







Bahasa
Halaman
Hukum


1
Updated Search Strategy (1 October 2010 to 30 May 2013):
Diagnosis of Obstructive Sleep Apnea: A Clinical Practice Guideline from the American College of
Physicians
Summary of Findings:
1. AHRQ Question-1: How do different available tests compare in their ability to diagnose
OSA in adults with symptoms suggestive of disordered sleep?
a. Comparison of portable devices and polysomnography
i. New Reports: 39 reports describing 36 populations
ii. Major Changes/Updates to ACP’s Clinical Practice Guidelines: None
b. Comparison of questionnaires and polysomnography
i. New Reports: 41 reports describing 40 populations
ii. Major Changes/Updates to ACP’s Clinical Practice Guidelines: None
c. Clinical prediction rules and polysomnography
i. New Reports: 6 reports describing 6 populations
ii. Major Changes/Updates to ACP’s Clinical Practice Guidelines: None
2. AHRQ Question-2: How does phased testing (screening tests of battery of followed by full
test) compare to full testing alone?
i. New Reports: 1 report
ii. Major Changes/Updates to ACP’s Clinical Practice Guidelines: None
3. AHRQ Question-3: What is the effect of preoperative screening for OSA on surgical
outcomes?
i. New Reports: 2 reports describing 2 populations
ii. Major Changes/Updates to ACP’s Clinical Practice Guidelines: None
4. AHRQ Question-4: In adults being screened for OSA, what are the relationships between
AHI or oxygen desaturation index (ODI), and other patient characteristics with respect to
long-term clinical and functional outcomes?
i. New Reports: 3 reports
ii. Major Changes/Updates to ACP’s Clinical Practice Guidelines: None
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

2
METHODS
We used systematic methods to identify relevant studies, apply inclusion and exclusion criteria,
evaluate study quality and summarize the four AHRQ questions regarding the diagnosis of OSA:
1. AHRQ Question-1: How do different available tests compare in their ability to diagnose
OSA in adults with symptoms suggestive of disordered sleep?
a. Comparison of portable devices and polysomnography
b. Comparison of questionnaires and polysomnography
c. Clinical prediction rules and polysomnography
2. AHRQ Question-2: How does phased testing (screening tests of battery of followed by full
test) compare to full testing alone?
3. AHRQ Question-3: What is the effect of preoperative screening for OSA on surgical
outcomes?
4. AHRQ Question-4: In adults being screened for OSA, what are the relationships between
AHI or oxygen desaturation index (ODI), and other patient characteristics with respect to
long-term clinical and functional outcomes?
Literature search
An investigator (J.C.H.) performed a previously described computerized search strategy from the
AHRQ report (Figure 1.) to identify relevant studies published between 1 October 2010 and 30 May
2013 in the MEDLINE electronic databases (Ovid MEDLINE and MEDLINE(R) In-Process). Non-
English language articles were excluded.
Inclusion and exclusion criteria
Initial search strategy (Figures 1 and 2) yielded a total of 2,435 articles. Inclusion and exclusion
criteria for each AHRQ question were derived from the original AHRQ report (Figure 3). A careful
review of titles and abstracts eliminated 1,728 articles. A review of full reports by one investigator
(J.C.H.) excluded 622 studies.
Study quality
Methodological criteria for study quality were adapted from those proposed by Kent et al., to
identify high-quality studies of the diagnosis for OSA (Figure 4) and utilized for AHRQ Questions 1 and
2.The revised criteria cover seven assessment categories: technical quality of index test, technical quality
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

3
of the reference test, application of the reference test, independence of interpretations, clinical description,
cohort assembly and sample size.
Data abstraction
One investigator (J.C.H) abstracted primary data regarding patient characteristics and test
diagnostics (e.g. sensitivity and/or specificity).
Data synthesis and sensitivity/specificity calculations
We constructed 2 x 2 contingency tables for each study to summarize the results of the index test
and the reference test(s). For each study, the true positive rate (TPR; sensitivity), the false-positive rate
(FPR; 1-specificity), the diagnostic odds ratio, positive predictive value, negative predictive value,
positive likelihood ratio, negative likelihood ratio, diagnostic accuracy ([TP+TN]/N) and the kappa-1
statistic were calculated. We calculated a weighted kappa-1 coefficient (a generalization of the
unweighted or Cohen’s kappa coefficient) to assess accuracy with regards to avoiding false negative
results. Calculation of the kappa-1 coefficient does not require the false positive rate (1-specificity), but
does require knowledge of the marginal probabilities. Weighted kappa coefficient values close to one
suggest good test accuracy, while values less than 0.40 suggest only fair to poor test accuracy.
Statistical models
All biostatistical models were programmed in Excel 8.0 for Windows (Microsoft Corporation,
Redmond, Washington, USA). A normal approximation to the binomial of the standard error was used in
calculating all other CI’s, as appropriate. When making comparisons between groups of studies we used
an unpaired t-test or the Mann-Whitney U test as appropriate. A two-tailed p-value <0.05 was considered
statistically significant.
RESULTS
We identified 2,435 potentially relevant articles, of which 85 reports met inclusion criteria
(Figure 2, Tables 1-7). These included 36 reports describing 33 patient populations reporting the
diagnostic accuracy of portable testing (AHRQ Key Question 1a; Table 1), 3 reports describing 3 patient
population reporting outcomes other than diagnostic accuracy for portable testing (AHRQ Key Question
1a; Table 2), 41 reports describing 40 patient populations reporting diagnostic accuracy of screening
questionnaires (AHRQ Key Question 1b; Table 3), 6 reports describing 6 patient populations reporting
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

4
diagnostic accuracy for clinical prediction rules (AHRQ Key Question 1c; Table 4), 1 report reporting
how phased testing compares to full testing (AHRQ Key Question 2; Table 5), 2 reports describing 2
patient populations reporting the effect of preoperative OSA screening on surgical outcomes (AHRQ Key
Question 3; Table 6), and 3 reports describing 2 patient populations describing long-term clinical and
functional outcomes in adults screened for OSA (AHRQ Key Question 4; Table 7).
Study Quality
The overall quality of the included studies in assessing sleep outcomes was generally fair (Tables
1-5).
I. AHRQ Key Question 1a: Comparison of portable devices and polysomnography
Thirty-six reports describing 33 patient populations reporting the diagnostic accuracy of portable
testing (Table 1) were included: 4 describing Type II portable devices (Table 8); 5 describing Type III
portable devices (Table 10); 11 describing Type IV portable devices (other than oximetry alone; Table
12); 10 describing oximetry alone reporting an oxygen desaturation index (ODI; (Table 14); and 6
describing oximetry alone with measures other than ODI (Table 16). Additionally, 3 studies reported
outcomes other than diagnostic accuracy using portable monitors (Table 2): two of these studies assessed
OSA treatment adherence and/or functional outcomes between those diagnosed with portable vs in-lab
polysomnography; one study assessed agreement between in-lab and home testing with regards to
therapeutic decision making. Many included studies excluded subjects with clinically significant cardiac,
pulmonary and/or neurologic disorders.
A. Findings:
a. Type II monitors vs. PSG
i. Four studies reported diagnostic accuracy of Type II devices compared with PSG
(Tables 8 and 9). Studies were highly heterogeneous with respect to populations
assessed and OSA definitions (particularly hypopneas). Reported diagnostic
accuracy was generally high with AUC’s generally above 0.90 and two of four
reporting positive Likelihood ratios ≥10 in subjects with an AHI cut-points
≥15/hr and/or ≥30/hr. However, only one study reported a negative likelihood
ratio ≤0.1 in subjects with AHI cut-points ≥15/hr.
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

5
b. Type III monitors vs. PSG
i. Five studies reported diagnostic accuracy of Type III devices compared with
PSG (Tables 10 and 11). Studies were highly heterogeneous with respect to
populations assessed and OSA definitions (particularly hypopneas). Diagnostic
accuracy was reported as high with AUC’s generally above 0.89. However, only
one of six studies reported positive Likelihood ratios ≥10 in subjects with an AHI
cut-point ≥15/hr. Three of six studies reported a negative likelihood ratio ≤0.1 for
subjects with AHI cut-points of ≥5/hr and/or ≥15/hr.
c. Type IV monitors (other than oximetry alone) vs. PSG
i. Thirteen studies reported diagnostic accuracy of Type IV devices compared with
PSG (Tables 12 and 13). Studies were highly heterogeneous with respect to
populations assessed and OSA definitions (particularly AHI and hypopneas).
Diagnostic accuracy was reported as high with AUC’s generally above 0.85. Five
studies reported positive Likelihood ratios ≥10 in subjects with an AHI cut-point
≥5/hr and/or ≥15/hr. Five studies reported a negative likelihood ratio ≤0.1 in
subjects with an AHI cut-point ≥5/hr and/or ≥15/h.
d. Oximetry alone (reporting ODI) vs. PSG
i. Ten studies reported diagnostic accuracy of Oximetry (evaluating oxygen
desaturation index [ODI]) compared with PSG (Tables 14 and 15). Studies were
highly heterogeneous with respect to populations assessed and OSA definitions
(particularly AHI, hypopneas and ODI definitions). Diagnostic accuracy was
reported as high with AUC’s generally above 0.9. Four studies reported positive
Likelihood ratios ≥10 in subjects with an AHI cut-points ≥5/hr, ≥15/hr and/or
≥30/hr. Five studies reported a negative likelihood ratio ≤0.1 in subjects with an
AHI cut-point ≥5/hr and/or ≥15/hr.
e. Oximetry alone (reporting outcome other than ODI) vs. PSG
i. Six studies reported diagnostic accuracy of Oximetry (using outcomes other than
ODI) compared with PSG (Tables 16 and 17). Studies were highly
heterogeneous with respect to populations assessed, OSA definitions (particularly
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

6
AHI and hypopneas definitions) and oximetry outcome measures. Diagnostic
accuracy was reported as high with AUC’s generally above 0.9. Only one study
reported a positive Likelihood ratio ≥10 in subjects with an AHI cut-points ≥5/hr
and/or≥15/hr. Two studies reported a negative likelihood ratio ≤0.1 in subjects
with an AHI cut-point ≥5/hr and/or ≥10/h.
f. Comparison of portable testing with PSG reporting outcomes other than diagnostic
accuracy
i. Three studies reported outcomes other than diagnostic accuracy in the
comparison of portable vs PSG testing (Table 2).
ii. Two studies randomized consecutive patients with high clinical OSA suspicion to
either a home testing pathway (both used Type III devices) vs in-lab PSG.
Primary outcomes were CPAP compliance (3 or 6-months) and/or functional
outcomes. Both studies concluded that home testing was not inferior to PSG with
respect to functional outcomes and CPAP adherence.
iii. One study assessed degree of agreement in therapeutic decisions (per AASM
criteria) between home and in-lab testing by performing both tests in patients
with suspected OSA with sleep physicians providing CPAP recommendations
based on each study (in a blinded protocol). The authors concluded that home-
testing was adequate when the AHI was high.
B. Major Changes/Updates to ACP’s Clinical Practice Guidelines: None
II. AHRQ Key Question 2a: Comparison of questionnaires and polysomnography
Forty-one reports describing 40 patient populations reporting the diagnostic accuracy of sleep
questionnaires (Table 18-29) were included: 15 describing the Berlin Questionnaire (BQ) (Table 18); 22
describing the Epworth Sleepiness Scale (ESS) (Table 20); 3 describing the Multivariate Apnea
Prediction Index (MAPI) (Table 22); 3 describing the Pittsburgh Sleep Quality Index (PSQI) (Table 24);
5 describing the STOP-BANG Questionnaire (Table 26); and 8 studies describing various other
questionnaires (Table 28).
A. Findings:
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

7
a. Berlin Questionnaire vs Sleep Study Testing
i. Sixteen studies reported diagnostic accuracy of the Berlin Questionnaire
compared with a sleep study (Tables 18 and 19). Studies were highly
heterogeneous with respect to populations assessed, type of reference test used
and OSA definitions (particularly AHI and hypopneas). Reported diagnostic
accuracy was low with AUC’s ranging from 0.50 to 0.64. No study reported a
positive Likelihood ratio ≥10 or a negative likelihood ratio ≤0.1.
b. Epworth Sleepiness Scale vs Sleep Study Testing
i. Twenty-two studies reported diagnostic accuracy of the Epworth Sleepiness
Scale compared with a sleep study (Tables 20 and 21). Studies were highly
heterogeneous with respect to populations assessed, type of reference test used
and OSA definitions (particularly AHI and hypopneas). Reported diagnostic
accuracy was low with AUC’s ranging from 0.42 to 0.85. No study reported a
positive Likelihood ratio ≥10 or a negative likelihood ratio ≤0.1.
c. MAPI vs Sleep Study Testing
i. Three studies reported diagnostic accuracy of the Multivariate Apnea Prediction
Index compared with a sleep study (Tables 22 and 23). These three studies were
highly heterogeneous with respect to populations assessed, type of reference test
used and OSA definitions (particularly hypopneas). Only one study reported an
AUC of 0.77. No study reported a positive Likelihood ratio ≥10 or a negative
likelihood ratio ≤0.1.
d. PSQI vs Sleep Study Testing
i. Three studies reported diagnostic accuracy of the Pittsburgh Sleep Quality Index
compared with a sleep study (24 and25). These three studies were highly
heterogeneous with respect to populations assessed, type of reference test used
and OSA definitions (particularly hypopneas). No study reported an AUC. No
study reported a positive Likelihood ratio ≥10 or a negative likelihood ratio ≤0.1.
e. STOP-BANG vs Sleep Study Testing
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

8
i. Five studies reported diagnostic accuracy of the STOP-BANG compared with a
sleep study (Tables 26 and 27). Studies were highly heterogeneous with respect
to populations assessed, type of reference test used and OSA definitions
(particularly AHI and hypopneas). Reported diagnostic accuracy (using a BMI
cut-point >35 for the STOP-BANG) was low with AUC’s ranging from 0.49 to
0.77. No study reported a positive Likelihood ratio ≥10. Only one study reported
a negative likelihood ratio ≤0.1 for an AHI cut-point ≥30/hr and a STOP-BANG
≥2.
f. Other Questionnaires vs Sleep Study Testing
i. Eight studies reported diagnostic accuracy of various other questionnaires
compared with a sleep study (Tables 28 and 29). These eight studies were highly
heterogeneous with respect to populations assessed, type of reference test used
and OSA definitions (particularly AHI and hypopneas). Reported diagnostic
accuracy was low with AUC’s ranging from 0.32 to 0.96. No study reported a
positive Likelihood ratio ≥10. One study reported negative likelihood ratio ≤0.1
for the Friedman classification in patients with an AHI ≥15/hr and/or ≥30/hr.
B. Major Changes/Updates to ACP’s Clinical Practice Guidelines: None
III. AHRQ Key Question 3a: Comparison of clinical prediction rules and polysomnography
Six reports describing 6 patient populations reporting the diagnostic accuracy of clinical prediction
rules (Table A-1C) were included. For each prediction rule, only one study was identified.
A. Findings:
a. Clinical Prediction Rules vs Sleep Study Testing
i. Six studies reported diagnostic accuracy of various other questionnaires
compared with a sleep study (Tables 30 & 31). These six studies were highly
heterogeneous with respect to populations assessed, type of reference test used
and OSA definitions (particularly AHI and hypopneas). Reported AUC’s ranged
from 0.64 to 0.77. No study reported a positive Likelihood ratio ≥10 and no study
reported negative likelihood ratio ≤0.1.
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

9
B. Major Changes/Updates to ACP’s Clinical Practice Guidelines: None
IV. AHRQ Key Question 2: How does phased testing compare to full test alone?
Only one study reporting outcomes/diagnostic accuracy of phased testing (Table 5) was included.
A. Findings:
a. Phased testing vs Sleep Study Testing
i. One study compared phased testing (MAPI questionnaire or various OSA
symptoms followed by portable type 3) with a PSG (Tables 32 & 33). The
reported AUC was 0.85 (for an AHI ≥30 & ESS >10). The reported positive
Likelihood ratio was ≥3.9 and negative likelihood ratio was 0.06.
B. Major Changes/Updates to ACP’s Clinical Practice Guidelines: None
V. AHRQ Key Question 3: What is the effect of preoperative OSA screening on surgical
outcomes?
Only two studies reporting outcomes regarding preoperative OSA screening (Table 6).
A. Findings:
a. Preoperative Screening
i. One study performed PSG in 819 patients being evaluated for surgery and
compared the PSG findings with whether the anesthesiologist and surgeon
evaluating the patients (and blinded to the sleep study) correctly identified
patients at risk for OSA (Table 6). Anesthesiologists and surgeons failed to
identify those with moderate-severe OSA 60% and 92% respectively. The STOP-
BANG questionnaire correctly classified 92.5% and 93.1% of those misclassified
by the anesthesiologist and surgeon, respectively.
ii. Another study performed a Type IV study during propofol infusions during
surgery for transurethral resection of the bladder or prostate. The authors report
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

10
that presence or severity of OSA did not “significantly” affect any perioperative
outcomes evaluated including spinal anesthesia level, monitoring time, propofol
infusion rate, intra-operative blood pressure, heart-rate or oxygen saturation
score.
B. Major Changes/Updates to ACP’s Clinical Practice Guidelines: None
VI. AHRQ Key Question 4: Predictors of long-term clinical and functional outcomes
Only three studies reporting outcomes regarding long-term clinical and functional outcomes were
identified (Table 7).
A. Findings:
a. Predictors of long-term clinical and functional outcomes
i. One study in 2,505 elderly male participants in the MrOS longitudinal Sleep
Study reported that severe OSA was associated with increased risk of death
(multivariate OR 1.74, 95% CI 1.04-2.89)
ii. One study in 819 patients in the Sleep Health Study (mean age 62 years, 42%
male) reported that subjects with incident cardiovascular disease (over 5-years)
experienced larger increases in AHI between sleep studies.
iii. One study in 784 elderly male participants in the MrOS longitudinal Sleep study
excluding those with baseline hypertension found no statistically significant
difference in incident hypertension with respect to baseline AHI.
B. Major Changes/Updates to ACP’s Clinical Practice Guidelines: None
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

11
APPENDIX FIGURE LEGENDS
Figure 1. MEDLINE search strategy derived from AHRQ report.
Figure 2. Literature search and selection. Studies could meet one or more exclusion criteria. For
simplicity, only one primary exclusion criterion per study is shown.
Figure 3. Inclusion and exclusion criteria derived from AHRQ report.
Figure 4. Methodological quality questionnaire.
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

12
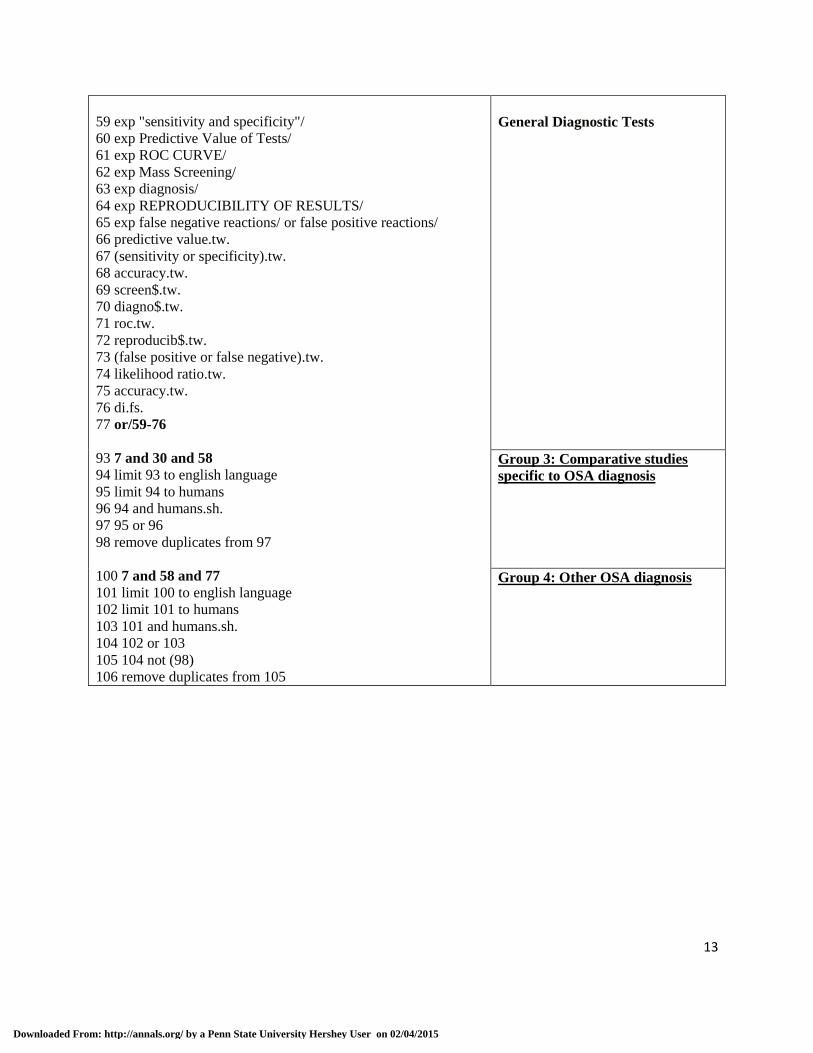
Figure 1. MEDLINE search strategy. Databases: OVID MEDLINE, MEDLINE(R) In-Process
1 exp Sleep Apnea Syndromes/ or exp Sleep Apnea, Obstructive/
2 exp Airway Resistance/
3 exp snoring/
4 Upper airway resistance syndrome.mp.
5 Respiratory disturbance.mp.
6 obstructive sleep apn?ea.mp.
7 or/1-6
8 randomized controlled trial.pt.
9 controlled clinical trial.pt.
10 randomized controlled trials/
11 Random Allocation/
12 Double-blind Method/
13 Single-Blind Method/
14 clinical trial.pt.
15 Clinical Trials.mp. or exp Clinical Trials/
16 (clinic$ adj25 trial$).tw.
17 ((singl$ or doubl$ or trebl$ or tripl$) adj (mask$ or
blind$)).tw.
18 Placebos/
19 placebo$.tw.
20 random$.tw.
21 trial$.tw.
22 (randomized control trial or clinical control trial).sd.
23 (latin adj square).tw.
24 Comparative Study.tw. or Comparative Study.pt.
25 exp Evaluation studies/
26 Follow-Up Studies/
27 Prospective Studies/
28 (control$ or prospectiv$ or volunteer$).tw.
29 Cross-Over Studies/
30 or/8-29
45 exp Polysomnography/
46 exp Oximetry/
47 exp Monitoring, Physiologic/
48 pulse transit time.mp.
49 exp Monitoring, Ambulatory/
50 peripheral Arterial Tonometry.mp.
51 exp Questionnaires/
52 exp Diagnostic Tests, Routine/
53 exp "Laboratory Techniques and Procedures"/
54 (Epworth or Stanford or Berlin or Pittsburgh or scale).af.
55 (friedman or surgical or staging).mp.
56 STOP-Bang.af.
57 Sleep Apnea, Obstructive/di
58 or/45-57
Sleep Apnea
Comparative Studies
Sleep Apnea Diagnostic Terms
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015
13
59 exp "sensitivity and specificity"/
60 exp Predictive Value of Tests/
61 exp ROC CURVE/
62 exp Mass Screening/
63 exp diagnosis/
64 exp REPRODUCIBILITY OF RESULTS/
65 exp false negative reactions/ or false positive reactions/
66 predictive value.tw.
67 (sensitivity or specificity).tw.
68 accuracy.tw.
69 screen$.tw.
70 diagno$.tw.
71 roc.tw.
72 reproducib$.tw.
73 (false positive or false negative).tw.
74 likelihood ratio.tw.
75 accuracy.tw.
76 di.fs.
77 or/59-76
93 7 and 30 and 58
94 limit 93 to english language
95 limit 94 to humans
96 94 and humans.sh.
97 95 or 96
98 remove duplicates from 97
100 7 and 58 and 77
101 limit 100 to english language
102 limit 101 to humans
103 101 and humans.sh.
104 102 or 103
105 104 not (98)
106 remove duplicates from 105
General Diagnostic Tests
Group 3: Comparative studies
specific to OSA diagnosis
Group 4: Other OSA diagnosis
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

14
Figure 2. Literature search and selection.
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

15
Figure 3. Inclusion and Exclusion criteria
GENERAL
Inclusion:
1. adults (>16 years).
2. only English-language, published, peer-reviewed articles.
Exclusion: 1. more than 20 percent of the participants had neuromuscular disease, Down syndrome, Prader-Willi
syndrome, major congenital skeletal abnormalities, narcolepsy, narcotic addiction, Alzheimer’s
disease, epilepsy, or who had experienced a disabling stroke.
2. abstracts, conference proceedings, or other unpublished ―grey‖ literature.
I. Diagnostic testing (AHRQ Key Questions 1 & 2).
Inclusion:
1. Adults (>16 years).with symptoms, findings, history, and comorbidities that indicated an
increased risk of sleep apnea.
2. Prospective cross-sectional or longitudinal studies of any follow-up duration.
3. At least 10 study participants had to be analyzed with each test of interest
4. We included all portable devices with any combination of two or more channels and those
that measured the following single channels: pulse transit time, peripheral arterial tone, and
pulse oximetry.
5. For the first analysis (portable versus PSG) we included only studies that performed an
overnight PSG.
6. For the second analysis (questionnaires, etc. versus standard testing), we included studies that
evaluated screening and other questionnaires, scales that included clinical criteria (e.g., signs,
symptoms, history, and comorbidities), and other clinical decision making tools. These tests
could be compared to either overnight PSG or portable testing.
7. For the second analysis (questionnaires, etc. versus standard testing), accepted studies either
validated their models in a separate subgroup of study participants or had their models
evaluated in subsequent studies.
8. Phased testing (Key Question 2). We included any study that directly compared phased
testing (a series of tests performed dependent on the results of initial tests) with full testing
(overnight PSG) alone.
9. OUTCOME OF INTEREST: We included all studies reporting concordance or agreement
among tests, predictive value (sensitivity, specificity) for diagnosis, change in clinical
management, and clinical outcomes.
Exclusion:
1. Studies conducted in only asymptomatic or healthy general-population participants, as well as
those in patients with known sleep apnea, were excluded.
2. Verification bias in which not everyone had PSG as the comparator.
3. We excluded studies on devices that used other single channel tests, specifically those that
measured only heart rate, heart rate variability, or actigraphy alone.
4. For the second analysis (questionnaires, etc. versus standard testing), We excluded studies
that assessed only single patient characteristics or risk factors.
5. For the second analysis (questionnaires, etc. versus standard testing), We also excluded tests
that were not validated in a group of participants separate from the sample used to develop the
test.
II. Preoperative screening (AHRQ Key Question 3).
Inclusion:
1. all preoperative adult (>16 years) patients, irrespective of the surgery to be performed, as long
as they were scheduled to receive general anesthesia.
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

16
2. assessed any test or predictor of sleep apnea.
3. prospective cross-sectional or longitudinal studies of any follow-up duration.
4. At least 10 study participants had to be analyzed with each test of interest
5. OUTCOME OF INTEREST: We included studies reporting all intraoperative events, surgical
recovery events, surgical recovery time, postsurgical events, length of intensive care or
hospital stay, and intubation or extubation failures.
Exclusion:
1. We excluded studies in which all patients were known to have sleep apnea. There were no
other restrictions based on patient symptoms or existing diagnoses.
III. Predictors of long-term outcomes (AHRQ Key Question 4).
1. We included studies of adults, regardless of health status, who had a baseline sleep study
performed for any reason.
2. Assessed AHI (or similar sleep study measures) together with other potential predictors of
long-term outcomes.
3. longitudinal studies enrolling ≥500 participants with a follow-up ≥1 year
4. report a multivariable analysis
5. OUTCOME OF INTEREST: We included analyses of long-term clinical outcomes of interest,
including all-cause mortality, cardiovascular-death, non-fatal cardiovascular disease, incident
hypertension, quality of life measures, incident stroke, and incident type 2 diabetes mellitus.
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

17
Figure 4. Methodological quality questionnaire.
A. Index Test Quality (3 points)
a. Was diagnostic technique described in sufficient detail to reproduce the procedure?
b. Was the AHI or RDI defined?
c. Were hypopneas defined?
B. Reference Test Quality (1 point)
a. Was confirmatory diagnostic procedure clearly described?
C. Application of Reference Test (2 points)
a. Were both positive and negative results compared to a gold standard?
b. Was the reference test applied consistently within those with and without OSA?
D. Independence of Test Interpretation (1 point)
a. Was there blinding of polysomnography (Reference Test) diagnosis?
E. Clinical Description (3 points)
a. Did the study include complete demographic information as per the following:
i. Were age, gender and BMI of subjects noted?
ii. Was the severity of sleep apnea (either overall or per individual subject)
noted?
b. Were inclusion and exclusion criteria clearly specified and drop-outs noted?
F. Cohort Assembly (4 points)
a. Were subjects enrolled prospectively?
b. Were subjects enrolled consecutively?
c. Did more than 90% of enrolled sample complete the study?
d. Multi-center trial?
G. Sample Size (2 points)
a. Were at least 35 participants with OSA analyzed?
b. Were at least 35 participants without OSA analyzed?
Total Possible Score: 16 points
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

18
Table 1. Studies on AHRQ Key Question 1a – Comparison of Diagnostic Accuracy Between Portable Devices and Polysomnography: Study Characteristics
Author, Year,
Study, Population,
Reference
Study Design/
Population
Num Study
Type
OSA Definition/
Comments
Quality Criteria
Index Test
Quality
Reference Test
Quality
Application of
Reference
Test
Independence
of Test
Interpretation
Clinical
Description
Cohort
Assembly
Sample
Size
Typ
e II
T
yp
e II
I T
yp
e IV
O
xim
etry
- O
DI
Oth
er O
xim
etry
Mea
sure
s
Was
dia
gn
ost
ic t
echn
iqu
e
des
crib
ed i
n s
uff
icie
nt
det
ail
to
rep
rodu
ce t
he
pro
cedu
re?
Was
th
e A
HI
or
RD
I d
efin
ed?
Wer
e h
ypo
pn
eas
def
ined
?
Was
con
firm
ato
ry d
iagno
stic
Pro
cedu
re c
lear
ly d
escr
ibed
?
Wer
e b
oth
po
siti
ve
and
neg
ativ
e
Res
ult
s co
mp
ared
to
a
gold
sta
nd
ard
?
Was
th
e re
fere
nce
tes
t ap
pli
ed
con
sist
entl
y w
ithin
tho
se w
ith
and
wit
hou
t O
SA
?
Was
th
ere
bli
nd
ing
of
poly
som
no
gra
phy
dia
gn
osi
s?
Ag
e, G
ender
Rep
ort
ed
OS
A S
ever
ity
Rep
ort
ed
Incl
usi
on
/Excl
usi
on
Cri
teri
a
Su
bje
cts
enro
lled
pro
spec
tiv
ely?
Su
bje
cts
enro
lled
con
secu
tivel
y?
≥90
% e
nro
lled
com
ple
te
Mult
i-ce
nte
r T
rial
≥35
Par
tici
pan
ts w
ith
OS
A
≥35
Par
tici
pan
ts w
itho
ut
OS
A
Ov
erall
Qu
ali
ty S
core
(0
-16
)
1. Nigro, 2013;
Hospital Aleman,
Buenos Aires,
Argentina
Search Strategy
Group 4
Prospective study of consecutive adult (age ≥18
years) patients referred to a
sleep clinic for possible OSA (snoring with/without apneas
and/or somnolence).
Exclusion criteria: use of oxygen, CPAP or NIPPV
during PSG, inadequate
PSG, <2 hours of recording (July2010 – Jan2011).
Age: 48.2 ±14.5 years Male: 69%
BMI: 30 ±7.2 kg/m2
ESS: NR RDI: 15.1/hr (median, IQR
6.3-34.6)
No OSA (RDI <5): 22% (12/55)
OSA (RDI ≥5/hr): 78% (43/55)
55 ˚ ̊ • ̊ ˚
AHI: NR RDI: sum of apneas,
hypopneas and RERA’s per
hour of sleep Hypopneas: NR; “in
agreement with international
criteria” RERA: NR
OSA: RDI ≥5/hr
Validation: Type I Polysomnography
(Harmonie or MiniPC)
•Type IV Sleep Study -
ApneaLink Ox
•Analyzed automatic vs
manual scoring. Only
manual scoring outcome(2) reported for this report.
• • ˚ • • • • • • • • • • ˚ • ˚ 13
2. Alvarez, 2012;
University of
Valladolid, Valladolid, Spain
Search Strategy
Group 4
Sleep clinic patients with
high clinical suspicion for
OSA undergoing sleep study testing.
Age: 52.3 ±13.7 years Male: 78%
240 ˚ ̊ ˚ • •
AHI: sum of apneas and
hypopneas per hour of sleep
Hypopneas: ≥50% decrease in nasal flow with either a >3%
oxygen desaturation or an
EEG arousal OSA: AHI ≥10/hr
• • • • • • ˚ • ˚ • • • • ˚ • • 13
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

19
BMI: 29.8 ±4.4 kg/m2
ESS: NR AHI: 25.7 ±26.1/hr
No OSA (AHI <10): 33%
(80/240) OSA (AHI ≥10/hr): 67%
(160/240)
Validation: Type I
Polysomnography (Alice 5, Respironics)
•Nonin Puresat pulse oximeter (≤3 sec averaging
signal; sampling rate 1 Hz)
3. Chung, 2012;
University Health Network, Toronto,
ON, Canada
(ref Singh 2013)
Search Strategy
Group 3
Consecutive preoperative
adults (age ≥18 years) scheduled for surgery.
Excluded patients expected
to have abnormal EEG findings (e.g. brain tumors,
epilepsy patients, patients
with deep brain stimulators)
Age: 60.3 ±12.7 years
Male: 54% BMI: 30.5 ±6.8 kg/m2
ESS: NR
AHI: 9.1/hr (median, IQR 3.8-21.4)
No OSA (AHI <5): 36%
(171/475) OSA (AHI ≥5/hr): 64%
(337/475)
25 ˚ ̊ ˚ • ̊
AHI: sum of apneas and
hypopneas per hour of sleep Hypopneas: 30 to 90%
decrease in nasal flow with a
>4% oxygen desaturation OSA: AHI ≥5/hr
Validation: Type II Sleep
Study (Embletta X100)
•PULSOX-300i (Konica
Minolta)
• • • • • • • • • • • • • ˚ • • 15
4. Danzie-Soares,
2012; University of
Sao Paulo Medical
School, Sao Paulo,
Brazil
Search Strategy
Group 3
Consecutive patients with severe CAD age ≥40 years
referred for CABG.
Excluded patients with prior
OSA diagnosis, history of
stroke, severe disability,
clinical instability, decompensated heart failure,
changes in medication within
prior one month or using supplemental oxygen.
Age: 58 ±7 years Male: 76%
BMI: 27.6 ±27.6 kg/m2
ESS: 7 (range 5-11) AHI: 22.9 ±20.0/hr
No OSA (AHI <5): 12.9%
(9/70) OSA (AHI ≥5): 87.1%
(61/70)
70 ˚ • ̊ ˚ ˚
AHI: sum of apneas and hypopneas per hour of sleep
Hypopneas: 50 to 90%
decrease in nasal flow with a
>3% oxygen desaturation
OSA: AHI ≥5/hr
Validation: Type I Polysomnography
•Type III Sleep Study (Stardust II, Respironics)
• • • • • • ˚ • • • • • • ˚ • ˚ 13
5. Ferre, 2012;
Hospital Universitari
Vall d’Hebron,
Consecutive patients referred to a sleep unit for suspected
OSA. Excluded significant
68 • ̊ ˚ ˚ ˚
AHI: sum of apneas and hypopneas per hour of sleep
Hypopneas: ≥50% decrease
• • • • • • • • • • • • • ˚ • ˚ 14
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

20
Barcelona, Spain
Search Strategy
Group 3
comorbidities (dialysis-
dependent renal failure, CHF, severe COPD,
previous stroke or
psychiatric disorder)
Age: 55.9 ±14.5 yrs
Male: 57% BMI: 28.5 ±4.8 kg/m2
ESS: 8.6 ±9.5
AHI: 21.7 ±19.0/hr No OSA (AHI <5): 19%
(13/68)
OSA (AHI ≥5/hr): 81% (55/68)
in nasal flow with either a
≥3% oxygen desaturation or an arousal
OSA: AHI ≥5/hr
Validation: Type I Polysomnography
•Type II Sleep Study (Somte polygraph)
6. Ling, 2012; West
Australian Sleep
Disorders Research Institute, Australia
Search Strategy
Group 3
Sleep disorder clinic patients
referred for diagnostic PSG
between Feb2001 and June2010. Excluded studies
where PAP therapy was
used. If >1 PSG performed, only initial diagnostic PSG
included. Excluded PSG
studies with insufficient oxygen data or in patients
with insufficient data to determine BMI.
Age: 51.2 ±14.0 years Male: 65%
BMI: 32.5 ±9.0 kg/m2
ESS: NR AHI: 31.3 ±29.3/hr
OSA (AHI ≥15): 64%
(7327/11448) No OSA (AHI <15): 36%
(4121/11448)
11,448 ˚ ̊ ˚ • ̊
AHI: “Respiratory events
were scored using Chicago
criteria” Hypopneas: ≥50% decrease
in nasal flow with either a
≥3% oxygen desaturation or an arousal
OSA: AHI ≥5/hr
Validation: Type I Polysomnography
•Integrated pulse oximeter
(Nonin Xpod 3011)
•Provided separate test
diagnostics at various BMI
cut-points
• • • • • • ˚ • • • • • • ˚ • • 14
7. Marcos, 2012;
University of Valladolid,
Valladolid, Spain
Search Strategy
Group 3
Symptomatic patients
(sleepiness, snoring, witnessed apneas) suspected
of sleep apnea. Initial
population randomly divided into training and test sets.
Age: 52.2 ±13.7 years Male: 78%
BMI: 29.8 ±4.5 kg/m2
ESS: NR AHI: 26.4 ±26.7/hr
OSA (AHI ≥5): 80%
144 ˚ ̊ ˚ ˚ •
AHI: “Per rules proposed by
Rechtschaffen and Kales” Hypopneas: NR
OSA: AHI ≥5/hr
Validation: Type I Polysomnography
•Nonin PureSat pulse oximeter
• ˚ ˚ • • • ˚ • • ˚ ˚ ˚ • ˚ • ˚ 8
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

21
(115/144)
No OSA (AHI <5): 20% (29/144)
8. Morales, 2012;
University of
Pennsylvania, Pennsylvania, PA,
USA
Search Strategy
Group 4
Elderly subjects (recruited
from Penn Partners in
Healthy Living, a consumer membership for older adults)
with and without sleepiness
(2001-2005). Recruited an equal number of study
participants for each decile
of the multivariable apnea prediction (MAP)
instrument. Exclusion
criteria: unable to speak
English, cognitive
impairment, alcoholism, use
of sedative hypnotics, medical conditions that
would alter breathing pattern
(e.g. stroke, CHF), prior OSA diagnosis or treatment,
had Cheyne-Stokes or
primary central sleep apnea.
Age: 71.3 ±5.9 years Male: 34%
BMI: 30.5 ±7.6 kg/m2
ESS: NR (30% ESS >10) AHI: NR
OSA (AHI ≥5 & ESS >10):
27% (22/92) No OSA: 73% (70/92)
92 ˚ ̊ • ̊ ˚
AHI: sum of apneas and
hypopneas per hour of sleep
Hypopneas: ≥50% decrease in nasal flow with either a
≥3% oxygen or EEG
arousals OSA: AHI ≥30/hr and ESS
>10
Validation: Type I Polysomnography
(Sandman, Embla)
•Type IV sleep study
(Rescare AutoSet, Resmed)
• • • • • • • • • • • • • ˚ • ˚ 14
9. Morillo, 2012;
Universidad de
Cadiz, Cadiz, Spain
Search Strategy
Group 3
Patients referred to a sleep
clinic for suspected OSA.
Inclusion criteria: age >14 years, medically stable
status. Exclusion criteria:
severe lung disease, severe daytime hypoxemia, known
coronary artery disease,
chronic insomnia, restless legs syndrome or psychiatric
disorder requiring
tranquillizers. First 37 patients formed training set
and remaining 78 patients
made up test set.
Age: 58.3 ±12.5 years
78 ˚ ̊ ˚ • •
AHI: sum of apneas and
hypopneas per hour of sleep
Hypopneas: ≥50% decrease in nasal flow with a ≥4%
oxygen
OSA: AHI ≥5/hr Validation: Type I
Polysomnography
•Jaeger 70750A19 oximeter
• • • • • • ˚ • ˚ • • • • ˚ • ˚ 12
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

