regarding the memory re-presentations of skilled tool use. Some researchers argue that tooluse can be mediated through sensorimotor processes (i.e., me-chanical problem-solving) along with physical affordances andthat declarative tool knowledge is not necessary (Gibson, 1977;Goldenberg and Spatt, 2009; Hartmann et al., 2005). Studies havealso shown that patients with semantic dementia and other de-clarative memory impairment are still able to use familiar toolsefficiently (Negri, et al., 2007). However, another perspective ar-gues that semantic tool knowledge is required in order to use toolsin a conventional manner. Advocates of this position have arguedthat people with semantic dementia often have some residualsemantic memory which may explain preserved tool use for fa-miliar tools (Buxbaum et al., 1997). This theory of residual se-mantic memory guiding tool use was supported by a study inwhich more severe semantic memory impairment was associatedwith greater impairment in tool use (Silveri and Ciccarelli, 2009).
While the role of semantic memory continues to be debated,the role of procedural memory in skilled tool use has not receivedmuch focus in the literature. However, there has been suggestionthat skilled tool use may rely on a cooperative interaction of bothdeclarative and procedural memory systems (Buxbaum et al.,1997; Negri et al., 2007; Silveri and Ciccarelli, 2009). Roy and Park(2010) proposed that declarative memory may be encode task-related details whereas procedural memory supports expression oflearned motor skills. However, the specific roles of both memorysystems in skilled tool use require further investigation.
1.2.3. Tool graspingPrevious research has suggested that grasping a tool for the
purpose of moving it, versus using it, rely on different cognitivemechanisms; however, there has been limited research directlyinvestigating the memory representations of tool grasping (Bux-baum et al., 2006). Existing research suggests that tool graspinghas strong declarative involvement. In a behavioral study, Creemand Proffit (2001) showed that healthy participants were lesslikely to grasp familiar tools appropriately, by their handles, whenthey concurrently performed a semantic secondary task comparedto when they performed a visuomotor secondary task. The authorsconcluded that grasping a tool for the purpose of using it, but notsimply moving it, requires semantic knowledge about the tool. In asubsequent neuroimaging study, Creem-Regehr and Lee (2005)reported greater activation in the middle temporal gyrus and fu-siform gyrus for images of familiar tools with handles compared tounfamiliar graspable shapes, suggesting that functional knowledgeof tools influences neural representations associated with graspingthe tool for use. Further evidence comes from the earlier describedstudy by Roy and Park (2010) in which an amnesic individual wasimpaired in his grasp demonstration for novel tools after beingtrained to use them. Thus, previous research with both novel andfamiliar tools suggests that grasping a tool for the purpose of usingit requires declarative knowledge of the tool. It could be arguedthat tool grasping involves skilled motor processes as well andtherefore, may involve the procedural memory system. However, itis unclear at this point whether the procedural memory systemand related subcortical structures are involved in tool grasping.
1.2.4. Memory for tool featuresIt is generally accepted that retrieval of knowledge related to
object features (e.g., function, color) is mediated primarily by de-clarative memory. It has been shown that people with temporallobe damage have difficulty remembering object-specific char-acteristics as this information is semantically represented (War-rington, 1975; Hodges et al., 2000). Studies have also investigatedthe neural representations of different categories of objects andshowed that retrieval of tool features appears to be centralized inthe medial fusiform gyrus, further demonstrating a declarativerepresentation of object features (Chao et al., 1999; Martin andChao, 2001). Lastly, the amnesic individual studied in Roy and Park(2010) was severely impaired in his ability to recall attributes ofnovel tools that he had been trained to use over several trials.Thus, the ability to recall properties of both familiar and noveltools appears to be primarily mediated by declarative memory.
2. Overview and rationale of experiment
Results from Roy and Park (2010), along with other existing re-search, suggest that intact declarative memory is necessary for theacquisition of tool attributes, tool grasping, and skilled tool use.However, the precise role of procedural memory in mediating as-pects of tool-related knowledge and skills has not yet been in-vestigated. While it has been proposed that motor skill acquisitionassociated with complex tools requires procedural memory, it isunclear which form of procedural memory supports this type oflearning (e.g., cortico-striatal versus cortico-cerebellar). There is alsogrowing evidence to suggest that, in addition to procedural memory,both motor skill acquisition and skilled tool use rely on declarativememory to a certain extent. In other words, these aspects of tool-related knowledge and skills may rely on an interaction of bothmemory systems. However, it is unclear what form this interactiontakes (e.g., competitive, compensatory, cooperative) for differentmeasures of tool-related knowledge and skills.
The current study was conducted as an extension to Roy and Park(2010), in order to investigate the specific role of the proceduralmemory system, as well as the interaction of the declarative andprocedural memory across various measures of tool knowledge andskills. We investigated memory for the same aspects of tool-relatedknowledge and skills (i.e., motor skill acquisition, recall of tool fea-tures, tool grasping, and skilled tool use) in a sample of people withPD and healthy age-matched controls. Participants were tested overtwo sessions, with a 3-week delay between sessions. Based on thepresumption that motor skill learning associated with complex toolsis striatally mediated, the following hypotheses were put forth. First,it was hypothesized that participants with PD would show a slowerrate of motor skill acquisition relative to controls across sessions, inaddition to generalized slowing. Second, it was predicted thatmemory for tool attributes would be unimpaired in individuals withPD relative to healthy controls. Third, it was predicted that in-dividuals with PD would be impaired in their tool grasping andskilled tool use relative to healthy controls. This prediction was basedon the argument that these latter aspects of tool knowledge rely onan interaction of both memory systems (Roy and Park, 2010). Fourth,it was predicted that, after the 3-week delay, all participants wouldshow decreased recall of aspects of tool knowledge that are re-presented declaratively (e.g., function of the tool) and that theamount of decline would be equivalent for both individuals with PDand controls. Finally, based on existing evidence of unimpaired initialskill learning, but impaired long-term retention, it seemed plausibleto predict that participants with PD would show this same pattern ofperformance (i.e., intact skill learning within session, but impairedretention over the 3-week delay; Doyon et al., 2009; Mochizuki-Kawai et al., 2004).

Table 1Participant characteristics.
Variable PD (n¼18) CON (n¼18) p-Value
M SD M SD
Age 67.3 6.6 70.8 6.8 .13Education (years) 14.8 2.7 14.5 3.6 .78Gender (M/F) 10/8 10/8MMSE (/30) 28.2 1.4 28.8 1.0 .11HADS – total (/42) 9.8 6.4 7.2 6.2 .23HADS – depression (/21) 4.3 3.1 2.6 3.5 .14HADS – anxiety (/21) 5.5 3.6 4.6 3.6 .46Years since onset 4.6 3.4
UPDRS motor sectionSession 1 24.9 6.7Session 2 23.18 6.3Side affected (L/R/B) 10/7/1LED (mg/day) 516.7 168.7
PD, Parkinson's disease; CON, Controls; MMSE, Mini-mental, State Examination;HADS, Hospital Anxiety and Depression, Scale; UPDRS, Unified Parkinson's DiseaseRating Scale; L/R/B, Left/Right/Both; and LED, levodopa-equivalent dose.
S. Roy et al. / Neuropsychologia 66 (2015) 55–6658
3. Method
3.1. Participants
A sample of 18 participants with a clinical diagnosis of idio-pathic PD confirmed by a neurologist, and 18 healthy age-matchedcontrols completed the study. Data from these 36 participants areincluded in the analyses. One other participant from the PD sam-ple withdrew due to inability to establish mental set. All partici-pants with PD were recruited from the Sun Life Financial Move-ment Disorders Research Centre (MDRC) in Waterloo, Ontario,Canada. Seven control participants were recruited from the Uni-versity of Waterloo's healthy older adult research participant pooland the other eleven control participants were spouses of patientsat the MDRC. A summary of participant characteristics can befound in Table 1. Participants with PD did not differ significantlyfrom controls on any participant characteristics.
