







Bahasa
Halaman
Hukum


Assessing cost-effectiveness of drug interventions for schizophrenia
Anne Magnus, Vaughan Carr, Cathrine Mihalopoulos, Rob Carter, Theo Vos
Objective:
To assess from a health sector perspective the incremental cost-effectiveness ofeight drug treatment scenarios for established schizophrenia.
Method:
Using a standardized methodology, costs and outcomes are modelled over thelifetime of prevalent cases of schizophrenia in Australia in 2000. A two-stage approach toassessment of health benefit is used. The first stage involves a quantitative analysis basedon disability-adjusted life years (DALYs) averted, using best available evidence. Therobustness of results is tested using probabilistic uncertainty analysis. The second stageinvolves application of ‘second filter’ criteria (equity, strength of evidence, feasibility andacceptability) to allow broader concepts of benefit to be considered.
Results:
Replacing oral typicals with risperidone or olanzapine has an incremental cost-effectiveness ratio (ICER) of A$48 000 and A$92 000/DALY respectively. Switching fromlow-dose typicals to risperidone has an ICER of A$80 000. Giving risperidone to peopleexperiencing side-effects on typicals is more cost-effective at A$20 000. Giving clozapine topeople taking typicals, with the worst course of the disorder and either little or cleardeterioration, is cost-effective at A$42 000 or A$23 000/DALY respectively. The least cost-effective intervention is to replace risperidone with olanzapine at A$160 000/DALY.
Conclusions:
Based on an A$50 000/DALY threshold, low-dose typical neuroleptics areindicated as the treatment of choice for established schizophrenia, with risperidone beingreserved for those experiencing moderate to severe side-effects on typicals. The moreexpensive olanzapine should only be prescribed when risperidone is not clinically indicated.The high cost of risperidone and olanzapine relative to modest health gains underlie thisconclusion. Earlier introduction of clozapine however, would be cost-effective. This work islimited by weaknesses in trials (lack of long-term efficacy data, quality of life and consumersatisfaction evidence) and the translation of effect size into a DALY change. Somestakeholders, including SANE Australia, argue the modest health gains reported in theliterature do not adequately reflect perceptions by patients, clinicians and carers, of improvedquality of life with these atypicals.
Key words:
Australian and New Zealand Journal of Psychiatry 2005; 39:44–54
clozapine, DALY, olanzapine, outcomes, risperidone, side-effects.
Schizophrenia involves multiple disturbances of psy-chological processes and runs an episodic or chroniccourse. It can cause major disruption to a person’s and
their family’s well-being and lifestyle, and carries con-siderable risk of premature mortality [1]. Drug treatmentof schizophrenia aims to reduce the severity, duration
Anne Magnus, Epidemiologist (Correspondence); Theo Vos, Senior Epi-demiologist
Health Surveillance and Evaluation Section, Public Health, Departmentof Human Services, Level 18, 120 Spencer St, Melbourne Vic. 3000,Australia. Email: [email protected]
Vaughan Carr, Professor, Director
Centre for Mental Health Studies, University of Newcastle, Australia
Cathrine Mihalopoulos, Senior Research Fellow (Health Economics); RobCarter, Associate Professor, (Health Economics) Deputy Director
Program Evaluation Unit, School of Population Health, University ofMelbourne, Melbourne, Australia
Received 17 October 2003; revised 26 June 2004; accepted 4 September2004.

A. MAGNUS, V. CARR, C. MIHALOPOULOS, R. CARTER, T. VOS 45
and frequency of psychotic symptoms, and the associ-ated levels of disability and mortality. Because of thenature of the disease, its early onset and low remissionrate, the lifetime costs are substantial [2]. Neurolepticmedication is a central element in the treatment ofschizophrenia [3]. However, the use of such medicationshas been linked with disabling side-effects [1]. The long-term management of schizophrenia includes optimalmedication, balancing the risk of relapse against theprofile of side-effects, together with appropriate psycho-social interventions, rehabilitation and social support.Drugs such as clozapine, risperidone and olanzapinehave raised expectations of improved patient outcomeswith reduced side-effect profiles, particularly extra-pyramidal symptoms, but at much higher cost. Clinicalpractice guidelines in Australia and overseas [4,5]recommend the newer drugs as first-line treatment forpatients with schizophrenia, relying on both expertopinion and limited trial evidence. However, the ques-tion arises as to whether the quality of life benefits ofthe newer drugs are sufficient to justify their additionalcost relative to traditional neuroleptics. This analysis hasbeen undertaken as part of the Assessing Cost Effective-ness – Mental Health (ACE-MH) project, funded by theAustralian Department of Health and Ageing, MentalHealth and Suicide Prevention Branch and the Depart-ment of Human Services, Mental Health Branch, Vic-toria. The project aim is to assess the options for changethat could improve the effectiveness and efficiency ofAustralia’s current mental health services by directingavailable resources toward ‘best practice’ cost-effectiveservices.
Method
All analyses undertaken in ACE-MH adhere to a detailed economicprotocol specifically designed for the study [6]. Briefly, the perspectiveis that of the health sector. Current practice is the comparator. The timehorizon is the remaining lifetime of prevalent cases of schizophreniaand related conditions in Australia in the year 2000. Discounting at 3%for both costs and benefits is incorporated. Benefits are measured indisability-adjusted life years (DALYs), an outcome measure combin-ing years of life lost to premature mortality (YLL) and years lived withdisability (YLD).
Schizophrenia is defined by ICD-10 codes and includes paranoid,hebephrenic, catatonic, undifferentiated, schizoaffective, delusionaldisorder and other non-organic nonaffective psychotic disorders. Wemodel the prevalent cases of schizophrenia by five-year age groups andsex, through a Markov model of annual cycles with relevant hazardsand marginal costs, until the whole cohort has died or reached100 years of age. The main benefits from the drug interventions comefrom differences in YLD calculated for each cycle by changing disa-bility weights.
Interventions
We model eight alternative interventions for people diagnosed withschizophrenia. Target groups differ depending on the intervention. Ris-peridone (5 mg/day) is evaluated as a replacement for oral typicalneuroleptics, for people with and without significant side-effects, andseparately, in comparison to taking low-dose typicals (< 300 chlor-promozine equivalents). Olanzapine (15 mg/day) is evaluated as areplacement for oral typical neuroleptics, for people with and withoutsignificant side-effects, and for those taking risperidone. Clozapine(400 mg/day) is evaluated for treatment-resistant cases (those identifiedas having a chronic course of disorder with either little or clear deterior-ation), taking typical neuroleptics.
Current practice
The treatment regimens and disability level of the prevalent casesof schizophrenia are extracted from the database of the 1997/98 LowPrevalence (Psychotic) Disorders Study (LPDS). The averagelength of illness in those surveyed was 15 years (range 0–54 years).A detailed account of the design and methods of the LPDS has beenpublished elsewhere [7]. The LPDS surveyed people in contact withspecialist mental health services in Australia in 1997/98, and under-represented community samples of people with schizophreniamanaged solely by general practitioners (GPs). A small communitystudy [8] estimated that the latter comprises about one in threepeople with schizophrenia in the population. We adjust for theundersampling by expanding the subsample of solely GP-managedschizophrenia cases from 3% to 33% of the total survey records. Weestimate there were 37 000 Australians in the year 2000 affected bythe condition [2,7]. We assume 1.5% remission rate based on themedian annualized remission rate reported in several longitudinalstudies [9–13]. Of the adjusted LPDS respondents, 20% of male and35% of female respondents were taking oral typical neurolepticsalone. Baseline adherence levels for people taking typical neuro-leptics are modelled at 54%, determined from community studies[14,15]. We derive a raised baseline general mortality risk forschizophrenia, retaining the age and sex pattern, from AustralianBureau of Statistics (ABS) mortality statistics with and withoutmention of schizophrenia for 1999, while constraining the relativerisk of all-cause mortality for ages 15+, to 1.56, as reported from ameta-analysis [16].
