







Bahasa
Halaman
Hukum


University of Massachusetts Amherst University of Massachusetts Amherst
ScholarWorks@UMass Amherst ScholarWorks@UMass Amherst
Masters Theses Dissertations and Theses
March 2022
A Simplified Fluid Dynamics Model of Ultrafiltration A Simplified Fluid Dynamics Model of Ultrafiltration
Christopher Cardimino University of Massachusetts Amherst
Follow this and additional works at: https://scholarworks.umass.edu/masters_theses_2
Recommended Citation Recommended Citation Cardimino, Christopher, "A Simplified Fluid Dynamics Model of Ultrafiltration" (2022). Masters Theses. 1152. https://doi.org/10.7275/28205018 https://scholarworks.umass.edu/masters_theses_2/1152
This Open Access Thesis is brought to you for free and open access by the Dissertations and Theses at ScholarWorks@UMass Amherst. It has been accepted for inclusion in Masters Theses by an authorized administrator of ScholarWorks@UMass Amherst. For more information, please contact [email protected].

A Simplified Fluid Dynamics Model of Ultrafiltration
A Thesis Presented
By
Christopher R Cardimino
Submitted to the Graduate School of the
University of Massachusetts Amherst in partial fulfillment
of the requirements for the degree of
Master of Science in Mechanical Engineering
February 2022
Mechanical and Industrial Engineering

A Simplified Fluid Dynamics Model of Ultrafiltration
A Thesis Presented
By
Christopher R. Cardimino
Approved as to style and content by:
________________________________________________
Yossi Chait, Chair
________________________________________________
Christopher Hollot, Member
________________________________________________
Govind Srimathveeravalli, Member
_____________________________________________
Sundar Krishnamurty, Department Head
Mechanical and Industrial Engineering

iii
ABSTRACT
A SIMPLIFIED FLUID DYNAMICS MODEL OF ULTRAFILTRATION
FEBRUARY 2022
CHRISTOPHER CARDIMINO, B.S. UNIVERSITY OF MASSACHUSETTS AMHERST
M.S.M.E., UNIVERSITY OF MASSACHUSETTS AMHERST
Directed by: Professor Yossi Chait
In end-stage kidney disease, kidneys no longer sufficiently perform their intended functions,
for example, filtering blood of excess fluid and waste products. Without transplantation or
chronic dialysis, this condition results in mortality. Dialysis is the process of artificially
replacing some of the kidney’s functionality by passing blood from a patient through an external
semi-permeable membrane to remove toxins and excess fluid. The rate of ultrafiltration – the
rate of fluid removal from blood – is controlled by the hemodialysis machine per prescription by
a nephrologist. While essential for survival, hemodialysis is fraught with clinical challenges. Too
high a fluid removal rate could result in hypotensive events where the patient blood pressure
drops significantly which is associated with adverse symptoms such as exhaustion, fainting,
nausea, and cramps, leading to decreased patient quality of life. Too low a fluid removal rate, in
contrast, could leave the patient fluid overloaded often leading to hypertension, which is
associated with adverse clinical outcomes.
Previous work in our lab demonstrated via simulations that it is possible to design an
individualized, model-based ultrafiltration profile with the aim of minimizing hypotensive events
during dialysis. The underlying model using in the design of the individualized ultrafiltration
profile is a simplified, linearized, continuous-time model derived from a nonlinear model of the
patient’s fluid dynamics system. The parameters of the linearized model are estimated from
actual patient’s temporal hematocrit response to ultrafiltration. However, the parameter
identification approach used in the above work was validated using limited clinical data and
often failed to achieve accurate estimation. Against this backdrop, this thesis had three goals: (1)
obtain a new, larger set of clinical data, (2) improve the linearized model to account for missing

iv
physiological aspects of fluid dynamics, and (3) develop and validate a new approach for
identification of model parameters for use in the design of individualized ultrafiltration profiles.
The first goal was accomplished by retrofitting an entire in-center, hemodialysis clinic in
Holyoke, MA, with online hematocrit sensors (CliC devices), Wi-Fi boards, and a laptop with a
radio receiver. Treatment data was wirelessly uploaded to a laptop and redacted files and manual
treatment charts were made available for our research per approved study IRB.
The second goal was accomplished by examining the nonlinear system of equations
governing the relevant dynamics and simplifying the model to an identifiable case.
Considerations of refill not accounted for fully in previous works were integrated into the
linearized model, adding terms but making it generally more accurate to the underlying
dynamics.
The third goal was accomplished by developing an algorithm to identify major system
parameters, using steady-state behavior to effectively reduce the number of parameters to
identify. The system was subsequently simulated over an established range for all remaining
parameters, compared to collected data, with the lowest RMS error case being taken as the set of
identified parameters.
While intra-patient identified individual model parameters were associated with a high
degree of variability, the system’s steady-state gain and time constants exhibited more consistent
estimations, though the time constants still had high variability overall. Parameter sensitivity
analysis shows high sensitivity to small changes in individual model parameters. The addition of
refill dynamics in the model constituted a significant improvement in the identifiability of the
measured dynamics, with up to 70% of data sets resulting in successful estimates. Unmodelled
dynamics, resulting from unmeasured input variables, resulted in about 30% of measured data
sets unidentifiable. The updated model and associated parameter identification developed in this
thesis can be readily integrated with the model-based design of individualized UFR profile.

v
TABLE OF CONTENTS Page
ABSTRACT……………………………………………………………………………………………….iii
List of Tables……………………………………………………………………………………………..vii
List of Figures……………………………………………………………………………………………viii
Nomenclature……………………………………………………………………………………………..ix
CHAPTER
1 INTRODUCTION ................................................................................................................ 1
2.1 Individualized UFR profiles ............................................................................................... 3
2 PROBLEM STATEMENT & THESIS CONTRIBUTIONS ..................................................... 4
3 CLINICAL DATA ACQUISITION ......................................................................................... 5
3.1 Clinical Data Collection ................................................................................................ 5
3.2 Clinical Data Analysis .................................................................................................. 6
4 MODELING ......................................................................................................................... 8
4.1 Literature Review ......................................................................................................... 8
4.2 Nonlinear Model in “Individualization of Ultrafiltration in Hemodialysis” ........................ 8
4.3 The Linearized Model in [8] .........................................................................................12
4.3.1 Accuracy of Linearization .....................................................................................14
4.4 Model Correction to Account for Refill Dynamics ........................................................15
5 PARAMETER IDENTIFICATION APPROACH ...................................................................17
5.1 Identification Method in “Individualization of Ultrafiltration in Hemodialysis” ................17
5.2 Nonlinear Least-Squares Parameter Iteration .............................................................17
5.2.1 Piecewise Analysis ..............................................................................................18
5.3 Final Approach ............................................................................................................20
5.4 Determination of Outlier Treatment Profiles ................................................................21
6 PARAMETER SENSITIVITY ..............................................................................................22
7 PARAMETER ESTIMATION RESULTS .............................................................................28
7.1.1 Patient 7 ..............................................................................................................28
7.1.2 Patient 6 ..............................................................................................................31
7.1.3 Patient 8 ..............................................................................................................33
7.1.4 Patient 11 ............................................................................................................34

vi
7.1.5 Patient 15 ............................................................................................................35
7.1.6 Patient 17 ............................................................................................................37
7.1.7 Patient 18 ............................................................................................................40
7.1.8 Patient 27 ............................................................................................................40
7.1.9 Patient 29 ............................................................................................................41
7.1.10 Patient 31 ............................................................................................................44
7.1.11 Patient 32 ............................................................................................................45
7.1.12 Patient 37 ............................................................................................................45
7.2 Summary of Key Intra-patient Estimation Results .......................................................46
8 DISCUSSION ....................................................................................................................48
8.1.1 Model Consistent with Clinical Data .....................................................................48
8.1.2 Transient Responses not Included in the Model ...................................................57
8.2 Long Term Projected Output .......................................................................................58
8.3 Parameter Estimation of a Second UFR Step Response ............................................59
8.4 Overall Limitations ......................................................................................................60
9 CONCLUSIONS .................................................................................................................62
10 FUTURE DIRECTIONS ..................................................................................................65
REFERENCES .........................................................................................................................66

vii
LIST OF TABLES Table Page
4.1 – Model Parameters and Definitions ................................................................................ 10
4.2 – Model Parameter Values Used in Figure 5.2 Plots ....................................................... 15
7.1 – Patient 7 Numerical Data ............................................................................................... 30
7.2 – Patient 6 Numerical Data ............................................................................................... 32
7.3 – Patient 8 Numerical Data ............................................................................................... 34
7.4 – Patient 11 Numerical Data ............................................................................................. 34
7.5 – Patient 15 Numerical Data ............................................................................................. 36
7.6 – Patient 17 Numerical Data ............................................................................................. 39
7.7 – Patient 18 Numerical Data ............................................................................................. 40
7.8 – Patient 27 Numerical Data ............................................................................................. 40
7.9 – Patient 29 Numerical Data ............................................................................................. 44
7.10 – Patient 31 Numerical Data ........................................................................................... 44
7.11 – Patient 32 Numerical Data ........................................................................................... 45
7.12 – Patient 37 Numerical Data ........................................................................................... 45
7.13 – Gain and Time Constants with Variabilities ............................................................... 47
8.1 - Gain and Time Constants with Variabilities ................................................................. 51

viii
LIST OF FIGURES Figure Page
1.1 – Diagram of Hemodialysis................................................................................................. 2
4.1 – Diagram of two-compartment modeling ......................................................................... 9
4.2 – Linearization Accuracy Assessment ............................................................................ 14
6.1 – Sensitivity of K vs. α ...................................................................................................... 23
6.2 – Sensitivity of K vs β ....................................................................................................... 24
6.3 – Sensitivity of K vs Kred ................................................................................................. 25
6.4 – Sensitivity of α vs τRED ................................................................................................... 26
7.1 – Patient 7 Day 105 ............................................................................................................ 29
7.2 – Patient 6 Day 107 ............................................................................................................ 31
7.3 – Patient 8 Day 107 ............................................................................................................ 33
7.4 – Patient 15 Day 133 .......................................................................................................... 35
7.5 – Patient 17 Day 107 .......................................................................................................... 37
7.6 – Patient 17 Day 107 Treatment Chart ............................................................................. 38
7.7 – Patient 17 Day 138 Long-Term Estimation ................................................................... 39
7.8 – Patient 29 Day 117 .......................................................................................................... 41
7.9 – Patient 29 Day 100 .......................................................................................................... 42
7.10 – Patient 29 Day 107 ........................................................................................................ 43

ix
NOMENCLATURE ESKD End-Stage Kidney Disease Vieu Initial interstitial compartment volume in
euhydrated state
ARA American Renal Associates mi Interstitial Protein Mass
HD Hemodialysis Ql Lymphatic Flow
IRB Institutional Review Board Pv Venous Pressure
VRBC Red Blood Cell Volume Pip Plasma Collid Osmotic Pressure (mmHg)
Kf Filtration Coefficient Δp Hydrostatic Pressure Gradient (mmHg)
Po Offset Pressure COV Coefficient of Variation
UF Ultrafiltration
UFR Ultrafiltration Rate
Vpeu Initial intravascular
compartment volume in
euhydrated state
mp Intravascular Protein Mass
Pc Hydrostatic Capillary
Pressure
Pi Interstitial Pressure
πi Interstitial Collid Osmotic
Pressure
Δπ Osmotic Pressure Gradient
x2 Interstitial Volume
a, b, c, d, r,
f, g, h, l,
Kc1, Kc2, Kc3
Dimensionless Parameters in
Nonlinear Fluid Dynamic
Model

1
1 INTRODUCTION In end-stage kidney disease (ESKD), the human body is unable to perform typical
functions in terms of filtering blood of excess fluid and toxins, as the kidneys have low operation
capacity noted in [1]. The shortage of kidneys for organ transplantation – currently the best
medical solution to this disease – remains a serious societal issue yet to be resolved. Long-term
management of ESKD relies on the artificial filtering of blood, a process known as hemodialysis
(HD). Developed in the early 20th century, HD can be performed by a variety of different
methods, one of which is ultrafiltration (UF), [2] which is the focus of this thesis. An initial
surgical intervention to create an external access to blood circulation is required for HD, with
treatments occurring multiple times per week for hours at a time. [2] While many medical
processes have seen major advances in the last several decades, treatments such as HD have
largely stagnated, and clinical outcomes have seen only limited improvements. [2]
The method of UF, shown in Figure 1.1, relies on passing a patient’s blood through a
closed, external circuit which includes a dialyzer – an artificial kidney of sorts – comprising a
blood compartment on one side of a semi-permeable membrane with a dialysate fluid on the
other side. [3] The filtration coefficient of the semi-permeable membrane separating the blood
and dialysate fluid, as well as the pressure gradient between the two fluids control the fluid-
removal rate. The amount of fluid to be removed in each treatment is prescribed by the treating
clinician but can be actively modified during the treatment if conditions require changed. Many
HD machines have 3-5 pre-programed ultrafiltration rate (UFR) profiles, but none are
individualized to the patient’s fluid dynamics.

