







Bahasa
Halaman
Hukum


PLEASE SCROLL DOWN FOR ARTICLE
This article was downloaded by: [Chang Gung Memorial Hospital]On: 25 June 2009Access details: Access Details: [subscription number 906386320]Publisher Informa HealthcareInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House,37-41 Mortimer Street, London W1T 3JH, UK
Scandinavian Journal of Infectious DiseasesPublication details, including instructions for authors and subscription information:http://www.informaworld.com/smpp/title~content=t713690438
Comparative proteomic studies of plasma from children with pneumococcalpneumoniaMing-Han Tsai ab; Tzou-Yien Lin cd; Sen-Yung Hsieh ce; Chih-Yung Chiu ab; Cheng-Hsun Chiu cd; Yhu-CheringHuang cd
a From the Department of Pediatrics, Chang Gung Memorial Hospital, Keelung b Graduate Institute of ClinicalMedical Sciences, Chang Gung University, Taoyuan c College of Medicine, Chang Gung University, Taoyuand Division of Pediatric Infectious Diseases, Department of Pediatrics, Chang Gung Children's Hospital,Taoyuan e Clinical Proteomics Center, Chang Gung Memorial Hospital, Taoyuan, Taiwan
First Published:2009
To cite this Article Tsai, Ming-Han, Lin, Tzou-Yien, Hsieh, Sen-Yung, Chiu, Chih-Yung, Chiu, Cheng-Hsun and Huang, Yhu-Chering(2009)'Comparative proteomic studies of plasma from children with pneumococcal pneumonia',Scandinavian Journal ofInfectious Diseases,41:6,416 — 424
To link to this Article: DOI: 10.1080/00365540902936909
URL: http://dx.doi.org/10.1080/00365540902936909
Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf
This article may be used for research, teaching and private study purposes. Any substantial orsystematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply ordistribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representation that the contentswill be complete or accurate or up to date. The accuracy of any instructions, formulae and drug dosesshould be independently verified with primary sources. The publisher shall not be liable for any loss,actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directlyor indirectly in connection with or arising out of the use of this material.

ORIGINAL ARTICLE
Comparative proteomic studies of plasma from children withpneumococcal pneumonia
MING-HAN TSAI1,2, TZOU-YIEN LIN3,4, SEN-YUNG HSIEH3,5, CHIH-YUNG CHIU1,2,
CHENG-HSUN CHIU3,4 & YHU-CHERING HUANG3,4
From the 1Department of Pediatrics, Chang Gung Memorial Hospital, Keelung, 2Graduate Institute of Clinical Medical
Sciences, Chang Gung University, Taoyuan, 3College of Medicine, Chang Gung University, Taoyuan, 4Division of Pediatric
Infectious Diseases, Department of Pediatrics, Chang Gung Children’s Hospital, Taoyuan, and 5Clinical Proteomics Center,
Chang Gung Memorial Hospital, Taoyuan, Taiwan
AbstractStreptococcus pneumoniae is the primary pathogen causing community acquired pneumonia in children. Despite medicalprogress, the prevalence of complicated pneumococcal pneumonia became increased without apparent explanations. Two-dimensional gel electrophoresis (2-DE) and mass spectrometry (MS) were used to compare the plasma protein profiles fromchildren with different severities of pneumococcal pneumonia. Plasma samples from 14 cases, 7 with complicated and theother 7 with uncomplicated pneumonia, were analyzed. Complicated pneumonia was defined by the presence of pleuralfluid parameters consistent with empyema, and/or a computed tomography compatible with necrotizing pneumonitis. Thenormal control group included 7 age-matched volunteers. By comparing the plasma proteins of patients with differentseverities, 4 proteins with significant differences were identified. The up-regulated proteins were haptoglobin andimmunoglobulin kappa chain. The down-regulated were apolipoprotein A-I (Apo-AI) and transthyretin. All these proteinsare known to take part in the inflammation reaction, which implicates the active innate immune responses in severeinfections of S. pneumoniae. In addition, the up-regulated haptoglobin, which protects lung tissues against oxidativedamage by the clearance of hemoglobin, can also act as an inflammatory inhibitor. Thus, our data seem to indicate thatinflammation balance may take place in the occurrence of complicated pneumococcal pneumonia.
Introduction
Streptococcus pneumoniae is the most common
cause of bacterial pneumonia in children [1,2]. The
formation of pneumatoceles or necrosis had been
previously considered a rare complication in children
with pneumococcal pneumonia. However, since the
1990s, an increase in the incidence of complicated
pneumonia has been observed among children,
especially in Taiwan, and the cause of this increase
is not well understood [1,3�6].
