INDIAN JOURNAL OF CLINICAL PSYCHOLOGY
92
Volume 44, Number - 1 March, 2017 ISSN 0303-2582 Editor K.S. Sengar Official Publication of INDIAN ASSOCIATION OF CLINICAL PSYCHOLOGISTS www.iacp.in RNI RN 26039/74 INDIAN JOURNAL OF CLINICAL PSYCHOLOGY Editorial Board, Journal Committee, Executive Council & Secretariat i-ii Instructions to Authors iii-vi Editorial Clinical Psychology beyond Mental Hospitals: Changing Role of Clinical Psychologists K. S. Sengar 1-5 Presidential Address Digital Technology and Clinical Psychology Amool R. Singh 6-8 Orations Cang Oration Challenges Concerning Adolescent Mental Health In India P. T. Sasi 9-13 H N Murthy Oration Experiences in Verbal Exposure for Stimulus Bound Anxiety Rakesh Kumar 14-20 Research Articles Relationship of Fluid and Crystallized Intelligence with Cognitive Insight in Persons with Schizophrenia Sandhyarani Mohanty and Sudhir Kumar 21-25 Stress-Coping and Factors Contributing to Resilience in College Students: An Exploratory Study from India Hesi S. Herbert and M. Manjula 26-34 Autistic Spectrum Disorders in Children with Intellectual Disability Saumyashree Mohapatra, Masroor Jahan and M. Thomas Kishore 35-40 Cognitive Retraining in Subdural Haematoma Richa Priyamvada, Rupesh Ranjan and Prabha Shukla 41-44 Efficacy of Behaviour Therapy in Internet Addiction Preeti Singh and Narendra Nath Samantaray 45-53 Indicators of Mental Illness in a North Indian Population Prachi Ghildyal and KomillaThapa 54-59 Toy Index of Children With or Without Developmental Disabilities S. Venkatesan and G Y Yashodharakumar 60-67 Mental Health Clinics A Case Study with Acceptance and Commitment Therapy Soheli Datta and Tilottama Mukherjee 68-74 Neuropsychological Functioning of Patient with Organic Personality Disorder with Caudate Nucleus Infarct: A Case Study Saniya Bhutani, Shweta Singh and Pooja Singh 75-78 Efficacy of Cognitive Behaviour Therapy in an Adult with Stammering Manoj Kumar Pandey, Prabha Mishra and Aradhana Shukla 79-82
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of INDIAN JOURNAL OF CLINICAL PSYCHOLOGY

83
Volume 44, Number - 1March, 2017
ISSN 0303-2582
Editor
K.S. Sengar
Official Publication of INDIAN ASSOCIATION OF
CLINICAL PSYCHOLOGISTSwww.iacp.in
RNI RN 26039/74
INDIAN JOURNAL OF CLINICAL PSYCHOLOGY
Editorial Board, Journal Committee, Executive Council & Secretariat i-ii
Instructions to Authors iii-viEditorialClinical Psychology beyond Mental Hospitals: Changing Role of Clinical Psychologists K. S. Sengar
1-5
Presidential AddressDigital Technology and Clinical PsychologyAmool R. Singh
6-8
OrationsCang OrationChallenges Concerning Adolescent Mental Health In IndiaP. T. Sasi
9-13
H N Murthy OrationExperiences in Verbal Exposure for Stimulus Bound AnxietyRakesh Kumar
14-20
Research ArticlesRelationship of Fluid and Crystallized Intelligence with Cognitive Insight in Persons with SchizophreniaSandhyarani Mohanty and Sudhir Kumar
21-25
Stress-Coping and Factors Contributing to Resilience in College Students: An Exploratory Study from India Hesi S. Herbert and M. Manjula
26-34
Autistic Spectrum Disorders in Children with Intellectual DisabilitySaumyashree Mohapatra, Masroor Jahan and M. Thomas Kishore
35-40
Cognitive Retraining in Subdural HaematomaRicha Priyamvada, Rupesh Ranjan and Prabha Shukla
41-44
Efficacy of Behaviour Therapy in Internet Addiction Preeti Singh and Narendra Nath Samantaray
45-53
Indicators of Mental Illness in a North Indian PopulationPrachi Ghildyal and KomillaThapa
54-59
Toy Index of Children With or Without Developmental DisabilitiesS. Venkatesan and G Y Yashodharakumar
60-67
Mental Health ClinicsA Case Study with Acceptance and Commitment TherapySoheli Datta and Tilottama Mukherjee
68-74
Neuropsychological Functioning of Patient with Organic Personality Disorder with Caudate Nucleus Infarct: A Case StudySaniya Bhutani, Shweta Singh and Pooja Singh
75-78
Efficacy of Cognitive Behaviour Therapy in an Adult with StammeringManoj Kumar Pandey, Prabha Mishra and Aradhana Shukla
79-82

84
We’re here to help you creategreater mental health and well-being,with our assessments that areadapted and standardized for India.
Wechsler AbbreviatedScale of Intelligence,Second Edition,India (WASI-IIINDIA)
Wechsler AdultIntelligence Scale,Fourth Edition,India (WAIS-IVINDIA)
Wechsler Memory Scale,Third Edition,India (WMS-IIIINDIA)
Wechsler IntelligenceScale for Children,Fourth Edition,India (WISC-IVINDIA)
Raven’s Educational CPM/CVS,India Edition
Raven’s CPM/ CVS HINDI, with Regional LanguageTranslations
Dyslexia Screening Test-JuniorIndia Edition (DST-JINDIA)
Beck Youth Inventories,Second Edition,India (BYI 2 India)
Many of our assessments are now available
on our digital assessment platform, Q-global.
Learn more about Q-global at www.pearsonclinical.in/q-global
Pearson Clinical India
@ThinkClinical
Pearson Clinical India
Copyright © 2016. Pearson India Education Services Private Limited. All Rights Reserved.
Pearson Clinical & Talent Assessment+91 924 360 0012 | [email protected] | www.pearsonclinical.in
Registered Office: 4th floor, Software Block, Elnet Software City, TS - 140, Block 2 & 9,Rajiv Gandhi Salai, Taramani, Chennai, Tamil Nadu 600113.

i
INDIAN JOURNAL OF CLINICAL PSYCHOLOGY
Volume 44 March 2017 No. 1
Editor : K. S. Sengar
Editorial Board
Anisha Shah (Bengaluru) Ashima N. Wadhawan (Delhi) D. K. Sharma (Delhi) Devvrata Kumar (Bengaluru) K. B. Kumar (NOIDA) K. Pramodu (Kozikode) L. S. S. Manickam (Mysuru)
Nawab Akhtar Khan (Mysuru)Shweta Singh (Lucknow)
Maitreyee Dutta (Tezpur) Manjari Srivastava (Mumbai) N. G. Desai (Delhi) Adarsh Kohli (Chandigarh) Rajeev Dogra (Rohtak) S. L. Vaya (Ahmedabad) U. K. Sinha (Delhi)
Sanjukta Das (Kolkata)Rushi Tamanna (Delhi)Anand Pratap Singh (Gautam Budh Nagar)Renuka Jena (UK)
Shweta (Singapore)
Sameeta, Ng
Statistical Consultants
Ram C. Bajpai (Singapore)
Himanshu K. Chaturvedi (Delhi)
Editorial Advisory Board
A. K. Srivastava (Kanpur)
Amool R. Singh (Ranchi)
B. L. Dubey (USA)
D. P. Sen Mazumdar (Delhi)
M. K. Mondal (Delhi)
M. S. Thimappa (Bengaluru)
R . G. Sharma (Varanasi)
S. C. Gupta (Lucknow)
T. B. Singh (Patna)
Distinguished Former Editors
S. K. Verma (1974 – 1983)
S. K. Maudgil (1984 – 1986)
S. C. Gupta (1987 – 1989)
D. K. Menon (1990 – 1991)
R. Kishore (1992)
K. Dutt (1993)
K. Rangaswami (1994 – 1995)
S. S. Nathawat (1996 – 2002)
Amool R. Singh (2002 – 2006)
Ashima N. Wadhawan (2007)
S. P. K. Jena (2008- 2011)
ii
JOURNAL COMMITTEEK. S. Sengar (Ranchi) ChairpersonS. Balakrishnan (Chennai) P. T. Sasi (Thrissur)
Rakesh Kumar (Agra) Jashobanta Mohapatra (Cuttak)Kalpana Srivatava (Pune) (Ex. Officio Member)
EXECUTIVE COUNCILPresidentAmool R. Singh RINPAS, Kanke, Ranchi (Jharkhand) [email protected], [email protected]
President Elect K. Gireesh (Thiruananthpuram)[email protected]
Immediate Past President V. C. [email protected]
Hon. General Secretary Kalpana SrivastavaDept of Psychiatry, AFMC, Pune (Mah.)[email protected] [email protected]
Immediate Past Hon. Gen. Secretary Masroor JahanRINPAS, Kanke, Ranchi (Jharkhand)[email protected]
Treasurer B. N. RoopeshNIMHANS, [email protected]
COUNCIL MEMBERSAll IndiaSanjukta Das [email protected]
Manoj K [email protected]
West Zone Smita [email protected]
Sudipta [email protected]
South Zone
Srihari, [email protected]
Jini K. [email protected]
East ZoneSameeta [email protected]
Bidita [email protected]
North Zone Vikas [email protected]
Atul [email protected]
President Nominee
S. L. [email protected]
Minkesh [email protected]
SECRETARIATDepartment of Psychiatry, Armed Forces Medical College (AFMC), Pune (Maharashtra) India.

iii
INSTRUCTIONS TO AUTHORSIJCP welcomes the submission of manuscript
in all areas of treatment, prevention and promotion of mental health especially on issues that appeal to clinicians, researchers, academicians and practitioners in the field of mental health. This journal publishes Research / Original Articles, Review Articles, Brief Communications, Case Reports, Letter to Editor, Book Reviews and News about conferences etc. Manuscript must be prepared in IJCP format outlined below. Before submission of a manuscript to IJCP it is mandatory that all authors have read the manuscript and owe the responsibility. The research that is reported in IJCP must be conducted after the approval of ethical committee and information regarding the same should be furnished in the method section. In general, at least fifty percent of the author should be member of IACP (any category)
Publication PolicyThe IJCP policy advice the author of
manuscript not to submit the same manuscript in two or more journals for concurrent consideration and the same must be stated in cover letter. IJCP requires the author to reveal any possible conflict of interest in the conduct and reporting of the study. They should also describe their role and participation in designing the study; data collection; analysis; interpretation of data; writing of report and / or in decision to submit the report for publication. Acknowledgement must be furnished in condition of participation in the study in any form or if the material (picture, tables or any other data, with permission) has been taken from any other place/source and is part of the study/ manuscript. Ethical standards must be followed in the treatment of their sample, human or animals, or to describe details of treatment and research must be approved from ethical committee. Approval letter should be submitted to editor, IJCP (for ethical principles one can visit www.apa.org/ethics).
IJCP requires from Author/ Authors to transfer copyright to IJCP for accepted manuscript before publication.
Guidelines for Manuscript PreparationLength and style of Manuscript
Full length manuscript length should not exceed more than 5000 words tentatively 15 typed pages total (including cover page, abstract, text, references, tables, and figures), with appropriate margins (at least 1 inch) on all sides and a standard font (e.g. Times New Roman) of 12 points ( not smaller). The entire manuscript (text, references, tables etc) must be double spaced, one side on a paper of good quality. The manuscript should conform the Horward style. The text of observational and experimental study should be divided into following sections: Title of the Paper, Name of the Author (s), Abstract, Introduction, Method, Results, Discussion and References. Manuscript should be prepared in following format:
a. Cover Page / Title Page (Page 1) should consist Title of the Article, name of the author (s) / corresponding author (s), institutional affiliation, telephone / mobile number, e mail addresses. It should also consist the source of support, if any, received in any form (grant, equipment, drugs etc.) and word count, number of tables, figures used in the article.
Conflict of Interest: Authors are required to complete a declaration
of competing interest on their cover letter or on separate page. They should also describe their role and participation in designing the study; data collection; analysis; interpretation of data; writing of report and / or in decision to submit the report for publication.
Acknowledgements: Acknowledge to them who have been involved
/ contributed substantially in conception, design, data collection, interpretation of data or any other significant contribution in study.
b. Page 2 should consist only title of the study abstract and key words (up to 6 key words).
For more details about manuscript preparation “Publication Manual of American Psychological Association (6th ed.)” can be consulted (also visit www.apastyle.org).

iv
AbstractAbstract up to 250 words should be given on
page 2 of the manuscript and must include: Aims / Objectives: A brief about the purpose of the study. Method: description of the data (e.g. N, age, sex, SES. etc) briefly procedure, tools used, statistical procedure, etc. and Results.
Abstract must communicate the glimpse of the study.Key Words
After the abstract, authors should provide key word (5-6 in numbers) which mainly deals with the study.
c. Page 3 should contain the actual article beginning with title, introduction and ending with references.
INTRODUCTIONProvide a context for the study. Focus on the
theoretical origin of the problem and its nature and significance in present scenario. Also deals with existing knowledge of present day.
METHODIncludes Aims/Objectives, Hypothesis, source
of population and selection criteria, participants, tools and techniques used. This section of each empirical report must contain the description of participants, detail description of measure used for study and statistical procedure applied. Statistical procedure should be described with enough detail by emphasizing the procedure used for processing the data including software package and its version. Statistical reporting must convey clinical significance. Author should report descriptive statistics for all continuous study variable and effect sizes for the primary study findings. Authors submitting review articles should describe the method used for locating, selecting, extracting and synthesizing data.
RESULTSAfter processing the data, obtained values to be
presented in table/graphic form or in illustrations. This should include the demographic correlates and study variables.
DISCUSSIONThis section should focus on the discussion of
the findings in the light of currently available literature whether supporting the results or contradictory. Findings to be concluded and limitation, implication of the findings on current clinical or academic set up and future direction should also be delineated clearly.
REFERENCESReferences should be listed in alphabetical
order as per guideline delineated in APA Manual. Each reference presented in reference list must appear in the text and references cited in text must be present in reference section. Some examples for citation of references are as under.
a. Article from Journal Singh., R. S., & Oberhummer, I. (1980).
Behaviour therapy within a setting of karma yoga. Journal of Behaviour Therapy and Experimental Psychiatry,11, 135-141
b. Journal Article in Press Kharitonov, S. A., & Barnes, P. J. (in Press),
Behavioural and social adjustment. Journal of Personality and Social Psychology.
c. Conference Proceedings Published Jones, X. (1996). Prevalence of Mental &
Behavioural disorder. In Proceedings of the First National Conference of World Psychiatry Association, 27-30 June; Baltimore. Edited by Smith Y. Sumeham: Butter \vorth-Heinemann; pp. 16-27.
d. Book Chapter or Article in Edited Books Singh, A K., Mishra, R S., & Banerjee, S
(2012). Pattern of perception of mental illness in North America and Central India : A cross cultural study. In Hutton, J., Devika, N., Mohd, S H., & Robert, L S. Perception of Mental Illness Across the Globe. (Pp 456-479), Print Vision Press, India.
f. Entire Issue or Special Section of Journal Ponder, B., Johnston, S., & Chodosh, L. (Eds.)
(2006). Innovative oncology. In Breast Cancer Research, 10, 1-72.
g. Whole Conference Proceedings Smith, Y. (Ed) (1996). Proceedings of the
First National Conference of World Psychiatry Association, 27-30 June : Baltimore. Edited by

v
Stoneham : Butterworth-Heinemann. Pp 16-27.
h. Complete Book Margulis, L. (2005) Cognitive Sciences. New
Haven: Yale University Press.
i. Monograph or Book in a Series Gupta, S.C., & Sethi B.B. (1987). Psychiatric
Morbidity in Uttar Pradesh. Monograph of Culture & Society, 10 (1, Serial No. - 25).
j. Technical & Research Reports Shankar, M., Dutta, K., & Tiwari, A. K. (1995).
Mental Health in Schools (DGHS Publication No. 10, 2), Delhi. Govt. Printing Press.
k. Ph. D. Thesis Kohavi, R. (1995). Psychosocial function in
diabetics, Ph.D. thesis. All India Institute of Medical Sciences. New Delhi.
I. Link/URL Morse, S.S. (1995). Factors in the emergence
of infectious diseases. F merg Infect Dis [serial on the Internet] Jan-Mar [cited 1996 Jun 5); 1(1). Available from: URL: http://www.cdc.gov/ncidod/EID/eid.htm.
TABLES AND ILLUSTRATIONS Table should be clearly prepared and double
space typed with proper margin, presented on separate sheet. All table should be numbered and the same must appear in text (e. g. table number .... to be inserted here). Each Table must carry brief title. Avoid long and multiple box / table. Sample is as under :
Conditions Schizo (n=30 Normal (n=30) t
Mean SD Mean SD
Visual 1.7 0.94 0.7 0.01 0.45**
Auditors 3.0 0.02 2.6 0.96 0.11*
p< 01*, p<001**Graphic files (figure) of good quality/ digital
print is required to be submitted in JPG or TIF format by hiding identity in case of person or place of importance.
For further details for preparation of manuscript, tables, figures, references, metrics authors are advised to consult Publication Manual of the American Psychological Association (6th ed.) or can also visit to www.apastyle.org.
MANUSCRIPT SUBMISSION Two sets of Manuscript, neatly typed in
double space, printed on one side on the paper of good quality along with soft copy (CD) should be submitted to the Editor, IJCP on address given below. Cover Letter, Declaration, Ethical Committee Approval and Letter of Conflict must be enclosed.
NB: After the receipt of the manuscript by editorial office it is mandatory to be reviewed by board of reviewers which may take time. Authors are requested to give some grace period to editorial office. As soon as the opinion / comments of the reviewer will be received by the editorial office, same will be forwarded to corresponding author. In case, manuscript is not found suitable for publication in IJCP, will not be returned to the Author. However, if some author is interested to take their manuscript back, need to send the Self Addressed and Stamped Envelope to the editorial office with request letter for taking manuscript back.
All Manuscript must be Submitted to:Dr. K. S. SengarEditorIndian Journal of Clinical Psychology.Additional Professor, Department of Clinical PsychologyRINPAS, Kanke, Ranchi – 834006Jharkhand (India)Mobile. : 91 94317 69001, 91 95700 93721
Submission of manuscript can also be done through mail on [email protected]

vi
INDIAN JOURNAL OF CLINICAL PSYCHOLOGY
The Indian journal of Clinical Psychology is an official publication of Indian Association of Clinical Psychologists. It is peer reviewed journal published biannual in the month of March and September. It was started in 1974 and is being published regularly.
The journal has long circulation amongst the various professionals like Clinical Psychologists, Psychiatrists, Psychiatric Social Workers and others who have interest in the area of mental health.
Journal publishes Research Articles, Review Articles, Case Reports, Book Reviews, Brief Communication and Letters to Editor. The journal encourages the articles related to theory based interventions, studies that investigate mechanism of change, effectiveness of treatment in real world setting. Journal also accepts the articles in the area of Women, Child & Adolescents and Community Mental Health. Articles related to epidemiology, critical analysis and meta analysis of treatment approaches, health care economics etc. are also accepted.
Journal is registered with Registrar of News Papers of India (RNI 26039/74) Subscription Institutional IndividualIndia Rs. 2000 per year Rs. 1000 per yearOverseas U.S. $ 200 per year U.S. $ 100 per year
Terms & Conditions/Mode of Payment: Payment should be made by multi city Cheque or Demand Draft, drawn in favour of the Editor, Indian Journal of Clinical Psychology, payable at Ranchi and to be sent to : Dr. K.S. Sengar, Editor, IJCP, RINPAS, Kanke, Ranchi - 834 006 (Jharkhand) INDIA. Payment can also be made online on following details:Name of Benificiary: Editor Indian Journal of Clinical PsychologyAccount No: 20993931473Name of the Bank & Branch: Allahabad Bank, RINPAS Branch, Kanke, RanchiIFSC Code: ALLA0212013 MICR Code: 834010007
Form IVINDIAN JOURNAL OF CLINICAL PSYCHOLOGY, 2017, Vol. 44, No. 1
Statement about the ownership and other particulars about Indian Journal of Clinical Psychology :1. Place of Publication : Ranchi2. Periodicity of Publication : Half-Yearly3. Printer's Name : Annapurna Press & Process, 5, Main Road,
Ranchi (Jharkhand)4. Editor's and Publisher's Name : Dr. K. S. Sengar5. Nationality : Indian6. Address : Department of Clinical Psychology,
Ranchi Institute of Neuro Psychiatry and Allied Sciences (RINPAS), Kanke, Ranchi -834 006 (Jharkhand), INDIA Phone : 91 94317 69001, 91 95700 93721
7. Name and address of individuals & Who own the Journal & partners or share holders holding more than one percent of the total capital. : Indian Association of Clinical Psychologists
I, Dr. K. S. Sengar, hereby declare that the particulars given above are true to the best of my knowledge and belief.
The information published in the journal reflects the views of the author and not of the journal or its editorial board or Association. Author will be solely responsible for the information presented herein and its accuracy or completeness. Journal represent that the information is presented herein is complete and accurate and not responsible for any errors or omission.
The copies of the journal to members of the association/subscribers are sent by ordinary post and editor or editorial board will not be responsible for non delivery of the journal. However, for ensured delivery of the journal it is mandatory to request the editorial office to send the journal by registered post or speed post by paying the necessary postal charges for speed post or registered post.
Claims for missing issues will be serviced without any additional cost. However, the claims must be made within stipulated period (2 months after the publication of journal).
All communication to be made on [email protected]

1
Indian Journal of Clinical Psychology2017, Vol. 44, No. 1, 1-5
Copyright, 2017, Indian Association ofClinical Psychologists (ISSN 0303-2582)
Editorial
Clinical Psychology beyond Mental Hospitals: Changing Role of Clinical Psychologists
K S Sengar“Psychology has a long past but short history”
quoted long back. Since the time of origin of life in planet understanding of behaviour/ psychology of individual remained the subject of interest and curiosity, either in structured or unstructured form. Since beginning, the psychology was functioning either as independent discipline or along with some other discipline as philosophy, physiology / neurophysiology, medicine etc.. But behaviour was always the subject of study either as the part of philosophical thoughts / concepts or the form of religion, belief and culture etc. It was not only remain confined to study the behaviour of human being rather psychological phenomenon was studied in behaviour of animals, plants and many more areas. The great Indian epics Mahabharata, Ramayana and also Quran, Bible etc. excellently narrate all the psychological phenomenon in relation to behaviour, characters and traits individual bears and also predict the behaviour thoughts and feelings of individuals on the basis of categorization they had made. They also guide for the remedial measures to eliminate the sufferings which are psychological in nature. Though, the psychology has long history since the time of philosopher physiologist Descartes (1596-1650) who significantly impacted the psychological thinking with his two important contribution by arguing that (1) animals are automata, that they act like machine, and that man do too in their irrational conduct. He further argued that “if you knew enough about the nervous system you can make a mechanical or electronic robot who could act and think like a man”. (2) Descartes second argument is that 'soul and body, consciousness, and nervous system' are quite separate (dualism) and forming different worlds which nevertheless interact, rather affecting each other”. This conceptualization of Descartes lead to modern common sense notion that mind is something within the head taking up no separate space of its own and responsible for thinking, controlling the actions of body and sending/ passing the set of information from one to other (Boring, 1948). These concepts further lead to study the concept of brain behaviour relationship (S-O-R) and germinated the roots of behaviouristic thought/school.
In first part of 19th century physiology was growing as a separate discipline of science. During this era some of the physiologists developed the
interests what are really the psychological problems. The pioneer are the Muller (1801 – 1858), known as father of experimental physiology postulated the thought that excitement of particular nerve is based on nature of sensory quality, and the same idea in long run converted in today’s behavioural neuropsychology which deals with physiological arousal in the brain leading to different types of behavioural and emotional manifestations in the individual. Transformation of thought from physiological perspective of nerve excitement solely depends on the intensity of stimuli to interpretation of human behaviour took enough time and multiple significant researches had contributed during this phase to understand the brain behaviour relationship. After the establishment of experimental laboratory by Wilhelm Wundt at Leipzig in 1879 the formal study of human behaviour was started in laboratory in structured form.
Even before Psychology became a science, people practiced- some form of psychology, thus providing some relief for psychologically distressed individuals, but under several different labels, such as phrenologist, physiognomist, graphologist, mesmerist, spiritualist, psychic, mental healer, seer and many more (Benjamin Jr., 2005). However, the problem was that no laws existed at that time to regulate the practice of these people, no professional standards to regulate the training of these individuals and to ensure competence, no laws to even protect the public from fraudulent practices. Everybody did what they liked. The field of Clinical Psychology on the contrary is governed by rules and regulations. There are standards of practice which also include regulation of training and professional ethics to ensure competence and the protection of the public. Clinical Psychology is also driven by research.
It was Lightner Witmer who was adventurous enough to venture into the assessment, diagnosis and treatment of abnormality in 1896 when he established his Psychological Clinic, where he treated children with learning disabilities and behaviour problems and in 1907, published his first journal in which he published his case studies from his clinic. It was in this journal that he coined the term ―Clinical Psychology which marked the beginning of the field of clinical psychology; a sub field of psychology. “Clinical Psychology discipline involves the provision of diagnostic assessment,

2
K. S. Sengar / Clinical Psychology beyond Mental Hospitals ...............................
evaluation, treatment plan, treatment, prevention, and consultative services to patients of emergency room, inpatient units, and clinics of hospitals (Benjamin Jr, 2005). Overall, the field of clinical psychology integrates science, theory and practice to understand, predict and alleviate maladjustment, disabilities, and discomfort as well as to promote human adaptation, adjustment, and personal development. It, therefore, focuses on the intellectual, emotional, biological, psychological, social, and behavioural aspects of human function in different cultures and at all socioeconomic levels.
The growth of clinical psychology can be traced to the first and second world wars in which clinical psychologists were engaged in treating-shell shock or Post Traumatic Stress disorder in victims at army hospitals. Today, the field of clinical psychology has grown so much that it also has other subfields, include; clinical health psychology, clinical neuropsychology, psychoneuroimmunology / psychoneuroendocrinoimmunology, clinical forensic psychology, clinical child psychology, psycho-oncology, clinical geriatric psychology among others. Roles of Clinical Psychologists in Health care to assess, diagnose, predict, prevent, and treat psychopathology, mental disorders, and other individual's or group problems to improve behaviour, adjustment, adaptation, personal effectiveness, and satisfaction. Clinical psychologists also do research and teach in schools. The relevance of the clinical psychologists in the health sector cannot be underestimated.
In India,beginning of today’s Clinical Psychology as profession is credited to Dr. Girindrasekhar Bose (1886-1953). After obtaining his MB degree from Calcutta Medical College in 1910, he started practicing medicine and during his practice he developed the interest in Psychology. After obtaining M. Sc. in Psychology from Calcutta University in 1917 and subsequently D. Sc. in Psychology from Calcutta University in 1921 (First Doctorate in Psychology) on the thesis “The Concept of Repression” which was published in book form before the translation of Freud lectures in English. This book attracted the people worldwide and appreciated by then luminaries of psychology. Dr. Bose developed his interest in understanding of human behaviour and focused on the extensive need of the knowledge and deeper understanding of human behaviour. He started the experimentation and research in human behavior in department of experimental psychology (1st Dept. of Psychology in India), Calcutta University. Dr. Bose had become interested in Psychoanalysis and was in correspondence with Freud. He formed the Indian
Psychoanalytic Society in 1921 which was recognized by International Psychoanalytic Society in 1922. He was accepted as a Psychoanalyst; and was only to achieve this status beside Freud and Ernest Jones without being analyzed themselves. The Indian Psychoanalytic Society attracted to medical doctors, psychologists and other educated persons for the knowledge and training in psychoanalysis. He emphasized the culture specific therapeutic module e.g., guru- shishya system of therapy (Prabhu GG, 2001a).
The recommendation of utilization of clinical psychologist’s services in diagnosis and management of psychiatric patients was made first time in India in 1920 by Indian Psychoanalytic Society which was headed by Dr. Bose. After this recommendation Dr. Berkley Hill then Superintendent of European Hospital, Ranchi (presently Central Institute of Psychiatry) who was analyzed by Freud and was second analyst in India after Bose, made psychologists part of team involved in diagnosis and management of psychiatric patients (Hartnack, 2001; Bose, 1931).
Advances in psychological, medical, and physiological research have led to a new way of thinking about health and illness. This is reflected in the biopsychosocial model that views health and illness as the product of a combination of factors including biological characteristics (e.g., genetic predisposition), behavioural factors, (e.g., lifestyle, stress, health, beliefs) and social conditions (e.g., cultural influences, family relationships and social support). This conceptualization of health and illness has many scientific and practical benefits. At the top of this list is the fact that people can reduce their risk of developing major medical problems, receive more effective treatment, and reduce their health care cost when they seek treatment from an interdisciplinary team including behavioural health service providers (clinical psychologist). Because behaviour plays a vital role in mental and physical health and now a days behavioural health is becoming the cornerstone of the biopsychosocial practice. Behaviour may positively or negatively affect the body by stating that lifestyles, life-events, and bad behaviour are directly related to health and illness; the way we think about events determines our response to them in developing healthy or unhealthy behaviour and changes in behaviour. Attitudes to health determine whether we hear or listen to advice from health professionals, and a person's personality may predispose the body to certain dysfunctions (Prabhu GG, 2001b).
Physicians often have difficulty to understand some behaviour of people visit to them for consultation - 'why people behave differently when they know the negative effect of smoking or drinking, why they are

3
K. S. Sengar / Clinical Psychology Beyond Mental Hospitals...........
reluctant to manage the stress, change life style and not serious about children's problems, why patients do not come to see me when nothing wrong or when something wrong. Why don't they visit timely to see me to prevent or treat the sufferings, they visit to me only when some thing is seriously wrong'. These questions can easily be answered by the clinical psychologist. Since psychism and human behaviour are complex and central in field of life, the role of clinical psychologist becomes more wider in health care system. The relevance of clinical psychologist in health care system is further highlighted by the fact that, it is now recognized that psychological issues play a crucial role in almost every health care condition, and that addressing these issues will increase well-being and quality of life. According to WHO one person out of Four is in psychological distress. Eight out of ten of the top causes of death have psychosocial components in their etiology and/or maintenance. Forty-five per cent of all causes of death are cardiovascular in nature (which is often stress-related). Sixteen out of twenty of the most frequently diagnosed conditions in primary care have some behavioural component which could be amenable to intervention by clinical psychologists. Approximately three million people world-wide die each year from a tobacco-related disease. Also, the growing diseases of civilization [cancer, coronary heart disease, stroke etc.] are mediated by social isolation, obesity and substance abuse. Chronic conditions are the main focus of health care (Sarfo, 2014). All these suggest that psychological issues must play an increasingly central role in the provision of health care in all types of settings, from primary care to specialist centres. Clinical psychologists are therefore needed to help to increase the range of treatments offered to patients
Clinical psychologists are mental health professionals and usually render services through mental health units and psychiatric hospitals. they also deal with the behavioural dimensions of the physical health and illnesses. They provide the clinical and health services to both inpatient and outpatient units as well as to patients who function independently and to new patients who need evaluation. They provide a variety of psychological interventions such as cognitive behaviour therapy; behavioural modification; family and couple therapy; biofeedback; rehabilitation; group psychotherapy; psychoanalysis; client-centered therapy; pain management; neuropsychological rehabilitation; interpersonal psychotherapy etc.
Researches across the world have indicated that substantial number of (approx. 25%) physical
complaints presented by the patient have no known or demonstrative organic or biological signs and these physical or medical symptoms presented by patients are unexplained medically (functional symptoms) that respond well to the psychological intervention. Therefore, psychological interventions are effective for the improvement of physical and mental health and the quality of life. Clinical psychologists also provide psychological consultation for health care professionals, businesspersons, schools, organizations, communities etc. For example, a competent clinical psychologist may help a physician to better manage noncompliance with unpleasant medical procedure. A businessman may consult a clinical psychologist to help to reduce conflicts among workers or provide stress management training. Clinical Psychologists’ consultation might include assessment, teaching, research, and therapy.
Many a time person comes in outdoor medical clinics with sick role in order to get attention from health practitioners. Such cases becomes difficult to diagnose and manage and at the same time they also put unnecessary burden on health care system. If clinical psychologists are employed, they can identify such people and separate them from those who really need medical care and manage them those need the psychological care. People suffering from chronic and terminal illness such as sickle cell anaemia, diabetes, cancer, HIV/AIDS etc. along with medical condition, also have psychological problems such as depression, anxiety and suicidal tendencies which are associated with their medical problems can be handled better by a clinical psychologist and their psychological needs could be met effectively. Aside the psychological needs, these people need to live with the consequences of their illnesses and the clinical psychologist can help them to manage these consequences by helping them with pain management and coping skills training so as to increase their functional abilities and to develop a wide range of methods of ensuring social and vocational engagement and support for them. This would go a long way to improve their quality of life considerably. It has also been established that certain medical conditions are mediated by psychological factors, for instance; Irritable Bowel Syndrome, Dysmenorrhoea, Obesity, headaches, bruxism, cancer among others, in that psychological factors influence the onset, course, severity, frequency or interfere with the treatment of such conditions (Smith & Nicassio, 1995). These conditions would therefore be successfully treated only if both medical and psychological treatments are used, and the clinical psychologist cannot be left out

4
in this case. Other roles clinical psychologist can play in general medical care include; Pre and post surgery counselling, pre and post natal counselling, care for the elderly and terminally-ill, Stress management and the prevention and adjunct treatment of lifestyle diseases such as hypertension , cardiovascular diseases etc. Mental health of the individual is very complex phenomenon includes multiple etiological reasons e.g., biological, psychological social, environmental, financial and many more. In such conditions it is not possible to deliver complete care by any single agency rather it needs the collaborative and cohesive efforts by medical professionals, clinical psychologists, health workers, nurses, public health engineer and other para professionals. The mental health and physical problems are highly interrelated and affects each other. For the delivery of complete health care the team work of the different professional is required and services of clinical psychologists can be useful in delivering the complete health care to the community.
Clinical Psychologist may also play a major role in in administration as they are experts in understanding and managing human behaviour. In western scenario, clinical psychologists/ psychologists are considered as efficient and competent administrators. Because the understanding of human behaviour in social contexts is considered the backbone of management, therefore clinical psychologists find themselves in administrative positions in hospitals and other residential treatment settings. Clinicians from psychology serve as chairpersons of departments, units, or divisions in hospitals e.g. neuropsychology, mental health, rehabilitation, and occupational health. They could be directors of graduate training programs in mental health, student counselling-psychological centers, hospital outpatient departments, and directors of hospitals. Moreover, they participate in assigned committees and are active members of their departments. In administration, psychologists manage budgets, lead multidisciplinary professional and support staff; they develop policies and procedures for planning and personnel issues etc. Finally, they participate and contribute to all quality management activities of hospitals and other care settings. But in India clinical psychologists are not involved in administration and planning of health care system at any level. In India, clinical psychologists most often do not like to be part of administrative functioning. Generally, they avoid bearing the responsibilities, taking challenges and extra burden except their professional responsibilities of evaluation and therapeutic work of mentally ill
people. They need to develop managerial competence, leadership quality and need to come forward to share the responsibilities either as member of health care planning and delivery system or independently for the good cause of health care delivery (Amool R Singh, 2014). Clinical psychologists need to prepare themselves to share/ own the administrative and financial responsibilities, hold the above positions, if offered. Basic knowledge and skills of accounts, planning and administration need to be developed and duties related to these areas can be performed within profession. They must take the responsibilities to develop and implement the plan and policies in relation to health care system especially mental health. It is important to look that today's life of the individuals' is very complicated and health problems are also becoming equally complicated to understand, diagnose and treat and this health care system can not be run only by hospitals only. Hospitals are already highly crowded/overloaded. Nevertheless, community cooperation and community care has become inseparable segment of health system. In such scenario clinical psychologists can play vigorous role in bridging the gap of community and hospitals through creating awareness about preventive measure for various illnesses and developing the concept of health hygiene community and also in implementing government sponsored health care schemes/program.
A considerable portion of the time of many clinical psychologists who work in medical settings, is spent in academic activities (teaching and training). They teach all courses of psychology, human behaviour and behavioural sciences included in the curricula of undergraduate and postgraduate medical, dental, nursing and other allied health courses as well as psychology students, interns and residents, and also train health professionals.
As a profession, clinical psychology should be represented in virtually every health care delivery system. In United States federal and state health system clinical psychologists / psychologists are recognized as providing needed, valuable and cost effective health services. The USA psychologists, however, are recognized as members of the hospital medical staff with full privileges. They have to provide the psychological care (behavioural health assessments and interventions) to patients with physical diagnosis, rather than just mental health diagnosis. Moreover, some states in USA (like Pennsylvania, California and some more) clinical psychologists have been granted prescription privileges to prescribe psychotropic medications. In this direction, military psychologists of the US Department of Defence
K. S. Sengar / Clinical Psychology beyond Mental Hospitals ...............................

5
K. S. Sengar / Clinical Psychology beyond Mental Hospitals ...............................
(DoD) are prescribing psychotropic medications since years. This initial program (prescription privileges for military psychologists) had been thoroughly evaluated by the American governmental bodies such as Vector Research, Inc., the US General Accounting Office, and the American College of Neuropsychopharmacology. The results were that the program has achieved the primary objective for which it was established by demonstrating that licensed clinical psychologists can be trained to provide safe, high-quality cost-effective pharmacological care. This project is strongly supported by the American Psychological Association that launched a task Force on psychopharmacology to train psychologists as prescribers (Dunivin, 2003).
It is now recognized that psychological issues play a crucial role in almost every health care condition, and that addressing these issues will increase well-being and quality of life. One important role is the prevention of diseases, through behaviour medicine (Ogden, 2000); whereby people can be helped to behave in healthier ways, given that many illnesses or disabilities could be prevented.
There is big query about claims clinical psychologists make for themselves and the actual commitments for delivery system they do. This might be one reason for which clinical psychologists confine their boundaries only up to the psychiatric establishment. This needs to be changed and for that change in training and teaching model, supervision and researches required to improve the competence level at par with other associated professionals/medical branches. The big issue of training, teaching and supervision of clinical psychology as profession in our country, needs to be addressed seriously and course curricula, duration of training, quality of training, available infrastructure in training institutions, needs to be readdressed. the clinical psychologists also need to acquire the training/ knowledge of the other related fields. The clinical psychologists working in other set up (except mental health) especially in association with medicine need to have some basic knowledge of physiology, pharmacology and medicine. Some specialized areas as obstetrics, surgery etc. require much broader knowledge than simply the field of clinical psychology. Learning and cognition now presents with enormous and complex phenomena and the area of cerebral functioning and some organic disorder like aphasias, apraxias, dementias and many more are highly unknown to most of clinical psychologists because of tertiary knowledge of neurophysiology and neuroanatomy. This need to be enhanced to depth and practical exposure of training in neuroanatomy/ neurophysiology required to be given.
So that they can be well equipped with knowledge to understand these complex areas of profession and feel confident in handling these patients with comp;et understanding and competence. The application of social psychology (social cognition) also have the great significance in profession of clinical psychology and so, social psychological concepts are also need to be addressed seriously (Prabhu, 2001a).
There is misconception that clinical psychologists are only meant for the mental hospitals which is due to ignorance about what exactly the field is about. Clinical psychologists can play very vital roles in general medicine, paediatrics, surgery, plastic surgery unit, obstetrics & gynaecology, terminal care units, amputee rehab units, cardiac after care units, oncology units and / or any other non psychiatric areas along with school settings and courts.
Further, the role of clinical psychologist is traditionally known for, - mental health service provider is not limited up to mental health area only, rather the role of clinical psychologist is enormous.
REFERENCESAmool R Singh (2014). Clinical Psychologist and Hospital
Administration. Indian journal of Clinical Psychology, 44 (1), 8-11.
Benjamin, L. T. Jr. (2005). A history of Clinical Psychology as profession in America (And a glimpse at in future). Ann. Rev. Clinical Psychology, 1, 1-30.
Boring, E G., Lensfeild, H S., & Weld, M P. (1948). Foundation of Psychology. John Willey & Sons, New York .
Bose, G (1931). New techniques of Psychoanalysis. International Journal of Psychoanalysis, 12, 387-388.
Dunivin, D., & Southwel, G. (2000). Psychopharmacology training in psychology internship. Professional Psy-chology, Research and Practice, 31, 610-614.
GG, Prabhu (2001a). Indian clinical psychologists of the millennium: the 3 G phenomena. Indian Journal of Clinical Psychology, 28,149-154.
Hartnack, C. Vishnu (2001) Psychoanalysis in Bengal. Psychoa-nalysis in Colonial India. Delhi-Oxford University Press.
Prabhu, GG (201b). Identifying limitation and gaps to the de-velopment of clinical psychology in India (symposium presentation II). Indian Journal of Clinical Psychology, 28, 164-172.
Sarfo, J. O. (2014). Role of clinical neuropsychologist in the evaluation and management of Diabetes Mellitus in Ghana. J. of Advocacy, Res. and Edu., 1 (1), 37-40.
Smith, P,. & Nicassio, P. (1995). Psychological Practice: Appli-cation of biopsychosocial model. In Smith, T., & Nicas-sio, P.: Managing the Chronic Illness. Washington, APA.

