







Bahasa
Halaman
Hukum

DERMATOPATHOLOGY
Carney complex: A clinicopathologic and molecularbiological study of a sporadic case, including
extracutaneous and cutaneous lesions and a novelmutation of the PRKAR1A gene
Denisa Kacerovska, MD, PhD,a Radek Sima, MSc,a Michal Michal, MD,a,e Ondrej Hes, MD, PhD,a
Patrik Roucka, MD,b Marta Zarybnicka, MD,b Milan Hora, MD, PhD,c Zdenek Chudacek, MD, PhD,d,f
and Dmitry V. Kazakov, MD, PhDa
Pilsen and Prague, Czech Republic
Background: Carney complex (CNC) is an autosomal dominant disorder associated with multipleneoplasms.
Objective: We report a case of a 40-year-old Caucasian man with a sporadic form of CNC.
Methods: This is a clinicopathologic description and molecular biological study with an emphasis onhistopathologic findings.
Results: The patient presented with multiple cutaneous myxomas, cardiac myxomas, and spottypigmentation at typical sites. Additionally, a blue nevus, a lipoma, multiple calcifications in both testes,and hypoechogenic areas suspected of being adenomas in the thyroid gland were found. Microscopically,the 2 cardiac and 6 cutaneous myxomas studied manifested a typical appearance, being composed ofscattered polygonal, stellate, plump and/or spindle cells in a mucinous matrix containing small, sometimesdilated blood vessels. Of the 6 cutaneous myxomas, only in one lesion was there an abnormal epithelialcomponent (tiny basaloid buds and a horn cyst). Molecular biologic study revealed a heterozygous shiftmutation c.796dupA in exon 10 of the PRKAR1A gene. Physical examination and genetic testing of familymembers (both parents and two brothers) for the PRKAR1A mutation were negative, as was analysis of theperipheral blood of 110 randomly selected, unrelated healthy individuals for the above mutation. Thesefindings suggest sporadic disease and a novel mutation in our patient.
Limitations: None.
Conclusion: Herein we report a case of sporadic CNC in which a novel mutation in PRKAR1A wasidentified. ( J Am Acad Dermatol 2009;61:80-7.)
Key words: blue nevus; cardiac myxomas; Carney complex; chromosome 17q24; cutaneous myxomas;novel mutation; PRKAR1A gene.
From Sikl’s Department of Pathology,a and the Departments of
Cardiosurgery,b Urology,c and Radiology,d Charles University,
Medical Faculty Hospital, and the Bioptical Laboratory,e Pilsen;
and the Department of Radiology, Charles University, First
Medical Faculty, Prague.f
Funding sources: None.
Conflicts of interest: None declared.
Reprint requests: Dmitry V. Kazakov, MD, PhD, Sikl’s Department of
Pathology, Charles University, Medical Faculty Hospital, Alej
Svobody 80, 304 60 Pilsen, Czech Republic. E-mail: kazakov@
medima.cz.
0190-9622/$36.00
ª 2009 by the American Academy of Dermatology, Inc.
doi:10.1016/j.jaad.2008.11.015
80
Carney complex (CNC) is an autosomal dom-inant disease characterized by multiple myx-omas, spotty pigmentation of the skin, and
endocrine abnormalities. Although a combination ofseveral components of this inherited condition wasdescribed as early as 1973,1 the disease was recog-nized as a distinct syndrome by Carney et al2 in1985. The clinical manifestations of CNC include (1)myxomas occurring in various organs such as theskin, superficial soft tissue, heart, and breast; (2)cutaneous and mucocutaneous lentiginous pigmen-tation; and (3) an endocrinopathy manifesting asprimary pigmented nodular adrenocortical disease
J AM ACAD DERMATOL
VOLUME 61, NUMBER 1
Kacerovska et al 81
causing adrenocorticotropic hormoneeindepend-ent Cushing syndrome and/or growth hormoneeproducing pituitary adenomas.3 Less commoncomponents of this disorder may include large-cellcalcifying Sertoli cell tumor of the testis,4 psammo-matous melanotic schwannoma,5-7 and epithelioidblue nevus.7,8 In the literature there have also beenreported rare cases of osteochondromyxoma,9 thy-roid gland abnormalities,10 ovarian lesions,11,12 andtetralogy of Fallot,13,14 although it is not clear atpresent whether these represent a component of thesyndrome or are merely coincidental.