There have been many studies on S. pneumoniae
itself, but few studies were performed on the
mechanisms in vivo in the affected patients [7,8].
Plasma is a widely used clinical resource that is
closely correlated with disease progression, and
analysis of the plasma protein profile alterations
in affected children is a promising way to elucidate
the mechanisms of complicated pneumococcal
pneumonia [9].
Proteomics, a large-scale study of gene expres-
sion at the protein level, is a rapidly developing area
of biomedical research [10]. Many studies have
demonstrated that determination of protein profiles
is useful in elucidating pathological pathways as well
as alterations associated with disease processes [11].
With the development of clinical proteomics, many
technologies have been employed to study plasma
proteomes [12]. In the present study, we used a
combination of techniques, including 2-dimensional
gel electrophoresis (2-DE), image analysis, and
mass spectrometry (MS), to compare the plasma
protein profiles among pneumococcal pneum-
onia children with different severities and hea-
lthy individuals. Potential markers associated with
Correspondence: T.-Y. Lin, Division of Pediatric Infectious Diseases, Department of Pediatrics, Chang Gung Children’s Hospital, No. 5 Fu-Hsin Street,
Kweishan 333, Taoyuan, Taiwan. Tel: �886 3 3281200, extn. 8002; Fax: �886 3 3288957. E-mail: [email protected]
Scandinavian Journal of Infectious Diseases, 2009; 41: 416�424
(Received 28 December 2008; accepted 30 March 2009)
ISSN 0036-5548 print/ISSN 1651-1980 online # 2009 Informa UK Ltd. (Informa Healthcare, Taylor & Francis As)
DOI: 10.1080/00365540902936909
Downloaded By: [Chang Gung Memorial Hospital] At: 07:32 25 June 2009

complicated pneumococcal pneumonia were also
identified.
Materials and methods
Patient enrollment and sample preparation
This study was approved by Institutional Review
Board of Chang Gung Memorial Hospital. From
January 2002 to June 2005, patients less than 18 y of
age with pneumococcal pneumonia were enrolled
into our study. Those with concomitant life-threaten-
ing diseases or immunodeficiency were excluded.
The study population was categorized into 3 groups
in accordance with the disease severity: group 1
(severe test group), patients with complicated pneu-
monia; group 2 (mild test group), patients with
uncomplicated lobar pneumonia; and group 3 (con-
trol group), children visiting our outpatient depart-
ment (OPD) for allergen survey without any
infectious diseases. We collected plasma specimens
on the first d of admission. To remove albumin and
immunoglobulin (IgG) from human plasma, the
samples were treated with a Proteoprep Immunoaffi-
nity Albumin and IgG Depletion Kit (SIGMA)
according to the manufacturer’s instructions.
Pneumonia was defined as the combination of
acute respiratory symptoms and a consolidation on
chest radiographic images, which were interpreted
by attending physicians and radiologists. Compli-
cated pneumonia was defined by the presence of
pleural fluid parameters consistent with empyema
(based on visual or biochemical characteristics) and/
or cavitations or pneumatoceles on a computed
tomographic image compatible with necrotizing
pneumonitis [1]. The diagnostic criteria of pneumo-
coccal infection were a culture (including blood or
pleural effusions) yielding Streptococcus pneumo-
niae or a positive result of pleural pneumococcal
antigen.
Two-dimensional electrophoresis (2-DE)
500 mg of plasma were diluted to 330 ml with
rehydration solution (8 M urea, 4% CHAPS,
50 mM DTT, 0.2% v/v (pH 3�10) IEF buffer, trace
bromophenol blue). The samples were loaded on
immobilized pH gradient gel strips (pH 3�10), and
isoelectric focusing (IEF) was performed using a
Protean IEF Cell system (BioRad). The gels were
rehydrated overnight at 50 V. Proteins were focused
subsequently for 1 h at 100 V; then a gradient was
applied from 100 to 8000 V for 1 h and finally at
10,000 V to give a total of 55,000 Vh. All IEFs were
carried out at 208C. After the first-dimensional IEF,
IPG strips were placed in an equilibration solution
(6 M urea, 2% SDS, 30% glycerol, 0.375 M Tris-
HCl, pH 8.8) containing 2% DTT and were shaken
for 20 min at 50 rpm in an orbital shaker. The strips
were then transferred to the equilibration solution
containing 2.5% iodoacetamide and shaken for
another 20 min before being placed on a 12.5%
polyacrylamide gel slab. Separation in the second
dimension was carried out using Protean II electro-
phoresis equipment. Afterwards, the gels were fixed
and SYPRO Ruby stained.