22
Male: 74%
BMI: 32.1 ±6.3 kg/m2 ESS: NR
AHI: 28.9 ±28.3/hr
OSA (AHI ≥5): NR No OSA (AHI <5): NR
10. Nigro, 2012;
Hospital Aleman,
Buenos Airesm Argentina
Search Strategy
Group 4
Consecutive patients referred
to sleep clinic for possible
OSA undergoing sleep testing.
Age: 53.7 ±15.4 years Male: 77%
BMI: 27.5 kg/m2(median,
IQR 24.7-31.2)
ESS: NR
AHI: 21.3/hr (median, IQR
8.8-43.5) RDI: 24/hr (median, IQR
11.5-45.3)
OSA (RDI ≥5): 86% (102/119)
No OSA (RDI <5): 14%
(17/119)
119 ˚ ̊ ˚ • ̊
AHI: NR
RDI: sum of apneas,
hypopneas and RERA’s per hour of sleep
Hypopneas: NR; “in
agreement with international criteria”
RERA: NR
OSA: RDI ≥5/hr
Validation: Type I
Polysomnography
(Neurotrace or MiniPC)
•Oximetry (Nonin)
•Combination of ODI and
clinical criteria (ESS and
comorbidity) evaluated simultaneously
• • ˚ • • • • • • • • • • ˚ • ˚ 13
11. O’Brien, 2012;
University of Michigan, Ann
Arbor, MI, USA
Search Strategy
Group 4
Women in third trimester of
pregnancy (≥28 weeks gestation) recruited from an
obstetric clinic.
Age: 30.2 ±7.1 years
Male: 100%
BMI: 31.9 ±3.0 kg/m2 ESS: NR
AHI: 5.4 ±8.5/hr
OSA (AHI ≥5): 26% (8/31) No OSA (AHI <5): 74%
(23/31)
31 ˚ ̊ • ̊ ˚
AHI: sum of apneas and
hypopneas per hour of sleep RDI: Number of respiratory
events (apnea, hypopnea,
and RERA) per hour of
sleep
Hypopneas: ≥50% decrease
in nasal flow with either a ≥3% oxygen desaturation or
EEG arousal
OSA: AHI ≥5/hr Validation: Type II
Polysomnography
(Medpalm)
•WatchPat 200 (Itamar)
• • • • • • • • • • • • • ˚ ˚ ˚ 13
12. Oliveria, 2012;
Universidade Federal
de Sao Paulo, Sao
Paulo, Brazil
Search Strategy
Group 4
Consecutive patients age ≥40 years attending a pulmonary
clinic with diagnosis of
GOLD Class II or III COPD with symptoms suggestive of
OSA (loud snoring, reported
apneas, excessive sleepiness). Exclusion
criteria: COPD exacerbation
26 • ̊ ˚ ˚ ˚
AHI: NR Hypopneas: ≥50% decrease
in nasal flow OR a <50%
reduction in nasal flow associated with either ≥3%
oxygen desaturation or an
EEG arousal OSA: AHI ≥5/hr
Validation: Type I
• ˚ • • • • • • ˚ • • • • ˚ ˚ ˚ 11
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

23
within 3 months, change in
bronchodilator therapy, other sleep-related disorders, prior
diagnosis or treatment for
OSA, severe cardiovascular disorders or neuromuscular
diseases, using oxygen,
psychotropic drugs, alcohol or drugs of abuse.
Age: 62.8 ±8.5 years Male: 50%
BMI: 31.0 ±5.6 kg/m2
ESS: 10.5 ±4.1 AHI: 23.0 ±3.5/hr
OSA (AHI ≥5): NR (90% of
enrolled patients had an AHI ≥5/hr; 41 of these were
excluded from the final
analysis) No OSA (AHI <5): NR
Polysomnography (Embla
N7000)
•Type II Polysomnography
(Stardust II, Philips-Respironics)
•High rate of inadequate portable Type II study
recordings notes (26 out of
67)
13. Onder, 2012;
Istanbul Training and
Research Hospital, Istanbul, Turkey
Search Strategy
Group 4
Sleep clinic patients
complaining of snoring and
apneas undergoing sleep study evaluations. Exclusion
criteria: peripheral vasculopathy, neuropathy,
DM, cardiac arrhythmias,
phalangeal deformity, bilateral cervical and
thoracic sympathectomy,
alpha adrenergic receptor blocker usage.
Age: 43.3 ±12.9 years Male: 64%
BMI: 30.5 ±4.5 kg/m2
ESS: NR AHI: 19.3 ±23.5/hr
OSA: NR
No OSA: NR
59 ˚ ̊ • ̊ ˚
AHI: sum of apneas and
hypopneas per hour of sleep
Hypopneas: ≥30% decrease in nasal flow with a ≥4%
oxygen desaturation OSA: NR
Validation: Type I
Polysomnography
•WatchPat 200 (Itamar)
• • • • • • ˚ • ˚ • • • • ˚ ˚ ˚ 11
14. Sommermeyer,
2012; University of
Gothenburg,
Gothenburg, Sweden
Search Strategy
Group 4
Sleep clinic patients with suspected sleep disordered
breathing recruited from four
sleep labs (Sweden and Germany).
Age: 54.0 ±14.0 years Male: 63%
BMI: 28.5 ±5.9 kg/m2
66 ˚ ̊ ˚ • ̊
AHI: sum of apneas and hypopneas per hour of sleep
Hypopneas: ≥50% decrease
in nasal flow with a ≥3% oxygen desaturation
OSA: AHI ≥5/hr
Validation: Type III Sleep Study (SOMNOcheck2)
• • • • • • ˚ • • • • • • • • ˚ 14
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

24
ESS: 10.0 ±5.0
AHI: 19.3 ±18.5/hr OSA (AHI ≥5): 65% (43/66)
No OSA (AHI <5): 35%
(23/66)
•Oximetry – ODI
automatically scored by either ≥4% SO2 drop or
≥3% SpO2 drop with an
autonomic arousal (pulse rate ≥20% from baseline or
pulse wave amplitude
(PWA) attenuation ≥40% from baseline or PWA
attenuation ≥35% with pulse
rate increase ≥15% from baseline.
15. Ward, 2012;
Royal Brompton
Hospital and Imperial
College, London, UK
Search Strategy
Group 3
Adult (age 18-90 years)
patients with low or
preserved EF heart failure
recruited from outpatient
cardiology clinic. Exclusion
criteria: change in medications preceding 4
weeks, receiving therapy for
SDB. Recruited irrespective of clinical suspicion for
SDB.
Age: 69.8 (median, IQR
58.8-76.8) Male: 86%
BMI: 29.1 kg/m2 (median, IQR
25.4-32.7) ESS: NR
AHI: NR; for SDB 27.0/hr
(median) OSA (AHI ≥15): 45%
(77/171)
No OSA (AHI <15): 56% (96/171)
173 ˚ ̊ ˚ • ̊
AHI: sum of apneas and
hypopneas per hour of sleep
Hypopneas: ≥50% decrease
in nasal flow with either a
≥3% oxygen or EEG arousal
OSA: AHI ≥15/hr Validation: Type II
Polysomnography
•Wrist worn pulse oximeter
• • • • • • ˚ • • • • • • ˚ • • 14
16. Bahammam,
2011; King Saudi
University, Riyadh, Saudi Arabia
Search Strategy
Group 3
Consecutive adult (age 18 to
65 years) patients referred to
a sleep clinic for suspected OSA (based on presence of
loud interrupted snoring,
daytime sleepiness or witnessed apneas. Excluded
patients with COPD,
elevated PaCO2, CHF, neuromuscular diseases and
those on home oxygen or
mechanical ventilation.
Age: 46.3 ±12.6 years
95 ˚ ̊ • ̊ ˚
AHI: sum of apneas and
hypopneas per hour of sleep
Hypopneas: ≥50% decrease in nasal flow with either a
≥3% oxygen desaturation or
EEG arousal OSA: AHI ≥5/hr
Validation: Type I
Polysomnography
•Type IV Sleep Study
(ApneaLink, Resmed)
• • • • • • ˚ • • • • • • ˚ • ˚ 13
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

25
BMI: 34.1 ±7.9 kg/m2
Male:61% ESS:NR
AHI: 39.5 ±30.4/hr
OSA (AHI ≥5): 15% (14/95) No OSA (AHI <5): 85%
(81/95)
17. Batchelder,
2011; Clayton Sleep Institute of
Maplewood, MO;
Sleep Medicine Center of West
Seneca, NY, Sleep
Fit of Broomfield,
CO, USA
Search Strategy
Group 3
Consecutive patients referred
for suspected SDB. Excluded patients if they had
participated in an
investigational drug study within 7 days of enrollment.
Age: 52.7 ±13 years
Male: 61%
BMI:36.0 ±9.6 kg/m2
ESS: NR AHI: NR
OSA: NR
No OSA: NR
104 ˚ ̊ ˚ ˚ •
AHI: NR
Hypopneas: ≥40% decrease in nasal flow with a ≥3%
oxygen desaturation
OSA: AHI ≥5/hr Validation: Type III Sleep
Study
•Pulse oximetry saturation
patterns recognition
algorithm (OxiMax SPD) designed to detect specific
signatures of SpO2 trend
associated with repetitive reductions in airflow (RRiA)
•Respiratory event and not
patient was the unit of analysis
• • • • • ˚ • • ˚ • • • • • ˚ ˚ 12
18. Bohning, 2011;
Karl-Hansen-Klinik, Bad Lippspringe,
Germany
Search Strategy
Group 4
Consecutive sleep clinic
patients (Jan2007-Sept2007). Exclusion criteria: dementia,
intolerance of pulse-
oximetry, severe
neurological conditions,
severe endocrinological
disorders.
Age: 55 ±13 years
Male: 82% BMI:31.6 ±5.9 kg/m2
ESS: NR
AHI: NR OSA: 87% (117/135)
No OSA: 13% (18/135)
135 ˚ ̊ ˚ • ̊
AHI: NR
Hypopneas: NR OSA: AHI ≥5/hr
Validation: Type I
Polysomnography
•Oximetry: ODI (undefined)
˚ ˚ ˚ ˚ • • ˚ • ˚ • • • • ˚ • ˚ 8
19. Bruyneel, 2011;
Saint-Pierre Hospital,
Brussels, Belgium
Search Strategy
Group 4
Consecutive adult (age ≥18 years) sleep clinic patients
with suspected OSA (all
complained of snoring and daytime sleepiness or had ≥2
other OSA symptoms).
Exclusion criteria: prior PSG, restrictive respiratory
diseases, distance >30 miles
66 • ̊ ˚ ˚ ˚
AHI: sum of apneas and hypopneas per hour of sleep
Hypopneas: ≥50% decrease
in nasal flow with either a ≥3% oxygen desaturation or
EEG arousal
OSA: AHI ≥5/hr Validation: Type I
Polysomnography (Medatec)
• • • • • • ˚ • • • • • • ˚ • ˚ 13
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

26
from sleep clinic.
Age: 48.9 ±12.1 years
Male: 59%
BMI: 30.5 ±7.3 kg/m2 ESS: NR
AHI: 26.4 ±30/hr
OSA (AHI ≥5): 81% (50/66) No OSA (AHI <5): 19%
(16/66)
•Type II device (Pamela V 3.631, Medatec)
20. Campbell, 2011;
Otago University Wellington,
Wellington, New
Zealand
Search Strategy
Group 4
Consecutive adult (Age >18
years) sleep clinic patients with suspected OSA
undergoing PSG. Exclusion
criteria: significant
psychiatric or cardiovascular
morbidity, limited mobility
or referred for an alternative sleep disorder.
Age: 49.1 ±13.8 years Male: 80%
BMI: 31.0 ±6.1 kg/m2
ESS: NR AHI: 34.5 ±29.0/hr
OSA (AHI ≥5): 80% (24/30) No OSA (AHI <5): 20%
(6/30)
30 • ̊ ˚ ˚ ˚
AHI: sum of apneas and
hypopneas per hour of sleep Hypopneas: A visible
decrease in nasal flow and
either a ≥3% oxygen
desaturation or an EEG
arousal
OSA: AHI ≥5/hr Validation: Type I
Polysomnogram (S=series,
Compumedics)
•Type II Sleep Study (Siesta
System, Compumedics)
• • • • • • ˚ • • • • • • ˚ ˚ ˚ 12
21. Chai-Coetzer,
2011; Repatriation
General Hospital and
Flinders Medical
Centre, South Australia
Search Strategy
Group 3
Adult patients (age 25-70
years) attending six primary
care clinics were recruited
(June2007-April2008).
Exclusion criteria: pregnancy, significant
cognitive impairment, poorly
controlled psychiatric disorder or prior OSA
treatment
Age: 55 years (range 45-62)
Male:53%
BMI: 31.7 kg/m2 (range 28.8-36.1)
ESS: 8 (range 4-10)
AHI: 26.9/hr (range 13.1-41.3)
OSA (AHI ≥30): 39%
(31/77) No OSA (AHI <30): 61%
(46/77)
77 ˚ ̊ • • ̊
AHI: NR
Hypopneas: Either ≥50%
decrease in nasal flow and
either a ≥3% oxygen
desaturation or an EEG arousal
OSA: AHI ≥30/hr
Validation: Type I Polysomnogram
•Type IV Sleep Study
(ApneaLink, Resmed)
•ODI (3%)
• • • • • • ˚ • ˚ • • • • ˚ • ˚ 12
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

27
22. Cheliout-Heraut,
2011; Versailles-Saint-Quentin
University, Garches
Hospital, Garches, France
Search Strategy
Group 4
Patients with suspected OSA
based on daytime sleepiness and snoring. Exclusion
criteria: neurologic disorders,
parasomnias, RLS, PLM’s, severe respiratory disorder or
recent medication use
(dopamine agonists, benzodiazepines, opioids,
substance of abuse including
alcohol).
Age: 55.4 ±8.7 years
BMI: NR Male: 67%
ESS: NR
AHI: NR OSA (AHI ≥5/hr): 92%
(83/90)
No OSA (AHI <5/hr): 8% (7/90)
90 ˚ • ̊ ˚ ˚
AHI: sum of apneas and
hypopneas per hour of sleep Hypopneas: either ≥50%
decrease in nasal flow OR
≥30 decrease in nasal flow and either a ≥3% oxygen
desaturation or an EEG
arousal OSA: AHI ≥5/hr
Validation: Type 1
Polysomnography (Embla)
• Type III portable study (Somnolter device, Nomics)
• • • • • • ˚ ˚ • • • • • ˚ • ˚ 12
23. Chouchou, 2011;
Universite Claude
Bernard, Lyon, France
Search Strategy
Group 4
Subjects enrolled in the
PROOF study (a prospective,
observational, population cohort study assessing
Prognostic indicator of cardiovascular and
cerebrovascular events;
inclusion age ≥65 years; exclusion cardiovascular and
general morbidity) were
enrolled into the SYNAPSE (Systeme Nerveux
Autonome – Physiologie –
Sommeil -Epidemiologie) study
Age: 65.8 ±1.1years Male: 43%
BMI: 25.4 ±4.0 kg/m2
ESS: 5.5 ±3.4 AHI: NR
OSA (AHI ≥5/hr): 91%
(710/780)
No OSA (AHI <5/hr): 9%
(70/780)
780 ˚ ̊ • ̊ ˚
AHI: sum of apneas and
hypopneas per hour of sleep
Hypopneas: ≥50% decrease in nasal flow and a ≥3%
oxygen desaturation OSA: AHI ≥15/hr
Validation: Type 3 Sleep
Study (HypnoPTT, Tyco Healthcare)
•Pulse Transit Time (PTT)
measured on the Type III
sleep study and an autonomic activation index
(AAI) was obtained using
the manufacturer’s analysis software.
• • • • • • • • ˚ • • • • ˚ • • 14
24. Driver, 2011;
Kingston General Hospital and Queen’s
University, Kingston,
Patients referred to a sleep
lab for diagnostic sleep testing. Exclusion criteria:
high-care needs, known
73 ˚ • ̊ ˚ ˚
AHI: sum of apneas and
hypopneas per hour of sleep Hypopneas: 50 to 90%
decrease in nasal flow and a
• • • • • • • • • • • • • ˚ • ˚ 14
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

28
Ontario, Canada
Search Strategy
Group 4
hypercapnia or
hypoventilation
Age: 52.9 ±12.2 years
BMI: 32.2 ±6.8 kg/m2 Male: 41%
ESS: NR
AHI: 26.0 ±25.9/hr OSA (AHI ≥5/hr): 84%
(61/73)
No OSA (AHI <5/hr): 16% (12/73)
≥3% oxygen desaturation
AND an EEG arousal OSA: AHI ≥5/hr
Validation: Type I
Polysomnogram
•Type III portable study (MediByte)
25. Gjevre, 2011;
University of
Saskatchewan,
Saskatoon,
Saskatchewan,
Canada
Search Strategy
Group 4
Consecutive adult (age 21 to
70 years) women scheduled
for routine PSG to evaluate
clinically suspected OSA.
Exclusion criteria: strong
suspicion for another primary sleep disorder (e.g.
insomnia, narcolepsy, RLS,
parasomnia, nocturnal seizures), regular shift work,
lung disease CHF, unstable
angina, CVA or pregnancy in prior 6 months,
neuromuscular disease, renal failure.
Age: 52 ±11.0 years Male: 100%
BMI: 34.9 ±9.0 kg/m2
ESS: 9.6 ±4.4 AHI: 15.1 ±16.3/hr
OSA (AHI ≥5/hr): 68%
(32/47) No OSA (AHI <5/hr): 32%
(15/47)
47 ˚ • ̊ ˚ ˚
AHI: sum of apneas and
hypopneas per hour of sleep
Hypopneas: ≥50% decrease
in nasal flow and a ≥3%
oxygen desaturation
OSA: AHI ≥5/hr Validation: Type I
Polysomnogram
•Type III portable study
(Embletta 2601-1)
• • • • • • ˚ • • • • • • ˚ ˚ ˚ 12
26. Hedner, 2011;
Sahlgrenska University Hospital
Gothenburg, Sweden;
Brigham and Women’s Hospital
and Harvard Medical
School, Boston, MA , USA; Israel Institute
of Technology, Haifa,
Israel
Search Strategy
Multi-center study cohort
consisting of 139 sleep clinic patients referred for
suspected OSA, 17 normal
volunteers and 71 subjects randomly drawn from a
population study undergoing
ambulatory PSG studies in the evaluation between OSA
and hypertension.
Age: 49 ±14 years
BMI: 29 ±6 kg/m2
227 ˚ ̊ • ̊ ˚
RDI: Number of respiratory
events (apnea, hypopnea, and RERA) per hour of
sleep
Hypopneas: NR OSA: RDI ≥10/hr
Validation: Type I
Polysomnogram
•WatchPat 100 (Itamar)
• • ˚ • • • ˚ ˚ • • • ˚ • • • • 11
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

29
Group 3 Male: NR
ESS: NR RDI: 30 ±23/hr
OSA (RDI ≥10/hr):83%
(189/227) No OSA (RDI <10/hr): 17%
(38/227)
27. Marcos, 2011;
University of Valladolid,
Valladolid, Spain
Search Strategy
Group 3
Subjects suspected of OSA
due to daytime sleepiness, loud snoring or reported
apnea events.
Age: 52.4 ±13.8 years
Male: 77%
BMI: 29.8 ±4.2 kg/m2
ESS: NR
AHI: 24.8 ±25.2/hr
OSA (AHI ≥10/hr): 67% (64/96)
No OSA (AHI <10/hr): 33%
(32/96)
96 ˚ ̊ ˚ ˚ •
AHI: “According to the
rules proposed by Rechtschaffen and Kales”
Hypopneas: NR
OSA: AHI ≥10/hr Validation: Type I
Polysomnogram
•Nonin PurseSat pulse
oximeter
• ˚ ˚ • • • ˚ • • • • ˚ • ˚ • ˚ 10
28. Masa, 2011;
CIBER de
Enfermedades Respiratorias, Madrid
Spain
Search Strategy
Group 4
*Two published
papers in 2011 on same population*
Patients with suspected OSA
(snoring, observed apneas,
ESS>10, morning tiredness, no other suspected sleep
disorders) age 18 to 70 were
recruited from eight sleep centers in Spain (Dec2008-
Dec2009). Exclusion criteria:
unstable heart disease.
Age: 48.7 ±11.8 years
Male: 76% BMI: 31.0 ±6.6kg/m2
ESS: 11.6 ±5
AHI: 38.3 ±28.5/hr OSA: 90% (313/348)
No OSA: 10% (35/348)
348 ˚ • ̊ ˚ ˚
AHI: sum of apneas and
hypopneas per hour of sleep
Hypopneas: ≥30% decrease in airflow and either ≥3%
oxygen desaturation or an
EEG arousal OSA: AHI ≥5/hr
Validation: Type I
Polysomnogram
•Type III sleep study
(BreastSC20 or Breat Medial AB)
• • • • • • ˚ • • • • • • • • • 15
29. Nigro, 2011;
Hospital Aleman,
Buenos Aires,
Argentina
Search Strategy
Group 4
*Two published
papers 2012 and 2011 on same population*
Prospective study of consecutive adult (age ≥18
years) patients referred to
sleep clinic for possible OSA (snoring with or without
apneas and/or somnolence).
Exclusion criteria: use of oxygen, CPAP, noninvasive
PAP during PSG;
uninterruptable PSG, recording time <2 hours
(Mar 2008-Nov 2008).
90 ˚ ̊ • ̊ ˚
AHI: sum of apneas and hypopneas per hour of sleep
RDI: sum of apneas,
hypopneas and RERA’s per hour of sleep
Hypopneas: NR; “In
agreement with international criteria”
OSA: RDI ≥5/hr
Validation: Type I Polysomnogram (BiOPC or
NEUROTRACE)
• • ˚ • • • ˚ • • • • • • ˚ • ˚ 12
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

30
Age: 49.6 ±15.1 years Male: 77%
BMI: 29.3 kg/m2 (median,
IQR 25.2-32.5) ESS: NR
AHI: 11.8/hr (median; IQR
5.8-32.3) RDI: 13.9/hr (median, IQR
7-34.1)
OSA (RDI ≥5): 83% (75/90) No OSA (RDI <5): 27%
(15/90)
•Type IV sleep study (ApneaLink, Resmed)
•evaluated auto vs manual scoring
30. Yang, 2011;
Buddhist Tzu Chi
General Hospital,
Hualien, Taiwan
Search Strategy
Group 4
Cross-sectional study of
adult Chinese sleep clinic
patients (Feb2007-Dec2007).
Exclusion: diagnosis of
narcolepsy, central sleep apnea, non-Asians, age <18,
chronic pulmonary and heart
disease.
Age: 50.3 ±14.8 years
Male: 70% BMI: 26.8 ±5.7 kg/m2
ESS: 8.0 ±4.6 AHI: 18.5 ±19.7/hr
OSA (AHI ≥5): 63% (54/86)
No OSA (AHI <5): 37% (32/86)
86 ˚ ̊ • ̊ ˚
AHI: sum of apneas and
hypopneas per hour of sleep
Hypopneas: ≥50% decrease
in airflow and either ≥4%
oxygen desaturation or an EEG arousal
OSA: AHI ≥5/hr
Validation: Type I Polysomnogram (Embla
A10)
•Type IV sleep study
(Oximetry and RIP-derived X-flow)
• • • • • • ˚ • • • • • • ˚ • ˚ 13
31. Alvarez, 2010;
University of
Valladolid, Valladolid, Spain
Two references
Search Strategy
Group 3
Subjects suspected of OSA
due to daytime sleepiness,
loud snoring, nocturnal choking and awakenings or
reported apnea events.
Age: 52.9 ±14.1 years
Male: 78%
BMI: 29.8 ±5.6 kg/m2 ESS: NR
AHI: 29.0 ±28.5/hr
OSA (AHI ≥10/hr): 68% (100/148)
No OSA (AHI <10/hr): 32%
(48/148)
148 ˚ ̊ • • •
AHI: sum of apneas and
hypopneas per hour of sleep
Hypopneas: ≥50% decrease in airflow and either ≥3%
oxygen desaturation or an
EEG arousal OSA: AHI ≥10/hr
Validation: Type I
Polysomnogram
•Type IV sleep study (Single
channel airflow and Oximetry)
•Oximetry
• • • • • • ˚ • • • • ˚ • ˚ • • 13
32. Nigro, 2010;
Hospital Aleman,
Buenos Aires, Argentina
Consecutive adult (age ≥18
years) sleep clinic patients
with suspected OSA (July 2007-Nov2007). Exclusion
criteria: use of supplemental
66 ˚ ̊ • ̊ ˚
AHI: sum of apneas and
hypopneas per hour of sleep
RDI: sum of apneas, hypopneas and RERA’s per
hour of sleep
• • • • • • ˚ • • • • • • ˚ • ˚ 13
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

31
Search Strategy
Group 4
oxygen or CPAP or other
modality of noninvasive positive airway pressure
during the PSG, inadequate
sleep studies.
Age: 51.6 ±14.1 years
Male: 71% BMI: 29.3 ±5.4 kg/m2
ESS: NR
AHI: 9.5/hr (median, IQR 4.1-34.1)
RDI: 10.6/hr (median, IQR
5.4-34.1) OSA (RDI ≥5): 77% (51/66)
No OSA (RDI <5): 23%
(15/66)
Hypopneas: Discernible
decrease in airflow and either ≥3% oxygen
RERA: an EEG arousal
associated with an alteration of the inspiratory contour in
the waves from the
thoracoabdominal bands OSA: RDI ≥5/hr
Validation: Type I
Polysomnogram (BIOPC or NEUROTRACE, Akonic)
•Type IV sleep study (ApneaLink, Resmed)
33. Yadollahi, 2010;
University of
Manitoba, Winnipeg,
MB, Canada
Search Strategy
Group 4
Sleep clinic patients undergoing in-lab PSG were
recruited.
Age: 51.4 ±11.9 years
Male: 71%
BMI: 31.9 ±6.4 kg/m2 ESS: NR
AHI: 23.6 ±30.3/hr OSA: NR
No OSA: NR
66 ˚ ̊ • ̊ ˚
AHI: sum of apneas and hypopneas per hour of sleep
Hypopneas: NR
OSA: AHI ≥5/hr Validation: Type I
Polysomnogram
•Type IV sleep study
(Oximetry and tracheal sound signals)
• • ˚ ˚ • • ˚ • ˚ • • • • ˚ ˚ ˚ 10
* Abbreviations: ˚ (No), • (Yes), afib (atrial fibrillation), AHI (apnea-hypopnea index), AASM (American Academy of Sleep Medicine), ASA (American Society of Anesthesiologists), BMI (body mass index), BQ (Berlin
questionnaire), CABG (coronary artery bypass graft), CAD (coronary artery disease), CHF (congestive heart failure), COPD (chronic obstructive pulmonary disease), CPAP (continuous positive airway pressure), CSA (central
sleep apnea), CV (cardiovascular), DM (diabetes mellitus), ECG (electrocardiograph), EEG (electroencephalographic arousal), EF (ejection fraction), ESS (Epworth sleepiness scale), FOSQ (functional outcomes sleep questionnaire), GFR (glomerular filtration rate), GOLD (global initiative for COPD), hr (hour), IIH (idiopathic intracranial hypertension), IQR (interquartile range), NA (not applicable), NIPPV (noninvasive positive airway
pressure), NR (not reported), Num (number), MAPI (multivariate apnea prediction index), MI (myocardial infarction), ODI (oxygen desaturation index), OSA (obstructive sleep apnea), PaCO2 (arterial partial pressure of
carbon dioxide), PAP (positive airway pressure), PLMS (periodic limb movements of sleep), PSG (polysomnography), RERA (respiratory effort related arousal), RDI (respiratory disturbance index), RLS (restless legs syndrome), SDB (sleep disordered breathing), VA (veterans administration)
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

32
Table 2. Studies on AHRQ Key Question 1a – Comparison of Outcomes Other Than Diagnostic Accuracy Between Portable Devices and Polysomnography: Study
Characteristics
Author, Year,
Study, Reference
Study Design Num Population OSA Definition/
Comments
Outcome(s)
1. Andreu, 2012;
Hospital of Sant
Joan d’Alacant,
Madrid, Spain
Search Strategy
Group 4
Sleep clinic patients referred for high level of
clinical OSA suspicion (ESS ≥12 and Sleep
Apnoea Clinical Score (SACS) ≥15. Exclusion
criteria: impaired lung function (COPD,
obesity-hypoventilation, restrictive disorders),
associated pathologies (psychiatric disorders,
neoplasms, RLS, other dyssomnias or
parasomnias), prior CPAP therapy. Patients
were randomized into three
diagnostic/treatment groups: 1) Portable sleep
study with home follow-up with a sleep unit
nurse (at 1, 3 and 6 months); 2) Portable sleep
study with hospital follow-up with a sleep
pulmonologist (at 1, 3 and 6 months); or 3) In-
lab polysomnography with hospital follow-up
with a sleep pulmonologist (at 1, 3 and 6
months). CPAP pressure was chosen via a
prediction formula and was not changed
during follow-up. Study was planned/powered
as a non-inferiority trial.
Primary Outcomes measured: CPAP
compliance at 6-months.
Secondary Outcomes measured: daytime
sleepiness (ESS), quality of life (FOSQ),
symptoms and cost per patient.
65 Age: 52 ±10 years
Male: 83%
BMI: 34 ±7 kg/m2
ESS: 15 ±3
AHI: 43 ±20/hr
No OSA (AHI <15/hr):
0% (0/65)
OSA (AHI ≥15/hr):
100% (65/65)
•Severe (AHI ≥30):
69% (45/65)
AHI: NR
Hypopneas: Not
defined
OSA: AHI ≥15/hr
•Type I
Polysomnogram
(Somnostar Alpha
41000,
SensorMedics)
•Type 3 sleep study
(Stardust polygraph,
Phillips Respironics)
•At 6-months, CPAP compliance (% used at least
4hr/night for 70% of days) was similar between each
treatment group (73% vs 68% vs 57%, p>0.05). At 6-
months, no statistically significant difference in ESS,
global FOSQ score, FOSQ activity score or FOSQ
symptoms score was noted between the three
treatment groups. The most expensive strategy was
group 2 (in-lab PSG with pulmonologist follow-up;
849 Euros) followed by group 3 (portable sleep study
with pulmonologist follow-up; 644 Euros) with the
least expensive being group 1 (portable sleep study
with home nurse follow-up; 590 Euros; ANOVA
p<0.001; direct comparison Group 1 and 3, p<0.05).
•Author’s conclusions: Patients with a high clinical
OSA probability can be diagnosed and treated in a
home setting with a high level of CPAP compliance
and lower costs than using either a hospital-based
approach or home RP/hospital follow-up.
2. Kuna, 2011;
Philadelphia VA
Medical Center,
Philadelphia, PA,
USA
Search Strategy
Consecutive patients referred to the
Philadelphia VA Medical Center and Veterans
Affairs Pittsburgh Healthcare System
(multicenter) with suspected OSA were
randomized to either ambulatory
management using a portable monitor (n=148)
or standard in-laboratory testing (n=148).
296 Age: 53.5 ±10.5 years
Male: 95%
BMI: 34.6 ±6.5 kg/m2
ESS: 12.4 ±5.2
AHI: 45.1 ±26.5/hr
No OSA (AHI <15/hr):
9% (26/296)
AHI: NR
Hypopneas: Not
defined
OSA: AHI ≥15/hr
•Type I
Polysomnogram
•No clinical or statistically significant difference in
CPAP adherence (3.5 ±2.5 hours/day vs 2.9 ±2.3
hours/day; p=0.08) between home group vs in-
laboratory group. A statistically significant
improvement in functional outcomes in both the home
group (mean FOSQ improvement 1.74 ±2.81;
p<0.001) and the in-laboratory groups (mean FOSQ
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

33
Group 4
Home testing pathway involved a type 3
portable diagnostic sleep study with
individuals with an AHI ≥15/hr started on
home autoCPAP for 4 to 5 days with CPAP
pressure selected based on pressure spent 90%
of time resulting in an AHI <10/hr. Patients
with an AHI <15/hr on home study underwent
in in-lab PSG for confirmation.
In-laboratory testing pathway involved in-
lab polysomnography with individuals with an
AHI ≥15/hr undergoing in-lab CPAP titration
per “recommended” guidelines and CPAP
prescribed at the lowest pressure associated
with an AHI <10/hr.
Primary Outcomes measured: functional
outcomes (FOSQ score) and CPAP treatment
adherence at 3-months.
OSA (AHI ≥15/hr): 91%
(270/296)
•Mild: NR
•Moderate: NR
•Severe: NR
•Type 3 sleep study
(Embletta, Embla)
improvement to 1.85 ±2.46; p<0.001). Similar
improvements in ESS (-2.6 ±5.2 vs -2.9 ±4.4),
psychomotor vigilance task, SF-12 and Center fir
Epidemiologic Studies Depression Scale (CES-D)
were observed between both testing pathways. Mean
percentage of days CPAP used at least 4 hours/day
was 52 ±34% in home tested group vs 49 ±35% in the
in-laboratory tested group (p= 0.42). The mean
residual AHI on CPAP downloads was 4.3 ±3.4/hr in
the home tested group and 4.7 ±3.5/hr in the in-
laboratory tested group (p=0.51)
•Lower bound of the one-sided 95% noninferiority CI
was -0.54 for the FOSQ and 0.03 for the CPAP
adherence.
•Author’s conclusions: Functional outcomes and
treatment adherence in patients evaluated according to
a home testing algorithm is not clinically inferior to
that in patients receiving standard in-laboratory
polysomnography.
3. Masa, 2011;
CIBER de
Enfermedades
Respiratorias,
Madrid Spain
Search Strategy
Group 4
Patients with suspected OSA (snoring,
observed apneas, ESS>10, morning tiredness,
no other suspected sleep disorders) age 18 to
70 were recruited from eight sleep centers in
Spain (Dec2008-Dec2009). Exclusion criteria:
unstable heart disease. All patients underwent
in-lab PSG and home-testing in random order
(within 3 days of each other) with tests scored
separately by blinded technicians. Authors
performed a masked post hoc analysis to
ascertain the agreement in therapeutic
decision-making between in-lab PSG and
home testing. Therapeutic decisions (CPAP,
no CPAP, impossible decision) were made by
a researcher in a random order (each patient
presented twice with either PSG or home
based testing information) blinded to
participant identification or other data. CPAP
recommendations based on AASM criteria:
348 Age: 48.7 ±11.8 years
Male: 76%
BMI: 31.0 ±6.6kg/m2
ESS: 11.6 ±5
AHI: 38.3 ±28.5/hr
No OSA (AHI <5/hr) 9%
(33/348)
OSA (AHI ≥5/hr): 91%
(315/348)
•Mild (AHI 5-15):
37% (129/315)
•Moderate (AHI 15-
30): 12% (42/215)
•Severe (AHI≥30):
41% (144/315)
AHI: sum of apneas
and hypopneas per
hour of sleep
Hypopneas: ≥30%
decrease in airflow
and either ≥3%
oxygen desaturation
or an EEG arousal
OSA: AHI ≥5/hr
Validation: Type I
Polysomnogram
\•Type 3 sleep study
(BreastSC20 or Breat
Medial AB)
•Therapeutic decision using home based testing had a
sensitivity of 77%, a specificity of 77% and accuracy
of 76%. Patients with more severe OSA (AHI ≥30/hr)
had a sensitivity of 94% and specificity 44% and
accuracy of 91% with home based testing.
•Author’s conclusions: Home-based therapeutic
decision was adequate when AHI was high, but
deficient in the large population in patients with mild
to moderate AHI.
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

34
AHI (on either in-lab PSG or home sleep
study) ≥15/hr or AHI ≥5 with significant
symptoms or consequences.
Primary Outcomes measured: determine
agreement between home sleep testing and in-
hospital PSG for therapeutic decision making
in a large sample.
* Abbreviations: O
(No), • (Yes), afib (atrial fibrillation), AHI (apnea-hypopnea index), AASM (American Academy of Sleep Medicine), ASA (American Society of
Anesthesiologists), BMI (body mass index), BQ (Berlin questionnaire), CABG (coronary artery bypass graft), CAD (coronary artery disease), CHF (congestive heart failure),
COPD (chronic obstructive pulmonary disease), CPAP (continuous positive airway pressure), CSA (central sleep apnea), CV (cardiovascular), DM (diabetes mellitus), ECG
(electrocardiograph), EEG (electroencephalographic arousal), EF (ejection fraction), ESS (Epworth sleepiness scale), FOSQ (functional outcomes sleep questionnaire), GFR
(glomerular filtration rate), GOLD (global initiative for COPD), hr (hour), IIH (idiopathic intracranial hypertension), IQR (interquartile range), NA (not applicable), NIPPV
(noninvasive positive airway pressure), NR (not reported), Num (number), MAPI (multivariate apnea prediction index), MI (myocardial infarction), ODI (oxygen desaturation
index), OSA (obstructive sleep apnea), PaCO2 (arterial partial pressure of carbon dioxide), PAP (positive airway pressure), PLMS (periodic limb movements of sleep), PSG
(polysomnography), RERA (respiratory effort related arousal), RDI (respiratory disturbance index), RLS (restless legs syndrome), SDB (sleep disordered breathing), VA (veterans
administration)
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

35
Table 3. Studies on AHRQ Key Question 1b – Comparison of Diagnostic Accuracy Between Questionnaires and Polysomnography: Study Characteristics
Author, Year,
Study, Reference
Study Design/
Population
Num Study
Type
OSA Definition/
Comments
Quality Criteria
Index Test
Quality
Reference Test
Quality
Application of
Reference
Test
Independence
of Test
Interpretation
Clinical
Description
Cohort
Assembly
Sample
Size
Ber
lin Q
ues
tionn
aire
E
pw
ort
h S
leep
ines
s S
cale
M
ult
ivar
iate
Apn
ea P
red
icti
on
S
TO
P-B
AN
G
Oth
er
Was
dia
gn
ost
ic t
echn
iqu
e
des
crib
ed i
n s
uff
icie
nt
det
ail
to
rep
rodu
ce t
he
pro
cedu
re?
Was
th
e A
HI
or
RD
I d
efin
ed?
Wer
e h
ypo
pn
eas
def
ined
?
Was
con
firm
ato
ry d
iagno
stic
Pro
cedu
re c
lear
ly d
escr
ibed
?
Wer
e b
oth
po
siti
ve
and
neg
ativ
e
Res
ult
s co
mp
ared
to
a
gold
sta
nd
ard
?
Was
th
e re
fere
nce
tes
t ap
pli
ed
con
sist
entl
y w
ithin
tho
se w
ith
and
wit
hou
t O
SA
?
Was
th
ere
bli
nd
ing
of
poly
som
no
gra
phy
dia
gn
osi
s?
Ag
e, G
ender
, B
MI,
AH
I R
epo
rted
OS
A S
ever
ity
Rep
ort
ed
Incl
usi
on
/Excl
usi
on
Cri
teri
a
Su
bje
cts
enro
lled
pro
spec
tiv
ely?
Su
bje
cts
enro
lled
con
secu
tivel
y?
≥90
% e
nro
lled
com
ple
te
Mult
i-ce
nte
r T
rial
≥35
Par
tici
pan
ts w
ith
OS
A
≥35
Par
tici
pan
ts w
itho
ut
OS
A
Ov
erall
Qu
ali
ty S
core
(0
-16
)
1. Geiger-Brown,
2013; University of Maryland School of
Medicine, Maryland,
USA
Search Strategy
Group 3
Chronically partially sleep-
deprived shift-work registered nurses.
Age: 40 ±13 years Male: 0%
BMI: NR
ESS: NR AHI: 2.3 ±5.4/hr
OSA (AHI ≥5): 14% (3/21)
No OSA (AHI<5): 86% (17/21)
21 • ̊ ˚ ˚ ˚
RDI: sum of apneas,
hypopneas and RERA’s per hour of sleep
AHI: sum of apneas and
hypopneas per hour of sleep Hypopneas: 50 to 90%
decrease in nasal flow with a
>4% oxygen desaturation RERA’s: 30 to 90%
decrease in nasal flow with a
>3% oxygen desaturation OSA: AHI ≥5/hr
Validation: Type I
Polysomnography
• • • • • • ˚ ˚ • • • ˚ • ˚ ˚ ˚ 10
2. Sharkey, 2013;
Rhode Island
Hospital and Alpert Medical School of
Brown University,
Providence, RI, USA
Search Strategy
Group 4
Patients evaluated for bariatric
surgery (Jan 2003-Dec2005).
Retrospective chart review. Excluded patients who did not
complete PSG or ESS/FOSQ.
Age: 42.0 ±9.5 years
Male: 11%
BMI: 50.2 ±7.7 kg/m2 ESS: 6.3 ±4.8
AHI: 29.5 ±31.5/hr
OSA (AHI ≥15): 58% (157/269)
No OSA (AHI <15): 42%
(112/269)
269 ˚ • ̊ ˚ •
AHI: sum of apneas and
hypopneas per hour of sleep
Hypopneas: ≥50% decrease in nasal flow with a >3%
oxygen desaturation
OSA: AHI ≥15/hr Validation: Type I
Polysomnography
•Other: Functional
Outcomes of Sleep
Questionnaire (FOSQ)
• • • • • • ˚ • • • ˚ • • ˚ • • 13
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

