






Bahasa
Halaman
Hukum

International Journal of Public Health and Clinical Sciences e-ISSN : 2289-7577. Vol. 3:No. 5
September/October 2016
Arinah W. D. S., Faisal I., Muhamad Hanafiah Juni, Ismail, I., Mohamed, A. S 159
IJPHCS
Open Access: e-Journal
FACTORS ASSOCIATED WITH EMERGENCY
DEPARTMENT GREEN ZONE UTILIZATION IN HOSPITAL
Arinah W. D. S.1, Faisal I.
1, Muhamad Hanafiah Juni
1*,
Ismail, I.2, Mohamed, A. S.
3
1 Department of Community Health, Faculty of Medicine and Health Sciences, Universiti
Putra Malaysia. 2 Department of Medicine, Faculty of Medicine and Health Sciences, Universiti Putra
Malaysia. 3Department of Emergency, Serdang Hospital, Ministry of Health Malaysia.
*Corresponding author: AP Muhamad Hanafiah Juni, Department of Community Health,
Faculty of Medicine and Health Sciences, Universiti Putra Malaysia 40300 UPM Serdang,
Selangor Darul Ehsan, MALAYSIA; Email: [email protected]
ABSTRACT
Introduction: In hospital, emergency departments are highly utilized by patients.
Overcrowding, congestion and long waiting time were among the issues highlighted resulting
from it. In Selangor, there has been a steady increase in utilization of emergency department
of government hospitals over the past five (5) years. Utilization of green zone was the highest
in these hospitals. Being a department that provides a comprehensive emergency service and
provides easy access for the community, issues of appropriateness utilization arise. This study
aims to determine the level of appropriateness of green zone utilization by patients attending
Emergency Department in Serdang Hospital and factors influencing its utilization.
Methodology: A cross-sectional study was conducted in Emergency Department of Serdang
Hospital. Sample size of green zone adult patients were obtained by systematic random
sampling. Emergency Medicine and Trauma Services Policy Malaysia 2012 were used to
classify patients to appropriate and inappropriate utilization of green zone. Pre-tested self-
administered questionnaire were used to interview patients. Descriptive statistics, chi-square
test and logistic regression used to analyse the data collected. Data analysis conducted using
IBM SPSS Statistics version 22 and p value significant at <0.05.
Result: There were 793 (90.7%) patients in this study. It was found that level of
appropriateness utilization in green zone emergency department was 83.6% appropriate and
16.4% was inappropriate. Median age of patients were 29 years old (IQR ± 25th, 75th; 23,
40). Majority were Malays (74%). The results of chi-square test indicated that there were
significant association between marital status (p=0.032), patients attending emergency
department because treatment cost is cheap (p=0.025), emergency department operates 24
hours (p=0.045) and time of patient presentation to emergency department (p=0.001). From
the study, the multivariate results revealed that the odds of married patients (AOR=1.481,
95% CI: 1.008, 2.174) to utilize the emergency department were higher than not married
patients, the odds of patients utilize emergency department not because of the cheap treatment
(AOR=1.614, 95% CI: 1.073, 2.469) was almost two times more and lastly the odds of
International Journal of Public Health and Clinical Sciences e-ISSN : 2289-7577. Vol. 3:No. 5
September/October 2016
Arinah W. D. S., Faisal I., Muhamad Hanafiah Juni, Ismail, I., Mohamed, A. S 160
IJPHCS
Open Access: e-Journal
utilization after office hours were two times more than during office hours (AOR=2.117, 95%
CI: 1.388, 3.227).
Conclusion: The study revealed majority of patients utilized green zone appropriately.
Married patient, patient attend emergency department not because treatment cost is cheap and
patient attending after office hour were significantly associated with appropriateness
utilization of emergency department. Further study needed to determine the cause and effect
relationship.
Keywords: Emergency department, utilization, appropriateness, green zone.
1.0 Introduction
Emergency medicine and trauma services provide resuscitation and stabilization, diagnosis
and management of life-threatening conditions, early definitive care management and patient
disposition in emergency department. The scope of services and quality of care have
continued to grow along with the advancement of technology. It is one of the most important
ambulatory care in hospital as it is the gatekeeper of all illnesses.
In order to provide total quality management, triage service was established (Emergency
Medicine and Trauma Services Policy Malaysia, 2012). In Malaysia, government hospitals
must provide pre-hospital services and hospital-based services for the community. This
includes triage service (Emergency Medicine and Trauma Services Policy Malaysia, 2012).
The triage service counter shall be the first point of contact for all patients accessing the
Emergency and Trauma Department care. Patients are triage into red zone, yellow zone and
green zone according to priority of treatment. Red zone also known as critical zone, yellow
zone as semi-critical zone and green zone as non-critical zone.
Over the past five years there have been a steady upward trend in the total emergency
department of government hospitals utilization in Selangor State (Ministry of Health
Malaysia, 2010 – 2013). Out of the total emergency department utilization in Selangor State,
utilization of the green zone was the highest which constituted of 843,366 patients (77.2%) in
2013 (Ministry of Health Malaysia, 2013). In Serdang Hospital, the utilization of green zone
in the emergency department showed an average of 70 – 75% of the total utilization of
emergency department over the past 5 years (Ministry of Health Malaysia, 2016).
High emergency department utilization is a worrying fact and could explain the current
condition in emergency department such as overcrowding (Cunningham, 2011), longer patient
waiting time (Erenler et al, 2015) and reduced quality of care (Moskop, 2010). There have
been several studies in the literature reporting regarding appropriateness utilization of
emergency department all over the world. Unfortunately, it has not been given great attention
by the researchers in Malaysia and this motivated the present study. This study aimed to
determine the appropriateness utilization of green zone among adult patients attending
Emergency Department in Serdang Hospital and factors influencing the utilization.
International Journal of Public Health and Clinical Sciences e-ISSN : 2289-7577. Vol. 3:No. 5
September/October 2016
Arinah W. D. S., Faisal I., Muhamad Hanafiah Juni, Ismail, I., Mohamed, A. S 161
IJPHCS
Open Access: e-Journal
2.0 Methodology
2.1. Study design and patients
This was a cross-sectional study carried out among green zone adult patients in Emergency
Department of Serdang Hospital. The inclusion criteria were Malaysian, all patients registered
as green zone patients and adult patients (age 18 – 60). The exclusion criteria were foreigners
and patients refused to participate.
2.2. Green Zone
In Serdang Hospital, the Emergency Medicine and Trauma Services (EMTS) Policy Malaysia
2012 [MOH/P/PAK/228.12(BP)] was adopted into more specific guidelines in green zone.
