







Bahasa
Halaman
Hukum


GcHN
Obo
Sermca
Rr
C3
Cfwp
FJ(DAS
PS
R
RN
TCUHapCirCS
D
0©d
AGOS Papers www.AJOG.org
3
PR30: a novel indicator of poor survival for endometrialarcinomaarriet O. Smith, MD; Kimberly K. Leslie, MD; Meenakshi Singh, MD; Clifford R. Qualls, PhD; Chetana M. Revankar, PhD;ancy E. Joste, MD; Eric R. Prossnitz, PhD
BJECTIVE: This study was undertaken to evaluate the relationshipetween GPR30, classical steroidal receptor expression, and clinicalutcome in patients with endometrial carcinoma.
TUDY DESIGN: Immunohistochemistry was used to investigate thexpression of GPR30, estrogen, progesterone, epidermal growth factoreceptors and Ki-67 in 47 consecutive consenting patients with endo-etrial carcinoma diagnosed between 1997 and 2001. Results were
orrelated with clinical and pathologic predictors of adverse outcomend survival.
ESULTS: GPR30 correlated positively with epidermal growth factor
oi: 10.1016/j.ajog.2007.01.004
86.e1 American Journal of Obstetrics & Gynecology APRIL 2007
eptor expression. GPR30 overexpression occurred more frequently inumors with deep myometrial invasion, high-grade, biologically ag-ressive histologic subtypes, and advanced stage. In patients withPR30 overexpression, survival was significantly poorer (65.2% vs00%, P � .005).
ONCLUSION: GPR30 represents an alternative estrogen-responsiveeceptor that is overexpressed in tumors where estrogen and proges-erone receptors are downregulated, and in high-risk endometrial can-er patients with lower survival rates.
ey words: endometrial carcinoma, estrogen receptor, GPR30,
eceptor (P � .005), but negatively with progesterone (P � .05) re- progesterone receptor, survivalite this article as: Smith HO, Leslie KK, Singh M, et al. GPR30: a novel indicator of poor survival for endometrial carcinoma. Am J Obstet Gynecol 2007;196:86.e1-386.e11.
arcinoma of the endometrium isthe most common malignancy af-
ecting the female reproductive tract,ith an estimated 41,200 new cases ex-ected in the United States in 2006.1 Ap-
proximately 75-80% of endometrial car-cinomas are of endometrioid histology,2
arise within a background of hyperpla-sia,3 and are associated with high levels ofestrogen (ER), progesterone (PR), and
epidermal growth factor receptor(EGFR) expression.4-6 Type I endome-trial carcinomas, which have a more fa-vorable prognosis, result from continu-ous exposure to estrogen without thedifferentiating effects of progesterone.Type II cancers are not usually associatedwith estrogen, and tend to have a moreaggressive phenotype.7 Although low-grade, early-stage endometrial carci-noma is usually curable, the 5-year sur-vival rate for stage III and IV disease isonly approximately 34%.8,9 Recurrentdisease not amenable to surgery is usu-ally fatal; in 2006, it is estimated that7350 women in the United States will diefrom this disease.1
Recently, we described a novel intra-cellular 7-transmembrane G protein-coupled estrogen receptor (GPR30) thatappears to function alongside the tradi-tional estrogen receptor to regulatephysiologic responsiveness to estro-gen.10 G protein-coupled receptors rep-resent the largest class of signaling mol-ecules in the human genome.11 They areheptahelical transmembrane proteins12
traditionally expressed on the cell sur-face, where the binding of agonists ini-tiates activation of heterotrimeric gua-
rom the Departments of Obstetrics and Gynecology (Drs Smith and Leslie), Pathology (Droste), and Cell Biology and Physiology and the Cancer Research and Treatment CenterDrs Revankar and Prossnitz), University of New Mexico Health Sciences Center, and theepartment of Mathematics and Statistics, University of New Mexico (Dr Qualls),lbuquerque, NM; and the Department of Pathology, University of Colorado Healthciences Center, Denver, CO (Dr Singh).
resented at the 25th Annual Meeting of the American Gynecological and Obstetrical Society,ept. 14-16, 2006, Williamsburg, VA.
eceived Nov. 15, 2006; accepted Jan. 2, 2007.
eprints: Harriet O. Smith, MD, Department of Obstetrics and Gynecology, 2211 Lomas Blvd,E, Albuquerque, NM 87131-5286; [email protected].
his study was supported by Pilot Research Funds (H.O.S.) from the University of New Mexicoancer Research and Treatment Center; National Cancer Institute Grant NCI P30 CA118110; theniversity of New Mexico School of Medicine Grant C-2279-RAC (H.O.S.); National Institutes ofealth Grants CA11666 (E.R.P.), R01CA99908-1 (K.K.L.), CA27469 (Gynecologic Oncology Groupnd K.K.L.), and DHHS/NIH/NCRR/GCRC Grant 5M01 RR00997; the Cory Beach Foundation;rivate donations (Shirley Leslie; Dean and Alice Irvin); and the Biostatistics Shared Resource of theancer Research and Treatment Center, University of New Mexico Health Sciences Center. Images
n this article were generated in the UNM Cancer Center Fluorescence Microscopy Facility, whicheceived support from NCRR 1 S10 RR14668, NSF MCB9982161, NCRR P20 RR11830, NCI R24A88339, NCRR S10 RR19287, NCRR S10 RR016918, the University of New Mexico Healthciences Center, and the University of New Mexico Cancer Center.
rs Leslie and Prossnitz share equal credit as senior investigators.
002-9378/$32.002007 Mosby, Inc. All rights reserved.
ctgG1
Crtc
K
n
ine nucleotide binding proteins (G
pltaptpsdglcpgtn
PfirbEassrlHmcecuct
ecsEpcprfvtidvshet
ar
MSTbUeapctantIavatwtbcdtatocvfdthLmrsfN
IGtNi4tp(sI
cal1GrmMDc(MarraKcrbEEEtr
tpdrKKEthmdmtftCmfwnMa
iUtc02
www.AJOG.org AGOS Papers
roteins) and downstream effectors, fol-owed by rapid receptor phosphoryla-ion, desensitization, internalization,nd recycling.13 Unlike virtually all Grotein-coupled receptors characterizedo date, GPR30 is localized to the endo-lasmic reticulum, where, as demon-trated with a novel fluorescent estrogenerivative, it specifically binds estro-en.10 Stimulation of GPR30 by estrogeneads to calcium mobilization and nu-lear phosphatidylinositol 3,4,5-triphos-ate accumulation. In addition to estro-en, classic ER antagonists such asamoxifen activate multiple cellular sig-aling pathways via GPR30.10,14
In stage I and II tumors, both ER andR status correlate inversely with many
actors predictive of adverse outcome,ncluding histology, adnexal spread, andecurrence15; PR, but not ER status haseen shown to predict survival.15,16
GFR is expressed in both endometrioidnd nonendometrial cell types,17 and inome clinical trials, expression has beenhown to correlate with lower survivalates.17,18 EGFR is expressed in equiva-ent amounts in Ishikawa H and
ec50co cells, prototypic cell cultureodels for type I and type II endometrial
arcinomas,19 whereas GPR30 is prefer-ntially expressed in Hec50co cells.10 Re-ent results suggest that GPR30 may reg-late proliferation of endometrialarcinoma cell lines by estrogen andamoxifen.20
The purpose of this investigation is tovaluate expression of GPR30 and toorrelate these findings with the expres-ion of classic steroid receptors (ER, PR),GFR, and Ki-67, a proliferative markerredictive of survival in endometrial car-inoma,21 as well as to clinical andathologic predictors of outcome in a se-ies of patients with at least 5 years ofollow-up. GPR30-mediated transacti-ation of EGFR may result in constitu-ive EGFR activation. In type II tumorsn which classical estrogen receptors areownregulated, preferential GPR30 acti-ation may lead to chronic signaling re-ulting in tumor proliferation. If so, weypothesized that patients with high lev-ls of GPR30 expression may exhibit fea-
ures predictive of adverse outcome such ps high-grade, advanced-stage, and high-isk histologic subtypes.