Protein visualization and image analysis
For SYPRO Ruby staining, gels were initially fixed for
60 min in a buffer containing 10% methanol and 7%
acetic acid. The gels then were stained for 4 h in a
commercially available SYPRO Ruby buffer (Mole-
cular Probes, Eugene, OR) followed by washing in the
fixation buffer. Protein patterns in the gels were
recorded as digitalized images using a high-resolution
scanner (ProExpress, PerkinElmer, Boston, MA).
The SYPRO Ruby stained gels were used for image
analysis using the Progenesis software package (Pro-
genesis Discovery, Nonlinear Dynamics, Durham,
NC).
Protein analysis by mass spectrometry
The spots of interest were manually excised
from the gels. Proteins selected for analysis were
in-gel digested with trypsin. Briefly, the spots were
destained using 50 mM NH4HCO3 in 50% ACN
and dried in a SpeedVac concentrator. Subsequently
the samples were digested with trypsin (Promega,
Madison, WI) at 0.002 mg/ml in 25 mM NH4HCO3
(pH 8.5). After digestion, the supernatant was
collected and 1.5 ml was spotted onto a matrix-
assisted laser desorption/ionization (MALDI) target
plate.
Measurements were performed using the MALDI
time-of-flight mass spectrometry (Ultraflex; Bruker
Daltonics, Germany) and its settings were as follows:
ion source 1, 25.0 kV; ion source 2, 22.15 kV; lens,
6 kV; reflector, 26.3 kV; reflector 2, 14.65 kV; pulse
ion extraction, 120 ns. Ionization was achieved by
irradiation with a 337-nm nitrogen laser (l�337 nm)
and the high purity nitrogen gas (99.999%) was
maintained at 2050 mbar. The laser was operated at
25 Hz with laser power of 30%. For matrix suppres-
sion, we used a high gating factor with signal
suppression up to 400 Da. The mass calibration
was executed with the peptides in a mass range of
760�3100 Da. For each MALDI spot, spectra were
accumulated to the intensity of 2.5�10�4 arbitrary
intensity. We then used the flexAnalysis 2.0 and
BioTools 2.2 (Bruker Daltonics, Germany) to process
Plasma proteome in complicated pneumococcal pneumonia 417
Downloaded By: [Chang Gung Memorial Hospital] At: 07:32 25 June 2009

the raw data and search the processed peak lists via
MASCOT software 2.1 (in-house version) from
matrix science (www.matrixscience.com) to identify
the proteins.
Enzyme-linked immunosorbent assay
An enzyme-linked immunosorbent assay (ELISA)
was used to detect the antibodies to the recombinant
protein antigens. Briefly, 100 ml of the diluted
antigens (2�5 mg/ml) in PBS buffer, pH 7.4, was
added to the wells of the flat-bottomed ELISA
plates, and incubated overnight at 48C in a moist
chamber. The wells were then washed with a PBS
solution, pH 7.4, containing 0.05% Tween 20
(PBST) and blocked by the addition of 200 ml
PBST-0.1% BSA at room temperature for 1 h. After
emptying the wells, 100 ml sera with serial 2-fold
diluted in PBST-1% BSA was added to the wells,
which were then incubated at room temperature for
2 h. After washing the wells, 100 ml of the strepta-
vidine conjugated to horseradish-peroxidase diluted
1:5000 in PBST-1% BSA was added and the
incubation was continued at room temperature for
1 h. After an additional wash, 100 ml of the substrate
solution (TMB(tetramethylbenzidine)) was added to
the wells, which were then incubated at room
temperature for approximately 15 min. The reaction
was then stopped with 50 ml 2.0 N H2SO4 and the
absorbance was read at 450 nm. Each test was
performed in duplicate, and the mean absorbance of
the wells with no antigen was subtracted from that of
the wells with the protein antigens prior to analysis.
The criteria for sensitivity were determined by
adding 2 SD to the mean absorbance in the sera
from the healthy controls in this study.
Western blot analysis
Each plasma sample was loaded with the same
quantity. Protein from plasma was electrophoresed
on a 12% SDS-polyacrylamide gel and then trans-
ferred onto PVDF membrane. Actin was used as a
reference (internal control). The membranes were
blocked 1 h at 378C in 20 mM Tris-base, 150 mM
NaCl, pH 7.4, 0.05% Tween-20 (TBST) containing
10% skimmed milk. The primary antibodies used
were anti-fetuin polyclonal antibody or anti-alpha-1
anti-chymotrypsin (ACT). Membranes were incu-
bated overnight at 48C with each primary antibody,
and then were washed 3 times with TBST and
incubated with horseradish peroxidase-conjugated
secondary antibody for 1 h at room temperature.
