Continuous positive airway pressure reduces blood pressure in patients with obstructive sleep apnea;...
12
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. Continuous positive airway pressure reduces blood pressure in patients with obstructive sleep apnea; a systematic review and meta-analysis with 1000 patients Andressa S.O. Schein a , Alessandra C. Kerkhoff a,b , Christian C. Coronel a , Rodrigo D.M. Plentz a,c , and Graciele Sbruzzi a,b Background: Obstructive sleep apnea (OSA) may lead to the development of hypertension and therapy with continuous positive airway pressure (CPAP) can promote reduction in blood pressure. Objective: The objective of this study is to review systematically the effects of CPAP on blood pressure in patients with OSA. Methods: The search was conducted in the following databases, from their beginning until February 2013: MEDLINE, Embase, Cochrane CENTRAL, Lilacs and PEDro. In addition, a manual search was performed on references of published studies. Randomized clinical trials (RCTs) that used CPAP compared with placebo CPAP or subtherapeutic CPAP for treatment of patients with OSA and that evaluated office systolic blood pressure (SBP) and diastolic blood pressure (DBP) and 24-h ambulatory blood pressure were selected. Results: Sixteen RCTs were included among 3409 publications, totaling 1166 patients. The use of CPAP resulted in reductions in office SBP [3.20 mmHg; 95% confidence interval (CI) 4.67 to 1.72] and DBP (2.87 mmHg; 95% CI 5.18 to 0.55); in night-time SBP (4.92 mmHg; 95% CI 8.70 to 1.14); in mean 24-h blood pressure (3.56 mmHg; 95% CI 6.79 to 0.33), mean night-time blood pressure (2.56 mmHg; 95% CI 4.43 to 0.68) and 24-h DBP (3.46 mmHg; 95% CI 6.75 to 0.17). However, no significant change was observed in daytime SBP (0.74 mmHg; 95% CI 3.90 to 2.41) and daytime DBP (1.86 mmHg; 95% CI 4.55 to 0.83). Conclusion: Treatment with CPAP promoted significantly but small reductions in blood pressure in individuals with OSA. Further studies should be performed to evaluate the effects of long-term CPAP and the impact on cardiovascular risk. Keywords: arterial pressure, continuous positive airway pressure, hypertension, sleep apnea, obstructive sleep apnea syndromes Abbreviations: 95%CI, 95% confidence interval; AHI, apnea–hypopnoea index; CPAP, continuous positive airway pressure; DBP, diastolic blood pressure; OSA, obstructive sleep apnea; RCTs, randomized clinical trials; SBP, systolic blood pressure INTRODUCTION O bstructive sleep apnea (OSA) is characterized by repetitive episodes of complete or partial airway obstruction during sleep. Its prevalence is higher than 10% [1,2], and it is associated with increased cardio- vascular mortality and with all causes of mortality [3–6]. In addition, this sleep disorder can cause a variety of physio- logical disturbances such as hypoxemia, carbon dioxide retention, decrease in baroreflex sensitivity and increased activity of the sympathetic nervous system [7–10]. These systemic disturbances can lead to sustained increase in blood pressure [10–12]. According to the Joint National Committee [13], OSA is one of the identifiable causes of hypertension, which is responsible for approximately 50% of ischemic heart dis- ease and 60% of cerebrovascular accidents [14]. Therefore, the prevention of these events depends on the appropriate control and reduction of blood pressure levels. Continuous positive airway pressure (CPAP) represents an effective treatment option for OSA patients, with positive effects such as mortality reduction and improvement in quality of life, benefits to the autonomic nervous system, reduction of sympathetic nervous activity and increase of the baroreflex sensitivity [15 – 20]. Some studies have shown that the use of CPAP promotes reduction in blood pressure in individuals with OSA [16,18,21]. Drager et al. [22] conducted a randomized study with 36 OSA patients with prehypertension or masked hyperten- sion, observing that the use of CPAP resulted in significant reduction in the 24-h SBP and arterial pressure. However, other investigations found no changes in blood pressure after treatment with CPAP [15,23,24]. Campos-Rodriguez et al. [25] evaluated the effect of CPAP on the blood pressure Journal of Hypertension 2014, 32:000–000 a Instituto de Cardiologia do Rio Grande do Sul/Fundac ¸a ˜ o Universita ´ ria de Cardiologia, b Universidade Federal do Rio Grande do Sul and c Universidade Federal de Cie ˆ ncias da Sau ´ de de Porto Alegre, Porto Alegre, Brazil Correspondence to Graciele Sbruzzi, ScD, R Felizardo, 750. Bairro, Jardim Bota ˆ nico. Porto Alegre, RS 90690-200, Brazil. Tel: +55 51 33085885; e-mail: graciele.sbruzzi @ufrgs.br Received 13 January 2014 Revised 28 April 2014 Accepted 28 April 2014 J Hypertens 32:000–000 ß 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. DOI:10.1097/HJH.0000000000000250 Journal of Hypertension www.jhypertension.com 1 Original Article
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Continuous positive airway pressure reduces blood pressure in patients with obstructive sleep apnea;...

CE: Namrta; JH-D-14-00062; Total nos of Pages: 12;
JH-D-14-00062
Original Article
Continuous positive airway pressure reduces bloodpressure in patients with obstructive sleep apnea; asystematic review andmeta-analysis with1000 patients
Andressa S.O. Scheina, Alessandra C. Kerkhoffa,b, Christian C. Coronela, Rodrigo D.M. Plentza,c, andGraciele Sbruzzia,b
Journal of Hypertension 2014, 32:000–000aInstituto de Cardiologia do Rio Grande do Sul/Fundacao Universitaria de Cardiologia,bUniversidade Federal do Rio Grande do Sul and cUniversidade Federal de Ciencias daSaude de Porto Alegre, Porto Alegre, Brazil
Correspondence to Graciele Sbruzzi, ScD, R Felizardo, 750. Bairro, Jardim Botanico.Porto Alegre, RS 90690-200, Brazil. Tel: +55 51 33085885; e-mail: [email protected]
Received 13 January 2014 Revised 28 April 2014 Accepted 28 April 2014
J Hypertens 32:000–000 � 2014 Wolters Kluwer Health | Lippincott Williams &Wilkins.
DOI:10.1097/HJH.0000000000000250
Background: Obstructive sleep apnea (OSA) may lead tothe development of hypertension and therapy withcontinuous positive airway pressure (CPAP) can promotereduction in blood pressure.
Objective: The objective of this study is to reviewsystematically the effects of CPAP on blood pressure inpatients with OSA.
Methods: The search was conducted in the followingdatabases, from their beginning until February 2013:MEDLINE, Embase, Cochrane CENTRAL, Lilacs and PEDro.In addition, a manual search was performed on referencesof published studies. Randomized clinical trials (RCTs) thatused CPAP compared with placebo CPAP orsubtherapeutic CPAP for treatment of patients with OSAand that evaluated office systolic blood pressure (SBP) anddiastolic blood pressure (DBP) and 24-h ambulatory bloodpressure were selected.
Results: Sixteen RCTs were included among 3409publications, totaling 1166 patients. The use of CPAP resultedin reductions in office SBP [�3.20 mmHg; 95% confidenceinterval (CI)�4.67 to�1.72] and DBP (�2.87 mmHg; 95% CI�5.18 to�0.55); in night-time SBP (�4.92 mmHg; 95% CI�8.70 to�1.14); in mean 24-h blood pressure(�3.56 mmHg; 95% CI �6.79 to �0.33), mean night-timeblood pressure (�2.56 mmHg; 95% CI�4.43 to�0.68) and24-h DBP (�3.46 mmHg; 95% CI�6.75 to�0.17). However,no significant change was observed in daytime SBP(�0.74 mmHg; 95% CI �3.90 to 2.41) and daytime DBP(�1.86 mmHg; 95% CI �4.55 to 0.83).
Conclusion: Treatment with CPAP promoted significantlybut small reductions in blood pressure in individuals withOSA. Further studies should be performed to evaluate theeffects of long-term CPAP and the impact oncardiovascular risk.
Keywords: arterial pressure, continuous positive airwaypressure, hypertension, sleep apnea, obstructive sleepapnea syndromes
Abbreviations: 95%CI, 95% confidence interval; AHI,apnea–hypopnoea index; CPAP, continuous positive airwaypressure; DBP, diastolic blood pressure; OSA, obstructivesleep apnea; RCTs, randomized clinical trials; SBP, systolicblood pressure
Copyright © Lippincott Williams & Wilkins. UnauthJournal of Hypertension
INTRODUCTION
Obstructive sleep apnea (OSA) is characterized byrepetitive episodes of complete or partial airwayobstruction during sleep. Its prevalence is higher
than 10% [1,2], and it is associated with increased cardio-vascular mortality and with all causes of mortality [3–6]. Inaddition, this sleep disorder can cause a variety of physio-logical disturbances such as hypoxemia, carbon dioxideretention, decrease in baroreflex sensitivity and increasedactivity of the sympathetic nervous system [7–10]. Thesesystemic disturbances can lead to sustained increase inblood pressure [10–12].
According to the Joint National Committee [13], OSA isone of the identifiable causes of hypertension, which isresponsible for approximately 50% of ischemic heart dis-ease and 60% of cerebrovascular accidents [14]. Therefore,the prevention of these events depends on the appropriatecontrol and reduction of blood pressure levels.
Continuous positive airway pressure (CPAP) representsan effective treatment option for OSA patients, with positiveeffects such as mortality reduction and improvement inquality of life, benefits to the autonomic nervous system,reduction of sympathetic nervous activity and increase ofthe baroreflex sensitivity [15–20]. Some studies have shownthat the use of CPAP promotes reduction in blood pressurein individuals with OSA [16,18,21].
Drager et al. [22] conducted a randomized study with 36OSA patients with prehypertension or masked hyperten-sion, observing that the use of CPAP resulted in significantreduction in the 24-h SBP and arterial pressure. However,other investigations found no changes in blood pressureafter treatment with CPAP [15,23,24]. Campos-Rodriguezet al. [25] evaluated the effect of CPAP on the blood pressure
orized reproduction of this article is prohibited.www.jhypertension.com 1

CE: Namrta; JH-D-14-00062; Total nos of Pages: 12;
JH-D-14-00062
Schein et al.
of 68 individuals with OSA and hypertension who weretreated with antihypertensives. The results showed thatshort-term CPAP did not improve the 24-h blood pressure,but the results of a long-term treatment were not explored.