Inclusion criteria included being right-handed, fluent in Eng-lish, and between the ages of 55 and 85. Exclusion criteria in-cluded history of serious head injury, history of any neurologicalillnesses (other than PD in the patient group), psychotic symptoms(e.g., hallucinations), color-blindness, clinical diagnosis of mildcognitive impairment, general cognitive deterioration as evi-denced by a score below 26 on the Mini-Mental State Examination(MMSE; Folstein et al., 2010) as would be indicative of cognitiveimpairment according to the Movement Disorders Society TaskForce (Dubois et al., 2007), current depression or anxiety as as-sessed by the Hospital Anxiety and Depression Scale (HADS; Zig-mond and Snaith, 1983), inability to use the right hand freely dueto injury or any other condition such as arthritis. In addition,participants with PD were not included if they had severe tremorin the right hand, severe rigidity in the right hand or wrist which
Fig. 1. Examples of novel tools d
would affect ability to manipulate small objects, or severe brady-kinesia (i.e., slowed movement). Patients were asked a series ofquestions about their daily functioning to assess these features(e.g., Does your tremor affect your ability to write? Use a hammer?Hold a toothbrush?). In addition, current scores from the motorsection of the Unified Parkinson's Disease Rating Scale were re-viewed prior to inclusion to determine severity of motor symp-toms (UPDRS III; Fahn and Elton, 1987; see Table 1).
Seventeen of the participants with PD were taking dopami-nergic drugs and they continued with their regular medicationregimen throughout the study. One participant with PD was nottaking any medication at all. Three participants with PD weretaking anti-depressant medication; however, their symptoms didnot meet criteria for depression or anxiety on the HADS at thetime of testing. None of the participants were taking antic-holinergic drugs or amphetamines. The experiment was approvedby the relevant ethics review boards and each participant providedwritten consent prior to participation.
3.2. Materials
3.2.1. Experimental materialsA set of fifteen novel complex tools were constructed from
K'NEX, a children's construction toy (see Fig. 1). The tools wereoriginally developed for Roy and Park (2010) and were modelledafter novel tools used in an earlier study by Weisberg et al. (2007).For the current study, a subset of nine tools were selected from theoriginal set of 15. These nine tools were included because theywere found to be less susceptible to motor disturbance duringpilot testing with a separate sample of PD patients. Each tool wasdesigned to act on a unique object, hereafter called a recipient(e.g., small plastic wheel), in order to perform a specific function(e.g., guide a plastic wheel down a curved path). Each tool waspainted a different color, and previous research established thatneither the function of the tool nor manner of grasp were apparentfrom physical appearance (Roy and Park, 2010). All tools weredesigned to be used uni-manually. Brief training videos of thetools were created which demonstrate the use of each tool. Thevideos also included an audio track which directed the partici-pant's attention to specific details about the task as it was viewed(e.g., how to grasp the tool, where to position the recipient). Thenine tools were divided randomly into three sets of three tools (SetA, Set B, and Set C).
3.2.2. Recall testA set of gray-scale images of the tools were used to develop a
recall test of tool attributes. Three photographs of each tool weretaken from three different, approximately equidistant, angles.During the recall test, participants were shown the three picturesof each tool, one tool at a time, and were asked to answer thefollowing five questions about each tool: (1) What is the functionof the tool/What is it used for? (2) What is the color of the actualphysical tool? (3) What is the recipient that the tool interacts
eveloped for this research.
Table 2Standardized z-scores for participants with Parkinson's Diseasea.
Neuropsychological test M (SD) p-Valueb
WAIS-IV (selected subtests)Digit span .074 (.63) .62Matrix reasoning .16 (.90) .47Information .41 (.93) .08
HVLT-RTotal recall (T1-T3) � .57 (.98) .02Delayed recall � .41 (1.05) .11Percent retained � .09 (1.28) .77
BVMT-RTotal recall (T1-T3) � .20 (1.19) .48Delayed recall � .00 (1.06) .99Percent retained .06 (.46) .57
ROCF-copy � .12 (1.33) .72
Trail making testPart A � .38 (.72) .07Part B � .63 (1.11) .05
Stroop test (Victoria version)Dots .06 (.88) .78Words .10 (.78) .59Color words .31 (1.09) .25
Phonemic fluency .28 (.87) .18Semantic fluencyAnimals .53 (1.15) .07Supermarket .00 (1.03) .99
Boston naming test .62 (.71) o .001
Grooved pegboardDominant hand � .83 (.89) .001Non-dominant hand �1.08 (.86) o .001
WAIS-IV¼Wechsler Adult Intelligence Scale – Fourth Edition; HVLT-R¼HopkinsVerbal Learning Test – Revised; BVMT-R¼Brief Visuospatial Memory Test – Re-vised; and ROCF¼Rey Osterrieth Complex Figure.
a Scores represent mean z-scores across participants for each cognitive test.Raw scores on each test were first scored according to appropriate normative datafor each participant and were then converted to z-scores.
b A one-sample t-test was conducted to obtain p-values.
1 Participants with PD had one additional session, scheduled on a separate day,for neuropsychological testing.
S. Roy et al. / Neuropsychologia 66 (2015) 55–66 59
with? (4) What is the color of the recipient? and (5) How manyrecipients does the tool act on? Once the participant completedthe five questions for a tool, they were not allowed to go back andreview previous responses. Participants were asked to verballyprovide their responses and the experimenter recorded these re-sponses verbatim.
3.2.3. Grasp-to-command testEach tool was placed on the table in front of the participant
without its associated recipient(s). In order to control for the po-sition of the tool's handle, the tool was presented in one of threeorientations. To use the analogy of a clock, if the participant weresitting at the hour-hand position of 6 o'clock, the tool handle wasplaced at approximately 1 o'clock, 4 o'clock, or 7 o'clock, in nopredetermined order. The tool was not presented at 11 o'clock(furthest away from participant's right hand) to minimize dis-comfort and awkward hand positioning that may have interferedwith scoring. The participant was instructed, “With your righthand, showme how you would grasp this tool if you were to use it.Show me the first thing that comes to mind.” The participant wasallowed to rotate the tool in order to make the handle more ac-cessible. After the participant demonstrated the grasp, the parti-cipant was asked to release the tool.
3.2.4. Use-to-command testAfter the participant demonstrated the grasp of a tool, the ex-
perimenter set up the entire task with all associated materials. Thetool was positioned in front of the participant in the proper or-ientation for use and the recipient(s) was placed in a small outlinedsquare, next to the tool. The participant was instructed, “Again, usingyour right hand, I'd like you to showme how you would use the tool.Show me the first thing that comes to mind. Please let me knowwhen you've completed the task.” Participants were expected to firstposition the recipient in the correct starting location. Then, they weregiven a limit of 90 s to demonstrate correct use of the tool from startto finish. Timing began when the tool made contact with the re-cipient and ended when either the task was completed without erroror when the time limit was up. During use-to-command, participantswere informed that the experimenter would not be providing themwith any assistance or feedback on any aspect of their performance.Further details on the experimental materials and procedures can befound in Roy and Park (2010).