2
Figure 1.1: Diagram of hemodialysis process, detailing the path of blood from removal to return
to the body. Retrieved from Shutterstock with appropriate licensing. [4]
The process of removing excess fluid from ESKD patients using HD, while essential for
lifesaving, can have adverse short- and long-term clinical outcomes. Short term outcomes
include hypotension and the associated events, and long-term outcomes range from fatigue and
decreased quality of life, to shortened life span. [5] While longer HD treatments, which results in
lower UFR values, have been associated with improved clinical outcomes, this option is not
practical for in-center treatments due to logistical constraints and patient resistance. [6] There is
an increased interest in improving fluid management during HD treatments in order to improve
outcomes. [7] It has been suggested that individualization of UFR profiles should be a key

3
strategy in an overall effort to improve fluid management outcomes. [7][8] This state of affairs
provided the motivation for the research described in this thesis.
1.1 Individualized UFR profiles
Individualized UFR profile in [8] can be designed, for example, to maintain patient
hematocrit below a specified time-dependent critical level throughout treatment. An overall
critical value of hematocrit has been proposed as part of improved fluid management [refs].
Current pre-programmed UFR profiles in many HD machines (e.g., linear and exponential) fail
to offer such an individualization goal due a patients’ intra- and inter-treatment fluid dynamics
variability. Such an individualization would be a function of many factors including, amount of
fluid volume to be removed, treatment time, and maximal allowed UFR, and other unmeasurable
physiological and pathophysiological responses. [8]
Recently, a new method for the design of individualized UFR profiles was proposed in
[8] which relies on a patient’s fluid dynamics model during HD. The model used in [8] is a
nonlinear system of equations governing the interstitial and intravascular fluid dynamics in a
patient. The dynamics is driven by osmotic and static pressure differentials created by the
initiation of UF and is a function of a number of biological variables. These include amounts of
proteins in the body, a generalized inter-compartmental filtration coefficient, and initial fluid
volumes, all of which are difficult or not feasible to measure on a routine basis. The large
number of unknown parameters in this nonlinear model make it a poor candidate for use in UFR
profile design, given the paucity of available measurements. Therefore, Rammah in [7][8]
proposed a simplified model with reduced number of parameters obtained by a linearization of
the nonlinear system about initial volumes, with the assumption of constant parameter values.
Parameters were identified through a linear-least squares algorithm applied to the discrete-time
linearized model [8].
We have shown in a recent numerical study that the system identification approach used
in [8] exhibits technical challenges stemming from noisy data, parameters at different scales, and
a linearization. The focus of this thesis is on the development and experimental validation of a
new methodology for optimal parameter estimation of patient hemodynamics model from
measured data.

4
2 PROBLEM STATEMENT & THESIS CONTRIBUTIONS The main hypothesis of this thesis is that the complex hemodynamics of a patient’s
interstitial and intravascular spaces during HD can be accurately identified by a linearized
system model only knowing patient hematocrit and UF rate step changes during treatment. The
aims of this thesis are:
(1) To design a system identification scheme for identifying parameters of a patient
hematocrit dynamics model during HD which can be readily used in connection with the
individualized UFR profile design method of [8], and
(2) To analyze intra- and inter-patient estimated fluid dynamics models over several HD
treatments.
Achieving these goals involved the following three tasks:
1. Collection of clinical data from hemodialysis sessions,
2. Updating the model and devising a parameter identification method to conform with
measured hematocrit behavior, and
3. Analysis of model identification results.

5
3 CLINICAL DATA ACQUISITION The success of the ultrafiltration design in [8] relies on establishing a suitable system model
and accurately identifying parameters. We also wish to gain an understanding of intra-patient
variability, which can only be studied with several collected instances of patient data, requiring a
clinical setting. Central to the success of this research topic is the adequate collection of data for
subsequent analysis. The ARA clinic in Holyoke was graciously retrofitted by the manufacturer
with CliC units for just this purpose, which enabled the high-quality collection of data for use in
model development and analysis. All procedures of research were approved by the attached IRB
filing, (supplemental document 1).
3.1 Clinical Data Collection
Data collection took place in the ARA Holyoke, MA clinic, conducted alongside the
normal personnel and medical professionals of the site. Patients enrolled in the study had been
receiving treatment from the site prior to the commencement of the study, with treatment profiles
having been determined through previous treatments. Staff at the clinic were instructed to not use
the CliC monitoring devices to drive changes in treatment initially. Each patient was assigned a
unique four-digit identifying number to distinguish them from other patients.
A laptop, disconnected for the internet, was positioned within wireless range of all
treatment chairs, equipped with a radio receiver and CLM Printer software which together served
to receive and save Clic data files. After a patient is seated and connected to the HD machine,
and immediately before the start of UF, the nurse would enter appropriate commands into the
HD machine software to enable data collection and transfer at a later time, including a 4-digit
patient identifier. Upon conclusion of HD treatment, the staff member in charge of turning over
the machine to prepare it for the next patient selected print in the machine software in order to
send the treatment data file of the prior patient to the computer. Upon receiving the data, a
MATLAB script entitled “clean_data.m” (attached in code repository) opened each file in
succession, stripped out identifying markers, extracted only the relevant columns, and saved the
data in a new file. Additionally, this script added a further layer of obfuscation to the patient
identification by converting the four-digit number to a two-digit number. Patient treatment sheets
were also scanned with identifying or sensitive information redacted off and relabeled with the
patient’s two-digit identifier for reference.

6
This process did not go without difficulties. For different reasons many data files from
many treatments did not transmit to the laptop. The reasons for this include operator error, I/O
software issues on the laptop, and other unknown issues. In other cases, in the raw data files, the
patient’s four-digit identifier was missing. In such cases, an effort was made to correlate the
treatment start time as noted on the data file with the treatment start times on the treatment
charts. As the number on the charts is recorded from the screen at commencement of treatment,
most cases of incomplete data files were identified. Patient data files and chart-recorded
ultrafiltration rates were separated into folders named for each two-digit patient number for
analysis. Timestamp data was likewise stripped out to prevent patient correlation. Any data
stored on this researcher laptop fully satisfy the IRB guidelines with any HIPPA the identifying
information permanently stripped from patient charts and data files. Overall, many of these
difficulties contributed to limited data sets being collected for each patient.
The data collection ran from March 2020 to June 2020, which correlated to the start of the
COVID-19 pandemic. As a result, many considerations previously thought unproblematic were
thrown into flux. The clinic was forced to shift many patients and appointments around between
days and facilities, introducing new patients for only a single treatment or two each, rendering
data file collection problematic at best. Some early patients that were being examined no longer
had data files collected, and I was unable to visit the clinic to examine progress. Thus, data
collection relied on internal staff who were coping with the swift changes brought on. With each
of these factors in mind, an average patient only had 4.4 measurements collected, following the
elimination of patients with only a single data set to process. I would like to extend my greatest
thanks to the staff of the clinic who aided in the collection of this data throughout this process,
despite the additional strains put on them due to this pandemic.
3.2 Clinical Data Analysis
A second MATLAB 2020a code “folder_analysis.m” was used to open each patient folder in
sequence and run the identification algorithm detailed in Section 6. The output of the analysis
code included all relevant identified parameters, as well as identified plots (examples of which
may be seen in section 8 as well as Appendix A). Identified parameters were also saved in
spreadsheet form with associated day to an excel file to facilitate result comparisons. Examples
of these excel spreadsheets for each patient may be seen in section 8. Analysis of these results as

7
detailed in Section 9 was then preformed manually or with the assistance of codes structured
specifically for the analysis at hand using these generated files.

8
4 MODELING
4.1 Literature Review
In this thesis we focus on modeling work originated in [9], which aimed to develop and
validate a model for the fluid dynamic system between interstitial and intravascular space during
hemodialysis. The model was identified in this study by determining the various parameters
included in the equations through clinical methods on 13 patients and comparing the model
output to collected volume change data when excess blood volume is removed.
In [10], changes in relative blood volume were modelled a simplified system model based
on a smaller number of, and appropriateness of the model was established using again using
clinical data.
In [11], parameter sensitivity analysis of the model in [10] was carried out. A simulation
model was developed in [11], based on the equations in [9], and modified 13 parameter values
from their determined baseline values to match responses in the linearized function analyzed in
[10].
More recently, [8] proposed a new method for the design of individualized UF profiles
based on the model in [11]. The model was further simplified using linearization around
equilibrium (UF=0) followed by discretization. This model comprised of 3 parameters which are
functions of the 13 parameters in the underlying nonlinear model of [11]. The parameters of the
simplified model in [8] were estimated using a linear least-squares problem. Subsequent analysis
at our lab revealed that this algorithm was fraught with technical issues and could not
successfully estimate parameters in many data sets.
Next, we describe through analysis of the underlying assumptions taken in the derivation
of the simplified model in [8], our model refinements made for purposes of achieving a more
accurate parameter identification.
4.2 Nonlinear Model in “Individualization of Ultrafiltration in Hemodialysis”
A two-compartment model for patient fluid volume shown in Figure 5.1 (as illustrated in
and extracted from [8]) is used to approximate the complex fluid dynamics system in the human
body. This model incorporates static and oncotic pressure differences between the interstitial and
intravascular compartments, as well as flow through the lymphatic system. The following

9
equations describe the dynamics with the nomenclature described below in table 5.1. These
equations are derived from the first appearance in the linearization model described in [7].
Figure 4.1: A schematic of the simplified of the two-compartment fluid dynamic model.[8]

10
Table 4.1: Modeling variables and parameters used in both nonlinear and linearized systems, as
well as their respective meanings.
x1 Intravascular Volume (L) x2 Interstitial Volume (L)
VRBC Red Blood Cell Volume (L) a, b, c, d, r,
f, g, h, l,
Kc1, Kc2, Kc3
Dimensionless Parameters
Kf Filtration Coefficient
(L/min/mmHg)
Po Offset Pressure (mmHg)
U Ultrafiltration Rate (L/min) Vieu Initial interstitial compartment
volume in euhydrated state (L)
Vpeu Initial intravascular
compartment volume in
euhydrated state (L)
mi Interstitial Protein Mass (g)
mp Intravascular Protein Mass (g) Ql Lymphatic Flow (L/min)
Pc Hydrostatic Capillary
Pressure (mmHg)
Pv Venous Pressure
Pi Interstitial Pressure (mmHg) Pip Plasma Collid Osmotic Pressure
(mmHg)
πi Interstitial Collid Osmotic
Pressure (mmHg)
Δp Hydrostatic Pressure Gradient
(mmHg)
Δπ Osmotic Pressure Gradient
(mmHg)
1 1 10
2 2 20
(0)
(0)
= − + − =
= − =
f l
f l
x Q Q u x x
x Q Q x x (4.1)
In Eq. 4.1, x1 denotes intravascular volume and x2 denotes interstitial volume. With the
equations for the osmotic and oncotic pressure differentials (Δπ and Δp, respectively) the flow
volume per minute across the capillary membrane may be determined which forms the basis of
most of the refill flow (Qf).
( )f fQ K p = − (4.2)
The lymphatic flow (Ql), limited using hyperbolic tangent term to a maximum flow of g, is
driven by oncotic pressure differentials.
tanh( )l iQ g h P l= + (4.3)

11
The oncotic and osmotic pressure differentials driving the refill and lymphatic flow are described
as follows:
1
,
2
, 2
,
2 3
1 2 3
2 3
1 1 1
2 3
1 2 3
2 3
2 2 2
100
100
100
= +
+= + +
= + +
= + +
= + +
c v o
f
RBCv
RBC P eu
i
i eu
i eu
c p c p c p
p
c i c i c ii
P P P
V xP d r
V V
a x bP
V xc
V
k m k m k m
x x x
k m k m k m
x x x
(4.4)
with the flow from interstitial (x2) to intravascular (x1) being well defined through these
equations, and UFR being known, it is possible to track the hematocrit changes, this being a
function of the intravascular compartment volume alone.
1
RBC
RBC
VHCT
V x=
+ (4.5)
Equations (4.1) -(4.5) form our model relating the input UFR and the output hematocrit,
assuming the knowledge of initial conditions. In this time-invariant model, the parameters are
fixed throughout the treatment, and initial flow between compartments is assumed to be zero for
identification purposes. Each of the compartments is assumed to have an initial static volume
prior to UF beginning.
We note that [8] discussed the identifiability of the unknown parameters in the model (4.1) -
(4.5) when only HCT and UFR data is available. Weak parameter sensitivity is noted within
patients for the parameters of the nonlinear model, and as a result [8] fixed all parameters outside
of compartment volumes in the nonlinear model a priori based on data from earlier papers.