The reader is referred to Haby
et al
. [6] for the full rationale,description and distribution of the disability scores of the LPDSrespondents, which are used to indicate the baseline severity levels inthe eligible population. In short, severity was measured by interview inthe LPDS using six selected items from the WHO Disability Assess-ment Schedule (DAS), the Lancashire Quality of Life Profile andthe Social Contact Questionnaire, plus two questions capturing therespondents’ self-rating of satisfaction with independence and with lifein general [17]. Assuming a linear relationship between the disabilityscores in the survey (ranging from 0 best to 16 worst) and extremevalues of the four disability weights (DW) used in the Dutch Burdenof Disease study [18], we derive a DW for each of the LPDS respond-ents (ranging from 0.21 for the mildest health state to 0.96 for theworst).

46 COST-EFFECTIVENESS OF DRUGS FOR SCHIZOPHRENIA
Assessment of benefit
Benefits are calculated using a two-stage process. The first stageinvolves the estimation of the health gain that could be attributed toeach intervention using the disability-adjusted life year (DALY). Thesecond stage involves the assessment of issues that either influencethe degree of confidence that can be placed in the cost-effectivenessratios or broader issues that need to be taken into account in decision-making about resource allocation in mental health.
Stage one: measurement of health gain
We scrutinized systematic reviews and more recent randomizedcontrolled trials published in peer reviewed journals up to 2002, forevidence of differences in quality of life, short- and long-term side-effects of medication, compliance change, symptom reduction andweight gain, under each of the eight intervention scenarios [19–26].
Symptom reduction
Consistent with other ACE-MH analyses, we summarize the impactof each intervention on severity of psychotic symptoms using the effectsize (Hedge’s g) [27], which relies on the reporting of continuousoutcome measures. The outcome measures used to determine thepooled effect size differ by study and most commonly include the BriefPsychiatric Rating Scale (BPRS), Positive and Negative SyndromeScale (PANSS) and Clinical Global Impression Scale (CGI). First weaverage effect size within studies, and then pool them across studiesusing the random effects method of DerSimonian and Laird [27]. Thepooled effect size is translated into a DW change by each of the twomethods referred to as the ‘Conversion Factor’ (CF) method and the‘Survey Severity’ (SS) method described elsewhere [6]. The results ofthe two methods are combined and taken into account in the uncertaintyanalysis as a reflection of the lack of established practice in translatinghealth outcomes relevant to cost-utility studies of schizophrenia.
Side-effects
The impact of the change in side-effects due to a switch in medica-tion is estimated separately and translated into an additional change in
DW. We determine the proportion of people reporting moderate orsevere impairment in daily life due to medication in the LPDS fromtheir response to the question: ‘How much has everyday life beenaffected by these medication-related side-effects?’ We calculate themean DW based on the disability score as described above, in respond-ents on typical medication with no or mild (0.32), moderate (0.42) andsevere (0.45) problems due to side-effects. We assume these dif-ferences in DW reflect the additional disability due to side-effects.The change in health benefit due to side-effects is then determined bythe difference in the proportions reporting moderate and severe side-effects on different drug regimens in the LPDS.
For clozapine, we model no difference in disability due to haemato-logical side-effects as the mandatory frequent blood checks ensurepatients are taken off the drug before more serious illness ensues.
Weight gain
We include an estimate of the mortality and morbidity risks associ-ated with weight gain. From a number of studies of the impact of weightgain on ischaemic heart disease, ischaemic stroke, diabetes mellitus andcolorectal cancer [28–31] we derive a relative risk of mortality orincidence per kilo of weight gain. The mean relative risks range from1.03 for colon cancer, 1.04 for ischaemic heart disease and stroke, to1.11 for diabetes. The disability from diseases associated with weightgain is extrapolated from the ratio of morbidity to mortality ratio forthese conditions, in the 1996 Burden of Disease estimates [32].
Suicide
We found evidence for a reduction in suicide risk (by 50%) forpatients on clozapine [33], but not for any of the other drugs.
Adherence
From differences in the published rates of leaving trials early, wedetermine the difference in adherence between drug regimens. If com-pliance levels improve with the intervention, we model that the compa-rator for the additional compliers, is no neuroleptic medication,resulting in a greater effect size (as assessed in trials of neurolepticsagainst placebo) and DW change. The modelled components of DWchange and the effect sizes for each intervention appear in Table 1.
Table 1. Determination of disability weight change by intervention
Intervention Effect size (SE) Improvement due to symptom
reduction
Improvement due to side-effect profile
Combined improvement in Disability weight (95% CI)
Risperidone
vs
typicals 0.219 (0.09) 0.033 0.010 0.043 (0.018–0.079)Risperidone
vs
typicals with side-effects 0.219 (0.09) 0.031 0.073 0.105 (0.077–0.142)Risperidone
vs
low dose typicals 0.126 (0.118) 0.019 0.008 0.027 (–0.001–0.060)Olanzapine
vs
typicals 0.251 (0.079) 0.038 0.010 0.046 (0.027–0.078)Olanzapine
vs
typicals with side-effects 0.251 (0.079) 0.038 0.073 0.109 (0.086–0.143)Olanzapine
vs
risperidone 0.096 (0.095) 0.015 0.0 0.015 (–0.014–0.046)Clozapine
vs
typicals little deterioration 0.416 (0.107) 0.064 0.007 0.071 (0.042–0.131)Clozapine
vs
typicals clear deterioration 0.63 (0.163) 0.104 0.010 0.109 (0.065–0.188)
CI, confidence interval; SE, standard error.

A. MAGNUS, V. CARR, C. MIHALOPOULOS, R. CARTER, T. VOS 47
Stage two: the second filter criteria
As with other ACE-MH analyses, apart from the cost-effectivenessof results, we take four second filter criteria into account: level ofevidence; equity; acceptability to stakeholders; and feasibility afterconsultation with Steering Committee members [6].
Costs of intervention
The marginal cost of changing from one medication regimen toanother is calculated using year 2000 prices. Cost-offsets are not fac-tored into the analyses because we were unable to determine a fall inresource utilization associated with a reduction of illness severity dueto a particular intervention. We investigated the potential costs of psy-chotic relapse versus the costs of people diagnosed with psychosis whodo not relapse in Australia in the LPDS by regressing illness severityagainst resource utilization. None of the proxy variables for illnessseverity predicts resource utilization. SOFAS scores, DWs anddiagnostic categories in the survey, each predict less than 5% of thevariation in health service utilization, whether inpatient or outpatientcare. The number of GP visits or contacts with mental health teams isassumed constant, except for the clozapine intervention which requiresweekly blood tests for the first 18 weeks, and monthly thereafter. Unitcost data sources and assumptions are shown in Table 2. Costs thatwould have been incurred under current practice are subtracted fromthe intervention costs to obtain the incremental cost.
