







Bahasa
Halaman
Hukum

DRD3 Ser9Gly Polymorphism Is Related to Thermal Pain Perception
and Modulation in Chronic Widespread Pain Patients and Healthy
Controls
Stephane Potvin,* Annie Larouche,y Edith Normand,* Juliana Barcellos de Souza,*Isabelle Gaumond,z Sylvain Grignon,y and Serge Marchand**Service of Neurosurgery, Faculty of Medicine, University of Sherbrooke, Sherbrooke, Canada.yDepartments of Psychiatry and Physiology, Faculty of Medicine, University of Sherbrooke, Sherbrooke, Canada.zDepartment of Health Sciences, Universite du Quebec en Abitibi-Temiscamingue, Rouyn-Noranda, Quebec, Canada.
Abstract: Experimental studies showed that dopamine influences pain perception in healthy volun-
teers. Dopamine dysfunctions have been linked to the physiopathology of fibromyalgia (FM), which
is associated with hyperalgesia and deficient pain inhibition. We sought to investigate the relationships
between catecholamine-related polymorphisms [dopamine-D3 receptor (DRD3) Ser9Gly and catechol-
O-methyltransferase (COMT) Val158Met] and thermal pain measures in healthy subjects and FM pa-
tients. Seventy-three subjects (37 FM patients and 36 controls) participated in this study. Thermal
pain thresholds (TPTs) were measured using a Peltier thermode. Inhibitory systems were elicited using
a thermal tonic pain stimulation administered before and after activation of the diffuse noxious inhib-
itory controls (DNIC) by means of a cold-pressor test. Genetic analyses were performed using polymer-
ase chain reaction. Regression analyses were performed across and within groups. FM was associated
with lower TPTs and deficient pain inhibition. DRD3 Ser9Gly polymorphism predicted (1) DNIC efficacy
across groups and (2) thermal TPTs in FM patients. COMT Val158Met and thermal pain measures were
not related. These preliminary results suggest that the DRD3 Ser9Gly polymorphism influences DNIC ef-
ficacy and TPTs and that this latter relationship is present only in FM patients. Two core psychophysical
features of FM appear to be significantly influenced by limbic dopamine functioning.
Perspective: This experimental study is the first to relate DNIC and TPTs to a functional polymor-
phism of limbic dopamine-D3 receptors. As lowered pain thresholds and deficient pain inhibition
are 2 core features of fibromyalgia, these preliminary results may help identify a subgroup of FM
patients who require closer medical attention.
ª 2009 by the American Pain Society
Key words: Chronic widespread pain, COMT, diffuse noxious inhibitory controls, DRD3, hyperalgesia.
The Journal of Pain, Vol 10, No 9 (September), 2009: pp 969-975Available online at www.sciencedirect.com
Despite (very) low concentrations of dopamine re-ceptors at the spinal level,23 mounting evidencesuggests that dopamine significantly influences
Received August 14, 2008; Revised January 19, 2009; Accepted March 18,2009.Drs Potvin and Larouche contributed equally to this work.Dr Marchand is holder of the Pain Chair from the University of Sher-brooke and UQAT and a supported member of the Centre de rechercheclinique Etienne-Le Bel du Centre Hospitalier Universitaire de Sherbrooke(Fonds de Recherche en Sante du Quebec). Dr Potvin is holder of a post-doctoral scholarship from the Canadian Institute of Health Research(CIHR). Dr Marchand holds grants from the CIHR. Dr Grignon is a memberof the Centre de Recherches Cliniques Etienne-Le Bel and of the Centredes Neurosciences de Sherbrooke. Genotyping studies were funded inpart by an unrestricted grant from Novartis Canada to the Departmentof Psychiatry, Sherbrooke University.Address reprint requests to Dr Serge Marchand, University of Sherbrooke,Faculty of Medicine, Axe Douleur CRC-CHUS, 3001, 12e Avenue Nord,Sherbrooke, Canada, J1H 5N4. E-mail: [email protected]
1526-5900/$36.00
ª 2009 by the American Pain Society
doi:10.1016/j.jpain.2009.03.013
pain perception. In rodents, psychostimulants havebeen shown to enhance morphine-induced analgesia.3
It has also been demonstrated that psychostimulantsproduce pain-relieving effects in models of tonic pain(eg, formalin test)1 and that these effects can be reversedby lesions of dopaminergic cells in the ventral tegmentalarea (VTA).24 Recently, these promising preclinical find-ings translated into human studies suggesting that dopa-mine may be a key supraspinal modulator of painperception.
Over the last few years, positron emission tomography(PET) studies have been conducted among healthy volun-teers and produced converging evidence of correlationsbetween striatal D2/D3 receptor binding potential (atrest) and pain perception (mostly pain thresholds).21,25,27
That is, these studies showed that increased dopamineactivity in the striatum is associated with less subjectivepain. Interestingly, the potential role of dopamine in
969

endogenous pain modulation systems has also beenexplored by Hagelberg et al.10 Using the cold-pressortest as a conditioning stimulus, this group demonstrateda positive relationship between striatal dopaminerelease and pain inhibition.