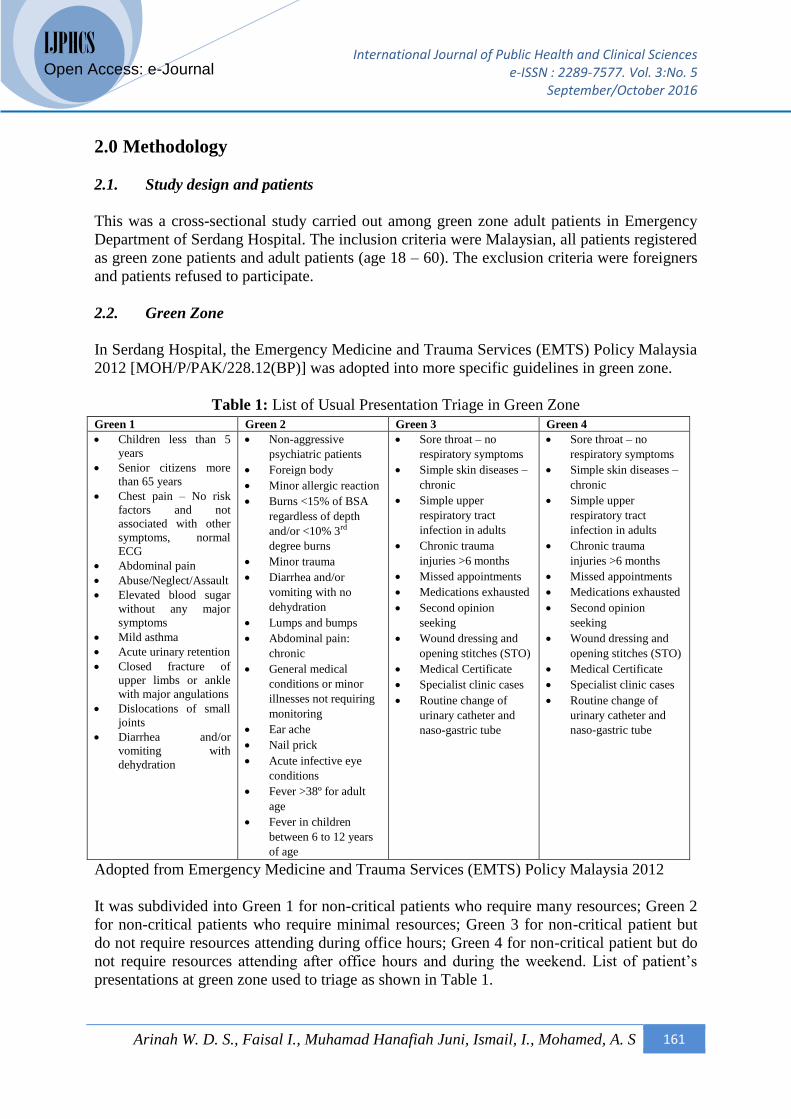
Table 1: List of Usual Presentation Triage in Green Zone
Green 1 Green 2 Green 3 Green 4
Children less than 5
years
Senior citizens more
than 65 years
Chest pain – No risk
factors and not
associated with other
symptoms, normal
ECG
Abdominal pain
Abuse/Neglect/Assault
Elevated blood sugar
without any major
symptoms
Mild asthma
Acute urinary retention
Closed fracture of
upper limbs or ankle
with major angulations
Dislocations of small
joints
Diarrhea and/or
vomiting with
dehydration
Non-aggressive
psychiatric patients
Foreign body
Minor allergic reaction
Burns <15% of BSA
regardless of depth
and/or <10% 3rd
degree burns
Minor trauma
Diarrhea and/or
vomiting with no
dehydration
Lumps and bumps
Abdominal pain:
chronic
General medical
conditions or minor
illnesses not requiring
monitoring
Ear ache
Nail prick
Acute infective eye
conditions
Fever >38º for adult
age
Fever in children
between 6 to 12 years
of age
Sore throat – no
respiratory symptoms
Simple skin diseases –
chronic
Simple upper
respiratory tract
infection in adults
Chronic trauma
injuries >6 months
Missed appointments
Medications exhausted
Second opinion
seeking
Wound dressing and
opening stitches (STO)
Medical Certificate
Specialist clinic cases
Routine change of
urinary catheter and
naso-gastric tube
Sore throat – no
respiratory symptoms
Simple skin diseases –
chronic
Simple upper
respiratory tract
infection in adults
Chronic trauma
injuries >6 months
Missed appointments
Medications exhausted
Second opinion
seeking
Wound dressing and
opening stitches (STO)
Medical Certificate
Specialist clinic cases
Routine change of
urinary catheter and
naso-gastric tube
Adopted from Emergency Medicine and Trauma Services (EMTS) Policy Malaysia 2012
It was subdivided into Green 1 for non-critical patients who require many resources; Green 2
for non-critical patients who require minimal resources; Green 3 for non-critical patient but
do not require resources attending during office hours; Green 4 for non-critical patient but do
not require resources attending after office hours and during the weekend. List of patient’s
presentations at green zone used to triage as shown in Table 1.
International Journal of Public Health and Clinical Sciences e-ISSN : 2289-7577. Vol. 3:No. 5
September/October 2016
Arinah W. D. S., Faisal I., Muhamad Hanafiah Juni, Ismail, I., Mohamed, A. S 162
IJPHCS
Open Access: e-Journal
2.3. Appropriateness of Utilization
In this study, appropriateness of green zone utilization in emergency department was
determined by two steps: begin with triage of green zone patients according to patient’s
presentation upon arrival and finally end status of patient after consulted and examined by
attending doctor. Patients triaged to Green 1 and Green 2 were considered as appropriate
utilization regardless of the end status of patient (admitted or discharged). Patients triaged to
Green 3 and Green 4 were seen by attending doctor for consultation and examination. Then
the attending doctor decide the end status of the patient to determine the level of
appropriateness. If patients required admission to ward, they were considered as appropriate
utilization. If patients discharge home, they were considered as inappropriate utilization. In
Green 3 and Green 4 decided by attending doctor to be admitted to ward, they were
considered as appropriate utilization.
2.4. Data Collection
Patients were randomly selected using systematic random sampling over the period of two
weeks. Data obtained from the hospital system on the attendance of green zone adult patients
in January 2016 at Emergency Department Serdang Hospital per week. Simple random
sampling for the first number and systematically with the sampling fraction of two (2) until
completing the required number of sample size. Total number of patients required were 874
patients. However, 81 questionnaires were either not collected as the patients did not show up
for consultation or incomplete form thus giving the overall response rate of 90.7% (793
patients).
2.5. The study instrument
A structured questionnaire adapted from Selasawati et al. (2007) was pre-tested and used as
self-administered questionnaire for data collection. The questionnaire consists of four (4)
sections. Section A contained 7 questions on socio-demographic. Section B was on patient’s
knowledge on the roles and functions of emergency department and were measured as “yes”,
“unsure” and “no”. For the purpose of analysis, the answers were classified into “correct
knowledge” and “wrong knowledge” and analysed individually. Section C consisted of 9
questions on patient’s perceptions of emergency department. The answers ranges from
“strongly agree”, “agree”, “neutral”, “disagree” and “strongly disagree”. Each questions were
analysed individually and the results were collapsed into “disagree”, “neutral” and “disagree”
when perform analytical study. Section D component on reasons patients attend emergency
department over other healthcare facilities. Patients chose one or more reasons. Section E
recorded the time of presentation of patients to green zone emergency department.
Questionnaire was discussed with the experts in the field for content validity. Internal
consistency method used to determine the reliability of the questionnaire with Cronbach’s
Alpha values of 0.73 for knowledge and 0.74 for perception.
2.6. Data analysis
Data analyzed using IBM SPSS Statistics version 22. Descriptive statistics used to measure
frequency, percentage, mean and median. Chi-square test used to measure association
International Journal of Public Health and Clinical Sciences e-ISSN : 2289-7577. Vol. 3:No. 5
September/October 2016
Arinah W. D. S., Faisal I., Muhamad Hanafiah Juni, Ismail, I., Mohamed, A. S 163
IJPHCS
Open Access: e-Journal
between two categorical of dependent variables (level of appropriateness utilization) and
independent variables (socio-demographic, knowledge of patients on roles and functions of
emergency department, patient’s perceptions of emergency department, reasons for preferring
emergency department and time of presentation). Logistic regression test conducted to
determine the predictors of green zone utilization in Emergency Department, Serdang
Hospital.