6
Presidential Address
Digital Technology and Clinical PsychologyAmool R. Singh
The theme of the conference is apt for the current era of digital technology. Like other disciplines, the technology has influenced the field of Clinical Psychology also. Active use of the technology mainly started during 80s, since then it is expanding day by day. It has influenced education/ teaching/research, assessment and intervention approaches in the form of technology-based educational and research strategies, diagnostic equipment specialization and technology-based therapy / rehabilitation.
Technology has made recording system easy, sustainable and accessible. Data-base is created easily and it can be shared with concerned persons and authorities in time-effective and cost-effective manner. It has boosted up research and comparison of data from various sources. Easy accessibility of database and research inputs have paved the way for systematic research. With the help of technical support, the quality of teaching and training have improved. Recording devices provide opportunities for later analysis of data, analyzing it more objectively and data remains available when and where required.
Today in my address, I will delineate the application of technology in the core domains of Clinical Psychology i.e., assessment, therapy and research. It will be followed by a realistic evaluation that how far one can be dependent on technology.
ASSESSMENTStarting with assessment, the role of technology
has increased in this field in last three decades exponentially. Be it assessment of cognitive functions, personality or any other specific clinical constructs, we have tools that can be administered and interpreted with the help of computers. For example, there are neuropsychological batteries like CANTAB which can be administered, scored and interpreted (with the help of international database)using computer. Even testes like Luria-Nebraska Neuropsychological Battery which depends extensively on bed-side clinical examination procedures, can be scored and interpreted within seconds with the help of software. Likewise, now-a-days, most of the personality tests
are computer administered. There are softwares for MMPI, MCMI and various other internationally acclaimed personality assessment tools. Even there are attempts to develop computer versions of interpretation of Rorschach test.
At this juncture, I would like to have a specific mention of the domain of the fields of Clinical Forensic Psychology and neuroscience in context of Clinical Psychology. In the area of forensic psychology, there are tools that assist in predicting recidivism (likelihood of repeat offending), detection of deception through Autonomic Nervous System and Central Nervous System indicators and so on. Likewise, EEG, fMRI and other such technologies have enriched our understanding of brain-behaviour relationship.
THERAPYTraditionally, psychotherapy is a face-to-face
interaction with a client (or a group of clients) and therapist. However, technology has blurred this boundary significantly. Thus, there are internet and telephone based therapy protocols and practices, therapies using Virtual Reality (VR) technology and so on. All sorts of therapy paradigms and client population have been tried using these methods and often they have been found to be effective. In a meta-analysis, internet-based therapies have been found to have medium effect size which matches with the average effect size of traditional face-to-face therapies (Barak et al., 2008).
Of late, VR technology based therapies are being extensively tried. In VR technology based therapy, the patient is provided an immersive environment in which he goes through therapy process with the help of virtual situations and even therapist. For example, Avatar therapy has been developed for auditory hallucination in which the patient enters into dialogue with his virtual avatar which gradually assists him in understanding and controlling the hallucination (Leff et al., 2014). Likewise, there are VR based therapies to treat phobia and PTSD. Telephone- based interventions and telephonic helplines are also being used for providing clinical services effectively.
Prof. of Clinical Psychology & Former Director, RINPAS, Kanke, Ranchi Presidential Address was delivered in Inaugural Function of 43rd National Annual Conference of Indian Association of Clinical Psychologists held at Coimbatore, Tamil Nadu on Jan. 27-29 2017. E-mail : [email protected]
Indian Journal of Clinical Psychology2017, Vol. 44, No. 1, 6-8
Copyright, 2017, Indian Association ofClinical Psychologists (ISSN 0303-2582)
7
Computer based intervention offers excellent platform for psychotherapy process research. The intervention may be specified, and if administered by trained professionals, human variability and error do not affect the operation of the programme. Thus, the process becomes standardized and is provided uniformly. It also facilitates evidence-based research.
Apart from these, technology has substantial role in psychotherapy training. Thomas Berger (2004) described technological applications in psychotherapy training. He distinguished between:
• An objectivistic approach with an emphasis on tools facilitating the passing of information from teachers/ trainers to trainees. The emphasis here is on declarative knowledge and on learning contents.
• A constructive approach with an emphasis on supporting active information processing taking place within trainees, that is, rather on processes and on using contents in processes than on contents themselves.Computer-based therapeutic interventions
are gaining acceptability and promising evidences have been provided by researchers mainly for use of psycho-educational materials, cognitive behaviour therapy, cognitive rehabilitation etc. Studies comparing computer-based intervention and face-to-face CBT suggest that gains of both intervention strategies may be comparable. Telephone- based interventions and telephonic helplines are also being used for providing clinical services effectively. Computer-based interventions have been mainly used for depression, anxiety and addiction etc. However, studies are also available that suggest advantage of face-to-face therapy over computerized intervention. For example, a study by Stoner and colleagues in 2015 on mobile phone intervention for improving drug compliance concluded that it is feasible to implement mobile phone intervention, however, text message reminders were not effective for adherence.
RESEARCHResearch requires objectivity and replicability
and technology has made these requirements more easily attainable. Computers and softwares decrease the confounding effect of human variability in any assessment procedures. Thus, a given tool is administered in same way (in terms
of time, stimulus presentation rate and so on depending on the requirements of a given research) to all the participants. Further, sophisticated statistical softwares such as SPSS have made the statistical analysis of the data pretty easy. Also, some sophisticated research; for example, the neurobiological effect of psychotherapy, neural changes after cognitive remediation and so on have become possible only because of the availability of sophisticated technologies such as fMRI and PET.
ADVANTAGES AND DISADVANTAGESVarious advantages and disadvantages of
technological development have been delineated by Franz Caspar in 2004.
The technology has specific advantages in the sense of requiring no or limited personal contact when the physical access to a suitable therapist is particularly difficult, especially for handicapped patients. It has made easier access for the underprivileged. People with limited resource and limited possibilities of direct, physical contact may also be benefitted.
Convenience in this context mainly means that technical applications allow consumers to choose the time, location and circumstances under which they access and use clinical services. Inhibited patients, patients having problem in face to face communication may find it more comfortable. In face to face intervention setting, clients need to respond immediately, however, response may be delayed in computer-based technologies. The possibility of not having to respond immediately, may give clinicians as well as client an advantage whenever necessary reflection is limited or threatened by the perceived need of reacting immediately in natural conversation. Thus, telepresence facilitates communication and gives opportunity for delayed response. Because of access to computer-based database and limited need to access to services physically, technical applications give, in one form or other, access to best experts for the respective problems.
Along with consumers, it is convenient for service providers as well. Providing psycho-educational information and other routines may be carried out by technological assistance and the clinician can concentrate on more subtle tasks which actually require human involvement thus preventing burnout from excessive routine.
Amool R. Singh / Digital Technology and Clinical Psychology

8
Further, replication of stimuli or problem-solving situations is a major advantage of using machines.
However, there are various limitations also that we should keep in mind.
• In administering interventions using technology, computer-based skills are required from the provider’s side. Clinician have been trained over many years to value the ‘human connections’ and talking in contrast to technical applications. Hence, new skills should be developed.
• Clients also require skills related to use of technology. Moreover, those who need the service most may not have access to computers. There may subjective barriers in using computer-based technologies. Clinicians in face to face situations may have a special appeal for many clients while technical applications are lacking such an appeal.
• In many situations missing nonverbal signs in communication may induce misunderstanding or communication gap.The delay in therapist answers may be a subjective as well as objective disadvantage. Delay responses from side of service providers and consumer has limitations in situations requiring crisis intervention.
• Clients may develop adaptability to devices however, there is risk of dependence on devices. Technical application may seduce incompetent providers to offer services they could not provide based on their personal competence.
• Ethical problems are related to the equal access to applications, to a possible monopolization of services, to the risk of cultural imperialism.Legal problems are not only related to data protection but also to qualification/ certification of service providers across state and national borders and to copy right issues.
INDIAN CONTEXTWhile translating western experiences in
Indian context, we should be careful and sensitive in considering socio-cultural aspects and infrastructure limitations. Although people have access to various technology, however, its use is still limited in India.
Few telephonic helpline services are available in India, however, it is not being used to its maximum potential. Sensitization and awareness programmes
are required for disseminating information about various programmes and educating public for accessing such services.
Legal and ethical guideline for professional practice should be developed so that service providers are answerable to the system.
Moreover, our training curriculums are designed focusing of face-to-face psychological services. Hence, training manuals for providing technology-based services, short-term courses for qualified mental health professionals, and workshops for first-hand experience should be conducted to develop expertise in clinicians.
CONCLUSIONTechnology is playing role in all spheres of
life and our profession is not an exception. It has tremendous potentials in terms of making services available to mass, overcoming the difficulties caused by distance, time and so on. However, as in any other field, we must remain cautious about the blind use of technology. It must be used judiciously so that the need for empathic relationship and the enormous effects of human bonds are not neglected. Any technology has potentials to bring metamorphic changes provided there is human touch!! Furthermore, never forget that “technology is a good servant but a bad master”.
REFERENCESBarak, A., Hen, L., Boniel-Nissim, M., & Shapira, N. (2008).
A comprehensive review and a meta-analysis of the effectiveness of internet-based psychotherapeutic interventions. Journal of Technology in Human Services, 26 (2-4), 109-160.
Berger, T. (2004). Computer-based technological applica-tions in psychotherapy training. Journal of Clinical Psychology, 60 (3), 301-315.
Caspar, F. (2004). Technological developments and applications in clinical psychology and psychother-apy: Introduction (Editorial). Journal of Clinical Psychology, 60 (3), 221-238.
Leff, J., Williams, G., Huckvale, M., Arbuthhonot, M., & Leff, a. P. (2014). Avatar therapy for persecutory auditory hallucinations: What is it and how does it work. Psychosis, 6 (2), 166-176.
Stoner, A. A., Arenella, P. B., & Hendershot, C. S. (2015). Randomized controlled trail of a mobile phone intervention for improving adherence to naltrexone for alcohol use disorders. PLoS One, 10(4):e0124613, doi:10.1371/Journal.pone.0124613.e collection 2015.
Amool R. Singh / Digital Technology and Clinical Psychology

9
Indian Journal of Clinical Psychology2017, Vol. 44, No. 1, 9-13
Copyright, 2017, Indian Association ofClinical Psychologists (ISSN 0303-2582)
Challenges Concerning Adolescent Mental Health In India*P. T. Sasi
Cang Oration
I consider myself very fortunate to be among this August gathering of beloved teachers, class mates and batch mates of older times, younger and elder members of our psychology family, to deliver the Kang Oration. I am thankful to chair person and the members of the award committee for giving me the opportunity to deliver this oration, instituted by Dr. Gurminder Sahasi, a Senior Clinical Psychologist in the fond memory of her father, C. S. Kang. The topic that I have selected for my presentation is ‘Challenges Concerning Adolescent Mental Health in India’.
Adolescent Population in India: In India, children in the age category of 10- 19
Years, constitute 21 % of the total population. Every 5th person in the country is an adolescent. State wise UP has the largest share of adolescent population (24.25%) and Kerala has the lowest rate (16.2%). Similarly India has the largest adolescent population (20%) in the world (Sivagurunathan et al, 2015).
Adolescent Health Problems:Road traffic injuries were the leading cause of
death among adolescents (WHO, 2014). About 15% of global maternal death occurs among adolescent girls (Abouzahr, 2013). Injuries and neuropsychiatric disorders were the major issues in adolescents. There is an increasing trend in adolescent obesity due to great shift in diet and activity pattern (UNICEF, 2012). Half of all mental health disorders in adulthood starts by the age of 14 years, and most of the cases are either undetected or untreated. In the South East Asian Region (SEAR), Unipolar depressive illness in females, and road traffic injuries in males were the major health issues and it remains at the top throughout the years. AIDS has emerged as third leading cause of Disability Adjusted Life Years (DALY) in the last decade (WHO, 2014).
Adolescent Health Problems in India:Even though India has the largest adolescent
population in the world, there were few studies done on the prevalence and various other aspects of adolescent health problems in India.
Sexual and Reproductive Health Problems:2.7% of boys and 8% girls reported sexual
debut before the age of 15 and most of the sexual activity happens in the context of marriage, this
leads to early pregnancy due to social pressure (IIPS, 2007).
NFHS-03 shows steady increase in the percentage of 1st pregnancy among adolescents. Early marriage and low contraceptive usage are the reasons behind this trend. Early marriage carries the risk of subjecting girls to physical, emotional and sexual violence (Ganchimeg, 2014). Similarly awareness regarding transmission of STI is low among adolescents. Due to inadequate knowledge adolescents are at greater risk of exposure to unprotected sex, unethical sexual practice and STI. In the age group of 15 - 19 Years among those who had sexual intercourse, 10.5% of girls and 10.8 % of boys reported having STI or symptom of STI and 0.07% of girls and 0.01% boys were found to be HIV+ve (IIPS, 2014).
Problems Related to Food Habits:Studies indicate that 2.4% adolescent girls and
31.7% boys were overweight and 2/1000 adolescent girls and 1/1000 adolescent boys suffer from diabetes. They are also highly prone for eating disorders like anorexia nervosa or binge eating due to body dissatisfaction and depression (Sivagurunathan, 2013). A study from Chennai done in the age group of 11 to 17 years shows that, 90% eat either food or snacks while watching TV, 82% buy food products and snacks based on advertisement, 59% skipped outdoor activities for TV (Priyadarshini, 2013). Television viewing in childhood and adolescence is associated with overweight, poor fitness, smoking and raised cholesterol in adulthood.
Adolescent Psychiatric Problems:There is mounting evidence that many, if not
most, life time psychiatric disorders will first appear
*Chief Consultant Clinical Psychologist, Sun Medical and Research Centre, Thrissur, Kerala. Email: [email protected] was delivered in 43rd National Annual Conference of Indian Association of Clinical Psychologists held at Coimbatore from Jan 27-29, 2017.

10
in childhood or adolescence. The median prevalence estimate of functionally impairing child and adolescent psychiatric disorders is 12%, although the range of estimate is wide. Disorders that often appear first in childhood or adolescence are among those ranked highest in the World Health Organization estimates of the global burden of disease (WHO, 2014., UNICEF, 2014). Mortality and morbidly due to mental health problems in the adolescents increased and topped in recent years. Prevalence rate of adolescent psychiatric disorders in the community has been found to be 6.46% (Rani & Karunanidhi, 2010., Patel, et. al., 2013., Malhothra & Patra, 2014). Anxiety disorders, Depression, ADHD, and behaviour disorders including Anti social behaviours are common. Substance induced mood disorder, internet addiction, social media addiction, cyber sex addiction etc are on increase.
Suicide:In India suicide among adolescents is higher
than any other age group. 40% of suicide in men and 56% of suicide death in women occurred in the age category of 15-29 years. 4% of adolescent shows suicide behaviours, females are 4 times more prone than males. Suicidal behaviour is associated with absenteeism, independent decision making, premarital sex, unfulfilling wishes for vehicles and high cost phones, academic problems and mental disorders (Pillai et al., 2009., Patel et al., 2012).
Road Traffic Accidents:Road traffic injuries emerged as a leading
cause of death among adolescents. Rash driving, driving without license, drunken driving and use of mobile phones while driving are factors associated with road traffic injuries in young drivers. In India in 2001- 2003 deaths due to unintentional injuries constituted nearly 20% of the deaths in 15- 29 age group (Jagnoor et al., 2005).
Sexual Abuse:A statement released by Louis- Georges
Arsenguir, UNICEF representative to India, states “It is alarming that too many of these cases are children. One in three rape victims is a child. More than 7200 children including infants are raped every year; experts believe that many more cases go unreported.
Tulir- CPHCSA’s study in 2006, conducted
among 2211 school going children in Chennai, indicates a CSA prevalence rate of 42%. Children of all socio-economic group were found to be equally vulnerable. While 48% of boys reported having been abused, the prevalence rate among girls was 39%. 15% of both the boys and girls were severely abused (RAHI, 1998., TULIR- CPHCSA, 2006). In 2007, the Indian government backed a survey of 12500 children in thirteen states, of the children interviewed, more than half (53%) said they had been subjected to one or more forms of sexual abuse. Over 20% of those interviewed said they were subjected to severe forms of abuse. Of those who said they were sexually abused 50% were boys. Mostly victims suffer in silence because of fear and social stigma. Sexual abuse indirectly affects the physical health, mental health, sexual health, academic performance and personality (Paras et al., 2009).
Substance Abuse:The use of alcohol, nicotine and illegal drugs
among adolescents has shown significant increase throughout India over the past few years. 44% of under- graduate students in the age group of 17 to 19 years had already initiated alcohol consumption out of these 79% are boys and 21% girls. Beer is the most frequently consumed alcoholic beverage by boys and girls. Among students studying for Medicine and Engineering 24% smoke cigarettes and 29% drank alcohol and 11% abuse cannabis regularly. Initiating cannabis at this age is strongly associated with the development schizophrenic spectrum disorders in adulthood. A study conducted in Kerala in the year 1986 found substance abuse starts at the age of 19 years, when it repeated in 1990’s it has come down to 17 years, and of late we come across children studying in 6th and 7th standard are abusing various substances like Panparag, Hans, gum, whitener etc (Ray et al., 2004., Kirmani & Suman, 2010., Anglin et al., 2012., Tikkoo et al., 2013).
Net Addiction:The internet has become basic tool for trading,
entertainment, communication, as well as education in the contemporary world. Internet addiction results in personal, family, academic, financial and occupational problems that are characteristics of other addiction. Many persons who attempt to quit their internet use experience withdrawal
P. T. Sasi / Challenges Concerning Adolescent Mental Health In India

11
including anger, depression, mood swings, anxiety, fear, irritability, sadness, loneliness, boredom, restlessness, procrastination and upset stomach. Being addicted to the internet can also cause physical discomfort or medical problems such as, Carpal Tunnel Syndrome, dry eyes, backaches, severe headaches, eating irregularities, decreased personal hygiene and sleep disturbance (Byun et al., 2009., Moreno, 2011., Moreno et al., 2013., Cheng, 2014).
Social Media Addiction: Social net working sites such as Face
book and Twitter are now used by 1 in 4 people worldwide. Social media is delivering reinforcement every time when a person logs on. For those who post status updates, the reinforcement keeps coming in the form of supportive comments and likes. So it becomes hard for a person who has developed this habit to simply stop. This behaviour can lead to FB addiction. Social networks are massively addictive among adolescents. Most people check and interact on social sites consistently throughout the day. And they have no idea how much actual time they spend on social media. 95% of teenagers who use social media have witnessed forms of cyber bullying on social networking sites and 33 % have been victims of cyber bulling (Masters, 2015). Similarly face book depression occurs when young users see status updates and wall posts and photos that make them feel unpopular.
Selfie Addiction Disorder:With the advent of smart phones equipped
with high resolution selfie cameras, there is growing tendency especially among adolescents, posting the selfie photographs on social networking sites for comments of friends and others. The Americian Psychatric Association has officially confirmed this behaviour as a mental disorder. APA called this disorder as selfities, and is defined as obsessive compulsive desire to take photos of one’s self and post them on social media as a way to make up for the lack of self esteem and to fill a gap in intimacy. Many times children met with accidents and death while snapping picture of adventurous nature.
Adolescent Health Programmes in the Country:Although the magnitude of adolescent
problems in the country is too large, unfortunately
we do not have a separate adolescent mental health policy in India. However, Government has initiated many adolescent health programmes under various ministries. Adolescent health programmes, their ministries and the services provided are described in the table below.
Table 1: Adolescent's Health Program run by Different Departments of Govt. of India:
Sr No Ministries & Adolescent's Program /Services
1 Ministry of Health & Family Welfare
aAdolescents Reproductive & Sexual Health (ARSH)
Preventive, promotive, curative & counselling services for reproductive & sexual Problems
b School Health ProgramNutritional interventions, promoting health, life style, counselling & immunization
2 Women and Child Development
a Kishori Shakti YojanaServices improving health, nutritional and educational status of Girls
b Balika Samridhi Yojana
Services to raise the age of marriage and to improve enrolment and retention of girls at school
cRajiv Gandhi Scheme for Empowerment of Adolescents Girls
Iron & Folic acid supplementation, nutritional and health education, ARSH, life skill education and vocational training fro girls aged 16 & above under Nutritional Skill Development Program
d Integrated program for street Children
Shelter, nutrition, education health care and recreation facilities to street children Child Help Line Services (1098)
3 Human Resource Development
a Sarva Suraksha Abhiyan
Free & Compulsory education to 6-14 years age group
b Mahila Samakhya Program
Provides equal educational opportunities for women
c Adolescents Education Program
Creates awareness and positive attitude to develop skills to enable them to respond to real life situation.
4 Youth Affairs and Sports
a Nehru Yuva Kendra Sangathan Empowerment of rural youth
b National Services Scheme
Personality development of children through community service
cNational Program for Youth & Adolescents Development
Leadership Qualities and personality development of youth
P. T. Sasi / Challenges Concerning Adolescent Mental Health In India
12
Sr No Ministries & Adolescent's Program /Services
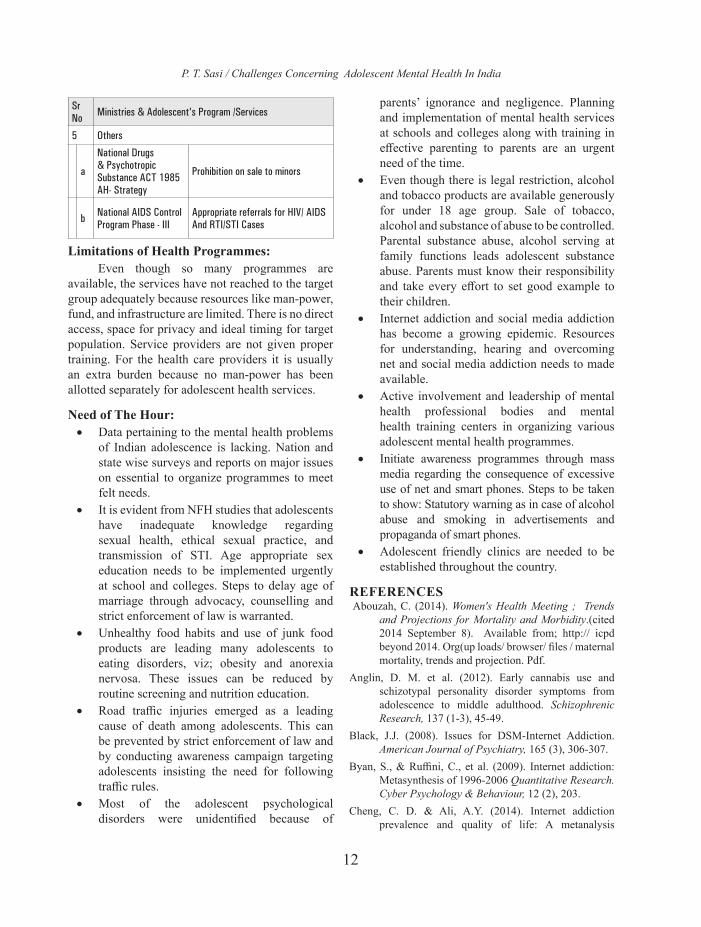
5 Others
a
National Drugs & Psychotropic Substance ACT 1985 AH- Strategy
Prohibition on sale to minors
b National AIDS Control Program Phase - III
Appropriate referrals for HIV/ AIDS And RTI/STI Cases
Limitations of Health Programmes:Even though so many programmes are
available, the services have not reached to the target group adequately because resources like man-power, fund, and infrastructure are limited. There is no direct access, space for privacy and ideal timing for target population. Service providers are not given proper training. For the health care providers it is usually an extra burden because no man-power has been allotted separately for adolescent health services.
Need of The Hour: • Data pertaining to the mental health problems
of Indian adolescence is lacking. Nation and state wise surveys and reports on major issues on essential to organize programmes to meet felt needs.
• It is evident from NFH studies that adolescents have inadequate knowledge regarding sexual health, ethical sexual practice, and transmission of STI. Age appropriate sex education needs to be implemented urgently at school and colleges. Steps to delay age of marriage through advocacy, counselling and strict enforcement of law is warranted.
• Unhealthy food habits and use of junk food products are leading many adolescents to eating disorders, viz; obesity and anorexia nervosa. These issues can be reduced by routine screening and nutrition education.
• Road traffic injuries emerged as a leading cause of death among adolescents. This can be prevented by strict enforcement of law and by conducting awareness campaign targeting adolescents insisting the need for following traffic rules.
• Most of the adolescent psychological disorders were unidentified because of
parents’ ignorance and negligence. Planning and implementation of mental health services at schools and colleges along with training in effective parenting to parents are an urgent need of the time.
• Even though there is legal restriction, alcohol and tobacco products are available generously for under 18 age group. Sale of tobacco, alcohol and substance of abuse to be controlled. Parental substance abuse, alcohol serving at family functions leads adolescent substance abuse. Parents must know their responsibility and take every effort to set good example to their children.
• Internet addiction and social media addiction has become a growing epidemic. Resources for understanding, hearing and overcoming net and social media addiction needs to made available.
• Active involvement and leadership of mental health professional bodies and mental health training centers in organizing various adolescent mental health programmes.
• Initiate awareness programmes through mass media regarding the consequence of excessive use of net and smart phones. Steps to be taken to show: Statutory warning as in case of alcohol abuse and smoking in advertisements and propaganda of smart phones.
• Adolescent friendly clinics are needed to be established throughout the country.
REFERENCES Abouzah, C. (2014). Women's Health Meeting ; Trends
and Projections for Mortality and Morbidity.(cited 2014 September 8). Available from; http:// icpd beyond 2014. Org(up loads/ browser/ files / maternal mortality, trends and projection. Pdf.
Anglin, D. M. et al. (2012). Early cannabis use and schizotypal personality disorder symptoms from adolescence to middle adulthood. Schizophrenic Research, 137 (1-3), 45-49.
Black, J.J. (2008). Issues for DSM-Internet Addiction. American Journal of Psychiatry, 165 (3), 306-307.
Byan, S., & Ruffini, C., et al. (2009). Internet addiction: Metasynthesis of 1996-2006 Quantitative Research. Cyber Psychology & Behaviour, 12 (2), 203.
Cheng, C. D. & Ali, A.Y. (2014). Internet addiction prevalence and quality of life: A metanalysis
P. T. Sasi / Challenges Concerning Adolescent Mental Health In India

13
of 31 nations across seven world region. Cyber Psychology, Behavoiur and Social Networking, 17 (12), 755.
Ganchimeg (2014). Pregnancy and child birth outcomes among adolescent mothers: A WHO Multi Country study. BJOG, 121, 40-48.
International Institute for Population Sciences. (IIPS) and Macro International. (2014). National Family Health Survey (NFHS-3), 2005-06; India. Volume 1. (cited 2014 November 20). Available from: http:// www. Rchipps.org /nfhs/ NFHS-3%. 20Data/ Vol-1volume—corrected 17 October 2008. Pdf.
Jagnoor, J., & Suraweera, L . (2012). Unintentional injury mortality in India, 2005: Nationally representative mortality survey of 1.1 million homes. BMC Public Health, 12 (1), 487.
Kirmani, M. N. & Suman. L. N. (2010). Gender differences in alcohol related attitudes and expectances among college students. Journal of Indian Academy of Applied Psychology, 36, 19-24.
Malhotra, S. P. (2014). Prevalence of child and Adolescent Psychiatric disorders in India. A systematic review and meta-analysis. Child and Adolescent Psychiatry and Mental Health, 89 (1), 22.
Masters, K. (2015). Social Networking Addiction among Health Science Students in Oman. Sulthan Gaboos University Medical Journal, 15 (3), 357-363.
Moreno, N.A. (2011). Problematic internet use among US youth. Archives of Paediatrics & Adolescent Medicine, 165 (9),797.
Paras, M. L. (2009). Sexual abuse and life time diagnosis of somatic disorders; A systematic review and meta-analysis. Journal of American Medical Association (JAMA), 302, 550- 561.
Patel, V. (2012). Suicide mortality in India: a nationally representative survey. The Lancet, 379, 2343-51.
Pillai, A., Andrews, T., & Patel, V. (2009). Violence, psychological distress and the risk of suicidal behaviour in young people in India. International Journal of Epidemiology, 38 (2), 459-469.
Priyadarshini, R., Jasmine, S., Valarmathi, S., Kalpana, S., & Parameswari, S. (2013). Impact of media on the physical health of urban school children age group 11- 17 Years in Chennai. A cross-sectional study. IOSR Journal of Humanities and Social Science, 9 (5), 30-35.
Rani, M., & Karunanidhi, S. (2010). Prevalence of depressive symptoms among urban adolescents in South India. Journal of Indian Association of Child & Adolescent Mental Health, 6 (2), 33-43.
Ray, R., Mondal, A. B. (2004). The extent, pattern and trends of drug abuse in India- National Survey. United Nations Office on Drugs and Crimes and Ministry of Social Justice and Empowerment (GOI), New Delhi.
Sivagurunathan, C., Umadevi, R., & Gopalakrishnan, S. (2015). Adolescent Health : Present Status and Related Programmes in India. Are we in the right direction?. Journal of Clinical Diagnostic Research, 9 (3) LE01-LE06.
Suman, L.N. (2012). Substance use: A psychological perspective. Indian Journal of Clinical Psychology, 39 (1), 10-18.
Tikoo, V., Dhawan, A., Pattnayak, R., & Chopra, A. (2014). Assessment of Pattern and profile of substance use among children in India (cited 2014 September 8). Available from: http:// www.ncper. Govt. in/ view file. php. Fid+17.
UNICEF (2012). Progress for Children: A Report Card on Adolescents. Adolescent Mortality, morbidly and Health Related Behaviours.(cited 2014 November 20). Available at: http:// www. Unicef. Org/publications/ files /progress for children No. 10 EN 04232012.pdf.
UNICEF (2014). Progress for Children: A Report Card on Adolescents. Adolescent Mortality, Morbidly and Health Related Behaviours.(cited 2014 November 20). Available at: http:// www. Unicef. Org/publications/ files /progress for children No. 10 EN 04232012.pdf.
WHO (2014). Mortality, Morbidly and Disability in Adolescence: Health for the World’s Adolescents, top 10 Cause of Death among Adolescents by Sex. (cited 2014 November 20). Available from: http:// apps.who.inr/adolescent/seconddecade/section3/
level3-2.php.WHO (2014). Health for Worlds Adolescents: Disability
Adjusted Life Years, Combining Mortality and Morbidly. (cited 2014 November 20). Available from: htt:// public Fabuleausoftware.com/profile/digitalteam# 1/vizhome/shared/ FPYZ7PPMR.
P. T. Sasi / Challenges Concerning Adolescent Mental Health In India

14
Experiences in Verbal Exposure for Stimulus Bound AnxietyRakesh Kumar
In India, we are seeing a major shift in the practice of clinical psychology from a predominantly psychodiagnostic exercises to the primacy of the applications of principles of psychology in successfully modifying the dysfunctional thinking, emotions and behaviours which either determine the abnormal expressions or develop in response to the conditions like chronic and incurable physical and psychological illnesses. Management of irrational fears and anxiety reactions forms a major portion of our working in clinical settings. These painful emotions spoil peace and harmony both within the individual and in interpersonal context. A person affected even with a specific phobia can have intense turmoil which can affect and modify his/her functioning and even impact the family members.
A lady with intense fear and disgust of lizard reported that she asked only two questions from her would be husband at the time of engagement. First, whether he was scared of lizards and second, if he smokes. The motive behind this enquiry was that if he was also phobic to the lizards, then who would remove the fear of lizards if both of them were scared. Also, she would like to seal all the ventilators and openings in bedroom to prevent lizard creeping in; and in that case if he smokes, then the room would be filled with smoke.
It is a common observation that persons with specific phobia do make extensive arrangements to prevent exposure to their phobic stimuli. A couple having a teenage boy shared that the husband is a claustrophobic and does not use lifts. He would climb staircase in multistory buildings. Both wife and the boy do follow him on the staircase for social
reasons. At times, wife observed him extremely tired due to climbing staircases for 4th floors and upwards. Another person with claustrophobia shared weird imaginary situations which could make him scared. He imagined what would happen if someone ties him and put into the dickey of a car, or seal him in a jute bag, or put a drum over him. He went beyond it and shared that he is terribly scared for the possibility of next birth, how he would manage himself in womb for nine months if he is to take next birth.
Social anxiety has a high prevalence and can be seen in all developmental stages from childhood to the old age. Becoming conscious and fearing the evaluations reduce the participation of persons having social anxiety in social activities. Students shy away and get blushed when they are required to ask questions, respond to queries and express their opinion in academic activities. Many of them could be bright and talented. The low participation in group academic activities limits expression of their talents. In a social function, they feel awkward and embarrassed suffering silently. If we could successfully address social anxiety in childhood and adolescents then such persons would make qualitative changes in the lives. Such persons even tend to suppress their creativity for fears of being judged negatively. Reduction in social anxiety could liberate them and make confident so that they express themselves. In adult life persons with social anxiety shy away from fellow workers and group participations. An adult male manager of a finance company at division level got a promotion offer to the level of the manager at State level. He got scared that if he accepted the promotion, he would have to
Indian Journal of Clinical Psychology2017, Vol. 44, No. 1, 14-20
Copyright, 2017, Indian Association ofClinical Psychologists (ISSN 0303-2582)
H N Murthy Oration
Dear Chairperson and Distinguished Delegates,I am feeling honoured and grateful to Indian Association of Clinical Psychologists (IACP) for
my nomination to deliver the most prestigious oration in the memory of late Prof. H. N. Murthy, former, HOD, Clinical Psychology, NIMHANS who contributed immensely in the field of clinical psychology and in particular Behaviour Therapy and Biofeedback in India. The field of behaviour therapy has evolved tremendously over the years. From behaviour therapy we have moved up to Cognitive Therapies and from Biofeedback to Neurofeedback. Still we are continually evolving and coming up with newer methodologies and conceptualization to heal the troubled mind.
Senior Clinical Psychologist, Institute of Mental Health and Hospital, Agra, Email: [email protected] Oration was delivered in 43rd NACIACP held in Coimbatore from Jan. 27- 29, 2017

15
address larger audience quite frequently and interact with authorities at higher level. He approached me for seeking help through hypnosis to enhance his level of confidence so that he could face challenges of social interactions; else he was contemplating to decline the offer.
Theories of psychology have an answer to most of such problems. We have been successfully addressing irrational fears through the applications of the principles of cognitive and behavioural therapies. Cognitive restructuring and exposure therapies produce remarkable results in both phobia and OCD. With advancements in conceptualization of psychological problems and their handling through psychological methods, psychologists are coming up with newer models which add values to the methodologies and healing potentials.
For dealing with the problems of phobia and OCD, we rely mostly on exposures to the objects and situations that elicit fear reactions. This exposure is typically done by exposing to feared cues in actual situations and/or in imagination. If a person has a phobia of dogs, then an exposure would involve forming mental images of dogs or exposing him/her to the images, videos or actual dogs. Such an exposure elicits fear reaction and with continued exposure it leads to habituation. Exposure and bearing the discomfort without avoiding is the key to success of such exposure based treatments. On the other hand, cognitive therapy makes an appeal to the reason of the person to evaluate his/her dysfunctional thoughts related to the objects and situations that elicit fear reactions. Objects and situations by themselves are not the problem but the meaning ascribed by a person to those objects/situations is considered as cognitive determinant of the fear reaction. When a person successfully makes corrections in his/her dysfunctional patterns of thinking, then substantial relief in irrational fears take place. The affected persons having cognitive sophistication to conceptualize their problems at cognitive level can derive maximum benefits from a combination of cognitive restructuring and exposure therapies.
We are continually evolving in our understanding of human behaviour; its determinants and methods of modifications. Our patients are the best teachers in our pursuits for innovation. About 10
years ago, while working with an adult patient with more than 15 years h/o of fear of the term ‘ruin’, I realized the importance of verbal exposure. This patient was troubled by specific word that implies ‘ruin’. He was avoiding all places, persons, situations, conversations and objects that represented ‘ruin’. Exposure to the stimuli that represented ‘ruin’ used to trigger sympathetic arousal; he felt palpitations, shortness of breath, restlessness, dry mouth, sweating and the like. The pervasive avoidance left him almost isolated and he began to live a life of seclusion. He was terrified of the probabilities of actual ‘ruin’ by having the idea of ‘ruin’ in the content of his consciousness. He would keep on trying and trying to eliminate the term ‘nash’ (ruin) from his conscious awareness. He was unsuccessful in eliminating the term from his mind. He consulted me with a specific request of removal of this term from his conscious awareness through hypnosis. I engaged him in therapy with full awareness that his request of removal of ‘nash’ term through hypnosis cannot be accomplished by me given the nature of his disorder.
I listened to his story and got stuck on his linguistic patterns. His description contained following statements: (1) ‘Nash’ ho jayega (ruin will take place) (2) vansh nash ho jayega (entire family will be ruined) (3) guldiva ho jayega (equivalent to ruin according to him) (4) punja chhip jayega (again equivalent to ruin for him). He held the belief that by having this term in his conscious awareness by itself could be the cause of ‘ruin’.
My attention got focused on the usage of future tense in his expressions. Quickly, I considered options of (a) verbal exposure by changing the tense of the same statements (b) words as conditioned stimuli (c) addressing magical thinking. I disputed his magical thinking that merely having the word ‘nash’ in the content of consciousness cannot actually cause ‘ruin’ to him or his family. Mental repetitions of the words cannot cause physical events by themselves. Considering words as conditioned stimuli and principles of exposure and habituation, I was all set in to make him repeat the ‘nash’ word until habituation takes place. Instead of prescribing the ditto statements for repetition, I modified the tense of the statements which were formulated as follows: (1) Nash ho chuka hai (2) vansh nash ho
Rakesh Kumar / Experiences in Verbal Exposure for Stimulus Bound Anxiety

16
chukka hai (3) guldiva ho chukka he (4) punja chhip chuka hai.
When I asked him to repeat these tense converted statements, he displayed escape behaviour by turning his face. He could not dare to repeat. Then I resorted to modelling of the repetitions. I verbalized and repeated above statements. Gradually, he took over from me and began to repeat above statements. The repetitions of above statements quickly elicited fear reaction which gradually began to resolve. Subjective Reports of felt distress and its resolution followed a typical anxiety curve. Daily sessions of this procedure were conducted. In between sessions homework assignments of similar repetitions and writing these statements were prescribed. He complied to the homework and designed his own real time exposure to the situations that could involve usage of ‘nash’ word. He needed only seven sessions and he was fully comfortably in listening and speaking all the words and statements related to ‘nash’ word. Treatment was terminated with mutual consent and follow up advice. His social and occupational functioning improved tremendously. He maintained his improvement for one and half-years and again presented with same problem. This time he needed only three days to recover from the relapse. In last 10 years he presented with relapse for two more times and took only two days on each relapse to recover. He is maintaining well and continuing his maintenance medicines. While drafting this oration, I called him to enquire his status, he reported that intermittently he gets that fear in mild doses and he by himself repeats above statements covertly and it cools down within a span of about 5-10 minutes indicating that this is a potentially efficient procedure to produce improvement and a promising approach even for relapse management.
Encouraged by the results and patterns of improvement and maintenance in this case, I began to apply similar approach in other patients of stimulus bound anxiety which include persons affected by obsessions and phobias like agoraphobia, claustrophobia, phobia of animals, social anxiety, fear of skin disease, fear of pointed objects, fear of fatal disease. In the course of my applications, I have now formalized this approach of verbal exposure which I am labelling as Cognitive Drill Therapy (CDT).
Applicability: CDT is applicable in stimulus bound anxiety
specifically phobia and some cases of OCD in clinical and sub-syndromal conditions in neurotic patients and in general population. It may not be applicable in Generalized Anxiety Disorder and Major Psychiatric Disorders.
Structure of Stimulus Bound Anxiety: This form of anxiety has a readily discernable
structure consisting of four components. (1) Objects of fear (2). Body-Mind Reactions (3). Safety Behaviours (4). Danger Ideation. These four components in short are called as OBSD. It follows a straightforward conceptualization. That is, exposure to objects of fear elicit body-mind reactions such as palpitations, shortness of breath, sweating, trembling, butterfly in stomach, nausea, mind going blank, feelings of fainting and so on. To get rid of these painful body-mind reactions (BMR), the person engages in safety behaviour by making elaborate preparations to deal with the exposure, by escaping or avoiding the objects of fear. At the core of it lies threat perception reflected in the thoughts of some kind of threat and danger. This threat perception reflects imagined feared consequences. Four components can be understood clearly with a real case example.
A middle aged person had a phobia of dog since childhood. Specifically, he was troubled by street dogs (Objects of fear). If he came across a street dog he would experience palpitation, trembling, uneasy, sweating, butterfly in stomach etc. (Body-Mind Reactions). He would keep distance from street dog and even change the route if he anticipated a dog on the way (Safety behaviour). In response to actual or imagined encounter with street dogs he thought that the dog may lick or bite him, he may get rabies and even die (danger ideation).
An OBSD analysis of phobia and OCD yields a comprehensive and explicit picture of the problems of a person. To further refine the conceptualization, I categorized four components in two layers (1) Overt Layer and (2) Covert Layer. Overt layer consists of first three components of OBSD i.e. Objects of fear, Body-Mind Reactions and Safety behaviour. Covert layer consists of danger ideation; which is cognitive appraisal of the objects of fear.
Rakesh Kumar / Experiences in Verbal Exposure for Stimulus Bound Anxiety