As the literature presents controversial results on theeffects of CPAP on blood pressure in individuals with OSA,a more complete analysis and updating of existing infor-mation are necessary. Thus, the objective of the presentstudy was to review systematically the effects of CPAP onblood pressure in patients with OSA.
MATERIALS ANDMETHODSThis study was approved by the Ethics Committee inResearch of Instituto de Cardiologia do Rio Grande doSul/Fundacao Universitaria de Cardiologia, number 4665/11, and follows the recommendations proposed by theCochrane Collaboration and Preferred Reporting Itemsfor Systematic Review and Meta-Analyses: The PRISMAStatement [26].
Eligibility criteriaThis review included randomized clinical trials (RCTs) thatinvestigated patients with OSA treated with CPAP com-pared with placebo CPAP, sham CPAP or subtherapeuticCPAP (pressure lower than the therapeutic level).Parameters evaluated were office SBP and DBP and 24-hambulatory blood pressure.
Studies in which the control group was treated withCPAP with therapeutic pressure, conservative treatment,placebo drug treatment or no treatment were excluded. Incases of studies with multiple publications (or substudies),the study was included only once.
Search strategyThe search was conducted until February 2013, using thefollowing electronic databases: MEDLINE accessed byPubMed, Cochrane Central Register of Controlled Trials(Cochrane CENTRAL), EMBASE, LILACS and PhysiotherapyEvidence Database (PEDro). In addition, we performed amanual search of references in published studies about thesubject. We used the following keywords to search: ‘sleepapnea, obstructive’, ‘continuous positive airway pressure’,‘nasal continuous positive airway pressure’ associated witha list of sensitive terms to search for RCTs [27]. There wereno language restrictions. The complete search strategy usedin PubMed is summarized in Table 1.
Copyright © Lippincott Williams & Wilkins. Unaut
TABLE 1. Search strategy used in PubMed
#1 "Sleep Apnea, Obstructive"[Mesh] OR ‘‘Apnea, Obstructive Sleep’’ OR ‘‘ApneasObstructive’’ OR ‘‘Obstructive Sleep Apnea Syndrome’’ OR ‘‘Syndrome, Sleep‘‘Obstructive Sleep Apnea’’ OR ‘‘Sleep Apnea Syndrome, Obstructive’’ OR ‘‘UAirway Resistance, Sleep Apnea’’
#2 (randomized controlled trial[pt] OR controlled clinical trial[pt] OR randomized coOR single-blind method[mh] OR clinical trial[pt] OR clinical trials[mh] OR ("cliAND (mask�[tw] OR blind�[tw])) OR ("latin square"[tw]) OR placebos[mh] ORstudies[mh] OR prospective studies[mh] OR cross-over studies[mh] OR contro
#3 "Continuous Positive Airway Pressure"[Mesh] OR ‘‘CPAP Ventilation’’ OR ‘‘Ven‘‘Bilevel Continuous Positive Airway Pressure’’ OR ‘‘Nasal Continuous Positive‘‘Airway Pressure Release Ventilation’’ OR ‘‘APRV Ventilation Mode’’ OR ‘‘APModes, APRV’’
#4 #1 AND #2 AND #3
2 www.jhypertension.com
Study selection and data extractionTitles and abstracts of all articles identified by the searchstrategy were independently evaluated by two investi-gators, in duplicate (A.S.O.S. and A.C.K.). Abstracts thatdid not provide sufficient information regarding theinclusion and exclusion criteria were selected for full-textevaluation. In the second phase, the same reviewers inde-pendently evaluated these full-text articles and made theirselection in accordance with the eligibility criteria. Dis-agreements between reviewers were solved by consensus,and, if disagreement persisted, by a third reviewer (G.S.).Although the study did not have all the necessary data formeta-analysis, the corresponding author was contacted torequest the missing data. Only two articles required revisionof the third reviewer [28,29].
The data extraction was performed by the same tworeviewers independently via a standardized form. Infor-mation on interventions, outcomes and patients werecollected. Discordances between reviewers were resolvedby consensus or by a third reviewer (G.S.). The primaryoutcomes analysed were office SBP and DBP (mmHg)assessed through three measures, and secondary outcomeswere mean 24-h, nighttime and daytime blood pressureassessed by 24-h ambulatory blood pressure monitoring(mmHg).
Assessment of risk of biasThe methodological quality assessment was also performedby two investigators independently (A.S.O.S. and A.C.K.)and took into consideration the following characteristics ofincluded studies: randomization sequence generation, allo-cation concealment, blinding, blinding of outcome asses-sors, description of losses and exclusions and intention-to-treat analysis. Studies without a clear description of thesefeatures were considered as unclear or not reporting.
Data analysisThe meta-analysis was performed using a random effectsmodel and the measures of effect were obtained by post-intervention values with 95% confidence interval (95% CI).It was considered a statistically significant alpha value of0.05. Statistical heterogeneity of the treatment effectsamong studies was assessed using the Cochran’s Q testand the inconsistency I2 test: values above 25 and 50% wereconsidered indicative of moderate and high heterogeneity,respectively. All analyses were conducted using softwareReview Manager 5.2 (Cochrane Collaboration).
horized reproduction of this article is prohibited.
, Obstructive Sleep’’ OR ‘‘Obstructive Sleep Apneas’’ OR ‘‘Sleep Apneas,Apnea, Obstructive’’ OR ‘‘Syndrome, Obstructive Sleep Apnea’’ ORpper Airway Resistance Sleep Apnea Syndrome’’ OR ‘‘Syndrome, Upper
ntrolled trials[mh] OR random allocation[mh] OR double-blind method[mh]nical trial"[tw]) OR ((singl�[tw] OR doubl�[tw] OR trebl�[tw] OR tripl�[tw])
placebo�[tw] OR random�[tw] OR research design[mh:no exp] OR follow-upl�[tw] OR prospectiv�[tw] OR volunteer�[tw]) NOT (animal[mh] NOT human[mh])tilation, CPAP’’ OR ‘‘Biphasic Continuous Positive Airway Pressure’’ OR
Airway Pressure’’ OR ‘‘nCPAP Ventilation’’ OR ‘‘Ventilation, Ncpap’’ ORRV Ventilation Modes’’ OR ‘‘Ventilation Mode, APRV’’ OR ‘‘Ventilation
Volume 32 � Number 1 � Month 2014
CE: Namrta; JH-D-14-00062; Total nos of Pages: 12;
JH-D-14-00062
Effects of CPAP in OSA
Sensitivity analyses were conducted considering thecharacteristics of patients included, such as severity ofOSA assessed through the apnea-hypopnea index (AHI),BMI and studies that included only hypertensive or normo-tensive patients, or studies that included both hypertensiveand normotensive patients. The AHI was considered mild incases of 5–14 episodes per hour, moderate in cases of15–29 episodes per hour and severe when in cases of 30 ormore episodes per hour [30]. Separate calculations wereredone considering each characteristic.
RESULTS
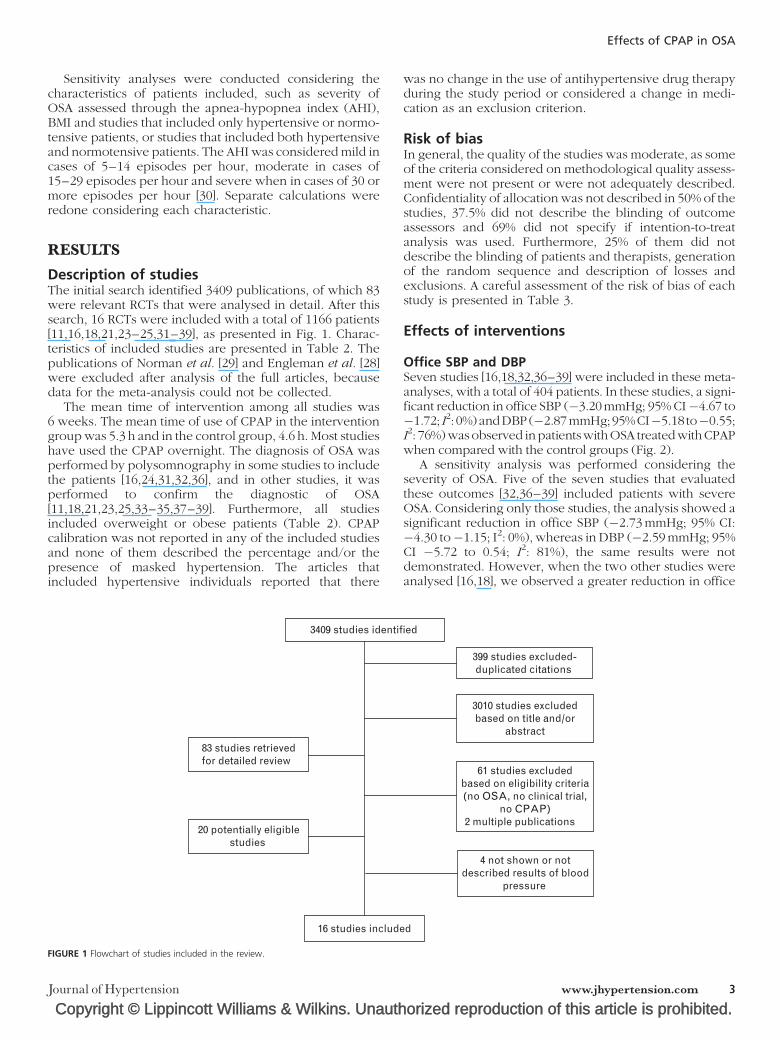
Description of studiesThe initial search identified 3409 publications, of which 83were relevant RCTs that were analysed in detail. After thissearch, 16 RCTs were included with a total of 1166 patients[11,16,18,21,23–25,31–39], as presented in Fig. 1. Charac-teristics of included studies are presented in Table 2. Thepublications of Norman et al. [29] and Engleman et al. [28]were excluded after analysis of the full articles, becausedata for the meta-analysis could not be collected.