3.0 Results
3.1. Level of appropriateness utilization
This study revealed that out of 793 patients in green zone, 660 were triaged to G1 and G2
(appropriate utilization). Remaining 133 patients were triaged to G3 and G4. Out of the 133
patients, three were admitted to ward (appropriate utilization) and 130 were allowed home
(inappropriate utilization). Therefore, total appropriate utilization were 663 (83.6%) and
inappropriate utilization were 130 (16.4%)
3.2 Socio-demographic characteristics
More than half (53.5%) of the patients had their ages within the range 18 to 30 years with
median age 29 years old (IQR ± 25th, 75th; 23, 40). Male and female gender both showed
almost an equal number of patients with male at 53.5% and female 46.5%. Malays constituted
the majority ethnic group among patients 587 (74%). Patients’ level of education were mainly
till secondary school (55.4%). In employment status, working in private sectors (45.9%) were
the most. About two third of patients (60.9%) with income per month less than RM1500.00.
3.3 Factors associated with appropriateness utilization of emergency department
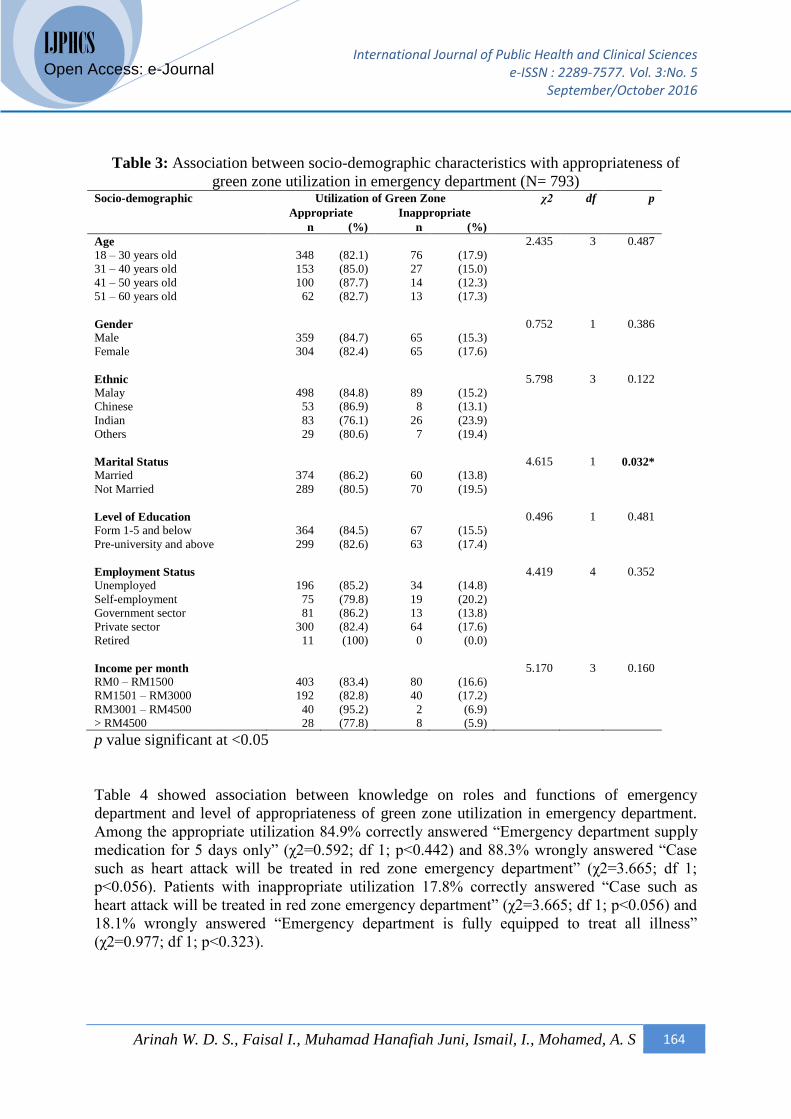
Table 3 below showed an association between socio-demographic characteristics and level of
appropriateness of green zone utilization in emergency department. Appropriate utilization of
emergency department was among patients aged 41-50 years old (87.7%), male (84.7%),
Chinese (86.9%), married (86.2%), patients with education until secondary school (84.5%),
patients working in government sectors (86.2%) and patients with income per month of RM
3001 – RM4500 (95.2%). Highest inappropriate utilization was patients age 18-30 years of
age (17.9%), female (17.6%), Indian (23.9%), not married (19.5%), patients with education
level of pre-university and above (17.4%), self-employment patients (20.2%) and those with
income per month of RM1501 – RM3000 (17.2%). Marital status (χ2=4.615; df 1; p<0.032)
was significantly association with the level of appropriateness of green zone utilization in
emergency department.
International Journal of Public Health and Clinical Sciences e-ISSN : 2289-7577. Vol. 3:No. 5
September/October 2016
Arinah W. D. S., Faisal I., Muhamad Hanafiah Juni, Ismail, I., Mohamed, A. S 164
IJPHCS
Open Access: e-Journal
Table 3: Association between socio-demographic characteristics with appropriateness of
green zone utilization in emergency department (N= 793) Socio-demographic Utilization of Green Zone χ2 df p
Appropriate Inappropriate
n (%) n (%)
Age
18 – 30 years old
31 – 40 years old
41 – 50 years old
51 – 60 years old
348
153
100
62
(82.1)
(85.0)
(87.7)
(82.7)
76
27
14
13
(17.9)
(15.0)
(12.3)
(17.3)
2.435 3
0.487
Gender
Male
Female
359
304
(84.7)
(82.4)
65
65
(15.3)
(17.6)
0.752 1 0.386
Ethnic
Malay
Chinese
Indian
Others
498
53
83
29
(84.8)
(86.9)
(76.1)
(80.6)
89
8
26
7
(15.2)
(13.1)
(23.9)
(19.4)
5.798 3 0.122
Marital Status
Married
Not Married
374
289
(86.2)
(80.5)
60
70
(13.8)
(19.5)
4.615 1 0.032*
Level of Education
Form 1-5 and below
Pre-university and above
364
299
(84.5)
(82.6)
67
63
(15.5)
(17.4)
0.496 1 0.481
Employment Status
Unemployed
Self-employment
Government sector
Private sector
Retired
196
75
81
300
11
(85.2)
(79.8)
(86.2)
(82.4)
(100)
34
19
13
64
0
(14.8)
(20.2)
(13.8)
(17.6)
(0.0)
