






Bahasa
Halaman
Hukum


For Peer ReviewCUTANEOUS ANTHRAX IN EASTERN TURKEY: A REVIEW OF 85 CASES
Journal: Clinical and Experimental Dermatology
Manuscript ID: CED-2007-0254.R1
Manuscript Type: Clinical Original Article
Date Submitted by the Author:
11-Jul-2007
Complete List of Authors: Karahocagil, Mustafa; Yüzüncü Yýl University, Faculty of Medicine, Infectious Diseases and Clinical Microbiology Akdeniz, Necmettin; Yüzüncü Yýl University, Faculty of Medicine, Dermatology Akdeniz, Hayrettin; Yüzüncü Yýl University, Faculty of Medicine, Infectious Diseases and Clinical Microbiology Çalka, Ömer; Yüzüncü Yýl University, Faculty of Medicine, Dermatology Karsen, Hasan; Yüzüncü Yýl University, Faculty of Medicine, Infectious Diseases and Clinical Microbiology Bilici, Adnan; Yüzüncü Yýl University, Faculty of Medicine, Infectious Diseases and Clinical Microbiology Bilgili, Serap; Yüzüncü Yýl University, Faculty of Medicine, Dermatology Evirgen, Ömer; Yüzüncü Yýl University, Faculty of Medicine, Infectious Diseases and Clinical Microbiology
keywords: Anthrax, Cutaneous anthrax, Bacillus anthracis
Clinical and Experimental Dermatology
For Peer Review
CUTANEOUS ANTHRAX IN EASTERN TURKEY:
A REVIEW OF 85 CASES
Mustafa Kasım KARAHOCAGİL*
Necmettin AKDENİZ**
Hayrettin AKDENİZ*
Ömer ÇALKA**
Hasan KARSEN*
Adnan BİLİCİ*
Serap G. BİLGİLİ**
Ömer EVİRGEN***
* Yüzüncü Yıl University Department of Infectious Diseases and Clinical Microbiology
** Yüzüncü Yıl University Department of Dermatology
*** Adıyaman State Hospital Department of Infectious Diseases and Clinical Microbiology
Correspondence
Mustafa Kasım KARAHOCAGİL
Yüzüncü Yıl University Department of Infectious Diseases and Clinical Microbiology
65200 VAN / TÜRKİYE
Telephone: + 90 432 2164705
Fax: + 90 432 2167519
E-mail: [email protected]
Page 1 of 16 Clinical and Experimental Dermatology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
CUTANEOUS ANTHRAX IN EASTERN TURKEY:
A REVIEW OF 85 CASES
ABSTRACT
Background: Anthrax is a zoonotic disease diminishing worldwide. Although a very rare
disease in developed countries, anthrax is still endemic in developing countries.
Aim: To evaluate clinical history and features, treatment and outcome of our anthrax cases
and emphasize the importance of the disease in our region.
Method: In this study, the records of the 85 patients diagnosed with cutaneous anthrax,
admitted to our hospital between March 2002 and March 2007 were reviewed; age, sex, occupation,
clinical symptoms and findings, location and type of lesions, clinical history, laboratory findings,
treatment and outcome were recorded.
Results: Of 85 patients, 46 (54.1%) were male, 39 (45.9%) female; with age range 6-72
years (mean age: 30.6 years). All the patients had a history of contact with infected animals or
animal products. The agent was observed through direct examination of Gram-stained smears in 17
patients (20%). B. anthracis was isolated from vesicle fluid cultures in 11 patients (12.9%).
Diagnosis was based on clinical findings in remainder 57 patients (67.1%). All the patients, except
for two patients with respiratory tract obstruction, were discharged from the hospital with full
recovery.
Conclusion: Anthrax continues to be an endemic disease in Turkey. Anthrax should be
considered in patients with proper contact history having a painless ulcer and vesicular skin lesions
surruonded by a zone of edema. Gram-staining and simple culture methods before initiation of the
antibiotic therapy will easily reveal the diagnosis in these patients.
Key Words: Anthrax, Cutaneous anthrax, Bacillus anthracis
Page 2 of 16Clinical and Experimental Dermatology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
CUTANEOUS ANTHRAX IN EASTERN TURKEY:
A REVIEW OF 85 CASES
INTRODUCTION
Anthrax is a zoonosis that essentially affects grazing herbivorous animals. Humans are
incidental hosts, and are infected through direct or indirect contact with animals or contaminated
products.1 The causative agent, B. anthracis, is a Gram positive aerobic or facultatively anaerobic,
non-motile, spore-forming bacterium. Characteristically, chains of bacilli resemble bamboo shots.
Virulence depends on sporulation and the production of toxins, both under genetic control.1,2
The incidence of anthrax is diminishing worldwide, but it has not been entirely eradicated.