The mean time of intervention among all studies was6 weeks. The mean time of use of CPAP in the interventiongroup was 5.3 h and in the control group, 4.6 h. Most studieshave used the CPAP overnight. The diagnosis of OSA wasperformed by polysomnography in some studies to includethe patients [16,24,31,32,36], and in other studies, it wasperformed to confirm the diagnostic of OSA[11,18,21,23,25,33–35,37–39]. Furthermore, all studiesincluded overweight or obese patients (Table 2). CPAPcalibration was not reported in any of the included studiesand none of them described the percentage and/or thepresence of masked hypertension. The articles thatincluded hypertensive individuals reported that there
Copyright © Lippincott Williams & Wilkins. Unauth
3409 studies identif
83 studies retrievedfor detailed review
20 potentially eligiblestudies
16 studies include
FIGURE 1 Flowchart of studies included in the review.
Journal of Hypertension
was no change in the use of antihypertensive drug therapyduring the study period or considered a change in medi-cation as an exclusion criterion.
Risk of biasIn general, the quality of the studies was moderate, as someof the criteria considered on methodological quality assess-ment were not present or were not adequately described.Confidentiality of allocation was not described in 50% of thestudies, 37.5% did not describe the blinding of outcomeassessors and 69% did not specify if intention-to-treatanalysis was used. Furthermore, 25% of them did notdescribe the blinding of patients and therapists, generationof the random sequence and description of losses andexclusions. A careful assessment of the risk of bias of eachstudy is presented in Table 3.
Effects of interventions
Office SBP and DBPSeven studies [16,18,32,36–39] were included in these meta-analyses, with a total of 404 patients. In these studies, a signi-ficant reduction in office SBP (�3.20mmHg; 95% CI�4.67 to�1.72; I2: 0%)andDBP(�2.87mmHg;95%CI�5.18 to�0.55;I2: 76%)wasobserved inpatientswithOSA treatedwithCPAPwhen compared with the control groups (Fig. 2).
A sensitivity analysis was performed considering theseverity of OSA. Five of the seven studies that evaluatedthese outcomes [32,36–39] included patients with severeOSA. Considering only those studies, the analysis showed asignificant reduction in office SBP (�2.73 mmHg; 95% CI:�4.30 to�1.15; I2: 0%), whereas in DBP (�2.59 mmHg; 95%CI �5.72 to 0.54; I2: 81%), the same results were notdemonstrated. However, when the two other studies wereanalysed [16,18], we observed a greater reduction in office
orized reproduction of this article is prohibited.
ied
399 studies excluded-duplicated citations
3010 studies excludedbased on title and/or
abstract
61 studies excludedbased on eligibility criteria(no OSA, no clinical trial,
no CPAP)2 multiple publications
4 not shown or notdescribed results of blood
pressure
d
www.jhypertension.com 3

Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
CE: Namrta; JH-D-14-00062; Total nos of Pages: 12;
JH-D-14-00062
TA
BLE
2.
Ch
ara
cteri
stic
so
fin
clu
ded
stu
die
s
Stu
dy,
year
Part
icip
an
ts(n
)I/
C
Ag
ed
(years
)I/
C
BM
I(k
g/m
2)
I/C
Loss
es
du
rin
gtr
eatm
en
t(n
)I/
C
Pati
en
ts’
com
pli
an
cew
ith
CPA
Ptr
eatm
en
t(n
)I/
C
AH
Im
ean
I/C
Hyp
ert
en
sive
an
d/o
rn
orm
o-
ten
sive
pati
en
tsPara
mete
rso
fC
PA
P
Alo
nso
-Fer
nan
dez
etal
.[3
1]
31/3
152
a30.5�
4.0
/28.7�
4.7
6/6
25/2
543.8
aN
orm
ote
nsi
ve;
Inte
rven
tion:
-D
aytim
eSB
P:126�
10
mm
Hg
–D
aytim
eD
BP:
79�
6m
mH
g;
Contr
ol:
-D
aytim
eSB
P:122�
9m
mH
g;
-D
aytim
eD
BP:
78�
5m
mH
g
Inte
rven
tion:
-Pr
essu
reC
PAP:
10
cmH
2O
;-
Tim
e:6.2�
1.1
h/n
ight
/12
wee
ks;
Contr
ol:
Plac
ebo
CPA
P;-
Tim
e:6.3�
1.6
h/n
ight
/12
wee
ks
Bar
be
etal
.[2
3]
29/2
654/5
229�
1/
29�
0.4
0/1
29/2
554/5
7H
yper
tensi
vean
dnorm
ote
nsi
ve;
Inte
rven
tion:
-24-h
SBP:
126�
2m
mH
g;
-24-h
DBP:
79�
1m
mH
g;
Contr
ol:
-24-h
SBP:
123�
2m
mH
g;
-24-h
DBP:
77�
2m
mH
g
Inte
rven
tion:
-Pr
essu
reC
PAP:
8cm
H2O
;-
Tim
e:5�
0.4
h/d
ay/6
wee
ks;
Contr
ol:
Plac
ebo
CPA
P;-
Tim
e:4�
0.5
h/d
ay/6
wee
ks
Bec
ker
etal
.[1
1]
30/3
054.4
/52.3
33.3�
5.1
/33.5�
614/1
416/1
614.4
/14.1
Hyp
erte
nsi
vean
dnorm
ote
nsi
ve;
Inte
rven
tion:
-SB
P:135.9�
17.5
mm
Hg;
-D
BP:
83.4�
15.9
mm
Hg;
Contr
ol:
-SB
P:136.2�
13.1
mm
Hg;
-D
BP:
81.1�
12.3
mm
Hg
Inte
rven
tion:
-Pr
essu
reC
PAP:
9.1�
2.3
cmH
2O
;-
Tim
e:5.5�
2.0
/nig
ht/
9w
eeks
;C
ontr
ol:
Subth
erap
eutic
CPA
P;-
Pres
sure
:3
–4
cmH
2O
;-
Tim
e:5.4�
2.2
/nig
ht/
9w
eeks
Cam
pos-
Rodriguez
etal
.[2
5]
36/3
655.3
/58
35.7�
5.6
/33.8�
6.3
2/2
34/3
4�
10
even
ts/h
aH
yper
tensi
ve;
Inte
rven
tion:
-24-h
SBP:
131.9�
13.5
mm
Hg;
-24-h
DBP:
78.4�
10.3
mm
Hg;
Contr
ol:
-24-h
SBP:
130.4�
15.9
mm
Hg;
-24-h
DBP:
77.6�
8.7
mm
Hg
Inte
rven
tion:
-Pr
essu
reC
PAP:
9.5�
1.9
cmH
2O
;-
Tim
e:5�
1.4
h/d
ay/
4w
eeks
;C
ontr
ol:
Subth
erap
eutic
CPA
P;-
Pres
sure
:2
cmH
2O
;-
Tim
e:4.4�
1.9
h/d
ay/
4w
eeks
Cro
sset
al.
[32]
29/2
948
a37�
1a
27/2
72/2
63
aH
yper
tensi
vean
dnorm
ote
nsi
ve;
-SB
P:143.2�
3.3
mm
Hg
a;
-D
BP:
80.4�
2.0
2m
mH
ga
Inte
rven
tion:
-Pr
essu
reC
PAP:
The
fixe
dpre
ssure
det
erm
ined
from
the
CPA
Ptitr
atio
n;
-Ti
me:
4.4
9�
0.4
h/d
ay/6
wee
ks;
Contr
ol:
Plac
ebo
CPA
P;-
Tim
e:3.0
8�
0.4
8h
/day
/6w
eeks
Dim
sdal
eet
al.
[33]
21/1
847.7
/48.9
32.7�
4.9
/28.5�
5N
ot
info
rmed
21/1
8N
ot
info
rmed
Hyp
erte
nsi
vean
dnorm
ote
nsi
ve;
Inte
rven
tion:
-SB
P:128�
15
mm
Hg;
-D
BP:
82�
8m
mH
g;
Contr
ol:
-SB
P:123�
12
mm
Hg;
-D
BP:
78�
9m
mH
g
Inte
rven
tion:
-Pr
essu
reC
PAP:
8to
10
cmH
2O
;C
ontr
ol:
Plac
ebo
CPA
P;-
Pres
sure
:2
cmH
2O
;-
Tim
e:>
5h/n
ight
/1w
eek
Dura
n-C
anto
llaet
al.
[21]
169/1
71
53.2
/51.7
31.9�
5.7
/31.9�
5.8
32/3
6137/1
35
44.5
/42.5
Hyp
erte
nsi
vean
dnorm
ote
nsi
ve;
Inte
rven
tion:
-SB
P:131.1�
11.6
mm
Hg;
-D
BP:
82.5�
8m
mH
g;
Contr
ol:
-SB
P:128.8�
11.4
mm
Hg;
-D
BP:
81.8�
8.6
mm
Hg
Inte
rven
tion:
-Pr
essu
reC
PAP:
8.8�
1.6
cmH
2O
;-
Tim
e:4.5�
1.7
h/
nig
ht/
12
wee
ks;
Contr
ol:
Plac
ebo
CPA
P;-
Pres
sure
:<
1cm
H2O
;-
Tim
e:4.2�
1.8
h/
nig
ht/
12
wee
ks
Schein et al.
4 www.jhypertension.com Volume 32 � Number 1 � Month 2014

Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
CE: Namrta; JH-D-14-00062; Total nos of Pages: 12;
JH-D-14-00062
Huiet
al.
[34]
28/2
850.3
/51.1
27.4�
0.7
/26.9�
0.8
5/5
23/2
331.2
aH
yper
tensi
vean
dnorm
ote
nsi
ve;
Inte
rven
tion:
-24-h
SBP:
125.9�
3.0
mm
Hg;
-24-h
DBP:
82.5�
2.2
mm
Hg;
Contr
ol:
-24-h
SBP:
122�
3.0
mm
Hg;
-24-h
DBP:
79.6�
2.2
mm
Hg
Inte
rven
tion:
-Pr
essu
reC
PAP:
10.7�
0.4
cmH
2O
;-
Tim
e:5.1�
0.4
h/n
ight/
12
wee
ks;
Contr
ol:
Subth
erap
eutic
CPA
P;-
Pres
sure
:4
cmH
2O
;-
Tim
e:2.6�
0.4
h/n
ight/
12
wee
ksK
ohle
ret
al.