4.419 4 0.352
Income per month
RM0 – RM1500
RM1501 – RM3000
RM3001 – RM4500
> RM4500
403
192
40
28
(83.4)
(82.8)
(95.2)
(77.8)
80
40
2
8
(16.6)
(17.2)
(6.9)
(5.9)
5.170 3
0.160
p value significant at <0.05
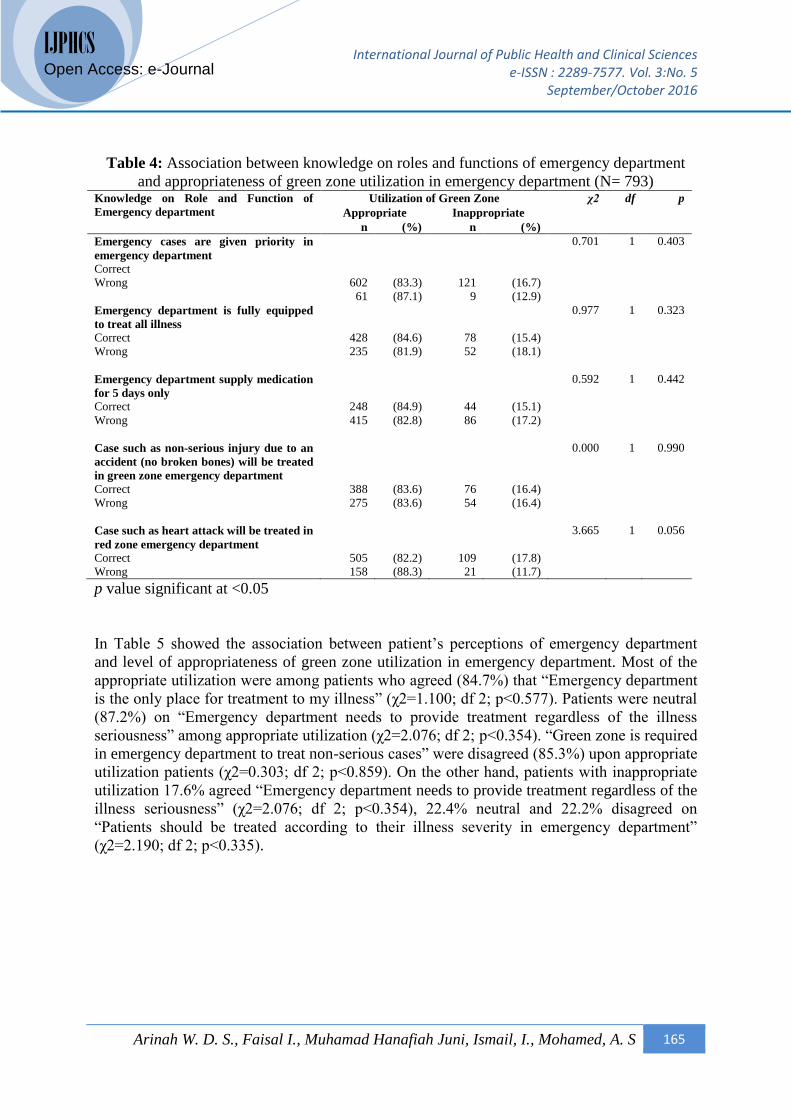
Table 4 showed association between knowledge on roles and functions of emergency
department and level of appropriateness of green zone utilization in emergency department.
Among the appropriate utilization 84.9% correctly answered “Emergency department supply
medication for 5 days only” (χ2=0.592; df 1; p<0.442) and 88.3% wrongly answered “Case
such as heart attack will be treated in red zone emergency department” (χ2=3.665; df 1;
p<0.056). Patients with inappropriate utilization 17.8% correctly answered “Case such as
heart attack will be treated in red zone emergency department” (χ2=3.665; df 1; p<0.056) and
18.1% wrongly answered “Emergency department is fully equipped to treat all illness”
(χ2=0.977; df 1; p<0.323).
International Journal of Public Health and Clinical Sciences e-ISSN : 2289-7577. Vol. 3:No. 5
September/October 2016
Arinah W. D. S., Faisal I., Muhamad Hanafiah Juni, Ismail, I., Mohamed, A. S 165
IJPHCS
Open Access: e-Journal
Table 4: Association between knowledge on roles and functions of emergency department
and appropriateness of green zone utilization in emergency department (N= 793) Knowledge on Role and Function of
Emergency department
Utilization of Green Zone χ2 df p
Appropriate Inappropriate
n (%) n (%)
Emergency cases are given priority in
emergency department
Correct
Wrong
602
61
(83.3)
(87.1)
121
9
(16.7)
(12.9)
0.701 1 0.403
Emergency department is fully equipped
to treat all illness
Correct
Wrong
428
235
(84.6)
(81.9)
78
52
(15.4)
(18.1)
0.977 1 0.323
Emergency department supply medication
for 5 days only
Correct
Wrong
248
415
(84.9)
(82.8)
44
86
(15.1)
(17.2)
0.592 1 0.442
Case such as non-serious injury due to an
accident (no broken bones) will be treated
in green zone emergency department
Correct
Wrong
388
275
(83.6)
(83.6)
76
54
(16.4)
(16.4)
0.000 1 0.990
Case such as heart attack will be treated in
red zone emergency department
Correct
Wrong
505
158
(82.2)
(88.3)
109
21
(17.8)
(11.7)
3.665 1 0.056
p value significant at <0.05
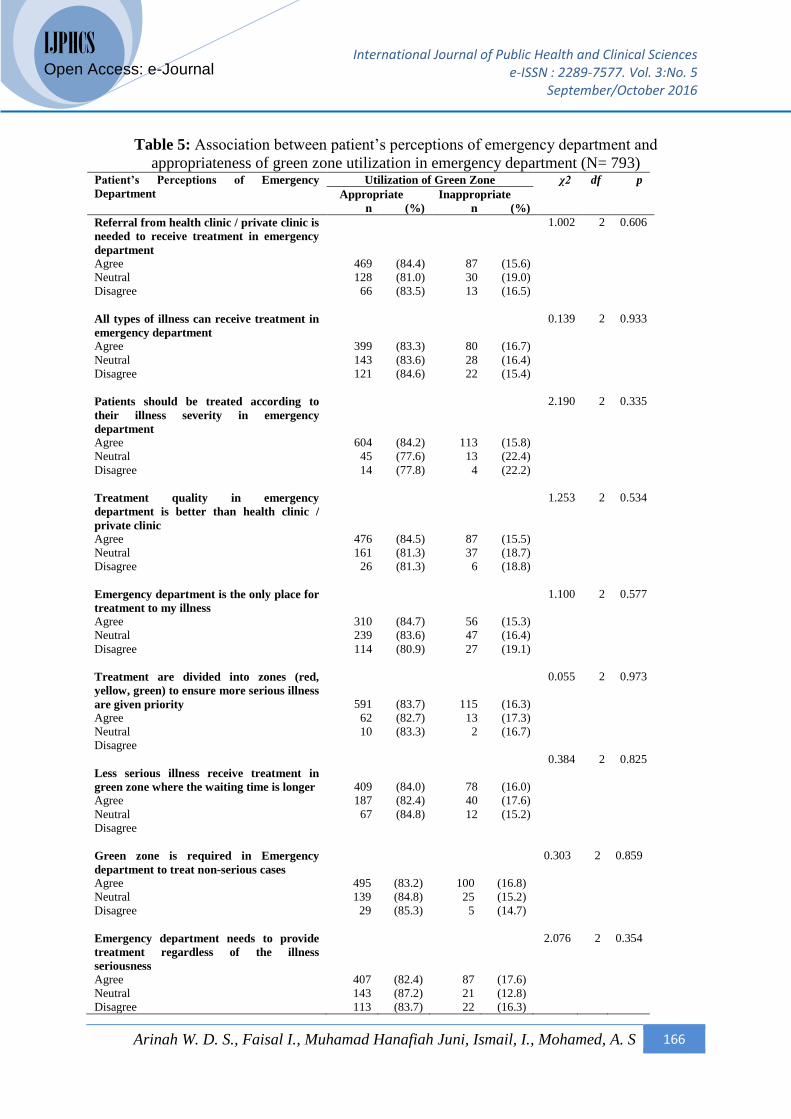
In Table 5 showed the association between patient’s perceptions of emergency department
and level of appropriateness of green zone utilization in emergency department. Most of the
appropriate utilization were among patients who agreed (84.7%) that “Emergency department
is the only place for treatment to my illness” (χ2=1.100; df 2; p<0.577). Patients were neutral
(87.2%) on “Emergency department needs to provide treatment regardless of the illness
seriousness” among appropriate utilization (χ2=2.076; df 2; p<0.354). “Green zone is required
in emergency department to treat non-serious cases” were disagreed (85.3%) upon appropriate
utilization patients (χ2=0.303; df 2; p<0.859). On the other hand, patients with inappropriate
utilization 17.6% agreed “Emergency department needs to provide treatment regardless of the
illness seriousness” (χ2=2.076; df 2; p<0.354), 22.4% neutral and 22.2% disagreed on
“Patients should be treated according to their illness severity in emergency department”
(χ2=2.190; df 2; p<0.335).