Apart from these PET investigations, genetic studieshave also highlighted a role of dopamine in humanpain perception. So far, the most frequently assessedpolymorphism has been the catechol-O-methyltransfer-ase (COMT) Val158Met polymorphism. COMT is a cata-bolic enzyme degrading catecholamines (dopamineand norepinephrine) in the frontal lobe, and its gene islocated on chromosome 22q11. COMT Val158Met isa single nucleotide polymorphism (SNP), which consistsof a G / A transition at codon 158, the result of whichis an amino acid change. Val/val, val/met, and met/metgenotypes are, respectively, associated with high, inter-mediate, and low activity of the enzyme.36 The relation-ship between the COMT Val1158Met polymorphism andpain perception has been investigated in healthy volun-teers, consistently showing that carriers of the met/metgenotype experience the most intense experimentallyinduced pain.4,5,37
On the basis of the results from these experimentalstudies, the role of dopamine in chronic pain conditionshas been explored. Although preliminary results havelinked dopamine dysfunctions to burning mouth syn-drome,12 the most frequently studied chronic pain disor-der has been fibromyalgia (FM). Of unknown etiology,FM is characterized by chronic widespread pain (>3months).31 Experimental studies repetitively showedthat FM is associated with lowered mechanical/thermalpain thresholds, indicative of hyperalgesia.22 FM hasalso been related to abnormal endogenous pain modula-tion systems. Diffuse nociceptive inhibitory control (DNIC)is 1 of the principal endogenous inhibitory pain systems.The DNIC theory postulates that a nociceptive stimulationwill trigger descending inhibitory neurons from the brain-stem, inducing diffuse inhibition throughout the body(eg ‘‘pain inhibits pain’’ phenomenon).18,19 Using a spatialsummation paradigm,20 our group found a deficit in DNICin FM patients but not in low back pain patients,14 sug-gesting a pathology-specific deficit.
Recently, Wood34 hypothesized that dopaminergicdysfunctions may contribute to the pathophysiology ofthis chronic widespread pain disorder. In support of thehypothesis, a pharmacological double-blinded, pla-cebo-controlled study showed the efficacy of pramipex-ole, a D2/D3 receptor agonist, for the treatment ofFM.11 In addition, it has been shown that presynaptic do-pamine activity is reduced in FM patients, relative tohealthy controls, in brain regions such as the thalamus,hippocampus, and anterior cingulate cortex.32 It hasalso been found that striatal dopamine release is not cor-related with subjective pain in FM, although this correla-tion is observed in healthy controls.33 Moreover, anassociation study demonstrated that the COMT val/valgenotype is less frequent in FM patients relative to con-trols.9 Garcia-Fructuoso et al7 found that FM patientswith the met/met genotype have a more severe form ofthe disease. Finally, Vargas-Alarcon et al29 showed an
970
association between 3 SNPs of the COMT gene and FMin Spanish but not Mexican patients.
Genetic studies involving FM patients have not com-prised psychophysical measures so far. Also noteworthy,these genetic studies focused mainly on COMT genepolymorphisms, which regulate dopamine (catechol-amines) activity mainly in the frontal lobe. The objectiveof the current endophenotyping study was to deter-mine the influence of dopamine-related gene polymor-phisms on thermal pain thresholds (TPT) and DNICefficacy in FM patients and healthy controls. To untan-gle the influence of frontal and limbic dopamine activ-ity, we assessed COMT Val158Met and dopamine-D3
receptor (DRD3) Ser9Gly polymorphisms because D3 re-ceptors are preferentially localized within the limbic sys-tem. D3 receptors are also localized in the prefrontalcortex and basal ganglia, but their highest concentra-tions are found in the limbic system.36 The DRD3 geneis located on chromosome 3p13.3.3. DRD3 Ser9Gly isan SNP, whose mutated genotype (homozygous ‘‘gly-gly’’) is linked to the highest activity of the receptor.6
To our knowledge, this is the first study to investigatethe relationships between DRD3 Ser9Gly and experi-mental pain.
Methods
ParticipantsThirty-seven patients with FM and 36 healthy volun-
teers participated in this study. Patients were recruitedthrough newspaper ads, FM associations, and referralsfrom physicians. Patients were diagnosed with FM usingAmerican Association of Rheumatology criteria30 byneurosurgeons, rheumatologists, or physicians on theward, specialized in the treatment of chronic pain. Par-ticipants who were pregnant or breast-feeding, whohad diabetes, lupus, rheumatoid arthritis, or a cardiacpathology were excluded from the study. Substanceabuse was also an exclusion criterion. The Human EthicsCommittees of the Universite du Quebec en Abitibi-Te-miscamingue and Universite de Sherbrooke approvedthe research protocol, and all participants gave theirwritten informed consent. Groups did not differ interms of age [FM = 50.6 6 7.4; controls = 47.9 6 5.3;t = � 1.746; P = .085], sex (89% of females in FM; 81%of females in controls; c2 = 1.063; P = .303), and the pres-ence or absence of a regular menstrual cycle (c2 = 5.164;P = .076). Eighteen FM patients were treated withantidepressants (tricyclics, selective serotonin reuptakeinhibitors, or serotonin/norepinephrine reuptake inhib-itors) None were taking antidepressants acting on dopa-mine (eg bupropion). None of the healthy volunteerswere receiving medications acting on the central ner-vous system.