ATERIALS AND METHODSpecimenshis study was reviewed and approvedy the Institutional Review Board of theniversity of New Mexico Health Sci-
nce Center. Although tissue acquisitionnd surveillance is ongoing, the studyopulation consisted of 47 consecutiveonsenting patients who had endome-rial carcinoma diagnosed between 1997nd 2001. For each case, preoperative ve-ous serum samples were collected on
he day of surgery and stored at �20°C.mmediately after hysterectomy, benignnd tumor uterine tissues were har-ested, snap frozen in liquid nitrogen,nd frozen at �80°C. A portion of theumor was blocked in paraffin, andhere feasible, ten 5-�m sections from
he most representative available tissuelocks were prepared for immunohisto-hemistry. Clinical and pathologic pre-ictors of adverse outcome, such as In-ernational Federation of Gynecologynd Obstetrics (FIGO) stage, histology,umor grade, and depth of invasion werebtained from pathology reports andonfirmed by secondary pathology re-iew by 2 pathologists. Epidemiologicactors known to be associated with en-ometrial carcinogenesis and relevantreatment data were abstracted fromospital and clinic medical records.ong-term follow-up was obtained fromultiple sources, including medical
ecords, correspondence with local phy-icians, and for cases otherwise lost toollow-up, by using the University ofew Mexico Tumor Registry.
mmunohistochemistryPR30 immunostaining and interpreta-
ion were performed at the University ofew Mexico Health Sciences Center us-
ng the C- and N-terminal antibodies in6 and 9 cases, respectively. Immunohis-ochemistry and quantification of ex-ression for ER, PR, Ki-67, and EGFR45 cases) were performed at the Univer-ity of Colorado Health Sciences Center.nterpretation of immunoreactivity was
erformed by 2 pathologists, who re- cAPRIL 2007 America
orded the intensity (0, 1�, 2�, 3�)s ordinal and the percentage of epithe-ial cells stained as continuous data (0-00%). Rabbit antisera directed againstPR30 were generated from peptides
epresenting the amino and carboxy ter-ini of GPR30 (MDVTSQARGVGLE-YPGTAQPAAC and CAVIPDSTEQS-VRFSSAV, respectively) with an added
ysteine residue for KLH conjugationNew England Peptide, Inc, Gardner,
A). The anti-GPR30 carboxy-terminalntiserum from 1 rabbit was affinity pu-ified by using a peptide-conjugatedesin and used in these studies. The otherntibodies used were directed againsti-67 (a mouse monoclonal antibody,
lone MIB-1, DakoCytomation, Carpinte-ia, CA), PR (a mouse monoclonal anti-ody, clone PgR 636 DakoCytomation),R (a monoclonal antibody specific forR-�, clone 1D5, DakoCytomation), andGFR (a monoclonal antibody detecting
otal EGFR, clone 31G7, Zymed Laborato-ies, Inc, San Francisco, CA).
ER, PR, Ki-67, and EGFR. In brief, af-er deparaffination, antigen retrieval waserformed by incubating the slides in aecloacking chamber with Dako targetetrieval solution (DakoCytomation) fori-67, ER, and PR, and with a proteinase
solution (DakoCytomation) forGFR, for 20 and 10 minutes, respec-
ively. Tissues were incubated with 3%ydrogen peroxide in methanol for 30inutes to quench endogenous peroxi-
ase. The Dako Autostainer (DakoCyto-ation) was programmed to incubate
he tissue slides with primary antibodiesor 1 hour at room temperature for all ofhe assays. The EnVision Plus Kit (Dako-ytomation) was used to complete im-unostaining according to the manu-
acturer’s instructions; antibody bindingas detected by the chromogen diami-obenzadine (Sigma-Aldrich, St. Louis,O). Slides were then counterstained
nd evaluated.GPR30. Sections were deparaffinized
n Citrosolve (Paco Systems, Devon,nited Kingdom), followed by rehydra-
ion in ethanol. Antigen retrieval was ac-omplished by microwaving slides in.01 mol/L Na citrate buffer (pH 6.0) for5 minutes, followed by incubation of
ooled slides in fresh 2% H2O2 for 10n Journal of Obstetrics & Gynecology 386.e2
mw3Xlbib3Bat(mbrmbwdhrcmctwVf2tp
gplcststicrcmv
SCiUsiisaSicspo
mpmwufu.s
RTbttt1r1Epsbsaom1nw
lls w
AGOS Papers www.AJOG.org
3
inutes. Permeabilization and blockingere performed incubating the slides for0 minutes in 200 �L of 0.1% triton-100 in phosphate-buffered saline so-
ution (PBS) with 3% bovine serum al-umin in a humid chamber. Slides were
ncubated with the primary GPR30 anti-ody or isotype control diluted 1:100 in% normal goat serum overnight at 4°C.ound antibody was detected using thevidin-biotin immunoperoxidase sys-em, incubating with biotinylated-GAR1:200 in 3% normal goat serum) for 60inutes at room temperature, followed
y incubation with strepatvidin-horse-adish peroxidase (diluted 1:250 in nor-al goat serum) for 45 minutes. Anti-
ody binding was detected by stainingith enzyme substrate diaminobenza-ine (DAB; Sigma-Aldrich). Immuno-istochemistry was performed in 2 sepa-ate sessions with the use of positiveontrols shown to express GPR30 by im-unofluroescence and negative controls
onsisting of normal and tumor tissueshat express GPR30 that were incubatedith the rabbit isotype control antibody.alidation of GPR30 expression was per-
ormed by comparing interpretation byindependent reviewers. In 10 samples,
here was 100% agreement regarding the
TABLE 1Intensity of staining and number (
Receptor
Intensity of staining
3� 2�
GPR30H 23 9...................................................................................................................
n � 46 50.0% 19.6%...................................................................................................................
GPR30L 0 6...................................................................................................................
n � 46 0.0% 13.0%...................................................................................................................
EGFR 17 15...................................................................................................................
n � 45 37.8% 33.3%...................................................................................................................
Ki-67 40 4...................................................................................................................
n � 45 88.9% 8.9%...................................................................................................................
PR 28 4...................................................................................................................
n � 45 62.2% 8.9%...................................................................................................................
ER 22 8...................................................................................................................
n � 45 48.9% 17.8%...................................................................................................................