Visualization of the immunoreactive proteins was
accomplished using ECL reagents. All the mem-
branes were exposed on the same X-ray film; then, 1
semi-quantitative analysis based on OD was
performed for Western blot films by Bio 1D��software (Vilber Lourmat, France).
Statistical methods
Data were analyzed with the SPSS Statistical Pack-
age (version 11.0). Fisher’s exact test was used to
analyze categorical data, and the Wilcoxon rank-sum
test or ANOVA was used to analyze continuous data.
A p-valueB0.05 was considered to be statistically
significant.
Results
Comparative proteomic analysis using 2-DE
Considering individual variability, we chose cases
with similar age distribution in each experimental
group and there were 7 cases in each group. The
average timing of sample collection was 8.594.2 d
after onset of disease. Table I shows the clinical
features of our patients. There were no significant
differences in the demographic and laboratory data
among the 3 groups. However, all cases in group 1
(complicated pneumonia cases) were admitted to the
pediatric intensive care unit (PICU) and received
invasive procedures (i.e. chest tube drainage or
operation), but in group 2 (uncomplicated lobar
pneumonia cases), only 1 case received invasive
procedure and neither of them was admitted to
PICU during hospitalization.
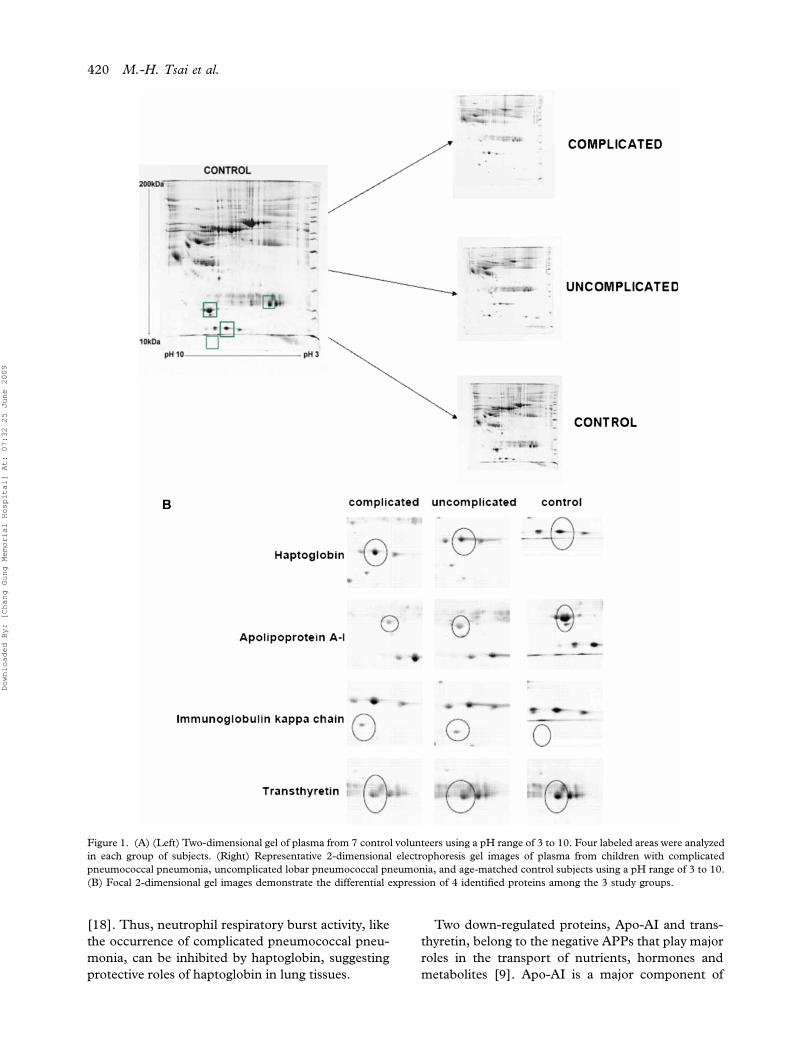
2-DE was used to study the alterations of plasma
protein profiles among the 3 study groups. The
representative 2-DE images are shown in Figure 1A.