36
3. Vana, 2013;
Arizona State University, Phoenix,
AZ, USA
Search Strategy
Group 4
Consecutive new adult (age
≥18 years) patients referred to clinic for sleep evaluations.
Exclusion criteria: prior
diagnosis of OSA, health conditions that could affect
EEG tracings and sleep
staging (e.g. dementia, severe brain injuries, developmental
delay or stimulant use).
Age: 46.4 ±13.2 years
Male: 34%
BMI: 36.3 ±9.2 kg/m2 ESS: 8.0 (median, range 0-24)
AHI: 8.9/hr (median, range 0 -
99.9) OSA (AHI ≥5): 68% (32/47)
No OSA (AHI <5): 32%
(15/47)
47 ˚ • ̊ • •
AHI: sum of apneas and
hypopneas per hour of sleep Hypopneas: ≥30% decrease
in nasal flow with a ≥4%
oxygen desaturation OSA: AHI ≥5/hr
Validation: Type I
Polysomnography (diagnostic or split-night
protocols)
•Other: Combination of high
risk on STOP-BANG or
ESS >10
•Evaluated STOP-BANG
using various BMI cut-points: BMI >30, BMI >35
• • • • • • ˚ • • • • • • ˚ ˚ ˚ 12
4. Albuquerque,
2012; Mayo Clinic
Center, Rochester,
MN, USA
Search Strategy
Group 4
Prospective study of Afib patients referred for direct
current cardioversion
treatment.
Age: 69.1 ±11 years Male: 76%
BMI: 34.1 ±8.6 kg/m2
ESS: 8.9 ±4.4 AHI: 23.1 ±22.6/hr
SDB (AHI ≥5): 78%
(118/151) No SDB (AHI <5): 22%
(33/151)
(Pure OSA: 57%, Pure CSA: 10.6%, Mixed sleep apnea:
18.6%)
151 ˚ • ̊ ˚ ˚
AHI: sum of apneas and hypopneas per hour of sleep
Hypopneas: 50 to 90%
decrease in nasal flow with a ≥4% oxygen
OSA: AHI ≥5/hr (obstructive events)
SDB: AHI ≥5/hr
(obstructive, central or mixed events)
• • • • • • ˚ • • • • • • ˚ • ˚ 13
5. Asha’ari, 2012;
Beserah Health Polyclinic, Kuantan,
Pahang, Malaysia
Search Strategy
Group 4
Adult (age 18 to 40) patients
recruited into a case-control study to assess the
association of OSA and HTN
in a younger population. Exclusion criteria:
pregnancy, unstable or
decompensated cardiorespiratory disease,
airway cancer, recent upper
respiratory tract surgery, prior OSA treatment,
inadequate/uninterpretable
240 ˚ • ̊ ˚ ˚
AHI: not reported
Hypopneas: “according to the AASM 2007 guidelines”
OSA: AHI ≥5/hr
Validation: Type I Polysomnography
•provides outcome data separately for hypertensive
and nonhypertensive
participants
• • • • • • ˚ • • • • • • ˚ • • 14
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

37
sleep study.
Age: 26.7 ±6.2 years
Male: 72%
BMI: 30.8 ±7.5 kg/m2 ESS: NR (32% ESS ≥10)
AHI: 25.9 ±4.5/hour
OSA (AHI ≥5): 68% (162/240)
No OSA (AHI <5): 33%
(78/240)
6. Chung, 2012;
University of
Toronto, Toronto,
ON, Canada
Search Strategy
Group 4
Adult (age ≥18 years) patients scheduled for
elective surgery attending
preoperative clinic at two
hospitals (Toronto Western
Hospital and Mount Sinai
Hospital). Exclusion criteria: expected abnormal EEG
findings (e.g. brain tumour,
epilepsy, deep brain stimulator)
Age: 60 years (range 51-68) Male: 48%
BMI: 30 kg/m2 (range 26-34) ESS: NR
AHI:NR
OSA: (AHI ≥5): 68% (510/746)
No OSA (AHI<5): 32%
(236/746)
746 ˚ ̊ ˚ • ̊
AHI: sum of apneas and hypopneas per hour of sleep
Hypopneas: “scored
according to the American
Academy of Sleep Medicine
Task Force
recommendations” OSA:AHI ≥5/hr
Validation: Type 2 Portable
Sleep Study (Embletta X-100)
• • • • • • • ˚ • • • ˚ • ˚ • • 13
7. Danzie-Soares,
2012; University of
Sao Paulo Medical
School, Sao Paulo, Brazil
Search Strategy
Group 3
Consecutive patients with severe CAD age ≥40 years
referred for CABG.
Excluded patients with prior OSA diagnosis, history of
stroke, severe disability,
clinical instability, decompensated heart failure,
changes in medication within
prior one month or using supplemental oxygen.
Age: 58 ±7 years Male: 76%
BMI: 27.6 ±27.6 kg/m2
ESS: 7 (range 5-11) AHI: 22.9 ±20.0/hr
OSA (AHI ≥5): 87.1%
70 • • ̊ ˚ ˚
AHI: sum of apneas and hypopneas per hour of sleep
Hypopneas: 50 to 90%
decrease in nasal flow with a >3% oxygen desaturation
OSA: AHI ≥5/hr
Validation: Type I Polysomnography
• • • • • • ˚ • • • • • • ˚ • ˚ 13
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

38
(61/70)
No OSA (AHI <5): 12.9% (9/70)
8. Facco, 2012;
Northwestern
University Prentice Women’s Hospital,
Chicago, IL, USA
Search Strategy
Group 3
Pregnant women at high risk
for sleep apnea
(hypertension, pregestational diabetes, BMI ≥30, prior
preeclampsia)
Age: 33.0 ±6.5 years
Male: 0%
BMI: 31.9 ±9.1 kg/m2 ESS: 7.5 ±4.3 (0-19)
AHI: 1.5/hr (median, IQR
0.6-6.0)
OSA (AHI ≥5): 28%
(28/100)
No OSA (AHI<5): 72% (72/100)
100 • • ̊ ˚ ˚
AHI: “analysis of the WP
100 signals allows for
determination of the AHI” Hypopneas: Not defined
OSA: AHI ≥5/hr
Validation: Type IV Sleep Study (Watch-PAT100,
Itamar Medical)
•Developed a four-variable
model to predict OSA –
however was not validated
in separate population
(excluded from ACP
systematic review)
• ˚ ˚ • • • ˚ • ˚ • • ˚ • ˚ ˚ • 9
9. Feng, 2012;
Tianjin Medical University General
Hospital, Tianjin,
China
Search Strategy
Group 4
Consecutive patients referred
to several sleep centers (n=20) for suspected OSA
(Jan2004 – Apr2006)
Age: 45.9 ±12.1 years
Male: 86%
BMI: 27.6 ±3.9 kg/m2 ESS: 9.4 ±5.0
AHI: 35.2 ±25.2/hr
OSA (AHI ≥5): 91%
(2084/2297)
No OSA (AHI<5): 9%
(213/2297)
˚ • ̊ ˚ ˚
AHI: sum of apneas and
hypopneas per hour of sleep Hypopneas: ≥50% decrease
in nasal flow with either a
>3% oxygen desaturation or signs of a physiologic
arousal
OSA: AHI ≥5/hr Validation: Type I
Polysomnography
• • • • • • ˚ • • • • • • • • • 15
10. Gjevre, 2012;
University of
Saskatchewan, Saskatoon, SK
Canada
Search Strategy
Group 3
12 Rheumatoid arthritis
patients with abnormal scores
on the ESS and/or Pittsburgh Sleep Quality Index were
age/gender matched to 13 RA
patients with normal ESS and PSQI. Exclusions: use of
anti-TNF-alpha agents, age
<18 years, pregnancy within prior 6-months.
Age: 60.4 ±9.8 years Male: 28%
BMI: 29.7 ±4.2 kg/m2
ESS: NR AHI: 14.7 ±14.8/hr
OSA (AHI ≥5): 68% (17/25)
25 • • ̊ ˚ ˚
AHI: sum of apneas and
hypopneas per hour of sleep
Hypopneas: Not defined OSA: AHI ≥5/hr
Validation: Type I
Polysomnography
• • ˚ • • • • • ˚ • • • • ˚ ˚ ˚ 11
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

39
No OSA (AHI<5): 32%
(8/25)
11. Knutson, 2012;
National Institutes of
Health, Bethesda,
MD, USA
Search Strategy
Group 3
Obese (BMI 30-55) men and premenopausal women aged
18-50 years reporting less
than 6.5 hrs of sleep were analyzed from an ongoing,
randomized, prospective,
intervention trial (sleep extension study) from
11Sept2006 to 3Nov2009.
Recruited using advertisements. Self-reported
weight and thyroid hormonal
replacement therapy had to
be stable for preceding 6-
months.
Age: 40.8 ±6.9 years
Male: 30.2%
BMI: 38.2 ±5.9 kg/m2 ESS: 8.6 ±4.4
AHI: NR
OSA: (RDI ≥5) 66% (92/139)
No OSA (RDI<5): 34%
(47/139)
139 ˚ • ̊ ˚ •
RDI: sum of abnormal respiratory events per hour
of sleep
Hypopneas: 50 to 90% decrease in nasal flow with a
>3.5% oxygen desaturation
OR ≥1% desaturation with ≥1surrogate arousal
indicator
OSA: RDI ≥15/hr Validation: Type IV Sleep
Study (Apnea Risk
Evaluation System,
Advanced Brain Monitoring,
Inc)
•Other: Pittsburgh Sleep
Quality Index
• • • • • • ˚ • • • • • • ˚ • • 14
12. Koyama, 2012;
Universidade Federal
de Sao Paulo, Sao
Paulo, Brazil
Search Strategy
Group 3
Male railroad workers employed by a Brazilian
railroad company. Jan2008
to Nov2010.
Age: 35.6 ±9.6 years Male: 100%
BMI: 26.7 ±4.1 kg/m2
ESS: 7.9 ±3.6 AHI: NR
OSAS: 35% (261/745)
No OSAS: 65% (484/745)
745 • • ̊ ˚ ˚
AHI: Not defined Hypopneas: Not defined
OSAS: AHI ≥15/hr or (AHI
≥5/hr and ESS ≥10)
Validation: Type I
Polysomnography
• ˚ ˚ • • • ˚ • • • • • • ˚ ˚ ˚ 10
13. Laporta, 2012;
Western New York
Respiratory Research
Center, Buffalo, NY, USA
Search Strategy
Group 4
Consecutive veterans with ischemic heart disease
(documented MI, coronary
angiography, coronary artery bypass grafts) presenting to a
cardiology clinic at the VA
Western New York Healthcare System from
Oct2010-Sept2011.
Exclusion criteria: prior OSA diagnosis or treatment,
91 • ̊ ˚ ˚ ˚
AHI: sum of apneas and hypopneas per hour of sleep
Hypopneas: ≥50 decrease in
nasal flow with a >3% oxygen
OSA: AHI ≥5/hr
Validation: Type I Polysomnography
• • • • • • ˚ • • • • • • ˚ • ˚ 13
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

40
neurologic disease, systolic
CHF (EF<45%), receiving opiates.
Age: 67.7 ±11.8 years Male: 100%
BMI: 29.9 ±5.0 kg/m2
ESS: 9.3 ±4.8 AHI: 19.9 ±19.0/hr
OSA (AHI ≥5): 75% (69/91)
No OSA (AHI <5): 25% (22/91)
14. Martinez, 2012;
Universidade Federal
do Rio Grande do
Sul, Porto Alegre,
Brazil
Search Strategy
Group 3
Cross sectional analysis of
consecutive patients with
prior angina (age <65, BMI
≤40, no COPD or DM,
nonsmoker, prior CAD
intervention, recent angina, use of anxiolytic medication,
previous coronary
intervention). From Mar2007 to Feb2008
Age: 54 ±6.9 years Male: 46%
BMI: 23 ±11 kg/m2 ESS: NR
AHI: 17 ±14/hr
OSA (AHI ≥5): 79% (45/57) No OSA (AHI<5): 21%
(12/57)
57 • ̊ ˚ ˚ ˚
AHI: sum of apneas and
hypopneas per hour of sleep
Hypopneas: ≥50% decrease
in nasal flow with a ≥3%
oxygen desaturation
OSA: AHI ≥5/hr Validation: Type III Home
Sleep Study
(SOMNOcheck)
• • • • • • ˚ • • • • • • ˚ • • 14
15. Morales, 2012;
University of Pennsylvania,
Pennsylvania, PA,
USA
Search Strategy
Group 4
Elderly subjects (recruited
from Penn Partners in Healthy Living, a consumer
membership for older adults)
with and without sleepiness (2001-2005). Recruited an
equal number of study
participants for each decile of the multivariable apnea
prediction (MAP)
instrument. Exclusion criteria: unable to speak
English, cognitive
impairment, alcoholism, use of sedative hypnotics,
medical conditions that
would alter breathing pattern (e.g. stroke, CHF), prior
OSA diagnosis or treatment,
92 ˚ ̊ • ̊ ˚
AHI: sum of apneas and
hypopneas per hour of sleep Hypopneas: ≥50% decrease
in nasal flow with either a
≥3% oxygen or EEG arousals
OSA: AHI ≥30/hr and ESS
>10 Validation: Type I
Polysomnography
(Sandman, Embla)
• • • • • • • • • • • • • ˚ • ˚ 14
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

41
had Cheyne-Stokes or
primary central sleep apnea.
Age: 71.3 ±5.9 years
Male: 34% BMI: 30.5 ±7.6 kg/m2
ESS: NR (30% ESS >10)
AHI: NR OSA (AHI ≥5 & ESS >10):
27% (22/92)
No OSA: 73% (70/92)
16. Morrell, 2012;
Dept of Population
Health Sciences,
University of
Wisconsin-Madison,
Madison, WI, USA
Search Strategy
Group 3
Wisconsin state employees (of four state agencies) aged
30-60 years evaluated in
1988.
Age: 50.4 years
Male: 74% BMI: 31.1 ±7.1 kg/m2
ESS: 8.7 ±4.1
AHI: NR OSA: (AHI ≥15): 84%
(606/3695)
No OSA (AHI<15): 16% (3089/3695)
3,695 ˚ • ̊ ˚ ˚
AHI: sum of apneas and hypopneas per hour of sleep
Hypopneas: discernible
decrease in nasal flow with a
≥4% oxygen
OSAS: AHI ≥15/hr or on
CPAP Validation: Type II Sleep
Study (Polygraph model 78)
• • • • • • ˚ • ˚ • • • • ˚ • • 13
17. Nicholl, 2012;
Dept of University of Calgary, Calgary,
Alberta, Canada
Search Strategy
Group 3
Adults (age ≥18 years) with
chronic kidney disease (GFR <60 mL/min/1.73 m2)
attending an outpatient
nephrology clinic. Exclusion
criteria: current supplemental
oxygen, tracheostomy,
inability to provide informed consent.
Age: 65 ±12 years Male: 63%
BMI: 31.2 ±8.3 kg/m2
ESS: 7.9 ±4.7 ODI(4%): 21.1 ±25.1/hr
OSA: (ODI ≥15): 39%
(46/119) No OSA (ODI<15): 61%
(73/119)
119 ˚ • ̊ ˚ •
ODI: sum of number of
episodes of desaturation ≥4% per hour of recording
OSA: ODI(4%) ≥15/hr
Validation: Type IV Sleep
Study (Remmers Sleep
Recorder Model 4.2)
•Also compared to a control
group with OSA but without
history of kidney disease (n=230).
•Other: Pittsburgh Sleep
Quality Index
• ˚ ˚ • • • • • ˚ • • • • ˚ • • 12
18. Ravesloot, 2012;
St. Lucas Andreas
Hospital, Amsterdam,
Netherlands
Search Strategy
Prospective study of consecutive adult (age 18-65
years) bariatric candidates.
Age: 43.0 ±10.0 years
Male: 28%
279 ˚ • ̊ ˚ ˚
AHI: sum of apneas and hypopneas per hour of sleep
Hypopneas: ≥30% decrease
in nasal flow with a ≥4% oxygen desaturation
OSA: AHI ≥5/hr
˚ • • • • ˚ ˚ • • • • • • ˚ • • 12
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

42
Group 4 BMI: 46.1 ±5.8 kg/m2
ESS: 8.0 ±5.0 AHI: NR
OSA: (AHI ≥5): 30%
(84/279) No OSA (AHI<5): 70%
(195/279)
Validation: Type I
Polysomnography
19. Senchak, 2012; San Antonio Military Medical Center, Fort
Sam Houston, TX,
USA
Search Strategy
Group 4
Multi-institutional,
prospective clinical trial in adult (age ≥18 years) patients
(active duty army)
undergoing tonsillectomy for chronic, recurrent tonsillitis.
Exclusion criteria: prior OSA
diagnosis.
Age: 26.8 ±8.0 years
Male: 48% BMI: 27.7 ±5.8 kg/m2
ESS: NR
AHI: 4.7 ±9.6/hr OSA: (AHI ≥5): 80% (52/77)
No OSA (AHI<5): 20%
(15/77)
77 ˚ ̊ ˚ ˚ •
AHI: NR
Hypopneas: NR OSA: AHI ≥5/hr
Validation: Type IV Sleep
Study (ApneaLink Plus, Resmed)
•Other: Two questionnaires
used to assess pretest
probability of OSA – High
pretest probability for OSA defined as an ESS ≥8 and a
positive Berlin snore score
(Berlin category 1 score ≥2)
• ˚ ˚ • • • ˚ • ˚ • • • ˚ • ˚ • 10
20. Sharwood, 2012; The George Institute
for Global Health, Sydney, Australia
Search Strategy
Group 4
Random sample of long
distance commercial truck
drivers
Age: 46.4 years
Male: 99%
BMI: 30.6 kg/m2
ESS: 5.9
AHI: 19.5 ±15/hr MAPI: NR
OSA: (AHI ≥18): 59%
(193/325) No OSA (AHI<18): 41%
(132/325)
325 ˚ ̊ • ̊ ˚
AHI: NR
Hypopneas: NR
OSA: AHI ≥18/hr Validation: Type IV sleep
study (flow monitor,
DiagnoseIT)
Multivariable Apnea
Prediction Index (MAPI)
• ˚ ˚ • • • ˚ • ˚ • • • ˚ ˚ • • 10
21. Bertolazi, 2011; Universidade Federal
do Rio Grande do Sul
(UFRGS), Brazil
Search Strategy
Group 4
Consecutive sleep clinic patients undergoing sleep
study evaluations
Age: 46.6 ±11.0 years
Male: 42%
BMI: 38.3 ±6.8.8 kg/m2 ESS: NR
AHI: 16.3 ±23.0/hr
PSQI: 10.8 ±4.7 OSA: (AHI ≥5): 48% (40/83)
No OSA (AHI<5): 52%
83 ˚ ̊ ˚ ˚ •
AHI: NR Hypopneas: NR
OSA: “per standards
established by the American Academy of Sleep Medicine
(AASM)”
Validation: “Polysomnography”
•Other: Pittsburgh Sleep Quality Index (PSQI)
• ˚ ˚ ˚ • • ˚ • ˚ • • • • ˚ • • 10
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

43
(43/83)
22. Chai-Coetzer,
2011; Repatriation
General Hospital and
Flinders Medical Centre, South
Australia
Search Strategy
Group 3
Adult patients (age 25-70 years) attending six primary
care clinics were recruited
(June2007-April2008). Exclusion criteria:
pregnancy, significant
cognitive impairment, poorly controlled psychiatric
disorder or prior OSA
treatment
Age: 50 years (range 40-58)
Male:44%
BMI: 29.3 kg/m2 (range
25.5-33.8)
ESS: 7 (range 5-10) AHI: 16.5/hr (range 9.6-
28.2)
OSA (AHI ≥30): 21% (16/78)
No OSA (AHI <30): 79%
(62/78)
78 ˚ ̊ ˚ ˚ •
AHI: NR Hypopneas: Either ≥50%
decrease in nasal flow or a
≥3% oxygen desaturation or an EEG arousal
OSA: AHI ≥30/hr
Validation: Type I Polysomnogram
•Other: Two-stage model - OSA 50 questionnaire
(≥5/10) and ODI (3%)
(≥16/hr)
• • • • • • ˚ • ˚ • • • • ˚ • ˚ 12
23. Enciso, 2011;
University of
Southern California,
Los Angeles, CA, USA
Search Strategy
Group 4
Patients of the USC School of Dentistry
Age: 54.9 ±12.1 years Male: 77%
BMI: 26.6 ±18.1 kg/m2
ESS: NR
RDI: 24.3 ±18.1/hr
OSA (RDI ≥15): 63% (53/84)
No OSA (RDI<15): 37%
(31/84)
84 • ̊ ˚ ˚ •
RDI: Not reported Hypopneas: Not reported
OSA: RDI ≥15/hr
Validation: Type IV Home Sleep Study
•Other: Apnea Risk
Evaluation System (ARES)
questionnaire
• ˚ ˚ • • • ˚ • • ˚ • • • ˚ • ˚ 10
24. Farney, 2011;
LDS Hospital, Salt
Lake City, UT, USA
Search Strategy
Group 3
Consecutive patients referred to a sleep clinic who
underwent PSG testing for any
reason (1/2006-12/2008). Exclusion criteria: on
supplemental oxygen, prior
diagnosis or treatment for OSA, incomplete
questionnaire or demographic
data, insufficient/inadequate sleep study data.
Age: 49.7 ±15.2 years Male: 57.2%
1,426 ˚ ̊ ˚ • ̊
AHI: sum of apneas and hypopneas per hour of sleep
Hypopneas: studies prior to
4/2007, scoring based on “earlier” ‘Chicago’ criteria;
after this date based on
AASM 2007 standards OSA: AHI ≥5/hr
Validation: Type I
Polysomnogram
• • • • • • ˚ • • • • • • ˚ • • 14
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

44
BMI: 33.8 ±8.1 kg/m2
ESS: NR AHI: 32.9 ±30.1/hr
OSA(AHI≥5): 89.5%
(1274/1424) No OSA (AHI<5): 10.5%
(150/1424)
25. Gasa, 2011;
Hospital Universitari de Bellvitge,
Barcelona, Spain
Search Strategy
Group 4
Prospective multicenter cross-
sectional study of consecutive adult (age 18-60 years)
bariatric candidates from
Jan2009toFeb2010. Exclusion criteria: prior OSA diagnosis
or treatment, unstable CV
conditions, acute or chronic
inflammatory diseases in prior
6 months, chronic
immunosuppressant therapy, severe CHF, COPD,
psychiatric disorder,
pregnancy or current Alcohol abuse.
Age: 43.0 ±10.0 years Male: 28%
BMI: 46.1 ±5.8 kg/m2 ESS: 8.0 ±5.0
AHI: NR
OSA (AHI≥15): 72% (115/159)
No OSA (AHI<15): 28%
(44/159)
159 ˚ • ̊ ˚ ˚
AHI: Not defined
Hypopneas: Not defined OSA: AHI ≥15/hr
Validation: Type I
Polysomnography
• • • • • • ˚ ˚ ˚ • • • • • • • 13
26. Hrubos-Strom,
2011; Akerhus
University Hospital,
Lorenskog, Norway
Search Strategy
Group 3
Cross-sectional study of subjects residing in three
counties in central Norway
(age 30 to 65) randomly selected from the National
Population Register.
Age: 48.3 ±11.2 years
Male: 54.8%
BMI: 27.9 ±4.8 kg/m2 ESS: 8.8 ±4.6
AHI: 6.4/hr (median, IQR 1.7-
18.3) OSA (AHI ≥5): 16% (83/518)
No OSA (AHI <5): 84%
(435/518)
518 • ˚ ̊ ˚ ˚
AHI: sum of apneas and hypopneas per hour of sleep
Hypopneas: ≥70% decrease
in nasal flow with a >4% oxygen desaturation
OSA: AHI ≥5/hr
Validation: Type I Polysomnography
• • • • • • ˚ • • • • • • ˚ • • 14
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

45
27. Khoo, 2011;
National University of Singapore,
Singapore
Search Strategy
Group 4
Consecutive patients referred
to a sleep clinic (Dec 2005 –Dec 2007).
Age: 47.5 ±13.9 years Male:79%
BMI: 28.5 ±5.8
ESS: NR AHI: 40.8 ±29.3/hr
OSA (AHI ≥20): 66%
(77/117) No OSA (AHI <20): 34%
(40/117)
117 ˚ • ̊ ˚ ˚
AHI: sum of apneas and
hypopneas per hour of sleep Hypopneas: ≥20% reduction
in nasal flow with a >3%
oxygen desaturation OSA: AHI ≥20/hr
Validation: Type 1
Polysomnography
• • • • • • ˚ • ˚ • • • • ˚ • • 13
28. Kopitovic, 2011;
Institute for
Pulmonary Diseases
of Vojvodina, Serbia
Search Strategy
Group 4
Sleep clinic patients with OSA
symptoms undergoing sleep
study evaluations (June2006 –
Sept2009)
Age: 53 (median, IQR 43-59)
Male: 78%
BMI: 28 kg/m2 (median, IQR 25-32)
ESS: 9 (median, IQR 6-12)
AHI: 17.4/hr (median, IQR 1.4-43.7)
OSA (AHI ≥5): 62% (70/112)
No OSA (AHI<5): 38%
(42/112)
112 ˚ • ̊ ˚ ˚
AHI: sum of apneas and
hypopneas per hour of sleep
Hypopneas: ≥50% decrease
in nasal flow
OSA: AHI ≥5/hr Validation: Type 1
Polysomnography
(SomnoStar, Viasys)
• • • • • • ˚ • • • • • • ˚ • • 14
29. Martinez, 2011;
Universidade Federal
do Rio Grande do Sul
(UFRGS), Porto Alegre, RS, Brazil
Search Strategy
Group 4
Cross-sectional, prospective
study of consecutive adult (age
≥18 years) patients undergoing
sleep study testing for suspected OSA
Age: 46 ±14 years Male: 63.5%
BMI: 27 ±5.3 kg/m2
ESS: 10 ±5.1 AHI: 24 ±22/hr
OSA (AHI ≥5): 84%
(780/929) No OSA (AHI<5): 16%
(149/929)
929 ˚ • ̊ ˚ ˚
AHI: sum of apneas and
hypopneas per hour of sleep
Hypopneas: ≥50% decrease
in nasal flow with a ≥3% oxygen desaturation or a 3-s
arousal
OSA: AHI ≥5/hr Validation: Type 1
Polysomnography
•performed ESS
immediately before and day
after PSG. Pre-PSG ESS used in this analysis.
• • • • • • ˚ • • • • • • ˚ • • 14
30. Sareli, 2011;
University of
Pennsylvania,
Philadelphia, PA, USA
Consecutive bariatric surgery candidates referred for a sleep
study (11/2005-1/2007) at the
Penn Sleep Clinic for various reasons (irrespective of clinical
symptoms or findings
342 ˚ • • ̊ ˚
AHI: sum of apneas and hypopneas per hour of sleep
Hypopneas: 30 to 99%
decrease in nasal flow with either a ≥3% oxygen
desaturation or an EEG
• • • • • • ˚ • • ˚ • • • ˚ • • 13
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

46
Search Strategy
Group 3
suggestive of OSA).
Age: 43.8 ±10.9 years
Male: 18.4%
BMI: 49.5 ±10.0 kg/m2 ESS: 8.7 ±5
AHI: 24.9 ±30.3/hr
OSA (AHI ≥5): 77% (264/342) No OSA (AHI <5): 23%
(78/342)
arousal
OSA: AHI ≥5/hr Validation: Type I
Polysomnography
31. Sert Kuniyoshi,
2011; Mayo Clinic and Foundation,
Rochester, MN, USA
Search Strategy
Group 3
Cross-sectional study of recent
MI patients (1 to 3 months prior). Excluded patients with
prior OSA diagnosis receiving
CPAP treatment.
Age: 62 ±13 years
Male: 81% BMI: 30 ±5 kg/m2
ESS: 9.1 ±4.2
AHI: NR OSA (AHI ≥5): 74% (73/99)
No OSA (AHI<5): 26%
(26/99)
99 • • ̊ ˚ ˚
AHI: sum of apneas and
hypopneas per hour of sleep Hypopneas: 30 to 90%
decrease in nasal flow with a
≥4% oxygen desaturation
OSA: AHI ≥5/hr
Validation: Type I
Polysomnography
• • • • • • • • • • • • • ˚ • ˚ 14
32. Sforza, 2011;
Universite Jean
Monnet, Saint-Etienne, France
Search Strategy
Group 3 & Group 4
Prospective study of
participants aged ≥65 from the
PROOF study (French population). Exclusion criteria:
prior diagnosis or treatment for
OSA, MI, CHF, stroke,
neurologic or psychiatric
disorders.
Age: 65.6 ±0.8 years
Male: 40.9%
BMI: 25.3 ±5.1 kg/m2 ESS: 5.6 ±5.1
AHI: 21.6 ±16.0/hr
OSA: (AHI ≥15): 57% (369/643)
No OSA (AHI<15): 43%
(274/643)
643 • ˚ ̊ ˚ ˚
AHI: sum of apneas and
hypopneas per hour of sleep
Hypopneas: ≥50% decrease in nasal flow with a ≥3%
oxygen desaturation
OSA: AHI ≥15/hr
Validation: Type III Sleep
Study
•Provided data/outcomes
separately by gender and
Mini-Mental-State Examination
• • • • • • • • • • • • • ˚ • • 15
33. Silva, 2011;
Arizona State
University, Tucson, AZ, USA
Search Strategy
Group 4
Prospective multicenter cohort
population study (Sleep Heart
Health Study) in subjects age >40 years.
Age:62.4 ±10.3 years Male: 52%
BMI: NR (35% had BMI ≥30
4,770 ˚ • ̊ ˚ •
AHI: sum of apneas and
hypopneas per hour of sleep
Hypopneas: ≥25% decrease in nasal flow with a ≥4%
oxygen desaturation
OSA: AHI ≥5/hr Validation: Type II Sleep
Study (Compumedics
• • • • • • ˚ • • • • • • • • • 15
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

47
kg/m2)
ESS: NR (28% ESS >11) AHI: NR
OSA (AHI ≥5): 13%
(603/4770) No OSA (AHI<5): 87%
(4167/4770)
portable PS-2 system)
•Other: Takegami 4-variable
screening tool, STOP
questionnaire
34. Subramanian,
2011; Baylor College of Medicine,
Houston, TX, USA
Search Strategy
Group 3
Consecutive adult (age ≥18
years) patients referred to a sleep clinic for suspected sleep
apnea. Exclusion criteria:
prior OSA diagnosis, failed to perform an adequate sleep
study, did not complete study
questionnaire. Data collected
prospectively but analyzed
retrospectively.
Age: 55 ±14years
Male: 59%
BMI: 35 ±9 kg/m2 ESS: NR
RDI: 38 ±8/hr
OSA: (RDI ≥5): 85% (432/509)
No OSA (RDI<5): 15% (77/509)
509 • • ̊ ˚ •
RDI: sum of apneas,
hypopneas and RERA’s per hour of sleep
Hypopneas: required ≥4%
oxygen desaturation in addition to defined reduction
in airflow per 2007
American Academy of Sleep
Medicine Scoring
Guidelines
RERA’s: NR OSA: RDI ≥5/hr
Validation: Type I
Polysomnography
•Other: NAMES assessment
(Neck circumference, airway classification, comorbidities,
Epworth scale, snoring)
• • • • • • ˚ • • • • ˚ • ˚ • • 13
35. Thurtell, 2011;
Emory University
School of Medicine,
Atlanta, Georgia,
USA
Search Strategy
Group 3
Newly diagnosed idiopathic
intracranial hypertension (IIH).
Retrospectively included all
patients with newly diagnosed
IIH (by Dandy criteria) and
completing BQ, sleep study. Exclusion criteria: age <16,
pregnancy, prior IIH diagnosis,
another cause for increased intracranial pressure.
Age: 32 (median, range 16-54) Male: 20%
BMI: 39.8 kg/m2 (median, range
27-52) ESS: NR
AHI: NR
OSA (AHI ≥5): 60% (18/30) No OSA (AHI<5): 40%
(12/30)
30 • ˚ ̊ ˚ ˚
AHI: sum of apneas and
hypopneas per hour of sleep
Hypopneas: “determined
using conventional criteria.”
Reference to 2007 AASM
scoring criteria. OSA: AHI ≥5/hr
Validation: Type I
Polysomnography
• ˚ ˚ • • • • • • • • • • ˚ ˚ ˚ 11
36. Vaz, 2011;
University of Porto
Medical School,
Consecutive sleep clinic patients with suspected OSA.
Back translated Berlin
95 • ˚ ̊ ˚ ˚
AHI: sum of apneas and hypopneas per hour of sleep
Hypopneas: 20 to 50%
• • • • • • ˚ • • • • • • ˚ • ˚ 13
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

48
Porto, Portugal
Search Strategy
Group 4
Questionnaire into
Portuguese language by two bilingual translators (both
sleep specialists) working
independently and then back translated into English by
two other bilingual
translators and then compared with original
English language version
with necessary adjustments to obtain a single Portuguese
version.
Age: 51 ±13 years
Male: 67%
BMI: NR (55% had BMI >30 kg/m2)
ESS:10 ±6
AHI: 24 ±17/hr OSA (AHI ≥5): 83% (79/95)
No OSA (AHI<5): 17%
(16/95)
decrease in nasal flow with a
≥4% oxygen desaturation. OSA: AHI ≥5/hr
Validation: Type 3 Sleep
Study (alpha screen; Vyasis)
37. Ong, 2010;
Singapore General
Hospital, Singapore
Search Strategy
Group 4
Consecutive sleep clinic patients (95% evaluated for
suspected sleep apnea) undergoing PSG testing
(Nov 2008 – April 2009)
Age: 47 ±15.2 years
Male: 71%
BMI: 27.8 ±5.9 kg/m2 ESS: 9.4 ±5.2
AHI: 26.2 ±26.9/hr
OSA: 75% (239/317) No OSA (AHI<5): 25%
(78/317)
317 ˚ ˚ ̊ • ̊
AHI: sum of apneas and hypopneas per hour of sleep
Hypopneas: ≥30% decrease in nasal flow with either a
≥4% oxygen desaturation
OR ≥3% oxygen and an EEG arousal
OSA: AHI ≥5/hr
Validation: Type 1 Polysomnogram
•Evaluated STOP-BANG using various BMI cut-
points: BMI ≥26, BMI ≥30,
BMI ≥35
• • • • • • ˚ • • • • • • ˚ • • 14
38. Patt, 2010; Ohio State University,
Columbus, OH, USA
Search Strategy
Group 4
Patients with new lower extremity non-healing
wounds from April to Sept
2009. No prior screening for symptoms or risk factors for
sleep apnea.
Age: NR
Male: NR
BMI: NR ESS: NR
AHI: 15.6/hr
46 • ˚ ̊ ˚ ˚
AHI: sum of apneas and hypopneas per hour of sleep
Hypopneas: ≥50% decrease
in nasal flow with a ≥4% oxygen
OSA: AHI ≥15/hr
Validation: Type 3 Polysomnography
• • • • • • ˚ ˚ • • • ˚ • ˚ • ˚ 11
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

49
OSA (AHI ≥5): 83% (38/46)
No OSA (AHI<5): 17% (12/46)
39. Rodrigues, 2010;
Santa Casa de
Limeira, Brazil
Search Strategy
Group 3
Patients complaining of
snoring and clinical history
suggestive of OSA and symptoms of daytime
sleepiness, non-restful sleep
and snoring were evaluated by sleep study.
Age: 48.0 ±11.3 years Male: NR
BMI: 29.4 ±5.6 kg/m2
ESS: 11.3 ±5.1
AHI: NR
OSA (AHI ≥5): 90%
(101/112) No OSA (AHI <5): 10%
(11/112)
101 ˚ ̊ ˚ ˚ •
AHI: NR
Hypopneas: NR
OSA: AHI ≥5/hr Validation: Type I
Polysomnography
•Other: Friedman’s
classification (modified
Mallampati scale, pharyngeal tonsil size and
BMI)
• ˚ ˚ ˚ • • ˚ ˚ • • • • • ˚ • ˚ 9
40. Tanaka, 2010;
Hyogo College of
Medicine, Hyogo,
Japan
Search Strategy
Group 3
Male passenger transportation workers (train and bus drivers,
rail conductors, mechanics)
age 20 to 50 years from April2005 to March2006
Age: 39.9 ±8.2 years Male: 100%
BMI: NR
ESS: NR
AHI: NR
OSA: (ODI(3%) ≥15): 15%
(108/715) No OSA (ODI(3%)<15): 85%
(607/715)
75 ˚ • ̊ ˚ ˚
ODI: sum of ≥3% desaturations per hour of
recording
OSA: ODI(3%) ≥15/hr Validation: Type IV sleep
study (Pulse Oximeter -
Pulsox-3, Konica Minolta)
• • • • • • ˚ ˚ • • • • • ˚ • • 13
* Abbreviations: O
(No), • (Yes), afib (atrial fibrillation), AHI (apnea-hypopnea index), AASM (American Academy of Sleep Medicine), ASA (American Society of Anesthesiologists), BMI (body mass index), BQ (Berlin
questionnaire), CABG (coronary artery bypass graft), CAD (coronary artery disease), CHF (congestive heart failure), COPD (chronic obstructive pulmonary disease), CPAP (continuous positive airway pressure), CSA (central sleep apnea), CV (cardiovascular), DM (diabetes mellitus), ECG (electrocardiograph), EEG (electroencephalographic arousal), EF (ejection fraction), ESS (Epworth sleepiness scale), FOSQ (functional outcomes sleep
questionnaire), GFR (glomerular filtration rate), GOLD (global initiative for COPD), hr (hour), IIH (idiopathic intracranial hypertension), IQR (interquartile range), NA (not applicable), NIPPV (noninvasive positive airway
pressure), NR (not reported), Num (number), MAPI (multivariate apnea prediction index), MI (myocardial infarction), ODI (oxygen desaturation index), OSA (obstructive sleep apnea), OSAS (obstructive sleep apnea syndrome), PaCO2 (arterial partial pressure of carbon dioxide), PAP (positive airway pressure), PLMS (periodic limb movements of sleep), PSG (polysomnography), RERA (respiratory effort related arousal), RDI (respiratory disturbance
index), RLS (restless legs syndrome), SDB (sleep disordered breathing), VA (veterans administration)
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