Clinical AssessmentThe symptoms of FM were assessed using the self-ad-
ministered Fibromyalgia Impact Questionnaire (FIQ)2
that measures the components of health the mostaffected by FM over the last week. This 10-item
DRD3 Polymorphism and Pain Modulation

Potvin et al
questionnaire is composed of 3 questions rated on a Lik-ert-type scale and 7 questions rated on visual analogscales ranging from 0 to 10, where higher scores indicatea higher negative impact and/or a greater severity ofsymptoms. Depressive symptoms were evaluated withthe depression item from the FIQ.
Thermal Pain MeasuresIn a pretest session, TPTs were measured by applying
a thermode on the left forearm of participants. The Pelt-ier thermode used (TSA II; Medoc, Advanced Medical Sys-tems, Minneapolis, MN) was a heating plate connectedto a computer that allowed a precise setting of experi-mental temperature. Subjects were advised that thethermode temperature would gradually increase from32�C to 51�C by a rate of 0.3�C per second. Subjectswere instructed to verbally report when their sensationschanged from heat to pain.
Afterward, a continuous heat pulse was administeredwith a thermode for 2 minutes on the left forearm of par-ticipants. Experimental temperature reached a predeter-mined fixed value and remained constant during the2-minute testing period (time 0 to time 120). It was setat a value corresponding to a temperature individuallypredetermined to induce a 50% pain rating during thepretest. During thermal stimulation (pretest and test),pain intensity was measured using a computerized visualanalog scale (COVAS) that ranged from 0% (no pain) to100% (most intense pain imaginable). To capture the ef-fects of DNIC, we administered the tonic heat pain proce-dure twice and conducted a cold-pressor test (CPT)between administrations. The CPT consisted of theimmersion of the opposite (right) arm (up to the shoul-der) for 2 minutes in a bath of cold water. Temperatureof the water was set at 12�C to ensure that the CPT wassufficiently painful to elicit DNIC but tolerable for 2 min-utes. The CPT recruits the DNIC because it is a strong no-ciceptive stimulation which takes place during a lengthytime span30 and is applied over a large body surfacearea.20 By comparing the pain evaluation induced bythe thermode, acquired before and after the cold-pres-sor test, we were able to measure the inhibitory effectof the DNIC response.
GenotypingGenomic DNA was extracted from peripheral blood
collected from patient using DNeasy spin columns(Qiagen, Mississauga, Ontario, Canada) and quantifiedusing a Nanodrop ND-1000 spectrophotometer. The tar-get region of the DRD3 gene was amplified with PCR us-ing the primers (50-30) F-GCT CTA TCT CCA ACT CTC ACAand R-AAG TCT ACT CAC CTC CAG GTA (GenebankU25441). Genomic DNA (30 to 60 ng) was added to 0.4mM of each dNTP, 1 mM of each primer pair and 1U ofTaq DNA polymerase (Roche) completed with Taq buffer.Conditions for PCR were 94�C for 2 minutes, 35 cycles of94�C for 20 seconds, 55�C for 20 seconds, and 72�C for 20seconds and a final extension at 72�C 7 minutes. The PCRproducts were digested with MscI restriction enzyme(BioLabs) for 16 hours at 37�C and analyzed on a 4%
agarose gel containing ethidium bromide.26 Digestionof the 462 bp PCR product revealed a 304 bp fragmentif the serine allele was present or 206 and 98 bp frag-ments if the glycine allele was present. Constant bandsof 111 and 47 bp were also produced. PCR for COMTgene was carried out using the primers (50-30) F-TCG TGGACG CCG TGA TTC AGG and R-AGG TCT GAC AAC GGGTCA GGC (Genebank Z26491). Conditions were: 94�C for2 minutes, 34 cycles of 94�C for 45 seconds, 58�C for 45 sec-onds, and 72�C for 30 seconds and a final extension at72�C for 7 minutes. The PCR products were digestedwith NlaIII restriction enzyme for 16 hours at 37�C and an-alyzed on a 4% agarose gel containing ethidium bro-mide.17 The digested 217 bp PCR product revealed 136and 81 bp fragments if the valine allele was present or96, 81, and 40 bp if the methionine allele was present.
Statistical AnalysesFor our analyses, the dependent variables were TPTand
DNIC efficacy (percentage of change between post- andpre-DNIC mean COVAS scores [time 0 to time 120]). TheKolmogorov-Smirnov test was applied to verify the nor-mal distribution of data. TPT and DNIC efficacy bothhad a normal distribution (TPT: Z = 1.177; P = .125; DNIC:Z = 0.629; P = .824). Between-group differences in psycho-physical measures (TPT and DNIC) were calculated usinganalyses of variance. The influence of genotypes (COMTand DRD3) on psychophysical measures was assessedwith linear regression analyses, using genotypes as pre-dictors (wild-type homozygous genotype = 0; heterozy-gous genotype = 1; mutated homozygous genotype = 2).Regression analyses were performed across or withingroups based on the significance of group�genotype in-teractions, which was evaluated using mixed-effectmodels. For the regression analyses, a power analysiswas performed, and it was estimated that 81 participantsare required to detect a moderate relationship (r = 0.3)between experimental pain measures and dopaminegene polymorphisms, using an a level of 0.05 and statisti-cal power of 80%. Finally, between-group differences inallelic frequencies were evaluated using c2 tests. The levelof significance was set at P < .05.