* Number (%) with � 25% of positive epithelial cells, � 25the greatest intensity of staining; GPR30L, number (%) of ce
resence or absence of staining, and d
86.e3 American Journal of Obstetrics & Gynecol
ood correlation (within 1 quartile) withercent and intensity (0-3�) of epithe-
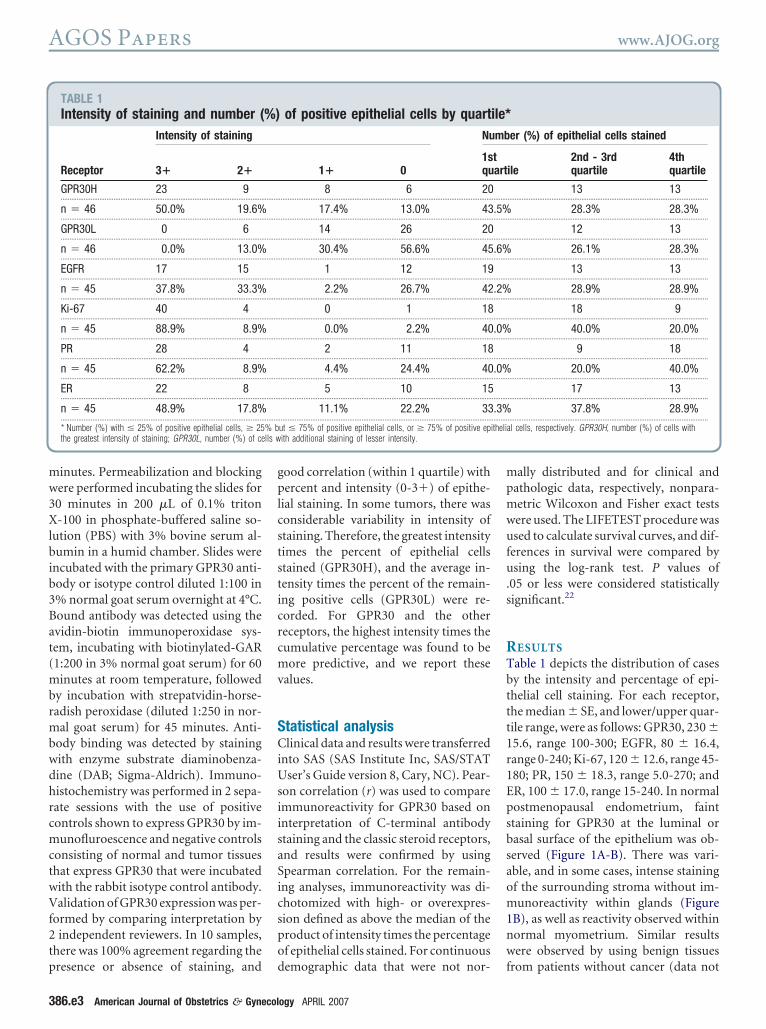
ial staining. In some tumors, there wasonsiderable variability in intensity oftaining. Therefore, the greatest intensityimes the percent of epithelial cellstained (GPR30H), and the average in-ensity times the percent of the remain-ng positive cells (GPR30L) were re-orded. For GPR30 and the othereceptors, the highest intensity times theumulative percentage was found to beore predictive, and we report these
alues.
tatistical analysislinical data and results were transferred
nto SAS (SAS Institute Inc, SAS/STATser’s Guide version 8, Cary, NC). Pear-
on correlation (r) was used to comparemmunoreactivity for GPR30 based onnterpretation of C-terminal antibodytaining and the classic steroid receptors,nd results were confirmed by usingpearman correlation. For the remain-ng analyses, immunoreactivity was di-hotomized with high- or overexpres-ion defined as above the median of theroduct of intensity times the percentagef epithelial cells stained. For continuous
of positive epithelial cells by quartNu
1� 01squ
8 6 20.........................................................................................................................
17.4% 13.0% 43.........................................................................................................................
14 26 20.........................................................................................................................
30.4% 56.6% 45.........................................................................................................................
1 12 19.........................................................................................................................
2.2% 26.7% 42.........................................................................................................................
0 1 18.........................................................................................................................
0.0% 2.2% 40.........................................................................................................................
2 11 18.........................................................................................................................
4.4% 24.4% 40.........................................................................................................................
5 10 15.........................................................................................................................
11.1% 22.2% 33.........................................................................................................................
ut � 75% of positive epithelial cells, or � 75% of positive epith additional staining of lesser intensity.
emographic data that were not nor- f
ogy APRIL 2007
ally distributed and for clinical andathologic data, respectively, nonpara-etric Wilcoxon and Fisher exact testsere used. The LIFETEST procedure wassed to calculate survival curves, and dif-
erences in survival were compared bysing the log-rank test. P values of
05 or less were considered statisticallyignificant.22
ESULTSable 1 depicts the distribution of casesy the intensity and percentage of epi-helial cell staining. For each receptor,he median � SE, and lower/upper quar-ile range, were as follows: GPR30, 230 �5.6, range 100-300; EGFR, 80 � 16.4,ange 0-240; Ki-67, 120 � 12.6, range 45-80; PR, 150 � 18.3, range 5.0-270; andR, 100 � 17.0, range 15-240. In normalostmenopausal endometrium, fainttaining for GPR30 at the luminal orasal surface of the epithelium was ob-erved (Figure 1A-B). There was vari-ble, and in some cases, intense stainingf the surrounding stroma without im-unoreactivity within glands (Figure
B), as well as reactivity observed withinormal myometrium. Similar resultsere observed by using benign tissues
er (%) of epithelial cells stained
ile2nd - 3rdquartile
4thquartile
13 13..................................................................................................................
28.3% 28.3%..................................................................................................................
12 13..................................................................................................................
26.1% 28.3%..................................................................................................................
13 13..................................................................................................................
28.9% 28.9%..................................................................................................................
18 9..................................................................................................................
40.0% 20.0%..................................................................................................................
9 18..................................................................................................................
20.0% 40.0%..................................................................................................................
17 13..................................................................................................................
37.8% 28.9%..................................................................................................................
al cells, respectively. GPR30H, number (%) of cells with
%) ile*mb
tart
......... .........
.5%......... .........
......... .........
.6%......... .........
......... .........
.2%......... .........
......... .........
.0%......... .........
......... .........
.0%......... .........
......... .........
.3%......... .........