17
Typically, a patient operates at overt layer. An exposure to the objects of fear, trigger BMR which he/she learns to deal with through safety behaviour. The affected person does not deal with the covert layer. Engaging in safety behaviour negatively reinforces his/her patterns of safety behaviour and does not provide him/her an opportunity to correct underlying danger ideation. The problem persists with a fallacy that avoidance is the best solution for dealing with his/her problems.
From a psychological perspective, covert layer is the basis of overt layer, hence, we are required to effectively address the danger ideation. When an affected person is asked what would happen if exposure to the objects of fear no longer triggers danger thoughts, he/she readily responds that the problem will disappear. In above case, when this person was asked what will happen if he was in proximity of a street dog and the thoughts of licking, biting, rabies and dying did not occur in his mind! He immediately replied problem would be solved.
Psycho-education: A psycho-education of the patient regarding
nature and psychological determinants of his behaviour sets in the background for successful applications of this approach. All forms of psychotherapies would lead to a change in covert structure. It is the methodology of accomplishing the change that distinguishes the nature of an intervention. In Cognitive Restructuring we are likely to make an appeal to the reason to correct the underlying danger thoughts and in behavioural exposure we would plan an exposure to the objects of fear for cognitive changes to occur.
Intervention Protocol: In Cognitive drill, a person is required to
verbally repeat his/her danger thoughts by converting future tense into past or present. A prototype protocol of cognitive drill is ‘imagine the objects of fear and verbally repeat the tense converted danger thought’. In above case, ‘the person was required to imagine a street dog and verbally repeat that the dog has licked me, bitten me, I have caught rabies and died of it’.
From a theoretical perspective, actual object of fear, mental representations of an object of fear and even the words representing the object of fear; all are
conditioned stimuli. Habituation can be attained by exposing a person to the objects of fear in any of the modalities. Technically, an affected person is not scared of the objects of fear instead he/she is scared of the feared consequences represented by the objects of fear. By accessing and subjecting the feared consequences to verbal exposure can quickly and efficiently facilitate the attainment of therapeutic goals.
Anxiety Curve: Verbal exposure through drill statements,
typically elicits fear reaction which rises to the peak and then resolve forming a pattern of anxiety curve. In response to drill, within a few minutes, anxiety tends to resolve.
Generalization: When drill leads to substantial reduction of
fear from one object, then a generalization to non-drilled objects does not occur spontaneously. It then implies that drill need be practiced for each identified object of fear and danger ideation.
Homework Assignment: A patient is encouraged to practice verbal
exposure in-between sessions. This exposure can be done in any modalities which include sub-vocal drill, writing drill statements on a sheet of paper, listening to the drill statements in an audio. Also, it is recommended that a drill diary be maintained in which the patient records his/her experiences and practice of drill on daily basis. A review of the drill diary can provide valuable feedback to the patient as well as the therapist.
Drill and Daring: Actual physical stimuli involved in the
patient’s phobia and OCD are neutral and harmless barring the natural probability of harm they could cause. The problem lies with the cognitive appraisal and the emotional conditioning having its own neurophysiology and patterns of neural activation. Verbal drill efficiently addresses the problem at cognitive and neuro-physiological level. Hence, behavioural experiments do indicate generalization effect from verbal drill to real objects. A patient is encouraged to design his/her own daring as far as possible by exposing oneself to the feared objects. Hurry is not the key. Patient is allowed to adjust the
Rakesh Kumar / Experiences in Verbal Exposure for Stimulus Bound Anxiety

18
limits of exposure. If still, exposure to the actual physical stimuli elicits fear reaction, then additional verbal drill or drill on the spot can be recommended.
Maintenance:Verbal exposure leads to durable changes in fear
reactions. The case based data suggest maintenance of acquired gains over months and years.
Outcomes: Like any exposure therapy, cognitive drill results in three important and desired outcomes. (1) Habituation (2) Cognitive Reinterpretation (3) Enhanced Self-efficacy.
The available case data (Kumar et al, 2012; Dwivedi & Kumar, 2015; Arya et al., 2017) and the cases being worked out so far suggest that cognitive drill can be potentially efficient and effective form of intervention which produce durable results in phobia and some cases of OCD.
AREAS OF RESEARCH Cognitive Drill Therapy is of very recent origin hence, extensive empirical researches are required to establish its efficacy, mechanisms of action, durability and generalization of acquired therapeutic gains. Followings could be considered while contemplating researches on this form of treatment.
1. Single Subject Designs: While working with individual cases of phobia
and OCD we could consider the scientific methodology of Applied Behaviour Analysis i.e. Single-Subject Designs. There are many variants in Single-Subject Designs. In particular, we could consider going for Multiple Baseline Designs across Stimulus Conditions and Multiple Baseline Designs across Individuals. During the course of applications of verbal exposure, it is being noticed that the patients show little generalization across stimulus conditions. A successful drill to one stimulus shows little or incomplete generalization to other stimuli. This observation of little generalization provides an opportunity to empirically test the efficacy of verbal exposure across stimulus conditions.
2. Psycho-physiological Measurement: Significant advancements have taken place in
psycho-physiological measurement. Verbal exposure provides us an opportunity to obtain moment to moment data through subjective reports of distress and psycho-physiological measurements. Such measurements would allow us to compare changes between periods of baseline arousal vis-à-vis during real time application of verbal exposure. This would serve the purpose of objective clinical validation of changes in sympathetic arousal as well as an objective assessment of research findings.
3. Within Group Designs: Pre-post and follow up studies of one
homogeneous clinical group such as social anxiety, obsessions, specific phobias, agoraphobia could generate the data of effectiveness of verbal exposure in achieving improvements and maintenance in phobia and OCD.
4. Between Group Designs: Such designs could be used to generate
comparative data of the effectiveness of verbal exposure against a waitlisted control group, only medicine vs. medicine plus verbal exposure and comparisons of verbal exposure with other forms of psychological treatments.
5. Group Intervention: OBSD data within a diagnostic category is
likely to be very similar. For instance, the persons affected by social anxiety have similar sets of situations of fear, BMR, safety behaviour and danger ideation. Similar is the case with other phobic conditions and OCD. We can form groups of persons affected with a specific disorder and provide verbal exposure in groups with on the spot supervision and assistance by therapists to explore if this form of exposure could efficiently be used in groups. If a group format becomes effective, this would help us to reach the mass and address the massive magnitude of problems of phobia and OCD prevalent in the population.
6. Physiological Mechanisms: The study of neuro-physiological mechanisms
involved in drill specifically neurotransmitters and neural pathways can open up a new area
Rakesh Kumar / Experiences in Verbal Exposure for Stimulus Bound Anxiety

19
of real time monitoring and research into the mechanisms of action from psychology to biology. It would be immensely useful if we could establish what kind of changes take place during and after verbal exposure in neuro-chemical and neural networks in the brain.
7. Mechanisms of Action: It is hypothesized that primarily three
mechanisms of action operate in verbal exposure. (1). Habituation (2). cognitive appraisal (3) .time reference. We need to establish these mechanisms and explore additional mechanisms of action involved in verbal exposure.Generally, people ask me questions related to
generalization of the therapeutic gains from clinic setting to real life, maintenance of therapeutic effects, relapse and whether it is a symptomatic treatment. My observations suggest that verbal exposure produce lasting improvements with more or less smooth generalization to real life situations. If spontaneous generalization does not happen then drill and daring accomplish the job. Cognitive Drill Therapy addresses the cognitive determinants of fears through behavioural principles. It directly, modifies underlying danger ideation. I term it as ‘experiential realization’. In the process of drill, a realization takes place that the objects of fear are neutral and danger ideation lies at imagination level of the patient. The strings of danger ideation elicited during OBSD analysis and cognitive drill permeate deeper layers of cognitive structures. Drill commences with an initial working OBSD analysis which keeps on updating as deeper layers of cognitions surface. It penetrates layer by layer. When drill normalizes a specific string of danger ideation, the next deeper layer of danger ideation string becomes apparent. It can descend down to the initial sensitizing event. Accessing non-conscious cognition through working on danger ideation leads to insight. But this insight by itself may not be enough to disengagement of fear reactions from objects of fears. Still drill could be required to achieve habituation. Symptom substitution is not being seen in the treated patients. Future researches would help us in determining comprehensive indications, contra-indications and other aspects of this form of verbal exposure therapy.
At this point of time, I am taking liberty to share my own personal experiences of social anxiety. I myself had been experiencing severe social anxiety since early days. I never participated in any discussions in seminars/ conferences/ journal club during my training in Central Institute of Psychiatry in 1987-1989 except my own presentations which were done with great distress. Also, I never presented any paper/symposium in National Conferences of Indian Association of Clinical Psychologists. This anxiety in me had shaped my pervasive avoidance of presentations to the extent that the present president of IACP had organized National Conference of IACP in Ranchi Institute of Neuropsychiatry and Allied Sciences (RINPAS) and I was keen to participate as a passive participant. But I received an invitation to chair a scientific session in that conference which escalated social anxiety in me to the extent that I had to decide not to participate. It was a difficult and painful face saving option for me. This oration is the very first presentation of mine in any National Conference of my own association. I am attributing part of this courage to my self-application of the principles of verbal exposure which enabled me to stand up on the podium. I am getting similar reports from my students who are learning verbal exposure therapy from me. They too are applying on their own fears including social anxiety. One of them says that she has been working to inculcate courage in herself and others too through verbal exposure therapy.
Millions of people across world are affected by clinical and sub-clinical conditions of stimulus bound anxiety. These conditions mostly require input of psychological theories and can effectively be treated by available methods of psychological treatment. In reality, significantly less number of affected persons are aware that their suffering is a recognized problem which can be treated. We have a massive professional responsibility and obligation to create awareness of these conditions and treat efficiently. We also need to introspect ourselves, how many such cases we are seeing in our clinical practice per year and in our entire active professional career. We are lacking authoritative epidemiological data on the prevalence of anxiety disorders and the magnitude of emotional, behavioural, social and financial burden that flows from having such disorders.
Rakesh Kumar / Experiences in Verbal Exposure for Stimulus Bound Anxiety

20
Every emotional disorder is a punch in the wellbeing and optimum productivity of an individual. Anxiety disorders could also be a precursor to other problems like substance abuse and depression. Hence, there is a calling for us to develop effective service delivery models to reach the millions of affected individuals. Time has come when we should get prepared to super-specialized service centers dealing with such conditions. I have a vision to see centers for social anxiety, specific phobias, agoraphobias, OCD and the like across the country involved in service delivery, training and researches. We could contemplate for developing resource centers for these disorders and transfer skills of managing these conditions to psychologists, family members, educators, community workers, patients and other professionals.
In addition to that, we also could think of developing self-help material for various anxiety disorders specifically for patients and their family members. Self-help literature can provide an opportunity for us to create awareness of the prevalent anxiety disorders, impressing the mass that these are recognized psychological disorders amenable to change through psychological input. Such an approach could possible help us to disengage the stigma attached with our profession and make us more accessible to the public at large. It is we, who are required to reach to the millions of affected persons. If we keep on waiting such persons to come to us, it will take many more years.
Let us first reach to as many affected persons as possible so that they open up themselves and begin to flow to us in mass. Verbal exposure is a lightweight form of treatment. The affected persons as well as therapists are required to acquire specific set of concepts and skills which can easily be transferred to others. We can integrate core features of all forms of therapies available to us to heal the people silently suffering from anxiety disorders. I
have recorded many of my experiences, concepts and procedures of verbal exposure in the book ‘Cognitive Drill Therapy’. However, crafting and application of verbal exposure is a highly skilled and specialized task which would need properly supervised training. I wish if verbal exposure could form a part of regular training of exposure therapies to the students of clinical psychology so that they contribute substantially to most major dimensions of this therapy.
REFERENCESArya, B., Verma, S., & Kumar, R. (2017). Efficacy of
Cognitive Drill Therapy in Treatment of Specific Phobia. SIS Journal of Projective Psychology and Mental Health, 24, 48-51.
Dwivedi, S., & Kumar, R. (2015). Efficacy of Cognitive Drill Therapy in Agoraphobia with Panic Disorder: A Case Study. SIS Journal of Projective Psychology and Mental Health, 22, 139-146.
Kumar, R., Sameer, A., & Singh, B. (2012).Preliminary Test of Cognitive Drill as an Intervention. Indian Journal of Clinical Psychology, 39, 67-74.
Kumar, R., & Dubey, B. L. (2016). Cognitive Drill Therapy: A Potent Application of the Principles of Psychology for OCD and Phobia. SIS Journal of Projective Psychology and Mental Health,, 23, 125-126.
Jain, R. (2016) Cognitive Drill Therapy. ISBN-13:978-1539554219
Jain, R. (2015). Manual of Cognitive Drill Therapy on website: www.cognitivedrill.com/ www.cdt.oo.gd
Sameer, A (2007). Case Studies in Cognitive Drill Therapy, Unpublished Postgraduate Dissertation, Barkatullah University, Bhopal.
Verma, S., & Kumar, R. (2016). Cognitive Drill Technique: A novel approach to manage fear of height. Symposium on Psychological Assessment in Military: The Indian Scenario in 26th Annual convention of National Academy of Psychology (NAOP), 29-31 December 2016.
Rakesh Kumar / Experiences in Verbal Exposure for Stimulus Bound Anxiety

21
1. Research Officer 2. Director, Institute of Mental Health and Hospital, Agra - 282002 (UP). *Corresponding Author: Sandhya Rani Mohanti Email: [email protected]
General intelligence is said to consists of two distinct factors – Fluid intelligence (Gf) and Crystallized Intelligence (Gc) (Cattell, 1971;1987). Fluid intelligence, also called as fluid reasoning is involved in solving novel problems which has little impact of learning. It includes abilities such as pattern recognition, abstract reasoning, and problem-solving. The tools like Raven's matrices are used to tap fluid reasoning. Crystallized intelligence on the other hand, reflects the outcome of acquired cognitive processes and it is best assessed with tests that emphasize scholastic and cultural knowledge. However, crystallized intelligence is not merely equivalent of memory and knowledge but it heavily relies on the usage of information stored in long term memory.
Neuropsychological and brain researches are suggesting a strong link between activity in prefrontal cortex (PFC) and tasks of fluid reasoning, executive function and working memory. The persons having a damage in prefrontal cortex also show severe impairment in fluid reasoning tasks such as Raven’s Progressive Matrices (Duncane et al., 1995; Waltz et al., 1999). On the other hand,
these researches also demonstrated that such persons with PFC damage show little changes in the learned tasks such as vocabulary which are grouped under crystallized intelligence. A discrepancy between fluid reasoning tasks and crystallized reasoning tasks can co-exist to the extent that persons with average crystallized intelligence can have fluid functioning as much as 2 SD below average (Blair, 2006). It is suggested that PFC is involved in solving novel and non-semantic problems but PFC plays little role in tasks of crystallized intelligence. Furthermore, the brain imaging researches suggested that the performance on the tasks of crystallized intelligence were associated with specific frontal and posterior temporal and parietal areas (Sowell et al., 2004).
The concept of insight has been refined over time. Early accounts categorized insight into two dichotomous categories (Lewis, 1934). Subsequently, it was revised into a multi- dimensional and continuous construct (Mintz, Dobson & Romney, 2003). Measure for evaluation of multiple dimensions of insight such as awareness of illness, awareness of signs and symptoms, need for treatment etc. has also been developed (Amador & Kronengold, 2004).
Indian Journal of Clinical Psychology2017, Vol. 44, No. 1, 21-25
Copyright, 2017, Indian Association ofClinical Psychologists (ISSN 0303-2582)
Research Article
ABSTRACTCognitive Insight addresses the evaluative and interpretative processes involved in anomalous experiences. A degree of self-certainty in one’s own abnormal thinking is associated with psychotic symptoms and indicates poor insight whereas self-reflection on one’s thought processes involved in production of aberrant experiences leads to regulation and corrective experiences. In present study, we examined the role of fluid and crystallized intelligence in cognitive insight in persons with schizophrenia. 30 patients with schizophrenia were sampled from Institute of Mental Health and Hospital, Agra. Following tools were individually administered: (1) Beck Cognitive Insight Scale for measuring cognitive insight (2) Raven’s Colored Progressive Matrices as a measure of fluid reasoning (3) Weschler Adult Performance Intelligence Scale-PR for fluid intelligence and (4) Verbal Adult Intelligence Scale of PGI Battery of Brain Dysfunction for Crystallized Intelligence (5) Vocabulary Sub-test of Binet-Kulshresth Test of Intelligence for crystallized intelligence. The correlational analysis revealed that self-reflectiveness dimension of cognitive insight is positively associated with both fluid and crystallized intelligence whereas self-certainty dimension does not have any significant relationship with either of the factors of intelligence.Key Words: Fluid Intelligence, Crystallized Intelligence, Insight, Cognitive Insight, Schizophrenia
Relationship of Fluid and Crystallized Intelligence with Cognitive Insight in Persons with Schizophrenia
*Sandhyarani Mohanty1 and Sudhir Kumar2

22
An important dimension of insight was introduced by Beck (2004) which he labelled as ‘Cognitive Insight’ and defined as “a patient's current capacity to evaluate his or her anomalous experiences and atypical interpretations of events” . They described four aspects of cognitive insight that can be disrupted in psychosis: (a) impairment of ability to be objective about delusional experiences and cognitive distortions, (b) reduced capacity to put these experiences into perspective, (c) unresponsiveness to corrective information from others, and (d) overconfidence in delusional judgments (Beck & Warman, 2004).
Beck et al. (2004) developed ‘Beck Cognitive Insight Scale’ (BCIS) which has two dimensions (a) Self-reflectiveness (b) Self-certainty. Research findings suggest that psychotic patients have low self-reflectivenss and high degree of self-certainty. Engh, Friis, & Birkenaes et al. (2010) reported that delusions irrespective of the presence or absence of hallucinations were associated with low self-reflectiveness and high self-certainty, reflecting low cognitive insight in the patients of schizophrenia. Mohanty and Kumar (2012) also reported that schizophrenic persons with positive or negative psychopathology have greater self-certainty and decreased capacity for self-reflectiveness.
Recent neuropsychological and neuro-imaging researches are including assessment of cognitive insight. Lysaker et al. (2008) reported that there is a significant association between cognitive insight, executive function, understanding one’s own mind. The role of neurocognitive and metacognitive processes is being implicated. Lepage et al. (2008) observed that verbal learning, memory and attention were significantly correlated with Self-Certainty.
Cognitive insight is essentially based on cognitive endowment. A certain degree of cognitive capacity is required to examine one’s own thought processes and their outcomes. Given this proposition, it flows that intellectual function play a role in the processes grouped under ‘cognitive insight’. The present study was designed to empirically examine the role of fluid and crystallized intelligence in cognitive insight in persons with schizophrenia.
METHODAims and Objectives:1. To explore relationship of fluid intelligence
with cognitive insight2. To explore relationship of crystallized
intelligence with cognitive insight.
Sample:A sample of 30 patients with schizophrenia
diagnosed through ICD-10 Diagnostic Criteria was drawn from inpatients of Institute of Mental Health and Hospital, Agra. The patients in the age range of 20-44 years with two or more years duration of illness and not having any major co-morbid psychiatric disorder were selected.
Measures:Following tools were administered on the
participants: • Wechsler Adult Performance Intelligence
Scale (Ramalingaswami, 1974). • Verbal Adult Intelligence Scale (VAIS) of
PGI Battery of Brain Dysfunction (Pershad &Verma,1990).
• Vocabulary Test of Stanford Binet Intelligence Scale: Hindi Adaptation (Kulshrestha, 1971).
• Raven’s Colored Progressive Matrices (Raven, Court & Raven, 2002).
• Beck’s Cognitive Insight Scale (Beck et al., 2004).
RESULTS AND DISCUSSIONTable-1: Sample Characteristics.
Characteristics Patients (n=30)
Age (in Years) 34.17±7.23
Education (in years) 11.06±2.04
Duration of Illness (in Years) 8.16±4.19
Age of Onset (in Years) 26.00±6.51
DomicileRural 50%
Urban 50%
Family TypeNuclear 66.7%
Joint/Extended 33.33%
Table-1 depicts the demographic and clinical characteristics of the same. The mean age of the participants was 34.17 (7.23) years. The mean years of education was 11.06 (2.04) years. The duration of schizophrenic illness was 8.16 (4.19) years. The mean age of onset of schizophrenic illness was 26.00 (6.51) years. There was equal representation from
Sandhyarani et al.,............. / Relationship of Fluid and Crystallized Intelligence ................

23
rural/urban domicile (50%). 66.70% participants hailed from nuclear families and only 33.33% participants were from joint/extended families.
Table-2: Mean and S.D. of VAIS, WAPIS, RCPM, Vocabulary and BCIS Domains.
Measures Min. Max. Mean S DVAIS TQ: Information 60.00 135.00 92.56 17.75VAIS TQ: Arithmetic 64.00 121.00 84.60 13.80
VAIS TQ: Digit Span 102.00 158.00 125.00 14.95
VAIS TQ: Comprehension 61.00 124.00 97.10 15.45VAIS: Total VQ 85.00 126.00 100.00 10.41BKT: Vocabulary 11 26 20.90 3.43
WAPIS Scaled Score: Picture Completion 3.00 12.00 7.86 2.35
WAPIS Scaled Score: Object Assembly 0.00 12.00 5.36 3.25
WAPIS Scaled Score: Block Design 0.00 13.00 7.26 2.87
WAPIS Scaled Score: Picture Arrangement 0.00 8.00 5.13 3.07
WAPIS Scaled Score: Digit Symbol 3.00 10.00 5.63 1.67
WAPIS: Total PQ 50 92 75.46 10.48RCPM: Total Correct 11.00 33.00 21.06 5.70BCIS:Self-reflectiveness 15.00 26.00 20.20 2.63BCIS: Self-certainty 2.00 7.00 4.46 1.27
Table - 2 indicates that average Verbal IQ was 100. The mean Table Quotient (TQ) on digit span subtest was 125 (14.95) which was highest among four sub-scales of VAIS. The mean TQ on arithmetic was 84.60 (13.80) which was lowest. The mean Performance Quotient (PQ) was 75.46 (10.48) which was lower than the average. The scores on self-reflectiveness was 20.20 (2.63) was quite higher than the scores (4.46±1.27) on self-certainty dimension of Cognitive Insight.
Table-3: Correlation Coefficients between VAIS & Vocabulary Scores and BCIS Scores.
VAIS Domains BCIS: Self-reflectiveness
BCIS: Self-certainty
VAIS: Information .625** - .138VAIS: Arithmetic .477** - .018VAIS: Digit Span .267 - .150VAIS: Comprehension .145 - .219VAIS: VQ .577** - .210BKT: Vocabulary .448* .058
*0 .05 level; ** 0 .001 level
VAIS and Vocabulary tests were used as measures of crystallized intelligence. Table-3 indicates that Verbal IQ and Vocabulary test scores are significantly and positively correlated with self-reflectiveness dimension of BCIS. Only two sub-scales of VAIS, Information and Arithmetic are significantly associated with self-reflectiveness dimension of BCIS. The other two sub-scales, digit span and comprehension were not correlated significantly with self-reflectiveness dimension of BCIS. None of the measures were found to have any significant correlation with self-certainty dimension of BCIS.
Table-4: Correlation Coefficients between WAPIS & RCPM Scores and BCIS Scores.
WAPIS Domains BCIS: self-reflectiveness
BCIS: Self-
certainty
WAPIS: Picture Completion .632** -.276
WAPIS: Object Assembly .394** -.374*
WAPIS: Block Design .508* .012
WAPIS: Picture Arrangement .598** .045
WAPIS: Digit Symbol .080 .163
WAPIS: PQ .693** -.215
RCPM .334 .081
* 0.05 level; ** 0.001 levelWAPIS and RCPM were used as measures of
fluid intelligence. Table - 4 indicates that PQ was significantly and positively associated with self-reflectiveness dimension of BCIS. WAPIS has five sub-scales. Except digit symbol, four sub-scales of WAPIS were having significant positive correlation with self-reflectiveness dimension of BCIS. For self-certainty object assembly sub-test of WAPIS emerged to have a significant but negative correlation. Other sub-scales including PQ were not found to have any significant correlation with self-certainty dimension of BCIS. For RCPM a correlation coefficient of .334 was present with self-reflectiveness dimension of BCIS but it could not reach statistical significance. For self-certainty dimension of BCIS negligible correlation was present with RCPM scores.
The results are suggestive of a positive association of self-reflectiveness dimension of
Sandhyarani et al.,............. / Relationship of Fluid and Crystallized Intelligence ................

24
BCIS with both fluid and crystallized factors of intelligence. Self-certainty appeared to be independent of intellectual processes. The results of self-certainty and IQ are in agreement with the observations of Cooke et al. (2010) who reported lack of significant correlation between self-certainty and general intellectual ability, verbal fluency, sustained attention and memory. These researchers further suggested that poor executive functioning may contribute more strongly than general cognitive ability to individuals with schizophrenia making over-confident decisions. But for self-reflectiveness also, no association with general cognitive ability was observed. But the present study indicates significant association between general cognitive ability and self-reflectiveness.
The dimension of BCIS recognized as indicative of cognitive insight i.e., Self-reflectiveness, is an expression of introspection and the willingness to acknowledge fallibility (Beck et al., 2004). The ability to introspect into one’s reasoning and its reality check certainly needs general cognitive abilities without which it is unlikely that a person would be able to examine his/her own mental processes and the faults in reasoning process. Self-reflectiveness capitalizes at least on following specific cognitive abilities, a storage of experiential database, ability to retrieve the relevant data from the cognitive storage, matching of current cognitive experiences with the past experiences, social norms, considering multiple alternative interpretation about one’s experiences and probabilities of anomalous cognitive experiences being valid and objective. Therefore, an association between self-reflectiveness and general cognitive abilities seem to be a plausible one.
Van Camp, Oldenburg, & Sabbe (2016) observed that in patients with bipolar disorder, following variables were having significant positive associations with self-reflectiveness dimension of BCIS-speed of processing, attention, working memory, visual learning, reasoning and problem solving. The self-certainty dimension of BCIS correlated negatively to working memory, but, this correlation was explained by confounding variables. This observation also supports that a host of cognitive variables are associated with self-reflectivity dimension of BCIS rather than self-certainty.
Studies examining the association of specific neuropsychological functioning such as executive function, verbal memory, meta-cognition etc should also consider the role of general cognitive abilities in cognitive insight of the patients. The present study included chronic patients who were mostly stable. Their strength of self-certainty was quite lesser than the level of self-reflectiveness as indicated by the mean scores on two dimensions of BCIS. It would be of interest to examine the relationship of general cognitive abilities with cognitive insight in patients having lesser duration of illness and higher scores on self-certainty dimension which would indicate poor cognitive insight. Also, more recently developed measures of general cognitive abilities could be used in future researches to further examine the role of general cognitive abilities in cognitive insight.
In conclusion, the results of the present study suggest significant association of both fluid and crystallized cognitive abilities in cognitive insight in persons with chronic schizophrenia. Studies on cognitive abilities and cognitive insight should consider this general abilities to partial out the contribution of specific cognitive abilities in cognitive insight.
REFERENCESAmador, X.F., & Kronengold, H. (2004). Understanding
and assessing insight. In: Amador XF, David AS, editors. Insight and Psychosis: Awareness of Illness in Schizophrenia and Related Disorders. 2nd ed. Oxford, UK: Oxford University Press. p. 3-30
Beck, A.T, & Warman, D.M. (2004). Cognitive insight: theory and assessment. In: Amador XF, David AS, editors. Insight and Psychosis: Awareness of Illness in Schizophrenia and Related Disorders. 2nd ed. New York, NY: Oxford University Press. p. 79-87.
Beck A.T., Baruch E., Balter J.M., Steer R.A., & Warman D.M. (2004) A new instrument for measuring insight: the Beck Cognitive Insight Scale. Schizophrenia Research, 68, 319–329
Blair, C. (2006). How similar are fluid cognition and general intelligence? A developmental neuroscience perspective on fluid cognition as an aspect of human cognitive ability. Behavioural and Brain Sciences, 29, 109 –125.
Sandhyarani et al.,............. / Relationship of Fluid and Crystallized Intelligence ................

25
Cattell, R. B. (1971). Abilities: Their Structure, Growth, and Action. New York: Houghton Mifflin. ISBN 0-395-04275-5.
Cattell, R. B. (1987). Intelligence: Its Structure, Growth, and Action. New York: Elsevier Science.
Cooke, M.A., Peters, E.R., Fannon, D., Aasen, I., Kuipers, E. & Kumaria, V. (2010) Cognitive insight in psychosis: The relationship between self-certainty and self-reflection dimensions and neuropsychological measures. Psychiatry Research, 178 (2), 284–289.
Duncan, J., Burgess, P., & Emslie, H. (1995).Fluid intelligence after frontal lobe lesions.Neuropsychologia, 33, 261–268.
Engh, J.A., Friis, S., & Birkenaes, A.B. (2010) Delusions Are Associated With Poor Cognitive Insight in Schizophrenia. Schizophrenia Bulletin, 36 (4), 830-835.
Kulshrestha, S.K. (1971) Stanford Binet Intelligence Scale: Hindi Adaptation of Third Revision. Form L-M. Allahbad: Manav Seva Sansthan
Lepage, M., Buchy, L., Bodnar, M., Bertrand, M.C., Joober, R.,& Malla, A. (2008) Cognitive insight and verbal memory in first episode psychosis. European Psychiatry, 23, 368-374.
Lewis, A. (1934) The psychopathology of insight. British Journal of Medical Psychology,14, 332-348.
Lysaker, P.H., Warman, D.M., & Dimaggio, G. (2008) Metacognition in schizophrenia: associations with multiple assessments of executive function. Journal of Nervous and Mental Disease, 196, 84-389.
Mintz, A.R., Dobson, K.S., & Romney, D.M. (2003) Insight in schizophrenia: a meta-analysis. Schizophrenia Research. 61,75-88.
Mohanty, S. & Kumar, S. (2012) Psychopathology and cognitive insight in patients with chronic schizophrenia. Indian Journal of Clinical Psychology. 39, 124-127
Pershad, D, and Verma, S.K. (1990) Handbook of PGI Battery of Brain Dysfunction (PGI-BBD) National Psychological Corporation, Agra.
Ramalingaswami, P. (1974). The Weschler Adult Performance Intelligence Scale-PR. Manasayan, New Delhi.
Raven, J. C., Court, J. H. & Raven, J. (2002). Raven’s Colored Progressive Matrices. Dr. G. Schuhfried Ges M. B. H. Austria.
Sowell, E. R., Thompson, P. M., Leonard, C. M., Welcome, S. E., Kan, E., & Toga, A. W. (2004). Longitudinal mapping of cortical thickness and brain growth in normal children. Journal of Neuroscience, 24 (38), 8223– 8231.
Van Camp, L.S., Oldenburg, J.F., & Sabbe, B.G. (2016) How self-reflection and self-certainty are related to neuro cognitive functioning: an examination of cognitive insight in bipolar disorder. Cognitive Neuropsychiatry, 21 (2),130-45.
Waltz, J. A., Knowlton, B. J., Holyoak, K. J., Boone, K. B., Mishkin, F. S., & de Menezes Santos, M. (1999). A system for relational reasoning in human prefrontal cortex. Psychological Science, 10 (2), 119 –125.
Sandhyarani et al.,............. / Relationship of Fluid and Crystallized Intelligence ................

26
1. Research Associate, Dept. of Psychiatry, 2. Additional Professor, Deptt. of Clinical Psychology, NIMHANS, Bangalore -560 029, *Corresponding Author: M Manjula. Email: [email protected]
INTRODUCTION College education phase in young adult’s
life is characterized by transitional changes and adjustments in the areas of academics, physiological, sexual, emotional and spiritual domains. The most commonly and consistently reported areas of stress are academics, relationships and work (Baldwin, Chambliss, & Towler, 2003; Narayanan & Rao, 2002; Shiraishi, 2000). However, the stressful experiences can have differential impact. Some students adapt well, while others become vulnerable to psychological problems. Studies on students have traditionally been focusing on impact of the stress on mental health problems such as depression, anxiety, somatoform disorders, adjustment disorders, alcohol and drug abuse and personality disorders (Chandrashekar, 2007; Narayanan & Rao, 2002). High level of distress is observed across studies (Narayanan & Rao, 2002; Nikhil & Manjula, 2009) with a heightened suicidal risk (Singh & Manjula, 2012). Professional students were found to have more stress compared to non- professional students. Also
they were poorly emotionally adjusted in comparison to non-professional group (Singh & Singh 2008). According to Abhay, Krishnakumar, Paul, and Shashidhar (2011), prevalence of perceived stress was found to be 50 % in the professional students. Engineering and management students were found to be experiencing role overload, role stagnation and self-role distance (Agrawal & Chahar, 2007).
Coping strategies among the students also have been explored to a greater extent. A study by Marykutty (2001) showed that social support was perceived as most useful. Distressed students had a tendency to engage in maladaptive coping. In a study by Paradkar (2006), suicidal ideators were found to be using more maladaptive coping strategies. Gender differences were observed in the coping styles used. Females preferred distress reducing strategies, social support utilization and religious coping while males used negative distraction strategies and active behavioural methods including high risk coping behaviours (Paradkar & Rao, 2006; Rao, Moudid & Subbakrishna, 2000).
Indian Journal of Clinical Psychology2017, Vol. 44, No. 1, 26-34
Copyright, 2017, Indian Association ofClinical Psychologists (ISSN 0303-2582)
Research Article
ABSTRACT College students encounter stress in various aspects of life. While some students adapt well, others may become vulnerable. Hence it is important to recognize the important factors that contribute to resilience in college students. Aim of the study is to explore stress and coping and the association between resilience and psychosocial variables of theoretical relevance in college students. A sample of 200 students doing engineering course from engineering colleges in Bengaluru was assessed using Socio-demographic data sheet, The Connor-Davidson Resilience scale, Positive and Negative Affect Schedule, NEO Five Factor Inventory, Rosenberg Self-Esteem Scale, Relationship Scale Questionnaire, The Coping Checklist, Psychological Well Being scale and Depression Anxiety and Stress Scale. Result shows majority of them experienced high stress in the area of relationship. Social support and distraction positive were used as the main coping strategies. Majority of them were found to have medium resilience. Resilience had significant positive correlation with positive affect, extraversion, conscientiousness, self-esteem, secure attachment, dismissive attachment, problem solving coping, social support and psychological well-being. Positive affect, conscientiousness and dismissive attachment style predicted resilience in positive direction. The findings throw light on the factors that are to be addressed in the promotive intervention programs with college students.Key words: Resilience, College Students, Stress, Coping
Stress-Coping and Factors Contributing to Resilience in College Students: An Exploratory Study from India
Hesi S. Herbert1 and *M. Manjula2

27
Various factors were associated with coping such as high sense of humour, use of deliberate efforts at resolving the problem causing stress and reappraisal of the stressful situation by positively interpreting its meaning for personal growth (Abel, 2002). Though it is an important perspective, this deficit oriented approach provides a limited view of individuals and their range of possible outcomes (Tedeschi & Kilmer, 2005) Recently, researchers have shifted their focus towards positive changes resulting from the stressful situation (Tedeschi & Calhoun, 2004). This paradigm shift towards strength model from a problem oriented model is referred to as resiliency research (Richardson, 2002). Even though early studies have looked at those exposed to serious form of adversity, recent studies indicate that the concept of resilience has relevance not only to those undergoing significant life challenges but also to those experiencing daily stressors (Li, 2008). Resilience is the ability to show positive adaptation despite significant life adversities and the ability to adapt to difficult and challenging life experiences (Luther, Cicchetti, & Becker, 2000; Masten & Reed, 2002).
Studies on resilience started with the focus on vulnerability and protective factors in children who were exposed to adversity. Vulnerability factors are those indices that exacerbate the negative effects of the risk condition. Protective factors are those that modify the effects of risk in a positive direction. The protective factor model of resilience states that protective factors reduce the effect of risk and promote resilience (Masten, 2001; O‟Leary, 1998; Rutter, 1989). Though the resilience research started with children, recently, research has focused on the adults as well (Pedhazur & Schmelkin, 1991). Studies on resilience over the transition to adulthood suggested the term “late- emerging resilience” to refer to the changes that occur during adulthood in response to the adverse life events. The transition to adulthood serves as an opportunity for positive development through the actions of self and others.
Various factors are associated with resilience. Positive affect is one such factor that expands the range of cognitions and behaviour to build on resources (Singh & Yu, 2010). Similarly positive self-esteem is a buffer against the effects of adversity (Gilligan, 2009; Newman & Blackburn, 2002). Active coping is found to have positive relation with resilience
(Li, 2008). Positive peer relations characterized by pro-social interactions, peer acceptance and support were found to promote successful adaptation (Criss, Pettit, Bates, Dodge, & Lapp, 2002; Kokko & Pulkkinen, 2000). In addition, personality traits such as emotional stability, conscientiousness, openness, extraversion and agreeableness have also found to be the sources of resilience (Campbell-Sills, Sharon,& Stein, 2006; Singh & Yu, 2010).
Rationale of the Present Study:From the literature it is evident that young
adults exposed to stressors when coupled with their developmental gaps in coping ability make them vulnerable to psychological problems. Similarly there are certain protective factors that contribute to successful adjustment and resulting resilience. Various factors contributing to resilience have been identified across studies. However, many of these factors are not easily amenable to change. Therefore, it is necessary to understand the factors contributing to resilience and are amenable to change in order to develop intervention programmes which would enhance the resilience in college students. Resilience literature largely comes from children and adolescents, and very little attention is being paid to young adults. Also, most of the knowledge on resilience comes from western literature. Given the role of cultural context it is very important to study factors associated with resilience in Indian context. Considering the high levels of stress experienced among the students doing professional courses, engineering students are considered in order to explore the factors contributing to stress and resilience. The objectives of the study were to study stress and coping and resilience in college students and also to examine the association between resilience and variables such as positive and negative affect, personality, self esteem, relationship and psychological well being.
METHODParticipants and Procedure:
A total of 200 engineering students (157 males, 43 females; mean age: 19.8; age range: 18- 23 years) were selected for the study. One college was chosen randomly from the list of engineering colleges at Bengaluru using lottery method. One
Hesi S. et al......., / Stress-Coping and Factors Contributing ..........

28
class each from 1-4 years of the course, including different branches was again selected randomly. The study was exploratory in nature with a single group design. All students who gave consent were included. Ethical clearance was obtained from NIMHANS Ethics Committee. The study was conducted during December 2010 to May 2011. The questionnaires were administered by researcher in groups of 15 to 50 students. The size of the group varied as the strength of the class also varied due to the specialization they belonged to. Administration of the tools took around 1 to 1 ½ hrs. Confidentiality and anonymity was ensured and maintained. Feedback about any student was not given to the authorities. Current study was conducted as the initial phase of a larger study which examined the effect of resilience based intervention program for the students.
MEASURESSocio Demographic Data Sheet: It consisted 2 sections
a) Socio-demographic Details: Age, sex, religion, marital status, family type,
satisfaction with the family functioning, and course details.
b) Stressful Life Event: Open ended questions were used to assess
specific issues contributing to stress and the coping strategies used them. The questions covered presence of life event, its impact, and factors which helped in overcoming the stress.
The Connor-Davidson Resilience Scale (CD-RISC; Connor & Davidson, 2003):
CD-RISC is a 25- item scale rated on a 5- point scale (0–4). The total scores ranges from 0–100, with higher scores reflecting greater resilience. It has 5 subscales such as (1) personal competence, high standards, and tenacity; (2) trust in one’s instincts, tolerance of negative affect, and strengthening effects of stress; (3) positive acceptance of change, and secure relationships; (4) control and (5) spiritual influences. Internal consistency (Cronbach’s Alpha) was 0.89. Test-retest reliability was 0.87. Convergent and discriminant validity is established.
Positive and Negative Affect Schedule (PANAS; Rao & Mehrotra, 2006):
The scale includes items tapping unpleasant
activated, pleasant activated, pleasant deactivated and unpleasant deactivated dimensions of affect. There are 13 pleasant and 13 unpleasant affect related statements tapping the experience of positive and negative affect in general. High scores on the respective scales indicate the corresponding affect. The measure has sound psychometric properties. Internal consistency was .88.
NEO Five Factor Inventory (NEO-FFI; Costa & Mc Crae, 1992)
The NEO-FFI is a 60-item self-report measure of the ‘‘big five’’ dimensions of personality. It consists of five 12-item scales measuring neuroticism, extraversion, openness, agreeableness, and conscientiousness. Respondents rate each item on a five-point scale. Highest score indicates highest in that personality dimension. The NEO-FFI has demonstrated good internal consistency, test–retest reliability and validity. The reliability coefficients for the subscales were 0.69 for Agreeableness, 0.75 for Extraversion, 0.72 for Openness, 0.80 for Conscientiousness and 0.83 for Neuroticism.
Rosenberg Self-Esteem Scale (Rosenberg, 1965):It is a unidimensional measure of global self-
esteem. The items represent a continuum of self-worth statements ranging from statements that are endorsed by individuals with low self-esteem to those endorsed only by persons with high self-esteem. The scale has 10- questions with four response choices, ranging from strongly agree to strongly disagree. Internal consistency reliability ranges from 0.85 to 0.88 for college samples.
Relationship Scale Questionnaire (RSQ; Griffin & Bartholomew, 1994):
The RSQ contains 17 short statements, rated on a 5-point scale. These items reflect the degree of security, fearfulness, preoccupiedness, and dismissiveness. The reliability coefficients of the scale were calculated by the Retest Method and varied between 0.54 and 0.78.
The Coping Checklist (CCL; Rao, 1985):CCL involves components of both problem
focused and emotion focused coping. It has 6 subscales: one of problem focused coping (problem solving), four of emotion focused coping (denial,
Hesi S. et al......., / Stress-Coping and Factors Contributing ..........