12
Therefore, reducing the number of parameters for identification as well as determining a fixed
range of uncertainty was a goal in the design of the linearized model as presented in [8].
4.3 The Linearized Model in [8]
The model-based design of an individualized UFR profile at the initial segment of an HD
treatment requires the model (Eq. 4.1-45.5) to be parameterized in real time which is an
impossible task. In [8] a simplified model to facilitate fast online parameter estimation using
from data at the start of an HD treatment was introduced, as required for a design of UF profiles.
To that end, [8] proposed using a linearized model, described about a given equilibrium point.
For example, assuming that the 2-pool fluid dynamics model is in steady-state with no UFR or
refill flows, the following model is derived by assuming small changes in all states about their
equilibrium values, x10 and x20 (see Appendix B for details of linearization).
( ) ( )
( ) ( )
( )
1 1 10 2 20 10 0
2 1 10 2 20 20
0 1 10
10
20
0
0
0
(0)
x x x x x x u u
x x x x x x
HCT HCT K x x
x
x
HCT HCT
− − + − + − +
− − − +
− −
=
=
=
(4.6)
The terms K, α, and β, are functions of the parameters in the nonlinear model as described below
(see Appendix A for details).

13
( )2
10
12 3
1 2 310
2 3 4
, , 10 10 10
2 3
1 2 3
2 3 4
20 20 20 , 20
,
100 2 3100
1002 3
100
−
=+
+= + + + + +
= + + + −
+
RBC
RBC
f
f c p c p c pRBCf
RBC p eu RBC p eu
fc i c i c if
i eu
i eu
VK
V x
K d f k m k m k mV xK
V V V V x x x
Kk m k m k m bK a
x x x V x
V c
2 20
, ,20 20,
, ,
100 100sech 100
100 100
+
− + + +
i eu i eu
i eu
i eu i eu
xh a h b h bg h a
V Vx xV c
V V c
(4.7)
The final input-output relation between the input UFR and the output HCT can be derived
using Laplace transform. Transforming the linearized model above results in:
10 201 10 1 2
10 202 20 1 2
100 1
( ) ( ) ( ) ( )
( ) ( ) ( )
( ) ( )
− − + + − −
− − − +
− +
x xX s s x X s X s U s
s s
x xX s s x X s X s
s s
K xHCT s HCT K X s
s
(4.8)
Finally, using straightforward algebraic steps we arrive at the simplified transfer function model.
( )
( )
( )
( )
K sHCT s
U s s s
+=
+ +(4.9)
Note that this model has only three variables, K, α, and β.

14
4.3.1 Accuracy of Linearization
By definition, the linearization is accurate only for small perturbations in all signals about
their respective equilibrium levels. To validate this assumption, we simulated the nonlinear
model (4.1) -(4.5) at various UFR profiles with model parameters as defined in Table 4.1 and
compared the corresponding responses with those obtained from the linear model (4.9) using
identical UFR profiles and K, α, and β computed from the parameters in Table 4.1 and equations
(4.7).
Figure 4.2: Linearization accuracy assessment of the model (YY) for model parameters and
UFR data in Table 5.1. 1: UFR of 1500 mL/hr transitioning to 1800 mL/hr at 60 minutes, initial
HCT of 38.54%. 2: UFR of 1200 mL/hr transitioning to 900 mL/hr at 60 minutes, initial HCT of
38.54%. 3: UFR of 900 mL/hr transitioning to 1200 mL/hr at 60 minutes, initial HCT of 32.69%.

15
Table 4.2: Model parameters for nonlinear-linearization comparison.
a 0.006 b -198
c -45 d 0.01
r -30 f 1.46
g 0.045 Kc1 0.21
Kc2 0.0016 Kc3 9*10-6
h 0.7672 Kf 0.0057
l 0.045 mi 210 g
mi 210 g Vrbc 2 L
Po 13.2 mmHg Vpeu 3 L
Vieu 11 L
An excellent agreement between HCT responses from the nonlinear (4.1) -(4.5) and
linearized (4.9) models is observed in Figure 5.2 at various UFR steps at t = 0 and different
initial conditions. An excellent agreement is also observed in the response to a second UFR step
at a later time during treatment, t = 60 min. Between 0-60 minutes, the maximum absolute
difference in hematocrit for each case 1, 2, and 3 respectively were 0.05%, 0.02%, and 0.09%
within the first 60 minutes after a UFR step change which are each extremely low. This confirms
the suitability of the linearized model for this application. When examining clinically gathered
data, more significant deviations were noted in the refill rate, leading to a correction in the model
described next.
4.4 Model Correction to Account for Refill Dynamics
The simplified model (4.9), derived about an equilibrium state, does not include refill term.
Clearly, even under the assumption of small perturbation, any UF change would induce refill
which is an instantaneous function of pressure differential.
( )f fQ K p = − (4.10)

16
Actual refill dynamics, not explicit in (4.9), is reported to exhibit lag of 15-30 minutes to reach
its maximal value for a constant UF step change. To capture refill yet enjoy the simplification
offered by linearization, one can think of a single input to the linearized model (4.9) which is the
net flow to the intravascular compartment x1, i.e., the difference between UFR and refill flows
(by assumption UFR results in Qf flowing into x1)
( ) ( )0 0f f fUFR UFR Q Q UFR Q− − − = − (4.11)
We further assume that the final value of refill is a between 0% (no refill) and 100% (max refill)
of the value of the UFR step, and that its dynamics can be modeled as first order system:
( )0( ) 1 reduction
t
f REDQ t UFR UFR K e
− = − −
(4.12)
where Kred is a reduction factor on the overall UFR scaled between 0 and 1 and tau is a rime
constant set to give an exponential curvature to this term. Therefore, the net flow, or a modified
input Umod can be described by
mod R( ) [1 (1 )]reduction
t
EDU t K e
−
= − − (4.13)
Steady state flat HCT response, i.e., negligible to no hematocrit change over time, corresponds to
a reduction factor of KRED = 1. While this modification now accounts for actual refill dynamics,
it adds two additional parameters, KRED and τreduction, that must be identified.
For future sections, the following will be referenced as functions of combined
parameters:
1
SYS
RED reduction
KGain
=
+
=+
=
(4.14)

17
5 PARAMETER IDENTIFICATION APPROACH
The model developed in Chapter 5, while simplified, requires an estimation of unknown
parameters in order to design an individualized UF profile. The parameter identification
approach in [8], which was based on least squares formulation, suffered several technical issues.
In this thesis, we examined several identification methods with particular consideration was paid
to having a “simple” to implement algorithm easily integrated into hemodialysis machines.
These factors all came into consideration in the design process of our system identification
approach as described next.
5.1 Identification Method in “Individualization of Ultrafiltration in Hemodialysis”
In [8] a linear least-squares identification approach was defined using the discrete-time
model of the fluid dynamics model described in Eqn. (5.9). Examination of this method revealed
some drawbacks, particularly one assumption that was applied in ill-conditioned cases but could
not be supported on a technical level. In addition, identification in the presence of noisy data
would often result in estimated parameters outside their expected range, [8] and/or the overall
agreement between simulated response and data would suffer. As a result, there was a clear need
to adopt and/or develop a different algorithm. Section 4 motivated to desire to reduce the number
of parameters, and next we describe several parameter identification methods considered for this
purpose.
5.2 Nonlinear Least-Squares Parameter Iteration
In this approach, a nonlinear, iterative least squares formulation was considered. This
approach would function by perturbing the parameters a small amount to gauge the change in fit
of simulated response vs. data via RMS error from the alteration of parameters, then computing
and applying a small change iteratively until the RMS error in the system is minimized. This
approach allowed for each of the parameters to be modified gradually, however, it tended to
converge to a local minima often resulting in nonphysical values of beta being computed. Since β
is directly proportional to the steady state solution, it rendered the estimated parameters
unusable.
To rectify this problem, β was initially scaled within the iterative approach such that it
would not change as much through each iteration of the algorithm. While scaling has helped with

18
the convergence of β, it did not remove the problem of it being pushed to nonphysical ranges in
iteration. It appeared to be the case that as beta was so low (on the order of 10-2), iterative
approaches converging on parameter values were ill-equipped to converge to adequate problem
solutions due to the small values in question. Other approaches were briefly considered without
much success and will not be reviewed here.
Based on the initial experience with several parameter estimation approaches, it was
decided to examine the model in order to exploit specific characteristics of the response with the
aim of developing a more suitable approach.
5.2.1 Piecewise Analysis
The response of the fluid dynamics model, Eq. (4.9), to a constant UF step comprises two
segments, transient and steady-state. Specifically, at steady state, the relation between the input
and the response, so-called system’s gain, can be rewritten as a function to compute β in terms of
the steady state slope, K, α, and the UF profile applied. The β parameter has been observed in
numerical computations using table 5.1 to generally compute to one order of magnitude
compared to K and α, and thus this is an invaluable exploitation of model behavior to inform on
identification approach. Using this approach, it was possible to define the entire estimation of the
hemodynamic system response in terms of K and α, as well as known input quantities. Among
the major impacts of this change is the ability to use methods of identifying the system once
deemed to be computationally intensive, as now there are only two major parameters to iterate on
(K and α), instead of three (K, α, and β).
For practical future use in HD units, solutions that do not require proprietary parameter
identification software are desired instead of packaged algorithms that add complexity and cost.
As such, a grid-search approach becomes practical to use now, in which a large grid is created
with all possible permutations of K and α, the grids then being applied to the problem and used
to compute the minimum-error parameter set. When three parameters were present in the system,
this approach was somewhat intensive, as to even generate matrices of sufficient resolution to be
meaningful, the size would be unsupportable by MATLAB (and incidentally the RAM of the
computer in question).
The benefits to using a grid search system are twofold when using only two parameters in
it – firstly, the problem of converging to a local minima is resolved. As long as the grid

19
boundaries are sufficiently large and the resolution sufficiently small, then the reached global
minima can be assumed to be sufficiently accurate. Secondly, the identification process itself
runs far faster than all prior approaches, with no iteration involved or non-converging loops
possible, the system being a strict computation of the simulation output, and subsequent
comparison to the hematocrit data set input. This gridding approach relies on the grid being high
enough resolution between parameters to accurately identify the global-minima parameter
values.
Use of the grid search system proved highly effective in the identification of parameters,
working well and yielding accurate results when applied to noise-added simulated system
models. As these were simulated sets with the underlying parameters known, it was possible to
compare converged upon parameter results with the theoretical computed ones. With the
establishment of a working identification approach with regards to simulated data sets, this
approach may be applied to actual collected data sets to determine any problems or differences,
if present. As the simulation model represents an idealized version of the system, some
differences are generally expected. In the case of the patient data, what is observed in many cases
that is substantially different from our model is the existence of ‘flat’ profiles, where despite a
substantial UFR, patient hematocrit remains constant throughout or after a short transient.