% b itheli
rom patients without cancer (data not

stw1pgahdmvsatus
g(tcccst(ui
tp0
n.s�c���d�e
6Bw
IaFam
www.AJOG.org AGOS Papers
hown). Low levels of expression similaro benign endometrium were seen inell-differentiated carcinomas (Figure, D-E). In contrast, high immunoex-ression was observed in stage IIIC,rade 1 disease (Figure 1, G). In this ex-mple, the primary tumor lacked manyigh-risk features predictive of advancedisease (grade 1, depth of myometrial tu-or invasion 40%, absence of lympho-
ascular space or cervical stromal inva-ion). The negative control (isotypentibodies) using sections from this pa-ient defined background staining (Fig-re 1, I). High levels of GPR30 expres-
FIGURE 1GPR30 in benign and malignant en
BE
BE
Gr 1
A
D
G
mmunohistochemistry for GPR30 (C terminal) odenocarcinoma with 1 mm invasion C, stage II, stage IIA UPSC; G, stage IIIC, grade 1 endomentibody). BE, Benign endometrium; Gr, grade.agnification).
ion were observed in tumors of high- e
rade (Figure 1, C,H), advanced stageFigure 1, C,G,H), and high-risk sub-ypes, including uterine papillary serousarcinomas (UPSC, Figure 1, F), clearell carcinomas (Figure 2, C,F), and car-inosarcomas (Figure 2, H-I). In 9 pairedamples, no significant differences in in-ensity times percentage of cells stainedpaired t test, P � .57) were observed bysing C-terminal vs N-terminal antibod-
es (Figure 3).GPR30 expression (determined with
he C-terminal antibody) correlatedositively with EGFR expression (r �.42, P � .005), and negatively with PR
metrial tissues
BE
Gr 1
Gr 3
B
E
H
nign and malignant endometrial glands from patgrade 3 mixed endometrioid and serous carcinoid adenocarcinoma; H, stage IVB grade 3 endom, G, H, I, 10� original magnification; B, C, E
xpression (r � �0.30, P � .05), and had t
APRIL 2007 America
o correlation with Ki-67 (r � 0.09, P �57) or ER (r � �0.09, P � .54). ERtrongly correlated with PR expression (r
0.65, P � .0001). There was an inverseorrelation between Ki-67 and ER (r �0.46, P � .0013) and PR (r � �0.36, P.016), but no correlation with EGFR (r�0.03, P � .82) expression. EGFR also
id not correlate with ER (r � �0.12, P.44) or PR (r � � 0.16, P � .30)
xpression.The mean age of diagnosis (� SD) was
1.4 (� 11.3) years (range, 33-84 years).y race/ethnicity, 22 (46.8%) werehite, 20 (42.6%) were Hispanic, and
Negative Control
UPSC
Gr 3
C
F
I
ts with A, D, Stage IA and B, E, IB endometrioidwith extensive lymphovascular space invasion;oid adenocarcinoma; I negative control (isotype� original magnification; D, F, 40� original
do
f be ienIC, matrio etri(A , 20
he remainder were black (2), American
n Journal of Obstetrics & Gynecology 386.e4

I((mwB1pi4mw.m(
s�owp
nasw((eg
pr[wdg[d.Etwg[
InaepC
AGOS Papers www.AJOG.org
3
ndian (2), or Asian (1). Thirty-nine83%) were postmenopausal; 1429.8%) had used hormone therapy. Theean body mass index (BMI in kg/cm2)as 32.9 � 9.9 (range 18.1-58.1), with aMI � 25, � 25.1 but � 29.9, or � 30 in2 (25.3%), 9 (19.2%), and 26 (34.0%)atients, respectively. The mean weight
n kilograms was 84.9 � 26.9 (range5.2-151 kg). PR overexpression wasore common in heavier patients, usingeight (Wilcoxon, P � .02) or BMI (P �
03). ER overexpression was more com-on using weight (P � .02) but not BMI
FIGURE 2GPR30 and EGFR expression in hig
EGFR
A
EGFR
EGFR
D
G
mmunohistochemistry for GPR30 and EGFR in pegative but strongly positive for Ki-67 (not shnd positive for Ki-67 within glands and strompithelial cells were negative, whereas malignanlasma membrane whereas the subcellular expr, G, H, 20� original magnification; B, D, E, I
P � .10). Differences in Ki-67 expres- r
86.e5 American Journal of Obstetrics & Gynecol
ion by weight (P � .07) but not BMI (P.26) approached significance. No
ther differences in expression levelsere found by these epidemiologicarameters.As determined by histologic exami-
ation, 36 (72.3%) were endometrioiddenocarcinomas, including 4 withquamous differentiation; of these, 7ere grade 3 tumors. Ten cases
21.3%) were either carcinosarcomas3), UPSC (3), clear cell (1), or mixedpithelial (3) cell types. Comparingrade 1 � 2 with grade 3 � other high-
risk endometrial tumors
EGFR
GPR30
EGFR
B
E
H
nts with A-C, F clear cell carcinomas and D-E,), A, B, EGFR and C, F, GPR30. Carcinosarcomata not shown). Malignant mesenchymal cells
ands and stroma were both intensely positive fion pattern of GPR30 is consistent with its prev� original magnification; F, 63� original ma
isk cell types, GPR30 was overex- G
ogy APRIL 2007
ressed more frequently in the high-isk tumors (10/30 [33.3%] vs 13/1681.3%], Fisher exact test, P � .005)hereas PR expression above the me-ian occurred more frequently in low-rade tumors (18/30 [60.0%] vs 2/1414.3%], P � .008), with no significantifferences observed for Ki-67 (P �
21), EGFR (P � .35), or ER (P � .21).xcluding high-risk histologic sub-
ypes, PR expression above the medianas more common in grade 1 � 2 vsrade 3 tumors (18/29 [62.1%] vs 1/714.3%], P � .037), and differences in
GPR30
GPR30
GPR30
C
F
I
carcinosarcomas. Clear cell tumors were ER/PRwere ER negative, predominantly PR negative,
re strongly positive for D, E, G, EGFR but the, I, GPR30 ; EFGR expression is clearly in thesly characterized intracellular expression.10 (A,cation).
h
atie G-Iown asa (d wet gl or Hess iou, 40 gnifi
PR30 overexpression by tumor grade

(a
tsctwarm.
fPv
nv(
IAmgCtm
www.AJOG.org AGOS Papers
10/29 [34.5%] vs 5/7 [71.4%], P � .07)pproached statistical significance.
Clinical and pathologic characteristicshat predict outcome in patients areummarized in Table 2. The majority ofases (63.8%) had stage I disease. Illus-rated in Table 3, both GPR30 and EGFRere more frequently overexpressed in
dvanced disease (P � .001 and P � .035,espectively) and in tumors with deepyometrial invasion (P � .001 and P �
FIGURE 3Detection of GPR30 using N-and C-terminal antibodies
Negative Control
N-GPR30
C-GPR30
A
B
C
mmunoexpression for GPR30 was similar using, the C-terminal antibody; and B, the N- ter-inal antibody; C, negative control; stage IB,
rade 1 endometrial adenocarcinoma. C-GPR30,-terminal antibody for GPR30; N-GPR30, N-
erminal antibody for GPR30 (A, C, 40� originalagnification; C, original magnification 20�).
059, respectively), but no significant dif- (
erences were observed for Ki-67, ER, orR. There was pelvic lymph node in-olvement in 6 of 35 patients sampled
TABLE 2Clinical and pathologic criteria tha
Stage of disease..........................................................................................................
I..........................................................................................................
IA..........................................................................................................
IB..........................................................................................................
IC..........................................................................................................
II..........................................................................................................
IIA..........................................................................................................
IIB..........................................................................................................
III..........................................................................................................
IIIA..........................................................................................................
IIIC..........................................................................................................
IV...................................................................................................................
Tumor grade (FIGO)..........................................................................................................
1..........................................................................................................
2..........................................................................................................
3 (including high-risk cell types)...................................................................................................................
Depth of myometrial invasion...................................................................................................................
None..........................................................................................................