[16]
51/5
148.1
/48.7
35.8�
7.3
/34.5�
5.0
2/1
50/4
9N
ot
info
rmed
Hyp
erte
nsi
vean
dnorm
ote
nsi
veIn
terv
ention:
-SB
P:135.8�
16.0
mm
Hg;
-D
BP:
89.3�
10.8
mm
Hg
Contr
ol:
-SB
P:141.6�
17.4
mm
Hg;
-D
BP:
92.9�
11.4
mm
Hg
Inte
rven
tion:
-Pr
essu
reC
PAP:
10�
1.9
cmH
2O
;-
Tim
e:3.9�
2.5
h/n
ight/
4w
eeks
;C
ontr
ol:
Subth
erap
eutic
CPA
P;-
Pres
sure
:<
1cm
H2O
;-
Tim
e:4.7�
2.1
h/n
ight/
4w
eeks
Kohle
ret
al.
[35]
20/2
163.6
/61.8
32.9�
6.5
/33.1�
4.4
0/1
20/2
05.1
/4.3
Hyp
erte
nsi
vean
dnorm
ote
nsi
ve;
Inte
rven
tion:
-D
aytim
eSB
P:133.3�
16.6
mm
Hg;
-D
aytim
eD
BP:
82.3�
7.8
mm
Hg;
Contr
ol:
-D
aytim
eSB
P:129.2�
12.7
mm
Hg;
-D
aytim
eD
BP:
82.2�
8.2
mm
Hg
Inte
rven
tion:
-Pr
essu
reC
PAP:
not
info
rmed
;C
ontr
ol:
Plac
ebo
CPA
P;-
Pres
sure
:not
info
rmed
;-
Tim
e:2
wee
ks
Lam
etal
.[3
6]
31/3
046.5
/46.1
27.8�
3.7
/27.2�
3.7
2/0
29
and
30
33.4
/31.3
Norm
ote
nsi
veIn
terv
ention:
-SB
P:130.8�
14.7
mm
Hg;
-D
BP:
80.1�
10.8
mm
Hg;
Contr
ol:
-SB
P:129.5�
16.5
mm
Hg;
-D
BP:
82.0�
11.6
mm
Hg
Inte
rven
tion:
-Pr
essu
reC
PAP:
not
info
rmed
;C
ontr
ol:
Plac
ebo
CPA
P;-
Pres
sure
:0
–1
cmH
2O
;-
Tim
e:1
wee
k
Mill
set
al.
[37]
17/1
647.6
/49
31.7�
1.4
/32.2�
1.7
Not
info
rmed
Not
info
rmed
65/6
1.2
Hyp
erte
nsi
vean
dnorm
ote
nsi
ve;
Inte
rven
tion:
-SB
P:155.2�
4.5
mm
Hg;
-D
BP:
84.2�
2.6
mm
Hg;
Contr
ol:
-SB
P:149�
5.8
mm
Hg;
-D
BP:
83.6�
3.4
mm
Hg
Inte
rven
tion:
-Pr
essu
reC
PAP:
Pres
sure
was
incr
ease
dfr
om
1to
2cm
H2O
untilap
nea
san
dhyp
opnea
sw
ere
contr
olle
d;
Contr
ol:
Plac
ebo
CPA
P;-
Pres
sure
:3
cmH
2O
;-
Tim
e:2
wee
ksN
guye
net
al.
[38]
10/1
052.9
/52.3
30.1�
4.7
/29.6�
5.6
Not
info
rmed
Not
info
rmed
38.8
/31.6
Hyp
erte
nsi
vean
dnorm
ote
nsi
ve;
Inte
rven
tion:
-SB
P:121.0�
11.6
mm
Hg;
-D
BP:
75.2�
11.1
mm
Hg
Contr
ol:
-SB
P:127�
10.3
mm
Hg;
-D
BP:
78.9�
11.4
mm
Hg
Inte
rven
tion:
-Pr
essu
reC
PAP:
Was
modifie
duntilth
ere
spirat
ory
dis
turb
ance
sw
ere
contr
olle
d.
-Ti
me:
12
wee
ks;
Contr
ol:
Plac
ebo
CPA
P;-
Pres
sure
:Fi
xed
and
osc
illat
ing
in0.5
cmH
2O
;-
Tim
e:12
wee
ksPa
truno
etal
.[3
9]
9/
948.1
/45.4
36.7�
5.2
/35.1�
6.7
Not
info
rmed
Not
info
rmed
45.8
/43.6
Hyp
erte
nsi
vean
dnorm
ote
nsi
ve;
Inte
rven
tion:
-SB
P:141�
10
mm
Hg;
-D
BP:
83�
6m
mH
g;
Contr
ol:
-SB
P:139�
14
mm
Hg;
-D
BP:
86�
5m
mH
g
Inte
rven
tion:
-Pr
essu
reC
PAP:
12�
3cm
H2O
;C
ontr
ol:
auto
CPA
P;-
Tim
e:12
wee
ks
(Continued
)
Effects of CPAP in OSA
Journal of Hypertension www.jhypertension.com 5

Copyright © Lippincott Williams & Wilkins. Un
CE: Namrta; JH-D-14-00062; Total nos of Pages: 12;
JH-D-14-00062
TA
BLE
2(C
on
tin
ued
)
Stu
dy,
year
Part
icip
an
ts(n
)I/
C
Ag
ed
(years
)I/
C
BM
I(k
g/m
2)
I/C
Loss
es
du
rin
gtr
eatm
en
t(n
)I/
C
Pati
en
ts’
com
pli
an
cew
ith
CPA
Ptr
eatm
en
t(n
)I/
C
AH
Im
ean
I/C
Hyp
ert
en
sive
an
d/o
rn
orm
o-
ten
sive
pati
en
tsPara
mete
rso
fC
PA
P
Pepper
ellet
al.
[18]
59/5
950.1
/50.1
34.6�
8.5
/35.3�
6.0
6/8
53/5
1N
ot
info
rmed
Hyp
erte
nsi
vean
dnorm
ote
nsi
ve;
Inte
rven
tion:
-SB
P:132.5�
15.3
mm
Hg;
-D
BP:
85.1�
8.7
mm
Hg
Contr
ol:
-SB
P:134.9�
18.7
mm
Hg;
-D
BP:
85.1�
8.9
mm
Hg
Inte
rven
tion:
-Pr
essu
reC
PAP:
9.8�
1.9
cmH
2O
;C
ontr
ol:
Subth
erap
eutic
CPA
P;-
Pres
sure
:1
cmH
2O
;-
Tim
e:5
h/n
ight/
4w
eeks
Robin
son
etal
.[2
4]
18/1
754/5
433.2�
5.3
a2/1
16/1
6N
ot
info
rmed
Hyp
erte
nsi
ve;
Inte
rven
tion:
-24-h
SBP:
140.3�
16.1
mm
Hg;
-24-h
DBP:
85.3�
11.2
mm
Hg;
Contr
ol:
-24-h
SBP:
143.0�
17.3
mm
Hg;
-24-h
DBP:
86.7�
11.1
mm
Hg
Inte
rven
tion:
-Pr
essu
reC
PAP:
10.4�
1.5
cmH
2O
;-
Tim
e:5.2�
2.1
h/n
ight/
4w
eeks
;C
ontr
ol:
Subth
erap
eutic
CPA
P;-
Pres
sure
:1
cmH
2O
;-
Tim
e:4.3�
2.4
h/n
ight/
4w
eeks
AH
I,ap
nea
–hyp
opnea
index
;C
,co
ntr
olgro
up;
CPA
P,co
ntinuous
posi
tive
airw
aypre
ssure
;I,
inte
rven
tion
gro
up.
aV
alue
for
the
tota
lsa
mple
.
Schein et al.
6 www.jhypertension.com
aut
SBP (�6.51 mmHg; 95% CI �10.70 to �2.32; I2: 0%) andDBP (�3.41 mmHg; 95% CI �5.77 to �1.05; I2: 0%), inpatients treated with CPAP. Thus, the severity of OSA couldexplain the heterogeneity found in the analysis of DBP, asno heterogeneity was found when analysing only thestudies with no severe OSA.
Most of the studies that were considered in this meta-analysis included only hypertensive and normotensivepatients in both treatment groups, or only hypertensivepatients in the same sample. However, only one study [36]included only normotensive patients. The exclusion of thispublication did not modify the overall result of the meta-analysis (SBP �3.36 mmHg; 95% CI �4.86 to �1.86; I2: 0%and DBP �2.85 mmHg; 95% CI �5.39 to �0.31; I2: 79%).
Twenty-four-hour SBP and DBP and 24-h meanarterial pressureSix studies [11,16,21,24,25,34] totalling 620 patients, eval-uated 24-h SBP and DBP. The comparison of CPAP treat-ment with control groups showed a nonsignificantreduction in 24-h SBP (�3.57 mmHg; 95% CI �8.58 to1.44; I2: 66%), and a significant reduction in 24-h DBP(�3.46 mmHg; 95% CI �6.75 to �0.17; I2: 71%) (Fig. 3).
Considering the sensitivity analysis for individuals withsevere OSA, two articles presented this characteristic[21,34]. Analysing only these studies, no significant reductionof these variables was observed, but there was an absence ofheterogeneity (24-hDBP�1.00mmHg; 95% CI�2.82 to 0.82;I2: 0%and 24-h SBP 0.12mmHg; 95% CI�2.59 to 2.83; I2: 0%),showing that the severity of OSA could explain the hetero-geneity found in these analyses. Similarly, in the sensitivityanalysisofpatientswithmildOSA,twoarticles[11,25] includedpatients with this characteristic and, when only these wereanalysed, no significant change was found in these variables(24-h SBP �4.66mmHg; 95% CI �16.41 to 7.08; I2: 77% and24-h DBP �4.14mmHg; 95% CI �12.93 to 4.65; I2: 80%).