More than 400 protein spots were detected on the
2-DE gels, which localized in the ranges of pI 3�10
and Mr 10�200 kDa. The 2-DE images were
analyzed by Progenesis 2D Elite software to esti-
mate the abundance of proteins in each sample and
to generate quantitative data. Based on a threshold
ratio of 2.0, the software detected the spots of
interest that revealed a significant change among the
3 groups. Protein spots that could not be identified
were excluded. Four different protein spots, includ-
ing 2 up-regulated and 2 down-regulated spots in
plasma of complicated pneumonia children, were
observed showing differences between the 3 experi-
mental groups (Figure 1B).
Protein identification
After scanning, the gels were stained with SYPRO-
Ruby and 4 protein spots with significant change
were picked using a SpotCutter and then subjected
to in-gel digestion for MALDI-TOF MS analysis.
418 M.-H. Tsai et al.
Downloaded By: [Chang Gung Memorial Hospital] At: 07:32 25 June 2009

MALDI-TOF MS was then used to analyze the
peptides after in-gel digestion. Table II reveals the
identified proteins, including Swiss-Pro accession
number, protein description, protein coverage, iden-
tification method, score, fold changes and functional
classification. The changes in the identified proteins
in 3 different groups can be summarized into 2
modes: 1) haptoglobin and immunoglobulin kappa
chain C region, which were up-regulated in the
group with complicated pneumonia compared to the
other 2 groups; and 2) apolipoprotein A-I (Apo-AI)
and transthyretin, which were down-regulated in the
group with complicated pneumonia compared to the
other 2 groups.
Validation of the up-regulated expression proteins and
down-regulated expression proteins by ELISA and
Western blot
To validate the results of our study, ELISA and
Western blot were used for further confirmation of
4 differential proteins. Initially, we investigated the
seroreactivity of 4 differential proteins using ELISA
and the relative concentration levels of these pro-
teins are shown as Table III and Figure 2. The
ELISA results verified the significant up-regulation
of haptoglobin/immunoglobulin kappa chain and
down-regulation of Apo-AI/transthyretin in group 1
(complicated pneumonia group). We selected 2
differentially expressed proteins, haptoglobin and
Apo-AI, for further confirmation using Western blot
analysis. Figure 3 shows the scanned Western blot
films (Figure 3A, 3B). The OD of each band in the
film was evaluated by Bio1D�� software (Vilber
Lourmat, France) (Figure 3C). Compared to that
derived from normal control group and cases with
uncomplicated lobar pneumonia, up-regulation of
haptoglobin and down-regulation of Apo-AI in the
sera of complicated pneumonia group were verified.
Discussion
In this study, we used the comparative proteomics
technology, 2-DE and MS, to demonstrate the
characteristic changes of the plasma proteins in
different severities of pneumococcal pneumonia.
Several plasma proteins altered significantly in cases
with complicated pneumococcal pneumonia. The
up-regulated proteins were haptoglobin and immu-
noglobulin kappa chain C region, and the down-
regulated proteins were Apo-AI and transthyretin.
All of the altered proteins are acute phase proteins
(APPs) and known to take part in the inflammation
reaction [13].
Like other acute respiratory infections, S. pneumo-
niae can induce the activation of immune response,
and this activation may cause lung tissue damage,
airway occlusion and then extravasation of erythro-
cytes into the lower respiratory tract [9,14,15]. Free
iron released from hemoglobin after hemolysis can
catalyze the formation of reactive oxygen species and
lead to oxidative damage in lung tissue [16]. Hence it
is very important to keep the balance of the immune
system between the ability to clear the pathogen and
the damage to the delicate structure of lungs [9].
Haptoglobin, 1 of the up-regulated proteins found in
our complicated pneumococcal pneumonia patients,
is a member of the acute-phase reactants [15]. It has
long been known as a major hemoglobin-binding
protein associated with hemoglobin catabolism [17].
Plasma haptoglobin could contribute significantly to
the clearance of hemoglobin and thus protect the
lower respiratory tract against hemoglobin mediated
oxidative damage [15]. Another important biologic
function of haptoglobin is the modulation of the
immune response [15]. In a previous study, hapto-
globin has been shown to decrease the reactivity of
lymphocytes and neutrophils toward a variety of
stimuli, and may act as a natural antagonist for
receptor-ligand activation of the immune system
Table I. Clinical characteristics of selected children analyzed with proteomic methods stratified by different severities of pneumococcal
pneumonia.
Parameters Group 1 n�7 complicated Group 2 n�7 lobar Group 3 n�7 control p-valuea
Age (months) mean9SD 34.3911.7 44.499.1 46.3910.8 0.102
Gender (male/total) 2/7 5/7 5/7 0.174
WBC (/mm3) mean9SD 16371.497763.1 17700.098644.1 � 0.767
Segment (%) 75.798.4 67.1919.2 � 0.314
CRP (mg/l) mean9SD 173.0968.0 175.09133.7 � 0.972
Operation 7/7 0 � 0.001
Chest tube 7/7 1/7 � 0.005
PICU admission 7/7 0 � 0.001
WBC: white blood cell; CRP: C-reactive protein; SD: standard deviation; PICU: pediatric intensive care unit.