�50%..........................................................................................................
�50%...................................................................................................................
Serosal involvement...................................................................................................................
Lymphovascular space involvement..........................................................................................................
No..........................................................................................................
Yes...................................................................................................................
Pelvic lymph node status..........................................................................................................
Negative..........................................................................................................
Positive..........................................................................................................
Not sampled...................................................................................................................
Paraaortic lymph node status..........................................................................................................
Negative..........................................................................................................
Positive..........................................................................................................
Not sampled...................................................................................................................
Tumor volume within uterus..........................................................................................................
�2 cm..........................................................................................................
2-4 cm..........................................................................................................
�4 cm, but � 8 cm..........................................................................................................
�8 cm
14.3%). Although not statistically sig- a
APRIL 2007 America
ificant, more patients with positive pel-ic lymph nodes overexpressed GPR3015/29 [51.7%] vs 5/6 [83.3%], P � .17)
redict survivalNumber (%)
..................................................................................................................
30 (63.8%)..................................................................................................................
12 (25.5%)..................................................................................................................
15 (31.9%)..................................................................................................................
3 (6.4%)..................................................................................................................
8 (17.0%)..................................................................................................................
5 (10.6%)..................................................................................................................
3 (6.4%)..................................................................................................................
7 (14.9%..................................................................................................................
1 (2.1%)..................................................................................................................
6 (12.8%)..................................................................................................................
2 (4.3%)..................................................................................................................
..................................................................................................................
22 (46.8%)..................................................................................................................
9 (19.2%)..................................................................................................................
16 (34.0%)..................................................................................................................
..................................................................................................................
16 (34.0%)..................................................................................................................
16 (34.0%)..................................................................................................................
11 (23.4%)..................................................................................................................
4 (8.5%)..................................................................................................................
..................................................................................................................
34 (72.3%)..................................................................................................................
13 (27.7%)..................................................................................................................
..................................................................................................................
29 (61.7%)..................................................................................................................
6 (12.8%)..................................................................................................................
12 (25.5%)..................................................................................................................
..................................................................................................................
31 (66.0%)..................................................................................................................
1 (2.1%)..................................................................................................................
15 (31.9%)..................................................................................................................
..................................................................................................................
8 (17.0)..................................................................................................................
13 (23.4%)..................................................................................................................
19 (40.4%)..................................................................................................................
7 (14.9%)
t p
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
nd EGFR (13/27 vs 5/6, P � .13),
n Journal of Obstetrics & Gynecology 386.e6

w6Pcwni�.tlvpc.E/.Eqsb1[sv(efGPKP
faodevwmsw6rdv(79dmvtP
et4wGrop
Iw(sswsaI(Hpi((
CPmtt8ehta(illms
AGOS Papers www.AJOG.org
3
hereas there was no difference for Ki-7, PR, or ER (3 of 6 patients, all P � .64).eritoneal washings were negative in 41ases (87.2%), positive in 2 (4.3%) andere either not obtained or indetermi-ate in 4 (8.5%). Both women with pos-
tive peritoneal cytology had GPR30 (P.20), EGFR (P � .23), and ER (P �
23) expression above the median. Six-een cases had cervical involvement,imited to the cervical glands (7), or in-ading the stroma (9). GPR30 overex-ression was found in 12/15 (80%) ofases with cervical involvement (P �005), with no significant differences forGFR, Ki-67, ER or PR (10/15, P � .11; 7
15, P � .76; 6/14, P � .99; and 6/14, P �99, respectively). Both GPR30 andGFR were overexpressed more fre-uently in cases with uterine tumor mea-urements more than 4 cm in diametery gross examination (16/24 [66.7%] vs5/22 [31.8%], P � .012 and 16/2466.7%] vs 15/21 [28.6%], P � .012, re-pectively). Lymphovascular space in-olvement (LVI) was identified in 1327.7%) cases. Comparisons of receptorxpression by LVI were not significantor ER, PR, or EGFR (all P �.50), orPR30 (14/33 [42.4%] vs 9/13 [69.2%],� .19), but approached significance fori-67 (12/33 [36.4%] vs 8/12 [66.7%],
TABLE 3Immunohistochemistry results byParameter No. posit
Surgical stage I..........................................................................................................†GPR30 �230 9/30 (30..........................................................................................................†EGFR �80 10/29 (34..........................................................................................................†Ki-67 �120 13/29 (44..........................................................................................................†PR �150 14/29 (48..........................................................................................................†ER �100 14/29 (48
...................................................................................................................
Myometrial invasion 0%..........................................................................................................†GPR30 �230 7/16 (48..........................................................................................................†EGFR �80 8/16 (50..........................................................................................................†Ki-67 �120 7/16 (43..........................................................................................................†PR �150 5/16 (31..........................................................................................................†ER �100 6/16 (37
...................................................................................................................
* Fisher exact tests.† Receptor expression above the median.
� .09). G
86.e7 American Journal of Obstetrics & Gynecol
There were 9 deaths in this series, 8rom recurrent or progressive diseasend 1 within 6 months of diagnosis fromrgan failure. Because there was no evi-ence that this patient had recurrent dis-ase, this case was censored from the sur-ival analysis. The disease-free survivalas 82.2% (median survival time 62.5onths, range 0-113 months). The ob-
erved survival was 100% in 22 patientsith low/normal GPR30 compared with5.2% with GPR30 overexpression (log-ank, P � .005). In all 8 cancer-relatedeaths, GPR30 was overexpressed. Sur-ival rates by expression for Ki-6773.7% vs 88.0%, P � .15), ER (88.4% vs7.3%, P � .37), or EGFR (72.7% vs0.1%, P � .20) were not significantlyifferent, but expression of PR above theedian was associated with higher sur-
ival rates, a difference bordering on sta-istical significance (95.0% vs 69.6%,� .057).Stratified by stage (I/II vs III/IV), as
xpected, survival rates were lower in pa-ients with advanced disease (91.9% vs4.4%, log-rank, P � .002). The 1 patientith stage III/IV disease and low/normalPR30 expression remains free of recur-
ence. By stage and GPR30 expression,bserved survival rates were 100% foratients with stage I/II, low/normal
ical and pathologic parameters(%) No. positive (%)
II.........................................................................................................................
) 6/7 (85.7%).........................................................................................................................
) 5/7 (71.4%).........................................................................................................................
) 2/7 (28.6%).........................................................................................................................
) 3/6 (50.0%).........................................................................................................................
) 4/7 (57.1%).........................................................................................................................
� 50%.........................................................................................................................
) 3/16 (19.8%).........................................................................................................................
) 4/15 (26.7%).........................................................................................................................
) 7/15 (46.7%).........................................................................................................................
) 10/14 (71.4%).........................................................................................................................
) 7/15 (46.7%).........................................................................................................................
PR30, 80.0% for patients with stage 1
ogy APRIL 2007
/II, high GPR30, and 37.5% for patientsith stage III/IV high GPR30 expression
log-rank, P � .002). In post hoc analy-es, the difference in survival was alsoignificant for patients with stage I/IIith low/normal vs high GPR30 expres-
ion (100.0% vs 80.0%, P � .045) as wells for stage I/II with low/normal vs stageII/IV with high GPR30 expression100% vs 37.5%, log-rank, P � .001).owever, in patients with GPR30 ex-
ression above the median, differencesn survival by stage were not significant80.0% vs 37.5%, log-rank, P � .09)Figure 4).