Although a very rare disease in western Europe and the United States, anthrax is still a common
disease in parts of Africa, Latin America, Asia and eastern Europe.1,2 In Europe, the major afflicted
regions continue to be Mediterranean countries such as Spain, Greece and Turkey.3,4 It is an
endemic zoonosis in the east and southeast parts of Turkey where animal husbandry is the main
source of living.5-10
The initial clinical manifestation of anthrax depends on the way of entrance of B.anthracis
spores: cutaneous, inhalational or gastrointestinal. Cutaneous anthrax accounts for more than 95%
of disease instances and, in most cases, develops on exposed skin sites, such as face, neck or arms,
associated with animal outbreaks.1,2
Recently, the bioterrorist attacks in USA in 2001, demonstrated the possibility of the use of
B. anthracis as a biological weapon: The modern experience with inhalational anthrax is based on a
considerable extent of the 1979 outbreak in Sverdlovsk, Russia, after the accidental escape and
windborne spread of spores of B. anthracis from a biological weapons factory, that produced 68
deaths.11-13
Page 3 of 16 Clinical and Experimental Dermatology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
In this study, we evaluated the clinical history and features, therapy and outcome of 85
cutaneous anthrax cases followed up in our clinic over the last 5-year period. The importance of the
disease in Eastern Aanatolia region of Turkey is also emphasized.
MATERIAL AND METHODS
Eigthy-five patients clinically diagnosed with cutaneous anthrax in the Departments of
Infectious Diseases and Dermatology at Yüzüncü Yıl University Medical Faculty between March
2002 and March 2007 were included in this study. The records of the patients were reviewed, age,
sex, occupation, clinical symptoms and findings, location and type of lesions, clinical history,
laboratory findings, treatment and outcome were recorded. Routine blood analysis, peripheral blood
smear, blood biochemistry, erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP)
were examined in all patients. Bacteriological analyses including Gram staining and cultures from
skin lesions in all patients were done, in addition to blood cultures in some patients with fever. The
diagnosis of anthrax was based upon history, clinical findings and/or microbiological procedures.
Clinical diagnosis was done by demonstrating the presence of a typical anthrax skin lesion (an ulcer
covered by a characteristic black eschar) in a patient with appropriate history, microbiological
diagnosis was performed by demonstrating encapsulated Gram positive bacilli from the lesion
material, followed by recovery of the agent from the culture medium. Sheep’s blood agar was used,
and large non-hemolytic white-gray colonies with irregularly tapered outgrowths (a medusa’s head
appearance) were evaluated. Gram-stained smears from the culture showed rod-shaped bacteria
growing as long chains. A Gram-positive breakpoint ID panel (Becton-Dickinson Diagnostic
Instrument Systems) was used in the identification.
A detailed history included the occupation of the patient or parents, exposure to sick animals
or animal products, the time of onset of the first lesion and antibiotic therapy prior to admission.
The presence of purulent discharge in cutaneous lesion and its vicinity was accepted as secondary
infection. Patients were followed up for 2 months after completion of treatment.
Page 4 of 16Clinical and Experimental Dermatology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
RESULTS
A total of 85 patients, 46 male (54.1%), 39 female (45.9%); whose age range: 6-72 years
(mean age: 30.6 years) were admitted to our hospital. All the patients were from Van, an ancient
city which is located in estern Anatolia region of Turkey on the eastern coast of Lake Van, or other
cities, county or villages located on the basin of Lake Van. 3 of the cases (3.5%) were from city
center, 17 (20%) from county center and 65 (76.5%) were from villages. The majority of the
patients was in the 11-40 years age group (64.7%). Generally there was no gender difference in the
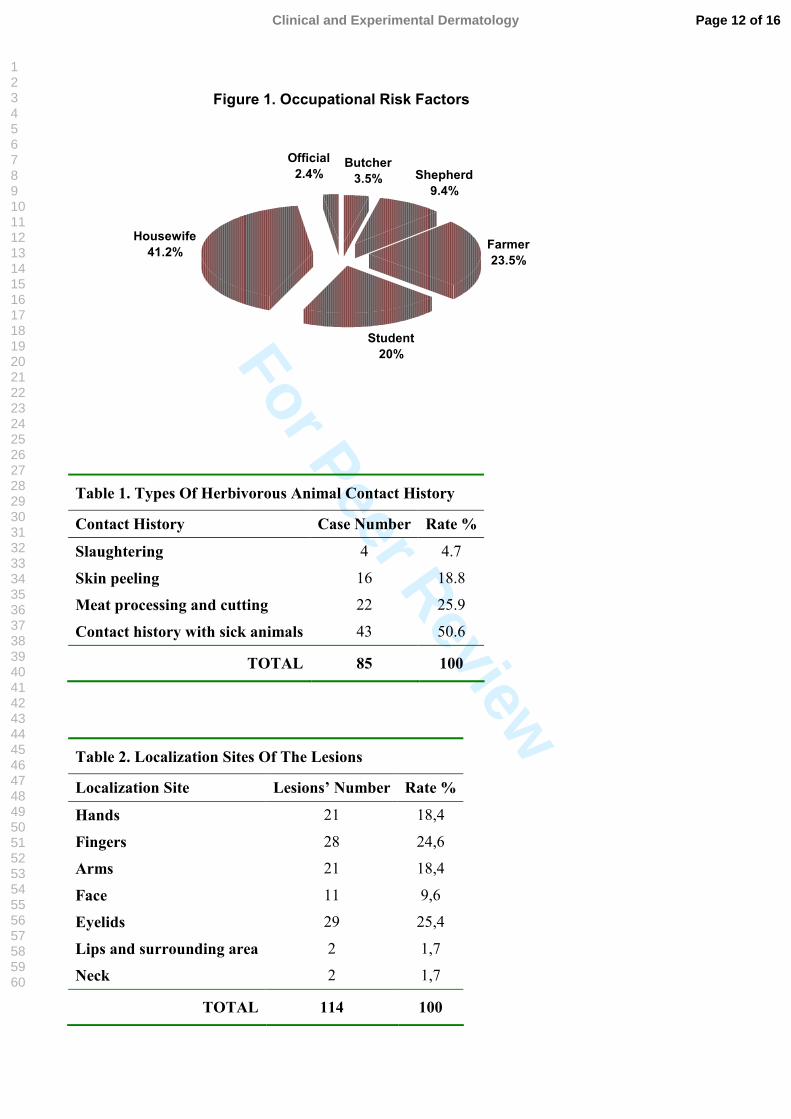
groups. The distribution of the patients by their occupation is shown in Figure 1. The distribution of
the cases did not differ by year but showed a density in the months from July to September (85.9%),
August (49.4%) being the most intensive month.