Data presented as no/total or mean9standard deviation.apB0.05 was considered to be statistically significant; Fisher’s exact test and Wilcoxon rank-sum test used for analysis.
Plasma proteome in complicated pneumococcal pneumonia 419
Downloaded By: [Chang Gung Memorial Hospital] At: 07:32 25 June 2009
[18]. Thus, neutrophil respiratory burst activity, like
the occurrence of complicated pneumococcal pneu-
monia, can be inhibited by haptoglobin, suggesting
protective roles of haptoglobin in lung tissues.
Two down-regulated proteins, Apo-AI and trans-
thyretin, belong to the negative APPs that play major
roles in the transport of nutrients, hormones and
metabolites [9]. Apo-AI is a major component of
Figure 1. (A) (Left) Two-dimensional gel of plasma from 7 control volunteers using a pH range of 3 to 10. Four labeled areas were analyzed
in each group of subjects. (Right) Representative 2-dimensional electrophoresis gel images of plasma from children with complicated
pneumococcal pneumonia, uncomplicated lobar pneumococcal pneumonia, and age-matched control subjects using a pH range of 3 to 10.
(B) Focal 2-dimensional gel images demonstrate the differential expression of 4 identified proteins among the 3 study groups.
420 M.-H. Tsai et al.
Downloaded By: [Chang Gung Memorial Hospital] At: 07:32 25 June 2009

high-density lipoproteins (HDL) [19]. Recently,
lipoproteins have been found to play a key role in
innate immunity, and changes in lipoprotein levels
have been reported in a variety of inflammatory
disorders [20]. Of all lipoproteins, HDL has the
highest lipopolysaccharide (LPS, a component of
the outer membrane of Gram-negative bacteria)
and lipoteichoic acid (LTA, a major cell wall
component of Gram-positive bacteria) binding
capacity [21,22]. In vivo and in vitro experiments
have shown that bacterial substances such as LPS
and LTA are neutralized by HDL or Apo-AI,
suggesting anti-inflammatory properties of HDL
[21�23].
Our study revealed that the concentrations of
Apo-AI, the major component of HDL, were
markedly reduced and the changes were closely
related to the severity of the pneumococcal
pneumonia. The diminution of HDL in severe
infections has been well known, but the mechan-
isms are not well understood [20,24]. One possi-
bility is that HDL is consumed significantly by
binding bacterial substances [21,22]. Another
possibility is that high concentrations of proin-
flammatory cytokines during sepsis suppress HDL
production and facilitate HDL degradation
[25,26]. The decline in HDL renders the host
tissue more susceptible to bacterial substance-
mediated injury, resulting in cytokine overproduc-
tion and a further depletion of HDL (vicious
circle) [24]. Further prospective, randomized
designed studies are needed because it remains
unclear whether a lower Apo-AI level in children
with complicated pneumococcal pneumonia is
only an epiphenomenon or has a causal relation-
ship with adverse clinical outcomes.
Although our results cannot completely resolve
‘‘the cause of the increase of complicated pneu-
mococcal pneumonia in Taiwan’’, we still derived
the important concept that a defense homeostasis
may occur during the progression of complicated
pneumococcal pneumonia. This phenomenon is
not only specifically found in complicated pneu-
mococcal pneumonia, but also found in other
severe pathogen-infectious pneumonia such as
SARS coronavirus-associated pneumonia [9].
Thus, we can utilize these identified proteins as
markers to predict the clinical outcomes, espe-
cially during the treatment of severe respiratory
tract infection.
In conclusion, we reported an application of
proteomic approaches to elucidate the possible
pathological process for complicated pneumococcalTab
leII
.Id
enti
fica
tion
of
the
an
aly
zed
pro
tein
s.
Sw
iss-
Pro
acc
essi
on
no.