50
Table 4. Studies on AHRQ Key Question 1c – Comparison of Diagnostic Accuracy Between Clinical Prediction Rules and Polysomnography: Study Characteristics
Author, Year,
Study, Population,
Reference
Study Design Num Predictors OSA Definition/
Comments
Quality Criteria
Index Test
Quality
Reference Test
Quality
Application of
Reference
Test
Independence
of Test
Interpretation
Clinical
Description
Cohort
Assembly
Sample
Size
Was
dia
gn
ost
ic t
echn
iqu
e
des
crib
ed i
n s
uff
icie
nt
det
ail
to
rep
rodu
ce t
he
pro
cedu
re?
Was
th
e A
HI
or
RD
I d
efin
ed?
Wer
e h
ypo
pn
eas
def
ined
?
Was
con
firm
ato
ry d
iagno
stic
Pro
cedu
re c
lear
ly d
escr
ibed
?
Wer
e b
oth
po
siti
ve
and
neg
ativ
e
Res
ult
s co
mp
ared
to
a
gold
sta
nd
ard
?
Was
th
e re
fere
nce
tes
t ap
pli
ed
con
sist
entl
y w
ithin
tho
se w
ith
and
wit
hou
t O
SA
?
Was
th
ere
bli
nd
ing
of
poly
som
no
gra
phy
dia
gn
osi
s?
Ag
e, G
ender
, B
MI,
AH
I R
epo
rted
OS
A S
ever
ity
Rep
ort
ed
Incl
usi
on
/Excl
usi
on
Cri
teri
a
Su
bje
cts
enro
lled
pro
spec
tiv
ely?
Su
bje
cts
enro
lled
con
secu
tivel
y?
≥90
% e
nro
lled
com
ple
te
Mult
i-ce
nte
r T
rial
≥35
Par
tici
pan
ts w
ith
OS
A
≥35
Par
tici
pan
ts w
itho
ut
OS
A
Ov
erall
Qu
ali
ty S
core
(0
-16
)
1. Jauhar, 2012;
Glasgow Dental
Hospital, Glasgow, Scotland, UK
Search Strategy
Group 4
Consecutive adult (age >18
years) patients who
required a sleep study were recruited.
Age: 46.6 ±11.2 years Male: 75%
BMI: 32.5 ±8.7 kg/m2
ESS: 11.1 ±5.4
ODI: NR (for those with
OSA, median ODI 24, IQR
11,68) OSA (ODI ≥10/hr and ESS
≥10): 52% (37/71)
No OSA: 48% (34/71)
71 BMI, neck
circumference,
palatal height, maxillary and
mandibular
intermolar distance, overjet
ODI: NR
OSA: ODI ≥10/hr and ESS
≥10 Validation: Type IV Sleep
Study (Somnoscreen)
•Kushida Index developed
previously to predict clinically
suspected OSA
• ̊ ˚ • • • ˚ • • • • • • ˚ • ˚ 11
2. Morales, 2012;
University of
Pennsylvania, Pennsylvania, PA,
USA
Search Strategy
Group 4
Elderly subjects (recruited
from Penn Partners in
Healthy Living, a consumer membership for older
adults) with and without
sleepiness (2001-2005). Recruited an equal number
of study participants for
each decile of the
multivariable apnea
prediction (MAP)
instrument. Exclusion criteria: unable to speak
English, cognitive
impairment, alcoholism,
92 Apnea symptoms,
neck circumference,
age
AHI: sum of apneas and
hypopneas per hour of sleep
Hypopneas: ≥50% decrease in nasal flow with either a
≥3% oxygen or EEG
arousals OSA: AHI ≥30/hr and ESS
>10
Validation: Type I
Polysomnography
(Sandman, Embla)
•Optimal parameters set as
one that minimized total
prediction errors, computed as
• • • • • • • • • • • • • ˚ • ˚ 14
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

51
use of sedative hypnotics,
medical conditions that would alter breathing
pattern (e.g. stroke, CHF),
prior OSA diagnosis or treatment, had Cheyne-
Stokes or primary central
sleep apnea.
Age: 71.3 ±5.9 years
Male: 34% BMI: 30.5 ±7.6 kg/m2
ESS: NR (30% ESS >10)
AHI: NR OSA (AHI ≥5 & ESS >10):
27% (22/92)
No OSA: 73% (70/92)
sum of false-positives and
false-negative predictions.
3. Su, 2012; Cathay General Hospital,
Taipei City, Taiwan
Search Strategy
Group 3
Consecutive patients with suspected OSA recruited
from Oct2007 to July2008.
Age: 48.3 ±11.9 years
Male:77%
BMI: 24.8 ±3.1 kg/m2 ESS: 10.1 ±6.4
AHI: NR OSA (RDI ≥5): 72%
(21/29)
No OSA (RDI <5): 28% (8/29)
29 Age, weight, SBP, DBP, DI3, DI4
RDI: “Number of events per hour”
Hypopnea: NR
OSA: RDI ≥5/hr Validation: Type 1
polysomnogram
•Applied multiclass
Mahalanobis-Taguchi system (MMTS) based on
anthropometric information
and questionnaire data to predict OSA.
• • • • • • ˚ ˚ • • • • • ˚ ˚ ˚ 11
4. Khoo, 2011;
National University
of Singapore, Singapore
Search Strategy
Group 4
Consecutive patients
referred to a sleep clinic
(Dec 2005 –Dec 2007).
Age: 45.5 ±13.5 years
Male:81% BMI: 29.6 ±5.7 kg/m2
ESS: NR
AHI: 40.8 ±29.5/hr OSA (AHI ≥20): 65%
(34/52)
No OSA (AHI <20): 35% (18/52)
52 Flemons Index: 4-
variable model (neck
circumference, HTN, habitual snoring and
gasping or choking)
Koo Model: age,
male gender, neck
circumference, frequent awakenings
with unrefreshing
sleep
AHI: sum of apneas and
hypopneas per hour of sleep
Hypopneas: ≥20% reduction in nasal flow with a >3%
oxygen desaturation
OSA: AHI ≥20/hr Validation: Type 1
polysomnogram
•Flemons Index developed
previously to predict
clinically suspected OSA
•Koo Model developed and
validated in current study
• • • • • • ˚ • ˚ • • • • ˚ • • 13
5. Kolotkin, 2011;
LDS Hospital, Salt
Lake City, UT, USA
Search Strategy
Bariatric surgery candidates
(BMI >40 or ≥35 with 2 co-
morbidities). Exclusion criteria: prior weight loss
surgery, gastric/duodenal
310 BMI, age, HgA1C,
insulin level,
gender, neck circumference
AHI: sum of apneas and
hypopneas per hour of sleep
Hypopneas: “A reduction” in nasal flow with a >4%
oxygen desaturation
• • • • • • ˚ • • • • • • ˚ • • 14
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

52
Group 3 ulcers or MI within prior 6
months, active cancer within prior 5 years, history
of alcohol/narcotics use,
use of supplemental oxygen or CPAP for OSA.
Age: 41.6 ±10.4 years Male:16%
BMI:46.8 ±7.5 kg/m2
ESS: NR AHI: NR
OSA (AHI ≥5): 81%
(252/310) No OSA (AHI <5): 19%
(58/310)
OSA: AHI ≥5/hr
Validation: Type III Sleep Study
•Dixon prediction model developed previously to
predict clinically suspected
OSA in bariatric surgery candidates.
6. Sun, 2011; Tapai
Medical University, Tapai, Taiwan
Search Strategy
Group 3
Patients from a teaching
hospital; suspected of sleep disordered breathing
referred for sleep study.
Age: 43.4 ±12.7 years
Male: 76%
BMI: NR (20% BMI >25 kg/m2)
ESS: NR (39% ESS >10) AHI: NR
OSA (AHI ≥5): 77%
(85/110) No OSA (AHI <5):23%
(25/110)
110 29 variables AHI: NR
Hypopneas: NR OSA: AHI ≥5/hr
Validation:
“Polysomnography test”
•Genetic algorithm was used
to build the five best models based on questions taken
from the Berlin Questionnaire, Rome
Questionnaire, ESS and
BASH’IM score
˚ ˚ ˚ ˚ • • ˚ ˚ • • ˚ ˚ • ˚ • ˚ 6
* Abbreviations: O
(No), • (Yes), afib (atrial fibrillation), AHI (apnea-hypopnea index), AASM (American Academy of Sleep Medicine), ASA (American Society of Anesthesiologists), BMI (body mass index), BQ (Berlin
questionnaire), CABG (coronary artery bypass graft), CAD (coronary artery disease), CHF (congestive heart failure), COPD (chronic obstructive pulmonary disease), CPAP (continuous positive airway pressure), CSA (central sleep apnea), CV (cardiovascular), DM (diabetes mellitus), ECG (electrocardiograph), EEG (electroencephalographic arousal), EF (ejection fraction), ESS (Epworth sleepiness scale), FOSQ (functional outcomes sleep questionnaire), GFR
(glomerular filtration rate), GOLD (global initiative for COPD), hr (hour), IIH (idiopathic intracranial hypertension), IQR (interquartile range), NA (not applicable), NIPPV (noninvasive positive airway pressure), NR (not reported),
Num (number), MAPI (multivariate apnea prediction index), MI (myocardial infarction), ODI (oxygen desaturation index), OSA (obstructive sleep apnea), PaCO2 (arterial partial pressure of carbon dioxide), PAP (positive airway pressure), PLMS (periodic limb movements of sleep), PSG (polysomnography), RERA (respiratory effort related arousal), RDI (respiratory disturbance index), RLS (restless legs syndrome), SDB (sleep disordered breathing), VA
(veterans administration)
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

53
Table 5. Studies on AHRQ Key Question 2 – How does phased testing compare to full test alone: Study Characteristics
Author, Year, Study,
Population, Reference
Study Design Num Phase Testing
Algorithm
OSA Definition/
Comments
Quality Criteria
Index Test
Quality
Reference Test
Quality
Application of
Reference
Test
Independence
of Test
Interpretation
Clinical
Description
Cohort
Assembly
Sample
Size
Was
dia
gn
ost
ic t
echn
iqu
e
des
crib
ed i
n s
uff
icie
nt
det
ail
to
rep
rodu
ce t
he
pro
cedu
re?
Was
th
e A
HI
or
RD
I d
efin
ed?
Wer
e h
ypo
pn
eas
def
ined
?
Was
con
firm
ato
ry d
iagno
stic
Pro
cedu
re c
lear
ly d
escr
ibed
?
Wer
e b
oth
po
siti
ve
and
neg
ativ
e
Res
ult
s co
mp
ared
to
a
gold
sta
nd
ard
?
Was
th
e re
fere
nce
tes
t ap
pli
ed
con
sist
entl
y w
ithin
tho
se w
ith
and
wit
hou
t O
SA
?
Was
th
ere
bli
nd
ing
of
poly
som
no
gra
phy
dia
gn
osi
s?
Ag
e, G
ender
, B
MI,
AH
I R
epo
rted
OS
A S
ever
ity
Rep
ort
ed
Incl
usi
on
/Excl
usi
on
Cri
teri
a
Su
bje
cts
enro
lled
pro
spec
tiv
ely?
Su
bje
cts
enro
lled
con
secu
tivel
y?
≥90
% e
nro
lled
com
ple
te
Mult
i-ce
nte
r T
rial
≥35
Par
tici
pan
ts w
ith
OS
A
≥35
Par
tici
pan
ts w
itho
ut
OS
A
Ov
erall
Qu
ali
ty S
core
(0
-16
)
1. Morales, 2012;
University of Pennsylvania,
Pennsylvania, PA,
USA
Search Strategy Group
4
Elderly subjects (recruited
from Penn Partners in Healthy Living, a consumer
membership for older
adults) with and without sleepiness (2001-2005).
Recruited an equal number
of study participants for each decile of the
multivariable apnea
prediction (MAP)
instrument. Exclusion
criteria: unable to speak English, cognitive
impairment, alcoholism,
use of sedative hypnotics, medical conditions that
would alter breathing
pattern (e.g. stroke, CHF), prior OSA diagnosis or
treatment, had Cheyne-
Stokes or primary central sleep apnea.
Age: 71.3 ±5.9 years
Male: 34%
BMI: 30.5 ±7.6 kg/m2
ESS: NR (30% ESS >10) AHI: NR
OSA (AHI ≥5 & ESS >10):
27% (22/92)
92 Phase testing:
1. MAP (multivariate
apnea
prediction instrument)
and/or apnea
symptoms and clinical
findings
2. Portable
Type IV sleep study based on
prior test
results (if “intermediate”
OSA
probability
AHI: sum of apneas and
hypopneas per hour of sleep
Hypopneas: ≥50%
decrease in nasal flow with either a ≥3% oxygen
or EEG arousals
OSA: AHI ≥30/hr and ESS >10
Validation: Type I
Polysomnography
(Sandman, Embla)
•Two-stage algorithm (3
parameters): 1) MAP lower
bound below which sleep apnea could be excluded;
2) MAP upper bound above
which study participants can be assessed to have
OSA; and 3) home study
AHI cut-points (to be used in study participants with
intermediate MAP values)
above which study
participants can be assessed
to have OSA.
• • • • • • • • • • • • • ˚ • ˚ 14
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

54
No OSA: 73% (70/92)
* Abbreviations: O (No), • (Yes), afib (atrial fibrillation), AHI (apnea-hypopnea index), AASM (American Academy of Sleep Medicine), ASA (American Society of Anesthesiologists), BMI (body mass index), BQ (Berlin
questionnaire), CABG (coronary artery bypass graft), CAD (coronary artery disease), CHF (congestive heart failure), COPD (chronic obstructive pulmonary disease), CPAP (continuous positive airway pressure), CSA (central sleep
apnea), CV (cardiovascular), DM (diabetes mellitus), ECG (electrocardiograph), EEG (electroencephalographic arousal), EF (ejection fraction), ESS (Epworth sleepiness scale), FOSQ (functional outcomes sleep questionnaire),
GFR (glomerular filtration rate), GOLD (global initiative for COPD), hr (hour), IIH (idiopathic intracranial hypertension), IQR (interquartile range), NA (not applicable), NIPPV (noninvasive positive airway pressure), NR (not reported), Num (number), MAPI (multivariate apnea prediction index), MI (myocardial infarction), ODI (oxygen desaturation index), OSA (obstructive sleep apnea), PaCO2 (arterial partial pressure of carbon dioxide), PAP
(positive airway pressure), PLMS (periodic limb movements of sleep), PSG (polysomnography), RERA (respiratory effort related arousal), RDI (respiratory disturbance index), RLS (restless legs syndrome), SDB (sleep disordered
breathing), VA (veterans administration)
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

55
Table 6. Studies on AHRQ Key Question 3 – What is the effect of preoperative screening for OSA on surgical outcomes: Study Characteristics
Author, Year,
Study, Reference
Study Design Num Population OSA Definition/
Comments
Outcome(s)
1. Singh, 2013;
University Health
Network, Toronto,
ON, Canada
Search Strategy
Group 3
Adult (age >18) patients
visiting two preoperative
surgery clinics were
recruited. Excluded patients
expected to have abnormal
EEG findings (e.g. brain
tumors, epilepsy patients,
patients with deep brain
stimulators). October 2005 to
November 2009.
Anaesthetists and surgeons
blinded to preoperative sleep
study and Berlin
Questionnaire
819 Age: 59 (median; IQR
50,68)
Male: 48%
BMI: 29.1 kg/m2
(median; IQR 25.6-
33.4)
ESS: NR
AHI: NR
OSA (AHI ≥5/hr) :
69% (465/819)
AHI: sum of
apneas and
hypopneas per hour
of sleep
Hypopneas: >30 to
90% decrease in
nasal flow with a
>4% oxygen
desaturation
OSA: AHI ≥5/hr
•Of 267 preoperative patients with undiagnosed symptomatic moderate-
severe OSA (AHI ≥15/hr), 92% were unidentified by surgeons and 60% by
anaesthetists prior to surgery.
•Anesthesiologists did not identify 76% of those with mild, 65% moderate
and 53% with severe OSA prior to surgery – 60% of those with moderate-
severe OSA. 69.2% of those missed complained of snoring, daytime
sleepiness or witnessed apneas. 92.5% of those missed were classified as
high-risk by the STOP-BANG questionnaire.
•Surgeons did not identify 97% of those with mild, 93% moderate and 90%
with severe OSA prior to surgery – 92% of those with moderate-severe OSA.
94.9% of those missed complained of snoring, daytime sleepiness or
witnessed apneas. 93.1% of those missed were classified as high-risk by the
STOP-BANG questionnaire.
2. Kim, 2012;
Samsung Medical
Centre,
Sungkyunkwan
University, School
of Medicine,
South Korea
Search Strategy
Group 4
Men (age 40 to 75 years)
undergoing spinal anesthesia for
transurethral resection of the
bladder or prostate (ASA
physical status 1-2) were
recruited. Exclusion criteria:
ECG or chest radiographic
abnormalities, prior OSA
diagnosis or taking a medication
that might affect sleep pattern.
ApneaLink (Type IV monitor)
was recorded and auto-analyzed
AHI-indexes during propofol
sedation for surgery/.
29 Age: NR
Male: 100%
BMI: NR
ESS: NR
AHI: 17/hr (median;
IQR 0 to 70)
OSA (AHI ≥10/hr) :
66% (19/29)
AHI: sum of
apneas and
hypopneas per hour
of sleep
Hypopneas: >50%
decrease in nasal
flow
OSA: AHI ≥10/hr
•Presence or severity of OSA did not ‘significantly’ affect spinal anesthesia
level, BIS, monitoring time, analysis time, propofol infusion, intra-
operative blood pressure, heart rate and oxygen saturation score.
* * Abbreviations: O
(No), • (Yes), afib (atrial fibrillation), AHI (apnea-hypopnea index), AASM (American Academy of Sleep Medicine), ASA (American Society of
Anesthesiologists), BMI (body mass index), BQ (Berlin questionnaire), CABG (coronary artery bypass graft), CAD (coronary artery disease), CHF (congestive heart failure), COPD
(chronic obstructive pulmonary disease), CPAP (continuous positive airway pressure), CSA (central sleep apnea), CV (cardiovascular), DM (diabetes mellitus), ECG
(electrocardiograph), EEG (electroencephalographic arousal), EF (ejection fraction), ESS (Epworth sleepiness scale), FOSQ (functional outcomes sleep questionnaire), GFR (glomerular
filtration rate), GOLD (global initiative for COPD), hr (hour), IIH (idiopathic intracranial hypertension), IQR (interquartile range), NA (not applicable), NIPPV (noninvasive positive
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

56
airway pressure), NR (not reported), Num (number), MAPI (multivariate apnea prediction index), MI (myocardial infarction), ODI (oxygen desaturation index), OSA (obstructive sleep
apnea), PaCO2 (arterial partial pressure of carbon dioxide), PAP (positive airway pressure), PLMS (periodic limb movements of sleep), PSG (polysomnography), RERA (respiratory
effort related arousal), RDI (respiratory disturbance index), RLS (restless legs syndrome), SDB (sleep disordered breathing), VA (veterans administration)
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

57
Table 7. Studies on AHRQ Key Question 4 – In adults screened for OSA, what is the relationship between OSA with respect to long-term clinical and functional outcomes? :
Study Characteristics
Author, Year,
Study, Reference
Study Design Num Population OSA Definition/
Comments
Outcome(s)
1. Ensrud, 2012;
Minneapolis
Veterans Affairs
Health Care
System,
Minneapolis, MN,
USA
Search Strategy
Group 4
Study subjects were
participants in the MrOS
Longitudinal Sleep Study
conducted 2003-2005
(ancillary study to identify
outcomes of sleep disorders
in older men). Inclusion
criteria: age ≥65 years,
classifies as “non-frail” at
baseline; Exclusion criteria:
missing repeat frailty status.
Objective: “test the
hypothesis that non-frail
older men with poorer sleep
at baseline are at increased
risk of frailty and death at
follow-up”
2,505 Age: 75.7 ±5.2 years
Male: 100%
BMI: 27.2 ±3.7 kg/m2
ESS: NR (12% had
ESS >10)
AHI: NR
OSA (AHI ≥30/hr) :
9% (209/2505)
AHI: sum of
apneas and
hypopneas per hour
of sleep
Hypopneas: >30%
decrease in nasal
flow with a >4%
oxygen
desaturation
OSA: AHI ≥30/hr
Sleep Study: Type
2 Polysomnogram
(in-home,
unattended)
•Severe OSA was associated with increased risk of death at follow-up
(multivariable OR 1.74, 95% CI 1.04-2.89).
2. Chami, 2011;
Boston University
School of
Medicine, Boston,
USA
Search Strategy
Group 4
Population cohort study
(Sleep Heart Health Study) of
adults (age ≥40 years)
recruited in several ongoing
cohort studies of
cardiovascular and
pulmonary disease in USA.
Excluded patients who had
surgery for OSA.
819 Age: 61.9 ±10.2 years
Male: 43%
BMI: 28.7 ±5.3 kg/m2
ESS: NR
AHI: NR
OSA (AHI ≥5/hr) :
NR
AHI: sum of
apneas and
hypopneas per hour
of sleep
Hypopneas: >30%
decrease in nasal
flow with a >3%
oxygen
desaturation
OSA: AHI ≥5/hr
•Patients with incident cardiovascular disease (over 5-years) experienced
larger increases in AHI between PSG’s
3. Fung, 2011;
San Diego
Veterans Affairs
Healthcare
System, San
Diego, CA, USA
Study subjects were
participants in the MrOS
Longitudinal Sleep Study
conducted 2003-2005
(ancillary study to identify
outcomes of sleep disorders
784 Age: 75.1 ±4.9 years
Male: 100%
BMI: 26.4 ±3.4 kg/m2
ESS: NR
AHI: 10.0 ±12.0/hr
OSA (AHI ≥5/hr) :
AHI: sum of
apneas and
hypopneas per hour
of sleep
Hypopneas: >30%
decrease in nasal
•No statistically significant difference with incident HTN with respect
to baseline RDI.
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

58
Search Strategy
Group 4
in older men). Objective was
to assess whether incident
hypertension is associated
with polysomnography
measures of sleep disordered
breathing in older men.
Inclusion criteria: age ≥65
years. Exclusion criteria:
hypertension.
54% (423/784) flow with a >4%
oxygen
desaturation
OSA: AHI ≥5/hr
Sleep Study: Type
2 Polysomnogram
(in-home,
unattended)
* Abbreviations: O
(No), • (Yes), afib (atrial fibrillation), AHI (apnea-hypopnea index), AASM (American Academy of Sleep Medicine), ASA (American Society of Anesthesiologists),
BMI (body mass index), BQ (Berlin questionnaire), CABG (coronary artery bypass graft), CAD (coronary artery disease), CHF (congestive heart failure), COPD (chronic obstructive
pulmonary disease), CPAP (continuous positive airway pressure), CSA (central sleep apnea), CV (cardiovascular), DM (diabetes mellitus), ECG (electrocardiograph), EEG
(electroencephalographic arousal), EF (ejection fraction), ESS (Epworth sleepiness scale), FOSQ (functional outcomes sleep questionnaire), GFR (glomerular filtration rate), GOLD
(global initiative for COPD), hr (hour), IIH (idiopathic intracranial hypertension), IQR (interquartile range), NA (not applicable), NIPPV (noninvasive positive airway pressure), NR
(not reported), Num (number), MAPI (multivariate apnea prediction index), MI (myocardial infarction), ODI (oxygen desaturation index), OSA (obstructive sleep apnea), PaCO2
(arterial partial pressure of carbon dioxide), PAP (positive airway pressure), PLMS (periodic limb movements of sleep), PSG (polysomnography), RERA (respiratory effort related
arousal), RDI (respiratory disturbance index), RLS (restless legs syndrome), SDB (sleep disordered breathing), VA (veterans administration)
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

59
Table 8 - AHRQ Question 1a – Summary of Type II Portable Sleep Study Diagnostic Studies
Study Search
Strategy
Sample Demographics N Index/Validation OSA Definition OSA Prevalence Portable
Cut-
point(s)
PSG
Cut-Point(s)
Ferre, 2012 Group 3 Consecutive
patients referred to
a sleep unit for
suspected sleep
apnea
Age: 55.9
±14.5 years
Male: 57%
BMI: 28.5 ±4.8
kg/m2
ESS: 8.6 ±9.5
AHI: 21.7
±19.0/hr
68 •Type II Portable Study
(Somte polygraph,
Compumedics)
•Type I
Polysomnography
AHI: sum of apneas
and hypopneas per
hour of sleep
Hypopneas: ≥50
decrease in nasal flow
with either a ≥3%
oxygen desaturation or
an arousal
OSA: AHI ≥5/hr
No OSA (AHI <5): 19%
(13/68)
OSA (AHI ≥5):: 81%
(55/68)
•Mild (AHI 5-15): 28%
(19/68)
•Moderate (AHI 15-30):
26% (18/68)
•Severe (AHI ≥30): 26%
(18/68)
Various:
AHI
>5/hr
AHI
>15/hr
AHI
>30/hr
Various:
AHI >5/hr
AHI
>15/hr
AHI
>30/hr
Oliveria,
2012
Group 4 Consecutive
COPD patients
with suspected
OSA
•High rate of
inadequate
portable Type II
study recordings
reported (26 out of
67)
Age: 62.8 ±8.5
years
Male: 50%
BMI: 31.0 ±5.6
kg/m2
ESS: 10.5 ±4.1
AHI: 23.0
±3.5/hr
26 •Type II Portable Study
(Stardust II, Philips-
Respironics)
•Type I
Polysomnography
(Embla N7000)
AHI: NR
Hypopneas: ≥50%
decrease in nasal flow
OR a <50% reduction
in nasal flow
associated with either
≥3% oxygen
desaturation or an
EEG arousal
OSA: AHI ≥5/hr
No OSA (AHI <5): NR
OSA (AHI ≥5): NR (90%
of enrolled patients had an
AHI ≥5/hr; 41 of these
were excluded from the
final analysis)
Various:
AHI >5-
15/hr
AHI
>30/hr
Various:
AHI >5-
15/hr
AHI
>30/hr
Bruyneel,
2011
Group 4 Consecutive
patients referred to
a sleep unit for
suspected sleep
apnea
Age: 48.9
±12.1 years
Male: 59%
BMI: 30.5 ±7.3
kg/m2
ESS: NR
AHI: 26.4
±30/hr
66 •Type II Portable Study
(Pamela V 3.631,
Medatec)
•Type I
Polysomnography
(Medatec)
AHI: sum of apneas
and hypopneas per
hour of sleep
Hypopneas: ≥50%
decrease in nasal flow
with either a ≥3%
oxygen desaturation or
EEG arousal
OSA: AHI ≥5/hr
No OSA (AHI <5): 23%
(14/66)
OSA (AHI ≥5): 77%
(48/66)
•Mild (AHI 5-15): 42%
(20/48)
•Moderate (AHI 15-30):
23% (11/48)
•Severe (AHI ≥30): 35%
(17/48)
Various:
AHI
>5/hr
AHI
>15/hr
AHI
>30/hr
Various:
AHI >5/hr
AHI
>15/hr
AHI
>30/hr
Campbell, Group 4 Consecutive Age: 49.1 30 •Type II Portable Study AHI: sum of apneas No OSA (AHI <5): 20% Various: Various:
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

60
2011 patients referred to
a sleep unit for
suspected sleep
apnea
±13.8 years
Male: 80%
BMI: 31.0 ±6.1
kg/m2
ESS: NR
AHI: 34.5
±29.0/hr
(Siesta System,
Compumedics)
•Type I
Polysomnogram
(S=series,
Compumedics)
and hypopneas per
hour of sleep
Hypopneas: A visible
decrease in nasal flow
and either a ≥3%
oxygen desaturation or
an EEG arousal
OSA: AHI ≥5/hr
(6/30)
OSA (AHI ≥5): 80%
(24/30)
•Mild (AHI 5-15): 29%
(7/24)
•Moderate/Severe (AHI
≥15): 71% (17/24)
AHI
>5/hr
AHI
>10/hr
AHI
>15/hr
AHI >5/hr
AHI
>10/hr
AHI
>15/hr
* Abbreviations: AHI (apnea-hypopnea index), BMI (body mass index), CABG (coronary artery bypass graft), CAD (coronary artery disease), COPD (chronic obstructive
pulmonary disease), CPAP (continuous positive airway pressure), DM (diabetes mellitus), EEG (electroencephalogram), ESS (Epworth sleepiness scale), hr (hour), IQR
(interquartile range), MI (myocardial infarction), N (number), NR (not reported), OSA (obstructive sleep apnea), OSAS (obstructive sleep apnea syndrome), mod (moderate), PSG
(polysomnogram), RDI (respiratory disturbance index), RERA (respiratory effort related arousal), SDB (sleep disordered breathing)
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

61
Table 9 - AHRQ Question 1a – Diagnostic Accuracy of Type II Portable Sleep Study Diagnostic Studies
Study N Cut-Point OSA
Prevalence
Population TP FN FP TN Diagnostic
Odds Ratio
p-
value
Sens Spec PPV NPV +LR -LR Accuracy AUC Pos
Posttest
Probability
Neg
Posttest
Probability
Kappa(1)
Coefficient
Ferre, 2012 68 PSG: AHI ≥5/hr
Type II Study: AHI
≥5/hr
0.809 Sleep clinic patients
with suspected OSA
50 5 3 10 33.3 <0.001 0.909 0.769 0.943 0.667 3.94 0.118 0.882 0.81 0.943 0.333 0.704
68 PSG: AHI ≥15/hr
Type II Study: AHI
≥15/hr
0.529 Sleep clinic patients
with suspected OSA
31 5 1 31 192.2 <0.001 0.861 0.969 0.969 0.861 27.56 0.143 0.912 0.91 0.969 0.139 0.934
68 PSG: AHI ≥30/hr
Type II Study: AHI
≥30/hr
0.265 Sleep clinic patients
with suspected OSA
11 7 2 48 <0.001 0.611 0.960 0.846 0.873 15.29 0.405 0.868 0.86 0.846 0.127
Oliveria, 2012 26 PSG: AHI 5-15/hr
Type II Study: AHI 5-
15/hr
NR COPD patients with
suspected OSA
. . . . . . . . . . . . . . . 0.350
26 PSG: AHI ≥30/hr
Type II Study: AHI
≥30/hr
NR COPD patients with
suspected OSA
. . . . . . . . . . . . . . . 0.560
Bruyneel,
2011
66 PSG: AHI ≥5/hr
Type II Study: AHI
≥5/hr
0.774 Sleep clinic patients
with suspected OSA
45 3 9 5 8.33 0.004 0.938 0.357 0.833 0.625 1.458 0.175 0.806 NR 0.833 0.375 0.262
66 PSG: AHI ≥15/hr
Type II Study: AHI
≥15/hr
0.452 Sleep clinic patients
with suspected OSA
22 6 10 24 8.80 <0.001 0.786 0.706 0.688 0.800 2.671 0.304 0.742 NR 0.688 0.200 0.430
66 PSG: AHI ≥30/hr
Type II Study: AHI
≥30/hr
0.274 Sleep clinic patients
with suspected OSA
13 4 1 44 <0.001 0.765 0.978 0.929 0.917 34.41 0.241 0.919 NR 0.929 0.083
Campbell,
2011
30 PSG: AHI ≥5/hr
Type II Study: AHI
≥5/hr
0.800 Sleep clinic patients
with suspected OSA
21 3 1 1 128.0 0.092 0.875 0.500 0.955 0.250 1.750 0.250 0.733 0.900 0.875 0.500 0.409
30 PSG: AHI ≥10/hr
Type II Study: AHI
≥10/hr
0.700 Sleep clinic patients
with suspected OSA
19 2 1 8 <0.001 0.905 0.889 0.950 0.800 8.143 0.107 0.900 0.921 0.950 0.l200
30 PSG: AHI ≥15/hr
Type II Study: AHI
≥15/hr
0.567 Sleep clinic patients
with suspected OSA
16 1 3 10 384.0 <0.001 0.941 0.769 0.842 0.909 4.078 0.076 0.867 0.942 0.842 0.091 0.636
* Abbreviations: +LR (positive likelihood ratio), -LR (negative likelihood ratio), AHI (apnea-hypopnea index), AUC (area under the curve), CABG (coronary artery bypass graft), CAD (coronary artery disease), COPD (chronic
obstructive pulmonary disease), CPAP (continuous positive airway pressure), FN (false negative), FP (false positive), N (number), NR (not reported), NPV (negative predictive value), MI (myocardial infarction), OSA (obstructive sleep apnea), OSAS (obstructive sleep apnea syndrome), PPV (positive predictive value), PSG (polysomnogram), RDI (respiratory disturbance index), Sen (sensitivity), Spec (specificity), TN (true negative), TP (true positive)
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

62
Table 10 - AHRQ Question 1a – Summary of Type III Portable Sleep Study Diagnostic Studies
Study Search
Strategy
Sample Demographics N Index/Validation OSA Definition OSA Prevalence Portable
Cut-point(s)
PSG
Cut-
Point(s)
Danzi-
Soares,
2012
Group 3 Consecutive
patients
referred for
CABG
Age: 58 ±7 years
Male: 76%
BMI: 27.6 ±27.6
ESS: 7 (range 5-
11)
AHI: 22.9 ±20.0
70 •Type III portable study
(Stardust II, Respironics)
•Type I Polysomnography
AHI: sum of apneas and
hypopneas per hour of
sleep
Hypopneas: 50 to 90%
decrease in nasal flow
with a >3% oxygen
desaturation
OSA: AHI ≥5/hr
No OSA (AHI <5/hr):
12.9% (9/70)
OSA (AHI ≥5/hr):
87.1% (61/70)
•Mild (AHI 5-15):
32.9% (23/70)
•Moderate (AHI 15-
30): 27.1% (19/70)
•Severe (AHI≥30):
27.1% (19/70)
Various:
AHI >5/hr
AHI >15/hr
Various:
AHI
>5/hr
AHI
>15/hr
Cheliout-
Heraut,
2011
Group 4 Patients with
suspected
OSA based
on daytime
sleepiness
and snoring
Age: 55.4 ±8.7
years
BMI: NR
Male: 67%
ESS: NR
AHI: NR
90 • Type III portable study
(Somnolter device,
Nomics) – automated
scoring
• Type 1
Polysomnography
(Embla)
AHI: sum of apneas and
hypopneas per hour of
sleep
Hypopneas: either ≥50
decrease in nasal flow OR
≥30 decrease in nasal
flow and either a ≥3%
oxygen desaturation or an
EEG arousal
OSA: AHI ≥5/hr
No OSA (AHI <5/hr):
8% (7/90)
OSA (AHI ≥5/hr): 92%
(83/90)
•Mild (AHI 5-15):
25% (21/83)
•Moderate (AHI 15-
30): 34% (28/83)
•Severe (AHI≥30):
41% (34/83)
AHI >5/hr
AHI
>5/hr
Driver,
2011
Group 4 Patients
referred to a
sleep lab for
diagnostic
sleep testing
Age: 52.9 ±12.2
years
BMI: 32.2 ±6.8
kg/m2
Male: 41%
ESS: NR
AHI: 26.0
±25.9/hr
73 • Type III portable study
(MediByte)
•Type 1
Polysomnography
AHI: sum of apneas and
hypopneas per hour of
sleep
Hypopneas: 50 to 90%
decrease in nasal flow and
a ≥3% oxygen
desaturation AND an
EEG arousal
OSA: AHI ≥5/hr
No OSA (AHI <5/hr)
16% (12/73)
OSA (AHI ≥5/hr): 84%
(61/73)
•Mild (AHI 5-15):
28% (17/61)
•Moderate (AHI 15-
30): 34% (21/61)
•Severe (AHI≥30):
38% (23/61)
Various:
AHI >5/hr
AHI >10/hr
AHI >15/hr
AHI >20/hr
AHI >30/hr
Various:
AHI
>5/hr
AHI
>10/hr
AHI
>15/hr
AHI
>20/hr
AHI
>30/hr
Gjevre, Group 4 Consecutive Age: 52 ±11.0 47 •Type III portable study AHI: sum of apneas and No OSA (AHI <5/hr): Various: AHI
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

63
2011 adult (age 21
to 70 years)
women
scheduled
for routine
PSG to
evaluate
clinically
suspected
OSA
years
Male: 100%
BMI: 34.9 ±9.0
kg/m2
ESS: 9.6 ±4.4
AHI: 15.1
±16.3/hr
(Embletta 2601-1)
•Type I Polysomnography
hypopneas per hour of
sleep
Hypopneas: ≥50 decrease
in nasal flow and a ≥3%
oxygen desaturation
OSA: AHI ≥5/hr
32% (15/47)
OSA (AHI ≥5/hr): 68%
(32/47)
•Mild/Mod (AHI 5-
30): 75% (24/47)
•Severe (AHI ≥30):
25% (8/47)
AHI >5/hr
AHI >10/hr
AHI >15/hr
AHI >20/hr
AHI >30/hr
>5/hr
Masa,
2011
Group 4 Sleep clinic
patients with
suspected
OSA
Age: 48.7 ±11.8
years
Male: 76%
BMI: 31.0
±6.6kg/m2
ESS: 11.6 ±5
AHI: 38.3
±28.5/hr
348 •Type III sleep study
(BreastSC20 or Breat
Medial AB)
•Type I Polysomnography
AHI: sum of apneas and
hypopneas per hour of
sleep
Hypopneas: ≥30%
decrease in airflow and
either ≥3% oxygen
desaturation or an EEG
arousal
OSA: AHI ≥5/hr
No OSA (AHI <5/hr)
9% (33/348)
OSA (AHI ≥5/hr): 91%
(315/348)
•Mild (AHI 5-15):
37% (129/315)
•Moderate (AHI 15-
30): 12% (42/215)
•Severe (AHI≥30):
41% (144/315)
Various:
AHI >5/hr
AHI >10/hr
AHI >15/hr
AHI >20/hr
AHI >25/hr
Various:
AHI
>5/hr
AHI
>10/hr
AHI
>15/hr
* Abbreviations: AHI (apnea-hypopnea index), BMI (body mass index), CABG (coronary artery bypass graft), CAD (coronary artery disease), COPD (chronic obstructive
pulmonary disease), CPAP (continuous positive airway pressure), DM (diabetes mellitus), EEG (electroencephalogram), ESS (Epworth sleepiness scale), hr (hour), IQR
(interquartile range), MI (myocardial infarction), N (number), NR (not reported), OSA (obstructive sleep apnea), OSAS (obstructive sleep apnea syndrome), mod (moderate),
PSG (polysomnogram), RDI (respiratory disturbance index), RERA (respiratory effort related arousal), SDB (sleep disordered breathing)
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

