






Bahasa
Halaman
Hukum


This article appeared in a journal published by Elsevier. The attachedcopy is furnished to the author for internal non-commercial researchand education use, including for instruction at the authors institution
and sharing with colleagues.
Other uses, including reproduction and distribution, or selling orlicensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of thearticle (e.g. in Word or Tex form) to their personal website orinstitutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies areencouraged to visit:
http://www.elsevier.com/copyright

Author's personal copy
REVIEW
Educational Strategies to Reduce SerumPhosphorus in Hyperphosphatemic PatientsWith Chronic Kidney Disease: SystematicReview With Meta-analysisDaniel Caldeira, MD,* Tiago Amaral, MD,† Cl�audio David, MD,*‡
and Cristina Sampaio, MD, PhD*§
Objective: To systematically review educational strategies for phosphorus reduction in patients with hyperphos-
phatemia and chronic kidney disease (CKD).
Design: Systematic review with meta-analysis.
Data Sources: CENTRAL, MEDLINE, EMBASE, and mRCT databases were assessed in June 2010.
Study Selection: Randomized controlled trials evaluating educational strategies related to diet in hyperphospha-
temic patients with CKD.
Data Extraction and Synthesis Method: Study characteristics, phosphorus levels, and calcium–phosphorus
product levels were retrieved. Jadad scale was used for quality assessment. Mean difference (MD) and 95% confi-
dence intervals (CIs) were calculated by random effects method.
Results: Seven randomized controlled trials were retrieved with a total of 524 patients with hyperphosphatemia
and CKD. Educational strategies reduced phosphorus levels with an MD of 20.72 mg/dL (95% CI: 21.11 to
20.33, P, .01). Sensitivity analysis of trials with follow-up of,4months did not show any benefit of the intervention,
but educational intervention for $4 months showed an MD of 21.07 (95% CI: 21.49 to 20.64, P , .01). Calcium–
phosphorus product level was improved in 227 evaluated patients from 5 trials with an MD of 25.22 mg2/dL2
(95% CI: 29.48 to 20.98, P 5 .02, and I2 5 58%). Sensitivity analysis removed the source of heterogeneity and re-
sulted in an MD of 23.02 (95% CI: 26.51 to 0.47, P 5 .09).
Conclusions: Education helped reduce phosphorus levels in hyperphosphatemic patients with CKD, particularly
those on dialysis.
� 2011 by the National Kidney Foundation, Inc. All rights reserved.
PATIENTS WITH CHRONIC kidney dis-ease (CKD) often have impairment of min-
eral metabolism, and phosphorus levels increaseas the disease advances.1,2 Hyperphosphatemiais associated with increased mortality3,4 andmorbidities such as high turnover bone disease5
and hyperparathyroidism.6 Increased serum phos-phorus level is also associated with progression ofCKD.7 Elevated calcium–phosphate (Ca 3 P)product level is related to calciphylaxis.8
Hyperphosphatemia management includes die-tary restriction, use of phosphate-binding agents,and dialysis.9
Patients’ knowledge about high-phosphoruscontaining food and compliance to an adequatediet regimen are essential to maintain phosphorus
*Clinical Pharmacology and Therapeutics Laboratory, Faculty of
Medicine, Lisbon, Portugal.
†Nephrology Department, Hospital Santa Cruz, Centro Hospi-
talar Lisboa Ocidental, Lisbon, Portugal.
‡Department of Cardiology, Hospital Santa Maria, Centro Hos-
pitalar Lisboa Norte, Lisbon, Portugal.
§Neurological Clinic Research Unit, Institute of Molecular Med-
icine, Lisbon, Portugal.
This research received no specific grant from any funding agency in
the public, commercial or not-for-profit sectors.
Address reprint requests to Daniel Caldeira, MD, Laborat�orio deFarmacologia Cl�ınica e Terap̂eutica, Faculdade de Medicina da Uni-
versidade de Lisboa, Av. Prof. Egas Moniz, Lisboa 1649-028,
Portugal. E-mail: [email protected]� 2011 by the National Kidney Foundation, Inc. All rights
reserved.
1051-2276/$36.00
doi:10.1053/j.jrn.2010.11.006
Journal of Renal Nutrition, Vol 21, No 4 (July), 2011: pp 285–294 285

Author's personal copy
in acceptable levels. Previous studies suggested thatpatient education may improve phosphate con-trol.10,11 Certain techniques, such as educationalprograms or nutritional counseling, may improvehyperphosphatemia and its complications.
The objective of this review is to assess theefficacy through randomized controlled trials(RCTs) of educational and/or nutritional coun-seling to decrease phosphorus and Ca 3 P prod-uct levels in patients with hyperphosphatemiaand CKD.