All publications considered for the analysis of thesevariables included hypertensive and normotensive patients,with the exception of two studies [24,25] that included onlypatients with hypertension. After exclusion of these articles,no significant reduction was seen in the two variables (datanot shown). And, considering only these two articles in themeta-analysis, the same behaviour was observed (data notshown).
Furthermore, seven studies [11,16,18,21,24,25,34] eval-uated the mean 24-h arterial pressure in 738 patients andobserved a significant reduction in this variable(�3.56 mmHg; 95% CI �6.79 to �0.33; I2: 74%) (Fig. 3).
Considering the high statistical heterogeneity found in thismeta-analysis,weobservedthat in threestudies [11,16,18], theresults were more significant than in the other publicationsincluded in this analysis. When excluding these studies fromthe analyses, the heterogeneity disappeared, but the differ-ence in mean 24-h arterial pressure observed between CPAPtreatedandcontrolgroupswasnonsignificant (�0.18mmHg;95% CI �1.86 to 1.50; I2: 0%).
Daytime and night-time SBP and DBPSix studies [11,21,23,31,34,35] totalling 563 patients eval-uated the daytime SBP and DBP. The studies did not show asignificant reduction after treatment with CPAP as
horized reproduction of this article is prohibited.Volume 32 � Number 1 � Month 2014

CE: Namrta; JH-D-14-00062; Total nos of Pages: 12;
JH-D-14-00062
TABLE 3. Assessment of risk of bias
Study, year
Generation ofthe randomsequence
Concealedallocation Blinding
Blinding ofoutcomeassessors
Description oflosses andexclusions
Intention totreat analysis
Alonso-Fernandez [31] No Not informed Yes Yes Yes Not informed
Barbe et al. [23] Yes Yes Not informed Not informed Yes Yes
Becker et al. [11] Yes Yes Yes Not informed Yes Not informed
Campos-Rodriguez [25] Yes Not informed Yes Yes Yes Yes
Cross et al. [32] No Yes Yes Yes Yes No
Dimsdale et al. [33] Yes Not informed No No No No
Duran-Cantolla et al. [21] Yes Yes Yes Yes Yes Yes
Hui et al. [34] Yes Not informed Not informed Not informed Yes No
Kohler et al. [16] Yes Yes Yes Yes Yes Yes
Kohler et al. [35] Yes Not informed Yes Yes Yes Not informed
Lam et al. [36] Yes Yes Yes Yes Yes No
Mills et al. [37] Not informed Not informed Yes Not informed Not informed Not informed
Nguyen et al. [38] Not informed Not informed Yes Yes Not informed Not informed
Patruno et al. [39] Yes Not informed No No No No
Pepperell et al. [18] Yes Yes Yes Yes Yes Yes
Robinson et al. [24] Yes No No No Yes No
Effects of CPAP in OSA
compared with control groups (daytime SBP �0.74 mmHg;95% CI �3.90 to 2.41; I2: 37% and daytime DBP�1.86 mmHg; 95% CI �4.55 to 0.83; I2: 61%) (Fig. 4).
Similarly, the studies that evaluated the effect of CPAP inpatients with severe OSA [21,23,31,34] did not show asignificant effect on these variables (data not shown).However, in mild OSA [11,16], the sensitivity analysis dem-onstrated significant reduction in daytime DBP with noheterogeneity (�7.84 mmHg; 95% CI �12.05 to �3.63; I2:
Copyright © Lippincott Williams & Wilkins. Unauth
Study or Subgroup1.1.1 Systolic blood pressure
1.1.2 Diastolic blood pressure
Mean SDCPAP Control
Total Mean SD Total Weig
Cross, 2008 141 3 27 144 4 27 61.2Kohler, 2008 133 13 51 140 17 51 6.3Lam, 2010 128 14 29 127 16 30 3.7Mills, 2006 145 5 17 147 5 16 18.7Nguyen, 2010 126 16 10 130 14 10 1.3Patruno, 2005 124 6 9 130 12 9 2.8Peppperell, 2002 130 15 –59 136 18 59 6.1Subtotal (95% CI) 202 202 100.0
Heterogeneity: Tau2 = 0.00; chi2 = 4.53, df = 6 (P = 0.61); I2 = 0%Test for overall effect: Z = 4.25 (P < 0.0001)
Cross, 2008 82 2 27 82 2 27 21.8Kohler, 2008 87 9 51 91 10 51 14.5Lam, 2010 76 8 29 79 12 30 10.6Mills, 2006 79 3 17 83 3 16 19.4Nguyen, 2010 84 11 10 79 12 10 4.3Patruno, 2005 76 4 9 83 5 9 13.1Peppperell, 2002 83 9 59 86 8 59 16.3Subtotal (95% CI) 202 202 100.0
Heterogeneity: Tau2 = 6.08; chi2 = 24.54, df = 6 (P = 0.0004); I2 = 76Test for overall effect: Z = 2.43 (P = 0.02)
FIGURE 2 Effect of continuous positive airway pressure on office SBP and DBP.
Journal of Hypertension
0%), whereas the daytime SBP (�6.61 mmHg; 95% CI�13.24 to 0.03; I2: 29%) was unchanged compared withthe global analysis.
Results for night-time blood pressures were described inthe same six studies. The results showed a significantdecrease in night-time SBP (�4.92 mmHg; 95% CI �8.70to �1.14; I2: 55%) but not in DBP (�2.87 mmHg; 95% CI�6.14 to 0.40; I2: 69%) in patients treated with CPAP ascompared with the control groups (Fig. 4).
orized reproduction of this article is prohibited.
htMean differenceIV, Random, 95% CI
Mean differenceIV, Random, 95% CI
–20 –10
Favours CPAP Favours control
0 10 20
% –3.00 [–489, –1.11]% –7.00 [–12.87, 1.13]% 1.00 [–6.66, 8.66]% –2.00 [–5.41, 1.41]% –4.00 [–17.18, 9.18]% –6.00 [–14.77, 2.77]% –6.00 [–11.98, –0.02]% –3.20 [–4.67, –1.72]
% 0.00 [–1.07, 1.07]% –4.00 [–7.69, –0.31]% –3.00 [–8.19, 2.19]% –4.00 [–6.05, –1.95]% 5.00 [–5.09, 15.09]% –7.00 [–11.18, –2.82]% –3.00 [–6.07, 0.07]% –2.87 [–5.18, –0.55]
%
www.jhypertension.com 7

CE: Namrta; JH-D-14-00062; Total nos of Pages: 12;
JH-D-14-00062
Study or Subgroup1.2.1 24-h systolic blood pressure
Mean SDCPAP Control
Total Mean SD Total WeightMean differenceIV, Random, 95% CI
Mean differenceIV, Random, 95% CI
–20 –10
Favours CPAP Favours control
0 10 20
Becker, 2003 126 14 16 137 11 16 15.3% –11.00 [–19.72, –2.28]Campos-Rodrigues, 2006 131 12 34 130 16 34 18.9% –1.00 [–5.72, 7.72]Duran-Cantola, 2010 128 13 169 128 13 171 26.3% 0.00 [–2.76, 2.76]Hui, 2006 123 15 23 120 30 23 9.1% –3.00 [–10.71, 16.71]Kohler, 2008 128 14 51 139 19 51 19.3% –11.00 [–17.48, –4.52]Robinson, 2006 137 16 16 139 18 16 11.1% –2.00 [–13.80, 9.80]Subtotal (95% CI) 309 311 100.0% –3.57 [–8.58, 1.44]Heterogeneity: Tau2 = 22.86; chi2 = 14.78, df = 5 (P = 0.01); I2 = 66%Test for overall effect: Z = 1.40 (P = 0.16)
1.2.2 24-h diastolic blood pressure
1.2.3 24-h mean arterial pressure
Becker, 2003 73 10 16 82 9 16 12.8% –9.00 [–15.59, –2.41]Campos-Rodrigues, 2006 77 9 34 77 9 34 18.3% 0.00 [–4.28, 4.28]Duran-Cantola, 2010 81 9 169 82 9 171 24.3% –1.00 [–2.91, 0.91]Hui, 2006 80 11 23 81 9 23 14.5% –1.00 [–6.81, 4.81]Kohler, 2008 81 10 51 89 8 51 20.3% –8.00 [–11.51, –4.49]Robinson, 2006 84 12 16 87 12 16 9.8% –3.00 [–11.32, 5.32]Subtotal (95% CI) 309 311 100.0% –3.46 [–6.75, –0.17]Heterogeneity: Tau2 = 10.64; chi2 = 17.08, df = 5 (P = 0.004); I2 = 71%Test for overall effect: Z = 2.06 (P = 0.04)
Becker, 2003 91 10 16 100 9 16 11.4% –9.00 [–15.59, –2.41]Campos-Rodrigues, 2006 96 9 34 96 11 34 14.7% 0.00 [–4.78, 4.78]Duran-Cantola, 2010 97 9 169 97 9 171 20.1% 0.00 [–1.91, 0.91]Hui, 2006 94 11 23 95 11 23 11.8% –1.00 [–7.36, 5.36]Kohler, 2008 97 10 51 106 10 51 16.5% –9.00 [–12.88, –5.12]Pepperell, 2002 98 9 59 102 11 59 17.0% –4.00 [–7.63, –0.37]Robinson, 2006 101 12 16 104 13 16 8.5% –3.00 [–11.67, 5.67]Subtotal (95% CI) 368 370 100.0% –3.56 [–6.79, –0.33]Heterogeneity: Tau2 = 12.51; chi2 = 22.88, df = 6 (P = 0.0008); I2 = 74%Test for overall effect: Z = 2.16 (P = 0.03)
FIGURE 3 Effect of continuous positive airway pressure on 24-h SBP and DBP and 24-h mean blood pressure.
Schein et al.