Uncertainty analysis
We perform Monte Carlo simulation-modelling techniques using the@RISK Software (Palisade, 4.0) Newfield, NY and present uncertaintyranges as well as point estimates for benefits and cost-effectivenessratios that reflect all the main sources of uncertainty in the calculations.Parameters and distributions for the uncertainty assumptions of oneintervention as an example, appear in Table 3. The probability distribu-tions around the input variables are based on: (i) standard errors quoted
in, or calculated from, the literature; (ii) a range of parameter valuesquoted in, or calculated from, the literature; or (iii) expert advice. Allresults are presented to two significant digits.
Results
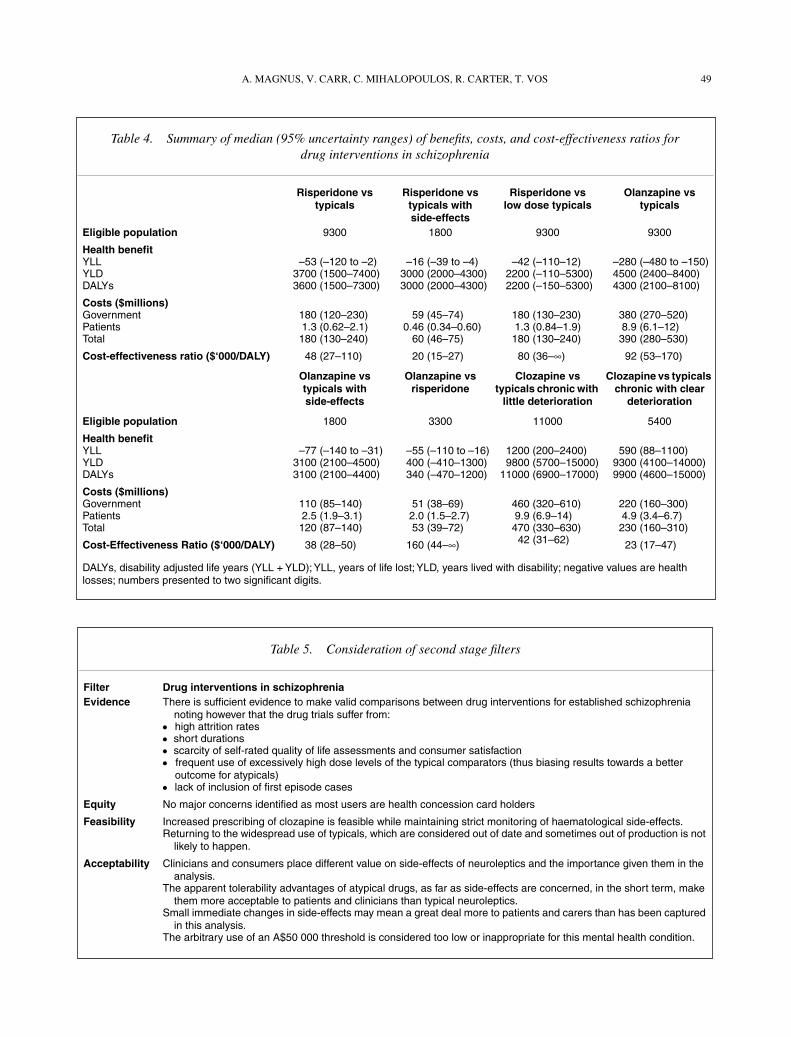
To change all people taking oral typicals to risperidone has anincremental cost-effectiveness ratio (ICER) of A$48 000 (Table 4). Tochange people taking oral typicals to olanzapine has an ICER ofA$92 000. Limiting the change to only those people taking typicalswith side-effects yields an ICER of A$20 000 for risperidone andA$38 000 for olanzapine. The ICER of changing those people currentlytaking low-dose typicals to risperidone is A$80 000. Changing thepeople currently taking risperidone to olanzapine has an ICER ofA$160 000. Giving clozapine to people with the worst course of thedisorder taking typicals, results in an ICER of A$42 000 and A$23 000depending on their subclassification in the LPDS on levels of functionaldeterioration (little or clear), respectively. Consideration of the secondstage filters for these interventions is shown in Table 5. Acceptabilityto stakeholders of a reduction in the use of atypicals emerged as the keyconcern in this analysis.
Discussion
Replacing typical neuroleptics with risperidone fallsjust below the ‘value for money’ threshold of A$50 000per DALY, which is used in all ACE-MH analyses. If thecomparison is made against low doses of typical neuro-leptics, a change to risperidone is less cost-effective atA$80 000. For those on typicals with significant side-effects, risperidone is cost-effective at A$20 000. However,to extend risperidone from those patients on typicals exper-iencing side-effects to include all the remaining patientson typicals has an ICER of A$120 000. Results for olan-zapine are less favourable. While providing olanzapine
Table 2. Summary of annual unit costs, data sources and assumptions
Element costed Cost to government
Cost to patient
Assumptions
Oral typical medications $116 $43 The surveyed mix of typicals on the LPDS is current practice.Risperidone (5 mg/day) $2185 $65 Script volumes and costs to government and patient on the PBS and
RPBS were provided by DHA for financial year 1999/2000.Olanzapine (15 mg/day) $4085 $140 Recommended daily doses taken from Carr
et al
. [50]Clozapine (400 mg/day) $3732 $107Cogentin (4 mg/day) $50 $35 28.5% of people using oral typicals use anticholinergic medication
compared to 10% of those taking risperidone [51]Blood testing for clozapine: 95% of blood testing in Victoria is performed out of hospital for which
AMHS take responsibility. Includes 15 mins of psychiatric nurse (RPN Grade 2–4), and psychiatrist (at Specialist to Senior Specialist year 5) time. Advice provided by Mental Health Branch.
– first year $1079 $67– subsequent years $501 $31
PBS, Pharmaceutical Benefit Scheme; RPBS, Repatriation Pharmaceutical Benefit Scheme; DHA, Australian Department of Health and Ageing; LPDS, Low Prevalence Disorders Study; AMHS, Area Mental Health Services; RPN, registered nurse.

48 COST-EFFECTIVENESS OF DRUGS FOR SCHIZOPHRENIA
to patients with side-effects on typicals costs A$38 000per DALY, the true decision-making issue is what theadded benefits are relative to the greater cost of prescrib-ing olanzapine rather than risperidone. As the additionalbenefits are very small and the cost difference great,olanzapine should never be chosen on cost-effectivenessgrounds. Similarly, choosing to switch patients currentlyon risperidone to olanzapine is not cost-effective(A$120 000) and should not be considered unless thereis a compelling clinical indication. The use of clozapine inpreference to typical neuroleptics for patients with themore severe course of illness is a cost-effective interven-tion and this suggests that earlier identification and treat-ment of these patients with clozapine is warranted. Theextensive uncertainty modelling which has provided rangesrather than point estimates for these cost-effectivenessratios indicates that the above conclusions are justifieddespite the difficulties in estimation.
We have relied heavily on the evidence providedin Cochrane systematic reviews of drug interventions inschizophrenia because randomized controlled trials are
the ‘gold standard’ in comparisons of relative drugefficacy. To this was added more recent trial evidencewhere available. Where evidence is missing we havechosen to highlight research gaps rather than use lowerlevel evidence for efficacy. This is in contrast torecently developed clinical practice guidelines [4,5].