64
Table 11 - AHRQ Question 1a – Diagnostic Accuracy of Type III Portable Sleep Study Diagnostic Studies
Study N Cut-Point OSA
Prevalence
Population TP FN FP TN Diagnostic
Odds Ratio
p-
value
Sens Spec PPV NPV +LR -LR Accuracy AUC Pos Posttest
Probability
Neg Posttest
Probability
Kappa(1)
Coefficient
Danzi-Soares, 2012 70 •PSG: AHI ≥5/hr
•Type III Study: AHI
≥5/hr
0.871 CABG patients 56 5 3 6 22.40 <0.001 0.918 0.667 0.949 0.545 2.754 0.123 0.886 0.900 0.949 0.455 0.605
70 •PSG: AHI ≥15/hr
•Type III Study: AHI
≥15/hr
0.543 CABG patients 25 13 7 25 <0.001 0.658 0.781 0.781 0.658 3.01 0.520 0.714 0.790 0.781 0.342
Cheliout-Heraut,
2011
90 •PSG: AHI ≥5/hr
•Type III Study: AHI
≥5/hr
0.922 Sleep clinic patients
with suspected OSA
69 14 1 6 29.57 <0.001 0.831 0.857 0.986 0.300 5.819 0.197 0.833 NR 0.986 0.700 0.816
Driver, 2011 73 •PSG: AHI ≥5/hr
•Type III Study: AHI
≥5/hr
0.836 Sleep clinic patients 59 2 4 8 22.59 <0.001 0.967 0.667 0.937 0.800 2.902 0.049 0.918 0.940 0.937 0.200 0.614
73 •PSG: AHI ≥15/hr
•Type III Study: AHI
≥15/hr
0.603 Sleep clinic patients 35 9 1 28 <0.001 0.795 0.966 0.972 0.757 23.07 0.212 0.863 0.926 0.972 0.243
73 •PSG: AHI ≥30/hr
•Type III Study: AHI
≥30/hr
0.315 Sleep clinic patients 16 7 0 50 <0.001 0.696 1.00 1.00 0.877 NA 0.304 0.904 0.870 NA 0.123
Gjevre, 2011 47 •PSG: AHI ≥5/hr
•Type III Study: AHI
≥5/hr
0.681 Sleep clinic patients
with suspected OSA
31 1 6 9 30.69 <0.001 0.969 0.600 0.838 0.900 2.42 0.052 0.851 0.879 0.838 0.100 0.492
Masa, 2011 348 •PSG: AHI ≥5/hr
•Type III Study: AHI
≥5/hr
0.905 Sleep clinic patients
with suspected OSA
302 13 14 19 30.13 <0.001 0.959 0.576 0.956 0.594 2.260 0.072 0.922 0.917 0.956 0.406 0.533
348 •PSG: AHI ≥10/hr
•Type III Study: AHI
≥5/hr
0.905 Sleep clinic patients
with suspected OSA
274 41 5 28 <0.001 0.870 0.848 0.982 0.406 5.741 0.153 0.868 0.917 0.982 0.594
348 •PSG: AHI ≥5/hr
•Type III Study: AHI
≥10/hr
0.830 Sleep clinic patients
with suspected OSA
280 9 36 23 <0.001 0.969 0.390 0.886 0.719 1.588 0.080 0.871 0.883 0.886 0.281
348 •PSG: AHI ≥10/hr
•Type III Study: AHI
≥20/hr
0.830 Sleep clinic patients
with suspected OSA
205 84 6 53 <0.001 0.709 0.898 0.972 0.387 6.975 0.324 0.741 0.883 0.972 0.613
348 •PSG: AHI ≥15/hr
•Type III Study: AHI
≥10/hr
0.534 Sleep clinic patients
with suspected OSA
175 11 65 97 <0.001 0.941 0.599 0.729 0.898 2.345 0.099 0.782 0.891 0.729 0.102
348 •PSG: AHI ≥15/hr
•Type III Study: AHI
≥25/hr
0.534 Sleep clinic patients
with suspected OSA
125 61 13 149 <0.001 0.672 0.920 0.906 0.710 8.375 0.357 0.787 0.891 0.906 0.290
* Abbreviations: +LR (positive likelihood ratio), -LR (negative likelihood ratio), AHI (apnea-hypopnea index), AUC (area under the curve), CABG (coronary artery bypass graft), CAD (coronary artery disease), COPD (chronic
obstructive pulmonary disease), CPAP (continuous positive airway pressure), FN (false negative), FP (false positive), N (number), NR (not reported), NPV (negative predictive value), MI (myocardial infarction), OSA (obstructive sleep apnea), OSAS (obstructive sleep apnea syndrome), PPV (positive predictive value), PSG (polysomnogram), RDI (respiratory disturbance index), Sen (sensitivity), Spec (specificity), TN (true negative), TP (true positive)
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

65
Table 12 - AHRQ Question 1a – Summary of Type IV Portable Sleep Study Diagnostic Studies
Study Search
Strategy
Sample Demographics N Index/Validation OSA Definition OSA Prevalence Portable
Cut-point(s)
PSG
Cut-Point(s)
Nigro, 2013 Group
4
Sleep clinic
patients with suspected OSA
Age: 48.2 ±14.5 years
Male: 69% BMI: 30 ±7.2 kg/m2
ESS: NR
RDI: 15.1/hr (median, IQR 6.3-34.6)
55 •Type IV Sleep Study
(ApneaLink Ox)
•Type I Polysomnography
(Harmonie or MiniPC)
•Automatic analysis was also
assessed; manual scoring results reported for this report
AHI: NR
RDI: sum of apneas, hypopneas and RERA’s per
hour of sleep
Hypopneas: NR; “in agreement with international
criteria”
RERA: NR OSA: RDI ≥5/hr
OSA (RDI ≥5/hr): 78% (43/55)
No OSA (RDI <5): 22% (12/55) •Mild (RDI 5-15): 35% (15/55)
•Moderate (RDI 15-30): 30%
(13/55) •Severe (RDI ≥30): 35% (15/55)
AHI ≥5/hr RDI ≥5/hr
Morales,
2012
Group
4
Elderly patients
(population
study) with and
without sleepiness
Age: 71.3 ±5.9 years
Male: 34%
BMI: 30.5 ±7.6 kg/m2
ESS: NR (30% ESS >10) AHI: NR
92 •Type IV Sleep Study
(ResCare AutoSet, ResMed)
•Type I Polysomnography (Sandman, Embla)
AHI: sum of apneas and
hypopneas per hour of sleep
Hypopneas: ≥50% decrease
in nasal flow with either a ≥3% oxygen or EEG
arousals
OSA: AHI ≥30/hr and ESS >10
No OSA: 73% (70/92)
OSA (AHI ≥5 & ESS >10): 27%
(22/92)
•Mild (AHI 5-15 & ESS >10): 32% (7/22)
•Moderate (AHI 15-30 & ESS
>10): 23% (5/22) •Severe (AHI ≥30 & ESS >10):
45% (10/22)
AHI ≥20.9/hr AHI ≥30/hr
& ESS >10
O’Brien,
2012
Group
4
Women in third
trimester of
pregnancy
Age: 30.2 ±7.1 years
Male: 100%
BMI: 31.9 ±3.0 kg/m2 ESS: NR
AHI: 5.4 ±8.5/hr
31 •WatchPat 200 (Itamar)
•Type II Polysomnography (Medpalm)
AHI: sum of apneas and
hypopneas per hour of sleep
RDI: Number of respiratory events (apnea, hypopnea,
and RERA) per hour of
sleep Hypopneas: ≥50% decrease
in nasal flow with either a
≥3% oxygen or EEG arousal OSA: AHI ≥5/hr
No OSA (AHI <5): 74% (23/31)
OSA (AHI ≥5): 26% (8/31)
•Mild: 63% (5/8) •Moderate: 38% (3/8)
•Severe: 0% (0/8)
Various:
AHI ≥5/hr
AHI ≥6.1/hr
Various:
AHI ≥5/hr
RDI ≥10/hr
Onder, 2012 Group
4
Sleep clinic
patients with suspected OSA
Age: 43.3 ±12.9 years
Male: 64% BMI: 30.5 ±4.5 kg/m2
ESS: NR
AHI: 19.3 ±23.5/hr
59 •WatchPat 200 (Itamar)
•Type I Polysomnography
AHI: sum of apneas and
hypopneas per hour of sleep Hypopneas: ≥30% decrease
in nasal flow with a ≥4%
oxygen OSA: NR
No OSA: NR
OSA: NR
AHI ≥20/hr AHI ≥20/hr
Bahammam
2011
Group
3
Patients with
suspected OSA
Age: 46.3 ±12.6 years
BMI: 34.1 ±7.9 Male:61%
ESS:NR
AHI: 39.5 ±30.4/hr
97 •Type IV portable study
(ApneaLink)
•Type I Polysomnography
(Alice , Respironics)
AHI: sum of apneas and
hypopneas per hour of sleep Hypopneas: ≥50% decrease
in nasal flow with either a
≥3% oxygen or EEG arousal OSA: AHI ≥5/hr
No OSA (AHI <5): 85% (81/95)
OSA (AHI ≥5): 15% (14/95) •Mild: 27% (22/81)
•Moderate: 22% (18/81)
•Severe: 51% (41/81)
Various:
AHI ≥5/hr AHI ≥10/hr
AHI ≥15/hr
AHI ≥30/hr
Various:
AHI ≥5/hr AHI ≥10/hr
AHI ≥15/hr
AHI ≥30/hr
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

66
Chai-
Coetzer,
2011
Group
3
Adult patients
attending six primary care
clinics
Age: 55 years (range 45-
62) Male:53%
BMI: 31.7 kg/m2 (range
28.8-36.1) ESS: 8 (range 4-10)
AHI: 20.9/hr (range 13.1-
41.3)
77 •Type IV portable study
(ApneaLink)
•Type I Polysomnogram
AHI: NR
Hypopneas: Either ≥50% decrease in nasal flow or a
≥3% oxygen desaturation or
an EEG arousal OSA: AHI ≥30/hr
No OSA (AHI <30): 79% (62/78)
OSA (AHI ≥30): 21% (16/78) •Mild: NR
•Moderate: NR
•Mild: NR
AHI ≥30/hr AHI ≥30/hr
Chouchou,
2011
Group
4
Adult (Age ≥65
years) subjects
enrolled in the PROOF study
Age: 65.8 ±1.1years
Male: 43%
BMI: 25.4 ±4.0 kg/m2 ESS: 5.5 ±3.4
AHI: NR
780 •Pulse Transit Time (PTT)
measured on the Type 3 sleep
study –autonomic activation index (AAI) obtained from
PTT signal and broken down
into respiratory events.
• Type III Sleep Study
(HypnoPTT, Tyco Healthcare)
AHI: sum of apneas and
hypopneas per hour of sleep
Hypopneas: ≥50 decrease in nasal flow and a ≥3%
oxygen desaturation
OSA: AHI ≥15/hr
No OSA (AHI <5/hr): 9% (70/780)
OSA (AHI ≥5/hr): 91% (710/780)
•Mild (AHI 5-15): 37% (263/710) •Moderate (AHI 15-30): 38%
(270/710)
•Severe (AHI ≥30): 25% (177/710)
Various:
AAI ≥32.3/hr
AAI ≥56.3/hr
Various:
AHI ≥15/hr
AHI ≥30/hr
Hedner,
2011
Group
3
Multi-center
study cohort consisting of
139 sleep clinic
patients referred for suspected
OSA, 17 normal
volunteers and 71 subjects
randomly drawn
from a population
study
Age: 49 ±14 years
BMI: 29 ±6 kg/m2 Male: NR
ESS: NR
RDI: 30 ±23/hr
227 •WatchPat 100 (Itamar)
•Type I Polysomnography
RDI: Number of respiratory
events (apnea, hypopnea, and RERA) per hour of
sleep
Hypopneas: Not defined OSA: RDI ≥10/hr
No OSA: 17% (38/227)
OSA:83% (189/227) •Mild: 29% (54/189)
•Moderate: 43% (82/189)
•Severe: 28% (53/189)
RDI ≥10/hr
RDI ≥10/hr
Nigro, 2011 Group 4
Consecutive sleep clinic
patients with
suspected OSA (Mar 2008-Nov
2008).
Age: 49.6 ±15.1 years Male: 77%
BMI: 29.3 kg/m2
(median, IQR 25.2-32.5) ESS: NR
AHI: 11.8/hr (median; IQR
5.8-32.3) RDI: 13.9/hr (median,
IQR 7-34.1)
OSA (RDI ≥5): 83%
(75/90)
No OSA (RDI <5): 27%
(15/90)
90 •Type IV sleep study (ApneaLink, Resmed)
•Type I Polysomnogram (BiOPC or NEUROTRACE)
AHI: sum of apneas and hypopneas per hour of sleep
RDI: sum of apneas,
hypopneas and RERA’s per hour of sleep
Hypopneas: NR for PSG;
“In agreement with international criteria”
OSA: RDI ≥5/hr
No OSA (RDI <5): 27% (15/90) OSA (RDI ≥5): 83% (75/90)
Various: AHI ≥5/hr
AHI ≥10/hr
AHI ≥15/hr AHI ≥20/hr
AHI ≥30/hr
Various: RDI ≥5/hr
RDI ≥10/hr
RDI ≥15/hr RDI ≥20/hr
RDI ≥30/hr
Yang, 2011 Group
4
Chinese sleep
clinic patients
Age: 50.3 ±14.8 years
Male: 70%
86 •Type IV sleep study
(Oximetry and RIP-derived
AHI: sum of apneas and
hypopneas per hour of sleep
No OSA (AHI <5): 37% (32/86)
OSA (AHI ≥5): 63% (54/86)
Various:
AHI ≥5/hr
Various:
AHI ≥5/hr
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

67
BMI: 26.8 ±5.7 kg/m2
ESS: 8.0 ±4.6 AHI: 18.5 ±19.7/hr
X-flow)
•Type I Polysomnography
(Embla A10)
Hypopneas: ≥50% decrease
in airflow and either ≥4% oxygen desaturation or an
EEG arousal
OSA: AHI ≥5/hr
•Mild (AHI 5-15): 24% (13/54)
•Moderate (AHI 15-30): 39% (21/54)
•Severe (AHI ≥30): 37% (20/54)
AHI ≥15/hr
AHI ≥15/hr
Alvarez,
2010
Group
3
Symptomatic
patients with suspected OSA
Age: 52.9 ±14.1years
Male: 78% BMI: 29.8 ±5.6 kg/m2
ESS: NR
AHI: 29.0 ±28.5/hr
148 • Type IV sleep study
(Oximetry [sampling rate 1 Hz] and airflow derived from
PSG
•Type I Polysomnogram
(Alice 5, Respironics)
•Relationship between
changes in airflow and SpO2
(particularly peak amplitude and relative power in the very
low frequency band) were
analyzed via magnitude squared coherence function to
predict AHI
•Logistic regression was
performed on common
oximetry statistics in the time and frequency domains,
conventional spectral
characteristics from the
power spectral density
function and nonlinear
features. Variables assessed in model: relative power (PR),
fourth order statistical
moments in the time domain (M4t), Lempel-Ziv
complexity (LZC), second
order statistical moments in the time domain(M2t)
AHI: “sum of apneas and
hypopneas per hour of sleep Hypopneas: ≥50% decrease
in airflow and either ≥3%
oxygen desaturation or an EEG arousal
OSA: AHI ≥10/hr
No OSA (AHI <10/hr): 32%
(48/148) OSA (AHI ≥10/hr): 68% (100/148)
Peak
amplitude (PA), and
Relative
Power (PR) assessed for
SpO2, flow
and magnitude
squared
coherence;
relative power (PR), fourth
order
statistical moments in
the time
domain (M4t), Lempel-Ziv
complexity
(LZC), second order
statistical
moments in
the time
domain(M2t)
AHI ≥10
Nigro, 2010 Group
4
Consecutive
sleep clinic patients with
suspected OSA
(July 2007-Nov2007).
Age: 51.6 ±14.1 years
Male: 71% BMI: 29.3 ±5.4 kg/m2
ESS: NR
AHI: 9.5/hr (median, IQR 4.1-34.1)
RDI: 10.6/hr (median,
IQR 5.4-34.1)
66 •Type IV sleep study
(ApneaLink, Resmed)
•Type I Polysomnogram
(BIOPC or NEUROTRACE, Akonic)
AHI: sum of apneas and
hypopneas per hour of sleep RDI: sum of apneas,
hypopneas and RERA’s per
hour of sleep Hypopneas: Discernible
decrease in airflow and
either ≥3% oxygen RERA: an EEG arousal
No OSA (RDI <5): 23% (15/66)
OSA (RDI ≥5): 77% (51/66) •Mild (RDI 5-15): 39% (20/51)
•Moderate (RDI 15-30): 27%
(14/51) •Severe (RDI ≥30): 33% (17/51)
Various:
AHI ≥5/hr AHI ≥10/hr
AHI ≥15/hr
AHI ≥30/hr
Various:
RDI ≥5/hr RDI ≥10/hr
RDI ≥15/hr
RDI ≥30/hr
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

68
associated with an alteration
of the inspiratory contour in the waves from the
thoracoabdominal bands
OSA: RDI ≥5/hr
Yadollahi,
2010
Group
4
Sleep clinic
patients
Age: 51.4 ±11.9 years
Male: 71%
BMI: 31.9 ±6.4 kg/m2 ESS: NR
AHI: 23.6 ±30.3/hr
66 •Type IV sleep study
(Oximetry and tracheal sound
signals)
•Type I Polysomnogram
AHI: sum of apneas and
hypopneas per hour of sleep
Hypopneas: NR OSA: AHI ≥5/hr
No OSA: NR
OSA: NR
Various:
AHI ≥8.6/hr
AHI ≥13.0/hr AHI ≥18.5/hr
AHI ≥23.0/hr
Various:
AHI ≥5/hr
AHI ≥10/hr AHI ≥15/hr
AHI ≥20/hr
* Abbreviations: AHI (apnea-hypopnea index), BMI (body mass index), CABG (coronary artery bypass graft), CAD (coronary artery disease), COPD (chronic obstructive pulmonary disease), CPAP (continuous
positive airway pressure), DM (diabetes mellitus), EEG (electroencephalogram), ESS (Epworth sleepiness scale), hr (hour), IQR (interquartile range), MI (myocardial infarction), N (number), NR (not reported), OSA
(obstructive sleep apnea), OSAS (obstructive sleep apnea syndrome), mod (moderate), PSG (polysomnogram), RDI (respiratory disturbance index), RERA (respiratory effort related arousal), SDB (sleep disordered
breathing)
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

69
Table 13 – AHRQ Question 1a – Diagnostic Accuracy of Type IV Portable Sleep Study Diagnostic Studies
Study N Cut-Point OSA
Prevalence
Population TP FN FP TN p-value Sens Spec PPV NPV +LR -LR Accuracy AUC Pos Posttest
Probability
Neg Posttest
Probability
Nigro, 2013 55 •PSG: AHI ≥5/hr •Type IV Study: RDI
≥5/hr
0.782 Patients with suspected OSA
40 3 1 11 <0.001 0.930 0.917 0.976 0.786 11.16 0.076 0.927 0.923 0.976 0.214
O’Brien,
2012
31 •PSG: AHI ≥5/hr •WatchPAT: AHI
≥5/hr
0.258 Pregnant Women 7 1 3 20 <0.001 0.875 0.870 0.700 0.952 6.708 0.144 0.871 0.960 0.700 0.048
31 •PSG: AHI ≥5/hr
•WatchPAT: AHI ≥6.1/hr
0.258 Pregnant Women 7 1 2 21 <0.001 0.875 0.913 0.778 0.955 10.063 0.137 0.903 0.960 0.778 0.045
31 •PSG: RDI ≥10/hr
•WatchPAT: RDI ≥10/hr
0.258 Pregnant Women 5 0 5 21 <0.001 1.000 0.808 0.500 1.000 5.200 0.000 0.839 0.940 0.500 0.000
Morales,
2012
92 •PSG: RDI ≥20.9/hr
•Type IV Study: AHI ≥30/hr & ESS >10
0.109 Elderly patients
with and without daytime sleepiness
8 2 21 61 <0.001 0.800 0.744 0.276 0.968 3.124 0.269 0.750 0.791 0.276 0.032
Onder, 2012 59 •PSG: AHI ≥20/hr
•WatchPAT: AHI ≥20/hr
0.375 Sleep clinic
patients with suspected OSA
15 6 5 33 <0.001 0.714 0.868 0.750 0.846 5.429 0.329 0.857 NR 0.765 0.165
BaHammam,
2011
95 •PSG: AHI ≥5/hr
•Type IV Study: AHI
≥5/hr
0.853 Patients with
suspected OSA
81 0 8 6 <0.001 1.00 0.429 0.910 1.00 1.75 0.000 0.916 0.971 0.910 0.000
95 •PSG: AHI ≥15/hr
•Type IV Study: AHI ≥15/hr
0.621 Patients with
suspected OSA
58 1 15 21 <0.001 0.983 0.583 0.795 0.955 2.359 0.029 0.832 0.924 0.795 0.045
95 •PSG: AHI ≥30/hr
•Type IV Study: AHI
≥30/hr
0.432 Patients with
suspected OSA
41 0 11 43 <0.001 1.00 0.796 0.788 1.00 4.91 0.000 0.884 0.997 0.788 0.000
Chai-Coetzer,
2011
77 •PSG: AHI ≥30/hr
•Type IV Study: AHI
≥30/hr
0.210 Primary care
clinic patients
. . . . . . . . . . . . 0.950 . .
Chouchou,
2011
780 •PSG: AHI ≥15/hr
•Type IV Study: AAI
≥32.3/hr
0.573 Elderly patients 315 132 151 182 <0.001 0.705 0.547 0.676 0.580 1.554 0.540 0.637 0.670 0.676 0.420
780 •PSG: AHI ≥30/hr
•Type IV Study: AAI
≥56.3/hr
0.227 Elderly patients 57 120 32 571 <0.001 0.322 0.947 0.640 0.826 6.068 0.716 0.805 0.740 0.640 0.174
Hedner, 2011 227 •PSG: RDI ≥10/hr NR Suspected OSA, . . . . . . . . . . . . 0.960 . .
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

70
• WatchPAT: RDI
≥10/hr
healthy volunteers
and population study subjects
Nigro, 2011 90 •PSG: RDI ≥5/hr
•Type IV Study: AHI ≥5/hr
0.833 Sleep clinic
patients
67 8 2 13 <0.001 0.893 0.867 0.971 0.619 6.700 0.123 0.889 0.880 0.971 0.381
90 •PSG: RDI ≥10/hr
•Type IV Study: AHI
≥10/hr
0.744 Sleep clinic
patients
49 18 2 21 <0.001 0.731 0.913 0.961 0.538 8.410 0.294 0.778 0.822 0.961 0.462
90 •PSG: RDI ≥15/hr
•Type IV Study: AHI
≥15/hr
0.478 Sleep clinic
patients
31 12 1 46 <0.001 0.721 0.979 0.969 0.793 33.88 0.285 0.856 0.850 0.969 0.207
90 •PSG: RDI ≥20/hr •Type IV Study: AHI
≥20/hr
0.367 Sleep clinic patients
29 4 1 56 <0.001 0.879 0.982 0.967 0.933 50.09 0.123 0.944 0.931 0.967 0.067
90 •PSG: RDI ≥30/hr •Type IV Study: AHI
≥30/hr
0.289 Sleep clinic patients
22 4 1 63 <0.001 0.846 0.984 0.957 0.940 54.15 0.156 0.944 0.915 0.957 0.060
Yang, 2011 86 •PSG: AHI ≥5/hr •Type IV Study: AHI
≥5/hr
0.628 Chinese sleep clinic patients
53 1 0 32 <0.001 0.981 1.000 1.000 0.970 NA 0.019 0.988 NR NA 0.030
86 •PSG: AHI ≥15/hr
•Type IV Study: AHI ≥15/hr
0.477 Chinese sleep
clinic patients
35 6 1 44 <0.001 0.854 0.978 0.972 0.880 38.41 0.150 0.919 NR 0.972 0.120
Alvarez, 2010 148 •PSG: AHI ≥10/hr •Type IV Study:
PAFlow
0.676 Symptomatic patients with
suspected OSA
84 16 7 41 <0.001 0.840 0.854 0.923 0.719 5.760 0.187 0.845 0.904 0.923 0.281
148 •PSG: AHI ≥10/hr
•Type IV Study: PFlow
0.676 Symptomatic
patients with suspected OSA
68 32 13 32 <0.001 0.680 0.729 0.840 0.522 2.511 0.439 0.696 0.739 0.840 0.478
148 •PSG: AHI ≥10/hr
•Type IV Study: PAMSC
0.676 Symptomatic
patients with suspected OSA
81 19 7 41 <0.001 0.810 0.854 0.920 0.683 5.554 0.222 0.824 0.903 0.920 0.317
148 •PSG: AHI ≥10/hr
•Type IV Study: PMSC
0.676 Symptomatic
patients with
suspected OSA
77 23 7 41 <0.001 0.770 0.854 0.917 0.641 5.280 0.269 0.797 0.884 0.917 0.359
Nigro, 2010 66 •PSG: RDI ≥5/hr
•Type IV Study: AHI
≥5/hr
0.773 Patients with
suspected OSA
45 6 2 13 <0.001 0.882 0.867 0.957 0.684 6.618 0.136 0.879 0.875 0.957 0.316
66 •PSG: RDI ≥10/hr
•Type IV Study: AHI
≥10/hr
0.545 Patients with
suspected OSA
32 4 3 27 <0.001 0.889 0.900 0.914 0.871 8.889 0.123 0.894 0.890 0.914 0.129
66 •PSG: RDI ≥15/hr •Type IV Study: AHI
≥15/hr
0.470 Patients with suspected OSA
29 2 3 32 <0.001 0.935 0.914 0.906 0.941 10.91 0.071 0.924 0.925 0.906 0.059
66 •PSG: RDI ≥30/hr 0.258 Patients with 17 0 5 44 <0.001 1.000 0.898 0.773 1.000 9.800 0.000 0.924 NR 0.773 0.000
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

71
•Type IV Study: AHI
≥30/hr
suspected OSA
35 •PSG: RDI ≥5/hr •Type IV Study: AHI
≥5/hr
0.303 Patients with suspected OSA
found to have mild
or no OSA
15 5 2 13 <0.001 0.750 0.867 0.882 0.722 5.625 0.288 0.424 NR 0.710 0.111
49 •PSG: RDI ≥5/hr
•Type IV Study: AHI
≥15/hr
0.286 Patients with
suspected OSA
excluding those found to have
severe OSA
12 2 3 32 <0.001 0.857 0.914 0.800 0.941 10.00 0.156 0.898 NR 0.800 0.059
Yadollahi,
2010
66 •PSG: AHI ≥5/hr •Type IV Study: AHI
≥8.6/hr
NR Sleep clinic patients
. . . . . 0.743 0.824 . . . . . 0.870 . .
66 •PSG: AHI ≥10/hr
•Type IV Study: AHI ≥13/hr
NR Sleep clinic
patients
. . . . . 0.828 0.911 . . . . . 0.950 . .
66 •PSG: AHI ≥15/hr
•Type IV Study: AHI ≥18.5/hr
NR Sleep clinic
patients
. . . . . 0.846 0.960 . . . . . 0.960 . .
66 •PSG: AHI ≥20/hr
•Type IV Study: AHI
≥23.0/hr
NR Sleep clinic
patients
. . . . . 0.916 0.978 . . . . . 0.990 . .
* Abbreviations: +LR (positive likelihood ratio), -LR (negative likelihood ratio), AHI (apnea-hypopnea index), AUC (area under the curve), CABG (coronary artery bypass graft), CAD (coronary artery disease), COPD (chronic obstructive
pulmonary disease), CPAP (continuous positive airway pressure), FN (false negative), FP (false positive), N (number), NR (not reported), NPV (negative predictive value), MI (myocardial infarction), OSA (obstructive sleep apnea), OSAS (obstructive sleep apnea syndrome), PPV (positive predictive value), PSG (polysomnogram), RDI (respiratory disturbance index), Sen (sensitivity), Spec (specificity), TN (true negative), TP (true positive)
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

72
Table 14 - AHRQ Question 1a – Summary of Oximetry Diagnostic Studies (Oxygen Desaturation Index)
Study Search
Strategy
Sample Demographics N Index/Validation OSA Definition OSA Prevalence Oximetry
Cut-point(s)
PSG
Cut-Point(s)
Alvarez, 2012 Group 4 Sleep clinic patients with
high clinical
suspicion for OSA
Age: 52.3 ±13.7 years Male: 78%
BMI: 29.8 ±4.4 kg/m2
ESS: NR AHI: 25.7 ±26.1/hr
96 •Nonin Puresat pulse oximeter (≤3 sec averaging signal;
sampling rate 1 Hz)
• Type I Polysomnography
(Alice 5, Respironics)
AHI: sum of apneas and hypopneas per hour of sleep
Hypopneas: ≥50% decrease in
nasal flow with either a >3% oxygen desaturation or an
EEG arousal
OSA: AHI ≥10/hr
OSA (AHI ≥10/hr): 67% (160/240)
No OSA (AHI <10): 33%
(80/240)
ODI (3%) ≥10/hr
AHI ≥10/hr
Chung, 2012 Group 3 Consecutive
preoperative
adults scheduled for
surgery.
Age: 60.3 ±12.7 years
Male: 54%
BMI: 30.5 ±6.8 kg/m2 ESS: NR
AHI: 9.1/hr (median, IQR 3.8-
21.4)
475 •PULSOX-300i pulse
oximeter wristwatch
(averaging time 3 seconds)
•Type II Polysomnography
(Embletta X100)
AHI: sum of apneas and
hypopneas per hour of sleep
Hypopneas: 30 to 90% decrease in nasal flow with a
>4% oxygen desaturation
OSA: AHI ≥5/hr
No OSA (AHI <5): 36%
(171/475)
OSA (AHI ≥5): 64% (337/475) •Mild (AHI 5-15): 29%
(138)
•Moderate (AHI 15-30): 19% (92)
•Severe (AHI ≥30): 16%
(74)
Various:
ODI (4%)
>5/hr ODI (4%)
>10/hr
ODI (4%) >15/hr
ODI (4%)
>30/hr
Various:
AHI >5/hr
AHI >15/hr AHI >30/hr
Ling, 2012 Group 3 Sleep disorder
clinic patients
referred for diagnostic
PSG
Age: 51.2 ±14.0 years
Male: 65%
BMI: 32.5 ±9.0 kg/m2 ESS: NR
AHI: 31.3 ±29.3/hr
11,448 •Integrated oximeter (Nonin
Xpod 3011, Nonin medical)
•Type I Polysomnography
(Compumedics E-series)
AHI: “Respiratory events
were scored using Chicago
criteria” Hypopneas: ≥50% decrease
in nasal flow with either a
≥3% oxygen desaturation or
an arousal
OSA: AHI ≥5/hr
No OSA (AHI <15): 36%
(4121/11448)
OSA (AHI ≥15): 64% (7327/11448)
Various:
ODI (2%)
≥10/hr ODI (2%)
≥15/hr
ODI (2%)
≥20/hr
ODI (3%)
≥10/hr ODI (3%)
≥15/hr
ODI (3%) ≥20/hr
ODI (4%)
≥10/hr ODI (4%)
≥15/hr
ODI (4%) ≥20/hr
Various:
AHI ≥15/hr
AHI ≥30/hr
Morillo, 2012 Group 3 Sleep disorder
clinic patients with suspected
OSA
Age: 58.3 ±12.5 years
Male: 74% BMI: 32.1 ±6.3 kg/m2
ESS: NR
AHI: 28.9 ±28.3/hr
78 •Jaeger 70750A19 oximeter
(8 cycles per second)
•Type I Polysomnography
(Erich Jaeger)
AHI: sum of apneas and
hypopneas per hour of sleep Hypopneas: ≥50% decrease
in nasal flow with a ≥4%
oxygen OSA: AHI ≥5/hr
No OSA (AHI <5): NR
OSA (AHI ≥5): NR
Various:
ODI (4%) ≥9/hr
ODI (4%)
≥12/hr ODI (4%)
Various:
AHI ≥5/hr AHI ≥10/hr
AHI ≥15/hr
AHI ≥20/hr
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

73
•Chose optimal threshold
cut-point for ODI to comparison with PSG AHI
≥13/hr
ODI (4%) ≥19/hr
Nigro, 2012 Group 4 Sleep disorder
clinic patients with suspected
OSA
Age: 53.7 ±15.4 years
Male: 77% BMI: 27.5 kg/m2 (median, IQR
24.7-31.2)
ESS: NR AHI: 21.3/hr (median, IQR
8.8-43.5)
RDI: 24/hr (median, IQR 11.5-45.3)
119 •Oximetry (Nonin)
• Type I Polysomnography
(Neurotrace or MiniPC)
AHI: NR
RDI: sum of apneas, hypopneas and RERA’s per
hour of sleep
Hypopneas: NR; “in agreement with international
criteria”
RERA: NR OSA: RDI ≥5/hr
No OSA (RDI <5): 14%
(17/119) OSA (RDI ≥5): 86%
(102/119)
Various:
ODI (3%) ≥15/hr OR
ODI (3%)
≥5/hr and ESS ≥12 or
comorbidity
ODI (4%)
≥15/hr OR
ODI (4%)
≥5/hr and ESS
≥12 or
comorbidity
RDI ≥15/hr
OR RDI ≥5/hr and
ESS ≥12 or
comorbidity (HTN,
cardiac
arrhythmias, CAD,
CVD, DM)
Sommerymeyer,
2012
Group 4 Sleep disorder
clinic patients
with suspected SDB
Age: 54.0 ±14.0 years
Male: 63%
BMI: 28.5 ±5.9 kg/m2 ESS: 10.0 ±5.0
AHI: 19.3 ±18.5/hr
66 • Oximetry – ODI
automatically scored by either
≥4% SO2 drop or ≥3% SpO2 drop with an autonomic
arousal (pulse rate ≥20%
from baseline or pulse wave amplitude (PWA) attenuation
≥40% from baseline or PWA
attenuation ≥35% with pulse rate increase ≥15% from
baseline.
• Type III Sleep Study
(SOMNOcheck2)
AHI: sum of apneas and
hypopneas per hour of sleep
Hypopneas: ≥50% decrease in nasal flow with a ≥3%
oxygen
OSA: AHI ≥5/hr
No OSA (AHI <5): 35%
(23/66)
OSA (AHI ≥5): 65% (43/66) •Mild (AHI 5-15): 33%
(14/43)
•Moderate (AHI 15-30): 33% (14/43)
•Severe (AHI ≥30): 35%
(15/43)
ODI (3% &
4%) ≥15/hr
AHI ≥15/hr
Ward, 2012 Group 3 Adult patients with low or
preserved
ejection fraction heart
failure
Age: 69.8 years (median, IQR 58.8-76.8)
Male: 86%
BMI: 29.1 kg/m2 (median, IQR 25.4-32.7)
ESS: NR
AHI: NR; for SDB 27.0 (median)
171 •Wrist worn pulse oximeter (Pulsox 3i, Konica Minolta,
sampling time 5s & data
storage frequency 0.2 Hz)
•Type II Polysomnography
(SOMNOscreen, SOMNOmedics)
AHI: sum of apneas and hypopneas per hour of sleep
Hypopneas: ≥50% decrease
in nasal flow with either a ≥3% oxygen or EEG arousal
OSA: AHI ≥15/hr
•reported data separately for
with and without very low
frequency increment of heart
rate variability
No OSA (AHI <15): 56% (96/171)
OSA (AHI ≥15): 45%
(77/171)
Various: ODI (3%)
≥7.5/hr
ODI (3%) ≥12.5/hr
AHI ≥15/hr
Bohning, 2011 Group 4 Consecutive
sleep clinic patients
Age: 55 ±13 years
Male: 82% BMI:31.6 ±5.9 kg/m2
ESS: NR
135 •Oximetry (Nonin model
3100 WristOx): ODI (undefined)
AHI: NR
Hypopneas: NR OSA: AHI ≥5/hr
No OSA (AHI <5): 13%
(18/135) OSA (AHI ≥5): 87%
(117/135)
Various:
ODI ≥5/hr ODI ≥15/hr
Various:
AHI ≥5/hr AHI ≥15/hr
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

74
AHI: NR •Type I Polysomnography •Mild (AHI 5-15): 34%
(40/117) •Moderate (AHI 15-30):
21% (25/117)
•Severe (AHI ≥30): 44% (52/117)
Chai-Coetzer,
2011
Group 3 Adult
patients attending six
primary care
clinics
Age: 55 years (range 45-62)
Male:53% BMI: 31.7 kg/m2 (range 28.8-
36.1)
ESS: 8 (range 4-10) AHI: 20.9/hr (range 13.1-41.3)
77 • Oximetry recorded from
ApneaLink device
•Type I Polysomnogram
AHI: NR
Hypopneas: Either ≥50% decrease in nasal flow or a
≥3% oxygen desaturation or
an EEG arousal OSA: AHI ≥30/hr
No OSA (AHI <30): 79%
(62/78) OSA (AHI ≥30): 21% (16/78)
•Mild: NR
•Moderate: NR •Mild: NR
AHI ≥30/hr AHI ≥30/hr
Alvarez, 2010 Group 3 Symptomatic
patients with suspected
OSA
Age: 52.9 ±14.1 years
Male: 78% BMI: 29.8 ±5.6 kg/m2
ESS: NR
AHI: 29.0 ±28.5/hr
148 • Oximetry derived from PSG
(sampling rate 1 Hz)
•Type I Polysomnogram
(Alice 5, Respironics)
AHI: “sum of apneas and
hypopneas per hour of sleep Hypopneas: ≥50% decrease
in airflow and either ≥3%
oxygen desaturation or an EEG arousal
OSA: AHI ≥10/hr
No OSA (AHI <10/hr): 32%
(48/148) OSA (AHI ≥10/hr): 68%
(100/148)
Various:
ODI(2%) ≥10/hr
ODI(3%)
≥10/hr ODI(4%)
≥10/hr
AHI ≥10/hr
* Abbreviations: AHI (apnea-hypopnea index), BMI (body mass index), CABG (coronary artery bypass graft), CAD (coronary artery disease), COPD (chronic obstructive pulmonary disease), CPAP (continuous positive
airway pressure), DM (diabetes mellitus), EEG (electroencephalogram), ESS (Epworth sleepiness scale), hr (hour), IQR (interquartile range), MI (myocardial infarction), N (number), NR (not reported), OSA (obstructive sleep
apnea), OSAS (obstructive sleep apnea syndrome), mod (moderate), PSG (polysomnogram), RDI (respiratory disturbance index), RERA (respiratory effort related arousal), SDB (sleep disordered breathing)
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