OMMENTathologic, clinical, and cell cultureodels support the division of endome-
rial carcinoma into type I and type IIumors, with 5-year survival rates of5.6% and 58.8%, respectively.7 Type IIndometrial carcinomas are usually ofigh grade (grade 3 nuclear and/or archi-ectural), contain phenotypic featuresssociated with lower survival ratesUPSC, clear cell, and mixed epithelial),nvade deeply into the myometrium,ymphatic, and vascular spaces, are lessikely to be ER or PR positive, and are
ore likely to recur. Because the classicalteroid receptors are expressed in only
No. positive (%) P value*
III/IV..................................................................................................................
8/9 (88.9%) �.001..................................................................................................................
7/9 (77.8%) .035..................................................................................................................
5/9 (55.6%) .56..................................................................................................................
3/9 (33.3%) .46..................................................................................................................
4/9 (44.4%) �.99..................................................................................................................
� 50%..................................................................................................................
12/14 (92.9%) �.001..................................................................................................................
10/14 (71.4%) .059..................................................................................................................
6/14 (42.9%) �.99..................................................................................................................
5/14 (35.7%) .07..................................................................................................................
9/14 (64.3%) .37..................................................................................................................
clinive
......... .........
.0%......... .........
.5%......... .........
.8%......... .........
.3%......... .........
.3%......... .........
......... .........
.8%......... .........
.0%......... .........
.8%......... .........
.3%......... .........
.5%......... .........
5-20% of recurrent tumors, response to

papcdr
pGpaasvDsseaEEtGhdspfactfwgaumEasMssebigeiP
lpess
botttmohFct2i
ptcawftctouawwEsm
Gwaadtcao
AWRopiufd
R1t12c3cbpC4MD
O3G
www.AJOG.org AGOS Papers
rogestational therapy is usually poor,16
nd in those who do respond, ligand-de-endant activation of the receptor islosely linked to progesterone receptorownregulation and loss ofesponsiveness.5
In this series of 47 well-characterizedatients with endometrial carcinoma,PR30 expressed above the median wasredictive of many parameters associ-ted with adverse outcome (high gradend biologically aggressive histologicubtypes, cervical involvement, ad-anced stage) and lower survival rates.ifferences in survival by GPR30 expres-
ion persisted when further stratified bytage of disease (I/II vs III/IV). GPR30xpression inversely correlated with ERnd PR, and correlated positively withGFR expression. Both GPR30 andGFR were overexpressed in stage III/IV
umors. Although the function ofPR30 in relation to ER, PR, and EGFRas only begun to be elucidated, theseata support the hypothesis that GPR30ignaling is a critical pathway for tumorroliferation and progression, especially
or type II endometrial carcinomas. Rel-tively new discoveries emphasize theomplexity of ER signaling and its mul-iple regulatory interactions with growthactor and other kinase signaling path-ays. Both genomic (nuclear) and non-enomic (membrane and cytoplasmic)ctivities mediated by estrogen contrib-te to this intimate cross-talk, a funda-ental factor in endocrine resistance.
strogen, as well many of the classic ERntagonists (including tamoxifen) activateignaling pathways via GPR30.10,14,20
odulation of GPR30 function/expres-ion should further elucidate interrelation-hips that may serve as targets for moreffective treatment strategies. This possi-ility is closer to realization with our recent
dentificationof thefirstGPR30-specific li-and.23 GPR30 activation may also partlyxplain higher phosphorylated AKT levelsn type II tumors, despite lower ER-� andR expression.24
There are, however, also importantimitations of this study. Although theeriod of follow-up is sufficient to gen-rate survival data, the sample size ismall and largely comprised of early-
tage disease. Currently, more cases are peing analyzed to determine the impactf receptor status on epidemiologic fea-ures (age at diagnosis, menopausal sta-us, and use of hormone therapy). Addi-ional samples are needed to perform a
ultivariate analysis of the relationshipf GPR30 expression on tumor grade,istology, depth of myometrial invasion,IGO stage, and survival. Immunohisto-hemistry is by nature subjective, al-hough interpretation was performed byindependent observers without clinical
dentifiers.To our knowledge, this is the first re-
ort of GPR30 that uses human archivalumor samples from patients with gyne-ologic tumors. This study links GPR30,
newly discovered estrogen receptor,ith many of the clinical and pathologic
eatures associated with type II endome-rial tumors, and its overexpression isorrelates with poor survival rates. Fu-ure studies will examine the expressionf GPR30 in other solid tumors, partic-larly those linked to estrogen (breastnd ovarian carcinomas). In patientsith recurrent endometrial carcinoma,e plan to evaluate both GPR30 andGFR expression with respect to re-ponse to EGFR antagonists to deter-
ine whether GPR30 and EGFR overex-
FIGURE 4Survival by GPR30 expression and
bserved survival stratified by GPR30 expression7.5% for patients with stage I/II-low/normal GPR30 expression, respectively.
ression are predictive of response. c
APRIL 2007 America
iven that stage I/II disease associatedith GPR30 overexpression was associ-
ted with lower survival rates, we plan toddress expression of GPR30 in interme-iate-risk endometrial carcinoma to de-ermine whether GPR30 molecularlyharacterizes those patients in need ofdjuvant therapy from those who can bebserved. f
CKNOWLEDGMENTe thank Drs Gloria E. Sarto, Carolyn D.unowicz, and William F. Rayburn, for their rec-mmendations, modifications, and editorial ex-ertise, and also thank Dr Larry A. Sklar, who
ntellectually and financially (EB00264) contrib-ted to studies determining that GPR30 as aunctional estrogen receptor as well as in theevelopment of the first GPR30 agonist.