The trials reviewed and included in this report sufferedin several ways that limit their usefulness for this analy-sis. First, schizophrenia drug trials are characterized byvery high drop-out rates that can severely limit theirconclusions. Second, none of the included trials measurepatient-rated quality of life. Clinician-rated quality oflife measures were undertaken in some trials [34–36].Hamilton [34] found significant between-treatment dif-ferences in favour of olanzapine in some subscales of theQLS instrument, but importantly not in the total scores.A non-randomised observational study [37] comparingthe atypicals of interest in this paper to typicals, whileshowing some advantages in subjective tolerability onsome scales for the atypicals, is prone to selection biasand would need to be repeated in well-designed RCTs
Table 3. Uncertainty parameters and sources used in the analysis specific to schizophrenia
Parameter Uncertainty distribution SourcePrevalence and current practice
Remission rate Uniform (0.01, 0.02) Calculated from long-term follow-up studies [9–13,52]:
Disability weight Conversion factor Uniform (0.158, 0.204) [53]Disease prevalence – male Triangular (0.0016, 0.0023, 0.0031) Dismod
±
30% assumed [7]Disease prevalence – female Triangular (0.0010, 0.0015, 0.0019) Dismod
±
30% assumedBaseline adherence all typical neuroleptics users Normal (54%, 5%) [54]Baseline adherence risperidone Triangular (48%,60%,71%) [54]Percent on typicals with moderate side-effects Triangular (12.7%, 15.0%, 17.3%) Analysis of LPDSPercent on typicals with severe side-effects Triangular (8.1%, 10.0%, 11.9%) Analysis of LPDSPercent on atypicals with moderate side-effects Triangular (7.1%, 9.0%, 10.9%) Analysis of LPDSPercent on atypicals with severe side-effects Triangular (4.5%, 6.0%, 7.5%) Analysis of LPDSRelative risk of a person on typicals with side-effects also
getting side-effects on atypicalsTriangular (1,1.5,2) Expert opinion of steering
committee membersPercent of persons on typicals taking low dose (< 300 cpz
equivalents/day)70% Analysis of BEACH [55] and
unpublished EPPIC resource use data
Relative risk per kilo weight gain – diabetes Triangular (1.07, 1.11, 1.14) Analysis based on [31]Relative risk per kilo weight gain – colorectal cancer Triangular (1.01, 1.03, 1.05) Analysis based on [30]Relative risk per kilo weight gain – ischaemic heart
diseaseTriangular (1.02, 1.04, 1.06) Analysis based on [28]
Relative risk per kilo weight gain – ischaemic stroke Triangular (1.02, 1.04, 1.05) Analysis based on [29]
Health benefit: example intervention – risperidone compared to typicals
†
Additional adherence Normal (9%, 4%) Drop out rates in trials [21]Reduction in cogentin use Triangular (–0.09, –0.18, –0.26) [51,56]Effect size Normal (0.219, 0.09) [21]Effect size of additional compliers with intervention Normal (0.496, 0.089) [57]Weight gain in those adherent to typicals Normal (0.5, 0.35) [58]Weight gain in additional compliers Normal (2.1, 0.21) [58]
†
Detailed assumptions of other interventions available from the authors; Normal, RiskNormal (mean, standard error); Triangular, RiskTriang (minimum, mean, maximum); Uniform, RiskUniform (minimum, maximum); BEACH, Bettering the Evaluation and Care of Health; EPPIC, Early Psychosis Prevention and Intervention Centre.
A. MAGNUS, V. CARR, C. MIHALOPOULOS, R. CARTER, T. VOS 49
Table 4. Summary of median (95% uncertainty ranges) of benefits, costs, and cost-effectiveness ratios for drug interventions in schizophrenia
Risperidone vs typicals
Risperidone vs typicals with side-effects
Risperidone vs low dose typicals
Olanzapine vs typicals
Eligible population
9300 1800 9300 9300
Health benefit
YLL –53 (–120 to –2) –16 (–39 to –4) –42 (–110–12) –280 (–480 to –150)YLD 3700 (1500–7400) 3000 (2000–4300) 2200 (–110–5300) 4500 (2400–8400)DALYs 3600 (1500–7300) 3000 (2000–4300) 2200 (–150–5300) 4300 (2100–8100)
Costs ($millions)
Government 180 (120–230) 59 (45–74) 180 (130–230) 380 (270–520)Patients 1.3 (0.62–2.1) 0.46 (0.34–0.60) 1.3 (0.84–1.9) 8.9 (6.1–12)Total 180 (130–240) 60 (46–75) 180 (130–240) 390 (280–530)
Cost-effectiveness ratio ($‘000/DALY)
48 (27–110) 20 (15–27) 80 (36–
∞
) 92 (53–170)
Olanzapine vs typicals with side-effects
Olanzapine vs risperidone
Clozapine vs typicals chronic with
little deterioration
Clozapine vs typicals chronic with clear
deterioration
Eligible population
1800 3300 11000 5400
Health benefit
YLL –77 (–140 to –31) –55 (–110 to –16) 1200 (200–2400) 590 (88–1100)YLD 3100 (2100–4500) 400 (–410–1300) 9800 (5700–15000) 9300 (4100–14000)DALYs 3100 (2100–4400) 340 (–470–1200) 11000 (6900–17000) 9900 (4600–15000)
Costs ($millions)
Government 110 (85–140) 51 (38–69) 460 (320–610) 220 (160–300)Patients 2.5 (1.9–3.1) 2.0 (1.5–2.7) 9.9 (6.9–14) 4.9 (3.4–6.7)Total 120 (87–140) 53 (39–72) 470 (330–630) 230 (160–310)
Cost-Effectiveness Ratio ($‘000/DALY)
38 (28–50) 160 (44–
∞
) 42 (31–62) 23 (17–47)
DALYs, disability adjusted life years (YLL + YLD); YLL, years of life lost; YLD, years lived with disability; negative values are health losses; numbers presented to two significant digits.
Table 5. Consideration of second stage filters
Filter Drug interventions in schizophreniaEvidence
There is sufficient evidence to make valid comparisons between drug interventions for established schizophrenia noting however that the drug trials suffer from:
●
high attrition rates
●
short durations
●
scarcity of self-rated quality of life assessments and consumer satisfaction
●
frequent use of excessively high dose levels of the typical comparators (thus biasing results towards a better outcome for atypicals)
●
lack of inclusion of first episode cases
Equity
No major concerns identified as most users are health concession card holders
Feasibility
Increased prescribing of clozapine is feasible while maintaining strict monitoring of haematological side-effects.Returning to the widespread use of typicals, which are considered out of date and sometimes out of production is not
likely to happen.
Acceptability
Clinicians and consumers place different value on side-effects of neuroleptics and the importance given them in the analysis.
The apparent tolerability advantages of atypical drugs, as far as side-effects are concerned, in the short term, make them more acceptable to patients and clinicians than typical neuroleptics.
Small immediate changes in side-effects may mean a great deal more to patients and carers than has been captured in this analysis.
The arbitrary use of an A$50 000 threshold is considered too low or inappropriate for this mental health condition.