29
distraction, faith, acceptance) and one of social support seeking. Items are scored dichotomously. Internal consistency is 0.79 and test – retest reliability is 0.74.
Psychological Well Being (PWB; Bhogle & Jaiprakash, 1995):
The Scale has 28 items representing different components of well being such as positive affect, satisfaction, loneliness, general efficacy, satisfaction in daily activities, life satisfaction, meaningfulness and suicidal ideas. There are 13 factors in the scale. The answers were obtained in Yes – No format. The scores range from 0-28. Higher scores indicate better psychological well being. The Test re-test reliability (after 3 months) is 0.72, and split half co-efficient is 0.91.
Depression Anxiety and Stress Scale (DASS; Lovibond & Lovibond, 1995):
The DASS is a set of three self- report scales designed to measure the negative emotional states of depression, anxiety and stress. Each of the three DASS scales contains 7 items, divided into subscales of 2-5 items with similar content, rated on 4-point severity. Internal consistency reliability coefficients for Depression, Anxiety, Stress subscales and full Scale were Cronbach’s alphas of 0.79, 0.71, 0.76, and 0.89 respectively.
Statistical Analysis:Statistical analysis was done using the Statistical
Package for Social Sciences (SPSS version 16). Quantitative analysis included descriptive statistics such as mean, standard deviation and range which were used to analyse socio-demographic data and other variables. Correlation was done for finding the relationships among variables. Regression analysis was carried out for identifying factors that predict resilience. For some of the items in socio-demographic data sheet, qualitative analysis was carried out in which the data obtained was coded for themes and analysed.
RESULTSSocio demographic Details of the Sample:
Majority of the sample were males (78%), from Hindu religious background (87%) and from nuclear families (76%). Most of them (80%) reported satisfaction with family functioning (Table 1).
Table1: Socio demographic Details of the Sample (n=200).
Socio-demographic Variable
Mean (SD)
Frequency %
Age 19.79±1.17
SexMale 157 78.5
Female 43 21.5
Religion
Christian 7 3.5
Hindu 174 87.0
Muslim 11 5.5
Other 5 2.5
Atheist 3 1.5
Family Type
Nuclear 152 76.0
Joint 10 5.0
Extended 38 19.0
Satisfaction
with Family
Yes 160 80.0
No 40 20.0
Stress and Coping: Based on the qualitative analysis of the life
events and coping, majority of life events reported were in the area of relationship (27.5%) which included relationship with peers and heterosexual relationship, illness (8.5%) and academic stress (6.5%). Academic achievement (9%) was the main positive life event. With regard to coping strategies used, mostly used coping was seeking social support (12.5%) and distraction strategies which were adaptive (10.5%). Other strategies included using acceptance (4.5%) and meditation (3%), taking action (1.5%) and positive thinking (1%).
On DASS, almost 16% of sample had severe depression, 26% has severe anxiety and 12% has severe stress. Around 28% of students fell in the normal category of depression, 20% for anxiety and 36% for stress. While mild level of depression and stress was reported in about 50% of the students; moderate level of anxiety was reported by about 50% of the sample. On CCL, frequently used coping strategies were acceptance, problem solving, social support and distraction positive. Distraction negative and religious coping were the least used coping strategies (Table 2).
Hesi S. et al......., / Stress-Coping and Factors Contributing ..........

30
Table 2: Mean and SD of Variables Taken for the Study.
Variables Mean S D
Resilience 68.36 12.68
Coping Strategies
Problem solving
Distraction positive 54.70 18.33
Distraction negative 28.03 20.95
Acceptance 70.12 16.83
Religious 29.99 24.94
Denial 49.26 21.54
Social Support 56.42 24.56
Positive Affect 44.24 6.86
Negative Affect 34.99 8.24
Self esteem 17.39 4.49
Psychological Well Being 16.73 2.67
Personality
Neuroticism 23.36 6.41
Extraversion 30.26 5.1
Openness 26.57 5.19
Agreeableness 26.21 5.21
Conscientiousness 28.68 5.23
Relationship
Secure Attachment 3.25 0.5
Fearful Attachment 2.92 0.72
Pre occupied Attachment 2.89 0.65
Dismissive Attachment 3.24 0.62
Resilience and Other Variables: Based on the mean score on resilience scale
the sample was classified into low, medium and high resilient group by taking mean + 1 SD. Majority of them (69.2%) were found to have medium resilience. It is evident from the table that the positive affect was higher compared to negative affect. Among the personality dimension, they got highest score in extraversion and lowest score in neuroticism. With regard to the relationships, Secure and dismissive attachment style had higher score compared to fearful and preoccupied attachment style (table 2). The mean value of self esteem was higher than mid point indicating that the sample had moderate to higher self esteem. Similarly, the mean value of
psychological well being was slightly above the median indicating higher psychological functioning.
CORRELATES OF RESILIENCE Table 3 shows that, resilience had significant
positive correlation with positive affect, extraversion, conscientiousness, self esteem, secure attachment, dismissive attachment, problem solving coping, social support and psychological well being. Resilience was negatively correlated with negative affect, neuroticism, depression, stress and denial coping.
Table 3 : Correlation between Resilience and Other Variables.
Variable Resilience
Positive affect 0.54**
Negative Affect -0.25**
Personality Neuroticism
Extraversion -0.26**
Openness 0.31**
Agreeableness 0.08
Conscientiousness 0.11
0.37**
Self esteem 0.33**
Depression Anxiety Stress
Depression -0.16*
Anxiety -0.10
Stress -0.19**
Relationship Secure attachment 0.19**
Fearful attachment -0.09
Pre occupied attachment -0.11
Dismissive attachment 0.18**
Coping Problem solving 0.20**
Distraction positive 0.06
Distraction negative -0.12
Acceptance 0.04
Religious 0.056
Denial -0.29**
Social Support 0.20**
Psychological Well Being 0.17*
*p<0.05, **p<0.01
Hesi S. et al......., / Stress-Coping and Factors Contributing ..........

31
Predictors of Resilience: Regression analysis shows (Table 4) that,
variables such as positive affect, conscientiousness, negative affect, and dismissive attachment style accounted for 38% of variance. Positive affect, conscientiousness and dismissive attachment style predicted resilience in positive direction whereas negative affect in negative direction.
Table 4 : Stepwise Regression Analysis Showing Predictors of Resilience.
Dependent Variable: Resilience
Predictors Beta Coefficient Significance R2
Positive Affect .54 .00
.39Conscientiousness .23 .00
Negative Affect -.20 .00
Dismissiveness .12 .02
DISCUSSIONThe findings of the present study give a
comprehensive picture of stress, coping and resilience in college students. In line with the existing literature, majority of the life events reported were in the domain of relationship and academics (Baldwin, Chambliss, Towler, 2003; Nikhil & Manjula, 2009; Paradkar & Rao, 2006; Shiraishi, 2006). The findings throw light on the importance of relationships especially the heterosexual relationships at this phase of life. Further, it also emphasizes the need for support and guidance to handle relationships since this is one of the significant factors contributing to stress. Almost half of the participants had mild levels of depression and stress and moderate level of anxiety. Compared to other student population, the sample in the current study had higher distress (Nikhil & Manjula, 2009). The findings indicate that professional students experience more stress compared to other students. The demands of the professional course were reported to be the reason for high stress (Abhay et al., 2011; Schneider, 2005).
Despite experiencing high levels of stress, majority of the students showed positive outcomes. They used adaptive coping strategies such as social support seeking, problem solving and distraction positive. Previous literature also showed that college students used mostly adaptive coping strategies
(Abhay, Krishnakumar, Paul & Shashidhar, 2011; Marykutty & Rao, 2001; Paradkar & Rao, 2007). They were found to have moderate to high resilience, which might have been contributed by good family functioning and adaptive coping (Table 3). Similar findings are reported in a study on healthy adult offsprings of parents diagnosed with schizophrenia, adaptive coping and social support contributed to their resilience (Herbert & Manjula, 2012). The self esteem was found to be moderate to high in the sample. One of the possible contributors to the self esteem may be the active coping methods used by the majority of students (Orth, Robins & Meier, 2009). In line with the other findings, current study also showed adequate psychological functioning (Shadap, & Manjula 2011; Singh, Manjula & Philip, 2012). With regard to the relationships, more participants reported to have secure and dismissive attachment styles. The findings were slightly different from those reported in other studies. A study by Narayanan and Rao (2002) on undergraduate students found that the four attachment styles were present more or less equally in the sample. While other studies have reported that half of the sample had secure attachment style (Bartholomew, & Horowitz, 1991; Brennan, Clark & Shaver, 1998). Overall, despite the stress experienced in areas such as academics and relationships, the college students mostly used adaptive coping, showed moderate to high resilience and self esteem, and had secure and dismissive styles of attachment with parents.
Resilience showed positive correlation with positive affect and negative correlation with negative affect. The findings are in commensurate with the literature that occurrence of positive affect served to moderate stress reactivity and mediate stress recovery (Ong, Bergeman, Bisconti & Wallace, 2006). It is also noted that individuals with high levels of resilience are likely to use positive affect to bounce back from adverse experiences (Carle & Chassin, 2004). Personality traits such as extraversion and conscientiousness were positively correlated while neuroticism was negatively correlated with resilience. This result was in line with other findings (Shiner & Masten, 2012; Yu & Zhang, 2007). The tendency of extraverted individuals to become resilient was explained by the fact that extraverted people tend to experience more positive affect, form attachments
Hesi S. et al......., / Stress-Coping and Factors Contributing ..........

32
to others easily, and seek out social interaction (Costa & Mc Crae, 1992). Highly conscientious persons take an active problem-solving approach in dealing with stress (Campbell-Sills, Sharon & Stein, 2006). However, people with high neuroticism were vulnerable to emotional distress and become less resilient (Kling, Ryff, Love & Essex, 2003; Ormel, Oldehinkel & Vollebergh, 2004). The positive relationship between resilience and self esteem similarly may be understood in the background of a well established finding that positive self esteem acts as a buffer against the effects of adversity (Gilligan, 2009; Newman & Blackburn, 2002).
The finding that resilience is positively associated with active coping and negatively related to emotion- focused coping was consistent across studies (Campbell-Sills, Sharon & Stein, 2006; Southwick, Vythilingam & Charney, 2005). Successful coping resulted in adaptation leading to enhancement of an individual’s existing resilience (Garvie, 1997; Kumpfer, 1999). Thus findings of the current study indicated that for the youth pursuing professional course, problem solving and social support plays an important role in contributing to their resilience.
Current study found positive relationship between resilience and secure attachment. Secure attachment served as protective factor in mediating stressful environments and situations thus enhancing resilience (Karreman & Vingerhoets, 2012; Simeon et al. 2007). The role of relationship was also emphasised in the context of self esteem which again showed positive relation with resilience. The self esteem which was based on relationships, as opposed to an achievement-based sense of self-esteem strengthened resilience (Hartertling, 2008). Surprisingly, dismissive attachment style also had shown positive correlation with resilience. This finding throws light on the fact that avoidance of attachment may also contribute to develop resilience when the individual found it difficult to make and maintain healthy and secure attachments (Bartholomew, 1991). However, the finding needs further exploration to understand the context in which it is helpful and its effects in long term. Similar to established results, positive affect, conscientiousness and dismissive attachment style predicted resilience in positive direction whereas negative affect in negative direction (Campbell-Sills et al., 2006; Ong et al., 2006).
The study has few limitations such as the sample was obtained from an urban college and hence limits the generalizability of the findings to other settings. However, the findings reflect the general pattern of stress, coping and resilience in students pursuing professional courses. The study has explored the various correlates of resilience which has received less attention in India. Information regarding stress and coping was collected qualitatively which added to richness of the information obtained. Large sample size adds to the strength of the study.
CONCLUSIONThe current study adds to the understanding of
stress and resilience of the college students belonging to professional courses which is given less attention in India. The study highlights the importance of certain factors such as active coping, positive affect, self esteem, healthy relationship and personality traits such as extraversion and conscientiousness in contributing to resilience. The findings have important implications for enhancing resilience and mental health promotion among college students.
ACKNOWLEDGEMENTSWe thank Dr. D. K. Subbakrishna, Professor
and Head, Department of Biostatistics, NIMHANS & Dr. Mariamma Philip, Assistant Professor, Department of Biostatistics NIMHANS, for guiding us in analyzing the data.
REFERENCESAbhay, M. B., Krishnakumar, M. K., Paul, N. C., &
Shashidhar, H. G. (2011). Differences in perceived stress and its correlates among students in professional courses. Journal of Clinical and Diagnostic Research, 5 (6), 1228-1233.
Agrawal, R. K., & Chahar, S. S. (2007). Examining role stress among technical students in India. Social Psychology of Education, 10 (1), 77-91.
Baldwin, D. R., Chambliss, L. N., & Towler, K. (2003). Optimism and stress: An African American college student perspective. College Student Journal, 37, 276-285.
Bartholomew, K., & Horowitz, L.M. (1991). Attachment styles among young adults: A test of four-category model. Journal of Personality and Social Psychology, 61, 226-244.
Bhogle, S., & Jaiprakash, I. J. (1995). Development of the Psychological Wellbeing (PWB) Questionnaire. Journal of Personality and Clinical Studies, 11, 5-9.
Hesi S. et al......., / Stress-Coping and Factors Contributing ..........

33
Bienvenu, O. J., & Stein, M. B. (2003). Personality and anxiety disorders: A review. Journal of Personality Disorders,17, 139–151.
Brennan, K. A., Clark, C. L., & Shaver, P. R. (1998). Self-report measurement of adult attachment: An integrative overview. In J. A. Simpson &W. S. Rholes (Eds.), Attachment Theory and Close Relationships (pp. 46–76). New York: Guilford.
Campbell-sills, L., Sharon, L. C., & Stein, M. B. (2006). Relationship of resilience to personality, coping, and psychiatric symptoms in young adults. Behaviour Research and Therapy 44, 585–599.
Carle, A. C., & Chassin, L. (2004). Resilience in a Community Sample of Children of Alcoholics: Its Prevalence and Relation to Internalising Symptomatology and Positive Affect. Journal of Applied Developmental Psychology, 25, 577–596.
Chandrashekar, C. R. (Ed.) (2007). Manual on Student’s Counseling for Teachers (3rded.). Bangalore: NIMHANS
Connor, K. M., & Davidson, J. R. (2003). Development of a new resilience scale: The Connor Davidson Resilience Scale (CD-RISC). Depression and Anxiety, 18 (2), 76-82.
Costa, P. T. Jr., & McCrae, R. R. (1992). Revised NEO Personality Inventory (NEO-PI-R) and NEO Five Factor Inventory (NEO-FFI) Professional Manual. Odessa, FL: Psychological Assessment Resources.
Coutu, D. (2002). How resilience works. Harvard Business Review, 5, 46-55.
Criss, M., M., Pettit, G., S., Bates, J.,E., Dodge, K., A., & Lapp, A.,L. (2002). Family adversity, positive peer relationships, and children’s externalizing behaviour: A longitudinal perspective on risk and resilience. Child Development, 73, 1220 – 1237.
Dumont, M. (1999). Resilience in adolescents: protective role of social support, coping strategies, self esteem, and social activities on experience of stress and depression. Journal of Youth and Adolescence, 28 (3), 343.
Fredrickson, B. L. (2000). Cultivating positive emotions to optimise health and well-being. Prevention and Treatment, 3, 1-25.
Garvie, P. A. (1997). The effects of difficult tasks on resilience in young adults. Dissertation Abstract International, 58, 5642.
Gilligan, R. (2009). Promoting Resilience: Supporting Children and Young People Who are in Care, Adopted or in Need. London: BAAF.
Griffin, D., & Bartholomew, K. (1994). Models of the self and other: Fundamental dimensions underlying measures of adult attachment. Journal of Personality and Social Psychology, 67 (3), 430-445.
Hartertling, L. M. (2008). Strengthening Resilience in a Risky World: It's All About Relationships, Women & Therapy, 31 (2-4), 51-70.
Herbert, H. S., Manjula, M., & Philip, M. (2013). Resilience and Factors Contributing to Resilience among the Offsprings of Parents with Schizophrenia, Psychological Studies, 58 (1), 80-88.
Herrman, H., Stewart, D. E., Diaz-Grandos, N., Berger, E. L., Jackson, B., & Tracy, Y. (2011). What is Resilience? Canadian Journal of Psychiatry, 56 (5), 258-265.
Karreman, A., &Vingerhoets, Ad. J. J. M. (2012). Attachment and well-being: The mediating role of emotion regulation and resilience. Personality and Individual Differences, 53 (7), 821-826.
Kling, K.C., Ryff, C. D., Love, G., & Essex, M. (2003).Exploring the influence of personality on depressive symptoms and self-esteem across a significant life transition. Journal of Personality and Social Psychology, 85, 922-932.
Kokko, K., & Pulkkinen, L. (2000). Aggression in childhood and long-term unemployment in adulthood: A cycle of maladaptation and some protective factors. Developmental Psychology, 36, 463-472.
Kumpfer, L. K. (1999). Factors and processes contributing to resilience: The resilience framework. In M. D. Glantz& J. L. Johnson (Eds.), Resilience and Development: Positive Life Adaptations (pp. 179-224). New York: Academic/Plenum.
Li, M. H. (2008). Relationships among stress coping, secure attachment, and the trait of resilience among Taiwanese college students. College Student Journal, 42, 312- 325.
Lovibond, S. H., & Lovibond, P.F. (1995). Manual for the Depression Anxiety Stress Scales. (2nded.) Sydney: Psychology Foundation.
Luthar, S.S., Cicchetti, D. and Becker, B. (2000). The construct of resilience: A critical evaluation and guidelines for future work. Child Development, 71, 543-562.
Marikutty, P. J.,& Rao, K. (2001). Process of Coping with Stressful Life Events among College Students. (Unpublished M.Phil Dissertation). NIMHANS, Bangalore.
Masten, A. S. (2001). Ordinary magic: Resilience processes in development. American Psychologist, 56 (3), 227-238.
Masten, A. S., & Reed, M. (2002). Resilience in development. In C.R. Synder & S.J. Lopez (Eds.), Handbook of Positive Psychology. New York, NY: Oxford University Press.
Monasterio, E. B. (2002). Enhancing resilience in the adolescent. Nursing Clinic of North America,37, 373–379.
Narayanan, G., & Rao, K. (2002). Attachment styles,
Hesi S. et al......., / Stress-Coping and Factors Contributing ..........

34
Personality and Coping in Young Adults. (Unpublished MPhil Dissertation). NIMHANS, Bangalore.
Newman, T., & Blackburn, S. (2002). Transitions in the lives of children and young people: Resilience factors. Interchange 78. Edinburgh: Scottish Executive.
Nikhil D, & Manjula M. (2009). Mental Health Issues, Psychological Functioning and Attitude Towards Help Seeking in Pre- University College Students. NIMHANS, Bangalore: (Unpublished MPhil Dissertation)..
O’Leary, V. E. (1998). Strength in the face of adversity: Individual and Social Thriving. Journal of Social Issues, 54, 425–446.
Ong, A.D., Bergeman, C.S., Bisconti, T.L., & Wallace, K. (2006).Psychological resilience, positive emotions, and successful adaptation to stress in later life. Journal of Personality and Social Psychology, 91, 730–749.
Ormel, J., Oldehinkel, A.J., & Vollebergh, W. (2004).Vulnerability before, during, and after a major depressive episode: a 3-wave population-based study. Archives of General Psychiatry, 61, 990–996.
Orth, U., Robins, R., & Meier, L. L. (2009). Disentangling the effects of low self-esteem and stressful life events on depression: Findings from three longitudinal studies. Journal of Personality and Social Psychology, 97, 307–321.
Paradkar, A., & Rao, K. (2006). Psychological Distress, Suicidal and Help Seeking Behaviour in College Students. Unpublished M Phil Thesis. Bangalore : NIMHANS (Deemed University).
Pinjarkar, R., &Mehrotra, S. (2007). Experience of positive affect and meaning in life : An exploratory study. Unpublished M Phil Thesis. Bangalore : NIMHANS (Deemed University).
Rao, D., & Mehrotra, S. (2006). Negotiation of life-tasks and subjective well-being in young adults pursuing professional courses. Psychological Studies, 51, 144-152.
Rao, K., Subbakrishna, D. K., & Prabhu, G. G. (1989). Development of a Coping Checklist: A Preliminary Report. Indian Journal of Psychiatry, 31, 128–133.
Resnick, M. D., Bearman, P. S., Blum, R. W., Bauman, K. E., Harris, K. M., Jones, J., Udry, J. R. (1997) Protecting adolescents from harm. Findings from the National Longitudinal Study on Adolescent Health. Journal of the American Medical Association, 278 (10), 823-32.
Rosenberg, M. (1965). Society and the Adolescent Self-Image. Princeton, NJ: Princeton.
Rutter, M. (1999). Resilience concepts and findings: Implications for family therapy. Journal of Family Therapy, 21 (2), 119-144.
Rutter, M. (2000). Resilience reconsidered: Conceptual
considerations, empirical findings, and policy implications. In J. P. Shonkoff, & S. J. Meisels (Eds.). Handbook of Early Childhood Intervention- 2 (pp. 651-682). New York, NY: Cambridge University Press.
Schneider, L. (n.d.) Perceived Stress among Engineering Students. Retrieved from http://asee.morrisville.edu.
Shadap, I. M. B., & Manjula, M. (2011). The Psychological Functioning, Self Efficacy and Family Functioning in College Students. (Unpublished MPhil Dissertation). NIMHANS, Bangalore.
Shiner, R. L. & A. S. Masten (2012). Childhood personality as a harbinger of competence and resilience in adulthood. Development and Psychopathology, 24 (2), 507-528.
Shiraishi, Y. (2000). Attributional patterns and adjustment in the college transition: A cross cultural study. Dissertation Abstract International, 61 (6B), 3292.
Simeon, D., Yehuda, R., Cunill, R., Knutelska, M., Putnam, F. W., & Smith, L. M. (2007). Factors associated with resilience in healthy adults. Psychoneuroendocrinology, 32, 1149–1152.
Singh, K., & Yu, X. (2010). Psychometric Evaluation of the Connor-Davidson Resilience Scale (CD-RISC) in a Sample of Indian Students. Journal of Psychology, 1 (1), 23-30.
Singh, S. & Manjula M. (2010). Suicidal Risk, Childhood Adversity and Psychological Functioning in College Students. (Unpublished M Phil Dissertation). NIMHANS, Bangalore.
Singh. A., & Singh. S. (2008). Stress and Adjustment Among Professional and Non professional Students. Indian Psychiatry Journal, 17, 26-7.
Southwick, S. M., Vythilingam, M., & Charney, D.S. (2005). The psychobiology of Depression and Resilience to Stress: Implications for prevention and treatment. Annual Review of Clinical Psychology, 1, 255–291.
Tedeschi, R. G., & Calhoun, L. G. (2004). Post traumatic growth: Conceptual foundations and empirical evidence. Psychological Inquiry, 15, 1–18.
Tedeschi, R. G., & Kilmer, R. P. (2005). Assessing strengths, Resilience, and Growth to Guide Clinical Interventions. Professional Psychological Research and Practice, 36, 230-237.
Tugade , M.M., & Fredrickson, B.L. (2004) Resilient Individuals Use Positive Emotions to Bounce Back from Negative Emotional Experiences. Journal of Personality & Social Psychology, 86 (2), 320–333.
Yu, X., & Zhang, J. (2007). Factor analysis and psychometric evaluation of the Connor-Davidson Resilience Scale (CD-RISC)with Chinese people. Social Behaviour and Personality, 35 (1), 19–30.
Hesi S. et al......., / Stress-Coping and Factors Contributing ..........

35
INTRODUCTIONIntellectual disability (ID) is associated with
many behavioural and emotional disorders. Well-constructed community-based population studies suggest that 35-40% of children and adolescents with intellectual disabilities are likely to have a diagnosable psychiatric disorder. And autism spectrum disorders (ASD) are one of the prominent comorbid conditions in ID with a point prevalence of 8% (Emerson & Hatton, 2007). It is generally reported that the chance of autistic features increases with the severity of ID (Beitchman, & Peterson, 1986; Kar, Khanna & Kar, 1997; Srinath, et al., 1989). But there are not many studies in the Indian context to address this issue. In this backdrop the present paper attempts to briefly review the construct of autism and its relation with ID before proceeding to explain the objectives of the study.
Kanner (1943) described a few children whose relation to people was ‘altogether different’ and instances in which they would barely notice when other people entered a room. He also noted that these children tended to use language in a very literal fashion and that they failed to relate to other people physically. Since the time Kanner noted that extreme autism, obsessiveness, stereotypy, and echolalia’ are
Research Article
Autistic Spectrum Disorders in Children with Intellectual DisabilitySaumyashree Mohapatra1, *Masroor Jahan2 and M. Thomas Kishore3
1 . Clinical Psychologist, Dept. of Clinical Psychology, SCB Med College, Cuttuck. 2. Additional Prof. of Clinical Psychology, Ranchi Institute of Neuro Psychiatry and Allied Sciences (RINPAS), Ranchi 3. Assoc. Prof. of Clinical Psychology, National Institute of Mental Health and Neuro Sciences (NIMHANS), Bengaluru. *Corresponding Author: Masroor Jahan Email: [email protected].
ABSTRACTAutistic features unless at the level of syndrome are usually ignored in people with
intellectual disabilities. It is more evident as the severity of intellectual disabilities increases. The present study was designed to assess the type and severity of autistic features among children with intellectual disabilities. Fifty children with intellectual disabilities, aged 3 to 18 years, were recruited from a local special school as well as the outpatient services of a tertiary psychiatric hospital by using purposive sampling. Stanford - Binet Intelligence Scale, Seguin Form Board, Gilliam Autism Rating Scale were used for assessment. Results indicate that 84% of the participants had very low to below average autistic features while 6% (n=3) had scores above the cutoff suggesting a possible comorbidity of autism spectrum disorder. All core features of autism spectrum disorder such as stereotype behaviours, communication, social interactions and developmental concerns were noted in the study group in the range of 8 to 10%. Developmental concerns shared a significant negative correlation with the intellectual level (r= -.28; p <.05). The study implies that children with intellectual disabilities can have autistic features independent of comorbid diagnosis of autism and they need appropriate interventions to manage the same. Key words: Autism Spectrum Disorder, Intellectual Disability, GARS.
features of infantile autism, some held the view that specific features such as social and communication difficulties and repetitive behaviours could be part of intellectual difficulties hence ASD could not be differentiated from ID. Later studies clearly indicate specific features of autism are clearly independent of associated intellectual impairment.
Rutter (1978) was clear that the social and communication difficulties were not just a function of associated intellectual disability. These various issues were considered as autism was first included in the landmark, third edition of DSM (DSM-III; American Psychiatric Association, 1980). Most of the nuclear characteristics described by Kanner such as ‘autistic aloofness’ and ‘insistence on sameness’ are still part of the criteria to diagnose ASD in current classifications. The fourth edition of DSM (DSM-IV; American Psychiatric Association, 1994) identifies autism along with four other disorders as part of pervasive developmental disorders (PDD) that are characterized by severe, pervasive impairments in specific developmental areas, such as social interactions and communication, or stereotyped behaviours, interests and activities. However, later studies revealed that separate diagnoses of pervasive developmental disorders were not consistently applied across different
Indian Journal of Clinical Psychology2017, Vol. 44, No. 1, 35-40
Copyright, 2017, Indian Association ofClinical Psychologists (ISSN 0303-2582)

36
clinics and treatment centers. The fifth edition of DSM (DSM-5; American Psychiatric Association, 2013) recognized that autism is a spectrum disorder implying that PDD not otherwise specified, autism and Apserger’s disorder are on the same continuum. DSM-5 also refined the symptoms criteria for ASD as it truncated the social and communication domains into one. Thus for a diagnosis of autism spectrum disorders the DSM-5 requires that there is evidence for persistent deficits in social communication and social interaction across contexts, not accounted for by general developmental delays and restricted, repetitive patterns of behaviour, interests, or activities. These symptoms must be present in early childhood but may not fully manifest ed until social demands exceed limited capacities. The ASD symptoms will fall on a continuum, with some individuals showing mild symptoms and others having much more severe symptoms. This spectrum will allow clinicians to account for the variations in symptoms and behaviours from person to person. Symptoms together limit and impair everyday functioning.
The tenth version of the International Classification of Diseases (ICD-10; World Health Organization, 1992) identifies autism as a pervasive developmental disorders characterized by qualitative abnormalities in reciprocal social interactions and in patterns of communication, and by restricted, stereotyped, repetitive repertoire of interests and activities. These qualitative abnormalities are a pervasive feature of the individual's functioning in all situations, although they may vary in degree. ICD-10 also recognizes that it is usual, but not invariable, for there to be some degree of general cognitive impairment suggestive of ID; and there is some disagreement on the subdivision of this overall group of pervasive developmental disorders. ICD-10 specified that behaviours could be defined in terms of the associated mental age. If ID is present it is important that it is separately coded because it is not a universal feature of PDD.
Autistic Features in ID: Rutter (1978) provided an important and
influential synthesis of Kanner’s original report with subsequent research. Rutter’s work provided evidence for four essential features autism: (1) early onset, (2) distinctively impaired social development, (3) distinctively impaired communication, and (4)
unusual behaviors of the type suggested in Kanner’s concept of “insistence on sameness”. This provided enough impetus to differentiate between autism and ID and for the former’s entry into the diagnostic system, that is, the third edition of DSM (DSM-III; American Psychiatric Association, 1980).
Wing and Gould (1979) studied 132 children under 15 years of age, who has significant social impairment and, in more than 50% of cases, intellectual impairment. They found that 12.8% of the sample had autistic syndrome. The study also revealed that mutism or echolalia, and repetitive stereotyped behaviour were found in almost all the socially impaired children, but to a less marked extent in a minority of the sociable severely retarded. A subgroup with a history of Kanner's early childhood autism could be identified reliably but shared many abnormalities with other socially impaired children. These findings imply that it is possible and even necessary to distinguish between ID, typical autism, and other conditions involving social impairment.
Cantú, Stone, Wing, Langee and Williams (1990) screened 780 children with ID and identified 9.3% as having autism or autistic behaviour. Kar and Khanna (1993) observed autistic disorder in 13% of 55 children with ID, with majority of them having an IQ less than 50. Kar et al. (1997) conducted a study to assess the autistic features in 52 children with ID. They found it was possible to diagnose the syndrome of autism in children with ID in a significant number (9.6%) by using structured interview schedule, that is, the Ritvo Freeman Real Life Rating Scale, as compared to limited instances of clinical diagnosis (1.9%). Kar et al. (1997) also found that more number of children with severe or profound ID had a diagnosis of autism or autistic features. Purkayastha, Girimaji, Srinath and Seshadri (1997) conducted a study to know the clinical profile in a group of 874 children with ID, which revealed that co-morbid autistic features were present in 4.7% of the cases. The prevalence may increase up to 18% in adult population with ID (Corbett, 1979). Autism can virtually affect all the psychological and behavioural domains with prominent disturbances in social, communicative and cognitive spheres (Malhotra & Vikas, 2005). La Malfa et al. (2004) identified a strong relationship between ID and autism spectrum, with 40% of people with ID also presenting with a
Saumyashree et al.,...... / Autistic Spectrum Disorders in Children with Intellectual Disability

37
pervasive developmental disorder (PDD) and nearly 70 % of those with PDD having ID. However, studies indicate that less than one-half of the individuals with ID, who met diagnostic criteria for autism, were previously diagnosed as such. It suggests that individuals with ID should be carefully evaluated for presence of autism instead of passing the observed behavioural issues as a characteristic feature of low intelligence (Bryson et al., 2008).
Significance of the Present Study:Gillberg (2010) found that there could be some
bias to ignore the presence of neurodevelopmental disorders on clinical examination. And it is more common in case of ID as it decreases the prominence of associated emotional and behavioural disorders (Reiss, Levitan, & Szyszko, 1982) and not to say about sub-syndromal features. In India where the quantum of social benefits and service provisions are determined by the percentage of disability, which understandably goes up with additional condition, detecting additional conditions in ID has direct relevance for service delivery. Until recently when India did not have specific provisions to diagnose and quantify the disability associated with autism, presence of autism in ID was not given any additional consideration while estimating the disability or providing the social benefits. Conversely, it is in the common knowledge that autism, at times, is certified as ID to secure social benefits for the individuals with autism. Since there are specific policies and provisions to diagnose and quantify the disability associated with autism, there is a need to systematically study autistic features in ID. The data generated may hopefully be useful in panning appropriate services for people with ID and ASD. In this context, the objective of the study was to assess the frequency and type of autistic features in children with intellectual disability.
METHODThis study adopted the cross- sectional, post-
facto research design. It included 50 children with an ICD-10 diagnosis of intellectual disability without any comorbid syndrome, who were in the age range of 3 to 18 years. Children with associated sensory-motor impairments and known cases of organic brain impairment and neurological disorder like epilepsy were not included in the study. The participants were
selected by using purposive sampling technique from a community-based, not-for-profit day care facility (n= 30) and from the outpatient unit of a tertiary care psychiatry facility (n = 20). After obtaining the clearance from the Institute’s Ethics Review Board, prospective children were identified and informed consent was obtained from the parents. Wherever possible, assent to participate in the study was obtained from the children as well. Parents were interviewed with a semi-structured schedule to gather the minimum required socio-demographic and clinical details of the child. And each child was individually assessed with the Seguine Form Board Test (Indian adaptation by Bharatraj, 1971) and the Stanford - Binet Intelligence Scale (Hindi adaptation by Kulshrestha, 1971) for general intellectual functioning; and with Gilliam Autism Rating Scale (GARS; Gilliam, 1995) for identification of autistic features. On GARS, those with average and above-average scores were considered to have ASD. All these scales were used in earlier studies without any cultural limitations in India.
DATA ANALYSISData were analyzed using Statistical Package for
Social Sciences for Windows Version 16.0. Frequency, percentage and product moment correlation were used for the analysis of the data.
RESULTTable 1: Showing Characteristics of the Sample.
Variables n %
SexMale 35 70Female 15 30
Education
Illiterate 16 32
Pre-Primary 20 40
Primary 7 14
Secondary 7 14
Socio- economic Status
Upper 2 4Middle 21 42Lower 27 54
DomicileUrban 13 26Semi-urban 8 16Rural 29 58
Level of IDMild 21 42Moderate 17 34Severe to Profound 12 24
Mean age of participants was 10.46 (SD = 3) years. Table 1 indicates that the majority of the study
Saumyashree et al.,...... / Autistic Spectrum Disorders in Children with Intellectual Disability

38
group was males (70%), who belonged to lower socio-economic status (54%) and rural background (58%) and had minimum of pre-primary level education (40%). Majority of them had mild ID (42%).
Table 2: Presence of Autistic Features among Children with Intellectual Disability.
Categories on GARS n %
Very low 42 84Low 2 4Below Average 3 6Average 2 4Above average 1 2Total 50 100
Table 2 shows the prevalence of autistic features in the study group. Only three (6%) people had significant level of autistic features- two with an average level and one with above average level of autistic features, indicating caseness for autism. A separate analysis indicates that among the three, who were positive for autism, one each had mild, moderate and severe level of ID.
Table 3: Autistic Features among Children with Intellectual Disability as Assessed by GARS.
GARS Domains
Levels of Symptoms
Stereotype Behaviour
Commu-nication
Social Interaction
Developmental Disturbances
n % n % n % n %
Absent 21 42% 17 34% 22 44% 0 0%
Very low 16 32% 17 34% 14 28% 0 0%
Low 9 18% 7 14% 7 14% 1 2%
Below Average 0 0% 4 8% 3 6% 8 16%
Average 3 6% 5 10% 4 8% 36 72%
Above Average 1 2% 0 0% 0 0% 5 10%
Table 3 shows the severity of autistic features in the study group across different domains of GARS such as, stereotype behaviour, communication, social interactions, and developmental disturbances. On Stereotype Behaviour domain, 6% had average level and 2% had above average level of symptoms. In the communication domain, 10% of the children had average level of symptoms. In the area of Social Interaction, 8%
of the children had average level of deficits. In the area of Developmental disturbances, 72% of children had average level of symptoms and another 10% had above average level of symptoms.
Table 4: Showing Correlation between Intelligence Quotient and Autistic Features.
Intelligence Quotient
GARS Domains
Stereotype Behaviour
Commu-nication
Social Interaction
Developmental Disturbances
- .10 - .17 - .15 - .28*
*p < .05 Table 4 shows the correlation between
intelligence quotient (IQ) and autistic features. The results revealed a significant negative between IQ and developmental disturbances. No significant correlation was observed between IQ and stereotype behaviour, communication and social interaction problems. However, developmental disturbances was found significantly negatively correlated with Intelligence Quotient.
DISCUSSIONThe result of the present study is based on the
detailed assessment of 50 children with ID. The study revealed that three children (6%) had probable caseness for autism on GARS as opposed to none on clinical examination. The three had three different levels of ID. Together these findings indicate that autism could be found across various levels of ID (Kar & Khanna, 1993; Kar et al., 1997) and structured rating scales may pick up autism better than mere clinical examination (Kar et al. 1997). Findings also show however that all the children in the study had some kind of autistic features in varying levels. Significant problems were noted in the domain of developmental concerns. Since the group has a primary diagnosis of ID, it was beyond the scope of this study to comment whether the developmental concerns reflected on GARS were primarily due to ID or attributable to ASD. Nonetheless, the findings imply that developmental concerns typical of autism could also be found in those with ID.
The finding of 6% of children as having autistic disorder is similar to the study by Cantu et al. (1990). These findings are somewhat similar to an epidemiologically-derived, population-based study of
Saumyashree et al.,...... / Autistic Spectrum Disorders in Children with Intellectual Disability

39
adolescents with ID, which indicates that overall, 28% of individuals, or 2.0 of the 7.1/1000 with ID in the target population were identified with autism (Bryson et al., 2008). It also supports that ASD could be found across all levels of ID (Bryson et al., 2008), but more difficult to identify it in children with severe and profound intellectual disability due to diagnostic over shadowing phenomena observed in ID. There seems to be consensus that children with ID have deficits in language and communication and both variables share an inverse correlation (Beitchman, 1986). Absence of speech, idiosyncratic use, echolalia and lack of communicative use of language was marked, similar to those described in previous studies (Kar et al., 1997; Srinath et al., 1989). In general, it appears that ASD may not be clinically easily identifiable in ID but on application of structured interview schedules and rating scales stresses the importance of use of structured methods for identifying ASD in the backdrop of ID (Kar et al., 1997).
Findings of the present study are consistent with the study by Purkayastha et al. (1997), who had reported that only 4.7% of children have significant autistic features. Consistent with earlier studies, the present study revealed that developmental delay, stereotype behaviour, communication deficit and deficit in social interaction are commonly seen features in children with ID (American Psychiatric Association, 2000; Corbett, 1979; Wing & Gould, 1979). Corbett (1979) has estimated that stereotype is seen in as many as 40% of children under 16 with severe mental retardation and 18% of adults with ID. Among those residing institutions, the incidence of abnormal stereotypes may be even greater. Berkaon and Davenport (1962) have observed that about two thirds of their samples engaged in some form of rhythmical movement. The present study reveals that nearly 2% had above-average range of autistic features. Besides the developmental concerns, social and communication impairments were commonly noted in this study. This finding is consistent with previous studies that social and language impairment could be reliably identified as autistic features in ID as low intelligence cannot explain the atypical and diverse presentation (Kar et al., 1997). And a high correlationship between ID and autism calls for a new approach in order to elaborate a new integrated model for people with ID (La Malfa et al., 2004).
In conclusion, symptoms of autism could be expected in children with ID without a
diagnosis of co-morbid autism. Developmental delay, Stereotype behaviour, communication deficit and deficit in social interaction part of the symptom clusters. The correlation between intelligence quotient and probability of autism for developmental disturbances significantly increase with lower intelligent quotient.
REFERENCESAmerican Psychiatric Association. (1980). Diagnostic
and Statistical Manual of Mental Disorders (3rd ed.). Washington, DC: Author.
American Psychiatric Association. (1994). Diagnostic and Statistical Manual of Mental Disorders (4th ed.). Washington, DC: Author.
American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders (5th ed.). Washington, DC: Author.
Beitchman, J.H. & Peterson, M. (1986) Disorders of language communication and behaviour of mentally retarded children. Some ideas on their co-occurrence. Psychiatric Clinics of North America, 9(4), 689-698
Berkson, G. & Davenport, R. K. (1962). Stereotyped movements of mental defectives: Initial Survey. American Journal of Mental Deficiency, 66, 849-851.
Bharat Raj, J., (1971). A.H.S.H. norms on Seguin form board with Indian children. Journal of All India Institute of Speech and Hearing , 2, 34-39.
Bryson, S.E., Bradley, E.A., Thompson, A., & Wainwright, A. (2008). Prevalence of autism among adolescents with intellectual disabilities. Canadian Journal of Psychiatry, 53(7), 449-459.
Cantú, E.S., Stone, J.W., Wing, A.A., Langee, H.R. & Williams, C.A. (1990). Cytogenetic, survey for autistic fragile X Carriers in mental retardation. American Journal on Mental Retardation , 94 (4), 442 - 447.
Corbett, J.A. (1979). Psychiatric morbidity and mental retardation. In F. James & R. Snaith (Eds.). Psychiatric Illness and Mental Handicap. London: Gaskell Press, 11-25.
Emerson, E. & Hatton, C. (2007). Mental health of children and adolescents with intellectual disabilities in Britain. The British Journal of Psychiatry, 191 (6), 493-499. doi: 10.1192/bjp.bp.107.038729
Saumyashree et al.,...... / Autistic Spectrum Disorders in Children with Intellectual Disability