Types of contact history with herbivorous animals are shown in Table 1. 26 patients (30.5%)
had contact only with sheep, 23 (27.3%) with goats, 13 (15.3%) with cows and 23 (27.1%) with
cows, sheep and goats together.
All of the patients had cutaneous anthrax, malignant edema (lesions on the face and neck)
was observed in 44 patients (51.8%) (Fig. 2) and malignant pustule (lesions on the arms and) hands
in 41 patients (48.2%) (Fig. 3-4). There were two lesions totally in 19 patients: on the upper
extremity in 12, on the eyelid and face in 5, and on the eyelid and upper extremity in 2 patients. The
distribution of the lesions by localization sites is shown in Table 2.
Two of our cases showed a clinical picture of sepsis and findings of respiratory tract
obstruction. These two patients were followed up in the Intensive Care Unit and underwent
tracheostomy. Although connected to the ventilator, they died probably because of delayed
admission. They had a clinical picture of malignant edema and sepsis, the lesions were on the right
eyelid and its surrounding in one patient and on the neck in the other. Sepsis was suspected with
clinical findings with no culture positivity in blood. The patients were connected to the mechanical
ventilator due to respiratory obstruction and altered consciousnees probably because of toxemia.
Page 5 of 16 Clinical and Experimental Dermatology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
The clinical and laboratory findings of the patients are shown in Table 3. The agent was
observed through direct examination of Gram-stained smears in 17 patients (20%). B. anthracis was
isolated from vesicle fluid cultures in 11 patients (12.9%). 45 patients (52.9%) had received an
antibiotic before admission to our clinic, with a period ranging from 1 to 10 days (meanly 2.7 days).
Diagnosis was based on clinical findings in 57 patients (67.1%). Serological tests could not be
conducted. Following medical treatment, reconstructive surgery was required for the scar lesions in
a total of 6 patients (7%): these were on the eyelids in 3 patients, on the right hand in one, on the
index finger in one and on the face (maxillary region) in one patient
In the treatment of malignant pustule, procaine penicilin was used (2x800.000 units IM in
adults and 2x400.000 units IM in children) for one week. 5 patients (5.9%) with peripheral and
small lesions who received prior oral treatment were given amoxicillin (3x500-1000mg/day). The
treatment was started with crystallised penicilin G (6x2-4 million units in adults and 500.000
U/kg/day in children) in cases with malignant edema. After about 5 days, the treatment was
changed to procaine penicillin and continued through the tenth day. Systemic corticosteroids were
added to the antibiotic treatment in 24 patients (54.5%) with the malignant edema and 2 patients
(4.9%) with malignant pustule. For this purpose, prednisolone (1-2 mg/kg/day) was used for 3 days.
In addition, the lesions were topically covered with gauze embedded with rivanol. Rivanol was used
to prevent a secondary infection in our patients because of their poor hygienic conditions in general.
The second purpose of our rivanol use was medical debridement, for removal of the crusts, necrotic
tissues and purulent materials in the wound. Ciprofloxacin was added to the standard treatment in
11 patients (12.9%) having a secondary infection. The mean hospitalization period was 7.9 days in
cases with malignant pustule and 12.8 days in cases with malignant edema. All of the patients,
except for two patients who presented with clinically anthrax sepsis and findings of respiratory tract
obstruction were discharged from the hospital with full recovery.