50 COST-EFFECTIVENESS OF DRUGS FOR SCHIZOPHRENIA
Tabl
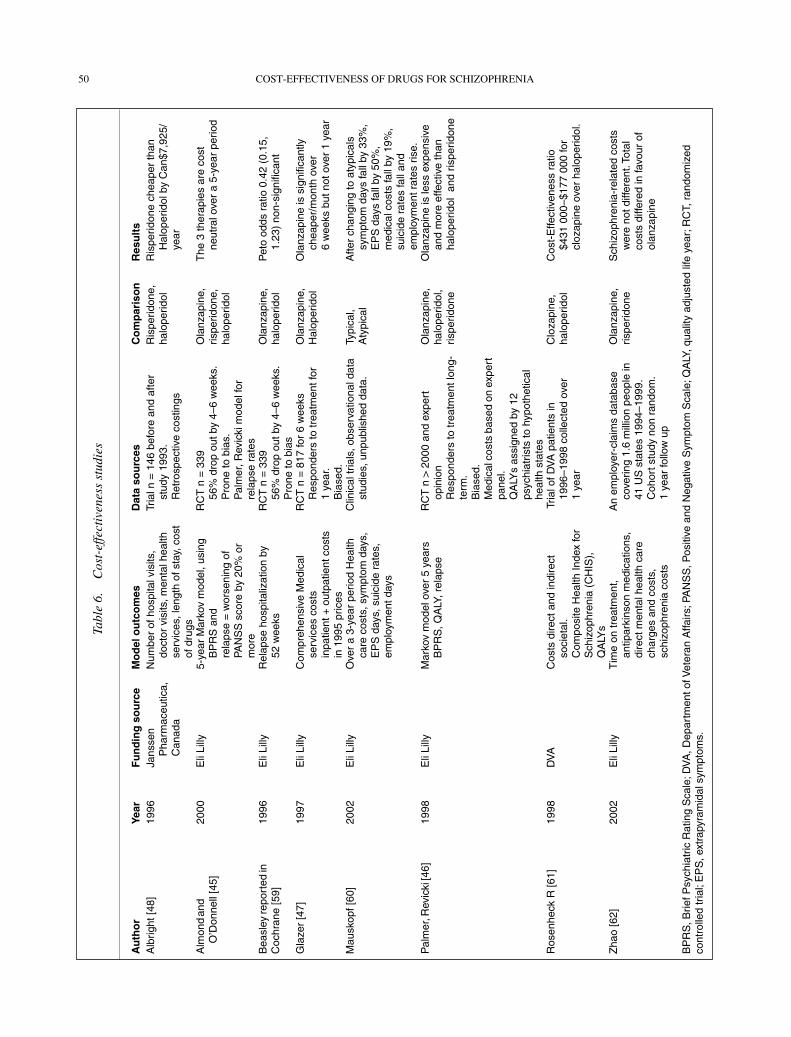
e 6.
Cos
t-ef
fect
iven
ess
stud
ies
Au
tho
rYe
arF
un
din
g s
ou
rce
Mo
del
ou
tco
mes
Dat
a so
urc
esC
om
par
iso
nR
esu
lts
Alb
right
[48]
1996
Jans
sen
Pha
rmac
eutic
a,
Can
ada
Num
ber
of h
ospi
tal v
isits
, do
ctor
vis
its, m
enta
l hea
lth
serv
ices
, len
gth
of s
tay,
cos
t of
dru
gs
Tria
l n =
146
bef
ore
and
afte
r st
udy
1993
. R
etro
spec
tive
cost
ings
Ris
perid
one,
ha
lope
ridol
Ris
perid
one
chea
per
than
H
alop
erid
ol b
y C
an$7
,925
/ye
ar
Alm
ond
and
O’D
onne
ll [4
5]20
00E
li Li
lly5-
year
Mar
kov
mod
el, u
sing
B
PR
S a
nd
rela
pse
= w
orse
ning
of
PAN
SS
sco
re b
y 20
% o
r m
ore
RC
T n
= 3
39
56%
dro
p ou
t by
4–6
wee
ks.
Pro
ne to
bia
s.
Pal
mer
, Rev
icki
mod
el fo
r re
laps
e ra
tes
Ola
nzap
ine,
ris
perid
one,
ha
lope
ridol
The
3 th
erap
ies
are
cost
ne
utra
l ove
r a
5-ye
ar p
erio
d
Bea
sley
repo
rted
in
Coc
hran
e [5
9]19
96E
li Li
llyR
elap
se h
ospi
taliz
atio
n by
52
wee
ksR
CT
n =
339
56
% d
rop
out b
y 4–
6 w
eeks
. P
rone
to b
ias
Ola
nzap
ine,
ha
lope
ridol
Pet
o od
ds r
atio
0.4
2 (0
.15,
1.
23)
non-
sign
ifica
nt
Gla
zer
[47]
1997
Eli
Lilly
Com
preh
ensi
ve M
edic
al
serv
ices
cos
ts
inpa
tient
+ o
utpa
tient
cos
ts
in 1
995
pric
es
RC
T n
= 8
17 fo
r 6
wee
ks
Res
pond
ers
to tr
eatm
ent f
or
1 ye
ar.
Bia
sed.
Ola
nzap
ine,
H
alop
erid
olO
lanz
apin
e is
sig
nific
antly
ch
eape
r/m
onth
ove
r 6
wee
ks b
ut n
ot o
ver
1 ye
ar
Mau
skop
f [60
]20
02E
li Li
llyO
ver
a 3-
year
per
iod
Hea
lth
care
cos
ts, s
ympt
om d
ays,
E
PS
day
s, s
uici
de r
ates
, em
ploy
men
t day
s
Clin
ical
tria
ls, o
bser
vatio
nal d
ata
stud
ies,
unp
ublis
hed
data
.Ty
pica
l, A
typi
cal
Afte
r ch
angi
ng to
aty
pica
ls
sym
ptom
day
s fa
ll by
33%
, E
PS
day
s fa
ll by
50%
, m
edic
al c
osts
fall
by 1
9%,
suic
ide
rate
s fa
ll an
d em
ploy
men
t rat
es r
ise.
Pal
mer
, Rev
icki
[46]
19
98
Eli
Lilly
Mar
kov
mod
el o
ver
5 ye
ars
BP
RS
, QA
LY, r
elap
seR
CT
n >
200
0 an
d ex
pert
op
inio
n R
espo
nder
s to
trea
tmen
t lon
g-te
rm.
Bia
sed.
M
edic
al c
osts
bas
ed o
n ex
pert
pa
nel.
QA
LYs
assi
gned
by
12
psyc
hiat
rists
to h
ypot
hetic
al
heal
th s
tate
s
Ola
nzap
ine,
ha
lope
ridol
,ris
perid
one
Ola
nzap
ine
is le
ss e
xpen
sive
an
d m
ore
effe
ctiv
e th
an
halo
perid
ol a
nd r
ispe
ridon
e
Ros
enhe
ck R
[61]
1998
DV
AC
osts
dire
ct a
nd in
dire
ct
soci
etal
. C
ompo
site
Hea
lth In
dex
for
Sch
izop
hren
ia (
CH
IS),
Q
ALY
s
Tria
l of D
VA
pat
ient
s in
19
96–1
998
colle
cted
ove
r 1
year
Clo
zapi
ne,
halo
perid
olC
ost-
Effe
ctiv
enes
s ra
tio
$431
000
–$17
7 00
0 fo
r cl
ozap
ine
over
hal
oper
idol
.