Methods
Searching
A searching strategy was developed using CEN-TRAL (Cochrane Library issue April 2010),MEDLINE (until June 2010), and EMBASE(until June 2010) databases for identification ofRCTs. Database mRCT (June 2010) was alsosearched for completed and/or unpublished clini-cal trials. The following termswere used and com-bined with Boolean operators AND and OR:‘‘education*,’’ ‘‘counsel*,’’ ‘‘phosphorus,’’ ‘‘phos-phate,’’ ‘‘hyperphosph*,’’ ‘‘chronic,’’ ‘‘end-stage,’’‘‘renal,’’ ‘‘kidney,’’ ‘‘failure,’’ ‘‘injury,’’ ‘‘dialysis,’’and ‘‘hemodialysis.’’ No language limitation wasapplied. Articles references were also searched inan attempt to identify any missing study.
Selection
Search method was developed to obtain RCTsassessing educational interventions to reducephosphorus levels in patients with CKD andhyperphosphatemia. We included all patientswith CKD considered to be hyperphosphatemicby the authors, irrespective of the cutoff value.
Any kind of educational or counseling inter-vention related to diet was allowed in the interven-tional group. Passive and active comparators, suchas standard renal dietitian advice, were allowed.
Primary outcome was phosphorus level,whereas secondary outcome was Ca 3 P productlevel. End-study results were used for pooledanalysis.
Validity Assessment
Studies were evaluated according to the Jadadscale. No studies were excluded on the basis ofthe reported quality.
Data Abstraction
Studies that met the criteria outlined previouslywere assessed byone reviewauthor and checked byanother. Patients’ data, study size, population age,follow-up, interventions, and outcomes wereretrieved. Serum phosphorus and Ca3 P productlevels were converted to mg/dL and mg2/dL2,respectively (conversion ratios: 1 mmol/L 5 3.10mg/dL; 1 mmol2/L2 5 12.35 mg2/dL2). Dataentry into software was also double-checked. Alldisagreements were solved by consensus.
Quantitative Data Synthesis
The statistical analyses were performed usingthe RevMan software (version 5.0.23) developedby The Nordic Cochrane Center. Outcomeswere analyzed by the Mantel–Haenszel methodand themean difference (MD)was calculated. Re-sult uncertainty was expressed using 95% confi-dence intervals (CIs). The results estimates werebased on a fixed-effects model or random-effectsmodel in accordance with heterogeneity. Hetero-geneity was assessed using the I2 test. Heterogene-ity was assumed when I2 was .50%.Subgroup analysis was performed accordingly
in either dialysis or nondialysis state. Sensitivityanalysis was conducted in accordance with eitherfollow-up period ($4 months or ,4 months) orheterogeneity source.
Results
Search filters were applied in MEDLINE,CENTRAL, EMBASE, and mRCT and weobtained 48 citations in the different databases.Duplicated records were removed leaving a totalof 28 studies. From these, 17 studies were rejectedon the basis of abstract evaluation. From theremaining 11 studies, full-text assessment was per-formed for possible study eligibility. Four trialswere then excluded because they involved testingof phosphate-binding agents (2 studies), enteralnutrients, or education in patients without hyper-phosphatemia. Seven trials12–18 were included forqualitative and quantitative analysis. Two of themwere unpublished studies retrieved from mRCT(Fig. 1).14,18 Data from the study by Foley wereobtained after contacting the study coordinator.Table 1 shows the main characteristics of trials
and their conclusions. All trials were randomized.The study by Degen18 was the only one with
CALDEIRA ET AL286

Author's personal copy
adequate allocation concealment, whereas allother studies were unclear about this information.
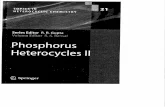
Table 2 showsmethodological assessment of tri-als’ quality with Jadad score ranging from 1 to 3.
The 7 selected studies had 524 patients withhyperphosphatemia and CKD—6 studies assessed509 patients on dialysis and 1 study reported out-comes that evaluated 15 predialysis patients.Mean age of the patients was .50 years andfollow-up period ranged between 4 weeks and12 months. Methods used in the interventionswere variable, but they aimed to reduce phospho-rus levels through counseling or education in die-tary changes (Table 1).
The trial by Ashurst and Dobbie12 reportedmean serum phosphorus and Ca 3 P productlevels but did not report their standard deviations(SDs). For serum phosphorus level, mean SD ofboth intervention was calculated considering theP value to be .02 (authors reported a P value of,.02). For Ca3 P product level, because P valuewas nonsignificant, the worst known scenario wasconsidered. In the trial by Yokum et al.,15 SD wasused for educational intervention, whereas in thetrial by Morey et al.16 it was used for control.