3.3. Neuropsychological tests
A battery of standardized neuropsychological tests was ad-ministered to characterize participants with PD. This battery in-cluded the Hopkins Verbal Learning Test-Revised (HVLT-R; Bene-dict et al., 1998), Brief Visuospatial Memory Test Revised (BVMT-R;Benedict, 1997), Stroop test-Victoria version (Troyer et al., 2006),Boston Naming Test (BNT; Kaplan et al., 1983), Rey-OsterriethComplex Figure Test – Copy only (ROCF; Osterrieth, 1944), TrailMaking Test (Reitan and Wolfson, 1985), FAS Verbal Fluency Test(Spreen and Benton, 1977), Animal Naming Test (Tombaugh et al.,1999), selected tests from the Wechsler Adult Intelligence Scale(WAIS-IV; Wechsler, 2009), Grooved-Pegboard test (Matthews andKlove, 1964), and the Pantomime test from the Waterloo-Sunny-brook Apraxia Battery. The Pantomime test was performed at theend of the session. The results from the Pantomime test will beused in another related study and are therefore not presented inthe current study. The entire battery took approximately 50 min tocomplete, and it was administered on a separate day, apart fromthe two experimental sessions. Test results of individuals werecombined to create a cognitive profile of the patient group (seeTable 2). As a group, participants with PD performed within theaverage range across all cognitive domains tested, including tests
of declarative memory. Control participants did not undergo for-mal cognitive testing.
3.4. Design and procedure
Each participant was tested individually over two 60-min ses-sions (S1 and S2), three weeks apart.1 Prior to each session, par-ticipants with PD underwent assessment of their motor symptoms(i.e., UPRDS) as well. Each session was composed of three phases:Pre-test, Training, and Post-test. The three tool sets (i.e., A, B, andC) were counterbalanced in their presentation across the threephases (see Appendix A). In order to reduce fatigue for participantswith PD, the number of tools trained was limited to two sets (i.e.,six tools) and participants were trained twice on each of thesetools. One of the two trained sets was tested in the Pre- and Post-tests. The remaining untrained tool set was reserved for a singletraining trial at the end of Session 2. This design allowed for eachsession to fit within one hour, while still obtaining data on allmeasures. The implementation of this design will be outlined inthe Pre-test, Training, and Post-test sections that follow.

2 In order to ensure that average time scores were not inflated by incompleteattempts (i.e., maximum time scores of 90 s) these incomplete attempts were re-moved before conducting analyses on completion time for both Training and Use-to-command.
S. Roy et al. / Neuropsychologia 66 (2015) 55–6660
3.4.1. Pre-testThe Pre-test began with the recall test, followed by grasp-to-
command and, finally, use-to-command tests described earlier.The Pre-test was conducted on only one set of the tools (e.g., SetA). The purpose of the Pre-test in S1 was to confirm that partici-pants were not able to infer attributes, grasp, or use of the toolsprior to formal training.
3.4.2. TrainingAfter the Pre-test, participants were trained to use six of the
tools, one at a time. In other words, they were trained on two setsof tools, one of which included the set used in the Pre-test (e.g., SetA and Set B). First, participants viewed the training video for thetool. Prior to starting the video, participants were instructed to payclose attention to the video as they would only be able to watch itonce. During the video, the actual tool shown in the video waspositioned in front of participants on the table in the proper or-ientation for use and the recipient(s) was placed in a small out-lined square to the side of the tool. Materials were positioned inthe same locations in the videos as well. Participants were askednot to handle the tool while the video was playing. Immediatelyafter viewing the video, participants were asked to perform thetask in the same manner as in the video. They were instructed toperform the task as quickly as possible, from start to finish,without making any errors, and to restart the task if they madeany errors. They were given a 90 s limit to complete one errorlesstrial. In order to perform the task in the same manner as shown inthe video, participants first had to position the recipient in thecorrect location and then complete the task using the tool. Timingbegan when the tool made contact with the recipient and endedonce an errorless (successful) trial was completed or when thetime limit was up. The experimenter provided verbal feedback toparticipants to correct the initial grasp as well as errors during thetask. Once the task was completed, or after the time limit wasreached, the tool and all materials were reset to their originalposition and the participant was asked to perform the task againwith the same tool for a second trial. Thus, participants performedtwo consecutive trials for each of the six tools. The order in whichthe tools were presented was fixed within each set; however, theorder of tool sets was counterbalanced across participants.
3.4.3. Post-testAfter completing the training phase, the Post-test was adminis-
tered which included the same test measures as the Pre-test. How-ever, the Post-test was performed on the set of trained tools that wasnot used in the Pre-test (see Appendix A). As example, for Participant1, the pre-test was administered for Set A in S1. Then the participantwas trained on Sets B and A, respectively. After training, the S1 post-test was administered on Set B. The post-test was administered onSet B, and not Set A, in order to minimize recency recall effects. S2Pre-test was then administered on Set B again, which allowed for theeffect of delay to be examined on the same tools.
After Post-test in S2, participants were given one training trialwith the remaining third set of tools that had not been presentedearlier in the experiment (see Appendix A). The purpose of thistrial with previously untrained tools was to investigate whetherthe training provided during the experiment generalized, and re-sulted in improved performance with novel tools.
3.5. Scoring
The following scoring procedures were implemented for allmeasures in the current study. Inter-rater reliability is also pre-sented for those measures which do not have an objective scoringsystem and therefore, may have required experimenter judgment.Inter-rater scores reflect the percentage of agreement between the
two raters for a given measure. Further details on scoring proce-dures can be found in Roy and Park (2010).
For Training performance, two scores were obtained for eachtool task. The number of attempts reflects the number of errorsmade before performing the full task without errors (i.e., errorlesstrial). Completion time reflects total time of the single errorlessattempt for each tool task from the moment the tool made contactwith the recipient to the point where the task was completedsuccessfully, without error. If a participant was unable to completethe task successfully within the 90-s time limit, a maximum scoreof 90 s was recorded.
Performance on the recall test was measured as the percentageof correct responses to items in each test trial. Total recall accuracywas measured as the percentage of correct items out of the totalnumber of items. A scoring rubric was developed for the recall testwhich contains a set of acceptable responses for each item. Thisrubric is based on responses obtained from participants duringinitial pilot testing of the materials.
Grasp-to-command performance was scored as the percentageof correct grasp demonstrations to command in each test trial.Each correct demonstration was given one point. As describedearlier, each tool has a unique functional manner of grasping thatparticipants learn during the training phase. A second in-dependent rater scored 30% of the data and an inter-rater relia-bility score of 92.4% was obtained for grasp-to-command.
Performance on the use-to-command test can be broken downinto two components, accuracy and completion time. Tool use ac-curacy was measured as the percentage of correct tool use demon-strations to command (e.g., whether or not a participant was able tocomplete the task successfully within 90 s) while completion timeprovided a measure of how quickly the participant was able tocomplete the task, in seconds. In terms of accuracy, if a participantwas able to accurately demonstrate the tool's use within the 90 stime limit, the demonstration was scored as correct and one pointwas given. If the task was performed incorrectly, or was not com-pleted within the 90 s time limit, the demonstration was scored asincorrect. A second independent rater scored 30% of the data and aninter-rater reliability score of 94.5% was obtained for use-to-com-mand accuracy. Completion time for use-to-command performancewas measured in the same manner as in Training.
3.6. Statistical analyses
All experimental measures were analyzed using parametricstatistical techniques. Analyses for each measure were divided intowithin-session and between-session components. Primary ana-lyses for each measure included a two-way mixed ANOVA withgroup and trial as factors for the interaction and a one-way ANOVAfor main effects of group and trial. Bonferroni error correction wasapplied in all follow-up pairwise comparisons.