Page 6 of 16Clinical and Experimental Dermatology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
DISCUSSION
While there is a general decrease in the number of anthrax outbreaks worldwide, and thus of
human cases, anthrax is still a disease that is extensively underdiagnosed and underreported.7,11 The
regions with widespread infection include African countries, Latin America and the Mediterranean
countries.3,4,11,14
Cutaneus anthrax constitues more than 95% of all clinical forms throughout the world and is
generally associated with animal husbandry.1,2 In our series, all the cases were in the form of
cutaneous disease, all associated with sick livestock. Whereas industrial cases account for most of
the anthrax cases in developed countries in which there is no conventional exposure to infected
animals or animal products, the spread of anthrax in developing countries such as Turkey occurs
most frequently by direct contact.15,16 We found that in all of our cases the disease was contracted
by direct or indirect contact with infected animals or animal products. Nevertheless, we can not
exclude the possibility that some cases of gastrointestinal and inhalational anthrax may have been
missed especially in regions such as ours that cutaneous anthrax cases are widespread and contact
with infected animals is intensive.2,7
The organism gains access through a break in the skin. Subcutaneously inoculated anthrax
spores grow rapidly, producing organisms that release toxins and form a primary lesion surrounded
by a red edematous area. While direct contact of the hands and arms with infected materials gives
rise to lesions in the form of malignant pustule, lesions which develop by inoculation of
contaminated material transported from the hands and fingers onto eyes, face or neck are generally
in the form of malignant edema.1,17 The fact that the lesions on the eyes and face constituted the
majority of the cases (35.1 %) in our series, most of them seen in children, may be explained by the
inattentiveness to hygienic care in children compared to adults.
The most important means of subsistence for the people in our region, not only in villages
but also in rural areas and even city centers, is animal husbandry performed by traditional methods.
In our region, animal anthrax incrases in arid seasons especially in summer months and early
Page 7 of 16 Clinical and Experimental Dermatology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
spring.1,18 This explains the intensity of human anthrax cases in July to September (85.9%), August
being the most intensive month (49.4%). This finding is correlated with the literature.5-10 Maguina
et al.11 have reported in their series of 71 cases that the disease was associated with direct contact
with beef cattle (78.9%), goats (14.1%) and swine (7%), and they associated outbreaks of human
anthrax with cases in cattle. However, in our series, types of contacted animals were only sheep in
26 cases, goats in 23 cases, and cattle in 13 cases, being in 23 cases with cows, sheep and goats
together. This finding is associated with widespread stockbreeding of sheep and goats rather than
cattle in our region. However, the fact that the control of these animals is more difficult and the
region is close to Iran frontier where the animal traffic is uncontrolled made us consider that these
animals can be more important as a source of infection in our country.
Anthrax is an endemic disease in our country although its incidence is decreasing. In
Turkey, 4423 human anthrax cases were reported between the years 1980-89. About 300 cases were
reported annually from 1990 on.16,19 Recently Turkish Ministry of Health, General Directorate of
Basic Health Services reported 396 and 532 anthrax cases for years 2000 and 2001, respectively.20
Not all the anthrax cases that occur in our region are referred to our clinic, with some cases,
especially those presenting in malignant pustule form, being treated in the first-step health care
facilities.6 Therefore, the majority of the patients (52.9%) are admitted to our clinic after receiving
an antibiotic. When we take into consideration that some of the patients recover with the treatment
available from the first-step health care facilities, it is well understood that the incidence of anthrax
in our region is much higher than our own caseload suggests.
There was no gender difference in the groups in our series. Alhough Irmak et al.6 have
reported in their series of 39 cases that women constituted a majority of 65.4% and they attributed
this to women in rural areas dealing with animal husbandry rather than men, there does not appear
such a gender difference in two previous studies performed in our region by other authors.7,8
Page 8 of 16Clinical and Experimental Dermatology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
In cases the lesions were located on face, eyes and neck, in the form of malignant edema,
clinical prognosis was more severe and hospital stay was longer (12.8 days vs 7.9 days) than the
malignant pustule form, because antibiotic treatment was completed to 10 days in edema form.
Diagnosis of cutaneous anthrax requires clinical suspicion. The clue to the diagnosis of
cutaneous anthrax is the history and rapid development of a painless ulcer surrounded by a zone of
edema. However, plague, tularemia, glanders, ecthyma gangrenosum, ulcerative skin lesions,
rickettsial pox, rat-bite fever, orf, syphilitic chancre, staphylococcal furuncle, lymphangitis,
vasculitis, cutaneous tuberculosis, cutaneous diphteria, leprosy and spider bites must be considered
in differential diagnosis of cutaneous anthrax.1,2,8,11 The diagnosis is confirmed by bacteriological
examination of infected tissue (Gram-staining and culture) or isolation of the bacillus from blood
cultures in systemic infections. In 32.9% of our cases (28 cases), the agent could be demonstrated
by direct examination of Gram-stained smears and/or by culture methods. The fact that the
causative agent could not be detected in 67.1% of the cases can be explained by the use of
antibiotics by some patients (52,9%) before their admission to our clinic. Also in the literature, the
rate of positive anthrax cultures from skin lesions does not exceed 60-65%, the low rate being
attributed to use of antibiotics prior to culture.6,7,21 As a matter of fact, cultures taken from the
lesions of patients who were treated with penicilin have become negative within a few hours after
the initiation of the therapy.22 Therefore, we can conclude that the diagnosis can clinically be
achieved in patients with proper history and physical examination findings.