These SD values were the highest among alltrials.19
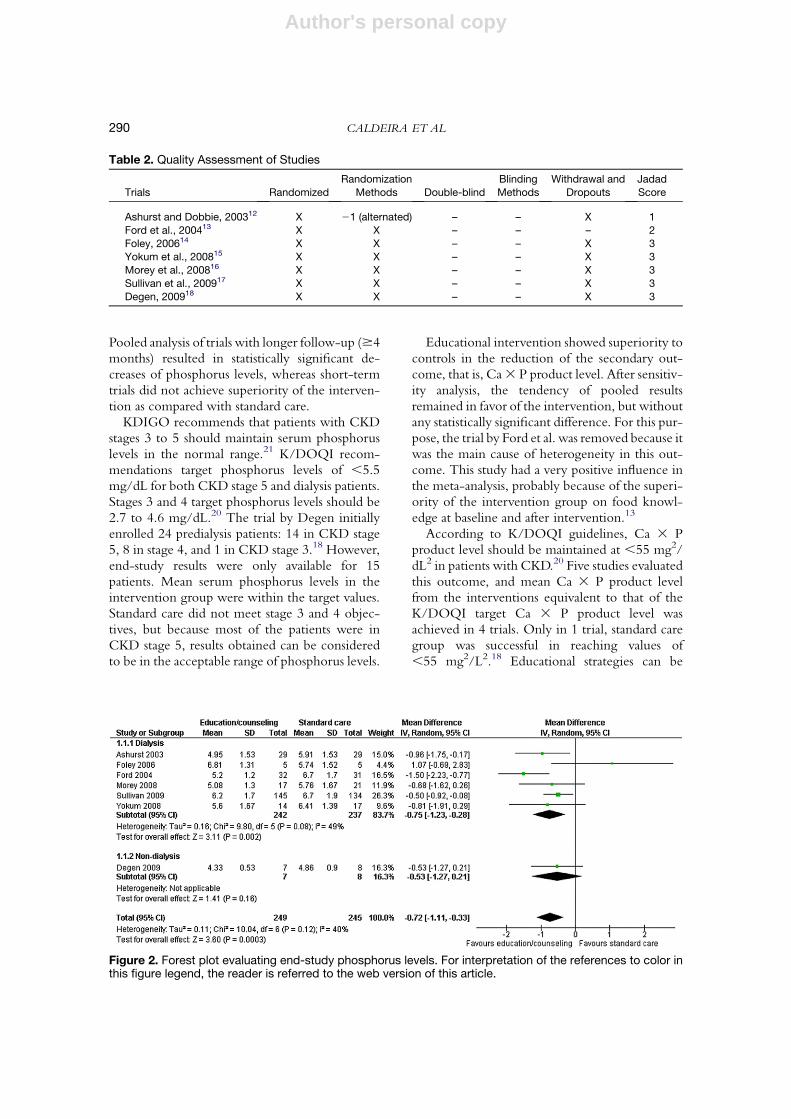
End-study results were analyzed by random-effects methods because of the different nature ofeducational interventions.For the primary outcome, there was no hetero-
geneity in overall and subgroups pooled analysis.MD for phosphorus levels was 20.72 mg/dLand 95% CI ranged from 21.11 to 20.33 (P 5.0003). Although subgroup analysis showed thatthe intervention was effective for patients on dial-ysis with an MD of 20.75 mg/dL and 95%CI ranging from 21.23 to 20.28 (P 5 0.002), itdid not show statistical significance in patientsnot on dialysis who had an MD of 20.53 with95% CI ranging from 21.27 to 0.21 (P 5 .16)(Fig. 2).Sensitivity analysis of phosphorus level was con-
ducted in accordance with follow-up periods ofthe trials (Fig. 3). Trials with follow-up periodsof ,4 months did not show superiority of educa-tional intervention (MD: 20.38; 95% CI: 20.91to 0.15, P 5 .16), whereas those with longerfollow-up periods showed the benefits of a longereducational intervention with a weighted MD of
Figure 1. Flow chart ofstudies selection.