4. Results
4.1. Training
4.1.1. Within session effectsThere was a main effect of group showing that participants
with PD were slower relative to controls, F(1,34)¼8.51, p¼ .006, η2
¼ .20 (see Fig. 2).2 There was also a main effect of trial, showingthat all participants became faster from T1 to T2, F(1, 34)¼13.35,
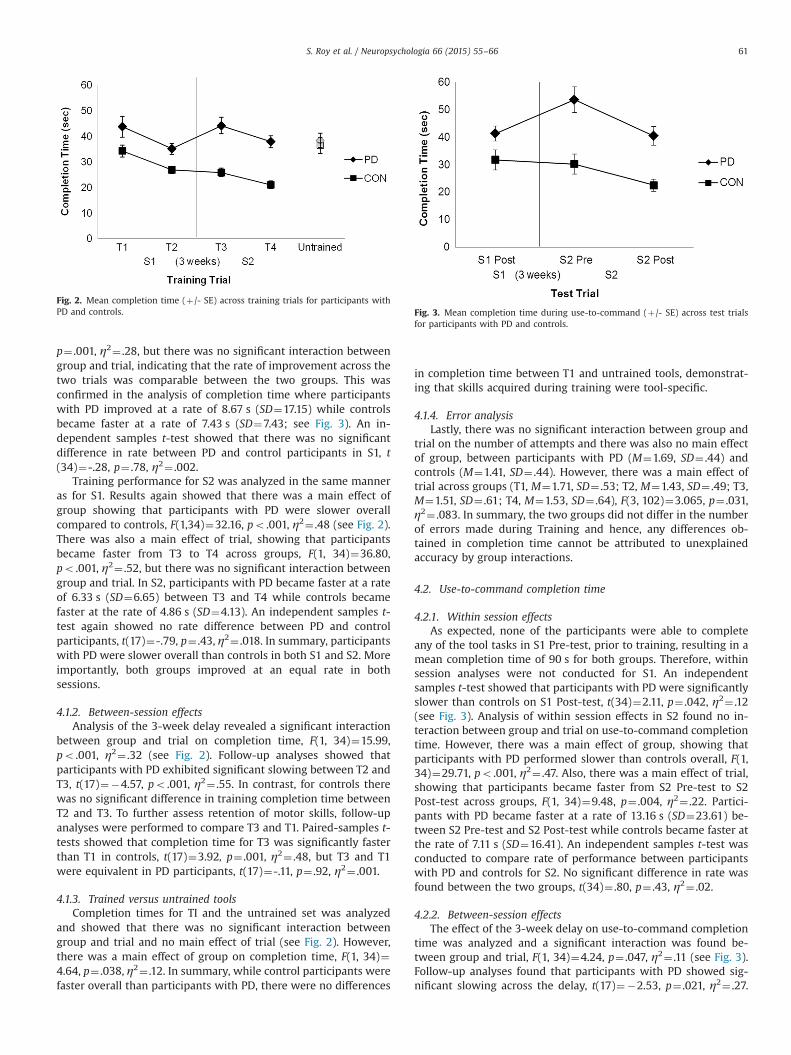
Fig. 2. Mean completion time (þ/- SE) across training trials for participants withPD and controls. Fig. 3. Mean completion time during use-to-command (þ/- SE) across test trials
for participants with PD and controls.
S. Roy et al. / Neuropsychologia 66 (2015) 55–66 61
p¼ .001, η2¼ .28, but there was no significant interaction betweengroup and trial, indicating that the rate of improvement across thetwo trials was comparable between the two groups. This wasconfirmed in the analysis of completion time where participantswith PD improved at a rate of 8.67 s (SD¼17.15) while controlsbecame faster at a rate of 7.43 s (SD¼7.43; see Fig. 3). An in-dependent samples t-test showed that there was no significantdifference in rate between PD and control participants in S1, t(34)¼-.28, p¼ .78, η2¼ .002.
Training performance for S2 was analyzed in the same manneras for S1. Results again showed that there was a main effect ofgroup showing that participants with PD were slower overallcompared to controls, F(1,34)¼32.16, po .001, η2¼ .48 (see Fig. 2).There was also a main effect of trial, showing that participantsbecame faster from T3 to T4 across groups, F(1, 34)¼36.80,po .001, η2¼ .52, but there was no significant interaction betweengroup and trial. In S2, participants with PD became faster at a rateof 6.33 s (SD¼6.65) between T3 and T4 while controls becamefaster at the rate of 4.86 s (SD¼4.13). An independent samples t-test again showed no rate difference between PD and controlparticipants, t(17)¼-.79, p¼ .43, η2¼ .018. In summary, participantswith PD were slower overall than controls in both S1 and S2. Moreimportantly, both groups improved at an equal rate in bothsessions.
4.1.2. Between-session effectsAnalysis of the 3-week delay revealed a significant interaction
between group and trial on completion time, F(1, 34)¼15.99,po .001, η2¼ .32 (see Fig. 2). Follow-up analyses showed thatparticipants with PD exhibited significant slowing between T2 andT3, t(17)¼�4.57, po .001, η2¼ .55. In contrast, for controls therewas no significant difference in training completion time betweenT2 and T3. To further assess retention of motor skills, follow-upanalyses were performed to compare T3 and T1. Paired-samples t-tests showed that completion time for T3 was significantly fasterthan T1 in controls, t(17)¼3.92, p¼ .001, η2¼ .48, but T3 and T1were equivalent in PD participants, t(17)¼-.11, p¼ .92, η2¼ .001.
4.1.3. Trained versus untrained toolsCompletion times for TI and the untrained set was analyzed
and showed that there was no significant interaction betweengroup and trial and no main effect of trial (see Fig. 2). However,there was a main effect of group on completion time, F(1, 34)¼4.64, p¼ .038, η2¼ .12. In summary, while control participants werefaster overall than participants with PD, there were no differences
in completion time between T1 and untrained tools, demonstrat-ing that skills acquired during training were tool-specific.
4.1.4. Error analysisLastly, there was no significant interaction between group and
trial on the number of attempts and there was also no main effectof group, between participants with PD (M¼1.69, SD¼ .44) andcontrols (M¼1.41, SD¼ .44). However, there was a main effect oftrial across groups (T1, M¼1.71, SD¼ .53; T2, M¼1.43, SD¼ .49; T3,M¼1.51, SD¼ .61; T4, M¼1.53, SD¼ .64), F(3, 102)¼3.065, p¼ .031,η2¼ .083. In summary, the two groups did not differ in the numberof errors made during Training and hence, any differences ob-tained in completion time cannot be attributed to unexplainedaccuracy by group interactions.
4.2. Use-to-command completion time
4.2.1. Within session effectsAs expected, none of the participants were able to complete
any of the tool tasks in S1 Pre-test, prior to training, resulting in amean completion time of 90 s for both groups. Therefore, withinsession analyses were not conducted for S1. An independentsamples t-test showed that participants with PD were significantlyslower than controls on S1 Post-test, t(34)¼2.11, p¼ .042, η2¼ .12(see Fig. 3). Analysis of within session effects in S2 found no in-teraction between group and trial on use-to-command completiontime. However, there was a main effect of group, showing thatparticipants with PD performed slower than controls overall, F(1,34)¼29.71, po .001, η2¼ .47. Also, there was a main effect of trial,showing that participants became faster from S2 Pre-test to S2Post-test across groups, F(1, 34)¼9.48, p¼ .004, η2¼ .22. Partici-pants with PD became faster at a rate of 13.16 s (SD¼23.61) be-tween S2 Pre-test and S2 Post-test while controls became faster atthe rate of 7.11 s (SD¼16.41). An independent samples t-test wasconducted to compare rate of performance between participantswith PD and controls for S2. No significant difference in rate wasfound between the two groups, t(34)¼ .80, p¼ .43, η2¼ .02.
4.2.2. Between-session effectsThe effect of the 3-week delay on use-to-command completion
time was analyzed and a significant interaction was found be-tween group and trial, F(1, 34)¼4.24, p¼ .047, η2¼ .11 (see Fig. 3).Follow-up analyses found that participants with PD showed sig-nificant slowing across the delay, t(17)¼�2.53, p¼ .021, η2¼ .27.