CNC is a genetically heterogeneous entity, with atleast two known genes responsible for the disease,namely the CNC1 gene located on chromosome17q22-24 and the CNC2 gene mapped to 2p16.15,16
The CNC1 gene, also known as the PRKAR1A gene, atumor suppressor gene, encodes the type 1A regula-tory subunit of c-AMP-dependent protein kinase A,which is known to be an important effector moleculein many endocrine signaling pathways.17 Inactivatingmutations of PRKAR1A have been found in approx-imately half of all patients with CNC.18 The CNC2gene is less well characterized but may be involved inregulating genomic stability.19,20
Hereinwe report a caseof sporadic CNC inwhich anovel mutation in the PRKAR1A gene was identified.
MATERIAL AND METHODSThe removed tissue was fixed in 4% formaldehyde
and embedded in paraffin. The paraffin blocks were
Table I. Primers used for amplification of codingexons of the PRKAR1A gene
Exon Name Sequence 59/39
3 PRKAR-3F TGCCAGATTGACATTTTGCTPRKAR-3R CCTCATCATCTCCCCACATT
4 PRKAR-4F CATGCCGAAGGATCTCATTTPRKAR-4R AGTGGGTCCCAAAAGCATC
5 PRKAR-5F CAGGTTGCAAACGTGAAATGPRKAR-5R TTGGGATCACACCCTTACTTG
6 PRKAR-6F TTCACGGAAGAGACATGTGAAPRKAR-6R GCCTCCTCTCCCGTAACAAT
7 PRKAR-7F TTCTTTCTTTAATTTGGAATATGCTTCPRKAR-7R TGCTCGGAAGCGATCAATA
8 PRKAR-8F AAAAAGGTTTGAGGGTTTTTAACATPRKAR-8R TTCTAAATCACACTCTCAAACACCA
9 PRKAR-9F CACGTCTTGGGGATATCACTTPRKAR-9R CTTTTCCCAAGTCCATCCAA
10 PRKAR-10F GCAGTTATTTTGATTCTTGTCTTTCAPRKAR-10R TTAGCCCACTCTTTCCCTCTT
11 PRKAR-11F CCCTGGGTTTGAGAGTGTGTPRKAR-11R AACCATGTATTTATTGTGAGGGAAT
12 PRKAR-12F GGAAATGTTTTTCATAGAAGTTAGCCPRKAR-12R GAAAAGGGAGGCACAGGAG
cut into 5-�m thick sections and stained with hema-toxylin and eosin.
DNA from the patient’s peripheral blood wasextracted by the NucleoSpin Tissue Kit (Macherey-Nagel, Duren, Germany) according to the manufac-turer’s protocol. Ten coding exons (exons 3-12according to the reference sequence NG 007093) ofthe PRKAR1A gene were amplified by polymerasechain reaction (PCR) using primers listed in Table I.PCR conditions were as follows: 12.5 �L of HotStartTaq PCR Master Mix (QIAgen, Hilden, Germany), 10
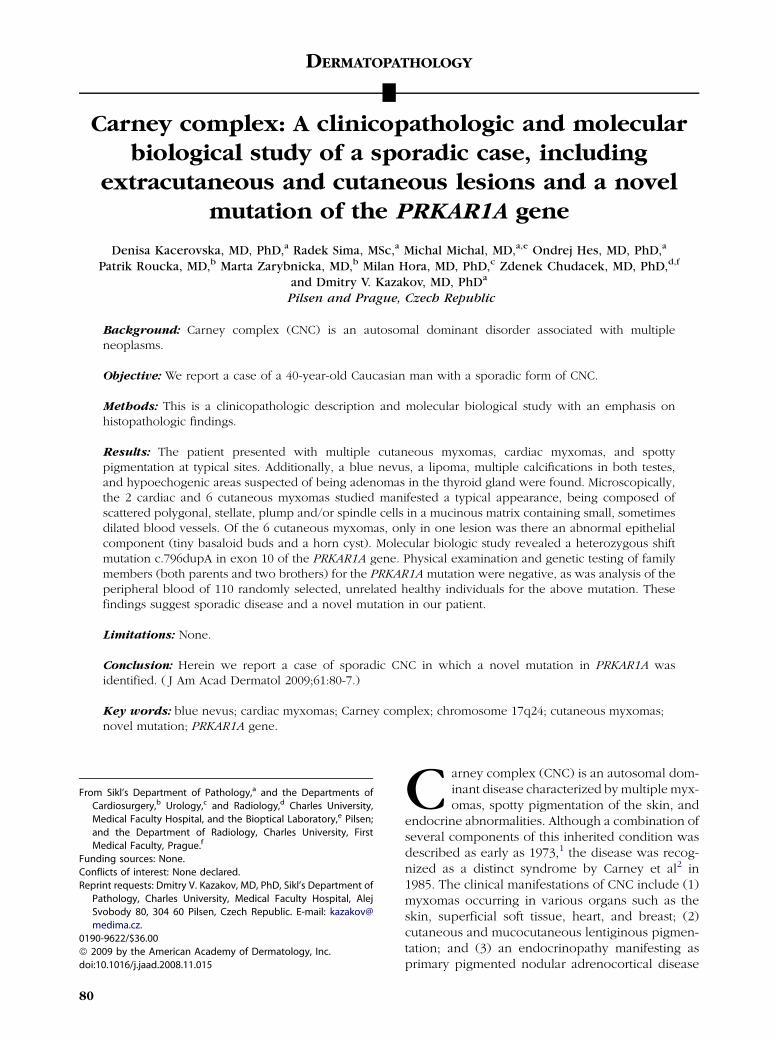
Fig 1. A, Transthoracic echocardiography of two myxo-mas located in right ventricular chamber. B, Cardiacmyxoma is nonencapsulated and poorly circumscribed.C, Round to polygonal and stellate cells surrounded byabundant loose stroma rich in acid mucopolysaccharidesFocally, areas with many siderophages and extravasatederythrocytes are present. (B and C, Hematoxylin-eosinstain.)