Results
Group DifferencesA deficit in DNIC efficacy was observed in FM patients,
relative to controls [FM = 5.7% 6 43.0%; controls = 25.16 35.7; F(1,72) = 4.355; P = .040]. In addition, TPT weresignificantly lower in FM patients, relative to controls[FM = 37.7�C 6 4.1; controls = 42.4 6 3.6; F(1,72) =25.720; P = .0001]. There was no difference in DNIC effi-cacy (P = .704) and TPT (P = .459) between FM patientstreated with antidepressants and those who were not.
DRD3 and COMT Polymorphisms
Genotype Frequencies
There were no differences in genotype frequenciesbetween FM patients and controls in DRD3 Ser9Gly
971
(c2 = 2.002; P = .359) and COMT Val158Met (c2 =0.136;.934) (Table 1).
DRD3 Ser9Gly
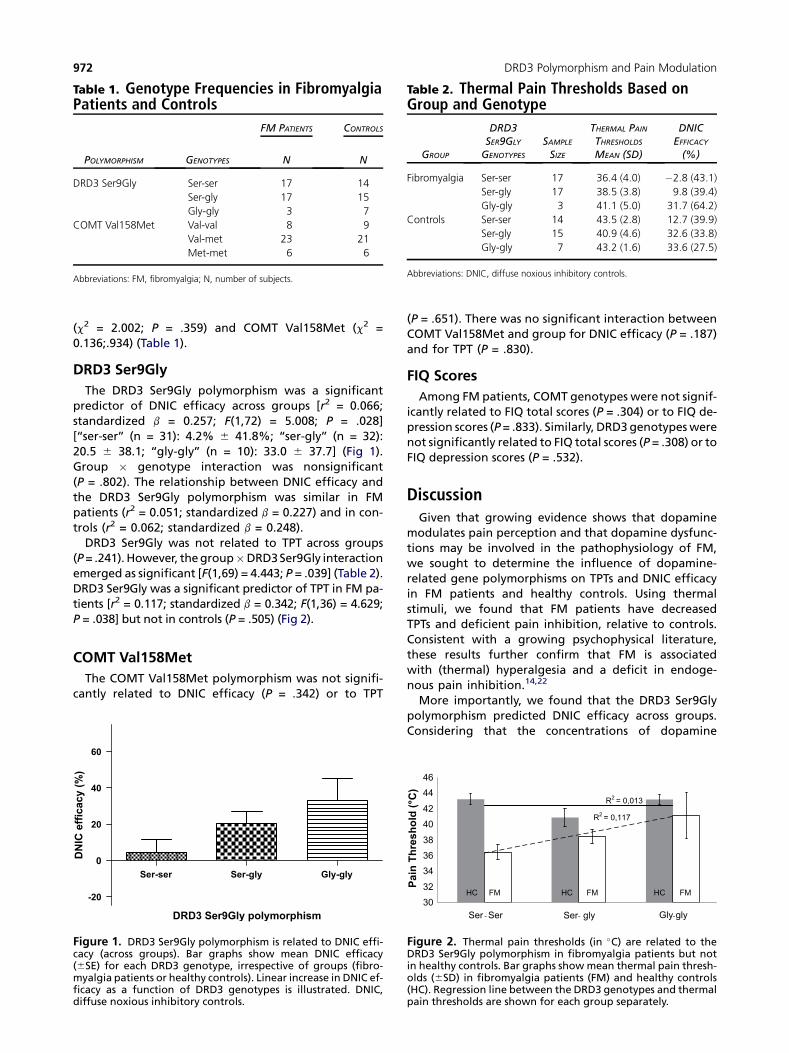
The DRD3 Ser9Gly polymorphism was a significantpredictor of DNIC efficacy across groups [r2 = 0.066;standardized b = 0.257; F(1,72) = 5.008; P = .028][‘‘ser-ser’’ (n = 31): 4.2% 6 41.8%; ‘‘ser-gly’’ (n = 32):20.5 6 38.1; ‘‘gly-gly’’ (n = 10): 33.0 6 37.7] (Fig 1).Group � genotype interaction was nonsignificant(P = .802). The relationship between DNIC efficacy andthe DRD3 Ser9Gly polymorphism was similar in FMpatients (r2 = 0.051; standardized b = 0.227) and in con-trols (r2 = 0.062; standardized b = 0.248).