EFERENCES. Jemal A, Siegel R, Ward E, et al. Cancer sta-istics, 2006. CA Cancer J Clin 2006;56:06-30.. Prat J. Prognostic parameters of endometrialarcinoma. Hum Pathol 2004;35:649-62.. Trimble CL, Kauderer J, Zaino R, et al. Con-urrent endometrial carcinoma in women with aiopsy diagnosis of atypical endometrial hyper-lasia: a Gynecologic Oncology Group study.ancer 2006;106:812-9.. Creasman WT, Soper JT, McCarty KS Jr,cCarty KS Sr, Hinshaw W, Clarke-PearsonL. Influence of cytoplasmic steroid receptor
GO stage
d stage (I/II vs III/IV) were 100.0%, 80.0%, and0, stage I/II-high GPR30, and stage III/IV-high
FI
anPR3
ontent on prognosis of early stage endometrial
n Journal of Obstetrics & Gynecology 386.e8

c15gsG6Ses17d18Wtms9ddtGc1bcs1rt1rJ1pr1Bpcen1Got11Omcc11W2pc1Pcc1Rd
ht22Taec2npe12r2Va22tmlG
DHHmdS
b3ecrttpphupaw
awtadestgc
fktfEftDeirgmaadpHt
tewpagpdus
slamieb2ctbG
mdenamPt2(
AGOS Papers www.AJOG.org
3
arcinoma. Am J Obstet Gynecol 1985;51:922-32.. Leslie KK, Stein MP, Kumar NS, et al. Pro-esterone receptor isoform identification andubcellular localization in endometrial cancer.ynecol Oncol 2005;96:32-41.. Khalifa MA, Abdoh AA, Mannel RS, HarawayD, Walker JL, Min KW. Prognostic utility ofpidermal growth factor receptor overexpres-ion in endometrial adenocarcinoma. Cancer994;73:370-6.. Bokhman JV. Two pathogenetic types of en-ometrial carcinoma. Gynecol Oncol 1983;5:10-7.. Sutton G, Axelrod JH, Bundy BN, et al.hole abdominal radiotherapy in the adjuvant
reatment of patients with stage III and IV endo-etrial cancer: a gynecologic oncology group
tudy. Gynecol Oncol 2005;97:755-63.. Randall ME, Filiaci VL, Muss H, et al. Ran-omized phase III trial of whole-abdominal irra-iation versus doxorubicin and cisplatin chemo-herapy in advanced endometrial carcinoma: aynecologic Oncology Group Study. J Clin On-ol 2006;24:36-44.0. Revankar CM, Cimino DF, Sklar LA, Arter-urn JB, Prossnitz ER. A transmembrane intra-ellular estrogen receptor mediates rapid cellignaling. Science 2005;307:1625-30.1. Ji TH, Grossmann M, Ji I. G protein-coupledeceptors: I, diversity of receptor-ligand interac-ions. J Biol Chem 1998;273:17299-302.2. Gether U, Kobilka BK. G protein-coupledeceptors: II, mechanism of agonist activation.Biol Chem 1998;273:17979-82.3. Prossnitz ER. Novel roles for arrestins in theost-endocytic trafficking of G protein-coupledeceptors. Life Sciences 2004;75:893-9.4. Filardo EJ, Quinn JA, Frackelton AR Jr,land KI. Estrogen action via the G protein-cou-led receptor, GPR30: stimulation of adenylylyclase and cAMP-mediated attenuation of thepidermal growth factor receptor-to-MAPK sig-aling axis. Mol Endocrinol 2002;16:70-84.5. Ehrlich CE, Young PC, Stehman FB, SuttonP, Alford WM. Steroid receptors and clinicalutcome in patients with adenocarcinoma ofhe endometrium. Am J Obstet Gynecol988;158:796-807.6. Thigpen JT, Brady MF, Alvarez RD, et al.ral medroxyprogesterone acetate in the treat-ent of advanced or recurrent endometrial car-
inoma: a dose-response study by the Gyne-ologic Oncology Group. J Clin Oncol 1999;7:1736-44.7. Khalifa MA, Mannel RS, Haraway SD,alker J, Min KW. Expression of EGFR, HER-
/neu, P53, and PCNA in endometrioid, serousapillary, and clear cell endometrial adenocar-inomas. Gynecol Oncol 1994;53:84-92.8. Niikura H, Sasano H, Matsunaga G, et al.rognostic value of epidermal growth factor re-eptor expression in endometrioid endometrialarcinoma. Hum Pathol 1995;26:892-6.9. Albitar L, Laidler LL, Abdallah R, Leslie KK.egulation of signaling phosphoproteins by epi-
ermal growth factor and Iressa (ZD1839) in m86.e9 American Journal of Obstetrics & Gynecol
uman endometrial cancer cells that modelype I and II tumors. Mol Cancer Ther005;4:1891-9.0. Vivacqua A, Bonofiglio D, Recchia AG, et al.he G protein-coupled receptor GPR30 medi-tes the proliferative effects induced by 17beta-stradiol and hydroxytamoxifen in endometrialancer cells. Mol Endocrinol 2006;20:631-46.1. Salvesen HB, Iversen OE, Akslen LA. Prog-ostic significance of angiogenesis and Ki-67,53, and p21 expression: a population-basedndometrial carcinoma study. J Clin Oncol999;17:1382-90.2. Collett D. Modeling survival data in medicalesearch. London: Chapman & Hall; 1994.3. Bologa CG, Revankar CM, Young SM, et al.irtual and biomolecular screening converge onselective agonist for GPR30. Nat Chem Biol
006;2:207-12.4. Rice LW, Stone RL, Xu M, et al. Biologicargets for therapeutic intervention in endo-etrioid endometrial adenocarcinoma and ma-
ignant mixed mullerian tumors. Am J Obstetynecol 2006;194:1119-28.
ISCUSSION
olly H. Gallion, MD. Dr Muellereubach, Dr Eberhard, Dr Ferguson,embers, and guests. It is my pleasure to
iscuss the research presented by Drmith.I read her manuscript with interest,
eing most intrigued by the title, “GPR0: a novel indicator of poor survival forndometrial carcinoma.” Primarily, be-ause most of the major advances occur-ing in cancer treatment right now are inhe area of individualizing medicine, get-ing away from the 1 shoe fits all ap-roach of the past. There is tremendousotential for biomarkers to improveealth outcomes by allowing for individ-alization of therapy. Both throughrognostic markers, which tell us who’st risk as well as predictive markershich tell us how to treat.As Dr Smith described, there is clearlysubset of endometrial cancer patientsho do extremely poorly with standard
herapy. A marker that could reliably,nd I emphasize the word reliably, couldifferentiate poor from good prognosisndometrial cancer patients would havetrong clinical utility. Allowing us toreat the poor prognosis subset more ag-ressively and to potentially avoid theosts and toxicity, of unnecessary treat-
ent in the good prognosis group. gogy APRIL 2007
Breast cancer is the current paradigmor individualized medicine. As younow, the presence of a BRCA1 or 2 mu-ation is a powerful prognostic markeror cancer risk. For women with cancer,R, and Her 2 are powerful prognostic
actors that have been incorporated intohe 21 gene profile, known as OncotypeX test. This panel of markers separates
arly stage ER� breast cancer patientsnto low-, medium-, and high-recur-ence risk categories. In the case of estro-en receptor, the marker is also a treat-ent target, identifying women who will
nd will not benefit from endocrine ther-py. Likewise in the case of metastaticisease, HER 2 amplification/overex-ression, is used to select patients forerceptin therapy. Her 2 receptor is also
he target for Herceptin therapy.Dr Smith has just described the iden-
ification of a novel GPCR protein that isxpressed in endometrial cancer. GPR30as correlated with other known poorrognostic factors, including lack of ERnd PR expression, advanced stage, andrade. Moreover, it was associated withoor prognosis. This is exactly the sameiscovery pathway that led to the clinicalse of the Her 2 protein in breast cancerome years ago.
She and her colleagues at the Univer-ity of New Mexico are to be congratu-ated on their work. They developed thentibody, validated the methodology foreasuring the protein, and then applied
t to samples from a tissue bank Dr Smithstablished in 1996. I understand thisank now has samples from more than00 endometrial cancer cases with out-omes. Thus, they were able to marryheir laboratory efforts with their tumorank to perform correlative studies ofPR30.Dr Smith speculates that this markeray ultimately be used as a marker to
ifferentiate between intermediate-riskndometrial cancer patients who are ineed of adjuvant therapy and those whore not. Morevoer, that it may be a treat-ent target for GPR30 blockade therapy.
articularly in light of the fact that of theop 200 best-selling drugs on the market,5% target G-protein coupled receptorsGPCRs), making this class of drug tar-
ets 1 of the most heavily investigated by
pc
ltwtcdapspiim
ontHnwtnpmpt
mgHuOtpstn
dSlcts
ewtTcfa
tPt
imlqswpt
Dlfvfimatpfs
dvnt8rRtrteHdPwpp(bdaat(tttntMiaumimditadNsdbthpwtauifw
www.AJOG.org AGOS Papers
harmaceutical companies for drug dis-overy and development.