J AM ACAD DERMATOL
JULY 2009
82 Kacerovska et al
Fig 2. A-C, Spotty pigmentation around eyes and lips with several pigmented dots on lower lipand on palm. D, Two small, pink, sessile myxomas with smooth, nonulcerated surface locatedon right cheek.
pmol of each primer, 100 ng of template DNA, anddistilled water up to 25 �L. Amplification programconsisted of an initial denaturation at 958C for 15minutes, then 40 cycles of denaturation at 958C for1 minute, annealing at 608C for 1 minute, andextension at 728C for 1 minute. Program was finishedby a final extension at 728C for 7 minutes.
Amplified fragments were purified by MontagePCR Filter Units (Millipore, Billerica, MA) and se-quenced using a Big Dye Terminator SequencingKit (PE/Applied Biosystems, Foster City, CA) on anautomated sequencer ABI Prism 3130xl (PE/AppliedBiosystems) at a constant voltage of 11.3 kV for20 minutes.
After identification of an apparently novel muta-tion (see below), peripheral blood from 110 ran-domly selected healthy individuals was tested toexclude the possibility that the PRKAR1A abnormal-ity might represent a polymorphism rather than amutation.
CASE REPORTThe patient was a 40-year-old Caucasian man with
a medical history of a cardiac myxoma of the rightventricle with penetration into the pulmonary trunkwhenhewas 14 years old. Themyxomawas removed
surgically. In addition, he was diagnosed with acutaneous myxoma involving the external ear canalat the age of 30 years. He was admitted to our hospitalbecause of two newly developed heart masses lo-cated in the right ventricular chamber, which ontransthoracic echocardiography appeared as sessileor pedunculated masses measuring 1.98 3 1.78 cmand 4.87 3 2.16 cm, respectively (Fig 1, A). Surgicalexcision of both tumors was performed; histologicalexamination confirmed cardiac myxomas.
On physical examination, spotty pigmentationaround the eyes and lips and several pigmentedlesions on his lower lip were observed (Fig 2, A andB). Additionally, similar lentiginous pigmentationwas present on the palms and the palmar side ofthe fingers (Fig 2, C ). On the right cheek and temple,there were small, pink, sessile papules with smooth,nonulcerated surface (Fig 2, D); similar lesions werenoted on the left shoulder, thigh, and back. A subcu-taneous nodule measuring 3.0 3 2.5 cm was presenton the posterior aspect of the neck (Fig 3, A). A smallblue nevus was situated on the back (Fig 3, B).