75
Table 15 - AHRQ Question 1a – Diagnostic Accuracy of Oximetry Diagnostic Studies (Oxygen Desaturation Index)
Study N Cut-Point OSA
Prevalence
Population TP FN FP TN p-
value
Sens Spec PPV NPV +LR -LR Accuracy AUC Pos
Posttest
Probability
Neg
Posttest
Probability
Alvarez, 2012 96 •PSG: AHI ≥10/hr
•Oximetry: ODI(3%) ≥10/hr
0.667 Sleep clinic patients
with suspected OSA
57 7 4 28 <0.001 0.891 0.875 0.934 0.800 7.125 0.125 0.885 NR 0.934 0.200
Chung, 2012 475 •PSG: AHI ≥5/hr
•Oximetry: ODI(4%) ≥5/hr
0.640 Preoperative patients 293 11 56 115 <0.001 0.964 0.673 0.840 0.913 2.943 0.054 0.859 0.908 0.840 0.087
475 •PSG: AHI ≥15/hr
•Oximetry: ODI(4%) ≥5/hr
0.349 Preoperative patients 165 1 190 119 <0.001 0.994 0.385 0.465 0.992 1.617 0.016 0.598 NR 0.465 0.008
475 •PSG: AHI ≥30/hr
•Oximetry: ODI(4%) ≥5/hr
0.156 Preoperative patients 74 0 285 116 <0.001 1.00 0.289 0.206 1.00 1.407 0.000 0.156 NR 0.206 0.000
475 •PSG: AHI ≥5/hr
•Oximetry: ODI(4%) ≥15/hr
0.640 Preoperative patients 137 167 3 168 <0.001 0.451 0.982 0.979 0.501 25.69 0.559 0.642 NR 0.979 0.499
475 •PSG: AHI ≥15/hr
•Oximetry: ODI(4%) ≥15/hr
0.349 Preoperative patients 116 50 23 286 <0.001 0.699 0.926 0.835 0.851 9.388 0.325 0.846 0.931 0.835 0.149
475 •PSG: AHI ≥30/hr
•Oximetry: ODI(4%) ≥15/hr
0.156 Preoperative patients 70 4 74 327 <0.001 0.946 0.815 0.486 0.988 5.126 0.066 0.836 NR 0.486 0.012
475 •PSG: AHI ≥5/hr
•Oximetry: ODI(4%) ≥30/hr
0.640 Preoperative patients 66 238 1 170 <0.001 0.217 0.994 0.985 0.417 37.13 0.788 0.497 NR 0.985 0.583
475 •PSG: AHI ≥15/hr
•Oximetry: ODI(4%) ≥30/hr
0.349 Preoperative patients 64 102 2 307 <0.001 0.386 0.994 0.970 0.751 59.57 0.618 0.781 NR 0.970 0.249
475 •PSG: AHI ≥30/hr
•Oximetry: ODI(4%) ≥30/hr
0.156 Preoperative patients 56 18 11 390 <0.001 0.757 0.973 0.836 0.956 27.59 0.250 0.939 0.958 0.836 0.044
Ling, 2012 11,448 •PSG: AHI ≥15/hr
•Oximetry: ODI(3%) ≥15/hr
0.640 Sleep clinic patients 4521 2806 346 3775 <0.001 0.617 0.916 0.929 0.574 7.349 0.418 0.725 NR 0.929 0.426
11,448 •PSG: AHI ≥30/hr
•Oximetry: ODI(3%) ≥30/hr
0.386 Sleep clinic patients 2576 1843 309 6720 <0.001 0.583 0.956 0.893 0.785 13.26 0.436 0.812 NR 0.893 0.215
11,448 •PSG: AHI ≥15/hr
•Oximetry: ODI(4%) ≥15/hr
0.640 Sleep clinic patients 3121 4206 70 4051 <0.001 0.426 0.983 0.978 0.491 25.08 0.584 0.626 NR 0.978 0.509
11,448 •PSG: AHI ≥30/hr
•Oximetry: ODI(4%) ≥30/hr
0.386 Sleep clinic patients 1706 2713 42 6987 <0.001 0.386 0.994 0.976 0.720 64.61 0.618 0.759 NR 0.976 0.280
Morillo, 2012 78 •PSG: AHI ≥5/hr
•Oximetry: ODI (4%) ≥9/hr
NR Sleep clinic patients
with suspected OSA
. . . . . 0.832 0.790 . . 2.97 0.19 . 0.910 . .
78 •PSG: AHI ≥10/hr
•Oximetry: ODI (4%) ≥12/hr
NR Sleep clinic patients
with suspected OSA
. . . . . 0.872 0.805 . . 4.47 0.16 . 0.910 . .
78 •PSG: AHI ≥15/hr
•Oximetry: ODI (4%) ≥13/hr
NR Sleep clinic patients
with suspected OSA
. . . . . 0.923 0.769 . . 3.43 0.11 . 0.910 . .
78 •PSG: AHI ≥20/hr
•Oximetry: ODI (4%) ≥19/hr
NR Sleep clinic patients
with suspected OSA
. . . . . 0.848 0.828 . . 4.92 0.18 . 0.930 . .
Nigro, 2012 119 •PSG: RDI ≥15/hr OR RDI ≥5/hr and
ESS ≥12 or comorbidity
•Oximetry ODI (3%) ≥15/hr OR ODI
(3%) ≥5/hr and ESS ≥12 or
comorbidity
0.798 Sleep clinic patients
with suspected OSA
88 7 2 22 <0.001 0.926 0.917 0.978 0.759 11.12 0.080 0.924 0.923 0.978 0.241
119 •PSG: RDI ≥15/hr OR RDI ≥5/hr and
ESS ≥12 or comorbidity
•Oximetry: ODI (4%) ≥15/hr OR
ODI (4%) ≥5/hr and ESS ≥12 or
comorbidity
0.790 Sleep clinic patients
with suspected OSA
75 19 1 24 <0.001 0.798 0.960 0.987 0.558 19.95 0.211 0.832 0.879 0.987 0.442
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

76
Sommerymeyer,
2012
66 •PSG: AHI ≥15/hr
•Oximetry: ODI (3% and 4%) ≥15/hr
0.439 Sleep clinic patients
with suspected SDB
28 1 2 35 <0.001 0.966 0.946 0.933 0.972 17.86 0.036 0.955 0.980 0.933 0.028
Ward, 2012 171 •PSG: AHI ≥15/hr
•Oximetry: ODI(3%) ≥7.5/hr
0.444 CHF patients 74 2 65 30 <0.001 0.974 0.316 0.532 0.938 1.423 0.083 0.608 0.920 0.532 0.062
171 •PSG: AHI ≥15/hr
•Oximetry: ODI(3%) ≥12.5/hr
0.444 CHF patients 71 5 26 69 <0.001 0.934 0.726 0.732 0.932 3.413 0.091 0.819 NR 0.732 0.068
Bohning, 2011 134 •PSG: AHI ≥5/hr
•Oximetry: ODI (undefined) ≥5/hr
0.873 Sleep clinic patients
with suspected OSA
117 0 11 6 <0.001 1.000 0.353 0.914 1.000 1.545 0.000 0.918 NR 0.914 0.000
134 •PSG: AHI ≥15/hr
•Oximetry: ODI (undefined) ≥15/hr
0.784 Sleep clinic patients
with suspected OSA
51 26 1 56 <0.001 0.662 0.982 0.981 0.683 37.75 0.344 0.799 NR 0.981 0.317
Chai-Coetzer,
2011
77 •PSG: AHI ≥30/hr
•Oximetry: ODI (3%) ≥30/hr
0.210 Primary care clinic
patients
. . . . . . . . . . . . 0.960 . .
Alvarez, 2010 148 •PSG: AHI ≥10/hr
•Oximetry: ODI (2%) ≥10/hr
0.676 Sleep clinic patients
with suspected OSA
85 15 6 42 <0.001 0.850 0.875 0.934 0.737 6.80 0.171 0.858 0.943 0.934 0.263
148 •PSG: AHI ≥10/hr
•Oximetry: ODI (3%) ≥10/hr
0.676 Sleep clinic patients
with suspected OSA
86 14 7 41 <0.001 0.860 0.854 0.925 0.745 5.90 0.164 0.858 0.932 0.925 0.255
148 •PSG: AHI ≥10/hr
•Oximetry: ODI (4%) ≥10/hr
0.676 Sleep clinic patients
with suspected OSA
85 15 6 42 <0.001 0.850 0.875 0.934 0.737 6.80 0.171 0.858 0.922 0.934 0.263
* Abbreviations: +LR (positive likelihood ratio), -LR (negative likelihood ratio), AHI (apnea-hypopnea index), AUC (area under the curve), CPAP (continuous positive airway pressure), FN (false negative), FP (false positive), N
(number), NR (not reported), NPV (negative predictive value), ODI (oxygen desaturation index), OSA (obstructive sleep apnea), PPV (positive predictive value), PSG (polysomnogram), RDI (respiratory disturbance index), Sen (sensitivity), Spec (specificity), TN (true negative), TP (true positive)
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

77
Table 16 – Summary of Oximetry Diagnostic Studies (Other than Oxygen Desaturation Index)
Study Search
Strategy
Sample Demographics N Index/Validation OSA Definition OSA Prevalence Oximetry
Cut-point(s)
PSG
Cut-Point(s)
Alvarez,
2012
Group 4 Sleep clinic patients with
high clinical
suspicion for OSA
Age: 52.3 ±13.7 years
Male: 78%
BMI: 29.8 ±4.4 kg/m2
ESS: NR
AHI: 25.7 ±26.1/hr
144 •Nonin Puresat pulse oximeter (≤3 sec averaging signal; sampling rate 1 Hz)
• Type I Polysomnography (Alice 5, Respironics) •16 features (time and frequency statistics and
spectral and nonlinear features) were computed
using a genetic algorithm. Optimal model contained 6 variables: time domain statistics (M1t,
M3t, M4T), frequency domain statistics (MF),
conventional spectral measures (PA) and nonlinear
measures (CTM).
AHI: sum of apneas and hypopneas per hour of
sleep
Hypopneas: ≥50% decrease in nasal flow
with either a >3% oxygen
desaturation or an EEG arousal
OSA: AHI ≥10/hr
No OSA (AHI <10): 33% (80/240)
OSA (AHI ≥10/hr): 67%
(160/240)
NR
AHI ≥10/hr
Marcos,
2012
Group 3 Symptomatic
patients (sleepiness,
snoring,
witnessed apneas)
suspected of
sleep apnea. Initial
population
randomly divided into
training and
test sets.
Age: 52.2 ±13.7
years Male: 78%
BMI: 29.8 ±4.5
kg/m2 ESS: NR
AHI: 26.4
±26.7/hr
144 •Nonin Puresat pulse oximeter (averaging time 3
seconds)
•Type I Polysomnography (Alice 5, Respironics,
Philips Healthcare) •Multiple linear regression and multilayer
perceptron neural networks evaluated oximetry
data ( time-domain, frequency-domain parameters) to derive oximetry algorithm predictive of OSA
AHI: “Per rules proposed
by Rechtschaffen and Kales”
Hypopneas: NR
OSA: AHI ≥5/hr
No OSA (AHI <5): 80%
(115/144) OSA AHI ≥5):: 20%
(29/144)
•Mild (AHI 5-15): 30% (35/115)
•Moderate (AHI 15-30):
26% (30/115) •Severe (AHI ≥30): 43%
(50/115)
Various:
AHI ≥5/hr AHI ≥10/hr
AHI ≥15/hr
AHI ≥30/hr
Various:
AHI ≥5/hr AHI ≥10/hr
AHI ≥15/hr
AHI ≥30/hr
Morillo,
2012
Group 3 Sleep disorder
clinic patients
with suspected OSA
Age: 58.3 ±12.5
years
Male: 74% BMI: 32.1 ±6.3
kg/m2
ESS: NR AHI: 28.9
±28.3/hr
78 •Jaeger 70750A19 oximeter (8 cycles per second)
•Type I Polysomnography (Erich Jaeger) •An alternative frequency desaturation index
(FDI) was obtained by regression analysis
•Chose optimal threshold cut-point for FDI to comparison with PSG AHI
AHI: sum of apneas and
hypopneas per hour of
sleep Hypopneas: ≥50%
decrease in nasal flow
with either a ≥4% oxygen OSA: AHI ≥5/hr
No OSA (AHI <5): NR
OSA (AHI ≥5): NR
Various:
FDI ≥7.45/hr
FDI ≥15.5/hr FDI ≥19.1/hr
FDI ≥22.0/hr
Various:
AHI ≥5/hr
AHI ≥10/hr AHI ≥15/hr
AHI ≥20/hr
Batchelder,
2011
Group 3 Consecutive patients
referred for
suspected SDB
Age: 52.7 ±13 years
Male:
BMI:36.0 ±9.6 kg/m2
ESS: NR AHI: NR
104 •Nellcor OxiMax Max-A digit sensor and Nellcor N-600x pulse oximeter (Covidien)
•Type III sleep study (in-lab study; although additional PSG channels were captured; only
airflow, oximetry and respiratory inductance plethysmography were evaluated).
•Pulse oximetry saturation patterns recognition
AHI: NR Hypopneas: ≥40%
decrease in nasal flow
with a ≥3% oxygen desaturation
OSA: AHI ≥5/hr
No OSA: NR OSA: NR
NA (unit of analysis
was respiratory
event – not patient; various threshold
were High, Medium and Low
saturation pattern
detection)
NA (unit of
analysis
was respiratory
event – not patient;
various
threshold
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

78
algorithm (OxiMax SPD) designed to detect
specific signatures of SpO2 trend associated with repetitive reductions in airflow (RRiA)
were High,
Medium and Low
saturation
pattern detection)
Marcos,
2011
Group 3 Patients
suspected of OSA
Age: 52.4 ±13.8
years Male: 77%
BMI: 29.8 ±4.2
kg/m2 ESS: NR
AHI: 24.8
±25.2/hr
96 • Nonin PurseSat pulse oximeter (sampling
frequency of 1 Hz)
•Type I Polysomnography (Alice 5, Respironics)
•KerEnt analysis (nonlinear measure) of SpO2
signals to evaluate degree of irregularity to predict
AHI
AHI: “According to the
rules proposed by Rechtschaffen and Kales”
Hypopneas: NR
OSA: AHI ≥10/hr
No OSA (AHI <10/hr): 33%
(32/96) OSA (AHI ≥10/hr): 67%
(64/96)
Oximetry KerEnt
Analysis: -0.02 threshold
AHI ≥10/hr
Alvarez,
2010
Group 3 Symptomatic patients with
suspected
OSA
Age: 52.9 ±14.1years
Male: 78%
BMI: 29.8 ±5.6 kg/m2
ESS: NR
AHI: 29.0 ±28.5/hr
148 • Oximetry derived from PSG (sampling rate 1 Hz)
•Type I Polysomnogram (Alice 5, Respironics)
•Relationship between changes in airflow and
SpO2 (particularly peak amplitude and relative
power in the very low frequency band) were analyzed via magnitude squared coherence
function to predict AHI
•Logistic regression was performed on common
oximetry statistics in the time and frequency domains, conventional spectral characteristics from
the power spectral density function and nonlinear
features. Variables assessed in model: relative
power (PR), fourth order statistical moments in the
time domain (M4t), Lempel-Ziv complexity (LZC),
second order statistical moments in the time domain(M2t)
AHI: “sum of apneas and hypopneas per hour of
sleep
Hypopneas: ≥50% decrease in airflow and
either ≥3% oxygen
desaturation or an EEG arousal
OSA: AHI ≥10/hr
No OSA (AHI <10/hr): 32% (48/148)
OSA (AHI ≥10/hr): 68%
(100/148)
Peak amplitude (PA), and Relative
Power (PR)
assessed for SpO2, flow and
magnitude squared
coherence; relative power (PR), fourth
order statistical
moments in the time domain (M4t),
Lempel-Ziv complexity (LZC),
second order
statistical moments
in the time
domain(M2t)
AHI ≥10/hr
* Abbreviations: AHI (apnea-hypopnea index), BMI (body mass index), CABG (coronary artery bypass graft), CAD (coronary artery disease), COPD (chronic obstructive pulmonary disease), CPAP (continuous positive
airway pressure), DM (diabetes mellitus), EEG (electroencephalogram), ESS (Epworth sleepiness scale), hr (hour), IQR (interquartile range), MI (myocardial infarction), N (number), NR (not reported), OSA (obstructive sleep
apnea), OSAS (obstructive sleep apnea syndrome), mod (moderate), PSG (polysomnogram), RDI (respiratory disturbance index), RERA (respiratory effort related arousal), SDB (sleep disordered breathing)
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

79
Table 17 – Diagnostic Accuracy of Oximetry Diagnostic Studies (Other than Oxygen Desaturation Index)
Study N Cut-Point OSA
Prevalence
Population TP FN FP TN p-value Sens Spec PPV NPV +LR -LR Accuracy AUC Pos Posttest
Probability
Neg Posttest
Probability
Alvarez, 2012 144 •PSG: AHI≥10/hr •6 Variable Oximetry
Model
0.667 Sleep clinic patients with
suspected OSA
87 9 9 39 <0.001 0.906 0.813 0.906 0.813 4.833 0.115 0.875 NR 0.906 0.188
Marcos, 2012 144 •PSG: AHI≥5/hr •Oximetry MLP:
≥5/hr
0.799 Symptomatic patients with
suspected OSA
101 14 9 20 <0.001 0.878 0.690 0.918 0.588 2.83 0.177 0.840 NR 0.918 0.412
144 •PSG: AHI≥15/hr
•Oximetry MLP: ≥15/hr
0.556 Symptomatic
patients with suspected OSA
74 6 4 60 <0.001 0.925 0.938 0.949 0.909 14.80 0.080 0.931 NR 0.949 0.091
144 •PSG: AHI≥30hr
•Oximetry MLP: ≥30/hr
0.427 Symptomatic
patients with suspected OSA
45 5 3 64 <0.001 0.900 0.955 0.938 0.928 20.10 0.105 0.932 NR 0.938 0.072
Morillo, 2012 78 •PSG: AHI ≥5/hr
•Oximetry: FDI ≥7.5/hr
NR Sleep clinic
patients with suspected OSA
. . . . . 0.900 0.750 0.930 0.595 3.60 0.130 . 0.890 . .
78 •PSG: AHI ≥10/hr
•Oximetry: FDI ≥15.5/hr
NR Sleep clinic
patients with suspected OSA
. . . . . 0.833 0.804 0.890 0.720 4.27 0.210 . 0.900 . .
78 •PSG: AHI ≥15/hr
•Oximetry: FDI
≥19.1/hr
NR Sleep clinic
patients with
suspected OSA
. . . . . 0.846 0.769 0.810 0.800 3.67 0.200 . 0.910 . .
78 •PSG: AHI ≥20/hr
•Oximetry: FDI
≥22/hr
NR Sleep clinic
patients with
suspected OSA
. . . . . 0.864 0.828 0.860 0.820 5.01 0.160 . 0.920 . .
Batchelder,
2011
104 “High” SPD
assessment setting
NR Sleep clinic
patients with
suspected OSA
498 123 384 2912 . 0.802 0.883 . . . . 0.871 0.870 . .
104 “Medium” SPD assessment setting
NR Sleep clinic patients with
suspected OSA
202 419 113 3183 . 0.325 0.966 . . . . 0.966 0.870 . .
104 “Low” SPD assessment setting
NR Sleep clinic patients with
suspected OSA
63 558 11 3285 . 0.101 0.997 . . . . 0.855 0.870 . .
Marcos, 2011 96 •PSG: AHI ≥10/hr
•Oximetry KerEnt
Analysis: --0.02
threshold
0.667 Symptomatic
patients with
suspected OSA
52 12 6 26 <0.001 0.813 0.813 0.897 0.684 4.33 0.231 0.813 0.870 0.897 0.316
Alvarez, 2010 148 •PSG: AHI ≥10/hr
•Oximetry: PASPO2
0.676 Symptomatic
patients with
84 16 8 40 <0.001 0.840 0.833 0.913 0.714 5.040 0.192 0.838 0.901 0.913 0.286
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

80
suspected OSA
148 •PSG: AHI ≥10/hr
•Oximetry: PSPO2
0.676 Symptomatic
patients with suspected OSA
84 16 9 39 <0.001 0.840 0.813 0.903 0.709 4.480 0.197 0.831 0.996 0.903 0.291
148 •PSG: AHI ≥10/hr
•Oximetry: LR (PR, M4t, LZC, M2t)
0.676 Symptomatic
patients with suspected OSA
92 8 7 41 <0.001 0.920 0.854 0.929 0.837 6.309 0.094 0.899 0.967 0.929 0.163
* Abbreviations: +LR (positive likelihood ratio), -LR (negative likelihood ratio), AHI (apnea-hypopnea index), AUC (area under the curve), CABG (coronary artery bypass graft), CAD (coronary artery disease), COPD (chronic
obstructive pulmonary disease), CPAP (continuous positive airway pressure), FN (false negative), FP (false positive), N (number), NR (not reported), NPV (negative predictive value), MI (myocardial infarction), ODI (oxygen desaturation index), OSA (obstructive sleep apnea), OSAS (obstructive sleep apnea syndrome), PPV (positive predictive value), PSG (polysomnogram), RDI (respiratory disturbance index), Sen (sensitivity), Spec (specificity), TN (true
negative), TP (true positive)
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

81
Table 18 - AHRQ Question 1b – Summary of Berlin Questionnaire (BQ) Diagnostic Studies
Study Search
Strategy
Sample Demographics N Validation OSA Definition OSA Prevalence Berlin
Cut-point(s)
AHI
Cut-Point(s)
Geiger-Brown,
2013
Group 3 Chronically partially
sleep-deprived shift-work nurses.
Age: 40 ±13 years
Male: 0% BMI: NR
ESS: NR
AHI: 2.3 ±5.4/hr
21 Type I
Polysomnography
RDI: sum of apneas,
hypopneas and RERA’s per hour of sleep
AHI: sum of apneas and
hypopneas per hour of sleep Hypopneas: 50 to 90%
decrease in nasal flow with a
>4% oxygen desaturation RERA’s: 30 to 90%
decrease in nasal flow with a >3% oxygen desaturation
OSA: AHI ≥5/hr
SDB (RDI ≥5): 43% (9/21) - 24%
mild, 19% moderate, 0% severe
No OSA (AHI<5): 86% (17/21)
OSA (AHI ≥5): 14% (3/21) •Mild (AHI 5-15): 100% (21/21)
•Moderate (AHI 15-30): 0%
•Severe (AHI ≥30): 0%
BQ ≥2 Various:
AHI ≥5/hr RDI ≥5/hr
Danzi-Soares,
2012
Group 3 Consecutive patients referred for CABG
Age: 58 ±7 years Male: 76%
BMI: 27.6 ±27.6 kg/m2
ESS: 7 (range 5-11) AHI: 22.9 ±20.0/hr
70 Type I Polysomnography
AHI: sum of apneas and hypopneas per hour of sleep
Hypopneas: 50 to 90%
decrease in nasal flow with a >3% oxygen desaturation
OSA: AHI ≥5/hr
No OSA (AHI <5): 12.9% (9/70) OSA (AHI ≥5): 87.1% (61/70)
•Mild (AHI 5-15): 32.9% (23/70)
•Moderate (AHI 15-30): 27.1% (19/70)
•Severe (AHI ≥30): 27.1% (19/70)
BQ ≥2 Various: AHI ≥5/hr
AHI ≥15/hr
Facco, 2012 Group 3 Pregnant women at high risk for sleep apnea
(hypertension,
pregestational diabetes, BMI ≥30, prior
preeclampsia)
Age: 33.0 ±6.5 years Male: 0%
BMI: 31.9 ±9.1 kg/m2
ESS: 7.5 ±4.3 (0-19) AHI: 1.5/hr (median, IQR
0.6-6.0)
100 Type IV Sleep Study (Watch-
PAT100, Itamar
Medical)
AHI: “analysis of the WP100 signals allows for
the determination of the
AHI” Hypopneas: Not defined
OSA: AHI ≥5/hr
No OSA (AHI<5): 72% (72/100) OSA (AHI ≥5): 28% (28/100)
•Mild: NR
•Moderate: NR •Severe: NR
BQ ≥2 AHI ≥5/hr
Gjevre, 2012 Group 3 Rheumatoid arthritis patients with and
without abnormal scores
on the ESS and/or Pittsburgh Sleep Quality
Index
Age: 60.4 ±9.8 years Male: 28%
BMI: 29.7 ±4.2 kg/m2
ESS: NR AHI: 14.7 ±14.8/hr
25 Type I Polysomnography
(15 channel,
Sandman software)
AHI: sum of apneas and hypopneas per hour of sleep
Hypopneas: Not defined
OSA: AHI ≥5/hr
No OSA (AHI<5): 32% (8/25) OSA (AHI ≥5): 68% (17/25)
•Mild: NR
•Moderate: NR •Severe: NR
BQ ≥2 AHI ≥5/hr
Koyama, 2012 Group 3 Male railroad workers Age: 35.6 ±9.6 years Male: 100%
BMI: 26.7 ±4.1 kg/m2
ESS: 7.9 ±3.6 AHI: NR
745 Type I Polysomnography
(EMBLA Titanium)
AHI: Not defined Hypopneas: Not defined
OSAS: AHI ≥15/hr or (AHI
≥5/hr and ESS ≥10)
No OSAS: 65% (484/745) OSAS: 35% (261/745)
•Mild: 54%
•Moderate: 25% •Severe: 20%
BQ ≥2 AHI ≥15/hr or (AHI
≥5/hr and
ESS ≥10)
Laporta, 2012 Group 4 Veterans with ischemic
heart disease
Age: 67.7 ±11.8 years
Male: 100% BMI: 29.9 ±5.0 kg/m2
ESS: 9.3 ±4.8
AHI: 19.9 ±19.0/hr
91 Type I
Polysomnography
AHI: sum of apneas and
hypopneas per hour of sleep Hypopneas: ≥50 decrease in
nasal flow with a >3%
oxygen OSA: AHI ≥5/hr
No OSA (AHI <5): 25% (22/91)
OSA (AHI ≥5): 75% (69/91) •Mild (AHI 5-15): 41% (28/69)
•Moderate (AHI 15-30): 28%
(19/69) •Severe (AHI ≥30): 31% (21/69)
BQ ≥2 Various:
AHI ≥5/hr AHI ≥10/hr
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

82
Martinez, 2012 Group 3 Consecutive patients
with prior angina (age <65, BMI ≤40, no
COPD or DM,
nonsmoker, prior CAD intervention, recent
angina)
Age: 54 ±6.9 years
Male: 46% BMI: 23 ±11 kg/m2
ESS: NR
AHI: 17 ±14/hr
57 Type III Home
Sleep Study (SOMNOcheck)
AHI: sum of apneas and
hypopneas per hour of sleep Hypopneas: ≥50% decrease
in nasal flow with a ≥3%
oxygen desaturation OSA: AHI ≥5/hr
No OSA (AHI<5): 21% (12/57)
OSA (AHI ≥5): 79% (45/57) •Moderate-severe (AHI ≥15): 55%
(25/45)
BQ ≥2 AHI ≥15/hr
Enciso, 2011 Group 4 Patients of the USC School of Dentistry
Age: 54.9 ±12.1 years Male: 77%
BMI: 26.6 ±18.1 kg/m2
ESS: NR RDI: 24.3 ±18.1/hr
84 Type IV Home Sleep Study (ARES
Unicorder)
RDI: Not reported Hypopneas: Not reported
OSA: RDI ≥15/hr
No OSA (RDI<15): 37% (31/84) OSA (RDI ≥15): 63% (53/84)
BQ ≥2 Various: RDI ≥10/hr
RDI ≥15/hr
Hrubos-Strom,
2011
Group 3 Norwegian general
population
Age: 48.3 ±11.2 years
Male: 54.8% BMI: 27.9 ±4.8 kg/m2
ESS: 8.8 ±4.6
AHI: 6.4/hr (median, IQR 1.7-18.3)
518 Type I
Polysomnography
AHI: sum of apneas and
hypopneas per hour of sleep Hypopneas: ≥70% decrease
in nasal flow with a >4%
oxygen desaturation OSA: AHI ≥5/hr
No OSA (AHI <5): 84% (435/518)
OSA (AHI ≥5): 16% (83/518) •Mild (AHI 5-15): 51% (42/83)
•Moderate-Severe (AHI ≥15): 49%
(41/83))
BQ ≥2 Various:
AHI ≥5/hr AHI ≥15/hr
Sert
Kuniyoshi,
2011
Group 3 Cross-sectional study of
recent MI patients (1 to 3 months prior).
Excluded patients with prior OSA diagnosis
receiving CPAP
treatment.
Age: 62 ±13years
Male: 81% BMI: 30 ±5 kg/m2
ESS: 9.1 ±4.2 AHI: NR
99 Type I
Polysomnography (Compumedics)
AHI: sum of apneas and
hypopneas per hour of sleep Hypopneas: 30 to 90%
decrease in nasal flow with a ≥4% oxygen desaturation
OSA: AHI ≥5/hr
No OSA (AHI<5): 26% (26/99)
OSA (AHI ≥5): 74% (73/99) •Mild (AHI 5-15): 37% (27/73)
•Moderate (AHI 15-20): 34% (25/73)
•Severe (AHI ≥30): 29% (21/73)
BQ ≥2 Various:
AHI ≥5/hr AHI ≥15/hr
AHI ≥30/hr
Sforza, 2011 Both:
Group 3
Group 4
Prospective study of
participants age ≥65
from the PROOF study (French population)
Age: 65.6 ±0.8years
Male: 40.9%
BMI: 25.3 ±5.1 kg/m2 ESS: 5.6 ±5.1
AHI: 21.6 ±16.0/hr
643 Type III Home
Sleep Study
(HypnoPTT, Tyco Healthcare, Puritan
Bennett Co, USA)
AHI: sum of apneas and
hypopneas per hour of sleep
Hypopneas: ≥50% decrease in nasal flow with a ≥3%
oxygen desaturation
OSA: AHI ≥15/hr
•Provided data/outcomes
separately by gender and Mini-Mental-State
Examination
No OSA (AHI<15): 43% (274/643)
OSA: (AHI ≥15): 57% (369/643)
BQ ≥2 Various:
AHI ≥15/hr
AHI ≥30/hr
Subramanian,
2011
Group 3 Consecutive patients referred for suspected
sleep apnea (no prior
OSA Diagnosis)
Age: 55 ±14 years Male: 59%
BMI: 35 ±9 kg/m2
ESS: NR RDI: 38 ±8/hr
509 •Type I Polysomnography
RDI: sum of apneas, hypopneas and RERA’s per
hour of sleep
Hypopneas: required ≥4% oxygen desaturation in
addition to defined reduction
in airflow per 2007 American Academy of Sleep
No OSA (RDI<5): 15% (77/509) OSA: (RDI ≥5): 85% (432/509)
•Mild: 31% (134/432)
•Moderate/Severe (RDI ≥15): 69% (298/432)
BQ ≥2 Various: RDI ≥5/hr
RDI ≥15/hr
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

83
Medicine Scoring
Guidelines RERA’s: NR
OSA: RDI ≥5
Thurtell, 2011 Group 3 Newly diagnosed idiopathic intracranial
hypertension
Age: 32 years (median, range 16-54)
Male: 20%
BMI: 39.8 kg/m2 (median, range 27-52)
ESS: NR
AHI: NR
30 Type I Polysomnography
AHI: sum of apneas and hypopneas per hour of sleep
Hypopneas: “determined
using conventional criteria.” Reference to 2007 AASM
scoring criteria.
OSA: AHI ≥5/hr
No OSA (AHI<5): 40% (12/30) OSA (AHI ≥5): 60% (18/30)
•Mild (AHI 5-15): 39% (7/18)
•Moderate (AHI 15-20): 22% (4/18)
•Severe (AHI ≥30): 39% (7/18)
BQ ≥2 AHI ≥5/hr
Vaz, 2011 Group 4 Consecutive sleep clinic
patients referred for
suspected sleep apnea
•Also assessed a
“modified” Berlin Questionnaire (no
previously validated)
Age: 51 ±13 years
Male: 67%
BMI: NR (55% had BMI >30 kg/m2)
ESS:10 ±6
AHI: 24 ±17/hr
95 Type III Sleep
Study (alpha screen;
Vyasis)
AHI: sum of apneas and
hypopneas per hour of sleep
Hypopneas: 20 to 50% decrease in nasal flow with a
≥4% oxygen desaturation.
OSA: AHI ≥5/hr
No OSA (AHI<5): 17% (16/95)
OSA (AHI ≥5): 83% (79/95)
•Mild (AHI 5-15): 42% (33/79) •Moderate (AHI 15-20): 25%
(20/79)
•Severe (AHI ≥30): 33% (26/79)
BQ ≥2 Various:
AHI ≥5/hr
AHI ≥15/hr AHI ≥30/hr
Patt, 2010 Group 4 Patients with chronic wounds
Age: 55±16.1 years Male: 48%
BMI: 32 ±16.1 kg/m2
ESS: 8.9 ±4.8 AHI: 15.6/hr
46 Type III Home Sleep Study
(Stardust II,
Respironics)
AHI: sum of apneas and hypopneas per hour of sleep
Hypopneas: ≥50% decrease
in nasal flow with a ≥4% oxygen
OSA: AHI ≥15/hr
No OSA (AHI<5): 17% (12/46) OSA (AHI ≥5): 83% (38/46)
•Mild (AHI 5-15): 32% (12/38)
•Moderate-Severe (AHI 15-30): 68% (26/38)
BQ ≥2 AHI ≥15/hr
* Abbreviations: AHI (apnea-hypopnea index), BMI (body mass index), CABG (coronary artery bypass graft), CAD (coronary artery disease), COPD (chronic obstructive pulmonary disease), CPAP (continuous positive
airway pressure), DM (diabetes mellitus), EEG (electroencephalogram), ESS (Epworth sleepiness scale), hr (hour), IQR (interquartile range), MI (myocardial infarction), N (number), NR (not reported), OSA (obstructive sleep
apnea), OSAS (obstructive sleep apnea syndrome), mod (moderate), PSG (polysomnogram), RDI (respiratory disturbance index), RERA (respiratory effort related arousal), SDB (sleep disordered breathing)
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

84
Table 19 - AHRQ Question 1b – Diagnostic Accuracy of Berlin Questionnaire (BQ) Diagnostic Studies
Study N Cut-Point OSA
Prevalence
Population TP FN FP TN Diagnostic
Odds Ratio
p-
value
Sens Spec PPV NPV +LR -LR Accuracy AUC Pos Posttest
Probability
Neg
Posttest
Probability
Kappa(1)
Coefficient
Geiger-Brown,
2013
21 BQ ≥2
AHI ≥5/hr
0.143 Sleep
deprived shift
workers
2 1 15 3 0.40 <0.001 0.667 0.167 0.118 0.750 0.800 2.00 0.238 NR 0.118 0.250 -0.029
21 BQ ≥2
RDI ≥5/hr
0.429 Sleep
deprived shift
workers
3 6 2 10 0.375 0.333 0.833 0.600 0.625 2.00 0.800 0.619 NR 0.600 0.375
Danzi-Soares,
2012
70 BQ ≥2
AHI ≥5/hr
0.871 CABG 44 17 5 4 2.07 0.311 0.721 0.444 0.898 0.190 1.298 0.627 0.686 NR 0.898 0.810 0.206
70 BQ ≥2
AHI ≥15/hr
0.543 CABG 28 10 21 11 1.47 0.464 0.737 0.344 0.571 0.524 1.123 0.766 0.557 NR 0.571 0.476 0.063
Facco, 2012 100 BQ ≥2
AHI ≥5/hr
0.280 Pregnant
women
11 17 23 49 22.59 0.487 0.393 0.681 0.324 0.742 1.23 0.892 0.600 0.540 0.324 0.258 0.060
Gjevre, 2012 25 BQ ≥2
AHI ≥5/hr
0.680 Rheumatoid
arthritis
7 10 2 6 1.86 0.432 0.412 0.750 0.778 0.375 1.647 0.784 0.520 NR 0.778 0.625 0.306
Koyama, 2012 745 AHI ≥15/hr
or (AHI
≥5/hr and
ESS≥10
0.350 Male railroad
workers
103 158 387 97 <0.001 0.395 0.200 0.210 0.380 0.494 3.021 0.268 NR 0.210 0.620
Laporta, 2012 91 BQ ≥2
AHI ≥5/hr
0.747 Male veterans
with IHD
56 12 14 9 2.96 0.035 0.824 0.391 0.800 0.429 1.353 0.451 0.714 NR 0.800 0.571 0.209
Martinez, 2012 57 BQ ≥2
AHI ≥15/hr
0.439 Angina
patients
18 7 16 16 2.57 <0.001 0.720 0.500 0.529 0.696 1.440 0.560 0.596 NR 0.529 0.304 0.162
Enciso, 2011 84 BQ ≥2
RDI ≥10/hr
0.774 Dentistry
patients
44 21 6 13 0.005 0.677 0.684 0.880 0.382 2.144 0.472 0.679 NR 0.880 0.618
84 BQ ≥2
RDI ≥15/hr
0.631 Dentistry
patients
36 17 14 17 22.59 0.040 0.679 0.548 0.720 0.500 1.504 0.585 0.631 NR 0.720 0.500 0.241
Hrubos-Strom,
2011
518 BQ ≥2
AHI ≥5/hr
0.160 Norwegian
population
31 52 70 365 3.11 <0.001 0.373 0.839 0.307 0.875 2.321 0.747 0.764 NR 0.307 0.125 0.175
518 BQ ≥2
AHI ≥15/hr
0.079 Norwegian
population
18 23 97 380 3.07 <0.001 0.439 0.797 0.157 0.943 2.159 0.704 0.768 NR 0.157 0.057 0.084
Sert Kuniyoshi,
2011
99 BQ ≥2
AHI ≥5/hr
0.737 Recent MI 50 23 14 12 1.85 0.179 0.685 0.462 0.781 0.343 1.272 0.683 0.626 0.580 0.781 0.657 0.167
99 BQ ≥2
AHI ≥15/hr
0.465 Recent MI 30 16 34 19 1.04 0.912 0.652 0.358 0.469 0.543 1.017 0.970 0.495 0.500 0.469 0.457 0.008
99 BQ ≥2
AHI ≥30/hr
0.212 Recent MI 15 6 49 29 0.464 0.714 0.372 0.234 0.829 1.137 0.768 0.444 0.540 0.234 0.171
Sforza, 2011 643 BQ ≥2
AHI ≥15/hr
0.574 Age ≥65 283 86 166 108 2.14 <0.001 0.767 0.394 0.630 0.557 1.266 0.591 0.608 NR 0.630 0.443 0.132
643 BQ≥2
AHI ≥30/hr
NR Age ≥65 . . . . . 0.234 0.766 . . . . . . . .
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

85
Subramanian,
2011
509 BQ ≥2
RDI ≥5/hr
0.849 Suspected
OSA
397 35 63 14 2.56 0.006 0.919 0.182 0.863 0.286 1.123 0.446 0.807 NR 0.863 0.714 0.095
509 BQ ≥2
RDI ≥15/hr
0.585 Suspected
OSA
277 21 181 30 2.17 0.008 0.930 0.142 0.605 0.588 1.084 0.496 0.603 NR 0.605 0.412 0.047
Thurtell, 2011 30 BQ ≥2
AHI ≥5/hr
0.600 Intracranial
HTN
15 3 5 7 6.04 0.018 0.833 0.583 0.750 0.700 2.000 0.286 0.733 NR 0.750 0.300 0.375
Vaz, 2011 95 BQ ≥2
AHI ≥5/hr
0.832 Suspected
OSA
57 22 8 8 2.56 0.082 0.722 0.500 0.877 0.267 1.443 0.557 0.684 0.611 0.877 0.733 0.269
95 BQ ≥2
AHI ≥15/hr
0.484 Suspected
OSA
38 8 27 22 3.17 0.004 0.826 0.448 0.585 0.733 1.499 0.387 0.632 0.637 0.585 0.267 0.195
95 BQ≥2
AHI ≥30/hr
0.274 Suspected
OSA
23 3 58 37 <0.001 0.885 0.389 0.284 0.925 1.449 0.296 0.632 0.638 0.353 0.100
Patt, 2010 46 BQ ≥2
AHI ≥15/hr
0.565 Chronic
wounds
15 11 11 9 1.11 0.855 0.577 0.450 0.577 0.450 1.049 0.940 0.522 NR 0.577 0.550 0.027
* Abbreviations: +LR (positive likelihood ratio), -LR (negative likelihood ratio), AHI (apnea-hypopnea index), AUC (area under the curve), CABG (coronary artery bypass graft), CAD (coronary artery disease),
COPD (chronic obstructive pulmonary disease), CPAP (continuous positive airway pressure), FN (false negative), FP (false positive), N (number), NR (not reported), NPV (negative predictive value), MI (myocardial infarction), ODI (oxygen desaturation index), OSA (obstructive sleep apnea), OSAS (obstructive sleep apnea syndrome), PPV (positive predictive value), PSG (polysomnogram), RDI (respiratory
disturbance index), Sen (sensitivity), Spec (specificity), TN (true negative), TP (true positive)
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