40
Gillberg, C. (2010). The ESSENCE in child psychiatry: Early Symptomatic Syndromes Eliciting Neurodevelopmental Clinical Examinations. Research in Developmental Disabilities, 31 (6), 1543-51.
Gilliam, J.E. (1995). Gilliam Autism Rating Scale: Examiner’s Manual. Austin, TX: Pro- ED
Kanner L (1943). Autistic disturbances of affective contact. The Nervous Child, 2, 217-250 (Reprinted in Acta Paedopsychiatrica, 1968, 35, 100-136).
Kar, N., & Khanna, R. (1993). Mental health problems among children with mental retardation. Indian Journal of Psychiatry, 9 (1-4), 24-26.
Kar, N., Khanna, R. & Kar G.C. (1997). Autistic features in children with mental retardation. Indian Journal of Psychiatry, 39 (4), 304-308.
Kulshrestha S., (1960). Stanford- Binet Intelligence Scale Hindi Adaptation, 3rd Revision- Form L-M. New Delhi: Prasad Psycho Corporation.
La Malfa, G., Lassi S., Bertelli, M., Salvini, R., & Placidi, G.F. (2004). Autism and intellectual disability: a study of prevalence on a sample of the Italian population. Journal of Intellectual Disability Research, 48 (3): 262-267
Lotter,V. (1978). Childhood autism in Africa. Journal of Child Psychology and Psychiatry, 19, 231-244.
Malhotra, S. & Vikas, A. (2005). Pervasive Developmental Disorders: Indian Scene. Journal of the Indian Academy of Child and Adolescent Mental Health, 1 (3), 5. Available from: http://
www.jiacam.org/0103/Jiacam05_3_5.pdf.Purkayastha, M., Girimaji, S., Srinath, S. & Seshadri,
S.P (1997). Clinical profile in mental retardation. In Research Endeavours in Child and Adolescent Psychiatry in India. The Proceeding of the 4th Biennial conference of the Indian Association for child and Adolescent Mental Health, Goa, pp. 48-53.
Reiss, S., Levitan, G.W., & Szyszko, J. (1982). Emotional disturbance and mental retardation: diagnostic overshadowing. American Journal of Mental Deficiency, 86(6), 567-574.
Rutter, M. (1978). Diagnosis and definition of childhood autism. Journal of Autism and Childhod Schizophrenia, 8 (2):, 139-161.
Srinath, S., Choudhuri, J., Bhide, A.V., Narayanan, H.S. & Shivaprakash (1989). Descriptive study of infantile autism. NIMHANS Journal, 7 (1), 77-81.
Wing, L. & Gould, J. (1979).Severe impairment of social interaction and associated abnormalities in children: Epidemiology and classification. Journal of Autism and Developmental Disorder. 9 (1), 11-29.
World Health Organization. (1992) The ICD-10 International Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines. World Health Organization, Geneva.
Saumyashree et al.,...... / Autistic Spectrum Disorders in Children with Intellectual Disability

41
1. Post Doctoral Fellow (UGC), Deptt. of Psychology, Patna University Patna, 2. Clinical Neuropsychologist, Deptt.of Psychiatry, B M H & R C, Bhopal, 3. Ex Professor, Patna University, Patna, India *Corresponding Author: Richa Priyamvada. Email: [email protected] Paper was presented in 43rd NACIACP 2017 held on 27-29 Jan 2017 at Coimbatore, Tamil Nadu, India
INTRODUCTIONAs we know it is the practice of training
techniques that facilitate improvement in targeted cognitive areas; and focus on functional outcome. Cognitive retraining is a systematic, functionally oriented service of therapeutic cognitive activities and an understanding of the person’s behavioural deficits. Services are directed to achieve functional changes by
• Reinforcing strengthening or establishing previously learned patterns of behaviour, or
• Establishing new patterns of cognitive activity or mechanism to compensate for impaired neurological systems.Cognitive retraining is based on the theory
proposed by Luria that the recovery of function can occur through new learned connections established through cognitive retraining exercises. The process of cognitive rehabilitation involves assessment of cognitive functions, goal setting, and applying appropriate cognitive exercise to improve the cognitive function.
It may involve internally focused interventions, meaning the direct process-specific training of a
function, e. g. Like attention and /or memory training as well as learning compensatory techniques. Another aspect of internally focused interventions often included in cognitive retraining programs involves facilitation of insight and self-awareness with regard to cognitive abilities, which includes instruction in the use of meta cognitive strategies. Externally focused interventions, on the other hand, involve adapting to environmental demands, making environmental modifications and the use of specialized teaching strategies. Subdural haematoma is a collection of blood outside the brain. Subdural haematomas are usually caused by severe head injuries. In a subdural haematoma, blood collects between the layers of tissue that surrounds the brain. The outermost layer is called the dura. In a subdural haematoma, bleeding occurs between the dura and the next layer, the arachnoid. The present study was conducted with an aim to see the efficacy of cognitive retraining in Subdural Haematoma
METHODOLOGYSample:
The sample comprised of 5 patients of Subdural Hematoma. The mean age was 25 years educated upto graduate level. All patients were right
Indian Journal of Clinical Psychology2017, Vol. 44, No. 1,41-44
Copyright, 2017, Indian Association ofClinical Psychologists (ISSN 0303-2582)
Research Article
ABSTRACT Head injury survivors may experience a range of neuropsychological problems following a brain injury either through a road accident or due to any other injuries. Depending on the part of the brain affected and the severity of the injury, the result on any one individual can vary greatly. Personality changes, memory deficits, lack of impulse control, and poor concentration are all common. Cognitive Retraining is a technique that is designed to enhance perception, attention, comprehension, learning, remembering, reasoning and problem solving in individuals who are impaired in these areas. The present study was conducted to see the impact of Cognitive Retraining in Subdural Haematoma. The sample comprised of 5 patients of Subdural Haematoma. The mean age was 25 years educated up to graduate level. All patients were right handed, Cases were referred from Neuro surgeon. The study was pre and post intervention with follow-up. Firstly socio demographic data was filled, for Cognitive assessment LNNB-I was used. Total 36 sessions with homework assignment was given i. e. pre-assessment, cognitive retraining after that Post assessment was done to see the outcome of cognitive retraining with four month follow up. Results suggests that there was significant improvement found in the patients after the intervention in the area of attention, recall, recognition and planning. Along with these deficits their basic living skills of the patients were improved as reported by their parents and relatives. Cognitive Retraining are quite useful in remediating cognitive deficits.Keywords: Cognitive Retraining, Subdural Haematoma, Cognitive Functions, LNNB
Cognitive Retraining in Subdural Haematoma*Richa Priyamvada1, Rupesh Ranjan2 and Prabha Shukla3

42
handed, Case were referred from Neuro surgeon. The study was pre and post intervention with follow-up assessment design.
Assessment Tools: • Socio demographic Data Sheet • Annet’s Hand Preference Scale (1970) • Luria Nebraska Neuropsychological Battery
(LNNB-I; Golden et al., 1985)
Procedure:5 patients of Subdural Haematoma were
selected for study. Initial session includes Clinical interview and required history, Socio-demographic sheet were filled. Since all the patient was right handed which was also screened out through Annet’s Hand Preference Battery. To assess the cognitive deficits LNNB-I was administered. After Pre-assessment, cognitive retraining was given to patients. Three sessions per week with homework assignment was given which includes pre assessment, cognitive retraining and after that post assessment was done to see the outcome of cognitive retraining after four month follow up.
COGNITIVE RETRAINING PROGRAMTable 1: Showing the Various Areas Deals
Cognitive Functions are Studied. Areas Name of the Activities Area Focused
Attention
Daily Activities Fine Motor Control, Attention Difficulties
Cancellation tasks Attention/Concentration
Maze drawing Attention/Concentration
Word search Attention/Concentration
Grain sorting Attention /Concentration
Memory and ProblemSolving
Orientation TaskMemory, Attention/Concentration
Number Sequencing Memory Orientation
Colour Discrimination Tasks
Visuo Spatial, Memory
Recall of Pictures & PlacesMemory Orientation, Reasoning, Problem Solving Skills
Location Information Memory, Planning
Number Sequencing Memory Orientation
Areas Name of the Activities Area Focused
Recall andRecognition
Picture Recall, Family Pictures
Recall And Recognition
Recall Places, Road Maps
Memory, Recognition
Following Commands Planning, Recognition
Language Skills and Reasoning
Reading Comprehension
Visual Spatial Skills, Attention /Concentration, Language Skills
Drawing Figures Visual Spatial
Arithmetic Reasoning, Memory
Word Search Reasoning, Language
Puzzles, Crosswords Reasoning
Picture Recall, Family Pictures
Recall And Recognition
Recall Places, Road Maps
Memory, Recognition
Following Commands Planning, Recognition
Reading ComprehensionVisual Spatial Skills, Attention/Concentration, Language Skills
Drawing Figures Visual Spatial
Arithmetic Reasoning, Memory
Word Search Reasoning, Language
Puzzles, Crosswords Reasoning
RESULTS Table 1: Showing the Socio-demographic Details.
Variable Mean±SD
Age 25±1.58
Sex Male 05(100)
Education 16±0.83
Marital Status Single 05(100)
Domicile Urban 05(100)
Table 1 describes the socio-demographic details of the Subdural Haematoma patients.
Richa Priyamvada et al.,........ / Cognitive Retraining in Subdural Haematoma

43
Table 2: Showing Pre and Post Assessment Findings of Subdural Haematoma on LNNB-I.
LNNB-I ScalesPretest Score
Mean ± SD
Post test Score
Mean ± SD
pValue
Motor Functions (C1) 74.40± 5.17 54.20±3.63 2.032
Rhthym Functions (C2) 46.80±3.96 33.80±3.63 2.032*
Tactile Functions (C3) 69.80±4.43 50.60±1.14 2.032*
Visual Functions (C4) 53.20±3.27 46.20±1.48 2.032*
Receptive Speech (C5) 51.40±1.14 48.40±1.14 2.032*
Expressive Speech (C6) 55.80±6.22 49.40±1.14 2.032*
Writing (C7) 56.20±4.14 48.80±1.30 1.67*
Reading (C8) 59.20±1.64 48.40±4.56 2-032*
Arithmetic(C9) 51.20±0.83 45.80±3.11 2-032*
Memory Functions (C10) 62.00±2.12 48.80±1.30 2-032*
Intellectual Functions (C11) 59.40±3.28 50.40±1.81 2-041*
Pathognomic (S1) 55.20±6.14 43.80±4.38 2-032*
Left Hemisphere (S2) 60.80±6.79 48.80±3.11 2-032*
Right Hemisphere (S3) 75.80±4.60 57.60±7.76 2-032*
Profile elevation (S4) 69.20±2.58 53.40±3.43 2-032*
Impairment (S5) 67.00±5.70 54.20±3.76 2-032*
*Significant at 0.05 levelTable no 5 shows the pre and post assessment
findings of Subdural Haematoma. The scale assesses the cognitive deficits in patients of Subdural Haematoma. The result revels patient’s significantly differ on Wilcoxon sign rank test on Motor functions (C1), Rhythm Functions Scale (C2), Tactile Functions (C3), Visual Functions (C4). Receptive Speech (C5), Expressive Speech (C6), Writing (C7), Reading (C8), Arithmetic (C9), Memory (C10), Intellectual Process (C11), Left Hemisphere, (S2), Right Hemisphere (S3), Profile Elevation (S4)), and Impairment Scale (S5), which shows the efficacy of cognitive retraining program. The post test score were significantly reduced on above areas suggest the problem severity was significantly reduced after behavioural intervention.
DISCUSSIONIn the present study the aim was to decipher the
improvement in cognitive functioning of the patient through cognitive retraining techniques. Therefore a pretest was done to assess cognitive deficits in patients of Subdural Haematoma. After four month of regular intervention all areas were again assessed (post test) by using same tests i. e. as in pre test.
SDH (n=5)
Pre Assessment LNNB
Cognitive Retraining Programme
Thrice/ week with home work Assignment
4 months follow up
Post assessment LNNB
Positive Out come
Results reveals there was a significant improvement in Motor functions (C1), Rhythm functions scale (C2), Tactile functions (C3), Visual Functions (C4), Receptive speech (C5), Expressive Speech (C6), Writing (C7), Reading (C8) Arithmetic (C9), Memory (C10), Intellectual Process (C11), left hemisphere, (S2), Right hemisphere (S3), Profile Elevation (S4)), and Impairment Scale (S5) which shows the efficacy of cognitive retraining which is consistent with findings of Jamuna et al., 2010. Similarly Nehra et al. (2012) reported three
Richa Priyamvada et al.,........ / Cognitive Retraining in Subdural Haematoma

44
confirmed cases of effective cognitive retraining in moderate and severe traumatic brain injury. As Subdural Haematoma patient’s exhibit significant disability due to cognitive deficits particularly in attention, learning and memory, and higher-order executive functions. Individuals who sustain brain injuries frequently have difficulties in arousal, attention, concentration, memory, problem solving, decision making, insight and other areas of cognition that impede their ability to perform their occupation in everyday life. Alterations in perception, motor control, balancing, emotional functioning, social interaction and control of behaviour are also common after brain injury and are closely linked with cognitive issues (Bell & Sandell, 1998). Cognitive retraining or Brain injury rehabilitation (Sohlberg & Mateer, 2001) is based on the nature and scope of neuropsychological symptoms identified on special batteries of test designed to measure brain functioning following brain injury practicing various cognitive tasks--doing arithmetic problems, solving logic puzzles, concentration skills, or reading may help brain rehabilitation. The study of Arciniegas et al. (2002) reveals disturbances of attention and memory are particularly problematic, as disruption of these relatively basic cognitive functions may cause or exacerbate additional disturbances in executive function, communication, and other relatively more complex cognitive functions Thus Cognitive rehabilitation may also be useful for the treatment of impaired attention, interpersonal communication skills, and executive function following TBI. This form of treatment is most useful for patients with mild to moderate cognitive impairments, and may be particularly useful for those who are still relatively functionally independent and motivated to engage in and rehearse these strategies. The significant differences show that cognitive retraining is useful in remediating cognitive deficits in haematoma patient along with improvement in daily living activity.
CONCLUSIONCognitive retraining is an effective method for
rehabilitating Subdural Hepatoma cases suffering from various cognitive deficits. Also this training
is beneficial only with the patient’s compliance; family support and long term follow up. However, larger sample may be needed for generalization of the results.
REFERENCESAnnett, M. (1970). A classification of hand preference
by association analysis. British Journal of Psychology, 61, 303-321.
Arciniegas, D B., Held, K., & Wagner, P. (2002) Cognitive Impairment Following Traumatic Brain Injury Treat Options. Neurol. 2002 Jan, 4 (1), 43-57.
Ashima, Nehra., & Swati, Bajpai (2012) Effectiveness of Cognitive Retraining after Brain Trauma― Case Studies Activitas Nervosa Superior, 54, No. 3-4
Bell, K. R., & Sandell, M.E., (1998). Brain injury rehabilitation. Post-acute rehabilitation and community integration. Archives of Physical Medicine and Rehabilitation, 79, S21–5.
Golden, C J., Grabber, B., Coffman, J A., Berg, R A., Newlin, D B., & Block, S. (1981). Structural brain deficits in schizophrenia;identification by CT scan density measurements. Archives of General Psychiatry, 38, 1014-1017
Golden, C. J., Purish, A. D., & Hammeke, T. A. (1985). Luria –Nebraska Neuropsychological Battery: Forms I & II (Manual). Western Psychological Services, Los Angeles
Jamuna, N., & Shibu, Pillai. (2010). Home based cognitive retraining in traumatic brain injury. Indian Journal of Neurotrauma (IJNT) 7, No. 1, 93-96
Sohlberg, M. M., & Mateer, C. A. (2001). Cognitive Rehabilitation: An Integrated Neuropsychological Approach. 1st Edition. Vol. 16, United States of America: Guilford Press.
Richa Priyamvada et al.,.......... / Cognitive Retraining in Subdural Haematoma

45
INTRODUCTION Now a days it is common that many individuals
have become so dependent on internet that possibly it seems difficult to imagine a day without it. The internet was first time launched in India on 15 August 1995 at Mumbai. It took ten years to become access of general population through computers and within five years internet spread their wings very rapidly through laptops, tablets, smartphones etc. Now the addiction term is too frequently used for internet because the researches describes many underlying similarities with substance addictions such as tolerance, withdrawal, repeated unsuccessful attempts to cut back or quit, and impairment in normal functioning (Young, 1998; Beard & Wolf, 2001; Shapira et al., 2003; Aboujaoude et al., 2006; Block, 2008; Chang & Hung, 2012).
The term Internet Addiction (IA) was first time introduced in 1995 by Goldberg to describe the negative effects of excessive Internet use on personal lives. Thereafter, Young (1998) used the term “Pathological Internet Use” when presenting a paper
at the American Psychological Association’s (APA) meeting. But later, she used the phrase “Internet Addiction” when talking with the general public.
The Internet Addiction is characterised as preoccupation about the Internet, internet usage more than intended, Internet use regardless of the negative consequences, rapidly increasing amount of time engaged in internet activities (tolerance), withdrawal symptoms (irritability, anxiety, sadness) when internet use prevented (Davis, 2001), unsuccessful attempts to control the Internet use (Rau et al., 2006), loss of interests in previous hobbies and entertainment as a result of internet use, and with the exception, deceiving family members, therapists, or others regarding the amount of Internet use and increase amount of Internet use to escape or relieve from negative mood (feelings of helplessness, guilt, anxiety). As a result IA peoples was found to have risked or lost a significant relationship, job, or educational or career opportunity than normal controlled populations.
The harmful effects of IA includes social
Indian Journal of Clinical Psychology2017, Vol. 44, No. 1, 45-53
Copyright, 2017, Indian Association ofClinical Psychologists (ISSN 0303-2582)
Research Article
ABSTRACTLiterature has been receiving many studies on the rise of internet addiction recently. The harmful effects of the Internet Addiction are well documented in Indian youths. Various psychological therapies are being researched and utilised for managing this concern. Hence, present study was planned to see the applicability of Behaviour Therapy for the management of Internet Addiction. In this study ten PG students were selected by using purposive sampling from Institute of Mental Health and Hospital, Agra. Participants were equally divided into two groups (Experimental & Control) and their pre and post assessment has been done by using Young’s Internet Addiction Test and a semi structured self-monitoring data sheet was specifically developed to assess the frequency, time and activities of Internet use. The experimental group received 8 sessions of the Behaviour Therapy intervention. The results of present study suggest that the behaviour therapy is significantly (U 0.00, Z 2.61, Sig 0.01) effective for the management of Internet Addiction and it was also revealed that students were spending their maximum time with social chatting sites, watching and downloading videos and browsing other than studies. Conclusion: Behaviour therapy is found significantly effective in managing Internet addiction. The high positive reinforcement of internet use changed into punishment and rapid conditioning with boredom, loneliness, social interaction, stress and free time with Internet deconditioned by using behaviour therapy techniques. Key words: Internet Addiction, Behaviour Therapy, Internet Chatting, Online Shopping, online, Video Watching, Classical Conditioning, Operant Conditioning
Efficacy of Behaviour Therapy in Internet Addiction *Preeti Singh¹ and Narendra Nath Samantaray²
1. Astt Prof., Dept. of Clinical Psychology, Inst. of Mental Health and Hospital, Agra, India 2. Clinical Psychologist, Dept. of Clinical Psychology, Mental Health Institute (COE), SCB Med. Coll. & Hospital, Cuttack, India *Corresponding Author: Priti Singh. E mail: [email protected]. The Paper was presented in 43rd NACIACP 2017 held in Coimbatore on Jan 27-29,2017 and Awarded SC Gupta Best Paper Award

46
dysfunctions such as social isolation, poor social skill, difficulty to perform given tasks and responsibilities, less time for work and family commitments, poor interpersonal relationships, family discord, divorce, job loss, academic failure, poor academic grades, academic probation and sometime expulsion from schools (Leung, 2007; Mythily et al., 2008; Kim et al., 2010; Wang et al., 2012; Azher et al., 2014; Rajeev et al., 2015). Whereas bodily manifestations of it varies from sleep deprivation, tension headache, physical pain, blurred vision, malnutrition, fatigue (White, 2011), low eye sight, disturbed digestion (Azher et al., 2014) and cognitive impairment too (Davis, 2001).
The several studies reveals that IA is significantly correlated with depression (Sanders et al., 2000; Ha et al., 2007; Ni et al., 2009; Stetina et al., 2011), anxiety (Ni et al., 2009), social phobia (Koet al., 2009), loneliness (Ozcan and Buzlu, 2007), low self-esteem (Ko et al., 2005; Ko et al., 2007), hostility (Ko et al., 2007; Yen et al., 2008), substance use (Koet et al., 2006; Korkeila et al., 2010), harmful alcohol use (Yen et al.,2009; Ohannessian, 2009), low frustration tolerance (Ko et al., 2008), attention deficit and hyperactivity disorder (Yen et al., 2007) and high impulsivity (Cao et al., 2007).
The high prevalence of IA was found in Japan - 25.43% followed by Hong Kong - 24.71% and also found high addiction of social networking sites - 34.8% followed by instant messenger - 27.98% (Kwok et al., 2014). Among college students the high prevalence was found in UK - 18.3% (Niemz et al., 2005) followed by South America – 13% (Scherer, 1997) and among high school highest prevalence found in Korea – 39.6% (Kim et al., 2006). A Pakistan study of college students reported 34% problematic IA with 2.7% severe IA and among them males - 48.42 are high as compare to females - 38.73% (Azher et al., 2014). The Internet in India (I-Cube) 2011 reported, Internet users in India has crossed the landmark 100 million mark in September 2011 and more than three quarters of Internet using population driven by young men (27%), school (21%) and college going kids (27%) (Dholakia, 2011). The Indian statistics compiled by Ethinos Digital Marketing, 2012 (United States of America) shows that Face book has crossed 50 million users, Twitter grows to 13 million and LinkedIn has over
15 million users in India. An Indian study of college students reported high prevalence of IA in medical students (49.5%) and also found highest prevalence 89.2% in 4th year students followed by 31.1% 3rd year students and the lowest 5% in 2nd year (Mishra et al., 2015).
Psychotherapeutic Management of Internet Addiction:
There were several psychotherapeutic techniques which has been identified, designed and developed to help the IA peoples such as time management skills (Du et al., 2010), solution focused brief therapy (Fang-ru et al., 2005), group therapy (Jager et al., 2012), social skill training (Jager et al., 2012), cognitive behaviour therapy (Greenfield, 2000; Orzack, 1999; Davis, 2001; Hansen, 2002; Young, 2007), addiction counselling (Chang et al., 2005) and family therapy. Among them a comprehensive CBT program is developed by Young was frequently used and found to be significantly effective for the management of IA (Young, 2007 & 2011). However Young’s CBT for IA started with behaviour modification and proceeded towards cognitive intervention but as compare to comprehensive CBT programs, efficacy studies of using behaviour dominated therapies on IA has not been significantly studied.
Hence, this study was planned to find the objective, problem focused and less cost effective intervention for IA by using Behaviour Therapy.
Behaviour Therapy Conceptualization of Internet Addiction:
The behaviour therapy has been suggested in early stage treatment of IA with specific focus on behaviours and situations (Hall & Parsons, 2001). Present study conceptualized the Classical conditioning and Operant Conditioning models in the development and management of IA behaviour.
Behaviour therapy intervenes and alters the stimulus (external environment and situations) to change the maladaptive behaviour into adaptive behaviour. Some of external and situational factors are considered as maintaining factors of IA such as visual attraction of sites, need to chat someone, free time, need to purchase something, want to make listen others (sharing one’s thought without inhibition and
Preeti et al.,............ / Efficacy of Behaviour Therapy in Internet Addiction
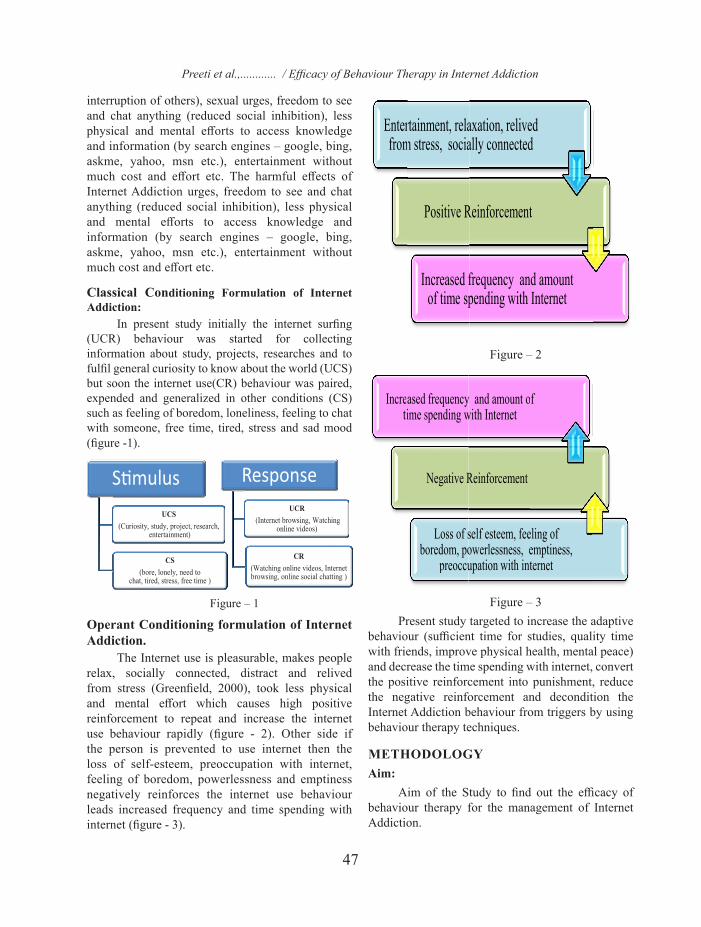
47
interruption of others), sexual urges, freedom to see and chat anything (reduced social inhibition), less physical and mental efforts to access knowledge and information (by search engines – google, bing, askme, yahoo, msn etc.), entertainment without much cost and effort etc. The harmful effects of Internet Addiction urges, freedom to see and chat anything (reduced social inhibition), less physical and mental efforts to access knowledge and information (by search engines – google, bing, askme, yahoo, msn etc.), entertainment without much cost and effort etc.
Classical Conditioning Formulation of Internet Addiction:
In present study initially the internet surfing (UCR) behaviour was started for collecting information about study, projects, researches and to fulfil general curiosity to know about the world (UCS) but soon the internet use(CR) behaviour was paired, expended and generalized in other conditions (CS) such as feeling of boredom, loneliness, feeling to chat with someone, free time, tired, stress and sad mood (figure -1).
Figure – 1
Operant Conditioning formulation of Internet Addiction.
The Internet use is pleasurable, makes people relax, socially connected, distract and relived from stress (Greenfield, 2000), took less physical and mental effort which causes high positive reinforcement to repeat and increase the internet use behaviour rapidly (figure - 2). Other side if the person is prevented to use internet then the loss of self-esteem, preoccupation with internet, feeling of boredom, powerlessness and emptiness negatively reinforces the internet use behaviour leads increased frequency and time spending with internet (figure - 3).
Enterfrom
rtainment, relam stress, socia
Positive R
Increased fof time sp
axation, reliveally connected
Reinforcement
frequency andpending with I
ed d
t
d amount Internet
Incretiased frequencyime spending w
Negative R
Loss of sboredom, po
preoccu
y and amount owith Internet
Reinforcement
self esteem, feeowerlessness, eupation with int
f
eling of emptiness, ternet
Figure – 2
Enterfrom
rtainment, relam stress, socia
Positive R
Increased fof time sp
axation, reliveally connected
Reinforcement
frequency andpending with I
ed d
t
d amount Internet
Incretiased frequencyime spending w
Negative R
Loss of sboredom, po
preoccu
y and amount owith Internet
Reinforcement
self esteem, feeowerlessness, eupation with int
f
eling of emptiness, ternet
Figure – 3
Present study targeted to increase the adaptive behaviour (sufficient time for studies, quality time with friends, improve physical health, mental peace) and decrease the time spending with internet, convert the positive reinforcement into punishment, reduce the negative reinforcement and decondition the Internet Addiction behaviour from triggers by using behaviour therapy techniques.
METHODOLOGYAim:
Aim of the Study to find out the efficacy of behaviour therapy for the management of Internet Addiction.
Preeti et al.,............ / Efficacy of Behaviour Therapy in Internet Addiction

48
Hypothesis: There is no significant difference between post
assessment of the Internet Addiction in experimental and control group.
Design: Before and after with control group design.
Sample: The 10 PG students having Internet Addiction
were selected by using purposive sampling technique from Institute of Mental Health and Hospital, Agra. The ten (6 females and 4 males) samples were equally divided into experimental group (3 female and 2 male) and control group (3 female and 2 male). The age range of students is between 25-30 years. The inclusion criteria was living in single rooms at hostel for last one year, unmarried, knowledge of Hindi and English language, weekly spending 35 to 50 hours with internet other than studies. Students having any psychiatric comorbidity, significant disabling physical illness, organic pathology and substance abuse were excluded from the study.
Tools: For the present study following tools were used:
Socio-demographic Data Sheet: It was semi structured Performa especially
designed for this study. It contains information about socio-demographic variables like age, sex, education, marital status, residence, occupation and religion.
Young Internet Addiction Test: Developed by Dr. Kimberly Young in 1996.
The psychometric properties was analysed by factor analysis of six factors (salience, excessive use, neglecting work, anticipation, lack of control and neglecting social life) and found good internal consistency (.62-.226) and concurrent validity, with salience being the most reliable (Widyanto & Mcmurran, 2004).
Self-Monitoring Data Sheet: This is a semi-structure self-monitoring data
sheet specifically developed for the present study to assess the frequency, time and activities of Internet use. The content validity has been evaluated on the basis of five professionals response.
Behaviour Therapy Techniques Used in Present Study:
Present study used the following behaviour therapy techniques for the management of IA:
Activity Scheduling: Changing the time of Internet use, using
alarms, set time limits, and prioritise the work.
Graded Task Assignment: To reduce the procrastination about studies and
other significant tasks.
Stimulus Control: Mobile free a day in week, switch-off, flight
mode, silent and hide the phone. • Distraction• Flash cards• Alternate Problem Solving focused behaviour • Relaxation, exercise and play outdoor games
or outing with friends
Procedure:Initially the clinical interview has been done to
identify the level and severity of Internet Addiction. Thereafter 10 students meeting the inclusion criteria were selected for the study. Then socio-demographic data sheet, Young Internet Addiction Test and Self –monitoring data sheet had been applied on the students. Afterwards the drawn samples were divided into two groups (Control and Experimental Group) with 5 samples in each group. The therapy session has been started with psycho-education about nature, causes, prevalence, comorbidity and management of Internet Addiction. Thereafter the Activity Scheduling, Graded Task Assignment, Stimulus Control, Distraction, Flash Cards, Alternate Problem Solving Focused Behaviour, Relaxation, Exercise and Play Outdoor Games or outing with friend’s behavioural techniques were applied on experimental group biweekly for 8 sessions. After completion of intervention program both groups were reassessed by using Young Internet Addiction Test and Self-Monitoring data sheet. The Mean, SD and the Mann Whitney statistical measures has been used for the statistical analysis of the study.
Preeti et al.,............ / Efficacy of Behaviour Therapy in Internet Addiction

49
RESULTSTable 1: The Average Time Spending with
Internet Activities Each Day Before and After Treatment.
Internet Activities
Minutes Spending with Internet in a day
Pre Assessment Scores Post Assessment Scores
Exp. Group(Pre) N=5
Control Group(Pre) N=5
Exp. Group(Post) N=5
Control Group(Post) N=5
Mean±SD Mean±SD Mean±SD Mean±SD
Social Chatting (SC) 149±29.10 170.80±13.37 40.00±14.21 169.60±9.76
Watching and Downloading Videos (WDV)
146±44.96 161.40±38.70 20.00±15.81 160.60±35.77
Video Calling (VC) 35.20±48.72 38.80±56.95 14.00±19.49 35.80±53.27
Shopping Sites (SS) .00.±00 .00±.00 .00±.00 .00±.00
Email (E) .00.±00 .00±.00 .00±.00 .00±.00
Browsing other than studies (BOS)
107±29.98 83.60±30.87 22.20±11.58 80.60±23.21
Figure – 4
The table-1 suggest significant reduction of each day time spending with internet other than studies of experimental group participants after one month therapeutic intervention. However, there are slight reductions also observed in control group participants, which is only for few minutes. The table-1 also suggest that majority of participants were spending more time with social chatting sites followed by watching and downloading videos and browsing other than study material. None of the participants reported using shopping sites and checking e mails for the one month period (figure - 4).
Table 2: The average Internet Addiction Before and After Treatment.
Young’s
Internet
Addiction
Test
Pre Assessment Scores Post Assessment Scores
Exp. Group N=5
Mean±SD
Control Group
N=5Mean±SD
Exp.Group
N=5Mean±SD
Control Group
N=5Mean±SD
77.60±5.37 76.60± 5.50 35.00±5.57 74.60± .67
Figure - 5
Table - 2 reveals significant reduction of internet addiction score and criteria from problematic use to average use of experimental group. While slight reduction also observed in control group participants but they keep maintain on problematic use category of internet addiction severity (figure - 5).
Table 3 : The Difference Between Time Spending with Internet Activities Each Day Before and After Treatment.
Internet Activities
Pre Assessment (N=10) Post Assessment (N=10)Mean Rank Mann Whitney Mean
Rank Mann Whitney
Exp. Con-trol U value Z
ScoreSig.(2- tailed) Exp. Con-
trol U value Z Score
Sig. (2- tailed)
Social Chatting 21 34 6.00 1.36 .175 15 40 .00 2.62 .01
Watching & Down-loading Videos
22 33 7.00 1.15 .251 15 40 .00 2.61 .01
Video Calling 27 27 12.50 .00 1.00 25 30 10.50 .47 .638
Shopping Sites 27 27 12.50 .00 1.00 27 27 12.50 .00 1.00
Email 27 27 12.50 .00 1.00 27 27 12.50 .00 1.00Browsing other than Studies
35 19 4.50 1.68 .094 15 40 .00 2.61 .01
Table – 3 revealed that there is no significant difference was obtained of different internet activities in pre-assessment of experimental and control group except browsing other than study material
Preeti et al.,............ / Efficacy of Behaviour Therapy in Internet Addiction
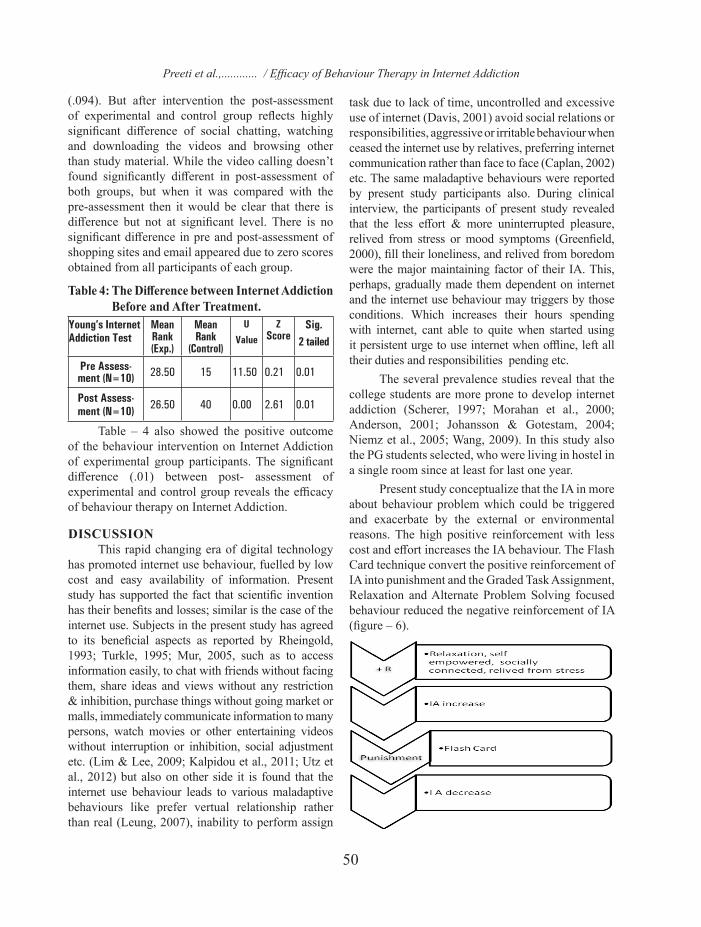
50
(.094). But after intervention the post-assessment of experimental and control group reflects highly significant difference of social chatting, watching and downloading the videos and browsing other than study material. While the video calling doesn’t found significantly different in post-assessment of both groups, but when it was compared with the pre-assessment then it would be clear that there is difference but not at significant level. There is no significant difference in pre and post-assessment of shopping sites and email appeared due to zero scores obtained from all participants of each group.
Table 4: The Difference between Internet Addiction Before and After Treatment.
Young’s Internet Addiction Test
Mean Rank (Exp.)
Mean Rank
(Control)
U Value
Z Score
Sig.2 tailed
Pre Assess-ment (N=10) 28.50 15 11.50 0.21 0.01
Post Assess-ment (N=10) 26.50 40 0.00 2.61 0.01
Table – 4 also showed the positive outcome of the behaviour intervention on Internet Addiction of experimental group participants. The significant difference (.01) between post- assessment of experimental and control group reveals the efficacy of behaviour therapy on Internet Addiction.
DISCUSSION This rapid changing era of digital technology
has promoted internet use behaviour, fuelled by low cost and easy availability of information. Present study has supported the fact that scientific invention has their benefits and losses; similar is the case of the internet use. Subjects in the present study has agreed to its beneficial aspects as reported by Rheingold, 1993; Turkle, 1995; Mur, 2005, such as to access information easily, to chat with friends without facing them, share ideas and views without any restriction & inhibition, purchase things without going market or malls, immediately communicate information to many persons, watch movies or other entertaining videos without interruption or inhibition, social adjustment etc. (Lim & Lee, 2009; Kalpidou et al., 2011; Utz et al., 2012) but also on other side it is found that the internet use behaviour leads to various maladaptive behaviours like prefer vertual relationship rather than real (Leung, 2007), inability to perform assign
task due to lack of time, uncontrolled and excessive use of internet (Davis, 2001) avoid social relations or responsibilities, aggressive or irritable behaviour when ceased the internet use by relatives, preferring internet communication rather than face to face (Caplan, 2002) etc. The same maladaptive behaviours were reported by present study participants also. During clinical interview, the participants of present study revealed that the less effort & more uninterrupted pleasure, relived from stress or mood symptoms (Greenfield, 2000), fill their loneliness, and relived from boredom were the major maintaining factor of their IA. This, perhaps, gradually made them dependent on internet and the internet use behaviour may triggers by those conditions. Which increases their hours spending with internet, cant able to quite when started using it persistent urge to use internet when offline, left all their duties and responsibilities pending etc.
The several prevalence studies reveal that the college students are more prone to develop internet addiction (Scherer, 1997; Morahan et al., 2000; Anderson, 2001; Johansson & Gotestam, 2004; Niemz et al., 2005; Wang, 2009). In this study also the PG students selected, who were living in hostel in a single room since at least for last one year.
Present study conceptualize that the IA in more about behaviour problem which could be triggered and exacerbate by the external or environmental reasons. The high positive reinforcement with less cost and effort increases the IA behaviour. The Flash Card technique convert the positive reinforcement of IA into punishment and the Graded Task Assignment, Relaxation and Alternate Problem Solving focused behaviour reduced the negative reinforcement of IA (figure – 6).
Preeti et al.,............ / Efficacy of Behaviour Therapy in Internet Addiction