Ultrasonography and computed tomography ofthe testes revealed bilateral multiple lumpy calcifi-cations (Fig 4); no tumorous mass was detected.Ultrasonography of the thyroid gland disclosed

J AM ACAD DERMATOL
VOLUME 61, NUMBER 1
Kacerovska et al 83
several hypoechogenic areas suspected as adeno-mas. Biopsy of the testes and thyroid gland was notdone.
RESULTSGross features
Grossly, both cardiac myxomas were well circum-scribed, soft, whitish, lobulated masses. On cutsection, the tumors appeared solid, homogeneous,and white with a focus of hemorrhage in the centerof the larger lesion.
Grossly, the cutaneous myxomas were 2- to 8-mmsessile papules with a gelatinous cut surface. The
Fig 3. A, Subcutaneous nodule on posterior aspect ofneck. The lesion proved to be lipoma by microscopy. B,Small blue nevus on back. C, Microscopic appearance ofthe blue nevus: highly pigmented spindle melanocytesin superficial and reticular dermis. (Hematoxylin-eosinstain.)
myxoma from the external ear canal appeared as apolypoid lesion.
Histopathologic findingsAvailable for histopathologic review were two
cardiac myxomas, 6 cutaneous myxomas includingone myxoma from the external ear canal, one bluenevus, and one lipoma.
Microscopically, both cardiac myxomas werenonencapsulated and poorly circumscribed lesions(Fig 1, B). They showed round to polygonal andstellate cells surrounded by abundant loose stromarich in acid mucopolysaccharides (Fig 1, C ), growingaround vessels. Focally, areas with a high number ofsiderophages and extravasated erythrocytes werepresent. Mitoses, pleomorphism, and areas of necro-sis were absent.
All cutaneous myxomas were relatively well-cir-cumscribed nonencapsulated lesions (Fig 5, A andB). Four of them were superficial and located in theupper dermis, one was situated deep in the reticulardermis with extension to the subcutis, and the onefrom the external ear canal was a polypoid lesion. Allwere composed of scattered polygonal, stellate,plump, and/or spindle cells with small or inconspic-uous nucleoli growing in a copious mucinous matrixcontaining small, sometimes slightly dilated blood
Fig 4. A, Computed tomography: multifocal, dispersed,and bilateral testicular calcifications in slightly atrophictesticles. B, Ultrasonography: discrete hypoechogenicityof testicle with multiple lumpy calcifications.

J AM ACAD DERMATOL
JULY 2009
84 Kacerovska et al
Fig 5. A and B, Cutaneous myxomas are relatively well-circumscribed nonencapsulatedlesions. C, All of the myxomas are composed of scattered polygonal, stellate, plump, and/orspindle cells with small or inconspicuous nucleoli growing in a copious mucinous matrixcontaining small, sometimes slightly dilated blood vessels. D, Miniature area of the mucinousstroma with a few mesenchymal cells in direct contact with a hair follicle, apparently replacingthe follicular papilla. (A-D, Hematoxylin-eosin stain.)