International Journal of Public Health and Clinical Sciences e-ISSN : 2289-7577. Vol. 3:No. 5
September/October 2016
Arinah W. D. S., Faisal I., Muhamad Hanafiah Juni, Ismail, I., Mohamed, A. S 166
IJPHCS
Open Access: e-Journal
Table 5: Association between patient’s perceptions of emergency department and
appropriateness of green zone utilization in emergency department (N= 793) Patient’s Perceptions of Emergency
Department
Utilization of Green Zone χ2 df p
Appropriate Inappropriate
n (%) n (%)
Referral from health clinic / private clinic is
needed to receive treatment in emergency
department
Agree
Neutral
Disagree
469
128
66
(84.4)
(81.0)
(83.5)
87
30
13
(15.6)
(19.0)
(16.5)
1.002 2 0.606
All types of illness can receive treatment in
emergency department
Agree
Neutral
Disagree
399
143
121
(83.3)
(83.6)
(84.6)
80
28
22
(16.7)
(16.4)
(15.4)
0.139 2 0.933
Patients should be treated according to
their illness severity in emergency
department
Agree
Neutral
Disagree
604
45
14
(84.2)
(77.6)
(77.8)
113
13
4
(15.8)
(22.4)
(22.2)
2.190 2 0.335
Treatment quality in emergency
department is better than health clinic /
private clinic
Agree
Neutral
Disagree
Emergency department is the only place for
treatment to my illness
Agree
Neutral
Disagree
Treatment are divided into zones (red,
yellow, green) to ensure more serious illness
are given priority
Agree
Neutral
Disagree
Less serious illness receive treatment in
green zone where the waiting time is longer
Agree
Neutral
Disagree
476
161
26
310
239
114
591
62
10
409
187
67
(84.5)
(81.3)
(81.3)
(84.7)
(83.6)
(80.9)
(83.7)
(82.7)
(83.3)
(84.0)
(82.4)
(84.8)
87
37
6
56
47
27
115
13
2
78
40
12
(15.5)
(18.7)
(18.8)
(15.3)
(16.4)
(19.1)
(16.3)
(17.3)
(16.7)
(16.0)
(17.6)
(15.2)
1.253
1.100
0.055
0.384
2
2
2
2
0.534
0.577
0.973
0.825
Green zone is required in Emergency
department to treat non-serious cases
Agree
Neutral
Disagree
495
139
29
(83.2)
(84.8)
(85.3)
100
25
5
(16.8)
(15.2)
(14.7)
0.303 2 0.859
Emergency department needs to provide
treatment regardless of the illness
seriousness
Agree
Neutral
Disagree
407
143
113
(82.4)
(87.2)
(83.7)
87
21
22
(17.6)
(12.8)
(16.3)
2.076 2 0.354
International Journal of Public Health and Clinical Sciences e-ISSN : 2289-7577. Vol. 3:No. 5
September/October 2016
Arinah W. D. S., Faisal I., Muhamad Hanafiah Juni, Ismail, I., Mohamed, A. S 167
IJPHCS
Open Access: e-Journal
p value significant at <0.05
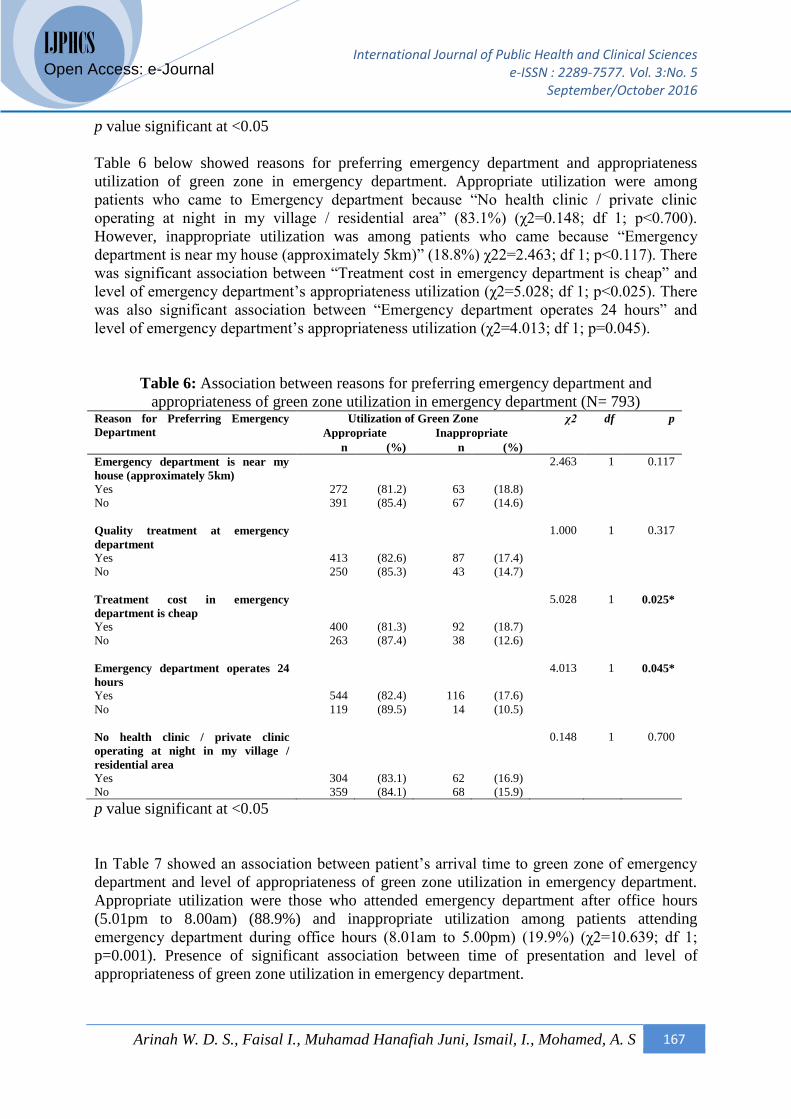
Table 6 below showed reasons for preferring emergency department and appropriateness
utilization of green zone in emergency department. Appropriate utilization were among
patients who came to Emergency department because “No health clinic / private clinic
operating at night in my village / residential area” (83.1%) (χ2=0.148; df 1; p<0.700).
However, inappropriate utilization was among patients who came because “Emergency
department is near my house (approximately 5km)” (18.8%) χ22=2.463; df 1; p<0.117). There
was significant association between “Treatment cost in emergency department is cheap” and
level of emergency department’s appropriateness utilization (χ2=5.028; df 1; p<0.025). There
was also significant association between “Emergency department operates 24 hours” and
level of emergency department’s appropriateness utilization (χ2=4.013; df 1; p=0.045).