Zha
o [6
2]20
02E
li Li
llyT
ime
on tr
eatm
ent,
antip
arki
nson
med
icat
ions
, di
rect
men
tal h
ealth
car
e ch
arge
s an
d co
sts,
sc
hizo
phre
nia
cost
s
An
empl
oyer
-cla
ims
data
base
co
verin
g 1.
6 m
illio
n pe
ople
in
41 U
S s
tate
s 19
94–1
999.
C
ohor
t stu
dy n
on r
ando
m.
1 ye
ar fo
llow
up
Ola
nzap
ine,
ris
perid
one
Sch
izop
hren
ia-r
elat
ed c
osts
w
ere
not d
iffer
ent.
Tota
l co
sts
diffe
red
in fa
vour
of
olan
zapi
ne
BP
RS
, Brie
f Psy
chia
tric
Rat
ing
Sca
le; D
VA
, Dep
artm
ent o
f Vet
eran
Affa
irs; P
AN
SS
, Pos
itive
and
Neg
ativ
e S
ympt
om S
cale
; QA
LY, q
ualit
y ad
just
ed li
fe y
ear;
RC
T, r
ando
miz
ed
cont
rolle
d tr
ial;
EP
S, e
xtra
pyra
mid
al s
ympt
oms.

A. MAGNUS, V. CARR, C. MIHALOPOULOS, R. CARTER, T. VOS 51
before informing this type of analysis. The literature onquality of life in schizophrenia identifies that uncertaintyremains surrounding the determinants of subjective sat-isfaction with treatment in schizophrenia [38]. We choseto model disability based on symptoms and treatmentadverse effects for reasons of data availability. We rec-ognize that the well-being of people with schizophreniadepends on more than a narrow health focus and ourfindings are limited by not considering other elementsof quality of life such as safety, employment, financialsupport, family and social relationships.
Third, the included trials are largely conducted onpatients with established schizophrenia. Emsley [39] isthe only first-episode psychosis trial contributing to theanalysis. We can therefore not generalize the findingsto newly diagnosed or first-episode psychosis patients.Fourth, trials measuring the longer-term health status orsuicide risk of people with schizophrenia on medicationare lacking. Fifth, comparison of the levels of side-effects from risperidone, olanzapine, clozapine or typicalneuroleptic drugs in trials is compromised by the factthat many of these trials compare excessively high dosesof typicals (e.g. up to 15–20 mg haloperidol) with moremoderate doses of these atypicals. Trials report an oddsratio of 0.5 for serious side-effects comparing theseatypicals with typicals (in other words, serious side-effects are twice as common in those taking typicals).In contrast, the observational data we use from the LPDSindicates that there is only about a 70% higher propor-tion of persons reporting moderate or severe impairmentin daily life due to side-effects in those on typicalscompared to those on atypicals. Due to the high dosesof typicals given to controls in trials we argue that theobservational data from the LPDS may be closer tothe true difference in side-effects, although we cannotexclude selection bias, recall bias and the potentialimpact of drug combinations in respondents. We havenot considered the possible association with myocarditisand cardiomyopathy as a side-effect of clozapine use[40,41]. Last, most of the trials exclude people with ahistory of substance abuse. Treatment outcome withantipsychotic drugs for patients who also abuse alcoholor illicit drugs is poor [42].
The use of a utility measure like the DALY in thisanalysis highlights the coarse nature of quality of lifemeasurement in schizophrenia in burden of diseasestudies. The crude categorizations of the DALY DWs donot easily lend themselves to the measurement of changeattributed to particular interventions. We have used twountested methods of translating evidence from trials intoDALYs. We used the work of Gureje [43] to classifyseverity by a combination of quality of life indicators(two self-reported) from the survey. Clearly there is
room for improvement, particularly in finding moreaccurate methods of evaluating severity and change inseverity in a utility measure. A recent meta-analysiscomparing the relative efficacy of typical and severalatypical neuroleptics largely confirms our effect sizeestimates [44].
The main drivers of the differences in cost-effectivenessare the much higher costs of risperidone and olanzapineand the modest effect sizes regardless of the method oftranslating the effect size into a change in DALYs. Thehigh cost of clozapine however, is combined with aclearly higher effect size.
When the patent period expires, the cost of a drug canchange considerably. All the drugs considered in thismodelling will come off patent within the next 10 years,but we have not incorporated a change in price to eithergovernment or patient. The Australian experience withclozapine suggests that price remains unchanged ingeneric drug forms in schizophrenia treatment. To theextent that the price of the drugs falls, the ICER resultswill become more favourable, but such lower ICERresults should only inform policy if, and when, the pricefalls. Other cost-effectiveness studies have reported thatthe additional cost of the atypical neuroleptics, is offsetby cost savings, due to fewer and shorter hospital admis-sions. However, the majority of these studies was fundedby pharmaceutical companies, with a vested interestin a particular atypical drug (Table 6). Furthermore,cost savings were sometimes based on expert opinion[45–47] or data from studies that were either not random-ised or subject to the previously discussed biases [48].The cost of hospitalization has not been incorporatedinto the analysis for two main reasons. We could find norelationship between illness severity and resource use inthe LPDS and the decision to hospitalize a person isinfluenced by many other variables (bed availability forexample), apart from the patient characteristics of need.
We base much of our analysis of current practice inAustralia on the LPDS. Without the survey these analy-ses would have been very difficult. However, the surveyis limited in a number of ways. It was not a representa-tive community sample, it suffered a low response rate,it included no validated quality of life instrument, normedication dosage data, duration of medication treat-ment, or compliance data. Further, people with schizo-phrenia who were not in contact with specialist mentalhealth services were under-represented. We were able toovercome some of these shortcomings with referenceto other smaller Australian community samples, givinggreater weight to the GP-managed cases.
This work has drawn upon, but is also limited by theavailable research and the assumptions necessary to com-plete the work. Notwithstanding the many shortcomings

52 COST-EFFECTIVENESS OF DRUGS FOR SCHIZOPHRENIA
in data sources and study methods, we conclude that weare able to make valid comparisons of cost-effectivenessresults between drug interventions for schizophrenia.Comparisons of results with other ACE-MH interven-tions are more problematic and it is even more difficultto compare these results with cost per DALY estimatesin other health areas where health gain is dominated byextension of life rather than quality of life. However,the absolute value of the ICERs is more influenced bythe methodological problems encountered and the untriedsolutions adopted. For this reason it is advisable to readthe range of values for each ICER along with the mid-point values, and to interpret them as indicative ratherthan definitive. The relative rankings of the drug inter-ventions are clearly identified and would remain con-stant at any threshold value.
There are no major equity concerns about differentchoices of drug treatment, as all drugs are available onthe Pharmaceutical Benefits Schedule (PBS). Minimalpatient contributions occur since most people with schizo-phrenia have healthcare concession cards. There aremore important issues with regards to feasibility andparticularly acceptability to stakeholders. We con-clude that the high cost of risperidone and very high costof olanzapine do not weigh up against the relativelymodest health benefits, except in the case of those exper-iencing moderate to severe side-effects on typicals. Thisconclusion may not conform with values held by clini-cians, carers and people with schizophrenia. We may nothave adequately estimated all benefits in our analysesand we acknowledge that there is likely to be morevariation in the effect of drugs on individuals than wehave captured by analysing the mean treatment effectsreported in the literature. Hence, these findings cannotbe imposed rigidly on clinical practice. However, adopt-ing the A$50 000 threshold, and year 2000 drug prices,current practice seems far removed from cost-effectiveprescribing.