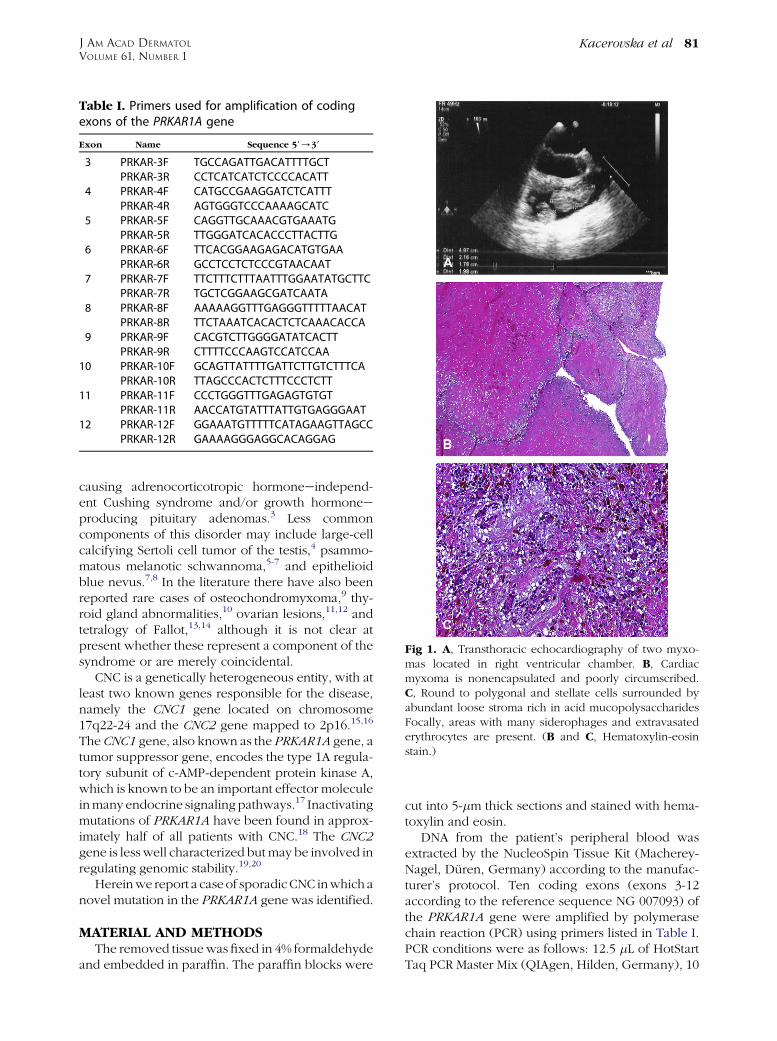
vessels (Fig 5, C ). Many cells contained pseudonu-clear inclusions. The epidermis above all but onemyxoma (the exception being the myxoma of theexternal ear canal) was unremarkable. The overlyingepithelium in the external ear canal lesion exhibitedtiny buds and interconnected strands of epithelialcells with peripheral palisading (Fig 6). Few lym-phocytes or mast cells were observed in the myxoidstroma.
In one specimen, in addition to an incipientmyxoma in the upper dermis, there was anotherminiature area of the mucinous stroma with a fewmesenchymal cells in direct contact with a hairfollicle, apparently replacing the follicular papilla(Fig 5, D).
The blue nevus (Fig 3, C ) and the lipoma showedtypical appearances.
PRKAR1A mutation analysisThewhole coding sequenceof thePRKAR1A gene,
including exon-intron junctions, was amplified, se-quenced, and compared with the reference sequence(GenBank accession number NG 007093), whichrevealed a heterozygous shift mutation c.796dupA
in exon 10 (Fig 7). This mutation leads to a frameshiftstarting at threonine 266 and creating a new stopcodon (UGA) at position 269 (p.Thr266AsnfsX4). Inaddition, the peripheral blood of both parents of thepatient (aged 66 and68) andhis twobrothers (aged45and 30), none of whom showed clinical features ofCNC, was studied for PRKAR1A mutation, but noalteration was found.
DISCUSSIONThe clinical features of the patient fulfilled the
diagnostic criteria of CNC (Table II).21 He had spottypigmentation of the skin at typical sites, multiplecutaneousmyxomas, and cardiacmyxomas. Locationof the myxomas involving the external auditory canalare very specific for this syndrome. Additionally,multiple testicular calcifications were found. Theseare included in the criteria for CNC. The calcificationsmay be found in coexistence with a large-cell calci-fying Sertoli cell tumor or they may occur separatelyin the testes in the absence of this tumor.9,22-25
Testicular microcalcifications set within scarred stro-mal tissue may also represent remnants of regressedgerm cell tumors, especially choriocarcinomas,
J AM ACAD DERMATOL
VOLUME 61, NUMBER 1
Kacerovska et al 85
which should be taken into consideration whenconstructing the differential diagnosis.26,27
The histologic picture of all tumors in our patientwas typical, including the epithelial proliferations inthe lesion that came from the external ear canal.25 Aninteresting feature was the presence of an incipientmyxoma in the vicinity of a hair follicle, with thespecific stroma of the follicular papilla seeminglyreplaced by the myxomatous elements that appearedto be part of the myxoma (see Fig 5, D). Althoughmucin can occasionally be recognized in otherwisenormal follicular papillae, never has this feature hadsuch a prominent presentation. We believe that theassociation of myxomas and hair follicle differentia-tion in CNC is not a simple coincidence and thesignificance of this association maybe under-recog-nized. Although commonly referred to as ‘‘epithelialcomponents,’’ these epithelial proliferations, on
Fig 6. A-C, In external ear canal lesion, overlying epithe-lium exhibits tiny buds and interconnected strands ofepithelial cells with peripheral palisading. (A-C, Hematox-ylin-eosin stain.)