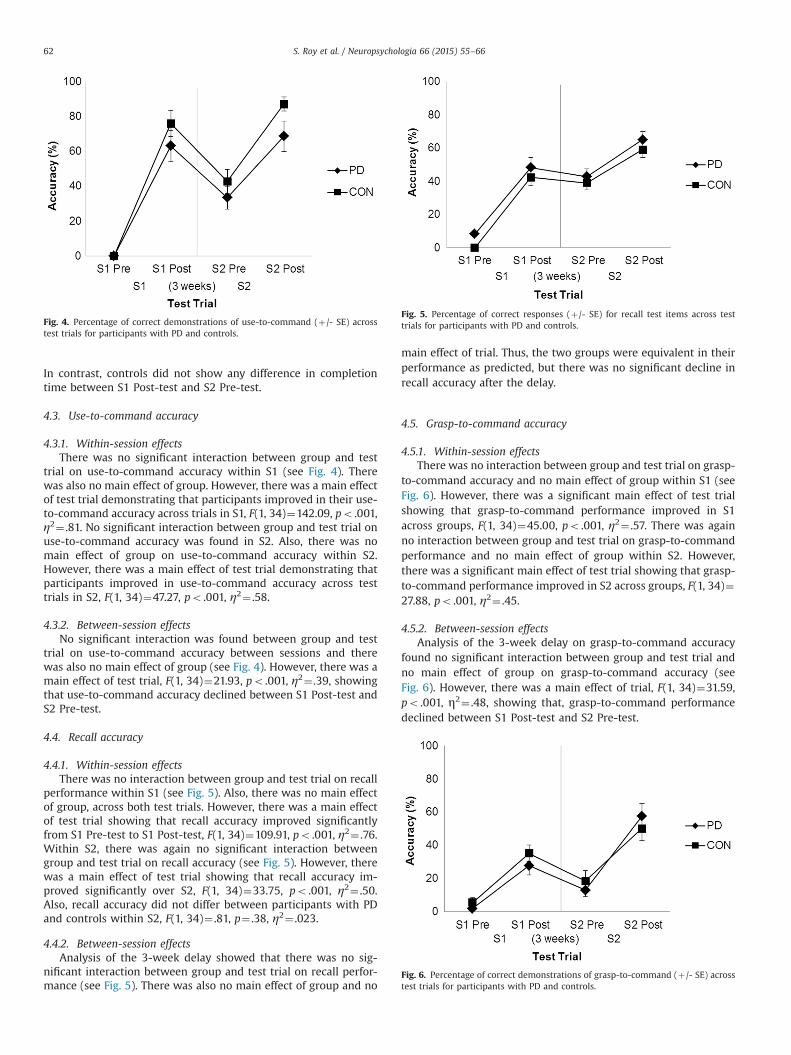
Fig. 4. Percentage of correct demonstrations of use-to-command (þ/- SE) acrosstest trials for participants with PD and controls.
Fig. 5. Percentage of correct responses (þ/- SE) for recall test items across testtrials for participants with PD and controls.
Fig. 6. Percentage of correct demonstrations of grasp-to-command (þ/- SE) acrosstest trials for participants with PD and controls.
S. Roy et al. / Neuropsychologia 66 (2015) 55–6662
In contrast, controls did not show any difference in completiontime between S1 Post-test and S2 Pre-test.
4.3. Use-to-command accuracy
4.3.1. Within-session effectsThere was no significant interaction between group and test
trial on use-to-command accuracy within S1 (see Fig. 4). Therewas also no main effect of group. However, there was a main effectof test trial demonstrating that participants improved in their use-to-command accuracy across trials in S1, F(1, 34)¼142.09, po .001,η2¼ .81. No significant interaction between group and test trial onuse-to-command accuracy was found in S2. Also, there was nomain effect of group on use-to-command accuracy within S2.However, there was a main effect of test trial demonstrating thatparticipants improved in use-to-command accuracy across testtrials in S2, F(1, 34)¼47.27, po .001, η2¼ .58.
4.3.2. Between-session effectsNo significant interaction was found between group and test
trial on use-to-command accuracy between sessions and therewas also no main effect of group (see Fig. 4). However, there was amain effect of test trial, F(1, 34)¼21.93, po .001, η2¼ .39, showingthat use-to-command accuracy declined between S1 Post-test andS2 Pre-test.
4.4. Recall accuracy
4.4.1. Within-session effectsThere was no interaction between group and test trial on recall
performance within S1 (see Fig. 5). Also, there was no main effectof group, across both test trials. However, there was a main effectof test trial showing that recall accuracy improved significantlyfrom S1 Pre-test to S1 Post-test, F(1, 34)¼109.91, po .001, η2¼ .76.Within S2, there was again no significant interaction betweengroup and test trial on recall accuracy (see Fig. 5). However, therewas a main effect of test trial showing that recall accuracy im-proved significantly over S2, F(1, 34)¼33.75, po .001, η2¼ .50.Also, recall accuracy did not differ between participants with PDand controls within S2, F(1, 34)¼ .81, p¼ .38, η2¼ .023.
4.4.2. Between-session effectsAnalysis of the 3-week delay showed that there was no sig-
nificant interaction between group and test trial on recall perfor-mance (see Fig. 5). There was also no main effect of group and no
main effect of trial. Thus, the two groups were equivalent in theirperformance as predicted, but there was no significant decline inrecall accuracy after the delay.
4.5. Grasp-to-command accuracy
4.5.1. Within-session effectsThere was no interaction between group and test trial on grasp-
to-command accuracy and no main effect of group within S1 (seeFig. 6). However, there was a significant main effect of test trialshowing that grasp-to-command performance improved in S1across groups, F(1, 34)¼45.00, po .001, η2¼ .57. There was againno interaction between group and test trial on grasp-to-commandperformance and no main effect of group within S2. However,there was a significant main effect of test trial showing that grasp-to-command performance improved in S2 across groups, F(1, 34)¼27.88, po .001, η2¼ .45.
4.5.2. Between-session effectsAnalysis of the 3-week delay on grasp-to-command accuracy
found no significant interaction between group and test trial andno main effect of group on grasp-to-command accuracy (seeFig. 6). However, there was a main effect of trial, F(1, 34)¼31.59,po .001, η2¼ .48, showing that, grasp-to-command performancedeclined between S1 Post-test and S2 Pre-test.

S. Roy et al. / Neuropsychologia 66 (2015) 55–66 63
5. Discussion
Participants with PD and healthy age-matched controls weretrained to use a set of novel complex tools over two sessions andwere tested on their memory for various aspects of each tool's useand its features. Previous research has shown that both declarativeand procedural memory systems contribute to tool use (Roy andPark, 2010). Previous research has also presented evidence ofcompetitive, compensatory, as well as cooperative interactionbetween the declarative and procedural memory systems; how-ever, these different forms of interaction have not yet been in-vestigated in the domain of tool use. Thus, the aim of the currentstudy was to directly investigate the role of procedural memory,and the nature of interaction between declarative and proceduralmemory, in mediating tool-related knowledge and skills in PDcompared to a healthy control group.
5.1. Training
It was predicted that motor skill acquisition associated withnovel complex tools was striatally mediated and that participantswith PD would therefore show impairment in learning of motorskills relative to controls. Within-session analysis suggested thatalthough participants with PD were slower overall than controls,their performance improved at the same rate. However, between-session analysis showed slowing over the 3-week delay in parti-cipants with PD. In addition, comparison of the first trial from eachsession (i.e., T1 and T3) demonstrated that participants with PDfailed to retain gains from Session 1 over the delay. In contrast,control participants did not show slowing after a 3-week delay andtheir Trial 3 completion time was also significantly faster than Trial1 completion time. This suggests that controls, but not participantswith PD, retained motor skills over the 3-week delay. As previousresearch has shown, procedural skills are generally resistant tointerference and decay (Matsuzaka et al., 2006; Penhune andDoyon, 2002). Therefore, the current pattern of performance de-monstrates that the striatal regions are not required for initial skilllearning associated with use of complex tools, but appear to play acritical role in the retention of these skills.