A sensitivity analysis was also performed considering theseverity of OSA. In four studies [21,23,31,34] that includedpatients with severe OSA, there was no significant reductionin night-time SBP (�3.23 mmHg; 95% CI �7.33 to 0.86; I2:53%) and DBP (�0.72 mmHg; 95% CI�2.44 to 1.00; I2: 0%).However, the analysis of mild OSA [11,16] was significant inboth SBP (�9.42 mmHg; 95% CI �14.99 to �3.85; I2: 0%)and DBP (�8.93 mmHg; 95% CI �12.67 to �5.19; I2: 0%)and this analysis could explain the heterogeneity observedin the global analysis.
One study [31] considered only normotensive individ-uals, differing from the others in which hypertensive andnormotensive patients were included. Excluding this pub-lication, the results for night-time and daytime blood pres-sure observed in the general analysis remained unchanged(data not shown).
Mean night-time and daytime blood pressureFive studies [11,21,24,33,34] investigated the mean night-time and daytime blood pressure in 489 patients. The meannight-time blood pressure was significantly reduced inindividuals treated with CPAP when compared with controlgroups (�2.56 mmHg; 95% CI �4.43 to �0.68; I2: 31%),
Copyright © Lippincott Williams & Wilkins. Unaut8 www.jhypertension.com
which was not observed in the mean daytime blood pres-sure (�1.85 mmHg; 95% CI �4.77 to 1.07; I2: 65%) (Fig. 5).
The high heterogeneity that was also observed in themeta-analysis of mean night-time and daytime blood press-ures can be explained by two studies [11,33], which alsoreport more significant results. After exclusion of thesestudies, the heterogeneity disappeared, but the differencerelated to these variables also became nonsignificant (datanot shown).
All publications considered for analysis of these variablesincluded hypertensive and normotensive individuals,except for one study [24] that included only patients withhypertension. Exclusion of this study did not change theresult of the analysis (data not shown).
In the sensitivity analysis for OSA severity, only twostudies [21,34] included individuals with severe OSA. Ana-lysing only these, it was observed that neither mean day-time nor night-time blood pressure presented anysignificant changes (mean daytime blood pressure:0.83 mmHg; 95% CI �1.20 to 2.86; I2: 0%; mean night-timeblood pressure:�1.00 mmHg; 95% CI�3.02 to 1.02; I2: 0%),but the severity of OSA could explain the heterogeneityfound in the global analyses.
horized reproduction of this article is prohibited.Volume 32 � Number 1 � Month 2014

CE: Namrta; JH-D-14-00062; Total nos of Pages: 12;
JH-D-14-00062
Study or Subgroup1.3.1 Daytime systolic blood pressure
1.3.2 Daytime systolic blood pressure
Mean SDCPAP Control
Total Mean SD Total WeightMean differenceIV, Random, 95% CI
Mean differenceIV, Random, 95% CI
–20 –10
Favours CPAP Favours control
0 10 20
Alonso-Fernández, 2009 127 9 27 126 12 25 17.9% 1.00 [–4.88, 6.88]Barbe, 2001 127 11 29 124 15 26 14.2% 3.00 [–4.02, 10.02]Becker, 2003 132 16 16 143 11 16 8.9% –11.00 [–20.51, –1.49]Duran-Cantola, 2010 133 13 169 132 13 171 34.8% 1.00 [–1.76, 3.76]Hui, 2006 127 16 23 128 18 23 8.5% –1.00 [–10.84, 8.84]Kohler, 2011 131 10 20 135 11 20 15.7% –4.00 [–10.52, 2.52]Subtotal (95% CI) 282 281 100.0% –0.74 [–3.90, 2.41]Heterogeneity: Tau2 = 5.47; chi2 = 7.94, df = 5 (P = 0.16); I2 = 37%Test for overall effect: Z = 0.46 (P = 0.64)
Alonso-Fernández, 2009 78 5 25 77 6 25 21.8% 1.00 [–2.06, 4.06]Barbe, 2001 81 5 29 80 10 26 17.2% 1.00 [–3.25, 5.25]Becker, 2003 76 12 16 86 11 16 8.3% –10.00 [–17.98, –2.02]Duran-Cantola, 2010 84 9 169 85 10 171 25.9% 1.00 [–3.02, 1.02]Hui, 2006 82 11 23 83 10 23 11.9% –1.00 [–7.08, 5.08]Kohler, 2011 80 8 20 87 8 20 14.9% –7.00 [–11.96, –2.04]Subtotal (95% CI) 282 281 100.0% –1.86 [–4.55, 0.83]Heterogeneity: Tau2 = 6.23; chi2 = 12.97, df = 5 (P = 0.02); I2 = 61%Test for overall effect: Z = 1.35 (P = 0.18)
1.3.3 Night-time systolic blood pressure
1.3.4 Night-time diastolic blood pressure
Alonso-Fernández, 2009 117 7 25 126 12 25 19.4% –9.00 [–14.45, –3.55]Barbe, 2001 117 11 29 116 15 26 15.3% 1.00 [–6.02, 8.02]Becker, 2003 118 14 16 130 13 16 10.9% –12.00 [–21.36, –2.64]Duran-Cantola, 2010 119 14 169 121 15 171 26.8% –2.00 [–5.08, 1.08]Hui, 2006 114 15 23 116 15 23 12.0% –2.00 [–10.67, 6.67]Kohler, 2011 127 13 20 135 9 20 15.5% –8.00 [–14.93, –1.07]Subtotal (95% CI) 282 281 100.0% –4.92 [–8.70, –1.14]Heterogeneity: Tau2 = 11.37; chi2 = 11.09, df = 5 (P = 0.05); I2 = 55%Test for overall effect: Z = 2.55 (P = 0.01)
Alonso-Fernández, 2009 69 9 25 70 6 25 17.9% –1.00 [–5.24, –3.24]Barbe, 2001 73 11 29 72 10 26 14.7% 1.00 [–4.55, 6.55]Becker, 2003 70 10 16 77 8 16 13.2% –7.00 [–13.27, –0.73]Duran-Cantola, 2010 74 10 169 75 10 171 23.1% –1.00 [–3.13, 1.13]Hui, 2006 74 11 23 74 9 23 14.2% 0.00 [–5.81, 5.81]Kohler, 2011 74 8 20 84 7 20 16.9% –10.00 [–14.66, –5.34]Subtotal (95% CI) 282 281 100.0% –2.87 [–6.14, –0.40]Heterogeneity: Tau2 = 10.88; chi2 = 16.37, df = 5 (P = 0.0006); I2 = 69%Test for overall effect: Z = 1.72 (P = 0.09)
FIGURE 4 Effect of continuous positive airway pressure on daytime and night-time SBP and DBP.
Effects of CPAP in OSA
In addition, sensitivity analyses were performed toevaluate the effect of obesity and overweight for all vari-ables in this study. There was no significant differencebetween the results of the global analysis and results ofthese sensitivity analyses (data not shown) for BMI.
DISCUSSIONThis systematic review with meta-analysis showed thattreatment with CPAP as compared with control groupspromoted significant reductions in office SBP and DBP,24-h DBP, 24-h mean blood pressure, night-time SBP andnight-time mean blood pressure in patients with OSA butwith a small effect size. We also observed that the night-timeSBP was the variable with the greatest reduction after
Copyright © Lippincott Williams & Wilkins. UnauthJournal of Hypertension
treatment with CPAP (�4.92 mmHg), followed by the24-h mean blood pressure (�3.56 mmHg) and 24-h DBP(�3.46 mmHg).
Recent studies [3,4,19] demonstrated that the use ofCPAP reduces mortality and cardiovascular risks forpatients with OSA, and that one of the mechanismsinvolved may be the reduction in blood pressure as dem-onstrated in this study. This reduction in blood pressure isdue to the fact that the use of CPAP, as already shown in theliterature, promotes increased baroreflex sensitivity,decreased arterial stiffness and reduced sympathetic nerveactivity [20,40]. A systematic review of the effect of treat-ment with CPAP on blood pressure of patients with OSA,published in 2007 [41], observed a positive effect of thistherapy in lowering blood pressure, with not only greater
orized reproduction of this article is prohibited.www.jhypertension.com 9

CE: Namrta; JH-D-14-00062; Total nos of Pages: 12;
JH-D-14-00062
Study or Subgroup Mean SDCPAP Control
Total Mean SD Total WeightMean differenceIV, Random, 95% CI
Mean differenceIV, Random, 95% CI
–20 –10
Favours CPAP Favours control
0 10 20
1.4.2 Night-time mean arterial pressure
1.4.3 Daytime mean arterial pressure
Becker, 2003 86 11 16 95 10 16 6.1% –9.00 [–16.28, –1.72]Dimsdale, 2000 88 2 21 91 3 18 45.5% –300 [–4.63, 1.37]Duran-Cantola, 2010 89 10 169 90 10 171 36.7% –1.00 [–3.13, 1.13]Hui, 2006 88 11 23 89 11 23 7.7% –1.00 [–7.36, 5.36]Robinson, 2006 93 12 16 98 14 16 4.1% –5.00 [–14.03, 4.03]Subtotal (95% CI) 245 244 100.0% –2.56 [–4.43, –0.68]Heterogeneity: Tau2 = 1.33; chi2 = 5.84, df = 4 (P = 0.21); I2 = 31%Test for overall effect: Z = 2.67 (P = 0.008)
Becker, 2003 94 11 16 105 11 16 10.8% –11.00 [–18.62, –3.38]Dimsdale, 2000 95 2 21 97 3 18 35.9% –2.00 [–3.63, –0.37]Duran-Cantola, 2010 101 10 169 100 10 171 33.3% 1.00 [–1.13, 3.13]Hui, 2006 97 11 23 98 13 23 12.3% –1.00 [–7.96, 5.96]Robinson, 2006 106 13 16 108 14 16 7.8% –2.00 [–11.36, 7.36]Subtotal (95% CI) 245 244 100.0% –1.85 [–4.77, 1.07]Heterogeneity: Tau2 = 5.50; chi2 = 11.42, df = 4 (P = 0.02); I2 = 65%Test for overall effect: Z = 1.24 (P = 0.021)
FIGURE 5 Effect of CPAP on mean nighttime and daytime blood pressure.