EDUCATION TO REDUCE SERUM PHOSPHORUS IN CKD 287

Author's personal copy
Table
1.Main
CharacteristicsoftheStudies
Study
Ashurstand
Dobbie,200312
Ford
etal.,
200413
Foley,200614
Yokum
etal.,
200815
Moreyetal.,
200816
Sullivanetal.,
200917
Degen,200918
Setting
Hemodialysis
Hemodialysis
Hemodialysis
Hemodialysis
Hemodialysis
Hemodialysis
Nonhemodialysis
Patients
Stable
hemodialysis
patients
with
hyperphosphatemia
Dialysis
patients
with
hyperphosphatemia
Hyperphosphatemic
ESRDondialysis
Stable
hyperphosphatemic
adultsundergoing
regularhemodialysis
Stable
adult
hemodialysis
patients
with
hyperphosphatemia
Hemodialysed
patients
with
hyperphosphatemia
Predialytic
hyperphosphatemic
patients
Numberof
patients
56
63
10
34
67
279
16
Hyperphosphatemia
criteria
Atleast1value
above1.7
mmol
(5.26mg/dL)of
serum
phosphate
inlast3months
Meanserum
phosphorusabove
6.0
mg/dLover3
months
Serum
phosphate
.5.5
mg/dLin
4of6laboratory
evaluationsover
6months
Atleast1Serum
phosphate
value
above.1.8
mmol/L
(5.57mg/dL)in
last
3months
Meanserum
phosphate
persistentlyabove
theUKRenal
Association
Standards
Committeetarget
,1.8
mmol/L,
(5.57mg/dL)
Recentserum
phosphoruslevel
andmeanserum
phosphoruslevelf
ortheprevious3
monthsgreater
than5.5
mg/dL
6-m
onthsmean
serum
phosphorus
.1.35mmol/L
(4.17mg/dL)
Age(years)
53(m
ean)
74%
above
50years
old
55(m
ean)
49(m
ean)
58(m
ean)
53(m
ean)
54(m
ean)
Follo
w-up
6months
6months
4weeks
4months
6/12months
3months
12weeks
Intervention
Educational
interventionand
one-to-onerenal
dietitianteaching
sessiongivenby
arenaldietitian
Monthly
additional
educational
sessionswith
educationaltools
suchasposters,
handouts,puzzles,
andan
individualized
phosphorus
trackingtool.
Weekly
nutritional
counseling
sessionsusing
amodified
versionof
motivational
interviewing
Pharm
acistandrenal
dietitianconsults
Monthly
dietetic
consultations
Educationon
avoidingfoods
withphosphorus
additiveswhen
purchasing
groceriesor
visitingfastfood
restaurants
Dietary
education
usingthe
PhosphorusPoint
System
Tool
Comparator
Norm
almanagement
onthedialysis
unit
withrenal
hemodialysis
dietitian.
Standard
dietitian
care
during
monthly
nutrition
rounds.
Traditionalmonthly
nutritional
counseling
Standard
care
with
renaldietitian
consultbutnot
pharm
acistconsult
Baselineandend-
study(6th
month)
renaldietitian
counseling
Standard
care
from
theirdietitiansand
nephrologists.
Dietitianprovidedlist
offoodshighin
phosphorusto
avoid,andlow
phosphorusfoods
toconsumemore
frequently
Outcomes
Serum
phosphate,
serum
calcium
andCa3
P
product
Before-and-after
knowledgetest
results,serum
calcium,
phosphorus,
parathyroid
horm
one,and
calcium/
phosphorus
productlevels.
Serum
phosphorus
levels
Changein
serum
phosphate
levels,
correctedcalcium,
Ca3
Pproduct
andiPTH
Serum
phosphate,
serum
calcium
andCa3
P
product
Phosphoruslevels,
foodknowledge
score,reads
ingredients
list
andreadsnutrition
facts
label
Serum
phosphorus
levels,dietary
intakeand
satisfactionand
knowledgeof
dietary
phosphorus
content
CALDEIRA ET AL288

Author's personal copy
21.07 and 95% CI ranging from21.49 to20.64(P , .00001).In 227 patients with hyperphosphatemia and
CKD (212 dialysis patients and 15 predialysispatients), Ca 3 P product level results were het-erogeneous with I2 5 58% for the dialysis sub-group. Education and/or counseling proved tobe superior to controls with an MD of 25.23mg2/dL2 (95% CI: 29.48 to 20.98, P 5 .02),but these results were not reproducible in the pre-defined subgroups. For patients on dialysis, MDwas 25.75 mg2/dL2, which was a statistically sig-nificant result with 95% CI ranging from 211.08to 20.42. The non-dialysis group did not havestatistically significant results with an MD of23.09 mg2/dL2 and 95% CI ranging from29.78 to 3.60 (Fig. 4).Sensitivity analysis of Ca 3 P product level in
accordance with follow-up periods of the trialscould not be conducted, although this outcomewas analyzed in accordance with heterogeneitysource (Fig. A1). Excluding the trial by Fordet al.13 helped remove heterogeneity, thus chang-ing the results in the overall and dialysis subgroups.Dialysis subgroup weighted MD was23.00 mg2/L2 with 95% CI ranging from 27.09 to 1.09.Overall mean reduction of Ca 3 P product levelwas 23.02 mg2/L2 (95% CI: 26.51 to 0.47),without any statistically significant differences.