With regards to the pattern of within and between sessionperformance, it appears that different processes may be under-lying these different stages of motor skill learning. A similar pat-tern of intact learning within sessions, but impaired retentionbetween-sessions, has been reported previously in individualswith PD (Bédard and Sanes, 2011; Leow et al., 2012; Marinelli et al.,2009; Mochizuki-Kawai et al., 2004). In terms of processes, it hasbeen argued that the cortico-cerebellar circuit along with thehippocampus and frontal regions are primarily involved in earlystages of learning and therefore, may support initial skill learning,but that the striatal system is particularly critical for long-termretention of motor skills after initial training (Albouy et al., 2013;Doyon et al., 2009; Mochizuki-Kawai et al., 2004). As noted earlier,between-session slowing over a three week delay in PD partici-pant performance supports the idea that striatal dysfunction isassociated with impaired retention of motor skills.
Although the above interpretation of training results is plau-sible, it is worth noting that the pattern of intact learning withinsession and a decline in performance after a delay is also char-acteristic of a declarative pattern of learning. Thus, another inter-pretation of training results is that in participants with PD, de-clarative memory compensated for an inefficient procedural sys-tem. This form of declarative compensation in participants with PDhas been shown previously in studies using other striatallymediated tasks including probabilistic classification learning andmotor sequence learning (Gobel et al., 2013; Moody et al., 2004). Ithas also been previously argued that the declarative and
procedural memory systems share a competitive interaction dur-ing motor skill learning in healthy individuals (Albouy et al., 2013).Therefore, it is possible that the lack of an efficient proceduralsystem, which would typically override the declarative system, ledto overuse of the declarative system as means of compensation.However, the extent to which the declarative system can effec-tively compensate for a dysfunctional procedural system duringmotor skill learning requires further investigation. Current find-ings would suggest that while declarative memory may be able tosupport initial skill learning, some aspect of performance wouldremain unfulfilled due to vulnerability of the declarative system toboth decay and interference. In summary, training performance ofparticipants with PD demonstrates impaired functioning of theprocedural memory system, but the possibility declarative com-pensation cannot be ruled out.
Given that individuals with PD typically show generalizedslowing, it is important to address the possibility of slowed re-trieval processes affecting performance. As noted, participantswith PD were slower overall relative to controls, but rate oflearning was equivalent to controls within sessions. Thus, gen-eralized motor slowing did not affect rate of learning. After thedelay, participants with PD demonstrated slower completion timerelative to controls, but were also slower than their own perfor-mance in Session 1. In other words, slowing demonstrated afterthe 3-week delay was greater than what would have been ex-pected simply from generalized slowing. Furthermore, resultsshowed that participants with PD did not show any savings incompletion time from Session 1. This pattern of results suggeststhat slower performance after the delay cannot be explained byslowed retrieval processes alone, but rather that slowing was re-lated to some disruption associated with the retention processover the delay. At this point, the cognitive and neural processesgiving rise to this impaired training performance after the delay inparticipants with PD are not entirely clear. As previously discussed,one explanation may be impaired skill retention due to striataldysfunction. Another possible explanation that has been offered isdeclarative compensation. If there is an overreliance on declarativememory in participants with PD during skill learning, it is possiblethat slowed retrieval of declarative task knowledge may have ledto slower task completion after the delay.
5.2. Use-to-command
The use-to-command accuracy measure indicates whether ornot a task was correctly performed, regardless of how quickly itwas performed. Use-to-command accuracy of participants with PDwas equivalent to that of controls. Both groups showed improvedaccuracy over test trials. Both groups also showed a significantdecline in use-to-command accuracy after the 3-week delay. Thispattern of performance is consistent with findings from Roy andPark (2010) and demonstrates that the use-to-command accuracymeasure is strongly declarative.
As described, the use-to-command accuracy measure indicateswhether or not a task is performed correctly, regardless of speed.In contrast, use-to-command completion time measures howquickly correctly performed tasks were completed. Results showedthat within session, participants with PD were slower than con-trols; however, they improved at the same rate as controls. Therewas also an effect of the 3-week delay for participants with PD, butnot for controls. Participants with PD were significantly slowerafter the delay while controls retained their speed. Thus, thepattern of use-to-command completion time within session isvery similar to that of training performance. For both measures,performance reflects intact learning within sessions, but impairedretention between sessions. It should also be noted that onlycorrect trials were included in analysis of completion time;

S. Roy et al. / Neuropsychologia 66 (2015) 55–6664
therefore, slower completion time cannot be attributed to loweraccuracy.
Based on the distinct patterns of performance, it appears thatuse-to-command accuracy and completion time may measuredistinct types of memory required for skilled tool use. That is, tooluse accuracy assesses whether declarative memory related to thetool task including critical contextual information (e.g., positioningof recipient) was retained whereas speed is a reflection of proce-dural learning. In the current study, participants with PD wereunimpaired on the declarative component of skilled tool use (i.e.,accuracy), but were impaired on the procedural component (i.e.,completion time). More specifically, participants with PD couldrecall contextual information about the task equally well as heal-thy controls; however, they lacked motor expertise associated withusing the tools. As with training results, it is possible that in ad-dition to learning contextual details with declarative memory,participants with PD also used a declarative strategy to performthe tool tasks. This would be indicative of a compensatory inter-action between declarative and procedural memory in the contextof skilled tool use. As with Training, it is possible that skilled tooluse performance in participants with PD reflects a greater relianceon declarative memory than procedural memory as a compensa-tory mechanism.
Overall, use-to-command results are consistent with the hy-pothesis that skilled tool use relies on a cooperative interaction ofboth declarative and procedural memory systems in healthy in-dividuals. It could be argued that declarative memory providestask-related knowledge (e.g., positioning of recipient, sequence ofsteps) and procedural memory represents the learned motor skillsassociated with complex tools. The current findings, taken to-gether with Roy and Park (2010) suggest that both systems arenecessary for proficient and accurate tool use. While other studieshave proposed that both memory systems are involved in skilledtool use, to our knowledge, this is the first study to provide directevidence of this interaction and speculate on the differential rolesof each system.
5.3. Recall
It was predicted that participants with PD would be unim-paired in their recall of tool attributes relative to controls, and thatboth PD and control participants would show a decline in recallaccuracy after a 3-week delay. As predicted, PD and control par-ticipants showed equivalent recall accuracy for tool attributes.Both groups showed evidence of learning various tool features(e.g., tool function, colors) across tests trials. Although a decline inrecall accuracy was predicted after the 3-week delay for bothgroups, this hypothesis was not supported by the data. Neithergroup showed evidence of forgetting tool features after the delay.This result is inconsistent with the findings from Roy and Park(2010) in which control participants had significantly worse recallof tool attributes after a 3-week delay, using the same tools.However, there are some methodological differences that mayexplain the lack of decline in recall accuracy in the current study.In Roy and Park (2010), participants were trained and tested (i.e.,Pre-test, and Post-test) on a set of ten tools. In the current study,only six tools were trained and three of these six tools were tested.Thus, it is possible that having a small tool set size meant thatparticipants had less information to learn about the tools andhence, less information to forget over the delay. Although no effectof delay was found for either group, participants with PD stillperformed as well as controls in their recall accuracy. Unimpairedrecall performance in the participants with PD is consistent withthe hypothesis that knowledge of tool attributes is primarilymediated by declarative memory and neuropsychological test re-sults showing that participants with PD were unimpaired on tests
of declarative memory. These findings are also consistent withprevious research showing that tool properties are declarative andthat declarative memory is relatively unimpaired in PD (War-rington and Shallice, 1984; Hay et al., 2002).