Table 6: Association between reasons for preferring emergency department and
appropriateness of green zone utilization in emergency department (N= 793) Reason for Preferring Emergency
Department
Utilization of Green Zone χ2 df p
Appropriate Inappropriate
n (%) n (%)
Emergency department is near my
house (approximately 5km)
Yes
No
272
391
(81.2)
(85.4)
63
67
(18.8)
(14.6)
2.463 1 0.117
Quality treatment at emergency
department
Yes
No
413
250
(82.6)
(85.3)
87
43
(17.4)
(14.7)
1.000 1 0.317
Treatment cost in emergency
department is cheap
Yes
No
400
263
(81.3)
(87.4)
92
38
(18.7)
(12.6)
5.028 1 0.025*
Emergency department operates 24
hours
Yes
No
544
119
(82.4)
(89.5)
116
14
(17.6)
(10.5)
4.013 1 0.045*
No health clinic / private clinic
operating at night in my village /
residential area
Yes
No
304
359
(83.1)
(84.1)
62
68
(16.9)
(15.9)
0.148 1 0.700
p value significant at <0.05
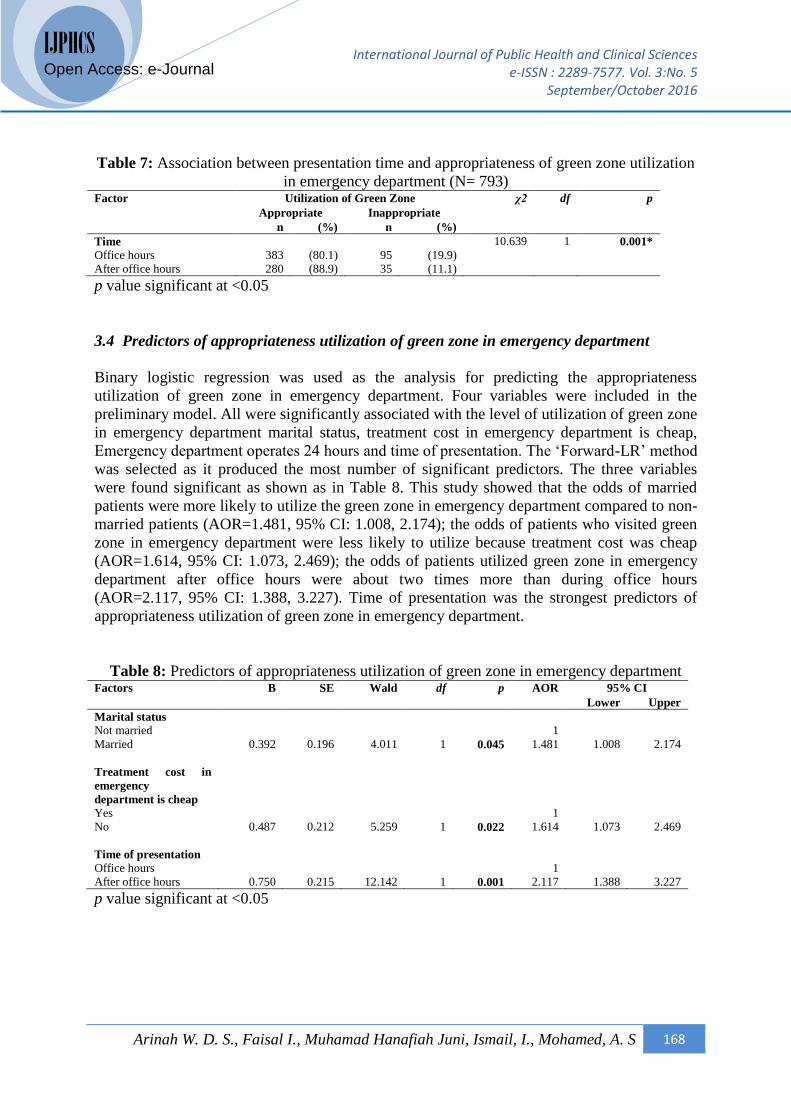
In Table 7 showed an association between patient’s arrival time to green zone of emergency
department and level of appropriateness of green zone utilization in emergency department.
Appropriate utilization were those who attended emergency department after office hours
(5.01pm to 8.00am) (88.9%) and inappropriate utilization among patients attending
emergency department during office hours (8.01am to 5.00pm) (19.9%) (χ2=10.639; df 1;
p=0.001). Presence of significant association between time of presentation and level of
appropriateness of green zone utilization in emergency department.
International Journal of Public Health and Clinical Sciences e-ISSN : 2289-7577. Vol. 3:No. 5
September/October 2016
Arinah W. D. S., Faisal I., Muhamad Hanafiah Juni, Ismail, I., Mohamed, A. S 168
IJPHCS
Open Access: e-Journal
Table 7: Association between presentation time and appropriateness of green zone utilization
in emergency department (N= 793) Factor Utilization of Green Zone χ2 df p
Appropriate Inappropriate
n (%) n (%)
Time
Office hours
After office hours
383
280
(80.1)
(88.9)
95
35
(19.9)
(11.1)
10.639 1 0.001*
p value significant at <0.05
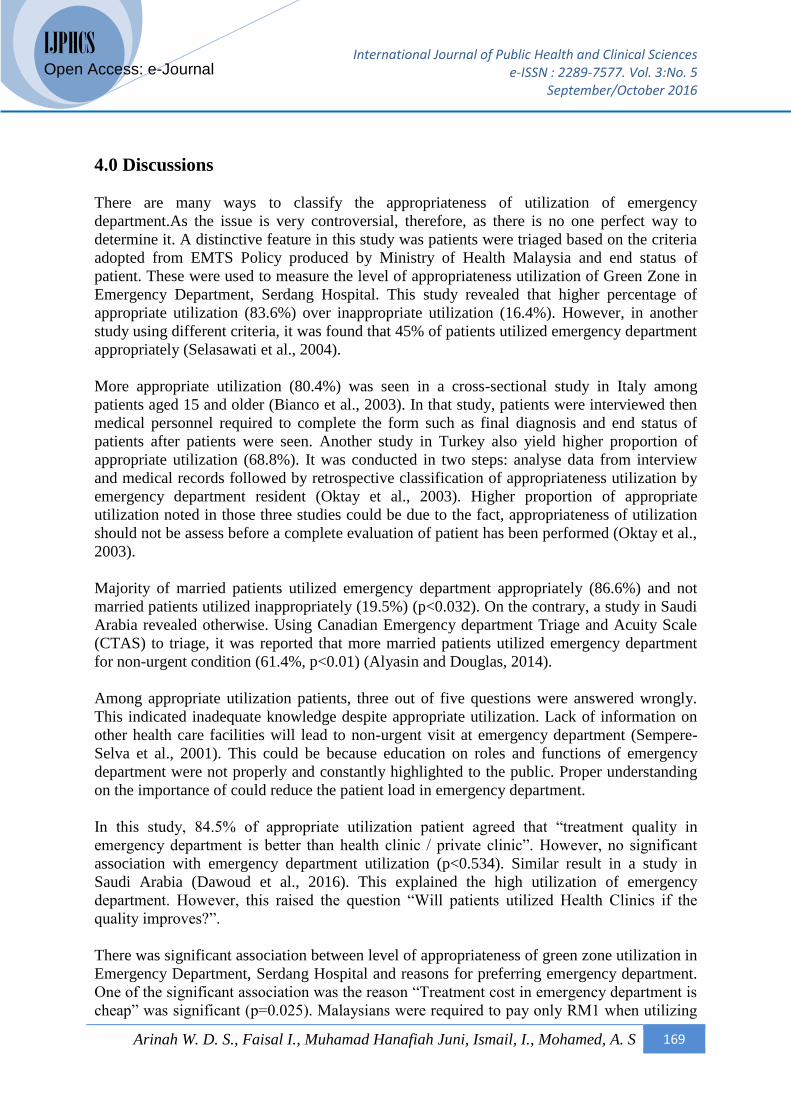
3.4 Predictors of appropriateness utilization of green zone in emergency department
Binary logistic regression was used as the analysis for predicting the appropriateness
utilization of green zone in emergency department. Four variables were included in the
preliminary model. All were significantly associated with the level of utilization of green zone
in emergency department marital status, treatment cost in emergency department is cheap,
Emergency department operates 24 hours and time of presentation. The ‘Forward-LR’ method
was selected as it produced the most number of significant predictors. The three variables
were found significant as shown as in Table 8. This study showed that the odds of married
patients were more likely to utilize the green zone in emergency department compared to non-
married patients (AOR=1.481, 95% CI: 1.008, 2.174); the odds of patients who visited green
zone in emergency department were less likely to utilize because treatment cost was cheap
(AOR=1.614, 95% CI: 1.073, 2.469); the odds of patients utilized green zone in emergency
department after office hours were about two times more than during office hours
(AOR=2.117, 95% CI: 1.388, 3.227). Time of presentation was the strongest predictors of
appropriateness utilization of green zone in emergency department.