Pro
tein
des
crip
tion
Pro
tein
cover
age
Iden
tifi
cati
on
met
hod
s
MA
SC
OT
score
Pea
k-v
olu
me
rati
o(f
old
s:
test
/con
trol)
Fu
nct
ion
al
class
ific
ati
on
P02766-0
0-0
0-0
0T
ran
sthyre
tin
(Pre
alb
um
in)
73%
PM
F107
1/2
.50
Thyro
idhorm
on
eb
ind
ing
pro
tein
;tr
an
sport
eract
ivit
y
P00738-0
0-0
0-0
0H
apto
glo
bin
30%
PM
F63
2.2
5D
efen
sere
spon
se
P02647-0
0-2
3-0
0A
polipopro
tein
A-I
57%
PM
F230
1/2
.74
Lip
idm
etabolism
;ci
rcu
lati
on
P01834-0
0-0
0-0
0Im
mu
noglo
bu
lin
kap
pa
chain
Cre
gio
n
82%
PM
F62
2.5
Imm
un
ere
spon
se
PM
F:
pep
tid
em
ass
fin
ger
pri
nti
ng.
Plasma proteome in complicated pneumococcal pneumonia 421
Downloaded By: [Chang Gung Memorial Hospital] At: 07:32 25 June 2009

pneumonia in childhood. Our studies demonstrate
that all of the altered proteins found in complicated
pneumococcal pneumonia children are APPs. They
are known to take part in the inflammation reaction
[13], which implicates the active innate immune
responses in severe infections with S. pneumoniae.
Due to the protective role of up-regulated haptoglo-
bin, our results also showed that there is some
Table III. Seroreactivity of 4 proteins among 3 study groups by ELISA testing.
Study group Complicated (mean9SD) Uncomplicated (mean9SD) Control (mean9SD) p-value
Haptoglobin (mg/ml) 0.73490.259 0.59390.296 0.24290.157 0.007
Apolipoprotein A-I (mg/ml) 4135.991763.1 4696.291829.7 6629.293583.7 0.208
Immunoglobulin kappa chain C region (mg/ml) 3.97690.877 3.21790.781 2.08590.621 0.001
Transthyretin (Prealbumin) (mg/ml) 2.53391.210 3.10691.751 7.01793.788 0.007
SD: standard deviation.
ANOVA was used to compare the mean levels of 4 proteins among the 3 study groups.
Figure 2. Seroreactivity of 4 proteins among 3 study groups by ELISA testing shown as scatter plots.
422 M.-H. Tsai et al.
Downloaded By: [Chang Gung Memorial Hospital] At: 07:32 25 June 2009

mechanism that sustains the inflammation balance
in the occurrence of complicated pneumococcal
pneumonia.
Acknowledgements
We thank the members of the Clinical Proteomics
Center of Chang Gung Memorial Hospital,
Taoyuan, Taiwan, for excellent technical assistance.
This work was supported by a grant from Chang
Gung Memorial Hospital (CMRPG 33061).
Declaration of interest: The authors report no
conflicts of interest. The authors alone are respon-
sible for the content and writing of the paper.
Figure 3. Western blot results validating the increased expression of haptoglobin in the group with complicated pneumococcal pneumonia
(A). The decreased expression of apolipoprotein in the group with complicated pneumococcal pneumonia (B). Actin was used as a
reference; the semi-quantitative analysis of Western blot films based on the OD of bands (C).
Plasma proteome in complicated pneumococcal pneumonia 423
Downloaded By: [Chang Gung Memorial Hospital] At: 07:32 25 June 2009

References
[1] Tan TQ, Mason EO Jr, Barson WJ, Wald ER, Schutze GE,
Bradley JS, et al. Clinical characteristics and outcome of
children with pneumonia attributable to penicillin-suscepti-
ble and penicillin-non-susceptible Streptococcus pneumo-
niae. Pediatrics 1998;/102:/1369�75.
[2] McCarthy VP, Patamasucon P, Gaines T, Lucas MA.
Necrotizing pneumococcal pneumonia in childhood. Pediatr
Pulmonol 1999;/28:/217�21.
[3] Kerem E, Bar Ziv Y, Rudenski B, Katz S, Kleid D, Branski
D. Bacteremic necrotizing pneumococcal pneumonia in
children. Am J Respir Crit Care Med 1994;/149:/242�4.
[4] McCarthy VP, Patamasucon P, Gaines T, Lucas MA.
Necrotizing pneumococcal pneumonia in childhood. Pediatr
Pulmonol 1999;/28:/217�21.
[5] Chen KC, Su YT, Lin WL, Chiu KC, Niu CK. Clinical
analysis of necrotizing pneumonia in children: 3-y experience
in a single medical center. Acta Paediatr Tw 2003;/44:/343�8.
[6] Hsieh YC, Hsueh PR, Lu CY, Lee PI, Lee CY, Huang LM.
Clinical manifestations and molecular epidemiology of
necrotizing pneumonia and empyema caused by Streptococ-
cus pneumoniae in children in Taiwan. Clin Infect Dis 2004;/
38:/830�5.