Discussion
These results show that educational strategies inpatients with hyperphosphatemia and CKD canbe useful in the reduction of serum phosphoruslevels. This was well documented in the dialysisgroup, whereas education and/or counseling inpatients not on dialysis was not statistical signifi-cant in both outcomes. Reduced sample sizewith 15 patients underpowered comparison inthis latter subgroup.Analyzing trials with patients on dialysis, end-
study mean serum phosphorus Kidney DiseaseOutcomes Quality Initiative (K/DOQI) targetlevel of ,5.5 mg/dL20 was achieved in 50% ofthe analyzed studies, whereas none of the controlswere able to reach these values (5.7426.70 mg/dL). The pooled analysis showed that a decreaseof 0.75 mg/dL in phosphorus levels can beobtained in these patients when compared withthe controls.Sensitivity analysis suggested that maintaining
a long-term intervention may be important.
Conclusions
Educational
intervention
decreased
phosphate
levels
Extraeducational
sessionshowed
decreaseof
phosphorus
levels
Aggressive
counselingdid
notresultin
lower
serum
phosphoruslevels
withthis
patient
population.Larger
sample
sizeand/
orlongerfollo
w-
upcould
have
beenshownto
bebeneficial
Thephosphate
management
protocolwas
effective,andits
implementationwas
associatedwith
significantlybetter
serum
phosphate
control
Monthly
dietetic
consultations
improvedshort-
term
phosphate
levels
Educationof
patients
with
ESRDresultsin
modest
improvements
in
hyperphosphatemia
Analyze
dpopulation
wasvery
smallfor
definite
conclusions,but
educationdid
notreduce
significantlythe
phosphoruslevels
iPTH,intactparathyroid
horm
one;ESRD,end-stagerenald
isease
.
EDUCATION TO REDUCE SERUM PHOSPHORUS IN CKD 289
Author's personal copy
Pooled analysis of trials with longer follow-up ($4months) resulted in statistically significant de-creases of phosphorus levels, whereas short-termtrials did not achieve superiority of the interven-tion as compared with standard care.
KDIGO recommends that patients with CKDstages 3 to 5 should maintain serum phosphoruslevels in the normal range.21 K/DOQI recom-mendations target phosphorus levels of ,5.5mg/dL for both CKD stage 5 and dialysis patients.Stages 3 and 4 target phosphorus levels should be2.7 to 4.6 mg/dL.20 The trial by Degen initiallyenrolled 24 predialysis patients: 14 in CKD stage5, 8 in stage 4, and 1 in CKD stage 3.18 However,end-study results were only available for 15patients. Mean serum phosphorus levels in theintervention group were within the target values.Standard care did not meet stage 3 and 4 objec-tives, but because most of the patients were inCKD stage 5, results obtained can be consideredto be in the acceptable range of phosphorus levels.
Educational intervention showed superiority tocontrols in the reduction of the secondary out-come, that is, Ca3 P product level. After sensitiv-ity analysis, the tendency of pooled resultsremained in favor of the intervention, but withoutany statistically significant difference. For this pur-pose, the trial by Ford et al. was removed because itwas the main cause of heterogeneity in this out-come. This study had a very positive influence inthe meta-analysis, probably because of the superi-ority of the intervention group on food knowl-edge at baseline and after intervention.13
According to K/DOQI guidelines, Ca 3 Pproduct level should be maintained at ,55 mg2/dL2 in patients with CKD.20 Five studies evaluatedthis outcome, and mean Ca 3 P product levelfrom the interventions equivalent to that of theK/DOQI target Ca 3 P product level wasachieved in 4 trials. Only in 1 trial, standard caregroup was successful in reaching values of,55 mg2/L2.18 Educational strategies can be
Table 2. Quality Assessment of Studies
Trials Randomized
Randomization
Methods Double-blind
Blinding
Methods
Withdrawal and
Dropouts
Jadad
Score
Ashurst and Dobbie, 200312 X 21 (alternated) – – X 1
Ford et al., 200413 X X – – – 2
Foley, 200614 X X – – X 3Yokum et al., 200815 X X – – X 3
Morey et al., 200816 X X – – X 3
Sullivan et al., 200917 X X – – X 3
Degen, 200918 X X – – X 3
Figure 2. Forest plot evaluating end-study phosphorus levels. For interpretation of the references to color inthis figure legend, the reader is referred to the web version of this article.
CALDEIRA ET AL290

Author's personal copy
beneficial to achieve K/DOQI target Ca 3 Pproduct level.