86
Table 20 - AHRQ Question 1b – Summary of Epworth Sleepiness Scale (ESS) Diagnostic Studies
Study Search
Strategy
Sample Demographics N Validation OSA Definition OSA Prevalence ESS
Cut-point(s)
AHI
Cut-Point(s)
Sharkey, 2013 Group 4 Patients evaluated for bariatric surgery
Age: 42.0 ±9.5 years Male: 11%
BMI: 50.2 ±7.7 kg/m2
ESS: 6.3 ±4.8 AHI: 29.5 ±31.5/hr
269 Type I Polysomnography
AHI: sum of apneas and hypopneas per hour of sleep
Hypopneas: ≥50% decrease in
nasal flow with a >3% oxygen desaturation
OSA: AHI ≥15/hr
No OSA (AHI <15): 42% (112/269) OSA (AHI ≥15): 58% (157/269)
•Moderate (AHI 15-30): 49%
(77/157) •Severe (AHI ≥30): 51% (80/157)
Various: ESS ≥10
ESS ≥16
Various: AHI ≥15/hr
AHI ≥30/hr
Vana, 2013 Group 4 New adult patients referred to clinic for
sleep evaluations
Age: 46.4 ±13.2 years Male: 34%
BMI: 36.3 ±9.2 kg/m2
ESS: 8.0 (median, range 0-24)
AHI: 8.9/hr (median,
range 0 -99.9)
47 Type I Polysomnography
(diagnostic or split-
night protocols)
AHI: sum of apneas and hypopneas per hour of sleep
Hypopneas: ≥30% decrease in
nasal flow with a ≥4% oxygen desaturation
OSA: AHI ≥5/hr
No OSA (AHI <5): 32% (15/47) OSA (AHI ≥5): 68% (32/47)
•Mild (AHI 5-15): 48% (15/47)
•Moderate (AHI 15-30): 25% (8/47)
•Severe (AHI ≥30): 28% (9/47)
ESS >10
AHI ≥5/hr
Albuquerque,
2012
Group 4 Afib patients
referred for direct
current cardioversion
Age: 69.1 ±11 years
Male: 76%
BMI: 34.1 ±8.6 kg/m2 ESS: 8.9 ±4.4
AHI: 23.1 ±22.6/hr
151 Type I
Polysomnography
(Nicolet Instrument Corp)
AHI: sum of apneas and hypopneas
per hour of sleep
Hypopneas: 50 to 90% decrease in nasal flow with a ≥4% oxygen
OSA: AHI ≥5/hr (obstructive
events) SDB: AHI ≥5/hr (obstructive,
central or mixed events)
No SDB (AHI <5): 22% (33/151)
SDB (AHI ≥5): 78% (118/151)
•Mild (AHI 5-15): 33% (39/118) •Moderate (AHI 15-30): 30%
(35/118)
•Severe (AHI ≥30): 37% (44/118)
(Pure OSA: 57%, Pure CSA: 10.6%,
Mixed sleep apnea: 18.6%)
Various:
ESS >10
ESS ≥10
Various:
AHI ≥5/hr
AHI ≥15/hr AHI ≥30/hr
Asha’ari, 2012 Group 4 Hypertensive (case)
and non-
hypertensive (control) groups
Age: 26.7 ±6.2 years
Male: 72%
BMI: 30.8 ±7.5 kg/m2 ESS: NR (32% ESS ≥10)
AHI: 25.9 ±4.5/hour
240 Type I
Polysomnography
AHI: not reported
Hypopneas: “according to the
AASM 2007 guidelines” OSA: AHI ≥5/hr
No OSA (AHI <5): 33% (78/240)
OSA (AHI ≥5): 68% (162/240)
•Mild (AHI 5-15): NR •Moderate (AHI 15-30): NR
•Severe (AHI ≥30): NR
Various:
ESS ≥10
ESS ≥14
AHI ≥5/hr
Danzi-Soares,
2012
Group 3 Consecutive patients referred for
CABG
Age: 58 ±7 years Male: 76%
BMI: 27.6 ±27.6 kg/m2
ESS: 7 (range 5-11) AHI: 22.9 ±20.0/hr
70 Type I Polysomnography
AHI: sum of apneas and hypopneas per hour of sleep
Hypopneas: 50 to 90% decrease in
nasal flow with a >3% oxygen desaturation
OSA: AHI ≥5/hr
No OSA (AHI <5): 12.9% (9/70) OSA (AHI ≥5): 87.1% (61/70)
•Mild (AHI 5-15): 32.9% (23/70)
•Moderate (AHI 15-30): 27.1% (19/70)
•Severe (AHI ≥30): 27.1% (19/70)
ESS >10
Various: AHI ≥5/hr
AHI ≥15/hr
Facco, 2012 Group 3 Pregnant women at high risk for sleep
apnea
(hypertension, pregestational
diabetes, BMI ≥30,
Age: 33.0 ±6.5 years Male: 0%
BMI: 31.9 ±9.1 kg/m2
ESS: 7.5 ±4.3 (0-19) AHI: 1.5/hr (median. IQR
0.6-6.0)
100 Type IV Sleep Study (Watch-
PAT100, Itamar
Medical)
AHI: “analysis of the WP100 signals allows for the determination
of the AHI”
Hypopneas: Not defined OSA: AHI ≥5/hr
No OSA (AHI<5): 72% (72/100) OSA (AHI ≥5): 28% (28/100)
•Mild: NR
•Moderate: NR •Severe: NR
Various: ESS ≥10
ESS ≥12
AHI ≥5/hr
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

87
prior preeclampsia)
Feng, 2012 Group 4 Consecutive patients referred to
a sleep center for
suspected OSA
Age: 45.9 ±12.1 years Male: 86%
BMI: 27.6 ±3.9 kg/m2
ESS: 9.4 ±5.0 AHI: 35.2 ±25.2/hr
2,297 Type I Polysomnography
AHI: sum of apneas and hypopneas per hour of sleep
Hypopneas: ≥50% decrease in
nasal flow with either a >3% oxygen desaturation or signs of a
physiologic arousal
OSA: AHI ≥5/hr
No OSA (AHI<5): 9% (213/2297) OSA (AHI ≥5): 91% (2084/2297)
•Mild: 20% (420/2297)
•Moderate: 22% (460/2297) •Severe: 58% (1204/2084)
ESS >10
Various: AHI ≥5/hr
AHI ≥15/hr
AHI ≥30/hr
Gjevre, 2012 Group 3 Rheumatoid
arthritis patients
with and without abnormal scores on
the ESS and/or
Pittsburgh Sleep Quality Index
Age: 60.4 ±9.8 years
Male: 28%
BMI: 29.7 ±4.2 kg/m2 ESS: NR
AHI: 14.7 ±14.8/hr
25 Type I
Polysomnography
(15 channel, Sandman software)
AHI: sum of apneas and hypopneas
per hour of sleep
Hypopneas: Not defined OSA: AHI ≥5/hr
No OSA (AHI<5): 32% (8/25)
OSA (AHI ≥5): 68% (17/25)
•Mild: NR •Moderate: NR
•Severe: NR
ESS >10 AHI ≥5/hr
Knutson, 2012 Group 3 Obese (BMI 30-55)
men and premenopausal
women aged 18-50
years reporting less than 6.5 hrs of sleep
Age: 40.8 ±6.9
Male: 30.2% BMI: 38.2 ±5.9 kg/m2
ESS: 8.6 ±4.4
AHI: NR
139 Type IV Sleep
Study (Apnea Risk Evaluation System,
Advanced Brain
Monitoring, Inc)
RDI: sum of abnormal respiratory
events per hour of sleep Hypopneas: 50 to 90% decrease in
nasal flow with a >3.5% oxygen
desaturation OR ≥1% desaturation with ≥surrogate arousal indicator
OSA: RDI ≥15/hr
No OSA (RDI<5): 34% (47/139)
OSA: (RDI ≥5) 66% (92/139) •Mild (AHI 5-15): 37% (52/139)
•Moderate-Severe (AHI ≥15): 29%
(40/139)
ESS ≥10 RDI ≥15/hr
Koyama, 2012 Group 3 Male railroad workers
Age: 35.6 ±9.6 years Male: 100%
BMI: 26.7 ±4.1 kg/m2
ESS: 7.9 ±3.6
AHI: NR
745 Type I Polysomnography
(EMBLA Titanium)
AHI: Not defined Hypopneas: Not defined
OSAS: AHI ≥15/hr or (AHI ≥5/hr
and ESS ≥10)
No OSAS: 65% (484/745) OSAS: 35% (261/745)
•Mild: 54%
•Moderate: 25%
•Severe: 20%
ESS >10 AHI ≥15/hr or (AHI ≥5/hr and
ESS >10)
Morrell, 2012 Group 3 Wisconsin state
employees age 30-60 years
Age: 50.4 years
Male: 74% BMI: 31.1 ±7.1 kg/m2
ESS: 8.7 ±4.1
AHI: NR
3,695 Type II
Polysomnography (Polygraph model
78)
AHI: sum of apneas and hypopneas
per hour of sleep Hypopneas: discernible decrease in
nasal flow with a ≥4% oxygen
OSAS: AHI ≥15/hr or on CPAP
No OSA (AHI<15): 16%
(3089/3695) OSA: (AHI ≥15): 84% (606/3695)
ESS ≥10 AHI ≥15 (or
CPAP)
Nicholl, 2012 Group 3 Adults with chronic
kidney disease
attending an outpatient
nephrology clinic
Age: 65 ±12 years
Male: 63%
BMI: 31.2 ±8.3 kg/m2 ESS: 7.9 ±4.7
ODI(4%): 21.1 ±25.1/hr
119 Type IV Sleep
Study (Remmers
Sleep Recorder Model 4.2)
ODI: sum of number of episodes of
desaturation ≥4% per hour of
recording OSA: ODI(4%) ≥15/hr
No OSA (ODI<15): 61% (73/119)
OSA: (ODI ≥15): 39% (46/119)
ESS >10 ODI (4%)
≥15/hr
Ravesloot,
2012
Group 4 Consecutive bariatric candidates
Age: 45.1 ±10.6 years Male: 23.3%
BMI: 44.2 ±6.4 kg/m2
ESS: 4.3 ±3.8 AHI: 23.9 ±27.7/hr
279 Type I Polysomnography
(Flaga Medical)
AHI: sum of apneas and hypopneas per hour of sleep
Hypopneas: ≥30 decrease in nasal
flow with a ≥4% oxygen desaturation
OSA: AHI ≥5/hr
No OSA (AHI<5): 30% (84/279) OSA (AHI ≥5): 70% (195/279)
•Mild (AHI 5-15): 35% (67/195)
•Moderate (AHI 15-20): 25% (48/195)
•Severe (AHI ≥30): 40% (78/195)
ESS >10 (??)
Various: AHI ≥5/hr
AHI ≥15/hr
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

88
Gasa, 2011 Group 4 Consecutive
bariatric candidate
Age: 43.0 ±10.0 years
Male: 28% BMI: 46.1 ±5.8 kg/m2
ESS: 8.0 ±5.0
AHI: NR
159 Type I
Polysomnography
AHI: Not defined
Hypopneas: Not defined OSA: AHI ≥15/hr
No OSA (AHI<15): 28% (44/159)
OSA (AHI ≥15): 72% (115/159)
ESS ≥10 AHI ≥15/hr
Khoo, 2011 Group 4 Consecutive
patients referred to
a sleep clinic
Age: 47.5 ±13.9 years
Male:79%
BMI: 28.5 ±5.8 kg/m2 ESS: NR
AHI: NR
117 Type I
Polysomnography
(Compumedics E Series)
AHI: sum of apneas and hypopneas
per hour of sleep
Hypopneas: ≥20% reduction in nasal flow with a >3% oxygen
desaturation
OSA: AHI ≥20/hr
No OSA (AHI <20): 34% (40/117)
OSA (AHI ≥20): 66% (77/117)
ESS ≥10 AHI ≥20/hr
Kopitovic,
2011
Group 4 Sleep clinic patients
with OSA
symptoms undergoing sleep
study evaluations
Age: 53 (median, IQR 43-
59)
Male: 78% BMI: 28 kg/m2 (median,
IQR 25-32)
ESS: 9 (median, IQR 6-12) AHI: 17.4/hr (median, IQR
1.4-43.7)
112 Type I
Polysomnography
(SomnoStar, Viasys)
AHI: sum of apneas and hypopneas
per hour of sleep
Hypopneas: ≥50% decrease in nasal flow
OSA: AHI ≥5/hr
No OSA (AHI<5): 38% (42/112)
OSA (AHI ≥5): 62% (70/112)
•Mild (AHI 5-15): NR •Moderate (AHI 15-20): NR
•Severe (AHI ≥30): NR
Various:
ESS ≥5
ESS ≥10
AHI ≥5/hr
Martinez, 2011 Group 4 Consecutive adult patients undergoing
sleep study testing for suspected OSA
•performed ESS immediately before
and day after PSG.
Pre-PSG ESS used in this analysis.
Age: 46 ±14 years Male: 63.5%
BMI: 27 ±5.3 kg/m2 ESS: 10 ±5.1
AHI: 24 ±22/hr
929 Type I Polysomnography
AHI: sum of apneas and hypopneas per hour of sleep
Hypopneas: ≥50% decrease in nasal flow with either a ≥3%
oxygen desaturation or a 3-s EEG
arousal OSA: AHI ≥5/hr
No OSA (AHI<5): 16% (149/929) OSA (AHI ≥5): 84% (780/929)
•Mild (AHI 5-15): 29.8% (232/780)
•Moderate (AHI 15-20): 26.4%
(206/780) •Severe (AHI ≥30): 43.8%
(342/780)
ESS >10 AHI ≥5/hr
Sareli, 2011 Group 3 Consecutive
patients evaluated for bariatric surgery
and referred for a
sleep study (11/2005-1/2007) at
the Penn Sleep
Clinic for various reasons
Age: 43.8 ±10.9 years
Male: 18.4% BMI: 49.5 ±10.0 kg/m2
ESS: 8.7 ±5
AHI: 24.9 ±30.3/hr
342 Type I
Polysomnography (Sandman Elite
software)
AHI: sum of apneas and hypopneas
per hour of sleep Hypopneas: 30 to 99% decrease in
nasal flow with either a ≥3%
oxygen desaturation or an EEG arousal
OSA: AHI ≥5/hr
No OSA (AHI<5): 23% (78/342)
OSA (AHI ≥5): 77% (264/342) •Mild (AHI 5-15): 40% (105/264)
•Moderate (AHI 15-20): 25%
(66/264) •Severe (AHI ≥30):35% (93/264)
Various:
ESS >10 ESS ≥10
ESS ≥16
Various:
AHI ≥5/hr AHI ≥15/hr
AHI ≥30/hr
Sert
Kuniyoshi,
2011
Group 3 Cross-sectional
study of recent MI patients (1 to 3
months prior).
Excluded patients with prior OSA
Age: 62 ±13 years
Male: 81% BMI: 30 ±5 kg/m2
ESS: 9.1 ±4.2
AHI: NR
99 Type I
Polysomnography (Compumedics)
AHI: sum of apneas and hypopneas
per hour of sleep Hypopneas: 30 to 90% decrease in
nasal flow with a ≥4% oxygen
desaturation OSA: AHI ≥5/hr
No OSA (AHI<5): 26% (26/99)
OSA (AHI ≥5): 74% (73/99) •Mild (AHI 5-15): 37% (27/73)
•Moderate (AHI 15-20): 34%
(25/73) •Severe (AHI ≥30): 29% (21/73)
ESS ≥10
AHI ≥5/hr
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

89
diagnosis receiving
CPAP treatment.
Silva, 2011 Group 4 Sleep Heart Health
Study (SHHS) –
Population study in subjects age >40
years
Age:62.4 ±10.3 years
Male: 52%
BMI: NR (35% had BMI ≥30 kg/m2)
ESS: NR (28% ESS >11)
AHI: NR
4770 Type II
Polysomnography
(Compumedics portable PS-2
system)
AHI: sum of apneas and hypopneas
per hour of sleep
Hypopneas: ≥25% decrease in nasal flow with a ≥4% oxygen
desaturation
OSA: AHI ≥5/hr
No OSA (AHI<5): 87% (4167/4770)
OSA (AHI ≥5): 13% (603/4770)
>Moderate (AHI 15-20): 43% (258/603)
>Severe (AHI ≥30): 57%
(345/603)
ESS >10 Various:
AHI ≥15/hr
AHI ≥30/hr
Subramanian,
2011
Group 3 Consecutive
patients referred for
suspected sleep apnea (no prior
OSA Diagnosis)
Age: 55 ±14 years
Male: 59%
BMI: 35 ±9 kg/m2 ESS: NR
RDI: 38 ±8/hr
509 •Type I
Polysomnography
RDI: sum of apneas, hypopneas
and RERA’s per hour of sleep
Hypopneas: required ≥4% oxygen desaturation in addition to defined
reduction in airflow per 2007
American Academy of Sleep Medicine Scoring Guidelines
RERA’s: NR
OSA: RDI ≥5
No OSA (RDI<5): 15% (77/509)
OSA: (RDI ≥5): 85% (432/509)
•Mild: 31% (134/432) •Moderate/Severe (RDI ≥15): 69%
(298/432)
ESS >10 Various:
RDI ≥5/hr
RDI ≥15/hr
Tanaka, 2011 Group 3 Male passenger
transportation
workers (train and bus drivers, rail
conductors,
mechanics)
Age: 39.9 ±8.2 years
Male: 100%
BMI: NR ESS: NR
AHI: NR
75 Pulse Oximeter
(Pulsox-3, Konica
Minolta)
ODI: sum of ≥3% desaturations
per hour of recording
OSA: ODI(3%) ≥15/hr
No OSA (ODI(3%) <15): 85%
(607/715)
OSA: (ODI(3%) ≥15): 15% (108/715)
ESS >10 ODI (3%)
≥15/hr
* Abbreviations: AHI (apnea-hypopnea index), BMI (body mass index), CABG (coronary artery bypass graft), CAD (coronary artery disease), COPD (chronic obstructive pulmonary disease), CPAP (continuous positive
airway pressure), DM (diabetes mellitus), EEG (electroencephalogram), ESS (Epworth sleepiness scale), hr (hour), IQR (interquartile range), MI (myocardial infarction), N (number), NR (not reported), OSA (obstructive sleep
apnea), OSAS (obstructive sleep apnea syndrome), mod (moderate), PSG (polysomnogram), RDI (respiratory disturbance index), RERA (respiratory effort related arousal), SDB (sleep disordered breathing)
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

90
Table 21 - AHRQ Question 1b – Diagnostic Accuracy of Epworth Sleepiness Scale (ESS) Diagnostic Studies
Study N Cut-Point(s) OSA
Prevalence
Population TP FN FP TN Diagnostic
Odds Ratio
p-
value
Sens Spec PPV NPV +LR -LR Accuracy AUC Pos Posttest
Probability
Neg
Posttest
Probability
Kappa(1)
Coefficient
Sharkey, 2013 269 AHI ≥15/hr
ESS ≥10
0.584 Bariatric
surgery
candidates
50 107 20 84 0.224 0.318 0.750 0.641 0.440 1.274 0.909 0.498 NR 0.641 0.560
269 AHI ≥30/hr
ESS ≥10
0.297 Bariatric
surgery
candidates
29 51 49 140 0.088 0.363 0.741 0.372 0.733 1.398 0.861 0.628 NR 0.372 0.267
Vana, 2013 47 AHI ≥5/hr
ESS >10
0.681 New sleep
clinic patients
10 22 7 8 0.519 0.305 0.313 0.533 0.588 0.267 0.670 1.289 0.383 0.423 0.588 0.733 -0.290
Albuquerque,
2012
151 AHI ≥5/hr
ESS >10
0.781 Afib patients
for DCCV
38 80 15 18 0.570 0.159 0.322 0.545 0.717 0.184 0.708 1.243 0.371 NR 0.717 0.816 -0.295
151 AHI ≥15/hr
ESS >10
0.523 Afib patients
for DCCV
23 56 30 42 0.575 0.107 0.291 0.429 0.434 0.429 0.699 1.215 0.430 NR 0.434 0.571 -0.187
151 AHI ≥5/hr
ESS ≥10
0.781 Afib patients
for DCCV
46 72 18 15 0.532 0.109 0.390 0.455 0.719 0.172 0.715 1.342 0.404 NR 0.719 0.828 -0.287
Asha’ari, 2012 240 AHI ≥5/hr
ESS ≥10
0.675 HTN and non-
HTN patients
56 106 24 54 1.19 0.559 0.346 0.692 0.700 0.338 1.123 0.945 0.458 NR 0.700 0.663 0.077
230 AHI ≥5/hr
ESS ≥14
0.675 HTN and non-
HTN patients
38 124 14 64 0.332 0.235 0.821 0.731 0.340 1.307 0.933 0.425 NR 0.731 0.660
Danzi-Soares,
2012
70 AHI ≥5/hr
ESS >10
0.871 CABG
patients
16 45 1 8 22.59 <0.001 0.262 0.889 0.941 0.151 2.361 0.830 0.343 NR 0.941 0.849 0.542
70 AHI ≥15/hr
ESS >10
0.543 CABG
patients
8 30 9 23 0.681 0.492 0.211 0.719 0.471 0.434 0.749 1.098 0.443 NR 0.471 0.566 -0.158
Facco, 2012 100 AHI ≥5/hr
ESS ≥10
0.280 Pregnant
women at
high risk for
OSA
10 18 17 55 22.59 0.221 0.357 0.764 0.370 0.753 1.513 0.742 0.650 0.57 0.370 0.247 0.126
Feng, 2012 2297 AHI ≥5/hr
ESS >10
0.907 Sleep clinic
patients
808 1276 24 189 4.899 <0.001 0.388 0.887 0.971 0.129 3.44 0.690 0.434 NR 0.971 0.871 0.689
2297 AHI ≥15/hr
ESS >10
0.724 Sleep clinic
patients
725 939 107 526 22.59 <0.001 0.436 0.831 0.871 0.359 2.578 0.679 0.545 NR 0.871 0.641 0.533
2297 AHI ≥30/hr
ESS >10
0.524 Sleep clinic
patients
607 597 225 868 <0.001 0.504 0.794 0.730 0.592 2.449 0.624 0.642 NR 0.730 0.408
Gjevre, 2012 25 AHI ≥5/hr
ESS >10
0.680 Rheumatoid
arthritis
patients
8 9 2 6 2.326 0.294 0.471 0.750 0.800 0.400 1.882 0.706 0.560 NR 0.800 0.600 0.375
Knutson, 2012 134 RDI ≥15/hr
ESS >10
0.299 Obese patients
reporting <6.5
hrs of sleep
14 26 29 65 1.215 0.638 0.350 0.691 0.326 0.714 1.134 0.940 0.590 NR 0.326 0.286 0.039
Koyama, 2012 745 AHI ≥15/hr or
(AHI ≥5/hr and
0.350 Male railroad
workers
114 147 122 362 <0.001 0.437 0.748 0.483 0.711 1.73 0.753 0.639 NR 0.483 0.289
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

91
ESS ≥10)
ESS ≥10
Morrell, 2012 3695 AHI ≥15 (or CPAP)
ESS ≥10
0.164 Wisconsin
state
employees
304 302 1208 1881 <0.001 0.502 0.609 0.201 0.862 1.283 0.818 0.591 NR 0.201 0.138
Nicholl, 2012 119 ODI (4%)
≥15/hr
ESS >10
0.387 Chronic
kidney disease
patients
18 28 14 59 2.664 0.017 0.391 0.808 0.563 0.678 2.040 0.753 0.647 NR 0.563 0.322 0.287
Ravesloot, 2012 279 AHI ≥5/hr
ESS >10 (??)
0.699 Bariatric
patients
. . . . . . . . . . . . . 0.540 . . .
279 AHI ≥15/hr
ESS >10 (??)
0.451 Bariatric
patients
. . . . . . . . . . . . . 0.590 . . .
Gasa, 2011 159 AHI ≥15/hr
ESS >10
0.723 Bariatric
patients
32 83 10 34 1.279 0.514 0.278 0.773 0.762 0.291 1.224 0.934 0.415 NR 0.762 0.709 0.140
Khoo, 2011 117 AHI ≥20/hr
ESS ≥10
0.658 Sleep clinic
patients
56 21 26 14 0.387 0.727 0.350 0.683 0.400 1.119 0.779 0.598 NR 0.683 0.600
Kopitovic, 2011 112 AHI ≥5/hr
ESS ≥5
0.625 Sleep clinic
patients
67 3 30 12 <0.001 0.957 0.286 0.691 0.800 1.34 0.15 0.705 NR 0.691 0.200
112 AHI ≥5/hr
ESS ≥10
0.625 Sleep clinic
patients
50 20 5 37 16.79 <0.001 0.714 0.881 0.909 0.649 6.00 0.324 0.777 0.850 0.909 0.351 0.758
Martinez, 2011 929 AHI ≥5/hr
ESS >10
0.840 Sleep clinic
patients
421 359 55 94 1.996 <0.001 0.540 0.631 0.884 0.208 1.462 0.730 0.554 NR 0.884 0.792 0.280
Sareli, 2011 342 AHI ≥5/hr
ESS >10
0.772 Bariatric
patients
93 171 18 60 1.783 0.044 0.352 0.769 0.838 0.260 1.527 0.842 0.447 NR 0.838 0.740 0.289
342 AHI ≥5/hr
ESS ≥10
0.772 Bariatric
patients
110 154 23 55 1.689 0.053 0.417 0.705 0.827 0.263 1.413 0.827 0.482 NR 0.827 0.737 0.242
342 AHI ≥15/hr
ESS >10
0.465 Bariatric
patients
60 99 51 132 1.564 0.052 0.377 0.721 0.541 0.571 1.354 0.863 0.561 NR 0.541 0.429 0.141
342 AHI ≥15/hr
ESS ≥10
0.465 Bariatric
patients
71 88 62 121 0.042 0.447 0.661 0.534 0.579 1.318 0.837 0.561 NR 0.534 0.421
Sert Kuniyoshi,
2011
99 AHI ≥5/hr
ESS >10
0.737 Recent MI 26 47 8 18 1.214 0.655 0.356 0.692 0.765 0.277 1.158 0.930 0.444 0.58 0.765 0.723 0.104
Silva, 2011 4770 AHI ≥15/hr
ESS >10
0.126 Population
study (SHHS)
235 368 1192 2975 1.595 <0.001 0.390 0.714 0.165 0.890 1.362 0.855 0.673 0.53 0.165 0.110
4770 AHI ≥30/hr
ESS >10
0.072 Population
study (SHHS)
159 186 1310 3115 <0.001 0.461 0.704 0.108 0.944 1.557 0.766 0.686 0.58 0.108 0.056 0.044
Subramanian,
2011
509 RDI ≥5/hr
ESS >10
0.849 Suspected
OSA
233 199 34 43 1.476 0.113 0.539 0.558 0.873 0.178 1.221 0.825 0.542 NR 0.873 0.822 0.158
509 RDI ≥15/hr
ESS >10
0.585 Suspected
OSA
170 128 99 112 1.500 0.024 0.570 0.531 0.632 0.467 1.216 0.809 0.554 0.591 0.632 0.533 0.112
Tanaka, 2011 715 ODI (3%)
≥15/hr
ESS >10
0.151 Male
transportation
workers
18 90 107 500 0.952 0.809 0.167 0.824 0.144 0.847 0.945 1.012 0.724 NR 0.144 0.153 -0.008
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

92
* Abbreviations: +LR (positive likelihood ratio), -LR (negative likelihood ratio), AHI (apnea-hypopnea index), AUC (area under the curve), CABG (coronary artery bypass graft), CAD (coronary artery disease), COPD
(chronic obstructive pulmonary disease), CPAP (continuous positive airway pressure), FN (false negative), FP (false positive), N (number), NR (not reported), NPV (negative predictive value), MI (myocardial infarction), ODI (oxygen desaturation index), OSA (obstructive sleep apnea), OSAS (obstructive sleep apnea syndrome), PPV (positive predictive value), PSG (polysomnogram), RDI (respiratory disturbance index), Sen (sensitivity),
Spec (specificity), TN (true negative), TP (true positive)
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

93
Table 22 - AHRQ Question 1a – Summary of Multivariate Apnea Prediction Index (MAPI) Diagnostic Studies
Study Search
Strategy
Sample Demographics N Validation OSA Definition OSA Prevalence MAP
Cut-point(s)
AHI
Cut-Point(s)
Morales,
2012
Group 4 Elderly patients (population study) with
and without sleepiness
Age: 71.3 ±5.9 years Male: 34%
BMI: 30.5 ±7.6
kg/m2 ESS: NR (30% ESS
>10)
AHI: NR
92 •Type I Polysomnography
(Sandman, Embla)
AHI: sum of apneas and hypopneas per hour of sleep
Hypopneas: ≥50% decrease
in nasal flow with either a ≥3% oxygen or EEG
arousals
OSA: AHI ≥30/hr and ESS >10
No OSA: 73% (70/92) OSA (AHI ≥5 & ESS >10): 27%
(22/92)
•Mild (AHI 5-15 & ESS >10): 32% (7/22)
•Moderate (AHI 15-30 & ESS >10):
23% (5/22) •Severe (AHI ≥30 & ESS >10):
45% (10/22)
MAPI >0.5 AHI ≥30/hr & ESS >10
Sharwood,
2012
Group 4 Random sample of long distance commercial truck
drivers
Age: 46.4 years Male: 99%
BMI: 30.6 kg/m2
ESS: 5.9 AHI: 19.5 ±15/hr
MAPI: NR
325 Type IV sleep study (flow monitor,
DiagnoseIT)
AHI: NR Hypopneas: NR
OSA: AHI ≥18/hr
No OSA (AHI<18): 41% (132/325) OSA: (AHI ≥18): 59% (193/325)
>Severe (AHI ≥30): 39%
(52/193)
MAPI >0.5 AHI ≥18/hr
Sareli, 2011 Group 3 Consecutive patients evaluated for bariatric
surgery and referred for a sleep study (11/2005-
1/2007) at the Penn Sleep
Clinic for various reasons
Age: 43.8 ±10.9 years
Male: 18.4% BMI: 49.5 ±10.0
kg/m2
ESS: 8.7 ±5 AHI: 24.9 ±30.3/hr
342 Type I Polysomnography
(Sandman Elite software)
AHI: sum of apneas and hypopneas per hour of sleep
Hypopneas: 30 to 99% decrease in nasal flow with
either a ≥3% oxygen
desaturation or an EEG arousal
OSA: AHI ≥5/hr
No OSA (AHI<5): 23% (78/342) OSA (AHI ≥5): 77% (264/342)
•Mild (AHI 5-15): 40% (105/264)
•Moderate (AHI 15-20): 25%
(66/264) •Severe (AHI ≥30):35% (93/264)
Various: MAPI
score > and/or =
0.1 to 1.0
Various: AHI ≥5/hr
AHI ≥15/hr AHI ≥30/hr
* Abbreviations: AHI (apnea-hypopnea index), BMI (body mass index), CABG (coronary artery bypass graft), CAD (coronary artery disease), COPD (chronic obstructive pulmonary disease), CPAP (continuous
positive airway pressure), DM (diabetes mellitus), EEG (electroencephalogram), ESS (Epworth sleepiness scale), hr (hour), IQR (interquartile range), MI (myocardial infarction), N (number), NR (not reported), OSA
(obstructive sleep apnea), OSAS (obstructive sleep apnea syndrome), mod (moderate), PSG (polysomnogram), RDI (respiratory disturbance index), RERA (respiratory effort related arousal), SDB (sleep disordered
breathing)
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

94
Table 23 - AHRQ Question 1b – Diagnostic Accuracy of Multivariate Apnea Prediction Index (MAPI) Diagnostic Studies
Study N Cut-Point(s) Population OSA
Prevalence
TP FN FP TN p-value Sens Spec PPV NPV +LR -LR Accuracy AUC Pos Posttest
Probability
Neg Posttest
Probability
Morales, 2012 92 •AHI ≥30/hr & ESS >10
•MAPI ≥0.5
Elderly patients with
and without
sleepiness
0.109 9 1 29 53 <0.001 0.900 0.646 0.237 0.981 2.545 0.155 0.674 0.776 0.237 0.019
Sharwood, 2012 325 •AHI ≥18/hr
•MAPI ≥0.5
Commercial
truck drivers
0.406 74 58 81 112 0.013 0.561 0.580 0.477 0.659 1.366 0.757 0.572 NR 0.477 0.341
Sareli, 2011 258 •AHI ≥5/hr
•MAPI ≥0.5
Bariatric
candidates
0.779 168 33 31 26 <0.001 0.836 0.456 0.844 0.441 1.537 0.360 0.752 NR 0.844 0.559
258 •AHI ≥15/hr
•MAPI ≥0.5
Bariatric
candidates
0.481 106 18 93 41 0.002 0.855 0.306 0.533 0.695 1.232 0.474 0.570 NR 0.533 0.305
* Abbreviations: +LR (positive likelihood ratio), -LR (negative likelihood ratio), AHI (apnea-hypopnea index), AUC (area under the curve), CABG (coronary artery bypass graft), CAD (coronary artery disease), COPD (chronic
obstructive pulmonary disease), CPAP (continuous positive airway pressure), FN (false negative), FP (false positive), N (number), NR (not reported), NPV (negative predictive value), MI (myocardial infarction), ODI (oxygen
desaturation index), OSA (obstructive sleep apnea), OSAS (obstructive sleep apnea syndrome), PPV (positive predictive value), PSG (polysomnogram), RDI (respiratory disturbance index), Sen (sensitivity), Spec (specificity), TN (true negative), TP (true positive)
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

95
Table 24 - AHRQ Question 1b – Summary of Pittsburgh Sleep Quality Index (PSQI) Diagnostic Studies
Study Search
Strategy
Sample Demographics N Validation OSA Definition OSA Prevalence PSQI
Cut-point(s)
AHI
Cut-Point(s)
Knutson,
2012
Group 3 Obese (BMI 30-55) men and premenopausal
women aged 18-50 years
reporting less than 6.5 hrs of sleep
Age: 40.8 ±6.9 years
Male: 30.2%
BMI: 38.2 ±5.9 kg/m2
ESS: 8.6 ±4.4
AHI: NR PSQI: 9.0 ±3.4
139 Type IV Sleep Study (Apnea Risk
Evaluation System,
Advanced Brain Monitoring, Inc)
RDI: sum of abnormal respiratory events per hour of
sleep
Hypopneas: 50 to 90% decrease in nasal flow with a >3.5%
oxygen desaturation OR ≥1%
desaturation with ≥surrogate arousal indicator
OSA: RDI ≥15/hr
No OSA (RDI<5): 34% (47/139) OSA: (RDI ≥5) 66% (92/139)
•Mild (AHI 5-15): 37% (52/139)
•Moderate-Severe (AHI ≥15): 29% (40/139)
PSQI >5 AHI ≥15/hr
Nicholl,
2012
Group 3 Adults with chronic kidney disease attending
an outpatient nephrology
clinic
Age: 65 ±12 years Male: 63%
BMI: 31.2 ±8.3
kg/m2 ESS: 7.9 ±4.7
ODI(4%): 21.1
±25.1/hr
119 Type IV Sleep Study (Remmers
Sleep Recorder
Model 4.2)
ODI: sum of number of episodes of desaturation ≥4%
per hour of recording
OSA: ODI(4%) ≥15/hr
No OSA (ODI<15): 61% (73/119) OSA: (ODI ≥15): 39% (46/119)
PSQI >5 ODI(4%) ≥15/hr
Bertolazi,
2011
Group 4 Consecutive sleep clinic
patients undergoing sleep
study evaluations
Age: 46.6 ±11.0
years
Male: 42% BMI: 38.3 ±6.8
kg/m2
ESS: NR AHI: 16.3
±23.0/hr
PSQI: 10.8 ±4.7
83 “Polysomnography” AHI: NR
Hypopneas: NR
OSA: “per standards established by the American
Academy of Sleep Medicine
(AASM)”
No OSA (AHI<5): 52% (43/83)
OSA: (AHI ≥5): 48% (40/83)
PSQI >5 AHI ≥5/hr
* Abbreviations: AHI (apnea-hypopnea index), BMI (body mass index), CABG (coronary artery bypass graft), CAD (coronary artery disease), COPD (chronic obstructive pulmonary disease), CPAP (continuous
positive airway pressure), DM (diabetes mellitus), EEG (electroencephalogram), ESS (Epworth sleepiness scale), hr (hour), IQR (interquartile range), MI (myocardial infarction), N (number), NR (not reported),
OSA (obstructive sleep apnea), OSAS (obstructive sleep apnea syndrome), mod (moderate), PSG (polysomnogram), RDI (respiratory disturbance index), RERA (respiratory effort related arousal), SDB (sleep
disordered breathing)
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

96
Table 25. AHRQ Question 1b – Diagnostic Accuracy of Pittsburgh Sleep Quality Index (PSQI) Diagnostic Studies
Study N Cut-Point OSA
Prevalence
Population TP FN FP TN p-value Sens Spec PPV NPV +LR -LR Accuracy AUC Pos
Posttest
Probability
Neg Posttest
Probability
Knutson,
2012
128 AHI ≥15/hr
PSQI >5
0.281 Obese patients
reporting <6.5 hrs
of sleep
5 31 13 79 0.972 0.139 0.859 0.278 0.718 0.983 1.003 0.656 NR 0.278 0.282
Nicholl,
2012
119 ODI(4%)
≥15/hr
PSQI >5
0.387 Chronic kidney
disease patients
21 25 31 42 0.733 0.457 0.575 0.404 0.627 1.075 0.945 0.529 NR 0.404 0.373
Bertolazi,
2011
83 AHI ≥5/hr
PSQI ≥5
0.518 Sleep clinic
patients
31 12 40 0 <0.001 0.721 0 0.437 0 0.721 2233.5 0.373 NR 0.437 1.0
* Abbreviations: +LR (positive likelihood ratio), -LR (negative likelihood ratio), AHI (apnea-hypopnea index), AUC (area under the curve), CABG (coronary artery bypass graft), CAD (coronary artery disease), COPD (chronic obstructive pulmonary disease), CPAP (continuous positive airway pressure), FN (false negative), FP (false positive), N (number), NR (not reported), NPV (negative predictive value), MI (myocardial infarction), ODI (oxygen
desaturation index), OSA (obstructive sleep apnea), OSAS (obstructive sleep apnea syndrome), PPV (positive predictive value), PSG (polysomnogram), RDI (respiratory disturbance index), Sen (sensitivity), Spec (specificity), TN
(true negative), TP (true positive)
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

97
Table 26 - AHRQ Question 1b – Summary of STOP-BANG Questionnaire Diagnostic Studies
Study Search
Strategy
Sample Demographics N Validation OSA Definition OSA Prevalence STOP-BANG
Cut-point(s)
AHI
Cut-Point(s)
Vana, 2013 Group 4 New adult (age ≥18 years) patients referred to clinic for
sleep evaluations.
•Evaluated STOP-BANG
using various BMI criteria
including >35 or >30
Age: 46.4 ±13.2 years Male: 34%
BMI: 36.3 ±9.2 kg/m2
ESS: 8.0 (median, range 0-24)
AHI: 8.9/hr (median,
range 0 -99.9)
47 Type I Polysomnography
(diagnostic or
split-night protocols)
AHI: sum of apneas and hypopneas per hour of sleep
Hypopneas: ≥30% decrease in
nasal flow with a ≥4% oxygen desaturation
OSA: AHI ≥5/hr
No OSA (AHI <5): 32% (15/47) OSA (AHI ≥5): 68% (32/47)
•Mild (AHI 5-15): 48% (15/47)
•Moderate (AHI 15-30): 25% (8/47)
•Severe (AHI ≥30): 28% (9/47)
≥3 points
AHI ≥5/hr
Chung, 2012 Group 4 Patients scheduled for surgery
attending preoperative clinic
Age: 60 years (range
51-68)
Male: 48% BMI: 30 kg/m2 (range
26-34)
ESS: NR AHI:NR
746 Type 2 Portable
Sleep Study
(Embletta X-100)
AHI: sum of apneas and
hypopneas per hour of sleep
Hypopneas: “scored according to the American Academy of
Sleep Medicine Task Force
recommendations” OSA:AHI ≥5/hr
No OSA (AHI<5): 32% (236/746)
OSA: (AHI ≥5): 68% (510/746)
•Mild (AHI 5-15): 44% (223/510)
•Moderate (AHI 15-30): 30%
(153/236) •Severe (AHI ≥30): 26%
(134/236)
Various:
≥2 points
≥3 points ≥5 points
Various:
AHI ≥5/hr
AHI ≥15/hr
AHI
≥30/hr:
Farney,
2011
Group 3 Consecutive patients referred to a sleep clinic who
underwent PSG testing for
any reason (1/2006-12/2008)
Age: 49.7 ±15.2 years Male: 57.2%
BMI: 33.8 ±8.1 kg/m2
ESS: NR AHI:32.9 ±30.1/hr
1,426 Type 1 Polysomnogram
(17 channel;
Cadwell lab)
AHI: sum of apneas and hypopneas per hour of sleep
Hypopneas: studies prior to
4/2007, scoring based on “earlier” ‘Chicago’ criteria; after
this date based on AASM 2007
standards
OSA: AHI ≥5/hr
No OSA (AHI<5): 10.5% (150/1424)
OSA: 89.5% (1274/1424)
•Mild (AHI 5-15): 24.7% (315/1424)
•Moderate (AHI 15-30): 29.7%
(379/1274)
•Severe (AHI ≥30): 45.5%
(580/1274)
Various: ≥1 points
≥2 points
≥3 points ≥4 points
≥5 points
≥6 points
Various: AHI ≥5/hr
AHI
≥15/hr AHI
≥30/hr
Silva, 2011 Group 4 Sleep Heart Health Study – Population study in subjects
age >40 years
Age:62.4 ±10.3 years Male: 52%
BMI: NR (35% had BMI
≥30 kg/m2) ESS: NR (28% ESS
>11)
AHI: NR
4770 Type II Polysomnography
(Compumedics
portable PS-2 system)
AHI: sum of apneas and hypopneas per hour of sleep
Hypopneas: ≥25% decrease in
nasal flow with a ≥4% oxygen desaturation
OSA: AHI ≥5/hr
No OSA (AHI<5): 87% (4167/4770)
OSA (AHI ≥5): 13% (603/4770)
•Moderate (AHI 15-20): 43% (258/603)
•Severe (AHI ≥30): 57%
(345/603)
≥3 points
Various: AHI
≥15/hr
AHI ≥30/hr
Ong, 2010 Group 4 Consecutive sleep clinic
patients (95% evaluated for
suspected sleep apnea)
•Evaluated STOP-BANG
using various BMI cut-points: BMI ≥26, BMI ≥30, BMI ≥35
Age: 47 ±15.2 years
Male: 71%
BMI: 27.8 ±5.9 kg/m2
ESS: 9.4 ±5.2
AHI: 26.2 ±26.9/hr
317 Type 1
Polysomnogram
AHI: sum of apneas and
hypopneas per hour of sleep
Hypopneas: ≥30% decrease in
nasal flow with either a ≥4%
oxygen desaturation OR ≥3%
oxygen and an EEG arousal OSA: AHI ≥5/hr
No OSA (AHI<5): 25% (78/317)
OSA: 75% (239/317)
•Mild (AHI 5-15): 33% (79/239)
•Moderate (AHI 15-30): 21%
(51/239)
•Severe (AHI ≥30): 46% (109/239)
≥3 points
Various:
AHI ≥5/hr
AHI
≥15/hr
AHI
≥30/hr
* Abbreviations: AHI (apnea-hypopnea index), BMI (body mass index), CABG (coronary artery bypass graft), CAD (coronary artery disease), COPD (chronic obstructive pulmonary disease), CPAP (continuous
positive airway pressure), DM (diabetes mellitus), EEG (electroencephalogram), ESS (Epworth sleepiness scale), hr (hour), IQR (interquartile range), MI (myocardial infarction), N (number), NR (not reported), OSA
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