Ciprofloxacin, doxycycline, and penicillin G are currently recommended by the Centers for
Disease Control and Prevention and the Food and Drug Administration as therapeutics for
inhalation and cutaneous anthrax.23 Penicilin has been the drug of choice for anthrax for many
decades although many antibiotics are efficient in vitro against B. anthracis. Öncül et al.8 have
found the penicilin susceptibility as 100% in 14 strains in their study performed in eastern Anatolia
region of Turkey in 2002. BakıcıMZ et al.24 have also reported in their study performed in the same
year that 28 B. anthracis strains were all susceptible to penicillin. Similarly, 11 strains of B.
Page 9 of 16 Clinical and Experimental Dermatology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
anthracis isolated from cultures in our series were susceptible to penicilin. Penicillin has been used
in all our cases except for 5 cases described below and has been found effective. However, the use
of oral antibiotics has been reported to be sufficient in the form of malignant pustule.1,2 Therefore,
in 5 cases with small peripheral lesions, oral amoxicillin was given because of prior oral treatment
and has been achieved good results. In the literature it has been reported that anthrax sepsis is not
fatal provided that the treatment is started early.25 In our series, 2 patients with clinically anthrax
sepsis who underwent thracheostomy needed connection to ventilator because of respiratory tract
obstruction. They did not respond to treatment and died probably because of delayed admission to
our clinic.
In conlusion, anthrax continues to be an important infectious disease endemic in developing
countries including Turkey. Anthrax should be considered in patients with proper contact history
with infected animals or animal products having a painless ulcer and vesicular skin lesions
surruonded by a zone of edema. Gram-staining and simple culture methods before initiation of the
antibiotic therapy will easily reveal the diagnosis of anthrax in these patients.
REFERENCES
1. Lew DP. Bacillus anthracis (Anthrax). In: Principles and Practice of Infectious Diseases
(Mandell GL, Bennett JE, Dolin R. eds) 5th edn. New York: Churchill Livingstone, 2000: 2215-
2220.
2. Doğanay M. Bacillus anthracis ve Diğer Bacillus Türleri. In: İnfeksiyon Hastalıkları ve
Mikrobiyolojisi (Topçu AW, Söyletir G, Doğanay M.eds), 2nd edn. İstanbul: Nobel Tıp
Kitabevi, 2002: 1533-1543.
3. Hugh-Jones M.1996-97 Global anthrax report. J Appl Microbiol 1999; 87: 189-91.
4. Velimirovic B. Anthrax in Europe. Rev Sci Tech Off Int Epiz 1984; 3: 527.
5. Doğanay M, Aydın N. Antimicrobial susceptibility of Bacillus anthracis. Scand J Infect Dis
1991; 23: 333-335.
6. Irmak H, Buzgan T, Karahocagil MK et al. Cutaneous manifestations of anthrax in eastern
Anatolia: a review of 39 Cases. Acta Medica Okayama 2003; 57: 235-240.
7. Demirdag K, Ozden M, Saral Y et al. Cutaneous anthrax in adults: a review of 25 cases in the
Eastern Anatolian Region of Turkey. Infection 2003; 31: 327-330.
Page 10 of 16Clinical and Experimental Dermatology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
8. Öncül O, Özsoy MF, Gül HC. Cutaneous anthrax in Turkey: a review of 32 cases Scand J Infect
Dis 2002; 34: 413-416.
9. Caksen H, Arabacı F, Abuhandan M et al. Cutaneous anthrax in Eastern Turkey. Cutis 2001;
67: 488-492.
10. Caksen H, Atas B, Odabas D, Irmak H. Anthrax of the eyelid in a Turkish girl. Pediatr
Dermatol. 2003; 20: 93-94.
11. Maguina C, del Pozo JF, Terashima A et al. Cutaneous anthrax in Lima, Peru: retrospective
analysis of 71 cases, includıng four with a menıngoencephalic complication. Rev Inst Med Trop
S Paulo 2005; 47: 25-30.
12. Abramova FA, Grinberg LM, Yampolskaya OV, Walker DH. Pathology of inhalational anthrax
in 42 cases from the Sverdlovsk outbreak of 1979. Proc Natl Acad Sci U S A. 1993; 90: 2291-
2294.
13. Meselson M, Guillemin J, Hugh-Jones M et al. Sverdlovsk anthrax outbreak of 1979. Science.
1994; 266: 1202-1208.
14. Pugh A O, Davies JCA. Human anthrax in Zimbabwe. Salisbury Med Bull 1990; 68: 32.
15. Doğanay M, Aygen B. Diagnosis: cutaneous anthrax. Clin Infect Dis 1997; 25: 607-725.
16. Kaya A, Taşyaran MA, Özkurt Z, et al. Şarbon:68 olgunun değerlendirilmesi. Flora 1997; 1:
51-54.
17. Mallon E, McKee PH. Extraordinary case report: Cutaneous anthrax. Am J Dermatopathol
1997; 19: 79-82.
18. Dragon DC, Rennie RP. The ecology of anthrax spores: tough but not invincible. Can Vet J
1995; 36: 295-301.