5.4. Grasp-to-command
It was predicted that if tool grasping to command was depen-dent on both declarative and procedural memory systems that itwould be impaired in participants with PD, due to their proceduralmemory impairment. However, results showed that grasp-to-command performance of participants with PD was equivalent tothat of controls. Both groups showed improvement over trials. Inaddition, both groups showed a significant decline in their grasp-to-command performance after the 3-week delay. Taken together,these results suggest that grasping a tool for use is strongly de-clarative in nature. These findings are also consistent with pre-vious research showing that tool grasping for use relies on thedeclarative memory system (Creem and Proffit, 2001; Roy andPark, 2010). Although participants with PD were not impaired, aprocedural component cannot be ruled out based on currentfindings. It is possible that the explicit manner of testing for toolgrasping (i.e., to command) may have biased participants to use amore declarative strategy. It is also possible that precise methodsof assessing grasp involving kinematic measures may reveal con-tributions of procedural memory in tool grasping.
5.5. Future directions
It was proposed that the declarative memory system was morestrongly activated in participants with PD compared to controls tocompensate for their impaired procedural system during trainingand possibly use-to-command as well. The possibility of someform of compensation holds important implications for re-habilitation purposes. For instance, it may be worth exploring ef-fects of inhibiting or limiting declarative involvement during skilllearning to test the limits of this compensatory mechanism. Futureresearch in this area would also benefit from more studies usingtools and other physical objects as stimuli. The majority of existingstudies investigating motor skill learning have used some form ofcomputer-based testing. These types of tests are highly valuedbecause of their standardization, ease of administration, and theirestablished neural correlates. However, the use of physical toolswould help to increase ecological validity and generalizability toeveryday activities.
6. Conclusion
The current study demonstrates that declarative and proce-dural memory systems are both involved in learning many aspectsof tool-related knowledge and skills. While memory for tool fea-tures and tool grasping appears to be predominantly declarative,findings suggest that motor skill acquisition and skilled tool userequire an interaction of both declarative and procedural memorysystems. In the case of tool use, findings demonstrate a co-operative interaction where the declarative system appears to beessential for encoding task-specific details while the striatal-basedprocedural system is critical for the acquisition and retention ofmotor skills. Findings also suggest that motor skill acquisition mayinvolve an interaction of both systems. However, the precise nat-ure of this interaction is less clear and may depend on variousfactors (e.g., nature of the task, measurement of performance; seePackard and Goodman, 2013). In general, the current findingssuggest that striatal-based procedural memory is not required forinitial stages of motor skill learning, and that this initial learning

S. Roy et al. / Neuropsychologia 66 (2015) 55–66 65
may be, at least partly, supported by the declarative system.However, declarative memory does not appear to be sufficient tomediate long-term retention of motor skills, which appears torequire striatal-based procedural memory. Current findings alsoraise the possibility that a declarative approach to skill learning,while not effective for all stages of learning, may be adopted byindividuals with striatal damage (e.g., individuals with PD) as ameans of compensation. From a clinical perspective, this com-pensatory tendency may have important implications for the de-velopment and modification of interventions that could improverehabilitation programs for participants with PD.
Acknowledgments
We would like to extend our sincerest gratitude to all in-dividuals who participated in this experiment. In particular, wethank the individuals with PD and their family members for par-ticipating in the study. We would also like to thank all studentsand research assistants at the Sun Life Financial Movement Dis-orders Research Centre for their help with participant recruitment.We would like to acknowledge Naveen Gnanabakthan for assis-tance with initial development of novel tool tasks and inter-raterscoring. In addition, we thank the reviewers of this manuscript fortheir helpful comments. This project was funded by an internalgrant awarded to Dr. Norman Park. It was also supported in part bySummer Student Fellowship No. PDF-SFW-1334, from the Parkin-son's Disease Foundation, awarded to Holly Fernandes who as-sisted with pilot testing and analyses.
Appendix A
see Table A1
Table A1Illustration of experiment design showing counterbalance oracross experimental phases.
Session 1
Participant Pre-test Training Post-test
1 A B A B
2 B A B A
3 B C B C
4 C B C B
5 C A C A
6 A C A C
3-week
References
Albouy, G., King, B.R., Maquet, P., Doyon, J., 2013. Hippocampus and striatum: dy-namics and interaction during acquisition and sleep-related motor sequencememory consolidation. Hippocampus 23, 985–1004.
Bédard, P., Sanes, J.N., 2011. Basal ganglia-dependent processes in recalling learnedvisual-motor adaptations. Exp. Brain Res. 209, 1–9.
Benedict, R.H.B., 1997. Brief Visuospatial Memory Test—Revised. ProfessionalManual. Fla: Psychological Assessment Resources., Odessa.
Benedict, R.H.B., Schretlen, D., Groninger, L., Brandt, J., 1998. The Hopkins VerbalLearning Test—revised: normative data and analysis of interform and test–retest reliability. Clin. Neuropsychol. 12, 3–5.
Brashers-Krug, T., Shadmehr, R., Bizzi, E., 1996. Consolidation in human motormemory. Nature 382, 252–255.
Buxbaum, L.J., Kyle, K.M., Tang, K., Detre, J.M., 2006. Neural substrates of knowledgeon hand postures for object grasping and functional object use: evidence fromfMRI. Brain Res. 1117, 175–185.
Buxbaum, L.J., Schwartz, M.F., Carew, T.G., 1997. The role of semantic memory inobjectuse. Cognit. Neuropsychol. 14, 219–254.
Chao, L.L., Haxby, J.V., Martin, A., 1999. Attribute-based neural substrates in tem-poral cortex for perceiving and knowing about objects. Nat. Neurosci., 2,913–919, 913–919.
Cohen, N.J., Squire, L.R., 1980. Preserved learning and retention of pattern-analyzingskill in amnesia: dissociation of knowing how and knowing that. Science 210,207–210.
Creem-Regehr, S.H., Lee, J.N., 2005. Neural representations of graspable objects: aretools special? Cognit. Brain Res. 22, 457–469.
Creem, S.H., Proffit, D.R., 2001. Grasping objects by their handles: a necessary in-teraction between cognition and action. J. Exp. Psychol.: Hum. Percept. Perform.27, 218–228.
Daprati, E., Sirigu, A., 2006. How we interact with objects: learning from brain le-sions. Trends Cognit. Sci. 10, 265–270.
Doyon, J., Bellec, P., Amsel, R., Penhune, V., Monchi, O., Carrier, J., et al., 2009.Contributions of the basal ganglia and functionally related brain structures tomotor learning. Behav. Brain Res. 199, 61–75.
Dubois, B., Burn, D., Goetz, C., Aarsland, D., Brown, R.G., Broe, G.A., et al., 2007.Diagnostic procedures for Parkinson's disease dementia: recommendationsfrom the Movement Disorder Society Task Force. Mov. Disord. 22, 2314–2324.
Fahn, S., Elton, R.L., 1987. Members of the UPDRS Development Committee. UnifiedParkinson's Disease Rating Scale. In: Fahn, S., Marsden, C.D., Goldstein, M.,Calne, D.B. (Eds.), Recent Developments in Parkinson's disease, vol. 2. Macmi-lian Healthcare Information, Florham Park, NJ, pp. 153–163.
Foerde, K., Shohamy, D., 2011. The role of the basal ganglia in learning and memory:insight from Parkinson’s disease. Neurobiol. Learn. Mem. 96, 624–636.
Folstein, M., Folstein, S., Folstein, J., 2010. The Mini-Mental State Examination: abrief cognitive assessment. Princ. Pract. Geriatr. Psychiatry, 145–146.
der of the three tool sets used in the study (A, B, and C)
Session 2
Pre-test Training Post-test Untrained
B A B A C
A B A B C
C B C B A
B C B C A
A C A C B
C A C A B
delay

S. Roy et al. / Neuropsychologia 66 (2015) 55–6666
Foundas, A.L., Macauley, B.L., Raymer, A.M., Maher, L.M., 1995. Ecological implica-tions of limb apraxia: Evidence from mealtime behavior. J. Int. Neuropsychol.Soc. 1, 62–66.