Schein et al.
reductions in the mean 24-h blood pressure, but also withreduced effect size. This finding suggests that patients withproblems for blood pressure control could benefit from thistherapy, corroborating with our results.
The reduction in blood pressure associated with the useof CPAP is a clinically relevant fact, because the SBP is astrong, continuous and independent risk predictor forcardiovascular disease [14]. A meta-analysis that included61 observational studies aiming at investigating the relation-ship between blood pressure and cardiovascular mortality[14] showed a strong and direct relationship of increasedblood pressure and age with mortality rate. This suggeststhat reductions in blood pressure could decrease the risk ofmortality and reinforce the importance of implementingprogrammes such as CPAP with this aim. Studies haveshown that reductions in SBP is associated with reductionin coronary heart disease, stroke, total cardiovascularmortality and all-cause mortality rates [42–44].
In our study, the night-time SBP was the variable morestrongly affected by treatment with CPAP. This is an import-ant result, as a systematic review of longitudinal studiesconducted by Hansen et al. [45] showed that night-time SBPwas a stronger predictor of cardiovascular outcomes thansystolic daytime blood pressure in hypertensive patients.This can be explained by alterations in the sympatheticmodulation of the night-time blood pressure, disturbedbaroreflex sensitivity [46] and sleep apnea [2]. Upper airwayocclusion in OSA patients reduces the supply of oxygen andincreases the concentration of carbon dioxide, in additionto increasing sympathetic activity [7,10]. This can result inperipheral vasoconstriction and blood pressure elevation[47]. As already demonstrated by other studies, the use ofCPAP promotes reduction of sympathetic activity andincreases the oxygen saturation [10]. These physiologicaleffects of CPAP can explain the reduction in night-timeblood pressure associated with the treatment.
Copyright © Lippincott Williams & Wilkins. Unaut10 www.jhypertension.com
Interestingly, through the sensitivity analyses performed,our study demonstrated that CPAP has a greater effect onpatients with mild OSA. Patients with more severe OSAgenerally present an associated hypertensive state, andthe more severe form of hypertension can promote struc-tural and functional changes. The more severe the disease,greater the injury to target organs [48,49]. Moreover, the lackof effect in more severe OSA patients could be explained bythe small number of studies included in the sensitivityanalyses regarding the severity of OSA, which may havereduced the power of the analyses, beyond the short inter-vention time conducted by the studies. Perhaps, for patientswith severe OSA, longer therapy is required to see an effect.
One of the limitations of the present review is themoderate methodological quality of most of the includedstudies. Half of the articles do not describe whether theallocation was concealed and whether the analyses wereperformed for intention to treat. Another fact to be con-sidered is the heterogeneity found in the meta-analysis,demonstrating a high variation among the included studiesin relation to the form of analysis of outcomes, character-istics of the patients included (inclusion of normotensiveand hypertensive patients and differences in the severity ofOAS), and especially in the time and parameters of CPAP.
Comparisons with other reviewsMontesi et al. [50] conducted a systematic review with ameta-analysis on the effects of CPAP on the SBP and DBP inOSA patients. The meta-analysis included 32 studies, with atotal of 1948 patients, and showed a beneficial effect ofCPAP therapy in these patients, with a mean reduction of2.58 mmHg in daytime SBP and 2.01 mmHg in daytimeDBP. However, this study had some methodological short-comings, such as searching publications in only one data-base and inclusion of studies with patients with othercomorbidities that could influence the results. In contrast,
horized reproduction of this article is prohibited.Volume 32 � Number 1 � Month 2014

CE: Namrta; JH-D-14-00062; Total nos of Pages: 12;
JH-D-14-00062
Effects of CPAP in OSA
the present systematic review consisted of a sensitive,comprehensive and systematic bibliographic search, withexplicit and reproducible eligibility criteria in differentdatabases, with a focus on a specific research question,with the inclusion of specific control groups, making thesample more homogeneous.
Recently, another systematic review with meta-analysiswas conducted [51] that included 32 RCTs (30 RCTs wereincluded in the meta-analysis), totalling 1906 patients. Theaim of this study was to analyse the efficacy of CPAP onblood pressure in individuals with OSA. The results of thisstudy demonstrated a reduction in blood pressure butwere a low effect size, with the mean reduction of 2.6�0.5 mmHg in SBP and 2.0� 0.4 mmHg in DBP favouringtreatment with CPAP. Furthermore, the reduction observedin studies that included outpatient monitoring of the 24-hblood pressure, which was divided into periods during theday and throughout the night, demonstrated a difference inthe mean daytime SBP of 2.2� 0.7 mmHg, although duringthe night-time, the mean SBP and DBP were 3.8 � 1.0 and1.8 � 0.6 mmHg, respectively. In our study, we foundsimilar reductions but with a bigger effect size. The differ-ence may be due to stricter criteria on inclusion in thestudies with control group performed in our study that onlyincluded studies with placebo or subtherapeutic CPAP,although in the study by Fava et al. [51], the control groupwas more heterogeneous, including other control measuresin addition to the sham CPAP. In our study, the real effect ofCPAP was emphasized.
In summary, this systematic review with meta-analysisshowed that treatment with CPAP promoted a significantlybut small reduction in office SBP and DBP, 24-h DBP, 24-hmean blood pressure, nighttime SBP and night-time meanblood pressure in patients with OSA. Thus, our results haveshown that CPAP is an effective therapy for lowering bloodpressure in individuals with OSA, but is not clear whetherthat reduction may improve the cardiovascular risk forthese patients. Therefore, further randomized clinical trialsshould be conducted with higher methodological standardsto confirm these findings and to evaluate the effects of long-term CPAP and the impact on cardiovascular risk.
ACKNOWLEDGEMENTS
Conflicts of interestThere are no conflicts of interest.
REFERENCES1. Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The
occurrence of sleep-disordered breathing among middle-aged adults.N Engl J Med 1993; 328:1230–1235.
2. Young T, Peppard PE, Gottlieb DJ. Epidemiology of obstructive sleepapnea: a population health perspective. Am J Respir Crit Care Med2002; 165:1217–1239.
3. Marin JM, Carrizo SJ, Vicente E, Agusti AG. Long-term cardiovascularoutcomes in men with obstructive sleep apnoea-hypopnoea with orwithout treatment with continuous positive airway pressure: an obser-vational study. Lancet 2005; 365:1046–1053.
4. Marshall NS, Wong KK, Liu PY, Cullen SR, Knuiman MW, Grunstein RR.Sleep apnea as an independent risk factor for all-cause mortality: theBusselton Health Study. Sleep 2008; 31:1079–1085.
5. Martinez-Garcia MA, Campos-Rodriguez F, Catalan-Serra P, Soler-Cat-aluna JJ, Almeida-Gonzalez C, De la Cruz Moron I, et al. Cardiovascular
Copyright © Lippincott Williams & Wilkins. UnauthJournal of Hypertension
mortality in obstructive sleep apnea in the elderly: role of long-termcontinuous positive airway pressure treatment: a prospective obser-vational study. Am J Respir Crit Care Med 2012; 186:909–916.
6. Young T, Finn L, Peppard PE, Szklo-Coxe M, Austin D, Nieto FJ, et al.Sleep disordered breathing and mortality: eighteen-year follow-up ofthe Wisconsin sleep cohort. Sleep 2008; 31:1071–1078.
7. Carlson JT, Hedner J, Elam M, Ejnell H, Sellgren J, Wallin BG. Aug-mented resting sympathetic activity in awake patients with obstructivesleep apnea. Chest 1993; 103:1763–1768.
8. Gapelyuk A, Riedl M, Suhrbier A, Kraemer JF, Bretthauer G, Malberg H,et al. Cardiovascular regulation in different sleep stages in the obstruc-tive sleep apnea syndrome. Biomed Tech (Berl) 2011; 56:207–213.
9. Mediano O, Barcelo A, de la Pena M, Gozal D, Agusti A, Barbe F.Daytime sleepiness and polysomnographic variables in sleep apnoeapatients. Eur Respir J 2007; 30:110–113.
10. Somers VK, Dyken ME, Clary MP, Abboud FM. Sympathetic neuralmechanisms in obstructive sleep apnea. J Clin Invest 1995; 96:1897–1904.
11. Becker HF, Jerrentrup A, Ploch T, Grote L, Penzel T, Sullivan CE, PeterJH. Effect of nasal continuous positive airway pressure treatment onblood pressure in patients with obstructive sleep apnea. Circulation2003; 107:68–73.
12. Kapa S, Sert Kuniyoshi FH, Somers VK. Sleep apnea and hypertension:interactions and implications for management. Hypertension 2008;51:605–608.
13. Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JLJr, et al. Seventh report of the Joint National Committee on Prevention,Detection, Evaluation, and Treatment of High Blood Pressure. Hyper-tension 2003; 42:1206–1252.
14. Lewington S, Clarke R, Qizilbash N, Peto R, Collins R. Age-specificrelevance of usual blood pressure to vascular mortality: a meta-analysisof individual data for one million adults in 61 prospective studies.Lancet 2002; 360:1903–1913.
15. Barnes M, McEvoy RD, Banks S, Tarquinio N, Murray CG, Vowles N,Pierce RJ. Efficacy of positive airway pressure and oral appliance inmild to moderate obstructive sleep apnea. Am J Respir Crit Care Med2004; 170:656–664.
16. Kohler M, Pepperell JC, Casadei B, Craig S, Crosthwaite N, Stradling JR,Davies RJ. CPAP and measures of cardiovascular risk in males withOSAS. Eur Respir J 2008; 32:1488–1496.
17. Narkiewicz K, Kato M, Phillips BG, Pesek CA, Davison DE, Somers VK.Nocturnal continuous positive airway pressure decreases daytimesympathetic traffic in obstructive sleep apnea. Circulation 1999;100:2332–2335.
18. Pepperell JC, Ramdassingh-Dow S, Crosthwaite N, Mullins R, Jenkin-son C, Stradling JR, Davies RJ. Ambulatory blood pressure aftertherapeutic and subtherapeutic nasal continuous positive airway pres-sure for obstructive sleep apnoea: a randomised parallel trial. Lancet2002; 359:204–210.