19. Doğanay M. Human anthrax in Turkey. Salisbury Med Bull 1995; 87: 8.
20. Turkish Ministry Of Health. (2001) Basic Health Services Annual Statistics Year of 2001
[WWW document]. URL http://www.saglik.gov.tr/TR/BelgeGoster.aspx? F6E10F8892433
CFF71BE64510F6C8BC9BCE6CB6771470A25 html [accessed on 29 June 2007]
21. Dixon TC, Meselson M, Guillemin J et al. Anthrax. N Engl J Med 1999; 341: 815-826.
22. Ronaghy HA, Azadeh B, Kohout E: Penicillin therapy of human cutaneous anthrax. Curr Ther
Res 1972; 14: 721-725.
23. Inglesby TV, O'Toole T, Henderson DA et al. Anthrax as a biological weapon, 2002: updated
recommendations for management. JAMA 2002; 287: 2236-2252.
24. Bakıcı, MZ, N. Elaldı N, Bakır M et al. Antimicrobial susceptibility of Bacillus anthracis in an
endemic area. Scand. J. Infect. Dis. 2002; 34: 564-566.
25. Felek S, Akbulut A, Kalkan A. A case of anthrax sepsis: non-fatal course. J Infect 1999; 38:
201-202.
Page 11 of 16 Clinical and Experimental Dermatology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
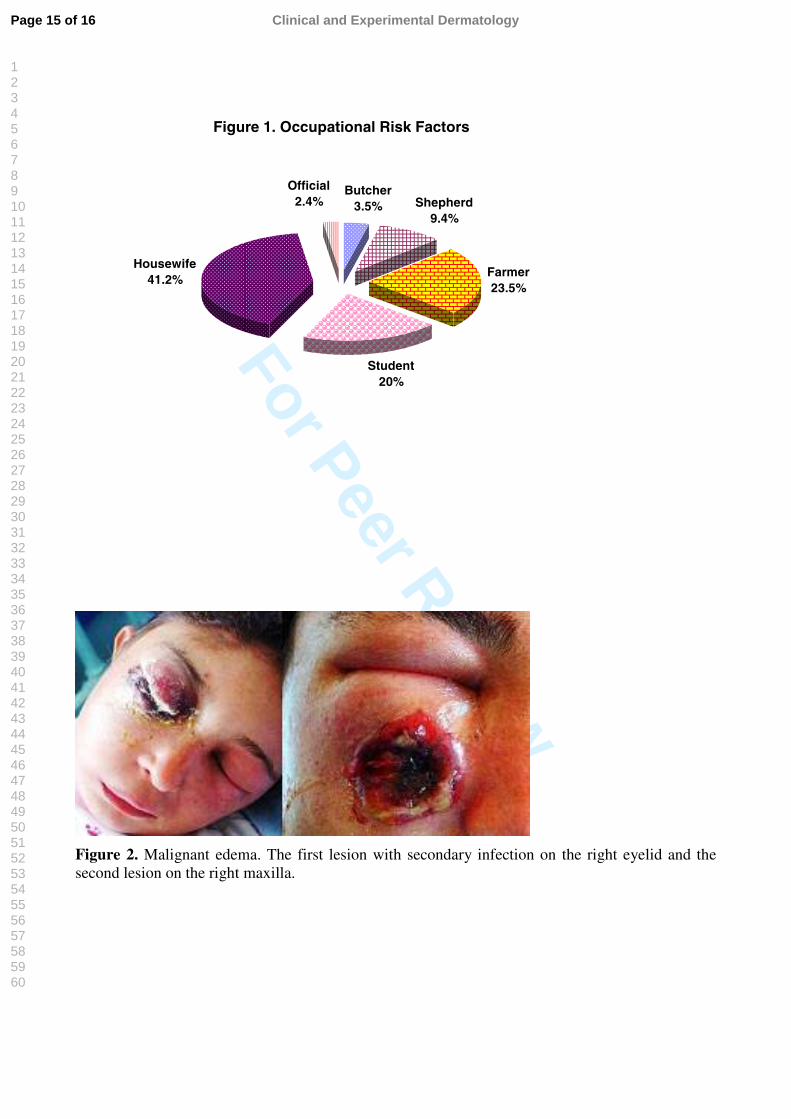
Figure 1. Occupational Risk Factors
Student20%
Housewife41.2% Farmer
23.5%
Shepherd9.4%
Official2.4%
Butcher3.5%