Frey, S.H., 2007. What puts the how in where? Tool use and the divided visualstreams hypothesis. Cortex 43, 368–375.
Gabrieli, J.D., Corkin, S., Mickel, S.F., Growdon, J.H., 1993. Intact acquisition andlong-term retention of mirror-tracing skill in Alzheimer's disease and in globalamnesia. Behav. Neurosci. 107, 899–910.
Gibson, J.J., 1977. The theory of affordances. In: Shaw, R., Bransford, J. (Eds.), Per-ceiving, Acting, and Knowing: Toward an Ecological Psychology. LawrenceErlbaum Associates Inc, Hillsdale, NJ.
Gobel, E.W., Blomeke, K., Zadikoff, C., Simuni, T., Weintraub, S., Reber, P.J., 2013.Implicit perceptual-motor skill learning in mild cognitive impairment andParkinson's disease. Neuropsychology 27, 314–321.
Goldenberg, G., Spatt, J., 2009. The neural basis of tool use. Brain 132, 1645–1655.Hartmann, K., Goldenberg, G., Daumüller, M., Hermsdörfer, J., 2005. It takes the
whole brain to make a cup of coffee: the neuropsychology of naturalistic ac-tions involving technical devices. Neuropsychologia 43, 625–637.
Hay, J.F., Moscovitch, M., Levine, B., 2002. Dissociating habit and recollection: evi-dence from Parkinson's disease, amnesia and focal lesion patients. Neu-ropsychologia 40, 1324–1334.
Heilman, K.L., 2002. Matter of mind. Oxford University Press, New York.Hodges, J.R., Bozeat, S., Lambon Ralph, M.A., Patterson, K., Spatt, J., 2000. The role of
conceptual knowledge in object use. Evidence from semantic dementia. Brain123, 1913–1925.
Kaplan, E., Goodglass, H., Weintraub, S., 1983. Boston Naming Test. Lea and Febiger,Philadelphia.
Knowlton, B.J., Mangels, J.A., Squire, L.R., 1996. A neostriatal habit learning systemin humans. Science 273, 1399–1402.
Leow, L., Loftus, A.M., Hammond, G.R., 2012. Impaired savings despite intact initiallearning of motor adaptation in Parkinson's disease. Exp. Brain Res. 218,295–304.
Marinelli, L., Crupi, D., Di Rocco, A., Bove, M., Eidelberg, D., Abbruzzese, G., Ghilardi,M.F., 2009. Learning and consolidation of visuo-motor adaptation in Parkin-son's disease. Parkinsonism Relat. Disord. 15, 6–11.
Martin, A., Chao, L.L., 2001. Semantic memory and the brain: structure and pro-cesses. Curr. Opin. Neurobiol. 11, 194–201.
Matsuzaka, Y., Picard, N., Strick, P.L., 2006. Skill representation in the primary motorcortex after long-term practice. J. Neurophysiol. 97, 1819–1832.
Matthews, C.G., Kløve, H., 1964. Instruction Manual for the Adult NeuropsychologyTest Battery. University of Wisconsin Medical School, Madison.
Mochizuki-Kawai, H., Kawamura, M., Hasegawa, Y., Mochizuki, S., Oeda, R., Yama-naka, K., et al., 2004. Deficits in long-term retention of learned motor skills inpatients with cortical or subcortical degeneration. Neuropsychologia 42,1858–1863.
Moody, T.D., Bookheimer, S.Y., Vanek, Z., Knowlton, B.J., 2004. An implicit learningtask activates medial temporal lobe in patients with Parkinson's disea. Behav.Neurosci. 118, 438–442.
Negri, G.A., Lunardelli, A., Gigli, G.L., Rumiati, R.I., 2007. Degraded se-manticknowledge and accurate object use. Cortex 43, 376–388.
Nissen, M.J., Bullemer, P., 1987. Attentional requirements of learning: evidence fromperformance measures. Cognit. Psychol. 19, 1–32.
Osterrieth, P.A., 1944. “Filetest de copie d'une figure complex: contribution a l'etudede la perception et de la memoire [The test of copying a complex figure: a
contribution to the study of perception and memory]. Arch. Psychol. 30,286–356.
Packard, M.G., Goodman, J., 2013. Factors that influence the relative use of multiplememory systems. Hippocampus 23, 1044–1052.
Packard, M.G., Knowlton, B.J., 2002. Learning and memory functions of the basalganglia. Ann. Rev. Neurosci. 25, 563–593.
Penhune, V.B., Doyon, J., 2002. Dynamic cortical and subcortical networks inlearning and delayed recall of timed motor sequences. J. Neurosci. 22,1397–1406.
Penhune, V.B., Steele, C.J., 2012. Parallel contributions of cerebellar, striatal and M1mechanisms to motor sequence learning. Behav. Brain Res. 226, 579–591.
Poldrack, R., Packard, M.G., 2003. Competition among multiple memory systems:converging evidence from animal and human brain studies. Neuropsychologia41, 245–251.
Poldrack, R.A., Clark, J., Pare-Blagoev, J., Shohamy, D., Creso Moyano, J., Myers, C.,et al., 2001. Interactive memory systems in the human brain. Nature 414,546–550.
Reitan, R.M., Wolfson, D., 1985. The Halstead-Reitan Neuropsychological Test Bat-tery: Theory and Clinical Interpretation. Neuropsychology Press, Tucson, AZ.
Roy, S., Park, N.W., 2010. Dissociating the memory systems mediating complex toolknowledge and skills. Neuropsychologia 48, 3026–3036.
Schendan, H.E., Searl, M.M., Melrose, R.J., Stern, C.E., 2003. An fMRI Study of the roleof the medial temporal lobe in implicit and explicit sequence learning. Neuron37, 1013–1025.
Siegert, R.J., Taylor, K.D., Weatherall, M., Abernethy, D.A., 2006. Is implicit sequencelearning impaired in Parkinson's disease? A meta-analysis. Neuropsychology20, 490–495.
Silveri, M.C., Ciccarelli, N., 2009. Semantic memory in object use. Neuropsychologia47, 2634–2641.
Song, S., Howard, J.H., Howard, D.V., 2007. Implicit probabilistic sequence learningis independent of explicit awareness. Learn. Mem. 14, 167–176.
Spreen, O., Benton, A.L., 1977. Neurosensory Center Comprehensive Examinationfor Aphasia. Neuropsychology Laboratory, University of Victoria, Victoria, BC.
Squire, L.R., 2009. Memory and brain systems: 1969–2009. J. Neurosci. 29,12711–12716.
Tombaugh, T.N., Kozak, J., Rees, L., 1999. Normative data stratified by age andeducation For two measures of verbal fluency: FAS and animal naming. Arch.Clin. Neuropsychol. 14, 167–177.
Troyer, A.K., Leach, L., Strauss, E., 2006. Aging and response inhbition: normativedata for the Victoria Stroop Test. Aging, Neuropsychol. Cognit. 13, 20–35.
Warrington, E.K., 1975. The selective impairment of semantic memory. Q. J. Exp.Psychol. 27, 635–657.
Warrington, E.K., Shallice, T., 1984. Category specific semantic impairments. Brain107, 829–854.
Wechsler, D., 2009. Wechsler Memory Scale, fourth edition Pearson, San Antonio,TX.
Weisberg, J., van Turrennout, M., & Martin, A. (2007). A neural system for learningabout object function. Cereb. Cortex, 17, 513-521.
Zigmond, A.S., Snaith, R.P., 1983. The Hospital Anxiety and Depression Scale. ActaPsychiatr. Scand. 67, 361–370.
Top Related
Copyright © 2022 FDOKUMEN