19. Stanchina ML, Welicky LM, Donat W, Lee D, Corrao W, Malhotra A.Impact of CPAP use and age on mortality in patients with combinedCOPD and obstructive sleep apnea: the overlap syndrome. J Clin SleepMed 2013; 9:767–772.
20. Toraldo DM, De Nuccio F, Nicolardi G. Effects of nCPAP therapy oncardiorespiratory outcomes in obstructive sleep apnea syndrome:compliance and technological advancements. Expert Rev Respir Med2011; 5:41–47.
21. Duran-Cantolla J, Aizpuru F, Montserrat JM, Ballester E, Teran-Santos J,Aguirregomoscorta JI, et al. Continuous positive airway pressure astreatment for systemic hypertension in people with obstructive sleepapnoea: randomised controlled trial. BMJ 2010; 341:c5991.
22. Drager LF, Pedrosa RP, Diniz PM, Diegues-Silva L, Marcondes B, CoutoRB, et al. The effects of continuous positive airway pressure onprehypertension and masked hypertension in men with severeobstructive sleep apnea. Hypertension 2011; 57:549–555.
23. Barbe F, Mayoralas LR, Duran J, Masa JF, Maimo A, Montserrat JM, et al.Treatment with continuous positive airway pressure is not effective inpatients with sleep apnea but no daytime sleepiness. A randomized,controlled trial. Ann Intern Med 2001; 134:1015–1023.
24. Robinson GV, Smith DM, Langford BA, Davies RJ, Stradling JR. Con-tinuous positive airway pressure does not reduce blood pressure innonsleepy hypertensive OSA patients. Eur Respir J 2006; 27:1229–1235.
25. Campos-Rodriguez F, Grilo-Reina A, Perez-Ronchel J, Merino-SanchezM, Gonzalez-Benitez MA, Beltran-Robles M, Almeida-Gonzalez C.
orized reproduction of this article is prohibited.www.jhypertension.com 11

CE: Namrta; JH-D-14-00062; Total nos of Pages: 12;
JH-D-14-00062
Schein et al.
Effect of continuous positive airway pressure on ambulatory BP inpatients with sleep apnea and hypertension: a placebo-controlled trial.Chest 2006; 129:1459–1467.
26. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting itemsfor systematic reviews and meta-analyses: the PRISMA statement. Int JSurg 2010; 8:336–341.
27. Robinson KA, Dickersin K. Development of a highly sensitive searchstrategy for the retrieval of reports of controlled trials using PubMed.Int J Epidemiol 2002; 31:150–153.
28. Engleman HM, Gough K, Martin SE, Kingshott RN, Padfield PL, DouglasNJ. Ambulatory blood pressure on and off continuous positive airwaypressure therapy for the sleep apnea/hypopnea syndrome: effects in‘nondippers’. Sleep 1996; 19:378–381.
29. Norman D, Loredo JS, Nelesen RA, Ancoli-Israel S, Mills PJ, Ziegler MG,Dimsdale JE. Effects of continuous positive airway pressure versussupplemental oxygen on 24-h ambulatory blood pressure. Hyperten-sion 2006; 47:840–845.
30. Sleep-related breathing disorders in adults: recommendations forsyndrome definition and measurement techniques in clinical research.The Report of an American Academy of Sleep Medicine Task, Force.Sleep 1999; 22:667–689.
31. Alonso-Fernandez A, Garcia-Rio F, Arias MA, Hernanz A, de la Pena M,Pierola J, et al. Effects of CPAP on oxidative stress and nitrate efficiencyin sleep apnoea: a randomised trial. Thorax 2009; 64:581–586.
32. Cross MD, Mills NL, Al-Abri M, Riha R, Vennelle M, Mackay TW, et al.Continuous positive airway pressure improves vascular function inobstructive sleep apnoea/hypopnoea syndrome: a randomised con-trolled trial. Thorax 2008; 63:578–583.
33. Dimsdale JE, Loredo JS, Profant J. Effect of continuous positive airwaypressure on blood pressure: a placebo trial. Hypertension 2000; 35 (1 Pt1):144–147.
34. Hui DS, To KW, Ko FW, Fok JP, Chan MC, Ngai JC, et al. Nasal CPAPreduces systemic blood pressure in patients with obstructive sleepapnoea and mild sleepiness. Thorax 2006; 61:1083–1090.
35. Kohler M, Stoewhas AC, Ayers L, Senn O, Bloch KE, Russi EW, StradlingJR. Effects of continuous positive airway pressure therapy withdrawalin patients with obstructive sleep apnea: a randomized controlled trial.Am J Respir Crit Care Med 2011; 184:1192–1199.
36. Lam JC, Lam B, Yao TJ, Lai AY, Ooi CG, Tam S, et al. A randomisedcontrolled trial of nasal continuous positive airway pressure on insulinsensitivity in obstructive sleep apnoea. Eur Respir J 2010; 35:138–145.
37. Mills PJ, Kennedy BP, Loredo JS, Dimsdale JE, Ziegler MG. Effects ofnasal continuous positive airway pressure and oxygen supplement-ation on norepinephrine kinetics and cardiovascular responses inobstructive sleep apnea. J Appl Physiol 2006; 100:343–348.
38. Nguyen PK, Katikireddy CK, McConnell MV, Kushida C, Yang PC.Nasal continuous positive airway pressure improves myocardial
Copyright © Lippincott Williams & Wilkins. Unaut12 www.jhypertension.com
perfusion reserve and endothelial-dependent vasodilation in patientswith obstructive sleep apnea. J Cardiovasc Magn Reson 2010; 12:50.
39. Patruno V, Beghi AS, Chiesa G, Malianni L, Montano AN. Differentefficacy of CPAP and Auto CPAP therapy in patients with sleep apneasyndrome (SAOS): preliminary results. Rass Di Patol Dell‘apparato Resp2005; 20:107–116.
40. Buchner NJ, Quack I, Stegbauer J, Woznowski M, Kaufmann A, RumpLC. Treatment of obstructive sleep apnea reduces arterial stiffness.Sleep Breath 2012; 16:123–133.
41. Haentjens P, Van Meerhaeghe A, Moscariello A, De Weerdt S, Poppe K,Dupont A, Velkeniers B. The impact of continuous positive airwaypressure on blood pressure in patients with obstructive sleep apneasyndrome: evidence from a meta-analysis of placebo-controlledrandomized trials. Arch Intern Med 2007; 167:757–764.
42. He J, Whelton PK. Elevated systolic blood pressure and risk ofcardiovascular and renal disease: overview of evidence from obser-vational epidemiologic studies and randomized controlled trials. AmHeart J 1999; 138 (3 Pt 2):211–219.
43. Goff DC Jr, Lloyd-Jones DM, Bennett G, O’Donnell CJ, Coady S,Robinson J, et al. 2013 ACC/AHA Guideline on the Assessment ofCardiovascular Risk. J Am Coll Cardiol 2014; doi: 10.1016/j.jacc.2013.11.005.
44. James PA, Oparil S, Carter BL, Cushman WC, Dennison-Himmelfarb C,Handler J, et al. 2014 evidence-based guideline for the management ofhigh blood pressure in adults: report from the panel membersappointed to the Eighth Joint National Committee (JNC 8). JAMA2014; 311:507–520.
45. Hansen TW, Li Y, Boggia J, Thijs L, Richart T, Staessen JA. Predictiverole of the nighttime blood pressure. Hypertension 2011; 57:3–10.
46. Vaile JC, Stallard TJ, al-Ani M, Jordan PJ, Townend JN, Littler WA. Sleepand blood pressure: spontaneous baroreflex sensitivity in dippers andnondippers. J Hypertens 1996; 14:1427–1432.
47. Phillips CL, O’Driscoll DM. Hypertension and obstructive sleep apnea.Nat Sci Sleep 2013; 5:43–52.
48. Frattola A, Parati G, Cuspidi C, Albini F, Mancia G. Prognostic value of24-h blood pressure variability. J Hypertens 1993; 11:1133–1137.
49. White WB, Dey HM, Schulman P. Assessment of the daily bloodpressure load as a determinant of cardiac function in patients withmild-to-moderate hypertension. Am Heart J 1989; 118:782–795.
50. Montesi SB, Edwards BA, Malhotra A, Bakker JP. The effect of con-tinuous positive airway pressure treatment on blood pressure: asystematic review and meta-analysis of randomized controlled trials.J Clin Sleep Med 2012; 8:587–596.
51. Fava C, Dorigoni S, Dalle Vedove F, Danese E, Montagnana M, GuidiGC, et al. Effect of continuous positive airway pressure (Cpap) onblood pressure in patients with obstructive sleep apnea/hypopnea. Asystematic review and meta-analysis. Chest 2014; 145:762–771.
Reviewer’s Summary Evaluation
Reviewer 1Is treatment of obstructive sleep apnea (OSA) syndromewith positive airway pressure (CPAP), an effective treat-ment for hypertension? This comprehensive meta-analysisaddresses that question with a thorough and carefullystructured approach. The results pooled from appropriatelyselected trials indicate a small, but statistically significantreduction in blood pressure related to CPAP. However, alltrials are brief, mostly 6 weeks length, so that the durabilityof the pressure response is unknown. Dropout rates arehigh and those with sleep apnea are overweight with othercardiovascular risk factors. It remains to be shown thatCPAP therapy for sleep apnea is an effective preventiveintervention for cardiovascular disease.
Reviewer 2This meta-analysis of randomized controlled trials ofCPAP on blood pressure in patients with OSA includedonly studies that employed placebo CPAP, sham CPAPand subtherapeutic CPAP in the control groups. Anotherstrength was the careful analysis for bias in each study.The dominant effect seen was on nighttime blood pres-sure, not surprising given the contemporaneous therapyoffsetting the hypoxic insult of OSA, but of great import-ance as nocturnal hypertension is associated withincreased cardiovascular morbidity. A number of unre-solved questions remain: What is the durability of effect?How do patients with masked hypertension respond?Is hypertension in patients with severe OSA resistant toCPAP or is there a response to prolonged treatment?
horized reproduction of this article is prohibited.Volume 32 � Number 1 � Month 2014