The market share of atypicals as a group, and the shareof olanzapine within the group, has grown since 1997,the year of the LPDS survey. Reversing this trend maynot be feasible as pharmaceutical companies are alreadystarting to withdraw some of the typicals. However, it isvery difficult to identify economic justification for thetwo-fold difference in price, minimal differences in effi-cacy and longer-term side-effect profiles of olanzapinecompared to risperidone. Furthermore, the PBS maybenefit from a review of drug pricing policies/practicesafter patent expiration with the high price of genericclozapine as an example.
To overcome weakness in trial evidence, longer-termnon-industry-funded trials of existing and new atypicalneuroleptics, in comparison with lower dose typical
neuroleptics, in both first-episode and established schizo-phrenia, are desirable. Until then, clinical doubt con-tinues to exist regarding alternative drug therapies.The development of clinical practice guidelines basedon lower levels of evidence may inhibit the establish-ment of trial evidence [49]. Importantly, to enable cost-effectiveness to be better evaluated, we recommend thatoutcome measurement in such studies include qualityof life (both patient- and clinician-rated), social andeconomic functioning, drug tolerability, compliance,satisfaction and side-effects.
Acknowledgements
We thank members of the ACE–MH Steering Com-mittee for their input to the project. The present reporthas drawn from data collected in the framework of theCollaborative Study on Low-Prevalence (Psychotic)Disorders, an epidemiological and clinical investigationwhich is part of the National Survey of Mental Healthand Well-being, Australia 1997–1998. The views of theauthors may not necessarily reflect those of the LowPrevalence (Psychotic) Disorders Study Group.
References
1. American Psychiatric Association.
Practice Guidelines for the Treatment of Schizophrenia.
Washington DC: American Psychiatric Press, 1996.
2. Access Economics.
Schizophrenia: costs an analysis of the burden of schizophrenia and related suicide in Australia.
Melbourne: SANE Australia, 2002.
3. Awad AG, Voruganti LNP. Quality of life and new antipsychotics in schizophrenia. Are patients better off?
International Journal of Social Psychiatry
1999; 45:268–275.4. McGorry P, Killackey E, Lambert M, Lambert T. Summary
Australian and New Zealand clinical practice guideline for the treatment of schizophrenia (2003).
Australasian Psychiatry
2003; 11:136–147.
5. National Institute for Clinical Excellence.
Schizophrenia. Core interventions in the treatment and management of schizophrenia in primary and secondary care.
London: National Collaborating Centre for Mental Health, 2002
6. Haby M, Carter R, Mihalopoulos C
et al.
Assessing cost-effectiveness – Mental health. Introduction to the study and methods.
Australian and New Zealand Journal of Psychiatry
2004; 38: 569–578.
7. Jablensky A, McGrath J, Herrman H
et al.
People living with psychotic illness: an Australian study 1997–98.
Canberra: Department of Health and Aged Care, 1999.
8. Lewin TJ, Carr VJ. Rates of treatment of schizophrenia by general practitioners. A pilot study.
Medical Journal of Australia
1998; 168:166–169.
9. Harding CM, Brooks GW, Ashigawa T, Strauss JS, Breier A. The Vermont Longitudinal Sudy of persons with severe mental illness, 1: Methodology, study sample, and overall status 32 years later.
American Journal of Psychiatry
1987; 144:718–726.10. Ciompi L. Three lectures in schizophrenia. The natural history of
schizophrenia in the long term.
British Journal of Psychiatry
1980; 136: 413–420.
A. MAGNUS, V. CARR, C. MIHALOPOULOS, R. CARTER, T. VOS 53
11. Helgason L. Twenty years’ follow-up of first psychiatric presentation for schizophrenia: what could have been prevented?
Acta Psychiatrica Scandinavica
1990; 81:231–235.12. Harrison G, Hopper K, Craig T, Laska E, Siegel C,
Wanderling J. Recovery from psychotic illness: a 15- and 25-year international follow-up study.
British Journal of Psychiatry
2001; 178:506–517.13. Huber G, Gross G, Schuttler R, Linz M. Longitudinal studies of
schizophrenic patients.
Schizophrenia Bulletin
1980; 6:592–605.14. Gaebel W. Towards the improvement of compliance: the
significance of psycho-education and new antipsychotic drugs.
International Clinical Psychopharmacology
1997; 12:S37–S42.15. Marder SR. Facilitating compliance with antipsychotic
medication.
Journal of Clinical Pharmacology
1998; 58:21–25.16. Harris E, Barraclough B. Excess mortality of mental disorder.
British Journal of Psychiatry
1998; 173:11–53.17. Gureje O, Herrman H, Harvey C, Morgan V, Jablensky A. The
Australian national survey of psychotic disorders: profile of psychosocial disability and its risk factors.
Psychological Medicine
2002; 32:639–647.18. Stouthard M, Essink-Bot M, Bonsel G
et al.
Disability Weights for Diseases in the Netherlands
. Rotterdam: Department of Public Health Erasmus University, 1997.
19. Kennedy E, Song F, Hunter R, Clarke A, Gilbody S. Risperidone versus typical antipsychotic medication for schizophrenia (Cochrane Review). In:
The Cochrane Library.
Oxford: Update Software, 2003.
20. Duggan L, Fenton M, Dardennes RM, El-Dosoky A, Indran S. Olanzapine for schizophrenia (Cochrane Review). In:
The Cochrane Library.
Oxford: Update Software, 2003.21. Gilbody SM, Bagnall AM, Duggan L, Tuunainen A. Risperidone
versus other atypical antipsychotic medication for schizophrenia (Cochrane Review). In:
The Cochrane Library.
Oxford: Update Software, 2003.
22. Tuunainen A, Wahlbeck K, Gilbody S. Newer atypical antipsychotic medication versus clozapine for schizophrenia (Cochrane Review). In:
The Cochrane Library.
Oxford: Update Software, 2003.
23. Wahlbeck K, Cheine M, Essali M. Clozapine versus typical neuroleptic medication for schizophrenia (Cochrane Review). In:
The Cochrane Library.
Oxford: Update Software, 2003.24. Geddes J, Freemantle N, Harrison P, Bebbington P. Atypical
antipsychotics in the treatment of schizophrenia: systematic overview and meta-regression analysis.
British Medical Journal of
2000; 321:1371–1376.25. Waraich P, Adams CE, Roque M, Hamill K, Marti J. Haloperidol
dose for the acute phase of schizophrenia (Cochrane Review). In:
The Cochrane Library.
Oxford: Update Software, 2003.26. Csernansky JG, Mahmoud R, Brenner R. A comparison of
risperidone and haloperidol for the prevention of relapse in patients with schizophrenia.
The New England Journal of Medicine
2002; 346:16–22.27. Egger M, Smith G, Altman D.
Systematic reviews in health care: meta-analysis in context
, 2nd edn. London: BMJ, 2001.28. Willett W, Manson J, Stampfer M
et al.
Weight, weight change and coronary heart disease in women: risk within the ‘normal’ weight range.
Journal of the American Medical Society
1995; 273:461–465.
29. Rexrode K, Hennekens C, Willett W
et al.