20
5.3 Final Approach
To account for the effects of flat steady-state profiles, the gain of the model is expanded
to be a function of both the reduction factor (KRED) introduced in Eq. 5.12 and the steady state
gain of equation 5.9, the rationale of which is described in chapter 5. Therefore, a method must
be determined to provide an a priori estimate for either of these factors to maintain the capability
to compute the identification within a reasonable timeframe. As the gain in Eq. 5.9 is based off
of internal model parameters, the reduction factor KRED is chosen for this estimation. In order to
do so, we examine the relative angle trajectory of the steady state of the hematocrit (y) vs. time
(x) when plotted. An angle of 55 degrees or higher is determined as the ‘baseline’ where no
reduction in steady state is applied. For angles below this, scaling down to zero degrees (flat
profiles), we define an arctangent term that linearly scales a reduction factor (KRED), scaling up
to 1. To account for variance in the flat profiles caused by noise, any computed reduction factor
of 0.95 or above was reset to 1, such that there is no effective UFR on the system in steady state.
With this reduction factor being determined, we may apply algorithmic methods to
determine the remaining parameters, K, α, β, and τreduction. Worthy of note is that the combined
parameter:
1
+ (5.1)
also is the internal time constant of the system and may affect the terms in the estimation when
the reduction factor time constant is introduced. Term 1.1 is defined as τsys. As before, a grid-
search approach is defined which creates a grid containing all possible combinations of K and α,
with β being calculated from the steady state slope, and KRED being determined from the angular
approach defined above. The time constant on the reduction factor, τreduction, is looped through,
with the grid approach being conducted for each value of τreduction. This results in the
determination of the global minimum RMS error between collected data and simulated response,
the parameters of which are stored as the identified system. This approach is robust enough to
determine parameters through noise consistently, and by using the gridded approach, forces all
parameters to remain in the physical regime. As the reduction factor is determined in advance

21
and the simulation must start from a specific initial hematocrit, this method is susceptible to
influences from outlier treatment profiles caused by errors in treatment or starting conditions.
5.4 Determination of Outlier Treatment Profiles
As expected, actual responses measured during HD treatments can exhibit dynamics that cannot
be accounted for with the model under same UFR input (5.9). As a result, such responses should
be recognized prior to applying identification to avoid inaccurate or misleading results.
Conditions that are known to results in unmodelled dynamics include needle misplacement (Fig
8.5) which affect local recirculation and lead to very different hematocrit profiles. While
treatment sheets note any such events, since they are not integrated with most electronic health
records, we are able to recognize such instances manually on a case-by-case basis.
Outlier dynamics, those exhibiting significant refill dynamics without any change in
treatment UFR profile, are especially challenging. For example, a patient hematocrit can reach
expected equilibrium rate, then at some point later in the treatment change its slope indicating a
corresponding refill change. Figure 8.3 depicts such an instance. While changes in hemodynamic
response to treatment are expected as fluid is removed, they are not included in our model (5.9)
as the required variables necessary to be added are not available. Specifically, factors such as
changes in blood pressure, caused either by treatment or simply by nervousness can drive some
of these changes, factors which cannot be easily integrated into the two-compartment model
used. Additional, similar impacts can be caused by initial conditions existing in the HD system.
While the CliC monitoring devices do not flag beginning treatment until one minute of consistent
hematocrit readings, so-called ‘false starts’ are still possible, and lead to inaccurate readings.
These cases are typically characterized by very low starting hematocrit, or very rapid changes in
hematocrit within the first few minutes of treatment. While somewhat harder to isolate than the
prior cases, these are nonetheless eliminated from analysis where noted.

22
6 PARAMETER SENSITIVITY In modelling the response of a system, it is essential to avoid over-parameterization. That
is, the model includes more parameters than are needed based on either the actual model or the
nature of the data available for estimation. As a result, an over-parametrized model is more likely
to have worse fit to the data. Therefore, sensitivity analysis which analyzes over parametrization
is paramount in any parameter estimation process. For example, the sensitivity analysis tool in
Simulink accomplishes this by generating simulations with randomized parameters and
comparing the RMS error to generate a 2-dimensional heat map of most accurate to least model
fit measure. By comparing the heat maps, with a parameter on each axis over multiple data sets
to ensure this is consistently observed in the same manner, it is possible to analyze the model fits
sensitivity with respect to the 2 parameters in the map. Observing Figure 7.1 as an example case,
we can observe the lowest error (most accurate region) is within the bottom right corner in the
darkest blue, marked by the black circumscribed region. This indicates that the lowest error is
observed for high K and low α values. Error values increase, and therefore the accuracy gets
worse, in a stratified pattern with increasing α value and decreasing K value, until reaching the
highest error, in the regions indicated by the red perimeter. These indicators are used for each of
the following plots, Figures 7.1-7.4.

23
Figure 6.1: Heatmap comparing the influence of parameters K and α on the system model
compared to a data set of patient 29. Blue indicates higher accuracy to the data set utilized. The
region surrounded in black indicates high sensitivity in that region, and the region circumscribed
in red indicates low sensitivity.

24
Figure 6.2: Heatmap comparing the influence of parameters K and β on the system model
compared to a data set of patient 29. Blue indicates higher accuracy to the data set utilized. The
region surrounded in black indicates high sensitivity in that region, and the region circumscribed
in red indicates low sensitivity.

25
Figure 6.3: Heatmap comparing the influence of parameters K and the reduction factor (Kred)
on the system model compared to a data set of patient 29. Blue indicates higher accuracy to the
data set utilized. The region surrounded in black indicates high sensitivity in that region, and the
region circumscribed in red indicates low sensitivity.

26
Figure 6.4: Heatmap comparing the influence of parameters α and the reduction factor time
constant (τRED) compared to a data set of patient 29. Blue indicates higher accuracy to the data
set utilized. The region surrounded in black indicates high sensitivity in that region, and the
region circumscribed in red indicates low sensitivity.
As indicated by the heat maps above, there is a narrow band of the K and alpha parameter
values that produce the most accurate estimation results in the regime of high K and low α.
Additionally, when examining β vs. either K or α, β does not seem to have an overall impact on
the accuracy, seen by the broad value sets of β for which accuracy is highest. This is particularly
notable since due to β’s low value it is assumed that there would be a great degree of sensitivity
to this parameter, but this does not seem to be the case here.
It is observed in Figure 6.4 that there is a far greater sensitivity to α in the model
compared to the time constant from refill/reduction factor. While the τSYS parameter ranges from
7-14 minutes for optimal accuracy, α is highly restricted to below 0.05, less than 5% of its
allowed range. In a similar manner, the KRED and K parameter are examined in relation to one
another. Notably, when comparing the two there appears to be a triangular region (maximum
reduction and maximum K to zero reduction and medium K). This indicates as expected a

27
proportional relationship between the parameters, as at steady state the reduction effectively acts
as a multiplier on K.

28
7 PARAMETER ESTIMATION RESULTS In this chapter we report parameter estimation results using the ID method presented in
Chapter 6. A total of 77 measurements were collected from 25 patients, with each treatment
being recorded as a single measurement. Of these patients, due to several data collection
limitations, only a single data file was recorded for 8 patients and those were removed from
analysis for reasons noted in Section 4.1. Each subsection contains the identification results of a
single patient. In some cases, identified data sets were excluded from the statistical analysis, the
main reasons being a) the initial hematocrit data point does not coincide with the first UF step, b)
the data set is identified as flat in steady-state, or c) other reasons such as needle misplacement.
The results for each patient are presented in terms of plots that compare measure data
with the simulated response from the estimated model (4.8) and a table summarizing identified
parameters and other key variables at each measurement day available for that patient. For
brevity, except for representative plots, all other plots can be found in Appendix A. In particular,
a plot representing good data is shown in section 8.1.1, and a plot representing known external
effects such as needle adjustment in section 8.1.6.
Following the intra-patient results, we describe intra-patient parameter variability using
means and standard deviations. Finally, we briefly present prediction results and estimation
results for subsequent UFR step change later in the HD treatment.
7.1.1 Patient 7
Figure 8.1 shows a comparison between measured HCT data at one of the measured treatments
vs. the estimation. The data in Figure 8.1 includes the initial time span used for parameter
estimation and the subsequent 25 minutes for validation purpose. Overall parameter estimation
results for all measured treatment days are presented in Table 8.1. The 5 identified model
parameters, Kred, K, α, β, and τreduction, along with key computed variables, Gain, τRED, and τSYS as
defined in Equation 5.14. Replications of day number (column 1) indicate that the patient
underwent changes in UFR, the new value of which can be seen in the corresponding column
and row. Each UFR change was a step change, which are processed and implemented near-
instantaneously. To protect PHI, per IRB, day represents the difference between actual treatment
date and an unrelated start date.

29
Figure 7.1: Measured Hematocrit (HCT), identified HCT and UFR profile. The black solid line
indicates the region used for parameter identification, the green dashed line indicates the
validated response using identified parameters, and ultrafiltration rate. Time of 0 corresponds to
start of HD treatment.

30
Table 7.1: Patient 7 numerical data from system identification. Time constant (τ) terms are in
units of minutes, and Gain is defined as HCT*hr/mL.
DAY HCT(0) UFR(mL/hr) Kred K α β Gain τsys τreduction
105 0.35 1120 0.28 0.06 0.01 0.01 0.03 52.74 14
133 0.38 1200 0.84 0.07 0.04 0.02 0.02 16.54 12
138 0.36 1100 0.89 0.20 0.31 0.05 0.03 2.81 4
147 0.35 1120 1.00 0.62 0.01 0.00 0.00 100.00 1
152 0.35 1100 0.55 0.04 0.04 0.08 0.03 8.24 13
77 0.28 1100 0.94 0.15 0.05 0.01 0.03 16.57 11
84 0.32 750 1.00 0.33 0.01 0.00 0.00 100.00 1
84 0.32 1130 1.00 1.00 1.00 0.00 0.00 1.00 1
Mean 0.70 0.10 0.09 0.03 0.03 0.35 2.48
Standard Deviation 0.25 0.06 0.11 0.03 0.00 0.03 1.94

31
7.1.2 Patient 6
Table 7.2 summarizes the results of model parameter estimation and key parameter
values. An example of near-flat hematocrit response at steady-state, typical to this patient, is
shown in Figure 7.2.
Figure 8.2: Hematocrit (left axis) vs. time (bottom) for measured data, as well as corresponding
identified profile. The black solid line indicates the region used for profile identification, with the
green dashed line indicating the projection into the future of this model. Ultrafiltration rate is
indicated on the right axis and is a fixed rate throughout this treatment period.

32
Table 7.2: Parameter estimation results for Patient 6. Time constant (τ) terms are in units of
minutes, and Gain is defined as HCT*hr/mL.
DAY HCT(0) UFR(mL/hr) Kred K α β Gain τsys τreduction
107 0.33 1240 0.90 0.06 0.01 0.01 0.02 61.91 14
107 0.33 1340 0.00 0.04 0.75 1.55 0.03 0.44 15
138 0.33 1380 0.70 0.13 0.02 0.00 0.02 41.97 1
142 0.32 670 0.15 0.09 0.35 0.44 0.05 1.27 6
142 0.33 1410 1.00 0.01 1.00 0.00 0.00 1.00 1
142 0.34 1470 0.73 0.02 0.28 11.40 0.02 0.09 4
152 0.32 1110 0.87 0.06 0.04 0.03 0.03 14.35 15
Mean 0.65 0.09 0.11 0.12 0.03 29.87 9.00
Standard Deviation 0.30 0.03 0.14 0.18 0.01 23.62 5.79

33
7.1.3 Patient 8
Table 7.3 shows the results of patient parameter identification, as well as other key
parameter values. Figure 7.3 displays treatment data and identification for patient 8, day 107.
This case depicts an abrupt change in hematocrit at 50 minutes from an unknown source,
meriting the key inclusion here.
Figure 7.3: Hematocrit (left axis) vs. time (bottom) for measured data, as well as corresponding
identified profile. The black solid line indicates the region used for profile identification, with the
green dashed line indicating the projection into the future of this model. Ultrafiltration rate is
indicated on the right axis and is a fixed rate throughout this treatment period.

34
Table 7.3: Patient 8 numerical data from system identification. Time constant (τ) terms are in
units of minutes, and Gain is defined as HCT*hr/mL.
DAY HCT(0) UFR(mL/hr) Kred K α β Gain τsys τreduction
107 0.38 1270 0.37 0.03 1.00 4.22 0.02 0.19 12
138 0.33 1400 1.00 0.35 0.01 0.00 0.00 100.00 1
147 0.35 1290 0.31 0.03 0.04 0.17 0.02 4.72 10
154 0.33 1300 0.69 0.05 0.01 0.01 0.02 55.62 14
89 0.35 1250 1.00 0.36 0.01 0.00 0.00 100.00 1
96 0.38 1220 0.02 0.03 1.00 39.08 0.03 0.02 1
Mean 0.46 0.04 0.35 1.47 0.02 20.18 12.00
Standard Deviation 0.17 0.01 0.46 1.95 0.00 25.13 1.63
7.1.4 Patient 11
Table 7.4 indicates system identification results for patient 11.
Table 7.4: Patient 11 numerical data from system identification Time constant (τ) terms are in
units of minutes, and Gain is defined as HCT*hr/mL.
DAY HCT(0) UFR(mL/hr) Kred K α β Gain τsys τreduction
112 0.3194 800 0.2 0.17 0.08 0.005669 0.01125 11.67279 15
112 0.3253 620 0.9 0.16 0.19 94.05 0.159677 0.010611 3
112 0.3256 300 1 0.86 0.01 0.006226 0.33 61.62791 1
114 0.3099 550 0.6 0.45 0.01 0.000827 0.034364 92.36364 1
Mean 0.4 0.31 0.045 0.003248 0.022807 52.01822 8
Standard Deviation 0.282843 0.19799 0.049497 0.003424 0.016344 57.05704 9.899495

35
7.1.5 Patient 15
Table 7.5 contains the system identification results for patient 15. Figure 7.4 indicates the
identified response for patient 15, day 133 compared to collected data. Note the scaling on the
left y-axis, indicating that the hematocrit does not appreciably vary over 70 minutes of treatment.
Figure 7.4: Hematocrit (left axis) vs. time (bottom) for measured data, as well as corresponding
identified profile. The black solid line indicates the region used for profile identification, with the
green dashed line indicating the projection into the future of this model. Ultrafiltration rate is
indicated on the right axis and is a fixed rate throughout this treatment period.