Table 8: Predictors of appropriateness utilization of green zone in emergency department Factors B SE Wald df p AOR 95% CI
Lower Upper
Marital status
Not married
Married
0.392
0.196
4.011
1
0.045
1
1.481
1.008
2.174
Treatment cost in
emergency
department is cheap
Yes
No
0.487
0.212
5.259
1
0.022
1
1.614
1.073
2.469
Time of presentation
Office hours
After office hours
0.750
0.215
12.142
1
0.001
1
2.117
1.388
3.227
p value significant at <0.05
International Journal of Public Health and Clinical Sciences e-ISSN : 2289-7577. Vol. 3:No. 5
September/October 2016
Arinah W. D. S., Faisal I., Muhamad Hanafiah Juni, Ismail, I., Mohamed, A. S 169
IJPHCS
Open Access: e-Journal
4.0 Discussions
There are many ways to classify the appropriateness of utilization of emergency
department.As the issue is very controversial, therefore, as there is no one perfect way to
determine it. A distinctive feature in this study was patients were triaged based on the criteria
adopted from EMTS Policy produced by Ministry of Health Malaysia and end status of
patient. These were used to measure the level of appropriateness utilization of Green Zone in
Emergency Department, Serdang Hospital. This study revealed that higher percentage of
appropriate utilization (83.6%) over inappropriate utilization (16.4%). However, in another
study using different criteria, it was found that 45% of patients utilized emergency department
appropriately (Selasawati et al., 2004).
More appropriate utilization (80.4%) was seen in a cross-sectional study in Italy among
patients aged 15 and older (Bianco et al., 2003). In that study, patients were interviewed then
medical personnel required to complete the form such as final diagnosis and end status of
patients after patients were seen. Another study in Turkey also yield higher proportion of
appropriate utilization (68.8%). It was conducted in two steps: analyse data from interview
and medical records followed by retrospective classification of appropriateness utilization by
emergency department resident (Oktay et al., 2003). Higher proportion of appropriate
utilization noted in those three studies could be due to the fact, appropriateness of utilization
should not be assess before a complete evaluation of patient has been performed (Oktay et al.,
2003).
Majority of married patients utilized emergency department appropriately (86.6%) and not
married patients utilized inappropriately (19.5%) (p<0.032). On the contrary, a study in Saudi
Arabia revealed otherwise. Using Canadian Emergency department Triage and Acuity Scale
(CTAS) to triage, it was reported that more married patients utilized emergency department
for non-urgent condition (61.4%, p<0.01) (Alyasin and Douglas, 2014).
Among appropriate utilization patients, three out of five questions were answered wrongly.
This indicated inadequate knowledge despite appropriate utilization. Lack of information on
other health care facilities will lead to non-urgent visit at emergency department (Sempere-
Selva et al., 2001). This could be because education on roles and functions of emergency
department were not properly and constantly highlighted to the public. Proper understanding
on the importance of could reduce the patient load in emergency department.
In this study, 84.5% of appropriate utilization patient agreed that “treatment quality in
emergency department is better than health clinic / private clinic”. However, no significant
association with emergency department utilization (p<0.534). Similar result in a study in
Saudi Arabia (Dawoud et al., 2016). This explained the high utilization of emergency
department. However, this raised the question “Will patients utilized Health Clinics if the
quality improves?”.
There was significant association between level of appropriateness of green zone utilization in
Emergency Department, Serdang Hospital and reasons for preferring emergency department.
One of the significant association was the reason “Treatment cost in emergency department is
cheap” was significant (p=0.025). Malaysians were required to pay only RM1 when utilizing
International Journal of Public Health and Clinical Sciences e-ISSN : 2289-7577. Vol. 3:No. 5
September/October 2016
Arinah W. D. S., Faisal I., Muhamad Hanafiah Juni, Ismail, I., Mohamed, A. S 170
IJPHCS
Open Access: e-Journal
government health facility such as emergency department and outpatient clinic. Services
provided inclusive of examination, consultation, treatment and medication. Patients utilizing
emergency department inappropriately stated the reason for choosing emergency department
over other health care facilities was because it was cheap (18.7%, p<0.025).
The other significant reason was “Emergency department operates 24 hours” (p=0.045).
Emergency department provides wide range of services and comprehensive care for patients
as well as having feasible operating hours, which is of great convenience to the community. A
department with health staff and operating 24 hours resulting in 83.2% (p=0.045) of patients
utilized emergency department inappropriately (Khan et al., 2011). A cross-sectional study
among 28 hospitals revealed that one of the most cited and important reason and for patients
utilizing emergency department was the hours of operation. The hours include during
evening, weekend and patients unable to leave work (Ragin et al., 2005).
It was noted 88.9% of appropriate utilization of green zone in emergency department were
after office hours (1701hrs to 800hrs) and 80.1% during office hours (0801hrs – 1700hrs)
(p=0.001). It is understandable that in Malaysia, government health clinics operate during
weekdays until 1700hrs. In some of the clinics, it operates until 2200hrs and some even on
Saturdays. Klinik 1 Malaysia (K1M) on the other hand, operates everyday until 2200hrs.
Despite the government’s effort of providing access of health care to the community, it seems
insufficient. This can be reflected in this study as high utilization was among those who
attended emergency department appropriately after office hours (p=0.001).
Current study revealed that marital status was one of the significant predictor of
appropriateness utilization of green zone in emergency department (p=0.045, AOR=1.481). In
contrast to this study, a study in Taiwan found out that odds of unmarried patients utilized
emergency department inappropriately higher compared to married patients (Tsai et al.,
2010). Both studies used triage to determine the appropriateness of emergency department
utilization.
Another significant predictor was treatment cost in emergency department is cheap in this
study. Unlike certain countries, patients are not assigned to certain healthcare provider.