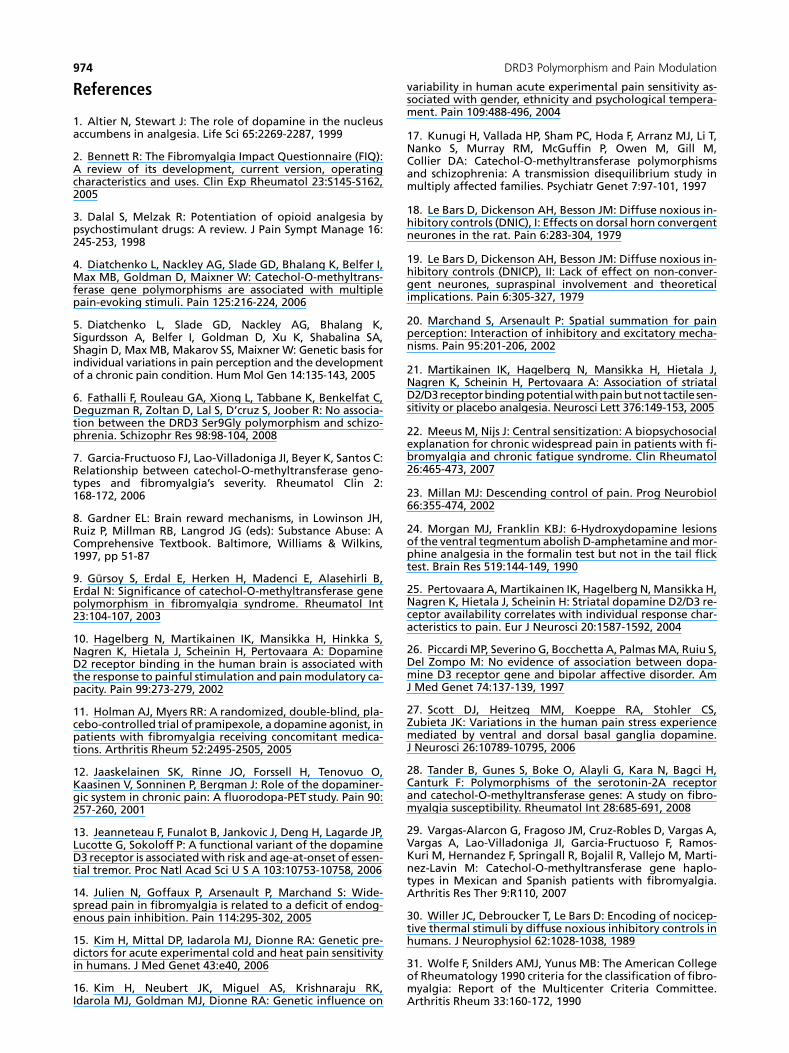
DRD3 Ser9Gly was not related to TPT across groups(P = .241). However, the group�DRD3 Ser9Gly interactionemerged as significant [F(1,69) = 4.443; P = .039] (Table 2).DRD3 Ser9Gly was a significant predictor of TPT in FM pa-tients [r2 = 0.117; standardized b = 0.342; F(1,36) = 4.629;P = .038] but not in controls (P = .505) (Fig 2).
COMT Val158Met
The COMT Val158Met polymorphism was not signifi-cantly related to DNIC efficacy (P = .342) or to TPT
(P = .651). There was no significant interaction betweenCOMT Val158Met and group for DNIC efficacy (P = .187)and for TPT (P = .830).
FIQ Scores
Among FM patients, COMT genotypes were not signif-icantly related to FIQ total scores (P = .304) or to FIQ de-pression scores (P = .833). Similarly, DRD3 genotypes werenot significantly related to FIQ total scores (P = .308) or toFIQ depression scores (P = .532).
DiscussionGiven that growing evidence shows that dopamine
modulates pain perception and that dopamine dysfunc-tions may be involved in the pathophysiology of FM,we sought to determine the influence of dopamine-related gene polymorphisms on TPTs and DNIC efficacyin FM patients and healthy controls. Using thermalstimuli, we found that FM patients have decreasedTPTs and deficient pain inhibition, relative to controls.Consistent with a growing psychophysical literature,these results further confirm that FM is associatedwith (thermal) hyperalgesia and a deficit in endoge-nous pain inhibition.14,22
More importantly, we found that the DRD3 Ser9Glypolymorphism predicted DNIC efficacy across groups.Considering that the concentrations of dopamine
Table 1. Genotype Frequencies in FibromyalgiaPatients and Controls
FM PATIENTS CONTROLS
POLYMORPHISM GENOTYPES N N
DRD3 Ser9Gly Ser-ser 17 14
Ser-gly 17 15
Gly-gly 3 7
COMT Val158Met Val-val 8 9
Val-met 23 21
Met-met 6 6
Abbreviations: FM, fibromyalgia; N, number of subjects.
-20
0
20
40
60
Ser-ser Ser-gly Gly-gly
DRD3 Ser9Gly polymorphism
DN
IC
efficacy (%
)
Figure 1. DRD3 Ser9Gly polymorphism is related to DNIC effi-cacy (across groups). Bar graphs show mean DNIC efficacy(6SE) for each DRD3 genotype, irrespective of groups (fibro-myalgia patients or healthy controls). Linear increase in DNIC ef-ficacy as a function of DRD3 genotypes is illustrated. DNIC,diffuse noxious inhibitory controls.
R2 = 0,013
R2 = 0,117
303234363840424446
Ser Ser Ser gly Gly gly
Pa
in
T
hre
sh
old
(°C
)
FM FM FM HC HC HC
Figure 2. Thermal pain thresholds (in �C) are related to theDRD3 Ser9Gly polymorphism in fibromyalgia patients but notin healthy controls. Bar graphs show mean thermal pain thresh-olds (6SD) in fibromyalgia patients (FM) and healthy controls(HC). Regression line between the DRD3 genotypes and thermalpain thresholds are shown for each group separately.