Interfering factors, such as parathyroid hor-mone (PTH) levels and drug-use, were similar be-tween control and intervention groups in most ofthe studies. Only in the study by Sullivan et al.,was the PTH lower in the control group. Inter-group use of phosphate-binding drugs was similarwithin the studies that reported this informa-tion.13,14,16–18 Three studies reported the use of
vitamin D analogs. Two of them showed nodifferences between groups,16,17 whereas in thestudy by Ford et al., the use of vitamin D analogswas lower in the control group.13 Only 1 trialshowed baseline use of calcimimetics, but no dif-ferences were stated between intervention andstandard care groups.17
There is a close relationship between phospho-rus and protein intake.22 K/DOQI recommendsprotein intake of 0.6 to 0.75 g/kg/day for patients
Figure 3. Forest plot of sensitivity analysis of phosphorus levels in accordance with the follow-up periods ofthe trials. For interpretation of the references to color in this figure legend, the reader is referred to the webversion of this article.
Figure 4. Forest plot evaluating calcium–phosphorus product levels. For interpretation of the references tocolor in this figure legend, the reader is referred to the web version of this article.
EDUCATION TO REDUCE SERUM PHOSPHORUS IN CKD 291

Author's personal copy
with CKD stages 1 to 4.23 Protein restriction forthese patients can slow down disease progres-sion.24 Same guidelines recommendminimal dailyprotein intake of 1.2 g/kg/day for patients ondialysis to maintain good nutritional status becauselow protein intake can increase morbidity rate.25
Patients on dialysis often suffer from anorexia,and phosphorus-based food additives can be usedas flavor enhancers to help reach nutritional objec-tives,26 but they can also worsen phosphorus levels.Further, some studies showed that the recommen-ded amount of protein intake can lead to hyper-phosphatemia.27 In the selected trials, Morey et al.showed that educational strategy did not changenutritional parameters such as body mass index,albumin, handgrip strength, and mid-upper-armcircumference.16 In the study by Degen, serumcreatinine, albumin, weight, and body mass indexwere found to be similar between interventions.18
However, the follow-up periods in these studieswere short, preventing speculation of its resultsin long-term interventions, thus suggesting thateducational intervention may reduce serum phos-phorus without interfering with nutritional status.Some studies have showed that ingestion ofproteins with low phosphorus contents (lowphosphorus to protein ratio) could avoidmalnutri-tion and reduce mortality rate.28,29 Only 1 trialfrom the selected studies evaluated educationalintervention without a clear focus on protein–phosphorus restriction; Sullivan et al. successfullyused an intervention to avoid phosphorus-basedfood additives.17
Therefore, adequate balance should be individ-ually maintained on the basis of nutritional status,phosphorus, and calcium levels. Patients shouldnot consume processed foods, snacks, and softdrinks with large amounts of inorganic phospho-rus, and high phosphorus-to-protein ratio such asdairy products, sausages, or egg yolk. Counselingshould be conducted to reduce total phosphorusintake and to address preference of organic proteinswith low phosphorus-to-protein ratio to avoidmalnutrition. Relatively high phosphorus contentof vegetarian proteins is less absorbable because ofthe interference by phytates.29,30 Boiled food canalso reduce phosphorus content.31
Because only 45% of patients on hemodialysishave acceptable phosphorus levels according toDialysis Outcomes and Practice Patterns Study(DOPPS),32 additional therapeutic options suchas education or counseling are needed.
Psychoeducational interventionswere shown toimprove overall and postdialysis survival in 172predialysis patients versus 163 patients with pre-dialysis standard care, in a RCT with a meanfollow-up of 8.5 years.33 This result was also sup-ported by an observational study that analyzed 287predialysis patients assigned to multidisciplinaryeducation and 286 without this intervention.Mean follow-up was 11.7 months. Patients withmultidisciplinary education had lower mortalityand were less likely to initiate dialysis. Multidisci-plinary predialysis education was an independentprognostic factor for mortality rate in patientsnot on dialysis.34 Although the referred trialspointed out that education can be useful in pre-dialysis,33–35 RCTs are required to elucidatewhether education can improve phosphorusand Ca 3 P product levels in patients withhyperphosphatemia and CKD, irrespective ofwhether or not they are on dialysis.Independently of the methods used in educa-
tional and/or nutritional counseling actions, ourstudy showed that these nonpharmacologicalinterventions related to diet were effective in theimprovement of phosphorus levels in patientswith CKD and hyperphosphatemia. Educationmay also play an important role in reducing Ca 3P product level.
Implications to the Practice
These results are important for patients andhealthcare providers because beyond pharmaco-logical interventions, educational and/or counsel-ing interventions can be an additional resource toachieve desired phosphorus and/or Ca3 P prod-uct levels. For policy makers, this may be an effec-tive intervention to decrease high phosphorusburdens in CKD.Presented data support the fact that educational
interventions related to diet might be beneficial ifmaintained for a period of $4 months.
Implications to Research
Further studies using Ca3 P product level as anoutcome are required to possibly establish the ben-efit of the intervention in this outcome. The effectof education and/or counseling for patients onperitoneal dialysis is still unknown; therefore,more studies are needed to assess the efficacy ofthis intervention in peritoneal dialysis.