Patients can opt to attend government health clinics or private GP. Despite charging only
RM1 for Malaysian utilizing government health facility, our findings revealed that the odds of
patients utilized emergency department not because of the cheap treatment was 1.6 (p=0.022).
Another study in Hong Kong revealed similar results where the odds of patients utilizing
emergency department for general practitioner cases because of the lower cost was less likely
(Lee et al., 2000).
The strongest predictor of green zone utilization in emergency department was time of
presentation. The odds of utilization after office hours (1701hrs – 0800hrs) were two times
more than during office hours (0801hrs – 1700hrs). The finding was consistent with the
closure of health clinics, extended hours health clinics and K1M. This was again seen in a
study conducted in a University Hospital where the highest peak for both appropriate and
inappropriate cases were around 2000hrs (Selasawati et al., 2004). In addition, another study
reported time of presentation from 800hrs until 1800hrs was significantly associated with
inappropriate utilization of emergency department (Tsai et al., 2010).
International Journal of Public Health and Clinical Sciences e-ISSN : 2289-7577. Vol. 3:No. 5
September/October 2016
Arinah W. D. S., Faisal I., Muhamad Hanafiah Juni, Ismail, I., Mohamed, A. S 171
IJPHCS
Open Access: e-Journal
5.0 Conclusion and recommendation
Taking into consideration 70 – 75% of the total utilization of Emergency Department in
Serdang Hospital over the past 5 years was green zone, this study revealed higher appropriate
utilization than inappropriate utilization. Therefore, future study is needed on the
development of a more pragmatic guideline to determine the appropriateness of green zone
utilization in emergency department.
One of the most significant factors associated with the level of appropriateness of green zone
utilization in emergency department was patient time of presentation. However, future studies
needed to determine the cause-effect relationship between these two variables.
Acknowledgement
The manuscript was prepared as part of requirement of graduation in Master of Public Health
degree in Department of Community Health, Faculty of Medicine and Health Sciences,
Universiti Putra Malaysia.
This study obtained approval from University Research Ethical Committee (JKEUPM),
Universiti Putra Malaysi (Reference number: UPM/TNCPI/RMC/JKEUPM/1.4.18.2), from
the Ministry of Health via National Medical Research Register (NMRR) (ID: NMRR-15-
2227-28389), from Selangor State Health Office, Ministry of Health (Reference number:
(50)JKNS (P) 130/4 Jld 9), from Serdang Hospital, Ministry of Health (Reference number:
UPM/FPSK/JKK/100-3) and from Dr. Selasawati binti Hj. Ghazali for using questionnaire.
The authors would like to thank the Director General of Health Malaysia for permission to
publish this manuscript, Dr. Rosidah Ibrahim and staff of Emergency Department, Serdang
Hospital for their cooperation and support during data collection, and to
Declaration
Author(s) declare that there is no conflict of interest regarding publication of this article.
Author’s contribution
Author 1 : information gathering, preparation and editing of manuscript
Author 2 : review of manuscript
Author 3 : final review of manuscript and final editing
Author 4 : review of manuscript
Author 5 : review of manuscript
International Journal of Public Health and Clinical Sciences e-ISSN : 2289-7577. Vol. 3:No. 5
September/October 2016
Arinah W. D. S., Faisal I., Muhamad Hanafiah Juni, Ismail, I., Mohamed, A. S 172
IJPHCS
Open Access: e-Journal
References
Alyasin, A. R. N., & Douglas, C. (2014). Reasons for non-urgent presentations to the
emergency department in Saudi Arabia. International Emergency Nursing,
22(4):220-225.
Ministry of Health Malaysia (2010). Selangor State Health Department Annual Report 2010.
Report prepared at Selangor State Health Department, Ministry of Health.
Ministry of Health Malaysia (2012). Selangor State Health Department Annual Report 2010.
Report prepared at Selangor State Health Department, Ministry of Health.
Ministry of Health Malaysia (2013). Selangor State Health Department Annual Report 2010.
Report prepared at Selangor State Health Department, Ministry of Health.
Bianco, A., Pileggi, C., Angelillo, I. F. (2003). Non-urgent visits to a hospital Emergency
department in Italy. Journal of the Royal Institute of Public Health, 117(4):250-255.
Cunningham, P. (2011). Nonurgent use of hospital emergency department. Statement before
the U.S. Senate for the hearing on “Diverting non-urgent Emergency Room use: Can
it provide better care and lower Costs?”. May 2011.
Dawoud, S. O., Ahmad, A. M. K., Alsharqi, O. Z., Al-Raddadi, R. M. (2016). Utilization of
the Emergency department and predicting factors associated with its use at the Saudi
Ministry of Health General Hospitals. Global Journal of Health Science, 8(1):90-106.
Emergency Medicine and Trauma Services Policy (2012). Medical Development Division:
Ministry of Health, Malaysia. 2012.
Ministry of Health Malaysia (2016). Annual report on outpatient attendances by category
code, case type and total in emergency department / unit. Report prepared for
Serdang Hospital at Serdang Hospital, Ministry of Health Malaysia.
Erenler, A. K., Ozel, I., Ece, Y., Karabulut, M., Orucoglu, A., Ciftci, E. (2015). Analysis of
triage application in emergency department. Open Journal of Emergency Medicine,
3(3):13-17.
Khan, Y., Glazier, R. H., Moeneddin, R., Schull, M. J. (2011). A Population-based study of
the association between socioeconomic status and emergency department Utilization
in Ontario, Canada. Academy Emergency Medicine, 18(8):836-843.
Lee, A., Lau, F. L.,Hazlett, C. B., Kam, C. W., Wong, P., Wong, T. W., Chow, S. (2000).
Factors associated with non-urgent utilization of Accident and Emergency Services:
A case-control study in Hong Kong. Social Science & Medicine, 51(7):1075-1085.
Moskop, J. C. (2010). Nonurgent care in the emergency department — bane or boon? Virtual
Mentor, 12(6):476-482
International Journal of Public Health and Clinical Sciences e-ISSN : 2289-7577. Vol. 3:No. 5
September/October 2016
Arinah W. D. S., Faisal I., Muhamad Hanafiah Juni, Ismail, I., Mohamed, A. S 173
IJPHCS
Open Access: e-Journal
Oktay, C., Cete, Y., Eray, O., Pekdemir, M., Gunerli, A. (2003). Appropriateness of
emergency department visits in a Turkish University Hospital. Croatian Medical
Journal, 44(5):585-591.
Selasawati, H. G., Naing, L., Wan Aasim, W. A., Winn, T., Rusli, B. N. (2004). Inappropriate
utilization of emergency department services in Universiti Sains Malaysia Hospital.
Med J Malaysia, 59(1):26-33.
Selasawati, H. G., Naing, L., Wan Aasim, W. A., Winn, T., Rusli, B. N. (2007). Factors
associated with inappropriate utilisation of emergency department services. Asia-
Pacific Journal of Public Health, 19(2):29-36.
Sempere-Selva, T., Peiro, S., Sendra-Pina, P., Martinez-Espin, C., Lopez-Aguilera, I. (2001).
Inappropriate use of an accident and emergency department: Magnitude, associated
factors and reasons – an approach with explicit criteria. Annals of Emergency
Medicine, 37(6):568-579.
Tsai, J. C. H., Liang, Y. W., Pearson, W. S. (2010). Utilization of emergency department in
patients with non-urgent medical problems: patient preference and emergency
department convenience. Journal of the Formosan Medical Association, 109(7):533-
542.
Top Related
Copyright © 2022 FDOKUMEN