Table 1. Types Of Herbivorous Animal Contact History
Contact History Case Number Rate %
Slaughtering 4 4.7
Skin peeling 16 18.8
Meat processing and cutting 22 25.9
Contact history with sick animals 43 50.6
TOTAL 85 100
Table 2. Localization Sites Of The Lesions
Localization Site Lesions’ Number Rate %
Hands 21 18,4
Fingers 28 24,6
Arms 21 18,4
Face 11 9,6
Eyelids 29 25,4
Lips and surrounding area 2 1,7
Neck 2 1,7
TOTAL 114 100
Page 12 of 16Clinical and Experimental Dermatology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
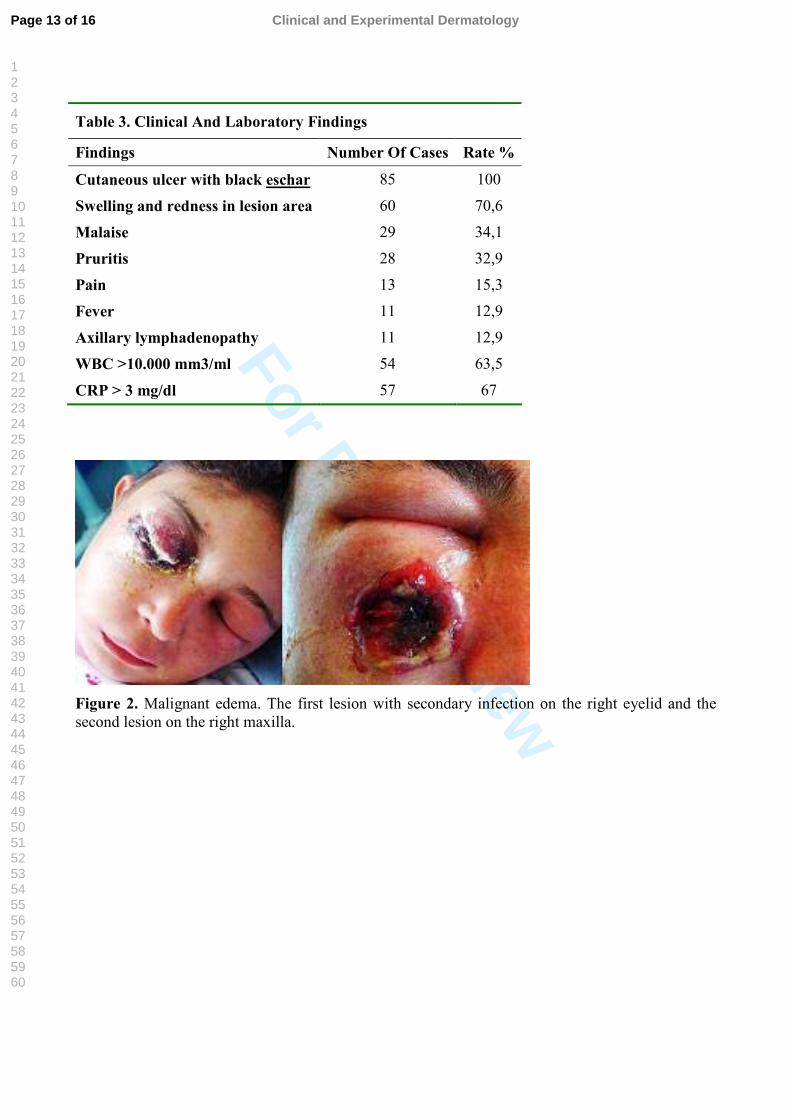
Table 3. Clinical And Laboratory Findings
Findings Number Of Cases Rate %
Cutaneous ulcer with black eschar 85 100
Swelling and redness in lesion area 60 70,6
Malaise 29 34,1
Pruritis 28 32,9
Pain 13 15,3
Fever 11 12,9
Axillary lymphadenopathy 11 12,9
WBC >10.000 mm3/ml 54 63,5
CRP > 3 mg/dl 57 67
Figure 2. Malignant edema. The first lesion with secondary infection on the right eyelid and the second lesion on the right maxilla.
Page 13 of 16 Clinical and Experimental Dermatology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
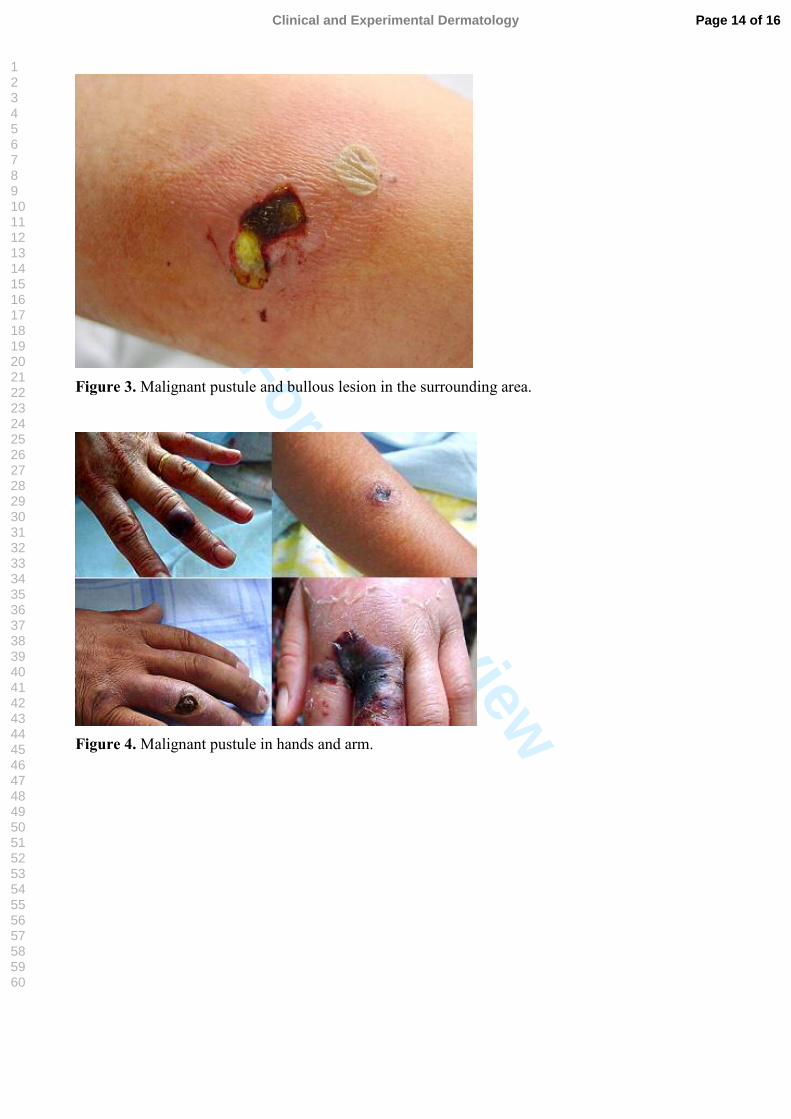
Figure 3. Malignant pustule and bullous lesion in the surrounding area.