98
(obstructive sleep apnea), OSAS (obstructive sleep apnea syndrome), mod (moderate), PSG (polysomnogram), RDI (respiratory disturbance index), RERA (respiratory effort related arousal), SDB (sleep disordered
breathing)
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

99
Table 27 - AHRQ Question 1b – Diagnostic Accuracy of STOP-BANG (BMI >35) Questionnaire Diagnostic Studies
Study N Cut-Point OSA
Prevalence
Population TP FN FP TN Diagnostic
Odds Ratio
p-
value
Sens Spec PPV NPV +LR -LR Accuracy AUC Pos Posttest
Probability
Neg
Posttest
Probability
Kappa(1)
Coefficient
Vana, 2013 47 STOP-BANG ≥3
points
AHI ≥5/hr
0.681 New sleep clinic
patients
30 2 10 5 7.500 0.015 0.938 0.333 0.750 0.714 1.406 0.188 0.745 0.490 0.750 0.286 0.217
Chung,
2012
746 STOP-BANG ≥2
points
AHI ≥5/hr
0.684 Elective surgery
candidates
488 22 194 42 <0.001 0.957 0.178 0.716 0.656 1.164 0.242 0.710 0.650 0.716 0.344
746 STOP-BANG ≥2
points
AHI ≥15/hr
0.385 Elective surgery
candidates
283 4 399 60 <0.001 0.986 0.131 0.415 0.938 1.134 0.107 0.460 0.670 0.415 0.063
746 STOP-BANG ≥2
points
AHI ≥30/hr
0.180 Elective surgery
candidates
134 0 548 64 <0.001 1.00 0.105 0.196 1.00 1.117 0.000 0.265 0.710 0.196 0.000
746 STOP-BANG ≥3
points
AHI ≥5/hr
0.684 Elective surgery
candidates
429 81 141 95 3.568 <0.001 0.841 0.403 0.753 0.540 1.408 0.395 0.702 0.650 0.753 0.460 0.218
746 STOP-BANG ≥3
points
AHI ≥15/hr
0.385 Elective surgery
candidates
256 31 314 145 3.813 <0.001 0.892 0.316 0.449 0.824 1.304 0.342 0.538 0.670 0.449 0.176 0.105
746 STOP-BANG ≥3
points
AHI ≥30/hr
0.180 Elective surgery
candidates
127 7 443 169 6.921 <0.001 0.948 0.276 0.223 0.960 1.309 0.189 0.397 0.710 0.223 0.040 0.053
746 STOP-BANG ≥5
points
AHI ≥5/hr
0.684 Elective surgery
candidates
185 325 48 188 <0.001 0.363 0.797 0.794 0.366 1.783 0.800 0.500 0.650 0.794 0.634
746 STOP-BANG ≥5
points
AHI ≥15/hr
0.385 Elective surgery
candidates
126 161 107 352 <0.001 0.439 0.767 0.541 0.686 1.883 0.731 0.641 0.670 0.541 0.314
746 STOP-BANG ≥5
points
AHI ≥30/hr
0.180 Elective surgery
candidates
75 59 158 454 <0.001 0.560 0.742 0.322 0.885 2.168 0.594 0.709 0.710 0.475 0.130
Farney,
2011
1424 STOP-BANG ≥2
points
AHI ≥5/hr
0.895 Sleep clinic patients 1240 34 115 35 <0.001 0.973 0.233 0.915 0.507 1.270 0.114 0.895 NR 0.915 0.493
1424 STOP-BANG ≥2
points
AHI ≥15/hr
0.673 Sleep clinic patients 942 17 413 52 <0.001 0.982 0.112 0.695 0.754 2.281 0.327 0.698 NR 0.695 0.246
1424 STOP-BANG ≥2
points
AHI ≥30/hr
0.407 Sleep clinic patients 573 7 782 62 <0.001 0.988 0.073 0.423 0.899 1.066 0.164 0.446 NR 0.423 0.101
1424 STOP-BANG ≥3
points
AHI ≥5/hr
0.895 Sleep clinic patients 1139 135 63 87 22.588 <0.001 0.894 0.580 0.948 0.392 2.129 0.183 0.861 NR 0.948 0.608 0.502
1424 STOP-BANG ≥3
points
AHI ≥15/hr
0.673 Sleep clinic patients 895 64 307 158 7.197 <0.001 0.933 0.340 0.745 0.712 1.414 0.196 0.739 NR 0.745 0.288 0.218
1424 STOP-BANG ≥3
points
0.372 Sleep clinic patients 555 25 782 197 5.593 <0.001 0.957 0.201 0.415 0.887 1.198 0.214 0.482 NR 0.415 0.113 0.069
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

100
AHI ≥30/hr
1424 STOP-BANG ≥5
points
AHI ≥5/hr
0.895 Sleep clinic patients 654 620 16 134 <0.001 0.513 0.893 0.976 0.178 4.813 0.545 0.553 NR 0.976 0.822
1424 STOP-BANG ≥5
points
AHI ≥15/hr
0.665 Sleep clinic patients 523 400 111 354 <0.001 0.567 0.761 0.825 0.469 2.374 0.569 0.632 NR 0.825 0.531
1424 STOP-BANG ≥5
points
AHI ≥30/hr
0.407 Sleep clinic patients 385 195 285 559 <0.001 0.664 0.662 0.575 0.741 1.966 0.508 0.663 NR 0.575 0.259
Silva, 2011 4770 STOP-BANG ≥3
points
AHI ≥15/hr
0.126 Population study
(SHHS)
525 78 2363 1804 4.923 <0.001 0.871 0.433 0.182 0.959 1.535 0.299 0.488 0.640 0.182 0.041 0.063
4770 STOP-BANG ≥3
points
AHI ≥30/hr
0.072 Population study
(SHHS)
243 102 1792 2633 3.765 <0.001 0.704 0.595 0.119 0.963 1.739 0.497 0.603 0.660 0.119 0.037 0.051
Ong, 2010 317 STOP-BANG ≥3
points
AHI ≥5/hr
0.754 Consecutive
sleep clinic
patients
203 36 37 41 6.170 <0.001 0.849 0.526 0.846 0.532 1.791 0.287 0.770 0.775 0.856 0.468 0.373
317 STOP-BANG ≥3
points
AHI ≥15/hr
0.505 Consecutive
sleep clinic
patients
146 14 94 63 7.032 <0.001 0.913 0.401 0.608 0.818 1.524 0.218 0.659 0.775 0.608 0.182 0.209
317 STOP-BANG ≥3
points
AHI ≥30/hr
0.344 Consecutive
sleep clinic
patients
104 5 136 72 11.101 <0.001 0.954 0.346 0.433 0.935 1.459 0.133 0.555 0.772 0.433 0.065 0.136
* Abbreviations: +LR (positive likelihood ratio), -LR (negative likelihood ratio), AHI (apnea-hypopnea index), AUC (area under the curve), CABG (coronary artery bypass graft), CAD (coronary artery disease), COPD (chronic obstructive pulmonary disease), CPAP (continuous positive airway pressure), FN (false negative), FP (false positive), N (number), NR (not reported), NPV (negative predictive value), MI (myocardial infarction), ODI (oxygen
desaturation index), OSA (obstructive sleep apnea), OSAS (obstructive sleep apnea syndrome), PPV (positive predictive value), PSG (polysomnogram), RDI (respiratory disturbance index), Sen (sensitivity), Spec (specificity), TN
(true negative), TP (true positive)
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

101
Table 28 - AHRQ Question 1b – Summary of Other OSA Diagnostic Questionnaires
Study Search
Strategy
Sample Demographics N Validation OSA Definition OSA Prevalence Cut-point(s) AHI
Cut-Point(s)
Sharkey, 2013 Group 4 Patients evaluated for bariatric
surgery
•Evaluated Functional Outcomes
of Sleep Questionnaire (FOSQ)
Age: 42.0 ±9.5 years
Male: 11% BMI: 50.2 ±7.7 kg/m2
ESS: 6.3 ±4.8
AHI: 29.5 ±31.5/hr
269 Type I
Polysomnography
AHI: sum of apneas and
hypopneas per hour of sleep Hypopneas: ≥50% decrease in
nasal flow with a >3% oxygen
desaturation OSA: AHI ≥15/hr
No OSA (AHI <15): 42%
(112/269) OSA (AHI ≥15): 58%
(157/269)
•Moderate (AHI 15-30): 49% (77/157)
•Severe (AHI ≥30): 51%
(80/157)
Various:
FOSQ ≤90 FOSQ ≤70
Various:
AHI ≥15/hr
AHI
≥30/hr
Vana, 2013 Group 4 New adult (age ≥18 years)
patients referred to clinic for sleep
evaluations.
•Evaluated ESS >10 or STOP-
BANG ≥3
•Evaluated STOP-BANG using
various BMI criteria including
>35 or >30
Age: 46.4 ±13.2 years
Male: 34%
BMI: 36.3 ±9.2 kg/m2
ESS: 8.0 (median, range 0-24)
AHI: 8.9/hr (median,
range 0 -99.9)
47 Type I
Polysomnography
(diagnostic or split-
night protocols)
AHI: sum of apneas and
hypopneas per hour of sleep
Hypopneas: ≥30% decrease in
nasal flow with a ≥4% oxygen desaturation
OSA: AHI ≥5/hr
No OSA (AHI <5): 32% (15/47)
OSA (AHI ≥5): 68% (32/47)
•Mild (AHI 5-15): 48%
(15/47) •Moderate (AHI 15-30): 25%
(8/47)
•Severe (AHI ≥30): 28% (9/47)
ESS >10 or
STOP-BANG
≥3 points
AHI ≥5/hr
Senchak, 2012 Group 4 Multi-institutional, prospective
clinical trial in adult (age ≥18
years) patients (active duty army) undergoing tonsillectomy for
chronic, recurrent tonsillitis
•Two questionnaires used to
assess pretest probability of OSA
– High pretest probability for OSA defined as an ESS ≥8 and a
positive Berlin snore score
(Berlin category 1 score ≥2)
Age: 26.8 ±8.0 years
Male: 48%
BMI: 27.7 ±5.8 kg/m2 ESS: NR
AHI: 4.7 ±9.6/hr
77 Type IV Sleep Study
(ApneaLink Plus,
Resmed)
AHI: NR
Hypopneas: NR
OSA: AHI ≥5/hr
No OSA (AHI<5): 20% (15/77)
OSA: (AHI ≥5): 80% (52/77)
•Mild: NR •Moderate: NR
•Mild: NR
ESS ≥8 and a
positive Berlin
snore score (Berlin
category 1
score ≥2)
AHI ≥5/hr
Chai-Coetzer,
2011
Group 3 Adult patients attending six
primary care clinics
•Evaluated two-stage screening
model incorporating BOTH OSA
50 questionnaire (Obesity,
snoring, apnea, age 50; ≥5/10)
and 3%ODI (≥16/hr)
Age: 50 years (range 40-
58)
Male:44% BMI: 29.3 kg/m2 (range
25.5-33.8)
ESS: 7 (range 5-10)
AHI: 16.5/hr (range 9.6-
28.2)
78 Type I
Polysomnogram
AHI: NR
Hypopneas: Either ≥50%
decrease in nasal flow or a ≥3% oxygen desaturation or an
EEG arousal
OSA: AHI ≥30/hr
No OSA (AHI <30): 79%
(62/78)
OSA (AHI ≥30): 21% (16/78) •Mild: NR
•Moderate: NR
•Mild: NR
OSA 50
questionnaire
(≥5/10) AND 3%ODI
(≥16/hr)
AHI
≥30/hr
Enciso, 2011 Group 4 Patients of the USC School of Dentistry
Age: 54.9 ±12.1 years Male: 77%
BMI: 26.6 ±18.1 kg/m2
84 Type IV Sleep Study (ARES Unicorder)
RDI: Not reported Hypopneas: Not reported
OSA: RDI ≥15/hr
No OSA (RDI<15): 37% (31/84)
OSA (RDI ≥15): 63% (53/84)
“High Risk” on ARES
Various: RDI
≥10/hr
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

102
•Evaluated the Apnea Risk
Evaluation System (ARES) questionnaire that combines
features of three validated
questionnaires: Berlin, Flemon’s Index and ESS.
ESS: NR
RDI: 24.3 ±18.1/hr
RDI
≥15/hr
Silva, 2011 Group 4 Sleep Heart Health Study –
Population study in subjects age >40 years
• Evaluated the Takegami 4-item
Screen
Age:62.4 ±10.3 years
Male: 52% BMI: NR (35% had BMI
≥30 kg/m2)
ESS: NR (28% ESS >11)
AHI: NR
4,770 Type II Sleep Study
(Compumedics portable PS-2 system)
AHI: sum of apneas and
hypopneas per hour of sleep Hypopneas: ≥25% decrease in
nasal flow with a ≥4% oxygen
desaturation OSA: AHI ≥5/hr
No OSA (AHI<5): 87%
(4167/4770) OSA (AHI ≥5): 13%
(603/4770)
•Moderate (AHI 15-20): 43% (258/603)
•Severe (AHI ≥30): 57%
(345/603)
•Takegami 4-
Variable Screening tool
≥14
•STOP ≥2
Various-
AHI ≥15/hr
AHI
≥30/hr
Subramanian,
2011
Group 3 Consecutive patients referred for
suspected sleep apnea (no prior
OSA Diagnosis)
•NAMES (Neck circumference,
airway classification, comorbidities, Epworth scale,
snoring) and NAMES2 (NAMES
criteria and gender, BMI ≥30) Scores
Age: 55 ±14 years
Male: 59%
BMI: 35 ±9 kg/m2 ESS: NR
RDI: 38 ±8/hr
509 •Type I
Polysomnography
RDI: sum of apneas,
hypopneas and RERA’s per
hour of sleep Hypopneas: required ≥4%
oxygen desaturation in addition
to defined reduction in airflow per 2007 American Academy
of Sleep Medicine Scoring
Guidelines RERA’s: NR
OSA: RDI ≥5
No OSA (RDI<5): 15%
(77/509)
OSA: (RDI ≥5): 85% (432/509) •Mild: 31% (134/432)
•Moderate/Severe (RDI ≥15):
69% (298/432)
NAMES ≥3
NAMES2 ≥4
Various-
RDI ≥5/hr
RDI ≥15/hr
Rodrigues,
2010
Group 3 Patients complaining of snoring and clinical history suggestive of
OSA and symptoms of daytime
sleepiness, non-restful sleep and snoring were evaluated by sleep
study.
•Friedman’s classification
(modified Mallampati scale,
pharyngeal tonsil size and BMI)
Age: 48.0 ±11.3 years Male: NR
BMI: 29.4 ±5.6 kg/m2
ESS: 11.3 ±5.1 AHI: NR
101 •Type I Polysomnography
AHI: NR Hypopneas: NR
OSA: AHI ≥5/hr
No OSA (AHI <5): 10% (11/112)
OSA (AHI ≥5): 90% (101/112)
Various- Friedman ≥2
Friedman ≥3
Friedman =4
Various- AHI ≥5/hr
AHI
≥15/hr AHI
≥30/hr
* Abbreviations: AHI (apnea-hypopnea index), BMI (body mass index), CABG (coronary artery bypass graft), CAD (coronary artery disease), COPD (chronic obstructive pulmonary disease), CPAP (continuous positive
airway pressure), DM (diabetes mellitus), EEG (electroencephalogram), ESS (Epworth sleepiness scale), hr (hour), IQR (interquartile range), MI (myocardial infarction), N (number), NR (not reported), OSA (obstructive
sleep apnea), OSAS (obstructive sleep apnea syndrome), mod (moderate), PSG (polysomnogram), RDI (respiratory disturbance index), RERA (respiratory effort related arousal), SDB (sleep disordered breathing)
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

103
Table 29 - AHRQ Question 1b – Diagnostic Accuracy of Other OSA Diagnostic Questionnaires
Study N Cut-Point OSA
Prevalence
Population TP FN FP TN p-
value
Sens Spec PPV NPV +LR -LR Accuracy AUC Pos Posttest
Probability
Neg
Posttest
Probability
Sharkey, 2013 269 •FOSQ ≤90
•PSG: AHI ≥15/hr
0.584 Bariatric surgery
candidates
52 105 31 81 0.341 0.331 0.723 0.627 0.435 1.197 0.925 0.494 NR 0.627 0.565
269 •FOSQ ≤70
•PSG: AHI ≥15/hr
0.584 Bariatric surgery
candidates
21 136 11 101 0.375 0.134 0.902 0.656 0.426 1.362 0.961 0.454 NR 0.656 0.574
Vana, 2013 47 •ESS >10 or STOP-BANG ≥3 points
(BMI >35 rule)
•PSG: AHI ≥5/hr
0.681 Patients referred to
clinic for sleep
evaluations.
30 2 12 3 0.154 0.938 0.200 0.714 0.600 1.172 0.313 0.702 0.569 0.714 0.400
Senchak, 2012 77 •ESS ≥8 and a positive Berlin snore
score (Berlin category 1 score ≥2)
•PSG: AHI ≥5/hr
0.195 Patients undergoing
tonsillectomy for
chronic, recurrent
tonsillitis
12 3 25 37 0.006 0.800 0.597 0.324 0.925 1.984 0.335 0.636 NR 0.324 0.075
Chai-Coetzer,
2011
78 •OSA 50 questionnaire (≥5/10) AND
3%ODI (≥16/hr)
•PSG: AHI ≥30/hr
0.205 Adult patients
attending six
primary care clinics
14 2 11 51 <0.001 0.875 0.823 0.560 0.962 4.932 0.15 0.833 0.75 0.560 0.038
Enciso, 2011 84 •ARES High Risk
•PSG: RDI ≥10/hr
0.774 Dentistry patients 48 5 17 14 <0.001 0.906 0.452 0.738 0.737 1.651 0.209 0.738 NR 0.738 0.263
84 •ARES High Risk
•PSG: RDI ≥15/hr
0.631 Dentistry patients 57 8 8 11 <0.001 0.877 0.579 0.877 0.579 2.083 0.213 0.810 NR 0.877 0.421
Silva, 2011 4,770 •Takegami 4-item Screen ≥14
•PSG: AHI ≥15/hr
0.126 SHHS Population
Study
149 454 283 3,884 <0.001 0.247 0.932 0.345 0.895 3.638 0.808 0.845 0.590 0.345 0.105
4,770 •Takegami 4-item Screen ≥14
•PSG: AHI ≥30/hr
0.072 SHHS Population
Study
143 202 301 4124 <0.001 0.414 0.932 0.322 0.953 6.093 0.628 0.895 0.670 0.322 0.047
4,770 •STOP ≥2
•PSG: AHI ≥15/hr
0.126 SHHS Population
Study
374 229 1821 2346 <0.001 0.620 0.563 0.170 0.911 1.419 0.675 0.570 0.580 0.170 0.089
4,770 •STOP ≥2
•PSG: AHI ≥30/hr
0.072 SHHS Population
Study
237 108 1792 2633 <0.001 0.687 0.595 0.117 0.961 1.696 0.526 0.602 0.670 0.117 0.039
Subramanian,
2011
509 •PSG: RDI ≥5/hr
•NAMES ≥3
0.849 Suspected OSA 380 52 55 22 <0.001 0.880 0.286 0.874 0.297 1.231 0.421 0.790 NR 0.874 0.703
509 •PSG: RDI ≥15/hr
•NAMES ≥3
0.585 Suspected OSA 271 27 162 49 <0.001 0.909 0.232 0.626 0.645 1.184 0.390 0.629 0.643 0.626 0.355
509 •PSG: RDI ≥5/hr
•NAMES2 ≥4
0.849 Suspected OSA 367 65 45 32 <0.001 0.850 0.416 0.891 0.330 1.454 0.362 0.784 NR 0.891 0.670
509 •PSG: RDI ≥15/hr
•NAMES2 ≥4
0.585 Suspected OSA 274 24 139 72 <0.001 0.919 0.341 0.663 0.750 1.396 0.236 0.680 0.669 0.663 0.250
Rodrigues, 2010 101 •PSG: AHI ≥5/hr
•Friedman ≥2
0.902 Suspected OSA 99 2 11 0 0.638 0.980 0.000 0.900 0.000 0.980 NA 0.884 NR 0.900 NA
101 •PSG: AHI ≥15/hr
•Friedman ≥2
0.482 Suspected OSA 54 0 56 2 0.169 1.000 0.034 0.491 1.000 1.036 0.000 0.500 NR 0.491 0.000
101 •PSG: AHI 30/hr
•Friedman ≥2
0.313 Suspected OSA 35 0 75 2 0.336 1.000 0.026 0.318 1.000 1.027 0.000 0.330 NR 0.318 0.000
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

104
101 •PSG: AHI ≥5/hr
•Friedman ≥3
0.902 Suspected OSA 63 38 4 6 0.275 0.624 0.545 0.926 0.136 1.372 0.690 0.616 NR 0.926 0.864
101 •PSG: AHI ≥15/hr
•Friedman ≥3
0.482 Suspected OSA 39 15 29 29 0.016 0.722 0.500 0.574 0.659 1.444 0.556 0.607 NR 0.574 0.341
101 •PSG: AHI ≥30/hr
•Friedman ≥3
0.313 Suspected OSA 25 10 43 34 0.118 0.714 0.442 0.368 0.773 1.279 0.647 0.527 NR 0.368 0.227
101 •PSG: AHI ≥5/hr
•Friedman =4
0.902 Suspected OSA 8 93 1 10 0.892 0.079 0.909 0.889 0.097 0.871 1.013 0.161 NR 0.889 0.903
101 •PSG: AHI ≥15/hr
•Friedman =4
0.482 Suspected OSA 6 48 3 55 0.248 0.111 0.948 0.667 0.534 2.148 0.937 0.545 NR 0.667 0.466
101 •PSG: AHI ≥30/hr
•Friedman =4
0.313 Suspected OSA 5 30 4 73 0.101 0.143 0.948 0.556 0.709 2.750 0.904 0.696 NR 0.556 0.291
* Abbreviations: +LR (positive likelihood ratio), -LR (negative likelihood ratio), AHI (apnea-hypopnea index), AUC (area under the curve), CABG (coronary artery bypass graft), CAD (coronary artery disease), COPD (chronic obstructive pulmonary disease), CPAP (continuous positive airway pressure), FN (false negative), FP (false positive), N (number), NR (not reported), NPV (negative predictive value), MI (myocardial infarction),
ODI (oxygen desaturation index), OSA (obstructive sleep apnea), OSAS (obstructive sleep apnea syndrome), PPV (positive predictive value), PSG (polysomnogram), RDI (respiratory disturbance index), Sen (sensitivity),
Spec (specificity), TN (true negative), TP (true positive)
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

105
Table 30 - AHRQ Question 1C – Summary of OSA Clinical Prediction Rule Diagnostic Studies
Study Search
Strategy
Sample Demographics N Index/Validation OSA Definition OSA Prevalence Prediction Rule PSG
Cut-Point(s)
Jauhar,
2012
Group 4 Consecutive patients
with
suspected OSA
Age: 46.6 ±11.2 years
Male: 75%
BMI: 32.5 ±8.7 kg/m2
ESS: 11.1 ±5.4
ODI: NR (for those with OSA, median
ODI 24/hr, IQR 11-
68)
71 •Kushida Index developed previously to predict clinically
suspected OSA (variables: BMI,
neck circumference, palatal height, maxillary and mandibular
intermolar distance, overjet)
• Type IV Sleep Study
(Somnoscreen)
ODI: NR OSA: ODI ≥10/hr and
ESS ≥10
No OSA: 48% (34/71) OSA (ODI ≥10 and ESS ≥10): 52%
(37/71)
•Mild or Borderline: 46% (17/37) •Moderate: 19% (7/37)
•Severe: 35% (13/37)
Kushida Index ≥70
ODI ≥10 AND ESS
≥10
Morales,
2012
Group 4 Elderly
patients
(population study) with
and without
sleepiness
Age: 71.3 ±5.9 years
Male: 34%
BMI: 30.5 ±7.6 kg/m2
ESS: NR (30% ESS
>10) AHI: NR
92 •Optimal parameters set as one
that minimized total prediction
errors, computed as sum of false-positives and false-negative
predictions. 3-variables chosen:
Apnea symptoms, neck circumference, age
•Type I Polysomnography (Sandman, Embla)
AHI: sum of apneas
and hypopneas per
hour of sleep Hypopneas: ≥50%
decrease in nasal flow
with either a ≥3% oxygen or EEG
arousals
OSA: AHI ≥30/hr and ESS >10
No OSA: 73% (70/92)
OSA (AHI ≥5 & ESS >10): 27%
(22/92) •Mild (AHI 5-15 & ESS >10):
32% (7/22)
•Moderate (AHI 15-30 & ESS >10): 23% (5/22)
•Severe (AHI ≥30 & ESS >10):
45% (10/22)
Rule ≥0.676 AHI
≥30/hr &
ESS >10
Su, 2012 Group 3 Consecutive
patients
with
suspected
OSA
Age: 48.3 ±11.9
years
Male:77%
BMI: 24.8 ±3.1
kg/m2 ESS: 10.1 ±6.4
AHI: NR
144 •Multiclass Mahalanobis-Taguchi
(MMTS) based anthropometric
information and questionnaire
data to predict OSA (6 variables:
age, weight, SBP, DBP, DI3, DI4)
• Type 1 polysomnogram
RDI: “Number of events
per
hour of sleep”
Hypopnea: NR
OSA: RDI ≥5/hr
No OSA (RDI <5): 28% (8/29)
OSA (RDI ≥5): 72% (21/29)
•Mild (RDI 5-15): 29% (6/21)
•Moderate (RDI 15-30): 43%
(9/21) •Severe (RDI ≥30): 29% (6/21)
Various:
AHI ≥5/hr
AHI ≥15/hr
AHI ≥30/hr
Various:
AHI ≥5/hr
AHI
≥15/hr
AHI ≥30/hr
Kolotkin,
2012
Group 3 Bariatric
surgery
candidates
Age: 41.6 ±10.4
years
Male:16% BMI:46.8 ±7.5 kg/m2
ESS: NR
AHI: NR
310 • Dixon prediction model
developed previously to predict
clinically suspected OSA in bariatric surgery candidates. (6
variables: BMI ≥45 kg/m2, age
≥38 years, HgA1C ≥6%, insulin level ≥28 μU/mL, male gender,
neck circumference ≥43 cm)
• Kolotkin alternative prediction
model developed and validated a prediction model to predict OSA
in bariatric surgery candidates.
(10 variables: neck
AHI: sum of apneas
and hypopneas per
hour of sleep Hypopneas: “A
reduction” in nasal
flow with a >4% oxygen desaturation
OSA: AHI ≥5/hr
No OSA (AHI <5): 19% (58/310)
OSA (AHI ≥5): 81% (252/310)
•Mild (RDI 5-15): 47% (115/252) •Moderate (RDI 15-30): 26%
(65/252)
•Severe (RDI ≥30): 29% (72/252)
Dixon Model
Various:
Cut-points between 0
and 6 points
Alternate
Model
Various: Cut-points
between 0 and 10 points
Various:
AHI
≥15/hr AHI
≥30/hr
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

106
circumference ≥40.75 cm, SBP
≥123.5, waist/hip ratio≥0.956, waist ≥134.4 cm, glucose, ≥96.5
loud snoring, age ≥41.5 years,
frequent snoring, BMI ≥45.17 kg/m2, male gender))
• Type III Sleep Study (Embletta portable system without EEG)
Khoo, 2011 Group 4 Consecutive
patients referred to a
sleep clinic
Age: 45.5 ±13.5
years Male:81%
BMI: 29.6 ±5.7
kg/m2
ESS: NR
AHI: 40.8 ±29.5/hr
52 Koo Model (developed and
validated in current study): age, male gender, neck circumference,
frequent awakenings with
unrefreshing sleep
Type I Polysomnography
(Compumedics E Series)
Flemons Index (previously
validated 4-variable model to predict clinically suspected OSA):
neck circumference, HTN, habitual
snoring and gasping/ choking
AHI: sum of apneas
and hypopneas per hour of sleep
Hypopneas: ≥20%
reduction in nasal flow
with a >3% oxygen
desaturation
OSA: AHI ≥20/hr
No OSA (AHI <20): 34% (18/52)
OSA (AHI ≥20): 65% (34/52)
Koo Model:
0.6
Flemons
Index: 17
AHI
≥20/hr
Sun, 2011 Group 3 Suspected
OSA
Age: 43.4 ±12.7
years Male: 76%
BMI: NR (20% BMI
>25 kg/m2) ESS: NR (39% ESS
>10)
AHI: NR
110 •Genetic algorithm was used to
build the five best models based on questions taken from the
Berlin Questionnaire, Rome
Questionnaire, ESS and BASH’IM score
• “Polysomnography test”
AHI: NR
Hypopneas: NR OSA: AHI ≥5/hr
No OSA (AHI <5):23% (25/110)
OSA (AHI ≥5): 77% (85/110) •Mild (AHI 5-15): 38% (32/85)
•Moderate (AHI 15-30): 32%
(27/85) •Severe (AHI ≥30): 31% (26/85)
AHI ≥15/hr
AHI
≥15/hr
* Abbreviations: AHI (apnea-hypopnea index), BMI (body mass index), CABG (coronary artery bypass graft), CAD (coronary artery disease), COPD (chronic obstructive pulmonary disease), CPAP
(continuous positive airway pressure), DM (diabetes mellitus), EEG (electroencephalogram), ESS (Epworth sleepiness scale), hr (hour), IQR (interquartile range), MI (myocardial infarction), N (number),
NR (not reported), OSA (obstructive sleep apnea), OSAS (obstructive sleep apnea syndrome), mod (moderate), PSG (polysomnogram), RDI (respiratory disturbance index), RERA (respiratory effort related
arousal), SDB (sleep disordered breathing)
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

107
Table 31 - AHRQ Question 1C – Diagnostic Accuracy of OSA Clinical Prediction Rule Diagnostic Studies
Study N Cut-Point OSA
Prevalence
Population TP FN FP TN p-
value
Sens Spec PPV NPV +LR -LR Accuracy AUC Pos Posttest
Probability
Neg
Posttest
Probability
Jauhar,
2012
71 •Rule: ≥71
•PSG: ODI ≥10 AND
ESS ≥10
0.521 Patients with
suspected OSA
25 12 10 24 0.001 0.676 0.706 0.714 0.667 2.297 0.459 0.690 NR 0.714 0.333
Moreales,
2012
92 •Rule: ≥0.676
•PSG: AHI ≥30 AND
ESS >10
0.109 Elderly subjects
with and without
sleepiness
9 1 29 53 <0.001 0.900 0.646 0.237 0.981 2.545 0.155 0.674 0.774 0.237 0.019
Su, 2012 144 •Rule: AHI ≥5/hr
•PSG: AHI ≥5/hr
0.724 Patients with
suspected OSA
. . . . . . . . . . . 0.844 . . .
Kolotkin,
2012
310 •Dixon Rule: ≥2 criteria •PSG: AHI ≥15/hr
0.442 Bariatric surgery candidates
103 34 74 99 <0.001 0.752 0.572 0.582 0.744 1.758 0.434 0.652 NR 0.582 0.256
310
•Dixon Rule: ≥3 criteria
•PSG: AHI ≥15/hr
0.442 Bariatric surgery
candidates
71 66 31 142 <0.001 0.518 0.821 0.696 0.683 2.892 0.587 0.687 NR 0.696 0.317
310 •Dixon Rule: ≥2 criteria •PSG: AHI ≥30/hr
0.232 Bariatric surgery candidates
60 12 117 121 <0.001 0.833 0.508 0.339 0.910 1.695 0.328 0.584 NR 0.339 0.090
310 •Dixon Rule: ≥3 criteria
•PSG: AHI ≥30/hr
0.232 Bariatric surgery
candidates
46 26 56 182 <0.001 0.639 0.765 0.451 0.875 2.715 0.472 0.735 NR 0.451 0.125
155 •Kolotkin Rule: ≥5 criteria
•PSG: AHI ≥15/hr
NR Bariatric surgery candidates
. . . . . 0.761 0.716 . . . . . 0.780 . .
155 •Kolotkin Rule: ≥5 criteria
•PSG: AHI ≥30/hr
NR Bariatric surgery candidates
. . . . . 0.839 0.597 . . . . . NR . .
Khoo, 2011 52 •Koo Model: 0.6 •PSG: AHI ≥20/hr
0.654 Sleep clinic patients
13 21 3 17 0.073 0.382 0.850 0.813 0.447 2.549 0.727 0.577 0.690 0.828 0.579
52 •Flemons Index: 17
•PSG: AHI ≥20/hr
0.654 Sleep clinic
patients
25 7 11 9 0.079 0.781 0.450 0.694 0.563 1.420 0.486 0.654 0.642 0.694 0.438
Sun, 2011 43 •Rule: AHI ≥15/hr •PSG: AHI ≥15/hr
NR Patients with suspected OSA
. . . . . 0.818 0.952 0.947 0.833 . . 0.884 . . .
* Abbreviations: +LR (positive likelihood ratio), -LR (negative likelihood ratio), AHI (apnea-hypopnea index), AUC (area under the curve), CABG (coronary artery bypass graft), CAD (coronary artery disease), COPD (chronic obstructive pulmonary disease), CPAP (continuous positive airway pressure), FN (false negative), FP (false positive), N (number), NR (not reported), NPV (negative predictive value), MI (myocardial infarction),
ODI (oxygen desaturation index), OSA (obstructive sleep apnea), OSAS (obstructive sleep apnea syndrome), PPV (positive predictive value), PSG (polysomnogram), RDI (respiratory disturbance index), Sen (sensitivity),
Spec (specificity), TN (true negative), TP (true positive)
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

108
Table 32 - AHRQ Question 2 – Phased testing compared with full testing alone
Study Search
Strategy
Sample Demographics N Phased Testing/Validation OSA Definition OSA Prevalence Prediction Rule PSG
Cut-Point(s)
Morales,
2012
Group 4 Elderly patients
(population
study) with and without
sleepiness
Age: 71.3 ±5.9 years Male: 34%
BMI: 30.5 ±7.6 kg/m2
ESS: NR (30% ESS >10)
AHI: NR
92 •Two-stage algorithm (3 parameters): 1) MAP lower bound
below which sleep apnea could be
excluded; 2) MAP upper bound above which study participants can
be assessed to have OSA; and 3)
home study AHI cut-points (to be used in study participants with
intermediate MAP values) above
which study participants can be assessed to have OSA.
•Phase testing: 1. MAPI (multivariate apnea
prediction instrument) and/or apnea
symptoms and clinical findings 2. Portable Type IV sleep study
based on prior test results (if
“intermediate” OSA probability
•Optimal parameters set as one that minimized total prediction errors,
computed as sum of false-positives
and false-negative predictions. 3-variables chosen: Apnea symptoms,
neck circumference, age
•Validation: Type I
Polysomnography (Sandman, Embla)
AHI: sum of apneas and hypopneas per hour of
sleep
Hypopneas: ≥50% decrease in nasal flow
with either a ≥3%
oxygen or EEG arousals OSA: AHI ≥30/hr and
ESS >10
No OSA: 73% (70/92) OSA (AHI ≥5 & ESS >10): 27%
(22/92)
•Mild (AHI 5-15 & ESS >10): 32% (7/22)
•Moderate (AHI 15-30 & ESS >10):
23% (5/22) •Severe (AHI ≥30 & ESS >10): 45%
(10/22)
Rule ≥0.676 AHI ≥30/hr & ESS >10
* Abbreviations: AHI (apnea-hypopnea index), BMI (body mass index), CABG (coronary artery bypass graft), CAD (coronary artery disease), COPD (chronic obstructive pulmonary disease), CPAP (continuous
positive airway pressure), DM (diabetes mellitus), EEG (electroencephalogram), ESS (Epworth sleepiness scale), hr (hour), IQR (interquartile range), MI (myocardial infarction), N (number), NR (not reported), OSA
(obstructive sleep apnea), OSAS (obstructive sleep apnea syndrome), mod (moderate), PSG (polysomnogram), RDI (respiratory disturbance index), RERA (respiratory effort related arousal), SDB (sleep disordered
breathing)
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015

109
Table 33 -AHRQ Question 2 – Phased testing compared with full testing alone
Study N Cut-Point OSA
Prevalence
Population TP FN FP TN p-
value
Sens Spec PPV NPV +LR -LR Accuracy AUC Pos Posttest
Probability
Neg
Posttest
Probability
Morales, 2012 92 •PSG: AHI ≥30/hr & ESS >10
•1st Stage prediction model (apnea
symptoms, neck circumference, age,
gender): Lower bound <0.5; Upper
Bound >0.80
•2nd Stage: Type IV sleep study AHI
>25/hr
0.109 Elderly patients
with and without
sleepiness
10 0 21 61 <0.001 0.952 0.747 0.323 1.00 3.905 0.064 0.772 0.850 0.323 0.005
92 •PSG: AHI ≥30/hr & ESS >10
•1st Stage prediction model (MAPI):
Lower bound <0.4; Upper Bound
>0.90
•2nd Stage: Type IV sleep study AHI
>15/hr
0.109 Elderly patients
with and without
sleepiness
9 1 20 62 <0.001 0.900 0.756 0.310 0.984 3.690 0.132 0.772 0.833 0.310 0.016
* Abbreviations: +LR (positive likelihood ratio), -LR (negative likelihood ratio), AHI (apnea-hypopnea index), AUC (area under the curve), CABG (coronary artery bypass graft), CAD (coronary artery disease), COPD (chronic obstructive pulmonary disease), CPAP (continuous positive airway pressure), FN (false negative), FP (false positive), N (number), NR (not reported), NPV (negative predictive value), MI (myocardial infarction),
ODI (oxygen desaturation index), OSA (obstructive sleep apnea), OSAS (obstructive sleep apnea syndrome), PPV (positive predictive value), PSG (polysomnogram), RDI (respiratory disturbance index), Sen (sensitivity),
Spec (specificity), TN (true negative), TP (true positive)
Downloaded From: http://annals.org/ by a Penn State University Hershey User on 02/04/2015
Top Related
Copyright © 2022 FDOKUMEN