While I share her enthusiasm, I wouldike to insert a work of caution regardinghe path to clinical utility, it is fraughtith landmines. As we all know, despite
he virtual explosion of research in on-ology biomarkers over the past severalecades, there are only a few that havectually been incorporated into clinicalractice. This is despite massive infu-ions of research resources and countlessresentations and publications, includ-
ng as I might add some of my own, tout-ng the discovery of novel tumor
arkers.In fact, in the practice of gynecologic
ncology, we can count on one hand, theumber of tumor markers that we rou-
inely use in clinical practice (CA 125,er 2). This is in stark contrast to theumber of presentations such as the onee heard this morning touting the iden-
ification of the newest and greatestovel prognostic factors. In fact, mostromising initial reports of novel tumorarkers are followed by subsequent re-
orts of inconsistent or even contradic-ory results.
In recognition of this problem, severalembers of the ASCO tumor marker
uidelines working group, led by Danayes, have developed a tumor markertility grading system to achieve 2 goals.ne, to provide a framework for analyze
he quality of biomarkers studies and 2,rovide a guide for planning clinicaltudies, similar to that of the phase I-IIIrial schema used for the evaluation ofew chemotherapy agents.The Hayes level of evidence criteria are
epicted here, and as you can see, Drmith’s work would be categorized as aevel 4 study. I am assuming, she and herolleagues will steadfastly march upwardhrough the levels of evidence in her sub-equent work with this marker.
In addition to levels of evidence, Hayest al note that although a good markerith a high level of evidence is necessary
o be clinically useful, it is not sufficient.he marker must also lead to an actuallinical decision that results in a moreavorable clinical outcome. Specifically,
clinical decision that is based on using Bhe marker must have a positive affect onFI, survival, QOL, or cost of care for it
o have any clinical utility.In view of the guidance provided to
nvestigators through the Hayes and Re-ark criteria for tumor markers, I would
ike Dr Smith to address the following 3uestions: The first 2 relate to study de-ign issues that are commonly associatedith overly optimistic estimates of therognostic significance of markers, andhe third to future study design:
1. What percentage of endometrialcancer cases treated at her institu-tion during the study period wasactually entered onto this proto-col? Were there significant differ-ences between the study popula-tion and the general population ofcases in terms of clinical, patho-logic prognostic factors, andtreatment. If so, how would thisbias the study findings.
2. The second related to the assay it-self. Was the cutpoint to definepositivevsnegativeGPR30definedbefore correlation with clinico-pathologic factor analysis? If not,multiple testing with cutpoint op-timization used has lead to overlyoptimistic estimates of the prog-nostic significance of this marker.
3. In your manuscript, you lay outmultiple future studies you plan,including breast and ovarian can-cer, intermediate-risk endometrialcancer and correlation with re-sponse to EGFR antagonists in pa-tients with recurrent disease. If youwere allowed to focus and followonly 1 route of future investigationwhat would you do?
r Smith (closing). Thank you, Dr Gal-ion, for your insightful comments andor providing me with questions in ad-ance of the scientific session. This is therst investigation of GPR30 using im-unohistochemistry in any solid tumor,
nd the results support the hypothesishat GPR30 expression is increased inatients with lower survival rates. We
ully acknowledge that our sample size ismall, and our results must be validated.
etween 1997 and 2001, 85 patients un- wAPRIL 2007 American
erwent primary surgical therapy at Uni-ersity Hospital for endometrial carci-oma, 76.5% of whom consented to par-
icipate. During the same time period,24 new endometrial carcinomas wereegistered by the New Mexico Tumoregistry. Thus, our sample is representa-
ive of 10% of cases in New Mexico. Aelated issue is the unique distribution ofhe study population stratified by race/thnicity: non-Hispanic white (46.8%),ispanic white (42.6%), American In-
ian (4.3%), black (4.3%), and Asian,acific South Island descent (2.1%),hich is similar to ethnically diverseopulation of New Mexico: non-His-anic white (44%), Hispanic white45%), American Indian (8%), andlack, Asian, or of Pacific-South Islandescent (3%). It is feasible that clinicalnd pathologic prognostic factors anddjuvant treatment may have influencedhe results of this study. For example, 1838.3%) received adjuvant radiationherapy and 2, chemotherapy. Stratifica-ion by use of adjuvant therapy prospec-ively or with a larger sample size iseeded to address the impact of addi-
ional treatment. About 30% of Newexico’s population has no healthcare
nsurance and the median income ismong the lowest in the nation. Mostninsured patients receive cancer treat-ent at our center. For these reasons, it
s feasible that the study population hadore severe comorbidities and greater
elays in diagnosis and treatment. To ben the database, at least 1 g of tissue hado have been collected; on this basislone, patients with small tumor bur-ens were not included. Data from theew Mexico Tumor Registry indicate no
ignificant differences in survival for en-ometrial carcinoma by race/ethnicity,ut SEER data indicate that US black pa-ients have mortality rates 2.4-foldigher than white and other nonwhiteatients. Our study included only 2 blackomen, a potential limitation. Before
he analysis, staining was graded by usingmodified H score, defined by the prod-ct of intensity and the percentage of ep-
thelial cells stained. The median valueor all of the receptors, including GPR30,as chosen as the cut score. No attempt
as made to “fit” the data to the cutJournal of Obstetrics & Gynecology 386.e10

swfBGcpagno
rktctcpssh
wGftMtbpmR
AGOS Papers www.AJOG.org
3
core. In summary, Dr Gallion asked, if Iere to focus, and pursue only 1 route of
uture investigation, what would I do?ecause we are funded to investigatePR30 in breast carcinoma, I plan to
ontinue this investigation. The dataresented today need to be validated,nd an RO1 to support further investi-ation of GPR30 in endometrial carci-oma has been submitted. Although
ur preliminary results support the u86.e11 American Journal of Obstetrics & Gyneco
ole of GPR30 as a potential biomar-er, we do not understand the func-ional relationship of GPR30 and thelassical estrogen receptors in humanissues, including normal epithelialells during embryonic development,regnancy, and throughout the men-trual cycle. Therefore, if I were to pur-ue this work based on that part of theuman spirit that longs to explore and
nderstand the unknown, my goal slogy APRIL 2007
ould be to elucidate mechanisms ofPR30 function in mullerian tissues
rom birth to senescence. I would likeo express my thanks to President
ueller-Heubach, Secretary Ferguson,he Program Committee, and mem-ers and guests for inviting me toresent these data, and to acknowledgey mentors (Drs Gloria Sarto, Carolynunowicz, and Bill Rayburn) for their
upport. Thank you.
Top Related
Copyright © 2022 FDOKUMEN