scrutiny, often evidence various features that canbe interpreted as signs of follicular differentiationtoward the follicular germ, trichogenic stroma, in-cluding follicular papilla, isthmus, infundibulum,and mantle.19,25,28,29
Application of a rigorous screening protocol forall first-degree relative of patients affected with CNSshowed an increase in a number of familial cases.In a recent review, Stratakis, Kirschner, and Carney21
identified 338 patients with CNC reported world-wide, a majority of whom (70%) belonged to 67affected families, whereas only 88 individuals had noknown affected relative. The authors suggested thatsome familial cases may have gone unrecognized,resulting in an ‘‘increase’’ of ‘‘sporadic’’ cases. Theclinical variability of the disease and the small size ofaffected CNC families because of infertility arethought to contribute to this under-recognition.
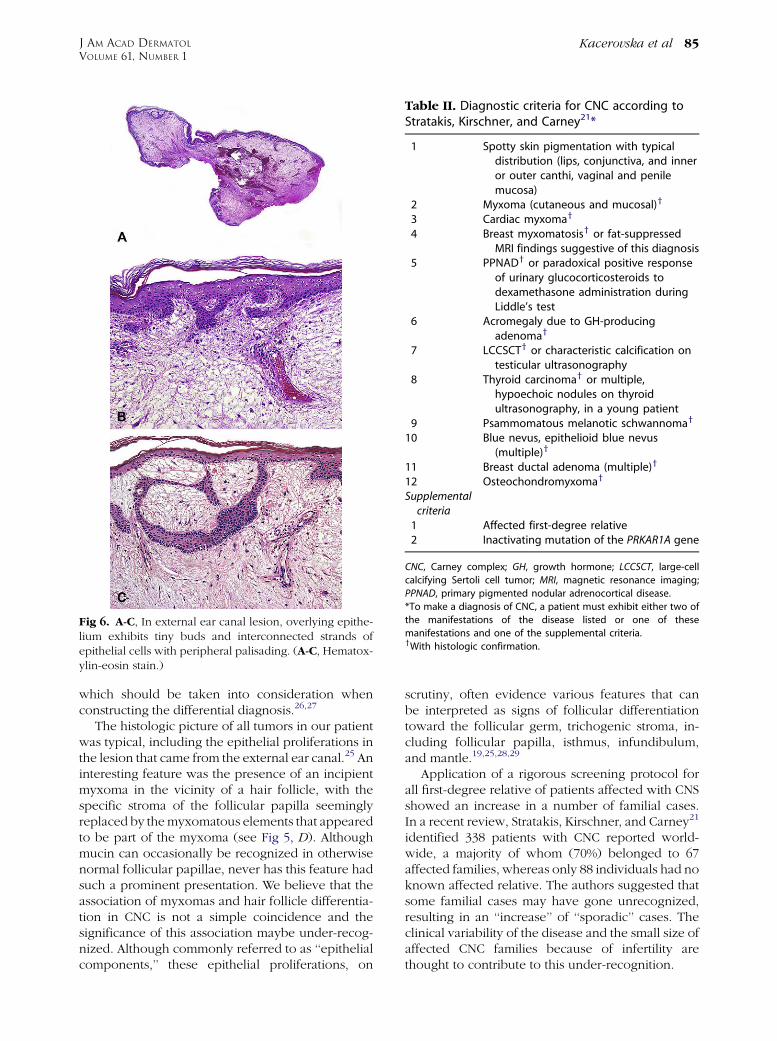
Table II. Diagnostic criteria for CNC according toStratakis, Kirschner, and Carney21*
1 Spotty skin pigmentation with typicaldistribution (lips, conjunctiva, and inneror outer canthi, vaginal and penilemucosa)
2 Myxoma (cutaneous and mucosal)y
3 Cardiac myxomay
4 Breast myxomatosisy or fat-suppressedMRI findings suggestive of this diagnosis
5 PPNADy or paradoxical positive responseof urinary glucocorticosteroids todexamethasone administration duringLiddle’s test
6 Acromegaly due to GH-producingadenomay
7 LCCSCTy or characteristic calcification ontesticular ultrasonography
8 Thyroid carcinomay or multiple,hypoechoic nodules on thyroidultrasonography, in a young patient
9 Psammomatous melanotic schwannomay
10 Blue nevus, epithelioid blue nevus(multiple)y
11 Breast ductal adenoma (multiple)y
12 Osteochondromyxomay
Supplementalcriteria
1 Affected first-degree relative2 Inactivating mutation of the PRKAR1A gene
CNC, Carney complex; GH, growth hormone; LCCSCT, large-cell
calcifying Sertoli cell tumor; MRI, magnetic resonance imaging;
PPNAD, primary pigmented nodular adrenocortical disease.