Figure 4. Malignant pustule in hands and arm.
Page 14 of 16Clinical and Experimental Dermatology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
Figure 1. Occupational Risk Factors
Student20%
Housewife41.2%
Farmer23.5%
Shepherd9.4%
Official2.4%
Butcher3.5%
Figure 2. Malignant edema. The first lesion with secondary infection on the right eyelid and thesecond lesion on the right maxilla.
Page 15 of 16 Clinical and Experimental Dermatology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
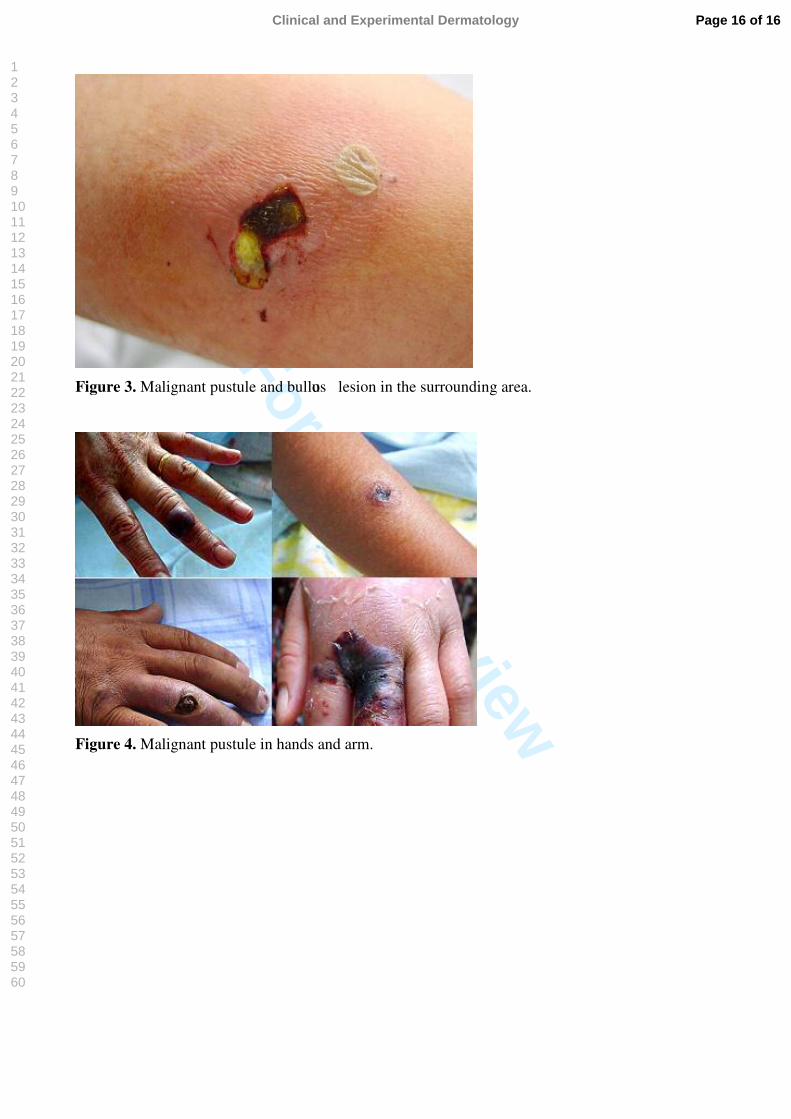
Figure 3. Malignant pustule and bullous lesion in the surrounding area.
Figure 4. Malignant pustule in hands and arm.
Page 16 of 16Clinical and Experimental Dermatology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Copyright © 2022 FDOKUMEN