51
On the other side the rapid conditioning of IA with mood symptoms, loneliness, free time, boredom, stress, tired, need to chat someone etc. (CS) works as a cue to perpetuating the IA behaviour and could cause relapses also. Therefore the management of CS is planned to break the conditioning between CS and CR (IA) by using behaviour therapy techniques such as Activity Scheduling, Distraction, Stimulus control, Alternative Problem Solving focused behaviour, Relaxation, exercise and play outdoor games or outing with friends. And the result findings suggest that these behaviour therapy techniques significantly decondition the pairing between CS and CR (figure - 7).
•Infostud
•Infofulf
•Ente
ormation for dy purposes ormation to fill Curiosity ertainment
UCS
Activity Scbehaviour,
••••••
cheduling, DisRelaxation, e
•Bore •Free time•Loneliness•Stress •Tired•Need to chatsomeone
CS
straction, Stimexercise and p
t
mulus control, lay outdoor g
•Internetbrowsin
•Watchinonline v
U
Alternative Pames or outin
t ng ng videos
UCR
Problem Solvinng with friends
•Watchionline v
•Internebrowsin
•Social csites
ng focused s.
ing videos
et ng chatting
CR
Figure - 7: Figure 7 shows flow chart of Activity Scheduling, Distraction, Stimulus Control, Alternative Problem Solving Focused Behaviour, Relaxation, Exercise and Play Outdoor Games or Outing with Friends.
The findings of the present study also reveals that the majority of students from both groups were spending their maximum time with social chatting, watching and downloading videos, browsing other than study material and none of them were spending time with internet shopping sites and checking emails was consistent with other Indian studies (Dholakia, 2011;
Ethinos Digital Marketing, 2012). The result findings also showed the significant reduction of time spending with social chatting and watching and downloading videos of experimental group participants after one month behaviour therapy intervention. The significant reduction of the YIAT scores and level of severity in experimental group participants was also observed after behaviour therapy intervention suggests the efficacy of behaviour therapy for the management of internet addiction (Hall & Parsons, 2001).
CONCLUSION Internet Addiction is an emerging new mental
health problem (DSM-V) causes significant personal, social, educational and occupational impairment. The Internet Addiction have high amount of positive and negative reinforcement and rapid conditioning with boredom, loneliness, social interaction, stress and free time. The present study used behaviour therapy techniques to change the positive reinforcement into punishment, reduce negative reinforcement and decondition the Internet Addiction behaviour. The result shows significant efficacy of behaviour therapy for the management of Internet Addiction.
Future DirectionsFuture studies can be targeted to use behaviour
therapy for the management of internet addiction in chronicity, different age groups, gender, psychiatric co-morbidity, personality features, cognitive ability, educational background etc.
Clinical Implication Behaviour therapy is an economical and
objective evidence based psychotherapy gives more outcome in less effort can be useful in this rapid growing and scientific era to manage internet addiction. The behaviour therapy techniques required less cognitive ability so could be highly generalized to maximum number of populations.
No conflict of interest was among authors. All the authors contributed significantly on study. the study was approved by ethical committee of the institute.
REFERENCES Aboujaoude, E., Koran, L. M., Gamel, N., Large, M. D., &
Serpe, R. T. (2006). Potential markers for problematic internet use: a telephone survey of 2,513 adults. CNS Spectrums, 11 (10), 750-755.
Preeti et al.,............ / Efficacy of Behaviour Therapy in Internet Addiction

52
Anderson, K. J. (2001). Internet use among college students: An exploratory study. Journal of American College Health, 50 (1), 21-26.
Azher, M., Khan, R. B., Salim, M., Bilal, M., Hussain, A., & Haseeb, M. (2014). The relationship between internet addiction and anxiety among students of University of Sargodha. International Journal of Humanities and Social Science, 4 (1), 288-293.
Beard, K. W., & Wolf, E. M. (2001). Modification in the proposed diagnostic criteria for Internet addiction. Cyber Psychology & Behavior, 4 (3), 377-383.
Block, J. J. (2008). Issues for DSM-V: Internet addiction. American Journal of Psychiatry, 165 (3), 306-307.
Cao, F., Su, L., Liu, T., & Gao, X. (2007). The relationship between impulsivity and Internet addiction in a sample of Chinese adolescents. European Psychiatry, 22 (7), 466-471.
Caplan, S. E. (2002). Problematic Internet use and psychosocial well-being: development of a theory-based cognitive–behavioral measurement instrument. Computers in Human Behavior, 18 (5), 553-575.
Chang, D. F., Tong, H., Shi, Q., & Zeng, Q. (2005). Letting a hundred flowers bloom: Counselling and psychotherapy in the People's Republic of China. Journal of Mental Health Counselling, 27 (2), 104.
Chang, J. P. C., & Hung, C. C. (2012). Problematic internet use. IACAPAP e-Textbook of Child and Adolescent Mental Health. Geneva: International Association for Child and Adolescent Psychiatry and Allied Professions.
Davis, R. A. (2001). A cognitive-behavioural model of pathological Internet use. Computers in human behaviour, 17 (2), 187-195.
Dholakia V. (2011). India crosses 100 million internet users landmark. Retrieved from: http://trak.in/tags/business/2011/11/08/internet-user-growth-india-report/
Du, Y. S., Jiang, W., & Vance, A. (2010). Longer term effect of randomized, controlled group cognitive behavioural therapy for Internet addiction in adolescent students in Shanghai. Australian and New Zealand Journal of Psychiatry, 44 (2), 129-134.
Ethinos Digital Marketing (2012). A snapshot of digital India Retrieved from: http://www.slideshare.net/Ethinos/a-snapshot-of-digital-india-may-2012
Fang-ru, Y., & Wei, H. (2005). The effect of integrated psychosocial intervention on 52 adolescents with Internet addiction disorder. Chinese Journal of Clinical Psychology, 13 (3), 343-5.
Greenfield, D. N. (2000). Virtual Addiction: Help for Netheads, Cyberfreaks, and Those Who Love Them. Adolescence, 35 (137), 223.
Ha, J. H., Kim, S. Y., Bae, S. C., Bae, S., Kim, H., Sim, M., & Cho, S. C. (2007). Depression and Internet addiction in adolescents. Psychopathology, 40 (6), 424-430.
Hall, A. S., & Parsons, J. (2001). Internet addiction: College
student case study using best practices in cognitive behaviour therapy. Journal of Mental Health Counselling, 23 (4), 312.
Jager, S., Muller, K. W., Ruckes, C., Wittig, T., Batra, A., Musalek, M.,&Beutel, M. E. (2012). Effects of a manualized short-term treatment of internet and computer game addiction (STICA): study protocol for a randomized controlled trial. Trials, 13 (1), 1.
Johansson, A., &Gotestam, K. G. (2004). Internet addiction: characteristics of a questionnaire and prevalence in Norwegian youth (12–18 years). Scandinavian Journal of Psychology, 45 (3), 223-229.
Kalpidou, M., Costin, D., & Morris, J. (2011). The relationship between Facebook and the well-being of undergraduate college students. Cyber Psychology, Behaviour, and Social Networking, 14 (4), 183-189.
Kim, K., Ryu, E., Chon, M. Y., Yeun, E. J., Choi, S. Y., Seo, J. S., & Nam, B. W. (2006). Internet addiction in Korean adolescents and its relation to depression and suicidal ideation: a questionnaire survey. International Journal of Nursing Studies, 43 (2), 185-192.
Kim, Y., Park, J. Y., Kim, S. B., Jung, I. K., Lim, Y. S., & Kim, J. H. (2010). The effects of Internet addiction on the lifestyle and dietary behaviour of Korean adolescents. Nutrition Research and Practice, 4 (1), 51-57.
Ko, C. H., Yen, J. Y., Chen, C. C., Chen, S. H., & Yen, C. F. (2005). Gender differences and related factors affecting online gaming addiction among Taiwanese adolescents. The Journal of Nervous and Mental Disease, 193 (4), 273-277.
Ko, C. H., Yen, J. Y., Chen, C. C., Chen, S. H., Wu, K., & Yen, C. F. (2006). Tridimensional personality of adolescents with internet addiction and substance use experience. The Canadian Journal of Psychiatry, 51 (14), 887-894.
Ko, C. H., Yen, J. Y., Chen, C. S., Yeh, Y. C., & Yen, C. F. (2009). Predictive values of psychiatric symptoms for internet addiction in adolescents: a 2-year prospective study. Archives of Paediatrics & Adolescent Medicine, 163 (10), 937-943.
Ko, C. H., Yen, J. Y., Yen, C. F., Chen, C. S., & Wang, S. Y. (2008). The association between Internet addiction and belief of frustration intolerance: the gender difference. Cyber Psychology & Behaviour, 11 (3), 273-278.
Ko, C. H., Yen, J. Y., Yen, C. F., Lin, H. C., & Yang, M. J. (2007). Factors predictive for incidence and remission of internet addiction in young adolescents: a prospective study. Cyber Psychology & Behaviour, 10 (4), 545-551.
Korkeila, J., Kaarlas, S., Jaaskelainen, M., Vahlberg, T., &Taiminen, T. (2010). Attached to the web—harmful use of the Internet and its correlates. European Psychiatry, 25 (4), 236-241.
Leung, L. (2006). Stressful life events, motives for Internet use, and social support among digital kids. Cyber Psychology & Behaviour, 10 (2), 204-214.
Preeti et al.,............ / Efficacy of Behaviour Therapy in Internet Addiction

53
Lim, S., & Lee, J. E. R. (2009). When playing together feels different: effects of task types and social contexts on physiological arousal in multiplayer online gaming contexts. Cyber Psychology & Behaviour, 12 (1), 59-61.
Mak, K. K., Lai, C. M., Watanabe, H., Kim, D. I., Bahar, N., Ramos, M., & Cheng, C. (2014). Epidemiology of internet behaviors and addiction among adolescents in six Asian countries. Cyberpsychology, Behaviour, and Social Networking, 17 (11), 720-728.
Mishra, S., Rout, R. P., & Jayakrishnan, K. (2015). A Correlative Study to Assess the Internet Addiction and Health Status among the Students of SOA University Bhubaneswar. International Journal of Nursing Education, 7 (4), 82-86.
Morahan-Martin, J., & Schumacher, P. (2000). Incidence and correlates of pathological Internet use among college students. Computers in Human Behaviour, 16 (1), 13-29.
Mur, C. (Ed.). (2005). Does the Internet benefit society?.Greenhaven Pr.
Mythily, S., Qiu, S., & Winslow, M. (2008). Prevalence and correlates of excessive Internet use among youth in Singapore. Annals Academy of Medicine Singapore, 37 (1), 9.
Ni, X., Yan, H., Chen, S., & Liu, Z. (2009). Factors influencing internet addiction in a sample of freshmen university students in China. Cyberpsychology & Behaviour, 12 (3), 327-330.
Niemz, K., Griffiths, M., &Banyard, P. (2005). Prevalence of pathological Internet use among university students and correlations with self-esteem, the General Health Questionnaire (GHQ), and disinhibition. Cyber Psychology & Behaviour, 8 (6), 562-570.
Ohannessian, C. M. (2009). Does technology use moderate the relationship between parental alcoholism and adolescent alcohol and cigarette use?. Addictive Behaviour, 34 (6), 606-609.
Orzack, M. (1999). Computer addiction: Is it real or is it virtual. Harvard Mental Health Letter, 15 (7), 8.
Rajeev M.M. & Jobilal (2015). Effects of Social Media on Social Relationships: A Descriptive Study on the Impact of Mobile Phones among Youth Population. International Research Journal of Social Sciences, Vol. 4 (2), 11-16.
Rau, P. L. P., Peng, S. Y., & Yang, C. C. (2006). Time distortion for expert and novice online game players. Cyber Psychology & Behaviour, 9 (4), 396-403.
Rheingold, H. (1993). The Virtual Communication: Homesteading on the Electronic Frontier Reading. MA: Addison-Wesley.
Sanders, C. E., Field, T. M., Miguel, D., & Kaplan, M. (2000). The relationship of Internet use to depression and social isolation among Adolescents. Adolescence, 35 (138), 237.
Scherer, K. (1997). College life online of College life and
Development. Healthy and Unhealthy Internet use Journal, 38, 655-665.
Shapira, N. A., Lessig, M. C., Goldsmith, T. D., Szabo, S. T., Lazoritz, M., Gold, M. S., & Stein, D. J. (2003). Problematic internet use: proposed classification and diagnostic criteria. Depression and Anxiety, 17 (4), 207-216.
Sherer, K. (1997). College life on-line: Healthy and unhealthy Internet use. Journal of College Student Development, 38, 655-665.
Stetina, B. U., Kothgassner, O. D., Lehenbauer, M., & Kryspin-Exner, I. (2011). Beyond the fascination of online-games: Probing addictive behaviour and depression in the world of online-gaming. Computers in Human Behaviour, 27 (1), 473-479.
Turkle, S. (1995). Life Behind the Screen: Identity in the Age of the Internet. New York, NY: Simon & Schuster.
Utz, S., Jonas, K. J., & Tonkens, E. (2012). Effects of passion for massively multiplayer online role-playing games on interpersonal relationships. Journal of Media Psychology.
Wang, L., Luo, J., Gao, W., & Kong, J. (2012). The effect of Internet use on adolescents’ lifestyles: A national survey. Computers in Human Behaviour, 28 (6), 2007-2013.
Wang, S. (2009). The relationship of online game addiction and cognitive distortions and intervention in adolescents. Unpublished master's thesis. Guangzhou, Guangdong, China: Sun-Yat Sen University.
Widyanto, L., & McMurran, M. (2004). The psychometric properties of the internet addiction test. Cyber Psychology & Behaviour, 7 (4), 443-450.
Yen, J. Y., Ko, C. H., Yen, C. F., Chen, C. S., & Chen, C. C. (2009). The association between harmful alcohol use and Internet addiction among college students: comparison of personality. Psychiatry and Clinical Neurosciences, 63 (2), 218-224.
Yen, J. Y., Ko, C. H., Yen, C. F., Chen, S. H., Chung, W. L., & Chen, C. C. (2008). Psychiatric symptoms in adolescents with Internet addiction: Comparison with substance use. Psychiatry and Clinical Neurosciences, 62 (1), 9-16.
Yen, J. Y., Ko, C. H., Yen, C. F., Wu, H. Y., & Yang, M. J. (2007). The comorbid psychiatric symptoms of Internet addiction: attention deficit and hyperactivity disorder (ADHD), depression, social phobia, and hostility. Journal of Adolescent Health, 41 (1), 93-98.
Young, K. S. (1998). Internet addiction: The emergence of a new clinical disorder. Cyber Psychology & Behaviour, 1 (3), 237-244.
Young, K. S. (2007). Cognitive behaviour therapy with Internet addicts: treatment outcomes and implications. Cyber Psychology & Behaviour, 10 (5), 671-679.
Young, K. S. (2011). CBT-IA: The first treatment model for internet addiction. Journal of Cognitive Psychotherapy, 25 (4), 304-312.
Preeti et al.,............ / Efficacy of Behaviour Therapy in Internet Addiction

54
1. Assistant Professor, North East Regional Institute of Education, (NCERT), Shillong 2. Professor, Dept. of Psychology, University of Allahabad. Corresponding Author: *Prachi Ghildial, e-mail : [email protected]
INTRODUCTION The anti-positivist focus on multiple realities,
subaltern voices and local-cultural understandings has found its way into the discourse on mental illness as it has into the definition, understanding and theorizing of several other phenomena. Acknowledging, and actively espousing, the role of the perceiver’s context in the way reality is perceived, made sense of and dealt with, has become the mainstay of constructionist perspective. Hence, the emphasis on culture as a determining principle in most transactions with the ‘objective’ world. This culture is a ‘patterned’ and ‘programmed’ way of responding to the context in which one is and which also is unique to members of different collective groups (Kluckhohn, 1951; Hofstede, 1980). Geertz (1973) gives the concept of culture a semiotic interpretation equating it with historically transmitted and symbolic meanings and conceptions which enable men to ‘communicate, perpetuate, and develop their knowledge about and attitudes toward life.” Thus culture would be an independent variable in studying various phenomenon. Since cultures vary, the conceptions as well as perceptions of members of these cultures would vary with respect to various phenomena. Culture has been found to influence the way people make attributions, categorization and similarity judgments, somatization, depression and pain, moral judgment and processes of school
learning (Angel & Guarnaccia, 1981; Angel & Idler,1992; Angel & Thoits, 1987; Kleinman, 1986; Markus & Kitayama, 1992; Miller & Bersoff, 1992; Miller, 1984; Pepitone & Triandis, 1987).
As with other phenomenon, mental illness is also a function of the time and place of its origin. With Szasz (1974) denying the very existence of it, the definitions of mental illness have been changing across time and they differ across cultures. Clare (1976) has talked about attempts to replace the term mental illness by one with a less medical connotation like ‘deviance, maladaptation, social disturbance, problems of living or community disorder”. This attempt has the rudiments of an acknowledgement of the mental illness being a cultural-social rather than an exclusively medical or biological phenomenon. Culture becomes important when the symptoms of mental illness have to be construed, interpreted and made sense of. There are symptoms that are universally construed as mental illness (Lin, 1996) and there are culture-specific syndromes (Marsella, 1993).
Even so called universal illnesses like depression and schizophrenia have different manifestation and prognosis in different cultures (Marsella, 1980; Katz et al, 1988; Sartorius et al, 1986, Warner 1994) though the core symptoms of Schizophrenia are universally manifested (WHO, 1973). This paper focuses on how culture influences the recognition or identification of mental illness.
Indian Journal of Clinical Psychology2017, Vol. 44, No. 1, 54-59
Copyright, 2017, Indian Association ofClinical Psychologists (ISSN 0303-2582)
Research ArticleIndicators of Mental Illness in a North Indian Population
*Prachi Ghildyal1 and KomillaThapa2
ABSTRACTCulture plays an important role in cognitive process that mediate the social interaction in the
behaviour of individual. Fundamental cognitive process e.g., emotions, self esteem, self concept, self enhancement, attitude, prejudice, memory processes etc. are influenced and shaped by individual's culture. These are the important determinants of mental illnesses. Understanding, interpretations, and acceptability of symptoms of mental illnesses may varies from one culture to other, Present study try to find out how cultural influence affect the recognition and identification of mental illnesses. The sample of present study include 28 patients suffering from various mental disorders 24 relatives of the patients and 64 lay persons from Northern India. The semi structured interview procedure and semi structured questionnaire was used to collect the data. Responses obtained were qualitatively interpreted. Result shows that deviance from set norms of the community was considered as symptoms of mental illnesses without consideration whether the deviance is of due to mental illness or is of physical aspect of the problem. Some unusual phenomenon as sneezia was also considered a sign of mental illness. Behavioural excess in any form e.g., excess eating excess quietness etc was also considered as sign of mental illness in Noth Indian population. Keywords: Mental Illness, Culture, North India, Schizophrenia

55
METHOD Sample:
RESULTSThis study was carried out within the qualitative
paradigm because herein the attempt was to explore ideas and understand them rather than to focus on how many of the respondents give a particular response. Thus, every different response was given place in the cultural construction of mental illness. The responses obtained are being presented in the following tables.
Table 1: Showing the Distribution of Males and Females, Age Range in Years and the Average Age of the Respondents in Each of the Respondent Groups.
Patients Relatives Hindus Muslims ChristiansMale 18 18 22 8 4Female 10 6 19 7 4Total 28 24 41 15 8Age Range 20-65 22-75 16-68 16-53 23-71Average Age 35.39 41.25 33.06 29.46 42.38
Table 2: Showing the Distribution of the Patient Group into the Diagnostic Categories.
Bipolar Mood Disorder Schizophrenia Anxiety Disorders10 14 4
Table 3: Showing the Sample Distribution in Terms of Socio-Economic Status (Included Both Educational Level and Income).
Middle - High SES Low SESPatients 22 6Relatives 19 5
Laypersons 45 19
Table No. 4: Showing the Symptoms of Mental Illness Generated in All Three Groups.
Patients Relatives Laypersons
Physical or Somatic Physical or SomaticComplaints Impaired Intellect
Cognitive Dysfunction a) Irrational Thinkingb) Intellectual Slowing
Lowered Self Awareness
Appearance and Manner of Speech
Emotional Distress
a) Emotional excessesb) Emotional blunting
Behavioural Excesses
Behavioural Abnormalitiesa) Inappropriate behaviourb) Behavioural odditiesc) Behavioural excessesd) Withdrawal
Alienation from Interpersonal/ Social Situations
Irrational thoughts and Fears
Emotional Dysfunction
Anxiety related symptoms
Negative Affect Thought Aberrations
Faulty Perceptions
Impaired Interpersonaland Social Relations
Absence of Volition and Purpose in ActionsInterpersonal and Social Unconcern
Table 5: Showing the Cultural Symptoms Identified by Each of the Groups.Patients Relatives Laypersons
Physical or Somatic Physical or Somatic, Physical problems
Uljhan or a sense of apprehensiveness
Behavioural Eccentricities (praying, singing & crying in excess)
Appearance and Manner of Speech
Somatic hallucinations e.g. liver being jammed, Head filled with water
Uljhan
Delusions of a cultural nature e.g considering oneself as ‘Devi’
Stubbornness in interpersonal relationsNo belongingness
DISCUSSIONAs Maretzki (1981) points out, “Culture is a
super biological characteristic of the species which therefore must pertain to every human”. Thus, in this study, to get to the cultural construction of indicators of mental illness, rather than going to the religious-philosophical texts and some experts on culture, constructions of the laypersons were accessed with the belief that it is neither possible nor desirable to restrict the idea of culture to what obtains only in codified knowledge or belief systems. Herein the definition of culture as including the most humble people and the most menial acts (Hofstede, 1980) is used. Culture is not only what some elite groups profess and practice. It is as Geertz (1973) points out, the “total way of life of a people”. Therefore looking for culture beyond the lay and ordinary is not warranted. Since culture permeates all acts and behaviours, it is inseparable from the persons in a given society and it influences their way of thinking, feeling and believing (Kluckhohn, 1951).
There are several models to understand the relationship between culture and psychopathology. The first of these, the relativistic model states that the normality and abnormality of behaviour can be seen in relation to the cultural context and opportunities and preferences for certain behaviour in that culture. In this model, mental illness seems to be a label
Prachi et al., .............../ Indicators of Mental Illness in Norht Indian Population.

56
reserved for those whose characteristic reactions are denied validity by their society (Benedict 1934). An evolutionary perspective (Levine, 1973) under the functional- adaptive model stresses on adaptive qualities in relation to environmental pressures and selective processes in relation to the development and functioning of personality. Culture is seen ideationally where, among other things, the cognitive dimensions of culture which contain the principles or rules of behaviour and interactions are stressed. These shared unconscious and conscious cognitions rather than shared motivations maintain the social fabric and social actions of individuals, and are therefore relevant in situations of stress and disturbed relationships as well as in treatment strategies and effectiveness.
The social structure and social relations model (Henry, 1973) talks about shared assumptions between all other ‘sane’ people about how reality is constituted. In families with disturbed inter personal patterns the “as if-ness” or illusions do not conform to, or are different from, the “average illusion”. The symptoms that have come up in the study reflect that mental illness, madness or abnormality as it is variously referred to, is an entity that is constructed by people as an aberration and deviation from what is dictated by the norms of society for typical behaviour. It refers to people who have failed to adjust to the social mores and who do not fit in with the dominant ways and the basic ethos of that particular culture.
The responses in present study suggested that any deviance from the routine and socially approved mode of behaviour, thinking and feeling is seen as a sign of mental illness whether it is related to physical aspects, cognition, emotion or interpersonal relationships. When asked to come up with the indicators of mental illness, the respondents came up with the two extremes of any behaviour as mental illness for e.g., eating too much as well as not feeling hungry or crying always or not crying at all. Anything which most others do and the person does not or is unable to, and everything that he does which the majority does not is seen as a deviance and consequently a symptom of mental illness.
Mental illness thus is defined by the patients, relatives and laypersons as the "autonomous assertion of pure spontaneous self". At times labels rather than symptoms were used to describe mental illness. It was also believed that the patient attempts to draw others’
attention towards himself – a startling echo of the view held by many that a patient’s symptoms are in fact his cry for help. Although all the three groups have come up with certain common symptoms and those that can be placed together in certain overlapping categories, there is discernible a difference in the extent to which the members of each group are able to penetrate the layers of personality in their attempts to understand what is wrong with the person. The context in which each of the persons are determines the way in which the symptoms are construed as indicators of mental illness.
The laypersons have focused mainly on the overt signs of mental illness probably because they are the most obvious and easily accessible to an outsider. This is probably why this group alone has come up with symptoms relating to appearance and dress. This is an example of the layperson’s tendency to judge the patient’s mental and functional state by his outward appearance only. However, the laypersons have also talked about certain symptoms which are common to those cited by the other two groups which suggests that they have accurate information as to what might constitute mental illness. Mental illness is synonymous with abnormality or deviance from the norm and laypersons have come up with almost all kinds of such deviance as symptoms. When confronted with the task of defining the indicators of mental illness, people first try to define what is normally expected and then enumerate all that is contrary to this expectation as a sign of abnormality.
Thus, culture defines what is expected and normal and therefore, also by implication what is abnormal. This preference for culturally or socially acceptable behaviour as the yardstick against which abnormality is measured is seen in the responses of relatives as well as laypersons. The relatives of the patients have emphasized deviance from the acceptable mode of behaving and living. In terms of depth, this stance penetrates deeper into the patients’ inner distress than the laypersons who had judged illness on the basis of appearance. The patients themselves talk more in terms of personal distress – the deepest and the inner most aspect if seen in terms of depth and the layers which need to be pierced to reach this.
The symptoms that have come up in this study are similar to those categories that emerged in the Kota study of Carstairs and Kapur (1976). This study had
Prachi et al., .............../ Indicators of Mental Illness inNorht Indian Population.

57
detected symptoms categorized as somatic, anxiety and worries, irritability and tension, forgetfulness and poor concentration, depressive and psychotic symptoms. In keeping with the transitional state of Indian culture, the indicators that were reported are a mix of both universally observed indicators and some uniquely cultural ones. Some of the uniquely cultural ways of understanding mental illness are presented in the table no 5.
As often stated in literature about the somatisation of complaints amongst Indians, this study also revealed an emphasis on somatic symptoms to express the mental distress amongst all the three groups of respondents. Amongst the uniquely cultural somatic symptoms that emerged were somatic complaints, burning sensation in the head, stomach and feet, headache, cramps and weakness. Though sleeplessness was the most frequent complaint, in one case it was drowsiness that was mentioned as a symptom of mental illness. Rastogi et al. (1976) found that 96 percent of neurotic patients in India had somatic symptoms in their clinical picture. They concluded that patients who are unsophisticated and are unable to use the psychological language and mention symptoms like anxiety, worry, sadness etc. use a somatic language to express their difficulties. Similar findings have been reported by Verma& Wig (1974); Verma et al. (1974), and Agarwal et al. (1973).
In developing countries, psychological distress is experienced and communicated through physical complaints (Kapur, 2001). These could include complaints of pain, dizziness, fatigue, decreased sleep and appetite etc. Apart from the somatic complaints, influence of culture can be seen in the hallucinations and delusions also as one person had the delusion that she was a goddess. ‘Uljhan’, translated as a kind of unease or apprehension was another cultural symptom that came up very frequently in data. This was the indicator of personal distress that both the patients and their relatives referred to.
Some of the respondents were unable to differentiate between mental illness and mental retardation and included low IQ and slow information processing as an indicator of mental illness. Another view stated that many a times it is difficult to identify mentally sick people because they show no outward symptoms but may be extremely irritable, confused or under great stress and despair. This statement appears
insightful since it is almost always that the more florid symptoms of distress are the ones that are most frequently identified and that too often when the illness has reached a stage where it spills over into various aspects of the individual’s functioning, going unnoticed in the earlier and the more manageable stage.
The universally accepted symptom of withdrawal as an indicator of depression was interpreted by one of the respondents as being an indicator of being engrossed and happy in one's own self, and being unconcerned about the external world implying that cutting oneself off from the world around is not necessarily distressing for the person, he might be choosing to do it not for any other reason but because that is a better way of life for him and he enjoys it. This way of interpreting a widely accepted symptom is unique to the Indian cultural context since withdrawing from the world is considered a step towards a more evolved existence and is culturally sanctioned here and so it is probable that some people see it as not an illness but a desirable thing. In contrast to the modern concept of normality as a culturally bound statistical average, the traditional Indian concept is based on the ideal even though unattainable (Palsane et al., 2002). Becoming one with the ‘parabrahman’ and losing one’s identity (Samadhi, Nirvana, Self-Realization) is seen as the way out of all misery and suffering (Rao, 1983).
Though there are certain categories of symptoms that are unique to each group; there is considerable overlap on a number of others. For example, all the three groups have come up with symptoms relating to emotional, cognitive (in the form of irrational thoughts) and somatic symptoms. Sleeplessness is the most cited symptom across groups. Only the laypersons have talked about the illness being identified by the person’s appearance.
Inability to maintain interpersonal and social relationships is also viewed as an indicator of mental illness. Not relating to people as their own- or the absence of the feeling of belongingness is a uniquely cultural way of understanding deviance in a culture which lays premium on relatedness and embeddedness in a group be it family or community. It has come up in all groups as a major indicator of abnormality. An unconcern for interpersonal relations would be expected to be construed as a sign of abnormality in a culture that is characterised by relatedness and simultaneous dwelling in various orders of being.
Prachi et al., .............../ Indicators of Mental Illness inNorht Indian Population.

58
The Hindu view of the person, which colours the traditional perceptions of the nature of man, holds the person to be ‘dividual’ i.e. divisible (Marriot, 1980, 1990). He derives his personal nature interpersonally. As Kakar (1997) states, all affects, needs and motives are relational and distress is experienced when relationships (with the human, natural as well as the cosmic world) are disordered. Even the urbanized and literate individuals view the self and the world in a ‘relational’ manner. Kakar points out cases where an individual’s autonomy is viewed by his relatives (accompanying him for the psychiatric interview further evidencing his ‘relational’ self) as a symptom of his disorder.
Herein Roland (1988) views the Indian self as familial, having the distinctive features of symbiosis-reciprocity, narcissistic configurations of we-self regard, a socially contextual ego-ideal, a superego that structures expression of strong drives according to the exigencies of hierarchical extended family and group relationships, two different levels of mode of communication, and modes of cognition and ego functioning that are highly contextual and oriented towards symbols, signs and influences. Thus, the Indian self is characterized by intensely emotional connectedness, empathy and receptivity to others, an experiential sense of self as ‘we-self’, strong identification with family and deriving self-esteem from family honour and reputation, idealization of elders and reciprocal responsibilities that are traditionally defined.
Impaired intellectual functioning as form of mental illness has been suggested by the patients and the laypersons but not the patients’ relatives. This might be an indication of the patients’ lowered self-awareness and insight and inability to monitor and control their activities. Also, it is not always that laypersons stick to the stereotypes of mental illness. At times they go beyond these prejudices and show remarkable insight coming up with both positive and negative but non-stereotypical aspects of mental illness. They believe for example that the patient is happy in his own reclusive world and he is actually not suffering but content in such a state. This is another echo of the cultural belief or rather premium given to renunciation as the highest form of individualistic striving and the way to escape from the karmic cycle. Contrary to the obvious and easily apparent ‘relational ness’ of the self, the Indian self is also more individual in its unconscious than is overtly apparent and, at least in fantasy, Indians are
capable of conceiving and desiring a self that is free of all attachments and relationships (Kakkar, 1997).
Alternately, they view it as his communication to an indifferent social and interpersonal world. This is a more positive perspective. On the negative side, they view pathology as an attempt to camouflage one’s weaknesses rather than accepting them. An important point that emerges is that laypersons also view some of these symptoms as being beyond the patient’s volition. This realization is significant because that denotes a somewhat, though very rudimentary, sympathy and acceptance for the patient’s condition. Accepting that these behaviours are not deliberate and conscious indicates an understanding and a favourable perspective towards the patient’s problems- at least a willingness to understand.
To conclude it can be said that the construction of mental illness involves identifying ‘anomalous’ behaviour for which no rule or set of instructions can be found (Smith, 1978). Normal and abnormal behaviour is socially constructed. Deviance from social norms is seen as mental illness. Psychiatric symptoms as withdrawal, hallucinations, continual muttering, posturing etc. maybe categorized as violations of certain social norms- these norms are so taken- for- granted that they are not explicitly verbalized, and are called residual rules (Scheff, 1966). Mental illness is thus determined by the incomprehensibility, irrationality, or unintelligibility of an individual’s behaviour (Coulter, 1973; Foucault, 1965; Horwitz 1982; Ingleby, 1982).
REFERENCESAgarwal, A.K., Rajkumar, & Kapur, R.N. (1973). Somatic
symptoms of neurosis: Index of body- image. Indian Journal of Psychiatry, 15, 367-373
Angel, R.., & Guarnaccia, P. (1981). Mind, body and culture: Somatization among Hispanics. Social Science Medicine. 12 (28), 1229-38
Angel, R.., & Idler, E. L. (1992). Somatization and hypochon-driasis: Sociocultural factors in subjective experience. Research in Community Mental Health.7, 71-93
Angel, R. &Thoits, P. (1987). The impact of culture on the cognitive structure of illness. Culture, Medicine and Psychiatry, 11, 465-494
Benedict, R.(1934). Patterns of Culture. London: Routledge & Kegan Paul Ltd.
Carstairs, G.M., & Kapur, R.L. (1976). The Great Universe of Kota. London: The Hogarth Press.
Clare, Anthony. (1976). Psychiatry in Dissent: Controversial Issues in Thought and Practice. Tavistock Publications.
Prachi et al., .............../ Indicators of Mental Illness in Norht Indian Population.

59
Coulter, J. (1973). Approaches to Insanity: A Philosophical and Sociological Study. New York: Wiley.
Foucault, M. (1965). Madness and Civilization: A History of In-sanity in the Age of Reason. New York: Random House.
Geertz, C. (1973). The Interpretation of Cultures: Selected Essays. London: Fontana Press.
Henry, J. (1973). Pathways to Madness. New York: Vintage Books Edition.
Hofstede, G. (1980). Culture’s Consequences: International Differences in Work Related Values. California: Sage
Horwitz, A.V. (1982). The Social Control of Mental Illness. New York: Academic Press.
Ingleby, D. (1982). The social construction of mental illness. In P. Wright & A. Treacher (eds.) The Problem of Medical Knowledge: Examining the Social Construction of Medicine. Edinburgh University Press.
Kakar, S. (1997). Culture and Psyche: Selected Essays. Delhi: Oxford University Press
Kapur, M.(2001). Mental health, illness and therapy. In J. PAndey (ed.) Psychology in India Revisited- Developments in the Discipline. Vol. 2. New Delhi: Sage
Katz, H. M., Marsella, A. J., Dube, K. C., Olatawura, M., Taka-hashi, R., Nakane, Y., et al.. (1988). On the expression of psychosis in different cultures: Schizophrenia in an Indian and in a Nigerian community: A report from the W H O project on determinants of outcome of severe mental disorders. Culture, Medicine and Psychiatry, 12, 331-355
Kleinman, A. (1986). Social origins of distress and disease: Depression, neurasthenia, and pain in modern China. Culture, Medicine and Psychiatry, 6, 117-189
Kluckhohn, C. (1951). The study of culture. In D. Lerner and H.D. Laswell (eds.) The Policy Sciences. Stanford, CA: Stanford University Press
Levine, R. (1973). Culture, Behaviour and Personality. Chicago: Aldine Publishing Company
Lin, K. M., (1996). Cultural influences on the diagnosis of psychotic and organic disorders. In J. E. Mezzich, A. Kleinman, H. Fabrega, and D.L. Parron (eds.) Culture and psychiatric diagnosis: A DSM IV Perspective. Schizophrenia Bulletin, 14, 555-567
Maretzki, T. W. (1981). The cultural paradigm. In C. Eisdorfer, D. Cohen, A. Kleinman and P. Maxim (eds.)Models for Clinical Psychopathology. New York: S.P. Medical and Scientific Books.
Markus, H. R. & Kitayama, S. (1992). The what, why and how of Cultural Psychology. Psychological Inquiry, 3 (3), 208-11.
Marriot, M. (1980). The Open Hindu Person and Interpersonal Fluidity. Unpublished paper read at Association for Asian Studies Meetings, Washington, D.C.
Marriot, M. (1990). India Through Hindu Categories. New Delhi: Sage.
Marsella, A. J. (1980). Depressive experience and disorder across cultures.In H.C. Triandis& J.G. Draguns (eds.) Handbook of Cross-Cultural Psychology, 6. Boston: Allyn& Bacon.
Marsella, A.J. (1993). Sociocultural foundations of psychopathology: An historical overview of concepts, events, and pioneers prior to 1970. Trans cultural Psychiatric Review, 30 (2), 97-142
Miller, J.G. & Bersoff, D.M. (1992). Culture and moral judgement: How are conflicts between justice and interpersonal responsibility resolved? Journal of Personality & Social Psychology, 62, 541-554
Miller, J.G. (1984). Culture and the development of everyday social explanation. Journal of Personality Social Psychology, 46, 961-78
Palsane, M. N., Bhavsar, S. N., Goswami, R. P., & Evans, G. W.(2002). The concept of stress in the Indian tradition. In G. Misra & A. K. Mohanty (eds.) Perspectives on Indigenous Psychology. New Delhi: Concept
Pepitone, A. & Triandis, H. C. (1987).On the universality of social psychological theories. Journal of Cross Cultural Psychology, 18, 471-498
Rao, S.K.R. (1983). The conception of stress in Indian thought: I. The theoretical aspects of stress in Sankhya and Yoga systems, and I the practical involvement in Gita and Ayurveda. NIMHANS Journal, 115-131.
Rastogi , V. S., Jindal, R. C., Gupta, M. P., Rana, S. S. & Singhal, S. (1976). Somatic symptoms in neurosis: A cross cultural study. Indian Journal of Psychiatry, 18, 103-108
Sartorius, N., Jablensky, A., Korten, A., & Ernberg, G. (1986). Early manifestation and first contact incidence of schizophrenia. Psychological Medicine, 16, 909-928
Scheff, T. J. (1966). Being Mentally Ill: A Sociological Theory. Chicago: Aldine (reprinted 1984)
Smith, D. (1978). K is mentally ill. Sociology, 12, 23-53Szasz, T.S. (1974). The Second Sin. London: Routledge and
Kegan PaulSVerma, S.K & Wig, N. N (1974).A cross cultural comparison of
psychiatric patients on some of the parameters of Cornell Medical Index. Indian Journal of Clinical Psychology, 1, 109-113 (IPA, 5, 365)
Verma, S. K., Wig, N. N & Pershad, D.(1974). A comparative study of medical and psychiatric patients on Cornell Medical Index. Indian Journal of Clinical Psychology, 1, 109-113 (IPA, 5, 365)
Warner, R. (1994). Recovery from Schizophrenia: Psychiatry and Political Economy (2nded.) New York: Routledge.
World Health Organization (1973). Report of the International Pilot Study of Schizophrenia. Geneva: World Health Organization.’
Prachi et al., .............../ Indicators of Mental Illness in Norht Indian Population.