Table 2. Thermal Pain Thresholds Based onGroup and Genotype
GROUP
DRD3SER9GLY
GENOTYPES
SAMPLE
SIZE
THERMAL PAIN
THRESHOLDS
MEAN (SD)
DNICEFFICACY
(%)
Fibromyalgia Ser-ser 17 36.4 (4.0) �2.8 (43.1)
Ser-gly 17 38.5 (3.8) 9.8 (39.4)
Gly-gly 3 41.1 (5.0) 31.7 (64.2)
Controls Ser-ser 14 43.5 (2.8) 12.7 (39.9)
Ser-gly 15 40.9 (4.6) 32.6 (33.8)
Gly-gly 7 43.2 (1.6) 33.6 (27.5)
Abbreviations: DNIC, diffuse noxious inhibitory controls.
972 DRD3 Polymorphism and Pain Modulation

Potvin et al
receptors at the spinal level are (very) low, Wood35 pro-posed that dopamine may play a role in descendingpain inhibition via the mesolimbic (reward) system,whose neurons project from the VTA to the nucleus ac-cumbens (ventral striatum).8 To our knowledge, thePETstudy from Hagelberg et al10 is the only study that di-rectly tested this hypothesis. In this study, our resultsprovide the first genetic evidence that mesolimbic dopa-mine is indeed implicated in DNIC efficacy because D3
receptors are preferentially localized within the (meso)-limbic system. More precisely, we observed that the mu-tated homozygous genotype (‘‘gly-gly’’) was associatedwith the strongest DNIC efficacy, whereas the wild-type‘‘ser-ser’’ genotype was associated with the weakest.Because ‘‘gly-gly’’ genotype is linked with highest D3 re-ceptor functioning, our results suggest that enhancedmesolimbic dopamine activity is associated with thestrongest DNIC efficacy. As such, our results confirmWood’s hypothesis, and they are compatible with theresults from Hagelberg et al,10 who showed a positiverelationship between striatal dopamine release andthe magnitude of pain inhibition. In rodents, there isreliable evidence demonstrating that DNIC recruitsopioidergic, serotoninergic, and noradrenergic neuronslocated in brainstem structures (periaqueductal graymatter, raphe magnus nucleus, and locus coeruleus, re-spectively), which project to the spinal cord anddampen the intensity of incoming afferents.18,19 Futurestudies will need to better delineate the pathwayslinking the brain reward system and these brainstemstructures.
Interestingly, we found that DRD3 Ser9Gly was a signif-icant predictor of TPTs in FM patients but not in controls.Given that there was no association between DRD3Ser9Gly and FM, this polymorphism does not appear tobe a risk factor for FM. However, for those who haveFM, DRD3 Ser9Gly significantly influences thermal hyper-algesia. In rodents, dopamine release in the brain rewardsystem produces antihyperalgesic effects.1 We foundthat the ‘‘gly-gly’’ genotype, which might be linked tothe highest activity of the receptor,13 is associated withhigher TPTs; that is, less hyperalgesia. This finding isthus coherent with results from preclinical research. Ifconfirmed, this finding may help identify subgroup ofFM patients, namely the ‘‘ser-ser’’ carriers, who requirecloser medical attention.
We found that ‘‘gly-gly’’ carriers had greater DNIC effi-cacy, and we also observed that FM patients (but not con-trols) carrying the same genotype had less thermalhyperalgesia. Taken together, these findings suggestthat endogenous pain inhibition systems dampen hyper-algesic responses in those exposed to traumatic physicalexperiences and sustained pain, as it is the case in FM.Conversely, efficient endogenous pain inhibition systemsmay not influence pain sensitivity (TPTs) in those whohave not been exposed to enduring pain.
Surprisingly, COMT Val158Met exerted no influenceon DNIC efficacy and TPTs. These negative results con-trast with previous studies showing a relationship be-tween this polymorphism and experimentally inducedpain.4,5,37 There are at least 2 reasons for this discrep-
ancy. First, our measures differed from the ones usedby other groups, who did not measure DNIC efficacy.Second, we cannot exclude that other COMT SNPs mayhave produced positive results. In this vein, it must bementioned that Kim et al16 reported no relationship be-tween COMT Val158Met and experimental pain butobserved positive results for COMT haplotypes.15 Alter-natively, it is tempting to consider that our results actuallysuggest that the relationship between experimentallyinduced pain perception and dopamine depends on thelimbic system (DRD3) rather than the frontal lobe(COMT).
No differences were found in allelic/genotypic fre-quencies between FM patients and controls for theCOMT Val158Met polymorphism. This result contrastswith the study from Gursoy et al,9 who showed an asso-ciation between COMT Val158Met and FM, but it is in parwith recent results from Tander et al,28 who failed todescribe such an association. As for the lack of associa-tion between DRD3 Ser9Gly and FM, it suggests thatthis polymorphism is not a risk factor for FM. However,the lack of association between DRD3 Ser9Gly andCOMT Val158Met polymorphisms and FM must beinterpreted cautiously. Our endophenotyping studywas underpowered to detect between-group differencesin allelic/genotypic frequencies, as this was simply notthe objective of the study.