A prospective study of body mass index, weight change and risk of stroke in women.
Journal of American Medical Association
1997; 275:447–451.30. Lee I, Paffenbarger RJ. Quetelet’s index and risk of colon cancer
in college alumni.
Journal of the National Cancer Institute
1992; 84:1326–1331.
31. Colditz G, Willett W, Rotnitsky A, Manson J. Weight gain as a risk factor for clinical diabetes mellitus in women.
Annals of Internal Medicine
1995; 122:481–486.
32. Department of Human Services.
Victorian Burden of Disease Study: morbidity.
Melbourne: Department of Human Services, 1999.
33. Duggan A, Warner J, Knapp M, Kerwin R. Modelling the impact of clozapine on suicide in patients with treatment-resistant schizophrenia in the UK.
British Journal of Psychiatry
2003; 182:505–508.
34. Hamilton SH, Edgell ET, Revicki DA, Breier A. Functional outcomes in schizophrenia: a comparison of olanzapine and haloperidol in a European subsample.
International Clinical Psychopharmacology
2000; 15:245–255.35. Tran PV, Hamilton SH, Kuntz AJ
et al.
Double-blind comparison of olanzapine versus risperidone in the treatment of schizophrenia and other psychotic disorders.
Journal of Clinical Psychopharmacology
1997; 17:407–418.36. Rosenheck R, Cramer J, Xu W
et al.
A comparison of clozapine and haloperidol in hospitalized patients with refractory schizophrenia.
New England Journal of Medicine
1997; 337:809–815.
37. Voruganti L, Cortese L, Oyewumi L, Cernovsky Z, Zirul S, Awad A. Comparative evaluation of conventional and novel antipsychotic drugs with reference to their subjective tolerability, side-effect profile and impact on quality of life.
Schizophrenia Research
2000; 43:135–145.38. Hellewell J. Patients’ subjective experiences of antipsychotics.
Clinical relevance.
CNS Drugs
2002; 16:457–471.39. Emsley RA, Risperidone Working Group. Risperidone in the
treatment of first-episode psychotic patients: a double-blind multicenter study.
Schizophrenia Bulletin
1999; 25:721–729.40. Coulter DM, Bate A, Meyboom RHB, Lindquist M, Edwards IR.
Antipsychotic drugs and heart muscle disorder in international pharmacovigilance: data mining study.
British Medical Journal
2001; 322:1207–1209.
41. Kilian JG, Kerr K, Lawrence C, Celermajer DS. Myocarditis and cardiomyopathy associated with clozapine.
Lancet
1999; 354:1841–1845.
42. Owen RR, Fischer EP, Booth BM, Cuffel BJ. Medication noncompliance and substance abuse among patients with schizophrenia.
Psychiatric Services
1996; 47:853–858.43. Gureje O, Herrman H, Harvey C, Trauer T, Jablensky A.
Defining disability in psychosis: Performance of the diagnostic interview for psychosis-disability module (DIP-DIS) in the Australian national survey of psychotic disorders.
Australian and New Zealand Journal of Psychiatry
2001; 35:846–851.44. Davis J, Chen N, Glick I. A Meta-analysis of the efficacy of
second-generation antipsychotics.
Archives of General Psychiatry
2003; 60:553–564.45. Almond S, O’Donnell O. Cost analysis of the treatment of
schizophrenia in the UK. A simulation model comparing olanzapine, risperidone and haloperidol.
Pharmacoeconomics
2000; 17:383–389.
46. Palmer CS, Revicki DA, Genduso LA, Hamilton SH, Brown RE. A cost-effectiveness clinical decision analysis model for schizophrenia.
American Journal of Managed Care
1998; 4:345–355.
47. Glazer WM, Johnstone BM. Pharmacoeconomic evaluation of antipsychotic therapy for schizophrenia.
Journal of Clinical Psychiatry
1997; 58:50–54.48. Albright P, Livingstone S, Keegan DL, Ingham M,
Shrikhande S, Le Lorier J. Reduction of healthcare resource utilisation and costs following the use of risperidone for patients with schizophrenia previously treated with standard antipsychotic therapy.
Clinical Pharmacoeconomics
1996; 11:289–299.
49. Geddes J. Generating evidence to inform policy and practice: The example of the second generation ‘atypical’ antipsychotics.
Schizophrenia Bulletine
2003; 29:105–114.
54 COST-EFFECTIVENESS OF DRUGS FOR SCHIZOPHRENIA
50. Carr VJ, Neil AL, Halpin SA, Holmes S, Lewin TJ. Costs of schizophrenia and other psychoses in urban Australia: findings from the low prevalence (psychotic) disorders study.
Australian and New Zealand Journal of Psychiatry
2003; 37:31–40.
51. Davies A, Adena MA, Keks NA, Catts SV, Lambert T, Schweitzer I. Risperidone versus haloperidol: I. Meta-analysis of efficacy and safety.
Clinical Therapeutics
1998; 20:58–71.52. Jablensky A. Epidemiology of schizophrenia.
Australasian Epidemiologist
2002; 9:2–8.53. Sanderson K, Andrews G, Corry J, Lapsley H. Using the effect
size to model change in preference values from descriptive health states.
Quality of Life Research
2004; 13:1255–1264.54. Carr VJ, Neil AL, Halpin SA, Holmes S.
Costs of psychosis in urban Australia. A bulletin of the low prevalence disorders study.
Newcastle: Centre for Mental Health Studies and the Universtity of Newcastle. 2000.
55. Britt H, Miller G, Knox C
et al.
General practice activity in Australia 2000–01.
AIHW Cat. No. GEP8. Canberra: Australian Institute of Health and Welfare, 2001. (General Practice Series no. 8.)
56. Davies A, Langley PC, Keks NA, Catts SV, Lambert T, Schweitzer I. Risperidone versus haloperidol: II. Cost-effectiveness.
Clinical Therapeutics
1998; 20:196–212.
57. Leucht S, Pitschel-Walz G, Abraham D, Kissling W. Efficacy and extrapyramidal side-effects of the new antipsychotics olanzapine, quetiapine, risperidone, and sertindole compared to conventional antipsychotics and placebo. A meta-analysis of randomised control trials. Schizophrenia Research 1999; 35:51–68.
58. Allison DB, Mentore JL, Heo M et al. Antipsychotic-induced weight gain: a comprehensive research synthesis. American Journal of Psychiatry 1999; 156:1686–1696.
59. Beasley CM, Tollefson GD, Tran PV, Satterlee W, Sanger T, Hamilton SH. Olanzapine versus placebo and haloperidol. Acute phase results of the North American double-blind olanzapine trial. Neuropsychopharmacology 1996; 14:111–123.
60. Mauskopf JA, Muroff M, Gibson PJ, Grainger DL. Estimating the costs and benefits of new drug therapies: atypical antipsychotic drugs for schizophrenia. Schizophrenia Bulletin of the 2002; 28:619–635.
61. Rosenheck R, Cramer J, Xu W et al. Multiple outcome assessment in a study of the cost-effectiveness of clozapine in the treatmnent of refractory schizophrenia. Health Services Research 1998; 33:1237–1267.
62. Zhao Z. A retrospective evaluation of olanzapine versus risperidone in the treatment of schizophrenia. Managed Care Interface 2002; 15:75–81.
Top Related
Copyright © 2022 FDOKUMEN