[7] Wu TT, Hsueh PR, Lee LN, Yang PC, Luh KT. Pneumonia
caused by penicillin-non-susceptible Streptococcus pneumo-
niae: clinical characteristics, prognostic factors, and out-
comes. J Formos Med Assoc 2000;/99:/18�23.
[8] Weiser JN, Kapoor M. Effect of intrastrain variation in the
amount of capsular polysaccharide on genetic transforma-
tion of Streptococcus pneumoniae: implications for viru-
lence studies of encapsulated strains. Infect Immun 1999;/67:/
3690�2.
[9] Wan J, Sun W, Li X, Ying W, Dai J, Kuai X, et al.
Inflammation inhibitors were remarkably up-regulated in
plasma of severe acute respiratory syndrome patients at
progressive phase. Proteomics 2006;/6:/2886�94.
[10] Hsieh SY, Shih TC, Yeh CY, Lin CJ, Chou YY, Lee YS.
Comparative proteomic studies on the pathogenesis of
human ulcerative colitis. Proteomics 2006;/6:/5322�31.
[11] Hanash S. Disease proteomics. Nature 2003;/422:/226�32.
[12] Anderson NL, Anderson NG. The human plasma proteome:
history, character, and diagnostic prospects. Mol Cell
Proteomics 2002;/1:/845�67.
[13] Gruys E, Toussaint MJM, Niewold TA, Koopmans SJ.
Acute phase reaction and acute phase proteins. J Zhejiang
Univ SCI 2005;/11:/1045�56.
[14] Kadioglu A, Gingles NA, Grattan K, Kerr A, Mitchell TJ,
Andrew PW. Host cellular immune response to pneumo-
coccal lung infection in mice. Infect Immun 2000;/68:/
492�501.
[15] Yang F, Ghio AJ, Herbert DC, Weaker FJ, Walter CA,
Coalson JJ. Pulmonary expression of the human haptoblogin
gene. Am J Respir Cell Mol Biol 2000;/23:/277�82.
[16] Balla J, Nath KA, Balla G, Juckett MB, Jacob HS, Vercellotti
GM. Endothelial cell heme oxygenase and ferritin induction
in rat lung by hemoglobin in vivo. Am J Physiol 1995;/268:/
321�7.
[17] Yang F, Haile DJ, Berger FG, Herbert DC, Beveren EV,
Ghio AJ. Haptoglobin reduces lung injury associated with
exposure to blood. Am J Physiol Lung Cell Mol Physiol
2003;/284:/402�9.
[18] Oh SK, Pavlotsky N, Tauber AI. Specific binding of
haptoglobin to human neutrophils and its function conse-
quences. J Leukoc Biol 1990;/47:/142�8.
[19] Mateos-Caceres PJ, Garcıa-Mendez A, Lopez Farre A,
Macaya C, Nunez A, Gomez J, et al. Proteomic analysis of
plasma from patients during an acute coronary syndrome.
J Am Coll Cardiol 2004;/44:/1578�83.
[20] van Leeuwen HJ, Heezius EC, Dallinga GM, van Strijp JA,
Verhoef J, van Kessel KP. Lipoprotein metabolism in
patients with severe sepsis. Crit Care Med 2003;/31:/
1359�66.
[21] Levels JH, Abraham PR, van den Ende A, van Deventer SJ.
Distribution and kinetics of lipoprotein-bound endotoxin.
Infect Immun 2001;/69:/2821�8.
[22] Levels JH, Abraham PR, van Barreveld EP, Meijers JC, van
Deventer SJ. Distribution and kinetics of lipoprotein-bound
lipoteichoic acid. Infect Immun 2003;/71:/3280�4.
[23] Wu A, Hinds CJ, Thiemermann C. High-density lipopro-
teins in sepsis and septic shock: metabolism, actions, and
therapeutic applications. Shock 2004;/21:/210�21.
[24] Chien JY, Jerng JS, Yu CJ, Yang PC. Low serum level of
high-density lipoprotein cholesterol is a poor prognostic
factor for severe sepsis. Crit Care Med 2005;/33:/1688�93.
[25] Cohen J. The immunopathogenesis of sepsis. Nature 2002;/
420:/885�91.
[26] Fraunberger P, Pilz G, Cremer P, Werdan K, Walli AK.
Association of serum tumor necrosis factor levels with
decrease of cholesterol during septic shock. Shock 1998;/
10:/359�63.
424 M.-H. Tsai et al.
Downloaded By: [Chang Gung Memorial Hospital] At: 07:32 25 June 2009
Top Related
Copyright © 2022 FDOKUMEN