CALDEIRA ET AL292

Author's personal copy
Efficacy trials of these interventions with clini-cal outcomes, such as hyperphosphatemia-associatedmorbidities, are also essential to establisha definite role for educational strategies in thesepatients.
Assessment of mortality rate on educationand/or counseling evaluating patients withhyperphosphatemia and CKD is lacking, andgeneral CKD requires more powerful studiesthan those published for psychoeducationalinterventions.33,35
Limitations
Reduced number of trials with small number ofpatients and short-term follow-up periods werethe limitations for this study.
Overall, included studies had low quality (Jadadscore between 1 and 3), with a small number ofstudies reporting allocation concealment.
Studies by Foley and Yokum et al. could under-estimate effects of intervention because baselinephosphorus and Ca3 P product (in the latter trial)levels were lower in the control group and werenot statistically different.14,15
Patients not on dialysis were evaluated in only 1trial and its sample size was very small (n 5 15),thus making results in this subgroup inadequateto draft reliable conclusions.
Morey et al. enrolled 67 patients but phospho-rus levels of both intervention and control groupswere only supplied at the 12-month follow-up for48 patients.16 These were the results applied in thepooled analysis.
Conclusions
Educational interventions were effective inreducing phosphorus levels in patients with hyper-phosphatemia on dialysis. In comparison withcontrols, longer interventions ($4 months) wereefficient, whereas those with ,4 months follow-up were not. Education might play a role indecrease of Ca 3 P product levels.
AcknowledgmentsWe thank Dr. Sharon Foley for providing unpublished data.
References
1. Hsu CY, ChertowGM: Elevations of serum phosphorus and
potassium in mild to moderate chronic renal insufficiency. Neph-
rol Dial Transplant 17:1419-1425, 2002
2. Uribarri J: Phosphorus homeostasis in normal health and in
chronic kidney disease patients with special emphasis on dietary
phosphorus intake. Semin Dial 20:295-301, 2007
3. Block GA, Klassen PS, Lazarus JM, et al: Mineral metabo-
lism, mortality, and morbidity in maintenance hemodialysis.
J Am Soc Nephrol 15:2208-2218, 2004
4. Kestenbaum B, Sampson JN, Rudser KD, et al: Serum phos-
phate levels and mortality risk among people with chronic kidney
disease. J Am Soc Nephrol 16:520-528, 2005
5. Hruska KA, Saab G, Mathew S, et al: Renal osteodystrophy,
phosphate homeostasis, and vascular calcification. Semin Dial 20:
309-315, 2007
6. Llach F, Forero FV: Secondary hyperparathyroidism in
chronic renal failure: pathogenic and clinical aspects. Am J Kidney
Dis 38:S20-S33, 2001
7. Norris KC, Greene T, Kopple J, et al: Baseline predictors of
renal disease progression in the African American study of hyper-
tension and kidney disease. J Am Soc Nephrol 17:2928-2936,
2006
8. Ahmed S, O’Neill KD, Hood AF, et al: Calciphylaxis is asso-
ciated with hyperphosphatemia and increased osteopontin expres-
sion by vascular smooth muscle cells. Am J Kidney Dis 37:
1267-1276, 2001
9. Coladonato JA: Hyperphosphatemia management includes
phosphorus-restriction diet, phosphorus-binding agents and dial-
ysis. Control of hyperphosphatemia among patients with ESRD.
J Am Soc Nephrol 16:S107-S114, 2005
10. Poduval RD,WolgemuthC, Ferrell J, et al: Hyperphospha-
temia in dialysis patients: is there a role for focused counseling?