36
Table 7.5: Patient 15 numerical data from system identification. Time constant (τ) terms are in
units of minutes, and Gain is defined as HCT*hr/mL.
DAY HCT(0) UFR(mL/hr) Kred K α β Gain τsys τreduction
133 0.30 750 0.86 0.10 0.01 0.01 0.04 62.16 1
133 0.30 300 1.00 0.18 0.99 0.00 0.00 1.01 1
142 0.31 400 1.00 0.67 0.01 0.00 0.00 100.00 1
142 0.31 470 0.28 0.12 0.97 1.25 0.07 0.45 3
147 0.32 500 1.00 0.01 1.00 0.00 0.00 1.00 1
152 0.32 550 1.00 0.57 0.01 0.00 0.00 100.00 1
Mean 0.57 0.11 0.49 0.63 0.05 31.30 4.00
Standard Deviation 0.29 0.01 0.48 0.62 0.01 30.85 1.00

37
7.1.6 Patient 17
Figure 7.5 compares measured with simulated hematocrit responses to UF over estimation
and validation spans. Figure 7.6 is the redacted treatment chart for day 107 (Figure 7.5) and
indicates a needle readjustment. Figure 7.7 depicts the long-term tracking of identified system to
collected data over the entire treatment span. Table 7.6 reports all identified parameters for each
treatment day of patient 17.
Figure 7.5: Patient 17 day 107 hematocrit and system identification simulation. Subplot
indicates long term data and corresponding identified system simulation.

38
Figure 7.6: Patient 17 day 107 patient treatment chart, indicating a needle adjustment taking
place between 7:00 and 7:35, 39-74 minutes following treatment start.

39
Figure 7.7: Patient 17 long-term behavior for day 138. Patient data is indicated by blue dots. The
region used to estimate parameters is denoted by the green line, while the long-term projection is
indicated in yellow. Subplot zooms in on region of estimation.
Table 7.6: Patient 17 numerical data from system identification. Time constant (τ) terms are in
units of minutes, and Gain is defined as HCT*hr/mL.
DAY HCT(0) UFR(mL/hr) Kred K α β Gain τsys τreduction
107 0.31 510 0.00 0.13 0.10 0.12 0.07 4.58 15
112 0.30 490 0.47 0.29 0.05 0.01 0.06 15.78 1
119 0.27 510 0.48 0.96 0.35 0.02 0.06 2.68 1
135 0.30 690 0.55 0.31 0.07 0.01 0.04 12.32 5
138 0.32 850 0.28 0.12 0.07 0.03 0.04 9.84 4
154 0.37 310 0.90 0.34 0.01 0.00 0.09 73.12 15
154 0.39 390 1.00 1.00 1.00 0.00 0.00 1.00 1
Mean 0.45 0.42 0.14 0.02 0.05 10.15 2.75
Standard Deviation 0.10 0.32 0.12 0.01 0.01 4.80 1.79

40
7.1.7 Patient 18
Table 7.7 records the system identification results for patient 18.
Table 7.7: Patient 18 numerical data from system identification. Time constant (τ) terms are in
units of minutes, and Gain is defined as HCT*hr/mL.
DAY HCT(0) UFR(mL/hr) Kred K α β Gain τsys τreduction
119 0.32 860 0.50 0.03 0.05 0.00 0.00 20.00 14
135 0.31 730 0.46 0.01 1.00 0.00 0.00 1.00 3
135 0.31 560 1.00 0.01 1.00 0.00 0.00 1.00 15
138 0.34 1070 0.79 0.73 0.31 0.01 0.03 3.11 1
138 0.36 950 0.63 0.15 1.00 0.26 0.03 0.80 4
154 0.36 860 0.47 0.02 0.08 0.00 0.00 12.50 9
70 0.35 570 1.00 0.74 0.01 0.00 0.00 100.00 1
70 0.35 510 1.00 1.00 1.00 0.00 0.00 1.00 1
Mean 0.71 0.44 0.66 0.13 0.03 1.95 2.50
Standard Deviation 0.08 0.29 0.35 0.12 0.00 1.16 1.50
7.1.8 Patient 27
Table 7.8 records the system identification results for patient 27.
Table 7.8: Patient 27 numerical data from system identification. Time constant (τ) terms are in
units of minutes, and Gain is defined as HCT*hr/mL.
DAY HCT(0) UFR(mL/hr) Kred K α β Gain τsys τreduction
107 0.35 480 1.00 1.00 0.01 0.00 0.00 100.00 1
119 0.36 740 0.27 0.30 0.19 0.03 0.04 4.51 13
119 0.37 600 -0.21 0.07 0.12 11.24 0.07 0.09 15
138 0.37 860 0.80 0.41 0.01 0.00 0.03 91.91 1
138 0.40 560 1.00 0.01 1.00 0.00 0.00 1.00 1
0 0.00 0 0.00 0.00 0.00 0.00 0.00 0.00 0
149 0.35 340 0.35 0.24 0.03 0.02 0.09 20.67 15
149 0.36 350 0.82 0.09 1.00 9.41 0.08 0.10 15
Mean 0.31 0.27 0.11 0.03 0.07 12.59 14.00
Standard Deviation 0.04 0.03 0.08 0.01 0.02 8.08 1.00

41
7.1.9 Patient 29
Figures 7.8-7.10 depict identified responses compared with collected hematocrit data, as
well as providing the UFR. Note the scaling on the hematocrit indicates that these responses
occur over a very small hematocrit range and are broadly flat. Table 7.9 records the identified
parameters and corresponding statistics.
Figure 7.8: Hematocrit (left axis) vs. time (bottom) for measured data, as well as corresponding
identified profile. The black solid line indicates the region used for profile identification, with the
green dashed line indicating the projection into the future of this model. Ultrafiltration rate is
indicated on the right axis and is a fixed rate throughout this treatment period.

42
Figure 7.9: Hematocrit (left axis) vs. time (bottom) for measured data, as well as corresponding
identified profile. The black solid line indicates the region used for profile identification, with the
green dashed line indicating the projection into the future of this model. Ultrafiltration rate is
indicated on the right axis and is a fixed rate throughout this treatment period.

43
Figure 7.10: Hematocrit (left axis) vs. time (bottom) for measured data, as well as corresponding
identified profile. The black solid line indicates the region used for profile identification, with the
green dashed line indicating the projection into the future of this model. Ultrafiltration rate is
indicated on the right axis and is a fixed rate throughout this treatment period.

44
Table 7.9: Patient 29 numerical data from system identification. Time constant (τ) terms are in
units of minutes, and Gain is defined as HCT*hr/mL.
DAY HCT(0) UFR(mL/hr) Kred K α β Gain τsys τreduction
100 0.35 670 0.84 0.26 0.15 0.03 0.04 5.58 3
107 0.34 670 0.86 0.05 0.02 0.11 0.04 7.62 12
117 0.33 940 0.75 0.06 0.05 0.05 0.03 9.84 12
0 0.00 0 0.00 0.00 0.00 0.00 0.00 0.00 0
121 0.33 800 0.78 0.15 0.02 0.01 0.04 38.10 1
121 0.33 840 0.49 1.00 0.68 0.03 0.04 1.42 1
140 0.33 870 0.69 0.08 0.04 0.03 0.03 14.64 13
145 0.34 1030 1.00 0.17 0.01 0.00 0.00 100.00 1
Mean 0.783845 0.12 0.056 0.045341 0.036824 15.15561 8.2
Standard Deviation 0.06101 0.07823 0.048415 0.035963 0.004841 11.86252 5.114685
7.1.10 Patient 31
Table 7.10 reports system identification results for patient 31.
Table 7.10: Patient 31 numerical data from system identification. Time constant (τ) terms are in
units of minutes, and Gain is defined as HCT*hr/mL.
DAY HCT(0) UFR(mL/hr) Kred K α β Gain τsys τreduction
121 0.3259 1050 0.190916 0.12 0.28 0.098601 0.031252 2.641301 9
145 0.3237 1250 0.284581 0.03 0.02 0.108883 0.025345 7.758992 11
149 0.3356 1130 1 0.26 0.01 0 0 100 1
Mean 0.237749 0.075 0.15 0.103742 0.028298 5.200147 10
Standard Deviation 0.046833 0.045 0.13 0.005141 0.002954 2.558846 1

45
7.1.11 Patient 32
Table 7.11 reports system identification results for patient 32.
Table 7.11: Patient 32 numerical data from system identification. Time constant (τ) terms are in
units of minutes, and Gain is defined as HCT*hr/mL.
DAY HCT(0) UFR(mL/hr) Kred K α β Gain τsys τreduction
112 0.3271 680 1 0.72 0.01 0 0 100 1
119 0.3091 600 0.740517 0.21 0.07 0.020622 0.047787 11.03488 1
135 0.3098 830 0.761958 0.13 0.08 0.028864 0.034468 9.18577 10
135 0.3325 710 0.535774 0.05 1 5.01453 0.041687 0.166264 1
138 0.3171 800 0.318961 0.16 0.48 0.155497 0.03915 1.573571 5
Mean 0.607146 0.166667 0.21 0.068328 0.040468 7.264739 5.333333
Standard Deviation 0.249805 0.040415 0.23388 0.075603 0.006757 5.014663 4.50925
7.1.12 Patient 37
Table 7.12 reports system identification results for patient 37.
Table 7.12: Patient 37 numerical data from system identification. Time constant (τ) terms are in
units of minutes, and Gain is defined as HCT*hr/mL.
DAY HCT(0) UFR(mL/hr) Kred K α β Gain τsys τreduction
105 0.3614 750 0 0.12 0.34 0.235506 0.049106 1.7376 15
112 0.3518 600 0.899412 0.97 0.05 0.002559 0.047222 19.02635 1
133 0.352 1000 0.899412 0.52 0.01 0.000576 0.028333 94.55129 1
133 0.3903 690 0.523778 1 0.19 0.008537 0.043001 5.036834 10
82 0.3356 800 0.614287 0.11 0.02 0.009918 0.036465 33.42487 11
Mean 0.136667 0.082661 0.044264 0.3496 716.6667 18.06294 9
Standard Deviation 0.144299 0.10812 0.005568 0.010647 84.98366 12.9542 5.887841

46
7.2 Summary of Key Intra-patient Estimation Results
Table 7.13 combines the reduction factor at steady state with the gain within the model
transfer function from equation (4.9) and reports the mean and standard deviation of this
combined parameter for each patient. The time constant term from the model is also reported
here again, for ease of comparison. This provides a clean and clear way to examine the inter-
patient differences in the relevant parameters, as well as a quick reference for the inter-patient
variability. Inclusion of coefficient of variation here also allows a reference for the relative
impact of the standard deviation as compared to the mean.