The most important limitation of our study is the sizeof the sample involved. Even though the study producedsignificant results, we cannot rule out that our findingswere the result of a lack of representativeness of thesample involved in the study. To our knowledge, this isthe first study to describe a link between the DRD3Ser9Gly polymorphism and experimental pain measures.However, for the moment, our results must be consid-ered as exploratory. Clearly, these results need to be cor-roborated by other research teams in larger groups ofparticipants (�105 subjects; a posteriori power analysis;b = 80%, a = 0.05) before the relationship between theDRD3 Ser9Gly polymorphism and DNIC efficacy—ourmain finding—can be confirmed.
Consistent with previous findings, FM was associatedwith lower TPTs and deficient pain inhibition. DRD3Ser9Gly polymorphism but not COMT Val158Metemerged as a significant predictor of (1) DNIC efficacyacross groups and (2): thermal TPTs only in FM patients.The results from this endophenotyping study providepreliminary evidence that the DRD3 Ser9Gly polymor-phism influences DNIC efficacy and TPTs and that thislatter relationship is only present in FM patients. Assuch, these findings show that 2 of the core psycho-physical features of FM are significantly influencedby limbic dopamine functioning. These preliminaryfindings must be confirmed in a larger group ofparticipants.
AcknowledgmentsThe authors thank Dr Christian Cloutier and Dr Pierre
Arsenault for their assistance in patient recruitment.
973
974 DRD3 Polymorphism and Pain Modulation
References
1. Altier N, Stewart J: The role of dopamine in the nucleusaccumbens in analgesia. Life Sci 65:2269-2287, 1999
2. Bennett R: The Fibromyalgia Impact Questionnaire (FIQ):A review of its development, current version, operatingcharacteristics and uses. Clin Exp Rheumatol 23:S145-S162,2005
3. Dalal S, Melzak R: Potentiation of opioid analgesia bypsychostimulant drugs: A review. J Pain Sympt Manage 16:245-253, 1998
4. Diatchenko L, Nackley AG, Slade GD, Bhalang K, Belfer I,Max MB, Goldman D, Maixner W: Catechol-O-methyltrans-ferase gene polymorphisms are associated with multiplepain-evoking stimuli. Pain 125:216-224, 2006
5. Diatchenko L, Slade GD, Nackley AG, Bhalang K,Sigurdsson A, Belfer I, Goldman D, Xu K, Shabalina SA,Shagin D, Max MB, Makarov SS, Maixner W: Genetic basis forindividual variations in pain perception and the developmentof a chronic pain condition. Hum Mol Gen 14:135-143, 2005
6. Fathalli F, Rouleau GA, Xiong L, Tabbane K, Benkelfat C,Deguzman R, Zoltan D, Lal S, D’cruz S, Joober R: No associa-tion between the DRD3 Ser9Gly polymorphism and schizo-phrenia. Schizophr Res 98:98-104, 2008
7. Garcia-Fructuoso FJ, Lao-Villadoniga JI, Beyer K, Santos C:Relationship between catechol-O-methyltransferase geno-types and fibromyalgia’s severity. Rheumatol Clin 2:168-172, 2006
8. Gardner EL: Brain reward mechanisms, in Lowinson JH,Ruiz P, Millman RB, Langrod JG (eds): Substance Abuse: AComprehensive Textbook. Baltimore, Williams & Wilkins,1997, pp 51-87
9. Gursoy S, Erdal E, Herken H, Madenci E, Alasehirli B,Erdal N: Significance of catechol-O-methyltransferase genepolymorphism in fibromyalgia syndrome. Rheumatol Int23:104-107, 2003
10. Hagelberg N, Martikainen IK, Mansikka H, Hinkka S,Nagren K, Hietala J, Scheinin H, Pertovaara A: DopamineD2 receptor binding in the human brain is associated withthe response to painful stimulation and pain modulatory ca-pacity. Pain 99:273-279, 2002
11. Holman AJ, Myers RR: A randomized, double-blind, pla-cebo-controlled trial of pramipexole, a dopamine agonist, inpatients with fibromyalgia receiving concomitant medica-tions. Arthritis Rheum 52:2495-2505, 2005
12. Jaaskelainen SK, Rinne JO, Forssell H, Tenovuo O,Kaasinen V, Sonninen P, Bergman J: Role of the dopaminer-gic system in chronic pain: A fluorodopa-PET study. Pain 90:257-260, 2001
13. Jeanneteau F, Funalot B, Jankovic J, Deng H, Lagarde JP,Lucotte G, Sokoloff P: A functional variant of the dopamineD3 receptor is associated with risk and age-at-onset of essen-tial tremor. Proc Natl Acad Sci U S A 103:10753-10758, 2006
14. Julien N, Goffaux P, Arsenault P, Marchand S: Wide-spread pain in fibromyalgia is related to a deficit of endog-enous pain inhibition. Pain 114:295-302, 2005
15. Kim H, Mittal DP, Iadarola MJ, Dionne RA: Genetic pre-dictors for acute experimental cold and heat pain sensitivityin humans. J Med Genet 43:e40, 2006