*To make a diagnosis of CNC, a patient must exhibit either two of
the manifestations of the disease listed or one of these
manifestations and one of the supplemental criteria.yWith histologic confirmation.

J AM ACAD DERMATOL
JULY 2009
86 Kacerovska et al
Fig 7. Heterozygous shift mutation c.796dupA in exon 10 of PRKAR1A gene using forwardprimer.
Mutations in the PRKAR1A gene have been iden-tified in approximately 65% of the CNC patients,in both familial and sporadic cases.18 In our case,we detected a novel heterozygous shift mutationc.796dupA in exon 10 of the PRKAR1A gene. Thismutation leads to a frameshift creating a new stopcodon. The biologic effect of this mutation is pro-duction of a truncated and probably inactive protein.To our knowledge, this mutation has not beendescribed. Neither was this alteration detected in110 unrelated healthy individuals we investigated.The parents and two brothers of the patient had noclinical features of CNC, and the analysis of theirblood for PRKAR1A mutations showed no alteration,thus indicating that our patient had a sporadic formof the disease.
In summary, we have described a sporadic case ofCNC, with a novel mutation in exon 10 of thePRKAR1A gene, with typical clinical features includ-ing cardiac myxomas, cutaneous myxomas, a bluenevus, and multiple testicular calcifications.
REFERENCES
1. Rees JR, Ross FG, Keen G. Lentiginosis and left atrial myxoma.
Br Heart J 1973;35:874-6.
2. Carney JA, Gordon H, Carpenter PC, Shenoy BV, Go VL. The
complex of myxomas, spotty pigmentation, and endocrine
overactivity. Medicine (Baltimore) 1985;64:270-83.
3. Carney DF, Koski CL, Shin ML. Elimination of terminal com-
plement intermediates from the plasma membrane of nucle-
ated cells: the rate of disappearance differs for cells carrying
C5b-7 or C5b-8 or a mixture of C5b-8 with a limited number of
C5b-9. J Immunol 1985;134:1804-9.
4. Washecka R, Dresner MI, Honda SA. Testicular tumors in
Carney’s complex. J Urol 2002;167:1299-302.
5. Carney JA. Psammomatous melanotic schwannoma. A distinc-
tive, heritable tumor with special associations, including
cardiac myxoma and the Cushing syndrome. Am J Surg Pathol
1990;14:206-22.
6. Martin-Reay DG, Shattuck MC, Guthrie FW Jr. Psammomatous
melanotic schwannoma: an additional component of Carney’s
complex. Report of a case. Am J Clin Pathol 1991;95:484-9.
7. Carney JA, Stratakis CA. Epithelioid blue nevus and psammo-
matous melanotic schwannoma: the unusual pigmented skin
tumors of the Carney complex. Semin Diagn Pathol 1998;15:
216-24.
8. Carney JA, Ferreiro JA. The epithelioid blue nevus. A multi-
centric familial tumor with important associations, including
cardiac myxoma and psammomatous melanotic schwannoma.
Am J Surg Pathol 1996;20:259-72.
9. Carney JA, Boccon-Gibod L, Jarka DE, Tanaka Y, Swee RG, Unni
KK, et al. Osteochondromyxoma of bone: a congenital tumor
associated with lentigines and other unusual disorders. Am J
Surg Pathol 2001;25:164-76.
10. Stratakis CA, Courcoutsakis NA, Abati A, Filie A, Doppman JL,
Carney JA, et al. Thyroid gland abnormalities in patients with
the syndrome of spotty skin pigmentation, myxomas, endo-
crine overactivity, and schwannomas (Carney complex). J Clin
Endocrinol Metab 1997;82:2037-43.