47
Table 7.13: Gains and time constant averaged and standard deviations for all patient initial steps
for which the steady-state slope is nonzero.
Patient Number Gain
Mean ± SD
(COV)
Time Constant (system),
Minutes Mean ± SD
(COV)
Time Constant (refill),
Minutes Mean ± SD
(COV)
6 0.014 ± 0.019
(1.36)
29.9 ± 23.6
(0.789)
9.00 ± 5.79
(0.64)
7 0.0081 ± 0.0080
(0.987)
19.4 ± 17.5
(0.902)
2.48 ± 1.94
(0.78)
8 0.013 ± 0.0053
(0.41)
20.2 ± 25.1
(1.24)
12.00 ± 1.63
(0.14)
11 0.011 ± 0.0034
(0.31)
34.7 ± 41.1
(1.18)
6.33 ± 6.18
(0.98)
15 0.027 ± 0.022
(0.81)
31.3 ± 30.85
(0.986)
4.00 ± 1.00
(0.25)
17 0.027 ± 0.005
(0.021)
10.2 ± 4.8
(0.471)
2.75 ± 1.79
(0.65)
18 0.0084 ± 0.0029
(0.35)
1.95 ± 1.16
(0.595)
2.50 ± 1.50
(0.6)
27 0.045 ± 0.019
(0.42)
12.6 ± 8.1
(0.643)
14.00 ± 1.00
(0.11)
29 0.0077 ± 0.0018
(0.24)
15.2 ± 11.9
(0.783)
8.20 ± 5.11
(0.62)
31 0.022 ± 0.005
(0.23)
5.2 ± 2.6
(0.5)
10.00 ± 1.00
(0.1)
32 0.016 ± 0.0097
(0.61)
7.3 ± 4.1
(0.562)
5.33 ± 4.51
(0.85)
37 0.023 ± 0.019
(0.83)
18.1 ± 12.9
(0.713)
9.00 ± 5.89
(0.65)

48
8 DISCUSSION
The results presented in Chapter 8 highlight the challenges associated with modelling
human physiology. Here, we discuss intra- and inter-patient parameter estimation results, then
follow with a description of strengths and limitations of our modelling and parameter estimations
approach.
Not unexpectedly, we observed that the response of a patient to UF can vary significantly
from one HD treatment to another. On any given day, the measured HCT response can nicely
supports our model, Eq. (4.7), leading to successful parameter estimation, while the measured
HCT response at a different HD treatment – a week later but under similar treatment parameters
– can exhibit dynamics that is not included in our model. Unfortunately, such unmodelled
dynamics cannot be simply added to the model under the constraint of having only HCT
measurements and UFR input.
By construction, the expected hematocrit response of the system model described by Eq.
(4.7) to a step UFR change from equilibrium comprises two parts: (a) the initial transients
modelled by a 1st-order exponential rise, and (b) the steady state response modelled by a constant
HCT increase which parallels the constant UFR profile. When the measured response follows
both parts within reasonable accuracy – in approximately 70% of data sets -- our ID algorithm
(Chapter 4) can successfully estimate model parameters. The remaining approximately 30% of
data sets pose a challenge to our approach for reasons as discussed below. We first discuss
results from successful estimations, followed by examining limitations of our approach.
8.1.1 Model Consistent with Clinical Data
The model (5.7) supported the measured dynamics in approximately 70% the data sets: a
mono-exponential transient followed by a constant positive steady-state HCT slope, albeit with
some noise. To test if a data set conforms to (5.7) model, we initially fit a line to the response
starting 10-15 minutes following the initiation of HD treatment as detailed in section 6.3. For
positive slope cases, the system identification algorithm (Chapter 6.1) checks in place for poor
fitting and large variability on the linear slope fit. Subsequently, the time constant for the initial
exponential transients is estimated as described in Section 6. Extremely low or high time
constant estimations were eliminated from the analysis due to high time constants creating

49
effects violating our assumptions of dynamics having settled when steady-state slope is
estimated, and extremely low time constants being indicative of poorly isolated transient
dynamics as detailed in Section 6.
Next, we discuss results from model parameter estimations in terms of key input-output
parameters system time constant τSYS, and gain, Gain, with the gain notably being modified with
the reduction factor term to conform to the true steady state value identified as in (8.1).
1
(1 )
sys
REDK KGain
=+
− =
+
(8.1)
Additionally, we will examine the reduction factor time constant KRED to determine the effect it
has on the identified system. Analysis of individual parameter statistics follows. We begin our
analysis by examining responses of few patients, 17, 7, and 29, to illustrate intra-patient
parameter variability and potential outlier data sets skewing statistics in results.
Observations from patient 17 along with brief discussions of patients 7 and 29 will lead
into a broader discussion of the variance in Gain and τSYS terms. These parameters will be
examined across all patients for variance intra-patient, as well as discussing the variations of the
mean parameter values inter-patient. Fast and slow time constants are discussed with reference to
patient 31, which will branch into a discussion of the impact of ultrafiltration rate on identified
parameter values. The effect of different ultrafiltration rates on estimated parameters is presented
using patients 32 and 29. Finally, we discuss data sets corresponding to the same patient with
similar conditions which result in different estimated parameters.
The Gain of patient 17 exhibits small variability across 5 treatment data sets. The
coefficient of variation is 0.21 despite larger differences in UFR and initial hematocrit across the
5 data sets (see Table (7.6)). This relatively low Gain variability was initially unexpected, as it is
a function of individual parameters which have large variability. Specifically, mean ± SD of ,
Kred and β, are 0.05 ± 0.04, 0.53 ± 0.34, and 0.24 ± 0.35, respectively. The parameter K has
larger variability (0.42 ± 0.32). Days 119 and 154 seem to drive up the SD and call into question
the strength of examining individual parameters in the model for identifying the system.

50
The estimate of τSYS is strongly affected by the estimate of τRED made at the initial step.
Two of the 5 estimates were fixed at the maximum allowed value of 15 min and one at the
minimum allowed 1 min, with an overall mean ± SD of 10.15 ± 4.80 min. In contrast, the other 2
estimates were 4 and 5 min, which are considered reasonably close to one another. There are
considerations on two of the 15-minute cases that provide additional context to the specific
results, day 112 having a low β parameter which reduced the Gain, and day 154 having an
unusually long system time constant as well. Effectively, these disparities indicate that these two
cases may not be representative of data sets for which the converged parameters are accurate to
the broad index of cases. The variability in these parameters, particularly in τSYS, is seen in the
sensitivity analysis as well (Chapter 7), where τSYS could vary by a large amount yet have
negligible impact on the accuracy of the result, as long as the α parameter was maintained within
a specific range.
This pattern is further confirmed by examining patient 29’s data, with dynamics ranging
from cases matching (4.7), flat response cases, and cases that do not conform to the model (4.7).
Gain is again noted to have a low coefficient of variation 0.24 (0.0077 ± 0.0018), while the
variance in system time constant remains high (15.1 ± 11.9 min), coefficient of variation of
0.783. The reduction factor time constant (τRED) fares no better (8.20 ± 5.11) minutes and a
coefficient of variation of 0.62. These observations provide an indication of low variability in the
Gain parameter, though having mixed results in both time constants, observing generally high
variability.
The observations above made in terms of specific patients, can be extended for the entire
cohort using Table 8. For ease of reference, Table 8.13 is copied into Table 9.1 below.
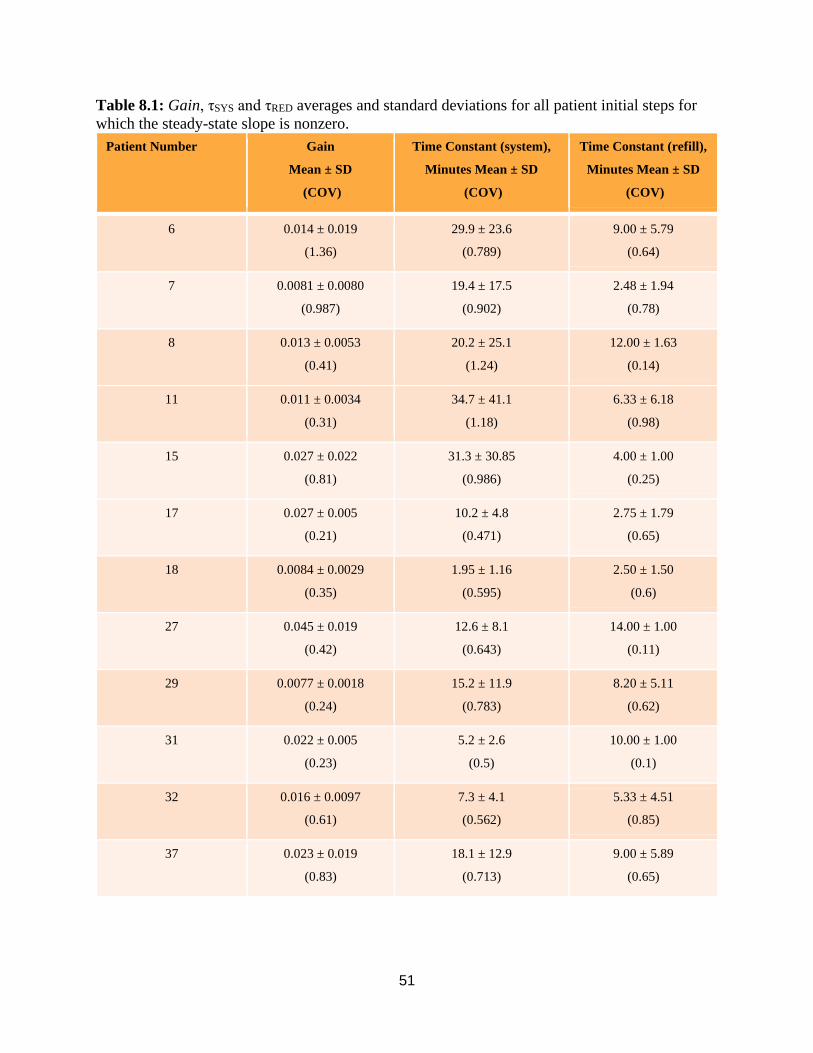
51
Table 8.1: Gain, τSYS and τRED averages and standard deviations for all patient initial steps for
which the steady-state slope is nonzero.
Patient Number Gain
Mean ± SD
(COV)
Time Constant (system),
Minutes Mean ± SD
(COV)
Time Constant (refill),
Minutes Mean ± SD
(COV)
6 0.014 ± 0.019
(1.36)
29.9 ± 23.6
(0.789)
9.00 ± 5.79
(0.64)
7 0.0081 ± 0.0080
(0.987)
19.4 ± 17.5
(0.902)
2.48 ± 1.94
(0.78)
8 0.013 ± 0.0053
(0.41)
20.2 ± 25.1
(1.24)
12.00 ± 1.63
(0.14)
11 0.011 ± 0.0034
(0.31)
34.7 ± 41.1
(1.18)
6.33 ± 6.18
(0.98)
15 0.027 ± 0.022
(0.81)
31.3 ± 30.85
(0.986)
4.00 ± 1.00
(0.25)
17 0.027 ± 0.005
(0.21)
10.2 ± 4.8
(0.471)
2.75 ± 1.79
(0.65)
18 0.0084 ± 0.0029
(0.35)
1.95 ± 1.16
(0.595)
2.50 ± 1.50
(0.6)
27 0.045 ± 0.019
(0.42)
12.6 ± 8.1
(0.643)
14.00 ± 1.00
(0.11)
29 0.0077 ± 0.0018
(0.24)
15.2 ± 11.9
(0.783)
8.20 ± 5.11
(0.62)
31 0.022 ± 0.005
(0.23)
5.2 ± 2.6
(0.5)
10.00 ± 1.00
(0.1)
32 0.016 ± 0.0097
(0.61)
7.3 ± 4.1
(0.562)
5.33 ± 4.51
(0.85)
37 0.023 ± 0.019
(0.83)
18.1 ± 12.9
(0.713)
9.00 ± 5.89
(0.65)

52
With notable exceptions, mainly patients with response data sets with low gain, it can be
observed that for the aggregated gain parameter, Gain, the coefficient of variation remains
generally below 0.35 in 5 of the cases and is above 0.35 in the remaining patients. The
coefficient of variation only goes above one in a single case, patient 6. As the reduction factor is
bundled into this gain calculation, this provides a true indication of how refill plays into the
system in the long-term and is the best measure in our model of steady-state behavior. Note
when discussing system reduction factor’s role, it must remain between 0 and 1, as refill cannot
be reversed in our model, or more simply, drawing from a pool cannot cause more fluid to enter
than was removed. The τRED was chosen to be a value between 1 and 15 minutes, which was
chosen due to the general time observed for transients to die out in initial modeling and
simulations. While this can lead to cases when reduction factor time constant runs up right
against the limits, it is overall the best current estimate of where the bounds of the time constant
should lie.
Patient 17, returning to as a representative sample an example, has a gain of (0.027 ±
0.005) a coefficient of variability of 0.21. This is in a patient with 6 data sets, indicating that this
patient has low overall variability in gain identification. The system time constant is less
consistent, having a mean of 10.2 minutes, and a standard deviation of 4.2 minutes, variability
coefficient of 0.471. This variance being more substantial indicates that the patient’s refill is
stimulated at various rates on different days or possibly due to differing initial conditions, with
no time constant in particular being consistent. Further information bolstering this assessment is
seen in examining the refill time constant, with a mean of 2.75 min and a coefficient of variation
of 0.65. The difference in these time constants indicates some inconsistency in patient
hemodynamics, affirming the high variability compared to gain.
Such system time constant variability also occurs in 4 other patients (Patients 7, 8, 11,
and 15) with the coefficients of variation of the time constants often equaling up to 0.8 or more.
Similarly, the reduction factor time constant has such a coefficient of variation in patients 11 and
32. Only two system time constants coefficients of variation are equal to or below 0.5 (patients
17 and 31) indicating a high level of variance across patients in the trial for the system time
constant term, which in turn indicates somewhat of an unpredictability in the rate the system
settles into steady-state. 4 patients (8, 15, 27, and 31) exhibit coefficients of variation below 0.5
for the reduction factor time constant, slightly better than the system time constant. This could be