60
1. Professor in Clinical Psychology, 2. Clinical Psychologist-Grade II, AIISH, Manasagangotri, Mysore: 570006, Corresponding Author: S Venkatesan Email:[email protected]
Although inter-related, distinctions are made between sports, play, games and toys. All of them are usually dumped under the paraphernalia of what is called as extra-scholastic activities in children. In that sense, they are viewed as ‘additional’ or ‘secondary’ to some other presumably ‘primary’ educational activity. All children require and desire greater educational inputs via individualized, informal, play-driven or functional activities instead of a rigorous, regimented, and formal, classroom or curriculum based teaching (Venkatesan, 2015a; 2015b). Ongoing efforts to organize events like ‘special’ arts, sports or games for Children with Developmental Disabilities (CWDD) is testimony to the fact that they benefit by such means (Hsieh-Chun, 2008; Murphy, Carbone, 2008; Weiss et al. 2003).
Toys help children to discover the world around. It forms a wonderful outlet as means of recreation, education and entertainment. It inspires curiosity, provides opportunity for social and emotional growth. It stimulates creativity, intellect and imagination in children (Tomopoulos et al., 2006; Goldstein, 1994). The scarcity of research on toys vis-a-vis children is lamented (Lieber & Beckman,
1991; Rubin & Howe, 1985).Research on some aspects of play behavior is available (Venkatesan & Ravindran, 2012; Khoshali & Venkatesan, 2010; 2007; Venkatesan, 2000), whereas use of toys by CWDD is minimally explored (Venkatesan, 2014; 2012).
Toy availability, ownership and use are different. One is unsure whether children are given the play materials that they are entitled. The chances are that CWDD might not be provided toys at all. Given their generally poor record of limited repertoire of responses, lack of reciprocity, curiosity, diversity, monotony, and failure to demand toys, they may not be given toys. There are questions on how they use toys, how long or how many times they are used, or whether they are used. Toys maybe kept away from children fearing it might be broken or because they are expensive. There are questions on how much or how frequently money is spent on toys for a given child. Toys may not be purchased. They might be given homemade toys or they may be simply passed on from a senior to junior generation. There are doubts,if parents appreciate that toys are needed as much as food, clothing, shelter and/or medical attention. It would
Indian Journal of Clinical Psychology2017, Vol. 44, No. 1, 60-67
Copyright, 2017, Indian Association ofClinical Psychologists (ISSN 0303-2582)
Research ArticleToy Index of Children With or Without Developmental Disabilities
*S. Venkatesan1 and G Y Yashodharakumar2
ABSTRACTToys are integral ingredients in the lives of children. Contrasting assistive devices, they enable and empower them. This study attempts to develop and determine a toy index based on identified parameters as reported by parent respondents. The index was intended to serve as contemporary benchmarks for targeted children with or without developmental disabilities. Using a cross sectional exploratory survey design, a sample of 267 children including 158 boys (Mean Age: 3.89; SD: 1.32) and 109 girls (Mean Age: 4.13; SD: 1.48) distributed across gender and age groups below six years was drawn from varied socio-demographic backgrounds. Both, formal and informal open-ended data elicitation tools, such as, exploratory interview with significant others, field visit and observations, verbatim recording of informant responses was undertaken. The obtained data was codified, categorized, compiled, collated and analyzed across parameters, such as, ownership, availability, usage and expenditure incurred on toys per child. Results show an overall impoverished mean toy index of 8.60 (SD: 4.14) with varying metrics across age, gender, area of residence, and types of developmental disabilities especially against typical children taken as standard comparison group. Boys than girls show greater ownership and parents spend more money on toys for them as also children from urban than those from rural areas secure higher toy index. The findings highlight the need to provide toys and encourage their use as mandated by child rights rather than as an option for convenience.
Key words: Toys,Toy Index, Play, Developmental Disabilities

61
be worthwhile to explore how or to what extent such toy demands are met, how are the choices made, what considerations are involved in their procurement and dispensing, and ultimately, how they are eventually put into use or handled by the CWDD for whom they are intended. There are many unanswered questions on how toys can be classified or which category of toys is apt for which developmental age or stage in children. It is unknown, how many toys such children actual own, how they are acquired, who makes choices for their procurement, how much time the child is allowed to be with them, whether there are safety norms or practices that govern their making and use, how much time, effort or money is expended on toys vis-à-vis CWDD (Blakemore & Centers, 2005; Ae-Hwa et al. 2003).
In short, there is need to devise objective observable and measurable metrics of what may be called as toy index to benchmark each child or group of children with or without developmental disabilities. Against this background, it was the specific objective of this study to develop and determine a toy index based on respondent reports on identified parameters as point of reference for targeted children with or without developmental disabilities.
METHODThis study employed a cross sectional
randomized survey design. Toy denotes an object used for play. It may
be a model or miniature replica for something. The various attributes of toy need to be demarcated and understood. ‘Toy availability’ is distinguished from ‘toy handling’, ‘toy ownership’, ‘toy possession’ ‘toy accessibility’, and/or ‘toy sharing’. Further, aspects related to ‘toy utility’, ‘toy budgeting’, ‘toy time’, ‘toy life’ and ‘types, classification or taxonomy of toys’ are differentiated. At present, there is no formal or official taxonomy of toys. Informal distinctions are made, if any, on the basis of age: baby, infant, toddler, preschool, adolescent or adult toys. Some classify by content, such as: soft, hard, stuffed, clay, paper, rubber, metal, wooden or plastic toys. A few tell between toys on gender while others denounce this as sexist. Others classify toys by their purpose and functional-utilitarian value to its owner as: sensory, educational, entertainment, personalized fetish-private or public. Operations
based classification of toys is attempted as manual, mechanized, techno-savvy, computer enabled, hand or leg-driven, etc.
Toy Availability is a quality, state or condition of being at hand or easily obtainable. Accessibility appears close and synonymous, but this is not true. For example, a hand operated toy may be made available to a child who is physically challenged. Thus, it may not be ‘accessible’. In this sense, accessibility is the strength and degree to which persons with disability are provided for and enabled to live independently and participate in all aspects of life. In this context, ‘toy handling’ refer to ‘the mechanical process or manner by which one touches, feels, manipulates, deals or treats an object or thing’. Another allied term, ‘toy ownership’ (or ‘possession’) is the ‘state, fact or right to proprietorship as one’s own belonging’. The term ‘toy sharing’ denotes ‘the act of apportioning or allowing somebody to use something or have part of something’. This study delves into all these related but distinct terms in the development of ‘toy index’ (Smith, 2010).
Participants:A purposive sample of 267 children (Mean
Age: 3.99± 1.39) below six years including 158 boys (Mean Age: 3.89±1.32) and 109 girls (Mean Age: 4.13±1.48) were recruited for this study (t: 1.353; p: 0.18; NS). It covered children with and without developmental disabilities drawn from the clinical population seeking services in the investigating agency, a national level institution serving such a cause. Additional sample was drawn from special schools in the city. Typical children were recruited from neighbourhood crèches, play pens, preschools, kindergartens and Montessori schools. The various categories of CWDD included those with specific or global developmental delays, sensory, multiple or intellectual disabilities, cerebral palsy, specific speech delays, at risk cases and autistic disturbances with or without associated problem behaviour, seizure disorders, etc. Children from the limits of Municipal Corporation were considered urban and those from village Panchayats were deemed rural. The distribution of sample characteristics is given in Table 1. To ascertain the socio-demographic status, an adapted, updated, revised and truncated version of NIMH Socio-Economic Status Scale (NIMH-SES;
S. Venkatesan et al.,...................... / Toy Index of Children With or Without ....................

62
Venkatesan, 2011) was used. The original 5-tier SES was reduced to 3-tier scale by clubbing the first and last two layers as ‘low’, ‘middle’ and ‘high’ class. However, the 4 - point criteria of deciding on the SES level based on (i) pooled monthly income; (ii) highest education in family; (iii) occupation; and, (iv) immovable-movable familial properties was retained.
Table 1: Distribution of Sample Characteristics.Variables N HI DD ESD MD TC Probability
GenderBoys 158 30 49 31 23 25 Cramer’s:0.188; P: 0.052;
X2: 9.408; df: 4; p: 0. 052Girls 109 26 16 25 20 22Age Groups0-2 years 34 5 13 10 3 3
Cramer’s: 0.225; p: 0.001;
X2: 27.075; df: 8; p: 0.0012-4 years 81 21 8 14 23 154-6 years 152 30 44 32 17 29Residence Rural 150 36 40 26 26 22 Cramer’s:0.184;P: 0.059;
X2: 9.080; df: 4; p: 0.059Urban 117 20 25 21 17 34SESLow 149 39 44 23 14 29
Cramer’s: 0.348;P: 0.000;
X2: 64.661; df: 8; p: 0.00Middle 89 15 15 31 15 13High 29 2 6 2 18 1Total 267 56 65 47 43 56
[HI: Hearing Impairment; D D: Developmental Disa-bilities; ESD: Expressive Speech Delays; MD: Multiple Disabilities; TC: Typical Children]
Tools:The following tools were used for data
collection: (i) Socio-demographic Data Sheet; and, (ii) Data Elicitation Probe on Toys.
The socio-demographic data sheet is investigator constructed device to elicit details from respondents including fathers, mothers, or caregivers about themselves and/or their CWDD. It covered questions related to the child’s age, gender, diagnosis, and area of residence.
Another 25-item Data Elicitation Probe on Toys, exclusively developed for this study, covered questions on or about toys vis-a-vis CWDD. The probe opened with a question on or about toy availability (or otherwise) for a given child, before proceeding to list them along with information on the frequency or expenditure incurred on their purchase, criteria for their selection, manner of their dispensing
it to the child, etc. The statements were phrased in simple language. The placement of questions was randomized although it was ensured that all of them were covered either by personal interview or by respondents themselves. Examiners made behaviour observation of respondents during data collection. The tool was piloted on a sample of 30 parents before editing, rewording, rephrasing or simplifying the statements to its final form. In pilot phase, apart from using unstructured interview technique, the preliminary format of this tool was deliberately kept open ended and filled with cafeteria questions to allow respondents to select statements or answers best representing their view.
An illustrative sample of the open ended probes included: Does the child own any toys which can be deemed as his/her personal belongings? If YES, how did the child get these toys? What is the cost of the toys owned by the child? Since when does the child own the toy/s? In case, the toys are purchased, who or how was the decision taken to procure them? How frequently are they purchased? Which of the toys, do you think, is the favourite for your child? How does s/he engage with the favourite toy? What or which toy based activities you think is appropriate for your child? Once a toy has run through its use, how or where do you dispose them? Does the child recognize, preserve and protect his or her toys? Does the child share his/her toys? Does the child handle the toys safely? Are you aware of any toy bank or toy library in your vicinity? Are there any toys which you will never purchase for your child? According to you, which are the most lovable toys? Which are the most hateful toys? What are the attributes you see when purchasing a toy: looks and appearance, cost or price, educational value, entertainment value, safety, brand name, durability, design, eco-friendly, value for money, quality, reinforcement value, supporting manual, time used up, packaging, functional use, learning opportunity, maintenance, washable, etc. Additional questions pertained to: Are you aware of any brand names in the toy industry? How often do you buy toys: every week, month, on special occasions, etc? How much would you be willing to spend on children’s toy? Toys come in different forms, which one would you prefer? How long do you expect the child’s toy to last? Which type of play does your child show interest in? How many hours in
S. Venkatesan et al.,..............., / Toy Index of Children With or Without ....................

63
a day does the child play with toys? Typically, where do you buy your children’s toys?
Procedure: Following informed consent and strict
adherence to the mandated ethical guidelines for research in the investigating agency (Venkatesan, 2009), data collection involved individualized interview and verbatim recording of answers given by respondents. The collected data, by way of transcripts, were subjected to category classification, coding and analysis. Consensual validation between examiners not below the rank of post graduation in clinical psychology was undertaken.
The concept of index owes its origin to the fields of statistics, mathematics and economics (Ralph, O’Neill & Winston, 2015). Applied to this study, the toy index is denoted as the mean number of toys made available per child across age, condition, gender, and/or area of residence. The matter is not as simple as this. It is not simply a matter of owning toys or making them available to a given child or groups of children. Toys may be made available but rarely put to use. Further, there is a question of economics. How much money is spent for its procurement? Certain branded toys are expensive for the short span of shelf life that they are likely to have. All this needs to be meaningfully and coherently combined as inclusion parameters within the toy index.
Going by this rationale, toy index is defined as ‘an objective measurable sum total value derived against four parameters identified, explained and weighed before transforming it into a meaningful whole as overall mean and variance for given child’. The identified parameters for inclusion in the index were: ownership, availability, usage and expenditure. For example, if a child ‘owned two toys’ (Score: 1) ‘received as gift’ (Score: 0), which was ‘given to calm’ him (Score: 2)‘at least 3-4 times in a week’(Score: 3), the sum total toy score for that child is calculated as 6 out of 20. Thus, individual, subgroup and overall scores of toy index was calculated and tabulated across the studied socio-demographic variables. The parameters and scheme of scoring to derive the Toy Index is given in Table 2.
S. Venkatesan et al.,..............., / Toy Index of Children With or Without ....................
Table 2: Parameters and Scoring Used for Toy Index.Score Ownership Availability Usage Expenditure
0 No Toys Not made available
Never used Nil-Await as gifts
1 1-2 Toys Kept in showcase
Used once a week
Ad hoc purchases
2 3-4 Toys Given to calm child
Used twice a week
<Rs. 100 a month
3 5-6 Toys Given on demand
Used 3-4 times a week
Rs. 101-200 a month
4 6-7 Toys Given conditionally
Used 5 times a week
Rs. 201-300 a month
5 >7 Toys Access left to child
Used daily > Rs. 301 per month
(Maximum Score: 20)
RESULTSThe mean toy index for overall sample of
children with and without developmental disabilities (N: 267) is 8.60±4.14). Within the parameters used to determine the toy index, the mean scores on reported ownership (Mean 1.93±0.95) and expenditure (Mean: 1.97±1.09) appears to be lower than for their availability (Mean 2.43±1.23) and usage (Mean 2.27± 1.54). This is interpreted as children making better use of the limited toys made available to them. The number of toys owned is fewer and the expenditure incurred by parents is also less. Analysis of results on the measured toy index for various parameters against various socio-demographic variables is given in Tables 3 & 4.
Table 3: Mean Scores of Toy Index by Gender and Residence.
VariablesGender
t Value
Residence
t valueBoysMean±SD
Girls Mean±SD
Rural Mean±SD
Urban Mean±SD
N 158 109 150 117
Ownership 2.06±1.03 1.73±0.8 2.81** 1.83±0.93 2.06± 0.98 1.99*
Availability 2.58±1.27 2.22±1.14 2.33* 2.26±1.2 2.65± 1.24 2.59**
Usage 2.33±1.53 2.33±1.56 0.53 ns 2.02±1.42 2.59± 1.62 3.05**
Expenditure 2.23±1.09 1.61±0.99 4.74** 1.77±1.00 2.24± 1.16 3.57**
Toy Index 9.09±4.22 7.89±3.92 2.36* 7.87± 3.82 9.54± 4.35 3.32**
**>p.01 *>p05
On the whole, results show that boys in this sample (N: 158; Mean 9.09±4.22) than girls (N: 109; Mean 7.89±3.92) and children from urban (N: 117; Mean 9.54±4.35) rather than rural areas (N: 150;

64
UsageM 2.43c 1.12b 3.89d 0.33a 3.51d
193.0
*** 2.03 2.15 2.39 2.27
1.12SD 0.78 0.67 0.97 0.61 0.8 1.7 1.52 1.51 1.54
Ex-pendi-ture
M 1.96b 1.38a 2.66c 1.35a 2.55c 1.97
22.51
1.62 2.07 2 1.97
2.20SD 0.85 0.91 0.98 1.11 0.93 1.09 1.13 1.05 1.1 1.09
Toy Index
M 8.36c 5.71b 13.16e 4.09a 11.6d 8.6
127.6
6 7.47 8.43 8.95 8.6
1.88
SD 2.32 2.47 2.7 2.31 2.26 4.14 4.11 3.81 4.28 4.14
***>p.001 **>p.01 *>p05
In terms of response content taken from the protocols of interview records, it is seen that no answers were forthcoming several questions from the respondents. ‘Who or how was the decision taken to procure toys’ or ‘How frequently they are purchased’ was rarely answered. Respondent awareness on the ‘favourite’ and/or ‘most hated’ toys for your child was low. They confessed ignorance on age appropriateness of toys, safety norms in use of toys, about toy bank or neighbourhood toy lending libraries. While the procurement of toys for their child was left to chance, they were unaware of brand names, toy-disposal, eco-friendly attributes and educational value or about their maintenance.
DISCUSSIONResearch on toys vis-a-vis children with or
without disabilities is admittedly irregular, inchoate and incomplete. The beneficial role of toys for children is conceded (Lear, 1996; Riddick, 1982; Clark & Roberta, 1979; Kawin, 1934). A noteworthy development on this theme in India is the development and standardization of ‘Activity Checklist for Preschool Children with Developmental Disabilities’ (ACPC-DD; Venkatesan, 2004) with its accompanying ‘Toy Kits for Infants, Toddlers and Preschoolers with Developmental Disabilities’ (Venkatesan, 2010). Despite positive reviews on ‘toy kits’ (Venkatesan, 2012; Karande, 2011; Srivastava, 2011), one is unsure whether the children are indeed being given play materials. In seeking to develop, determine or prepare contemporary benchmarks for the targeted children, this study finds an almost impoverished overall toy index (N: 267; Mean 8.60±4.14) against standard comparison group of typical children (N: 56; Mean 13.6±2.70) out of maximum possible score of 20 on this measurement.
Ae-Hawa et al. (2003) reviewed findings of 13 intervention studies published between 1975-1999 on 3-5 year children with disabilities to conclude that positive outcome is associated with play using
S. Venkatesan et al.,............... / Toy Index of Children With or Without ....................
Mean 7.87±3.82) secure higher toy index (p: <0.01). More specifically, boys show greater ownership and parents appear to spend significantly more money for them compared to girls (p: < 0.05). However, there are no differences with respect to availability and usage of toys in relation to gender (p: > 0.05). In relation to area of residence, the children from urban areas consistently show high scores across all parameters of ownership, availability, usage, and expenditure than their rural counterparts.
In relation to their condition (Table 3), if the typical children are deemed as standard comparison group (N: 56; Mean 13.16±2.70), those with expressive speech delays (N: 47; Mean: 11.60±2.26) appear to trail closest behind albeit with lower toy index. This is followed by children with hearing impairment (N: 56; Mean 8.36±2.32) and those with developmental disabilities (N: 65; Mean 5.71±2.47). The children with multiple disabilities appear to be the most disadvantaged (N: 43; Mean 4.09±2.31) with the least toy index (p: <0.001). Scheffe’s Post-hoc Analysis was additionally carried out as a posterior test to discover patterns and/or relationships, if any, between sub groups of the sample conditions. By doing so, no significant mean differences were observed between any of the sub groups (p: >0.05).
Analysis of results against age variable (Table 4) show a linear increasing trend with younger children measuring lower toy index compared to their older peers. The children between 0-2 years (N: 34; Mean 7.47± 4.11) show the lowest mean toy index compared to those between 2-4 years (N: 81; Mean 8.43±3.81)and 4-6 years(N: 152; Mean 8.95±4.28). Once again, on Scheffe’s Post-hoc Analysis, no significant mean differences were observed between any of the sub groups against the various parameters except in the area of toy ownership (p: >0.05).
Table 4: Mean Scores of Toy Index by Condition and Age.
Vari-ables
Condition Age Group
HI DD TC MD ESD Ove rall
F Value 0-2y 2-4y 4-6y Ove
rallF
Value
N 56 65 56 43 47 267 34 81 152 267
Own-ership
M 1.73b 1.43ab 2.82c 1.07a 2.57c 1.93
58.72
*** 1.59a 1.81ab 2.07b 1.93
4.43
**
SD 0.67 0.64 0.88 0.55 0.68 0.95 0.74 0.74 1.07 0.95
Avail-ability
M 2.23b 1.77ab 3.79d 1.35a 2.96c 2.43
62.39
*** 1.59a 1.81ab 2.07b 1.93
0.65SD 0.89 0.86 0.93 0.95 0.81 1.23 0.74 0.74 1.07 0.95

65
• In relation to their condition, against the benchmark of a standard comparison group in typical children, those with expressive speech delays appear to trail closest behind them with lower toy index, followed by children with hearing impairments, those with developmental disabilities,and eventually, the most disadvantaged are children with multiple disabilities with the least toy index; and,
• There is a linear trend with younger and rural children measuring lowest toy index compared to their older peers and/or those from urban areas.To conclude, the availability of toys, its usage,
purchase and procurement against various types of disability as well as typical children is still an uncharted terrain. This study sought to focus on a neglected theme by deriving and developing baseline bench marks or tentative estimates on contemporary status of toys vis-à-vis CWDDs. This pioneering development of toy index across various age groups is likely to throw up bench marks that may be sooner or later linked to providing, ownership or usage of toys as a matter of child rights rather than as sheer option to appease them (Johnson, 2012). Thereby, it has opened vistas for purchase, provision and use of toys necessary for informal, individualized, developmentally appropriate, activity-oriented, learner paced, ecologically interactive and educational interventions for children in the country.
ACKNOWLEDGEMENTSThe authors seek to place on record the gratitude
due to Dr. S. R. Savithri, Director, All India Institute of Speech and Hearing, Mysore: Karnataka, India, for financial grant received through ‘AIISH Research Fund’ for completion of the project titled ‘Development of Toy Index for Children with Developmental Disabilities’ (2014-15). The present work is part of the series of research papers in the project.
REFERENCESAe-Hwa, K., Vaughn, S., Elbaum, B., Hughes, M. T., Sloan,
C. V. M., & Sridhar, D. (2003). Effects of toys or group composition for children with disabilities: a synthesis. Journal of Early Intervention, 25, 189-205.
Allen, A. (1968). Criteria for selecting gifts. Childhood Education. 45 (3), 118-121.
Blakemore, J. E., & Centers, R. E. (2005). Characteristics of
S. Venkatesan et al.,............... / Toy Index of Children With or Without .....
social toys. Beneficial effects of toy play in children with multiple disabilities in inclusive classroom setting are recorded (DiCarlo & Reid, 2004; DiCarlo, Reid & Stricklin, 2003). Research has focused on toy preferences in children (Thomas, 1984; Frashner, Naurss, & Brogan, 1980), toy selection by parents (Christensen & Stockdale, 1991; Peretti & Sydney, 1984; Kesner & Sunal, 1980; Allen, 1968), the need or utility of toy libraries (Brodin & Bjorck-Akerson, 1992; Jackson, Robey, Watjus & Chadwick, 1991; Johnson, 1978) and toy safety issues (Wu et al. 2013; Taylor, Morris & Rogers, 1997; Hillery, 1994; Dawson, 1990) in the context of CWDD. It appears that parents in the Indian scene are typically unaware of these several important nuances related to toys and children.
As derived in this study, gender stereotyping appears is a crucial variable in choice or dispensing of toys, their made availability and patterns of use (Venkatesan, 2014; Martin, Eisenbud & Rose, 1995; Caldera, Huston & O’Brien, 1989; Robinson & Morris, 1986). Cherney and London (2006), for instance, found that boys spent more time on leisure activities like engagement in sports, watching television and playing computer games than girls. Giddings and Halverson (1981) noted that children spent 20 per cent of their waking time in play, wherein boys played more with vehicles and girls spent more time with dolls involving domestic role play and dressing up. Although common sense tells that different age groups of children are attracted by different types of toys, it is now shown that older children and/or those from urban areas show higher toy index than younger ones. In sum, this study shows that
• The mean toy index for overall sample of children with and without developmental disabilities is 8.60 for a maximum score of 20, which is much lower than 13.6 derived for typical children;
• Children appear to make better use of the limited toys made available, while the number of toys owned by them is fewer and the expenditure incurred by parents is also less;
• Boys than girls and children from urban than those from rural areas secure higher toy index;
• Boys show greater ownership and parents appear to spend more money on toys for them compared to girls;

66
boys’ and girls’ toys. Sex Roles, 53, 9 & 10, 619-633.Brodin, J., & Bjorck-Akesson, E. (1992). Toy libraries/
Lekoteks in an international perspective. Euro Rehab, 2, 97-102
Caldera, Y. M., Huston, A. C., & O’Brien, M. (1989). Social interactions and play patterns of parents and toddlers with feminine, masculine, and neutral toys. Child Development, 60, 70-76. .
Cherney, I. D., & London, K. (2006). Gender linked differences in the toys, television shows, computer games, and outdoor activities of 5- to 13-year old children. Sex Roles, 54, 717.
Christensen, K.E., & Stockdale, D.F. (1991). Predictors of toy selection criteria of preschool children parents. Children’s Environments Quarterly, 8, 1, 25-36.
Clark, W., & Roberta, B. (1979). Improving the leisure-time behaviour of severely/profoundly mentally retarded children through toy play. AAESPH Review. 4, 3, 237-250.
Dawson, C. (1990). Choosing safe toys for children. Consumers Research Magazine, 73 (12), 15.
DePauw, K. P., & Gavron, S. J. (2005). Disability sport. Champaign, Illinois: Human Kinetics.
DiCarlo, C. F., & Reid, D.H. (2004). Increasing pretend toy play of toddlers with disabilities in an inclusive setting. Journal of Applied Behaviour Analysis, 37, 197–207. doi: 10.1901/jaba.2004.37-197
DiCarlo, C. F., Reid, D. H., & Stricklin, S. B. (2003). Increasing toy play among toddlers with multiple disabilities in an inclusive classroom: a more-to-less, child-directed intervention continuum. Research in Developmental Disabilities. 24, 3, 195-209.
Frashner, R. S., Nurss, J. R., & Brogan, D. R. (1980). Children’s toy preferences revisited: Implications for early childhood education. Child Care Quarterly, 9, 26-31.
Giddings, M., & Halverson, C. F. (1981). Young children’s use of toys in home environments. Family Relations, 30, 1, 69-74.
Goldstein, J.H. (Ed.). (1994). Toys and Child Development. Cambridge: Cambridge University Press.
Hillery, N. (1994). Rub a dub dub, many toys in the tub, How do we keep them clean? Child's Play, 10, 3, 4-5
Hsieh-Chun, H. (2008). Effects of ordinary and adaptive toys on pre-school children with developmental disabilities. Research in Developmental Disabilities, 29, 5, 459-466.
Jackson, S. C., Robey, L., Watjus, M., & Chadwick, E. (1991). Play for all children: The toy library solution. Childhood Education, 68, 1, 27-31.
Johnson, E. (1978). The toy library—A how-to handbook, Minnesota: Toys 'n Things, Maine: Training Resource Centre
Johnson, E. (2012). The Children’s Bill of Emotional
Rights: A Guide to the Needs of Children. Plymouth, UK: Jason Aronson.
Karande, S. (2011). Toy kit for kids with developmental Rehab, 2, 97-102
Caldera, Y. M., Huston, A. C., & O’Brien, M. (1989). Social interactions and play patterns of parents and toddlers with feminine, masculine, and neutral toys. Child Development, 60, 70-76. .
Cherney, I. D., & London, K. (2006). Gender linked differences in the toys, television shows, computer games, and outdoor activities of 5- to 13-year old children. Sex Roles, 54, 717.
Christensen, K.E., & Stockdale, D.F. (1991). Predictors of toy selection criteria of preschool children parents. Children’s Environments Quarterly, 8, 1, 25-36.
Clark, W., & Roberta, B. (1979). Improving the leisure-time behaviors of severely/profoundly mentally retarded children through toy play. AAESPH Review. 4, 3, 237-250.
Dawson, C. (1990). Choosing safe toys for children. Consumers Research Magazine, 73 (12), 15.
DePauw, K. P., & Gavron, S. J. (2005). Disability sport. Champaign, Illinois: Human Kinetics.
DiCarlo, C. F., & Reid, D.H. (2004). Increasing pretend toy play of toddlers with disabilities in an inclusive setting. Journal of Applied Behaviour Analysis, 37, 197–207. doi: 10.1901/jaba.2004.37-197
DiCarlo, C. F., Reid, D. H., & Stricklin, S. B. (2003). Increasing toy play among toddlers with multiple disabilities in an inclusive classroom: a more-to-less, child-directed intervention continuum. Research in Developmental Disabilities. 24, 3, 195-209.
Frashner, R. S., Nurss, J. R., & Brogan, D. R. (1980). Children’s toy preferences revisited: Implications for early childhood education. Child Care Quarterly, 9, 26-31.
Giddings, M., & Halverson, C. F. (1981). Young children’s use of toys in home environments. Family Relations, 30, 1, 69-74.
Goldstein, J.H. (Ed.). (1994). Toys and Child Development. Cambridge: Cambridge University Press.
Hillery, N. (1994). Rub a dub dub, many toys in the tub, How do we keep them clean? Child's Play, 10, 3, 4-5
Hsieh-Chun, H. (2008). Effects of ordinary and adaptive toys on pre-school children with developmental disabilities. Research in Developmental Disabilities, 29, 5, 459-466.
Jackson, S. C., Robey, L., Watjus, M., & Chadwick, E. (1991). Play for all children: The toy library solution. Childhood Education, 68, 1, 27-31.
Johnson, E. (1978). The toy library—A how-to handbook,
S. Venkatesan et al.,..............., / Toy Index of Children With or Without .....

67
Minnesota: Toys 'n Things, Maine: Training Resource CenterJohnson, E. (2012). The Children’s Bill of Emotional
Rights: A Guide to the Needs of Children. Plymouth, UK: Jason Aronson.
Karande, S. (2011). Toy kit for kids with developmental disabilities, user manual. Mysore: All India Institute of Speech and Hearing. Indian Paediatrics, 48, 10, 830.
Kawin, E. (1934). The function of toys in relation to child development. Journal of Childhood Education, 11, 3, 122-132.
Kesner, J. R., & Sunal, C. S. (1980). Choosing the right toy: A checklist. International Journal of Early Childhood. 12, 2, 76-80.
Khoshali, A.K., & Venkatesan, S. (2007). Play behaviour in children with mental retardation. Psychological Studies. 52,1, 90-94.
Khoshali, A.K., & Venkatesan, S. (2010). Development of play activity checklist for children with mental retardation. Indian Journal of Clinical Psychology. 37, 2, 101-107.
Lear, R. (1996). Play Helps: Toys and Activities for Children with Special Needs. Butterworth/Heinemann.
Lieber, J., & Beckman, P. J. (1991). The role of toys in individual and dyadic play among young children with handicaps. Journal of Applied Developmental Psychology, 12, 2, 189-203.
Martin, C.L., Eisenbud, L., & Rose, H. (1995). Children’s gender based reasoning about toys. Child Development, 66: 1453-1471. Doi: 10.1111/j.1467-8624.1995.tb00945.x
Murphy, N. A., & Carbone, P. S. (2008). Promoting the participation of children with disabilities in sports, recreation, and physical activities. Pediatrics, 121, 5, 1057-1061.
Peretti, P. O., & Sydney, T. M. (1984). Parental toy choice stereotyping and its effects on child toy preference and sex-role typing. Social Behaviour and Personality, 12, 213-216.
Riddick, B. (1982). Toys and Play for the Handicapped Child. New York: Routledge. Pp. 149.
Robinson, C.C., & Morris, J.T. (1986). The gender stereotyped nature of Christmas toys received by 36-, 48-and 60-month-old children: A comparison between non-requested vs. requested toys. Sex Roles, 25, 21-32.
Rubin, K.H., & Howe, N. (1985). Toys and play behaviour: An overview. Topics in Early Childhood Special Education, 5, 3, 1-9.
Smith, P. K. (2010). Children and Play: Understanding Children’s World. West Sussex, UK: John Wiley. P. 89-94.
Srivastava, A. K. (2011). Toy Kit for Kids with Developmental Disabilities, User Manual. Mysore: All India Institute of Speech and Hearing. Journal of Disability Management and Special Education, 1, 1, 87-88
Taylor, S.I., Morris, V.G., & Rogers, C.S. (1997). Toy safety and selection. Early Childhood Education Journal, 24, 4, 235-238.
Thomas, B. (1984). Early toy preferences of four year old readers and nonreaders. Child Development. 55: 424-430.
Tomopoulos, S., Dreyer, B.P., Tamis-LeMonda, C., Flynn, V., Rovira, I., Tineo, W., & Mendelsohn, A.L. (2006). Books, toys, parent-child interactions and development of young latino children. Ambulatory Paediatrics, 6, 2, 72-78.
Venkatesan, S. (2000). Play activities in children with mental retardation. Indian Journal of Clinical Psychology. 27, 1, 124-128.
Venkatesan, S. (2004). Children with Developmental Disabilities: A Training Guide for Parents, Teachers & Caregivers. New Delhi: Sage.
Venkatesan, S. (2009). Ethical Guidelines for Bio Behavioral Research. Mysore: All India Institute of Speech and Hearing.
Venkatesan, S. (2010). Toy Kit for Kids with Developmental Disabilities: User Manual. Mysore: All India Institute of Speech and Hearing.
Venkatesan, S. (2012). Utility analysis of assembled toy kits for kids with developmental disabilities. Journal of Disability Management and Special Education, 2, 2, 27-37.
Venkatesan, S. (2014). Availability of toys for children with developmental disabilities. Journal of Disability Management and Special Education. 4, 1, 58-70.
Venkatesan, S. (2015a). Evaluation of teaching objectives earmarked for children with developmental disabilities. Disabilities and Impairments, 29, 2, 85-95.
Venkatesan, S. (2015b). Revisiting goal setting for children with developmental disabilities. Journal of Disability Management and Special Education, 5, 2, 19-27.
Venkatesan, S., & Ravindran, N. (2012). Play behaviour and activities in siblings of children with developmental disabilities. Journal of Indian Academy of Applied Psychology. 38, 1, 69-78.
Weiss, J., Diamond, T., Denmark, J., & Lovald, B. (2003). Involvement in Special Olympics and its relations to self-concept and actual competency in participants with developmental disabilities. Research in Developmental Disabilities, 24, 4, 281-305.
Wu, R.S., Chan, J.X., Chong, S.L., Ong, G.Y., & Ng, K.C. (2013). Toy safety in Singapore: where are we now? Singapore Medical Journal, 54, 11, 639-642.
S. Venkatesan et al.,...... / Toy Index of Children With or Without Developmental Disabilities

68
A Case Study with Acceptance and Commitment Therapy*Soheli Datta1 and Tilottama Mukherjee2
ABSTRACTAcceptance and Commitment Therapy (ACT) is one of the new interventions from both behavioural and cognitive wings purporting to create a rich and meaningful life and also accepting the pain that goes with it. It is a highly structured package for the treatment of patients suffering from depression. The present case study is an attempt to provide therapeutic intervention programme to a 12 years old boy of Hindu origin suffering from depression. The child was treated by using ACT techniques. The presenting symptoms, assessment strategies and treatment elements have been covered in details. After 16 sessions of therapeutic intervention, significant improvement was found in the client. The sessions include assessments, psycho-education, ACT principles and techniques and mindfulness practices.
Keywords: Psychological Inflexibility, Depression, Values, Defusion, Payoffs, Mindfulness.
INTRODUCTIONThe first wave of behaviour therapy has so far
countered the excesses and scientific weakness of existing non-empirical clinical traditions. The second wave was also characterized by similar change efforts guided by social learning and cognitive principles that included cognitive components in addition to the behavioural and emotive targets. Acceptance and Commitment Therapy is one of the new interventions from both behavioural and cognitive wings. It seem to be moving the field in a different direction and including itself in the third wave and is based on a basic experimental analysis of human cognition.
Acceptance and Commitment Therapy also pronounced as the word ‘ACT’, is a model applied for change in psychological inflexibility. This was propounded in the United States of America by the Psychologist, Steven Hayes. This has been largely effective in helping patients with various problems, from depression and anxiety disorder, to chronic pain and even addiction. To be more specific, one’s abilities to plan, predict, evaluate, verbally communicate, and relate events and stimuli to one another both help and hurt them (Hayes et al., 1999). Moreover, research has demonstrated that the more one attempts to suppress thoughts and feelings, the more present they become (Abramowitz, Tolin, & Street, 2001; Campbell Sills, Barlow, Brown, & Hofmann, 2006).
ACT is one of the mindfulness based behavioural therapy and utilizes an eclectic approach of metaphors, paradox, and mindfulness skills,
1. Asstt. Prof., Dept. of Applied Psychology, University of Calcutta 2. Asstt. Prof., Dept. of Psychology, University of Calcutta. *Corresponding Author: Soheli Dutta E-mail:[email protected]
along with a wide range of experiential exercises and values-guided behavioural interventions in its process. The goal of ACT is to create a rich and meaningful life and also accepting the pain that goes with it. ACT is about taking effective action guided by one’s deepest values and in which one is fully present and engaged. ACT teaches mindfulness skills as an effective way to handle barriers, in the form of unpleasant and unwanted experiences. Through six core therapeutic processes, namely, acceptance and willingness, cognitive defusion exercises, the present-moment awareness, self as the context, values, and committed action, the clients are guided to open up to and act upon actual experiences rather than what the mind or the body demands. The principles of ACT focuses on acceptance, cognitive defusion practices, contact with the present moment, the observing self, its values and committed action.
The World Health Organization estimates that depression is currently one of the most debilitating diseases in the world. A pilot study by Wicksell, Melin, & Olsson (2007) suggested that ACT treatment resulted in significant improvements in functional ability in adolescents. Adolescents treated with ACT reported less catastrophizing and lowered perceived pain (Wicksell et al., 2009), providing some encouragement toward pursuing ACT as a treatment for depression. In the school setting, an ACT to with adolescents has reported significantly improved outcomes up to two years later on measures of stress and psychological flexibility (Livheim, 2004). ACT is also found to be effective
Case Report
Indian Journal of Clinical Psychology2017, Vol. 44, No. 1, 68-74
Copyright, 2017, Indian Association ofClinical Psychologists (ISSN 0303-2582)

69
in adolescents experiencing depressive symptoms in clinical population treated in community health and an early intervention program in schools (Hayes, Bach & Boyd, 2010)
CASE PRESENTATION
The child, a 12 years old boy, Bengali speaking Hindu, studying in class VII had been slow in all activities for the last 8 years 6 months. He always had to be pushed by his parents to do all the activities otherwise he got late for his school and tuitions. He lacked interest in every activities, got easily distracted while studying and took more time than usual to complete his tasks and his academic performance was also poor. For the last 6 months, the child had been threatening his mother that he would commit suicide by consuming sleeping pills. His family presented the child for treatment after he had tried to be aggressive with his sister for twice in the last one month. The parents shared non-congenial relationship with the child. The mother being a working woman showed warmth towards him but did not spend enough time. However as per the child, his father who was in emergency duty, also paid less time, and was at times critical and punitive. Their communication was indirect. He was referred from a local government hospital for counselling. Mental status examination revealed well kempt and tidy appearance, presence of touch with surroundings, proper eye contact, and cooperative attitude towards examiner. Motor behaviour was normal and his speech was audible with normal reaction time to stimulus, normal speed, normal productivity, relevant, coherent and goal directed. Orientation to time, place and person was intact and attention could not be sustained for prolonged period of time. General intelligence seemed to be average along with conceptual abstraction, satisfactory social, and personal and test judgement. His subjective affect and objective affect were depressed. There were no abnormalities in thought stream, form and possession, with ideas of helplessness and death wishes in thought content, and there were no perceptual disturbances present. Moreover, his insight was at grade II (slight awareness of being sick but denying at the same time) and led to the
provisional diagnosis of Moderate Depressive Episode with Sibling Rivalry.
IMPLEMENTING ACCEPTANCE AND COMMITMENT THERAPY (ACT)
The purpose of using ACT includes presence of marked psychological inflexibility in the child, significant disturbances about current problems and is amenable to the use of value and diffusion based interventions required for psychotherapy. Areas to be focussed were to increase understanding and insight into depressive experiences, improve coping and creating hope, reduction in distress associated with sibling rivalry, reducing payoffs, modifying psychological inflexibility, correcting negative self-esteem, enable restore self-worth, maintenance of gains and prevention of relapse. The Session details are as follows-
Session 1-4:Detailed case history was taken from the
parents and mental status examination of the child was conducted. The Malin’s Intelligence Scale for Indian Children (MISIC), was administered for assessing the child’s present level of intellectual functioning and his IQ (95) was found to be average.
Junior Temperament and Character Inventory (JTCI) was administered to assess the child’s general temperament and character and the findings revealed Above Average range in the ‘Harm Avoidance’ domain, which reveals that the child might be worrying, pessimistic, fearful, shy and fatigable. His score in the ‘Reward Dependence’ and ‘Self-Directedness’ domain fell in the ‘Below Average’ category, which indicates a tendency to be withdrawn and detached, and a tendency to be immature, fragile and ineffective.
Childhood Depression Inventory (CDI) was administered to assess the child’s level of negative mood, interpersonal problems and difficulties, ineffectiveness, anhedonia and negative self esteem where, in the domain of Interpersonal Problems and Negative Self-Esteem his score was much above average, which reflects difficulties in interaction with people including trouble getting along with people, social isolation and social avoidance and a tendency to have thoughts of suicide. The score on the domain of Ineffectiveness was much above average,
Soheli et al.,.......... / A Clinical Case Study with Acceptance and ................

70
indicating negative evaluation of one’s ability and school performance.
Devereux Scale of Mental Disorder (D.S.M.D) was administered to assess the child’s presence of any features of internalizing, externalizing and critical pathology. The child’s score in the scale of ‘Attention’ was ‘Elevated’, indicating problems with concentration and distractibility. The Externalizing composite was in the ‘Borderline’ range, indicating conflicts with others in his environment. ‘Elevated’ score in ‘Depression’ indicated a tendency to withdraw from social contacts, depressed mood and decreased interest in activities. Score on ‘Acute Problems’ was in the ‘Borderline’ range indicating psychological disturbances in the child currently. The pre intervention DSMD profile was as follows:
Rorschach Inkblot Test was administered to provide an expression of the structure of personality of the child which revealed disturbances when environmental stimuli touch on the area of affectional need and little responsiveness to influences from the environment along with depressive tendencies.
Thematic Apperception Test (TAT) was administered to assess dynamics and content of personality. Results indicated severe morbidity and self to be inquisitive, hostile, dissocial, guilty and defiant. There was need for achievement, cognizance, isolation, power, aggression, autonomy and succorance. The environment was perceived as threatening. An ambivalent attitude was perceived toward authority figures. The conflicts were autonomy versus compliance and morality versus conscience and there is a dominance of id impulses over superego. The hero’s nature of anxiety was of physical harm, punishment and rejection. The main defenses used by the hero were denial, wish fulfilment, rationalization and regression.
Session 5 and 6: Psycho-education on the Disorder: this
provides an opportunity for the patient to increase their understanding of their own symptoms and the context in which they occur. Psycho-education given to the child and mother on the topics: like, the term depression and sibling rivalry, their symptoms and aetiology, epidemiology, vulnerability factors, life stress factors and the various protective factors. Psycho-education of Therapeutic Intervention
was given on the various treatment modes, about ACT, Need for ACT, importance of homework and treatment expectations.
Session 7 and 8 (Case Conceptualization):
A Case formulation was done using the Model of Functional Analysis (Harris, 2013).
TRIGGERS: Situations, thoughts and feelings that precede the
behaviour.
BEHAVIOUR: What do you do?
PAYOFFS:Immediate outcomes of the behaviour that keeps
it going.• If my mother loves my sister- seeing it and
thinking about it• If my parents ask me to sit for studying• If I ask for anything from my mother (pen,
pencil or colours)• If my mother scold me for my studies or results
I get very angry, avoid thinking about that, and try seeing cartoons more
• I refuse to do so and irritate them often• My mother refuses to give, I keep on insisting• I threaten her for committing suicide, I did try
once too I avoid the place and the situation, I hate that, I watch cartoons, it makes me feel good
• They ask me go and watch cartoons, it helps me avoid studying
• If she does not pay, grandmother gives money, I buy whatever I like to buy
• My mother has stopped scolding me as before, thus I can easily avoid studying On a 10 point scale, of Subjective Unit of
Distress (SUD), starting from 0–10, with 0 being having no subjective distress and 10 having the greatest subjective distress, the child was asked to rate his distress on the scale. The child rated 6 out of 10. Moreover, a “No harm contract” was made with the child, to deal with what the child tried to deal or control his problems, which says: “I S.G., 12 years
Soheli et al.,.......... / A Clinical Case Study with Acceptance and ................