11. Cohen C, Turner ML, Stratakis CA. Pigmented lesions of the
conjunctiva in Carney’s complex. J Am Acad Dermatol 2000;
42:145.
12. Papageorgiou T, Stratakis CA. Ovarian tumors associated with
multiple endocrine neoplasias and related syndromes (Carney
complex, Peutz-Jeghers syndrome, von Hippel-Lindau disease,
Cowden’s disease). Int J Gynecol Cancer 2002;12:337-47.
13. Akbas H, Kirali K, Daglar B, Kutay V, Isik O, Yakut C. Surgical
treatment of left-atrial myxoma in Carney’s complex. Thorac
Cardiovasc Surg 1997;45:148-50.
14. Yarman S, Gurbuz L, Tanakol R, Kapran Y, Alagol F. Association
of Fallot tetralogy with Carney’s complex. Ir Med J 2001;94:
305-7.
15. Stratakis CA, Carney JA, Lin JP, Papanicolaou DA, Karl M, Kastner
DL, et al. Carney complex, a familial multiple neoplasia and
lentiginosis syndrome. Analysis of 11 kindreds and linkage to
the short arm of chromosome 2. J Clin Invest 1996;97:699-705.
16. Casey M, Mah C, Merliss AD, Kirschner LS, Taymans SE, Denio
AE, et al. Identification of a novel genetic locus for familial
cardiac myxomas and Carney complex. Circulation 1998;98:
2560-6.
17. Sassone-Corsi P. Coupling gene expression to cAMP signal-
ling: role of CREB and CREM. Int J Biochem Cell Biol 1998;30:
27-38.
18. Kirschner LS, Carney JA, Pack SD, Taymans SE, Giatzakis C,
Cho YS, et al. Mutations of the gene encoding the protein
kinase A type I-alpha regulatory subunit in patients with the
Carney complex. Nat Genet 2000;26:89-92.
19. LeBoit PE, Gunter B, Weedon D, Sarasin A. Pathology &
Genetics Skin Tumours. World Health Organization Classifica-
tion of Tumours. Lyon: IARC Press; 2006.
20. Matyakhina L, Pack S, Kirschner LS, Pak E, Mannan P, Jaikumar J,
et al. Chromosome 2 (2p16) abnormalities in Carney complex
tumours. J Med Genet 2003;40:268-77.
21. Stratakis CA, Kirschner LS, Carney JA. Clinical and molecular
features of the Carney complex: diagnostic criteria and
recommendations for patient evaluation. J Clin Endocrinol
Metab 2001;86:4041-6.
22. Kennedy RH, Waller RR, Carney JA. Ocular pigmented spots
and eyelid myxomas. Am J Ophthalmol 1987;104:533-8.
23. Grossniklaus HE, McLean IW, Gillespie JJ. Bilateral eyelid
myxomas in Carney’s complex. Br J Ophthalmol 1991;75:
251-2.
24. Palva T, Saksela E, Ramsay H. Myxoma of the external auditory
meatus. J Laryngol Otol 1991;105:364-6.
25. Ferreiro JA, Carney JA. Myxomas of the external ear and their
significance. Am J Surg Pathol 1994;18:274-80.

J AM ACAD DERMATOL
VOLUME 61, NUMBER 1
Kacerovska et al 87
26. Azzopardi JG, Mostofi FK, Theiss EA. Lesions of testes
observed in certain patients with widespread choriocarcinoma
and related tumors. The significance and genesis of hematox-
ylin-staining bodies in the human testis. Am J Pathol 1961;38:
207-25.
27. Renshaw AA. Testicular calcifications: incidence, histology and
proposed pathological criteria for testicular microlithiasis.
J Urol 1998;160:1625-8.
28. Carney JA, Headington JT, Su WP. Cutaneous myxomas. A
major component of the complex of myxomas, spotty pig-
mentation, and endocrine overactivity. Arch Dermatol 1986;
122:790-8.
29. Bennett KR, Heath BJ, Creswell LL, Veugelers MA, McDermott
DA, Barksdale S, et al. The Carney complex: unusual skin
findings and recurrent cardiac myxoma. Arch Dermatol 2005;
141:916-8.
Top Related
Copyright © 2022 FDOKUMEN