53
due to the limiting of the reduction factor time constant to the 1-15 minute range, while the
system time constant is theoretically allowed to range up to 100 minutes. Rationale for the time
constant variance will be explored further in long term estimation accuracy, as well as when
algorithmic limitations are discussed in further detail.
Examining more specific days in patients yields interesting considerations in the behavior
of refill over time, as it is clearly not consistent and may bias results. Patient 31 has two data
sets, day 121 and 135, (the third day 149 is erroneously identified as a flat profile in steady state)
where the identified plot is visually offset from the collected data in places, possibly due to the
patient having an especially extended time constant that is not identified (particularly in Figure
A126). Additionally, at 30 minutes on day 121 (Figure A124) we observe the hematocrit profile
flattens to have near-zero slope even though the UFR profile is relatively high at 1050 mL/hr.
Prior to this, however, both profiles track with limited visual error, meriting deeper examination
of initial conditions (Table 7.1.10). The initial hematocrit in these cases is very similar, and the
ultrafiltration rate is also comparable, days 121 and 135 being 1050 and 1250 mL/hr,
respectively. The estimated Gain, in both cases, approximately 0.31 and 0.25, are similar. The
identifications of τSYS and τRED are also similar enough, apart from the system time constant for
day 121 at 2.6 minutes. As this is low, this will cause the system portion to settle quickly and any
transient being more subject to the reduction factor. In examining specific parameters, the β
parameters are extremely similar, while the K and α parameters having a large disparity. The
reduction factor is substantially similar for these cases. Overall, this again indicates the concept
that the gain and time constants are often easier to identify than individual parameters, and may
be meaningful quantities, though in general time constant variability remains high.
Patient 32 (Figs. A130 – A138) exhibits mixed identification results due to limited
hematocrit change, which will be used as an example for such cases. For the cases of day 119,
135, and 138, it visually appears that the identification was successful, with the simulation
tracking to the collected data. Day 135 is particularly of note, since the simulation exhibits
behavior consistent with two very different time constants, and the collected data has behavior
consistent with refill changing 30 minutes into treatment. Day 119 indeed has two different time
constants of 11 minutes for the system, and 1 minute for the system time constant, which is
exceptionally low.

54
Patient 32’s system gain estimates (no reduction factor applied) vary between 0.035 and
0.048 (0.040 ± 0.0067), with the reduction factor having a large range of approximately 0.3-0.75
(0.61 ± 0.25). Hematocrit remains about the same for each case, around 0.305. Patient 32
exhibits more variance in parameters than other cases observed, with the α (0.21 ± 0.23) and β
(0.068 ± 0.076) parameters having a standard deviation exceeding the mean. Interestingly, the
Ksys parameter (0.17 ± 0.040) has a lower variance than the other parameters, standing somewhat
unique alongside the intra-patient statistics of other patients. Day 119 and day 135 are both
similar across all parameters, reduction factor, K, α, and β. This is a particularly interesting point,
as the only major difference between these two cases is the reduction factor time constant, which
due to the high reduction factor is non-negligible in this analysis. Nonetheless, this parameter
similarity indicates that parameters can be identified similarly between data sets of a patient,
though due to observations in other patients this seems to be a rare occurrence.
Figures such as 7.8 (patient 29 day 117) has a middling to high UFR of 940 mL/hr, which
is more than sufficient to instigate refill, based on observations made in analyzing patient data.
Identification can proceed, as the profile is not entirely flat, and is identified with a 0.75
reduction factor. Similar cases are seen for this patient where all their reduction factors are high
due to relatively flat recorded profiles. Similar initial hematocrits are observed each day for this
patient, being between 33% and 34%, and similar UFRs are present on each day. When
comparing aggregate parameters, the gain is very low compared to other patients, and the
standard deviation is very low for the gain. This indicates that this patient’s gain is consistent,
and very low throughout the data sets analyzed. Again, more substantial variance is observed in
time constant results. Despite the low variance in gain, each individual parameter displays
substantial variance, with the mean values for K, α, and β nearly equaling the standard deviation
of each in the identification. Through this, it can be discerned that for profiles with limited
hematocrit change (high refill) more of a challenge is presented than for cases with higher gain.
Overall, both system and reduction factor time constant have a more pronounced
variability than the gain parameter intra-patient. It seems to be the case for the patients observed
that individual parameters are very ill-suited to forming statistics for, with the examination of
combined parameters being the more ideal approach. Due to the low variability on the gain
parameter generally, along with the higher variability on τRED and τSYS, it seems to be indicative

55
of more predictability in steady-state behavior for a patient than behavior in transient. This is due
to dynamics not accounted for in our modeling as will be further explored in section 9.4.
8.1.1.1 The Estimation Algorithm Does Not Apply to Flat HCT Steady State Behavior
While flat, or near-flat, steady-state HCT slopes are consistent with expected responses,
that is, when refill matches UFR, such cases pose a numerical limitation on our system
identification. When examining the data obtained, one of the results found was the prevalence of
‘flat’ hematocrit profiles, cases where despite the application of UF, patient hematocrit does not
appreciably change, either initially or at steady state after some transient. In these cases, by
definition, during identification the reduction factor was set to 1. Mathematically speaking, this
indicates that the rate of refill in the system matches the rate of fluid removal precisely. As this is
only in steady state, this approach allows the time constant for reduction factor, τRED, to still be
present, allowing the system to still have a transient before settling into a flat steady state
hematocrit. This approach clearly will make the estimation of steady state gain more difficult, as
there is none in this system, and as the identification process couples the steady state gain to time
constant results are affected.
The numerical limitation posed by flat steady-state slopes stems from how the parameter
is estimated. Specifically, the gain of the system is computed using the slope of the system,
corrected for the reduction factor. For flat cases, this slope can only be zero. As a result, when β
is computed as a function of K and alpha, the result is that beta can only be zero, due to the
computed slope being used as a multiplier in the function as seen in Eq. 9.2 below.
0( )
0 ( )
K
K
=
+
+=
(8.2)
With β = 0, the response simplifies to:
(1 (1 ))
( ) (1 )
t
tautUFR e K
HCT t e
−
− − − = − (8.3)
which acts as an exponential decay term with an associated gain, reaching zero gain in steady
state. As the system hematocrit does not appreciably change, a poor estimate of the reduction

56
factor’s time constant is obtained, leading to inaccurate evaluations of when steady state is
reached.
As an example of this occurring, in the case of patient 7, two individual day cases (Figs
A19 and A21) are noted where the hematocrit profiles are not entirely flat but have very high
reduction factors (Kred) (0.84 and 0.89, respectively) comparative to other data sets between
patients and within patient 7. These were chosen as they allow for estimation to take place fully,
as opposed to reduction factors of 1 where the gain can only be computed as zero. As with
agreement in data sets where steady state was a clearly positive and linear slope, similar Gain is
observed across the identifications of the parameters, the grouping being even closer than patient
17, being (0.026 ± 0.0005) (no reduction factor), though the systems have vastly different time
constants (τSYS, [19.4 ± 17.5, COV 0.902] and τRED, [2.48 ± 1.94 COV 0.78]) despite the Gain
being nearly identical, which remain consistent with other patients observed in terms of accurate
gain estimation and variable time constants.
While patient 29 has a data set appearing as flat, it is not quite as extreme as seen in other
patients, with a reduction factor of 0.85. Interestingly day 107 and day 100 have the same UFR,
comparable initial hematocrits, and similar computed reduction factors but show drastically
different responses. Day 117 has a response that is not flat, and is consistent with the
expectations of the model, and has a higher UFR. A lower gain factor of 0.75 is also computed
for day 117. Notable differences between day 117 and the other patient 29 data sets are a higher
UFR, as well as slightly different starting hematocrits between all three cases. This difference
could point to slight differences in refill instigating these variations in hematocrit response to
UF, especially in the day 117 case. Effectively, the higher UFR could be sufficient in these cases
at the level they are to overcome the refill amount that would typically generate a flat profile.
The responses seen in the numerical results indicates that flat data sets are not simple to
identify despite initially promising results on the Gain parameter combination. This is an
unanticipated result as initially it would seem that the gain parameter combination would be the
most difficult to get right in a flat data set. The likely reason for this parameter coming out
consistently is in fact the use of the reduction factor to estimate refill, as it allows for a
normalization of system behavior in steady state, leading to a better estimate of gain. This cannot
make up for the fact that in flat profiles the transient is not as distinct, and if the transient is

57
indistinct, the K and α parameters will have worse estimations, leading to a poor calculation of β,
leading in turn to poor Gain, τSYS and τRED calculations.
8.1.2 Transient Responses not Included in the Model
In approximately 30% of measured data sets, the observed HCT dynamics is notably
different from the expected behavior described by the model (5.9). Causes, general unknown, but
may include food intake, patient keeps moving on the chair, and hypotensive events. Other
causes are related to the dialysis procedure itself. Misleading initial hematocrit data is possible
under certain conditions: initially, the external lines an access is connected to passes through are
filled with saline solution, and as treatment initiates the blood mixes with the saline until the line
is filled entirely with blood. This is determined by when the hematocrit reading is stable for a
period, at which point a signal is given to start treatment. Dialysis staff is instructed to wait few
minutes for HCT stabilization before UF is turned on. If the saline is not completely cleared from
the line, a false initial hematocrit reading is observed, invalidating the applicability of our model
(5.9). Needle mis- and re-placement, often at the start of HD session, introduce HCT transients
not otherwise predicted by (5.9), especially when UFR is fixed. The challenge with such
instances is that it still might be possible to estimate model parameters, however, the underlying
dynamics is not expected from out model. an example of which can be seen in Figures 7.5-7.6.
The chart indicates a needle adjustment sometime between 7-7:30. The hematocrit profile shows
a change around the 15 minutes mark (actual treatment time of 7:15), while the UFR profile
remained fixed. Therefore, our model does not match the dynamics observed in this treatment.
This case is particularly notable as visually the agreement of the estimation to the patient data
indicates a well-identified system over the estimation span, but examining the variables obtained
yields a near-zero reduction and a slightly higher gain than normal. Without knowledge of the
initial needle misplacement, it would be difficult to determine that the variables identified were
subject to abnormal data conditions, and as patient data and estimation align initially, there is
nothing obviously wrong on the surface of the estimation. This is a key point to address, as not
all data sets that conform to the expectations of the model on their surface conform to the
modeling in practice, and their limitation in the modeling process that must be accounted for as
well. Additionally, as this was the only case of needle misplacement noted, it cannot be
determined here if all data sets with needle misplacement have this hematocrit behavior, or if

58
other behavior can occur. It is even possible that there are data sets we have with minor needle
misplacement we remain unaware of.
A certain behavior is noted particularly in the identified systems of patient 29 (Figure
7.9) that merits further discussion, the small dip in the estimate during the response. The reason
for this dip is a result of the additional time constant associated with reduction factor (τRED) for
refill in the system. As the reduction factor in these cases is so high and the time constant is
relatively slow, the reduction takes a significant amount of time to affect the system and the
additional dynamics can be clearly seen. While in the nonlinear model derived for the system this
sort of behavior is impossible, the modifications made to the linearized model to account for
refill create these dynamics. While this does not affect the data, it is an aspect to keep in mind
when analyzing the parameters converged upon. As the RMS error of the model response
compared to the data is used to establish the ‘best’ parameters, this may be established by having
a significant time delay in the system which visually may not represent the exact behavior of the
data. As such it remains an important step to visually verify the model response compared to the
data in cases to ensure consistency and accuracy of findings.
In addition to these behaviors, patient 33 (Figures A139-A146) exhibits behavior opposed
to the expectations of the ultrafiltration process, where hematocrit drops when ultrafiltration
begins in each case. This is likely due to overload state of the patient, as their hematocrit is very
low starting out (27.5% - 30%). This is a clear case where the system identification cannot
function due to the expected behavior from modeling not matching with the behavior of the data
collected. Ultrafiltration draws excess fluid from the intravascular compartment, and therefore it
is expected that the volume will deplete as fluid is removed, even with refill from the interstitial
compartment. In this patient’s cases, this refill exceeds the rate of fluid loss, and therefore causes
compartment volume to increase, thus decreasing hematocrit. This is a clear reversal of
expectations from the model as developed, and therefore cannot be properly analyzed at this
stage.
8.2 Long Term Projected Output
The system identification process takes place over the initial, short span of time,
approximately up to thirty minutes following the imitation of UFR. This leaves out much of the
remaining dynamics taking place later during treatment, generally after the first sixty minutes.