71
of age, studying in class VII, reside with my father, mother, sister and grandmother. I have come to the Department of Psychology, University of Calcutta, for therapeutic intervention. Here, I have informed my clinician about my death wishes and suicidal ideation as I do not feel life to be worth living. However, I declare that, as long as my therapeutic sessions will be continuing, I would cause no harm to myself and if any thought about committing harm comes to my mind, I would definitely inform my clinician about it and would also inform my parents”. Case Conceptualization was there after done using the principles of ACT (Harris, 2013)
Q. What valued direction does the child want to move in? (What domain of life and what values seem most important to this child? Does he has any values which are congruent goals or ongoing valued activities?)
A. I have a great deal of therapeutic expectations. I want to come out as a good and well-to-do individual. I want to be a scientist in future. Hope I would be able to become so. I want to follow that direction only keeping it in focus. I have to study a lot. I have to keep my mood well so that I can study well.
Q. What stands in the child’s way? (Identify the barriers to valued living: fusion, avoidance, and unworkable action.)
A. Parents and Sister
Q. What is he fusing with? (Identify problematic fusion, including reasons, rules, judgments regarding past, future, and self-description)
A. I do not; rather I refuse to listen to my parents. They love my sister more than they love me. Before she came to our lives, parents used to love me a lot, now, their love is getting shared because of my sister. I am not able to tolerate this. Hence, I feel life is not worth living and I feel like ending my life
Q. What is he avoiding? (Identify thoughts, feelings, memories, urges, sensations, and emotions that this child is trying to avoid or get rid of.)
A. Thoughts: of lack of love from parents, distant and disturbed relation with parents.
Feelings: of sadness and helplessness, negative
self esteem, Memories: of past days, when his sister was not with them
Urges: of love, affection and nurturance from parents,
Sensations: being unloved and Emotions: depressiveness
Q. What unworkable actions is he taking? (What is the child doing that makes his life worse or keeps him stuck?)
A. Irritating his parents, refusing to listen to them, outward hostility towards sister, getting angry himself and increase in lack of self esteem
Session 9-10 (Confronting the System):The child rated 5 on SUD. Review about how
the child was during the last week was done and a Cost Benefit Analysis was done thereafter
COST BENEFITIf I commit suicide, I will not be able to talk to
people anymore. It would definitely bring peace to my life, then nobody can see me and I would no more feel sad or they can never make me sad.
I would no more be able to get love and affection from my parents. I would become a soul and would be able to roam around freely as I like and nobody can catch me.
I would not be able to back up my own things that I do not share with anybody, like my colour pencil set. Even I do not allow my sister to get hold of it. I would be able to view my parents when I become a soul, I can poke them, make them fearful, I would say them that My body is no more present but my soul is there to frighten you all. They would only be able to see me in a mirror.
My sister would catch hold of many things, like my pencil box, my collection of Indian Currency I can go anywhere and anytime I like
The client was asked to fill up an ACT worksheet and was also explained various metaphors. Therapy metaphors use a story or illustration to view alternative ways of looking at something. Every culture uses these types of stories, analogies to improve understanding, make a point more memorable, and help us make positive changes. Metaphor was used to help get a different view
Soheli et al.,.......... / A Clinical Case Study with Acceptance and ................

72
of his thoughts, feelings and self evaluation. The metaphors “life is like a cake”, “don’t think about the puppy” and “ball in a pool” were used along with the defusion exercise of “kicking soccer balls”. For the homework worksheet, metaphor used was: “passengers on the bus”, “the circus act” and “eating an apple” was used along with defusion exercise of boat on the water (Stoddard & Afari, 2014). Introduction to the exercise of clarifying the child’s values was employed which revealed that the values which were most important for the present client were that of, to be caring toward myself, others, the environment, act kindly toward himself and others in pain, be cooperative and collaborative with others, encourage and reward behavior that he values in himself or others, choose how he lives and help others do likewise, be friendly, companionable, or agreeable toward others, to seek, create, and engage in fun-filled activities, to create or enjoy pleasurable and sensual experiences and family.
Session 11-14: (Assessment of values and committed action and steps to pursue new goals)
SUD was rated to be 5. The child’s values and committed action were assessed. Important life domains: Friends, family and health, Values: Love, support, caringness and acceptance, Goals & actions: Already have: none, Want to pursue: more love from mother and father as well, Need for skills-training: Time management, Problem solving, Self-soothing and Relaxation, Need for training attention skills: The child has the ability, although support from family is needful, Resources: He is attentive and gets easily persuaded by love and affection, My personal barriers: Distance from mother. However, based on the session’s evaluation of values, the agenda for motivating the child to practice new skills or pursue important goals was done
Step 1: Linking the Goals to Values: The child was taught that, if he values family
and his health then taking sudden decisions may cost him more than he has thought of. This would never bring a positive change in his life.
Step 2: Setting Goals Effectively: Specific: I would sit to study on the right time and
obey my parents.
Meaningful: doing this would be living my values of being lovable and parent would be caring.
Adaptive: this would help me handle my distress more effectively.
Realistic: it would bring me back the lost respect and trust from my parents, Time framed: I would start from today itself, will continue as long as I live.
Step 3: Taking Small Steps: The child was made aware that - A journey of
thousand miles begins with one step. Thus he was asked to begin with small steps towards a better future. If the goal seems much bigger, he should make it smaller, rather than not focusing on the goal anymore.
Step 4: Carrot versus Stick: The child was taught that, many people try
to motivate themselves through being harsh, judgmental, self-critical, or punitive. But if beating yourself up were a good way to change behaviour, wouldn’t you be perfect by now? Learn to “drop the stick”: unhook yourself from excessive expectations and harsh self-judgments, and instead practice self acceptance and self-compassion. Then he was asked to link his actions to values, and reflecting on the likely positive outcomes.
Step 5: Anticipate Obstacles: The child was asked, if he is really trying to
meet his values to his goal, then what are the obstacles coming in his way?: The possible obstacles enlisted by the child were the superiority of his sister and lack of love from his mother. To this, he has asked to concentrate on his studies and do well in his upcoming examinations; this would not make him feel inferior and moreover, would bring back the lost love from his mother.
Step 6: Confronting the Costs - What is costing him in terms of: Health: getting distressed day by day.
Wellbeing: having lack of pleasure and interest in activities.
Soheli et al.,.......... / A Clinical Case Study with Acceptance and ................

73
Relationships: more and more distancing from family.
Life: What will be his life: One year from now: the distance will increase, if I
die, then my parents will mourn for me.Two years from now: they would live their own
life, busy with their daily routines, I will be forgotten, my own things will no more be my own, and
Ten years from now: nobody will remember me. Confronting the costs helped the child view how inflexible he has been, and that avoidance or escape is not the solution and problem solving might lead to a better result. To this, the metaphors “the tunnel” and “the beach ball” (Stoddard & Afari, 2014) were used.
The child was asked to imagine how his life will be if he successfully comes out of his distressing period and ignoring the benefits: One year from now: I would be in class VIII, parents would get a bit old, there would be a decrease in their energy, grandmother would become more weak, sister would be in class I, I would look brightly into my future, Two years from now: I would be in Class IX, preparing for my board examination, father would be nearing his retirement, mother would work more hard, don’t know about grandmother, sister will still be little one. My responsibilities for my family would increase. I have to be more positive and Ten years from now: my mother would be nearing her retirement, father would have got retired, sister would be in higher secondary grade, and I would probably do a service. I would be the only earning family member to look forward, only possible support for my family, hence I must live to my parent’s desire
Step 7: Cultivating Willingness: The child was willing to make room for his
inevitable discomfort, hence he was educated on- Working on acceptable skills: he was asked to continue his attentiveness with studies, to focus on his works, reducing hostility towards his sister, love her and care for her, Enhancing the link to his values: The area he values more is his family, friends and his health. He was
made to link the valued objects by himself, and how he has been maintaining with this was enhanced. Moreover, his active uses of coping strategies were reinforced and discussing easier goals that elicits less discomfort like proper scheduling of study time, enough of leisure time to spend on extracurricular activities.
Step 8: Defusing from Reason Giving: It was found that fusion with reason giving was
a major barrier to his action, hence naturally it was targeted with defusion techniques like: “The Boat on the Water”.
Step 9: Enlist Support: Mother, father and best friend were found to be
the social support to the child
Step 10: Use Reminders: Activity scheduling was done where the to-
do list was included so that the child gets reminded of his necessary actions and goals to be accomplished. The schedule included time for studying, going to school, playing with neighbour mates and most important being the time that he would spend with his family.
Session 15-16 (Mindfulness Practice)a. Contact with the Present: Mindfulness exercise, focused on the
experience of feeling and sensing. The child was made to sit comfortably. He was given a freshly plucked leaf and was asked to feel the leaf slowly with a total focus on the smell and texture and, sensations and movements in his fingers. While he was doing this, all sorts of distracting thoughts and feelings may arise. The aim is simply to let the thoughts come and go, and allow his feelings to be there, and keep his attention focused on the leaf. He was amazed that he felt so many sensations through one single leaf. An analogy with social situations was then done through the use of a mindfulness exercise of “floating leaves on a moving stream” (Stoddard & Afari, 2014).
b. The Observing Self: Accessing a transcendent sense of self,
a continuity of conscious process that is
Soheli et al.,.......... / A Clinical Case Study with Acceptance and ................

74
unchanging, is ever-present, and impervious to harm. The child was taken through a mindfulness exercise. First, he was asked to close his eyes and observe his thoughts and sensations: the form the thoughts took, their apparent location in space and the speed with which they were moving. Then I asked him to be aware of what he was noticing. There were thoughts, and there was his self noticing them. Again and again, his attention was drawn to the distinction between the thoughts that arise, and the self who observes those thoughts. This was made analogous to social situations through mindfulness exercise of “watching the mind train” (Stoddard & Afari, 2014)
DISCUSSIONIn ACT, the therapeutic relationship is based
on a stance toward oneself and others that is curative, and allows that stance to be modelled. It creates a social context in which important issues can be evoked and strong, open, and loving relationships usually are a natural expression of values in the client and the therapist. ACT is also a powerful and intrusive intervention in depression. It raises basic issues of values, meaning, and self-identity to the clients. By implementing ACT on the child, there was a decrease in subjective unit of distress (Booztin & Stevens, 2005) and also a decrease in negative self esteem, increase in self confidence and reduction in death wishes. It helped in bringing back more of the lost confidence in the child and developing a social support network. It has been found that the fundamental problem in this case was that of an unwillingness to remain in contact with particular experiences coupled with an attempt to avoid or escape these experiences (Hayes & Gifford, 1997; Hayes et al., 1996). Thus across the duration of therapy sessions, ACT principles sought to weaken attempts of control of particular experiences as an explicit treatment goal. The post intervention DSMD profile is as follows:
However, much progress could have been done with greater number of sessions. Goals that need to be focussed include increasing more of psychological flexibility, working out more on interpersonal problems, relapse prevention and termination.
CONCLUSIONThis case study provides one example of how
ACT works with complex histories and how it can be effectively treated in this present context. The key ingredients to treatment success likely included flexibility with fidelity in implementing an ACT treatment; attention to individual and cultural factors; the use of creative strategies for carrying out of the underlying theoretical principles of the treatment.
REFERENCESAbramowitz, J. S., Tolin, D. F., & Street, G. P. (2001).
Paradoxical effects of thought suppression: A meta- analysis of controlled studies. Clinical Psychology Review, 21, 683– 703. doi:10.1016/S0272- 7358(00)00057- X.
Campbell- Sills, L., Barlow, D. H., Brown, T. A., & Hofmann, S. G. (2006). Effects of suppression and acceptance on emotional responses of individuals with anxiety and mood disorders. Behaviour Research and Therapy, 44, 1251– 1263. doi: 10.1016/j.brat.2005. 10.001.
Hayes, L., Bach, P. A. & Boyd, C. P. (2011). Psychological Treatment for Adolescent Depression:Perspectives on the Past, Present, and Future. Behaviour Change,Volume 27 Pp,123-137
Harris, R. (2013). Getting Unstuck in ACT: A Clinician's Guide to Overcoming Common Obstacles in Acceptance and Commitment Therapy, pp. 2, 6.
Hayes S.C. & Gifford E.V. ( 1997). The trouble with language: Experiential avoidance, rules, and the nature of verbal events. Psychological Science, 8, 170 -173.
Hayes S.C, Wilson K.G, Gifford E.V, Follette V.M, & Strosahl K.D (1996). Emotional avoidance and behavioral disorders: A functional dimensional approach to diagnosis and treatment.Journal of Consulting and Clinical Psychology. 64,1152–1168.
Hayes, S. C., Strosahl, K. D., & Wilson, K. G. (1999). Acceptance and Commitment Therapy: An Experiential Approach to Behavior. Change.New York: Guilford Press.
Livheim, F. (2004). Acceptance and commitment therapy in schools to cope with stress and promote health: A randomized controlled trial. University of Uppsala, Sweden.
Stoddard. J.A. & Afari. N., (2014). The Big Book of ACT Metaphors. New Harbinger Publications, Oakland, CA.
Wicksell, R., Melin, L., & Olsson, G. (2007). Exposure and acceptance in the rehabilitation of ado-lescents with idiopathic chronic pain: A pilot study. European Journal of Pain, 11(3), 267–274.
Soheli et al.,.......... / A Clinical Case Study with Acceptance and ................

75
1. M. Phil Clinical Psychology Trainee, 2. Assoc. Prof., Clinical Psychology 3. Jr. Resident, Deptt. of Psychiatry, K G M U, Lucknow. *Corresponding Author; Shweta Singh. Email: [email protected]
Brain damage is caused as a result of a trauma, cerebrovascular accident or degenerative process. Studies indicate that any damage to the sub-cortical structures of the brain may cause varying degree of neuropsychological as well as emotional and behavioural changes in a person (Grönholm, 2016).
A significant alteration of the habitual patterns of behaviour displayed by the subject premorbidly, involving the expression of emotions, needs and impulses is referred to as Organic Personality Disorder (OPD) in ICD 10 (WHO,1992). Whereas, DSM-5 addresses OPD as Personality changes due to another medical conditions and described as ‘personality disturbance representing a change the individual's previous characteristic personality pattern’(APA, 2013).
Impairment of cognitive and thought functions, and altered sexuality may also be part of the clinical picture (ICD-10,WHO,1992). Literature reports usually OPD occurs with frontal lobe lesions or lesions in other circumscribed areas of the brain (Schwarzbold, 2008). In addition Fronto-temporal regions of the brain have also been indicated (Mahoney et al., 2011).
In addition to determination of the presence or absence of organic pathology, Neuropsychological assessment is also used to assist in identification of disrupted psychological components, determine the interaction between organic and non-organic processes which lead to pathology and to plan cognitive rehabilitation.
Case History:
A 20 years old male belonging to low SES was admitted with complaints of bodily weakness, abnormal movements in left hand and leg and socially inappropriate behaviour following a cerebrovascular accident which took place 14 months back.
The patient was apparently asymptomatic and was well adjusted to personal, social and occupational life before the stroke. He was working in a garment shop when he suddenly developed weakness in left upper and lower limb and delineation of face towards right. It was associated with fever, headache, loss of consciousness, abnormal body movement, incontinence of urine and feces and speech disturbance. The weakness
Indian Journal of Clinical Psychology2017, Vol. 44, No. 1, 75-78
Copyright, 2017, Indian Association ofClinical Psychologists (ISSN 0303-2582)
Case Report
ABSTRACT Organic Personality Disorder is characterized by significant changes in the personality of the individual in terms of affect, behaviour and cognition due to an organic basis. The present paper investigates about the neuropsychological functioning of a young male with organic personality disorder with caudate nucleus infarct caused by cerebrovascular accident. The neuropsychological assessment done by using standardized tools revealed the patient to have an average level of intellectual functioning. However, significant deficits were found in mental Speed, sustained attention, executive functioning, verbal retention, visual retention, visuo-motor coordination and visuo-spatial construction. Mild deficit was found in recent memory and recognition. No deficits were found in attention and concentration, remote memory, immediate recall and delayed recall. A diffused involvement of frontal, temporal and parietal lobes is being discussed and implicated for neuropsychological rehabilitation.Keywords: Neuropsychological Assessment, Organic Personality Disorder, Caudate Nucleus, Infarct, Executive Function, Neuropsychological Battery
Neuropsychological Functioning of Patient with Organic Personality Disorder with Caudate Nucleus Infarct: A Case Study
Saniya Bhutani1, *Shweta Singh2 and Pooja Singh3

76
persisted and the patient could not walk properly without assistance and could not use his left hand properly.
He developed abnormal body movements which affected the muscles of the face, tongue, neck, distal part of hands and legs and it was not associated with pain or any abnormal discomfort. The patient developed significant behavioural changes in the form of irritability, impulsivity, odd eating behaviour, indifference and difficulty in execution of task.
Patient was not bothered about his appearance and personal hygiene. Socially inappropriate behaviour was also reported and observed by family members in form of micturating and masturbating in public. Patient was observed to eat in odd ways and the quantity of the food was increased than his usual self. On being prompted to do routine chores either he would escape from the situation or become abusive and assaultive.
Both behavioural change and abnormal body movements persisted. For the above complaints the family members sought treatment from multiple physicians but as they did not find improvement, would stop medication all the time. Eventually, he was brought to Department of Psychiatry, KGMU and was admitted for detailed evaluation and management.
MRI indicated acute infarct with haemorrhagic foci in right caudate nucleus, anterior limb of internal capsule and lentiform nucleus. Small acute infarct in head of caudate nucleus on left side was observed. Old infarct with encephalomalacic changes were noted in bilateral head of caudate.
Premorbid personality suggested that the patient was attached to family members and had many friends. His mood was stable, calm and relaxed. He held a positive attitude towards work and responsibility and could make decisions easily. He was methodical and meticulous in his approach. He was self-confident, insensitive to criticism, emotionally controlled, tolerant and adaptable. His meal habits were regular and proper. He would have
regular sleeping hours. Bowel habits were within normal limits.
On mental status examination, eye to eye contact could not be maintained consistently. The rate of speech was increased. The motor activity was increased as the patient stood multiple times during the course of assessment. Abnormal involuntary movements like movement of fingers, frequent change of posture, getting up and sitting back was observed. Attention was aroused but could not be sustained. Affect was cheerful. Flow of thinking was normal and form was relevant and coherent. There were no perceptual abnormalities observed. Personal and social judgment was impaired. Mental status examination of the patient was collaborative with the history of the patient revealing behavioural change, increased rate and tone of speech along with impaired judgment. On the basis of History, Mental Status Examination and ICD-10 criteria, a diagnosis of Organic Personality Disorder (F07.0) was made. The patient was referred for neuro-psychological assessment to understand the brain behaviour pathology and magnitude of neuropsychological deficits in the patient and to plan rehabilitation.
Neuropsychological Tools:The areas investigated were Intellectual
Functioning, Attention, Memory Functioning, Executive Functioning and Perceptuo-motor abilities. Tests selected from PGI- BBD were Verbal Adult Intelligence Scale and Battery of Performance Test of Intelligence including Digit Span (Forward and Backward) Recent Memory, Remote Memory, Immediate Recall, Delayed Recall, Verbal Retention, Visual Retention, Recognition, Nahor-Benson Test and Bender Gestalt Test (Prasad & Verma 1990).
Tests selected from NIMHANS neuropsy-chological battery were -Digit symbol substitution (Mental speed), Digit vigilance test (Sustained at-tention), Executive functioning-Controlled oral word association test (COWA)(Phonemic Fluency), Animal names' test (Category fluency) and Verbal N Back test (Verbal working memory) ( Shobhini et al., 2004)
Saniya et al.,.................., / Neuropsychological Functioning of Patient ..................... ....

77
RESULTSTable 1: Test Findings
Function Test Administered Scores Interpretation
Intelligence
Verbal Tests
InformationComprehensionArithmeticDigit Span
88 89 92 97
Average Intellectual Functioning
Perfo
r-ma
nce
Test
s Koh’s Block Design Alexander Pass Along
92 109
(IQ=96,VQ=92, PQ=109)
Attention & Concentration Digit Span (F & B) 7 No dysfunction
Sustained Attention Digit Symbol Substitution
Time Taken: 535 seconds
Significant dysfunction
Executive Functions Significant dysfunction
Verbal Fluency COWA (Controlled Oral Word Test Association Test)
2
Category Fluency Animal Names Test 8
Working Memory N Back Test1 Back
Hit: 3Error: 5
2 Back Hit: 1Error: 9
Learning and Memory
Remote MemoryRecent MemoryImmediate RecallDelayed RecallVerbal RetentionVisual RetentionRecognition
63782-similar pairs2 dissimilar pairs27
Dysfunction in verbal and visual reten-tion. Mild defi-cits in recent memory & recognition.
Visuo-spatial Construction
Nahor-Benson TestBender Gestalt Test
59
Significant Dysfunction
Table 1 shows the test findings for various tests administered. There was absence of the focal signs.
DISCUSSIONThe neuropsychological profile of the patient
with OPD and caudate neucli infarct in terms of haemorrhagic foci in right caudate nucleus and small acute infarct in left caudate nucleus caused by cerebrovascular accident is suggestive of diffused
involvement of frontal, parietal and temporal lobe with significant deficits in Mental Speed, sustained attention, visuo-motor coordination, Executive Functioning, Verbal retention, Visual Retention and visuo-spatial construction.
The role of caudate nucleus has been implicated in the conceptual integration of memories (Mendez et al., 1989). Benke et al. (2010) suggest neuropsychological deficits in executive functioning, drive, attention and memory are associated with left caudate nucleus. The neurons of dorsolateral prefrontal circuit project to the regions of caudate nucleus are clinically and experimentally linked to executive functions (Bonelli, 2007). Deficits in visuo-spatial construction can be associated with temporal and parietal regions of right hemisphere (Corbetta & Shulman, 2002). Studies indicate the involvement of right frontal and parietal cortices in sustained attention, hence deficit would lead to poor sustained attention (Pardo, Fox & Raichle,1991). The prefrontal cortex mediates the role of motor speed, response speed, visuo-motor coordination and motor persistence (Joseph, 1996).
Literature suggests that patients with OPD are presented with frontal syndrome characterized by lack of inhibitions, inappropriate mood, decreased control over inhibition. The interconnections between caudate nucleus and frontal lobe can jointly explain the personality changes in the patient.
The frontosubcortical circuit that is linked to the caudate nucleus is involved in the personality changes and the neuropsychological functioning deficits.
CONCLUSIONNeuropsychological findings in patient of
OPD with caudate nucleus infarct indicate that the patient had average level of intelligence with IQ about 95-100. Cerebrovascular accident involving caudate nucleus lead to significant deficits in mental Speed, sustained attention, visuo-motor coordination, Executive Functioning, Verbal retention, Visual Retention and visuo-spatial construction. Deficits have been found in recent memory, recognition.
Saniya et al.,.................., / Neuropsychological Functioning of Patient ..................... ....

78
REFERENCESAmerican Psychiatric Association. (2013). Diagnostic
and Statistical Manual of Mental Disorders (5th ed.). Washington, DC:
Benabarre A, Ibáñez J, Boget T, et al. (2001). Neuropsychological and psychiatric complications in endoscopic third ventriculostomy: a clinical case report. Journal of Neurology, Neurosurgery & Psychiatry 2001, 71, 268-271.
Benke T, Delazer M, Bartha L & Auer A (2010). Basal Ganglia Lesions and the Theory of Fronto-Subcortical Loops: Neuropsychological Findings in Two Patients with Left Caudate Lesions. Neurocase: The Neural Basis of Cognition
Bonelli, R. M., & Cummings, J. L. (2007). Frontal-subcortical circuitry and behaviour. Dialogues in Clinical Neuroscience, 9(2), 141–151.
Corbetta M, Shulman GL.(2002). Control of goal-directed and stimulus-driven attention in the brain. Nat Rev Neurosci. 3, 201–215.
Damasio AR (1996). Descartes’ error: emotion, reason, and the human brain. London: Papermac, 1996.
Hallett, S. (1993). Neuropsychology. In Morgan, G.& Butler, S. (Eds.) Seminars in Basic Neurosciences, pp. 151-186. Available from: URL: http://www.rcpsych.ac.uk/pdf/semBasNeuro_chapter5.pdf
Joseph, R. (1996). Neuropsychiatry, Neuropsychology and Clinical Neuroscience (2nd ed.). Williams Wilkins, USA
Joseph R.G. The Head of the Caudate Nucleus. Retrieved from http://brainmind.com/CaudateHead.html
Kolb, B., & Whishaw, I. Q. (2003). Fundamentals of Human Neuropsychology. New York, NY: Worth Publishers.
Mas-Exposito L, Amador-Campos JA, Lalucat-Jo L., & Villegas-Miranda F. (2014). Neuropsychological functioning of a patient with organic personality disorder. Actas Esp Psiguiatr 2014 Jul-Aug;42(4):196-200. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/25017497.1
Mendez, M.F., Adams, N.L., & Lewandowski, K.S. (1989). Neurobehavioural changes associated with caudate nucleus. Neurology, 39, 349
Pardo, P.V., Fox, P.T., & Raichle, M.E. (1991). Localization of a human system for sustained attention by positron emission topography. Nature, 349, 61-65
Pershad D, Verma SK.(1990). Handbook of PGI Battery of Brain Dysfunction (PGI-BBD) Agra: National Psychological Corporation.
Rao, S. L., Subbakrishna, D. K. & Gopukumar, K. (2004) NIMHANS Neuropsychology Battery – 2004.Bangalore: NIMHANS Publications.
Sadock, B. J., Sadock, V. A., & Ruiz, P. (2015). Synopsis of Comprehensive Text Book of Psychiatry: Behavioural Sciences/Clinical Psychiatry (Eleventh edition.). Philadelphia: Wolters Kluwer.
World Health Organization. (1993). ICD-10, the ICD-10 International Classification of Mental and Behavioural Disorders: Diagnostic Criteria for Research. Geneva: World Health Organization.

79
1. Asst. Prof. of Clinical Psychology, 2 M.Phil. (Clinical Psychology), Deptt. of Clinical Psychology, PGIBAMS, Raipur, 3. Prof & Head, Deptt. of Psychology, Kumaun University, Nainital, U. K. *Corresponding Author: Manoj Kumar Pandey. Email: [email protected]
INTRODUCTIONStammering is a speech disorder characterized
by involuntary disruptions to speech which hinder the capacity to communicate effectively (Iverach & Rapee, 2014). Stammering is accompanied by various negative consequences in the lifespan which increase the susceptibility to social and psychological difficulties (Schneier, Wexler, & Liebowitz, 1997).These negative consequences are likely to lead the individual in shame and embarrassment, low self-esteem, and withdrawal (Langevin & Prasad, 2012). Stammering has negative effects on aspects of life such as education, employment, family and marital relationship and social life of the individual (Klompas & Ross, 2004). Literature puts forth the evidence of presence of social anxiety or social phobia in people who stutter (Stein, Baird, & Walker, 1996; Schneier, Wexler, & Liebowitz, 1997). Studies also indicate adults who stutter have demonstrated significantly greater expectancy of social harm than those who do not stutter (Davis, Shisca & Howell, 2007). Thus, there seem to be a reciprocal relationship among expectance of social harm, social anxiety and stammering. Although, there has been plenty of studies (Gil, Carrillo &Meca, 2001) investigating the use of cognitive behavioural therapy in social anxiety disorder, there has been few studies (Menzies et al., 2008) assessing the use of cognitive behaviour
therapy in stammering as a primary disorder while simultaneously dealing with social anxiety. The present case report is prepared with the objective of assessing the use of cognitive behaviour therapy in patient with stammering as a primary disorder.
CLINICAL HISTORYThe index patient X, 28 years unmarried
female,bachelor in Dental Surgery belong to upper socio-economic status, hailing from urban area of Bahraich district, U.P. was brought to Sahara Hospital, Lucknow with complaints of involuntary repetition of syllables when starting to speak, eye blinking, facial grimacing, jerking of head while trying to speak, shyness, high anxiety in social situation, avoiding speaking in social situations and to strangers since childhood. Mother reported that patient is having this problem in public speaking since about ten years of age. These problems in speaking also used to occur while speaking to father and during talking about emotional issues. As per the patient, her difficulty in speaking had negative influence on interpersonal relationship, quality of relationship with father and on group academic activity. She used to avoid the family and social gathering. She had a pessimistic outlook about recovery from this problem. She has been treated by three speech therapists. Each time she discontinued
Indian Journal of Clinical Psychology2017, Vol. 44, No. 1, 79-82
Copyright, 2017, Indian Association ofClinical Psychologists (ISSN 0303-2582)
Case Report
Efficacy of Cognitive Behaviour Therapy in an Adult with Stammering*Manoj Kumar Pandey1, Prabha Mishra2 and Aradhana Shukla3
ABSTRACT The present investigation is a case report which was aimed at studying the use of cognitive behaviour therapy (CBT) in reducing the stammering and social anxiety associated with it. An adult female patient along with her parents visited Clinical Psychology OPD in a private hospital in Lucknow, for psychotherapeutic treatment of stammering. Detail clinical history was taken and pre assessment for stammering and social anxiety was carried out. Therapeutic intervention was conducted using CBT with a structured program. After the completion of 13 weeks intervention sessions post assessment data and at 3 months,follow up data was also obtained. Assessment at pre, post intervention and follow up was carried out using Perceptions of Stuttering Inventory (Woolf, 1967) and Social Anxiety Questionnaire for Adults-30 (Caballo et al., 2010). This case intervention revealed that CBT is helpful in reducing stammering and social anxiety when both conditions are treated simultaneously. To conclude, it is suggestive that finding from this case report need to be investigated in random control trial to treat the adult stammering.Key words: Cognitive Behaviour Therapy, Stammering, Social Anxiety.
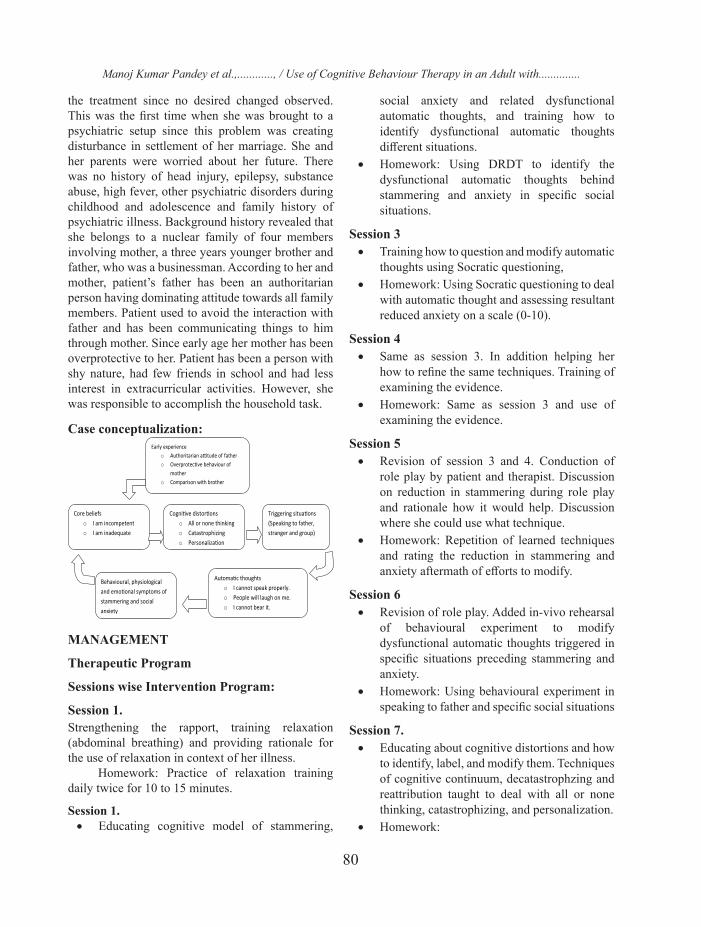
80
the treatment since no desired changed observed. This was the first time when she was brought to a psychiatric setup since this problem was creating disturbance in settlement of her marriage. She and her parents were worried about her future. There was no history of head injury, epilepsy, substance abuse, high fever, other psychiatric disorders during childhood and adolescence and family history of psychiatric illness. Background history revealed that she belongs to a nuclear family of four members involving mother, a three years younger brother and father, who was a businessman. According to her and mother, patient’s father has been an authoritarian person having dominating attitude towards all family members. Patient used to avoid the interaction with father and has been communicating things to him through mother. Since early age her mother has been overprotective to her. Patient has been a person with shy nature, had few friends in school and had less interest in extracurricular activities. However, she was responsible to accomplish the household task.
Case conceptualization:
MANAGEMENT
Therapeutic Program
Sessions wise Intervention Program:
Session 1. Strengthening the rapport, training relaxation (abdominal breathing) and providing rationale for the use of relaxation in context of her illness.
Homework: Practice of relaxation training daily twice for 10 to 15 minutes.
Session 1. • Educating cognitive model of stammering,
social anxiety and related dysfunctional automatic thoughts, and training how to identify dysfunctional automatic thoughts different situations.
• Homework: Using DRDT to identify the dysfunctional automatic thoughts behind stammering and anxiety in specific social situations.
Session 3 • Training how to question and modify automatic
thoughts using Socratic questioning, • Homework: Using Socratic questioning to deal
with automatic thought and assessing resultant reduced anxiety on a scale (0-10).
Session 4 • Same as session 3. In addition helping her
how to refine the same techniques. Training of examining the evidence.
• Homework: Same as session 3 and use of examining the evidence.
Session 5 • Revision of session 3 and 4. Conduction of
role play by patient and therapist. Discussion on reduction in stammering during role play and rationale how it would help. Discussion where she could use what technique.
• Homework: Repetition of learned techniques and rating the reduction in stammering and anxiety aftermath of efforts to modify.
Session 6 • Revision of role play. Added in-vivo rehearsal
of behavioural experiment to modify dysfunctional automatic thoughts triggered in specific situations preceding stammering and anxiety.
• Homework: Using behavioural experiment in speaking to father and specific social situations
Session 7. • Educating about cognitive distortions and how
to identify, label, and modify them. Techniques of cognitive continuum, decatastrophzing and reattribution taught to deal with all or none thinking, catastrophizing, and personalization.
• Homework:
Manoj Kumar Pandey et al.,............, / Use of Cognitive Behaviour Therapy in an Adult with..............

81
• Labelling and modifying cognitive distortions. Rating the resulting reduced anxiety and stammering.
Session 8 • Revision of session 7. • Homework: Same as session 7.
Session 9 • Recapitulation of learned techniques, felt
difficulties, and perceived reduction in rating of stammering and anxiety.
• Homework: Speaking out in group situations in dental clinic, social gathering, and with father.
Session 10 - 13 • Educating about dysfunctional core belief.
Training how to identify and deal them. Same techniques were generalized to deal with core beliefs which were applied in previous sessions.
Session 14-15 • Homework: Continued dealing with
dysfunctional automatic thoughts, cognitive distortions, identification and modification of dysfunctional core beliefs.
PROCEDUREDetailed clinical history of the patient was taken
in first intake interview. Frequency and intensity of stammering and anxiety in social situation was recorded. In second meeting baseline assessment of stammering and social anxiety was carried out and psycho-education was conducted. Psycho-education included informing about illness, psychological management methods, rationale how psychological management could help, duration of treatment, role of patients and therapist in treatment, expected recovery, and prognosis of the problem. Perceptions of Stuttering Inventory (Woolf, 1967) for assessment of stammering and Social Anxiety Questionnaire for Adults-30 (Caballo et al., 2010) were used to assess social anxiety. Therapy was carried out in 13 weekly sessions and one follow up session on 3 months taken. The duration of individual session was 45 to 60 minutes. Each weekly session started with feedback from patient about reduction in frequency and intensity (using scaling) of stammering and anxiety and difficulties in accomplishing homework.
In session 6, 7 and 8 three attempts of behavioural experiment of speaking in front of group with assistance of therapist was conducted in hospital. Patient’s father, mother and brother were involved in therapy only for observation of change in stammering and asked to report on phone before the each individual session. After the completion of 13 sessions and 3 months follow up an assessment for stammering and social anxiety was conducted. Comparison of stammering and social anxiety is at pre, post intervention and 3 months follow up is depicted in figure 1 and 2. Stammering is shown as scores on three domains of perception of stuttering inventory i.e., struggle, avoidance and expectancy.
02468
101214161820
Pre Post F ollow Up
Struggle
Avoidance
Expectancy
Figure 1: Perceptions of Stuttering Inventory
Figure 2: Social Anxiety Questionnaire for Adults.
Manoj Kumar Pandey et al.,.......... / Title “Use of Cognitive Behaviour Therapy in an Adult with...

82
DISCUSSIONCBT has been found to be effective in treating
social anxiety disorder as a major treatment method (Gil, Carrillo & Meca, 2001). However, few studies denote the effectiveness of CBT in managing stammering (Reddy, Sharma & Shivashankar, 2010). This case intervention is suggestive that CBTis useful in reducing the frequency and intensity of stammering when co-morbid social anxiety is also simultaneously treated. In adult who had developed the stammering at childhood are most likely to have social anxiety disorder in life time. People with social anxiety frequent report problems of stammering while facing groups (Messenger, Onslow, Packman & Menzies, 2004). Tendency of avoidance remains a core maintaining factor in social anxiety and avoidance may create a hurdle in compliance with exposure based homework provided in CBT for stammering. Therefore, CBT in management of stammering can be started with relaxation and cognitive strategies to deal with dysfunctional cognition. Whereas, behavioural exposure based methods can be applied in later on enhance the rate of improvement. In conclusion, it is indicative from this case investigation that CBT is helpful in reducing stammering. There should be random control trials to further establish its effectiveness and efficacy in management of stammering.
REFERENCES: Caballo, V. E., Salazar, I. C., Irurtia, M. J., Arias, B.,
Hofmann, S. G., & the CISO-A Research Team (2010a). Measuring social anxiety in 11 countries: Development and validation of the Social Anxiety Questionnaire for Adults. European Journal of Psychological Assessment, 26, 95-107.
Davis, S., Shisca, D., & Howell, P. (2007). Anxiety in speakers who persist and recover from stuttering. Journal of Communication Disorders, 40, 398–417.
Gil, P. J. M., Carrillo, F. X. M. & Meca, J. S. (2001). Effectiveness of Cognitive-Behavioural Treatment in Social Phobia: A Meta-Analytic Review. Psychology in Spain, 5, 1, 17-25
Iverach, L. & Rapee, R. M. (2014). Social anxiety disorder and stuttering: Current status and future directions. Journal of Fluency Disorders 40, 69–82.
Klompas, M. & Ross, R. (2004). Life experiences of people who stutter, perceived impact of stuttering on quality of life: Personal accounts of South African individuals. Journal of Fluency Disorders, 29, 275-305.
Langevin, M., & Prasad, N. G. (2012). A stuttering education and bullying awareness and prevention resource: A feasibility study. Language, Speech and Hearing Services in Schools, 43, 344–358.
Menzies, R. G., O’Brian, S., Onslow, M., Packman, A., St Clare, T., & Block, S. (2008). An experimental clinical trial of a Cognitive Behaviour Therapy package for chronic stuttering. Journal of Speech, Language and Hearing Research, 51, 1451–146 4.
Messenger, M., Onslow, M., Packman, A. & Menzies, R. (2004). Social anxiety in stuttering: measuring negative social experiences. Journal of Fluency Disorders, 29, 3, 201-212.
Reddy, R. P., Sharma, M. P. & Shivashankar, N. (2010). Cognitive Behaviour Therapy for Stuttering: A Case Series. Indian Journal of Psychological Medicine, 32, 1, 49-53.
Schneier, F. R., Wexler, K. B., & Liebowitz, M. R. (1997). Social phobia and stuttering. The American Journal of Psychiatry,154, 131.
Stein, M. B., Baird, A., & Walker, J. R. (1996). Social phobia in adults with stuttering. American Journal of Psychiatry, 153, 278–280.
Woolf, G. (1967). The Assessment of Stuttering As Struggle, Avoidance and Expectancy. British Journal of Disorders of Communication, 2, 158-171.
Manoj Kumar Pandey et al.,.......... / Use of Cognitive Behaviour Therapy in an Adult with.............
Official Publication of INDIAN ASSOCIATION OF
CLINICAL PSYCHOLOGISTSwww.iacp.in

85
86
3052
_(05
-17)
_Ann
apur
na P
ress
• 06
51-2
3318
00
IND
IAN JO
UR
NAL O
F CLIN
ICAL PSYC
HO
LOG
Y, 44 (1), March-2017