16. Kim H, Neubert JK, Miguel AS, Krishnaraju RK,Idarola MJ, Goldman MJ, Dionne RA: Genetic influence on
variability in human acute experimental pain sensitivity as-sociated with gender, ethnicity and psychological tempera-ment. Pain 109:488-496, 2004
17. Kunugi H, Vallada HP, Sham PC, Hoda F, Arranz MJ, Li T,Nanko S, Murray RM, McGuffin P, Owen M, Gill M,Collier DA: Catechol-O-methyltransferase polymorphismsand schizophrenia: A transmission disequilibrium study inmultiply affected families. Psychiatr Genet 7:97-101, 1997
18. Le Bars D, Dickenson AH, Besson JM: Diffuse noxious in-hibitory controls (DNIC), I: Effects on dorsal horn convergentneurones in the rat. Pain 6:283-304, 1979
19. Le Bars D, Dickenson AH, Besson JM: Diffuse noxious in-hibitory controls (DNICP), II: Lack of effect on non-conver-gent neurones, supraspinal involvement and theoreticalimplications. Pain 6:305-327, 1979
20. Marchand S, Arsenault P: Spatial summation for painperception: Interaction of inhibitory and excitatory mecha-nisms. Pain 95:201-206, 2002
21. Martikainen IK, Hagelberg N, Mansikka H, Hietala J,Nagren K, Scheinin H, Pertovaara A: Association of striatalD2/D3 receptorbinding potentialwithpainbutnot tactile sen-sitivity or placebo analgesia. Neurosci Lett 376:149-153, 2005
22. Meeus M, Nijs J: Central sensitization: A biopsychosocialexplanation for chronic widespread pain in patients with fi-bromyalgia and chronic fatigue syndrome. Clin Rheumatol26:465-473, 2007
23. Millan MJ: Descending control of pain. Prog Neurobiol66:355-474, 2002
24. Morgan MJ, Franklin KBJ: 6-Hydroxydopamine lesionsof the ventral tegmentum abolish D-amphetamine and mor-phine analgesia in the formalin test but not in the tail flicktest. Brain Res 519:144-149, 1990
25. Pertovaara A, Martikainen IK, Hagelberg N, Mansikka H,Nagren K, Hietala J, Scheinin H: Striatal dopamine D2/D3 re-ceptor availability correlates with individual response char-acteristics to pain. Eur J Neurosci 20:1587-1592, 2004
26. Piccardi MP, Severino G, Bocchetta A, Palmas MA, Ruiu S,Del Zompo M: No evidence of association between dopa-mine D3 receptor gene and bipolar affective disorder. AmJ Med Genet 74:137-139, 1997
27. Scott DJ, Heitzeg MM, Koeppe RA, Stohler CS,Zubieta JK: Variations in the human pain stress experiencemediated by ventral and dorsal basal ganglia dopamine.J Neurosci 26:10789-10795, 2006
28. Tander B, Gunes S, Boke O, Alayli G, Kara N, Bagci H,Canturk F: Polymorphisms of the serotonin-2A receptorand catechol-O-methyltransferase genes: A study on fibro-myalgia susceptibility. Rheumatol Int 28:685-691, 2008
29. Vargas-Alarcon G, Fragoso JM, Cruz-Robles D, Vargas A,Vargas A, Lao-Villadoniga JI, Garcia-Fructuoso F, Ramos-Kuri M, Hernandez F, Springall R, Bojalil R, Vallejo M, Marti-nez-Lavin M: Catechol-O-methyltransferase gene haplo-types in Mexican and Spanish patients with fibromyalgia.Arthritis Res Ther 9:R110, 2007
30. Willer JC, Debroucker T, Le Bars D: Encoding of nocicep-tive thermal stimuli by diffuse noxious inhibitory controls inhumans. J Neurophysiol 62:1028-1038, 1989
31. Wolfe F, Snilders AMJ, Yunus MB: The American Collegeof Rheumatology 1990 criteria for the classification of fibro-myalgia: Report of the Multicenter Criteria Committee.Arthritis Rheum 33:160-172, 1990

32. Wood PB, Patterson JC, Sunderland JJ, Tainter KH,Glabus MF, Lilien DL: Reduced presynaptic dopamine activityin fibromyalgia syndrome demonstrated with positron emis-sion tomography: A pilot study. J Pain 8:51-58, 2007
33. Wood PB, Schweinhardt P, Jaeger E, Dagher A,Hakyemez H, Rabiner EA, Bushnell CM, Chizh BA: Fibromyal-gia patients show an abnormal dopamine response to pain.Eur J Neurosci 25:3576-3582, 2007
34. Wood PB: A reconsideration of the relevance of systemiclow-dose ketamine to the pathophysiology of fibromyalgia.J Pain 7:611-614, 2006
Potvin et al
35. Wood PB: Mesolimbic dopaminergic mechanisms andpain control. Pain 120:230-234, 2006
36. Zinkstok J, van Amelsvoort T, de Haan L, Baas F,Linszen D: The Catechol-O-Methyltransferase Gene andSchizophrenia, in Lang MV (ed): Trends in SchizophreniaResearch. New York, Nova Biomedical Books, 2005, pp45-78
37. Zubieta JK, Heitzeg MM, Smith YR, Bueller JA, Xu K,Xu Y, Koeppe RA, Stohler CS, Goldman D: COMT Val158Metgenotype affects m-opioid neurotransmitter responses toa pain stressor. Science 299:1240-1243, 2003
975
Top Related
Copyright © 2022 FDOKUMEN