59
We observe, for example Figure 8.5, where refill either seems to stop or slow down suddenly,
and drastic increases in slope occurs. In contrast, there are instances where refill suddenly
increases without apparent cause, causing a flattening in the HCT response, in some cases even
drops in hematocrit, as in Figure A106.
Long-term results are intrinsically tied to the steady-state behavior of the patient, and
therefore the more accurate that estimation is in the patient the more viable long-term results will
be for practical use. However, in most patients, other factors, primarily the nonlinearity of the
response and ANS response to dialysis, but also factors such as albumin level and oxygen
saturation, none are part of our model, will influence response of this longer time frame. For
example, Figure 8.7 shows the long-term behavior of the model identified for a case with a
relatively linear slope in steady-state. Despite matching up precisely in the region used for
identification, following this region there is offset between the estimated and actual slopes. Even
outside of drastic refill changes such as are in figures A124 and A106 among others, Figure 8.7
shows a case where even a seemingly linear slope can have a slightly inaccurate identification.
The region of estimation for the steady-state slope can be expanded to attempt to isolate this
slope more accurately, however in doing so the problem of measurement noise affecting results
is again encountered. Ultimately, as expected due to the limited time range over which our model
is effective, the identification seems to be more effective in determining short-term behavior near
the transient then in determining the longer-term trends of patient hematocrit. The response over
the longer time range will therefore require a separate estimation which should result in different
parameters.
8.3 Parameter Estimation of a Second UFR Step Response
In some HD treatment, there is a UF step change at some point in the treatment. Parameter
estimation of this response is significantly more difficult to estimate due to several factors.
Nevertheless, some observations can be made concerning the parameters and combinations of
parameters during transitions. The primary of these is that without exception, the system time
constant following a UFR step change is extremely fast, effectively approaching zero. Given that
refill has already reached its steady state from the initial UFR step, it appears to respond rapidly
to the new UFR. Further research is required on this topic to determine specific implications and
factors involved in estimating model parameters after a second UFR step change.

60
8.4 Overall Limitations
There are several limitations of our study as follows. The first among these is the
incapability of the identification to accurately estimate flat or near-flat data sets. As the
identification requires the use of the steady-state slope to estimate the overall parameters, a
steady-state slope of zero leaves numerical deficiencies in the solution, and thus these cases are
unidentifiable at this stage. It is worthy of note that flat hematocrit profiles indicate strong refill
from interstitial to intravascular space, and this refill is often indicative of fewer hypotensive
events, the overall goal of profile individualization. In addition to cases with strong refill,
systemic errors in treatment also interfere with identification, and in practice can only be noted
through treatment notes.
There are treatment-related factors that adversely affect the validity of our approach. Such
factors, including needle misplacement, food intake, and initial transients in refill between our
modeled compartments, are not part of the original nonlinear model, and therefore, not part of
the linearized model. Other factors can translate into time-varying parameters, also not
unaccounted for in the modeling. The most notable of these is the filtration coefficient, Kf, which
regulates the flow between interstitial and intravascular space. This parameter has been shown to
have substantial fluctuations over treatment periods, and substantial changes in this parameter
will lead to differences in patient response. As noted in Section 2.3, this broadly has influence on
the long-term output, which can influence the accuracy of identifications over the course of an
entire treatment.
Algorithmic limitations are also presented, with Figure A27 being representative of these.
As the algorithm functions by determining the steady-state slope, errors in the determination of
this term can lead to vast errors in the overall identification. In A27, what can be observed is
behavior where despite visual indications to the contrary, the steady state slope is identified as
being zero, which in turn results in the algorithm failing to identify any meaningful parameters.
This misidentification is due to the small fluctuations lowering the hematocrit in places in
steady-state, which in turn causes the linear fit slopes of hematocrit over time to be both negative
and positive, eventually converging to a most-often occurrence of zero. This behavior is noted in
Figure A128 as well, for patient 31, day 149 where a dip in hematocrit at approximately 25
minutes seems to generate the image of a flat profile in the analysis algorithm. Visual assistance

61
in the identification of slope would assist in eliminating these edge-cases, while pointing to
minor flaws in the identification algorithm.
Despite the limitations of the modelling and system identification approach, parameters are
shown to be identifiable in the aggregate gain and time constant parameters in 70% of measured
data sets. The model is sensitive to each of the parameters identified, indicating the importance
of accurate identification of each.

62
9 CONCLUSIONS
Dialysis is a critical treatment method for end-stage kidney disease, replacing the
function of kidneys when they can no longer filter excess fluid and toxins on their own. While
the treatment is very common, it has not seen much modernization or evolution in methods,
which this thesis addresses in part.
In this thesis, we focused on extending recent results derived in our lab which developed
a method for computing an individualized UFR profile based on a simplified model of a patient’s
fluid dynamics during hemodialysis. Specifically, we focused on the development and validation
of a dedicated parameter identification technique that can be integrated with the UFR profile
design method. The contributions of this thesis are threefold: (1) acquisition of unique clinical
data, (2) improving the simplified fluid dynamics model, and (3) development of a new system
identification technique. This study was approved by the IRB at the University of Massachusetts,
Amherst.
Actual treatment data was acquired via a collaboration with Crit-Line Technologies, a
division of Fresenius Medical Care North America, which enabled the construction of an
autonomous data acquisition system. The company’s device (CliC) is integrated within its
hemodialysis machine giving clinical staff real-time hematocrit data at a one-minute interval.
These devices were located at the American Renal Associates Inc. (ARA) in-center dialysis
facility in Holyoke, Massachusetts. Special Wi-Fi boards were retrofitted into each HD machine,
and at the end of each HD treatment, treatment data was downloaded to a dedicated laptop with a
special radio board. Downloaded data files included coded patient study ID, relative blood
volume change and oxygen level at a 1-minute interval. Separately, we collected redacted charts
from each treatment comprising UFRs and other treatment notes at a 30-minute interval. In all,
20 HD patients participated in the study, and a total of 77 treatment data sets were collected over
a 3-month period.
A key limitation of the simplified model used in the UFR profile design method was its
restriction to a no refill condition. To overcome this limitation, since a step UFR is expected to
elicit fluid refill from the interstitial compartment as observed in clinical data, we modified the
simplified fluid dynamics model to explicitly include refill term dynamics. However, the
modified model comprises 5 unknown parameters compared with 3 in the original model.

63
The main goal in the development of our parameter identification technique was an
automatic estimation from measured data of the 5 model parameters. To determine the steady-
state and transient regions on an autonomous basis, linear fits are performed over 10-minute-long
regions beginning 10 minutes following initiation of UF. Each slope is stored, and a histogram of
slopes is used to determine the most frequent occurrence, which serves as the identified slope.
From the beginning of the data to the first instance of this slope serves as the transient portion of
data. Certain measured data cannot be used with this technique. Data that exhibits unmodelled
dynamics, such as when patient intakes food, moves, misplaced needle placement, and
autonomic nervous system input, resulting in significant effect on the fluid dynamics. In
addition, the modified model included a linear combination of UFR and refill which makes
system ID mathematically impossible when HCT is flat, i.e., refill rate being equal to the UFR.
There was significant intra-patient estimated parameters variability, particularly related to
the fluid dynamics time-constant which varied by up to a factor of 5. This large variability could
be related to patient not being in true steady-state following priming – possibly due to priming
fluid not fully circulated in the system – something we are unable to verify. In contrast, steady
state properties of the model, steady-state gain and refill reduction factor had only moderate
intra-patient variability. Steady-state gain is identified with consistent values intra-patient, when
there is sufficient data following the model’s predicted response, with low variability even with
different UFRs. Both the gain and reduction factor when combined have low coefficient of
variation in patients despite differences in initial hematocrit and fluid removal rate during
treatment. Combined, these two factors indicate that when patients reach steady state, their
hematocrit responses to constant UFRs are more predictable as refill transients are not
confounding our results. The system time constant is not identified with consistent values intra-
patient, exhibiting high coefficient of variation for all but two patients for the system time
constant and four for reduction factor time constant. A potential explanation for this is there are
assumptions of transient dynamics made such as the presence of steady-state compartment
volume and these may not be present in patients, affecting the transient with factors that are not
accounted for in the modeling. Comparing parameters inter-patient shows large differences
between each patient’s identified parameters, as well as the combination of parameters such as
gain and time constant. This variability confirms different patients having different responses to
treatment, even when examining cases with similar initial hematocrit and UFRs. Similar gain

64
values intra-patient indicates the possibility for treatment to be predictable and individualized in
select patient cases, however, identification of time constants requires future work to determine
if better prediction of this term can be achieved.
The design of an individualized UFR profile could prove to be a key step to improving
the lives and treatment outcomes of patients undergoing dialysis, and a key point of that process
is the identification of an accurate system model. The identification procedure detailed here is
shown to have low variability in the identification of Gain and reduction parameters in steady
state, indicating a capability to predict short term treatment trajectories, with long-term cases
remaining less predictable likely due to unmodeled hemodynamics. By integrating observations
from clinical data into the development of the system model, we can better model the dynamics
of the patient, and better able to predict patient response to treatment application.

65
10 FUTURE DIRECTIONS
There are several possible topics for future work in this area. Flat steady-state HCT
responses cannot be handled by the algorithm, hence a fast estimation algorithm that can
overcome this limitation would constitute an important contribution. Several factors could be
involved such as O2 Sat and patient Albumin levels, and a determination of a possible correlation
between these parameters and steady-state response could potentially assist in the determination
of model reduction factor, ultimately leading to more accurate results in parameter estimation in
such cases and in all cases, in general.
Better understanding of the long term HCT dynamics, especially following a second UFR
step change, would constitute another contribution. Our initial analysis showed that such cases
are characterized by fast system time constants, that is, transitional behavior being all but non-
existent.
Finally, as this thesis resulted in an updated model to be used with the method for design of
the individualized ultrafiltration profile, the profile design method necessitates an appropriate
update for this model change.

66
REFERENCES
[1] Facts About Chronic Kidney Disease. (2020, September 01). Retrieved December 10, 2020,
from https://www.kidney.org/atoz/content/about-chronic-kidney-disease
[2] Bosch J.P., Geronemus R., Glabman S., Moutoussis G., Kahn T., von Albertini B. (1980)
Ultrafiltration in Patients with Endstage Renal Disease. In: Cooper A.R. (eds)
Ultrafiltration Membranes and Applications. Polymer Science and Technology, vol
13. Springer, Boston, MA. https://doi.org/10.1007/978-1-4613-3162-9_37
[3] Ofsthun NJ, Leypoldt JK. Ultrafiltration and backfiltration during hemodialysis. Artif
Organs. 1995 Nov;19(11):1143-61. doi: 10.1111/j.1525-1594.1995.tb02276.x. PMID:
8579527.
[4] Dialysis Process Illustration. Retrieved December 22, 2020, from
https://www.shutterstock.com/image-vector/dialysis-process-illustration-767190277
[5] Hemodialysis. (2019, July 23). Retrieved December 22, 2020, from
https://www.mayoclinic.org/tests-procedures/hemodialysis/about/pac-20384824
[6] Frequent Long Dialysis : Why Do Length and Frequency Help? (n.d.). Retrieved December
22, 2020, from https://www.kidneynews.org/kidney-news/features/frequent-long-dialysis-
why-do-length-and-frequency-help
[7] Abohtyra, R., Hollot, C., Germain, M., Chait, Y., & Horowitz, J. (2018). Personalized
Ultrafiltration Profiles to Minimize Intradialytic Hypotension in End-Stage Renal Disease.
2018 IEEE Conference on Decision and Control (CDC). doi:10.1109/cdc.2018.8619152
[8] Abohtyra R, Chait Y, Germain MJ, Hollot CV, Horowitz J. Individualization of
Ultrafiltration in Hemodialysis. IEEE Trans Biomed Eng. 2019 Aug;66(8):2174-2181.
doi: 10.1109/TBME.2018.2884931. Epub 2018 Dec 4. PMID: 30530307; PMCID:
PMC6691497.
[9] Schneditz, D. Pathophysiology of refilling. Issues in Nephrosciences 6.96. 1996. ISBN – 88-
85453-57-0.
[10] Zhu F, Kappel F, Leonard EF, Kotanko P, Levin NW. Modeling of change in blood volume
and extracellular fluid volume during hemodialysis. Annu Int Conf IEEE Eng Med Biol
Soc. 2013;2013:1506-9. doi: 10.1109/EMBC.2013.6609798. PMID: 24109985.
[11] Goncalves, A. Model-Based Feedback Control for Hemodialysis Treatment of Chronic
Kidney Disease Patients. 2015. Unpublished.
Top Related
Copyright © 2022 FDOKUMEN