J Ren Nutr 13:219-223, 2003
11. Sun CY, Chang KC, Chen SH, et al: Patient education: an
efficient adjuvant therapy for hyperphosphatemia in hemodialysis
patients. Ren Fail 30:57-62, 2008
12. Ashurst Ide B, Dobbie H: A randomized controlled trial of
an educational intervention to improve phosphorus levels in
hemodialysis patients. J Ren Nutr 13:267-274, 2003
13. Ford JC, Pope JF, Hunt AE, et al: The effect of diet educa-
tion on the laboratory values and knowledge of hemodialysis
patients with hyperphosphatemia. J Ren Nutr 14:36-44, 2004
14. Foley S: Nutrition counseling to lower serum phosphorus
levels; 2006. Available at: http://www.controlled-trials.com/
mrct. Identifier NCT00296439. Register found in June 2010
15. YokumD, Glass G, Cheung CF, et al: Evaluation of a phos-
phate management protocol to achieve optimum serum phos-
phate levels in hemodialysis patients. J Ren Nutr 18:521-529,
2008
16. Morey B,WalkerR, Davenport A:More dietetic time, bet-
ter outcome? A randomized prospective study investigating the
effect of more dietetic time on phosphate control in end-stage kid-
ney failure haemodialysis patients. Nephron Clin Pract 109:
c173-c180, 2008
17. Sullivan C, Sayre SS, Leon JB, et al: Effect of food additives
on hyperphosphatemia among patients with end-stage renal dis-
ease: a randomized controlled trial. JAMA 301:629-635, 2009
18. Degen JA: Intensive dietary education using the Phospho-
rus Point System Tool to improve hyperphosphatemia in patients
with chronic kidney disease. Available at: http://hdl.handle.net/
1807/18272. Accessed June, 2010
19. Higgins JPT, Deeks JJ, Altman DG: Special topics in statis-
tics. In: Higgins JPT, Green S (eds.): CochraneHandbook for Sys-
tematic Reviews of Interventions Version 5.0.1. The Cochrane
EDUCATION TO REDUCE SERUM PHOSPHORUS IN CKD 293

Author's personal copy
Collaboration, 2008. Available at: www.cochrane-handbook.org.
Accessed June, 2010; Updated September 2008
20. National Kidney Foundation: KDOQI clinical practice
guidelines for bone metabolism and disease in chronic kidney
disease. Available at: http://www.kidney.org/Professionals/
kdoqi/guidelines_bone/. Accessed June, 2010
21. KDIGO guideline for chronic kidney disease—mineral
and bone disorder (CKD-MBD). Available at: http://www.
kdigo.org/clinical_practice_guidelines/. Accessed October, 2010
22. Boaz M, Smetana S: Regression equation predicts dietary
phosphorus intake from estimate of dietary protein intake. J Am
Diet Assoc 96:1268-1270, 1996
23. National Kidney Foundation: KDOQI clinical practice
guidelines for nutrition in chronic renal failure. Available at:
http://www.kidney.org/professionals/kdoqi/guidelines_updates/
doqi_nut.html. Accessed June, 2010
24. Klahr S, Levey AS, Beck GJ, et al, Modification of Diet in
Renal Disease Study Group: The effects of dietary protein restric-
tion and blood-pressure control on the progression of chronic
renal disease. N Engl J Med 330:877-884, 1994
25. Acchiardo SR, Moore LW, Burk L: Morbidity and mortal-
ity in hemodialysis patients. ASAIO Trans 36:M148-M151, 1990
26. Lopes AA, Lopes GB: Reducing serum phosphorus con-
centration in patients with end-stage renal disease. JAMA 301:
2443-2444, 2009
27. Uribarri J, CalvoMS: Hidden sources of phosphorus in the
typical American diet: does it matter in nephrology? Semin Dial
16:186-188, 2003
28. Noori N, Kalantar-Zadeh K, Kovesdy CP, et al: Associa-
tion of dietary phosphorus intake and phosphorus to protein ratio
with mortality in hemodialysis patients. Clin J Am Soc Nephrol 5:
683-692, 2010
29. Kalantar-Zadeh K, Gutekunst L, Mehrotra R, et al:
Understanding sources of dietary phosphorus in the treatment
of patients with chronic kidney disease. Clin J Am Soc Nephrol
5:519-530, 2010
30. Noori N, Sims JJ, Kopple JD, et al: Organic and inorganic
dietary phosphorus and its management in chronic kidney disease.
Iran J Kidney Dis 4:89-100, 2010
31. Cupisti A, D’Alessandro C, Baldi R, et al: Dietary habits
and counseling focused on phosphate intake in hemodialysis
patients with hyperphosphatemia. J Ren Nutr 14:220-225, 2004
32. Young EW, Albert JM, Satayathum S, et al: Predictors and
consequences of altered mineral metabolism: the dialysis out-
comes and practice patterns study. Kidney Int 67:1179-1187,
2005
33. Devins GM, Mendelssohn DC, Barr�e PE, et al: Predial-
ysis psychoeducational intervention extends survival in CKD:
a 20-year follow-up. Am J Kidney Dis 46:1088-1098, 2005
34. Wu IW,Wang SY, Hsu KH, et al: Multidisciplinary predial-
ysis education decreases the incidence of dialysis and reduces
mortality—a controlled cohort study based on the NKF/DOQI
guidelines. Nephrol Dial Transplant 24:3426-3433, 2009
35. Binik YM, Devins GM, Barre PE, et al: Live and learn:
patient education delays the need to initiate renal replacement
therapy in end-stage renal disease. J Nerv Ment Dis 181:
371-376, 1993
Figure A1. Forest plot of sensitivity analysis of calcium–phosphorus product levels.
Appendix
CALDEIRA ET AL294
Top Related
Copyright © 2022 FDOKUMEN

